In chronic lateral epicondylitis, apoptosis and autophagic cell death occur in the extensor carpi...
8
ELBOW In chronic lateral epicondylitis, apoptosis and autophagic cell death occur in the extensor carpi radialis brevis tendon Jimin Chen, MD, MMS, Allan Wang, MD, Jiake Xu, MD, Minghao Zheng, MD, PhD* Unit of Orthopaedic Research, School of Surgery, University of Western Australia, Perth, Australia Hypothesis: Despite its common occurrence, lateral epicondylitis is poorly understood from a cellular and molecular perspective. We hypothesize that apoptosis and autophagic cell death are involved in the devel- opment of chronic lateral epicondylitis. Materials and methods: In 10 patients undergoing surgery for chronic recalcitrant lateral epicondylitis, tendon samples were taken from the extensor carpi radialis brevis (ECRB) tendon and were processed for hematoxylin and eosin, terminal deoxynucleotidyl transferase-mediated deoxy uridine triphosphate nick- end labeling (TUNEL) assay, and immunostaining. Extracellular matrix structure was graded I to III accord- ing to collagen fiber structure and arrangement. Apoptotic rate, autophagic cell death rate, cell density, and type I collagen content were measured and compared between areas with different collagen grade. Results: Apoptotic and autophagic cell death occur in the ECRB tendon and varied with the grade of collagen structure. In grade I matrix with relatively less disrupted collagen structure, the apoptosis rate was 23.2% 4.8% and the autophagy cell death rate was 7.6% 2.2%. In grade II matrix with more advanced breakdown of collagen structure, the apoptosis rate increased to 34.4% 4% (P < .05) and the autophagic cell death rate to 13.7% 3% (P < .05). Discussion: This study demonstrated that apoptosis and autophagic cell death occur in the ECRB tendon in chronic lateral epicondylitis. The markedly elevated apoptotic rate and autophagic cell death rate in the grade II matrix may be responsible for the decrease in cellularity and further deterioration of collagen quality seen in end-stage grade III matrix, and this eventually compromised the tendon’s ability to maintain its integrity and resulted in tendon tear. Conclusion: Both apoptosis and autophagic cell death play an important role in the development of tendon degeneration in chronic lateral epicondylitis. Level of evidence: Basic science study. Ó 2010 Journal of Shoulder and Elbow Surgery Board of Trustees. Keywords: Autophagic cell death; apoptosis; tendon degeneration; tennis elbow; chronic lateral epicondylitis; tendinopathy The pathology of lateral epicondylitis has been described as degenerative tendinopathy characterized by disruption of extra cellular matrix (ECM) and angiofibroblastic hyper- plasia. 16 Despite its common occurrence as a sporting and *Reprint requests: Prof. Ming-Hao Zheng, Unit of Orthopaedic Research, School of Surgery, University of Western Australia, M Block, QE2 Medical Centre, Nedlands, WA 6009, Australia. E-mail address: [email protected] (M. Zheng). J Shoulder Elbow Surg (2010) 19, 355-362 www.elsevier.com/locate/ymse 1058-2746/2010/$36.00 - see front matter Ó 2010 Journal of Shoulder and Elbow Surgery Board of Trustees. doi:10.1016/j.jse.2009.07.064
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of In chronic lateral epicondylitis, apoptosis and autophagic cell death occur in the extensor carpi...

*Reprint re
Research, Schoo
QE2 Medical C
E-mail addre
J Shoulder Elbow Surg (2010) 19, 355-362
1058-2746/2010
doi:10.1016/j.jse
www.elsevier.com/locate/ymse
ELBOW
In chronic lateral epicondylitis, apoptosis and autophagiccell death occur in the extensor carpi radialis brevistendon
Jimin Chen, MD, MMS, Allan Wang, MD, Jiake Xu, MD, Minghao Zheng, MD, PhD*
Unit of Orthopaedic Research, School of Surgery, University of Western Australia, Perth, Australia
Hypothesis: Despite its common occurrence, lateral epicondylitis is poorly understood from a cellular andmolecular perspective. We hypothesize that apoptosis and autophagic cell death are involved in the devel-opment of chronic lateral epicondylitis.Materials and methods: In 10 patients undergoing surgery for chronic recalcitrant lateral epicondylitis,tendon samples were taken from the extensor carpi radialis brevis (ECRB) tendon and were processed forhematoxylin and eosin, terminal deoxynucleotidyl transferase-mediated deoxy uridine triphosphate nick-end labeling (TUNEL) assay, and immunostaining. Extracellular matrix structure was graded I to III accord-ing to collagen fiber structure and arrangement. Apoptotic rate, autophagic cell death rate, cell density, andtype I collagen content were measured and compared between areas with different collagen grade.Results: Apoptotic and autophagic cell death occur in the ECRB tendon and varied with the grade ofcollagen structure. In grade I matrix with relatively less disrupted collagen structure, the apoptosis ratewas 23.2% � 4.8% and the autophagy cell death rate was 7.6% � 2.2%. In grade II matrix with moreadvanced breakdown of collagen structure, the apoptosis rate increased to 34.4% � 4% (P < .05) andthe autophagic cell death rate to 13.7% � 3% (P < .05).Discussion: This study demonstrated that apoptosis and autophagic cell death occur in the ECRB tendonin chronic lateral epicondylitis. The markedly elevated apoptotic rate and autophagic cell death rate in thegrade II matrix may be responsible for the decrease in cellularity and further deterioration of collagenquality seen in end-stage grade III matrix, and this eventually compromised the tendon’s ability to maintainits integrity and resulted in tendon tear.Conclusion: Both apoptosis and autophagic cell death play an important role in the development of tendondegeneration in chronic lateral epicondylitis.Level of evidence: Basic science study.� 2010 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: Autophagic cell death; apoptosis; tendon degeneration; tennis elbow; chronic lateral
epicondylitis; tendinopathyquests: Prof. Ming-Hao Zheng, Unit of Orthopaedic
l of Surgery, University of Western Australia, M Block,
entre, Nedlands, WA 6009, Australia.
