What is the current optimal fat grafting processing technique ...
Upload
independentCategory
view
2download
0
Long-Term Results of Split-Skin Grafting in Combination withExcimer Laser for Stable Vitiligo
NAWAF AL-MUTAIRI, MD, FRCPC,� YASHPAL MANCHANDA, MD, DNB,y AZARI AL-DOUKHI, MD,z AND
AHMAD AL-HADDAD, MDz
BACKGROUND Some cases of focal or segmental vitiligo are refractory to medical treatment, and surgi-cal management is the treatment of choice. Postsurgical exposure to ultraviolet B rays can lead to fasterand better cosmetic results.
OBJECTIVE To determine the long-term results of combination therapy with split-skin-thickness graft-ing and 308-nm excimer laser for the management of stable focal or segmental vitiligo.
PATIENTS AND METHODS Seventeen patients (8 female, 9 male) with stable focal or segmental vitiligonot responding to nonsurgical modalities were treated with split-skin-thickness grafting and postgraft-ing with 32 sessions of 308-nm excimer laser, beginning 2 weeks after surgery. The patients werefollowed up every year for evaluation of results.
RESULTS All seventeen (100%) patients showed repigmentation, and overall results were graded asexcellent in 12 patients and good in the other five at the end of excimer laser therapy. Final evaluationdone at the end of 1 year revealed excellent results in all 17 patients. Two patients developed new vitiligolesion on other parts of the body during follow-up. None of the patients developed depigmentation ofthe transplanted skin.
CONCLUSION Combination treatment with split-skin-thickness grafting and postsurgical exposure to308-nm excimer laser in patients with stable focal or segmental vitiligo can lead to fast, cosmeticallygood, long-lasting results.
The authors have indicated no significant interest with commercial supporters.
Vitiligo is an idiopathic acquired pigmentary
disorder clinically characterized by solitary or
multiple depigmented macules that may arise in a
localized, segmental, or generalized distribution.1 It
is cosmetically disfiguring, especially in dark-skinned
individuals, and can cause significant psychological
morbidity. Some degree of spontaneous repigmenta-
tion occurs in 10% to 20% of patients, but rarely is
it cosmetically acceptable,2 often occurring in a
perifollicular pattern. The duration of vitiligo and
the body site of depigmented lesions seem to play an
important role in the overall response rate achievable
with different treatment modalities.3 The treatment
of vitiligo is challenging; although medical therapies
are the primary treatments, some patients are
refractory to medical treatment. In such patients,
surgical therapies can be used alone or in conjunc-
tion with medical therapy to achieve repigmentation,
provided the disease is stable. In 1964, Behl4 was the
first to report the use of thin Thiersch’s skin grafts to
treat vitiligo. Since then, various surgical techniques
and modifications have been used to treat recalci-
trant but stable vitiligo with permanent and almost
complete regimentation.5 Also, a combination of
grafting and other nonsurgical modalities such as
psoralen plus ultraviolet (UV) radiation (PUVA)6,7
and narrow-band (NB) UV-B8,9 have been used to
achieve better and faster results. Ideally, the aim of
vitiligo treatment should be to achieve complete and
permanent repigmentation toward the color of the
surrounding normal skin in the shortest possible time
with minimal or no side effects.
& 2010 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2010;36:499–505 � DOI: 10.1111/j.1524-4725.2010.01477.x
4 9 9
�Department of Medicine, Faculty of Medicine, Kuwait University, Kuwait; yDepartments of Dermatology andzVenereology, Farwaniya Hospital, Kuwait

Subjects and Methods
Seventeen patients (9 male; 8 female) aged 18 to 40
with focal, segmental, stable vitiligo seen between
2005 and 2007 were enrolled in the study (Table 1)
The duration of their disease ranged from 5 to 20
years. All the patients had received various therapies
in the past, including psoralens, NB UV-B, excimer
laser, and steroids, with minimal benefit. None of the
patients had received surgical treatment. Five
patients had a family history of vitiligo, and three
had associated systemic diseases (2 diabetes mellitus;
1 thyroid disorder). None had a history of keloidal
tendency or bleeding diathesis. Eight of the lesions
were on the head and neck, three on the hands,
five on the foot, and one on the trunk). The disease
was stable in all the patients for at least 1 year (range
1–10 years) at the time of enrollment. The follow-up
period ranged from 2 years to 4 years.
