
Focal nodular hyperplasia and hepatic adenoma: current diagnosis and management
15
1 23 Updates in Surgery Official Journal of the Italian Society of Surgery ISSN 2038-131X Volume 66 Number 1 Updates Surg (2014) 66:9-21 DOI 10.1007/s13304-013-0222-3 Focal nodular hyperplasia and hepatic adenoma: current diagnosis and management Agustin Cristiano, Agustin Dietrich, Juan Carlos Spina, Victoria Ardiles & Eduardo de Santibañes
Transcript of Focal nodular hyperplasia and hepatic adenoma: current diagnosis and management

1 23
Updates in SurgeryOfficial Journal of the Italian Society ofSurgery ISSN 2038-131XVolume 66Number 1 Updates Surg (2014) 66:9-21DOI 10.1007/s13304-013-0222-3
Focal nodular hyperplasia and hepaticadenoma: current diagnosis andmanagement
Agustin Cristiano, Agustin Dietrich,Juan Carlos Spina, Victoria Ardiles &Eduardo de Santibañes

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer-
Verlag Italia. This e-offprint is for personal
use only and shall not be self-archived
in electronic repositories. If you wish to
self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.

REVIEW ARTICLE
Focal nodular hyperplasia and hepatic adenoma: currentdiagnosis and management
Agustin Cristiano • Agustin Dietrich •
Juan Carlos Spina • Victoria Ardiles •
Eduardo de Santibanes
Received: 25 March 2013 / Accepted: 16 June 2013 / Published online: 27 June 2013
� Springer-Verlag Italia 2013
Abstract Benign liver tumors are common lesions that
can be classified into cystic and solid lesions. Cystic lesions
are the most frequent; however, they rarely represent a
diagnostic or therapeutic challenge. In contrast, solid
lesions are more difficult to characterize and management
remains controversial. The wide availability and use of
advanced imaging modalities, including ultrasonography,
computed tomography, and magnetic resonance imaging
have led to increased identification of incidental liver
masses. Although some of these incidentally discovered
masses are malignant, most are benign and must be
included in the differential diagnosis. In this article we
review FNH and HA. Its etiology, biological behavior,
diagnosis, and treatment will be highlighted.
Keywords Benign liver tumors � Focal nodular
hyperplasia � Hepatocellular adenoma � Diagnosis �Management � Treatment
Introduction
Benign liver tumors are common lesions that can be found
in 20–52 % of the population according to different
autopsy-based series [1, 2]. Cystic lesions are the most
frequent; however, they rarely represent a diagnostic or
therapeutic challenge. In contrast, solid lesions are more
difficult to characterize and their management remains
controversial.
Solid liver lesions may originate from blood vessels, the
epithelium of the bile ducts, or liver parenchymal cells.
After simple cysts, hepatic hemangiomas are the most
common tumors, followed by focal nodular hyperplasia
and hepatocellular adenomas [3, 4].
Over the past few decades the diagnosis of solid liver
lesions has risen. Although there is an increase in the risk
factors for developing these lesions, such as the use of
hormonal treatments, the advent of better diagnostic
imaging methods has led to an improvement in the inci-
dental diagnosis of these diseases. Now there are more and
better studies that allow us to detect smaller lesions, earlier
and with superior anatomic and spatial resolution. With the
advent of positron emission tomography (PET–CT) and
new magnetic resonance imaging (MRI) techniques,
information on the metabolic activity of the lesions can be
obtained. These advances have improved the diagnosis of
benign and malignant liver lesions.
It is sometimes difficult to elucidate the malignant or
benign condition of liver tumors only by their character-
istics with just one imaging method. In these situations, it is
necessary to use multiple studies that complement one
another to make the best therapeutic decision. The risk of
conservative treatment in malignant tumors is much higher
than the risk of benign liver tumor resection.
To arrive at a correct diagnosis we should not only rely
on imaging studies: the past medical history, physical
examination and laboratory tests are also of vital impor-
tance. Personal history of previous cancer disease, alcohol
consumption, viral infections, cirrhosis, and use of oral
A. Cristiano � A. Dietrich � V. Ardiles (&) � E. de Santibanes
Liver Transplant Unit and General Surgery Department,
Hospital Italiano de Buenos Aires, Gascon 450,
1181 Buenos Aires, Argentina
e-mail: [email protected]
E. de Santibanes
e-mail: [email protected]
J. C. Spina
Radiology Department, Hospital Italiano de Buenos Aires,
Buenos Aires, Argentina
123
Updates Surg (2014) 66:9–21
DOI 10.1007/s13304-013-0222-3
Author's personal copy

contraceptives or other steroids can help guide the diag-
nosis as well.
In this article we review focal nodular hyperplasia and
hepatocellular adenoma. Its etiology, biological behavior,
diagnosis, and treatment will be highlighted.
Focal nodular hyperplasia
Focal nodular hyperplasia (FNH) is the second solid liver
tumor in order of frequency, representing approximately
8 % of all primary hepatic neoplasms and is present in
0.3–3 % of the general population [5–7]. These tumors are
more frequent in women (10:1) aged between 20 and
50 years [8]. Despite the increased prevalence of FNH in
women there is no evidence linking these tumors with the
use of oral contraceptives (OC) [9]. However, in our
clinical experience we have observed growth of these
tumors in patients consuming OC; therefore, we suggest
discontinuing the medication.
Pathogenesis
The genesis of FNH is probably secondary to a vascular
malformation that produces blood hyper-perfusion in an
area of liver parenchyma, which determines a hyperplastic
response to this phenomenon without risk of malignant
transformation, [5, 10] or bleeding, justifying no aggressive
treatment [11]. Furthermore, FNH is associated with other
vascular malformations and hemangiomas in the liver and
brain, reinforcing the theory of the vascular etiology [10].
At present, the pathophysiology of FNH remains
unclear. However, in the past few years, the biomolecular
study of B-catenin, glutamine synthetasa (GS), and TGF-
beta, which are involved in liver proliferation, has led to a
better understanding of the genetic pathways of these
tumors.
Due to the major role of B-catenin in the regulation of
hepatocyte proliferation [12], its activation could conse-
quently contribute to tumor formation. Moreover, there are
several genes that are up-regulated in FNH, almost all of
them regulated by the B-catenin. The biomolecular study
of its over-expression in FNH showed heterogeneous dis-
tribution due to the polyclonal nature of the disease [13]. In
contrast, a subtype of HCA (activated b-catenin), which
presents a monoclonal origin, has a completely different
pattern of staining [13, 14].
Nowadays, the histopathological study of the GS has
also become a very useful tool for rapid identification of
FNH. For Bioulac-Sage et al. [15] GS immunostaining was
similar in all FNH cases. GS was present in large hepato-
cytic areas, anastomosed in a ‘map-like’ pattern, often
surrounding hepatic veins; whereas GS was not expressed
in hepatocytes close to fibrotic bands containing arteries
and ductules. In HCA or well-differentiated hepatocellular
carcinoma (HCC) presenting b-catenin mutation, GS was
positive but with a completely different pattern that
appeared diffuse and not ‘map-like’.
Histopathology
Histopathologically, FNH are well-differentiated tumors
without capsule, consisting of hepatocellular nodules
accompanied by stromal tissue [16]. FNH can be divided
into classical (80 %) and atypical (20 %), and within the
latter three subtypes can be distinguished: telangiectatic,
with cell atypia, and mixed (hyperplastic and adenomatous)
[17]. The abnormal hystoarchitecture or vascular malfor-
mations may be absent in non-classical forms, but bile duct
proliferation is always present [18]. The clinical relevance
of these three subtypes of FNH is not yet defined. Nowa-
days, the telangiectatic form as a variant of HNF is dis-
cussed. They often present clinical and morphologic signs
of hemorrhage like patients with adenomas [19]. Due to
this behavior, this variant may be treated as a HCA.
Diagnosis
Patients are generally asymptomatic and FNH manifests as
an incidental finding on an imaging study. However, 25 %
of the patients may have related symptoms. The most
common symptoms include epigastric pain, early satiety,
and/or a palpable abdominal mass [20].
The differential diagnosis with other hepatic tumors is
not easy, especially with other hypervascular tumors such
as HCA, HCC, and hypervascular metastases. MRI and CT
are able to provide some information for the diagnosis of
FNH, especially when the lesion depicts typical features,
such as uniform hypervascularity after intravenous contrast
administration and a central scar of fibro vascular tissue,
but unfortunately they are not always present [18, 21]. In a
series of 305 FNH, Nguyen et al. [17] describe that a
central scar could only be found in about 50 % of the cases.
At ultrasound FNH appears as a hypo or isoechoic solid
lesion and may rarely present as a hyperechoic lesion [22].
