
High resolution magnetic resonance imaging application in anatomy: the extensor digitorum muscle...
7
MAGMA (1997) 5, 21-27 High resolution magnetic resonance imaging application in anatomy: the extensor digitorum muscle insertion on the first phalanx Serge Van Sint Jan, 1 Johan Van Audekerke, 2 Annemie Van der Linden, 2. and Marcel Rooze 1 1Department for Human Anatomy and Embryology, University of Brussels (ULB), Brussels, Belgium 2Bio-Imaging Laboratory, University of Antwerp (RUCA), Antwerp, Belgium Classical dissection may give unsatisfactory results because of the presence of artifacts due to both the embalming process and displacement of the anatomical structures. This spatial disturbance could explain the divergent descriptions found in the literature about the presence, or the absence, of an insertion of the extensor digitorum muscle (ED) at the base of the first phalanx (P1). Prelimi- nary experiments by Van Sint Jan et al. (1996) found the same contradiction: dissections did not show a real tendon attachment, whereas a functional experiment seemed to show that "something" should exist between ED and P1 to explain the results. This paper presents the results of an in vitro MRI study of this anatomical area. A 7-T NMR microscope was used to collect accurate, noninvasive data. Subsequently, surface rendering was performed to visualize the structures in a three- dimensional manner. The results of this MRI study, together with functional data obtained in an earlier study, showed that no real insertion of ED on P1 exists. However, some collagenic fibers were occasionally observed running from the ventral aspect of ED to both P1 and the metacarpo- phalangeal joint capsule. Those few collagenic fibers would play a secondary role in the extension of P1. Keywords: magnetic resonance imaging microscopy, tendon, finger, image analysis, three- dimensional reconstruction, diagnosis. INTRODUCTION Classical dissection does not always yield fully satis- fying anatomical description. In the first place, dissec- tion is often performed on embalmed specimens and artifacts may be present. Second, dissection disturbs the spatial relationships of the anatomical structures. This must explain why contradictory descriptions are found in the literature about the insertion of the extensor digitorum muscle (ED) on the first phalanx (P1) [1]. The two most frequently encountered points * To whom all correspondenceshould be addressed, at Bio-Imaging Lab, RUCA, University of Antwerp, Groenenborgerlaan 171, B-2020 Antwerp, Belgium. Date received: November 28, 1996; date accepted: December 5, 1996. 1352-8661 1997 Chapman & Hall of disagreement in the literature are the hypothetical existence and the role of a tendon insertion of ED on P1. Some authors describe a tendon insertion, whereas others do not. A third category of authors do not as- sign a major action to this tendon and call it the "sleeping attachment" [1]. However, since this area is often affected in degen- erative diseases such as rheumatoid arthritis and in orthopedic traumatology as well, a clear anatomical description is necessary for efficient diagnosis. The present study was aimed at bringing in new data about the ED insertion on P1 and consisted of three parts: dissection of the region for a morphologi- cal description (part I), a functional anatomy study (part II), and high-gradient magnetic resonance imag- ing (part III). Parts I and II have been published else- where [1], and the methods and results sections of these parts are therefore less extensively discussed in this paper.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of High resolution magnetic resonance imaging application in anatomy: the extensor digitorum muscle...

MAGMA (1997) 5, 21-27
High resolution magnetic resonance imaging application in anatomy: the extensor digitorum muscle insertion on the
first phalanx
Serge Van Sint Jan, 1 Johan Van Audekerke, 2 Annemie Van der Linden, 2. and Marcel Rooze 1
1Department for Human Anatomy and Embryology, University of Brussels (ULB), Brussels, Belgium 2Bio-Imaging Laboratory, University of Antwerp (RUCA), Antwerp, Belgium
Classical dissection may give unsatisfactory results because of the presence of artifacts due to both the embalming process and displacement of the anatomical structures. This spatial disturbance could explain the divergent descriptions found in the literature about the presence, or the absence, of an insertion of the extensor digitorum muscle (ED) at the base of the first phalanx (P1). Prelimi- nary experiments by Van Sint Jan et al. (1996) found the same contradiction: dissections did not show a real tendon attachment, whereas a functional experiment seemed to show that "something" should exist between ED and P1 to explain the results. This paper presents the results of an in vitro MRI study of this anatomical area. A 7-T NMR microscope was used to collect accurate, noninvasive data. Subsequently, surface rendering was performed to visualize the structures in a three- dimensional manner. The results of this MRI study, together with functional data obtained in an earlier study, showed that no real insertion of ED on P1 exists. However, some collagenic fibers were occasionally observed running from the ventral aspect of ED to both P1 and the metacarpo- phalangeal joint capsule. Those few collagenic fibers would play a secondary role in the extension of P1.
