
Inefficient Cytotoxic T Lymphocyte–Mediated Killing of HIV-1–Infected Cells In Vivo
Upload
independentCategory
view
0download
0
Acce
pted M
anus
cript
1
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected].
Incidence and Risk Factors for Invasive Pneumococcal Disease in HIV-infected and non-HIV infected Individuals Before and After the Introduction of Combination Antiretroviral Therapy: Persisting High Risk among HIV-infected Injecting Drug Users Zitta Barrella Harboe1,2, Mette Vang Larsen3, Steen Ladelund3, Gitte Kronborg3,4, Helle Bossen Konradsen2, Jan Gerstoft1, Carsten Schade Larsen5, Court Pedersen6, Gitte Pedersen7, Niels Obel1,4, Thomas Benfield3,4 1Department of Infectious Diseases, Righospitalet 2Department of Microbiology & Infection control, Meningtis and Respiratory Tract Infections, Statens Serum Institut 3Department of Infectious Diseases and Clinical Research Center, Copenhagen University Hospital, Hvidovre 4Faculty of Health and Medical Sciences, University of Copenhagen 5Department of Infectious Diseases, Aarhus University Hospital 6Department of Infectious Diseases, Odense University Hospital 7Department of Infectious Diseases, Aalborg University Hospital Corresponding Author: Zitta Barrella Harboe, M.D, Ph.D. Meningtis and Respiratory Tract Infections, Department of Microbiology & Infection control, Statens Serum Institut, Artillerivej 5, DK-2300 S Copehangen, Denmark, Tel: +45- 3268 3268, Email: [email protected] Summary HIV-infected adults have a substantially high risk of IPD compared to those without HIV-infection. The risk was reduced among HIV-infected individuals who were on antiretroviral treatment and who had favorable markers of immunosuppression, but not for HIV-infected IDUs.
Clinical Infectious Diseases Advance Access published July 17, 2014 by guest on M
ay 29, 2016http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
2
ABSTRACT Background: Invasive pneumococcal disease (IPD) is an important cause of morbidity among HIV-infected individuals. We described incidence and risk factors for IPD in HIV-infected and uninfected individuals. Methods: Nationwide population-based cohort study of HIV-infected adults treated at all Danish HIV-treatment centers during 1995-2012. Nineteen population-matched controls per HIV-infected individual were retrieved. The risk of IPD (RR, [95% CI]) was assessed using Poisson regression. Results: The incidence of IPD was 304.7 cases/100,000 PYFU in HIV-infected and 12.8/100,000 PYFU in HIV-uninfected individuals. After adjusting for confounders, HIV-infection (RR 24.4 [23.7-25.1]), male sex (RR 1.20 [1.16-1.24]), increasing age (per year) (RR 1.03 [1.03-1.04]) and calendar period (pre-cART [RR 2.80 [2.70-2.91] compared to late cART) were significantly associated with an increased risk of IPD. Among HIV-infected individuals, male sex (RR 1.57 [1.49-1.66]), smoking (RR 1.34 [1.26-1.42]), and intravenous drug use (RR 2.51 [2.26-2.67]) were associated with an increased risk of IPD. Detectable viral loads (RR 1.88 [1.79-1.98]) and a relative fall in CD4 T-cell counts were also associated with an increased risk (≥500 to 350-<500 CD4 T-cells/µl RR 1.29 [1.21-1.37], and <100 cells/µl RR 7.4 [6.87-8.02]). The risk of IPD declined over time though this was not the case for IDUs where the risk remained unchanged. Conclusions: The incidence of IPD in HIV-infected individuals remained significantly higher than the incidence observed in non-HIV-infected, in spite of the widespread use of cART. IDUs have a persisting high risk of IPD. IDU, smoking, the receipt of cART are suitable targets for preventive measures in the future.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
3
INTRODUCTION Streptococcus pneumoniae is an important cause of severe bacterial disease in HIV and HIV-
uninfected individuals [1-4]. Incidence rates of invasive pneumococcal disease (IPD) have been
reported to be up to 100 times higher among HIV-infected patients compared to the background
population, and recurrences are common[5-8].
The widespread use of combination antiretroviral therapy (cART) during the last decades has
changed the epidemiology of IPD in HIV-infected patients. Several studies have reported a
decreased incidence of IPD after the implementation of cART that is presumed to be related to
immune reconstitution [7, 9-11]. We have previously shown that the risk of pneumonia in HIV-
infected individuals decreased significantly after the introduction of cART [12] but that the overall
incidence of pneumonia remained significantly higher than in a HIV-uninfected matched
population. In the US, the incidence of IPD in HIV-infected patients continued to be 35-fold higher
than in the general population after the introduction of cART [11]. Other studies have indicated that
the incidence of IPD has remained quite unchanged after the introduction of cART [1, 13, 14].
Clinical presentation, risk factors and outcomes after IPD differ between HIV-infected and HIV-
uninfected individuals. Ethnicity, income level, injecting drug use (IDU), alcohol abuse, smoking,
prior hospitalization, comorbidity, hepatitis C co-infection, low CD4 T-cell counts, and high HIV-
RNA viral load (VL) have all been associated with an increased risk of IPD [1, 7, 10, 15], while the
use of cART and a conjugate pneumococcal vaccine have been associated with protection [2, 10,
15, 16]. In particular, IDUs are at higher risk of recurrent bacterial infections, including pneumonia
[17, 18]. Several of these factors have also been associated with higher risk of IPD in the general
population [10, 19]. A large, multicenter, observational study on risk factors and outcomes after
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
4
pneumococcal pneumonia in HIV-infected and HIV-uninfected patients found an increased 14-days
mortality in HIV-infected patients after adjustment for age and severity of disease [4]. Another
study indicated that HIV-infected patients without comorbidities have a lower mortality than HIV-
uninfected patients with higher levels of comorbidity [20].
