
Pathogenesis of lymphoid lesions in murine experimental listeriosis
Upload
rbhs-rutgersCategory
view
0download
0
Robert C. Wilson, Hartmut Hanauske-Abel and Timothy A. McCaffreyPaula J. Bray, Baoheng Du, Victor M. Mejia, Steven C. Hao, Ezra Deutsch, Chenzhong Fu,
in Cells From Human Vascular LesionsGlucocorticoid Resistance Caused by Reduced Expression of the Glucocorticoid Receptor
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1999 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.19.5.11801999;19:1180-1189Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/19/5/1180World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from by guest on October 27, 2013http://atvb.ahajournals.org/Downloaded from

Glucocorticoid Resistance Caused by Reduced Expression ofthe Glucocorticoid Receptor in Cells From
Human Vascular LesionsPaula J. Bray, Baoheng Du, Victor M. Mejia, Steven C. Hao, Ezra Deutsch, Chenzhong Fu,
Robert C. Wilson, Hartmut Hanauske-Abel, Timothy A. McCaffrey
Abstract—Mechanisms that control the balance between cell proliferation and death are important in the development ofvascular lesions. Rat primary smooth muscle cells were 80% inhibited by low microgram doses of hydrocortisone (HC)and 50% inhibited by nanogram concentrations of transforming growth factor-b1 (TGF-b1), although some linesacquired resistance in late passage. However, comparable doses of HC, or TGF-b1, failed to inhibit most humanlesion-derived cell (LDC) lines. In sensitive LDC, HC (10mg/mL) inhibited proliferation by up to 50%, with obviousapoptosis in some lines, and TGF-b1 inhibited proliferation by more than 90%. Collagen production, as measured by[3H]proline incorporation or RIA for type III pro-collagen, was either unaffected or increased in the LDCs by HC. Thesedivergent responses between LDC lines were partially explained by the absence of the glucocorticoid receptor (GR) andheat shock protein 90 mRNA in 10 of 12 LDC lines, but the presence of the mineralocorticoid receptor and11b-hydroxysteroid dehydrogenase type II. Western blot analysis confirmed the absence of the GR protein in cellslacking GR mRNA. Immunohistochemistry of human carotid lesions showed high levels of GR in the tunica media, butlarge areas lacking GR in the fibrous lesion. Considering the absence of the GR in most lines, the effects of HC maybe elicited through the mineralocorticoid receptor. Functional resistance to the antiproliferative and antifibrotic effectsof HC may contribute to excessive wound repair in atherosclerosis and restenosis.(Arterioscler Thromb Vasc Biol.1999;19:1180-1189.)
Key Words: glucocorticoid receptorn transforming growth factor-b1 n atherosclerosisn cell proliferationn collagenproductionn smooth muscle cellsn restenosis
Restenotic narrowing of arteries after angioplasty orendarterectomy is caused principally by fibroprolifera-
tive intimal hyperplasia and contractile remodeling by a cellresembling both the vascular smooth muscle cell (SMC) andmyofibroblast.1,2 Serial angiography after angioplasty sug-gests that almost all patients will exhibit a fibroproliferativenarrowing after angioplasty, although in most patients thestenosis will spontaneously regress to exhibit a net luminalgain.3 However, in 40% of patients, this lesion fails toregress, but instead progresses to clinical restenosis (reviewedin Reference 4). Restenosis appears to be caused by themigration of cells into the intima, subsequent proliferation,and extracellular matrix deposition. In animal models, neo-intimal regression is caused by apoptosis of the lesion cells.5
In humans, growing evidence suggests that restenosis may becaused by a failure in growth inhibitory and apoptoticsystems that would normally mediate lesion regression.6,7
Thus, the persistence and slow proliferation of cells in theinjured vessel wall may be caused by a failure in endogenousinhibitory systems.
One defective inhibitory system involves the transforminggrowth factor-b1 (TGF-b1) receptor pathway. Lesion-derived cells (LDCs) from human atherosclerotic plaques areresistant to the inhibitory effects of TGF-b1 because of adecrease in the TGF-b type II signaling receptor.7 In somepatients, microsatellite instability in the TGF-b type IIreceptor is responsible for the resistance to TGF-b1 inLDCs.8 Another major inhibitory system of SMC prolifera-tion are glucocorticoids (GCs). When the hormone is boundto the glucocorticoid receptor (GR) complex, a fibrosuppres-sant effect is exerted, which is elicited in several ways:inhibition of SMC proliferation in vitro,9,10 inhibition ofcollagen production,11–13 induction of apoptosis in lympho-cytes and fibroblasts (for review see Reference 14), andanti-inflammatory or immunosuppressive actions.15,16 Giventhese diverse antifibrotic and antiproliferative actions, GCsshould be good candidates for preventing restenosis.
Animal studies have generally supported a beneficial effectof GCs on both primary, cholesterol-induced atherosclerosisand postangioplasty restenosis. In cholesterol models of
Received September 11, 1998; revision accepted November 16, 1998.From the Divisions of Hematology/Oncology (P.J.B., B.D., V.M.M., C.F., T.A.M.) and Cardiology (S.C.H., E.D.), Department of Medicine, and the
Division of Pediatric Endocrinology (R.C.W., H.H.-A.), Department of Pediatrics, Cornell University Medical College, New York, NY.Correspondence to Timothy A. McCaffrey, PhD, Cornell University Medical College, Division of Hematology/Oncology, Room C606, 1300 York Ave,
New York, NY 10021. E-mail [email protected]© 1999 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol.is available at http://www.atvbaha.org
1180

atherosclerosis, treatment with hydrocortisone has consis-tently been shown to lessen the severity of atherosclerosis invarious rabbit models.17–20 In models of balloon-catheterinjury, GCs typically inhibit neointimal proliferation in vivoin both rat21 and rabbit models,22–24although shorter, 1-weektreatments with dexamethasone have failed to inhibit intimalhyperplasia in rabbits.25
Despite these in vivo effects of steroids, 2 clinical trialshave failed to observe a beneficial role of GCs in preventingrestenosis in humans.26,27 Both studies administered highdoses of prednisolone, a synthetic GC, after successfulcoronary angioplasty, and both concluded that high-dosesteroid therapy does not influence the overall rate of resteno-sis after coronary angioplasty when compared with theuntreated control groups.
In vitro studies have observed that corticosteroids inhibitproliferation of SMCs derived from atherosclerotic arteries.28
However, to see any significant decrease in cell number (60%to 70%), highly concentrated doses of steroids were needed.In the case of hydrocortisone, 10 000-fold higher than phys-iological levels were required to see a 70% inhibition of SMCproliferation. Some diseases are known to involve acquiredresistance to GCs with time, and this resistance results fromthe relative inability of GCs to exert their effects on targettissues. Such diseases include asthma,29 rheumatoid arthri-tis,30 and acute lymphoblastic leukemia.31 The present studiesexamine the hypothesis that arteriosclerosis may also involveacquired resistance to GCs. The results indicate that themajority of cell lines from human endarterectomy lesions areresistant to the antiproliferative effects of hydrocortisone andthis may be caused by the absence of the GR or othermembers of the GR multiprotein complex.
MethodsVascular SpecimensVascular lesions were acquired as waste surgical material, underInstitutional Review Board approved protocols, from patients under-going surgical endarterectomy at the New York Hospital/CornellMedical Center. Portions of the vascular lesions were explanted forcell culture, and the remainder was fixed in 4% buffered formalde-hyde and paraffin-embedded for immunohistochemical analysis.
