
CCR2 and CCR5 genes polymorphisms in benign prostatic hyperplasia and prostate cancer
6
CCR2 and CCR5 genes polymorphisms in benign prostatic hyperplasia and prostate cancer Francis Maria Báo Zambra a , Vanderlei Biolchi b , Ilma Simoni Brum b , José Artur Bogo Chies a,⇑ a Department of Genetics, Instituto de Biociências, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil b Department of Physiology, Instituto de Ciências Básicas da Saúde, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil article info Article history: Received 9 November 2012 Accepted 10 April 2013 Available online 28 April 2013 abstract Benign prostatic hyperplasia (BPH) and prostate cancer (PCa) are two chronic conditions, very common in aged men, that have been associated to inflammatory process. Chemokines and their receptors are rec- ognized as critical mediators of inflammatory responses, they regulate immune cell migration and are implicated in tumor pathogenesis. The impact of two chemokine receptor gene polymorphisms, CCR2- 64I (rs1799864) and CCR5-D32 (rs333), was evaluated in BPH and PCa. 385 DNA samples (130 BPH, 136 PCa, 119 healthy control) were genotyped. The allele frequencies were similar among control, BPH and PCa groups. Median of serum PSA levels was different between groups: 0.79, 1.45 and 6.91 ng/mL in control, BPH and PCa groups, respectively (all p < 0.001). The prostate volume median was 20.00 cm 3 in the control group, thus, lower than BPH (35.35 cm 3 ) and PCa (35.80 cm 3 ) (both p < 0.001), nevertheless no statistical significant difference was observed between BPH and PCa patients (p = 0.172). Remarkably, CCR2-64I was a protective factor to PCa when compared with BPH (OR = 0.550; 95%CI = 0.311–0.975), although the statistically significant difference was lost after correc- tion for multiple comparisons. No significant associations of CCR5-D32 variant were observed with BPH, PCa or PCa clinicopathologic status. Our data suggest the influence of CCR2-64I variant in the devel- opment of prostate cancer. Ó 2013 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved. 1. Introduction Prostate cancer (PCa) is one of the most common cancers in adult male and represents a leading cause of cancer deaths among men worldwide [1,2]. Benign prostatic hyperplasia (BPH) is one of the most frequent proliferative diseases affecting aged men [3,4]. Both conditions are considered chronic diseases with early onset and slow progression [5]. BPH and PCa are also conditions associ- ated with prostatic inflammation, are hormone dependent, their incidence and prevalence rise with the advance of age and, even though there is no clear genetic and molecular relationship be- tween them and considering that both conditions present two dif- ferent pathogenetic pathways, a possible common denominator between them was suggested [6]. Chemokines and chemokine receptors are among factors that may influence PCa and BPH incidence and progression [7,8]. Che- mokines are small chemotactic soluble proteins recognized as crit- ical mediators of inflammatory responses by regulating the migration of immune cells through the interaction with chemokine receptors present on the surface of these cells [9]. These molecules, due to their immunomodulatory activities, are critically involved in processes that allow the development of effective immune re- sponses [9]. Although it is already known that chemokines and chemokine receptors can be involved in tumor pathogenesis, it is not yet clear how they affect human cancer progression. Some con- troversial data exists, since these molecules were already reported as being involved in both tumor development and cancer metasta- sis, as well as in antitumor immune responses [10]. Chemokine receptors are molecules that present seven trans- membrane domains and couples to G-protein for signal transduc- tion [11]. CCR2 is a CC chemokine receptor that can bind CCL2, CCL7, CCL8 and CCL13 chemokines (reviewed by [11]). Among im- mune cells, CCR2 is mainly expressed in macrophages, T lympho- cytes, dendritic cells, B cells and basophils (reviewed by [12]). Recent investigations about PCa and BPH have focused in the CCR2 and its CCL2 ligand, and suggested that CCR2 may contribute to tumor progression [8,13–15]. Regarding this, it was observed 0198-8859/$36.00 - see front matter Ó 2013 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.humimm.2013.04.031 Abbreviations: BPH, benign prostatic hyperplasia; PCa, prostate cancer; CCR, chemokine (C–C motif) receptor; CCL, chemokine (C–C motif) ligand; PSA, prostate- specific antigen. ⇑ Corresponding author. Address: Universidade Federal do Rio Grande do Sul, Departamento de Genética, Instituto de Biociências, Avenida Bento Gonçalves 9500, Prédio 43323, Lab. 212, CEP 91501-970 Agronomia, Porto Alegre, RS, Brazil. Fax: +55 51 3308 7311. E-mail addresses: [email protected] (F.M.B. Zambra), [email protected] (V. Biolchi), [email protected] (I.S. Brum), [email protected] (J.A.B. Chies). Human Immunology 74 (2013) 1003–1008 Contents lists available at SciVerse ScienceDirect www.ashi-hla.org journal homepage: www.elsevier.com/locate/humimm
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of CCR2 and CCR5 genes polymorphisms in benign prostatic hyperplasia and prostate cancer

Human Immunology 74 (2013) 1003–1008
Contents lists available at SciVerse ScienceDirect
www.ashi-hla.org
journal homepage: www.elsevier .com/locate /humimm
CCR2 and CCR5 genes polymorphisms in benign prostatic hyperplasiaand prostate cancer
0198-8859/$36.00 - see front matter � 2013 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.humimm.2013.04.031
Abbreviations: BPH, benign prostatic hyperplasia; PCa, prostate cancer; CCR,chemokine (C–C motif) receptor; CCL, chemokine (C–C motif) ligand; PSA, prostate-specific antigen.⇑ Corresponding author. Address: Universidade Federal do Rio Grande do Sul,
Departamento de Genética, Instituto de Biociências, Avenida Bento Gonçalves 9500,Prédio 43323, Lab. 212, CEP 91501-970 Agronomia, Porto Alegre, RS, Brazil. Fax: +5551 3308 7311.
E-mail addresses: [email protected] (F.M.B. Zambra), [email protected](V. Biolchi), [email protected] (I.S. Brum), [email protected] (J.A.B. Chies).
