Naturally Occurring Radioactive Materials (NORM) in Class II ...
Upload
independentCategory
view
0download
0
C©2007, University of Texas Southwestern Medical School at DallasJournal compilation C©2007, Blackwell Publishing, Inc.
DOI: 10.1111/j.1540-8183.2007.00309.x
Incidence and Treatment of Arterial Access Dissections Occurring duringCardiac Catheterization
AMIT PRASAD, M.D.,1 P. ALEXANDER COMPTON, M.D.,1 ANAND PRASAD, M.D.,2
MICHELE ROESLE, R.N.,2 LORENZA MAKKE, R.C.I.S.,2 SHARON ROGERS, R.N.,2
SUBHASH BANERJEE, M.D.,2 and EMMANOUIL S. BRILAKIS, M.D., PH.D.2
From the 1Department of Internal Medicine, University of Texas Southwestern Medical School; and 2Division of Cardiovascular Diseases,University of Texas Southwestern Medical School, and Department of Cardiology, Dallas VA Medical Center, Dallas, Texas
Background: Arterial access dissections may complicate cardiac catheterization and can often be treated percu-taneously. The goal of this study was to examine the incidence, consequences, and the treatment of arterial accessdissections at a tertiary referral hospital with an active training program.Methods: Patients experiencing arterial access dissection during coronary angiography or intervention at ourinstitution between October 1, 2004, and January 31, 2007, were identified and their records were retrospectivelyreviewed.Results: Thirteen of the 3,062 consecutive patients (0.42%) had arterial access dissection during the study period.The location of the dissection was in the common femoral artery (CFA) (n = 6), the external iliac artery (EIA)(n = 6), or in an aortobifemoral graft (n = 1). Three of the six patients with CFA dissection were diagnosedduring coronary angiography, and because of significant comorbidities were treated with self-expanding stents.After a mean follow-up of 7 months, they experienced no stent fracture or other complication. Six patients hadEIA dissections. In one such patient, the dissection was not flow limiting and was treated conservatively. Theremaining five patients underwent successful implantation of self-expanding stents, and during a mean follow-upof 9.6 months, no patient had any symptoms or events related to lower extremity ischemia. Finally, one patient hadan aortobifemoral graft dissection. Due to the patient’s critical condition, secondary to sepsis, his family electedto withdraw care, and he subsequently expired.Conclusions: Arterial access dissections occur infrequently during cardiac catheterization. Routine femoral arteryangiography may help identify vascular access complications, often allowing simultaneous endovascular treatment,with excellent short-term outcomes. (J Interven Cardiol 2008;21:61–66)
Introduction
Arterial access complications, such as bleeding,infection, arteriovenous fistula, neuropathy, pseudo-aneurysm, and dissections, can complicate diagnosticand therapeutic cardiac catheterization. Even thoughmultiple vascular access complication reports havebeen published,1–12 most studies have focused on
Address for reprints: Emmanouil S. Brilakis, M.D., Ph.D., Dal-las VA Medical Center (111A) 4500 South Lancaster Road,Dallas, TX 75216. Fax: (214) 302–1341; e-mail: [email protected]
bleeding, pseudoaneurysms, arteriovenous fistulas, andthrombosis, with little data available on arterial accessdissections.13 The goal of this study was to examine theincidence, treatment, and the consequences of arterialdissections complicating transfemoral cardiac catheter-ization at a large, tertiary referral hospital with an activecardiology fellowship training program.
Methods
We retrospectively reviewed the records of consec-utive patients undergoing transfemoral coronary an-giography or percutaneous coronary intervention at the
Vol. 21, No. 1, 2008 Journal of Interventional Cardiology 61
PRASAD, ET AL.
