Gambia report final
67
ANTAKI LAB Travel Report On-site assessment of healthcare systems and mPharesis integration feasibility in The Gambia Molly Blank, Jackie Brackett 9/19/2012 From September 3-7, students Molly Blank and Jackie Brackett travelled to The Gambia to study the healthcare system in a malaria-endemic country. Findings from interviews, site visits, and discussions were used to assess the potential implementation of a device currently under development; the mPharesis. This device would be used to filter red blood cells infected with malaria out of a patient’s system to improve patient outcomes for severe malaria. Although the concept of rapid parasite reduction in a clinical context was cautiously well-received, it was resolved that infrastructural challenges device use will require concept refinement. The following document includes details on the trip, findings, and recommendations based on information gathered.
Transcript of Gambia report final

ANTAKI LAB
Travel Report On-site assessment of healthcare systems and mPharesis
integration feasibility in The Gambia
Molly Blank, Jackie Brackett
9/19/2012
From September 3-7, students Molly Blank and Jackie Brackett travelled to The Gambia to study the healthcare system in a malaria-endemic country. Findings from interviews, site visits, and discussions were used to assess the potential implementation of a device currently under development; the mPharesis. This device would be used to filter red blood cells infected with malaria out of a patient’s system to improve patient outcomes for severe malaria. Although the concept of rapid parasite reduction in a clinical context was cautiously well-received, it was resolved that infrastructural challenges device use will require concept refinement. The following document includes details on the trip, findings, and recommendations based on information gathered.

INTRODUCTION 2
Malaria 2
mPharesis 2
Site Visits 3
Royal Victoria Teaching Hospital 3
Brikama Health Center 5
Serrekunda Health Center 6
Interviews 8
Cultural and contextual observations 8
SYNTHESIZED DELIVERABLES 9
Patient profiles 9
Urban dweller 9
Rural dweller 10
Severe malaria – the waiting period 10
Facility profiles 10
Personas 11
IMPLICATIONS ON DESIGN 12
Clinical use 12
Supply 12
Cost 12
Maintenance, training 12
Logistical concerns 13
Human factors considerations 13
Preliminary cost analysis 13
Transfusion 13
Malaria Treatments 13
RECOMMENDATIONS FOR DEVICE DEVELOPMENT 14
Addressing the need 14
Future development 14
APPENDICES 15
Appendix 1- References 15
Appendix 2– Malaria Statistics in The Gambia 17
Appendix 3- Royal Victoria Teaching Hospital Complete Notes 19
Appendix 4– Notes from Brikama Health Center visit 21
Brikama Antenatal 23
Brikama Labor Ward 23
Brikama Public Health 23
Brikama General Ward 23
Hands-on care clinic 23
Appendix 5 -Baseline Questionnaire 24
Appendix 6– Interview Transcript, Umberto D’Alessandro 26
Appendix 7 - Interview Transcript, Dr. Readon Ideh 39
Appendix 8 - Interview Transcript, Dr. Kalfa Bojang 46
Appendix 9 - Interview Transcript from Dr. Joseph Okebe 55
Appendix 10- Images from the Serrekunda Clinic 60

Introduction
Malaria Across the globe, hundreds of tropical and poorer countries suffer from endemic levels of malaria; a disease caused by a Plasmodium parasite. Of the Plasmodium genus, four species are responsible for malaria in humans. The most severe presentations of malaria stem from infection by Plasmodium falciparum and continue to be a significant cause of mortality in children and adults alike. Despite increased efforts to control and eradicate malaria, many factors continue to contribute to its endemic stronghold. Among these factors are the pervasiveness of the parasite in regions and the robustness of the mosquito transmission vector. An Anopheles mosquito feeds on the blood of someone carrying malaria (people can contribute to transmission without being symptomatic) then transmits the parasite to the next host on which it feeds. Although simple in its transmission mechanism, the specific pathophysiology and life stages of the parasite make successful immune responses difficult and interventions complex. The initial infection by mosquito introduces sporozoites, a motile form of the parasite that migrates to the host’s liver cells to multiply. After days, the infected liver cells will rupture and release the asexually reproducing merozoite form of the parasite which invade red blood cells and continue reproducing. Some merozoites differentiate into the sexual forms of the parasite, gametocytes, which are transmitted to a mosquito to perpetuate the parasite. The parasites that reside in erythrocytes damage the cells as they feed and reproduce which causes fundamental changes in the mechanical and physical behaviors of the cell. The pathophysiology for uncomplicated malaria stems from parasites in the bloodstream, anemia from infected red blood cells, and toxins in the blood from the ruptured cells as parasites reproduce. For a majority of cases, malaria resolves itself with appropriate therapy and minimal intervention. In some cases, however, the infection can take a turn for the worse and become severe, or complicated, malaria. In these cases, infected cells begin to occlude flow into vital organs and cause greater systemic failures. Recommended treatments, preventions, and interventions for malaria vary widely, with even greater variation in adherence to recommendations in different regions and socioeconomic statuses (as will be discussed in greater depth in the following sections). Prevailing strategies endorsed by the WHO include the use of insecticide-treated bed nets to prevent transmission and supplying effective drugs to patients showing symptoms of malaria. Specific treatments are recommended based on patient characteristics and clinical symptoms [1].
mPharesis The World Health Organization reported that international funding for malaria rose to record levels of US $2 billion in 2011 [2]. Although tremendous resources are being committed to eliminating malaria, the targets for the Global Malaria Action Plan needed revision since rates of mortality and incidence fell short of their initial goals for 2010. Although there were signs of improvement around the globe for many indicators, mortality is still a significant problem. The mPharesis is a device developed by the company AccelDx that was proposed to directly address the mortality of severe malaria.
Blue
Highlight
Blue
Highlight

As parasites feed and reproduce within red blood cells, the parasite consumes parts of the hemoglobin in the cell and reconfigures the remaining toxic elements into hemozoin, a paramagnetic crystal. Since exclusively infected cells have this inherent magnetic property, it provides a unique opportunity for filtration. The mPharesis proposes the laminar flow of red blood cells through a magnetic field to leverage the magnetic properties of hemozoin and remove infected cells from the bloodstream. Since only infected cells are removed, healthy ones are returned to combat anemia and minimize the volume of blood required for transfusion.
On-Site Work in The Gambia
AccelDx was represented at a conference by Dr. Alberto Gandini, where he met Umberto D’Alessandro. After some discussion, the work by AccelDx on malaria and diagnostics piqued Dr. D’Alessandro’s interest and he agreed to support the effort. Since this introduction, we leveraged the contact to conduct intensive, on-site research in a malaria-endemic region where Dr. D’Alessandro regularly works. This facility is the Medical Research Council (MRC) in The Gambia. The MRC collaborates closely with the London School of Hygiene and Tropical Medicine and is the largest medical research investment in a developing country.
With the MRC as our host site, we were able to visit nearby facilities where the MRC recruits for and conducts clinical trials. Although there were more sites inland (“upcountry”), we were assured that the sites visited demonstrated an excellent representative breadth of resources and conditions for healthcare in The Gambia.
Site Visits
Royal Victoria Teaching Hospital
Figure 1 - Front gate of the Royal Victoria Teaching Hospital
Due to concerns with restrictions on government facilities, this image is courtesy of Hayley, at lifeasabutterfly.com/

Our visit to the Royal Victoria Teaching Hospital (RVTH) was hosted by Dr. Uduak Okomo, a consulting pediatrician from the MRC. RVTH is the primary referral center for The Gambia and is the best-equipped public facility in the country. This is one of the few sites equipped for surgical procedures, although there are no resident medical specialists (of primary concern are cardiology and oncology). Dr. Okomo guided us through the pediatric, emergency, and pediatric wards and full notes from the tour are included in Appendix 3. During this visit, an important theme emerged: although this is the most developed, sophisticated and largest medical facility in the country, it still visibly suffers from staffing, technical, and supply limitations. For instance, complex surgeries and cancer patients are referred to Senegal because of insufficient lab equipment and expertise. Many of these referred patients will never seek the necessary treatment. A patient can be referred multiple times, travel to seek care, and ultimately be left untreated and out of achievable options. If the patient happens to have enough money to pay for private care, sometimes they are still unable to receive the ideal treatment since private practitioners are scarce and may even decline treatment due to post-operative risks. For ailments within the scope of RVTH, patients’ treatments can be cut short because healthcare is a free service space and resources are limited. Logistical challenges such as immobile oxygen support also affect care. If oxygen support is needed for a patient who also needs diagnostic imaging, there are no portable oxygen systems so the patient is taken off support while diagnostic images are taken. Risk is minimized by coordinating with the imaging technicians and doing as many preparations in advance as possible to reduce the amount of time the patient is unsupported. RVTH is not exempt from the infrastructural irregularities in The Gambia, either. Electrical power can be inconsistent although to a lesser extent than other regions of the country. Bed sharing is also common in pediatrics, so cross-contamination can occur. Finally, the cleaning of supplies is theoretically executed by the biomedical technician team but this is not consistent and nurses often clean equipment by hand with soap, water, and ethanol. Other limitations from the facility included:
Oxygen concentrators are generally split between up to five patients and oxygen delivered to each patient is unknown which is not ideal for treatment
Oxygen concentrator is shared between the emergency and pediatric wards
Fingertip pulse oximeter generally does not work and is the only one for the pediatric ward
A wing of the neonatal ward was recently closed due to staff and equipment shortages
Some shifts lack a nurse to receive emergency patients and the nurse attendant on call must be called
Not enough incubators to fill the need Although unanimously agreed to be the best healthcare facility in the country, resource limitations at RVTH affect patients and care provided on a daily basis.

Brikama Health Center
Figure 2 -Photograph of the Brikama Health Center
To visit the Brikama Health Center, a shuttle from the MRC was arranged with a translator and guide to ensure that we were able to navigate the center without interfering with the clinic. Upon arrival, we spoke with both the hospital director and the resident business manager who was working at the clinic while pursuing a degree at the University of The Gambia in public health policy. This interview revealed more facets of the increasingly consistent theme: the facility is constantly overwhelmed by patients so staff do their best to overcome the severe shortages in both personnel and equipment. They declined audio recording so complete notes from the interview are included in Appendix 4.
Some notable findings and information from this interview:
They estimated that this health center sees approximately 6000-8000 patients per month
Supplies are managed by the central government system and are often insufficient o The day prior to our arrival, they ran out of HIV testing equipment
Although beating the national average of 5 birth attendants per 1000 births, Brikama has 6 midwives per 1000 births and is considered by the director to suffer staff shortages
Referrals to RVTH are sometimes due to exhaustion of supplies for patients
They own an x-ray machine but lack the expertise and staff to use it
Many communities lack access to healthcare due to transportation issues, water covering roads o Other delays in treatment stem from native treatments, perceived success of self-
treatment, and the long lines and waiting at clinics After developing a basic understanding of the Brikama Health Center facilities, we asked more specific questions pertaining to malaria and the mPharesis. This discussion leads to the following findings:
Blood supply is constantly a problem
Blue
Highlight
o 4 people in a month received donated blood, and the other 50 cases or so requiring blood received it from family members
Drugs are largely available for malaria, but bed space is at a premium o Reducing the length of stay for severe malaria would be a strong value proposition, the
long patient stays are expensive
At peak season, up to 40 patients in a day with malaria, 5-10 of whom are severe/complicated After the interview with the director, we conducted brief interviews with the nurses in charge of each the maternity ward, neonatal ward, public health ward, general ward, and hands-on care clinic.
Serrekunda Health Center
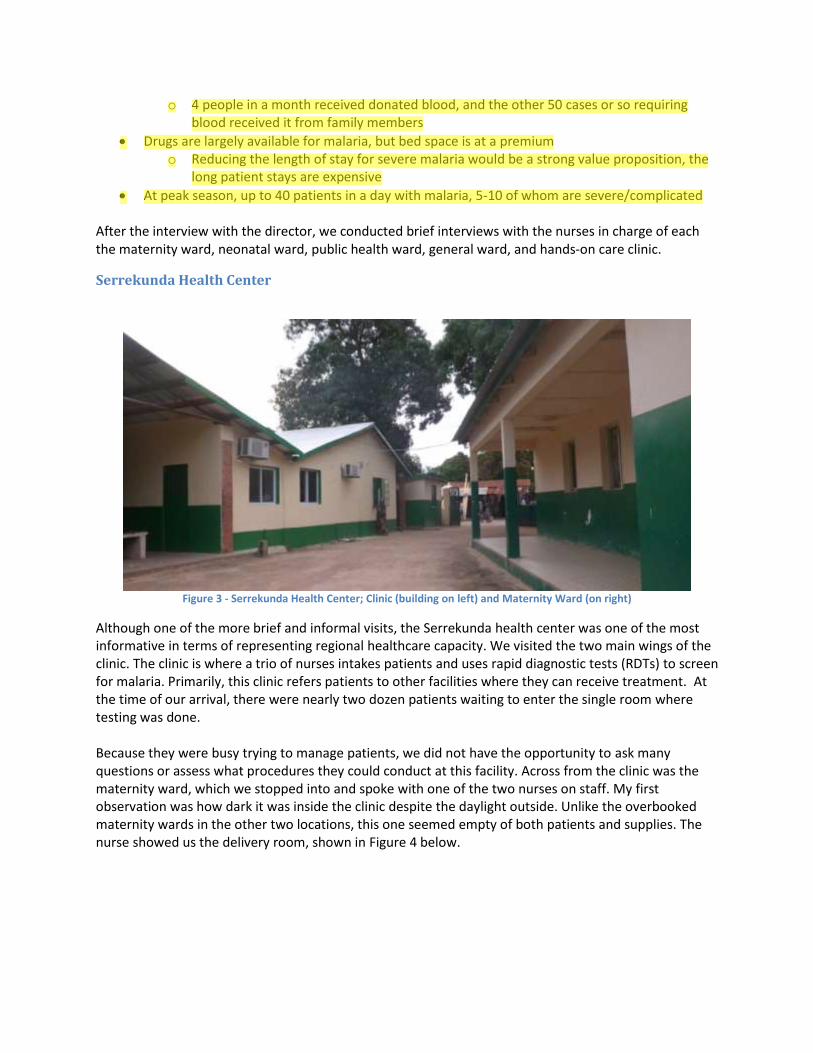
Figure 3 - Serrekunda Health Center; Clinic (building on left) and Maternity Ward (on right)
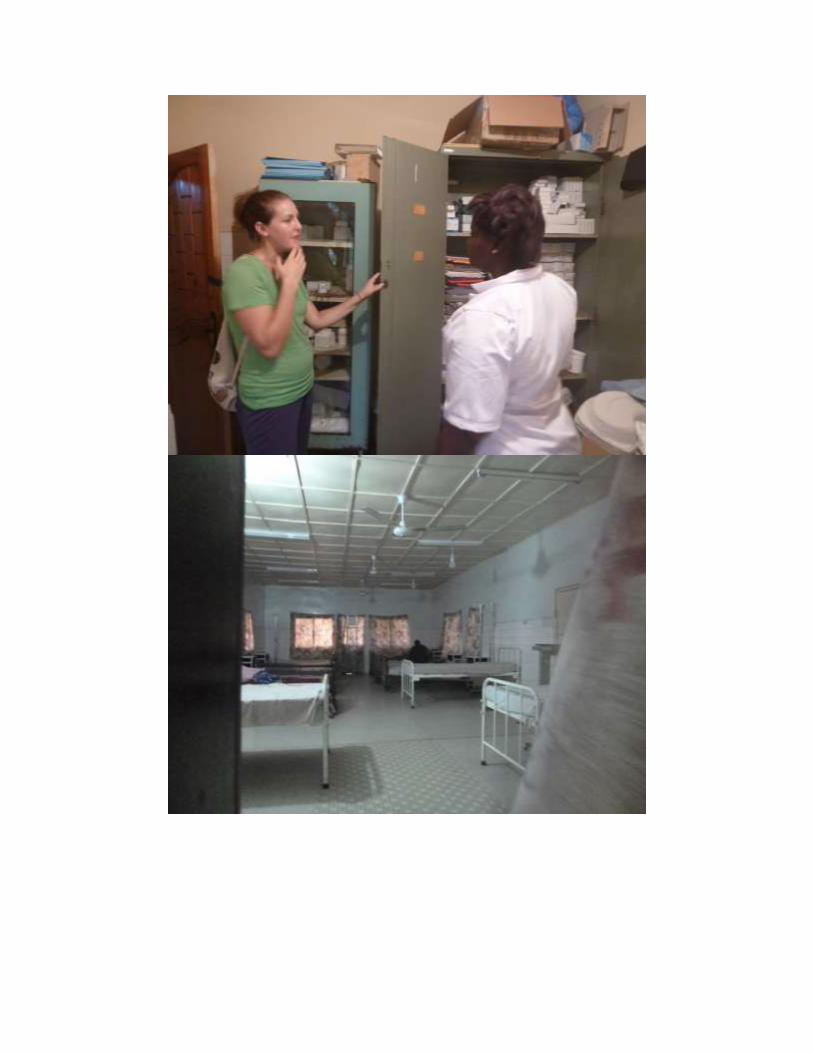
Although one of the more brief and informal visits, the Serrekunda health center was one of the most informative in terms of representing regional healthcare capacity. We visited the two main wings of the clinic. The clinic is where a trio of nurses intakes patients and uses rapid diagnostic tests (RDTs) to screen for malaria. Primarily, this clinic refers patients to other facilities where they can receive treatment. At the time of our arrival, there were nearly two dozen patients waiting to enter the single room where testing was done. Because they were busy trying to manage patients, we did not have the opportunity to ask many questions or assess what procedures they could conduct at this facility. Across from the clinic was the maternity ward, which we stopped into and spoke with one of the two nurses on staff. My first observation was how dark it was inside the clinic despite the daylight outside. Unlike the overbooked maternity wards in the other two locations, this one seemed empty of both patients and supplies. The nurse showed us the delivery room, shown in Figure 4 below.
Blue
Highlight

