COMPUGIRLS: Stepping stone to future computer-based technology pathways
Upload
khangminh22Category
view
0download
0
2007 AANEM Plenary
AANEM 54thAnnual MeetingPhoenix, Arizona
plenary SeSSIon:gaIT In moTIon: STeppIng
InTo The 21ST CenTury
Gerald J. Herbison, MD
Mark Hallett, MD
Catherine Lomen-Hoerth, MD, PhD
H. Kerr Graham, MD, FRCS (Ed), FRACS
Kenton R. Kaufman, PhD, PE
James K. Richardson, MD
Am
eric
an
Ass
oc
iati
on
of
Neu
ro
mu
scu
lar
& E
lec
tro
dia
gn
ost
ic M
edic
ine
�����


2007 PLENARY SESSION AANEM 54th Annual Meeting
Phoenix, Arizona
Copyright © October 2007 American Association of Neuromuscular & Electrodiagnostic Medicine
2621 Superior Drive NW Rochester, MN 55901
Printed by Johnson Printing ComPany, inC.
Gerald J. Herbison, MDMark Hallett, MD
Catherine Lomen-Hoerth, MD, PhDH. Kerr Graham, MD, FRCS (Ed), FRACS
Kenton R. Kaufman, PhD, PEJames K. Richardson, MD
Plenary Session:Gait in Motion: Stepping into the 21st Century

Plenary Session: Gait in Motion: Stepping into the 21st Century
Faculty
ii
Gerald Herbison, MDProfessorDepartment of Rehabilitation MedicineJefferson Medical College of Thomas Jefferson UniversityPhiladelphia, PennsylvaniaDr. Herbison is a professor in the Department of Rehabilitation Medicine at Jefferson Medical College of Thomas Jefferson University in Philadelphia, Pennsylvania. Dr. Herbison earned his medical degree from Stritch School of Medicine at Loyola University in 1962. He has been the director of the clinical electrophysiology clinic at Thomas Jefferson University since 1970 and was the Director of Research for 25 years and the Director of Pediatric Rehabilitation for 20 years. He presently teaches electromyo-graphy part-time as well as gross anatomy and kinesiology to residents. Dr. Herbison was on the Editorial Board of the Archives of Physical Medicine and Rehabilitation for more than 20 years, and he served for 6 years as Editor-in-Chief. He also served as a member of the editorial board of Muscle & Nerve from 1983 to 1986. Dr. Herbison has published 98 peer-reviewed publications, 10 textbook chapters, and 135 abstracts. He has also been the recipient of numerous honors and awards including the American Academy of Physical Medicine and Rehabilitation’s Annual Walter J. Zeiter Lectureship and Distinguished Clinician Award, the American Association of Neuromuscular & Electrodiagnostic Medicine’s Distinguished Physician Award, and the Excellence in Teaching Award from the Graduating Residents of the Department of Rehabilitation Medicine at Thomas Jefferson University.
Mark Hallett, MDChiefHuman Motor Control SectionNational Institute of Neurological Disorders and StrokeNational Institute of HealthBethesda, MarylandDr. Hallett is Chief of the Human Motor Control Section, National Institute of Neurological Disorders and Stroke (NINDS), National Institutes of Health (NIH), where he does research on the physiology of human movement and the pathophysiology of movement disorders. The work in the laboratory currently includes studies on focal dystonias, Tourette’s syndrome, Parkinson’s disease, essential tremor, cerebellar ataxia, and psychogenic movement disorders. He is currently Editor-in-Chief of Clinical Neurophysiology and is one of the Associate Editors of Brain. He is a past-president of the AANEM and the Movement Disorder Society, and a former vice-president of the American Academy of Neurology. He just finished his 8-year term on the American Board of Electrodiagnostic Medicine. Dr. Hallett obtained his medical degree at Harvard University and trained in neurology at Massachusetts General Hospital. He per-formed fellowships in neurophysiology at the NIH and at the Institute of Psychiatry in London. From 1976 to 1984, Dr. Hallett was the Chief of the Clinical Neurophysiology Laboratory at the Brigham and Women’s Hospital and Associate Professor of Neurology at Harvard Medical School. Since 1984, he has been at the NINDS where he also served as Clinical Director of NINDS until July 2000.
Plenary Chair: Michael T. Andary, MD, MS
The ideas and opinions expressed in this publication are solely those of the specific authors and do not necessarily represent those of the AANEM.

Catherine Lomen-Hoerth, MD, PhDAssistant ProfessorDepartment of NeurologyUniversity of California, San FranciscoSan Francisco, CaliforniaDr. Lomen-Hoerth is an assistant professor in residence in the Department of Neurology at the University of California, San Francisco (UCSF). She directs the Amyotrophic Lateral Sclerosis (ALS) Treatment and Research Center at UCSF and teaches clinical neurophysiology. She obtained a medical degree and doctorate degree from Stanford University, working in the laboratory of Dr. Eric Shooter on neurotrophic factor receptors. She went on to the UCSF for her internship and residency in neurology, finishing her last year as chief resident. After a year of training in clinical neurophysiology working under Dr. Richard K. Olney, she joined the faculty at UCSF in 1999. She received the Golseth Young Investigator Award from the AANEM in 1999 for her paper comparing multiple point and statistical motor unit number estimation. The ALS Center at UCSF received certification in 2001 as an ALS Association Center of Excellence and as a Muscular Dystrophy Association center in 2007. Currently she follows over 250 ALS patients in this center annually. Her research is now focused on identifying genetic and environmental risk factors for ALS and developing neuroimaging techniques for earlier diagnosis of ALS. She also discovered the overlap syndrome of ALS with frontotemporal dementia. Recognition of this dementia overlap syndrome is leading to new treat-ment strategies for ALS patients and is helping their families to better understand and cope.
Kenton R. Kaufman, PhD, PEDirectorBiomechanics-Motion Analysis LaboratoryMayo ClinicRochester, MinnesotaDr. Kaufman is Director of the Biomechanics-Motion Analysis Laboratory at Mayo Clinic Rochester and a consultant in the Departments of Orthopedic Surgery, Physiology, and Biomedical Engineering. He holds the academic rank of Professor of Biomedical Engineering and is recog-nized with the distinction of a named professorship, the W. Hall Wendel, Jr., Musculoskeletal Research Professorship. Dr. Kaufman earned his bachelor of science degree and masters degree in agricultural engineer-ing at South Dakota State University. He was a visiting scientist at Mayo Graduate School of Medicine, and he earned a PhD in biomechanical engineering at North Dakota State University. Dr. Kaufman completed a post-doctoral fellowship in biomechanical engineering at Mayo Graduate School of Medicine.He has memberships in numerous professional societ-ies and has participated in journal review and editorial activities for many publications. He has also received several honors and awards during his training and career. He has given numerous invited presentations and is often invited to serve as a visiting professor. He has authored more than 350 articles, book chapters, and abstracts. Dr. Kaufman focuses his re-search on the biomechanics of human movement. He also has conducted research to decrease overuse injuries in military recruits and has developed the combat boots worn by the United States Marine Corps. Dr. Kaufman holds four United States patents and one international patent.
iii
Please be aware that some of the medical devices or pharmaceuticals discussed in this handout may not be cleared by the FDA or cleared by the FDA for the specific use described by the authors and are “off-label” (i.e., a use not described on the product’s label). “Off-label” devices or pharmaceuticals may be used if, in the judgement of the treating physician, such use is medically indi-cated to treat a patient’s condition. Information regarding the FDA clearance status of a particular device or pharmaceutical may be obtained by reading the product’s package labeling, by contacting a sales representative or legal counsel of the manufacturer of the device or pharmaceutical, or by contacting the FDA at 1-800-638-2041.

iv
H. Kerr Graham, MD, FRCS, FRACSProfessorDepartment of Orthopaedic SurgeryThe Royal Children’s HospitalMelbourne, AustraliaDr. Graham is the University of Melbourne’s Professor of Orthopaedic Surgery at The Royal Children’s Hospital in Melbourne, Australia. He is Director of the Hugh Williamson Gait Laboratory, the first motion analysis laboratory to be established in Australia. The Hugh Williamson Gait Laboratory conducts an extensive program of biomechanical and clinical research as the lead center in the National Health and Medical Research Council of Australia Clinical Centre of Research Excellence in Gait Rehabilitation. Dr. Graham’s clinical interests include movement disorders in children, the relationship between gross motor function and musculoskeletal deformities and population-based studies in cerebral palsy. Dr. Graham was responsible for setting up integrated spasticity manage-ment programs at The Royal Children’s Hospital including the use of bot-ulinum toxin-A, introduction of selective dorsal rhizotomy, and intrathecal Baclofen pump programs. Dr. Graham has received a number of research awards including the Norman Martin medal in 1986 and the John Mitchell Crouch fellowship in 2001, which is the highest research award of the Royal Australasian College of Surgeons. He has served as Visiting Professor in North America, South America, Europe, and Southeast Asia. He is an associate editor of Developmental Medicine & Child Neurology and has an extensive publication record. He has supervised many PhD students to completion in a wide range of research areas and is delighted to be presenting the 20th Annual Stuart Reiner lecture.
James K. Richardson, MDAssociate ProfessorDepartment of Physical Medicine and RehabilitationUniversity of MichiganAnn Arbor, MichiganDr. Richardson received his medical degree from the University of Cincinnati College of Medicine in 1984. He completed separate resi-dencies in internal medicine (1984 to 1987) and physical medicine and rehabilitation (1987 to 1990) and is board-certified in those fields as well as in electrodiagnostic medicine. He has been a member of the faculty at the University of Michigan since 1990 and was promoted to Associate Professor with tenure in 2005. His clinical appointments have included directing the Inpatient Rehabilitation Service until 2000 and, more re-cently, co-directing the Electrodiagnostic Laboratory. Much of the research presented was performed with Dr. Richardson’s friend and mentor, and director of the University of Michigan Biomechanical Laboratory, James A. Ashton-Miller, PhD. Although Dr. Richardson has been fortunate to receive a variety of recognitions, he has been most honored by the annual teaching awards (6 Silver Crutch Awards, 1 Gold Crutch and, finally, 1 Platinum Crutch Award) that various classes of superb University of Michigan resident physicians have awarded him.
Authors had nothing to disclose.

v
Plenary Session: Gait in Motion: Stepping into the 21st Century
Contents
Faculty ii
Objectives iii
Preactivity Questions v
Course Committee vi
Gait in Peripheral Neuropathies 1Gerald J. Herbison, MD
Neurological Gait Disorders 17Mark Hallett, MD
Mobility and Amyotrophic Lateral Sclerosis 25Catherine Lomen-Hoerth, MD, PhD
High-Tech Versus Low-Tech in the Assessment of Gait and Function 29H. Kerr Graham, MD, FRCS (Ed), FRACS
Measuring Muscle Function During Gait 39Kenton R. Kaufman, PhD, PE
The Sluggish Sheepdog and the Incredible Shrinking Foot: Understanding and Managing Neuropathic Gait 49James K. Richardson, MD
Activity and Faculty Evaluation 57
CME Self-Assessment Test 59
Objectives—At the conclusion of the plenary session participants will be able to: (1) identify abnormalities of gait associated with peripheral nerve abnormalities; (2) understand central nervous system physiological effects on gait; (3) explain mobility problems in the management of motor neuron disease; (4) review surgical options to improve gait; (5) discuss the use of gait lab in diagnosing and managing gait disorders; and (6) identify gait abnormalities and treatment strategies associated with peripheral neuropathy.
Prerequis ite—This course is designed as an educational opportunity for residents, fellows, and practicing clinical EDX physi-cians at an early point in their career, or for more senior EDX practitioners who are seeking a pragmatic review of basic clinical and EDX principles. It is open only to persons with an MD, DO, DVM, DDS, or foreign equivalent degree.
AccreditAtiOn stAtement—The AANEM is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians.
cme credit—The AANEM is accredited by the ACCME to provide continuing medical education (CME) for physicians. The AANEM designates this educational activity for a maximum of 3 AMA PRA Category 1 Credit(s) TM. Each physician should only claim credit commensurate with the extent of their participation in the activity. This event is an Accredited Group Learning Activity as defined by the Maintenance of Certification Program of The Royal College of Physicians and Surgeons of Canada. CME for this activity is available 10/07 - 10/10.

vi AANEM Plenary

A. Extremely
B. Somewhat
C. Very Little
D. Not at all
It is important that the CME activity:
1. Address my most pressing questions.
2. Address competencies identified by my specialty.
3. Provide fair and balanced content.
4. Provide clear evidence to support content.
5. Include opportunities to learn interactively from faculty and par-ticipants.
6. Provide me with supporting materials or tools for my office (re-minders, patient materials, etc.).
7. Include opportunities to solve patient cases.
8. Translate trial data to patients I see in my practice.
9. Address barriers to my optimal patient management.
AANEM Plenary vii
Pre-AcTIVITy QUeSTIoNS
BeFore yoU BeGIN THIS AcTIVITyWe need your feedback in order to improve future educational activities.
On the scantron sheet provided, please rate how important each of the following aspects of the CME activity are to you using this scale:
Fill
in an
swer
s here
Instructions for filling out
your parScore sheet
Using a #2 pencil, fill in your answers beginning with ques-tion #1.
After completion of this activity, go to the back of the book and fill in your answers beginning with ques-tion #10.

viii
Charles G. Burgar, MDTemple, Texas
John E. Chapin, MDAlbuquerque, New Mexico
Nayan P. Desai, MDSan Diego, California
Eric P. Gierke, MDEverett, Washington
Ghazala Riaz Hayat, MDSaint Louis, Missouri
Robert W. Irwin, MDMiami, Florida
Rajasekhar V. Kandala, MDLong Beach, California
Kathleen D. Kennelly, MDJacksonville, Florida
Christina M. Marciniak, MDChicago, Illinois
Elizabeth A. Sekul, MDAugusta, Georgia
Benn E. Smith, MDScottsdale, Arizona
Jeffrey A. Strommen, MD Rochester, Minnesota
2006-2007 AANEM PRESIDENT
Kathryn A. Stolp, MD, MSDurham, North Carolina
2006-2007 AANEM PROGRAM COMMITTEE
Michael T. Andary, MD, MS, ChairEast Lansing, Michigan

INTroDUcTIoN
The manual muscle test (MMT) is the cornerstone of evaluating gait dysfunction caused by peripheral neuropathies. This manu-script identifies key features of gait dysfunction caused by lower motor neuron disorders leading to weakness of the hip, knee, and ankle muscles. Not all major muscle groups of the lower limb are identified; only muscle groups that impact directly on this manu-script’s discussion of gait dysfunction are presented. This author’s preference for muscle testing is based on Muscle Testing: Techniques of Manual Examination by Daniels, Williams, and Worthingham, which was first published in 1946 to aid in evaluating patients weakened by poliomyelitis. The most recent edition was published in 2007.3
Muscle Testing
Lovett and Martin first described the use of gravity in muscle testing.6 They graded muscles from “totally paralyzed” to “normal” with a fair grade muscle being able to overcome gravity. This was subsequently modified by the Medical Research Council10 (Table).
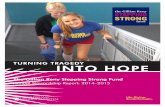
If the patient is unable to maintain the limb in a position against gravity, the muscle is graded less than 3. The “break test” method is described below for each muscle group. In addition, the following figures included demonstrate both an initial and final position. The examiner should push the limb out of an initial position to gain an appreciation of the patient’s strength. As gait is primarily tested in
patients who can sit, the muscle testing described below is with the patient in the sitting position.
Hip flexion (L2, L3, L4). The patient sits with the knee bent and flexes the hip. The examiner forces the hip out of the flexed posi-tion (Figure 1a,b).
Hip internal rotation/abduction (superior gluteal nerve, L4, L5, S1). The hip abductor muscles are the same muscles that internally rotate the hip. For this reason internal rotation can be tested as a surrogate for abduction. In this test, the patient sits with the knees bent and touching, and spreads their feet apart. The examiner grasps the ankles and pushes the feet together (Figure 2 a,b). Abduction is tested with the patient in the side lying posi-tion, elevating the lower limb toward the ceiling. The examiner places one hand on the hip and pushes the hip into adduction
Gait in Peripheral Neuropathies
Gerald J. Herbison, MDProfessor
Jefferson Medical CollegeThomas Jefferson UniversityPhiladelphia, Pennsylvania
Table Medical Research Council Grading Scale
0: No contraction1: Flicker muscle contraction2: Full range of motion3: Active motion against gravity4: Active motion against gravity and resistance5: Normal
(Figure 3 a,b). The examiner prevents the patient from rolling toward the back and using the hip flexor muscles as pseudo-abduc-tors. This author is opposed to having the patient either sit or lie in the supine position to spread the legs apart with the examiner resisting because the patient in all likelihood will appear to spread the legs apart by externally rotating the hips.
Hip extension (Inferior gluteal, L5, S1, S2). To test hip exten-sion, the patient lies prone, flexes the knee, and elevates the limb toward the ceiling. The examiner places the hand on the posterior
thigh, just proximal to the knee and pushes the thigh toward the examining table (Figure 4 a,b). The knee is flexed to relatively weaken the hamstring muscles. This author’s preference for testing the hip extensors is to have the patient lie supine, with the limb to be tested flexed and over the end of the examining table, with the opposite limb flexed to the chest. The patient attempts to hold the hip extended while the examiner attempts to pull the hip into flexion (Figure 5 a,b). The hip extensors can be tested when the patient is positioned supine on the examining table with their legs extended. The examiner attempts to flex the hip while the patient
2 Gait in Peripheral Neuropathies AANEM Plenary
Figure 1 Hip flexion manual muscle test
Figure 2 Hip internal rotation manual muscle test
Figure 1a Initial position
Figure 2a Initial position
Figure 1b Final position
Figure 2b Final position

resists. However, the problem with this technique is that the gluteus maximus is assisted by the full force of the hamstring muscles.
Knee extension (Femoral, L2, L3, L4). In the knee extension test, the patient sits with the knee bent to approximately 70 degrees.
The examiner positions a forearm under the thigh being tested and places the hand of the same limb on top of the opposite thigh. The examiner grasps the ankle of the patient with the other hand, placing the elbow of that limb against the inner aspect of the thigh (Figure 6 a,b). This position provides the examiner with the use of the force of lower limb muscles to counter the force of contraction of the very strong quadriceps muscles.
AANEM Plenary Gait in Motion: Stepping into the 21st Century 3
Figure 3 Hip abduction manual muscle test
Figure 4 Hip extension prone manual muscle test
Figure 3a Initial position
Figure 4a Initial position
Figure 3b Final position
Figure 4b Final position

