ORIGINAL ReseARches Isolated renal hydatid cyst ... - Zenodo
Upload
independentCategory
view
2download
0
1
VEGF receptor inhibition blocks liver cyst growth in pkd2(WS25/-) mice
Claudia R. Amura1, Kelley S. Brodsky1, Rachel Groff1, Vincent H. Gattone2,Norbert F. Voelkel1 and R. Brian Doctor1
1 Department of Medicine University of Colorado Health Sciences Center
Denver, CO 80262
2 Department of Anatomy and Cell Biology Indiana University School of Medicine
Indianapolis, IN 46202
Running Head: VEGF induces liver cyst growth
Corresponding Author: R. Brian Doctor, Ph.D. Box B158 4200 E. 9th Avenue Denver, CO 80262 [email protected]: 303-315-3507
Page 1 of 29 Articles in PresS. Am J Physiol Cell Physiol (May 2, 2007). doi:10.1152/ajpcell.00038.2007
Copyright © 2007 by the American Physiological Society.

2ABSTRACT
Proliferation of the cyst lining epithelial cells is an integral part of ADPKD cyst growth. Cytokines
and growth factors within cyst fluids are positioned to induce cyst growth. Vascular endothelial growth
factor (VEGF) is a pleitropic growth factor present in ADPKD liver cyst fluids (human: 1,128 + 78 pg/ml;
mouse: 2,787 + 136 pg/ml) and, to a lesser extent, in ADPKD renal cyst fluids (human: 294 + 41 pg/ml;
mouse: 191 + 90 pg/ml). Western blotting showed receptors for VEGF (VEGFR1 and VEGFR2) were
present in both normal mouse bile ducts and pkd2(WS25/-) liver cyst epithelial cells. Treatment of
pkd2(WS25/-) liver cyst epithelial cells with VEGF (50–50,000 pg/ml) or liver cyst fluid induced a
proliferative response. The effect on proliferation from liver cyst fluid was inhibited by SU5416, a potent
VEGF receptor inhibitor. Treatment of pkd2(WS25/-) mice between 4 and 8 months of age with SU5416
markedly reduced the cyst volume density of the liver (Vehicle: 9.9 + 4.3 % of liver; SU5416: 1.8 + 0.7 %
of liver). SU5416 treatment between 4 and 12 months of age markedly protected against increases in
liver weight (pkd2(+/+): 4.8 + 0.2 %BW; pkd2(WS25/-)-Vehicle: 10.8 + 1.9 %BW; pkd2(WS25/-)-
SU5416: 4.8 + 0.4 %BW). The capacity of VEGF signaling to induce in vitro proliferation of pkd2(WS25/-)
liver cyst epithelial cells and inhibition of in vivo VEGF signaling to retard liver cyst growth in
pkd2(WS25/-) mice indicates the VEGF signaling pathway is a potentially important therapeutic target in
the treatment of ADPKD liver cyst disease.
KEYWORDS Autosomal dominant polycystic kidney disease
SU5416
Growth factors
cytokines
Page 2 of 29

3INTRODUCTION Autosomal dominant polycystic kidney disease (ADPKD) is a genetic disease that occurs in ~1 in
800 individuals. The clinical symptoms generally appear after the third decade of life. The most prevalent
clinical manifestation of ADPKD is the development of renal cysts and loss of renal function. ADPKD
accounts for >5% of all end stage renal disease. The most common extrarenal manifestation, accounting
for up to 10% of ADPKD morbidity and mortality, is the development of liver cysts. Within a clinically
affected liver, the liver parenchymal volume does not change significantly (1) but the liver can have
hundreds of distinct cysts with cysts reaching several centimeters in diameter. In the liver, the clinical
manifestations of ADPKD are associated directly with the compression of the surrounding tissues,
organs and vasculature. Consequently, growth of liver cysts is considered a key element in the onset of
the clinical features. Medical therapies that block liver cyst growth are predicted to largely eliminate the
clinical consequences of ADPKD liver cyst disease.
ADPKD is considered a molecular recessive disease and is linked to mutations in either the
PKD1 or PKD2 genes. Affected individuals are predicted to have a germ line mutation in one copy of the
gene and, during their lifetime, undergo a somatic mutation in individual cells in the second copy of the
gene. In the kidney, cysts emerge from epithelial cells lining the nephron. In the liver, cysts emerge from
cholangiocytes, the epithelial cells lining the intrahepatic bile duct. Following the gene mutation,
individual epithelial cells undergo clonal expansion to initially form an outpocket from the nephron or duct
and, subsequently detach from the original nephron or duct to form an autonomous, enclosed cyst within
the body of the organ. Lined by a single layer of epithelial cells, these cysts continue to grow and emerge
from the organs as superficial cysts. In the case of the ADPKD liver, cysts can enlarge to the point where
the total liver volume more than doubles.
While cystogenesis is linked to mutations in the PKD1 and PKD2 genes, the development of the
disease is markedly heterogeneous. Part of this heterogeneity may be influenced by the nature of the
germline mutation and the nature of the second, somatic mutation. However, sibship studies and linkage
analyses indicate much of the heterogeneity is likely due to modifier genes and extragenetic factors (2).
One potential source of extragenetic influence is autocrine/paracrine signaling by cytokines and growth
factors synthesized and released by epithelial cells that line the cysts (3; 4). Vascular endothelial growth
factor (VEGF) is among these identified factors. Under physiologic conditions, VEGF promotes
angiogenesis in developing tissues and helps maintain the status of established endothelial cells (5).
VEGF also contributes to the pathophysiology of specific tumors by promoting their neovascularization
(6). Accordingly, the present study investigated the contribution of VEGF to the growth of ADPKD cysts.
It showed that [1] VEGF accumulates in ADPKD liver cyst fluid to levels that can drive the proliferation of
liver cyst epithelial cells in culture and [2] inhibition of the VEGF signaling pathway in vivo markedly
inhibits liver cyst growth in a mouse model of ADPKD.
Page 3 of 29