Francis Maria Báo Zambra a, Vanderlei Biolchi b, Ilma Simoni Brum b, José Artur Bogo Chies a,⇑a Department of Genetics, Instituto de Biociências, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazilb Department of Physiology, Instituto de Ciências Básicas da Saúde, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
a r t i c l e i n f o
Article history:Received 9 November 2012Accepted 10 April 2013Available online 28 April 2013
a b s t r a c t
Benign prostatic hyperplasia (BPH) and prostate cancer (PCa) are two chronic conditions, very common inaged men, that have been associated to inflammatory process. Chemokines and their receptors are rec-ognized as critical mediators of inflammatory responses, they regulate immune cell migration and areimplicated in tumor pathogenesis. The impact of two chemokine receptor gene polymorphisms, CCR2-64I (rs1799864) and CCR5-D32 (rs333), was evaluated in BPH and PCa. 385 DNA samples (130 BPH,136 PCa, 119 healthy control) were genotyped. The allele frequencies were similar among control, BPHand PCa groups. Median of serum PSA levels was different between groups: 0.79, 1.45 and 6.91 ng/mLin control, BPH and PCa groups, respectively (all p < 0.001). The prostate volume median was20.00 cm3 in the control group, thus, lower than BPH (35.35 cm3) and PCa (35.80 cm3) (both p < 0.001),nevertheless no statistical significant difference was observed between BPH and PCa patients(p = 0.172). Remarkably, CCR2-64I was a protective factor to PCa when compared with BPH(OR = 0.550; 95%CI = 0.311–0.975), although the statistically significant difference was lost after correc-tion for multiple comparisons. No significant associations of CCR5-D32 variant were observed withBPH, PCa or PCa clinicopathologic status. Our data suggest the influence of CCR2-64I variant in the devel-opment of prostate cancer.� 2013 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights
reserved.
1. Introduction
Prostate cancer (PCa) is one of the most common cancers inadult male and represents a leading cause of cancer deaths amongmen worldwide [1,2]. Benign prostatic hyperplasia (BPH) is one ofthe most frequent proliferative diseases affecting aged men [3,4].Both conditions are considered chronic diseases with early onsetand slow progression [5]. BPH and PCa are also conditions associ-ated with prostatic inflammation, are hormone dependent, theirincidence and prevalence rise with the advance of age and, eventhough there is no clear genetic and molecular relationship be-tween them and considering that both conditions present two dif-ferent pathogenetic pathways, a possible common denominatorbetween them was suggested [6].
Chemokines and chemokine receptors are among factors thatmay influence PCa and BPH incidence and progression [7,8]. Che-mokines are small chemotactic soluble proteins recognized as crit-ical mediators of inflammatory responses by regulating themigration of immune cells through the interaction with chemokinereceptors present on the surface of these cells [9]. These molecules,due to their immunomodulatory activities, are critically involvedin processes that allow the development of effective immune re-sponses [9]. Although it is already known that chemokines andchemokine receptors can be involved in tumor pathogenesis, it isnot yet clear how they affect human cancer progression. Some con-troversial data exists, since these molecules were already reportedas being involved in both tumor development and cancer metasta-sis, as well as in antitumor immune responses [10].
Chemokine receptors are molecules that present seven trans-membrane domains and couples to G-protein for signal transduc-tion [11]. CCR2 is a CC chemokine receptor that can bind CCL2,CCL7, CCL8 and CCL13 chemokines (reviewed by [11]). Among im-mune cells, CCR2 is mainly expressed in macrophages, T lympho-cytes, dendritic cells, B cells and basophils (reviewed by [12]).Recent investigations about PCa and BPH have focused in theCCR2 and its CCL2 ligand, and suggested that CCR2 may contributeto tumor progression [8,13–15]. Regarding this, it was observed
1004 F.M.B. Zambra et al. / Human Immunology 74 (2013) 1003–1008
that CCR2 mRNA expression is significantly higher in metastaticPCa tissue as compared to localized PCa (intermediary expression)or benign prostate tissue (low expression) [16]. The CCR2 allelicvariant, CCR2-64I (rs1799864), has a G-to-A nucleotide substitu-tion at position 190 that substitutes the amino acid residue valine(V) at position 64 by isoleucine (I) within the first transmembranedomain of the CCR2 receptor [17]. The CCR2-64I variant has beenreported as a risk factor for hepatocellular cancer [18], bladder can-cer [19] and, in contrast, as a protective factor for breast cancer[20]. The role of this genetic variant in tumor progression isuncertain.
CCR5 is another member of the CC chemokine receptor classand is capable to bind CCL3, CCL4, CCL5 and CCL8 (reviewed by[11]). CCR5 regulates trafficking and effector functions of mem-ory/effector T cells, macrophages, immature dendritic cells andNK cells [21]. The CCR5/CCL5 axis has been investigated at recentstudies in PCa and BPH progression [22–24]. The CCR5-D32(rs333) is a variant allele whose 32 bp deletion in the coding regionof CCR5 gene results in a nonfunctional receptor [25–27]. TheCCR5-D32 was reported as a risk factor for gallbladder cancer[28], but conversely, as a protective factor for prostate cancer[29]. CCR5 can regulate immune responses by mediating therecruitment of regulatory T cells (which are essential to immunehomeostasis) [30], as observed in studies with pathological condi-tions such as chronic intestinal inflammation [31] and in a pancre-atic cancer model [32]. Interestingly, it should be pointed out thatchemokine receptors such as CCR2 and CCR5 can be involved inboth cancer development and in chronic inflammatory diseases[33].
Considering that CCR2 and CCR5 are involved in inflammatoryprocesses and in immune system regulation, that such processesmay be related to pro- or antitumor activity in the host, and thatthere are still many questions about its functional significance intumor development and progression, our aim was to investigatethe impact of two chemokine receptor gene polymorphisms,CCR2-64I and CCR5-D32, in BPH and PCa development.
2. Materials and methods
2.1. Study population
In this case-control study 385 samples provided from the Labo-ratório de Biologia Molecular Endócrina e Tumoral (UFRGS) wereanalyzed (130 from BPH patients, 136 PCa patients and 119healthy control subjects). All individuals were diagnosed at theHospital de Clínicas de Porto Alegre, Rio Grande do Sul, the south-ernmost state of Brazil, between 2004 and 2009. The ethnicity(White, Brown, Black or other, according to the national IBGE –Instituto Brasileiro de Geografia e Estatística – classification system[34]) was self-categorized by the individuals when data was col-lected. The ethnic distribution did not differ significantly betweencontrol, BPH and PCa groups, and included predominantly White/Euro-descendant individuals. Although some ethnic admixture de-gree can exist in these individuals classified as Euro-descendants,Santos et al. [35] reported an almost exclusive European geneticcontribution in a sample of individuals from South Brazil [35].The researchers, using a 48-insertion–deletion ancestry-informa-tive marker panel to assess individual interethnic admixture, iden-tified a very high level of European contribution (94%) and lowNative American (5%) and African (1%) contribution in these indi-viduals [35]. In other study, using a panel of 40 validated ances-try-informative insertion–deletion DNA polymorphisms, Penaet al. [36] estimated individually the European, African and Amer-indian ancestry components of self-categorized White, Brown orBlack individuals from South Brazil [36]. In this study, individuals
classified as White had around 85.5% European, 5.3% African and9.3% Amerindian ancestry, while individuals classified as Brownand Black have approximately 45% of African, 44% of Europeanand 11% of Amerindian ancestry [36]. Therefore, these data to-gether validated our classification of ethnicity.
