AT2 receptors: functional relevance in cardiovascular disease
Upload
independentCategory
view
0download
0
Thyroid Disease and theCardiovascular System
Sara Danzi, PhDa,*, Irwin Klein, MDb,c
INTRODUCTION
There is an intimate relationship between the thyroid gland and the heart. Thyroiddysfunction, including subclinical thyroid disease, has significant effects on cardiovas-cular function and health. Likewise, chronic disease states, such as heart disease,may lead to reduced serum thyroid hormone levels, specifically T3 (low T3 syndrome)causing a synergistic negative effect on cardiac and cardiovascular function. There-fore, diagnosis and treatment of the patient with heart disease may benefit from anal-ysis of thyroid status, including levels of serum total T3.
THYROID HORMONE REGULATION AND METABOLISM
The thyroid gland produces 2 biologically active hormones, thyroxine (T4) and triiodo-thyronine (T3). Although T4 has some documented nongenomic effects, it is largelyconsidered a prohormone. Most of T4 is converted to T3 by 50-monodeiodination inthe liver, kidneys, and skeletal muscle.1,2 T3 is then delivered to the circulation sothat it is available for tissues and organs that rely solely or predominantly on serumT3, such as the heart.
a Department of Biological Sciences and Geology, Queensborough Community College, 222-0556th Avenue, Bayside, NY 11364, USA; b Department of Medicine and Cell Biology, NYU Schoolof Medicine, New York, NY 10016, USA; c Private Office, 935 Northern Boulevard, Great Neck,NY 11021, USA* Corresponding author.E-mail address: [email protected]
KEYWORDS
! Hypothyroidism ! Hyperthyroidism ! Subclinical ! Thyroid hormone! Triiodothyronine ! Heart ! Cardiac myocyte
KEY POINTS
! Thyroid dysfunction may significantly impair cardiac and cardiovascular health.
! Chronic diseases, such as heart disease, may lead to the low T3 syndrome.
! More severe heart disease (NYS Heart Association classification stages 3 and 4) is asso-ciated with an increased prevalence of low T3 syndrome.
! Regardless of the cause, in this context decreased serum T3 levels are associated withpoor prognosis, especially in heart disease.
Endocrinol Metab Clin N Am 43 (2014) 517–528http://dx.doi.org/10.1016/j.ecl.2014.02.005 endo.theclinics.com0889-8529/14/$ – see front matter ! 2014 Elsevier Inc. All rights reserved.
Expression and activity of relevant monodeiodinases are also regulated in part byT3.
3 Serious chronic illness, such as heart disease, is often associated with decreasedserum T3 levels. This is known as low T3 syndrome or nonthyroidal illness and isfrequently caused by impaired deiodinase activity, primarily from congestion in theliver.1 The hepatic type 1 iodothyronine deiodinase (D1) is induced at the transcrip-tional level by T3, but in illness, a cytokine-mediated effect blocks the induction, result-ing in decreased serum T3 levels.
4
The regulation of thyroid hormone synthesis and secretion is primarily dependent onthyrotropin (thyroid stimulating hormone or TSH), synthesized and released by theanterior pituitary in a negative feedback loop. This feedback is largely driven by serumT4 levels and thus, serum T3 levels decline without promoting a compensatoryresponse from the pituitary. In the low T3 syndrome, however, increased T4 productionwould not be beneficial because it is the conversion to T3 that is impaired. The conse-quences of this and potentially significant implications for the heart and cardiovascularsystem are discussed.
THYROID HORMONE ACTION AT THE CELLULAR LEVEL
The actions of T3 include genomic transcriptional activation and repression and non-genomic actions targeted to specific membrane proteins, organelles, and cytoskeletalcomponents. Membrane proteins include solute transporters for ions (Ca21, Na1) andglucose among many others.5 Together, the nongenomic and genomic actions of T3on cardiac myocytes and vascular smooth muscle are responsible for significanteffects on the heart and cardiovascular system function.The transcriptional actions of T3 are mediated by nuclear receptor proteins that bind
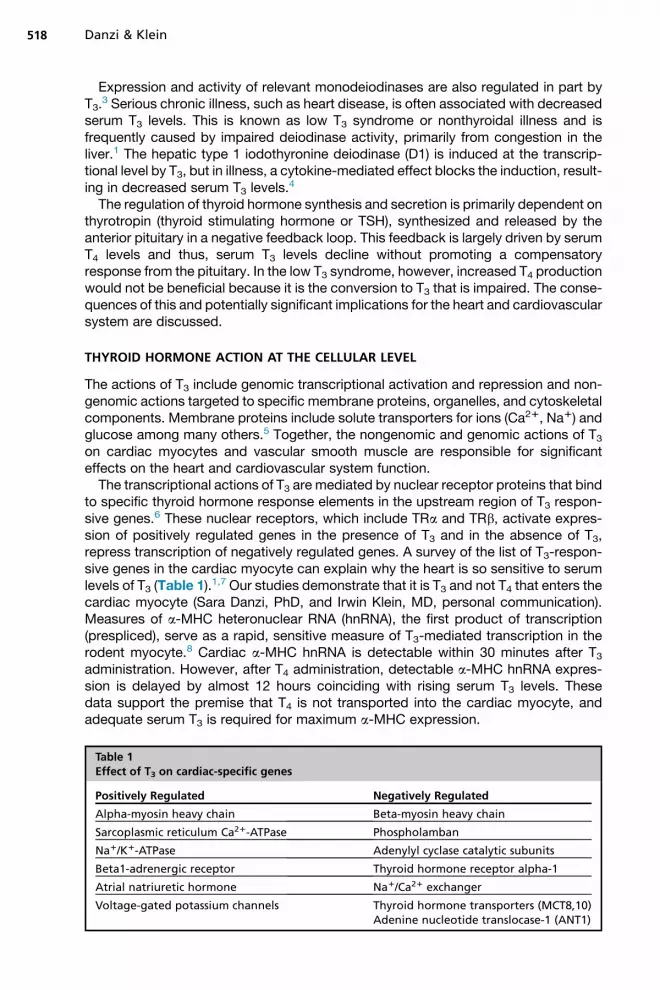
to specific thyroid hormone response elements in the upstream region of T3 respon-sive genes.6 These nuclear receptors, which include TRa and TRb, activate expres-sion of positively regulated genes in the presence of T3 and in the absence of T3,repress transcription of negatively regulated genes. A survey of the list of T3-respon-sive genes in the cardiac myocyte can explain why the heart is so sensitive to serumlevels of T3 (Table 1).1,7 Our studies demonstrate that it is T3 and not T4 that enters thecardiac myocyte (Sara Danzi, PhD, and Irwin Klein, MD, personal communication).Measures of a-MHC heteronuclear RNA (hnRNA), the first product of transcription(prespliced), serve as a rapid, sensitive measure of T3-mediated transcription in therodent myocyte.8 Cardiac a-MHC hnRNA is detectable within 30 minutes after T3administration. However, after T4 administration, detectable a-MHC hnRNA expres-sion is delayed by almost 12 hours coinciding with rising serum T3 levels. Thesedata support the premise that T4 is not transported into the cardiac myocyte, andadequate serum T3 is required for maximum a-MHC expression.
