
Hypoglycemia and Insular Hyperplasia: Review of 748 Cases
6
Hypoglycemia and Insular Hyperplasia: Review of 148 Cases PARIDE STEFANINI, M.D., MANLIO CARBONI, M.D., NERI PATRASSI, M.D., ANTONIO BASOLI, M.D. On the bases of personal experience and the series of 148 cases from an international inquiry and a review of the literature, the relation between insular hyperplasia and hypoglycemia was examined. The fundamental points in this investigation included: age, diagnostic investigations, histo- logical findings and postoperative results. The data on the patients with insular hyperplasia indicates that 83% were of adult age. Insular hyperplasia was the only abnormal factor determined to be present. Through treatment a high percentage of cases (71% ) was cured. From a practical sur- gical point of view, differentiation between occult insulomas and insular hyperplasia is not critical. Consequently, good results can be achieved in botlh diseases by practicing a pro- gressive blind resection guided by examination of the op- erated specimen and by intra-operative blood sugar levels. H YPERINSULINISM of pancreatic origin may be caused by either a benign 8 cell adenoma, carcinoma, or diffuse hyperplasia of the islet cells. Of these causes, the adenoma is by far the most common. Occasionally however, the only recognizable patho- logic lesion in the pancreas is islet hyperplasia. Many cases of hypoglycemia with islet hyperplasia have been reported. Some authors hesitate to accept islet cell hyper- plasia as the cause of hypoglycemia. When only diffuse hyperplasia of the islets is found they feel that the hypoglycemia is caused by a missed insuloma. In the child, however, the existence of islet hyperplasia and its capacity to determine hypoglycemia is generally ac- cepted.42 Cases have been reported in which pancreatic hypoglycemia exists with insular hyperplasia in the ab- sence of insulomas and other hypoglycemia-inducing Submitted for publication June 12, 1973. Address correspondence to: Paride Stefanini, M.D., 2nd Surgical Clinic of The University of Rome Medical School, Policlinico Umberto 10, 00161, Rome, Italy. From the 2nd Surgical Clinic and Surgical Anatomy of the University of Rome Medical School, Rome, Italy diseases.29 Many authors have reported relief of hypo- glycemia after pancreatic resections without finding a beta islet-cell tumor.8644'49'3 Our experience in management of hyperinsulinism of pancreatic origin consists of 11 adenomas, one carcinoma and five insular hyperplasias. The observation of these cases of hyperplasia induced us to investigate this still much discussed topic. We reviewed the literature and carried out an international inquiry (Table 1). An anal- ysis of these cases and of our own experience is reported in this paper. Material On the basis of our research we observed that of a total of 1137 cases of organic hypoglycemia, 1067 (93.8%) were caused by insulomas and 70 (6.2%) by insular hy- perplasia. In seven cases (0.6%) there was a combina- tion of the two diseases. Of the 149 authors who communicated their experi- ence on hypoglycemia of pancreatic origin, 30 (20%) report cases of insular hyperplasia. Yet seven (4%) of these have doubts on the connection between hypo- glycemia and insular hyperplasia in their patients. Of 148 cases of insular hyperplasia documented from a histological and clinical point of view, 122 had under- gone surgical intervention with immediate and long term relief of hypoglycemia. In the series collected from 140 cases documented, there were 78 (56%) females and 62 (44%) males: only 16 were children, while all the others were adults with an age ranging from 19 to 65 years. 130
Transcript of Hypoglycemia and Insular Hyperplasia: Review of 748 Cases

Hypoglycemia and Insular Hyperplasia:
Review of 148 Cases
PARIDE STEFANINI, M.D., MANLIO CARBONI, M.D., NERI PATRASSI, M.D.,ANTONIO BASOLI, M.D.
On the bases of personal experience and the series of 148cases from an international inquiry and a review of theliterature, the relation between insular hyperplasia andhypoglycemia was examined. The fundamental points in thisinvestigation included: age, diagnostic investigations, histo-logical findings and postoperative results. The data on thepatients with insular hyperplasia indicates that 83% wereof adult age. Insular hyperplasia was the only abnormalfactor determined to be present. Through treatment a highpercentage of cases (71% ) was cured. From a practical sur-gical point of view, differentiation between occult insulomasand insular hyperplasia is not critical. Consequently, goodresults can be achieved in botlh diseases by practicing a pro-gressive blind resection guided by examination of the op-erated specimen and by intra-operative blood sugar levels.