The quadriceps are not the only knee extensors during gait. During gait there are three major muscle groups that extend the knee. On heel contact, immediately after the swing phase of gait, the quadri-ceps assist in preventing the knee from flexing. It is obvious that the quadriceps participate in this action, however the hip extensors also extend the knee at the moment the heel touches the floor. With the foot on the floor the posterior pull of hip extensors pull the knee into extension. By a similar mechanism the plantar flexors extend the knee when the foot is on the ground. During gait, when the fore foot is on the ground, the plantar flexors prevent the leg from
dorsiflexing on the foot by pulling the tibia posteriorly. This assists in preventing the knee from bending.15 Simply, the plantar flexors extend the knee when the foot is on the ground. In summary, there are three groups of muscles that can extend the knee when the foot is on the ground, the hip extensors, the quadriceps, and the plantar flexors.4
Ankle dorsiflexors (deep peroneal, primarily L4, L5, S1). The tibialis anterior and toe dorsiflexors contribute to this motion. To test the ankle dorsiflexors, the patient sits with the knee bent and
4 Gait in Peripheral Neuropathies AANEM Plenary
Figure 5a Initial position Figure 5b Final position
Figure 6b Final position
Figure 5 Hip extension supine manual muscle test
Figure 6 Knee extension manual muscle test
Figure 6a Initial position

dorsiflexes the ankle preferably with the heel on a stool or on the floor. The examiner places the hand on top of the foot, proximal to the toes, and forcefully plantar flexes the foot (Figure 7 a,b). If the patient cannot put the heel on the floor, the examiner cups the heel in the palm of one hand and forces the ankle into plantar flexion with the other hand.
Ankle plantar flexion/eversion (superficial peroneal, L5, S1). The peroneus longus and brevis pass posterior to the lateral mal-leolus. The toe dorsiflexors also evert the foot but do not plantarflex the foot. The plantar flexor/everters are tested by having the patient sit with the knees bent. The patient plantar flexes and everts the foot. The examiner grasps the ankle with one hand and the lateral forefoot with the other hand and forces the foot into inversion and very slight dorsiflexion (Figure 8a,b). The examiner should watch the toes to be sure the patient is not using the toe dorsiflexors to assist with eversion of the foot.
Ankle plantar flexion/inversion (tibial, L5, S1). The patient plantar flexes and inverts the foot. The examiner grasps the ankle with one hand and the medial forefoot with the other and forces the foot into eversion and very slight dorsiflexion (Figure 9 a,b). The examiner should observe the tibialis anterior muscle tendon at the ankle just lateral to the crest of the tibia to be sure the patient is not using that muscle to assist with inversion of the foot.
Ankle plantar flexors (tibial, L5, S1, S2). The plantar flexors are powerful muscles. Unless the patient is extremely weak it is futile to
use the hand to push on the sole of the foot to test these muscles. The patient stands on one foot holding the hands of the examiner. The patient raises the heel from the floor 20 times for a muscle grade of 5/53 (Figure 10 a,b). Previous editions of Muscle Testing: Techniques of Manual Examination suggested five repetitions, which would be more reasonable for a busy clinical practice. If the patient has difficulty standing, this author instructs the patient to sit with the knees bent and the foot touching the floor. The patient plantar flexes the heel 1 inch from the floor and the examiner force-fully pushes on top of the thigh just proximal to the patella in order to forcefully plantar flex the foot (Figure 10 c,d). At times it is dif-ficult to be sure the patient is not using the hip flexors to prevent the examiner from pushing the thigh down towards the floor. In this instance, this author places his foot under the patient’s forefoot and pushes. If considerable pressure is felt on the top of the author’s foot, it indicates the patient is forcefully plantar flexing the foot.
GAIT SceNArIoS
The following gait scenarios include a relevant history, physical ex-amination, description of gait, an explanation of the gait problem, and a general differential of the causes of such a gait problem. Past medical history, review of systems, family history, strength, pinprick and touch sensation, and reflexes are mentioned if the in-formation is helpful in understanding the gait dysfunction in each case scenario. Any action to prevent hip flexion, knee flexion, or ankle flexion (dorsiflexion) will be called hip extension, knee exten-
AANEM Plenary Gait in Motion: Stepping into the 21st Century 5
Figure 7b Final position
Figure 7 Ankle dorsiflexion manual muscle test
Figure 7a Initial position

6 Gait in Peripheral Neuropathies AANEM Plenary
Figure 9b Final position
Figure 9 Ankle plantar flexion - inversion manual muscle test
Figure 9a Initial position
Figure 8b Final position
Figure 8 Ankle plantar flexion – eversion manual muscle test
Figure 8a Initial position

AANEM Plenary Gait in Motion: Stepping into the 21st Century 7
Figure 10b Sitting final position
Figure 10 Plantar flexion manual muscle test
Figure 10a Sitting initial position
Figure 10c Standing initial position Figure 10d Standing final position

sion, or ankle extension (plantar flexion) respectively. See Perry and Schoneberger for a review of gait.14
Case 1. The patient is a 32-year-old woman who was evaluated November 7, 2002 when she complained of unchanging ankle weakness, and numbness and tingling (but no burning) on the top of the foot and halfway up the lateral aspect of the left leg. This developed immediately after tripping and falling face-first to the sidewalk on September 22, 2002. She did not recall twisting her ankle. The strength was 3/5 for the ankle dorsiflexors and 3+/5 for the peroneus longus and brevis muscles. Touch and pinprick were decreased along the left lateral leg and top of the foot. The patient walked with a left foot slap, but no evidence of inversion of the ankle or steppage during gait.
The patient had a foot slap because the dorsiflexors were weak, but not paralyzed.7,9 By inference the patient was a robust walker. If she walked slowly and/or with short steps, there would be no foot slap. Secondly, the hip extensor and quadriceps muscles had to be strong enough to sustain robust heel strike at the onset of the stance phase of gait or the patient would have flexed at the hip and/or knee at that phase of gait.
The differential diagnosis of a patient with foot slap, in the absence of steppage, includes partial weakness of the dorsiflexors such as a radiculopathy isolated to the L5 nerve root. A radiculopathy iso-lated to a single root would not cause paralysis of the dorsiflexors because they are supplied by two roots. Partial weakness of the dorsiflexors could also be caused by an incomplete peroneal neu-ropathy. The patient in this case was recovering from a complete peroneal neuropathy.
Case 2. The patient is a 55-year-old man who was evaluated January 15, 2002. He complained of severe sharp and dull pain in the left foot, ankle, and lateral leg and mild pain in the knee for a period of 2 years. The pain worsened over the previous 2 months. There was no history of trauma. The pain was associated with ankle weakness and numbness, tingling, and burning on the top of the foot from the ankle to the tips of the toes, exclusive of the little toe. The patient had periodic back pain for 20 years. The strength was 0/5 for the left ankle dorsiflexors and 3/5 for the peroneus longus and brevis muscles. Touch and pinprick were decreased on the top of the left foot. The patient walked with a left steppage gait (Figure 11 a,b) and foot slap. There was no inversion of the ankle during the swing phase of gait. The patient had a magnetic resonance
8 Gait in Peripheral Neuropathies AANEM Plenary
Figure 11a Normal side Figure 11b Steppage side
Figure 11 Steppage gait

imaging (MRI) examination which disclosed a cyst at the fibular head. The cyst was removed on February 27, 2002, after which the patient had some recovery of dorsiflexion strength when seen on July 23, 2002.
The patient had a steppage gait because of absent dorsiflexors. This gait is characterized by excessive hip flexion during the swing phase of gait.1,11 Steppage allows the patient to clear the toe during this phase of gait. With some recovery of the dorsiflexors some pa-tients continue to have a steppage gait until secure enough to walk without the steppage gait deviation. Although a patient with step-page gait may slap the foot on the ground at the onset of the stance phase of gait, this is not what characterizes the gait of a person with total paralysis of the dorsiflexors.11 As previously stated in Case 1, foot slap is a better characterization for partial dorsiflexion weak-ness whereas steppage is the gait deviation of a patient with total dorsiflexion paralysis.
The differential diagnosis of a patient with a steppage gait is not likely to be a single radiculopathy because the dorsiflexors are supplied by two nerve roots. A monoradiculopathy would cause weakness—not paralysis—of the dorsiflexor muscles. A total per-oneal neuropathy at the fibular head is the primary reason, but not the only reason for unilateral paralysis of the dorsiflexors.
Case 3. The patient is a 67-year-old man who was seen December 11, 2003, when he complained of severe sharp and dull pain in the right knee, anterior leg, and top of the foot which began in September 2003 following no trauma. At the onset of symptoms, he also had very severe pain in the buttocks and posterior thigh, but not the low back. From the onset he had tingling, but no numbness or burning on the top of the right foot. At the time he developed the pain, he also developed weakness in the right lower limb. From September to December of 2003, he lost 20 pounds. In September of 2002 he developed pain in the left buttocks and leg followed by left drop foot, which gradually improved over the subsequent months. The patient had leukemia diagnosed in 1994, Type II dia-betes mellitus diagnosed in 1998, and a recent loss of erections. The leukemia had been in remission for several years. When evaluated on December 11, 2003, his right quadriceps strength was 3+/5, left quadriceps strength was 5/5, right ankle dorsiflexor strength was 2/5, and left dorsiflexor strength was 4/5. Touch was decreased over the right anterior thigh, anterior, medial, and lateral leg, and the top of the foot. Pinprick was decreased over the right anterior thigh and medial leg. The right knee jerk and both ankle jerks were absent. The patient’s gait problem was limited to a foot slap on the left. The patient underwent a lumbosacral MRI which did not explain the weakness and gait problem.
The patient had a foot slap on the stronger left side because the left quadriceps were strong. With strong quadriceps, the patient could tolerate a vigorous heel contact at the beginning of the stance phase of gait without fear of the left knee buckling. On the right side, however, where the quadriceps were very weak (3+/5), the patient compensated by decreasing the vigor of heel contact. This decreased the force driving the forefoot into foot slap, while at the same time reducing the chances of buckling at the knee.
The differential diagnosis of a patient with 3+/5 ankle dorsiflexors without a foot slap includes any condition that would weaken the quadriceps force of contraction in the same limb. The patient was thought to have diabetic lumbosacral radiculoplexus neuropathy2 as a cause of muscle weakness. Myopathies and arthritis of the knee could weaken the force of knee extension and reduce the chances of observing a foot slap in a patient who otherwise would be expected to have one.
Case 4. The patient is a 79-year-old man who was evaluated on July 18, 2002, for moderate to severe sharp and dull pain over the low back and the right greater than the left hip. He had many falls from decreased balance. These symptoms began approximately 8 months prior to his evaluation. Approximately 4 months prior to evaluation he developed progressively worsening weakness of the left greater than the right knee, and numbness, tingling, and burning on the bottom greater than the top of the foot. Symptoms were greater in the left foot. He had a total knee arthroplasty in 2000, but con-tinued to have left greater than right knee pain. The patient had 3+/5 left dorsiflexors and 0/5 right and left plantar flexor muscles, decreased pinprick in the little toe, and absent deep tendon reflexes (DTRs) in the lower limbs. The patient walked with poor balance, flexed knees (Figure 12), and was unable to walk on his toes.
The patent walked with flexed knees because of the profound plantar flexor weakness. The plantar flexors are active from foot flat, shortly after the beginning of the stance phase of gait, to push off at the end of the stance phase of gait. During the middle of the stance phase of gait, the plantar flexors prevent the foot from dorsiflexing. If the foot dorsiflexes when the foot is on the ground, the knee flexes or the patient falls forward. The patient in this case stated that he had weak knees. The sensation of weak knees was caused by the profound plantar flexion weakness5,12,13,15 in the presence of strong quadriceps muscles. If he did not have strong quadriceps the knees would have buckled.
The differential diagnosis of knee flexion during the stance phase of gait, apart from joint disease and upper motor neuron problems, is any lower motor neuron disease causing weakness of the plantar flexors in the presence of strong quadriceps. The patient in this case had intact L3, L4 nerve roots but the L5 and S1 and S2 nerve roots were compressed. Spina bifida commonly causes this type of gait deviation.
Case 5. The patient is a 62-year-old man who was seen August 22, 2002, 1 month after developing a right retroperitoneal bleed, as-sociated with right groin and thigh pain, after being anticoagulated for a deep venous thrombosis. He had 2/5 hip flexion and 0/5 thigh adductors and knee extension. The strength of all other major muscle groups was normal. Pinprick and touch were decreased along the anterior thigh and medial leg. He could walk unassisted with his right leg slightly externally rotated. Heel impact was de-creased at the beginning of the stance phase of gait.
This case reinforces the concept that the hip and knee extensors and plantar flexors all contribute to knee extension and knee stabil-ity during the stance phase of gait. As long as the patient’s foot was
AANEM Plenary Gait in Motion: Stepping into the 21st Century 9

on the floor, the hip extensors8 and ankle plantar flexors5,12,13,15
could pull the femur and tibia in a posterior direction and help maintain the knee in extension.
The differential diagnosis of total knee paralysis of the quadriceps includes a femoral neuropathy with or without an obturator neu-ropathy. The patient in this case had a retroperitoneal bleed as a cause of his weakness. Retractors can also cause femoral neuropa-thies during surgery. A monoradiculopathy is not a likely cause of complete paralysis of the quadriceps muscles because they are sup-plied by more than one nerve root.
Case 6. The patient is a 92-year-old woman who was evaluated in July 2002 for moderate pain in the left hip and knee. The patient had Paget’s disease of the entire left femur with 4 inches of shorten-ing of that limb. Left hip internal rotation was decreased (Figure 13) and the flexion, abduction, external rotation, and extension (FABERE) test (Figure 14) was positive. The patient ambulated with a 4-inch heel and 3-inch sole lift with an antalgic gait favor-ing the left hip.
10 Gait in Peripheral Neuropathies AANEM Plenary
Figure 13 Passive internal rotation of the hip. Internal rotation is tested by placing the hip and knee in 90 degree of flexion. The hip is rotated as pictured above. Abnormal rotation is characterized by decreased internal rotation in the symptomatic hip, compared to the asymptomatic hip or rotation of less than about 30 degrees bilaterally.
Figure 14 Flexion, Abduction, External Rotation, Extension (FABERE) test. The FABERE test is positive if the patient has groin pain in this position.
Figure 12 Weak plantar flexors causes instability of the knee

The patient leaned laterally over the left hip while bearing weight on the left lower limb. During the stance phase of gait the hip ab-ductors contract to prevent the body from falling to the opposite side of the weight-bearing limb. The pressure between the acetabu-lum and femur arises from two sources: the weight of the body bearing down on the joint and the contraction of the hip abduc-tors. If the patient leans over the hip joint using the trunk muscles, there is no need for the hip abductors to contract to prevent the body from falling to the opposite side of the weight-bearing limb. This reduces hip pain by decreasing the pressure between the ac-etabulum and the head of the femur during the stance phase of gait. This gait can be indistinguishable from the compensated gluteus gait16 described later. The patient in this case had an antalgic gait because of degeneration of the hip joint. Hip pain, independent of the cause, can result in this gait deviation.
Case 7. The patient is a 32-year-old man who was evaluated August 3, 2006, for moderate to severe sharp and dull pain on the top of the left midfoot to the tips of the great and second toes following a gunshot injury to the right lower quadrant on May 21, 2006. Initially he had numbness in the same area as the pain. He also had foot weakness. The patient had 3+/5 hip internal rotators, abductors, ankle dorsiflexors, and plantar flexor muscles. Touch was decreased on the top of the foot. The patient ambulated with a compensated gluteus medius gait (Figure 15 a,b).
Normal hip abductor muscles eccentrically contract during the stance phase of gait to prevent the pelvis on the swing side from excessively tilting toward the floor. The patient in this case leaned laterally over the left hip while bearing weight on the left lower limb to compensate for the weak left hip abductors. This compen-
AANEM Plenary Gait in Motion: Stepping into the 21st Century 11
Figure 15a Normal side Figure 15b Compensated side
Figure 15 Compensated gluteus medius gait

satory motion prevented excessive tilt of the right pelvis toward the floor each time the left lower limb supported the body weight. Some patients prefer compensating for weak abductors by leaning over the weight-bearing limb rather than allowing the pelvis to tilt toward the floor as described later in Case 8.
The differential diagnosis of a compensated gluteus medius gait includes any cause of weak hip abduction. As previously stated, this gait can be indistinguishable from the antalgic gait deviation described in this case. The patient in this case had hip pain due to degeneration of the hip joint.
Case 8. The patient is a 69-year-old woman who was evaluated February 25, 2003, for mild to severe sharp and dull pain in the low back and the left, greater than right, hip, thigh, knee, leg, and ankles. The pain was associated with tingling, but there was no
numbness or burning in the legs. She had weakness of the right, greater than the left, leg. The symptoms had been present for several months following no trauma. The patient had 3+/5 right hip abductors and ankle dorsiflexors, and 4/5 right and left quad-riceps and left ankle dorsiflexors. The pinprick and touch sensation was decreased on the right, greater than the left, lower extremity from the inguinal ligament to the toes. The knee jerks were absent, but the ankle jerks were present. The patient ambulated with a right uncompensated gluteus medius gait (Figure 16 a,b).
The patient’s pelvis tilted excessively toward the floor on the left side, during the swing phase of gait, because of the weakness of the right hip abductors. This is called an uncompensated gluteus medius gait because there was no attempt to prevent excessive tilt of the pelvis toward the floor on the left side by truncal bending over the right lower limb during the stance phase of gait. Although this
12 Gait in Peripheral Neuropathies AANEM Plenary
Figure 16a Normal side Figure 16b Uncompensated side
Figure 16 Uncompensated gluteus medius gait

AANEM Plenary Gait in Motion: Stepping into the 21st Century 13
gait is called an uncompensated gluteus medius gait, the gluteus minimus and tensor fascia latae are also weak. All three muscles also internally rotate the hip and are innervated by the superior gluteal nerve and the L4,5 and S1 nerve roots.
The differential diagnosis of an uncompensated gluteus medius gait includes all the reasons for weakness of the hip abductors. This patient had bilateral L4, L5, S1 radiculopathies, worse on the right than the left. Degenerative disease of the hip joint is an unlikely cause of an uncompensated gluteus gait because the passive pull of the abductors would increase the pressure between the acetubulum and the head of the femur and increase the patient’s pain.
Case 9. The patient is a 71-year-old man who was evaluated on January 7, 2004, for periodic pain in the right thigh and progres-sive weakness in the same area. He had poliomyelitis at the age of 4 with residual weakness primarily affecting the right shoulder.
The patient had previous electrodiagnostic (EDX) testing at which time post-polio syndrome was considered as a cause of his recent onset weakness and pain. On January 7, 2004, he had 0/5 deltoid, internal, and external shoulder rotation, and 2+/5 hip flexion and abduction on the right side. There was no passive internal rotation (Figure 13) and he had a positive FABERE test of the right hip. The patient tilted the trunk over the right lower limb each time the right foot was on the ground. He used crutches to prevent this gait deviation.
The gait deviation of tilting the trunk over the right lower limb each time the foot was on the ground could be explained on the basis of weak abductors and or degenerative changes in the right hip. If the gait problem was due to weak abductors, it would be called a compensated gluteus gait, but if it was due to degenera-tive changes in the right hip, it would be called an antalgic gait (Figure 17 a,b). The marked decrease in hip internal rotation and
Figure 17a Normal side Figure 17b Antalgic side
Figure 17 Antalgic gait

