Synthetic osteochondral grafting of ankle osteochondral lesions.
6
Synthetic osteochondral grafting of ankle osteochondral lesions Christopher J. Pearce (FRCS(Tr&Orth), MFSEM(UK)) a, *, Louise E. Gartner (BSc, MRCP, FRCR) b , Adam Mitchell (FRCS, FRCR) c , James D. Calder (MD, FRCS(Tr&Orth), FFSEM(UK)) c a Department of Trauma and Orthopaedic Surgery, Egerton Road, Guildford, Surrey GU2 7XX, UK b Department of Radiology, Watford Road, Harrow HA1 3UJ, UK c Department of Radiology, 369 Fulham Road, London SW10 9NH, UK 1. Introduction The incidence and recognition of osteochondral lesions (OCLs), particularly in young, sporting individuals, is rising [1– 4]. It is known that such lesions have a limited repair capacity [5,6], especially in skeletally mature individuals [7]. Persistent osteochondral defects gradually lead to degeneration of the articular cartilage [8] and may eventually lead to osteoarthritis (OA) [7,9,10]. A number of surgical interventions have been employed in the treatment of patients with osteochondral defects. These include arthroscopic debridement and microfracture [11,12], autogenous osteochondral grafting (OATS procedure) [13], Matrix-Induced Autologous Chondrocyte Implantation (MACI) [14], and Autolo- gous Chondrocyte Implantation (ACI) [15]. When an OCL presents with a significant sub-chondral cystic lesion, simple debridement and microfracture may not be sufficient and an attempt to restore the congruence of the weight-bearing surface may yield superior results [13,16–18]. The ideal procedure would also restore hyaline cartilage to the joint surface. Synthetic grafts offer a number of potential benefits over other treatment options in that they require only a single procedure as opposed to two-staged treatment for MACI and ACI [14,15]. There is also no morbidity to healthy host tissue as seen in the OATS procedure [13,19]. In our experience, the surgery is technically easier to perform with a small learning curve. Tru-fit TM (Smith & Nephew, Andover, Massachusetts) (Fig. 1) is a biphasic osteochondral biodegradable substitute currently available for treatment of articular osteochondral defects. The osseous substitute consists of a matrix of calcium triphosphate. The cartilaginous substitute consists of poly (DL-lactide-co- glycolide) (PLGA). It is licensed in the UK for use as an osteochondral graft for osteochondral lesions. We present a small series of osteochondral lesions in the ankle treated with the Tru- fit TM synthetic graft with a minimum follow up of one year. 2. Method Five men and one woman, all of whom had sustained a traumatic inversion injury to the ankle whilst playing sports were treated. All had either failed to improve after arthroscopic debridement and microfracture in the past or had presented with Foot and Ankle Surgery 18 (2012) 114–118 A R T I C L E I N F O Article history: Received 14 September 2010 Received in revised form 1 April 2011 Accepted 7 April 2011 Keywords: Ankle OCL Synthetic graft A B S T R A C T Background: The treatment of osteochondral lesions, especially those with a cystic component or those that have failed the standard arthroscopic procedures can be challenging. Synthetic grafts have several potential advantages over other second line treatments including the fact that only one operation is required and no other joint is violated. Method: We report the results of the first series of synthetic grafts used in the treatment of osteochondral lesions of the ankle with a minimum of one year follow up. Results: There was significant improvement in the American Orthopaedic Foot & Ankle Society (AOFAS) Hindfoot and Ankle Osteoarthritis Scale (AOS) scores and all patients were satisfied with the results of surgery. Magnetic Resonance Imaging (MRI) scans at one year have demonstrated resolution of the bony cysts and surrounding bone marrow oedema but, worryingly, continued to show high signal on the T2 weighted images within the plugs themselves. Qualitative T2 mapping has suggested a fibrous rather than hyaline appearance of the cartilage portions of the plugs. Conclusions: The clinical results have been encouraging but more patients and longer follow up are required before firm conclusions can be drawn. ß 2011 European Foot and Ankle Society. Published by Elsevier Ltd. All rights reserved. * Corresponding author at: 20 Topiary Square, Stanmore Road, Richmond TW9 2DB, UK. Tel.: +44 07976356076. E-mail addresses: [email protected], [email protected] (C.J. Pearce). Contents lists available at ScienceDirect Foot and Ankle Surgery jou r nal h o mep age: w ww.els evier .co m/lo c ate/fas 1268-7731/$ – see front matter ß 2011 European Foot and Ankle Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.fas.2011.04.001
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Synthetic osteochondral grafting of ankle osteochondral lesions.

