
Mantle cell lymphoma as a component of composite lymphoma: clinicopathologic parameters and biologic...
14
Progress in pathology Mantle cell lymphoma as a component of composite lymphoma: clinicopathologic parameters and biologic implications ☆ Thomas G. Papathomas MD a,b , Ioannis Venizelos MD a , Cherie H. Dunphy MD c , Jonathan W. Said MD d , Michael L. Wang MD e , Elias Campo MD f , Steven H. Swerdlow MD g , John C. Chan MD h , Carlos E. Bueso-Ramos MD, PhD i , Dennis D. Weisenburger MD h , L. Jeffrey Medeiros MD i , Ken H. Young MD, PhD i, ⁎ a Department of Pathology, Hippokration General Hospital of Thessaloniki, 54642 Thessaloniki, Greece b Department of Pathology, Erasmus MC University Medical Center Rotterdam, 3015 GE Rotterdam, The Netherlands c Department of Pathology and Laboratory Medicine, University of North Carolina, Chapel Hill, NC 27599, USA d Department of Pathology and Laboratory Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, USA e Department of Myeloma/Lymphoma, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA f Department of Anatomic Pathology, Hospital Clinic, University of Barcelona, 08014 Barcelona, Spain g Department of Pathology, University of Pittsburgh Medical Center, Pittsburgh, PA 15213, USA h Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE 68198, USA i Department of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA Received 10 July 2011; revised 30 August 2011; accepted 31 August 2011 Keywords: Mantle cell lymphoma; Composite lymphoma; Clonal relationship; Small lymphocytic lymphoma; Chronic lymphocytic leukemia; Follicular lymphoma; Plasma cell neoplasm; Marginal zone lymphoma; Classical Hodgkin lymphoma; Plasmablastic lymphoma; Burkitt lymphoma Summary Composite lymphoma is a rare circumstance in which 2 or more distinct types of lymphoma occur in a single anatomical location. Although composite lymphoma has been increasingly identified with the advent of molecular genetic techniques, this topic has only rarely been a specific focus of the medical scientific literature. In this review, we focus on mantle cell lymphoma occurring as a major pathologic component of composite lymphoma and emphasize the clinicopathologic features of these tumors and associated biologic implications. To date, 26 cases of composite lymphoma including a component of mantle cell lymphoma have been previously published. Issues of clonal relatedness between the individual lymphoma components and emerging biologic implications as well as potential diagnostic pitfalls are evaluated. © 2012 Elsevier Inc. All rights reserved. ☆ The study is supported by The University of Texas MD Anderson Cancer Center Institutional R&D Fund, The University of Texas MD Anderson Cancer Center Institutional Research Grant Award, The myeloma SPORE Research Development Program Award, Gundersen Medical Foundation Award, and Forward Lymphoma Fund. This study is also partially supported by NCI/NIH (R01CA138688 and 1RC1CA146299). ⁎ Corresponding author. The University of Texas MD Anderson Cancer Center, Department of Hematopathology, Houston, Texas 77230-1439. E-mail address: [email protected] (K. H. Young). www.elsevier.com/locate/humpath 0046-8177/$ – see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.humpath.2011.08.024 Human Pathology (2012) 43, 467–480
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Mantle cell lymphoma as a component of composite lymphoma: clinicopathologic parameters and biologic...
www.elsevier.com/locate/humpath
Human Pathology (2012) 43, 467–480
Progress in pathology
Mantle cell lymphoma as a component of compositelymphoma: clinicopathologic parameters andbiologic implications☆
Thomas G. Papathomas MDa,b, Ioannis Venizelos MDa, Cherie H. Dunphy MDc,Jonathan W. Said MDd, Michael L. Wang MDe, Elias Campo MDf,Steven H. Swerdlow MDg, John C. Chan MDh, Carlos E. Bueso-Ramos MD, PhDi,Dennis D. Weisenburger MDh, L. Jeffrey Medeiros MDi, Ken H. Young MD, PhDi,⁎
aDepartment of Pathology, Hippokration General Hospital of Thessaloniki, 54642 Thessaloniki, GreecebDepartment of Pathology, Erasmus MC University Medical Center Rotterdam, 3015 GE Rotterdam, The NetherlandscDepartment of Pathology and Laboratory Medicine, University of North Carolina, Chapel Hill, NC 27599, USAdDepartment of Pathology and Laboratory Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, USAeDepartment of Myeloma/Lymphoma, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USAfDepartment of Anatomic Pathology, Hospital Clinic, University of Barcelona, 08014 Barcelona, SpaingDepartment of Pathology, University of Pittsburgh Medical Center, Pittsburgh, PA 15213, USAhDepartment of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE 68198, USAiDepartment of Hematopathology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA
Received 10 July 2011; revised 30 August 2011; accepted 31 August 2011
CF
0d
Keywords:Mantle cell lymphoma;Composite lymphoma;Clonal relationship;Small lymphocyticlymphoma;Chronic lymphocyticleukemia;Follicular lymphoma;Plasma cell neoplasm;Marginal zone lymphoma;Classical Hodgkinlymphoma;Plasmablastic lymphoma;Burkitt lymphoma
Summary Composite lymphoma is a rare circumstance in which 2 or more distinct types of lymphomaoccur in a single anatomical location. Although composite lymphoma has been increasingly identifiedwith the advent of molecular genetic techniques, this topic has only rarely been a specific focus of themedical scientific literature. In this review, we focus on mantle cell lymphoma occurring as a majorpathologic component of composite lymphoma and emphasize the clinicopathologic features of thesetumors and associated biologic implications. To date, 26 cases of composite lymphoma including acomponent of mantle cell lymphoma have been previously published. Issues of clonal relatednessbetween the individual lymphoma components and emerging biologic implications as well as potentialdiagnostic pitfalls are evaluated.© 2012 Elsevier Inc. All rights reserved.
☆ The study is supported by The University of Texas MD Anderson Cancer Center Institutional R&D Fund, The University of Texas MD Anderson Cancerenter Institutional Research Grant Award, The myeloma SPORE Research Development Program Award, Gundersen Medical Foundation Award, andorward Lymphoma Fund. This study is also partially supported by NCI/NIH (R01CA138688 and 1RC1CA146299).
⁎ Corresponding author. The University of Texas MD Anderson Cancer Center, Department of Hematopathology, Houston, Texas 77230-1439.E-mail address: [email protected] (K. H. Young).046-8177/$ – see front matter © 2012 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2011.08.024

468 T. G. Papathomas et al.
1. Introduction
The term composite lymphoma (CL), first proposed byCuster in 1954, has been inconsistently used over the yearsbut is most commonly used to describe the occurrence of2 unrelated types of lymphoma involving the same anatomi-cal site [1]. Traditionally, the definition of CL has been basedon morphological and immunophenotypic examination [2].The application of molecular genetic techniques to the anal-ysis of CLs, however, has shown clonal relatedness in a subsetof CL cases in which the components were thought to beindependent based on traditional criteria. Müller-Hermelinket al [3] recognizing these issues have attempted to provide amore up-to-date and practical definition, stating “the termcomposite lymphoma should be reconsidered as a merelydescriptive term for one morphological manifestation encom-passing at least 2 different biologic processes, namely, clonaltransformation and coexistence of 2 clonally unrelatedtypes of lymphoma, which may have the same pathogeneticbackground (eg, immunodeficiency-related) or may occurindependently by chance.” Of note, it is suggested that ahematopathologist should designate and quantify each indi-vidual component [1], particularly in the context of differentnatural histories, prognosis, and therapeutics. In-depth molec-ular understanding of CLs also may shed new light on ourunderstanding of lymphomagenesis.
In this review, we focus on and provide a comprehensivereview of mantle cell lymphoma (MCL) occurring as a com-ponent of CL, with a special emphasis on the clinicopathol-ogic features and biologic implications of this circumstanceand the aim of identifying some of the research questions thatneed to be addressed for this rare manifestation of lymphoma.
Relevant articles were obtained using the followingdatabase: National Library of Medicine's Pubmed coveringthe period up to the present day (May 2011) using thekeywords composite mantle cell lymphoma, synchronousmantle cell lymphoma, mantle cell lymphoma transforma-tion, extranodal mantle cell lymphoma, and compositelymphoma. References within these articles were alsoreviewed. Because the term MCL was first widely acceptedin 1992 [4], a few cases of MCL designated by older names(eg, centrocytic lymphoma and intermediate differentiatedlymphocytic lymphoma) potentially may not have beencaptured in the search.
2. CL with an MCL as major pathologiccomponent
MCL occurring in the context of a CL is exceedingly rare.In this comprehensive, retrospective literature review, weidentified 26 cases of CL in which MCL was 1 component.Almost all documented cases (Table 1) were case reports[13-28] or included as a part of small case series with adifferent focus from that of this study. The other component
in these CL cases included follicular lymphoma (FL),chronic lymphocytic leukemia/small lymphocytic lymphoma(CLL/SLL), classical Hodgkin lymphoma (cHL), plasma cellneoplasms (PCN), marginal zone lymphoma (MZL), plas-mablastic lymphoma (PBL), and Burkitt lymphoma (BL).The age range extended from the 5th to 10th decades, with amedian age of 69.5 years. These were 13 women and 13men. Sixteen CLs involved lymph nodes, and 9 involvedextranodal sites including spleen (n = 3), soft tissues of thehead region (n = 3), gastrointestinal tract (n = 2), and bonemarrow (n = 1). One patient with CL had simultaneousinvolvement of lymph node and eyelid.
