
The Healing of Tibial Fracture and Response of the Local Lymphatic System
6
The Healing of Tibial Fracture and Response of the Local Lymphatic System Grzegorz Szcze ˛sny, MD, PhD, Waldemar L. Olszewski, MD, PhD, Magdalena Gewartowska, MSci, Marzanna Zaleska, and Andrzej Go ´recki, MD, PhD Background: Damage of tissues by mechanical injury and inflammation is followed by reaction of the regional lym- phoid tissue, lymphatics, and lymph nodes. In our previous lymphoscinti- graphic studies, we showed that closed fractures of a lower limb cause reaction of the local lymphoid tissue. There was dilation of lymphatics draining the site of the fracture and enlargement of in- guinal lymph nodes. These changes per- sisted even after clinical healing of the fracture. In the long-lasting nonhealing fractures, the lymphoscintigraphic pic- tures were different. The draining lym- phatics became obliterated, and the lymph nodes disappeared. Methods: In this study, we tried to correlate the lymphoscintigraphic images, reflecting the immune events at the fracture site, with the immunohistochemical obser- vations of the biopsy specimens obtained during corrective operations from the heal- ing and nonhealing fracture gaps. Thirty- eight patients with closed fracture of the tibia without traumatic skin changes were studied. Results: We confirmed that closed tibial fracture evokes response of the re- gional lymphatic system. Normal fracture healing with immune cell infiltrates and foci of ossification was accompanied by dilated lymphatics and enlarged lymph nodes. Prolonged nonhealing fracture with lack of cellular reaction in the gap proceeded with decreased mass of lymph nodes. Conclusion: This study provides ev- idence for existence of a functional axis between wound of bone and surrounding soft tissue and the local lymphatic (im- mune) system. We hypothesize that the fast healing is regulated by influx into the wound of lymph node regulatory cells, whereas prolonged healing causes gradual exhaustion of the regional lymph node functional elements, and reciprocally im- pairment in sending regulatory cells to the fracture gap. Key Words: Tibia, Fracture, Lymph nodes, Lymphoscintigraphy, Healing. J Trauma. 2007;63:849 – 854. D amage of tissues by mechanical injury and inflamma- tion is followed by reaction of the regional lymphoid tissue, lymphatics, and lymph nodes. This is a physio- logic response of the first line of defense system not only against penetrating foreign antigens, as microorganisms, but also spread of the individual’s own antigens released from the damaged cells and preventing development of autoimmune disease. Lower extremities are exposed to trauma and infec- tions and each episode of injury is reflected in the lymphatics, lymph flow and popliteal, and inguinal and iliac lymph nodes. 1–3 Open injuries of soft tissues and bone cause damage to blood vessels and tissue cells and contamination of the wound with environmental microorganisms. Closed injuries are usually not infected; however, the cellular debris freed from the damaged cells can also evoke response of the local lymphoid tissue. 4 In our previous lymphoscintigraphic stud- ies, we showed that closed fractures of a lower limb cause reaction of the local lymphoid tissue. 2 There was dilation of lymphatics draining the site of the fracture and enlargement of inguinal lymph nodes. In a number of cases, enlargement of the popliteal nodes was also observed. These changes persisted even after clinical healing of the fracture. In the long-lasting nonhealing fractures, the draining lymphatics became obliterated and the lymph nodes disappeared. 2 The question arises regarding what kind of reactions proceed simultaneously in the fracture gap and lymphatics and lymph nodes and whether the lymph node reaction re- flects the cellular and molecular events in the healing and nonhealing gaps. Another interesting question is whether the immune process ongoing in the nodes has a reciprocal effect on healing of the injured tissues. In this study, we correlated the lymphoscintigraphic im- ages, reflecting the immune events at the fracture site, with the immunohistochemical observations in the biopsy speci- mens obtained from the healing and nonhealing fracture gaps. In addition to a better understanding of the local immune response to damaged bone, the obtained results would under- line the advantageousness of lymphoscintigraphic images in evaluating the fracture healing process. PATIENTS AND METHODS Patients Thirty-eight patients with fracture of the tibia were included into the study in the order they were admitted to the department Submitted for