Foot and Ankle Surgery 18 (2012) 114–118
Synthetic osteochondral grafting of ankle osteochondral lesions
Christopher J. Pearce (FRCS(Tr&Orth), MFSEM(UK))a,*, Louise E. Gartner (BSc, MRCP, FRCR)b,Adam Mitchell (FRCS, FRCR)c, James D. Calder (MD, FRCS(Tr&Orth), FFSEM(UK))c
a Department of Trauma and Orthopaedic Surgery, Egerton Road, Guildford, Surrey GU2 7XX, UKb Department of Radiology, Watford Road, Harrow HA1 3UJ, UKc Department of Radiology, 369 Fulham Road, London SW10 9NH, UK
A R T I C L E I N F O
Article history:
Received 14 September 2010
Received in revised form 1 April 2011
Accepted 7 April 2011
Keywords:
Ankle
OCL
Synthetic graft
A B S T R A C T
Background: The treatment of osteochondral lesions, especially those with a cystic component or those
that have failed the standard arthroscopic procedures can be challenging. Synthetic grafts have several
potential advantages over other second line treatments including the fact that only one operation is
required and no other joint is violated.
Method: We report the results of the first series of synthetic grafts used in the treatment of
osteochondral lesions of the ankle with a minimum of one year follow up.
Results: There was significant improvement in the American Orthopaedic Foot & Ankle Society (AOFAS)
Hindfoot and Ankle Osteoarthritis Scale (AOS) scores and all patients were satisfied with the results of
surgery. Magnetic Resonance Imaging (MRI) scans at one year have demonstrated resolution of the bony
cysts and surrounding bone marrow oedema but, worryingly, continued to show high signal on the T2
weighted images within the plugs themselves. Qualitative T2 mapping has suggested a fibrous rather
than hyaline appearance of the cartilage portions of the plugs.
Conclusions: The clinical results have been encouraging but more patients and longer follow up are
required before firm conclusions can be drawn.
� 2011 European Foot and Ankle Society. Published by Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Foot and Ankle Surgery
jou r nal h o mep age: w ww.els evier . co m/lo c ate / fas
1. Introduction
The incidence and recognition of osteochondral lesions(OCLs), particularly in young, sporting individuals, is rising [1–4]. It is known that such lesions have a limited repair capacity[5,6], especially in skeletally mature individuals [7]. Persistentosteochondral defects gradually lead to degeneration of thearticular cartilage [8] and may eventually lead to osteoarthritis(OA) [7,9,10].
A number of surgical interventions have been employed in thetreatment of patients with osteochondral defects. These includearthroscopic debridement and microfracture [11,12], autogenousosteochondral grafting (OATS procedure) [13], Matrix-InducedAutologous Chondrocyte Implantation (MACI) [14], and Autolo-gous Chondrocyte Implantation (ACI) [15].
When an OCL presents with a significant sub-chondral cysticlesion, simple debridement and microfracture may not be sufficientand an attempt to restore the congruence of the weight-bearing
* Corresponding author at: 20 Topiary Square, Stanmore Road, Richmond TW9
2DB, UK. Tel.: +44 07976356076.
E-mail addresses: [email protected], [email protected]
(C.J. Pearce).
1268-7731/$ – see front matter � 2011 European Foot and Ankle Society. Published b
doi:10.1016/j.fas.2011.04.001
surface may yield superior results [13,16–18]. The ideal procedurewould also restore hyaline cartilage to the joint surface.
Synthetic grafts offer a number of potential benefits over othertreatment options in that they require only a single procedure asopposed to two-staged treatment for MACI and ACI [14,15]. Thereis also no morbidity to healthy host tissue as seen in the OATSprocedure [13,19]. In our experience, the surgery is technicallyeasier to perform with a small learning curve.
Tru-fitTM (Smith & Nephew, Andover, Massachusetts) (Fig. 1) isa biphasic osteochondral biodegradable substitute currentlyavailable for treatment of articular osteochondral defects. Theosseous substitute consists of a matrix of calcium triphosphate.The cartilaginous substitute consists of poly (DL-lactide-co-glycolide) (PLGA). It is licensed in the UK for use as anosteochondral graft for osteochondral lesions. We present a smallseries of osteochondral lesions in the ankle treated with the Tru-fitTM synthetic graft with a minimum follow up of one year.
