Expression of thyroid hormone receptor/erbA genes is altered in human breast cancer
10
Expression of thyroid hormone receptor/erbA genes is altered in human breast cancer Jose´ M Silva 1 , Gemma Domı´nguez 1 , Jose´ M Gonza´lez-Sancho 4 , Jose´ M Garcı´a 1 , Javier Silva 1 , Carmen Garcı´a-Andrade 2 , Antonia Navarro 3 , Alberto Mun˜oz* ,4 and Fe´lix Bonilla* ,1 1 Department of Medical Oncology, Clı´nica Puerta de Hierro, E-28035 Madrid, Spain; 2 Department of Pathology, Hospital Santa Cristina, E-28009 Madrid, Spain; 3 Department of Pathology, Clı´nica Puerta de Hierro, E-28035 Madrid, Spain; 4 Instituto de Investigaciones Biome´dicas ‘Alberto Sols’, Consejo Superior de Investigaciones Cientı´ficas-Universidad Auto ´noma de Madrid, E-28029 Madrid, Spain The relation between thyroid status and diseases and cancer is unclear. No detailed analysis of thyroid hormone receptor (TR) expression in human breast cancer has been reported. We have analysed the expression and mutational status of the TRa1, encoded by the c-erbA proto-oncogene, TRb1 and TRb2 isoforms in 70 sporadic breast cancers. Alterations in the RNA level of TRb1, TRa1, or both were found in a number of patients. No expression of TRb2 RNA was detected. Western blotting analysis confirmed the dierences in expression at the protein level in those cases where sucient tumor sample was available. Additionally, tumor-specific truncated TRb1 RNA was found in six patients. Strikingly, three transcripts shared the same breakpoint. Only one tumor carried the corresponding deletion at the genomic DNA level, suggesting that the remaining abnormal TRb1 tran- scripts are aberrant splicing products. Though no significant correlation was found between TRb1 altera- tion and any clinical parameter, it showed a tendency to associate with early age of onset (550 years). Our results reveal specific alterations in the expression of TRb and TRa genes in a subset of breast cancer patients, suggesting that deregulation of thyroid hormone target genes may be involved in the generation of this neoplasia. Oncogene (2002) 21, 4307 – 4316. doi:10.1038/sj.onc. 1205534 Keywords: erbA; thyroid receptor genes; thyroid hor- mone; breast cancer; mutation Introduction Breast cancer is the most common neoplasia and the second cause of cancer deaths in women in western countries (Kelsey and Horm-Ross, 1993; Alberg and Helzlsouer, 1997). Numerous physiological agents and pathological conditions as well as environmental risk factors have been proposed to influence the develop- ment of this neoplasia. Among them, thyroid hormone (triiodothyronine, T3, and its precursor thyroxine, T4) has long been postulated since Beatson described the use of thyroid extracts for metastatic breast cancer treatment more than a century ago (Beatson, 1896). However, the relation between thyroid status and diseases and the pathogenesis of human breast cancer is not understood (Hedley et al., 1981; Guernsey, 1993; Strain et al., 1997; Smyth, 1997). T3 binds to specific high anity receptors (TR, thyroid receptors) which belong to the superfamily of nuclear receptors (Mangelsdorf et al., 1995). They function as ligand-modulated transcription factors regulating the expression of target genes upon binding to specific sequences named hormone re- sponse elements (Mun˜oz and Bernal, 1997). TRs are encoded by two genes, TRa and TRb, located on human chromosomes 17 and 3, respectively. By alternative splicing and dierential promoter usage these two genes yield up to nine polypeptides, only four of which bind T3 and are functional receptors: TRa1, TRb1, TRb2, and TRb3 (Mun˜oz and Bernal, 1997; Chassande et al., 1997; Williams, 2000; Dressel and Baniahmad, 2001). Every cell type in the organism expresses a defined pattern of receptor isoforms depending on its developmental and physio- logical state. Remarkably, the retroviral v-erbA oncogene encoding a mutated TRa1 gene induces erythroleukemia and sarcomas in birds (Sap et al., 1986) and hepatocarcinomas in transgenic mice (Barlow et al., 1994). Data on the integrity of TR genes in human breast tumors are very scarce. Two studies reporting allelic losses suggested that TR genes may function as tumor suppressors. In one study TRb gene was located in the 3p21 – 25 region of somatic homo- zygosity in breast carcinomas (Ali et al., 1989). In another study, TRa locus was reported in a region of chromosome 17 lost in 11 out of 14 sporadic breast carcinomas (Futreal et al., 1992). However, no point Oncogene (2002) 21, 4307 – 4316 ª 2002 Nature Publishing Group All rights reserved 0950 – 9232/02 $25.00 www.nature.com/onc *Correspondence: F Bonilla; E-mail: [email protected] and A Mun˜oz Received 3 January 2002; revised 20 March 2002; accepted 27 March 2002
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Expression of thyroid hormone receptor/erbA genes is altered in human breast cancer

Expression of thyroid hormone receptor/erbA genes is altered in humanbreast cancer
Jose M Silva1, Gemma Domõ nguez1, Jose M Gonza lez-Sancho4, Jose M Garcõ a1, Javier Silva1,Carmen Garcõ a-Andrade2, Antonia Navarro3, Alberto MunÄ oz*,4 and Fe lix Bonilla*,1
1Department of Medical Oncology, ClõÂnica Puerta de Hierro, E-28035 Madrid, Spain; 2Department of Pathology, Hospital SantaCristina, E-28009 Madrid, Spain; 3Department of Pathology, ClõÂnica Puerta de Hierro, E-28035 Madrid, Spain; 4Instituto deInvestigaciones BiomeÂdicas `Alberto Sols', Consejo Superior de Investigaciones Cientõ®cas-Universidad AutoÂnoma de Madrid,E-28029 Madrid, Spain
The relation between thyroid status and diseases andcancer is unclear. No detailed analysis of thyroidhormone receptor (TR) expression in human breastcancer has been reported. We have analysed theexpression and mutational status of the TRa1, encodedby the c-erbA proto-oncogene, TRb1 and TRb2isoforms in 70 sporadic breast cancers. Alterations inthe RNA level of TRb1, TRa1, or both were found in anumber of patients. No expression of TRb2 RNA wasdetected. Western blotting analysis con®rmed thedi�erences in expression at the protein level in thosecases where su�cient tumor sample was available.Additionally, tumor-speci®c truncated TRb1 RNA wasfound in six patients. Strikingly, three transcriptsshared the same breakpoint. Only one tumor carriedthe corresponding deletion at the genomic DNA level,suggesting that the remaining abnormal TRb1 tran-scripts are aberrant splicing products. Though nosigni®cant correlation was found between TRb1 altera-tion and any clinical parameter, it showed a tendency toassociate with early age of onset (550 years). Ourresults reveal speci®c alterations in the expression ofTRb and TRa genes in a subset of breast cancerpatients, suggesting that deregulation of thyroidhormone target genes may be involved in the generationof this neoplasia.Oncogene (2002) 21, 4307 ± 4316. doi:10.1038/sj.onc.1205534
Keywords: erbA; thyroid receptor genes; thyroid hor-mone; breast cancer; mutation
Introduction
Breast cancer is the most common neoplasia and thesecond cause of cancer deaths in women in westerncountries (Kelsey and Horm-Ross, 1993; Alberg and
Helzlsouer, 1997). Numerous physiological agents andpathological conditions as well as environmental riskfactors have been proposed to in¯uence the develop-ment of this neoplasia. Among them, thyroidhormone (triiodothyronine, T3, and its precursorthyroxine, T4) has long been postulated since Beatsondescribed the use of thyroid extracts for metastaticbreast cancer treatment more than a century ago(Beatson, 1896). However, the relation betweenthyroid status and diseases and the pathogenesis ofhuman breast cancer is not understood (Hedley et al.,1981; Guernsey, 1993; Strain et al., 1997; Smyth,1997).