Inclusion criteria for BPH, according to Biolchi et al. [37], were:age between 40 and 80 years, prostate volume larger than 30 cm3
(evaluated by abdominal ultrasound to define BPH group), no pastor current hormone-ablation therapy or 5a-reductase inhibitortherapy, and absence of any neoplasia. Patients were submittedto surgery and the diagnosis of BPH was confirmed by pathologicalexamination. According to Neto et al. [38], inclusion criteria for thePCa group were: age 45–80 years old, no current hormone-ablativetherapy and no other concomitant neoplasia. Controls were se-lected from a prostate cancer prevention program conducted since2004. Inclusion criteria for controls were age between 40 and80 years, prostate volume smaller than 30 cm3, PSA value less than2.0 ng/mL, digital rectal examination with normal result and ab-sence of any neoplasia. Factors such as age, ethnic origin, tumorstage, Gleason score and total serum PSA levels at diagnosis wererecorded. The study was approved by the local and national EthicsCommittee and informed consent was obtained from every subject.
2.2. Genotyping
CCR2 typing was performed by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay. TheCCR2-64I polymorphism was genotyped using specific primerspreviously described by Smith et al. [17]. The PCR samples wereprepared to a final volume of 25 ll, according to Vargas et al.[39], as follows: 1 ll of DNA (0.2–0.5 lg), 2.5 ll of 10� PCR buffer[200 mM Tris–HCl (pH 8.4), 500 mM KCl], 1 ll of 50 mM MgCl2,1 ll of 3 mM dNTP mix, 1 ll of 10 pmol primer mix and 0.2 llTaq DNA polymerase 5 U/ll (Invitrogen Corporation, California,USA). Samples were submitted to 40 cycles of 1 min at 94 �C,1 min at 55 �C, and 1 min at 72 �C. The PCR product resulting wasa 128 bp fragment. Then, it was digested with 4 U of the BsaBIrestriction enzyme for 16 h at 60 �C, producing 110 bp and 18 bpfragments (CCR2-64I allele) or a single undigested 128 bp fragment(wild-type allele), which were visualized under UV irradiation in a8% polyacrylamide gel stained with ethidium bromide.
CCR5 genotyping was performed by conventional PCR and thegenotypes were visualized on 3% agarose gel stained with ethidiumbromide, as described in Chies & Hutz [40]. Amplification of theCCR5-wt allele generates a 137 bp band and the CCR5-D32 allelegenerates a 105 bp band.
2.3. Statistical analysis
Hardy–Weinberg equilibrium was assessed using a Chi-squaretest. Differences between means in the continuous variables wereanalyzed by ANOVA one way test, with 95% significance. The Krus-kal–Wallis non-parametric test, following by Dunn’s test was per-formed to analyze the median differences of serum PSA andprostate volume values between groups. For analysis, the genotypefrequencies of CCR2-64I as well as CCR5-D32 were grouped for thepresence of at least one variant allele versus wt genotypes, whilehaplotypes were compounds by the presence of at least one variantallele versus double wild-type genotypes, considering a smallnumber of homozygous individuals to CCR2-64I and CCR5-D32in the sample and a dominant effect to the genetic variants. Theindividuals with PCa were classified in two groups based in tumorstage, as having evidence of localized PCa (T1 and T2 stages) orextraprostatic disease (T3 and T4 stages), while to biopsy Gleasonscore patients were divided in two groups: 66(3 + 3) andP7(3 + 4), as representative of less or more aggressive disease,

F.M.B. Zambra et al. / Human Immunology 74 (2013) 1003–1008 1005
respectively. Logistic regression models (age-adjusted) or Chi-square tests were used to provide odds ratio (OR), 95% confidenceintervals (CI) and P-values for the risk of CCR2-64I, CCR5-D32 andhaplotypes with diseases, tumor stage and Gleason score. With asample size of 385 individuals, the power to detect differences be-tween groups in this study range from 15% to 50%. All tests weretwo-sided and 5% level was used as threshold for statistical signif-icance. Data analysis was performed using the computer softwareSPSS version 17.0 for windows (SPSS Inc., Chicago, Illinois, USA).
3. Results
3.1. Population
In the study of the polymorphic variants CCR2-64I and CCR5-D32, 385 samples divided into three groups were analyzed: control(119 individuals), BPH (130) and PCa (136). The characteristics ofthe studied population are shown in Table 1. The participants arepredominantly euro-descendants (83.5% control, 91.6% BPH and86.0% PCa) and the ethnic distribution did not differ significantlybetween the studied groups (Pglobal = 0.164). The mean age ob-served at diagnosis in the control group was 57.21 ± 7.91 years(range: 41–75 years), in the BPH group was 63.08 ± 8.99 (range:42–82) and in PCa group was 63.30 ± 6.97 (range: 46–75). Theaverage age of the control group was lower than the other groups(both P < 0.001), but did not differ significantly between BPH andPCa groups (P = 0.975) (Table 1).
The serum PSA median was 0.79 (0.56–1.11) ng/mL in the con-trol group, 1.45 (0.70–3.91) ng/mL in the BPH group and 6.91
Table 1Characteristics of the sample assesseda in the CCR2-64I and CCR5-D32 study.
Control(n = 119)
BPH(n = 130)
PCa(n = 136)
Ethnicity(euro-descendant)b,f
96 (83.5%) 109 (91.6%) 104 (86.0%)
Age (years)f
Mean ± SDg 57.21 ± 7.91 63.08 ± 8.99 63.30 ± 6.97Range 41–75 42–82 46–75
PSA (ng/mL)c,f,h 0.79(0.56 – 1.11)
1.45(0.70–3.93)
6.91(5.41–10.33)
Prostate volume(cm3)c,f
20.00(16.65–25.00)
35.35(30.00–50.00)
35.80(28.70–44.52)
Tumor stageb,d,e
(T1 + T2) 71 (55.5%)(T3 + T4) 52 (40.6%)
Gleason scoreb
4 (2 + 2) 1 (0.8%)5 (3 + 2) 1 (0.8%)6 (3 + 3) 70 (54.3%)7 (3 + 4) 23 (17.8%)7 (4 + 3) 21 (16.3%)8 (3 + 5) 1 (0.8%)8 (4 + 4) 6 (4.7%)9 (4 + 5) 5 (3.9%)9 (5 + 4) 1 (0.8%)
a Sample assessed (n = 385): 119 control subjects, 130 BPH patients and 136 PCapatients. PCa, prostate cancer, BPH, benign prostatic hyperplasia.
b Number of cases and percentages.c Medians and 25/75 percentiles.d There was no information available on pathologic tumor stage for 8 (5.9%)
patients and on grade stage for 7 (5.1%) patients.e Five (3.9%) patients were submitted to radiotherapy.f P value – ethnicity – PCa vs. BPH vs. control: Pglobal = 0.164. Age – BPH or PCa vs.
control: P < 0.001; PCa vs. BPH: P = 0.975. PSA – BPH or PCa vs. control and PCa vs.BPH: P < 0.001. Prostate volume – BPH or PCa vs. control: P < 0.001; PCa vs. BPH:P = 0.556.
g SD, standard deviation.h PSA, prostate-specific antigen.
