
Prevention of anterior cruciate ligament injuries in soccer
13
SPORTS MEDICINE Prevention of anterior cruciate ligament injuries in sports—Part I: Systematic review of risk factors in male athletes Eduard Alentorn-Geli • Jurdan Mendiguchı ´a • Kristian Samuelsson • Volker Musahl • Jon Karlsson • Ramon Cugat • Gregory D. Myer Received: 6 August 2013 / Accepted: 14 October 2013 Ó Springer-Verlag Berlin Heidelberg 2013 Abstract Purpose The purpose of this study was to report a com- prehensive literature review on the risk factors for anterior cruciate ligament (ACL) injuries in male athletes. Methods All abstracts were read and articles of potential interest were reviewed in detail to determine on inclusion status for systematic review. Information regarding risk factors for ACL injuries in male athletes was extracted from all included studies in systematic fashion and classi- fied as environmental, anatomical, hormonal, neuromus- cular, or biomechanical. Data extraction involved general characteristics of the included studies (type of study, characteristics of the sample, type of sport), methodologi- cal aspects (for quality assessment), and the principal results for each type of risk factor. Results The principal findings of this systematic review related to the risk factors for ACL injury in male athletes are: (1) most of the evidence is related to environmental and anatomical risk factors; (2) dry weather conditions may increase the risk of non-contact ACL injuries in male athletes; (3) artificial turf may increase the risk of non- contact ACL injuries in male athletes; (4) higher posterior tibial slope of the lateral tibial plateau may increase the risk of non-contact ACL injuries in male athletes. Conclusion Anterior cruciate ligament injury in male athletes likely has a multi-factorial aetiology. There is a lack of evidence regarding neuromuscular and biome- chanical risk factors for ACL injury in male athletes. Future research in male populations is warranted to provide adequate prevention strategies aimed to decrease the risk of this serious injury in these populations. Level of evidence Systematic review on level I–IV stud- ies, Level IV. Keywords Prevention Á ACL injury Á Risk factors Á Male athletes E. Alentorn-Geli (&) Department of Orthopaedic Surgery, Hospital del Mar—Parc de Salut Mar, Universitat Autonoma de Barcelona and Universitat Pompeu Fabra, Passeig Marı ´tim 25-29, 08003 Barcelona, Spain e-mail: [email protected] J. Mendiguchı ´a Department of Physical Therapy, Zentrum Rehab and Performance Center, Baran ˜ain, Navarre, Spain K. Samuelsson Á J. Karlsson Department of Orthopaedics, Sahlgrenska University Hospital, Mo ¨lndal, Sweden V. Musahl Department of Orthopaedic Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA, USA R. Cugat Garcı ´a-Cugat Foundation, Barcelona, Spain R. Cugat Mutualidad de Futbolistas, Federacio ´n Espan ˜ola de Fu ´tbol— Delegacio ´n Catalun ˜a, Barcelona, Spain G. D. Myer Division of Sports Medicine, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA G. D. Myer Departments of Pediatrics and Orthopaedic Surgery, University of Cincinnati, Cincinnati, OH, USA G. D. Myer The Micheli Center for Sports Injury Prevention, Boston, MA, USA 123 Knee Surg Sports Traumatol Arthrosc DOI 10.1007/s00167-013-2725-3
-
Upload
pointblanklondon -
Category
Documents
-
view
5 -
download
0
Transcript of Prevention of anterior cruciate ligament injuries in soccer

SPORTS MEDICINE
Prevention of anterior cruciate ligament injuries in sports—PartI: Systematic review of risk factors in male athletes
Eduard Alentorn-Geli • Jurdan Mendiguchıa •
Kristian Samuelsson • Volker Musahl •
Jon Karlsson • Ramon Cugat • Gregory D. Myer
Received: 6 August 2013 / Accepted: 14 October 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract
Purpose The purpose of this study was to report a com-
prehensive literature review on the risk factors for anterior
cruciate ligament (ACL) injuries in male athletes.
Methods All abstracts were read and articles of potential
interest were reviewed in detail to determine on inclusion
status for systematic review. Information regarding risk
factors for ACL injuries in male athletes was extracted
from all included studies in systematic fashion and classi-
fied as environmental, anatomical, hormonal, neuromus-
cular, or biomechanical. Data extraction involved general
characteristics of the included studies (type of study,
characteristics of the sample, type of sport), methodologi-
cal aspects (for quality assessment), and the principal
results for each type of risk factor.
Results The principal findings of this systematic review
related to the risk factors for ACL injury in male athletes
are: (1) most of the evidence is related to environmental
and anatomical risk factors; (2) dry weather conditions may
increase the risk of non-contact ACL injuries in male
athletes; (3) artificial turf may increase the risk of non-
contact ACL injuries in male athletes; (4) higher posterior
tibial slope of the lateral tibial plateau may increase the risk
of non-contact ACL injuries in male athletes.
Conclusion Anterior cruciate ligament injury in male
athletes likely has a multi-factorial aetiology. There is a
lack of evidence regarding neuromuscular and biome-
chanical risk factors for ACL injury in male athletes.
Future research in male populations is warranted to provide
adequate prevention strategies aimed to decrease the risk of
this serious injury in these populations.
Level of evidence Systematic review on level I–IV stud-
ies, Level IV.
Keywords Prevention � ACL injury � Risk factors �Male athletes
E. Alentorn-Geli (&)
Department of Orthopaedic Surgery, Hospital del Mar—Parc de
Salut Mar, Universitat Autonoma de Barcelona and Universitat
Pompeu Fabra, Passeig Marıtim 25-29, 08003 Barcelona, Spain
e-mail: [email protected]
J. Mendiguchıa
Department of Physical Therapy, Zentrum Rehab and
Performance Center, Baranain, Navarre, Spain
K. Samuelsson � J. Karlsson
Department of Orthopaedics, Sahlgrenska University Hospital,
Molndal, Sweden
V. Musahl
Department of Orthopaedic Surgery, University of Pittsburgh
Medical Center, Pittsburgh, PA, USA
R. Cugat
Garcıa-Cugat Foundation, Barcelona, Spain
R. Cugat
Mutualidad de Futbolistas, Federacion Espanola de Futbol—
Delegacion Cataluna, Barcelona, Spain
G. D. Myer
Division of Sports Medicine, Cincinnati Children’s Hospital
Medical Center, Cincinnati, OH, USA
G. D. Myer
Departments of Pediatrics and Orthopaedic Surgery, University
of Cincinnati, Cincinnati, OH, USA
G. D. Myer
The Micheli Center for Sports Injury Prevention,
Boston, MA, USA
123
Knee Surg Sports Traumatol Arthrosc
DOI 10.1007/s00167-013-2725-3
Introduction
Anterior cruciate ligament (ACL) injuries are a common
and debilitating injury in competitive sports [10, 37, 67].
The costs of this injury are very high from both the
patient’s health and economic standpoints [33, 35, 36, 49].
The high incidence of ACL injury along with the poten-
tially devastating long-term consequences on the knee has
led to great research efforts focused on prevention and
management of injuries. Many studies have been con-
ducted to better understand the inciting mechanisms of
ACL injury and the associated risk factors that contribute
to increased risk for injury [3, 17, 38, 42]. While sub-
stantive research efforts have been made to improve
diagnosis and treatment strategies [5, 15, 19, 24, 45, 53, 55,
56, 72, 77], the long-term consequence of ACL injuries is
likely osteoarthritis, even in cases undergoing surgical
treatment [49]. Therefore, the most effective strategy to
avoid joint damage is prevention.
There has been a growing awareness on the relevance
of prevention of ACL injuries in athletes from health care
providers who are faced to manage the injuries. Women
have a higher risk of non-contact ACL injuries compared
to their male counterparts [6, 10]; therefore, research on
mechanisms of injury, risk factors and prevention strate-
gies of these injuries has predominately focused on the
female athlete [3, 4, 17, 18, 40, 42]. Most of the inves-
tigations only included females or compared females and
males [3, 4, 17, 18, 40, 42, 56]. However, the overall
incidence of ACL injuries is high in males as well [54],
especially considering that males may be more exposed to
high-risk sports [33]. Unfortunately, the available infor-
mation on risk factors for non-contact ACL injuries spe-
cifically in male has not been well documented to date.
Thus, the exact information regarding the factors that
place a male athlete at greater risk of ACL injury is not
well understood and data from female athletes are often
extrapolated to their male counterparts, which likely leads
to sub-optimal intervention and management strategies for
the male athlete. Therefore, the purpose of this systematic
review was to assimilate and synthesize the existing
evidence on the risk factors for ACL injuries in male
athletes.
