
Biologic, histologic and densitometric effects of oral risedronate on bone in patients with multiple...
9
Pergamon Bone, Vol. 15, No. 1, pp. 41-49, 1994 Copyright 0 1994 Elsevier Science Ltd Printed in the USA. All rights reserved 8756-3282/94 $66.00 + .OO Biologic, Histologic and Densitometric Effects of Oral Risedronate on Bone in Patients with Multiple Myeloma C. ROUX,’ P. RAVAUD,’ M. COHEN-SOLAL,2 M. C. DE VERNEJOUL,2 S. GUILLEMANT,3 B. CHERRUAU,4 P. DELMAS,5 M. DOUGADOS’ and B. AMOR’ ’ Department of Rheumatology, Rent Descartes University, Paris, France ’ INSERM lJ349, Centre Viggo Petersen, France 3 Department of Biochemisrry, Pierre and Marie Curie University, Paris, France 4 Department of Biochemistry, RenC Descartes University, Paris, France ’ INSERM V 234, HGpital E. Herriot, Lyon, France Address for correspondence and reprints: C. Roux, M.D., Department of Rheumatology, Cochin Hospital, 27 me du Faubourg Saint Jacques, 75014 P-&is, France. Abstract Recent studies have shown that treatment with bisphospho- nates could be effective against the myelomatous skeletal de- terioration. However, the mechanisms of action of these drugs in multiple myeloma (MM) have been poorly studied. In the present study, 11 patients with MM and bone lesions were treated orally with 30 mg/day of risedronate for 6 months, and monitored for 6 additional months. Mean se- rum calcium decreased from day 4, with a concomitant in- crease in circulating levels of PTH (l-84) and ~,~Fv(OH)~D. These parameters reached their nadir on day 7 and returned to baseline value during the treatment period. Markers of bone resorption, pyridinoline and deoxypyridinoline de- creased from day 7; they were at 50% and 78% of their basal value at the end of treatment and follow-up periods, respec- tively. A signiicant reduction of estimates of bone formation (serum alkalbe phosphatase and osteocalcin) appeared at month 3 and persisted for the remainder of the 9-month period. Histomorphometric analysis showed a significant re- duction of activation frequency, number of osteoclasts and erosion depth. Bone turnover was high at baseline, and nor- mal after treatment, without mineralisation defects. Mean wall thickness was not diierent before and after treatment. Spinal bone mineral density measured by dual energy X-ray absorptiometry increased (5.3%) at the end of treatment. We conclude that oral risedronate in multiple myeloma induces a noticeable and rapid inhibition of bone resorption. Key Words: Risedronate-Bisphosphonates-Multiple my- eloma-Collagen cross-links-Histomorphometry-Densitometry. Introduction Bone lesions are frequent in multiple myeloma: two thirds of patients experience bone pain, and up to one third present with This work was presented in part at the Fourteenth Annual Meeting of the American Society for Bone and Mineral Research (September 30 to October 4, 1992, Min- neapolis, Minnesota) and Sixth International Congress on Bone Morphometry (Ck- tober 69, 1992, Lexington, Kenmcky). 41 hypercalcemia (Kyle 1975). These lesions are related to bone lysis and osteoporosis. Skeletal complications are major prob- lems in the management of patients, even in those responding to alkylating agents (Belch et al. 1991). Prevention of multiple myeloma-induced skeletal lesions may therefore decrease dis- ease morbidity. Bone lesions in multiple myeloma derive in part from in- creased bone resorption because of excess of osteoclastic activ- ity. Drugs known to increase bone mineral density, i.e., sodium fluoride alone or in combination with calcium, and androgenic steroids, were proven to be ineffective to aid in bone repair (Harley et al. 1972; Kyle et al. 1975; Cohen et al. 1984). Intra- nasal calcitonin, a pharmacological inhibitor of osteoclastic ac- tivity, improved some histomorphometric parameters 3 months after a short-term treatment in multiple myeloma (Rico et al. 1990). Several studies have described the efficacy of some bisphosphonates in inhibiting metastasis-induced bone resorption (Paterson et al. 1993), and in conecting malignant hypercalce- mia (Ralston et al. 1989). Myelomatous hypercalcemia has also been effectively treated with bisphosphonates (Paterson et al. 1983). Some studies (Siris et al. 1980; Delmas et al. 1982; Merlini et al. 1990; Lahtinen et al. 1992) reported effectiveness of clodronate in preventing the myelomatous skeletal deteriora- tion. However, a long-term, double-blind study with oral eti- dronate did not demonstrate a clinically significant impact in this indication (Belch et al. 1991). This may be explained by the low dose employed; on the other hand, the degree of activity of bisphosphonates varies greatly from compound to compound (Fleisch 1989), depending of their actual chemical configuration. Risedronate is a new bisphosphonate, designated as l- hydroxy-2-(3-pyridinyl) ethylidene bisphosphonic acid monoso- dium salt. In vitro and in vivo animal studies have demonstrated a selective antiosteoclastic activity of this compound. In an open study of pagetic patients, treatment with risedronate induced a dose-dependent decrease in the excess of serum alkaline phos- phatase (Kylstra et al. 1991). Although the histologic bone ef- fects of risedronate have been documented in animal studies, no human data are yet available. We conducted an explorative study of the antiosteoclastic activity of risedronate in multiple my- eloma, in order to know if beneficial effects could be expected in this disease. We report here the biologic, histologic and densi- tometric results of this l-year open study.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Biologic, histologic and densitometric effects of oral risedronate on bone in patients with multiple...

Pergamon
Bone, Vol. 15, No. 1, pp. 41-49, 1994 Copyright 0 1994 Elsevier Science Ltd Printed in the USA. All rights reserved
8756-3282/94 $66.00 + .OO
Biologic, Histologic and Densitometric Effects of Oral Risedronate on Bone in Patients with Multiple Myeloma C. ROUX,’ P. RAVAUD,’ M. COHEN-SOLAL,2 M. C. DE VERNEJOUL,2 S. GUILLEMANT,3 B. CHERRUAU,4 P. DELMAS,5 M. DOUGADOS’ and B. AMOR’
’ Department of Rheumatology, Rent Descartes University, Paris, France ’ INSERM lJ349, Centre Viggo Petersen, France 3 Department of Biochemisrry, Pierre and Marie Curie University, Paris, France 4 Department of Biochemistry, RenC Descartes University, Paris, France ’ INSERM V 234, HGpital E. Herriot, Lyon, France
Address for correspondence and reprints: C. Roux, M.D., Department of Rheumatology, Cochin Hospital, 27 me du Faubourg Saint Jacques, 75014 P-&is, France.
Abstract
Recent studies have shown that treatment with bisphospho- nates could be effective against the myelomatous skeletal de- terioration. However, the mechanisms of action of these drugs in multiple myeloma (MM) have been poorly studied. In the present study, 11 patients with MM and bone lesions were treated orally with 30 mg/day of risedronate for 6 months, and monitored for 6 additional months. Mean se- rum calcium decreased from day 4, with a concomitant in- crease in circulating levels of PTH (l-84) and ~,~Fv(OH)~D. These parameters reached their nadir on day 7 and returned to baseline value during the treatment period. Markers of bone resorption, pyridinoline and deoxypyridinoline de- creased from day 7; they were at 50% and 78% of their basal value at the end of treatment and follow-up periods, respec- tively. A signiicant reduction of estimates of bone formation (serum alkalbe phosphatase and osteocalcin) appeared at month 3 and persisted for the remainder of the 9-month period. Histomorphometric analysis showed a significant re- duction of activation frequency, number of osteoclasts and erosion depth. Bone turnover was high at baseline, and nor- mal after treatment, without mineralisation defects. Mean wall thickness was not diierent before and after treatment. Spinal bone mineral density measured by dual energy X-ray absorptiometry increased (5.3%) at the end of treatment. We conclude that oral risedronate in multiple myeloma induces a noticeable and rapid inhibition of bone resorption.