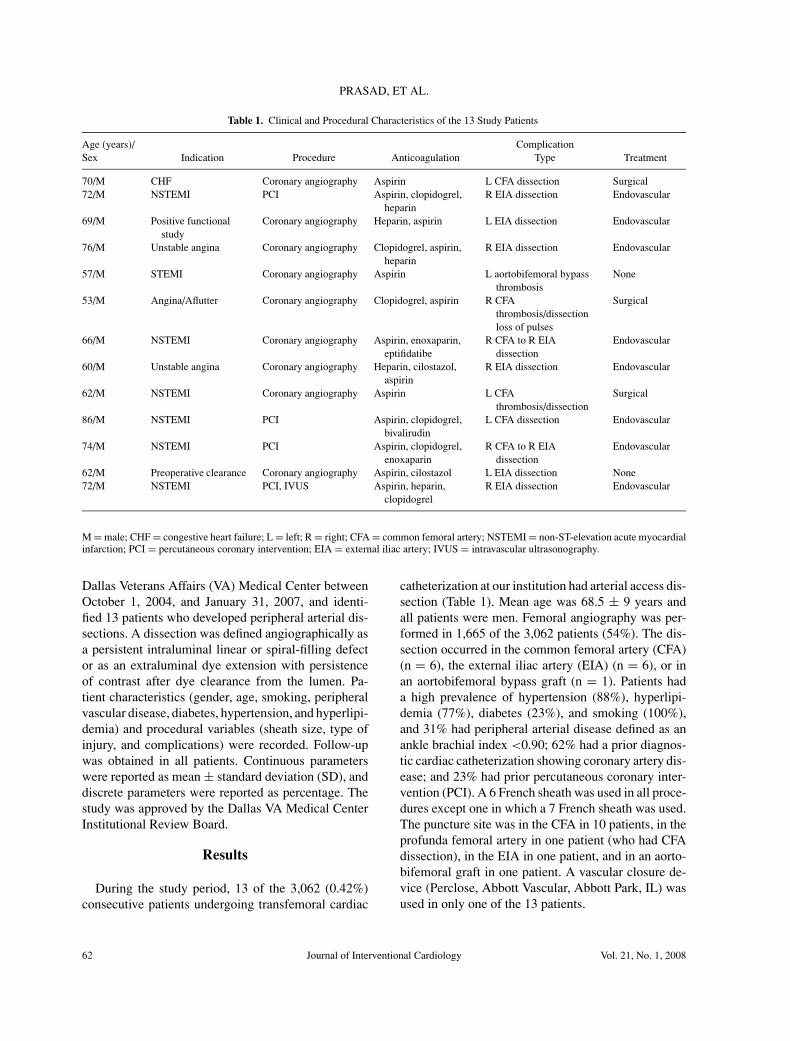
Table 1. Clinical and Procedural Characteristics of the 13 Study Patients
Age (years)/ ComplicationSex Indication Procedure Anticoagulation Type Treatment
70/M CHF Coronary angiography Aspirin L CFA dissection Surgical72/M NSTEMI PCI Aspirin, clopidogrel,
heparinR EIA dissection Endovascular
69/M Positive functionalstudy
Coronary angiography Heparin, aspirin L EIA dissection Endovascular
76/M Unstable angina Coronary angiography Clopidogrel, aspirin,heparin
R EIA dissection Endovascular
57/M STEMI Coronary angiography Aspirin L aortobifemoral bypassthrombosis
None
53/M Angina/Aflutter Coronary angiography Clopidogrel, aspirin R CFAthrombosis/dissectionloss of pulses
Surgical
66/M NSTEMI Coronary angiography Aspirin, enoxaparin,eptifidatibe
R CFA to R EIAdissection
Endovascular
60/M Unstable angina Coronary angiography Heparin, cilostazol,aspirin
R EIA dissection Endovascular
62/M NSTEMI Coronary angiography Aspirin L CFAthrombosis/dissection
Surgical
86/M NSTEMI PCI Aspirin, clopidogrel,bivalirudin
L CFA dissection Endovascular
74/M NSTEMI PCI Aspirin, clopidogrel,enoxaparin
R CFA to R EIAdissection
Endovascular
62/M Preoperative clearance Coronary angiography Aspirin, cilostazol L EIA dissection None72/M NSTEMI PCI, IVUS Aspirin, heparin,
clopidogrelR EIA dissection Endovascular
M = male; CHF = congestive heart failure; L = left; R = right; CFA = common femoral artery; NSTEMI = non-ST-elevation acute myocardialinfarction; PCI = percutaneous coronary intervention; EIA = external iliac artery; IVUS = intravascular ultrasonography.
