Gender Differences in Lymphocyte Populations, Plasma HIV RNA Levels, and Disease Progression in a...
12
DOI: 10.1542/peds.2005-0294 2006;118;146 Pediatrics Katherine Luzuriaga, Mary Paul and Clemente Diaz Marc Foca, Jack Moye, Clara Chu, Yvonne Matthews, Ken Rich, Ed Handelsman, Disease Progression in a Cohort of Children Born to Women Infected With HIV Gender Differences in Lymphocyte Populations, Plasma HIV RNA Levels, and http://pediatrics.aappublications.org/content/118/1/146.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2006 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at Iraq:AAP Sponsored on June 3, 2013 pediatrics.aappublications.org Downloaded from
Transcript of Gender Differences in Lymphocyte Populations, Plasma HIV RNA Levels, and Disease Progression in a...

DOI: 10.1542/peds.2005-0294 2006;118;146Pediatrics
Katherine Luzuriaga, Mary Paul and Clemente DiazMarc Foca, Jack Moye, Clara Chu, Yvonne Matthews, Ken Rich, Ed Handelsman,
Disease Progression in a Cohort of Children Born to Women Infected With HIVGender Differences in Lymphocyte Populations, Plasma HIV RNA Levels, and
http://pediatrics.aappublications.org/content/118/1/146.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2006 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

ARTICLE
Gender Differences in Lymphocyte Populations,Plasma HIV RNA Levels, and Disease Progression in aCohort of Children Born to Women InfectedWith HIVMarc Foca, MDa, Jack Moye, MDb, Clara Chu, PhDc, Yvonne Matthewsc, Ken Rich, MDd, Ed Handelsman, MDe, Katherine Luzuriaga, MDf,
Mary Paul, MDg, Clemente Diaz, MDh, Women and Infants Transmission Study
aDepartment of Pediatrics, Columbia University, New York, New York; bNational Institute of Child Health and Human Development, Bethesda, Maryland; cClinical Trialsand Surveys Corp, Baltimore, Maryland; dDepartment of Pediatrics, University of Illinois, Chicago, Illinois; eDepartment of Pediatrics, State University of New York,Brooklyn, New York; fDepartment of Pediatrics, University of Massachusetts, Worcester, Massachusetts; gDepartment of Pediatrics, Baylor University College of Medicine,Houston, Texas; hDepartment of Pediatrics, University of Puerto Rico, San Juan, Puerto Rico
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.We sought to document gender differences in lymphocyte subsets andplasma RNA levels in a pediatric cohort with presumed minimal hormonal differ-ences (on the basis of age).
METHODS.Blood samples from antiretroviral therapy-treated, HIV-infected children(n � 158) and HIV-uninfected children (n � 1801) who were enrolled in theWomen and Infants Transmission Study were analyzed at specified study intervalswith consensus protocols, and various parameters were compared.
RESULTS.Antiretroviral therapy-treated, HIV-infected female children had, on aver-age, 0.38 log10 copies per mL lower plasma RNA levels than did their malecounterparts, but lymphocyte differences were not noted in this cohort. Despitetheir higher plasma RNA level, a greater proportion of male children survivedthrough 8 years of age. There were no gender differences with respect to the ageof diagnosis of HIV, time to antiretroviral therapy after diagnosis of HIV, or type ofantiretroviral therapy. Lymphocyte differences were noted for uninfected chil-dren.
CONCLUSIONS. Plasma RNA levels differed among antiretroviral therapy-treated, HIV-infected children according to gender, in a manner similar to that noted inprevious pediatric and adult studies. Lymphocyte subsets varied according togender in a cohort of HIV-exposed but uninfected children. Most importantly,overall mortality rates for this cohort differed according to gender.
www.pediatrics.org/cgi/doi/10.1542/peds.2005-0294
doi:10.1542/peds.2005-0294
This work was presented at the 8thConference on Retroviruses andOpportunistic Infections; February 4–8,2001; Chicago, IL.
KeyWordsHIV, gender
AbbreviationsWITS—Women and Infants TransmissionStudyECS—European Collaborative StudyCDC—Centers for Disease Control andPreventionART—antiretroviral therapyREACH—Reaching for Excellence inAdolescent Care and Health
Accepted for publication Jan 19, 2006
Address correspondence to Marc Foca, MD,Department of Pediatrics, Division ofInfectious Diseases, Morgan Stanley Children’sHospital of New York Presbyterian, 622 W.168th St, VC-4 East, Room 449H, New York, NY10032. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2006 by theAmerican Academy of Pediatrics
146 FOCA et al at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

GENDER DIFFERENCES IN lymphocyte populations andplasma HIV RNA copy number have been exam-
ined in multiple large cohort studies involving adoles-cents and adults. In general, HIV-infected women havegreater CD4� cell counts (�70–100 cells per �L) andpercentages (�5%)1,2 and lower HIV RNA values (0.17–0.78 log units),3,4 compared with HIV-infected men, inthe first 4 to 5 years of infection. Those analyses werelimited largely to treatment-naive or minimally treatedpatients, and rates of disease progression were not con-sistently different.5,6 Other studies examined gender dif-ferences in response to potent combination therapies,with similarly mixed results.7–9 In addition, althoughCD4� cell counts were found to be higher in cohorts ofHIV-negative women, compared with HIV-negativemen,10 such differences were not noted in a large cross-sectional analysis of healthy children.11
One hypothesis for the observed differences in HIVRNA copy number and lymphocyte subsets betweenfemale and male patients with HIV infection has beenthe effect of postpubertal sex hormones. The currentstudy was undertaken with the supposition that thehormonal environment of infants and of prepubertalchildren varies less than that of adults. We examinedgender differences with respect to lymphocyte subsetsand with respect to HIV RNA copy number and diseaseprogression (for patients with perinatally acquired HIV)among children born to HIV-infected women in theWomen and Infants Transmission Study (WITS) cohort.
