
VEGF receptor inhibition blocks liver cyst growth in pkd2(WS25/-) mice

●
bc●
●
vlu(2mfdoia●
icwma3c.ws●
zippdm©
A
OcmEG
Aj
0d
Inhibition of Corneal Neovascularization by TopicalBevacizumab (Anti-VEGF) and Sunitinib (Anti-VEGF and
Anti-PDGF) in an Animal Model
JUAN J. PÉREZ-SANTONJA, EZEQUIEL CAMPOS-MOLLO, MARIOLA LLEDÓ-RIQUELME, JAIME JAVALOY,
AND JORGE L. ALIÓAioutf
rfV1semVVatam
drcBasr
VmvmmrrRbact
PURPOSE: To evaluate the effects of topically appliedevacizumab and sunitinib on experimentally inducedorneal neovascularization.DESIGN: Experimental animal study.METHODS: Thirty-six New Zealand rabbits were in-
olved. One eye per rabbit was used. Corneal neovascu-arization was induced by placing 5 silk sutures in thepper cornea. Rabbits were randomized to 1 of 3 groups12 rabbits each): Group 1 received saline 0.9%, Group
bevacizumab 5 mg/mL, and Group 3 sunitinib 0.5g/mL. All treatments were administered 3 times daily
or 14 days. Photographs were taken on a slit lamp onays 7 and 14, and angiographic photographs were takenn day 14. The area of neovascularization was measuredn mm2, percentage of the total corneal area, and percent-ge of the corneal surface covered by sutures.RESULTS: On day 14, corneal neovascularization area
n Group 1 (25.92 � 5.08 mm2, 18.78% � 3.5% oforneal surface, 105.59% � 18.9% of corneal surfaceith sutures) was larger than in Groups 2 (18.52 � 7.94m2, 13.67% � 5.8%, 76.35% � 33.2%) (1-way
nalysis of variance, P � .041) and 3 (4.57 � 2.32 mm2,.40% � 1.7%, 18.94% � 9.2%)(P < .001). Neovas-ularization in Group 2 was larger than in Group 3 (P <001). Compared to saline, corneal neovascularizationas inhibited 28.5% by bevacizumab and 82.3% by
unitinib. Sunitinib settled on the iris.CONCLUSIONS: Topical administration of both bevaci-
umab and sunitinib inhibits corneal neovascularizationn rabbits. But vascular endothelial growth factor (VEGF)athway blockade by bevacizumab was not sufficient for arofound inhibition. Blocking both VEGF and platelet-erived growth factor pathways using sunitinib was 3-foldore effective. (Am J Ophthalmol 2010;150:519–528.2010 by Elsevier Inc. All rights reserved.)
ccepted for publication Apr 18, 2010.From the Refractive Surgery and Cornea Unit, Alicante Institute ofphthalmology/Vissum, Miguel Hernández University School of Medi-
ine, Alicante, Spain (J.J.P.S., J.J., J.L.A.); the Department of Ophthal-ology, Virgen de los Lirios Hospital, Alcoy, Alicante, Spain (J.J.P.S.,.C.M.); and the Department of Ophthalmology, Elche Universityeneral Hospital, Elche, Alicante, Spain (M.L.R.).Inquiries to Juan J. Pérez-Santonja, Instituto Oftalmológico de
slicante/Vissum, Avda. Denia s/n, 03016-Alicante, Spain; e-mail:
© 2010 BY ELSEVIER INC. A002-9394/$36.00oi:10.1016/j.ajo.2010.04.024
NGIOGENESIS IS THE FORMATION OF NEW BLOOD
vessels from preexisting vascular structures.1 In thecornea, it is a not-infrequent consequence of var-
ous inflammatory, infectious, and traumatic corneal dis-rders.2 Corneal neovascularization, however, has thenwanted consequence of opacification of adjacent cornealissue and thus can result in significant reduction in visualunction.1,3
Angiogenesis is a complex multistep process tightlyegulated by the action of both stimulatory (angiogenicactors) and inhibitory (angiogenic inhibitors) molecules.4
ascular endothelial growth factor (VEGF) appears to beof the most important regulators of corneal angiogene-
is.5,6 Corneal epithelial and endothelial cells, vascularndothelial cells of limbal vessels, and fibroblasts andacrophages in scar tissue all have been found to excreteEGF, especially in inflamed and vascularized corneas.1,6
EGF and its tyrosine kinase receptors VEGFR1 (flt-1)nd, particularly, VEGFR2 (flk-1) promote many aspects ofhe angiogenic process. VEGF increases vascular perme-bility of venules and induces vascular endothelial cellitosis and migration.1,7
A second important regulator of angiogenesis is platelet-erived growth factor (PDGF). Newly formed vessels willegress spontaneously unless they are enveloped by peri-ytes, an event promoted by platelet-derived growth factor(PDGFB).8 Vascular endothelial cells produce PDGFB,
nd the surrounding mural cells (pericytes and vascularmooth muscle cells) express platelet-derived growth factoreceptor type � (PDGF receptor type � or PDGFR�).9
Bevacizumab is a monoclonal antibody that binds toEGF with high specificity, thereby blocking VEGF-ediated signaling pathways and thus angiogenesis.10 Be-
acizumab, approved originally for the treatment ofetastatic colorectal cancer,11 has been used in ophthal-ology (off-label) for the treatment of exudative age-
elated macular degeneration, proliferative diabeticetinopathy, and iris rubeosis, with promising results.12,13
ecently, topical and subconjunctival administration ofevacizumab has been reported in experimental modelsnd in human clinical cases for inhibition or regression oforneal neovascularization.14–19 Corneal neovasculariza-ion was inhibited or regressed significantly in the above
tudies, although it was not completely eliminated.LL RIGHTS RESERVED. 519
iI(nptwtsoarba
tiiWbunu
T
oUtHac
tiSutlv1mltptrdpmp
i0zCsldacitto(d
Fp1ao
5
Sunitinib is a small molecule receptor tyrosine kinasenhibitor with antitumor as well as antiangiogenic activity.t is approved by the US Food and Drug AdministrationFDA) for use in the treatment of renal and gastrointesti-al tumors. Sunitinib selectively inhibits VEGFR2 andlatelet-derived growth factor receptor � phosphoryla-ion.20 In ophthalmology, orally administered sunitinibas able to reduce significantly choroidal neovasculariza-
ion in mice.21 As far as we know, there are no previoustudies on topical administration of sunitinib for inhibitionf corneal neovascularization or any other form of ocularngiogenesis. Inhibition of both VEGF and platelet-de-ived growth factor signaling could be more effective inlocking angiogenesis than targeting the VEGF systemlone.