Dallas Veterans Affairs (VA) Medical Center betweenOctober 1, 2004, and January 31, 2007, and identi-fied 13 patients who developed peripheral arterial dis-sections. A dissection was defined angiographically asa persistent intraluminal linear or spiral-filling defector as an extraluminal dye extension with persistenceof contrast after dye clearance from the lumen. Pa-tient characteristics (gender, age, smoking, peripheralvascular disease, diabetes, hypertension, and hyperlipi-demia) and procedural variables (sheath size, type ofinjury, and complications) were recorded. Follow-upwas obtained in all patients. Continuous parameterswere reported as mean ± standard deviation (SD), anddiscrete parameters were reported as percentage. Thestudy was approved by the Dallas VA Medical CenterInstitutional Review Board.
Results
During the study period, 13 of the 3,062 (0.42%)consecutive patients undergoing transfemoral cardiac
catheterization at our institution had arterial access dis-section (Table 1). Mean age was 68.5 ± 9 years andall patients were men. Femoral angiography was per-formed in 1,665 of the 3,062 patients (54%). The dis-section occurred in the common femoral artery (CFA)(n = 6), the external iliac artery (EIA) (n = 6), or inan aortobifemoral bypass graft (n = 1). Patients hada high prevalence of hypertension (88%), hyperlipi-demia (77%), diabetes (23%), and smoking (100%),and 31% had peripheral arterial disease defined as anankle brachial index <0.90; 62% had a prior diagnos-tic cardiac catheterization showing coronary artery dis-ease; and 23% had prior percutaneous coronary inter-vention (PCI). A 6 French sheath was used in all proce-dures except one in which a 7 French sheath was used.The puncture site was in the CFA in 10 patients, in theprofunda femoral artery in one patient (who had CFAdissection), in the EIA in one patient, and in an aorto-bifemoral graft in one patient. A vascular closure de-vice (Perclose, Abbott Vascular, Abbott Park, IL) wasused in only one of the 13 patients.
62 Journal of Interventional Cardiology Vol. 21, No. 1, 2008
INCIDENCE AND TREATMENT OF ARTERIAL DISSECTIONS
