
Differential sensitivity of the Brattleboro rat to glutamatergic and dopaminergic perturbation

0892-663819010004-27451$01.50. © FASEB 2745
Is the neuronal basis of Alzheimer’s disease
cholinergic or glutamatergic?ALAN M. PALMER1 AND SAMUEL GERSHON
Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh, Pittsburgh,
Pennsylvania 15213, USA
ABSTRACT
The hypothesis that the symptomatology of Alzheimer’sdisease is attributable to cholinergic dysfunction issupported by postmortem studies that have demon-strated reduced choline acetyltransferase (ChAT) ac-
tivity across all areas of cerebral cortex and diminishednumbers of perikarya in the basal forebrain nucleusbasalis of Meynert. Biopsy studies of ChAT activity,choline uptake, and acetylcholine synthesis also sug-gest that cholinergic denervation occurs relatively earlyin the course of the disease, and in confirmation ofpostmortem data, correlates with the severity of cogni-tive impairment. An alternative hypothesis to explainthe dementia of Alzheimer’s disease is the glutamater-gic hypothesis. This is based largely on postmortemevidence indicating reduced binding and uptake ofD[3H]aspartate, as well as loss of a number of otherputative markers, such as phosphate-activated gluta-minase activity, glutamate concentration, and thenumber of pyramidal cell perikarya, with this latterchange correlating with the severity of dementia. Short-comings of each hypothesis are discussed and the merits
of single neuron hypotheses to explain the dementia ofAlzheimer’s disease are considered. -PALMER, A. M.;GERSHON, S. Is the neuronal basis of Alzheimer’s dis-ease cholinergic or glutamatergic? FASEBJ. 4: 2745-2752; 1990.
Key Words: acetylcholine Alz/zeimer’s disease d.enwntia
glutamate N-methyl-D-asparate receptor
ALZHEIMER’S DISEASE, THE MOST COMMON cause of de-mentia in the elderly, is characterized clinically by aprogressive deterioration in memory, personality, andintellect, and neuropathologically by the presence oflarge numbers of senile plaques and neurofibrillary tan-gles. Plaques consist of clusters of dystrophic neuritesand glial cell processes around a central core of amyloid,and are usually located in association areas of neocortex,the hippocampus, and amygdala. Neurofibrillary tangles,abnormal intraneuronal protein arranged in bundles ofpaired helical filaments, are usually found in the same
cortical regions as plaques together with subcorticalregions such as the nucleus basalis of Meynert, the lo-cus ceruleus, and the dorsal raphe nuclei (1). AlthoughAlzheimer’s disease has been recognized and clinicallydifferentiated since the turn of the century, the emer-gence of testable hypotheses to explain its associatedsymptomatology is relatively recent. This review willfocus on two such hypotheses, each based on abnormal-ities in specific neurons in the brain. The first focus isthe cholinergic hypothesis of Alzheimer’s disease, whichargues that the fundamental feature of this disorder, thesyndrome of dementia, is attributable to loss of corticalcholinergic innervation from neurons in the nucleusbasalis of Meynert. Second is the glutamatergic hy-pothesis of Alzheimer’s disease, which suggests that thedementia is caused by loss of glutamatergic neurons fromthe neocortex and hippocampus. Supporting evidence de-rived from postmortem studies of the human brain will bedescribed, and each hypothesis will be assessed.
THE CHOLINERGIC HYPOTHESIS OF
ALZHEIMER’S DISEASE
Neurochemical studies of cholinergic neurons
The cholinergic hypothesis of Alzheimer’s diseaseemerged as a direct consequence of three reports pub-lished in 1976/1977, which indicated that the activity ofthe enzyme responsible for the synthesis of acetyicho-line, ChAT,2 was substantially reduced in Alzheimer’sdisease neocortex and hippocampus (2). This dysfunc-tion has been confirmed in all subsequent studies andis evident throughout the cerebral cortex (2) (Table 1).However, the prospect of obtaining meaningful data fromdiseased postmortem brain may be questioned, asparameters under scrutiny may be influenced by factorssuch as patient’s age, sex, drug history, immediate pre-
‘To whom correspondence should be addressed.2Abbreviations: ACh, acetylcholine; ChAT, choline acetyltransfer-
ase; CNS, central nervous system; LTP, long-term potentiation;MK-801, (+ )-5-methyl-lO,ll-dihydro-5H-dibenzo[ad]cyclophenten-5,10-imine maleate; NMDA, N-methyl-D-aspartate; PAG, phosphate-activated glutaminase; TCP, 1-[l-(2-thienyl)cydohexylpiperidine; a-KG, a-ketoglutarate; WAIS, Wechsler Adult Intelligence Scale.