2. Method
Five men and one woman, all of whom had sustained atraumatic inversion injury to the ankle whilst playing sports weretreated. All had either failed to improve after arthroscopicdebridement and microfracture in the past or had presented with
y Elsevier Ltd. All rights reserved.
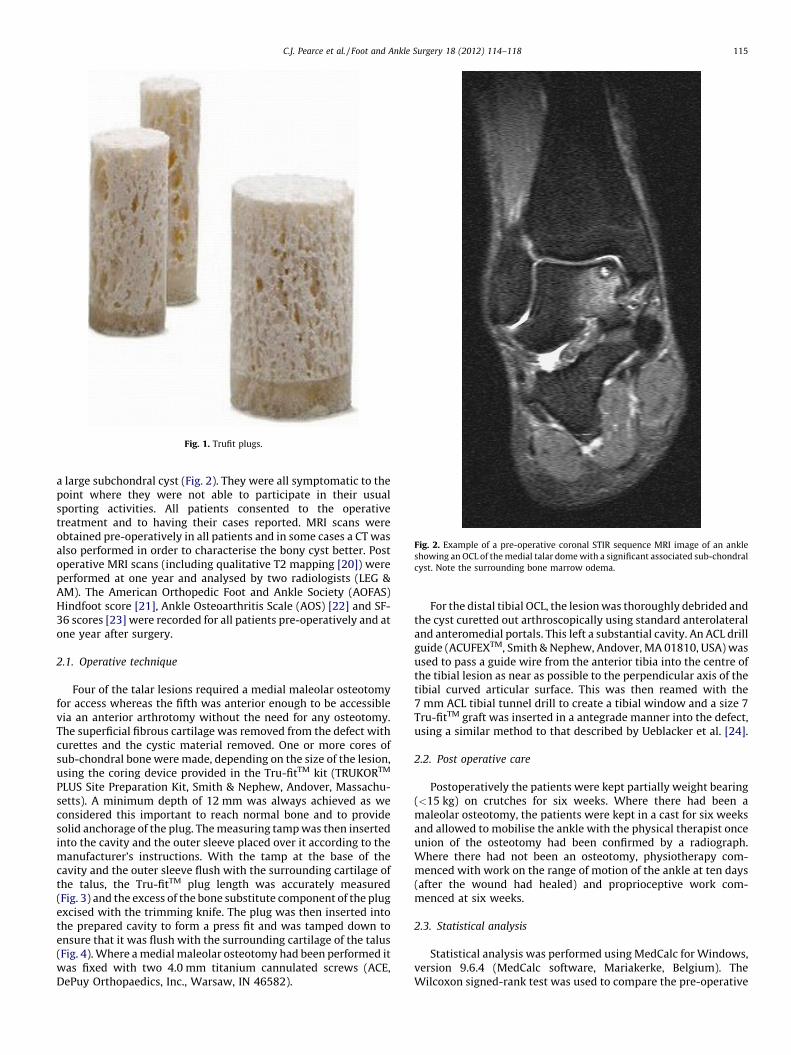
Fig. 1. Trufit plugs.
Fig. 2. Example of a pre-operative coronal STIR sequence MRI image of an ankle
showing an OCL of the medial talar dome with a significant associated sub-chondral
cyst. Note the surrounding bone marrow odema.
C.J. Pearce et al. / Foot and Ankle Surgery 18 (2012) 114–118 115
a large subchondral cyst (Fig. 2). They were all symptomatic to thepoint where they were not able to participate in their usualsporting activities. All patients consented to the operativetreatment and to having their cases reported. MRI scans wereobtained pre-operatively in all patients and in some cases a CT wasalso performed in order to characterise the bony cyst better. Postoperative MRI scans (including qualitative T2 mapping [20]) wereperformed at one year and analysed by two radiologists (LEG &AM). The American Orthopedic Foot and Ankle Society (AOFAS)Hindfoot score [21], Ankle Osteoarthritis Scale (AOS) [22] and SF-36 scores [23] were recorded for all patients pre-operatively and atone year after surgery.
