Genetic Diversity and Drug Resistance Profiles in HIV Type 1- and HIV Type 2-Infected Patients from...
15
Genetic Diversity and Drug Resistance Profiles in HIV Type 1- and HIV Type 2-Infected Patients from Cape Verde Islands Va ˆ nia Oliveira, 1,2 Ine ˆs Ba ´ rtolo, 2,3 Pedro Borrego, 2,3 Cheila Rocha, 2,3 Emı ´lia Valadas, 4 Jorge Barreto, 5 Elsa Almeida, 5 Francisco Antunes, 4 and Nuno Taveira 2,3,6 Abstract Our aim was to characterize for the first time the genetic diversity of HIV in Cape Verde Islands as well as the drug resistance profiles in treated and untreated patients. Blood specimens were collected from 41 HIV-1 and 14 HIV-2 patients living in Santiago Island. Half of the patients were on antiretroviral treatment (ART). Pol and env gene sequences were obtained using in-house methods. Phylogenetic analysis was used for viral subtyping and the Stanford Algorithm was used for resistance genotyping. For HIV-1, the amplification of pol and env was possible in 27 patients (66%). HIV-1 patients were infected with subtypes G (13, 48%), B (2, 7%), F1 (2, 7%), and CRF02_AG (2, 7%), and complex recombinant forms including a new C/G variant (n = 8, 30%). Drug resistance mutations were detected in the PR and RT of three (10%) treated patients. M41L and K103N transmitted drug resistance mutations were found in 2 of 17 (12%) untreated patients. All 14 HIV-2 isolates belonged to group A. The origin of 12 strains was impossible to determine whereas two strains were closely related to the historic ROD strain. In conclusion, in Cape Verde there is a long-standing HIV-2 epidemic rooted in ROD-like strains and a more recent epidemic of unknown origin. The HIV-1 epidemic is caused by multiple subtypes and complex recombinant forms. Drug resistance HIV-1 strains are present at moderate levels in both treated and untreated patients. Close surveillance in these two populations is crucial to prevent further transmission of drug-resistant strains. Introduction C ape Verde is an archipelago located offshore Senegal in the West African coast with a population of 491,575 individuals. 1 The first AIDS case in a Cape Verdian individual was identified in 1982 and was caused by HIV-2. 2 Similarly to neighboring countries such as Senegal and Gambia, HIV seroprevalence is low, estimated at less than 1% according to the national surveys from 1989 and 2005. 3 At the end of 2005, approximately 1710 cases of HIV infection were determined, and half were already the in AIDS stage. Similar to other West African countries, both types of HIV circulate, with 72% of the cases caused by HIV-1, 22% by HIV-2, and 6% by both viruses (potential double infections). 3 Since the advent of highly active antiretroviral therapy in developed countries we have seen an improved prognosis of HIV-1-infected patients, with a significant decrease in mor- bidity and mortality rates associated with this infection. 4,5 Combined antiretroviral therapy (cART) has been introduced recently in resource-limited countries. 6 However, there are concerns about the low efficacy of cART in these countries, which could lead to the rapid and uncontrolled emergence and transmission of drug-resistant viruses. 7 Three factors that can lead to low cART efficacy are the limited HIV-RNA monitoring of patients undergoing therapy, the unregulated and unmonitored use of antiretroviral drugs bought on the black market or abroad, and the lack of drug resistance sur- veillance systems. 7–10 Despite these limitations, transmitted 1 Laborato ´ rio de Hemato-Oncologia, Instituto Portugue ˆs de Oncologia, Lisbon, Portugal. 2 Unidade dos Retrovı ´rus e Infecc ¸o ˜ es Associadas, Centro de Patoge ´nese Molecular, Faculdade de Farma ´cia de Lisboa, Lisbon, Portugal. 3 Centro de Investigac ¸a ˜ o Interdisciplinar Egas Moniz (CiiEM), Instituto Superior de Cie ˆncias da Sau ´ de Egas Moniz, Monte de Caparica, Portugal. 4 Clı ´nica Universita ´ ria de Doenc ¸as Infecciosas/Servic ¸o de Doenc ¸as Infecciosas, Faculdade de Medicina de Lisboa/Hospital de Santa Maria, Lisbon, Portugal. 5 Hospital Dr. Agostinho Neto, Delegacia de Sau ´ de, Cidade da Praia, Cabo Verde. 6 Instituto de Medicina Molecular, Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal. AIDS RESEARCH AND HUMAN RETROVIRUSES Volume 27, Number 00, 2011 ª Mary Ann Liebert, Inc. DOI: 10.1089/aid.2011.0174 1 AIDS-2011-0174-ver9-Oliveira_1P Type: note AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 1
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Genetic Diversity and Drug Resistance Profiles in HIV Type 1- and HIV Type 2-Infected Patients from...

Genetic Diversity and Drug Resistance Profiles in HIV Type1- and HIV Type 2-Infected Patients from Cape Verde Islands
Vania Oliveira,1,2 Ines Bartolo,2,3 Pedro Borrego,2,3 Cheila Rocha,2,3 Emılia Valadas,4
Jorge Barreto,5 Elsa Almeida,5 Francisco Antunes,4 and Nuno Taveira2,3,6
Abstract
Our aim was to characterize for the first time the genetic diversity of HIV in Cape Verde Islands as well as thedrug resistance profiles in treated and untreated patients. Blood specimens were collected from 41 HIV-1 and 14HIV-2 patients living in Santiago Island. Half of the patients were on antiretroviral treatment (ART). Pol and envgene sequences were obtained using in-house methods. Phylogenetic analysis was used for viral subtyping andthe Stanford Algorithm was used for resistance genotyping. For HIV-1, the amplification of pol and env waspossible in 27 patients (66%). HIV-1 patients were infected with subtypes G (13, 48%), B (2, 7%), F1 (2, 7%), andCRF02_AG (2, 7%), and complex recombinant forms including a new C/G variant (n = 8, 30%). Drug resistancemutations were detected in the PR and RT of three (10%) treated patients. M41L and K103N transmitted drugresistance mutations were found in 2 of 17 (12%) untreated patients. All 14 HIV-2 isolates belonged to group A.The origin of 12 strains was impossible to determine whereas two strains were closely related to the historic RODstrain. In conclusion, in Cape Verde there is a long-standing HIV-2 epidemic rooted in ROD-like strains and amore recent epidemic of unknown origin. The HIV-1 epidemic is caused by multiple subtypes and complexrecombinant forms. Drug resistance HIV-1 strains are present at moderate levels in both treated and untreatedpatients. Close surveillance in these two populations is crucial to prevent further transmission of drug-resistantstrains.