2746 Vol. 4 July 1990 The FASEB Journal PALMER AND GERSHON
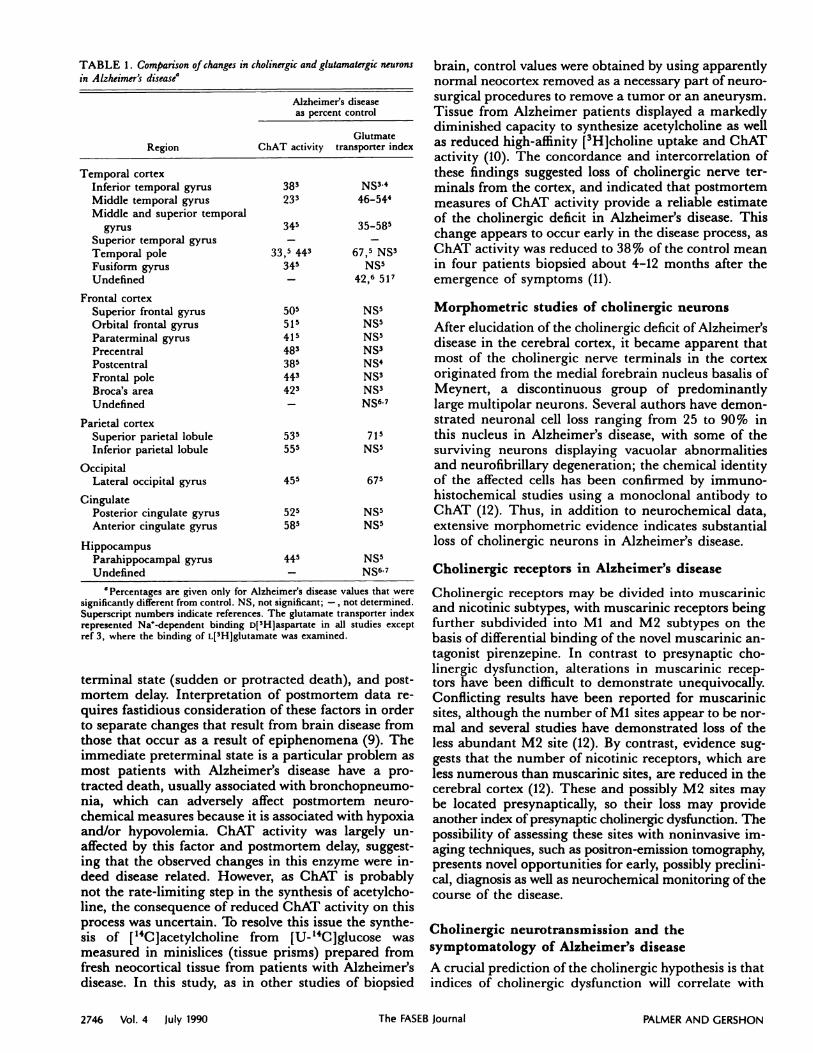
TABLE I. Comparison of changes in cholznergic and glutamatergic neuronsin A lzheimer’s disease’
Alzheimer’s diseaseas percent control
GlutmateRegion ChAT activity transporter index
Temporal cortex
Inferior temporal gyrus 38 NS34
Middle temporal gyrus 23 46-54k
Middle and superior temporal
gyros 345 35-58
Superior temporal gyrus - -
Temporal pole 33,5 443 67, NS3
Fusiform gyrus 345 NS5
Undefined - 42,6 5l
Frontal cortexSuperior frontal gyros 50 NS5
Orbital frontal gyros 5l NS5
Paraterminal gyrus 4l NS5
Precentral 48 NS3
Postcentral 38 NS4
Frontal pole 443 NS3
Broca’s area 42 NS3
Undefined - NS67
Parietal cortex
Superior parietal lobule 535 7lInferior parietal lobule 555 NS5
Occipital
Lateral occipital gyrus 455 67
Cingulate
Posterior cingulate gyrus 52 NS5Anterior cingulate gyros 58 NS5
Hippocampus
Parahippocampal gyrus 445 NS5
Undefined - NS67
‘Percentages are given only for Alzheimer’s disease values that weresignificantly different from control. NS, not significant; -, not determined.Superscript numbers indicate references. The glutamate transporter indexrepresented Na’-dependent binding D[3Hjaspartate in all studies exceptref 3, where the binding of L[3H]glutamate was examined.
terminal state (sudden or protracted death), and post-mortem delay. Interpretation of postmortem data re-quires fastidious consideration of these factors in orderto separate changes that result from brain disease fromthose that occur as a result of epiphenomena (9). Theimmediate preterminal state is a particular problem asmost patients with Alzheimer’s disease have a pro-tracted death, usually associated with bronchopneumo-nia, which can adversely affect postmortem neuro-chemical measures because it is associated with hypoxiaand/or hypovolemia. ChAT activity was largely un-affected by this factor and postmortem delay, suggest-ing that the observed changes in this enzyme were in-deed disease related. However, as ChAT is probablynot the rate-limiting step in the synthesis of acetyicho-line, the consequence of reduced ChAT activity on thisprocess was uncertain. To resolve this issue the synthe-sis of [‘4Cjacetylcholine from [U-14C]glucose wasmeasured in minislices (tissue prisms) prepared fromfresh neocortical tissue from patients with Alzheimer’sdisease. In this study, as in other studies of biopsied
brain, control values were obtained by using apparentlynormal neocortex removed as a necessary part of neuro-surgical procedures to remove a tumor or an aneurysm.Tissue from Alzheimer patients displayed a markedlydiminished capacity to synthesize acetylcholine as wellas reduced high-affinity [3H]choline uptake and ChATactivity (10). The concordance and intercorrelation ofthese findings suggested loss of cholinergic nerve ter-minals from the cortex, and indicated that postmortemmeasures of ChAT activity provide a reliable estimateof the cholinergic deficit in Alzheimer’s disease. Thischange appears to occur early in the disease process, asChAT activity was reduced to 38% of the control meanin four patients biopsied about 4-12 months after theemergence of symptoms (11).
Morphometric studies of cholinergic neurons
After elucidation of the cholinergic deficit of Alzheimer’sdisease in the cerebral cortex, it became apparent thatmost of the cholinergic nerve terminals in the cortexoriginated from the medial forebrain nucleus basalis ofMeynert, a discontinuous group of predominantlylarge multipolar neurons. Several authors have demon-strated neuronal cell loss ranging from 25 to 90% inthis nucleus in Alzheimer’s disease, with some of thesurviving neurons displaying vacuolar abnormalities
and neurofibrillary degeneration; the chemical identityof the affected cells has been confirmed by immuno-histochemical studies using a monoclonal antibody toChAT (12). Thus, in addition to neurochemical data,extensive morphometric evidence indicates substantialloss of cholinergic neurons in Alzheimer’s disease.
Cholinergic receptors in Alzheimer’s disease
Cholinergic receptors may be divided into muscarinicand nicotinic subtypes, with muscarinic receptors beingfurther subdivided into Ml and M2 subtypes on thebasis of differential binding of the novel muscarinic an-tagonist pirenzepine. In contrast to presynaptic cho-linergic dysfunction, alterations in muscarinic recep-tors have been difficult to demonstrate unequivocally.Conflicting results have been reported for muscarinicsites, although the number of Ml sites appear to be nor-mal and several studies have demonstrated loss of theless abundant M2 site (12). By contrast, evidence sug-gests that the number of nicotinic receptors, which areless numerous than muscarinic sites, are reduced in thecerebral cortex (12). These and possibly M2 sites maybe located presynaptically, so their loss may provideanother index of presynaptic cholinergic dysfunction. Thepossibility of assessing these sites with noninvasive im-aging techniques, such as positron-emission tomography,presents novel opportunities for early, possibly preclini-cal, diagnosis as well as neurochemical monitoring of thecourse of the disease.