ss: [email protected] (M. Zheng).
/$36.00 - see front matter � 2010 Journal of Shoulder and Elbo
.2009.07.064
The pathology of lateral epicondylitis has been describedas degenerative tendinopathy characterized by disruptionof extra cellular matrix (ECM) and angiofibroblastic hyper-plasia.16 Despite its common occurrence as a sporting and
w Surgery Board of Trustees.

356 J. Chen et al.
occupational injury, the process of tendinopathy is poorlyunderstood from a cellular and molecular perspective.
Programmed cell death (PCD) is an important physio-logic process that maintains homeostasis in many tissues.The 2 main types of PCD are type I apoptosis and type IIautophagy.7 Apoptosis is a series of biochemical events,including blebbing, loss of membrane asymmetry, cellshrinkage, nuclear fragmentation, chromatin condensation,and chromosomal DNA fragmentation, all of which even-tually lead to the termination of the cell.9 Autophagy isa process of nutrition redistribution that involves degrada-tion of a cell’s nonessential organelles through the lyso-somal mechanism.13,26 Both are tightly regulated processesthat are important in regulating cell growth, organ devel-opment, and tissue homeostasis, but excessive PCD couldalso be pathogenic.
Recent studies suggest that apoptosis is important in thedevelopment of tendon degeneration in rotator cuff,28,30
patellar23 and Achilles tendons.19 Likewise, excessiveautophagic cell death is involved in many degenerativediseases such as Parkinson disease,2 Alzheimer disease,5,6
and aortic valve disease.14 The involvement of these 2 typesof PCD in lateral epicondylitis has not been studied. Weproposed that excessive PCD may be important in thedevelopment of chronic lateral epicondylitis and is thecause of the depletion of tenocytes and disruption of extracellular matrix. Thus the aim of this study was to investi-gate the involvement of apoptosis and autophagic cell deathin chronic lateral epicondylitis and their role in cellularalteration and ECM disruption.
Materials and methods
Institutional ethics committee approval was granted by Sir CharlesGairdner Hospital Human Ethic committee for this study thatanalyzed extensor carpi radialis brevis (ECRB) tendon samplesobtained during surgical debridement and lateral epicondylarrelease, as treatment for refractory and severe lateral epicondylitis.
Patients and tissue collection
The study recruited 10 patients (6 men, 4 women), who were anaverage age of 50 years (range, 39-63 years). Patients had a clin-ical diagnosis of lateral epicondylitis (left, 6; right, 4; Table I) thathad been confirmed with ultrasound or magnetic resonanceimaging scans revealing ECRB tendinosis. A nonoperative courseof treatment had failed in all patients. Two patients had receiveda corticosteroid injection and 1 had received 2 steroid injections,but none of the patients responded sufficiently. All patients weretreated with the Nirschl procedure.16 The tendon samples con-sisted of the debrided ECRB where it was released at the lateralepicondyle. All samples were fixed, embedded, and cut into 5-mm-thick sections for hematoxylin and eosin (H&E) staining, terminaldeoxynucleotidyl transferase-mediated deoxy uridine triphosphatenick-end labeling (TUNEL) assay, and immunohistochemicalstaining.