Figure 4 - Serrekunda delivery room
During our small tour, the nurse pointed out an incubator in the corner of the delivery room without a blanket. She described it as inadequate although it was unclear if it operated poorly or not at all. The operating room was also minimal with less than a dozen instruments laid out in the open on a table, most of which were pans. One of the two facility autoclaves was in this room, shown in Figure 5, although the nurse said it had been broken for some time and they had to use a smaller one that had electrical problems in the ward. There was a single small sink in the room for hand washing and supplies for more than basic sanitation seemed to be absent. The nurse then showed us the supply closet where all medications and consumables were stored. Although the cupboard seemed to be stocked, she said that often supplies are insufficient and that requests for more are often not fulfilled. Because it is a government clinic, they are at the mercy of the Ministry of Health for what and when their supplies get re-stocked.
This clinic was more fortunate than many because they had an ambulance. During our stay, however, we met a man who told a story of finding someone who had been hit by a car, came to this clinic, and they were unable to treat his injuries and unable to transport him because the ambulance was out of gas. He filled up the gas tank out of pocket to help the patient survive although he was unclear as to whether or not the victim did, in fact, survive.
The complete set of photographs from this visit are included in Appendix 10.
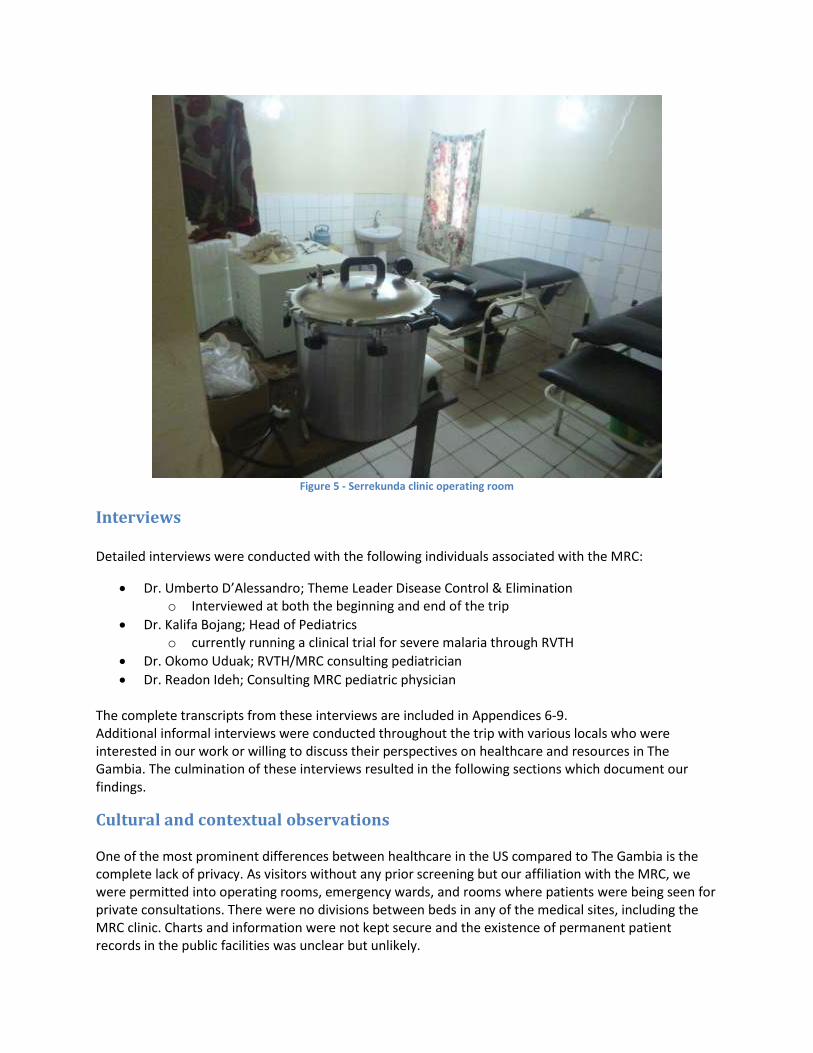
Figure 5 - Serrekunda clinic operating room
Interviews Detailed interviews were conducted with the following individuals associated with the MRC:
Dr. Umberto D’Alessandro; Theme Leader Disease Control & Elimination o Interviewed at both the beginning and end of the trip
Dr. Kalifa Bojang; Head of Pediatrics o currently running a clinical trial for severe malaria through RVTH
Dr. Okomo Uduak; RVTH/MRC consulting pediatrician
Dr. Readon Ideh; Consulting MRC pediatric physician The complete transcripts from these interviews are included in Appendices 6-9. Additional informal interviews were conducted throughout the trip with various locals who were interested in our work or willing to discuss their perspectives on healthcare and resources in The Gambia. The culmination of these interviews resulted in the following sections which document our findings.
Cultural and contextual observations One of the most prominent differences between healthcare in the US compared to The Gambia is the complete lack of privacy. As visitors without any prior screening but our affiliation with the MRC, we were permitted into operating rooms, emergency wards, and rooms where patients were being seen for private consultations. There were no divisions between beds in any of the medical sites, including the MRC clinic. Charts and information were not kept secure and the existence of permanent patient records in the public facilities was unclear but unlikely.

We did not witness any tensions between patients and healthcare workers because people in The Gambia are exposed to a high degree of western culture during the dry season due to tourism. So concepts from Western culture and medicine are not generally a problem in The Gambia. At the MRC, we attended a lecture in their weekly series that did address cultural considerations of blood-contacting devices and studies in areas of Africa that are far more skeptical of Western healthcare practices from cultural beliefs. The case study addressed the belief in Cameroon that if you have someone’s blood, you can control their fate to an extent because of the mystical powers that blood contains. So when a child had blood drawn at a clinic for a test and their condition worsened until the child eventually died, it was the blood draw that was determined to be the cause by the local population. This clinical trial for malaria was almost shut down because tensions between the health workers and local population became too high. This was an excellent example of how cultural understanding and trust are an essential part of successful clinical work. English is the official language of The Gambia, but we quickly realized in speaking with people that the local, tribal languages are far more prominent and are the preferred languages for native Gambians. Mandinka and Wolof are the most frequently spoken in the coastal region, but we were told they are merely two of the seven tribal languages in The Gambia. English was generally spoken, but uncomfortable and challenging for some people. This did not seem to be a major barrier for people to communicate, but this may not be the case in all regions of Gambia. Because we spent most of our time in largely urban areas, some work in a rural setting would be necessary to understand how much of a problem communication would be. Finally, the relationship between the hundreds of patients seen in these clinics each day and their caretakers was minimal. Although this is only reasonable to expect by virtue of logistics, the reality of it seemed to have an impact on the healthcare provided. Weary mothers with their sick children sat long hours in shared beds. It looked like they were given little choice or discussion in the course of treatment if they had any choice at all. Even in the US, people can have difficulty advocating their own health and understanding the methods behind the white coats, but this divide was even more pronounced in the clinics in Gambia. I believe this represents a far more challenging educational and cultural issue that likely defies technical interventions yet is important to acknowledge nonetheless.
Synthesized Deliverables
Patient profiles
Urban dweller Access to clinics largely available
Access to local pharmacies o Self-treatment not uncommon, although not always with appropriate drugs (painkillers,
or other self-palliative care) For example, several people we spoke with touted marijuana as a treatment for
asthma
Cost of treatment is less a barrier than taking the time to go to a clinic o Government facilities offer free or nearly free service
Blue
Highlight
Blue
Highlight
Blue
Highlight

o To visit MRC, people wake up around 4am to get a clinic ticket and still have to wait all day to receive care
Challenge for a woman taking care of children, etc. Taking a full day to receive care is a significant deterrent and inevitable There is a large chance they will simply be referred
Rural dweller Not uncommon to use local and homeopathic treatments
Literacy, language barriers a potential issue with receiving treatment
Frequently, homes will be several kilometers from the nearest health outpost or clinic, even in small country like Gambia
o Problem is understood to be more exaggerated in other, larger countries
Roads washed out o Peak transmission and malaria season is due to the rains which cause the floods and
damages to infrastructure o Even more of an issue during rainy season when malaria transmission peaks o Limited supply or access to insecticide-treated bed nets
Cost of transport to the clinic more of a financial barrier than the care itself
Severe malaria – the waiting period
As we conducted interviews, it became evident that people waiting too long to come in to the clinics was one of the root causes of death by severe malaria. Malaria is a treatable condition in The Gambia, so we asked: why do people wait too long? Our interviews revealed a pattern of factors that contribute to people waiting until it’s nearly too late. First is quite simply the pervasiveness of malaria. Dr. D’Alessandro likened the disease to having a cold in the United States or Europe. It expected that at the end of rainy season, people will be sick for some time and then recover. Because this is generally true and so few cases become truly life-threatening, it’s a gamble that people are willing to take. Another barrier in reaching care is the set of logistical challenges associated with getting care. People require transportation to the clinic, have to wait to be seen, then receive treatment. Self-care can also contribute to waiting for treatment. Symptoms can be masked as the malaria worsens and finally when the malaria takes a turn for the severe, there is very little time to seek appropriate treatment. The most prominent cause of mortality appeared to be the rapid speed of onset for severe malaria. On the order of hours, the patient can go from mild symptoms to sequestration, occlusion of blood flow, and organ failure. Because getting to clinics presents a challenge to patients in any circumstance, it can be particularly lethal for such a time-sensitive condition.
Facility profiles Although we were unable to visit a facility representing each tier of the public healthcare system, we were able to span a significant number in a short period of time and through interviews were able to gain a broad understanding of the hierarchy. Across the entirety of the public healthcare system in The
Blue
Highlight
Blue
Highlight
Blue
Highlight
Gambia, there are no specialists. Cancer and cardiac cases are referred to facilities outside the country. Dakar in Senegal has larger facilities and is the main site for referrals.
Of the system we were able to observe and discuss, the following hierarchy was described:
RVTH – primary teaching hospital o Most reliable infrastructure o One of the rare facilities equipped to conduct surgeries o Still short-handed with staff and equipment
Health clinics o Referral and basic care centers o Lacking equipment, staff o Primarily used for vaccinations, antenatal, maternity care, screening and referrals
Health outposts o Outreach, primarily
Village workers o Dynamic role, the first line of support for villages
Pharmacies o No prescription system o Counterfeits are not as significant problem in The Gambia as many countries
Personas o Patient
Generally getting to clinics can be a struggle
Transportation distance and cost
Challenges of travel with children
They need to take the day off work, which is not always possible
Clinic waiting times are long even for checking in Significant range of education, literacy Receptive to western medicine if they come to clinics
o Doctor Few and far between, their time is in high demand
o Nurse Nursing staff are the strong majority in clinics Do most of the work, monitoring, and patient care
o Technician Extent of training unknown Uncommon Generally are unable to conduct all of their duties when present
Cleaning, maintenance, repairs o Village healthcare worker
Role was unclear Trendy role to address in healthcare intervention programs
Currently working with the Malaria Control Programme in Gambia to use RDTs and help treat malaria sooner and more broadly
o Government Funds public clinics
Allocation and distribution of clinic supplies
Implications on design
Because the underlying reason for our excursion to The Gambia was to observe the context for the mPharesis, this section delineates our findings with regard to the implementation of the device. We list the different contextual challenges for the device as it is currently envisioned.
A bold emphasis has been placed on areas of particular concern.
Clinical use Will it improve outcomes? Exchange transfusion therapy isn’t shown to improve clinical
outcomes definitively yet [3] o Recent studies of artesunate in Europe of severe malaria recorded deaths only after
parasites were cleared; one by iatrogenic complication 4 days after parasite clearance when an IV catheter was removed and the patient hemorrhaged, and the other was suspected to be a lung embolism 8 days after clearance. [4]
o Does not target sequestered parasites, which the drugs do [5]
Real problem is getting treatment in time, less the efficacy of the treatment
Risk introduced by blood-contacting devices o Infection o Blood compatibility issues
Treatment must be easily administered to both adults and children o Introduces issues of dosage, rate, and scaling
Time consuming to find donor, screen for blood compatibility o Surrounding logistics may be a rate-limiting step in therapy utility
Complexity of treatment is a challenge for managing clinical treatment
Dosage calculations are a challenge for many treatments, maintaining appropriate levels of both heparin and antimalarial therapies would be a challenge for healthcare providers
Monitoring of therapy burdens the limited staff
Supply Blood supply is a constant problem
o Blood/family members must also be tested on a time scale that will still be acceptable for patients in the throes of severe malaria
Heparin, consumables, in addition to conventional malaria treatments
Inconsistent re-supply in government facilities
Cost Always a limitation
Consumables
Transfusion cost estimated in the range of hundreds of dollars, while artesunate treatments can be administered completely for less than $100
o This type of cost may be prohibitive for use in Africa
Maintenance, training Must require minimal expertise to maintain and use
o Robust design o Streamlined settings that minimize risk, maximize efficacy o Equipment repairs are not consistent, staff not always qualified for repairs
Blue
Highlight
Blue
Highlight
Blue
Sticky Note
See Kreeftmeijer-Vegter et al 2013 Manual blood exchange transfusion etc
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

o Demanding environment through both dust, water, and frequent use
Cleaning protocols are not reliably followed o Infection, blood-borne pathogens, thrombosis o Less an issue of compliance than supply
When alcohol is not available, soap and water are used
Logistical concerns Use for multiple patients
o During peak season, double-digit numbers of patients may come in with severe malaria at a time
o Demand will far exceed the capacity of the device Increased risk of improper cleaning and treatment
Human factors considerations User capacity
o Complex treatments can’t be sustained by limited staff in peak season o Quinine treatments (a controlled IV drip line) are too complex in many regions due to
the high number of admissions and need to monitor the treatment [6] o Incorrect treatment is already a concern with drug administration [7] [8]
User training o Not perceived as a significant barrier for use
Controlled factors o Significant impact for flow rate, heparin, other treatment settings
Seasonal robustness o Rainy season and electrical power o Dry season, low demand but solar power an option
Preliminary cost analysis
Transfusion Although there is no well-established, consistent price for transfusion, approximate costs of
$278 per unit of blood and a total of $1,100 including acquisition, storage, testing, and transport have been recorded [9]
Reported transfusion costs variation due to a variety of factors including ease of blood access, staffing
Surgical transfusions are reported: o “The total cost of a unit of RBC was US$ 1,158 (2007 value), of which, indirect overhead,
total transfusion process cost, weighted average acquisition cost and direct overhead cost per unit accounted for 40.6%, 34.0%, 21.5% and 3.9%, respectively. “ [10]
Malaria Treatments Artesunate treatment for a child with severe malaria (US $3.3) [7]
o Quinine is $1.3
Artesunate cost for 100mg of oral preparation in 2010 from the UN Population Fund is $2.00 for a 6 tab-cap package [11]
Artesunate treatment cost of US$ 66.5 across four different sites in Tanzania, Uganda and Nigeria for 2300 patients. The recorded cost includes the cost of treatment, diagnostic testing, medical equipment, hotel cost of inpatient care [12]
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Sticky Note

o Also showed that the all-inclusive price of Artesunate is not significantly more than quinine
Transfusion therapies have inherent risk Especially in underdeveloped healthcare systems where equipment is rarely cleaned up
to standards Even has a degree of risk in the US [9]
Recommendations for device development
There are potential advantages to the development of the mPharesis how it is currently envisioned. These include the rapid removal of parasites from the blood resulting in a shorter parasite clearance time, the fundamental concept relies on physical changes in the cell so the therapy is independent of drug resistance, and it could reduce the amount of time patients spend in already overburdened health facilities. However, for all the benefits, we believe that the technology has an application with even more promise for disrupting how malaria is measured and monitored now.
Addressing the need The real problem is not really the treatment of severe malaria; it’s getting effective treatment to people before it gets beyond the “point of no return”. Severe malaria deaths are very seldom an issue with ineffective treatments and drug resistance currently only affects south Asia and even then merely delays the drug’s effects.
When I read articles about malaria in Europe, I find that it’s not the treatment that doesn’t work but instead the accuracy and timing of diagnosis. The expertise in malaria microscopy is much rarer in Europe than areas where the disease is endemic. So why fix the part that already works? The treatments are effective and ever-improving.
Future development “It has been discussed whether the evidence from endemic regions can be generalized to the European population. Patients’ characteristics, clinical manifestations and supportive care may differ greatly between developing and industrialized countries. It has also been debated whether this would justify or even require a trial comparing artesunate and quinine for European patients. Our current view is that severe malaria is such a rare disease in Europe that sufficient sample sizes cannot be obtained. Furthermore, the question remains whether European physicians would be willing to participate in such a trial now that artesunate is recommended as the treatment of choice for severe malaria by WHO” [4] Existing methods of rapidly detecting malaria are microscopy, which requires trained technicians and supplies, or rapid diagnostic tests (RDTs) which tend to be either expensive or lower in specificity and sensitivity. Our complete understanding of the parasite clearance curve is limited by the microscopy detection lower limit [5]. Using the same magnetic filtration of infected cells, it is possible to develop a robust detection platform that could be used in field testing with high specificity and sensitivity.
Use the same magnetic filtration technology to create a robust, field testing device
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Sticky Note
citation?
o Intervene at the clinic level, a relevant point of intervention Tool for research, potentially replace POC RDTs for malaria clinics where malaria
is tested for each and every patient No shelf life issues
o Won’t require any more training than currently needed for POC devices
Appendices
Appendix 1- References
[1] World Health Organization, "Guidelines for the treatment of malaria - 2nd edition," WHO Library,
vol. 1, pp. 1-194, 2010.
[2] World Health Organization, "World Health Statistics 2012," World Health Library, vol. 1, pp. 1-175,
2012.
[3] L. Auer-Hackenberg, T. Staudinger, A. Bojic, G. Locker, G. Leitner, W. Graninger, S. Winkler, M.
Ramharter and N. Worel, "Automated red blood cell exchange as an adjunctive treatment for
severe Plasmodium falciparum malaria at the Vienna General Hospital in Austria: a retrospective
cohort study," Malaria Journal, vol. 11, no. 158, pp. 1-7, 2012.
[4] A. R. Kreeftmeijer-Vegter, P. J. van Genderen, L. G. Visser, W. F. Vierman, J. Clerinx, C. K. van
Veldhuizen and P. J. de Vries, "Treatment outcome of intravenous artesunate in patients with
severe malaria in the Netherlands and Belgium," Malaria Journal, vol. 11, no. 102, pp. 1-11, 2012.
[5] N. White, "The parasite clearance curve," Malaria Journal, vol. 10, no. 278, 2011.
[6] Medecins sans frontieres, "Making the Switch - Ensuring access to improved treatment for severe
malaria in Africa," Campaign for Access to Essential Medicines, Geneve, 2011.
[7] The Lancet, "Artesunate for severe malaria," The Lancet, vol. 377, no. 9776, p. 1466, 2011.
[8] U. Mehta, D. Durrheim, L. Blumberg, S. Donohue, F. Hansford, A. Mabuza, P. Kruger, J. Gumede, E.
Immelman, S. Canal, J. Hugo, G. Swart and K. Barnes, "Malaria deaths as sentinal events to monitor
healthcare delivery and antimalarial drug safety," Tropical Medicine and International Health, vol.
12, no. 5, pp. 617-628, 2007.
[9] E. Mullin, "Study: Blood transfusions costly, used too often," Dorland Health, 2012.
[10] A. Shander, A. Hofmann, S. Ozawa and M. Javidroozi, "The true cost of red blood cell transfusion in
surgical patients," in American Society of Hematology Annual Meeting and Exposition, San
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