publication January 26, 2006. Accepted for publication June 30, 2006. Copyright © 2007 by Lippincott Williams & Wilkins From the Department of Surgical Research and Transplantology (G.S., W.L.O., M.G., M.Z.), Medical Research Centre, Polish Academy of Sci- ences; and Department of Orthopedics and Traumatology (G.S., A.G.), Medical University, Warsaw, Poland. Address for reprints: Grzegorz Szcze ˛sny, MD, PhD, Department for Surgical Research and Transplantology, Medical Research Centre, Polish Academy of Sciences, 5 Pawin ´skiego St., 02-106 Warsaw, Poland; email: [email protected]. DOI: 10.1097/01.ta.0000236641.51515.8f The Journal of TRAUMA Injury, Infection, and Critical Care Volume 63 • Number 4 849
Transcript of The Healing of Tibial Fracture and Response of the Local Lymphatic System

The Healing of Tibial Fracture and Response of the LocalLymphatic SystemGrzegorz Szczesny, MD, PhD, Waldemar L. Olszewski, MD, PhD, Magdalena Gewartowska, MSci,Marzanna Zaleska, and Andrzej Gorecki, MD, PhD
Background: Damage of tissues bymechanical injury and inflammation isfollowed by reaction of the regional lym-phoid tissue, lymphatics, and lymphnodes. In our previous lymphoscinti-graphic studies, we showed that closedfractures of a lower limb cause reactionof the local lymphoid tissue. There wasdilation of lymphatics draining the siteof the fracture and enlargement of in-guinal lymph nodes. These changes per-sisted even after clinical healing of thefracture. In the long-lasting nonhealingfractures, the lymphoscintigraphic pic-tures were different. The draining lym-phatics became obliterated, and thelymph nodes disappeared.
Methods: In this study, we tried tocorrelate the lymphoscintigraphic images,reflecting the immune events at the fracturesite, with the immunohistochemical obser-vations of the biopsy specimens obtainedduring corrective operations from the heal-ing and nonhealing fracture gaps. Thirty-eight patients with closed fracture of thetibia without traumatic skin changes werestudied.
Results: We confirmed that closedtibial fracture evokes response of the re-gional lymphatic system. Normal fracturehealing with immune cell infiltrates andfoci of ossification was accompanied bydilated lymphatics and enlarged lymphnodes. Prolonged nonhealing fracture
with lack of cellular reaction in the gapproceeded with decreased mass of lymphnodes.
Conclusion: This study provides ev-idence for existence of a functional axisbetween wound of bone and surroundingsoft tissue and the local lymphatic (im-mune) system. We hypothesize that thefast healing is regulated by influx into thewound of lymph node regulatory cells,whereas prolonged healing causes gradualexhaustion of the regional lymph nodefunctional elements, and reciprocally im-pairment in sending regulatory cells to thefracture gap.
Key Words: Tibia, Fracture, Lymphnodes, Lymphoscintigraphy, Healing.
J Trauma. 2007;63:849–854.
Damage of tissues by mechanical injury and inflamma-tion is followed by reaction of the regional lymphoidtissue, lymphatics, and lymph nodes. This is a physio-
logic response of the first line of defense system not onlyagainst penetrating foreign antigens, as microorganisms, butalso spread of the individual’s own antigens released from thedamaged cells and preventing development of autoimmunedisease. Lower extremities are exposed to trauma and infec-tions and each episode of injury is reflected in the lymphatics,lymph flow and popliteal, and inguinal and iliac lymphnodes.1–3 Open injuries of soft tissues and bone cause damageto blood vessels and tissue cells and contamination of thewound with environmental microorganisms. Closed injuriesare usually not infected; however, the cellular debris freedfrom the damaged cells can also evoke response of the locallymphoid tissue.4 In our previous lymphoscintigraphic stud-
ies, we showed that closed fractures of a lower limb causereaction of the local lymphoid tissue.2 There was dilation oflymphatics draining the site of the fracture and enlargementof inguinal lymph nodes. In a number of cases, enlargementof the popliteal nodes was also observed. These changespersisted even after clinical healing of the fracture. In thelong-lasting nonhealing fractures, the draining lymphaticsbecame obliterated and the lymph nodes disappeared.2
The question arises regarding what kind of reactionsproceed simultaneously in the fracture gap and lymphaticsand lymph nodes and whether the lymph node reaction re-flects the cellular and molecular events in the healing andnonhealing gaps. Another interesting question is whether theimmune process ongoing in the nodes has a reciprocal effecton healing of the injured tissues.