Cell CultureVascular lesions from carotid and femoral or iliac endarterectomyspecimens were finely diced, and the explants placed in 25-cm2
tissue culture flasks containing medium 199 (M199; Gibco BRL)
supplemented with 10% FBS and gentamicin sulfate (50mg/mL).LDCs from the explants were subcultured with trypsin/EDTA (GibcoBRL) at a 1:2 split ratio. Cells were obtained in approximately 30%of the patient specimens acquired and could typically be maintainedfor 5 to 8 passages (p5 through p8), although most analyses wereconducted as soon as sufficient cell numbers were obtained (p2through p4). Rat SMCs were explanted from the aorta of 3-month-old Fisher 344 (Harlan Sprague Dawley, Indianapolis, IN) rats andalso grown in M199 with 10% FBS and gentamicin sulfate for up to40 passages.
Cell ProliferationThe effect of the steroids on the rate of DNA synthesis was examinedby semiautomated methods. Cells were plated at 13104 cells/well of96-well microtiter plates at least 24 hours before the assay. Hydro-cortisone (0.01 to 10mg/mL) was added to M199 plus 1% FBS for20 hours before the cells were pulsed with [3H]thymidine (1mCi/mL;NEN) for 4 hours. Cells were collected with trypsin/EDTA and a cellharvester (Wallac, Inc), and the DNA-incorporated label was deter-mined by scintillation counting (Betaplate; Wallac, Inc) (n53 perpoint). Cell proliferation was also determined over a 5-day periodwith exposure to hydrocortisone or TGF-b1, or both, followed bytrypsinization and physical counting of the cells using a particlecounter (Coulter ZBI).
Protein SynthesisThe rate of protein synthesis was measured by [3H]proline incorpo-ration, which is partially incorporated into proline-rich proteins suchas collagen. Cells were plated as described for cell proliferation.Hydrocortisone was added to the cells (M199/1%FBS) at least 4hours before the cells were pulsed with [3H]proline (4 mCi/mL;L-[5-3H]proline; NEN) for 24 hours. The supernatants were precip-itated in 10% trichloroacetic acid (TCA). The adherent cell mono-layer was washed twice with PBS and then dissolved with 1 mol/LNaOH for 30 minutes at 37°C. The TCA-precipitated supernatantand cell monolayer were counted using a scintillation counter. Allconcentrations were tested in replicates of 3 wells.
Collagen SecretionPooled triplicate supernatants from the cell proliferation assays wereanalyzed further by radioimmunoassay techniques for the presenceof antigenic material derived from the N-terminal pro-peptide of typeIII (PIIINP; Incstar) collagen. A 1-step equilibrium-type assay usingpolyclonal rabbit antibodies against purified human pro-peptideantigen was used. All samples were measured in duplicate, interpo-lated to a standard curve, and expressed in nanograms3104 cells.
RNA ExtractionTotal RNA was extracted from cell cultures by RNAzol B (Tel Test).Briefly, the supernatant was removed and RNAzol B was added tothe cells and rapidly harvested (0°C to 4°C) with a sterile scraper.The cell suspension was collected, chloroform was added, and themixture was centrifuged at 14 000g for 15 minutes at 4°C. The
Oligonucleotide Primers Used for RT-PCR
Primer Forward No. Reverse No. PCR Product Accession No. Reference
Human GR 249–270 657–676 428 bp M10901 54
Rat GR 1088–1111 1468–1497 404 bp M14053 35
MR 2769–2795 3168–3194 426 bp M16801 36
11b-HSD2 278–299 676–697 304 bp (RNA) U27318 37
Hsp 70 493–516 913–936 443 bp L12723 38
Hsp 90 344–366 517–526 182 bp X15183 57
hGRa 3325–3346 3617–3638 314 bp M10901 54
hGRb 2500–2522 2930–2951 452 bp M11050 54
TGF-b receptor I 1260–1283 1491–1514 255 bp L11695 58
MR indicates mineralocorticoid receptor; Hsp, heat shock protein; hGR, human GR; and 11b-HSD2,11b-hydroxy steroid dehydrogenase type II.
Bray et al May 1999 1181

aqueous phase was collected and mixed with an equal volume ofisopropanol and centrifuged at 14 000g for 15 minutes at 4°C, andthe resulting pellet was washed with ethanol.
Reverse Transcription–Polymerase ChainReaction (RT-PCR)The oligonucleotide primers used for RT-PCR analysis of selectedsteroid hormone receptors are listed in the Table. Total RNA (500ng) was reverse transcribed into cDNA with MuLV reverse tran-scriptase at 42°C with random hexamers (Perkin Elmer) followed byPCR with Taq polymerase in a 100-mL reaction containing0.2 mmol/L of dNTPs and 0.15mmol/L of each primer. The PCRprofile varied for particular primer pairs but generally consisted of aninitial 1-minute denaturation at 95°C, then 35 cycles of 1-minutedenaturation at 95°C, 2-minute annealing at 60°C, 1-minute exten-sion at 72°C, and finally a 10-minute extension at 72°C. Fifteenmicroliters of PCR product were separated in 1.5% (wt/vol) agarosegel and stained with ethidium bromide.
Western Blot AnalysisThe conditioned media of the LDCs was removed and concentrated(Centricon 10; Amicon), and protein lysates were made from theLDCs. Lysis buffer (40 mmol/L Tris-base, 1% Triton X-100,2 mmol/L MgCl2, 0.1 mmol/L PMSF, 5mg/mL leupeptin; pH 8.8)was added to the LDCs, which were then harvested and sonicated for5 s. Protein content was determined by the bicinchoninic acid (BCA)assay (Pierce), and 30mg was used for analysis. Samples were boiledfor 10 minutes, analyzed by SDS-PAGE, and electroblotted ontopolyvinylidene difluoride (PVDF membranes) (NEN Life Science)in 160 mmol/L glycine, 25 mmol/L Tris base, and 20% methanoltransfer buffer. The PVDF membrane was then blocked in Tris-buffered saline (TBS)-milk (20 mmol/L Tris-HCl, 150 mmol/LNaCl, and 4% powdered milk; pH 7.4) for 2 hours. The membranewas exposed to the anti-GR antibody (diluted 1:100, NovacastraLaboratories) overnight, then washed in TBS before application ofthe peroxidase-conjugated anti-mouse IgG (diluted 1:1000), whichwas detected by chemiluminescence (NEN Life Science).
Apoptosis Assays
Terminal Deoxyribonucleotide Transferase-MediateddUTP Nick-End LabelingFragmented DNA was labeled in situ by use of the terminaldeoxyribonucleotide transferase-mediated dUTP nick-end labeling(TUNEL) method (Boehringer-Mannheim). Briefly, LDCs wereplated on 8-well chambered glass slides at least 24 hours beforetreatment. Hydrocortisone (10mg/mL) was added to the cells for 24and 48 hours before the TUNEL assay (M199/1%FBS). The cellswere fixed in 4% buffered formaldehyde and permeabilized (0.1%Triton X-100, 0.1% sodium citrate). The fragmented DNA waslabeled with fluorescein dUTP at strand breaks identified by terminaldeoxynucleotide transferase (TdT) for 1 hour in the dark at 37°C.The cells were then analyzed directly under a fluorescence micro-scope. Negative controls were performed by omitting the TdT. Foreach treatment group 10 fields (approximately 400 cells) werecounted and the percentage of TUNEL-positive cells calculated.
Colorimetric MTT AssayThe MTT reduction by mitochondria is a measure of metabolism andtherefore only detects living cells.39a Inhibition of MTT reductionhas been used as a quantitative assay for apoptosis. Cells were platedas described for cell proliferation. Hydrocortisone was added to thecells (M199/1%FBS) at least 20 hours before the cells were pulsedwith MTT (0.5 mg/mL) for 4 hours. The medium was removed andDMSO was added to dissolve the dark blue crystals; the mixture wasthoroughly shaken at room temperature for 30 minutes. The opticaldensity of each well was determined by absorbance at 540 nm.