Material and methods
The methodology of this study was reported following the
Preferred Reporting Items for Systematic Reviews and
Meta-Analyses (PRISMA) Statement for systematic
reviews [52]. This is an evidence-based minimum set of
items that serve as a guide for authors when reporting
systematic reviews or meta-analyses, and include: title,
abstract, introduction (rationale and objectives), methods
(protocol and registration, eligibility criteria, information
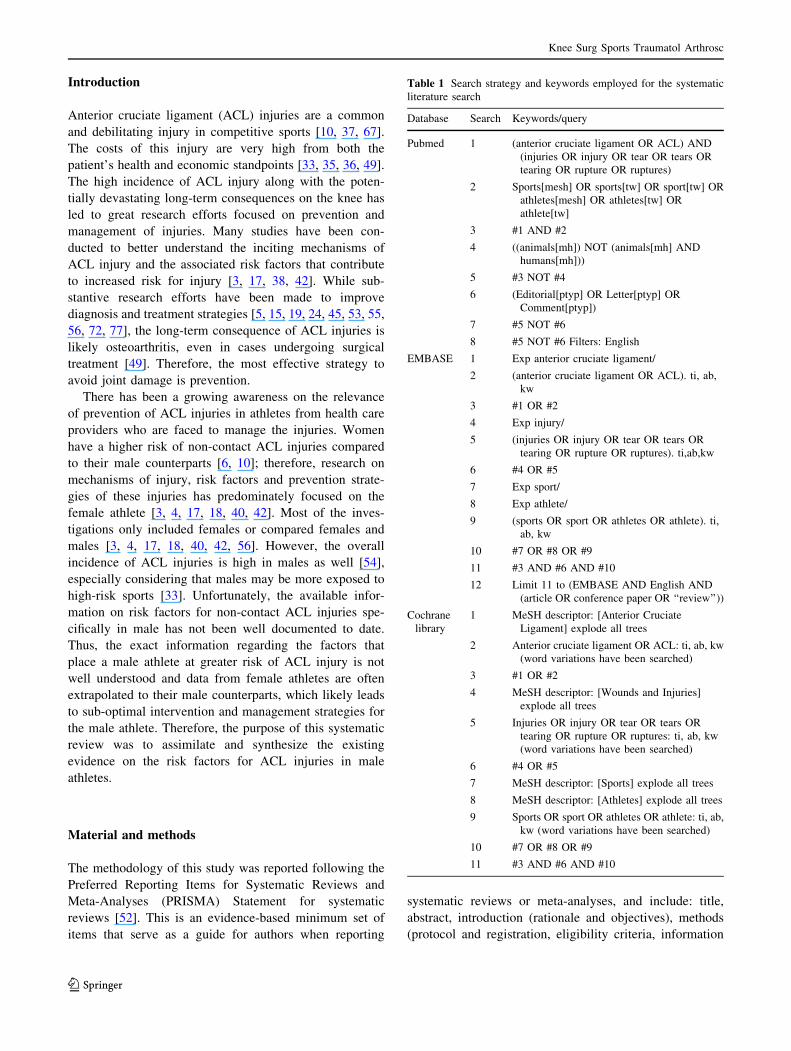
Table 1 Search strategy and keywords employed for the systematic
literature search
Database Search Keywords/query
Pubmed 1 (anterior cruciate ligament OR ACL) AND
(injuries OR injury OR tear OR tears OR
tearing OR rupture OR ruptures)
2 Sports[mesh] OR sports[tw] OR sport[tw] OR
athletes[mesh] OR athletes[tw] OR
athlete[tw]
3 #1 AND #2
4 ((animals[mh]) NOT (animals[mh] AND
humans[mh]))
5 #3 NOT #4
6 (Editorial[ptyp] OR Letter[ptyp] OR
Comment[ptyp])
7 #5 NOT #6
8 #5 NOT #6 Filters: English
EMBASE 1 Exp anterior cruciate ligament/
2 (anterior cruciate ligament OR ACL). ti, ab,
kw
3 #1 OR #2
4 Exp injury/
5 (injuries OR injury OR tear OR tears OR
tearing OR rupture OR ruptures). ti,ab,kw
6 #4 OR #5
7 Exp sport/
8 Exp athlete/
9 (sports OR sport OR athletes OR athlete). ti,
ab, kw
10 #7 OR #8 OR #9
11 #3 AND #6 AND #10
12 Limit 11 to (EMBASE AND English AND
(article OR conference paper OR ‘‘review’’))
Cochrane
library
1 MeSH descriptor: [Anterior Cruciate
Ligament] explode all trees
2 Anterior cruciate ligament OR ACL: ti, ab, kw
(word variations have been searched)
3 #1 OR #2
4 MeSH descriptor: [Wounds and Injuries]
explode all trees
5 Injuries OR injury OR tear OR tears OR
tearing OR rupture OR ruptures: ti, ab, kw
(word variations have been searched)
6 #4 OR #5
7 MeSH descriptor: [Sports] explode all trees
8 MeSH descriptor: [Athletes] explode all trees
9 Sports OR sport OR athletes OR athlete: ti, ab,
kw (word variations have been searched)
10 #7 OR #8 OR #9
11 #3 AND #6 AND #10
Knee Surg Sports Traumatol Arthrosc
123

sources, search, study selection, data collection process,
data items, risk of bias in individual studies, summary
measures, synthesis of results, risk of bias across studies,
and additional analyses), results (study selection, study
characteristics, risk of bias within studies, results of indi-
vidual studies, synthesis of results, risk of bias across
studies, and additional analysis), discussion (summary of
evidence, limitations, and conclusions), and funding.
Eligibility criteria
All prospective, cross-sectional or retrospective prognos-
tic human studies investigating risk factors for ACL
injury were evaluated for eligibility. Studies were inclu-
ded if they were: level of evidence between I and IV,
written in English language, and contained results speci-
fied for males. Studies only reporting issues other than
risk factors or studies investigating only female sample
were excluded. Studies not including ACL-injured sub-
jects or ACL injury as an outcome measure were exclu-
ded. Therapeutic and diagnostic studies were excluded.
Review articles, systematic reviews, and meta-analyses
were not included, but reference lists were examined to
ensure completeness of relevant studies. To avoid selec-
tion bias, studies comparing females and males were
reviewed in detail to assess for intra-group comparison in
males.
Information sources and search
Electronic search
A systematic electronic literature search was conducted
using the PubMed (MEDLINE) database and The Coch-
rane Library up to September 2012 (no start date), EM-
BASE database from 1980 to September 2012. Two expert
librarians in electronic search methods performed the lit-
erature search. The search strategy and keywords employed
in this study are summarized in Table 1.
Other search methods
The reference lists of all included articles were reviewed to
search for potential studies not previously identified.
Data collection and analysis
Study selection
All abstracts were read and articles of potential interest were
reviewed in detail (full text) by 3 authors (EAG, JM, and
GDM) to decide on inclusion or exclusion from this sys-
tematic review. In cases of disagreement, all three authors
reviewed and discussed the study and a final decision in
consensus. In all cases where the information regarding the
sex of the subject was not provided, a contact with the cor-
responding author was established to determine the sex of
the investigation subjects.
Data collection process
Information regarding risk factors for ACL injuries in
male athletes was extracted by the first author from all
included studies in systematic fashion following the
classification of risk factors suggested in the Hunt Valley
meeting [38]. Thus, risk factors were classified as envi-
ronmental, anatomical, hormonal, neuromuscular, and
biomechanical. Data extraction involved general charac-
teristics of the included studies (type of study, charac-
teristics of the sample, type of sport), methodological
aspects (for quality assessment), and the principal results
for each type of risk factor. One author (EAG) performed
all data extraction, which was then verified by two
authors (JM and GDM).
Assessment of the risk of bias
The methodological quality of all included studies was
evaluated with the assessment of the risk of bias in several
areas of a research project. This assessment was performed
by answering yes, no, unknown, or not applicable to the
following information from each study: prospective, con-
cealed allocation (yes = assignment was made by an
independent person who had no information about study
participants), similarities at baseline between groups
(yes = study groups were similar in demographic charac-
teristics), blinding of participants (yes = study population
blinding was clearly described and acceptable), blinding of
data collectors (yes = data collectors were blinded
regarding group assignments), blinding of outcome asses-
sors (yes = outcome assessors who evaluated the partici-
pants were blinded regarding group assignments), previous
knee injuries excluded, results specified for non-contact
injuries, influence of other risk factors controlled, accept-
able compliance (yes = compliance was regularly checked
or otherwise strictly supervised by someone other than
study participants, and it was more than 70 % in every
study group), dropout reasons reported, acceptable dropout
rate (yes = dropout rate was \30 %), duration of inter-
vention comparable between groups, and intention-to-treat
analysis (yes = all subjects assigned to a group at the
beginning of the study were included in the analysis). A
final quality score was given for each study, where ‘yes’
was 1 point and the other response was 0 points. The
assessment of the risk of bias in included studies was based
on the article by Aaltonen et al. [1].
Knee Surg Sports Traumatol Arthrosc
123
Results
Study selection
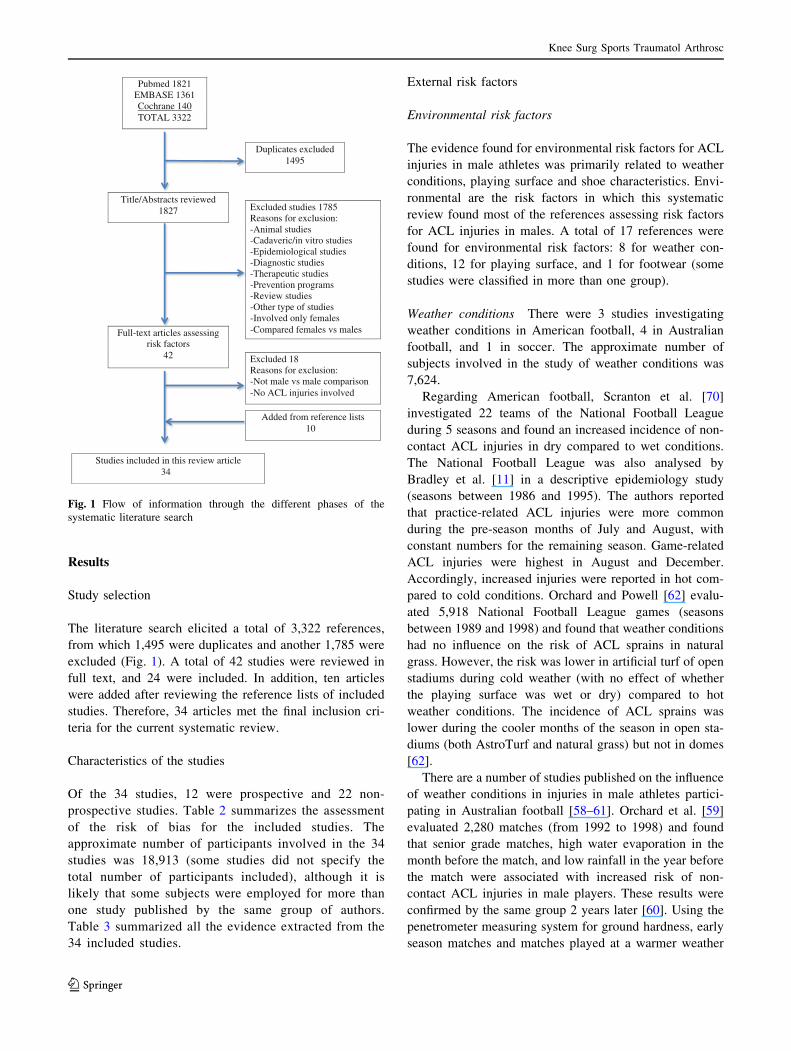
The literature search elicited a total of 3,322 references,
from which 1,495 were duplicates and another 1,785 were
excluded (Fig. 1). A total of 42 studies were reviewed in
full text, and 24 were included. In addition, ten articles
were added after reviewing the reference lists of included
studies. Therefore, 34 articles met the final inclusion cri-
teria for the current systematic review.