Key Words: Risedronate-Bisphosphonates-Multiple my- eloma-Collagen cross-links-Histomorphometry-Densitometry.
Introduction
Bone lesions are frequent in multiple myeloma: two thirds of patients experience bone pain, and up to one third present with
This work was presented in part at the Fourteenth Annual Meeting of the American Society for Bone and Mineral Research (September 30 to October 4, 1992, Min- neapolis, Minnesota) and Sixth International Congress on Bone Morphometry (Ck- tober 69, 1992, Lexington, Kenmcky).
41
hypercalcemia (Kyle 1975). These lesions are related to bone lysis and osteoporosis. Skeletal complications are major prob- lems in the management of patients, even in those responding to alkylating agents (Belch et al. 1991). Prevention of multiple myeloma-induced skeletal lesions may therefore decrease dis- ease morbidity.
Bone lesions in multiple myeloma derive in part from in- creased bone resorption because of excess of osteoclastic activ- ity. Drugs known to increase bone mineral density, i.e., sodium fluoride alone or in combination with calcium, and androgenic steroids, were proven to be ineffective to aid in bone repair (Harley et al. 1972; Kyle et al. 1975; Cohen et al. 1984). Intra- nasal calcitonin, a pharmacological inhibitor of osteoclastic ac- tivity, improved some histomorphometric parameters 3 months after a short-term treatment in multiple myeloma (Rico et al. 1990). Several studies have described the efficacy of some bisphosphonates in inhibiting metastasis-induced bone resorption (Paterson et al. 1993), and in conecting malignant hypercalce- mia (Ralston et al. 1989). Myelomatous hypercalcemia has also been effectively treated with bisphosphonates (Paterson et al. 1983). Some studies (Siris et al. 1980; Delmas et al. 1982; Merlini et al. 1990; Lahtinen et al. 1992) reported effectiveness of clodronate in preventing the myelomatous skeletal deteriora- tion. However, a long-term, double-blind study with oral eti- dronate did not demonstrate a clinically significant impact in this indication (Belch et al. 1991). This may be explained by the low dose employed; on the other hand, the degree of activity of bisphosphonates varies greatly from compound to compound (Fleisch 1989), depending of their actual chemical configuration.
Risedronate is a new bisphosphonate, designated as l- hydroxy-2-(3-pyridinyl) ethylidene bisphosphonic acid monoso- dium salt. In vitro and in vivo animal studies have demonstrated a selective antiosteoclastic activity of this compound. In an open study of pagetic patients, treatment with risedronate induced a dose-dependent decrease in the excess of serum alkaline phos- phatase (Kylstra et al. 1991). Although the histologic bone ef- fects of risedronate have been documented in animal studies, no human data are yet available. We conducted an explorative study of the antiosteoclastic activity of risedronate in multiple my- eloma, in order to know if beneficial effects could be expected in this disease. We report here the biologic, histologic and densi- tometric results of this l-year open study.

42 C. Roux et al.: Risedronate and multiple myeloma
Patients and Methods Clinical and radiologic assessment
Patients
Patients fulfilling the diagnostic criteria for multiple myeloma of the U.S. Southwest Oncology Group (SWOG) (Durie et al. 1977) were recruited for the study, at the Rheumatology Depart- ment of Cochin Hospital. Excluded from the study were patients with previous treatment with bisphosphonates, fluoride, calcito- nin, calcium or vitamin D. The disease could be in plateau or progression phase. Chronic renal failure was not an exclusion criteria.
Thirteen patients were included in the trial and 11 of them completed the study.
A 59-year-old man died during month 9 of study, in the immediate course of a high dose chemoradiotherapeutic regimen supported by autologous transplantation. During the study, the disease developed with ganglionic , cutaneous, muscular and he- matological complications, but without new skeletal lesions.
A 68-year-old man developed malignant hypercalcemia and a new osteolytic lesion of the ilium during the third month of risedronate treatment. The diagnosis of multiple myeloma was made 13 months before. He received six courses of chemother- apy with a good biological response. He was untreated for 3 months at the beginning of the study. A new course of che- motherapy was initiated because of hypercalcemia which was cured in 3 days. The patient died 2 months later of septic complications.
So, data on 11 patients are the basis of this report. There were 8 women and 3 men, aged 65.3 & 6.9 years (57-76). All the women were menopausal without hormonal replacement ther- apy. The myeloma protein was IgG-kappa in 5 patients, IgG- lambda in 3 patients, light chain kappa in 1 patient and non- secretory in 2 patients. All patients had normal kidney function, except one with chronic renal failure (serum creatinine at 160 pmol/l) for 4 years. At the beginning of the study, the disease was in plateau phase in 7 patients.
Before the onset of this trial, patients had been followed for multiple myeloma for an average of 21 months (3-77). They had received an average of 11 (2-26) course chemotherapy. None of them was previously untreated. Four patients received chemo- therapy regimens while also on risedronate treatment, on a 4-week interval basis: 3 patients received melphalan + cyclo- phosphamide + prednisone, and 1 patient received vincristine + cyclophosphamide + melphalan + prednisone. During the 6-month treatment period, the average cumulative dose of pred- nisone for these 4 patients was 1572 mg (360-2670).
Study design and drug administration
The study was an open-label single-site trial of 12 months du- ration approved by the Ethical Review Board of Cochin Hospital (Paris).
After confirming that the patient fulfilled the entry criteria defined above, and after written informed consent was obtained, the study drug was supplied. Patients received three capsules of the study drug, once daily, each capsule containing 10 mg of active drug. The administration was continuous for 6 months. After completion of 6-month treatment, patients were followed up for the next 6-month period. Patients were instructed to take the three capsules at bedtime, standing, with approximately 120 cc of water, and to have nothing to eat or drink 2 h before or 2 h following dosing. They were also instructed not to ingest within 2 h of absorbing risedronate any dairy products, or antacids.
A clinical assessment was made by the same investigator for each patient at each monthly visit; this included physical exam- ination, vital signs, height and weight. The patients were sys- tematically asked for presence of bone pain, and oral temperature was measured at each visit. The clinical evaluation was made before any chemotherapy course, during a daycase admission.
Skeletal X-rays including the thoracic and lumbar spine, long bones of both arms and legs and pelvis were realised within 90 days before the entry visit. A complete skeletal X-ray survey was not repeated. Standard X-rays were performed only in cases of acute bone pain.
General laboratory assessment
Laboratory assessment (according to standard methods) was made upon entry visit, twice during the first week (days 4 and 7). then twice monthly during the first 6 months, and thereafter monthly. It included the following evaluations: routine hemato- logical variables, Westergren sedimentation rate and liver and renal function tests. Serum electrophoresis of proteins, and uri- nalysis, including protein and red and white blood cells were evaluated monthly. P,-Microglobulin and serum immunoglobu- lin quantification was carried out upon entry visit, and at months 6, 9 and 12.
Laboratory assessment of bone metabolism
Laboratory assessment of bone metabolism was made upon entry visit, then twice during the first week, then monthly during the first 6 months and 3 and 6 months after the end of treatment. The determination of urinary excretion of pyridinium cross-links was made at the entry visit, on days 4 and 7 and on months 1, 3, 6, 9 and 12.
Blood and urine samples were taken after a 12-h overnight fast, before any chemotherapy course. The mine assessment was made on a 2-h fasting urine collection: the patients were in- structed to void and discard the first urine upon arising at 7 a.m. Thereafter, they were allowed to drink water but to remain fast- ing, and to collect all the urine for the next 2 h. The fasting sample avoids the need for low-gelatin diet. All urine samples were obtained by voluntary voiding.