ImmunocytochemistryPortions of endarterectomy specimens were fixed in phosphate-buffered 4% formaldehyde, paraffin-embedded, and immunostainedby standard procedures for the avidin-biotin enhanced immunoper-
oxidase detection (Vector Laboratories). Primary antibodies includeda monoclonal antibody to detect the GR (NCL-GCR; NovacastraLaboratories), HAM56 to detect macrophages, a mouse IgG controlantibody (Cappel Cooper Diagnostics), and HHF35 to detect SMC-specific actin (kindly provided by A. Gown40). Positive immuno-staining was detected with DAB, and tissues were counterstainedwith hematoxylin.
In Situ HybridizationLDC lines were plated onto glass multichamber slides (Labtek) andallowed to adhere for at least 24 hours before fixation withDEPC-treated 4% buffered formaldehyde for 20 minutes. The fixedmonolayer was prehybridized with hybridization buffer (2 mg/mLnuclease-free BSA, 20% dextran sulfate, 20 mmol/L EDTA, 1mg/mL yeast tRNA, 200mg/mL poly(A), 43 SSC in Denhardt’ssolution), and then the mRNA for the GR was detected in LDC by insitu hybridization (ISH) of a digoxigenin-labeled probe in hybrid-ization buffer at 45°C overnight. Free probe was washed with 23SSC at 37°C. Hybrids were detected with anti-digoxigenin/alkalinephosphatase visualized with Fast Red substrate.
ResultsRat SMC Sensitivity to GCsPrimary SMCs isolated from Fisher 344 rat aortas weresignificantly growth-inhibited (P,0.05) by treatment withincreasing concentrations of hydrocortisone for 20 hours(Figure 1A), as measured by [3H]thymidine incorporation. Inboth of the rat lines tested (R8 and R13), strong inhibition(approximately 60% to 90%) occurred at low doses ofhydrocortisone, 0.125 to 1.25mg/mL. Higher doses of hydro-cortisone further inhibited proliferation, which was maximalat 1250 mg/mL of hydrocortisone with an 80% to 90%decrease in DNA synthesis. Later passages of one of the ratSMC lines (R13-P32) were resistant to the antiproliferativeeffects of hydrocortisone, suggesting an acquired resistanceto hydrocortisone in these SMCs. Essentially identical resultswere obtained with dexamethasone when corrected for the30-fold greater potency of this synthetic steroid (not shown).Further, the inhibitory effect of GCs on DNA synthesis wascorroborated by marked decreases in cell numbers over a6-day period. Dexamethasone, at 0.040mg/mL (equivalent to1.2 mg/mL of hydrocortisone) caused a 62% decrease in cellproliferation of R8 and 40% decrease in R13.
The inset in Figure 1 demonstrates the presence of the GRby RT-PCR (404 bp) in both early (P4) and late passages (P29or P32) of these 2 rat SMC lines. Thus, serial subpassage can,
Figure 1. Antiproliferative responses to hydrocortisone orTGF-b1 in rat aortic SMC. SMC from rat aorta were exposed toincreasing concentrations of hydrocortisone for 20 hours andthen the rate of DNA synthesis was measured by [3H]thymidineincorporation (n53, bars5SEM). Insets represent RT-PCR analy-sis of the rat GR in early and late passages of the same ratSMC line.
1182 Glucocorticoid Resistance in Lesion-Derived Cells

but need not, cause rat SMCs to become resistant to hydro-cortisone, and in this case, the functional resistance isapparently not caused by the loss of the GR mRNA.
Both rat SMC lines were also sensitive to the antiprolif-erative effects of TGF-b1 in early passages, with a 65%decrease in cell proliferation at 10 ng/mL TGF-b1. Laterpassages of R13, but not R8, became resistant to the antipro-liferative effects of TGF-b1, thus paralleling the response tohydrocortisone and dexamethasone. TGF-b resistance with invitro aging of the R13 line could be attributed to loss of thetype II receptor (not shown), in a manner similar to the knownloss of the type II receptor in SMCs derived from aged rats.41
TGF-b resistance may also explain the acquired resistance tohydrocortisone in R13 because hydrocortisone has beenreported to inhibit cell proliferation via activation ofTGF-b.42
Effects of Hydrocortisone on DNA Synthesisin LDCsLDCs were treated with increasing concentrations of hydro-cortisone or TGF-b1 under conditions similar to the ratstudies. After 20 hours of low-dose hydrocortisone treatment(1 mg/mL), LDC proliferation was not inhibited (as measuredby [3H]thymidine incorporation) in 5 of 8 lesion-derivedSMC lines (Figure 2C; LDC sensitivity is defined as.50%inhibition of DNA synthesis). This low dose of hydrocorti-sone is 10 times higher than the physiological levels ofcortisol in the body (average cortisol levels at NY Hospitalare 0.1260.03 mg/mL). Much higher concentrations of hy-drocortisone (10mg/mL; 100-fold higher than physiological),were needed to produce any detectable inhibition of cellproliferation in 5 of 8 LDC lines. At the highest tested dose,3 of 8 cell lines remained resistant to the antiproliferativeeffects of hydrocortisone (Figure 2C). Only 2 cells lines,E12sc (a clone ofsmall cells) and late passage E137, were
inhibited strongly (75%) with high-dose hydrocortisone treat-ment (Figure 2A), a result comparable with the sensitive ratSMCs. In a third line, E47sc (also clonal), hydrocortisoneinhibited DNA synthesis by 50% (Figure 2A).
Our laboratory previously has shown that LDCs are resis-tant to the inhibitory effects of TGF-b1.7 Figure 2D confirmsthat 6 of 8 LDC lines were resistant to the effects of TGF-b1.The majority of these resistant cell lines were also resistant tohydrocortisone (ie, E60, E64, E63, E145, and E137 early).Two hydrocortisone-sensitive cell lines, E47sc and E137 latepassage, were also extremely sensitive to TGF-b1, exhibiting75% to 90% inhibition of DNA synthesis (Figure 2B).
GC-Induced ApoptosisGCs have been reported in the literature to induce apoptosisin fibroblasts and lymphocytes;14 however, their effect onapoptosis of human vascular SMCs has not been reported.Exposure to hydrocortisone (10mg/mL) for 48 hours in anormal human neonatal SMC line (CRL1999) causes a smallincrease in the rate of apoptosis compared with untreatedcontrol cells (Figure 3A). A small increase in cell death wasalso observed in the E12sc and E47sc LDC lines treated withhydrocortisone. However, the E85 LDC line, after 48 hours ofhigh-dose hydrocortisone treatment (10mg/mL), had thegreatest increase of cell death with a 3-fold increase abovebasal levels (Figure 3A).
The MTT assay was used as a second method of measuringcell death. After 20 hours of exposure of the normalCRL1999 SMC line to increasing concentrations of hydro-cortisone, a dose of 10mg/mL hydrocortisone decreased cellsurvival by 30% (Figure 3B). Both E12sc and E47sc LDClines were resistant to the hydrocortisone-induced effects on
Figure 2. Antiproliferative responses to hydrocortisone orTGF-b1 in LDCs. A, Inhibition of DNA synthesis in 3 LDC linesafter 20 hours of treatment with increasing concentrations ofhydrocortisone. B, Sensitivity to increasing concentrations ofTGF-b1 in 2 LDC lines. C, Resistance to the inhibitory effects ofhydrocortisone in 5 LDC lines. D, Resistance to the antiprolifera-tive effects of TGF-b1 in 6 LDC lines.
Figure 3. Apoptotic responses to hydrocortisone in LDCs. A,TUNEL analysis of LDC treated for 48 hours with 10 mg/mL ofhydrocortisone (grey bars) (n52 to 3). For each treatment group,10 fields (approximately 400 cells) were counted and the per-centage of TUNEL-positive cells calculated. B, MTT assay is ameasure of cell survival, and thus a decrease in MTT absor-bance is reflective of cell death. Cells were treated with increas-ing concentrations of hydrocortisone, and after 20 hours MTTactivity was measured. All results are expressed as a percent-age of control, with no hydrocortisone treatment given as 100%(n52 to 3).
