
9 is Always on top: Assessing the automaticity of synaesthetic number-forms

B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r . com/ loca te /b ra i n res
Research Report
Evidence for motor learning in Parkinson's disease:Acquisition, automaticity and retention of cued gaitperformance after training with external rhythmical cues
Lynn Rochestera,b,⁎, Katherine Bakerb, Victoria Hetheringtonb, Diana Jonesb,Anne-Marie Willemsc, Gert Kwakkeld, Erwin Van Wegend, Inge Limd, Alice Nieuwboerc
aInstitute for Ageing and Health, Newcastle University, UKbNorthumbria University, Newcastle, UKcKatholieke Universiteit, Leuven, BelgiumdVrije Universiteit Medisch Centrum, Amsterdam, the Netherlands
A R T I C L E I N F O
⁎ Corresponding author. Professor of HumanResearch Unit, Campus for Ageing and Vitali
E-mail address: [email protected]
0006-8993/$ – see front matter. Crown Copyrdoi:10.1016/j.brainres.2010.01.001
A B S T R A C T
Article history:Accepted 2 January 2010Available online 11 January 2010
People with Parkinson's disease (PD) have difficulty learning new motor skills. Evidencesuggests external stimuli (cues) may enhance learning; however, this may be specific tocued rather than non-cued performance. We aimed to test effects of cued training on motorlearning in PD. We defined motor learning as acquisition (single task), automaticity (dualtask) and retention of single- and dual-task performance (follow-up). 153 subjects with PDreceived 3 weeks cued gait training as part of a randomised trial (the RESCUE trial). Wemeasured changes in cued gait performance with three external rhythmical cues (ERC)(auditory, visual and somatosensory) during single and dual tasks after training and 6weeksfollow-up. Gait was tested without cues to compare specificity of learning (transfer).Subjects were ‘on’ medication and were cued at preferred step frequency duringassessment. Accelerometers recorded gait and walking speed, step length and stepfrequency were determined from raw data. Data were analysed with SAS using linearregressionmodels. Walking speed and step length significantly increased with all cues aftertraining during both single- and dual-task gait and these effects were retained. Trainingeffects were not specific to cued gait and were observed in dual-task step length, andwalking speed however was more limited in single-task non-cued gait. These resultssupport the use of ERC to enhance motor learning in PD as defined by increased acquisition,automaticity and retention. They also highlight the potential for sustained improvement inwalking and complex task performance.
Crown Copyright © 2010 Published by Elsevier B.V. All rights reserved.
Keywords:Motor learningExternal rhythmical cueGaitParkinson's diseaseDual taskAutomaticityRetention
Movement Science, Institute for Ageing and Health, Newcastle University, Clinical Ageingty, Newcastle upon Tyne, NE4 5PL, UK. Fax: 0191 248 1251.(L. Rochester).
ight © 2010 Published by Elsevier B.V. All rights reserved.

104 B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
1. Introduction
Research has highlighted a role for the basal ganglia inlearning, raising questions regarding the capacity for peoplewith Parkinson's disease (PD) to acquire and retain motorskills (Doyon, 2008). Motor skills and sequences of movementare acquired through a process of implicit learning, becomingautomatic with practice and performed with little consciousawareness as opposed to explicit learning which refers toacquisition of factual knowledge. Automatic movements havefunctional benefits, allowing dual- and multiple-task perfor-mance, and are impaired in PD (Bond and Morris, 2000; O'Sheaet al., 2002; Rochester et al., 2004). The main method ofmanaging the symptoms of Parkinson's disease (PD) isthrough levodopa therapy providing highly effective symp-tomatic treatment. However, after a variable period of time,motor complications develop that cannot be adequatelycontrolled with medication. These complications includeunpredictable and extended ‘off’ periods, dyskinesias, poorgait and balance which contribute to reduced mobility andincreased risk of falls. Rehabilitation strategies that result insustained change in function in PD may therefore offer animportant contribution to patient management. Knowledge ofmotor learning is therefore critical for the optimal design ofrehabilitation interventions (Abbruzzese et al., 2009).
Motor skill acquisition, automaticity and retention areconsidered hallmarks ofmotor learning. Learning amotor skillhas two phases in which the skill is acquired over a short timescale (a few hours) and then consolidated (retained) into long-term memory with practice over several weeks (Karni et al.,1995). During the early stage attention is required and withrepeated practice this is reduced such that performance canoccur automatically with relatively little attention. Whilst arecent meta-analysis concluded that implicit sequence learn-ing was impaired in PD (Siegert et al., 2006) others havereported that it was possible but attenuated compared tocontrols (Wu and Hallet, 2008; Wilkinson and Jananshanhi,2007; Mentis et al., 2003; Carbon and Eidelberg, 2006). In PD thefast stage of learning where skills are acquired may bepreserved; however, transference of skills into later stages oflearning with increased automaticity and retention of skill isless efficient compared to age matched controls (Doyon et al.,1998; Wu and Hallet, 2008; Wilkinson and Jananshanhi, 2007;Muslimovic et al., 2007).
Motor learning studies demonstrate that there is capacityfor people with PD to learn a variety of motor tasks rangingfrom upper limb movement to functional tasks (Smiley-Oyenet al., 2006; Jessop et al., 2006; Mak and Hui-Chan, 2008). Acommon feature of these studies is the use of augmentedfeedback such as auditory pacing cues or visual cues fortraining. External information in the form of visual or auditorystimuli improves motor performance and motor learning innormal subjects (Heremans et al., 2009; Semjen et al., 2000).Augmented visual feedback also facilitatedmotor learning in anovel upper limb task in PD (Verschueren et al., 1997).Interestingly in this study, the effects were not retained inthe absence of sensory information, highlighting the possibil-ity that learning in PD is context specific with externalfeedback being incorporated into the motor program
(Verschueren et al., 1997). The study by Verschueren et al.(1997) also highlights an important point in relation tomethods of evaluating training as some studies test the effectof training with the cue and others test without the cue andtherefore measure transfer of skill. This is an importantdistinction as cue specific learning (described by Verschuerenet al., 1997) may be missed.
