Influence of high-frequency cyclical stimulation on the bone fracture-healing process: mathematical...
18
doi: 10.1098/rsta.2011.0153 , 4278-4294 369 2011 Phil. Trans. R. Soc. A Jorge Grasa, Belén Seral and José Manuel García-Aznar María José Gómez-Benito, Libardo Andrés González-Torres, Esther Reina-Romo, and experimental models the bone fracture-healing process: mathematical Influence of high-frequency cyclical stimulation on References l.html#ref-list-1 http://rsta.royalsocietypublishing.org/content/369/1954/4278.ful This article cites 71 articles, 1 of which can be accessed free Subject collections (27 articles) mathematical modelling collections Articles on similar topics can be found in the following Email alerting service here in the box at the top right-hand corner of the article or click Receive free email alerts when new articles cite this article - sign up http://rsta.royalsocietypublishing.org/subscriptions go to: Phil. Trans. R. Soc. A To subscribe to on November 14, 2012 rsta.royalsocietypublishing.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Influence of high-frequency cyclical stimulation on the bone fracture-healing process: mathematical...

doi: 10.1098/rsta.2011.0153, 4278-4294369 2011 Phil. Trans. R. Soc. A
Jorge Grasa, Belén Seral and José Manuel García-AznarMaría José Gómez-Benito, Libardo Andrés González-Torres, Esther Reina-Romo, and experimental modelsthe bone fracture-healing process: mathematical Influence of high-frequency cyclical stimulation on
Referencesl.html#ref-list-1http://rsta.royalsocietypublishing.org/content/369/1954/4278.ful
This article cites 71 articles, 1 of which can be accessed free
Subject collections
(27 articles)mathematical modelling collectionsArticles on similar topics can be found in the following
Email alerting service herein the box at the top right-hand corner of the article or click Receive free email alerts when new articles cite this article - sign up
http://rsta.royalsocietypublishing.org/subscriptions go to: Phil. Trans. R. Soc. ATo subscribe to
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

Phil. Trans. R. Soc. A (2011) 369, 4278–4294doi:10.1098/rsta.2011.0153
Influence of high-frequency cyclical stimulationon the bone fracture-healing process:
mathematical and experimental modelsBY MARÍA JOSÉ GÓMEZ-BENITO1, LIBARDO ANDRÉS GONZÁLEZ-TORRES1,
ESTHER REINA-ROMO2, JORGE GRASA1, BELÉN SERAL1 ANDJOSÉ MANUEL GARCÍA-AZNAR1,*
1Aragón Institute of Engineering Research (I3A), Universidad de Zaragoza,María de Luna s/n, 50018 Zaragoza, Spain
2Department of Mechanical Engineering, University of Seville,41092 Seville, Spain
Mechanical stimulation affects the evolution of healthy and fractured bone. However,the effect of applying cyclical mechanical stimuli on bone healing has not yet beenfully clarified. The aim of the present study was to determine the influence of a high-frequency and low-magnitude cyclical displacement of the fractured fragments on thebone-healing process. This subject is studied experimentally and computationally fora sheep long bone. On the one hand, the mathematical computational study indicatesthat mechanical stimulation at high frequencies can stimulate and accelerate the processof chondrogenesis and endochondral ossification and consequently the bony union of thefracture. This is probably achieved by the interstitial fluid flow, which can move nutrientsand waste from one place to another in the callus. This movement of fluid modifies themechanical stimulus on the cells attached to the extracellular matrix. On the other hand,the experimental study was carried out using two sheep groups. In the first group, staticfixators were implanted, while, in the second one, identical devices were used, but with anadditional vibrator. This vibrator allowed a cyclic displacement with low magnitude andhigh frequency (LMHF) to be applied to the fractured zone every day; the frequencyof stimulation was chosen from mechano-biological model predictions. Analysing theresults obtained for the control and stimulated groups, we observed improvements inthe bone-healing process in the stimulated group. Therefore, in this study, we show thepotential of computer mechano-biological models to guide and define better mechanicalconditions for experiments in order to improve bone fracture healing. In fact, bothexperimental and computational studies indicated improvements in the healing processin the LMHF mechanically stimulated fractures. In both studies, these improvementscould be associated with the promotion of endochondral ossification and an increase inthe rate of cell proliferation and tissue synthesis.
Keywords: bone healing; low-magnitude high-frequency mechanical stimulation;mechano-biological model
*Author for correspondence ([email protected]).
One contribution of 11 to a Theme Issue ‘Towards the virtual physiological human: mathematicaland computational case studies’.
This journal is © 2011 The Royal Society4278
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4279
1. Introduction
Fracture healing is a complex process that involves decision-making in manyaspects, such as the optimum external fixator to use or the specific treatmentto follow. As this process is mechanically driven, both experimental andcomputational studies have been performed in an attempt to improve theunderstanding of this process. In fact, external fixators have usually been designedfrom biomechanical [1] and clinical [2] considerations; similarly, treatments forbone healing are based on either mechanical or biological processes [3].
This mechanical and biological coupling has motivated the development ofmore complex computational models that are normally known as mechano-biological models [4]. These models have succeeded in predicting the outcomeof fracture healing and distraction osteogenesis under different loading regimesor external fixators. This highlights the close relationship that is needed betweenengineers and clinicians. For a complete review of fracture-healing biology andmodels, see Geris et al. [5].
Nevertheless, mechano-biological models have not normally been used to defineand drive treatments or experiments. Therefore, in this study, as a further step wepropose the design of a new bone-healing treatment based on the prediction ofa mechano-biological model [6]. This treatment was applied in a sheep animalmodel in order to evaluate its functionality. With this aim, we initially andbriefly describe the use of computer biomechanical-based models for the designof clinical treatments and protheses. Next, mechano-biological-based modelsand applications are widely revised, distinguishing between tissue differentiationtheories and their application to bone healing and distraction osteogenesis. And,finally, a revision of the influence of the stimulation type (mechanical, biophysical,biochemical or low-magnitude high-frequency (LMHF) mechanical stimulation)on the course of bone healing is also discussed.
2. Background
(a) Biomechanical computer design of clinical treatments and implants
Biomechanical principles have been widely used in the design of implants andorthopaedic treatments such as fracture healing. Here, only a brief revision ofsome biomechanical computer models is shown. Models have evolved from thefirst analytical developments [7,8] and experimental studies [9] to the use ofcomputer-oriented techniques such as the finite-element method. Finite-elementmodels, probably initiated by Brekelmans et al. [10], have become increasinglywidespread in recent decades [11,12]. In fact, finite-element models have beenused in orthopaedics in the design of prostheses such as for the knee [13], hip[14], pelvis [15], femur [16], tibia [17], hand [18] and foot [19]. In all these studies,the stress and strain states in one or several fixed time points are analysed tocorrelate them with the suitability of the implant or treatment.