Bray et al May 1999 1183

cell death (Figure 3B). E85 was very sensitive to theapoptotic effects of hydrocortisone, with a 30% increase incell death at 10mg/mL hydrocortisone, a similar pattern asthat seen with the TUNEL assay (Figure 3A). In general, theTUNEL assay underestimates the number of apoptotic cellsbecause cells detach and are lost in subsequent washing steps.The MTT assay is more accurate as only live cells reduce theMTT, but is confounded by the effect of proliferation innonapoptotic cells.
Pro-Collagen III Production by LDCsA major antifibrotic effect of GCs is a decrease in type I andIII collagen synthesis in many cell types, including fibro-blasts12,13 and ureteral SMCs.43 However the effects of GCson cells derived from atherosclerotic lesions are unknown.Given the resistance of most LDC lines to HC, the effect onprotein and collagen synthesis was examined.
After 5 days’ treatment of the E47sc LDCs with eitherhydrocortisone alone or in the presence of TGF-b1, the cellswere counted and the supernatants removed for the pro-collagen III RIA (PCNPIII). Both TGF-b1 (1 ng/mL) andhydrocortisone (10mg/mL) inhibited cell proliferation by upto 50% (Figure 4A). Analyzing the supernatants from thesecells for pro-collagen III synthesis, hydrocortisone (10mg/mL) increased pro-collagen III production by 2-fold(Figure 4B). This effect was further exaggerated with theaddition of TGF-b1. To confirm this increase in collagensynthesis, proline incorporation (an indirect measure of col-lagen production) was increased markedly in TGF-b1- andhydrocortisone-treated cells (Figure 4C). Related studiesobserved similar increases in proline incorporation indepen-dent of changes in cell number (not shown). These resultssuggest that GCs enhance, not reduce, collagen production inLDCs.
Analysis of the GR mRNA in LDCs by RT-PCRTo determine the molecular basis for the resistance tohydrocortisone, RNA extracted from LDCs was analyzed forthe presence of the human GR by RT-PCR. The primers weredirected to exon 2, giving a 428-bp product, and after 35cycles of PCR, mRNA for the GR was absent in 10 of 14LDC lines (Figure 5A; only 6 cell lines shown). LDCs frompatient E137 expressed the GR in early (E137E) but not late(E137L) passage. Only 3 other lines were observed withdetectable GR mRNA levels, E12sc, E145, which expresseda low level, and normal SMCs derived from internal mam-mary arteries (IMA) (Figure 5B).
Two GR isoforms have been identified, hGRa and hGRb,which originate by alternative splicing of exon 9. hGRa isfully functional and hGRb has no hormone-binding activityand is thought to act as a dominant-negative inhibitor of GRfunction.44 The cell lines that expressed the GR mRNA in theprior study (IMA, E12sc, E137E, and E145) were tested forexpression of the 2 receptor isoforms. PCR primers todistinguish between the 2 receptor isoforms were directed toexon 9a or 9b, and in all cases the functional hGRa (314-bpPCR product) was present and hGRb absent (452 bp; Figure5B). As in the prior study, E137E expressed the highest levelof GR mRNA expression.
To confirm the absence of the GR in LDC lines, in situhybridization for the GR was performed on a receptor-
positive LDC line (E12sc) and a negative cell line (E47sc).Figure 5C illustrates positive staining for the GR (anti-sense)in the E12sc LDC line but not E47sc. The sense controls werenegative both in E12sc and E47sc, suggesting the positivehybridizations were not caused by nonspecific annealing ofprobe.
Presence of Heat Shock Protein 70 But Not HeatShock Protein 90 in LDCsThe unliganded GR is part of a multiprotein complex,comprising 2 molecules of heat shock protein 90 (Hsp 90), 1molecule of Hsp 70, 1 molecule of Hsp 56, and 1 molecule ofHsp 26. Abnormal Hsp 70 and Hsp 90 have been reported insteroid-resistant acute lymphoblastic leukemia,31 suggestingthat if these proteins are absent or dysfunctional, the GRmultiprotein complex is unable to form and enter the nucleus,rendering the cells resistant to GCs. RT-PCR analysis of 6LDCs and 1 normal SMC line (IMA) indicated that Hsp 90(Figure 6, top) was detected only faintly in 1 line (E85) andwas absent in all other lines (182-bp product). Hsp 70 (Figure6, middle) was strongly positive in 5 of the cell lines (443 bp)but undetectable in E137 and E47sc. The presence of the type
Figure 4. Proliferative and fibrotic responses to hydrocortisonein LDCs. A, Cell numbers after 20 hours of treatment withTGF-b (1 ng/mL) alone or TGF-b plus hydrocortisone (0.1 to 10mg/mL), or hydrocortisone alone (10 mg/mL) in E47sc LDCs. B,The supernatants from A were analyzed by RIA for pro-collagentype III (n52) and corrected for differences in cell number. C,[3H]proline incorporation was determined after 20 hours ofhydrocortisone treatment (n53) in the presence of TGF-b (1ng/mL).
1184 Glucocorticoid Resistance in Lesion-Derived Cells
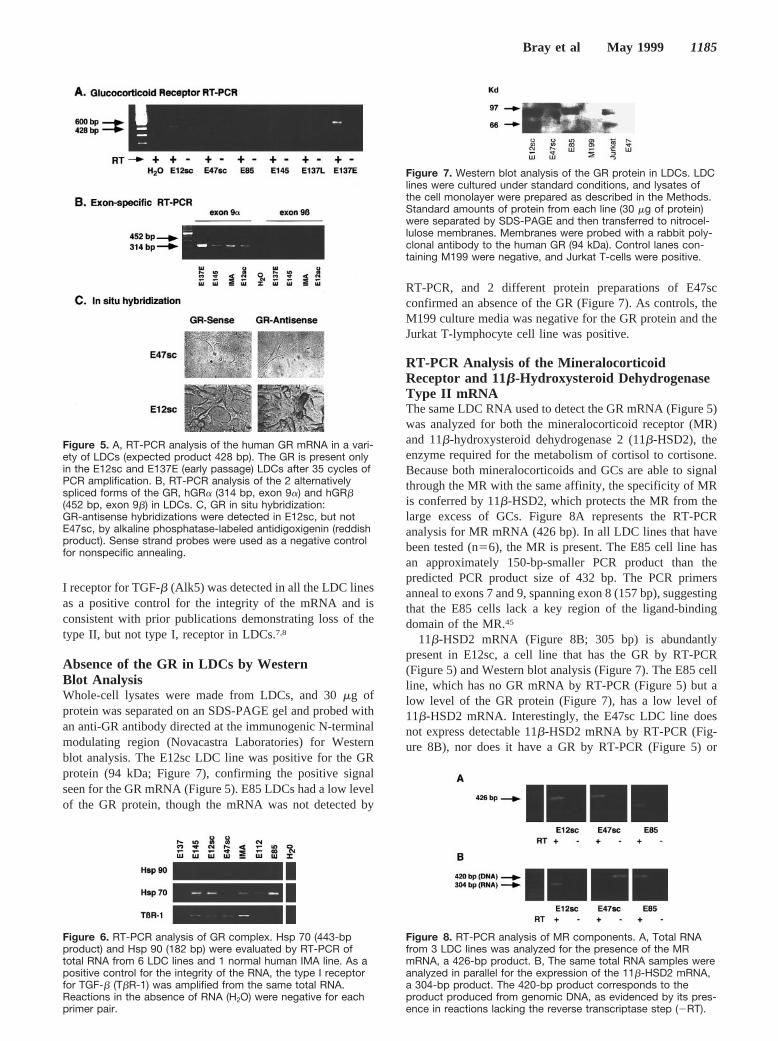
I receptor for TGF-b (Alk5) was detected in all the LDC linesas a positive control for the integrity of the mRNA and isconsistent with prior publications demonstrating loss of thetype II, but not type I, receptor in LDCs.7,8
Absence of the GR in LDCs by WesternBlot AnalysisWhole-cell lysates were made from LDCs, and 30mg ofprotein was separated on an SDS-PAGE gel and probed withan anti-GR antibody directed at the immunogenic N-terminalmodulating region (Novacastra Laboratories) for Westernblot analysis. The E12sc LDC line was positive for the GRprotein (94 kDa; Figure 7), confirming the positive signalseen for the GR mRNA (Figure 5). E85 LDCs had a low levelof the GR protein, though the mRNA was not detected by
RT-PCR, and 2 different protein preparations of E47scconfirmed an absence of the GR (Figure 7). As controls, theM199 culture media was negative for the GR protein and theJurkat T-lymphocyte cell line was positive.