Fransisco, 2008.
[11] International Drug Price Indicator Guide, "Drug Price Search," Management Sciences for Health,
2010. [Online]. Available: http://erc.msh.org/dmpguide/. [Accessed 1 October 2012].
[12] Y. Lubell, A. Riewpaiboon, A. M. Dondorp, L. von Seidlein, O. A. Mokuolu, M. Nansumba, S. Gesase,
A. Kent, G. Mtove, R. Olaosebikan, W. Pan Ngum, C. I. Fanello, I. Hendriksen, N. P. Day, N. J. White
and S. Yeung, "Cost-effectiveness of parenteral artesunate for treating children with severe malaria
in sub-Saharan Africa," Bulletin of the World Health Organization, vol. 89, no. 7, pp. 504-512, 2011.
[13] J. Forbes, M. Anderson, G. Anderson, G. Bleecker, E. Rossi and G. Moss, "Blood transfusion costs: a
multicenter study," Transfusion, vol. 31, no. 4, pp. 318-23, 1991.

Appendix 2– Malaria Statistics in The Gambia Gambia and malaria, from WHO statistics report in 2011
o 479,409 reported Malaria cases in 2009 o Malaria-specific mortality (per 100,000 population, 2008): 93
African region: 94, global: 12 o Percent of deaths in children under 5 from malaria in 2008: 22%
African region: 18, global: 9 o Children under 5 years sleeping under insecticide-treated bed nets from 2000-2009:
49% African region average: 17%
o Children under 5 with fever who received treatment with any antimalarial: 63% African region average not reported
Health burden by geography, financial status
From WHO health statistics 2011: Under-five mortality rate (probability of dying by age 5 per 1000 live births)
o By place of residence Rural: 150, Urban: 96
o By wealth quintile Lowest: 158, Highest: 72
o Educational level of mother Lowest: 140, Highest: 66
o Gambia Gambia, from WHO statistics report in 2011
Physicians per 10,000 population from 2000-2010: 0.4 (total 62) o African region average: 2.3 o Global average: 14.0
Nursing and midwife personnel per 10,000 from 2000-2010: 5.7 (total 927) o African region average: 10.9 o Global average: 29.7
Pharmaceutical personnel per 10,000 from 2000-2010: 0.3 (total of 49) o African region average: 0.8 o Global average: 4.1
Environment and public health workers per 10,000 from 2000-2010: 1.1 (total 150) o African region average: 0.4 o Global average: not reported
Community health workers per 10,000 from 2000-2010: 0.7 (total 117) o African region average: not reported o Global average: 4.0
Hospital beds per 10,000 from 2000-2009: 11 o African region average: 9 o Global average: 29
Radiotherapy units per 1,000,000 in 2010: 0 o African region average: 0.1 o Global average: 1.8
Health systems overview
Structure, governing powers
Comparison to other health systems
o Qualitative from interviews
Financials o Payment systems o WHO Health expenditure statistics
Total expenditure on health as % of GNP
2000: 5.8 (African region: 5.5; global: 8.3)
2008: 5.5 (African region: 6.0; global 8.5) General government expenditure on health as % of total health expenditure
2000: 33.6 (African region: 43.7; global: 56.4)
2008: 48.1 (African region: 49.8; global: 60.5) Private expenditure on health as % of total health expenditure
2000: 66.4 (African region: 56.3; global: 43.5)
2008: 51.9 (African region: 50.2; global: 38.4) General government expenditure on health as % of total government
expenditure
2000: 8.8 (African region: 8.2; global: 13.3)
2008: 11.6 (African region: 9.6; global: 13.9) External resources for health as % of total expenditure on health
2000: 22.2 (African region: 6.6; global: 0.3)
2008: 38.0 (African region: 9.5; global: 0.3) Social security expenditure on health as % of general government
expenditure on health:
2000/2008: 0 (2008 African region: 9.4; global: 42.2) Out-of-pocket expenditure as % of private expenditure on health
2000: 53.7 (African region: 57.3 ; global: 50.7)
2008: 48.4 (African region: 60.9; global: 50.7) Private prepaid plans as % of private expenditure on health
2000: 2.3 (African region: 34.8; global: 38.5)
2008: 3.1 (African region: 30.8; global: 41.5) Per capita total expenditure on health at average exchange rate (US$)
2000: 19 (African region: 34; global: 484)
2008: 27 (African region: 83; global: 854) Per capita government expenditure on health at average exchange rate
(US$)
2000: 6 (African region: 15; global: 280)
2008: 13 (African region: 41; global: 517)
Appendix 3- Royal Victoria Teaching Hospital Complete Notes The following notes were taken by hand while following Dr. Uduak Okomo on a tour of the Royal Victoria Teaching Hospital (RVTH). Points we believe should be emphasized are highlighted in blue.
Oxygen gas is expensive, potentially dangerous o They do use O2 concentrators, but have problems with reliability and servicing o People are generally not trained for use o Broken ones are sent to the biomedical unit but don’t always get fixed and returned
Oxygen requires transport, cylinders o Significant patient demand o Depletion is a problem
Only one O2 plant in the country for supply
Concentrators don’t have specific percentages for the amount of oxygen being delivered o Exacerbated by the use of a splitter, no guarantee of equal O2 distribution
Shown the emergency pediatric and general pediatric wards o Approximately 16 beds in each o Most beds were shared between 2 and even 3 patients
Cross-contamination occurs
Stable electricity is a device limiting factor
Children develop pneumonia after upper respiratory infection o Common cause for oxygen demand
O2 is not portable, requires patients to disconnect for diagnostic imaging (x-ray, etc.) o Minimize patient time off oxygen support by close coordination with receiving
department to reduce waiting time and ensure everything is prepped for the patient Risky, but the best option that they have
Leading causes of O2 demand o Heart problems leading to respiratory tract infection o Lung problems
#1: pneumonia #2: bronchiolitis
Nebulizers are useful, too but people often lack training and they break often
Equipment cleaned with methylated spirits [denatured alcohol, ethanol in a form that renders it undrinkable]
o Inconsistent, and lots of things are cleaned by hand when the biomedical team can’t come by to sterilize
In this case, nursing staff clean with soap/water/alcohol
She wasn’t familiar with the training/experience level of biomedical staff
Pulse oximeter for hypoxia, but the device generally doesn’t work o Diagnosis for hypoxia is then largely symptomatic
Nose flaring, significant lower rib action while breathing indicate respiratory distress -> patient is put on O2 support
NEED: a smaller, mobile O2 unit so patients can take home O2 support for chronic issues
Patients are on O2 support for 48-72 hours in general
Seasonal admissions o 40-50 admissions in a day, peaks during rainy season o Multiple patients per bed is standard
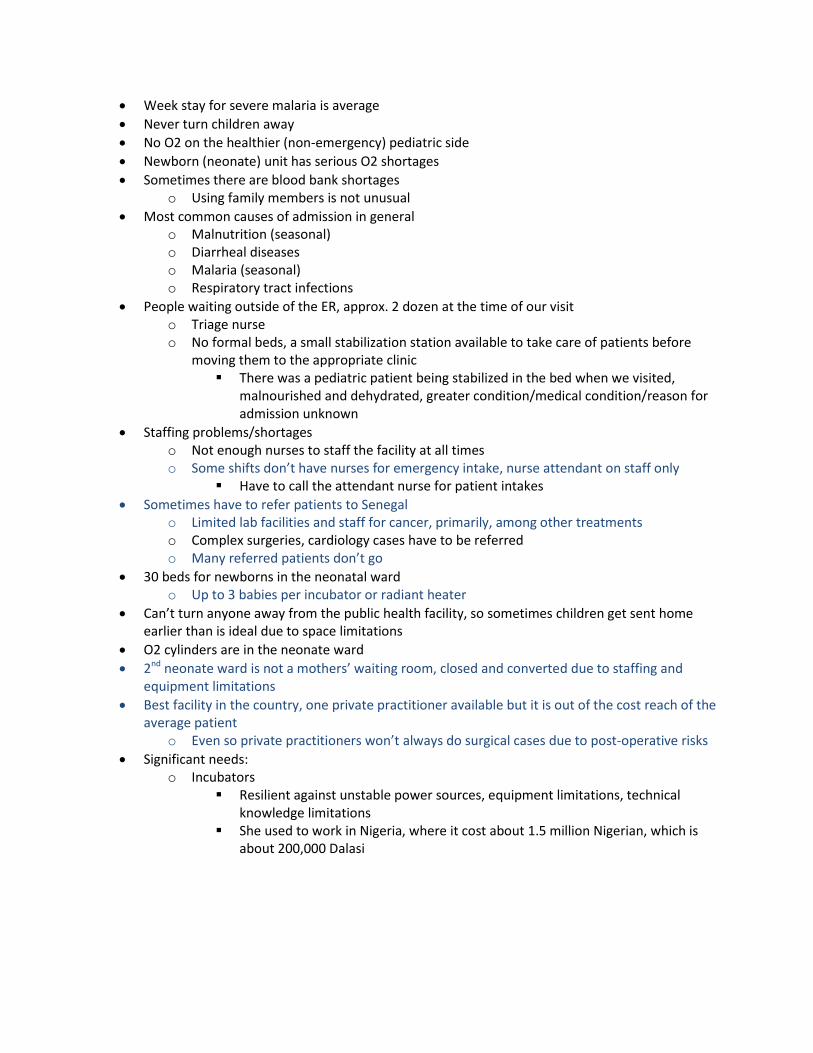
Week stay for severe malaria is average
Never turn children away
No O2 on the healthier (non-emergency) pediatric side
Newborn (neonate) unit has serious O2 shortages
Sometimes there are blood bank shortages o Using family members is not unusual
Most common causes of admission in general o Malnutrition (seasonal) o Diarrheal diseases o Malaria (seasonal) o Respiratory tract infections
People waiting outside of the ER, approx. 2 dozen at the time of our visit o Triage nurse o No formal beds, a small stabilization station available to take care of patients before
moving them to the appropriate clinic There was a pediatric patient being stabilized in the bed when we visited,
malnourished and dehydrated, greater condition/medical condition/reason for admission unknown
Staffing problems/shortages o Not enough nurses to staff the facility at all times o Some shifts don’t have nurses for emergency intake, nurse attendant on staff only
Have to call the attendant nurse for patient intakes
Sometimes have to refer patients to Senegal o Limited lab facilities and staff for cancer, primarily, among other treatments o Complex surgeries, cardiology cases have to be referred o Many referred patients don’t go
30 beds for newborns in the neonatal ward o Up to 3 babies per incubator or radiant heater
Can’t turn anyone away from the public health facility, so sometimes children get sent home earlier than is ideal due to space limitations
O2 cylinders are in the neonate ward
2nd neonate ward is not a mothers’ waiting room, closed and converted due to staffing and equipment limitations
Best facility in the country, one private practitioner available but it is out of the cost reach of the average patient
o Even so private practitioners won’t always do surgical cases due to post-operative risks
Significant needs: o Incubators
Resilient against unstable power sources, equipment limitations, technical knowledge limitations
She used to work in Nigeria, where it cost about 1.5 million Nigerian, which is about 200,000 Dalasi

Appendix 4– Notes from Brikama Health Center visit During this site visit, we had the opportunity to interview the director of the health center and one of his associates who is working there while pursuing a degree in public health policy. The notes from the interview are as follows:
This facility sees between 6000-8000 patients in a month regularly
Different units for public health, maternity, outpatient (general ward)
Surgeries are OBGYN only
Conduct screening of pregnant women
Lab facilities include serology testing, hemoglobin, blood work, microbio o Also test for various STIs although it can be difficult to differentiate between them
Gonorrhea/syphilis/etc. ; hepatitis B not testable in facility o Because Hepatitis B cannot be tested for, blood transfusion will be done anyway rather
than allowing a patient in need to die
Central medical from government for restocking o Don’t always get the desired volume or type of equipment – mismatch between what’s
asked for and what’s delivered o The day prior to our visit, ran out of HIV testing equipment
Shortage of staff o 6 midwives for 1000 deliveries
5 midwives per 1000 is the national average, so better than other facilities
Brikama receives from local clinics o Will refer to RVTH (hypertensive cases, severe traumas, etc.) o Will also refer when supplies are exhausted o O2 is in constant demand here, too
Blood shortages a constant problem o 4 people in a month received donated blood, the other 50 or so cases received blood
from family members o The blood bank attempted a centrally organized effort in the past but it wasn’t
sustainable
Malaria cases can be up to 40 in a day for malaria in peak season o 5-10 cases of severe malaria daily
Primary problem at that point is space, drugs are largely available o Severe cases can be treated for 2 days on average o Once they are “out of the woods,” they are given oral medication and released o Fluids, admissions, stay time are expensive
Far preferred to do a rapid test and treat
Some communities simply lack access o Roads covered in water o People have to come in on foot o Sometimes severe cases come in because people believe they have been treated and
are well, then once they make it back to the clinic it’s too late o People will sometimes seek native treatments, and education is an issue o Long wait times can play a role in severity o People will seek symptomatic self-treatment
POC testing only available to health centers
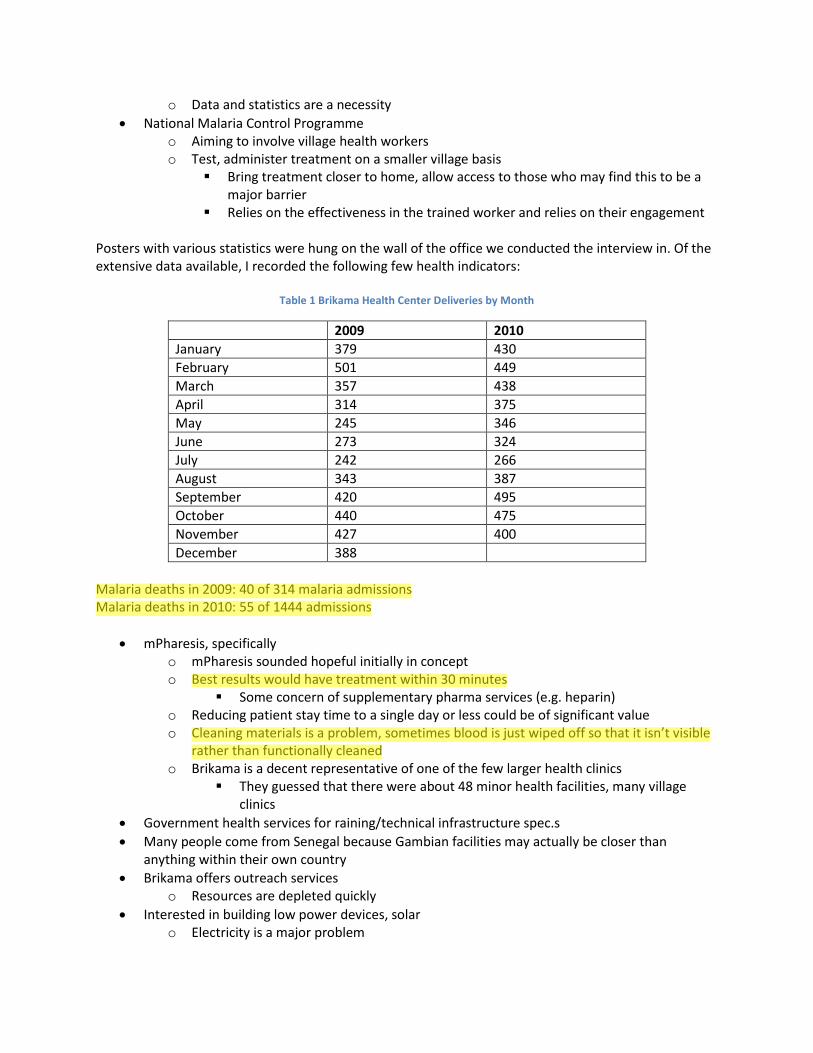
o Data and statistics are a necessity
National Malaria Control Programme o Aiming to involve village health workers o Test, administer treatment on a smaller village basis
Bring treatment closer to home, allow access to those who may find this to be a major barrier
Relies on the effectiveness in the trained worker and relies on their engagement Posters with various statistics were hung on the wall of the office we conducted the interview in. Of the extensive data available, I recorded the following few health indicators:
Table 1 Brikama Health Center Deliveries by Month
2009 2010
January 379 430
February 501 449
March 357 438
April 314 375
May 245 346
June 273 324
July 242 266
August 343 387
September 420 495
October 440 475
November 427 400
December 388
Malaria deaths in 2009: 40 of 314 malaria admissions Malaria deaths in 2010: 55 of 1444 admissions
mPharesis, specifically o mPharesis sounded hopeful initially in concept o Best results would have treatment within 30 minutes
Some concern of supplementary pharma services (e.g. heparin) o Reducing patient stay time to a single day or less could be of significant value o Cleaning materials is a problem, sometimes blood is just wiped off so that it isn’t visible
rather than functionally cleaned o Brikama is a decent representative of one of the few larger health clinics
They guessed that there were about 48 minor health facilities, many village clinics
Government health services for raining/technical infrastructure spec.s
Many people come from Senegal because Gambian facilities may actually be closer than anything within their own country
Brikama offers outreach services o Resources are depleted quickly
Interested in building low power devices, solar o Electricity is a major problem
Blue
Highlight
Blue
Highlight
Blue
Highlight