T3 binds to speci®c high a�nity receptors (TR,thyroid receptors) which belong to the superfamily ofnuclear receptors (Mangelsdorf et al., 1995). Theyfunction as ligand-modulated transcription factorsregulating the expression of target genes uponbinding to speci®c sequences named hormone re-sponse elements (MunÄ oz and Bernal, 1997). TRs areencoded by two genes, TRa and TRb, located onhuman chromosomes 17 and 3, respectively. Byalternative splicing and di�erential promoter usagethese two genes yield up to nine polypeptides, onlyfour of which bind T3 and are functional receptors:TRa1, TRb1, TRb2, and TRb3 (MunÄ oz and Bernal,1997; Chassande et al., 1997; Williams, 2000; Dresseland Baniahmad, 2001). Every cell type in theorganism expresses a de®ned pattern of receptorisoforms depending on its developmental and physio-logical state. Remarkably, the retroviral v-erbAoncogene encoding a mutated TRa1 gene induceserythroleukemia and sarcomas in birds (Sap et al.,1986) and hepatocarcinomas in transgenic mice(Barlow et al., 1994).
Data on the integrity of TR genes in human breasttumors are very scarce. Two studies reporting alleliclosses suggested that TR genes may function astumor suppressors. In one study TRb gene waslocated in the 3p21 ± 25 region of somatic homo-zygosity in breast carcinomas (Ali et al., 1989). Inanother study, TRa locus was reported in a region ofchromosome 17 lost in 11 out of 14 sporadic breastcarcinomas (Futreal et al., 1992). However, no point
Oncogene (2002) 21, 4307 ± 4316ã 2002 Nature Publishing Group All rights reserved 0950 ± 9232/02 $25.00
www.nature.com/onc
*Correspondence: F Bonilla; E-mail: [email protected] and A MunÄ ozReceived 3 January 2002; revised 20 March 2002; accepted 27March 2002
mutations were found thus excluding this locus as acommon tumor suppressor gene in breast cancer(Futreal et al., 1994). The validity of these studieshas, however, been criticized, since they were basedon markers whose location is not mapped precisely(Huber-Gieseke et al., 1997). Additionally, frequentco-ampli®cation of TRa with the c-erbB2/neu onco-gene was reported in human mammary tumors;although overexpression was not detected (van deVijver et al., 1987). Little is known about TRexpression in human breast cancer patients. Only afew reports have described the presence of unchar-acterized TR in breast tumors (Smallridge andLatham, 1980; Cerbon et al., 1981; Alvarado-Pisaniet al., 1986).
Here we analyse the pattern of expression andintegrity of the RNA encoding TRa1, TRb1, andTRb2 in human breast cancer. A series of matchedsamples of tumoral and control tissue from 70 patientswith known clinicopathological parameters were ana-lysed by semi-quantitative reverse transcription-poly-merase chain reaction (RT ±PCR) and single-strandedconformational polymorphism (SSCP), and thosesuspected of harboring alterations were sequenced.Several patients showed alterations in TRb1 and TRa1expression levels that were con®rmed by real-time PCRand Western blotting, while expression of TRb2 wasnot detected. Expression of truncated TRb1 transcriptswere found in six patients. Only one abnormaltranscript correlated with a genomic deletion, whilethe remaining ®ve most probably result from alter-native or aberrant splicing events.
Results
TR RNA expression is altered in a subset of breast tumors
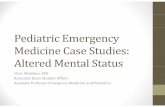
We ®rst analysed the pattern of expression of TR genesin normal breast samples by semi-quantitative PCR.Primers used as shown in Table 1. Both TRa1 andTRb1 were expressed in normal breast tissue (Figure1). In contrast, no expression of TRb2 RNA was foundin any of the 70 samples studied.
