
Risedronate did not block the maximal anabolic effect of PTH in aged rats
7
Risedronate did not block the maximal anabolic effect of PTH in aged rats Wei Yao a , Ming Su a , Qing Zhang a , Xiaoyan Tian a , Rebecca B. Setterberg a , Cindy Blanton b , Mark W. Lundy b , Roger Phipps b , Webster S.S. Jee a, ⁎ a Division of Radiobiology, University of Utah School of Medicine, 729 Arapeen Dr., Suite 2338, Salt Lake City, UT 84108, USA b Procter & Gamble Pharmaceuticals, Mason, OH, USA Received 16 February 2007; revised 15 June 2007; accepted 4 July 2007 Available online 17 July 2007 Abstract The study was designed to investigate if pre-treating rats with a therapeutic equivalent dose of risedronate blunted the anabolic effects of PTH, and whether a withdrawal period prior to PTH treatment would alter any effect of risedronate on PTH treatment. Skeletally mature rats were treated for 18 weeks with vehicle, risedronate, or risedronate for 8 weeks followed by vehicle for 10 weeks (withdrawal period). At the end of this period, animals were treated for a further 12 weeks with PTH or PTH vehicle. Trabecular and cortical bone mass were monitored by serial pQCT, or by DXA and microCT. Bone histomorphometry was performed on the proximal tibiae and tibial shafts for bone turnover parameters at week 40. Risedronate alone moderately increased while PTH alone markedly increased trabecular bone mass at the proximal tibial (35% and 200%, respectively) and lumbar vertebral body (14% and 36%, respectively). The maximum bone gains were similar with and without pretreatment with risedronate as compared to the PTH alone. Continuous administration of risedronate for 18 weeks prior to PTH treatment had lower percentage increases in proximal tibial BMD during the first 8 weeks of PTH treatments, and had lower active bone forming surface and bone formation rates after being treated with PTH 12 weeks as compared to the PTH alone group. However, with the 10-week withdrawal period, risedronate did not blunt the stimulatory effect of PTH on osteoblast activity as shown by similar bone formation rates as with PTH alone. Our findings suggest that while risedronate pretreatment may slow the bone anabolic response to PTH, a withdrawal period prior to PTH treatment allows osteoblastic activity to respond normally to PTH stimulation. © 2007 Elsevier Inc. All rights reserved. Keywords: Risedronate; PTH; Withdrawal; Bone morphology Introduction Anti-resorptive agents have been available as the “first-line” therapeutic agents for the prevention and treatment for osteopo- rosis in the past decade [1–5]. The development of parathyroid hormone and its analogs has provided a new approach of anabolic therapy for osteoporosis [6–9]. How best to use the combination of anti-resorptive and anabolic drugs is not clear. When PTH was given to estrogen-deficient animals [10–13] or to post-menopausal subjects [14–17] who had been treated with estrogen or the selective estrogen receptor modulator raloxifene, the anabolic effects of PTH were not altered as reflected by increases in bone formation markers and bone mineral density (BMD). Similarly, a trial in glucocorticoid- induced osteoporosis subjects who received both estrogen and hPTH(1–34) revealed that bone formation markers, spinal and hip BMD increased as expected [18]. However, there are conflicting reports concerning the effects of more potent anti- resorptive agents on the skeletal response to PTH. In studies with rats, pretreatment with alendronate blunted the PTH induced increase in BMD, even if a withdrawal period was applied [19]. Three randomized, placebo controlled clinical trials also showed that alendronate pretreatment significantly blunted the PTH stimulated increase in bone density [6,20,21]. However, other studies have reported that PTH could stimulate bone formation even if the patients had been previously treated with alendronate for over 1 year [22,23] or in estrogen deficient rats treated with alendronate for 10 months [12]. The majority of studies have so far focused on alendronate. Preliminary pre-clinical data suggested that co-treatment of Bone 41 (2007) 813 – 819 www.elsevier.com/locate/bone ⁎ Corresponding author. Fax: +1 801 581 7008. E-mail address: [email protected] (W.S.S. Jee). 8756-3282/$ - see front matter © 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.bone.2007.07.005
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Risedronate did not block the maximal anabolic effect of PTH in aged rats

813–819www.elsevier.com/locate/bone
Bone 41 (2007)
Risedronate did not block the maximal anabolic effect of PTH in aged rats
Wei Yao a, Ming Su a, Qing Zhang a, Xiaoyan Tian a, Rebecca B. Setterberg a, Cindy Blanton b,Mark W. Lundy b, Roger Phipps b, Webster S.S. Jee a,⁎
a Division of Radiobiology, University of Utah School of Medicine, 729 Arapeen Dr., Suite 2338, Salt Lake City, UT 84108, USAb Procter & Gamble Pharmaceuticals, Mason, OH, USA
Received 16 February 2007; revised 15 June 2007; accepted 4 July 2007Available online 17 July 2007
Abstract
The study was designed to investigate if pre-treating rats with a therapeutic equivalent dose of risedronate blunted the anabolic effects of PTH,and whether a withdrawal period prior to PTH treatment would alter any effect of risedronate on PTH treatment. Skeletally mature rats weretreated for 18 weeks with vehicle, risedronate, or risedronate for 8 weeks followed by vehicle for 10 weeks (withdrawal period). At the end of thisperiod, animals were treated for a further 12 weeks with PTH or PTH vehicle. Trabecular and cortical bone mass were monitored by serial pQCT,or by DXA and microCT. Bone histomorphometry was performed on the proximal tibiae and tibial shafts for bone turnover parameters at week 40.Risedronate alone moderately increased while PTH alone markedly increased trabecular bone mass at the proximal tibial (35% and 200%,respectively) and lumbar vertebral body (14% and 36%, respectively). The maximum bone gains were similar with and without pretreatment withrisedronate as compared to the PTH alone. Continuous administration of risedronate for 18 weeks prior to PTH treatment had lower percentageincreases in proximal tibial BMD during the first 8 weeks of PTH treatments, and had lower active bone forming surface and bone formation ratesafter being treated with PTH 12 weeks as compared to the PTH alone group. However, with the 10-week withdrawal period, risedronate did notblunt the stimulatory effect of PTH on osteoblast activity as shown by similar bone formation rates as with PTH alone. Our findings suggest thatwhile risedronate pretreatment may slow the bone anabolic response to PTH, a withdrawal period prior to PTH treatment allows osteoblasticactivity to respond normally to PTH stimulation.© 2007 Elsevier Inc. All rights reserved.
Keywords: Risedronate; PTH; Withdrawal; Bone morphology
Introduction
Anti-resorptive agents have been available as the “first-line”therapeutic agents for the prevention and treatment for osteopo-rosis in the past decade [1–5]. The development of parathyroidhormone and its analogs has provided a new approach of anabolictherapy for osteoporosis [6–9]. How best to use the combinationof anti-resorptive and anabolic drugs is not clear.
