
Current drug targets for Alzheimer's disease treatment
15
Research Overview Current Drug Targets for Alzheimer’s Disease Treatment Debomoy K. Lahiri, 1,n Martin R. Farlow, 1 Nigel H. Greig, 2 and Kumar Sambamurti 3 1 Department of Psychiatry, Institute of Psychiatric Research, Indiana University School of Medicine, Indianapolis, Indiana 2 Drug Design and Development Section, Laboratory of Neurosciences, National Institute on Aging, Baltimore, Maryland 3 Department of Neuroscience, Mayo Clinic, Jacksonville, Florida Strategy, Management and Health Policy Venture Capital Enabling Technology Preclinical Research Preclinical Development Toxicology, Formulation Drug Delivery, Pharmacokinetics Clinical Development Phases I-III Regulatory, Quality, Manufacturing Postmarketing Phase IV Abstract Alzheimer’s disease (AD), the most common form of dementia among the elderly, is a progressive, degenerative disorder of the brain with a loss of memory and cognition. A defining characteristic of AD is the deposition of amyloid fibrils and neurofibrillary tangles in the brain of afflicted individuals. Biochemically, they are mainly composed of b-amyloid protein (Ab) and phosphorylated tau proteins, respectively. There is also a loss of the presynaptic markers of the cholinergic system, such as acetylcholine, in the brain areas related to memory and learning. The biochemical pathways leading to AD are presently unknown and are a subject of intensive study with current theories favoring a hypothesis where Ab aggregates to toxic forms that induce tau phosphorylation and aggregation. It is believed that this ultimately leads to dysfunction and death of cholinergic neurons, and compensation for this loss had been the primary focus of first generation therapeutic agents. The amyloid and tau hypotheses have lead to a focus on amyloid and tau as therapeutic targets. The current therapeutic goals are to reduce amyloid levels, prevention of amyloid aggregation/toxicity and tau phosphorylation/aggregation. AD has a heterogeneous etiology with a large percentage termed sporadic AD arising from unknown causes and a smaller fraction of early onset familial AD (FAD) caused by mutations in several genes, such as the b- amyloid precursor protein (APP) and presenilins (PS1, PS2). Other genes, such as apolipoprotein E (APOE), are considered to be risk factors for AD. Several proteins, such as APP, APOE, BACE (b-amyloid cleaving enzyme), PS1/2, secretases, and tau play important roles in the pathology of AD. Therefore, attempts are being made to develop new inhibitors for BACE, PS-1 and g-secretase for treatment of AD. There is also a significant advancement in understanding the function of cholinesterase (ChE) in the brain and the use of ChE inhibitors in AD. The mechanism of a new generation of acetyl- and butyrylChE inhibitors is being studied and tested in human clinical trials for AD. Other strategies, such as vaccination, anti-inflammatory agents, cholesterol-lowering agents, anti-oxidants and hormone therapy, are also being studied for treating or slowing the progression of AD. Developments of early diagnostic tools based on quantitative biochemical markers will be useful to better follow the course of the disease and to evaluate different therapeutic strategies. In the present review, we attempt to critically examine recent trends in AD research from neurochemical to clinical areas. We analyze various neurobiological mechanisms that provide the basis of new targets for AD drug development. These current research efforts should lead to a deeper understanding of the pathobiochemical processes that occur in the AD brain to effectively diagnose and prevent their occurrence. Drug Dev. Res. 56:267–281, 2002. c 2002 Wiley-Liss, Inc. Key words: Alzheimer’s disease; amyloid; anticholinesterases; APP gene; cholesterol; cholinergic agents; cholinomi- metic drugs; donepezil; estrogen; exelon; galantamine; microtubule-associated protein; NSAIDs; oxidative damage; phenserine; vaccine DDR n Correspondence to: D.K. Lahiri, Indiana University School of Medicine, Institute of Psychiatric Research, Rm. PR-313, 791 Union Drive, Indianapolis, IN 46202-4887. E-mail: [email protected] Published online in Wiley InterScience (www.interscience. wiley.com) DOI: 10.1002/ddr.10081 DRUG DEVELOPMENT RESEARCH 56:267–281 (2002) c 2002 Wiley-Liss, Inc.
Transcript of Current drug targets for Alzheimer's disease treatment

Research Overview
Current Drug Targets for Alzheimer’s Disease TreatmentDebomoy K. Lahiri,1,n Martin R. Farlow,1 Nigel H. Greig,2 and Kumar Sambamurti3
1Department of Psychiatry, Institute of Psychiatric Research,Indiana University School of Medicine, Indianapolis, Indiana
2Drug Design and Development Section, Laboratory of Neurosciences,National Institute on Aging, Baltimore, Maryland
3Department of Neuroscience, Mayo Clinic, Jacksonville, Florida
Strategy, Management and Health Policy
Venture Capital
Enabling
Technology
Preclinical
Research
Preclinical Development
Toxicology, Formulation
Drug Delivery,
Pharmacokinetics
Clinical Development
Phases I-III
Regulatory, Quality,
Manufacturing
Postmarketing
Phase IV
Abstract Alzheimer’s disease (AD), the most common form of dementia among the elderly, is aprogressive, degenerative disorder of the brain with a loss of memory and cognition. A definingcharacteristic of AD is the deposition of amyloid fibrils and neurofibrillary tangles in the brain of afflictedindividuals. Biochemically, they are mainly composed of b-amyloid protein (Ab) and phosphorylated tauproteins, respectively. There is also a loss of the presynaptic markers of the cholinergic system, such asacetylcholine, in the brain areas related to memory and learning. The biochemical pathways leading to ADare presently unknown and are a subject of intensive study with current theories favoring a hypothesiswhere Ab aggregates to toxic forms that induce tau phosphorylation and aggregation. It is believed that thisultimately leads to dysfunction and death of cholinergic neurons, and compensation for this loss had beenthe primary focus of first generation therapeutic agents. The amyloid and tau hypotheses have lead to afocus on amyloid and tau as therapeutic targets. The current therapeutic goals are to reduce amyloidlevels, prevention of amyloid aggregation/toxicity and tau phosphorylation/aggregation. AD has aheterogeneous etiology with a large percentage termed sporadic AD arising from unknown causes and asmaller fraction of early onset familial AD (FAD) caused by mutations in several genes, such as the b-amyloid precursor protein (APP) and presenilins (PS1, PS2). Other genes, such as apolipoprotein E (APOE),are considered to be risk factors for AD. Several proteins, such as APP, APOE, BACE (b-amyloid cleavingenzyme), PS1/2, secretases, and tau play important roles in the pathology of AD. Therefore, attempts arebeing made to develop new inhibitors for BACE, PS-1 and g-secretase for treatment of AD. There is also asignificant advancement in understanding the function of cholinesterase (ChE) in the brain and the use ofChE inhibitors in AD. The mechanism of a new generation of acetyl- and butyrylChE inhibitors is beingstudied and tested in human clinical trials for AD. Other strategies, such as vaccination, anti-inflammatoryagents, cholesterol-lowering agents, anti-oxidants and hormone therapy, are also being studied for treatingor slowing the progression of AD. Developments of early diagnostic tools based on quantitativebiochemical markers will be useful to better follow the course of the disease and to evaluate differenttherapeutic strategies. In the present review, we attempt to critically examine recent trends in AD researchfrom neurochemical to clinical areas. We analyze various neurobiological mechanisms that provide thebasis of new targets for AD drug development. These current research efforts should lead to a deeperunderstanding of the pathobiochemical processes that occur in the AD brain to effectively diagnose andprevent their occurrence. Drug Dev. Res. 56:267–281, 2002. �c 2002 Wiley-Liss, Inc.
Key words: Alzheimer’s disease; amyloid; anticholinesterases; APP gene; cholesterol; cholinergic agents; cholinomi-metic drugs; donepezil; estrogen; exelon; galantamine; microtubule-associated protein; NSAIDs; oxidative damage;phenserine; vaccine
DDR
nCorrespondence to: D.K. Lahiri, Indiana University Schoolof Medicine, Institute of Psychiatric Research, Rm. PR-313, 791Union Drive, Indianapolis, IN 46202-4887.E-mail: [email protected]
Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/ddr.10081
DRUG DEVELOPMENT RESEARCH 56:267–281 (2002)
�c 2002 Wiley-Liss, Inc.

ALZHEIMER’S DISEASE:SIGNS, SYMPTOMS, AND CAUSE
Alzheimer’s disease (AD) is a progressive, neuro-degenerative disease of the brain, and is the mostcommon form of dementia among the elderly popula-tion. It has recently been found that patients withprogressive amnesia without impairment in activity ofdaily living (mild cognitive impairment, MCI) canprogress to AD at a rate of about 12% per year. AD ischaracterized by more than just memory loss; it alsoresults in other cognitive and behavioral symptoms thatprogressively impair function in activities of daily living.The cognitive symptoms include memory loss, disor-ientation, confusion, problems with reasoning andthinking. Behavioral symptoms include agitation, anxi-ety, delusions, depression, hallucinations, insomnia,and wandering.
The major hallmarks of AD are clinically general-ized progressive dementia and, neuropathologically, thepresence of two characteristic lesions: the extraneur-onal amyloid plaque and the intraneuronal neurofi-brillary tangle in the post-mortem brain [Burns et al.,1970; Selkoe, 2000]. Although the substantial advancesmade over the years have identified amyloid plaques asa potential cause of AD, the sequence of events thatlead to neuronal loss or dysfunction and dementia arestill unclear. An understanding of these underlyingmechanisms will certainly form the basis for devisingbetter strategies for diagnosis, prevention, and treat-ment. During the last couple of years, much has beenlearned about factors that may contribute to the onsetof AD [De Strooper and Annaert, 2000; Selkoe, 2000].For example, the recent discovery of a previouslyunknown lesion that is characteristic of AD hasidentified a third component that may help us tofurther understand the disease process and discovernovel therapeutic targets. This lesion, called the AMYplaque, most likely plays a role in the onset andprogression of AD [Lippa et al., 2000].
AD appears to have a heterogeneous etiology andcan be caused by mutations in the b-amyloid proteinprecursor (APP) gene on chromosome 21, the pre-senilin 1 (PS1) gene on chromosome 14, and presenilin2 (PS2) gene on chromosome 1 [Tanzi and Bertram,2001]. However, these mutations account for only asmall percentage of AD patients with an early age ofonset and a family history of the disease. The vastmajority of AD patients do not have a family history ofthe disease and do not show mutations in these genes.Studies suggest that in the typical late-onset AD family,there are genetic factors that may increase the level ofamyloid deposition. However, it is important to notethat this disease occurs with increasing frequency with
aging in the general population, even in the absence ofa family history.
