
Human adenoma cells are highly susceptible to the genotoxic action of 4-hydroxy-2-nonenal
Upload
independentCategory
view
7download
0
Huh AYriMIkNk'UfNIVHrIiIW,¶ DUdU
Results of a Multidisciplinary Strategy forManagement of Mediastinal ParathyroidAdenoma as a Cause of PersistentPrimary Hyperparathyroidism
GERARD M. DOHERTY, M.D.,* JOHN L. DOPPMAN, M.D.,4 DONALD L. MILLER, M.D.,4 MIMI S. GEE, M.D.,*STEPHEN J. MARX, M.D.,§ ALLEN M. SPIEGEL, M.D.,|| GERALD D. AURBACH, M.D.,§ HARVEY 1. PASS, M.D.,t
MURRAY F. BRENNAN, M.D.,¶ and JEFFREY A. NORTON, M.D.*
Persistent primary hyperparathyroidism due to mediastinalparathyroid adenoma was effectively treated by either angio-graphic ablation or median sternotomy in this study of49 patientsmanaged at the National Institutes of Health since 1977. Eachpatient presented here with symptomatic persistent primary hy-perparathyroidism after failed initial surgical procedures doneat other institutions. Each patient underwent extensive parathy-roid localization procedures, including selective angiography, andmost had a parathyroid adenoma localized to the mediastinum.Angiographic ablation, the deliberate injection of large doses ofcontrast material into the artery that selectively perfuses theadenoma, was initially successful in 22 of 30 procedures (73%)in 27 patients. Long-term control of persistent primary hyper-parathyroidism was achieved in 17 of 27 patients (63%) by an-giographic ablation. Each unsuccessful ablation could be easilysalvaged by surgical resection. Surgical resection of the para-thyroid adenoma by median sternotomy achieved immediatesuccess in 24 of 24 procedures (p2 < 0.02 versus ablation), andlong-term cure in 23 of 23 evaluable patients (P2 < 0.001 versusablation). However, ablation did have benefits for the patientsin whom it was successfully performed. It was associated witha significantly shorter hospital stay (median, 6 days versus 9days for sternotomy, P2 < 0.003), much less pain, and easierrecuperation. Complications of each procedure were transientand similar in both groups. Operative resection is the most ef-fective single means to eradicate mediastinal parathyroid ade-noma; however, angiographic ablation can provide similar long-term control of hyperparathyroidism in 63% of patients with lesspain and shorter convalescence than that seen in patients aftermedian sternotomy. Our results suggest that angiographic abla-tion should be attempted as the initial procedure for patientswith persistent primary hyperparathyroidism caused by an an-giographicaHly identified mediastinal parathyroid adenoma. Op-eration can be reserved for those who fail ablation.
From the Surgical Metabolism Section* and the ThoracicOncology Section,t Surgery Branch, National Cancer
Institute, the Diagnostic Radiology Department,f WarrenGrant Magnuson Clinical Center, the Metabolic DiseasesBranch§ and the Moiecular Pathophysiology Branch, ||National Institute of Diabetes and Digestive and Kidney
Diseases, National Institutes of Health, Bethesda, Maryland;and the Memorial Sloan-Kettering Cancer Center,¶
New York, New York
P RIMARY HYPERPARATHYROIDISM IS the mostcommon cause ofhypercalcemia, and can usuallybe cured by surgical excision of a single parathy-
roid adenoma." 2 The adenoma is most commonly locatedwithin or near the usual anatomic location of the para-thyroid glands on the posterior capsule of the thyroidgland. In a small proportion ofpatients, however, cervicalexploration for primary hyperparathyroidism fails becauseof ectopically located adenomatous parathyroid tissuewithin the mediastinum.3 The mediastinal parathyroidadenoma usually can be localized at subsequent evalua-tion with noninvasive and invasive radiographic studies.'
Standard therapy for persistent primary hyperparathy-roidism secondary to a mediastinal parathyroid adenomais surgical resection; however, at the National Institutesof Health (NIH), some patients with mediastinal para-thyroid adenomas have been successfully managed by se-lective infusion of large doses of ionic radiographic con-trast into the vessel feeding the tumor.4'9~12 This procedurehas been described previously to demonstrate the feasi-bility and the immediate success rates.10 " Initially, an-giographic ablation was performed serendipitously by in-advertently wedging the catheter into a selective feedingartery. The procedure has been thought to be safest and
101
Address reprint requests to Jeffrey A. Norton, M.D., Head, SurgicalMetabolism Section, Surgery Branch, National Cancer Institute/NIH,Building 10, Room 2B07, Bethesda, MD 20892.