Sometimes there is a pseudocapsule caused by compression
of the underlying liver parenchyma. The central scar can be
seen in approximately 20 % of cases and looks slightly
hyperechoic [18]. Using Doppler, a central artery with
branches with a star pattern can be seen [21, 23]. Often the
information obtained through the abdominal ultrasound is
non-specific; however, when performed with IV contrast
the revenue of the study is better [21, 22, 24]. Most lesions
10 Updates Surg (2014) 66:9–21
123
Author's personal copy

demonstrate enhancement during the arterial phase with the
presence of central stellate arteries and a centrifugal con-
trast pattern with a transient peripheral unenhanced zone
that reflects a peripheral part of the lesion that is not ini-
tially enhanced [25, 26]. In portal and delayed phases, FNH
shows isoechogenicity compared with adjacent paren-
chyma [18, 27, 28].
CT should be performed with and without IV contrast in
arterial, portal, and equilibrium phases for a proper char-
acterization of the lesion. Early studies, dating from the
late 1980s, reported the usefulness of CT for the diagnosis
of FNH and showed a sensitivity of 75 % and specificity of
92 % [29, 30]. In unenhanced series FNH appears hypo or
isodense to normal liver parenchyma. In the context of
steatosis, FNH could appear as a hyperdense lesion because
of the parenchymal attenuation caused by hepatic steatosis
[31]. After an injection of IV contrast, FHN enhances
homogeneously during the arterial phase due to the pre-
dominant arterial vascularization. The arterial enhance-
ment allows the identification of a hypodense central scar
that becomes evident in up to 60 % of cases [32]. During
the portal venous phase, FNH is less conspicuous and
becomes isoattenuating with the rest of the liver. In the
equilibrium phase, approximately 5 min after the bolus
injection, the lesion remains isoattenuating and the central
scar may enhance slightly due to uptake of contrast mate-
rial by the fibroconective tissue [33, 34]. Generally, it is
easier to observe the central scar and other characteristics
as vascular abnormalities in lesions larger than 3 cm
(Fig. 1). In smaller lesions, these features are less obvious
and may be absent in up to 70 % of cases [34].
Other features of FNH also appear to be related to its
size. Smaller lesions invariably enhance homogeneously,
rarely distort liver architecture, and rarely have displaced
or enlarged peritumoral blood vessels. Larger lesions may
be slightly heterogeneous (mostly attributable to the pres-
ence of fibrous septa) and demonstrate dilated feeding
arteries or draining veins in 34 % of lesions. Enlarged
vessels on the surface of a FNH penetrating to the central
scar are a well-recognized pathologic feature of FNH, and
the demonstration of such vessels on CT scans should not
be regarded as suggestive of malignancy [31].
A pseudocapsule has been reported by Brancatelli et al.
[31] in 8 % of FNH. In patients with fatty liver, a
pseudocapsule may become evident due to compressed
liver and mild fibrosis along the periphery of the lesion
may be denser than the rest the liver [35]. Other sources of
a pseudocapsules are the dilated vessels and sinusoids that
can be present around the FNH [29]. Hence, the presence
of a pseudocapsule should not be regarded as an invariable
sign of malignancy. On the other hand, calcification is a
rare finding in FNH, suggesting the need for further eval-
uation [31].
Currently, MR imaging is considered a highly accurate,
non-ionizing radiation diagnostic procedure for the detec-
tion and characterization of focal liver lesions and is often
used as a problem-solving modality when equivocal find-
ings are obtained with other imaging techniques. It should
Fig. 1 MDCT showing typical
FNH in segment IV. a Hepatic
arterial phase: shows FNH
enhancing brightly except for
the central scar and thin septa.
Note enlarged feeding artery
penetrating to the center of the
lesion. b Portal venous phase:
FNH is less conspicuous and
becomes isoattenuating with the
rest of the liver. Scar begins to
fade toward isoattenuation.
c Equilibrium phase: the lesion
remains isoattenuating and the
central scar shows slight
enhancement. d Coronal
maximum intensity projection
(MIP) during arterial phase
shows enlarged feeding artery
branches along the surface of
the lesion and penetrating to the
center
Updates Surg (2014) 66:9–21 11
123
Author's personal copy
be used instead of CT for the characterization of liver
lesions, in particular, for asymptomatic young women.
At MRI, FNH is typically homogeneously isointense or
slightly hyperintense with respect to the normal surrounding
liver parenchyma on T2-weighted images, and isointense or
slightly hypointense on T1-weighted images before admin-
istration of gadolinium [36]. However, these characteristics
are shared by other benign and malignant liver tumors. The
administration of IV contrast allows a definitive diagnosis if a
typical behavior is present. The enhancement pattern parallels
that of contrast-enhanced CT, with a rapid and homogeneous
enhancement during the arterial phase that becomes isoin-
tense during the portal venous phase and equilibrium images.
A central scar, when present, is hyperintense on T2-weighted
images and hypointense on T1-weighted images. During the
dynamic phase of contrast enhancement, it is hypointense
during the arterial and portal venous phases and slightly
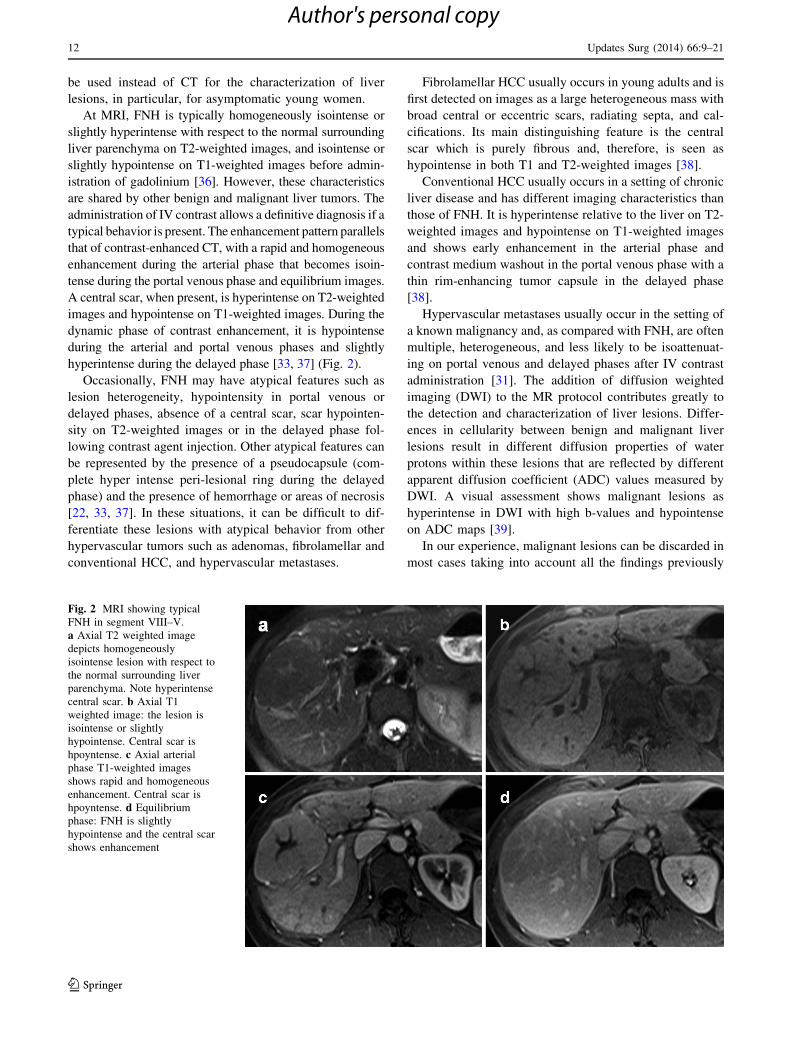
hyperintense during the delayed phase [33, 37] (Fig. 2).
Occasionally, FNH may have atypical features such as
lesion heterogeneity, hypointensity in portal venous or
delayed phases, absence of a central scar, scar hypointen-
sity on T2-weighted images or in the delayed phase fol-
lowing contrast agent injection. Other atypical features can
be represented by the presence of a pseudocapsule (com-
plete hyper intense peri-lesional ring during the delayed
phase) and the presence of hemorrhage or areas of necrosis
[22, 33, 37]. In these situations, it can be difficult to dif-
ferentiate these lesions with atypical behavior from other
hypervascular tumors such as adenomas, fibrolamellar and
conventional HCC, and hypervascular metastases.
Fibrolamellar HCC usually occurs in young adults and is
first detected on images as a large heterogeneous mass with
broad central or eccentric scars, radiating septa, and cal-
cifications. Its main distinguishing feature is the central
scar which is purely fibrous and, therefore, is seen as
hypointense in both T1 and T2-weighted images [38].