(b) Mechano-biological models of bone healing and their applications
Given that this study aims to demonstrate the potential to drive experimentsthrough mechano-biological models, a wide revision has been developed.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4280 M. J. Gómez-Benito et al.
This revision has been divided by distinguishing between theories for tissuedifferentiation and evolutionary models of bone healing and distractionosteogenesis.
(i) Tissue differentiation theories
Many researchers have attempted to establish the relationship between themechanical level of an undifferentiated tissue and the ultimate tissue phenotypeformed. Pauwels [20] proposed the first rigorous mechano-regulation theory whichhypothesized that the invariants of the strain and stress tensors guided thedifferentiation pathway. Later, a simpler idea, strain-based, was proposed byPerren [21] and Perren & Cordey [22] to predict the evolution of tissues in a bonefracture gap. They developed the concept of ‘interfragmentary strain’. Also basedon the ideas of Pauwels, Carter [23] proposed a combination of octahedral shearstress and hydrostatic stress for his differentiation theory [24]. Unlike Pauwels,Carter [23] recognized the influence of vascularization and proposed that lowoxygen tension favours chondrogenesis. Claes & Heigele [25], using an elasticfinite-element model, proposed a mechano-regulation theory similar to that ofCarter [23], but presented in quantitative terms. Unlike the previous models,Prendergast et al. [26] developed a mechano-regulation concept assuming thattissues are poroelastic, and thus comprise both fluid and solid phases. Theyproposed a mechano-regulation pathway regulated by two biophysical stimuli, theoctahedral shear strain of the solid and the interstitial fluid velocity relative tothe solid. Finally, Gómez-Benito et al. [27] and García-Aznar et al. [28] proposeda mathematical model exclusively driven by the second invariant of the deviatoricstrain tensor (proportional to the octahedral shear strain), assuming that tissuesare poroelastic.
(ii) Evolutionary models of bone healing and distraction osteogenesis
The previous tissue differentiation theories have been successfully used inseveral computational studies to reproduce the main patterns of fracture healingin specific mechanical environments. For instance, Lacroix & Prendergast [29]have developed a bone-healing model based on the mechano-regulation theorypreviously formulated by Prendergast et al. [26]. This model was then taken upby Andreykiv et al. [30], Isaksson et al. [31], Byrne [32] and Boccaccio et al.[33]. Gómez-Benito et al. [27] and García-Aznar et al. [28] succeed in simulatingthe main processes that occur during fracture healing and improved on existingnumerical models of fracture healing by providing a mathematical formulation ofcallus growth.
All these models are related to mechanical stimuli, which are definitelyperceived by cells whose biological sensing and signalling activities are implicitlyassumed but not directly considered. In contrast, other mechano-biological modelshave introduced biological factors in addition to the mechanical ones. Forinstance, Ament & Hofer [34] proposed a biomechanical model based on a setof fuzzy logic rules to describe the tissue transformation during healing. Theyintroduced a biological factor that accounted for the vascularization in additionto the mechanical stimulus (the strain energy density). This approach has beentaken up by Simon et al. [35,36] and Shefelbine et al. [37], who simulated, usingfinite-element analysis and fuzzy logic, fracture healing, based on local mechanical
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4281
factors, as described by Claes & Heigele [25], and the local vascularity. Recently,Chen et al. [38] introduced the supply of nutrients to the previous computationalalgorithm. Bailón-Plaza & van der Meulen [39] presented the first two-dimensionaltemporo-spatial mathematical model of the bone-healing process that considersthe effect of growth factors. This model was later modified to incorporate theeffects of mechanical stimulation on cell differentiation [40] and angiogenesisand directed cell migration with a continuous mathematical model [41] thathas been recently improved by introducing a deterministic hybrid modellingframework [42].
Fracture and distraction repair proceed through the same cellular healingprocess [43], and, therefore, most existing mechano-biological models ofdistraction osteogenesis are based on existing models of fracture healing, either onthe mechano-regulation theory presented earlier by Prendergast et al. [26,44–46]or on that proposed by Gómez-Benito et al. [27,47,48].
(c) Experimental analysis of the influence of the load type in bone healing:low-magnitude high-frequency mechanical stimulus
Although it seems that there exists an optimal mechanical environment foreach specific fracture to heal [49], more insight is needed in order to definethe type, magnitude and time history of the optimal mechanical load foreach kind of fracture. Different authors have tried to identify the influenceof the mechanical environment on fracture healing, by determining the effectof the different load types (axial, bending, shear and torsion) on the outcomeof the process. Nevertheless, we should mention the difficulty in avoiding anaxial load component due to the animal’s weight; this compression componentwill represent a stimulus for the healing process [50]. In addition, the axialinterfragmentary movement reduces the gap size, promoting the healing process[51]. Finally, it is important to underline the difficulty in quantitatively comparingthe different loading conditions. For example, when a bone is under compressivemotion, the gap distance is shortened; in contrast, tensile motion lengthensit [52].
(i) Axial loads
It is generally accepted that some amount of axial movement between fracturefragments stimulates callus formation and favours the quality and quantity ofthe new tissue [53]. In contrast, excessive interfragmentary movement delays thehealing process and may result in the non-union of bone fragments, causing, insome cases, pseudoarthrosis [51].
The effect of tensile axial loads on the process of distraction osteogenesishas been widely studied. Through the application of tensional stress, a dynamicmicroenvironment is created, with the formation of tissue parallel to the tractionvector [54]. This environment stimulates changes at the cellular and sub-cellularlevels [55]. There is a prolongation of angiogenesis with an increase in tissueoxygenation and an increase in the proliferation of spindle-shaped fibroblast-likecells. This type of spindle-shaped cell and its secreted collagen, mostly type I,becomes longitudinally oriented along the axis of tension. The collagen fibres ofthe fibrous interzone seem to play a critical role in bone formation in tensileenvironments by providing mechanical stability and facilitating the formation
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4282 M. J. Gómez-Benito et al.
of early bone spicules [2,56]. It has also been observed that these cells canexpress osteocalcin, osteopontin and alkaline phosphate, which is evidence of someosteoblastic differentiation.
(ii) Shear loads
Bishop et al. [57,58] compared the bone-healing process under pure interfrag-mentary torsional shear, pure axial compression and no applied motion. Thetorsional load group resulted in more intercortical mineralized callus and bridgingthan the axial group, and more callus area than the non-stimulated group.Through this experiment, they analysed the effect of octahedral normal andshear strains on fracture healing. The mass of the periosteal callus in theanimals subjected to a history of torsional load was twice the mass of theperiosteal callus in the animals subjected to axial load. This fact may justifythe choice of the second invariant of the deviatoric strain tensor as the mechanicalstimulus that controls the mechano-biological processes involved in boneregeneration.
