
Combination of Alfuzosin and Tadalafil Exerts an Additive Relaxant Effect on Human Detrusor and...
10
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Combination of Alfuzosin and Tadalafil Exerts an Additive Relaxant Effect on Human Detrusor and...
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Voiding Dysfunction
Combination of Alfuzosin and Tadalafil Exerts an Additive
Relaxant Effect on Human Detrusor and Prostatic Tissues In Vitro
Stephanie Oger a, Delphine Behr-Roussel a, Diane Gorny a, Thierry Lebret b,Yves Denoux b, Laurent Alexandre a, Francois Giuliano c,*
a Pelvipharm, Orsay Parc, Batiment Cedre, 86 rue de Paris, 91400 Orsay, Franceb Foch Hospital, Department of Urology, Suresnes, Francec AP-HP, Neuro-Uro-Andrology, Department of Physical Medicine and Rehabilitation Raymond Poincare Hospital, Garches, France
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted April 21, 2009Published online ahead ofprint on May 3, 2009
Keywords:
PDE5 inhibitor
a1-adrenoceptor antagonist
Lower urinary tract symptoms
Bladder
Prostate
Smooth muscle
Abstract
Background: Lower urinary tract symptoms (LUTS) suggestive of benign prostatic
hyperplasia (BPH) and erectile dysfunction (ED) are highly prevalent in aging menand are strongly linked. Alpha1-blockers such as alfuzosin are effective monotherapiesfor LUTS. Phosphodiesterase type 5 (PDE5) inhibitors such as tadalafil are the first-line
treatment for ED. Both drugs act by two different mechanisms of action on commonurogenital target organs and, thus, may have additive effects.Objectives: We evaluated in vitro the effects of alfuzosin, tadalafil, and the combinationof both on human detrusor and prostatic smooth muscle.
Design, setting, and participants: Prostatic and bladder tissue were obtained frompatients (n = 20 and n = 17, respectively) undergoing cystoprostatectomy for bladdercancer.Measurements: In organ baths, isolated prostatic strips and isolated bladder strips were
incubated with vehicle, tadalafil (10�6 M and 10�5 M), alfuzosin (3 � 10�8 M or 10�6 Mand 10�5 M) or a combination. Concentration-response curves (CRCs) to norepinephrinewere generated on prostatic strips and detrusor strips precontracted with carbachol.
Strips were also submitted to electrical field stimulation (EFS).Results and limitations: When alfuzosin and tadalafil were combined, the maximalrelaxation to norepinephrine on carbachol-precontracted detrusor strips was signifi-cantly increased compared with tadalafil alone, and EFS-induced detrusor contractions
were better inhibited compared with each compound alone. Tadalafil significantlyinhibited norepinephrine-induced prostatic strip contractions by reducing the maximaleffect, whereas alfuzosin shifted the CRC of norepinephrine to the right. Combining bothtadalafil and alfuzosin resulted in a greater relaxant effect. Likewise, the combination
was more effective at reducing EFS-induced contractions compared with each com-pound alone.Conclusions: The combination of alfuzosin and tadalafil exerts an additive effect of
inhibiting adrenergic smooth muscle tone of prostatic tissue and EFS-induced detrusorcontractions and conversely, of enhancing adrenergic relaxation of detrusor precontractedwith carbachol. These experiments provide experimental support for the clinical inves-tigation of the combination of a1-blockers and PDE5 inhibitors in the treatment of LUTS.
# 2009 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. AP-HP, Neuro-Uro-Andrology, Department of Physical Medicine and Reha-bilitation, Raymond Poincare Hospital, 104 bd Raymond Poincare, 92380 Garches, France.Tel. +33147107748; Fax: +33147104443.E-mail address: [email protected] (F. Giuliano).
0302-2838/$ – see back matter # 2009 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2009.04.039
Author's personal copy
1. Introduction
Lower urinary tract symptoms (LUTS) increase with
advancing age [1]. LUTS comprise storage symptoms, often
related to detrusor overactivity, and voiding symptoms. The
latter could result either from bladder outlet obstruction as
a result of benign prostatic enlargement resulting from the
histologic condition of benign prostatic hyperplasia (BPH)
or from impaired detrusor contractility.
Alpha-adrenoceptor antagonists are considered to be the
most effective monotherapy for LUTS suggestive of BPH [2].
They improve both voiding and storage symptoms of BPH
and are characterized by a rapid onset of action [3]. All
a1-adrenoceptor antagonists are considered to have a
comparable efficacy in LUTS. Nevertheless, alfuzosin offers
the advantages of good cardiovascular tolerability, even in
elderly and hypertensive patients, and less deleterious effect
on sexual function [4].
Phosphodiesterase type 5 (PDE5) inhibitors are the first-
line treatment of erectile dysfunction (ED) [5]. Moreover,
randomized placebo-controlled trials have shown that the
three available PDE5 inhibitors (ie, sildenafil, vardenafil, or
tadalafil), also improve voiding and storage LUTS in patients
with BPH [6–9]. A recent pilot study has also shown that a
single vardenafil administration (20 mg) can improve
urodynamic parameters in men with spinal cord injuries
[10].
LUTS and ED are strongly linked independent of age and
cardiovascular comorbidities, as shown in several epide-
miologic studies [11,12]. Thus, coprescription of a-adreno-
ceptor antagonists and PDE5 inhibitors is likely to increase.
The concept is currently emerging that treatment with a
combination of an a1-adrenoceptor antagonist and a PDE5
inhibitor is the most effective therapy to treat LUTS related
to BPH. Specific precautions, however, should be taken
regarding the concomitant use of these two therapeutic
classes due to their potential additive hypotensive effects.
Interestingly, alfuzosin (10 mg once daily [OD]) shows no
relevant hemodynamic interaction with tadalafil at the
highest prescribed dose (20 mg OD) [13]. Moreover, very
recent reports of combination of a-adrenoceptor antagonists
and PDE5 inhibitors have each reported no symptomatic
hemodynamic effects [14,15]. Finally, a pilot clinical study
has shown that combining sildenafil 25 mg OD with alfuzosin
10 mg OD was superior to each therapy alone (same dosages)
in relieving LUTS and ED in BPH patients [16].