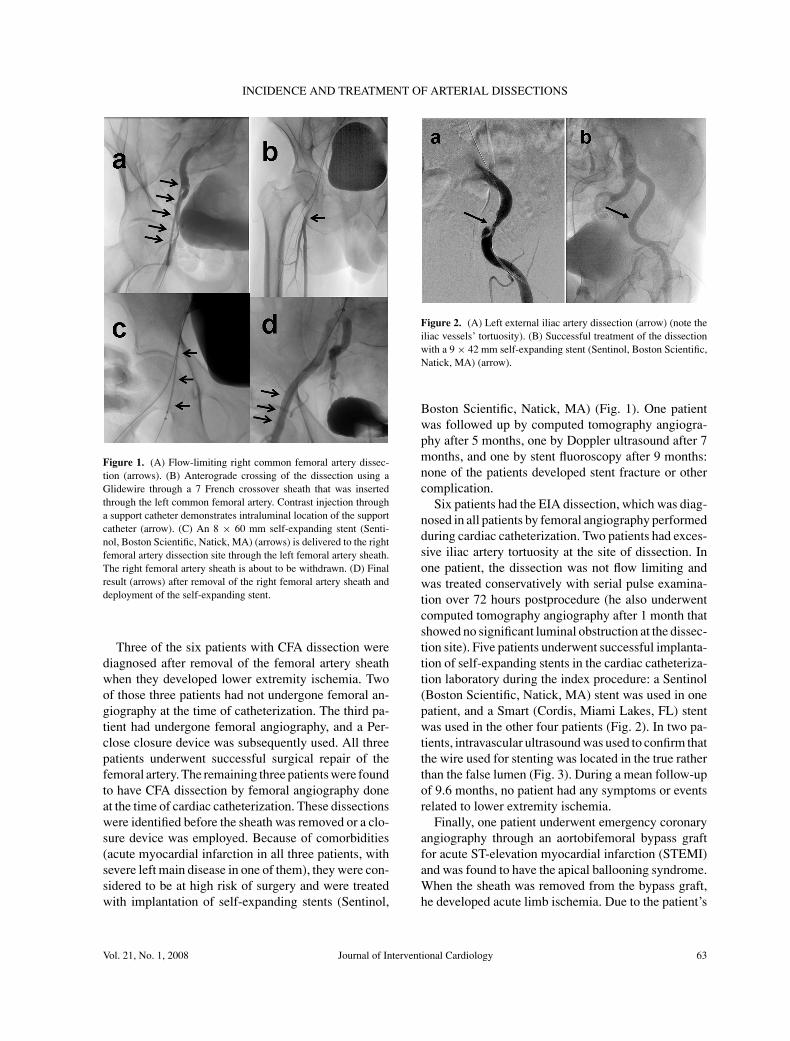
Figure 1. (A) Flow-limiting right common femoral artery dissec-tion (arrows). (B) Anterograde crossing of the dissection using aGlidewire through a 7 French crossover sheath that was insertedthrough the left common femoral artery. Contrast injection througha support catheter demonstrates intraluminal location of the supportcatheter (arrow). (C) An 8 × 60 mm self-expanding stent (Senti-nol, Boston Scientific, Natick, MA) (arrows) is delivered to the rightfemoral artery dissection site through the left femoral artery sheath.The right femoral artery sheath is about to be withdrawn. (D) Finalresult (arrows) after removal of the right femoral artery sheath anddeployment of the self-expanding stent.
Three of the six patients with CFA dissection werediagnosed after removal of the femoral artery sheathwhen they developed lower extremity ischemia. Twoof those three patients had not undergone femoral an-giography at the time of catheterization. The third pa-tient had undergone femoral angiography, and a Per-close closure device was subsequently used. All threepatients underwent successful surgical repair of thefemoral artery. The remaining three patients were foundto have CFA dissection by femoral angiography doneat the time of cardiac catheterization. These dissectionswere identified before the sheath was removed or a clo-sure device was employed. Because of comorbidities(acute myocardial infarction in all three patients, withsevere left main disease in one of them), they were con-sidered to be at high risk of surgery and were treatedwith implantation of self-expanding stents (Sentinol,
Figure 2. (A) Left external iliac artery dissection (arrow) (note theiliac vessels’ tortuosity). (B) Successful treatment of the dissectionwith a 9 × 42 mm self-expanding stent (Sentinol, Boston Scientific,Natick, MA) (arrow).
Boston Scientific, Natick, MA) (Fig. 1). One patientwas followed up by computed tomography angiogra-phy after 5 months, one by Doppler ultrasound after 7months, and one by stent fluoroscopy after 9 months:none of the patients developed stent fracture or othercomplication.