14 Gait in Peripheral Neuropathies AANEM Plenary
positive FABERE test in the same hip indicates that his ambulatory problem should be referred to as an antalgic gait.
The differential diagnosis of a patient who walks by tilting the trunk over the supporting limb includes weakness of the hip ab-ductors and or hip joint pathology on that side. The treatment implications are significant. This patient had imaging studies which demonstrated that the acetabular bone abutted the bone of the femoral head. He had a total hip arthroplasty and subsequently walked without canes or crutches.
Case 10. The patient is a 70-year-old man who was evaluated June 10, 2004, for progressively worsening proximal muscle weak-ness that began in childhood. His brother had the same history. Recently the patient developed difficulty breathing. This required a tracheotomy and supplemental oxygen. The plantar flexors were tight allowing -10 degrees of ankle dorsiflexion. He had marked weakness proximally with good strength distally in the upper limbs. The hip and knee muscle strength was 0/5. The ankle dorsiflexors were 4/5 and the plantar flexors were 3+/5 tested in the sitting posi-tion (Figure 10c). The patient maintained increased lumbar lordosis throughout the gait cycle and tilted the trunk over the weight-bear-ing limb. When the right or left foot was on the ground, the knee of the same side was maintained in slight hyperextension.
The increased lumbar lordosis placed his trunk weight behind the hip joint and prevented that joint from precipitously flexing. This is called a gluteus maximus gait. The tilt of the pelvis from side to side, as previously noted, is referred to as the compensated gluteus medius gait, due to weak hip abductors. The knees were extended each time the patient placed a foot on the ground by the tight plantar flexors. If the patient came down on his heels, the knees would have buckled. The plantar flexor tightness assured that the ball of his foot bore the weight of the body, which forced his knees into extension. The patient’s brother, who was confined to a wheel-chair, had commented that the problem with his brother’s walking was his tight heel cords and that his brother’s Achilles tendons should have been cut. If the patient’s Achilles tendons were cut, he would drop to the ground, immediately buckling at the hips and knees. This case reinforces the point mentioned above of the im-portance of the plantar flexors as knee extensors. In this patient, the plantar flexion force came from a contracture of the plantar flexors, not from active plantar flexion.
The differential diagnosis of the gait deviation is any neuropathy or myopathy that causes weakness of the hip and knee muscles. This patient and his brother had primary muscular atrophy.
Case 11. The patient is a 25-year-old woman who was evaluated June 1, 2004, for difficulty walking. She initially developed pain on October 12, 2003, that started after participating in a breast cancer walk. The pain was moderate and dull in the anterior right thigh, and severe and sharp across the low back. About a week later, she began to notice that her legs started to give out, initially worse on the right side, but subsequently worse on the left side, resulting in several falls. She had difficulty walking up and down stairs, and
getting in and out of chairs. The past medical history, review of systems, and family history were unremarkable except for the fol-lowing: EDX testing performed in April 2004 was normal, as was an MRI of the brain, cervical, thoracic, and lumbar spine, and the thighs. A week prior to the evaluation she was seen in an emergency room for severe low back pain for which she was given flexeril and naprosyn. She had 2/5 strength of the right and left hip flexors, abductors, and extensors and 4/5 strength of all other major muscle groups of the upper and lower limbs. The patient ambulated with a profound bilateral gluteus medius (Figure 18) and maximus gait (Figure 19). The patient had profound postexercise facilitation on repeat EDX studies.
The patient’s bilateral gluteus medius and maximus gait was due to the marked hip abductor and extensor weakness respectively. It is highly unlikely that this type of gait would ever be seen with low back pain or as a result of psychogenic disorder. Secondly, such
Figure 18 Compensated gluteus medias gait

AANEM Plenary Gait in Motion: Stepping into the 21st Century 15
focal weakness would not likely be caused by low back pain, a ra-diculopathy, or a psychogenic disorder.
The differential diagnosis of the gait disorder and weakness in-cludes any myopathy that causes proximal weakness. This patient has Lambert-Eaton myasthenic syndrome and Sjögren’s syndrome.
No cancer was diagnosed prior to or since 2003. The patient has not responded to treatment.
coNcLUSIoN
Characteristic gait disorders result from identifiable weakness of specific muscle groups. Paralysis of the ankle dorsiflexors is charac-terized by a steppage gait whereas partial paralysis is typified by a foot slap. A patient’s complaint of “weak knees” warrants an exami-nation of the strength of the hip extensors and plantar flexors. With practice, patients with quadriceps paralysis can walk on flat surfaces with almost normal gait, because they have two of the three knee extensors intact (hip extensors and ankle plantar flexors). Paralysis of the hip extensors results in a gluteus maximus gait. This gait is characterized by increased lumbar lordosis. This posture places the trunk behind the hip joint and prevents precipitous hip flexion. Weak hip abductors cause either an uncompensated or compen-sated gluteus medius gait. A compensated gluteus medius gait appears the same as an antalgic gait due to hip joint pathology.
Acknowledgments
Thank you to all the patients that allowed me to make videotapes, Theera Vachranukunkeit, MD and Jeremy Simon, MD for their help in making the manual muscle test figures, and Patricia and Matt Herbison for technical support.
reFereNceS
1. Campbell WW. DeJong’s the neurologic examination, 6th edition. Philadelphia: Lippincott Williams & Wilkins; 2005. p 531.
2. Dyck PJB, Windebank AJ. Diabetic and nondiabetic lumbosacral radiculoplexus neuropathies: new insights into pathology and treat-ment. Muscle Nerve 2002;25:477-491.
3. Hislop HJ, Montgomery J. Daniels & Worthingham’s muscle testing: techniques of manual examination. Edinburgh: Elsevier-Saunders; 2007.
4. Hollinshead WH. Anatomy for surgeons: the limbs and back. New York. Harper & Row; 1964.
5. Lehmann JF, Condon SM, deLateur BJ, Smith JC. Gait abnormali-ties in tibial nerve paralysis: a biomechanical study. Arch Phys Med Rehabil 1985;66:80-85.
6. Lovett RW, Martin EG. Certain aspects of infantile paralysis and a description of a method of muscle testing. JAMA 1916;66:729- 733.
7. Lower-limb orthotics. New York University Medical Center. Post-Graduate Medical School Prosthetics and Orthotics. 1981. p 62.
8. Lower-limb prosthetics. New York University Medical Center. Post-Graduate Medical School Prosthetics and Orthotics. 1980. p 147, 234.
9. Malanga G, DeLisa JA. Clinical observation. In: DeLisa J, editor. Med. gait analysis in the science of rehabilitation: monograph 002. Department of Veterans Affairs, Veterans Health Adminnistration, Rehabilitation Research and Development Service. Scientific and Technical Publications Section. Baltimore. p 9.
10. Medical Research Council: War Memorandum No 7. Aids to the investigation of peripheral nerve injuries. 2nd rev. ed. London, Her Majesty’s Stationery Office 1943 (Reprinted 1973)
Figure 19 Gluteus maximus gait
16 Gait in Peripheral Neuropathies AANEM Plenary
11. Murray MP, Clarkson BH. The vertical pathways of the foot during level walking. II. Clinical examples of distorted pathways. Phys Ther 1966; 46: 585-9
12. Murray MP, Guten GN, Sepic SB, Gardner GM, Baldwin JM. Function of the triceps surae during gait. Compensatory mecha-nisms for unilateral loss. J Bone Joint Surg. 1978; 60-A:473-6
13. Perry J, Schoneberger B. Gait analysis: normal and pathological func-tion. Thorofare, NJ: SLACK, Inc; 1992.
14. Perry J, Fontaine JD, Mulroy, S. Findings in the post-poliomyelitis syndrome. Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg. 1995; 77-A:1148-53
15. Sutherland DH, Cooper L, Dale D. The role of the ankle plantar flexors in normal walking. J Bone Joint Surg. 1980; 62-A: 354-63
16. Peltier LF. The classic: Trendelenburg’s test 1895. Clin Orthop 1998;355:3-7.

A common patient complaint particularly in the elderly is difficulty with walking. The ability to get around is important to indepen-dence, and falls can get patients into considerable trouble with everything from fractured hips to subdural hematomas. Moreover, walking is not easy; it is a difficult motor control task that requires both balancing on two legs and executing locomotion. While often the diagnosis is clear, other times it can be difficult, and the difficulty is magnified because the problem can be multifactorial. Recognizing the principle patterns of gait abnormalities is valuable in establishing the diagnosis and pointing the way to appropriate therapy.
NorMAL GAIT
Human gait is a complex, rhythmic, cyclic movement.1 The move-ments are generated to some extent by a locomotor generator in the spinal cord, but they are under control by supraspinal mechanisms. The spinal cord generator can produce only simple, primitive step-ping and react to perturbations in stereotypic fashion.2 Supraspinal mechanisms are required for a person to go in desired directions, with desired velocities, and to deal well with perturbations. An important supraspinal control center is the mesencephalic locomo-tor region, which includes the pedunculopontine nucleus. The pe-dunculopontine nucleus is an important integrator of activity from basal ganglia, cerebellum, and motor cortex and projects to reticu-lar nuclei in the brainstem. The fastigial nucleus of the cerebellum seems also important.3 Supraspinal control signals are conveyed to the spinal cord by reticulospinal and vestibulospinal tracts.
A number of terms useful in describing gait are defined here:
Stance phase: When the foot is on the floor.
Swing phase: When the foot is in the air.
Stance time: The time that the foot is on the floor, measured as the time between heel strike and toe or heel off, whichever is last.
Swing time: The time that the foot is in the air, measured as the time between toe off and heel strike.
Cadence: The number of steps per minute.
Step length: The distance advanced by one foot compared to the position of the other.
Stride length: The sum of two consecutive step lengths or the dis-tance advanced by one foot compared to its prior position.
Step time: The time between heel strike of one foot to the subse-quent heel strike of the contralateral foot.
Gait cycle: One complete cycle of events, often considered the time between two consecutive heel strikes of the same foot. Hence, a gait cycle would begin at the beginning of stance phase of one foot, go through stance and swing, and end at the end of swing (which is the beginning of the next stance phase).
Stride time: The time for a full gait cycle.
Average gait velocity: The stride length divided by the stride time.
Neurological Gait Disorders
Mark Hallett, MDChief
Human Motor Control SectionNational Institute of Neurological Disorders and Stroke,
National Bethesda, Maryland
17

The gait cycle is illustrated in Figure 1. Note that the gait cycle for the two legs is not exactly 180 degrees out of phase. For this reason, and because the stance phase is longer than the swing phase, there are several periods when both feet are on the ground; these are called double support. With normal gait, when the foot contacts the ground, the heel contacts first, and then the foot rotates to flat, with the heel as the point of rotation. When the foot leaves the floor for swing, the foot rotates over the toe, and the heel leaves the ground first.
The joint angles of a normal gait cycle and the muscle activities during gait are normally stereotyped. These are commonly quan-tified in the gait laboratory and can be useful. At least the joint angles can be appreciated somewhat visually.
GAIT DISorDerS
epidemiology
In the elderly population, the common causes for gait problems are stroke, peripheral neuropathy, brain or spinal cord trauma, and Parkinson’s disease.4 The term senile gait is sometimes used, but it does not exist as a distinct entity. Multiple medical problems accumulate with age, including visual difficulties and arthritis, that become additive. Sudarsky evaluated a series of patients who were referred for an unknown gait disorder.5 After careful neu-rologic evaluation, he was able to make a diagnosis in most. The most common entities were sensory deficits (18.3%), myelopathy (16.7%), multiple infarcts (15.0%), parkinsonism (11.7%), and unknown (14.2%).
18 Neurological Gait Disorders AANEM Plenary
Figure 1. Diagram of the gait cycle. From <www.laboratorium.dist.unige.it> by Gerard Malanga, MD and Joel A. DeLisa, MD.

evaluation of Gait
When evaluating gait, the gait itself should of course be observed, but special attention should be paid to different aspects, including the nature of the steps, including the stride length and cadence, deviations from the direction of progression, the width of the feet from each other during periods of double support, the variability of the stepping, and the angular movements at the joints. Any stiff-ness of motion should be noted. Additionally, the ability to initiate stepping and the ability to turn should be observed. In looking for more subtle abnormalities, individuals can be asked to walk a straight line, heel to toe. In the case of dystonia, the patients might be asked to walk backward to determine whether this improves the performance. Balance should be assessed as well, with observation of quiet standing with eyes open and eyes closed and performance of the pull test. Of course, it is critical to evaluate patients for non-neurologic features such as arthritis, limitation of motion, pain (antalgic gait), and asymmetries of leg length.
A number of important observations have implications for the dif-ferential diagnosis6:
Weakness: Weakness should ordinarily be noted on general neu-rologic examination. Depending on the muscles that are affected, certain patterns will be identified, such as steppage and waddling, which are described later. Weakness is commonly due to neuropa-thy or myopathy.
Dysmetria of stepping: Steps that are abnormal by virtue of being the wrong length or direction and that are also highly variable are dysmetric. This is characteristic of ataxia and chorea. Ataxia looks mostly clumsy, while chorea often has a dancing quality.
Stiffness or rigidity: A reduction of joint movement produces stiffness and rigidity. It is seen with spasticity, parkinsonism, and dystonia.
Veering: Deviations from a direct line of progression, or veering, are due to either vestibular or cerebellar disorders.
Freezing: Freezing is also known as motor blocks and is character-ized by lack of movement, with the feet looking as though they are glued to the floor. Patients often look as though they are trying to move, but they cannot. This might be due to an inability to generate sufficient postural shifting to initiate forward movement.7 Freezing can occur in trying to initiate gait, and is also called start hesitation. Freezing can also interrupt walking, and in this circum-stance, it is sometimes precipitated by a sensory stimulus such as a doorway, the ring of a doorbell, or a traffic light changing color. Curiously, sensory stimuli can also be used to improve freezing. They appear to act in this regard by providing external triggers for movement. In addition to the absence of movement, another
form of freezing is characterized by rapid side-to-side shifting of weight but no lifting of the feet and no forward progression. This has been called slipping clutch syndrome. In this situation, physi-ologic studies show cocontraction activity in antagonist muscles, apparently not permitting effective forward movement.8 Freezing is very common in idiopathic Parkinson’s disease but is also seen in other parkinsonian states, such as progressive supranuclear palsy, vascular parkinsonism, and normal pressure hydrocephalus. It seems less common in multiple-system atrophy and drug-induced parkinsonism.9
Marché à petit pas: Walking with very short, often shuffling, steps is called marché à petit pas. This is most typical of a multi-infarct state, but can be seen with parkinsonism.
Festination: Festination is described as short steps becoming pro-gressively more rapid. This extension of marché à petit pas is also characteristic of parkinsonism. The stepping may even become much more rapid than normal. This can also be called a propulsive gait.
Anatomic/Physiologic classification
This manuscript follows the classification of Nutt, Marsden, and Thompson, proposed in 1993, since that has been the most commonly used.6 Some more recent refinements have been suggested,10,11 and some modifications have been made.
LoWeST LeVeL
The lowest level refers to elemental disorders such as those result-ing from muscle, nerve, or root disorders. This would also include the consequences of sensory deficits, such as peripheral neuropa-thy, vestibular disorder, or visual disorder. Severe sensory loss can produce a gait similar to that of cerebellar ataxia; these patients have particular difficulty walking in the dark.
One set of examples relates to disturbances generated by particular patterns of weakness. For example, the steppage gait is the result of a foot drop. The hip and knee have to be excessively flexed to bring the leg up high enough that the toes do not scrape the floor. Another example is the waddling gait, in which weakness of the hip abductors leads to dropping of the pelvis toward the swing leg and compensatory lean toward the stance leg.
MIDDLe LeVeL
The middle level refers to central nervous system disorders arising from standard parts of the motor system.
AANEM Plenary Gait in Motion: Stepping into the 21st Century 19

Hemiparetic Gait
Owing to a unilateral lesion of the corticospinal tract, most com-monly seen with stroke, hemiparetic gait is a stiff extended leg that circumducts during swing with scraping of the toe. Typically, of course, there should be some weakness in a pyramidal distribution and increased reflexes. The earliest sign might be reduced knee flexion during swing.12
Paraparetic Gait
Paraparetic gait is a bilateral hemiparetic gait and shows stiffness of both legs with scissoring (excessive hip adduction). Conditions in which this is prominent include spinal cord injury, hereditary spastic paraparesis, and primary lateral sclerosis.
Stiff-legged Gait
Stiff-legged gait includes the spastic syndromes of hemiparetic and paraparetic and also the disorder that is seen with stiff-man syn-drome. There is particular stiffness of the spine with hyperlordosis, but all joints of the lower extremity will have reduced range of motion as well.
Ataxic Gait
Patients with cerebellar ataxia have difficulty with motor control by virtue of dysmetria, dyssynergia, variability of performance, and poor balance. All these features contribute to their disorder of gait. Clinically, the gait is characterized by irregularity of stepping, in direction, distance, and timing. Patients may lurch in different directions. Stability of upright stance is poor, and patients may fall. Just as with standing balance, the base, or distance between the feet, is said to be broad.
Palliyath and colleagues13 studied the gait pattern in 10 patients with cerebellar degenerations. Gait at natural speed was studied by using a video-based kinematic data acquisition system for measur-ing body movements. Patients showed a reduced step and stride length with a trend toward reduced cadence. Heel off time, toe off time, and time of peak flexion of the knee in swing were all delayed. Range of rotation of ankle, knee, and hip were all reduced, but only ankle range of rotation reached significance. Multijoint coordination was impaired, as indicated by a relatively greater delay of plantar flexion of the ankle compared with flexion of the knee and a relatively late knee flexion compared with hip flexion at the onset of swing. Patients also showed increased variability of almost all measures. While some of the deviations from normal were due simply to the slowness of walking, the gait pattern of patients with
cerebellar degeneration showed incoordination similar to that pre-viously described for their multijoint limb motion. A wide base was not seen in this study, but it was seen in another study.14
Patients with essential tremor have a mild gait abnormality that is ataxic in type.15 This forms part of the evidence that essential tremor results from cerebellar dysfunction.
Parkinsonian Gait
Parkinson patients often have a stooped posture, and they stand and walk on a narrow base.16,17 Sometimes there is marked flexion of the trunk called camptocormia, a condition also seen in dystonia and in psychogenic conditions.18 Balance is poor. They have short, shuffling steps, the marché à petit pas, which can be associated with festination. They turn en bloc, and important associated signs are lack of armswing and tremor of the hands. Freezing is common and can occur both in the “off ” and “on” states. Freezing is seen in about a quarter of patients by 4 years after diagnosis.19
Gait speed in Parkinson’s disease is slow. If trying to walk faster, patients increase step rate proportionately more than stride length (compared with normal subjects).20,21 Electromyography studies have illuminated the pathophysiology.22
Variability of stride length is a gait feature that has been associated with falls. Stride time and variability were studied in patients with Parkinson’s disease and compared with other clinical measures.23 Variability was independent of tremor, rigidity, and bradykinesia but somewhat responsive to levodopa. Gait variability markedly in-creases with a simultaneous cognitive task, and this certainly would make patients more prone to falls.24 Patients with more freezing also have more variability, suggesting that this might be a factor in the etiology of freezing.25 Abnormalities of electromyographic pattern have been described.26
Dystonic Gait
An early common manifestation of dystonic gait is inversion of the foot with walking. The great toe can be flexed or extended. It is an action dystonia and would not be present at rest. As the dystonia worsens, there can be more abnormal posturing of the legs, trunk, and arms. Sometimes, there is so much abnormal movement that the gait looks like the dancing gait of chorea. The disorder is task specific, so walking backward might be much better than walking forward, and running can be spared. Dystonic gaits can look very unusual, and care is needed to distinguish them from psychogenic. Camptocormia—flexion of the spine—is one such abnormal posture in which a principal differential diagnosis is psychogenic.
20 Neurological Gait Disorders AANEM Plenary