4METHODS Pkd2(WS25/-) Mouse Model C57BL/6 pkd2(WS25/-) mice were developed by Stefan
Somlo (Yale University) and breeding pairs were provided for this project (7). The animals were cared for
in the Center for Laboratory Animal Research at UCHSC and all experimental protocols were approved
by the UCHSC Animal Care and Use Committee. C57BL/6 Pkd2(+/-) and C57BL/6 pkd2(WS25/+) mice
were used as breeding pairs to generate pkd2(WS25/-) mice for the study. Mice were genotyped by
Southern blotting (7). Briefly, DNA was isolated from tail snips (Gentra Systems; Minneapolis, MN) and
digested overnight with Pst-1 restriction enzyme (Promega; Madison, WI). The cut DNA was run out on a
0.7% agarose gel and transferred onto nylon membranes overnight. A DNA probe specific to the
recombinant region was labeled with 32P by random priming (Decaprime II/Ambion; Austin, TX). The
probes were incubated with the blots overnight. Labeled blots were washed and developed by
autoradiography. Pkd2(WS25/-) mice closely model the human condition by having one copy of pkd2
knocked out and having a second, recombinant-sensitive allele (i.e. WS25) that undergoes high rates of
recombination to yield knock outs of the second copy of the gene in somatic cells during the life span of
the animals. By four months of age, pkd2(WS25/-) mice develop discernible kidney and liver cysts. Over
the subsequent four to eight months, these cysts grow and emerge from the tissues.
Culture of pkd2(WS25/-) liver cyst epithelial cells Liver cyst epithelial cells (termed pkd2
cells) were isolated from pkd2(WS25/-) mice and grown in culture (8). Unless otherwise noted, media
and reagents for cell cultures were obtained from Gibco-Invitrogen (Carlsbad, CA). Pkd2(WS25/-) mice
were grown to 10-12 months of age to allow the liver cysts to grow out from the liver. Mice were
euthanized and superficial liver cyst wall tissues were excised and finely minced under clean conditions.
The minced tissue was suspended in 20 ml of Growth Media (DMEM-F12; 5% fetal bovine serum
(Hyclone; Logan, UT), 2 mM glutamine, 1% non-essential amino acids, 1% lipid concentrate, 1% vitamin
solution, 393 ng/ml dexamethasone (Sigma; St. Louis, MO), 25 ng/ml epidermal growth factor (Upstate
Biologics, Lake Placid, NY), 30 µg/ml bovine pituitary extract (Upstate Biologics, Lake Placid, NY), 3.4
µg/ml triiodothyrodine, 1% insulin-transferrin-Se, 0.4 µg/ml forskolin (Sigma; St. Louis, MO), 50 µg/ml
soybean trypsin inhibitor; pH 7.5) and placed above a 2 mm slab of rat tail collagen. Epithelial cells were
allowed to grow out onto the collagen slab for 4-5 days prior to refeeding. Biochemical, histologic and
physiologic assessment have shown these cells have the characteristics of cholangiocytes, the
progenitor cell of liver cyst epithelia (8). Cells were passaged by digesting the collagen from beneath the
cells (1 mg/ml collagenase (Sigma; St. Loius, MO), 2 mg/ml dispase; 60 min at 37 oC), disrupting the
monolayer into small epithelial ‘islands’ and reseeding with these ‘islands’. Liver cyst epithelial cells were
similarly isolated from Balb/c cpk(+/-) mice, genetic model with mutations in the Cys-1 gene that similarly
gives rise to liver cysts (8).
Page 4 of 29

5Polarized model of liver cyst epithelial cells To develop a polarized epithlelial model of
liver cyst lining epithelial cells, pkd2 liver cyst epithelial cells were seeded and grown into confluent
monolayers on semi-permeable supports. After developing high transepithelial resistances (>1,000
Ω.cm2), the polarity of cytokine and growth factor secretion was determined by exchanging the apical and
basal media and sampling the apical and basal media were over the following three days. The
concentration of VEGF was determined by ELISA analysis, as described below.
Isolation of intrahepatic bile ducts Normal bile ducts were enriched by an extended
collagenase digestion of the liver (9). Livers of pkd2(+/+) mice were perfused for 45-60 min with
collagenase solution (DMEM-F12, 0.05% type I collagenase (Worthington; Lakewood, NJ); 37 oC). The
bulk of the hepatocytes were lightly teased away from the biliary tree. The biliary tree was further shaken
in the collagenase solution for 15-30 min to dissociate hepatocytes from the biliary tissue. Western
blotting for bile salt export protein (BSEP; hepatocyte marker) and ezrin (cholangiocyte marker) showed
the preparations to be enriched a minimum of 5-fold for cholangiocytes (data not shown).
Collection of liver and kidney cyst fluids Human kidney and liver cyst fluids were collected
from individuals undergoing laproscopic fenestration procedures. Fluids were drawn into a 10 cc syringe,
transferred into sterile tubes, frozen in liquid nitrogen and stored at –80 oC prior to ELISA analysis.
Protocols for collection and use of the materials were approved by the Colorado Multiple Institution
Review Board and all patients provided consent for participation in the study. Similarly, liver and kidney
cyst fluids from euthanized pkd2(WS25/-) mice were drawn into a 1 cc or 5 cc syringe, transferred, frozen
in liquid nitrogen and stored at -80 oC prior to analysis.
Cell proliferation assays The rates of proliferation of the pkd2 liver cyst epithelial cells were
measured by Alamar Blue assay (Biosource/Invitrogen; Carlsbad, CA). The proliferative response of
these cells was measured in response to treatment with recombinant mouse VEGF (R&D Systems;
Minneapolis, MN) or liver cyst fluid. Pkd2(WS25/-) liver cyst epithelial cells were passaged onto collagen-
treated 6-well plates (BD Bioscience; San Jose, CA), allowed to seed overnight in Growth Media,
incubated for 24 hours in serum-free DMEM-F12 and then cultured for 24 hours in DMEM-F12 media
with no serum (baseline control; value set at 0%), 10% fetal bovine serum (Hyclone; Logan, UT; positive
control; value set at 100%), serum-free media containing 0.05 – 50 ng/ml recombinant mouse VEGF
(R&D Systems; Minneapolis, MN) or serum-free media containing 10% pkd2(WS25/-) liver cyst fluid .
Subsequently, as detailed by the manufacturer, serum-free media containing 10% Alamar Blue was
added to the cells for 18 hours, the media evaluated for absorbance at 540 nm and 600 nm and the
reduction of Alamar Blue calculated, as described by the manufacturer. The proliferative effect of liver
cyst fluid was confirmed by Western blotting for PCNA (data not shown).
Page 5 of 29

6
Cytokine array and ELISA assays The broad pattern of growth factor and cytokine expression
in mouse liver cyst fluid was evaluated by cytokine array analysis, as described by the manufacturer
(Panomics; Redwood City, CA). The concentrations of VEGF in mouse liver cyst fluids were measured
by ELISAs on 96-well VEGF ELISA plates purchased from ELISA Tech (Aurora, CO). Recombinant
mouse VEGF was used to calibrate the responses.
Western blotting assays Western blots were performed by standard methods (10). Tissue or
cell culture samples were solubilized in 5xPAGE (5% sodium dodecyl sulfate, 25% sucrose, 50 mM Tris,
5 mM EDTA, 200 mM dithiothreitol; pH 8.0), the protein content was measured by bicinchoninic acid
assay (Pierce; Rockford, IL) and 40 µg of protein was loaded per lane. Nitrocellulose blots were probed
with commercial antibodies against PCNA (BD Bioscience; San Jose, CA; 1:5,000), VEGFR1 (a.k.a. Flt-
1; Epitomics; Burlingame, CA; 1:5,000), VEGFR2 (a.k.a. Flk-1/KDR; Affinity Bioreagents; Golden, CO;
1:2,000) and actin (Calbiochem; LaJolla, CA; 1:5,000). Primary antibodies were detected with
horseradish peroxidase-labeled goat anti-rabbit or anti-mouse secondary antibodies (Bio-Rad; Hercules,
CA; 1:10,000). The chemiluminescence signals (Pierce; Rockford, IL) were detected by a UVP
Bioimaging System (Upland, CA).
In vivo pkd2(WS25/-) treatment regimens Male pkd2(WS25/-) mice were treated in vivo out to
12 months of age with SU5416, a lipophilic, long-acting VEGF receptor inhibitor (11). All animals were
raised to 4 months of age without treatment. This avoided potential developmental complications from
SU5416 that can occur in rodents and, more importantly, allowed the process of cystogenesis to occur
unabated. Beginning at 4 months of age, mice were split into two groups, Control and SU5416, that were
treated by subcutaneous injection (300 µl) at two week intervals. The vehicle consisted of 0.5%
carboxymethylcellulose (CMC), 0.9% NaCl, 0.4% polysorbate 80, 0.9% benzoyl alcohol). The
experimental group received 0.75 mg SU5416 in 300 µl of vehicle. Mice were treated and studied at 8
months (4 months of treatment) and 12 months (8 months of treatment) of age. At the end of the study,
animals were euthanized, the animal was weighed, liver and kidneys were weighed, sections of liver and
kidney were frozen in liquid nitrogen, fixed in formaldehyde (3% formaldehyde in phosphate buffered
saline; pH 7.4) or fixed in glutaraldehyde (1% glutaraldehyde, 2% sucrose, 100 mM cacodylate; pH 7.4).
Determination of liver and kidney cyst volume densities Cyst volume densities
were quantified in livers and kidneys. After fixation, slabs were cut from the middle of the main liver lobe
and middle of one kidney, sequentially equilibrated into 5%, 10% and 25% sucrose, immersed in OCT
(TissueTek; Torrence, CA), frozen in liquid nitrogen and sectioned (10 µm). Sections were then stained
(1% toluidine blue, 1% borax, 30% EtOH) and digitally imaged (UVP Bioimaging System; Upland, CA).
Page 6 of 29