In this study, we correlated the lymphoscintigraphic im-ages, reflecting the immune events at the fracture site, withthe immunohistochemical observations in the biopsy speci-mens obtained from the healing and nonhealing fracture gaps.In addition to a better understanding of the local immuneresponse to damaged bone, the obtained results would under-line the advantageousness of lymphoscintigraphic images inevaluating the fracture healing process.
PATIENTS AND METHODSPatients
Thirty-eight patients with fracture of the tibia were includedinto the study in the order they were admitted to the department
Submitted for publication January 26, 2006.Accepted for publication June 30, 2006.Copyright © 2007 by Lippincott Williams & WilkinsFrom the Department of Surgical Research and Transplantology (G.S.,
W.L.O., M.G., M.Z.), Medical Research Centre, Polish Academy of Sci-ences; and Department of Orthopedics and Traumatology (G.S., A.G.),Medical University, Warsaw, Poland.
Address for reprints: Grzegorz Szczesny, MD, PhD, Department forSurgical Research and Transplantology, Medical Research Centre, PolishAcademy of Sciences, 5 Pawinskiego St., 02-106 Warsaw, Poland; email:[email protected].
DOI: 10.1097/01.ta.0000236641.51515.8f
The Journal of TRAUMA� Injury, Infection, and Critical Care
Volume 63 • Number 4 849

of orthopedic surgery for the check-up. The inclusion criteriacomprised closed fracture without traumatic skin changes.Exclusion criteria were leg dermatitis, chronic venous insuffi-ciency, ulcers and additional injuries in the past as well aschronic atherosclerotic limb ischemia and diabetes. The patients’data and applied therapy are presented in Table 1. All patientswere evaluated radiologically immediately after fracture andlater at 2 months intervals. The delay in fracture repair wasdiagnosed clinically according to the pathologic mobility be-tween bone fragments, and from X-ray films in the anteropos-terior and lateral positions. The diagnosis was further confirmedon the basis of computed tomography scans as lack of callusformation between bone fragments. Routine lower limb isotopelymphography was performed before surgery. Ten patients haduneventful healing (group 1), and 28 had delayed healing or lackof union (group 2). Patients with indications for surgical correc-tion (n � 28) were divided into two groups: group 1A, unevent-ful healing (21–42 days after fracture) (n � 7); and group 2A,nonhealing fracture (43 days to 15 months after fracture) (n �21). All these patients were operated upon because of either lackof bone fragments alignment or nonunion. Tissue specimenswere taken from the fracture gap for immunohistochemical in-vestigations. The wounds were inspected daily. There was nowound suppuration or dehiscence during the follow-up period.The institute ethical committee approved the study.
LymphoscintigraphyLymphoscintigrams were obtained on the day of appear-
ance in the outpatients department, on both extremities aftersubcutaneous injection of 99mTc-Nanocol (3 mCi) into thefirst web space using a gamma camera (Orbiter ZLC 750,Siemens, Earlangen, Germany). The image of the lower legand thigh lymphatics and lymph nodes was evaluated quan-titatively. Lymphoscintigrams were scanned and analyzedusing specialized PC software (Olympus Micro Image, Ver-sion 3.0.0., Olympus Optical, Hamburg, Germany). The sur-face area of the lymphatics (Lv) and inguinal lymph nodes(LN) of both extremities was evaluated in the inguinal area,thigh, and calf (Fig. 1). Data were expressed as indexesobtained from the equations ILv or LN � STrLv or LN/SCLv or LN,where SLv or LN were surface of lymph vessels or lymph nodesmeasured on the injured (Tr) and contralateral (C) extremity.The obtained data were compared between groups.