Table 1Effect of T3 on cardiac-specific genes
Positively Regulated Negatively Regulated
Alpha-myosin heavy chain Beta-myosin heavy chain
Sarcoplasmic reticulum Ca21-ATPase Phospholamban
Na1/K1-ATPase Adenylyl cyclase catalytic subunits
Beta1-adrenergic receptor Thyroid hormone receptor alpha-1
Atrial natriuretic hormone Na1/Ca21 exchanger
Voltage-gated potassium channels Thyroid hormone transporters (MCT8,10)Adenine nucleotide translocase-1 (ANT1)
Danzi & Klein518
Despite the fact that the regulation of a-MHC has been carefully studied in rodentcardiac myocytes, it is the calcium cycling proteins in the human heart that appear tobe the most important target of thyroid hormone action. The sarcoplasmic reticulumcalcium ATPase (SERCA2) functions to sequester calcium in the sarcoplasmic retic-ulum during the relaxation phase of myocyte contraction. The SERCA2 ion transporteris regulated by the presence and phosphorylation state of membrane protein phos-pholamban (PLB). Phosphorylation of PLB alters the conformational state of the pro-tein, which in turn affects SERCA2 function.9,10 Expression of both these proteins isregulated by T3. SERCA2 expression is positively regulated and PLB expression isnegatively regulated. In addition, the degree of PLB phosphorylation is regulated byT3. The net effect is that, in the presence of T3, myocyte calcium cycling is enhancedleading to improved cardiac myocyte relaxation and improved overall cardiac dia-stolic function. This is the mechanism by which T3 acts as a unique lusitropic agent.With insufficient serum T3 levels, impaired diastolic function may result. The low T3syndrome may be a significant factor in heart disease, specifically diastolicdysfunction.Thyroid hormone analogues are of clinical interest for potential therapeutic value in
lipid lowering and weight loss. The development for clinical use has heretofore beenhampered by the untoward cardiac effects despite being designed for thyroid hor-mone receptor selectivity.11 However, a recent study of the TRb specific ligand, epro-tirome, has shown the novel ability to lower serum cholesterol levels without affectingheart rate or cardiac function.12 This class of drugs will require further study as a noveladdition to the therapeutic armamentarium for reducing cardiovascular risk throughlowered low density lipoprotein (LDL) cholesterol and Lp(a).13 To date, the develop-ment of eprotirome has been halted as a result of untoward histologic findings in carti-lage from animals treated with the drug for 12 months.
THYROID HORMONE ACTION ON THE HEART AND CARDIOVASCULAR SYSTEM
Thyroid function can be assessed in variousways includingmeasurement of thyroid hor-mones, free and total T4 and T3 and of TSH. Most often, the measurement of serum TSHlevels is the only test ordered, as TSH is considered the gold standard for thyroid func-tion. However, despite the narrowing of the reference range for TSH (from 0.3–3.5mU/L),variations in thyroid hormone levels within the normal range are associated with predict-able affects on cardiac function.14,15 Measurement of other thyroid hormones, specif-ically total T3, demonstrates associations with impaired cardiac function and serumbrain natriuretic peptide in patients with cardiac disease and heart failure (especiallydiastolic dysfunction).16
Cellular T3 uptake from serum depends on members of the monocarboxylate trans-porter (MCT) and organic anion transporter family of plasma membrane trans-porters.16,17 These proteins transport a variety of ligands but only MCT8 andMCT10 (also known as TAT1) are highly specific for iodothyronines and are expressedin heart (Sara Danzi, PhD, and Irwin Klein, MD, personal communication).18 Most dataindicate that the cardiac myocyte cannot metabolize T4 to T3. The observed cardiacmyocyte nuclear actions and changes in gene expression result from changes in bloodlevels of T3.