METHODS
Patient Group and Study DesignThe population studied included all singleton and first-born twin infants of HIV-infected pregnant women re-cruited into the WITS between 1989 and September2003. These mother-infant pairs were recruited andstudied at 6 clinical sites in Boston, New York City (2sites), Chicago, Houston, and Puerto Rico. Infant infec-tion status was determined with HIV DNA polymerasechain reaction assays and/or HIV cultures. Infants with�2 positive determinations from samples drawn on dif-ferent dates were considered infected. One infant wascategorized as HIV infected through consultation with aclinical working group set up to review clinical andlaboratory information for children for whom inade-quate laboratory diagnostic data had been obtained. Thisinfant was not included in the mortality analysis, be-cause the exact date when this infant became HIV pos-itive was not available. Infants with �2 negative deter-minations (at �1 month of age and �1 at �4 months ofage) and no positive determinations were considereduninfected.
Clinical and laboratory assessments were performedat birth, at 1, 2, 4, 6, 12, 18, and 24 months of age, andthen yearly for uninfected children and every 6 months
for HIV-infected children. These analyses were restrictedto data from birth through 8 years of age, to minimizethe potential impact of pubertal change on outcomes.Flow cytometry was performed by laboratories with ap-proved performance in the National Institute of Allergyand Infectious Diseases, Division of AIDS, immunologyquality assurance program, with AIDS Clinical TrialsGroup consensus protocols for 2- and 3-color flow cy-tometry.12 HIV RNA quantification was performed withthe Roche Amplicor HIV-1 monitor test, in laboratorieswith approved performance in the National Institute ofAllergy and Infectious Diseases, Division of AIDS, virol-ogy quality assurance program, with the AIDS ClinicalTrials Group consensus protocol.13 These tests were per-formed for HIV-infected infants at every visit. Diseaseprogression was measured with clinical and immuno-logic criteria set forth in the Centers for Disease Controland Prevention (CDC) classification of disease for HIV-infected children.14
Statistical AnalysesAnalyses of baseline characteristics were performed witheither a �2 test for categorical variables or an F test forcontinuous variables, to determine whether there weregender differences at baseline. These analyses were per-formed separately for 3 subgroups, namely, HIV-infectedchildren who were treated with antiretroviral therapy(ART), HIV-infected but untreated children, and HIV-exposed but uninfected children.
Longitudinal data analyses were performed for thefollowing measures: total lymphocyte counts, white bloodcell counts, absolute and relative counts of lymphocyteswith CD3�CD4�, CD3�CD8�, CD3�CD16�CD56�, andCD19� immunophenotypes, and log10 HIV RNA levelsfor HIV-infected children. The same measures, with theexception of log10 HIV RNA levels, were also analyzedfor HIV-uninfected children. Gender differences wereexamined by fitting a generalized estimating equationsmodel,15 which included terms for gender, age, and gen-der-age interaction, to each of the measures. The pur-pose of including the interaction term was to determinewhether the gender effect changed with age. Becausethe measures were not linear with age, we modeled witha set of dummy variables to account for the nonlinearityof the effect. Modeling the age effect in this mannerallows for changes in the shape of the adjusted meanprofiles with respect to age. Additional covariates in-cluded in the generalized estimating equations modelsfor ART-treated, HIV-infected children were time-de-pendent ART use, birth group (defined according towhen a child was born, ie, on or before February 28,1994, between March 1, 1994, and July 31, 1996, or onor after August 1, 1996), mother’s race, mother’s use ofillicit hard drugs during pregnancy, mother’s use of al-cohol during pregnancy, and preterm birth. Maternalhard drug use was defined as the use of cocaine, meth-
PEDIATRICS Volume 118, Number 1, July 2006 147 at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

adone, heroin, or any illicit injectable drugs. Maternaldrug use was ascertained through self-reports and/orurine toxicologic tests. Preterm birth was defined as �37weeks of gestation. For the HIV-infected but untreatedchildren, gender differences were evaluated after adjust-ment for age, mother’s race, mother’s hard drug useduring pregnancy, maternal alcohol use during preg-nancy, and preterm birth.
The birth group covariate defines the time period inwhich children were born and reflects the level of ARTexposure a child might have acquired in utero. Adjust-ment with this covariate was necessary because of thechanging use of ART in the 3 different time periods. ARTprophylaxis of perinatal transmission was not provenbefore 1994, and only a limited number of women usedART for their own health. From 1994 to the middle of1996, zidovudine monotherapy was used by almost allwomen to prevent perinatal HIV transmission. From themiddle of 1996 onward, zidovudine continued to beused for prevention of perinatal HIV transmission butthe protease inhibitor class of antiretroviral agents be-came available and many pregnant women receivedcombination ART for their own health. Adjustment ac-cording to birth group ensured that comparisons werenot made between the 3 different time periods. Clinical
site was also examined, to confirm that there was nosignificant intersite laboratory effect.
Analysis of disease progression was performed withthe Kaplan-Meier method; the gender difference wasassessed with the log-rank test. A sensitivity analysis toevaluate more thoroughly the gender difference in dis-ease progression was performed with stratified Cox pro-portional-hazards regression analyses. Mortality risk fac-tor analysis was performed with Wilcoxon rank-sumtests.
RESULTS
Demographic Features of HIV-Uninfected SubjectsThe uninfected group consisted of 1801 children, ofwhom 896 were male and 905 were female. Forty-eightpercent of the population was black, 35% Hispanic, 11%white, and 6% other or unknown. Twenty-six percent ofthe children were born before March 1, 1994, 22%between March 1, 1994, and July 31, 1996, and 52% onor after August 1, 1996. The mean number of visits was9 during the study period. There was no difference in thedistribution of any of the baseline variables tested be-tween male and female infants (Table 1).