Several alterations were found in TRa1 and TRb1RNA expression in the matched tumor tissues. Sixsamples displayed changes in TRa1 RNA levels (twoup-regulated and four down-regulated), and four inTRb1 RNA (one up-regulated and three down-regulated), while two neoplastic tissues displayedconcomitant alterations in both (down-regulation ofTRb1 and up- or down-regulation of TRa1) (Figure2a). Additionally, six tumor samples, but not theirnormal counterparts, presented novel TRb1 transcripts,
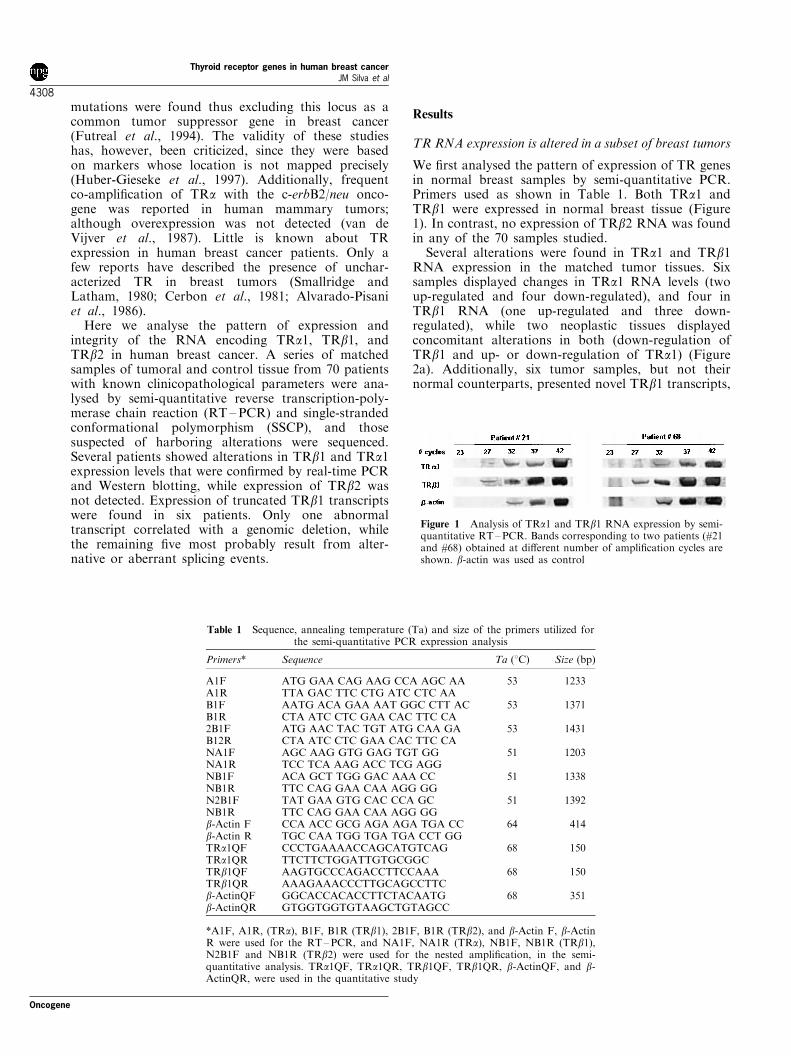
Table 1 Sequence, annealing temperature (Ta) and size of the primers utilized forthe semi-quantitative PCR expression analysis
Primers* Sequence Ta (8C) Size (bp)
A1F ATG GAA CAG AAG CCA AGC AA 53 1233A1R TTA GAC TTC CTG ATC CTC AAB1F AATG ACA GAA AAT GGC CTT AC 53 1371B1R CTA ATC CTC GAA CAC TTC CA2B1F ATG AAC TAC TGT ATG CAA GA 53 1431B12R CTA ATC CTC GAA CAC TTC CANA1F AGC AAG GTG GAG TGT GG 51 1203NA1R TCC TCA AAG ACC TCG AGGNB1F ACA GCT TGG GAC AAA CC 51 1338NB1R TTC CAG GAA CAA AGG GGN2B1F TAT GAA GTG CAC CCA GC 51 1392NB1R TTC CAG GAA CAA AGG GGb-Actin F CCA ACC GCG AGA AGA TGA CC 64 414b-Actin R TGC CAA TGG TGA TGA CCT GGTRa1QF CCCTGAAAACCAGCATGTCAG 68 150TRa1QR TTCTTCTGGATTGTGCGGCTRb1QF AAGTGCCCAGACCTTCCAAA 68 150TRb1QR AAAGAAACCCTTGCAGCCTTCb-ActinQF GGCACCACACCTTCTACAATG 68 351b-ActinQR GTGGTGGTGTAAGCTGTAGCC
*A1F, A1R, (TRa), B1F, B1R (TRb1), 2B1F, B1R (TRb2), and b-Actin F, b-ActinR were used for the RT±PCR, and NA1F, NA1R (TRa), NB1F, NB1R (TRb1),N2B1F and NB1R (TRb2) were used for the nested ampli®cation, in the semi-quantitative analysis. TRa1QF, TRa1QR, TRb1QF, TRb1QR, b-ActinQF, and b-ActinQR, were used in the quantitative study
Figure 1 Analysis of TRa1 and TRb1 RNA expression by semi-quantitative RT±PCR. Bands corresponding to two patients (#21and #68) obtained at di�erent number of ampli®cation cycles areshown. b-actin was used as control
Thyroid receptor genes in human breast cancerJM Silva et al
4308
Oncogene

shorter than wild-type (Figure 2b). Three of them(patients #12, #22 and #56) were of similar size.
TR protein levels correlate with RNA expression
To con®rm at the protein level the di�erences in RNAexpression found by using semi-quantitative RT±PCR,we performed Western analysis of the cases wheretumor and normal tissues were available, ®ve withnormal RNA expression and patients #24 and #76 withaltered expression. According to previous reports, aband of 48 kDa was detected using an antibody (a-144)against TRa1, while two di�erent anti-TRb antibodies(b-62 and b-82) detected a band of 55 kDa (Falcone etal., 1992). The results were in good concordance withthose obtained by semi-quantitative RT±PCR: nochanges in protein levels were detected in any of the®ve patients with normal TR RNA expression, whilelower expression of TRb1 but not TRa1 polypeptideswas found in patient #24, and reduction in both TRa1and TRb1 was clear in patient #76 (Figure 3).
Quantitative PCR analysis confirms alterations in TRRNA expression
We did not have su�cient sample to analyse theexpression of TR polypeptides in the 12 cases withaltered RNA expression, so we performed real-timequantitative PCR in these cases and also in 10 othersexpressing normal RNA levels. The results wereconsistent with those obtained by semi-quantitativePCR in 10 out of 12 cases displaying altered TRa1and/or TRb1 RNA levels, and also in the cases with
normal expression (Figure 4). However, only minordi�erences in expression were found in the two cases inwhich concomitant alterations in both TRb1 and TRa1RNAs had been found by semi-quantitative RT ±PCR(not shown). The linear relationship between thefractional cycle and the ¯uorescent threshold wasstrong (r2=1).
SSCP analysis suggests the expression of abnormal TRtranscripts in breast tumor tissue
Restriction fragments from TRa1 and TRb1 cDNAsobtained from all patients were analysed (Table 2).Five tumor samples showed a di�erential band whencompared to matched normal tissue (not shown). Fourof the changes in mobility corresponded to TRb1cDNA fragments, and the remaining to TRa1 cDNA.Three of the tumor samples showing changes in TRb1cDNA fragments mobility corresponded to thoseexpressing shorter transcripts (patients #12, #22, and#71).
Truncated TRb1 RNAs are expressed in breast tumors
Sequencing of the six selected short TRb1 cDNAscon®rmed the presence of truncations of variablelength, ranging from 135 to 705 bp. A scheme of theencoded transcripts with the location of the deletionsand the a�ected domains in the correspondingproducts is shown in Figure 5. The aminoterminal A/B domain responsible for the ligand-independenttransactivation activity were not included in anydeletion. In one patient (#12) the deletion links G369with C724 without altering the reading frame. As aconsequence, the mutant TRb1 lacked exons 4 and 5which encode respectively part of the DNA-binding Cdomain (the second zinc ®nger) and the hinge Ddomain. Another mutant (#71) had an internal deletionin exon 7 corresponding to part of the heterodimeriza-tion and hormone binding E domain, which linkedA958 to T1094 and caused the change of Ser320 intoan Ile without a�ecting the reading frame.