Cholinergic neurotransmission and thesymptomatology of Alzheimer’s disease
A crucial prediction of the cholinergic hypothesis is thatindices of cholinergic dysfunction will correlate with

NEURONAL BASIS OF ALZHEIMER’S DISEASE 2747
the severity of dementia. Relating neurochemical meas-ures to assessments of the behavioral changes in
Alzheimer’s disease is problematical in postmortem tis-sue because of the variable, often prolonged, time be-tween clinical assessment and death together with thelikelihood that such tissue reflects the end stages of thedisease. A correlation between mean cortical ChAT ac-tivity and an overall measure of cognitive function as-sessed 6 months before death was reported for a groupof subjects with either Alzheimer’s disease or depres-sion (2). However, no relationship was apparent within
the Alzheimer’s disease group, and the use of mean cor-tical ChAT activity failed to provide a specific anatomi-cal basis for these associations. Nonetheless in a popu-
lation of 15 Alzheimer subjects, a subsequent study in-
dicated a significant negative relationship between ChATactivity and an overall assessment of cognitivedecline (2). This has been confirmed by a biopsy studyof 17 Alzheimer’s disease subjects in which [14C]acetyl-
choline synthesis (but not ChAT activity) was found tocorrelate with an overall assessment of the severity ofdementia (Table 2). It is not possible to form conclu-sions regarding cause and effect from the observed rela-tionships, as the two may be independently related todisease severity, but at least they are consistent with
there being a cholinergic contribution to the develop-ment of the dementia of Alzheimer’s disease. Studies of
the behavioral consequences of cholinergic drugs or
cholinergic lesions in experimental animals also lendcredence to the hypothesis that memory loss is a symp-tom of cholinergic dysfunction (14), as do studies of theeffect of cholinergic drugs on human cognitive perfor-
mance (15).
GLUTAMATERGIC NEURONS IN THE BRAIN
Glutamate neurotransmission
The ability of glutamate, aspartate, and a number ofrelated amino acids to directly activate CNS neuronswas first demonstrated more than 30 years ago and
formed the basis of the proposed neurotransmitter rolefor these substances. Subsequent biochemical and elec-trophysiological studies have substantiated this postu-
late and indicated a major role for acidic amino acids
as excitatory neurotransmitters in the mammalian CNS.This is based on the following evidence for glutamate
and aspartate: 1) both are present in relatively highconcentrations in the brain, 2) they are released in a
calcium-dependent manner upon membrane depolari-zation, 3) they are rapidly removed from the extracellu-lar space by a high-affinity uptake system, and 4) bothhave selective binding sites that can be demonstrated byradioligand binding studies and receptor sites that canbe identified pharmacologically in vivo (8, 16). Gluta-mate is synthesized by several biochemical routes:1) from a-ketoglutarate by the action of both trans-aminase and glutamic acid dehydrogenasc, 2) fromglutamine by the action of glutaminase, 3) from orni-thine by the action of ornithine amino transferase viaglutamate semialdehyde, and 4) from proline by pro-line oxidase coupled with subsequent oxidation of theintermediate i-1-pyrroline-5-carboxylic acid. The pre-cise role of each of these routes is not yet known. Meta-bolic studies have led to the simplified model (illus-trated in Fig. 1) that indicates the existence of one large(neuronal) and one small (glial) pool of neurotransmit-ter glutamate. After its release from the nerve terminal,glutamate is partially taken up into the nerve terminalsor into glial cells where it is converted into glutamineby the glial cell-specific enzyme glutamine synthetase.This glutamine is then transported into the nerve ter-minal where it is converted back to glutamate by the ac-tion of the phosphate-activated glutaminase (8).
Pyramidal neurons
Quantitative electron microscopic studies have indi-cated that pyramidal cells constitute about 70% of thetotal neuron population in the mammalian cerebralcortex, which emphasizes their pivotal role in corticalcircuitry (18). These cells are characterized by a singledominant apical dendrite, several basal dendrites, andone main axon; they connect cortical areas both withina hemisphere (association fibers) and betwen hemi-
spheres (callosal fibers) and connect the cortex with
other regions of the brain (corticofugal fibers). Themain axon of pyramidal cells emits several axon col-laterals that ramify within proximity of the parent cellbody and may also ascend, descend, or travel long
TABLE 2. Relationships between indices of the severity of dementia and neurochemical measures of cholinergic neurons and a putative morphometric marker
of glutamatergic neurons in the temporal cortex of Alzheimer patients examined antemortem’
Cholinergic
Putative glutamatergic
(Pyramidal cell loss)
Layer III Layer VChAT activity ACh synthesis
Dementia score NS (11) -0.63 (17) 0.67 (17) 0.71 (17)WAIS verbal subscale NS (9) NS (13) -0.61 (13) -0.63 (13)
WAIS performance subscale NS (8) NS (10) -0.53 (10) -0.59 (10)Token test NS (10) NS (12) -0.58 (12) -0.81 (12)Visual reaction time test NS (10) -0.45 (12) 0.67 (12) 0.70 (12)
‘Modified from ref 13. Numbers represent Spearman correlation coefficients for significant relationships (P < 0.05) with number of patientsexamined indicated in parentheses. NS, not significant. WAIS, Weschler Adult Intelligence Scale; ACh, acetylcholine. Dementia score represents anassessment of the severity of dementia on a 0-9 integer scale, based on cumulative scores of measures of impairments of language, perceptuospatialfunction, and memory, each scored on a 0-3 scale.

2748 Vol. 4 July 1990 The FASEB Journal PALMER AND GERSHON
horizontal distances in the cortex. Electron microscopicevidence indicates that the most (if not all) axon col-laterals of superficial pyramidal cells form synapseswith other pyramidal cells (19). Thus the synapse thatdirectly connects different pyramidal cells probably,constitutes the major component of the total number ofsynapses in the cerebral cortex.