External cues have received much interest as a rehabilita-tion tool to improve function such as gait in PD (for review, seeRubinstein et al., 2002; Lim et al., 2005; Nieuwboer et al., 2008).External cues have been defined as temporal (e.g., auditorytones to step in time to) or spatial (lines on the ground to stepon or over) stimuli associated with the ongoing facilitation ofmovement (Nieuwboer et al., 2007). In PD, where practice wasgiven in a single training session external cues improvedwalking speed and step length (Morris et al., 1996; Rochester etal., 2007; Baker et al., 2007; Hausdorff et al., 2007). Dual-taskwalking speed and step length also improve suggesting thatgait had become more automatic (Rochester et al., 2005, 2007;Baker et al., 2007). Furthermore a one off-training session withexternal cues had a short-term carryover effect to non-cuedgait (up to 2 h) (Morris et al., 1996; Rochester et al., 2005, 2007;Baker et al., 2007, 2008; Hausdorff et al., 2007), which mayindicate the early stages of learning or heightened attention.These studies measure cued gait and underscore the potentialfor cueing training as a motor learning paradigm. Howeverthey also raise the question as to whether a longer period oftraining may facilitate the later phase of motor learning in PDto enhance automaticity and retention.
Clinical studies have shown that externally cued practiceover more extended periods (3–6 weeks) show significantbenefits of training with a range of different external cues ongait, balance and transfers (Thaut et al., 1996; Nieuwboer et al.,2007; Mak and Hui-Chan, 2008; Sidaway et al., 2006). Cuedtraining has also been shown to be more effective than otherinterventions such as non-cued exercise (Mak et al., 2007;Marchese et al., 2000). Evidence for retention is inconclusivehowever with some studies reporting retention of between 2and 4 weeks (Mak and Hui-Chan, 2008; Sidaway et al., 2006)whilst others of longer duration (6 weeks) do not (Nieuwboeret al., 2007). In all of these studies, training effects weremeasured without the external cue; therefore, they primarilyconcentrated on generalisation to a range of functional skillsand motor symptoms. It may be that learning in PD is cuespecific as reported by Verschueren et al. (1997) and theeffect of training on cued performance is therefore not clearto date.
As stated above, we have shown that gait training withexternal rhythmical cues (ERC) (the RESCUE trial) (Nieuwboeret al., 2007) improved a variety of functional tests relating to abroad range of mobility outcomes. These effects were notretained at 6weeks; however, themethod of assessment couldbe insensitive to learning effects specific to cued performance.We were therefore also interested in the specificity of trainingwith ERC on cued gait performance, which we evaluated usinga specially designed protocol that measured cued single- anddual-task gait performance (Rochester et al., 2007). We usedthree different ERC modalities (visual, auditory and somato-sensory) and found ERC (especially auditory) immediatelyenhanced dual-task gait performance before training and had

105B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
a short-term carryover to non-cued gait but these effects werenot retained when measured 3 weeks later (Rochester et al.,2007). Here we extend our findings to report the effect oftraining with ERC on cued gait performance during single- anddual-task gait and retention of performance. These are newdata and have not been previously reported. In this study wedefined motor learning as acquisition, automaticity andretention of skill. We hypothesized that an extended periodof training with ERCs would further enhance cued gaitperformance during single (acquisition) and dual tasks(automaticity) and would be retained. We also tested trainingeffects during non-cued single- and dual-task gait to seelearning was specific to cued trials only.
2. Results
Demographic subject data are shown in Table 1. There was nodifference between the characteristics of the early and lategroups. Most patients had mild to moderate disease severityas 46.4% of patients (n=71) were in Hoehn and Yahr stage II,41.8% (n=64) in stage III and 11.8% (n=18) in stage IV. Duringthe 3-week training period, 102 (67%) trainedwith the auditorycue, 51 (33%) with the somatosensory cue and no one selected
Table 1 – Comparison between early and late cueingtraining groups for demographic and clinicalcharacteristics (n=153). Data are described as median andinterquartile range (Q1–Q3) values except for age andfreezers/non-freezers where the total number of each isgiven. Significance level is p=0.05.
Early n=76median(Q1–Q3)
Late n=77median(Q1–Q3)
p-value
DemographyMale/female ⁎ 48/28 40/37 0.16Age 67.5 (61.5–72) 69 (62.5–73) 0.7
PD characteristicsDisease duration 7 (4–11) 8 (4–12) 0.59H&Y (on) 2.5 (2.5–3) 3 (2.5–3) 0.56H&Y II/III/IV ⁎ 39/29/8 32/35/10 0.48Freezers/N-freezers ⁎ 31/45 32/45 0.92
Clinical dataUPDRS-total (on) 54 (46–65.5) 56 (49–63) 0.62UPDRS I (on) 4 (2–5) 3 (2–4) 0.1UPDRS II (on) 16 (12–19.5) 16 (12–20) 0.67UPDRS III (on) 31 (25–37) 34 (28–41) 0.32UPDRS IV (on) 3 (1–5) 2 (1–5) 0.43Levodopa (mg) 500 (300–700) 350 (200–550) 0.07MMSE 28.5 (27–30) 29 (27–30) 0.99Brixton 4 (2–6) 4.0 (2–6) 0.45HADS anxiety 6.5 (4–10) 6 (4–10) 0.97HADS depression 7.5 (5–10) 6 (4.5–9) 0.45
H&Y=Hoehn and Yahr stages during on; UPDRS=UnifiedParkinson's Disease Rating Scale; PD= Parkinson's disease;MMSE=Mini Mental State Examination; HADS=Hospital Anxietyand Depression Scale.⁎ Expressed as number of patients and p values based on Chi-squaredtest.
the visual cue. During assessment however cued gait wastested with all ERC types (see Fig. 1).
