Incidence, clinical features, treatment and outcome of primary central nervous system lymphoma in...
10
Incidence, Clinical Features, Treatment and Outcome of Primary Central Nervous System Lymphoma in Norway A Ten-year National Survey Ingfrid Salvesen Haldorsen, Jan Harald Aarseth, Aase Hollender, John Ludvig Larsen, Ansgar Espeland and Olav Mella From the Department of Radiology (I.S. Haldorsen, J.L. Larsen, A. Espeland), the Department of Neurology (J.H. Aarseth), the Department of Oncology and Medical Physics (O. Mella), Haukeland University Hospital, Bergen, Norway, and the Department of Oncology, the Norwegian Radium Hospital, Oslo, Norway (A. Hollender) Correspondence to: Ingfrid Salvesen Haldorsen, Department of Radiology, Haukeland University Hospital, 5021 Bergen, Norway. Tel: 47-55972327. Fax: 47-55975140. E-mail: [email protected] Acta Oncologica Vol. 43, No. 6, pp. 520 /529, 2004 The incidence of primary central nervous system lymphoma (PCNSL) has been reported to increase in some parts of the world, while being stable in other regions. In an attempt to characterize the incidence rate, clinical features, treatment, outcome, and prognostic factors of PCNSL in Norway, we report our experience in a large unselected series of patients. Clinical features, histological diagnosis, radiological findings, treatment, and outcome of all patients diagnosed with PCNSL in Norway in the years 1989 /1998 were registered. During the 10-year period 58 new cases of histologically verified PCNSL were registered in Norway. The annual incidence rate of PCNSL was on average 1.34 cases per million people with a non-significant increasing trend (p /0.069). For patients diagnosed before death (n /45) the estimated survival following histological diagnosis was 55%, 47%, and 23% at 1, 2, and 5 years, respectively. In Cox-regression analysis age, WHO performance status and treatment had independent prognostic impact on survival. In the studied decade, there was a non-significant trend towards increased incidence of PCNSL, perhaps due to increased availability of diagnostic imaging, especially magnetic resonance imaging. Received 29 December 2003 Accepted 10 May 2004 Primary central nervous system lymphomas (PCNSL) are extranodal malignant lymphomas arising in the brain, the spinal cord, the leptomeninges or the eyes, with the absence of lymphoma outside the nervous system at the time of diagnosis. In the last two decades an increase in incidence of PCNSL in immunologically normal as well as in immuno-compromised individuals has been reported in the US (1, 2), Southeast England (3) and Southeast Netherlands (4). In the same period, a stable incidence of PCNSL has been found in studies from the province of Alberta (Canada) (5), western Denmark (6), Southeast Scotland (7), Hong Kong (8) and northern India (9). These divergent findings suggest regional differences in PCNSL incidence during the last decades. PCNSL may affect all age groups with a peak incidence in the fifth to seventh decade and a median age in the sixth decade in non-AIDS patients (10). The most common clinical symptoms at time of diagnosis are personality change, focal neurological deficit and symp- toms of raised intracranial pressure (6, 10 /12). Prognosis of PCNSL in patients receiving only sympto- matic therapy is extremely poor with a median survival of 2 /3 months (13). After short-term steroid treatment 15 /25% of the tumours show dramatic volume shrinkage but this lasts only a few weeks in the majority of patients (14). Radiotherapy was earlier considered the mainstay of therapy, and it will normally induce complete or partial tumour regression. Few patients, however, are cured with radiation alone and the survival time is often reported to be 12 /16 months, with only 3 /4% long-term survivors (15). A combination of radiotherapy and chemotherapy has sub- stantially improved survival in the last decade with a reported median survival of up to 42 months and a 5-year survival of 22 /40% (16, 17). The disadvantage of this combination is the well-documented long-term treatment- induced neurotoxicity, especially affecting the age group of over 60 (16, 18). Chemotherapy alone has a well-documen- ted effect on PCNSL and seems to cause less neurotoxic sequelae than the combination of radio- and chemotherapy, perhaps at the cost of a little decreased median survival (19, 20). æ ORIGINAL ARTICLE æ # Taylor & Francis 2004. ISSN 0284-186X Acta Oncologica DOI: 10.1080/02841860410015640 Acta Oncol Downloaded from informahealthcare.com by 190.201.225.93 on 05/20/14 For personal use only.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Incidence, clinical features, treatment and outcome of primary central nervous system lymphoma in...

Incidence, Clinical Features, Treatment and Outcome ofPrimary Central Nervous System Lymphoma in Norway
A Ten-year National Survey
Ingfrid Salvesen Haldorsen, Jan Harald Aarseth, Aase Hollender, John Ludvig Larsen,Ansgar Espeland and Olav Mella
From the Department of Radiology (I.S. Haldorsen, J.L. Larsen, A. Espeland), the Department of Neurology (J.H.Aarseth), the Department of Oncology and Medical Physics (O. Mella), Haukeland University Hospital, Bergen,Norway, and the Department of Oncology, the Norwegian Radium Hospital, Oslo, Norway (A. Hollender)
Correspondence to: Ingfrid Salvesen Haldorsen, Department of Radiology, Haukeland University Hospital, 5021Bergen, Norway. Tel: 47-55972327. Fax: 47-55975140. E-mail: [email protected]
Acta Oncologica Vol. 43, No. 6, pp. 520�/529, 2004
The incidence of primary central nervous system lymphoma (PCNSL) has been reported to increase in some parts of the world, while beingstable in other regions. In an attempt to characterize the incidence rate, clinical features, treatment, outcome, and prognostic factors ofPCNSL in Norway, we report our experience in a large unselected series of patients. Clinical features, histological diagnosis, radiologicalfindings, treatment, and outcome of all patients diagnosed with PCNSL in Norway in the years 1989�/1998 were registered. During the10-year period 58 new cases of histologically verified PCNSL were registered in Norway. The annual incidence rate of PCNSL was on average1.34 cases per million people with a non-significant increasing trend (p�/0.069). For patients diagnosed before death (n�/45) the estimatedsurvival following histological diagnosis was 55%, 47%, and 23% at 1, 2, and 5 years, respectively. In Cox-regression analysis age, WHOperformance status and treatment had independent prognostic impact on survival. In the studied decade, there was a non-significant trendtowards increased incidence of PCNSL, perhaps due to increased availability of diagnostic imaging, especially magnetic resonance imaging.