8 The cardiac myocyte is very sensitive to changes in serum T3, and this isevidenced by rapid changes in the expression of T3 mediated genes.8
Through effects on cardiac myocytes and vascular smooth muscle cells, increasedserum T3 levels are associated with enhanced contractility and diastolic function andlower systemic vascular resistance (SVR).1,19 Data from the Framingham Heart Studyconfirm that TSH is inversely related to left ventricular contractility.20 Clearly heart rate
Thyroid Disease and the Cardiovascular System 519
is positively associated with serum T3 levels and heart rate remains one of the mostsensitive physiologic measures of thyroid hormone action.The effects of thyroid hormone on the heart and cardiovascular system are the most
informative and sensitive signs of thyroid dysfunction. Thyroid disease states havepredictable cardiac and hemodynamic consequences. These are discussed later.
HYPERTHYROIDISM
Many of the classic signs and symptoms of hyperthyroidism are the cardiac and he-modynamic manifestations and include palpitations, tachycardia, exercise intoler-ance, dyspnea on exertion, widened pulse pressure, and sometimes atrial fibrillation(Table 2).21,22 In patients with hyperthyroidism, whether endogenous or exogenousin origin, cardiac output may be increased by 50% to 300% over that of normal sub-jects due to the combined effect of increased resting heart rate, contractility, ejectionfraction, and blood volume with decreased SVR.1 Vascular tissue in the pulmonarysystem does not appear to respond similarly, and pulmonary hypertension has beennoted with hyperthyroidism.23 Pulmonary artery hypertension in hyperthyroidismmay be associated with signs of right-sided heart failure, including neck vein disten-sion and peripheral edema.24,25
Cardiac contractility is enhanced, including both systolic and diastolic function, andcardiac output and resting heart rate are increased in hyperthyroidism.26 A decrease inSVR decreases afterload and improves myocardial efficiency. An increase in bloodvolume and an increase in venous return cause the preload of the heart to increase,further augmenting cardiac output. The increase in cardiovascular hemodynamicsallows for increased blood flow leading to enhanced perfusion to provide for the sub-strate and oxygen demands of peripheral tissues (Fig. 1).The cardiovascular manifestations of hyperthyroidism are independent of the cause
of the increased levels of thyroid hormone.27 Tachycardia is the most common finding.Heart rate is increased both at rest and with exercise and palpitations are common.Atrial arrhythmias, including atrial fibrillation can occur but this is more common inolder patients. Other findings include widened pulse pressure, increased systolicand lowered diastolic pressure, and dyspnea on exertion. Exercise intolerance withlimitations such as climbing one flight of stairs results from both skeletal muscleand respiratory weakness as well as a decrement in cardiac reserve capacity.
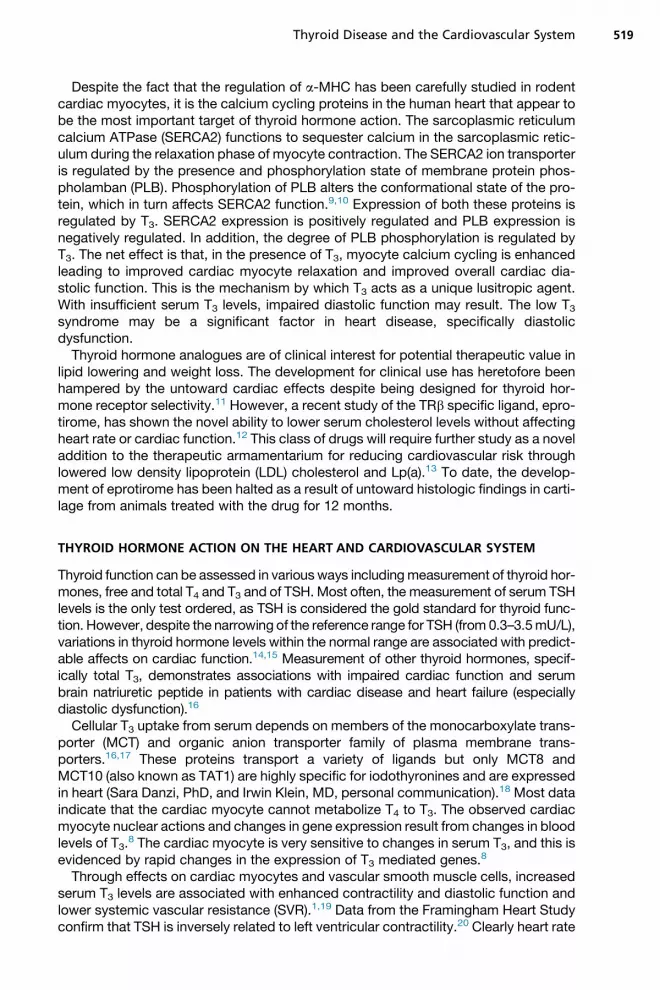
Table 2Cardiovascular signs and symptoms associated with hyperthyroidism and hypothyroidism
Hyperthyroidism Hypothyroidism
Palpitations Fatigue
Anginal chest pain Decreased endurance
Exercise intolerance Increased serum cholesterol
Atrial fibrillation Impaired cardiac contractility
Exertional dyspnea Impaired diastolic function
Cardiac hypertrophy Increased SVR
Systolic hypertension Bradycardia
Peripheral edema Decreased endothelial-derived relaxation factor
Hyperdynamic precordium Increased homocysteine
Pulmonary hypertension Increased C-reactive protein
Heart failure
Danzi & Klein520

Signs and symptoms of heart failure may rarely occur in patients with thyrotoxicosis,usually in the setting of prolonged and severe hyperthyroidism or after the onset ofatrial fibrillation. Because cardiac output at rest is increased in hyperthyroidism, theincreased output that normally accompanies exercise is blunted. Pulmonary and pe-ripheral edema can occur as atrial filling pressure increases, causing a congested cir-culation.13 True heart failure in hyperthyroidism, characterized by decreased cardiaccontractility, abnormal diastolic compliance, and pulmonary congestion, is most likelythe result of rate-related heart failure because sustained tachycardia impairs leftventricular contractility. This finding should be confirmed by noninvasive cardiac mea-sures such as echocardiography followed by the usual course of diuretics. Beta-adrenergic blocking drugs are indicated to control the heart rate and should beused as part of the initial therapy within an intensive care unit setting if the degreeof heart failure is significant enough to impair cardiovascular hemodynamics. Althoughpropranolol is the most commonly used agent, intravenous use should be avoided andthe short-acting agent esmolol can be used if concern about negative inotropy out-weighs the goal of rate reduction. Attention to other potential medical comorbidities,such as infection, should also be addressed. Although b-adrenergic blockade can pro-vide improvement in many, if not all of the cardiovascular findings, definitive treatmentis necessary to normalize serum T4, T3, and TSH. Treatment of the hyperthyroidism inthese circumstances is best accomplished with 131Iodine or alternatively methimazole,and in almost all cases, this returns cardiac function to normal.28 In the setting of multi-nodular goiter, pretreatment with methimazole may be beneficial, but this does notappear to be the case in patients with classical Grave disease.Sinus tachycardia is the most common rhythm disturbance in young, otherwise
healthy patients with hyperthyroidism. Atrial fibrillation caused by hyperthyroidism
Fig. 1. Effects of thyroid hormone on cardiovascular hemodynamics. T3 affects tissue ther-mogenesis, systemic vascular resistance, blood volume, cardiac contractility, heart rate,and cardiac output as indicated by the arrows.