Walking speed, step length and cadence were estimatedfrom rawdata obtainedwith accelerometers as shown in Fig. 1.These data were collected during single- and dual-taskwalking. Descriptive data (mean and SD) for all gait variablesare shown in Table 2. We estimated the effect of cueingtraining using multiple linear regression models whichaccounted for repeated measures inherent in the studydesign (Fig. 2). During single and dual tasks the training effectfor each ERC (visual, auditory and somatosensory) wasestimated using the first three assessments (T1, T2, T3).Statistical models corrected for differences between earlyand late groups at baseline, time effects (T1–T2 late group)and carryover effects (T2–T3 early group) (Fig. 2 for studydesign). The sameprocedurewasused for each variable (speed,step length and cadence). The change scores reported inTable 3 are therefore the estimates of training effects on cuedperformance with baseline, time and carryover effects con-trolled for (Table 3). Data from early and late groups are pooledfor descriptive purposes before, after and at follow-up. Missingdata were due to equipment failure or recording difficultieswhich occurred in a random fashion and the characteristics ofthose patients were not different from those included in theanalysis. Motor learning was defined as acquisition, automa-ticity and retention and the results are presented according tothis definition.
2.1. Acquisition (single task)
Following cueing training single-task walking speed signifi-cantly increased with each ERC and this was largely achievedby a significant increase in step length. Therewas a significantincrease with all ERC modalities (visual, auditory, somatosen-sory) despite the fact that no one chose to train with the visualcue. There was no significant difference in training effectbetween cue types. Unsuprisingly cadence did not changesignificantly following training due to the fact that gait wascued at preferred rate and effectively controlled this param-eter. There was limited transfer to non-cued gait in the singletask with significant improvement in step length; however,walking speed did not change significantly and cadencedecreased.
2.2. Automaticity (dual task)
We used gait performance under dual-task conditions as ameasure of automaticity and change in attentional resourceswith increased proficiency in performance (Doyon, 2008;Jueptner et al., 1997; Wu and Hallett, 2008). Firstly, weidentified the attentional demands of the dual task bycomparing single- and dual-task non-cued gait using pooleddata from early and late groups at T1. Walking speed (prep<.0001; post p<.0001) and step length (pre p<.0001; postp<.0001) were significantly reduced during the dual-taskcompared to single-task gait; however, cadence remainedunchanged. The baseline characteristics of the early and lategroups are shown in Table 2, and again differences betweengroups at baseline were adjusted for in the analysis. Thetraining effects on cued gait during dual tasks are shown in
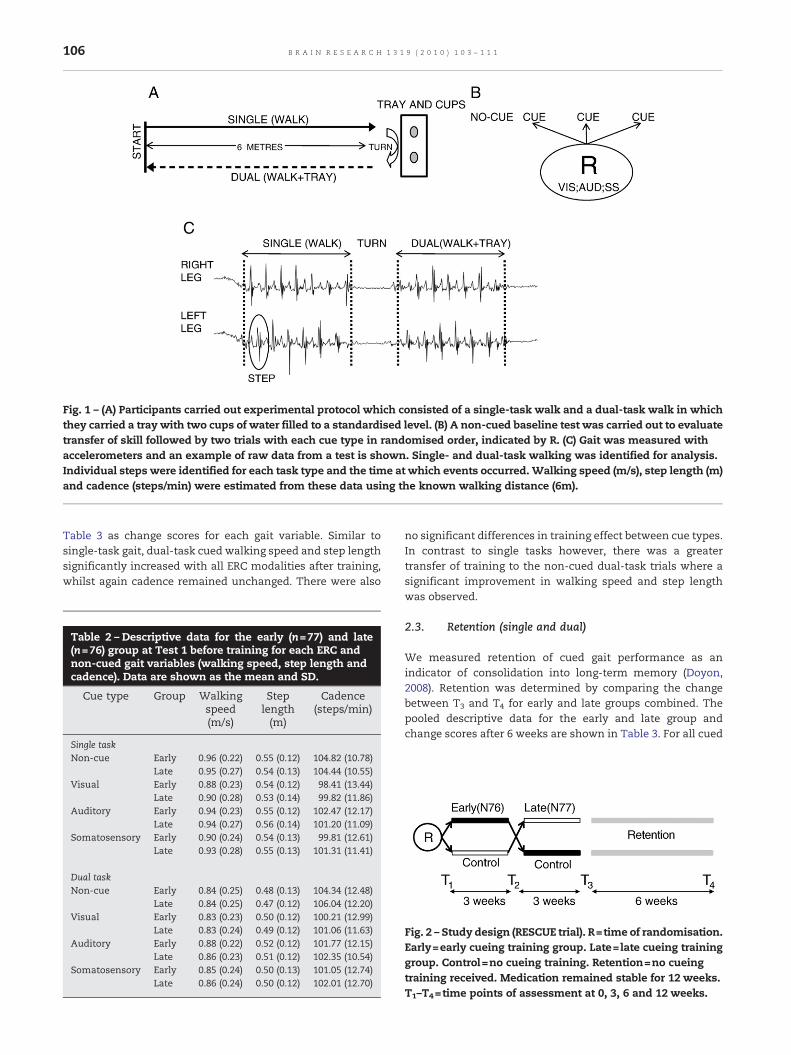
Fig. 1 – (A) Participants carried out experimental protocol which consisted of a single-task walk and a dual-task walk in whichthey carried a tray with two cups of water filled to a standardised level. (B) A non-cued baseline test was carried out to evaluatetransfer of skill followed by two trials with each cue type in randomised order, indicated by R. (C) Gait was measured withaccelerometers and an example of raw data from a test is shown. Single- and dual-task walking was identified for analysis.Individual steps were identified for each task type and the time at which events occurred.Walking speed (m/s), step length (m)and cadence (steps/min) were estimated from these data using the known walking distance (6m).