Introduction
Cape Verde is an archipelago located offshore Senegalin the West African coast with a population of 491,575
individuals.1 The first AIDS case in a Cape Verdian individualwas identified in 1982 and was caused by HIV-2.2 Similarly toneighboring countries such as Senegal and Gambia, HIVseroprevalence is low, estimated at less than 1% according tothe national surveys from 1989 and 2005.3 At the end of 2005,approximately 1710 cases of HIV infection were determined,and half were already the in AIDS stage. Similar to other WestAfrican countries, both types of HIV circulate, with 72% of thecases caused by HIV-1, 22% by HIV-2, and 6% by both viruses(potential double infections).3
Since the advent of highly active antiretroviral therapy indeveloped countries we have seen an improved prognosis ofHIV-1-infected patients, with a significant decrease in mor-bidity and mortality rates associated with this infection.4,5
Combined antiretroviral therapy (cART) has been introducedrecently in resource-limited countries.6 However, there areconcerns about the low efficacy of cART in these countries,which could lead to the rapid and uncontrolled emergenceand transmission of drug-resistant viruses.7 Three factors thatcan lead to low cART efficacy are the limited HIV-RNAmonitoring of patients undergoing therapy, the unregulatedand unmonitored use of antiretroviral drugs bought on theblack market or abroad, and the lack of drug resistance sur-veillance systems.7–10 Despite these limitations, transmitted
1Laboratorio de Hemato-Oncologia, Instituto Portugues de Oncologia, Lisbon, Portugal.2Unidade dos Retrovırus e Infeccoes Associadas, Centro de Patogenese Molecular, Faculdade de Farmacia de Lisboa, Lisbon, Portugal.3Centro de Investigacao Interdisciplinar Egas Moniz (CiiEM), Instituto Superior de Ciencias da Saude Egas Moniz, Monte de Caparica,
Portugal.4Clınica Universitaria de Doencas Infecciosas/Servico de Doencas Infecciosas, Faculdade de Medicina de Lisboa/Hospital de Santa Maria,
Lisbon, Portugal.5Hospital Dr. Agostinho Neto, Delegacia de Saude, Cidade da Praia, Cabo Verde.6Instituto de Medicina Molecular, Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal.
AIDS RESEARCH AND HUMAN RETROVIRUSESVolume 27, Number 00, 2011ª Mary Ann Liebert, Inc.DOI: 10.1089/aid.2011.0174
1
AIDS-2011-0174-ver9-Oliveira_1P
Type: note
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 1

HIV drug resistance is still residual (< 5%) in most sub-Sa-haran countries.11–17
Worldwide strains of HIV-1 are phylogenetically classi-fied into four very divergent groups, M, N, O, and P.18
Amino acid sequences of Gag and Env can differ betweengroups up to 30% and 47%, respectively. HIV-1 group M, theonly pandemic group, has diversified into nine divergentsubtypes (A, B, C, D, F, G, H, K, and J), six subsubtypes (F1,F2, A1–A5), and multiple circulating recombinant forms.19,20
Amino acid sequences of Env can differ by up to 20% withina particular subtype and over 35% between subtypes. As forHIV-2, which is mostly restricted to a few West Africancountries including Cape Verde, despite the existence ofeight genetic groups named A to H only groups A and Bseem to be spreading, with group A much more commonthan group B.21–23
The extraordinary HIV diversity is seen as a major hurdleto the development of a prophylactic vaccine.24 HIV diver-sity and its rapid evolution may present significant problemsto diagnosis and to antiviral therapy. For example, signifi-cant antigenic changes in HIV-1 group O viruses have re-cently been shown to hinder the diagnostic performance ofseveral serodiagnostic assays.25 Likewise, many compara-tive studies have shown that the sensitivity and specificity ofviral load assays vary depending on HIV-1 group or sub-type.18,26–29 Regarding antiviral therapy, there are majordifferences in the susceptibility of HIV-1 and HIV-2 to thecurrent available drugs. Indeed, HIV-2 is naturally resistantto nonnucleoside reverse transcriptase inhibitors (NNRTIs)and it presents a diminished sensitivity to certain proteaseinhibitors (PI).30 Moreover, most cART regimens used inHIV-1 patients are unable to fully suppress HIV-2 replica-tion, to increase the number of CD4 cells, or to prevent theaccumulation of drug-resistant mutations.31 Diversityamong HIV-1 isolates also affects antiviral therapy. For in-stance, like HIV-2, group O strains are resistant toNNRTIs.32,33 Natural polymorphisms found in the proteaseand reverse transcriptase of some non-B subtypes may lowertheir genetic barrier to resistance to some protease and re-verse transcriptase inhibitors.17,34 Finally, certain drug-resistant mutations accumulate more frequently and rapidlyin some non-B subtypes than in HIV-1 B (e.g., K65R, L90M,and V106M in subtype C and I54V/L in subtype G).34–36
Hence, HIV diversity has major implications for the devel-opment of resistance, for the genotypic evaluation of drugresistance, and for the selection of therapeutic regimens, atleast in countries in which both HIV-1 and HIV-2 circulatesuch as Cape Verde.
Cape Verde, like most other resource-limited countries,adopted the World Health Organization (WHO) public healthapproach in antiretroviral therapy (ART) utilization.37 cARThas been available free of charge since December 2004 andwas initially given to a group of 148 patients. The preferentialfirst line regime adopted includes a combination of lamivu-dine (3TC), stavudine (d4T), and nevirapine (NVP). Presently,there are no data concerning the genetic diversity of HIV inCape Verde. Moreover, there is no information about theprevalence and nature of primary and secondary drug resis-tance in this country. The aim of the present work was todetermine, for the first time, the HIV-1 and HIV-2 geneticforms present in Cape Verde and the drug resistance profilesin treated and untreated patients.
Materials and Methods
Patients
Blood samples were collected during 2005 (n = 37), 2006(n = 14), and 2007 (n = 4) from 41 HIV-1- and 14 HIV-2-infectedpatients living in Santiago Island and attending the Delegaciade Saude, Cidade da Praia, Cape Verde. Nineteen of the HIV-1individuals had received cART, 18 were drug naıve, and forfour there were no indication on the drug regimen. Half of theHIV-2 patients were on cART. The epidemiological charac-teristics of the HIV-1 and HIV-2 patients are described in
b T1Table 1. Plasma samples were preserved at - 20�C in Cidadeda Praia and thereafter at - 80�C in Lisbon, Portugal. Ser-ologic diagnosis of HIV infection and CD4 + T cell counts weredone in Cape Verde; plasma viral load was determined withthe Cobas Amplicor HIV-1 Monitor test version 1.5 (Roche) inLisbon, Portugal. Written informed consent was obtainedfrom all participants and the study was approved by theethics committees of the participating institutions.