H YPERINSULINISM of pancreatic origin may be causedby either a benign 8 cell adenoma, carcinoma, or
diffuse hyperplasia of the islet cells. Of these causes, theadenoma is by far the most common.
Occasionally however, the only recognizable patho-logic lesion in the pancreas is islet hyperplasia. Manycases of hypoglycemia with islet hyperplasia have beenreported. Some authors hesitate to accept islet cell hyper-plasia as the cause of hypoglycemia. When only diffusehyperplasia of the islets is found they feel that thehypoglycemia is caused by a missed insuloma. In thechild, however, the existence of islet hyperplasia and itscapacity to determine hypoglycemia is generally ac-cepted.42 Cases have been reported in which pancreatichypoglycemia exists with insular hyperplasia in the ab-sence of insulomas and other hypoglycemia-inducing
Submitted for publication June 12, 1973.Address correspondence to: Paride Stefanini, M.D., 2nd Surgical
Clinic of The University of Rome Medical School, PoliclinicoUmberto 10, 00161, Rome, Italy.
From the 2nd Surgical Clinic and Surgical Anatomyof the University of Rome Medical School, Rome, Italy
diseases.29 Many authors have reported relief of hypo-glycemia after pancreatic resections without finding abeta islet-cell tumor.8644'49'3Our experience in management of hyperinsulinism of
pancreatic origin consists of 11 adenomas, one carcinomaand five insular hyperplasias. The observation of thesecases of hyperplasia induced us to investigate this stillmuch discussed topic. We reviewed the literature andcarried out an international inquiry (Table 1). An anal-ysis of these cases and of our own experience is reportedin this paper.
Material
On the basis of our research we observed that of atotal of 1137 cases of organic hypoglycemia, 1067 (93.8%)were caused by insulomas and 70 (6.2%) by insular hy-perplasia. In seven cases (0.6%) there was a combina-tion of the two diseases.Of the 149 authors who communicated their experi-
ence on hypoglycemia of pancreatic origin, 30 (20%)report cases of insular hyperplasia. Yet seven (4%) ofthese have doubts on the connection between hypo-glycemia and insular hyperplasia in their patients.Of 148 cases of insular hyperplasia documented from
a histological and clinical point of view, 122 had under-gone surgical intervention with immediate and long termrelief of hypoglycemia.
In the series collected from 140 cases documented,there were 78 (56%) females and 62 (44%) males: only16 were children, while all the others were adults withan age ranging from 19 to 65 years.
130

HYPOGLYCEMIA AND INSULAR HYPERPLASIA
TABLE 1. Insular Hyperplasias: Case Material
No. ofSeries Cases Authors (cases)
Gathered by 65 Biancalana 1, Blomquist 1, Bloodworth 1,Internat. Inquiry Carrington 1, Creutzfeldt 1, De Cesare 1,