Thyroid Disease and the Cardiovascular System 521
(especially subclinical hyperthyroidism) is observed more frequently with advancingage.29 Although the prevalence of abnormal thyroid function testing, including a sub-normal serum TSH level, is low in patients with new onset atrial fibrillation, the benefitassociated with the ability to restore thyrotoxic patients to a euthyroid state and sinusrhythm justifies routine TSH testing in this setting.Symptomatic treatment of thyrotoxic atrial fibrillation includes b-adrenergic
blockade13; this can be accomplished rapidly whereas treatments including radioio-dine and methimazole leading to restoration of the euthyroid state require a longertime. Digitalis has been used to control the ventricular response in hyperthyroidism-associated atrial fibrillation but usually requires higher doses of this medication. Antico-agulation in patients with hyperthyroidism and atrial fibrillation is controversial becausethe potential for systemic or cerebral embolization must be weighed against the risk ofbleeding and complications. The major risk factor for systemic embolization in thyro-toxicosis seems to be age and not the presence of atrial fibrillation. Therefore, unlessthere is a separate cardiac indication for warfarin or other forms of anticoagulation,either no treatment or aspirin can be used especially in younger individuals, as needed.Successful treatment of hyperthyroidism to restore normal serum levels of T4 and T3
leads to reversion to sinus rhythm in most younger patients within a fewmonths. In thesetting of atrial fibrillation of longer duration and in older patients, the rate of reversionto sinus rhythm is lower and electrical or pharmacologic cardioversion should there-fore be attempted after the patient has been rendered euthyroid.
HYPOTHYROIDISM
In contrast to the dramatic clinical signs and symptoms of hyperthyroidism, the car-diovascular manifestations of hypothyroidism are more subtle.22 Thus, althoughbradycardia, diastolic hypertension, a narrow pulse pressure, and a relatively quietprecordium are characteristic findings, the correct diagnosis is often establishedwhen a serum TSH level is obtained for one of a variety of clinical indications. Thesemay include fatigue, myalgias, elevated cholesterol, or the feeling of puffiness (seeTable 2). Hemodynamic changes of hypothyroidism are diametrically opposite tothose of hyperthyroidism.30 Treatment of hypothyroid patients with restoration of aeuthyroid state resolves these changes in parallel with a resolution of clinicalsymptoms.Hypothyroidism also produces increases in total and LDL cholesterol as well as
apolipoprotein B through multiple mechanisms, but in general, in magnitude propor-tional to the severity of the hypothyroidism. Thus, the finding of a direct relationshipbetween the level of TSH as a measure of hypothyroidism and serum total cholesteroland LDL cholesterol is not surprising.31
Serum creatine kinase is elevated by 50% to 10-fold in as many as 30% of patientswith hypothyroidism. Isoform specificity indicates that more than 96% is the muscleform, consistent with a skeletal muscle origin of increased enzyme release.32 Pericar-dial effusions can occur, consistent with the observation that patients with hypothyroid-ism have an increase in volume of distribution of albumin and a decrease in lymphaticclearance function. Occasionally, the pericardial effusions are quite large, and echocar-diography demonstrates small to moderate effusions in as many as 30% of overtlyhypothyroid patients. The presence of pericardial fluid in hypothyroid patients doesnot usually compromise cardiac output. Cardiac tamponade is exceedingly rare, andafter initiation of T4 therapy, the effusion resolves over a period of weeks to months.The electrocardiogram in hypothyroidism is characterized by sinus bradycardia, low
voltage, and prolongation of the action potential duration and the QT interval. The
Danzi & Klein522
latter, in turn, predisposes patients to ventricular arrhythmias. There are case reportsof patients with acquired torsades de pointes that completely resolved with thyroidhormone therapy.1
As a result of an increase in risk factors, including hypercholesterolemia, hyperten-sion, and elevated levels of homocysteine, patients with hypothyroidism may haveincreased risk for atherosclerosis.32,33 Studies have shown increases in abdominalaortic atherosclerosis in patients with even mild hypothyroidism.34 Whether patientswith hypothyroidism have an increase in coronary artery disease is an important clin-ical issue.In otherwise healthy patients younger than 50 years, it is possible to initiate full
replacement doses of L-thyroxine (100–150 mg/d or 1.5 mg/kg). In patients older than50 years with known or suspected coronary artery disease, the issue is more compli-cated and treatment should be started with low dose (25–50 mg) T4 and increasedslowly, no more than every 6 to 12 weeks.In all patients, thyroid hormone replacement should continue until serum TSH is
normal and the patients are clinically euthyroid. The concept that these patientsbenefit from maintenance of “mild hypothyroidism” is not supported by the knowneffects of thyroid hormone on the heart and cardiovascular system. Thyroid hormonereplacement should be accomplished with purified preparations of levothyroxinesodium. Preparations containing T4 with T3 (eg, thyroid extract) or the existing purifiedpreparations of T3 do not appear to offer benefit in the majority of patients. The shorthalf-life of T3 and the inability to maintain serum levels within normal range in patientsso treated can add to cardiac risk.35,36
