
On estimating the directionality distribution in pedicle trabecular bone from micro-CT images

Bone 43 (2008) 238–248
Contents lists available at ScienceDirect
Bone
j ourna l homepage: www.e lsev ie r.com/ locate /bone
Mechanical loading enhances the anabolic effects of intermittent parathyroidhormone (1–34) on trabecular and cortical bone in mice
Toshihiro Sugiyama ⁎, Leanne K. Saxon, Gul Zaman, Alaa Moustafa, Andrew Sunters,Joanna S. Price, Lance E. LanyonDepartment of Veterinary Basic Sciences, The Royal Veterinary College, University of London, Royal College Street, London NW1 0TU, UK
⁎ Corresponding author.E-mail address: [email protected] (T. Sugiyama).
8756-3282/$ – see front matter © 2008 Elsevier Inc. Aldoi:10.1016/j.bone.2008.04.012
a b s t r a c t
a r t i c l e i n f oArticle history:
The separate and combined Received 18 December 2007Revised 11 March 2008Accepted 13 April 2008Available online 1 May 2008Edited by: S. Ralston
Keywords:Mechanical loadingAdaptationParathyroid hormoneMouseMicro-computed tomography
effects of intermittent parathyroid hormone (iPTH) (1–34) andmechanical loadingwere assessed at trabecular and cortical sites ofmouse long bones. Female C57BL/6mice from13 to 19weeks ofage were given daily injections of vehicle or PTH (1–34) at low (20 μg/kg/day), medium (40 μg/kg/day) orhigh (80 μg/kg/day) dose. For three alternate days per week during the last two weeks of this treatment,the tibiae and ulnae on one side were subjected to a single period of non-invasive, dynamic axial loading(40 cycles at 10 Hz with 10-second intervals between each cycle). Two levels of peak load were used; onesufficient to engender an osteogenic response, and the other insufficient to do so. The whole tibiae and ulnaewere analyzed post-mortem by micro-computed tomography with a resolution of 5 μm. Treatment withiPTH (1–34)modified bone structure in a dose- and time-dependentmanner, whichwas particularly evident inthe trabecular region of the proximal tibia. In the tibia, loading at a level sufficient by itself to stimulateosteogenesis produced an osteogenic response in the low-dose iPTH (1–34)-treated trabecular bone and in theproximal and middle cortical bone treated with all doses of iPTH (1–34). In the ulna, loading at a level thatdid not by itself stimulate osteogenesis was osteogenic at the distal site when combined with high-doseiPTH (1–34). At both levels of loading, there were synergistic effects in cortical bone volume of the proximaltibia and distal ulna between loading and high-dose iPTH (1–34). Images of fluorescently labelled bonesconfirmed that such synergism resulted from increases in both endosteal and periosteal bone formation.Nowoven bone was induced by iPTH (1–34) or either level of loading alone, whereas the combination of iPTH(1–34) and the “sufficient” level of loading stimulated woven bone formation on endosteal and periostealsurfaces of the proximal cortex in the tibiae. Together, these data suggest that in female C57BL/6 mice,under some but not all circumstances, mechanical loading exerts an osteogenic response with iPTH (1–34) intrabecular and cortical bone.
© 2008 Elsevier Inc. All rights reserved.
Introduction
Fragility fracture associated with osteoporosis is a major healthproblem especially for women [1–3]. Although anti-resorptive agentssuch as bisphosphonates have played a central role in the manage-ment of osteoporosis, anabolic therapies have the potential tostrengthen the fragile skeleton by enhancing bone formation [4]. Atpresent, intermittent parathyroid hormone (iPTH) [5–15] is the onlytreatment licensed for this purpose. Patients who fail anti-resorptivetherapy and are at high risk of fracture, would be candidates for suchtherapy. However, one possible concern [16–18] is that the effects ofiPTH might be attenuated under conditions of low physical activity,which is itself a risk factor for fracture of the hip in postmenopausalwomen [19].
l rights reserved.
Mechanical loading is the major natural anabolic factor thatinfluences bone structure and strength [20–22]. However, prescribingosteogenic levels of load-bearing exercise for osteoporotic patientsalready at high risk of fracture is problematic. There would thereforebe benefit if iPTH could reduce the loading level necessary to stimulatea loading-related anabolic effect [23]. Clinical evidence shows thattreatment with iPTH increases cortical width at some skeletal sites[24,25]. This site specificity has been attributed to differences in thebones' local mechanical environment [25]. Since iPTH increasesremodelling turnover within the bone, it is associated with areduction in overall bone mineralization [25,26]. This decrease couldcontribute to the stimulus for cortical expansion by a compensatoryeffect through increasedmechanical strain from loading [27,28]. If thiswere so, it would suggest that in the human skeleton iPTH isstimulating an osteogenic response, at least in part, as a secondaryeffect.
No such secondary effect is possible in vitro, where PTH promotesthe response of bone-forming osteoblastic cells to mechanical
Materials and methods
239T. Sugiyama et al. / Bone 43 (2008) 238–248
stimulation [29,30]. Consistent with this in vitro observation, severalexperimental in vivo studies using rats have shown that iPTH andmechanical loading act synergistically in both trabecular and corticalbone [31–36]. These experiments include the effects of loading on thevertebra of the tail [32,36]; mediolateral bending of the tibia [34,35];and axial compression of the ulna [35]. Although, to our knowledge,there is no direct evidence of such synergistic actions in mice, iPTHtreatment has been reported to increase periosteal bone formationand cortical thickness in the tibia but not in the vertebral body in thisspecies. The authors ascribed this regional difference to the differentmechanical environment at the two sites [37].
Since, in rodents such as rat and mouse, intracortical boneremodelling only occurs at very low levels, any potential effects ofiPTH on mineralization due to increased remodelling can probably bediscounted in these animals. This means that any possible secondaryeffect on bone's response to loading such as that mentioned above canbe excluded. In this situation, the responses of the skeleton of wild-type and genetically modified mice to iPTH and mechanical loadingshould provide significant mechanistic insights into their primary andcombined effects.
C57BL/6 mice have been extensively used as the background ofgeneticallymodified animals in the field of bone research [38] and alsoshow a good response to mechanical loading [39]. The present studywas therefore designed to assess the effects of mechanical loading ontrabecular and cortical sites of long bones in female C57BL/6 micetreated with low, medium or high dose of iPTH (1–34). These micewere pre-treated with iPTH (1–34) before loading in order toapproximate to the most likely clinical situation where iPTH wouldhave been prescribed and exercise then introduced to provide anadditional osteogenic stimulus. It would be unlikely for both exerciseand iPTH therapy to be introduced together, or exercise before iPTHtherapy. The tibia and ulna on one side were subjected to non-invasive, dynamic axial loading using methods previously reported
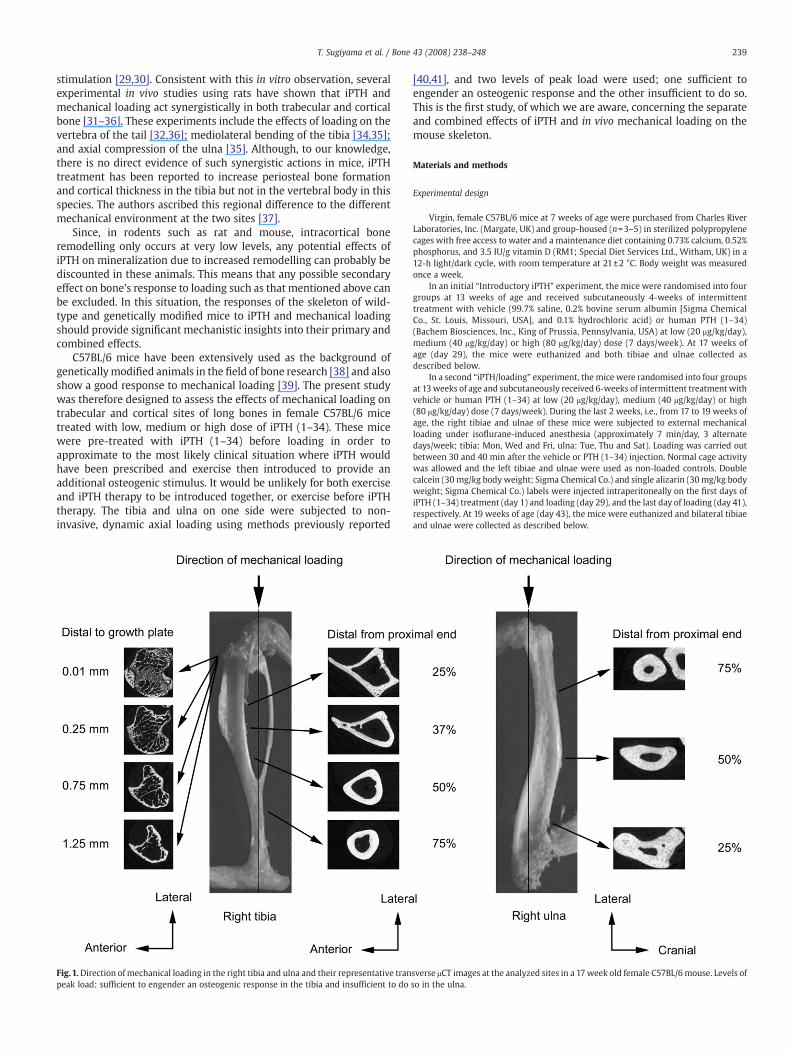
Fig.1.Direction ofmechanical loading in the right tibia and ulna and their representative tranpeak load: sufficient to engender an osteogenic response in the tibia and insufficient to do
[40,41], and two levels of peak load were used; one sufficient toengender an osteogenic response and the other insufficient to do so.This is the first study, of which we are aware, concerning the separateand combined effects of iPTH and in vivo mechanical loading on themouse skeleton.