The purpose of this study was to evaluate the effect ofopical administration of bevacizumab and topical admin-stration of sunitinib in the prevention of experimentallynduced corneal neovascularization in a rabbit model.
ith this approach, we test the hypothesis that blockingoth VEGF and platelet-derived growth factor pathwayssing sunitinib is more effective in inhibiting cornealeovascularization than blocking the VEGF system alonesing bevacizumab.
METHODS
HIS EXPERIMENTAL STUDY INVOLVED 36 MALE 2.5-MONTH-
ld New Zealand white rabbits that weighed 2.5 to 3.0 kg.nder general anesthesia induced by intramuscular injec-
ion of ketamine HCl (20 mg/kg body weight) and xylazineCl (6 mg/kg body weight), supplemented by topical
nesthesia (0.4% oxybuprocaine hydrochloride), a modifi-
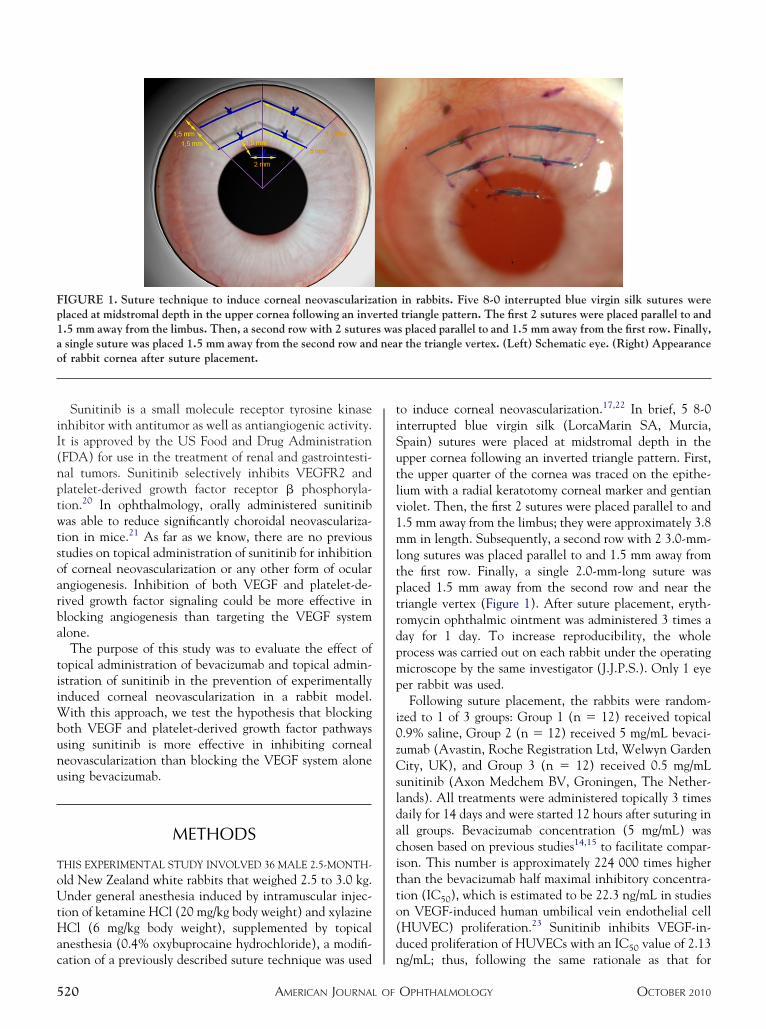
IGURE 1. Suture technique to induce corneal neovascularizalaced at midstromal depth in the upper cornea following an inv.5 mm away from the limbus. Then, a second row with 2 suturesingle suture was placed 1.5 mm away from the second row andf rabbit cornea after suture placement.
ation of a previously described suture technique was used n
AMERICAN JOURNAL OF20
o induce corneal neovascularization.17,22 In brief, 5 8-0nterrupted blue virgin silk (LorcaMarin SA, Murcia,pain) sutures were placed at midstromal depth in thepper cornea following an inverted triangle pattern. First,he upper quarter of the cornea was traced on the epithe-ium with a radial keratotomy corneal marker and gentianiolet. Then, the first 2 sutures were placed parallel to and.5 mm away from the limbus; they were approximately 3.8m in length. Subsequently, a second row with 2 3.0-mm-
ong sutures was placed parallel to and 1.5 mm away fromhe first row. Finally, a single 2.0-mm-long suture waslaced 1.5 mm away from the second row and near theriangle vertex (Figure 1). After suture placement, eryth-omycin ophthalmic ointment was administered 3 times aay for 1 day. To increase reproducibility, the wholerocess was carried out on each rabbit under the operatingicroscope by the same investigator (J.J.P.S.). Only 1 eye
er rabbit was used.Following suture placement, the rabbits were random-
zed to 1 of 3 groups: Group 1 (n � 12) received topical.9% saline, Group 2 (n � 12) received 5 mg/mL bevaci-umab (Avastin, Roche Registration Ltd, Welwyn Gardenity, UK), and Group 3 (n � 12) received 0.5 mg/mL
unitinib (Axon Medchem BV, Groningen, The Nether-ands). All treatments were administered topically 3 timesaily for 14 days and were started 12 hours after suturing inll groups. Bevacizumab concentration (5 mg/mL) washosen based on previous studies14,15 to facilitate compar-son. This number is approximately 224 000 times higherhan the bevacizumab half maximal inhibitory concentra-ion (IC50), which is estimated to be 22.3 ng/mL in studiesn VEGF-induced human umbilical vein endothelial cellHUVEC) proliferation.23 Sunitinib inhibits VEGF-in-uced proliferation of HUVECs with an IC50 value of 2.13
in rabbits. Five 8-0 interrupted blue virgin silk sutures weretriangle pattern. The first 2 sutures were placed parallel to and
s placed parallel to and 1.5 mm away from the first row. Finally,r the triangle vertex. (Left) Schematic eye. (Right) Appearance
tionerteds wanea
g/mL; thus, following the same rationale as that for
OPHTHALMOLOGY OCTOBER 2010

bczmpT(fpi
ccv(
aRFss�dd
(aee�
V
evacizumab (224 000 � 2.13), a 0.5 mg/mL approximateoncentration is obtained. Topical formulation of bevaci-umab consisted of the intravenous solution (25 mg/mL)ixed with 0.9% sterile saline. The final formulation
rovided 5 mL of bevacizumab 5 mg/mL and a pH of 6.4.opical sunitinib consisted of sunitinib malate powder
99% chemical purity) mixed with sterile saline. Finalormulation provided 5 mL of sunitinib 0.5 mg/mL and aH of 6.7. All eye drops were prepared every day before usen the hospital pharmacy and were stored at �4°C.