The TUNEL assay
The standard TUNEL assay (Cell Death Detection-AP Kit1684817, Roche Diagnostics GmbH, Mannheim, Germany) wasused to identify apoptotic cells by labeling nuclear DNA frag-ments. In brief, after removal of paraffin and rehydration, sectionswere incubated with the following reagents: proteinase K (20 mg/mL) for 15 minutes, 0.1% Triton X-100 for 8 minutes, TUNELreaction mixture (provided in kit 9:1; negative control slide wasadded by label solution without enzyme solution) for 60 minutes,convert-AP (provided in kit) for 30 minutes, and dia-minobenzidine (DAB k3468, DAKO, Glostrup, Denmark) for5 minutes. Sections were counterstained with Mayer’s hematox-ylin. Phosphate-buffered saline was used to rinse or wash thesections between reagents. All procedures were performed atroom temperature, and all reagents were prepared with DNA-freesolution. Cells positive for TUNEL assay were stained brown.
Immunohistochemistry staining
Serial sections were stained for ubiquitin (autophagic cell death)and type I collagen. After removal of paraffin and rehydration,sections were incubated in following reagents: 0.1% trypsin for20 minutes, 3% hydrogen peroxide for 5 minutes, 20% fetalbovine serum for 30 minutes, antiubiquitin antibody (Z0458,DAKO, Glostrup, Denmark 1:200) or antihuman type I collagenantibody (MP Biomedicals, Solon, OH, 1:3000) for 3 hours(negative controls were prepared by omitting the primary anti-body), secondary anti-body (K0675, DAKO, Glostrup, Denmark)for 15 minutes, and DAB (DAB k3468, DAKO, Glostrup, Den-mark) for 5 minutes. Tris-buffered saline was used to rinse orwash the section between reagents, and all procedures wereperformed at room temperature. Sections were counterstainedwith Mayer’s hematoxylin. Cells positive for autophagy celldeath and tendon matrix positive for type I collagen were stainedbrown.
Section evaluation
Collagen structure gradingSlides of different staining were scanned and analyzed by Aperio’s120-slide ScanScope XT system (Aperio Technologies, Vista,CA), which was able to zoom freely up to �40 magnification.According to the ECM structure, all samples were graded into I,II, and III areas using the following criteria, which were modifiedfrom previous studies (Figure 1, A).8,15,21 The process of gradingwas done separately by 2 individuals and the 2 results werecompared. If an inconsistency existed, the field was reassessed anda final grade was agreed upon.
� Grade I: Slightly degraded collagen structure with slightwaviness and minimal splitting between contiguous fiberbundles (Figure 1, B).� Grade II: Moderately degraded collagen structure with some
separation between bundles, increased waviness, loss ofparallel arrangement and moderate fibre fragmentation(Figure 1, C).� Grade III: Severely degraded collagen structure with total loss
of fibre orientation and severely fragmented fibers (Figure 1,D).
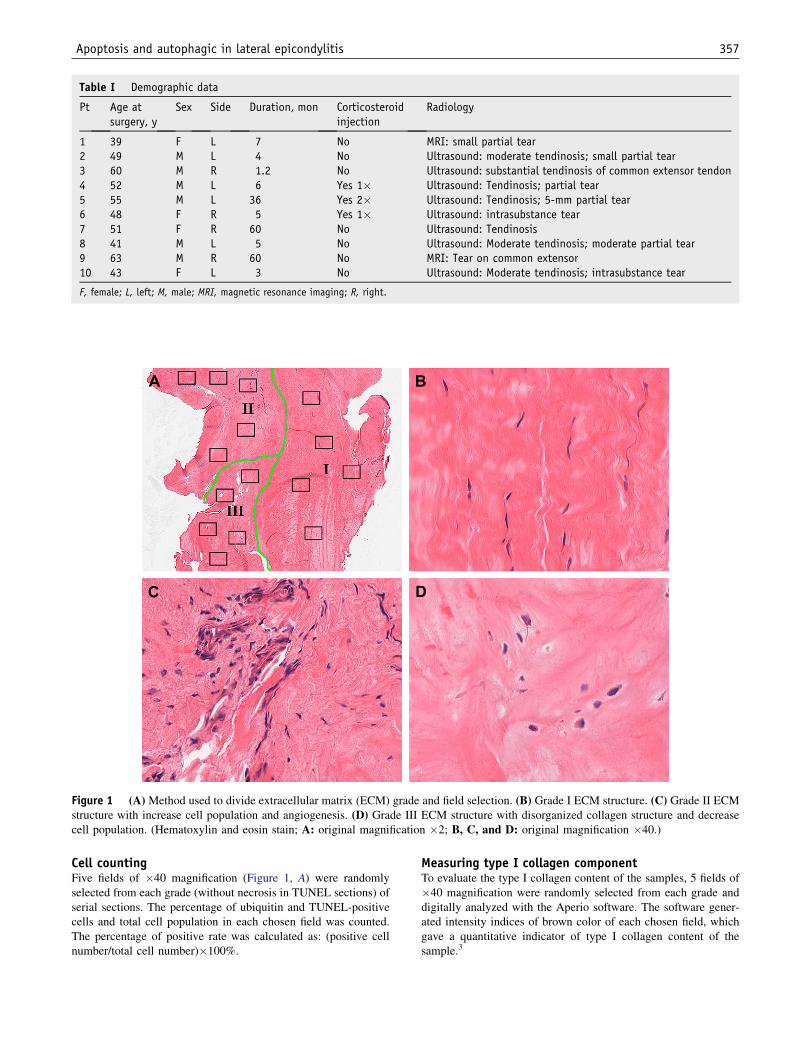
Table I Demographic data
Pt Age atsurgery, y
Sex Side Duration, mon Corticosteroidinjection
Radiology
1 39 F L 7 No MRI: small partial tear2 49 M L 4 No Ultrasound: moderate tendinosis; small partial tear3 60 M R 1.2 No Ultrasound: substantial tendinosis of common extensor tendon4 52 M L 6 Yes 1� Ultrasound: Tendinosis; partial tear5 55 M L 36 Yes 2� Ultrasound: Tendinosis; 5-mm partial tear6 48 F R 5 Yes 1� Ultrasound: intrasubstance tear7 51 F R 60 No Ultrasound: Tendinosis8 41 M L 5 No Ultrasound: Moderate tendinosis; moderate partial tear9 63 M R 60 No MRI: Tear on common extensor10 43 F L 3 No Ultrasound: Moderate tendinosis; intrasubstance tear