Selection criteria were clinically stable lesion for
at least 1 year and focal or segmental vitiligo.
Exclusion criteria were generalized vitiligo, presence
of koebnerization, keloidal tendency, and bleeding
diathesis.
The study protocol conformed to the ethical guide-
lines of the 1975 Declaration of Helsinki, and the
institutional ethics committee approved the study.
All participants provided signed informed consent.
Stable disease was defined as no new lesions or
expansion of the preexisting lesions in the previous
1 year. All patients had a baseline photograph taken.
Information about each patient’s name, age, sex,
occupation, and contact details were noted on a
form. A detailed history regarding the disease, such
as duration, site, progression, type, distribution, and
stability of the lesions, was recorded. Any previous
history of systemic disease, endocrinological distur-
bances, keloidal or bleeding tendency, or herpes
labialis (especially in the patients with facial lesions)
was noted. A detailed history of past treatments was
also obtained. A general physical examination and
systemic evaluation was then performed in all
the patients to exclude any other concomitant
dermatological or medical disorders. A baseline
examination, including complete blood count,
differential count, coagulation profile, liver function
tests, and renal function tests, was performed on all
patients.
Procedure
Split-Skin-Thickness Grafting
Preparation of Donor Site. The site used was the
lateral aspect of thigh. After shaving off the hairs and
proper cleansing with povidone iodine and 70%
ethanol, the area was anaesthetized with 1%
xylocaine without adrenalin. The area was then
stretched, and thin epidermal grafts were taken
using a sterilized platinum razor blade. The blade
was held in a medium-sized straight artery forceps.
The length of the cutting edge of the blade and the
angle at which the blade was held were adjusted to
obtain a uniformly thin graft. The adjusted artery
forceps were then slid against the stretched donor
skin at an appropriate angle, and normal saline was
used if necessary to reduce friction between the blade
and skin. The grafts obtained were transferred to a
petri dish containing normal saline. The area of
the recipient site determined the number of grafts
taken.
Preparation of Recipient Site. After proper cleansing
with povidone iodine and 70% ethanol, the area was
abraded using an electrical dermabrader fitted with a
diamond fraise. The recipient site was abraded until
pinpoint hemorrhages were seen uniformly all over
the lesion. The area was then cleaned with normal
sterile saline and covered with a gauze piece soaked
in normal saline. The grafts obtained were then
spread upside down on the sterile glass slides. Iris
forceps were used to spread the graft. The slide was
placed on the recipient area and pressed against the
skin. The graft was adjusted according to the shape
of the recipient site. Any blood or exudates between
the graft and recipient area were evacuated by firmly
pressing the positioned graft with the help of wet
gauze, without displacing the graft. After properly
covering the recipient site with the grafts, the area
D E R M AT O L O G I C S U R G E RY5 0 0
S P L I T- S K I N G R A F T I N G A N D E X C I M E R I N S TA B L E V I T I L I G O

was dressed with paraffin-based antiseptic dressing
followed by wet gauzes and adhesive tape and then
bandaged to secure the site. A pressure bandage was
used at the recipient site to ensure immobilization.
Postoperative Care. Patients were advised to avoid
excessive movement of the grafted area and to follow
up after 1 week for a change of dressing. All
patients were prescribed prophylactic antibiotics for
1 week and a pain killer if required. Patients
with facial lesions were also given prophylactic
acyclovir to prevent the reactivation of herpes
labialis. The dressing was changed after 1 week,
and redressing was done using the same method.
Two weeks after surgery, the dressing was removed,
and patients were asked to apply topical antibiotic
cream twice daily.