De Peyster 5, Fonkaisrud 1, Fraser 1, Fuchsig2, Goffrini 3, Hess 1, Huguet 1, Juvara 7,Leger 15, Mandache 1, McGarity 1, Mc-Govern 1, Passaro 1, Pellegrini 1, Poli 1,Porter 6, Ritchie 1, Saegesser 1, Sato 2,Shamiyeh 1, Singleton 1, Solcia 1, White 3,Zenker 1
Gathered from 78 Auguston 1,1 Barbarino 1,2 Becker 6,3-4 BellReview of the 1,5 Bernhard 3,6 Boone 1,7 Broq 6,9 CallawayLiterature 1,10 Conn 1,11 David 1,12 Deucher 2,14 Deuil
1,'5 Edwards 1,16 Fish 1,17 Geraud 1,19Gilchrist 1,29 Graham 1,21 Greenle 1,22Grotzinger 2,23 Haworth 8,25 Hellstrom 1,26Hill 1,27 Holman 1,28 Kalbfleisch 1,30 Kjaer-gaard 2,32 Koutras 4,33 Leriche 1,37 Linder1,38 McCaughan 4,3940 Magner 1,"3 Martin1,46 Maxeiner 1,47 Mengoli 1,48 Milone 1,49Mosenthal 1,50 Orr 1,12 Pfeiffer 1,53 Phillips1,54 Richardson 1,55 Sawyer 1,57 Sendrail 2,69Simon 1,60 Sloper 2,61 Spencer 1,62 Walters 1,64Whipple 365
Personal Cases 5Total 148
Our patients had an average age of 35 years. Fourwere females and one was a male.The symptomatology of our cases with insular hyper-
plasia was practically the same as that presented bypatients with insulomas. The only conclusion we can
draw from our experience is that, in comparison to in-sulomas, patients with hyperplasia presented hypogly-cemia crises at less frequent intervals. However, cardio-vascular and gastrointestinal symptoms were more oftennoted (Table 2). Neurological symptoms were frequentand often resulted in diagnostic errors, with admittanceof patients to mental hospitals. Gastrointestinal symp-
toms, consisted mainly in hunger while the cardiovas-cular symptoms consisted mainly of sinus tachycardia.On the average, there elapsed four-and-a-half years
from the onset of symptoms to the diagnosis of hypogly-cemia. Epilepsy was diagnosed three times and numer-
ous E.E.G.'s were carried out with negative results.The same investigations were useful in evaluating
patients with hyperplasia and in those with insulomas.In particular, the prolonged fasting test (five out of five)and the tolbutamide test (three out of four) had a
high degree of diagnostic accuracy. Blood insulin levels,measured by radioimmunological assay, were very highin the three cases tested. The clinical symptoms and thebiochemical data of our patients do not differ greatlyfrom those communicated to us by the authors. Twenty-one reported that in their opinion, clinical findings andlaboratory data showed no differences between theircases of insulomas and those of hyperplasia.The surgical treatment of our patients is summarized
in Table 3. The preoperative diagnosis in our patientshas always been that of hypoglycemia from insulomaand the finding of insular hyperplasia was unexpected.The type of intervention, the death rate, and longterm
