Localized carcinoma of the prostate (Stages T1B, T1C, T2, and T3). Review of management with...
18
3156 Review Article Localized Carcinoma of the Prostate (Stages TI 6, TIC, T2, and T3) Review of Management with External Beam Radiation Therapy Carlos A. Perez, M.D.,* Gerald E. Hanks, M.D.,? Steven A . Leibel, M.D.,$ Anthony L. Zietman, M.D.,§ Zvi Fuks, M.D.,S and W. Robert Lee, M.D.7 Background. Optimal treatment for patients with lo- calized carcinoma of the prostate is controversial. Radia- tion therapy is an established modality in the manage- ment of these patients, and several reports indicate the results are comparable to those achieved with radical prostatectomy. Recently effectiveness of therapy for car- cinoma of the prostate is being evaluated in light of post- treatment prostate-specific antigen (PSA) determina- tions. Methods. A review was performed of multiple publi- cations and data from selected institutions with large ex- perience in the management of carcinoma of the prostate. Survival and clinical incidence of local recurrence and distant metastases were analyzed as well as preliminary data on postirradiation PSA levels. Factors that affect the outcome of therapy and relevant clinical trials are dis- cussed. Results. Reported differences in the age of patients treated with radical prostatectomy (59-63 years), irradia- tion (63-69 years), or observation (69-75.5 years) were identified. The effect of surgical staging on outcome of irradiation was significant. In multiple series of patients clinically and radiographically staged, the 5-year dis- ease-free survival (DFS) with external irradiation was 95-100% for clinical stage Tla, 80-90% for Stage Tlb,c, and 50-70'/0 for clinical Stage T3. A correlation has been identified between the initial PSA levels and the probabil- ity from freedom of chemical failure (PSA elevation) after definitive irradiation. In five series comprising 814 patients with Stage Tlc and T2 tumors, the DFS (end point chemical failure) was 95%, with initial PSA of less than 4 ng/ml, 83-92% with 4.1-10 ng/ml, 35-85% with From the *Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, Missouri; tDepartment of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, Pennsylvania; $Department of Radiation Oncol- ogy, Memorial Sloan-Kettering Cancer Center, New York, New York; and §Department of Radiation Oncology, Massachusetts General Hospital, Boston, Massachusetts. Address for reprints: Carlos A. Perez, M.D., Radiation Oncology Center, 4511 Forest Park, St. Louis, MO 63108. Accepted for publication September 9, 1993. 10.1-20 ng/ml, and 10-63% with PSA higher than 20 ng/ ml. In the various series, follow-up ranged from a median of 1.5 years to a minimum of 4 years. In two series of 225 and 201 patients receiving doses of 7500-8000 cGy, less morbidity has been observed with three-dimensional treatment planning conformal radiation therapy than with conventional irradiation. New directions for future clinical trials are discussed, including dose escalation studies; use of high linear energy transfer to improve lo- coregional tumor control; and combination of irradiation and androgen suppression to enhance local tumor con- trol, decrease distant metastasis, and improve survival. Preliminary results of a randomized study recently re- ported by RTOG strongly suggest that the use of goserelin acetate and flutamide decreases the incidence of clinical local recurrence (12.4% in 225 patients) compared with a control group treated with irradiation alone (25.2% in 230 patients) and enhances disease-free survival. Conclusions. Although modern approaches to the management of patients with localized carcinoma of the prostate with irradiation are effective, investigators must continue to critically assess policies of treatment, develop appropriately designed prospective clinical trials, and define the optimal management of patients with localized carcinoma of the prostate. Cancer 1993; 72~3156-73. Key words: carcinoma of the prostate, irradiation, pros- tate-specific antigen, clinical trials. Effectiveness of any therapy in localized carcinoma of the prostate is always scrutinized against the back- ground of what many believe is a fairly indolent clinical course of the disease. Whitmore' pointed out that the end results of treatment in these patients may be a com- bined consequence of host factors, tumor natural his- tory and behavior, and therapy efficacy; he further stated that there is no best treatment for all patients but rather a variety of methods, one of which is best for a particular patient and his tumor. The Consensus Devel- opment Conference on Management of Localized Pros-
Transcript of Localized carcinoma of the prostate (Stages T1B, T1C, T2, and T3). Review of management with...

3156 Review Article
Localized Carcinoma of the Prostate (Stages T I 6, TIC, T2, and T3) Review of Management with External Beam Radiation Therapy
Carlos A. Perez, M.D.,* Gerald E. Hanks, M.D.,? Steven A . Leibel, M.D.,$ A n t h o n y L. Zietman, M.D.,§ Z v i Fuks, M.D.,S and W. Robert Lee, M.D.7
Background. Optimal treatment for patients with lo- calized carcinoma of the prostate is controversial. Radia- tion therapy is an established modality in the manage- ment of these patients, and several reports indicate the results are comparable to those achieved with radical prostatectomy. Recently effectiveness of therapy for car- cinoma of the prostate is being evaluated in light of post- treatment prostate-specific antigen (PSA) determina- tions.
Methods. A review was performed of multiple publi- cations and data from selected institutions with large ex- perience in the management of carcinoma of the prostate. Survival and clinical incidence of local recurrence and distant metastases were analyzed as well as preliminary data on postirradiation PSA levels. Factors that affect the outcome of therapy and relevant clinical trials are dis- cussed.
Results. Reported differences in the age of patients treated with radical prostatectomy (59-63 years), irradia- tion (63-69 years), or observation (69-75.5 years) were identified. The effect of surgical staging on outcome of irradiation was significant. In multiple series of patients clinically and radiographically staged, the 5-year dis- ease-free survival (DFS) with external irradiation was 95-100% for clinical stage Tla, 80-90% for Stage Tlb,c, and 50-70'/0 for clinical Stage T3. A correlation has been identified between the initial PSA levels and the probabil- ity from freedom of chemical failure (PSA elevation) after definitive irradiation. In five series comprising 814 patients with Stage Tlc and T2 tumors, the DFS (end point chemical failure) was 95%, with initial PSA of less than 4 ng/ml, 83-92% with 4.1-10 ng/ml, 35-85% with
From the *Radiation Oncology Center, Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, Missouri; tDepartment of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, Pennsylvania; $Department of Radiation Oncol- ogy, Memorial Sloan-Kettering Cancer Center, New York, New York; and §Department of Radiation Oncology, Massachusetts General Hospital, Boston, Massachusetts.
Address for reprints: Carlos A. Perez, M.D., Radiation Oncology Center, 4511 Forest Park, St. Louis, MO 63108.
Accepted for publication September 9, 1993.
10.1-20 ng/ml, and 10-63% with PSA higher than 20 ng/ ml. In the various series, follow-up ranged from a median of 1.5 years to a minimum of 4 years. In two series of 225 and 201 patients receiving doses of 7500-8000 cGy, less morbidity has been observed with three-dimensional treatment planning conformal radiation therapy than with conventional irradiation. New directions for future clinical trials are discussed, including dose escalation studies; use of high linear energy transfer to improve lo- coregional tumor control; and combination of irradiation and androgen suppression to enhance local tumor con- trol, decrease distant metastasis, and improve survival. Preliminary results of a randomized study recently re- ported by RTOG strongly suggest that the use of goserelin acetate and flutamide decreases the incidence of clinical local recurrence (12.4% in 225 patients) compared with a control group treated with irradiation alone (25.2% in 230 patients) and enhances disease-free survival.
Conclusions. Although modern approaches to the management of patients with localized carcinoma of the prostate with irradiation are effective, investigators must continue to critically assess policies of treatment, develop appropriately designed prospective clinical trials, and define the optimal management of patients with localized carcinoma of the prostate. Cancer 1993; 72~3156-73.
Key words: carcinoma of the prostate, irradiation, pros- tate-specific antigen, clinical trials.
Effectiveness of any therapy in localized carcinoma of the prostate is always scrutinized against the back- ground of what many believe is a fairly indolent clinical course of the disease. Whitmore' pointed out that the end results of treatment in these patients may be a com- bined consequence of host factors, tumor natural his- tory and behavior, and therapy efficacy; he further stated that there is no best treatment for all patients but rather a variety of methods, one of which is best for a particular patient and his tumor. The Consensus Devel- opment Conference on Management of Localized Pros-

Irradiation in Management of Prostate Cancer/Perez et al. 3157
tate Cancer2 concluded that radical prostatectomy and radiation therapy are clearly effective treatments for tu- mors limited to the prostate in appropriately selected patients. It was further asserted that patients should be informed of the various options of therapy with the accompanying side effects and that physicians must make an effort to properly select patients for a given type of treatment.
Several authors, including Adolfsson et al.,3 G e ~ r g e , ~ Johansson et aL5 and Whitmore et a1.,6 have reported on patients age 60 and older who on histologic diagnosis of carcinoma of the prostate were managed conservatively and followed up without specific anti- cancer treatment until symptoms developed. However, interpretation of these reports is difficult because of lack of details on patient selection and tumor character- istics and clear definition of end points (e.g., survival, cause of death, symptoms, quality of life). For example, in a recent metaanalysis by Adolfsson et al.,3 in a review of the literature (22 reports comprising 2567 patients) the authors concluded that these tumors have a pro- tracted course associated with a significant competing mortality and marginal benefit from radical prostatec- tomy at 10 years. They reported the number of person- years at risk, showing a calculated 10-year disease-spe- cific survival of 93% for radical prostatectomy, 83% for deferred treatment, and 62% for external radiation ther- apy. Noteworthy, no emphasis was placed on the dif- ferent ages, clinical stages, or histologic degree of dif- ferentiation of the tumors in the various treatment groups. Patient ages ranged from 59 to 63 years with radical prostatectomy, 63 to 69 years with radiation therapy, and 65 to 75.5 years with observation. The cancer-specific survival rates published by these au- thors do not state whether disease-free or cause-specific survival data were reported by some of the authors of the radiation therapy series. Additionally, there was no accounting for imbalance in prognostic factors, and in such a review a multivariate analysis cannot be used to assess the effectiveness of different treatments after ad- justing for other factors.
Fleming et al.7 recently described the results of a decision analysis model based on published data on therapy results and concluded that observation is rea- sonable management for patients older than 75 years of age, whereas, using optimistic assumptions, either radi- cal prostatectomy or radiation therapy offers the same therapeutic benefits to patients 60 to 65 years old with moderately or poorly differentiated tumors. Lu-Yao et a1.' examined chronologic and geographic trends in the use of radical prostatectomy in a selected sample of Medicare beneficiaries treated between 1984 and 1990 and found that the rate of performance of the operation increased by 5.75 times in all age groups during that
period; morbidity and mortality rates were similar in the 65-69-year and the 70-74-year age groups but were appreciably higher in those older than 75 years. In an editorial, Whitmore' pointed out that the conclu- sions of Fleming et aL7 challenge prevailing conceptions of many urologists and radiation oncologists regarding the effectiveness of their respective modalities in the treatment of some patients. He noted that the optimal management of clinically localized prostatic cancer may be more a matter of opinion than a fact. Similarly, Moore et a1.I' provided evidence that urologists and oncologists recommend treatment consistent with their respective disciplines (i.e., surgery, irradiation, or che- motherapy).
Identification of specific costs and tumor features that predict natural behavior and response to therapy of an individual tumor in a given patient may thus be nec- essary for a fully rational approach to therapy. In to- day's health environment, it is practically impossible in the United States to delay definitive therapy in most patients with localized carcinoma of the prostate, ex- cept in selected elderly patients or those with less-than- ideal general health with well-differentiated Stage A or B1 tumors. Properly designed prospective clinical trials are critically needed to better define the efficacy and cost-effectiveness of various therapeutic approaches for localized carcinoma of the prostate.
Role of Definitive Irradiation
External irradiation is used as definitive therapy in a large proportion of patients with clinical Stage A and B carcinoma of the prostate and, in most institutions, in most patients with Stage C or more locally extensive tumors." Tumor doses have ranged from 6000 to 6400 cGy for Stage A1 (Tla), 6500 to 7000 cGy for A2 (Tlb) and B (T2), and 7000 to 7200 cGy for Stage C (T3) tumors. Several retrospective studies indicate that dose affects local tumor control. Perez et al.12,13 reported im- proved local control rates with doses greater than 6500 cGy, particularly in Stage C patients. Hanks et aI.,l4 in 1348 patients with Stage B and C tumors, reported an actuarial 5-year local recurrence rate of 37% for pa- tients with Stage C tumor treated with doses of less than 6000 cGy, 36% for 6000-6490 cGy, 29% for 6500-6990 cGy, and 19% for 7000 cGy or more. By 7 years, 32% of patients receiving 6500-6900 cGy and 24% treated with higher doses had local recurrences.
Controversy regarding elective pelvic lymph node irradiation and its effect on survival is not settled. M ~ G o w a n ' ~ reported better survival and fewer pelvic failures in patients with Stage B2 or C tumors treated with larger fields encompassing the pelvic lymph nodes compared with patients receiving treatment to the pros-

3158 CANCER December 1,1993, Volume 72, No. 11
tate and periprostatic tissues only. Ploysongsang et a1.16 described, in 126 patients receiving treatment to the prostate and whole pelvis, a 5-year survival rate of 92% in Stage B and 72% in Stage C compared with 70% and 40%, respectively, in 116 patients with irradiation to the prostatic area only. Perez et aL13 noted a 20% inci- dence of pelvic recurrences in patients with Stage C disease receiving treatment to the pelvic lymph nodes (5000 cGy) compared with 37% in 137 patients receiv- ing treatment to the pelvic area with portals smaller than 14 cm2 after 4000 cGy. Bagshaw" described a trend toward improved survival in patients with Stage B1 tumors with negative staging lymphadenectomy when the lymph nodes were irradiated, the results be- ing superior to those observed in patients with positive nodes. However, in a later report, Spaas et al." showed no significant advantage for pelvic lymph node irradia- tion over prostatic field irradiation in pathologically staged patients. Likewise, Asbell et al.19 reported no difference in survival or patterns of failure in a random- ized study of 445 patients with Stage A2 or B carcinoma of the prostate receiving treatment to the pelvic lymph nodes (4500 cGy) and the prostate (additional 2000 cCy) or to the prostate and adjacent tissues only (6500 cGy).