ALZHEIMER’S DISEASE: PREVALENCE ANDECONOMIC COSTS
Alzheimer’s disease is an age-dependent disorderand the projected increase in the population over 65 fromB14% to B25% is expected to not only increase theaffected population but also place the burden of care on asmaller population of young adults [Hebert et al., 2001].Alzheimer’s disease affects approximately 4 millionAmericans. It is projected that 14 million Americansand 22 million individuals worldwide will have AD by themiddle of the next century unless preventive or curativemedications are found. Epidemiological surveys show awide variation (4–12%) in the incidence of AD inAmericans over 65, presumably due to differences inthe diagnostic methodology, which highlights the need forconsistent diagnostic strategies and criteria. Nevertheless,the prevalence of AD increases exponentially with agewith estimates showing that it increases from 10% at 65years to nearly 50% at 85 years. A person with AD livesan average of 8 years, but some patients live as many as20 years or more from the onset of symptoms. The cost ofAD has been estimated at $100 billion a year in theUnited States, costing American businesses more than$33 billion annually, $26 billion to lost productivity ofcaregivers, plus $7 billion related to costs for health andlong-term care (source: Alzheimer’s Association, Chica-go). Diagnostic testing for AD is only expected tocontribute marginally to this cost. The development ofmore reliable and sensitive methods may likely improvecare and better target therapy in the future. Thus, betterdiagnosis may allow more accurately targeted futuretherapies and potentially, by delaying or preventingdisability, may reduce the costs associated with the illness.
CURRENT LINES OF RESEARCH AND SCOPE OF THEPRESENT REVIEW
Research in AD is rapidly expanding and itcurrently encompasses various cellular, molecular,genetic, clinical, and therapeutic aspects. Reviewingall these diverse areas is beyond the scope of thepresent work. However, we will briefly mention thesalient features of the definitive review work of otherinvestigators in different AD fields. The moleculargenetics of AD [St. George-Hyslop, 2000; Tanzi andBertram, 2001] and its relationship to other primaryneurodegenerative disease have recently been re-viewed [Hardy, 2001]. There are also recent reviewsof the role of key protein molecules that are believed toparticipate in AD pathogenesis. For example, the cellbiology of AD, particularly the roles of secretases[Walter et al., 2001; Sambamurti et al., 2002a,b;
268 LAHIRI ET AL.

Sisodia, 2002], presenilin and notch [Fraser et al., 2001;Selkoe, 2001] have also been reviewed (Table 1).Similarly, the role of tau gene mutations and neurode-generation on AD pathology has recently beensummarized [Goedert and Spillantini, 2001]. In addi-tion to APP and PS-1, there is a recent spotlight onBACE as a target for treatment in AD [Dingwall, 2001].Lately, APP has been proposed to link kinesin-I to adifferent, also unknown, class of axonal vesicles. Thisfinding of a possible functional interaction betweenkinesin-I and APP may implicate kinesin-I basedtransport in the development of AD [Goldstein, 2001].
THERAPEUTIC STRATEGIES
Regarding therapeutic strategies, several recentreviews are worth mentioning. The immunotherapeuticstrategies for prevention and treatment of AD [Solomon,2000], and specifically immunotherapy with Ab for AD[Schenk, 2001] are examples of new frontiers. Nasalvaccination with Ab peptide for the treatment of AD isalso under study [Lemere et al., 2001]. Recent studies ofthe inflammatory processes in the brain have led topreliminary work suggesting anti-inflammatory agents,such as ibuprofen, may treat or slow the progression ofthe disease. Inflammatory drug prospects for AD [DeStrooper and Konig, 2001] and effects of estrogen on thebrain [Friedrich, 2002] have been reviewed. Celastrol,which is a potent antioxidant and anti-inflammatory drug,has also been studied as a possible treatment for AD[Allison et al., 2001]. Newer technologies, such as theDNA microarray technique to study a gene expressionprofile of AD [Loring et al., 2001; Pasinetti et al., 2001],proteomics to analyze the protein profiling of AD braintissues, and transgenic mouse models of AD [Bales et al.,1999; Janus and Westaway, 2001; Price et al., 1998], mayyield clues to the pathobiochemical processes of thedisease, which may generate novel therapies.
THEORIES OF AD
Alternative theories about AD, such as consider-ing the AD process as similar to cancer due to a loss ofcell-cycle control [Herrup and Yang, 2001] or viewing
AD as a result of a dysfunctional signaling pathwaymediated by APP [Neve et al., 2001], have also beenproposed. Other approaches, such as nutritional factors[Reynish et al., 2001] and genetic and environmentalfactors in AD [Tol et al., 1999] are also being studied.In addition, there are recent reviews of the roles of glialcells [Van Eldik, 2001], CD40 signaling [Town et al.,2001], neuronal ERK, JNK/SAPK, and p38 pathways[Zhu et al., 2001] in AD. Roles for oxidation of Abpeptide [Head et al., 2001], and of oxidative damage[Butterfield et al., 2001] in AD have also beendocumented. Indeed, our current understanding ofthe role of oxidative stress in AD has resulted indeveloping the beneficial use of antioxidants, such asvitamin E, in preventing or delaying disease onset.Depressive symptoms [Purandare et al., 2001] andsleep disturbances [Vitiello and Borson, 2001] inpatients with AD have been investigated andcharacterized. The striking association of AD withvascular dementia and the cardiovascular illnesses hasbeen reviewed [Jagust, 2001], and has led to coining ofthe popular phrase, ‘‘what is bad for the heart is bad forthe mind’’ [Marx, 2001].
Many other lines of ongoing research may alsolead to a deeper understanding of the processes thatoccur in the AD brain. Promising areas include: (1)neurotransmitter deficiencies and dysfunction in braincell communication, (2) beta amyloid protein andsenile plaques and their role in the disease process, (3)tau protein and neurofibrillary tangles and their role inthe disease process, (4) the role of estrogen in thebrain, (5) inflammation and its effect on brain cellactivity, (6) oxidative stress and its effect on brain cellprocess, and (7) genetic factors related to onset of thedisease (source: Alzheimer’s Association, Chicago). Wewill briefly review the current state of knowledge inAlzheimer’s research, and the potential basis for newdiagnostic and treatment strategies for AD. Thepresent review will focus mainly on advances relatedto testing and development of three current hypothesesof AD, ‘‘amyloid,’’ ‘‘tangles,’’ and ‘‘cholinergic,’’ andhow they lead to the development of new potentialdrug targets for AD treatment.
GENETICS OF ALZHEIMER’S DISEASE
Alzheimer’s disease is believed to result from aseries of steps in pathogenic pathways leading toamyloid deposition and neurodegeneration in key areasof the brain involved in cognition and memory[Sambamurti et al., 2002a,b; Shastry, 1998]. Theemerging picture is that AD is a genetically complex,heterogeneous disorder. Mutations and or polymorph-isms in several genes located in at least four differentchromosomes (1, 14, 19, 21) are involved in AD
TABLE 1. Selected Genes Implicated in Alzheimer’s Disease
Gene Chromosome Onset of AD
APP 21q21 Early (B50s)APOE 19q13 Late (E4 earlier than E3)S182/PS1 14q24 Early (B40s and 50s)STM2/PS2 1q31-42 Early (B50s)a-2 macroglobulin 12 Late-onsetIDE (Insulindegrading enzyme)
10 ? Late-onset AD
UPA 10 (gene unknown) ? Late-onset AD
DRUG TARGETS FOR ALZHEIMER’S DISEASE 269

[St George-Hyslop, 2000; Tanzi and Bertram, 2001](Table 1). Besides APP, other gene products are knownto be involved in AD. Recent studies have identifiedpoint mutations in at least seven genes that contribute toor cause the disease. Mutations in three of these genes,APP on chromosome 21, PS1 on chromosome 14, PS2on chromosome 1, are dominant and lead to AD withvirtually 100% penetrance, while inheritance of certainalleles of the APOE gene (e4) strongly increases the riskfor developing AD at an earlier age. There are recentreports of (1) a susceptibility locus for AD onchromosome 10 [Myers et al., 2000] and (2) a geneticlinkage of AD to chromosome 10q [Bertram et al.,2000]. A linkage of plasma Ab42 to a quantitative locuson chromosome 10 in a late onset AD pedigree has alsobeen shown [Ertekin-Taner et al., 2000] (Table 1).
RISK FACTORS FOR AD
Many risk factors are under investigation forassociation with AD. For example, certain genes makesome families vulnerable, head injuries may increaserisk, and high blood pressure is a new suspect [Kalaria,2001; Mark, 2001]. But the biggest risk for AD is age:cases double with every 5 years as patients age between65 and 85. Up to now, there are several risk factors thatare known to lead to an earlier onset of AD. One ofthese is, in some rare familial form, a mutation in theAPP gene, the second is an additional copy of this genein individuals with Down’s syndrome, and the third is amutation in a gene on chromosome 14. However, themechanism by which these genetic alterations influ-ence beta-amyloid formation remains to be deter-mined. Additionally, the E4 allele of APOE constitutesa major susceptibility factor for the development of thefamilial and sporadic forms of late-onset AD. As only afew cases of AD can be explained in this way and sincethe prevalence of AD exceeds 20% among people over80 years of age, still other risk factors must have toexist. As an example, the transcriptional control of theAPP gene has not yet been fully explored.
ALZHEIMER’S DISEASE: NEUROPATHOLOGY ANDAFFECTED PATHWAYS
Alzheimer’s disease is characterized by selectiveneuronal cell death, the presence of extracellularamyloid deposits in the core of neuritic plaques andthe formation of intraneuronal neurofibrillary tangles inthe brain of afflicted individuals [Selkoe, 2001; Terry,1998]. Neurochemically, these deficits are associatedwith dramatic losses of cortically projecting cholinergicneurons and by a reduction in the presynaptic markersof the cholinergic system, particularly in the areas ofthe brain related to memory and learning [Bartus et al.,1982; Davies and Maloney, 1976].
AMYLOID HYPOTHESIS
The major component of the amyloid plaque coreis the pathologically deposited amyloid-beta-peptide(Ab), which is derived from APP [Younkin, 1998]. Ab, aself-aggregating peptide of 39–43 residues, is synthe-sized as part of the larger 110–120 kDa APP, which is atype I integral membrane glycoprotein with a large N-terminal extracellular domain, a single transmembranedomain and a short cytoplasmic tail. The Ab sequencespans portions of the extracellular and transmembranedomains of APP. The amyloid plaque is also seen in asubset of cognitively normal aged individuals and isbelieved to precede other lesions during the pathogen-esis of AD.
The major evidence linking AD neuropathologywith APP and/or its Ab-containing derivatives werefindings that (1) virtually all individuals carrying anextra copy of chromosome 21, which contains the APPgene, show an AD-like neurodegeneration as early asthe middle of their third decade (trisomy 21; Downsyndrome), (2) specific point mutations in the APPgene cause some forms of familial AD (FAD), (3)specific point mutations in the presenilin genes (PS1and PS2), which cause some forms of FAD, also showalterations in APP processing to secrete higher levels ofthe longer Ab42 peptide, and (4) a clinical correlationbetween elevated levels of amyloid b-peptide in thebrain and cognitive decline has recently been reported[Naslund et al., 2000].