results which were obtained from the different authors,are summarized in Table 4. The types of operation mostused were corpocaudal pancreatectomy (63.8%) and sub-total pancreatectomy (24.3%). Twice, following a sub-total resection, a total resection was carried out withrecovery in one case and the persistence of hypoglycemiain the other. The follow up period was of six months tofive years except in five cases. Pancreatic biopsy led tothe diagnosis of insular hyperplasia in four cases. Oneof these cases had insular carcinoma associated withhyperplasia.
In four cases, insular hyperplasia was diagnosed atpost-mortem examination.
Case Report
L.G., a 32-year-old woman had experienced increasingly fre-quent episodes of wealness, memory loss, mental confusion andcoma over a 5-year period.Her symptoms were most prominent when fasting and after
physical effort. The first physician she consulted diagnosed epi-lepsy. She was admitted to the 2nd Surgical Clinic of the Uni-versity of Rome in September 1969. There were no significantphysical findings, except tachycardia during hypoglycemic attacks.An oral glucose tolerance test, tolbutamide test, prolonged fasting
TABLE 2. Insular Hyperplasias: Symptoms and Diagnosis (personal cases)
Previous PreviousCase Age Sex Principal Symptoms Diagnosis Admissions Blood Sugar IRI Fasting Tolbutamide
1 50 M 5 years neuropsychic epilepsy 2 0.30 +cardiovascular
2 39 F 11 years neuropsychic epilepsy 4 0.40 + +3 36 F 7 months neuropsychic 0.45 69 + i
gastrointest.4 32 F 4 years neuropsychic epilepsy 3 0.25 91 + +
cardiovascular5 20 F 4 years neuropsychic 1 0.40 72 + +
cardiovasculargastrointest.
Vol. 180 * No. I 131
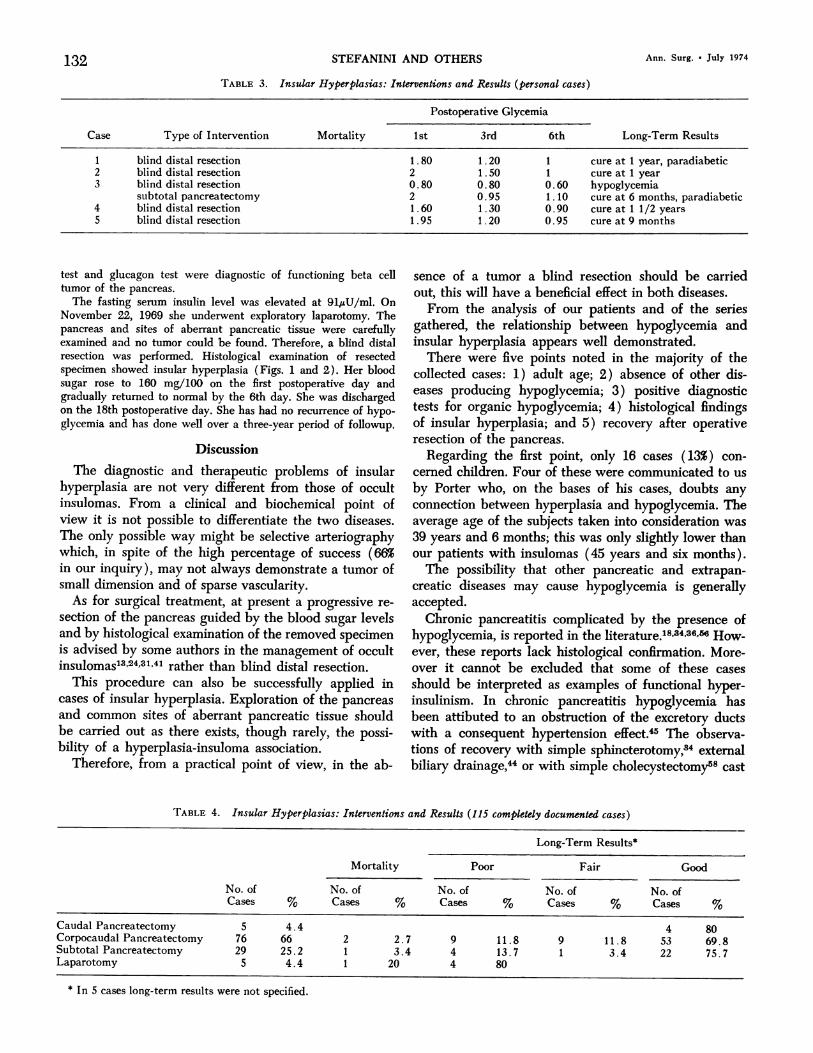
TABLE 3. Insular Hyperplasias: Interventions and Results (personal cases)
Postoperative Glycemia
Case Type of Intervention Mortality 1st 3rd 6th Long-Term Results
1 blind distal resection 1.80 1.20 1 cure at 1 year, paradiabetic2 blind distal resection 2 1.50 1 cure at 1 year3 blind distal resection 0.80 0.80 0.60 hypoglycemia
subtotal pancreatectomy 2 0.95 1.10 cure at 6 months, paradiabetic4 blind distal resection 1.60 1.30 0.90 cure at 1 1/2 years5 blind distal resection 1 .95 1 .20 0.95 cure at 9 months
test and glucagon test were diagnostic of functioning beta celltumor of the pancreas.
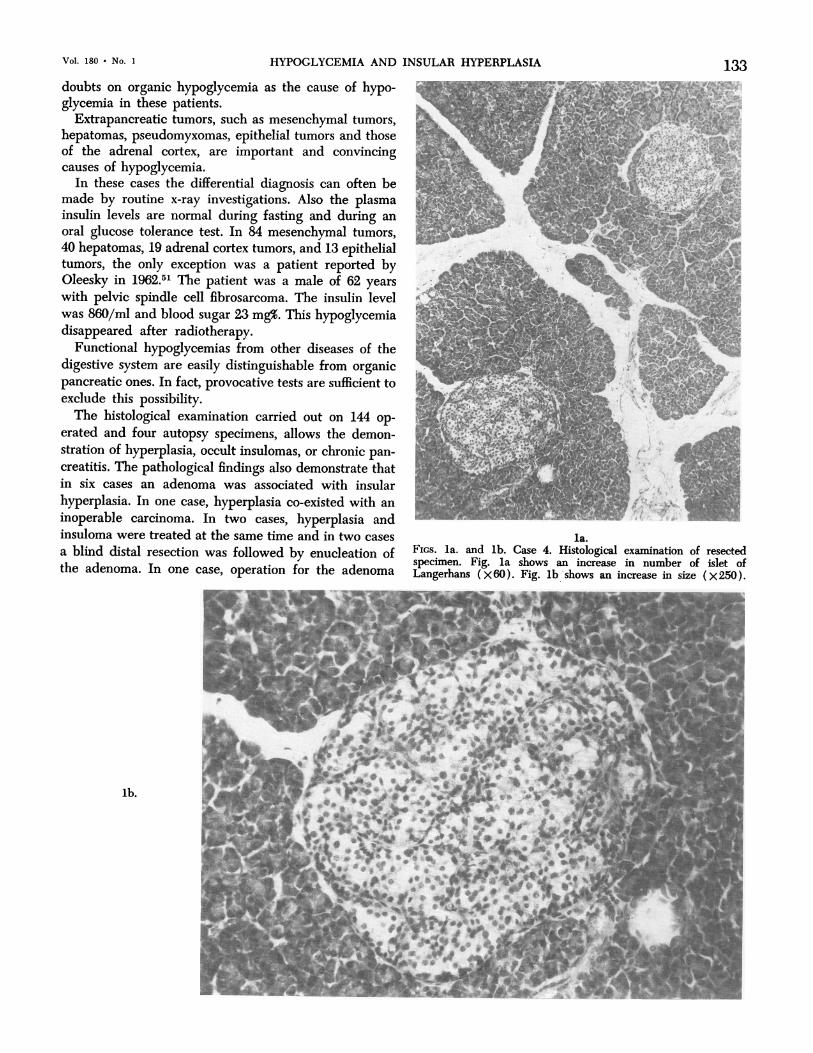
The fasting serum insulin level was elevated at 91l,uU/ml. OnNovember 22, 1969 she underwent exploratory laparotomy. Thepancreas and sites of aberrant pancreatic tissue were carefullyexamined and no tumor could be found. Therefore, a blind distalresection was performed. Histological examination of resectedspecimen showed insular hyperplasia (Figs. 1 and 2). Her bloodsugar rose to 160 mg/100 on the first postoperative day andgradually returned to normal by the 6th day. She was dischargedon the 18th postoperative day. She has had no recurrence of hypo-glycemia and has done well over a three-year period of followup.