When PTH was given to estrogen-deficient animals [10–13]or to post-menopausal subjects [14–17] who had been treatedwith estrogen or the selective estrogen receptor modulatorraloxifene, the anabolic effects of PTH were not altered asreflected by increases in bone formation markers and bone
⁎ Corresponding author. Fax: +1 801 581 7008.E-mail address: [email protected] (W.S.S. Jee).
8756-3282/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.bone.2007.07.005
mineral density (BMD). Similarly, a trial in glucocorticoid-induced osteoporosis subjects who received both estrogen andhPTH(1–34) revealed that bone formation markers, spinal andhip BMD increased as expected [18]. However, there areconflicting reports concerning the effects of more potent anti-resorptive agents on the skeletal response to PTH. In studieswith rats, pretreatment with alendronate blunted the PTHinduced increase in BMD, even if a withdrawal period wasapplied [19]. Three randomized, placebo controlled clinicaltrials also showed that alendronate pretreatment significantlyblunted the PTH stimulated increase in bone density [6,20,21].However, other studies have reported that PTH could stimulatebone formation even if the patients had been previously treatedwith alendronate for over 1 year [22,23] or in estrogen deficientrats treated with alendronate for 10 months [12].
The majority of studies have so far focused on alendronate.Preliminary pre-clinical data suggested that co-treatment of
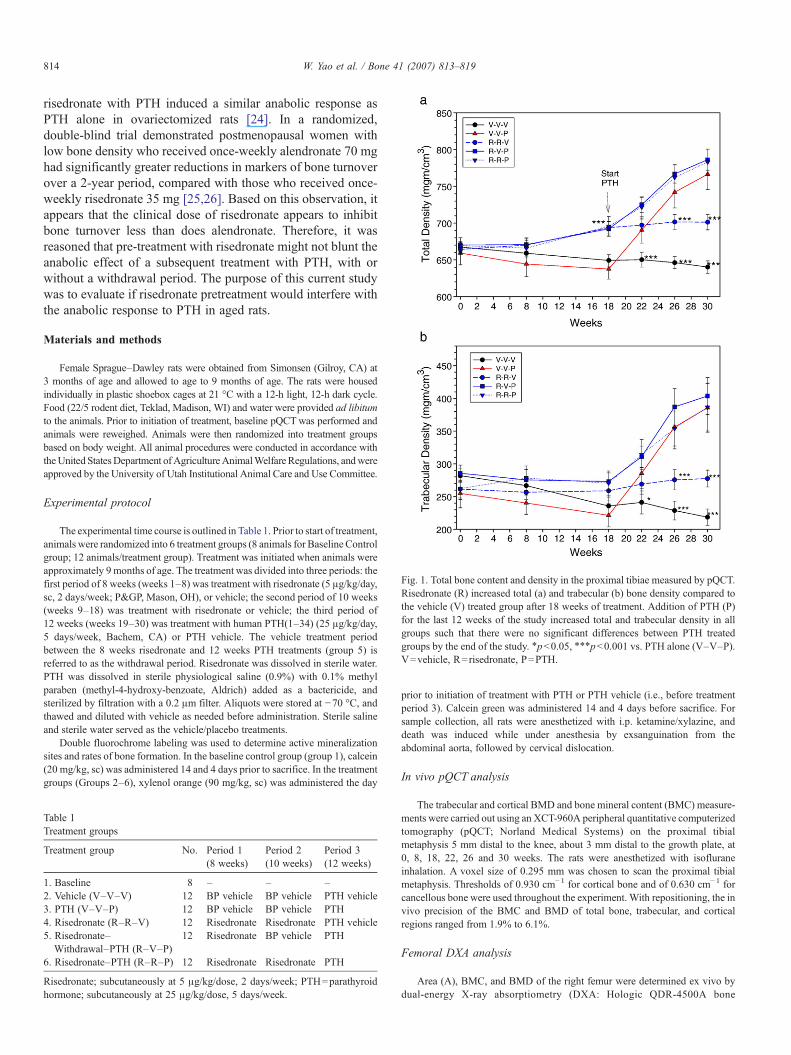
Fig. 1. Total bone content and density in the proximal tibiae measured by pQCT.Risedronate (R) increased total (a) and trabecular (b) bone density compared tothe vehicle (V) treated group after 18 weeks of treatment. Addition of PTH (P)for the last 12 weeks of the study increased total and trabecular density in allgroups such that there were no significant differences between PTH treatedgroups by the end of the study. ⁎pb0.05, ⁎⁎⁎pb0.001 vs. PTH alone (V–V–P).V=vehicle, R=risedronate, P=PTH.
814 W. Yao et al. / Bone 41 (2007) 813–819
risedronate with PTH induced a similar anabolic response asPTH alone in ovariectomized rats [24]. In a randomized,double-blind trial demonstrated postmenopausal women withlow bone density who received once-weekly alendronate 70 mghad significantly greater reductions in markers of bone turnoverover a 2-year period, compared with those who received once-weekly risedronate 35 mg [25,26]. Based on this observation, itappears that the clinical dose of risedronate appears to inhibitbone turnover less than does alendronate. Therefore, it wasreasoned that pre-treatment with risedronate might not blunt theanabolic effect of a subsequent treatment with PTH, with orwithout a withdrawal period. The purpose of this current studywas to evaluate if risedronate pretreatment would interfere withthe anabolic response to PTH in aged rats.
Materials and methods
Female Sprague–Dawley rats were obtained from Simonsen (Gilroy, CA) at3 months of age and allowed to age to 9 months of age. The rats were housedindividually in plastic shoebox cages at 21 °C with a 12-h light, 12-h dark cycle.Food (22/5 rodent diet, Teklad, Madison, WI) and water were provided ad libitumto the animals. Prior to initiation of treatment, baseline pQCTwas performed andanimals were reweighed. Animals were then randomized into treatment groupsbased on body weight. All animal procedures were conducted in accordance withtheUnited StatesDepartment ofAgricultureAnimalWelfare Regulations, andwereapproved by the University of Utah Institutional Animal Care and Use Committee.
Experimental protocol
The experimental time course is outlined in Table 1. Prior to start of treatment,animals were randomized into 6 treatment groups (8 animals for Baseline Controlgroup; 12 animals/treatment group). Treatment was initiated when animals wereapproximately 9 months of age. The treatment was divided into three periods: thefirst period of 8 weeks (weeks 1–8) was treatment with risedronate (5 μg/kg/day,sc, 2 days/week; P&GP, Mason, OH), or vehicle; the second period of 10 weeks(weeks 9–18) was treatment with risedronate or vehicle; the third period of12 weeks (weeks 19–30) was treatment with human PTH(1–34) (25 μg/kg/day,5 days/week, Bachem, CA) or PTH vehicle. The vehicle treatment periodbetween the 8 weeks risedronate and 12 weeks PTH treatments (group 5) isreferred to as the withdrawal period. Risedronate was dissolved in sterile water.PTH was dissolved in sterile physiological saline (0.9%) with 0.1% methylparaben (methyl-4-hydroxy-benzoate, Aldrich) added as a bactericide, andsterilized by filtration with a 0.2 μm filter. Aliquots were stored at −70 °C, andthawed and diluted with vehicle as needed before administration. Sterile salineand sterile water served as the vehicle/placebo treatments.