The mechanism of action responsible for the greater
benefit of the combination in LUTS is not yet fully
understood and should be explored. Increasing recent data
indicate that the benefit observed from the combination in
clinical practice on LUTS could be due to an effect of both
drugs, not only on the prostate but also on the smooth
muscle of the bladder [17–19]. Thus, our goal was to
evaluate in vitro whether the combination of alfuzosin and
tadalafil was more effective than each compound alone in
inhibiting pharmacologically induced or electrical field
stimulation (EFS)–induced contractions of human prostatic
smooth muscle and/or in enhancing pharmacologically
induced relaxation of human bladder smooth muscle.
2. Materials and methods
2.1. Preparation of human prostatic strips and detrusor
strips
Prostatic samples (from the transition zone) and bladder samples (from
the dome) were obtained from 20 patients (age: 69 � 3 yr) and from 17
patients (age: 67 � 2.5 yr), respectively, undergoing cystoprostatectomy for
infiltrating bladder cancer. The subjects had no history of bladder
dysfunction according to their medical charts and had not received
radiotherapy. All patients provided their informed consent.
Tissue samples were stored at 4 8C in Krebs-HEPES buffer (118 mM
sodium chloride, 4.7 mM potassium chloride (KCl), 1.2 mM magnesium
sulfate, 1.2 mM potassium dihydrogen phosphate, 2.5 mM calcium
chloride, 4.2 mM sodium bicarbonate, 11.1 mM glucose, and 20.8 mM
HEPES; pH: 7.4) containing penicillin (100 IU/ml) and streptomycin
(0.1 mg/ml) for optimal conservation until use (within 24 h maximum).
Samples were cleaned of adherent tissue and blood, and sections
(4 � 2 � 2 mm) were excised from each donor sample for each
experiment.
Strips were suspended in 5-ml organ chambers filled with Krebs-
HEPES buffer (37 8C, pH: 7.4) that was continuously bubbled with 95% O2
and 5% CO2. They were connected to force transducers for isometric
tension recording (Pioden Controls Ltd, UK) and an initial tension was
applied (0.5–1 g). Following amplification, the tension changes were
computerized with Mac Lab/8 using Chart 5 software (ADInstruments
Ltd, Oxfordshire, UK). The tissue preparations were allowed to
equilibrate for 60 min while being washed periodically with fresh
Krebs-HEPES buffer, and they were primed by KCl (100 mM, 10 min).
2.2. In vitro contractile experiments with prostatic strips
Concentration-response curves (CRCs) to norepinephrine (10�8 M to
10�4 M) were constructed on each strip. Then, after washings, and
following a 20-min incubation period with either vehicle (corresponding
to the high dose combination), tadalafil (10�6 M or 10�5 M), alfuzosin
(3 � 10�8 M), or two combinations of both compounds (10�6 M tadalafil
plus 3 � 10�8 M alfuzosin or 10�5 M tadalafil plus 3 � 10�8 M alfuzosin),
CRCs to norepinephrine were repeated.
In another set of experiments, frequency response curves (FRCs) (at
5 Hz, 10 Hz, 15 Hz, 20 Hz, 30 Hz, and 40 Hz; 5-ms pulse duration, 5-s
train duration; 300 mA) were constructed. After washings, and following
a 20-min incubation period with the same conditions as for norepi-
nephrine CRCs, FRCs were repeated.
The concentrations used for alfuzosin were in the same range as its
pKi determined for the a1-adrenoceptor in human prostate [20].
The concentrations used for tadalafil were previously reported to be
efficient concentrations in prostatic tissue [21] and were used to
evaluate whether the combination could improve the efficacy of each
compound.
2.3. In vitro contractile experiments with detrusor strips
Strips were incubated for a 20-min period with alfuzosin alone (at 10�6
and 10�5 M), tadalafil alone (at 10�6 M and 10�5 M), or both compounds
combined at two different concentrations (10�6 M tadalafil plus 10�6 M
alfuzosin or 10�5 M tadalafil plus 10�5 M alfuzosin) and vehicle
(corresponding to the dosage combination). Strips were then precon-
tracted with carbachol (10�6 M) and allowed to reequilibrate until a
stable response was obtained (20 min), and then CRCs for norepinephr-
ine (10�9 M to 3 � 10�5 M) were performed.
In a second set of experiments, the detrusor strips were submitted to
