
Arterial Line dr cindy
28
Arterial Line Cindy E. Boom Cindy E. Boom National Cardiovascular Center National Cardiovascular Center Harapan Kita, Jakarta 2007 Harapan Kita, Jakarta 2007
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Arterial Line dr cindy

Arterial Line
Cindy E. BoomCindy E. BoomNational Cardiovascular CenterNational Cardiovascular CenterHarapan Kita, Jakarta 2007Harapan Kita, Jakarta 2007

IntroductionIntroduction
Performed in 100% of all patients undergo cardiac surgery
Performed in 50-70% of all ICU patients

HistoricHistoricalal
1.Farinas (1941): aorta cannulation with urethral catheter introduced through a surgically exposed femoral artery.
2.Strain gauge manometer introduced (1947).
3.Peterson et al. (1949) described on-line arterial monitoring.
4.Seldinger (1953): percutaneous placement using a guidewire.

Indications for Arterial Indications for Arterial CannulationCannulation
1.Hemodynamic monitoring.2.Frequent arterial blood gas sampling.
3.Arterial administration of drugs.
4.Intraaortic baloon pump use.
Patient will require three or more measurements daily

EquipmentEquipment
1.An appropriate intravascular catheter.
2.Fluid-filled noncompliant tubing with stopcocks.
3.A transducer and dome.4.A constant flush device.5.Electronic monitoring equipment, consisting of a connecting cable, monitor with amplifier, oscilloscope display screen, and recorder.

Intravascular pressure changes are transmitted through
Hydraulic (fluid-filled) element
Transducer
Convert mechanical displacement
Proportional electrical signal

The major problems:
1. Inadequate dynamic response.
2. Improper zeroing and zero drift
3. Improper transducer/ monitor calibration (12-15)

Site Selection
The ideal artery has extensive collateral
circulation that will maintain the
viability of distal tissues of thrombosis occurs

The site should be:1.Comfortable for the patient2.Accessible for nursing care 3.Close to the monitor equipment4.No infection5.No disruption in the epidermal barrier
6.Larger arteries and catheters provide more accurate (central aortic)

Surgical cut down at any site is no longer recommended due to increased risk of complications, especially infection and thrombosis

Radial & femoral artery constitute more than 90% of all arterial catheterizationsFemoral artery is preferred siteLong term
cannulation
Brachial artery is not commonly used because
↓good collateral circulation
↑risk of distal ischemia
Axillary artery has
many attractive features

Radial Artery Radial Artery CannulationCannulation
Understanding of arterial anatomy
Modified Allen’s Test (1929); technique of diagnosing occlusive arterial disease

Fig. Anatomy of the radial artery. Note the collateral circulation to the ulnar artery thought the deep volar arterial arch and dorsal arch.
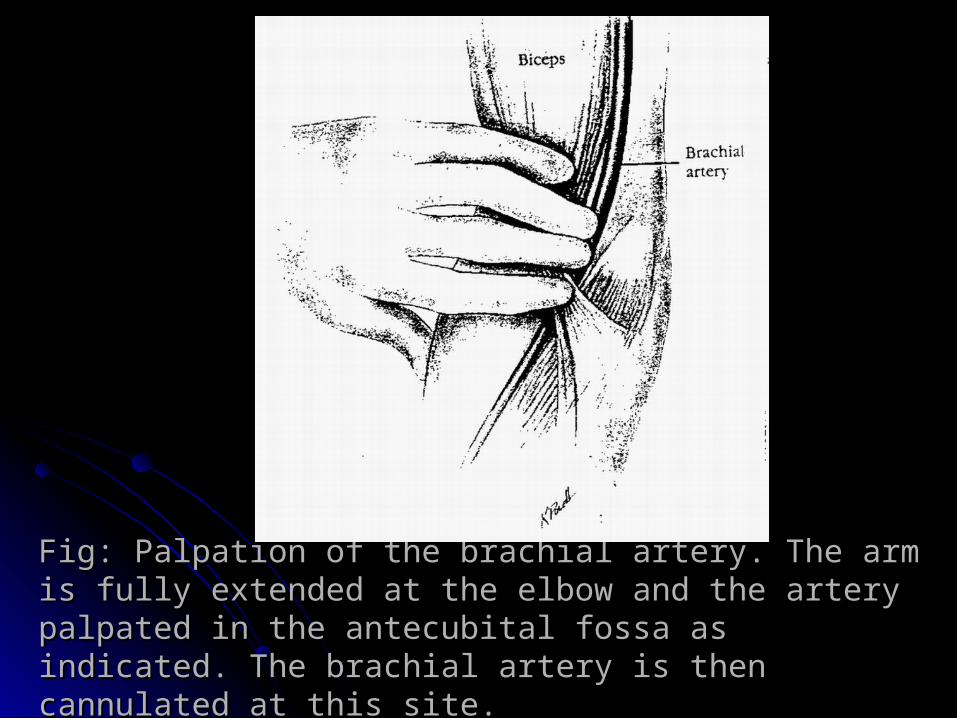
Fig: Palpation of the brachial artery. The arm Fig: Palpation of the brachial artery. The arm is fully extended at the elbow and the artery is fully extended at the elbow and the artery palpated in the antecubital fossa as palpated in the antecubital fossa as indicated. The brachial artery is then indicated. The brachial artery is then cannulated at this site.cannulated at this site.