Serum and urinary calcium, phosphate, serum and urinary creatinine, total alkaline phosphatases were measured using stan- dard laboratory methods. In the fasting 2-h urine sample, the calciumcreatinine ratio (Ca/Cr) and hydroxyproline/creatinine ratio (Hp/Cr) was determined. Tubular reabsorption of phosphate (TmP/GFR) was expressed as the estimated maximal tubular reabsorption divided by the glomerular filtration rate, according to Walton and Bijvoet (1975).
Aliquots of serum and plasma were frozen for subsequent determinations: plasma intact human PTH [PTH (l-84) normal range (lo-60 pg/ml], serum osteocalcin (normal range lo-45 ng/ml), serum 25-hydroxyvitamin D [25-(OH)D, normal range 5-30 ng/ml] and 1,25-dihydroxyvitamin D [ 1,25-(OH), D, nor- mal range 15-60 pg/ml]. The stored samples of each patient were assayed within the same batch. PTH (l-84) was measured by a commercially available immunoradiometric assay (Intact PTH, Nichols Institute, San Juan Capistrano, CA). Osteocalcin was measured by a solid-phase two-site immunoradiometric assay (ELSA-OSTEO, CIS Bio International, Gif-sur-Yvette, France) using human osteocalcin as a standard and two monoclonal an- tibodies raised against osteocalcin purified from human cortical bone, a solid phase anti 25-37 monoclonal antibody and a i2’I-

C. Roux et al.: Risedronate and multiple myeloma
labelled anti-513 monoclonal antibody (within-assay variation less than 4%, between-assay variation less than 6%) (Garner0 et al. 1992). Serum 25(0H)D concentrations were measured by a competitive protein binding assay after extraction and chromato- graphic purification; the coefficient of variation for this method was 9% for low and normal values (Guillemant et al. 1979). Serum 1,25-(OH), D was measured by a radioreceptor assay involving extraction and purification on C 180H cartridges; a calf thymus receptor specific for both 1,25-(OH), D, and 1,25-(OH), D, was used in a nonequilibrium competitive protein binding assay (Insctar, Stillwater, MN). Within- and between-assay vari- ation is less than 10% in the range of concentrations measured in this study.
Aliquots of urine were frozen ( - 70” C) for determination of urinary excretion of pyridinium cross-links, pyridinoline and deoxypyridinoline, as previously described (Uebelhart et al. 1990). Normal ranges for pyridinoline/creatinine ratio (Pyr/Cr) and deoxypyridinoline/creatinine ratio (DPyr/Cr) have been de- termined as 49.8 +- 18.7 and 8.2 + 3.4 pmollpmol, respec- tively, in postmenopausal women (Uebelhart et al. 1990). Inter- and intraassay variations for pyridinoline and deoxypyridinoline measurements were 9.6%, 10% and 14.98, 13%, respectively.
Histologic assessment
Paired transiliac bone biopsies were obtained under local anes- thesia from each patient, using an 8-mm inner diameter trephine. Prerequisite double labeling was effected with tetracycline chlor- hydrate (500 mg twice daily), administered according to a sched- ule of 4 days on, 12 days off, 2 days on and 5 days off. The first biopsy was obtained upon entry visit; the second was taken on the opposite iliac crest, on the last day of the six month period of treatment. For each patient, the paired biopsies were analysed together. The biopsies were fixed in 70% alcohol, then embed- ded at low temperature in methyl-methacrylate. Sections were cut with a heavy microtome (type Jung K). The sections were stained using naphtol ASTR phosphate as a substrate for tartate- resistant acid phosphatases, and counterstained with toluidine blue (pH 2.4). The histomorphometric measurements were per- formed on two or three distant sections using an objective eye- piece Zeiss Intergratte Plate II and a semiautomatic image ana- lyzer (Biocom, France) (Cohen-Solal et al. 1991).
Trabecular bone histomorphometric parameters were evalu- ated and labelled according to the American Society for Bone and Mineral Research nomenclature (Pa&t et al. 1987): bone volume/tissue volume (BVITV, %), mean wall thickness (Wth, pm), osteoid volume/bone volume (OV/BV, %), osteoid sur- faces/bone surface (OS/BS, %), osteoid thickness (O.Th, pm), osteoblast surfaces/bone surface (Obl.S/BS, %), mineral appo- sition rate (MAR, pm/d), bone formation rate/bone surface (BFRBS, pm3/pm2/d), activation frequency (Acf, y), eroded surfaces/bone surface (ES/BS, %), number of osteoclasts/mm* tissue (N.OC/T.Ar/rnm*). osteoclast surfaces (OC.S/BS, %). The following bone microstructural indices were calculated from the surface and volume measurements: trabecular number (Tb.Nb/mm*), trabecular separation (TbSp, pm) and trabecular width (Tb.Wi, km) according to Parfitt et al. (1983). Depth of eroded cavities devoided of osteoid at their base (EDe, pm) was measured as previously described (Cohen-Solal et al. 1991). An average of 5.9 +- 3.3 resorption lacunaelpatient were measured.
Twenty-four women without any bone disease (mean age 61 2 8 years) were used as controls (Garcia-Carasco et al. 1989). Normal values for erosion depth have been reported previously (Cohen-Solal et al. 1991).
43
Bone mineral density assessment
Bone mineral density (BMD, g/cm*) and bone mineral content (BMC, g) were measured by dual energy X-ray absorptiometry (DXA) (Hologic QDR 1000). A 2 score, i.e., the number of standard deviations related to normal age- and sex-matched sub- jects, was calculated for each BMD measurement. At the lumbar spine level, the second, third and fourth vertebrae were measured (antero-posterior view). At the upper extremity of the femurs, three sites were measured: neck, trochanteric area and Ward’s triangle. Ward’s triangle was automatically determined by the software as the area of lower density (Roux et al. 1990). Three DXA measurements were performed for each patient: upon entry visit, on the last day of the 6-month period of treatment and 6 months after the end of treatment. In our department, the preci- sion of DXA measurements are 1% and 1.2% for spine and femur levels, respectively. All exams were performed by the same observer, with strict, standardized positioning of patients. For each patient, all exams were analysed with the same region of interest. At the femur level, the mean values of the right and left were calculated.
Statistical analysis
The significance of changes in the biological values was calcu- lated using the Wilcoxon Signed-Rank test for the following end points: days 4 and 7 and months 1, 3, 6, 9 and 12. The com- parison of histomorphometric data to controls, at baseline and at the end of treatment was assessed by the Mann-Whitney test. Changes in histomorphometric values and BMD after treatment were assessed by the Wilcoxon Signed-Rank test. Spearman’s coefficient of correlation was used as appropriate. p Values above 0.05 were not considered significant.
Results
Clinical and radiologic assessment
At the study entry, patients reported no bone pain related to multiple myeloma. Baseline skeletal X-rays showed multiple lytic bone lesions in all patients except 1, and vertebral fractures in 8 patients. During the study, no changes in height were ob- served. All temperature variations were due to septic complica- tions of myeloma or chemotherapy.
During the study, new bone pain was reported by 3 patients. In 1 case, pain was related to a new lytic lesion of a clavicula, during the last month of follow-up. A second patient, with chronic renal function failure, had a symptomatic localisation of histologically proven amyloidosis in the lumbar epidural space and ilium, during the second month of the study. The third patient complained of lumbar spine pain, without osteolytic X-ray lesions, related to a disease relapse, during month 5 of the study.
One patient reported a side effect related to risedronate: ep- igastric pain while taking the three capsules, on the second day of treatment. This side effect was subsequently avoided by in- creasing the volume of water taken with the study drug.
General laboratory assessment
All the variations of general laboratory variables could be related to the disease or the chemotherapy. Neither renal failure nor increase in creatinine level in the patient with chronic renal fail- ure were observed. The mean value (*standard deviation) of myeloma protein was 20.2 -C 12.9 g/l (7.4-48.6) at the begin-

Tab
le
I.