TABLE 1 Comparison of Demographic Characteristics According to Gender for HIV-Uninfected Childrenin WITS, as of September 30, 2003
Male (N � 896) Female (N � 905) P
N n Proportion, %,or Mean
N n Proportion, %,or Mean
Clinical siteUniversity of Massachusetts 160 17.85 161 17.79Columbia University 114 12.72 97 10.71University of Illinois at Chicago 154 17.18 159 17.56University of Puerto Rico 201 22.43 185 20.44State University of New Yorkat Brooklyn
132 14.73 140 15.46
Baylor University 896 135 15.06 905 163 18.01 .423a
RaceWhite 109 12.16 93 10.27Black 406 45.31 450 49.72Hispanic 324 36.16 307 33.92American Indian 5 0.55 3 0.33Asian 0 0.00 1 0.11Other 30 3.34 32 3.53Unknown 896 22 2.45 905 19 2.09 .454a
Birth groupBefore February 28, 1994 242 27.00 225 24.86March 1, 1994, to July 31, 1996 192 21.42 207 22.87After August 1, 1996 896 462 51.56 905 473 52.26 .530a
Preterm delivery 885 161 18.19 902 139 15.41 .115a
ART at anytime 896 658 73.43 905 681 75.24 .378a
Mother used hard drugs 889 258 29.02 901 257 28.52 .816a
Mother drank alcohol 889 317 35.65 901 338 37.51 .415a
No. of visits 896 9.61 905 9.47 .475b
a �2 test.b F test.
148 FOCA et al at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

Demographic Features of HIV-Infected InfantsThe infected group consisted of 178 children, of whom88 were male and 90 were female. Among the 178HIV-infected children, there were 158 individuals whohad been treated with ART. Of the 158 ART-treated,HIV-infected children, 80 were male and 78 were fe-male. Sixty-six percent experienced a CDC class A event,72% a class B event, and 37% a class C event, and 27%were delivered preterm. There were no statistical differ-ences between male and female subjects for any of thedemographic variables tested (Table 2). For the set ofinfants (n � 20, 11%) who had never been treated withART, no differences between male and female infantswere seen in the parameters described above (data notshown).
Immunologic Parameters for ART-Treated, HIV-InfectedChildrenAfter adjustment for age, ART use, birth group, mother’srace/ethnicity, maternal hard drug use during preg-nancy, maternal alcohol use during pregnancy, and pre-term birth, gender-based differences were not seen withrespect to total lymphocyte count, total white blood cellcount, CD4� cell count and percentage, CD8� cell countand percentage, CD16�CD56� cell count and percent-
age, and CD19� cell percentage. A trend toward lowerCD19� cell counts was demonstrated for female children(� � �146; P � .08) (Table 3). Of the other parameterstested, maternal hard drug use during pregnancyshowed a trend toward children having lower CD4� cellcounts (� � �186; P � .06). The physiologic explanationfor this phenomenon is unclear, but this was reportedpreviously by the WITS.16 Of interest, children whosemothers did not use hard drugs during pregnancy alsohad, on average, greater CD16�CD56� natural killer cellcounts (� � �75; P � .04) and percentages (� � �1.97;P � .03). There were no hard drug effects on the otherparameters analyzed. Maternal alcohol use during preg-nancy had no effect on CD4� cell counts or percentages;however, ART-treated, HIV-infected children whosemothers did not use alcohol during pregnancy had, onaverage, higher absolute CD19� cell counts (� � �172;P � .04). Racial/ethnic differences were also noted, withchildren of black mothers having a lower mean totallymphocyte count (� � �909; P � .01) and a lowermean CD4� cell count (� � �565; P � .002), comparedwith children of white mothers. No differences werenoted in CD4� cell percentage, CD8� cell count or per-centage, CD16�CD56� cell count or percentage, orCD19� cell count or percentage. Differences between
TABLE 2 Comparison of Demographic Characteristics According to Gender for ART-Treated, HIV-Infected Children in WITS, as of September 30, 2003
Male (N � 80) Female (N � 78) P
N n Proportion, %,or Mean
N n Proportion, %,or Mean
Clinical siteUniversity of Massachusetts 17 21.25 20 25.64Columbia University 12 15.00 7 8.97University of Illinois at Chicago 17 21.25 17 21.79University of Puerto Rico 18 22.50 14 17.94State University of New York 12 15.00 14 17.94Baylor University 80 4 5.00 78 6 7.69 .763a
RaceWhite 10 12.50 13 16.66Black 33 41.25 33 42.30Hispanic 28 35.00 24 30.76American Indian 1 1.25 4 5.12Asian 0 0.00 1 1.28Other 4 5.00 2 2.56Unknown 80 4 5.00 78 1 1.28 .429a
Birth groupBefore February 28, 1994 50 62.50 51 65.38March 1, 1994, to July 31, 1996 13 16.25 18 23.07After August 1, 1996 80 17 21.25 78 9 11.53 .196a
Preterm delivery 78 22 28.20 76 20 26.31 .792a
Mother used hard drugs 77 35 45.45 77 38 49.35 .628a
Mother drank alcohol 77 31 40.25 77 35 45.45 .514a
Had class A event 80 52 65.00 78 53 67.94 .694a
Had class B event 80 54 67.50 78 60 76.92 .186a
Had class C event 80 27 33.75 78 31 39.74 .434a
No. of visits 80 19.36 78 18.07 .362b
a �2 test.b F test.