The most common hypothesis [Selkoe, 2000] thatinvokes the participation of APP in the neuronal celldeath in AD is the amyloid hypothesis, whichpostulates that plaque amyloid depositions or partiallyaggregated soluble Ab trigger a neurotoxic cascade,thereby causing neurodegeneration and AD. Thistheory is based on studies suggesting that Ab is toxicto neurons and on the measurements of increased Abrelease by transfected cell lines expressing FAD mutantproteins. There is a support of the amyloid hypothesisfrom a study showing a correlation between memorydeficits, Ab elevation, and amyloid plaques in trans-genic mice [Hsiao et al., 1996].
MODIFIED VERSION OF THE AMYLOIDHYPOTHESIS
A modified version of the amyloid hypothesispostulates that the primary contributor to the etiologyof AD lies within the cytoplasmic domain of APP [Neveet al., 2001]. This has also been used to explain theneurotoxicity of the carboxyl-terminal 99-amino acidfragment of the APP (APP-C100), which includes the42-amino acid Ab peptide and 57 adjacent amino acidsin the carboxyl-terminus of APP. The mechanism
270 LAHIRI ET AL.

behind the amyloidogenic and the neurotoxic propertyof APP-100 is not known [Yankner et al., 1990].However, recently a model has been suggested inwhich intracellular amyloidogenic fragments, such asAPP-C100, kill neurons ‘‘from inside,’’ in contrast tothe popular hypothesis that extracellular Ab causesneurodegeneration ‘‘from outside.’’ APP-C100 is anormal metabolic product of APP in the human brain.More recently, Bredessen and coworkers showed that a31-residue C-terminal fragment was generated bycaspase cleavage of APP within its cytoplasmic domainin cells undergoing apoptosis. Expression of this 31-residue fragment was sufficient to induce apoptosis.Deletion of the 31 residues from APP-C100 removedits neurotoxicity suggesting that this region maymediate toxicity. The proteolysis of APP to Ab40 andAb42 should also yield a cognate C-terminal fragment(CTFg) of 59 and 57 residues, respectively. Allconditions that increase production of Ab42 shouldtherefore automatically increase CTFg57. Thus, theobserved high correlation between AD and Ab42 levelsshould naturally extend to CTFg57 [Pinnnix et al.,2001; Gao and Pimplikar, 2001].
TANGLE HYPOTHESIS
The second major lesion characteristic of AD isthe intracellular deposition of the microtubule-bindingprotein, tau, in the form of neurofibrillary tangles(NFTs) [Goedert and Spillantini, 2001]. Reportssuggest that the load of this lesion may be more closelylinked to the dementia characteristic of AD thanamyloid plaque burden [Terry, 1996]. The tau modelsuggests that the creation of the NFTs is the mostimportant characteristic of AD and that the density ofNFTs correlates positively with disease severity.According to the tau hypothesis, structural modificationof tau such as hyperphosphorylation and aggregationinterferes with tau function leading to the neuronaldysfunction that may cause AD. In support of thishypothesis, abnormally phosphorylated tau has beenobserved in the CSF of AD patients at a very earlystage. Furthermore, mutations in tau have been foundthat do lead to dementia and neurofibrillary tangleformation [Spillantini et al., 1997]. However, it isimportant to note that these mutations do not lead toamyloid deposition characteristic of AD. Recently aunified approach of ‘‘tau’’ and ‘‘beta-amyloid’’ pathwayshas been proposed [Lee, 2001] based on two recentstudies. First, a recent report has suggested that theformation of NFTs in P301l tau transgenic mice isinduced by Ab42 fibrils [Gotz et al., 2001], and thesecond report has observed enhanced neurofibrillarydegeneration in transgenic mice expressing mutant tauand APP [Lewis et al., 2001].
CHOLINERGIC HYPOTHESIS
In AD, the severe loss of cholinergic neurons inthe nucleus basalis and associated areas that form thecholinergic forebrain area, and their projections to thecerebral cortices are marked with decreased levels ofacetylcholine and its rate-limiting synthetic enzyme,choline acetyltransferase, in the cortex [Bartus et al.,1982]. There is also a matching reduction in the level ofthe enzyme, acetylcholinesterase, and in particular theG4 form [Atack et al., 1986], which is responsible forterminating the physiological role of acetylcholine atcholinergic synapses. The reduction of cholinergicactivity in the central nervous system (CNS) of ADpatients correlates with their deterioration in scores ondementia rating scales. Coincidental with thesechanges, a rise in the level of the sister enzyme,butyrylcholinesterase, occurs. Butyrylcholinesterasebares some 65% homology to acetylcholinesterase,likewise metabolizes acetylcholine, but bares a differ-ent topology. It is predominantly localized to glial cells,which increase during AD progression, and likelyfunctions to hydrolyze excess acetylcholine in thehealthy brain. The change in the normal relationshipbetween acetylcholinesterase and butyrylcholinester-ase, from an abundance ratio of 0.3 to as high as 11 insome brain areas as AD develops, undoubtedly resultsin a mismatching between acetylcholine release and itsoptimal metabolism that likely contributes to choliner-gic dysfunction [Greig et al., 2000b]. In addition, arecent study has demonstrated that some 10 to 15% ofcholinergic neurons in the hippocampus and amygdalaof healthy human brain have butyrylcholinesterase,rather than acetylcholinesterase, at the synapse as theirmetabolizing enzyme [Darvesh et al., 1998]. One can,therefore, hypothesize that specific neuronal pathwaysmay function via butyrylcholinesterase, and thisprompted the recent development of selective rever-sible agents to inhibit butyrlcholinesterase to both aug-ment these pathways and to normalize the butyryl vs.acetylcholinesterase ratio in the AD brain [Yu et al.,1999; 2001].
All these findings, along with the known role ofcholinergic neurotransmission in memory processingand storage, led to the hypothesis that cholinergicaugmentation might improve cognition in AD, via theamplification of acetylcholine’s action through inhibi-tion of its metabolizing enzymes, and by the use ofdirect agonists, both muscarinic and nicotinic [Giaco-bini, 2000]. Currently, cholinesterase inhibition is themost effective, widely studied, and developed approachfor treating the symptoms of AD [Becker et al., 2001;Imbimbo, 2001]. In this regard, four currentlyadministered drugs for AD, tacrine, donepezil, riva-
DRUG TARGETS FOR ALZHEIMER’S DISEASE 271

stigmine, and galantamine have been approved by U.S.Food and Drug Administration (FDA) for prescriptionuse, and belong to the drug category of cholinesteraseinhibitors (Table 2). All are centrally active and havebeen shown to improve memory and cognition in somepatients with mild to moderate AD. Their effectsbecome more apparent after several weeks of therapyand, interestingly, although all are members of thesame drug class, they vary from one another in someunexpected ways. For instance, their adverse effectprofiles differ; tacrine can cause hepatic dysfunction,donepezil diarrhea, and rivastigmine vomiting. Thisdissimilarity likely derives from their divergent chemi-cal structures and hence different binding sites withinacetyl- and butyrylcholinesterase, and different pharma-cokinetics. Resulting from this, donepezil and galanta-mine possess selectivity for the acetyl form ofcholinesterase, whereas both tacrine and rivastigmineco-inhibit both acetyl- and butyrylcholinesterase.Furthermore, likely due to their mechanisms of bindingand long half-lives, the former two agents graduallyinduce up-regulation of their target, acetylcholinester-ase, whereas the latter do not, and these as well as otherdifferences plausibly account for the observation thatpatients not benefiting from one agent may benefit fromanother, although all are of the same class.
The relationship between the cholinergic neuro-nal loss and the causative amyloid trigger is a majorarea that has been under intensive research. In thisregard, several recent studies using cell culture andanimal models have shed light onto the effects ofanticholinesterase drugs on levels of amyloid proteins[Haroutunian et al., 1997; Lahiri et al., 2000a, Shawet al., 2001]. Specific agents possess amyloid loweringactions as a consequence of their cholinergic as well asnon-classical, non-cholinergic activities [Shaw et al.,2001]. This overlap in actions of particular agents maybe critical in light of the extensive co-localizationbetween the G1 forms of acetyl- and butyrylcholines-terase and amyloid plaques, which correlate withplaque load and disease progression [Arendt et al.,1992]. Indeed, there is a co-localization of butyrylcho-linesterase and all of the pathological hallmarksassociated with AD pathology; amyloid plaques, NFTs,and dystrophic neurons [Guillozet et al., 1997;
Mesulam, 2000; Moran et al., 1993]. The reasonsunderpinning such co-localization have yet to beelucidated, but may relate to a host of non-cholinergicactions associated with acetyl- and butyrylcholinester-ase. For example, both enzymes are known to play arole in cell proliferation and differentiation in embryo-nic brain as well as to bear a structural similarity toadhesion molecules (e.g., neurotactin, neuroligin, andgliotactin) that possess trophic and regenerative func-tions [Snow et al., 1988; Stropa et al., 1990]. Inaddition, butyrylcholinesterase has been reported tocleave substrates other than choline esters, and likelyhas amidase and protease activities [Small et al., 1996;Greenfield, 1996]. Unfortunately, the co-existence ofacetyl and butyrylcholinesterase with Ab peptide mayamplify the toxicity associated with the latter [Barber etal., 1996] to potentially cause a spiraling of deleteriousevents within the brain. Whether or not cholinesteraseinhibitors can block the interaction between theenzymes and Ab peptide remains to be elucidated,and likely will depend on the commonality of bindingsites involved in the enzyme/drug and enzyme/peptideinteractions.
CURRENT ALZHEIMER DRUGS BASED ON THECHOLINERGIC HYPOTHESIS:
ANTICHOLINESTERASE DRUGS
As described, the four currently available drugsfor treating AD subjects in the United States belong tothe same drug category, cholinesterase inhibitors(Table 2). All have been approved by the FDA toprimarily treat the symptoms of AD, and include:tacrine (Cognexs), available by prescription since1993; donepezil (Aricepts), available since 1996;rivastigmine (Exelon), available since 2000, and galan-tamine (Reminyls), approved in 2001. All work byincreasing the brain’s supply of acetylcholine, which, asdescribed, is deficient in AD. They thus temporarilytreat the cognitive loss to improve the quality of life.However, none cure AD, nor do they halt diseaseprogression, although particular ones may reduce therate of progression via some of the mechanismsdescribed above. Interestingly, despite being from thesame class, the agents differ in a number of respects.Differences in their adverse effect profiles, targets, and
TABLE 2. FDA Approved Drug for Alzheimer’s Disease
Drug Marketing time Company Type
Tacrine Cognex Park-Davis Acetylcholinesterase inhibitorDonepezil Aricept Eisai Acetylcholinesterase inhibitorRivastigmine Exelon Novartis Acetylcholinesterase inhibitorGalantamine Reminyl Janssen Acetylcholinesterase inhibitor
272 LAHIRI ET AL.

regulation [Nordberg et al., 2001] potentially allowsome ability for switching between the agents to findthe one with best activity in specific individuals. All areapproved and effective for treatment of mild tomoderate AD and are currently being assessed insubjects with advanced disease as well as with MCI.
GENERAL FACTS OF THE DRUGS ANDAD MARKET DYNAMICS
Currently, there is no known way to predictwhether one will benefit from these drugs. Because ofthis uncertainty, it is important to take into account thepossible results of treatment including the potentialbenefits, risks, and costs associated with their use.These drugs are currently the only ones available byprescription for the treatment of AD, but several otherdrugs are under investigation.