The importance of adequate radiation therapy tech- niques to achieve optimal tumor control in the pelvis has been emphasized recently. l3 Furthermore, a lower incidence of distant metastases and improved survival have been reported in patients with locoregional tumor control compared with patients with pelvic failure in reports by Fuks et aL2' in patients treated with intersti- tial irradiation, by Kaplan et aL2* and Perez et aLl3 with external beam irradiation, and by Kuban et aLZ2 with either treatment modality.
Results of Treatment
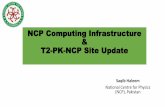
The 5-year disease-free survival (DFS) rates with exter- nal irradiation reported in multiple series are approxi- mately 95-100% for clinical Stage A1 (Tla), 80-90% for clinical Stage A2 (Tlb,c), and 50-7070 for clinical Stage C (T2). The corresponding 10-year rates are 95%, 65-8070, and 40-50%, respectively. The cause-specific survival or overall survival rates in most series are ap- proximately 10% higher than the DFS rates at various times after treatment. Tables 1 and 2 summarize re- ported survival results for the various clinical stages.
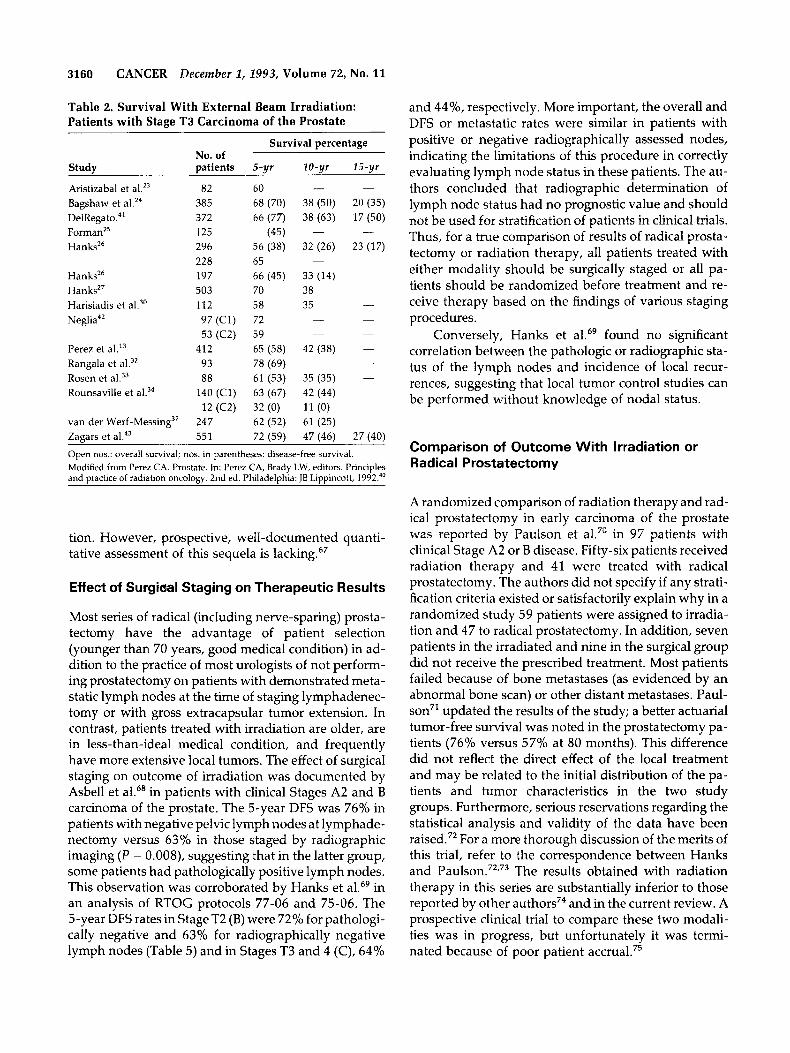
The clinically assessed incidence of local recur- rences after definitive irradiation has ranged from 0% to 20% for Stage Tlb, 5% to 30% for T2, and 12% to 40% for T3 tumors (Tables 3 and 4). However, when the data are analyzed using actuarial methods, the inci- dence of clinically detected local recurrences is some-
what higher (at 10 years, 20% for stage Tlb, 24% for T2, and 40% for T3 lesion^).'^,^^ These figures are com- parable to the reported incidence of histologically posi- tive routine prostate biopsy results, as will be discussed later.
The incidence of distant metastases is approxi- mately 20% in patients with Stage Tlb,c and T2 tumors and 40% in patients with T3 lesions (Tables 3 and 4). Distant dissemination is closely correlated with histo- logic degree of tumor differentiation (Gleason s ~ o r e ) . ~ ~ , ' ~ , ~ ~ Additionally, as noted by Adolfsson et aL3 the calculated weighted mean number of distant metas- tases was 29 per 1000 person-years at risk and for deaths due to intercurrent disease 36.3 per 1000 per- son-years at risk for patients treated with radiation ther- apy, compared with 12.6 and 9.9, respectively, for pa- tients treated with radical prostatectomy, a strong re- flection of patient selection.
Numerous reports have been published of results of treatment of localized carcinoma of the prostate with interstitial therapy using lZ5I, 198A~, I9'Ir, or, more re- cently, lo3Pd; results are comparable to those obtained with external irradiation alone.3b,4b-58 Interstitial brachy- therapy is not discussed further in the current review.
Morbidity of External Irradiation
As reported by Lawton et al.59 and Perez et al.," the incidence of fatal complications in localized carcinoma of the prostate treated with external irradiation is ap- proximately 0.2%, demonstrating the low risk of this therapy. The overall incidence of significant urinary or rectosigmoid sequelae is approximately 3% severe and 7-10% moderate.24,3b,59,61-63 Th e most frequent urinary sequelae are urethral stricture and cystitis with inter- mittent hematuria (3-6'70). Bladder fistula, hemorrhagic cystitis, or ureteral stricture occur in fewer than 0.5% of patients. A higher incidence of urethral stricture (about 5% versus 3%) has been described in patients irradiated after a transurethral resection of the prostate." Some degree of urinary incontinence, in some cases related to stress, is noted in about 2% of patients, more frequently after transurethral resection. The incidence of severe anal/rectal injury requiring colostomy is less than 1%. Perez et aL6' reported one rectovesical and one vesico- sigmoid fistula in 738 patients (.27%), and Lawton et al.59 recorded 11 (1 YO) Grade 4 and 5 rectal injuries in 1020 patients. The incidence of proctitis or rectal ulcer causing bleeding is approximately 5%; occasionally, a perianal abscess or anal stricture is noted.
Perez et aI.l3 described a higher incidence of Grade 2 and 3 rectosigmoid sequelae in patients receiving treatment to the pelvic lymph nodes and the prostate (10% actuarial at 10 years) compared with 3% in pa-
Irradiation in Management of Prostate Cancer/Perez et al. 3159
Table 1. Survival With External Beam Irradiation: Patients with Stage Tlb and T2 Carcinoma of the Prostate
No. of patients Survival percentage
Stage Stage Stages Study T l b T2 T l b 6 T 2 5-yr 10-yr 15-yr
Aristizabal et aIz3
As b e 11 '
BagshawZ4
Formanz5 Hanksz6 Hanksz6 Hanksz6 Hanks27 Hanksz6 Hanks et Hanks et Harisiadis et
Kurup et aL3'
Perez et
Rangala et
Rosen et al.33
Rounsaville et
Sagerman et
S h i ~ l e y ~ ~ van der Werf-Messing et Zagars et
17
84
308
116
84
313
13 24
48
10
25
37
34
3071
32
101
361
218
415
312
25
65
252
25
85
SO
100
24
82
113
60
104*
100 82 79 (66)
85 (90) 83 (87)
85 (74)
84 (76) 86 74 (56) 77 (87) 87 (96) 87 88
(63)
75 (53)
(95)
85 (78) 82 (76)
100 (56) 90 (59) 96 (84) 77 (68) 81 (82) 84 (71) 91 (77)
85 (85) 78 (61) 74 (90) 93 (89)
65 (70) 40 (65) 55 (65) 35 (50)
63 (52) 46 (34) 54 (53) 41 (39) 64 43 (27) 22 (15)
63 (86) (52)
(76) 70 (60) 65 (56)
80 (68) 43 (60) 67 (69) 53 (52)
86 (72) 66 (70) 50 78 (61)
70 (85) 68 (-1
Zietman39 164 94 (92) 66 (70) (52) Open no.: overall survival; no. in parentheses: disease-free survival. * Surgically staged patients. t Includes T2a tumors. Modified from Perez CA. Prostate. In: Perez CA, Brady LW, editors. Principles and practice of radiation oncology. 2nd ed. Philadelphia: JB Lippincott, 1992.
tients receiving treatment to the prostate bed only, yet the size of the prostatic volume portals did not affect morbidity, regardless of association with pelvic lymph node irradiation. Kurup et al.,31 Mameghan et al.,64 and Rosen et al.65 made similar observations.
Some reports have suggested that doses of more than 7000 cGy may be associated with a higher inci- dence of morbidity. Pilepich et a1.62 noted no increase in incidence of proctitis or other late rectal injuries with doses up to 7000 cGy. Conversely, Smit et a1.66 de- scribed a 2-year actuarial incidence of moderate or se- vere proctitis in 22% of patients receiving less than 7000 cGy to the anterior rectal wall, 20% with 7000-
7500 cGy, and 60% with doses higher than 7500 cGy. Hanks et a1.61 and Lawton et al.59 observed a signifi- cantly increased incidence of Grades 3, 4, and 5 uri- nary toxicity in patients receiving more than 7000 cGy (P = 0.03).
Leg, scrotal, or penile edema is extremely rare in patients treated with irradiation alone (less than 1 %), but its incidence ranges from 10% to 30%, depending on extent of lymph node dissection in patients under- going this procedure.62 Erectile dysfunction, a signifi- cant treatment sequela affecting quality of life, particu- larly in younger men, has been described in 14-50% of patients, depending on age and techniques of irradia-
3160 CANCER December 2, 2993, Volume 72, No. 11
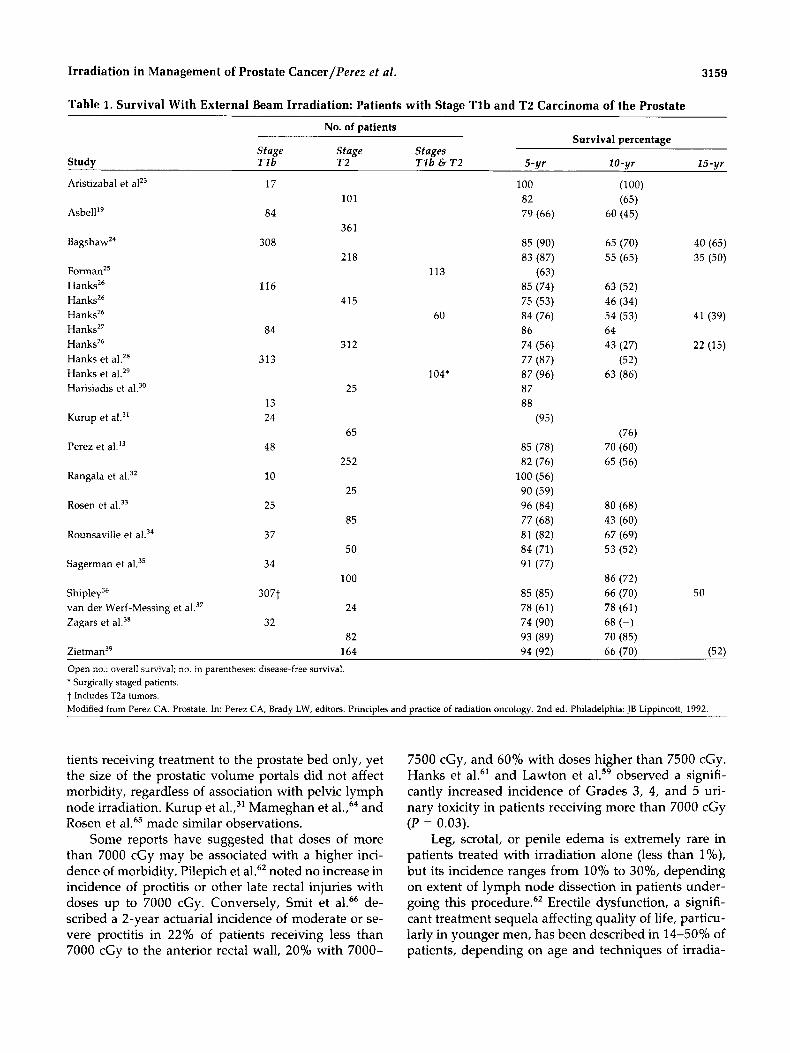
Table 2. Survival With External Beam Irradiation: Patients with Stage T3 Carcinoma of the Prostate
Study
Aristizabal et al.23 Bagshaw et DelRega to?' Forrnan2' Hanksz6
Hanks26 Hanksz7 Harisiadis et al.30 Neglia42
Perez et Rangala et al.32 Rosen et al.33 Rounsaville et al.34
van der Wer f -Me~s ing~~ Zaears et al.43
Survival percentage No. of patients 5-yr 10-yr 15-yr
- - 82 60 385 68 (70) 38 (50) 20 (35) 372 66 (77) 38 (63) 17 (50) 125 (451 -
296 56 (38) 32 (26) 23 (17) 228 65 197 66 (45) 33 (14) 503 70 38 112 58 35
-
-
- 97(C1) 72 - -
53 (C2) 59
93 78 (69) -
88 61 (53) 35 (35) -
- -
412 65 (58) 42 (38) - -
140 (Cl ) 63 (67) 42 (44) 12 (C2) 32 (0) 11 (0)
247 62 (52) 61 (25) 55 1 72 159) 47 (46) 27 (40)
Open nos.: overall survival; nos. in parentheses: disease-free survival. Modified from Perez CA. Prostate. In: Perez CA, Brady LW, editors. Principles and uractice of radiation oncoloev. 2nd ed. Philadeluhia: IB Liuuincott. 1992."
and 44%, respectively. More important, the overall and DFS or metastatic rates were similar in patients with positive or negative radiographically assessed nodes, indicating the limitations of this procedure in correctly evaluating lymph node status in these patients. The au- thors concluded that radiographic determination of lymph node status had no prognostic value and should not be used for stratification of patients in clinical trials. Thus, for a true comparison of results of radical prosta- tectomy or radiation therapy, all patients treated with either modality should be surgically staged or all pa- tients should be randomized before treatment and re- ceive therapy based on the findings of various staging procedures.