a
b
Figure 2 Expression of TR RNA in breast tumors. (a) Gelsshowing the di�erences in TRa1 and TRb1 RNA expressionbetween normal (N) and tumoral (T) tissue in two patients.Higher TRb1 RNA expression was found in patient #8 tumor;lower TRa1 RNA expression was found in patient #15; and bothalterations, higher TRa1 and lower TRb1 RNA expression wasfound in patient #31. Patient #62 showed normal level ofexpression of both TR RNAs in the tumor. (b) Sizes of theTRb1 RNAs expressed. Six tumors (patient # are indicated)showed expression of shorter TRb1 transcripts as compared tothat found in normal tissue (wild-type, WT). Note the distinct,tumor-speci®c relation between the expression levels of normaland mutant TRb1 RNAs
Figure 3 Expression of TR polypeptides in breast tumors.Western blot analysis of normal (N) and tumor (T) samplesfrom representative cases in which no di�erences in TRa1 orTRb1 (patient #63), down-regulation of TRb1 (patient #24), ordown-regulation of TRa1 and TRb1 (patient #76) was found.Conditions and antibodies used were as described in Materialsand methods. Sizes of the major bands detected are indicated
Oncogene
Thyroid receptor genes in human breast cancerJM Silva et al
4309

Remarkably, three patients (#22, #56, and #86)expressed truncated TRb1 RNA which shared nearlythe same breakpoint located close to the end of exon 4,a result that may indicate the presence of a fragile siteor, alternatively, a cryptic splicing site. These deletionsled to the expression of short transcripts encoding onlythe aminoterminal A/B and C domains. One of mutanttranscripts (patient #86) linked T498 to A1024 andrestored the wild-type frameshift 120 nucleotides beforethe stop codon. Though this RNA includes thecarboxyterminal AF-2 motif, it is highly improbablethat its encoded product can retain transactivating
activity since it lacks most of the ligand-binding andheterodimerization domain. The TRb1 transcript ofpatient #76 was similar to this one but with a smallerdeletion linking T542 to T1143. This patient alsoshowed a reduced level of TRa1 RNA. Therefore, atleast ®ve of the six mutant TRb1 transcripts encodedseverely truncated receptor proteins which, if stablyexpressed, may be either non-functional or exhibitaltered biological activities.
None of the 10 tumor samples which gave bandswith normal mobility in SSCP and neither of the othertwo patients (#10 and #16) with an abnormal SSCPpattern showed any sequence alteration (not shown).
Only one tumor contained a mutation at the TRb1 locus
To explore whether the aberrant TRb1 transcriptsresulted from deletions at the DNA level, we attemptedto amplify the genomic sequences bearing the putativeintragenic TRb deletions by using ¯anking primers(Table 3). These primers were designed in such a waythat an ampli®ed PCR product would be expected inthe case of a deletion in the genomic DNA, while nosuch product is expected if the TRb gene is intact dueto the very large DNA sequence to be ampli®ed. Withthe exception of patient #71, no ampli®ed productswere obtained (not shown). Subsequent sequencingcon®rmed an internal deletion in exon 7 of TRb genein the tumor sample of patient #71, which was absentin the normal breast tissue. In patient #12, whichexpressed an abnormal TRb1 transcript lacking exons4 and 5, we searched by the same method formutations in the splice acceptor site of exon 4 thatcould give rise to exon skipping. However, noalterations in the genomic sequence were found.
Clinicopathological correlations
None of the parameters analysed revealed signi®cantassociation with alterations in TR genes in tumorbreast tissue (abnormal expression or deletion). How-ever, four of the six patients with mutated TRb1 wereunder 50 years of age at diagnosis, while in contrastonly 16 of the remaining 64 patients (25%) werediagnosed before this age (P=0.05). The family historyof the six patients expressing aberrant TRb1 transcriptswas irrelevant with respect to breast cancer, with onlyone patient (#22) having a second-degree relativea�ected.
Figure 4 Quantitative analysis in LightCycler-PCR by usingSYBRGreen. The ®gure shows the plot of the intensity of the¯uorescence signal vs number of cycles. (a) TRa1 expression. Asan example, T and N correspond respectively to tumor andnormal tissue of patient #31 indicating a 10-fold higher expressionin the tumor. (b) TRb1 expression. N and T correspond tonormal and tumor tissue of patient #24 showing a lowerexpression in the tumor. (c) b-actin expression. Tumor andnormal tissue of patients #31 and #24 are shown. All of 27 breastcancer patients studied showed the same ampli®cation pro®les
Table 2 Enzymes used to obtain TR cDNA fragments suitable forSSCP analysis
PCR fragment SSCP Fragments(bp) Enzyme (bp)
443 BbvI 208, 70, 162473 Tsp45I 210, 265408 Tsp45I 105, 200, 105356 SspI 167, 189593 Tsp45I 110, 210, 275476 NciI 268, 218
Thyroid receptor genes in human breast cancerJM Silva et al
4310
Oncogene

Discussion
This study shows alterations in TR expression inhuman breast tumors. Six out of 70 patients expressedtruncated TRb1 RNA in tumor but not in controltissue. The reason for the appearance of abnormalTRb1 transcripts was, in one case, a genomic deletion(patient #71) and, in another, could be exon skippingby alternative splicing (patient #12), while in theremaining four cases it is unknown. We speculate thatthe neoplastic transformation alters the normal splicingmechanism, producing aberrant spliced messengers.Additional point mutations, however, cannot be ruledout given the possibility of false negatives associatedwith the SSCP technique. We also detected changes inthe level of TRb1 and TRa1 RNAs in a number ofpatients, which were con®rmed at the protein level inthose cases where su�cient material was available. Nosigni®cant correlation was found to any clinicopatho-
logical parameter, which is not surprising given the sizeof the series and the percentage of mutations.
To our knowledge this is the ®rst description ofthe expression of altered TR genes in human breastcancer. Abnormalities in TR genes have beendescribed in other human malignancies such ashepatocellular carcinomas, colon, thyroid, lung,pituitary and gastrointestinal tumors (Arbuthnot etal., 1989; Lin et al., 1999; McCabe et al., 1999;Markowitz et al., 1989; Wallin et al., 1992; Dobrovicet al., 1988). However, none of these studies includeda systematic analysis of TRs expression in asubstantial number of patients. More recently, TRexpression was studied in 20 cases of human renalclear cell carcinoma (Puzianowska-Kuznicka et al.,2000). While TRa RNA level was decreased, theTRa1 protein was increased in tumors. TRb1 proteinwas barely detectable even in those (30%) cancersshowing TRb RNA overexpression. In a subsequent
Figure 5 Schematic representation of the six truncated TRb1 RNA found. The domains and respective functions, and exonpattern in TRb1 are indicated. AF(Activation Function)-1 and -2 are the regions responsible respectively for the hormone-independent and -dependent transactivation functions of the receptor; the CoR-box is a sequence in the hinge region implicated intranscriptional co-repressor recruitment (Collingwood et al., 1998); and the signature motif is a sequence highly conserved amongnuclear receptors which has been proposed to stabilize the folding of the receptor molecule and play a role in dimerization andperhaps transcriptional activation and repression (O'Donnell and Koenig, 1990; Busch et al., 1997; Collingwood et al., 1998).Numbers below the sequences refer to the aminoacids linked in the mutated transcripts. Deleted areas are in large brackets. Dottedlines represent the non-in frame new sequences with numbers of aminoacids in small brackets, and STOP indicates the appearanceof abnormal termination codons
Oncogene
Thyroid receptor genes in human breast cancerJM Silva et al
4311

work, these authors have reported mutations in sevenTRb and three TRa RNAs in a series of 22 renalcarcinomas (Kamiya et al., 2002).