FL was found to be the most frequent partner of MCL inthese CLs, in 8 (30.8%). In decreasing order of frequency,other partners of MCL included CLL/SLL, 5 (19%); cHL, 5(19%); PCN, 4 (15.4%); MZL, 2 (7.6%); PBL, 1 (3.8%); andBL, 1 (3.8%). Seven patients (27%) had a history oflymphoma before diagnosis of CL: 4 MCLs, 2 FLs, and 1designated as a chronic lymphoproliferative disease.
2.1. FL-MCL
Among the 8 known CL cases of FL-MCL in theliterature, 5 were mainly nodal, whereas 3 involvedextranodal sites: small intestine, orbit, and spleen (Fig. 1).All but 1 (case 4) were clonally unrelated or indefinite [5-12].However, there is no definite proof of clonal independencein FL-MCL CLs for a few reasons. First, there is no con-tinuity among the techniques used to determine clonalrelatedness, and microdissection was performed in only 3cases (all of which were in the unrelated/indefinite subset)[5-7]. Second, Roullet et al [6] found some evidence ofclonal relatedness, as analysis of IGK by PCR (VK-Kderegion) revealed the same monoclonal rearrangement, incontrast with other data emerging from their investigation,such as (1) separate translocations in immunophenotypicallydifferent cell subpopulations and (2) IGH analysis by PCRdetected monoclonality only in the MCL component,supporting clonal unrelatedness. Therefore, in an effort toreconcile these findings, a common (ancestral) clonal originwith subsequent divergence could be speculated as suggestedby Roullet et al [6].
The MCL component demonstrated an in situ growthpattern in 3 cases, a mixed mantle zone and nodular growthpattern in 2 cases, a diffuse growth pattern in 2 cases, and amantle zone growth pattern in 1 case (Table 2). The find-ing of an in situ MCL component in these CL cases addsfurther to the notion that in situ MCL (along with in situFL/intrafollicular neoplasia) is increasingly recognized in theroutine clinical practice, either as an incidental finding in thesetting of lymphoid hyperplasia or rarely with an unrelatedlymphoproliferative disorder or metastatic nonlymphoidmalignancy [29]. Whether these lesions will ever progressto clinically significant disease or simply correspond torelatively stable clonal proliferations of lymphoid cells is as

Table 1 Clinicopathologic features of CLs with a MCL component with a special emphasis on the clonal relationship between the individual lymphoma components
Caseno./Ref
Subtypes oflymphoma
Age/sex
Medical history/clinicalpresentation and signs
Anatomical site Clonalrelationship
Methods used to detect anyevidence of clonal relationship
1 [5] MCL + FL 58/F NA/small bowel obstruction Small intestine, mesentericlymph nodes: MCL involvement
Unrelated Microdissection, IgVH sequencing
2 [6] MCL + FL 84/F Recurrent rectal carcinoma/multiple radiologicallydetected splenic masses, suggestive of metastaticcarcinoma
Spleen Unrelated Microdissection, FISH andimmuno-FISH, IgH andIgK PCR analysis
3 [7] MCL + FL 65/M NA/persistent left inguinal lymphadenopathy Lymph node spleen, liver, PB:MCL involvement
Unrelated Microdissection, FISH, IGHPCR analysis
4 [8] MCL + FL 70/F Long-standing history (17 y) of nodalFL/chronic peripheral lymphadenopathy
Lymph node of the left cervicalregion
Related Microdissection, IgVH sequencing
5 [9] MCL + FL 67/F 1-y history of MCL involving the Waldeyerring/right cervical lymphadenopathy
Lymph node of the right cervicalregion
Indefinitea IgH PCR analysis
6 [10] MCL + FL 40/M 6-y history of FL/generalized lymphadenopathy Lymph node of the cervical region NA NA7 [11] MCL + FL 56/M Unremarkable/generalized lymphadenopathy
(laterocervical, supraclavicular, axillary,retroperitoneal, inguinal)
Lymph node of the inguinal region Indefiniteb FISH, IgH PCR analysis
8 [12] MCL + FL 73/M NA/retrobulbar ache, proptosis (3 mm), chemosis,lymphangiectasis, slight limitation of downgaze
Intraconal and superonasal orbit,mid- and posterior orbit
Unrelated FISH
9 [13] MCL + CLL/SLL 73/M Long-standing history (22 y) of malignantmelanoma/4-mo history of a lump in his left thighwith multiple hard left inguinal lymph nodes
Lymph node of the left inguinalregion PB/BM: CLL
Unrelated FISH
10 [14] MCL + CLL/SLL 86/F Alzheimer disease, elevated blood pressure, arthritis/bilateral cervical and axillary lymphadenopathy and on CTscan: mediastinal and retroperitoneal lymphadenopathy
Lymph node PB: CLL/SLL + MCL Unrelated FISH, conventional cytogenetics, IgHand IgK PCR analysis
11 [15] MCL + CLL/SLL 86/M NA/cervical, axillary and inguinallymphadenopathy and hepatomegaly
Lymph node: MCL + CLL/SLL PB:CLL/SLL +MCL
Unrelated IgH PCR analysisc
12 [16] MCL + CLL/SLL 84/F Diabetes, coronary artery disease, and stage2 chronic kidney disease/anemia, thrombocytopeniaand splenomegaly
Bone Marrow PB: CLL/SLL + MCL Unrelated FISH
13 [5] MCL + CLL/SLL 69/F NA/laryngectomy and bilateral neck dissectionfor a T3 squamous cell carcinoma of the vocal cords
Lymph nodes PB: CLL/SLL + MCL Unrelated Microdissection, IgVH sequencing
14 [17] MCL + cHL 45/M 3-y history of MCL/residual disease, resectionof an abdominal lymph node and the spleen
Lymph node Related Microdissection, IgVH sequencing [17]LDI PCR analysis of IgH-associatedchromosomal translocations [18]
15 [19] MCL + cHL 61/M 10-y history of chronic lymphoproliferativedisorder/isolated splenomegaly
Spleen Unrelated Microdissection, IgVH sequencing
16 [19] MCL + cHL 66/M Unremarkable/left cervical lymphadenopathy,a left tonsillar mass, and a nodular eyelid mass
Eyelid and lymph node of the leftcervical region
Unrelated Microdissection, IgVH sequencing
17 [20] MCL + cHL 69/F Rheumatoid arthritis, asthma, posttherapeutichypothyroidism/right cervical and bilateralaxillary, lymphadenopathy
Lymph node of the axillary region NA NA
(continued on next page)
469Mantle
celllym
phomaas
acom
ponentof
composite
lymphom
a
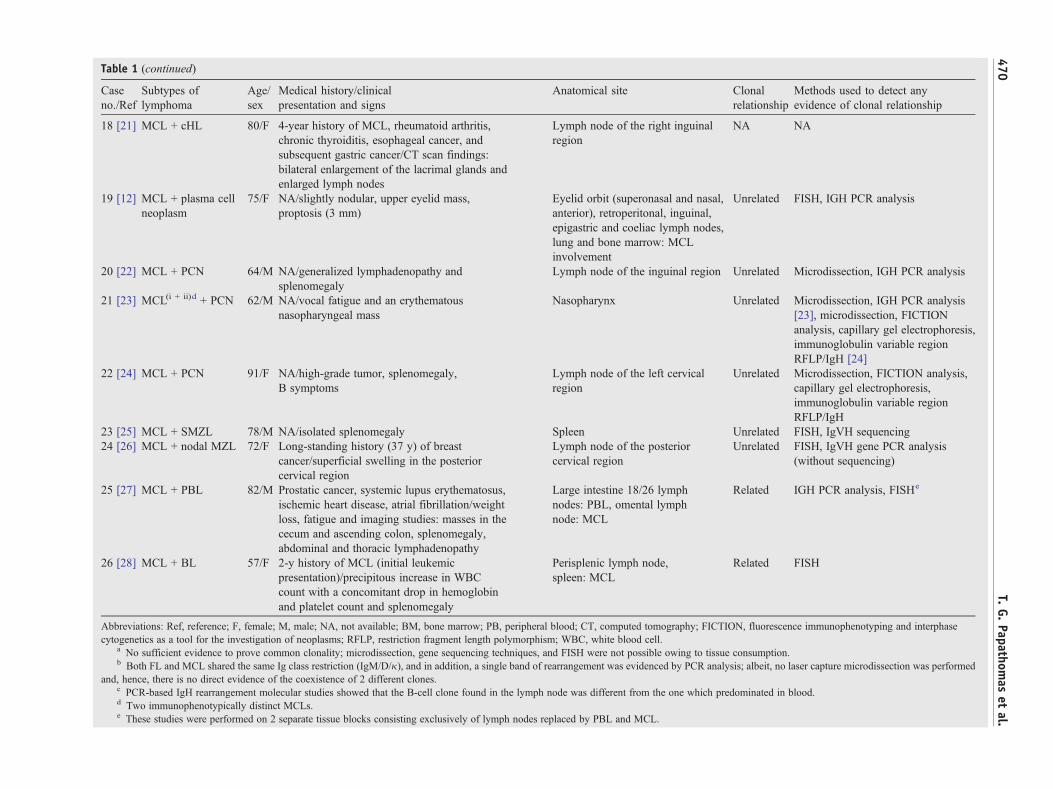
Table 1 (continued)
Caseno./Ref
Subtypes oflymphoma
Age/sex
Medical history/clinicalpresentation and signs
Anatomical site Clonalrelationship
Methods used to detect anyevidence of clonal relationship
18 [21] MCL + cHL 80/F 4-year history of MCL, rheumatoid arthritis,chronic thyroiditis, esophageal cancer, andsubsequent gastric cancer/CT scan findings:bilateral enlargement of the lacrimal glands andenlarged lymph nodes
Lymph node of the right inguinalregion
NA NA
19 [12] MCL + plasma cellneoplasm
75/F NA/slightly nodular, upper eyelid mass,proptosis (3 mm)
Eyelid orbit (superonasal and nasal,anterior), retroperitonal, inguinal,epigastric and coeliac lymph nodes,lung and bone marrow: MCLinvolvement
Unrelated FISH, IGH PCR analysis
20 [22] MCL + PCN 64/M NA/generalized lymphadenopathy andsplenomegaly
Lymph node of the inguinal region Unrelated Microdissection, IGH PCR analysis
21 [23] MCL(i + ii)d + PCN 62/M NA/vocal fatigue and an erythematousnasopharyngeal mass
Nasopharynx Unrelated Microdissection, IGH PCR analysis[23], microdissection, FICTIONanalysis, capillary gel electrophoresis,immunoglobulin variable regionRFLP/IgH [24]
22 [24] MCL + PCN 91/F NA/high-grade tumor, splenomegaly,B symptoms
Lymph node of the left cervicalregion
Unrelated Microdissection, FICTION analysis,capillary gel electrophoresis,immunoglobulin variable regionRFLP/IgH
23 [25] MCL + SMZL 78/M NA/isolated splenomegaly Spleen Unrelated FISH, IgVH sequencing24 [26] MCL + nodal MZL 72/F Long-standing history (37 y) of breast
cancer/superficial swelling in the posteriorcervical region
Lymph node of the posteriorcervical region
Unrelated FISH, IgVH gene PCR analysis(without sequencing)