F, female; L, left; M, male; MRI, magnetic resonance imaging; R, right.
Figure 1 (A) Method used to divide extracellular matrix (ECM) grade and field selection. (B) Grade I ECM structure. (C) Grade II ECMstructure with increase cell population and angiogenesis. (D) Grade III ECM structure with disorganized collagen structure and decreasecell population. (Hematoxylin and eosin stain; A: original magnification �2; B, C, and D: original magnification �40.)
Apoptosis and autophagic in lateral epicondylitis 357
Cell countingFive fields of �40 magnification (Figure 1, A) were randomlyselected from each grade (without necrosis in TUNEL sections) ofserial sections. The percentage of ubiquitin and TUNEL-positivecells and total cell population in each chosen field was counted.The percentage of positive rate was calculated as: (positive cellnumber/total cell number)�100%.
Measuring type I collagen componentTo evaluate the type I collagen content of the samples, 5 fields of�40 magnification were randomly selected from each grade anddigitally analyzed with the Aperio software. The software gener-ated intensity indices of brown color of each chosen field, whichgave a quantitative indicator of type I collagen content of thesample.3

Figure 2 Ubiquitin staining (original magnification �40) for autophagy of tenocytes showed (A) the average ubiquitin-positive rate ofgraded I area was at its lowest post of 7.6% � 2.2%, (B) peaked at 13.7% � 3% in grade II area, and (C) then slightly decreased to 12.1% �4% in grade III area. The arrow indicates cells stained positive for ubiquitin. (D) The ubiquitin-positive rate of grade II and III area wassignificantly higher than that of grade I area (P < .01). The error bars designate the standard deviation.
358 J. Chen et al.
Statistical analysis
All values are expressed as mean � standard deviation. Statisticalanalysis among the different graded areas was performed usinganalysis of variance with SPSS 12.0 software (SPSS Inc, Chicago,IL). The confidence limit was predetermined at a probability levelof P � .05.
Results
General histology
On H&E staining, the degenerated ECRB samples revealeda highly variable collagen structure and cellularmorphology. In grade I areas, collagen fibers were contin-uously packed in a parallel pattern with slight splittingbetween bundles, and nearly all tendon cells were spindleshaped and aligned along the fiber orientation (Figure 1, B).In grade II areas, splitting and fragmentation of fiberbundles were common, with intense small blood vessel
genesis and cellular proliferation. A large proportion of thecells had lost the parallel alignment and became morerounded (Figure 2, C). In grade III areas, the parallelcollagen fiber pattern of normal tendon was totally lost andreplaced by a haphazard arrangement of highly fragmentedfiber and round tendon cell (Figure 3, D). The proliferationof blood vessel and cells were diminished in grade III areas.In addition, no calcification or inflammatory cells infiltra-tion was observed in any tendon samples.