Received 29 December 2003Accepted 10 May 2004
Primary central nervous system lymphomas (PCNSL)
are extranodal malignant lymphomas arising in the
brain, the spinal cord, the leptomeninges or the eyes,
with the absence of lymphoma outside the nervous system
at the time of diagnosis. In the last two decades an
increase in incidence of PCNSL in immunologically
normal as well as in immuno-compromised individuals
has been reported in the US (1, 2), Southeast England (3)
and Southeast Netherlands (4). In the same period, a
stable incidence of PCNSL has been found in studies
from the province of Alberta (Canada) (5), western
Denmark (6), Southeast Scotland (7), Hong Kong (8)
and northern India (9). These divergent findings suggest
regional differences in PCNSL incidence during the last
decades.
PCNSL may affect all age groups with a peak incidence
in the fifth to seventh decade and a median age in the
sixth decade in non-AIDS patients (10). The most
common clinical symptoms at time of diagnosis are
personality change, focal neurological deficit and symp-
toms of raised intracranial pressure (6, 10�/12).
Prognosis of PCNSL in patients receiving only sympto-
matic therapy is extremely poor with a median survival
of 2�/3 months (13). After short-term steroid treatment
15�/25% of the tumours show dramatic volume shrinkage
but this lasts only a few weeks in the majority of patients
(14). Radiotherapy was earlier considered the mainstay of
therapy, and it will normally induce complete or partial
tumour regression. Few patients, however, are cured with
radiation alone and the survival time is often reported to be
12�/16 months, with only 3�/4% long-term survivors (15). A
combination of radiotherapy and chemotherapy has sub-
stantially improved survival in the last decade with a
reported median survival of up to 42 months and a 5-year
survival of 22�/40% (16, 17). The disadvantage of this
combination is the well-documented long-term treatment-
induced neurotoxicity, especially affecting the age group of
over 60 (16, 18). Chemotherapy alone has a well-documen-
ted effect on PCNSL and seems to cause less neurotoxic
sequelae than the combination of radio- and chemotherapy,
perhaps at the cost of a little decreased median survival
(19, 20).
�ORIGINAL ARTICLE �
# Taylor & Francis 2004. ISSN 0284-186X Acta Oncologica
DOI: 10.1080/02841860410015640
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

The aims of this retrospective study were to investigate
the incidence rate, clinical features and therapeutic outcome
of a population of patients with PCNSL comprising all
patients with histologically verified diagnosis in Norway
during a 10-year period. Our material represents an
unselected patient population from a well-defined and
circumscribed geographical region, comprising an entire
country with a population of 4.4 million (1998). The
registration of cancer in Norway is very reliable because
all new cases of cancer are required by law to be reported to
the Norwegian Cancer Registry by involved physicians and
pathology laboratories. The unselected nature of the
material in this study makes it suitable for investigating
trends such as alterations of incidence.
MATERIAL AND METHODS
A complete list of all patients recorded as PCNSL in
Norway from 1 January 1989 to 31 December 1998 (n�/
101) was obtained from the Norwegian Cancer Registry.
The majority of the patients (n�/95) were diagnosed and
treated at one of the 5 major university hospitals in Norway.
During a period of 4 months the first author visited all the
university hospitals in order to go through the complete
medical records of these patients. The medical records of
the remaining 6 patients diagnosed at other hospitals were
sent to the authors by mail. Clinical features, morphologic
diagnosis, radiological findings, medical treatment, and
outcome were registered.
A total of 58 patients with histologically or cytologically
verified PCNSL were diagnosed and treated in Norway in
the studied decade. We excluded 27 of the 101 patients
recorded as PCNSL because we found they had lymphoma
in other locations at the time of diagnosis (n�/10),
intraspinal extradural tumour involving vertebral corpora
(n�/6), plasmocytoma (n�/3), Langerhans cell histiocytosis
X (n�/3), or only clinical and radiological signs of PCNSL
without histologic verification (n�/5). A further 16 HIV-
infected patients diagnosed with AIDS-related PCNSL were
also excluded from the following evaluation.
For the present study, we analysed data from the
remaining 58 patients with histologically or cytologically
verified PCNSL diagnosed in 1989 to 1998. The histo-
pathological material has been re-examined and the
findings will be presented in a separate publication. In
none of the patients has this review led to a change in
diagnosis.
Statistical analysis
Calculation of the incidence rates was based on the number
of new cases with primary central nervous system lym-
phoma each year and the population in Norway as at 1
January in the same year. The trend test and 95%
confidence intervals for incidence were calculated according
to the Poisson distribution.
Duration of survival was calculated as time between date
of procedure (operation/biopsy/cytology) that led to con-
clusive histologic diagnosis and date of death or 1 May 2002
if still alive. Survival curves were calculated and plotted
using the method of Kaplan and Meier (21). For univariate
comparison of survival curves the log-rank test was used.
The Cox Proportional Hazard Model was used to study the
effect on survival of several factors simultaneously and to
estimate hazard ratios (22). The assessment of the propor-
tional hazard assumption was done by comparing the Cox
model with a time dependent model (23). All p-values in the
analyses are two-sided. The analyses were performed with
StatXact, SPSS, and S-plus.