Phototherapy
Method. The grafted area was then treated with
excimer laser twice a week with a fluence starting
from 100 J/cm2. The fluence was raised at every
session until a persistent erythema was noted,
after which the laser was used at the same fluence
until 16 weeks (32 sessions).
Machine. The laser used was a 308-nm excimer laser
(Talos, Wavelight Laser Technology AG, Erlangen,
Germany). The Talos excimer laser is a xenon chlo-
ride (XeCl) gas laser. Talos always operates at the
same pulse repetition frequency of 200 Hz. The
energy per pulse also remains constant in operating
mode. The laser device offers an assortment of three
different hand pieces with diameters of 15, 20, and
25 mm that encompass treatment zones of 1.8, 3.1,
and 4.9 cm2. The pulse length of the Talos excimer
laser is 60 ns, with a repetition frequency of 200 Hz
and an energy-per-pulse emission of 4.6 mJ. The
average output density is 200 mW/cm2.
Response Assessment. The patient and the physician
evaluated the response twice. The first evaluation
was done at the end of the treatment (after 32 ses-
sions with the 308-nm excimer laser), and the second
evaluation was done 1 year after surgery. After that,
Figure 1. Complete repigmentation of localized vitiligo lesion on left medial malleolus. (A) Preoperative localized vitiligo.(B) One week postoperative photo showing well-placed graft. (C) Four-year postoperative photo showing complete repig-mentation.
3 6 : 4 : A P R I L 2 0 1 0 5 0 1
A L - M U TA I R I E T A L
the patients were followed at least once a year, but
there was no change in the evaluation.
Results
The maximum area treated in one operative session
was 55 cm2, and the minimum was 2 cm2. The total
area transplanted in 17 patients was 441 cm2, with
an average of 26 cm2.
Response Assessment
Patient Response Assessment. All patients were
asked to grade their response after completion of 32
sessions of excimer laser treatment using a visual
analogue scale, with responses of excellent, good,
fair, and poor. At the first evaluation, 12 (70.5%)
patients rated their response as excellent, and the
remaining five (29.4%) as good. The five patients
with a response of good at the initial evaluation
graded their response as excellent at the time of final
evaluation 1 year after the surgery. Thus, at the
final evaluation, all 17 (100%) patients graded their
response as excellent.
Physician Response Assessment. We evaluated the
results using the scoring system suggested by Gupta
and colleagues10 for the evaluation of autologous
transplants. The scoring was done once at the end of
32 exposures of 308-nm excimer laser and again 1
year after surgery. At the first evaluation, 12 of the
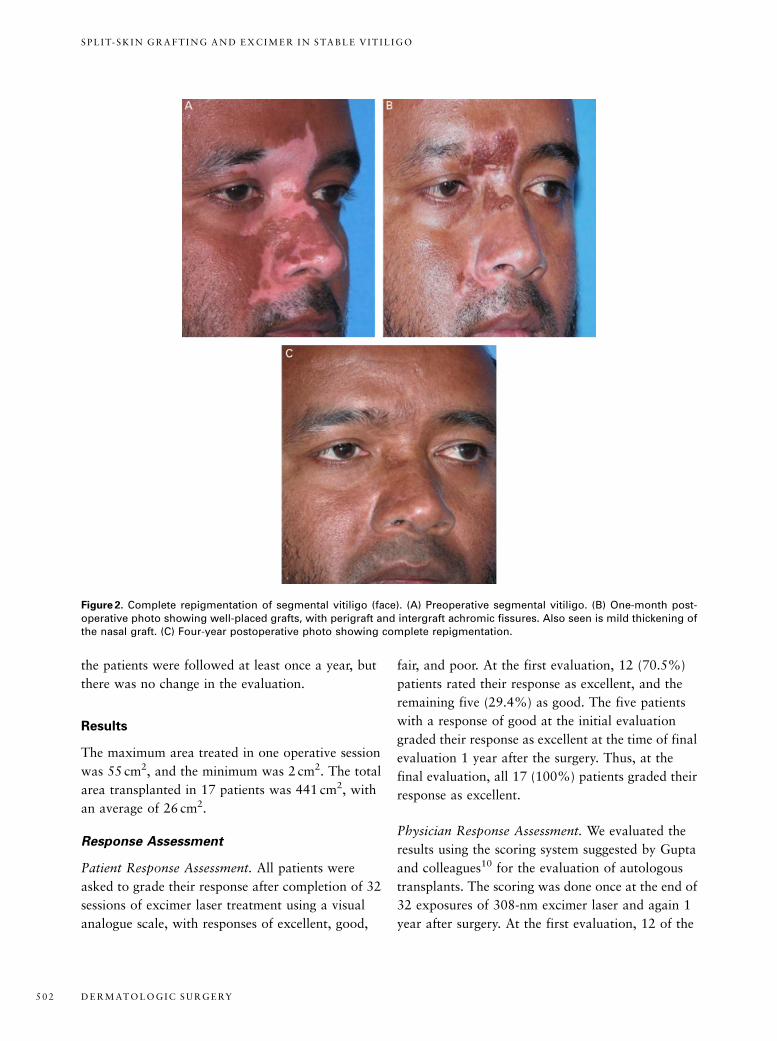