choreic Gait
Choreic gait is often called dancing gait and represents the super-imposition of chorea on the locomotor movements. Stepping is also uncoordinated and appears dysmetric, like an ataxic gait.
Bouncing Gait (Myoclonus)
When myoclonus affects stance and gait, it gives rise to a charac-teristic bouncing. The appearance is due more to frequent negative myoclonus than positive myoclonus.
HIGHeST LeVeL
The highest-level disorders come from malfunction of the cerebral hemispheres and include disorders arising from psychiatric origin, including cautious gait and psychogenic gait. These disorders are not completely distinct from each other; patients may have characteristics of more than one or may progress from one to another.10,11,27
Frontal Gait Disorder
This disorder comprises three conditions from the original Nutt and colleagues classification—frontal disequilibrium, isolated gait ignition failure, and frontal gait disorder. These are difficult to separate from each other and it seems unnecessary to do so, since the etiologies are also similar.
Patients with frontal gait disorder, at first, look as though they have a parkinsonian gait with short, shuffling steps; poor balance; initiation failure; and hesitations on turns. Differentiating features are a more upright stance, lack of tremor, frontal lobe signs, and apparent involvement of only the lower part of the body.27 This last feature gives rise to the term lower half parkinsonism or lower body parkinsonism. The disorder does not respond to levodopa.
The etiologies of frontal gait disorder include subcortical arte-riosclerotic encephalopathy (Binswanger’s disease), multi-infarct state, anterior cerebral artery stroke, normal pressure hydrocepha-lus, Pick’s disease, Alzheimer’s disease, frontotemporal dementia, subdural hematoma, brain tumor, multiple sclerosis, progressive supranuclear palsy, and corticobasal degeneration.27
The gait in normal pressure hydrocephalus has been the most studied. These patients have freezing and gait apraxia. Quantitative gait studies show decreased stride length and reduced foot floor clearance.28,29 Evidence-based guidelines have been pub-lished. “The diagnosis of idiopathic normal-pressure hydrocephalus (INPH) requires convergent evidence from the clinical history, physical examination, and brain imaging. Gait and/or balance impairments are usual symptoms, and findings may also include disturbances in cognition and control of urination. Documentation of ventricular enlargement by brain imaging is necessary but not sufficient in itself to establish a diagnosis of INPH.”30
Factor and colleagues31 using the term primary progressive freezing gait reported a series of 30 patients and found a clinically distinct progressive neurologic disorder that primarily affected gait, initially resulting in freezing and later in postural instability. A wheelchair-bound state often developed within 5 years. It was accompanied by other parkinsonian features, particularly bradykinesia, but was un-responsive to dopaminergic medications. Because of its stereotyped manner, they suggested that it be considered a specific entity within the parkinsonism-plus disorders.
cautious Gait
Cautious gait is a common disorder, especially in the elderly or with patients who have already experienced a fall for some reason. The term space phobia has been used. Patients become cautious because of anxiety that they will fall. The gait is like what it would be for normal people who are walking on ice. There is a wide base with slow, short steps; turns are en bloc; arms are tense. Patients try to find support, and when they have it, there is marked improvement. These individuals do not have overt freezing or shuffling.
Psychogenic Gait
A gait disorder is a common way for psychogenic movement disor-ders to present.32,33,34 This is also called astasia-abasia or acrobatic gait. There are unusual patterns of stance and gait, often incon-sistent, often dramatic, with lurching but only rarely falls (and then without patients hurting themselves). Sudden knee buckling without falling is a common pattern.32 Extreme slow motion can be seen, and there is a sense that energy is being wasted. Camptocormia is one of the patterns that is commonly psychogenic. Careful ob-servation will show that the person typically demonstrates excellent balance. There might well be wide fluctuations over short periods of time. As with other psychogenic movement disorders, positive psychiatric features are frequent and can be important in making a clear diagnosis. A possible clue to this is a suffering or strained facial expression, with moaning and hyperventilation.32
Apraxia of Gait
The term apraxia of gait is used is so many ways that it has become largely a confusion. Most commonly it has been applied to frontal gait disorders. Apraxia generally refers to a loss of skilled movement in the absence of a more elemental abnormality that might explain it. This term might well be restricted to situations where there is a gait abnormality in the presence of limb apraxia demonstrated in other ways. One situation where this is seen is in patients with corticobasal degeneration.
Failures of Multitasking
Walking does require a certain amount of attention. Attention is needed, for example, to decide where to go, how to avoid obstacles, what to do about obstacles if not avoidable, when to start and stop. Humans have a limited amount of attention and when trying to do two tasks at the same time, attention has to be shared and each
AANEM Plenary Gait in Motion: Stepping into the 21st Century 21

22 Neurological Gait Disorders AANEM Plenary
task has less of it. If attention is impaired, or there is difficulty in rapid shifting of attention, then there might be difficulty with gait. This is a problem in patients with Parkinson disease35 and Alzheimer disease.36,37 The problem can be quantified by assessing gait parameters with and without a dual task.24 Clinically, the “stop walking while talking test” can be used.38 Subjects are asked to talk while they are walking. If they stop walking, then this is positive. It has been demonstrated that persons with difficulty in multitask-ing are at a greater risk of falling.
Multifactorial etiology
It was mentioned earlier but is worth noting again at this point that disorders of gait are often multifactorial, particularly in the elderly. It is useful to continue searching for etiologies even after one has been identified. This is certainly true of psychogenic gait, since many of these patients have organic neurologic disturbances.
THerAPeUTIc coNSIDerATIoNS
Etiologic considerations come first. Is there a treatable neuropa-thy? Can vision be improved? Parkinson’s disease can be treated, as can normal pressure hydrocephalus. The second consideration would be symptomatic treatments. Physical therapy can help with strengthening exercises or practice with elemental coordinations. There is a variety of walking aids, from canes to walkers. There are weighted walkers and rolling walkers that help in special circum-stances. It is also critical to know when to suggest that the patient no longer should be trying to walk without assistance.
Acknowledgment
This syllabus is the work of the United States Government and is not copyrighted. It is modified and updated from a chapter in press, in Principles and Practice of Movement Disorders, S. Fahn and J. Jankovic (Editors), Elsevier.
reFereNceS
1. Winter DA. The biomechanics and motor control of human gait: normal, elderly and pathological. Waterloo: University of Waterloo Press; 1991. 143 p.
2. Burke RE. The central pattern generator for locomotion in mammals. Adv Neurol 2001;87:11-24.
3. Mori S, Matsuyama K, Mori F, Nakajima K. Supraspinal sites that induce locomotion in the vertebrate central nervous system. Adv Neurol 2001;87:25-40.
4. Sudarsky L. Gait disorders: prevalence, morbidity, and etiology. Adv Neurol 2001;87:111-117.
5. Sudarsky L. Clinical approaches to gait disorders of aging. In: Masdeu J, Sudarsky L, Wolfson L, editors. Gait disorders of aging: falls and therapeutic strategies. Philadelphia: Lippincott-Raven; 1997. p 147-158.
6. Nutt JG, Marsden CD, Thompson PD. Human walking and higher-level gait disorders, particularly in the elderly. Neurology 1993;43:268-279.
7. Elble RJ, Cousins R, Leffler K, Hughes L. Gait initiation by patients with lower-half parkinsonism. Brain 1996;119:1705-1716.
8. Yanagisawa N, Hayashi R, Mitoma H. Pathophysiology of frozen gait in Parkinsonism. Adv Neurol 2001;87:199-207.
9. Giladi N. Freezing of gait. Clinical overview. Adv Neurol 2001;87:191-197.
10. Jankovic J, Nutt JG, Sudarsky L. Classification, diagnosis, and etiol-ogy of gait disorders. Adv Neurol 2001;87:119-133.
11. Nutt JG. Classification of gait and balance disorders. Adv Neurol 2001;87:135-141.
12. Kerrigan DC, Karvosky ME, Riley PO. Spastic paretic stiff-legged gait: joint kinetics. Am J Phys Med Rehabil 2001;80:244-249.
13. Palliyath S, Hallett M, Thomas SL, Lebiedowska MK. Gait in patients with cerebellar ataxia. Mov Disord 1998;13:958-964.
14. Hudson CC, Krebs DE. Frontal plane dynamic stability and co-ordination in subjects with cerebellar degeneration. Exp Brain Res 2000;132:103-113.
15. Stolze H, Petersen G, Raethjen J, Wenzelburger R, Deuschl G. The gait disorder of advanced essential tremor. Brain 2001;124:2278-2286.
16. Morris ME, Huxham F, McGinley J, Dodd K, Iansek R. The biome-chanics and motor control of gait in Parkinson disease. Clin Biomech (Bristol, Avon) 2001;16:459-470.
17. Morris ME, Huxham FE, McGinley J, Iansek R. Gait disorders and gait rehabilitation in Parkinson’s disease. Adv Neurol 2001;87:347-361.
18. Azher SN, Jankovic J. Camptocormia: pathogenesis, classification, and response to therapy. Neurology 2005;65:355-359.
19. Rascol O, Brooks DJ, Korczyn AD, De Deyn PP, Clarke CE, Lang AE. A five-year study of the incidence of dyskinesia in patients with early Parkinson's disease who were treated with ropinirole or levodopa. 056 Study Group. N Engl J Med 2000;342:1484-1491.
20. Morris ME, Iansek R, Matyas TA, Summers JJ. Ability to modulate walking cadence remains intact in Parkinson’s disease. J Neurol Neurosurg Psychiatry 1994;57:1532-1534.
21. Morris M, Iansek R, Matyas T, Summers J. Abnormalities in the stride length-cadence relation in parkinsonian gait. Mov Disord 1998;13:61-69.
22. Albani G, Sandrini G, Kunig G, Martin-Soelch C, Mauro A, Pignatti R, Pacchetti C, Dietz V, Leenders KL. Differences in the EMG pattern of leg muscle activation during locomotion in Parkinson’s disease. Funct Neurol 2003;18:165-170.
23. Schaafsma JD, Giladi N, Balash Y, Bartels AL, Gurevich T, Hausdorff JM. Gait dynamics in Parkinson's disease: relationship to Parkinsonian features, falls and response to levodopa. J Neurol Sci 2003;212:47-53.
24. Hausdorff JM, Balash J, Giladi N. Effects of cognitive challenge on gait variability in patients with Parkinson’s disease. J Geriatr Psychiatry Neurol 2003;16:53-58.
25. Hausdorff JM, Schaafsma JD, Balash Y, Bartels AL, Gurevich T, Giladi N. Impaired regulation of stride variability in Parkinson’s disease subjects with freezing of gait. Exp Brain Res 2003;149:187-194.
26. Nieuwboer A, Dom R, De Weerdt W, Desloovere K, Janssens L, Stijn V. Electromyographic profiles of gait prior to onset of freezing episodes in patients with Parkinson’s disease. Brain 2004;127:1650-1660.
27. Thompson PD. Gait disorders accompanying diseases of the frontal lobes. Adv Neurol 2001;87:235-241.
28. Stolze H, Kuhtz-Buschbeck JP, Drucke H, Johnk K, Illert M, Deuschl G. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J Neurol Neurosurg Psychiatry 2001;70:289-297.

AANEM Plenary Gait in Motion: Stepping into the 21st Century 23
29. Stolze H, Kuhtz-Buschbeck JP, Drucke H, Johnk K, Diercks C, Palmie S, Mehdorn HM, Illert M, Deuschl G. Gait analysis in idio-pathic normal pressure hydrocephalus--which parameters respond to the CSF tap test? Clin Neurophysiol 2000;111:1678-1686.
30. Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 2005;57:S4-S16.
31. Factor SA, Jennings DL, Molho ES, Marek KL. The natural history of the syndrome of primary progressive freezing gait. Arch Neurol 2002;59:1778-1783.
32. Lempert T, Brandt T, Dieterich M, Huppert D. How to identify psy-chogenic disorders of stance and gait. A video study in 37 patients. J Neurol 1991;238:140-146.
33. Hayes MW, Graham S, Heldorf P, de Moore G, Morris JG. A video review of the diagnosis of psychogenic gait: appendix and commen-tary. Mov Disord 1999;14:914-921.
34. Bhatia KP. Psychogenic gait disorders. Adv Neurol 2001;87:251-254.
35. Yogev G, Giladi N, Peretz C, Springer S, Simon ES, Hausdorff JM. Dual tasking, gait rhythmicity, and Parkinson’s disease: which aspects of gait are attention demanding? Eur J Neurosci 2005;22:1248-1256.
36. Pettersson AF, Olsson E, Wahlund LO. Effect of divided attention on gait in subjects with and without cognitive impairment. J Geriatr Psychiatry Neurol 2007;20:58-62.
37. Sheridan PL, Solomont J, Kowall N, Hausdorff JM. Influence of ex-ecutive function on locomotor function: divided attention increases gait variability in Alzheimer’s disease. Journal of the American Geriatrics Society 2003;51:1633-1637.
38. Bloem BR, Grimbergen YA, van Dijk JG, Munneke M. The “posture second” strategy: a review of wrong priorities in Parkinson’s disease. J Neurol Sci 2006;248:196-204.

24 AANEM Plenary

INTroDUcTIoN
Amyotrophic lateral sclerosis (ALS) was first described in the late 1800s in France. It is a progressive, fatal disease causing weakness of the voluntary muscles with no known cure. It usually starts in the limbs and spreads contiguously, causing mobility to be one of the first functions affected. Bulbar onset is less common and respiratory onset is very rare. Death from respiratory failure occurs on average 3-5 years after the first symptom, but the range is very broad with some people dying 2 months after their first symptom while others are still walking 10-15 years after their first symptom. ALS was first made aware to the general public in the 1930s when Lou Gehrig, the famous New York Yankees baseball player, developed the disease and rapidly declined over the course of 2 years. The incidence of ALS is 1-3 cases per 100,000 without any geographic or ethnic preferences. ALS is found more commonly in men and has its onset on average at age 56, but onset ranges from age 20 to age 80. ALS is usually a sporadic disease, but 10% of the time it is familial, typically with autosomal dominant inheritance. There is only one medication approved by the United States Food and Drug Administration to treat ALS—riluzole. The drug prolongs survival by 10% and delays disease progression modestly but is expensive and sometimes causes a hardship for patients without supplemental prescription coverage. It is usually fairly well tolerated, however, and approximately 50% of ALS patients typically take the drug.7
cLINIcAL FeATUreS
ALS is a clinical diagnosis with a combination of progressive upper and lower motor neuron findings (Figure 1). Upper motor neuron (UMN) findings include slow speech, brisk gag and jaw jerk, brisk reflexes, spasticity, and Hoffman’s or Babinski signs. Lower motor
neuron (LMN) findings include atrophy, fasciculations, and weak-ness. Patients may also have a pure UMN syndrome, typically termed primary lateral sclerosis (PLS) when the needle electromyo-graphy (EMG) examination is normal and symptoms have been present for over 3 years. A pure LMN syndrome is typically termed progressive muscular atrophy (PMA) variant of ALS. Either PLS or PMA may evolve over time to ALS and have a progression typical of ALS. At other times, PLS or PMA patients may have a more slowly progressive course.
It is important to exclude mimics of ALS, which are many. Strokes, brain tumors, multiple sclerosis, and B12 deficiency are common causes of UMN damage and must be excluded in the work-up of a potential ALS patient. Multifocal motor neuropathy (MMN), para-neoplastic syndromes, monoclonal gammopathies, lyme disease, HIV, hereditary neuropathies, lead toxicity, and polio may mimic ALS causing an LMN syndrome. Spine disease is one condition which can cause a combination of UMN and LMN findings in the limbs if there is spinal stenosis compressing the cord and foraminal narrowing compressing nerve roots, but usually the pattern of the weakness and neuroimaging helps distinguish this possibility from ALS. A brainstem tumor could also cause both UMN and LMN findings depending on where it is located, and neuroimaging with gadolinium is critical for patients with brainstem findings on ex-amination.
In addition to neuroimaging and blood work, a needle EMG is critical in making a definitive diagnosis of ALS. Nerve conduction studies with proximal stimulation can help identify conduction block which is typical of MMN as well as identify any subclinical sensory involvement or features characteristic of a hereditary neu-ropathy or monoclonal gammopathy. Kennedy’s disease, another motor neuron disease which is caused by trinucleotide repeats in
Mobility and Amyotrophic Lateral Sclerosis
catherine Lomen-Hoerth, MD, PhDAssistant Professor
Department of NeurologyUniversity of California, San Francisco
San Francisco, California
25

the androgen receptor, may have absent or low amplitude sensory nerve action potentials. Bulbar onset cases may be confused with myasthenia gravis, and repetitive nerve stimulation may aid in the diagnosis along with testing acetylcholine receptor antibodies. The EMG portion of the study is necessary to exclude myopathies which can sometimes mimic ALS, although rapidly progressive cases of ALS may sometimes have myopathic units on EMG. Even in clear-cut cases of ALS with extensive UMN and LMN findings, the EMG is useful for prognosis based on the degree of denervation present as well as for determining subclinical disease in areas not yet obviously clinically affected.
MoBILITy AND AMyoTroPHIc LATerAL ScLeroSIS
Once a diagnosis of ALS is established, difficulty with mobility is one of the first issues to address, since limb onset weakness is most common first symptom. There are several aspects to managing mo-
bility problems. The patient, home, and work environment need to be assessed for equipment that may aid in improving function and safety. Driving needs to be assessed for safety. Medications need to be considered to help manage spasticity if present. Other symptoms that need to be optimized to improve mobility are: (1) breathing, (2) communication, (3) mood, and (4) good nutrition. Cognitive problems bring a special challenge in managing the patient with mobility problems due to ALS. Lastly, exercise may play an impor-tant role in preserving function, managing spasticity, and helping elevate mood as the disease advances.
equipment for Patients With Mobility Problems
Technological advances allow for many options for patients as their weakness progresses. Ankle foot orthodics are often a first step, and options now include flexible braces that allow driving. Walkers, canes, and crutches have also advanced in terms of mate-rials to allow for sturdier devices that provide better support and
26 Mobility and ALS AANEM Plenary
Figure 1 El Escorial Revisited: Revised Criteria for the Diagnosis of Amyotrophic Lateral Sclerosis3
Last Modified: 25 Mar 2003©1997-2006 World Federation of Neurology. All rights reserved.
Disclaimer | contact Webmaster