25 [27] MCL + PBL 82/M Prostatic cancer, systemic lupus erythematosus,ischemic heart disease, atrial fibrillation/weightloss, fatigue and imaging studies: masses in thececum and ascending colon, splenomegaly,abdominal and thoracic lymphadenopathy
Large intestine 18/26 lymphnodes: PBL, omental lymphnode: MCL
Related IGH PCR analysis, FISHe
26 [28] MCL + BL 57/F 2-y history of MCL (initial leukemicpresentation)/precipitous increase in WBCcount with a concomitant drop in hemoglobinand platelet count and splenomegaly
Perisplenic lymph node,spleen: MCL
Related FISH
Abbreviations: Ref, reference; F, female; M, male; NA, not available; BM, bone marrow; PB, peripheral blood; CT, computed tomography; FICTION, fluorescence immunophenotyping and interphasecytogenetics as a tool for the investigation of neoplasms; RFLP, restriction fragment length polymorphism; WBC, white blood cell.
a No sufficient evidence to prove common clonality; microdissection, gene sequencing techniques, and FISH were not possible owing to tissue consumption.b Both FL and MCL shared the same Ig class restriction (IgM/D/κ), and in addition, a single band of rearrangement was evidenced by PCR analysis; albeit, no laser capture microdissection was performed
and, hence, there is no direct evidence of the coexistence of 2 different clones.c PCR-based IgH rearrangement molecular studies showed that the B-cell clone found in the lymph node was different from the one which predominated in blood.d Two immunophenotypically distinct MCLs.e These studies were performed on 2 separate tissue blocks consisting exclusively of lymph nodes replaced by PBL and MCL.
470T.
G.Papathom
aset
al.

A
G
CD10
CD3 CD5 CD5
Cyclin D1 Cyclin D1
MCL
MCL
MCL
B C
FED
G H I
Fig. 1 Histologic and immunophenotypic features of MCL with FL. A, B and C, Nodular pattern of atypical lymphoid cells with variablyexpanded mantle zones (hematoxylin and eosin stain, original magnification ×20, ×40, and ×100). D, CD3 staining normal small T cells in theinterfollicular areas (immunoperoxidase stain, original magnification ×20). E and F, CD5 staining normal small T cells in the interfollicularareas and B cells in the focally expanded mantle zone. Arrows in F show the MCL in situ component (immunoperoxidase stain, originalmagnification ×20 and ×100). G, Strong CD10 staining of atypical centrocytes and centroblasts within a follicle (immunoperoxidase stain,original magnification ×20). H and I, Cyclin D1 staining of atypical lymphoid cells in the mantle zones (immunoperoxidase stain, originalmagnification ×20 and ×100).
471Mantle cell lymphoma as a component of composite lymphoma
yet unclear [30-33]. Given the uncertain clinical behavior, ithas been recently proposed for these tissue-based lesionsto be designated as FL- or MCL-like B cells of uncertainsignificance, respectively [33]. As in situ MCL can occur in alymphoid organ that appears normal by routine histologicexamination, to prevent in situ MCL being missed, it may bevaluable that cyclin D1, CD5, and BCL-2 (for in situ FL) beincluded in the diagnostic panel for revealing potentialcoexistence. From a histopathologic perspective, it is notuncommon to see partial involvement by an overt lymphomabefore this particular diagnosis is rendered [33].
2.2. CLL/ SLL-MCL
The occurrence of either diffuse large B-cell lymphoma orcHL arising in the setting of CLL/SLL is well known [34]. In
contrast, CLL/SLL has only rarely been reported to occursimultaneously with MCL (Fig. 2). To date, 10 CLL/SLL-MCL cases have been described in the literature. In 5 of thesepatients, CLL/SLL and MCL were synchronous and in-volved the same anatomical site and are thus included here astrue CLL/SLL-MCL CL [5,13-16,35,36]. All of the lattercases displayed clonal unrelatedness, indicating differentclonal origins for the 2 components.
Given that (1) a subset of CLL/SLL cases shows CD23negativity or aberrant expression of cyclin D1 within pro-liferation centers [37] and (2) 1 case of CLL/SLL-MCL (case11) displayed only a few CD23+ B cells in the absence ofpseudofollicles, although flow cytometry showed that 10%of lymph node cells were CD5−/CD23+high/Ig− B cells [15],pathologists attempting to pinpoint the type of lymphomashould be aware of such immunophenotypic variations anduse an integrated approach to establish the correct diagnosis

Table 2 Clinicopathologic features of CLs with an MCL component with a special emphasis on histology growth pattern and immunophenotypic profile of MCL component
Caseno./Ref
Subtypes oflymphoma
Morphology (MCLc) Immunophenotypic studies (MCLc) Clinical follow-up
1 [5] MCL + FL Diffuse growth pattern CD20+, CD5+, cyclin D1−, CD23−, CD43+,bcl-2+, κ−, λ−, p53−, p27−, Ki-67expression: 1%-2%
22 cycles of polychemotherapy over a period of 2 y;ANED at 8 y
2 [6] MCL + FL In situ MCL CD20+, CD5−, cyclin D1+, CD23−, CD43−,bcl-2+, Ki-67 expression: b5%a
The patient refused staging and therapy; dead ofunknown causes at 13 mo
3 [7] MCL + FL Mantle zone and nodulargrowth pattern
CD20+, CD79a+, CD5+, cyclin D1+, CD23−,CD10−, p27
Splenectomy at 2 y; AWD at 4.5 y
4 [8] MCL + FL Diffuse growth pattern CD20+, cyclin D1−b No chemotherapy; ANED at 4 mo5 [9] MCL + FL Mantle zone and nodular
growth patternCD20+, CD5+, cyclin D1+, IgD+, bcl-2+,bcl-6−, CD10−, CD3−, Ki-67 expression: b20%
NA
6 [10] MCL + FL In situ MCL CD20+, CD5−, cyclin D1+, IgD+, bcl-2+,bcl-6−, CD3−, CD23−, CD43−, CD10−,MUM-1−, Ki-67 expression: b5%
NA
7 [11] MCL + FL In situ MCL CD20+, CD5+, cyclin D1+, IgDWI, bcl-2WI,bcl-6−, CD10−, CD3−, p27PWI, Ki-67 expression: 8%
R-CHOP chemotherapy; alive in complete remissionat 27 mo
8 [12] MCL + FL Mantle zone growth pattern CD20+, CD5+, cyclin D1+ Radiotherapy and CHOP chemotherapy; DOD at 20 mo9 [13] MCL + CLL/SLL Diffuse growth pattern CD20+, CD5+, cyclin D1+, CD23− A watch-and-wait policy adopted; NA10 [14] MCL + CLL/SLL Nodular growth pattern CD20+, CD5+, cyclin D1+, CD23− 12 cycles of palliative oral chemotherapy
(chlorambucil) and prednisone; AWD at 16 mo11 [15] MCL + CLL/SLL NA CD20+, CD5+, CD23− NA12 [16] MCL + CLL/SLL Multifocal nodular and
interstitial growth patterncCD5+brightly, CD19+high, CD20+high, CD22+ ,FMC-7+, IgM κ+, CD10−, CD23−d
6 cycles of bendamustine and rituximab in the first-linesetting + maintenance therapy in the form of rituximab;alive in complete remission at 18 mo
13 [5] MCL + CLL/SLL Nodular growth pattern CD20+, CD5+/−, cyclin D1+, CD23−, CD43+, bcl-2+,IgD+, κ−, λ+, p53−, p27 −, Ki-67 expression: 3%-10%
NA
14 [17] MCL + cHL Sinusoidal growth pattern withan extracapsular extension
CD20+, cyclin D1+, Oct-2+, BOB1+ NA
15 [19] MCL + cHL Nodular growth pattern CD20+, CD5 −, cyclin D1+, CD23−, bcl-2+, CD43+,IgD+, CD10−, bcl-6 −, CD15−, CD30−, EBV−, LMP−
Diagnostic splenectomy; NA
16 [19] MCL + cHL Diffuse growth pattern CD20+, CD5−/+, cyclin D1+, CD23−, bcl-2+,CD43+, IgD+, CD10 −, bcl-6−, CD15−, CD30−,EBV−−, LMP−
Surgical resection of the eyelid tumor and cervical lymphnode; NA
17 [20] MCL + cHL Diffuse and vaguely nodulargrowth pattern
CD20+, CD79a+, CD3−, CD5−, cyclin D1+,CD23−, κ−, λ+
CHOP chemotherapy and fludarabine/cyclophosphamide/AWD after chemotherapy and finally dead of pneumoniaat 11 mo
18 [21] MCL + cHL Diffuse growth pattern CD20+, cyclin D1+ Reduced-dose 2-CdA and mitoxantrone (R-CdM) regimenfor MCL; conventional therapy for CL/dead of traumaticsubdural hematoma at 7 mo
19 [12] MCL + PCN Diffuse growth pattern CD20+, CD5WI, cyclin D1+, p53− Chemotherapy—chlorambucil; DOD at 56 mo
472T.