Accepted for publication July 25, 1991.

DOHERTY AND OTHERS
have the best results when "staining" mediastinal ade-nomas. The role of purposeful selective angiographicablation in the management of patients with persistentprimary hyperparathyroidism secondary to a mediastinalparathyroid adenoma is unclear, because no studies havecompared ablation with surgery. We have chosen pur-poseful ablation in patients with mediastinal parathyroidadenoma as a cause of persistent primary hyperparathy-roidism, if it is angiographically identifiable, and if, basedon the records of the prior operations, the patient doesnot appear to be at high risk for the development of post-operative hypoparathyroidism. We now compare our
long-term results in patients treated with angiographicablation with those in a concurrent group of patients whounderwent surgical resection via median sternotomy, todetermine the role of ablation in the management ofme-diastinal parathyroid adenomas.
Methods
Patients with either persistent or recurrent primary hy-perparathyroidism are managed at the NIH according toan approved protocol that has been described in detail.'2Briefly, the diagnosis of primary hyperparathyroidism isconfirmed in each patient by demonstration of elevatedserum levels of both calcium and parathyroid hormone,and the indications for reoperation are evaluated. Recordsand pathology specimens from the initial surgical pro-cedures done at the referring institution are carefully re-
viewed to determine a working diagnosis of parathyroidadenoma, hyperplasia, or cancer and whether the patienthas persistent (no disease-free interval) or recurrent (dis-ease-free period of at least 6 months) primary hyperpara-thyroidism. After the identification of either persistent or
recurrent symptomatic primary hyperparathyroidism,each patient that warrants reoperation then undergoesnoninvasive localizing procedures including computedtomography (CT), magnetic resonance imaging, ultra-sound and technetium-thallium scintigraphy; if the out-come of noninvasive studies are inconclusive, these are
followed by selective angiography and venous sam-
pling.5"3"14Since 1977, patients who could be identified as having
a mediastinal parathyroid adenoma as a cause for persis-tent primary hyperparathyroidism have been managedeither by deliberate angiographic ablation via injection ofionic contrast into a feeding vessel or by planned surgicalexcision via median sternotomy. In general, if angio-graphic ablation was feasible, it was performed instead ofmedian sternotomy because it appeared easier to undergoand was less painful. If two or three normal parathyroidglands had been removed at the initial procedure, how-ever, median sternotomy and surgical resection of theparathyroid adenoma were performed because this al-
lowed cryopreservation ofremoved parathyroid tissue thatcould be reimplanted if the patient developed long-termhypoparathyroidism. Angiographic ablation was per-formed by superselective catheterization of the arterysupplying the adenoma, and infusion of ionic contrastmedia to stain the tumor as previously described.4""' 5
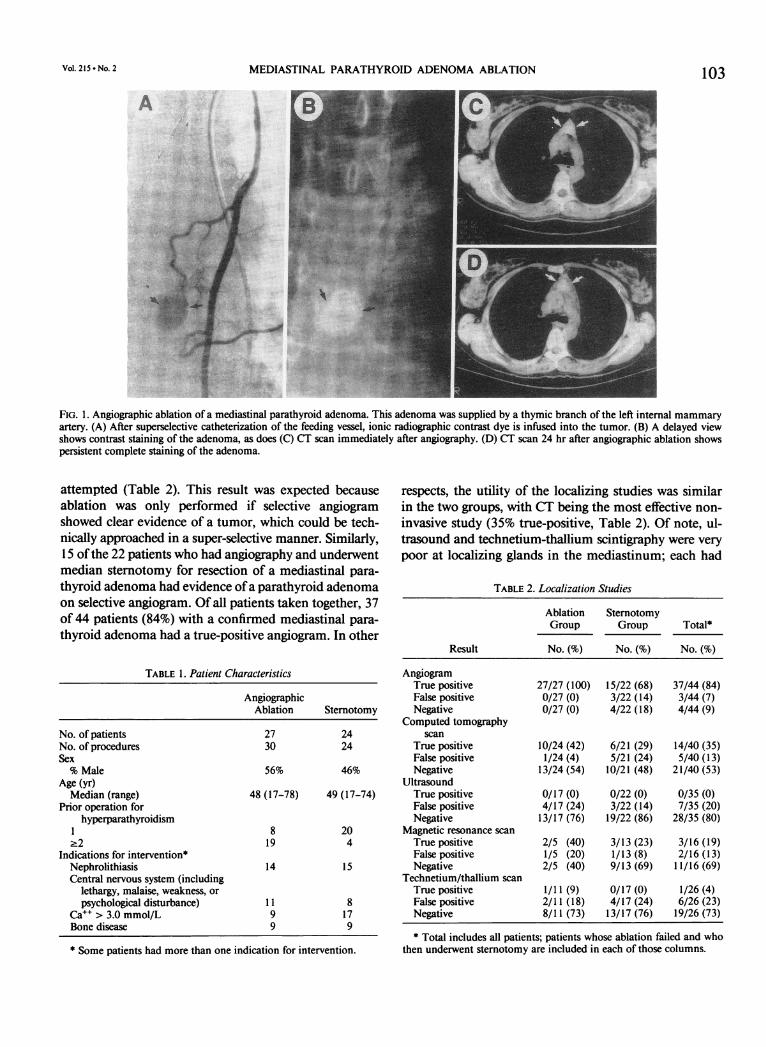
Most patients who had a tumor deliberately stained withcontrast had a CT scan 24 hours after staining to deter-mine if the parathyroid adenoma retained the contrast as
a predictor of procedure efficacy (Fig. 1). When ablationwas not technically possible, or if it failed to correct thepersistent primary hyperparathyroidism, adenomas weresurgically resected.