DiscussionThe diagnostic and therapeutic problems of insular
hyperplasia are not very different from those of occultinsulomas. From a clinical and biochemical point ofview it is not possible to differentiate the two diseases.The only possible way might be selective arteriographywhich, in spite of the high percentage of success (66%in our inquiry), may not always demonstrate a tumor ofsmall dimension and of sparse vascularity.As for surgical treatment, at present a progressive re-
section of the pancreas guided by the blood sugar levelsand by histological examination of the removed specimenis advised by some authors in the management of occultinsulomas'3 24813'41 rather than blind distal resection.
This procedure can also be successfully applied incases of insular hyperplasia. Exploration of the pancreasand common sites of aberrant pancreatic tissue shouldbe carried out as there exists, though rarely, the possi-bility of a hyperplasia-insuloma association.
Therefore, from a practical point of view, in the ab-
sence of a tumor a blind resection should be carriedout, this will have a beneficial effect in both diseases.From the analysis of our patients and of the series
gathered, the relationship between hypoglycemia andinsular hyperplasia appears well demonstrated.There were five points noted in the majority of the
collected cases: 1) adult age; 2) absence of other dis-eases producing hypoglycemia; 3) positive diagnostictests for organic hypoglycemia; 4) histological findingsof insular hyperplasia; and 5) recovery after operativeresection of the pancreas.
Regarding the first point, only 16 cases (13%) con-cerned children. Four of these were communicated to us
by Porter who, on the bases of his cases, doubts anyconnection between hyperplasia and hypoglycemia. Theaverage age of the subjects taken into consideration was39 years and 6 months; this was only slightly lower thanour patients with insulomas (45 years and six months).The possibility that other pancreatic and extrapan-
creatic diseases may cause hypoglycemia is generallyaccepted.
Chronic pancreatitis complicated by the presence ofhypoglycemia, is reported in the literature.18,3436,66 How-ever, these reports lack histological confirmation. More-over it cannot be excluded that some of these casesshould be interpreted as examples of functional hyper-insulinism. In chronic pancreatitis hypoglycemia hasbeen attibuted to an obstruction of the excretory ductswith a consequent hypertension effect.45 The observa-tions of recovery with simple sphincterotomy,34 externalbiliary drainage,44 or with simple cholecystectomy58 cast
TABLE 4. Insular Hyperplasias: Interventions and Results (115 completely documented cases)
Long-Term Results*
Mortality Poor Fair Good
No. of No. of No. of No. of No. ofCases % Cases % Cases % Cases % Cases %
Caudal Pancreatectomy 5 4.4 4 80Corpocaudal Pancreatectomy 76 66 2 2.7 9 11.8 9 11.8 53 69.8Subtotal Pancreatectomy 29 25.2 1 3.4 4 13.7 1 3.4 22 75.7Laparotomy 5 4.4 1 20 4 80
* In 5 cases long-term results were not specified.
132 STEFANINI AND OTHERS Ann. Surg. * July 1974
HYPOGLYCEMIA AND INSULAR HYPERPLASIA 133doubts on organic hypoglycemia as the cause of hypo-glycemia in these patients.
Extrapancreatic tumors, such as mesenchymal tumors,hepatomas, pseudomyxomas, epithelial tumors and thoseof the adrenal cortex, are important and convincingcauses of hypoglycemia.