Nevertheless, the influence of shear interfragmentary movements on fracturehealing is still controversial [59,60]. On the one hand, Augat et al. [60]demonstrated that shear loads delay the healing process, and could result ina non-union. In their experiments they compared the effect of axial and shearloads on the fracture callus of sheep, for interfragmentary movements of similarmagnitude. All fractures that healed under axial load resulted in successfulunion; nevertheless, only partial healing was achieved under shear loads. On theother hand, Park et al. [59] postulated that shear loads are beneficial for bonehealing; when small shear strains are permitted the healing process is accelerated,generating different effects on tissues in the interfragmentary space.
(iii) Bending loads
Hente et al. [61] studied the healing process under pure bending loads.Important differences were observed on the side of the callus subjected tocompressive and tension loads in both shape and tissue distribution; indeed, thetension side was bigger than the compression one.
(iv) Additional external stimulation
Different external stimuli have been applied to stimulate and accelerate bonehealing [62], such as low-intensity ultrasound, electromagnetic fields, electriccurrents of low potential and, more recently, LMHF mechanical stimulations.Results support the assumption of the beneficial effects of external biophysicalstimulations on bone healing. However, there are still only a few commercialdevices able to apply external mechanical stimulations [62]. In contrast tobiochemical stimulations [63], LMHF mechanical stimulation is safer.
The idea of LMHF mechanical stimulation was originally proposed to mimicmuscle activity, which presents a signal of strain lower than 10 m3 in a range offrequencies of 10–50 Hz [64]. In fact, these researchers assumed that age reducesmuscle activity [64] and this effect could be one of the factors causing bone mass
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4283
loss. Rubin et al. [64] determined that the muscle activity in frequencies higherthan 20 Hz decreases by a factor of three in elderly people compared with youngadults.
LMHF mechanical stimulation with a frequency of 30–35 Hz has beenapplied to stimulate fracture healing in long bones of healthy and osteoporoticrats [65–67] and sheep [68]. It also has beneficial effects on the healing ofnon-weight-bearing bone defects in rats [69] and in distraction osteogenesis[70]. A frequency of 45 Hz was used to stimulate scaffolded and non-scaffolded cranial defects in rats, showing a clear beneficial effect with respectto the non-stimulated defects [71]. This effect was even greater when ascaffold was present. Nevertheless, lower frequencies of stimulation (20 Hz)have been demonstrated to have no beneficial effects on bone healing [72].The idea of applying LMHF to stimulate bone matrix production is notnew. It has been previously applied to strengthen healthy and osteoporoticbones [64,73] and on the growing skeleton [74]. Regarding the beneficialeffects on bone mass, higher frequencies of stimulation have been tested(90 Hz), showing a much more beneficial effect than moderate frequencies ofstimulation [75].
As it is still not clear which is the most appropriate frequency of stimulation,in this study, we used a mechano-biological model of tissue differentiation [26] topredict the most appropriate frequency of stimulation [6], and we applied it toan animal experiment on sheep to test the reliability of the proposed hypothesisin the mechano-biological model.
3. Mathematical modelling and experiments
The main aim of this study was to design an external fixator that is ableto monitor and stimulate fracture healing. A fixator was designed, followingbiomechanical and mechano-biological principles, and was implanted in sheepin order to evaluate its functionality (see the work scheme summarized in figure1). In fact, this design was developed using the following protocol:
— Biomechanical functionality. The geometrical configuration of the fixatorwas defined in order to promote natural healing. Finite-element modelswere used for its design under biomechanical principles.
— Design of the external device for mechanical stimulation. After validation ofthe biomechanical design, we decided to carry out active treatment of thefracture in order to reduce the healing time and improve the quality of boneregeneration. To do so, we incorporated in the fixator a small dimensionmotor able to stimulate the fracture by LMHF mechanical stimulation.
— Design of the fixator based on mechano-biological modelling. As there issome controversy about the most appropriate frequency of stimulation tofavour bone healing, we performed a mechano-biological computationalanalysis to determine the effect of the frequency of stimulation on bonefracture healing [6].
— Experimental validation. Experiments were performed to corroborate thefindings of the biomechanical and mechano-biological models.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4284 M. J. Gómez-Benito et al.
design concept
validation
biomechanicalmodel
mechano-biologicalmodel
computationalprediction
prototype definition
tissueresponse
implantgeometry
experimentalevaluation
instrumentation
monitoringquantification
Figure 1. Scheme of the process for designing the external fixator based on biomechanicaland mechano-biological principles.
More details of all these steps for both computational and experimental studiesare described in order to achieve the main objective of this work: the design ofan active fixator from mechano-biological mathematical models.
(a) Biomechanical model: fixator design
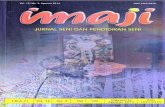
First, we designed an external static fixator from a biomechanical perspective[1]. The mechanical environment in the fracture gap was previously analysedat different time points in the healing process by means of static finite-elementanalyses (figure 2). Different mechanical tests were computationally simulated inthe fixator bone system. The same simulated mechanical tests were performed in amechanical test Instron machine to correctly calibrate the system. An appropriatemechanical environment was used at each time point. In this way, we designeda fixator that ensured a maximum interfragmentary strain of 10 per cent withinthe fracture gap [1]. Design criteria also included low weight of the fixator, ease ofimplantation, biocompatibility and comfort for the animal during the surgery andrecovery. The fixator incorporated a monitoring device to quantify the fracture-healing process. This specifically designed fixator was mechanized and implantedin a group of sheep (control or static group). These sheep were monitored, andsuccessful healing was achieved in all the animals.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4285
max. principalstrain3.000e–017.000e–046.300e–045.600e–044.900e–044.200e–043.500e–042.800e–042.100e–041.400e–047.000e–050.000e+00
Figure 2. Maximum principal strain in the tibia and external fixator 1 day after surgery.