In Denmark, the incidence of IPD had steadily increased in the general population since the late
1980s, mainly due to an increment in the number of cases diagnosed with pneumococcal bacteremia
[21]. More recently, the epidemiology of IPD has dramatically changed after the introduction of
pneumococcal conjugate vaccination in 2007 in the national childhood immunization program [22].
The total incidence of IPD has declined in approximately 20%, mainly due to a 70% reduction in
IPD in children younger than 2 years, but also a 20% reduction in adults older than 65 years was
seen [23]. It is not known whether these changes similarly have affected HIV-infected individuals
since the incidence of IPD has not yet been assessed nor has the effect on the risk of IPD after the
widespread implementation of cART.
The aim of this study was to examine changes in the incidence of IPD in a nationwide cohort of
HIV-infected individuals after the implementation of cART in Denmark, and compare these with
the incidence of IPD observed in a population of matched controls. We also assessed risk factors
associated with the occurrence of IPD and mortality related to it.
MATERIAL AND METHODS
Study Design and Setting: Nationwide population-based cohort study of HIV-1-infected and HIV-
uninfected individuals in Denmark from January 1, 1995 to December 31, 2010. The estimated
prevalence of HIV among adults in Denmark, a country with a population of 5.4 million, is ~0.09%
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
5
[24]. Treatment for HIV-infection is provided at only eight specialized HIV-centers. The Danish
health care system provides free, tax-supported medical care for all residents, including
antiretroviral treatment for HIV-infection.
The study was based on the linkage of national laboratory surveillance data on IPD, the Danish HIV
Cohort Study (DHCS), and the Danish Civil Registration System (CRS). The linkage between data
sources was done by using the unique ten-digit identification number provided to all residents in
Denmark. We identified 19 control-individuals from the background population per HIV-infected
individual included in DHCS. Population controls were not registered in the DHCS and then
assumed to be HIV-uninfected individuals [25], so an individual known to be HIV-infected could
not be a selected as a control. Controls were matched to the corresponding HIV-infected individual
on the day the patient received the HIV-diagnose according to date of birth and sex. Death was
considered to be related to IPD when the date of death was registered within 30-days after the
clinical sample was obtained from the patient.
The study was approved by the Danish Data Protection Agency (record. nr. 2007-41-0229 and
2007-41-1196).
Data sources and Definitions
National laboratory surveillance data on IPD: The characteristics and completeness of the
national surveillance system for IPD have previously been described and centralized at the National
Neisseria and Streptococcus Reference Laboratory (NSR), Statens Serum Institut (SSI) [26, 27].All
isolates are routinely serotyped as previously described [28, 29].
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
6
We included cases of IPD defined as the isolation of S. pneumoniae from a patients’ cerebrospinal
fluid (CSF), blood or both. When both CSF and blood isolates were received simultaneously, the
case was categorized as meningitis. Recurrences were defined as new episodes of IPD occurring at
least 30-days after the first IPD episode.
In October 2007, the 7-valent pneumococcal conjugate vaccine (PCV7) was introduced in the
Danish childhood immunization program in a 2+1 schedule, but in April 2010, PCV13 gradually
started to replace PCV7 [30, 31].
The Danish HIV Cohort Study (DHCS): The cohort includes all HIV-infected individuals
followed at Danish HIV-treatment centers after January 1, 1995 [24, 32]. HIV-infected individuals
are followed on an outpatient basis at intended intervals of 12-24 weeks. Baseline characteristics
and HIV-related parameters are registered at inclusion in DHCS and updated annually. HIV-related
parameters include, among others, the route of infection, information on cART, development of
opportunistic infections and other AIDS-defining illnesses, and laboratory values including CD4 T-
cell counts and VL.The completeness and reliability of DHCS has been estimated to be as high as
99% for patients diagnosed with HIV-infection, when comparing it to other national hospital
databases [25]. Only HIV-1-infected individuals aged 16 years or older and living in Denmark were
included in the study.
The Danish Civil Registration System (CRS): National register that contains information on birth,
emigration, address, and vital status of all residents in Denmark [33]. Every person in the CRS is
identified by a unique 10-digit personal number, assigned at birth or immigration.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
7
Statistical analysis: Median and inter quartile ranges (IQR) were determined for age, duration of
HIV-infection and CD4 T-cell counts. Intergroup baseline characteristics were compared using the
chi square-test for dichotomous variables and Wilcoxon two-sample test for continuous variables.
Two-tailed p-values <0.05 were considered statistically significant. The person-years at risk were
counted from the day HIV-infected patients entered DHCS (earliest 1 January 1995, or a later date
of HIV-diagnose or immigration, whichever was last) to the date of IPD, emigration, death, or 31
December 2012, which ever was first.
Incidence rates of IPD were calculated as events per 100,000 person-years of follow-up (PYFU). In
order to investigate the effect of the introduction of cART, we studied three clinically relevant
periods that corresponded to the use of increasingly effective antiretroviral therapy: 1995 to 1996
(pre-cART), 1997 to 1999 (early-cART), and 2000 to 2012 (late-cART). Incidence rates were
compared by estimating incidence rate ratios (IRR) with 95% confidence intervals (95% CI).
We used a Poisson regression model to assess risk factors for the occurrence of IPD, both in the
total study population and for HIV-infected individuals only. Estimates are presented as relative risk
(RR) with 95% CIs. To account for changes over time in age, CD4 T-cell counts and different time
period of initiation of cART, we adjusted for these variables as time-dependent covariates by the
method described by Rostgaard [34]. For the total study population, the variables entered into the
model were HIV-infection (yes vs. no), age, and time period (pre-, early- and late-cART). For HIV-
infected individuals the variables entered into the model were: ethnicity (Caucasian vs. non-
Caucasian), sex (female vs. men), age (per-year increment), smoking (current or previous vs.
never), HIV transmission group, (IDUs, heterosexuals, and others vs. men who have sex with men
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
8
(MSM)), and time period (pre-cART, early-cART and late-cART). Latest CD4 T-cell count before
IPD, latest VL measurement (undetectable <500 copies/mL vs. detectable ≥500 copies/mL), and
being on cART before IPD (cART vs. none) were included in the model as a time-dependent
variable.