Conventional HCC usually occurs in a setting of chronic
liver disease and has different imaging characteristics than
those of FNH. It is hyperintense relative to the liver on T2-
weighted images and hypointense on T1-weighted images
and shows early enhancement in the arterial phase and
contrast medium washout in the portal venous phase with a
thin rim-enhancing tumor capsule in the delayed phase
[38].
Hypervascular metastases usually occur in the setting of
a known malignancy and, as compared with FNH, are often
multiple, heterogeneous, and less likely to be isoattenuat-
ing on portal venous and delayed phases after IV contrast
administration [31]. The addition of diffusion weighted
imaging (DWI) to the MR protocol contributes greatly to
the detection and characterization of liver lesions. Differ-
ences in cellularity between benign and malignant liver
lesions result in different diffusion properties of water
protons within these lesions that are reflected by different
apparent diffusion coefficient (ADC) values measured by
DWI. A visual assessment shows malignant lesions as
hyperintense in DWI with high b-values and hypointense
on ADC maps [39].
In our experience, malignant lesions can be discarded in
most cases taking into account all the findings previously
Fig. 2 MRI showing typical
FNH in segment VIII–V.
a Axial T2 weighted image
depicts homogeneously
isointense lesion with respect to
the normal surrounding liver
parenchyma. Note hyperintense
central scar. b Axial T1
weighted image: the lesion is
isointense or slightly
hypointense. Central scar is
hpoyntense. c Axial arterial
phase T1-weighted images
shows rapid and homogeneous
enhancement. Central scar is
hpoyntense. d Equilibrium
phase: FNH is slightly
hypointense and the central scar
shows enhancement
12 Updates Surg (2014) 66:9–21
123
Author's personal copy

described. Therefore, the main differential diagnosis is
with adenomas when the lesions enhance strongly during
the arterial phase and then either retain a hyperintense
appearance or demonstrate isointensity with the normal
liver parenchyma during subsequent portal venous and
delayed phases. Unfortunately, DWI does not contribute to
this differential diagnosis because both quantitative and
qualitative assessment of ADC values for FNH and ade-
nomas are similar.
In these patients, MRI hepato-specific contrast agents
(gadobenatedimeglumine, MultiHance, Bracco, Milan,
Italy, formerly known as Gd-BOPTA and gadoxetate,
Primovist, Bayer-Schering, Berlin, Germany, formerly
known as Gd-EOB-DTPA) can be used as a problem
solving tool [40]. They are gadolinium-based agents with
combined perfusion and hepatocyte-specific properties.
Both gadobenate and gadoxetate are taken up by the
hepatocytes and excreted by the biliary system. These
agents are useful in differentiating FNH from other
hypervascular lesions, particularly adenoma [40]. The key
lies in the histological absence of bile ducts in adenomas
and malignant lesions against the histological structure of
FNH that is similar to that of normal hepatic parenchyma.
Hence, on delayed phase images (acquired at 15–20 min to
3 h depending on the type of contrast used) a substantial
hepatocellular enhancement is noted in FNH that is iden-
tified as iso-hyperintense lesion while adenomas, hepato-
carcinomas, and metastases are identified as hypointense
lesions [41]. This typical pattern makes these agents very
effective in the characterization of FNH. Indeed, the
combination of strong enhancement on arterial phase
images and iso or hyperintensity on hepatobiliary phase
images showed 83.8 % sensitivity and 98.5 % specificity
for the diagnosis of FNH [40].
Treatment
Due to the lack of randomized clinical trials assessing the
benefits of elective surgery versus conservative treatment,
management of patients with diagnosis of FNH remains
controversial.
However, the absence of malignant transformation and
the low rate of tumor complications support the indication
of a conservative treatment, especially in the case of small,
asymptomatic FNH without enlargement during follow-up
[42].
On the other side, the inability to rule out malignancy,
tumor enlargement (3–5 cm/year), and symptomatic
patients should undergo surgical resection [43–46].
Several studies have demonstrated that elective surgery
for the treatment of FNH is a safe procedure in selected
cases, with low morbidity and long-term relief of symp-
toms [42, 47, 48].
Adenoma
HCAs are uncommon benign tumors. In the 1970s, with the
development of oral contraception, there was an increased
incidence of HCA in women consuming OC [49–51].
Further studies specified this relationship by showing that
those patients treated with high estrogenic doses and/or for
prolonged periods of time have a risk of developing HCA
25 times higher (3–4 cases per 100,000 people) than the
general population [50, 51]. More controversial is the
hypothesis that the lesion can have regression after dis-
continuation of treatment, although there are publications
that support it [52, 53]. Another risk factor for development
of HCA is pregnancy, which is related to increased
endogenous steroids, which are related to the formation of
these tumors [54, 55]. There are other less common pre-
disposing factors such as consumption of anabolic steroids,
iron metabolic diseases, endocrine disorders, or glycogen
storage diseases (especially type I) [56, 57]. A recent study
showed that being overweight/obese represents a novel
factor favoring the emergence of HCA [58]. These patients
would also have an increased risk of having a complicated
tumor (bleeding and malignant transformation).
Hepatic adenomas are generally located in the right lobe
of the liver and are mostly single, but several simultaneous
lesions in the liver parenchyma can be seen [59–61]. The
term Hepatic adenomatosis was classically reserved for
those patients with over ten lesions separated by normal
parenchyma that could be present in 10–24 % of patients
with HCA [60, 61]. Nowadays, the adenomatosis is not
considered a specific type of HCA and the number of
nodules would not have therapeutic implications [62].
Pathogenesis
The pathogenesis is controversial although some reports
associate the presence of steatosis with this form of the
disease [63]. In this situation of multiple adenomas, the
relationship with the use of oral contraceptives or steroids
is controversial, but some authors suggested an association
between hepatic adenomatosis and glycogen storage dis-
eases [60, 64].
Histopathology
Macroscopically, most HCAs are solitary, unencapsulated
tumors that vary from \1 cm to up to 20 cm in size that
may have central areas of necrosis or hemorrhage [65, 66].
In the histological study, there are plates of two or three
cells with high intracellular lipid content grouped into
cords, with no portal spaces, separated by dilated
Updates Surg (2014) 66:9–21 13
123
Author's personal copy

sinusoidal vessels supplied only by arterial blood [67, 68].
The lack of portal space and bile ducts differentiates HCA
from FNH (86).
HCA had been classified into three histopathological
varieties: steatosic, telangiectatic, and indeterminate,
which have different clinical and biological behaviors.
Telangiectatic and indeterminate varieties have an
increased risk of complications such as bleeding and
malignancy [56, 60, 69, 70]. However, nowadays hepato-
cellular adenomas are classified into three distinct sub-
types: HCAs with hepatocyte nuclear factor 1 (HNF1)
mutated (HNF-HCAs), HCAs characterized by B-catenin
mutations, and inflammatory HCAs (I-HCAs) due to
mutations involving interleukin-6 (IL-6) signal transducer.
Inflammatory HCAs and HNF-HCAs are the two major
subgroups of HCAs [6, 65]. I-HCAs represent the most
common variant (35–50 % of HCAs). They present an
increased risk of bleeding and small risk of malignant
transformation and are associated with obesity. HNF-HCAs
represent 30–45 % of HCAs, with risk of bleeding but no
risk of malignant transformation. These two subtypes are
more frequent in women in treatment with OCs. The third
group is HCAs with activation of B-catenin and represents
10–17 % of HCAs. In this form of HCA there is no sex
distinction, and it presents a relationship with glycogene
storage disease and treatment with androgens [65].
B-catenin-activated lesions seem to have a higher risk of
malignant transformation in patients with HCA. Therefore,
identifying a b-catenin mutation is of major interest.
Additional markers may help to discriminate these lesions.
As mentioned above, glutamine synthetase (GS) is another
useful marker in tumor liver pathology. A strong and
homogeneous GS staining is shown in b-catenin-mutated
HCA [11]. This pattern can be also seen in hepatocelullar
carcinoma (HCC), in which even 50 % of the HCC,
including early forms, present diffuse and strong GS
immunostaining [71]. During the past decade, new tissue
markers have become available, especially to identify
malignant lesions like Glypican-3 and Heat Shock Protein-
70 (HSP-70) (see Table 1). Although these markers have a
low sensibility (35–50 %), they are highly specific when
combined (95–100 %) [72–75].
However, despite the importance of histopathological
analyses to confirm the subtypes of HCAs, GS and
b-catenin immunohistochemical staining are not sensitive
enough to detect all b-catenin mutations in HCA, and the
interpretation of b-catenin staining may also be difficult
because of the heterogeneous staining pattern [76].