Bon
e m
etab
olis
m
asse
ssm
ent
in s
erum
of
11
pat
ient
s w
ith
mul
tiple
m
yelo
ma
trea
ted
with
ri
sedr
onat
e
Tre
atm
ent
Follo
w-u
p
Firs
t w
eek
Mon
th
Mon
th
Ent
ry
visi
t D
ay
4 D
ay
7 I
3 6
9 12
Seru
m
Cal
cium
(m
moh
l)
2.24
t
0.19
2.
19
? 0.
188
2.11
f
0.16
” 2.
14
t 0.
11”
2.23
i
0.12
2.
17
r+_ 0
.12
2.21
2
0.13
2.
23
+ 0.
11
Phos
phat
e (m
mol
/l)
1.25
5
0.23
1.
14
? 0.
27
1.02
+
0.20
1.
02
* 0.
17h
1.10
t
0.18
” 1.
13
i-
0.20
b 1.
20
? 0.
18
1.14
t
0.18
a A
lkal
ine
phos
phat
ase
(NJ/
I)
59.6
4 2
20.0
9 66
.18
i 24
.43
61.0
0 2
18.4
8 61
.55
-t
18.2
0 47
.27
+ 15
.95h
41
.36
2 0.
34h
46.2
7 +
7.63
” 48
.00
I 9.
84
Ost
eoca
lcin
(n
g/m
l)
32.8
6 +
IO.1
4 27
.45
-c
16.4
4 28
.45
2 13
.91
31.3
5 t
14.2
0 23
.89
1-
10.8
6”
17.9
0 2
l.92b
20
.37
+ 9.
19h
19.5
0 +
10.7
9b
PTH
(l
-84)
(p
glm
l)
40.0
5 2
14.2
1 63
.82
2 43
.07”
85
.91
-c 6
0.91
’ 76
.64
t 34
.20h
58
.82
5 24
.44”
40
.50
+- 1
5.24
34
.45
t 11
.42
35.1
4 t
16.2
2 25
(0H
)D
(ngi
ml)
7.
13
” 4.
22
7.66
f
4.31
6.
69
t-
3.81
6.
72
-t
3.86
8.
11
” 5.
02
12.2
9 f
7.21
b 13
.42
2 6~
12~
8.40
‘-
4.
13b
1,25
-(O
H),
D
(pgl
mf)
21
.55
? 6.
68
26.3
6 5
6.17
’ 32
.95
t 12
.07b
36
.00
2 12
.79h
30
.55
+ 11
.21b
24
.75
+- 1
1.87
25
.23
2 7.
86
23.5
5 4
9.25
Val
ues
give
n ar
e m
ean
? st
anda
rd
devi
atio
n.
The
st
atis
tical
si
gnif
ican
ce
of c
hang
es
from
pr
etre
atm
ent
valu
es
is d
eter
min
ed
by t
he W
ilcox
on
test
. A
p v
alue
le
ss t
han
0.05
is
con
side
red
sign
ific
ant.
ap < 0.05.
bp <
0.01
.

C. Roux et al.: Risedronate and multiple myeloma 45
Table II. Bone metabolism assessment in 2-h fasting urine of 11 patients with multiple myeloma treated with risedronate
Treatment Follow-up
First week Month Month
Entry visit Day 4 Day I 1 3 6 9 12
2-hour fasting urine CalciumIcreat. 0.21 0.18 0.20 0.18 0.15 0.18 0.29 0.24
(mmol/mmol) 2 0.15 * 0.19 2 0.31 ?I 0.21 2 0.15” + 0.10” f 0.21 * 0.16 Hydroxyprolinelcreat. 31.12 21.39 25.43 32.14 13.99 24.38 33.20 31.88
(umoYmmo1) 2 38.28 2 12.81 ? 18.67 ? 26.65 2 11.43 2 23.20 -+ 31.94 -t 31.02 Pyridinolinelcreat. 76.65 67.50 54.07 65.11 56.01 49.82 51.23 60.01
(pmob~mol) f 39.46 f 39.05 + 25.09” f 36.39 f 29.18 f 20.46b ? 25.85b 2 39.23 Deoxypyridinohnefcreat. 14.18 13.08 9.39 7.91 8.39 6.99 9.04 10.86
(pmoY~mo1) 2 6.02 2 6.07 2 3.90b t- 3.69b ? 4.25b * 3.11s 2 4.20b -c 6.94 TmF’GFB (mmohl) 1.19 1.07 0.94 0.93 1.07 1.10 1 .Ol 1.10
f 0.35 2 0.24 2 0.25 t 0.22” * 0.15 ? 0.48 2 0.21 * 0.20
Values given are mean 2 standard deviation. The statistical significance of changes from pretreatment values is determined by the Wilcoxon test. A p value less than 0.05 is considered significant. “p < 0.05. “p < 0.01.
ning, 17.3 ? 8.1 (7.1-30.8) after 6 months of treatment and 22.1 2 10.9 (7.6-37.0) after 6 months of follow-up. The mean serum level of P,-microglobulin was 3.8 * 3.9 mg/l (1.6-14.7) upon entry visit, 2.7 t 1.1 (1.6-5.1) after 6 months of treatment and 2.9 t 1.3 (1.7-6.0) after 6 months of follow-up.
Laboratory assessment of bone metabolism
Changes of the measured parameters of bone metabolism with time are reported in Tables I and II and Figures 1 and 2.
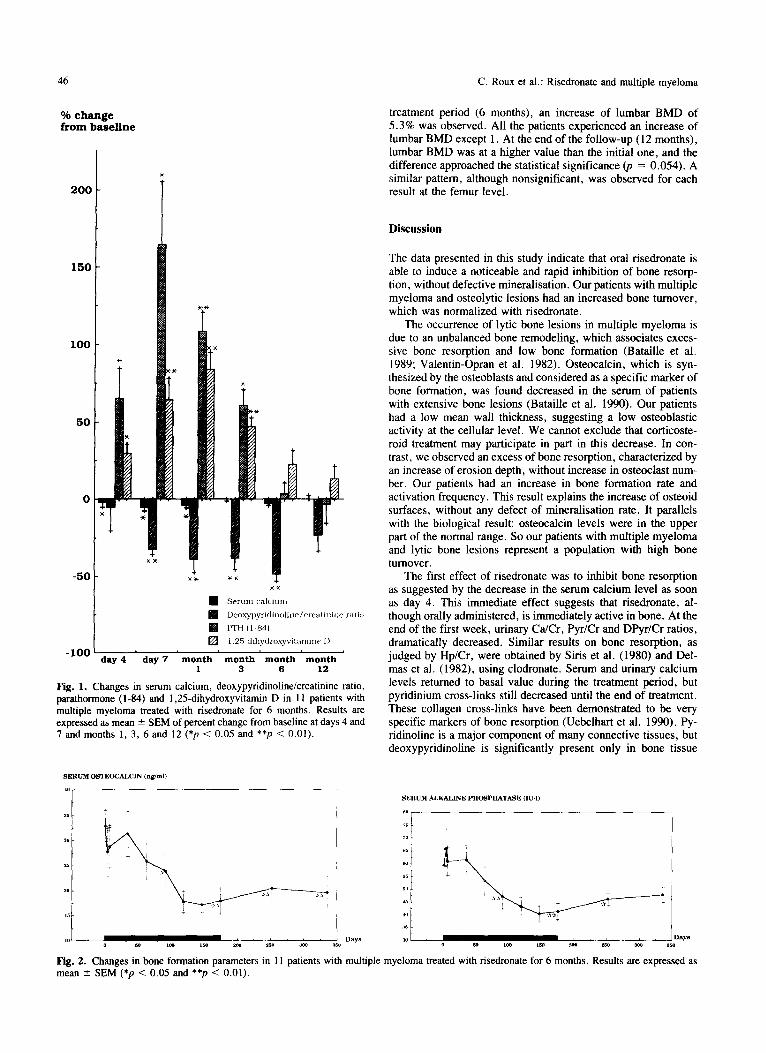
Upon entry visit, only 1 patient was hypercalcemic (2.75 mmol/l); normalisation of serum calcium was obtained after 2 days of risedronate treatment, during a course of chemotherapy. Alkaline phosphatases and osteocalcin were normal in all pa- tients. Mean urinary collagen cross-links were in the upper nor- mal range, suggesting a high level of bone resorption. Serum 25(0H)D was below the normal values in 4 patients; this result was associated with prolonged hospitalisation periods. Treat- ment was associated with a decrease of mean serum calcium from day 4 (-2%) and a concomitant increase in circulating levels of PTH (l-84) ( + 65%) and 1,25-(OH), D (+ 30%). The variations of serum calcium and PTH (l-84) levels were corre- lated during the first week (r = - 0.88, p = 0.02). Mean serum calcium and PTH (l-84) changes reached their nadir on day 7 ( - 5% and + 165%, respectively), and returned to pretreatment levels during the treatment period. All the patients (except 1 with hypercalcemia upon entry visit) experienced asymptomatic hy- pocalcemia. PTH (l-84) exceeded normal values during the treatment period in 9 of 11 patients. The same pattern was ob- served for 1,25-(OH), D level, with a nadir during the first month ( + 84%). Serum phosphate began to decrease on day 7, and returned to pretreatment values during follow-up. Similar changes were seen in the tubular reabsorption of phosphate. An increase in the 25-(0H)D level was observed during follow-up, i.e., during the summer, and was related to usual seasonal change (Stamp et al. 1974).