Conversely, Hanks et al.69 found no significant correlation between the pathologic or radiographic sta- tus of the lymph nodes and incidence of local recur- rences, suggesting that local tumor control studies can be performed without knowledge of nodal status.
Comparison of Outcome With Irradiation or Radical Prostatectomy
tion. However, prospective, well-documented quanti- tative assessment of this sequela is lacking.67
Effect of Surgical Staging on Therapeutic Results
Most series of radical (including nerve-sparing) prosta- tectomy have the advantage of patient selection (younger than 70 years, good medical condition) in ad- dition to the practice of most urologists of not perform- ing prostatectomy on patients with demonstrated meta- static lymph nodes at the time of staging lymphadenec- tomy or with gross extracapsular tumor extension. In contrast, patients treated with irradiation are older, are in less-than-ideal medical condition, and frequently have more extensive local tumors. The effect of surgical staging on outcome of irradiation was documented by Asbell et aL6* in patients with clinical Stages A2 and B carcinoma of the prostate. The 5-year DFS was 76% in patients with negative pelvic lymph nodes at lymphade- nectomy versus 63% in those staged by radiographic imaging (P = 0.008), suggesting that in the latter group, some patients had pathologically positive lymph nodes. This observation was corroborated by Hanks et al.69 in an analysis of RTOG protocols 77-06 and 75-06. The 5-year DFS rates in Stage T2 (B) were 72% for pathologi- cally negative and 63% for radiographically negative lymph nodes (Table 5) and in Stages T3 and 4 (C), 64%
A randomized comparison of radiation therapy and rad- ical prostatectomy in early carcinoma of the prostate was reported by Paulson et aL7' in 97 patients with clinical Stage A2 or B disease. Fifty-six patients received radiation therapy and 41 were treated with radical prostatectomy. The authors did not specify if any strati- fication criteria existed or satisfactorily explain why in a randomized study 59 patients were assigned to irradia- tion and 47 to radical prostatectomy. In addition, seven patients in the irradiated and nine in the surgical group did not receive the prescribed treatment. Most patients failed because of bone metastases (as evidenced by an abnormal bone scan) or other distant metastases. Paul- son7' updated the results of the study; a better actuarial tumor-free survival was noted in the prostatectomy pa- tients (76% versus 57% at 80 months). This difference did not reflect the direct effect of the local treatment and may be related to the initial distribution of the pa- tients and tumor characteristics in the two study groups. Furthermore, serious reservations regarding the statistical analysis and validity of the data have been raised.72 For a more thorough discussion of the merits of this trial, refer to the correspondence between Hanks and P a ~ l s o n . ~ ~ , ~ ~ The results obtained with radiation therapy in this series are substantially inferior to those reported by other authors74 and in the current review. A prospective clinical trial to compare these two modali- ties was in progress, but unfortunately it was termi- nated because of poor patient accrual.75
Irradiation in Management of Prostate Cancer/Perez ef al. 3161
Table 3. Incidence of Local Recurrence, Distant Metastases, and Intercurrent Disease in Patients with Stages Tlb and T2 Treated With External Radiation Therapy
Local recurrence Distant No. of patients (%) metastases (%)
Intercurrent Study T l b T2 T l b T 2 T l b T 2 disease
Aristizabal et aLZ3 Asbell" Bagshaw et aLZ4
Hanks26 Hanks26 Hanksz6 Hanksz6 Hanks et aLz8 Hanks et al.z9 a
Kuban et al.44
Kurup et al?'
Perez et aI.l3
17 84
308
60$ 116
313 16 41
24
48
101 361
218
312 415
88
118
65
252 Rosen et al.33 25
Rounsaville et al.34 37 85
50
100 Shipley et al.36 307 162 ZagarP 32
Sagerman et aL3' 34
6 5 6 19 26/218* (12%) 11 16
20t 30 t
4 15§
35" 29§
11 221 0 15t 2
0 19
3 20 t
24 t
0
0 9
21
0
5 19
9 17
20t
20 36
15 8
16 t 1st 0
7 Yo
18%
82 12t a Surgically staged patients. *All stages. t 10-yr actuarial $ Includes T2 tumors. 5 At 10 years. " At 15 years. ll5-Year actuarial.
The effect of surgcal staging on therapeutic out- come and the implications of comparing reported sur- vival with radiation therapy or radical prostatectomy are illustrated in a report by Hanks et aLZ9 on 104 pa- tients with clinical Stage Tlb or T2 carcinoma of the prostate who were surgically staged, had negative lymph nodes, and were treated with definitive radia- tion therapy. The DFS rates at 5 and 10 years were 85% and 67'10, respectively. The corresponding overall sur- vival rates were 87% and 63%, respectively. The proba- bility of clinical control of the tumor in the prostate was 96% at 5 years and 87% at 10 years. These results are similar to those obtained with radical pro~tatectomy.~~
The DFS and cause-specific survival (or overall sur- vival) reported in many radiation therapy series are comparable to those obtained with radical prostatec- tomy, as illustrated in Figure 1. The role and results of
radical prostatectomy are discussed in a companion ar- ticle by Gibbons.77
Positive Prostate Biopsy Results After Definitive Radiation Therapy
Several authors have reported histologic evidence of viable adenocarcinoma in the prostate at various times after completion of radiation therapy. Cox and Stoffe17' noted that there was a decreasing incidence of positive biopsy results as a function of time after irradiation (from 70% at 6 months to 20% after 24 months). These data should be interpreted in light of radiobiologic data indicating that cell death after radiation exposure is a postmitotic event. In view of the long doubling time of many prostate tumors in early biopsies, cells that harbor lethal damage but have not had an opportunity to mor-
3162 CANCER December 2 , 1993, Volume 72, No. 11
Table 4. Incidence of Locoregional Recurrence, Distant Metastases, and Intercurrent Disease in Patients with Stage T3 Treated With External Radiation Therapy
No. Locoregional Distant Intercurrent of recurrence metastases disease
Study patients (YO) (YO) (010)
Aristizabal et al.23 82 12 33 12*
Bagshaw et 385 38t 25$ Del Regato4' -
Hanksz6 296 3ot Hanksz6 197 429
-
Kuban et al.44 136 24 Kurup et a ~ ~ ' 74 12 39 6 Perez et aI.I3 412 40t 42 Rosen et al.33 88 30t R o ~ n s a v i l l e ~ ~ 152 23 39 12 Sagerman et al.35 63 23 29 Zietrnan3' 30t 'Total in all stages. t 10-yr actuarial.
At 10 yr. 4 At 15 yr.
phologically express it may be misinterpreted as viable cells. There was no significant correlation between the status of the prostatic biopsy results (positive or nega- tive) and subsequent survival. scar din^^^ confirmed this observation, reporting that 32% of his patients with a positive biopsy result at 12 months had a negative pathologic specimen at 24 months.
The rate of positive specimens is also related to the initial clinical stage of the tumor; scar din^'^ noted a positivity of 28% for Stage B1, 41% for Stage B2, and
62% for Stage C lesions. Likewise, Freiha and Bag- shawe0 reported no positive biopsy results in patients with Stages A2 and B, but rates of 38%, 59%, and 74% for small Stage B2, large Stage B2, and Stage C tumors, respectively.
In Kuban et al.'s analysis" of 94 patients with clini- cally negative digital examination of the prostate who did not receive hormonal therapy until documented evi- dence of recurrence and on whom routine biopsies of the prostate were performed 18 months or more after irradiation, the incidence of positive biopsy results was related to the initial stage: 1 of 10 (loo/,) for Stage A2,lO of 55 (18%) for Stage B, and 6 of 29 (21%) for Stage C lesions. By 10 years, clinical local failure developed in 75% of the patients with positive biopsy results; DFS was 20% compared with 30% and 6O%, respectively, in patients with negative biopsy results.
Postirradiation biopsy findings were closely related to the clinical status of the prostate gland in the experi- ence of Freiha and Bagshaw" and scar din^,^^ who re- ported 89% and 64% incidence, respectively, of posi- tive biopsy results in patients with suspected or definite clinical evidence of tumor regrowth, whereas the same authors noted 25% and 20% positivity, respectively, in patients with negative clinical examination of the pros- tate. In a publication by Scardino and Wheeler," the local recurrence rate was 52% at 5 years with a positive biopsy result versus 12% with a negative specimen and at 10 years, 72% and 30%, respectively (P < 0.001). When only patients with normal results from a digital rectal examination were considered, the risk of local recurrence at 10 years was 50% with a positive and 25% with a negative biopsy result. Thus, timing of post-
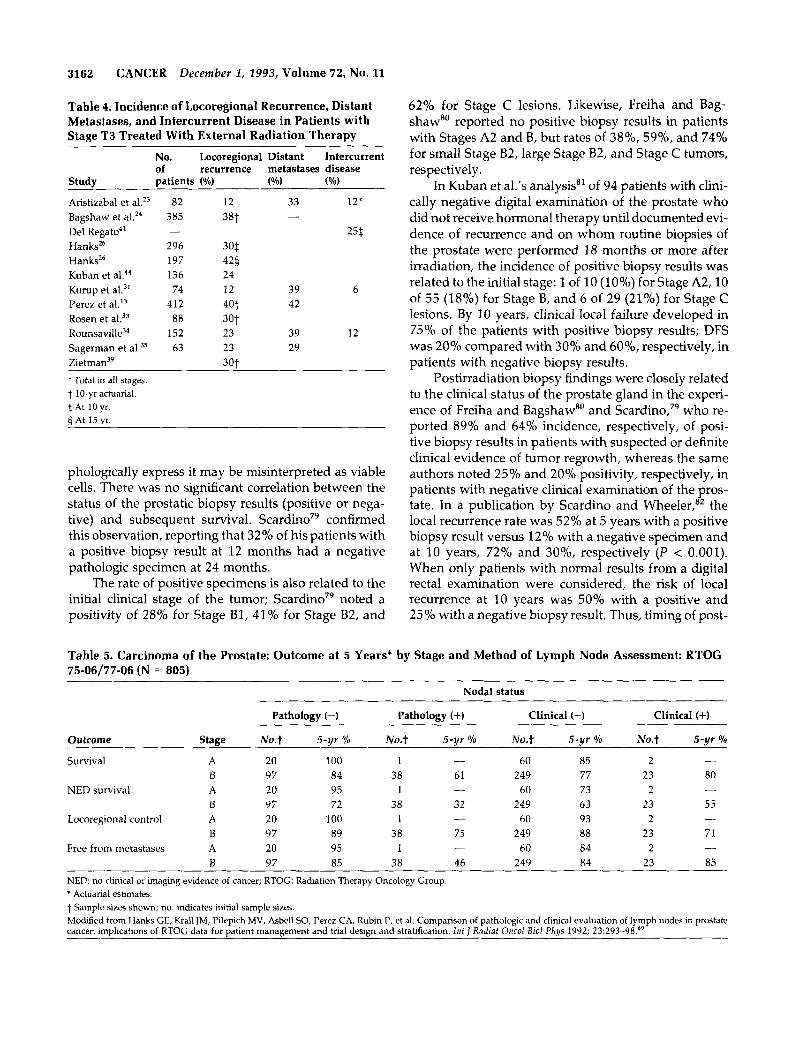
Table 5. Carcinoma of the Prostate: Outcome at 5 Years* by Stage and Method of Lymph Node Assessment: RTOG 75-06/77-06 (N = 805)
Nodal status
Pathology (-) Pathology (+) Clinical (-) Clinical (+)
Outcome Stage N0.t 5-yr YO No. t 5-yr Yo N0.t 5-yr ?h No.t 5-yr YO
Survival A 20 100 1 - 60 85 2
NED survival A 20 95 1 - 60 73 2
- B 97 84 38 61 249 77 23 80
B 97 72 38 32 249 63 23 55
B 97 89 38 75 249 88 23 71
B 97 85 38 46 249 84 23 85
-
- Locoregional control A 20 100 1 - 60 93 2
- Free from metastases A 20 95 1 - 60 84 2
NED: no clinical or imaging evidence of cancer; RTOG: Radiation Therapy Oncology Group. * Actuarial estimates. t Sample sizes shown; no. indicates initial sample sizes. Modified from Hanks GE, Krall JM, Pilepich MV, Asbell SO, Perez CA, Rubin P, et al. Comparison of pathologic and clinical evaluation of lymph nodes in prostate cancer: implications of RTOG data for patient manaaement and trial desian and stratification. I n t I Radiat Oncol B i d Phvs 1992; 23:293-98.69
Irradiation in Management of Prostate CancerlPerez et ai. 3163
100
W c3 2
-0 ~tiw. , ,nlr ;uur~3~w.,rnu. A @whew, M.. IS92 v nu.c,1eeo
EXPECTED SURVIVORSHIP (Genaol Population) MICROSCOPICALLY LOCALIZED (861 .wLmeLE NODULE ( 1031
"0 5 10 15 YEARS AFTER OPERATION
MGH (Initial PSA S15) ....... . . -.-\:. (T kz-T B z , NX ; n=57)
U C U fl A.C, N ; n-230) € 6 0 c .- 8 n do
yaars from therapy
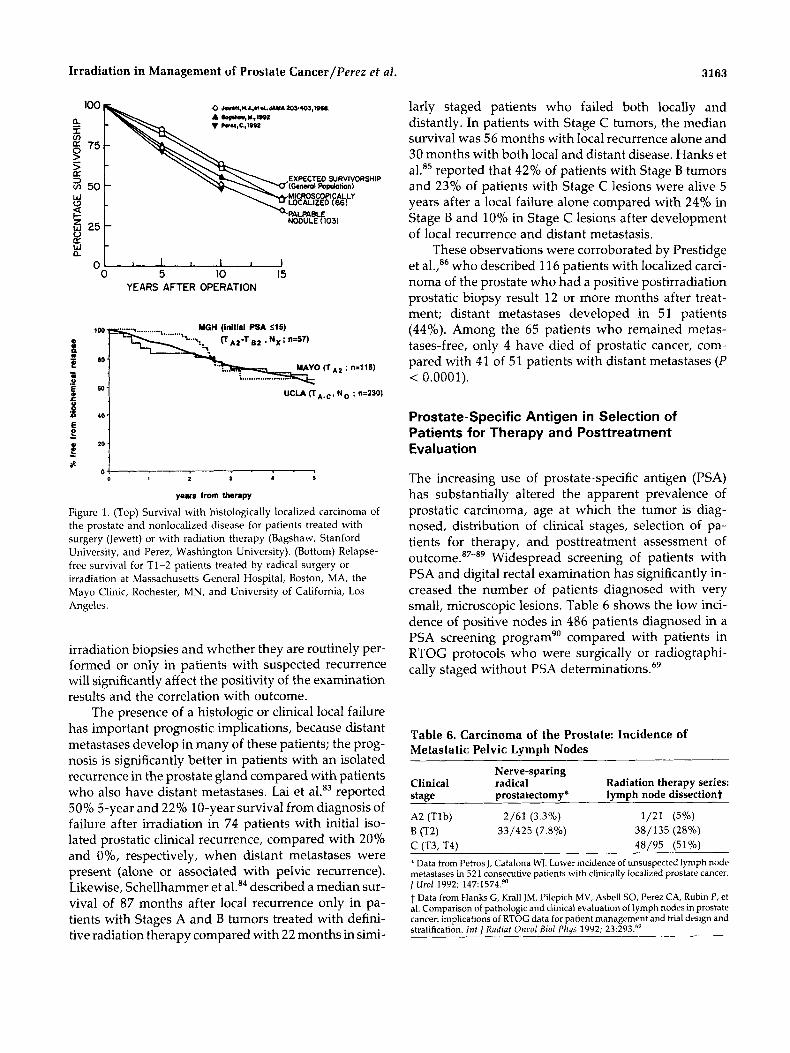
Figure 1. (Top) Survival with histologically localized carcinoma of the prostate and nonlocalized disease for patients treated with surgery (Jewett) or with radiation therapy (Bagshaw, Stanford University, and Perez, Washington University). (Bottom) Relapse- free survival for T1-2 patients treated by radical surgery or irradiation at Massachusetts General Hospital, Boston, MA, the Mayo Clinic, Rochester, MN, and University of California, Los Angeles.