Keywords: magnetic resonance imaging microscopy, tendon, finger, image analysis, three- dimensional reconstruction, diagnosis.
INTRODUCTION
Classical dissection does not a lways yield fully satis- fying anatomical description. In the first place, dissec- tion is often pe r fo rmed on em ba l m ed specimens and artifacts may be present. Second, dissection disturbs the spatial relat ionships of the anatomical structures.
This mus t explain w h y contradictory descript ions are found in the l i terature about the insertion of the extensor d ig i torum muscle (ED) on the first pha lanx (P1) [1]. The two mos t f requently encountered points
* To whom all correspondence should be addressed, at Bio-Imaging Lab, RUCA, University of Antwerp, Groenenborgerlaan 171, B-2020 Antwerp, Belgium. Date received: November 28, 1996; date accepted: December 5, 1996.
1352-8661 �9 1997 Chapman & Hall
of d isagreement in the li terature are the hypothet ical existence and the role of a tendon insertion of ED on P1. Some authors describe a tendon insertion, whereas others do not. A third category of authors do not as- sign a major action to this t endon and call it the "s leeping a t t achment" [1].
However , since this area is often affected in degen- erat ive diseases such as rheumato id arthritis and in or thopedic t raumato logy as well, a clear anatomical descript ion is necessary for efficient diagnosis.
The present s tudy was a imed at br inging in new data about the ED insertion on P1 and consisted of three parts: dissection of the region for a morphologi - cal descript ion (part I), a functional ana tomy s tudy (part II), and high-gradient magnet ic resonance imag- ing (part III). Parts I and II have been publ i shed else- where [1], and the methods and results sections of these par ts are therefore less extensively discussed in this paper.

22 S VAN SINT JAN et al.
MATERIAL AND METHODS
Cadaver hands and upper limbs from Caucasian indi- viduals over age 60 were used in the three parts of the study.
Morphologic study
Dissection of 20 embalmed and 10 fresh-frozen (FF) hands was performed to observe the relationships of the ED tendon in the metacarpophalangeal (MP) joint area [1]. The embalming process occurred according to Dankmeyer's method [2]. Special care-was taken to avoid any damage to the structures underlying the ED tendon.
Functional study
Ten additional FF upper limbs from recently deceased donors were used for the functional part of the study [1]. The limbs were sectioned above the distal epiph- ysis of the humeral bone and frozen (-7~ until 24 hours before the experiment. The experimental proto- col was the following: each limb was mounted on an experimental device that allowed only finger joint mo- tions. Any other joint motions (wrist and elbow) were avoided thanks to several pins drilled into the joints. A system of markers was stuck in P1. Then a camera recorded the marker displacement amplitude during the extension of P1. Motion recording was performed before and after removal of the subtendinous struc- tures. The dorsal aponeurosis (Fig. 1, structure 6a; ana- tomic structures are hencefore denoted by curly brack- ets: {6a}) was always respected. Statistical data were compared using Student's t-test. (Table 1 lists the in- dex numbers for all structures illustrated in the fig- ures.)
MRI study
MRI was used as a virtual dissection tool to collect new data. Five embalmed and five FF nondissected fingers were used. Before imaging, the flexor and ex- tensor tendons were slightly stretched with a constant tension to keep them in a more physiological position. This tension was maintained throughout the imaging. All finger joints were extended, with a slight hyper- extension of the MP joint. Each finger was then posi- tioned in a birdcage radiofrequency (RF) coil (diam- eter: 30 mm). MRI was performed on a 7-T system from SMIS (Surrey Medical Imaging Systems) with a horizontal bore of 8 cm. A multislice SE sequence with the following parameters was used: matrix, 256 x 256; slice thickness, I mm; number of slices, 16. The field of view (FOV) varied between 20 mm and 45 mm, TE = 22 ms, and TR varied among 500, 1000, and 1200 ms.
MAGMA (I997) 5(1)
Fig. 1. Finger anatomy, adapted from Sobotta [3]. Top, Musculoskeletal structures, lateral view (soft tissue has been removed). Middle, Digital nerves and arteries, lat- eral view. Bottom, Transverse view (at the level of the first phalanx). See Table 1 for key to the numerical des- ignations.
The MR images were compared with the dissection results and used to obtain three-dimensional isosur- face models, as explained in the next section.