Six patients had the EIA dissection, which was diag-nosed in all patients by femoral angiography performedduring cardiac catheterization. Two patients had exces-sive iliac artery tortuosity at the site of dissection. Inone patient, the dissection was not flow limiting andwas treated conservatively with serial pulse examina-tion over 72 hours postprocedure (he also underwentcomputed tomography angiography after 1 month thatshowed no significant luminal obstruction at the dissec-tion site). Five patients underwent successful implanta-tion of self-expanding stents in the cardiac catheteriza-tion laboratory during the index procedure: a Sentinol(Boston Scientific, Natick, MA) stent was used in onepatient, and a Smart (Cordis, Miami Lakes, FL) stentwas used in the other four patients (Fig. 2). In two pa-tients, intravascular ultrasound was used to confirm thatthe wire used for stenting was located in the true ratherthan the false lumen (Fig. 3). During a mean follow-upof 9.6 months, no patient had any symptoms or eventsrelated to lower extremity ischemia.
Finally, one patient underwent emergency coronaryangiography through an aortobifemoral bypass graftfor acute ST-elevation myocardial infarction (STEMI)and was found to have the apical ballooning syndrome.When the sheath was removed from the bypass graft,he developed acute limb ischemia. Due to the patient’s
Vol. 21, No. 1, 2008 Journal of Interventional Cardiology 63

PRASAD, ET AL.
Figure 3. (A) Right external iliac artery dissection (arrow). (B) Intravascular ultrasound showing the presence of an intimalflap and a false lumen (arrows) and confirming that the wire is in the true lumen. (C) Successful treatment of the dissectionwith a self-expanding 12 × 40 mm self-expanding stent (Smart, Cordis, Miami Lakes, FL) (arrows).
critical condition, secondary to sepsis, his familyelected to withdraw care, and he subsequently expired.
Discussion
In published case series with >1,000 patients, the in-cidence of vascular access complications is 0.6–1.8%for diagnostic coronary catheterization and 0.9–2.9%for PCIs.1–12 The incidence of arterial dissections was0.06–0.3%, but was only reported in a few studies andmay be underreported because some arterial occlusionsmay develop as a result of prior dissections (Table 2).The reported combined incidence of arterial occlusionand dissection was 0.12–0.4% (Table 2), which is sim-ilar to the incidence in our study (0.42%). Our studymay have underestimated the true incidence of arterialdissections, as only approximately half of the 3,062patients undergoing transfemoral cardiac catheteriza-tion had femoral angiography. However, major arterialaccess dissections are unlikely to have been missed, be-cause they would likely lead to limb ischemia. Femoralcannulation for cardiopulmonary bypass during mini-mally invasive cardiac surgery resulted in femoral ar-
Table 2. Frequency of Vascular Access Complications and Dissections.
Frequency of Frequency of Frequency ofAll Femoral Access Access Arterial Dissection and
Author Year Complications Dissections Thrombosis Risk Factors
Messina et al.7 1991 106/6,912 (1.5%) 4/6,912 (0.06%) 32/6,912 (0.4%) Hypertension, peripheral vascular diseaseMuller et al.8 1992 69/2,400 (2.9%) NA 3/2,400 (0.12%) Age >65 years, peripheral vascular diseaseSherev et al.12 2005 33/1,570 (2%) 5/1,570 (0.3%) NA High anatomic arteriotomy locationAgostoni et al.1 2006 34/1,288 (2.6%) 1/1,288 (0.08) NA Age >65 years, female gender
NA = not available.
terial injuries (likely dissections) in seven of the 739patients (0.9%).14
The likely cause of dissection varied in our patients.The high and low puncture could have contributed toit in one patient each. In one patient, dissection waslikely related to the use of the Perclose vascular clo-sure device. Femoral artery dissection is a recognizedcomplication of the Perclose (and other) closure de-vices and could occur if the needles are deployed tooearly and they interact with the posterior wall of thevessel or if the needles are deployed through a plaquein the anterior wall of the vessel.15,16 In two of the sixpatients with iliac artery dissection, tortuosity appearedto be the major contributor. Even though it cannot beassessed in a retrospective study, meticulous attentionand gentle manipulations while puncturing the arteryand advancing the wire may lower the risk of accesssite complications. Compared to the femoral or brachialaccess, the transradial access has the lowest risk of ac-cess site complications.17 Whether cardiology traineeparticipation resulted in more complications could notbe examined in our study as a fellow participated inalmost all procedures.