Immunohistochemical Investigations of FractureGap Tissue
Tissue specimens from the fracture were snap-frozen at�70°C, sectioned, and stained immunohistochemically withantibodies against human leukocyte antigen (HLA)-DR(HLA class II), CD68 (monocytes/macrophages), CD4
Table 1 The Clinical Parameters and Treatment of Patients With Tibial Fracture
Age Mean � SD Type of FracturePrimary Treatment
Type of Surgery Duration of Follow-up (mo)Mean � SD (Range)Conservative Surgical
Group 1 (n � 10) 41.3 � 9.43 Tibial shaft (10) 3 7 ORIF (7) 8.0 � 6.5 (3–24)Group 2 (n � 28) 41.0 � 17.4 Tibial shaft (28) 7 21 ORIF (16), external
fixation (7), bonetransplantation (5)
28.6 � 49.19 (3–204)
ORIF, open reduction internal fixation.
Fig. 1. Lymphoscintigram of lower limbs of a 49-year-old man 3months after closed fracture of the proximal haft of the left tibia.Uneventful healing seen on X-ray film (upper left), validated by thecomputed tomography scan ( lower left). Lymphoscintigraphic pic-ture (right) shows dilated calf and thigh lymph vessels and enlargedinguinal lymph nodes. Dilation of lymphatics occurs in tissues withincreased capillary filtration of plasma and formation of interstitialfluid (local swelling) and lymph. Enlargement of lymph nodes is anindicator of antigenic stimulation and subsequent recruitment ofcells from the drained tissues and blood.
The Journal of TRAUMA� Injury, Infection, and Critical Care
850 October 2007

(helper) and CD8 (cytotoxic T lymphocytes), CD25 (receptorfor interleukin-2), CD22 (B lymphocytes), CD34 (stem cellsand thymocytes), and elastase (granulocytes) (all DAKO,Glostrup, Denmark). Staining with antibodies against bonemorphogenetic proteins 2 and 4 (BMP-2 and 4), collagen type1 and 2, SDF-1 (stromal derived factor-1), and OPG (osteo-protegerin) was performed (SantaCruz Biotechnology, CA).Stainings were performed using LSAB or LSAB-2 HRP kit(DAKO) according to the manufacturer’s procedures. Micro-scopical slides were analyzed under optical microscope(Olympus, BX40F, Nagano, Japan). Trichrome stainingallowed visualization of collagen and elastin deposition. His-tologic scoring of cells from 0� to ��� (0–3) was per-formed, where 1 (1–25 cells), 2 (26–50 cells), and 3 (�50cells/�200 magnification field). The intensity of staining ofproteins in the intercellular space was scored 0 to 3, where 1was weak, 2 intermediate, and 3 strong, compared with thestrong in a control gap tissue.
Statistical AnalysisThe lymph vessel and node surface area values of the
affected and healthy limb were presented as means indexes(affected versus normal). The differences were analyzedusing the Student t test for pairs. Differences between theunion and nonunion groups were evaluated using theMann-Whitney test for nonparamateric values. Two inves-tigators blinded to the study evaluated the tissue sections.The mean densities of cells and intensity of protein stain-ing were compared using the Monte Carlo permutationexact test. Differences were considered significant at the plevel �0.05.