Experimental design
Virgin, female C57BL/6 mice at 7 weeks of age were purchased from Charles RiverLaboratories, Inc. (Margate, UK) and group-housed (n=3–5) in sterilized polypropylenecages with free access to water and a maintenance diet containing 0.73% calcium, 0.52%phosphorus, and 3.5 IU/g vitamin D (RM1; Special Diet Services Ltd., Witham, UK) in a12-h light/dark cycle, with room temperature at 21±2 °C. Body weight was measuredonce a week.
In an initial “Introductory iPTH” experiment, the mice were randomised into fourgroups at 13 weeks of age and received subcutaneously 4-weeks of intermittenttreatment with vehicle (99.7% saline, 0.2% bovine serum albumin [Sigma ChemicalCo., St. Louis, Missouri, USA], and 0.1% hydrochloric acid) or human PTH (1–34)(Bachem Biosciences, Inc., King of Prussia, Pennsylvania, USA) at low (20 μg/kg/day),medium (40 μg/kg/day) or high (80 μg/kg/day) dose (7 days/week). At 17 weeks ofage (day 29), the mice were euthanized and both tibiae and ulnae collected asdescribed below.
In a second “iPTH/loading” experiment, the mice were randomised into four groupsat 13weeks of age and subcutaneously received 6-weeks of intermittent treatmentwithvehicle or human PTH (1–34) at low (20 μg/kg/day), medium (40 μg/kg/day) or high(80 μg/kg/day) dose (7 days/week). During the last 2 weeks, i.e., from 17 to 19 weeks ofage, the right tibiae and ulnae of these mice were subjected to external mechanicalloading under isoflurane-induced anesthesia (approximately 7 min/day, 3 alternatedays/week; tibia: Mon, Wed and Fri, ulna: Tue, Thu and Sat). Loading was carried outbetween 30 and 40 min after the vehicle or PTH (1–34) injection. Normal cage activitywas allowed and the left tibiae and ulnae were used as non-loaded controls. Doublecalcein (30 mg/kg body weight; Sigma Chemical Co.) and single alizarin (30mg/kg bodyweight; Sigma Chemical Co.) labels were injected intraperitoneally on the first days ofiPTH (1–34) treatment (day 1) and loading (day 29), and the last day of loading (day 41),respectively. At 19 weeks of age (day 43), the mice were euthanized and bilateral tibiaeand ulnae were collected as described below.
sverse μCT images at the analyzed sites in a 17week old female C57BL/6mouse. Levels ofso in the ulna.
240 T. Sugiyama et al. / Bone 43 (2008) 238–248
All procedures complied with the UK Animals (Scientific Procedures) Act 1986 andwere reviewed and passed by the ethics committee of The Royal Veterinary College(London, UK).
In vivo mechanical loading
The apparatus and protocol for dynamically loading the mouse tibia and ulnahave been reported previously [40,41]. Dynamic cyclical loads are applied betweenthe flexed knee and ankle or the flexed elbow and wrist. The flexed joints arepositioned in concave cups; the upper cup, into which the knee or wrist ispositioned, is attached to the actuator arm of a servo-hydraulic loading machine(Model HC10; Zwick Testing Machines Ltd., Leominster, UK) and the lower cup to adynamic load cell. The servo-hydraulic mechanism of the loading machine operatesto apply controlled dynamic compressive loads axially to the tibia/fibula or ulna/radius (Fig. 1).
In the “Introductory iPTH” experiment, the right fore and hind limbs including alltissues were stored at −20 °C in sealed, air-tight plastic bags immediately after sacrifice.When ready for measurement, these limbs were put in saline solution at roomtemperature for at least 3 h. Soft tissues were dissected to expose the medial surface ofthe proximal tibia (37% along the shaft) and the lateral surface of the ulna mid-shaft,and trimmed single element strain gauges (EA-06-015DJ-120; Vishay MeasurementsGroup, Basingstoke, UK) were bonded to these surfaces in longitudinal alignment. Thegauges were connected to a strain conditioner/amplifier system and mechanical load-induced strains were measured as previously described [40,41].
In the “iPTH/loading” experiment, the right tibia and ulna of each mouse washeld in the upper and lower cups of the loading apparatus and dynamic axial loads(trapezoidal-shaped pulse period=0.1 s [loading 0.025 s, hold 0.05 s and unloading0.025 s]; rest time between pulses=10 s; cycles/day=40) were applied between theknee and ankle or the elbow and wrist. In the mice treated with vehicle, peak loads of12.0 N (engendering approximately 1200 µε at the medial surface of the tibiae 37%along the bone shafts from their proximal end) and 2.5 N (engenderingapproximately 1350 µε at the lateral surface of the ulna midshafts) were applied tothe tibia and ulna, respectively. These peak loads were sufficient and insufficient,respectively, to stimulate an osteogenic response in the present loading regimen[40,41]. The peak loads applied to the iPTH (1–34)-treated bones were adjusted toinduce similar peak levels of bone strain by using data of the bone length and
Table 1Structural parameters in the tibia and ulna of 17 week old female C57BL/6 mice treated wit
Dose of PTH (1–34) 0 μg/kg/day
Trabecular bone of proximal tibiaSecondary spongiosaPercent bone volume (%) 10.9±0.4Trabecular number (mm−1) 2.09±0.08Trabecular thickness (mm) 0.0523±0.0012
Cortical bone of tibiaProximal (25%)Periosteally-enclosed volume (mm3) 2.88±0.04Cortical bone volume (mm3) 1.55±0.04Medullary volume (mm3) 1.32±0.02
Middle (50%)Periosteally-enclosed volume (mm3) 2.04±0.02Cortical bone volume (mm3) 1.20±0.02Medullary volume (mm3) 0.832±0.022
Distal (25%)Periosteally-enclosed volume (mm3) 1.53±0.02Cortical bone volume (mm3) 1.08±0.02Medullary volume (mm3) 0.450±0.018
Cortical bone of ulnaProximal (25%)Periosteally-enclosed volume (mm3) 0.886±0.020Cortical bone volume (mm3) 0.814±0.016Medullary volume (mm3) 0.0726±0.0052
Middle (50%)Periosteally-enclosed volume (mm3) 0.584±0.010Cortical bone volume (mm3) 0.484±0.008Medullary volume (mm3) 0.101±0.007
Distal (25%)Periosteally-enclosed volume (mm3) 0.408±0.006Cortical bone volume (mm3) 0.360±0.008Medullary volume (mm3) 0.0486±0.0024
Mean±S.E. (n=8–10).a pb0.05 vs 0 μg/kg/day (one-way ANOVA followed by a post hoc Bonferroni or Dunnettb pb0.05 vs 20 μg/kg/day (one-way ANOVA followed by a post hoc Bonferroni or Dunnetc pb0.05 vs 40 μg/kg/day (one-way ANOVA followed by a post hoc Bonferroni or Dunnet
“average” polar mean moment of inertia at proximal (25%), middle (50%) and distal(75%) sites in the “Introductory iPTH” experiment. As a result, in mice treated withiPTH (1–34) at low, medium or high dose, peak loads for the tibiae sufficient toengender osteogenesis, and for the ulnae insufficient to do so were 13.7, 14.7 and15.8 N, and 2.8, 3.0 and 3.3 N, respectively.
High-resolution micro-computed tomography (μCT) analysis
The left tibiae and ulnae in the “Introductory iPTH” experiment and the bilateraltibiae and ulnae in the “iPTH/loading” experiment were stored in 70% ethanol.These tibiae and ulnae were scanned at high-resolution μCT (SkyScan 1172; SkyScan,Kontich, Belgium) with a pixel size of 5 μm. The images of the whole bones werereconstructed by the SkyScan software (version 1.4.4) and their lengths weremeasured. The analyzed regions were 1) in trabecular bone of the proximal tibiae,between 0.01 and 0.25 mm (containing primary spongiosa) and 0.25 and 1.25 mm(secondary spongiosa) distal to growth plate, 2) in cortical bone of the tibiae,0.5 mm long centered across the proximal (25% and 37%), middle (50%) and distal(75%) sites, and 3) in cortical bone of the ulnae, 0.5 mm long sections across theproximal (25%), middle (50%) and distal (75%) sites (Fig. 1). In the tibiae, the 37%proximal cortical bone site was selected because this was where the strain gaugeswere positioned. Three-dimensional structural analysis for these trabecular andcortical bone sites were performed by the SkyScan software (version 1.6.1.1).Percent bone volume, trabecular number and trabecular thickness in the trabecularbone, and periosteally-enclosed volume, cortical bone volume, medullary volumeand cross-sectional polar mean moment of inertia, a parameter of structural bonestrength, in the cortical bones were evaluated.
Calcein and alizarin labels imaging by confocal microscopy
In the “iPTH/loading” experiment, both left non-loaded and right loaded tibiaeand ulnae were maintained in 70% ethanol after scanning by μCT. These bones werethen dehydrated, cleared and embedded in methyl methacrylate as previouslydescribed [42], and 500 μm-thick serial transverse segments of the whole tibiae andulnae were obtained by cutting with an annular diamond saw. Images of calcein andalizarin labelled transverse bone sections were visualized using argon 488 nm laserand HeNe 543 nm laser, respectively, of a confocal laser scanning microscope (LSM
h 4-weeks of intermittent parathyroid hormone (iPTH) (1–34)
20 μg/kg/day 40 μg/kg/day 80 μg/kg/day
16.0±0.4a 17.8±0.3a,b 29.2±1.3a,b,c
3.24±0.05a 3.81±0.09a,b 6.68±0.34a,b,c
0.0494±0.0007 0.0468±0.0005a 0.0438±0.0008a,b
3.10±0.04a 3.22±0.08a 3.34±0.06a,b
1.81±0.02a 1.84±0.05a 1.92±0.05a
1.30±0.03 1.39±0.04 1.43±0.03b
2.12±0.04 2.18±0.04a 2.24±0.04a
1.27±0.02 1.31±0.02a 1.38±0.03a,b
0.856±0.024 0.872±0.018 0.868±0.018
1.58±0.02 1.63±0.03 1.69±0.03a,b
1.16±0.02a 1.22±0.04a 1.30±0.04a,b
0.424±0.016 0.402±0.018 0.388±0.022
0.916±0.012 0.962±0.016a 0.984±0.010a,b
0.846±0.012 0.886±0.016a 0.904±0.010a,b
0.0708±0.0052 0.0754±0.0056 0.0788±0.0076
0.616±0.010 0.648±0.012a 0.672±0.012a,b
0.528±0.006a 0.546±0.010a 0.568±0.010a,b
0.088±0.005 0.101±0.004 0.104±0.007
0.460±0.010a 0.456±0.006a 0.478±0.006a
0.406±0.006a 0.412±0.004a 0.428±0.006a
0.0520±0.0030 0.0450±0.0038 0.0496±0.0030
T3 test).t T3 test).t T3 test).