RESULTS
Incidence of PCNSL
During the 10-year period from 1 January 1989 to 31
December 1998 58 patients were identified with morpholo-
gically verified non-AIDS related PCNSL. The average
annual incidence rate of PCNSL in the population of
Norway during the period was 1.34 cases per million (95%
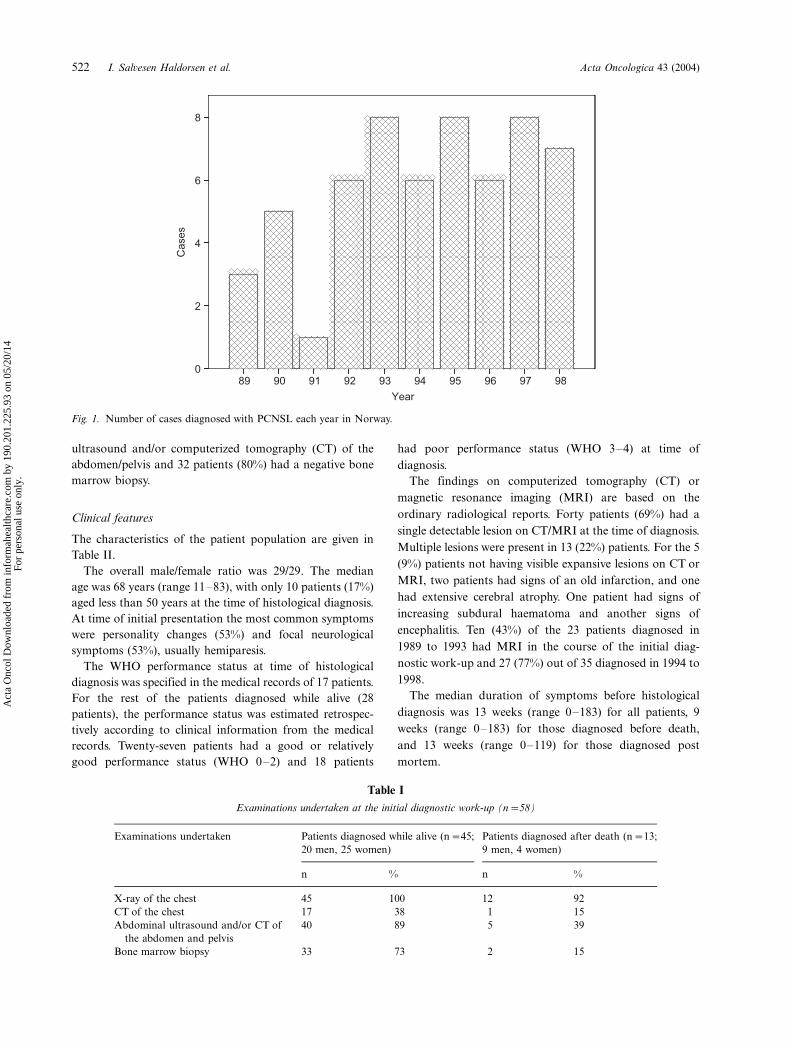
confidence interval: 1.02�/1.74). Fig. 1 shows the number of
patients diagnosed with PCNSL each year. There was a
trend towards but not significant increase in annual
incidence (p�/0.069).
Clinical and histological assessment
The diagnosis of PCNSL in our material was established
pathologically by either open biopsy (n�/29), stereotactic
biopsy (n�/14), or cytology of cerebrospinal fluid (n�/2). In
13 patients the diagnosis was first established by autopsy.
The diagnosis was based on both routine light microscopic
and in most cases (n�/44) also immunohistochemical
examinations performed at the time of initial presentation.
Fifty-three out of 58 specimens were analysed at university
hospital pathology laboratories.
Three of the patients had received immuno-suppressive
medication prior to diagnosis. One patient used sulfasalazin
for ulcerative colitis and one patient azathioprin after a
renal transplant. One patient used systemic steroids and
azathioprin for uveitis for one year prior to diagnosis.
In addition to a thorough physical examination, most
patients went through a list of supplementary radiological
and medical examinations at the initial diagnostic work-up
(Table I). In none of the patients was systemic lymphoma
found.
In addition to the 13 patients whose diagnosis was
established by autopsy, 5 of the patients had their diagnoses
confirmed by autopsy. In all of the cases the autopsies
confirmed that lymphoma was restricted to the central
nervous system. Of the remaining 40 patients without
autopsies confirming that lymphoma was restricted to the
central nervous system, 38 patients (95%) had a negative
Acta Oncologica 43 (2004) Primary nervous system lymphoma in Norway 521
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.
ultrasound and/or computerized tomography (CT) of the
abdomen/pelvis and 32 patients (80%) had a negative bone
marrow biopsy.
Clinical features
The characteristics of the patient population are given in
Table II.
The overall male/female ratio was 29/29. The median
age was 68 years (range 11�/83), with only 10 patients (17%)
aged less than 50 years at the time of histological diagnosis.
At time of initial presentation the most common symptoms
were personality changes (53%) and focal neurological
symptoms (53%), usually hemiparesis.
The WHO performance status at time of histological
diagnosis was specified in the medical records of 17 patients.
For the rest of the patients diagnosed while alive (28
patients), the performance status was estimated retrospec-
tively according to clinical information from the medical
records. Twenty-seven patients had a good or relatively
good performance status (WHO 0�/2) and 18 patients
had poor performance status (WHO 3�/4) at time of
diagnosis.
The findings on computerized tomography (CT) or
magnetic resonance imaging (MRI) are based on the
ordinary radiological reports. Forty patients (69%) had a
single detectable lesion on CT/MRI at the time of diagnosis.
Multiple lesions were present in 13 (22%) patients. For the 5
(9%) patients not having visible expansive lesions on CT or
MRI, two patients had signs of an old infarction, and one
had extensive cerebral atrophy. One patient had signs of
increasing subdural haematoma and another signs of
encephalitis. Ten (43%) of the 23 patients diagnosed in
1989 to 1993 had MRI in the course of the initial diag-
nostic work-up and 27 (77%) out of 35 diagnosed in 1994 to
1998.
The median duration of symptoms before histological
diagnosis was 13 weeks (range 0�/183) for all patients, 9
weeks (range 0�/183) for those diagnosed before death,
and 13 weeks (range 0�/119) for those diagnosed post
mortem.
Fig. 1. Number of cases diagnosed with PCNSL each year in Norway.
Table I
Examinations undertaken at the initial diagnostic work-up (n�/58)
Examinations undertaken Patients diagnosed while alive (n�/45;
20 men, 25 women)
Patients diagnosed after death (n�/13;
9 men, 4 women)
n % n %
X-ray of the chest 45 100 12 92
CT of the chest 17 38 1 15
Abdominal ultrasound and/or CT of
the abdomen and pelvis
40 89 5 39
Bone marrow biopsy 33 73 2 15
522 I. Salvesen Haldorsen et al. Acta Oncologica 43 (2004)
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

Primary treatment
There was no consensus on primary treatment concerning
PCNSL in Norway in the period studied, although some
patients were treated in accordance with joint Nordic
protocols in the later part of the interval. Twelve of the
13 patients diagnosed after death had received no chemo-
or radiotherapy and one patient had received chemo-
therapy.
