From the salivary proteome to the OralOme: Comprehensive molecular oral biology
12
From the salivary proteome to the OralOme: Comprehensive molecular oral biology Nuno Rosa a, *, Maria Jose ´ Correia a , Joel P. Arrais c , Pedro Lopes c , Jose ´ Melo c , Jose ´ Luı ´s Oliveira c , Marlene Barros a,b a Health Sciences Institute, Portuguese Catholic University – Viseu, Portugal b Centre for Neurosciences and Cell Biology, University of Coimbra, Portugal c Department of Electronics, Telecommunications and Informatics (DETI), Institute of Electronics and Telematics Engineering of Aveiro (IEETA), University of Aveiro, Portugal 1. Introduction The human oral cavity is a complex ecosystem where host, microbial and external factors combine in a dynamic equilibrium which is reflected in saliva. The understanding of oral biology hinges upon the compilation and integration of all information generated by high-throughput techniques, particularly proteomic studies of saliva. Saliva is an aqueous biological fluid, with many and diverse functions, essential for the maintenance of healthy oral tissues. 1 It consists predominantly of water (99%) but includes a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x a r t i c l e i n f o Article history: Accepted 28 December 2011 Keywords: Saliva Salivary proteome Oralome Bioinformatics Oral biology Oral pathology Systems biology a b s t r a c t Objectives: There have been several efforts to identify the protein components of saliva. Some of these studies were conducted in healthy individuals and other in individuals with different oral and systemic disorders. However, a resource compiling and reviewing all of the proteins identified in proteomic studies is still lacking. The aim of this project is to develop such a resource. Design: The proteins identified by proteomic studies were compiled and all information concerning them was manually curated according to ‘‘IPI History search’’ and UniProt. Proteins were classified according to gene ontology using PANTHER. The involvement of each protein in disease was scrutinized using DAVID and a classification into protein disease classes was performed. Results: This survey of proteins in the oral cavity lead to the identification of 3397 non- redundant proteins, 605 altered in pathological conditions and 51 present only in disease. These proteins originate from different sources: 3115 from saliva, 990 from oral mucosa and 1929 from plasma. All protein sources contribute with different numbers and types of proteins to identical functions. However, each source produces specific proteins. Examples of the use of this proteomics database of saliva included the analysis of the changes in the proteome associated with periodontitis and a survey of systemic disease potential biomarkers in saliva. Conclusion: The database generated with this work and the information therein stands as a resource for investigators/clinicians studying the oral biology, searching for molecular disease markers, developing diagnostic and prognostic tests, and contributing to the dis- covery of new therapeutic agents. # 2012 Elsevier Ltd. All rights reserved. * Corresponding author at: Health Sciences Institute, Catholic Portuguese University, Estrada da Circunvalac ¸a ˜o, 3504-505 Viseu, Portugal. Tel.: +351 232430200; fax: +351 232428344. E-mail address: [email protected] (N. Rosa). AOB-2738; No. of Pages 12 Please cite this article in press as: Rosa N, et al. From the salivary proteome to the OralOme: Comprehensive molecular oral biology. Archives of Oral Biology (2012), doi:10.1016/j.archoralbio.2011.12.010 Available online at www.sciencedirect.com journal homepage: http://www.elsevier.com/locate/aob 0003–9969/$ – see front matter # 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.archoralbio.2011.12.010
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of From the salivary proteome to the OralOme: Comprehensive molecular oral biology
AOB-2738; No. of Pages 12
From the salivary proteome to the OralOme: Comprehensivemolecular oral biology
Nuno Rosa a,*, Maria Jose Correia a, Joel P. Arrais c, Pedro Lopes c,Jose Melo c, Jose Luıs Oliveira c, Marlene Barros a,b
aHealth Sciences Institute, Portuguese Catholic University – Viseu, PortugalbCentre for Neurosciences and Cell Biology, University of Coimbra, PortugalcDepartment of Electronics, Telecommunications and Informatics (DETI), Institute of Electronics and Telematics Engineering of Aveiro (IEETA),
University of Aveiro, Portugal
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x
a r t i c l e i n f o
Article history:
Accepted 28 December 2011
Keywords:
Saliva
Salivary proteome
Oralome
Bioinformatics
Oral biology
Oral pathology
Systems biology
a b s t r a c t
Objectives: There have been several efforts to identify the protein components of saliva.
Some of these studies were conducted in healthy individuals and other in individuals with
different oral and systemic disorders. However, a resource compiling and reviewing all of the
proteins identified in proteomic studies is still lacking. The aim of this project is to develop
such a resource.
Design: The proteins identified by proteomic studies were compiled and all information
concerning them was manually curated according to ‘‘IPI History search’’ and UniProt.
Proteins were classified according to gene ontology using PANTHER. The involvement of
each protein in disease was scrutinized using DAVID and a classification into protein disease
classes was performed.
Results: This survey of proteins in the oral cavity lead to the identification of 3397 non-
redundant proteins, 605 altered in pathological conditions and 51 present only in disease.
These proteins originate from different sources: 3115 from saliva, 990 from oral mucosa and
1929 from plasma. All protein sources contribute with different numbers and types of proteins
to identical functions. However, each source produces specific proteins. Examples of the use of
this proteomics database of saliva included the analysis of the changes in the proteome
associated with periodontitis and a survey of systemic disease potential biomarkers in saliva.
Conclusion: The database generated with this work and the information therein stands as a
resource for investigators/clinicians studying the oral biology, searching for molecular
disease markers, developing diagnostic and prognostic tests, and contributing to the dis-
covery of new therapeutic agents.
# 2012 Elsevier Ltd. All rights reserved.
Available online at www.sciencedirect.com
journal homepage: http://www.elsevier.com/locate/aob
1. Introduction
The human oral cavity is a complex ecosystem where host,
microbial and external factors combine in a dynamic
equilibrium which is reflected in saliva. The understanding
* Corresponding author at: Health Sciences Institute, Catholic PortugueTel.: +351 232430200; fax: +351 232428344.
E-mail address: [email protected] (N. Rosa).
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
0003–9969/$ – see front matter # 2012 Elsevier Ltd. All rights reservedoi:10.1016/j.archoralbio.2011.12.010
of oral biology hinges upon the compilation and integration of
all information generated by high-throughput techniques,
particularly proteomic studies of saliva.
Saliva is an aqueous biological fluid, with many and diverse
functions, essential for the maintenance of healthy oral
tissues.1 It consists predominantly of water (99%) but includes
se University, Estrada da Circunvalacao, 3504-505 Viseu, Portugal.
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
d.

a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x2
AOB-2738; No. of Pages 12
a complex mixture of electrolytes (sodium, potassium,
calcium, chloride, magnesium, bicarbonate and phosphate),
proteins (enzymes, immunoglobulins and other antimicrobial
factors, mucosal glycoproteins, albumin and other polypep-
tides and oligopeptides) and, in even smaller amounts, glucose
and nitrogenous products (urea and ammonia).2
The proteins present in whole saliva are secreted mainly
from 3 pairs of major salivary glands: the parotid, the
submandibular, and the sublingual, making up approximately
90% of total salivary secretion. The remaining proteins result
from the minor salivary glands (located at various oral mucosal
sites),3 the gingival crevicular fluid (GCF) and the oral mucosa
(including tongue and other oral mucosae). Saliva also has
plasmatic proteins. There are several ways by which plasma
proteins can reach saliva. The most common include passive
diffusion, ultrafiltration (which occurs through the tight
junctions between the cells) and as a result of GCF outflow.4
The complete role of salivary proteins in oral physiology
and as indicators of disease states is still poorly understood.
The determination of the salivary proteome enables not only
the functional characterisation of saliva, and thus the
clarification of its role in oral biology, but also the identifica-
tion of disease biomarkers. The fact that whole saliva includes
plasma derived proteins and exfoliated epithelial cells, has led
to the suggestion that it may in the future provide a means for
diagnosis of conditions that currently require blood or tissue
samples.
In the last decade, the development of powerful and
discriminating proteomics techniques, allowed an exponen-
tial increase in the identification of protein components of
saliva. Some studies include exclusively samples from healthy
individuals5–23 and others use samples from individuals with
several oral24–39 and systemic27,40–50 disorders. Despite the
vast amount of data generated, these are still scattered and
there is, no database publicly available with a compilation and
characterisation of the proteins identified by proteomic
studies. Bioinformatics tools have a key role in exploring
these data by modelling the inter-relationships between the
sequences, structures and functions of proteins, extracting
biological meaning from the data generated by these studies.51
The aim of this work was to compile and curate the
proteins reported in proteomic studies of saliva and charac-
terize the saliva proteome (OralOme). An integrated database
was created in a local repository and will be publically
available to the scientific community shortly.