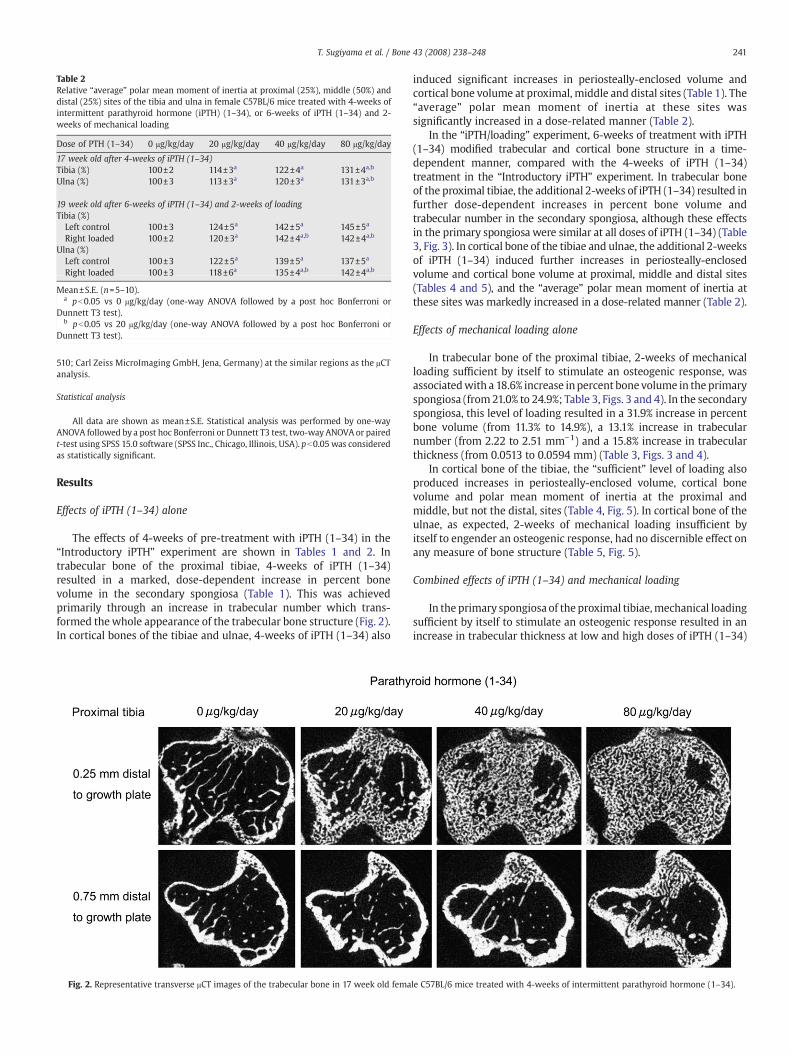
Table 2Relative “average” polar mean moment of inertia at proximal (25%), middle (50%) anddistal (25%) sites of the tibia and ulna in female C57BL/6 mice treated with 4-weeks ofintermittent parathyroid hormone (iPTH) (1–34), or 6-weeks of iPTH (1–34) and 2-weeks of mechanical loading
Dose of PTH (1–34) 0 μg/kg/day 20 μg/kg/day 40 μg/kg/day 80 μg/kg/day
17 week old after 4-weeks of iPTH (1–34)Tibia (%) 100±2 114±3a 122±4a 131±4a,b
Ulna (%) 100±3 113±3a 120±3a 131±3a,b
19 week old after 6-weeks of iPTH (1–34) and 2-weeks of loadingTibia (%)Left control 100±3 124±5a 142±5a 145±5a
Right loaded 100±2 120±3a 142±4a,b 142±4a,b
Ulna (%)Left control 100±3 122±5a 139±5a 137±5a
Right loaded 100±3 118±6a 135±4a,b 142±4a,b
Mean±S.E. (n=5–10).a pb0.05 vs 0 μg/kg/day (one-way ANOVA followed by a post hoc Bonferroni or
Dunnett T3 test).b pb0.05 vs 20 μg/kg/day (one-way ANOVA followed by a post hoc Bonferroni or
Dunnett T3 test).
241T. Sugiyama et al. / Bone 43 (2008) 238–248
510; Carl Zeiss MicroImaging GmbH, Jena, Germany) at the similar regions as the μCTanalysis.
Statistical analysis
All data are shown as mean±S.E. Statistical analysis was performed by one-wayANOVA followed by a post hoc Bonferroni or Dunnett T3 test, two-way ANOVA or pairedt-test using SPSS 15.0 software (SPSS Inc., Chicago, Illinois, USA). pb0.05 was consideredas statistically significant.
Results
Effects of iPTH (1–34) alone
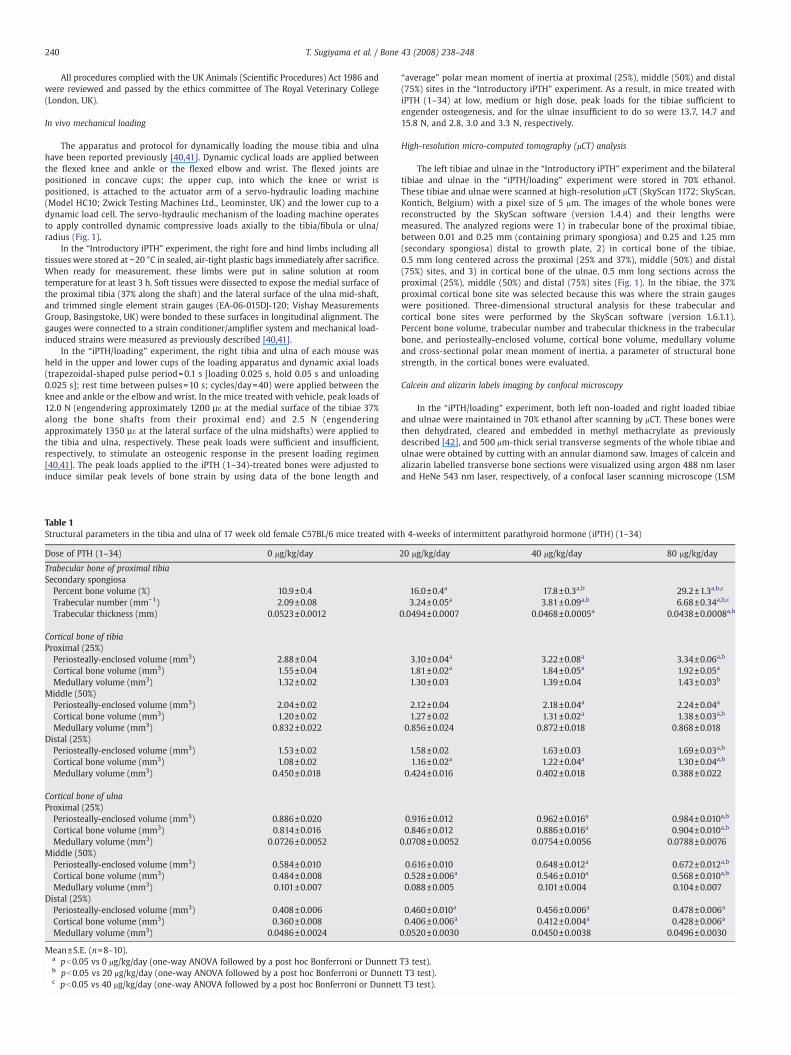
The effects of 4-weeks of pre-treatment with iPTH (1–34) in the“Introductory iPTH” experiment are shown in Tables 1 and 2. Intrabecular bone of the proximal tibiae, 4-weeks of iPTH (1–34)resulted in a marked, dose-dependent increase in percent bonevolume in the secondary spongiosa (Table 1). This was achievedprimarily through an increase in trabecular number which trans-formed thewhole appearance of the trabecular bone structure (Fig. 2).In cortical bones of the tibiae and ulnae, 4-weeks of iPTH (1–34) also
Fig. 2. Representative transverse μCT images of the trabecular bone in 17 week old fema
induced significant increases in periosteally-enclosed volume andcortical bone volume at proximal, middle and distal sites (Table 1). The“average” polar mean moment of inertia at these sites wassignificantly increased in a dose-related manner (Table 2).
In the “iPTH/loading” experiment, 6-weeks of treatment with iPTH(1–34) modified trabecular and cortical bone structure in a time-dependent manner, compared with the 4-weeks of iPTH (1–34)treatment in the “Introductory iPTH” experiment. In trabecular boneof the proximal tibiae, the additional 2-weeks of iPTH (1–34) resulted infurther dose-dependent increases in percent bone volume andtrabecular number in the secondary spongiosa, although these effectsin the primary spongiosa were similar at all doses of iPTH (1–34) (Table3, Fig. 3). In cortical bone of the tibiae and ulnae, the additional 2-weeksof iPTH (1–34) induced further increases in periosteally-enclosedvolume and cortical bone volume at proximal, middle and distal sites(Tables 4 and 5), and the “average” polar mean moment of inertia atthese sites was markedly increased in a dose-related manner (Table 2).