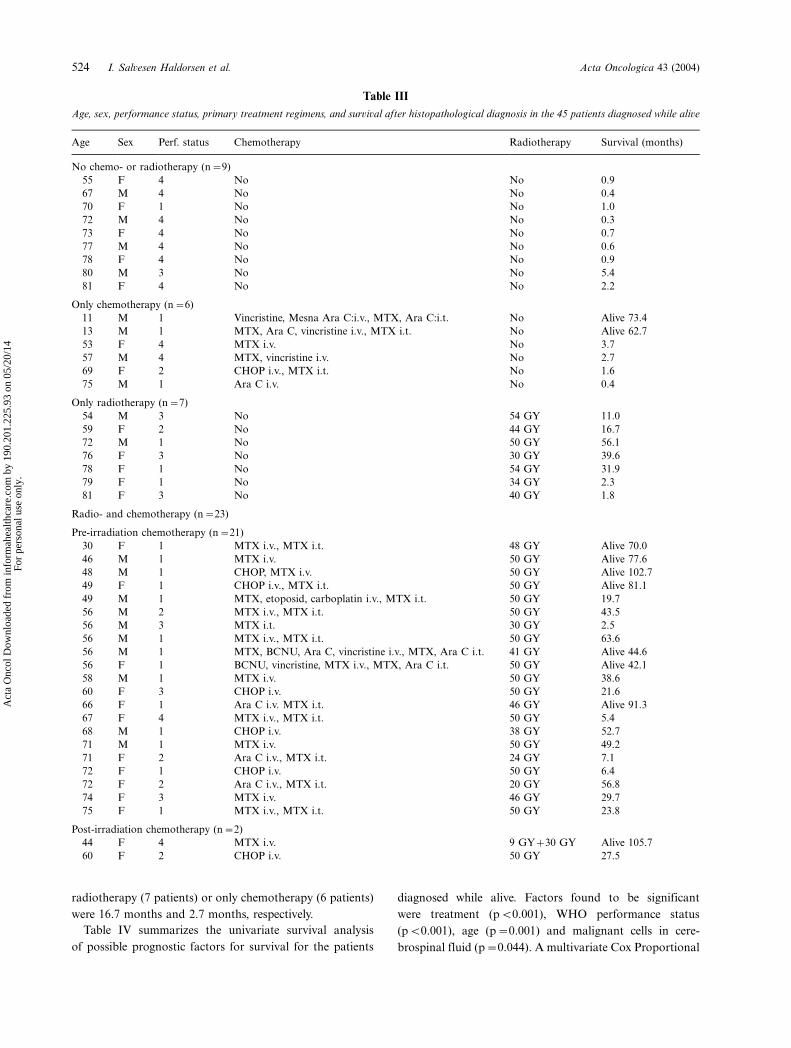
The 45 patients whose diagnosis was verified histologi-
cally before death had received a wide spectrum of
treatment (Table III). Nine (20%) of the 45 patients did
not receive any chemo- or radiotherapy. These patients had
a mean age of 72.6 years (compared with 62.9 in the
material as a whole). Two of them died suddenly in the
postoperative period; the other 7 had a poor general
condition, which excluded them from active therapy.
Six (13%) of the 45 patients received chemotherapy alone
with various regimens. Three patients had received a
combination of intravenous (i.v.) chemotherapy and in-
trathecal (i.t.) chemotherapy, while three patients had only
i.v. chemotherapy.
Seven (16%) of the 45 patients received only radiotherapy
consisting of total brain irradiation with an average dose of
43 Gy (range 30�/54 GY) given in 10�/28 fractions. In two of
the patients the therapy included booster fractions towards
the tumour.
Twenty-three (51%) of the 45 patients had received both
chemo- and radiotherapy. In 21 patients the treatment with
various chemotherapy regimens preceded the radiotherapy.
In two cases the chemotherapy was preceded by radiation.
Twelve of the patients had intrathecal (i.t.) methotrexate
and/or cytarabin in addition to intravenous (i.v.) regimens.
One patient had only i.t. methotrexate and 10 patients only
i.v. chemotherapy. Of the 22 patients who received i.v.
chemotherapy, 13 received high-dose methotrexate with
folic acid rescue either alone or in combination with other
chemotherapy. Six of the regimens included the CHOP
(cyclophosphamide, adriamycin, vincristine, and predni-
sone) and four included cytarabin. One patient had addi-
tional chemotherapy with i.v. etoposid and carboplatin at
the time of recurrence 6 months after initial therapy. The
radiotherapy consisted initially of total brain irradiation
with an average dose of 45 Gy (range 20 Gy�/50 Gy) given
in 5�/28 fractions. In 17 of the patients the dosage was
partly given as a booster towards the macroscopic tumour.
One patient received an additional radiation of the spine (30
Gy) and one patient received fractions towards the eyes (30
Gy and 40 Gy) months after the initial brain irradiation.
Of the 30 patients who received chemotherapy, the
treatments had been initially well tolerated in 20 patients.
Four patients had elevation of blood creatinine after i.v.
high-dose methotrexate, and one patient developed a rash
secondary to methotrexate therapy. Two patients had
septicaemia and another patient meningitis. One patient
had a deep venous thrombosis and another patient
pulmonary oedema with resulting death after a few days.
Data on late neurotoxicity have not been available for
evaluation.