(5.47–10.27) ng/mL in the PCa group, differing significantly be-tween them (all P < 0.001). The prostate volume median was20.00 (17.00–20.00) cm3 in the control group, thus, lower thanthe BPH group with 35.35 (30.00–50.00) cm3 and the PCa groupwith 35.80 (28.00–44.35) cm3 (both P < 0.001). However, therewas no significant difference in prostate volume between BPHand PCa groups (P = 0.172). Among the PCa patients, 71 (55.5%)men had organ-confined disease (T1 or T2) at the time of surgery,while 52 (40.6%) men had extraprostatic tumor (T3 or T4). Thebiopsy Gleason score was 66(3 + 3) in 72 (52.9%) and P7(3 + 4)in 57 (41.9%) PCa patients (Table 1).
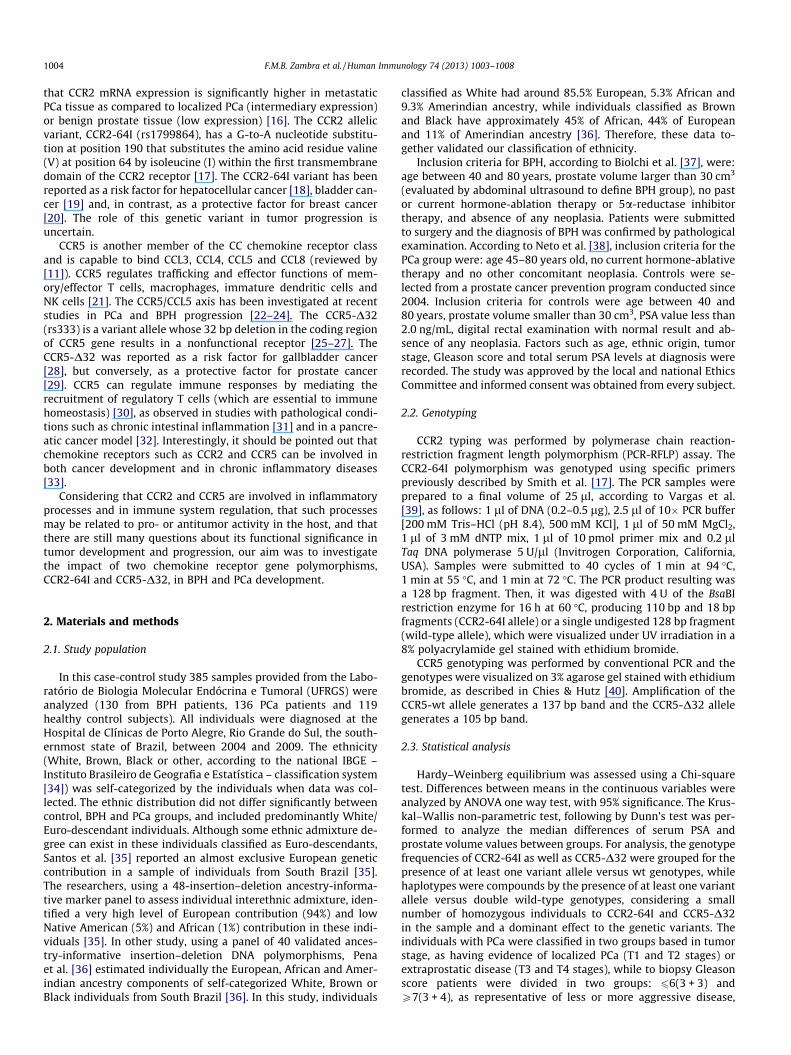
The allele and genotype frequencies of CCR2-64I and CCR5-D32among control, BPH and PCa groups are presented in Table 2. Theallele frequencies of CCR2-64I were 14.0%, 15.8% and 11.1% in con-trol, BPH and PCa groups, respectively; while of CCR5-D32 were5.1%, 7.1% and 6.2%, respectively. The genotype frequencies distri-bution was in agreement with the Hardy–Weinberg equilibrium inall sample groups (CCR2-64I – control: v2 = 0.281, P = NS; BPH:v2 = 2.173, P = NS; PCa: v2 = 0.084, P = NS); (CCR5-D32 – control:v2 = 1.757, P = NS; BPH: v2 = 0.739, P = NS; PCa: v2 = 0.582, P = NS).
3.2. CCR2-64I and CCR5-D32 influence in BPH and PCa risk
The association between CCR2-64I or CCR5-D32 with BPH orPCa risk was evaluated by logistic regression analysis. Consideringthat the average age was different between the control group andBPH or PCa groups, and that such variable is associated with therisk of these diseases, age at diagnosis was included as a covariatein this analysis. Comparison for the presence (64I/64I + wt/64I) orthe absence (wt/wt) of the CCR2-64I allele between BPH vs. controlgroups (OR = 1.428, 95%CI = 0.787–2.591, P = 0.241) and betweenPCa vs. control groups (OR = 0.786, 95%CI = 0.422–1.464,P = 0.448) do not yield statistically significant differences. Thesame comparison age-adjusted to PCa vs. BPH suggested CCR2-64I as a protective factor to PCa (OR = 0.550, 95%CI = 0.311–0.975, P = 0.041), although the statistically significant differencewas lost after correction for multiple comparisons (P-value ad-justed = 0.369 by Bonferroni correction) (Table 3). Comparison forthe presence (D32/D32 + wt/D32) or the absence (wt/wt) of theCCR5-D32 allele between BPH vs. control groups (OR = 1.534,95%CI = 0.656–3.582, P = 0.323), PCa vs. control groups(OR = 1.142, 95%CI = 0.476–2.739, P = 0.767) or PCa vs. BPH groups(OR = 0.746, 95%CI = 0.357–1.563, P = 0.438) do not yield statisti-cally significant differences (Table 3). The association of haplotypesbetween BPH vs. control groups (OR = 1.412, 95%CI = 0.809–2.467,P = 0.225), PCa vs. control groups (OR = 0.870, 95%CI = 0.492–1.538,P = 0.632) or PCa vs. BPH groups (OR = 0.617, 95%CI = 0.365–1.043,P = 0.072) do not yield statistically significant differences (Table 3).
3.3. CCR2-64I and CCR5-D32 influence in PCa clinicopathologic status
The association between CCR2-64I or CCR5-D32 with risk forPCa clinicopathologic status was evaluated by Chi-square analysis.When analyzing the association of the CCR2-64I and CCR5-D32genotypes or haplotypes with pathologic stages (T1–T2 and T3–T4) in PCa patients no association was observed (Table 4). Also,no association between the presence or absence of the studied alle-lic variants or haplotypes were observed considering the Gleasonscore [66(3 + 3) and P7(3 + 4)] of PCa patients (Table 5).