RESULTSLymphatic Response to Bone Fracture
Lymphoscintigraphies performed in patients from group1 (bone union) revealed in the affected limb of all patientsdilated lymphatics of the superficial system and enlargedinguinal lymph nodes (Fig. 1). The surface area of calf lymphvessels was 3.24 � 3.25 times, of thigh lymphatics 3.14 �2.95 times, and of lymph nodes 1.76 � 0.67 times larger thanin the nonfractured limb (all p � 0.05). In group 2 (nonunion)lymphoscintigraphies revealed decrease of inguinal lymphnode surface area in all patients, when compared with con-tralateral limb. The surface area of calf lymph vessels was1.70 � 2.28 times (not significant [NS]) of thigh lymphatics,0.57 � 0.50 times (NS) of lymph nodes, and 0.49 � 0.40times of that of the nonfractured limb (lymph nodes p � 0.001) (Fig. 2). Deep lymphatics and popliteal lymph nodesappeared on lymphoscintigrams in six patients (43%).
Immunohistochemical Evaluation of Gap TissueFoci of Osteogenesis
The pictures of healing fractures showed cellular infil-trates and foci of ossification. In contrast, there was lack ofchondrocytes and osteoblasts, and only a few fibroblasts
could be seen in the nonhealing gap tissue. Trichrome stain-ing was weak in this group.
Phenotypes of Infiltrating Cells
There were major differences between the healing and non-healing fractures. In the healing gaps, dense infiltrates withHLA-DR� cells, CD68� macrophages, CD4� (helper), CD8(cytotoxic) lymphocytes, and some granulocytes were seen.There were also many large CD34� (stem cells). The endothe-lial cells were CD34�. In the nonhealing gap tissue there wasstatistically less of HLA-DR�, macrophages, CD4, CD8, CD25(IL2 receptor), CD22 (B cells), elastin � (granulocytes andmacrophages) cells, and fibroblasts than in the healing gap (Figs.3 and 4). There was no difference in the density of CD34� cellswith the healing cases; however, the intensity of this moleculeon endothelial cells was decreased.
Fig. 2. Lymphoscintigram of the lower limbs of a 35-year-old manwith pseudarthrosis of the distal part of the right tibia, 23 monthsafter closed fracture. Edema of the whole limb. There is no outlineof lymphatics and lack of opacified inguinal lymph nodes. Periph-eral lymphatics most likely underwent inflammatory obliterationand lymph nodes became fibrotic.
Tibial Fracture and Regional Lymph Nodes
Volume 63 • Number 4 851

Fig. 3. Immunohistopathologic pictures of the tibial fracture gap tissue harvested during corrective surgery in a uneventful (A) and delayedhealing (B). (a) hematoxylin-eosin staining, (b) trichrome staining for collagen and elastin, (c) expression of HLA-DR antigen on infiltratingcells, (d) CD68 macrophages, (e) staining for OPG (brown areas), and (f) SDF-1 (brown areas). Osteogenesis pictures were seen in allspecimens from uneventful healing. There was no osteogenesis and little deposition of collagen as well as lack of OPG and SDF-1 in tissuesfrom delayed healing. Also, there were fewer cells with HLA-DR and CD68 phenotype in the gap tissue (CD nomenclature of cellularpopulations clarified in text).