Autophagic cell death of tenocytes
We have used ubiquitin as a marker for autophagic celldeath according to previous publications.10,11,24 In ECRBtendon samples, ubiquitin-positive cells were staineda brown color (Figure 2, A, B, C). The average ubiquitin-positive rate of all counted fields was 11.2% � 3.2%(Table II). The average ubiquitin-positive rate was lowest ingrade I areas at 7.6% � 2.2%, peaked at 13.7% � 3% ingrade II areas, and then slightly decreased to 12.1% � 4%in grade III areas. The ubiquitin-positive rate of grade II

Figure 3 The TUNEL assay for apoptotic tenocyte (original magnification �40) showed a (A) similar pattern as autophagic cell deathwas observed, with the lowest apoptotic rate found in graded I area of 23.2% � 4.8%, which (B) dramatically increased to 34.4% � 4% ingrade II area and (C) then slightly decreased to 28.4% � 5% in grade III area. The arrows designate cells stained positive for TUNEL assay.(D) The apoptotic rate in the grade II and III areas was significantly higher than that of the grade I area (P < .05). The error bars designatethe standard deviation.
Table II Analysis of apoptosis and autophagic cell death in the extensor carpi radialis brevis
Extensor carpiradialis brevis, mean�SD
Variable Grade I Grade II Grade III Mean
Autophagic celldeath, %
7.6� 2.2 13.7� 3 12.1� 4 11.2� 3.2
Apoptosis, % 23.2� 4.8 34.4� 4 28.4� 5 28.7� 5.6Cell density, cells/field 49� 19 107� 44 48� 17 .Collagen I intensity index 63.8� 9 58.�þ6.7 47.9� 4.8 .
SD, standard deviation.
Apoptosis and autophagic in lateral epicondylitis 359
and III areas was significantly higher than that of grade Iarea (P < .01; Figure 2, D).
Apoptotic cell death of tenocytes
Next, we used the TUNEL assay to determine the rate ofapoptotic cells in the ECRB tendon samples,28,30 and the
nuclei of apoptotic cells were stained brown (Figure 3 A,B, C). The average apoptotic rate of all counted fields was28.7% � 5.6% (Table II). A similar pattern to autophagiccell death was observed: the lowest average apoptotic ratewas found in grade I areas of 23.2% � 4.8%, it dramati-cally increased to 34.4% � 4% in grade II areas, and thenslightly decreased to 28.4% � 5% in grade III areas.
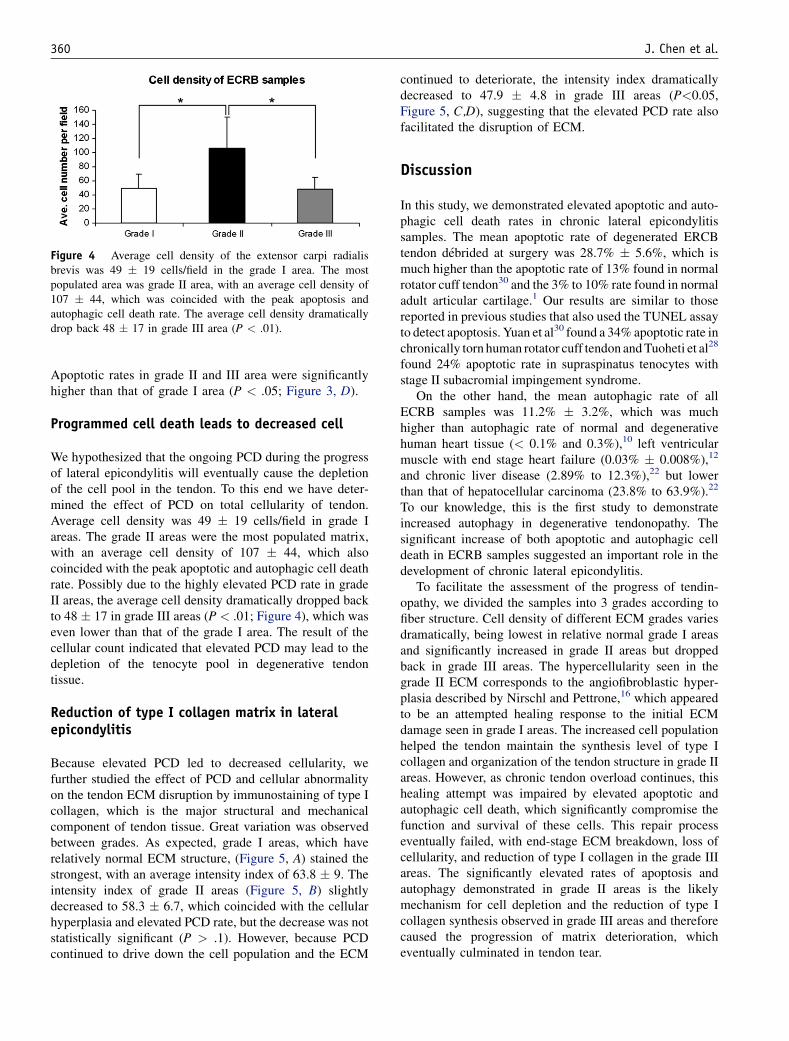
Figure 4 Average cell density of the extensor carpi radialisbrevis was 49 � 19 cells/field in the grade I area. The mostpopulated area was grade II area, with an average cell density of107 � 44, which was coincided with the peak apoptosis andautophagic cell death rate. The average cell density dramaticallydrop back 48 � 17 in grade III area (P < .01).