We expect this study and the associated database to be a
valuable resource for investigators aiming to clarify the oral
biology, identify molecular disease markers, develop diagnos-
tic tests and improve prognostic, as well as providing
information for the design of biological pathways setting
the ground for the discovery of new therapeutic agents.
2. Materials and methods
2.1. Compilation and curation of human OralOme
To create the database the first step was to compile the
proteins identified in published proteomic studies of saliva
samples. We analysed several bibliographic references of
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
proteomic studies in which a complete lists of proteins was
provided.5–50 These studies used saliva from different sources
and are classified in Table 1 regarding sample type.
Because proteins present in whole saliva could originate
from blood transudates, we checked plasma proteomic
studies52,53 to verify which of the proteins present in salivary
proteomic results could have originated from the plasma. To
this subset of proteins we called the salivary plasma.
In this paper, ‘‘saliva’’ is the set of proteins identified by
proteomics techniques, obtained from salivary glands, crevi-
cular fluid and whole saliva samples. ‘‘Whole saliva’’ is
understood as saliva whose samples were not collected
directly from the gland ducts or the gingival crevice. The
proteins identified in the different studies were compared and
repeated entries eliminated. All proteins showing expression
changes in certain pathologies were stored with an indication
of up-regulation or down-regulation under these conditions.
Since there are differences in expression of proteins depen-
dent on donor age, whenever possible we also recorded the age
group for the sample donors.
We registered the existence and type of post translational
modifications of salivary proteins due to the crucial role these
may have in protein function and consequently in oral
physiology.
From the first publication of saliva proteomes, many of the
original identified proteins, catalogued as different entries in
biological databases, have been merged with others and some
were deleted due to misidentification. Therefore, all informa-
tion concerning the identified proteins was manually curated
and updated as of February 2011. The update of the IPI
(International Protein Index) entries was carried out with ‘‘IPI
History search’’ tool (http://www.ebi.ac.uk/IPI/IPIhelp.html).54
All other updates have been made according to UniProt
database (http://www.uniprot.org/).55,56 The curated list of
proteins identified in this work was stored in the database
OralCard—Web Information System for Oral Health developed
for this purpose.
2.2. Human saliva proteome cataloguing
2.2.1. Gene ontology (GO) analysisThe proteins in the database were classified according to
molecular function, biological process and cellular component
by using the PANTHER database (http://www.pantherdb.org/
).57,58 PANTHER is a unique resource that classifies genes and
proteins by their functions, using published scientific experi-
mental evidence and evolutionary relationships inferred by
curators with the goal of predicting function even in the
absence of direct experimental evidence. PANTHER applies
both software tools and manual curation to perform these
inferences as accurately as possible, and to keep them up-to-
date as new experimental results accumulate. To accomplish
this task we conducted a Batch ID Search with the PANTHER
Classification Tool for each group of proteins, using the AC
UniProtKB identifiers (without protein isoforms). We also used
the PANTHER gene expression data analysis tool to compare
classifications of multiple clusters of lists with a reference list
(total number of human proteins in PANTHER database) to
statistically determine over- or under-representation of
PANTHER classification categories. Each list is compared to
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
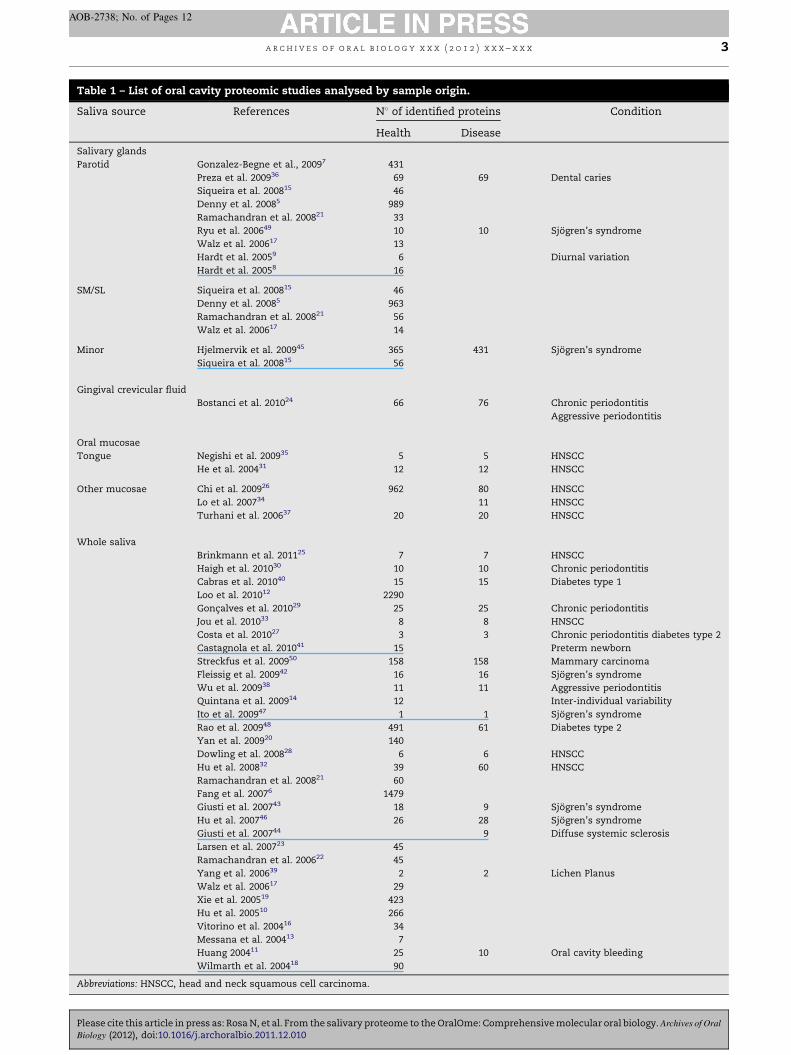
Table 1 – List of oral cavity proteomic studies analysed by sample origin.
Saliva source References N8 of identified proteins Condition
Health Disease
Salivary glands
Parotid Gonzalez-Begne et al., 20097 431
Preza et al. 200936 69 69 Dental caries
Siqueira et al. 200815 46
Denny et al. 20085 989
Ramachandran et al. 200821 33
Ryu et al. 200649 10 10 Sjogren’s syndrome
Walz et al. 200617 13
Hardt et al. 20059 6 Diurnal variation
Hardt et al. 20058 16
SM/SL Siqueira et al. 200815 46
Denny et al. 20085 963
Ramachandran et al. 200821 56
Walz et al. 200617 14
Minor Hjelmervik et al. 200945 365 431 Sjogren’s syndrome
Siqueira et al. 200815 56
Gingival crevicular fluid
Bostanci et al. 201024 66 76 Chronic periodontitis
Aggressive periodontitis
Oral mucosae
Tongue Negishi et al. 200935 5 5 HNSCC
He et al. 200431 12 12 HNSCC
Other mucosae Chi et al. 200926 962 80 HNSCC
Lo et al. 200734 11 HNSCC
Turhani et al. 200637 20 20 HNSCC
Whole saliva
Brinkmann et al. 201125 7 7 HNSCC
Haigh et al. 201030 10 10 Chronic periodontitis
Cabras et al. 201040 15 15 Diabetes type 1
Loo et al. 201012 2290
Goncalves et al. 201029 25 25 Chronic periodontitis
Jou et al. 201033 8 8 HNSCC
Costa et al. 201027 3 3 Chronic periodontitis diabetes type 2
Castagnola et al. 201041 15 Preterm newborn
Streckfus et al. 200950 158 158 Mammary carcinoma
Fleissig et al. 200942 16 16 Sjogren’s syndrome
Wu et al. 200938 11 11 Aggressive periodontitis
Quintana et al. 200914 12 Inter-individual variability
Ito et al. 200947 1 1 Sjogren’s syndrome
Rao et al. 200948 491 61 Diabetes type 2
Yan et al. 200920 140
Dowling et al. 200828 6 6 HNSCC
Hu et al. 200832 39 60 HNSCC
Ramachandran et al. 200821 60
Fang et al. 20076 1479
Giusti et al. 200743 18 9 Sjogren’s syndrome
Hu et al. 200746 26 28 Sjogren’s syndrome
Giusti et al. 200744 9 Diffuse systemic sclerosis
Larsen et al. 200723 45
Ramachandran et al. 200622 45
Yang et al. 200639 2 2 Lichen Planus
Walz et al. 200617 29
Xie et al. 200519 423
Hu et al. 200510 266
Vitorino et al. 200416 34
Messana et al. 200413 7
Huang 200411 25 10 Oral cavity bleeding
Wilmarth et al. 200418 90
Abbreviations: HNSCC, head and neck squamous cell carcinoma.