a smoother gait. Manual wheelchairs are now ultra-light and can even tilt and recline for patient comfort. Electronic wheelchairs have become smaller and lighter, and some can be folded into a car. Newer models advertise “thought” controlled wheelchairs that can also be used to produce speech. Stair climbers and portable ramps allow more patients to live in their original homes even if stairs are present. Newer rail systems allow patients to be transported in the air from the bed to the bathroom independently. Specialized beds allow for greater comfort and safety. A home safety assessment is useful at the onset of mobility difficulties to discuss all options available as remodeling is planned and in order to determine future needs and anticipate problems before serious falls occur. Later, home physical therapy and occupational therapy can aid in stretching exercises and transfer safety training for caregivers as function declines. Even once a patient is in hospice, it is possible to order home physical therapy and occupational therapy for patients through hospice to ensure patient comfort and safety.
Driving With Mobility Problems
It is critical to determine if patients are safe to drive for their protec-tion and others. Driving safety can be difficult to assess and often if it is not clear based on a clinical assessment, a driving assessment is needed. This assessment is typically recommended at 6-month intervals and consists of a detailed evaluation by the Department of Motor Vehicles (DMV) using the patient’s modified vehicle if modifications are made. For patients with greater leg weakness than arm weakness, hand controls may be an option in order to continue driving. Wheelchair vans can be modified to allow the patients to drive in addition to being a passenger. If patients are resistant to a driving assessment and safety is an issue, then reporting by the physician to the DMV is required.1 Most public transportation systems have been modified to allow safe transport via wheelchairs as an option. Lastly, many towns have services which offer free transportation to those who are disabled, as many may not have the resources to purchase a wheelchair van.
MeDIcATIoNS For SPASTIcITy
Spasticity is a very disabling problem in ALS, and with medication management, it is often a balance between relief of spasticity and loosening the legs too much to cause difficulty walking. Valium at night is often effective at doses of 10-20 mg. Baclofen in doses up to 100 mg per day is effective, but the titration upwards or downwards needs to be slow, at a rate of no more than half of a pill per day. Tizanidine is sometimes effective when used in combination with baclofen or alone, and again slow titration upwards and downwards is important. When medications are at their maximum tolerated doses and spasticity is still a significant problem, a baclofen pump may be considered. A trial is often performed first in the hospital with gradually increasing doses administered until a bell-shaped curve of response is produced indicating a dose-dependent effect. A pump is then implanted and the dose started at their peak efficacy. This therapy often allows patients to completely eliminate their oral medication and is most effective for patients with primarily UMN involvement. For focal areas of spasticity, botulinum toxin is an option for some patients.8
oPTIMIZING SyMPToMS
If other ALS symptoms are not managed, particularly nutrition and breathing, there is a significant impact on mobility. Good nutri-tion is critical, because even overweight patients can easily become malnourished and lose muscle mass if they are not able to take in enough calories, either from difficulty swallowing or difficulty eating due to arm weakness. Malnourished patients will have dif-ficulty having the energy to move well. Along with the difficulties in food delivery associated with this disease, the metabolism is increased due to the increased work of breathing and moving. A high-protein, high-calorie diet is recommended with modifications of food consistency as needed for swallowing safety, and ultimately a feeding tube is required in many cases to maintain adequate nutri-tion and hydration.
Maintaining good breathing is necessary and oxygen needs to be avoided since it can trigger CO2 retention and even cause coma. Noninvasive positive pressure ventilation is recommended in cases where the forced vital capacity is less than 50%, when the maximum inspiratory force is low, or when there are significant nocturnal de-saturations. Patients are encouraged to exercise with their breathing machines to help improve endurance. Eventually the diaphragm strength weakens to the point that noninvasive ventilation is no longer effective and unless the patient chooses tracheostomy and mechanical ventilation, they ultimately die of respiratory failure. Some patients with respiratory onset disease chose tracheostomy and mechanical ventilation. This creates mobility concerns even if walking is strong due to the risk of extubation if a patient trips and falls while carrying their ventilator.
IMPAcT oF coGNITIVe AND BeHAVIorAL ProBLeMS oN MoBILITy
One of the largest challenges in managing ALS patients is caring for those patients with associated frontotemporal dementia or the more subtle form of cognitive or behavioral dysfunction that occurs in nearly 50% of patients. Cognitive or behavioral problems can be caused by sleep deprivation, noctural hypooxygenation, medica-tion side effects, and depression, so it is important to recognize and screen for these treatable conditions. However, often when these conditions are corrected, there is still underlying cognitive or behavioral dysfunction associated with the disease. These patients are poor in complying with treatment recommendations, lack good judgment when walking, and have poor insight into their disease process, which can shorten their life span by as much as 1 year.6
IMPorTANce oF eXercISe
Animal studies support the role of exercise in ALS for helping prolong disease survival, even with vigorous exercise.4,5 In humans with ALS, recent studies support moderate exercise with resistance training in slowing disease progression and in improving quality of life.2 While it is important to avoid extreme exercise of weak muscles which could cause irreversible damage, and exercising in settings where falling could be dangerous, moderate exercise has
AANEM Plenary Gait in Motion: Stepping into the 21st Century 27

the advantages of reducing spasticity, strengthening muscles, and elevating mood.
SUMMAry
Today there is more hope for ALS patients in terms of medications to help manage the symptoms of the disease, and equipment to enable them to be as independent as possible and to have a greater quality of life. Critical in this process is a connection with a certi-fied multidisciplinary ALS center with specialists trained in ALS who are familiar with all the options available for patients. With technological advances, patients with this disease are living longer, more productive lives.
reFereNceS
1. Bacon D, Fisher RS, Morris JC, Rizzo M, Spanaki MV. American Academy of Neurology position statement on physician reporting of medical conditions that may affect driving competence. Neurology 2007;68:1174-1177.
2. Bello-Haas VD, Florence JM, Kloos AD, Scheirbecker J, Lopate G, Hayes SM, Pioro EP, Mitsumoto H. A randomized controlled trial of resistance exercise in individuals with ALS. Neurology 2007;68:2003-2007.
3. Brooks BR, Miller RG, Swash M, Munsat TL. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:293-299.
4. Kirkinezos IG, Hernandez D, Bradley WG, Moraes CT. Regular ex-ercise is beneficial to a mouse model of amyotrophic lateral sclerosis. Ann Neurol 2003;53:804-807.
5. Liebetanz D, Hagemann K, von Lewinski F, Kahler E, Paulus W. Extensive exercise is not harmful in amyotrophic lateral sclerosis. Eur J Neurosci 2004;20:3115-3120.
6. Olney RK, Murphy J, Forshew D, Garwood E, Miller BL, Langmore S, Kohn MA, Lomen-Hoerth C. The effects of executive and behav-ioral dysfunction on the course of ALS. Neurology 2005;65:1774-1777.
7. Rowland LP. Diagnosis of amyotrophic lateral sclerosis. J Neurol Sci 1998;160:S6-24.
8. Simmons Z. Management strategies for patients with amyotrophic lateral sclerosis from diagnosis through death. The neurologist 2005;11:257-270.
28 Mobility and ALS AANEM Plenary

INTroDUcTIoN
Neuromuscular diseases are common in both children and adults and present an enormous clinical challenge in terms of management and a substantial economic burden to healthcare systems through-out the world. For example, cerebral palsy (CP) affects 764,000 children and adults in the United States1 and is the most common cause of disability affecting children in developed countries with an incidence of 2/1000 live births2 based on 2003 estimates. The economic burden of CP includes $1.18 billion in direct medical costs, $1.05 billion in direct nonmedical costs, and an additional $9.24 billion in indirect costs, for a total cost of $11.5 billion or $921,000 average cost per person.3
The assessment and management of children and adults with neuromuscular disorders is therefore an important clinical prior-ity. However, there is little agreement as to which tools are most useful. Even within common diagnostic groups such as CP, there is enormous variation in access to sophisticated investigations, such as instrumented gait analysis, both within and between countries. For instance, in 2006, Narayanan and colleagues conducted a survey of the members of the Pediatric Orthopaedic Society of North America reported that 40% of orthopaedic surgeons in North America did not have access to a gait laboratory for the
management of children with CP.4 In this manuscript, a range of technologies will be described which have been found to be useful in the evaluation of children with neuromuscular disease, particularly cerebral palsy. These tools range from “low tech” to “high tech.”
Low-tech approaches include widely available low-cost technolo-gies such as mobility scales and video recording. Higher technol-ogy includes three-dimensional gait analysis and metabolic testing. Some of these tools are useful in routine clinical practice, others are restricted to research settings. The use of these tools will be illustrated by reference to specific clinical cases in which the evalu-ation has contributed to patient management. Given the prevalence of CP, and the fact that this contributes to approximately 80% of this author’s gait laboratory workload, there will be a substantial focus on CP. However, other neuromuscular conditions will also be discussed.
HISTorIcAL BAcKGroUND
In 1994, the first clinical gait analysis laboratory in an Australian hospital was opened at The Royal Children’s Hospital in Melbourne. This facility was endowed by a philanthropic trust and is known
High-Tech Versus Low-Tech in the Assessment of Gait and Function
H. Kerr Graham MD, FrcS (ed), FrAcSProfessor of Orthopaedic Surgery
The Royal Children’s HospitalThe University of Melbourne
Murdoch Childrens Research InstituteMelbourne, AustraliaAdrienne Harvey
M Physio. Doctoral student, The University of Melbourne School of Physiotherapy
Parkville, Australia
29

30 High-Tech Versus Low-Tech in the Assessment of Gait and Function AANEM Plenary
as the Hugh Williamson Gait Laboratory. Following the success-ful introduction of clinical management programs based on gait analysis, the state government provided a specified grant for recur-rent funding of the Hugh Williamson Gait Laboratory. In 2005, the National Health and Medical Research Council of Australia awarded the Hugh Williamson Gait Laboratory and three affiliated gait laboratories in Melbourne the status of a “Clinical Centre of Research Excellence in Gait Rehabilitation.” This brings together four gait laboratories within a 10 km radius to share technology, improve measurement reliability, and to train clinicians and re-searchers in sophisticated motion analysis techniques. The labora-tory at The Royal Children’s Hospital has a principal focus in the management of children with CP, myelomeningocele as well as research programs in Rett syndrome and Dravet syndrome. By contrast, the Kingston Centre has programs in adult neurological disorders including Parkinson’s disease and stroke.
BAcKGroUND To THe MoTor DISorDer IN cereBrAL PALSy
The motor problems associated with CP can be classified accord-ing to three main criteria: type of motor disorder, topographical distribution, and gross motor function.
Type of Motor Disorder
CP is part of a larger group of disorders in which injury to the motor pathways of the central nervous system (CNS) is involved. Traditionally, motor disorders of central origin have been divided into “pyramidal” and “extrapyramidal” depending on the presumed anatomical location of the brain injury and its resulting symptoms.5 The pyramidal disorders, better known as the “upper motoneuron (UMN) syndrome,” involve lesions in any part of the corticospi-nal tracts and their connections resulting in a disruption of the spinal motor centers and a net loss of inhibition of the “stretch” reflex. These tracts and their involvement in the reflex circuits as-sociated muscle movement are shown in Figure 1. Clinically, the UMN syndrome is manifested by muscle weakness with a typical distribution (extensors > flexors), loss of selective motor control, spasticity, hyperreflexia, and Babinski sign. Spasticity is character-ized by muscle resistance at rest that is velocity dependent and associated with an increase in tonic stretch reflexes resulting from hyperexcitability of the stretch reflex.6 Spasticity predominates in the antigravity muscles (flexors greater than extensors). Over the long term, patients with this disorder will develop bony deformities and musculoskeletal abnormalities that are the result of the muscle imbalance around the joint.
The extrapyramidal motor syndrome, also called “dyskinetic motor syndrome,” results from injury to the basal ganglia and their con-nections. The motor symptoms associated with this type of disorder include dystonia, choreoathetosis, and other involuntary move-ments. Muscle tone may be decreased, normal, or increased. The hypertonia seen in patients with this disorder is not velocity de-pendent and affects both agonist and antagonist muscles. Dystonia is a hyperkinetic movement disorder characterized by sustained muscle contractions that cause twisting or repetitive movements
and abnormal postures or positions. Dystonia is characterized by an excessive co-contraction of antagonist muscles during voluntary movement, overflow of muscle contraction to remote muscles not normally employed for that particular movement, and spontaneous muscle spasms that are influenced by the patient’s emotional and conscious state. Because of the variability in tone and movement, fixed contractures may take longer to develop in patients with dyskinetic motor disorders. However, joint dislocations may occur at any stage. Tendon releases have a poor prognosis, and selective dorsal rhizotomies (SDR) do not improve the hypertonia seen in these patients because the hypertonia is not due to an exaggerated stretch reflex. Although more than 80% of patients with CP have spasticity, many have a mixed motor picture showing signs of spas-ticity and dystonia.7,8
Proper identification and understanding of these motor disorders is essential to formulating a successful treatment strategy.
The symptoms of CP are not usually evident at birth but instead emerge as the child develops.9 The symptoms that may be mani-fested in CP are highlighted in Table 1. Delgado and Albright8 and Sanger and colleagues10 offer fuller discussions on classification of movement disorders associated with CP.
Many of the clinically significant phenomena associated with CP, such as dystonia and spasticity, result from a net imbalance of dynamic and static forces that affect the position of the joints stati-cally and the movement of limbs dynamically. These changes alter the functionality of the muscle, joint, and surrounding soft tissue.
Although the CNS damage in CP is not progressive, some evidence indicates that the secondary musculoskeletal pathology is progres-sive.11 Increased bone growth and increased muscle tone in the child with CP may lead to contractures and joint subluxation/dislo-cation, which can complicate movement. Therefore, it is important that these children are repeatedly screened for problems, such as silent hip subluxation, as they age.10
Topographical Distribution
As shown in Table 1, CP has a topographical distribution defined by the location of its musculoskeletal symptoms (although there is a substantial overlap of affected areas). Hemiplegia, diplegia, and quadriplegia are the common topographical types, with monople-gia and triplegia being relatively uncommon.
Most children with CP can be classified using a combination of movement disorder type with a topographic location—for example, spastic diplegia, spastic hemiplegia with athetosis, dystonia quad-riplegia, etc. Perhaps the most common motor disorder is a mixed disorder—for example, spastic dystonia.
Gross Motor Function: The Gross Motor Function classification System
Gross motor function in children with CP can be easily classified using the Gross Motor Function Classification System (GMFCS). The GMFCS is a five-level grading system based on the assessment

AANEM Plenary Gait in Motion: Stepping into the 21st Century 31
of self-initiated movement, with emphasis on function during sitting and walking. Distinctions between levels are based on func-tional limitations, the need for walking aids or wheeled mobility, and the quality of movement (Table 3). This system is a reliable and valid method for the classification and prediction of motor func-tion in children with CP aged 2 to 12 years.12
Combining classification of the movement disorder and topo-graphical distribution with grading of gross motor function results in a comprehensive description of the individual child with CP. This classification can be a useful communication aid between phy-sicians and allied health personnel in providing the right treatment for a child with CP. It is also helpful in clinical research. Presented here are two examples where this classification is effective.
Example 1: Ben is a 4-year-old boy with a right spastic hemiplegia, GMFCS Level I.
This classification describes a younger child with unilateral spastic-ity and a very high level of independent function. Such children often have a unilateral spastic equinus that can be effectively managed by intramuscular injection of botulinum neurotoxin type A (BoNT-A).
Example 2: Amy is a 12-year-old girl with spastic-dystonic quad-riplegia. She is GMFCS Level V.
This classification describes a child with a generalized movement disorder and a very low level of function. Such children may benefit
Figure 1 Neuronal pathway. This diagram shows the neuronal pathways associated with the response to a stretch reflex. In the UMN syndrome, lesions in any part of the corticospinal tracts or their connections result in a loss of inhibition of the stretch reflex.
Table 2 The Gross Motor Function Classification System
GMFCS Level DefinitionsI Children walk indoors and outdoors, and climb stairs without
limitations. They perform gross motor skills, including running and jumping, but speed, balance, and coordination are reduced.
II Children walk indoors and outdoors, and climb stairs holding onto a rail, but experience limitations walking on uneven surfaces and inclines, and walking in crowds and confined spaces. These children have at best only minimal ability to perform gross motor skills, such as running and jumping.
III Children walk indoors or outdoors on a level surface with an assistive mobility device. They may climb stairs holding onto a rail. Depending on upper limb function, these children propel a wheelchair manually or are transported (pushed by another person) when travelling long distances or outdoors on uneven terrain.
IV Children may maintain levels of function achieved when they were younger than 6 years or rely more on wheeled mobility when at home, or at school, or in the community. Children may achieve self-mobility using a powered wheelchair.
V Physical impairments restrict voluntary control of movement and the ability to maintain antigravity head and trunk postures. All areas of motor function are limited. Functional limitations in sitting and standing are not fully compensated through the use of adaptive equipment and assistive technology. Children have no means of independent mobility and are transported (pushed by another person). Some children achieve self-mobility using a powered wheelchair with extensive modifications.
Table 1 Topographical Distribution of Cerebral Palsy
Topographical Descriptor Area affectedMonoplegia One limb involvedHemiplegia Involvement of one side of the bodyDiplegia Lower extremities more involved than
the upper extremitiesTriplegia Three extremities involvedQuadriplegia or tetraplegia All four extremities involved

32 High-Tech Versus Low-Tech in the Assessment of Gait and Function AANEM Plenary
from complex interdisciplinary care, including physical therapy, communication aids, suitable seating, a wheelchair for mobility, and perhaps intrathecal baclofen (ITB) pump for the control of generalized spastic dystonia.
Assessment of children with cerebral Palsy
To assess children with CP, the following are used:
1. Functional scales2. Physical examination3. Two-dimensional video recording4. Kinematics5. Kinetics6. Electromyography7. Pedobarography8. Radiology9. Physiological testing10. Activity Monitoring11. Questionnaires addressing Function, Participation and Quality of Life
Given the previous discussion in relation to the diagnosis and clas-sification of cerebral palsy, the value of a careful history (pregnancy, birth history, perinatal history, neonatal history) and physical examination are obvious. It is very important to establish the di-agnosis as robustly as possible and for the majority of children this involves an expert assessment with a developmental pediatrician, a pediatric neurologist, and imaging of the brain (computerized tomography or magnetic resonance imagine).
Characterizing the movement disorder is important because the natural history maybe different and certain interventions are in-dicated in specific motor types and contraindicated in others. For example, SDR is considered to be a reliable and useful procedure in a small subset of children with spastic diplegia of prematurity. However, SDR is unpredictable in children with mixed movement disorders and especially in dystonia.
1. Functional Scales
In the approach to the assessment and management of children with CP, reliable assessments of gross motor function and the use of the scales of gross motor function are crucial. The most widely used scales are the GMFCS,13 Functional Mobility Scale (FMS)14 and the Functional Assessment Questionnaire (FAQ).15 The GMFCS can be used to describe gross motor function in children with CP in four discrete age bands. The descriptors for the aged 6-12 band are found in Table 2. The illustrations for the 6-12 age group are found in Appendix 1. GMFCS predicts long-term motor func-tion, musculoskeletal complications such as hip displacement, and functions as a template for planning rehabilitation and long term management strategies.
The FMS is the only current scale which addresses different envi-ronmental conditions (home, school, and community) by describ-ing the level of assistance the child needs to achieve mobility over
three specific distances: 5, 50, and 500 yards.14 These distances have been chosen to correspond to mobility at home, school, and the community. Unlike the GMFCS, the FMS provides a more comprehensive view of the child’s requirement for support and mobility in different settings and is responsive to change after inter-vention. A goal of certain interventions such as multilevel surgery may be to reduce the level of assistance required in the community, e.g., from using a walker to using walking sticks.
The FAQ provides additional information in respect of walking and community activities.15
2. Standardized Physical examination
Given that children with motor disorders are often seen in a stage of evolution due to the plasticity of the CNS, the effects of growth, and intervention, standardized physical examination is a “low tech” but core component of assessment. In the gait laboratory, this is relatively straightforward. Physical therapists are trained in standardized examination techniques and achieve good reliability by formal training and quality review processes.16 Measures under-taken include assessments of motor type, dynamic measurements of spasticity, scaling of spasticity by the modified Ashworth Scale and Modified Tardieu Scale. In addition, joint range of motion looking for overt and occult contractures, measurement of bony torsion (femur and tibia) as well as assessments of motor strength and selec-tive motor control are all part of the standard assessment package. The use of a standardized physical examination record sheet is key to systematic data collection, archiving and longitudinal clinical follow-up, and research.
3. Two-dimensional Video recording
In neuromuscular disorders, physicians are concerned with move-ment, gait, and function. Even though three-dimensional instru-mented gait analysis is the gold standard for assessment, a core component of such an assessment remains two-dimensional vid-eo.17 Given the low cost and wide availability of video recorders and DVD recorders, as well as the ability to store large volumes of digital information on optical drives, the utility of video recording is clear.
The value of two-dimensional video recording is enhanced if a systematic approach is employed including:
• Use of a standard recording space
• Appropriate lighting
• Standardized walkway
• Standardized sequence of video recording: split screen, sagittal and coronal, full length, and half frame.
Even the most comprehensive written report of a child’s walking pattern is completely trumped by 30 seconds of well-recorded videotape! In addition, issues related to gait and function which