Just before suture placement, the dimensions of eachornea were measured so that corneal surface area could bealculated. These dimensions included horizontal andertical corneal diameters and anterior chamber depth
TABLE 1. Basic Corneal Dimensions, Calculated CornealExperimental G
Group 1 (Saline)
Horizontal corneal diameter (mm) 12.93 � 0.22
Vertical corneal diameter (mm) 12.03 � 0.33
Mean corneal diameter (mm) 12.48 � 0.22
Corneal radius (mm) 6.24 � 0.11
Anterior chamber depth (mm) 2.22 � 0.23
Corneal surface area (mm2) 138.1 � 6.6
Corneal surface covered by sutures (mm2) 24.63 � 2.48
ANOVA � analysis of variance; SD � standard deviation.
TABLE 2. Corneal Neovascularization by Slit-Lamp
Group 1 (Saline
Square mm 16.96 � 2.5
Percentage of neovascularized area to total
corneal area 12.31 � 1.9
Percentage of neovascularized area to corneal
area covered by sutures 69.18 � 9.7
Inhibition rate 0%
ANOVA � analysis of variance; SD � standard deviation.
TABLE 3. Corneal Neovascularization by Slit-Lamp
Group 1 (Saline
Square mm 25.92 � 5.0
Percentage of neovascularized area to total
corneal area 18.78 � 3.5
Percentage of neovascularized area to corneal
area covered by sutures 105.59 � 18.
Inhibition rate 0%
ANOVA � analysis of variance; SD � standard deviation.
ACD). Corneal diameters were measured using a caliper, (
BEVACIZUMAB/SUNITINIBOL. 150, NO. 4
nd ACD using standard ultrasound biometry (OcuscanxP, Alcon Laboratories Inc, Fort Worth, Texas, USA).or corneal surface area calculation, we considered thehape of the cornea as a spheroidal dome, applying thetraightforward spheroidal dome surface formula S �(r2 � h2), where r represents the radius of the base (r �/2, d � corneal diameter), h represents height of theome (anterior chamber depth), and � � 3.14159.All animals were evaluated by slit-lamp biomicroscopy
slit-lamp biomicroscopy study), once animals had beennesthetized as described above. Rabbit corneas werevaluated by slit-lamp biomicroscopy on the third, sev-nth, and 14th days. Corneal photographs were taken with10 magnification using a FinePrix S2Pro digital camera
ce Area, and Corneal Surface Covered by Sutures in All(Mean � SD)
Group 2 (Bevacizumab) Group 3 (Sunitinib) 1-Way ANOVA
12.80 � 0.25 12.82 � 0.16 P � .270
11.83 � 0.38 11.90 � 0.16 P � .292
12.31 � 0.29 12.36 � 0.10 P � .183
6.15 � 0.14 6.18 � 0.06 P � .183
2.32 � 0.23 2.12 � 0.07 P � .050
136.3 � 7.4 134.2 � 2.8 P � .290
24.37 � 2.23 24.04 � 2.05 P � .818
icroscopy After 7 Days of Treatment (Mean � SD)
Group 2 (Bevacizumab) Group 3 (Sunitinib) 1-Way ANOVA
11.38 � 4.47 2.46 � 0.90 P � .001
8.39 � 3.2 1.82 � 0.6 P � .001
46.65 � 18.4 10.11 � 3.2 P � .001
33% 85.5%
icroscopy After 14 Days of Treatment (Mean � SD)
Group 2 (Bevacizumab) Group 3 (Sunitinib) 1-Way ANOVA
18.52 � 7.94 4.57 � 2.32 P � .001
13.67 � 5.8 3.40 � 1.7 P � .001
76.35 � 33.2 18.94 � 9.2 P � .001
28.5% 82.3%
Surfaroups
Biom
)
1
Biom
)
8
9
Fuji Photo Film Co. Ltd, Tokyo, Japan) attached to the
AND NEW VESSELS 521

spwsamvNe
apVTmmcs
Foc(a
5
lit-lamp microscope (SL-D7; Topcon Corp, Tokyo, Ja-an). On day 3, 2 different calibrated color photographsere taken from each cornea to measure the corneal
urface covered by the sutures. On days 7 and 14, 2 colornd 1 red-free calibrated photographs were taken toeasure the corneal surface covered with neovascular
essels. The mean value from all 3 pictures was used.eovascularization of each cornea was evaluated by an
IGURE 2. Color and red-free photographs of rabbit corneas shn treatment in all experimental groups. (Top) Control group (overed by sutures (stimulating area). (Middle) Inhibition of cGroup 2), with neovascular tissue covering the first 2 rows of sfter administration of topical sunitinib (Group 3), with little
xaminer who was masked to the treatment groups. Image s
AMERICAN JOURNAL OF22
nalysis of each photograph was performed using an imagerocessing and analysis software program (Image-Pro Plus.6.0; Media Cybernetics Inc, Bethesda, Maryland, USA).he corneal surface covered with neovascularization waseasured on the calibrated photographs in terms of squarem, as well as the percentage of the total area of the
ornea and the percentage of the corneal area covered byutures, which might facilitate comparison with previous
g the corneal neovascularization area (yellow line) after 14 dayse) (Group 1) with new vessels covering all the corneal surfaceal neovascularization after topical bevacizumab administrations only. (Bottom) Corneal neovascularization was almost absentts emerging from the limbus.
owinsalinorneuturesprou
tudies.