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x 3
AOB-2738; No. of Pages 12
Please cite this article in press as: Rosa N, et al. From the salivary proteome to the OralOme: Comprehensive molecular oral biology. Archives of Oral
Biology (2012), doi:10.1016/j.archoralbio.2011.12.010
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x4
AOB-2738; No. of Pages 12
the reference list using the binomial test59 for each GO cellular
component, molecular function or biological process term in
PANTHER.
2.2.2. Disease associationHuman saliva and plasma proteins were scrutinized for their
involvement in diseases and grouped into protein disease
classes by the use of DAVIDBioinformatics Resources 6.7 (http://
david.abcc.ncifcrf.gov/home.jsp).60,61 DAVID bioinformatics
resources consist of an integrated biological knowledgebase
and analytic tools aimed at systematically extracting biological
meaning from large gene/protein lists. For this task, the lists of
proteins derived from the saliva, salivary plasma (plasma
proteins found in saliva) and total plasma (all plasma proteins)
were subjected to Functional Annotation Tool. The proteins
were annotated according to ‘‘genetic association database
disease class’’ and presented as a ‘‘chart report’’. This is an
annotation-term-focused view which lists annotation terms
and their associated genes under study. To avoid over counting
duplicated genes, the Fisher exact statistics is calculated based
on corresponding DAVID gene IDs by which all redundancies in
original IDs are removed. All results of the Chart Report have to
pass the thresholds (by default, Max.Prob. � 0.1 and Min.-
Count � 2) in the Chart Option section to ensure only statisti-
cally significant ones are displayed.
3. Results
3.1. Compilation and curation of human oral proteome
This work leads to the documentation of 3397 non-
redundant proteins that may be found in the oral cavity.
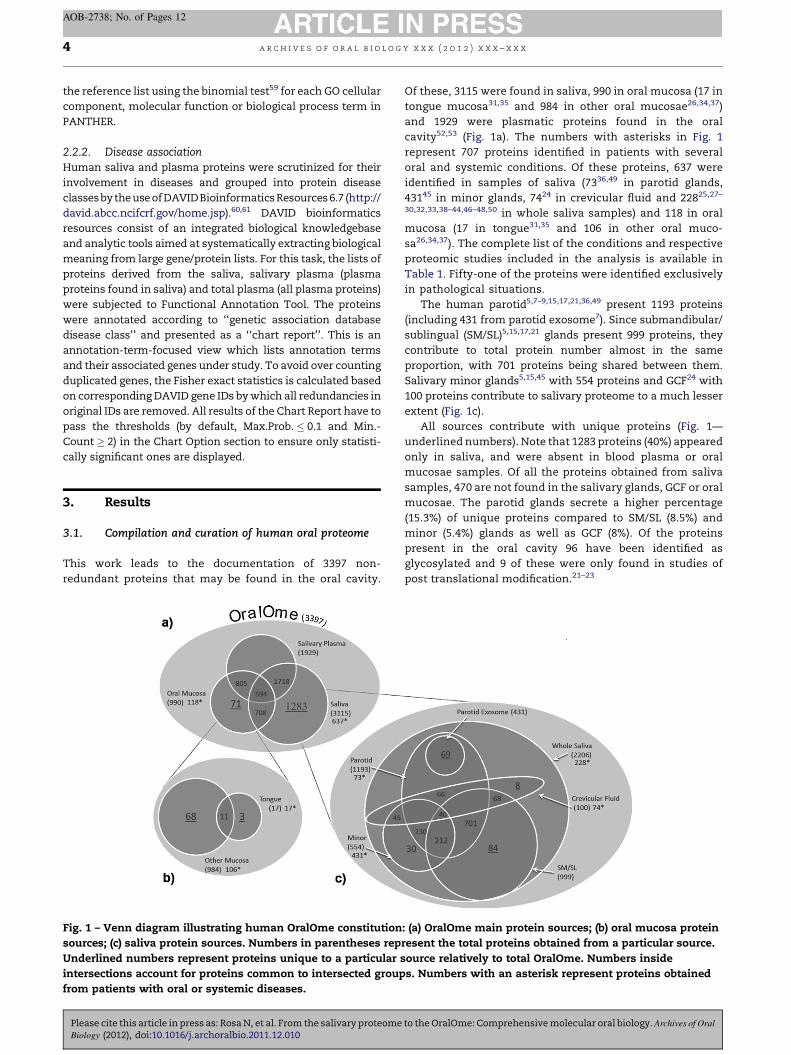
Fig. 1 – Venn diagram illustrating human OralOme constitution
sources; (c) saliva protein sources. Numbers in parentheses rep
Underlined numbers represent proteins unique to a particular s
intersections account for proteins common to intersected group
from patients with oral or systemic diseases.
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
Of these, 3115 were found in saliva, 990 in oral mucosa (17 in
tongue mucosa31,35 and 984 in other oral mucosae26,34,37)
and 1929 were plasmatic proteins found in the oral
cavity52,53 (Fig. 1a). The numbers with asterisks in Fig. 1
represent 707 proteins identified in patients with several
oral and systemic conditions. Of these proteins, 637 were
identified in samples of saliva (7336,49 in parotid glands,
43145 in minor glands, 7424 in crevicular fluid and 22825,27–
30,32,33,38–44,46–48,50 in whole saliva samples) and 118 in oral
mucosa (17 in tongue31,35 and 106 in other oral muco-
sa26,34,37). The complete list of the conditions and respective
proteomic studies included in the analysis is available in
Table 1. Fifty-one of the proteins were identified exclusively
in pathological situations.
The human parotid5,7–9,15,17,21,36,49 present 1193 proteins
(including 431 from parotid exosome7). Since submandibular/
sublingual (SM/SL)5,15,17,21 glands present 999 proteins, they
contribute to total protein number almost in the same
proportion, with 701 proteins being shared between them.
Salivary minor glands5,15,45 with 554 proteins and GCF24 with
100 proteins contribute to salivary proteome to a much lesser
extent (Fig. 1c).
All sources contribute with unique proteins (Fig. 1—
underlined numbers). Note that 1283 proteins (40%) appeared
only in saliva, and were absent in blood plasma or oral
mucosae samples. Of all the proteins obtained from saliva
samples, 470 are not found in the salivary glands, GCF or oral
mucosae. The parotid glands secrete a higher percentage
(15.3%) of unique proteins compared to SM/SL (8.5%) and
minor (5.4%) glands as well as GCF (8%). Of the proteins
present in the oral cavity 96 have been identified as
glycosylated and 9 of these were only found in studies of
post translational modification.21–23
: (a) OralOme main protein sources; (b) oral mucosa protein
resent the total proteins obtained from a particular source.
ource relatively to total OralOme. Numbers inside
s. Numbers with an asterisk represent proteins obtained
to the OralOme: Comprehensive molecular oral biology. Archives of Oral

a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x 5
AOB-2738; No. of Pages 12
3.2. Characterisation of human oral proteome
The human proteins present in the oral cavity have several
origins including the salivary glands, oral mucosa and even
blood plasma. The proteins associated to each of these
compartments were characterised according to diverse
aspects including cellular component, molecular function
and biological process in order to understand their functional
organization.
3.2.1. Saliva, oral mucosae and salivary plasma proteinscomparisonWhen the different sources of oral cavity proteins are
compared according to cellular component (GO: 0005575 –
‘‘The part of a cell or its extracellular environment in which a gene
product is located’’) (Fig. 2a) we found that most of the proteins
in the OralOme are intracellular. Most of these intracellular
proteins are derived from the oral mucosa (60.2%), which also
contributes to the oral proteome with a higher percentage of
ribonucleoprotein complexes (12.4%) than saliva (5.9%) and
salivary plasma (7.7%). Furthermore, we can see that the oral
cavity has a large percentage of protein complexes (almost
twice what would be expected relative to total human
proteins).