However, regarding these specific histopathologic
characteristics, there are potential problems regarding
biopsy, like sampling errors, risk of hemorrhage or tumor
seeding along the needle-track [77]. Limited core biopsies
may present difficulties in differentiating HCA from
normal hepatocytes, FNH, and well-differentiated hepato-
cellular carcinoma, making the indication of biopsy con-
troversial [78, 79].
Clinical presentation
In the past, most of the HCA were diagnosed in symp-
tomatic patients [71]; however, with the improvement of
radiological techniques, the number of incidentalomas
increased and, therefore, the number of sympomatic
patients decrease [80].
Chronic upper-right quadrant and epigastric pain asso-
ciated with nausea or early satiety are common symptoms
and are produced by the tumor size and mass effect [59,
81]. Less frequently, patients may present sudden pain
followed by hypotension which translates into subcapsular
or intraperitoneal bleeding as a complication of the tumor
[59].
Diagnosis
Ultrasound is certainly one of the first methods in the study
of a liver mass. In the case of HCA its value is debated.
Although some authors report up to 50 % in diagnostic
sensitivity, specificity is low [60, 82]. The lesions may be
hypo-iso or hyperechoic, and this depends on the tumor
characteristics (amount of lipids, calcification, intratumoral
hemorrhage, necrosis, etc.) and underlying liver paren-
chyma [68, 82]. Doppler demonstrated intratumoral arterial
flow and peritumoral arterial and venous flow, showing a
continuous plane wave [68, 83]. The combination of ultra-
sound associated with IV contrast infusion enhances the
ability to differentiate HCA from other liver lesions.
According to tumor histology, HCAs show homogeneous
enhancement during the hepatic arterial phase preceding
enhancement of normal liver parenchyma, sometimes with
centripetal filling, with no radial vascular structures. Rapid
wash out and no portal venous enhancement during the
hepatic portal venous phase is seen, with isoechoic or, more
often, slight hypoechoic appearance in the later parenchy-
mal phases. This pattern allows its differentiation from FNH
that enhances both in arterial and portal phase [26, 28].
CT findings of adenomas depend on the characteristics
of the lesion and surrounding liver parenchyma. Therefore,
they can show hyperattenuation on unenhanced images in
patients with steatosis or hypoattenuation in high lipid
content lesions surrounded by normal parenchyma [68, 84].
If necrosis or hemorrhage is present, as described in 25 %
of lesions, a more heterogeneous pattern can be seen
showing hyperattenuation in regions with recent bleeding,
and hypoattenuation in region with previous bleeding. The
incidence of calcification varies from 5 to 10 % and a
tumor capsule was described in 25 % of lesions [68].
14 Updates Surg (2014) 66:9–21
123
Author's personal copy

Therefore, at CT, HCAs are usually isodense prior to the
injection of IV contrast, but may often be heterogeneous
with hyperdense areas through the presence of bleeding or
hypodense areas through the presence of lipid or fat [85].
After IV contrast administration, the lesions enhance rap-
idly and relatively homogeneously during the arterial phase
in the case of small tumors (\3 cm) and heterogeneously in
the larger lesions that usually present bleeding complica-
tion or fat deposition. In the portal venous and delayed
phases adenomas became more homogeneous and similar
in attenuation to normal liver. Nevertheless, in 19 % of
cases they can be hypoattenuated in delayed phase images
[68, 84].
At MRI the imaging features of hepatocellular adeno-
mas vary on the basis of the histopathologic findings and
associated complications, so there are also various
appearances either due to the presence of fat, old or recent
hemorrhage, necrosis, or calcification foci [68]. On T1-
weighted images, HCA tend to appear as hyperintense
lesions although there are publications in which these
findings were present in only a minority of cases [86–88].
Such hyper intensity is due to the presence of fat, glycogen,
or bleeding. Since fat is present in the intracellular space,
adenomas show significant signal intensity drop due to fat
content on opposed-phase images [86–88]. On T2-weigh-
ted images, most of these lesions are slightly hyperintense
and heterogeneous because of a combination of hyper and
hypointense areas that correspond to hemorrhage and
necrosis [86–88]. After IV contrast, they enhance quickly
and heterogeneously during arterial phase and tend to
homogenize with the surrounding parenchyma during the
portal venous and delayed phases, sometimes showing
wash out [88]. These features preclude making a differ-
ential diagnosis with other malignant lesions featuring
similar behavior (HCC or hypervascular metastases).
Unlike what happens with FNH, the use of gadolinium-
based hepato-specific contrast agents does not provide
additional information to differentiate between adenomas
and malignant lesions since both are hypointense on
delayed phase images (acquired at 15–20 min to 3 h
depending on the type of contrast used) [40].
As previously mentioned for FNH, diffusion weighted
images can help to differentiate HCAs from metastases but
are not useful in differentiating HCA from FNH.
MRI is the imaging modality of choice for subtype char-
acterization of hepatocellular adenomas. Laumonier et al.
[89] described that HNF-HCA and I-HCA are associated
with specific MR imaging patterns that are related to diffuse
fat distribution and to sinusoidal dilatation, respectively [89].
Inflammatory hepatocellular adenomas are diffusely
hyperintense on T2-weighted images, with higher signal
intensity in the periphery of the lesion, correlating with
dilated sinusoids. On T1-weighted images, they are isoin-
tense or mildly hyperintense, with minimal or no signal
drop on opposed-phase images. After the administration of
gadolinium, they usually show intense enhancement during
the arterial phase, which persists in the portal venous and
delayed phases [90] (Fig. 3).
Marked T2 hyper intensity associated with delayed,
persistent enhancement showed 85 % sensitivity and 87 %
specificity for the diagnosis of inflammatory hepatocellular
adenomas [89].
HNF-HCAs are isointense to slightly hyperintense on
T2-weighted images and predominantly hyper or isointense
on T1-weighted images, with diffuse signal drop on
opposed-phase because of intracellular steatosis. They
show moderate enhancement in the arterial phase with no
persistent enhancement in the portal venous or delayed
phases [90] (Fig. 4).
The presence of signal drop on opposed-phase images
showed 86 % sensitivity and 100 % specificity for the
diagnosis of this subtype of HCA [89].
No specific MR imaging patterns have yet been pro-
posed to identify either b-catenin-mutated hepato-cellular
adenomas or unclassified hepatocellular adenomas.
Figure 5 shows a flow-chart for the imaging diagnosis of
focal hepatic lesion.
Treatment
Liver resection for treatment of HCA has a morbidity of
10–25 % and mortality lower than 2 % [44, 60, 91], and
Table 1 Pathological features/
immunohistochemistry
HCA hepatocellular adenoma,
FNH focal nodular hyperplasia,
HCC hepatocellular carcinoma
HCA FNH HCC
Glypican-3 Negative staining Negative staining Diffuse cytoplasmatic staining.
HSP-70 Negative staining Negative staining Focal nucleocytoplasmatic
staining
GS Diffuse cytoplasmatic
staining
Cytoplasmatic
staining. ‘Map-
like’ pattern
Diffuse staining
B-catenine Homogeneous nuclear
staining, especially in
B-catenine-activated
subtype
Heterogeneous distribution Homogenous nuclear staining.
Updates Surg (2014) 66:9–21 15
123
Author's personal copy

should be performed on all patients with risk of bleeding
(20–30 and up to 50 %) or malignant transformation.
In non-surgical cases, the suspension of OC and imaging
follow-up is mandatory [56, 92]. Patients with HCA\5 cm
in size are rarely associated with risk of hemorrhage or
malignant transformation and hence can safely be managed
conservatively with imaging follow-up. Many authors
recommend early surveillance with multiphase CT or MRI
[93]. Some authors suggest adding to the follow-up peri-
odic dosage of alpha-feto protein [94].
To the present, there is no evidence in the literature, of
well-established protocols of surveillance in patients with
HCA. We recommend a close follow-up. Surveillance with
periodical US (every 3 month) can be a useful tool to detect
Fig. 3 MRI showing
inflammatory hepatocellular
adenoma in segment III. a Axial
T2 weighted image depicts a
diffusely hyperintense lesion.
b Axial T1 weighted image in-
phase and oppose phase shows
the lesion with heterogeneous
hypointensity but with no signal
drop on opposed-phase images.
c Axial arterial phase T1-
weighted image shows intense
enhancement. d Axial portal
venous phase T1-weighted
image showing persistent
enhancement of the lesion
during portal venous and
delayed phases (not shown)
Fig. 4 MRI showing HNF-1a–
mutated hepatocellular adenoma
in segment VI. a Axial T2
weighted image depicts a
slightly hyperintense focal
lesion. b Axial T1 weighted in-
phase and opposed phase
images: The lesion is isointense
on T1-weighted images (in-
phase), with diffuse signal drop
on oppose-phase. c Axial
arterial phase T1-weighted
image shows mild enhancement,
particularly in the anterior
region of the lesion. d Axial
portal venous phase T1-
weighted image shows no
persistent enhancement in the
portal venous and delayed
phases (not shown)
16 Updates Surg (2014) 66:9–21
123
Author's personal copy

change in size or tumor’s characteristics in those patients
with small and asymptomatic HCA.