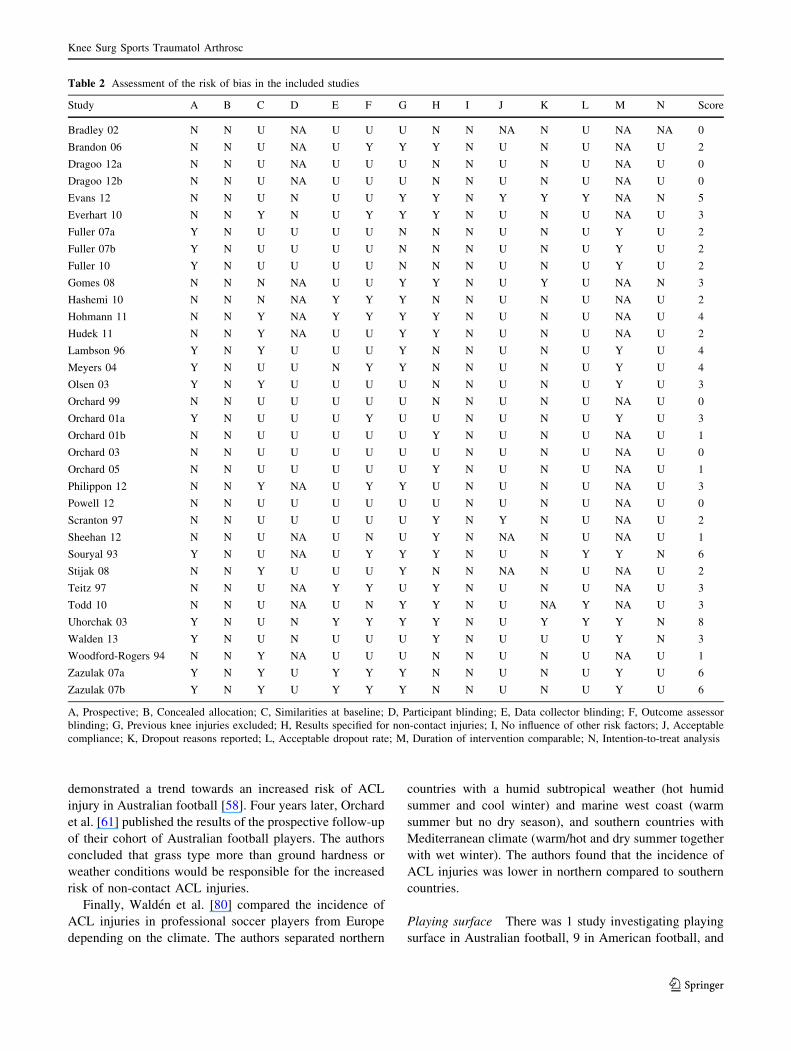
Characteristics of the studies
Of the 34 studies, 12 were prospective and 22 non-
prospective studies. Table 2 summarizes the assessment
of the risk of bias for the included studies. The
approximate number of participants involved in the 34
studies was 18,913 (some studies did not specify the
total number of participants included), although it is
likely that some subjects were employed for more than
one study published by the same group of authors.
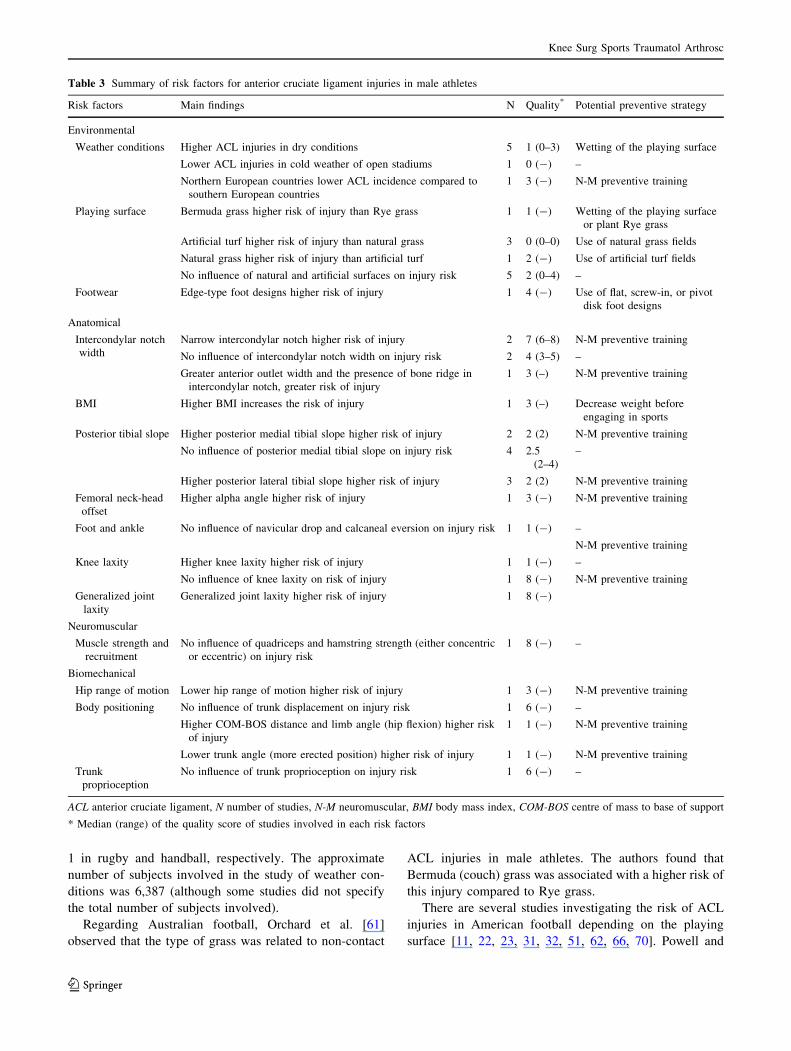
Table 3 summarized all the evidence extracted from the
34 included studies.
External risk factors
Environmental risk factors
The evidence found for environmental risk factors for ACL
injuries in male athletes was primarily related to weather
conditions, playing surface and shoe characteristics. Envi-
ronmental are the risk factors in which this systematic
review found most of the references assessing risk factors
for ACL injuries in males. A total of 17 references were
found for environmental risk factors: 8 for weather con-
ditions, 12 for playing surface, and 1 for footwear (some
studies were classified in more than one group).
Weather conditions There were 3 studies investigating
weather conditions in American football, 4 in Australian
football, and 1 in soccer. The approximate number of
subjects involved in the study of weather conditions was
7,624.
Regarding American football, Scranton et al. [70]
investigated 22 teams of the National Football League
during 5 seasons and found an increased incidence of non-
contact ACL injuries in dry compared to wet conditions.
The National Football League was also analysed by
Bradley et al. [11] in a descriptive epidemiology study
(seasons between 1986 and 1995). The authors reported
that practice-related ACL injuries were more common
during the pre-season months of July and August, with
constant numbers for the remaining season. Game-related
ACL injuries were highest in August and December.
Accordingly, increased injuries were reported in hot com-
pared to cold conditions. Orchard and Powell [62] evalu-
ated 5,918 National Football League games (seasons
between 1989 and 1998) and found that weather conditions
had no influence on the risk of ACL sprains in natural
grass. However, the risk was lower in artificial turf of open
stadiums during cold weather (with no effect of whether
the playing surface was wet or dry) compared to hot
weather conditions. The incidence of ACL sprains was
lower during the cooler months of the season in open sta-
diums (both AstroTurf and natural grass) but not in domes
[62].
There are a number of studies published on the influence
of weather conditions in injuries in male athletes partici-
pating in Australian football [58–61]. Orchard et al. [59]
evaluated 2,280 matches (from 1992 to 1998) and found
that senior grade matches, high water evaporation in the
month before the match, and low rainfall in the year before
the match were associated with increased risk of non-
contact ACL injuries in male players. These results were
confirmed by the same group 2 years later [60]. Using the
penetrometer measuring system for ground hardness, early
season matches and matches played at a warmer weather
Pubmed 1821EMBASE 1361Cochrane 140TOTAL 3322
Title/Abstracts reviewed1827
Duplicates excluded1495
Full-text articles assessing risk factors
42
Excluded studies 1785Reasons for exclusion:-Animal studies-Cadaveric/in vitro studies-Epidemiological studies-Diagnostic studies-Therapeutic studies-Prevention programs-Review studies-Other type of studies-Involved only females-Compared females vs males
Studies included in this review article34
Added from reference lists10
Excluded 18Reasons for exclusion:-Not male vs male comparison-No ACL injuries involved
Fig. 1 Flow of information through the different phases of the
systematic literature search
Knee Surg Sports Traumatol Arthrosc
123
demonstrated a trend towards an increased risk of ACL
injury in Australian football [58]. Four years later, Orchard
et al. [61] published the results of the prospective follow-up
of their cohort of Australian football players. The authors
concluded that grass type more than ground hardness or
weather conditions would be responsible for the increased
risk of non-contact ACL injuries.