Outcome
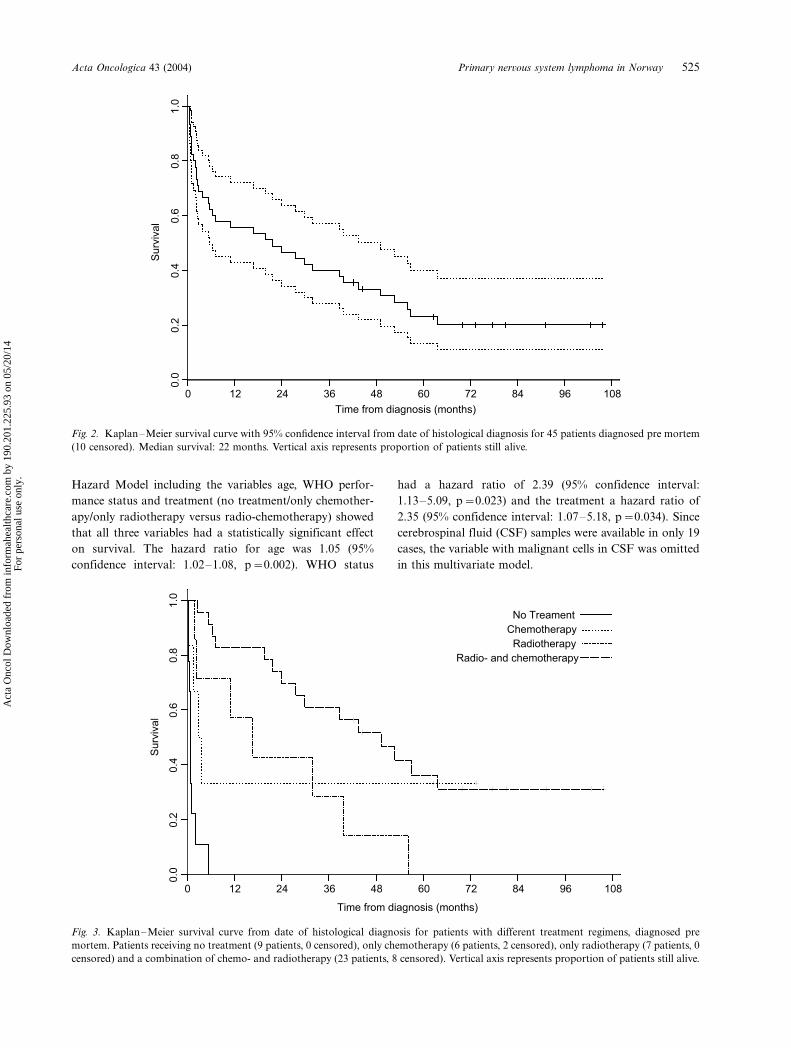
For the 45 patients diagnosed before death the overall
estimated survival following histological diagnosis was 55%,
47%, and 23% at 1, 2, and 5 years, respectively (Fig. 2) and
the median survival was 22 months. For the 13 patients
diagnosed post mortem the median survival from initial
symptoms was 3 months and only 15% were alive 1 year
after initial symptoms.
In the group of patients diagnosed while alive the survival
curve seemed greatly influenced by the treatment (Fig. 3).
The 23 patients receiving both chemo- and radiotherapy
had a median survival of 49.2 months, compared with 0.9
months in the untreated group (9 patients). The correspond-
ing median survival times for the patients receiving only
Table II
Clinical features of patients with primary central nervous system
lymphoma
Categorical variables n %
Sex, n�/58
Female 29 (50)
Male 29 (50)
Symptoms on admission, n�/58
Focal neurological 31 (53)
Personality change 31 (53)
Cerebellar symptoms/vertigo 24 (41)
Increased intracranial pressure 23 (40)
Visual disturbance 9 (16)
Epilepsy 7 (12)
Performance status at histological
diagnosis, n�/45
WHO 0�/2 27 (60)
WHO 3�/4 18 (40)
Cerebrospinal fluid examination
with regard to
Malignant cells, n�/24 3 (13)
Elevation of cell count, n�/18 12 (67)
Elevation of total protein, n�/14 8 (57)
Decrease of glucose, n�/3 1 (33)
Lesions on CT/MR, n�/58
No detectable expansive lesion 5 (9)
Single 40 (69)
Multiple 13 (22)
Opthalmologic examination, n�/12
Normal or irrelevant pathology 8 (67)
Uveitis 4 (33)
Continuous variables Mean Median Range
Age at diagnosis (years), n�/58 62.9 68.3 11�/83
Time until diagnosis (weeks), n�/58 21.7 12.8 0�/183
Acta Oncologica 43 (2004) Primary nervous system lymphoma in Norway 523
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.
radiotherapy (7 patients) or only chemotherapy (6 patients)
were 16.7 months and 2.7 months, respectively.
Table IV summarizes the univariate survival analysis
of possible prognostic factors for survival for the patients
diagnosed while alive. Factors found to be significant
were treatment (pB/0.001), WHO performance status
(pB/0.001), age (p�/0.001) and malignant cells in cere-
brospinal fluid (p�/0.044). A multivariate Cox Proportional
Table III
Age, sex, performance status, primary treatment regimens, and survival after histopathological diagnosis in the 45 patients diagnosed while alive
Age Sex Perf. status Chemotherapy Radiotherapy Survival (months)
No chemo- or radiotherapy (n�/9)
55 F 4 No No 0.9
67 M 4 No No 0.4
70 F 1 No No 1.0
72 M 4 No No 0.3
73 F 4 No No 0.7
77 M 4 No No 0.6
78 F 4 No No 0.9
80 M 3 No No 5.4
81 F 4 No No 2.2
Only chemotherapy (n�/6)
11 M 1 Vincristine, Mesna Ara C:i.v., MTX, Ara C:i.t. No Alive 73.4
13 M 1 MTX, Ara C, vincristine i.v., MTX i.t. No Alive 62.7
53 F 4 MTX i.v. No 3.7
57 M 4 MTX, vincristine i.v. No 2.7
69 F 2 CHOP i.v., MTX i.t. No 1.6
75 M 1 Ara C i.v. No 0.4
Only radiotherapy (n�/7)
54 M 3 No 54 GY 11.0
59 F 2 No 44 GY 16.7
72 M 1 No 50 GY 56.1
76 F 3 No 30 GY 39.6
78 F 1 No 54 GY 31.9
79 F 1 No 34 GY 2.3
81 F 3 No 40 GY 1.8
Radio- and chemotherapy (n�/23)
Pre-irradiation chemotherapy (n�/21)
30 F 1 MTX i.v., MTX i.t. 48 GY Alive 70.0
46 M 1 MTX i.v. 50 GY Alive 77.6
48 M 1 CHOP, MTX i.v. 50 GY Alive 102.7
49 F 1 CHOP i.v., MTX i.t. 50 GY Alive 81.1
49 M 1 MTX, etoposid, carboplatin i.v., MTX i.t. 50 GY 19.7
56 M 2 MTX i.v., MTX i.t. 50 GY 43.5
56 M 3 MTX i.t. 30 GY 2.5
56 M 1 MTX i.v., MTX i.t. 50 GY 63.6
56 M 1 MTX, BCNU, Ara C, vincristine i.v., MTX, Ara C i.t. 41 GY Alive 44.6
56 F 1 BCNU, vincristine, MTX i.v., MTX, Ara C i.t. 50 GY Alive 42.1
58 M 1 MTX i.v. 50 GY 38.6
60 F 3 CHOP i.v. 50 GY 21.6
66 F 1 Ara C i.v. MTX i.t. 46 GY Alive 91.3
67 F 4 MTX i.v., MTX i.t. 50 GY 5.4
68 M 1 CHOP i.v. 38 GY 52.7
71 M 1 MTX i.v. 50 GY 49.2
71 F 2 Ara C i.v., MTX i.t. 24 GY 7.1
72 F 1 CHOP i.v. 50 GY 6.4
72 F 2 Ara C i.v., MTX i.t. 20 GY 56.8
74 F 3 MTX i.v. 46 GY 29.7
75 F 1 MTX i.v., MTX i.t. 50 GY 23.8
Post-irradiation chemotherapy (n�/2)
44 F 4 MTX i.v. 9 GY�/30 GY Alive 105.7
60 F 2 CHOP i.v. 50 GY 27.5
524 I. Salvesen Haldorsen et al. Acta Oncologica 43 (2004)
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.