Glutamate as the neurotransmitter ofpyramidal neurons
Evidence to indicate that glutamate and aspartate aretransmitters of pyramidal neurons has been derivedfrom studies of the corticostriatal pathway, the massiveprojection system that links virtually the entire neo-cortex with the neostriatum. This is based on evidencefor 1) selective retrograde labeling of cortical pyramidalneurons after injection of D-[3H]aspartate, a non-metabolized glutamate analog, into rat neostriatum; 2)electrophysiological responsiveness of the neostriatumin response to electrical stimulation of the cortex, whichcan be mimicked by direct application of glutamate
Figure 1. Schematic model of a glutamatergic nerve terminal, post-synaptic process, and glial cell. The steps indicated are as follows.1) a-ketoglutarate (a-KG), derived from the oxidation of glucosewithin nsitochondria, is converted to L-glutamate by the enzyme a-ketoglutarate transarninase. 2) Phosphate-activated glutaminase
catalyzes the conversion of glutamine to glutamate. 3) L-Glutamateis stored in synaptic vesicles. 4) L-Glutamate is released from thenerve ending in a calcium-dependent fashion to interact with post-synaptic receptors. 5) L-Glutamate in the extracellular space istransported by a sodium-dependent process into glutamatergicnerve terminals and glial cells. 6) Glutamate in glial cells is con-verted into glutamine by the action of glutamine synthetase.7) Glutamine in glial cells is transferred back into glutamatergicnerve endings (18).
agonists to the neostriatum and blocked by glutamateantagonists; 3) reduced glutamate neurotransmissionin the neostriatum after ablation or undercutting of thefrontal cortex; and 4) increased extracellular concentra-tions of both radiolabeled and endogenous glutamateand aspartate in the neostriatum in response to bothelectrical stimulation and application of epileptogeniccompounds to the prefrontal cortex (17). Evidence toindicate a neurotransmitter role for glutamate in cor-ticocortical neurons is less advanced, but has been de-rived from retrograde transport studies in conjunctionwith D-[3H]aspartate autoradiography and aspartateand glutamate immunocytochemistry (20), as well asstudies of the release of glutamate from areas of the cor-tex during electrical stimulation of known input path-ways (21).
Glutamate receptors
Membrane binding studies of glutamate sites have ad-vanced rapidly in recent years, largely because of 1) theuse of subcellular fractions highly enriched in postjunc-tional membranes; 2) elucidation of the effects of deter-gent and freeze-thaw pretreatments and the effects ofions on the properties of L-[5H]glutamate binding; and3) the introduction of more selective radioligands. It isgenerally considered that three receptor subtypes medi-ate the excitatory effects of glutamate. These areNMDA, quisqualate, and kainate receptors, namedafter their potent and selective agonists (see ref 16 fora recent comprehensive review). The NMDA subtypeis the best-characterized glutamate receptor and existsas a receptor-channel complex, with its response depen-dent on the membrane potential of the neuron. Anotherunique feature of this complex is the allosteric modula-tion of receptor activity by glycine, zinc, and poly-amines. The receptor complex also has binding sites forboth agonists and psychoactive drugs such as phencycli-dine and the novel agent MK-801. Recent studies haveshown that phencyclidine-like drugs bind most readilyto the activated state of the NMDA receptor. Thusbinding of radiolabeled TCP and MK-801 can be in-creased by the addition of glutamate and enhanced fur-ther by the coapplication of low concentrations ofglycine.
THE GLUTAMATERGIC HYPOTHESIS OF
ALZHEIMER’S DISEASE
Neurochemical studies of glutamatergic neurons
in Alzheimer’s disease
Assessment of glutamatergic neurons in human braintissue is much less straightforward than for other neurontypes, primarily because of the major role of L-glutamatein brain metabolism. Thus, the neurotransmitter poolof L-glutamate makes a relatively small contribution tothe total pool of this substance, making it difficult to at-tribute changes in the concentration of L-glutamate inAlzheimer’s disease to either neurotransmitter or meta-bolic pools of L-glutamate. Indeed, it has been arguedthat the elevated concentration of L-glutamate and

NEURONAL BASIS OF ALZHEIMER’S DISEASE 2749
reduced concentration of L-aspartate reflect abnormalmetabolism in Alzheimer’s disease (22). This difficultywas overcome in the study by Hyman et al. (23), wherethe perforant path zone of the hippocampus, an areaenriched in glutamatergic nerve terminals, was shownto display a marked reduction in the concentration ofL-glutamate. This probably reflects loss of neurotrans-mitter L-glutamate, and thus indicates loss of the per-forant pathway in Alzheimer’s disease.
Indirect evidence to suggest loss of glutamatergicneurons in Alzheimer’s disease arose from the observa-tion of elevated [3H]glutamate binding in the neostria-tum (24), as it was argued that [3H]glutamate bindingin the striatum increases to compensate for loss ofglutamatergic corticostriatal neurons. The first directevidence to suggest loss of glutamatergic nerve termi-nals from the neocortex arose from the demonstrationof reduced sodium-dependent binding of D-[3H]aspar-tate to the glutamate/aspartate transporter in a combi-nation of middle and superior gyri of the temporal lobe(4). Subsequent studies confirmed this observation,although most other areas of the cerebral cortex (in-cluding areas of the temporal lobe) appear to be un-affected (Table 2). This is surprising in view of morpho-metric evidence that suggests a pronounced loss ofpyramidal cells in a number of areas of the cortex andthe proposed involvement of putative glutamatergic cor-ticocortical connections in Alzheimer’s disease (25, 26).
Three factors may have complicated postmortem de-terminations of D-[3H]aspartate binding. First, uptakeinto glial cells may have confounded all determina-tions, because as illustrated in Fig. 1, glial cells have asodium-dependent glutamate uptake mechanism aswell as glutamatergic nerve terminals, and evidencesuggests increased numbers of fibrous astrocytes inneocortex from Alzheimer subjects (1). Astrocyticproliferation is virtually an unavoidable consequence ofmost conditions associated with neuronal injury. Thus,in Alzheimer’s disease, the areas of neocortex withthe most pronounced neuronal injury may also beexpected to be associated with the most intense astro-cytic proliferation. Second, although the binding ofD-[3H]aspartate has been proposed as a suitablemarker of the glutamatergic nerve terminal, bindingexperiments with homogenates, and more recently inautoradiographic studies, have begun to question this.Danbolt and Storm-Mathisen (27) have suggested thatbinding of D-[3H]aspartate in homogenates representsuptake into rnembranous saccules rather than bindingto the glutamate/aspartate transporter. Similarly, auto-radiographic studies have demonstrated that lesions ofglutamatergic pathways do not reduce D-[3H]aspartatebinding in the terminal fields of these pathways (28).Third, evidence suggests that compensatory changesoccur in Alzheimer’s disease in the cerebral cortex inresponse to loss of synapses (29), which may serve tomask the true magnitude of loss of glutamatergic nerveterminals.