Some general facts about tacrine: it is adminis-tered four times a day, co-inhibits both acetyl- andbutyrylcholinesterase and its most common side effectsare changes in blood test indicators of liver function,especially elevation of the enzyme, transaminase.Hence, liver function is monitored every 2 weeksduring titration in individuals on tacrine. Indeed,tacrine’s high incidence of hepatotoxicity and theavailability of other anticholinesterases that lack thisadverse action have all but removed the agent from themarket place. Pertaining to donepezil: it is available in5- or 10-mg tablets. It is usually administered oncedaily, at bedtime, owing to its long pharmacokinetic andpharmacodynamic half-life. It is a selective inhibitor ofacetylcholinesterase and, to date, individuals with ADoften respond well to donepezil, showing improvementin cognition, general function, and behavior, withgenerally few serious side effects. Its common sideeffect is diarrhea, and the drug has thus far occupiedthe most dominant position in AD market share (64%)(Table 3). However, more recently FDA-approveddrugs are gradually eroding this position (Table 3).Regarding rivastigmine: it is supplied in capsulestrengths of 1.5, 3.0, 4.5, and 6.0 mg, requires agradual dose escalation, and, in three separate 6-monthpivotal trials, proved effective in slightly more than ahalf of treated individuals. The most common sideeffects are nausea and vomiting, with a corresponding
loss of appetite, fatigue, and weight loss. In most cases,these adverse effects are temporary, decline withcontinuing treatment, and are less common with slowerdose escalation schedules (source: Alzheimer’s Associa-tion, Chicago). Rivastigmine co-inhibits both acetyl-and butyrylcholinesterase, and has a selectivity for theG1 vs. G4 form of the enzyme [Enz et al., 1993]. Unlikethe other approved agents, it is not subject to hepaticmetabolism, and hence lacks the potential of adversedrug interactions with a number of agents that arecommonly prescribed to the elderly [Grossman et al.,2000]. Its current market share is 24% (Table 3).Finally, there is galantamine, which is available in 4-, 8-,12-mg capsules. It is given twice/day and 16 mg/day ina therapeutic dose with the option to increase to 24mg/day. In a recent large trial, treated patients, onaverage, had little progression in cognitive decline foralmost one year. It has a low selectivity for acetyl- vs.butyrylcholinesterase and its most common side effectsare nausea and vomiting during titration, which areusually self-limited and abate with continued therapy.Unlike the other approved agents, however, it possessesactions to modulate nicotinic receptors.
CURRENT DRUGS UNDER CLINICAL TRIALS FORTHE TREATMENT OF ALZHEIMER’S DISEASE
In addition to these large-scale clinical drug trialsas mentioned in Table 3, over two dozen othercompounds are under investigation for the treatmentof AD. More information concerning different clinicaldrug trials can be obtained from the web site of theNational Institute on Aging, National Institutes ofHealth, and the Alzheimer’s Association, Chicago. The
TABLE 4. Drugs Under Clinical Trial for Alzheimer’s Disease
Drug Status Company Type
Phenserine Phase II (USA) Axonyx Acetylcholinesterase inhibitorAIT-082 Phase III (Europe) NeoTherapeutics Neutrophic factorsMemantine Phase II (USA) Forest Pharmaceuticals NMDA receptorsAN-1792 (AD vaccine) Phase I (USA) Elan Corporation Amyloid neutralizing property
TABLE 3. AD Market Dynamicsn
Population/market share 2002 (millions)
US population 65–85 yrs old 30.6US population 85+yrs old 4.5US Alzheimer population 4.3Worldwide Alzheimer population 15.7Aricept market share 64%Exelon market share 24%Reminyl market share 12%Cognex market share o1%
nSource: Lexis-Nexis, Inc.
DRUG TARGETS FOR ALZHEIMER’S DISEASE 273

drugs listed in Table 4 are in varying phases of drugassessment; some are in preclinical testing, while othersare in Phases I, II, and III clinical trials of the drugdevelopment process. These drugs can broadly begrouped into 3 or 4 groups. The first includes agents,such as phenserine, that are third-generation anticholinesterases. The second group includes com-pounds, such as AIT-082 and propentophylline, thatprotect neurons against damage by virtue of theirneurotrophic action. The third includes agents thatshow amyloid-modifying properties due to their actionon the APP processing enzymes, such as inhibiting thebeta and gamma-secretases. The final group representsa ‘‘grab bag’’ of compounds that possess specific actionagainst other enzymes and targets involved in thedisease course. In addition, several other targets, whichare based on APP pathway, APOE genetics, and growthfactor-mediated repair, are currently being developedby different companies for AD treatment (Table 5).
An exciting new development is the finding byElan pharmaceuticals that vaccination with Ab pre-vents and or reverses deposition of this protein inamyloid plaques in a transgenic mouse model and evenhelps to reverse some of these lesions, therebyspawning a plethora of vaccination strategies. Thetreatment was undergoing phase-II trials but has beenhalted due to apparent encephalitis in some patients.The strategy, nevertheless, holds significant promiseand, once the mechanisms underlying its adverseactions are understood and potentially abated, its truevalue in AD treatment can be assessed. If, indeed, afuture version of this approach was to delay progressionof the disease, it would increase the need for preclinicaldiagnosis using biomarkers, to allow earliest imple-mentation of treatment.
Other remarkable recent findings include theobservation that cholesterol in the diet can affectamyloid load in an animal model and that cholesterollowering drugs may help reduce amyloid [Refolo et al.,2001]. In this regard, there is retrospective clinical datasupporting the hypothesis that lowering cholesterollevels may protect against AD [Wolozin et al., 2000].Similarly, a currently prescribed non-steroidal drug,ibuprofen, appears to modify APP processing in cellline studies. As several epidemiological studies havesuggested that it may affect progression to AD, it couldpossibly reduce or eliminate amyloid deposition.
MOLECULAR TARGETS
Amyloid-b Peptide Production: Alpha Secretase
Ab is generated by the proteolytic cleavage ofAPP by a group of enzymes known as secretases [Eslerand Wolfe, 2001; Samabamurti et al., 2002]. APP is
processed by alternative proteolytic pathways thatgenerate different breakdown products. In the secre-tory pathway, at least three different secretases appearto be active. The majority of APP is cleaved at Ab16 by‘‘a-secretase’’ to generate soluble amino-terminal deri-vatives of APP (sAPPa). This cleavage bisects the Abpeptide and thus prevents the formation of amyloido-genic fragments. Secreted derivatives of APP (sAPP)lacking the cytoplasmic tail, transmembrane domainand a small portion of the extracellular domaingenerated by the proteolytic processing of full-lengthAPP, have been detected in the conditioned medium ofseveral cell cultures, human plasma and in cerebrosp-inal fluid (CSF). An alternative secretase cleavageproduces truncated sAPP containing a potentiallyamyloidogenic sequence. This product sAPPg presum-ably is a result of the cleavage by g-secretase. Secretionof APP cleaved at the amino-terminus of Ab (sAPPb)has also been seen in several systems, which is as aresult of cleavage by b-secretase.
Beta Secretase Enzyme (BACE)
The enzymes involved in the generation of Ab arekey components of APP metabolism that are targets fordrug development [Hussein et al., 1999; Sinha et al.,1999; Vassar et al., 1999; Dingwall, 2001]. Excitingdevelopments in the last year have identified keycandidate enzymes with these activities. The identifica-tion of these proteins should lead to an understandingof the agents that regulate these activities to over-produce Ab42 in AD, and serve as useful therapeutictargets. Two novel aspartyl proteases were identified byseveral approaches and were shown to be capable of b-secretase activity. The major activity appears to bemediated by the enzyme named BACE, Asp-2, orMemapsin by different workers. This enzyme fulfillsseveral criteria for b-secretase activity including itssubstrate specificity and effects of modulating cellularexpression.
TABLE 5. Selected Target/Products From Different Companies
Company Product(s)/target(s)
Amgen Nerve growth and repairBrsitol-Myers Squibb Gamma secretase inhibitorCephalon Gamma secretase inhibitorElan Beta amyloid inhibitor vaccineEli Lilly SERM; gamma secretase inhibitorGlaxo Wellcome APOE modification, geneticsMerck Gamma secretase inhibitorPfizer Acetylcholinesterase and gamma
secretase inhibitorSchering-Plogh Presenilin gene functionVertex Nerve growth and repair
nSource: Lexis-Nexis, Inc.
274 LAHIRI ET AL.
Gamma Secretase: Presenilin I
The presenilins have been implicated in AD byvirtue of their key role in the proteolysis of APP [Haassand De Strooper, 1999]. It has been proposed thatpresenilins are g-secretases [Fraser et al., 2001]. Recentstudies showing that g-secretase activity can beimmunoprecipitated with presenilins in vitro strengthenthis hypothesis. This activity is in a large multisubunitcomplex indicating that other proteins may also play anessential role in the g-secretase activity, and inhibitorsof g-secretase activity have been reported that appar-ently do not affect Notch signaling; reported to beassociated with presenilin activity. The processing ofAPP by different secretase enzymes and the resultantproducts are schematically shown in Fig. 1.
Amyloid-b Peptide Aggregation
Amyloid plaques are derived from soluble amy-loid by aggregation into b-pleated sheet structures.One hypothesis suggests that the plaque or aggregatedamyloid is actually responsible for triggering theneurodegeneration in AD brain. If this hypothesis iscorrect, agents that break up the plaques or interfere inprotein folding to allow their aggregation can serve asuseful therapeutic agents [Soto et al., 1998, 2000;Cherny et al., 2001]. An endogenous melatonin-relatedindole structure, indole-3-propionic acid, has shown
potent neuroprotective properties against Ab [Chyanet al., 1999] and, also, it appears that melatonin mayreverse the profibrillogenic activity of apolipoprotein e4on Ab peptide [Poeggeler et al., 2001].
Amyloid-b Peptide Turnover
The net yield of Ab for deposition of plaques isdependent both on its production and its turnover inthe brain. Recent studies have identified severalpathways for Ab turnover including the insulin-degrading enzyme and neprilysin [Iwata et al., 2001].