7Using NIH Image, the areas of the observable cysts within the tissue as well as the total area of the
tissue section were obtained. The values were expressed as the cumulative cyst volume densities as a
percentage of the total tissue area.
Statistical analysis All values are reported as the mean + the standard error of the
mean. Statistical analyses of the differences in the means of experimental pairs were evaluated by t-test.
Studies with three or more groups were evaluated by an analysis of variance (ANOVA). The ANOVA
included a Tukey-Kramer multiple comparison test. P values <0.05 were considered statistically
significant.
Page 7 of 29
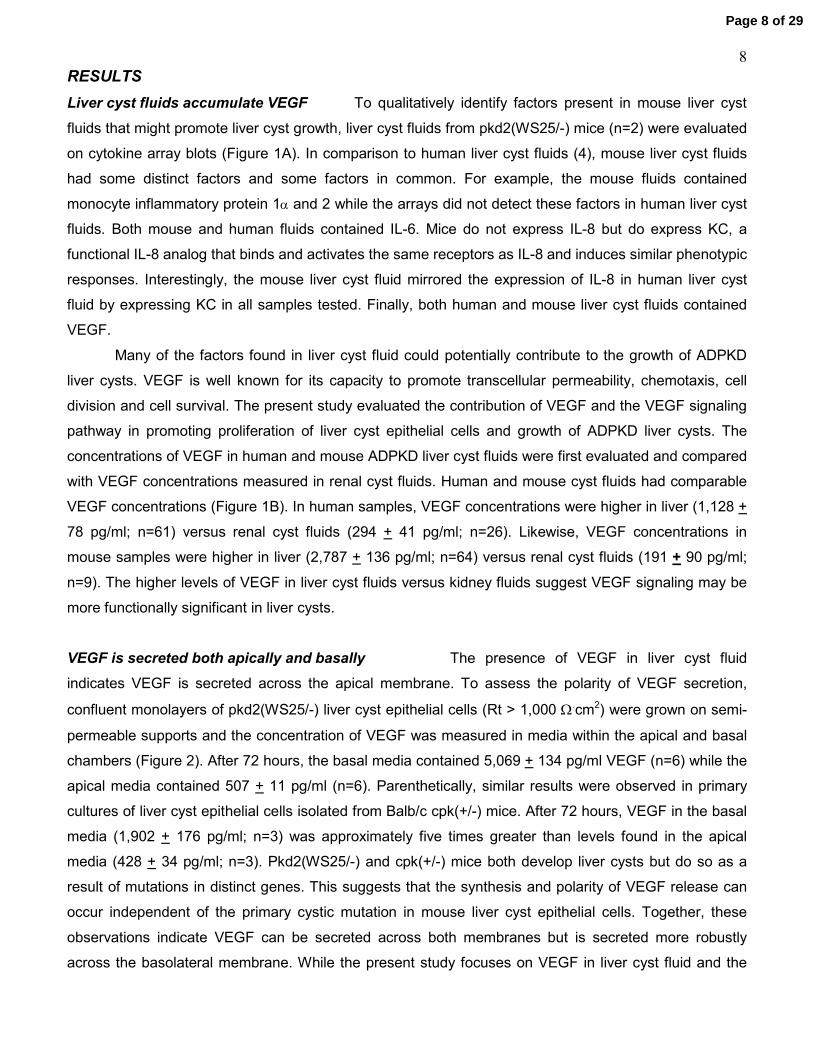
8RESULTS Liver cyst fluids accumulate VEGF To qualitatively identify factors present in mouse liver cyst
fluids that might promote liver cyst growth, liver cyst fluids from pkd2(WS25/-) mice (n=2) were evaluated
on cytokine array blots (Figure 1A). In comparison to human liver cyst fluids (4), mouse liver cyst fluids
had some distinct factors and some factors in common. For example, the mouse fluids contained
monocyte inflammatory protein 1α and 2 while the arrays did not detect these factors in human liver cyst
fluids. Both mouse and human fluids contained IL-6. Mice do not express IL-8 but do express KC, a
functional IL-8 analog that binds and activates the same receptors as IL-8 and induces similar phenotypic
responses. Interestingly, the mouse liver cyst fluid mirrored the expression of IL-8 in human liver cyst
fluid by expressing KC in all samples tested. Finally, both human and mouse liver cyst fluids contained
VEGF.
Many of the factors found in liver cyst fluid could potentially contribute to the growth of ADPKD
liver cysts. VEGF is well known for its capacity to promote transcellular permeability, chemotaxis, cell
division and cell survival. The present study evaluated the contribution of VEGF and the VEGF signaling
pathway in promoting proliferation of liver cyst epithelial cells and growth of ADPKD liver cysts. The
concentrations of VEGF in human and mouse ADPKD liver cyst fluids were first evaluated and compared
with VEGF concentrations measured in renal cyst fluids. Human and mouse cyst fluids had comparable
VEGF concentrations (Figure 1B). In human samples, VEGF concentrations were higher in liver (1,128 +
78 pg/ml; n=61) versus renal cyst fluids (294 + 41 pg/ml; n=26). Likewise, VEGF concentrations in
mouse samples were higher in liver (2,787 + 136 pg/ml; n=64) versus renal cyst fluids (191 + 90 pg/ml;
n=9). The higher levels of VEGF in liver cyst fluids versus kidney fluids suggest VEGF signaling may be
more functionally significant in liver cysts.
VEGF is secreted both apically and basally The presence of VEGF in liver cyst fluid
indicates VEGF is secreted across the apical membrane. To assess the polarity of VEGF secretion,
confluent monolayers of pkd2(WS25/-) liver cyst epithelial cells (Rt > 1,000 Ω.cm2) were grown on semi-
permeable supports and the concentration of VEGF was measured in media within the apical and basal
chambers (Figure 2). After 72 hours, the basal media contained 5,069 + 134 pg/ml VEGF (n=6) while the
apical media contained 507 + 11 pg/ml (n=6). Parenthetically, similar results were observed in primary
cultures of liver cyst epithelial cells isolated from Balb/c cpk(+/-) mice. After 72 hours, VEGF in the basal
media (1,902 + 176 pg/ml; n=3) was approximately five times greater than levels found in the apical
media (428 + 34 pg/ml; n=3). Pkd2(WS25/-) and cpk(+/-) mice both develop liver cysts but do so as a
result of mutations in distinct genes. This suggests that the synthesis and polarity of VEGF release can
occur independent of the primary cystic mutation in mouse liver cyst epithelial cells. Together, these
observations indicate VEGF can be secreted across both membranes but is secreted more robustly
across the basolateral membrane. While the present study focuses on VEGF in liver cyst fluid and the
Page 8 of 29