SAS statistical software version 9.1 (SAS Institute Inc, Cary, NC, USA) was used for analysis.
RESULTS
Baseline Characteristics: 5362 HIV-infected individuals fulfilled inclusion criteria for the study,
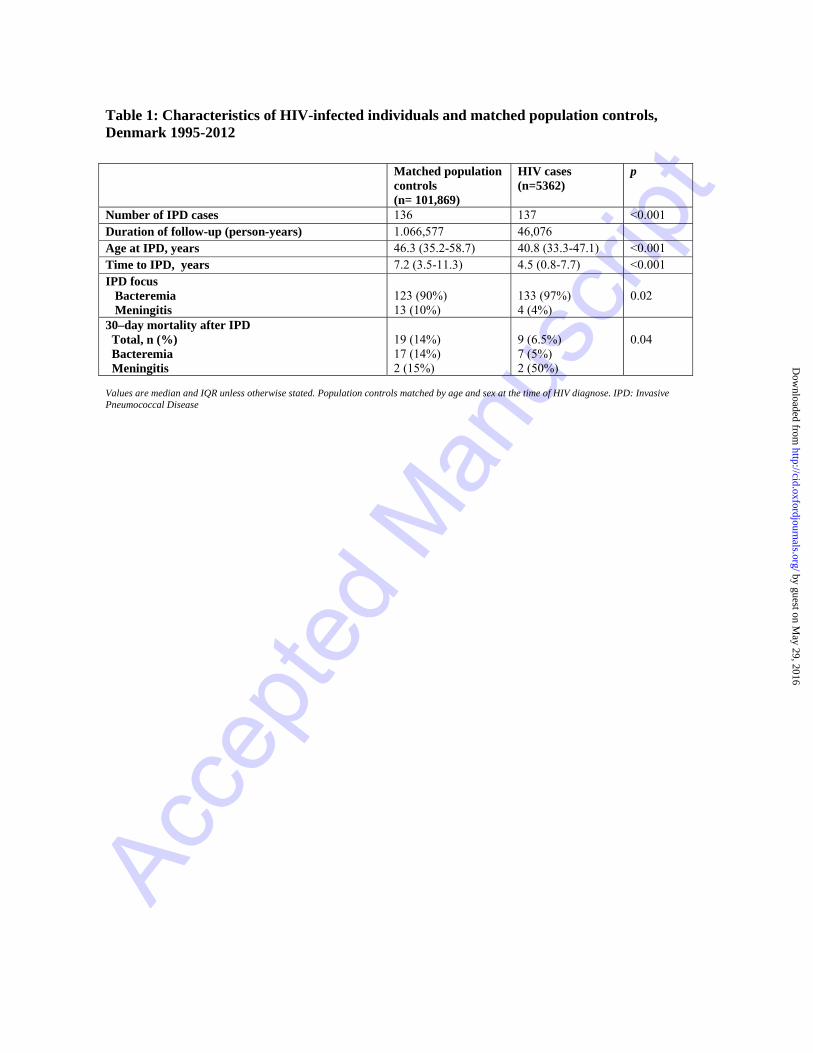
and were individually matched to 101.869 controls. Of these, 137 HIV-infected patients and 136
controls experienced an episode of IPD (Table 1). The mean of CD4 T-cell counts/VL
measurements available per patient was 30 (IQR 13-47) and the mean time between the last
measurement before the event was 4 months (IQR 22 days-3.4 years). HIV-infected individuals
were younger at the time of IPD, and had fewer episodes of meningitis. HIV-infected individuals
with IPD were more often males, IDUs, and had a lower nadir CD4 T-cell count compared to HIV-
infected individuals without IPD (Table 2). Just over half of HIV-infected patients were on cART at
the time of IPD.
Incidence of IPD: The incidence in HIV-infected and uninfected individuals declined significantly
between pre-cART and early/late-cART periods (Table 3).
No IPD recurrences were observed among controls. In contrast, 13 out of 137 HIV-infected patients
had a at new IPD episode (range 1-3). Five of the recurrences were due to a PCV13-serotype, six of
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
9
them were among IDUs, seven patients had CD4 T-cell counts <350 cells/µl and five had detectable
VL.
Factors associated with IPD: After adjusting for confounders (sex, age and calendar period) we
found that HIV-infected individuals had an overall 24-fold increased relative risk of IPD compared
to HIV-uninfected individuals from the background population (Table 4). In addition to this, male
sex, age, and the earliest calendar period were independently associated to an increased risk of IPD
in the total population.
Among HIV-infected individuals, we found that the risk of IPD was independently associated with
sex, smoking, HIV exposure group, treatment, lower CD4 T-cell counts, detectable VL and earlier
calendar periods (Table 4). The risk of IPD fell over time, being 22% higher in the pre-cART period
compared with the years 2000-2012, though this was not the case for IDUs (Figure 1).
Case fatality rate after IPD: The crude mortality proportion in HIV-uninfected individuals was
higher than among the HIV-infected individuals (14 vs. 6.5%, p=0.04). Controls tended to be older
and had more often pneumococcal meningitis than HIV-infected patients (Table 1). In the adjusted
analysis, age at IPD (increase per year: RR 1.05 [1.02–1.09]) was the only independent factor
associated with death, while sex (male RR 5.52 [0.7–43.1]), focus (meningitis vs. bacteremia: RR
2.67 [0.73–9.76]) and HIV-infection per se (RR 1.01[0.38–2.63]) did not reach statistical
significance.