irradiation biopsies and whether they are routinely per- formed or only in patients with suspected recurrence will significantly affect the positivity of the examination results and the correlation with outcome.
The presence of a histologic or clinical local failure has important prognostic implications, because distant metastases develop in many of these patients; the prog- nosis is significantly better in patients with an isolated recurrence in the prostate gland compared with patients who also have distant metastases. Lai et aLB3 reported 50% 5-year and 22% 10-year survival from diagnosis of failure after irradiation in 74 patients with initial iso- lated prostatic clinical recurrence, compared with 20% and O%, respectively, when distant metastases were present (alone or associated with pelvic recurrence). Likewise, Schellhammer et al.84 described a median sur- vival of 87 months after local recurrence only in pa- tients with Stages A and B tumors treated with defini- tive radiation therapy compared with 22 months in simi-
larly staged patients who failed both locally and distantly. In patients with Stage C tumors, the median survival was 56 months with local recurrence alone and 30 months with both local and distant disease. Hanks et aLB5 reported that 42% of patients with Stage B tumors and 23% of patients with Stage C lesions were alive 5 years after a local failure alone compared with 24% in Stage B and 10% in Stage C lesions after development of local recurrence and distant metastasis.
These observations were corroborated by Prestidge et a1.,86 who described 116 patients with localized carci- noma of the prostate who had a positive postirradiation prostatic biopsy result 12 or more months after treat- ment; distant metastases developed in 51 patients (44%). Among the 65 patients who remained metas- tases-free, only 4 have died of prostatic cancer, com- pared with 41 of 51 patients with distant metastases ( P < 0.0001).
Prostate-Specific Antigen in Selection of Patients for Therapy and Posttreatment Evaluation
The increasing use of prostate-specific antigen (PSA) has substantially altered the apparent prevalence of prostatic carcinoma, age at which the tumor is diag- nosed, distribution of clinical stages, selection of pa- tients for therapy, and posttreatment assessment of o u t c ~ m e . ~ ~ - ~ ~ Widespread screening of patients with PSA and digital rectal examination has significantly in- creased the number of patients diagnosed with very small, microscopic lesions. Table 6 shows the low inci- dence of positive nodes in 486 patients diagnosed in a PSA screening program" compared with patients in RTOG protocols who were surgically or radiographi- cally staged without PSA determination^.^^
Table 6. Carcinoma of the Prostate: Incidence of Metastatic Pelvic Lymph Nodes
Nerve-sparing Clinical radical Radiation therapy series: stage prostatectomy* lymph node dissectiont
A2 (Tlb) 2/61 (3.3%) 1/21 (5%) 33/425 (7.8%) 38/135 (28%)
- 48/95 (51%) B (T2) C fT3. T4) * Data from Petros J, Catalona WJ, Lower incidence of unsuspected lymph node metastases in 521 consecutive patients with clinically localized prostate cancer. j Urol 1992; 147:1574.90 t Data from Hanks G, Krall JM, Pilepich MV, Asbell SO, Perez CA, Rubin P, et al. Comparison of pathologic and clinical evaluation of lymph nudes in prostate cancer: implications of RTOG data for patient management and trial design and stratification. Jnt j Radiaf Oncoi B i d Phys 1992; 23:293.6'

3164 CANCER December 1, 2993, Volume 72, NO. 11
Several authors have shown a close correlation be- tween PSA levels, clinical and pathologic tumor stage, and, in conjunction with the Gleason score, a predict- able correlation with incidence of lymph node metasta- sis. Partin et aL9' noted that patients with PSA below 2.8 ng/ml and a Gleason score below 4 had approxi- mately 19'0 incidence of nodal disease or seminal vesicle involvement, whereas patients with PSA above 40 ng/ ml and a Gleason score higher than 8 had 60% probabil- ity of lymph node metastasis and seminal vesicle in- volvement at the time of prostatectomy. Although PSA levels vary within each clinical stage and overlap in some adjacent stages, they correlate with tumor volume (number of clonogenic cells). To integrate PSA levels and size of the prostate gland, the PSA index, or PSA density, has been p r o p o ~ e d . ~ ~ , ~ ~
In patients treated with radiation therapy, Russell et Zagars et al.,95 Fijuth et al.,96 Landmann and H ~ n i g , ~ ~ and Zentner et aL9' reported worse outcome after external irradiation in patients with initial PSA above normal levels. In patients with an initial normal PSA level, the probability of a chemical failure was be- low 5%, with median follow-up of up to 30 months, whereas with initial PSA greater than 10 ng/ml it ranged from 20% to 90%, depending on the pretreat- ment PSA level.
Meek et a ~ , ' ~ Ritter et al.,'" Vijayakumar et al.,"' and Zagars et al.95 have reported on PSA levels during and after radiation therapy. Transient increase of PSA during radiation therapy, even as soon as the first frac- tion, has been reported in some patient^.^^,'^' According to Ritter et al.'s'OO calculations, PSA half-life duringradi- ation therapy ranges from 43 to 58.5 days, with an ex- pected decline of 1.6% per day, or as reported by Zagars et a decline from 30 ng/ml to 4.7 ng/ml at 3 months after irradiation.
"Gold standard" PSA values after irradiation have not been established.lo2 Because the prostate gland re- mains in place and it is possible that some nonclono- genic cells continue to produce PSA, values are not ex- pected to decline to postprostatectomy levels (less than 0.6 ng/ml) in many patients. The "normal" postirradia- tion PSA may be defined as that value associated with long-term DFS'". Russell and Boileau noted that, using this approach, Stamey et al.'03 observed a mean PSA of 2.9 ng/ml (normal, 0 to 2.5 ng/ml) in 33 patients; Za- gars et al.,95 a median of 1.2 ng/ml (normal, 0 to 4 ng/ml); and Ritter et al.,loO a mean value of 1.1 ng/ml (normal, 0 to 3.2 ng/ml). Kaplan et al.'04,'05 described mathematical methods for estimating disease recur- rence in patients treated with radiation therapy based on the absolute value, rates of decline of posttreatment,
and subsequent rise of PSA. Hanks et al.'06 reported a correlation of PSA rise doubling time and clinical behav- ior including outcome with radiation therapy.
In any comparison of treatment series, stratification for PSA is as important as stratification for tumor size and grade. Thirty-three percent of T1-2 patients receiv- ing irradiation at Massachusetts General Hospital be- tween 1988 and 1992 had serum PSA values greater than 15 ng/ml compared with only 16% in the prosta- tectomy series reported by the Johns Hopkins g r o ~ p . " ~ The proportion of radiation-treated patients with occult micrometastatic disease is also correspondingly higher; in the Massachusetts General Hospital study, 65% of patients with preirradiation PSA levels below 15 ng/ml exhibited freedom from chemical failure 4 years after treatment, a value comparable to that following radical prostatectomy, when there are no known metastases in the pelvic lymph
Zagars and von Eschenbach,"' in 314 patients with clinically localized prostate cancer treated by definitive radiation therapy (28%, Stage A2; 34%, Stage B; and 389'0, Stage C), reported that 38% of the patients showed posttreatment increase in serum PSA levels by 4 years. As in other reports, the 4-year risk of chemical failure was closely related to the initial PSA level: 5%, less than or equal to 4 ng/ml; 20'30, greater than 4 to less than or equal to 10 ng/ml; 6O%, 10.1-30 ng/ml; and 8O%, greater than 30 ng/ml. The chemical failure pre- cedes a clinical recurrence by several years; even in pa- tients with initial PSA of 4-30 ng/ml, 80% were clini- cally tumor free 4 years after treatment. Others have reported shorter lead time from rising PSA to clinical evidence of relapse (an average of approximately 6
Patients with elevated pretreatment PSA levels, stable posttreatment levels, and subsequent ele- vation have a 33-44% risk of subsequent distant me- tastasis in less than 3 years.'04 Rising PSA levels after irradiation have been correlated with clinical progres- sion, although the time course has not been defined adeq~ate ly . '~~ ,"~ Failure of PSA to decrease to below normal serum levels by 6 months is associated with a significantly higher risk of postirradiation f a i l ~ r e . ~ ~ , ~ ~ , ' ~ ~
Zietman et al.,'I4 in 161 patients treated with defin- itive radiation therapy for localized carcinoma of the prostate, noted that 54% achieved a postirradiation na- dir value of 0-1 ng/ml, and 29% had an undetectably low value (less than 0.5 ng/ml). As in other reports, a significantly higher proportion of patients with Stage T1 or T2a lesions had initial (preirradiation) PSA values less than 10 ng/ml(65-72%) compared with those with more extensive tumors (45% in Stage T2b, 40% in Stage T3, and 17% in Stage T4). Lower initial PSA values were seen in patients with well and moderately differ-
Irradiation in Management of Prostate Cancer/Perez et al. 3165
L !
8 0
6 0 initial PSA
4 0
<15 (n=57)
initial PSA >15 (n=28) 1 D=O.O001 (3 ) I
8- 0 12 24 36 4 0
months from radical radiotherapy
"'b 8 0
6 o 1 40.1 (n=36)
initial PSA >15 (n=40) p=0.0003
L
al
c 0 1 2 2 4 36 4 0 i+!
months from radical radiotherapy
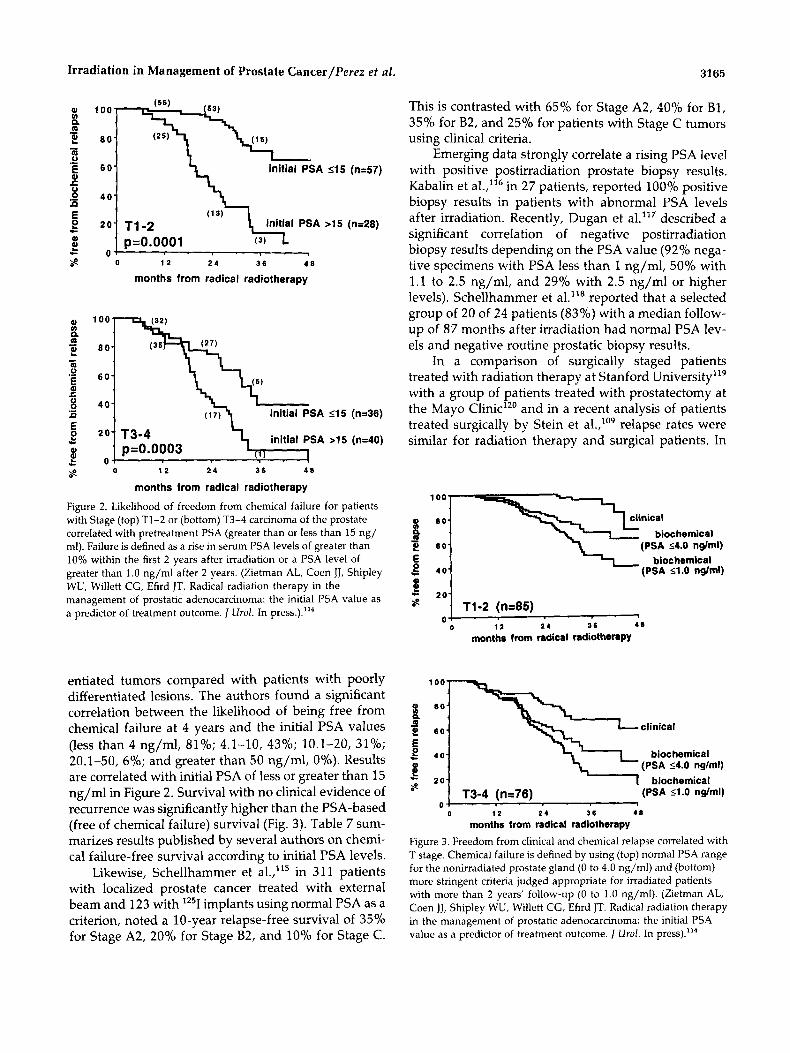
Figure 2 . Likelihood of freedom from chemical failure for patients with Stage (top) T1-2 or (bottom) T3-4 carcinoma of the prostate correlated with pretreatment PSA (greater than or less than 15 ng/ ml). Failure is defined as a rise in serum PSA levels of greater than 10% within the first 2 years after irradiation or a PSA level of greater than 1.0 ng/ml after 2 years. (Zietman AL, Coen JJ, Shipley WU, Willett CG, Efird JT. Radical radiation therapy in the management of prostatic adenocarcinoma: the initial PSA value as a predictor of treatment outcome. 1 Urol. In pre~s.) ."~
entiated tumors compared with patients with poorly differentiated lesions. The authors found a significant correlation between the likelihood of being free from chemical failure at 4 years and the initial PSA values (less than 4 ng/ml, 81%; 4.1-10, 43%; 10.1-20, 31%; 20.1-50, 6%; and greater than 50 ng/ml, 0%). Results are correlated with initial PSA of less or greater than 15 ng/ml in Figure 2 , Survival with no clinical evidence of recurrence was significantly higher than the PSA-based (free of chemical failure) survival (Fig. 3). Table 7 sum- marizes results published by several authors on chemi- cal failure-free survival according to initial PSA levels.