106 B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
Table 3 as change scores for each gait variable. Similar tosingle-task gait, dual-task cued walking speed and step lengthsignificantly increased with all ERC modalities after training,whilst again cadence remained unchanged. There were also
Table 2 – Descriptive data for the early (n=77) and late(n=76) group at Test 1 before training for each ERC andnon-cued gait variables (walking speed, step length andcadence). Data are shown as the mean and SD.
Cue type Group Walkingspeed(m/s)
Steplength(m)
Cadence(steps/min)
Single taskNon-cue Early 0.96 (0.22) 0.55 (0.12) 104.82 (10.78)
Late 0.95 (0.27) 0.54 (0.13) 104.44 (10.55)Visual Early 0.88 (0.23) 0.54 (0.12) 98.41 (13.44)
Late 0.90 (0.28) 0.53 (0.14) 99.82 (11.86)Auditory Early 0.94 (0.23) 0.55 (0.12) 102.47 (12.17)
Late 0.94 (0.27) 0.56 (0.14) 101.20 (11.09)Somatosensory Early 0.90 (0.24) 0.54 (0.13) 99.81 (12.61)
Late 0.93 (0.28) 0.55 (0.13) 101.31 (11.41)
Dual taskNon-cue Early 0.84 (0.25) 0.48 (0.13) 104.34 (12.48)
Late 0.84 (0.25) 0.47 (0.12) 106.04 (12.20)Visual Early 0.83 (0.23) 0.50 (0.12) 100.21 (12.99)
Late 0.83 (0.24) 0.49 (0.12) 101.06 (11.63)Auditory Early 0.88 (0.22) 0.52 (0.12) 101.77 (12.15)
Late 0.86 (0.23) 0.51 (0.12) 102.35 (10.54)Somatosensory Early 0.85 (0.24) 0.50 (0.13) 101.05 (12.74)
Late 0.86 (0.24) 0.50 (0.12) 102.01 (12.70)
no significant differences in training effect between cue types.In contrast to single tasks however, there was a greatertransfer of training to the non-cued dual-task trials where asignificant improvement in walking speed and step lengthwas observed.
2.3. Retention (single and dual)
We measured retention of cued gait performance as anindicator of consolidation into long-term memory (Doyon,2008). Retention was determined by comparing the changebetween T3 and T4 for early and late groups combined. Thepooled descriptive data for the early and late group andchange scores after 6 weeks are shown in Table 3. For all cued
Fig. 2 – Study design (RESCUE trial). R=time of randomisation.Early=early cueing training group. Late=late cueing traininggroup. Control=no cueing training. Retention=no cueingtraining received. Medication remained stable for 12 weeks.T1–T4=time points of assessment at 0, 3, 6 and 12 weeks.

Table 3 –Motor learning: acquisition, automaticity and retention.
Trials Variables Before trainingpooled data(early + late)
After trainingpooled data(early + late)
Training effectchange score(in units)
p value Follow-uppooled data(early + late)
Follow-upchange score
in units (T4–T3)
p value
Single taskNon-cue Speed .95 (.25) 1.02 (.25) .03 (.03) .25 1.05 (.26) 0.006 (0.025) 0.81
Step length .55 (.13) .59 (.13) .03 (.01) .023⁎ .59 (.13) -0.002 (0.013) 0.90Cadence 104.71 (10.73) 104.50 (10.90) -3.35 (1.50) .03⁎ 106.79 (13.44) 0.823 (1.17) 0.48
Visual Speed .89 (.26) .99 (.25) .06 (.03) .03⁎ 1.01 (.25) 0.007 (0.024) 0.77Step length .54 (.13) .59 (.13) .05 (.01) .001⁎ .58 (.13) -0.002 (0.012) 0.75Cadence 99.23 (12.65) 101.15 (12.27) -2.56 (1.76) .15 104.15 (12.02) 1.705 (1.077) 0.11
Auditory Speed .94 (.25) 1.03 (.24) .06 (.02) .02⁎ 1.05 (.26) -0.001 (0.025) 0.98Step length .55 (.13) .60 (.12) .04 (.01) .005⁎ .60 (.13) -0.0004 (0.012) 0.97Cadence 102.08 (11.99) 103.58 (12.00) -1.98 (1.84) .28 105.06 (11.90) 0.196 (1.059) 0.85
Somatosensory Speed .92 (.26) 1.01 (.24) .08 (.02) .0004⁎ 1.03 (.26) -0.003 (0.025) 0.91Step length .55 (.13) .59 (.12) .04 (.01) .002⁎ .59 (.12) -0.005 (0.012) 0.71Cadence 100.64 (12.22) 102.65 (12.08) .35 (1.76) .84 104.69 (12.11) 0.81 (1.083) 0.75
Dual taskNon-cue Speed .84 (.25) .93 (.23) .06 (.03) .04⁎ .94 (.24) -0.013 (0.021) 0.53
Step length .48 (.17) .53 (.11) .04 (.01) .004⁎ .53 (.12) 0.006 (0.025) 0.81Cadence 105.02 (12.93) 104.78 (12.50) -1.85 (1.74) .29 107.66 (12.50) 0.851 (1.087) 0.43
Visual Speed .83 (.23) .92 (.23) .07 (.02) .002⁎ .93 (.23) 0.002 (0.020) 0.92Step length .50 (.12) .54 (.11) .05 (.01) .0001⁎ .54 (.12) 0.007 (0.025) 0.77Cadence 100.79 (12.28) 101.80 (13.53) -2.29 (1.67) .17 104.63 (12.34) 1.249 (1.07) 0.24
Auditory Speed .87 (.23) .94 (.23) .05 (.02) .03⁎ .97 (.24) 0.010 (0.012) 0.62Step length .51 (.12) .55 (.11) .03 (.01) .01⁎ .55 (.11) -0.001(0.025) 0.98Cadence 102.10 (11.94) 103.43 (12.20) -1.23 (1.56) .43 105.75 (11.83) 1.018 (1.006) 0.31
Somatosensory Speed .85 (.24) .93 (.22) .08 (.02) .0004⁎ .94 (.23) -0.010 (0.012) 0.62Step length .50 (.13) .54 (.12) .04 (.01) .0004⁎ .54 (.11) -0.003 (0.025) 0.91Cadence 100.85 (13.53) 102.69 (13.19) -.44 (1.48) .77 105.00 (11.37) 0.201 (1.02) 0.84
Data for early and late groups are pooled to give the mean (SD) walking speed, step length and cadence expressed as the mean (SD) for non-cueand cued trials (visual, auditory, somatosensory). The training effect and follow-up changes scores are shown as estimatedmeans±SE in units ofmeasurement (speed (m/s); step length (m); cadence (steps/min)). Change scores are corrected for baseline differences, time and carryovereffects in the statistical model. Single-task gait (n=130) and dual-task gait (n=132). Significance level is p=0.05 and significant differences areshown by ⁎. To address the hypothesis of motor learning in this table: Acquisition=Single-Task Training Effect Change Score;Automaticity=Dual-Task Training Effect Change Score; Retention=Follow-up Change Score for Single and Dual Tasks.