Table 1. Comparison of Demographic, Immunologic,
and Virologic Characteristics Between HIV-1-and HIV-2-Infected Patients
Variables HIV-1 HIV-2 p value
N (%) 41 (75) 14 (25) —
Gender N (%)Male 12 (29) 6 (43) 0.5253a
Female 25 (61) 8 (57)Unknown 4 (10) —
Age group (years) N (%)10–19 1 (3) 0 0.5217b
20–29 3 (7) 1 (7)30–39 12 (29) 3 (21)40–49 14 (34) 6 (43)50–59 7 (17) 4 (29)Unknown 4 (10) — —
Transmission routeSexual 33 (81) 13 (93) 1.000c
Sexual/bloodtransfusion
1 (2) 1 (7)
Sexual/intravenousdrug user
2 (5) —
Vertical 1 (2) —Unknown 4 (10) — —
CD4 (median,range),cells/ll
417 (14–820) 487 (35–1420) 0.4115d
HIV RNA(mean, SD),copies/ml(N = 23)
9.4 · 104 (1.3 · 105) nd —
ART (N, %) 19 (46) 7 (50) 1.000e
aFisher exact test.bFisher exact test comparing the number of patients below or
above 40 years old.cFisher exact test comparing sexual transmission with other routes
of transmission.dMann–Whitney test.eFisher exact test comparing the number of patients on ART with
untreated patients.ART, antiretroviral therapy; nd, not done.
2 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 2

Viral RNA extraction, PCR amplification, andsequencing
HIV-1 viral RNA was extracted from 140 ll of plasma usingthe QIAamp Viral RNA miniKit (QIAGEN). Reverse tran-scriptase polymerase chain reaction was performed with the
TitanOne Tube reverse transcriptase polymerase chain reac-tion System (Roche). Nested polymerase chain reaction wasdone to obtain a 409-bp fragment from the C2V3C3 env re-gion, a 532-bp fragment containing the part of the gag geneand all the PR region, and a 1026-bp fragment from the RTregion. Thermal cycling conditions and primers sequence and
FIG. 1. Genetic subtypesand evolutionary relation-shipsAU3 c of the HIV-1 viruses se-quenced in this study basedon maximum likelihood phy-logenetic trees of the PR (A),RT (B), and C2V3C3 env generegion (C). The phylogenetictrees were constructed withreference sequences from allHIV-1 genetic forms obtainedfrom different locations. Se-quences from Cape Verdeisolates are shown in boldletters.
HIV INFECTION IN CAPE VERDE ISLANDS 3
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 3

position were described elsewhere.38,39 HIV-2 viral RNA wasextracted from plasma as described above. Nested polymer-ase chain reaction was done to obtain a 373-bp fragment fromthe C2V3C3 env region as described elsewhere.40 DNA se-quences were obtained with Big Dye Terminator Cycle Se-quencing Kit (Applied Biosystems) and an automatedsequencer.
Phylogenetic and recombination analysis
Sequences were aligned with sequences from referencestrains collected from the Los Alamos Sequence Database(http://www.hiv.lanl.gov/content/sequence/NEWALIGN/align.html) using Clustal X 1.8.41 Maximum likelihood phy-logenetic analyses42 were performed using the best-fit modelof molecular evolution estimated by Modeltest v3.7 under theAkaike Information Criterion.43 The chosen models wereK81uf + I + G for the env gene and GTR + I + G for the polgene of HIV-1 sequences and the TrN + I + G for both PR andC2V3C3 HIV-2 regions. Tree searches were conducted inPAUP v4.0b10 using a nearest-neighbor interchange heuristicsearch strategy44 and bootstrap resampling.45 Bootstrap val-ues ‡ 70% were considered definitive for significantFIG. 1. (Continued).
FIG. 1. (Continued).
4 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 4

clustering.46 All sequences were checked for hypermutation atthe Los Alamos website using the program Hypermut.47
Resistance mutation analysis
Genotypic analysis of HIV-1 drug resistance was per-formed using the Stanford Genotypic Resistance Interpreta-tion Algorithm (http://hivdb.stanford.edu/index.html). Atfirst, we considered all resistance mutations and unusualpolymorphisms. Mutations associated with transmitted HIVdrug resistance were then selected from a recently publishedlist.48
Statistical analysis
The Mann–Whitney test was used to compare groups. Thefrequencies of drug resistance mutations of viruses from CapeVerde were compared with those of all subtype B and G se-quences available at the Stanford HIV Drug Resistance Da-tabase using the Fisher exact test. p values < 0.05 wereconsidered significant.
Results
We analyzed samples from 55 patients, 41 (75%) infectedwith HIV-1 and 14 (25%) infected with HIV-2. There were nosignificant epidemiological or immunological differences be-tween HIV-1- and HIV-2-infected patients (Table 1). Mostpatients (60%) were female and were aged 40–49 years. Theinfection was mostly transmitted by the sexual route. Mostpatients had less than 500 CD4 + T cells, which is suggestive oflong-term infection. As expected, viral load was significantlylower in treated HIV-1 patients (N = 18) than in untreatedpatients (N = 19) (median HIV RNA copies per ml of plasma;range, 400; 400–93,000 vs. 43,900; 400–513,000; p < 0.0001).
For HIV-1, the amplification of the PR, RT, and/or C2V3C3genomic regions was possible in 27 HIV-1 samples (66%). Tenof these patients (37%) were on cART and 17 (63%) were drug-naive individuals. PR and RT sequences were obtained in 26(63%) and 27 (66%) patients, respectively. C2V3C3 env genesequences were obtained in 24 (59%) patients. All sequenceswere checked using the program Hypermut and none showedevidence of hypermutation.
Phylogenetic analyses revealed that 13 (48%) viral isolateswere subtype G, six (22%) were non-G [two (7%) subtype B,
two (7%) subtype F1, and two (7%) CRF02_AG], four (15%)were recombinants between subtype G and other subtypesor U strains [1 G (PR)/G (RT)/H (C2V3C3); 1 G/G/B; 1 C/C/G; 1 U/G/-], two (7%) were recombinants betweenCRF02_AG and subtype B and/or U strains [1 U/B/CRF02_AG; 1 U/CRF02_AG/CRF02_AG], and two (7%)were recombinants between the A subtype and U strains (U/A/U) ( b F1Fig. 1).
There were no major mutations associated with PI resis-tance in the naive population. The minor mutations associ-ated with PI resistance, L10I (6%) and A71V (6%), weredetected in two unrelated drug-naive patients ( b T2Table 2). TheM41L, K103N, and Y318F mutations conferring resistance toNRTIs or NNRTIs were found in 3 of 17 untreated patients.Only M41L and K103N are considered transmitted drugresistance mutations.48–50 Hence, our results reveal a 12% (2out of 17 patients) rate of transmitted drug resistance in CapeVerde.