PEDIATRICS Volume 118, Number 1, July 2006 149 at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

TABLE3
MultivariateAna
lysisof
Hem
atolog
icVa
riab
lesforA
RT-Treated
,HIV-In
fected
Child
ren
Covariate
Parameter(P)
Total
Lymphocyte
Count,
Cellsper�
L
WhiteBlood
CellCount,
Cells
�10
�3
per�
L
CD4�
Cell
Count,
Cellsper�
L
CD4�
Cell
Proportion,
%
CD8�
Cell
Count,
Cellsper�
L
CD8�
Cell
Proportion,
%
CD16
�/CD56
�
CellCount,
Cellsper �
L
CD16
�/CD56
�
CellProportion,
%
CD19
�Cell
Count,
Cellsper�
L
CD19
�Cell
Proportion,
%
HIVRN
ALevel,log
10
Copiesperm
L
Femalegender
�175(.41)
�0.18
(.57)
65(.48)
2.28
(.11)
�126(.23)
�1.74
(.20)
�49
(.11)
0.30
(.71)
�146(.08)
�1.16
(.36)
�0.38
(.03)a
Maternalprenatal
harddrug
use
�345(.15)
�0.08
(.83)
�186(.06)
�2.60
(.10)
�54
(.65)
0.54
(.72)
75(.04)a
1.97
(.03)a
�92
(.30)
�0.17
(.90)
0.37
(.03)a
Maternalprenatal
alcoholuse
124(.60)
0.10
(.77)
29(.77)
�1.10
(.47)
�15
(.90)
�1.25
(.41)
�2(.96)
�0.64
(.49)
172(.04)a
1.96
(.14)
�0.20
(.24)
Race/ethnicity
Blackb
�909(.01)a
�0.94
(.07)
�565(.002)a
�2.64
(.28)
�166(.29)
0.32
(.89)
�39
(.37)
0.52
(.69)
�152(.22)
0.65
(.74)
0.003(.99)
Hispanicb
�316(.36)
�0.14
(.77)
�367(.04)a
�3.65
(.14)
63(.65)
2.46
(.26)
25(.58)
�0.04
(.97)
�47
(.69)
�0.92
(.60)
0.04
(.88)
Pretermbirth
541(.01)a
0.73
(.01)a
120(.21)
�0.55
(.75)
318(.001)a
3.46
(.01)a
27(.42)
�1.60
(.13)
200(.02)a
0.15
(.92)
0.02
(.94)
aStatisticallysig
nificant.
bComparedwith
infantso
fwhitemothers.
TABLE4
MultivariateAna
lysisof
Hem
atolog
icVa
riab
lesforH
IV-In
fected
Child
renWho
DidNot
ReceiveART
Covariate
Parameter(P)
Total
Lymph
ocyte
Coun
t,Cells
per�
L
WhiteBlood
CellCo
unt,
Cells
�10
�3
per�
L
CD4�
Cell
Coun
t,Cells
per�
L
CD4�
Cell
Prop
ortio
n,%
CD8�
Cell
Coun
t,Cells
per�
L
CD8�
Cell
Prop
ortio
n,%
CD16
�/CD56
�
CellCo
unt,
Cells
per�
L
CD16
�/CD56
�
CellProp
ortio
n,%
CD19
�Cell
Coun
t,Cells
per�
L
CD19
�Cell
Prop
ortio
n,%
HIVRN
ALevel,log 1
0
Copies
perm
L
Femalegender
508(.36)
�0.73
(.44)
986(�
.0001)a
12.69(.001)a
�337(.26)
�7.04
(.02)a
�49
(.61)
�1.33
(.5)
49(.77)
�1.97
(.35)
0.2(.67)
Maternalprenatal
harddrug
use
�1254
(.01)a
�3.39
(.006)a
�170(.57)
2.95
(.66)
�888(.0004)a
�4.46
(.15)
�551(.002)a
�1.48
(.42)
�135(.56)
2.87
(.44)
�0.41
(.51)
Maternalprenatal
alcoholuse
612(.4)
0.23
(.87)
�343(.12)
�6.57
(.13)
369(.18)
�1.27
(.67)
386(.03)a
0.56
(.75)
472(.007)a
5.44
(.07)
0.41
(.47)
Race/ethnicity
Blackb
�1456
(.02)a
�3.15
(.03)a
�191(.52)
13.39(.04)a
�685(.04)a
1.47
(.74)
�560(.005)a
�3.81
(.39)
�663(.005)a
�7.60
(.12)
0.32
(.64)
Hisp
anicb
1026
(.41)
�0.55
(.80)
629(.27)
8(.37)
439(.44)
6.67
(.27)
�535(.03)a
�8.60
(.11)
268(.49)
�4(.45)
�0.54
(.6)
Pretermbirth
561(.43)
2.6(.02)a
�125(.65)
�5.20
(.32)
570(.13)
4.75
(.19)
369(.0002)a
5.51
(.008)a
�50
(.81)
�4(.11)
�0.23
(.6)
aStatisticallysig
nificant.
bComparedwith
childrenofwhitemothers.
150 FOCA et al at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

children born to white mothers and children born toHispanic mothers showed that children born to Hispanicmothers had a lower mean CD4� cell count (� � �367;P � .04), compared with children born to white moth-ers. Preterm birth did not affect CD4� cell counts orpercentages, but infants who were born at term had ahigher mean total lymphocyte count (� � �541; P �.01), white blood cell count (� � �0.73; P � .01), CD8�
cell count (� � �318; P � .001), CD8� cell percentage(� � �3.46; P � .03), and CD19� cell count (� � �200;P � .02).
Immunologic Parameters for HIV-Infected, Untreated ChildrenGender differences in CD4� cell counts and percentageswere pronounced, with female subjects having, on av-erage, 986 more cells per �L, compared with male sub-jects (P � .0001), and a 12.69-percentage point higherrelative CD4� cell percentage (P � .001) (Table 4). Smallsample size might have lead to greater variation in thisgroup. This observation deserves additional analysis.
Virologic Parameters and Mortality Rates for HIV-Infected,ART-Treated ChildrenAfter adjustment for other covariates, the RNA copynumber for female subjects was, on average, 0.38 log10
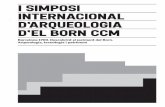
unit lower than that for male subjects (P � .03). Race/ethnicity did not affect these results. Children whosemothers used hard drugs during pregnancy had a highermean log RNA level (� � �0.37; P � .03). Kaplan-Meieranalysis of time until death revealed a significant in-crease (P � .02) in survival time for male children to 8years of age, despite their higher RNA values (Fig 1). Thesurvival difference remained after adjustment for clinicalsite and stratification according to birth group in a Coxproportional-hazards regression analysis. In these anal-
yses, children who survived beyond 8 years after enroll-ment were censored at either their date of death, if theydied, or their last follow-up date, if they were still alive.