Serotype distribution of pneumococcal isolates causing IPD: The serotype coverage of
pneumococcal conjugates vaccines differed slightly for HIV-infected and uninfected individuals.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
10
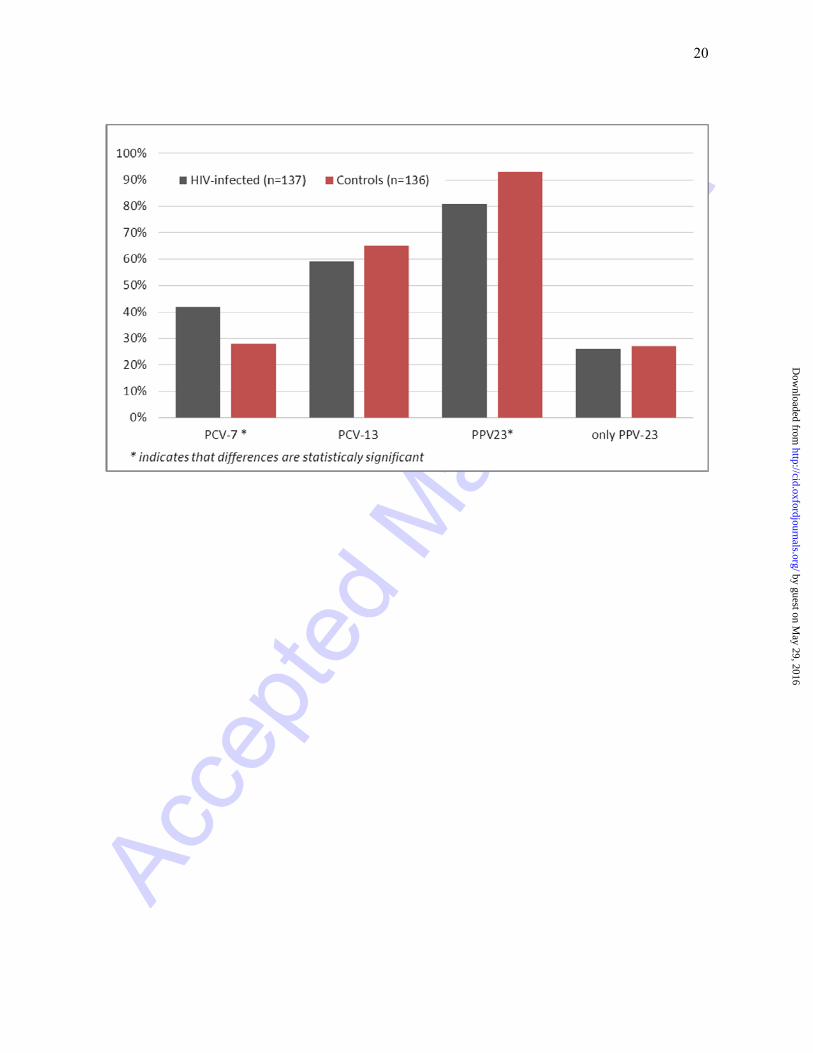
The overall coverage was ~30% for PCV7, 60% for PCV13, and 80% for PPV23 (Figure 2). The
higher serotype coverage of PCV7 in HIV-infected individuals was statistically significant
(p=0.02), and due to a higher prevalence of paediatric pneumococcal serotypes in this population.
DISCUSSION
In this nationwide population-based cohort study covering an 18-year period, we found that the
excess risk of IPD among HIV-infected individuals remained high compared to the risk of IPD
among HIV-uninfected individuals. Although the risk of IPD declined after the introduction of
cART, HIV-infection was associated with a 20-fold higher risk of IPD in the latest decade.
Remarkably, the risk of IPD in HIV-infected IDUs was unchanged over time and 300-fold higher
than in the background population.
In our cohort, the incidence of IPD was similar to that described in other studies on HIV-infected
populations [2, 7, 11, 13]. In the US, the availability of cART has significantly reduced the burden
of IPD in AIDS patients by approximately 50%, but the remaining risk of IPD was still ~35-fold
higher than in the general population [11]. Several factors, including secular trends of
pneumococcal disease; changes in blood culturing methods or clinical assessment protocols of HIV-
patients [13]; and changes in host related risk factors, such as an increasing proportion of HIV-
patients with comorbidities and IDUs [1, 13, 20] can at least partially explain this finding. A
limited effect of cART in reestablishing efficient antibody responses and preventing pneumococcal
disease has also been suggested [13, 35, 36].
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
11
HIV-infection is an important risk factor for IPD in our and other study populations [5, 37], and
also increasing age and being a male were identified as factors independently associated to IPD [19,
38]. Among HIV-infected patients, the risk of IPD was additionally associated to IDU, smoking,
lower CD4 T-cell counts and higher VL, in agreement with findings from other studies [1, 10, 15,
39]. The receipt of cART at the individual level was protective. The association of IDU and
smoking was not possible to address in the control population in this study.
We observed a lower mortality among patients with IPD among HIV-infected individuals compared
to the HIV-uninfected population. In our study, HIV-uninfected individuals were older at the time
of IPD and had a relatively higher proportion of pneumococcal meningitis (Table 1), all known risk
factors associated with mortality after IPD [19, 40]. A previous study from the US similarly found
that mortality after IPD in HIV-infected patients was approximately one-fifth of that of the HIV-
uninfected patients [20]. The investigators attributed the lower mortality to a younger age and less
comorbidity among IPD cases in HIV-infected patients. However, due to limitations in our study
design we were not able to verify the effect of comorbidity on mortality after IPD and further
studies are needed in order to clarify this hypothesis. Also, the number of deaths after IPD was
relatively small. HIV-infected individuals in ambulatory care may have earlier access to care by
specialized infectious disease physicians, and, thus, may have received adequate care at an earlier
time point.
The effectiveness of PPV23-vaccination on HIV-infected individuals receiving cART remains
controversial, and research on the impact of conjugate vaccines on IPD in HIV-infected patients is
still needed [3, 13, 35, 41]. A recent study from Malawi, showed that PCV7 was effective in
protecting HIV-infected individuals from recurrent IPD caused by PCV7-serotypes and 6A [16].