The leading causes of hypothyroidism include Hashimoto disease, previous radio-iodine therapy for Graves’ disease, and iodine deficiency (in parts of the world wherethat remains a public health problem). Thyroid gland failure in turn produces diag-nostic elevations in serum TSH.14 Thus, the finding of elevated TSH is sufficientto establish the diagnosis and form the basis for treatment. Thus, TSH screeningcan be advised for all adults and particularly patients demonstrating hypertension, hy-percholesterolemia, hypertriglyceridemia, coronary or peripheral vascular disease,unexplained pericardial or pleural effusions, and a variety of musculoskeletalsyndromes.1,32
SUBCLINICAL THYROID DISEASE
In contrast to overt symptomatic thyroid disease, subclinical thyroid disease impliesthe absence of classical hyper- or hypothyroidism-related symptoms in patientswith thyroid dysfunction. The definition has been further refined to include the demon-stration of an abnormal TSH level in the presence of normal serum levels of total T4 andfree T4.
37,38 A recent study confirmed that heart failure risks are increased in subclin-ical thyroid disease, with both higher and lower TSH levels.39 With the advent of wide-spread TSH screening, the prevalence of subclinical thyroid disease may exceed thatof overt disease by three- to four-fold.
SUBCLINICAL HYPOTHYROIDISM
Subclinical hypothyroidism, defined by a TSH level above the upper range of the refer-ence population (usually >5 mU/L), is seen in as many as 9% of unselected popula-tions, and prevalence clearly increases with advancing age.40 In contrast to youngerpatients, in whom there is a strong female predilection, this difference is lost in olderpopulations. Studies of lipid metabolism, atherosclerosis, cardiac contractility, andSVR are altered in subclinical hypothyroidism. Cholesterol levels rise in parallel with
Thyroid Disease and the Cardiovascular System 523
increments in TSH elevations starting at 5 mU/L. In a large study of women in Rotter-dam, it was noted that atherosclerosis and myocardial infarction were increased withodds ratios of 1.7 and 2.3, respectively, in women with subclinical hypothyroidism.Interestingly, the presence of antithyroid antibodies indicated heightened risk.34
Restoration of serum TSH to normal after thyroid hormone replacement improved lipidlevels, lowered SVR, and improved cardiac contractility.38 In patients with subclinicalhypothyroidism, isovolumic relaxation times are prolonged, whereas systolic contrac-tile function is unchanged. Replacement with L-thyroxine sodium at a mean dose of68 ug/d (range 50–100 ug/d) restored isovolumic relaxation times to normal, andcompared with those in the same patients before therapy, SVR declined and systolicfunction was significantly improved.38 A variety of studies have indicated that thechanges in SVR may result from alterations in endothelium-dependent vasodila-tion.41,42 Taking these findings together, it seems appropriate to recommend thyroidhormone replacement for all patients with subclinical hypothyroidism from a cardio-vascular perspective.13,43,44 The lack of untoward cardiac effects observed whenserum TSH levels have been restored to normal indicates that the potential benefitsfar outweigh the risks of treatment.1,33,37,44
Because hypothyroidism is known to produce a variety of modifiable cardiovascularrisk factors, it seemed quite attractive to suggest that thyroid hormone treatment of alldegrees of hypothyroidism would result in a cardiovascular benefit.1 However, a pro-spective randomized, controlled trial to test this hypothesis would be potentiallyunethical to undertake in overtly hypothyroid patients and require an inordinate num-ber of subjects to study subclinical hypothyroidism. With the increasing magnitude ofhealth care costs related to the diagnosis and treatment of heart failure, especially inthe aging population, this has important clinical implications. Similarly, the increasingprevalence of subclinical hypothyroidism in the aging population makes the questionof when and for whom thyroid hormone therapy should be recommended, an ongoingclinical challenge.As a test of this hypothesis, the report from Razvi and colleagues44 using The United
Kingdom General Practitioner research database to identify individuals with subclini-cal hypothyroidism and serum TSH levels in a range of 5 to 10 mU/L was of specialinterest. In that “real-world” study, 53% of the subclinical hypothyroid patients weretreated with levothyroxine and treatment led to a significant reduction in both ischemicheart disease events and cardiovascular mortality. In contrast, the older patients (olderthan 70 years) did not demonstrate the same therapeutic benefit.
DIAGNOSIS AND TREATMENT
Several studies have attempted to address the possibility of combination T4, T3 ther-apy for hypothyroidism with mixed results. The potential application in a small per-centage of hypothyroid patients with impaired deiodinase (D2) function has beenacknowledged. A properly conducted study with these selected patients may indicatea benefit of combination therapy where deiodinase activity has been compro-mised.45,46 (This seems in contrast to your statement above that combinationT4 and T3 should not be used; also contrary to ATA guidelines, but I think correctly re-flects the discussions of last year’s Spring ATA meeting.)