Given its complex array of biological activities, amutated TR can compromise cell growth or thedi�erentiated phenotype in multiple ways. Conceivably,abnormal TR carrying deletions such as thosedescribed here, which mostly a�ect the carboxyterminalhalf of the molecule, may inhibit the induction (orrepression) of target genes by T3 acting as dominantnegative over the normal cellular receptors. Suppo-sedly, except #12 which has a deleted second zinc®nger, the mutant TRb can bind DNA and so,competitively inhibit the access of co-expressed wild-type receptors to response elements in target promo-ters. This situation is reminiscent of what happens inpatients with the syndrome of generalized thyroidhormone resistance, most of whom carry mutations inthe TRb gene that produce non-hormone bindingpolypeptides with dominant negative activity (Dresseland Baniahmad, 2001). Moreover, mutated TR mayalter other cellular control systems or signaling path-ways through an abnormal interaction with theircomponent elements such as p53 or AP-1 (c-Jun, c-Fos).
The fact that TRb1 in patient #12 lacks exons 4 and5 suggests an alteration in the splicing of thistranscript. Alternatively, this RNA species might be aminor natural splice variant, though the loss of thesecond zinc ®nger makes this unlikely. The presence ofalterations in the splicing of TRb gene in breast tumors
is further indicated by the expression of severalaberrant transcripts in which the splicing does notoccur at de facto splicing sites. The ®nding of agenomic deletion in only one case supports thishypothesis. These results are in line with those recentlyreported for the mdm2 oncogene in human breastcancer (Lukas et al., 2001). These authors found bothalternative and aberrant mdm2 RNAs in some tumors.Alternative spliced variants of the estrogen receptor-a(ERa) mRNA have also been widely reported (Fasco etal., 2000), indicating that the splicing process issometimes altered in this neoplasia. To what extentmutant proteins encoded by splicing variants of these(TRb1, ERa, mdm2) and other RNAs a�ect thebiology of the mammary epithelial cells is unknown.It will probably depend on how the level of expressionof each variant modulates the activity of the wild-typeprotein.
The ®nding of TRb1 and TRa1 RNA expression inall samples analysed is consistent with the proposedaction of T3 in the breast, and supports the interest ofstudies on the e�ect of this hormone and its receptorsin mammary epithelial cells. Also, the lack of TRb2RNA agrees with the more restricted expression of thisisoform (Forrest and VennstroÈ m, 2000, and referencestherein). Quantitative di�erences found in TR RNAexpression with respect to normal tissue were neveroverwhelming, and only in one case was no wild-typeTRb1 RNA found. These ®ndings indicate that largedeletions covering the whole TR genes are notfrequent, and contradict two previous reports suggest-
Table 3 Sequence, annealing temperature (Ta), and size of the primers utilized forRTM±PCR±SSCP analysis and in the DNA genomic study*. The ®rst three pairsof primers were used for TRa1 ampli®cation and the second three pairs for TRb1(three set of primers were used in each region to obtain an appropriate size for theSSCP). The last ®ve sets of primers were used in the genomic DNA analysis of thesix tumors expressing truncated transcripts, being 12F8 and 22-56R* common for
cases #22 and #56
Primers Sequence Ta (8C) Size (bp)
NA1F AGC AAG GTG GAG TGT GG 51 443A3R GAT CGG ATC ATC TCC TCA2F AAG CGG GTG GCC AAG CG 51 473A2R AGC TGC TCC CGC TTG ACA3F AGCGAC ACC CTG ACG CT 51 408A1R TTA GAC TTC CTG ATC CTC AANB1F ACA GCT TGG GAC AAA CC 51 356B3R AAA CCC TTG CAG CCT TCB2F TAC CGC TGT ATC ACG TG 51 593B2R CGA AGG GAC ATG ATC TCB3F CTG CAA TGT GAA GAC CA 51 476NB1R TTC CAG GAA CAA AGG GG12F* ATGAAACTGTTGTCTTGGGTC 51 22212R* CATTCCTTGAATATGAAGCAAGB3F* (described above) 53 259b
71R* CTGAAGACATCAGCAGGAC12F* (described above) 56 13788b
22-56R* GAAAAACAACATCCTCACCTC12F* (described above) 51 24217b
NB1R* (described above)76F* GGTGCTGGATGACAGCAAG 51 21063b
NB1R* (described above)
bSize of the expected ampli®ed product in case of no deletion
Thyroid receptor genes in human breast cancerJM Silva et al
4312
Oncogene

ing loss of heterozygosity (LOH) of either TRb or TRain a high proportion of patients (Ali et al., 1989;Futreal et al., 1992). Our data do not support the ideathat TRb or TRa are tumor suppressor genes. Rather,they indicate that expression of altered TR maycontribute to the appearance or progression of breasttumors.
In mouse EpH4 mammary epithelial cells expressingexogenous TRa1, T3 regulates expression of stromely-sin-1 and -2, collagenase IVB, and tenascin-C andmodulates the di�erentiated phenotype (Lo pez-Bara-hona et al., 1995; Gonza lez-Sancho et al., 1999). TRare also present in human breast cancer cell lines(Burke and McGuire, 1978; Zhou-Li et al., 1992), butcon¯icting reports describe both mitogenic and anti-mitogenic e�ects of T3 (Nogueira and Brentani, 1996;Martõ nez et al., 2000). A role of T3 in the physiologyof ®brocystic breast disease has been suggested(Martõ nez et al., 1995). Although there is little evidencethat overt thyroid disease causes breast cancer,hypothyroidism has been proposed to favor thedevelopment of breast cancer by sensitizing breasttissue to the growth promoting action of estrogen,prolactin, and carcinogens (Smyth et al., 1996; Smyth,1997). Hypothyroidism or sick euthyroid syndrome arefrequently found in cancer patients perhaps as aconsequence of an increased level of cytokines suchas IL-6 (Yokoe et al., 1997), and low circulatingthyroid hormone has also been associated with poorresponse to therapy and prognosis (Yokoe et al., 1996).Normal mammary epithelium expresses TR genes, andis thus sensitive to T3. T3 regulates lobulo-alveolardevelopment, increases prolactin binding, and aug-ments milk production induced by insulin, prolactinand hydrocortisone (Singh and Bern, 1969; Vonderhaarand Greco, 1979; Selliti et al., 1983), probably byinducing the expression of genes such as a-lactalbumin,casein and epidermal growth factor receptor (Vonder-haar, 1977; Houdebine et al., 1978; Vonderhaar et al.,1986; Hudson et al., 1990).