9potential for autocrine/paracrine signaling of the cyst lining epithelial cells by VEGF in the apical media,
the accumulation of VEGF in the basal media indicates that VEGF signaling of liver cyst epithelial cells
along the basal membrane as well as signaling of the underlying vasculature may contribute profoundly
to any in vivo affect of VEGF.
Liver cyst epithelial cells express VEGF receptors In order for VEGF in the liver cyst fluid
to induce proliferation of the liver cyst lining epithelial cells, VEGF receptors must be present on the cells
to bind VEGF and transduce the VEGF signal to the cell interior. There are three characterized VEGF
receptors. VEGFR1 and VEGFR2 are the more broadly expressed and well defined of these receptors.
Western blotting showed that both VEGFR1 and VEGFR2 are expressed in the kidneys and livers of
both pkd2(+/+) and pkd2(WS25/-) mice (Figure 3A; n=1). In the ADPKD liver, cysts emerge from the
epithelial cells lining the intrahepatic bile duct. Termed cholangiocytes, these cells make up only 2-4% of
the liver cell mass. In order to determine if VEGFR1 and VEGFR2 are expressed in ‘normal’
cholangiocytes, normal bile ducts were enriched from the liver and evaluated by Western blotting.
Similarly, liver cyst epithelial cells were obtained by excising liver cyst wall tissue that had emerged from
the body of the liver. To further enrich the ‘cystic’ cholangiocytes, epithelial cells from the superficial cyst
walls were cultured. These epithelial cell cultures display a number of molecular, biochemical and
physiologic characteristics that demonstrate they originated from cholangiocytes (8). Compared to whole
liver samples (n=3), Western blotting showed both ‘normal’ (n=3) and ‘cystic’ cholangiocytes (cyst wall:
n=4; pkd2 cells: n=3) expressed both VEGFR1 and VEGFR2 (Figure 3B).
VEGF induces proliferation of liver cyst epithelial cells Given the presence of VEGF
in liver cyst fluids and VEGF receptors in liver cyst epithelial cells, the capacity of VEGF to induce cell
proliferation was measured in pkd2(WS25/-) liver cyst epithelial cells (Figure 4A). When compared to the
proliferative response derived from 10% FBS, an insignificant effect was measured with 50 pg/ml VEGF
(14 + 10%; n=4) but significant proliferative responses were measured with 500 pg/ml (61 + 15%; n=4),
5,000 pg/ml (108 + 4%; n=4) and 50,000 pg/ml (93 + 13%; n=4) of VEGF. In a parallel study, Mz-ChA1
cells, a human cholangiocarcinoma cell line that has successfully served as a model of human
cholangiocytes, showed a similar proliferative response to VEGF (data not shown). Consequently, the
VEGF concentrations present in liver cyst fluid of pkd2(WS25/-) mice (2,787 + 136 pg/ml) would likely be
sufficient to promote proliferation of liver cyst epithelial cells.
To evaluate if liver cyst fluid can induce proliferation of liver cyst epithelial cells, pkd2 cells were
treated with serum-free media containing 10% liver cyst fluid from pkd2(WS25/-) mice (mLCF). The
contribution of VEGF signaling to this proliferative response was also evaluated by pretreating paired
sets of pkd2 cells with 10 µM SU5416 (Figure 4B). Cultures treated with mLCF induced a significant
increase in cell proliferation (84 + 3 % of FBS response; n=8; p<0.05). Interestingly, in paired pkd2 cells
Page 9 of 29

10receiving aliquots of the same mLCF, pretreatment with SU5416 significantly reduced the proliferative
response to mLCF (37 + 3% of FBS response; n=8; p< 0.05).
Long-term SU5416 treatment does not affect weight gain The above biochemical and
cell culture studies indicate the VEGF signaling pathway is positioned to contribute significantly to the
proliferation of ADPKD liver cyst epithelial cells and growth of ADPKD liver cysts. To test this directly,
pkd2(WS25/-) mice were allowed to grow up to 4 months of age and then were treated with SU5416, a
VEGF receptor inhibitor, for an additional 4 months and 8 months. All pkd2(WS25/-) mice have
discernible kidney and liver cysts by 4 months of age (7). By raising the mice to 4 months of age prior to
treatment, the process of cystogenesis had been initiated and the study focused on the contributions of
VEGF signaling on the growth of cysts. SU5416 has some known deleterious effects on lung
development in juvenile rodents but is well tolerated in adult rodents (12; 13). The potential for
detrimental effects of SU5416 on the mice were screened for by following the rates of increase in body
weights in mice treated with SU5416 versus vehicle (Figure 5). When compared with 12 month old
vehicle-treated controls (44.3 + 2.0 gm; n=5), there was no significant difference in the body weight of
mice treated with SU5416 (42.0 + 4.7 gm; n=6). Parenthetically, the difference in the absolute values for
the weights of the SU5416-treated versus the vehicle-treated controls (2.3 gm) may be influenced by the
difference in the liver weights between the two groups at 12 months of age (6.0 gm; see below).
SU5416 inhibits the growth of liver cysts The effect of SU5416 treatment on liver cyst
growth was evaluated by measuring the cystic area of the liver at 8 months of age (4 months of
treatment) and liver weights at 8 months and 12 months of age (4 months and 8 months of treatment). In
cross sections of the primary liver lobe from the 8 month old mice, sections from pkd2(+/+) mice (n=4)
showed the liver parenchyma was homogeneous with no evidence of liver cysts (Figure 6A). In vehicle-
treated pkd2(WS25/-) mice, however, the body of the liver sections contained a number of cystic areas of
varying sizes. The cystic areas comprised 9.9 + 4.3% (n=4) of the total parenchymal area (Figure 6B). In
SU5416-treated animals, small putative cysts were observed but there was an absence of any large
cysts in the sections examined. Quantification shows the cystic areas in the sections from SU5416-
treated animals (1.8 + 0.7%; n=3) were significantly lower than the vehicle-treated group.
The liver weights in the 8 month old vehicle-treated animals (8.7 + 2.3% of body weight; n=4)
were also significantly greater than the livers from age-matched pkd2(+/+) animals (4.6 + 0.1% of body
weight; n=9). These elevated values resulted primarily from the expansion of a few cysts from the
surface of the livers while much of the liver parenchyma did not appear grossly affected. Interestingly, the
livers of the paired 8 month old pkd2(WS25/-) mice treated for four months with SU5416 were not
significantly increased (5.1 + 0.4% of body weight; n=3) when compared with the livers from pkd2(+/+)
mice. Further, liver weights from the 8 month old SU5416-treated mice were significantly lower than the
vehicle-treated mice. This protective effect of SU5416 against liver weight gain persisted at 12 months of
Page 10 of 29