Double fluorochrome labeling was used to determine active mineralizationsites and rates of bone formation. In the baseline control group (group 1), calcein(20 mg/kg, sc) was administered 14 and 4 days prior to sacrifice. In the treatmentgroups (Groups 2–6), xylenol orange (90 mg/kg, sc) was administered the day
Table 1Treatment groups
Treatment group No. Period 1(8 weeks)
Period 2(10 weeks)
Period 3(12 weeks)
1. Baseline 8 – – –2. Vehicle (V–V–V) 12 BP vehicle BP vehicle PTH vehicle3. PTH (V–V–P) 12 BP vehicle BP vehicle PTH4. Risedronate (R–R–V) 12 Risedronate Risedronate PTH vehicle5. Risedronate–Withdrawal–PTH (R–V–P)
12 Risedronate BP vehicle PTH
6. Risedronate–PTH (R–R–P) 12 Risedronate Risedronate PTH
Risedronate; subcutaneously at 5 μg/kg/dose, 2 days/week; PTH=parathyroidhormone; subcutaneously at 25 μg/kg/dose, 5 days/week.
prior to initiation of treatment with PTH or PTH vehicle (i.e., before treatmentperiod 3). Calcein green was administered 14 and 4 days before sacrifice. Forsample collection, all rats were anesthetized with i.p. ketamine/xylazine, anddeath was induced while under anesthesia by exsanguination from theabdominal aorta, followed by cervical dislocation.
In vivo pQCT analysis
The trabecular and cortical BMD and bone mineral content (BMC) measure-ments were carried out using an XCT-960A peripheral quantitative computerizedtomography (pQCT; Norland Medical Systems) on the proximal tibialmetaphysis 5 mm distal to the knee, about 3 mm distal to the growth plate, at0, 8, 18, 22, 26 and 30 weeks. The rats were anesthetized with isofluraneinhalation. A voxel size of 0.295 mm was chosen to scan the proximal tibialmetaphysis. Thresholds of 0.930 cm−1 for cortical bone and of 0.630 cm−1 forcancellous bone were used throughout the experiment. With repositioning, the invivo precision of the BMC and BMD of total bone, trabecular, and corticalregions ranged from 1.9% to 6.1%.
Femoral DXA analysis
Area (A), BMC, and BMD of the right femur were determined ex vivo bydual-energy X-ray absorptiometry (DXA: Hologic QDR-4500A bone
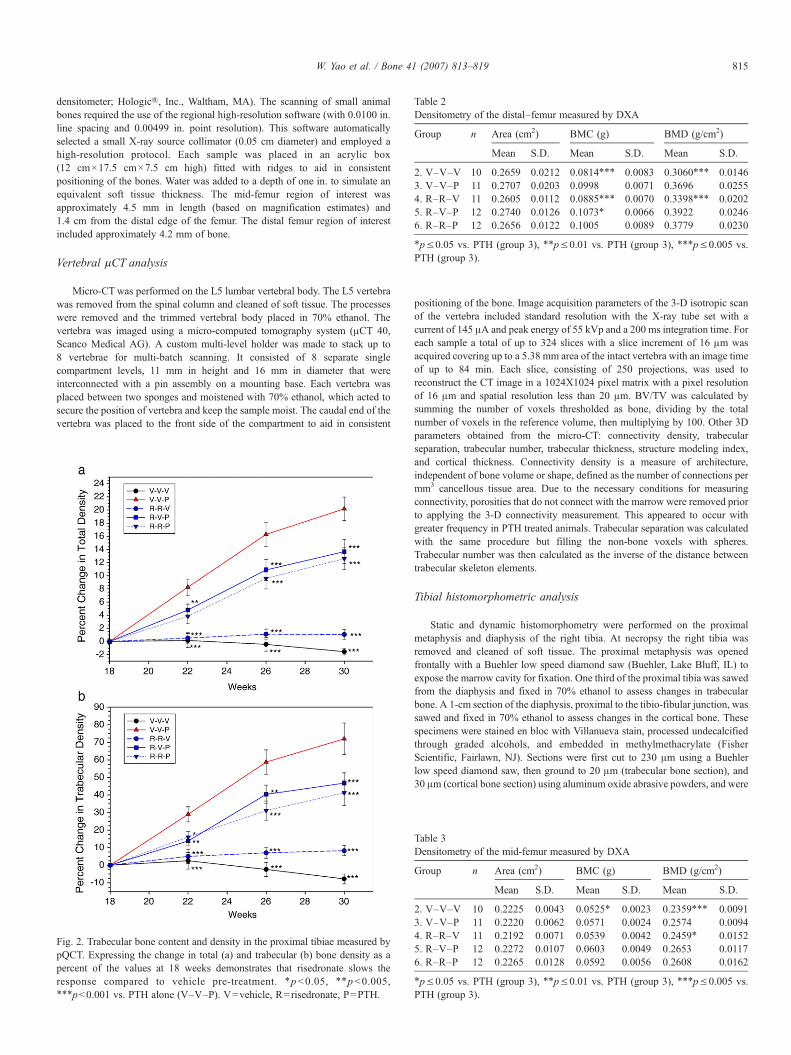
Table 2Densitometry of the distal–femur measured by DXA
Group n Area (cm2) BMC (g) BMD (g/cm2)
Mean S.D. Mean S.D. Mean S.D.
2. V–V–V 10 0.2659 0.0212 0.0814⁎⁎⁎ 0.0083 0.3060⁎⁎⁎ 0.01463. V–V–P 11 0.2707 0.0203 0.0998 0.0071 0.3696 0.02554. R–R–V 11 0.2605 0.0112 0.0885⁎⁎⁎ 0.0070 0.3398⁎⁎⁎ 0.02025. R–V–P 12 0.2740 0.0126 0.1073⁎ 0.0066 0.3922 0.02466. R–R–P 12 0.2656 0.0122 0.1005 0.0089 0.3779 0.0230
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs.PTH (group 3).