2.1. Operative technique
Four of the talar lesions required a medial maleolar osteotomyfor access whereas the fifth was anterior enough to be accessiblevia an anterior arthrotomy without the need for any osteotomy.The superficial fibrous cartilage was removed from the defect withcurettes and the cystic material removed. One or more cores ofsub-chondral bone were made, depending on the size of the lesion,using the coring device provided in the Tru-fitTM kit (TRUKORTM
PLUS Site Preparation Kit, Smith & Nephew, Andover, Massachu-setts). A minimum depth of 12 mm was always achieved as weconsidered this important to reach normal bone and to providesolid anchorage of the plug. The measuring tamp was then insertedinto the cavity and the outer sleeve placed over it according to themanufacturer’s instructions. With the tamp at the base of thecavity and the outer sleeve flush with the surrounding cartilage ofthe talus, the Tru-fitTM plug length was accurately measured(Fig. 3) and the excess of the bone substitute component of the plugexcised with the trimming knife. The plug was then inserted intothe prepared cavity to form a press fit and was tamped down toensure that it was flush with the surrounding cartilage of the talus(Fig. 4). Where a medial maleolar osteotomy had been performed itwas fixed with two 4.0 mm titanium cannulated screws (ACE,DePuy Orthopaedics, Inc., Warsaw, IN 46582).
For the distal tibial OCL, the lesion was thoroughly debrided andthe cyst curetted out arthroscopically using standard anterolateraland anteromedial portals. This left a substantial cavity. An ACL drillguide (ACUFEXTM, Smith & Nephew, Andover, MA 01810, USA) wasused to pass a guide wire from the anterior tibia into the centre ofthe tibial lesion as near as possible to the perpendicular axis of thetibial curved articular surface. This was then reamed with the7 mm ACL tibial tunnel drill to create a tibial window and a size 7Tru-fitTM graft was inserted in a antegrade manner into the defect,using a similar method to that described by Ueblacker et al. [24].
2.2. Post operative care
Postoperatively the patients were kept partially weight bearing(<15 kg) on crutches for six weeks. Where there had been amaleolar osteotomy, the patients were kept in a cast for six weeksand allowed to mobilise the ankle with the physical therapist onceunion of the osteotomy had been confirmed by a radiograph.Where there had not been an osteotomy, physiotherapy com-menced with work on the range of motion of the ankle at ten days(after the wound had healed) and proprioceptive work com-menced at six weeks.
2.3. Statistical analysis
Statistical analysis was performed using MedCalc for Windows,version 9.6.4 (MedCalc software, Mariakerke, Belgium). TheWilcoxon signed-rank test was used to compare the pre-operative

Fig. 4. Intra-operative photograph showing the plugs after implantation via a
medial maleolar osteotomy.
Fig. 3. Intra-operative photograph demonstrating the sizing of the TrufitTM plug.
C.J. Pearce et al. / Foot and Ankle Surgery 18 (2012) 114–118116
and post-operative scores. Statistical significance was accepted ifp < 0.05.
3. Results
All of the lesions of the talus involved the medial talar domeand, as previously mentioned, four required a medial maleolarosteotomy. At 12 months the postoperative AOFAS, AOS and SF36scores have improved (Table 1) and all of the patients are satisfied.There was statistically significant improvements in the AOFAS andAOS disability scores. With the small numbers of patients
Table 1Median scores pre and post operatively and results of the Wilcoxon test.
AOFAS AOS
Pain
AOS
Disability
SF-36
Pre op 70 30 26 58
Post op 92 11 6 71
p value 0.0312* 0.0937 0.0312* 0.0625
* Indicates statistical significance.
involved, the other results did not reach statistical significance.The medial maleolar osteotomies all united uneventfully by sixweeks on the radiographs. There were no surgical complicationsbut one patient injured his peroneal tendons playing football at 9months post operatively. All patients have returned to work andsports.
Follow up MRI scans in all cases demonstrate resolution ofthe cysts and markedly reduced surrounding bone marrowoedema (Fig. 5). They all however continue to show high signalon the T2 sequences within the plugs themselves. Thequalitative T2 maps revealed a disorganized pattern of T2 signalfrom the deep to superficial zones of the cartilage portion of theplugs (Fig. 6), suggesting a fibrous rather than hyaline cartilagecomposition [20].
Fig. 5. T2 fat-suppressed saggital MRI scan of the ankle 1 year post op. Note the high
signal within the plug itself and the resolution of the bone marrow odema that was
seen pre-operatively.