In this study, we included all patients who had at-tempted angiographic ablation of mediastinal adenomasfrom 1977 to 1989. They are compared with all patients.in the same period who underwent median sternotomyfor parathyroid adenoma. Data were collected by retro-spective chart review and telephone interviews with pa-tients and their referring physicians. Endpoints evaluatedinclude initial and long-term correction of hypercalcemia,need for subsequent interventions for hypercalcemia,postprocedure length of hospital stay, and complicationsof therapy.
Statistical methods applied include the Wilcoxon ranksum test for comparison ofnonparametric data, student'st test for comparison ofparametric data, and Fisher's exacttest for analysis of proportions. Significance was definedat P2 < 0.05.
ResultsPatient Characteristics
The 27 patients who underwent angiographic ablationto manage persistent primary hyperparathyroidism andthe 24 patients who underwent median stemotomy werevery similar with respect to age, gender, and signs andsymptoms of primary hyperparathyroidism (Table 1). Ahigher proportion of patients in the ablation group hadhad two or more prior operations for hyperparathyroidismcompared with the sternotomy group (P2 < 0.01, Fisher'sexact test). None ofthe 27 ablation patients had had priormedian sternotomy for primary hyperparathyroidism.Five patients who had failed ablation subsequently un-
derwent successful median sternotomy; these five patientswere included in both groups. Each patient had persistentprimary hyperparathyroidism and each had a diagnosisof parathyroid adenoma, based on prior pathology andeither pathology at curative surgical resection or correctionof hypercalcemia by angiographic ablation of a singlegland.
Localization StudiesSelective angiography correctly identified a mediastinal
parathyroid adenoma in each patient who had ablation
102 Ann. Surg. * February 1992
MEDIASTINAL PARATHYROID ADENOMA ABLATION 103
FIG. 1. Angiographic ablation of a mediastinal parathyroid adenoma. This adenoma was supplied by a thymic branch of the left internal mammaryartery. (A) After superselective catheterization of the feeding vessel, ionic radiographic contrast dye is infused into the tumor. (B) A delayed viewshows contrast staining of the adenoma, as does (C) CT scan immediately after angiography. (D) CT scan 24 hr after angiographic ablation showspersistent complete staining of the adenoma.
attempted (Table 2). This result was expected becauseablation was only performed if selective angiogramshowed clear evidence of a tumor, which could be tech-nically approached in a super-selective manner. Similarly,15 ofthe 22 patients who had angiography and underwentmedian sternotomy for resection of a mediastinal para-
thyroid adenoma had evidence ofa parathyroid adenomaon selective angiogram. Of all patients taken together, 37of 44 patients (84%) with a confirmed mediastinal para-
thyroid adenoma had a true-positive angiogram. In other
TABLE 1. Patient Characteristics
AngiographicAblation Sternotomy
No. of patients 27 24No. of procedures 30 24Sex% Male 56% 46%
Age (yr)Median (range) 48 (17-78) 49 (17-74)
Prior operation forhyperparathyroidism
1 8 2022 19 4
Indications for intervention*Nephrolithiasis 14 15Central nervous system (including
lethargy, malaise, weakness, or
psychological disturbance) 11 8Ca" > 3.0 mmol/L 9 17Bone disease 9 9
* Some patients had more than one indication for intervention.