815W. Yao et al. / Bone 41 (2007) 813–819
densitometer; Hologic®, Inc., Waltham, MA). The scanning of small animalbones required the use of the regional high-resolution software (with 0.0100 in.line spacing and 0.00499 in. point resolution). This software automaticallyselected a small X-ray source collimator (0.05 cm diameter) and employed ahigh-resolution protocol. Each sample was placed in an acrylic box(12 cm×17.5 cm×7.5 cm high) fitted with ridges to aid in consistentpositioning of the bones. Water was added to a depth of one in. to simulate anequivalent soft tissue thickness. The mid-femur region of interest wasapproximately 4.5 mm in length (based on magnification estimates) and1.4 cm from the distal edge of the femur. The distal femur region of interestincluded approximately 4.2 mm of bone.
Vertebral μCT analysis
Micro-CTwas performed on the L5 lumbar vertebral body. The L5 vertebrawas removed from the spinal column and cleaned of soft tissue. The processeswere removed and the trimmed vertebral body placed in 70% ethanol. Thevertebra was imaged using a micro-computed tomography system (μCT 40,Scanco Medical AG). A custom multi-level holder was made to stack up to8 vertebrae for multi-batch scanning. It consisted of 8 separate singlecompartment levels, 11 mm in height and 16 mm in diameter that wereinterconnected with a pin assembly on a mounting base. Each vertebra wasplaced between two sponges and moistened with 70% ethanol, which acted tosecure the position of vertebra and keep the sample moist. The caudal end of thevertebra was placed to the front side of the compartment to aid in consistent
Fig. 2. Trabecular bone content and density in the proximal tibiae measured bypQCT. Expressing the change in total (a) and trabecular (b) bone density as apercent of the values at 18 weeks demonstrates that risedronate slows theresponse compared to vehicle pre-treatment. ⁎pb0.05, ⁎⁎pb0.005,⁎⁎⁎pb0.001 vs. PTH alone (V–V–P). V=vehicle, R=risedronate, P=PTH.
positioning of the bone. Image acquisition parameters of the 3-D isotropic scanof the vertebra included standard resolution with the X-ray tube set with acurrent of 145 μA and peak energy of 55 kVp and a 200 ms integration time. Foreach sample a total of up to 324 slices with a slice increment of 16 μm wasacquired covering up to a 5.38 mm area of the intact vertebra with an image timeof up to 84 min. Each slice, consisting of 250 projections, was used toreconstruct the CT image in a 1024X1024 pixel matrix with a pixel resolutionof 16 μm and spatial resolution less than 20 μm. BV/TV was calculated bysumming the number of voxels thresholded as bone, dividing by the totalnumber of voxels in the reference volume, then multiplying by 100. Other 3Dparameters obtained from the micro-CT: connectivity density, trabecularseparation, trabecular number, trabecular thickness, structure modeling index,and cortical thickness. Connectivity density is a measure of architecture,independent of bone volume or shape, defined as the number of connections permm3 cancellous tissue area. Due to the necessary conditions for measuringconnectivity, porosities that do not connect with the marrow were removed priorto applying the 3-D connectivity measurement. This appeared to occur withgreater frequency in PTH treated animals. Trabecular separation was calculatedwith the same procedure but filling the non-bone voxels with spheres.Trabecular number was then calculated as the inverse of the distance betweentrabecular skeleton elements.
Tibial histomorphometric analysis
Static and dynamic histomorphometry were performed on the proximalmetaphysis and diaphysis of the right tibia. At necropsy the right tibia wasremoved and cleaned of soft tissue. The proximal metaphysis was openedfrontally with a Buehler low speed diamond saw (Buehler, Lake Bluff, IL) toexpose the marrow cavity for fixation. One third of the proximal tibia was sawedfrom the diaphysis and fixed in 70% ethanol to assess changes in trabecularbone. A 1-cm section of the diaphysis, proximal to the tibio-fibular junction, wassawed and fixed in 70% ethanol to assess changes in the cortical bone. Thesespecimens were stained en bloc with Villanueva stain, processed undecalcifiedthrough graded alcohols, and embedded in methylmethacrylate (FisherScientific, Fairlawn, NJ). Sections were first cut to 230 μm using a Buehlerlow speed diamond saw, then ground to 20 μm (trabecular bone section), and30 μm (cortical bone section) using aluminum oxide abrasive powders, and were
Table 3Densitometry of the mid-femur measured by DXA
Group n Area (cm2) BMC (g) BMD (g/cm2)
Mean S.D. Mean S.D. Mean S.D.
2. V–V–V 10 0.2225 0.0043 0.0525⁎ 0.0023 0.2359⁎⁎⁎ 0.00913. V–V–P 11 0.2220 0.0062 0.0571 0.0024 0.2574 0.00944. R–R–V 11 0.2192 0.0071 0.0539 0.0042 0.2459⁎ 0.01525. R–V–P 12 0.2272 0.0107 0.0603 0.0049 0.2653 0.01176. R–R–P 12 0.2265 0.0128 0.0592 0.0056 0.2608 0.0162
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs.PTH (group 3).

Table 4Lumbar vertebral body changes measured by micro-CT
Group n Bone volume/tissue volume (%)
Connectivitydensity (1/mm3)
Structuremodel index
Trabecularthickness (um)
Trabecularnumber (mm−1)
Corticalthickness (μm)
Mean S.D. Mean S.D. Mean S.D. Mean S.D. Mean S.D. Mean S.D.
2. V–V–V 9 42.52⁎⁎⁎ 5.15 56.86⁎ 7.74 −2.61⁎⁎⁎ 0.87 98.06⁎⁎⁎ 6.04 4.80⁎⁎⁎ 0.51 177.67⁎⁎⁎ 13.343. V–V–P 11 58.00 9.05 46.04 15.25 −6.83 3.13 124.98 15.97 5.65 0.77 223.18 26.264. R–R–V 11 48.35⁎⁎⁎ 4.80 53.12 12.30 −3.43⁎⁎⁎ 1.06 110.43⁎⁎⁎ 9.04 5.25 0.29 199.09⁎⁎⁎ 18.545. R–V–P 12 63.76 5.06 37.87⁎ 6.30 −8.16 2.24 140.93⁎⁎⁎ 9.05 6.14⁎ 0.62 239.83⁎ 14.676. R–R–P 12 62.18 6.39 38.55 5.10 −7.67 2.71 138.08⁎⁎⁎ 12.31 6.06 0.60 244.17⁎⁎ 27.48
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs. PTH (group 3).
816 W. Yao et al. / Bone 41 (2007) 813–819
cover slipped with Eukitt's mounting medium (Calibrated Instruments, Inc.,Hawthorn, NY).