EFS (20 Hz; 5-ms pulse duration, 5-s train duration; 300 mA) applied by
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7700
Author's personal copy
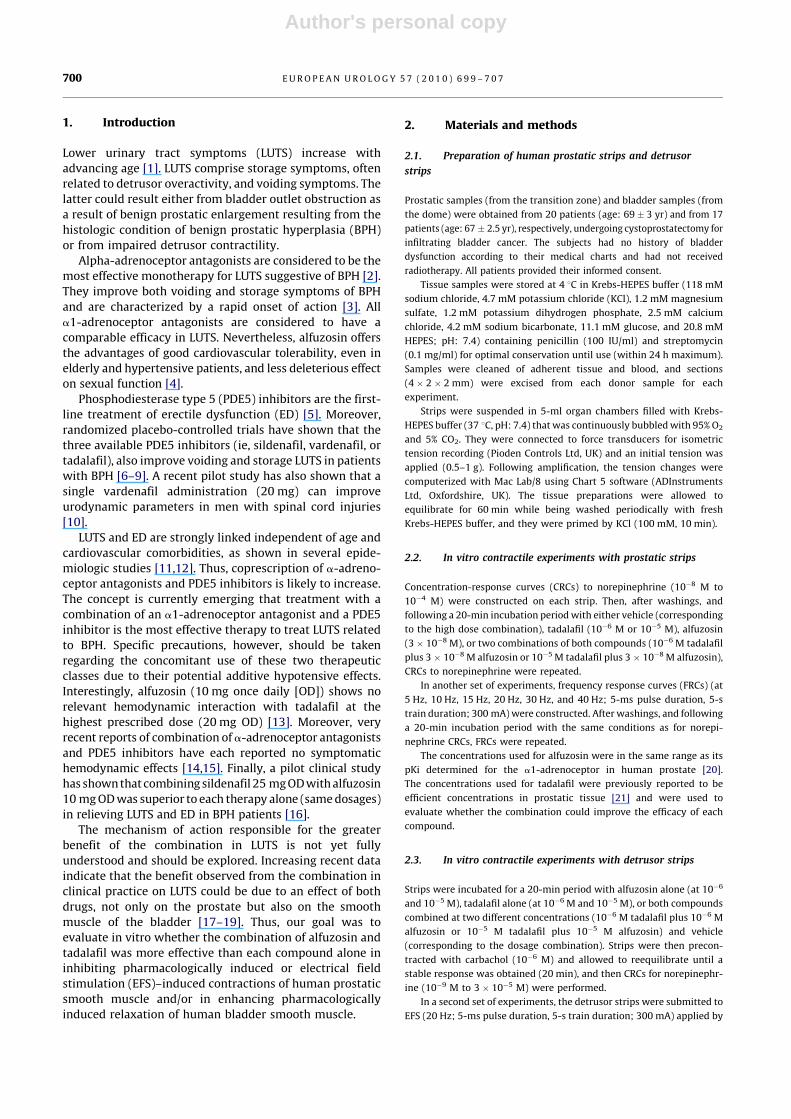
Table 1 – Maximal effect (Emax) and pD2� values of norepinephrine-induced contractions of human prostatic strips in presence of tadalafil,
alfuzosin, or a combination of both
Pretreatment pD2 Emax, %
Vehicle (n = 9) 5.6 � 0.1 65.4 � 3.0
Tadalafil 10�6 M (n = 7) 5.5 � 0.1 64.6 � 3.3
Tadalafil 10�5 M (n = 8) 5.7 � 0.2 48.4 � 4.6y
Alfuzosin 3.10�8 M (n = 7) 5.1 � 0.1yy 79.2 � 5.1y
Tadalafil 10�6 M plus alfuzosin 3.10�8 M (n = 5) 5.2 � 0.1yy,§ 68.9 � 4.4
Tadalafil 10�5 M plus alfuzosin 3.10�8 M (n = 7) 5.0 � 0.1yy,**,## 68.3 � 3.1*
� pD2 value is the negative log concentration of compound that produces 50% reduction of the maximal response. Data are the mean plus or minus standard
error of the mean of (n) experiments using prostate samples from (n) patients.y p < 0.05.yy p < 0.001 versus vehicle.§ p < 0.05 versus tadalafil 10�6.* p < 0.05.** p < 0.01 versus tadalafil 10�5M.## p < 0.01 versus tadalafil 10�6M plus alfuzosin 10�6 M.
Fig. 1 – Effect of combinations of tadalafil and alfuzosin on norepinephrine-induced contractions of human prostatic tissue. Concentration-responsecurves (CRCs) to norepinephrine were performed on human prostatic strips in presence of vehicle (n = 9) or of (A) tadalafil at 10S6 M (n = 7) or alfuzosin at3 T 10S8 M (n = 7) or a combination of both (n = 5), (B) tadalafil at 10S5 M (n = 8) or alfuzosin at 3 T 10S8 M (n = 7) or a combination of both (n = 7), or (C)combination of tadalafil 10S6 M plus alfuzosin 3 T 10S8 M (n = 5) or tadalafil 10S5 M plus alfuzosin 3 T 10S8 M (n = 7). Data are the mean plus or minusstandard error of the mean of (n) experiments using prostate samples from (n) patients.* p < 0.05.** p < 0.01, two-way analysis of variance (ANOVA) followed by Bonferroni post tests, d p < 0.05.### p < 0.001, two-way ANOVA followed by a modified student t test with the Bonferroni adjustment for multiple comparisons because of interaction inthe two-way ANOVA analysis, §p < 0.05.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7 701
Author's personal copy
groups of three stimulations at 1-min intervals and followed by a 3-min
period of rest. After 20 min of equilibration to obtain stable twitch
contractions, strips were incubated with vehicle or alfuzosin (20 min at
10�6 M and at 10�5 M). CRCs for tadalafil (10�7 M to 10�5 M) or vehicle in
log increments were then performed every 18 min.
The concentrations used for alfuzosin were higher than the one used
in experiments with prostate tissue because a-adrenoceptors play a
lesser role in human bladder contraction [20].
2.4. Data analysis
For experiments on detrusor strips using norepinephrine, results were
expressed as a percentage of inhibition of the contractile response to
carbachol. For experiments using EFS on detrusor tissue, results were
expressed in percentage of the initial contractile response before
addition of tadalafil or vehicle.
For experiments on prostatic strips, results were expressed as a
percentage of maximal contraction obtained during the first CRCs to
norepinephrine or the first FRCs. For each CRC for norepinephrine, a pD2
value (negative log concentration of compound that produces 50%
reduction of the maximal response) and a maximal effect were
determined in each experimental condition using the four-parameter
logistic model. Statistical comparisons were performed according to the
extra sum of squares F-test principle with GraphPad Prism 4.03 software
(GraphPad Software, La Jolla, CA, USA). The data were expressed as mean
plus or minus standard error of the mean of the number (n) of
experiments performed with different bladder or prostatic human
samples. Statistical comparisons of norepinephrine CRCs and EFS
experiments were performed with a two-way analysis of variance
(ANOVA) followed by Bonferroni posttest. In case of interaction between
the two factors (concentration and drug) in the two-way ANOVA, a
modified student t test with the Bonferroni adjustment for multiple
comparisons was performed.