Finally, Walden et al. [80] compared the incidence of
ACL injuries in professional soccer players from Europe
depending on the climate. The authors separated northern
countries with a humid subtropical weather (hot humid
summer and cool winter) and marine west coast (warm
summer but no dry season), and southern countries with
Mediterranean climate (warm/hot and dry summer together
with wet winter). The authors found that the incidence of
ACL injuries was lower in northern compared to southern
countries.
Playing surface There was 1 study investigating playing
surface in Australian football, 9 in American football, and
Table 2 Assessment of the risk of bias in the included studies
Study A B C D E F G H I J K L M N Score
Bradley 02 N N U NA U U U N N NA N U NA NA 0
Brandon 06 N N U NA U Y Y Y N U N U NA U 2
Dragoo 12a N N U NA U U U N N U N U NA U 0
Dragoo 12b N N U NA U U U N N U N U NA U 0
Evans 12 N N U N U U Y Y N Y Y Y NA N 5
Everhart 10 N N Y N U Y Y Y N U N U NA U 3
Fuller 07a Y N U U U U N N N U N U Y U 2
Fuller 07b Y N U U U U N N N U N U Y U 2
Fuller 10 Y N U U U U N N N U N U Y U 2
Gomes 08 N N N NA U U Y Y N U Y U NA N 3
Hashemi 10 N N N NA Y Y Y N N U N U NA U 2
Hohmann 11 N N Y NA Y Y Y Y N U N U NA U 4
Hudek 11 N N Y NA U U Y Y N U N U NA U 2
Lambson 96 Y N Y U U U Y N N U N U Y U 4
Meyers 04 Y N U U N Y Y N N U N U Y U 4
Olsen 03 Y N Y U U U U N N U N U Y U 3
Orchard 99 N N U U U U U N N U N U NA U 0
Orchard 01a Y N U U U Y U U N U N U Y U 3
Orchard 01b N N U U U U U Y N U N U NA U 1
Orchard 03 N N U U U U U U N U N U NA U 0
Orchard 05 N N U U U U U Y N U N U NA U 1
Philippon 12 N N Y NA U Y Y U N U N U NA U 3
Powell 12 N N U U U U U U N U N U NA U 0
Scranton 97 N N U U U U U Y N Y N U NA U 2
Sheehan 12 N N U NA U N U Y N NA N U NA U 1
Souryal 93 Y N U NA U Y Y Y N U N Y Y N 6
Stijak 08 N N Y U U U Y N N NA N U NA U 2
Teitz 97 N N U NA Y Y U Y N U N U NA U 3
Todd 10 N N U NA U N Y Y N U NA Y NA U 3
Uhorchak 03 Y N U N Y Y Y Y N U Y Y Y N 8
Walden 13 Y N U N U U U Y N U U U Y N 3
Woodford-Rogers 94 N N Y NA U U U N N U N U NA U 1
Zazulak 07a Y N Y U Y Y Y N N U N U Y U 6
Zazulak 07b Y N Y U Y Y Y N N U N U Y U 6
A, Prospective; B, Concealed allocation; C, Similarities at baseline; D, Participant blinding; E, Data collector blinding; F, Outcome assessor
blinding; G, Previous knee injuries excluded; H, Results specified for non-contact injuries; I, No influence of other risk factors; J, Acceptable
compliance; K, Dropout reasons reported; L, Acceptable dropout rate; M, Duration of intervention comparable; N, Intention-to-treat analysis
Knee Surg Sports Traumatol Arthrosc
123
1 in rugby and handball, respectively. The approximate
number of subjects involved in the study of weather con-
ditions was 6,387 (although some studies did not specify
the total number of subjects involved).
Regarding Australian football, Orchard et al. [61]
observed that the type of grass was related to non-contact
ACL injuries in male athletes. The authors found that
Bermuda (couch) grass was associated with a higher risk of
this injury compared to Rye grass.
There are several studies investigating the risk of ACL
injuries in American football depending on the playing
surface [11, 22, 23, 31, 32, 51, 62, 66, 70]. Powell and
Table 3 Summary of risk factors for anterior cruciate ligament injuries in male athletes
Risk factors Main findings N Quality* Potential preventive strategy
Environmental
Weather conditions Higher ACL injuries in dry conditions 5 1 (0–3) Wetting of the playing surface
Lower ACL injuries in cold weather of open stadiums 1 0 (-) –
Northern European countries lower ACL incidence compared to
southern European countries
1 3 (-) N-M preventive training
Playing surface Bermuda grass higher risk of injury than Rye grass 1 1 (-) Wetting of the playing surface
or plant Rye grass
Artificial turf higher risk of injury than natural grass 3 0 (0–0) Use of natural grass fields
Natural grass higher risk of injury than artificial turf 1 2 (-) Use of artificial turf fields
No influence of natural and artificial surfaces on injury risk 5 2 (0–4) –
Footwear Edge-type foot designs higher risk of injury 1 4 (-) Use of flat, screw-in, or pivot
disk foot designs
Anatomical
Intercondylar notch
width
Narrow intercondylar notch higher risk of injury 2 7 (6–8) N-M preventive training
No influence of intercondylar notch width on injury risk 2 4 (3–5) –
Greater anterior outlet width and the presence of bone ridge in
intercondylar notch, greater risk of injury
1 3 (–) N-M preventive training
BMI Higher BMI increases the risk of injury 1 3 (–) Decrease weight before
engaging in sports
Posterior tibial slope Higher posterior medial tibial slope higher risk of injury 2 2 (2) N-M preventive training
No influence of posterior medial tibial slope on injury risk 4 2.5
(2–4)
–
Higher posterior lateral tibial slope higher risk of injury 3 2 (2) N-M preventive training
Femoral neck-head
offset
Higher alpha angle higher risk of injury 1 3 (-) N-M preventive training
Foot and ankle No influence of navicular drop and calcaneal eversion on injury risk 1 1 (-) –
N-M preventive training
Knee laxity Higher knee laxity higher risk of injury 1 1 (-) –
No influence of knee laxity on risk of injury 1 8 (-) N-M preventive training
Generalized joint
laxity
Generalized joint laxity higher risk of injury 1 8 (-)
Neuromuscular
Muscle strength and
recruitment
No influence of quadriceps and hamstring strength (either concentric
or eccentric) on injury risk
1 8 (-) –
Biomechanical
Hip range of motion Lower hip range of motion higher risk of injury 1 3 (-) N-M preventive training
Body positioning No influence of trunk displacement on injury risk 1 6 (-) –
Higher COM-BOS distance and limb angle (hip flexion) higher risk
of injury
1 1 (-) N-M preventive training
Lower trunk angle (more erected position) higher risk of injury 1 1 (-) N-M preventive training
Trunk
proprioception
No influence of trunk proprioception on injury risk 1 6 (-) –
ACL anterior cruciate ligament, N number of studies, N-M neuromuscular, BMI body mass index, COM-BOS centre of mass to base of support
* Median (range) of the quality score of studies involved in each risk factors
Knee Surg Sports Traumatol Arthrosc
123

Schootman found an increased risk of ACL injuries in
artificial turf compared to natural grass after evaluating
National Football League games between 1980 and 1989
[66]. In contrast, Scranton et al. [70] found an increased
risk of non-contact ACL injuries in natural grass compared
to artificial turf during games of the National Football
League. A more recent investigation reported no differ-
ences in rates of non-contact ACL injuries between natural
grass and artificial surface throughout games of a 9-year
period [11]. These results were supported in the study by
Orchard and Powell [62], who found no increased risk of
ACL sprains in natural grass compared to dome and open
turf. However, when considering practice sessions, an
increased proportion of ACL injuries was reported on
natural (82 %) compared to artificial (18 %) surface [11].
Meyers et al. [51] evaluated male football of 8 high schools
over 5 competitive seasons and found non-significant dif-
ferences for both isolated and non-isolated ACL injuries
between artificial turf and natural. Similarly, Fuller et al.
[32] found no differences between artificial turf and natural
grass for the incidence of ACL injuries in male players,
either in practice and games [31]. Dragoo et al. [22, 23]
reported a descriptive epidemiology study over a period of
5 years in National Collegiate Athletic Association football
male athletes. The rate of ACL injuries in artificial surfaces
was increased relative to natural grass for both pre-season
and in-season periods, but not in the post-season period
[22, 23]. The increased risk of ACL injury in artificial
surfaces compared to natural grass was present in games,
scrimmages, and practices, and across all divisions [23].
The risk was higher in games compared to practice, and in
scrimmages compared to regular practice and walk-
throughs [22]. Regarding the specific type of artificial turf,
third-generation surfaces (with fill) had more risk of ACL
injury compared to first- and second-generation surfaces
(without fill) [23].