G.Papathom
aset
al.

20[22]
MCL+PCN
Diffuse
andfocally
vagu
ely
nodu
largrow
thpattern
CD20
+,CD5−,cyclin
D1+,IgD+,IgM
+,κ+,λ−
CHOPchem
otherapy
;dead
ofun
know
ncauses
with
indays
oftheendof
thefirstcycle
21[23]
MCL+PCN
Diffuse
grow
thpattern
CD20
+,CD5+,cyclin
D1+,IgM
+e
CD20
+,CD5+,cyclin
D1+,IgA+f
Surgicalresectionandradiotherapy
;ANED
at55
mo[23,24]
22[24]
MCL+PCN
Nod
ular
grow
thpattern
CD20
+,CD5+,cyclin
D1+,CD3−,CD23
−,
CD13
8−,IgG
−,IgM
−,κ−,λ−
Ritu
xan(w
ithdraw
alfrom
atrial);DOD
at28
mo
23[25]
MCL+SMZL
Nod
ular
grow
thpattern
CD20
+,CD5+,cyclin
D1+,CD23
−,CD10
−,Ig
λ+g
Diagn
ostic
splenectom
y;ANED
at1y
24[26]
MCL+no
dalMZL
Mantle
grow
thpattern
CD20
+,CD5+,cyclin
D1+,CD23
−,IgD+,IgM
+,bcl-2+
Radiotherapy;
ANED
at2y
25[27]
MCL+PBL
Nod
ular
grow
thpattern
CD20
+,CD79
a+,C
D5+,cyclin
D1+,bcl-2+,
CD10
−,CD13
8−,MUM1−
Chemotherapy
/NA
26[28]
MCL+BL
Nod
ular
grow
thpattern
CD20
+,CD5+,cyclin
D1+,bcl-2+,CD43
+,
CD10
−,Ki-67
expression
:30
%Fludarabine
for6mo,
splenectom
y;DOD
at4mo
Abb
reviations:M
CLc,MCLcompo
nent;A
WD,aliv
ewith
disease;ANED,aliv
ewith
noevidence
ofdisease;DOD,diedof
disease;NA,notavailable;ND,notdo
nedu
etoadvanced
age;NE,notevaluable;WI,
weakim
mun
ostaining;
PWI,partially
weakim
mun
ostaining;
R,rituximab;CHOP,cyclop
hosphamide,hy
drox
yldaun
orub
icin
(dox
orub
icin),on
covin(vincristin
e)andprednisone.
aIn
situ
hybridizationforκandλfailedto
displaydetectable
immun
oglobu
lintranscriptsin
themantle
zones(orin
follicularlymph
omano
dules).
bCD5+
,CD23
−,IgM/Dκisotyp
e(immun
opheno
typing
profile
ofthelymph
node
determ
ined
byflow
cytometricanalysisof
isolated
cells).
cExtensive
bone
marrowinvo
lvem
entb
ysm
allcelln
on-H
odgk
inlymph
oma;lymph
omatou
sinvo
lvem
entaccou
ntingforaminim
umof
65%
oftheprov
ided
sample.Neoplastic
lymph
ocytes
rang
ingfrom
smallto
medium
insize
andshow
ingroun
dto
indented
nuclearcontou
rs,mod
eratelyclum
pedchromatin,andscantclearcytoplasm.
dPeripheralbloo
dandbo
nemarrow
flow
cytometry
analysisdemon
strated2im
mun
opheno
typically
distinct
CD5+
mon
oclonalB-cellpo
pulatio
ns:κmon
otyp
icMCLandλmon
otyp
icB-cellchronic
lymph
ocytic
leuk
emia
(CD19
+,CD20
+dim,CD22
+,CD23
+,mon
otyp
icλlig
htchains
+dim,CD10
−andFMC-7
−).
e+fMon
otyp
icλandκlig
htchainrestrictionrespectiv
elybasedon
flow
cytometricanalysis.
gIm
mun
ohistochem
istryforIg
λwas
performed
onfrozen
section.
473Mantle cell lymphoma as a component of composite lymphoma
in the context of a CL, including detailed histopathologicanalysis, immunophenotypic studies, cytogenetics, andmolecular investigation. One case of CLL/SLL-MCLdescribed by Addada et al [13] consisted of a metastaticmelanoma and CLL/SLL-MCL together in a single lymphnode, an extremely rare example of 3 synchronous tumorwithin the same anatomical compartment [38-40].
2.3. cHL-MCL
Five cases of CL consisting of MCL and cHL have beenreported to date including 3 nodal, 1 extranodal (spleen), and1 displaying nodal as well as extranodal (eyelid) involvement[17-21]. There have been no reported CL cases of MCL andnodular lymphocyte predominant Hodgkin lymphoma(NLPHL). NLPHL also rarely coexists with other B-celllymphoproliferative disorders [41-43]. To our knowledge,only 1 case of a FL-NLPHL CL has been reported [43].
Another interesting issue is the description of a case ofcHL-MCL CL with synchronized dissemination of 2components in 2 separate anatomical locations (eyelid andlymph node) [19]. This rare case, along with an additionalCL case with cHL and peripheral T-cell lymphoma in 2distinct anatomical sites (liver and lymph node) [44],suggests a key role of microenvironmental factors [45,46].Another intriguing observation concerns 2 cases of cHL-MCL CL developing sequentially in the setting of MCL,which occurred 3 and 4 years earlier, respectively [17,21].Such a patient reinforces and further expands the concept thatpatients with non-Hodgkin lymphoma (NHL) have anincreased frequency of developing cHL [41]. As either thecHL or MCL component can be prevalent [17,21], a highindex of suspicion is required when dealing with a lympho-proliferative disorder after the occurrence of MCL in order tonot miss the diagnosis of an unusual CL (Fig. 3).
Epstein-Barr virus (EBV) infection is a known contribu-tor to the pathogenesis of a proportion of cHL cases. Thepresence EBV in the cHL component of some case reported(Table 3) provides additional evidence that EBV can play arole in the development of cHL in CLs, irrespective ofclonal relatedness [19,41,47-50]. Two other studies havereported that a subset of cHL-NHL CLs displayed EBVpositivity in each component, implying an origin from acommon EBV-infected progenitor cell [41,50]. However, itremains possible that EBV infection (or reactivation)functions as a nonpathogenic epiphenomenon given that(1) EBV infection might occur secondarily at the same timeor after cHL transformation [49], in a way analogous to thatpreviously described in a malignant T-cell clone [51] and(2) a subset of clonally related cHL-NHL CLs were actuallyEBV negative [52-56], suggesting a different pathogenesisindependent of EBV.
Of note, Tinguely et al [17,18] reported a unique caseof a clonally related cHL-MCL CL with EBV+ and EBV−
Hodgkin and Reed-Sternberg (HRS) cells (Table 3), the
A B C
FED
CD20 CD3
Cyclin D1
Clonality Analysis
CD5
MCL
SLL region
Fig. 2 Histologic and phenotypic features of MCL with small lymphocytic lymphoma. A, Nodular pattern of atypical lymphoid cells withexpanded mantle zone and internodular areas (hematoxylin and eosin stain, original magnification ×20). B, Differential CD20 staining ofatypical lymphoid cells in the nodular and internodular areas (immunoperoxidase stain, original magnification ×20). C, CD3 staining small Tcells in the internodular areas (immunoperoxidase stain, original magnification ×20). D, Weak CD5 staining of atypical lymphoid cells in thenodular and internodular areas (immunoperoxidase stain, original magnification ×20). E, Cyclin D1 staining of atypical lymphoid cells in theexpanded mantle zone and internodular areas with focal negative area of small lymphocytic lymphoma (immunoperoxidase stain, originalmagnification ×20). F, IgH PCR analysis on a MCL–small lymphocytic lymphoma composite case showing that the 2 lymphoid populationsare clonally unrelated.