Mean urinary C&r decreased on day 4 (- 33%); the nadir was observed at month 2 (- 63%). The return of this parameter to baseline was obtained during the treatment period. Mean uri- nary Hp/Cr pattern had a similar decrease, although nonsignifi- cant. Mean urinary Pyr/Cr and DPyr/Cr showed a decrease at day 7 (- 22% and - 32%, respectively). The lowest values were obtained at the end of the treatment period ( - 30% and - 49%,
respectively). These parameters were still decreased at 12% and 23%, respectively, at the end of follow-up.
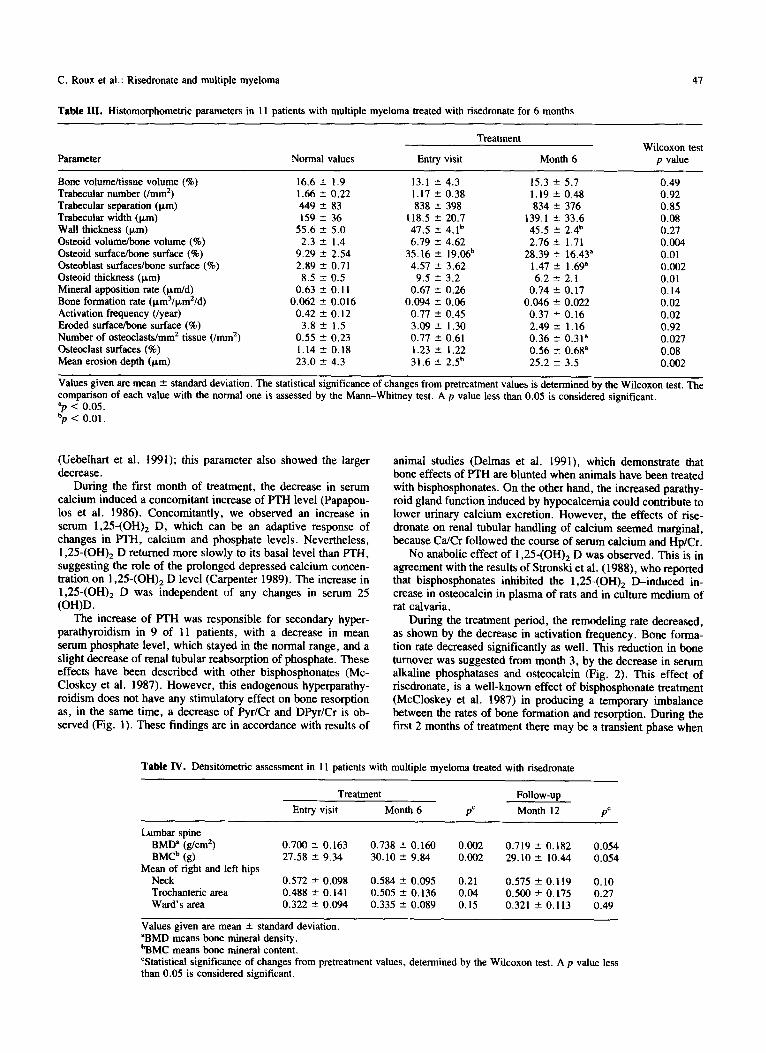
A decrease in alkaline phosphatases and serum osteocalcin appeared at month 3. They reached their nadir at the end of the treatment ( - 27% and -44%, respectively) and persisted for the remainder of the study. During the follow-up, osteocalcin level still decreased in 3 of 11 patients, and at the end of the study, the mean value of serum osteocalcin was 60% of the initial one.
Histologic assessment
Table III shows the changes with time in the means and standard deviations of the measured parameters.
At baseline, histomorphometric data showed a normal, al- though low, bone volume. None of the patients had a bone volume above the normal range. The results were obtained in areas where bone cannot be considered as totally invaded by the abnormal plasma cell proliferation. The osteoclast surfaces and the osteoclast number/mn?, the bone formation rate and activa- tion frequency, were at the upper limit of the normal range, although not different from controls. The mean erosion depth and the osteoid surfaces were significantly higher in our patients than in controls. Mean wall thickness was lower in multiple myeloma patients compared with controls.
After treatment, there was a marked decrease in bone tum- over, indicated by the result of activation frequency, and bone formation rate. There was a decrease in osteoid parameters, whereas trabecular width and mineralizing rate were unchanged. Mean wall thickness was not different before and after treatment. Therefore, the decreased rate of collagen synthesis, as suggested by the significant decrease in osteoid thickness, must have been counterbalanced by increased osteoblast lifespan. The osteoclast number/mm’ was lower after treatment. Moreover, erosion depth decreased to reach normal values.
None of the patients had or developed osteomalacia, as de- fined by increased osteoid volume with decreased mineral appo- sition rate and low mineralizing surface.
Bone mineral density assessment
The results are reported in Table IV. At the entry visit, mean Z score was - 1.58 + 1.26 and - 1.61 ‘- 1.25 at the lumbar spine and upper part of left femur, respectively. At the end of the
46
% change from baseline
2oc
15c
1oa
50
0
-50
-100 day 4 day 7 month month month month
1 3 6 12
Fig. 1. Changes in serum calcium, deoxypyridinolinelcreatinine ratio, parathormone (l-84) and 1,25-dihydroxyvitamin D in 11 patients with multiple myeloma treated with risedronate for 6 months. Results are expressed as mean 2 SEM of percent change from baseline at days 4 and 7 and months 1, 3, 6 and 12 (*p < 0.05 and **p < 0.01).
C. Roux et al.: Risedronam and multiple myeloma
treatment period (6 months), an increase of lumbar BMD of 5.3% was observed. All the patients experienced an increase of lumbar BMD except 1. At the end of the follow-up (12 months), lumbar BMD was at a higher value than the initial one, and the difference approached the statistical significance (p = 0.054). A similar pattern, although nonsignificant, was observed for each result at the femur level.