Regarding the evidence for other sports, an investigation
was performed to compare the risk of ACL injury between
artificial turf and natural grass in male rugby players during
2 seasons of match injuries sustained by 6 teams competing
in Hong Kong’s Division 1 and training injuries sustained
by 2 teams in the English Premiership [30]. The authors
reported no significant differences in ACL injuries between
artificial surface and natural grass. The risk of ACL injuries
in male handball athletes of the 3 top divisions of Norway
during 7 seasons was evaluated relative to the playing
surface (wooden floors, generally with lower friction, and
artificial floors, generally with higher friction) [57]. The
authors found that the type of floor was not a risk factor for
ACL injury in male handball players.
Footwear There is only 1 study included in this section.
Lambson et al. [48] reported a prospective study aimed to
evaluate torsional resistance of football cleats and its
relationship to ACL injuries in high school American
football players. The study included a sample of 3,119
players during the 1989–1991 competitive seasons. The
foot cleat designs evaluated were: edge (longer irregular
cleats placed at the peripheral margin of the sole with a
number of smaller pointed cleats positioned interiorly), flat
(cleats on the forefoot are the same height, shape, and
diameter, such as found on the soccer-style shoe), screw-in
(seven screw-in cleats of 0.5 inch height and 0.5 inch
diameter), and pivot disk (a 10-cm circular edge is on the
sole of the forefoot, with one 0.5-inch cleat in the centre)
[48]. The authors reported that the edge designs produced
significantly higher torsional resistance than the other
designs. In addition, this foot cleat design was significantly
associated with a higher risk of ACL injuries compared to
the other designs.
Internal risk factors
Anatomical risk factors
The evidence found for anatomical risk factors for ACL
injuries in male athletes was mainly related to morphologic
characteristics and knee laxity. The former has to do with
both knee (intercondylar notch and posterior tibial slope
characteristics) and hip morphology. A total of 13 refer-
ences were found for anatomical risk factors: 5 for in-
tercondylar notch width, 1 for body mass index, 9 for tibial
slope, 2 for knee laxity, and 1 for each hip morphology,
foot and ankle morphology, and generalized joint laxity.
Morphologic characteristics The 14 studies included in
morphologic characteristics involved approximately 3,891
participants, distributed in the following activities: Amer-
ican football (1 study), military subjects (3 studies), com-
bination of sports (2 studies), and undetermined activities
(3 studies).
The principal morphologic characteristics related to
ACL injuries reported for males are intercondylar notch
and posterior tibial slope. Regarding intercondylar notch
morphology, Souryal et al. [73] compared, in a prospective
(level II evidence) cohort study, the notch width index
between injured and uninjured high school male athletes.
The authors reported that ACL-injured males had signifi-
cantly narrower intercondylar notch compared to uninjured
subjects. In contrast, a similar investigation involving a
sample of 40 males (mean age 39 years, range 19–70)
found that in subjects with non-contact ACL injuries, there
were no differences in notch width index between the
injured and uninjured side [76]. In 2003, Uhorchak et al.
[79] reported in a prospective study with young military
cadets that injured subjects had significantly lower notch
Knee Surg Sports Traumatol Arthrosc
123

width, tibial eminence width, notch width index, and tibial
eminence width index compared to non-injured males
cadets. The authors found no differences in notch width/
eminence width ratio were reported [79]. Interestingly, the
authors found a 7.8-fold increased risk for non-contact
ACL injury in men with both narrow femoral notch and
generalized joint laxity compared to those without both
factors [79]. Evans et al. [26] reported a retrospective
comparative study with young, athletic subjects, and found
no differences between both injured and non-injured males
for height, condylar width, notch width, and notch width
index. Injured subjects had significantly higher weight and
body mass index compared to uninjured subjects. A narrow
notch width was associated with elevated body mass index
and was also a significant risk factor for males. Everhart
et al. [27] compared the notch morphology between sub-
jects with non-contact ACL injuries (cases) and a sample of
matched controls for age, sex, height, and weight. The
authors found that healthy men had greater anterior femoral
notch outlet width compared to injured men. The presence
of an anteromedial bone ridge in the femoral notch
increased the risk of non-contact ACL injury in men. In
addition, healthy men had a ridge thickness significantly
lower compared to injured men.
There are several retrospective investigations that have
evaluated the influence of posterior tibial slope on the risk
of non-contact ACL injuries in males. Brandon et al. [12]
reported a prognostic case–control study where they found
that males with ACL injuries demonstrated increased
posterior-inferior medial tibial slope when compared to
male controls. In contrast, another study reported ACL-
injured young males (not necessarily athletes) demon-
strated increased posterior tibial slope of the lateral plateau
(but not medial plateau) along with increased difference of
the tibial slope on the lateral and medial tibial plateaus
compared to non-injured control males [74]. In a similar
study, Hashemi et al. [39] compared the morphology of the
proximal tibia between ACL-injured (cases) and uninjured
(controls) males (not necessarily athletes). The authors
reported that injured males demonstrated increased medial
tibial slope, lateral tibial slope, and medial tibial depth
compared to uninjured males. In another case–control
study, Todd et al. [78] found no differences in posterior
tibial slope of the medial plateau between injured and
uninjured males. Similarly, Hudek et al. [46] found that
posterior lateral (but not medial) tibial slope in men with
non-contact ACL injuries was significantly higher relative
to control males. The authors also found that the meniscal
slope of injured subjects in medial and lateral plateaus was
significantly different compared to control subjects [46].
These authors introduced the measure of the meniscal slope
(marked by the superior margins of the anterior and pos-
terior horns in each meniscus). A comparison of the values
of the posterior tibial slope of the medial plateau between
males with and without ACL injuries was also reported by
Hohmann et al. [44]. As previously reported by other
authors [46, 74, 78], no significant differences in posterior
medial tibial slope between ACL-injured and control
groups were noted [44].
Recently, a retrospective investigation was performed to
determine the potential influence of the femoral neck-head
offset in the risk of ACL injuries [63]. The sample included
50 consecutive patients with primary ACL rupture and 50
consecutive patients with non-ACL injury (i.e. meniscus
tear, cartilage defect) [63]. The authors reported that male
patients with alpha-level angle over 60� were at a signifi-
cantly higher risk of ACL injury compared to male patients
with an alpha angle of 60� or less [63].
Finally, some aspects related to foot and ankle align-
ment were evaluated by Woodford-Rogers et al. [82]. The
authors compared the navicular drop (millimetre) and
calcaneal eversion in stance (degrees) of high school and
college male football players between the healthy limb of
non-contact ACL-injured and ACL-non-injured subjects.
They found no differences in navicular drop and calcaneal
eversion between injured and non-injured male football
players [82].
Knee laxity There were 2 studies reporting information
on the effects of knee laxity and generalized joint laxity on
the risk of ACL injuries. Both studies involved a total
sample of 767 individuals (28 American football players
and 739 military cadets).
Woodford-Rogers et al. [82] found that knee laxity (KT-
1000) of the uninvolved knee of subjects with an ACL
injury was increased relative to uninjured subjects. In
contrast, Uhorchak et al. [79] found no significant differ-
ences in specific knee laxity (KT-2000) between injured
and uninjured young male subjects. The authors also
reported that males with generalized joint laxity had a
relative risk of non-contact ACL injuries significantly
higher compared to subjects without generalized joint
laxity. They presented the relative risk of non-contact ACL
injuries in subjects with the combination of risk factors: the
risk of injury was significantly higher in subjects with
narrow notch width associated to generalized joint laxity
and specific knee laxity.
Neuromuscular risk factors
There was only 1 study included in this section. Uhorchak
et al. [79] reported a prospective investigation evaluating
several potential risk factors for non-contact ACL injuries
in a sample of 739 young male West Point cadets from the
United States Military Academy. Among other parameters,
the authors assessed the concentric and eccentric isokinetic
Knee Surg Sports Traumatol Arthrosc
123

strength of the knee extensors and flexors at 60 deg/sec
[79]. They observed no significant differences in quadri-
ceps and hamstrings strength, in either concentric or
eccentric muscle contractions, between non-contact ACL-
injured and non-injured males [79].
Biomechanical risk factors
The evidence found for biomechanical risk factors for ACL
injuries in male athletes was related to trunk and hip. Only 4
studies were found, which investigated the role of hip range
of motion (1 study), trunk and hip position (2 studies), and
trunk proprioception (1 study) on the risk of injury.
Trunk The investigation on the influence of trunk bio-
mechanics on the risk of ACL injuries in male athletes has
been reported in 3 studies. These studies involved a total
sample of 177 subjects from several types of sports (results
not specified by sport).
Zazulak et al. [85] reported a prospective biomechani-
cal-epidemiological prognosis study aimed to investigate
the influence of deficits in neuromuscular control of the
trunk to predict knee injury. Male athletes were tested for
trunk displacement after sudden force release and followed
for 3 years. Of the 137 male athletes initially evaluated, 14
male had knee injuries but there were only 2 ACL injuries.
The authors found no significant associations in maximal
trunk displacement (lateral, extension, and flexion trunk
displacement) between ACL-injured and uninjured males.
[85]. In a parallel publication, the same group found that
there were no significant differences in average error of
active proprioceptive repositioning of the trunk between
ACL-injured and ACL-uninjured male athletes [86].
In a recent publication, a case–control study was per-
formed that aimed to assess dynamic sagittal plane trunk
control during ACL injuries [71]. The authors conducted a
video analysis that compared movie captures of 20 athletes
performing a one-legged landing manoeuvre that resulted
in a torn ACL with matched movie captures of 20 athletes
performing a similar manoeuvre that did not result in an
ACL disruption (controls) [71]. They measured the dis-
tance of the centre of mass to base of support (normalized
by femur length) and measured the limb and trunk angles.