Especially for surgery
Limited surgical capability due to surgical suite and power o They have an x-ray machine, but can’t use it due to power/space/personnel limitations
Last week, in the middle of surgery, the anesthesia machine broke during surgery Brikama Antenatal
Every patient is tested for malaria
First booking service for new antenatals they test for HIV/AIDS, do urine and blood analysis o Provide individual counseling service
Same day as first admissions, they collect everything for testing then do same-day counseling
anti-malarials generally given, ideally prophylaxis given twice during term
Return for post-test counseling based on results Brikama Labor Ward
1 sink, 8 beds, 16 incubators
Had 22 deliveries in a single night shift once; 3 shifts each day, 24 hours
A single baby warmer for the facility
Oxygen concentrator shared between the neonatal and main ward
24 hour observation after delivery, some opt to leave earlier
They hold patients after dialation more than 2 cm, check progression every 4 hours
O2 and beds are both problems o Shared beds
One blood pressure machine, one thermometer o This wing does have enough nurses, generally
Brikama Public Health Dogs in the waiting room with dozens of women, children waiting to receive vaccinations
Single health worker conducting vaccinations
Hepatitis, polio, meningitis, all manner of vaccination offered for free o If they are willing to come to/wait at the clinic
Recommendations on general health behaviors
Gambians and others, whoever comes into the clinic will be offered treatment Brikama General Ward
Divided into male/female/pediatric
Most admissions were malaria at the time of our visit o Not unusual for the time of year
80% of cases are severe, uncomplicated cases are outpatient o Hold severe cases for up to 72 hours
Many people are pretty good about bringing kids in, they don’t chance it with a child and a fever o Getting less common for mortality in the very young
O2 is quite limited here as well o Cylinders are idea (although can be dangerous) but expensive and hard to replenish o Electricity is unreliable
Standby ambulance available 24 hr Hands-on care clinic
Consultation rooms o Computer in the room, unused
Treat sexual and reproductive
Blue
Highlight
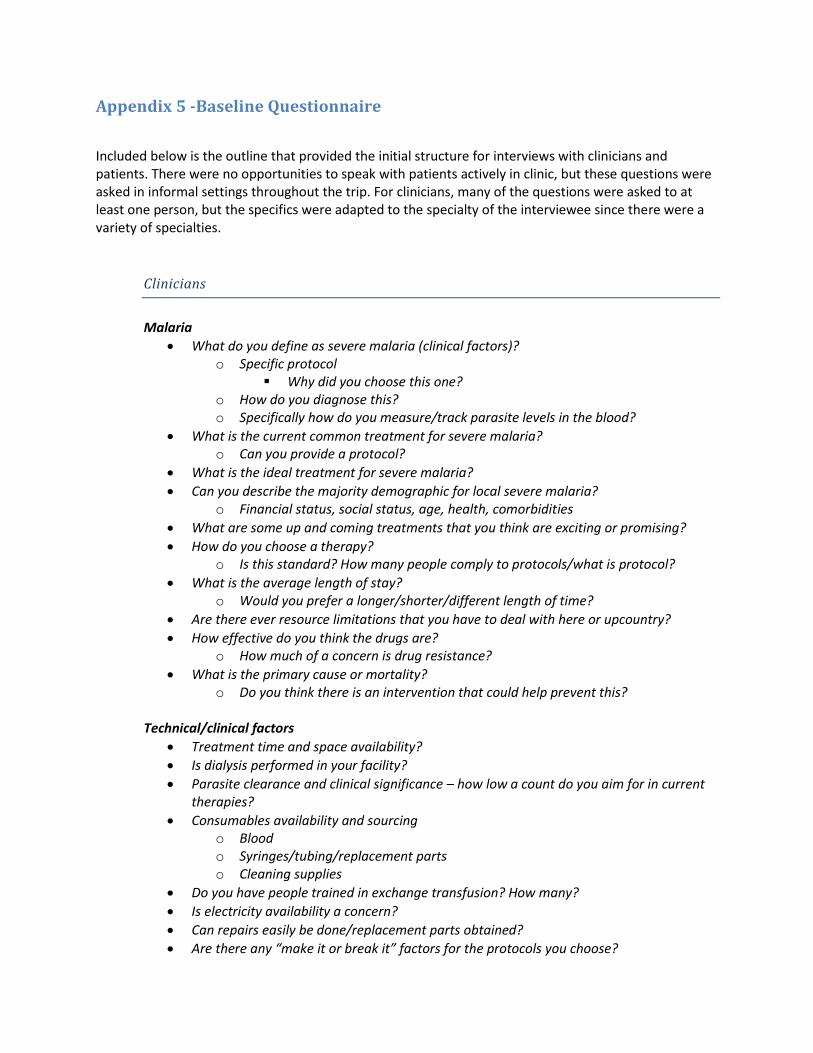
Appendix 5 -Baseline Questionnaire
Included below is the outline that provided the initial structure for interviews with clinicians and patients. There were no opportunities to speak with patients actively in clinic, but these questions were asked in informal settings throughout the trip. For clinicians, many of the questions were asked to at least one person, but the specifics were adapted to the specialty of the interviewee since there were a variety of specialties.
Clinicians
Malaria
What do you define as severe malaria (clinical factors)? o Specific protocol
Why did you choose this one? o How do you diagnose this? o Specifically how do you measure/track parasite levels in the blood?
What is the current common treatment for severe malaria? o Can you provide a protocol?
What is the ideal treatment for severe malaria?
Can you describe the majority demographic for local severe malaria? o Financial status, social status, age, health, comorbidities
What are some up and coming treatments that you think are exciting or promising?
How do you choose a therapy? o Is this standard? How many people comply to protocols/what is protocol?
What is the average length of stay? o Would you prefer a longer/shorter/different length of time?
Are there ever resource limitations that you have to deal with here or upcountry?
How effective do you think the drugs are? o How much of a concern is drug resistance?
What is the primary cause or mortality? o Do you think there is an intervention that could help prevent this?
Technical/clinical factors
Treatment time and space availability?
Is dialysis performed in your facility?
Parasite clearance and clinical significance – how low a count do you aim for in current therapies?
Consumables availability and sourcing o Blood o Syringes/tubing/replacement parts o Cleaning supplies
Do you have people trained in exchange transfusion? How many?
Is electricity availability a concern?
Can repairs easily be done/replacement parts obtained?
Are there any “make it or break it” factors for the protocols you choose?
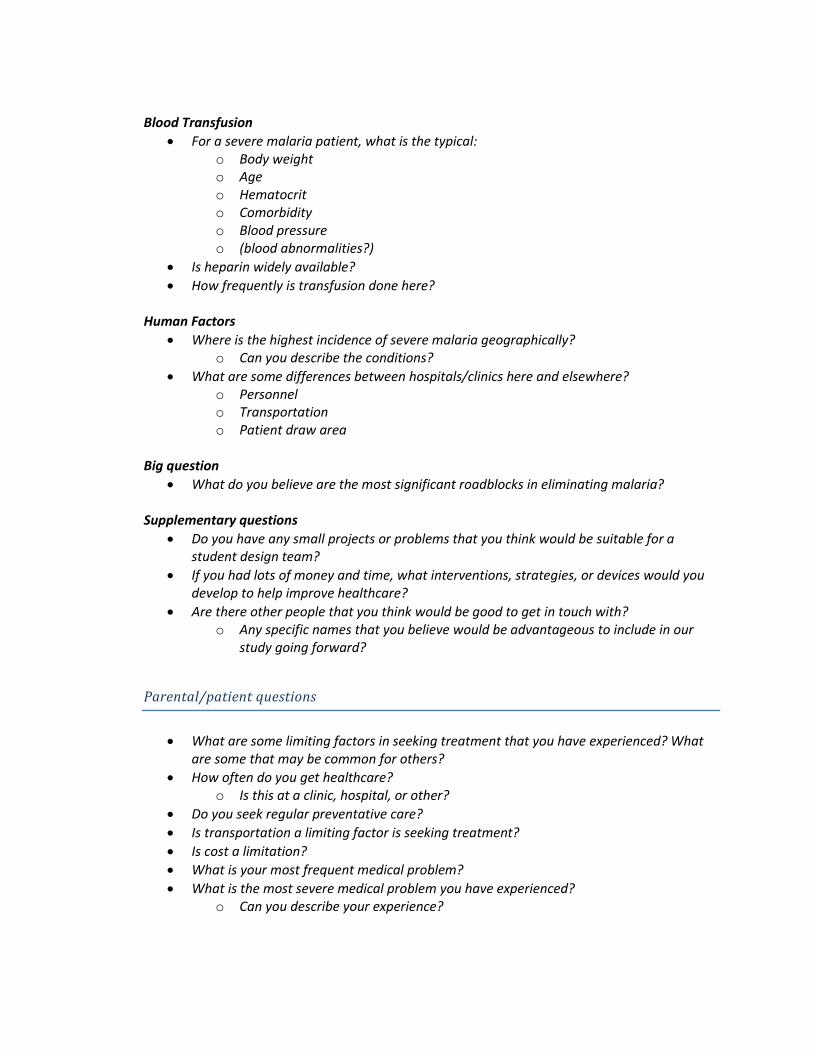
Blood Transfusion
For a severe malaria patient, what is the typical: o Body weight o Age o Hematocrit o Comorbidity o Blood pressure o (blood abnormalities?)
Is heparin widely available?
How frequently is transfusion done here?
Human Factors
Where is the highest incidence of severe malaria geographically? o Can you describe the conditions?
What are some differences between hospitals/clinics here and elsewhere? o Personnel o Transportation o Patient draw area
Big question
What do you believe are the most significant roadblocks in eliminating malaria?
Supplementary questions
Do you have any small projects or problems that you think would be suitable for a student design team?
If you had lots of money and time, what interventions, strategies, or devices would you develop to help improve healthcare?
Are there other people that you think would be good to get in touch with? o Any specific names that you believe would be advantageous to include in our
study going forward?
Parental/patient questions
What are some limiting factors in seeking treatment that you have experienced? What are some that may be common for others?
How often do you get healthcare? o Is this at a clinic, hospital, or other?
Do you seek regular preventative care?
Is transportation a limiting factor is seeking treatment?
Is cost a limitation?
What is your most frequent medical problem?
What is the most severe medical problem you have experienced? o Can you describe your experience?
Appendix 6– Interview Transcript, Umberto D’Alessandro During the trip, Dr. D’Alessandro was the subject of both the first and last interviews conducted.
FIRST MEETING:
Molly: So if I could ask a broad question I was wondering on what your opinion was as far as vector
control, versus developing immunizations against malaria, versus other treatments, versus getting drugs
to everybody? Is there specific kind of strategy for approaching malaria that that you think is most likely
to be successful?
Umberto: Yes there is an organizational strategy, which is prone to identifying efficacious treatment, in
this case artesunate-based combination treatment; then vector control, in this case in Africa, it is manly
insecticide-treated bed nets and now here they are doing spraying or they spray insecticide on the walls.
In this country it’s DDT, don’t be shocked, but it works for malaria and there are no health hazards for
humans, at least when used in this way. For pregnant woman we give intermediate prevention
treatment with a chemo-prophylactic drug and I think that is about it. At least in The Gambia and
several other countries it has been quite successful but the cost of transmission. In the last five years
we have passed from sort of depression, people have depression because malaria didn’t change. We are
unable to cover the population with bed nets and now there’s sort of a euphoria. Bill Gates announcing
2007 that we should go for elimination and education for malaria so a lot of people talk about
elimination of malaria.
Molly: How does that play into the work that you are doing at this facility?
Umberto: Well I am a team leader of disease control and elimination. I have a program grant who is
trying to look at the dynamics of malaria transmission and try to understand who are the people
transmitting. Because when malaria goes down, usually malaria is not uniform. You have small places,
what we call is hot spots, where there is more transmission for some reason we don’t understand and
there is places where there is less transmission. When transmission goes down these hot spots become
more apparent. We are doing a project, this year we selected the villages and the next year we are
going to follow very close these villages with the stream of the transmission but in the same area. A pair
of villages in six different areas but at the stream transmission, one low and one high transmission, and
we try to understand who transmits and how the parasite spreads in the population and so and so forth.
Also understand how the vector population behaves and if there is any difference. This is one thing,
another project we do which is funded but we haven’t started yet is to look at pregnant woman are
more vulnerable to malaria then others, than non-pregnant woman. I mentioned there is an
intermediate preventative treatment that should be given at the second and third trimester of
pregnancy, but the coverage is not very good. What we are going to try to do is a strategy in which we
compliment this with intermediate screening and treatment them if it’s positive for pregnant woman in
the villages with the village health worker. We will see if we can reduce malaria in this group. Then
another project that is just funded is the use of primaquine which is a drug that kills gametocytes, the
form that transfers to mosquitos. The problem with primaquine is that it causes hemolysis in people
with a certain genetic conformation it is called –(4:40)--- so they are deficient of some enzyme. If you
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