Discussion
The data presented in this study indicate that oral risedronate is able to induce a noticeable and rapid inhibition of bone resorp- tion, without defective mineralisation. Our patients with multiple myeloma and osteolytic lesions had an increased bone turnover, which was normalized with risedronate.
The occurrence of lytic bone lesions in multiple myeloma is due to an unbalanced bone remodeling, which associates exces- sive bone resorption and low bone formation (Bataille et al. 1989; Valentin-Opran et al. 1982). Osteocalcin, which is syn- thesized by the osteoblasts and considered as a specific marker of bone formation, was found decreased in the serum of patients with extensive bone lesions (Bataille et al. 1990). Our patients had a low mean wall thickness, suggesting a low osteoblastic activity at the cellular level. We cannot exclude that corticoste- roid treatment may participate in part in this decrease. In con- trast, we observed an excess of bone resorption, characterized by an increase of erosion depth, without increase in osteoclast num- ber. Our patients had an increase in bone formation rate and activation frequency. This result explains the increase of osteoid surfaces, without any defect of mineralisation rate. It parallels with the biological result: osteocalcin levels were in the upper part of the normal range. So our patients with multiple myeloma and lytic bone lesions represent a population with high bone turnover.
The first effect of risedronate was to inhibit bone resorption as suggested by the decrease in the serum calcium level as soon as day 4. This immediate effect suggests that risedronate, al- though orally administered, is immediately active in bone. At the end of the first week, urinary G&r, Pyr/Cr and DF’yr/Cr ratios, dramatically decreased. Similar results on bone resorption, as judged by Hp/Cr, were obtained by Siris et al. (1980) and Del- mas et al. (1982), using clodronate. Serum and urinary calcium levels returned to basal value during the treatment period, but pyridinium cross-links still decreased until the end of treatment. These collagen cross-links have been demonstrated to be very specific markers of bone resorption (Uebelhart et al. 1990). Py- ridinoline is a major component of many connective tissues, but deoxypyridinoline is significantly present only in bone tissue
Fig. 2. Changes in bone formation parameters in 11 patients with multiple myeloma treated with risedronate for 6 months. Results are expressed as mean k SEM (*p < 0.05 and **p < 0.01).
C. Roux et al.: Risedronate and multiple myeloma 47
Table III. Histomorphometric parameters in 11 patients with multiple myeloma treated with risedronate for 6 months
Parameter Normal values
Treatment Wilcoxon test
Entry visit Month 6 p value
Bone volume/tissue volume (%) 16.6 ? 1.9 13.1 I? 4.3 15.3 2 5.7 0.49
Trabecular number (/nun’) 1.66 * 0.22 1.17 +_ 0.38 1.19 f 0.48 0.92
Trabecular separation (wm) 449 2 83 838 ? 398 834 rt 376 0.85
Trabecular width (pm) 159 2 36 118.5 * 20.7 139.1 ? 33.6 0.08
Wall thickness (Fm) 55.6 2 5.0 47.5 2 4.1b 45.5 -+ 2.4b 0.27
Osteoid volume/bone volume (%) 2.3 + 1.4 6.79 ?I 4.62 2.76 * 1.71 0.004
Osteoid surface/bone surface (%) 9.29 * 2.54 35.16 ” 19X& 28.39 2 16.43” 0.01
Osteoblast surfaces/bone surface (%) 2.89 ” 0.71 4.57 2 3.62 1.47 + 1.69’ 0.002
Osteoid thickness (pm) 8.5 2 0.5 9.5 2 3.2 6.2 ?I 2.1 0.01
Mineral apposition rate (pm/d) 0.63 ” 0.11 0.67 2 0.26 0.74 -c 0.17 0.14
Bone formation rate (pm3/p,mZ/d) 0.062 ? 0.016 0.094 f 0.06 0.046 -+ 0.022 0.02
Activation fmquency (/year) 0.42 ? 0.12 0.77 2 0.45 0.37 * 0.16 0.02
Eroded surface/bone surface (%) 3.8 f 1.5 3.09 f 1.30 2.49 2 1.16 0.92
Number of osteoclasts/mm’ tissue (/mm*) 0.55 2 0.23 0.77 2 0.61 0.36 f 0.31” 0.027
Osteoclast surfaces (%) 1.14 2 0.18 1.23 2 1.22 0.56 If: 0.68” 0.08
Mean erosion depth (pm) 23.0 2 4.3 31.6 2 2.5b 25.2 2 3.5 0.002
Values given are mean f standard deviation. The statistical significance of changes from pretreatment values is determined by the Wilcoxon test. The comparison of each value with the normal one is assessed by the Mann-Whitney test. A p value less than 0.05 is considered significant. “p < 0.05. “p < 0.01.
(Uebelhart et al. 1991); this parameter also showed the larger decrease.
During the first month of treatment, the decrease in serum calcium induced a concomitant increase of PTH level (Papapou- 10s et al. 1986). Concomitantly, we observed an increase in serum 1,25-(OH), D, which can be an adaptive response of changes in PTH, calcium and phosphate levels. Nevertheless, I.25(OH), D returned more slowly to its basal level than PTH, suggesting the role of the prolonged depressed calcium concen- tration on 1,25-(OH), D level (Carpenter 1989). The increase in 1,25-(OH), D was independent of any changes in serum 25 (0H)D.
animal studies (Delmas et al. 1991), which demonstrate that bone effects of PTH are blunted when animals have been treated with bisphosphonates. On the other hand, the increased parathy- roid gland function induced by hypocalcemia could contribute to lower urinary calcium excretion. However, the effects of rise- dronate on renal tubular handling of calcium seemed marginal, because C&r followed the course of serum calcium and Hp/Cr.
No anabolic effect of 1,25-(OH), D was observed. This is in agreement with the results of Stronski et al. (1988), who reported that bisphosphonates inhibited the 1,25-(OH), &induced in- crease in osteocalcin in plasma of rats and in culture medium of rat calvaria.
The increase of PTH was responsible for secondary hyper- parathyroidism in 9 of 11 patients, with a decrease in mean
During the treatment period, the remodeling rate decreased,
serum phosphate level, which stayed in the normal range, and a as shown by the decrease in activation frequency. Bone forma-
slight decrease of renal tubular reabsorption of phosphate. These tion rate decreased significantly as well. This reduction in bone
effects have been described with other bisphosphonates (Mc- turnover was suggested from month 3, by the decrease in serum
Closkey et al. 1987). However, this endogenous hyperparathy- alkaline phosphatases and osteocalcin (Fig. 2). This effect of
roidism does not have any stimulatory effect on bone resorption risedronate, is a well-known effect of bisphosphonate treatment
as, in the same time, a decrease of Pyr/Cr and DPyr/Cr is ob- (McCloskey et al. 1987) in producing a temporary imbalance
served (Fig. 1). These findings are in accordance with results of between the rates of bone formation and resorption. During the first 2 months of treatment there may be a transient phase when
Table IV. Densitometric assessment in 11 patients with multiple myeloma treated with risedronate
Lumbar spine
BMD” (g/cm’) BMCb (g)
Mean of right and left hips
Neck Trochanteric area Ward’s area
Treatment
Entry visit Month 6
0.700 2 0.163 0.738 2 0.160 27.58 2 9.34 30.10 f 9.84
0.572 + 0.098 0.584 f 0.095 0.488 2 0.141 0.505 2 0.136 0.322 It 0.094 0.335 2 0.089
PC
0.002 0.002
0.21 0.04 0.15
Follow-up
Month 12
0.719 f 0.182 29.10 2 10.44
0.575 rt 0.119 0.500 f 0.175 0.321 ? 0.113
PC
0.054 0.054
0.10 0.27 0.49
Values given are mean * standard deviation. ‘BMD means bone mineral density. bBMC means bone mineral content. ‘Statistical significance of changes from pretreatment values, determined by the Wilcoxon test. A p value less than 0.05 is considered significant.