11age (Figure 7). Livers from vehicle-treated pkd2(WS25/-) mice had significant cystic involvement
including the presence of large superficial cysts extending from the lobes of the liver (Figure 7A – upper
panel). Livers from SU5416-treated pkd2(WS25/-) mice also had liver cysts present at the surface of the
liver but these cysts were far more modest in size (Figure 7A – lower panel). This is reflected in their liver
weights (Figure 7B). At 12 months of age, livers from vehicle-treated pkd2(WS25/-) mice were (10.8 +
1.9% of body weight; n=5) significantly enlarged compared to pkd2(+/+) mice (4.8 + 0.2% of body weight;
n=12) while livers from SU5416-treated pkd2(WS25/-) mice were not significantly different (4.8 + 0.4 % of
body weight; n=6) than livers from wild type animals. Furthermore, treatment of pkd2(WS25/-) mice with
SU5416 resulted in a significant reduction in liver weights when compared with vehicle treated
pkd2(WS25/-) mice. In short, SU5416 treatment blocked the growth of ADPKD liver cysts.
Effects of SU5416 on renal cysts are less pronounced While the protective effects of
SU5416 against liver cyst growth were profound, the effects of SU5416 on renal cyst growth are less
clear. Qualitatively, the kidneys from SU5416-treated mice had cyst involvement that was not apparently
different from vehicle-treated mice. This included kidneys that were grossly cystic despite receiving
SU5416 (Figure 8A). Efforts to quantify the cystic involvement did not provide a robust analysis. Cyst
areas in the analyzed slabs were markedly variable in kidneys from pkd2(WS25/-) mice and were not
different between vehicle-treated and SU5416-treated groups. This was likely influenced by two features.
First, there was significant localized variability in cysts within the bodies of the kidneys and the consistent
sampling of sections taken from the middle of the kidneys could have relatively normal kidney areas
analyzed despite the presence of cysts elsewhere in the body of the kidneys. Second, unlike the massive
enlargement of pkd2(WS25/-) livers, kidneys from vehicle-treated pkd2(WS25/-) mice (1.5 + 0.1% of
body wt; n=5) were not grossly enlarged so that their weights were not significantly different than kidneys
from pkd2(+/+) mice (1.3 + 0.1% of body wt; n=12; Figure 8B). Kidneys from pkd2(WS25/-) mice treated
with SU5416 for 8 months (i.e. 12 months of age) were 2.3 + 1.1% of body wt (n=6). Consequently, the
methodology to quantitatively evaluate the effects of SU5416 treatment on renal cyst growth was not
performed. Current evidence in the literature is similarly mixed regarding the contribution of VEGF
signaling to the growth of renal cysts. Treatment of developing CD-1 mice with antibodies against
VEGFR2 results in the development of renal cysts, suggesting inhibition of VEGF signaling could
promote renal cyst growth (14). Conversely, rapamycin treatment of Han:SPRD rats, a model for
ADPKD, retarded the growth of renal cysts (15; 16). Downstream effects of rapamycin included both
inhibiting the release of VEGF and blunting the sensitivity of cells to VEGF signaling (17). These studies
indicate that inhibition of VEGF signaling was a potential therapeutic strategy for the treatment of ADPKD
renal cyst disease.
Page 11 of 29

12DISCUSSION Clinical severity of ADPKD is impacted by extragenetic factors
While the genesis of the cysts is linked to mutations in the either the PKD1 or PKD2 genes, the
clinical presentation of ADPKD is markedly heterogeneous (18-20) and modifier genes and extragenetic
factors have significant impact on cyst progression and disease severity. For example, a comparative
analysis of the age of onset in end-stage renal disease showed a larger intraclass correlation in
monozygotic twins versus sibships (21). Furthermore, quantitative genetic analysis of specific phenotypic
traits in PKD1 families showed that inherited differences in modifier genes accounted for a substantial
portion of the variability in the phenotypic expression of ADPKD (2). One potential source of extragenetic
influence is the presence of signaling molecules, including growth factors and cytokines, in the
microenvironment in and around the cyst wall.
Epithelial cells that line ADPKD kidney and liver cysts differentially express a number of genes,
including upregulating the expression of genes for specific growth factors and cytokines (22). ADPKD
kidney and liver cyst fluids contain a number of specific cytokines and growth factors and treatment of
cultured renal epithelial cells with ADPKD renal cyst fluid promotes cell proliferation (4; 23). In ADPKD
renal cysts, cyst fluids have been shown to contain appreciable levels of EGF, EGF receptors redistribute
to the apical membrane of cyst lining epithelia and EGF receptor signaling promotes the growth of renal
cysts (24). The role of specific factors in promoting liver cyst growth is less clear but is of particular
interest since liver function persists even in grossly cystic livers. The clinical manifestations of ADPKD
liver cyst disease stems from the compression of surrounding tissues, organs and vasculature by the
enlarged livers. Like the human counterparts (4), liver cyst fluids from pkd2(WS25/-) mice accumulate
specific cytokines and growth factors including VEGF (Figure 1). VEGF and other pro-growth factors
within the cyst fluids represent attractive targets for therapeutic intervention to block the growth of
ADPKD livers.
It should be noted that the comparative level of VEGF expression by ‘normal’ versus ‘cystic’
cholangiocytes was not determined. The VEGF that accumulated in the liver cyst fluid could have arisen
simply due to constituitive levels of VEGF expression. VEGF expression is, however, induced by a
variety of mechanisms. The regulation of VEGF expression could potentially be directly influenced by the
primary mutation or driven by extragenetic stresses incurred by the cells. For example, polycystin-1
forms protein complexes with proteins in the mTOR pathway and loss of polycystin-1 could contribute to
activation of the mTOR pathway (25). Inhibition of the mTOR pathway by rapamycin can inhibit
angiogenesis and growth of tumors and does so, in part, through decreasing VEGF production (17).
Interest in the potential contributions of the mTOR-VEGF axis in impacting ADPKD is further heightened
by reports in Han:SPRD rats, a non-polycystin genetic rat model of kidney cyst disease, that demonstrate
a protective affect of rapamycin in renal cystogenesis and enlargement (15; 16). Elevated VEGF
expression may also be independent of the primary mutation leading to cyst formation. VEGF expression
Page 12 of 29

13is induced by various cell stressors and such stressors, including hypoxia and cell stretching, may be
experienced by the epithelial cells that line the liver cysts (4; 8). The present studies utilized the
pkd2(WS25/-) mice to test the hypothesis that the VEGF that is released by the liver cyst epithelial cells
promotes the growth of ADPKD liver cysts.
VEGF can promote cholangiocyte proliferation
Cholangiocytes are epithelial cells that line the intrahepatic bile duct and, when appropriately
mutated, give rise to liver cysts. Independent of any specific gene mutation, cholangiocytes retain a
robust capacity to undergo net proliferation. For example, cholangiocytes normally comprise 2-4% of the
liver cell mass. Two weeks following the ligation of the bile duct, cholangiocytes expanded in numbers to
comprise ~30% of the liver cell mass (26). For the lining epithelium, the formation of enclosed ADPKD
liver cysts has a number of similarities to the bile duct network upstream of the point of duct ligation. In a
study of VEGF signaling in proliferation of cholangiocytes from normal and bile duct ligated rat livers,
cholangiocytes expressed both VEGF and VEGF receptors (27). In these rat studies,
immunofluorescence showed the presence of VEGFR2 and VEGFR3. VEGFR1 was not detected.
Expression of VEGF and the VEGF receptors was upregulated in cholangiocytes from bile duct ligated
rat livers and in vitro proliferation assays showed the cholangiocytes had a proliferative response to
VEGF (27). In humans, VEGF and other angiogenic factors accumulate to appreciable levels in human
ADPKD liver cyst fluids (4) and immunohistology studies showed VEGFR1 and VEGFR2 were expressed
in cholangiocytes from normal livers as well as livers with ADPKD and Caroli’s disease (28). In mice,
Western blotting showed the presence of VEGFR1 and VEGFR2 (Figure 3) and administration of VEGF
to liver cyst epithelial cell cultures promotes cell proliferation (Figure 4A; (28)). Importantly, the
concentrations of VEGF measured in the liver cyst fluids were well within the range of VEGF
concentrations needed to induce cell proliferation. Furthermore, treatment of pkd2 cells with mouse liver
cyst fluid induced a robust proliferative response (Figure 4B). This proliferative response was inhibited by
blocking VEGF receptor activity (Figures 4B).
SU5416 suppresses liver cyst growth The in vitro studies indicate that the ADPKD liver cyst epithelial cells can synthesize and release
VEGF and induce proliferation of the liver cyst epithelial cells. In vivo studies using SU5416 were
performed to directly assess the significance of the VEGF signaling pathway in promoting ADPKD liver
cyst growth. SU5416 is a potent anti-angiogenic factor whose main activities include inhibition of
VEGFR2 (Flk-1/KDR) and VEGFR1 (Flt-1) (29; 30). Failure to significantly inhibit the tyrosine kinase
activities of EGF and FGF receptors demonstrates a relatively high specificity of SU5416 for VEGF
receptors (29). SU5416 has been shown to affect the PDGF receptor autophosphorylation but it remains
unclear if SU5416 impacts the activity of PDGF receptors in intact cells and tissues (29; 31). In addition
to the hormone receptor effects, SU5416 does potentially have a number of additional effects including
Page 13 of 29