AANEM Plenary Gait in Motion: Stepping into the 21st Century 33
can be readily appreciated on video include an estimate of walking speed and stability, balance, the ability to turn, the need for assistive devices and orthoses, an overall impression of spasticity in co-con-traction, or observation of dystonic movements in the extremities.
4. Instrumented Gait Analysis: Kinematics
Three-dimensional kinematics are in simple terms quantification of complex limb segmental motion resolved into three orthogonal axes x, y, and z. Light reflective markers are applied to standardized anatomical positions and the subject walks through a data capture area where infrared strobe lights record the motion of the markers in three dimensions in space with formidable accuracy. The data captured is then processed using anatomical and biomechanical models, and sophisticated software which generates standardized motion plots in the sagittal, coronal, and transverse planes. Gait laboratories maintain databases of normal subjects from which the gait patterns of individuals can be compared and gait deviations identified and described.
The accuracy of marker identification in space is to within 1 degree, but the weak link in the chain is the application of the markers and subsequent skin movement artifact. However, with standardized protocols, training programs, and quality assurance, impressive clinical reliability can be achieved which is certainly good enough for both clinical practice and research.
The amount of data from three-dimensional kinematics can at first sight be overwhelming, and both training and experience are required for accurate interpretation. However, movement pat-terns in most neuromuscular diseases are not random but highly stereotyped and can be characterized by recognition of “gait pat-terns.” For example, in CP there are clinically valid and reliable patterns for both spastic hemiplegia and spastic diplegia. These sagittal gait patterns reduce the complexity of kinematic data to a recognizable clinical pattern which can be recognized with a reasonable degree of accuracy from either clinical examination combined with video recording or from instrumented gait analysis with three-dimensional kinematics and kinetics. These sagittal gait patterns have been found to be most useful in characterizing gait, planning intervention, studying outcomes, and in clinical research and communication. The classification of sagittal gait patterns in spastic hemiplegia by Winters, Gage, and Hicks has been further developed by Dobson, Morris, Baker, and Graham to include both the coronal and transverse planes and to employ measures of foot alignment.18
In spastic diplegia, the classification developed by Rodda and colleagues has now been extended to include the hip and pelvis with further improvements in understanding gait and planning intervention.19
5. Instrumented Gait Analysis: Kinetics
During the process of data capture of limb segment motion, as the subject walks in the gait laboratory, kinetic data is gathered from force plates embedded in the gait laboratory floor. The measure-
ment of the ground reaction force can be used via biomechanical modeling to generate joint moments and powers by a process known as inverse dynamics. Joint moments and powers add greatly to the understanding of normal gait as well as pathological gait, but require additional training and expertise for appropriate uti-lization.20
6. Instrumented Gait Analysis: electromyography
Dynamic electromyography (EMG) is a useful component of in-strumented gait analysis because it contributes information regard-ing the timing of muscle activity. Information can be gained from electrodes mounted on the skin directly over major muscle groups such as the gastrocsoleus, tibialis anterior, quadriceps, and ham-strings. However, dynamic EMG does not give reliable information in respect of the strength of muscle activity but simply the timing. In addition, timing of muscle activity, in critically important muscles such as the tibialis posterior can only be reliably achieved using fine-wire electrodes inserted directly into the muscle. While this yields reliable and useful information, the invasiveness of the procedure in younger children limits its usefulness.
7. Pedobarography
A weakness of conventional gait laboratory biomechanical models is viewing the foot and ankle as a simple hinge with motion prin-cipally in the sagittal plane. The reality is that the foot is composed of segmental articulations which have a wide range of motions in all three anatomic planes. New approaches to foot kinematics are being developed by the use of multiple small markers and new biomechanical models. In addition, pressure distribution under the foot can be studied by means of pedabarography which gives an objective measure of foot pressures.21,22
8. radiology
Standardized radiological assessments are an essential component of overall assessment of gait and function in the gait laboratory. It is essential to know the status of hip development and stability for the appropriate interpretation of joint kinematics and kinetics. In ad-dition, axial imaging to measure torsional malalignment of femurs and tibias using computerized tomography is also extremely useful information in the interpretation of gait disorders.
Standing anterior/posterior and lateral foot radiographs are also extremely valuable to complement assessment of foot and ankle disorders as part of the overall movement disorder in CP.
9. Physiological Testing
Although instrumented gait analysis captures important tempo-rospatial data including walking speed, step length, and stride length, these data are captured during a short walk and not neces-sarily reflective of a subject’s walking speed and function in the community. The use of a portable metabolic cart was pioneered to measure the efficiency of gait by real time measurement of inspired and expired O2 and CO2.
23,24,25

34 High Tech Versus Low Tech in the Assessment of Gait and Function AANEM Plenary
The gait laboratory contains a circular walking track of known circumference. Children are requested to walk circular laps using their usual aids and orthoses, during which walking speed, oxygen consumption, and carbon dioxide production are continuously monitored. From these data, walking speed and distance over a 10-minute walk are readily measured. In addition, such parameters as oxygen cost and oxygen consumption are also derived. These measures give a guide to the overall efficiency (or inefficiency) of ambulation. This may provide information of prognostic value and also as useful in the longitudinal assessment of the value of inter-vention. For example, SDR in spastic diplegia may have a dramati-cally positive result in reducing oxygen consumption during gait. It is theorized that the reduction in spasticity and co-contraction reduces unwanted and unnecessary muscle contraction during walking, thereby improving overall gait efficiency. Other interven-tions such as multilevel surgery have a less dramatic benefit on reducing energy cost. However, the correction of crouch gait may be particularly beneficial.
10. Activity Monitoring
So far, the technologies discussed all relate to the measurement of gait and function within the artificial confines of the gait labora-tory. Using high-quality equipment and reliable protocols, much useful information can be gathered. However, laboratory based measurements are open to the criticism that they do not necessar-ily reflect what happens in the “real world.” In an effort to move outside the gait laboratory, many physicians have embarked on ambitious programs to measure activity in the community. A wide range of devices have been tested including accelerometer-based devices and uptimers.26,27,28
Most of this author’s experience has been with a simple device consisting of a mercury tilt switch, a microprocessor, and a battery housed in a small plastic container. This is attached to the subject’s thigh and worn for periods of 1 to 7 days. “Uptime” is recorded when the subject is standing or walking and “downtime” when the subject is sitting or lying. For the relatively low level of activities in which many children with neuromuscular disease engage, this has been a useful form of analysis. In addition to establishing a large normal database, there is now prospective data on a growing number of children with CP to establish both their natural history and to understand changes after intervention.
11. Questionnaires: Function, Participation, and Quality of Life
The majority of assessments in the gait laboratory and also mea-surements in the community of activity are objective but technical and do not always correlate with the patient and family view. The International Classification of Functioning provides a framework in which activity, activity limitations, and participation restrictions are key concepts. In an effort to understand the impact of neuro-muscular disability on function, participation and quality of life,
questionnaires have been developed which address these concepts to varying degrees. In the Hugh Williamson Gait Laboratory, the most widely used tools are the GMFCS, the FMS, and the FAQ. In addition, more extensive questionnaires are used in the context of clinical research including the Child Health Questionnaire, the Pediatric Orthopaedic Data Collection Instrument, and the Cerebral Palsy Quality of Life Questionnaire for Children (Primary Caregiver Questionnaire [4-12 years] and the Child Report Questionnaire [9-12 years]). The systematic gathering of such patient-oriented data is giving new insights into the understanding of neuromotor disability from the patient and family viewpoint. Counterintuitive findings have been found in which quality of life (from the point of view of both the child and parent) bears little relationship to the level of disability and level of gross motor func-tion. It is then not surprising that interventions to improve gross motor function may have variable effects on quality of life. This is an emerging area of great importance in clinical research and management.29,30
reFereNceS
1. Cerebral palsy—facts and figures. Available at: http://www.ucp.org/ucp_generaldoc.cfm/1/9/37/37-37/447. Accessed August 2, 2004.
2. Winter S, Autry A, Boyle C, Yeargin-Allsopp M. Trends in the prevalence of cerebral palsy in a population-based study. Pediatrics. 2002;110:1220-1225.
3. Centers for Disease Control and Prevention. Economic costs associ-ated with mental retardation, cerebral palsy, hearing loss and vision impairment-United States, 2003. MMWR Morb Mortal Wkly Rep. 2004;53:57-59.
4. Narayanan UG, Weir S, Morris A, Redekop S. Rates of utilization of gait analysis for surgical decision making for ambulatory cerebral palsy in North America. Paper No 42: Pediatric Orthopaedic Society Annual Meeting 2007, Florida USA.
5. Sanger TD, Delgado MR, Gaebler-Spira D, Hallett M, Mink JW, and the Task Force on Childhood Motor Disorders. Classification and definition of disorders causing hypertonia in childhood. Pediatrics 2003;111:89-97.
6. Dormans JP, Pellegrino L, Caring for children with cerebral palsy. A team approach. Baltimore: Paul H. Brooks Publishing Co., Inc.; 1998.
7. Lance JW. Symposium synopsis, in Feldman RG, Young RR, Koella WP, editors. Spasticity: disordered motor control. Chicago: Year Book Medical Publishers; 1980. p 485-494.
8. Brunstrom JE. Clinical considerations in cerebral palsy and spasticity. J Child Neurol 2001;16:10-15.
9. Delgado MR, Albright AL. Movement disorders in children: definitions, classifications, and grading systems. J Child Neurol. 2003;18:S1-S8.
10. Rang M, Silver R, De La Garza. Cerebral palsy. In: Morrissy RT, Weinstein SL, editors. Lovell and Winter’s pediatric orthopaedics, vol ume 1, 3rd edition. Philadelphia: JB Lippincott; 1990.
11. Boyd R, Graham HK. Botulinum toxin A in the management of children with cerebral palsy: indications and outcomes. Eur J Neurol. 1997;4:S15-S22.

AANEM Plenary Gait in Motion: Stepping into the 21st Century 35
12. Morris C, Bartlett D. Gross motor function classification system: impact and utility: Dev Med Child Neurol. 2004;46:60-65.
13. Palisano RJ, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;45:113-120.
14. Graham HK, Harvey A, Rodda J, Nattrass GR, Pirpiris M. The func-tional mobility scale (FMS). J Pediatr Orthop 2004;24:514-520.
15. Novacheck TF, Stout JL, Tervo R. Reliability and validity of the Gillette Functional Assessment Questionnaire as an outcome measure in children with walking disabilities. J Pediatr Orthop 2000;20:75-81.
16. Keenan WN, Rodda J, Wolfe R, Roberts S, Borton DC, Graham HK. The static examination of children and young adults with cerebral palsy in the gait analysis laboratory: technique and observer agree-ment. J Pediatr Orthop Br 2004;13:1-8.
17. Harvey A, Rodda J, Graham HK. Two dimensional video gait analysis: Applying the lessons from three dimensional gait analysis. Abstract accepted for presentation AACPDM Vancouver; October 2007.
18. Dobson F. Classification of gait in children with spastic hemiplegic cerebral palsy, PhD Thesis. Completed and awarded. The University of Melbourne; 2007.
19. Rodda JM, Graham HK, Carson L, Galea MP, Wolfe R. Sagittal gait patterns in spastic diplegia. J Bone Joint Surg Br 2004;86:251-258.
20. Gage JR. The treatment of gait problems in cerebral palsy. London, England: Cambridge University Press; 2004.
21. Miller F. Cerebral palsy. New York: Springer; 2005.
22. Chang CH, Miller F, Schuyler J. Dynamic pedobarograph in evaluation of varus and valgus foot deformities. J Pediatr Orthop 2002;22:813-818.
23. Duffy CM, Hill AE, Graham HK. The influence of flexed-knee gait on the energy cost of walking in children. Dev Med Child Neurol 1997;39:234-238.
24. Corry IS, Duffy CM, Cosgrove AP, Graham HK. Measurement of oxygen consumption in disabled children by the Cosmed K2 por-table telemetry system. Dev Med Child Neurol 1996;38:585-593.
25. Boyd R, Fatone S, Rodda J, Olesch C, Starr R, Cullis E, Gallagher D, Carlin JB, Nattrass GR, Graham HK. High- or low- technology measurements of energy expenditure in clinical gait analysis. Dev Med Child Neurol 1999;41:676-682.
26. Eldridge BJ, Galea M, McCoy AT, Wolfe R, Graham HK. Uptime normative values in children 8 to 15 years of age. Dev Med Child Neurol 2003;45:189-193.
27. Eldridge BJ, McCoy AT, Galea M, Wolfe R, Graham HK. Variability in the measurement of uptime in children; a preliminary study. Clin Rehab 2003;17:499-503.
28. Pirpiris M, Graham HK. Uptime in children with cerebral palsy. J Pediatr Orthop 2004;24:521-528.
29. Waters E, Davis E, Mackinnon A, Boyd R, Graham HK, Lo SK, and colleagues. Psychometric properties of the quality of life question-naire for children with CP. Dev Med Child Neurol 2007;49:49-55.
30. Davis E, Waters E, Mackinnon A, Reddihough D, Graham K, Mehmet Radji O, Boyd R. Paediatric quality of life instruments: a review of the impact of the conceptual framework on outcomes. Dev Med Child Neurol 2006;48:311-318.

36 High Tech Versus Low Tech in the Assessment of Gait and Function AANEM Plenary
GMFCS Level IChildren walk indoors and outdoors and climb stairswithout limitation. Children perform gross motor skillsincluding running and jumping, but speed, balance andco-ordination are impaired.
GMFCS Level IIChildren walk indoors and outdoors and climb stairsholding onto a railing but experience limitations walkingon uneven surfaces and inclines and walking in crowdsor confined spaces.
GMFCS Level IIIChildren walk indoors or outdoors on a level surface withan assistive mobility device. Children may climb stairsholding onto a railing. Children may propel a wheelchairmanually or are transported when traveling for longdistances or outdoors on uneven terrain.
GMFCS Level IVChildren may continue to walk for short distances on awalker or rely more on wheeled mobility at home andschool and in the community.
GMFCS Level VPhysical impairment restricts voluntary control ofmovement and the ability to maintain antigravity head andtrunk postures. All areas of motor function are limited.Children have no means of independent mobility andare transported.
Appendix 1. The Gross Motor Function Classification System (GMFCS) for children with cerebralpalsy, aged 6 to 12 years. Reproduced by permission from the Journal of Pediatric Orthopaedics.

AANEM Course Gait in Motion: Stepping into the 21st Century 37
Group IIIEquinus/jump knee
α >900
GastrocsoleusHamstrings/RF
PsoasSolid AFO/GRAFO
Group IVEquinus/jump knee/
hip flexion
Appendix 2: Sagittal Gait Patterns: Spastic Hemiplegia (Winters et al 1987)
α >900
Gastrocsoleus——
Hinged AFO
Group IITrue equinus
α >900
———
Hinged AFO
Group IDrop foot
α >900
GastrocsoleusHamstrings/RF
—Hinged AFO
α >900
GastrocHamstrings/RF
(Psoas)Hinged AFO
Group IIJump knee
α <900
—Hamstrings/RF
PsoasGRAFO
Group IVCrouch gait
α =900
(Gastroc)Hamstrings/RF
PsoasSolid AFO
Group IIIApparent equinus
α >900
Gastroc——
Hinged AFO
Group ITrue equinus
Appendix 3: Sagittal Gait Patterns: Spastic Diplegia (Rodda & Graham)

38 AANEM Course

AANEM Plenary 39
INTroDUcTIoN
The first systematic investigation of human movement was made by Leonardo da Vinci. Later, Borelli combined the sciences of mathematics, physics, and anatomy and published a mathematical description of movement in De Motu Animalium. This is the first biomechanical treatise which used established fundamental theories and principles of classical mechanics to understand human move-ment. Biomechanical studies of human movement are now a well established scientific field of investigation.
The main functions of the human musculoskeletal system are to sustain loads and provide mobility. Knowledge about joint motion and forces are important in sports training, patient functional evaluation, prosthetic and orthotic design, bone remodeling, and fracture healing. However, bones and joints do not produce move-ment. The muscular system provides this function.
Muscle strength tests are often used to evaluate a person’s ability for functional movement. Knowledge of muscle forces during dynamic activities of daily living can provide insight into muscle mechanics, muscle physiology, musculoskeletal mechanics, neurophysiology, and motor control. The attractiveness of muscle strength tests has been based on their obvious validity and analogous simplicity. However, commonly used methods for clinical examination or instrumented strength testing only provide information regarding muscle groups. Needle electromyography (EMG) can provide infor-mation regarding individual muscle function, but does not provide a quantitative measure of muscle force during dynamic activities. A method is emerging to quantify muscle tension during dynamic movement. This manuscript discusses the different methods used for assessing dynamic muscle function.
cLINIcAL eXAMINATIoN
Manual muscle testing (MMT) is the most common noninstru-mented method for measuring muscle strength. The examiner assesses the strength of individual muscle groups by applying a counterforce to the limb to resist the patients’ voluntary muscle contraction. This method was introduced by Lovett.1 The most often used clinic system for MMT is the 6-level scale (Table 1). This scoring system ranges from 5 (normal strength) to 0 (no evidence of contractility). Muscle grade is determined by the ability of the subject to move voluntarily against gravity and to resist a force applied by an examiner.2,3 This technique allows an experienced examiner to rapidly determine the distribution and severity of weakness over a large number of muscle groups. This
Measuring Muscle Function During Gait
Kenton r. Kaufman, PhD, PeProfessor
Department of Biomedical Engineering Director
Motion Analysis LaboratoryMayo Clinic
Rochester, Minnesota
Table 1 Scoring system for manual muscle testing
Muscle Grades Description5-Normal Complete range of motion against gravity with full resistance4-good Complete range of motion against gravity with some resistance3-Fair Complete range of motion against gravity2-Poor Complete range of motion with gravity eliminated1-Trace Evidence of slight contractility; no joint motion0-Zero No evidence of contractility