In these cases the differential diagnosis can often bemade by routine x-ray investigations. Also the plasmainsulin levels are normal during fasting and during anoral glucose tolerance test. In 84 mesenchymal tumors,40 hepatomas, 19 adrenal cortex tumors, and 13 epithelialtumors, the only exception was a patient reported byOleesky in 1962.51 The patient was a male of 62 yearswith pelvic spindle cell fibrosarcoma. The insulin levelwas 860/ml and blood sugar 23 mg%. This hypoglycemiadisappeared after radiotherapy.
Functional hypoglycemias from other diseases of thedigestive system are easily distinguishable from organicpancreatic ones. In fact, provocative tests are sufficient toexclude this possibility.The histological examination carried out on 144 op-
erated and four autopsy specimens, allows the demon-stration of hyperplasia, occult insulomas, or chronic pan-creatitis. The pathological findings also demonstrate thatin six cases an adenoma was associated with insularhyperplasia. In one case, hyperplasia co-existed with aninoperable carcinoma. In two cases, hyperplasia andinsuloma were treated at the same time and in two casesa blind distal resection was followed by enucleation ofthe adenoma. In one case, operation for the adenoma
la.FIGS. la. and lb. Case 4. Histological examination of resectedspecimen. Fig. la shows an increase in number of islet ofLangerhans (x60). Fig. lb shows an increase in size (X250).
lb.
Vol. 180 * No. I

Ann. Surg. * July 1974
was carried out and subsequently reoperation with thediagnosis of hvperplasia. The long term results in thisgroup of patients, records two failures; one of whichrelated to exploratory laparotomv for insular carcinoma,and five recoveries.Considering the results of surgical treatment the per-
centage of recoveries were 71%. Mortality of operationwas 4.5%. In many cases, surgical failure, after corpo-caudal resection can be attributed to an inadequate re-section of the pancreas. Yet one cannot deny that occultinsulomas could have been present in the 24.5% of thecases where hypoglycemia persisted.
AcknowledgmentsWe are greatly indebted to all those authors who sent us their
personal communications and to all those who collaborated withtheir valid information.
References1. Auguston, H.: Hyperinsulinism with Hyperplasia of Island
Langerhans. Lancet, 67:190, 1947.2. Barbarino, A., Orlandelli, E., Pizzolato, P. and Balducci, L.:
Crisi Ipoglicemiche Ricorrenti da Iperplasia delle CelluleBeta del Pancreas. Gazz, Int. Med. Chir., 19:1420, 1970.
3. Becker, W. H. and Nusselt, H.: Uber einige bemerkenswertebeobachtungen beim hyperinsulinismus. Dtsch med. Wschr.,76:1613, 1951.
4. Becker, W. H.: Indikatinsstellung zur Pankreatektomie oderPankresecktion bei nicht auffindbarem Inseldadenom.Arch. Klin. Chir., 273:699, 1952.
5. Bell, H. G., Goldman, I., Craig, L. S. and McGorkie, H.:Hyperinsulinism. Surgery, 15:681, 1944.
6. Bernhard, F.: Erkennung und Behandlung des Hyperinsulin-ismus. Dtsch. Med. Wschr., 74:1048, 1949.
7. Boone, J. A.: Case of Hyperinsulinism without DemonstrablePancreatic Changes in a 11-Year Old Child. N. Engl. J.Med., 211:49, 1934.
8. Breidhal, H. D., Priestley, J. T. and Rynearson, E. H.: Hyper-insulinism: Surgical Aspects and Results. Ann. Surg., 142:698, 1955.
9. Broq, P. and Verne, J.: Essai de classification des hypogli-cemies d'origine pancreatique: etude cytologique de 10pieces operatoires. Presse Med., 62:1770, 1954.
10. Callaway, E.: Subtotal Resection of Pancreas of an 8-Year OldChild for Hyperinsulinism. JAMA, 35:164, 1946.
11. Conn, J. W. and Seltzer, H. S.: Spontaneous Hypoglycemia.Am. J. Med., 19:460, 1955.
12. David, O.: Quoted by Whipple.13. De Peyster, F. A.: Planning the Appropriate Operations for
Islet-cell Tumors of the Pancreas. Surg. Clin. N. Am., 50:133, 1970.