Static and dynamic histomorphometry of the proximal tibial metaphysis wasperformed using a microscope with either transmitted or fluorescent light linkedto a computer-assisted image system (Osteomeasure; Osteometrics, Inc. Atlanta,GA). Measurements were collected from the area from 1 mm to 4 mm distal tothe growth plate/epiphyseal junction. Static measurements included total area(TAr), trabecular bone area (TbAr), and trabecular perimeter (TbPm) measuredby the digitizing system. From these data, static measurements were calculatedas previously defined [27]. Dynamic measurements included single and doublelabel perimeters (sLPm and dLPm, respectively), eroded perimeter (ErPm), andinterlabel width (IrWi). These indices were used to derive mineral appositionrate (MAR), mineralizing surface (MS/BS) and eroded surfaces (ES/BS) incancellous bone [27]. Mineralizing surface was calculated as % single-labeledsurface/2+ % double-labeled surface. BFR/BS was calculated by MAR×MS/BS.
Histomorphometry of cortical bone was performed using a digitizing imageanalysis system (DIAS) (KSS Image, Magna, UT), which consisted of anepifluorescent microscope and a digitizing pad coupled to a Macintosh SEcomputer (Apple Computer, Inc.; Cupertino, CA). Static measurements includedtotal area, periosteal perimeter (P.Pm), marrow area (Ma.Ar), endocorticalperimeter (E.Pm), and average cortical bone width (Ct.Wi). Static measurementswere calculated from these parameters as previously defined [27]. Dynamicmeasurements of the periosteal and endocortical surfaces included single anddouble label perimeters, inter-labeled width and endocortical eroded perimeter(En–Er.Pm). These indices were used to derive bone formation rates forperiosteal and endocortical surfaces.
Data handling and statistical analysis
Data in tables are expressed as group means±S.D.; in figures the densitydata are expressed as mean±S.E.M., absolute (mgm/cm3) or percent changescalculated from the start of study (week 0). The data were analyzed using JMPstatistical software (SAS Institute Inc., Cary, NC). Comparisons were made toPTH treatment (group 3) using ANOVAwith Fisher's protected two-sided LeastSignificant Difference (LSD) test. Differences were considered statisticallysignificant at p≤0.05 on a two-sided test.
Table 5Bone histomorphometry of the proximal tibia metaphysis
Group n Bone volume/tissue volume (%)
Trabecularthickness (μm)
Trabeculanumber (m
Mean S.D. Mean S.D. Mean
2. V–V–V 10 7.83⁎⁎⁎ 2.85 38.00⁎⁎⁎ 4.74 2.01⁎⁎⁎
3. V–V–P 11 24.07 6.54 82.17 10.06 2.904. R–R–V 11 10.56⁎⁎⁎ 2.73 44.79⁎⁎⁎ 5.48 2.35⁎
5. R–V–P 12 24.10 8.00 82.52 14.73 2.866. R–R–P 12 21.97 9.69 76.05 20.54 2.77
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs. PTH
Results
Body weights ranged from 400 to 500 g at the beginning ofthe study and they did not differ among vehicle and othertreatment groups at the initiation, during or at the end of thetreatment period 3 (data not shown).
Total bone density in the proximal tibia measured by pQCTdecreased with vehicle treatment throughout the study (Fig. 1a).Risedronate treatment increased bone density by 18 monthscompared to vehicle treatment. PTH treatment increased bonedensity to similar levels in groups previously treated withvehicle or risedronate. Similar results were observed fortrabecular bone density in the proximal tibia (Fig. 1b). Therewere greater increases in both the total tibial bone density (Fig.2a) and trabecular bone density (Fig. 2b) in the PTH treatedanimals previously treated with vehicle, as compared topretreated with risedronate, with or without a withdrawal period.
In the distal femur (Table 2) and lumbar vertebral body(Table 4), animals pretreated for 8 weeks with risedronatefollowed by “withdrawal” for 10 weeks prior to PTH treatmenthad higher trabecular bone mass than PTH alone, but thesechanges did not reach statistical significance. In contrast, al-though continuous risedronate followed by PTH increased bonedensity compared to vehicle alone, it did not significantly in-crease bone density compared to PTH alone. Cortical bonedensity in the mid-femur (Table 3), proximal tibiae (data notshown) and the tibial diaphysis (Table 7) were similar in all PTHtreated groups.
Fluorochrome labels revealed that the primary effect of PTHwas to increase double-labeled surfaces (Tables 5–7, Fig. 3),whereas risedronate alone markedly inhibited bone formation
rm−1)
Mineralapposition rate(μm/day)
Bone formationrate/bone surface(μm/day×100)
Eroded surface/bone surface (%)
S.D. Mean S.D. Mean S.D. Mean S.D.
0.52 0.50⁎⁎⁎ 0.07 13.25⁎⁎⁎ 2.85 3.27 0.750.56 0.79 0.05 23.18 6.82 3.16 1.200.45 0.00⁎⁎⁎ 0.00 0.00⁎⁎⁎ 0.00 1.42⁎⁎⁎ 0.620.56 0.82 0.05 19.31 6.77 2.50 1.020.61 0.79 0.05 15.01⁎⁎⁎ 5.28 2.52 0.95
(group 3).
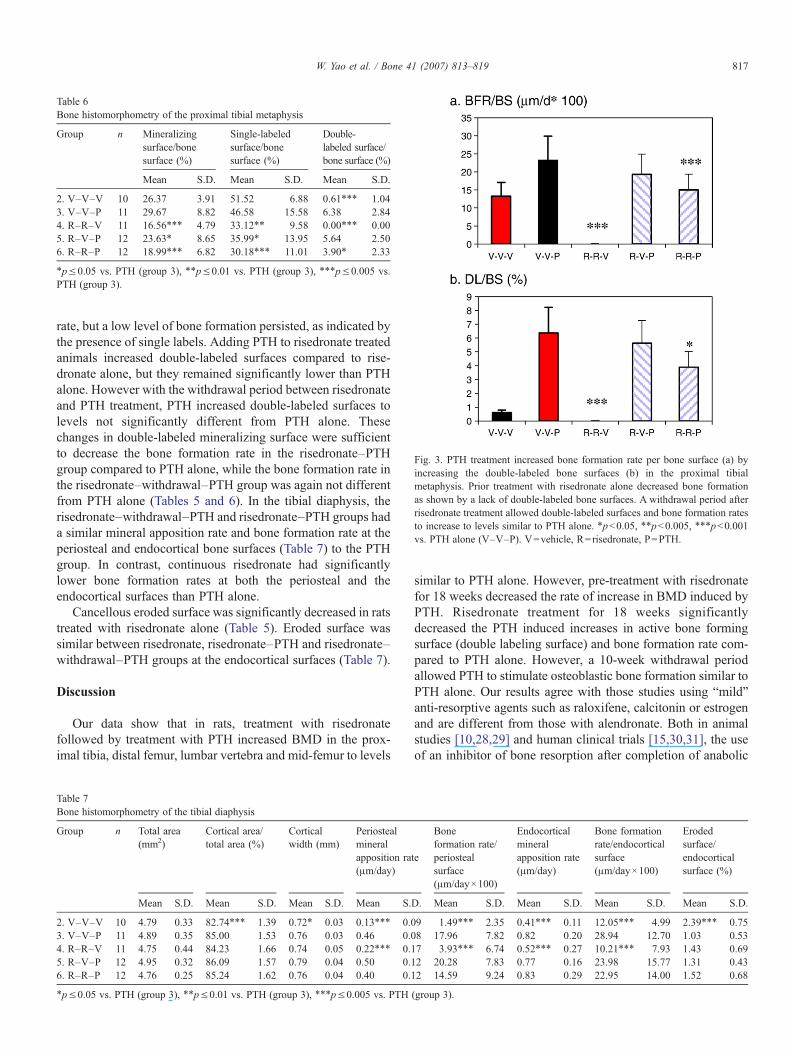
Table 6Bone histomorphometry of the proximal tibial metaphysis
Group n Mineralizingsurface/bonesurface (%)
Single-labeledsurface/bonesurface (%)
Double-labeled surface/bone surface (%)
Mean S.D. Mean S.D. Mean S.D.