Fig. 6. Qualitative T2 mapping MRI scan showing a disorganized pattern of T2 signal
from the deep to superficial zones of the cartilage portion of the plugs.
C.J. Pearce et al. / Foot and Ankle Surgery 18 (2012) 114–118 117
4. Discussion
Osteochondral lesions of the talus account for around 4% of allosteochondral lesions [25] and their incidence is rising as ourawareness of them increases and modern imaging techniques aidtheir diagnosis [2]. Tibial plafond lesions are much less common ashighlighted by the series by Mologne and Ferkel where, even in acomplex foot and ankle referral practice, only 23 tibial OCLs wereencountered in a series of 880 ankle arthroscopies (2.6%) [26].
Non-operative treatment and simple excision of the lesion havebeen shown in a systematic review of the literature to be inferior tomore active treatments [27]. Good clinical outcomes can beexpected in the majority of patients following arthroscopicdebridement and drilling or microfracture for osteochondral lesionsin the ankle [27–30]. Some authors however, have pointed out thatcystic lesions represent a structural defect that shaving or drillingalone will not adequately address [13]. Small cysts may still beamenable to arthroscopic treatment [31] but an attempt to restorethe congruence of the weight-bearing surface may yield superiorresults where there are larger cystic lesions [13,16–18]. Moreover,the results of repeated arthroscopic treatment of talar osteochondrallesions have traditionally been less encouraging [32,33], although amore recent paper challenged that view [18]. The numbers ofpatients in all of these series are small however and thereforecaution must be employed in interpreting the conclusions.
Good results have been reported in the treatment of type Vosteochondral lesions of the talus with an osteochondral autograftfrom the ipsilateral knee [13]. 50 patients were treated with a 90%satisfaction rate. 34% however required further surgery and onepatient later required an arthroscopic debridement of the knee toremove scar tissue following the harvest. Lee et al. [19] reported100% good to excellent results following osteochondral autograftsfrom the knee, however two of the seventeen patients continued tohave pain in the knee at final follow up. Another study evaluatingACI in the treatment of ten patients found that the Lysholm kneescores were still reduced (in some cases significantly) in two thirdsof the patients at a year post surgery [34].
The great potential advantages of a synthetic graft are that itrequires only a single operation, is technically easier to perform
than some of the other grafting techniques and does not violate anotherwise healthy joint. Another advantage is that angled graftsare available for corner lesions (though none of the patientsreported in this series required an angled graft).
Tru-fitTM is marketed as having the potential to induce hyaline-like cartilage and has been used for ‘‘back-filling’’ of autogenouscartilage-bone transplantation harvest sites. Its mechanicalproperties have been tested independently and, of course varywith the diameter of the plug used. Mechanical strength wasconsiderably higher under constrained rather than unconstrainedloading which the authors point out demonstrates the importanceof obtaining a close press fit on insertion. The modulus of elasticitywas calculated at 50 MPa for the 7 mm plug, 60 MPa for the 9 mmand 80 MPa for the 11 mm plug [35]. A case report of its successfuluse for grafting of a greater tuberosity cyst prior to rotator cuffrepair has been published [36]. Another study investigated asynthetic allograft analogous to Tru-fitTM in pigs as conduit for ACIwith some success [37]. In that study, at 6 months all of the 38implanted sites were filled with firm bone which was covered witheither fibrous or cartilaginous tissue. The distal tibial lesion in ourseries has been published as a case report highlighting the surgicaltechnique [38].
The patients in this small series are satisfied with the outcomeof their surgery and have stated that they would have theprocedure again. Clinically and functionally they have improvedafter the surgery. The AOFAS Hindfoot scores and AOS disabilityscales were significantly better at 1 year, however these are notvalidated outcome scores and this a small series of cases with nocontrol group. Radiographically, the cystic lesions and surroundingbone marrow oedema have resolved. Although the assessment ofthe cartilage regenerate on the qualitative T2 mapping MRI scans isquite subjective, our two radiologists agreed that the cartilage overthe plugs appeared to be of fibrous rather than hyaline morphologyat one year. Again due to the subjective nature of the assessmentno formal inter or intra-observer agreement calculation was madein this respect.
We believe that much of the symptomatic improvement is dueto the filling of the cystic lesion beneath the OCL allowing apossibly more stable scaffold for the hyaline-like or fibro-cartilageto form with a congruous joint surface. The osseous portions of theplugs remain high signal on the T2 images at one year however,suggesting a high fluid content, so it is unclear exactly how stablethis osseous portion is.