Hazard Model including the variables age, WHO perfor-
mance status and treatment (no treatment/only chemother-
apy/only radiotherapy versus radio-chemotherapy) showed
that all three variables had a statistically significant effect
on survival. The hazard ratio for age was 1.05 (95%
confidence interval: 1.02�/1.08, p�/0.002). WHO status
had a hazard ratio of 2.39 (95% confidence interval:
1.13�/5.09, p�/0.023) and the treatment a hazard ratio of
2.35 (95% confidence interval: 1.07�/5.18, p�/0.034). Since
cerebrospinal fluid (CSF) samples were available in only 19
cases, the variable with malignant cells in CSF was omitted
in this multivariate model.
Fig. 2. Kaplan�/Meier survival curve with 95% confidence interval from date of histological diagnosis for 45 patients diagnosed pre mortem
(10 censored). Median survival: 22 months. Vertical axis represents proportion of patients still alive.
Fig. 3. Kaplan�/Meier survival curve from date of histological diagnosis for patients with different treatment regimens, diagnosed pre
mortem. Patients receiving no treatment (9 patients, 0 censored), only chemotherapy (6 patients, 2 censored), only radiotherapy (7 patients, 0
censored) and a combination of chemo- and radiotherapy (23 patients, 8 censored). Vertical axis represents proportion of patients still alive.
Acta Oncologica 43 (2004) Primary nervous system lymphoma in Norway 525
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

DISCUSSION
In the 10-year period studied we have registered 58
new cases of non-AIDS related and morphologi-
cally verified PCNSL in Norway. Our study is one of few
population-based materials published, and as far as we
know the only material covering the entire population of a
country.
The average annual incidence rate of non-AIDS related
PCNSL in the population of Norway during the 10-year
period studied was 1.34 new cases per million inhabitants.
These findings are relatively similar to those of Krogh-
Jensen et al. (24) who estimated the average annual
incidence rate in the population of a region of Denmark
to be 1.56 per million in the 10-year period 1983�/1992.
Relatively similar incidence rates have been reported from
Hong Kong (1.03 per million, 1982�/1997) (8), Alberta,
Canada (age-standardized incidence rates 0.178�/1.631 per
million, 1975�/1996) (5) and Southeast Netherlands (World
Standardized Rate of 2.3 and 1.7 cases per million males
and females respectively, 1989�/1994) (4). These incidence
rates contrast with those of Olson et al. (1), who, having
excluded never-married patients and patients of unknown
marital status (to exclude possible HIV infection), reported
an annual incidence rate of 4.8 per million in the period
1985�/1997, based on epidemiological data covering about
10% of the US population. However, Olson et al. based
their findings on data from the nine Surveillance, Epide-
miology and End Results (SEER) registries without a
review of the medical records. The review of the medical
records performed in the present study has led to exclusion
of 27 out of 85 patients with incorrect registration of
PCNSL, such as patients with systemic lymphomas. Similar
experiences have been reported in the Danish (24) and
Canadian study (5).
Table IV
Prognostic factors for survival in PCNSL: univariate analyses
n Median survival in
months (95% CI)
Log-rank test
(p value)
Treatment, n�/45 B/0.001
No treatment 9 0.9 (0.5, 1.3)
Only chemotherapy 6 2.7 (0.2, 5.3)
Only radiotherapy 7 16.7 (2.1, 31.2)
Chemo- & radiotherapy 23 49.2 (29.7, 68.8)
Age at diagnosis, n�/45 0.001
0�/60 20 43.5 (0.0, 87.5)
Above 60 25 5.4 (0.0, 12.2)
Sex, n�/45 0.46
Female 25 16.7 (0.0, 41.4)
Male 20 38.6 (0.0, 90.6)
Performance status, n�/45 B/0.001
WHO 0�/2 27 49.2 (27.7, 70.7)
WHO 3�/4 18 2.5 (1.4, 3.6)
Time to diagnosis (weeks), n�/45 0.99
0�/5.6 15 19.7 (0.6, 38.9)
5.7�/14.3 15 38.6 (0.0, 90.3)
above 14.3 15 16.7 (0.0, 39.9)
Year of diagnosis, n�/45 0.23
1989�/1993 15 11.0 (0.0, 25.2)
1994�/1998 30 31.9 (5.3, 58.5)
Lesions on CT/MR, n�/43 0.32
Single 33 23.8 (9.1, 38.5)
Multiple 10 5.4 (0.0, 78.6)
Malignant cells in CSF, n�/19 0.044
No 16 23.8 (0.0, 63.9)
Yes 3 2.5 (0.0, 5.9)
Raised protein level in CSF, n�/11 0.18
No 5 56.1 (0.0, 117.5)
Yes 6 3.7 (0.0, 26.3)
Operation prior to diagnosis, n�/43 0.28
Tumor resection 29 19.7 (1.2, 38.3)
Stereotactic biopsy 14 27.5 (12.7, 42.3)
526 I. Salvesen Haldorsen et al. Acta Oncologica 43 (2004)
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

Despite mandatory cancer reporting to the Norwegian
Cancer Registry, some cases may not have been reported,
resulting in an underestimation of incidence. In addition, we
are aware of 5 patients in the Norwegian Cancer Registry
and 1 additional patient treated at a university hospital with
clinical and radiological signs of PCNSL that were never
histologically verified and are therefore not included in our
material. On the other hand, some of the patients in our
material could possibly have occult systemic lymphoma
since adequate staging regimens were not performed in all
of the patients. However, an autopsy that excluded systemic
lymphoma was performed in 18 of the patients. Of the
remaining 40 patients, 38 had a negative abdominal CT or
ultrasound and 32 a negative bone marrow biopsy, demon-
strating that the vast majority underwent relevant staging.