64 Journal of Interventional Cardiology Vol. 21, No. 1, 2008

INCIDENCE AND TREATMENT OF ARTERIAL DISSECTIONS
Routine femoral angiography during cardiaccatheterization could lead to early diagnosis not onlyof arterial dissections, but also of other complications,such as bleeding from laceration of the inferior epigas-tric artery.18 Femoral angiography may optimally bebest performed in two views,19 immediately after ob-taining access to facilitate procedural planning. For ex-ample, if the puncture is high or low, elective PCI mightbe best postponed to minimize the risk of bleeding af-ter anticoagulation administration.12 Femoral angiog-raphy was not performed in two of the three patientswho subsequently developed acute limb ischemia, andwere found to have femoral artery dissection at surgery.Had femoral angiography been performed during car-diac catheterization in those patients, then the diagnosisand the treatment of dissection could have been initi-ated earlier.
Open surgical repair has historically been the treat-ment of choice for flow-limiting femoral access dissec-tions,6,7 but percutaneous techniques are increasinglybeing used to treat these injuries. The CFA stentingis not recommended because of the high risk of stentfracture, except when no other treatment is feasible,20
as was the case with three of our patients. Balloon an-gioplasty or atherectomy of the CFA might be betteralternatives to stenting if they provide an acceptableangiographic result. In a small series, six patients whodeveloped critical limb ischemia after cardiac catheter-ization were treated with local thrombolysis followedby balloon angioplasty (n = 4) or stenting (n = 2) withgood short-term results.13
Patients with non-flow-limiting iliac artery dissec-tions can often be treated conservatively, because theblood flow tends to “tuck” iliac dissections caused dur-ing retrograde insertion of catheters, wires, or otherequipment. Conservative management for non-flow-limiting dissections consists of bed rest with follow-upnoninvasive imaging and clinical exams. If dissectionsare flow limiting, then stenting (using self-expandingstents for the EIA or either self-expanding or balloon-expandable stents for the common iliac artery) may bethe treatment of choice, as it can be completed withina short period of time in the cardiac catheterizationsuite, provided that the necessary equipment and ex-pertise are available. A recent series examined the useof stents in treating catheter-induced iliac dissections.In a series of 11 patients with iatrogenic iliac dissectionduring cardiac catheterization, self-expanding stentswere placed with good postprocedural flow, and a 90%patency rate at 24-month follow-up.21 Before stent de-
ployment, it is crucial to confirm that the guidewire is inthe true rather than the false lumen, which could be ac-complished with intravascular ultrasonography (IVUS)(Fig. 3).21,22
In summary, vascular access dissection (1) occur in-frequently during cardiac catheterization, (2) may beidentified promptly by routine femoral angiography,and (3) can often be treated endovascularly at the timeof the index catheterization.
References
1. Agostoni P, Anselmi M, Gasparini G, et al. Safety of percuta-neous left heart catheterization directly performed by cardiol-ogy fellows: A cohort analysis. J Invasive Cardiol 2006;18:248–252.
2. Applegate RJ, Sacrinty MT, Kutcher MA, et al. Propensityscore analysis of vascular complications after diagnostic car-diac catheterization and percutaneous coronary intervention,1998–2003. Catheter Cardiovasc Interv 2006;67:556–562.
3. Chandrasekar B, Doucet S, Bilodeau L, et al. Complicationsof cardiac catheterization in the current era: A single-centerexperience. Catheter Cardiovasc Interv 2001;52:289–295.
4. Khoury M, Batra S, Berg R, et al. Influence of arterial accesssites and interventional procedures on vascular complicationsafter cardiac catheterizations. Am J Surg 1992;164:205–209.