Cyclin D1
CD30 CD30 EBV
A B C
D E F
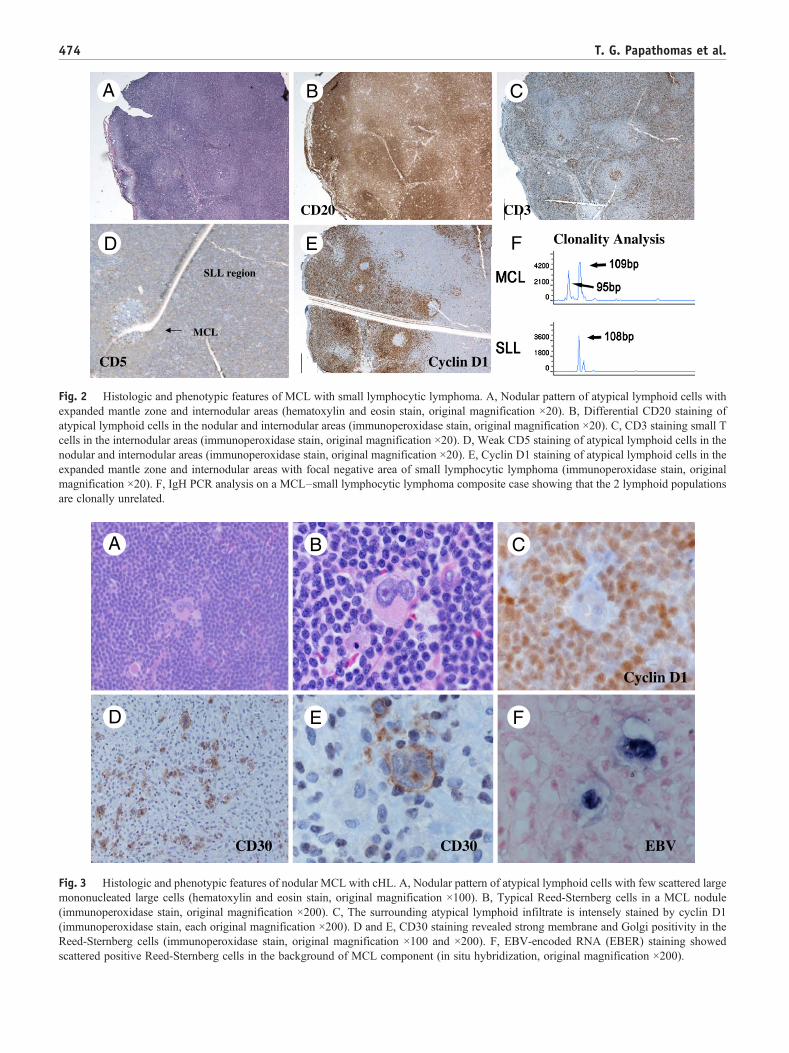
Fig. 3 Histologic and phenotypic features of nodular MCL with cHL. A, Nodular pattern of atypical lymphoid cells with few scattered largemononucleated large cells (hematoxylin and eosin stain, original magnification ×100). B, Typical Reed-Sternberg cells in a MCL nodule(immunoperoxidase stain, original magnification ×200). C, The surrounding atypical lymphoid infiltrate is intensely stained by cyclin D1(immunoperoxidase stain, each original magnification ×200). D and E, CD30 staining revealed strong membrane and Golgi positivity in theReed-Sternberg cells (immunoperoxidase stain, original magnification ×100 and ×200). F, EBV-encoded RNA (EBER) staining showedscattered positive Reed-Sternberg cells in the background of MCL component (in situ hybridization, original magnification ×200).
474 T. G. Papathomas et al.

475Mantle cell lymphoma as a component of composite lymphoma
only example of molecularly verified immunoglobulinheavy chain gene (IgH)–associated translocation in MCLand cHL. This case provides evidence that (1) IGH/CCND1translocation is an early step in the pathogenesis of cHL-MCL CL and most likely happens as a misguided VDJrecombination in a shared precursor during early B-celldevelopment; (2) a pregerminal center (GC) tumor cellprecursor gives rise to a HRS cell precursor. Whether thelatter shares a common precursor or is a direct descendant ofthe MCL clone has not been elucidated; (3) the GCmicroenvironment plays an important role in HodgkinLymphoma (HL) pathogenesis because mutated Ig variableregion (V) gene rearrangements were present only in HRScells; and (4) EBV infection of HRS cell precursors occursin the GC, contrasting experimental evidence supporting adifferent developmental (pre-GC) stage for this particularevent [57,58]. Given the distinctive mutation patternsobserved in EBV+ and EBV− HRS cells, coupled with thefact that only a subclone of HRS progenitor cell was EBVinfected [17], one could speculate that EBV infection playsan important role in the direct development of cHL, whereasother transforming events may reflect pathogenetic mech-anisms unrelated to EBV that account for the developmentof the EBV− cHL component of CLs.
Table 3 Histopathologic characteristics of Hodgkinlymphoma in the context of CLs with an MCL component,with a special emphasis on EBV status and the clonalrelatedness of the individual components
Case no./Ref Type of cHL EBV presencein HRS cells
Clonalrelatedness
14 [17] Lymphocyte-rich +/− Yes15 [19] Nodular sclerosis + No16 [19] Nodular sclerosis + No17 [20] Nodular sclerosis − NA18 [21] Unclassifiable + NA
2.4. PCN-MCL
We identified 4 clonally unrelated cases of MCLassociated with PCN, which are indeed bonafide CL, 2arising from the extranodal soft tissue of the head (eyelid andorbit and nasopharynx) [12,22-24]. One additional case of aconcomitant extranodal MCL and plasma cell myeloma wasreported [59]. As far as the latter case is concerned,Yamaguchi et al [59] performed clonality analysis usingpolymerase chain reaction (PCR) of the IgH gene comple-mentarity–determining region 3, including a single-cellassay, and confirmed clonal independence. However, thedesignation “PCN-MCL CL” should be used cautiously.First, clonal plasma cell differentiation in MCL has recentlybeen documented [24,60,61]. Others have proposed thatthese cases represent a novel morphological type of MCL[24,60], after no convincing evidence was found concerningthe differentiation of MCL cells into clonal PCs [62,63].Second, 4 (50%) of 8 patients with MCL associated with aclonal plasma cell population displayed a monoclonalparaprotein [24,61], and monoclonal IgM and IgG havebeen detected in 18% and 5% of MCL cases, respectively, in1 study [64]. Thus, given the potential difference between theprognosis and therapy of PCN-MCL CL compared withMCL with plasmacytic differentiation (Fig. 4), hemato-pathologists should always attempt to use a molecularapproach to determine the clonal relationship between the 2components with clonal independence establishing a diag-nosis of a PCN-MCL CL. However, it should be stressed thatneither immunohistochemistry nor the presence of the
t(11;14)(q13;q32) in both the MCL and the plasmacyticcomponent are sufficient to make this discrimination becausenot all clonally related cases display identical monotypic Iglight-chain expression between the 2 populations, in part,because of potential intraclonal variation [24,65], and thet(11;14)(q13;q32) can be observed in nonhyperdiploidplasma cell myeloma [66]. Instead, immunohistochemistryand fluorescence in situ hybridization (FISH) cytogeneticscan be used for the differential diagnosis of this uniquevariant of MCL from other low-grade B-cell lymphomaswith plasmacytic differentiation.
2.5. MZL-MCL
We identified 2 cases of MZL-MCL CL in the literature,1 case composed of nodal (N) MZL and the other splenic (S)MZL [25,26]. In an exploration of leukemic B-cell chroniclymphoproliferative disorders with more than 1 B-cell clone,Sanchez et al [36] described an additional case of syn-chronous extranodal MZL (mucosa-associated lymphoidtissue lymphoma) and MCL, and the presence of biclonalitywas confirmed by an IgH rearrangement molecular study.These 2 cases of MZL-MCL CL showed remarkable com-partmentalization of the 2 lymphomatous populations[25,26], providing strong evidence that these lymphomasarise from and remain confined to the discrete microana-tomical sites of their postulated nonneoplastic counterpartsduring the early stages of their development [26,34]. Apartfrom this topographic distribution, it is worth noting thatIgH VH gene mutations, indicative of the influence of themutational machinery of the follicular GC, characterize asubset of MCL (15%-40%) and SMZL (50%), whereas asubset of nodal marginal zone lymphoma (NMZL) (14%-25%) demonstrates an unmutated IgH VH gene sequence,implying a naïve B-cell origin for neoplastic cells [67,68].From a diagnostic standpoint, it is important to exclude thepossibility of a MZL-like MCL, and given the immunohis-tochemical aberrancies that have been described in bothMCL and MZL [69-71], a panel of immunostains (CD5 andcyclin D1) in combination with cytogenetics or FISHtechniques for t(11;14)(q13;q32) is highly recommended

Cyclin D1 Cyclin D1
Kappa Lambda
CD138
t(11;14)
A B C
FED
G H I
Fig. 4 Histologic and phenotypic features of MCL with clonal plasma cells. A and B, Nodular pattern of atypical lymphoid cells in theexpanded mantle zones. Clonal plasma cells are present within a nodule (hematoxylin and eosin stain, original magnification ×20 and×100). C, Cluster of clonal plasma cells in a nodule (hematoxylin and eosin stain, original magnification ×400). D and E, Cyclin D1 stainshowing nuclear positivity in the MCL component, whereas the staining in the plasma cells is undetermined or very weakly positive(immunoperoxidase stain, original magnification ×20 and ×400). F, CD138-positive clonal plasma cells within tumor nodules(immunoperoxidase stain, original magnification ×20). G and H, κ Light chain stain showing numerous positive plasma cells comparedwith only a rare positive cell with the corresponding λ light chain stain (messenger RNA in situ hybridization stains, original magnification×100). I, fluorescence immunophenotyping and interphase cytogenetics as a tool for the investigation of neoplasms analysis showing PCswith clonal κ light chain staining and the t(11;14). Clusters of κ light chain–positive plasma cells harbor the t(11;14) in their nuclei. Thered spots within the nuclei represent hybridization signals of the CCND1 gene on chromosome 11, whereas the green spots arehybridization signals of the IgH gene on chromosome 14. The t(11;14) fusion signals are identified as yellow or fused red-green signals, asillustrated by the arrows (fluorescence immunophenotyping and interphase cytogenetics as a tool for the investigation of neoplasms, originalmagnification ×1000).