Virologic Parameters and Mortality Rates for HIV-Infected,Untreated ChildrenHIV RNA copy numbers did not differ significantly andwere not affected by the other parameters tested. Sur-vival rates also did not differ according to gender, but thepower to detect differences was limited by the small sizeof the group (n � 20).
Additional Factors That Might Affect Mortality RatesTo investigate more thoroughly any potential differencesin survival rates according to gender, we examined sev-eral parameters that might have affected mortality ratesin this cohort. For the 79 male infants and 78 femaleinfants who were diagnosed as having HIV on the basisof laboratory studies and were treated with ART, themedian ages at diagnosis were 32 and 31 days, respec-tively (P � .68). Within this cohort, 109 patients startedART, at a median age of 111 days for male infants and115 days for female infants (P � .47). No differences inthe type of ART used were noted (ie, monotherapy, 48male and 42 female infants; dual therapy, 10 male and 8female infants; combination therapy, 1 male and 0 fe-male infants; P � .55). Overall, there were 58 CDC classC events (27 male and 31 female infants), with nostatistical differences according to gender in the types ofevents (P � .80) (Table 5). There seemed to be trendstoward a greater number of diagnoses of Candida esoph-agitis among female children and encephalopathyamong male children, but the numbers were small. Ofnote, death as a result of Pneumocystis pneumonia infec-tion occurred for 3 of 4 female patients and 2 of 5 male
FIGURE 1Time to death for ART-treated, HIV-infected children, ac-cording to gender.
PEDIATRICS Volume 118, Number 1, July 2006 151 at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

patients. All 9 case patients were born within the 4-yearperiod between February 1990 and February 1994, andthere was no gender difference in the median age atdiagnosis of Pneumocystis pneumonia (138 days for malepatients and 333 days for female patients; P � .30). Thesmall sample size limited the power to detect differencesof statistical significance.
Immunologic Parameters for HIV-Uninfected ChildrenStatistically significant gender effects were more numer-ous in the larger sample of HIV-uninfected children.Female children had, on average, higher total lympho-cyte counts (� � �239; P � .0004), white blood cell counts(� � �0.24; P � .01), CD4� cell counts (� � �238; P �.0001) and percentages (� � �2; P � .0001), andCD16�CD56� cell counts (� � �44; P � .002), comparedwith male children. The mean CD8� cell percentage waslower for female children (� � �1; P � .0001). Of theother parameters tested, maternal drug use affected onlyCD4� cell percentage. In contrast to findings for ART-treated, HIV-infected children, children who were ex-posed to hard drugs during pregnancy but were not HIVinfected tended toward a higher mean CD4� cell count(� � �72; P � .10) and had a higher mean CD4� cellpercentage (� � �0.81; P � .02). There were no differ-ences in any of the outcomes with respect to maternalalcohol use. Compared with children born to whitemothers, children born to black mothers had, on aver-age, significant decreases in total lymphocyte count,white blood cell count, CD4� cell count and percentage,CD8� cell count and percentage, CD16�CD56� cellcount, and CD19� cell count. The mean CD19� cellpercentage was significantly higher for children born toblack mothers. Children born to Hispanic mothers had,on average, significant decreases only in CD4� cell countand percentage (Table 6). Children who were born atterm had, on average, significantly higher white bloodcell count, CD8� cell count, CD8� cell percentage, andCD16�CD56� cell count and lower CD19� cell percent-age, compared with children who were born preterm. TA
BLE6
MultivariateAna
lysisof
Hem
atolog
icVa
riab
lesforH
IV-Exposed
butH
IV-UninfectedCh
ildren
Covariate
Parameter(P)
Total
Lymph
ocyte
Coun
t,Cells
per�
L
WhiteBlood
CellCo
unt,
Cells
�10
�3
per�
L
CD4�
CellCo
unt,
Cells
per�
LCD
4�Cell
Prop
ortio
n,%
CD8�
CellCo
unt,
Cells
per�
LCD
8�Cell
Prop
ortio
n,%
CD16
�/CD56
�
CellCo
unt,
Cells
per�
L
CD16
�/CD56
�
Prop
ortio
n,%
CD19
�CellCo
unt,
Cells
per�
LCD
19�Cell
Prop
ortio
n,%
Femalegender
239(.0004)a
0.24
(.01)a
238(�
.0001)a
2(�
.0001)a
�31
(.12)
�1(�
.0001)a
44(.002)a
0.27
(.13)
VariesW
ithTime
Maternalprenatalharddrug
use
53(.50)
0.02
(.87)
72(.1)
0.81
(.02)a
11(.62)
�0.11
(.67)
�4(.8)
�0.14
(.50)
�11
(.71)
�0.26
(.44)
Maternalprenatalalcoholuse
48(.52)
0.17
(.12)
�5(.90)
�0.34
(.29)
�10
(.65)
�0.07
(.78)
9(.57)
0.14
(.47)
�19
(.49)
�0.20
(.52)
Race/ethnicity
Blackb
�799(�
.0001)a
�1.35
(�.0001)a
�483(�
.0001)a
�1.84
(.0004)a
�218(�
.0001)a
�0.85
(.02)a
�91
(.0002)a
�0.01
(.97)
�109(.01)a
1.22
(.01)a
Hisp
anicb
9(.94)
�0.05
(.77)
�157(.02)a
�2.36
(�.0001)a
�37
(.31)
�0.42
(.26)
18(.49)
0.32
(.34)
60(.19)
0.98
(.05)
Pretermbirth
136(.15)
0.36
(.007)a
79(.13)
0.35
(.39)
62(.02)a
0.58
(.04)a
36(.04)a
0.45
(.05)
�44
(.22)
�1.28
(.001)a
aStatisticallysig
nificant.
bComparedwith
childrenofwhitemothers.