give primaquine they are going to get hemolysis. So that’s what prevents primaquine in a large scale. So
what we are going to do is we are going to first exclude these people form the trial, then we are going to
scale down different dosses of primaquine to see what is the minimum doss that can kill the
gametocytes because the problem with hemolysis is linked to the dose so if you decease the dose
probably you will have less risk, in a nutshell. For the vaccine, I am involved in the new vaccine from JSK
and RTSS the results have been published last year with 50% reduction in attaching children, but it is still
going. We are going to have vaccine in the next three of four years. But it is only 50% protection so but
it can compliment.
Molly: What kind of work are you doing with severe malaria? You said you were doing a clinical trial
here?
Umberto: Yes, there is a clinical trial but I am not directly involved in that, but there is my colleague Dr.
Bojang; I think you should meet him tomorrow. So this is a trial that is funded by the EDCTP and
basically try to see whether they can simplify the dose of artisinate; they are comparing different
schedules in children with severe malaria and this is done in the Royal Victoria Hospital in Banjul. So far
they haven’t recruited many patients because we are waiting for the peak, probably it is going to be this
month in October, there are not many patients. I think there are going to be with this rain, it is
absolutely crazy. It is very unusual to have so much rain. Yes!
Molly: A little more about the facility here, how many beds are here?
Umberto: As far as I know there are 40 beds. Oh 42. All the facilities are mainly for the staff. I mean, we
are more than 1000 staff and their family but it is also open to the public.
Molly: What kinds of services are available to the public?
Umberto: Well there are out patients and pediatrics and the internal medicine?
Molly: Do you do any blood transfusion or dialysis?
Umberto: That one I do not know because I am not directly involved in the clinic. I think blood
transfusion yes, dialysis probably not.
Molly: How is the management to the remote clinics done? Is it through project management teams
that head from hear and then do these clinical trials, remotely?
Umberto: No, the clinical trials are not done… for malaria they don’t do it here because transmission has
gone down quite a lot in the last few years so we haven’t had to many patients here. So what we
usually do is we go to Basse, we have a field station. When we do these kinds of trials and we
collaborate with the health centers which are small or smaller but they have beds. I mean, we can work
in any place in The Gambia, there is the Banjul referral hospital there is the RVTH; we work with the
government
Molly: what is the RVTH?
Umberto: Royal Victorian Teaching Hospital?
Molly: How do you do consumables, like just basic materials and how is blood availability?
Umberto: I can’t answer those kind of questions, you mean the bags of blood? I guess we buy them. It’s
not a problem.
Molly: That goes with replacement parts, do you have technical staff?
Umberto: Yes, there is a permanent service here, all the orders go through that.
Jackie: We have read in some places that if you have disposable parts that they tend to reuse them.
Have you heard of it happening in anywhere else in Gambia or outside of Gambia in Africa?
Umberto: It might occur but this is bad medical practice. So it is very difficult to know what’s going on. In
principle you should not do it but here for sure we do not do it. I can’t exclude that in government
hospitals they are not doing it but I am not sure. The Gambia health service is not as well off from the
rest of the work but it’s not bad either.
Molly: In general how does reimbursement work here because, I heard all these surfaces are free or at
low cost?
Umberto: As far as I know it is free for children and for the adults I am not sure.
Molly: Do you spend any of your time upcountry in any of the other clinics or are you mostly here?
Umberto: I go from time to time. I go according to the needs. I don’t do clinical work anymore because
I have too much to do. But there are several clinicians that work on the team.
Molly: I guess I don’t have a solid perception on what you do kind of day to day, I know there is a lot of
management involved in traveling in things but…?
Umberto: I write proposals, grant proposals, and papers I supervise PHD students. It is mainly
management research then hands on work.
Molly: What do you think are the most significant road blocks as far as getting malaria treatments and
getting them out there and distribution and things, if you could pick one?
Umberto: Well the first one is probably a management problem; sometime you have stock outs of the
tests and treatments. So it is more to do with how things are managed at the central level, it can
happen. It shouldn’t happen but it does happen. Sometimes you have facilities out of medication for
maybe one month. The second is that people sometimes don’t go very easily to the health facilities. It
depends what kind of services they offer but if the service is not good or for different reasons they don’t
attend.
Molly: That is one thing that we have really been wondering about. It sounds like there is a solid effort
to make these services affordable but it gets to the point of severe malaria. Severe malaria is a treatable
Blue
Highlight
Blue
Highlight
Blue
Highlight
disease for the most part and people know that it is around so what keeps people from coming in
sooner.
Umberto: Malaria is like a cold in the US or in Europe. It’s like oh I got malaria, I will just take a bit of
aspirin or go and get some drug because there is no prescription, so anybody can buy it you know
whatever they want it. That’s another problem, not in the royal areas but here, there are quite a few
pharmacies; they can go and buy and the quality of the drug is not guaranteed 100%. Sometimes you
have a drug that is not very good. The second point is that severe malaria can be very quick. A child can
start to faint when before he was perfectly ok. So sometimes it is so rapid that people don’t have time
to cope with it.
Jackie: What about transportation?
Umberto: Transportation is a problem as well a child that is very sick to bring them from peripheral area
to the health centers then referred to the RVTH, it can be a problem. Also because they need to pay for
the transportation; of course the services are free but not the transport. They have to provide money
for bringing the child or patient to the facility.
Molly: In general how do you imagine technical interventions to play a role in this, for the purpose of
our technology and also in general?
Umberto: We have to see how it can be integrated with what is already done. I think the first thing is to
show that there is an advantage in terms of case fatality, mortality. I don’t know what your plan in
terms of development but I think at the end of the day you need to show that is really beneficial. So
ideally you would have to do a large trial were you have a facility with or without or have the same
facility were children are going to introduced to this or not and show that benefits in mortalities. It is
going to be tough because probably you need a very, vary large trial.
Jackie: Do you know how many people that get the necessary medication and care and still die?
Umberto: I don’t know here but usually I think in the paper that was published on Artisinate I think it
was something like 8%. Eight percent or ten present, around that number
Jackie: Do you have a clue on why, did they come in to late?
Umberto: Yes, this is one of the problems, sometimes they just come in too late. Yes, if you look at all of
the data on mortality for malaria, most of that occurs on the first 24-48 hours; if you manage to go over
that you are likely to survive. Another problem is the secretion, neurological secretion. You know about
ten percent of the patient can have a neurological secretion after severe malaria
Molly: Is that permanent?
Umberto: yes, it is a brain damage.
Jackie: Yes, because of the clotting right?
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

Umberto: Yes you have some area of the brain that is not profuse anymore so you have damage on the
neurons.
Jackie: Do you know how long it takes for the drugs to start kicking in after you take them, if they come
in late to the hospital? Because we were thinking this device would be helpful for late minute, for
people who come in, it’s very last minute. We were thinking that drugs don’t have time to take into
advantage. So do you know how long it takes for drugs to kick in?
Umberto: Yea, Quinine takes a bit of time, but Artesunate is very, very quick. So you have a dramatic
decrease of parasite density in a very short time. I don’t know, I think it is one hour or two where you
have a very hug decrease in parasite density. I think the trouble there is the parasite that has secrete in
the deep circulation. Although, Artesunate is still effective for those points. But it is true that if you
could. How long does it take to filter the blood?
Jackie: Those numbers are not actually concrete yet we are still in developing. Right now we are trying
to see if there is actually a market for this, if this would be beneficial. Right now we are estimating it
would be something like dialysis maybe two to five hours.
Molly: We are hoping in the order of hours. As it is currently, it is scalable so we can adjust how much
blood flow is going through but it is limited by factors such as shock, how much you can take out of the
body at once. So it is physiologically limited.
Umberto: But it is not going to filter the drug?
Molly & Jackie: No
Umberto: So the drug is going to get back into the circulation again?
Molly & Jackie: Yes
Umberto: So you can use it at the same time?
Molly & Jackie: Yes
Jackie: That is the plan right now is to use it with the drug. I guess another problem we are facing right
now is cost. We are thinking the final device is going to cast maybe 20-30 thousand dollars; just one
time cost to buy the equipment. Is that something that seems like it would be useful if it saves maybe
50% of the people that would have died?
Umberto: Yes, of course it is a major cost. If you are sure there is a major advantage in the mortality. I
would be more concerned about the consumables, if you have to change a few parts. For if patient you
would have to change, if there is a filter or a membrane or a ..
Jackie: Right now blood flows through it, we could have reusable parts or disposable parts depending on
what kind of cleaning techniques they use in the clinics that are going to use it. We could make it all
Blue
Highlight
Blue
Highlight

reusable but we don’t know if sanitation and cleaning it is easy and if people do actually clean it
thoroughly, because there is HIV and all of that other diseases that come with blood.
Umberto: Yes, in the hospital we have everything, I mean we do surgeries. I guess you could possibly
could to reuse it if you autoclave...
Jackie: I mean, it could be reused but I don’t know if that would be better than disposable parts. I think
that if we were going to make it disposable then we would be like 5 dollars for each patient which is a
lot that we are hearing now.
Umberto: Yea it’s a lot. So it would be better to make it reusable. But it is true you would have to
guarantee that it is not dangerous.
Jackie: yes, correct
Molly: Do you imagine that this could fit in with a clinical trial here at some point, if it is developed?
Umberto: We could do a clinical trial but you we would need to use other centers because we will not
have enough. Hardly any facility would have enough patients. Just to give you an idea, the trial on
Artesunate they included something like five or six thousand patients, so you would need to be quite big
to show. If you do a small trial, even if there is some advantage, assuming you had an increase of ten
percent mortality or 20 percent it could be interesting, but to show that you need very very big numbers
Molly: How does funding clinical trials work? What is a ballpark cost for large scale?
Umberto: Well you have to apply. The medical counsel in the UK change the structure, so it gives us
something like six million pounds per year to maintain the platforms, but with this money we can’t do
any research so we would have to apply for additional.
Jackie: Do you know who to talk to get the best knowledge on how the hospital is run?
Umberto: Kalifa is going to be, Kalifa Bojung, because he is working with the MRC but he is a
pediatrician and he is sort of attached to the RTBH. He has a lot of experience on how it works.
Molly: As far as how to get a good idea on how a lot of rural clinics, the most number of clinics that are
in The Gambia or greater west Africa, is the teaching hospital kind of a good of resources that might be
available?
Umberto: This is for the teaching hospital if you want to see a clinic or health center it is a different
level.
Molly: One of them that is affiliated with here, we were told is a good representation of what kind of a
rural clinic would look like.
Umberto: Serrekunda?
Jackie & Molly: I don’t remember
Blue
Highlight
Blue
Highlight

Umberto: it is probably Serrekunda center.
Molly: is that close?
Umberto: It is not far. Yes, it is not far you can go. When do you leave?
Molly: Saturday
Umberto: Saturday. I think it is going to be difficult to organize a trip up country.
Molly: Yes, that is what we understand.
Jackie: Yes, we heard it is a half day travel.
Umberto: Yes, half day travel
Molly: We were hoping to get something that would be a good represented of what an upcountry clinic
would look more like so as long as we could get something that is similar representative, that would be
great.
Jackie: We are not selling this just to The Gambia we benefit of Africa so this is I hear is one of the best
hospitals in this country so
Umberto: The thing is the MRC, The Gambia, is not only for the health services, it is for the research.
There are a lot of research project that have been down here things that are now being taken out by the
health systems; The bed nets I did one of the first studs of bed nets here and now the bed nets are all
over the place in other countries. If you want to do a research project this is the right place but if you
want to do a big clinical trial we cannot in only The Gambia. You would have to go somewhere else.
Molly: How do you start developing those ties? Do you have to have a set of hospitals that already like
working in conjunction with you?
Umberto: Yea, we have a good network. We work with Senegal; we have a good network. I know a lot
of centers, research centers, in Africa that could be interested in doing this thing.
Molly: How do you handle some of the logistics of these clinical trials, when you are tracking things like
transmission?
Umberto: Malaria transmission?
Molly: Yea, so how do you actually measure that?
Umberto: It is very difficult to measure. There are different ways of measuring it. One is capturing
mosquitos for a certain amount of time and looking at how many of them are infectious. You can do
cross sectional surveys to see what is the prevalence of malaria in the population; it gives you sort of an
idea of how much, what is the transmission. For clinical trial, field based clinical trials, we have sort of
an organization; you have the field workers are at the community level so they maintain the contact
Blue
Highlight

between the community and the researcher, then we have clinician’s nurses at our facility, there is a
whole chain of people that link the researchers with the community. When you are talking about
clinical trials, for primaquine we have two insectaries were we raise mosquitos upcountry. What we do
we have two teams around this insectaries who are going to screen people in the villages and identify
those that are positive and for some of them we are going to take blood and we are going put the blood
in a container sweet membrane and then we feed it to mosquitos and we check how many of them get
infected. It is a quite big organization; we are talking about 30 to 40 people working on it
-Pause for Phone call—
Molly: What do you know about animal studies with malaria? I would imagine before doing a clinical
trial it would be wise to do some kind of animal studies to make sure it is totally safe and effective. Do
you know anything about effective protocols?
Umberto: I have never been involved in animal studies but I know there are people working on
monkeys.
Molly: There isn’t one broadly accepted malaria animal model?
Umberto: No, as far as I know. I mean you have the mouse as animal models for severe malaria you
have people working on monkeys for vaccine studies you know there are different models.
Molly: As a broad direction that malaria is moving, just numerically, is it on the rise or is it starting to get
under control?
Umberto: No, it is starting to go down. There are some countries where there is no change or actually
going a bit up but in overall. In The Gambia for example when I was here in the 90’s, when I was doing a
survey, we had something like 30-40 % of kids surveyed were positive with malaria infection. Now a
days you maybe have 10-15% so it is has changed a lot. Also what you are observing is the number of
cases is more in the older children because there is less transmission. The smaller children are more
likely to sleep under bed nets while the older children are not so you’ve more cases sort of 5 to 15 years
old.
Jackie: In literature we have read that it is increasing.
Umberto: Malaria. Well no if you look at the malaria which came out a few month ago it looks like there
is a decrease in transmission.
Jackie: yes, there is defiantly more of awareness now then there was before. So I can see it decreasing.
Umberto: Also the money for malaria control has increased dramatically. Also money for research has
increased dramatically that is reflected you know you have the funds for HIV and malaria who is giving a
huge amount of money to the malaria case. You can see things are moving.
Molly: Would you contribute that to any one intervention or just the sum of them?
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

Umberto: I think the sum of them. Bed nets, I think bed nets did a lot. Artesunate combination
treatment probably played a role because they also have some action against the gametocytes so they
also may decrease transmission not completely but some of them. So, the two combined and then of
course insecticides. The idea is that there is no one single intervention that can solve the problem so
the more you add the higher the impact
Molly: I am helping teach a capstone design class course. So if you have any baby design projects that
you think a student team could do.
Umberto: what do you mean by baby design project?
Molly: Anything like “gee I wish we would have something that could do this”. So, small technical
solutions or problems. Do you have anything that would be appropriate for a set of design students?
Umberto: like this one?
Molly: yes but a much smaller one. They have an entire year to do it but they are largely inexperienced.
But they can accomplish a lot but it is under guidance. So little engineering problems: keeping
something cold enough or helping transport things.
Umberto: Just like that I don’t know, but I can think about it. Can you send me some kind of example?
Molly: Ok so a couple from last year we had a team that built and designed a back brace that is
noninvasive to help prevent scoliosis in adolescence because the only ones they had were huge; they
build a streamline one. We had people that developed an inhaler for asthmatics except it was tiny and
you could fit it in your wallet rather than the clunky one; a single dose inhaler. We also had some teams
that built a diabetic ulcer detection system for feet.
Umberto: I think the best it to just circulate around this place. I mean they may have different ideas
because they have people working on TB working on material diseases so they may have an idea in that
particular field.
Blue
Highlight

SECOND MEETING:
Molly: I have had a really fantastic experience the fact that we were able to see different types of clinics
as well as what you do here at the facilities and really understanding more about the structure here and
how any kind of device could fit in with the infrastructure. That kind of insight was just, that was exactly
what we needed. Because that is what we totally don’t have in Pittsburgh so I would love to your
praises and also Dr. Okebe’s because I am so grateful that you made this happen for us
Umberto: Yes, I know for us it is good because I like the idea of Alberto and the diagnostic device and
this idea also could be good, it could end up in something that is useful as well. I mean for us it is also
good. From what you saw this week do you think you are going to go through with that of your
prototype
Molly: I think it needs some retargeting. As we envision it now I think there is a disconnect between
where the need for this device is and where the infrastructure is to support it is like blood availability
and reliable electricity, maybe we would need electricity maybe we could make it battery powered but
as for the design specifics we do need to find a way it would fit in better with the patient flow process
because as far as sever malaria is concerned I am just not sure that we would be able to get this product
to people any faster than the drugs.
Umberto: I mean any device won’t be able to because that depends on the ability of transport and other
things. But, I think the problem here is when they already are too late and they have huge parasitic
densities. If they use artesunate you can decrease the parasites load quite dramatically but the issue
here is whether this can improve that clearance of parasite. I don’t know but it could be useful in that
kind of view. Something that contracts that fact that people is coming late. I don’t know if this is going
to be useful in that point of view but it could be something that to think about. In the way of seeing the
thing.
Molly: so one of the other things that Jackie actually came up with was that I think could be brilliant is
an earlier intervention. Designing this so it is practically free to use and this could be something that
someone could use in one of the smaller clinics could use. Cause I could imagine some of the issues with
severe malaria is also the referral because I understand that there is a fabulous referral system but it
does add time delay and if we could perhaps get this device in a setting besides the hospitals so earlier
in the stages and get it more. But then selling it and getting it to be a functional business model and
developing it could be challenging. So do you think that if we designed it so that it was incredibly easy
to use and could rapidly decrease parasitic load that by the time they got to the hospital it could
improve outcomes.
Jackie: and that it was free so anyone could go in before they have severe malaria?
Umberto: Oh, so even in children with uncomplicated malaria?
Molly & Jackie: yea
Blue
Highlight
Umberto: my first reaction is that there is something similar which is I don’t know if you know --- it is
substitute to artesunate which are not policy here in The Gambia. But that showed a big study that
published something few years ago. I mean the results are not very wonderful. But basically show that
if you give a substitute artesunate in children for whom the referral is delayed more than six hours then
you have a gain but not for those that are referred immediately. As far as I know there are very few
countries that have implemented that. Now the issue here of this devise is that portable is in terms of
avoiding infections, sterilization, or if its disposable or not so there are several issues in feasibility or how
a nurse would be able to use it without putting the patient in additional danger. I am not clear on how
you plan on solving that.
Jackie: yes, risks vs. benefits
Molly: yes, we are suggesting taking all of the blood out of the patient and putting it back in and I am
not sure if that is ideal for these clinical settings
Umberto: yea but if you had something like some sort of cartage were you, instead of changing the
blood you, sort of filter sort of attract the parasitized red blood cells why not. So you have the cartage
and the parasitized red blood cells and those need to go back in those that are not parasitized I don’t
know. But something like that and very very simple like a sort of drip sort of perfusion line or glucose
solution they put a drip and they let the drip go. Can you do something as simple as that?
Jackie & Molly: Maybe will who knows.
Molly: So one of the other wild ideas we were thinking of toying with in the car was maybe we were
wondering if the magnetic properties of the cells were maintained after they start including blood flow.
And maybe we could use this magnetic concept to instead of reduce the parasite load help break up or
prevent these inclusions. Because that sounds like the real problem because if you can decrease
parasite load and deal with anemia because that would be a problem anyway and require blood the
toxicity level and anemia are the main causes of death besides the seclusion of flow. So, If we reduce
the seclusion of flow using magnets somehow.
Umberto: I don’t know if you have heard about rosetting. So that means you have a known percent of
Red blood cells who are stick to parasites red blood cells sort of bags with some kind of sticky wall. Of
course if you could sort of reverse this process and make the red blood cells less sticky that might help
but
Jackie: so we are still brainstorming. Currently I don’t think the way the business plan is working out. I
don’t think it would work because the cost of it is too much and were they would be able to use this
would only be in the main hospitals and it would only effect a very little population. So if we want to
make this a business plan we will defiantly have to change it. But I do think the design will defiantly
benefit people but it is just how much the risk benefit and cost so.
Molly: and the other question is we are racing vaccines
Blue
Highlight
Blue
Highlight