ALTERATIONS IN THYROID HORMONE METABOLISM THAT ACCOMPANY HEARTDISEASE
The intimate relationship between thyroid hormones and the heart are evident in thy-roid dysfunction with the observed effects on the heart and cardiovascular system. In
Danzi & Klein524
addition, altered thyroid hormone metabolism occurs in the setting of heart disease,after cardiac surgery, or after acute myocardial infarction, resulting in low serum T3levels despite normal TSH and T4 levels, which appears to result from a cytokine-induced blockade of iodothyronine deiodinase synthesis and activity, characteristicof chronic illness.4,47,48 Interleukin 6 and tumor necrosis factor a levels are increasedin the low T3 syndrome.In patients with heart failure, the decrease in serum T3 concentration is proportional
to the severity of the heart disease as assessed by the New York Heart Association(NYHA) functional classification.49 T3 is an important regulator of cardiac gene expres-sion and, in fact, the list of T3-mediated genes that are altered in overt hypothyroidismis almost identical to the changes in gene expression in heart failure.50,51 Theseinclude the genes that encode the contractile proteins, a-MHC and b-MHC, thesodium calcium exchanger (NCX1), SERCA2, PLB, and the b-adrenergic receptor(b-AR). The net effect of these alterations in gene expression is to alter cardiaccontractility, calcium cycling, and diastolic relaxation of the myocardium.The low T3 syndrome is a strong prognostic, independent predictor of death in pa-
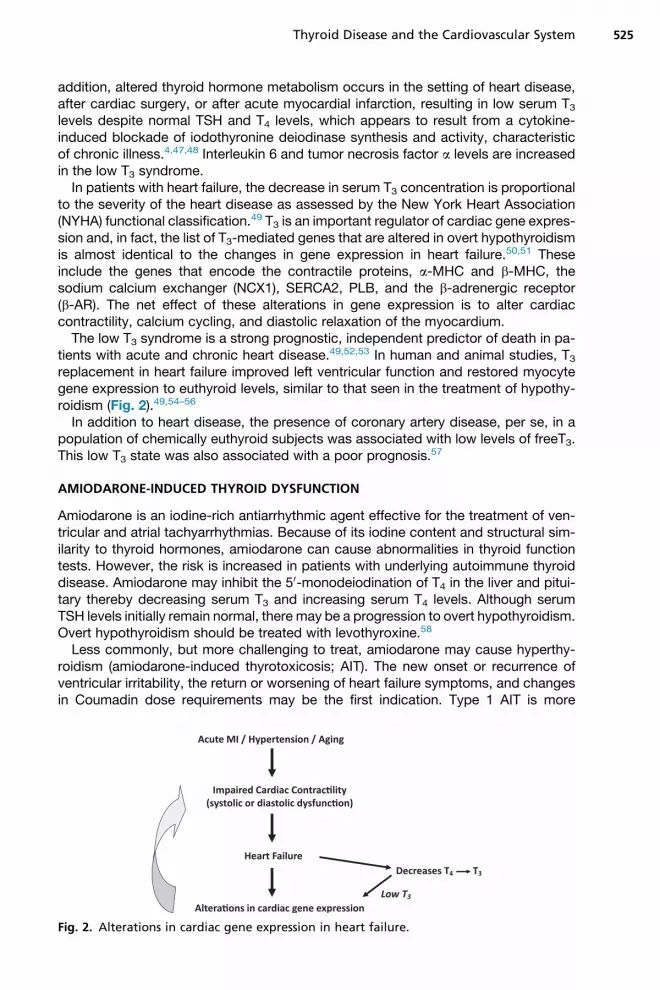
tients with acute and chronic heart disease.49,52,53 In human and animal studies, T3replacement in heart failure improved left ventricular function and restored myocytegene expression to euthyroid levels, similar to that seen in the treatment of hypothy-roidism (Fig. 2).49,54–56
In addition to heart disease, the presence of coronary artery disease, per se, in apopulation of chemically euthyroid subjects was associated with low levels of freeT3.This low T3 state was also associated with a poor prognosis.57
AMIODARONE-INDUCED THYROID DYSFUNCTION
Amiodarone is an iodine-rich antiarrhythmic agent effective for the treatment of ven-tricular and atrial tachyarrhythmias. Because of its iodine content and structural sim-ilarity to thyroid hormones, amiodarone can cause abnormalities in thyroid functiontests. However, the risk is increased in patients with underlying autoimmune thyroiddisease. Amiodarone may inhibit the 50-monodeiodination of T4 in the liver and pitui-tary thereby decreasing serum T3 and increasing serum T4 levels. Although serumTSH levels initially remain normal, there may be a progression to overt hypothyroidism.Overt hypothyroidism should be treated with levothyroxine.58
Less commonly, but more challenging to treat, amiodarone may cause hyperthy-roidism (amiodarone-induced thyrotoxicosis; AIT). The new onset or recurrence ofventricular irritability, the return or worsening of heart failure symptoms, and changesin Coumadin dose requirements may be the first indication. Type 1 AIT is more
Fig. 2. Alterations in cardiac gene expression in heart failure.
Thyroid Disease and the Cardiovascular System 525
common in iodine-deficient areas and is associated with preexisting thyroid abnormal-ities. Type II is a destructive thyroiditis. Treatment of AIT may include corticosteroidsor antithyroid drugs, but the discontinuation of amiodarone will not remedy the thyroiddysfunction because the half-life of amiodarone is quite long.59,60
REFERENCES
1. Klein I, Danzi S. Thyroid disease and the heart. Circulation 2007;116:1725–35.2. Koenig RJ. Regulation of type 1 iodothyronine deiodinase in health and disease.