Strikingly, T3 modulates ER expression and coreg-ulates gene expression with estrogen in non-mammarytissues (Cidlowski and Muldoon, 1975; Zhu et al.,1996). However data on mammary epithelial cells arelacking. Recently, TRa1, but neither of the TRbisoforms, has been reported to inhibit ERa transactiva-tion from consensus estrogen response element whereasit facilitates ERb-mediated transactivation (Vasudevanet al., 2001a). However, this interaction on the estrogenresponse element present in a physiological promoter isdi�erent (Vasudevan et al., 2001b). Given that ER andTR also share some transcriptional co-activators andthat alterations in expression of some of these such asAIB1 have been reported in breast cancers (Anzick etal., 1997; Bautista et al., 1998) alterations in TRexpression may a�ect estrogen action and breast tumorbiology.
In line with the view that the di�erent TRs exertonly partially redundant e�ects and act in a tissue-speci®c fashion (Forrest and VennstroÈ m, 2000), wespeculate that the more frequent alteration of TRb1
re¯ects a predominant biological role of this isoform inbreast cancer. The speci®city and alterations of TRexpression found in our study may help to explain thecon¯icting results published on the relation betweenthyroid status and disease and this neoplasia. Ourresults indicate the necessity to complement themeasurement of blood T3 and T4 concentrations withthe analysis of TR expression and integrity. Furtherstudies analysing TR expression at the protein level,and in larger series of patients may establish thesigni®cance of the presence of TRb1 variants in breasttumors and its putative correlation with any clinico-pathological parameter.
Material and methods
Tumor samples and clinicopathological parameters
Seventy sporadic breast carcinomas and normal breast tissuesamples from the same patients were snap-frozen in liquidnitrogen immediately after resection. All tumor samplescontained at least 75% tumor cells under histologicalexamination. The following parameters were obtained fromthe medical records of the 70 patients: birth date, tumor size,lymph node metastases, presence of steroid receptors(estrogen and progesterone), peritumoral vessel involvement,pathologic stage, histological grade, proliferation index, andc-ErbB2 status. Pathological stage was assessed using thetumor-node-metastasis (TNM) classi®cation. All tumors weregraded according to the Bloom-Richardson system. Steroidreceptor content (estrogen and progesterone), the prolifera-tive index and the c-ErbB2 expression were determined byimmunohistochemical procedures.
RNA extraction and semi-quantitative RT ±PCR
Total RNA was isolated from frozen tumor tissues of breastcarcinomas, matched with normal healthy breast tissue, usingRNeasy Mini Kit (Qiagen Inc., Hilden, Germany), andquanti®ed spectrophotometrically. Thirty ng of total RNAwas reverse-transcribed into ®rst strand cDNA and ampli®edin one step using the Gold RNA PCR Core Kit (PEBiosystems) according to the manufacturer's protocol. Theannealing temperature was 538C for the three cDNAs and theelongation time was 105 s. The ®nal volume was 20 ml and 40cycles of ampli®cation were used. We used b-actin as controlin the same conditions but the annealing temperature was648C instead of 538C, and the number of cycles was 35instead of 40 (Table 1). In order to increase the weak signalof the three TR genes, we performed a second, nested PCRampli®cation using a distinct set of primers (Table 1). Tothis, 3 ml of the product of the ®rst PCR was re-ampli®ed in a®nal volume of 25 ml, the annealing temperature was 51 ±568C (depending on the set of primers, see Table 1). The log-linear phase, used for semi-quantitative analysis, wasestablished at 32 cycles for TRa1 and at 35 cycles forTRb1 (Figure 1) (Corral-Debrinski et al., 1992; Ballinger etal., 1996). In these conditions the ampli®cation showedlinearity, as shown by serial dilutions. No signal was foundfor TRb2. Nested-ampli®ed products were analysed asdescribed above. Gel images were captured using a GS-690Imaging Densitometer (Bio-Rad Laboratories, Hercules, CA,U.S.A.), digitized in 400 d.p.i., and analysed using Multi-Analyst/PC (Bio-Rad laboratories). TR genes expression was
Oncogene
Thyroid receptor genes in human breast cancerJM Silva et al
4313

calculated as the expression ratio of tumor to normal tissueafter normalization to the corresponding b-actin levels. Thelog-linear phase was established at 30 cycles for b-actin. HighTR expression was arbitrarily de®ned as a fourfold or higherincrease over that of normal tissue, while reduced expressionwas considered when the value was 25% or less. Semi-quantitative RT±PCR from tumors and their matchednormal tissues was done three times to ensure reproducibilityof the results. Two additional TRb isoforms generated byalternative splicing, TRb3 and TRbD3, have been described(Williams, 2000). TRb3 and TRbD3 RNAs have di�erent 5'-sequences from TRb1 and TRb2, which excludes thepossibility of their ampli®cation in the conditions used inour study.
Quantitative PCR
Real-time quantitative PCR were performed using a Light-Cycler apparatus (Roche Diagnostics, Mannheim, Germany)using the LightCycler-FastStart DNA Master SYBR Green IKit (Roche Diagnostics). Each reaction was done in a ®nalvolume of 20 ml containing 2 ml of cDNA sample, 4 mM
MgCl2, 0.5 mM of each primer as well as 16reaction mixincluding FastStart DNA polymerase, reaction bu�er,dNTPs and SYBR green. PCR conditions were: 6 min at958C and 40 cycles of 958C for 20 s, 688C for 30 s and 728Cfor 15 s. The expression levels of TRa1 and TRb1 werenormalized to that of b-actin. A diluted sample of normaltissue was used to perform the standard curves for TRa1and TRb1. The primers used were designed with theassistance of the Primer Express TM 1.5 program (PEApplied Biosystems) (Table 1).