Umberto: no the vaccine is not going to. I mean it is a different area. The vaccine is preventing an
infection and this one is going to sort of make the survival people with severe malaria better. So they
would have escaped the vaccine and beneficial effect
Molly: I think it is the time line in developing this device and where that plays in other interventions that
are being developed because realistically I think designing and building a device with clinical trials that
puts us a few years out or about 10 years.
Jackie: so we don’t know if there is going to be a vaccination by the time this is up and running
Umberto: The current vaccination that is on trial probably will have a protection of about 50%. In places
like Uganda, demographic of republic of Congo, all the central Africa countries they are completely
hopeless. The transmission there is still so high that it is very unlikely that it is going to change
dramatically in the next five to 10 years. I mean here in The Gambia It might change and the idea really
is that you have this belt of transmission in Africa so it is to start from the edges and gradually reduce
and merge to the center. We don’t even know if it is possible and actually on of our projects is to try to
understand the transmission system. The malaria Parasite system with the vector system is very robust.
You still have people with low transmission with parasites floating in their blood. So we don’t know.
And this rainy season is absolutely crazy I would suspect that we would have probably we might have an
epidemics here because there is water everywhere and there is going to be breeding sites everywhere.
So transmission may even presume here at the coast. What I am saying is it is very difficult to predict. I
understand the problem because if you put 10 years into a study and it’s not going to be useful what is
the point but it is very difficult to predict. I am not sure what to tell you.
Molly: but we know more than we did at least.
Jackie: at least we have the questions to ask, we know were the flaws are.
Umberto: and for the diagnostic, do know were Alberto is in terms of the diagnostic
Molly: so I think right now they are working on developing consistency. They are trying to get that to be
more consistent results and outputs and continuing to optimize it. I know he does have a few staff on it
there is a post doc working almost exclusively on that and it sounds like it is making decent progress.
Right now I think they are working more towards a CD4 count for it.
Umberto: for HIV?
Molly: yea
Jackie: It is highly inaccurate. They still need to optimize stuff.
Umberto: well it depends on the currency because at the end of the day you want to know if the patent
is under a certain threshold. So if you cans distinguish those who are below 500 or below 300 that
would be already something. So it doesn’t have to be absolutely accurate
Blue
Highlight

Molly: I think it is getting consistent binding. Because it also used the occlusion of flow to determine.
The matter I think there is some microfluidics problems
Jackie: so they are getting the binding and making the chamber smaller but some reason it is not
changing the flow.
Molly: but they are making progress
Umberto: for countries like The Gambia were you have decrease transmission the major problem is to
find out people that are healthy but are still with parasites, so low parasite densities. I have a PHD
student that is trying to adapt molecular methods to the fields. Like simplify the BCI we have in the lab.
To have a diagnostic method that is very sensitive in the field. But if we could also have something that
uses magnetic force that would be great. So not a point of care test but really a test that you could
screen the whole population and find those that are positive and you treat them. At this moment our
diagnostic tests are not sensitive enough. You miss a lot of people with very very low parasitic densities.
Molly: so what is the overall problem is it the lack of sensitivities in devices or is it that you’re not getting
the microscopy slides.
Umberto: yes you have a threshold at which you cannot detect any more so it is something like 10
parasite per microliter. To get that you would need a very very good microscopy. So the ideal is about
ten parasites per microliter but there are people that are before that threshold and probably they still
transmit. And they are not sick that is one example of the adaptation of the parasite to the system. you
can detect people with PCR (polymerase chain reaction) which is amplify the DNA so it is very sensitive
you need a well-equipped lab
Molly: so using PCR you can detect parasite levels
Umberto: There are different types one type is a yes or no answer and the other type you can quantify
the density. But it doesn’t matter for the density what you want to know is to identify those who are
positive and treat them. One of our projects is to simplify as much as possible the PCR. Because with
the PCR it is a method that uses high temperature to replicated the DNA but you also have isothermal,
so normal temperature one so trying to adapt these one to the field so we could identify those who are
positive. But you know if we could get something simpler.
Molly: but you said it doesn’t have to be point of care?
Umberto: well it could be point of care
Molly: Just something reliable in a field
Umberto: The transformation, is very heterogeneous, so there are hot spots remaining says we want to
go into this region and we want to screen everybody and then we treat all of them. All those that are
positive. So by doing this we interrupt transmission.
Molly: and currently you have no way of knowing exactly who has parasites.
Blue
Highlight
Umberto: No
Molly: do you know of anything that is being developed or is that just untouched
Umberto: well there are isothermal molecular methods like LAMP but that’s it. And the RDT are also not
very sensitive, they have the sensitivity of the microscopy they will miss a lot of what you call sub-
parasitic infection so that means they are below the threshold of microscopy detection
Because I still think there is still so much unexplored territory where medical practitioners and engineers
if we could find a common vocabulary and a common problem to work on.
This is really an approach for were transmissions has decreased but not stopped you know relatively low
transmission area were identify the human reservoir it is different were the transmission is very high
and you would and to have a reliable test the facilities are simple that’s fine that’s a point of care. I
mean here it doesn’t mean point of care test but to go a bit farther
Appendix 7 - Interview Transcript, Dr. Readon Ideh
Molly: So can you tell us a little about your background and work here, just briefly.
Ideh: I am a pediatrician, and um, I am a general pedial consultant and we did clinical services, and um, I
also done some research in ammonia, in terms of the kind work I have done and closely I have managed
some children that have been emitted in the ward here
Molly: how many patients roughly get seen, like in a day here?
Ideh: The facility we have a good clinic were we receive the first point of contact with the patient from
the community. We do see a minimum of 150 new cases every day and we also see the follow up cases,
it’s a clinic so some follow up cases, but on average 150 new cases we see.
Molly: 150 a day
Ideh: A day
Molly: Do you accept all patients that come here
Ideh: Well our facility we do have limitations, we don’t do surgery, we don’t do trauma, but medical
cases we do accept and those cases that come here.
Molly: So when they come to the gate clinic if they do need something like surgery do you refer them?
Ideh: Yes, if they come through the gate clinic and it is for surgical cases we do refer them to the
teaching hospital
Molly: Do you offer services for free here or is there some kind of payment?

Ideh: It is essentially free
Molly: Essentially free?
Ideh: Yes, yes. Kids are completely free, adults are also free, consultations and all, but they do pay a
stipend of about five dalasi or ten dalasi for the medication. That why I say essentially free. But for the
children, it is completely free, they don’t pay a dime.
Jackie: Do you guys ever get like overbooked?
Ideh: We do get overbooked
Jackie: Do you send patients elsewhere or do you try to manage more than you can handle?
Molly: What happens in that case?
Ideh: Like I say, we have a restriction. We issue out tickets for those who come on their own and we take
150. But we do have referrals from other help facilities; for example, after our prior discussion was, if it
is a case we think we can handle. Than we also accept study participants. So, 150 is just for those who
are community patents, who come on their own. But any study participant, any participant that is
involved in any MRC study, have free access and they also can come with immediate family (siblings,
mom, and dad). So, those are outside the 150. Occasionally, like now we are entering our peak season,
most of our beds are filled up. We struggle to detach so we can create some room for some others. If
we are full, then we would have to ask that the patents go to the other health facilities, especially the
teaching hospital.
Molly: Are most of the clinical studies recruited through this clinic or through other hospitals?
Ideh: The MRC has field stations; they have got sites all over the country. We got post individual health
centers in the country, at least in the cost hear Faracunda, Serrekunda; we have very strong MRC
present there. At the teaching hospital, also MRC is there, Dr. Bojang is based there. So we do have
referrals from all those centers, as well as, all those who also come through our facility here, are
recruited.
Molly: So what are the most common procedures you do in this clinic or some of the most common
normality’s that come through the door, seasonally or otherwise?
Ideh: Well in the kids, of course axillary infections, ammonia, there is diarrheas, some UTI’s, severe
malnutrition; if you would go to the ward now you would see practically, more than half, 70% of the
patients at the moment have some form of malnutrition.
Molly: And is that seasonal or is that normal?
Ideh: Well it peeks, this is about the worst time because of the rains, the harvest has not started and the
old stalk is finishing. So this is the hungry season. This is when we have the worst of malnutrition cases.
The ammonia and the diarrheas are common. Then sickle cell patents and all sorts also. Right now
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

disease we do see quit a lot because in the facility we are doing some study on children with renal
diseases, so some how people know that we run such a clinic, we have a renal clinic, more or less. And
cardiac cases so we see the ones you were just struggling about, so we see cardiac cases nomadic
acquired and congenital heart diseases. We run a clinic, we do have a cardiac clinic which we run and
then we have some relationship with the charity that helps sponsor children for surgery at the general.
So those are the main stay. We also see asthmatics here, lots of asthmatics here; those are kids, in
adults: TB and all sorts DKs, diabetics, and heart failures.
Molly: So in the way of diagnostics when you have people come through the door is there a standard
procedure for evaluating them with diagnostic, is it all systematic, do you have lab facilities here that
you use for diagnostics:
Ideh: Yes it’s a research, it’s a research laboratory, we are equipt. Of course, you don’t grab patents
from the gate and process them through a lab. They are seen and then the clinician has an idea of what
and what he thinks he is dealing with, and then decides on what kind of investigations he wants to do
and then we do color the samples and run them through the lab. So we do have a clinical diagnostic lab
that can do everything practically: hematology and all of those biochemistry immune studies. We got
the works in terms of what we can do, malaria. Yea, we got a microbiology lab that is standard, we got
our imaging department, we got X-rays-we can do that contrasting, we got ultrasound and Doppler
machines and all, so we can do scans.
Jackie: so you have everything pretty much
Ideh: Except we don’t have CT scan, we don’t have MRI, we don’t have all of that. Because of the
studies we have here, like we have the hepatitis, peripheral study looking at liver, malaria season, and
we got some fancy equipment or so for scanning livers and all, we have all of that, so we got a
gastroenterologist here, so they do assist us in reviewing some of our in patients in that category.
Molly: Do you see a lot of patients with severe malaria come in?
Ideh: Oh yes this is malaria, it’s seasonal anyway. We are just worming up now because when the rain
seasons have come and about the peak of the rains. When the rains start going down, the malaria, they
starts coming. We started seeing how the child, young, right now so 401 malaria parasites. So we are
entering the season September, October peeks, November, and then December it starts going down, by
January it would not probably not see malaria again. We do have that season of intense transition,
starting September, October, November, then goes down.
Molly: Do you have a definition for sever malaria or is it kind of qualitative?
Ideh: Well of course it is the same standard definition that the WHO gives us. Its said that reducing the
parasite load, for example, or the clinical state of the patient was maybe frustrated child, you know so
week, other clinical things like if you suspect pulmonary edema or renal shutdown. The malaria
parasite, you need to identify that, sever malaria severe anemia. So we got so all of the criteria that is
“standard” clinical definition, that is what we follow.
Blue
Highlight

Molly: Is there a kind of majority demographic that comes through with sever malaria, is it mostly one
age group or gender?
Ideh: Well I would not be able to say at the top of my head because we do have incidentally, probably
when you do speak with the malaria, we do have a severe malaria team, we do have a team that is into
malaria.
-Pause for Phone Break-
Ideh: I am saying that for me, I have not sat down to look at maybe the age groups and all of that, but
we would say that the kids less than five. We hardly see young, middle-aged and 12 they don’t really
have the severe ones. Rarely do we see severe ones in less than six months but from two years to five
years and maybe ten years, that’s roughly. But, in the terms of tracking and demography, I think the
malaria team will be able to give you because they have all the data; they taken not of all the malaria
positive cases and the ages and all, people like Dr. Bojang and I think the malaria is on the Alexandra or
Prof. Umberto’s team could give you more concrete shop.
Molly: Are you familiar with exchange transfusion therapy and will you ever consider it?
Ideh: Exchange blood transfusion? I am a pediatrician that is what we do.
Molly & Jackie: For malaria, specifically
Ideh: I have not used that. I am not familiar with that as a treatment for sever malaria, No.
Molly: So we are actually researching the design of a device that will be used on sever malaria patients
that uses the magnetic properties of infected red blood cells to selectively filter out infected cells. Do
you think that would be valuable in the treatment of severe malaria that would have something to help
significantly reduce the parasite level, or are drugs enough? Because, this would be used in conjunction
with drug therapy.
Ideh: Well I think that whatever science comes up with, there usually will be pros and cons of every new
system. But at a glance, yes the problem is you have parasites in red cells, destroying the red cells, and
multiplying in the red cells so if you can withdraw them, that would be fine. That makes logical since
and of course you have the challenge of also knowing that removing the red cells that are parasitized
and you have to replace what you are removing. I would imagine the intelligent designers would also
think of or have to address the anemia that you would also be causing by the time you pulled off all such
red cells. I don’t know how it works, but at a glance it looks like something that should work; you
carried off the parasites within the red cells and probably deal with them in some way. Then if you were
able to replace those red call volume that you will be removing, with fresh, if that is the kind of
exchange you are talking about, then that is fine. You’re getting off load of parasites and you are trying
to replace with normal cells, fine. I don’t know how it works, but for me it’s good. But you need to
know, you are removing something which the normal body ideally has a way of dealing with. We give
the drugs, we kill the parasites. I know you would say the parasites are lysed I mean the red cells are
also lysed anyways so and there is still the anemia and all of that. I think it looks fancy, that’s why we
Blue
Highlight
still have mortalities in malaria because when you got so many parasites; even when you give the drugs,
you are destroying the red cells, destroying the parasites, you have all the debris and all of that, you
know all the inflammation and the whole processes. In a child, even when you give the adequate
antimalarial, they still die because there are a lot of other responses that is triggered. Probably if you
take away all the parasitized red cells you would just
Jackie: When you give the drug, and that parasitic load, what do you see people dying from?
Ideh: That is why people have tried to see if they could modulate the body’s response, inflammatory
markers, and all the things that are released.
-Pause for Phone Break-
Ideh: I mean for every disease process, the body responds to the pathogen, tries to get rid of it, you
understand. Your body does amount some kind of reaction to that and then you start trying to destroy
those pathogens for example. I’ll try a cue from what happens even in some kind of severe kind of
substance where you have organisms that have toxins within them and then you destroy, you lyse them.
Then when you lyse them, you have all the debris and all the toxins released into the system, into the
circulation. They also set up their own inflammatory reactions. The body is trying to deal with all of
these toxins and the debris. It’s like, the way I look at fighting pathogen and infections, a war; when you
have got the bad guys and you got the solders with the guns they are shooting through your bones, and
our bones are antimalarial and chemicals and throwing them into the body BOOM! Of course, you are
killing the bad guys but you are destroying your bridges, the explosions are hitting your houses,
everywhere is messed up. When you are finished killing the bad guy you have to go clear the debris,
clean up your roads and all of that that. That’s what happens when you fight. That’s practically what we
do when we use chemotherapy; we train chemicals to destroy some kind of parasite or some bacteria,
inside the body. The chemical is not exactly innocuous; the body has to deal with it. The chemical
destroys the organism or the pathogen, lyses it, the organism has its own foreign proteins and things all
that is exposed to the body. The body’s inflammatory system is triggered, and so a lot of things going
on. So that is the way I conceptualize and basically what happens, just in simple terms But if you can
get the bad guy out of the country, in the dessert, probably you would have less of destruction to your
bridges and things. I am only trying to say that from a simplified point of view. That seems to be some
of the advantages that comes from you taking out infected red cells with all of the parasites and I would
imagine the system would have a way to deal with it, more or less, maybe clean them out and perhaps
return it to the body whatever is still useful or totally replace it. Who knows what science is up to these
days, some fancy nice things.
Molly: To end with briefly, what do you think are some of the main problems that are being faced in
developing areas or low resourced areas, in general, with health care?
Ideh: When you talk about technology, because what you are bringing in now, it is probably something
nice. I don’t know how it is going to be, but if I tell you the troubles we have with even running even a
dialysis unit. Dialysis, which is kind of what you are doing, I mean it is a kind of dialysis for malaria
because you go, you get the blood, you wash it, and you return it. So we are going to do some kind of
Blue
Highlight
Blue
Highlight