A comparison of the different sources of oral cavity
proteins regarding molecular function (GO: 0003674 – ‘‘Elemen-
tal activities, such as catalysis or binding, describing the actions of a
gene product at the molecular level’’), using PANTHER Classifica-
tion System is presented in Fig. 2b. In saliva, oral mucosa and
salivary plasma, proteins participate in the same sort of
functions. However, each source contributes with a different
number and type of proteins that participate in common
functions, which reflects the specific role of each of these
sources to salivary functions.
Fig. 2b shows that a large percentage of the proteins present
in the oral cavity are involved in the molecular functions
‘‘catalytic activity’’ and ‘‘binding’’. Because some proteins can
have more than one function, we tried to find which of the
proteins with catalytic and binding activities are also involved
in other molecular functions (Fig. 2c). We confirmed that the
molecular functions ‘‘catalytic activity’’ and ‘‘binding’’ are
quite broad and redundant since the proteins involved in them
also have other activities. Note that many proteins with
catalytic activity also have binding activity. Likewise, many of
the proteins with binding activity are also structural mole-
cules, enzyme regulators or have catalytic activity, amongst
other functions.
Looking at the antioxidant function we see that, despite the
small percentage of proteins involved in it, all sources
contribute with proteins to carry out this important function
of saliva. Furthermore, the oral cavity has a higher percentage
(almost four times, p � 0.05) of proteins with antioxidant
activity than would be expected relative to total human proteins
(results not shown). The contribution of each source of OralOme
to the antioxidant activity function is almost the same (salivary
plasma 35%, saliva 30% and oral mucosae 30%). More interesting
is the fact that amongst the plasma proteins with antioxidant
function, almost all appear in the oral cavity (salivary plasma).
Only 5% of all plasma proteins with antioxidant function are not
present in the oral cavity (Fig. 2b—pie chart). We can also see
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
that some of these proteins with antioxidant function (e.g.
glutathione peroxidase and extracellular superoxide dismutase
[Cu–Zn]), are produced in all sources of saliva, except in the
crevicular fluid (Fig. 3b).
3.2.2. Human saliva protein sourcesMost of the proteins present in OralOme come directly from
saliva sources (major and minor salivary glands and GCF).
Thus, these proteins have a prominent role in saliva functions
and consequently in oral biology. In order to evaluate the
specific contribution of different saliva sources to the saliva
functions, we investigated the molecular functions of the
proteins produced from each source and the biological
processes (GO: 0008150 – ‘‘Any process specifically pertinent to
the functioning of integrated living units: cells, tissues, organs, and
organisms. A process is a collection of molecular events with a defined
beginning and end’’) in which they are involved, using PANTHER
Classification System (Fig. 3). The proteins produced by the
major and minor salivary glands contribute to the same
molecular functions. However, the number of proteins
dedicated to each molecular function varies slightly amongst
the major salivary gland proteins and at a greater degree,
between the proteins of all the major salivary glands and the
proteins of the minor ones. This variation consists mainly of
an increase in the number of proteins involved in catalytic and
structural activities and a decrease in the number of proteins
involved in enzyme regulatory and receptor activities (Fig. 3a).
The gingival crevicular fluid does not contain proteins
involved in ion channel and receptor activities neither
translation regulator activity. Furthermore, the number of
proteins from GCF with structural molecular activity is
markedly increased in relation to the proteins produced by
the salivary glands. We can also observe a sharp increase in
the number of unique proteins in GCF with transcription
regulatory activity (Fig. 3b).
Regarding biological processes involving proteins obtained
from each saliva source, it appears that they are very similar
and only the gingival crevicular fluid differs significantly
compared to other sources (Fig. 3c). Note that the GCF has an
increase of proteins involved in response to stimuli (8.4%
versus 5.9% of whole saliva) but has almost the same
percentage of proteins engaged in the ‘‘immune system
process’’ as other saliva sources. Moreover, we observed that
most proteins involved in immune response in saliva, were
also present in plasma (results not shown). Another difference
is that minor salivary glands produce a higher percentage
(25.1% versus 18% in parotid, 19.6% in SM/SL and 14.8% in GCF)
of proteins involved in metabolic processes.
3.3. Strategies for the analysis of molecular changes indisease
One of the most interesting uses of a database compiling all
the proteomic data available for the oral cavity is to enable the
analysis of proteomics data. This database is fundamental to
detect the possible changes in the quantity and type of
proteins present in saliva samples from diseased individuals.
This kind of approach allows the identification of functions/
biological processes compromised in the pathologies ana-
lysed. In Fig. 4 we show the classification of the proteins
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
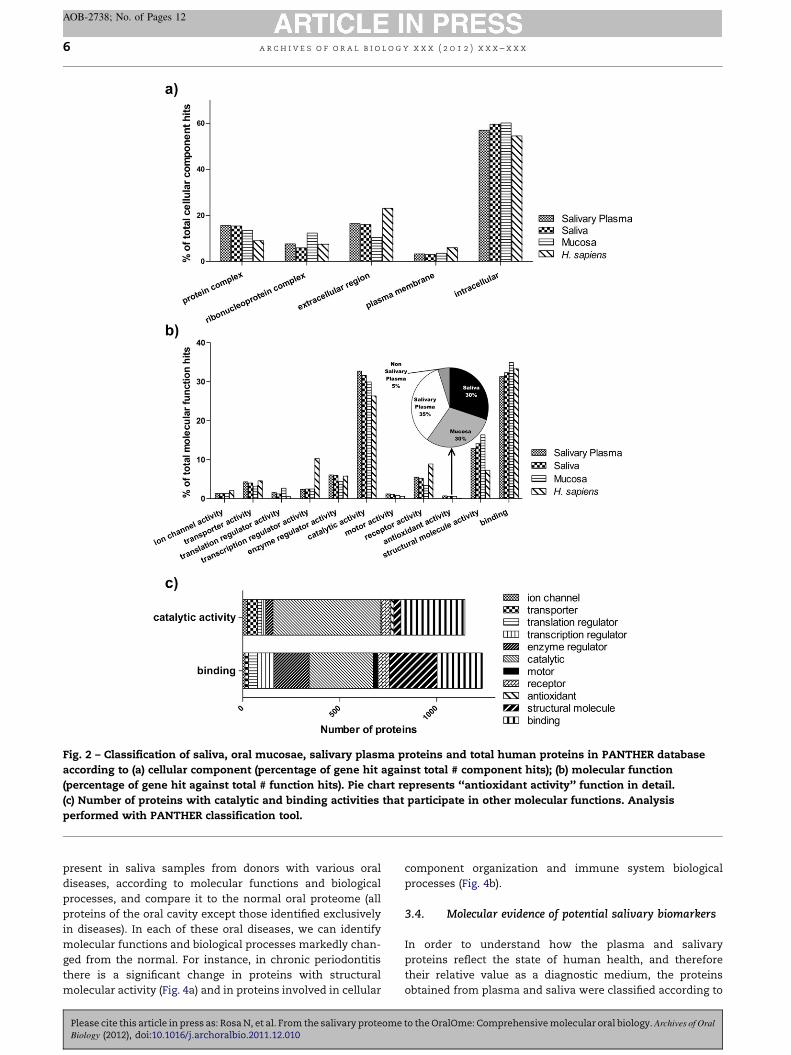
Fig. 2 – Classification of saliva, oral mucosae, salivary plasma proteins and total human proteins in PANTHER database
according to (a) cellular component (percentage of gene hit against total # component hits); (b) molecular function
(percentage of gene hit against total # function hits). Pie chart represents ‘‘antioxidant activity’’ function in detail.
(c) Number of proteins with catalytic and binding activities that participate in other molecular functions. Analysis
performed with PANTHER classification tool.
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x6
AOB-2738; No. of Pages 12
present in saliva samples from donors with various oral
diseases, according to molecular functions and biological
processes, and compare it to the normal oral proteome (all
proteins of the oral cavity except those identified exclusively
in diseases). In each of these oral diseases, we can identify
molecular functions and biological processes markedly chan-
ged from the normal. For instance, in chronic periodontitis
there is a significant change in proteins with structural
molecular activity (Fig. 4a) and in proteins involved in cellular
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
component organization and immune system biological
processes (Fig. 4b).