respects, the utility of the localizing studies was similarin the two groups, with CT being the most effective non-
invasive study (35% true-positive, Table 2). Of note, ul-trasound and technetium-thallium scintigraphy were very
poor at localizing glands in the mediastinum; each had
TABLE 2. Localization Studies
Ablation SternotomyGroup Group Total*
Result No. (%) No. (%) No. (%)
AngiogramTrue positive 27/27 (100) 15/22 (68) 37/44 (84)False positive 0/27 (0) 3/22 (14) 3/44 (7)Negative 0/27 (0) 4/22 (18) 4/44 (9)
Computed tomographyscan
True positive 10/24 (42) 6/21 (29) 14/40 (35)False positive 1/24 (4) 5/21 (24) 5/40 (13)Negative 13/24 (54) 10/21 (48) 21/40 (53)
UltrasoundTrue positive 0/17 (0) 0/22 (0) 0/35 (0)False positive 4/17 (24) 3/22 (14) 7/35 (20)Negative 13/17 (76) 19/22 (86) 28/35 (80)
Magnetic resonance scanTrue positive 2/5 (40) 3/13 (23) 3/16 (19)False positive 1/5 (20) 1/13 (8) 2/16 (13)Negative 2/5 (40) 9/13 (69) 11/16 (69)
Technetium/thallium scanTrue positive 1/1 1 (9) 0/17 (0) 1/26 (4)False positive 2/11 (18) 4/17 (24) 6/26 (23)Negative 8/11 (73) 13/17 (76) 19/26 (73)* Total includes all patients; patients whose ablation failed and who
then underwent sternotomy are included in each of those columns.
VOL. 215.- NO. 2
ii.4.xA'
i I
V
r

DOHERTY AND OTHERS
more false-positive than true-positive results. Computedtomography and magnetic resonance scans were slightlybetter than Tech-thal or ultrasound; however, nether ap-proached the accuracy of angiography (Table 2).
Angiographic Ablation
Thirty separate angiographic ablation procedures wereperformed in 27 patients with mediastinal parathyroidadenomas on selective angiogram. Three patients had re-peat ablation after an initial failure; one repeat ablationwas successful, whereas in two patients ablation failedagain and operation was required. The blood supply ofthe parathyroid adenoma arose from the internal mam-mary artery in 21 patients and the inferior thyroid arteryin six (Table 3, Fig. 1). Computed tomography scans wereperformed 24 hours after 21 of the 30 attempted ablationprocedures. Computed tomography evidence of persistentstaining of the parathyroid adenoma was thought to becomplete in 8, partial in 6, and not present in 7 (Table3). Of the 14 procedures that showed complete or partialstaining, the long-term outcomes of two are unknown.Eight procedures were successful, as demonstrated bylong-term resolution of hypercalcemia (8/12 evaluable,67%). Despite CT evidence of staining, four proceduressubsequently failed, as demonstrated by persistent hyper-calcemia (4 failed/ 12 evaluable, 33%). Furthermore, 5 ofthe 7 procedures in which the delayed CT scan showedno staining were unsuccessful as determined by persistenthypercalcemia, but two patients have remained normo-calcemic despite no CT evidence ofstaining after 24 hours.Therefore, persistent staining on the delayed CT scan mayhave some predictive value as to subsequent outcome,but some patients (33%) with evidence ofdelayed stainingmay fail and some patients (29%) without evidence ofdelayed staining may still be cured.