360 J. Chen et al.
Apoptotic rates in grade II and III area were significantlyhigher than that of grade I area (P < .05; Figure 3, D).
Programmed cell death leads to decreased cell
We hypothesized that the ongoing PCD during the progressof lateral epicondylitis will eventually cause the depletionof the cell pool in the tendon. To this end we have deter-mined the effect of PCD on total cellularity of tendon.Average cell density was 49 � 19 cells/field in grade Iareas. The grade II areas were the most populated matrix,with an average cell density of 107 � 44, which alsocoincided with the peak apoptotic and autophagic cell deathrate. Possibly due to the highly elevated PCD rate in gradeII areas, the average cell density dramatically dropped backto 48 � 17 in grade III areas (P < .01; Figure 4), which waseven lower than that of the grade I area. The result of thecellular count indicated that elevated PCD may lead to thedepletion of the tenocyte pool in degenerative tendontissue.
Reduction of type I collagen matrix in lateralepicondylitis
Because elevated PCD led to decreased cellularity, wefurther studied the effect of PCD and cellular abnormalityon the tendon ECM disruption by immunostaining of type Icollagen, which is the major structural and mechanicalcomponent of tendon tissue. Great variation was observedbetween grades. As expected, grade I areas, which haverelatively normal ECM structure, (Figure 5, A) stained thestrongest, with an average intensity index of 63.8 � 9. Theintensity index of grade II areas (Figure 5, B) slightlydecreased to 58.3 � 6.7, which coincided with the cellularhyperplasia and elevated PCD rate, but the decrease was notstatistically significant (P > .1). However, because PCDcontinued to drive down the cell population and the ECM
continued to deteriorate, the intensity index dramaticallydecreased to 47.9 � 4.8 in grade III areas (P<0.05,Figure 5, C,D), suggesting that the elevated PCD rate alsofacilitated the disruption of ECM.
Discussion
In this study, we demonstrated elevated apoptotic and auto-phagic cell death rates in chronic lateral epicondylitissamples. The mean apoptotic rate of degenerated ERCBtendon debrided at surgery was 28.7% � 5.6%, which ismuch higher than the apoptotic rate of 13% found in normalrotator cuff tendon30 and the 3% to 10% rate found in normaladult articular cartilage.1 Our results are similar to thosereported in previous studies that also used the TUNEL assayto detect apoptosis. Yuan et al30 found a 34% apoptotic rate inchronically torn human rotator cuff tendon and Tuoheti et al28
found 24% apoptotic rate in supraspinatus tenocytes withstage II subacromial impingement syndrome.
On the other hand, the mean autophagic rate of allECRB samples was 11.2% � 3.2%, which was muchhigher than autophagic rate of normal and degenerativehuman heart tissue (< 0.1% and 0.3%),10 left ventricularmuscle with end stage heart failure (0.03% � 0.008%),12
and chronic liver disease (2.89% to 12.3%),22 but lowerthan that of hepatocellular carcinoma (23.8% to 63.9%).22
To our knowledge, this is the first study to demonstrateincreased autophagy in degenerative tendonopathy. Thesignificant increase of both apoptotic and autophagic celldeath in ECRB samples suggested an important role in thedevelopment of chronic lateral epicondylitis.
To facilitate the assessment of the progress of tendin-opathy, we divided the samples into 3 grades according tofiber structure. Cell density of different ECM grades variesdramatically, being lowest in relative normal grade I areasand significantly increased in grade II areas but droppedback in grade III areas. The hypercellularity seen in thegrade II ECM corresponds to the angiofibroblastic hyper-plasia described by Nirschl and Pettrone,16 which appearedto be an attempted healing response to the initial ECMdamage seen in grade I areas. The increased cell populationhelped the tendon maintain the synthesis level of type Icollagen and organization of the tendon structure in grade IIareas. However, as chronic tendon overload continues, thishealing attempt was impaired by elevated apoptotic andautophagic cell death, which significantly compromise thefunction and survival of these cells. This repair processeventually failed, with end-stage ECM breakdown, loss ofcellularity, and reduction of type I collagen in the grade IIIareas. The significantly elevated rates of apoptosis andautophagy demonstrated in grade II areas is the likelymechanism for cell depletion and the reduction of type Icollagen synthesis observed in grade III areas and thereforecaused the progression of matrix deterioration, whicheventually culminated in tendon tear.