3.4. Molecular evidence of potential salivary biomarkers
In order to understand how the plasma and salivary
proteins reflect the state of human health, and therefore
their relative value as a diagnostic medium, the proteins
obtained from plasma and saliva were classified according to
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
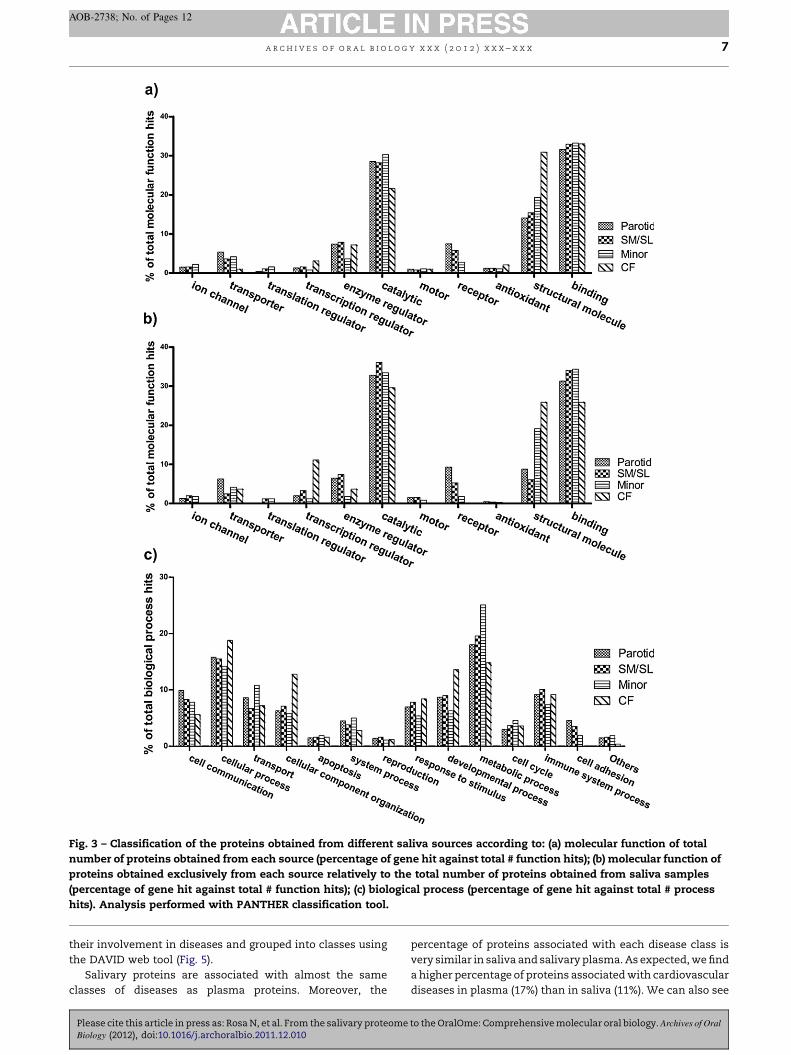
Fig. 3 – Classification of the proteins obtained from different saliva sources according to: (a) molecular function of total
number of proteins obtained from each source (percentage of gene hit against total # function hits); (b) molecular function of
proteins obtained exclusively from each source relatively to the total number of proteins obtained from saliva samples
(percentage of gene hit against total # function hits); (c) biological process (percentage of gene hit against total # process
hits). Analysis performed with PANTHER classification tool.
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x 7
AOB-2738; No. of Pages 12
their involvement in diseases and grouped into classes using
the DAVID web tool (Fig. 5).
Salivary proteins are associated with almost the same
classes of diseases as plasma proteins. Moreover, the
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
percentage of proteins associated with each disease class is
very similar in saliva and salivary plasma. As expected, we find
a higher percentage of proteins associated with cardiovascular
diseases in plasma (17%) than in saliva (11%). We can also see
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
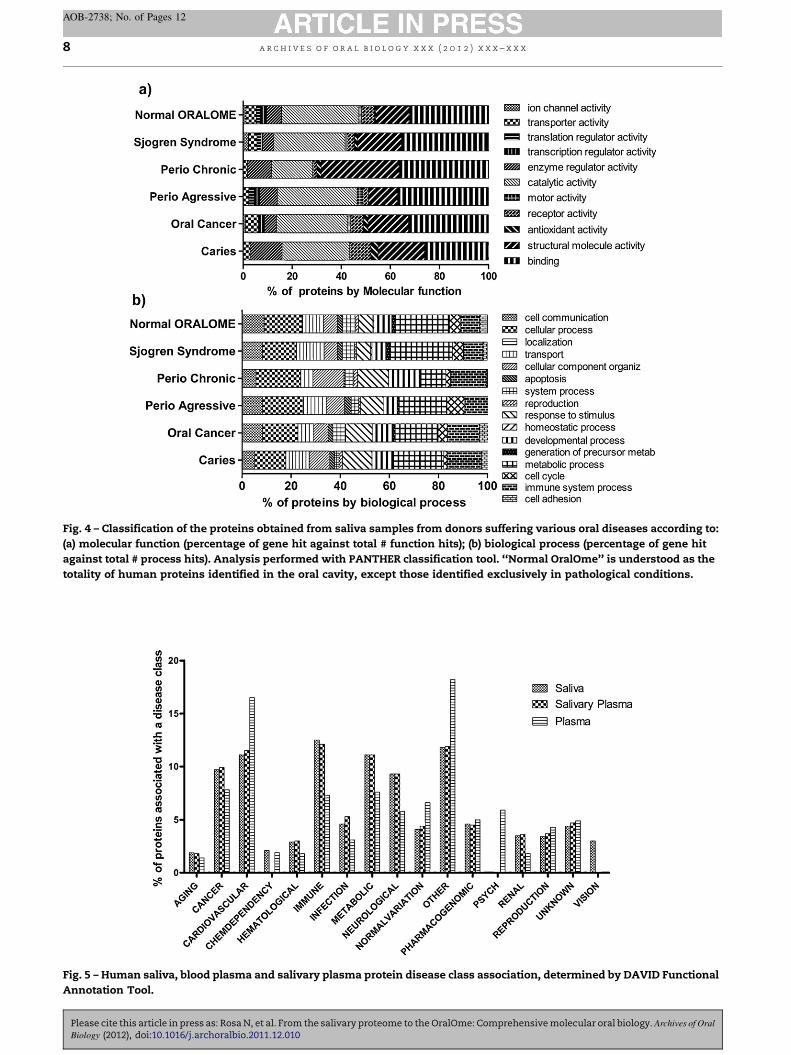
Fig. 4 – Classification of the proteins obtained from saliva samples from donors suffering various oral diseases according to:
(a) molecular function (percentage of gene hit against total # function hits); (b) biological process (percentage of gene hit
against total # process hits). Analysis performed with PANTHER classification tool. ‘‘Normal OralOme’’ is understood as the
totality of human proteins identified in the oral cavity, except those identified exclusively in pathological conditions.
Fig. 5 – Human saliva, blood plasma and salivary plasma protein disease class association, determined by DAVID Functional
Annotation Tool.
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x8
AOB-2738; No. of Pages 12
Please cite this article in press as: Rosa N, et al. From the salivary proteome to the OralOme: Comprehensive molecular oral biology. Archives of Oral
Biology (2012), doi:10.1016/j.archoralbio.2011.12.010

a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x 9
AOB-2738; No. of Pages 12
that there is a higher percentage of proteins associated with
immune system diseases in saliva (13%) than in plasma (7%).
More unusual is the presence of a higher percentage of proteins
related to neurological diseases in saliva (9.3%) than in plasma
(5.8%). In fact, we find, in saliva, an extensive range of proteins
involved in Alzheimer’s, Parkinson’s and Huntington’s disease.
Our analysis also identified salivary proteins involved in
diseases related to vision, which did not appear in plasma, as
is the case of ornithine aminotransferase (P04181), which, when
defective, is responsible for hyperornithinemia with gyrate
atrophy of choroid and retina (HOGA) [MIM:258870].
4. Discussion
4.1. Compilation and curation of human OralOme
Most of the attempts to elucidate the oral proteome, have
consisted of very specific studies focused on particular
situations24–50 or more general studies where saliva is
collected in well-defined conditions.7–20,24,25 Some attempts
were made at a broader approach. The first of these attempts
was by Denny et al. in 2008.5 They identified 1166 proteins
from saliva samples collected directly from major salivary
glands, developing the Salivary Proteome Knowledge Base.