Likewise, Schellhammer et al.,'15 in 31 1 patients with localized prostate cancer treated with external beam and 123 with lz5I implants using normal PSA as a criterion, noted a 10-year relapse-free survival of 35% for Stage A2, 20% for Stage B2, and 10% for Stage C.
This is contrasted with 65% for Stage A2, 40% for B1, 35% for B2, and 25% for patients with Stage C tumors using clinical criteria.
Emerging data strongly correlate a rising PSA level with positive postirradiation prostate biopsy results. Kabalin et a1.,lI6 in 27 patients, reported 100% positive biopsy results in patients with abnormal PSA levels after irradiation. Recently, Dugan et al."' described a significant correlation of negative postirradiation biopsy results depending on the PSA value (92% nega- tive specimens with PSA less than 1 ng/ml, 50% with 1.1 to 2.5 ng/ml, and 29% with 2.5 ng/ml or higher levels). Schellhammer et a1.It8 reported that a selected group of 20 of 24 patients (83%) with a median follow- up of 87 months after irradiation had normal PSA lev- els and negative routine prostatic biopsy results.
In a comparison of surgically staged patients treated with radiation therapy at Stanford University"' with a group of patients treated with prostatectomy at the Mayo Clinic'20 and in a recent analysis of patients treated surgically by Stein et al.,'09 relapse rates were similar for radiation therapy and surgical patients. In
biochemical 2 60 (PSA 54.0 nglml) E biochemical
4 0 (PSA s1.0 nslml)
1
0 1 2 2 4 36 4 8
months from radical radiotherapy
100-
\\clinical
'-L biochemical (PSA 54.0 ndrnl)
biochemical T3-4 (n=76) (PSA 51.0 nglml)
0 0 I2 2 4 36 4 0
months from radical radiotherapy
Figure 3. Freedom from clinical and chemical relapse correlated with T stage. Chemical failure is defined by using (top) normal PSA range for the nonirradiated prostate gland (0 to 4.0 ng/ml) and (bottom) more stringent criteria judged appropriate for irradiated patients with more than 2 years' follow-up (0 to 1.0 ng/ml). (Zietman AL, Coen JJ, Shipley WU, Willett CG, Efird JT. Radical radiation therapy in the management of prostatic adenocarcinoma: the initial PSA value as a predictor of treatment outcome. Urol. In press)."*
3166 CANCER December 2, 2993, Volume 72, No. 11
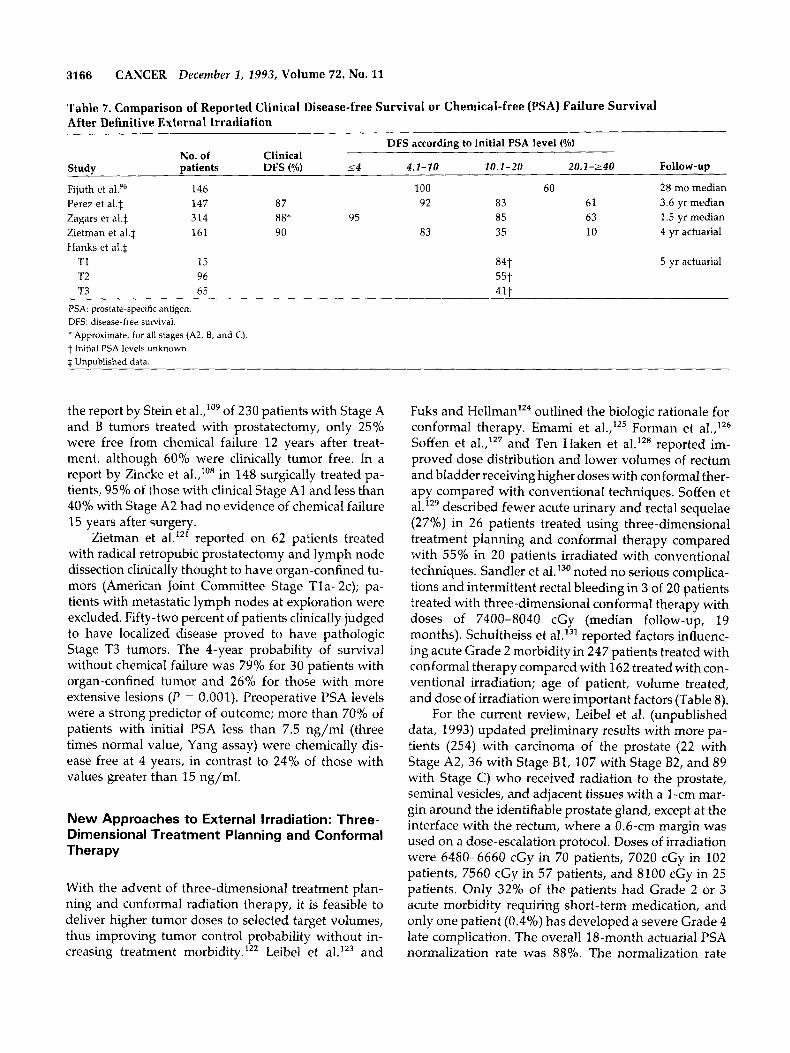
Table 7. Comparison of Reported Clinical Disease-free Survival or Chemical-free (PSA) Failure Survival After Definitive External Irradiation
DFS according to initial PSA level (%) No. of Clinical
Study patients DFS (%) s4 4.1-10 10.1-20 20.1-240 Follow-up
Fijuth et al.96 146 100 60 28 mo median Perez et a1.S 147 87 92 83 61 3.6 yr median Zagars et a1.S 314 88* 95 85 63 1.5 yr median Zietman et a1.S 161 90 83 35 10 4 yr actuarial Hanks et a1.S
T1 15 84t 5 yr actuarial T2 96 55t T3 65 41 t
PSA: prostate-specific antigen. DFS. disease-free survival. ' Approximate, for all stages (A2, B, and C). t Initial PSA levels unknown. t Unuublished data
the report by Stein et aI.,'O9 of 230 patients with Stage A and B tumors treated with prostatectomy, only 25% were free from chemical failure 12 years after treat- ment, although 60% were clinically tumor free. In a report by Zincke et al.,"' in 148 surgically treated pa- tients, 95% of those with clinical Stage A1 and less than 40% with Stage A2 had no evidence of chemical failure 15 years after surgery.
Zietman et al."' reported on 62 patients treated with radical retropubic prostatectomy and lymph node dissection clinically thought to have organ-confined tu- mors (American Joint Committee Stage Tla-2c); pa- tients with metastatic lymph nodes at exploration were excluded. Fifty-two percent of patients clinically judged to have localized disease proved to have pathologic Stage T3 tumors. The 4-year probability of survival without chemical failure was 79% for 30 patients with organ-confined tumor and 26% for those with more extensive lesions ( P = 0.001). Preoperative PSA levels were a strong predictor of outcome; more than 70% of patients with initial PSA less than 7.5 ng/ml (three times normal value, Yang assay) were chemically dis- ease free at 4 years, in contrast to 24% of those with values greater than 15 ng/ml.
New Approaches to External Irradiation: Three- Dimensional Treatment Planning and Conformal Therapy
With the advent of three-dimensional treatment plan- ning and conformal radiation therapy, it is feasible to deliver higher tumor doses to selected target volumes, thus improving tumor control probability without in- creasing treatment morbidity.'" Leibel et al.lZ3 and
Fuks and Hellman'24 outlined the biologic rationale for conformal therapy. Emami et al.,125 Forman et a1.,'26 Soffen et al.,lz7 and Ten Haken et al.'z6 reported im- proved dose distribution and lower volumes of rectum and bladder receiving higher doses with conformal ther- apy compared with conventional techniques. Soffen et allz9 described fewer acute urinary and rectal sequelae (27%) in 26 patients treated using three-dimensional treatment planning and conformal therapy compared with 55% in 20 patients irradiated with conventional techniques. Sandler et aI.I3' noted no serious complica- tions and intermittent rectal bleeding in 3 of 20 patients treated with three-dimensional conformal therapy with doses of 7400-8040 cGy (median follow-up, 19 months). Schultheiss et aI.I3' reported factors influenc- ing acute Grade 2 morbidity in 247 patients treated with conformal therapy compared with 162 treated with con- ventional irradiation; age of patient, volume treated, and dose of irradiation were important factors (Table 8).
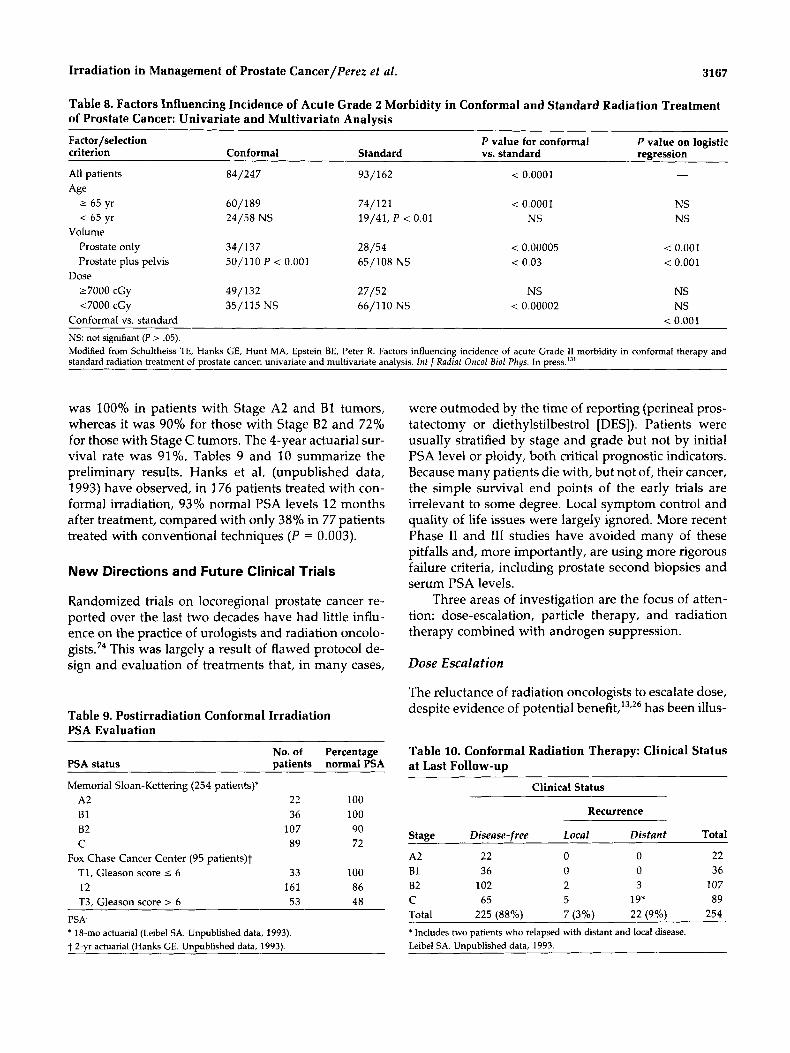
For the current review, Leibel et al. (unpublished data, 1993) updated preliminary results with more pa- tients (254) with carcinoma of the prostate (22 with Stage A2, 36 with Stage B l , 107 with Stage B2, and 89 with Stage C) who received radiation to the prostate, seminal vesicles, and adjacent tissues with a 1-cm mar- gin around the identifiable prostate gland, except at the interface with the rectum, where a 0.6-cm margin was used on a dose-escalation protocol. Doses of irradiation were 6480-6660 cGy in 70 patients, 7020 cGy in 102 patients, 7560 cGy in 57 patients, and 8100 cGy in 25 patients. Only 32% of the patients had Grade 2 or 3 acute morbidity requiring short-term medication, and only one patient (0.4%) has developed a severe Grade 4 late complication. The overall 18-month actuarial PSA normalization rate was 88%. The normalization rate
Irradiation in Management of Prostate Cancer/Perez et al. 3167
Table 8. Factors Influencing Incidence of Acute Grade 2 Morbidity in Conformal and Standard Radiation Treatment of Prostate Cancer: Univariate and Multivariate Analysis
~ ~~~~
Factor/selection P value for conformal P value on logistic criterion Conformal Standard vs. standard regression
AH patients
2 65 yr < 65 yr
Age
Volume
84/247
60/189 24/58 NS
93/162 < 0.0001
74/121 < 0.0001 19/41, P < 0.01 NS
Prostate only 34/137 28/54 Prostate plus pelvis 50/110 P < 0.001 65/108 NS
Dose
< 0.00005 < 0.03
-
NS NS
< 0.001 < 0.001
27000 cGy 49/132 27/52 NS NS ~ 7 0 0 0 cGy 35/115 NS 66/110 NS < 0.00002 NS
Conformal vs. standard < 0.001 NS: not signifiant (P > .05). Modified from Schultheiss TE, Hanks GE, Hunt MA, Epstein BE, Peter R. Factors influencing incidence of acute Grade II morbidity in conformal therapy and standard radiation treatment of prostate cancer: univariate and multivariate analysis. Inf Radiat Oncol B i d Phys. In pre~s. '~ '
was 100% in patients with Stage A2 and B1 tumors, whereas it was 90% for those with Stage 82 and 72% for those with Stage C tumors. The 4-year actuarial sur- vival rate was 91%. Tables 9 and 10 summarize the preliminary results. Hanks et al. (unpublished data, 1993) have observed, in 176 patients treated with con- formal irradiation, 93% normal PSA levels 12 months after treatment, compared with only 38% in 77 patients treated with conventional techniques (P = 0.003).