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
12
The introduction of general conjugate pneumococcal vaccination in young children in the US has
reduced the incidence of IPD in non-vaccinated persons, including HIV-infected individuals,
through the vaccines’ indirect effect [42]. HIV-infected individuals have higher rates of carriage
and infections caused by the so-called pediatric pneumococcal serotypes (groups 6, 14, 19 and 23)
[2, 43-45]. We found a similar pneumococcal serotype distribution in our study, thus providing
preventive opportunities for using conjugate pneumococcal vaccines. However, we did not take into
account seasonal variations and epidemiological trends of pneumococcal serotypes over the study
period [21]. Studies exploring the immunogenicity of conjugate pneumococcal vaccines in HIV-
infected individuals receiving cART are important, since pneumococcal vaccination is the only
available tool for preventing pneumococcal disease. On the light of our results, IDUs might be an
important target group for pneumococcal immunization, since they had the highest susceptibility to
the disease over time in spite of the availability of treatment.
The present study has certain limitations. It cannot be discarded that the greater absolute disease
incidence and relative lower mortality after IPD in the HIV-infected population could be affected by
referral bias, since febrile HIV-infected individuals are more likely to have taken blood cultures and
in our setting are often seen in infectious disease outpatient clinics. Also, the RR estimates for
HIV-infected individuals might be overestimated, since rates were obtained by comparing
incidences of IPD in HIV-infected individuals vs. those observed in controls, in whom the incidence
of IPD is relatively low compared to the incidence in youngest children and the elderly [21].
However, it is possible that the true incidence of IPD was probably underestimated in both HIV-
infected and non-HIV-infected individuals, since only cases with positive CSF or blood cultures
were included in the study. However, cases of pneumococcal infection of other sterile sites such as
pleural, synovial or peritoneal are not ascertained systematically in Denmark, and to maintain a high
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
13
order of specificity, we included only blood and CSF specimens. We were not able to retrieve
information regarding comorbidity; social factors like crowding, alcoholism, socio economic status
or pneumococcal vaccination status, all factors might influence the incidence of the IPD in the study
population. A sensitivity analysis to address the problem of potential residual confounding such as
comorbidity and the use of immunosuppressive therapy would be of great value in order to further
validate our findings and constitute a field for future analyses.
In conclusion, the incidence of IPD in HIV-infected individuals remained significantly higher than
the incidence observed in HIV-uninfected individuals, in spite of the widespread use of cART in
Denmark. IDUs have a remarkably high risk of IPD that hasn’t declined over time, and remain an
obvious group for targeted immunization because pneumococcal vaccination. Injecting drug use,
smoking and the receipt of cART are suitable targets for preventive measures in the future.
NOTES
ACKNOWLEDGEMENTS The authors thank the staff at the participating clinical departments and the clinical microbiological laboratories for their contribution in collecting data for the DHCS. We also thank all departments of clinical microbiology across the country for submitting invasive pneumococcal isolates to the NSR at the Statens Serum Institut for national surveillance. Centers in The Danish HIV Cohort Study: Departments of Infectious Diseases at Copenhagen University Hospitals, Rigshospitalet (J Gerstoft, N Obel) and Hvidovre (G Kronborg), Odense University Hospital (C Pedersen), Aarhus University Hospitals, Skejby (CS Larsen) and Aalborg (G Pedersen), Herning Hospital (A L Laursen), Helsingør Hospital (L Nielsen) and Kolding Hospital (J Jensen). Author Contributions: TB and ZBH conceived and designed the study. GK, NO, JG, CS, GP, CP, ZBH collected and quality controlled the data. ZBH, MVL and SL analyzed the data. ZBH, MVL, TB, GK, NO interpreted the results of the study. ZBH wrote the first draft of the paper. ZBH, MVL, TB, NO, GK, CP contributed to the writing of the paper. ZBH had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
14
Financial support: This study was supported by Statens Serum Institut, since data on Invasive Pneumococcal Disease were collected routinely with surveillance purposes through funding allocated to national surveillance. The funding entity did not have any influence in the study design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, writing of the paper; approval or decision to submit it for publication. The contents of the article are solely the responsibility of the authors and do not necessarily represent the official views of Statens Serum Institut. Potential conflicts of interest: ZBH has received travel grants and consultant fees from Pfeizer and GSK. TB reports receiving travel grants, research grants, honoraria, and consultancy fees from Bristol-Myers-Squibb, Gilead, GlaxoSmithKline, and Jannsen Pharmaceuticals. HBK as received consultant fees from both Pfeizer and GSK and research grants from Pfeizer NO has received research funding from Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, GlaxoSmithKline, Abbott, Boehringer Ingelheim, Janssen-Cilag and Swedish Orphan. JG reports receiving travel grants, research grants, honoraria, and consultancy fees from Bristol-Myers-Squibb, Gilead, ViiV, Abbvie, MSD, Medivir and Jannsen Pharmaceuticals. All other authors no conflicts of interest. Reference List (1) Barry PM, Zetola N, Keruly JC, Moore RD, Gebo KA, Lucas GM. Invasive pneumococcal
disease in a cohort of HIV-infected adults: incidence and risk factors, 1990-2003. AIDS 2006 Feb 14; 20(3):437-44.
(2) Dworkin MS, Ward JW, Hanson DL, Jones JL, Kaplan JE. Pneumococcal disease among human immunodeficiency virus-infected persons: incidence, risk factors, and impact of vaccination. Clin Infect Dis 2001 Mar 1; 32(5):794-800.
(3) Klugman KP, Madhi SA, Feldman C. HIV and pneumococcal disease. Curr Opin Infect Dis 2007 Feb; 20(1):11-5.
(4) Feldman C, Klugman KP, Yu VL, et al. Bacteraemic pneumococcal pneumonia: impact of HIV on clinical presentation and outcome. J Infect 2007 Aug; 55(2):125-35.
(5) Redd SC, Rutherford GW, III, Sande MA, et al. The role of human immunodeficiency virus infection in pneumococcal bacteremia in San Francisco residents. J Infect Dis 1990 Nov; 162(5):1012-7.