2.5. Drugs and chemicals
All drugs and chemicals were purchased from Sigma (St. Louis, MO, USA)
except tadalafil and alfuzosin, which were provided by Sanofi-Aventis
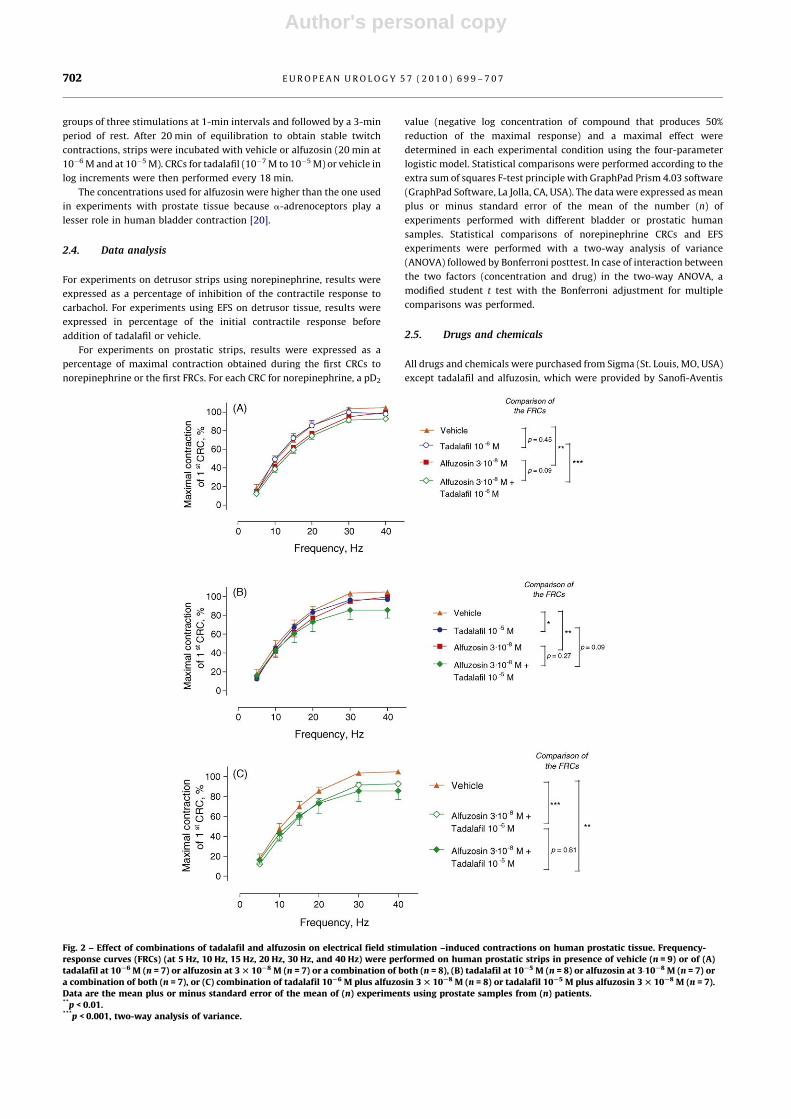
Fig. 2 – Effect of combinations of tadalafil and alfuzosin on electrical field stimulation –induced contractions on human prostatic tissue. Frequency-response curves (FRCs) (at 5 Hz, 10 Hz, 15 Hz, 20 Hz, 30 Hz, and 40 Hz) were performed on human prostatic strips in presence of vehicle (n = 9) or of (A)tadalafil at 10S6 M (n = 7) or alfuzosin at 3 T 10S8 M (n = 7) or a combination of both (n = 8), (B) tadalafil at 10S5 M (n = 8) or alfuzosin at 3�10S8 M (n = 7) ora combination of both (n = 7), or (C) combination of tadalafil 10S6 M plus alfuzosin 3 T 10S8 M (n = 8) or tadalafil 10S5 M plus alfuzosin 3 T 10S8 M (n = 7).Data are the mean plus or minus standard error of the mean of (n) experiments using prostate samples from (n) patients.**p < 0.01.***p < 0.001, two-way analysis of variance.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7702

Author's personal copy
(Paris, France). Tadalafil was prepared in dimethyl sulfoxide (DMSO).
Final concentrations of DMSO in the organ bath were 0.033 and 0.1% for
concentrations of 10�6 M and 10�5 M, respectively. Norepinephrine was
prepared in 0.1% ascorbic acid to avoid oxidation. Other drugs were
prepared in distilled water.
3. Results
3.1. Effect of tadalafil, alfuzosin, or a combination of both on
norepinephrine-induced contractions of human prostatic strips
In the presence of tadalafil 10�5 M, the maximal response to
norepinephrine was significantly decreased, whereas the
presence of tadalafil 10�6 M had no effect (Table 1).
Alfuzosin (at 3 � 10�8 M) significantly antagonized
norepinephrine-induced contractions of prostatic strips by
shifting the curve to the right by 3.2-fold (Table 1). The
combination of tadalafil (10�6 M) and alfuzosin (3� 10�8 M)
seemed to exert a greater inhibitory effect on norepine-
phrine-induced contractions compared with tadalafil 10�6 M
alone, although this comparison was not significant (Fig. 1A).
This combination did not further enhance the inhibitory
effect exerted by alfuzosin 3 � 10�8 M alone. The in-
hibitory effect on norepinephrine-induced contractions of
both compounds combined at high concentrations was
significantly greater than alfuzosin 3 � 10�8 M alone and
was also close to significantly greater than tadalafil alone
(Fig. 1B). The high-dose combination significantly dis-
placed further to the right, by 5-fold, the CRC for
norepinephrine obtained with tadalafil 10�5 M alone
(Table 1). Moreover, the maximal effect of norepinephrine
was lower with the high-dose combination compared with
alfuzosin 3 � 10�8 M alone, although the difference was
not significant (Table 1).
Combination of tadalafil and alfuzosin at high doses on
norepinephrine-induced contraction had greater relaxant
effects than the combination at the lower doses (Fig. 1C).
3.2. Effect of tadalafil, alfuzosin, or a combination of both on
electrical field stimulation–induced contractions of human
prostatic strips
Tadalafil (10�5 M) and alfuzosin (3� 10�8 M) significantly
inhibit EFS-induced prostatic-strip contractions (Fig. 2).
The combination of tadalafil (10�6 M) and alfuzosin
(3� 10�8 M) exerted a greater inhibitory effect on
EFS-induced contractions compared with tadalafil alone
but not with alfuzosin alone. The combination with tadalafil
at 10�5 M and alfuzosin at 3 � 10�8 M tended to exert a
greater inhibitory effect than each compound alone, although
these effects were not significantly different.