(b) Mechano-biological models: a computational prediction of the frequencyof stimulation
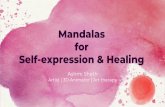
The influence of the frequency of the external load on the mechanical stimulusin the callus was computationally analysed [6] to determine the effect of LMHFmechanical stimulation on the healing outcome. An axisymmetric simplifiedmodel of the fracture callus in the metatarsus of a sheep was simulated [25]at two different time points, one and four weeks after fracture. The one-weekcallus was assumed to be fully formed by granulation tissue and the four weekcallus was formed by immature bone, cartilage and granulation tissue (see figure3). All tissues in the callus were assumed to be poroelastic [76]. The tissues underconsideration were: granulation tissue (Young’s modulus (E) 0.2 MPa, Poisson’sratio (n) 0.167 and permeability (k) 9.8 ! 10"8 mm seg"1); cartilage (E = 10 MPa,n = 0.167 and k = 4.9 ! 10"8 mm seg"1); immature bone tissue (E = 1000 MPa, n =0.3 and k = 9.8 ! 10"7 mm seg"1) and cortical bone tissue (E = 20 000 MPa, n =0.3 and k = 9.8 ! 10"11 mm seg"1) [6]. A displacement of 0.02 mm was appliedat the top of the cortical bone at different frequencies of stimulation (1, 50and 100 Hz) in order to evaluate their impact on tissue differentiation followingthe theory proposed by Prendergast et al. [26]. Nevertheless, it is important tonote that this displacement stimulus was applied for 15 min, which representsdifferent numbers of load cycles, i.e. 90 000, 45 000 and 900, respectively. Thecomputational model used here is the simplest model to quantify the effectof LMHF mechanical stimulation, although it is not able to represent thecomplete in vivo situation. To do so, a more realistic three-dimensional geometryshould be included as well as more complex loading regimes. Figure 3 showsthe evolution of the magnitudes of some mechanical variables when applyingan interfragmentary displacement of 0.02 mm at these frequencies and their
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4286 M. J. Gómez-Benito et al.
octahedral straincorticalboneimmaturebone
cartilage
granulationtissue
(a) (b)
one-week callus
four-week callus
cyclicstimulus
cyclicstimulus
0.02 mm
0.02 mm
null flux
null flux
free flux
free flux
second invariantof the deviatoric
strain tensor
fluid flow(mm seg–1)
P
P
01 Hz
50 Hz100 Hz
1 Hz50 Hz
100 Hz
1 Hz50 Hz
100 Hz
1 Hz50 Hz
100 Hz
1 Hz50 Hz
100 Hz
1 Hz50 Hz
100 Hz
–0.20
–0.40
–0.60
–0.80
–1.00
0 30 4844403632282420161284
0
25
20
15
10
5
0 0.20 0.40 0.60 0.80
–0.40
–0.80
–1.20
–1.60
0 0.20 0.40time (1¥103 s) time (1¥103 s) time (1¥103 s)oc
tahe
dral
str
ain
(1¥1
0–3 )
octa
ched
ral s
trai
n (1
¥10–
3 )
seco
nd in
vari
ant o
fth
e st
rain
tens
or (1
¥10–
3 )se
cond
inva
rian
t of
the
stra
in te
nsor
(1¥1
0–3 )
flui
d ve
loci
ty (1
¥10–3
)fl
uid
velo
city
(1¥1
0–3)
0.60 0.80
0 0.20 0.40
time (1¥103 s) time (1¥103 s)0.20 0.40 0.60 0.80
time (1¥103 s)0.60 0.80
–1.20
2035
30
25
20
15
10
5
0 0.20 0.40 0.60 0.80
16
12
8
4
0 0.20 0.40 0.60 0.80
Figure 3. (a) Tissue distribution and boundary conditions in the one- and four-week calluses(adapted from Claes & Heigele [25]). (b) Evolution of the mean mechanical stimulus at onepoint in the gap (see (a)) when stimulating with different frequencies (1, 50 and 100 Hz)for 15 min.
variations at two stages after the osteotomy. The fluid flow velocity variesin amplitude when the frequency of the external stimulus changes, whereasthe other mechanical variables (octahedral strain and second invariant of thedeviatoric strain tensor) are just slightly modified. These changes in the fluidflow velocity may induce movement of waste, nutrients or growth factors, whichcould also contribute to stimulating cellular activity (differentiation, proliferation,migration) by means of changes in the mechanical environment of the callus.As far as we know, the only differentiation law which takes into account thefrequency of stimulation is the one proposed by Prendergast et al. [26], by meansof the fluid flow since the other mechanical variables are just slightly modifiedwhen the frequency of stimulation is changed. Variations in this mechanicalvariable are important mainly for frequencies of stimulation higher than 50 Hz(figure 4). According to the differentiation rule proposed by Prendergast et al.[26], an increase in the frequency of stimulation may promote chondrogenesis andendochondral ossification. As our aim was to improve the bone-healing processin our experiments, we decided to stimulate the fracture site with a frequencyhigher than 50 Hz. As previous experimental studies have used frequencies up
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4287
10cartilage
bone
one-week callusstimulatedat 50 Hz
F > 50 Hz
F < 50 Hz
resorption
1
10–1
10–2
10–3
10–4
10–4 10–3 10–2 10–1
octahedral shear strain (%)1 10 102
flui
d fl
ow (m
m s
–1)
Figure 4. Differentiation theory proposed by Prendergast et al. [26]. The area outlined by thedashed line indicates the peak mechanical variables (octahedral shear strain and fluid flow) at allpoints in the fracture callus for a mechanical stimulation of 0.02 mm and frequency of 50 Hz in theone-week callus. Arrows show the tendency when the frequency (F) of stimulation is varied.
to 90 Hz [75] to stimulate bone mass formation in osteoporotic conditions, wedecided to use this frequency. Thus, we stimulated the fracture with a frequencyof 90 Hz for 15 min twice a day. The period of stimulation was chosen based onthe computational analysis as the mechanical stimulus stabilizes for a period ofstimulation longer than 15 min (figure 3). We further performed an eigenmodeanalysis of the bone and the external fixator at different time points in thehealing process in order to avoid stimulation at the natural frequencies of thebone–fixator system.
(c) Experimental follow-up
A monolateral external fixator, described previously [1], was developed in orderto study experimentally the process of fracture healing. This fixator allowed us tomonitor telemetrically the repair process in osteotomized long bones, correlatingthe load transmission through the main body of the system to the increasingstiffness of the regenerated bone. The monolateral external fixator that wasdeveloped was further improved to induce an interfragmentary displacement inthe osteotomized gap. This displacement was generated by means of vibrationproduced by a small electronic cylindrical motor (10 mm diameter and 20 mmlong) to obtain a LMHF displacement by a controlled stimulus [77]. This motorwas designed to always have the same excitation frequency. The interfragmentarymovement applied by the motor corresponds to 1 per cent, which is regulated bythe input power limitation of the battery, keeping the frequency the same. Athree-axis accelerometer was also included inside the fixator. This sensor, afterreal-time post-processing, could provide the actual displacement of the fixatorduring the stimulation.
Animals selected for the study were adult ‘Rasa Aragonesa’ female sheep. Thegap size was 2 mm and the monolateral external fixator was attached mediallyto the transversally osteotomized right tibiae [1]. Sheep were divided into twogroups of two sheep in each group: a stimulated group and a static or control
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4288 M. J. Gómez-Benito et al.