PAG has been localized to mitochondria, particularlysynaptosomal mitochondria, by subcellular fractiona-tion techniques. Immunohistochemical studies suggestan enrichment of this enzyme in pyramidal neurons
(30). In Alzheimer’s disease, PAG activity has beenfound to be reduced to 16 and 30% of control in a com-bination of the middle and superior temporal gyri andthe superior frontal gyms, respectively (22), and to18% of control in the cerebral cortex overall (30).However, PAG activity was found not to be affected intissue obtained either promptly after death or atcerebral biposy (22). Thus, it is unclear whether thereported changes in PAG activity reflect a disease-related change or a postmortem artifact, but studies ofPAG using immunohistochemical techniques shouldhelp to resolve this uncertainty.
Dynamic measures of neurotransmitter functioncannot be made postmortem unless the tissue is ob-tained either shortly after death and assayed immedi-ately or carefully frozen in isotonic media (9). Eventhen release processes appear vulnerable, as it has beendemonstrated in tissue obtained promptly after death(<3 h) and assayed immediately that it is not possibleto evoke calcium-dependent release of glutamate andaspartate (22). In a study of biopsy tissue, the releaseof endogenous aspartate and glutamate in sevenAlzheimer patients was not found to be different fromthat of seven controls (31). However, the calcium-dependency of this release was not determined in Alz-heimer tissue, and experiments were carried out understatic rather than superfused conditions. Thus theresults may have been complicated by uptake processes,particularly because evidence suggests impaired energymetabolism in Alzheimer’s disease (22).
The sodium-dependent uptake of glutamate or itsanalogs provides another marker of glutamatergicnerve terminals. Uptake of D-[3H]aspartic acid hasbeen a particularly useful marker because it is a goodsubstrate that is neither metabolized nor incorporatedinto proteins. The uptake of D-[3H]aspartate has beenshown to be reduced in Alzheimer’s disease in tissuefrom the temporal, frontal, parietal, and occipital cor-tex and hippocampus in tissue obtained 9 h after deathand frozen, thawed, and subfractionated (32). Thisstudy is complicated by the possibility that synapto-somes derived from Alzheimer and control brains havedifferent cryostability and fractionation characteristics,as reduced D-[3H]aspartate uptake in Alzheimer’s dis-ease may reflect a reduced final yield of synaptosomes.However, the changes observed showed some specificitybecause no significant difference between Alzheimer’sdisease and control is observed in the caudate nucleus,putamen, and the globus pallidus. Furthermore, asimilar study has demonstrated reduced uptake of D-
[3H]aspartate in unfractionated and unfrozen tissueobtained less than 3 h after death (22).
Morphometric studies of pyramidal neurons in
Alzheimer’s disease
Quantitative measurements of the number of perikaryain the cerebral cortex have indicated that large (pre-sumably pyramidal) neurons are depleted by 23-46%in Alzheimer’s disease. This work has been confirmedand extended by counts of the number of pyramidalneurons in cortical layers III and V (1). Pyramidal cells

2750 Vol. 4 July 1990 The FASEB Journal PALMER AND GERSHON
are the major site of neurofibrillary degeneration, andtheir abundance in the cerebral cortex makes it likelythat the terminal regions of these neurons make a sub-stantial contribution to the degenerating neurites thatpartially constitute senile plaques.
Glutamate receptors in Alzheimer’s disease
NMDA receptor-binding sites for both agonist andphencyclidine-like compounds appear to be unalteredin the hippocampus and most neocortical areas of Alz-heimer’s disease (28). Studies of subregions of the hip-pocampus have indicated various results, either bothsites reduced or unaltered (28, 33). Reduced glycinemodulation of the binding of [3H]MK-801 has been de-scribed for both the frontal and temporal lobes of Alz-heimer subjects, whereas the zinc allosteric site hasbeen found to be unaffected (Table 3). Scatchard anal-ysis with both [3H]MK-801 and [3H]TCP indicates thatreduced glycine modulation in Alzheimer’s diseasereflects a change in the number of glycine binding sitesand not a change in binding affinity (34, 35). Althoughevidence suggests that the changes observed may be at-tributable to a greater proportion of subjects dying aprotracted death in the Alzheimer’s disease group thanin controls, significant differences were observed whengroups were matched for this factor (33, 34). Moreover,binding of [3H]MK-801 in the presence of both gluta-mate and glycine was found to be reduced in Alzheimertissue obtained antemortem and therefore free of theinfluence of the immediate preterminal state (35).
Quisqualic acid and kainic acid binding sites havenot been thoroughly investigated in Alzheimer’s diseaseas NMDA sites. Quisqualate-sensitive [3H]glutarnatebinding has been found to be reduced in the hippo-campus (36), whereas kainate sites have been shown tobe unaltered in the temporal, frontal, and parietal cor-tex, hippocampus, and caudate nucleus (37).
TABLE 3. Glycine and zinc modulatory sites of the NMDA receptor inAlzheimer’s disease’
[‘H]MK-801 binding in Alzheimer’sdisease as a percentn of control
Glycine-dependentbinding Zinc IC,0
Temporal cortexInferior temporal gyrosSuperior and middle temporal
gyros
54* -
52 NS
Frontal cortex
Superior frontal gyrosFrontal pole
NS -
49 NS
Parietal cortexSuperior parietal lobule NS -
‘Modified from refs 33 and 34. NS, not significant; -, notdetermined. Glycine-dependent binding of [‘H]MK-801 is defined as thedifference between binding in the presence of 30 sM glutamate and 3 Mglycine and binding in the presence of 30 gM glutamate. ‘This value hasbeen calculated from the mean values in Table 1 from ref 34.