Effects of mechanical loading alone
In trabecular bone of the proximal tibiae, 2-weeks of mechanicalloading sufficient by itself to stimulate an osteogenic response, wasassociatedwith a 18.6% increase inpercent bone volume in the primaryspongiosa (from21.0% to 24.9%; Table 3, Figs. 3 and 4). In the secondaryspongiosa, this level of loading resulted in a 31.9% increase in percentbone volume (from 11.3% to 14.9%), a 13.1% increase in trabecularnumber (from 2.22 to 2.51 mm−1) and a 15.8% increase in trabecularthickness (from 0.0513 to 0.0594 mm) (Table 3, Figs. 3 and 4).
In cortical bone of the tibiae, the “sufficient” level of loading alsoproduced increases in periosteally-enclosed volume, cortical bonevolume and polar mean moment of inertia at the proximal andmiddle, but not the distal, sites (Table 4, Fig. 5). In cortical bone of theulnae, as expected, 2-weeks of mechanical loading insufficient byitself to engender an osteogenic response, had no discernible effect onany measure of bone structure (Table 5, Fig. 5).
Combined effects of iPTH (1–34) and mechanical loading
In the primary spongiosa of the proximal tibiae,mechanical loadingsufficient by itself to stimulate an osteogenic response resulted in anincrease in trabecular thickness at low and high doses of iPTH (1–34)
le C57BL/6 mice treated with 4-weeks of intermittent parathyroid hormone (1–34).
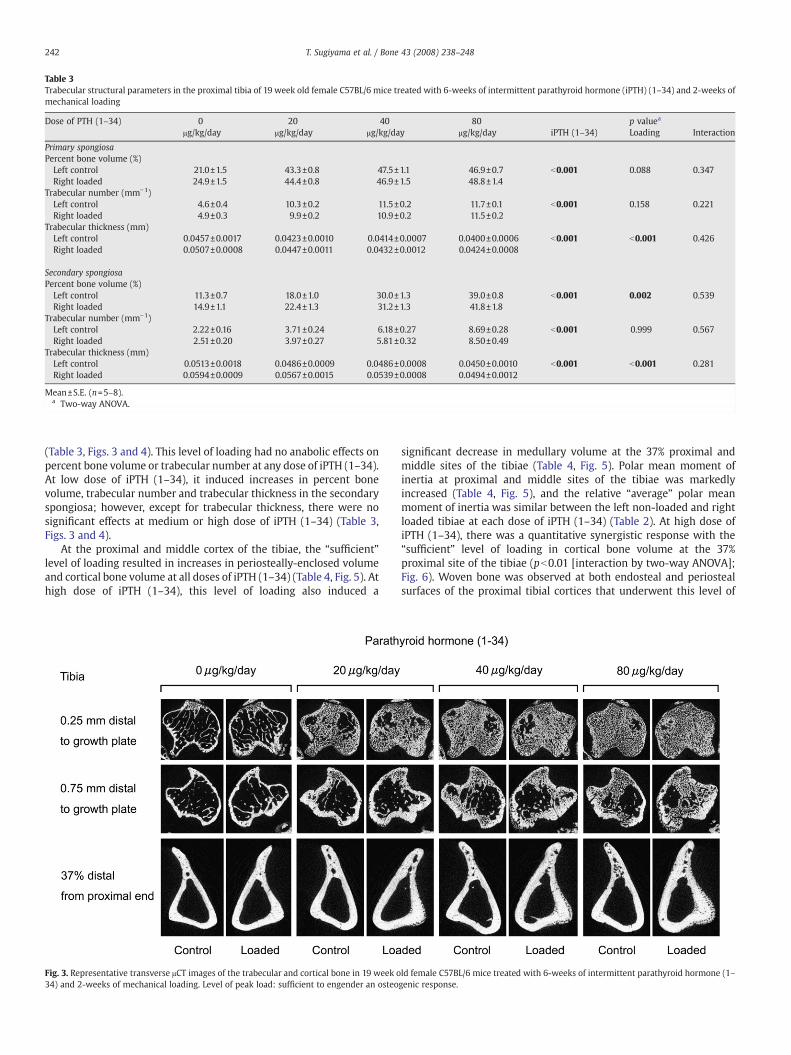
Table 3Trabecular structural parameters in the proximal tibia of 19 week old female C57BL/6 mice treated with 6-weeks of intermittent parathyroid hormone (iPTH) (1–34) and 2-weeks ofmechanical loading
Dose of PTH (1–34) 0 20 40 80 p valuea
μg/kg/day μg/kg/day μg/kg/day μg/kg/day iPTH (1–34) Loading Interaction
Primary spongiosaPercent bone volume (%)Left control 21.0±1.5 43.3±0.8 47.5±1.1 46.9±0.7 b0.001 0.088 0.347Right loaded 24.9±1.5 44.4±0.8 46.9±1.5 48.8±1.4
Trabecular number (mm−1)Left control 4.6±0.4 10.3±0.2 11.5±0.2 11.7±0.1 b0.001 0.158 0.221Right loaded 4.9±0.3 9.9±0.2 10.9±0.2 11.5±0.2
Trabecular thickness (mm)Left control 0.0457±0.0017 0.0423±0.0010 0.0414±0.0007 0.0400±0.0006 b0.001 b0.001 0.426Right loaded 0.0507±0.0008 0.0447±0.0011 0.0432±0.0012 0.0424±0.0008
Secondary spongiosaPercent bone volume (%)Left control 11.3±0.7 18.0±1.0 30.0±1.3 39.0±0.8 b0.001 0.002 0.539Right loaded 14.9±1.1 22.4±1.3 31.2±1.3 41.8±1.8
Trabecular number (mm−1)Left control 2.22±0.16 3.71±0.24 6.18±0.27 8.69±0.28 b0.001 0.999 0.567Right loaded 2.51±0.20 3.97±0.27 5.81±0.32 8.50±0.49
Trabecular thickness (mm)Left control 0.0513±0.0018 0.0486±0.0009 0.0486±0.0008 0.0450±0.0010 b0.001 b0.001 0.281Right loaded 0.0594±0.0009 0.0567±0.0015 0.0539±0.0008 0.0494±0.0012
Mean±S.E. (n=5–8).a Two-way ANOVA.
242 T. Sugiyama et al. / Bone 43 (2008) 238–248
(Table 3, Figs. 3 and 4). This level of loading had no anabolic effects onpercent bone volume or trabecular number at any dose of iPTH (1–34).At low dose of iPTH (1–34), it induced increases in percent bonevolume, trabecular number and trabecular thickness in the secondaryspongiosa; however, except for trabecular thickness, there were nosignificant effects at medium or high dose of iPTH (1–34) (Table 3,Figs. 3 and 4).
At the proximal and middle cortex of the tibiae, the “sufficient”level of loading resulted in increases in periosteally-enclosed volumeand cortical bone volume at all doses of iPTH (1–34) (Table 4, Fig. 5). Athigh dose of iPTH (1–34), this level of loading also induced a
Fig. 3. Representative transverse μCT images of the trabecular and cortical bone in 19 week o34) and 2-weeks of mechanical loading. Level of peak load: sufficient to engender an osteo
significant decrease in medullary volume at the 37% proximal andmiddle sites of the tibiae (Table 4, Fig. 5). Polar mean moment ofinertia at proximal and middle sites of the tibiae was markedlyincreased (Table 4, Fig. 5), and the relative “average” polar meanmoment of inertia was similar between the left non-loaded and rightloaded tibiae at each dose of iPTH (1–34) (Table 2). At high dose ofiPTH (1–34), there was a quantitative synergistic response with the“sufficient” level of loading in cortical bone volume at the 37%proximal site of the tibiae (pb0.01 [interaction by two-way ANOVA];Fig. 6). Woven bone was observed at both endosteal and periostealsurfaces of the proximal tibial cortices that underwent this level of
ld female C57BL/6 mice treated with 6-weeks of intermittent parathyroid hormone (1–genic response.
243T. Sugiyama et al. / Bone 43 (2008) 238–248
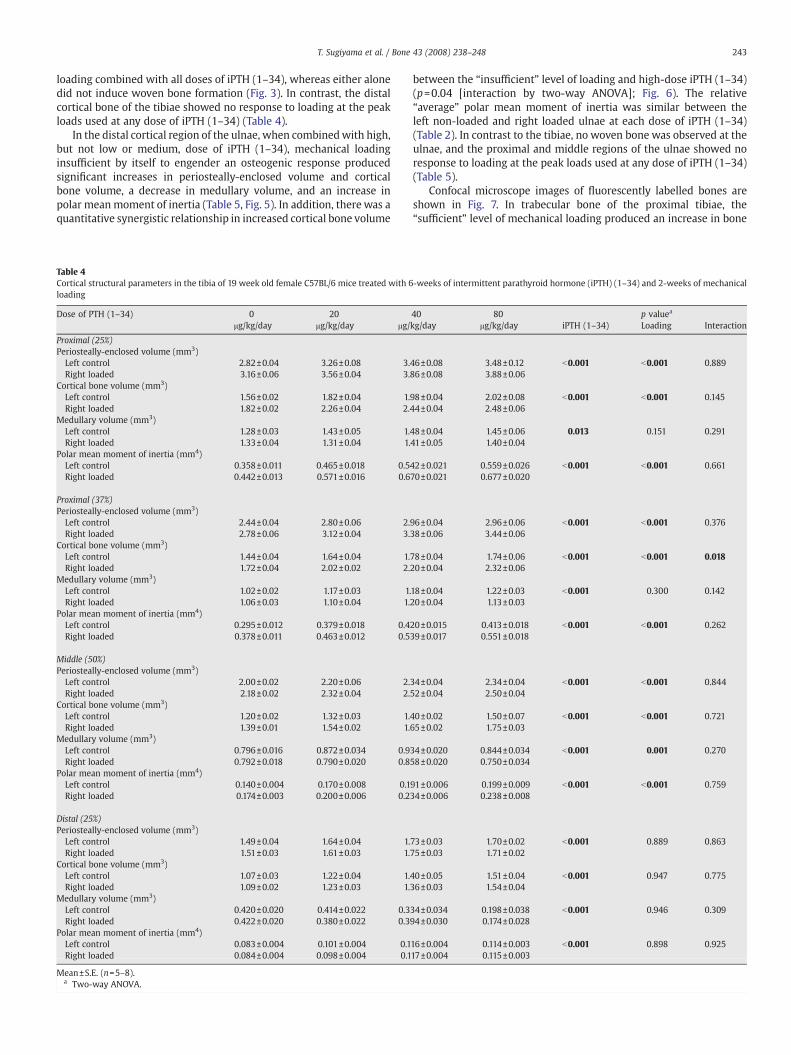
loading combined with all doses of iPTH (1–34), whereas either alonedid not induce woven bone formation (Fig. 3). In contrast, the distalcortical bone of the tibiae showed no response to loading at the peakloads used at any dose of iPTH (1–34) (Table 4).