14. Deucher, F.: Diffuse Adenomatose des LangherhanschenInselapparates. Arch. Klin. Chir., 282:556, 1955.
15. Devil, R. and Tugaye, A.: The Diagnosis of HypoglycemiaCaused by Malignant Tumours. Presse Med., 75:2178, 1967.
16. Edwards, M. H., Pessel, J. F., Rathmell, T. K. and Wise,J. S.: Hyperinsulinism and Premenstrual Tension: Report ofa Case of Hyperplasia of Islets of Langerhans. Am. J.Obstet. Gynecol., 70:1129, 1955.
17. Fish, G. D. Jr., Isham, W. H. and Tucker, F. C.: Hyper-insulinism Due to Hyperplasia of the Islets of Langerhans.Ill. Med. J., 120:290, 1961.
18. Friedlander, E. O.: Hyperinsulinism in Pancreatic or Biliarvand Gastrointestinal Tract Disease. JAMA, 177:300, 1961.
19. Geraud, J., Grimoud, M., Sendrail-Pesque, P., Rascol, A.and Bes, A.: Coexistence d'un adenome et d'une hyper-plasie langerhansienne diffuse. Toulouse Med., 65:71, 1964.
20. Gilchrist, A. R. and Linch, M. I. G.: Organic Hyperinsu-linism Treated with Alloxan. Lancet, 1:440, 1951.
21. Graham, G. and Oakley, W. G.: Treatment of Spontaneoushypoglycemia Due to Hyperplasia of Islets of Langerhans.Q. J. Med., 19:21, 1950.
22. Greenle, R. G., White, R. R. and Phillips, C.: ChronicHypoglycemia in an Infant Treated by Subtotal Pan-createctomy. JAMA, 149:272, 1952.
23. Grozinger, K. H.: Klinik der endokrinen Pankreasgeschwiilste.Mled. Welt., 44:261, 1967.
24. Hartsuck, J. M. and Brooks, J. R.: Functioning Beta Islet-cellTumours. Am. J. Surg., 117:541, 1969.
25. Haworth, J. C. and Coodin, F. J.: Idiopathic SpontaneousHypoglycemia in Children. Pediatrics, 25:748, 1960.
26. Hellstr6m, J.: Some Observations Based on Six Cases ofHyperinsulinism Treated Operatively. Acta Chir. Scand.,103:120, 1952.
27. Hill, R. M.: Hyperplasia of the Islets of Langerhans Asso-ciated with Spontaneous Hypoglycemia. J. Roy. Coll. Surg.Edinb., 6:126, 1961.
28. Holman, E., Wood, D. A. and Stockton, A. B.: Unusual Caseof Hyperinsulinism and Hypoglycemia. Arch. Surg., 47:165, 1943.
29. Howard, J. M., Moss, H. and Rhoads, J. E.: CollectiveReview: Hyperinsulinism and Islet Cell Tumors of thePancreas. With 398 Recorded Tumours. Surg. Gynecol.Obstet., 90:417, 1950.
30. Kalbfleisch, H. H.: Adenoma inkretorischer Drusen bei Hypo-glikamie. Frankfurt Z. Path., 50:462, 1937.
31. Kavlie, H. and White, T. T.: Pancreatic Islet Beta-cell Tu-mours and Hyperplasia. Experience in 14 Seattle Hospitals.Ann. Surg., 175:326, 1972.
32. Kjaergaard, S.: Partial Pancreatectomy for Hyperinsulinism.Acta Chir. Scand., 91:81, 1944.
33. Koutras, P. and White, R. R.: Insulin-secreting Tumours ofthe Pancreas. A Diagnostic and Therapeutic Challenge.Surg. Clin. N. Am., 52:299, 1972.
34. Lataste, J. and Neveux, J. Y.: Les pancreatites chroniquesavec hypoglycemie severe (a' propos d'une guerison parsphincterotomie). Presse Med., 72:389, 1964.
35. Laurent, J., Debry, G. and Floquet, J.: In Hypoglycaemictumours. 86, Amsterdam, Excepta Medica, 86, 1971.
36. Leger, L., Magdelaine, M. and Gillott, R.: Morphologie desilots Langerhans dans les hypoglycemies non tumorales.Presse Med., 70:313, 1962.
37. Leriche, R. and Schneider, H.: Deux pancreatectomies pourhyperinsulinisme. Presse Med., 49:569, 1941.
38. Linder, T. and Schmitz, W.: Die operative Behandlung desorganischen Hyperinsulinismus. Arztl. Wchnschr., 10:1,1955.
39. McCaughan, J. M. and Broun, G. O.: Value of Partial Pan-createctomy in Convulsive States Associated with Hvpo-glycemia. Ann. Surg., 105:354, 1937.