1.4
1.2
0.8
0.6
max
imum
axi
al lo
ad th
roug
h fi
xato
r(n
orm
aliz
ed w
ith th
e B
W)
0.4
0.2
1.0
07 9 11 13 15
days after fracture17 19 21 23
Figure 5. Evolution of mean maximum walking axial loads through the external fixator normalizedto the animal body weight (BW) in the control and stimulated groups (filled grey circles, control;filled black circles, stimulated).
group. The former received a daily stimulation of 90 Hz for 15 min twice a dayas the mechano-biological model had indicated (stimulated), while the latter didnot receive any external mechanical stimulation (static).
The fracture-healing outcome was evaluated by means of the force through thefixator each day. Animals were induced to walk for 10 min each day and the loadthrough the fixator was monitored during this period. The mean maximum axialload through the fixator at each step of walking was evaluated. Results for bothgroups are shown in figure 5. We should mention that the variations in the loadthrough the fixator during the first days after fracture could be attributed toadaptation to fixator. Even if a sheep walked normally during the first days afterfracture there was still no regular step for the sheep. Regarding the evolution ofthis load until day 15 after osteotomy, most of the load went through the fixatorin both the static group and the stimulated one. However, this load decreasedquickly from this time point until it reached 20 per cent of the body weight ofthe animal, a value that did not significantly vary during the following days.Thus, we assumed that, if the stiffness of the tissues does not vary significantly,tissues of the callus are mainly mineralized. This assumption was corroborated byradiographs of the injured leg. This occurred 30 days and 24 days after fracturefor the static and stimulated sheep, respectively. The quicker reduction of theload through the fixator in the stimulated sheep compared with the static sheepindicates an acceleration of the healing process in the stimulated sheep. Severalimage tests (radiographs during healing and micro-computed tomography afterthe sheep were killed) were performed in the operated tibiae. These tests indicatecomplete bony union in both groups at the time the sheep were killed. After death,torsion tests were performed in the healed calluses. The control calluses showed amean torsional stiffness of 0.8 N m per degree, while the average torsional stiffnessof the stimulated group was 2.2 N m per degree.
All these tests indicate a better quality of regenerated bone for the stimulatedsheep. These experimental results corroborate those predicted by the mechano-biological model: stimulation by a LMHF mechanical stimulus with a frequency
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4289
48444036322824
flui
d ve
loci
ty (1
¥10–
3 )
20161284
0 0.20 0.40
1 Hz20 Hz35 Hz50 Hz
time (1¥103 s)0.60 0.80
Figure 6. Mean fluid flow (mm seg"1) at one point of the gap with 1, 20, 35 and 50 Hz frequenciesof stimulation.
of 90 Hz improves the healing outcome, probably by means of the promotion ofchondrogenesis and endochondral ossification.
4. Concluding remarks
Both experimental and computational studies indicated improvements in thehealing process with LMHF mechanically stimulated fractures. On the one hand,the computational mechano-biological simulation showed an improvement in thebone-healing process when LMHF mechanical stimulation was applied to thehealing bone at frequencies higher than 50 Hz. This is attributed to changes inthe interstitial fluid flow velocity, which would promote endochondral ossification(following the differentiation rule proposed by Prendergast et al. [26]) and mayincrease cell activity (rates of cell proliferation, migration, differentiation andtissue synthesis) [6]. The LMHF mechanical signal could also be directly sensedby cells and could change its response. On the other hand, the experimentsconfirmed this improvement in the healing process by an acceleration of one weekin the healing process in the group stimulated by LMHF mechanical displacementat a frequency of 90 Hz compared with the non-stimulated control group. Theimprovement was further confirmed by the better quality of the callus in thestimulated group than that in the control group.
In addition, the results of the mechano-biological model (figure 6) could alsohelp to explain why no improvement was noted in the bone-healing process whenstimulating at a frequency of 20 Hz in previous studies [72] and why higherfrequencies could result in a better outcome of healing by means of the increaseof the fluid flow velocity [65–68]. Nevertheless, we have to keep in mind that thefrequency of stimulation is just one of the variables that could have an influenceon these experimental results. In fact, many other variables could also have someadditional effects.
Nevertheless, further animal experiments are needed to quantitativelydetermine the effect of LMHF mechanical stimulation on fracture callus andconfirm the results of both the computational simulations and the experiments.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4290 M. J. Gómez-Benito et al.
Also, different protocols of stimulation should be simulated computationally inorder to further improve this treatment. Moreover, although the potential ofmathematical models is very promising for the design of clinical treatments oncevalidated against experimental results, it is necessary to incorporate in the modelsthe coupling between mechanical and biochemical factors such as growth factors.Models based just on mechanical factors, such as the one proposed by Prendergastet al. [26], could represent qualitatively the behaviour of the system. Nevertheless,to obtain more realistic results, patient-specific variables should be introduced tothe models such as genetics, way of life or previous clinical history.
In this work, the mathematical modelling has provided guidelines for the designof a fracture-healing treatment and an external fixator. In fact, the combinationof mechano-biological and biomechanical models has led to the design of anexternal fixator able to monitor and stimulate fracture healing, reducing animalexperimentation. Just a few animals were tested in the experiments becausethe results have corroborated the outcome of the mechano-biological simulation.Thus, in this study, the mathematical model was used as a tool for thedesign of the experiments, not in the reverse way as has been done to date.Normally, experiments are used to validate the results of mathematical modelling.Nevertheless, more insight is needed in order to have a complete model that couldbe used by surgeons to determine patient-specific treatments.All the experiments and the animal care were carried out with the permission of the Universityof Zaragoza Ethics Commission and in accordance with the international guidelines for the use oflaboratory animals.
This research was supported by the Spanish Ministry of Science and Technology (grantDPI2009-07514). The project was part financed by the European Union, by means of the EuropeanRegional Development Fund.
References1 Grasa, J., Gómez-Benito, M. J., González-Torres, L. A., Asiaín, D., Quero, F. & García-Aznar,
J. M. 2010 Monitoring in vivo load transmission through an external fixator. Ann. Biomed.Eng. 38, 605–612. (doi:10.1007/s10439-009-9889-5)
2 Ilizarov, G. 1989 The tension-stress effect on the genesis and growth of tissues. Part I. Theinfluence of stability of fixation and soft-tissue preservation. Clin. Orthop. Relat. Res. 238,249–281.