Figure 5 (A) The grade I area stained the strongest on type I collagen staining, with an average intensity index of 63.8 � 9. (B) Theintensity index of grade II area slightly decreased to 58.3 � 6.7, but the decrease was not statistically significant. (C) The intensity indexdramatically decreased to in 47.9 � 4.8 in grade III area (A, B, C: original magnification �40). (D) Type I collagen content in extensorcarpi radialis brevis dramatically decreased (P < .05) in grade III area. The error bars show the standard deviation.
Apoptosis and autophagic in lateral epicondylitis 361
At present, what triggers the tenocytes to undergoapoptosis and causes tendon degeneration is still unclear.Several in vitro studies4,23 showed that cyclic mechanicalstimulation can activate the stress-activated protein kinase(SAPK)/Jun N-terminal kinase (JNK) signaling pathwayand modulate the apoptosis of human tendon fibroblasts.In an animal study, Scott et al20 showed apoptosis couldbe induced by high-strain mechanical loading in a rattibialis anterior tendon. In addition, Soslowsky et al25
showed that repetitive use induced tendon degeneration ina mouse model. Riek et al18 suggested that repetitiveeccentric contraction of the ECRB during tennis swing isthe likely cause of microtrauma that causes tears in thetendon. All of these studies suggested that ‘‘repetitivestrain’’ is the major cause of tenocytes PCD and tendondegeneration.
Tendon tissues are very poorly vascularized. Hypo-vascularity makes the tendon susceptible to malnutritionand subsequently tendon damage.17 A recent study sug-gested that autophagy might be a survival mechanism onbehalf of the cell during nutrient depletion,27 in which
increased levels of autophagy lead to the breakdown ofnonvital organelles and the release of nutrients, ensuringthat vital processes can continue.29 The elevated autophagiccell death rate seen in our ECRB samples is possiblya response to malnutrition. However, the initiating mecha-nisms for autophagic cell death in tendon degenerationrequire further study.
This study has some limitations. First, because all thesamples were collected from the edge of degeneratedtendon, even the grade I areas had some degree of degen-erative change and cannot actually represent normal tendontissue. However, we focused on studying the variationbetween different histologic grades and observing thepossible contribution of apoptosis and autophagy in theprocess of tendon degeneration (degenerate from grade I toII or III), so no normal tendon samples were required asa control. Also, because we only showed the variation ofPCD rate between different areas, it is still unclear if PCDis the cause or the result of ECM. Further research isnecessary to provide a better understanding on tendondegeneration at a cellular and molecular level.

362 J. Chen et al.
In summary, this study demonstrated that apoptotic andautophagic cell death occur in the ECRB tendon in chroniclateral epicondylitis and that elevated apoptotic and auto-phagic cell death rates vary with increasing ECM disrup-tion. The tendon is relatively hypercellular in grade II areas,but a markedly elevated apoptotic rate and autophagy celldeath rate was also observed. This may be responsible forthe decrease in cell population and deterioration of collagenquality seen in grade III areas, and this eventuallycompromised the ability of the tendon to maintain integrityand resulted in tendon tear. Further research to betterunderstand the cellular changes in tendinopathy may allowclinical cellular therapies to arrest the progression oftendinopathy or improve the quality of surgical repair.
Disclaimer
All authors, their immediate family, and any researchfoundation with which they are affiliated did not receiveany financial payments or other benefits from anycommercial entity related to the subject of this article.No external funding was received in assisting this study.
References
1. Adams CS, Horton WE Jr. Chondrocyte apoptosis increases with age
in the articular cartilage of adult animals. Anat Rec 1998;250:418-25.
2. Anglade P, Vyas S, Javoy-Agid F, et al. Apoptosis and autophagy in
nigral neurons of patients with Parkinson’s disease. Histol Histopathol
1997;12:25-31.
3. Aperio. http://www.aperio.com/download-imagescope-viewer.asp. 2008.
4. Arnoczky SP, Tian T, Lavagnino M, Gardner K, Schuler P, Morse P.
Activation of stress-activated protein kinases (SAPK) in tendon cells
following cyclic strain: the effects of strain frequency, strain magnitude,
and cytosolic calcium. J Orthop Res 2002;20:947-52.
5. Bahr BA, Bendiske J. The neuropathogenic contributions of lysosomal
dysfunction. J Neurochem 2002;83:481-9.
6. Bursch W. The autophagosomal-lysosomal compartment in programmed
cell death. Cell Death Differ 2001;8:569-81.
7. Bursch W, Ellinger A, Gerner C, Frohwein U, Schulte-Hermann R.
Programmed cell death (PCD). Apoptosis, autophagic PCD, or others?