We advocate standard arthroscopic debridement and micro-fracture/drilling techniques for OCLs in the ankle where there is nocystic formation.
5. Conclusion
We describe an alternative to autogenous osteochondralgrafting of an osteochondral lesion with an associated sub-corticalcyst in the ankle which eliminates the risks of harvesting from theknee. The preliminary clinical results of this procedure areencouraging but the MRI findings give cause for concern aboutthe stability of the osseous portion of the plugs and have failed todemonstrate hyaline-like cartilage on T2 mapping. More patientsand longer follow up are required before firm conclusions can bedrawn about this treatment.
Conflict of interest statement
The authors did not personally receive grants or outside fundingin support of their research or preparation of this manuscript. Theydid not receive payments or other benefits or a commitment toprovide such benefits from a commercial entity. A commercialentity paid benefits to a research fund, foundation, educational

C.J. Pearce et al. / Foot and Ankle Surgery 18 (2012) 114–118118
institution, or other charitable on non-profit organisation withwhich one of the authors are affiliated. Smith & Nephew paid forthe follow up MRI scans.
References
[1] Bohndorf K. Injuries at the articulating surfaces of bone (chondral, osteochon-dral, subchondral fractures and osteochondrosis dissecans). European Journalof Radiology 1996;22:22–9.
[2] Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooney T. Osteochondral lesions ofthe talus. The American Journal of Sports Medicine 1993;21:13–9.
[3] Loren GJ, Ferkel RD. Arthroscopic assessment of occult intra-articular injury inacute ankle fractures. Arthroscopy 2002;18:412–21.
[4] Vellet AD, Marks PH, Fowler PJ, Munro TG. Occult posttraumatic osteochondrallesions of the knee: prevalence, classification, and short-term sequelae evalu-ated with MR imaging. Radiology 1991;178:271–6.
[5] Jackson DW, Lalor PA, Aberman HM, Simon TM. Spontaneous repair of full-thickness defects of articular cartilage in a goat model. A preliminary study.The Journal of Bone and Joint Surgery 2001;83-A:53–64.
[6] McCullough CJ, Venugopal V. Osteochondritis dissecans of the talus: thenatural history. Clinical Orthopaedics and Related Research 1979;264–8.
[7] Prakash D, Learmonth D. Natural progression of osteo-chondral defect in thefemoral condyle. The Knee 2002;9:7–10.
[8] Guettler JH, Demetropoulos CK, Yang KH, Jurist KA. Osteochondral defects inthe human knee: influence of defect size on cartilage rim stress and loadredistribution to surrounding cartilage. The American Journal of Sports Medi-cine 2004;32:1451–8.
[9] Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatmentof deep cartilage defects in the knee with autologous chondrocyte transplan-tation. The New England Journal of Medicine 1994;331:889–95.
[10] Twyman RS, Desai K, Aichroth PM. Osteochondritis dissecans of the knee. Along-term study. Journal of Bone and Joint Surgery British 1991;73:461–4.
[11] Becher C, Thermann H. Results of microfracture in the treatment of articularcartilage defects of the talus. Foot & Ankle International 2005;26:583–9.
[12] Saxena A, Eakin C. Articular talar injuries in athletes: results of microfractureand autogenous bone graft. The American Journal of Sports Medicine 2007;35:1680–7.
[13] Scranton Jr PE, Frey CC, Feder KS. Outcome of osteochondral autograft trans-plantation for type-V cystic osteochondral lesions of the talus. The Journal ofBone and Joint Surgery British 2006;88:614–9.
[14] Schneider TE, Karaikudi S. Matrix-induced autologous chondrocyte implanta-tion (MACI) grafting for osteochondral lesions of the talus. Foot & AnkleInternational 2009;30:810–4.
[15] Giannini S, Buda R, Vannini F, Di Caprio F, Grigolo B. Arthroscopic autologouschondrocyte implantation in osteochondral lesions of the talus: surgical tech-nique and results. The American Journal of Sports Medicine 2008;36:873–80.
[16] Draper SD, Fallat LM. Autogenous bone grafting for the treatment of talar domelesions. Journal of Foot and Ankle Surgery 2000;39:15–23.