Glutamatergic neurotransmission and the
symptomatology of Alzheimer’s disease
Some of the symptoms of Alzheimer’s disease, particu-larly aphasia, agnosia, and apraxia, are often similar tothose associated with cortical disconnection syndromes.Recent quantitative data on the distribution of senileplaques and neurofibrillary tangles further suggest thatcorticocortical projection fibers are selectively affectedwithin association areas of the cortex (25, 26). This hasled to the hypothesis that Alzheimer’s disease representsa global cortical disconnection syndrome in which eachcortical region functions in isolation. Support for thishypothesis has come from a multidisciplinary antemor-tern study of Alzheimer’s disease, in which loss of theperikarya of pyramidal neurons from layers III and Vof the midtemporal gyrus of Alzheimer’s patients wasfound to correlate significantly with an assessment ofthe severity of dementia and scores on five psychometrictests (Table 2). As pyramidal neurons probably useglutamate as a neurotransmitter and receive prominentexcitatory inputs, the cortical disconnection hypothesisof Alzheimer’s disease predicts that changes in glutamateneurons and receptors are central to the production ofthe symptomatology of Alzheimer’s disease. Cortico-hippocampal neurons and a large proportion of hippo-campal neurons are also thought to use glutamate as aneurotransmitter (8). The phenomenon of long-termpotentiation, an enduring change in synaptic efficacy,has been extensively demonstrated in the hippocampusand has been proposed as a potential candidate for theneuronal basis of memory. Evidence to implicate glu-tamatergic neurotransmission both in LTP and inlearning and memory has come from observationsthat NMDA antagonists prevent the development ofLTP and impair the performance of experimental ani-mals in tasks that require learning and memory (38).These data, together with the data indicating impair-ments of glutamatergic neurons and the NMDA recep-tor in Alzheimer’s disease, suggest that glutamatergicneurons and receptors play a central role in higher cog-nitive processing. Thus glutamatergic dysfunction wouldbe expected to make a substantial contribution to theprogressive impairments of memory, personality, andintellect that characterize Alzheimer’s disease.
IS THE NEURONAL BASIS OF ALZHEIMER’S
DISEASE CHOLINERGIC OR
GLUTAMATERGIC?
Shortcomings of the cholinergic hypothesis
Although the evidence described above presents asomewhat convincing explanation for the neuronalbasis of Alzheimer’s disease, the cholinergic hypothesishas shortcomings. 1) Dysfunction of cholinergic neu-rons can account for the presence of neurofibrillarytangles in the nucleus basalis of Meynert and probablymakes a partial contribution to the total population ofsenile plaques in the cortex. However, the cholinergichypothesis fails to take account of neurofibrillary de-generation, pyramidal cell loss, and atrophy in the

NEURONAL BASIS OF ALZHEIMER’S DISEASE 2751
cerebral cortex and thus relegates major neuropatho-logical change to a subsidiary role. 2) Cholinergicmarkers have been shown to be normal in tissues re-moved at biopsy from a small group of demented pa-tients with none of the neuropathological features ofAlzheimer’s disease (10). Similarly, a postmortem studyhas indicated that a small subset of Alzheimer’s subjectswith typical Alzheimer’s pathology has normal ChATactivity in the cerebral cortex (4); activity in the amyg-dala of these subjects was markedly reduced, suggestingthat this region, at least in a subset of patients, may beparticularly important to the clinical development ofthe disease. 3) In olivopontocerebellar atrophy there isboth neurochemical and morphometric evidence tosuggest loss of cholinergic neurons, yet this is not a de-menting disorder (28). 4) Evidence indicating pre-synaptic cholinergic dysfunction in Alzheimer’s diseaseand the emergence of the cholinergic hypothesis led toattempts to ameliorate the symptoms of Alzheimer’sdisease by cholinergic pharmacotherapy. However,
despite more than 80 published attempts, such treat-ment has failed to clearly elicit clinical benefit (39).Substantial clinical benefit has been claimed for thepotent acetylcholinesterase inhibitor tetrahydro-9-aminoacridine (40), but this finding is controversialand awaits confirmation.
Shortcomings of the glutamatergic hypothesis
In contrast to the cholinergic hypothesis, the glu-tamatergic hypothesis is consistent with the formationof neurofibrillary tangles within the perikarya of pyra-midal neurons. However, the glutamatergic hypothesiscannot directly account for neurofibrillary degenera-tion in subcortical nuclei, although as affected nuclei allproject to the cortex, it has been argued that degenera-tion of these neurons occurs in a retrograde fashion inresponse to primary cortical injury (1). Glutamatergicneurons have not been extensively investigated in de-mentia, primarily because of the uncertain reliability ofneurochemical markers, so it is not yet clear whetherglutamatergic dysfunction is a prerequisite for demen-tia or if glutamatergic dysfunction is evident in non-dementing conditions. Moreover, it is not yet known ifthe pyramidal cells lost in Alzheimer’s disease (Table 2)are indeed glutamatergic. The prospect of glutamatepharmacotherapy in the treatment of Alzheimer’s dis-ease is limited by the possibility of excitotoxic or epilep-tic side effects, and it is unclear where glutamateagonists or antagonists should be used because of thepossibility that the neurodegeneration associated with
Alzheimer’s disease occurs as a consequence of glutamate-mediated excitotoxicity (28). Despite these uncertain-ties, evidence indicating reduced glycine modulationwithin the NMDA receptor in Alzheimer’s disease(Table 3) suggests that pharmacotherapy directed atthis site may be of clinical benefit and is likely to be freeof some of the side effects associated with directly act-ing agonist and antagonists.
The neuronal basis of Alzheimer’s disease
In addition to changes in cholinergic and glutamatergicsystems, Alzheirner’s disease is associated with dysfunc-
tion of cortical afferent noradrenergic and serotonergicneurons, which probably occurs early in the diseaseprocess. Cortical interneurons that release 7-amino-butyric acid and somatostatin also appear to be affected
but probably not until a relatively late stage of the dis-ease (9). It has been suggested that dysfunction of nor-adrenergic and serotonergic neurons contribute to non-cognitive changes in behavior, such as aggression and
depression, whereas cognitive changes are most readilyexplained by dysfunction of cholinergic and gluta-matergic neurons, the major cortical afferent, and in-trinsic cortical neurons, respectively (9).