Image processing and three- dimensional reconstruction
Initially, image filtering took place to eliminate some noise in the pictures and to increase the contrast be- tween the anatomical structures. A low-pass filter, the hybrid median filter, was applied to increase the sig- nal-to-noise ratio (SNR). This filter was preferred over the more classically used median and gaussian filters

EXTENSOR DIGITORUM MUSCLE INSERTION ON FIRST PHALANX
Table 1. Key to numerical designations used in all i l lustrations and throughout text.
23
Designation Structure Remarks
1 2 3 4 5 6 6a 7 8 9
10 10a
11 12 13 14 15 16 17 18 19 20 21 22 23 23a 23b 24 25 26 27 28 29 3O 31 32 33 34
Metacarpal bone First phalanx Volar plate Flexor digitorum profundus muscle tendon Flexor digitorum superficialis muscle tendon Extensor digitorum muscle tendon Dorsal aponeurosis Dorsal pad of the MP joint capsule {8} Metacarpophalangeal (MP) joint capsule Hyaline cartilage- Loose connective tissue Some collagenic fibers running through {10} and
ending in {8} and at the base of P1 {2} Third phalanx
. Vincula tendinum Tendon pulley Lumbricalis muscle Interosseous muscle Interosseous artery Dorsal digital artery Volar digital artery Dorsal digital nerve Volar digital nerve Annular tendon pulley Digital fat Lateral l igament Fibres of {23} ending at the base of P1 {2} Fibres of {23} ending in the volar plate {3} Circular tube filled with water Small artifact showing a very high intensity Second phalanx Medial band of ED {6} attached on P2 {26} Proximal interphalangeal joint cavity Attachment of FDS {5} on P2 {26} Lateral band of ED {6} running to P3 {30} Metacarpophalangeal joint cavity Cavities in the bone marrow Epidermis Deviation of the ED tendon {6} toward the MP cavity {31}
P1
FDP FDS ED Also called extensor hood
Indicated with arrows
P3 Function: blood supply support Also called fibrous flexor sheath
Adipocytes are sometimes visible One for each digital joint
O = 1 0 m m
P2
PIP
No attachment on P2 {26} MP
because the spatial position of the structure borders was better respected [4]. This was important to get good three-dimensional models. Then, a linear expansion (high-pass filter) of the image frequency histogram occurred to improve the image contrast. Finally, semi- automated image segmentation of the bone, extensor tendon {6} and hood {6a} was performed. The contrast between the structure borders was not high enough to allow fully automated threshold process [5].
At this stage, the contours of the structures were obtained and naturally defined in the spatial reference system of the MR device. Now, the three-dimensional surface models of the structures were obtained using
either bicubic B-spline or triangulation algorithms [6]. Surface modeling was used instead of volume render- ing because the former is more appropriate for real- time manipulation and joint motion simulation [7], which is planned for the future.
RESULTS Morphologic study It appeared that no real ED insertion [6] could be found on P1 {2} (Fig. 2). Only loose connective tissue {10} was found between the palmar aspect of the ED tendon and the MP joint capsule {8}. The range and
MAGMA (1997) 5(1)

24 S VAN SINT JAN et al.
Fig. 2. Dissection of the metacarpophalangeal (MP) area. The displayed fingers (fresh-frozen specimens) have been longitudinally cut to enable comparison with MR images. All pictures are lateral views of the MP area. A, General view. No loose connective tissue is present. B, Enlarged view of the dorsal part of the joint. A strong development of the loose connective tissue {10} is visible. Some collagenic fibers {10a} running from the tendon {6} to the joint capsule {8} are present. C, General view. Some loose connective tissue {10} is observable, but the collagenic expansion {10a} does not show a clear ending at the ventral aspect of the extensor tendon {6}. See Table 1 for key to the numerical designations.
development of the loose connective tissue was vari- able between the hands, but also between the fingers of a same hand. When a large, loose connective tissue {10} was present occasionally, some fibers {10a} were observed running from the ventral aspect of the ten- don to the joint capsule.
At this stage, the results seem to be in contradiction: on one hand, dissection did not show real tendinous relationships between P1 and ED, and on the other hand the functional s tudy seemed to indicate that "some- thing" must exist to explain the increased extension. MRI was then used to obtain supplementary data.
Functional study All of the fingers showed an increase in extension after resection of the subtendinous structure, which was the above-mentioned loose connective tissue {10}. This in- crease was statistically significant only for the fingers that showed a high development of loose connective tissue.