Most small HCAs remain stable during surveillance and
a small number of them may disappear [62].
Currently, liver resection is recommended in patients
with adenomas greater than 5 cm, inflammatory forms, and
patients unable to discontinue hormone therapy [70, 95–
97]. Also, due to the high risk of malignancy, HCAs in men
or evidence of B-catenin activation demonstrated on biopsy
are also indications of surgery [76, 98].
Patients presenting abdominal symptoms related to the
adenoma should be evaluated as candidates for surgery,
depending on their comorbidities. Most of previously
published series demonstrated low postoperative morbidity
and mortality [79, 80, 99].
The rupture of the HCA is a serious situation that
compromises the patient’s life. Resection in these cases has
a mortality rate of around 10 % [100–102]. Therefore,
resuscitation should be performed with hemodynamic sta-
bilization and angiographic embolization leaving hepatic
resection only for experienced surgeons [102, 103]. In case
of not having a specialized surgeon, damage control sur-
gery (liver packing) should be performed [101].
Although pregnancy is not contraindicated in patients
with HCAs, in women with HCAs greater than 5 cm
surgical resection is mandatory before conception [54, 55,
104]. Resection in the second trimester of pregnancy has a
low morbidity and mortality for both the mother and fetus
[105]. When the diagnosis is made in the third trimester,
we recommend a watchful waiting with strict clinical and
ultrasound follow-up, because in this period estrogen levels
are higher and the concomitant risk of bleeding is greater
[104]. Spontaneous rupture of the HCA during pregnancy
is a rare but extremely serious complication [106].
With regard to liver adenomatosis, a recent study
showed that the rates of intrahepatic bleeding and intra
tumoral bleeding in asymptomatic, incidentally discovered
HCA are 2 and 13 %, respectively, rates that are similar to
solitary HCAs [63].
Moreover, the potential risk of complications would be
related to the underlying histologic subtype and tumor size
rather than the number of HCAs [62, 76]. Resection of
large or complicated lesions is generally indicated with a
strict observance of those lesions left behind, as the risk of
complications in these is low [56, 60, 64, 93]. The indi-
cation for liver transplantation is reserved for those patients
who are symptomatic, who presented several episodes of
complications, and/or whose condition cannot be resolved
with surgical resection [60, 64, 93, 107, 108]. It is also
controversial whether the glycogen storage disease in these
Fig. 5 Flow-chart for the imaging diagnosis of focal hepatic lesion
Updates Surg (2014) 66:9–21 17
123
Author's personal copy

patients represents an indication for liver transplantation.
Some authors recommend it, but others only suggest this
procedure when the disease is accompanied by suspicion of
malignancy [109, 110].
Conflict of interest None.
References
1. Karhunen PJ (1986) Benign hepatic tumours and tumour like
conditions in men. J Clin Pathol 39(2):183–188 PMID: 3950039
PMCID: 499674
2. Ishak KG, Rabin L (1975) Benign tumors of the liver. Med Clin
North Am 59(4):995–1013
3. Heiken JP (2007) Distinguishing benign from malignant liver
tumours. Cancer Imaging 7 Spec No A: S1–S14. doi:10.1102/
1470-7330.2007.9084
4. Buell JF, Tranchart H, Cannon R, Dagher I (2010) Management
of benign hepatic tumors. Surg Clin North Am 90(4):719–735.
doi:10.1016/j.suc.2010.04.006
5. Maillette de Buy Wenniger L, Terpstra V, Beuers U (2010)
Focal nodular hyperplasia and hepatic adenoma: epidemiology
and pathology. Dig Surg 27(1):24–31. doi:10.1159/000268404
6. Bioulac-Sage P, Cubel G, Balabaud C, Zucman-Rossi J (2011)
Revisiting the pathology of resected benign hepatocellular
nodules using new immunohistochemical markers. Semin Liver
Dis 31(1):91–103. doi:10.1055/s-0031-1272837
7. Wanless IR, Mawdsley C, Adams R (1985) On the pathogenesis
of focal nodular hyperplasia of the liver. Hepatology 5(6):
1194–1200 (PMID: 4065824 pii: S0270913985001525)
8. Vilgrain V, Uzan F, Brancatelli G, Federle MP, Zappa M, Menu
Y (2003) Prevalence of hepatic hemangioma in patients with
focal nodular hyperplasia: MR imaging analysis. Radiology
229(1):75–79. doi:10.1148/radiol.2291021284
9. Kapp N, Curtis KM (2009) Hormonal contraceptive use among
women with liver tumors: a systematic review. Contraception
80(4):387–390. doi:10.1016/j.contraception.2009.01.021
10. Wanless IR, Albrecht S, Bilbao J, Frei JV, Heathcote EJ, Rob-
erts EA, Chiasson D (1989) Multiple focal nodular hyperplasia
of the liver associated with vascular malformations of various
organs and neoplasia of the brain: a new syndrome. Mod Pathol
2(5):456–462 PMID: 2813344
11. Rebouissou S, Bioulac-Sage P, Zucman-Rossi J (2008) Molec-
ular pathogenesis of focal nodular hyperplasia and hepatocel-
lular adenoma. J Hepatol 48(1):163–170. doi:10.1016/j.jhep.
2007.10.003
12. Tan X, Behari J, Cieply B, Michalopoulos GK, Monga SP
(2006) Conditional deletion of beta-catenin reveals its role in
liver growth and regeneration. Gastroenterology 131(5):1561–
1572. doi:10.1053/j.gastro.2006.08.042
13. Rebouissou S, Couchy G, Libbrecht L, Balabaud C, Imbeaud S,
Auffray C, Roskams T, Bioulac-Sage P, Zucman-Rossi J (2008)
The beta-catenin pathway is activated in focal nodular hyper-
plasia but not in cirrhotic FNH-like nodules. J Hepatol
49(1):61–71. doi:10.1016/j.jhep.2008.03.013
14. Chen YJ, Chen PJ, Lee MC, Yeh SH, Hsu MT, Lin CH (2002)
Chromosomal analysis of hepatic adenoma and focal nodular
hyperplasia by comparative genomic hybridization. Genes
Chromosom Cancer 35(2):138–143. doi:10.1002/gcc.10103
15. Bioulac-Sage P, Laumonier H, Rullier A, Cubel G, Laurent C,
Zucman-Rossi J, Balabaud C (2009) Over-expression of gluta-
mine synthetase in focal nodular hyperplasia: a novel easy
diagnostic tool in surgical pathology. Liver Int 29(3):459–465.
doi:10.1111/j.1478-3231.2008.01849.x
16. Sato Y, Harada K, Ikeda H, Fijii T, Sasaki M, Zen Y, Nakanuma
Y (2009) Hepatic stellate cells are activated around central scars
of focal nodular hyperplasia of the liver–a potential mechanism
of central scar formation. Hum Pathol 40(2):181–188. doi:
10.1016/j.humpath.2008.04.024
17. Nguyen BN, Flejou JF, Terris B, Belghiti J, Degott C (1999)
Focal nodular hyperplasia of the liver: a comprehensive patho-
logic study of 305 lesions and recognition of new histologic
forms. Am J Surg Pathol 23(12):1441–1454 (PMID: 10584697)
18. Vilgrain V (2006) Focal nodular hyperplasia. Eur J Radiol
58(2):236–245. doi:10.1016/j.ejrad.2005.11.043
19. Bioulac-Sage P, Rebouissou S, Sa Cunha A, Jeannot E, Lepreux
S, Blanc JF, Blanche H, Le Bail B, Saric J, Laurent-Puig P,
Balabaud C, Zucman-Rossi J (2005) Clinical, morphologic, and
molecular features defining so-called telangiectatic focal nodu-
lar hyperplasias of the liver. Gastroenterology 128(5):1211–
1218 (PMID: 15887105 pii: S0016508505001733)
20. Cherqui D, Rahmouni A, Charlotte F, Boulahdour H, Metreau
JM, Meignan M, Fagniez PL, Zafrani ES, Mathieu D, Dhumeaux
D (1995) Management of focal nodular hyperplasia and hepa-
tocellular adenoma in young women: a series of 41 patients with
clinical, radiological, and pathological correlations. Hepatology
22(6):1674–1681 (PMID: 7489973 pii: S0270913995004228)
21. Uggowitzer MM, Kugler C, Ruppert-Kohlmayr A, Groell R,
Raith J, Schreyer H (2000) Current status of diagnostic imaging
of focal nodular hyperplasia of the liver. Rofo 172(9):727–738.