OPHTHALMOLOGY OCTOBER 2010

raipfl5hsapiTmtcl
bamccsco
vUnvAessuLvwtTs
●
mgdsTT(ctng
●
C
litc
t19nmrsscof(
a3si(c
V
All animals were also evaluated by fluorescein angiog-aphy on day 14 (angiography study). Anterior segmentngiography was performed after intravenous injectionnto the ear vein of 0.3 mL/kg of 10% fluorescein. Cornealhotographs were taken between 2 and 3 minutes afteruorescein injection using a Nikon fundus camera (NFC-0; Nikon Corporation, Tokyo, Japan). Three differentigh-quality calibrated photographs were chosen to mea-ure the corneal surface covered with neovascular vessels,nd the mean value was used. The image analysis of eachhotograph was performed using the same image process-ng software program used for the biomicroscopy study.he corneal surface covered with neovascular vessels waseasured in terms of square mm (mm2), percentage of the
otal area of the cornea, and percentage of the corneal areaovered by sutures. After measuring the area of neovascu-arization, the animals were killed.
A screening for adverse ocular effects was also performedy slit-lamp biomicroscopy on days 7 and 14, and anydverse effects were recorded, as well as photographed andeasured if appropriate. Specifically, attention was paid to
onjunctival hyperemia, corneal epitheliopathy, anteriorhamber cellular reaction (number of inflammatory cellseen in a 1 � 3-mm high-powered beam), and iris and lenshanges. Fundus examination was performed by indirectphthalmoscopy before the animals were killed.Statistical analysis was performed using SPSS software
ersion 15.0 for Windows (SPSS, Inc, Chicago, Illinois,SA). Parametric statistical analyses were done, once theormal distribution of the data under consideration waserified by the 1-sample Kolmogorov-Smirnov procedure.nalysis was first performed on the changes over time in
ach group for corneal neovascularization using the paired-amples Student t test. Subsequently, group differences atpecific time points for continuous variables were testedsing the 1-way analysis of variance (1-way ANOVA).evene statistic was used to test the equality of groupariances in 1-way ANOVA. When the group variancesere equal pairwise multiple comparisons were tested using
he Tukey test, and when they were unequal using theamhane test. Differences were considered statistically
TABLE 4. Corneal Neovascularization by Fluorescei
Group 1 (Saline)
Square mm 26.39 � 4.54
Percentage of neovascularized area to total
corneal area 19.11 � 3.1
Percentage of neovascularized area to corneal
area covered by sutures 107.67 � 17.2
Inhibition rate 0%
ANOVA � analysis of variance; SD � standard deviation.
ignificant when P values were less than .05. c
BEVACIZUMAB/SUNITINIBOL. 150, NO. 4
RESULTS
BASIC CORNEAL DIMENSIONS: The basic corneal di-ensions and calculated corneal surface area for each
roup are shown in Table 1. There were no significantifferences in basic dimensions and calculated cornealurface area between groups (1-way ANOVA, P � .05).he corneal surface covered by sutures is also shown inable 1, with no significant differences between groups
1-way ANOVA, P � .818). These results show thatorneal dimensions were similar for all groups beforereatment. In addition, the amount of stimulus to induce aeovascular response in the cornea was also similar in allroups.
CORNEAL NEOVASCULARIZATION BY SLIT-LAMP BIOMI-
ROSCOPY: The corneal surface covered with neovascu-arization measured on the calibrated photographs is shownn Tables 2 and 3 in terms of square mm, percentage of theotal area of the cornea, and percentage of the corneal areaovered by sutures, for all 3 groups.
In Group 1 (saline), corneal neovascularization area onhe seventh day was 16.96 � 2.51 mm2, which represents2.31% � 1.9% of total corneal surface and 69.18% �.7% of all corneal surface covered by sutures. The cornealeovascular area increased significantly up to 25.92 � 5.08m2 on day 14 (paired-samples t test, P � .001), which
epresents 18.78% � 3.5% (P � .001) of total cornealurface and 105.59% � 18.9% (P � .001) of cornealurface covered by sutures. These results show that theorneal surface covered with neovascular vessels increasesver time in Group 1, and 14 days are more than enoughor the new vessels to cover all the stimulating areacorneal surface covered by sutures).