(6) Schuchat A, Broome CV, Hightower A, Costa SJ, Parkin W. Use of surveillance for invasive pneumococcal disease to estimate the size of the immunosuppressed HIV-infected population. JAMA 1991 Jun 26; 265(24):3275-9.
(7) Nuorti JP, Butler JC, Gelling L, Kool JL, Reingold AL, Vugia DJ. Epidemiologic relation between HIV and invasive pneumococcal disease in San Francisco County, California. Ann Intern Med 2000 Feb 1; 132(3):182-90.
(8) Ortqvist A, Hedlund J, Kalin M. Streptococcus pneumoniae: Epidemiology, Risk Factors, and Clinical Features. Semin Respir Crit Care Med 2005 Dec; 26(6):563-74.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
15
(9) Sullivan JH, Moore RD, Keruly JC, Chaisson RE. Effect of antiretroviral therapy on the incidence of bacterial pneumonia in patients with advanced HIV infection. Am J Respir Crit Care Med 2000 Jul; 162(1):64-7.
(10) Grau I, Pallares R, Tubau F, et al. Epidemiologic changes in bacteremic pneumococcal disease in patients with human immunodeficiency virus in the era of highly active antiretroviral therapy. Arch Intern Med 2005 Jul 11; 165(13):1533-40.
(11) Heffernan RT, Barrett NL, Gallagher KM, et al. Declining Incidence of Invasive Streptococcus pneumoniae Infections among Persons with AIDS in an Era of Highly Active Antiretroviral Therapy, 1995-2000. J Infect Dis 2005 Jun 15; 191(12):2038-45.
(12) Søgaard OS, Lohse N, Gerstoft J, et al. Hospitalization for pneumonia among individuals with and without HIV infection, 1995-2007: a Danish population-based, nationwide cohort study. Clin Infect Dis 2008 Nov 15; 47(10):1345-53.
(13) Jordano Q, Falco V, Almirante B, et al. Invasive pneumococcal disease in patients infected with HIV: still a threat in the era of highly active antiretroviral therapy. Clin Infect Dis 2004 Jun 1; 38(11):1623-8.
(14) Grau I, Ardanuy C, Linares J, Podzamczer D, Schulze MH, Pallares R. Trends in mortality and antibiotic resistance among HIV-infected patients with invasive pneumococcal disease. HIV Med 2009 May 6; 10(8):488-95.
(15) Gebo KA, Moore RD, Keruly JC, Chaisson RE. Risk factors for pneumococcal disease in human immunodeficiency virus-infected patients. J Infect Dis 1996 Apr; 173(4):857-62.
(16) French N, Gordon SB, Mwalukomo T, et al. A trial of a 7-valent pneumococcal conjugate vaccine in HIV-infected adults. N Engl J Med 2010 Mar 4; 362(9):812-22.
(17) Serraino D, Puro V, Boumis E, et al. Epidemiological aspects of major opportunistic infections of the respiratory tract in persons with AIDS: Europe, 1993-2000. AIDS 2003 Sep 26; 17(14):2109-16.
(18) Larsen MV, Harboe ZB, Ladelund S, et al. Major but differential decline in the incidence of Staphylococcus aureus bacteraemia in HIV-infected individuals from 1995 to 2007: a nationwide cohort study*. HIV Med 2012 Jan; 13(1):45-53.
(19) Harboe ZB, Thomsen RW, Riis A, et al. Pneumococcal serotypes and mortality following invasive pneumococcal disease: a population-based cohort study. PLoS Med 2009 May 26; 6(5):e1000081.
(20) Campo RE, Campo CE, Peter G, et al. Differences in presentation and outcome of invasive pneumococcal disease among patients with and without HIV infection in the pre-HAART era. AIDS Patient Care STDS 2005 Mar; 19(3):141-9.
(21) Harboe ZB, Benfield TL, Valentiner-Branth P, et al. Temporal trends in invasive pneumococcal disease and pneumococcal serotypes over 7 decades. Clin Infect Dis 2010 Feb 1; 50(3):329-37.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
16
(22) Harboe ZB, Valentiner-Branth P, Benfield TL, et al. Early effectiveness of heptavalent conjugate pneumococcal vaccination on invasive pneumococcal disease after the introduction in the Danish Childhood Immunization Programme. Vaccine 2010 Mar 19; 28(14):2642-7.
(23) Invasive pneumococcal disease and PCV coverage 2012 [Invasiv pneumokoksygdom og PCV-tilslutning 2012].Available at http://www.ssi.dk/English/News/EPI-NEWS/2013/No%2019%20-%202013.aspx, last accessed April 8. 2014.
(24) Lohse N, Hansen AB, Jensen-Fangel S, et al. Demographics of HIV-1 infection in Denmark: results from the Danish HIV Cohort Study. Scand J Infect Dis 2005; 37(5):338-43.
(25) Obel N, Reinholdt H, Omland LH, Engsig F, Sorensen HT, Hansen AB. Retrivability in The Danish National Hospital Registry of HIV and hepatitis B and C coinfection diagnoses of patients managed in HIV centers 1995-2004. BMC Med Res Methodol 2008; 8:25.
(26) Pebody RG, Hellenbrand W, D'Ancona F, Ruutu P. Pneumococcal disease surveillance in Europe. Euro Surveill 2006 Sep; 11(9):171-8.
(27) Harboe ZB, Valentiner-Branth P, Benfield TL, et al. Estimated effect of pneumococcal conjugate vaccination on invasive pneumococcal disease and associated mortality, Denmark 2000-2005. Vaccine 2008 Jul 4; 26(29-30):3765-71.
(28) Henrichsen J. Six newly recognized types of Streptococcus pneumoniae. J Clin Microbiol 1995 Oct; 33(10):2759-62.
(29) Sorensen UB. Typing of pneumococci by using 12 pooled antisera. J Clin Microbiol 1993 Aug; 31(8):2097-100.