476 T. G. Papathomas et al.
to distinguish this MCL variant from a true MZL-MCLCL (Fig. 5).
2.6. PBL-MCL and BL-MCL
According to the 2008 World Health Organization Clas-sification of Tumours of Haematopoietic and LymphoidTissues, histologic transformation of MCL to large celllymphoma does not occur [34]. It is acknowledged, however,that, at time of relapse, some MCL cases can display mor-phological features of histologic progression that potentiallyfulfill the criteria for being classified as pleomorphic MCL
variant [34]. We suggest, however, that this is a matter ofdefinition and is, in part, semantic. Certainly patients withMCL can progress to a histologic appearance that canoverlap with diffuse large B-cell lymphoma or even BL andmight be classified as such, if IGH/CCND1 and cyclin D1overexpression were not also identified. This being said, itseems to us that many cases reported as the pleomorphicvariant of MCL represent histologic transformation to ahigher grade B-cell lymphoma the same cases are clonallyrelated. In further support of this concept, Aukema et al [72]also have included neoplasms with t(11;14)(q13;q32)(CCND1/IGH) plus 8q24/MYC rearrangements as aform of double-hit B-cell lymphoma.

CD23MCL
NMZL
CD79a
Ki-67Cyclin D1BCL-2
A B C
FED
Fig. 5 Histologic and phenotypic features of nodular MCL with MZL. Nodular pattern of atypical lymphoid cells with variably confinedcentral regions and expanded marginal zones (hematoxylin and eosin stain, original magnification 40×) (A); weak CD23 staining highlighted asmall follicular dendritic cell network in an MCL nodule (immunoperoxidase stain, original magnification ×200) (B); both the nodules and thesurrounding infiltrate between the nodules displayed CD20 (not shown), CD79, and BCL-2 (C and D); note that the MCL component (both innodules and peripheral rim) is more intensely stained than the MZL component (immunoperoxidase stain, each original magnification ×20);cyclin D1 staining revealed a strong nuclear positivity for the nodular (MCL) component (immunoperoxidase stain, original magnification×100) (E); Ki-67 staining showed scattered atypical lymphoid cells in perinodular MZL areas but rare in the MCL component(immunoperoxidase stain, original magnification ×100) (F).
477Mantle cell lymphoma as a component of composite lymphoma
In the literature, we identified 2 cases reported as MCLtransforming into extranodal PBL or BL [27,28]. Althoughan increasing amount of evidence indicates a close rela-tionship between PBL and plasmablastic transformation ofPCN [73-77], the event of clonal plasmablastic transforma-tion has, to our knowledge, been reported only twice in otherB-cell NHL (FL and MCL) [27,78]. PBLs arising second-arily in the setting of CLL/SLL have been found to havedistinct clonal origins [79,80]. These highly unusual forms ofFL and MCL transformation are characterized by extranodallocalization; EBV negativity; retention of the t(14;18)(q32;q21) or the t(11;14)(q13;q32), respectively; and a commonclonal link, suggesting either divergent evolution from acommon progenitor cell or direct evolution from the FL orMCL clone [27,78,81]. In addition, Ouansafi et al [78]identified an MYC gene rearrangement in association withthe IGH/BCL-2 translocation in the transformed PBLcomponent, in accord with previously published studies[75,82,83], implying a pivotal role for MYC oncogenicdysregulation in the pathogenesis of PBL. Felten et al [28]documented an MCL transforming to BL containing anIGH/CCND1 translocation and MYC gene rearrangement.MYC gene abnormalities are uncommon secondary eventsthat occur in a subset of MCLs associated with leukemic
involvement; these cases have a characteristic morphology(blastoid, pleomorphic, or even BL-like) and an aggressiveclinical course with a poor prognosis [72,84-86].
3. Immunophenotypic profile of the MCLcomponent in the setting of CL
With regard to variations from the typical immunopheno-type of MCL, cyclin D1–negative (2 FL-MCL CLs) and/orCD5-immunonegative patterns (5/8) were the only aber-rancies displayed in the MCL component of CLs (Table 2).Two of these CD5− cases concerned in situMCLs, suggestingthat MCL is initially CD5 negative and that CD5 expressionoccurs later after the acquisition of additional genetic lesionsand evolution to overt MCL [10,29]. Nevertheless, CD5expression may be unstable and not necessarily related to theacquisition of genetic abnormalities. In fact, CD5 immuno-negativity has been reported in a subgroup of conventionalMCL along with a small subgroup of indolent MCL withperipheral blood involvement, t(11;14) translocation, andsomatic hypermutations [30,87]. Whether the latter subsetrepresents the favorable end of the spectrum in the evolution

478 T. G. Papathomas et al.
of MCL or an indolent form of MCL is uncertain [30]. In thiscontext, Fernàndez et al [88] recently provided evidencebased on genomic and expression profiling data that thisindolent MCL seems to correspond to a specific biologicMCL subtype characterized by a constellation of clinicobio-logic features encompassing (1) a predominant nonnodal andasymptomatic presentation; (2) stable disease; (3) high rate ofIGVH gene mutations; (4) lack of genomic complexity; and(5) absence of SOX11 expression. In addition, they showedthat indolent MCL cases had a small cell variant morphologyand exhibited CD5 negativity more frequently than conven-tional MCL cases [88].
4. Conclusion
In conclusion, we have provided a review of all knownCLs with an MCL component reported in the literature thusfar, providing further insight into the process of lymphoma-genesis and highlighting the heterogeneity of this poorlyunderstood circumstance. With the small number of casesand heterogeneous therapy, we cannot make definitive rec-ommendations. However, we have attempted to make sur-gical pathologists and hematopathologists aware of theclinicopathologic spectrum of MCL as a major pathologicpart of CL. We further show that a complete diagnosticworkup is needed in cases of MCL, not only to establish thecorrect diagnosis and exclude various morphological mimicsbut also in directing ancillary testing to detect clonal rela-tedness and, hence, provide prognostic and therapeuticimplications in CLs with an MCL component. To gain abetter understanding of this subtype of CL, further clonalitystudies are warranted.
Acknowledgments
The authors thank Dr Valerie A. White (Department ofPathology and Laboratory Medicine, Vancouver GeneralHospital and University of British Columbia, Vancouver,Canada), Machiko Tsukaguchi (Department of Hematology,Sakai Municipal Hospital, Osaka, Japan), and AlessandraStacchini (Flow Cytometry Unit, Department of Pathology,Molinette Hospital, Turin, Italy) for providing clinicopath-ologic data and follow-up information (cases 8/19 and cases18 and 7, respectively); Taxiarchis V. Kourelis (Departmentof Medicine, Saint Francis Hospital and Medical Center,Hartford, CT) as well as Michele R. Roullet and Adam Bagg(Pathology Sciences Medical Group/Eastern VirginiaMedical School, Norfolk, VA, & Department of Pathologyand Laboratory Medicine, Hospital of the University ofPennsylvania, Philadelphia, PA) for providing additionalhistopathologic and immunophenotypic data (cases 2 and12, respectively).
References
[1] Ioachim HL, Medeiros LJ. Composite lymphoma. In: Ioachim HL,Medeiros LJ, editors. Ioachim's lymph node pathology. Philadelphia,USA: Lippincott Williams & Wilkins; 2008. p. 452-9.
[2] Gonzalez CL, Medeiros LJ, Jaffe ES. Composite lymphoma—aclinicopathological analysis of 9 patients with Hodgkins disease andB-cell non-Hodgkin lymphoma. Am J Clin Pathol 1991;96:81-9.
[3] Müller-Hermelink HK, Zettl A, Pfeifer W, Ott G. Pathology oflymphoma progression. Histopathology 2001;38:285-306.
[4] Banks PM, Chan J, Cleary ML, et al. Mantle cell lymphoma. Aproposal for unification of morphologic, immunologic, and moleculardata. Am J Surg Pathol 1992;16:637-40.
[5] Fend F, Quintanilla-Martinez L, Kumar S, et al. Composite low gradeB-cell lymphomas with two immunophenotypically distinct cellpopulations are true biclonal lymphomas. A molecular analysis usinglaser capture microdissection. Am J Pathol 1999;154:1857-66.