In the distal cortical region of the ulnae, when combinedwith high,but not low or medium, dose of iPTH (1–34), mechanical loadinginsufficient by itself to engender an osteogenic response producedsignificant increases in periosteally-enclosed volume and corticalbone volume, a decrease in medullary volume, and an increase inpolar meanmoment of inertia (Table 5, Fig. 5). In addition, there was aquantitative synergistic relationship in increased cortical bone volume
Table 4Cortical structural parameters in the tibia of 19 week old female C57BL/6 mice treated with 6loading
Dose of PTH (1–34) 0 20μg/kg/day μg/kg/day μg/
Proximal (25%)Periosteally-enclosed volume (mm3)Left control 2.82±0.04 3.26±0.08 3.Right loaded 3.16±0.06 3.56±0.04 3.
Cortical bone volume (mm3)Left control 1.56±0.02 1.82±0.04 1.Right loaded 1.82±0.02 2.26±0.04 2.
Medullary volume (mm3)Left control 1.28±0.03 1.43±0.05 1.Right loaded 1.33±0.04 1.31±0.04 1.
Polar mean moment of inertia (mm4)Left control 0.358±0.011 0.465±0.018 0.5Right loaded 0.442±0.013 0.571±0.016 0.6
Proximal (37%)Periosteally-enclosed volume (mm3)Left control 2.44±0.04 2.80±0.06 2.Right loaded 2.78±0.06 3.12±0.04 3.
Cortical bone volume (mm3)Left control 1.44±0.04 1.64±0.04 1.Right loaded 1.72±0.04 2.02±0.02 2.
Medullary volume (mm3)Left control 1.02±0.02 1.17±0.03 1.Right loaded 1.06±0.03 1.10±0.04 1.
Polar mean moment of inertia (mm4)Left control 0.295±0.012 0.379±0.018 0.4Right loaded 0.378±0.011 0.463±0.012 0.5
Middle (50%)Periosteally-enclosed volume (mm3)Left control 2.00±0.02 2.20±0.06 2.Right loaded 2.18±0.02 2.32±0.04 2.
Cortical bone volume (mm3)Left control 1.20±0.02 1.32±0.03 1.Right loaded 1.39±0.01 1.54±0.02 1.
Medullary volume (mm3)Left control 0.796±0.016 0.872±0.034 0.9Right loaded 0.792±0.018 0.790±0.020 0.8
Polar mean moment of inertia (mm4)Left control 0.140±0.004 0.170±0.008 0.1Right loaded 0.174±0.003 0.200±0.006 0.2
Distal (25%)Periosteally-enclosed volume (mm3)Left control 1.49±0.04 1.64±0.04 1.Right loaded 1.51±0.03 1.61±0.03 1.
Cortical bone volume (mm3)Left control 1.07±0.03 1.22±0.04 1.Right loaded 1.09±0.02 1.23±0.03 1.
Medullary volume (mm3)Left control 0.420±0.020 0.414±0.022 0.3Right loaded 0.422±0.020 0.380±0.022 0.3
Polar mean moment of inertia (mm4)Left control 0.083±0.004 0.101±0.004 0.1Right loaded 0.084±0.004 0.098±0.004 0.1
Mean±S.E. (n=5–8).a Two-way ANOVA.
between the “insufficient” level of loading and high-dose iPTH (1–34)(p=0.04 [interaction by two-way ANOVA]; Fig. 6). The relative“average” polar mean moment of inertia was similar between theleft non-loaded and right loaded ulnae at each dose of iPTH (1–34)(Table 2). In contrast to the tibiae, no woven bone was observed at theulnae, and the proximal and middle regions of the ulnae showed noresponse to loading at the peak loads used at any dose of iPTH (1–34)(Table 5).
Confocal microscope images of fluorescently labelled bones areshown in Fig. 7. In trabecular bone of the proximal tibiae, the“sufficient” level of mechanical loading produced an increase in bone
-weeks of intermittent parathyroid hormone (iPTH) (1–34) and 2-weeks of mechanical
40 80 p valuea
kg/day μg/kg/day iPTH (1–34) Loading Interaction
46±0.08 3.48±0.12 b0.001 b0.001 0.88986±0.08 3.88±0.06
98±0.04 2.02±0.08 b0.001 b0.001 0.14544±0.04 2.48±0.06
48±0.04 1.45±0.06 0.013 0.151 0.29141±0.05 1.40±0.04
42±0.021 0.559±0.026 b0.001 b0.001 0.66170±0.021 0.677±0.020
96±0.04 2.96±0.06 b0.001 b0.001 0.37638±0.06 3.44±0.06
78±0.04 1.74±0.06 b0.001 b0.001 0.01820±0.04 2.32±0.06
18±0.04 1.22±0.03 b0.001 0.300 0.14220±0.04 1.13±0.03
20±0.015 0.413±0.018 b0.001 b0.001 0.26239±0.017 0.551±0.018
34±0.04 2.34±0.04 b0.001 b0.001 0.84452±0.04 2.50±0.04
40±0.02 1.50±0.07 b0.001 b0.001 0.72165±0.02 1.75±0.03
34±0.020 0.844±0.034 b0.001 0.001 0.27058±0.020 0.750±0.034
91±0.006 0.199±0.009 b0.001 b0.001 0.75934±0.006 0.238±0.008
73±0.03 1.70±0.02 b0.001 0.889 0.86375±0.03 1.71±0.02
40±0.05 1.51±0.04 b0.001 0.947 0.77536±0.03 1.54±0.04
34±0.034 0.198±0.038 b0.001 0.946 0.30994±0.030 0.174±0.028
16±0.004 0.114±0.003 b0.001 0.898 0.92517±0.004 0.115±0.003
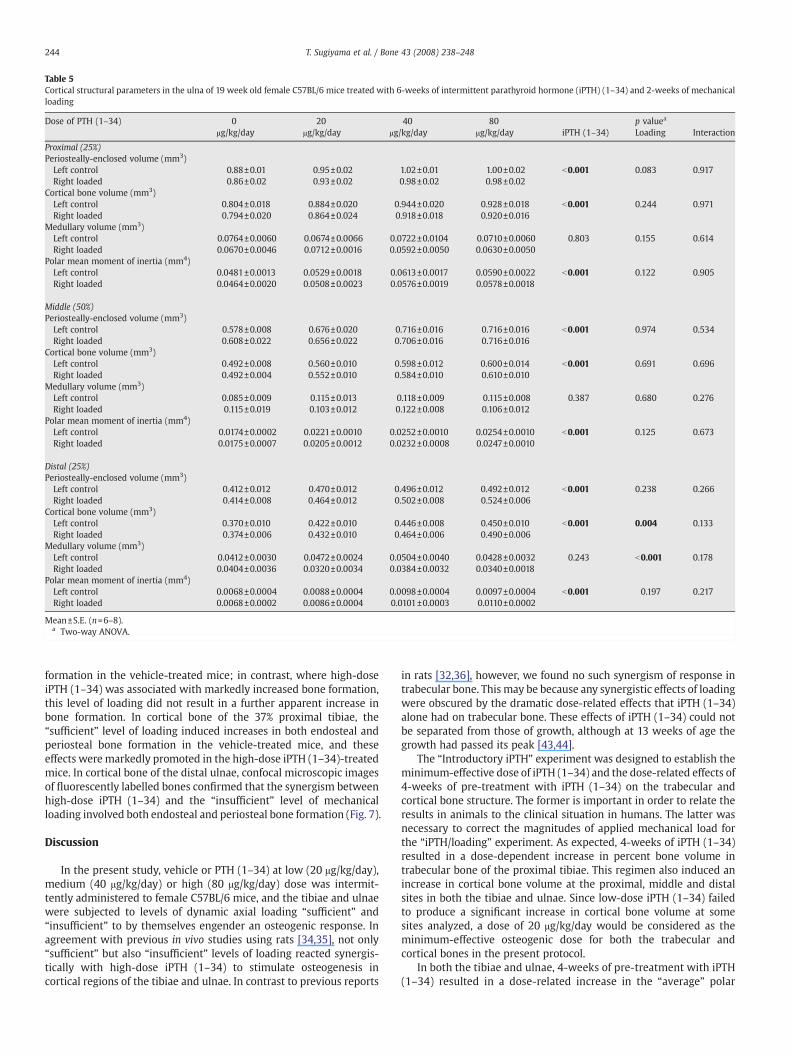
Table 5Cortical structural parameters in the ulna of 19 week old female C57BL/6 mice treated with 6-weeks of intermittent parathyroid hormone (iPTH) (1–34) and 2-weeks of mechanicalloading
Dose of PTH (1–34) 0 20 40 80 p valuea
μg/kg/day μg/kg/day μg/kg/day μg/kg/day iPTH (1–34) Loading Interaction
Proximal (25%)Periosteally-enclosed volume (mm3)Left control 0.88±0.01 0.95±0.02 1.02±0.01 1.00±0.02 b0.001 0.083 0.917Right loaded 0.86±0.02 0.93±0.02 0.98±0.02 0.98±0.02
Cortical bone volume (mm3)Left control 0.804±0.018 0.884±0.020 0.944±0.020 0.928±0.018 b0.001 0.244 0.971Right loaded 0.794±0.020 0.864±0.024 0.918±0.018 0.920±0.016
Medullary volume (mm3)Left control 0.0764±0.0060 0.0674±0.0066 0.0722±0.0104 0.0710±0.0060 0.803 0.155 0.614Right loaded 0.0670±0.0046 0.0712±0.0016 0.0592±0.0050 0.0630±0.0050
Polar mean moment of inertia (mm4)Left control 0.0481±0.0013 0.0529±0.0018 0.0613±0.0017 0.0590±0.0022 b0.001 0.122 0.905Right loaded 0.0464±0.0020 0.0508±0.0023 0.0576±0.0019 0.0578±0.0018
Middle (50%)Periosteally-enclosed volume (mm3)Left control 0.578±0.008 0.676±0.020 0.716±0.016 0.716±0.016 b0.001 0.974 0.534Right loaded 0.608±0.022 0.656±0.022 0.706±0.016 0.716±0.016
Cortical bone volume (mm3)Left control 0.492±0.008 0.560±0.010 0.598±0.012 0.600±0.014 b0.001 0.691 0.696Right loaded 0.492±0.004 0.552±0.010 0.584±0.010 0.610±0.010
Medullary volume (mm3)Left control 0.085±0.009 0.115±0.013 0.118±0.009 0.115±0.008 0.387 0.680 0.276Right loaded 0.115±0.019 0.103±0.012 0.122±0.008 0.106±0.012
Polar mean moment of inertia (mm4)Left control 0.0174±0.0002 0.0221±0.0010 0.0252±0.0010 0.0254±0.0010 b0.001 0.125 0.673Right loaded 0.0175±0.0007 0.0205±0.0012 0.0232±0.0008 0.0247±0.0010
Distal (25%)Periosteally-enclosed volume (mm3)Left control 0.412±0.012 0.470±0.012 0.496±0.012 0.492±0.012 b0.001 0.238 0.266Right loaded 0.414±0.008 0.464±0.012 0.502±0.008 0.524±0.006
Cortical bone volume (mm3)Left control 0.370±0.010 0.422±0.010 0.446±0.008 0.450±0.010 b0.001 0.004 0.133Right loaded 0.374±0.006 0.432±0.010 0.464±0.006 0.490±0.006
Medullary volume (mm3)Left control 0.0412±0.0030 0.0472±0.0024 0.0504±0.0040 0.0428±0.0032 0.243 b0.001 0.178Right loaded 0.0404±0.0036 0.0320±0.0034 0.0384±0.0032 0.0340±0.0018
Polar mean moment of inertia (mm4)Left control 0.0068±0.0004 0.0088±0.0004 0.0098±0.0004 0.0097±0.0004 b0.001 0.197 0.217Right loaded 0.0068±0.0002 0.0086±0.0004 0.0101±0.0003 0.0110±0.0002
Mean±S.E. (n=6–8).a Two-way ANOVA.
244 T. Sugiyama et al. / Bone 43 (2008) 238–248
formation in the vehicle-treated mice; in contrast, where high-doseiPTH (1–34) was associated with markedly increased bone formation,this level of loading did not result in a further apparent increase inbone formation. In cortical bone of the 37% proximal tibiae, the“sufficient” level of loading induced increases in both endosteal andperiosteal bone formation in the vehicle-treated mice, and theseeffects were markedly promoted in the high-dose iPTH (1–34)-treatedmice. In cortical bone of the distal ulnae, confocal microscopic imagesof fluorescently labelled bones confirmed that the synergism betweenhigh-dose iPTH (1–34) and the “insufficient” level of mechanicalloading involved both endosteal and periosteal bone formation (Fig. 7).