APP Regulatory Elements
From recent cellular, genetic, and clinical reports,there is strong support for the hypothesis that Ab42production followed by its aggregation is the centralprocess responsible for the neurodegeneration in AD.It is thus important to examine the pathways involvednot only in the regulation of Ab levels but also itsprecursor protein (APP). Moreover, studies of thehuman brain have suggested a higher APP gene-expression ratio than predicted between Down’ssyndrome (DS) and normal controls [Tanzi et al.,1987]. The apparent overexpression of the APP gene inDS and in certain areas of the brain in AD patientssuggests that overexpression might be an importantfactor in the neuropathology of AD [Johnson et al.,1990; Rumble et al., 1989] and that cell type-specificregulation of APP gene expression may be altered inAD. The structure and function of the APP regulatoryregions, such as promoter and enhancer elements, haverecently been investigated, and such studies indicatethat these APP regulatory regions may play a pivotalrole in the pathogenesis of AD [Lahiri and Robakis,1991; Salbaum et al., 1988]. In this regard, the human,mouse, rat, and monkey APP promoters have beenfunctionally characterized [Song and Lahiri, 1998].These recent studies have unveiled the role of differentcis-acting regulatory regions of the promoter on thetranscriptional control of APP gene expression. Severalgrowth factors and proinflammatory cytokines canincrease the expression of APP and augment Abdeposition [Lahiri et al., 2000b]. For example, the co-expression of transforming growth factors (TGF-b1) inhuman APP transgenic mice have been shown to causean increased production of APP and Ab deposition incerebral blood vessels and meninges [Mattson et al.,1997]. Ab has also been shown to induce theproduction and secretion of interferon-g (IFN-g) andinterleukin-1 (IL-1) in human vascular endothelial cells[Suo et al., 1998]. Studies with primary cultures[Goldgaber et al., 1989] and neuronal cells [Lahiriand Nall, 1995] have indicated that NGF, FGF, and IL-1 increase APP mRNA and promoter levels. Moreover,
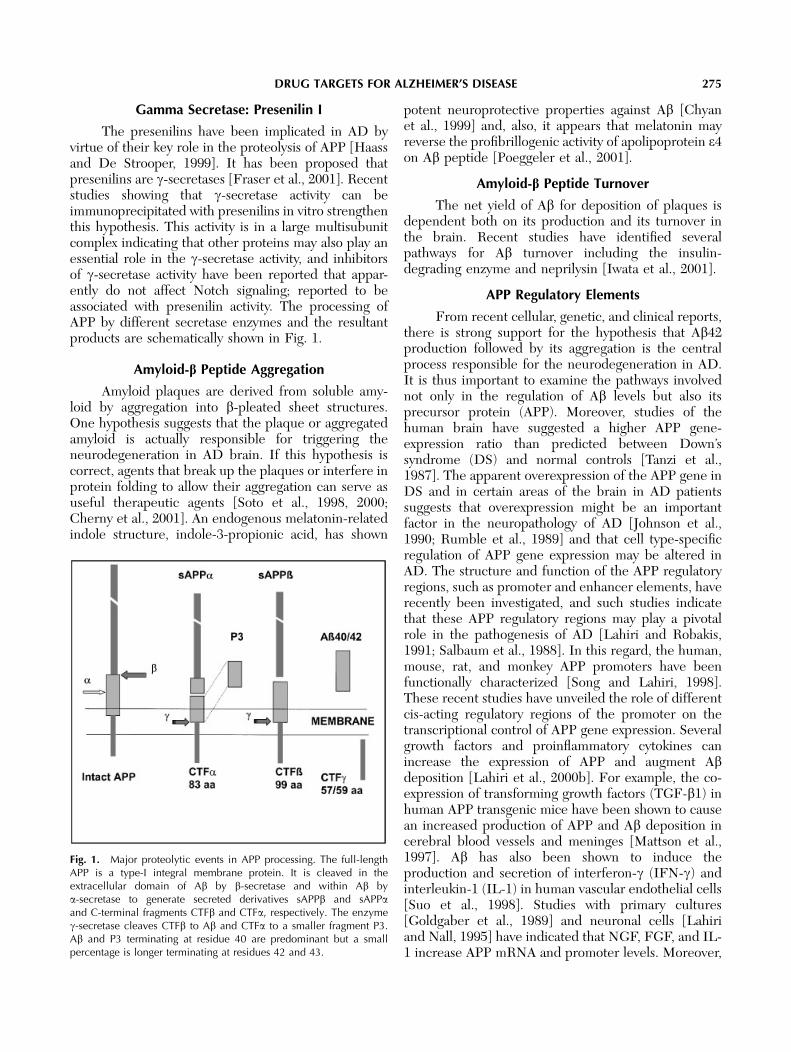
Fig. 1. Major proteolytic events in APP processing. The full-lengthAPP is a type-I integral membrane protein. It is cleaved in theextracellular domain of Ab by b-secretase and within Ab bya-secretase to generate secreted derivatives sAPPb and sAPPaand C-terminal fragments CTFb and CTFa, respectively. The enzymeg-secretase cleaves CTFb to Ab and CTFa to a smaller fragment P3.Ab and P3 terminating at residue 40 are predominant but a smallpercentage is longer terminating at residues 42 and 43.
DRUG TARGETS FOR ALZHEIMER’S DISEASE 275

NGF treatment induces transcription of TGF-b1through a specific promoter element on PC12 cells[Kim et al., 1994]. The regulation of a neural-specificgene is mediated by transcription factors that interactwith NGF-responsive elements [Luc and Wagner,1997]. These results suggest that Ab, acting in concertwith proinflammatory cytokines, could potentiallytrigger a self-propagating cycle of APP overexpressionresulting in an increased Ab deposition. Thus, factorsthat control both APP expression and processing are ofkey significance in AD pathogenesis.
In addition, it has recently been demonstratedthat the cytoplasmic tail of APP forms a multimericcomplex with the nuclear adaptor protein, Fe65, andthe histone acetyltransferase, Tip60 [Cao and Sudhof,2001]. This complex potently stimulates transcriptionvia heterologous Gal4- or LexA-DNA binding domains,and suggests that the release of the cytoplasmic tail ofAPP by gamma-cleavage may function in gene expres-sion. One can, therefore, postulate that it may be oftherapeutic benefit to block this interaction, openingup further avenues for drug design and development.
APP, Ab, and Cholinesterase Inhibitors
Cholinesterase inhibitors (ChEIs), which, asdescribed, are the only FDA approved drugs for thetreatment of AD patients, can regulate APP processingin cell lines [Lahiri et al., 2000]. For example, thetreatment of a human neuroblastoma cell line withtacrine or phenserine markedly suppressed the secre-tion of sAPPa and Ab [Lahiri et al., 1994; 1998; Shawet al., 2001]. For phenserine, this action is non-cholinergic as the antipode (the (þ)-enantiomer thatlacks anticholinesterase action) similarly reduces sAP-Pa and Ab, and is allowing the development of a newclass of agents that are cholinergically silent butpossesses Ab lowering properties. The lowering ofsAPP levels without a concomitant rise in Ab levels isanother novel property of certain cholinesteraseinhibitors, which can be further optimized for betterclinical effects. Indeed, the effect of anticholinesteraseson APP secretion is different from that of muscarinicagonists, such as carbachol, that stimulate sAPPasecretion after binding m1 receptors and activatingPKC [Nitsch et al., 1992]. The dual mechanism ofaction of specific cholinesterase inhibitors and mus-carinic agonists (i.e., cholinergic stimulation and Ablowering) remains an attractive therapeutic strategy forAD treatment that requires further optimization.
50-UTR of APPmRNA: A Novel Target
As discussed previously, studies with primarycultures and neuronal cells have shown that NGF,FGF, and IL-1 increase both APP mRNA and
promoter levels [Goldgaber et al., 1989; Lahiri andNall, 1995]. In addition, some factors can also regulateprotein levels by their effects at the post transcriptionallevel via the 50-untranslated region (UTR). Forexample, evidence for the regulation of translation ofthe APP mRNA by an IL-1 responsive element hasbeen reported [Rogers et al., 1999]. Notably, acholinesterase inhibitor, phenserine, has recently beenshown to reduce the translation of APP by takingadvantage of its translational regulation via the 50-UTR[Greig et al., 2000a; Shaw et al., 2001]. This 50-UTRthus represents a novel target for AD drug develop-ment. However, our current understanding of thecellular and molecular mechanisms that connectinflammatory cytokines to APP gene regulation islimited. Similarly, whether or not the large 30-UTR-APP mRNA can control protein levels and to whatextent the 30-UTR can be used as a potential drugtarget remains to be fully explored.
Tau Phosphorylation
The phosphorylated form of tau has been shownto be functionally inactive [Goedert and Spillantini,2001]. Recently, mutations in a splice site of tau havebeen shown to result in an increase in the ratio of four-repeat tau. This mutation is linked to a form ofdementia with NFT formation in the absence ofamyloid deposition. The finding that mutations in thetau protein, an important component of NFT, can alsolead to neurodegeneration suggests that NFT forma-tion may be the cause and not the consequence ofneurodegeneration. Secretion of abnormally glycosy-lated forms of tau into the CSF is reported to be anearly event in the AD brain and may eventually bedeveloped as an early diagnostic marker in AD.
Tau Aggregation
Although phosphorylated tau is known to bepresent in NFT, this cannot explain the deposition oftau as tangles. It has been reported that the four-repeattau that is generated by mutations in the tau geneassociated with dementia is due to the tau protein’scapacity to aggregate rapidly.
CHOLESTEROL
Recent studies indicate a link between heartdisease, cholesterol, and AD [Simons et al., 2001;Sparks et al., 2000]. Notably, cholesterol has beenshown to accumulate in senile plaques of AD patientsand in transgenic APP(SW) mice [Mori et al., 2001].This observation has strong therapeutic implications.For example, a cholesterol-lowering statin drug hasbeen shown to reduce beta-amyloid pathology in atransgenic mouse model of AD [Refolo et al., 2001].
276 LAHIRI ET AL.

Epidemiological studies have suggested that the takingof HMG-Coreductase inhibitors reduces the risk ofdeveloping AD in the normal elderly population.Finally, an independent study has reported thatSimvastatin strongly reduces levels of AD the beta-amyloid peptides, Ab-42 and Ab-40, both in vitro andin vivo [Fassbender et al., 2001].
NONSTEROIDAL ANTI-INFLAMMATORY DRUGSAND APP
Several recent studies suggest that the use ofnonsteroidal anti-inflammatory (NSAIDs) drugs areassociated with a reduced risk for developing AD [In t’Veld et al., 2001]. Moreover there is a report of usingcelastrol, which is a potent antioxidant and anti-inflammatory drug, as a possible treatment for AD[Allison et al., 2001]. Unfortunately, recent studies withPrednisone, Celebrex and Vioxx have not beenbeneficial in patients with established AD. Interest-ingly, other connections between NSAIDs and theamyloid pathways have been made. For example, it hasbeen recently shown that a subset of NSAIDs loweramyloidogenic Ab-42 independently of cyclooxygenaseactivity [Weggen et al., 2001]. These recent studieshave rekindled some enthusiasm for an anti-inflamma-tory drug to treat AD [De Strooper and Konig, 2001].
OXIDATIVE DAMAGE
There are reports of the role of oxidation of Abpeptide [Head et al., 2001], and of oxidative damage[Butterfield et al., 2001] playing a role in AD. Oxidativedamage has also been linked to neurodegeneration byselective alpha-synuclein nitration in synucleinopathylesions [Giasson et al., 2000]. Similarly, the productionof advanced glycation endproducts (AGES) has beenimplicated in brain aging and there is a proposalsupporting the use of AGE-inhibitors as neuroprotec-tive and anti-dementia drugs [Dukic-Stefanovic et al.,2001]. It has been hypothesized that nutrition andproper diet may protect the body from oxidativedamage [Mattson and Greig, 2001]. For example, ithas been shown that the curry spice, curcumin, appearsto reduce oxidative damage and amyloid pathology inan AD transgenic mouse model [Lim et al., 2001].