MRI study
The MR images clearly displayed structures such as tendons, arteries, nerves, ligaments, joint capsule, and volar plates (Fig. 3). The insertion of the medial band {27} of ED on the second phalanx {26} was clearly ob- servable (Fig. 4) and gave us a reference about what
MAGMA (1997) 5(1)
EXTENSOR DIGITORUM MUSCLE INSERTION ON FIRST PHALANX 25
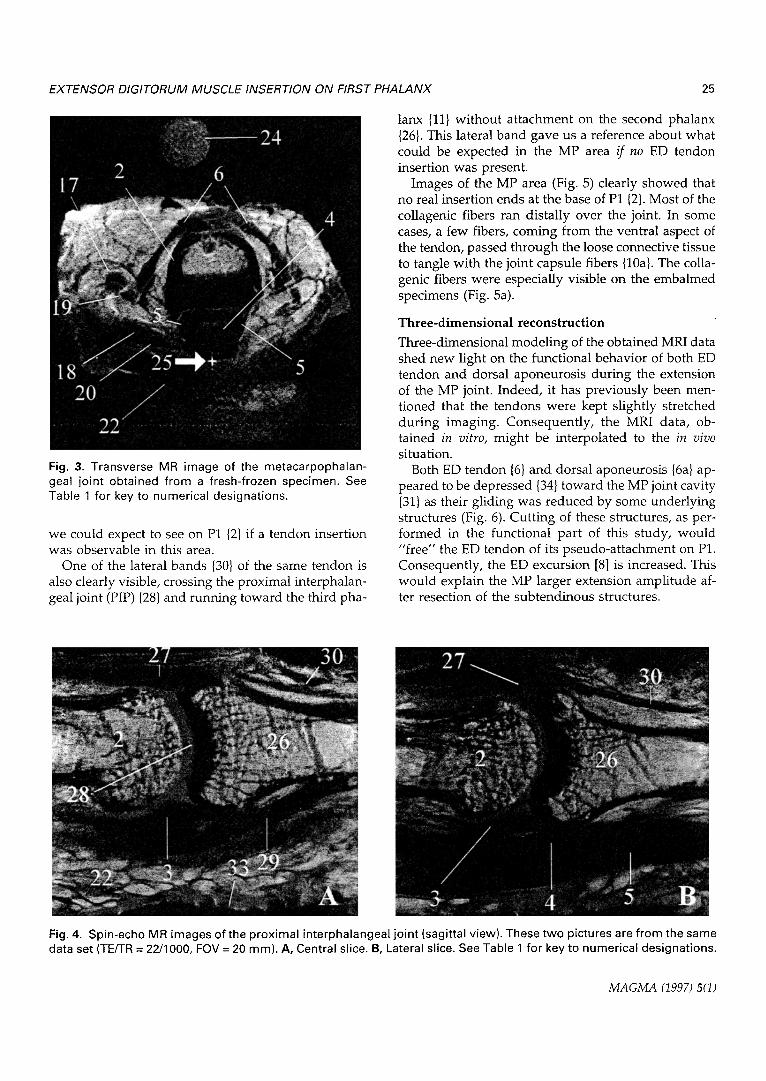
Fig. 3. Transverse MR image of the metacarpophalan- geal joint obtained from a fresh-frozen specimen. See Table 1 for key to numerical designations.
we could expect to see on P1 {2} if a tendon insertion was observable in this area.
One of the lateral bands {30} of the same tendon is also clearly visible, crossing the proximal interphalan- geal joint (PIP) {28} and running toward the third pha-
lanx {11} without attachment on the second phalanx {26}. This lateral band gave us a reference about what could be expected in the MP area /f no ED tendon insertion was present.
Images of the MP area (Fig. 5) clearly showed that no real insertion ends at the base of P1 {2}. Most of the collagenic fibers ran distally over the joint. In some cases, a few fibers, coming from the ventral aspect of the tendon, passed through the loose connective tissue to tangle with the joint capsule fibers {10a}. The colla- genic fibers were especially visible on the embalmed specimens (Fig. 5a).
Three-dimensional reconstruction
Three-dimensional modeling of the obtained MRI data shed new light on the functional behavior of both ED tendon and dorsal aponeurosis during the extension of the MP joint. Indeed, it has previously been men- tioned that the tendons were kept slightly stretched during imaging. Consequently, the MRI data, ob- tained in vitro, might be interpolated to the in vivo situation.
Both ED tendon {6} and dorsal aponeurosis {6a} ap- peared to be depressed {34} toward the MP joint cavity {31} as their gliding was reduced by some underlying structures (Fig. 6). Cutting of these structures, as per- formed in the functional part of this study, would "free" the ED tendon of its pseudo-attachment on P1. Consequently, the ED excursion [8] is increased. This would explain the MP larger extension amplitude af- ter resection of the subtendinous structures.
Fig. 4. Spin-echo MR images of the proximal interphalangeal joint (sagittal view). These two pictures are from the same data set (TE/TR = 22/1000, FOV = 20 mm). A, Central slice. B, Lateral slice. See Table 1 for key to numerical designations.