Western blotting
Protein extracts from tissue samples were obtained byhomogenization using the Dignam C bu�er supplementedwith 1% NP40 and protease inhibitors as described(Gonza lez et al., 2000) followed by 30 min incubation onice and centrifugation at 10 000 g at 48C for 10 min.Aliquots of the supernatants containing 40 mg protein wereelectrophoresed in 12% polyacrylamide gels and transferredto nylon PVDF membranes using a vertical BioRad transferapparatus at 1 mA/cm2 overnight. Equal loading ofindividual extracts was ensured by measuring proteinconcentration using the Bio-Rad Protein Assay. The ®lterswere washed, blocked with TBS (20 mM Tris base, 137 mM
Na Cl) pH 7.6, 0.1% Tween 20, 3% BSA, and incubatedovernight at 48C with the following anti-human TRantibodies (generously donated by Prof. L DeGroot,Chicago): a-144, recognizing TRa (1 : 200 dilution) and b-62 and b-82 (1 : 200 dilution), recognizing TRb1 and TRb2.As control we used an anti-histone antibody (BoehringerMannheim 1492-519, 1 : 1000 dilution). Blots were washed3615 min with TBS, 0.1% Tween-20 and incubated with ahorse anti-rabbit peroxidase secondary antibody (1 : 10.000;Sigma) for 1 h at room temperature. The blots weredeveloped by a peroxidase reaction using the Luminoldetection system (Pierce).
Single-stranded conformational polymorphism (SSCP)
Three fragments of each gene, TRa1 and TRb1, wereampli®ed using annealing temperatures that varied dependingon the pair primers (Table 3). PCR was performed under thesame conditions aforementioned using as template 3 ml fromthe ®rst PCR product. Ampli®ed products were incubatedwith restriction enzymes as indicated (Table 2) in order toobtain several fragments of appropriate sizes for SSCPanalysis. We followed the manufacturer's procedure (NewEngland Biolab, Inc.) including two modi®cations to ensure acomplete digestion: (i) three times higher restriction enzymesconcentrations, and (ii) overnight incubation. Completedigestion of all samples was checked by electrophoresis in8% polyacrylamide gels for 3 h at 400 V. The digestedsamples (10 ml) were denatured by mixing with 15 ml ofdenaturing stop solution (98% formamide, 0.02% xylenecyanol, and 0.02% bromophenol blue), heated to 958C for5 min, and cooled on ice. Samples were analysed on non-denaturing 10% polyacrylamide gels run for 12 ± 15 h at250 V, and stained by the silver staining method.
DNA sequencing
Tumor samples showing RNA of unexpected sizes during theexpression analysis were subjected to PCR, and the ampli®edmaterial was run in 1% low melting point agarose gels for2 h at 80 V. cDNAs of unusual size were puri®ed using theDNA and Gel Band Puri®cation Kit (Amersham BiotechInc.). Likewise, specimens that showed a di�erential band atSSCP were reampli®ed and PCR products were puri®ed usingthe High Pure PCR Product Puri®cation Kit (BoehringerMannheim Corp., USA). Both types of puri®ed DNAfragments were sequenced using an ABI PrismTM 377 DNASequencer apparatus (PE Applied Biosystem). To rule outfalse negative 10 tumor samples without abnormal SSCPpattern were also sequenced.
Statistical analysis
The variables analysed were contrasted using the w2 test, thew2 test with the Yates correction (Armitage and Berry, 1987),or Fisher's exact test when any of the expected frequencieswas less than ®ve. Two-tailed P values of 50.05 wereconsidered statistically signi®cant. Statistical analyses wereperformed using the EPI ± INFO package, version 6.04.
AcknowledgmentsWe thank Dr Leslie DeGroot from the University ofChicago for providing us with the anti-TR antibodies, DrsManuel Serrano and Angel Zaballos from Centro Nacionalde Biotecnologõ a, Madrid for their help with the real-timePCR and use of LightCycler facilities, Dr Ana Cuadradofor her help with the Western blot assays, and RobinRycroft for English language revision. This work wassupported by Grants 08.1/0042/1998 and 08.1/0069/20002from Comunidad Auto noma de Madrid, Spain.
References
Alberg AJ and Helzlsouer KJ. (1997). Curr. Opin. Oncol., 9,505 ± 511.
Ali I, Lidereau R and Callahan R. (1989). J. Natl. CancerInst., 81, 1815 ± 1820.
Thyroid receptor genes in human breast cancerJM Silva et al
4314
Oncogene

Alvarado-Pisani AR, Chacon RS, Betancourt LJ and Lo pez-Herrera L. (1986). Anticancer Res., 6, 1347 ± 1351.
Anzick SL, Kononen J, Walker RL, Azorsa DO, TannerMM, Guan XY, Sauter G, Kallionimi OP, Trent JM andMeltzer PS. (1997). Science, 277, 965 ± 968.
Arbuthnot P, Kew M, Parker I and Fitschen W. (1989).Anticancer Res., 9, 885 ± 888.
Armitage P and Berry G. (1987). Statistical Methods inMedical Research. Blackwell Scienti®c Publications:Oxford.
Ballinger SW, Bouder TG, Davis GS, Judice SA, Nicklas JAand Albertini RJ. (1996). Cancer Res., 56, 5692 ± 5697.
Barlow C, Meister B, Lardelli M, Lendhal U and VenntroÈ mB. (1994). EMBO J., 13, 4241 ± 4250.
Bautista S, ValleÁ s H, Walker RL, Anzick S, Zeillinger R,Meltzer P and Theillet XC. (1998). Clin. Cancer Res., 4,2925 ± 2929.
Beatson GT. (1896). Lancet, 2, 104 ± 107, 162 ± 165.Burke R and McGuire W. (1978). Cancer Res., 38, 3769 ±
3773.Busch K, Martin B, Baniahmad A, Renkawitz R and Muller
M. (1997). Mol. Endocrinol., 11, 379 ± 389.Cerbon M-A, Pichon M-F and Milgrom E. (1981). Cancer
Res., 41, 4167 ± 4173.Chassande O, Fraichard A, Gauthier K, Flamant F, Legarnd
C, Savatier P, Laudet V and Samarut J. (1997). Mol.Endocrinol., 11, 1278 ± 1290.
Cidlowski JA and Muldoon TG. (1975). Endocrinology, 97,59 ± 67.
Collingwood TN, Wagner R, Matthews CH, Clifton-BlighRJ, Gurner M, Rajanayagam O, Agostini M, FletterickRJ, Beck-Peccoz P, Reinhardt W, Binder G, Ranke MB,Hermus A, Hesch A, Lazarus J, Newrick P, Par®tt V,Raggatt P, de Zegher F and Chatterjee VKK. (1998).EMBO J., 17, 4760 ± 4770.
Corral-Debrinski M, Horton T, Lott M, Sho�ner JM, BealMF and Wallace DC. (1992). Nat. Genet., 2, 324 ± 329.
Dobrovic A, Houle B, Belouchi A and Bradley WE. (1988).Cancer Res., 48, 682 ± 685.
Dressel U and Baniahmad A. (2001). Nuclear Receptors inDisease. Burris TB and McCabe ERB (ed). IRL Press:London, pp. 59 ± 96.
Falcone M, Miyamoto T, Fierro-Renoy F, Macchia E andDeGroot L. (1992). Endocrinology, 131, 2419 ± 2429.