3 Giannoudis, P. V., Einhorn, T. A. & Marsh, D. 2007 Fracture healing: the diamond concept.Injury 38, S3–S6. (doi:10.1016/S0020-1383(08)70003-2)
4 van der Meulen, M. C. & Huiskes, R. 2002 Why mechanobiology? A survey article. J. Biomech.35, 401–414. (doi:10.1016/S0021-9290(01)00184-1)
5 Geris, L., Vander Sloten, J. & Van Oosterwyck, H. 2009 In silico biology of bone modelling andremodelling: regeneration. Phil. Trans. R. Soc. A 367, 2031–2053. (doi:10.1098/rsta.2008.0293)
6 González-Torres, L. A., Gómez-Benito, M. J., Doblaré, M. & García-Aznar, J. M. 2010 Influenceof the frequency of the external mechanical stimulus on bone healing: a computational study.Med. Eng. Phys. 32, 363–371. (doi:10.1016/j.medengphy.2010.01.010)
7 Koch, J. C. 1917 The laws of bone architecture. Am. J. Anat. 21, 177–298. (doi:10.1002/aja.1000210202)
8 Calderale, P. M., Gola, M. & Gugliotta, A. 1977 Analytical estimate of bone prosthesis coupling.In: Proc. VIth Int. Congr. Biomech., Copenhagen, Denmark, 11–14 July 1977 (eds E. Asmussen& K. Jorgensen), pp. 1–22. Baltimore, MD: University Park Press.
9 Martz, C. D. 1956 Stress tolerance of bone and metal. J. Bone Joint Surg. Am. 38, 827–834.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4291
10 Brekelmans, W. A. M., Poort, H. W. & Slooff, T. 1972 A new method to analyse the mechanicalbehaviour of skeletal parts. Acta Orthop. Scand. 43, 301–317.
11 Prendergast, P. J. 1997 Finite element models in tissue mechanics and orthopaedic implantdesign. Clin. Biomech. 12, 343–366. (doi:10.1016/S0268-0033(97)00018-1)
12 Juan, J. A., Prat, J., Vera, P., Hoyos, J. V., Sánchez-Lacuesta, J., Perís, J. L., Dejoz, R. &Alepuz, R. 1992 Biomechanical consequences of callus development in Hoffmann, Wagner,Orthofix and Ilizarov external fixators. J. Biomech. 25, 995–1006. (doi:10.1016/0021-9290(92)90035-Y)
13 Carr, B. C. & Goswami, T. 2009 Knee implants—review of models and biomechanics. Mater.Des. 30, 398–413. (doi:10.1016/j.matdes.2008.03.032)
14 Pérez, M. & Palacios, J. 2010 Comparative finite element analysis of the debonding process indifferent concepts of cemented hip implants. Ann. Biomed. Eng. 38, 2093–2106. (doi:10.1007/s10439-010-9996-3)
15 García, J. M., Doblaré, M., Seral, B., Seral, F., Palanca, D. & Gracia, L. 2000 Three-dimensionalfinite element analysis of several internal and external pelvis fixations. J. Biomech. Eng. 122,516–522. (doi:10.1115/1.1289995)
16 Seral, B., García, J. M., Cegoñino, J., Doblaré, M. & Seral, F. 2004 Finite element study ofintramedullary osteosynthesis in the treatment of trochanteric fractures of the hip: gamma andPFN. Injury 35, 130–135. (doi:10.1016/S0020-1383(03)00076-7)
17 Gómez-Benito, M. J., Fornells, P., García-Aznar, J. M., Seral, B., Seral-Iñigo, F. & Doblaré, M.2007 Computational comparison of reamed versus unreamed intramedullary tibial nails.J. Orthop. Res. 25, 191–200. (doi:10.1002/jor.20308)
18 Penrose, J. M., Williams, N. W., Hose, D. R. & Trowbridge, E. A. 1997 In situ simulation ofone-piece metacarpophalangeal joint implants using finite element analysis. Med. Eng. Phys.19, 303–307. (doi:10.1016/S1350-4533(96)00075-6)
19 Halloran, J. P., Ackermann, M., Erdemir, A. & van den Bogert, A. J. 2010 Concurrentmusculoskeletal dynamics and finite element analysis predicts altered gait patterns to reducefoot tissue loading. J. Biomech. 43, 2810–2815. (doi:10.1016/j.jbiomech.2010.05.036)
20 Pauwels, F. 1941 Grundriß einer Biomechanik der Frankturheilung (transl. Maquet, P. &Furlong, R. Berlin, Germany: Springer). In: Proc. 34th Kongress der Deutschen OrthopädischenGessellschaft. Stuttgart, Germany: Ferdinand Enke Verlag.
21 Perren, S. M. 1979 Physical and biological aspects of fracture healing with special reference tointernal fixation. Clin. Orthop. Relat. Res. 138, 175–196.
22 Perren, S. M. & Cordey, J. 1980 The concept of interfragmentary strain. In: Current conceptsof internal fixation of fractures (ed. H. K. Uhthoff), pp. 63–77. Berlin, Germany: Springer.
23 Carter, D. R. 1987 Mechanical loading history and skeletal biology. J Biomech. 20, 1095–1109.(doi:10.1016/0021-9290(87)90027-3)
24 Carter, D. R., Beaupré, G. S., Giori, N. J. & Helms, J. A. 1998 Mechanobiology of skeletalregeneration. Clin. Orthop. Relat. Res. 355S, 41–55. (doi:10.1097/00003086-199810001-00006)
25 Claes, L. E. & Heigele, C. A. 1999 Magnitudes of local stress and strain along bony surfacespredict the course and type of fracture healing. J. Biomech. 32, 255–266. (doi:10.1016/S0021-9290(98)00153-5)
26 Prendergast, P. J., Huiskes, R. & Søballe, K. 1997 Biophysical stimuli on cells duringtissue differentiation at implant interfaces. J. Biomech. 6, 539–548. (doi:10.1016/S0021-9290(96)00140-6)
27 Gómez-Benito, M. J., García-Aznar, J. M., Kuiper, J. H. & Doblaré, M. 2005 Influence offracture gap size on the pattern of long bone healing: a computational study. J. Theor. Biol.235, 105–119. (doi:10.1016/j.jtbi.2004.12.023)
28 García-Aznar, J. M., Kuiper, J. H., Gómez-Benito, M. J., Doblaré, M. & Richardson, J. B.2007 Computational simulation of fracture healing. J. Biomech. 40, 1467–1476. (doi:10.1016/j.jbiomech.2006.06.013)
29 Lacroix, D. & Prendergast, P. J. 2002 A mechano-regulation model for tissue differentiationduring fracture healing: analysis of gap size and loading. J. Biomech. 35, 1163–1171.(doi:10.1016/S0021-9290(02)00086-6)
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4292 M. J. Gómez-Benito et al.