doi:10.1055/s-2000-7227
22. van den Esschert JW, van Gulik TM, Phoa SS (2010) Imaging
modalities for focal nodular hyperplasia and hepatocellular
adenoma. Dig Surg 27(1):46–55. doi:10.1159/000268407
23. Uggowitzer MM, Kugler C, Mischinger HJ, Groll R, Ruppert-
Kohlmayr A, Preidler KW, Quehenberger F (1999) Echo-
enhanced Doppler sonography of focal nodular hyperplasia of
the liver. J Ultrasound Med 18(7):445–451 (quiz 453–444
[PMID: 10400046])
24. Quaia E (2011) The real capabilities of contrast-enhanced
ultrasound in the characterization of solid focal liver lesions. Eur
Radiol 21(3):457–462. doi:10.1007/s00330-010-2007-0
25. Kim MJ, Lim HK, Kim SH, Choi D, Lee WJ, Lee SJ, Lim JH
(2004) Evaluation of hepatic focal nodular hyperplasia with
contrast-enhanced gray scale harmonic sonography: initial
experience. J Ultrasound Med 23(2):297–305
26. Dietrich CF, Schuessler G, Trojan J, Fellbaum C, Ignee A
(2005) Differentiation of focal nodular hyperplasia and hepa-
tocellular adenoma by contrast-enhanced ultrasound. Br J Radiol
78(932):704–707. doi:10.1259/bjr/88181612
27. Kim TK, Jang HJ, Burns PN, Murphy-Lavallee J, Wilson SR(2008) Focal nodular hyperplasia and hepatic adenoma: differ-
entiation with low-mechanical-index contrast-enhanced sonog-
raphy. AJR 190(1):58–66. doi:10.2214/AJR.07.2493
28. Trillaud H, Bruel JM, Valette PJ, Vilgrain V, Schmutz G, Oyen
R, Jakubowski W, Danes J, Valek V, Greis C (2009) Charac-
terization of focal liver lesions with SonoVue-enhanced
sonography: international multicenter-study in comparison to
CT and MRI. World J Gastroenterol 15(30):3748–3756 (PMID:
19673015 PMCID: 2726452)
29. Procacci C, Fugazzola C, Cinquino M, Mangiante G, Zonta L,
Andreis IA, Nicoli N, Pistolesi GF (1992) Contribution of CT to
characterization of focal nodular hyperplasia of the liver. Gas-
trointest Radiol 17(1):63–73. doi:10.1007/BF01888511
30. Rogers JV, Mack LA, Freeny PC, Johnson ML, Sones PJ (1981)
Hepatic focal nodular hyperplasia: angiography, CT, sonogra-
phy, and scintigraphy. AJR 137(5):983–990 (PMID: 6975026)
18 Updates Surg (2014) 66:9–21
123
Author's personal copy

31. Brancatelli G, Federle MP, Grazioli L, Blachar A, Peterson MS,
Thaete L (2001) Focal nodular hyperplasia: CT findings with
emphasis on multiphasic helical CT in 78 patients. Radiology
219(1):61–68 (PMID: 11274535)
32. Carlson SK, Johnson CD, Bender CE, Welch TJ (2000) CT of
focal nodular hyperplasia of the liver. AJR 174(3):705–712
(PMID: 10701613)
33. Hussain SM, Terkivatan T, Zondervan PE, Lanjouw E, de Rave
S, Ijzermans JN, de Man RA (2004) Focal nodular hyperplasia:
findings at state-of-the-art MR imaging, US, CT, and pathologic
analysis. Radiographics 24(1):3–17. doi:10.1148/rg.241035050.
(discussion 18–19)
34. Blachar A, Federle MP, Ferris JV, Lacomis JM, Waltz JS,
Armfield DR, Chu G, Almusa O, Grazioli L, Balzano E, Li W
(2002) Radiologists’ performance in the diagnosis of liver
tumors with central scars by using specific CT criteria. Radiol-
ogy 223(2):532–539 (PMID: 11997564)
35. Vilgrain V, Flejou JF, Arrive L, Belghiti J, Najmark D, Menu Y,
Zins M, Vullierme MP, Nahum H (1992) Focal nodular hyper-
plasia of the liver: MR imaging and pathologic correlation in 37
patients. Radiology 184(3):699–703 (PMID: 1509052)
36. Mortele KJ, Praet M, Van Vlierberghe H, de Hemptinne B, Zou
K, Ros PR (2002) Focal nodular hyperplasia of the liver:
detection and characterization with plain and dynamic-enhanced
MRI. Abdom Imaging 27(6):700–707. doi:10.1007/s00261-001-
0140-6
37. Grazioli L, Morana G, Federle MP, Brancatelli G, Testoni M,
Kirchin MA, Menni K, Olivetti L, Nicoli N, Procacci C (2001)
Focal nodular hyperplasia: morphologic and functional infor-
mation from MR imaging with gadobenate dimeglumine.
Radiology 221(3):731–739 (PMID: 11719669)
38. Chung YE, Park MS, Park YN, Lee HJ, Seok JY, Yu JS,
Kim MJ (2009) Hepatocellular carcinoma variants: radiologic-
pathologic correlation. AJR 193(1):W7–W13. doi:10.2214/AJR.
07.3947
39. Taouli B, Koh DM (2010) Diffusion-weighted MR imaging of
the liver. Radiology 254(1):47–66. doi:10.1148/radiol.09090021
40. Ba-Ssalamah A, Uffmann M, Saini S, Bastati N, Herold C,
Schima W (2009) Clinical value of MRI liver-specific contrast
agents: a tailored examination for a confident non-invasive
diagnosis of focal liver lesions. Eur Radiol 19(2):342–357. doi:
10.1007/s00330-008-1172-x
41. Grazioli L, Morana G, Kirchin MA, Schneider G (2005)
Accurate differentiation of focal nodular hyperplasia from
hepatic adenoma at gadobenate dimeglumine-enhanced MR
imaging: prospective study. Radiology 236(1):166–177. doi:
10.1148/radiol.2361040338
42. Bonney GK, Gomez D, Al-Mukhtar A, Toogood GJ, Lodge JP,
Prasad R (2007) Indication for treatment and long-term outcome
of focal nodular hyperplasia. HPB (Oxford) 9(5):368–372. doi:
10.1080/13651820701504173
43. Nahm CB, Ng K, Lockie P, Samra JS, Hugh TJ (2011) Focal
nodular hyperplasia—a review of myths and truths. J Gastroin-
test Surg 15(12):2275–2283. doi:10.1007/s11605-011-1680-x
44. Belghiti J, Pateron D, Panis Y, Vilgrain V, Flejou JF, Benhamou
JP, Fekete F (1993) Resection of presumed benign liver
tumours. Br J Surg 80(3):380–383 (PMID: 8472159)
45. Chen MF (2000) Hepatic resection for benign tumours of the
liver. J Gastroenterol Hepatol 15(6):587–592 (PMID: 10921410)
46. Reddy KR, Kligerman S, Levi J, Livingstone A, Molina E,
Franceschi D, Badalamenti S, Jeffers L, Tzakis A, Schiff ER
(2001) Benign and solid tumors of the liver: relationship to sex,
age, size of tumors, and outcome. Am Surg 67(2):173–178
(PMID: 11243545)
47. Perrakis A, Demir R, Muller V, Mulsow J, Aydin U, Alibek S,
Hohenberger W, Yedibela S (2012) Management of the focal
nodular hyperplasia of the liver: evaluation of the surgical
treatment comparing with observation only. Am J Surg
204(5):689–696. doi:10.1016/j.amjsurg.2012.02.006
48. Ott R, Hohenberger W (1998) Focal nodular hyperplasia and
liver cell adenoma: operation or observation? Zentralbl Chir
123(2):145–153 (PMID: 9556887)
49. Baum JK, Bookstein JJ, Holtz F, Klein EW (1973) Possible
association between benign hepatomas and oral contraceptives.
Lancet 2(7835):926–929 (PMID: 4126557)
50. Rooks JB, Ory HW, Ishak KG, Strauss LT, Greenspan JR, Hill
AP, Tyler CW Jr (1979) Epidemiology of hepatocellular
adenoma. The role of oral contraceptive use. JAMA 242(7):
644–648 (PMID: 221698)
51. Rosenberg L (1991) The risk of liver neoplasia in relation to
combined oral contraceptive use. Contraception 43(6):643–652
(PMID: 1651205)
52. Buhler H, Pirovino M, Akobiantz A, Altorfer J, Weitzel M,
Maranta E, Schmid M (1982) Regression of liver cell adenoma.