107B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
trials and all gait variables the effects of trainingwere retainedduring both single and dual tasks with some evidence for aslight increase as shown by positive values. These changeswere very small however and difficult to interpret. In addition,retention was also observed for all gait variables during non-cued trials for both single and dual tasks.
3. Discussion
The key findings in this study were that gait training with ERCincreased single- and dual-task cued walking speed and steplength and these effects were retained at follow-up. Thesechanges were consistent with our definition of motor learningsupporting our hypothesis that cued training would increasemotor learning. Practice also transferred to non-cued gait,generalised across cue types and was retained. These data arerobust given the study design and novel and add to knowledgeregarding motor learning and its application to rehabilitationin PD.
We saw significant improvements in walking speed andstep length with all ERC during the single task, which wetermed acquisition of skill. Prior to training however, the effectof ERCduring a single taskwas limitedwith either no changeor
a small increase in walking speed or step length compared tonon-cued gait (Rochester et al., 2007). It is interesting thatsignificant improvementswith trainingwere seenwith all ERCdespite individuals electing to train with their preferred cuetype only (67% auditory and 33% somatosensory). These datasuggest that cued gait performance not only became moreproficient following training but also transferred to all cuetypes providing additional support formotor learning. The factthat cadence did not change significantly in response to ERC isnot surprising given that this temporal aspect of gait wasconstrained by the cueing frequency used. No other studieshave reported cued gait performance after a period of training.
We found that cued dual-task walking speed and steplength also significantly increased with all ERC after training.The dual-task was attentionally demanding (observed bysignificant reductions in walking speed and step lengthcompared to single-task gait) and therefore improved dual-task performance supports increased automaticity. We alsofound that cues had an immediate and significant effect ondual-task walking speed and step length before training(Rochester et al., 2007). It seems therefore that practiceincreased proficiency and generalized to all cue types asseen in the single task. Significant improvements in dual-taskgait performance in PD following training have also been

108 B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
reported by others (Canning et al., 2008) indicating improvedautomaticity of movement, this study was however un-cued.Studies in PD in the upper limb demonstrate that automaticitycan be achieved but with more difficulty and requires greateractivation of neural networks (Wu and Hallett, 2005). Activitywas increased in networks involving the cerebellum, premotorarea, parietal cortex, precuneus and dorsolateral prefrontalcortex (DLPFC) compared to normal subjects (Wu and Hallett,2005). Networks involved in the control of attention may alsocontribute. Increased activity in the DLPFC and anteriorcingulate is associated with attentional control of movementwhen learning a new task (Jueptner et al., 1996; Johanssen-Berg and Matthews, 2002) and disappears when the task isperformed automatically (Jueptner et al., 1996). When fingermovements are externally paced by ametronome the DLPFC isonly activated when the rhythm is modified and subjects arefully conscious of their movements (Stephan et al., 2002).These networks may therefore compensate for basal gangliadysfunction and contribute to motor learning in PD.
We demonstrated retention after 6 weeks, which is longerthan other studies of functional motor learning which rangefrom 15 min to 4 weeks (Chuma et al., 2006; Mak et al., 2007;Smiley-Oyen et al., 2006; Jessop et al., 2006). However, whilstwe report a relatively long retention period, studies overlonger time scales (1 year) in PD have shown that retention isimpaired (Doyon et al., 1998). Increased cued single-task gaitspeed and step lengthmay be related to a relatively fast phaseof learning (explicit learning) (Karni et al., 1995), however,retention of single- and dual-task cued gait performancesupports consolidation of training into long-term memory.
We found only limited transfer to non-cued single-task gaitwith no significant change in walking speed although steplength increased. These results agree in part with the findingsof Verschueren et al., (1997), who found no transfer of effect tonon-cued trials. However, we were surprised to find thattraining did transfer to non-cued dual-task walking speed andstep length. Farley and Koshland (2005) also found general-ization of amplitude training of limb movements to speedimprovements in non-cued in PD. Requirements for motorlearning (Schmidt and Wrisberg, 2000) advocate varied prac-tice which is functionally relevant and we adhered to theseprinciples, which may explain transfer of skill to non-cuedconditions and retention. Participants were required tosynchronize their gait with the cue and to practise this in avariety of different tasks and environments. Whether this isrelated to the type of training is uncertain. Transfer of trainingwas also observed across different cue modalities as seen byincreased gait speed and step length in visual cued trialsdespite the fact that this cue type was not selected for practiceby any participant. These results present the possibility thatmotor representation of rhythm may become stored incerebellar circuits providing a role for the cerebellum in howmovements are performed in relation to their timing (Ram-nani and Passingham, 2001). Whether different neural net-works contribute to augmented learning with rhythmical cuescannot be answered in this study as we did not have a controlgroup where gait without cues were practised. This questionstill needs to be addressed in future work.