In Group 2 (bevacizumab), corneal neovascularizationrea on the seventh day was 11.38 � 4.47 mm2 (8.39% �.2% of total corneal surface, 46.65% � 18.4% of cornealurface covered by sutures). The neovascular area alsoncreased significantly up to 18.52 � 7.94 mm2 on day 14paired-samples t test, P � .001) (13.67% � 5.8% of totalorneal surface and 76.35% � 33.2% of corneal surface
iography After 14 Days of Treatment (Mean � SD)
Group 2 (Bevacizumab) Group 3 (Sunitinib) 1-Way ANOVA
18.84 � 8.27 4.75 � 2.23 P � .001
13.92 � 6.1 3.53 � 1.6 P � .001
77.58 � 34.3 19.72 � 9.0 P � .001
28.6% 82%
n Ang
overed by sutures) (P � .001). Therefore, the corneal
AND NEW VESSELS 523

s1n
ooci(cccgw
it.siiFl(lisb(
cl(sciFlaAG(no
s
Fmlccbr(s
AMERICAN JOURNAL OF524
urface covered with new vessels increases over time, but at4 days only 76.35% of the stimulating area was covered byeovascular tissue.In Group 3 (sunitinib), corneal neovascularization area
n the seventh day was 2.46 � 0.90 mm2 (1.82% � 0.6%f total corneal surface, 10.11% � 3.2% of corneal surfaceovered by sutures). The corneal neovascular area alsoncreased significantly, up to 4.57 � 2.32 mm2 on day 14paired-samples t test, P � .002) (3.40% � 1.7% of totalorneal surface and 18.94% � 9.2% of corneal surfaceovered by sutures) (P � .001). The corneal surfaceovered with new vessels also increased over time in thisroup, but on day 14 only 18.94% of the stimulating areaas covered by new vessels.Seven days after treatment onset, corneal neovascular-
zation area (in terms of square mm) in Group 1 was largerhan in Groups 2 (1-way ANOVA, P � .005) and 3 (P �001). Similarly, neovascularization area in Group 2 wasignificantly larger than in Group 3 (P � .001). Therefore,n comparison with saline, corneal neovascularization wasnhibited 33% by bevacizumab and 85.5% by sunitinib.ourteen days after onset of treatment, corneal neovascu-arization area in Group 1 was also larger than in Groups 21-way ANOVA, P � .041) and 3 (P � .001). Neovascu-arization area in Group 2 was also significantly larger thann Group 3 (P � .001). Therefore, in comparison withaline, corneal neovascularization was inhibited 28.5% byevacizumab on the 14th day and 82.3% by sunitinibFigure 2).
In terms of percentage of the total area of the cornea,orneal neovascularization area on day 7 in Group 1 wasarger than in Groups 2 (1-way ANOVA, P � .007) and 3P � .001). Neovascularization surface in Group 2 was alsoignificantly larger than in Group 3 (P � .001). Inomparison with saline, corneal neovascularization wasnhibited 31.8% by bevacizumab and 85.2% by sunitinib.ourteen days after onset of treatment, corneal neovascu-arization area in Group 1 was larger than in Group 2,lthough this difference was not significant (1-wayNOVA, P � .055). However, neovascularization areas inroups 1 and 2 were significantly larger than in Group 3
P � .001). Therefore, in comparison with saline, cornealeovascularization was inhibited 27.2% by bevacizumabn day 14 and 81.9% by sunitinib.In terms of percentage of the corneal area covered by
utures, corneal neovascularization surface on day 7 in
IGURE 3. Angiographic photographs on day 14 after treat-ent onset in all experimental groups showing the neovascu-
arization area (outlined with a continuous line) in the upperornea. (Top) Control group (saline) (Group 1) with neovas-ular tissue extending throughout the corneal surface coveredy sutures. (Middle) Neovascular tissue covering the first 2ows of sutures after bevacizumab application (Group 2).Bottom) Little sprouts emerging from the limbus after
unitinib administration (Group 3).OPHTHALMOLOGY OCTOBER 2010

G.i(lbnGNcchs
●
A
sita
rsmas
tl(G.o2G.obrs8c
●
sia1s
iN5(
e
H(1(ispap(ya(iciedw
C
tqc
Fiaosg
V
roup 1 was larger than in Groups 2 (1-way ANOVA, P �005), and 3 (P � .001). The area with neovascularizationn Group 2 was also significantly larger than in Group 3P � .001). In comparison with saline, corneal neovascu-arization was inhibited 32.5% by bevacizumab and 85.4%y sunitinib. On day 14 after onset of treatment, cornealeovascularization area in Group 1 was larger than inroups 2 (1-way ANOVA, P � .049) and 3 (P � .001).eovascularization surface in Group 2 was also signifi-
antly larger than in Group 3 (P � .001). Therefore, asompared with saline, corneal neovascularization was in-ibited 27.7% by bevacizumab on day 14 and 82% byunitinib.
CORNEAL NEOVASCULARIZATION BY FLUORESCEIN
NGIOGRAPHY: The corneal area covered with new ves-els measured on the calibrated angiographic photographss shown in Table 4 in terms of square mm, percentage ofhe total area of the cornea, and percentage of the cornealrea covered by sutures, for all 3 groups.
Corneal neovascularization area by fluorescein angiog-aphy was not significantly different from that measured bylit-lamp biomicroscopy for all 3 groups, in terms of squarem (paired-samples t test, P � .1), percentage of the total
rea of the cornea (P � .1), and percentage of the cornealurface covered by sutures (P � .1).
On angiographic photographs, 14 days after onset ofreatment, corneal neovascularization area in Group 1 wasarger than in Groups 2 and 3, in terms of square mm1-way ANOVA, P � .039 for Group 2, P � .001 forroup 3), percentage of the total area of the cornea (P �
049 for Group 2, P � .001 for Group 3), and percentagef the corneal area covered by sutures (P � .045 for Group, P � .001 for Group 3). Neovascularization area inroup 2 was also significantly larger than in Group 3 (P �
001). As compared with saline, corneal neovascularizationn day 14 was inhibited 28.6% by bevacizumab and 82%y sunitinib, in terms of square mm (27.2% and 81.52%,espectively, when corneal neovascularization area istated as percentage of the total corneal area; 27.9% and1.7%, respectively, when stated as percentage of theorneal area covered by sutures) (Figure 3).