Figure 2. Complete repigmentation of segmental vitiligo (face). (A) Preoperative segmental vitiligo. (B) One-month post-operative photo showing well-placed grafts, with perigraft and intergraft achromic fissures. Also seen is mild thickening ofthe nasal graft. (C) Four-year postoperative photo showing complete repigmentation.
D E R M AT O L O G I C S U R G E RY5 0 2
S P L I T- S K I N G R A F T I N G A N D E X C I M E R I N S TA B L E V I T I L I G O

17 patients had excellent results, and the other five
had good results. At the second evaluation, 1 year
after surgery, all 17 patients had excellent results.
Two patients developed new vitiligo lesions in an
unaffected area, whereas the transplanted areas
retained the pigment. None of the patients developed
depigmentation of the transplanted skin during the
maximum follow-up period of 4 years.
Side Effects. Except for the mild hyperpigmentation
at the donor site visible on closer look, none of the
complications seen during the initial few months
persisted at the time of final evaluation (1 year after
surgery).
Discussion
Surgical treatment11–15 for vitiligo includes tissue
grafts (full- and split-thickness grafts, suction
blister grafts) and cellular grafts (noncultured kera-
tinocytes and melanocytes, cultured melanocytes,
autologous cultured epidermal cells), which basically
consist of transferring the autologous melanocytes
from normally pigmented donor skin to
depigmented skin. The use of surgical techniques
is restricted to the cases of stable, localized or
segmental vitiligo. A systematic review by Njoo
and colleagues16 on autologous transplantation
methods involving 63 studies (16 on punch
grafting, 13 on split-thickness grafting, 15 on
suction blister grafting, 17 on grafting of cultured
melanocytes) showed that the highest mean
success rates are achieved using split-thickness
skin grafting (87%). Khandpur and colleagues17
compared the results of split-thickness skin
grafting and minipunch grafting and had found
split-thickness skin grafting to be superior. After 1 to
2 weeks, the dressings are removed, and it might be
then combined with PUVA or psoralen with
solar ultraviolet light or NB UV-B treatment. The
success of this procedure reported by Gupta and
colleagues10 was 67% of patches with more than
75% repigmentation.
Figure 3. Complete repigmentation of localized vitiligo lesion on forehead. (A) Preoperative localized vitiligo. (B) One-weekpostoperative photo showing well-placed grafts, with a small area of hematoma beneath the graft. Single achromic fissureon the superior and medial aspect of the lesion because of possible side-wise shift of the supralateral graft. Six-monthspostoperative photo showing hypopigmented halo and small areas of graft thickening (C). One-year postoperative photoshowing complete repigmentation and no evidence of graft thickening (D).