The trunk angle was defined as the angle from the vertical
to the centre line of the trunk [71]. The limb angle was
defined as the angle between the vertical and the thigh
(represented as the line from the centre of the knee joint to
the centre of the hip joint) [71]. A positive trunk and/or
limb angle indicated that the trunk and/or limb was rotated
anteriorly relative to the vertical [71]. ACL-injured males
had higher centre of mass to base of support distance and
limb angle, and lower trunk ankle, compared to uninjured
subjects. Essentially, injured subjects landed with a more
erect trunk and with more hip flexion when compared to
uninjured subjects.
Hip There was only 1 study included in this section. Gomes
et al. [34] investigated the association between hip range of
motion and non-contact ACL injuries in a case–control study
involving 100 male non-professional soccer players. Hip
range of motion was assessed in a supine position and with 908of both hip and knee flexion. Findings were analysed
according to 2 cut-off points (70� and 80� of total internal-
external rotation sum) [34]. After adjusting for age, the
authors found reduced hip range of motion in injured com-
pared to control athletes, especially for internal rotation. Also,
there were significantly more subjects with\70� and\80� of
total internal-external hip rotation sum in the non-contact
ACL-injured group compared to the non-injured group [34].
Discussion
The principal findings of this systematic review related to
the risk factors for ACL injury in male athletes are: (1)
most of the evidence is related to environmental and ana-
tomical risk factors; (2) dry weather conditions may
increase the risk of non-contact ACL injuries in male
athletes; (3) artificial turf may increase the risk of non-
contact ACL injuries in male athletes; (4) higher posterior
tibial slope of the lateral tibial plateau may increase the risk
of non-contact ACL injuries in male athletes; and (5) there
is a lack of evidence regarding neuromuscular and bio-
mechanical risk factors for male athletes. The investigation
of both factors in relation to the risk of ACL injuries is an
area wide open for exploration in the future years.
The number of studies available in the literature evalu-
ating risk factors for ACL injuries in male athletes is much
lower compared to what is published for female athletes [3,
17, 38, 42, 65, 68]. Moreover, several of the reviewed
studies were not focused to compare injured and uninjured
male athletes, but to compare females vs. males for some
specific parameter [12, 26, 27, 63, 76, 85, 86]. These
studies were included because specific comparisons
between injured and uninjured males were also provided,
but it can be concluded that the investigation of risk factors
for ACL injuries in the male athlete has not awakened
much interest in the scientific community. Although the
risk of ACL injury is higher in the female athlete [3, 17, 38,
42, 65, 68], the relevance of the investigation of these
factors in males is important given the high overall number
of male athlete participants [33]. There are many studies
investigating neuromuscular and biomechanical risk factors
in males, but the data are limited which include ACL injury
as an outcome. Therefore, these studies could not be
included in this review because clear conclusions on the
Knee Surg Sports Traumatol Arthrosc
123
influence of these factors on the risk of ACL injuries in
males cannot be drawn [2, 7–9, 13, 14, 16, 20, 21, 25, 28,
29, 47, 50, 64, 75, 81, 83, 84]. Prospective coupled bio-
mechanical-epidemiological data are even more spars in
male athletes. Including only those studies comparing
either prospectively or retrospectively injured and unin-
jured males, the evidence is much more limited, and has
been summarized in Table 3. As shown, most of the
included studies belong to environmental and anatomical
risk factors. Although neuromuscular and biomechanical
risk factors offer the greatest potential to support injury
prevention and likely provide a significant contribution to
risk, there is limited evidence available on these related
risk factors in males at this point. Interestingly, biome-
chanical risk factors have strong evidence for their rela-
tionships to ACL injury risk in female athletes [43, 85], and
these risk factors appear interrelated [41].
The investigation on the influence of environmental risk
factors for non-contact ACL injuries in male athletes may
have some limitations which include potential confounding
factors for weather conditions (type of surface itself, type of
shoe, biomechanical or neuromuscular risk factors), lack of
control for weather conditions where injuries did not occur,
differing type of activity (games or practice) played in
different type of surface (natural grass vs. artificial turf),
limited number of ACL injuries observed, or the inclusion
of both contact and non-contact ACL injuries [22, 23, 30,
62, 69, 70]. It is important to consider in the investigations
that included contact injuries in their analyses may have
limited relevance relative to measurement of injury risk
reduction from training. With contact injuries, the influence
of potential risk factors may be hidden because an external
load from other players likely has limited potential to be
effected by neuromuscular training aimed to prevent injury
[59]. It would be, therefore, mandatory to include this
information in any study dealing with risk factors or
preventive strategies for ACL injuries in male athletes.
However, only 14 of 33 studies reported the results for non-
contact ACL injuries (Table 2). Cumulatively, there does
not appear to be consensus regarding the effects of extrinsic
factors on ACL injury risk in male athletes. In addition, the
extent to which these factors can be modified is limited
which supports future investigations focused on risk
reduction based on intrinsic risk factors, specifically mod-
ifiable causative factors for ACL injury in male athletes.
Anatomical risk factors for ACL injury in male athletes
may have the limitation of potential influence of other non-
controlled associated risk factors. Cases and controls are
often not matched for height, weight, and type of activities
at risk of non-contact ACL injury [39, 44]. Another con-
cern is the type of control ‘‘data’’ employed for the com-
parison with injured subjects [82]. In general, how
anatomical factors modify knee kinetics and kinematics are
not well understood. Overall, the study of the influence of
anatomical factors on the risk of non-contact ACL injuries
in males clearly needs more research, especially in athletes.
However, the potential for their modification via injury
prevention strategies is limited. The main interest of their
identification in an athlete would be to know those indi-
viduals in whom prevention programmes take even more
relevance to avoid ACL injury. Therefore, in athletes with
anatomical risk factors, prevention programmes empha-
sizing modification of neuromuscular and biomechanical
risk factors would be even more relevant to reduce injury
risk in male athletes.
As evidenced above, there is only 1 study pertaining to
neuromuscular control (level II evidence) [79]. Therefore,
there is not enough evidence to elaborate strong conclu-
sions on the influence of the neuromuscular system on non-
contact ACL injuries in male athletes. With respect to the
biomechanical risk factors category, the included studies
may have some limitations: low number of ACL injuries
observed, a mismatch between the time of injury and time
when the mechanism was assessed, difficulties at identi-
fying anatomical landmarks in clothed participants, and the
potential of a selection bias as the inclusion criteria were
based on a qualitative analysis [71, 85, 86]. Although there
is more information available for biomechanical compared
to neuromuscular risk factors (Table 3), this information is
still based on a low number of studies, therefore strong
conclusions can neither be elaborated.
Further research is clearly needed for neuromuscular and
biomechanical risk factors for non-contact ACL injuries in
male athletes. Some areas to be developed in the near future
regarding risk factors for non-contact ACL injury in males
are the comparison of injured and uninjured subjects for:
joint angles and moments during different playing actions
(landing, sidestep cutting, stop jump, etc.), muscle activa-
tion and recruitment patterns, muscle fatigue differences,
and trunk neuromuscular control, among others. Currently,
there is no clear explanation or robust model that consis-
tently demonstrates how all of the risk factors interact
because a reductionistic model does not consider the inter-
relationships and synergic interaction between them.
There are some potential limitations to this systematic
review. First, some studies may have been missed from the
current literature search. However, the employment of 3
databases and the thorough review of obtained references,
including a full-text reading of the most important refer-
ences, and the careful double-check of cited studies mini-
mized the risk. Second, many studies with the absence of
significance in the principal comparisons had a low number
of cases (ACL-injured males), so the risk of type-II error is
not negligible. Third, non-prospective studies may have a
high risk of bias, especially for those modifiable factors.
Case–control studies retrospectively look at some
Knee Surg Sports Traumatol Arthrosc
123

characteristics after cases (ACL-injured males) have been
identified. If the studied factors may be modified with time,
this comparison may be biased by the fact that the injury
elicited some changes in the knee. This is not the case for
most of the anatomical risk factors, but would be clearly
the case for neuromuscular and biomechanical risk factors.
In the latter, it is very important that adequate prospective
cohort studies are designed to assure confident conclusions,
controlling or adjusting the analysis for as much other risk
factors as possible. These types of studies would provide
the best causal-effect relationship between the factor and
the risk of non-contact ACL injuries.
Conclusions
The results of this systematic review indicate that ACL
injury in male athletes likely has a multi-factorial aetiol-
ogy. A thorough knowledge of these factors is crucial to
provide adequate prevention strategies aimed to decrease
the risk of this serious injury in the male athlete. The fol-
lowing conclusions may be elaborated regarding risk fac-
tors for non-contact ACL injuries.
• Most of the existing evidence is related to environ-
mental and anatomical risk factors for non-contact ACL
injuries.
• Dry weather conditions may increase the risk of non-
contact ACL injuries in male athletes.
• Artificial turf may increase the risk of non-contact ACL
injuries in male athletes compared to natural grass.
• Most of the studies of anatomical risk factors are not
specific for athletes.
• Higher posterior tibial slope of the lateral tibial plateau
may increase the risk of non-contact ACL injuries in
male athletes.
• The existing evidence for neuromuscular and biome-
chanical risk factors is low.
• The investigation of risk factors in male athletes,
especially neuromuscular and biomechanical, provides
possibility for future research.
References
1. Aaltonen S, Karjalainen H, Heinonen A, Parkkari J, Kujala UM
(2007) Prevention of sports injuries: systematic review of ran-
domized controlled trials. Arch Intern Med 167:1585–1592
2. Ahmad CS, Clark AM, Heilmann N, Schoeb JS, Gardner TR,
Levine WN (2006) Effect of gender and maturity on quadriceps-
to-hamstring strength ratio and anterior cruciate ligament laxity.