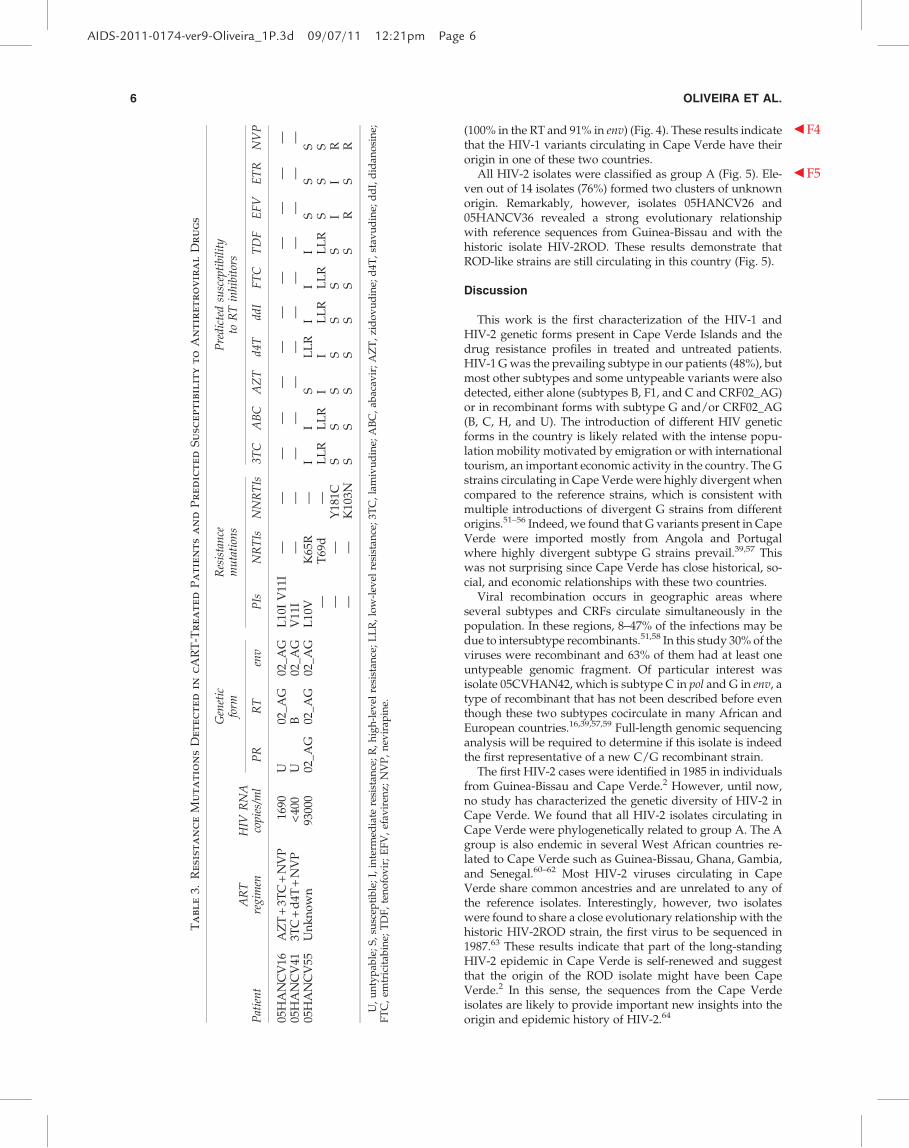
Resistance mutations were detected in 3 of 10 (30%) pa-tients undergoing cART ( b T3Table 3). No major mutations asso-ciated with PI resistance were found in this population. Theminor mutations L10I/V and V11I, associated with PI resis-tance, were found in two patients infected with complex re-combinant isolates. The K65R, T69d, K103N, and Y181Cmutations, which confer resistance to the NRTIs and NNRTIs,were all detected in patient 05HANCV55, who was infectedwith a CRF02_AG strain.
The frequency of some previously known PR polymor-phisms detected in subtype G isolates (29% of polymor-phisms) was significantly different ( p < 0.05) when comparedto isolates of similar subtype found throughout the world( b F2Fig. 2). Likewise, the frequency of the RT polymorphismsfound in the G subtype (38% of polymorphisms) was signif-icantly different ( p < 0.05) when compared to isolates fromworldwide treatment-naive patients infected with the samesubtype ( b F3Fig. 3). These results are a clear indication that the Gstrains circulating in Cape Verde are highly divergent andgenetically complex. The origin of the G strains from CapeVerde was investigated by phylogenetic analysis using RTand C2V3C3 env sequences from reference G sequences col-lected worldwide as well as sequences from Angola andPortugal deposited in the Los Alamos database. We foundthat the majority of the sequences from Cape Verde wereclosely related to sequences from Portugal and/or Angola
Table 2. Resistance Mutations Detected in Drug-Naıve Patients
and Predicted Susceptibility to Antiretroviral Drugs
Geneticform
Resistancemutations
Predicted susceptibilityto RT inhibitors
Patient PR RT env PI NRTI NNRTI 3TC ABC AZT d4T ddI FTC TDF EFV ETR NVP
05HANCV8 G G G K103N S S S S S S S R S R05HANCV11 B B — L10I05HANCV20 G G G A71V05HANCV31 G G B M41L S PLLR LLR LLR PLLR S PLLR S S S05HANCV45 G G G Y318F S S S S S S S PLLR PLLR I
PR, protease; RT, reverse transcriptase; PI, protease inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleosidereverse transcriptase inhibitor. S, susceptible; I, intermediate resistance; R, high-level resistance; LLR, low-level resistance; PLLR, potentiallow-level resistance; 3TC, lamivudine; ABC, abacavir; AZT, zidovudine; d4T, stavudine; ddI, didanosine; FTC, emtricitabine; TDF, tenofovir;EFV, efavirenz; NVP, nevirapine.
HIV INFECTION IN CAPE VERDE ISLANDS 5
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 5
(100% in the RT and 91% in env) ( b F4Fig. 4). These results indicatethat the HIV-1 variants circulating in Cape Verde have theirorigin in one of these two countries.
All HIV-2 isolates were classified as group A ( b F5Fig. 5). Ele-ven out of 14 isolates (76%) formed two clusters of unknownorigin. Remarkably, however, isolates 05HANCV26 and05HANCV36 revealed a strong evolutionary relationshipwith reference sequences from Guinea-Bissau and with thehistoric isolate HIV-2ROD. These results demonstrate thatROD-like strains are still circulating in this country (Fig. 5).