5. Koreny M, Riedmuller E, Nikfardjam M, et al. Arterial punc-ture closing devices compared with standard manual compres-sion after cardiac catheterization: Systematic review and meta-analysis. JAMA 2004;291:350–357.
6. McCann RL, Schwartz LB, Pieper KS. Vascular complicationsof cardiac catheterization. J Vasc Surg 1991;14:375–381.
7. Messina LM, Brothers TE, Wakefield TW, et al. Clinical char-acteristics and surgical management of vascular complicationsin patients undergoing cardiac catheterization: Interventionalversus diagnostic procedures. J Vasc Surg 1991;13:593–600.
8. Muller DW, Shamir KJ, Ellis SG, et al. Peripheral vascular com-plications after conventional and complex percutaneous coro-nary interventional procedures. Am J Cardiol 1992;69:63–68.
9. Nikolsky E, Mehran R, Halkin A, et al. Vascular complicationsassociated with arteriotomy closure devices in patients under-going percutaneous coronary procedures: A meta-analysis. JAm Coll Cardiol 2004;44:1200–1209.
10. Piper WD, Malenka DJ, Ryan TJ Jr, et al. Predicting vascu-lar complications in percutaneous coronary interventions. AmHeart J 2003;145:1022–1029.
11. Ricci MA, Trevisani GT, Pilcher DB. Vascular complicationsof cardiac catheterization. Am J Surg 1994;167:375–378.
12. Sherev DA, Shaw RE, Brent BN. Angiographic predictors offemoral access site complications: Implication for planned per-cutaneous coronary intervention. Catheter Cardiovasc Interv2005;65:196–202.
13. Tsetis DK, Kochiadakis GE, Hatzidakis AA, et al. Transcatheterthrombolysis with high-dose bolus tissue plasminogen activatorin iatrogenic arterial occlusion after femoral arterial catheteri-zation. Cardiovasc Intervent Radiol 2002;25:36–41.
14. Muhs BE, Galloway AC, Lombino M, et al. Arterial in-juries from femoral artery cannulation with port access cardiacsurgery. Vasc Endovascular Surg 2005;39:153–158.
15. Derham C, Davies JF, Shahbazi R, et al. Iatrogenic limb is-chemia caused by angiography closure devices. Vasc Endovas-cular Surg 2006;40:492–494.
Vol. 21, No. 1, 2008 Journal of Interventional Cardiology 65

PRASAD, ET AL.
16. Nehler MR, Lawrence WA, Whitehill TA, et al. Iatrogenic vas-cular injuries from percutaneous vascular suturing devices. JVasc Surg 2001;33:943–947.
17. Kiemeneij F, Laarman GJ, Odekerken D, et al. A ran-domized comparison of percutaneous transluminal coro-nary angioplasty by the radial, brachial, and femoral ap-proaches: The access study. J Am Coll Cardiol 1997;29:1269–1275.
18. Kawamura A, Piemonte TC, Nesto RW, et al. Retroperitonealhemorrhage from inferior epigastric artery: Value of femoralangiography for detection and management. Catheter Cardio-vasc Interv 2006;68:267–270.
19. Turi ZG. Optimizing vascular access: Routine femoral angiog-raphy keeps the vascular complication away. Catheter Cardio-vasc Interv 2005;65:203–204.
20. Silva JA, White CJ, Quintana H, et al. Percutaneous revascu-larization of the common femoral artery for limb ischemia.Catheter Cardiovasc Interv 2004;62:230–233.
21. Onal B, Ilgit ET, Akpek S, et al. Endovascular treatment ofobstructive iliac artery dissections. Acta Radiol 2005;46:359–365.
22. Babb JD, Collins TJ, Cowley MJ, et al. Revised guidelines forthe performance of peripheral vascular intervention. CatheterCardiovasc Interv 1999;46:21–23.
66 Journal of Interventional Cardiology Vol. 21, No. 1, 2008
Copyright © 2022 FDOKUMEN