Furthermore, experiences from others indicate that systemic
lymphoma masquerading as PCNSL is a relatively rare
occurrence (in the order of 4%) (25, 26). All taken
together, we consider our estimate of incidence to be fairly
reliable.
The rarity of PCNSL makes statistical assessment of
incidence alterations difficult. In our 10-year study period
there was a trend towards but not significant increase in
annual incidence of PCNSL (p�/0.069). During this period
(1989�/1998) diagnostic imaging with MRI has been
increasingly available in addition to CT at the hospitals in
Norway. Four hospitals had MRI in 1988, 6 in 1991, 8 in
1993, and 17 in 1998. The observed slight increase in
PCNSL could therefore be due to more sensitive and
accurate diagnostic evaluation. Patients receiving immuno-
suppressive therapy, such as transplant patients, carry an
increased risk of developing PCNSL (27). As only 3 of the
patients in our study had received immuno-suppressive
treatment, it would seem that this factor has little influence
on the findings. There was no reliable registration of the
entity PCNSL at the Norwegian Cancer Registry in the
decades prior to 1989, so that comparable data before 1989
are not available. Future studies, however, will, it is hoped,
be able to establish whether there is a real increase in non-
AIDS related PCNSL in Norway.
The 58 cases of morphologically verified PCNSL ac-
counted for 1.7% of all primary brain tumours (tumours in
meninges, corpus pineale, hypophysis, and cranial nerves
excluded) recorded at the Norwegian Cancer Registry in the
studied 10-year period. Similar percentages have been
reported from Denmark (6) and India (9), while studies
from The Netherlands (4) and the US (28) have reported a
percentage of 4�/6%. Morphologically verified PCNSL
accounted for 0.9% of newly diagnosed non-Hodgkin’s
lymphomas recorded at the Norwegian Cancer Registry in
the studied period.
The median age at time of diagnosis in our study was 68
years, which is 5�/15 years above the findings reported in
most other studies (6, 10, 11, 18, 19, 27). Compared with
those studies a relatively high percentage (22%) of our
patients were diagnosed after death. Varying autopsy
frequencies and different indications for autopsy in the
specific countries could possibly influence the age at which
the patients have their diagnosis established. In our study,
however, the median age of the patients diagnosed while
alive did not differ significantly from those diagnosed post
mortem (67 and 70 years respectively). Another explanation
of the differences in median age could be that older patients
in some countries go through less aggressive diagnostic
evaluation resulting in under-registration of PCNSL in
older age groups. The increased availability and geographi-
cal distribution of MRI during the time period must also be
taken into account. Finally, it is possible that our findings
reflect a real difference in age at diagnosis for Norwe-
gian PCNSL patients compared with those in other
countries.
We found a male/female ratio of 1.0, which is similar to
other findings (6, 11), although a male predominance also
has been reported (19, 29). In our study the median time
span between first symptom and diagnosis was found to be
13 weeks, which is consistent with reports from other
groups (11, 30). The lag time before diagnosis has been
found by others to have prognostic value (31), but this was
not apparent in the present study.
The clinical features in our patients corresponded well
with the literature (6, 10, 11). Personality change and focal
neurological symptoms, usually hemiparesis, were the most
frequent symptoms prior to diagnosis. The CSF was
examined less often than expected in our material. Eleva-
tion of cell count was found in 67% of the samples and
elevation of total protein in 57% of the samples. This
corresponds to the findings of other groups, reporting
elevated cell count in 35�/75% and increased total protein
in 54�/85% of samples (10, 29). Likewise, our finding of
malignant cells in CSF in 13% of the samples corresponds
with findings by the same groups and demonstrates that
CSF cytology is unreliable for the exclusion of PCNSL.
The prognosis of primary central nervous system lym-
phoma is considerably worse than for most other lympho-
mas in spite of advanced therapy. The comparison of the
mortality rates in different studies is hampered by selection
bias and the fact that only a few studies are population
based. In the present population-based study the median
survival of the patients diagnosed before death was 22
months. This compares favourably with other population-
based studies (4, 5, 24). Although treated patients are
positively selected, survival in our study seemed greatly
influenced by the treatment. In accordance with other
studies, patients receiving radiotherapy or both chemo-
and radiotherapy had a significantly better survival than
patients receiving no therapy at all (11, 12, 15�/17, 29). It
was not possible to demonstrate a significantly better
survival among patients receiving only chemotherapy than
Acta Oncologica 43 (2004) Primary nervous system lymphoma in Norway 527
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

among non-treated patients. However, this could be due to
the limited size of the series. The heterogeneity of the
chemotherapy and the radiation regimens applied and
the limited sample size makes it difficult to compare
the survival among patients receiving the different regim-
ens.
By univariate analysis we have demonstrated that young
age, good performance status, radiotherapy either alone or
in combination with chemotherapy, and lack of malignant
cells in CSF are associated with longer survival. Multi-
variate analysis confirmed the independent prognostic value
of age, therapy, and performance status. These findings
correspond with reports by other groups (11, 13, 15, 19, 29,
32).
In summary, the results of this national 10-year survey of
PCNSL are in agreement with data from single institutions
and regional surveys concerning clinical features and
response to therapy. The age at diagnosis is higher than in
most reports. There was a non-significant trend towards
increased incidence, perhaps related to increased availability
of diagnostic imaging, especially MRI.
ACKNOWLEDGEMENTS
This study was supported in part by grants from Amersham Health
AS and grants from Haakon and Sigrun Ødegaard’s Foundation.
Thanks are offered to the following institutions that have made
possible the review of the medical records of the patients treated at
their hospitals: Akershus University Hospital, Baerum Hospital,
Haukeland University Hospital, Hedmark Central Hospital, Laer-
dal Hospital, Rikshospitalet, Rogaland Central Hospital, St Olav
Hospital, the Norwegian Radiumhospital, Ullevaal University
Hospital, the University of Northern Norway Hospital and West-
Agder Central Hospital.
REFERENCES
1. Olson JE, Janney CA, Rao RD, et al. The continuing increase
in the incidence of primary central nervous system non-
Hodgkin lymphoma: a surveillance, epidemiology, and end
results analysis. Cancer 2002; 95: 1504�/10.
2. Corn BW, Marcus SM, Topham A, et al. Will primary central
nervous system lymphoma be the most frequent brain tumor
diagnosed in the year 2000? Cancer 1997; 79: 2409�/13.