Fasco MJ, Keyomarsi K, Arcaro KF and Gierthy JF. (2000).Mol. Cell. Endocrinol., 166, 156 ± 169.
Forrest D and VennstroÈ m B. (2000). Thyroid, 10, 41 ± 52.Futreal PA, Cochran C, Marks JR, Iglehart JD, Zimmerman
W, Barret JC and Wiseman RW. (1994). Cancer Res., 54,1791 ± 1794.
Futreal PA, SoÈ derkvist P, Marks JR, Iglehart JD, CochranC, Barret JC and Wiseman RW. (1992). Cancer Res., 52,2624 ± 2627.
Gonza lez MV, Jime nez B, Berciano MT, Gonza lez-SanchoJM, Caelles C, Lafarga M and MunÄ oz A. (2000). J. Cell.Biol., 150, 1199 ± 1208.
Gonza lez-Sancho JM, Alvarez-Dolado M and MunÄ oz A.(1999). Mol. Carcinogen., 24, 99 ± 107.
Guernsey DL. (1993). Cancer J., 6, 253 ± 256.Hedley AJ, Jones SJ, Spiegelhalter DJ, Clements P, Bewsher
PD, Simpson JG andWeir RD. (1981).Lancet, 1, 131 ± 133.Houdebine L, Delouis C and Devinoy E. (1978). Biochemie,
60, 809 ± 812.Huber-Gieseke T, Pernin A, Huber O, Burger AG and Meier
CA. (1997). Oncology, 54, 214 ± 219.Hudson LG, Stanton JB, Glass CK and Gill GN. (1990).
Cell, 62, 1165 ± 1175.
Kamiya Y, Puzianowska-Kuznicka M, McPhie P, NaumanJ, Cheng SY and Nauman A. (2002). Carcinogenesis, 23,25 ± 33.
Kelsey JL and Horm-Ross PL. (1993). Epidemiol. Rev., 15,7 ± 16.
Lin KH, Shieh HY, Chen SL and Hsu HC. (1999). Mol.Carcinog., 26, 53 ± 61.
Lo pez-Barahona M, Fialka I, Gonza lez-Sancho JM, Asun-cio n M, Gonza lez M, Iglesias T, Bernal J, Beug H andMunÄ oz A. (1995). EMBO J., 14, 1145 ± 1155.
Lukas J, Gao D-Q, Keshmeshian M, Wen W-H, Tsao-WeiD, Rosenberg S and Press MF. (2001). Cancer Res., 61,3212 ± 3219.
Mangelsdorf D, Thummel C, Beato M, Herrlich P, SchuÈ tz G,Umesono K, Blumberg B, Kastner P, Mark M, ChambonP and Evans R. (1995). Cell, 83, 835 ± 839.
Markowitz S, Haut M, Stellato T, Gerbic C and MolkentinK. (1989). J. Clin. Invest., 84, 1683 ± 1687.
Martõ nez L, Castilla JA, Gil T, Molina J, Alarco n JL,Marcos C and Herruzo A. (1995). Eur. J. Endocrinol., 132,673 ± 676.
MartõÂ nez MB, Ruan M and Fitzpatrick LA. (2000). CancerChemother. Pharmacol., 45, 93 ± 102.
McCabe CJ, Gittoes NJ, Sheppard MC and Franklyn JA.(1999). J. Clin. Endocrinol. Metab., 84, 649 ± 653.
MunÄ oz A and Bernal J. (1997). Eur. J. Endocrinol., 137,433 ± 445.
Nogueira CR and Brentani MMJ. (1996). Steroid Biochem.Mol. Biol., 59, 271 ± 279.
O'Donnell AM and Koenig RJ. (1990). Mol. Endocrinol., 4,715 ± 720.
Puzianowska-Kuznicka M, Nauman A, Madej A, Tanski Z,Cheng SY and Nauman J. (2000). Cancer Letts., 155,145 ± 152.
Sap J, MunÄ oz A, Damm K, Goldberg Y, Ghysdael J, LeutzA, Beug H and VennstroÈ m B. (1986). Nature, 324, 635 ±640.
Selliti D, Tseng Y and Latham K. (1983). Cancer Res., 43,1030 ± 1038.
Singh D and Bern H. (1969). J. Endocrinol., 45, 579 ± 583.Smallridge RC and Latham KR. (1980). Clin. Res., 28, 421.Smyth PPA. (1997). Ann. Med., 29, 189 ± 191.Smyth PPA, Smith DF, McDermott EWM, Murray MJ,
Geraghty JG and O'Higgins NJ. (1996). J. Clin.Endocrinol. Metab., 81, 937 ± 941.
Strain JJ, Bokje E, van't Veer P, Coulter J, Stewart C, LoganH, Odling-Smee W, Spence RAJ and Steele K. (1997).Nutr. Cancer, 27, 48 ± 52.
van de Vijver M, van de Bersselaar R, Devilee P, CornelisseC and Nusse R. (1987). Mol. Cell. Biol., 7, 2019 ± 2023.
Vasudevan N, Koibuchi N, Chin WW and Pfa� D. (2001a).Mol. Brain Res., 95, 9 ± 17.
Vasudevan N, Zhu YS, Daniel S, Koibuchi N, Chin WW andPfa� D. (2001b). J. Neuroendocrinol., 13, 779 ± 790.
Vonderhaar B. (1977). Endocrinology, 100, 1423 ± 1431.Vonderhaar B and Greco A. (1979). Endocrinology, 104,
409 ± 418.Vonderhaar B, Tang E, Lyster RR and Nascimento MCS.
(1986). Endocrinology, 119, 580 ± 585.Yokoe T, Iino Y, Takei H, Horiguchi J, Koibuchi Y,
Maemura M, Ohwada S and Morishita Y. (1997).Anticancer Res., 17, 695 ± 700.
Yokoe T, Iino Y, Takei H, Horiguchi J, Koibuchi Y,Maemura M, Ohwada S and Morishita Y. (1996).Anticancer Res., 16, 2069 ± 2072.
Wallin G, Bronnegard M, Grimelius L, MsGuire J andTorring O. (1992). Thyroid, 2, 307 ± 313.
Oncogene
Thyroid receptor genes in human breast cancerJM Silva et al
4315

Williams GR. (2000). Mol. Cell. Biol., 20, 8329 ± 8342.Zhou-Li F, Albaladejo V, Joly-Pharaboz MO, Nicolas B and
Andre J. (1992). Endocrinology, 130, 1145 ± 1152.
Zhu Y-S, Yen PM, Chin WW and Pfa� DW. (1996). Proc.Natl. Acad. Sci. USA, 93, 12587 ± 12592.
Thyroid receptor genes in human breast cancerJM Silva et al
4316
Oncogene