Loo et al. compiled 2290 proteins in saliva12 and compared
it with proteins identified in plasma. Another workgroup, led
by Li, published a body fluid database62 that includes salivary
proteins (Sys-BodyFluid). Despite the innovative attempt to
integrate information from the application of proteomics to
different body fluids, the data pertaining to saliva was limited
to eight studies conducted from 2004 to 2008, identifying 2161
proteins. In the Sys-BodyFluid database the proteins were
classified with the IPI code, which is now discontinued and
hinders the match of these proteins with those stored in the
major protein databases such as UniProtKB. It is known that
saliva is more complex than what is secreted by the salivary
glands and may have proteins from the oral mucosa and even
blood plasma. Our database includes proteins from all of these
sources both under physiological and pathological conditions.
This database offers more than just a list of proteins including
further information on each protein.
4.2. Saliva, oral mucosae and salivary plasma proteinscomparison
The amount and type of proteins obtained from each of the
oral protein sources, elucidates their contribution to the
physiology of the oral cavity leading to the interpretation of
the OralOme. Saliva, oral mucosa and plasma proteins
probably participate in the same sort of functions. However,
each source contributes with a different set of proteins. All
sources have unique proteins that may indicate specific
functions carried out by them and therefore, a particular role
in the oral cavity physiology. Since some proteins found in the
oral cavity are not found in the salivary glands, GCF or oral
mucosae, we set forth the hypothesis that, because the
salivary gland acinar complexes are ‘‘leaky’’ epithelia, many of
these proteins must come from plasma entering in saliva by
diffusion across tight junction complexes.
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
We noted that a large percentage of the proteins that
appear in the oral cavity are intracellular and are derived from
the oral mucosa, which is not surprising considering that
saliva collects a large number of proteins resulting from the
constant scaling that occurs in the oral cavity both from oral
mucosa and salivary gland ducts. Other evidence that
supports this is the fact that our results indicate that the
mucosa contributes to the oral proteome with a higher
percentage of ribonucleoprotein complexes than saliva and
salivary plasma, presumably due to cell lysis. It is well
established that ribosomes are abundant in the cell and it is
estimated that the majority of eukaryotic cellular RNA is
ribosomal RNA. So, there is a great contribution, in terms of
the mass, of these proteins to the whole cell content.
Moreover, we saw that the oral proteome has a percentage
of protein complexes higher than what would be expected
relative to total human proteins. We propose that this reflects
the supramolecular complexes existing in the complex
membrane organelle system and in the rough endoplasmic
reticulum and therefore structures which are intracellular.
Although most of the proteins present in the oral cavity are
involved in ‘‘catalytic activity’’ and ‘‘binding’’ these functions
are not necessarily the most representative. These functions
are quite broad and redundant since the proteins involved in
them also have other activities. This is a good example of the
difficulties that still exist in the cataloguing of protein
functions, as well as, the definition of the different ontologies,
that can lead to the misinterpretation of results.
The higher percentage of proteins with antioxidant activity
observed in the oral cavity in relation to total human proteins
is probably explained by the fact that the oral cavity is
particularly exposed to oxidative stress.63
4.3. Human saliva protein sources
The absence of proteins in gingival crevicular fluid involved in
ion channel and receptor activities can be explained by the
fact they are essentially integral membrane proteins, and
therefore cannot be released to the extracellular fluid which
composes the GCF. Moreover, the absence of proteins with
translation regulator activities from the GCF may be related to
the lower percentage of proteins with this function, found in
blood plasma, since the GCF is formed when fluid exudes from
the vessels of the microcirculation into the sulcus or dental
pocket.64 The GCF exhibits a marked increase in the number of
proteins with structural molecular activity when compared to
the proteins produced by the salivary glands. This fact is
probably due to the remodelling of extracellular matrix
occurring in healthy periodontium and to the increased
degradation of this matrix observed in oral diseases such as
periodontitis.65 Proteins resulting from this degradation
accumulate in the GCF.
The observed higher number of unique proteins in GCF
with transcription regulatory activity reflects the need for an
increased protein synthesis in order to offset the degradation
taking place in gingival crevice which is consistent with the
increase in cellular processes and cellular component organi-
zation processes observed in GCF.
The increase of proteins identified in GCF involved in the
response to stimuli could be explained by the fact that the
to the OralOme: Comprehensive molecular oral biology. Archives of Oral

a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x10
AOB-2738; No. of Pages 12
gingival sulcus is a ‘‘war zone’’ where the response of the host
tissue to microbial challenges is present.66 On the other hand, it
is strange that the GCF has almost the same percentage of
proteins engaged in the ‘‘immune system process’’ as other
saliva sources. These results suggest that, in the GCF the result
of ‘‘war’’ is more noticeable than the ‘‘warriors’’ themselves. In
other words, the GCF may be a good medium for studying the
degradome resulting from the host’s immune response to
microbial aggression. This is corroborated by the fact that there
is an increased amount of GCF produced in periodontal
disease24 and, in this instance, periodontal pockets comprise
not only the microorganisms growing in the sulcus, but also the
result of an overly aggressive immune response against these
microorganisms. Due to the equal participation of different
sources of saliva in the immune response, we can also speculate
that the participation in the ‘‘immune system process’’ is
shared by the whole saliva (because of its importance) and the
proteins involved can be recruited from plasma by infiltration in
the epithelium of glands and oral mucosa. The presence in
plasma of most of the proteins involved in immune response
carried out in saliva supports that idea.
With this work, we found that all sources of saliva,
especially the minor salivary glands, have a high percentage
of proteins involved in metabolism. This reveals the interest in
saliva as an object in metabolomics studies and in the
understanding of the molecular mechanisms of diseases
related to defects in metabolism, such as diabetes. Most of the
glycosylated proteins found in oral cavity, are involved in
metabolic diseases. This influence is through their role in the
complement and coagulation cascades pathways (results not
shown). Alterations in these pathways are known to be related
with poor wound healing.67 The characteristic diabetic
hyperglycaemic state may favour the glycosylation68 of the
proteins present in saliva and therefore be responsible for the
difficulty in healing observe in the oral cavity of diabetic
patients.
4.4. Strategies for the analysis of molecular changes indisease
The analysis of proteomics data revealing changes in the
quantity and type of proteins present in the saliva of diseased
patients can lead to the identification of functions/biological
processes compromised in these conditions. This analysis is
substantially easier and more reliable if there is a methodology
that can be reproduced in different situations, eliminating most
of the analyser’s subjectivity. We presented an example of how
proteomics data can be analysed and interpreted. This approach
allowed us to identify molecular support for the importance of
proteins involved in cellular component organization and
immune system biological processes as well as structural
molecular functions in the molecular mechanisms of periodon-
titis. Further analyses may lead to the identification of possible
molecular markers and even potential therapeutic targets.
4.5. Molecular evidence of potential salivary biomarkers
Salivary proteins are associated with nearly the same classes
of diseases as plasma proteins, indicating that molecular
markers for all these diseases can be found in saliva,
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
enhancing the possibility of its use for diagnosis of both oral
and systemic diseases.
The presence, in saliva, of a higher percentage of proteins
related to neurological, immune system and ophthalmic
diseases may be indicative of a strong potential of saliva as
a source of molecular markers essential for designing
strategies for non-invasive diagnosis of these diseases.
In spite of remarkable advances in bioinformatics techni-
ques used in systems biology, there are still clear gaps in the
path between proteomics results and the elucidation of
molecular mechanisms involving the identified proteins. This
void can only be overcome with studies, making use of
bioinformatics techniques, always based on human interpre-
tation in the light of existing literature.
Information about the oral cavity is dispersed through
different databases focused on more general systems. In
addition to being dispersed, the data are not always
standardized, which makes their integration and comprehen-
sive study a difficult task. The present work is the largest and
most comprehensive survey of proteins of the oral cavity,
covering proteins from all salivary sources both under
physiological and pathological conditions, organized in an
integrated database.
Funding
None.
Competing interests
None declared.
Ethical approval
Not required.
Appendix A. Supplementary data
Supplementary data associated with this article can be
found, in the online version, at doi:10.1016/j.archoralbio.
2011.12.010.
r e f e r e n c e s
1. Huq NL, Cross KJ, Ung M, Myroforidis H, Veith PD, Chen D,et al. A review of the salivary proteome and peptidome andsaliva-derived peptide therapeutics. Int J Pept Res Ther2007;13(September (4)):547–64.