ADVERSE OCULAR EFFECTS: In Group 1 (saline), noigns of conjunctival hyperemia, corneal epitheliopathy, orris or lens changes were observed on days 7 or 14. However,nterior chamber cellular reaction (between 5 and 10 cells/� 3-mm beam) was observed in 1 eye (8.3%) on the
eventh day. Fundus examination was normal.In Group 2 (bevacizumab), no conjunctival, corneal,
ris, or lens changes were observed on days 7 or 14.evertheless, anterior chamber cellular reaction (betweenand 10 cells/1 � 3-mm beam) was observed in 1 eye
8.3%) on day 7. Fundus examination was also normal.In Group 3 (sunitinib), no signs of conjunctival hyper-
mia or lens changes were observed on days 7 or 14. i
BEVACIZUMAB/SUNITINIBOL. 150, NO. 4
owever, on day 7 an anterior chamber cellular reactionbetween 5 and 10 cells/1 � 3-mm beam) was observed ineye (8.3%) and iris surface yellowish staining in 12 eyes
100%). Iris staining represents sunitinib deposits on theris surface, since sunitinib is yellow in color. Sunitinibettles on the inferior quadrant of the iris, starting at theupil rim and spreading to some extent between the pupilnd the anterior chamber angle. As measured on calibratedhotographs, iris staining area was 19.94 � 8.8 mm2
18.59% � 8.7% of total iris area) on day 7. On day 14, irisellowish staining was also observed in 12 eyes (100%),nd it had increased significantly up to 28.77 � 14.7 mm2
paired-samples t test, P � .021) (26.98% � 12.9% of totalris area) (P � .013) (Figure 4). On day 14, traces oforneal epithelium yellowish staining were also observedn 5 eyes (41.6%). Sunitinib deposits into the cornealpithelium were tiny, located at midperipheral cornea, andisappeared after epithelial scraping. Fundus examinationas normal.
DISCUSSION
ORNEAL NEOVASCULARIZATION REPRESENTS AN IMPOR-
ant cause of diminished corneal transparency and subse-uent reduction of vision.7 Diseases associated withorneal neovascularization include inflammatory disorders,
IGURE 4. Slit-lamp photograph showing iris surface yellow-sh staining in a rabbit eye after 14 days of sunitinib topicalpplication. Iris yellowish staining represents sunitinib depositsn the iris surface, since sunitinib is yellow in color. As shown,unitinib settles on the inferior quadrant of the iris because ofravity.
nfectious keratitis, contact lens–related hypoxia, alkali
AND NEW VESSELS 525

bCg
oirlvtVi
IabVsrcvisioiicrdctjtrii32sosc
liwtaoi
tl
rse(arvpon
kadPamadk(totctssn
rtorbpctmiwcitttai21sa
be
5
urns, stromal ulceration, and limbal stem cell deficiency.1
orneal neovascularization is also a major risk factor forraft rejection after penetrating keratoplasty.3
VEGF appears to be 1 of the most important regulatorsf corneal angiogenesis, both in experimental models andn the human cornea.5,6 VEGF and its tyrosine kinaseeceptors VEGFR1 and, mainly, VEGFR2 promote proteo-ytic degradation of the extracellular matrix and induceascular endothelial cell mitosis, migration, and capillaryube formation of the angiogenic process.1,7 Therefore,EGF antagonists might prevent or reduce neovascular-
zation, which would be of great clinical usefulness.Bevacizumab is a recombinant humanized monoclonal
gG1 antibody that binds to and inhibits the biologicalctivity of human VEGF in vitro and in vivo. Bevacizumabinds to all 5 VEGF-A isoforms, VEGF115, VEGF121,EGF165, VEGF189, and VEGF206.11 Recently, topical and
ubconjunctival administration of bevacizumab has beeneported in experimental animal models and in humanlinical cases for inhibition or regression of corneal neo-ascularization.14–19,24–27 Corneal neovascularization wasnhibited significantly between 32.2% and 88.5% after aingle subconjunctival injection of bevacizumab in exper-mental rabbit models.19,24 Several studies have also dem-nstrated the effects of topical bevacizumab in thenhibition of corneal neovascularization, with figures rang-ng from 20% to 79.7% in animal experiments.14,25 Re-ently, administration of bevacizumab has also beeneported in human clinical cases, either in the form ofrops or administered subconjunctivally. In these cases,orneal neovascularization was reduced significantly, be-ween 14.5% and 26.9% after single subconjunctival in-ection26 and between 28% and 48% after long-termopical administration.15,27 Similarly, our experimentalesults demonstrated that topical bevacizumab significantlynhibited corneal neovascularization in rabbits. In compar-son with saline, corneal neovascularization was inhibited3% by topical bevacizumab after 7 days of treatment and8% after 14 days, regardless of whether the results aretated in terms of square mm, percentage of the total areaf the cornea, or percentage of the corneal area covered byutures. Similar results were obtained by slit-lamp biomi-roscopy and fluorescein angiography.
In the above studies, including ours, corneal neovascu-arization was inhibited or regressed significantly, althought was not completely eliminated. Therefore, VEGF path-ay blockade prevents or reduces corneal neovasculariza-
ion, but it is not sufficient for a profound inhibition ofngiogenesis. This finding could be explained by presencef other regulators of angiogenesis, which might workrrespective of or in conjunction with VEGF.
Newly formed vessels will regress spontaneously unlesshey are enveloped by mural cells (pericytes around capil-
aries and smooth muscle cells around larger vessels).8 The lAMERICAN JOURNAL OF26
ecruitment of pericytes to the vascular bed increases thetability of the vessels.4 The recruitment of mural cells tondothelial cells requires platelet-derived growth factor BPDGFB), which is produced by vascular endothelial cells,nd signaling through the platelet-derived growth factoreceptor type � (PDGFR�) expressed by pericytes andascular smooth muscle cells.9 In mice, inhibition of thelatelet-derived growth factor signal pathway results in lossf pericytes and in reduction of vessel density in cornealeovascularization.28
Sunitinib is an oral small molecule receptor tyrosineinase inhibitor that exhibits potent antitumor and anti-ngiogenic activity. Sunitinib inhibits angiogenesis byiminishing signaling through VEGFR1, VEGFR2, andDGFR�, all of which are tyrosine kinase receptors,9
lthough VEGFR2 and PDGFR� seem to be the mainediators of angiogenesis.4 Sunitinib inhibits VEGFR2
nd PDGFR� phosphorylation in a time- and dose-depen-ent manner.20 Sunitinib inhibits other receptor tyrosineinases including stem cell factor receptor c-KIT, FLT3fms-related tyrosine kinase), and colony-stimulating fac-or 1 receptor (CSF-1R), which are involved in a numberf malignancies.29 Sunitinib was shown to be effective andolerated by patients in clinical trials for advanced renalell carcinoma and gastrointestinal stromal tumors, leadingo US FDA approval.29 In ophthalmology, a previous studyhowed that orally administered sunitinib was able toignificantly reduce the volume of experimental choroidaleovascularization membranes in mice.21
As far as we know, no previous studies have beeneported on topical administration of sunitinib for inhibi-ion of corneal neovascularization or any other form ofcular angiogenesis, after a PubMed search as literatureeview method. In our study, we test the hypothesis thatlocking both VEGF and platelet-derived growth factorathways using sunitinib is more effective in inhibitingorneal neovascularization in a rabbit model than blockinghe VEGF system alone using bevacizumab. Our experi-ental results showed that topical sunitinib significantly
nhibited corneal neovascularization, and this inhibitionas 2.9 times more profound than that by bevacizumab. Inomparison with saline, corneal neovascularization wasnhibited 85.5% by topical sunitinib after 7 days ofreatment and 82.3% after 14 days, regardless of whetherhe results are quoted in terms of square mm, percentage ofhe total area of the cornea, or percentage of the cornealrea covered by sutures. As compared with bevacizumab,nhibition of corneal neovascularization was 2.6-fold and.9-fold more profound with topical sunitinib, after 7 and4 days of treatment, respectively. The results obtained bylit-lamp biomicroscopy were similar to those observed byngiography.