2. V–V–V 10 26.37 3.91 51.52 6.88 0.61⁎⁎⁎ 1.043. V–V–P 11 29.67 8.82 46.58 15.58 6.38 2.844. R–R–V 11 16.56⁎⁎⁎ 4.79 33.12⁎⁎ 9.58 0.00⁎⁎⁎ 0.005. R–V–P 12 23.63⁎ 8.65 35.99⁎ 13.95 5.64 2.506. R–R–P 12 18.99⁎⁎⁎ 6.82 30.18⁎⁎⁎ 11.01 3.90⁎ 2.33
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs.PTH (group 3).
Fig. 3. PTH treatment increased bone formation rate per bone surface (a) byincreasing the double-labeled bone surfaces (b) in the proximal tibialmetaphysis. Prior treatment with risedronate alone decreased bone formationas shown by a lack of double-labeled bone surfaces. A withdrawal period afterrisedronate treatment allowed double-labeled surfaces and bone formation ratesto increase to levels similar to PTH alone. ⁎pb0.05, ⁎⁎pb0.005, ⁎⁎⁎pb0.001vs. PTH alone (V–V–P). V=vehicle, R=risedronate, P=PTH.
817W. Yao et al. / Bone 41 (2007) 813–819
rate, but a low level of bone formation persisted, as indicated bythe presence of single labels. Adding PTH to risedronate treatedanimals increased double-labeled surfaces compared to rise-dronate alone, but they remained significantly lower than PTHalone. However with the withdrawal period between risedronateand PTH treatment, PTH increased double-labeled surfaces tolevels not significantly different from PTH alone. Thesechanges in double-labeled mineralizing surface were sufficientto decrease the bone formation rate in the risedronate–PTHgroup compared to PTH alone, while the bone formation rate inthe risedronate–withdrawal–PTH group was again not differentfrom PTH alone (Tables 5 and 6). In the tibial diaphysis, therisedronate–withdrawal–PTH and risedronate–PTH groups hada similar mineral apposition rate and bone formation rate at theperiosteal and endocortical bone surfaces (Table 7) to the PTHgroup. In contrast, continuous risedronate had significantlylower bone formation rates at both the periosteal and theendocortical surfaces than PTH alone.
Cancellous eroded surface was significantly decreased in ratstreated with risedronate alone (Table 5). Eroded surface wassimilar between risedronate, risedronate–PTH and risedronate–withdrawal–PTH groups at the endocortical surfaces (Table 7).
Discussion
Our data show that in rats, treatment with risedronatefollowed by treatment with PTH increased BMD in the prox-imal tibia, distal femur, lumbar vertebra and mid-femur to levels
Table 7Bone histomorphometry of the tibial diaphysis
Group n Total area(mm2)
Cortical area/total area (%)
Corticalwidth (mm)
Periostealmineralapposition ra(μm/day)
Mean S.D. Mean S.D. Mean S.D. Mean S.
2. V–V–V 10 4.79 0.33 82.74⁎⁎⁎ 1.39 0.72⁎ 0.03 0.13⁎⁎⁎ 0.03. V–V–P 11 4.89 0.35 85.00 1.53 0.76 0.03 0.46 0.04. R–R–V 11 4.75 0.44 84.23 1.66 0.74 0.05 0.22⁎⁎⁎ 0.15. R–V–P 12 4.95 0.32 86.09 1.57 0.79 0.04 0.50 0.16. R–R–P 12 4.76 0.25 85.24 1.62 0.76 0.04 0.40 0.1
⁎p≤0.05 vs. PTH (group 3), ⁎⁎p≤0.01 vs. PTH (group 3), ⁎⁎⁎p≤0.005 vs. PTH
similar to PTH alone. However, pre-treatment with risedronatefor 18 weeks decreased the rate of increase in BMD induced byPTH. Risedronate treatment for 18 weeks significantlydecreased the PTH induced increases in active bone formingsurface (double labeling surface) and bone formation rate com-pared to PTH alone. However, a 10-week withdrawal periodallowed PTH to stimulate osteoblastic bone formation similar toPTH alone. Our results agree with those studies using “mild”anti-resorptive agents such as raloxifene, calcitonin or estrogenand are different from those with alendronate. Both in animalstudies [10,28,29] and human clinical trials [15,30,31], the useof an inhibitor of bone resorption after completion of anabolic
te
Boneformation rate/periostealsurface(μm/day×100)
Endocorticalmineralapposition rate(μm/day)
Bone formationrate/endocorticalsurface(μm/day×100)
Erodedsurface/endocorticalsurface (%)
D. Mean S.D. Mean S.D. Mean S.D. Mean S.D.
9 1.49⁎⁎⁎ 2.35 0.41⁎⁎⁎ 0.11 12.05⁎⁎⁎ 4.99 2.39⁎⁎⁎ 0.758 17.96 7.82 0.82 0.20 28.94 12.70 1.03 0.537 3.93⁎⁎⁎ 6.74 0.52⁎⁎⁎ 0.27 10.21⁎⁎⁎ 7.93 1.43 0.692 20.28 7.83 0.77 0.16 23.98 15.77 1.31 0.432 14.59 9.24 0.83 0.29 22.95 14.00 1.52 0.68
(group 3).

818 W. Yao et al. / Bone 41 (2007) 813–819
treatments is generally accepted as an appropriate way tomaintain the skeletal benefits gained during therapeutictreatment period. Co-treatments of anti-resorptive agents andPTH, particularly bisphosphonates, were found to have no morebeneficial effects than treatment with PTH alone [19,32].However, patients who are currently on anti-resorptive therapybut still have an active bone loss or have a high risk of fractureare candidates for treatment with an anabolic agent such asPTH.