3 6 : 4 : A P R I L 2 0 1 0 5 0 3
A L - M U TA I R I E T A L

The literature on successful use of the 308-nm
excimer laser dates to 2001. The 308-nm excimer laser
emits a monochromatic light of 308nm and induces
photobiological effects similar to NB UV-B, thus stimu-
lating adjacent melanocytes in the outer root sheath of
hair follicles and on the margins of lesions to migrate
and repopulate the vitiliginous areas. Several studies18–20
have shown the response of vitiligo patches to excimer
laser, and U.S. Food and Drug Administration has
approved it for the treatment of vitiligo and psoriasis.
Excimer laser permits the selective treatment of only
lesional skin in a small number of treatment sessions
over a short period of time and ensures no unnecessary
treatment of healthy skin. Thus the patient receives less
radiation, reducing the risk of skin aging and carcino-
genesis. Furthermore, the unsightly tanning of all
perilesional skin is avoided. Targeted phototherapy with
the 308-nm excimer laser can also reach areas inacces-
sible to conventional phototherapeutic modalities.
Combination treatment with grafting and postsur-
gical PUVA and NB UV-B therapy has been used in
the past. NB UV-B therapy has an advantage
over PUVA because no drugs are required for the
treatment, and the effect of photo-carcinogenesis
and photo-aging are probably reduced. However, the
use of NB UV-B leads to radiation of noninvolved
skin. With most of the suitable candidates for
surgery being cases of localized or segmental vitiligo,
we decided to combine split-thickness skin grafting
with the 308-nm excimer laser therapy postsurgi-
cally because our team has long experience in the
technique, and all of the patients selected in our
study had stable localized or segmental vitiligo
so we thought it was unnecessary to expose our
patients to excessive radiation. Hence, we used a
more targeted 308-nm excimer laser in our patients.
Conclusion
Split-skin grafting is a quick and effective modality
for the treatment of resistant cases of localized
vitiligo. The use of excimer laser after grafting min-
imizes the chances of developing perigraft halo or
achromic fissures, which is a common complication
of the surgery, particularly in a situation in which
TABLE 1. Patient Characteristics
Patient
Age/
Sex Site
Type of
Vitiligo
Duration
(Years)
Area
(cm2)
Grafts
Used, n
Physician Response
Assessment
Follow-Up
(Years)
Initial
Score
Final
Score
1 (Figure 1) 40/M Leg Focal 15 8 4 19 21 4
2 (Figure 3) 36/F Face Focal 20 38 8 18 21 2
3 30/M Leg Focal 10 2 2 13 18 2
4 28/M Face Segmental 15 55 9 18 21 3
5 18/F Neck Focal 5 30 6 18 21 3
6 30/F Hand Focal 8 20 5 13 18 2
7 18/M Trunk Segmental 6 42 7 19 21 2
8 18/M Face Segmental 4 36 11 18 18 4
9 22/M Hand Focal 10 15 8 19 21 3
10 20/F Face Segmental 8 10 6 13 21 3
11 (Figure 2) 40/F Face Segmental 15 5 3 19 21 4
12 19/M Leg Segmental 5 50 14 18 21 2
13 30/F Hand Focal 10 35 10 13 18 4
14 29/M Face Segmental 12 25 8 18 21 3
15 38/M Neck Focal 15 8 5 18 18 4
16 21/F Leg Focal 5 40 7 13 18 4
17 20/F Leg Focal 3 22 6 19 21 2
D E R M AT O L O G I C S U R G E RY5 0 4
S P L I T- S K I N G R A F T I N G A N D E X C I M E R I N S TA B L E V I T I L I G O

some of the grafts fail to survive for any reason.
Routine use of postgrafting excimer laser may lead
to fast, uniform, complete repigmentation of the
recipient area.
Our study shows that permanent cure of a stable,
localized vitiligo is achievable provided that patients
are selected judiciously, proper precautions are taken
during surgery and more importantly for the initial 2
weeks after surgery, and the surgeon has expertise in
the technique.
References
1. Goldinger SM, Dummer R, Schmid P, et al. Combination of 308-
nm xenon chloride excimer laser and topical calcipotriol in
vitiligo. J Eur Acad Dermatol Venereol 2007;21:504–8.