There are some limitations to this study which should beaddressed. Because of the study design (crossover) placebo
effects were not controlled for in this study. Also we did notcorrect for multiple comparisons in the analysis whichamounted to eight comparisons for each gait outcome. Theresults should therefore be interpreted cautiously. It is alsoimportant to note however that the statistical model used inthe analysis provided a conservative estimate of the trainingeffects as it corrected for time and carryover effects inherentin the study design, estimating training independently whichwill partly ameliorate the above limitations. The findings ofthis study cannot be generalized to people with PD who havesignificant cognitive decline and other co-morbidities andfuture studies should focus on these effects. It is highly likelythat subtle cognitive deficits and cognitive decline associatedwith PD will impair onmotor learning. The impact of differentstages of the disease and disease severity was also not a focusof this study and these factors are likely to impact on learningability.
Training increased cued gait performance for both singleand dual tasks and these effects were retained. This is the firstreport of learning in cued gait and also on automaticity andthe findings are therefore novel. These results together withlarge subject numbers and randomised controlled trial designprovide robust evidence regarding the capacity of people withPD for motor learning. The possibility to increase automaticperformance of dual tasks has functional implications forpeople with PD with potential impact on independence andsafety. The use of external cues to augment gait performancemay therefore be considered an effective motor learningparadigm for people with PD.
4. Experimental procedure
4.1. Subjects
153 participants with idiopathic PD were recruited from threecentres aroundNorthumbria University, Newcastle upon Tyne(UNN), Katholieke Universiteit of Leuven (UNL) and theDepartment of Neurology at Vrije Universiteit Medical Centreof Amsterdam (UNA). The study was approved by the ethicscommittee of each participating centre. All participants gaveinformed written consent to the study. Eligibility criteria were:a diagnosis of idiopathic PD, defined following the UK BrainBank Criteria ; stable medication usage; Hoehn and Yahr stageII, III or IV; at least one score >2 for one or both limbs for eitherthe tremor, rigidity or the bradykinesia items of the UPDRS;able to walk independently; age 18–80 years; no severecognitive impairments (Mini Mental State Examination(MMSE) >24; no other severe neurological, cardiopulmonaryor orthopaedic disorders; absence of drug-related fluctuationsmaking testing difficult, and no participation in a physiother-apy program two months prior to commencing the trial.Participants were excluded if they had undergone functionalneurosurgery.
4.2. Experimental protocol measuring the effect of ERCtraining (Fig. 1)
The effect of ERC training on cued gait performance with ERC(visual, auditory and somatosensory) was investigated using a

109B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
test of functional gait (Rochester et al., 2007) which incorpo-rated a single and a dual task. Participants started fromstanding andwere instructed towalk 6m to pick up a traywithtwo cups on it (filled to a standard level), turn around through180°, carry the tray back to the start position and stop.Participants were asked to walk at their preferred speed andconcentrate equally on all elements of the test. The test wasdivided into two conditions: walking without tray (single task)and walking with the tray (dual-task). Seven trials of the testwere carried out: non-cued; two cued trials with each cue type(visual, auditory, somatosensory). Trials were measuredwithout cues to determine transfer of cued training andspecificity of learning. A prototype cueing device worn on abelt around the waist provided three rhythmical cueingmodalities: (1) auditory (a beep delivered through an earpiece);(2) visual (light flashes delivered through a Light EmittingDiode attached to a pair of glasses); and (3) somatosensory(pulsed vibrations delivered by a miniature cylinder wornunder a wristband). The order of cue modalities was rando-mised by selecting cards; however, baseline gait was alwaystested before cued trials. Participants were asked to synchro-nize each step with the rhythm of the cue set at preferredstepping frequency determined during a 6m walk testconducted at preferred walking speed. Gait was measuredusing a Vitaport Activity MonitorR (VAM) (TEMEC InstrumentsInc.) which is a valid and reliable tool for measuring gait in PD(Lord et al., 2008). The activity monitor measured movementwith five accelerometers, one attached to each leg and threeplaced on the lower third of the sternum. Data were sampledat a frequency of 25 Hz and stored on a removable memorycard for later analysis. Data were analysed using a specificallydesigned software program (Vitagraph) (TEMEC InstrumentsInc.). Movement was not restricted in any way by either themonitor or the cueing device. Measurements were takenapproximately 1 h after medication to ensure participantswere in the ‘on’ phase of their medication. Walking speed,mean step length and cadence were estimated from analysisof the raw data collected by the VAM and validated in aprevious study (Lord et al., 2008) (Fig. 1C). The test was dividedinto two conditions (described above) for data analysis (Fig.1C): (1) walk only=single task; (2) walk + carry tray=dual task.Four trials were determined for each condition (single anddual): non-cued walking, visual, auditory and somatosensorycuedwalking, the cued trials being themean value of each pairof cued trials. The test of functional gait was carried out inparallel with a single-blind, randomised clinical trial with acrossover design (the RESCUE trial) (Fig. 2) (Nieuwboer et al.,2007). The experimental protocol was performed by a blindedassessor in the persons home immediately before randomisa-tion (T1) at 3 (T2), 6 (T3) and 12 (T4) weeks (Fig. 1) in the earlyand late groups.
4.3. ERC training
Participants were randomised to receive 3 weeks of cueingtraining either immediately (early) or after a 3-week delay(late) and both groups were followed-up for 6 weeks after cueswere withdrawn (Nieuwboer et al., 2007) (Fig. 2). A prototypecueing device (described above) was used to deliver the cuesduring training. This was worn on a belt around the waist and
provided three rhythmical cueing modalities: (1) auditory; (2)visual; and (3) somatosensory. Cueing was rhythmical,addressing temporal control of gait and aimed to improvestep length and walking speed. Participants used ERC toaugment gait performance during nine sessions which lastedfor 30min each. Participants tried all cuemodalities in the firstweek and then selected their preferred modality to train with.To assess the effect of cued training however, participantswere assessed with all three cues to evaluate generalisationfrom one cue type to another. A trained therapist facilitatedthe use of ERC during walking using the prototype cueingdevice, and this was carried out in the participants home. Gaitwas augmented by asking participants to step in time to therhythmical cues which were applied during single-, dual- andmulti-task walking. Cueing therapy consisted of the followingcomponents: gait initiation and termination, heel strike andpush-off, sideways and backwards stepping, walking whiledual tasking, and walking over various surfaces and longdistances. Complex tasks were used to reduce availableexplicit resources and encourage generalisation and automa-ticity. Evidence based cueing guidelines were used thatspecified cueing parameters and instructions (available onCD-ROM at http://www.rescueproject.org). Cues were deliv-ered at preferred frequency according to the environment inwhich the participant was practising. Medical treatmentcontinued unchanged throughout the study.