3.3. Effect of tadalafil, alfuzosin, or a combination of both
drugs on the relaxation induced by norepinephrine on
carbachol-precontracted human detrusor strips
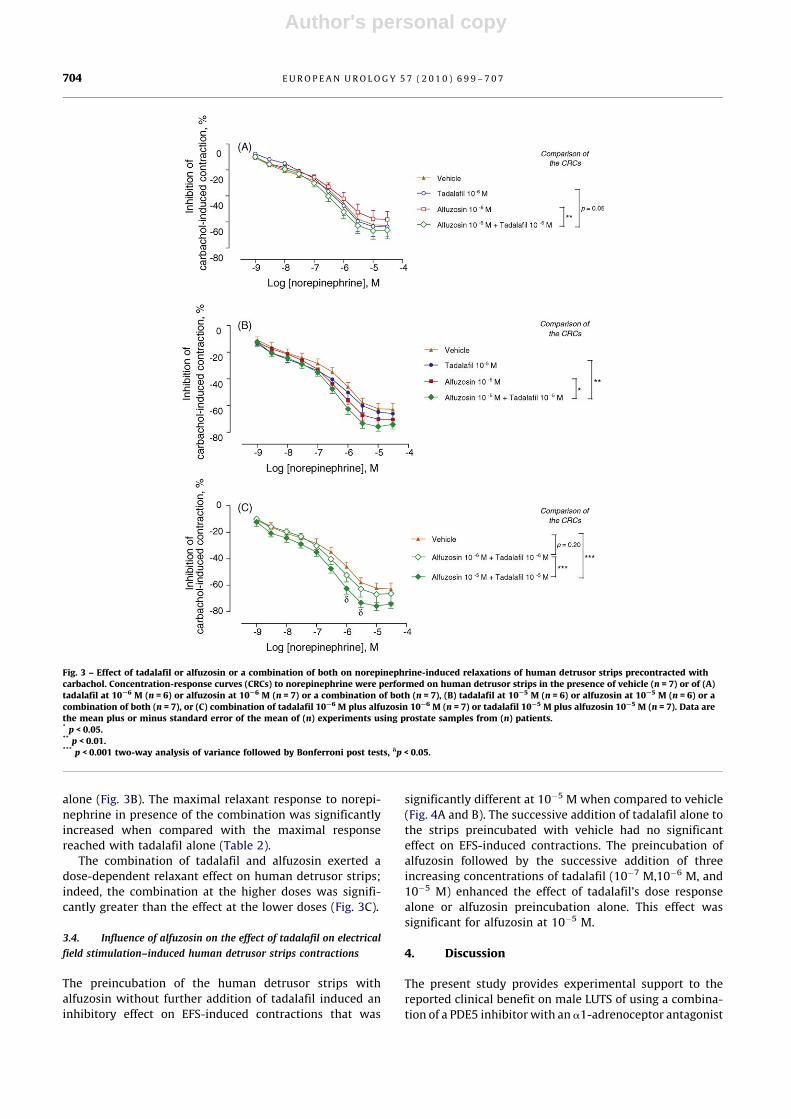
In presence of vehicle, norepinephrine induced a concen-
tration-dependent relaxation of carbachol-induced con-
traction of bladder strips when compared to the cumulative
addition of vehicle ( p < 0.0001; data not shown).
The presence of tadalafil (at both 10�6 M and 10�5 M) or
alfuzosin (10�6 M) in the organ bath did not modify the
relaxant effect of norepinephrine. Conversely, alfuzosin
(10�5 M) significantly enhanced the maximal relaxant
response of norepinephrine (Table 2).
In presence of the combination of tadalafil 10�6 M and
alfuzosin 10�6 M, norepinephrine exerted a greater
significant relaxant effect versus alfuzosin 10�6 M and
close to significantly greater effect versus tadalafil 10�6 M
alone (Fig. 3A). The maximal relaxant response of norepi-
nephrine when both drugs were combined was significantly
increased compared with alfuzosin alone (Table 2).
At higher concentrations (10�5 M), the combination of
tadalafil and alfuzosin further enhanced the relaxant effect
of norepinephrine when compared to tadalafil and alfuzosin
Table 2 – Maximal effect (Emax) and pD2� values of norepinephrine-induced relaxation of human detrusor strips precontracted with
carbachol in presence of tadalafil, alfuzosin, or a combination of both
Pretreatment pD2 Emax, %
Vehicle (n = 7) 6.3 � 0.1 �63.3 � 2.5
Tadalafil 10�6 M (n = 6) 6.4 � 0.1 �63.8 � 3.4
Tadalafil 10�5 M (n = 6) 6.5 � 0.1 �65.1 � 2.4
Alfuzosin 10�6 M (n = 7) 6.3 � 0.1 �58.2 � 2.7
Alfuzosin 10�5 M (n = 6) 6.5 � 0.1 �70.6 � 2.0y, *
Tadalafil 10�6 M plus alfuzosin 10�6 M (n = 7) 6.5 � 0.1 �66.8 � 2.8§
Tadalafil 10�5 M plus alfuzosin 10�5 M (n = 7) 6.5 � 0.1 �75.9 � 2.2yy,**,#
� pD2 value is the negative log concentration of compound that produces 50% reduction of the maximal response. Data are the mean plus or minus standard
error of the mean of (n) experiments using prostate samples from (n) patients.y p < 0.05.yy p < 0.001 versus vehicle.§ p < 0.05 versus alfuzosin 10�6 M.* p < 0.05.** p < 0.01 versus tadalafil 10�5 M.# p < 0.05 versus tadalafil 10�6 M plus alfuzosin 10�6 M.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7 703
Author's personal copy
alone (Fig. 3B). The maximal relaxant response to norepi-
nephrine in presence of the combination was significantly
increased when compared with the maximal response
reached with tadalafil alone (Table 2).
The combination of tadalafil and alfuzosin exerted a
dose-dependent relaxant effect on human detrusor strips;
indeed, the combination at the higher doses was signifi-
cantly greater than the effect at the lower doses (Fig. 3C).