Discussion
In the present study, vehicle or PTH (1–34) at low (20 μg/kg/day),medium (40 μg/kg/day) or high (80 μg/kg/day) dose was intermit-tently administered to female C57BL/6 mice, and the tibiae and ulnaewere subjected to levels of dynamic axial loading “sufficient” and“insufficient” to by themselves engender an osteogenic response. Inagreement with previous in vivo studies using rats [34,35], not only“sufficient” but also “insufficient” levels of loading reacted synergis-tically with high-dose iPTH (1–34) to stimulate osteogenesis incortical regions of the tibiae and ulnae. In contrast to previous reports
in rats [32,36], however, we found no such synergism of response intrabecular bone. This may be because any synergistic effects of loadingwere obscured by the dramatic dose-related effects that iPTH (1–34)alone had on trabecular bone. These effects of iPTH (1–34) could notbe separated from those of growth, although at 13 weeks of age thegrowth had passed its peak [43,44].
The “Introductory iPTH” experiment was designed to establish theminimum-effective dose of iPTH (1–34) and the dose-related effects of4-weeks of pre-treatment with iPTH (1–34) on the trabecular andcortical bone structure. The former is important in order to relate theresults in animals to the clinical situation in humans. The latter wasnecessary to correct the magnitudes of applied mechanical load forthe “iPTH/loading” experiment. As expected, 4-weeks of iPTH (1–34)resulted in a dose-dependent increase in percent bone volume intrabecular bone of the proximal tibiae. This regimen also induced anincrease in cortical bone volume at the proximal, middle and distalsites in both the tibiae and ulnae. Since low-dose iPTH (1–34) failedto produce a significant increase in cortical bone volume at somesites analyzed, a dose of 20 μg/kg/day would be considered as theminimum-effective osteogenic dose for both the trabecular andcortical bones in the present protocol.
In both the tibiae and ulnae, 4-weeks of pre-treatment with iPTH(1–34) resulted in a dose-related increase in the “average” polar

Fig. 4. Two-week mechanical load-induced changes ([right loaded− left control] / leftcontrol) of the trabecular structural parameters in 19 week old female C57BL/6 micetreated with 6-weeks of intermittent parathyroid hormone (iPTH) (1–34). Level of peakload: sufficient to engender an osteogenic response. Mean±S.E. (n=5–8). ⁎pb0.05 bypaired t-test between left control and right loaded. #pb0.05 by one-way ANOVAfollowed by a post hoc Bonferroni or Dunnett T3 test among four doses of PTH (1–34).
245T. Sugiyama et al. / Bone 43 (2008) 238–248
mean moment of inertia, a parameter of resistance to bending, at theproximal, middle and distal sites. These data as well as those forbone length were used to establish the necessary magnitudes ofmechanical load to produce the required bone strains. Since theadditional 2-weeks of treatment with iPTH (1–34) stimulated afurther increase in the “average” polar mean moment of inertia in adose-related manner, the corrected levels of mechanical load wouldresult in relatively lower peak strain in the bones of the iPTH (1–34)-treated mice than in those treated with vehicle during the latterduration of loading. Thus, the effects of mechanical loading are likelyto be under rather than overestimated. Nevertheless, the similarchanges in the relative “average” polar mean moment of inertiabetween the left non-loaded and right loaded tibiae and ulnae ateach dose of iPTH (1–34), as shown in Table 2, provides a validationof the corrected levels of applied mechanical load in the presentstudy.
In the “iPTH/loading” experiment, iPTH (1–34) and mechanicalloading at a level sufficient by itself to stimulate an osteogenicresponse were both associated with an increase in trabecularpercent bone volume in the proximal tibia. However, these effects
were produced in a different way; iPTH (1–34) increased trabecularnumber but had no anabolic effect on trabecular thickness, whereasthe “sufficient” level of loading increased both trabecular numberand thickness. This level of loading resulted in an additive increasein percent bone volume of the secondary spongiosa in mice alsotreated with low-dose iPTH (1–34), but we did not detect thesynergistic effects between iPTH (1–34) and loading reported inprevious in vivo studies in rats using axial compression of the tailvertebrae [32,36]. However, since these rats were not treated withiPTH before loading [32,36], the anabolic actions of mechanicalloading are likely to be restricted owing to the marked modificationof trabecular structure induced by the 4-weeks of pre-treatmentwith iPTH (1–34).
In cortical regions of the tibiae, iPTH (1–34) and the “sufficient”level of mechanical loading resulted in additive or synergisticincreases in periosteally-enclosed volume and cortical bone volumeat the proximal and middle sites; iPTH (1–34) induced an osteogenicresponse at all sites, whereas this level of loading had no effect at thedistal site. At the 37% proximal site of the tibiae where there was asynergistic effect in cortical bone volume between high-dose iPTH (1–34) and the “sufficient” level of loading, woven bone was produced atboth endosteal and periosteal surfaces in response to this level ofloading when combined with iPTH (1–34) at all doses but in nosituation in response to either stimulus alone. Since there is a strainthreshold above which woven bone formation occurs [45], theseresults suggest that iPTH (1–34) sensitizes bone cells to mechanicalstimulation and thus lowers the bone-modelling threshold of me-chanical strain. This concept is consistent with the confocal micro-scope images and previous findings in rats [34,35], both of whichshowed that iPTH (1–34) and mechanical loading synergisticallyincreased endosteal and periosteal bone formation.
As expected, in cortical regions of the ulna, mechanical loading at alevel insufficient by itself to stimulate an osteogenic response did notchange cortical bone structure in the vehicle-treatedmice. In contrast,inmice treatedwith high, but not low ormedium, dose of iPTH (1–34),this level of loading induced increases in the periosteally-enclosedvolume and cortical bone volume and a decrease in the medullaryvolume at the distal site. Together, these changes resulted in anincrease in the polar mean moment of inertia. Consistent with thedata from the proximal tibia, the synergistic relationship betweenhigh-dose iPTH (1–34) and the “insufficient” level of loading forcortical bone volume in the distal ulna also supports the concept thatiPTH (1–34) lowers the bone-modelling threshold of mechanicalstrain.