30 Andreykiv, A., van Keulen, F. & Prendergast, P. J. 2007 Simulation of fracture healingincorporating mechanoregulation of tissue differentiation and dispersal/proliferation of cells.Biomech. Model Mechanobiol. 7, 443–461. (doi:10.1007/s10237-007-0108-8)
31 Isaksson, H., van Donkelaar, C. C., Huiskes, R. & Ito, K. 2008 A mechano-regulatory bone-healing model incorporating cell-phenotype specific activity. J. Theor. Biol. 252, 230–246.(doi:10.1016/j.jtbi.2008.01.030)
32 Byrne, D. P. 2008 Computational modelling of bone regeneration using a three-dimensionallattice approach. PhD thesis, Trinity College, Dublin, Ireland.
33 Boccaccio, A., Kelly, D. J. & Pappalettere, C. 2011 A mechano-regulation model of fracturerepair in vertebral bodies. J. Orthop. Res. 29, 433–443. (doi:10.1002/jor.21231)
34 Ament, C. & Hofer, E. P. 2000 A fuzzy logic model of fracture healing. J. Biomech. 33, 961–968.(doi:10.1016/S0021-9290(00)00049-X)
35 Simon, U. et al. 2002 Dynamical simulation of the fracture healing process including vascularity.In: Proc. 13th Conf. of the European Society of Biomechanics (ESB), Wroclaw, Poland, 1–4September 2003.
36 Simon, U., Augat, P., Utz, M. & Claes, L. 2011 A numerical model of the fracture healing processthat describes tissue development and revascularization. Comp. Meth. Biomech. Biomed. Eng.14, 79–93. (doi:10.1080/10255842.2010.499865)
37 Shefelbine, S. J., Augat, P., Claes, L. & Simon, U. 2005 Trabecular bone fracture healingsimulation with finite element analysis and fuzzy logic. J. Biomech. 38, 2440–2450. (doi:10.1016/j.jbiomech.2004.10.019)
38 Chen, G., Niemeyer, F., Wehner, T., Simon, U., Schuetz, M., Pearcy, M. & Claes, L. 2009Simulation of the nutrient supply in fracture healing. J. Biomech. 42, 2575–2583. (doi:10.1016/j.jbiomech.2009.07.010)
39 Bailón-Plaza, A. & van der Meulen, M. 2001 A mathematical framework to study the effectsof growth factor influences on fracture healing. J. Theor. Biol. 212, 191–209. (doi:10.1006/jtbi.2001.2372)
40 Bailón-Plaza, A. & van der Meulen, M. 2003 Beneficial effects of moderate, early loading andadverse effects of delayed or excessive loading on bone healing. J. Biomech. 36, 1069–1077.(doi:10.1016/S0021-9290(03)00117-9)
41 Geris, L., Gerisch, A., Sloten, J. V., Weiner, R. & Oosterwyck, H. V. 2008 Angiogenesis inbone fracture healing: a bioregulatory model. J. Theoret. Biol. 251, 137–158. (doi:10.1016/j.jtbi.2007.11.008)
42 Peiffer, V., Gerisch, A., Vandepitte, D., Van Oosterwyck, H. & Geris, L. 2011 A hybridbioregulatory model of angiogenesis during bone fracture healing. Biomech. Model Mechanobiol.10, 383–395. (doi:10.1007/s10237-010-0241-7)
43 Lammens, J., Liu, Z., Aerssens, J., Dequeker, J. & Fabry, G. 1998 Distraction bone healingversus osteotomy healing: a comparative biochemical analysis. J. Bone Miner. Res. 13, 279–286.(doi:10.1359/jbmr.1998.13.2.279)
44 Idelsohn, S., Planell, J. A., Gil, F. J. & Lacroix, D. 2006 Development of a dynamic mechano-regulation model based on shear strain and fluid flow to optimize distraction osteogenesis.J. Biomech. 39S, S684.
45 Isaksson, H., Comas, O., Van Donkelaar, C. C., Mediavilla, J., Wilson, W., Huiskes, R. &Ito, K. 2007 Bone regeneration during distraction osteogenesis: mechano-regulation by shearstrain and fluid velocity. J. Biomech. 40, 2002–2011. (doi:10.1016/j.jbiomech.2006.09.028)
46 Boccaccio, A., Prendergast, P. J., Pappalettere, C. & Kelly, D. J. 2008 Tissue differentiationand bone regeneration in an osteotomized mandible: a computational analysis of the latencyperiod. Med. Biol. Eng. Comput. 46, 283–298. (doi:10.1007/s11517-007-0247-1)
47 Reina-Romo, E., Gómez-Benito, M. J., García-Aznar, J. M., Domínguez, J. & Doblaré, M. 2009Modeling distraction osteogenesis: analysis of the distraction rate. Biomech. Model Mechanobiol.8, 323–335. (doi:10.1007/s10237-008-0138-x)
48 Reina-Romo, E., Gómez-Benito, M. J., García-Aznar, J. M., Domínguez, J. & Doblaré, M.2010 Growth mixture model of distraction osteogenesis: effect of pre-traction stresses. Biomech.Model Mechanobiol. 9, 103–115. (doi:10.1007/s10237-009-0162-5)
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

LMHF stimulation in bone healing 4293
49 Goodship, A. E., Watkins, P. E., Rigby, H. S. & Kenwright, J. 1993 The role of fixator framestiffness in the control of fracture healing. An experimental study. J. Biomech. 26, 1027–1035.(doi:10.1016/S0021-9290(05)80002-8)
50 Klein-Nulend, J., Veldhuijzen, J. P. & Burger, E. H. 1986 Increased calcification of growth platecartilage as a result of compressive force in vitro. Arthritis Rheum. 29, 1002–1009. (doi:10.1002/art.1780290809)
51 Claes, L., Augat, P., Suger, G. & Wilke, H. J. 1997 Influence of size and stability of theosteotomy gap on the success of fracture healing. J. Orthop. Res. 15, 577–584. (doi:10.1002/jor.1100150414)
52 Park, S. H. 2004 Letter to the editor: ‘shear movement at the fracture site delays healing ina diaphyseal fracture model’ by Peter Augat, Johannes Buger, Sandra Schorlemmer, ThomasHenke, Manfred Peraus, Lutz Claes (J. Orthop. Res. 2003;21:1011–17). J. Orthop. Res. 22,1156–1157. (doi:10.1016/j.orthres.2004.02.003)
53 Claes, L., Heigele, C. A., Neidlinger-Wilke, C., Kaspar, D., Seidl, W., Margevicius, K. &Augat, P. 1998 Effects of mechanical factors on the fracture healing process. Clin. Orthop.Relat. Res. 355S, 132–147. (doi:10.1097/00003086-199810001-00015)
54 Delloye, C., Delefortrie, G., Coutelier, L. & Vincent, A. 1990 Bone regenerate formation incortical bone during distraction lengthening: an experimental study. Clin. Orthop. Relat. Res.250, 34–42.