2. de Almeida PDV, Gregio AMT, Machado MAN, de Lima AAS,Azevedo LR. Saliva composition and functions: acomprehensive review. J Contemp Dent Pract 2008;9(3):72–80.
3. Greabu M, Battino M, Mohora M, Totan A, Didilescu A, SpinuT, et al. Saliva—a diagnostic window to the body, both inhealth and in disease. J Med Life 2009;2(June (2)):124–32.
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x 11
AOB-2738; No. of Pages 12
4. Kaufman E, Lamster IB. The diagnostic applications ofsaliva—a review. Crit Rev Oral Biol Med 2002;13(2):197–212.
5. Denny P, Hagen FK, Hardt M, Liao L, Yan W, Arellanno M,et al. The proteomes of human parotid and submandibular/sublingual gland salivas collected as the ductal secretions. JProteome Res 2008;7(May (5)):1994–2006.
6. Fang X, Yang L, Wang W, Song T, Lee CS, DeVoe DL, et al.Comparison of electrokinetics-based multidimensionalseparations coupled with electrospray ionization-tandemmass spectrometry for characterization of human salivaryproteins. Anal Chem 2007;79(August (15)):5785–92.
7. Gonzalez-Begne M, Lu B, Han X, Hagen FK, Hand AR, MelvinJE, et al. Proteomic analysis of human parotid glandexosomes by multidimensional protein identificationtechnology (MudPIT). J Proteome Res 2009;8(March (3)):1304–14.
8. Hardt M, Thomas LR, Dixon SE, Newport G, Agabian N,Prakobphol A, et al. Toward defining the human parotidgland salivary proteome and peptidome: identification andcharacterization using 2D SDS-PAGE, ultrafiltration, HPLC,and mass spectrometry. Biochemistry 2005;44(March(8)):2885–99.
9. Hardt M, Witkowska HE, Webb S, Thomas LR, Dixon SE, HallSC, et al. Assessing the effects of diurnal variation on thecomposition of human parotid saliva: quantitative analysisof native peptides using iTRAQ reagents. Anal Chem2005;77(August (15)):4947–54.
10. Hu S, Xie Y, Ramachandran P, Ogorzalek Loo RR, Li Y, Loo JA,et al. Large-scale identification of proteins in humansalivary proteome by liquid chromatography/massspectrometry and two-dimensional gel electrophoresis-mass spectrometry. Proteomics 2005;5(April (6)):1714–28.
11. Huang C-M. Comparative proteomic analysis of humanwhole saliva. Arch Oral Biol 2004;49(December (12)):951–62.
12. Loo JA, Yan W, Ramachandran P, Wong DT. Comparativehuman salivary and plasma proteomes. J Dent Res2010;89(October (10)):1016–23.
13. Messana I, Cabras T, Inzitari R, Lupi A, Zuppi C, Olmi C, et al.Characterization of the human salivary basic proline-richprotein complex by a proteomic approach. J Proteome Res2004;3(4):792–800.
14. Quintana M, Palicki O, Lucchi G, Ducoroy P, Chambon C,Salles C, et al. Inter-individual variability of protein patternsin saliva of healthy adults. J Proteom 2009;72(July (5)):822–30.
15. Siqueira WL, Salih E, Wan DL, Helmerhorst EJ, OppenheimFG. Proteome of human minor salivary gland secretion. JDent Res 2008;87(May (5)):445–50.
16. Vitorino R, Lobo MJC, Duarte JAR, Ferrer-Correia AJ,Domingues PM, Amado FML. Analysis of salivary peptidesusing HPLC-electrospray mass spectrometry. BiomedChromatogr 2004;18(October (8)):570–5.
17. Walz A, Stuhler K, Wattenberg A, Hawranke E, Meyer HE,Schmalz G, et al. Proteome analysis of glandular parotid andsubmandibular-sublingual saliva in comparison to wholehuman saliva by two-dimensional gel electrophoresis.Proteomics 2006;6(March (5)):1631–9.
18. Wilmarth PA, Riviere MA, Rustvold DL, Lauten JD, MaddenTE, David LL. Two-dimensional liquid chromatographystudy of the human whole saliva proteome. J Proteome Res2004;3(October (5)):1017–23.
19. Xie H, Rhodus NL, Griffin RJ, Carlis JV, Griffin TJ. A catalogueof human saliva proteins identified by free flowelectrophoresis-based peptide separation and tandem massspectrometry. Mol Cell Proteomics 2005;4(November(11)):1826–30.
20. Yan W, Apweiler R, Balgley BM, Boontheung P, Bundy JL,Cargile BJ, et al. Systematic comparison of the human salivaand plasma proteomes. Proteom Clin Appl 2009;3(January(1)):116–34.
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
21. Ramachandran P, Boontheung P, Pang E, Yan W, Wong DT,Loo JA. Comparison of N-linked glycoproteins in humanwhole saliva, parotid submandibular, and sublingualglandular secretions identified using hydrazide chemistryand mass spectrometry. Clin Proteom 2008;4(December (3–4)):80–104.
22. Ramachandran P, Boontheung P, Xie Y, Sondej M, Wong DT,Loo JA. Identification of N-linked glycoproteins in humansaliva by glycoprotein capture and mass spectrometry. JProteome Res 2006;5(June (6)):1493–503.
23. Larsen MR, Jensen SS, Jakobsen LA, Heegaard NHH.Exploring the sialiome using titanium dioxidechromatography and mass spectrometry. Mol Cell Proteomics2007;6(October (10)):1778–87.
24. Bostanci N, Heywood W, Mills K, Parkar M, Nibali L, DonosN. Application of label-free absolute quantitativeproteomics in human gingival crevicular fluid by LC/MS E(gingival exudatome). J Proteome Res 2010;9(May (5)):2191–9.
25. Brinkmann O, Kastratovic DA, Dimitrijevic MV,Konstantinovic VS, Jelovac DB, Antic J, et al. Oral squamouscell carcinoma detection by salivary biomarkers in a Serbianpopulation. Oral Oncol 2011;47(January (1)):51–5.
26. Chi L-M, Lee C-W, Chang K-P, Hao S-P, Lee H-M, Liang Y,et al. Enhanced interferon signaling pathway in oral cancerrevealed by quantitative proteome analysis ofmicrodissected specimens using 16o/18o labeling andintegrated two-dimensional LC-ESI-MALDI tandem MS. MolCell Proteomics 2009;8(July (7)):1453–74.
27. Costa PP, Trevisan GL, Macedo GO, Palioto DB, Souza SLS,Grisi MFM, et al. Salivary interleukin-6, matrixmetalloproteinase-8, and osteoprotegerin in patients withperiodontitis and diabetes. J Periodontol 2010;81(March(3)):384–91.
28. Dowling P, Wormald R, Meleady P, Henry M, Curran A,Clynes M. Analysis of the saliva proteome from patientswith head and neck squamous cell carcinoma revealsdifferences in abundance levels of proteins associated withtumour progression and metastasis. J Proteom 2008;71(July(2)):168–75.
29. Goncalves LDR, Soares MR, Nogueira FCS, Garcia C,Camisasca DR, Domont G, et al. Comparative proteomicanalysis of whole saliva from chronic periodontitis patients.J Proteom 2010;73(May (7)):1334–41.
30. Haigh BJ, Stewart KW, Whelan JRK, Barnett MPG, SmolenskiGA, Wheeler TT. Alterations in the salivary proteomeassociated with periodontitis. J Clin Periodontol2010;37(March (3)):241–7.
31. He Q-Y, Chen J, Kung H-F, Yuen AP-W, Chiu J-F.Identification of tumor-associated proteins in oral tonguesquamous cell carcinoma by proteomics. Proteomics2004;4(January (1)):271–8.
32. Hu S, Arellano M, Boontheung P, Wang J, Zhou H, Jiang J,et al. Salivary proteomics for oral cancer biomarkerdiscovery. Clin Cancer Res 2008;14(October (19)):6246–52.
33. Jou Y-J, Lin C-D, Lai C-H, Chen C-H, Kao J-Y, Chen S-Y, et al.Proteomic identification of salivary transferrin as abiomarker for early detection of oral cancer. Anal Chim Acta2010;681(November (1–2)):41–8.