48 C. Roux et al.: Risedronate and multiple myeloma
bone formation is greater than bone resorption. This resulted in a decrease of the efflux of calcium from bone, with a consequent fall in serum and urinary calcium.
The reduction of the activation frequency of remodelling units, without any impairment of mineralisation, is responsible for two effects. First, completion of mineralisation of osteoid tissue is possible, and this is demonstrated by the reduction of the histomorphometric osteoid parameters. This explains the tran- sient increase in bone mineral density and bone mineral content observed with DXA. On the other hand, the reduction of the activation frequency may reduce the chances for thin trabecular plates to be perforated with a consequent loss of mechanical strength.
There are few human longitudinal histomorphometric studies of the effects of bisphosphonates. In women with osteoporosis, treated with cyclical etidronate for 2 years, a decrease in bone turnover was observed with lower bone resorption and formation (Ott et a!. 1990). Similar results, but with a decrease of mean wall thickness, was observed in another study during etidronate treatment (Pallot-Prades et al. 1991). Our data suggest that the mechanism of action of risedronate is similar, inducing a reduc- tion in both osteoclast number and activity with a maintained osteoblast activity.
Bisphosphonates are used extensively for treatment of Paget’s disease, and the marked effects on skeletal metabolism they in- duce persist for many months after stopping treatment (McClos- key et a!. 1987). This long-lasting effect authorizes short-course treatment for Paget’s disease (Thiebaud et al. 1988; O’Doherty et a!. 1992), although some patients do relapse within 3-12 months at the end of the treatment regime (Stone et a!. 1990). Admin- istration of etidronate has been proposed in osteoporosis with a cyclical regimen (Watts et a!. 1990). In our patients with mul- tiple myeloma, the decrease of bone resorption stopped when drug administration stopped. This cannot be explained by a re- lapse of the hematological disease in our patients. The fading of the effect of bisphosphonates on bone resorption in multiple myeloma was noticed by Merlini et a!. (1990), using short courses of intravenous clodronate. Persistence of multiple my- eloma cells in marrow ensures persistent secretion of cytokines which stimulate bone resorption. However, at the end of our study, the pyridinium cross-links did not return to baseline val- ues, although the difference was not significant.
Bone formation did not resume at the end of the follow-up. This can be a consequence of an unknown effect of risedronate on the production of proteins by osteoblasts (Stronski et a!. 1988). Most probably, because of the bone coupling process, it could be expected that bone formation will return to the pretreat- ment value several weeks following bone resorption (Netelenbos et al. 1991).
Our study was not designed to quantify clinical benefits of risedronate in multiple myeloma. Although the observed effects do not necessarily indicate any benefit in clinical terms, they suggest that this compound could be of interest for the manage- ment of this disease; our observation that a malignant hypercal- cemia can occur under treatment suggests that all the bone lytic lesions will not be controlled by bisphosphonates. The brief rem- nent effect raises the question of optimal treatment schedule of bisphosphonates in multiple myeloma. Oral risedronate reduces resorption depth, and may have utility in preventing trabecular perforation in disease states with accelerated bone remodelling.
Acknowfedgmenrs: We thank Mrs. Benayad for her expert secretarial
assistance.
References
Batwile, R.. Chappard. D.; Marcelli, C.; Dessauw. P.; Sany. J.; Bald&, P.; AI-
exandre. C. Mechanisms of bone deslruction in multiple myeloma: the impor-
tance of an unbalanced process in determining the severity of lytic bone dis- ease. J. Clin. Oncol 7:190!%1914; 1989.
Bataille, R.: Delmas, P. D.; Chappard, D.: Sany, J. Abnormal serum bone Gla
protein levels in multiple myeloma. Cancer 66:167-172; 1990.
Belch, A. R.: Bergsagel, D. E.; Wilson, K.; O’Reilly, S.; Wilson. 1.; Sutton, D.:
Pater. J.: Johnston. D.; Zee, B. Effect of daily etidronate on the osteolysis of
multiple myeloma. J. C/in. Oncol. 9:1397-1402; 1991.
Carpenter. T 0. Mmeral regulation of vttamin D metabolism. Bone Min 5:25%
269: 1989.
Cohen. H. I.; Silberman, H. R.; Tomyos, K.: Btiolucci, A. A., for the South-
eastern Cancer Study Group (SECSG). Comparison of two long-term chemo-
therapy regimens, with or without agents to modify skeletal repair, in multiple
myeloma. Blood 63:63%648: 1984.
Cohen-Solal, M.; Moneux, C.; de Vemejoul, M. C. Relationship between the
number of resorbing cells and the amount resorbed in metabolic bone disorders.
J. Bone Min. Res. 6~915-920; 1991.
Delmas, P. D.; Charhon, S.: Chapuy, M. C.: Vignon, E.; Brianqon, D.; Edouard,
C.: Meunier, P. 1. Long-term effects of dichloromethylene diphosphonate (Cl>
MDP) on skeletal lesions in multiple myeloma. Merabol. Bone Dis. Re/. Res. 4:163168: 1982.
Delmas, P. D.: Vergnaud. P.; Arlot. M. E.; Pastoureau, P.; Meunier, P. J. The m
viva anabolic effect of hPTH-( l-34) is blunted when bone resorption is blocked
by a bisphosphonate. J. Bone Min. Res. B(suppl. 1):214; 1991.
Durie, B. G. M.: Salmon, S. E. Multiple myeloma, macroglobulinemia and
monoclonal gammapathies. Recent advances in hematology. New York: Chur-
chill Livingstone; 1977; 243-261,
Fleisch, H. Bispbosphonates: a new class of drugs in diseases of bone and calcium
metabolism. Rec. Res. Cancer Res. 116:1-28; 1989.
Garcia-Carasco. M.; de Vemejoul, M. C.: Sterkers, Y .; Morieux, C.; Kuntz, D.:
Miravet. L. Decreased bone fomution in osteoporotic patients compared with
age matched controls. Cal@ Tissue Inr. 44: 173-175; 1989.
Gamero, P.; Grimaux, M.; Demiaux, B.; F’reaudat, C.; Seguin, P.; Delmas, P. D.
Measurement of serum osteocalcin with a human-specific two-site immunora-
diametric assay. J. Bone Min. Res 12:1389-1398; 1992.
Guillemant. S.; Kramer, R.; Eurin, J.; Guillemant, J. Radiocompetitive protein
binding assays for 25.hydroxyvitamin D, 24,25-dihydroxyvitamin D and 1,25-
dihydroxyvitamin D in human serum. Norman, A. W. et al., eds. Vifamin D: basic resrurch and its clinical application. Berlin: de Gruyter; 1979; 247-248.
Harley. J. 8.; Schilling, A.; Glidewell, 0. Ineffectiveness of fluoride therapy in
multiple myeloma. N. En&. J. Med. 286:1283-1288; 1972.
Kyle, R. A.; Jowsey, J.; Kelly, P. J. Multiple myeloma bone disease: the com-
parative effect of sodium fluoride and calcium carbonate or placebo. N. Engl.
J. Med. 293:133&1338; 1975.
Kyle. R. A. Multiple myeloma: review of 869 cases. Mayo C&I. Pax. 50~29110;
1975
Kylstra, J. W.. B&w. P. I.: Clemens, T. L.; Valentin, A.; Lepkowski. M. J.;
Axelrod, D. W.; Singer, F. R. Risedronate in resistant Paget’s: preliminary
results. J. Bone Min. Res. C(suppl. 1):851; 1991.
Lahtinen, R., La&o, M.; Palva, I.; Virkkunen, P.; Elomaa, I., for the Finnish
Leukemia group. Randomised, placebo-controlled multicentre trial of clo-
dronate in multiple myeloma. Lancet 340:104%1052; 1992.