Discussion
This work is the first characterization of the HIV-1 andHIV-2 genetic forms present in Cape Verde Islands and thedrug resistance profiles in treated and untreated patients.HIV-1 G was the prevailing subtype in our patients (48%), butmost other subtypes and some untypeable variants were alsodetected, either alone (subtypes B, F1, and C and CRF02_AG)or in recombinant forms with subtype G and/or CRF02_AG(B, C, H, and U). The introduction of different HIV geneticforms in the country is likely related with the intense popu-lation mobility motivated by emigration or with internationaltourism, an important economic activity in the country. The Gstrains circulating in Cape Verde were highly divergent whencompared to the reference strains, which is consistent withmultiple introductions of divergent G strains from differentorigins.51–56 Indeed, we found that G variants present in CapeVerde were imported mostly from Angola and Portugalwhere highly divergent subtype G strains prevail.39,57 Thiswas not surprising since Cape Verde has close historical, so-cial, and economic relationships with these two countries.
Viral recombination occurs in geographic areas whereseveral subtypes and CRFs circulate simultaneously in thepopulation. In these regions, 8–47% of the infections may bedue to intersubtype recombinants.51,58 In this study 30% of theviruses were recombinant and 63% of them had at least oneuntypeable genomic fragment. Of particular interest wasisolate 05CVHAN42, which is subtype C in pol and G in env, atype of recombinant that has not been described before eventhough these two subtypes cocirculate in many African andEuropean countries.16,39,57,59 Full-length genomic sequencinganalysis will be required to determine if this isolate is indeedthe first representative of a new C/G recombinant strain.
The first HIV-2 cases were identified in 1985 in individualsfrom Guinea-Bissau and Cape Verde.2 However, until now,no study has characterized the genetic diversity of HIV-2 inCape Verde. We found that all HIV-2 isolates circulating inCape Verde were phylogenetically related to group A. The Agroup is also endemic in several West African countries re-lated to Cape Verde such as Guinea-Bissau, Ghana, Gambia,and Senegal.60–62 Most HIV-2 viruses circulating in CapeVerde share common ancestries and are unrelated to any ofthe reference isolates. Interestingly, however, two isolateswere found to share a close evolutionary relationship with thehistoric HIV-2ROD strain, the first virus to be sequenced in1987.63 These results indicate that part of the long-standingHIV-2 epidemic in Cape Verde is self-renewed and suggestthat the origin of the ROD isolate might have been CapeVerde.2 In this sense, the sequences from the Cape Verdeisolates are likely to provide important new insights into theorigin and epidemic history of HIV-2.64
Ta
bl
e3.
Re
sist
an
ce
Mu
ta
tio
ns
De
te
ct
ed
in
cA
RT
-T
re
at
ed
Pa
tie
nt
sa
nd
Pr
ed
ic
te
dS
usc
ep
tib
il
it
yt
oA
nt
ir
et
ro
vir
al
Dr
ug
s
Gen
etic
form
Res
ista
nce
mu
tati
ons
Pre
dic
ted
susc
epti
bili
tyto
RT
inh
ibit
ors
Pat
ien
tA
RT
reg
imen
HIV
RN
Aco
pie
s/m
lP
RR
Ten
vP
IsN
RT
IsN
NR
TIs
3T
CA
BC
AZ
Td
4T
dd
IF
TC
TD
FE
FV
ET
RN
VP
05H
AN
CV
16A
ZT
+3T
C+
NV
P16
90U
02_A
G02
_AG
L10
IV
11I
——
——
——
——
——
——
05H
AN
CV
413T
C+
d4T
+N
VP
<400
UB
02_A
GV
11I
——
——
——
——
——
——
05H
AN
CV
55U
nk
no
wn
9300
002
_AG
02_A
G02
_AG
L10
VK
65R
—I
IS
LL
RI
II
SS
S—
T69
d—
LL
RL
LR
II
LL
RL
LR
LL
RS
SS
——
Y18
1CS
SS
SS
SS
II
R—
—K
103N
SS
SS
SS
SR
SR
U,
un
typ
able
;S
,su
scep
tib
le;
I,in
term
edia
tere
sist
ance
;R
,h
igh
-lev
elre
sist
ance
;L
LR
,lo
w-l
evel
resi
stan
ce;
3TC
,la
miv
ud
ine;
AB
C,
abac
avir
;A
ZT
,zi
do
vu
din
e;d
4T,
stav
ud
ine;
dd
I,d
idan
osi
ne;
FT
C,
emtr
icit
abin
e;T
DF
,te
no
fov
ir;
EF
V,
efav
iren
z;N
VP
,n
evir
apin
e.
6 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 6

The recent introduction of cART in Cape Verde promptedus to investigate drug resistance mutations in isolates fromtreated and untreated HIV-1-infected populations. We did notfind major PI resistance mutations in either population. Theminor mutations associated with PI resistance, L10I and A71V,were detected in two (6%) drug-naive patients. However, L10Ioccurs in 5–10% of untreated persons and A71V is a poly-morphism that appears in 2–3% of untreated individuals.Therefore these mutations are not considered transmitteddrug resistance mutations.49,50,65
In contrast, we detected NRTI or NNRTI resistance muta-tions in three unrelated drug-naive patients infected withsubtype G (05HANCV8, 05HANCV45) or a G/B recombinant
(05HANCV31). M41L, present in patient 05HANCV31, con-fers intermediate-to-high level resistance to AZT and d4T anda lower level of resistance to ddI, ABC, and TDF.50,66 K103N,present in patient 05HANCV08, causes high-level resistanceto NVP and EFV. It has a synergistic effect with L100I onetravirine (ETR) susceptibility.50,66 Y318F, present in patient05HANCV45, causes low/intermediate NVP resistance. It is arare mutation and, unlike M41L and K103N, it is not consid-ered a transmitted drug resistance mutation.48 Hence, overall,we found two cases of transmitted drug resistance in 17 pa-tients (12%). The finding of a moderate prevalence of trans-mitted HIV-1 drug resistance in Cape Verde was a surprise asfree access to cART was officially started at the end of 2004.3
FIG. 2. Minor mutationsand natural polymorphismsdetected in the protease ofdrug-naive patients fromCape Verde. Only the muta-tions whoseAU3 c frequency is sig-nificantly different ( p < 0.05,Fisher’s exact test) than thatfound in the Stanford data-base for untreated patientsare shown.
FIG. 3. Resistance muta-tions and natural polymor-phisms detected in the RT ofdrug-naive patients fromCape Verde.AU3 c Only the muta-tions whose frequency is sig-nificantly different ( p < 0.05,Fisher’s exact test) than thatfound in the Stanford data-base for untreated patientsare shown.