New Directions and Future Clinical Trials
Randomized trials on locoregional prostate cancer re- ported over the last two decades have had little influ- ence on the practice of urologists and radiation oncolo- g i s t ~ . ~ ~ This was largely a result of flawed protocol de- sign and evaluation of treatments that, in many cases,
Table 9. Postirradiation Conformal Irradiation PSA Evaluation
PSA status patients normal PSA
Memorial Sloan-Kettering (254 patients)*
No. of Percentage
A2 22 100 81 36 100 82 107 90 C 89 72
TI, Gleason score I 6 33 100 T2 161 86 T3, Gleason score > 6 53 48
Fox Chase Cancer Center (95 patients)t
PSA: * l8-mo actuarial (Leibel SA. Unpublished data, 1993). t 2-yr actuarial (Hanks GE. Unpublished data, 1993).
were outmoded by the time of reporting (perineal pros- tatectomy or diethylstilbestrol [DES]). Patients were usually stratified by stage and grade but not by initial PSA level or ploidy, both critical prognostic indicators. Because many patients die with, but not of, their cancer, the simple survival end points of the early trials are irrelevant to some degree. Local symptom control and quality of life issues were largely ignored. More recent Phase I1 and I11 studies have avoided many of these pitfalls and, more importantly, are using more rigorous failure criteria, including prostate second biopsies and serum PSA levels.
Three areas of investigation are the focus of atten- tion: dose-escalation, particle therapy, and radiation therapy combined with androgen suppression.
Dose Escalation
The reluctance of radiation oncologists to escalate dose, despite evidence of potential benefit,l3fz6 has been illus-
Table 10. Conformal Radiation Therapy: Clinical Status at Last Follow-up
Clinical Status
Recurrence
Stage Disease-free Local Distant Total
A2 22 0 0 22 B l 36 0 0 36 82 102 2 3 107 C 65 5 19* 89 Total 225 (88%) 7 (3%) 22 (9%) 254
* Includes two patients who relapsed with distant and local disease. Leibel SA. Unpublished data, 1993.

3168 CANCER December 1, 1993, Volume 72, No. 11
trated by a recent survey of radiation oncology centers in the United States.13* The doses prescribed for pros- tate cancer did not increase from 1984 to 1990, with the modal dose remaining at only 6000 cGy. A fear of po- tential increased morbidity and liability with conven- tional techniques keeps radiation oncologists cautious. Dose escalation is possible without an increase in mor- bidity using three-dimensional conformal planning (ul- trasound) or computed tomography-guided brachy- therapy (with or without h~perthermia) '~~; randomized trials testing this potential gain are in progress. The as- sumption of an advantage is such that the necessary trial may not be performed, and conformal therapy may slip into general use without formal testing, similar to the radical prostatectomy. The Massachusetts General Hospital recently completed a Phase 111 comparison of perineal proton boost versus conventional photon boost for patients with localized T3 and T4 prostate cancer. In both arms, the whole pelvis was treated to 5040 cGy with photons. The standard radiation therapy arm gave a total dose of 6000 cGy to the primary tumor. The experimental arm exploited the superior depth- dose characteristics of a 160 MV proton beam to bring the tumor volume to 7550 cGy. More than 180 patients have been recruited, and initial results will be reported in 1994.
Neutron Therapy
The neutron beam has potential biologic advantages over photons in killing slowly cycling or hypoxic cells. Its role in prostate cancer in a series of randomized stud- ies has been examined. The Neutron Therapy Collabo- rative Working Group Trial was opened in 1985 and closed in 1990; 182 T3-4 or pelvic node-positive pa- tients were treated with a pelvic field (5040 cGy in the photon arm at 180 cGy per fraction and 13.6 nGy at 1.7 nGy per fraction in the neutron arm). The prostate was boosted with 2000 cGy and 6.8 nGy, respectively. Five- year results show a significant pathologic local tumor control advantage for neutrons (82% versus 60%), but no difference in disease-free or overall survival has been 0 b ~ e r v e d . l ~ ~ If the node-positive patients are ex- cluded, the pathologic local control figures are 92% for neutrons and 59% for photons. Unlike in the RTOG mixed-beam predecessor there was significant morbidity in the neutron arm; 10 of 87 patients had Grade 4 morbidity (6 requiring colostomy) compared with only 1 of 85 treated with photons. Morbidity fig- ures such as these have made embracing neutrons for the treatment of pelvic malignancy less appealing.
Irradiation and Endocrine Therapy
The use of endocrine therapy in conjunction with radia- tion therapy has been explored in two contexts: (1) as
adjuvant therapy following irradiation for patients at high risk of occult metastatic disease and (2) as neoad- juvant cytoreductive therapy in patients with bulky pri- mary tumors to enhance likelihood of local control. In 1988, Zagars et al.136 reported a 15-year follow-up on .a randomized trial in which 78 T3-4NXMO patients were randomized to receive either irradiation alone or irra- diation plus DES until relapse or death. Actuarial dis8- ease-free survival was significantly improved in the adl- juvant DES group (63% versus 35%). Greater inter- current mortality in patients receiving DES, coupled with use of DES on relapse in the irradiation-only arm, resulted in no difference in overall survival or clinical local tumor control. This study made attractive further exploration of the combination of more modern and less morbid methods of androgen deprivation (luteiniz- ing hormone-releasing hormone agonists and testos- terone receptor antagonists) with radiation therapy.
RTOG protocol 8531 evaluated adjuvant goserelin acetate (Zoladex; ICA Pharma, Wilmington, DE) (3.6 mg subcutaneously every 28 days indefinitely) com- bined with irradiation in T3-4 and node-positive pa- tients or administered on relapse after identical irradia- tion alone. This study was closed in April 1992, having accrued 977 patients; early data are soon to be reported. The European Organization for Research on Treatment of Cancer (EORTC) activated a comparable protocol in March 1990. Patients at higher risk of metastatic dis- ease (T3-4 tumors or high Grade T1-2 tumors) are eligi- ble provided there is no evidence of gross distant meta- static disease or involved lymph nodes at or above the common iliac. Patients in the experimental arm receive cyproterone acetate (150 mg three times a day for 4 weeks) beginning 1 week before radiation therapy plus goserelin acetate (3.6 mg subcutaneously every 4 weeks) beginning on the first day of irradiation and continuing for 3 years or until progression, whichever occurs sooner.
The cytoreductive role of goserelin acetate and flu- tamide (Eulexin; Schering Corp., Kenilworth, NJ) in bulky primary disease (Stage T2b, 3, or 4) has been examined in RTOG protocol 8610. Pilepich et al.'37 re- cently completed analysis of 455 evaluable patients with large Stage T2b, T2c (B2, B3, B4, C, D1) adenocarci- noma of the prostate randomized to be treated with irradiation alone (4500 cGy to pelvic lymph nodes and an additional 2000-2500 cGy, depending on stage, to the prostatic area) or a combination of the same radia- tion therapy and adjuvant hormonal therapy consisting of goserelin acetate (3.6 mg subcutaneously every 4 weeks) and flutamide (250 mg orally three times a day), both drugs started 2 months before initiation of irradia- tion and continued throughout the entire course of radi- ation therapy. With a median observation period of 2.6
Irradiation in Management of Prostate Cancer/Perez et al. 3169
years, the local recurrence rate (clinical assessment) was significantly lower in patients treated with neoadjuvant hormonal therapy and radiation therapy (28 of 225 [12.4%]) compared with the control group (58 of 230 [25.2%]). The 4-year actuarial local failure rate was 13% in the study arm and 32% in the control arm. A decreasing incidence of distant metastasis was also noted in patients receiving hormonal therapy (47 of 225 [20.8%] versus 62 of 230 [26.9%]) (P = 0.05). The ac- tuarial DFS by cIinicaI assessment was 53% for the study arm and 41% for the control arm (P < 0.001). The corresponding chemical-free (PSA higher than 4 ng/ ml) recurrence survival rates were 35% for the study arm and 16% for the control arm. There were no sig- nificant differences in overall survival or morbidity in the two groups. The correlation of lower incidence of distant metastasis and improved survival in patients with local control of the prostatic t ~ m ~ r ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ pro- vides hope for improving the prognosis of these pa- tients with combined neoadjuvant hormonal and radia- tion therapy.
RTOG protocol 9202 was activated last year for pa- tients with T2b-4 disease and is rapidly accruing pa- tients. Neoadjuvant total androgen suppression, as in RTOG 8610, is given in both arms of the trial before irradiation; one group will receive 2 years of mainte- nance adjuvant goserelin acetate. The primary end point will be freedom from PSA recurrence. Patients will be stratified according to initial PSA level, which should help to further define the subpopulation, if any, that may gain from long-term total androgen suppres- sion.
The results of these randomized trials are eagerly awaited. The use of PSA and rebiopsy in defining treat- ment failure means that objective results will be more rapidly available; new strategies can be tested over 5 years rather than over 10-15 years. This will also help to limit the confounding effect of competing morbidity in this elderly population.
A trial similar to the original Veterans Administra- tion Cooperative Urological Research Group (VA- CURG) focal study13* comparing radical treatments with a policy of close observation (using PSA and transrectal ultrasound) and deferred treatment has be- come imperative. A sufficient number of large nonran- domized studies have been reported suggesting that men older than age 70 years with T1 and T2a well- or moderately differentiated tumors who are initially managed by observation and deferred treatment are unlikely to die of metastatic prostate cancer.5,139,140 These men could have their local disease controlled, if it ever became symptomatic, by transurethral resection of the prostate, irradiation, or endocrine therapy. Most U.S. physicians and their patients will, however, con-
tinue to opt for radical therapy until such a trial defines exactly which subgroups have little to lose by a conser- vative policy. Furthermore, well-designed clinical trials are highly desirable to compare radical prostatectomy and irradiation, considering such factors as patient se- lection, staging methods, tumor characteristics, and prognostic factors. End points should include survival, clinical or chemical failure, morbidity, and quality of life as well as cost-effectiveness of either therapeutic modality.
References
1. Whitmore WF. Overview. Historical and contemporary. NCZ Monogr 1988; 7:7-11.
2. National Institutes of Health Consensus Development Panel. Consensus statement: the management of clinically localized prostate cancer. NCZ Monogr 1988; 7:3-6.
3. Adolfsson J, Steineck G, Whitmore WF Jr. Recent results of man- agement of palpable clinical localized prostate cancer. Cancer
4. George NJR. Natural history of localized prostatic cancer man- aged by conservative therapy alone. Lancet 1988; 1:494-7.
5. Johansson J-E, Adami H-0, Anderson S-0, Bergstrom R, Holmberg L, Krusemo UB. High 10-year survival rate in patients with early, untreated prostatic cancer. IAMA 1992; 2672191-6.
6. Whitmore WF Jr., Warner ]A, Thompson IM Jr. Expectant man- agement of localized prostatic cancer. Cancer 1991; 67:1091-6.
7. Fleming C, Wasson JH, Albertsen PC, Barry MJ, Wennberg JE, for the Prostate Patient Outcomes Research Team. A decision analysis of alternative treatment strategies for clinically local- ized prostate cancer. J A M 1993; 269:2650-9.
8. Lu-Yao GL, McLerran D, Wasson JH, Wennberg JE, for the Pros- tate Patient Outcomes Research Team. An assessment of radical prostatectomy: time trends, geographic variation, and outcomes.
9. Whitmore WF. Management of clinically localized prostatic cancer: an unresolved problem, JAMA 1993; 269:2676-7.
10. Moore MJ, O’Sullivan B, Tannock IF. How expert physicians would wish to be treated if they had genitourinary cancer. ] Clin Oncol 1988; 6:1736-45.
11. Perez CA, Cosmatos D, Garcia DM, Eisbruch A, Poulter CA. Irradiation in relapsing carcinoma of the prostate. Cancer
12. Perez CA, Pilepich MV, Zivnuska F. Tumor control in definitive irradiation of localized carcinoma of the prostate. Int ] Radiat Oncol Biol Phys 1986; 12:523-31.
13. Perez CA, Lee HK, Georgiou A, Logsdon MD, Lai PP, Lockett MA. Technical and tumor-dated factors affecting outcome of definitive irradiation for localized carcinoma of the prostate. Int J Radiat Oncol Biol Phys 1993; 26:581-91.
14. Hanks GE, Martz KL, Diamond JJ. The effect of dose on local control of prostate cancer. Int ] Radiat Oncol Biol Phys 1988;
15. McGowan DG. The value of extended field radiation therapy in carcinoma of the prostate. Int ] Radiat Oncol Biol Phys 1981;
16. Ploysongsang SS, Aron BS, Shehata WM. Radiation therapy in prostate cancer: whole pelvis with prostate boost or small field to prostate? Urology 1992; 40:18-26.
1993; 72:310-22.
]AMA 1993; 269:2633-6.
1993;71: 1110-22.
15:1299-1305.
7:1333-9.

3170 CANCER December 1, 1993, Volume 72, No. 11
17. Bagshaw MA. Radiotherapeutic treatment of prostatic carci- noma with pelvic node involvement: 11. Urol Clin North A M
18. Spaas PG, Bagshaw MA, Cox RS. The volume of extended field irradiation in surgically staged carcinoma of the prostate. Int I Radiat Oncol B i d Phys 1988; 15(Suppl 1):133.