MAGMA (1997) 5(1)

26 S VAN SINT JAN et al.
Fig. 5. Spin-echo MR images of the metacarpophalangeal joint (sagittal view) of embalmed A and fresh-frozen (B through E) specimens. A, Same data set (TE/TR = 22/1200, FOV = 25 mm). A1, Central slice. A2, Intermediate slice. A3, Lateral slice. B and C, TE/TR = 22/1200, FOV = 20 ram. D and E, TE/TR = 22/500, FOV = 30 ram. See Table 1 for key to numerical designations.
MAGMA (1997) 5(1)

EXTENSOR DIGITORUM MUSCLE INSERTION ON FIRST PHALANX 27
Fig. 6. Lateral (left) and ventral (right) views of a three- dimensional surface rendering of the metacarpophalan- geal area from a MRI data set. See ,-Fable 1 for key to numerical designations.
DISCUSSION
Although neither the review of the literature nor new investigations gave us fully satisfactory results, the use of MRI and subsequent three-dimensional recon- struction brought in some new complementary and useful information about the ED insertion on P1.
No real tendinous insertion was found on dissection or on the MR images. Sometimes, some ED collagenic fibers ending in the MP joint capsule and at the base of P1 were observed on the MR images.
This inconstant tangling of some ED fibers with the MP joint capsule could explain the above-ment ioned contradictory results: some individuals have "a k ind" of ED insertion (actually, a few collagenic fibers) on P1, whereas others do not. When such an insertion is present, it has a secondary role in the extension of P1 [1]. This was confirmed by three-dimensional model- ing: when stretched, the ED tendon seems to be devi- ated ventrally toward the MP joint. An ED attachment on P1 is not biomechanically necessary to explain a MP extension [9].
MRI appeared to be useful for several reasons. At first, because of the noninvasive nature of the tech- nique, the structures of interest keep both their mutual relationships and spatial location. Also, the specimens are not ha rmed and can be used for further investiga- tion (e.g., functional experiment). Fur thermore, the resolution of the images is very high and therefore enables visualization of small anatomical structures. Even with cadaver specimens, the images are still of
interest and good three-dimensional models can be obtained.
On the other hand, the small size of the magnet bore did not allow in vivo human imaging, a l though the MR protocol used in this paper is also potentially very promising for human in vivo experiments on high- field whole-body systems. For example, tendon, liga- ment, and muscle injuries are classically diagnosed with echography, which has poor resolution for small structures such as those described in this paper. Thus, the diagnosis of hand and foot injuries is still very challenging in or thopedic practice. High-resolut ion MILl has been shown to be suitable for the observation of small anatomical s t ructures and should signifi- cantly improve the detection of musculoskeletal pa- thology. Also, such data would allow elaboration of complex three-dimensional models for medical edu- cation and surgical rehearsal [10].
REFERENCES
1. Van Sint Jan S, Rooze M, Van Audekerke J, Vico L (1996) The insertion of the extensor digitorum tendon on the proximal phalanx. J Hand Surg 21A 69-76.
2. Van Sint Jan S, Rooze M (1992) The thenar muscles: new findings. Surg Radiol Anat 14" 325-329.
3. Sobotta J (1985) Atlas d'anatomie humaine, 2nd ed. Mu- nich: Urban & Schwarzenberg.
4. Russ JC (1992) The Image Processing Handbook, 1st ed. Boca Raton: CRC Press.
5. HOhne KH, Pflesser B, Pommert A, Riemer M, Schier- mann T, Schubert R, Tiede U (1996) A new representa- tion of knowledge concerning human anatomy and function. Yearbook Med lnformatics 525-529.
6. Odesanya OS, Waggenspack WN, Thompson DE (1993) Construction of biological surface models from cross- sections. IEEE Trans Biomed Eng 40: 329-334.
7. Fujishiro I, Maeda Y, Sato H, Takeshima Y (1996) Volu- metric data exploration using interval volume. IEEE Vi- sualizat Comp Graph 2: 144-155.
8. Brand PW, Hollister A (1992) Clinical Mechanics of the Hand, 2nd ed. St. Louis: Mosby Year Book.
9. Tubiana R (1980) Trait# de chirurgie de la main. Paris: Mas- s o n .
10. H6hne KH, Pflesser B, Pommert A, Riemer M, Schie- mann T, Schubert R, Tiede U (1996) A "virtual body" model for surgical education and rehearsal. Computer 29: 25-31.
MAGMA (1997) 5(1)




