34. Lo W-Y, Tsai M-H, Tsai Y, Hua C-H, Tsai F-J, Huang S-Y, et al.Identification of over-expressed proteins in oral squamouscell carcinoma (OSCC) patients by clinical proteomicanalysis. Clin Chim Acta 2007;376(February (1–2)):101–7.
35. Negishi A, Masuda M, Ono M, Honda K, Shitashige M, SatowR, et al. Quantitative proteomics using formalin-fixedparaffin-embedded tissues of oral squamous cellcarcinoma. Cancer Sci 2009;100(September (9)):1605–11.
36. Preza D, Thiede B, Olsen I, Grinde B. The proteome of thehuman parotid gland secretion in elderly with and withoutroot caries. Acta Odontol Scand 2009;67(3):161–9.
to the OralOme: Comprehensive molecular oral biology. Archives of Oral
a r c h i v e s o f o r a l b i o l o g y x x x ( 2 0 1 2 ) x x x – x x x12
AOB-2738; No. of Pages 12
37. Turhani D, Krapfenbauer K, Thurnher D, Langen H,Fountoulakis M. Identification of differentially expressed,tumor-associated proteins in oral squamous cell carcinoma byproteomic analysis. Electrophoresis 2006;27(April (7)):1417–23.
38. Wu Y, Shu R, Luo L-J, Ge L-H, Xie Y-F. Initial comparison ofproteomic profiles of whole unstimulated saliva obtainedfrom generalized aggressive periodontitis patients andhealthy control subjects. J Periodont Res 2009;44(October(5)):636–44.
39. Yang L-L, Liu X-Q, Liu W, Cheng B, Li M-T. Comparativeanalysis of whole saliva proteomes for the screening ofbiomarkers for oral lichen planus. Inflamm res 2006;55(July(10)):405–7.
40. Cabras T, Pisano E, Mastinu A, Denotti G, Pusceddu PP,Inzitari R, et al. Alterations of the salivary secretorypeptidome profile in children affected by type 1 diabetes.Mol Cell Proteom 2010;9(10):2099–108.
41. Castagnola M, Inzitari R, Fanali C, Iavarone F, Vitali A,Desiderio C, et al. The surprising composition of the salivaryproteome of preterm human newborn. Mol Cell Proteomics2010;10(1). M110:003467.
42. Fleissig Y, Deutsch O, Reichenberg E, Redlich M, Zaks B,Palmon A, et al. Different proteomic protein patterns insaliva of Sjogren’s syndrome patients. Oral Dis2009;15(January (1)):61–8.
43. Giusti L, Baldini C, Bazzichi L, Ciregia F, Tonazzini I, MasciaG, et al. Proteome analysis of whole saliva: a new tool forrheumatic diseases—the example of Sjogren’s syndrome.Proteomics 2007;7(May (10)):1634–43.
44. Giusti L, Bazzichi L, Baldini C, Ciregia F, Mascia G,Giannaccini G, et al. Specific proteins identified in wholesaliva from patients with diffuse systemic sclerosis. JRheumatol 2007;34(October (10)):2063–9.
45. Hjelmervik TOR, Jonsson R, Bolstad AI. The minor salivarygland proteome in Sjogren’s syndrome. Oral Dis 2009;15(July(5)):342–53.
46. Hu S, Wang J, Meijer J, Ieong S, Xie Y, Yu T, et al. Salivaryproteomic and genomic biomarkers for primary Sjogren’ssyndrome. Arthritis Rheum 2007;56(November (11)):3588–600.
47. Ito K, Funayama S, Hitomi Y, Nomura S, Katsura K, Saito M,et al. Proteome analysis of gelatin-bound salivary proteinsin patients with primary Sjogren’s syndrome: identificationof matrix metalloproteinase-9. Clin Chim Acta 2009;403(May(1–2)):269–71.
48. Rao PV, Reddy AP, Lu X, Dasari S, Krishnaprasad A, Biggs E,et al. Proteomic identification of salivary biomarkers oftype-2 diabetes. J Proteome Res 2009;8(January (1)):239–45.
49. Ryu OH, Atkinson JC, Hoehn GT, Illei GG, Hart TC.Identification of parotid salivary biomarkers in Sjogren’ssyndrome by surface-enhanced laser desorption/ionizationtime-of-flight mass spectrometry and two-dimensionaldifference gel electrophoresis. Rheumatology (Oxford)2006;45(September (9)):1077–86.
50. Streckfus CF, Storthz KA, Bigler L, Dubinsky WP. Acomparison of the proteomic expression in pooled salivaspecimens from individuals diagnosed with ductalcarcinoma of the breast with and without lymph nodeinvolvement. J Oncol 2009:2009.
51. Fleming K, Kelley LA, Islam SA, MacCallum RM, Muller A,Pazos F, et al. The proteome: structure, function and
Please cite this article in press as: Rosa N, et al. From the salivary proteomeBiology (2012), doi:10.1016/j.archoralbio.2011.12.010
evolution. Philos Trans R Soc Lond B Biol Sci 2006;361(March(1467)):441–51.
52. Saha S, Harrison SH, Shen C, Tang H, Radivojac P, Arnold RJ,et al. HIP2: an online database of human plasma proteinsfrom healthy individuals. BMC Med Genomics 2008;1:1–12.
53. Nissum M, Kuhfuss S, Hauptmann M, Obermaier C, SukopU, Wildgruber R, et al. Two-dimensional separation ofhuman plasma proteins using iterative free-flowelectrophoresis. Proteomics 2007;7(December (23)):4218–27.
54. Kersey PJ, Duarte J, Williams A, Karavidopoulou Y, Birney E,Apweiler R. The International Protein Index: an integrateddatabase for proteomics experiments. Proteomics 2004;4(July(7)):1985–8.
55. Jain E, Bairoch A, Duvaud S, Phan I, Redaschi N, Suzek B,et al. Infrastructure for the life sciences: design andimplementation of the UniProt website. BMC Bioinform2009;10(1):136.
56. The UniProt Consortium. Ongoing and future developmentsat the Universal Protein Resource. Nucleic Acids Res2010;39(November (Database)):D214–9.
57. Mi H, Dong Q, Muruganujan A, Gaudet P, Lewis S, ThomasPD. PANTHER version 7: improved phylogenetic trees,orthologs and collaboration with the Gene OntologyConsortium. Nucleic Acids Res 2009;38(December(Database)):D204–10.
58. Thomas PD, Campbell MJ, Kejariwal A, Mi H, Karlak B,Daverman R, et al. PANTHER: a library of protein familiesand subfamilies indexed by function. Genome Res2003;13(9):2129–41.
59. Cho RJ, Campbell MJ. Transcription, genomes, function.Trends Genet 2000;16(September (9)):409–15.
60. Huang DW, Sherman BT, Lempicki RA. Systematic andintegrative analysis of large gene lists using DAVIDbioinformatics resources. Nat Protoc 2009;4(1):44–57.
61. Huang DW, Sherman BT, Lempicki RA. Bioinformaticsenrichment tools: paths toward the comprehensivefunctional analysis of large gene lists. Nucleic Acids Res2009;37(January (1)):1–13.
62. Li S-J, Peng M, Li H, Liu B-S, Wang C, Wu J-R, et al. Sys-BodyFluid: a systematical database for human body fluidproteome research. Nucleic Acids Res 2009;37(January(Database issue)):D907–D912.
63. Greabu M, Battino M, Mohora M, Totan A, Spinu T, Totan C,et al. Could constitute saliva the first line of defence againstoxidative stress? Rom J Intern Med 2007;45(2):209–13.
64. Delima AJ, Van Dyke TE. Origin and function of the cellularcomponents in gingival crevice fluid. Periodontology 20002003;31:55–76.
65. Sorsa T, Tjaderhane L, Konttinen YT, Lauhio A, Salo T, LeeH-M. Matrix metalloproteinases: contribution topathogenesis, diagnosis and treatment of periodontalinflammation. Ann Med 2006;38(5):306–21.
66. Vitkov L, Klappacher M, Hannig M, Krautgartner WD.Extracellular neutrophil traps in periodontitis. J Periodont Res2009;44(October (5)):664–72.
67. Grant PJ. Diabetes mellitus as a prothrombotic condition. JIntern Med 2007;262(August (2)):157–72.
68. Issad T. O-GlcNAc glycosylation and regulation of cellsignaling. Med Sci (Paris) 2010;26(September (8–9)):753–9.
to the OralOme: Comprehensive molecular oral biology. Archives of Oral