40 Measuring Muscle Function During Gait AANEM Plenary
method for grading strength has stood the test of time as being robust and clinically useful. However, the scale uses gravity as a benchmark against which strength is tested. Clearly, the weight of the limb and the length of the lever arm over which muscles operate differ across various joints. The proportion of maximum strength required to overcome gravity is markedly different between muscle groups. Therefore, MMT has limited value, particularly in the lower extremity (Figure 1). A normal muscle (Grade 5) ranges between 53% of nonparalytic normal strength for the knee to 80% for the ankle. The earliest display of weakness (Grade 4) represents 40% of normal strength.4 A Grade 3 muscle is approximately 15% of normal strength. During normal walking, muscles function at a 3+ level.5 This effort, averaging about 25% of normal strength, allows adequate reserves so that fatigue is avoided.6 However, people whose muscles only have fair strength (Grade 3) will have no endurance or reserve because they must function at a maximal effort level. Thus, manual muscle strength grading can be mislead-ing. Moreover, this scale is nonlinear and ordinal. This means that a change of scale from 4 to 3 does not imply the same loss of strength as from 3 to 2.7,8 These weaknesses have lead to other methods of assessing muscle strength.
NoNINSTrUMeNTeD MeASUreMeNT oF MUScLe STreNGTH
Several noninstrumented methods have been used for quantifying the strength of individuals with muscular weakness. These non-instrumented methods do not actually measure muscle strength, but rather provide a nonspecific indication of muscle capacity to perform an activity of daily living. The most commonly selected tasks are sit-to-stand9-11 and stair climbing.12,13 These tests are thought to test lower extremity muscle strength in a functional ca-pacity because the joint moment required to perform activities such as sit-to-stand, stair ascent, and stair descent is considerable.14-16 However, noninstrumented testing fails to predict the ability to walk because patients with muscle weakness can modify muscle action timing or alter upper extremity and trunk positions. Also, they find subtle ways to advance the limb in swing by postural substitution.6 Hence, while strength testing is critical, noninstru-mented muscle testing has serious limitations.
INSTrUMeNTeD STreNGTH TeSTING
Instrumented strength testing provides a more accurate indication of actual strength and is needed to define true functional capability. The use of an instrumented device to measure muscle force yields a quantitative value for a subject’s strength. This quantitative assess-ment has the advantage over MMT in that it is a continuous scale for which normal values can be determined.3,17,18 This scale also is equally accurate and sensitive over its entire range. A wide range of devices has been used. Instrumented methods include handheld dynamometers,19-21 load cells,22 handgrip dynamometers,23 and isokinetic dynamometers.24,25 Instrumented strength testing is a more accurate indication of actual strength status and is needed to define true capability. Instrumented measurement has been shown
to be more sensitive to differences in muscle strength than nonin-strumented manual measurement.26-29 Handheld dynamometers are held by the examiner, who then applies force to the patient being tested. The examiner must be strong enough to withstand the forces generated by the patient, otherwise the measurement tests the strength of the examiner rather than that of the patient. Load cells are fixed in position and only measure isometric strength. Handgrip dynamometers only measure handgrip strength and, thus, are limited in terms of applications. The most common strength-testing device is an isokinetic dynamometer, whose popularity may be attributed to the ease with which it provides information. Isokinetic testing, however, can only provide generalizations about muscle function. It cannot be used to comment on the function of an individual muscle. Also, the location of peak joint moment does not necessarily correspond to the position of maximum muscular output for a muscle.30 In general, instrumented methods are better than noninstrumented methods for providing information about muscular strength. However, these methods fail to provide detailed information about individual muscles. Needle EMG is commonly used to provide quantification of individual muscle function.
NeeDLe eLecTroMyoGrAPHy
Needle EMG has been used to assess muscle function. Methods have been developed to quantify electromyographic activity.31,32 However, the EMG provides a quantitative measurement of muscle tension only under isometric conditions.33-42 Inman and colleagues43 first observed changes in myoelectric signal amplitudes that corresponded to variations in muscle load. Since then, much work has been done to determine the degree to which EMG signals and muscle loads are related.44-49 Nonetheless, the EMG signal is a measure of the bioelectric events that occur in conjunction with contraction of muscle fibers. Thus, it is a phenomenon related to electrical aspects of muscle contraction rather than an effect of the muscle’s mechanical action.
Figure 1 Relative value of a manual muscle test for the lower limb extensor muscles (percent of true normal (From: Beasley, W.C., Quantitative muscle testing: Principles and applications to research and clinical services. Archives of Physical Medicine and Rehabilitation, 1961. 42: p. 398-425.)

AANEM Plenary Gait in Motion: Stepping into the 21st Century 41
Problems occur in dynamic situations when electromyographic activity is used as a measure of a muscle’s functional capability. The dynamic force produced by a muscle is not proportional to the degree of muscular activity. Other factors may affect muscle force, such as a change of muscle length,50-53 change of the muscle con-traction velocity,53-57 the rate and type of muscle contraction,6,58-60 joint position,61 and muscle fatigue.62,63 Because of these factors, the relationship between muscle force and EMG is not known for dynamic conditions.
DIrecT MUScLe Force MeASUreMeNT
In vivo internal muscle forces are difficult to measure directly. A tendon buckle transducer was proposed by Salmons64 to measure force from a single muscle or from a muscle group with a common tendon. This technique is limited to muscles with relatively long tendons that can be exposed surgically. Data from direct muscle force measurements in humans are very limited due to the invasive nature of the experiment. Direct muscle force measurements have been obtained from the human Achilles tendon65-70 and the patellar tendon.71 The results of these studies must be regarded cautiously, since the measurements obtained were from a group of muscles rather than individual muscles. Buckle transducers have also been implanted in the wrist flexors during carpal tunnel surgery.72 However, the usefulness of this technique for measuring muscle force during movement is severely limited.
INTrAMUScULAr PreSSUre MeASUreMeNT
Intramuscular pressure (IMP) measurement is an alternative me-chanical method to measure muscle force that is minimally inva-sive. The first reported measurement of interstitial fluid pressure was by Landerer in 1884.73 Since then many different measurement techniques have been used. Pressure measurement systems can be classified either as fluid filled or solid state. Fluid-filled pressure recording systems are sensitive to hydrostatic artifacts.74-76 Thus, fluid-filled systems may be used only with limited movements that do not involve position changes relative to the horizontal plane rendering this technology inappropriate for measurements during dynamic activities. In contrast, a fiber optic transducer is not sensitive to hydrostatic artifact77 and is effective for measuring intramuscular pressure during exercise.78 Willy and colleagues79 introduced an accurate self-calibrating, battery powered electronic transducer-tipped catheter. However, the catheter tip is quite large (0.99 mm). Commercially available fiber optic pressure transduc-ers are also too large for optimum comfort (0.55 mm) and may themselves induce pressure artifacts based on their large size. We have developed a pressure microsensor with a 360 μm diameter for measuring interstitial fluid pressure. This microsensor has been shown to have an accuracy, repeatability, and linearity better than 2% full scale output (FSO) and a hysteresis of 4.5% FSO.80 More
recently we have reduced the size of the microsensor to 250 μm (Figure 2).
Hill81 first reported that mechanical pressure is developed inside a muscle when it contracts. The increase in pressure is caused by the contracting muscle fibers applying pressure on the interstitial fluid volume. This observation led to the measurement of IMP as a direct measure of muscle force. Sylvest and Hvid82 used a needle technique to measure joint torque and IMP of human striated muscles under isometric conditions. They found a linear relation-ship between IMP and torque. Through animal studies81,83-85 and human studies63,82,86-93 investigators have shown that an approxi-mately linear relationship exists between IMP and muscle force during isometric contraction.
The IMP sensor was able to effectively measure in vivo intramuscu-lar pressure during muscle excitation (Figure 3). IMP measurements were taken in the tibialis anterior muscles of the rat during varying excitation frequencies at a supramaximal voltage. The shapes of the relative pressure curves are similar in shape to characteristic skeletal muscle force associated with contraction, further strengthening the hypothesis that intramuscular pressure correlates positively with in-tramuscular force. As the excitation frequency surpasses the relative and absolute refractory period, the muscles do not have the time to relax completely, resulting in tetanic contraction. Summation occurs as more motor units are recruited, leading to larger pressure amplitude. Tetanus is seen when the muscle is not allowed time to repolarize before the subsequent excitation pulse is administered. The IMP recordings accurately reflect these physiological events.
Figure 2 Microscopic view of a pressure microsensor used for measuring intramuscular pressure.

42 Measuring Muscle Function During Gait AANEM Plenary
The relationship between IMP and active and passive muscle tension has been quantified.94 The fiber length-isometric tension curve was characterized by an “ascending limb” at a length less than muscle optimum length (L0) and a “descending limb” at lengths greater than L0 (Figure 4). The shape of this curve presumable rep-resents a scaled and distorted version of a sarcomere length-tension curve previously published.95,96 Passive muscle tension increased in a fairly exponential fashion at lengths greater than L0. The length-pressure relationship generally mimicked the shape of the length-tension curve with an ascending limb at lengths less than L0 and descending limb at length greater than L0 (Figure 5). A positive linear relationship was found between IMP and muscle stress for both the ascending and descending limbs (Table 2). These data in-dicate that IMP measurement provides an accurate index of muscle tension under both active and passive conditions. These data agree with Baumann and colleagues97 who suggested that the IMP is related to the active and passive components of muscle tension.
A numerical model of skeletal muscle was developed to examine the mechanisms producing intramuscular pressure.98 The finite element technique was used to calculate the intramuscular pressure
Figure 3 In vivo isometric pressure measurements taken in the isolated tibialis anterior muscle of a rat. Relative pressures were measured as muscles were stimulated at a supramaximal voltage of 6V with 4ms pulses and a 2 ms delay at frequencies of 1,10,100, and 150 Hz.
Figure 4 Muscle length-tension relationship (Davis, Kaufman, Lieber, 2003)
AANEM Plenary Gait in Motion: Stepping into the 21st Century 43
and muscle stress during passive stretch and isometric contraction. Unipennate muscle was modeled as a two-dimensional material continuum that is incompressible and nonlinearly anisotropic. A novel element modeled the contractile portion of muscle, including the sarcomere length-force and velocity-force relationships.99 The muscle model agreed well with the experimental muscle stress data over the mid-range of muscle length, i.e., 0.8<L/L0 <1.15, for both active and passive conditions (Figure 6). The greatest discrepancy was for muscle lengths greater than 1.15, where the model overes-timated muscle stress. This may be due to sensor movement within the muscle specimen during testing. The muscle model accurately reflected intramuscular pressure for muscle lengths less than 1.15, but overestimated muscle passive intramuscular pressure at muscle lengths greater than 1.15 (Figure 7a). The active component of intramuscular pressure was modeled well by the simulation and showed a similar ascending and descending behavior centered around L0 (Figure 7b).
Table 2 Summary of Isometric Stress-Pressure Correlations*
Activation State Length-Tension curve rMS error (kPa) Pressure coefficients of Determination (r2) Mean ± SEM Range (min-max)Active Ascending Limb 175.2 ± 52.98 .60 ± .25 .138 - .963 Descending Limb 147.19 ± 47.46 .77 ± .16 .343 - .947Passive Ascending Limb 10.18 ± 4.21 .53 ± .36 .045 - .842 Descending Limb 20.19 ± 13.83 .86 ±.11 .672 - .982
*Values represent mean ± standard error for n=10 animal subjects. (From Davis, Kaufman, Lieber, 2003)
Figure 5 IMP-Length relationship (Davis, Kaufman, Lieber, 2003) imp = intramuscular pressure
Figure 6 Model data (solid line) and experimental (open diamonds) data for muscle (a) passive and (b) active stress. (From: Jenkyn, T., et al., Finite element model of intramuscular pressure during isometric contraction of skeletal muscle. Physics in Medicine and Biology, 2002. 47: p. 4043-4061.)

44 Measuring Muscle Function During Gait AANEM Plenary
Muscle function during gait has been quantified using IMP.100 IMP increased at the beginning of single-limb stance (opposite toe off ) (Figure 8). The increase of IMP corresponded with the increase in electromyographic activity of the gastrocnemius. The greatest muscle activity in the plantar flexors was required near the end of single-limb stance to meet the high intrinsic plantarflexion moment occurring at the ankle joint and to reverse the direction of ankle movement (Figure 9). The IMP reading continued briefly after cessation of the EMG. Furthermore, it can be noted that there is a lower-level IMP recording during the swing phase of gait. During the stance phase of gait, the peak IMP recording corresponded to the time when the ankle moment is at a maximum (opposite foot strike) (Figure 9). Furthermore, during the swing phase of gait, the peak of IMP corresponds to the point of time when the ankle is at peak dorsiflexion (Figure 9). Thus, the peaks in IMP during gait can be correlated with the peaks of active contraction and passive stretch of the gastrocnemius.
Figure 8 Raw data for a single subject during gait. Both electro-myogram activity and intramuscular pressure are being recorded from the gastrocnemius muscle. The stance phase of gait occurs from foot strike (FS) to toe-off (TO). The swing phase of gait occurs from TO to FW. Single-limb stance occurs from opposite toe-off (OTO) to opposite foot strike (OFS). (From Kaufman and Sutherland 1995. Dynamic intra-muscular pressure measurement during gait. Operative Techniques in Sports Medicine 2(4): 253.)t
Figure 7 Model data (solid line) and experimental (open diamonds) data for muscle (a) passive and (b) active intramuscular pressure. (From: Jenkyn, T., et al., Finite element model of intramuscular pressure during isometric contraction of skeletal muscle. Physics in Medicine and Biology, 2002. 47: p. 4043-4061.)
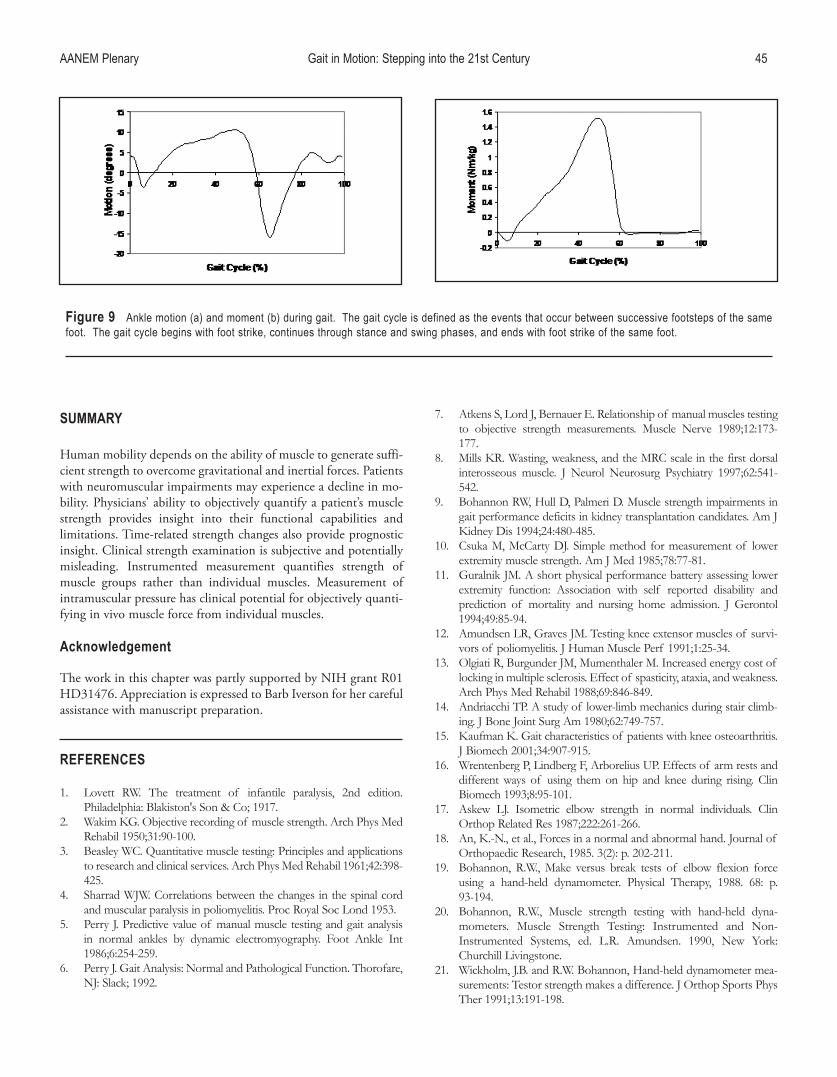
AANEM Plenary Gait in Motion: Stepping into the 21st Century 45
SUMMAry
Human mobility depends on the ability of muscle to generate suffi-cient strength to overcome gravitational and inertial forces. Patients with neuromuscular impairments may experience a decline in mo-bility. Physicians’ ability to objectively quantify a patient’s muscle strength provides insight into their functional capabilities and limitations. Time-related strength changes also provide prognostic insight. Clinical strength examination is subjective and potentially misleading. Instrumented measurement quantifies strength of muscle groups rather than individual muscles. Measurement of intramuscular pressure has clinical potential for objectively quanti-fying in vivo muscle force from individual muscles.
Acknowledgement
The work in this chapter was partly supported by NIH grant R01 HD31476. Appreciation is expressed to Barb Iverson for her careful assistance with manuscript preparation.
reFereNceS
1. Lovett RW. The treatment of infantile paralysis, 2nd edition. Philadelphia: Blakiston's Son & Co; 1917.
2. Wakim KG. Objective recording of muscle strength. Arch Phys Med Rehabil 1950;31:90-100.
3. Beasley WC. Quantitative muscle testing: Principles and applications to research and clinical services. Arch Phys Med Rehabil 1961;42:398-425.
4. Sharrad WJW. Correlations between the changes in the spinal cord and muscular paralysis in poliomyelitis. Proc Royal Soc Lond 1953.
5. Perry J. Predictive value of manual muscle testing and gait analysis in normal ankles by dynamic electromyography. Foot Ankle Int 1986;6:254-259.
6. Perry J. Gait Analysis: Normal and Pathological Function. Thorofare, NJ: Slack; 1992.
7. Atkens S, Lord J, Bernauer E. Relationship of manual muscles testing to objective strength measurements. Muscle Nerve 1989;12:173-177.
8. Mills KR. Wasting, weakness, and the MRC scale in the first dorsal interosseous muscle. J Neurol Neurosurg Psychiatry 1997;62:541-542.
9. Bohannon RW, Hull D, Palmeri D. Muscle strength impairments in gait performance deficits in kidney transplantation candidates. Am J Kidney Dis 1994;24:480-485.
10. Csuka M, McCarty DJ. Simple method for measurement of lower extremity muscle strength. Am J Med 1985;78:77-81.
11. Guralnik JM. A short physical performance battery assessing lower extremity function: Association with self reported disability and prediction of mortality and nursing home admission. J Gerontol 1994;49:85-94.
12. Amundsen LR, Graves JM. Testing knee extensor muscles of survi-vors of poliomyelitis. J Human Muscle Perf 1991;1:25-34.
13. Olgiati R, Burgunder JM, Mumenthaler M. Increased energy cost of locking in multiple sclerosis. Effect of spasticity, ataxia, and weakness. Arch Phys Med Rehabil 1988;69:846-849.
14. Andriacchi TP. A study of lower-limb mechanics during stair climb-ing. J Bone Joint Surg Am 1980;62:749-757.
15. Kaufman K. Gait characteristics of patients with knee osteoarthritis. J Biomech 2001;34:907-915.
16. Wrentenberg P, Lindberg F, Arborelius UP. Effects of arm rests and different ways of using them on hip and knee during rising. Clin Biomech 1993;8:95-101.
17. Askew LJ. Isometric elbow strength in normal individuals. Clin Orthop Related Res 1987;222:261-266.
18. An, K.-N., et al., Forces in a normal and abnormal hand. Journal of Orthopaedic Research, 1985. 3(2): p. 202-211.
19. Bohannon, R.W., Make versus break tests of elbow flexion force using a hand-held dynamometer. Physical Therapy, 1988. 68: p. 93-194.
20. Bohannon, R.W., Muscle strength testing with hand-held dyna-mometers. Muscle Strength Testing: Instrumented and Non-Instrumented Systems, ed. L.R. Amundsen. 1990, New York: Churchill Livingstone.
21. Wickholm, J.B. and R.W. Bohannon, Hand-held dynamometer mea-surements: Testor strength makes a difference. J Orthop Sports Phys Ther 1991;13:191-198.
Figure 9 Ankle motion (a) and moment (b) during gait. The gait cycle is defined as the events that occur between successive footsteps of the same foot. The gait cycle begins with foot strike, continues through stance and swing phases, and ends with foot strike of the same foot.