3. Lutz JM, Coleman MP. Trends in primary cerebral lymphoma.
Br J Cancer 1994; 70: 716�/8.
4. Van der Sanden GA, Schouten LJ, van Dijck JA, et al. Primary
central nervous system lymphomas: incidence and survival in
the Southern and Eastern Netherlands. Cancer 2002; 94: 1548�/
56.
5. Hao D, DiFrancesco LM, Brasher PM, et al. Is primary CNS
lymphoma really becoming more common? A population-
based study of incidence, clinicopathological features and
outcomes in Alberta from 1975 to 1996. Ann Oncol 1999; 10:
65�/70.
6. Krogh-Jensen M, D’Amore F, Jensen MK, et al. Clinicopatho-
logical features, survival and prognostic factors of primary
central nervous system lymphomas: trends in incidence of
primary central nervous system lymphomas and primary
malignant brain tumors in a well-defined geographical area.
Population-based data from the Danish Lymphoma Registry,
LYFO, and the Danish Cancer Registry. Leuk Lymphoma
1995; 19: 223�/33.
7. Yau YH, O’Sullivan MG, Signorini D, Ironside JW, Whittle
IR. Primary lymphoma of central nervous system in immuno-
competent patients in south-east Scotland. Lancet 1996; 348:
890.
8. Au WY, Chan AC, Srivastava G, et al. Incidence and pathology
of primary brain lymphoma in Hong Kong Chinese patients.
Leuk Lymphoma 2000; 37: 175�/9.
9. Powari M, Radotra B, Das A, et al. A study of primary central
nervous system lymphoma in northern India. Surg Neurol
2002; 57: 113�/6.
10. Herrlinger U, Schabet M, Bitzer M, et al. Primary central
nervous system lymphoma: from clinical presentation to
diagnosis. J Neurooncol 1999; 43: 219�/26.
11. Bataille B, Delwail V, Menet E, et al. Primary intracerebral
malignant lymphoma: report of 248 cases. J Neurosurg 2000;
92: 261�/6.
12. Schlegel U, Schmidt-Wolf IG, Deckert M. Primary CNS
lymphoma�/Clinical presentation, pathological classification,
molecular pathogenesis and treatment. J Neurol Sci 2000; 181:
1�/12.
13. Henry JM, Heffner RR, Jr., Dillard SH, et al. Primary
malignant lymphomas of the central nervous system. Cancer
1974; 34: 1293�/302.
14. Weller M. Glucocorticoid treatment of primary CNS lym-
phoma. J Neurooncol 1999; 43: 237�/9.
15. Nelson DF. Radiotherapy in the treatment of primary central
nervous system lymphoma (PCNSL). J Neurooncol 1999; 43:
241�/7.
16. Abrey LE, DeAngelis LM, Yahalom J. Long-term survival in
primary CNS lymphoma. J Clin Oncol 1998; 16: 859�/63.
17. Ferreri AJ, Reni M, Villa E. Therapeutic management of
primary central nervous system lymphoma: lessons from
prospective trials. Ann Oncol 2000; 11: 927�/37.
18. Herrlinger U, Schabet M, Brugger W, et al. Primary central
nervous system lymphoma 1991�/1997 �/ Outcome and late
adverse effects after combined modality treatment. Cancer
2001; 91: 130�/5.
19. Ferreri AJ, Blay JY, Reni M, et al. Prognostic scoring system
for primary CNS lymphomas: the International Extranodal
Lymphoma Study Group experience. J Clin Oncol 2003; 21:
266�/72.
20. Ferreri AJ, Abrey LE, Blay JY, et al. Summary statement on
primary central nervous system lymphomas from the Eighth
International Conference on Malignant Lymphoma, Lugano,
Switzerland, 12 to 15 June 2002. J Clin Oncol 2003; 21: 2407�/
14.
21. Kaplan EL, Meier P. Nonparametric estimation from incom-
plete observations. J Am Stat Assoc 1958; 53: 457�/81.
22. Cox DR. Regression models and life tables. J Roy Statist Soc
1972; 34: 187�/220.
23. Grambsch P, Therneau TM. Proportional hazards tests and
diagnostics based on weighted residuals. Biometrika 1994; 81:
515�/26.
24. Krogh-Jensen M, D’Amore F, Jensen MK, et al. Incidence,
clinicopathological features and outcome of primary central
nervous system lymphomas. Population-based data from a
Danish lymphoma registry. Danish Lymphoma Study Group,
LYFO. Ann Oncol 1994; 5: 349�/54.
25. O’Neill BP, Dinapoli RP, Kurtin PJ, et al. Occult systemic
non-Hodgkin’s lymphoma (NHL) in patients initially
diagnosed as primary central nervous system lymphoma
528 I. Salvesen Haldorsen et al. Acta Oncologica 43 (2004)
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.

(PCNSL): how much staging is enough?. J Neurooncol 1995;
25: 67�/71.
26. Herrlinger U. Primary CNS lymphoma: findings outside the
brain. J Neurooncol 1999; 43: 227�/30.
27. Schabet M. Epidemiology of primary CNS lymphoma. J
Neurooncol 1999; 43: 199�/201.
28. Miller DC, Hochberg FH, Harris NL, Gruber ML, Louis DN,
Cohen H. Pathology with clinical correlations of primary
central nervous system non-Hodgkin’s lymphoma. The Mas-
sachusetts General Hospital experience 1958�/1989. Cancer
1994; 74: 1383�/97.
29. Hayakawa T, Takakura K, Abe H, et al. Primary central
nervous system lymphoma in Japan*/A retrospective, co-
operative study by CNS-Lymphoma Study Group in Japan. J
Neurooncol 1994; 19: 197�/215.
30. Hochberg FH, Miller DC. Primary central nervous system
lymphoma. J Neurosurg 1988; 68: 835�/53.
31. Kim DG, Nam DH, Jung HW, et al. Primary central nervous
system lymphoma: variety of clinical manifestations and
survival. Acta Neurochir (Wien) 1996; 138: 280�/9.
32. Watne K, Scott H, Hager B, et al. Primary malignant
lymphoma of the brain. A report of 24 cases from
the Norwegian Radium Hospital. Acta Oncol 1992; 31:
545�/50.
Acta Oncologica 43 (2004) Primary nervous system lymphoma in Norway 529
Act
a O
ncol
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
190.
201.
225.
93 o
n 05
/20/
14Fo
r pe
rson
al u
se o
nly.