RT-PCR Analysis of the MineralocorticoidReceptor and 11b-Hydroxysteroid DehydrogenaseType II mRNAThe same LDC RNA used to detect the GR mRNA (Figure 5)was analyzed for both the mineralocorticoid receptor (MR)and 11b-hydroxysteroid dehydrogenase 2 (11b-HSD2), theenzyme required for the metabolism of cortisol to cortisone.Because both mineralocorticoids and GCs are able to signalthrough the MR with the same affinity, the specificity of MRis conferred by 11b-HSD2, which protects the MR from thelarge excess of GCs. Figure 8A represents the RT-PCRanalysis for MR mRNA (426 bp). In all LDC lines that havebeen tested (n56), the MR is present. The E85 cell line hasan approximately 150-bp-smaller PCR product than thepredicted PCR product size of 432 bp. The PCR primersanneal to exons 7 and 9, spanning exon 8 (157 bp), suggestingthat the E85 cells lack a key region of the ligand-bindingdomain of the MR.45
11b-HSD2 mRNA (Figure 8B; 305 bp) is abundantlypresent in E12sc, a cell line that has the GR by RT-PCR(Figure 5) and Western blot analysis (Figure 7). The E85 cellline, which has no GR mRNA by RT-PCR (Figure 5) but alow level of the GR protein (Figure 7), has a low level of11b-HSD2 mRNA. Interestingly, the E47sc LDC line doesnot express detectable 11b-HSD2 mRNA by RT-PCR (Fig-ure 8B), nor does it have a GR by RT-PCR (Figure 5) or
Figure 5. A, RT-PCR analysis of the human GR mRNA in a vari-ety of LDCs (expected product 428 bp). The GR is present onlyin the E12sc and E137E (early passage) LDCs after 35 cycles ofPCR amplification. B, RT-PCR analysis of the 2 alternativelyspliced forms of the GR, hGRa (314 bp, exon 9a) and hGRb(452 bp, exon 9b) in LDCs. C, GR in situ hybridization:GR-antisense hybridizations were detected in E12sc, but notE47sc, by alkaline phosphatase-labeled antidigoxigenin (reddishproduct). Sense strand probes were used as a negative controlfor nonspecific annealing.
Figure 6. RT-PCR analysis of GR complex. Hsp 70 (443-bpproduct) and Hsp 90 (182 bp) were evaluated by RT-PCR oftotal RNA from 6 LDC lines and 1 normal human IMA line. As apositive control for the integrity of the RNA, the type I receptorfor TGF-b (TbR-1) was amplified from the same total RNA.Reactions in the absence of RNA (H2O) were negative for eachprimer pair.
Figure 7. Western blot analysis of the GR protein in LDCs. LDClines were cultured under standard conditions, and lysates ofthe cell monolayer were prepared as described in the Methods.Standard amounts of protein from each line (30 mg of protein)were separated by SDS-PAGE and then transferred to nitrocel-lulose membranes. Membranes were probed with a rabbit poly-clonal antibody to the human GR (94 kDa). Control lanes con-taining M199 were negative, and Jurkat T-cells were positive.
Figure 8. RT-PCR analysis of MR components. A, Total RNAfrom 3 LDC lines was analyzed for the presence of the MRmRNA, a 426-bp product. B, The same total RNA samples wereanalyzed in parallel for the expression of the 11b-HSD2 mRNA,a 304-bp product. The 420-bp product corresponds to theproduct produced from genomic DNA, as evidenced by its pres-ence in reactions lacking the reverse transcriptase step (2RT).
Bray et al May 1999 1185

Western blot analysis (Figure 7). The 420-bp product corre-sponds to genomic DNA, confirmed by its presence inreactions lacking reverse transcription (2RT).
Immunohistochemical Analysis of the GR inEndarterectomy LesionsImmunohistochemical analysis of endarterectomy lesionspecimens from 3 patients demonstrated that the GR wasexpressed strongly by cells within the tunica media (Figure9A). In this patient, GR staining was also strongly positivearound a small branching blood vessel. However, withinthe atherosclerotic lesion, there was only scattered andrelatively weak immunoreactivity for the GR. This con-firms the in vitro observation of low levels of GRexpression detected by RT-PCR and Western blot analysis.The majority of the GR-positive cells were SMC/myofi-broblasts as indicated by thea-smooth muscle-actin stain-ing of adjacent sections of the same patient (Figure 9B).An antibody to detect macrophages in the lesion (HAM56)showed very little positive immunoreactivity (Figure 9C).The staining seen in the mouse IgG control section is onlythe hematoxylin counterstain (Figure 9D).
DiscussionSeverely narrowed carotid or coronary vessels are commonlyrevascularized by surgical endarterectomy or balloon angio-plasty, respectively. Although initially successful in restoringflow in almost all patients, the major limitation of theseprocedures is fibroproliferative restenosis of the arteriesduring the 6-month period after the procedure.4 The findingsof this paper illustrate that the majority of cell lines derived
from human endarterectomy lesions are resistant to theantiproliferative effects of hydrocortisone, because of de-creased expression of the GR, as determined by RT-PCR,Western blot analysis, and immunohistochemistry of the GRin endarterectomy lesions.
Prior studies have shown that cells derived from arteries ofaged rats41 and from human atherosclerotic lesions7 are bothresistant to the inhibitory effects of TGF-b1. This resistancecould be attributed to the loss of the type II TGF-b signalingreceptor, and in a subset of patients, this loss was caused bymicrosatellite instability in the TGF-b type II receptor gene.8
Although TGF-b1 is one of the key activating and suppress-ing factors in fibroproliferative disease, the GC system is alsorecognized as an important fibrosuppressive pathway. Exten-sive clinical and experimental evidence have suggested thathydrocortisone and its synthetic analogs (ie, dexamethasoneand prednisone) suppress fibroproliferative diseases by actingas antiproliferative agents,9,10 antifibrotic agents that reducecollagen production,11–13 anti-inflammatory agents,15,16 andapoptotic factors.14
Given these diverse suppressive effects on fibroprolifera-tive pathways, GCs should suppress restenosis, yet publishedclinical trials indicated that high-dose steroid therapy doesnot influence the overall rate of restenosis. Stone et al27
randomly assigned 102 patients with documented restenosisafter a prior successful coronary angioplasty to receivetreatment during repeat coronary angioplasty at the restenoticsite. Treated patients received 125 mg methylprednisoloneintramuscularly the evening before and the morning ofangioplasty and then oral prednisolone (60 mg/d) for 7 daysafter coronary angioplasty. Angiographic follow-up at 6months revealed the steroid-treated group had a 59% reste-nosis rate compared with the no-steroid control group, whichhad a 56% restenosis rate. A second randomized clinical trialexamined 915 patients in total. Treated patients (n5215)received a single dose of methylprednisolone (1 g IV; 2 to 24hours before coronary angioplasty). Again, angiography at 6months’ follow-up showed a 40% restenotic rate in thesteroid-treated group compared with 39% in the controlgroup.26
One possible explanation for the lack of a clinical benefitis insufficient local concentration of the drug at the site ofinjury. Intramural administration of hydrocortisone incorpo-rated into polymer microspheres caused a significant reduc-tion in post-angioplasty intimal hyperplasia in rabbits.46
Likewise, local delivery of dexamethasone via adventitialcuffs around the rat carotid artery produced a 75% reductionin balloon catheter–induced intimal hyperplasia.21 However,local delivery of dexamethasone by a novel polymer-coatedeluting stent in the porcine coronary injury model did notdecrease intimal hyperplasia.47
An alternate explanation for the clinical resistance tosteroid treatment may be offered by the relative resistance ofhuman LDCs to the antiproliferative effects of hydrocorti-sone. Analogous to TGF-b1 resistance caused by loss of thetype II receptor, these steroid-resistant cell lines typically lackkey elements of the GR complex. Restenotic lesions have alower rate of apoptotic SMCs and macrophages comparedwith primary lesions,6 implicating reduced apoptosis as animportant mechanism in restenotic lesion formation. Theresistance of some LDCs to the apoptotic effects of hydro-
Figure 9. Expression of the GR in human atheroscleroticlesions. The GR, smooth muscle-specific actin, and macro-phage markers were identified by immunostaining with specificantibodies in serial sections of a human carotid artery lesionacquired by endarterectomy (E158). A, GR antibody showedstrong reactivity in the tunica media (M) and wall of a branchingvessel (lower right of each panel), but showed only sparse andweak reaction in neointimal lesion (I), principally at the superfi-cial aspect of the lesion adjacent to the lumen (L). B, a-Smoothmuscle-actin staining identified almost all cells in this field asSMC/myofibroblasts. C, HAM56 staining for macrophages iden-tified small groups of positive staining marked by arrows. D,Control mouse IgG. These sections have been counterstainedwith hematoxylin.