2. Castanet J, Ortonne JP. Pathophysiology of vitiligo. Clin Dermatol
1997;15:845–51.
3. Gupta S, Kumar B. Epidermal grafting in vitiligo: influence of age,
site of lesion, and type of disease on outcome. J Am Acad
Dermatol 2003;49:99–104.
4. Behl PN. Treatment of vitiligo with homologous thin Thiersch’s
skin grafts. Curr Med Pract 1964;8:218–21.
5. Westerhof W, Lontz W, Vanscheidt W, Braathen L. Vitiligo news in
surgical treatment. J Eur Acad Dermatol Venereol 2001;15:510–1.
6. Skouge JW, Morison WL, Diwan RV, et al. Autografting and
PUVA. A combination therapy for vitiligo. Dermatol Surg Oncol
1992;18:357–60.
7. Hann SK, Im S, Bong HW, et al. Treatment of stable vitiligo with
autologous epidermal grafting and PUVA. J Am Acad Dermatol
1995;32:943–8.
8. Lahiri K, Malakar S, Sarma N, Banerjee U. Repigmentation
of vitiligo with punch grafting and narrow-band
UV-B (311nm)Fa prospective study. Int J Dermatol
2006;45:649–55.
9. Pianigiani E, Risulo M, Andreassi A, et al. Autologous epidermal
cultures and narrow-band ultraviolet B in the surgical treatment of
vitiligo. Dermatol Surg 2005;31:155–9.
10. Gupta S, Honda S, Kumar B. A novel scoring system for evalu-
ation of results of autologous transplantation methods in vitiligo.
Ind J Dermatol Venereol Leperol 2002;68:33–7.
11. Savant S. Surgical therapy of vitiligo: current status. Ind J
Dermatol Venereol Leperol 2005;71:307–10.
12. Rusfianti M, Yohanes WW. Dermatosurgical techniques for
repigmentation of vitiligo. Int J Dermatol 2006;45:411–7.
13. Mutalik S, Ginzburg A. Surgical management of stable vitiligo: a
review with personal experience. Dermatol Surg 2000;26:248–54.
14. Gupta S, Jain VK, Saraswat PK, et al. Suction blister epidermal
grafting versus punch skin grafting in recalcitrant and stable
vitiligo. Dermatol Surg 1999;25:955–8.
15. Kahn AM, Cohen MJ, Kaplan L. Vitiligo treatment by derm-
abrasion and epithelial sheet graftingFa preliminary report. J Am
Acad Dermatol 1993;28:773–4.
16. Njoo MD, Westerhof W, Boz JD, et al. A systematic review of
autologous transplantation methods in vitiligo. Arch Dermatol
1998;134:1543–9.
17. Khandpur S, Sharma VK, Manchanda Y. Comparison of
minipunch grafting versus split-skin grafting in chronic stable
vitiligo. Dermatol Surg 2005;31:436–41.
18. Nicolaidou E, Antoniou C, Stratigos A, Katsambas AD.
Narrowband ultraviolet B phototherapy and 308-nm excimer
laser in the treatment of vitiligo: a review. J Am Acad Dermatol
2009;60:470–7.
19. Hofer A, Hassan AS, Legat FJ, et al. The efficacy of excimer laser
(308 nm) for vitiligo at different body sites. J Eur Acad Dermatol
2006;20:558–64.
20. Casacci M, Thomas P, Pacifico A, et al. Comparison between 308-
nm monochromatic excimer light and narrow band UVB photo-
therapy (311-313 nm) in the treatment of vitiligoFa multicentre
controlled study. J Eur Acad Dermatol 2007;21:956–63.
Address correspondence and reprint requests to: NawafAl-Mutairi, MD, P.O. Box: 280, Farwaniya 80000,Kuwait, or e-mail: [email protected]
3 6 : 4 : A P R I L 2 0 1 0 5 0 5
A L - M U TA I R I E T A L
Copyright © 2022 FDOKUMEN