Am J Sports Med 34:370–374
3. Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D,
Lazaro-Haro C, Cugat R (2009) Prevention of non-contact ante-
rior cruciate ligament injuries in soccer players. Part 1: mecha-
nisms of injury and underlying risk factors. Knee Surg Sports
Traumatol Arthrosc 17:705–729
4. Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D,
Lazaro-Haro C, Cugat R (2009) Prevention of non-contact ante-
rior cruciate ligament injuries in soccer players. Part 2: a review
of prevention programs aimed to modify risk factors and to
reduce injury rates. Knee Surg Sports Traumatol Arthrosc
17:859–879
5. Araujo PH, Ahlden M, Hoshino Y, Muller B, Moloney G, Fu FH,
Musahl V (2012) Comparison of three non-invasive quantitative
measurement systems for the pivot shift test. Knee Surg Sports
Traumatol Arthrosc 20:692–697
6. Arendt E, Dick R (1995) Knee injury patterns among men and
women in collegiate basketball and soccer. NCAA data and
review of literature. Am J Sports Med 23:694–701
7. Besier TF, Lloyd DG, Ackland TR (2003) Muscle activation
strategies at the knee during running and cutting maneuvers. Med
Sci Sports Exerc 35:119–127
8. Besier TF, Lloyd DG, Ackland TR, Cochrane JL (2001) Antici-
patory effects on knee joint loading during running and cutting
maneuvers. Med Sci Sports Exerc 33:1176–1181
9. Besier TF, Lloyd DG, Cochrane JL, Ackland TR (2001) External
loading of the knee joint during running and cutting maneuvers.
Med Sci Sports Exerc 33:1168–1175
10. Bjordal JM, Arnly F, Hannestad B, Strand T (1997) Epidemiol-
ogy of anterior cruciate ligament injuries in soccer. Am J Sports
Med 25:341–345
11. Bradley JP, Klimkiewicz JJ, Rytel MJ, Powell JW (2002) Ante-
rior cruciate ligament injuries in the National Football League:
epidemiology and current treatment trends among team physi-
cians. Arthroscopy 18:502–509
12. Brandon ML, Haynes PT, Bonamo JR, Flynn MI, Barrett GR,
Sherman MF (2006) The association between posterior-inferior
tibial slope and anterior cruciate ligament insufficiency.
Arthroscopy 22:894–899
13. Brent J, Myer GD, Ford KR, Paterno M, Hewett T (2012) The
effect of sex and age on isokinetic hip abduction torques. J Sport
Rehabil 22:41–46
14. Chappell JD, Herman DC, Knight BS, Kirkendall DT, Garrett
WE, Yu B (2005) Effect of fatigue on knee kinetics and kine-
matics in stop-jump tasks. Am J Sports Med 33:1022–1029
15. Cheng T, Zhang GY, Zhang XL (2012) Does computer naviga-
tion system really improve early clinical outcomes after anterior
cruciate ligament reconstruction? A meta-analysis and systematic
review of randomized controlled trials. Knee 19:73–77
16. Cross MJ, Gibbs NJ, Bryant GJ (1989) An analysis of the sidestep
cutting manoeuvre. Am J Sports Med 17:363–366
17. Dai B, Herman D, Liu C, Garrett WE Jr, Yu B (2012) Prevention
of ACL injury, Part I: injury characteristics, risk factors, and
loading mechanism. Res Sports Med 20:180–197
18. Dai B, Herman D, Liu H, Garrett WE Jr, Yu B (2012) Prevention
of ACL injury, part II: effects of ACL injury prevention programs
on neuromuscular risk factors and injury rate. Res Sports Med
20:198–222
19. Dejour D, Ntagiopoulos PG, Saggin PR, Panisset JC (2013) The
diagnostic value of clinical tests, magnetic resonance imaging,
and instrumented laxity in the differentiation of complete versus
partial anterior cruciate ligament tears. Arthroscopy 29:491–499
20. Dempsey AR, Elliott BC, Munro BJ, Steele JR, Lloyd DG (2012)
Whole body kinematics and knee moments that occur during an
overhead catch and landing task in sport. Clin Biomech (Bristol,
Avon) 27:466–474
Knee Surg Sports Traumatol Arthrosc
123

21. Dempsey AR, Lloyd DG, Elliott BC, Steele JR, Munro BJ, Russo
KA (2007) The effect of technique change on knee loads during
sidestep cutting. Med Sci Sports Exerc 39:1765–1773
22. Dragoo JL, Braun HJ, Durham JL, Chen MR, Harris AH (2012)
Incidence and risk factors for injuries to the anterior cruciate
ligament in National Collegiate Athletic Association football:
data from the 2004–2005 through 2008–2009 National Collegiate
Athletic Association Injury Surveillance System. Am J Sports
Med 40:990–995
23. Dragoo JL, Braun HJ, Harris AH (2012) The effect of playing
surface on the incidence of ACL injuries in National Collegiate
Athletic Association American Football. Knee 20:191–195
24. Emond CE, Woelber EB, Kurd SK, Ciccotti MG, Cohen SB
(2011) A comparison of the results of anterior cruciate ligament
reconstruction using bioabsorbable versus metal interference
screws: a meta-analysis. J Bone Joint Surg Am 93:572–580
25. Escamilla RF, Fleisig GS, Zheng N, Lander JE, Barrentine SW,
Andrews JR, Bergemann BW, Moorman CT 3rd (2001) Effects
of technique variations on knee biomechanics during the squat
and leg press. Med Sci Sports Exerc 33:1552–1566
26. Evans KN, Kilcoyne KG, Dickens JF, Rue JP, Giuliani J, Gwinn
D, Wilckens JH (2012) Predisposing risk factors for non-contact
ACL injuries in military subjects. Knee Surg Sports Traumatol
Arthrosc 20:1554–1559
27. Everhart JS, Flanigan DC, Simon RA, Chaudhari AM (2010)
Association of noncontact anterior cruciate ligament injury with
presence and thickness of a bony ridge on the anteromedial aspect
of the femoral intercondylar notch. Am J Sports Med
38:1667–1673
28. Ford KR, Myer GD, Hewett TE (2010) Longitudinal effects of
maturation on lower extremity joint stiffness in adolescent ath-
letes. Am J Sports Med 38:1829–1837
29. Ford KR, Shapiro R, Myer GD, Van Den Bogert AJ, Hewett TE
(2010) Longitudinal sex differences during landing in knee
abduction in young athletes. Med Sci Sports Exerc 42:1923–1931
30. Fuller CW, Clarke L, Molloy MG (2010) Risk of injury associ-
ated with rugby union played on artificial turf. J Sports Sci
28:563–570
31. Fuller CW, Dick RW, Coriette J, Schmalz R (2007) Comparison of
the incidence, nature and cause of injuries sustained on grass and
new generation artificial turf by male and female football players.
Part 1: match injuries. Br J Sports Med 41(Suppl 1):i20–i26
32. Fuller CW, Dick RW, Coriette J, Schmalz R (2007) Comparison
of the incidence, nature and cause of injuries sustained on grass
and new generation artificial turf by male and female football
players. Part 2: training injuries. Br J Sports Med 41(Suppl
1):i27–i32
33. Gianotti SM, Marshall SW, Hume PA, Bunt L (2009) Incidence
of anterior cruciate ligament injury and other knee ligament
injuries: a national population-based study. J Sci Med Sport
12:622–627
34. Gomes JL, de Castro JV, Becker R (2008) Decreased hip range of
motion and noncontact injuries of the anterior cruciate ligament.
Arthroscopy 24:1034–1037
35. Gottlob CA, Baker CL (2000) Anterior cruciate ligament recon-
struction: socioeconomic issues and cost effectiveness. Am J
Orthop (BelleMead NJ) 29:472–476
36. Gottlob CA, Baker CL, Pellissier JM, Colvin L (1999) Cost
effectiveness of anterior cruciate ligament reconstruction in
young adults. Clin Orthop Relat Res 367:272–282
37. Granan LP, Bahr R, Steindal K, Furnes O, Engebretsen L (2008)
Development of a national cruciate ligament surgery registry: the
Norwegian national knee ligament registry. Am J Sports Med
36:308–315
38. Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD,
DeMaio M, Dick RW, Engebretsen L, Garrett WE Jr, Hannafin
JA, Hewett TE, Huston LJ, Ireland ML, Johnson RJ, Lephart S,
Mandelbaum BR, Mann BJ, Marks PH, Marshall SW, Myklebust
G, Noyes FR, Powers C, Shields C Jr, Shultz SJ, Silvers H,
Slauterbeck J, Taylor DC, Teitz CC, Wojtys EM, Yu B (2006)
Understanding and preventing noncontact anterior cruciate liga-
ment injuries: a review of the Hunt Valley II Meeting, January
2005. Am J Sports Med 34:1512–1532
39. Hashemi J, Chandrashekar N, Mansouri H, Gill B, Slauterbeck
JR, Schutt RC, Dabezies E, Beynnon BD (2010) Shallow medial
tibial plateau and steep medial and lateral tibial slopes. New risk
factors for anterior cruciate ligament injuries. Am J Sports Med
38:54–62
40. Hewett TE, Ford KR, Myer GD (2006) Anterior cruciate ligament
injuries in female athletes: part 2, a meta-analysis of neuromus-
cular interventions aimed at injury prevention. Am J Sports Med
34:490–498
41. Hewett TE, Myer GD (2011) The mechanistic connection
between the trunk, hip, knee, and anterior cruciate ligament
injury. Exerc Sport Sci Rev 39:161–166
42. Hewett TE, Myer GD, Ford KR (2006) Anterior cruciate ligament
injuries in female athletes: part 1, mechanisms and risk factors.