A follow-up study of three consecutive patients after discon-
tinuation of oral contraceptive use. Gastroenterology 82(4):
775–782 (pii: S0016508582000596, PMID: 6277724)
53. Edmondson HA, Reynolds TB, Henderson B, Benton B (1977)
Regression of liver cell adenomas associated with oral contra-
ceptives. Ann Intern Med 86(2):180–182 (PMID: 835939)
54. Noels JE, van Aalten SM, van der Windt DJ, Kok NF, de Man
RA, Terkivatan T, Ijzermans JN (2011) Management of hepa-
tocellular adenoma during pregnancy. J Hepatol 54(3):553–558.
doi:10.1016/j.jhep.2010.07.022
55. Terkivatan T, de Wilt JH, de Man RA, Ijzermans JN (2000)
Management of hepatocellular adenoma during pregnancy.
Liver 20(2):186–187 (PMID: 10847490)
56. Martin NM, Abu Dayyeh BK, Chung RT (2008) Anabolic ste-
roid abuse causing recurrent hepatic adenomas and hemorrhage.
World J Gastroenterol 14(28):4573–4575 (PMID: 18680242
PMCID: 2731289)
57. Reddy SK, Kishnani PS, Sullivan JA, Koeberl DD, Desai DM,
Skinner MA, Rice HE, Clary BM (2007) Resection of hepato-
cellular adenoma in patients with glycogen storage disease type
Ia. J Hepatol 47(5):658–663. doi:10.1016/j.jhep.2007.05.012
58. Bioulac-Sage P, Taouji S, Possenti L, Balabaud C (2012)
Hepatocellular adenoma subtypes: the impact of overweight and
obesity. Liver Int 32(8):1217–1221. doi:10.1111/j.1478-3231.
2012.02786.x
59. Shaked O, Reddy KR (2009) Approach to a liver mass. Clin
Liver Dis 13(2):193–210. doi:10.1016/j.cld.2009.02.004
60. Barthelmes L, Tait IS (2005) Liver cell adenoma and liver cell
adenomatosis. HPB (Oxford) 7(3):186–196. doi:10.1080/13651
820510028954
61. Lui AF, Hiratzka LF, Hirose FM (1980) Multiple adenomas of
the liver. Cancer 45(5):1001–1004 (PMID: 7260831)
62. Bioulac-Sage P, Laumonier H, Couchy G, Le Bail B, Sa Cunha
A, Rullier A, Laurent C, Blanc JF, Cubel G, Trillaud H, Zuc-
man-Rossi J, Balabaud C, Saric J (2009) Hepatocellular ade-
noma management and phenotypic classification: the Bordeaux
experience. Hepatology 50(2):481–489. doi:10.1002/hep.22995
63. Vetelainen R, Erdogan D, de Graaf W, ten Kate F, Jansen PL,
Gouma DJ, van Gulik TM (2008) Liver adenomatosis: re-eval-
uation of aetiology and management. Liver Int 28(4):499–508.
doi:10.1111/j.1478-3231.2008.01669.x
64. Chiche L, Dao T, Salame E, Galais MP, Bouvard N, Schmutz G,
Rousselot P, Bioulac-Sage P, Segol P, Gignoux M (2000) Liver
adenomatosis: reappraisal, diagnosis, and surgical management:
eight new cases and review of the literature. Ann Surg 231(1):
74–81 (PMID: 10636105 PMCID: 1420968)
65. Shanbhogue A, Shah SN, Zaheer A, Prasad SR, Takahashi N,
Vikram R (2011) Hepatocellular adenomas: current update on
Updates Surg (2014) 66:9–21 19
123
Author's personal copy

genetics, taxonomy, and management. J Comput Assist Tomogr
35(2):159–166. doi:10.1097/RCT.0b013e31820bad61
66. Rubin RA, Mitchell DG (1996) Evaluation of the solid hepatic
mass. Med Clin North Am 80(5):907–928 (PMID: 8804368)
67. Jenkins RL, Johnson LB, Lewis WD (1994) Surgical approach
to benign liver tumors. Semin Liver Dis 14(2):178–189. doi:
10.1055/s-2007-1007310
68. Grazioli L, Federle MP, Brancatelli G, Ichikawa T, Olivetti L,
Blachar A (2001) Hepatic adenomas: imaging and pathologic
findings. Radiographics 21(4):877–892 (discussion 892-874,
PMID: 11452062)
69. Bioulac-Sage P, Rebouissou S, Thomas C, Blanc JF, Saric J, Sa
Cunha A, Rullier A, Cubel G, Couchy G, Imbeaud S, Balabaud
C, Zucman-Rossi J (2007) Hepatocellular adenoma subtype
classification using molecular markers and immunohistochem-
istry. Hepatology 46(3):740–748. doi:10.1002/hep.21743
70. Paradis V, Benzekri A, Dargere D, Bieche I, Laurendeau I,
Vilgrain V, Belghiti J, Vidaud M, Degott C, Bedossa P (2004)
Telangiectatic focal nodular hyperplasia: a variant of hepato-
cellular adenoma. Gastroenterology 126(5):1323–1329 (PMID:
15131793, pii: S0016508504001544)
71. Pathologic diagnosis of early hepatocellular carcinoma: a report
of the international consensus group for hepatocellular neoplasia
(2009) Hepatology 49(2): 658–664. doi:10.1002/hep.22709
72. Lagana SM, Salomao M, Bao F, Moreira RK, Lefkowitch JH,
Remotti HE (2012) Utility of an Immunohistochemical Panel
Consisting of Glypican-3, Heat-shock Protein-70, and Gluta-
mine Synthetase in the Distinction of Low-grade Hepatocellular
Carcinoma From Hepatocellular Adenoma. Appl Immunohis-
tochem Mol Morphol. doi:10.1097/PAI.0b013e31825d527f
73. Libbrecht L, Severi T, Cassiman D, Van der Borght S, Pirenne J,
Nevens F, Verslype C, van Pelt J, Roskams T (2006) Glypican-3
expression distinguishes small hepatocellular carcinomas from
cirrhosis, dysplastic nodules, and focal nodular hyperplasia-like
nodules. Am J Surg Pathol 30(11):1405–1411. doi:10.1097/01.
pas.0000213323.97294.9a
74. Nassar A, Cohen C, Siddiqui MT (2009) Utility of glypican-3
and survivin in differentiating hepatocellular carcinoma from
benign and preneoplastic hepatic lesions and metastatic carci-
nomas in liver fine-needle aspiration biopsies. Diagn Cytopathol
37(9):629–635. doi:10.1002/dc.21075
75. Shafizadeh N, Kakar S (2011) Diagnosis of well-differentiated
hepatocellular lesions: role of immunohistochemistry and other
ancillary techniques. Adv Anat Pathol 18(6):438–445. doi:
10.1097/PAP.0b013e318234abb4
76. van Aalten SM, Verheij J, Terkivatan T, Dwarkasing RS, de
Man RA, Ijzermans JN (2011) Validation of a liver adenoma
classification system in a tertiary referral centre: implications for
clinical practice. J Hepatol 55(1):120–125. doi:10.1016/j.jhep.
2010.10.030
77. Terkivatan T, de Wilt JH, de Man RA, van Rijn RR, Zondervan
PE, Tilanus HW, IJ JN (2001) Indications and long-term out-
come of treatment for benign hepatic tumors: a critical appraisal.
Arch Surg 136(9):1033–1038 (PMID: 11529826,pii: soa0257)
78. Herman P, Pugliese V, Machado MA, Montagnini AL, Salem
MZ, Bacchella T, D’Albuquerque LA, Saad WA, Machado MC,
Pinotti HW (2000) Hepatic adenoma and focal nodular hyper-
plasia: differential diagnosis and treatment. World J Surg
24(3):372–376. doi:10.1007/s002689910059
79. Charny CK, Jarnagin WR, Schwartz LH, Frommeyer HS,
DeMatteo RP, Fong Y, Blumgart LH (2001) Management of
155 patients with benign liver tumours. Br J Surg 88(6):
808–813. doi:10.1046/j.0007-1323.2001.01771.x
80. Weimann A, Ringe B, Klempnauer J, Lamesch P, Gratz KF,
Prokop M, Maschek H, Tusch G, Pichlmayr R (1997) Benign
liver tumors: differential diagnosis and indications for surgery.