TABLE 5 Type of Class C Events According to Gender
No. (%)
Male Female
Serious bacterial infections 4 (14.81) 7 (22.58)Esophageal candidiasis 0 (0.00) 4 (12.90)CMV disease 1 (3.70) 1 (3.23)HIV encephalopathy 17 (62.96) 10 (32.26)Burkitt’s or immunoblastic lymphoma 0 (0.00) 1 (3.23)Mycobacterium avium complex 0 (0.00) 1 (3.23)PCP 5 (18.52) 4 (12.90)Wasting syndrome 0 (0.00) 3 (9.68)Total 27 (100) 31 (100)
CMV indicates cytomegalovirus; PCP, Pneumocystis pneumonia.
152 FOCA et al at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

DISCUSSIONIssues related to gender-specific differences in the patho-genesis and treatment of systemic disorders have be-come prominent in recent years. Differences in T lym-phocyte counts between women and men were seen forHIV-negative adults,10 as well as HIV-negative adoles-cents in the Reaching for Excellence in Adolescent Careand Health (REACH) study cohort.17 The REACH studycohort demonstrated differences in T cell subset valuesbetween HIV-negative and HIV-positive female subjectsand between HIV-negative and HIV-positive male sub-jects, but the authors did not compare HIV-infected fe-male and male subjects directly.18 The SEROCO studygroup1 demonstrated an absolute difference of 100 CD4�
cells between HIV-infected adult women and men thatpersisted for 5 years of follow-up monitoring. This resultwas of borderline significance, after adjustment for age.In addition, Prins et al2 found a statistical difference inT cell counts at the onset of AIDS, with women having 3times the absolute number of T cells as men (146 � 106
cells per L vs 49 � 106 cells per L; P � .004). Differencesin plasma RNA levels have also been noted.
Numerous studies documented lower plasma RNAvalues for HIV-infected women, compared with HIV-in-fected men, after adjustment for CD4� cell counts.3–5,19–24
Although it did not make a direct gender-based compari-son, the REACH study documented a negative correlationbetween plasma RNA levels and CD4� cell counts for bothadolescent men and women.25 CD4� cell count is usedgenerally as a surrogate measure for time since infection.Whether this is a valid approach has been questioned, andseveral reports compared plasma RNA levels with andwithout controlling for CD4� cell count, with similar con-clusions. These discrepancies have been noted in inci-dent4,21 and prevalent19,20,23 cases of disease. A recent meta-analysis26 of 15 published studies demonstrated a combined�0.23-log unit difference in plasma RNA values forwomen, compared with men. However, only 1 study5
showed a statistical difference in AIDS onset or mortalityrates relative to these 2 standard clinical laboratory param-eters. Several published reports indicated that mortalityrates related to HIV disease and responses to therapyseemed to be no different for women versus men, despitethe potential for women to begin ART later in their diseasecourse.9,21,27
The European Collaborative Study (ECS) examinedthese issues in a longitudinal pediatric cohort. In contrastto the adult studies, the ECS, examining 186 HIV-in-fected children up to 12 years of age, found higher CD4�
cell, CD8� cell, and total lymphocyte counts for boysthan for girls.28 In a separate analysis of the same cohortreported 1 year earlier,29 the investigators documented0.25- to 0.5-log unit lower plasma RNA levels for fe-males than for males, without evidence of statisticallydifferent rates of disease progression. We report gender-based differences in plasma RNA measurements be-
tween ART-treated, HIV-infected female and male chil-dren, similar to results reported previously for adultpatients. We noted a mean �0.38-log unit difference inplasma RNA values for female children, which falls wellwithin the ranges of values from adult studies and thevalues found by the ECS for pediatric patients.
Historically, survival advantages were seen for adultmale patients but, after controlling for other variables,including intravenous drug use, alcohol use, socioeco-nomic status, and access to care, these advantages dis-appeared. We found a significant survival advantage formale children despite their higher plasma RNA levels.This survival advantage remained statistically significantafter a sensitivity analysis was performed. The survivaldifference could not be explained on the basis of age atHIV diagnosis, age at initiation of ART, or type of therapyused. The potential role of adherence in these resultscould not be tested. Virtually all of the patients in thiscohort were receiving monotherapy or dual therapywith nucleoside analogues. The mortality results couldreflect the nature of the therapy (for example, the po-tency of zidovudine versus didanosine monotherapy). Itwas not possible to test this hypothesis with the currentdata set, because individual drugs were not recorded;only the drug class was specified. One child receivedcombination therapy. A larger cohort analysis might elu-cidate a factor or factors integral to these findings. Inaddition, a comparison of female and male children re-ceiving potent combination therapy may prove useful. Ifmortality differences persist among patients receivingcurrent standard-of-care treatment, then it may be nec-essary to reevaluate the approach to initiating therapyfor pediatric patients.
Currently, postpubertal hormonal differences havebeen invoked as one potential means of explaining gen-der differences in plasma RNA levels. In vitro, estrogeninhibits tumor necrosis factor-� production, and tumornecrosis factor-� has been shown to be important inHIV-1 expression.34 Our results seem to contradict thisassumption, because all of the children were prepuber-tal.
We found significant gender and racial differences inalmost all of the immunologic parameters tested for ourpopulation of HIV-exposed but uninfected children. Ofthe variables that were comparable to the ECS analysis,there was general agreement that female children hadgreater CD4� cell and total lymphocyte counts andlower CD8� cell counts, compared with male children.Children born to black mothers had lower overall lym-phocyte counts and subset counts than did children bornto white mothers. These results, in comparison with arecent cross-sectional analysis of healthy, HIV-nonex-posed children up to 18 years of age,11 raise some inter-esting issues.