[6] Roullet MR, Martinez D, Ma L, et al. Coexisting follicular and mantlecell lymphoma with each having an in situ component: a novel,curious, and complex consultation case of coincidental, composite,colonizing lymphoma. Am J Clin Pathol 2010;133:584-91.
[7] Zamò A, Zanotti R, Lestani M, et al. Molecular characterization ofcomposite mantle cell and follicular lymphoma. Virchows Arch 2006;448:639-43.
[8] Tsang P, Pan L, Cesarman E, Tepler J, Knowles DM. A distinctivecomposite lymphoma consisting of clonally related mantle celllymphoma and follicle center cell lymphoma. HUM PATHOL 1999;30:988-92.
[9] Ilgenfritz RB, Le Tourneau A, Arborio M, et al. Composite mantlecell and follicular lymphoma. A case report. HUM PATHOL 2009;40:259-63.
[10] Aqel N, Barker F, Patel K, Naresh KN. In-situ mantle cell lymphoma—a report of two cases. Histopathology 2008;52:256-60.
[11] Demurtas A, Aliberti S, Bonello L, et al. Usefulness of multiparametricflow cytometry in detecting composite lymphoma: study of 17 cases ina 12-year period. Am J Clin Pathol 2011;135:541-55.
[12] Looi A, Gascoyne RD, Chhanabhai M, et al. Mantle cell lymphoma inthe ocular adnexal region. Ophthalmology 2005;112:114-9.
[13] Addada J, Anoop P, Swansbury JG, et al. Synchronous mantle celllymphoma, chronic lymphocytic leukaemia and melanoma in a singlelymph node. Acta Haematol 2010;123:194-6.
[14] Perdigão J, Alaiz H, Lúcio P, et al. Mantle cell lymphoma and chroniclymphocytic leukemia: report of a rare disease association and reviewof the literature. J Hematopathol 2010;3:91-9.
[15] Lima M, Pinto L, Dos Anjos Teixeira M, et al. Guess what: chronic13q14.3+/CD5-/CD23+ lymphocytic leukemia in blood andt(11;14)(q13;q32)+/CD5+/CD23− mantle cell lymphoma in lymphnodes! Cytometry B Clin Cytom 2003;51:41-4.
[16] Kourelis TV, Kahl BS, Benn P, et al. Treatment of synchronous mantlecell lymphoma and small lymphocytic lymphoma with bendamustineand rituximab. Acta Haematol 2011;126:40-3.
[17] Tinguely M, Rosenquist R, Sundström C, et al. Analysis of a clonallyrelated mantle cell and Hodgkin lymphoma indicates Epstein-Barrvirus infection of a Hodgkin/Reed-Sternberg cell precursor in agerminal center. Am J Surg Pathol 2003;27:1483-8.
[18] Schmitz R, Renné C, Rosenquist R, et al. Insights into the multisteptransformation process of lymphomas: IgH-associated translocationsand tumor suppressor gene mutations in clonally related compositeHodgkin's and non-Hodgkin's lymphomas. Leukemia 2005;19:1452-8.
[19] Caleo A, Sánchez-Aguilera A, Rodríguez S, et al. Composite Hodgkinlymphoma and mantle cell lymphoma: two clonally unrelated tumors.Am J Surg Pathol 2003;27:1577-80.
[20] Hayes SJ, Banerjee SS, Cook Y, et al. Composite mantle-cell lym-phoma and classical Hodgkin lymphoma. Histopathology 2006;48:621-3.

479Mantle cell lymphoma as a component of composite lymphoma
[21] Senhara T, Aosasa K, Shibano S, Tsukaguchi M. [Picture in clinicalhematology no. 39: composite hodgkin lymphoma and mantle celllymphoma]. Rinsho Ketsueki 2009;50:517.
[22] Cachia AR, Diss TC, Isaacson PG. Composite mantle-cell lymphomaand plasmacytoma. HUM PATHOL 1997;28:1291-5.
[23] Wang HY, Karandikar N, Payne D, et al. A 3-way collision tumor ofthe upper respiratory tract: a composite of 2 immunophenotypicallydistinct mantle cell lymphomas and a plasmacytoma. HUM PATHOL2008;39:781-7.
[24] Visco C, Hoeller S, Malik JT, et al. Molecular characteristics of mantlecell lymphoma presenting with clonal plasma cell component. Am JSurg Pathol 2011;35:177-89.
[25] Lefebvre C, Fabre B, Vettier C, et al. Composite splenic marginal zonelymphoma and mantle cell lymphoma arising from 2 independentB-cell clones. HUM PATHOL 2007;38:660-7.
[26] Rodig SJ, Healey BM, Pinkus GS, et al. Mantle cell lymphoma arisingwithin primary nodal marginal zone lymphoma: a unique presentationof two uncommon B-cell lymphoproliferative disorders. Cancer GenetCytogenet 2006;171:44-51.
[27] Cooper CL, Joshua DE, Lee CS, et al. Extranodal plasmablasticlymphoma arising in mantle cell lymphoma. Histopathology 2007;51:856-9.
[28] Felten CL, Stephenson CF, Ortiz RO, Hertzberg L. Burkitt transforma-tion of mantle cell lymphoma. Leuk Lymphoma 2004;45:2143-7.
[29] Carbone A, Santoro A. How I treat: diagnosing and managing “in situ”lymphoma. Blood 2011;117:3954-60.
[30] Espinet B, Solé F, Pedro C, et al. Clonal proliferation of cyclin D1–positive mantle lymphocytes in an asymptomatic patient: an early-stage event in the development or an indolent form of a mantle celllymphoma? HUM PATHOL 2005;36:1232-7.
[31] Nodit L, Bahler DW, Jacobs SA, et al. Indolent mantle cell lymphomawith nodal involvement and mutated immunoglobulin heavy chaingenes. HUM PATHOL 2003;34:1030-4.
[32] Bassarova A, Tierens A, Lauritzsen GF, et al. Mantle cell lymphomawith partial involvement of the mantle zone: an early infiltrationpattern of mantle cell lymphoma? Virchows Arch 2008;453:407-11.
[33] Campo E, Swerdlow SH, Harris NL, et al. The 2008 WHOclassification of lymphoid neoplasms and beyond: evolving conceptsand practical applications. Blood 2011;117:5019-32.
[34] World Health Organization Classification of Tumours. In: SwerdlowSH, Campo E, Harris NL, et al, editors. World Health OrganizationClassification of Tumours of Haematopoietic and Lymphoid Tissues.Geneva: IARC Press; 2008. p. 233-68.
[35] Medlicott SA, Brown HA, Roland B, et al. Multiple lymphomatousdiverticulosis and comorbid chronic lymphocytic leukemia: novelmanifestations of ileocolic mantle cell lymphoma. Int J Surg Pathol2007;15:408-13.
[36] Sanchez ML, Almeida J, Gonzalez D, et al. Incidence and clinico-biologic characteristics of leukemic B-cell chronic lymphoproliferativedisorders with more than one B-cell clone. Blood 2003;102:2994-3002.
[37] Lu J, Chang KL. Practical immunohistochemistry in hematopathology:a review of useful antibodies for diagnosis. Adv Anat Pathol 2011;18:133-51.
[38] El Demellawy D, Ross C, Sur M, Alowami S. Synchronouslydiagnosed lymph nodal collision tumor of malignant melanoma andchronic lymphocytic leukemia/small lymphocytic lymphoma: casereport. Diagn Pathol 2007;2:34.
[39] Cantor AS, Moschos S, Jukic DM. A principal case of multiplelymphoid collision tumors involving both B-cell chronic lymphocyticleukemia and metastatic malignant melanoma. Dermatol Online J2010;16:6.
[40] St Peter SD, Roarke MC, Conley CR, Pockaj BA. Sentinel lymph nodebiopsy demonstrating concomitant melanoma and mantle celllymphoma. Surgery 2002;131:216-8.
[41] Jaffe ES, Zarate-Osorno A, Kingma DW, et al. The interrelationshipbetween Hodgkin's disease and non-Hodgkin's lymphomas. AnnOncol 1994;5(Suppl 1):7-11.
[42] Delabie J, Greiner TC, Chan WC, Weisenburger DD. Concurrentlymphocyte predominance Hodgkin's disease and T-cell lymphoma. Areport of three cases. Am J Surg Pathol 1996;20:355-62.
[43] Dargent JL, Lespagnard L, Meiers I, et al. Composite follicularlymphoma and nodular lymphocyte predominance Hodgkin's disease.Virchows Arch 2005;447:778-80.
[44] Sanchez S, Holmes H, Katabi N, et al. Composite lymphocyte-richHodgkin lymphoma and peripheral T-cell lymphoma associated withEpstein-Barr virus: a case report and review of the literature. ArchPathol Lab Med 2006;130:107-12.
[45] Coupland SE. The challenge of the microenvironment in B-celllymphomas. Histopathology 2011;58:69-80.
[46] Aldinucci D, Gloghini A, Pinto A, et al. The classical Hodgkin'slymphoma microenvironment and its role in promoting tumour growthand immune escape. J Pathol 2010;221:248-63.
[47] de Leval L, Vivario M, De Prijck B, et al. Distinct clonal origin in twocases of Hodgkin's lymphoma variant of Richter's syndromeassociated with EBV infection. Am J Surg Pathol 2004;28:679-86.