The Journal of TRAUMA� Injury, Infection, and Critical Care
852 October 2007
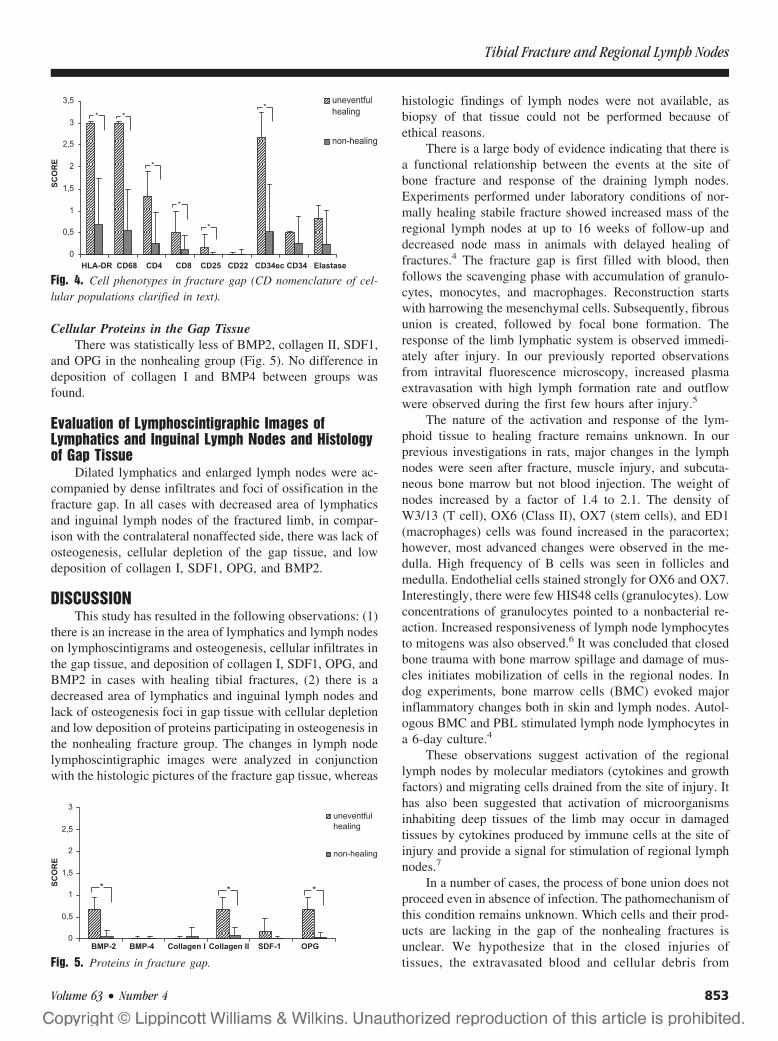
Cellular Proteins in the Gap TissueThere was statistically less of BMP2, collagen II, SDF1,
and OPG in the nonhealing group (Fig. 5). No difference indeposition of collagen I and BMP4 between groups wasfound.
Evaluation of Lymphoscintigraphic Images ofLymphatics and Inguinal Lymph Nodes and Histologyof Gap Tissue
Dilated lymphatics and enlarged lymph nodes were ac-companied by dense infiltrates and foci of ossification in thefracture gap. In all cases with decreased area of lymphaticsand inguinal lymph nodes of the fractured limb, in compar-ison with the contralateral nonaffected side, there was lack ofosteogenesis, cellular depletion of the gap tissue, and lowdeposition of collagen I, SDF1, OPG, and BMP2.
DISCUSSIONThis study has resulted in the following observations: (1)
there is an increase in the area of lymphatics and lymph nodeson lymphoscintigrams and osteogenesis, cellular infiltrates inthe gap tissue, and deposition of collagen I, SDF1, OPG, andBMP2 in cases with healing tibial fractures, (2) there is adecreased area of lymphatics and inguinal lymph nodes andlack of osteogenesis foci in gap tissue with cellular depletionand low deposition of proteins participating in osteogenesis inthe nonhealing fracture group. The changes in lymph nodelymphoscintigraphic images were analyzed in conjunctionwith the histologic pictures of the fracture gap tissue, whereas
histologic findings of lymph nodes were not available, asbiopsy of that tissue could not be performed because ofethical reasons.