Thyroid 2005;15:835–40.3. Bianco AC, Kim BW. Deiodinases: implications of the local control of thyroid
hormone action. J Clin Invest 2006;116:2571–9.4. Yu J, Koenig RJ. Induction of type 1 iodothyronine deiodinase to prevent the
nonthyroidal illness syndrome in mice. Endocrinology 2006;147:3580–5.5. Davis PJ, Davis FB. Nongenomic actions of thyroid hormone on the heart.
Thyroid 2002;12:459–66.6. Dillmann WH. Cellular action of thyroid hormone on the heart. Thyroid 2002;12:
447–52.7. Danzi S, Klein I, Portman MA. Effect of triiodothyronine on gene transcription
during cardiopulmonary bypass in infants with ventricular septal defect. Am JCardiol 2005;95:787–9.
8. Danzi S, Ojamaa K, Klein I. Triiodothyronine mediated myosin heavy chain genetranscription in the heart. Am J Physiol Heart Circ Physiol 2003;284:H2255–63.
9. Gustavsson M, Verardi R, Mullen DG, et al. Allosteric regulation of SERCA byphosphorylation-mediated conformational shift of phospholamban. Proc NatlAcad Sci U S A 2013;110:17338–43.
10. Ojamaa K, Kenessey A, Klein I. Thyroid hormone regulation of phospholambanphosphorylation in the rat heart. Endocrinology 2000;141:2139–44.
11. Danzi S, Klein I. Cardiac specific effects of thyroid hormone analogues. HormMetab Res 2011;43:1–6.
12. Ladenson PW, Kristensen JD, Ridgway EC, et al. Use of the thyroid hormoneanalogueeprotirome instatin-treateddyslipidemia.NEngl JMed2010;362:906–16.
13. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl JMed 2001;344:501–9.
14. DemersLM,SpencerCA.Laboratorymedicinepracticeguidelines: laboratory sup-port for the diagnosis and monitoring of thyroid disease. Thyroid 2003;13:3–126.
15. Roef GL, Taes YE, Kaufman JM, et al. Thyroid hormone levels within the refer-ence range are associated with heart rate, cardiac structure, and function inmiddle-aged men and women. Thyroid 2013;23:947–54.
16. Selvaraj S, Klein I, Danzi S, et al. Association of Serum Triiodothyronine withB-type natriuretic peptide and severe left ventricular diastolic dysfunction inheart failure with preserved ejection fraction. Am J Cardiol 2012;110:234–9.
17. Visser WE, Friesema EC, Visser TJ. Minireview: thyroid hormone transporters:the knowns and the unknowns. Mol Endocrinol 2011;25:1–14.
18. Friesema EC, Jansen J, Jachtenberg JW, et al. Effective cellular uptake andefflux of thyroid hormone by human monocarboxylate transporter 10. Mol Endo-crinol 2008;22:1357–69.
19. Danzi S, Klein I. Thyroid hormone and the cardiovascular system. Med ClinNorth Am 2012;96:257–68.
20. Pearce EN, Yang Q, Benjamin EJ, et al. Thyroid function and left ventricularstructure and function in the Framingham Heart Study. Thyroid 2010;20:367–73.
Danzi & Klein526
21. Dahl P, Danzi S, Klein I. Thyrotoxic cardiac disease. Curr Heart Fail Rep 2008;5:170–6.
22. Klein I. Endocrine disorders and cardiovascular disease. In: Bonow RO,Mann DL, Zipes DP, et al, editors. Braunwald’s heart disease, chapter 86. 9thedition. St. Louis (MO): WB Saunders and Company; 2011. p. 1829–43.
23. Marvisi M, Brianti M, Marani G, et al. Hyperthyroidism and pulmonary hyperten-sion. Respir Med 2002;96:215–20.
24. Ismail HM. Reversible pulmonary hypertension and isolated right-sided heartfailure associated with hyperthyroidism. J Gen Intern Med 2007;22:148–50.
25. Danzi S, Klein I. Thyroid hormone and blood pressure regulation. Curr Hyper-tens Rep 2003;5:513–20.
26. Mintz G, Pizzarello R, Klein I. Enhanced left ventricular diastolic function in hy-perthyroidism: noninvasive assessment and response to treatment. J Clin Endo-crinol Metab 1991;73:146–50.
27. Klein I, Danzi S. The cardiovascular system in thyrotoxicosis. In: Braverman L,Utiger R, editors. Werner & Ingbar’s the thyroid: a fundamental and clinical text,chapter 31. 10th edition. Philadelphia: Lippincott Williams & Wilkins; 2012.p. 559–68.
28. Bahn RS, BurchHB, Cooper DS, et al. Hyperthyroidism and other causes of thyro-toxicosis:management guidelines of theAmericanThyroidAssociation andAmer-ican Association of Clinical Endocrinologists. Endocr Pract 2011;17:456–520.
29. Sawin CT, Geller A, Wolf PA, et al. Low serum thyrotropin levels as a risk factorfor atrial fibrillation in older persons. N Engl J Med 1994;33:1249–52.
30. Klein I, Danzi S. The cardiovascular system in hypothyroidism. In: Braverman L,Utiger R, editors. Werner & Ingbar’s the thyroid: a fundamental and clinical text.10thedition.Philadelphia:LippincottWilliams&Wilkins;2012.p. 774–80Chapter53.
31. Parle JV, Maisonneuve P, Sheppard MC, et al. Prediction of all-cause and car-diovascular mortality in elderly people from one low serum thyrotropin result:a 10-year cohort study. Lancet 2001;358:861.