1186 Glucocorticoid Resistance in Lesion-Derived Cells

cortisone is another mechanism by which the lesion might failto regress. At higher concentrations of hydrocortisone, someLDCs exhibited cell death, possibly explaining the antipro-liferative effect of high doses of hydrocortisone. Interest-ingly, Sato et al.48 reported that human vascular SMCsisolated from IMAs decreased their GR expression after 1hour’s treatment with Lp(a), a risk factor for atherosclero-sis.49 These data, coupled with the present studies, suggestlesion cells may be less sensitive to the suppressive effects ofsteroids in an atherosclerotic environment.
Voisard et al28 cultured cells from human atheroscleroticlesions and found, in vitro, an antiproliferative effect ofcorticosteroids. However, high doses of hydrocortisone (1250mg/mL), or its synthetic analogs, prednisolone (750mg/mL)and dexamethasone (40mg/mL), were required to inhibitSMC proliferation by up to 70% after 5 days in culture.Correcting for the relative potency of these agents, theeffective dose was approximately 10 000-fold higher thanphysiological concentrations. Such high-dose steroid therapy,in vivo, could only be achieved for short periods by localadministration. Lesion cells that expressed a complete GRcomplex, such as E85, required a dose of only 10mg/mL ofhydrocortisone to significantly inhibit DNA synthesis by upto 80%, whereas most LDCs lacking the GR complex weredramatically resistant to steroid therapy. Although it ispossible that cells cultured from these plaques represent aselected subset of cells with resistance to GCs, 3 factsdiscount in vitro factors as the sole explanation for theresistance: (1) although serial subpassage can be associatedwith acquired resistance (Figure 1, R13), other lines (R8)show no decrease in sensitivity, suggesting the resistance iscaused by the expansion of a preexisting subset of resistantcells; (2) the LDCs exhibited resistance as soon as it waspossible to test, typically within 2 to 4 passages; and (3)immunostaining suggests the relative absence of the GR inhistological sections of human lesions (Figure 8).
Published evidence has indicated that GCs can act viastimulation of TGF-b activity,42 a possibility that wouldexplain the parallel resistance to these 2 factors in almost allrat (Figure 1) and human (Figure 2) lines examined. Anotable exception was the E12sc LDC line, which is partiallyhydrocortisone-sensitive, but TGF-b1-resistant, suggestingthat hydrocortisone can act via TGF-b–independent path-ways. An alternate explanation for the parallel resistance tothese 2 inhibitory systems is that a common factor is capableof modulating both the type II TGF-b receptor and membersof the GR complex. Such a factor would probably exert itseffects at the transcriptional level, because steady-statemRNA levels of both receptors is decreased.
The loss of the GR in the majority of endarterectomy celllines typically correlated with resistance to the antiprolifera-tive effects of GCs. However, 1 cell line (E47sc), wasextremely sensitive to the inhibitory effects of hydrocortisonebut lacked detectable levels of the GR. This cell line waspositive for the MR but not the enzyme 11b-HSD2, whichprotects the MR from the relative excess of circulating GCs.In the absence of 11b-HSD2, GCs bind to the MR withsimilar affinities as aldosterone.50 11b-HSD2 metabolizescortisol (hydrocortisone) to cortisone, which is inactive andcannot bind to the MR.39 Thus, in the absence of 11b-HSD2,as in E47sc, hydrocortisone should readily signal through the
MR, thus explaining the functional responses to hydrocorti-sone in a GR-negative line. The relationship between hydro-cortisone, 11-b-HSD2, and the MR or GR complex is shownschematically in Figure 10.
Typically, collagen synthesis is inhibited by GCs11–13;however, in vascular SMCs isolated from either bovine orhuman aortas, GCs enhance collagen protein synthesis,51,52
although the GR status of these SMCs was not determined.The present data raise the possibility that the relative loss ofthe GR signaling complex, or reduced expression of 11b-HSD2, would cause the GCs to interact with the MR andbehave as mineralocorticoids. A fibrotic response wouldresult because MR activation typically results in stronginduction of type I and type III collagen synthesis.32,53
The human GR gene contains a total of 10 exons and isapproximately 80 kb. There are 2 GR isoforms, hGRa andhGRb, which originate by alternative splicing of exon 9.44
hGRa is fully functional and hGRb has no hormone-bindingactivity.54 These 2 alternatively spliced forms of the GR areable to form heterodimers but are inactive compared withhGRa homodimers, and thus hGRb is thought to act as anendogenous inhibitor of GC action.55 The LDC lines that didexpress the GR only expressed detectable levels of the activeform, hGRa; therefore, the resistance to hydrocortisone inthese LDCs is probably not caused by hGRb inhibiting theactions of hGRa.
The unliganded GR is part of a multiprotein complex,comprising 2 molecules of Hsp 90 and 1 each of Hsp 70, Hsp56, and Hsp 26 (Figure 10). Hsp 90 molecules dissociate fromthe receptor complex on ligand binding,56 whereas Hsp 56 isrequired for directing the receptor complex to the nucleus,33
and Hsp 70 is a molecular chaperone for the GR entering thenucleus.34 Abnormal Hsp 70 and Hsp 90 have been reportedin steroid-resistant acute lymphoblastic leukemia.31 The ab-sence of the Hsp 90 complex in the LDC lines, and Hsp 70 in
Figure 10. Schematic model of steroid–steroid receptor interac-tions. Hydrocortisone (HC) does not typically interact with theMR because of rapid inactivation of HC to cortisone by 11b-HSD2. Normally, HC interacts with the GR as a member of amultiprotein cytoplasmic complex that includes Hsp 90, Hsp 70,Hsp 56, and Hsp 26. Hsp 90 dissociates from the GR on HCbinding, and the remaining complex traverses the nuclear mem-brane to exert transcriptional effects leading to suppression ofcollagen synthesis, inhibition of proliferation, and induction ofapoptosis. However, in the absence of the GR, it is hypothe-sized that HC levels can overwhelm 11b-HSD2 and signalthrough the MR. Likewise, in the absence of 11b-HSD2, HCreadily signals through the MR, leading to profibrotic effectsincluding the induction of collagen gene expression.