4. Discussion
PCa is the most common cancer type in adult men and BPH is anage-related proliferative abnormality that represents the mostcommon urologic diagnosis in men [3]. PCa shares a number of fea-
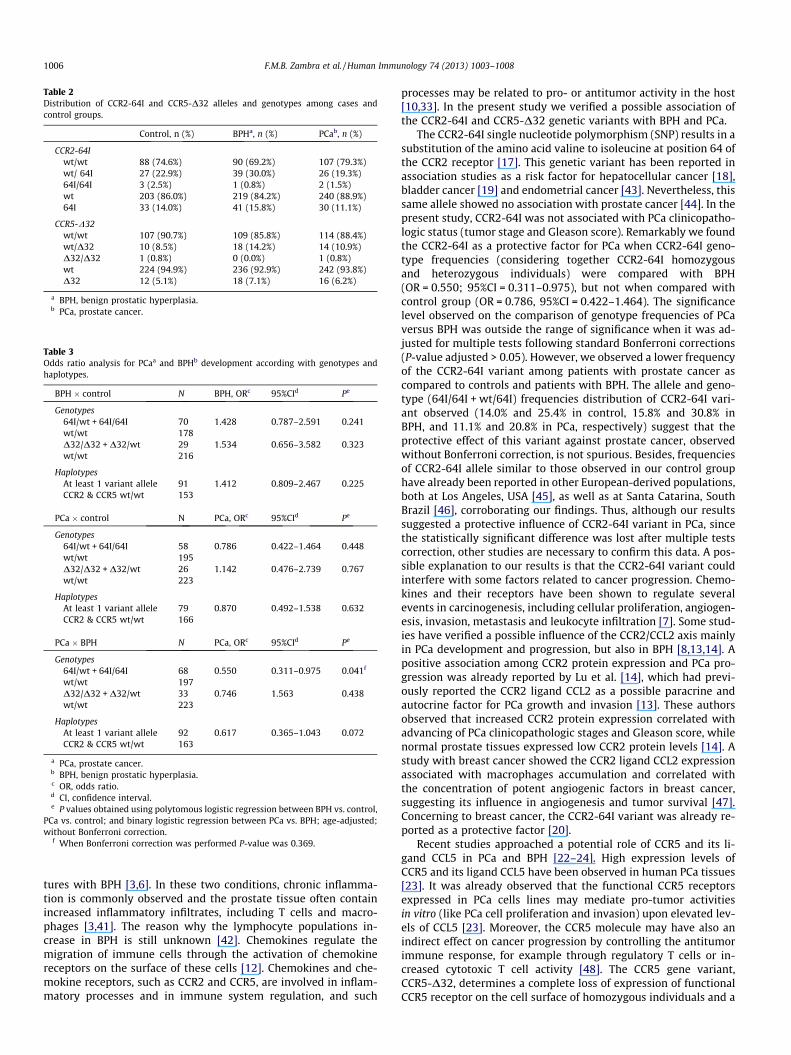
Table 2Distribution of CCR2-64I and CCR5-D32 alleles and genotypes among cases andcontrol groups.
Control, n (%) BPHa, n (%) PCab, n (%)
CCR2-64Iwt/wt 88 (74.6%) 90 (69.2%) 107 (79.3%)wt/ 64I 27 (22.9%) 39 (30.0%) 26 (19.3%)64I/64I 3 (2.5%) 1 (0.8%) 2 (1.5%)wt 203 (86.0%) 219 (84.2%) 240 (88.9%)64I 33 (14.0%) 41 (15.8%) 30 (11.1%)
CCR5-D32wt/wt 107 (90.7%) 109 (85.8%) 114 (88.4%)wt/D32 10 (8.5%) 18 (14.2%) 14 (10.9%)D32/D32 1 (0.8%) 0 (0.0%) 1 (0.8%)wt 224 (94.9%) 236 (92.9%) 242 (93.8%)D32 12 (5.1%) 18 (7.1%) 16 (6.2%)
a BPH, benign prostatic hyperplasia.b PCa, prostate cancer.
Table 3Odds ratio analysis for PCaa and BPHb development according with genotypes andhaplotypes.
BPH � control N BPH, ORc 95%CId Pe
Genotypes64I/wt + 64I/64I 70 1.428 0.787–2.591 0.241wt/wt 178D32/D32 + D32/wt 29 1.534 0.656–3.582 0.323wt/wt 216
HaplotypesAt least 1 variant allele 91 1.412 0.809–2.467 0.225CCR2 & CCR5 wt/wt 153
PCa � control N PCa, ORc 95%CId Pe
Genotypes64I/wt + 64I/64I 58 0.786 0.422–1.464 0.448wt/wt 195D32/D32 + D32/wt 26 1.142 0.476–2.739 0.767wt/wt 223
HaplotypesAt least 1 variant allele 79 0.870 0.492–1.538 0.632CCR2 & CCR5 wt/wt 166
PCa � BPH N PCa, ORc 95%CId Pe
Genotypes64I/wt + 64I/64I 68 0.550 0.311–0.975 0.041f
wt/wt 197D32/D32 + D32/wt 33 0.746 1.563 0.438wt/wt 223
HaplotypesAt least 1 variant allele 92 0.617 0.365–1.043 0.072CCR2 & CCR5 wt/wt 163
a PCa, prostate cancer.b BPH, benign prostatic hyperplasia.c OR, odds ratio.d CI, confidence interval.e P values obtained using polytomous logistic regression between BPH vs. control,
PCa vs. control; and binary logistic regression between PCa vs. BPH; age-adjusted;without Bonferroni correction.
f When Bonferroni correction was performed P-value was 0.369.
1006 F.M.B. Zambra et al. / Human Immunology 74 (2013) 1003–1008
tures with BPH [3,6]. In these two conditions, chronic inflamma-tion is commonly observed and the prostate tissue often containincreased inflammatory infiltrates, including T cells and macro-phages [3,41]. The reason why the lymphocyte populations in-crease in BPH is still unknown [42]. Chemokines regulate themigration of immune cells through the activation of chemokinereceptors on the surface of these cells [12]. Chemokines and che-mokine receptors, such as CCR2 and CCR5, are involved in inflam-matory processes and in immune system regulation, and such
processes may be related to pro- or antitumor activity in the host[10,33]. In the present study we verified a possible association ofthe CCR2-64I and CCR5-D32 genetic variants with BPH and PCa.