Modified Allen’s Test
Compresses both radial & ulnar arteries
Patient clinch & unclinch the fist
Until pallor of the palm
One artery is then released
Time to blushing of palm note
Procedure is repeated with the other artery
Normal < 7 seconds (+ test)Equivocal 8 – 14 secondsAbnormal >= 15 (- test)

Fig: The Allen test is performed before cannulation of the radial artery to ensure adequacy of the ulnar and radial arteries and patency of the deep palmar arch. I. The examiner compresses both arteries while the patient repeatedly makes a tight firs to squeeze blood out of the hand. 2. After the patient relaxes the fingers, the examiner observes the waxen hand. The patient sholud be instructed not to hyperextend the finger and wrist because this may result in a false-positive test. J, Compression of the ulnar artery is released and the hand is observed for a blush or hyperemia. If color does not return within 5 to 10 seconds, radial artery cannulation should not be done. If brisk filling occurs, the test is repeated with the radial artery to test radial artery competency. If both vessels are competent, the radial artery may used for puncture. (From Schwartz GR, editor: Principles and practice of emergency medicine, Philadelpiha, 1978, W.B. Saunders.)

Percutaneous insertion
Modified Allen’s Test
-Hand plated 30º-60º dorsiflexion; with the aid of a roll of gauze and armband.
-Not to hyperabduct the thumb (obliterate the pulse).
Volar aspect of the wrist is steriled
Approximately 0,5 ml of lidocaine is infiltrated (through 25-gauge needle)
20-gauge; 30º-60º angle entry to skin approximately 2-3 inches proximal to the distal wrist crease

20-gauge; 30º-60º angle entry to skin approximately 2-3 inches proximal to the distal wrist crease
Needle & cannulation advanced until blood return is noted (signifying intrarterial placement of the tip of the needle)
A small amount of further advancement for the cannula to enter the artery as well
With this accomplished, needle and cannula are brought flat to the skin and the cannula advanced to its hub with a firm, steady rotary action.
Correct positioning is confirmed by pulsatile blood return on removal of the needle
The catheter can then be advanced into the arterial lumen

Brachial artery cannulation
Infrequently performed
The lack of effective collateral circulationExperience in the
use of brachial artery catheters
Have reported complication rates no higher than with other routes
Doppler studies

Fig: Cannulation of the radial artery. Fig: Cannulation of the radial artery. A. A towel is placed behind the wrist, and the hand is A. A towel is placed behind the wrist, and the hand is immobilized with tape. immobilized with tape. The radial artery is fixated with a 20-gauge angiocath The radial artery is fixated with a 20-gauge angiocath connected to a 5-ml connected to a 5-ml syringe (optional). syringe (optional). B. The angiocath is withdrawn until pulsatile blood return B. The angiocath is withdrawn until pulsatile blood return is noted. is noted. C. The trocar is withdrawn as the Teflon catheter is C. The trocar is withdrawn as the Teflon catheter is simultaneously advancedsimultaneously advanced..

Femoral Femoral Artery Artery
CannulationCannulationFemoral artery catheters are gaining wider clinical use
The femoral artery is large and often palpable when other sites are not
The technique of cannulation is easy to learn

Fig. Anatomy of the femoral artery and adjacent structures. The artery is cannulated below the inguinal ligament.

Complications of Arterial CannulationArterial cannulation
Relatively safe
Estimate of total complication rate range 15% - 40% For infectious and
noninfectious complications have been identified

Complications Associated with Arterial Complications Associated with Arterial CannulationCannulationSiteSite ComplicationComplicationAll siteAll site Pain and swellingPain and swelling
ThrombosisThrombosisAsymptomaticAsymptomaticSymptomaticSymptomatic
EmbolizationEmbolizationHematomaHematomaHemorrhageHemorrhageLimb ischemiaLimb ischemiaCatheter-related infectionCatheter-related infection
LocalLocalSystemicSystemic
Diagnostic blood lossDiagnostic blood lossPseudoaneurysmPseudoaneurysmHeparin-associated thrombocytopeniaHeparin-associated thrombocytopenia
Radial arteryRadial artery Cerebral embolizationCerebral embolizationPeripheral neuropathyPeripheral neuropathy
Femoral arteryFemoral artery Retroperitoneal hemorrhageRetroperitoneal hemorrhageBowel perforationBowel perforationArteriovenous fistulaArteriovenous fistula
Axillary Axillary arteryartery
Cerebral embolizationCerebral embolizationBrachial plexopathyBrachial plexopathy
Brachial Brachial arteryartery
Median nerve damageMedian nerve damageCerebral embolizationCerebral embolization

Factor Predisposing to Complications with Arterial Factor Predisposing to Complications with Arterial CannulationCannulationLarge tapered cannulas Large tapered cannulas (> 20 gauge except at the large artery sites)(> 20 gauge except at the large artery sites)
HypotensionHypotensionCoagulopathyCoagulopathyLow cardiac outputLow cardiac outputMultiple puncture attemptsMultiple puncture attemptsUse of vasopressorsUse of vasopressorsAltherosclerosisAltherosclerosisHypercoagulable stateHypercoagulable statePlacement by surgical cutdownPlacement by surgical cutdownSite inflammationSite inflammationIntermittent flushing systemIntermittent flushing systemBacteremia Bacteremia

Recommendations
Most centers have more experience with radial artery cannulation, but femoral artery catheters are reliable and have a comparable incidence of complication

Thank you




