Am J Sports Med 34:299–311
43. Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ,
McLean SG, Van Den Bogert AJ, Paterno MV, Succop P (2005)
Biomechanical measures of neuromuscular control and valgus
loading of the knee predict anterior cruciate ligament injury risk
in female athletes: a prospective study. Am J Sports Med
33:492–501
44. Hohmann E, Bryant A, Reaburn P, Tetsworth K (2011) Is there a
correlation between posterior tibial slope and non-contact ante-
rior cruciate ligament injuries? Knee Surg Sports Traumatol
Arthrosc 19(Suppl 1):S109–S114
45. Hoshino Y, Araujo P, Ahlden M, Samuelsson K, Muller B,
Hofbauer M, Wolf MR, Irrgang JJ, Fu FH, Musahl V (2013)
Quantitative evaluation of the pivot shift by image analysis using
the iPad. Knee Surg Sports Traumatol Arthrosc 21:975–980
46. Hudek R, Fuchs B, Regenfelder F, Koch PP (2011) Is noncontact
ACL injury associated with the posterior tibial and meniscal
slope? Clin Orthop Relat Res 469:2377–2384
47. Huston LJ, Wojtys EM (1996) Neuromuscular performance
characteristics in elite female athletes. Am J Sports Med
24:427–436
48. Lambson RB, Barnhill BS, Higgins RW (1996) Football cleat
design and its effect on anterior cruciate ligament injuries. A
three-year prospective study. Am J Sports Med 24:155–159
49. Lohmander LS, Englund PM, Dahl LL, Roos EM (2007) The
long-term consequence of anterior cruciate ligament and menis-
cus injuries: osteoarthritis. Am J Sports Med 35:1756–1769
50. McLean SG, Myers PT, Neal RJ, Walters MR (1998) A quanti-
tative analysis of knee joint kinematics during the sidestep cutting
maneuver. Implications for non-contact anterior cruciate ligament
injury. Bull Hosp Jt Dis 57:30–38
51. Meyers MC, Barnhill BS (2004) Incidence, causes, and severity
of high school football injuries on FieldTurf versus natural grass.
A 5-year prospective study. Am J Sports Med 32:1626–1638
52. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009)
Preferred reporting items for systematic reviews and meta-anal-
yses: the PRISMA statement. Ann Intern Med 18:264–269
53. Mohtadi NG, Chan DS, Dainty KN, Whelan DB (2011) Patellar
tendon versus hamstring tendon autograft for anterior cruciate
ligament rupture in adults. Cochrane Database Syst Rev
9:CD005960
54. Mountcastle SB, Posner M, Kragh JF Jr, Taylor DC (2007)
Gender differences in anterior cruciate ligament injury vary withactivity: epidemiology of anterior cruciate ligament injuries in a
young, athletic population. Am J Sports Med 35:1635–1642
Knee Surg Sports Traumatol Arthrosc
123
55. Myer GD, Martin L Jr, Ford KR, Paterno MV, Schmitt LC, Heidt
RS Jr, Colosimo A, Hewett TE (2012) No association of time
from surgery with functional deficits in athletes after anterior
cruciate ligament reconstruction: evidence for objective return-
to-sport criteria. Am J Sports Med 40:2256–2263
56. Myer GD, Schmitt LC, Brent JL, Ford KR, Barber Foss KD,
Scherer BJ, Heidt RS, Divine JG, Hewett TE (2011) Utilization
of modified NFL combine testing to identify functional deficits in
athletes following anterior cruciate ligament reconstruction.
J Orthop Sports Phys Ther 41:377–387
57. Olsen OE, Myklebust G, Engebretsen L, Holme I, Bahr R (2003)
Relationship between floor type and risk of ACL injury in team
handball. Scand J Med Sci Sports 13:299–304
58. Orchard J (2001) The AFL penetrometer study: work in progress.
J Sci Med Sport 4:220–232
59. Orchard J, Seward H, McGivern J, Hood S (1999) Rainfall,
evaporation and the risk of non-contact anterior cruciate ligament
injury in the Australian Football League. Med J Aust 170:304–306
60. Orchard J, Seward H, McGivern J, Hood S (2001) Intrinsic and
extrinsic risk factors for anterior cruciate ligament injury in
Australian footballers. Am J Sports Med 29:196–200
61. Orchard JW, Chivers I, Aldous D, Bennell K, Seward H (2005) Rye
grass is associated with fewer non-contact anterior cruciate liga-
ment injuries than Bermuda grass. Br J Sports Med 39:704–709
62. Orchard JW, Powell JW (2003) Risk of knee and ankle sprains
under various weather conditions in American football. Med Sci
Sports Exerc 35:1118–1123
63. Philippon M, Dewing C, Briggs K, Steadman JR (2012)
Decreased femoral head–neck offset: a possible risk factor for
ACL injury. Knee Surg Sports Traumatol Arthrosc 20:2585–2589
64. Portes EM, Portes LA, Botelho VG, Souza Pinto S (2007) Is-
okinetic torque peak and hamstrings/quadriceps ratios in endur-
ance athletes with anterior cruciate ligament laxity. Clinics (Sao
Paulo) 62:127–132
65. Posthumus M, Collins M, September AV, Schwellnus MP (2011)
The intrinsic risk factors for ACL ruptures: an evidence-based
review. Phys Sportsmed 39:62–73
66. Powell JW, Schootman M (1992) A multivariate risk analysis of
selected playing surfaces in the National Football League: 1980
to 1989. An epidemiologic study of knee injuries. Am J Sports
Med 20:686–694
67. Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K (2007) A
meta-analysis of the incidence of anterior cruciate ligament tears
as a function of gender, sport, and a knee injury-reduction regi-
men. Arthroscopy 23:1320–1325
68. Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi T,
Garrett W, Georgoulis T, Hewett TE, Johnson R, Krosshaug T,
Mandelbaum B, Micheli L, Myklebust G, Roos E, Roos H,
Schamasch P, Shultz S, Werner S, Wojtys E, Engebretsen L
(2008) Non-contact ACL injuries in female athletes: an Interna-
tional Olympic Committee current concepts statement. Br J
Sports Med 42:394–412
69. Scranton PE Jr, Whitesel JP, Powell JW, Dormer SG, Heidt RS
Jr, Losse G, Cawley PW (1997) A review of selected noncontact
anterior cruciate ligament injuries in the National Football Lea-
gue. Foot Ankle Int 18:772–776
70. Scranton PE Jr, Whitesel JP, Powell JW, Dormer SG, Heidt RS
Jr, Losse G, Cawley PW (1997) A review of selected noncontact
anterior cruciate ligament injuries in the National Football Lea-
gue. Foot Ankle Int 18:772–776
71. Sheehan FT, Sipprell WH 3rd, Boden BP (2012) Dynamic sag-
ittal plane trunk control during anterior cruciate ligament injury.
Am J Sports Med 40:1068–1074
72. Smith TO, Davies L, Hing CB (2010) Early versus delayed sur-
gery for anterior cruciate ligament reconstruction: a systematic
review and meta-analysis. Knee Surg Sports Traumatol Arthrosc
18:304–311
73. Souryal TO, Freeman TR (1993) Intercondylar notch size and
anterior cruciate ligament injuries in athletes. A prospective
study. Am J Sports Med 21:535–539
74. Stijak L, Herzog RF, Schai P (2008) Is there an influence of the
tibial slope of the lateral condyle on the ACL lesion? Knee Surg
Sports Traumatol Arthrosc 16:112–117
75. Stoffel KK, Nicholls RL, Winata AR, Dempsey AR, Boyle JJ, Lloyd
DG (2010) Effect of ankle taping on knee and ankle joint biome-
chanics in sporting tasks. Med Sci Sports Exerc 42:2089–2097
76. Teitz CC, Lind BK, Sacks BM (1997) Symmetry of the femoral
notch width index. Am J Sports Med 25:687–690
77. Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M (2012)
Double-bundle versus single-bundle reconstruction for anterior
cruciate ligament rupture in adults. Cochrane Database Syst Rev
11:CD008413
78. Todd MS, Lalliss S, Garcia S, DeBerardino TM, Cameron KL
(2010) The relationship between posterior tibial slope and ante-
rior cruciate ligament injuries. Am J Sports Med 38:63–67
79. Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P,
Taylor DC (2003) Risk factors associated with noncontact injury of
the anterior cruciate ligament: a prospective four-year evaluation
of 859 West Point cadets. Am J Sports Med 31:831–842
80. Walden M, Hagglund M, Orchard J, Kristenson K, Ekstrand J
(2013) Regional differences in injury incidence in European
professional football. Scand J Med Sci Sports 23:424–430
81. Wojtys EM, Huston LJ, Schock HJ, Boylan JP, Ashton-Miller JA
(2003) Gender differences in muscular protection of the knee in
torsion in size-matched athletes. J Bone Joint Surg Am
85:782–789
82. Woodford-Rogers B, Cyphert L, Denegar CR (1994) Risk factors
for anterior cruciate ligament injury in high school and college
athletes. J Athl Train 29:343–346
83. Yeow CH, Lee PV, Goh JC (2010) Sagittal knee joint kinematics
and energetics in response to different landing heights and
techniques. Knee 17:127–131
84. Yeow CH, Lee PV, Goh JC (2011) An investigation of lower
extremity energy dissipation strategies during single-leg and
double-leg landing based on sagittal and frontal plane biome-
chanics. Hum Mov Sci 30:624–635
85. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J
(2007) Deficits in neuromuscular control of the trunk predict knee
injury risk: a prospective biomechanical-epidemiologic study.
Am J Sports Med 35:1123–1130
86. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J
(2007) The effects of core proprioception on knee injury: a
prospective biomechanical-epidemiological study. Am J Sports
Med 35:368–373
Knee Surg Sports Traumatol Arthrosc
123




