(30) Changed Pneumococcal Vaccine for Children [Ændret pneumokokvaccine til børn]. EPI-NEWS, No. 15, 2010. Available at http://www.ssi.dk/English/News/EPI-NEWS/2010/No%2015%20-%202010.aspx. 2010.
(31) PCV7 coverage & Invasive Pneumococcal Disease 2011. [PCV7-tilslutning og invasiv pneumokoksygdom 2011]. EPI-NEWS week 21, 2012. Available at http://www.ssi.dk/English/News/EPI-NEWS/2012/No%2021%20-%202012.aspx. Statens Serum Institut. 2012.
(32) Obel N, Engsig FN, Rasmussen LD, Larsen MV, Omland LH, Sorensen HT. Cohort Profile: The Danish HIV Cohort Study. Int J Epidemiol 2008 Sep 17.
(33) Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The Danish Civil Registration System. A cohort of eight million persons. Dan Med Bull 2006 Nov; 53(4):441-9.
(34) Rostgaard K. Methods for stratification of person-time and events - a prerequisite for Poisson regression and SIR estimation. Epidemiol Perspect Innov 2008; 5:7.
(35) Hart M, Steel A, Clark SA, et al. Loss of discrete memory B cell subsets is associated with impaired immunization responses in HIV-1 infection and may be a risk factor for invasive pneumococcal disease. J Immunol 2007 Jun 15; 178(12):8212-20.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
17
(36) Rodriguez-Barradas MC, Alexandraki I, Nazir T, et al. Response of human immunodeficiency virus-infected patients receiving highly active antiretroviral therapy to vaccination with 23-valent pneumococcal polysaccharide vaccine. Clin Infect Dis 2003 Aug 1; 37(3):438-47.
(37) Janoff EN, Breiman RF, Daley CL, Hopewell PC. Pneumococcal disease during HIV infection. Epidemiologic, clinical, and immunologic perspectives. Ann Intern Med 1992 Aug 15; 117(4):314-24.
(38) Alanee SR, McGee L, Jackson D, et al. Association of serotypes of Streptococcus pneumoniae with disease severity and outcome in adults: an international study. Clin Infect Dis 2007 Jul 1; 45(1):46-51.
(39) Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000 Mar 9; 342(10):681-9.
(40) Ortqvist A, Hedlund J, Kalin M. Streptococcus pneumoniae: epidemiology, risk factors, and clinical features. Semin Respir Crit Care Med 2005 Dec; 26(6):563-74.
(41) Nielsen H, Kvinesdal B, Benfield TL, Lundgren JD, Konradsen HB. Rapid loss of specific antibodies after pneumococcal vaccination in patients with human immunodeficiency virus-1 infection. Scand J Infect Dis 1998; 30(6):597-601.
(42) Flannery B, Heffernan RT, Harrison LH, et al. Changes in invasive Pneumococcal disease among HIV-infected adults living in the era of childhood pneumococcal immunization. Ann Intern Med 2006 Jan 3; 144(1):1-9.
(43) Hibbs JR, Douglas JM, Jr., Judson FN, McGill WL, Rietmeijer CA, Janoff EN. Prevalence of human immunodeficiency virus infection, mortality rate, and serogroup distribution among patients with pneumococcal bacteremia at Denver General Hospital, 1984-1994. Clin Infect Dis 1997 Aug; 25(2):195-9.
(44) Feldman C, Glatthaar M, Morar R, et al. Bacteremic pneumococcal pneumonia in HIV-seropositive and HIV-seronegative adults. Chest 1999 Jul; 116(1):107-14.
(45) Feldman C, Anderson R. New insights into pneumococcal disease. Respirology 2009 Mar; 14(2):167-79.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
18
FIGURE LEGENDS
Figure 1: Incidence of Invasive Pneumococcal Disease (IPD) per 100.000 person years of follow-up (PYFU) among HIV-infected patients by transmission groups, Denmark 1995-2012. IDU: injecting drug users, MSM: men who have sex with men. Periods: pre-HAART years 1995-1996, early HAART years 1997-1999, late-HAART years 2000-2012. Figure 2: Serotype distribution of pneumococcal isolates obtained from patients with invasive pneumococcal disease according to their HIV-status. Bars indicate the serotype coverage of three currently available pneumococcal vaccines. PCV-7: 7-valent pneumococcal conjugate vaccine (including serotypes 4, 6B, 9V, 14, 18C, 19F, 23F), PCV-13: 13-valent pneumococcal conjugate vaccine (including PCV7 serotypes plus serotypes 1, 3, 5, 6A, 19A), PPV-23: pneumococcal polysaccharide vaccine (including PCV13 serotypes but not 6A, plus serotypes 2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F, 33F), only-PPV23 serotypes: non PCV13 serotypes included in PPV23. *Indicates that differences among HIV-infected and non-infected are statistically significant.
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
19
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
20
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Acce
pted M
anus
cript
Table 1: Characteristics of HIV-infected individuals and matched population controls, Denmark 1995-2012
Values are median and IQR unless otherwise stated. Population controls matched by age and sex at the time of HIV diagnose. IPD: Invasive Pneumococcal Disease
Matched population controls (n= 101,869)
HIV cases (n=5362)
p
Number of IPD cases 136 137 <0.001 Duration of follow-up (person-years) 1.066,577 46,076 Age at IPD, years 46.3 (35.2-58.7) 40.8 (33.3-47.1) <0.001 Time to IPD, years 7.2 (3.5-11.3) 4.5 (0.8-7.7) <0.001 IPD focus Bacteremia Meningitis
123 (90%) 13 (10%)
133 (97%) 4 (4%)
0.02
30–day mortality after IPD Total, n (%) Bacteremia Meningitis
19 (14%) 17 (14%) 2 (15%)
9 (6.5%) 7 (5%) 2 (50%)
0.04
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
Table 2: Characteristics in HIV-infected individuals (n=5,362) with and without invasive pneumococcal disease (IPD) per December 31, 2012
Values are median and IQR unless otherwise stated. P are two tailed p-values from Fisher’s exact test. cART: combination antiretroviral therapy; MSM: Men who have sex with men; IDU: intravenous drug use; Other: blood transfusion, perinatal transmission, and unknown. MSM and individuals included in other HIV-exposure group who were active IDUs were considered as IDUs for the statistical analysis.