14inhibiting the expression of VEGF, HIF-1α and cycloxygenase-2 (32-34). The contribution of these
additional affects of SU5416 was not specifically evaluated in the present in vivo studies. As a sum of
these effects, studies on tumor vascularization and development of emphysema demonstrate directly
that SU5416 inhibits angiogenesis and vascular maintenance (29; 31; 35; 36).
The pkd2(WS25/-) mouse model was well suited for the study. First, the mutated pkd2(WS25/-)
mouse gene is directly homologous to the human PKD2 gene, one of two genes linked to ADPKD in
humans. Second, the liver cysts undergo significant and consistent enlargement by 12 months of life.
This gross enlargement parallels the primary clinical determinant in human ADPKD liver cyst disease
and permits the effects of SU5416 treatment on this key parameter to be assessed directly by measuring
liver weights. SU5416 treatment was initiated at 4 months of age and continued out to either 8 months (4
months of treatment) or 12 months (8 months of treatment) of age. The initial 4 month period without
treatment permitted the initial development of cysts in the kidneys and livers to occur (7) and,
consequently, have the study focus on the relative growth of cysts. Importantly, at 8 months of age, the
cystic area of the liver in pkd2(WS25/-) mice was markedly reduced in animals treated with SU5416
(Figure 6). This early effect persisted at 12 months of age where liver weights of untreated pkd2(WS25/-)
mice were twice as large as pkd2(WS25/-) mice that were treated with SU5416 (Figure 7). The livers of
SU5416-treated pkd2(WS25/-) mice did have cysts present at the surface but their sizes were
comparatively small and there was not a significant increase in liver weights compared to the livers of
pkd2(+/+) mice. These studies demonstrate that the VEGF signaling pathway contributes in a
pronounced way to the growth of ADPKD liver cysts in mice and supports further investigation into the
contribution of the VEGF signaling in the growth of mouse and human ADPKD liver cysts.
VEGF signaling may affect both the cyst epithelium and endothelium The primary
focus of the present study was on the autocrine/paracrine signaling by VEGF on the cyst lining epithelial
cells. Indeed, VEGF was present at relatively high concentrations in both human and mouse liver cyst
fluids (Figure 1), VEGF receptors were expressed in the cyst lining epithelium (Figure 3) and treatment of
primary liver cyst epithelial cells had increased rates of proliferation when treated with VEGF (Figure 4).
VEGF, however, is best known for its effects on the vasculature and capacity to induce angiogenesis.
Angiogenesis occurs in the walls of human ADPKD renal cysts and is likely influenced by VEGF
signaling (37). The present study did not characterize the potential effect of SU5416 treatment on
blocking angiogenesis and vascularization of the liver cyst walls but did show that VEGF is likely
secreted across the basolateral membrane of the cyst epithelium into the interstitial tissue of the liver
cyst wall (Figure 2). Compared to the apical release, there was substantially greater release of VEGF
across the basolateral membrane. This held for liver cyst epithelial cells from both cpk(+/-) and
pkd2(WS25/-) mice. Both mouse lines develop liver cysts but the cysts arise as a consequence of
mutations in distinct genes. In cpk(+/-) mice, cys-1, the gene encoding for the protein cystin, is mutated.
Page 14 of 29

15In pkd2(WS25/-) mice, pkd2, the gene encoding for polycystin-2, is mutated. The parallel results from
these two mouse lines suggest the release of VEGF may not be primarily modulated by the primary gene
mutation. Future studies will determine the effect of VEGF on angiogenesis and vascularization of the
liver cyst wall.
Therapeutic potential of inhibiting of the VEGF signaling pathway In summary, the
present mouse study demonstrates that VEGF is present in appreciable amounts in human and mouse
ADPKD liver cyst fluids (Figure 1), that cyst lining epithelial cells express VEGF receptors (Figure 3) and
that addition of VEGF at concentrations found in liver cyst fluid induces proliferation of the ADPKD liver
cyst lining epithelial cells in vitro (Figure 4). Importantly, these in vitro observations were extended in vivo
and showed that inhibition of the VEGF signaling pathway significantly blunts the growth of ADPKD liver
cysts (Figure 6 and 7). If inhibiting the VEGF signaling pathway in humans were similarly successful, the
VEGF signaling pathway could prove to be an important therapeutic target in the treatment of human
ADPKD liver cyst disease.
Page 15 of 29

16ACKNOWLEDGEMENTS Pkd2(WS25/-) mice used in this study were developed and graciously provided by Stefan Somlo
(Yale University). The presents studies were supported by grants to R.B.D. (NIH DK-34039; PKD
Foundation 109a2r) and V.H.G. (NIH DK-68581).
Page 16 of 29

17FIGURE LEGENDS Figure 1. Liver cyst fluid has physiologic levels of VEGF
(A) Cytokine array analysis of pkd2(WS25/-) mouse liver cyst fluid shows qualitatively that
specific cytokines and growth factors are present within the fluid. VEGF was among the detected factors.
(B) ELISAs of human and mouse liver and kidney cyst fluids found measurable levels of VEGF in liver
and kidney cyst fluids from both species. VEGF concentrations were significantly higher in human liver
cyst fluids (1,128 + 78 pg/ml; n=61) than human kidney cyst fluids (294 + 41 pg/ml; n=26). Likewise,
VEGF concentrations were significantly higher in mouse liver cyst fluids (2,787 + 136 pg/ml; n=64) than
mouse kidney cyst fluids (191 + 90 pg/ml; n=9). * p<0.05 Liver vs. Kidney
Figure 2. VEGF is secreted across both the basolateral and apical membranes
Pkd2 liver cyst epithelial cells were cultured on semi-permeable supports and allowed to form
confluent monolayers with transepithelial resistances >1,000 Ω.cm2. After 72 hours, VEGF was
significantly greater in the basal media (5,069 + 134 pg/ml; n=6) than in the apical media (507 + 11
pg/ml; n=6). *p<0.05 Apical vs media controls; ** p<0.05 Basal vs Apical or media controls.
Figure 3. Liver cyst epithelial cells express VEGF receptors
(A) Western blotting of kidney (K) and liver (L) tissue from pkd2(+/+) mmice (n=3) and
pkd2(WS25/-) mice (n=2) found that both VEGFR1 and VEGFR2 were expressed in each of these
tissues. Actin served as a loading control. (B) Within the liver, normal bile ducts from pkd2(+/+) mice
(Ducts; n=2), pkd2(WS25/-) liver cyst wall tissue (Cyst; n=4) and cultured liver cyst epithelial cells from
pkd2(WS25/-) mice (n=4) mice each expressed both VEGFR1 and VEGFR2. Actin served as a loading
control.
Figure 4. VEGF induces liver cyst epithelial cell proliferation
(A) To measure the capacity of VEGF to promote proliferation of pkd2(WS25/-) liver cyst epithelial
cells, cells were incubated in either serum-free media, media with 10% FBS or serum-free media
containing 50 to 50,000 pg/ml VEGF. An analysis of variance showed a significant proliferation response
occurred with 500 pg/ml VEGF (61 + 15% of FBS response; n=4) and a peak response was observed at
5,000 pg/ml (108 + 4% of FBS response; n=4). *p<0.05 vs Con. (B) Incubation of pkd2(WS25/-) cells in
serum-free media with 10% mouse liver cyst fluid (mLCF) also induced a significant increase in cell
proliferation (85 + 3% of FBS response; *p<0.05 vs Con; n=8). In paired studies, pretreatment of cells
with 10 µM SU5416 resulted in a significant inhibition of the proliferative response to 10% mLCF (35 +
2%; **p<0.05 vs Con and vs mLCF-Veh; n=8).
Page 17 of 29