3.4. Influence of alfuzosin on the effect of tadalafil on electrical
field stimulation–induced human detrusor strips contractions
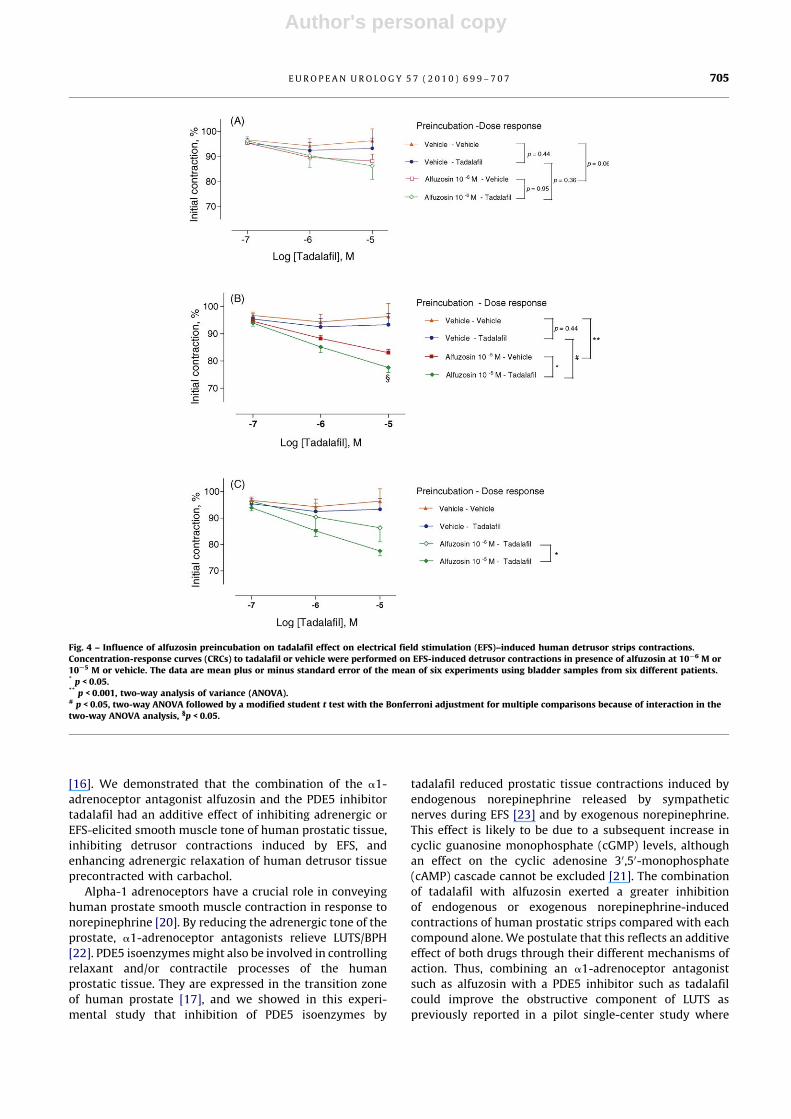
The preincubation of the human detrusor strips with
alfuzosin without further addition of tadalafil induced an
inhibitory effect on EFS-induced contractions that was
significantly different at 10�5 M when compared to vehicle
(Fig. 4A and B). The successive addition of tadalafil alone to
the strips preincubated with vehicle had no significant
effect on EFS-induced contractions. The preincubation of
alfuzosin followed by the successive addition of three
increasing concentrations of tadalafil (10�7 M,10�6 M, and
10�5 M) enhanced the effect of tadalafil’s dose response
alone or alfuzosin preincubation alone. This effect was
significant for alfuzosin at 10�5 M.
4. Discussion
The present study provides experimental support to the
reported clinical benefit on male LUTS of using a combina-
tion of a PDE5 inhibitor with an a1-adrenoceptor antagonist
Fig. 3 – Effect of tadalafil or alfuzosin or a combination of both on norepinephrine-induced relaxations of human detrusor strips precontracted withcarbachol. Concentration-response curves (CRCs) to norepinephrine were performed on human detrusor strips in the presence of vehicle (n = 7) or of (A)tadalafil at 10S6 M (n = 6) or alfuzosin at 10S6 M (n = 7) or a combination of both (n = 7), (B) tadalafil at 10S5 M (n = 6) or alfuzosin at 10S5 M (n = 6) or acombination of both (n = 7), or (C) combination of tadalafil 10S6 M plus alfuzosin 10S6 M (n = 7) or tadalafil 10S5 M plus alfuzosin 10S5 M (n = 7). Data arethe mean plus or minus standard error of the mean of (n) experiments using prostate samples from (n) patients.* p < 0.05.** p < 0.01.*** p < 0.001 two-way analysis of variance followed by Bonferroni post tests, dp < 0.05.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7704
Author's personal copy
[16]. We demonstrated that the combination of the a1-
adrenoceptor antagonist alfuzosin and the PDE5 inhibitor
tadalafil had an additive effect of inhibiting adrenergic or
EFS-elicited smooth muscle tone of human prostatic tissue,
inhibiting detrusor contractions induced by EFS, and
enhancing adrenergic relaxation of human detrusor tissue
precontracted with carbachol.
Alpha-1 adrenoceptors have a crucial role in conveying
human prostate smooth muscle contraction in response to
norepinephrine [20]. By reducing the adrenergic tone of the
prostate, a1-adrenoceptor antagonists relieve LUTS/BPH
[22]. PDE5 isoenzymes might also be involved in controlling
relaxant and/or contractile processes of the human
prostatic tissue. They are expressed in the transition zone
of human prostate [17], and we showed in this experi-
mental study that inhibition of PDE5 isoenzymes by
tadalafil reduced prostatic tissue contractions induced by
endogenous norepinephrine released by sympathetic
nerves during EFS [23] and by exogenous norepinephrine.
This effect is likely to be due to a subsequent increase in
cyclic guanosine monophosphate (cGMP) levels, although
an effect on the cyclic adenosine 30,50-monophosphate
(cAMP) cascade cannot be excluded [21]. The combination
of tadalafil with alfuzosin exerted a greater inhibition
of endogenous or exogenous norepinephrine-induced
contractions of human prostatic strips compared with each
compound alone. We postulate that this reflects an additive
effect of both drugs through their different mechanisms of
action. Thus, combining an a1-adrenoceptor antagonist
such as alfuzosin with a PDE5 inhibitor such as tadalafil
could improve the obstructive component of LUTS as
previously reported in a pilot single-center study where
Fig. 4 – Influence of alfuzosin preincubation on tadalafil effect on electrical field stimulation (EFS)–induced human detrusor strips contractions.Concentration-response curves (CRCs) to tadalafil or vehicle were performed on EFS-induced detrusor contractions in presence of alfuzosin at 10S6 M or10S5 M or vehicle. The data are mean plus or minus standard error of the mean of six experiments using bladder samples from six different patients.* p < 0.05.** p < 0.001, two-way analysis of variance (ANOVA).# p < 0.05, two-way ANOVA followed by a modified student t test with the Bonferroni adjustment for multiple comparisons because of interaction in thetwo-way ANOVA analysis, §p < 0.05.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7 705

Author's personal copy
the combination of alfuzosin 10 mg OD and sildenafil 25 mg
OD was superior to each compound taken in monotherapy
[16].