CONCLUSIONS AND FUTURE TRENDS
If dysfunction in both cholinergic and glutamatergicsystems contribute to the symptomatology of Alz-heimer’s disease, then hypotheses based on either neu-ronal system provide an inadequate explanation of theneuronal basis of dementia. Although there is substan-tial evidence to support the cholinergic hypothesis, seri-ous shortcomings are evident. Nonetheless, if the value
of a hypothesis is gauged by the amount of scientific en-deavor it stimulates, then the cholinergic hypothesis ofAlzheimer’s disease is one of the most successfulhypotheses in the history of neuroscience. The glu-tamatergic hypothesis offers an attractive, but notnecessarily mutally exclusive, alternative but it has notbeen as rigorously tested as its cholinergic counterpart.It has emerged together with morphometric studiesthat have implicated corticocortical association fibers inAlzheimer’s disease and advances with improved tech-niques to measure glutamatergic neurons in postmor-tem human brain. Further advances include the use ofglutamate (and aspartate) immunocytochemistry to ex-amine glutamatergic pyramidal neurons in Alzheimer’sdisease (20) and improved methodologies to determinethe binding of D-[3H]aspartate. If glutamatergic dys-function is a major contributor to the symptoms of Alz-heimer’s disease, then markers of glutamatergic neu-rons should correlate with measures of the severity of
dementia. An important task for future postmortemstudies is to establish whether such a relationship exists.This, together with attempts at glutamatergic pharma-cotherapy, will establish whether the glutamatergichypothesis provides an adequate explanation of the de-mentia of Alzheimer’s disease in addition to providinga powerful stimulus for future research. LI
REFERENCES
1. Mann, D. M. A. (1988) Neuropathological and neurochemicalaspect of Alzheimer’s disease. In Psychopharmacology of the AgingNervous System (Iversen, L. L., Iversen, S. D., and Snyder, S. H.,eds) pp. 1-67, Plenum, New York
2. Perry, E. K. (1986) The cholinergic hypothesis-ten years on.Br. Med. Bull. 42, 63-69
3. McGeer, E. G., Singh, E. A., and McGeer, P. L. (1987)Sodium-dependent glutamate binding in senile dementia. Neu-robiol. Aging 8, 219-223
4. Palmer, A. M., Procter, A. W., Stratmann, G. C., and Bowen,D. M. (1986) Excitatory amino acid-releasing and cholinergicneurons in Alzheimer’s disease. Neurosci. Lett. 66, 199-204

2752 Vol. 4 July 1990 The FASEB Journal PALMER AND GERSHON
5. Procter, A. W., Lowe, S. L., Palmer, A. M., Francis, P. T., Esiri,M. M., Stratmann, G. C., Najlerahim, A., Patel, A., Hunt, A.,and Bowen, D. M. (1988) Topographical distribution of neuro-chemical changes in Alzheimer’s disease. j Neurol. Sci. 84,125-140
6. Cowburn, R., Hardy, J., Roberts, P., and Briggs, R. (1988)Regional distribution of pre- and postsynaptic glutamatergicfunction in Alzheimer’s disease. Brain Res. 452, 403-407
7. Simpson, R. D. C., Royston, M. C., Deakin, J. F. W., Cross,A. J., Mann, D. M. A., and Slater, P. (1988) Regional changesin [‘H]D-aspartate and [‘H}TCP binding sites in Alzheimer’sdisease brains. Brain Res. 462, 76-82
8. McGeer, P. L., and McGeer, E. G. (1989) Amino acid neuro-transmitters. In Basic Neurochemistry (Siegel, G., Agranoff, B.,Albers, R. W., and Molinoff, P., eds) pp. 311-332, Raven, NewYork
9. Palmer, A. M., and Bowen, D. M. (1990) Neurochemical basisof dementia of the Alzheimer type: contribution of postmortem
and antemortem studies. In Biological Markers of Dementia ofAlzheimer Type: Proceedings of the St/ielsen Gamla Tjdnarinnor Sympo-sium on Aging and Aging Disorders No. 1. (Fowler, C., Carlson,L. A., Gottfries, C. G., and Winblad, B., eds) pp. 89-105,Smith-Gordon & Co. Ltd., London
10. Sims, N. R., Bowen, D. M., Allen, S. T., Smith, C. C. T.,Neary, D., Thomas, D. J., and Davison, A. N. (1983) Presynap-tic cholinergic dysfunction in patients with dementia. J. Neuro-chem. 40, 503-509
11. Bowen, D. M., Benton, J. S., Spillane, J. A., Smith, C. C. T.,and Allen, S. J. (1982) Choline acetyltransferase activity andhistopathology of frontal neocortex from biopsies of dementedpatients.]. NeuroL Sci. 57, 191-202
12. H#{246}hmann,C., Antuono, P., and Coyle, J. T. (1988) Basal fore-brain cholinergic neurons and Alzheimer’s disease. In Psycho-pharmacology of the Aging Nervous System (Iversen, L. L., Iversen,S. D., and Snyder, S. H., eds) pp. 69-106, Plenum, New York
13. Neary, D., Snowden, J. S., Mann, D. M. A., Bowen, D. M.,Sims, N. R., Northen, B., Yates, P. 0., and Davison, A. N.(1986) Alzheimer’s disease: a correlative study. j Neurol. Neuro-surg. Psychiair. 49, 229-237
14. Hagan, J. J., and Morris, R. G. M. (1988) The cholinergichypothesis of memory: a review of animal experiments. In Psy-chopharmacology of the Aging Nervous System (Iversen, L. L., Iver-sen, S. D., and Snyder, S. H., eds) pp. 237-323, Plenum, NewYork
15. Sahakian, B. J. (1988) Cholinergic drugs and human cognitive
performance. In Psychopharmacology of the Aging Nervous System(Iversen, L. L., Iversen, S. D., and Snyder, S. H., eds) pp.393-424, Plenum, New York
16. Collingridge, G. L., and Lester, R. A. (1989) Excitatory aminoacid receptors in the vertebrate central nervous system.Pharmacol. Rev. 40, 143-195
17. Palmer, A. M., Hutson, P. H., Lowe, S. L., and Bowen, D. M.(1989) Extracellular concentrations of aspartate and glutamatein rat neostriatum following chemical stimulation of frontalcortex. Exp. Brain Res. 75, 659-663.