Bray et al May 1999 1187

E47sc, suggests the resistance to hydrocortisone in these cellsis caused not only by an absent GR, but potentially by anabsence of other components of the GR multiproteincomplex.
To the extent that cells proliferating from human lesionsmay reflect the properties of cells that respond to vascularinjury, such as angioplasty, the results of the present studysuggest restenosis may be another disease involving acquiredresistance to GCs. The resistance of these LDCs to theantiproliferative and antifibrotic effects of hydrocortisonemay contribute to excessive wound repair in atherosclerosisand restenosis. These results may have therapeutic implica-tions if the GR can be replaced in GR-deficient vessels.Steroids are the first line, and in many cases the only line, oftherapy for a broad spectrum of inflammatory and fibroticdiseases. Thus, the ability to restore steroid responsivenessmight be adapted to treat steroid-resistant fibrosis in othersituations such as congestive heart failure, pulmonary fibro-sis, keloids, and arthritis.
AcknowledgmentsThis work was made possible in part by funds granted to P.J.B.through a fellowship program sponsored by The Charles H. RevsonFoundation. The statements made and views expressed, however, aresolely the responsibility of the author. The work was furthersupported by NIH grants to T.A.M. from the National Institutes onAging (AG12712) and the National Heart, Lung, and Blood Insti-tute (HL56987). H.H.A. was supported, in part, by NIH grantHD00072.
References1. Austin GE, Ratliff NB, Hollman J, Tabei S, Phillips DF. Intimal prolif-
eration of smooth muscle cells as an explanation for recurrent coronary.J Am Coll Cardiol. 1985;6:369–375.
2. Dartsch PC, Bauridel I, Schinko I, Weiss HD, Hfling B, Betz E. Cellconstitution and characteristics of human atherosclerotic plaques selec-tively removed by percutaneous atherectomy.Atherosclerosis. 1989;80:149–157.
3. Mehta VY, Jorgensen MB, Raizner AE, Wolde-Tsadik G, Mahrer PR,Mansukhani P. Spontaneous regression of restenosis: an angiographicstudy.J Am Coll Cardiol. 1995;26:696–702.
4. Herrman J-PR, Hermans WRM, Vos J, Serruys PW. Pharmacologicalapproaches to the prevention of restenosis following angioplasty: thesearch for the Holy Grail? (Part I).Drugs. 1993;46:18–52.
5. Bochaton-Piallat ML, Gabbiani F, Redard M, Desmouliere A, GabbianiG. Apoptosis participates in cellularity regulation during rat aortic intimalthickening.Am J Pathol. 1995;146:1059–1064.
6. Bauriedel G, Schluckebier S, Hutter R, Welsch U, Kandolf R, Luderitz B,Prescott MF. Apoptosis in restenosis versus stable-angina atherosclerosis:implications for the pathogenesis of restenosis.Arterioscler Thromb VascBiol. 1998;18:1132–1139.
7. McCaffrey TA, Consigli S, Du B, Falcone DJ, Sanborn TA, SpokojnyAM, Bush H. Decreased type II/type I TGF-b1 receptor ratio in cellsderived from human atherosclerotic lesions: conversion from an antipro-liferative to profibrotic response to TGF-b1. J Clin Invest. 1995;96:2667–2675.
8. McCaffrey TA, Du B, Consigli S, Szabo P, Bray PJ, Hartner L, WekslerBB, Sanborn TA, Bergman G, Bush HL. Genomic instability in the typeII TGF-b1 receptor gene in atherosclerotic and restenotic vascular cells.J Clin Invest. 1997;100:2182–2188.
9. Longenecker JP, Kilty LA, Johnson LK. Glucocorticoid influence ongrowth of vascular wall cells in culture.J Cell Physiol. 1982;113:197–202.
10. Berk BC, Vallega G, Griendling KK, Gordon JB, Cragoe E, Canessa M,Alexander RW. Effects of glucocorticoids of Na/H exchange and growthin cultured vascular smooth.J Cell Physiol. 1988;137:391–401.
11. Krane SM, Amento EP. Glucocorticoids and collagen disease.Adv ExpMed Biol. 1984;171:61–71.
12. Hamalainen l, Olkarinen J, Kivirikko KI. Synthesis and degradation oftype I procollagen mRNAs in cultured human skin fibroblasts and theeffect of cortisol.J Biol Chem. 1985;260:720–725.
13. Weiner FR, Cazja MJ, Jefferson DM, Giamvrone MA, Tur-Kaspa R, ReidLM, Zern MA. The effects of dexamethasone on in vitro collagen geneexpression.J Biol Chem. 1987;262:6955–6958.
14. Thompson EB. Apoptosis and steroid hormones.Mol Endocrinol. 1994;8:665–673.
15. Rohhut B, Russo-Marie F. Novel concepts in the mode of action ofanti-inflammatory steroids.Agents Actions. 1984;14:171–180.
16. Prescott M, McBride C, Court M. Development of intimal lesions afterleukocyte migration into the vascular wall.Am J Pathol. 1989;135:835–846.
17. Bailey JM, Butler J. Pathology: influence of anti-inflammatory agents ofexperimental atherosclerosis.Nature. 966; 212:731–732.
18. Gordon D, Kobernick SS, McMillan GC, Duff GL. The effect of cor-tisone on the serum lipids and on the development of experimentalcholesterol atherosclerosis in the rabbit.J Exp Med. 1954;99:371–386.
19. Hollander W, Kramsch DM, Franzblau C, Paddock J, Colombo MA.Suppression of atheromatous fibrous plaque formation by antiprolif-erative and anti-inflammatory drugs.Circ Res. 1974;34:I-131–I-141.
20. Makheja AN, Bloom S, Muesing R, Simon T, Bailey JM. Anti-inflammatory drugs in experimental atherosclerosis, 7: spontaneous ath-erosclerosis in WHHL rabbits and inhibition by cortisone acetate.Ath-erosclerosis. 1989;76:155–161.
21. Villa AE, Guzman LA, Chen W, Golomb G, Levy RJ, Topol EJ. Localdelivery of dexamethasone for prevention of neointimal proliferation in arat model of balloon angioplasty.J Clin Invest. 1994;93:1243–1249.
22. Oppenheim E, Bruger M. The effect of cortisone and ACTH on experi-mental cholesterol atherosclerosis in rabbits.Circulation. 1952;6:470–471.
23. Gordon JB, Berk BC, Bettmann MA, Selwyn AP, Rennke H, AlexanderRW. Vascular smooth muscle proliferation following balloon injury issynergistically inhibited by low molecular weight heparin and hydrocor-tisone.Circulation. 1987;76(suppl 4):IV-213. Abstract.
24. Petrik P, Law M, Moore W, Colburn M, Quinones-Baldrich W, GelabertH. Dexamethasone and enalapril suppress intimal hyperplasia indi-vidually but have no synergistic effect.Ann Vasc Surg. 1998;12:216–220.
25. Karim MA, Frizzell S, Inman L, Shinn M, Miller DD. In vivo role ofglucocorticoid hormone in barotrauma vascular repair and fibrosis.J MolCell Cardiol. 1997;29:1111–1122.
26. Pepine CJ, Hirshfeld JW, Macdonald RG, Henderson MA, Bass TA,Goldberg S, Savage MP, Vetrovec G, Cowley M, Taussig AS, WhitworthHB, Margolis JR, Hill JA, Bove AA, Jugo RA. A controlled trial ofcorticosteroids to prevent restenosis after coronary angioplasty.Circu-lation. 1990;81:1753–1761.
27. Stone GW, Rutherford BD, McConahay DR, Johnson WL, Giorgo LV,Ligon RW, Hartzler GO. A randomized trial of corticosteroids for theprevention of restenosis in 102 patients.Cathet Cardiovasc Diagn. 1989;18:227–231.