[17] Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revisedclassification. Foot & Ankle International 1999;20:789–93.
[18] Savva N, Jabur M, Davies M, Saxby T. Osteochondral lesions of the talus: results ofrepeat arthroscopic debridement. Foot & Ankle International 2007;28:669–73.
[19] Lee CH, Chao KH, Huang GS, Wu SS. Osteochondral autografts for osteochon-dritis dissecans of the talus. Foot & Ankle International 2003;24:815–22.
[20] White LM, Sussman MS, Hurtig M, Probyn L, Tomlinson G, Kandel R. CartilageT2 assessment: differentiation of normal hyaline cartilage and reparativetissue after arthroscopic cartilage repair in equine subjects. Radiology2006;241:407–14.
[21] Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M.Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes.Foot & Ankle International 1994;15:349–53.
[22] Domsic RT, Saltzman CL. Ankle osteoarthritis scale. Foot & Ankle International1998;19:466–71.
[23] Ware Jr JE, Gandek B. KM. SF-36 health survey: manual & interpretation guide.Lincoln, RI Quality Metric Incorporated; 1993. p. 2000.
[24] Ueblacker P, Burkart A, Imhoff AB. Retrograde cartilage transplantation on theproximal and distal tibia. Arthroscopy 2004;20:73–8.
[25] Alexander AH, Lichtman DM. Surgical treatment of transchondral talar-domefractures (osteochondritis dissecans). Long-term follow-up. The Journal ofBone and Joint Surgery 1980;62:646–52.
[26] Mologne TS, Ferkel RD. Arthroscopic treatment of osteochondral lesions of thedistal tibia. Foot & Ankle International 2007;28:865–72.
[27] Tol JL, Struijs PA, Bossuyt PM, Verhagen RA, van Dijk CN. Treatment strategiesin osteochondral defects of the talar dome: a systematic review. Foot & AnkleInternational 2000;21:119–26.
[28] Ferkel RD, Zanotti RM, Komenda GA, Sgaglione NA, Cheng MS, Applegate GR,et al. Arthroscopic treatment of chronic osteochondral lesions of the talus:long-term results. The American Journal of Sports Medicine 2008;36:1750–62.
[29] Parisien JS. Arthroscopic treatment of osteochondral lesions of the talus. TheAmerican Journal of Sports Medicine 1986;14:211–7.
[30] Kumai T, Takakura Y, Higashiyama I, Tamai S. Arthroscopic drilling for thetreatment of osteochondral lesions of the talus. The Journal of Bone and JointSurgery 1999;81:1229–35.
[31] Han SH, Lee JW, Lee DY, Kang ES. Radiographic changes and clinical results ofosteochondral defects of the talus with and without subchondral cysts. Foot &Ankle International 2006;27:1109–14.
[32] Robinson DE, Winson IG, Harries WJ, Kelly AJ. Arthroscopic treatment ofosteochondral lesions of the talus. The Journal of Bone and Joint SurgeryBritish 2003;85:989–93.
[33] Schimmer RC, Dick W, Hintermann B. The role of ankle arthroscopy in thetreatment strategies of osteochondritis dissecans lesions of the talus. Foot &Ankle International 2001;22:895–900.
[34] Whittaker JP, Smith G, Makwana N, Roberts S, Harrison PE, Laing P, et al. Earlyresults of autologous chondrocyte implantation in the talus. The Journal ofBone and Joint Surgery British 2005;87:179–83.
[35] Melton JTK, Bray L, Tong J, Cossey AJ. A biomechanical analysis of the materialproperties of the TRUFIT CB plug for osteochondral defects of the knee. TheJournal of Bone and Joint Surgery British 2010;92-B:420–1.
[36] Agrawal V, Stinson M. Arthroscopic grafting of greater tuberosity cyst androtator cuff repair. Arthroscopy 2007;23(904):e1–3.
[37] Jiang CC, Chiang H, Liao CJ, Lin YJ, Kuo TF, Shieh CS, et al. Repair of porcinearticular cartilage defect with a biphasic osteochondral composite. Journal ofOrthopaedic Research 2007;25:1277–90.
[38] Pearce CJ, Lutz MJ, Mitchell A, Calder JD. Treatment of a distal tibial osteo-chondral lesion with a synthetic osteochondral plug: a case report. Foot &Ankle International 2009;30:900–3.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具




