18. White, E. L. (1989) Cortical Circuits: Synaptic Organization of theCerebral Cortex. Birkhauser, Boston
19. Kisvarday, Z. F., Martin, K. A. C., Freund, T. F., Magloczky,Z., Whitteridge, D., and Somogyi, P. (1986) Synaptic targets ofHRP-IIlled layer III pyramidal cells in the rat striate cortex.Exp. Brain Res. 64, 541-552
20. Giuffrida, R., and Rustioni, A. (1989) Glutamate and asparateimmunoreactivity in corticocortical neurons of the sensori-motor cortex of rats. Exp. Brain Res. 78, 41-46
21. Hicks, T. P., Ruwe, W. D., Veale, W. L., and Veenhuizen, J.(1985) Aspartate and glutamate as synaptic transmitters ofparallel visual cortical pathways. Exp. Brain Res. 58, 421-425
22. Procter, A. W., Palmer, A. M., Francis, P. T., Lowe, S. L.,Neary, D., Murphy, E., Doshi, R., and Bowen, D. M. (1988)Evidence of glutamatergic denervation and possible abnormal
metabolism in Alzheimer’s disease. j Neurochem. 50, 790-80223. Hyman, B. T, Van Hoesen, G. W., and Damasio, A. R. (1987)
Alzheimer’s disease: glutamate depletion in the hippocampal
perforant pathway zone. Ann. NeuroL 22, 3 7-4024. Pearce, B. R., Palmer, A. M., Bowen, D. M., Wilcock, G. K.,
Esiri, M. M., and Davison, A. N. (1984) Neurotransmitter dys-function and atrophy of the caudate nucleus in Alzheimer’s dis-ease. Neurochem. Pathol. 2, 221-232
25. Pearson, R. C. A., Esiri, M. M., Hiorns, R. W., Wilcock,G. K., and Powell, T. P. S. (1985) Anatomical correlates of thedistribution of the pathological changes in the neocortex inAlzheimer’s disease. Proc. Natl. Acad. Sci. USA 82, 4531-4534
26. Rogers, J., and Morrison, J. H. (1985) Quantitative morphol-ogy and regional laminar distributions of senile plaques in Alz-heimer’s disease. Neuroscience 5, 2801-2808
27. Danbolt, N. C., and Storm-Mathisen,J. (1986) Inhibition by Kof Na’-dependent D-aspartate uptake into brain membranesaccules. j Neurochem. 47, 825-830
28. Greenamyre, T. J., and Young, J. B. (1989) Excitatory aminoacids and Alzheimer’s disease. Neurobiol. Aging 10, 593-602.
29. Geddes, J. W., Monaghan, D. T., Cotmam, C. W., Lott, I. T.,Kim, R. C., and Chai, H. -C. (1985) Plasticity of hippocampalcircuitry in Alzheimer’s disease. Science 230, 1179-1181
30. Akiyama, H., McGeer, P. L., Itagaki, S., McGeer, E. G., andKaneko, T. (1989) Loss of glutaminase-positive cortical neuronsin Alzheimer’s disease. Neurochem. Res. 14, 353-358
31. Smith, C. C. T., Bowen, D. M., Sims, N. R., Neary, D., andDavison, A. N. (1983) Amino acid release from biopsy samplesof temporal neocortex from patients with Alzheimer’s disease.Brain Res. 264, 138-141
32. Hardy,J., Cowburn, R., Barton, A., Reynolds, C. Lofdahl, E.,O’Carroll, A. M., Wester, P., and Winblad, B. (1987) Region-specific loss of glutamate innervation in Alzheimer’s disease.Neurosci. Lett. 73, 77-80
33. Steele, J. E., Palmer, A. M., Stratmann, G. C., and Bowen,D. M. (1989) The N-methyl-D-aspartate receptor complex inAlzheimer’s disease: reduced regulation by glycine but not byzinc. Brain Res. 500, 369-373
34. Procter, A. W., Wong, E. H. F., Stratmann, G. C., Lowe, S. C.,and Bowen, D. M. (1989) Reduced glycine stimulation of[5H]MK-801 binding in Alzheimer’s disease. J. Neurochem. 53,698-704
35. Procter, A. W., Sterling, J. H., Stratmann, G. C., Cross, A. J.,and Bowen, D. M. (1989) Loss of glycine-dependent radiologicalbinding to the N-methyl-D-aspartate-phencyclidine receptorcomplex in patients with Alzheimer’s disease. Neurosci. Lett. 101,62-66
36. Greenamyre, T. J., Penney, J. B., D’Amato, C. J., and Young,A. B. (1987) Dementia of the Alzheimer type: changes in hippo-
campal L-[3H]glutamate binding. j Neurochem. 48, 543-55137. Cowburn, R. F., Hardy, J. A., Briggs, R. S., and Roberts, P. J.
(1989) Characterization, density and distribution of kainatereceptors in normal and Alzheimer’s diseased human brain.
j Neurochem. 52, 140-14738. Bliss, T. V. P., and Lynch, M. A. (1988) Long-term potentiation
of synaptic transmission in the hippocampus: properties andmechanisms. In Long-term Potentiation: from Biophysics to Behavior(Landfield, P. W., and Deadwyler, S. A., eds) pp. 3-72, Alan R.Liss, New York
39. Collerton, D. (1986) Cholinergic function and intellectualdecline in Alzheimer’s disease. Neuroscience 19, 1-28
40. Summers, W. K., Majouski, L. V., Marsh, G. M., Tachiki, K.,and Kling, A. (1986) Oral tetrahydroaminoacridine in long-term treatment of senile dementia, Alzheimer type. N Engl. jMed. 315, 1241-1245
Copyright © 2022 FDOKUMEN




