PTH appears to stimulate bone formation through a numberof mechanisms including increasing osteoblast activity andlifespan [33], stimulating bone lining cells to differentiate intoosteoblasts [34] or inhibiting osteocytes from expressingsclerostin [35,36]. In addition, high bone turnover and rapidincreased resorption may contribute to the anabolic effects byhelping to release other growth factors, such as basic fibroblastgrowth factor and TGF-β1 from bone matrix [37–39].Continued risedronate might counteract the PTH effect onbone resorption and might contribute to the initial delay in theanabolic response of PTH. Other speculation included pretreat-ment with potent bisphosphonates such as alendronate mighthave toxic effects on mature osteoblasts or bone lining cells andtherefore prevented the uptake of PTH [19]. However, inestrogen-deficient rats that were pretreated with alendronate for10 months prior to switching to PTH, PTH's anabolic effectswere not affected [12]. Similar to the main finding of Ma et al.’sstudy on alendronate, we found that even in intact animals pre-exposed to risedronate, the maximal bone gain was not differentfrom that with PTH alone. The initial lower absolute increasesin total and trabecular BMD in R–R–P group might be due tothe fact that it had a higher baseline BMD before PTH wasinitiated. The percent increase of bone mineral density wassimilar within all the PTH-treated groups. Our findings agreedwith another pre-clinical study in which rats received concurrenttreatment with risedronate and PTH [24], where significant andsustained increases in vertebral bone mass and strength werefound. These results in animal studies agree with a clinical studyin which the increase in bone turnover with PTH in patientstreated with an anti-resorptive agent was similar to thatobserved in treatment-naive patients [40].
PTH primarily increased bone formation through increasesin MAR and mineralizing surface. A similar increase in MARoccurred whether or not risedronate was used prior to PTHtreatment. Risedronate significantly inhibited the PTH inducedincrease in double-labeled bone forming surfaces approximate-ly 40%, while with the withdrawal period this decrease in PTHinduced bone formation (~12% decrease) was not observed.Moreover, PTH did not increase bone resorption after 12 weeksof administration, at which time point it still increased boneformation. A positive bone balance was achieved in all groupstreated with PTH with bone formation exceeding boneresorption. Fuchs et al. recently observed that treatment ofrats with risedronate for 8 weeks significantly suppressed tra-becular bone formation rates; after discontinuation of treatmentfor 16 weeks the bone formation rates were not significantlydifferent from vehicle [41]. In the current study the increasedbone formation induced by the withdrawal period following
risedronate treatment, as demonstrated by the greater increase infemoral bone density and vertebral cancellous bone volume,suggest that a withdrawal period following risedronate treat-ment could increase the response to PTH treatment.
Since risedronate and PTH are used to treated osteoporoticpatients, it could be more clinically relevant to use estrogen-deplete rats rather than using intact rats. However, our purposeof the study was to look at the effects of risedronate on PTHresponse. It was a study to duplicate Gasser's protocol usingrisedronate [19]. Adding groups for estrogen deficiency thatmight increase bone turnover itself would have confused theissue. In addition, osteoporosis is not just the result of estrogenloss with aging plays an important role too. Therefore, ourconclusion on the interaction of PTH and bisphosphonate islimited to aging and not for those situations when bone turnoveris high during the acute phase of estrogen deficiency.
These results in rats indicate that while risedronate pretreat-ment may slow the bone anabolic response to PTH, awithdrawal period prior to PTH treatment allows osteoblasticactivity to respond normally to PTH stimulation. The datasuggest that parathyroid hormone should be considered forsubjects who have previously received risedronate, and thatadding a withdrawal period may result in a greater anabolicresponse to PTH.
References
[1] Gilchrist N. Antiresorptive agents, raloxifene, and PHARMAC. N ZMed J2006;119(1230):U1885.
[2] Cranney A, Adachi JD. Benefit–risk assessment of raloxifene in post-menopausal osteoporosis. Drug Saf 2005;28(8):721–30.
[3] Pande I, Hosking DJ. Oral antiresorptive therapy. Curr Rheumatol Rep2005;7(1):71–7.
[4] Babat LB, McLain R, Milks R, Ferrara L, Sohn MJ. The effects of theantiresorptive agents calcitonin and pamidronate on spine fusion in a rabbitmodel. Spine J 2005;5(5):542–7.
[5] Papapoulos SE. Who will benefit from antiresorptive treatment (bispho-sphonates)? Best Pract Res Clin Rheumatol 2005;19(6):965–73.
[6] Bilezikian JP, Rubin MR, Finkelstein JS. Parathyroid hormone as an anab-olic therapy for women and men. J Endocrinol Invest 2005;28(8 Suppl):41–9.
[7] Cosman F. Anabolic therapy for osteoporosis: parathyroid hormone. CurrRheumatol Rep 2006;8(1):63–9.
[8] HodsmanAB, Bauer DC, Dempster DW, Dian L,Hanley DA, Harris ST, et al.Parathyroid hormone and teriparatide for the treatment of osteoporosis: areview of the evidence and suggested guidelines for its use. Endocr Rev2005;26(5):688–703.
[9] Seeman E, Delmas PD. Reconstructing the skeleton with intermittentparathyroid hormone. Trends Endocrinol Metab 2001;12(7):281–3.
[10] Shen V, Birchman R, Xu R, Otter M, Wu D, Lindsay R, et al. Effects ofreciprocal treatment with estrogen and estrogen plus parathyroid hormoneon bone structure and strength in ovariectomized rats. J Clin Invest1995;96(5):2331–8.
[11] Hodsman AB, Drost D, Fraher LJ, Holdsworth D, Thornton M, Hock J,et al. The addition of a raloxifene analog (LY117018) allows for reducedPTH(1–34) dosing during reversal of osteopenia in ovariectomized rats.J Bone Miner Res 1999;14(5):675–9.
[12] Ma YL, Bryant HU, Zeng Q, Schmidt A, Hoover J, Cole HW, et al. Newbone formation with teriparatide [human parathyroid hormone-(1–34)] isnot retarded by long-term pretreatment with alendronate, estrogen, orraloxifene in ovariectomized rats. Endocrinology 2003;144(5):2008–15.
[13] Zhou H, Shen V, Dempster DW, Lindsay R. Continuous parathyroidhormone and estrogen administration increases vertebral cancellous bone

819W. Yao et al. / Bone 41 (2007) 813–819
volume and cortical width in the estrogen-deficient rat. J Bone Miner Res2001;16(7):1300–7.
[14] Cosman F, ShenV,Xie F, SeibelM,RatcliffeA, LindsayR. Estrogen protectionagainst bone resorbing effects of parathyroid hormone infusion. Assessment byuse of biochemical markers. Ann Intern Med 1993;118(5):337–43.