Surgery
Twenty-four patients underwent median sternotomyfor resection ofa parathyroid adenoma as a cause of per-
TABLE 3. Angiographic Ablation Procedures
No. Long-Term Cure
No. of procedures 30No. of patients 27Tumor vesselThymic branch of internal mammary 21Inferior thyroid artery 6
Successful vessel cannulation 2524° computed tomography-
demonstrated stainingPositive 8 4Partial 6 4Negative 7 2Not done 9 7
TABLE 4. Procedure Outcome
AngiographicAblation Sternotomy
No. of procedures 30 24No. of patients 27 24Hospital length of stay after
procedures (days) 6.0 (1-60)* 9.0 (5-60)median (range)
Serum calcium (mmol)Before proceduret 3.0 ± 0.3 3.0 ± 0.2Nadir after proceduret 2.2 ± 0.4 1.9 ± 0.1l§
Initially successful intervention 22/38 24/2411Long-term follow-up median
(range) 63 m (1-156) 42 m (1-122)Long-term parathyroid status
Hypoparathyroid 3 5Normoparathyroid 14 18Required subsequent
intervention forhyperparathyroidism 10 OT
Remains hyperparathyroid 1 0No follow-up 2 1
Long-term calcium or vitamin Dsupplements 3 5
Long-term serum calcium level(mmol) 2.5 ± 0.3 2.3 ± 0.1
* Shorter hospital stay vs. sternotomy, P2 < 0.003, Wilcoxon ranksum test. t Mean ± SD. Normal range 2.10-2.65 mmol. t Lower serumlevel ofcalcium vs. preprocedure level, P2 < 0.01, Student's t test, paired.§ Lower serum calcium level after procedure vs. ablation group, P2 < 0.01,Student's t test. || Higher proportion of initially successful interventionvs. ablation, P2 < 0.02, Fisher's exact test. ¶ Fewer patients required sub-sequent intervention compared with ablation, P2 < 0.002, Fisher's exacttest.
sistent primary hyperparathyroidism; the results ofsurgerywere compared with the results of angiographic ablation(Table 4). Patients who had angiographic ablation of amediastinal parathyroid adenoma had less postprocedurepain and a significantly shorter postprocedure hospitallength of stay when compared with patients who under-went sternotomy (median, 6 days versus 9 days, P2< 0.003, Wilcoxon rank sum test). Each group had sig-nificant diminution in the serum level of calcium afterthe intervention, as compared with initial levels (P2 < 0.01,paired Student's t test). However, the mean postprocedureserum level of calcium was significantly lower in the pa-tients who underwent stemotomy than in the patientswho underwent ablation (P2 < 0.01, Student's t test). Thisis accounted for by the presence of some unsuccessfulprocedures in the angioblation group. Twenty-two of thethirty ablation procedures (73%) were initially determinedto be successful, in other words, these procedures resultedin normocalcemia or hypocalcemia that was presentthroughout the postprocedure hospitalization. Each of the24 patients (100%) who underwent sternotomy also hadresolution of hypercalcemia, a significantly higher pro-portion than ablation P2 < 0.02, Fisher's exact test).
104 Ann. Surg. Februlary 1992

MEDIASTINAL PARATHYROID ADENOMA ABLATION 105Follow-Up
Long-term follow-up showed that 17 of the 28 (61%)evaluable angiographic ablation attempts were followedby durable relief of the hypercalcemia and primary hy-perparathyroidism and appear to be cured. Each of the24 evaluable patients managed with median sternotomy,however, was cured (better than ablation, P2 < 0.001,Fishers exact test). In addition, 3 of20 patients who wereinitially rendered normocalcemic by ablation subse-quently developed recurrent hyperparathyroidism morethan 6 months after ablation. Therefore, 10 ofthe ablationprocedures were followed by other interventions for per-sistent or recurrent hypercalcemia. Three patients had re-peat ablation; one was successful long-term. Seven failedablations were followed by successful surgical resectionof the adenoma. Five were included in the sternotomygroup, and two had a mediastinal parathyroid adenomaremoved through a cervical incision. Each ofthe patientswho had a failed ablation followed by surgical resectionwas cured.
Complications
Three patients in the angiographic ablation group havepersistent hypoparathyroidism that requires supplementalcalcium and vitamin D to maintain normal serum levelsofcalcium (Table 5). Seven patients had evidence of per-sistent hypoparathyroidism after successful resection ofaparathyroid adenoma by median sternotomy. Two ofseven patients are now normocalcemic after implantationoffragments ofcryopreserved autologous parathyroid ad-enoma into the muscle of the nondominant forearm. Ofthe five remaining hypoparathyroid patients, after surgicalresection of a parathyroid adenoma, two have no cry-opreserved tissue because the viability of the gland ap-peared compromised as a result of failed prior staining,whereas three patients have cryopreserved tissue availablebut have not yet had attempted autograft at 9 months,41 months, and 46 months after surgery.Two patients had complications after sternotomy for
adenoma excision (Table 5). Five patients in the ablationgroup had complications referable to the procedure. Allcomplications resolved with appropriate management.There were no deaths in either group.