Pediatric AIDS Clinical Trials Group 1009 studied im-munologic parameters, determined with 3-color flow
PEDIATRICS Volume 118, Number 1, July 2006 153 at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

cytometry, cross-sectionally in a large cohort of healthychildren and adolescents. The rationale for the study wasbased on the need for reference ranges of cell counts andsubsets for this population, for comparison in other anal-yses. After adjustment for laboratory variation, the re-searchers found no statistically significant gender or ra-cial differences, and they suggested that a single standardcould be used for all pediatric populations.11 Our analysisand the analysis by the ECS suggest that children whohave been exposed to HIV and ART but remain unin-fected have differences in lymphocyte subsets that arebased on gender and race. The WITS also adjusted forlaboratory variation and found that gender and racialeffects remained statistically significant, which is in con-trast to the Pediatric AIDS Clinical Trials Group 1009study. Among factors that might be invoked to explainthese observed differences are potential adverse mito-chondrial effects, resulting from HIV exposure, ART ex-posure, or both, on the developing fetus and the possi-bility of effects on immunologic parameters among thesechildren. In addition, the nature of the 2 studies (cross-sectional versus prospective) may have influenced theresults.
CONCLUSIONSWe report gender differences in plasma RNA levels be-tween ART-treated, HIV-infected, female and male chil-dren. This result is in agreement with previous workpublished by the ECS and is in general agreement withpublished adult literature. However, we found no differ-ence between male and female children with respect tolymphocyte counts. This result is in contrast to previouswork published by the ECS, and it may reflect the gen-erally small number of HIV-infected children analyzed inthis data set. This finding requires confirmation in otherpediatric cohorts, because of the implications for thera-peutic decision-making. We also noted gender and racialdifferences among HIV-uninfected children for most im-munologic parameters analyzed, which is in contrast toa previously published study of healthy children andadolescents.11 A comparison of these 2 cohorts mightresolve this controversy but, if the findings are validatedstatistically, then there is the possibility that HIV-ex-posed children have subtle immunologic perturbationsthat need to be characterized fully.
Finally, we report a significant survival advantage forHIV-infected male children treated with ART, despitetheir higher plasma RNA values. This advantage wassignificant even after a sensitivity analysis. It could notbe explained on the basis of readily available parameterssuch as age at HIV diagnosis or type of ART. However,few children were treated with more than monotherapyand, before the implications of these results are consid-ered more thoroughly, an analysis of children receivingpotent combination therapy should be performed. If the
data remain significant, then it may warrant a reevalu-ation of our treatment strategies.
ACKNOWLEDGMENTSAdditional support was provided by local clinical re-search centers, as follows: Baylor College of Medicine(Houston, TX), National Institutes of Health (NIH) grantGCRC RR000188; Columbia University (New York, NY),NIH grant GCRC RR000645.
Principal investigators, study coordinators, programofficers, and funding NIH were as follows: Clemente Diazand Edna Pacheco-Acosta (University of Puerto Rico,San Juan, PR; NIH grant U01 AI 034858); Ruth Tuo-mala, Ellen Cooper, and Donna Mesthene (Boston/Worcester site, Boston, MA; NIH grant 9U01 DA015054); Phil LaRussa and Alice Higgins (ColumbiaPresbyterian Hospital, New York, NY; NIH grant U01 DA015053); Sheldon Landesman, Edward Handelsman,and Ava Dennie (State University of New York, Brook-lyn, NY; NIH grant U01 HD 036117); Kenneth Rich andDelmyra Turpin (University of Illinois at Chicago, Chi-cago, IL; NIH grant U01 AI 034841); William Shearer,Susan Pacheco, and Norma Cooper (Baylor College ofMedicine, Houston, TX; NIH grant U01 HD 041983); JoanaRosario (National Institute of Allergy and Infectious Dis-eases, Bethesda, MD); Robert Nugent (National Instituteof Child Health and Human Development, Bethesda,MD); Vincent Smeriglio and Katherine Davenny (Na-tional Institute on Drug Abuse, Bethesda, MD); andBruce Thompson (Clinical Trials and Surveys Corp, Bal-timore, MD; NIH grant N01 AI 085339); scientific lead-ership core: Kenneth Rich (principal investigator) andDelmyra Turpin (study coordinator) (NIH grant 1 U01 AI050274-01).
REFERENCES1. Delmas MC, Jadand C, De Vincenzi I, et al. Gender difference
in CD4� cell counts persist after HIV-1 infection: SEROCOStudy Group. AIDS. 1997;11:1071–1073
2. Prins M, Robertson JR, Brettle RP, et al. Do gender differencesin CD4 cell counts matter? AIDS. 1999;13:2361–2364
3. Anastos K, Gange SJ, Lau B, et al. Association of race andgender with HIV-1 RNA levels and immunologic progression.J Acquir Immune Defic Syndr. 2000;24:218–226
4. Sterling TR, Lyles CM, Vlahov D, Astemborski J, Margolick JB,Quinn TC. Sex differences in longitudinal human immuno-deficiency virus type 1 RNA levels among seroconverters. J In-fect Dis. 1999;180:666–672
5. Farzadegan H, Hoover DR, Astemborski J, et al. Sex differencesin HIV-1 viral load and progression to AIDS. Lancet. 1998;352:1510–1514
6. Junghans C, Ledergerber B, Chan P, Weber R, Egger M. Sexdifferences in HIV-1 viral load and progression to AIDS: SwissHIV Cohort Study. Lancet. 1999;353:589
7. Moore AL, Mocroft A, Madge S, et al. Gender differences invirologic response to treatment in an HIV-positive population:a cohort study. J Acquir Immune Defic Syndr. 2001;26:159–163
8. Moore AL, Sabin CA, Johnson MA, Phillips AN. Gender andclinical outcomes after starting highly active antiretroviral