HIV INFECTION IN CAPE VERDE ISLANDS 7
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:21pm Page 7

FIG. 4. Origin of the HIV-1 subtype G iso-lates from Cape Verde. Phylogenetic trees werebuilt using RT (A) and b AU3C2V3C3 (B) genomicregions of the G isolates from this study as wellas G sequences from reference isolates andfrom Angolan (AO) and Portuguese (PT) pa-tients, all downloaded from the Los Alamosdatabase. Trees were built as described in theMaterials and Methods section. Bootstrap val-ues of 70% or greater indicate significant sup-port for the clusters. The scale represents thenumber of base substitutions per site.
8 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 8

FIG. 4. (Continued).
HIV INFECTION IN CAPE VERDE ISLANDS 9
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 9

Despite the relatively high prevalence of drug-resistantstrains found in treated individuals (30%), the K103N muta-tion was found in only one treated patient and M41L was notfound in treated patients. Hence, the most probable expla-nations for the origin of these resistant isolates in Cape Verdeare (1) the unregulated and unmonitorized use of anti-retroviral drugs previous to 2004 and (2) people displace-ments from countries in which ART has been available for alonger period of time.10,16
Resistance mutations were detected in 3 of 10 (30%) treatedpatients but there was clear evidence of virological failure inonly one of these patients (05HANCV55). The isolate from thispatient harbored mutations conferring resistance both toNRTIs (K65R, T69d) and NNRTIs (K103N, Y181C). K65Rcauses intermediate resistance to ddI, ABC, 3TC, FTC, andTDF, low resistance to d4T, and hypersusceptibility toAZT.50,66 Mutations at codon 69 usually occur as T69DS/A/I/N/G and are NRTI-selected mutations.50 T69d is a highlyunusual mutation at this position. Deletions at codon 69 occurat a frequency of about 0.1% and their phenotypic and clinicalsignificance are not known. Y181C confers high resistance toNVP and low resistance to EFV.50 Moreover, mutations atposition 181 compromise the ETR response and may providethe foundation for the development of high-level ETR resis-tance 50. K103N confers full resistance to EFV and NVP.50,67
Unfortunately, we had no access to the therapeutic regimen of
this patient. However, based on the resistance genotype only,this patient is a clear candidate for a PI-based second linetherapeutic regimen.
In conclusion, the long-standing HIV-2 epidemic in CapeVerde is partially rooted in the ROD strain, suggesting thatthe origin of this historic isolate was Cape Verde. The HIV-1epidemic results from the introduction of multiple subtypesand recombinant forms by migrant workers or tourists. Theprevailing and highly divergent HIV-1 subtype G has its or-igins in Portugal and Angola. We found a moderate preva-lence of primary and secondary HIV-1 drug resistance inCape Verde and evidence suggesting that most resistanceisolates showing primary resistance mutations were im-ported. In the actual context of access to standardized and freetherapeutic regimens, the development and implementationof drug resistance surveillance strategies in both treated anduntreated populations will be important to maximize the ef-ficacy of antiretroviral therapy and prevent further trans-mission of drug resistance isolates in Cape Verde.
GenBank Accession Numbers
Sequences have been assigned the following accessionnumbers: JF267400– JF267423 (HIV-1 env), JF267438–JF267463(HIV-1 PR), JF267464–JF267490 (HIV-1 RT), and JF267424–JF267437 (HIV-2 env).
FIG. 5. Genetic groups andAU3 c evolutionary relationships of the HIV-2 viruses sequenced in this study based on maximumlikelihood phylogenetic trees of the C2V3C3 env gene region. The phylogenetic tree was constructed with reference sequencesfrom all HIV-2 groups. Sequences from Cape Verde isolates start with 05HANCV.
10 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 10

Acknowledgments
This work was supported by Fundacao GlaxoSmithKlinepara as Ciencias da Saude, Portugal, Fundacao para a Cienciae Tecnologia (project PTDCSAU-FCF6767/2006), Portugal,and CHAIN (Collaborative HIV and Anti-HIV Drug Re-sistance Network), European Union. Pedro Borrego, CheilaRocha, and Ines Bartolo are supported by Ph.D. grants fromFundacao para a Ciencia e Tecnologia, Portugal.
Author Disclosure Statement
No competing financial interests exist.AU1 c
References
1. INECV: National Statistical Institute of Cape Verde. Preliminarydata of CENSO 2010. http://www.ine.cv/actualise/destaques/files/RELATORIO%20RESULTADOS%20PRELIMINARESR%20RGPH%202010%20final.pdf. Accessed November 2010.
2. Clavel F, Guetard D, Brun-Vezinet F, et al.: Isolation of a newhuman retrovirus from West African patients with AIDS.Science 1986;233(4761):343–346.
3. CCCS: II Plano Estrategico Nacional de Luta Contra o VIH-SIDA em Cabo Verde (2006–2010). http://www.minsaude.-gov.cv Accessed November 2010.
4. Mocroft A, Vella S, Benfield TL, et al.: Changing patternsof mortality across Europe in patients infected withHIV-1. EuroSIDA Study Group. Lancet 1998;352(9142):1725–1730.
5. Sterne JA, Hernan MA, Ledergerber B, et al.: Long-term ef-fectiveness of potent antiretroviral therapy in preventingAIDS and death: A prospective cohort study. Lancet2005;366(9483):378–384.
6. WHO. Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector: Progress report2009. WHO Library Cataloguing-in-Publication Data. Gen-eve http://www.who.int/hiv/pub/tuapr_2009_en.pdf. Ac-cessed November 2010.
7. Gupta RK, Hill A, Sawyer AW, et al.: Virological monitoringand resistance to first-line highly active antiretroviral ther-apy in adults infected with HIV-1 treated under WHOguidelines: A systematic review and meta-analysis. LancetInfect Dis 2009;9(7):409–417.
8. Bartlett JA and Shao JF: Successes, challenges, and limitationsof current antiretroviral therapy in low-income and middle-income countries. Lancet Infect Dis 2009;9(10):637–649.
9. Vijver vd, D, Wensing, A, and Boucher, C: The epidemi-ology of transmission of drugs resistant HIV-1. In: HIV Se-quence Compendium 2006/2007 (Leitner T, et al., eds.).Theoretical Biology and Biophysics Group, Los AlamosNational Laboratory, Los Alamos, NM, 2007, pp. 17–36.
10. Nkengasong JN, Adje-Toure C, and Weidle PJ: HIV anti-retroviral drug resistance in Africa. AIDS Rev 2004;6(1):4–12.
11. Abegaz WE, Grossman Z, Wolday D, et al.: Threshold sur-vey evaluating transmitted HIV drug resistance amongpublic antenatal clinic clients in Addis Ababa, Ethiopia.Antivir Ther 2008;13(Suppl 2):89–94.
12. Hedt BL, Wadonda-Kabondo N, Makombe S, et al.: Earlywarning indicators for HIV drug resistance in Malawi. An-tivir Ther 2008;13(Suppl 2):69–75.