There is a large body of evidence indicating that there isa functional relationship between the events at the site ofbone fracture and response of the draining lymph nodes.Experiments performed under laboratory conditions of nor-mally healing stabile fracture showed increased mass of theregional lymph nodes at up to 16 weeks of follow-up anddecreased node mass in animals with delayed healing offractures.4 The fracture gap is first filled with blood, thenfollows the scavenging phase with accumulation of granulo-cytes, monocytes, and macrophages. Reconstruction startswith harrowing the mesenchymal cells. Subsequently, fibrousunion is created, followed by focal bone formation. Theresponse of the limb lymphatic system is observed immedi-ately after injury. In our previously reported observationsfrom intravital fluorescence microscopy, increased plasmaextravasation with high lymph formation rate and outflowwere observed during the first few hours after injury.5
The nature of the activation and response of the lym-phoid tissue to healing fracture remains unknown. In ourprevious investigations in rats, major changes in the lymphnodes were seen after fracture, muscle injury, and subcuta-neous bone marrow but not blood injection. The weight ofnodes increased by a factor of 1.4 to 2.1. The density ofW3/13 (T cell), OX6 (Class II), OX7 (stem cells), and ED1(macrophages) cells was found increased in the paracortex;however, most advanced changes were observed in the me-dulla. High frequency of B cells was seen in follicles andmedulla. Endothelial cells stained strongly for OX6 and OX7.Interestingly, there were few HIS48 cells (granulocytes). Lowconcentrations of granulocytes pointed to a nonbacterial re-action. Increased responsiveness of lymph node lymphocytesto mitogens was also observed.6 It was concluded that closedbone trauma with bone marrow spillage and damage of mus-cles initiates mobilization of cells in the regional nodes. Indog experiments, bone marrow cells (BMC) evoked majorinflammatory changes both in skin and lymph nodes. Autol-ogous BMC and PBL stimulated lymph node lymphocytes ina 6-day culture.4
These observations suggest activation of the regionallymph nodes by molecular mediators (cytokines and growthfactors) and migrating cells drained from the site of injury. Ithas also been suggested that activation of microorganismsinhabiting deep tissues of the limb may occur in damagedtissues by cytokines produced by immune cells at the site ofinjury and provide a signal for stimulation of regional lymphnodes.7
In a number of cases, the process of bone union does notproceed even in absence of infection. The pathomechanism ofthis condition remains unknown. Which cells and their prod-ucts are lacking in the gap of the nonhealing fractures isunclear. We hypothesize that in the closed injuries oftissues, the extravasated blood and cellular debris from
Fig. 4. Cell phenotypes in fracture gap (CD nomenclature of cel-lular populations clarified in text).
Fig. 5. Proteins in fracture gap.
Tibial Fracture and Regional Lymph Nodes
Volume 63 • Number 4 853

local tissue are phagocytosed by macrophages and incor-porated by the migrating dendritic cells. The scavengingcells migrate to the afferent lymphatics and are draggedwith lymph stream to the regional lymph nodes. This lasthas been documented in a large series of studies.8 Inaddition to the migrating cells, their fragments, includingnuclei, flow with lymph to the nodes. In the nodes, presen-tation of self-antigens by dendritic cells to lymphocytes pro-ceeds. This results in priming of node cells and mobilizationof blood lymphocytes that enter the node via high endothelialvenules. Enlargement of lymph node cellular mass is ob-served. The question arises as to whether the antigen-specificclones of lymphocytes to self-antigens are being raised. If so,the primed cells would leave the lymph nodes via efferentlymphatics, and having flown through the thoracic duct, enterblood circulation. Then the antigen-specific cohorts of lym-phocytes home to the site of injury. There they may displaytheir cytotoxic and regulatory function. The cytotoxicity isnecessary for elimination of hyperproliferating granulationtissue cells. The regulatory CD4� and CD25� cells maydownregulate the process of uncontrolled growth of the gran-ulation tissue.9 This is an autoimmune type of response end-ing up when there is no more exposure of damaged andproliferating cells to the infiltrating immune cells. Such atype of protective autoimmunity process has been observedafter injury of the central nervous system and spinal cord. TheT cells directed against myelin-associated proteins accumu-lated at the site of injury, activated effector macrophages andB cells, which resulted in neuronal survival.10
As long as there is active healing of the wound, thedraining lymph nodes remain enlarged. However, a pro-longed healing process with cellular apoptosis and necrosismay lead to lymphocyte depletion and attenuation of nodefunction (unpublished). This in turn may result in lack ofproduction of antigen-specific lymphocytes and homing tothe wound and subsequently impaired regulation of the heal-ing mechanism. Whether the healing defect originates in thewound or the regional lymph node remains to be clarified.Nevertheless, observations indicate that there exists a func-tional axis between the wound and lymph nodes.