4.4. Data analysis
Data were analysed separately in one centre (Newcastle) by atesterwhowas not involved in data collection andwas blindedto cue order for the trials. The effect of training on cued gaitperformance was analysed as described below. To measureacquisition and automaticity cued gait performance with eachERC was compared to gait performance after training duringsingle (acquisition) and dual tasks (automaticity). In additionnon-cued gait was also measured to allow transfer from cuedto non-cued trial to be examined. The effects of cueingtraining on gait variables during single and dual tasks wereestimated using the first three assessments (T1, T2, T3).Multiple linear regression models were used to account forrepeatedmeasures. The linearmodels were fitted for each gaitvariable (walking speed, step length and cadence) with PROCMIXED in SAS (V8.2). In this model the effects of cueingtraining were corrected for differences of variables at baseline,time effects and carryover effects. Retention was assessed bycomparing the change between T3 and T4 using a model withtwo factors (time and group) fitted to the outcomes of tests 1–4for early and late groups combined. Results are reported asbeta estimates and standard errors (SE). Bonferroni correc-tions were not applied. Two-tailed analysis was performed onall tests with a significance level of p=0.05.
Acknowledgments
We gratefully acknowledge the financial support from theEuropean Commission Framework V funding; QLK6-2001-00120. We acknowledge the support of the UK NIHR Biomed-ical Research Centre for Ageing and Age-Related Disease

110 B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
award to the Newcastle upon Tyne Hospitals NHS FoundationTrust.
R E F E R E N C E S
Abbruzzese, G., Trompetto, C., Marinelli, L., 2009. The rationale formtoro learning in Parkinson's disease. Eur. J. Phys. Rehabil.Med. 45, 209–214.
Baker, K., Rochester, L., Nieuwboer, A., 2007. The effect of pairingauditory and attentional cues on the spatiotemporalparameters of gait in people with Parkinson's disease. Arch.Phys. Med. Rehabil. 88, 1593–1600.
Baker, K., Rochester, L., Nieuwboer, A., 2008. The effect of cues ongait variability — reducing the attentional cost of walking inpeople with Parkinson's disease. Parkinsonism Relat. Disord.14 (4), 314–320.
Bond, J., Morris, M., 2000. Goal-directed secondary motor tasks:their effects on gait in participants with Parkinson's disease.Arch. Phys. Med. Rehabil. 81, 110–116.
Carbon, M., Eidelberg, D., 2006. Functional imaging of sequencelearning in Parkinson's disease. J. Neurol. Sci. 248, 72–77.
Chuma, T., Faruque Reza, M., Ikoma, K., Mano, Y., 2006. Motorlearning of hands with auditory cues in patients withParkinson's disease. J. Neural Transm. 113, 175–185.
Doyon, J., 2008. Motor sequence learning andmovement disorders.Curr. Opin. Neurol. 21, 478–483.
Doyon, J., Laforce, J., Bouchard, G., Gandreau, D., Roy, J., Poirer, M.,Bedard, P.J., Bedard, F., Bouchard, J.P., 1998. The role of thestriatum, cerebellum and frontal lobes in the automatisationof a repeated visuomotor sequence of movements.Neuropsychologia 36 (7), 625–641.
Farley, B.G., Koshland, G.F., 2005. Training BIG to move faster: theapplication of the speed-amplitude relation as a rehabilitationstrategy for people with Parkinson's disease. Exp. Brain Res.167, 462–467.
Hausdorff, J.M., Lowenthal, J., Herman, T., Guendlinger, L., Peretz,C., Giladi, N., 2007. Rhythmic auditory stimulation modulatesgait variability in Parkinson's disease. Eur. J. Neurosci. 26,2369–2375.
Heremans, E., Helsen, W.F., De Poel, H.J., Alaerts, K., Meyns, P.,Feys, P., 2009. Facilitation ofmotor imagery throughmovementrelated cueing. Brain Res. 1278, 50–58.
Jessop, R.T., Horowicz, C., Dibble, L.E., 2006. Motor learning andParkinson's disease: refinement of movement velocity andendpoint excursion in a limits of stability balance task.Neurorehabil. Neural Repair 20, 459–467.
Johanssen-Berg, H., Matthews, P.M., 2002. Attention to movementmodulates activity in sensori-motor areas, including primarymotor cortex. Exp. Brain Res. 142, 13–24.
Jueptner, M., Stephan, K.M., Frith, C.D., Brooks, D.J., Frackpwiak,R.S.J., Passingham, R.E., 1997. Anatomy of motor learning. 1.Frontal cortex and attention to action. J. Neurophsiol. 77,1313–1324.
Karni, A., Meyer, G., Jezzard, P., Adams, M.M., Turner, R.,Ungerleider, L.G., 1995. Functional MRI evidence for adultmotor cortex plasticity during motor skill learning. Nature 377(14), 155–158.
Lord, S., Rochester, L., Baker, K., Hetherington, V., Nieuwboer, A.,2008. Concurrent validity of accelerometry to measure gait inParkinson's disease. Gait Posture 27 (2), 357–359.
Lim, I., van Wegen, E., de Goede, C., Duetekom, M., Nieuwboer, A.,Willems, A.M., Jones, D., Rochester, L., Kwakkel, G., 2005.Effects of external rhythmical cueing on gait in patients withParkinson's disease: a systematic review. Clin. Rehabil. (2005)19, 695–713.