13. Maphalala G, Okello V, Mndzebele S, et al.: Surveillance oftransmitted HIV drug resistance in the Manzini-Mbabanecorridor, Swaziland, in 2006. Antivir Ther 2008;13(Suppl 2):95–100.
14. Pillay V, Ledwaba J, Hunt G, et al.: Antiretroviral drug re-sistance surveillance among drug-naive HIV-1-infected in-dividuals in Gauteng Province, South Africa in 2002 and2004. Antivir Ther 2008;13(Suppl 2):101–107.
15. Somi GR, Kibuka T, Diallo K, et al.: Surveillance of trans-mitted HIV drug resistance among women attending ante-natal clinics in Dar es Salaam, Tanzania. Antivir Ther2008;13(Suppl 2):77–82.
16. Bartolo I, Casanovas J, Bastos R, et al.: HIV-1 genetic diver-sity and transmitted drug resistance in health care settings inMaputo, Mozambique. J Acquir Immune Defic Syndr2009;51(3):323–331.
17. Bartolo I, Rocha C, Bartolomeu J, et al.: Antiretroviral drugresistance surveillance among treatment-naive human im-munodeficiency virus type 1-infected individuals in Angola:Evidence for low level of transmitted drug resistance. An-timicrob Agents Chemother 2009;53(7):3156–3158.
18. Plantier JC, Leoz M, Dickerson JE, et al.: A new human im-munodeficiency virus derived from gorillas. Nat Med2009;15(8):871–872.
19. Buonaguro L, Tornesello ML, and Buonaguro FM: Humanimmunodeficiency virus type 1 subtype distribution in theworldwide epidemic: Pathogenetic and therapeutic impli-cations. J Virol 2007;81:10209–10219.
20. Vidal N, Bazepeo SE, Mulanga C, Delaporte E, and PeetersM: Genetic characterization of eight full-length HIV type 1genomes from the Democratic Republic of Congo (DRC)reveal a new subsubtype, A5, in the A radiation that pre-dominates in the recombinant structure of CRF26_A5U.AIDS Res Hum Retroviruses 2009;25(8):823–832.
21. Damond F, Worobey M, Campa P, et al.: Identification of ahighly divergent HIV type 2 and proposal for a change inHIV type 2 classification. AIDS Res Hum Retroviruses2004;20(6):666–672.
22. de Silva TI, Cotten M, and Rowland-Jones SL: HIV-2: Theforgotten AIDS virus. Trends Microbiol 2008;16(12):588–595.
23. Gao F, Yue L, Robertson DL, et al.: Genetic diversity of hu-man immunodeficiency virus type 2: Evidence for distinctsequence subtypes with differences in virus biology. J Virol1994;68(11):7433–7447.
24. Gaschen B, Taylor J, Yusim K, et al.: Diversity considerationsin HIV-1 vaccine selection. Science 2002;296(5577):2354–2360.
25. Plantier JC, Djemai M, Lemee V, et al.: Census and analysisof persistent false-negative results in serological diagnosis ofhuman immunodeficiency virus type 1 group O infections. JClin Microbiol 2009;47(9):2906–2911.
26. Parekh B, Phillips S, Granade TC, Baggs J, Hu DJ, and Re-spess R: Impact of HIV type 1 subtype variation on viralRNA quantitation. AIDS Res Hum Retroviruses 1999;15(2):133–142.
27. Antunes R, Figueiredo S, Bartolo I, et al.: Evaluation of theclinical sensitivities of three viral load assays with plasmasamples from a pediatric population predominantly in-fected with human immunodeficiency virus type 1 subtypeG and BG recombinant forms. J Clin Microbiol 2003;41(7):3361–3367.
28. Drexler JF, de Souza Luna LK, Pedroso C, et al.: Rates of andreasons for failure of commercial human immunodeficiencyvirus type 1 viral load assays in Brazil. J Clin Microbiol2007;45(6):2061–2063.
29. Church D, Gregson D, Lloyd T, et al.: HIV-1 viral load multi-assay comparison of the realtime HIV-1, COBAS TaqMan 48
HIV INFECTION IN CAPE VERDE ISLANDS 11
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 11

v 1.0, Easy Q v1.2 and Versant v3.0 assays in a cohort ofCanadian patients with diverse HIV subtype infections. JClin Microbiol. Nov 17 2010.AU2 c
30. Ntemgwa ML, d’Aquin Toni T, Brenner BG, Camacho RJ,and Wainberg MA: Antiretroviral drug resistance in humanimmunodeficiency virus type 2. Antimicrob Agents Che-mother 2009;53(9):3611–3619.
31. Soares RS, Tendeiro R, Foxall RB, et al.: Cell-associated viralburden provides evidence of ongoing viral replication inaviremic HIV-2 infected patients. J Virol 2011:85(5):2429–2438.
32. Descamps D, Collin G, Letourneur F, et al.: Susceptibility ofhuman immunodeficiency virus type 1 group O isolates toantiretroviral agents: In vitro phenotypic and genotypicanalyses. J Virol 1997;71(11):8893–8898.
33. Tuaillon E, Gueudin M, Lemee V, et al.: Phenotypic sus-ceptibility to nonnucleoside inhibitors of virion-associatedreverse transcriptase from different HIV types and groups. JAcquir Immune Defic Syndr 2004;37(5):1543–1549.
34. Wainberg MA and Brenner BG: Role of HIV subtype di-versity in the development of resistance to antiviral drugs.Viruses 2010;2(11):2493–2508.
35. Ariyoshi K, Matsuda M, Miura H, Tateishi S, Yamada K, andSugiura W: Patterns of point mutations associated with an-tiretroviral drug treatment failure in CRF01_AE (subtype E)infection differ from subtype B infection. J Acquir ImmuneDefic Syndr 2003;33(3):336–342.
36. Santos AF, Abecasis AB, Vandamme AM, Camacho RJ, andSoares MA: Discordant genotypic interpretation and phe-notypic role of protease mutations in HIV-1 subtypes B andG. J Antimicrob Chemother 2009;63(3):593–599.
37. Gilks CF, Crowley S, Ekpini R, et al.: The WHO public-healthapproach to antiretroviral treatment against HIV in re-source-limited settings. Lancet 2006;368(9534):505–510.
38. Bartolo I, Epalanga M, Bartolomeu J, et al.: High geneticdiversity of human immunodeficiency virus type 1 in An-gola. AIDS Res Hum Retroviruses 2005;21(4):306–310.
39. Bartolo I, Rocha C, Bartolomeu J, et al.: Highly divergentsubtypes and new recombinant forms prevail in the HIV/AIDS epidemic in Angola: New insights into the origins ofthe AIDS pandemic. Infect Genet Evol 2009;9(4):672–682.