18Figure 5. Body weights of pkd2(WS25/-) mice during SU5416 treatment
The body weights of pkd2(WS25/-) mice in the vehicle-treated (Control) or SU5416-treated
(SU5416) groups were not significantly different over the study period from 4 months to 12 months of
age. At 12 months of age, mice in the Control group weighed 44.3 + 2.0 gm (n=5) while mice in the
SU5416-treated group weighed 42.0 + 4.7 gm (n=6). Parenthetically, the difference in the absolute
values of the body weights in the Control and SU5416 is likely influenced by the significant increase in
liver weights in the Control group compared to the SU5416-treated group (see below).
Figure 6. Liver cyst areas of SU5416-treated pkd2(WS25/-) mice
(A) Shown are representative liver cross-sections from 8 month old mice that were used to
evaluate liver cyst volume densities. No cystic areas were observed in liver from pkd2(+/+) mice. In
contrast, in pkd2(WS25/-) mice treated with vehicle (Control), cysts of variable sizes were observed.
Livers from pkd2(WS25/-) mice treated with SU5415 had small putative cysts but large cysts were not
observed. (B) At 8 months of age, cysts comprised 9.9 + 4.3% (n=4) of the area of liver sections in
vehicle-treated pkd2(WS25/-) mice (Control). In SU5416-treated mice, cysts comprised a significantly
lower area of the livers (1.8 + 0.7%; n=3). *p<0.05 SU5416 vs Control.
Figure 7. Liver weights of SU5416-treated pkd2(WS25/-) mice
(A) Shown are livers taken from pkd2(WS25/-) mice at 12 months of age. The vehicle-treated
mice (Control; upper panel) display a profound growth of liver cysts that have emerged from the surface
of the liver. Livers from SU5416-treated mice also have a number of cysts on the surface of the liver
(arrowheads) but did not display the massive increase in cyst volumes. (bar = 1 cm) (B) This difference
in the development of massive superficial liver cysts is reflected in the liver weights. Liver weights,
expressed as a percentage of total body weight, were significantly elevated in vehicle-treated
pkd2(WS25/-) mice (Control; 10.8 + 1.9%; n=5) versus livers from pkd2(+/+) mice (+/+; 4.8 + 0.2%;
n=12). SU5416 treatment, however, profoundly blocked the increase in liver weights in pkd2(WS25/-)
mice (SU5416; 4.8 + 0.4%; n=6). This protection was such that liver weights from SU5416 were not
different in pkd2(+/+) mice . *p<0.05 Control vs pkd2(+/+) and SU5416.
Figure 8. Kidney weights in SU5416-treated pkd2(WS25/-) mice
(A) At 12 months of age, sections taken from the middle of the kidneys from vehicle-treated
(Control) and SU5416-treated (SU5416) pkd2(WS25/-) mice showed a range of cystic involvement in
both groups. This included kidneys with little or no cystic involvement (upper panels) to large cysts or
massive cyst involvement (lower panels). (B) Measurements of kidney weights, expressed as a percent
of body weight, was a relatively insensitive measure of kidney cyst disease since surface cysts were
observed in vehicle-treated pkd2(WS25/-) mice (Control) but the kidney weights (1.5 + 0.1%; n=5) were
Page 18 of 29

19not different from weights in pkd2(+/+) mice (1.3 + 0.1 %; n=12). Likewise, kidney weights from SU5416-
treated mice (2.3 + 1.1%; n=6) were not significantly different from weights in pkd2(+/+) mice.
Page 19 of 29

20REFERENCES 1. Everson GT, Scherzinger A, Berger-Leff N, Reichen J, Lezotte D, Manco-Johnson M and Gabow P.Polycystic liver disease: quantitation of parenchymal and cyst volumes from computed tomography images and clinical correlates of hepatic cysts. Hepatology 8: 1627-1634, 1988. 2. Fain PR, McFann KK, Taylor MRG, Tison M, Johnson AM, Reed B and Schrier RW. Modifier genes play a significant role in the phenotypic expression of PKD1. Kidney Int 67: 1256-1267, 2005. 3. Grantham JJ. Mechanisms of progression in autosomal dominant polycystic kidney disease. Kidney Int 63: S93-97, 1997. 4. Nichols MT, Gidey E, Matzakos T, Dahl R, Stiegmann G, Shah RJ, Grantham JJ, Fitz JG and Doctor RB.Secretion of cytokines and growth factors into ADPKD liver cyst fluid. Hepatology 40: 836-846, 2004. 5. Roy H, Bhardwaj S and Yla-Herttuala. BIology of vascular endothelial growth factor. FEBS Letters 580: 2878-2887, 2006. 6. Pandya NM, Dhalla NS and Santani DD. Angiogenesis: a new target of future therapy. Vasc Pharm 44: 265-274, 2006. 7. Wu G, D'Agati V, Cai Y, Markowitz GS, Park JH, Reynolds DM, Maeda Y, Le TC, Hou HJ, Kuchrlapati R, Edelmann W and Somlo S. Somatic inactivation of Pkd2 results polycystic kidney disease. Cell 93: 177-188, 1998. 8. Doctor RB, Johnson S, Brodsky KS, Amura CR, Gattone V and Fitz JG. Regulated ion secretion in liver cyst epithelia. Biochim Biophys Acta 1772: 345-354, 2007. 9. Gumpricht E, Devereaux MW, Dahl RH and Sokol RJ. Glutathione status of isolated rat hepatocytes affects bile acid-induced cellular necrosis but not apoptosis. Tox Appl Pharm 164: 102-111, 2000. 10. Doctor RB, Bennett V and Mandel LJ. Degradation of spectrin and ankyrin in the ischemic rat kidney. Am J Physiol 264: C1003-1013, 1993. 11. Arora A and Scholar EM. Role of tyrosine kinase inhibitors in cancer therapy. J Pharm Exp Therap 315: 971-979, 2005. 12. Voelkel NF, Cool C, Tarasevicinen-Stewart L, Geraci MW, Yeager M, Bull T, Kasper M and Tuder RM.Janus face of VEGF: The obligatory survival factor for lung vascular endothelium controls precapillary artery remodeling in severe pulmonary hypertension. Crit Care Med 30: S251-S256, 2002. 13. Tarasevicinen-Stewart L, Kashara Y, Alger L, Hirth P, McMahon G, Waltenberger J, Voelkel NF and Tuder RM. Inhibition of VEGF receptor 2 combined with chronic hypoxia causes cell death-dependent pulmonary endothelial cell proliferation and severe pulmonary hypertension. FASEB J 15: 427-438, 2001. 14. McGrath-Morrow S, Cho C, Molls R, Burne-Taney M, Haas M, Hicklin DJ, Tuder R and Rabb H. VEGF receptor 2 blockade leads to renal cyst formation in mice. Kidney Int 69: 1741-1748, 2006. 15. Tao Y, Kim J, Schrier RW and Edelstein CL. Rapamycin markedly slows disease progression in a rat model of PKD. J Am Soc Nephrol 16: 46-51, 2005. 16. Wahl PR, Serra AL, LeHir M, Molle KD, Hall MN and Wuthrich RP. Inhibition of mTOR with sirolimus slows disease progression in Han:SPRD rats with ADPKD. Nephrol Dial Transplant 21: 598-604, 2006. 17. Guba M, von Breitenbuch P, Steinbauer M, Koehl G, Flegel S, Hornung M, Bruns CJ, Zuelke C, Farkas S, Anthuber M, Jauch KW and Geissler EK. Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: involvement of vascular endothelial growth factor. Nature Med 8: 128-135, 2002. 18. Hateboer N, Lazarou LP, Williams AJ, Holman P and Ravine D. Familial phenotype differences in PKD1. Kidney Int 56: 34-40, 1999. 19. Milutinovic J, Rust PF, Fialkow PJ, Agodoa LY, Phillips LA, Rudd TG and SUtherland S. Intrafamilial phenotypic expression of autosomal dominant polycystic kidney disease. Am J Kidney Dis 19: 465-472, 1992. 20. Magistroni P, He N, Wang K, Andrew R, Johnson A, Gabow P, Dicks E, Parfrey P, Torra R, San-Millan JL and Pei Y. Genotype-renal function correlation in type 2 ADPKD. J Am Soc Nephrol 14: 1164-1174, 2003. 21. Persu A, Duyme M, Pirson Y, Lens X, Messiaen T, Breuning MH, Chauveau D, Levy M, Grunfeld JP and Devuyst O. Comparison between siblings and twins supports a role for modifier genes in ADPKD. Kidney Int 66: 2132-2136, 2004. 22. Husson H, Manavalan P, Akmaev VR, Russo RJ, Cook B, Richards B, Barbiero D, Liu D, Coao X, Landes GM, Wang CJ, Roberts BL, Klinger KW, Grubman SA, Jefferson DM and Ibraghimov-Beskrovnaya O. New insights into ADPKD molecular pathways using combination of SAGE and microarray techniques. Genomics 84: 497-510, 2004. 23. Ye M, Grant M, Sharma M, Elzinga L, Swan S, Torres V and Grantham J. Cyst fluid from human ADPKD promotes cyst formation by renal epithelial cells in vitro. J Am Soc Nephrol 3: 984-994, 1992. 24. Du J and Wilson PD. Abnormal polarization of EGF receptors and autocrine stimulation of cyst epithelial growth in human ADPKD. Am J Physiol 269: C487-495, 1995.
Page 20 of 29