The CCR2-64I single nucleotide polymorphism (SNP) results in asubstitution of the amino acid valine to isoleucine at position 64 ofthe CCR2 receptor [17]. This genetic variant has been reported inassociation studies as a risk factor for hepatocellular cancer [18],bladder cancer [19] and endometrial cancer [43]. Nevertheless, thissame allele showed no association with prostate cancer [44]. In thepresent study, CCR2-64I was not associated with PCa clinicopatho-logic status (tumor stage and Gleason score). Remarkably we foundthe CCR2-64I as a protective factor for PCa when CCR2-64I geno-type frequencies (considering together CCR2-64I homozygousand heterozygous individuals) were compared with BPH(OR = 0.550; 95%CI = 0.311–0.975), but not when compared withcontrol group (OR = 0.786, 95%CI = 0.422–1.464). The significancelevel observed on the comparison of genotype frequencies of PCaversus BPH was outside the range of significance when it was ad-justed for multiple tests following standard Bonferroni corrections(P-value adjusted > 0.05). However, we observed a lower frequencyof the CCR2-64I variant among patients with prostate cancer ascompared to controls and patients with BPH. The allele and geno-type (64I/64I + wt/64I) frequencies distribution of CCR2-64I vari-ant observed (14.0% and 25.4% in control, 15.8% and 30.8% inBPH, and 11.1% and 20.8% in PCa, respectively) suggest that theprotective effect of this variant against prostate cancer, observedwithout Bonferroni correction, is not spurious. Besides, frequenciesof CCR2-64I allele similar to those observed in our control grouphave already been reported in other European-derived populations,both at Los Angeles, USA [45], as well as at Santa Catarina, SouthBrazil [46], corroborating our findings. Thus, although our resultssuggested a protective influence of CCR2-64I variant in PCa, sincethe statistically significant difference was lost after multiple testscorrection, other studies are necessary to confirm this data. A pos-sible explanation to our results is that the CCR2-64I variant couldinterfere with some factors related to cancer progression. Chemo-kines and their receptors have been shown to regulate severalevents in carcinogenesis, including cellular proliferation, angiogen-esis, invasion, metastasis and leukocyte infiltration [7]. Some stud-ies have verified a possible influence of the CCR2/CCL2 axis mainlyin PCa development and progression, but also in BPH [8,13,14]. Apositive association among CCR2 protein expression and PCa pro-gression was already reported by Lu et al. [14], which had previ-ously reported the CCR2 ligand CCL2 as a possible paracrine andautocrine factor for PCa growth and invasion [13]. These authorsobserved that increased CCR2 protein expression correlated withadvancing of PCa clinicopathologic stages and Gleason score, whilenormal prostate tissues expressed low CCR2 protein levels [14]. Astudy with breast cancer showed the CCR2 ligand CCL2 expressionassociated with macrophages accumulation and correlated withthe concentration of potent angiogenic factors in breast cancer,suggesting its influence in angiogenesis and tumor survival [47].Concerning to breast cancer, the CCR2-64I variant was already re-ported as a protective factor [20].
Recent studies approached a potential role of CCR5 and its li-gand CCL5 in PCa and BPH [22–24]. High expression levels ofCCR5 and its ligand CCL5 have been observed in human PCa tissues[23]. It was already observed that the functional CCR5 receptorsexpressed in PCa cells lines may mediate pro-tumor activitiesin vitro (like PCa cell proliferation and invasion) upon elevated lev-els of CCL5 [23]. Moreover, the CCR5 molecule may have also anindirect effect on cancer progression by controlling the antitumorimmune response, for example through regulatory T cells or in-creased cytotoxic T cell activity [48]. The CCR5 gene variant,CCR5-D32, determines a complete loss of expression of functionalCCR5 receptor on the cell surface of homozygous individuals and a
Table 4Distribution of CCR2-64I and CCR5-D32 genotype and haplotype frequencies ingroups of tumor stage.
T1 + T2,n (%)
T3 + T4,n (%)
v2 ORb 95%CIc Pa
CCR2-64Iwt/64I + 64I/64I
12(17.1%)
12(23.1%)
0.665 1.450 (0.592–3.552)
0.492
wt/wt 58(82.9%)
40(76.9%)
CCR5-D32wt/D32 + D32/D32
7(10.6%)
7(14.0%)
0.309 1.372 (0.448–4.201)
0.581
wt/wt 59(89.4%)
43(86.0%)
HaplotypeAt least 1variant allele
17(26.2%)
18(36.0%)
1.294 1.588 (0.714–3.533)
0.308
CCR2 & CCR5wt/wt
48(73.8%)
32(64.0%)
a Values obtained using the Chi-square 2 � 2, with correction for continuity.b OR, odds ratio.c CI, confidence interval.
Table 5Distribution of CCR2-64I and CCR5-D32 genotype and haplotype frequencies ingroups of Gleason score.
66(3 + 3),n (%)
P7(3 + 4),n (%)
v2 ORb 95%CIc Pa
CCR2-64Iwt/64I + 64I/64I
14 (20.6%) 10 (18.5%) 0.082 0.877 0.355–2.165
0.822
wt/wt 54 (79.4%) 44 (81.5%)CCR5-D32
wt/D32 + D32/D32
10 (15.9%) 4 (7.5%) 1.880 0.433 0.127–1.470
0.253
wt/wt 53 (84.1%) 49 (92.5%)
HaplotypeAt least 1variantallele
21 (33.9%) 14 (26.4%) 0.750 0.701 0.313–1.569
0.422
CCR2 & CCR5wt/wt
41 (66.1%) 39 (73.6%)
a Values obtained using the Chi-square 2 � 2, with correction for continuity.b OR, odds ratio.c CI, confidence interval.
F.M.B. Zambra et al. / Human Immunology 74 (2013) 1003–1008 1007
greatly reduced expression in heterozygous [25–27]. By alteringCCR5 expression, the CCR5-D32 mutation should affect severalCCR5-mediated pathways in the immune response, as demon-strated by numerous studies [10,17,33]. Although often consideredas a ‘‘benign mutation’’ especially due to its role in HIV infectionresistance (reviewed by [49]) and more recently as a protective fac-tor against the development of endothelial dysfunction and cardio-vascular disease in patients with rheumatoid arthritis [50], severalassociations with this variant and negative effects were already re-ported, including cancer development (reviewed by [49]). In thepresent study no association of the CCR5-D32 variant was ob-served with PCa, PCa clinicopathologic status (tumor stage andGleason score) or BPH. Our results (relative to CCR5-D32 in PCa)corroborate data from a large Australian case-control study by Pet-ersen et al. [44], where CCR5-D32 variant was analyzed in a groupof 815 PCa patients and 738 healthy controls [44]. CCR5-D32 wasalready reported as a protective factor to PCa by Balistreri et al.[29], but in a quite small cohort (n = 50). To our knowledge, noother association study was performed that compare CCR5-D32with BPH.
A limitation of the present study is the sample size and also thefact that the functional role of CCR2-64I and CCR5-D32 in BPH andPCa development is still poorly understood. Due to inconsistencesin the scientific literature about the role of both polymorphisms,further investigations with functional assessments, meta-analysisand larger samples in different populations could clarify the roleof these genetic variants in prostate tumor development. Our studystands out by comparing three rather than two different groups,showing an important link among two prostatic tumor conditions.The understanding about CCR2-64I and CCR5-D32 genetic variantsmay be important to novel therapeutic approaches to PCa in the fu-ture and to survival improvement of affected subjects for thisdisease.