Concerning adverse ocular effects, mild anterior cham-er cellular reaction was observed in 1 eye of eachxperimental group after 7 days of treatment, which is
ikely related to the surgical technique used. In Group 3OPHTHALMOLOGY OCTOBER 2010

(asiaiefiugnrr
bs
magcrffidebsimuc
PlnicaDoC
V
sunitinib), iris surface yellowish staining was observed inll eyes, which represents sunitinib deposits on the irisurface. Sunitinib settled on the inferior quadrant of theris, likely induced by gravity, and the sunitinib depositrea increased significantly with time to up to 27% of totalris area. Traces of sunitinib deposits into the cornealpithelium were also observed in 41% of eyes. Thesendings indicate that sunitinib is able to reach the intraoc-lar space after topical application, a fact that could be ofreat clinical usefulness for the treatment of intraoculareovascular diseases, such as iris rubeosis, exudative age-elated macular degeneration, and proliferative diabeticetinopathy.
In summary, our study shows that topically administeredevacizumab, a VEGF antagonist, significantly inhibits
uture-induced corneal neovascularization in a rabbit e2036–2053.
1
1
1
1
1
1
1
1
BEVACIZUMAB/SUNITINIBOL. 150, NO. 4
odel, but it was not sufficient for a profound inhibition ofngiogenesis. A novel, topically administered, multitar-eted receptor tyrosine kinase inhibitor, sunitinib, signifi-antly and deeply inhibits corneal neovascularization inabbit eyes. This inhibition was almost 3-fold more pro-ound than that achieved by topical bevacizumab. Thesendings indicate that blocking both VEGF and platelet-erived growth factor pathways using sunitinib is moreffective in inhibiting corneal neovascularization thanlocking the VEGF system alone using bevacizumab. Ourtudy also shows that sunitinib is able to reach thentraocular space after topical application, a fact thatight be of clinical usefulness for the treatment of intraoc-
lar neovascular diseases. These results mandate furtherlinical investigation of topical sunitinib for neovascular
ye diseases, both corneal and intraocular.UBLICATION OF THIS ARTICLE WAS SUPPORTED IN PART BY A RESEARCH GRANT FROM THE CONSELLERIA DE SANITAT DEa Comunidad Valenciana, Dirección General de Ordenación, Evaluación e Investigación Sanitaria (AP-004/08), Valencia, Spain. The authors haveo financial conflict of interest. Involved in conception and design (J.J.P.S., E.C.M.); data collection (J.J.P.S., E.C.M., M.L.R.); analysis and
nterpretation (J.J.P.S., M.L.R., J.J.); statistical expertise (J.J., J.L.A.); writing the article (J.J.P.S., E.C.M.); literature search (J.J.P.S., E.C.M., M.L.R.);ritical revision (J.J., J.L.A.); and final approval (J.J.P.S., J.L.A.). Animal housing, feeding, and general care followed Association for Research in Visionnd Ophthalmology guidelines. Every procedure involving animals was conducted in accordance with the Declaration of Helsinki, with Councilirective 86/609/EEC of 24-11-1986 of the European Union, as well as Spanish laws and regulations (Royal Decree 1201/2005) regarding the protectionf animals used for experimental and other scientific purposes. The experimental protocol was approved by the Institutional Animal Care and Useommittee of Miguel Hernandez University, Alicante, Spain.
REFERENCES
1. Azar DT. Corneal angiogenic privilege: angiogenic andantiangiogenic factors in corneal avascularity, vasculogen-esis, and wound healing (an American OphthalmologicalSociety thesis). Trans Am Ophthalmol Soc 2006;104:264–302.
2. Cursiefen C, Kuchle M, Naumann GO. Angiogenesis incorneal diseases: histopathologic evaluation of 254 humancorneal buttons with neovascularization. Cornea 1998;17(6):611–613.
3. Dana MR, Schaumberg DA, Kowal VO, et al. Cornealneovascularization after penetrating keratoplasty. Cornea1995;14(6):604–609.
4. Kvanta A. Ocular angiogenesis: the role of growth factors.Acta Ophthalmol Scand 2006;84(3):282–288.
5. Gan L, Fagerholm P, Palmblad J. Vascular endothelialgrowth factor (VEGF) and its receptor VEGFR-2 in theregulation of corneal neovascularization and wound healing.Acta Ophthalmol Scand 2004;82(5):557–563.
6. Philipp W, Speicher L, Humpel C. Expression of vascularendothelial growth factor and its receptors in inflamed andvascularized human corneas. Invest Ophthalmol Vis Sci2000;41(9):2514–2522.