dialysis. Every bit of technology you need the experience. The people that will run it they need to be
trained. Fine, training is not a problem. You need to maintain the equipment that is where the problem
mainly is; you need to be able to supply the consumables for that equipment. For poor resource areas,
those are challenges. Those are huge challenges because we could get the machine it would work for six
months and nobody is able to maintain it. The government is not interested in paying some person to
come and surface it. The suppliers may say we will ok we will service it for you for one to two months
train up your people. But there are issues, we have them, real issues. Those are all the challenges that
can be worked through, but those are major problems I see with good technology and all. A place like
MRC for example, yes, we have a biomedical engineering department so we have the capacity to be able
to maintain it but if you go our labs you will see fancy things there, they maintain them. But outside a
place like MRC, it’s going to be difficult, the plan truth
Jackie: Do you see this being used outside of a main hospital, do you think it could be used in clinics or
do you think it could be some kind of technology you could only use in the hospitals?
Ideh: Well you know when technology starts you have the very big, let’s say when the first computer
was started, it started like four room or so and now we have phones that are practically a computer. It
depends on the unit because I am sure that if you make something that is so elaborate, like a proper
dialysis, you need to know then the kind of standard of the head facility that can accommodate it, of
course, would probably the major hospitals or referral centers. Well I think that is probably were you
will be starting from, the teaching hospitals, the general hospitals, and all them. Like special research
places like us, could have a unit. Fine, because that is anyways where most of the sever malaria cases
will go to. You want something that you will use in those kinds of places. It’s not just probably that you
are targeting sever malaria, those really bad ones, the normal ones probably may not be cost effective.
Carrying out such a procedure on somebody that you treat with Quinine for example. So yes, what you
are trying to design is something that looks like it’s going to be a specialties kind of facility. The people
that are going to run the facility and the machine itself, they need to be trained.
Jackie: But people with severe malaria all end up in the bigger hospital, correct?
Ideh: That is what I am saying; in a place like The Gambia for example, in my experience has a very good
referral system. That is one thing good for The Gambia, you can have cases referred from health centers
straight to the teaching hospital and the ambulance. That functions well and the country is small, it’s
not that big. In most of the very severe case, they end up in the teaching hospitals were they can have
this facility.
Jackie: How many sever malaria cases do you have at one time typically? I know it is different between
seasons, but at the peak season how many people do you see?
Ideh: I will speak for this facility because I can say how we have restrictions in how we take in clients; if
we are open 24 hour hospital where anyone can just come in it’s a different ball game, something like
the teaching hospital. You go there during the peak season you could see like six severe cases, some
being transfused, some being transfused on their mother’s laps it could be really chaotic. For us hear at
the peak, I know sometimes we could have four five or three four, like at once, with intense cases. But
Blue
Highlight
Blue
Highlight
during the peak you may end up having, who knows you could be up to five six. In terms of that we are
not the best place to give you true reflections, something like the teaching hospital/the head facilities.
Molly: On a separate note, for the kind of the up country clinics, smaller health facilities, what are some
of the technologies that you have here that you think would be very valuable there, but are not
appropriate for that setting? Like pulse examiners, things that are stable technologies in the clinics
Ideh: What we need for managing malaria is to be able to rapid make diagnosis in the first place. Most
of these health centers now they do have the RDT kits and all of that, which is fine. Then we moved
onto artesunate and injectable interactivities. It is the best treatment now for sever malaria these are
also available in the health centers, they do have them. But they may not have the intense monitoring,
where children convulse and they are having to receive fluids, were they need lots of care in terms of
the manpower capacity they would probably have the difficulty coping with such intensive monitoring of
very ill children. We are able to do here because we got a good compliment of nurse and staff. We
have very good doctors, that’s the difference.
Molly: What other kind of monitoring would help, are there specific vitals that you think would?
Ideh: Yes of course, you already mentioned that you want to be able to know that the pulsimetry is fine,
that the blood pressure monitoring is fine, you want to be able to look at the biochemistry in the blood
weather the acidic or not. Things that can tell us about the acid base thetas in the child. The blood
sugar monitor, because hypoglycemia is also something that very regularly complicates sever malaria.
You want to have your BM sticks to monitor the blood sugar. So if you can monitor the blood sugar, you
can monitor your acid base balance, your hemoglobin concentration, and your food intake and output
you are basically good with a severe case of malaria.
Jackie: What about other in general, not just focusing on malaria, any cases?
Ideh: The same thing again. Let’s say I have got a very bad cardiac patent, I want to know what is
happening with the central pressures and all. If I have all those central monitoring systems, that would
be fine.
Molly: Do they have ways of doing this now or is it problems with continuous monitoring that is lacking?
Ideh: Well we don’t have continuous monitoring, because if we have those that are very sick that would
be like high dependence or some intensive kind of setup. Where you would have a very sick child, let’s
say from sever malaria, you need to set with a continuous monitoring or a respirator and all of that. If it
goes up, it alarms. Yes, that would be helpful. We do have an intensive care unit at the teaching hospital
but quite frankly for children I don’t know how equipped it is to handle any serious cases. Those kinds
of equipment are needed in intensive monitoring are basically lacking.
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight

Appendix 8 - Interview Transcript, Dr. Kalfa Bojang
Molly: How long have you worked here?
Bojang: At the MRC? Since ‘95, that makes it how many years now, 17 years.
Molly; Your working with malaria specifically?
Bojang: Yes, mainly malaria.
Molly: How long have you been doing that?
Bojang: Since I have been here.
Molly: What do you think are some of the biggest problems that you have currently facing you in
treating malaria?
Bojang: In treating malaria, one of the biggest problems is in resistance to antimalarial drugs. But,
fortionally we’ve got drugs thsat are effective. But event then the concern is those drugs will not be
able to beat resistance again. Like it has been reported in Southwest Aisa, artesunate I am sure you have
heard about it, they are the best drugs we have. You know the resistance has been reported in this
location. I think that is one of the problems. The second one is access to treatment when patients
probably come in late for some instances, although it is getting better. One hopes that if they come
earlier and get treated appropriately, they won’t develop severe malaria.
Molly: Is the biggest problem for getting people to the hospital in time, that they are treating
themselves or that they are diagnosing themselves or simply when it gets severe it’s too late. What is
the biggest problem in getting people here in time for treating?
Bojang: I think the serious problem is too late and you can save some, but with the limited facilities we
can have for intensive care. I guess if you have the facilities for intensive care we would revise some of
those people that would die. For most instances, if you catch them early and treat them propriety, it is a
fairly curable disease. But the problem is some of them they don’t get treated appropriately or they
don’t come early enough. So those are the key problems.
Molly: So once people come to the hospital with severe malaria are there cases were they are treated
apropriatelly and they die anyway?
Bojang: When they come to big centers they are usually treated appropriately but you know the
problem with malaria is sometimes you can treat them appropriately and they still die; once they reach
a certain stage, because of some of the toxins being produced, your antimalarial can get rid of the
parasites but they still, some of them will still die. In those incidences I am sure if you can support them
you know with intensive care or in terms of ventilation you I think it is possible to save some of them.
But we don’t have those facilities.
Blue
Highlight
Blue
Highlight
Blue
Highlight

Molly: And how often does that happen? Is that frequent?
Bojang: Well the mortality associated with severe malaria is quite high it is between 9-10% to as high a
20%
Molly: That is simply because it is too late?
Bojang: Most of the time it is to late but you know once you get to a critical state there are some people
who, for various reasons I don’t know, how some people they develop some kind of immunity to it as
well. There are people that depend on the individual that they may be able to control the parasites
better. There are others we don’t quite understand, when you treat them even once they go to the
hospitals, they get treated appropriately but some of them die because it’s a point of therapy but still
does not prevent them from dying
Molly: So we are actually developing a device that will use the magnetic properties to of the infected red
blood cells to essentially use a dialysis like treatment to just exclusively remove the infected red blood
cells and we are hoping that, that might impact in people with severe malaria and it would help very
quickly reduce the parasite load without drugs or in conjunction with drugs. Do you think that would be
a useful device for improving outcomes?
Bojang: How do you anticipate this being done, I mean how you are going to remove the damaged. I
don’t understand how are you, could you just explain it a little more?
Molly: So it is very much like dialysis so you are taking the blood out of the patient you are running it
through a filter that essentially has a strong magnetic field and as these particles flow through that field
it takes out the ones with malaria because how the parasite affects the cell, it makes just those cells
magnetic. So it will just take out the infected cells from the blood stream and then replace or return the
healthy cells. It’s like an exchange transfusion therapy but with selective removal of the infected cells
Bojang: There are two issues there one is the cost
Molly: So it would have a significant cost upfront but we hope to make it very cheap per treatment and
it is even possible to have it just use an autoclave for all the blood contacted acting parts.
Bojang: Eventually it would only be useful in facilities that have and intensive care you cannot just use
this sort of thing in a rural area.
Molly: So you think there is an issue with a disconnect were the patients who need it most are and were
the centers are that would be able to afford this technology?
Bojang: Yes, I think it needs to have to be very user friendly. If it is going to be useful
Molly: So what is the most common treatment for sever malaria is there a constant drug combination
that is used everywhere?
Bojang: Well there is a recommended drug, it’s Quinine, that most places use.
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Molly: Is it faster than Artesunate?
Bojang: This is what is available, but recently WHO has recommendations that we use artesunate but
artesunate is not widely available, only very few sites. We hope with time everybody will be using
Artesunate but for now I think most people are using Quinine. Because Artesunate is not widely
available but Artesunate is one that is fast acting and have some reduced mortality.
Molly: So is that ideal or is there another treatment that you know of that exists?
Bojang: That is the best treatment that we have. Yea, Artesunate is the best treatment we have.
Molly: So is there a certain population that gets more severe malaria. Like is it like younger, older, male,
female, is thee a tendency for?
Bojang: Yea young children generally and pregnant women. We have seen in the past there has been
mainly under five but we have seen the mean age has shifted. We think that it is probably due to
malaria incidences going down so older children and immunity has shifted it but generally children.
Molly: How long do these therapy’s take once they are emitted to the hospital or clinic.
Bojang: how long before it works?
Molly: How long do you hold them and treat them for before sending them home?
Bojang: Well the treatment has different components. One is the antimalarial and the second part is the
supporting treatment. The antimalarial usually with Quinine, can go up to seven days maximum, and
with the Artesunate its in a seven dose regiment and we are doing a study not to try and make it a three
day regiment.
Jackie: Are they in the hospital for this whole time?
Bojang: If they are unconscious yes or if they are very ill yes but once they are better, they are able to
take other treatment and they are mobile, depending on the bed space we can tell them to go home
early. but of course its not only because of the malaria, you may treat the malaria tell you remove all
the parasites from the body but they remain unconscious and they remain very sick. So they may still
remain in the hospital for support. Some of them are there for maybe as long as three weeks, only if
they remain unconscious, obviously you can’t send them home.
Jackie: So how common is it to stay, like what is the average stay for someone that comes in with severe
malaria?
Bojang: An average stay is from is usually to four days.
Molly: What kind of resource limitations do you face; do you have issues getting the proper amount of
drugs, transporting them appropriately are there cold change issues?
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Bojang: The biggest limit in treatment is getting blood for those with severe anemia. That is the main
issue right now. It is mainly the supporting treatment that we have troubles with, the antimalarial most
of the time is readily available but there are cases were we run out of it. For example, we run out of
glucose which is treatment for children with low sugar, which is a well-known complication with severe
malaria. Other complications is with it is severe anemia and the limited blood transfusions.
Molly: So for how does getting blood work, are there established donations facilities?
Bojang: Well there are donation facilities but most of the time they won’t have the blood be the
demand is very high. So if that doesn’t work you would have to ask relatives to donate, again you
would have to bleed them, make sure they match, and have adequate blood to donate. You also have to
screen them to make sure they don’t have an infection. Most of the time it is actually relatives that
provide the blood.
Molly: Is exchange transfusion done anywhere around here, for malaria?
Bojang: No
Molly: Do you think that’s, just as a therapy in general, aside from all of the lack of blood availability, do
you think that that is a reasonable treatment?
Bojang: No
Molly: Ok, Why?
Bojang: Because of the instance level involved and in not sure that there has been any big trial that has
shown it makes a difference. I know in the west I know in some individuals with high intensive care
units they probably do transfusions but not in any endemic countries
Molly: So where is the highest incidence of sever malaria just kind of in the region. Is it more upcountry
primarily?
Bojang: Do you mean in the country or in the region?
Molly: Let’s go with region, so how does malaria show as far as were people are admitted to clinics. Is it
more rural area or cities?
Bojang: I think in general malaria is in rural areas it depends on the geography of the area. I mean if you
go to places like Morgen which is in the desert, you are not going to find any malaria there and if you go
to big cities you that is the breading place for the parasite is not there. You are not going to find many
mosquitos you’re not going to find much malaria there. But if you are in urban areas were the breading
place for the mosquitos are there, you would find it. It really varies in some places even in urban areas,
you would find it but in general it tends to be in more rural areas
Blue
Highlight

Molly: I know there are a bunch of different broad approaches in dealing with malaria, there is vector
control, there is antimalarial there is all of these things in trying to understand transmission. Do you
think that there is one approach that is going to be more effective in curving malaria as a whole?
Bojang: No, I think you have to use a combination there is not only one approach, depending on the
setting approaches. The only one that if it works would be vaccination
Molly: Do you think, I guess it is an unfair question but do you think it would be in the near future?
Bojang: There is a vaccination in the next five years but it is partially effective, it’s not fully effective, so
even you would still need to use other tools.
Molly: What do you think are some of the biggest challenges that we will face with in malaria in the
future. Even if a vaccine is developed do you think that distribution and treatment is still going to be an
issue?
Bojang: Well it depends on how effective this vaccine is I mean this current vaccine is partially effective
but if you have a vaccine that is 100% effective then that would solve most of our problems but that is
unlikely in this be short term. We still need to continue using tools. The problems that are likely to
occur: one resistance to a new parasite to the antimalarial, two is resistance to the insecticides we use. I
mean those are the two biggest challenges we will face. Of course the other challenge is funding,
money. Part of the reason there has been great success in malaria control in endemic countries is more
resources have become available by many multinational donors. So we hope they continue and provide
a lot of results for all of these countries. but recently they said they did not have enough because of the
crises in the west.
Molly: So if cost is not a problem, with drug resistance being an increasing problem do you think then
this dialysis type removal of parasites could be useful?
Bojang: I think it would only be useful in limited cases. I could not see using it on a wide scale, again this
is quite intensive. How many patients can you put on dialysis? If you go into a ward and you have 30
patients with malaria. From what I am hearing this cannot be used on a wide scale. I guess you could use
if for selective patients who are very ill or who your drugs are not particularly working very well, but I
don’t imagine such a treatment that we use on such a wide scale.
Molly: As engineers it is difficult to find places to begin helping in health care because doctors
approaches are much more based in medicine obviously in the development of vaccines and this kind of
cell based research so as builders of devices how do you think that engineers could we contribute to the
work your doing.
Bojang: I think one you have to work with the people evolved in health care. From the very beginning
just as you were doing, just going around looking at the needs and the practical problems involved.
Because its well to have a device that works but how do you use it in practice? I think that is going to
become increasingly important. Take the Dialysis machine, dialysis has a lot of problems: maintaining
the equipment (you need a competent person to maintain it), is limited to do three patients at a time,
Blue
Highlight
Blue
Highlight

and the resources that are required are very expensive and very few people can afford it. It is useful but
it can only benefit very few people. It has to be cheap, whatever you do, unless you find someone to
undermine the cost but anything that is expensive it may be useful in particular settings in the west for
example those with severe malaria going back to the US. but if it is mint to be used in developing
countries, cost has to be an important factor. Two you have to consider its ethicacy to establish
treatment. For example is it going to be in addition to using antimalarial or is it going to be capered
with, were direction is you going are not clear?
Molly: It would be an addition to. The whole objective would be to just help the patients with the most
severe malaria come off the break of death essentially just by helping reduce parasite load.
Bojang: To do that you need to do a trial to compare using this alone and then using established
treatment and see how much how this would benefit, in medical terms you would have to do a cost
benefit analysis. You know the cost of the whole thing compared to how many lives you can save using
this. That is going to be the since of I mean if it is useful or not. In the US cost, may not be as important
of a factor as much as it is here so remember the budgets we have are very limited.
Molly: So can you describe some of the work you are doing right now, with the clinical trial?
Bojang: We are doing a malaria vaccination trial. it’s a new generation of vaccine that antimalarial we
are doing a trial to looking at better ways in preventing malaria pregnancy. The current
recommendations said that in pregnant women to have two to three doses of antimalarial during
pregnancy because this is how to prevent them. We want to see whether this is still useful to do that.
Instead of doing that we are doing an intermediate screening and treatment, so instead of giving
antimalarial when they come, we screen them with the rapid test. If they come back positive then we
treat them. The third trial we are doing is at the main hospital and we are trying to simplify the
Artesunate treatment regimen so the standard treatment is usually seven doses but now we are trying
to see because of the difficulties in giving daily doses. So that is the trials we are doing.
Molly: For the rapid diagnostic. How reliable are they at this point?
Bojang: They are fairly reliable actually. This is now used in a wide use in many countries now. There
sensitive and there specificity is very high, more than 90%. They do have its limitations but they are very
reliable.
Molly: For secretion in places after treatment. Is there any work being done in trying to develop
therapy’s for that?
Bojang: For secretion usually you can only find that out after they have died. When they are alive and
are unconscious it is assumed that they have secretion in the brain. It is an assumption and most of the
time it is right. There are several of test you can do by looking at the back of the eye being the
indication of secretion. But what you tend to do is treat the symptoms. Those symptomatic treatments
have not been effective. People have tried but none of them have made any substantial differences.
Blue
Highlight
Blue
Highlight
Blue
Highlight