TABLE 5. Complications
Complication No.
StemotomyPneumonia IDeep venous thrombosis 1
Angiographic ablationPeripheral nerve symptoms 3Bradycardia IAcute renal failure I
Discussion
Although operative resection is the most effective singlemeans to eradicate functional mediastinal parathyroidadenomas and allows cryopreservation ofremoved tissue,many patients can have successful angiographic ablationwith minimal discomfort and complications. If ablationfails, then either repeat ablation or, more effectively, sur-gical resection, will cure them.
Angiographic ablation ofa mediastinal adenoma curedprimary hyperparathyroidism in 17 of 25 evaluable se-lected patients with symptomatic persistent primary hy-perparathyroidism. It was associated with a shorter hos-pital length-of-stay, and spared patients the greater painand longer convalescence associated with median ster-notomy. Although there was no substantial difference inmorbid complications of the two approaches, it is clearfrom observation ofthese patients after the two proceduresthat the recovery from the angiographic procedure wasmuch easier than that from median sternotomy. Thus,for the 17 patients whose ablation was curative, this ap-proach eliminated the need for sternotomy.
It has previously been stated4"'0 l that after ablationthe appearance ofthe parathyroid adenoma on subsequentCT (24 hours later) can predict whether the staining pro-cedure will be successful or unsuccessful. In general, thisstatement is true. The presence of persistent intense con-trast enhancement detected 1 day later by CT usually in-dicates that the patient will have a successful outcomewith resolution of hypercalcemia. This holds true in abouttwo of three cases, but some patients with persistent ev-idence of staining still may not have a successful outcome.The converse is also true. If there is no evidence of per-sistent staining ofthe abnormal parathyroid gland on fol-low-up CT, the serum level ofcalcium will usually remainelevated. However, a small proportion (29%) of patientswithout staining still may have a successful outcome andresolution of hypercalcemia.Median sternotomy for resection of parathyroid ade-
noma cured persistent primary hyperparathyroidism ineach patient studied here, including five patients who hadfailed angiographic ablation. Median sternotomy wasclearly a more effective treatment than ablation, both ininitial success rate and long-term control ofhypercalcemia(Table 4). Importantly, there was no apparent disadvan-tage in the ability to undergo subsequent curative medianstemotomy when patients have had prior attempted abla-tion. Each of the patients who had median sternotomyafter failed ablation was successfully salvaged, and therewere no complications ofthese operative procedures. Twopatients who had had prior ablation of a parathyroid ad-enoma, however, appeared to have decreased viability ofthe parathyroid adenoma at the time of resection, elim-inating our ability to cryopreserve some of the resected
Vol. 215 - No. 2

106 DOHERTY AND OTHERS
parathyroid adenoma. The ability to cryopreserve resectedparathyroid tissue during surgery to remove abnormalparathyroid glands appears to be a distinct advantage ofsurgery over ablation because the incidence of hypopara-thyroidism after successful reoperative parathyroid surgeryis high. A disadvantage of ablation is that no tissue canbe cryopreserved for potential delayed forearm autograftfor the correction of hypoparathyroidism.8"6 All patientswho come to ablation have had prior neck exploration asinitial attempted therapy for their primary hyperparathy-roidism. Most have had normal cervical parathyroidglands dissected and identified, often by biopsy. They areat risk for permanent hypoparathyroidism after ablationifthe adenoma represents their sole remaining functionalparathyroid tissue. Patients have a similar risk of hypo-parathyroidism after surgical resection; however, cry-opreservation of the tissue allows an autograft of para-thyroid adenoma tissue to the nondominant forearm, aswas successfully performed for two patients in the ster-notomy group described here.A concern that previously may have limited clinicians'
usage of this technique is the presumed risk of emboliccomplications to the brain or spinal cord.4 No patient inthis series experienced any embolic sequelae. Thus, at-tempted angiographic ablation ofmediastinal glands doesnot appear to add to the risk of diagnostic angiography.The theoretical risk of gland disruption by angioablationwith mediastinal tumor seeding was not seen.