55 Mosheiff, R., Cordey, J., Rahn, B. A., Perren, S. M. & Stein, H. 1996 The vascular supply tobone in distraction osteoneogenesis: an experimental study. J. Bone Joint Surg. Br. 78, 497–498.
56 Bouletreau, P. J., Warren, S. M. & Longaker, M. T. 2002 The molecular biology of distractionosteogenesis. J. Cranio maxillofac. Surg. 30, 1–11. (doi:10.1054/jcms.2001.0263)
57 Bishop, N. E., Schneider, E. & Ito, K. 2003 An experimental two degrees-of-freedom actuatedexternal fixator for in vivo investigation of fracture healing. Med. Eng. Phys. 25, 335–340.(doi:10.1016/S1350-4533(02)00250-3)
58 Bishop, N. E., van Rhijn, M., Tami, I., Corveleijn, R., Schneider, E. & Ito, K. 2006 Shear doesnot necessarily inhibit bone healing. Clin. Orthop. Relat. Res. 443, 307–314. (doi:10.1097/01.blo.0000191272.34786.09)
59 Park, S. H., O’Connor, K., McKellop, H. & Sarmiento, A. 1998 The influence of active shearor compressive motion on fracture-healing. J. Bone Joint Surg. Am. 80, 868–878.
60 Augat, P., Burger, J., Schorlemmer, S., Henke, T., Peraus, M. & Claes, L. 2003 Shear movementat the fracture site delays healing in a diaphyseal fracture model. J. Orthop. Res. 21, 1011–1017.(doi:10.1016/S0736-0266(03)00098-6)
61 Hente, R., Füchtmeier, B., Schlegel, U., Ernstbergert, A. & Perren, S. M. 2004 The influenceof cyclic compression and distraction on the healing of experimental tibial fractures. J. Orthop.Res. 22, 709–715. (doi:10.1016/j.orthres.2003.11.007)
62 Chao, E. Y. S. & Inoue, N. 2003 Biophysical stimulation of bone fracture repair, regenerationand remodelling. Eur. Cell Mater. 6, 72–85.
63 Dimitriou, R., Tsiridis, E. & Giannoudis, P. 2005 Current concepts of molecular aspects of bonehealing. Injury 36, 1392–1404. (doi:10.1016/j.injury.2005.07.019)
64 Rubin, C. T., Sommerfeldt, D. W., Judex, S. & Qin, Y. X. 2001 Inhibition of osteopenia by lowmagnitude, high-frequency mechanical stimuli. Drug. Discov. Today 6, 848–858. (doi:10.1016/S1359-6446(01)01872-4)
65 Leung, K. S., Shi, H. F., Cheung, W. H., Qin, L., Ng, W. K., Tam, K. F. & Tang, N. 2009 Low-magnitude high-frequency vibration accelerates callus formation, mineralization, and fracturehealing in rats. J. Orthop. Res. 27, 458–465. (doi:10.1002/jor.20753)
66 Shi, H. F., Cheung, W. H., Qin, L., Leung, A. H. C. & Leung, K. S. 2010 Low-magnitude high-frequency vibration treatment augments fracture healing in ovariectomy-induced osteoporoticbone. Bone 46, 1299–1305. (doi:10.1016/j.bone.2009.11.028)
67 Nizam, I., Oliver, R. & Walsh, W. 2009 The effects of high frequency, low magnitude mechanicalvibrations using the juvent dynamic motion therapy device on fracture healing in oestrogendeficient rodent models. J. Bone Joint. Surg. Br. 91, 448.
68 Goodship, A. E., Lawes, T. J. & Rubin, C. T. 2009 Low-magnitude high-frequency mechanicalsignals accelerate and augment endochondral bone repair: preliminary evidence of efficacy.J. Orthop. Res. 27, 922–930. (doi:10.1002/jor.20824)
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from

4294 M. J. Gómez-Benito et al.
69 Omar, H., Shen, G., Jones, A. S., Zoellner, H., Petocz, P. & Darendeliler, M. A. 2008 Effectof low magnitude and high frequency mechanical stimuli on defects healing in cranial bones.J. Oral Maxillofac. Surg. 66, 1104–1111. (doi:10.1016/j.joms.2008.01.048)
70 Bell, D., Oliver, R., Pincus, P. & Walsh, W. 2008 0r3: the effect of low-magnitude, high-frequency vibrations on regenerate bone in distraction osteogenesis. J. Bone Joint Surg. Br.92-B, 201.
71 Hwang, S. J., Lublinsky, S., Seo, Y.-K., Kim, I. S. & Judex, S. 2009 Extremely small-magnitudeaccelerations enhance bone regeneration: a preliminary study. Clin. Orthop. Relat. Res. 467,1083–1091. (doi:10.1007/s11999-008-0552-5)
72 Wolf, S., Augat, P., Eckert-Hubner, K., Laule, A., Krischak, G. D. & Claes, L. E. 2001 Effectsof high-frequency, low-magnitude mechanical stimulus on bone healing. Clin. Orthop. Relat.Res. 385, 192–198. (doi:10.1097/00003086-200104000-00030)
73 Rubin, C., Turner, A. S., Bain, S., Mallinckrodt, C. & McLeod, K. 2001 Low mechanical signalsstrengthen long bones. Nature 412, 603–634. (doi:10.1038/35088122)
74 Xie, L., Jacobson, J. M., Choi, E. S., Busa, B., Donahue, L. R., Miller, L. M., Rubin, C.T. & Judex, S. 2006 Low-level mechanical vibrations can influence bone resorption and boneformation in the growing skeleton. Bone 39, 1059–1066. (doi:10.1016/j.bone.2006.05.012)
75 Judex, S., Lei, X., Han, D. & Rubin, C. 2007 Low-magnitude mechanical signals that stimulatebone formation in the ovariectomized rat are dependent on the applied frequency but not onthe strain magnitude. J. Biomech. 40, 1333–1339. (doi:10.1016/j.jbiomech.2006.05.014)
76 Isaksson, H., Wilson, W., van Donkelaar, C. C., Huiskes, R. & Ito, K. 2006 Comparison ofbiophysical stimuli for mechano-regulation of tissue differentiation during fracture healing.J. Biomech. 39, 1507–1516. (doi:10.1016/j.jbiomech.2005.01.037)
77 Gómez-Benito, M. J., Grasa, J., Gonzalez-Torres, L., Seral, B. & García-Aznar, J. M. 2010Mechanical stimulation of fracture healing by low-amplitude and high frequency external loads.In Proc. 17th Congr. of the European Society of Biomechanics, Edinburgh, UK, 5–8 July 2010.
Phil. Trans. R. Soc. A (2011)
on November 14, 2012rsta.royalsocietypublishing.orgDownloaded from