19. Asbell SO, Krall JM, Pilepich MV, Baerwald H, Sause WT, Hanks GE, et al. Elective pelvic irradiation in stage A2, B carci- noma of the prostate: Analysis of RTOG 77-06. Int ] Radiat On- col B i d Phys 1988; 15:1307-16.
20. Fuks Z, Leibel SA, Wallner KE, Begg CB, Fair WR, Anderson LL, et al. The effects of local control on metastatic dissemination in carcinoma of the prostate: Long-term results in patients treated with Iz51 implantation. Int JRadiat Oncol Biol Phys 1991; 21:537- 47.
21. Kaplan ID, Prestidge BR, Bagshaw MA, Cox RS. The importance of local control in the treatment of prostatic cancer. ] Urol 1992;
22. Kuban DA, El-Mahdi AM, Schellhammer PF. Effect of local tu- mor control on distant metastasis and survival in prostatic adeno- carcinoma. Urology 1987; 30:420-6.
23. Aristizabal SA, Steinbronn D, Heusinkveld RS. External beam radiotherapy in cancer of the prostate: the University of Arizona experience. Radiofher Oncal 1984;l: 309-15.
24. Bagshaw MA, Cox RS, Ramback JE. Radiation therapy for local- ized prostate cancer: justification by long-term follow-up. Urol Clin North Am 1990; 17:787-802.
25. Forman JD, Wharam MD, Lee DJ, Zinreich ES, Order SE. Defini- tive radiotherapy following prostatectomy: results and compli- cations. Int J Radiat Oncol Bid Phys 1986; 12:185-9.
26. Hanks GE. Treatment of early stage prostate cancer: radiother- apy. In: Hellman S, DeVita V, Rosenberg S, Freeman S, editors. Important advances in oncology. Philadelphia: JB Lippincott, 1993. In press.
27. Hanks GE, Krall JM, Martz KL, Diamond JJ, Kramer S. The out- come of treatment of 313 patients with T-1 (UICC) prostate cancer treated with external beam irradiation. rnf J Radiat OncoI Biol Phys 1988; 14243-8.
29. Hanks GE, Asbell S, Krall JM, Perez CA, Doggett S, Rubin P, et al. Outcome for lymph node dissection negative T1-b, T2 (A- 2,B) prostate cancer treated with external beam irradiation in RTOG 77-06. Int Radiat Oncol Biol Phys 1991; 21:1099-103.
30. Harisiasdis L, Veenema RJ, Senyszyn JJ, Puchner PJ, Tretter P, Romas P, et al. Carcinoma of the prostate: treatment with exter- nal radiotherapy. Cancer 1978; 412131-42.
31. Kurup P, Kramer TS, Lee MS, Philips R. External beam irradia- tion of prostate cancer: experience in 163 patients. Cancer 1984; 53:37-43.
32. Rangala N, Cox JD, Byhardt RW, Wilson JF, Greenberg M, Lopes da Conceicao A. Local control and survival after external irra- diation for adenocarcinoma of the prostate. Int ] Radiat Oncol Biol Phys 1982; 8:1909-14.
33. Rosen EM, Cassady JR, Connolly J, Chaffey JT. Radiotherapy for localized prostate carcinoma. Int Radiat Oncol Bid Phys
34. Rounsaville MC, Green JP, Vaeth JM, Purdon RP, Heltzel MM. Prostatic carcinoma: limited field irradiation. Inf J Rudiat Oncol Biol Phys 1987; 13:1013-20.
35. Sagerman RH, Chun HC, King GA, Chung CT, Dalal PS. Exter- nal beam radiotherapy for carcinoma of the prostate. Cancer
36. Shipley WU, Prout Gr Jr., Coachman NM, McManus PL, Healey EA, Althausen AF, et al. Radiation therapy for localized prostate
1984; 2:297-303.
147:917-21.
1984; 10:2201-10.
1989; 63:2468-74.
carcinoma: experience at the Massachusetts General Hospital (1973-1981). NCI Monogr 1988; 7:67-73.
37. van der Werf-Messing BHP, Menon RS, van Putten WLJ. Pros- tatic cancer treated by external irradiation at the Rotterdam Ra- diotherapy Institute, Strahlentherapie 1984; 160:293-300.
38. Zagars GK, von Eschenback AC, Johnson DE, Oswald MJ. The role of radiation therapy in stages A2 and B adenocarcinoma of the prostate. Int ] Radiat Oncol Biol Phys 1988; 14:701-9.
39. Zietman AL, Shipley WU, Willett CG. Residual disease after radical surgery or radiation therapy for prostate cancer: clinical significance and therapeutic implications. Cancer 1993; 71:959- 69.
40. Perez CA. Prostate. In: Perez CA, Brady LW, editors. Principles and practice of radiation oncology. 2nd ed. Philadelphia: JB Lip- pincott, 1992;1067-116.
41. del Regato JA, Trailins AH, Pittman DD. Twenty years follow- up of patients with inoperable cancer of the prostate (stage C) treated by radiotherapy: report of a national cooperative study. Jnt J Radiat Oncol Biol Phys 1993; 26:197-201.
42. Neglia WJ, Hussey DH, Johnson DE. Megavoltage radiation ther- apy for carcinoma of the prostate. Inf J Radiat Oncoi Biol Phys
43. Zagars GK, von Eschenbach AC, Johnson DE, Oswald MJ. Stage C adenocarcinoma of the prostate: an analysis of 551 patients treated with external beam radiation. Cancer 1987; 60: 1489-99.
44. Kuban DA, El-Mahdi AM, Schellhammer PF. Prognosis in pa- tients with local recurrence after definitive irradiation for pros- tatic carcinoma, Cancer 1989; 63:2421-5.
45. Gleason DF, Veterans Administration Cooperative Urological Research Group. Histologic grading and clinical staging of pros- tatic carcinoma, In: Tannenbaum M, editor. Urologic pathology: the prostate. Philadelphia: JB Lippincott, 1977: 171-98.
46. Batata MA, Hilaris BS, Whitmore WF. Factors affecting tumor control. In: Hilaris BS, Batata MA, editors. Brachytherapy oncol- ogy 1983: advances in prostate and other cancer. New York: Memorial Sloan-Kettering Cancer Center, 198365-73.
47. Bosch PC, Forbes KA, Prassvinichai S, Miller JB, GoIji H, Martin DC. Preliminary observations on the results of combined tempo- rary '"Ir implantation and external beam irradiation for carci- noma of the prostate. ] Urol 1986; 135:722-5.
48. Brindle JS, Martinez A, Schray M. Pelvic lymphadenectomy and transperineal interstitial implantation of '"Ir combined with ex- ternal beam radiotherapy for bulky stage C prostatic carcinoma. Int J Radiat Oncol B i d Phys 1989; 17:1063-6.
49. Carlton CE Jr., Dawoud F, Hudgins P, Scott R Jr, Irradiation treatment of carcinoma of the prostate: a preliminary report based on 8 years of experience. ] Urol 1972; 18:924-7.
50. Carlton CE Jr., Hudgins PT, Guerriero WG, Scott R Jr. Radiother- apy in the management of stage C carcinoma of the prostate. Trans Am Assoc Geritourin Surg 1975; 67:70-4.
51. Hanks GE. External-beam radiation therapy for clinically local- ized prostate cancer: patterns of Care Studies in the United States. NCI Monogr 1988; 7:75-84.
52. Hilaris BS, Whitmore WF, Batata M, Barzell W. Behavioral pat- terns of prostate adenocarcinoma following an Iz5I implant and pelvic node dissection. Int ]Radial Oncol Biol Phys 1977; 2631- 7.
53. Hilaris BS, Whitmore WF, Batata MA, Barzell W, Tokita N. Iz5I implantation of the prostate: dose-response considerations. Fronf Radiat Ther Oncol 1978; 12:82-90.
54. Kuban DA, El-Mahdi AM, Schellhammer PF. I9'Ir interstitial implantation for prostate cancer. What have we learned 10 years later? Cancer 1989; 632415-20.
1977; 2:873-82.
Irradiation in Management of Prostate Cancer/Perez et al . 3171
55. Morton JD, Peschel RE. Iodine-125 implants versus external beam therapy for stages A2, B, and C prostate cancer. Int J Ra- diat Oncol Biol Phys 1988; 14x1153-7.
56. Puthawala AA, Syed AMN, Tansey LA, Shanberg A, Austin PA, McNamara CS. Temporary iridium-192 implant in the manage- ment of carcinoma of the prostate: an analysis of treatment re- sults and complications in the first 100 patients. Endocurie Hy- pertherm Oncol 1985; 1:25-34.
57. Sogani PC, DeCosse JJ Jr., Montie 1, Whitmore WF Jr., Grabstald H, Hilaris BS. Carcinoma of the prostate: treatment with pelvic lymphadenectomy and 1251 implants. Clin Bull 1979; 9:24-31.
58. Syed AMN, Puthawala A, Tansey LA, Shanberg AM, Neblett D, Mendez R, et al. Management of prostate carcinoma: combina- tion of pelvic lymphadenectomy, temporary Ir-192 implanta- tion, and external irradiation. Radiology 1983; 149:829-33.
59. Lawton CA, Won M, Pilepich MV, Asbell SO, Shipley WU, Hanks GE, et al. Long-term treatment sequelae following exter- nal beam irradiation for adenocarcinoma of the prostate: analy- sis of RTOG studies 7506 and 7706. Int J Radiat Oncol Biol Phys
60. Perez CA, Lee HK, Georgiou A, Lockett MA. Technical factors affecting morbidity in definitive irradiation for localized carci- noma of the prostate. Int J Radiat Oncol Biol Phys. In press.
61. Hanks GE, Leibel SA, Krall JM, Kramer S. Patterns of Care Stud- ies: dose-response observations for local control of adenocarci- noma of the prostate. Int J Radiat Oncol Biol Phys 1985; 11:153-7.
62. Pilepich MV, Asbell SO, Krall JM, Baerwald WH, Sause WT, Rubin P, et al. Correlation of radiotherapeutic parameters and treatment related morbidity: analysis of RTOG study 77-06. Int J Radiat Oncol Biol Phys 1987; 13:1007-13.
63. Pilepich MV, Krall JM, Sause WT, Johnson RJ, Russ HH, Hanks GE, et al. Correlation of radiotherapeutic parameters and treat- ment related morbidity in carcinoma of the prostate: analysis of RTOG study 75-06. Znt J Radiat Oncol Biol Phys 1987; 13:351-7.
64. Mameghan H, Fisher R, Mameghan J, Watt WH, Tynan A. Bowel complications after radiotherapy for carcinoma of the prostate: the volume effect. Int J Radiat Oncol Biol Phys 1990;
65. Rosen EM, Cassady JR, Connolly J, Chaffey JT. Radiotherapy for prostate carcinoma: the JCRT experience (1968-1978). 11. Factors related to tumor control and complications. Znt J Radiat Oncol Biol Phys 1985; 11:725-30.
66. Smit WGJM, Helle PA, van Putten WLJ, Wijnmaalen AJ, Sel- denrath JJ, van der Werf-Messing BHP. Late radiation damage in prostate cancer patients treated by high dose external radio- therapy in relation to rectal dose. Int J Radiat Oncol Biol Phys
67. Zinreich ES, Derogatis LR, Herpst J, Auvil G, Piantadosi S, Order SE. Pre and post-treatment evaluation of sexual function in patients with adenocarcinoma of the prostate. Int J Radiat Oncol Biol Phys 1990; 19:729-32.
68. Asbell SO, Martz ML, Pilepich MV, Baerwald H, Sause WT, Hanks GE, et al. Impact of surgical staging in evaluating the radiotherapeutic outcome in RTOG III study for A2 and B pros- tate carcinoma. In t ] Radiat Oncol B i d Phys 1989; 17:945-51.
69. Hanks GE, Krall JM, Pilepich MV, Asbell SO, Perez CA, Rubin P, et al. Comparison of pathologic and clinical evaluation of lymph nodes in prostate cancer: implications of RTOG data for patient management and trial design and stratification. Int ] Ra- diat Oncol Biol Phys 1992; 23:293-8.
70. Paulson DF, Lin GH, Hinshaw W, Stephani S, the Uro-Oncol- ogy Research Group. Radical surgery versus radiotherapy for adenocarcinoma of the prostate. J Urol 1982; 128:502-4.
1991; 21x935-9.
18:315-20.
1990; 18x23-9.
71. Paulson DF. Randomized series of treatment with surgery ver- sus radiation for prostate adenocarcinoma. NCI Monogr 1988;
72. Hanks GE. More on the Uro-Oncology Research Group report of radical surgery vs. radiotherapy for adenocarcinoma of the prostate [letter]. Znt J Radiat Oncol Biol Phys 1988; 14:1053.
73. Paulson DF. More on the Uro-Oncology Research Group report of radical surgery vs. radiotherapy for adenocarcinoma of the prostate: rebuttal [letterj. Int Radiat Oncol Biol Phys 1988;
74. Pilepich MV, Bagshaw MA, Asbell AO, Hanks GE, Krall JM, Emami B, et al. Definitive radiotherapy in resectable (stage A2 and B) carcinoma of the prostate: results of a nationwide over- view. Znt J Radiat Oncol Biol Phys 1987; 13:659-63.
75. Zietman AL, Shipley WU. Randomized trials in loco-regionally confined prostate cancer: past, present, and future. Semin Radiat Oncol 1993; 3:210-20.
76. Culp 0s. Radical perineal prostatectomy: its past, present, and possible future. J Urol 1967; 98:618-27.
77. Gibbons RP. Localized prostate carcinoma: surgical manage- ment. Cancer 1993; 72:2865-72.
78. Cox JD, Stoffel TJ. The significance of needle biopsy after irra- diation for stage C adenocarcinoma of the prostate. Cancer 1977;
79. Scardino PT. The prognostic significance of biopsies after radio- therapy for prostatic cancer. Semin Urol 1983; 1:243-52.