Ann N Y Acad Sci 2000;926:1-12.
8. Chen JM, Willers C, Xu J, Wang A, Zheng MH. Autologous tenocyte
therapy using porcine-derived bioscaffolds for massive rotator cuff
defect in rabbits. Tissue Eng 2007;13:1479-91.
9. Kerr JF, Wyllie AH, Currie AR. Apoptosis: a basic biological
phenomenon with wide-ranging implications in tissue kinetics. Br
J Cancer 1972;26:239-57.
10. Knaapen MW, Davies MJ, De Bie M, Haven AJ, Martinet W,
Kockx MM. Apoptotic versus autophagic cell death in heart failure.
Cardiovasc Res 2001;51:304-12.
11. Komatsu M, Waguri S, Chiba T, et al. Loss of autophagy in the central
nervous system causes neurodegeneration in mice. Nature 2006;441:
880-4.
12. Kostin S, Pool L, Elsasser A, et al. Myocytes die by multiple
mechanisms in failing human hearts. Circ Res 2003;92:715-24.
13. Kundu M, Thompson CB. Autophagy: basic principles and relevance
to disease. Annu Rev Pathol 2008;3:427-55.
14. Mistiaen WP, Somers P, Knaapen MW, Kockx MM. Autophagy as
mechanism for cell death in degenerative aortic valve disease: An
underestimated phenomenon in cardiovascular diseases. Autophagy
2006;2:221-3.
15. Movin T, Gad A, Reinholt FP, Rolf C. Tendon pathology in long-
standing achillodynia. Biopsy findings in 40 patients. Acta Orthop
Scand 1997;68:170-5.
16. Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of
lateral epicondylitis. J Bone Joint Surg Am 1979;61:832-9.
17. Rathbun JB, Macnab I. The microvascular pattern of the rotator cuff.
J Bone Joint Surg Br 1970;52:540-53.
18. Riek S, Chapman AE, Milner T. A simulation of muscle force and
internal kinematics of extensor carpi radialis brevis during backhand
tennis stroke: implications for injury. Clin Biomech (Bristol, Avon)
1999;14:477-83.
19. Scott A, Khan KM, Duronio V. IGF-I activates PKB and prevents
anoxic apoptosis in Achilles tendon cells. J Orthop Res 2005;23:
1219-25.
20. Scott A, Khan KM, Heer J, Cook JL, Lian O, Duronio V. High strain
mechanical loading rapidly induces tendon apoptosis: an ex vivo rat
tibialis anterior model. Br J Sports Med 2005;39:e25.
21. Shalabi A, Kristoffersen-Wiberg M, Papadogiannakis N, Aspelin P,
Movin T. Dynamic contrast-enhanced MR imaging and histopathology
in chronic Achilles tendinosis. A longitudinal MR study of 15 patients.
Acta Radiol 2002;43:198-206.
22. Shirahashi H, Sakaida I, Terai S, Hironaka K, Kusano N, Okita K.
Ubiquitin is a possible new predictive marker for the recurrence of
human hepatocellular carcinoma. Liver 2002;22:413-8.
23. Skutek M, van Griensven M, Zeichen J, Brauer N, Bosch U. Cyclic
mechanical stretching of human patellar tendon fibroblasts: activation
of JNK and modulation of apoptosis. Knee Surg Sports Traumatol
Arthrosc 2003;11:122-9.
24. Somers P, Knaapen M, Kockx M, Van Cauwelaert P, Bortier H,
Mistiaen W. Histological evaluation of autophagic cell death in
calcified aortic valve stenosis. J Heart Valve Dis 2006;15:43-7.
discussion 48.
25. Soslowsky LJ, Thomopoulos S, Tun S, et al. Neer Award 1999.
Overuse activity injures the supraspinatus tendon in an animal model:
a histologic and biomechanical study. J Shoulder Elbow Surg 2000;9:
79-84.
26. Stromhaug PE, Klionsky DJ. Approaching the molecular mechanism
of autophagy. Traffic 2001;2:524-31.
27. Tsujimoto Y, Shimizu S. Another way to die: autophagic programmed
cell death. Cell Death Differ 2005;12(Suppl. 2):1528-34.
28. Tuoheti Y, Itoi E, Pradhan RL, et al. Apoptosis in the supraspinatus
tendon with stage II subacromial impingement. J Shoulder Elbow Surg
2005;14:535-41.
29. Yorimitsu T, Klionsky DJ. Autophagy: molecular machinery for
self-eating. Cell Death Differ 2005;12(Suppl 2):1542-52.
30. Yuan J, Murrell GA, Wei AQ, Wang MX. Apoptosis in rotator cuff
tendonopathy. J Orthop Res 2002;20:1372-9.