Mak, M.K.Y., Hui-Chan, C.W.Y., 2008. Cued task-specific training isbetter than exercise in improving sit-to-stand in patients with
Parkinson's disease: a randomised controlled trial. Mov.Disord. 23 (4), 501–509.
Marchese, R., Diverio, M., Zucchi, F., Lentino, C., Abbruzzese, G.,2000. The role of sensory cues in the rehabilitation ofParkinsonian Patients: a comparison of two physical therapyprotocols. Mov. Disord. 15 (5), 879–883.
Mentis, M.J., Dhawan, V., Feigin, A., Delalot, D., Zgaljardic, D.,Edwards, C., Eidelberg, 2003. Early stage Parkinson's diseasepatients and normal volunteers: comparative mechanisms ofsequence learning. Hum. Brain Mapp. 20, 246–258.
Morris, M., Iansek, R., Matyas, T., Summers, J., 1996. Stride lengthregulation in Parkinson's disease. Normalization strategiesand underlying mechanisms. Brain 119, 551–568.
Muslimovic, D., Post, B., Speelman, J.D., Schmand, B., 2007. Motorprocedural learning in Parkinson's disease. Brain 130,2887–2897.
Nieuwboer, A., Rochester, L., Jones, D., 2008. Cueing gait andgait-related mobility in patients with Parkinson's disease:developing a therapeutic method based on the ICF. Top.Geriatr. Rehabil. 24 (2), 151–165.
Nieuwboer, A., Kwakkel, G., Rochester, L., Jones, D., van Wegen, E.,Willems, A.M., Chavert, F., Hetherington, V., Baker, K., Lim, I.,2007. Cueing training in the home improves gait-relatedmobility in Parkinson's diease: the RESCUE trial. J. Neurol.Neurosurg. Psychiatry 78, 134–140.
O'Shea, S., Morris, M., Iansek, R., 2002. Dual-task interferenceduring gait in people with parkinson's disease: effects ofmotor versus cognitive secondary tasks. Phys. Ther. 82,888–897.
Ramnani, N., Passingham, R.E., 2001. Changes in the human brainduring rhythm learning. J. Cogn. Neurosci. 13 (7), 952–966.
Rochester, L., Hetherington, V., Jones, D., Nieuwboer, A., Willems,A.M., Kwakkel, G., van Wegen, E., 2004. Attending to the task:Interference effects of functional tasks on walking inParkinson's disease and the role of cognition, depression,fatigue and balance. Arch. Phys. Med. Rehabil. 85 (10),1578–1585.
Rochester, L., Hetherington, V., Jones, D., Nieuwboer, A., Willems,A., Kwakkel, G., van Wegen, E., 2005. The effect of externalrhythmic cues (auditory and visual) on walking during afunctional task in homes of people with Parkinson's disease.Arch. Phys. Med. Rehabil. 86, 999–1006.
Rochester, L., Nieuwboer, A., Baker, K., Hetherington, V., Willems,A.M., Chavret, F., Kwakkel, G., van Wegen, E., Lim, I., Jones, D.,2007. The attentional cost of external rhythmical cues andtheir impact on gait in Parkinson's disease: effect of cuemodality and task complexity. J. Neural Transm. 114 (10),1243–1248.
Rubinstein, T., Giladi, N., Hausdorff, J., 2002. The power of cueingto circumvent dopamine deficits: a review of physical therapytreatment of gait disturbances in Parkinson's disease. Mov.Disord. 17 (6), 1148–1160.
Schmidt, R.A., Wrisberg, C.A., 2000. Motor learning andperformance. Human Kinetics, Champaign, IL.
Semjen, A., Schulze, H.H., Vorberg, D., 2000. Timing precision incontinuation and synchronisation tapping. Psychol. Res. 63,137–147.
Sidaway, B., Anderson, J., Danielson, G., Martin, L., Smith, G., 2006.Effects of long-term gait training using visual cues in anindividual with Parkinson's disease. Phys. Ther. 86 (2),186–194.
Siegert, R.J., Taylor, K.D., Weatherall, M., Abernethy, D.A., 2006. Isimplicit sequence learning impaired in Parkinson's disease? Ameta-analysis. Neuropsychology 20 (4), 490–495.
Smiley-Oyen, A.L., Lowry, K.A., Emerson, Q.R., 2006. Learning andretention of movement sequences in Parkinson's disease. Mov.Disord. 21 (8), 1078–1087.
Stephan, K.M., Thaut, M.H., Wunderlich, G., Schicks, W., Tian, B.,Tellmann, L., Schmitz, T., Herzog, H., McIntosh, G.C., Seitz, R.J.,

111B R A I N R E S E A R C H 1 3 1 9 ( 2 0 1 0 ) 1 0 3 – 1 1 1
Homberg, V., 2002. Conscious and subconscious sensorimotorsynchronisation — prefrontal cortex and the influence ofawareness. NeuroImage 15, 345–352.
Thaut, M.H., McIntosh, G.C., Rice, R.R., Miller, R.A., Rathburn, J.,Brault, J.M., 1996. Rhythmic auditory stimulation in gaittraining for Parkinson's disease patients. Mov. Disord. 11 (2),193–200.
Verschueren, S.M.P., Swinnen, S.P., Dom, R., De Weerdt, W., 1997.Interlimb coordination in patients with Parkinson's disease:motor learning deficits and the importance of
augmented information feedback. Exp. Brain Res. 113,497–508.
Wilkinson, L., Jananshahi, M., 2007. The striatum and probabilisticsequence learning. Brain Res. 1137, 117–130.
Wu, T., Hallett, M., 2005. A functional MRI study of automaticmovements in patients with Parkinson's disease. Brain 128,2250–2259.
Wu, T., Hallett, M., 2008. Neural correlates of dual taskperformance in patients with Parkinson's disease. J. Neurol.Neurosurg. Psychiatry 79 (7), 760–766.
Copyright © 2022 FDOKUMEN




