In the present study, the synergistic effects of iPTH (1–34) anddifferent levels of mechanical loading were observed at the 37%proximal tibia and distal ulna in mice treated with iPTH (1–34) at adose of 80 μg/kg/day, but not 20 or 40 μg/kg/day, suggesting that iPTH(1–34) sensitizes bone cells to mechanical stimulation only at higherdose. This possibility is supported by a previous report in rats thattreatment with iPTH (1–38) at a dose of 80 μg/kg/day, but not 30 μg/kg/day, induced a higher periosteal bone formation rate, whichresulted in larger cross-sectional total and bone areas, in remobilizedlimbs than in immobilized limbs [33].
On the other hand, the distal tibiae as well as the proximal andmiddle ulnae showed no response to mechanical loading at levelsapplied in the present study. The shape of the skeleton is controlled byits mechanical environment, and the differences among bone sites inresponse to any one loading configuration are likely to be determinedby how different this loading environment is from that to which thesite in question is habituated.
In conclusion, the present study in female C57BL/6 mice showsthat iPTH (1–34) and mechanical loading independently stimulateosteogenesis in both trabecular and cortical regions of long bones. Thedose-dependent effects of iPTH (1–34) on trabecular bone areparticularly marked, and the pre-treatment with iPTH (1–34) at
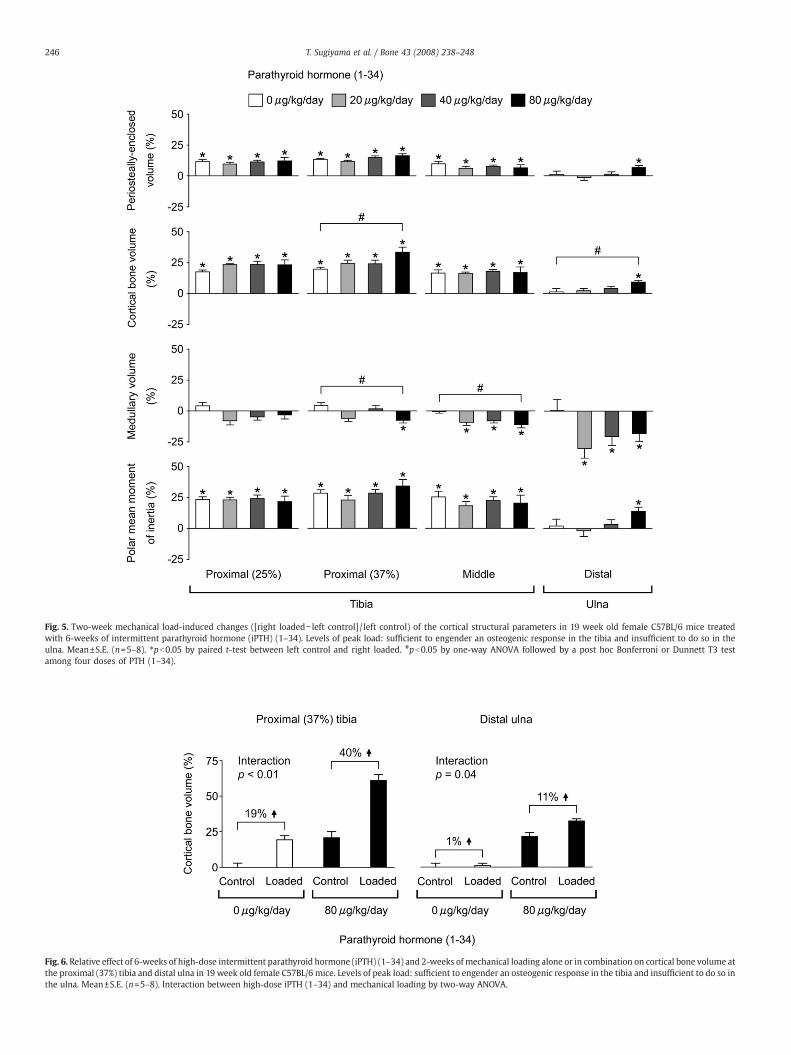
Fig. 5. Two-week mechanical load-induced changes ([right loaded− left control] / left control) of the cortical structural parameters in 19 week old female C57BL/6 mice treatedwith 6-weeks of intermittent parathyroid hormone (iPTH) (1–34). Levels of peak load: sufficient to engender an osteogenic response in the tibia and insufficient to do so in theulna. Mean±S.E. (n=5–8). ⁎pb0.05 by paired t-test between left control and right loaded. #pb0.05 by one-way ANOVA followed by a post hoc Bonferroni or Dunnett T3 testamong four doses of PTH (1–34).
Fig. 6. Relative effect of 6-weeks of high-dose intermittent parathyroid hormone (iPTH) (1–34) and 2-weeks ofmechanical loading alone or in combination on cortical bone volume atthe proximal (37%) tibia and distal ulna in 19 week old female C57BL/6 mice. Levels of peak load: sufficient to engender an osteogenic response in the tibia and insufficient to do so inthe ulna. Mean±S.E. (n=5–8). Interaction between high-dose iPTH (1–34) and mechanical loading by two-way ANOVA.
246 T. Sugiyama et al. / Bone 43 (2008) 238–248
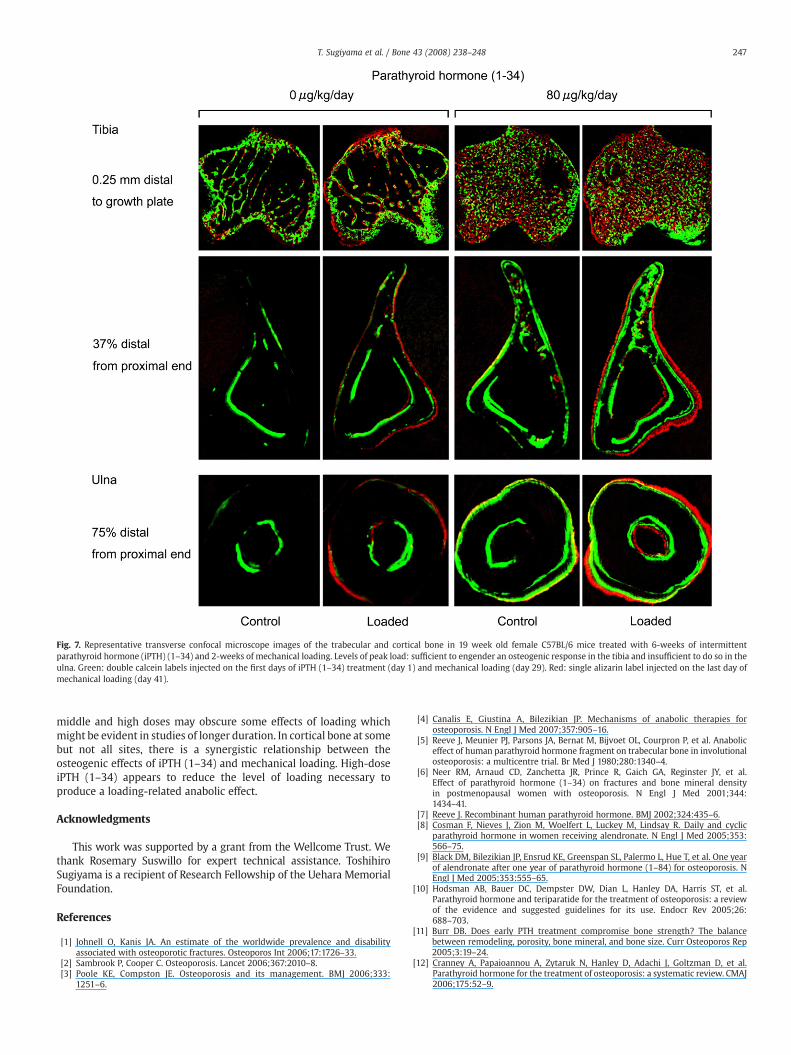
Fig. 7. Representative transverse confocal microscope images of the trabecular and cortical bone in 19 week old female C57BL/6 mice treated with 6-weeks of intermittentparathyroid hormone (iPTH) (1–34) and 2-weeks of mechanical loading. Levels of peak load: sufficient to engender an osteogenic response in the tibia and insufficient to do so in theulna. Green: double calcein labels injected on the first days of iPTH (1–34) treatment (day 1) and mechanical loading (day 29). Red: single alizarin label injected on the last day ofmechanical loading (day 41).
247T. Sugiyama et al. / Bone 43 (2008) 238–248
middle and high doses may obscure some effects of loading whichmight be evident in studies of longer duration. In cortical bone at somebut not all sites, there is a synergistic relationship between theosteogenic effects of iPTH (1–34) and mechanical loading. High-doseiPTH (1–34) appears to reduce the level of loading necessary toproduce a loading-related anabolic effect.
Acknowledgments
This work was supported by a grant from the Wellcome Trust. Wethank Rosemary Suswillo for expert technical assistance. ToshihiroSugiyama is a recipient of Research Fellowship of the Uehara MemorialFoundation.
References
[1] Johnell O, Kanis JA. An estimate of the worldwide prevalence and disabilityassociated with osteoporotic fractures. Osteoporos Int 2006;17:1726–33.
[2] Sambrook P, Cooper C. Osteoporosis. Lancet 2006;367:2010–8.[3] Poole KE, Compston JE. Osteoporosis and its management. BMJ 2006;333:
1251–6.
[4] Canalis E, Giustina A, Bilezikian JP. Mechanisms of anabolic therapies forosteoporosis. N Engl J Med 2007;357:905–16.