80. Freiha FS, Bagshaw MA. Carcinoma of the prostate: results of post-irradiation biopsy. Prostate 1984; 5:19-25.
81. Kuban DA, El-Mahdi AM, Schellhammer PF. The significance of post-irradiation prostate biopsy with long-term follow-up. Int ] Radiat Oncol Biol Phys 1993; 24:409-14.
82. Scardino PT, Wheeler TM. Local control of prostate cancer with radiotherapy: frequency and prognostic significance of positive results of post-irradiation prostate biopsy. NCI Monogr 1988;
83. Lai PP, Perez CA, Lockett MA. Prognostic significance of pelvic recurrence and distant metastasis in prostate carcinoma follow- ing definitive radiotherapy. Znt J Radiat Oncol Biol Phys 1992;
84. Schellhammer PF, El-Mahdi AM, Kuban DA. Therapeutic strate- gies for local failure after radiation therapy for stage A-C carci- noma of the prostate. Probl Urol. In press.
85. Hanks GE, Martz KL, Krall JM, Diamond JJ. Analysisof indepen- dent variables affecting survival after recurrence of prostate cancer. l n t J Radiat Oncol B i d Phys 1989; 16:1431-5.
86. Prestidge B, Kaplan 1, Cox RS, Bagshaw MA. Predictors of sur- vival after a positive post-irradiation prostate biopsy [abstract]. Int J Radiat Oncol Biol Phys 1992; 24(Suppl 1):151.
87. Catalona WJ, Smith DS, Ratliff TL, Dodds KM, Coplen DE, Yuan JJJ, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N Engl J Med 1991;
88. Oesterling JE, Chan DW, Epstein JL, Kimball AW Jr., Bruzck DJ, Rock RC, et al. Prostate specific antigen in the preoperative and postoperative evaluation of localized prostatic cancer treated with radical prostatectomy. J Urol 1988; 139:766-72.
89. Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Redwine E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N Engl J Med 1987; 317:909-16.
90. Petros ]A, Catalona WJ, Lower incidence of unsuspected lymph node metastases in 521 consecutive patients with clinically local- ized prostate cancer. J Urol 1992; 147:1574-5.
91. Partin AW, Lee BR, Chan DW, Epstein AW, Walsh PC. The use of prostate specific antigen (PSA) and Gleason score to predict
7127-31.
14:1053-4.
40:156-60.
7~95-103.
241423-30.
32411156-61.
3172 CANCER December 1, 1993, Volume 72, No. 11
pathologic stage in men with localized prostate cancer [abstract]. J Urol 1993; 149(Suppl):387A.
92. Andriole GL, Telle WB, Coplen DE, Catalona WJ. PSA index (PSAI) as a predictor of prostate cancer (Cap) in men with per- sistent serum PSA elevation [abstract]. J Urol 1992; 147(Suppl):387A.
93. Benson MC, Whang IS, Olsson CA, McMahan DJ, Conner WH. The use of prostate specific antigen density to enhance the pre- dictive value of intermediate levels of serum prostate specific antigen. ] Urol 1992; 1471817-21.
94. Russell KJ, Dunatov C, Hafermann MD, Griffith JT, Polissar L, Pelton J, et al. Prostate specific antigen in the management of patients with localized adenocarcinoma of the prostate treated with primary radiation therapy. ] Urol 1991: 1046-52.
95. Zagars GK, Sherman NE, Babaian RJ. Prostatic-specific antigen and external beam radiation therapy in prostatic cancer. Cancer
96. Fijuth J, Chauvet B, Vincent P, Felix-Faure C, Reboul F. Serum prostatic-specific antigen in monitoring the response of carci- noma of the prostate to radiation therapy. Radiofher Oncol 1992;
97. Landmann C, Hunig R. Prostatic specific antigen as an indicator of response to radiotherapy in prostate cancer. Int J Radiat Oncoi Biol Phys 1989; 17:1073-6.
98. Zentner PG, Pao LK, Benson MC, Schiff PB. PSA density: a new prognostic factor for the prediction of outcome in patients with prostate cancer. Znt ] Radiaf Oncol Biol Phys 1992; 24(Suppl 1):150.
99. Meek AG, Park TL, Oberman E, Wielopolski I. A prospective study of prostate-specific antigen levels in patients receiving ra- diotherapy for localized carcinoma of the prostate. Int ] Radiat Oncol Biol Phys 1990; 191733-41.
100. Ritter MA, Messing EM, Shanahan TG, Potts S , Chappell RJ, Porrs S, et al. Prostate-specific antigen as a predictor of radio- therapy response and patterns of failure in localized prostate cancer. ] Clin Oncol 1992; 10:1208-17.
101. Vijayakumar S, Quadri SF, Karrison TG, Trinidad CO, Chan S-K, Halpern HJ, et al. Localized prostate cancer: use of serial prostate-specific antigen measurements during radiation ther- apy. Radiology 1992; 184271-4.
102. Russell KJ, Boileau MA. Current status of prostate-specific anti- gen in the radiotherapeutic management of prostatic cancer. Se- rnin Radiat Oncol 1993; 31154-68.
103. Stamey TA, Kabalin JN, Ferrari M. Prostatic specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. ]
104. Kaplan I, Prestidge BR, Cox RS, Bagshaw MA. Prostate specific antigen after irradiation for prostatic carcinoma. J Uroi 1990;
105. Kaplan ID, Cox RS, Bagshaw MA. A model of prostatic carci- noma tumor kinetics based on prostate specific antigen levels after radiation therapy. Cancer 1991; 681400-5.
106. Hanks GE, Epstein BE, Peter R, Schultheiss TE. PSA doubling times in patients with prostate cancer, a potentially useful re- flection of tumor doubling time [abstract]. Znf ] Radiat Oncol Bid Phys 1992; 24:150.
107. Partin AW, Carter HB, Chan DW, Epstein JL, Oesterling JE, Rock RC, et al. Prostate specific antigen in the staging of local- ized prostate cancer: influence of tumor differentiation, tumor volume and benign hyperplasia. I Urol 1990; 143:747-52.
108. Zincke H, Blute ML, Fallen MJ, Farrow GM. Radical prostatec- tomy for stage A adenocarcinoma of the prostate: staging errors and their implications for treatment recommendations and dis- ease outcome. ] Urol 1991; 146:1053-8.
1991; 67:412-20.
231236-40.
U r d 1989; 141:1084-7.
144:1172-5.
109. Stein A, DeKernion JB, Smith RB, Dorey F, Patel H. Prostate specific antigen levels after radical prostatectomy in patients with organ confined and locally extensive prostate cancer. ] Urol
110. Frazier HA, Robertson JE, Humphrey PA, Paulson DJ. Is pros- tate specific antigen of clinical importance in evaluating out- come after radical prostatectomy. ] Urol 1993; 149:516-8.
111. Zagars GK, von Eschenbach AC. Prostate-specific antigen: an important marker for prostate cancer treated by external beam radiation therapy. Cancer 1993; 72538-48.
112. Kaplan ID, Cox RS, Bagshaw MA. Prostate specific antigen after external beam radiotherapy for prostatic cancer: followup. ] Urol
113. Killian CS, Yang N, Emrich LJ, Vargas FP, Kuriyama M, Wang MC, et al. Prognostic importance of prostate-specific antigen for monitoring patients with stages B2 to D1 prostate cancer. Cancer Res 1983; 45:886-91.
114. Zietman AL, Coen JJ, Shipley WU, Willett CG, Efird JT. Radical radiation therapy in the management of prostatic adenocarci- noma: the initial PSA value as a predictor of treatment outcome. ] Urol. In press.
115. Schellhammer PF, El-Mahdi AM, Wright GL Jr, Kolm P, Ragle R. Prostate-specific antigen to determine progress free survival after radiation therapy for localized carcinoma of prostate. Urol-
11 6. Kabalin JN, Hodge KK, McNeal JE, Freiha FS, Stamey TA. Iden- tification of residual cancer in the prostate following radiation therapy: role of transrectal ultrasound guided biopsy and pros- tate specific antigen. ] Urol 1989; 142:326-31.
117. Dugan TC, Shipley WU, Young RH, Verhey LJ, Althausen AF, Heney NM, et al. Biopsy after external beam radiation therapy for adenocarcinoma of the prostate: correlation with original histological grade and current prostate specific antigen levels. ]
118. Schellhammer PF, Schlossberg SM, El-Mahdi AM, Wright GL, Brassil DN. Prostate-specific antigen levels after definitive irra- diation for carcinoma of the prostate. ] Urol 1991; 145:1008-11.
119. Kaplan ID, Ccx RS, Bagshaw MA. Optimizing radiotherapy for prostatic cancer: issues of patient selection and the impact of local control. ] Urol. In press.
120. Blute ML, Nativ 0, Zinke H, Farrow GM, Therneau T, Lieber MM. Pattern of failure after radical retropubic prostatectomy for clinically and pathologically localized adenocarcinoma of the prostate: Influence of tumor deoxyribonucleic acid ploidy. ] Uroi
121. Zietman AL, Coen JJ, Shipley WU, Authausen AF. Adjuvant irradiation after radical prostatectomy for prostate adenocarci- noma: an analysis of freedom from PSA failure. Urology. In press.
122. Lichter AS, Sandler HM, Robertson Jm, Lawrence TS, Ten Ha- ken RK, McShan DL, et al. Clinical experience with three-di- mensional treatment planning. Sernin Radiat Oncol 1992; 2257- 66.
123. Leibel SA, Ling CC, Kutcher GJ, Mohan R, Cordon-Cordo C, Fuks 2. The biological basis for conformal three-dimensional radiation therapy. Znt [Radiat Oncol Biol Phys 1991; 21:805-11.
124. Fuks Z, Hellman S. Three-dimensional conformal radiotherapy. In: DeVita VT Jr, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 4th ed. Philadelphia: JB Lip- pincott, 1993: 2614-24.
125. Emami B, Purdy JA, Manolis JM, Gerber RL, Harms WB, Simp- son JR, et al. 3-D static conformal radiotherapy: preliminary re- sults of a prospective clinical trial [abstract]. Int ] Radiaf Oncol Biol Phys 1991; Zl(Supp1 1):147.
1992; 1471942-6.
1993; 149:5 19-22.
ogy 1993; 42:13-20.
Urol 1991; 146:1313-6.
1989; 14211262-5,
Irradiation in Management of Prostate Cancer/Perez et al. 3173
126. Forman JD, Lee Y, Lichter AS, Roberson PL. Lymph node irra- diation in carcinoma of the prostate: necessity of computerized tomography and three-dimensional treatment planning in por- tal design [abstract]. Int ] Radiat Oncol Biol Phys 1990; 19(Suppl 1):189.
127. Soffen EM, Hanks GE, Hwang CC, Chu JCH. Conformal static field therapy for low volume low grade prostate cancer with rigid immobilization. Znt ] Radiat Oncol Biol Phys 1991; 20:141-6.
128. Ten Haken RK, Perez-Tamayo C, Tesser RJ, McShan DL, Fraass BA, Lichter AS. Boost treatment of the prostate using shaped, fixed fields. Int J Radiat Oncol Biol Phys 1989; 16:193-200.
129. Soffen EM, Hanks GE, Hunt MA, Epstein BE. Conformal static field radiation therapy treatment of early prostate cancer versus non-conformal techniques: a reduction in acute morbidity. Znt J Radiat Oncol Bid Phys 1992; 24:485-8.
130. Sandler HM, Perez-Tamayo C, Ten Haken RK, Lichter AS. Dose escalation for stage C (T3) prostate cancer: minimal rectal toxic- ity observed using conformal therapy. Radiother Oncol 1992;
131. Schultheiss TE, Hanks GE, Hunt MA, Epstein BE, Peter R. Fac- tors influencing incidence of acute grade I1 morbidity in confor- mal therapy and standard radiation treatment of prostate cancer: univariate and multivariate analysis. Znt ] Radiat Oncol Biol Phys. In press.
132. Mettlin C, ]ones GW, Murphy GP. Trends in prostate cancer care in the United States, 1974-1990: observations from the pa- tient care evaluation studies of the American College of Sur- geons Commission on Cancer. C A Cancer] Clin 1993; 43:83-91.
133. Wallner K. Iodine 125 brachytherapy for early stage prostate cancer: New techniques may achieve better results. Oncology
23:53-4.
1991; 5:115-22.
134. Russell KJ, Krall JM, Laramore GE, Bumeson M, Maor MH, Davis LW, et al. Photon versus fast neutron external beam radio- therapy in the treatment of locally advanced prostate cancer: preliminary results of a randomized prospective trial of the Neu- tron Therapy Collaborative Working Group. lnt ] Radiat Oncol Biol Phys. In press.
135. Russell KJ, Laramore GE, Krall JM, Thomas FJ, Maor MH, Hen- drickson FR, et al. Eight years experience with neutron radiother- apy in the treatment of stages C and D prostate cancer: updated results of the RTOG 7704 randomized clinical trial. Prostate
136. Zagars GK, Johnson DE, von Eschenbach AC, Hussey DH. Ad- juvant estrogen following radiation therapy for stage C adeno- carcinoma of the prostate: long-term results of a prospective randomized study. Znt ] Radiat Oncol Biol Phys 1988; 14:1085- 91.
137. Pilepich MV, Krall JM, Al-Sarraf M, Roach M, Doggett RLS, Same WT, et al. Androgen suppression with radiation therapy compared with radiation therapy alone for locally advanced prostatic carcinoma: a RTOG randomized comparative trial. Int J Radiat Oncol Biol Phys. In press.
138. Byar DP, Veterans Administration Cooperative Urological Re- search Group. Survival of patients with incidentally found mi- croscopic cancer of the prostate: results of a clinical trial of con- servative treatment. J Urol 1972; 108:908-13.
139. Adolfsson J, Carstensen J . Natural course of clinically localized prostate adenocarcinoma in men less than 70 years old. ] Urol
140. Whitmore WF Jr., Adolfsson J, Steineck G. Conservative man- agement of localized prostatic cancer. Am ] Clin Oncol 1992;
1987; 11~183-93.
1991; 146:96-8.
15:446-52.




