[15] Dempster DW, Cosman F, Kurland ES, Zhou H, Nieves J, Woelfert L, et al.Effects of daily treatment with parathyroid hormone on bone micro-architecture and turnover in patients with osteoporosis: a paired biopsystudy. J Bone Miner Res 2001;16(10):1846–53.
[16] Lindsay R, Nieves J, Formica C, Henneman E, Woelfert L, Shen V, et al.Randomised controlled study of effect of parathyroid hormone onvertebral-bone mass and fracture incidence among postmenopausalwomen on oestrogen with osteoporosis. Lancet 1997;350(9077):550–5.
[17] Reeve J, Mitchell A, Tellez M, Hulme P, Green JR, Wardley-Smith B, et al.Treatment with parathyroid peptides and estrogen replacement for severepostmenopausal vertebral osteoporosis: prediction of long-term responsesin spine and femur. J Bone Miner Metab 2001;19(2):102–14.
[18] Lane N, Morris S. New perspectives on parathyroid hormone therapy. CurrOpin Rheumatol 2005;17(4):467–74.
[19] Gasser JA, Kneissel M, Thomsen JS, Mosekilde L. PTH and interactionswith bisphosphonates. J Musculoskel Neuronal Interact 2000;1:53–6.
[20] Black DM, Bilezikian JP, Ensrud KE, Greenspan SL, Palermo L, Hue T,et al. One year of alendronate after one year of parathyroid hormone (1–84)for osteoporosis. N Engl J Med 2005;353(6):555–65.
[21] Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, LangTF, et al. The effects of parathyroid hormone and alendronate alone or incombination in postmenopausal osteoporosis. N Engl J Med 2003;349(13):1207–15.
[22] Cosman F, Nieves J, Zion M, Woelfert L, Luckey M, Lindsay R. Daily andcyclic parathyroid hormone in women receiving alendronate. N Engl JMed 2005;353(6):566–75.
[23] Cosman F, Nieves J, Woelfert L, Shen V, Lindsay R. Alendronate does notblock the anabolic effect of PTH in postmenopausal osteoporotic women.J Bone Miner Res 1998;13(6):1051–5.
[24] Li M, Mosekilde L, Sogaard CH, Thomsen JS, Wronski TJ. Parathyroidhormone monotherapy and cotherapy with antiresorptive agents restorevertebral bone mass and strength in aged ovariectomized rats. Bone1995;16(6):629–35.
[25] Bonnick S, Saag KG, Kiel DP, McClung M, Hochberg M, Burnett SA, et al.Comparison of weekly treatment of postmenopausal osteoporosis withalendronate versus risedronate over two years 1. J Clin Endocrinol Metab2006;91(7):2631–7.
[26] Rosen CJ, Hochberg MC, Bonnick SL, McClungM,Miller P, Broy S, et al.Treatment with once-weekly alendronate 70 mg compared with once-weekly risedronate 35 mg in women with postmenopausal osteoporosis: arandomized double-blind study 3. J Bone Miner Res 2005;20(1):141–51.
[27] Parfitt AM, Drezner MK, Glorieux FH, Kanis JA, Malluche H, MeunierPJ, et al. Bone histomorphometry: standardization of nomenclature,
symbols, and units. Report of the ASBMR Histomorphometry Nomen-clature Committee. J Bone Miner Res 1987;2(6):595–610.
[28] Ma Y, Jee WS, Chen Y, Gasser J, Ke HZ, Li XJ, et al. Partial maintenanceof extra cancellous bone mass by antiresorptive agents after discontinu-ation of human parathyroid hormone (1–38) in right hindlimb immobilizedrats. J Bone Miner Res 1995;10(11):1726–34.
[29] RheeY,WonYY,BaekMH,LimSK.Maintenance of increased bonemass afterrecombinant human parathyroid hormone (1–84) with sequential zoledronatetreatment in ovariectomized rats. J Bone Miner Res 2004;19(6):931–7.
[30] Hodsman AB, Fraher LJ, Watson PH, Ostbye T, Stitt LW, Adachi JD, et al.A randomized controlled trial to compare the efficacy of cyclicalparathyroid hormone versus cyclical parathyroid hormone and sequentialcalcitonin to improve bone mass in postmenopausal women withosteoporosis. J Clin Endocrinol Metab 1997;82(2):620–8.
[31] Rittmaster RS, Bolognese M, Ettinger MP, Hanley DA, Hodsman AB,Kendler DL, et al. Enhancement of bone mass in osteoporotic women withparathyroid hormone followed by alendronate. J Clin Endocrinol Metab2000;85(6):2129–34.
[32] Garces C, Garcia LE. Combination of anabolic and antiresorptive agentsfor the treatment of osteoporosis. Maturitas 2006;54(1):47–54.
[33] Sowa H, Kaji H, Iu MF, Tsukamoto T, Sugimoto T, Chihara K. Parathyroidhormone–Smad3 axis exerts anti-apoptotic action and augments anabolicaction of transforming growth factor beta in osteoblasts. J Biol Chem2003;278(52):52240–52.
[34] Dobnig H, Turner RT. Evidence that intermittent treatment withparathyroid hormone increases bone formation in adult rats by activationof bone lining cells. Endocrinology 1995;136(8):3632–8.
[35] Bellido T, Ali AA, Gubrij I, Plotkin LI, Fu Q, O'Brien CA, et al. Chronicelevation of parathyroid hormone in mice reduces expression of sclerostinby osteocytes: a novel mechanism for hormonal control of osteoblastogen-esis. Endocrinology 2005;146(11):4577–83.
[36] Keller H, Kneissel M. SOST is a target gene for PTH in bone. Bone2005;37(2):148–58.
[37] Hurley M, Yao W, Lane NE. Changes in serum fibroblast growth factor 2in patients with glucocorticoid-induced osteoporosis treated with humanparathyroid hormone (1–34). Osteoporos Int 2005;16(12):2080–4.
[38] Hurley MM, Okada Y, Xiao L, Tanaka Y, Ito M, Okimoto N, et al.Impaired bone anabolic response to parathyroid hormone in Fgf2−/− andFgf2+/− mice. Biochem Biophys Res Commun 2006;341(4):989–94.
[39] Hurley MM, Tetradis S, Huang YF, Hock J, Kream BE, Raisz LG, et al.Parathyroid hormone regulates the expression of fibroblast growth factor-2mRNA and fibroblast growth factor receptor mRNA in osteoblastic cells.J Bone Miner Res 1999;14(5):776–83.
[40] Lecart MP, Bruyere O, Reginster JY. Combination/sequential therapy inosteoporosis. Curr Osteoporos Rep 2004;2(4):123–30.
[41] Fuchs RK, Phipps RJ, Burr DB. Trabecular bone turnover is reestablishedsooner in ovariectomized rats after withdrawal of treatment with risedronatevs alendronate. Bone 2006;38:S50.




