40. McCaughan, J. M. and Werner, A. A.: Fistulas and Cysts ofPancreas Following Operations of Hyperinsulinisms. Ann. J.Surg., 35:595, 1937.
41. McGarity, W. C. and Brantley, J. W.: Surgical Approach toInsulinomas. Am. J. Surg., 119:705, 1970.
42. McQuarrie, I.: Idiopathic Spontaneously Occurring Hypoglv-cemia in Infants. Am. J. Dis. Child, 87:399, 1954.
43. Magner, WV.: Hyperinsulinism. Can. Med. Ass. J., 45:49, 1941.
STEFANINI AND OTHERS134

HYPOGLYCEMIA AND INSULAR HYPERPLASIA
44. MIallet-Guy, P.: Hyperinsulinisme et pancreatite chroniqueavec ictere. Presse Med., 49:467, 1941.
45. Mansfield, G.: Versuche zu einer operativen Behandlung desDiabetes. Klin. Wschr., 6:195, 1924.
46. Mfartin, E. D. and Vu-Ngo-Kuyexi: Les hyperplasias et lestumeurs langerhansiennes a cellules beta. Histologie etultrastructure. Act. Hepato-Gastroent. Hotel-Dieu, 3:231,1967.
47. Maxeiner, S. R. and Bundy, H. E.: Islet-cell Tumours of thePancreas. Surgery, 18:171, 1945.
48. Mengoli, L. and Le Quesne, P.: Blind Pancreatic Resection forSuspected Insulinoma. A review of the Problem. Br. J.Surg., 54:749, 1967.
49. Milone, S.: Patologia e chirurgia delle sindromi ipoglicemichespontanee. Minerva Chir., 69:2141, 1961.
50. Mosenthal, H. O., Ashe, B. I., Poindexter, C. A. andMcBraver, R.: Spontaneous Hypoglycemia Occurring inCourse of Essential Hypertension. Med. Clin. N. Am.,17:41, 1933.
51. Oleesky, S., Bailey, I., Samols, E. and Bilkus, D.: A Fibro-sarcoma with Hypoglycemia and a High Serum InsulinLevels. Lancet, 2:378, 1962.
52. Orr, V.: Quoted by Hill.53. Pfeiffer, G. E. and Eisendorf, L. H.: Surgical Relief of
Hypoglycemic State Probably Due to Organic Hvperinso-linism. Am. J. Surg., 65:79, 1944.
54. Phillips, A. XV.: Hypoglycemia Associated with Hypertrophyof Islands of Langerhans. JANIA, 96:1195, 1931.
55. Richardson, J. E. and Russel, D. S.: Cerebral Disease Dueto Functioning Islet-cell Tumours. Lancet, 2:1054, 1952.
56. Savy, P., Blondet, P. and Buffard, P.: La reaction de l'hyper-glycemie provoquee au cours des pancreatites chroniques.14 cas de pancreatite chronique parahypoglycemianteJ. Med. Lyon, 662, 1947.
57. Sawyer, K. C., Proctor, H. M., Sawyer, R. B. and Sawyer,K. C. Jr.: The operative Mlanagement of Hypoglycemia.Rocky Mlt. Med. J., 59:31, 1962.
58. Schur, V. and Schurer A.: Quoted by Lataste and Neveux.59. Sendrail, M., Grimoud, M., Geraud, J., Bazex, A. and
Gleizes, L.: Les enseignements de l'etude cytologique dupancreas insulaire dans la chirurgie des hypoglycemieschroniques. Rev. Int. Hepat., 8:23, 1958.
60. Simon, H. E.: Surgery in Treatment of Hyperinsulinism.South. Surgeon, 3:211, 1934.
61. Sloper, J. C.: Small Pancreatic Islet Adenomata in Addison'sDisease. Arch. Path., 58:294, 1954.
62. Spencer, H.: Pancreatic Islet-cell Adenomata. J. Path. Bact.,69:259, 1955.
63. Stefanini, P. and Ermini, MI.: L'iperinsulinismo. ProceedingsXXI Congr. Soc. Int. Chir. Philadelphia, 128, 1965.
64. Walters, H.: Quoted by Whipple.65. Warren, K. W., Shields, A. J. and Le Compte, P. M.: The
Pathology of Diabetes Mellitus. Third edition. Philadelphia,Lea and Febiger, 1952.
66. Whipple, A. O.: Hyperinsulinism in Relation to PancreaticTumours. Surgery, 16:289, 1944.
135Vol. 180 * No. 1




