Although tadalafil was found to exert a relaxant effect in
vitro on human prostate strips, there was no effect of
tadalafil (5 mg, then 20 mg daily) on maximum flow rate in
patients with LUTS and ED [7,9]. It should be noted that in
the population studied, maximum flow rate was initially
elevated and, consequently, was difficult to further
improve, which may explain the lack of improvement
with tadalafil. Alternatively, the sites of action of
tadalafil in patients with LUTS could be extraprostatic.
Detrusor represents a potential site of action for tadalafil on
LUTS because PDE5 isoenzymes are expressed in human
detrusor [24] and a functional role of PDE5 isoenzymes in
rat bladder tissue has been described in vitro [18]. In our
experiments, however, tadalafil alone failed either to
enhance norepinephrine-induced relaxation of precon-
tracted human detrusor or to inhibit EFS-induced detrusor
contractions.
The concentrations of tadalafil used on both detrusor and
prostatic tissues were rather high; consequently, this raises
questions about whether the in vitro effects observed in the
present study are clinically relevant. Tadalafil was also
required at high concentrations to achieve relaxation of
human cavernosal strips [25], although its clinical benefit
on ED is clearly demonstrated. This highlights the difficulty
in determining the clinical relevance of the concentrations
used in in vitro experiments.
The combination of alfuzosin with tadalafil enhanced
norepinephrine-induced relaxation when compared with
each compound alone, suggesting that alfuzosin amplified
the relaxant effect of tadalafil which could not be identified
when it was used alone. This amplifying effect could be a
consequence of several modifications in signaling pathways.
First, in human detrusor, b-adrenoceptors predominate over
a-adrenoceptors; thus, the response to norepinephrine,
which does not discriminate between a-adrenoceptors and
b-adrenoceptors, is relaxation. Although a-adrenoceptors
are only weakly involved in human detrusor contraction,
high concentrations of a1-adrenoceptor agonists never-
theless evoke detrusor contractions [26,27]. By blocking the
signaling pathway mediating contraction induced by
norepinephrine, alfuzosin might even favor the cAMP-
dependent signaling pathway involved in the relaxation
mediated via b-adrenoceptors [28]. Consequently, alfuzosin
alone might enhance norepinephrine-induced relaxation of
human detrusor as shown in the present study. If the cAMP-
dependent signaling pathway is favored in the presence of
alfuzosin during norepinephrine-induced detrusor relaxa-
tion, this could increase cGMP levels initially stimulated by
tadalafil but that had remained, until then, functionally
silent. Such positive cross-talk mechanisms between cGMP
and cAMP signaling, previously described in other systems
[29], could be the origin of the enhanced relaxant effect of the
combination.
In parallel, the combination of alfuzosin and tadalafil
exerted a greater inhibitory effect on EFS-induced contrac-
tions compared with each compound alone. This benefit is
probably due to additive effects of both drugs. Indeed,
a1-adrenoceptors are expressed on cholinergic nerve term-
inals present in the bladder wall and facilitate acetylcholine
release to yield detrusor contraction [30]. Alfuzosin could
thus reduce acetylcholine release induced by EFS and
responsible for detrusor contractions, thereby indirectly
decreasing detrusor contractile tone and facilitating
tadalafil’s inhibitory effect.
5. Conclusions
The combination of alfuzosin and tadalafil has previously
been shown to exert an additive relaxant effect of human
corpus cavernosum [25], supporting the potential benefit of
such combination in ED patients not responding to PDE5
inhibitors as reported in pilot clinical studies [16,31,32].
These new experimental data suggest that the combination
of alfuzosin and tadalafil also shows an additive relaxant
effect on human prostate and detrusor tissue. This finding
suggests that the combination of alfuzosin and tadalafil
could be more effective than monotherapy in relieving LUTS
associated with BPH. Because LUTS and ED are strongly
linked, these results strengthen the concept that a
combination of a PDE5 inhibitor with an a1-adrenoceptor
antagonist might represent a promising pharmacologic
strategy to treat LUTS associated with BPH and ED. The
value of such a combination deserves further investigation
in placebo-controlled trials.
Author contributions: Francois Giuliano had full access to all the data in the
study and takes responsibility for the integrity of the data and the accuracy
of the data analysis.
Study concept and design: Oger, Behr-Roussel, Giuliano.
Acquisition of data: Gorny, Lebret, Denoux.
Analysis and interpretation of data: Gorny, Oger, Behr-Roussel.
Drafting of the manuscript: Oger, Behr-Roussel.
Critical revision of the manuscript for important intellectual content: Behr-
Roussel, Giuliano.
Statistical analysis: Gorny, Oger.
Obtaining funding: Alexandre, Giuliano.
Administrative, technical, or material support: Alexandre, Giuliano.
Supervision: Behr-Roussel, Giuliano.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest, including specific
financial interests and relationships and affiliations relevant to the subject
matter or materials discussed in the manuscript (eg, employment/affilia-
tion, grants or funding, consultancies, honoraria, stock ownership or
options, expert testimony, royalties, or patents filed, received, or pending),
are the following: None.
Funding/Support and role of the sponsor: This work was supported by
Sanofi-Aventis in the form of a restricted grant. Sanofi-Aventis approved
of the manuscript.
References
[1] Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human
benign prostatic hyperplasia with age. J Urol 1984;132:474–9.
[2] AUA guideline on management of benign prostatic hyperplasia
(2003). Diagnosis and treatment recommendations. J Urol 2003;
170:530–47.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7706

Author's personal copy
[3] Schwinn DA, Roehrborn CG. Alpha1-adrenoceptor subtypes and
lower urinary tract symptoms. Int J Urol 2008;15:193–9.
[4] Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the
treatment of lower urinary tract symptoms and clinical benign
prostatic hyperplasia: a randomized, placebo-controlled trial.
Urology 2001;58:953–9.
[5] Lue TF, Giuliano F, Montorsi F, et al. Summary of the recommenda-
tions on sexual dysfunctions in men. J Sex Med 2004;1:6–23.
[6] McVary KT, Monnig W, Camps Jr JL, Young JM, Tseng LJ, van den EG.
Sildenafil citrate improves erectile function and urinary symptoms
in men with erectile dysfunction and lower urinary tract symptoms
associated with benign prostatic hyperplasia: a randomized,
double-blind trial. J Urol 2007;177:1071–7.
[7] McVary KT, Roehrborn CG, Kaminetsky JC, et al. Tadalafil relieves
lower urinary tract symptoms secondary to benign prostatic hyper-
plasia. J Urol 2007;177:1401–7.