32. Rush J, Danzi S, Klein I. Role of thyroid disease in the development of statin-induced myopathy. Endocrinologist 2006;16:279.
33. Cappola AR, Ladenson PW. Hypothyroidism and atherosclerosis. J Clin Endo-crinol Metab 2003;88:2438.
34. Hak AE, Pols HA, Visser TJ, et al. Subclinical hypothyroidism is an independentrisk factor for atherosclerosis and myocardial infarction in elderly women: theRotterdam Study. Ann Intern Med 2000;132:270.
35. Kim SD, Kim SH, Park KS, et al. Regression of the increased common carotidartery-intima media thickness in subclinical hypothyroidism after thyroid hor-mone replacement. Endocr J 2009;56:753.
36. Garber JR, Cobin RH, Gharib H, et al. Clinical practice guidelines for hypothy-roidism in adults; cosponsored by the American Association of Clinical Endocri-nologists and the American Thyroid Association. Thyroid 2012;22:1200–35.
37. Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and therisk of coronary heart disease and mortality. JAMA 2010;304:1365.
38. Biondi B, Cooper DS. The clinical significance of subclinical thyroid dysfunction.Endocr Rev 2008;29:76.
39. Gencer B, Collet TH, Virgini V, et al. Subclinical thyroid dysfunction and the riskof heart failure events: an individual participant data analysis from 6 prospectivecohorts. Circulation 2012;126:1040–9.
40. Cappola AR, Fried LP, Arnold AM, et al. Thyroid status, cardiovascular risk, andmortality in older adults. JAMA 2006;295:1033.
Thyroid Disease and the Cardiovascular System 527
41. Biondi B, Klein I. Hypothyroidism as a risk factor for hypothyroidism. Endocrine2004;24:1–13.
42. Taddei S, Caraccio N, Virdis A, et al. Impaired endothelium-dependent vasodi-latation in subclinical hypothyroidism: beneficial effect of levothyroxine therapy.J Clin Endocrinol Metab 2003;88:3731.
43. Iervasi G, Molinaro S, Landi P, et al. Association between increased mortality andmild thyroid dysfunction in cardiac patients. Arch Intern Med 2007;167:1526–32.
44. Razvi S, Weaver JU, Butler TJ, et al. Levothyroxine treatment of subclinical hy-pothyroidism, fatal and nonfatal cardiovascular events, and mortality. ArchIntern Med 2012;172:811–7.
45. Wartofsky L. Combination L-T3 and L-T4 therapy for hypothyroidism. Curr OpinEndocrinol Diabetes Obes 2013;20:460–6.
46. Klein I, Danzi S. Thyroid hormone treatment to mend a broken heart. J ClinEndocrinol Metab 2008;93:1172–4.
47. Boelen A, Maas MA, Lowik CW, et al. Induced illness in interleukin-6 (IL-6)knock-out mice: a causal role of IL-6 in the development of the low 3,5,3’-triiodo-thyronine syndrome. Endocrinology 1996;137:5250–4.
48. Lubrano V, Pingitore A, Carpi A, et al. Relationship between triiodothyronine andproinflammatory cytokines in chronic heart failure. Biomed Pharmacother 2010;64:165–9.
49. Iervasi G, Pingitore A, Landi P, et al. Low-T3 syndrome: a strong prognostic pre-dictor of death in patients with heart disease. Circulation 2003;107:708–13.
50. Danzi S, Klein I. Changes in thyroid hormone metabolism and gene expressionin the failing heart: therapeutic implications. In: Iervasi G, Pingitore A, editors.Thyroid and heart failure, from pathophysiology to clinics. Italy: Springer-Verlag;2009. p. 97–107 Chapter 10.
51. Danzi S, Klein I. Alterations in thyroid hormones which accompany cardiovascu-lar disease. Clinical Thyroidology 2009;21:3–5.
52. Zhang B, Peng W, Wang C, et al. A low fT3 level as a prognostic marker inpatients with acute myocardial infarctions. Intern Med 2012;51:3009–15.
53. Nicolini G, Pitto L, Kusmic C, et al. New insights into mechanisms of cardiopro-tection mediated by thyroid hormones. J Thyroid Res 2013;2013:264387.
54. Henderson K, Danzi S, Paul JT, et al. Physiological replacement of T3 improvesleft ventricular function in an animal model of myocardial infarction-inducedcongestive heart failure. Circ Heart Fail 2009;2:243–52.
55. Pingitore A, Galli E, Barison A, et al. Acute effects of triiodothyronine (T3) replace-ment therapy in patients with chronic heart failure and low-T3 syndrome: a ran-domized, placebo-controlled study. J Clin Endocrinol Metab 2008;93:1351–8.
56. DeGroot LJ. Non-thyroidal illness syndrome is a manifestation of hypothalamic-pituitary dysfunction, and in view of current evidence, should be treated withappropriate replacement therapies. Crit Care Clin 2006;22:57–86.
57. Coceani M, Iervasi G, Pingitore A, et al. Thyroid hormone and coronary arterydisease: from clinical correlations to prognostic implications. Clin Cardiol2009;32:380–5.
58. Cohen-Lehman J, Dahl P, Danzi S, et al. Effects of amiodarone on thyroid func-tion. Nat Rev Endocrinol 2010;6:34–41.
59. Bogazzi F, Bartalena L, Cosci C, et al. Treatment of type II amiodarone-inducedthyrotoxicosis by either iopanoic acid or glucocorticoids: a prospective, ran-domized study. J Clin Endocrinol Metab 1999;88:2003.
60. Danzi S, Klein I. Amiodarone-induced thyroid dysfunction. J Intensive Care Med2013. [Epub ahead of print].
Danzi & Klein528
Copyright © 2022 FDOKUMEN