World J Surg 21(9):983–990 (discussion 990–981, PMID:
9361515)
81. Kerlin P, Davis GL, McGill DB, Weiland LH, Adson MA,
Sheedy PF 2nd (1983) Hepatic adenoma and focal nodular
hyperplasia: clinical, pathologic, and radiologic features.
Gastroenterology 84(5 Pt 1):994–1002 (PMID: 6299876,pii:
S0016508583000992)
82. Hussain SM, Semelka RC (2005) Hepatic imaging: comparison
of modalities. Radiol Clin North Am 43(5):929–947. doi:
10.1016/j.rcl.2005.05.006
83. Golli M, Van Nhieu JT, Mathieu D, Zafrani ES, Cherqui D,
Dhumeaux D, Vasile N, Rahmouni A (1994) Hepatocellular
adenoma: color Doppler US and pathologic correlations. Radi-
ology 190(3):741–744 (PMID: 8115621)
84. Ichikawa T, Federle MP, Grazioli L, Nalesnik M (2000) Hepa-
tocellular adenoma: multiphasic CT and histopathologic findings
in 25 patients. Radiology 214(3):861–868 (PMID: 10715059)
85. Hussain SM, van den Bos IC, Dwarkasing RS, Kuiper JW, den
Hollander J (2006) Hepatocellular adenoma: findings at state-of-
the-art magnetic resonance imaging, ultrasound, computed
tomography and pathologic analysis. Eur Radiol 16(9):1873–
1886. doi:10.1007/s00330-006-0292-4
86. Paulson EK, McClellan JS, Washington K, Spritzer CE, Meyers
WC, Baker ME (1994) Hepatic adenoma: MR characteristics
and correlation with pathologic findings. AJR 163(1):113–116
(PMID: 8010195)
87. Arrive L, Flejou JF, Vilgrain V, Belghiti J, Najmark D, Zins M,
Menu Y, Tubiana JM, Nahum H (1994) Hepatic adenoma: MR
findings in 51 pathologically proved lesions. Radiology 193(2):
507–512 (PMID: 7972769)
88. Chung KY, Mayo-Smith WW, Saini S, Rahmouni A, Golli M,
Mathieu D (1995) Hepatocellular adenoma: MR imaging fea-
tures with pathologic correlation. AJR 165(2):303–308 (PMID:
7618545)
89. Laumonier H, Bioulac-Sage P, Laurent C, Zucman-Rossi J, Bala-
baud C, Trillaud H (2008) Hepatocellular adenomas: magnetic
resonance imaging features as a function of molecular pathological
classification. Hepatology 48(3):808–818. doi:10.1002/hep.22417
90. Katabathina VS, Menias CO, Shanbhogue AK, Jagirdar J,
Paspulati RM, Prasad SR (2011) Genetics and imaging of
hepatocellular adenomas: 2011 update. Radiographics 31(6):
1529–1543. doi:10.1148/rg.316115527
91. Zucman-Rossi J, Jeannot E, Nhieu JT, Scoazec JY, Guettier C,
Rebouissou S, Bacq Y, Leteurtre E, Paradis V, Michalak S,
Wendum D, Chiche L, Fabre M, Mellottee L, Laurent C,
Partensky C, Castaing D, Zafrani ES, Laurent-Puig P, Balabaud
C, Bioulac-Sage P (2006) Genotype-phenotype correlation in
hepatocellular adenoma: new classification and relationship with
HCC. Hepatology 43(3):515–524. doi:10.1002/hep.21068
92. Terkivatan T, de Wilt JH, de Man RA, van Rijn RR, Tilanus HW,
IJ JN (2001) Treatment of ruptured hepatocellular adenoma. Br J
Surg 88(2):207–209. doi:10.1046/j.1365-2168.2001.01648.x
93. Ribeiro A, Burgart LJ, Nagorney DM, Gores GJ (1998) Man-
agement of liver adenomatosis: results with a conservative
surgical approach. Liver Transpl Surg 4(5):388–398 (PMID:
9724476, pii: S1527646598000690)
94. Ault GT, Wren SM, Ralls PW, Reynolds TB, Stain SC (1996)
Selective management of hepatic adenomas. Am Surg 62(10):
825–829
95. Edmondson HA, Henderson B, Benton B (1976) Liver-cell
adenomas associated with use of oral contraceptives. N Engl J
Med 294(9):470–472. doi:10.1056/NEJM197602262940904
96. Cho SW, Marsh JW, Steel J, Holloway SE, Heckman JT, Ochoa
ER, Geller DA, Gamblin TC (2008) Surgical management of
hepatocellular adenoma: take it or leave it? Ann Surg Oncol
15(10):2795–2803. doi:10.1245/s10434-008-0090-0
20 Updates Surg (2014) 66:9–21
123
Author's personal copy

97. Kent DR, Nissen ED, Nissen SE, Ziehm DJ (1978) Effect of
pregnancy on liver tumor associated with oral contraceptives.
Obstet Gynecol 51(2):148–151 (PMID: 622225)
98. Bioulac-Sage P, Balabaud C, Zucman-Rossi J (2010) Subtype
classification of hepatocellular adenoma. Dig Surg 27(1):39–45.
doi:10.1159/000268406
99. Perrakis A, Muller V, Oeckl K, Adamietz B, Demir R,
Hohenberger W, Yedibela S (2012) Indications and long-term
outcome after elective surgery for hepatocellular adenoma. Am
Surg 78(1):80–85 (PMID: 22273320)
100. Deneve JL, Pawlik TM, Cunningham S, Clary B, Reddy S,
Scoggins CR, Martin RC, D’Angelica M, Staley CA, Choti MA,
Jarnagin WR, Schulick RD, Kooby DA (2009) Liver cell
adenoma: a multicenter analysis of risk factors for rupture
and malignancy. Ann Surg Oncol 16(3):640–648. doi:10.1245/
s10434-008-0275-6
101. Ribeiro Junior MA, Chaib E, Saad WA, D’Albuquerque LA,
Cecconello I (2009) Surgical management of spontaneous
ruptured hepatocellular adenoma. Clinics (Sao Paulo) 64(8):
775–779. doi:10.1590/S1807-59322009000800011
102. Flowers BF, McBurney RP, Vera SR (1990) Ruptured hepatic
adenoma. A spectrum of presentation and treatment. Am Surg
56(6):380–383 (PMID: 2161632)
103. Choi BY, Nguyen MH (2005) The diagnosis and management of
benign hepatic tumors. J Clin Gastroenterol 39(5):401–412
(PMID: 15815209, pii: 00004836-200505000-00012)
104. Cobey FC, Salem RR (2004) A review of liver masses in
pregnancy and a proposed algorithm for their diagnosis and
management. Am J Surg 187(2):181–191. doi:10.1016/j.amjsurg.
2003.11.016
105. Gianopoulos JG (1995) Establishing the criteria for anesthesia
and other precautions for surgery during pregnancy. Surg Clin
North Am 75(1):33–45 (PMID: 7855716)
106. Stain SC, Woodburn DA, Stephens AL, Katz M, Wagner WH,
Donovan AJ (1996) Spontaneous hepatic hemorrhage associated
with pregnancy. Treatment by hepatic arterial interruption. Ann
Surg 224(1):72–78 (PMID: 8678621 PMCID: 1235249)
107. Dokmak S, Paradis V, Vilgrain V, Sauvanet A, Farges O, Valla
D, Bedossa P, Belghiti J (2009) A single-center surgical expe-
rience of 122 patients with single and multiple hepatocellular
adenomas. Gastroenterology 137(5):1698–1705. doi:10.1053/
j.gastro.2009.07.061
108. Marino IR, Scantlebury VP, Bronsther O, Iwatsuki S, Starzl TE
(1992) Total hepatectomy and liver transplant for hepatocellular
adenomatosis and focal nodular hyperplasia. Transpl Int 5(Suppl 1):
S201–S205 (PMID: 14621777 PMCID: 2993572)
109. Reddy SK, Austin SL, Spencer-Manzon M, Koeberl DD, Clary
BM, Desai DM, Smith AD, Kishnani PS (2009) Liver trans-
plantation for glycogen storage disease type Ia. J Hepatol
51(3):483–490. doi:10.1016/j.jhep.2009.05.026
110. Matern D, Starzl TE, Arnaout W, Barnard J, Bynon JS, Dhawan
A, Emond J, Haagsma EB, Hug G, Lachaux A, Smit GP, Chen
YT (1999) Liver transplantation for glycogen storage disease
types I, III, and IV. Eur J Pediatr 158(Suppl 2):S43–S48 (PMID:
10603098 PMCID: 3006437 pii: 9158S043.431)
Updates Surg (2014) 66:9–21 21
123
Author's personal copy




