In conclusion, this study suggests that the CCR2-64I variant is aprotective factor to PCa. No association of the chemokine receptorCCR5-D32 polymorphism was observed with BPH or PCa in thissample. There are still inconsistencies and doubts in the scientificliterature about the role of these genetic variants in prostate tumorprocesses, but the essential function of CCR2 and CCR5 in immuno-logical responses suggests that these genetic variants may havekey functions in cancer development and progression.
Acknowledgments
This study was supported by Conselho Nacional de Desenvolvi-mento Científico e Tecnológico CNPq grants (306349/2011-6,135450/2009-8, and 473115/2011-5), by Fundo do Incentivo à Pes-quisa e Eventos/Hospital de Clínicas de Porto Alegre FIPE/HCPAgrants (07-533), and by Fundação de Amparo à Pesquisa do Estadodo Rio Grande do Sul FAPERGS grants (10/1516-6). We gratefullyacknowledge to M.Sc. Caio C.S. Cerqueira for suggestions that en-riched this paper, to M.Sc. Paula Rohr, M.Sc. Caio C.S. Cerqueiraand Vania N. Hirakata for their usefull review of statistical analysisand to Patrícia Martiny for help in some data bank informations.
References
[1] Ferlay J, Shin HR, Bray F, Forman D, Mathers CD, Parkin D. GLOBOCAN 2008. In:Cancer incidence and mortality worldwide: IARC CancerBase No. 10.. Lyon,France: International Agency for Research on Cancer; 2012 [Online] http://globocan.iarc.fr (30 August 2012, date last accessed).
[2] Instituto Nacional de Câncer (INCA), http://www.inca.gov.br/estimativa/2012(09 February 2012, date last accessed).
[3] De Nunzio C, Kramer G, Marberger M, Montironi R, Nelson W, Schröder F, et al.The controversial relationship between benign prostatic hyperplasia andprostate cancer: the role of inflammation. Eur Urol 2011;60:106–17.
[4] Kirby RS. The natural history of benign prostatic hyperplasia what have welearned in the last decade. Urology 2000;56(Suppl. 1):3–6.
[5] Sciarra A, Di Silverio F, Salciccia S, Autran Gomez AM, Gentilucci A, Gentile V.Inflammation and chronic prostatic diseases: evidence for a link? Eur Urol2007;52:964–72.
[6] Alcaraz A, Hammerer P, Tubaro A, Schröder FH, Castro R. Is there evidence of arelationship between benign prostatic hyperplasia and prostate cancer?Findings of a literature review. Eur Urol 2009;55:864–75.
[7] Vindrieux D, Escobar P, Lazennec G. Emerging roles of chemokines in prostatecancer. Endocr Relat Cancer 2009;16:663–73.
[8] Fujita K, Ewing CM, Getzenberg RH, Parsons JK, Isaacs WB, Pavlovich CP.Monocyte chemotactic protein-1 (MCP-1/CCL2) is associated with prostaticgrowth dysregulation and benign prostatic hyperplasia. Prostate2010;70(5):473–81.
[9] Ruffini PA, Morandi P, Cabioglu N, Altundag K, Cristofanilli M. Manipulating thechemokine–chemokine receptor network to treat cancer. Cancer2007;109(12):2392–404.
[10] Mañes S, Mira E, Colomer R, Montero S, Real LM, Gómez-Moutón C, et al. CCR5expression influences the progression of human breast cancer in a p53-dependent manner. J Exp Med 2003;198:1381–9.
[11] Murphy PM, Baggiolini M, Charo IF, Hebert CA, Horuk R, Matsushima K, et al.International union of pharmacology. XXII. Nomenclature for chemokinereceptors. Pharmacol Ver 2000;52(1):145–76.
[12] Charo IF, Ransohoff RM. The many roles of chemokines and chemokinereceptors in inflammation. N Engl J Med 2006;354(6):610–21.
[13] Lu Y, Cai Z, Galson DL, Xiao G, Liu Y, George DE, et al. Monocyte chemotacticprotein-1 (MCP-1) acts as a paracrine and autocrine factor for prostate cancergrowth and invasion. Prostate 2006;66(12):1311–8.

1008 F.M.B. Zambra et al. / Human Immunology 74 (2013) 1003–1008
[14] Lu Y, Cai Z, Xiao G, Liu Y, Keller ET, Yao Z, et al. CCR2 expression correlates withprostate cancer progression. J Cell Biochem 2007;101(3):676–85.
[15] Zhang J, Lu Y, Pienta KJ. Multiple roles of chemokine (C–C motif) ligand 2 inpromoting prostate cancer growth. J Natl Cancer Inst 2010;102(8):522–8.
[16] Yu YP, Landsittel D, Jing L, Nelson J, Ren B, Liu L, et al. Gene expressionalterations in prostate cancer predicting tumor aggression and precedingdevelopment of malignancy. J Clin Oncol 2004;22:2790–9.
[17] Smith MW, Carrington M, Winkler C, Lomb D, Dean M, Huttley G, et al. CCR2chemokine receptor and AIDS progression. Nat Med 1997;3:1052–3.
[18] Yeh CB, Tsai HT, Chen YC, Kuo WH, Chen TY, Hsieh YH, et al. Geneticpolymorphism of CCR2-64I increased the susceptibility of hepatocellularcarcinoma. J Surg Oncol 2010;102(3):264–70.
[19] Narter KF, Agachan B, Sozen S, Cincin ZB, Isbir T. CCR2-64I is a risk factor fordevelopment of bladder cancer. Genet Mol Res 2010;9(2):685–92.
[20] Zafiropoulos A, Crikas N, Passam AM, Spandidos DA. Significant involvement ofCCR2-64I and CXCL12-3a in the development of sporadic breast cancer. J MedGenet 2004;41(5):e59.
[21] Balistreri CR, Caruso C, Grimaldi MP, Listì F, Vasto S, Orlando V, et al. CCR5receptor: biologic and genetic implications in age-related diseases. Ann NYAcad Sci 2007;1100:162–72.
[22] König JE, Senge T, Allhoff EP, Konig W. Analysis of the inflammatory network inbenign prostate hyperplasia and prostate cancer. Prostate 2004;58(2):121–9.
[23] Vaday GG, Peehl DM, Kadam PA, Lawrence DM. Expression of CCL5 (RANTES)and CCR5 in prostate cancer. Prostate 2006;66:124–34.
[24] Magnani M, Castro-Gomez RH, Aoki MN, Gregório EP, Libos F, Morimoto HK,et al. Analysis of peripheral T cells and the CC chemokine receptor (CCR5)delta32 polymorphism in prostate cancer patients treated withcarboxymethyl-glucan (CM-G). Nat Prod Res 2011. http://dx.doi.org/10.1080/14786419.2010.535159 [Epub ahead of print].