IPD (N=137) NON-IPD (N=5,225) p
Duration of follow-up (person-years) 1309 44,767 Age at HIV diagnosis, years 37.6 (30.0–43.4) 38.1 (30.5–44.5) 0.22 Male 93 (68%) 3,978 (76%) 0.03 Ethnicity Caucasian
109 (79%)
4137 (79%)
1.00
HIV-exposure group * Heterosexual MSM IDU Other Missing
47 (34%) 48 (35%) 36 (26%) 6 (5%) 0
1,912 (36%) 2,405 (46%) 533 (10%) 352 (7%) 23 (0.4%)
0.65 0.01 <0.001 0.38
Smoking status Current or ever smoker Never Missing
72 (52%) 18 (13%) 47 (20%)
2755 (52%) 1085 (21%) 1385 (26%)
0.1
cART at time of IPD 70 (51%) Median baseline CD4 T cell count, cells/µl 303 (IQR 87–450) 338 (120–484) 0.05 Median nadir CD4 T cell count, cells/µl 116 (IQR 20–189) 183 (53–263) <0.001
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
Table 3: Incidence rates of invasive pneumococcal disease among HIV-infected individuals and matched population controls during pre-cART, early-cART and late-cART periods
cART: combination antiretroviral therapy. Periods: pre-cART years 1995-1996, early c-ART years 1997-1999, late-cART years 2000-2012. IPD: invasive pneumococcal disease; PYFU: person-years of follow-up; IR (95% CI): incidence rates with 95% confidence interval estimated per 100.000 PYFU; IRR: Incidence Rate Ratio with 95% confidence interval estimated for the incidence of IPD among HIV-infected vs. controls.
Population controls HIV-infected individuals
Period IPD cases PYFU IR (95% CI) IPD cases PYFU IR (95% CI) IRR (95% CI) p
Pre-cART 13 76,914 16.9 (9.8-29.1) 33 3811 865.6 (615.4-1217.7) 51.2 (26.9-97.3) <0.001
Early-cART 11 145,580 7.5 (4.1-13.6) 16 6439 248.4 (152.2-405.5) 32.8 (15.2-70.8) <0.001
Late-cART 112 835,818 13.4 (11.1-16.1) 88 34,708 253.5 (205.7-312.4) 18.9 (14.3-25.0) <0.001
Total 136 1.058,314 12.8 (10.8-15-2) 137 44,959 304.7 (257.7-360.2) 23.7 (22.9-24.4) <0.001
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
Table 4: Crude and adjusted relative risk for invasive pneumococcal disease in the total study population and among HIV-infected individuals, Denmark 1995–2012 Crude Adjusted*
RR 95% CI P RR 95% CI p
Total study population
HIV-infection No Yes
1.00 23.7
22.9–24.4
<0.001
1.00 24.4
23.7–25.1
<0.001
Sex Female Male
1.00 1.00
0.76–1.33
0.96
1.00 1.20
1.16–1.24
<0.001
Age (per-year increment)
1.02 1.00-1.03 <0.001 1.03 1.03-1.04 <0.001
Time period Late-cART Early-cART Pre-cART
1.00 0.77 2.48
0.51–1.15 1.80–3.41
0.20 <0.001
1.00 0.87 2.80
0.83–0.91 2.70–2.91
<0.001 <0.001
HIV-infected individuals
Sex Female Male
1.00 1.39
1.33–1.46
<0.001
1.00 1.57
1.49–1.66
<0.001
Age (per-year increment)
0.98 0.98–0.99 <0.001 1.00 0.99–1.00 0.33
Ethnicity Non-caucasian Caucasian
1.00 0.96
0.91–0.1.02
0.22
1.00 0.96
0.91–1.03
0.95
Smoker No Yes
1.00 1.45
0.86-2.43
0.14
1.00 1.34
1.26–1.42
<0.001
HIV exposure group MSM IDU Heterosexual Other
1.00 3.48 1.00 1.21
3.29–3.68 0.89–1.12 1.15-1.28
<0.001 0.94 <0.001
1.00 2.51 0.68 0.80
2.26–2.67 0.61–0.76 0.75–0.85
<0.001 <0.001 <0.001
cART* No Yes
1.00 0.41
0.39–0.43
<0.001
1.00 0.81
0.77–0.86
<0.001
Viral Load* Non-detectable (< 500 copies/mL ) Detectable
1.00 3.22
3.07–3.38
<0.001
1.00 1.88
1.79–1.98
<0.001
CD4 T cell count* ≥ 500 cells/µl 350-499 cells/µl 100-349 cells/µl <100 cells/µl
1.00 1.64 3.52 11.8
1.52–1.77 3.30–3.75 11.0–12.7
<0.001 <0.001 <0.001
1.00 1.29 2.81 7.42
1.21–1.37 2.66–2.97 6.87–8.02
<0.001 <0.001 <0.001
Period Late-cART Early-cART Pre-cART
1.00 0.77 2.48
0.76–0.81 2.38–2.58
<0.001 <0.001
1.00 0.68 1.22
0.64–0.72 1.09–1.37
<0.001 <0.001
Multivariate model included all variables in the table. MSM. Men who sex with men; IDU: intravenous drug use. cART: combination antiretroviral therapy. Periods: pre-cART years 1995-1995, early c-ART years 1997-1999, late-cART years 2000-2012. HIV-RNA was only measurable since 1997 and onwards, the adjusted pre-cART estimate is then not adjusted for HIV-RNA in this table. *: time-updated variables
by guest on May 29, 2016
http://cid.oxfordjournals.org/D
ownloaded from
Copyright © 2022 FDOKUMEN




