DIAGNOSIS BASED ON AMYLOID ANDGENETIC ANALYSIS
As stated earlier, the senile plaque core consistsprimarily of the 4 kDa amyloid b peptide, which isderived from APP through proteolytic processing byrecently identified proteases b- and g-secretases. The Abpeptides of 40 and 42 residues are normally present inthe brain, CSF, and plasma of normal individuals and
are constitutively secreted from cultured cells, suggest-ing that these peptides do not intrinsically cause AD.However, the levels of Ab42, the major species of Abdeposited in AD brain, are increased by all identifiedmutations linked to familial AD. Furthermore, recentstudies have shown that in conventional sporadic AD, asin FAD, there are genetic determinants that result in anincrease in levels of Ab42 in the plasma [Younkin, 1998].Therefore, taking family history and other geneticfactors into account, high plasma Ab levels may serveas a useful diagnostic marker for predisposition to AD.Identification of the genes responsible for the increasein Ab linked to sporadic AD may provide additionalinformation to assess risk for AD in individual patients.
The currently popular hypothesis is that AD iscaused by the deposition of Ab42 forming toxicaggregates, which eventually form the core of senileplaques. Thus, the regulation of Ab42 to low physio-logical levels may be an important therapeutic goal forthe prevention of amyloidosis in AD. The mechanismby which amyloid deposition eventually leads toneurodegeneration and dementia currently remainsunknown. In fact, its role as the predominant cause ofAD has been questioned, as amyloid plaques have beenseen in healthy aged individuals with no signs ofdementia. Furthermore, the severity of dementia ismore closely correlated with numbers of NFTs thanwith senile plaques. Nevertheless, both these observa-tions can be readily explained by assuming that amyloiddeposition is an early step in a sequential cascade,which eventually leads to neuronal loss. The genesis ofthe NFT may be closely linked to the amyloid inducedneuron loss, either as a direct cause or as itsconsequence. Understanding the pathways for theinduction of NFTs by Ab may provide useful ther-apeutic targets and diagnostic markers.
SUMMARY AND FUTURE DIRECTIONS
Studies on neurobiological mechanisms to pro-vide new targets for drug development in AD areexpanding rapidly, and current investigations cover abroad area of cellular, molecular, genetic, and clinicalresearch. Herein, we have made an attempt to reviewrecent trends in AD research in these aforementionedareas. The molecular genetics of AD and the role of keyproteins (known and to be discovered) that arebelieved to participate in AD pathogenesis areimportant fields for further research. Similarly, the cellbiology of AD, particularly the roles of secretases,presenilin, notch and tau proteins should provide newlight on the cascade of AD neurodegenerative path-ways. In addition to APP and PS-1, there is significantactive research underway in the development of newinhibitors for BACE, PS-1, and g-secretase as targets
DRUG TARGETS FOR ALZHEIMER’S DISEASE 277

for treatment of AD. Research is also underway todissect and characterize APP genetic regulatoryelements and its 50-UTR for the development ofpotential drug targets. The immunotherapeutic strate-gies, specifically immunotherapy with Ab for AD,represent examples of an ‘‘out of the box’’ newapproach towards the treatment of AD [Ugen andMorgan, 2001]. Current studies of the inflammatoryprocesses of the brain are leading to preliminaryindications of the beneficial use of anti-inflammatoryagents, such as ibuprofen, in treating or slowing theprogression of the disease. Likewise, studies on theeffects of estrogen on the brain suggest that it, oranalogues thereof, may be of great potential foroffsetting or preventing AD in the future. Newertechnologies, such as DNA microarray technologies tostudy gene expression profiles in AD, proteomics toanalyze the protein profiling of AD brain tissues, andtransgenic mouse models of AD, should yield new anduseful clues to further characterize the pathobiochem-ical processes of the disease. Other approaches, such asnutritional, genetic, and environmental factors, mayalso highlight more effective preventive strategies forAD. Indeed, our current understanding of the role ofoxidative stress in AD has resulted in the wide use ofantioxidants, such as vitamin E, to potentially delay theprogression of AD. Finally, it should be stressed thatboth early diagnosis of AD and the development ofquantitative markers to better follow the course of thedisease are also extremely important for the evaluationand successful development of therapeutic strategies[Lahiri and Sambamurti, 2000]. Recent progress in thisarea has been quite remarkable and new techniqueshave been developed that allow the imaging of plaquesin live animals. Thus, it is hoped that all these lines ofongoing research, combined, should lead to a deeperunderstanding of the processes that occur in the ADbrain to allow us to effectively prevent their occurrence.
ACKNOWLEDGEMENTS
This work was supported in part by grants fromthe Alzheimer’s Association and Axonyx, Inc. to DKLand KS, and from the National Institutes of Health(AG18884 and AG18379) to DKL.
REFERENCES
Allison AC, Cacabelos R, Lombardi VR, Alvarez XA, Vigo C. 2001.Celastrol, a potent antioxidant and anti-inflammatory drug, as apossible treatment for Alzheimer’s disease. Prog Neuro-Psycho-pharmacol Biol Psychiat 25:1341–1357.
Arendt T, Bruckner MK, Lange M, Bigl V. 1992. Changes inacetylcholinesterase and butyrylcholinesterase in Alzheimer’sdisease resemble embryonic developmentFa study of molecularforms. Neurochem Int 21:381–396.
Atack JR, Perry EK, Bonham JR, Candy JM, Perry RH. 1986.Molecular forms of acetylcholinesterase and butyrylcholinesterasein the aged human central nervous system. J Neurochem 47:263–277.
Bales KR, Verina T, Cummins DJ, Du Y, Dodel RC, Saura J,Fishman CE, DeLong CA, Piccardo P, Petegnief V, Ghetti B,Paul SM. 1999. Apolipoprotein E is essential for amyloiddeposition in the APP(V717F) transgenic mouse model ofAlzheimer’s disease. Proc Natl Acad Sci USA 96:15233–15238.
Barber K, Mesullam MM, Kraft GA, Klein WL. 1996. Butyrylcho-linesterase alters the aggregation state of A-b amyloid. SocietyNeurosci Abst 22:1172.
Bartus RT, Dean RL III, Beer B, Lippa AS. 1982. The cholinergichypothesis of geriatric memory dysfunction. Science 217: 408–414.
Becker RE, Moriearty P, Unni L, Vicari S. 1997. Cholinesteraseinhibitors as therapy in Alzheimer’s disease:benefit to riskconsiderations in clinical application. In: Becker R, Giacobini,E, editors. Alzheimer’s Disease: from molecular biology totherapy. Boston: Brikhauser. p 257–266.
Bertram L, Blacker D, Mullin K, Keeney D, Jones J, Basu S, Yhu S,McInnis MG, Go RC, Vekrellis K, Selkoe DJ, Saunders AJ, TanziRE. 2000. Evidence for genetic linkage of Alzheimer’s disease tochromosome 10q. Science 290:2302–2303.
Butterfield DA, Drake J, Pocernich C, Castegna A. 2001. Evidenceof oxidative damage in Alzheimer’s disease brain: central role foramyloid b-peptide. Trends Mol Med 7:548–554.
Cao X, Sudhof TC. 2001. A transcriptionally active complex of APPwith Fe65 and histone cetyltransferase Tip60. Science 293:115–12.0
Cherny RA, Atwood CS, Xilinas ME, Gray DN, Jones WD, McLeanCA, Barnham KJ, Volitakis I, Fraser FW, Kim Y, Huang X,Goldstein LE, Moir RD, Lim JT, Beyreuther K, Zheng H, TanziRE, Masters CL, Bush AI. 2001. Treatment with acopper-zinc chelator markedly and rapidly inhibits beta-amyloidaccumulation in Alzheimer’s disease transgenic mice. Neuron30:665–676.
Chyan YJ, Poeggeler B, Omar RA, Chain DG, Frangione B, Ghiso J.Pappolla MA. 1999. Potent neuroprotective properties against theAlzheimer beta-amyloid by an endogenous melatonin-relatedindole structure, indole-3-propionic acid. J Biol Chem 274:21937–42192.
Darvesh S, Grantham DL, Hopkins DA. 1998. Distribution ofbutyrylcholinesterase in human amygdala and hippocampalformation. J Comp Neurol 393:374–390.
Davies P, Maloney AJ. 1976. Selective loss of central cholinergicneurons in Alzheimer’s disease. Lancet 2:140.
De Strooper B, Konig G. 2001. An inflammatory drug prospect.Nature 414:159–160.
Dingwall C. 2001. Spotlight on BACE: the secretases astargets for treatment in Alzheimer disease. J Clin Invest108:1243–1246.
Dukic-Stefanovic S, Schinzel R, Riederer P, Munch G. 2001. AGESin brain ageing: AGE-inhibitors as neuroprotective and anti-dementia drugs? Biogerontology 2:19–34.
Enz A, Amstutz R, Boddeke H et al. 1993. Brain selective inhibitionof acetylcholinesterase: a novel approach to therapy in Alzheimer’sdisease. Prog Brain Res 98:431–438.
Ertekin-Taner N, Graff-Radford N, Younkin LH, Eckman C, BakerM, Adamson J, Ronald J, Blangero J, Hutton M, Younkin SG.2000. Linkage of plasma Abeta42 to a quantitative locus onchromosome 10 in late-onset Alzheimer’s disease pedigrees.Science 290:2303–2304.
278 LAHIRI ET AL.

Esler WP, Wolfe MS. 2001. A portrait of Alzheimer secretases: newfeatures and familiar faces. Science 293:1449–1154.
Fassbender K, Simons M, Bergmann C, Stroick M, Lutjohann D,Keller P, Runz H, Kuhl S, Bertsch T, von Bergmann K, HennericiM, Beyreuther K, Hartmann T. 2001. Simvastatin stronglyreduces levels of Alzheimer’s disease beta-amyloid peptides Abeta42 and Abeta 40 in vitro and in vivo. Proc Natl Acad Sci USA98:5856–5861.
Fraser PE, Yu G, Levesque L, Nishimura M, Yang DS, Mount HT,Westaway D, St George-Hyslop PH. 2001. Presenilin function:connections to Alzheimer’s disease and signal transduction.Biochem Soc Symp 67:89–100.
Friedrich MJ. 2002. Teasing out effects of estrogen on the brain.JAMA 287:29–30.
Gao Y, Pimplikar SW. 2001. The gamma-secretase-cleaved C-terminal fragment of amyloid precursor protein mediates signal-ing to the nucleus. Proc Natl Acad Sci USA 98:14979–14984.
Giacobini E. 2000. Cholinesterase inhibitors: from the Calabar beanto Alzheimer therapy. In: Giacobini E, editor. Cholinesterases andcholinesterase inhibitors. London: Martin Dunitz. p 181–226.
Giasson BI, Duda JE, Murray IV, Chen Q, Souza JM, Hurtig HI,Ischiropoulos H, Trojanowski JQ, Lee VM. 2000. Oxidativedamage linked to neurodegeneration by selective alpha-synucleinnitration in synucleinopathy lesions. Science 290:985–989.