They have tried steroids to counter the toxins in the body but they have not worked terribly well. Fluid
have been tried, but they haven’t particularly worked.
Molly: and the train you are doing with the vaccine, Is this the one you imagine getting certified in the
next five years?
Bojang: No another one. This one is still very far away. This one is looking at if it is safe or if it illiterates
some response in the body. The one that is likely to be certified has been in trial for more than 20 years
now. So it is in the late stage trials and it has been shown to work in many different trials providing
between 30-50% protections.
Molly: Where is that being developed?
Bojang: ESK a company based in Belgium. That is in collaboration with gates foundation. Gates have
been supporting them but trials have been taken place in many countries. Many of different African
countries, six.
Jackie: Do you know how long it takes for the drugs to kick in?
Bojang: Some of them react very rapid. Take Artesunate for example takes 30 min or so. But they are
not one doses treatments, you have to give several doses before you. It takes 24 to 48 hours with
Artesunate to completely clear the parasite.
Jackie: from what we have read the infected red blood cells exponentially increase. So within 30 min of
taking the drug it stops increasing the parasite load?
Bojang: Generally within the first 24 hours you see a decrease in the parasitic load.
Jackie: do you know how much you have to decrease the parasitic load before your body can take over
and defend for itself?
Bojang: I think it is more complicated than that. Although the amount of parasite in the body is an
important factor, it is in fact one of the criteria we use in diagnosing severe malaria. But remember that
malaria in your blood produces toxins as well. You could have relatively low parasites in your body but
yet you could have severe malaria. You could have loads of parasites in your body but yet you are
walking around. Some of it may be secretion in the brain. Like I said before that it produces toxins. One
of those toxins makes you ill. There has been studies done with different parasites, some parasite are
more violent than others, they produce more toxins then all or most of the parasites. Or most off the
parasites can be secreted in your brain or in different organs. If you look at the blood flow, it may
appear that you have less number. We don’t have an effective way of measuring the total number of
parasites in your body because that is one of the problems. Are the all secreted in numerous organs?
When is sometimes the case, postmortem we look at organs of people that have dies from malaria they
will show secretion in the very small vessels in your brain, when test show they has a small number of
parasites.
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Blue
Highlight
Molly: how do you define severe malaria? Is it the parasites in your blood?
Bojang: That is one level. There are many criteria, if you are unconscious then you have sever malaria. If
you have got severe anemia, the blood level is very low, that is one criteria. If your blood sugar is very
low, as well. There are very standard definitions.
Jackie: we also here that sometimes you go through rough patches, for maybe a month, were you would
run out of the drugs you need to treat malaria. Do you see that occurring?
Bojang: For severe malaria at least here we hardly run out of antimalarial and drugs. There was a few
years ago when there was a shortage in supply during the peak season. The resources were made
available for antimalarial not to run out. It was an issue with distribution when you do run out. But that
is logistics maybe someone did not order them on time or the stock levels are not monitored.
Molly: so I know that in some places counterfeit drugs are an issue, are antimalarial concluded in that?
Bojang: Yes certainly, it is a big problem. Major problems there are some sources expectually from
southwest Asia. I think it is a major issue there, even parts of Nigeria.
Okebe: In places where there are mutable places to get drugs you are likely to have a lot of counterfeit
drugs. In The Gambia most of the drugs you would get in the hospital, the government controls how the
drugs going.
Bojang: But it is a major issue in some places. Counterfeit drugs in general, including malaria, are a
major issue.
Molly: What Kind of issues think face health care in general as far as improving outcome, is it going to be
derived from water, sanitation, or is it how things are managed, if you could pick one problem in health
as a whole?
Bojang: I think there is only one dimension. If think if you improve people’s sores of climates condition
(?) then I think you will improve health care. So I think if you are able to give poverty (laugher) then you
can. Of course there are other simpler measures as well that will improve. For example there is an
outbreak in (??), I am sure if you can improve the water supply, I think that would go a long way. You
have to have improved water supply. Then of course, making medicine, not only for malaria, available.
The other huge issue is the cost actually. In here there is free health care but that’s going to be very
difficult to sustain in the long run because health care is expensive. For patients even moving
themselves, transporting themselves, from where they are to health facilities can be an issue. Supply of
medications you know sometimes hospitals do run out of it. In places where you have to pay and you
don’t have the money and then you can’t access that health care. I think there are many diminutions,
One I think making the treatment readily available. Two I think the main one if I have to pick I think
improve society’s climate conditions. If you could do that I think that would go a long way in improving
health care there are individual programs with malaria: with distributing bed nets, chemical
prophylactics, vaccines, and all sorts of those approaches as well. I mean you got other diseases as well
where there are simple approaches as well. But I think all those things will help up to a point I mean
certain diseases have been controlled in the west because of the general improvement. I think in the
clement conditions, if you achieve that I think you would go a long way. Even take in example here, you
know his child my child are less likely to die with malaria then somebody in a rural area because maybe
we could access treatment and maybe we know a bit more about malaria so the general education as
well will help.
Molly: I am teaching an capstone design course for the biomedical engineers back at Carnegie Mellon. If
you have any projects that you have that involve designs like I wish I had some kind of tube that would
these things. If you would have any design projects and if you are willing to offer a little bit of time, we
would have some students that would love to have kind of something that is more applicable to work
on. So, if you or anyone you know would like to have something built I can be in touch.
Bojang: Ok well what are some of the issues that have been looked at in the past is how to provide
oxygen cheaply to
Molly: So like an oxygen concentrator?
Bojang: Yes we have an oxygen concentrator, but the problem is they don’t last very long or if you could
make it durable or if you could make a big oxygen concentrator somewhere that provides oxygen, like
path oxygen, to hospitals. I think that would be something that is useful.
Okebe: The small ones could only serve a maximum two people because it would have to run for long
periods, like for four hours so the chemical pack goes very easy.
Bojang: I think if you could do that it would make a difference in many countries. If you have something
that is relatively cheap but concentrates oxygen that can be supplied to multiple patients.
Molly: What cheap would cheap be in this case?
Jackie: How much are oxygen concentrators, now?
Bojang: Oxygen concentrators are expensive I think they cost about at least 1000 dolor’s but of course
that is just the initial cost, the running cost is very low. If you would have something very, I would say
five to ten thousand dollars but could supply multiple patients and is durable I am sure some hospitals
would consider that, even slightly more than that. like the hospital or the ward have four oxygen
concentrators but there the maximum is eight and they don’t last that long a well. But if you could say a
concentrator somewhere that could supply ten patients and would last long, I think that would be quite
helpful.
Molly: That sounds like a fabulous project if I could get a team to accept that project would you be
willing to let them get in touch with you for design specifications?
Bojang: Sure

Appendix 9 - Interview Transcript from Dr. Joseph Okebe
Ok I feel really silly asking this but I am not familiar with what your work is?
Okebe: I am a clinician, I started out as a clinician but at the moment I am a PHD student doing preology
work, mostly. I have been here for a few years. Lastly I am doing the clinical side of things, preology
clinical trials, more or else, everything except lab work. It is all malaria based.
Molly: So are you out in the field often or do you mostly organize from here?
Okebe: I think a bit of both. At the moment most of the work happens in the field, and the field is found
on the other side of the country. We plan and then we go out into the field.
Molly: For your work, are you working more on the tracking and transmission or treatment ethnicity?
Okebe: For the period it is mostly tracking and transmission. In the overall project it looks at how to
identify and, more or less, observe how transmission works across the county and trying to tease out all
the things that are related, to in terms of the human factors, the vector factors, and the parasite factors.
If we are able to kind of understand how those three factors work together, then you could now think of
ideas of how to interrupt transmission. It’s all about looking at ways to understand how transmission
works, so that you can potentially interrupt it. For me I am focusing on mostly around trying to identify
areas were they supposable have transmission and not have transmission ant trying to figure out why
that is so. There are a few theories around that weather this is a real difference or is it because the
monitoring systems are just slightly different.
Molly: What monitoring system do you use?
Okebe: Well, at the moment what we use to track transmission, we are doing it at a health facility based
surveillance or a field based surveillance. For both of these you would add to the presents of parasites,
yes or no, presence of gametocytes, yes or no, or you look at antibodies too and how the antibody
accumulate throughout in populations, in exposer to malaria. Before now, these methods have been
run more like stand-alone systems. After what I am trying to do, is see how you can put them together
in a way that you don’t have to use all three, you can see which of the three works best and then you
can apply them.
Molly: Do you work at all with government workers in this effort or is this all through the MRC?
Okebe: Most of them is through the government because the government have the structure. We have
a separate system for malaria, which is kind of under the government. We provide technical support.
That is part of what we do and then most of the field works with the collaboration with that.
Mollt: As I understand, you have the hospitals, there are the city clinics, and there is kind of the lower,
are they village health workers or are they smaller sites? That is the one area that we did not get a good
picture of, can you describe it to me?
Blue
Sticky Note
Study of planning human development
Okebe: If you go from the top down, there is the teaching hospital and then there are the, well they call
them regional hospitals, so it’s only between the main hospitals and the health centers; there are
probably two or three across the country.
Molly: Brikama is one of the district hospitals?
Okebe: No Brikama is a health center. There is a hospital that is why they call them hospitals. There is
one in banafenadal and brand central. So they are kind of intermediate between the teaching hospitals
and the health centers. You have the bigger hospitals, like Brikama, where you are able to have efficient
services and there are some other smaller health centers that do mostly admissions and prenatal care.
Then below that, you have the health posts that are more of dispenser units. They come under the
health centers. The health centers have what is called tracking clinics, kind of outage visits. When they
do outages visits they’re at the health posts. Then below that you have the village health worker which
is where the primary point of access care is.
Molly: What kind of facilities or technical expertise do they have, the village health workers? What kind
of training do they undergo?
Okebe: They more or less have training on IMCI (Integrated Management of Childhood Illness). It is very
basic training to try to recognize that this child is ill. Not so much on what the diagnosis is but this child
is ill, this child is very ill. If you pick up a child, you would say, if they are ill you do this and if very ill do
this, that level of training. I know for malaria particularly there is a move towards trying to train them to
be able to make proper diagnosis in RDTs. In principal they have been trained but I think that the wall is
in having them use it, store them, account for it, and give them treatment. It is kind of a new addition to
what they are normally used too. How that it degrades with the rest of the health system is probably
what is causing the delays in them using it.
Molly: That is one of the efforts that I hear the malaria control program is working on is getting those
diagnosis test. Your working with the village health care level, for yours?
Okebe: No, not consistently, so it depends on what the requirements of the project are. Most of the
projects are at the level of the health centers. For the transmission studies we will probably have to go
back to the village workers, but we will see. It’s difficult because if the system of using RDC was already
in place then it would be easier to pick up cases because that is not yet, it does create more challenges
working with them.
Molly: We visited the Serekunda health center and that will fall under the category of?
Okebe: Health center
Molly: So that is the second tear before the referral
Okebe: Yes
Molly: now I think I have a better understanding of the complete system. I thing going through the
MRC, I haven’t been able to peace everything fully together. That was helpful, thank you.
Molly: As a clinician and a researcher you have kind of a unique prospective on where you can invitation
our device working. We have been playing with different ideas of where this device could fit in that
chain. All the patients with severe malaria, when they are coming into these clinics, it would be ideal if
they could go to the smaller facilities and get this treatment. At least we could reduce the parasitic level
for when they do go to the hospital. The capabilities of those clinics may be mismatched with the needs
for the device. Where do you think a device for this will best fit in this kind of chain of referrals?
Okebe: In an ideal setting you need to have the requirements for the machine; you need to have readily
accessible blood and electricity. The health center will, more or less, have electricity but the blood
processing will be a big challenge, in most of them. That will determine how low you can go in the
health system. For children that are unconscious and have sever malaria, in principal, you could treat
them with some kind of supported care, weather if they have antimalarial. Then for any reason they
require transfusion, then they will have to be referred to where they have access to that. That would
put a cap on where you could actually put the facility.
Molly: That is the very disconnect that we are struggling with right now
Jackie: I think we can optimize this so you won’t need blood transfusions because ideally as the parasite
reproduces it essentially bursts the red blood cells so if we take only the infected red blood cells out you
are only do the same thing as if you did not get treatment but even better because you are not
exponentially growing the parasitic load. Kind of where I think the problem is in taking it into the
smaller clinics is the training they have in cleaning the equipment. We have learned that as long as they
have the cleaning supplies they will do it. We don’t know if this had to come with cleaning equipment.
We are worried because if we are going to make it cheap we are not using disposable parts, you would
have to just clean the chamber every time you use it and we don’t know if that would actually get done.
Right now we hear that they don’t have the cleaning supplies so a lot of the utensils they clean with
soap and water and then just reuse them. With ours there is blood contact so you would have to clean
it. So that’s where the problem is.
Okebe: Yes, yes, I agree. With whatever you put up you will have to be sure that it is safe and even if it is
not wonderful it does not increase the amount of risk that the person would get. For everyone that has
severe malaria you get a drop in Hb, whatever happens. It will not increase the relative drop in Hb as if
you don’t do anything. If it does pull all the red cells out in like a half an hour the body probably may
not be able to adjust to, let’s say 2% of its RBC content. As oppose to what the antimalarial would do
which is maybe take 2-3 days. That is probably one of the things to think about. The technical bits
would now be could you autoclave it. If you do autoclaving, then are kind of limited to the facilities that
can autoclave. Well bottom line is, you have to decide how low on the health system you want to really
pitch it. You probably would not get it as low as you would probably want. In a country like The Gambia
where, of course, most of the treatment will happen at the health center so you probably want to see if
you are going to pitch it has to be somewhere in the health centers. It would work in a teaching hospital
setting but whether it will work in the health centers is the question.
Molly: What are the different between the health systems in The Gambia and the greater West Africa?
How does this compare to other local systems? I know The Gambia as a country is not a huge as some
of them, so how does the system compare?
Okebe: The main differences are that most of the health services are provided by the government
system, so we got that. But in other of the bigger countries or continents, you have the option of the
private care or of government standard care; it varies depending on so many things. Do you want a
hotel suite for a hospital sweet or something to get by. This will also determine where you wanted to
pitch it. In a since, The Gambia will probably represent what happens in most semi-urban and rural
settings in bigger countries, because it would, more or less, have just the government health centers in
place. In bigger cities people would probably go to private care rather than going to the government
hospitals, more of less because it is more one to one care. So that is probably what would happen even
for severe malaria cases, as well.
Molly: So do you think there would be a market in private care in larger countries?
Okebe: There would be a market in larger countries in both the hospitals and private care.
Molly: How do you see engineering interventions combining with medical because it still feels, like to
me, that they are still very separate: doctors are pursuing vaccines and epidemiology and engineers are
trying to build toys and widgets that people may never use because they just don’t communicate with
each other. How do you think that engineering and medicine could play along a little better to make
more of an impact in more rural places or for tropical health?
Okebe: When it comes to tropical medicine, the clinician uses his brain cells like 95% of the time, he has
to really think everything through. But in western countries, you press a button and all your results out.
Most of the equipment wouldn’t work here for lots of reasons but there are really no alternative options
for these supposable wonderful things. I mean they work but you just simply can’t use them here, you
can’t run them, the facilities to support them are not there. I think adapting what is available for
tropical setting would make a whole lot of difference. For me, one thing I would really like to see what
happen is the diagnoses of malaria. If you are working in a research facility you use RDT but if you are in
rural hospitals you use your brain cells. Microscopy has been around longer than most people can
imagine and it is supposed to be the reference. The problem with microscopy is it depends a lot on who
does the readings. So if you got a good pair of eyes like mine you would be able to pick up parasites but
really in most places people don’t put the slide on the microscope and it would just tell you I think it is
yes or I think it is no I think you need to more opportunities in the of that. The RDT’s are good but the
RDTs tell you yes or no, yes or no, but they don’t give you a quantity which is the advantage the
microcopy has. I would probably like to see something that challenges the microscopy results with
malaria diagnostics.
Molly: the reliability and the degree of severity?
Okebe: Yes! Yes!
Molly: For converting devices, how do you priorities because there are so many things that are valuable
in US clinics: like how can you not get by without only one blood oxygen finger thing were everybody in
every bed has this all the time? How do you prioritize what is most useful, first? We have been talking
to people here, we keep hearing that we have everything we need we just don’t have enough of it. It is
like these O2 machines work fine we just need four more!
Okebe: Yea it is like the MRC we need like an extra three or four more. I have working in Nigeria before
coming here. One thing is the clinician needs a whole lot of support to put together his diagnostic, so he
probably has an idea on what it is but he is never really for sure, that this is what it is. We ran a few
trials a few years ago were we had this machine were you could do blood chemistry analysis, point of
view, drop of blood, comes out after two minutes so you got all of your readings. It works but the
machine itself cost 7000 pounds. It works, its fine, it just needs batteries and you could run as many
samples as you want. But it is just too expensive. I have worked in a hospital where it takes two days to
get basic chemistry of your results, if you get it. I mean it is useless if you want to know what the Hb is
and you have to wait six hours. I would say to push more of the standard things because the standard
things are expensive and they are fancy and are more difficult to maintain. You should really have
something that is close to it but cheaper and adapted to this kind of setting.
Molly: I am helping to teach the capstone course at CMU for biomedical engineering and we are starting
to look into brooding there horizons with local clinicians. I would like for them to start looking more
globally. Do you have any design projects or ideas that, you know “it would be cool if we could have
this,” specifically translated into some kind of setting. I am going to go back and see if someone wants
to work on a less power consumption oxygen concentrator. So if you have any design projects like that I
think it would be wonderful to have people that are interested in offering to help with good ideas for
these students to work on because we just have not have contacts for finding these projects urban
Pittsburgh, so if you or if anyone you would be interested in having a team of students.
Okebe: I would have to think about what could happen back home in Nigeria. What comes to mind, I
train as a pediatrician so I talk small sizes, everything has to be calibrated in kg or lb it is always a tricky
business in working out blood, how much fluids, how much drug and how fast, and so on. What comes
to mind is some way of delivering more precise quantities of whatever you are giving; probably
something that looks like a nutrition pump, so you want to give x over this amount of time and
calibrates and it does that for you. What happened is it is always too fast and you wind it down and it’s
too slow. Everything is trying to correct for low blood sugar because you just can’t get it right with what
is available. You want to transfuse children and you want to give 30 ml of blood and the pediatric bag
gives 250 ml so the option you turn in 250 and then other problems. So those problems to help monitor
or give their fluids efficiently, is what I would think of back home in Nigeria.
Appendix 10- Images from the Serrekunda Clinic