[8] Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. A randomised,
placebo-controlled study to assess the efficacy of twice-daily
vardenafil in the treatment of lower urinary tract symptoms sec-
ondary to benign prostatic hyperplasia. Eur Urol 2008;53:1236–44.
[9] Roehrborn CG, McVary KT, Elion-Mboussa A, Viktrup L. Tadalafil
administered once daily for lower urinary tract symptoms second-
ary to benign prostatic hyperplasia: a dose finding study. J Urol
2008;180:1228–34.
[10] Gacci M, Del Popolo G, Macchiarella A, et al. Vardenafil improves
urodynamic parameters in men with spinal cord injury: results
from a single dose, pilot study. J Urol 2007;178:2040–3.
[11] Rosen R, Altwein J, Boyle P, et al. Lower urinary tract symptoms and
male sexual dysfunction: the multinational survey of the aging
male (MSAM-7). Eur Urol 2003;44:637–49.
[12] McVary KT. Erectile dysfunction and lower urinary tract symptoms
secondary to BPH. Eur Urol 2005;47:838–45.
[13] Giuliano F, Kaplan SA, Cabanis MJ, Astruc B. Hemodynamic
interaction study between the alpha1-blocker alfuzosin and the
phosphodiesterase-5 inhibitor tadalafil in middle-aged healthy
male subjects. Urology 2006;67:1199–204.
[14] Bechara A, Romano S, Casabe A, et al. Comparative efficacy assess-
ment of tamsulosin versus tamsulosin plus tadalafil in the treat-
ment of LUTS/BPH. J Sex Med 2008;5:2170–8.
[15] Ng CF, Wong A, Cheng CW, Chan ES, Wong HM, Hou SM. Effect of
vardenafil on blood pressure profile of patients with erectile
dysfunction concomitantly treated with doxazosin gastrointestinal
therapeutic system for benign prostatic hyperplasia. J Urol 2008;180:
1042–6.
[16] Kaplan SA, Gonzalez RR, Te AE. Combination of alfuzosin and silde-
nafil is superior to monotherapy in treating lower urinary tract
symptoms and erectile dysfunction. Eur Urol 2007;51:1717–23.
[17] Uckert S, Oelke M, Stief CG, Andersson K-E, Jonas U, Hedlund P.
Immunohistochemical distribution of cAMP- and cGMP-phospho-
diesterase (PDE) isoenzymes in the human prostate. Eur Urol
2006;49:740–5.
[18] Tinel H, Stelte-Ludwig B, Hutter J, Sandner P. Pre-clinical evidence
for the use of phosphodiesterase-5 inhibitors for treating benign
prostatic hyperplasia and lower urinary tract symptoms. BJU Int
2006;98:1259–63.
[19] Filippi S, Morelli A, Sandner P, et al. Characterization and functional
role of androgen-dependent PDE5 activity in the bladder. Endocri-
nology 2007;148:1019–29.
[20] Michel MC, Vrydag W. Alpha1-, alpha2- and beta-adrenoceptors in
the urinary bladder, urethra and prostate. Br J Pharmacol
2006;147(Suppl 2):S88–119.
[21] Uckert S, Sormes M, Kedia G, et al. Effects of phosphodiesterase
inhibitors on tension induced by norepinephrine and accumulation
of cyclic nucleotides in isolated human prostatic tissue. Urology
2008;71:526–30.
[22] Jardin A, Andersson KE, Chapple C, et al. Alpha1-adrenoceptor
antagonist in the treatment of benign of prostatic hyperplasia.
In: Chatelain C, Denis L, Foo KT, Khoury S, Connell JM, editors.
5th International Consultation on Benign Prostatic Hyperplasia
(2000). Plymouth, UK: Health Publication Ltd; 2001. p. 459–77.
[23] Hieble JP, Ruffolo Jr RR. The use of alpha-adrenoceptor antagonists
in the pharmacological management of benign prostatic hypertro-
phy: an overview. Pharmacol Res 1996;33:145–60.
[24] Truss MC, Uckert S, Stief CG, Kuczyk M, Jonas U. Cyclic nucleotide
phosphodiesterase (PDE) isoenzymes in the human detrusor
smooth muscle. I. Identification and characterization. Urol Res
1996;24:123–8.
[25] Oger S, Behr-Roussel D, Gorny D, et al. Combination of alfuzosin and
tadalafil exerts in vitro an additive relaxant effect on human corpus
cavernosum. J Sex Med 2008;5:935–45.
[26] Nomiya M, Yamaguchi O. A quantitative analysis of mRNA expres-
sion of alpha1- and beta-adrenoceptor subtypes and their func-
tional roles in human normal and obstructed bladders. J Urol
2003;170:649–53.
[27] Bouchelouche K, Andersen L, Alvarez S, Nordling J, Bouchelouche P.
Increased contractile response to phenylephrine in detrusor of
patients with bladder outlet obstruction: effect of the alpha1A-
and alpha1D-adrenergic receptor antagonist tamsulosin. J Urol
2005;173:657–61.
[28] Uchida H, Shishido K, Nomiya M, Yamaguchi O. Involvement of cyclic
AMP-dependent and -independent mechanisms in the relaxation of
rat detrusor muscle via beta-adrenoceptors. Eur J Pharmacol
2005;518:195–202.
[29] Pelligrino DA, Wang Q. Cyclic nucleotide crosstalk and the regula-
tion of cerebral vasodilation. Prog Neurobiol 1998;56:1–18.
[30] Somogyi GT, Tanowitz M, De Groat WC. Prejunctional facilitatory
alpha 1-adrenoceptors in the rat urinary bladder. Br J Pharmacol
1995;114:1710–6.
[31] Yassin A, Saad F, Hoesl CE, Traish AM, Hammadeh M, Shabsigh R.
Alpha-adrenoceptors are a common denominator in the pathophy-
siology of erectile function and BPH/LUTS—implications for clinical
practice. Andrologia 2006;38:1–12.
[32] De Rose AF, Giglio M, Traverso P, Lantieri P, Carmignani G. Com-
bined oral therapy with sildenafil and doxazosin for the treatment
of non-organic erectile dysfunction refractory to sildenafil mono-
therapy. Int J Impot Res 2002;14:50–3.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 6 9 9 – 7 0 7 707


