[48] Mao Z, Quintanilla-Martinez L, Raffeld M, et al. IgVH mutationalstatus and clonality analysis of Richter's transformation: diffuse largeB-cell lymphoma and Hodgkin lymphoma in association with B-cellchronic lymphocytic leukemia (B-CLL) represent 2 different pathwaysof disease evolution. Am J Surg Pathol 2007;31:1605-14.
[49] Huang Q, Wilczynski SP, Chang KL, Weiss LM. Composite recurrenthodgkin lymphoma and diffuse large B-cell lymphoma: one clone, twofaces. Am J Clin Pathol 2006;126:222-9.
[50] Kingma DW, Medeiros LJ, Barletta J, et al. Epstein-Barr virus isinfrequently identified in non-Hodgkin's lymphomas associated withHodgkin's disease. Am J Surg Pathol 1994;18:48-61.
[51] Langer R, Geissinger E, Rüdiger T, et al. Peripheral T-cell lymphomawith progression to a clonally related, Epstein Barr virus+, cytotoxicaggressive T-cell lymphoma: evidence for secondary EBV infection ofan establishedmalignant T-cell clone.AmJSurg Pathol 2010;34:1382-7.
[52] Bräuninger A, Hansmann ML, Strickler JG, et al. Identification ofcommon germinal-center B-cell precursors in two patients with bothHodgkin's disease and non-Hodgkin's lymphoma. N Engl J Med1999;340:1239-47.
[53] Bellan C, Lazzi S, Zazzi M, et al. Immunoglobulin gene rearrangementanalysis in composite hodgkin disease and large B-cell lymphoma:evidence for receptor revision of immunoglobulin heavy chain variableregion genes in Hodgkin-Reed-Sternberg cells? Diagn Mol Pathol2002;11:2-8.
[54] van den Berg A, Maggio E, Rust R, et al. Clonal relation in a case ofCLL, ALCL, and Hodgkin composite lymphoma. Blood 2002;100:1425-9.
[55] Kanzler H, Küppers R, Helmes S, et al. Hodgkin and Reed-Sternberg-like cells in B-cell chronic lymphocytic leukemia represent theoutgrowth of single germinal-center B-cell–derived clones: potentialprecursors of Hodgkin and Reed-Sternberg cells in Hodgkin's disease.Blood 2000;95:1023-31.
[56] Küppers R, Sousa AB, Baur AS, et al. Common germinal-center B-cellorigin of the malignant cells in two composite lymphomas, involvingclassical Hodgkin's disease and either follicular lymphoma or B-CLL.Mol Med 2001;7:285-92.
[57] Babcock GJ, Hochberg D, Thorley-Lawson AD. The expressionpattern of Epstein-Barr virus latent genes in vivo is dependent upon thedifferentiation stage of the infected B cell. Immunity 2000;13:497-506.
[58] Bechtel D, Kurth J, Unkel C, Küppers R. Transformation of BCR-deficient germinal-center B cells by EBV supports a major role ofthe virus in the pathogenesis of Hodgkin and posttransplantationlymphomas. Blood 2005;106:4345-50.
[59] Yamaguchi M, Ohno T, Miyata E, et al. Analysis of clonal relationshipusing single-cell polymerase chain reaction in a patient with con-comitant mantle cell lymphoma and multiple myeloma. Int J Hematol2001;73:383-5.
[60] Young KH, Chan WC, Fu K, et al. Mantle cell lymphoma with plasmacell differentiation. Am J Surg Pathol 2006;30:954-61.

480 T. G. Papathomas et al.
[61] Naushad H, ChoiWW, Page CJ, et al. Mantle cell lymphoma with flowcytometric evidence of clonal plasmacytic differentiation: a casereport. Cytometry B Clin Cytom 2009;76:218-24.
[62] Weisenburger DD. Mantle-zone lymphoma. An immunohistologicstudy. Cancer 1984;53:1073-80.
[63] Swerdlow SH, Zukerberg LR, Yang WI, et al. The morphologicspectrum of non-Hodgkin's lymphomas with BCL1/cyclin D1 generearrangements. Am J Surg Pathol 1996;20:627-40.
[64] Preud'homme JL, Gombert J, Brizard A, et al. Serum Ig abnormalitiesin mantle cell lymphoma. Blood 1997;90:894-5.
[65] Nakamine H, Masih AS, Sanger WG, et al. Richter's syndrome withdifferent immunoglobulin light chain types. Molecular and cytogeneticfeatures indicate a common clonal origin. Am J Clin Pathol 1992;97:656-63.
[66] Fonseca R, Bergsagel PL, Drach J, et al. International MyelomaWorking Group molecular classification of multiple myeloma:spotlight review. Leukemia 2009;23:2210-21.
[67] Jares P, Campo E. Advances in the understanding of mantle celllymphoma. Br J Haematol 2008;142:149-65.
[68] Mollejo M, Camacho FI, Algara P, et al. Nodal and splenic marginalzone B cell lymphomas. Hematol Oncol 2005;23:108-18.
[69] Mozos A, Royo C, Hartmann E, et al. SOX11 expression is highlyspecific for mantle cell lymphoma and identifies the cyclin D1–negative subtype. Haematologica 2009;94:1555-62.
[70] Tasaki K, Shichishima A, Furuta M, et al. CD5-positive mucosa-associated lymphoid tissue (MALT) lymphoma of ocular adnexalorigin: usefulness of fluorescence in situ hybridization for distinctionbetween mantle cell lymphoma and MALT lymphoma. Pathol Int2007;57:101-7.
[71] Rymkiewicz G, Ptaszyński K, Walewski J, et al. Unusual cyclin D1positive marginal zone lymphoma of mediastinum. Med Oncol 2006;23:423-8.
[72] Aukema SM, Siebert R, Schuuring E, et al. Double-hit B-celllymphomas. Blood 2011;117:2319-31.
[73] Colomo L, Loong F, Rives S, et al. Diffuse large B-cell lymphomaswith plasmablastic differentiation represent a heterogeneous group ofdisease entities. Am J Surg Pathol 2004;28:736-47.
[74] Vega F, Chang CC, Medeiros LJ, et al. Plasmablastic lymphomas andplasmablastic plasma cell myelomas have nearly identical immuno-phenotypic profiles. Mod Pathol 2005;18:806-15.
[75] Taddesse-Heath L, Meloni-Ehrig A, Scheerle J, et al. Plasmablasticlymphoma with MYC translocation: evidence for a common path-way in the generation of plasmablastic features. Mod Pathol 2010;23:991-9.
[76] Qing X, Sun N, Chang E, et al. Plasmablastic lymphoma may occuras a high-grade transformation from plasmacytoma. Exp Mol Pathol2011;90:85-90.
[77] Lee CK, Ma ES, Shek TW, et al. Plasmablastic transformation ofmultiple myeloma. HUM PATHOL 2003;34:710-4.
[78] Ouansafi I, He B, Fraser C, et al. Transformation of follicularlymphoma to plasmablastic lymphoma with c-myc gene rearrange-ment. Am J Clin Pathol 2010;134:972-81.
[79] Robak T, Urbańska-Ryś H, Strzelecka B, et al. Plasmablasticlymphoma in a patient with chronic lymphocytic leukemia heavilypretreated with cladribine (2-CdA): an unusual variant of Richter'ssyndrome. Eur J Haematol 2001;67:322-7.
[80] Foo WC, Huang Q, Sebastian S, et al. Concurrent classical Hodgkinlymphoma and plasmablastic lymphoma in a patient with chroniclymphocytic leukemia/small lymphocytic lymphoma treated withfludarabine: a dimorphic presentation of iatrogenic immunodeficien-cy-associated lymphoproliferative disorder with evidence suggestiveof multiclonal transformability of B cells by Epstein-Barr virus. HUM
PATHOL 2010;41:1802-8.[81] Carlotti E, Wrench D, Matthews J, et al. Transformation of follicular
lymphoma to diffuse large B-cell lymphoma may occur by divergentevolution from a common progenitor cell or by direct evolution fromthe follicular lymphoma clone. Blood 2009;113:3553-7.
[82] Valera A, Balagué O, Colomo L, et al. IG/MYC rearrangements arethe main cytogenetic alteration in plasmablastic lymphomas. Am JSurg Pathol 2010;34:1686-94.
[83] Bogusz AM, Seegmiller AC, Garcia R, et al. Plasmablastic lymphomaswith MYC/IgH rearrangement: report of three cases and review of theliterature. Am J Clin Pathol 2009;132:597-605.
[84] Hao S, Sanger W, Onciu M, et al. Mantle cell lymphoma with 8q24chromosomal abnormalities: a report of 5 cases with blastoid features.Mod Pathol 2002;15:1266-72.
[85] Reddy K, Ansari-Lari M, Dipasquale B. Blastic mantle cell lymphomawith a Burkitt translocation. Leuk Lymphoma 2008;49:740-50.
[86] Au WY, Horsman DE, Viswanatha DS, et al. 8q24 translocations inblastic transformation of mantle cell lymphoma. Haematologica2000;85:1225-7.
[87] Orchard J, Garand R, Davis Z, et al. A subset of t(11;14) lymphomawith mantle cell features displays mutated IgVH genes and includespatients with good prognosis, nonnodal disease. Blood 2003;101:4975-81.
[88] Fernàndez V, Salamero O, Espinet B, et al. Genomic and geneexpression profiling defines indolent forms of mantle cell lymphoma.Cancer Res 2010;70:1408-18.




