154 FOCA et al at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

treatment: a cohort study. J Acquir Immune Defic Syndr. 2002;29:197–202
9. Moore AL, Kirk O, Johnson AM, et al. Virologic, immunologic,and clinical response to highly active antiretroviral therapy: thegender issue revisited. J Acquir Immune Defic Syndr. 2003;32:452–461
10. Maini MK, Gilson RJ, Chavda N, et al. Reference ranges andsources of variability of CD4 counts in HIV-seronegativewomen and men. Genitourin Med. 1996;72:27–31
11. Shearer WT, Rosenblatt HM, Gelman RS, et al. Lymphocytesubsets in healthy children from birth through 18 years of age:the Pediatric AIDS Clinical Trials Group P1009 study. J AllergyClin Immunol. 2003;112:973–980
12. AIDS Clinical Trials Group. Immunology. Available at: http://aactg.s-3.com/immlab.htm. Accessed January 21, 2006
13. AIDS Clinical Trials Group. Virology. Available at: http://aactg.s-3.com/virlab.htm. Accessed January 21, 2006
14. Centers for Disease Control and Prevention. 1994 revised clas-sification system for human immunodeficiency virus infectionin children less than 13 years of age. MMWR Recomm Rep.1994;43(RR-12):1–10
15. Zeger SL, Liang KY. Longitudinal data analysis for discrete andcontinuous outcomes. Biometrics. 1986;42:121–130
16. Neu N, Leighty R, Adeniyi-Jones S, et al. Immune parametersand morbidity in hard drug and human immunodeficiencyvirus-exposed but uninfected infants. Pediatrics. 2004;113:1260–1266
17. Rudy BJ, Wilson CM, Durako S, Moscicki AB, Muenz L, Doug-las SD. Peripheral blood lymphocyte subsets in adolescents: alongitudinal analysis from the REACH project. Clin Diagn LabImmunol. 2002;9:959–965
18. Douglas SD, Rudy B, Muenz L, et al. Peripheral blood mono-nuclear cell markers in antiretroviral therapy-naive HIV-infected and high risk seronegative adolescents: AdolescentMedicine HIV/AIDS Research Network. AIDS. 1999;13:1629–1635
19. Evans JS, Nims T, Cooley J, et al. Serum levels of virus burdenin early-stage human immunodeficiency virus type 1 disease inwomen. J Infect Dis. 1997;175:795–800
20. Lyles CM, Vlahov D, Farzadegan H, et al. Comparison of twomeasures of human immunodeficiency virus (HIV) type 1 loadin HIV risk groups. J Clin Microbiol. 1998;36:3647–3652
21. Sterling TR, Vlahov D, Astemborski J, Hoover DR, MargolickJB, Quinn TC. Initial plasma HIV-1 RNA levels and progressionto AIDS in women and men. N Engl J Med. 2001;344:720–725
22. Katzenstein DA, Hammer SM, Hughes MD, et al. The relationof virologic and immunologic markers to clinical outcomes
after nucleoside therapy in HIV-infected adults with 200 to 500CD4 cells per cubic millimeter: AIDS Clinical Trials GroupStudy 175 Virology Study Team. N Engl J Med. 1996;335:1091–1098
23. Rezza G, Lepri AC, d’Arminio Monforte A, et al. Plasma viralload concentrations in women and men from different expo-sure categories and with known duration of HIV infection:I.CO.N.A. Study Group. J Acquir Immune Defic Syndr. 2000;25:56–62
24. Donnelly CA, Bartley LM, Ghani AC, et al. Gender differencein HIV-1 RNA viral loads. HIV Med. 2005;6:170–178
25. Holland CA, Ellenberg JH, Wilson CM, et al. Relationship ofCD4� T cell counts and HIV type 1 viral loads in untreated,infected adolescents: Adolescent Medicine HIV/AIDS ResearchNetwork. AIDS Res Hum Retroviruses. 2000;16:959–963
26. Napravnik S, Poole C, Thomas JC, Eron JJ Jr. Gender differ-ence in HIV RNA levels: a meta-analysis of published studies.J Acquir Immune Defic Syndr. 2002;31:11–19
27. Nicastri E, Angeletti C, Palmisano L, et al. Gender differences inclinical progression of HIV-1-infected individuals during long-term highly active antiretroviral therapy. AIDS. 2005;19:577–583
28. European Collaborative Study. Are there gender and race dif-ferences in cellular immunity patterns over age in infected anduninfected children born to HIV-infected women? J AcquirImmune Defic Syndr. 2003;33:635–641
29. European Collaborative Study. Level and pattern of HIV-1RNA viral load over age: differences between girls and boys?AIDS. 2002;16:97–104
30. Friedland GH, Saltzman B, Vileno J, Freeman K, Schrager LK,Klein RS. Survival differences in patients with AIDS. J AcquirImmune Defic Syndr. 1991;4:144–153
31. Santoro-Lopes G, Harrison LH, Moulton LH, et al. Gender andsurvival after AIDS in Rio de Janeiro, Brazil. J Acquir ImmuneDefic Syndr Hum Retrovirol. 1998;19:403–407
32. Tu XM, Meng XL, Pagano M. Survival differences and trends inpatients with AIDS in the United States. J Acquir Immune DeficSyndr. 1993;6:1150–1156
33. Morgello S, Mahboob R, Yakoushina T, Khan S, Hague K.Autopsy findings in a human immunodeficiency virus-infectedpopulation over 2 decades: influences of gender, ethnicity, riskfactors, and time. Arch Pathol Lab Med. 2002;126:182–190
34. Shanker G, Sorci-Thomas M, Adams MR. Estrogen modulatesthe expression of tumor necrosis factor � mRNA in phorbolester-stimulated human monocytic THP-1 cells. LymphokineCytokine Res. 1994;13:377–382
PEDIATRICS Volume 118, Number 1, July 2006 155 at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2005-0294 2006;118;146Pediatrics
Katherine Luzuriaga, Mary Paul and Clemente DiazMarc Foca, Jack Moye, Clara Chu, Yvonne Matthews, Ken Rich, Ed Handelsman,
Disease Progression in a Cohort of Children Born to Women Infected With HIVGender Differences in Lymphocyte Populations, Plasma HIV RNA Levels, and
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/118/1/146.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/118/1/146.full.htat:This article cites 31 articles, 4 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/118/1/146.full.htThis article has been cited by 7 HighWire-hosted articles:
Subspecialty Collections
diseasehttp://pediatrics.aappublications.org/cgi/collection/infectious_Infectious Disease & Immunitythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2006 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Iraq:AAP Sponsored on June 3, 2013pediatrics.aappublications.orgDownloaded from