Goedert M, Spillantini MG. 2001. Tau gene mutations andneurodegeneration. Biochem Soc Symp 67:59–71.
Goldgaber D, Lerman MI, McBride OW, Saffiotti U, Gajdusek DC.1987. Characterization and chromosomal localization of a cDNAencoding brain-amyloid of Alzheimer’s disease. Science 235:877–880.
Goldstein LS. 2001. Kinesin molecular motors: transport pathways,receptors, and human disease. Proc Natl Acad Sci USA 98:6999–7003.
Gotz J, Chen F, van Dorpe J, Nitsch RM. 2001. Formation ofneurofibrillary tangles in P301l tau transgenic mice induced byAbeta 42 fibrils. Science 293:1491–1495.
Gozes I. 2001. Neuroprotective peptide drug delivery and develop-ment: potential new therapeutics. Trends Neurosci 24:700–705.
Greenfield S. 1996. Non-classical actions of cholinesterases: role incellular differentiation, tumorigenesis and Alzheimer’s disease.Neurochem Int 28:485–490.
Greig NH, De Micheli E, Holloway HW, Yu Q-S, Utsuki T, Perry T,Ingram DK, Deutsch J, Lahiri DK, Soncrant TT. 2000a. Theexperimental Alzheimer drug phenserine: pharmacokineticsand pharmacodynamics in the rat. Acta Neurol Scand 176:74–84.
Greig NH, Lahiri DK, Sambamurti K. 2000b. Butyrylcholinesterase:an important new target in Alzheimer’s disease therapy. IntPsychogeriat (in press).
Grossman GT, Stahelin HB, Messina JC, Anand R, Veach J. 2000.Lack of adverse pharmacodynamic drug interactions withrivastigmine and twenty-two classes of medications. Int J GerPsych 15:242–247.
Guillozet AL, Smiley JF, Mash DC, Mesulam MM. 1997.Butyrylcholinesterase in the life cycle of amyloid plaques. AnnNeurol 42:909–918.
Haass C, De Strooper B. 1999. The presenilins in Alzheimer’sdisease: proteolysis holds the key. Science 286:916–919.
Hardy J. 2001. Genetic dissection of primary neurodegenerativediseases. Biochem Soc Symp 67:51–57.
Haroutunian V, Greig NH, Pei XF, Utsuki T, Gluck R, Acevedo LD,Davis KL, Wallace WC. 1997. Pharmacological modulation ofAlzheimer’s b-amyloid precursor protein levels in the CSF of ratswith forebrain cholinergic system lesions. Brain Res Mol BrainRes 46:161–168.
Head E, Garzon-Rodriguez W, Johnson JK, Lott IT, Cotman CW,Glabe C. 2001. Oxidation of Ab and plaque biogenesis inAlzheimer’s disease and Down syndrome. Neurobiol Dis 8:792–806.
Hebert LE, Beckett LA, Scherr PA, Evans DA. 2001. Annualincidence of Alzheimer disease in the United States projected tothe years 2000 through 2050. Alz Dis Assoc Disord 15:169–173.
Herrup K, Yang Y. 2001. Pictures in molecular medicine:contemplating Alzheimer’s disease as cancer: a loss of cell-cyclecontrol. Trends Mol Med 7:527.
Hsiao K, Chapman P, Nilsen S, Eckman C, Harigaya Y, Younkin S,Yang F, Cole G. 1996. Correlative memory deficits, Abetaelevation, and amyloid plaques in transgenic mice. Science274:99–102.
Hussain I, Powell D, Howlett DR, Tew DG, Meek TD, Chapman C,Gloger IS, Murphy KE, Southan CD, Ryan DM, Smith TS,Simmons DL, Walsh FS, Dingwall C, Christie G. 1999.Identification of a Novel Aspartic Protease (Asp 2) as beta-Secretase. Mol Cell Neurosci 14:419–427.
Imbimbo BP. 2001. Pharmacodynamic-tolerability relationships ofcholinesterase inhibitors for Alzheimer’s disease. CNS Drugs15:375–390.
In t’ Veld BA, Ruitenberg A, Hofman A, Launer LJ, van Duijn CM,Stijnen T, Breteler MM, Stricker BH. 2001. Nonsteroidalantiinflammatory drugs and the risk of Alzheimer’s disease. NewEngl J Med 345:1515–1521.
Iwata N, Tsubuki S, Takaki Y, Shirotani K, Lu B, Gerard NP, GerardC, Hama E, Lee HJ, Saido TC. 2001. Metabolic regulation ofbrain Abeta by neprilysin. Science 292:1550–1552.
Jagust W. 2001. Untangling vascular dementia. Lancet 358:2097–2098.
Janus C, Westaway D. 2001. Transgenic mouse models ofAlzheimer’s disease. Physiol Behav 73:873–886.
Kalaria RN. 2001. Advances in molecular genetics and pathology ofcerebrovascular disorders. Trends Neurosci 24:392–400.
Kim SJ, Park K, Rudkin BB, Dey BR, Sporn MB, Roberts AB. 1994.Nerve growth factor induces transcription of transforming growthfactor-beta 1 through a specific promoter elementin PC12 cells.J Biol Chem 269:3739–3744.
Lahiri DK, Lewis S, Farlow MR. 1994. Tacrine alters the secretionof the beta-amyloid precurs or protein in cell lines. J Neurosci Res37:777–787.
Lahiri DK, Nall C. 1995. Promoter activity of the gene encoding thebeta-amyloid precursor protein is up-regulated by growth factors,phorbolester, retinoic acid and interleukin-1. Brain Res Mol BrainRes 32:233–240.
Lahiri DK, Robakis NK. 1991. The promote activity of the geneencoding Alzheimer beta amyloid precursor protein (APP) isregulated by two blocks of upstream sequences. Brain Res MolBrain Res 9:253–257.
Lahiri DK, Sambamurti K. 2000. Neurodiagnostics: focus onAlzheimer’s Disease. Spect Diagn Relat Tech 10:1–14.
Lahiri DK, Farlow MR, Sambamurti K. 1998. The secretion ofamyloid beta-peptides is inhibited in the tacrine-treated humanneuroblastoma cells. Mol Brain Res 62:131–140.
Lahiri DK, Farlow MR, Hintz N, Utsuki T, Greig NH. 2000a.Cholinesterase inhibitors, b-amyloid precursor protein and
DRUG TARGETS FOR ALZHEIMER’S DISEASE 279

amyloid b-peptides in Alzheimer’s disease. Acta Neurol Scand176:60–67.
Lahiri DK, Song W, Ge Y-W. 2000b. Analysis of the 50-flankingregion of the b-amyloid precursor protein gene that contributes toincreased promoter activity in differentiated neuronal cells. MolBrain Res 77:185–198.
Lee VM. 2001. Biomedicine. Tauists and beta-aptists united: wellalmost! Science 293:1446–1447.
Lemere CA, Maron R, Selkoe DJ, Weiner HL. 2001. Nasalvaccination with beta-amyloid peptide for the treatment ofAlzheimer’s disease. DNA Cell Biol 20:705–711.
Lewis J, Dickson DW, Lin WL, Chisholm L, Corral A, Jones G, YenSH, Sahara N, Skipper L, Yager D, Eckman C, Hardy J, HuttonM, McGowan E. 2001. Enhanced neurofibrillary degeneration intransgenic mice expressing mutant tau and APP. Science293:1487–1491.
Lim GP, Chu T, Yang F, Beech W, Frautschy SA, Cole GM. 2001.The curry spice curcumin reduces oxidative damage and amyloidpathology in an Alzheimer transgenic mouse. J Neurosci 21:8370–8377.
Lippa CF, Schmidt ML, Nee LE, Bird T, Nochlin D, Hulette C,Mori H, Lee VM, Trojanowski JQ. 2000. AMY plaques in familialAD: comparison with sporadic Alzheimer’s disease. Neurology54:100–104.
Loring JF, Wen X, Lee JM, Seilhamer J, Somogyi R. 2001. A geneexpression profile of Alzheimer’s disease. DNA Cell Biol 20:683–695.
Luc PV, Wagner JA. 1997. Regulation of the neural-specific geneVGF in PC12 cells. Identification of transcription factors interact-ing with NGF responsive elements. J Mol Neurosci 8:223–241.
Marx J. 2001. Alzheimer’s disease. Bad for the heart, bad for themind? Science 294:508–509.
Mattson MP, Barger SW, Furukawa K, Bruce AJ, Wyss-Coray T,Mark RJ, Mucke L. 1997. Cellular signaling roles of TGF beta,TNF alpha and beta APP in brain injury responses andAlzheimer’s disease. Brain Res Brain Res Rev 23:47–61.
Mattson MP, Greig NH. 2001. Slowing down cerebral degeneration.BioFutur Oct: 51–53.
Mesulam M. 2000. Neuroanatomy of cholinesterases in the normalhuman brain and in Alzheimer’s disease. In: Giacobini E, editor.Cholinesterases and cholinesterase inhibitors. London: MartinDunitz. p. 121–136.
Moran MA, Mufson EJ, Gomez-Ramos P. 1993. Colocalization ofcholinesterases with b amyloid protein in aged and Alzheimer’sbrains. Acta Neuropathol 85:362–369.
Mori T, Paris D, Town T, Rojiani AM, Sparks DL, Delledonne A,Crawford F, Abdullah LI,Humphrey JA, Dickson DW, MullanMJ. 2001. Cholesterol accumulates in senile plaques of Alzheimerdisease patients and in transgenic APP(SW) mice. J NeuropatholExp Neurol 60:778–785.
Myers A, Holmans P, Marshall H, Kwon J, Meyer D, Ramic D,Shears S, Booth J, DeVrieze FW, Crook R, Hamshere M,Abraham R, Tunstall N, Rice F, Carty S, Lillystone S,Kehoe P, Rudrasingham V, Jones L, Lovestone S, Perez-Tur J,Williams J, Owen MJ, Hardy J, Goate AM. 2000. Susceptibilitylocus for Alzheimer’s disease on chromosome 10. Science290:2304–2305.
Naslund J, Haroutunian V, Mohs R, Davis KL, Davies P, GreengardP, Buxbaum JD. 2000. Correlation between elevated levels ofamyloid b-peptide in the brain and cognitive decline. JAMA283:1571–1577.
Neve RL, McPhie DL, Chen Y. 2001. Alzheimer’s disease:dysfunction of a signalling pathway mediated by the amyloidprecursor protein? Biochem Soc Symp 67:37–50.
Nitsch RM, Slack BE, Wurtman RJ, Growdon JH. 1992. Release ofAlzheimer amyloid precursor derivatives stimulated by activationof muscarinic acetylcholine receptors. Science 258:304–307.
Nordberg A, Darreh-Shori T, Svenson A, Guan Z. 2001. AChE andBuChE activities in CSF of mild AD patients following 12 monthsof rivastigmine treatment. J Neurol Sci 187: P0144.