In summary, angiographic ablation of mediastinalparathyroid glands is a safe, reasonable option for themanagement of functional parathyroid adenomas in pa-tients with persistent primary hyperparathyroidism. Thisis accomplished by placing the catheter into the appro-priate feeding artery and deliberately perfusing the ade-noma with ionic contrast media. It can be performed withminimal pain, a short hospital stay, and a reasonable long-term cure rate. Although surgical resection offers higherinitial and long-term cure rates, ablation can cure 60% ofpatients, thus obviating the need for surgery. Surgical re-section after failed ablation is not more difficult and offersa 100% salvage rate for those not cured by angioblation.Finally, selection of patients who are likely to have func-tional parathyroid tissue remaining in the neck after theirinitial surgery may lower the incidence of permanent hy-poparathyroidism and thus render the absence of cry-opreserved tissue for autotransplantation less important.The strategy of attempting angiographic ablation in pa-tients with persistent primary hyperparathyroidism whohave failed prior neck surgery, have evidence of a me-diastinal adenoma on angiography, and have a low prob-ability ofpostoperative hypoparathyroidism appears war-
Ann. Surg. - February 1992
ranted. Median sternotomy can be reserved for those pa-tients in whom ablation is unsuccessful. This strategy willnot reduce the cure rate because median sternotomy andsurgical resection will cure the hyperparathyroidism inthe subgroup of patients who have an unsuccessful out-come with ablation. Angiographic ablation will eliminatethe pain and convalescent period required to recover frommedian sternotomy in the majority of patients for whomablation will be successful.
AcknowledgmentsThe authors thank Donald White, Alison McMullen, and Melissa
Corbitt for the storage and retrieval of data from the database maintainedfor these patients, and Barbara Owen for her expert preparation of themanuscript.
References
1. Segre GV, Potts JT. Differential diagnosis of hypercalcemia. InDeGroot U., ed. Endocrinology. Philadelphia: WB Saunders,1989, pp 984-1001.
2. Burt ME, Brennan MF. Incidence of hypercalcemia and malignantneoplasm. Arch Surg 1980; 115:704-707.
3. Clark OH. Mediastinal parathyroid tumors. Arch Surg 1988; 123:1096-1100.
4. Miller DL, Doppman JL, Chang R, et al. Angiographic ablation ofparathyroid adenomas: lessons from a 10-year experience. Ra-diology 1987; 165:601-607.
5. Miller DL, Doppman JL, Krudy AG, et al. Localization of para-thyroid adenomas in patients who have undergone surgery: PartII. Invasive procedures. Radiology 1987; 162:138-141.
6. Eisenberg H, Pallotta J, Sacks B, Brickman AS. Parathyroid local-ization, three-dimensional modeling, and percutaneous ablationtechniques. Endocrinol Metab Clin North Am 1989; 18:659-699.
7. Levin KE, Gooding GAW, Okerlund M, et al. Localizing studies inpatients with persistent or recurrent hyperparathyroidism. Surgery1987; 102:917-925.
8. Brennan MF, Norton JA. Reoperation for persistent and recurrenthyperparathyroidism. Ann Surg 1985; 201:40-44.
9. Norton JA, Schneider PD, Brennan MF. Median sternotomy inreoperations for primary hyperparathyroidism. World J Surg1985; 9:807-813.
10. Doppman JL, Marx SJ, Spiegel AM, et al. Treatment of hyperpara-thyroidism by percutaneous embolization of a mediastinal ade-noma. Radiology 1975; 115:37-42.
11. Doppman JL, Brown EM, Brennan MF, Spiegel A, Marx SJ, AurbachGD. Angiographic ablation ofparathyroid adenomas. Radiology1979; 130:577-582.
12. Norton JA. Reoperative parathyroid surgery: indication, intraoper-ative decision-making and results. Prog Surg 1986; 18:133-145.
13. Miller DL, Doppman JL, Shawker TH, et al. Localization of para-thyroid adenomas in patients who have undergone surgery: Part1. Noninvasive imaging methods. Radiology 1987; 162:133-137.
14. Miller DL. Preoperative localization and interventional treatmentof parathyroid tumors: when and how? World J Surg 1991 (inpress).
15. Doppman JL, Popovsky M, Girton M. The use of iodinated contrastagents to ablate organs: experimental studies and histopathology.Radiology 1981; 138:333-340.
16. Wells SA, Ross RJ, Dale JK, Gray RS. Transplantation of the para-thyroid glands. Surg Clin North Am 1979; 59:167-177.
Copyright © 2022 FDOKUMEN




