40. Barroso H and Taveira N: Evidence for negative selectivepressure in HIV-2 evolution in vivo. Infect Genet Evol2005;5(3):239–246.
41. Thompson JD, Gibson TJ, Plewniak F, Jeanmougin F, andHiggins DG: The CLUSTAL_X windows interface: flexiblestrategies for multiple sequence alignment aided by qualityanalysis tools. Nucleic Acids Res 1997;25(24):4876–4882.
42. Felsenstein J: Evolutionary trees from DNA sequences: Amaximum likelihood approach. J Mol Evol 1981;17(6):368–376.
43. Posada D and Crandall KA: MODELTEST: Testing the modelof DNA substitution. Bioinformatics 1998;14(9):817–818.
44. Phylogenetic analysis using parsimony (*and other meth-odes) [computer program]. Version 4. Sinauer Associates,Sunderland, Massachusetts. [computer program]. Version;2001.
45. Felsenstein J: Confidence limits on phylogenies: An ap-proach using the bootstrap. Evolution 1985;39:783–791.
46. Hillis DBJ: An empirical test for bootscanning as a method forassessing viral sequence relatedness. System Biol 1993;42:182–192.
47. Rose PP and Korber BT: Detecting hypermutations in viralsequences with an emphasis on G/A hypermutation.Bioinformatics 2000;16(4):400–401.
48. Bennett DE, Camacho RJ, Otelea D, et al.: Drug resistancemutations for surveillance of transmitted HIV-1 drug-resistance: 2009 update. PLoS One 2009;4(3):e4724.
49. Shafer RW, Rhee SY, Pillay D, et al.: HIV-1 protease andreverse transcriptase mutations for drug resistance surveil-lance. AIDS 2007;21(2):215–223.
50. Shafer RW and Schapiro JM: HIV-1 drug resistance muta-tions: An updated framework for the second decade ofHAART. AIDS Rev 2008;10(2):67–84.
51. Bartolo I, Rocha C, Bartolomeu J, et al.: Highly divergentsubtypes and new recombinant forms prevail in the HIV/AIDS epidemic in Angola: New insights into the origins ofthe AIDS pandemic. Infect Genet Evol 2009;9(4):672–682.
52. Entonu PE and Agwale SM: A review of the epidemiology,prevention and treatment of human immunodeficiency virusinfection in Nigeria. Braz J Infect Dis 2007;11(6):579–590.
53. Hamel DJ, Sankale JL, Eisen G, et al.: Twenty years of pro-spective molecular epidemiology in Senegal: Changes inHIV diversity. AIDS Res Hum Retroviruses 2007;23(10):1189–1196.
54. Ndongmo CB, Pieniazek D, Holberg-Petersen M, et al.: HIVgenetic diversity in Cameroon: Possible public health im-portance. AIDS Res Hum Retroviruses 2006;22(8):812–816.
55. Niama FR, Toure-Kane C, Vidal N, et al.: HIV-1 subtypesand recombinants in the Republic of Congo. Infect GenetEvol 2006;6(5):337–343.
56. Tebit DM, Ganame J, Sathiandee K, Nagabila Y, Coulibaly B,and Krausslich HG.: Diversity of HIV in rural Burkina Faso.J Acquir Immune Defic Syndr 2006;43(2):144–152.
57. Palma AC, Araujo F, Duque V, Borges F, Paixao MT, andCamacho R: Molecular epidemiology and prevalence ofdrug resistance-associated mutations in newly diagnosedHIV-1 patients in Portugal. Infect Genet Evol 2007;7(3):391–398.
58. Osmanov S, Pattou C, Walker N, Schwardlander B, andEsparza J: Estimated global distribution and regional spreadof HIV-1 genetic subtypes in the year 2000. J Acquir ImmuneDefic Syndr 2002;29(2):184–190.
59. Monno L, Brindicci G, Lo Caputo S, et al.: HIV-1 subtypesand circulating recombinant forms (CRFs) from HIV-infected patients residing in two regions of central andsouthern Italy. J Med Virol 2005;75(4):483–490.
60. Reeves JD and Doms RW: Human immunodeficiency virustype 2. J Gen Virol 2002;83(Pt 6):1253–1265.
61. Silva ZJ, Oliveira I, Andersen A, et al.: Changes in prevalenceand incidence of HIV-1, HIV-2 and dual infections in urbanareas of Bissau, Guinea-Bissau: Is HIV-2 disappearing? AIDS2008;22(10):1195–1202.
62. Berry N, Ariyoshi K, Balfe P, Tedder R, and Whittle H: Se-quence specificity of the human immunodeficiency virustype 2 (HIV-2) long terminal repeat u3 region in vivo allowssubtyping of the principal HIV-2 viral subtypes a and b.AIDS Res Hum Retroviruses 2001;17(3):263–267.
63. Guyader M, Emerman M, Sonigo P, Clavel F, Montagnier L,and Alizon M: Genome organization and transactivation ofthe human immunodeficiency virus type 2. Nature1987;326(6114):662–669.
64. Santiago ML, Range F, Keele BF, et al.: Simian immunode-ficiency virus infection in free-ranging sooty mangabeys(Cercocebus atys atys) from the Tai Forest, Cote d’Ivoire:Implications for the origin of epidemic human immunode-ficiency virus type 2. J Virol 2005;79(19):12515–12527.
65. Shafer RW, Rhee SY, and Bennett DE: Consensus drug re-sistance mutations for epidemiological surveillance: Basic
12 OLIVEIRA ET AL.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 12

principles and potential controversies. Antivir Ther2008;13(Suppl 2):59–68.
66. Johnson VA, Brun-Vezinet F, Clotet B, et al.: Update of thedrug resistance mutations in HIV-1: December 2009. TopHIV Med 2009;17(5):138–145.
67. Flys TS, Chen S, Jones DC, et al.: Quantitative analysis ofHIV-1 variants with the K103N resistance mutation aftersingle-dose nevirapine in women with HIV-1 subtypes A,C, and D. J Acquir Immune Defic Syndr 2006;42(5):610–613.
Address correspondence to:Nuno Taveira
Unidade dos Retrovırus e Infeccoes AssociadasCentro de Patogenese Molecular
Faculdade de FarmaciaUniversidade de Lisboa
Avenida das Forcas Armadas1649-019 Lisbon, Portugal
E-mail: [email protected]
HIV INFECTION IN CAPE VERDE ISLANDS 13
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 13

AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 14

AUTHOR QUERY FOR AIDS-2011-0174-VER9-OLIVEIRA_1P
AU1: Disclosure statement accurate? If not, amend as needed.AU2: Update and complete this reference.AU3: The text are not clear for figs. 1 to 5. Please provide a better quality artwork.
AIDS-2011-0174-ver9-Oliveira_1P.3d 09/07/11 12:22pm Page 15