[25] Liu R, Paxton WA, Choe S, Ceradini D, Martin SR, Horuk R, et al. Homozygousdefect in HIV-1 coreceptor accounts for resistance of some multiply-exposedindividuals to HIV-1 infection. Cell 1996;86(3):367–77.
[26] Samson M, Libert F, Doranz BJ, Rucker J, Liesnard C, Farber CM, et al. Resistanceto HIV-1 infection in caucasian individuals bearing mutant alleles of the CCR-5chemokine receptor gene. Nature 1996;382(6593):722–5.
[27] Dean M, Carrington M, Winkler C, Huttley GA, Smith MW, Allikmets R, et al.Genetic restriction of HIV-1 infection and progression to AIDS by a deletionallele of the CKR5 structural gene. Science 1996;273(5283):1856–62.
[28] Srivastava A, Pandey SN, Choudhuri G, Mittal B. CCR5D32 polymorphism:associated with gallbladder cancer susceptibility. Scand J Immunol2008;67:516–22.
[29] Balistreri CR, Carruba G, Calabrò M, Campisi I, Di Carlo D, Lio D, et al. CCR5proinflammatory allele in prostate cancer risk: a pilot study in patients andcentenarians from Sicily. Ann NY Acad Sci 2009;1155:289–92.
[30] Josefowicz SZ, Rudensky A. Control of regulatory T cell lineage commitmentand maintenance. Immunity 2009;30:616–25.
[31] Kang SG, Piniecki RJ, Hogenesch H, Lim HW, Wiebke E, Braun SE, et al.Identification of a chemokine network that recruits FoxP3(+) regulatory T cellsinto chronically inflamed intestine. Gastroenterology 2007;132:966–81.
[32] Tan MC, Goedegebuure PS, Belt BA, Flaherty B, Sankpal N, Gillanders WE, et al.Disruption of CCR5-dependent homing of regulatory T cells inhibits tumorgrowth in a murine model of pancreatic cancer. J Immunol 2009;182:1746–55.
[33] Hembruff SL, Cheng N. Chemokine signaling in cancer: Implications on thetumor microenvironment and therapeutic targeting. Cancer Ther2009;7:254–67.
[34] Osorio RG. O sistema classificatório de ’’cor ou raça’’ do IBGE. Brasília: Institutode Pesquisa Econômica Aplicada; 2003. 50 p..
[35] Santos NP, Ribeiro-Rodrigues EM, Ribeiro-Dos-Santos AK, Pereira R, Gusmão L,Amorim A, et al. Assessing individual interethnic admixture and populationsubstructure using a 48-insertion-deletion (INSEL) ancestry informativemarker (AIM) panel. Hum Mutat 2010;31(2):184–90. http://dx.doi.org/10.1002/humu.21159.
[36] Pena SD, Di Pietro G, Fuchshuber-Moraes M, Genro JP, Hutz MH, Kehdy Fde S,et al. The genomic ancestry of individuals from different geographical regionsof Brazil is more uniform than expected. PLoS One 2011;6(2):e17063. http://dx.doi.org/10.1371/journal.pone.0017063.
[37] Biolchi V, Neto BS, Koff W, Brum IS. Androgen receptor CAG polymorphism andthe risk of benign prostatic hyperplasia in a Brazilian population. Int Braz JUrol 2012;38:372–8.
[38] Neto BS, Koff WJ, Biolchi V, Brenner C, Biolo KD, Spritzer PM, et al. PolymorphicCAG and GGC repeat lengths in the androgen receptor gene and prostatecancer risk: analysis of a Brazilian population. Cancer Invest2008;26(1):74–80.
[39] Vargas AE, da Silva MA, Silla L, Chies JA. Polymorphisms of chemokinereceptors and eNOS in Brazilian patients with sickle cell disease. TissueAntigens 2005;66(6):683–90.
[40] Chies JA, Hutz MH. Hight frequency of the CCR5-delta32 variant amongindividuals from an admixed Brazilian population with sickle cell anemia. BrazJ Med Biol Res 2003;36:71–5.
[41] De Marzo AM, Platz EA, Sutcliffe S, Xu J, Grönberg H, Drake CG, et al.Inflammation in prostate carcinogenesis. Nat Rev Cancer 2007;7(4):256–69.
[42] Tang J, Yang J. Etiopathogenesis of benign prostatic hypeprlasia. Indian J Urol2009;25(3):312–7.
[43] Attar R, Agachan B, Kuran SB, Cacina C, Sozen S, Yurdum LM, et al. Associationof CCL2 and CCR2 gene variants with endometrial cancer in Turkish women. InVivo 2010;24:2243–8.
[44] Petersen DC, Severi G, Hoang HN, Padilla EJD, Southey MC, English DR, et al. Noassociation between common chemokine and chemokine receptor genevariants and prostate cancer risk. Cancer Epidemiol Biomarkers Prev2008;17(12):3615–7.
[45] Iyer RK, Kim PS, Bando JM, Lu KV, Gregg JP, Grody WW. A multiethnic study ofDelta32ccr5 and ccr2b-V64I allele distribution in four Los Angeles populations.Diagn Mol Pathol 2001;10(2):105–10.
[46] Acosta AX, Sampaio RG, Spínola JL, Galvão-Castro B. Distribution of the CCR2-64I allele in three Brazilian ethnic groups. Genet Mol Biol 2003;26:3. http://dx.doi.org/10.1590/S1415-47572003000300004. São Paulo.
[47] Ueno T, Toi M, Saji H, Muta M, Bando H, Kuroi K, et al. Significance ofmacrophage chemoattractant protein-1 in macrophage recruitment,angiogenesis, survival in human breast cancer. Clin Cancer Res2000;6:3282–9.
[48] Degerli N, Yilmaz E, Bardakci F. The D32 allele distribution of the CCR5 geneand its relationship with certain cancers in a Turkish population. Clin Biochem2005;38:248–52.
[49] Vargas AE, Cechim G, Correa JF, Gomes PA, Macedo Gde S, de Medeiros RM,et al. Pros and cons of a missing chemokine receptor-comments on ‘‘Is theEuropean spatial distribution of the HIV-1-resistant CCR5-D32 allele formedby a breakdown of the pathocenosis due to the historical Roman expansion?’’by Eric Faure and Manuela Royer-Carenzi (2008). Infect Genet Evol2009;9(4):387–9.
[50] Rodríguez-Rodríguez L, González-Juanatey C, García-Bermúdez M, Vázquez-Rodríguez TR, Miranda-Filloy JA, Fernández-Gutiérrez B, et al. CCR5D32variant and cardiovascular disease in patients with rheumatoid arthritis: acohort study. Arthritis Res Ther 2011;13(4):R133. http://dx.doi.org/10.1186/ar3444.




