Pasinetti GM. 2001. Use of cDNA microarray in the search formolecular markers involved in the onset of Alzheimer’s diseasedementia. J Neurosci Res 65:471–476.
Pinnix I, Musunuru U, Tun H, Sridharan A, Golde T, Eckman C,Ziani-Cherif C, Onstead L, Sambamurti K. 2001. A novel gamma -secretase assay based on detection of the putative C-terminalfragment-gamma of amyloid beta protein precursor. J Biol Chem276:481–487.
Poeggeler B, Miravalle L, Zagorski MG, Wisniewski T, Chyan YJ,Zhang Y, Shao H, Bryant-Thomas T, Vidal R, Frangione B, GhisoJ, Pappolla MA. 2001. Melatonin reverses the profibrillogenicactivity of apolipoprotein E4 on the Alzheimer amyloid Abetapeptide. Biochemistry 40:14995–15001.
Purandare N, Burns A, Craig S, Faragher B, Scott K. 2001.Depressive symptoms in patients with Alzheimer’s disease.Internat J Geriat Psychiatr 16:960–964.
Price DL, Sisodia SS, Borchelt DR. 1998. Genetic neurodegenera-tive diseases: the human illness and transgenic models. Science282:1079–1083.
Refolo LM, Pappolla MA, LaFrancois J, Malester B, Schmidt SD,Thomas-Bryant T, Tint GS, Wang R, Mercken M, Petanceska SS,Duff KE. 2001. A cholesterol-lowering drug reduces b-amyloidpathology in a transgenic mouse model of Alzheimer’s disease.Neurobiol Dis 8:890–899.
Reynish W, Andrieu S, Nourhashemi F, Vellas B. 2001. Nutritionalfactors and Alzheimer’s disease. J Gerontol Series A-Biol Sci MedSci 56:M675–680.
Rogers JT, Leiter LM, McPhee J, Cahill CM, Zhan SS, Potter H,Nilsson LN. 1999. Translation of the Alzheimer amyloid precursorprotein mRNA is up-regulated by interleukin-1 through 50-untranslated region sequences. J Biol Chem 274:6421–6431.
Rumble B, Retallack R, Hilbich C, Simms G, Multhaup G, MartinsR, et al. 1989. Amyloid A4 protein and its precursor in Down’ssyndrome and Alzheimer’s disease. N Engl J Med 320:14461–14462.
Salbaum JM, Weidemann A, Lemarie HG, Masters CL, BeyreutherK. 1988. The promoter of Alzheimer’s disease amyloid A4precursor gene. EMBO J 7:2807–2813.
Sambamurti K, Greig NH, Lahiri DK. 2002a. Advances in thecellular and molecular biology of the beta-amyloid protein inAlzheimer’s disease. NeuroMol Med 1:1–20.
Sambamurti K, Hardy J, Refolo LM, Lahiri DK. 2002b. TargetingAPP metobolism for the treatment of Alzheimer’s disease. DrugDev Res 56: 211–227.
Schenk D, Seubert P, Ciccarelli RB. 2001. Immunotherapy withbeta-amyloid for Alzheimer’s disease: a new frontier. DNA CellBiol 20:679–681.
Selkoe DJ. 2000. The origins of Alzheimer disease: A is for amyloid.JAMA 283:1615–1617.
Shastry BS. 1998. Molecular genetics of familial Alzheimer disease.Am J Med Sci 315:266–272.
Shaw KTY, Utsuki T, Rogers J, Yu Q-S, Sambamurti K, Brossi A, GeY-W, Lahiri DK, Greig NH. 2001. Phenserine regulates transla-
280 LAHIRI ET AL.

tion of b-amyloid precursor mRNA by a putative interleukin-1responsive element, a target for drug development. Proc NatlAcad Sci USA 98:7605–7610.
Simons M, Keller P, Dichgans J, Schulz JB. 2001. Cholesterol andAlzheimer’s disease: is there a link? Neurology 57:1089–1093.
Sinha S, Anderson JP, Barbour R, Basi GS, Caccavello R, Davis D,Doan M, Dovey HF, Frigon N, Hong J, Jacobson-Croak K, JewettN, Keim P, Knops J, Lieberburg I, Power M, Tan H, Tatsuno G,Tung J, Schenk D, Seubert P, Suomensaari SM, Wang S, WalkerD, John V, et al. 1999. Purification and cloning of amyloidprecursor protein beta-secretase from human brain. Nature402:537–540.
Sisodia SS. 2002. Biomedicine. A cargo receptor mystery APPar-ently solved? Science 295:805–807.
Snow AD, Mar H, Nochlin D, Kimata K, Kato M, Suzuki S, HassellJ, Wright TN. 1988. The presence of heparan sulfate proteogly-cans in the neuritic plaques and congophilic angiopathy inAlzheimer’s disease. Am J Pathol 133:156–463.
Small DH, Michaulson S, Sberna G. 1996. Non-classical actions ofcholinesterases: role in cellular differentiation, tumorigenesis andAlzheimer’s disease. Neurochem Int 453–483.
Solomon B. 2001. Immunotherapeutic strategies for preventionand treatment of Alzheimer’s disease. DNA Cell Biol20:697–703.
Song W, Lahiri DK. 1998. Functional identification of the promoterof the gene encoding the Rhesus monkey beta-amyloid precursorprotein. Gene 217:165–176.
Soto C, Sigurdsson EM, Morelli L, Kumar RA, Castano EM,Frangione B. 1998. Beta-sheet breaker peptides inhibit fibrillo-genesis in a rat brain model of amyloidosis: Implications forAlzheimer’s therapy. Nat Med 4:822–826.
Soto C, Saborio GP, Permanne B. 2000. Inhibiting the conversion ofsoluble amyloid-beta peptide into abnormally folded amyloido-genic intermediates: relevance for Alzheimer’s disease therapy.Acta Neurol Scand 102:90–95 (Suppl 176).
Sparks DL. Martin TA. Gross DR. Hunsaker JC 3rd.. 2000. Linkbetween heart disease, cholesterol, and Alzheimer’s disease: areview. Microsc Res Tech 50:287–290.
Spillantini MG, Goedert M, Crowther RA, Murrell JR, Farlow MR,Ghetti B. 1997. Familial multiple system tauopathy with preseniledementia: a disease with abundant neuronal and glial taufilaments. Proc Natl Acad Sci USA 94:4113–4118.
St George-Hyslop PH. 2000. Molecular genetics of Alzheimer’sdisease. Biol Psychiatr 47:183–199.
Suo Z, Humphrey J, Kundtz A, Sethi F, Placzek A, Crawford F,Mullan M. 1998. Soluble Alzheimers b-amyloid constricts thecerebral vasculature in vivo. Neurosci Lett 257:770–780.
Stropa EG, Gonzalez AM, Chorsky R, Corna RJ, Alvarez J, BirdED, Baird A. 1990. Basic fibroblast growth factor in Alzheimer’sdisease. Biochem Biophys Res Commun 171:690–696.
Tanzi RE, Bertram L. 2001. New frontiers in Alzheimer’s diseasegenetics. Neuron 32:181–184.
Tanzi RE, Gusella JF, Watkins PC, Bruns GA, St George-Hyslop P,Van Keuren ML., et al. 1987. Armyloid beta protein gene: cDNA,mRNA distribution, and genetic linkage near the Alzheimer locus.Science 235:880–884.
Terry RD. 1998. The cytoskeleton in Alzheimer disease. J NeuralTransm Suppl 53:1023–1025.
Tol J, Roks G, Slooter AJ, van Duijn CM. 1999. Genetic andenvironmental factors in Alzheimer’s disease. Rev Neurol (Paris)155:S10–S16.
Town T, Tan J, Mullan M. 2001. CD40 signaling and Alzheimer’sdisease pathogenesis. Neurochem Int 39:371–380.
Ugen KE, Morgan D. 2001. Alzheimer’s disease: molecularly basedimmunotherapeutics. DNA Cell Biol 20:677–678.
Van Eldik LJ. 2001. Glia and Alzheimer’s disease. Neurochem Int39:329–331.
Vassar R, Bennett BD, Babu-Khan S, Kahn S, Mendiaz EA, Denis P,Teplow DB, Ross S, Amarante P, Loeloff R, Luo Y, Fisher S,Fuller J, Edenson S, Lile J, Jarosinski MA, Biere AL, Curran E,Burgess T, Louis JC, Collins F, Treanor J, Rogers G, Citron M.1999. Beta-secretase cleavage of Alzheimer’s amyloid precursorprotein by the transmembrane aspartic protease BACE. Science286:735–741.
Vitiello MV, Borson S. 2001. Sleep disturbances in patients withAlzheimer’s disease: epidemiology, pathophysiology andtreatment. CNS Drugs 15:777–796.
Walter J, Schindzielorz A, Hartung B, Haass C. 2000. Phosphoryla-tion of the beta-amyloid precursor protein at the cell surface byectocasein kinases 1 and 2. J Biol Chem 275:523–529.
Weggen S, Eriksen JL, Das P, Sagi SA, Wang R, Pietrzik CU,Findlay KA, Smith TE, Murphy MP, Bulter T, Kang DE,Marquez-Sterling N, Golde TE, Koo EH. 2001. A subset ofNSAIDs lower amyloidogenic Abeta42 independently of cycloox-ygenase activity. Nature 414:212–216.
Wolozin B, Kellman W, Rousseau P, Celesia GG, Siegel G. 2000.Decreased prevalence of Alzheimer disease associated with 3-hydroxy-3-methyglutaryl coenzyme A reductase inhibitors. ArchNeurol 57:1439–1443.
Wong PC, Price DL, Cai H. 2001. The brain’s susceptibility toamyloid plaques. Science 293:1434.
Yan R, Bienkowski MJ, Shuck ME, Miao H, Tory MC, Pauley AM,Brashier JR, Stratman NC, Mathews WR, Buhl AE, Carter DB,Tomasselli AG, Parodi LA, Heinrikson RL, Gurney ME. 1999.Membrane-anchored aspartyl protease with Alzheimer’s diseasebeta-secretase activity. Nature 402:533–537.
Yankner BA, Duffy LK, Kirschner DA. 1990. Neurotrophic andneurotoxic effects of amyloid b protein: reversal by tachykininneuropeptides. Science 250:279–282.
Younkin SG. 1998. The role of A beta 42 in Alzheimer’s disease.J Physiol 92:289–92.
Yu C, Kim SH, Ikeuchi T, Xu H, Gasparini L, Wang R, Sisodia SS.2001. Characterization of a presenilin-mediated APP carboxylterminal fragment gammaCTFgamma: evidence for distinct me-chanisms involved in gamma-secretase processing of the APP andnotch 1 transmembrane domains. J Biol Chem 276:43756–43760.
Zhu X, Castellani RJ, Takeda A, Nunomura A, Atwood CS, Perry G,Smith MA. 2001. Differential activation of neuronal ERK, JNK/SAPK and p38 in Alzheimer disease: the ’two hit’ hypothesis.Mech Age Dev 123:39–46.
DRUG TARGETS FOR ALZHEIMER’S DISEASE 281




