7. Chang JH, Gabison EE, Kato T, Azar DT. Cornealneovascularization. Curr Opin Ophthalmol 2001;12(4):242–249.
8. Jo N, Mailhos C, Ju M, et al. Inhibition of platelet-derivedgrowth factor B signaling enhances the efficacy of anti-vascular endothelial growth factor therapy in multiple mod-els of ocular neovascularization. Am J Pathol 2006;168(6):
9. Roskoski R Jr. Sunitinib: a VEGF and PDGF receptor proteinkinase and angiogenesis inhibitor. Biochem Biophys ResCommun 2007;356(2):323–328.
0. Han YS, Lee JE, Jung JW, Lee JS. Inhibitory effects ofbevacizumab on angiogenesis and corneal neovasculariza-tion. Graefes Arch Clin Exp Ophthalmol 2009;247(4):541–548.
1. Kramer I, Lipp HP. Bevacizumab, a humanized anti-angio-genic monoclonal antibody for the treatment of colorectalcancer. J Clin Pharm Ther 2007;32(1):1–14.
2. Avery RL. Regression of retinal and iris neovascularizationafter intravitreal bevacizumab (Avastin) treatment. Retina2006;26(3):352–354.
3. Avery RL, Pieramici DJ, Rabena MD, Castellarin AA, NasirMA, Giust MJ. Intravitreal bevacizumab (Avastin) for neo-vascular age-related macular degeneration. Ophthalmology2006;113(3):363–372.
4. Bock F, Onderka J, Dietrich T, et al. Bevacizumab as a potentinhibitor of inflammatory corneal angiogenesis and lym-phangiogenesis. Invest Ophthalmol Vis Sci 2007;48(6):2545–2552.
5. Bock F, Konig Y, Kruse F, Baier M, Cursiefen C. Bevacizumab(Avastin) eye drops inhibit corneal neovascularization. GraefesArch Clin Exp Ophthalmol 2008;246(2):281–284.
6. DeStafeno JJ, Kim T. Topical bevacizumab therapy forcorneal neovascularization. Arch Ophthalmol 2007;125(6):834–836.
7. Kim TI, Kim SW, Kim S, Kim T, Kim EK. Inhibition ofexperimental corneal neovascularization by using subcon-junctival injection of bevacizumab (Avastin). Cornea 2008;
27(3):349–352.AND NEW VESSELS 527

1
1
2
2
2
2
2
2
2
2
2
2
5
8. Manzano RP, Peyman GA, Khan P, et al. Inhibition ofexperimental corneal neovascularisation by bevacizumab(Avastin). Br J Ophthalmol 2007;91(6):804–807.
9. Papathanassiou M, Theodossiadis PG, Liarakos VS, Rouvas A,Giamarellos-Bourboulis EJ, Vergados IA. Inhibition of cornealneovascularization by subconjunctival bevacizumab in an ani-mal model. Am J Ophthalmol 2008;145(3):424–431.
0. Mendel DB, Laird AD, Xin X, et al. In vivo antitumoractivity of SU11248, a novel tyrosine kinase inhibitortargeting vascular endothelial growth factor and platelet-derived growth factor receptors: determination of a pharma-cokinetic/pharmacodynamic relationship. Clin Cancer Res2003;9(1):327–337.
1. Takahashi H, Obata R, Tamaki I. A novel vascularendothelial growth factor receptor 2 inhibitor, SU11248,suppresses choroidal neovascularization in vivo. J OculPharmacol Ther 2006;22(4):213–218.
2. Schmidt-Erfurth U, Hasan T, Schomacker K, Flotte T,Birngruber R. In vivo uptake of liposomal benzoporphyrinderivative and photothrombosis in experimental cornealneovascularization. Lasers Surg Med 1995;17(2):178–188.
3. Wang Y, Fei D, Vanderlaan M, Song A. Biological activity ofbevacizumab, a humanized anti-VEGF antibody in vitro.
Angiogenesis 2004;7(4):335–345.AMERICAN JOURNAL OF28
4. Hosseini H, Nejabat M, Mehryar M, Yazdchi T, Sedaghat A,Noori F. Bevacizumab inhibits corneal neovascularization inan alkali burn induced model of corneal angiogenesis. ClinExperiment Ophthalmol 2007;35(8):745–748.
5. Yoeruek E, Ziemssen F, Henke-Fahle S, et al. Safety,penetration and efficacy of topically applied bevacizumab:evaluation of eyedrops in corneal neovascularization afterchemical burn. Acta Ophthalmol 2008;86(3):322–328.
6. You IC, Kang IS, Lee SH, Yoon KC. Therapeutic effect ofsubconjunctival injection of bevacizumab in the treatment ofcorneal neovascularization. Acta Ophthalmol 2009;87(6):653–658.
7. Koenig Y, Bock F, Horn F, Kruse F, Straub K, Cursiefen C.Short- and long-term safety profile and efficacy of topicalbevacizumab (Avastin) eye drops against corneal neovascu-larization. Graefes Arch Clin Exp Ophthalmol 2009;247(10):1375–1382.
8. Dell S, Peters S, Muther P, Kociok N, Joussen AM. The roleof PDGF receptor inhibitors and PI3-kinase signaling in thepathogenesis of corneal neovascularization. Invest Ophthal-mol Vis Sci 2006;47(5):1928–1937.
9. Chow LQ, Eckhardt SG. Sunitinib: from rational design to
clinical efficacy. J Clin Oncol 2007;25(7):884–896.OPHTHALMOLOGY OCTOBER 2010

JriOS
V
Biosketch
uan J. Pérez-Santonja received his medical degree from the University of Alicante (1987), Spain, and completed hisesidency training in Ophthalmology at Jiménez-Díaz Foundation Hospital in Madrid (1993). He completed a Fellowshipn Cornea and External Diseases at Moorfields Eye Hospital, London, UK (2001). He achieved European Board ofphthalmology Certification in 1996. He currently serves as Head of Ophthalmology Department at Alcoy Hospital,pain, and as Ophthalmic Surgeon at Alicante Institute of Ophthalmology/Vissum, Alicante, Spain.
BEVACIZUMAB/SUNITINIB AND NEW VESSELSOL. 150, NO. 4 528.e1
Copyright © 2022 FDOKUMEN




