A number of causative factors may play a role in im-paired wound healing of fractured bone. These may be excessof disintegrated cells by trauma and ischemia, impaired lym-phatic drainage, and transfer of signals to the lymph node,overloading of nodes by cellular debris from the peripheryresulting in apoptosis and necrosis of their cells, geneticdefects as point mutations of genes for interleukins andgrowth factors. Not properly cleared dead cells are dangerousfor the body. The dead cells accumulate, lose their membraneintegrity, danger signals are released, and nuclear antigens getaccessible in an inflammatory context. In times of increasedapoptosis, tolerance can be broken, and a chronic inflamma-
tion results, which can then lead to an autoimmune reactionagainst nuclear constituents. Many adaptor molecules andreceptors are involved in the clearance of dying cells. Com-plement components, serum DNAse I, phosphatidylserine,and modified glycoproteins participate crucially in the clear-ance of apoptotic and necrotic cells. Accumulation of nuclearmaterial in germinal centers of lymph nodes of some systemiclupus erythematosus (SLE) patients has been observed. Thenoningested nuclear material may provide survival signals forautoreactive B cells and consecutively antinuclear autoanti-bodies will be produced for wound cells.11
Taken together, the tibial fracture evokes response of theregional lymphatic system. Normal healing with immune cellinfiltrates and foci of ossification is accompanied by dilatedlymphatics and enlarged lymph nodes. Prolonged nonhealingfracture with lack of cellular reaction in the gap goes withdecreased mass of lymph nodes. We hypothesize that theprolonged healing process in the fracture gap causes gradualexhaustion of the lymph node functional elements, and recip-rocally deficient lymph node cannot produce and send regu-latory cells to the fracture gap.
REFERENCES1. Szczesny G, Olszewski WL. The pathomechanism of posttraumatic
edema of the lower limbs. II. Changes in the lymphatic system.J Trauma. 2003;55:350–354.
2. Szczesny G, Olszewski WL, Gorecki A. Lymphoscintigraphicmonitoring of the lower limb lymphatic system response to bonefracture and healing. Lymphat Res Biol. 2005;3:137–145.
3. Cakała M, Olszewski WL. The reaction of the regional lymph nodeson the skin bacterial and allogeneic antigens. Ann Transplant. 2004;9:59–62.
4. Szczesny G, Olszewski WL. The pathomechanism of posttraumaticedema of lower limbs. I. The effect of extravasated blood, bonemarrow cells, and bacterial colonization on tissues, lymphatics, andlymph nodes. J Trauma. 2002;52:315–322.
5. Szczesny G, Veihelmann A, Nolte D, Messmer K. Changes in thelocal blood and lymph microcirculation in response to directmechanical trauma applied to leg: in vivo study in an animal model.J Trauma. 2001;51:508–517.
6. Szczesny G, Olszewski WL, Zaleska M. Limb lymph node responseto bone fracture. Lymphat Res Biol. 2004;2:155–164.
7. Raasch W, Regunathan S, Li G, Reis DJ. Agmatine, the bacterialamine, is widely distributed in mammalian tissues. Life Sci. 1995;56:2319–2330.
8. Zatz MM, Lance EM. The distribution of 51Cr-labeled lymphocytesinto antigen-stimulated mice. Lymphocyte trapping. J Exp Med.1971;134:224–241.
9. Mittrucker HW, Kaufmann SH. Regulatory T cells and infection:suppression revisited. Eur J Immunol. 2004;34:306–312.
10. Hauben E, Nevo U, Yoles E, et al. Autoimmune T cells as potentialneuroprotective therapy for spinal cord injury. Lancet. 2000;355:286–287.
11. Munoz LE, Herrmann M, Gaipl US. Eine unzureichende erkennungund beseitigung von sterbenden zellen kann zur Entstehung vonchronischer autoimmunitat fuhren. Z Rheumatol. 2005;64:370–376.
The Journal of TRAUMA� Injury, Infection, and Critical Care
854 October 2007




