McCloskey, E. V.: Yates, A. J. P.: Beneton, M. N. C.; Galloway, J ,; Harris, S.:
Kanis. J. A. Comparative effects of intravenous diphosphonates on calcium
and skeletal metabolism in man. Bone E(supp1. l):S35-S41; 1987.
Merlini, G.: Attardo-Paninello. G.: Piccinini, L.: Crema, F.; Fiorentini, M. L.:
Riccardi, A.; Pavesi, F.; Nova& F.: Silingardi, V.; As&, E. Long-term
effects of parentera dichloromethylene bisphospbonate (Cl* MDP) on bone
disease of myeloma patients treated with chemotherapy. Hematol. Oncol. 8:23-30: 1990.
Netelenbos, J C.: Van Ginkel, F. C.; Lips. P.; Leeuwenkamp, 0. R.; Barto, R.:
Van Der Vijgh. W. J. F.; Van Der Wiel, H.; Hackeng, W. H. L. Effect of a
single infusion of aminohydroxypropylidene on calcium and bone metabolism
in healthy volunteers monitored during 2 months. J. Clin. Endocrinol. Me- tabol. 72:223228; 1991.
O’Doherty, D P.: Gertz, B. J.; Tindale, W.; Sciberras, D. G.; Survill, T. T.:
Kanis, J A. Effects of five daily I h infusions of alendronate in Paget’s disease of bone. J. Bone Min. Res. 7:81-87; 1992.
Ott, S. M.: Woodson, G. C.; Huffer. W. Bone histomorphometric changes in

C. Roux et al.: Risedronate and multiple myeloma 49
women with postmenopausal osteoporosis treated with etidronate. Chris- tiansen, C.; Overgaard, K., eds. Copenhagen: Osteopress; 1990; 1318-1322.
Pallot-Rades, B.; Chappard, D.; Tavan, P.; Prallet, B.; Riffat, G.; Alexandre, C. Etude histomorphometrique osseuse dam l’osttoporose fracturaire d’involution traitee par l’ethane-1, hydroxy- 1, 1 bisphosphonate (Etidronate) pendant 1 an. Rev. Rhum. Sk17 1-116; 1991.
Papapoulos, S. E.; Harinck, H. 1. J.; Bijvoet, 0. L. M.; Gleed, J. H.; Fraher, L. 1.; O’Riordan, I. L. H. Effects of decreasing serum calcium on circulating parathyroid hormone and vitamine D metabolites in normocalcemic and hy- percalcemic patients treatment with APD. Bone Min. 1:69-7X; 1986.
Part%, A. M.; Mathews, C. H. E.; Villanueva, A. R.; Kleerekoper, M.; Frame, B .; Rae. D. S. Relationships between surface, volume, and thickness of iliac uabecular bone in aging and in osteoporosis. J. CLin. Invest. 72:1396-1409; 1983.
Partitt, A. M.; Drezner, M. K.; Glorieux, F. H.; Kanis, J. A.; Mdluche, H.: Meunier, P. J., Ott, S. M.; Reeker, R. R. Bone histomorphometry: standard- ization of nomenclature, symbols and units. J. Bone Min. Res. 2~595-610; 1987.
Paterson, A. D.; Kanis, J. A.; Cameron, E. C.; Douglas, D. L.; Beard, D. J.: Preston, F. E.; Russel, R. C. G. The use of dichloromethylene diphosphonate for the management of hypercalcemia in multiple myeloma. Br. J. Hoemarol. 54:121-132; 1983.
Paterson, A. H. G.; Powles, T. J.; Kanis. 1. A.; McCloskey, E.; Hanson, J.; Ashley, S. Double-blind controlled trial of oral clodronate in patients with bone metastases from breast cancer. J. Clin. Oncol. 11:5%65; 1993.
Ralston, S. H.; Gallacher, S. I.; Patel, U.; Dryburgh, F. J.; Fraser, W. D.; Cowan, R. A.; Boyle, 1. T. Comparison of three intravenous bisphosphonates in cancer-associated hypercalcemia. Lancer 2: 118&l 182; 1989.
Rico, H.; Hermandez, E. R.; Diaz-Mediavilla. 1.; Alvarez, A.; Martinez, R.; Espinos, D. Treatment of multiple myeloma with nasal spray calcitonin: a histomorphometric and biochemical study. Bone Min. 8:231-237; 1990.
Roux, C.; Listrat, V.; Fechtenbaum, I.; Gibeault, P.; Saba, E.; Rabourdin, I. P.; Dougados, M.; Revel, M.; Amor, B. Bone mineral density of the proximal femur measured by dual-energy x-ray absorptiometry. Christiansen, C.; Over- gaard. K., eds. Copenhagen: Osteopress; 1990; 906-908.
Siris, E. S.; Sherman, W. H.; Baquiran, D. C.; Schlatterer, 1. P.; Osserman, E. F.; Canfield, R. E. Effects of dichloromethylene diphosphonate on skeletal
mobilization of calcium in multiple myeloma. N. Engl. J. Med. 302:31&315; 1980.
Stamp, T. C. B.; Round, J. M. Seasonal changes in human plasma levels of 25 hydroxyvitamine D. Nature 247:563-565; 1974.
Stone, M. D.; Hawthorne, A. B.; Kerr, D.; Webster, G.; Hosking, D. 1. Tmat- ment of Paget’s disease with intermittent low-dose infusions of disodium pa- midronate (APD). J. Bone Min. Res. 5:1231-1235; 1990.
Stronski, S. A.; Bettschen-Camin, L.; Wetterwald, A.; Felix, R.; Trechsel. U.; Ffeisch, H. Bisphosphonates inhibit 1,25-dihydroxyvitamine D3-induced in- crease of osteocalcin in plasma of rats in viva and in culture medium of rats calvaria in vitro. Calcif. Tissue Int. 42248254; 1988.
Tbiebaud, D.; Jaeger. P.; Gobelet, C.; Jacquet, A. F.; Burckhardt, P. A single infusion of the bisphosphonate AHPrBP (APD) as treatment of Paget’s disease of bone. Am. J. Med. 85:207-212; 1988.
Uebelhart, D.; Gineyts, E.; Chapuy, M. C.; Delmas, P. D. Urinary excretion of pyridinium cmsslinks: a new marker of bone resorption in metabolic bone disease. Bone Min. 8:X7-96; 1990.
Uebelhart, D.; Schlemmer, A.; Johansen, I. S.; Gineyts, E.; Christiansen, C.; Delmas, P. D. Effect of menopause and hormone replacement therapy on the urinary excretion of pyridinium cross-links. J. Clin. Endocrinol. Merobol. 72367-373; 1991.
Valentin-Opran, A.; Charhon, S. A.; Meunier, P. J.: Edouard, C. M.; Arlot, M. E. Quantitative histology of myeloma-induced bone changes. Br. J. Hae- marol. 52:60-610; 1982.
Walton, R. I.; Bijvoet, 0. L. M. Nomogram for derivation of renal threshold phosphate concentration. Lancer 1:30%310: 1975.
Watts, N. B.; Harris, S. T.; Genant. H. K.; Wasnich, R. D.; Miller, P. D.; Jack- son, R. D.; Licata, A. A.; Ross, P.: Woodson, G. C.; Yanover, M. J.; Mysiw , W. 1.; Kohse, L.; Rao, M. B.; Steiger, P.; Richmond, B.; Chesnut, C. H. Intermittent cyclical etidronate treatment of postmenopausal osteopom- sis. N. Engl. J. Med. 323:1%79; 1990.
Date Received: April 20, 1993 Dare Revised: June 7, 1993 Date Accepted: July 22, 1993




