[5] Reeve J, Meunier PJ, Parsons JA, Bernat M, Bijvoet OL, Courpron P, et al. Anaboliceffect of human parathyroid hormone fragment on trabecular bone in involutionalosteoporosis: a multicentre trial. Br Med J 1980;280:1340–4.
[6] Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, et al.Effect of parathyroid hormone (1–34) on fractures and bone mineral densityin postmenopausal women with osteoporosis. N Engl J Med 2001;344:1434–41.
[7] Reeve J. Recombinant human parathyroid hormone. BMJ 2002;324:435–6.[8] Cosman F, Nieves J, Zion M, Woelfert L, Luckey M, Lindsay R. Daily and cyclic
parathyroid hormone in women receiving alendronate. N Engl J Med 2005;353:566–75.
[9] Black DM, Bilezikian JP, Ensrud KE, Greenspan SL, Palermo L, Hue T, et al. One yearof alendronate after one year of parathyroid hormone (1–84) for osteoporosis. NEngl J Med 2005;353:555–65.
[10] Hodsman AB, Bauer DC, Dempster DW, Dian L, Hanley DA, Harris ST, et al.Parathyroid hormone and teriparatide for the treatment of osteoporosis: a reviewof the evidence and suggested guidelines for its use. Endocr Rev 2005;26:688–703.
[11] Burr DB. Does early PTH treatment compromise bone strength? The balancebetween remodeling, porosity, bone mineral, and bone size. Curr Osteoporos Rep2005;3:19–24.
[12] Cranney A, Papaioannou A, Zytaruk N, Hanley D, Adachi J, Goltzman D, et al.Parathyroid hormone for the treatment of osteoporosis: a systematic review. CMAJ2006;175:52–9.
248 T. Sugiyama et al. / Bone 43 (2008) 238–248
[13] Tashjian Jr AH, Gagel RF. Teriparatide [human PTH(1–34)]: 2.5 years of experienceon the use and safety of the drug for the treatment of osteoporosis. J Bone MinerRes 2006;21:354–65.
[14] Greenspan SL, Bone HG, Ettinger MP, Hanley DA, Lindsay R, Zanchetta JR, et al.Effect of recombinant human parathyroid hormone (1–84) on vertebral fractureand bone mineral density in postmenopausal women with osteoporosis: arandomized trial. Ann Intern Med 2007;146:326–39.
[15] Vestergaard P, Jorgensen NR, Mosekilde L, Schwarz P. Effects of parathyroidhormone alone or in combination with antiresorptive therapy on bone mineraldensity and fracture risk—a meta-analysis. Osteoporos Int 2007;18:45–57.
[16] Halloran BP, Bikle DD, Harris J, Tanner S, Curren T, Morey-Holton E. Regionalresponsiveness of the tibia to intermittent administration of parathyroid hormoneas affected by skeletal unloading. J Bone Miner Res 1997;12:1068–74.
[17] Tanaka S, Sakai A, Tanaka M, Otomo H, Okimoto N, Sakata T, et al. Skeletalunloading alleviates the anabolic action of intermittent PTH(1–34) in mouse tibiain association with inhibition of PTH-induced increase in c-fos mRNA in bonemarrow cells. J Bone Miner Res 2004;19:1813–20.
[18] Turner RT, Lotinun S, Hefferan TE, Morey-Holton E. Disuse in adult male ratsattenuates the bone anabolic response to a therapeutic dose of parathyroidhormone. J Appl Physiol 2006;101:881–6.
[19] Robbins J, Aragaki AK, Kooperberg C,Watts N, Wactawski-Wende J, Jackson RD, et al.Factors associated with 5-year risk of hip fracture in postmenopausal women. JAMA2007;298:2389–98.
[20] Lanyon L, Armstrong V, Ong D, Zaman G, Price J. Is estrogen receptor alpha key tocontrolling bones' resistance to fracture? J Endocrinol 2004;182:183–91.
[21] Skerry TM. One mechanostat or many? Modifications of the site-specific responseof bone to mechanical loading by nature and nurture. J Musculoskelet NeuronalInteract 2006;6:122–7.
[22] Rubin J, Rubin C, Jacobs CR. Molecular pathwaysmediating mechanical signaling inbone. Gene 2006;367:1–16.
[23] JeeWS, Tian XY. The benefit of combining non-mechanical agents withmechanicalloading: a perspective based on the Utah paradigm of skeletal physiology.J Musculoskelet Neuronal Interact 2005;5:110–8.
[24] Lindsay R, Zhou H, Cosman F, Nieves J, Dempster DW, Hodsman AB. Effects of aone-month treatment with PTH(1–34) on bone formation on cancellous,endocortical, and periosteal surfaces of the human ilium. J Bone Miner Res2007;22:495–502.
[25] Compston JE. Skeletal actions of intermittent parathyroid hormone: effects onbone remodelling and structure. Bone 2007;40:1447–52.
[26] Fox J, Miller MA, Newman MK, Recker RR, Turner CH, Smith SY. Effects of dailytreatment with parathyroid hormone 1–84 for 16 months on density, architectureand biomechanical properties of cortical bone in adult ovariectomized rhesusmonkeys. Bone 2007;41:321–30.
[27] Sugiyama T, Yamaguchi A, Kawai S. Effects of skeletal loading on bone mass andcompensation mechanism in bone: a new insight into the qmechanostatq theory.J Bone Miner Metab 2002;20:196–200.
[28] Sugiyama T, Takaki T, SakanakaK, SadamaruH,MoriK, Kato Y, et al.Warfarin-inducedimpairmentof cortical bonematerial quality and compensatory adaptation of corticalbone structure to mechanical stimuli. J Endocrinol 2007;194:213–22.
[29] Carvalho RS, Scott JE, Suga DM, Yen EH. Stimulation of signal transductionpathways in osteoblasts by mechanical strain potentiated by parathyroidhormone. J Bone Miner Res 1994;9:999–1011.
[30] Ryder KD, Duncan RL. Parathyroid hormone modulates the response of osteoblast-like cells to mechanical stimulation. Calcif Tissue Int 2000;67:241–6.
[31] Capozza R, Ma YF, Ferretti JL, Meta M, Alippi R, Zanchetta J, et al. Tomographic(pQCT) and biomechanical effects of hPTH(1–38) on chronically immobilized oroverloaded rat femurs. Bone 1995;17:233S–9S.
[32] Chow JW, Fox S, Jagger CJ, Chambers TJ. Role for parathyroid hormone inmechanical responsiveness of rat bone. Am J Physiol 1998;274:E146–54.
[33] Ma Y, Jee WS, Yuan Z, Wei W, Chen H, Pun S, et al. Parathyroid hormone andmechanical usage have a synergistic effect in rat tibial diaphyseal cortical bone.J Bone Miner Res 1999;14:439–48.
[34] Hagino H, Okano T, Akhter MP, Enokida M, Teshima R. Effect of parathyroidhormone on cortical bone response to in vivo external loading of the rat tibia.J Bone Miner Metab 2001;19:244–50.
[35] Li J, Duncan RL, Burr DB, Gattone VH, Turner CH. Parathyroid hormone enhancesmechanically induced bone formation, possibly involving L-type voltage-sensitivecalcium channels. Endocrinology 2003;144:1226–33.
[36] Kim CH, Takai E, Zhou H, von Stechow D, Muller R, Dempster DW, et al.Trabecular bone response to mechanical and parathyroid hormone stimula-tion: the role of mechanical microenvironment. J Bone Miner Res2003;18:2116–25.
[37] Zhou H, Iida-Klein A, Lu SS, Ducayen-Knowles M, Levine LR, Dempster DW, etal. Anabolic action of parathyroid hormone on cortical and cancellous bonediffers between axial and appendicular skeletal sites in mice. Bone2003;32:513–20.
[38] Davey RA, MacLean HE, McManus JF, Findlay DM, Zajac JD. Genetically modifiedanimal models as tools for studying bone and mineral metabolism. J Bone MinerRes 2004;19:882–92.
[39] Lau KH, Kapur S, Kesavan C, Baylink DJ. Up-regulation of the Wnt, estrogenreceptor, insulin-like growth factor-I, and bone morphogenetic protein path-ways in C57BL/6J osteoblasts as opposed to C3H/HeJ osteoblasts in partcontributes to the differential anabolic response to fluid shear. J Biol Chem2006;281:9576–88.
[40] Lee KC, Maxwell A, Lanyon LE. Validation of a technique for studying functionaladaptation of the mouse ulna in response to mechanical loading. Bone 2002;31:407–12.
[41] De Souza RL, Matsuura M, Eckstein F, Rawlinson SC, Lanyon LE, Pitsillides AA. Non-invasive axial loading of mouse tibiae increases cortical bone formation andmodifies trabecular organization: a new model to study cortical and cancellouscompartments in a single loaded element. Bone 2005;37:810–8.
[42] Baron R, Vignery A, Neff L, Silverglate A, Santa Maria A. Processing of undecalcifiedbone specimens for bone histomorphometry. In: Recker RR, editor. Bonehistomorphometry: techniques and interpretation. Boca Raton: CRC Press; 1983.13, 34.
[43] Iida-Klein A, Zhou H, Lu SS, Levine LR, Ducayen-Knowles M, Dempster DW, et al.Anabolic action of parathyroid hormone is skeletal site specific at the tissue andcellular levels in mice. J Bone Miner Res 2002;17:808–16.
[44] Iida-Klein A, Hughes C, Lu SS, Moreno A, Shen V, Dempster DW, et al. Effects ofcyclic versus daily hPTH(1–34) regimens on bone strength in association withBMD, biochemical markers, and bone structure in mice. J Bone Miner Res2006;21:274–82.
[45] Frost HM. Bone's mechanostat: a 2003 update. Anat Rec A DiscovMol Cell Evol Biol2003;275:1081–101.
Copyright © 2022 FDOKUMEN




