2125. Shillingford JM, Murcia NS, Larson CH, Low SH, Hedgepeth R, Brown N, Flask CA, Novick AC, Goldfarb DA, Kramer-Zucker A, Walz G, Piontek KB, Germino GG and Weinmbs T. The mTOR pathway is regulated by polycystin-1, and its inhibition reverses renal cystogenesis in polycystic kidney disease. Proc Natl Acad Sci USA 103: 5466-5471, 2006. 26. Alpini G, Lenzi R, Sarkozi L and Tavoloni N. Biliary physiology in rats with bile ductular cell hyperplasia. JClin Invest 81: 569-578, 1988. 27. Gaudio E, Barbaro B, Alvaro D, Glaser S, Francis H, Ueno Y, Meininger CJ, Franchitto A, Onori P, Marzioni M, Taffetani S, Fava G, Stoica G, Venter J, Reichenbach R, De Morrow S, Summers R and Alpini G.VEGF stimulates rat cholangiocyte proliferation via an autocrine mechanixm. Gastroenterol 130: 1270-1282, 2006. 28. Fabris L, Cadamuro M, Fiorotto R, Roskams T, Spirli C, Melero S, Sonzogni A, Joplin RE, Okolicsanyi L and Strazzabosco M. Effects of angiogenic factor overexpression by human and rodent cholangiocytes in polycystic liver diseases. Hepatology 43: 1001-1012, 2006. 29. Fong TAT, Shawver LK, Sun L, Tang C, App H, Powell TJ, Kim YH, Schreck R, Wang X, Risau W, Ullrich A, Hirth KP and McMahon G. SU5416 is a potent and selective inhibitor of the VEGF receptor (Flk-1/KDR) that inhibits tyrosine kinase catalysis, tumor vascularization and growth of multiple tumor types. Cancer Res 59: 99-106, 1999. 30. Itokawa T, Nokihara H, Nishioka Y, Sone S, Iwamoto Y, Yamada Y, Cherrington J, McMahon G, Shibuya M, Kuwano M and Ono M. Antiangiogenic effect by SU5416 is partly attributable to inhibition of Flt-1 receptor signaling. Mol Cancer Ther 1: 295-302, 2002. 31. Shaheen RM, Davis DW, Lin W, Zebrowski BK, Wilson MR, Bucana CD, McConkey DH, McMahon G and Ellis LM. Antiangiogenic therapy targeting the tyrosine kinase receptor for VEGF receptor inhibits the growth of colon cancer liver metastasis and induces tumor and endothelial cell apoptosis. Cancer Res 59: 5412-5416, 1999. 32. Litz J, Sakuntala G, Sulanke G, Lipson KE and Krystal GW. The multi-targeted kinase inhibitor SU5416 inhibits small cell lung cancer growth and angiogenesis, in part by blocking Kit-mediated VEGF expression. Lung Canc 46: 283-291, 2004. 33. Zhong XS, Zheng JZ, Reed E and Jiang BH. SU5416 inhibited VEGF and HIF-1a expression through the PI3K/AKT/p70S6K1 signaling pathway. Biochem Biophys Res Comm 324: 471-480, 2004. 34. Saha D, Sekhar KR, Cao C, Morrow JD, Choy H and Freeman ML. The antiangiogenic agent SU5416 down-regulates phorbol ester-mediated induction of cyclooxygenase 2 expression by inhibiting nicotinamide adenine dinucleotide phosphate oxidase activity. Cancer Res 63: 6920-6927, 2003. 35. Kasahara Y, Tuder RM, Taraseviciene-Stewart L, LeCras TD, Abman S, Hirth PK, Waltenberger J and Voelkel NF. Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J Clin Invest 106: 1311-1319, 2000. 36. Haspel HC, Scicli GM, McMahon G and Scicli AG. Inhibition of vascular endothelial growth factor-associated tyrosine kinase activity with SU5416 blocks sprouting in the microvascular endothelial cell spheroid model of angiogenesis. Microvasc Res 63: 304-315, 2002. 37. Bello-Reuss E, Holubec K and Rajaraman S. Angiogenesis in autosomal-dominant polycystic kidney disease. Kidney Int 60: 37-45, 2001.
Page 21 of 29

Figure 1.
A
B
Page 22 of 29

Figure 2.
Page 23 of 29

Figure 3.
A
B
Page 24 of 29

Figure 4.
A
B
Page 25 of 29

Figure 5.
Page 26 of 29

Figure 6.
A
Page 27 of 29

Figure 7.
A
B
Page 28 of 29

Figure 8.
A
B
Page 29 of 29
Copyright © 2022 FDOKUMEN