28. Voisard R, Seitzer U, Baur R, Dartsch PC, Osterhues H, Hoher M,Hombach V. Corticosteroid agents inhibit proliferation of smooth musclecells from human atherosclerotic arteries in vitro.Int J Cardiol. 1994;43:257–267.
29. Sher ER, Leung DY, Surs W, Sher ER, Zieg G, Kamada AK, Szefler SJ.Steroid-resistant asthma: cellular mechanisms contributing to inadequateresponse to glucocorticoid therapy.J Clin Invest. 1994;93:33–39.
30. Schlaghecke R, Kornely E, Wollenhaupt J, Specker C. Glucocorticoidreceptors in rheumatoid arthritis.Arthritis Rheum. 1992;35:740–744.
31. Kojika S, Sugita K, Inukai T, Saito M, Iijima K, Goi K, Shiraishi K, MoriT, Okazaki T, Kagami K, Ohyama K, Nakazawa S. Mechanisms ofglucocorticoid resistance in human leukemic cells: implication ofabnormal 90 and 70 kDa heat shock proteins.Leukemia. 1996;10:994–999.
32. Weber KT, Janicki JS, Shroff SG, Pick R, Chen RM, Bashey RI. Collagenremodeling of the pressure-overloaded hypertrophied nonhuman primate.Circ Res. 1988;62:757–765.
33. Czar MJ, Lyons RH, Welsh MJ, Renoir JM, Pratt WB. Evidence that theFK506-binding immunophilin heat shock protein 56 is required for traf-ficking of the glucocorticoid receptor from the cytoplasm to the nucleus.Mol Endocrinol. 1995;9:1549–1560.
34. Shi Y, Thomas JO. The transport of proteins into the nucleus requires the70-kilodalton heat shock protein or its cytosolic cognate.Mol Cell Biol.1992;12:2186–2192.
35. Miesfeld R, Rusconi S, Godowski PJ, Maler BA, Okret S, WikstroemAC, Gustafsson JA, Yamamoto KR. Genetic complementation to a glu-cocorticoid receptor deficiency by expression of cloned receptor cDNA.Cell. 1986;46:389–399.
36. Arriza JL, Weinberger C, Cerelli G, Claser TM, Handelin BL, HousmanDE, Evans RM. Cloning of human mineralocorticoid receptor: structural
1188 Glucocorticoid Resistance in Lesion-Derived Cells

and functional kinship with the glucocorticoid receptor.Science. 1987;237:268–275.
37. Agarwal AK, Rogerson FM, Mune T, White PC. Gene structure andchromosomal localization of the human HSD11K gene encoding thekidney (type 2) isozyme of 11b-hydroxysteroid dehydrogenase.Genomics. 1995;29:195–199.
38. Fathallah DM, Cherif D, Dellagi K, Arnaout MA. Molecular cloning of anovel human Hsp70 from a B cell line and its assignment to chromosome5. J Immunol. 1993;151:810–813.
39. Funder JW, Pearce PT, Smith R, Smith I. Mineralocorticoid action: targettissue specificity is enzyme, not receptor mediated.Science. 1988;242:583–585.
39a.Mosmann T. Rapid colorimetric assay for cellular growth and survival:application to proliferation and cytotoxicity assays.J Immunol Meth.1983;65:55–63.
40. Gown AM. Cell type and cell state specific antibodies in the analysis ofearly lesions of human atherosclerosis.Am J Hypertens. 1992; 5(suppl):114S–117S.
41. McCaffrey TA, Falcone DJ. Evidence for an age-related dysfunction inthe antiproliferative response to transforming growth factor-b in vascularsmooth muscle cells.Mol Biol Cell. 1993;4:315–322.
42. Boulanger J, Reyes-Moreno C, Koutsilieris M. Mediation of glucocor-ticoid receptor function by the activation of latent transforming growthfactor-b in MG-63 human osteosarcoma cells.Int J Cancer. 1995;61:692–697.
43. Wolf JS, Soble JJ, Ratliff TL, Clayman RV. Ureteral cell cultures, II:collagen production and response to pharmacologic agents.J Urol. 1996;156:2067–2072.
44. Encio IJ, Detera-Wadleigh SD. The genomic structure of the humanglucocorticoid receptor.J Biol Chem. 1991;266:7182–7188.
45. Geller DS, Rodriguez-Soriano J, Vallo Boado A, Schifter S, Bayer M,Chang SS, Lifton RP. Mutations in the mineralocorticoid receptor genecause autosomal dominant pseudohypoaldosteronism type I.Nat Genet.1998;19:279–281.
46. Valero F, Hamon M, Fournier C, Meurice T, Flautre B, Van Belle E,Lablanche J, Gosselin B, Bauters C, Bertrand M. Intramural injection ofbiodegradable microspheres as a local drug-delivery system to inhibitneointimal thickening in a rabbit model of balloon angioplasty.J Car-diovasc Pharmacol. 1998;31:513–519.
47. Lincoff AM, Furst JG, Ellis SG, Tuch RJ, Topol EJ. Sustained localdelivery of dexamethasone by a novel intravascular eluting stent toprevent restenosis in the porcine coronary injury model.J Am CollCardiol. 1997;29:808–816.
48. Sato A, Sheppard KE, Fullerton MJ, Sviridov DD, Funder JW. Glucocor-ticoid receptor expression is down-regulated by Lp(a) lipoprotein invascular smooth muscle cells.Endocrinology. 1995;136:3707–3713.
49. Dahlen GH. Lp(a) lipoprotein in cardiovascular disease.Atherosclerosis.1994;108:111–126.
50. Rupprecht R, Reul J, van Steensel B, Spengler D, Soder M, Berning B,Holsboer F, Damm K. Pharmacological and functional characterization ofhuman mineralocorticoid and glucocorticoid receptor ligands.EurJ Pharmacol. 1993;247:145–154.
51. Jarvelainen H, Halme T, Ronnemaa T. Effect of cortisol on the prolif-eration and protein synthesis of human aortic smooth muscle cells inculture.Acta Med Scand Suppl. 1982;660:114–122.
52. Leitman DC, Benson SC, Johnson LK. Glucocorticoids stimulatecollagen and noncollagen protein synthesis in cultured vascular smoothmuscle cells.J Cell Biol. 1984;98:541–549.
53. Medugorac I. Collagen content in different areas of normal and hyper-trophied rat myocardium.Cardiovasc Res. 1980;14:551–554.
54. Hollenberg SM, Weinberger C, Ong ES, Cerelli G, Oro A, Lebo R,Thompson EB, Rosenfeld MG, Evans RM. Primary structure andexpression of a functional human glucocorticoid receptor.Nature. 1985;318:635–641.
55. Bamberger CM, Bamberger AM, de Castro M, Chrousos GP. Glucocor-ticoid receptorb: a potential endogenous inhibitor of glucocorticoidaction in humans.J Clin Invest. 1995;95:2435–2441.
56. Pratt WB, Sanchez ER, Bresnick EH, Meshinchi S, Scherrer LC, DalmanFC, Welsh MJ. Interaction of the glucocorticoid receptor with theMr90 000 heat shock protein: an evolving model of ligand-mediated receptortransformation and translocation.Cancer Res. 1989;49:2222s–2229s.
57. Yamazaki M, Akaogi K, Miwa T, Imai T, Soeda E, Yokoyama K.Nucleotide sequence of a full-length cDNA for 90 kDA heat-shockprotein from human peripheral blood lymphocytes.Nucleic Acids Res.1989;17:7108.
58. Franzen P, Dijke P, Ichijo H, Yamashita H, Schulz H, Heldin C-H,Miyazono K. Cloning of a TGFb type I receptor that forms a heteromericcomplex with the TGFb type II receptor.Cell. 1993;75:681–692.
Bray et al May 1999 1189
Copyright © 2022 FDOKUMEN




