22. Fowler WM, Gardner GW. Quantitative strength measurements in muscular dystrophy. Arch Phys Med Rehabil 1967;48:629-644.
23. Sunderland A, Tinson D, Bradley L. Arm function after stroke: an evaluation of grip strength as a measure of recovery and a prognostic indicator. J Neurol Neurosurg Psychiatry 1989;752:1267-1272.
24. Armstrong LE. Using isokinetic dynamometry to test ambulatory patients with multiple sclerosis. Phys Ther, 1983. 63: p. 1274-1279.
25. Tripp EJ, Harris SR. Test-retest reliability of isokinetic knee exten-sion and flexion torque measurements in persons with spastic hemi-paresis. Physical Ther 1991;71:390-396.
26. Beasley WC. Influence of method on estimates of normal knee extensor force among normal and post-polio children. Phys Ther Review 1956;36:21-41.
27. Bohannon RW. Manual muscle test scores and dynamometer test scores of knee extension strength. Arch Phys Med Rehabil 1986;67:390-392.
28. Aitkens S, Lord J, Bernauer E. Relationship of manual muscle testing to objective strength measurements. Muscle Nerve 1989;12:173.
29. Schwartz S. Relationship between two measures of upper extremity strength: manual muscle test. Arch Phys Med Rehabil 1992;73:1063-1068.
30. Lieber RL, Boakes JL. Sarcomere length and joint kinematics during torque production in the frog hindlimb. Am J Physiol 1988;254:C759-C768.
31. Bogey RA, Barnes LA, Perry J. Computer algorithms to characterize individual subject EMG profiles during gait. Arch Phys Med Rehabil 1992;73:835-841.
32. Bogey RA, Barnes LA, Perry J. A computer algorithm for defining the group electromyographic profile from individual gait profiles. Arch Phys Med Rehabil 1993;74:286-291.
33. Bigland-Ritchie B, Kukulka CJ, Woods JJ. Surface EMG-force rela-tionships in human muscles of different fibre composition. J Physiol Lond 1980;308:103P-104P.
34. Dempster WT, Finerty JC. Relative activity of wrist moving muscles in static support of the wrist joint: An electromyographic study. Am J Physiol 1947;150:596-606.
35. deVries, H., Efficiency of electrical activity as a physical measure of the functional state of muscle tissue. Am J Phys Med 1968;47:10-22.
36. Lippold OCJ. The relation between integrated action potentials in a human muscle and its isometric tension. J Physiol Lond 1952;117:492-499.
37. Maton B, Bouisset S. The distribution of activity among the muscles of a single group during isometric contraction. Eur J App Physiol 1977;37:101-109.
38. Messier RH. The electromyogram as a measure of tension in the human biceps and triceps muscles. Int J Mech Sci 1971;13:585-598.
39. Metral S, Cassar G. Relationship between force and integrated EMG activity during voluntary isometric anistonic contraction. Eur J App Physiol 1981;46:185-198.
40. Moritani T, de Vries HA. Reexamination of the relationship between the surface integrated electromyogram (IEMG) and force of isomet-ric contraction. Am J Phys Med 1978;57:263-277.
41. Woods JJ, Bigland-Ritchie B. Linear and nonlinear surface EMG/force relationships in human muscles. Am J Phys Med 1983;62:287-299.
42. Zuniga EN, Simons DG. Nonlinear relationship between averaged electromyogram potential and muscle tension in normal subjects. Arch Phys Med Rehabil 1969;50:613-620.
43. Inman VT. Relationship of human electromyogram to muscular tension. Electroencephalogr Clin Neurophysiol 1952;4:187-194.
44. Bigland B, Lippold OCJ. The relationship between force, veloc-ity, and integrated electrical activity in human muscles. J Physiol 1954;123:214-224.
45. Bouisset S. EMG and muscle force in normal muscle activities. In: Desmedt JE, editor. New developments in EMG and clinical physiol-ogy. Basel, Switzerland: Karger; 1973.
46. Hatze H. A general myocybernetic control model of skeletal muscle. Biol Cybernetics 1978;28:143-157.
47. Hof AL, Vandenberg JW. Linearity between the weighted sum of the EMG's of the human triceps surae and the total torque. J Biomech 1977;10:529-539.
48. Komi PV. Relationship between muscle tension, EMG, and velocity of contraction under concentric and eccentric work. In: Desmedt JE, editor. New developments in clinical neurophysiology. Basel, Switzerland: Karger; 1973.
49. Milner-Brown HS, Stein RB. The relation between surface electro-myogram and muscle force. J Physiol 1975;246:549-569.
50. Komi PV, Buskirk ER. Effect of eccentric and concentric muscle conditioning on tension and electrical activity of human muscle. Ergonomics 1972;15:417-434.
51. Seliger V. Dolejs L, Karas V. A dynamometric comparison of maximum eccentric, concentric, and isometric conditions using EMG and energy expenditure measurements. Eur J App Physiol 1980;45:235-244.
52. Lunnen JD, Yack J, Le Veau BF. Relationship between muscle length, muscle activity, torque of the hamstring muscles. Phys Ther 1981;61:190-195.
53. Rosentswieg J, Hinson MM. Comparison of isometric, isotonic, and isokinetic exercises by electromyography. Arch Phys Med Rehabil 1972;68:249-252.
54. Barnes WS. The relationship of motor-unit activation to isokinetic muscular contraction at different contractile velocities. Phys Ther 1980;16:1152-1158.
55. Hinson MN, Rosentswieg J. Comparative electromyographic values of isometric, isotonic, and isokinetic contraction. Res Quart Exer Sport 1973;44:71-78.
56. Komi PV, Rusko H. Quantitative evaluation of mechanical and electrical changes during fatigue loadings of eccentric and concentric work. Scand J Rehab Med 1974;3:121-126.
57. Rothstein JM. Electromyographic, peak torque, and power relation-ships during isokinetic movement. Phys Ther 1983;63:926-933.
58. Osternig LR. Electromyographic patterns accompanying isokinetic exercise under varying speed and sequencing conditions. Am J Physical Med 1984;63:289-297.
59. Smidt G, Wadsworth JB. Floor reaction forces during gait: Comparison of patients with hip disease and normal subjects. Phys Ther 1973;53:1056-1062.
60. Vandervoort AA, Kramer JF, Wharram ER. Eccentric knee strength of elderly females. J Gerontol 1990;45:125-128.
61. Haffajee D, Maritz U, Suantesson G. Isometric knee extension strength as a function of joint angle, muscle length and motor unit activity. Acta Orthop Scand 1972;43:138-147.
62. Lippold OCJ, Redfearn J, Vuco J. Electromyography of fatigue. Ergonomics 1970;3:121-131.
63. Parker PA. Korner L, Kadefors R. Estimation of muscle force from intramuscular total pressure. Med Biol Eng Comput 1984;22:453-457.
64. Salmons S. Report on the 8th International Conference on Medical and Biological Engineering. Biomed Engineer 1969;4:467-474.
46 Measuring Muscle Function During Gait AANEM Plenary

AANEM Plenary Gait in Motion: Stepping into the 21st Century 47
65. Finni T, Komi PV, Lukkariniemi J. Achilles tendon loading during walking: Application of a novel optic fiber technique. Eur J Applied Physiol Occup Physiol 1998;77:289-291.
66. Fukashiro S. In-vivo Achilles tendon loading during jumping in humans. Eur J Applied Physiol 1995;71:453-458.
67. Gregor RJ. A comparison of the triceps surae and residual muscle moments at the ankle during cycling. J Biomech 1991;24:287-297.
68. Gregor RJ, Komi PU, Jarvinen M. Achilles tendon forces during cycling. Int J Sports Med 1987;8:9-14.
69. Komi PV. Relevance of in vivo force measurements to human bio-mechanics. J Biomech 1990;21:23-34.
70. Komi PV. In vivo registration of Achilles tendon forces in man: II. Methodological development. Int J Sports Med 1987;8:3-8.
71. Finni T, Komi PV, Lepola V. In-vivo human triceps surae and quadri-ceps femoris muscle function in a squat jump and counter movement jump. Eur J Applied Physiol 2000;83:416-426.
72. Schuind F. Flexor tendon forces: in vivo measurements. J Hand Surg Am 1992;17:291-298.
73. Landerer AS. Die Gewebesspannung in ihrem Einfluss auf die ortlich Blut-und-Lymphbewegung [Tissue contraction and its influ-ence on local blood and lymph flow]. Leipzig, Germany: Vogel; 1884.
74. Matsen FA. Monitoring of intramuscular pressure. Surgery 1976;79:702-709.
75. Rorabeck CH. Compartmental pressure measurements: an experi-mental investigation using the slit catheter. J Trauma 1981;21:446-449.
76. Styf JR. Evaluation of injection techniques in recording of intramus-cular pressure. J Orthop Res 1989;7:812-816.
77. Crenshaw AG. A new "transducer tipped" fiber optic catheter for measuring intramuscular pressures. J Orthop Res 1990;8:464-468.
78. Crenshaw AG, Styf JR, Hargens AR. Intramuscular pressures during exercise: An evaluation of a fiberoptic transducer-tipped catheter system. Eur J Applied Physiol 1992;65:178-182.
79. Willy C, Gerngross H, Sterk JC. Measurement of intracompartmen-tal pressure with use of a new electronic transducer-tipped catheter system. J Bone Joint Surg Am 1999;81:158-168.
80. Kaufman KR. Performance characteristics of a pressure microsen-sor. J Biomech 2003;36:283-287.
81. Hill AV. The pressure developed in muscle during contraction. J Physiol 1948;107:518-526.
82. Sylvest O, Hvid N. Pressure measurements in human striated muscles during contraction. Acta Rheumatol Scan 1959;5:216-222.
83. Kirkebö A, Wisnes A. Regional tissue fluid pressure in rat calf muscle during sustained contraction on stretch. Acta Physiol Scand 1982;11:551-556.
84. Mazella H. On the pressure developed by the contraction of striated muscle and its influence on muscular circulation. Arch Int Physiol 1954;62:334-347.
85. Sutherland DH. The potential application of a small solid state pres-sure transducer to measure muscle activity during gait. Trans Orthop Res Soc 1977;2:289.
86. Hargens AR. Intramuscular fluid pressure: a function of contraction force and tissue depth. Trans Orthop Res Soc 1982;7:371.
87. Hussain SNA, Magder S. Diaphragmatic intramuscular pressure in relation to tension, shortening, and blood flow. J App Physiol 1991;71:159-167.
88. Järvholm U. Intramuscular pressure and electromyography in the supraspinatus muscle at shoulder abduction. Clin Orthop Related Res 1989;245:102-109.
89. Körner L. Relationship on intramuscular pressure to the force output and myoelectric signal of skeletal muscle. J Orthop Res 1984;2:289-296.
90. Mubarak SJ. The wick catheter technique for measurement of intra-muscular pressure: a new research and clinical tool. J Bone Joint Surg Am 1976;58:1016-1020.
91. Owen CA. Relationship of intramuscular pressure to strength and muscular contraction. Trans Orthop Res Soc 1977;2:246.
92. Petrofsky JS, Hendershot DM. The interrelationship between blood pressure, intramuscular pressure, and isometric endurance in fast and slow twitch skeletal muscle in the cat. Eur J Applied Physiol Occup Physiol 1984;53:106-111.
93. Sejersted OM. Intramuscular fluid pressure during isometric contrac-tion of human skeletal muscle. J Applied Physiol Respir Environ Exer Physiol 1984;56:287-295.
94. Davis J, Kaufman KR, Lieber RL. Correlation between active and passive isometric force and intramuscular pressure in the isolated rabbit tibialis anterior muscle. J Biomech 2003;36:505-512.
95. Gordon AM, Huxley AF, Julian FJ. The variation in isometric tension with sarcomere length in vertebrate muscle fibres. J Physiol 1966;184:170-192.
96. Rack PMH, Westbury DR. The effects of length and stimulus rate on tension in the isometric cat soleus muscle. J Physiol 1969;204:443-460.
97. Baumann JU, Sutherland DH, Hanggi A. Intramuscular pressure during walking: An experimental study using the wick catheter tech-nique. Clin Orthop Relat Res 1979;145:292-299.
98. Jenkyn T. Finite element model of intramuscular pressure during iso-metric contraction of skeletal muscle. Phys Med Biol 2002;47:4043-4061.
99. van der Linden BJ. Mechanical modeling of skeletal muscle function, in PhD Thesis. Univ of Twente: Enschede, The Netherlands. 1988.
100. Kaufman KR, Sutherland DH. Dynamic intramuscular pressure measurement during gait. Operative Tech Sports Med 1995;3:250-255.

48 AANEM Plenary

THe IMPorTANce oF WALKING
According to Hippocrates, “walking is man’s best medicine.” Modern research confirms Hippocrates’ wisdom and suggests that exercise in the form of walking confers a significant health benefit, particularly for those with diabetes mellitus and lipid disorders. Men who walked regularly had reduced overall mortality11 and women who walked 3 or more hours per week had a reduction in coronary events similar in magnitude to women who performed more vigorous exercise.18 Moreover, older women who walked were less likely to demonstrate cognitive decline than more sedentary women40 and older persons of both genders who walk were less likely to show mobility loss.39 Relatively modest changes in lifestyle confer a benefit. It is estimated that by walking 30 or more minutes per day and reducing television time to less than 10 hours/week women could reduce new cases of obesity and diabetes mellitus by 30% and 43%, respectively.13 Lastly, there is evidence that weight-bearing activity may be protective against foot ulcer in persons with diabetic polyneuropathy (DPN).14
NeUroPATHy LeADS To BALANce IMPAIrMeNT
Neuropathy is one of the most common diagnoses made in the electrodiagnostic laboratory and it often subtly, but always sig-nificantly, impairs balance and gait. With regard to “static” balance such as quiet standing (which is not truly static given that the
center of mass rotates about the ankle in the manner of an inverted pendulum) neuropathic subjects show increased center of pressure excursions as compared to control subjects,32,37 and these excursions correlate with peripheral nerve conduction studies.38 Neuropathy also impairs transition from bipedal to unipedal balance, whether on command or subject-controlled.24 Neuropathic subjects also show greater difficulty recovering from perturbations in the forms of a tilting support surface or being released following a lateral lean2,10 (Table 1). Cavanagh and colleagues4 found that young adults with neuropathy were 15 times more likely to be injured while walking than a control group, and Sorock and Labiner34 confirmed prospectively that neuropathy increased fall risk in a cohort of older persons living in senior housing. Similarly, in two separate studies it was found that older persons with neuropathy were 23 and 17 times more likely to fall than age- and gender-matched controls.25,26 Resnick and colleagues22 demonstrated that peripheral neuropathy (PN), rather than the presence of diabetes, is responsible for lower extremity dysfunction among older persons with diabetes mellitus. Most falls in older persons with6 and with-out3 neuropathy fall during ambulation, especially on irregular surfaces. Such findings indicate that patients with neuropathy have a reasonably “stable” gait unless they encounter physical perturba-tions. Therefore, patients with neuropathy who wisely comply with Hippocrates’ recommendation, but do not have access to specific equipment or environments, will walk outside and encounter ir-regular surfaces or other perturbations that place these patients at increased fall risk.
The Sluggish Sheepdog and the Incredible Shrinking Foot: Understanding and Managing
Neuropathic Gait
James K. richardson, MDAssociate Professor
Department of Physical Medicine and RehabilitationCo-Director
Electrodiagnostic LaboratoryUniversity of Michigan Health Systems
Ann Arbor, Michigan
49

50 The Sluggish Sheepdog and the Incredible Shrinking Foot AANEM Plenary
Neuropathy at the Ankle
The ankle is the most distal joint with a significant influence on posture and, as would be expected, is the joint whose function is most impaired by the typical length-dependent neuropathy. Table 2 summarizes some of the studies that have identified functionally significant sensory and motor impairments among older persons with PN. Ankle proprioceptive thresholds are increased (worse) in the frontal and sagittal planes among DPN subjects as compared to controls.31,36 Similarly, maximal motor function is decreased in both planes at the ankle in subjects with DPN as compared to controls.1,10 Are these impairments sufficient to affect postural stability in neuropathic patients? To explore this question, this manuscript will first attempt to define postural stability and then apply that definition in the context of a patient with neuropathy trying to stand on one foot or walk.
WHAT IS STABILITy?
All would agree that an object or person that is difficult to push over is stable. This is true whether the object or person, or more generically the “system,” is static (e.g., a statue) or dynamic (e.g., a patient walking to the mailbox). According to Reeves and col-leagues, “To discuss the stability of a system, whether it is in equi-librium (static) or changing with time (dynamic), we must give a small perturbation and observe the new behavior.”21 If the behavior of the object in static equilibrium does not change, it is stable. If the behavior of the object in dynamic equilibrium quickly resumes its previous behavior following the perturbation (a fullback shed-ding a light defensive back without changing stride) then it is stable as well. A system in dynamic equilibrium that gradually resumes its previous behavior after a perturbation (a drunk who staggers after
encountering a lightpost but resumes his gait after several chaotic steps) is “asymptotically stable.” If the system does not resume its previous behavior after a perturbation (the patient with neuropathy who steps on a grandchild’s toy and falls), then it is unstable.
Quantifying Stability
How stable is a system? Stability cannot be quantified because it is, in reality, a dichotomous variable—a system is stable or it is not. There are no gradations of stability (Figure 1). However, it is intuitively obvious that a difference exists between a salt shaker balanced on edge and a pyramid, or between an older woman with neuropathy tottering on gravel and a running back burst-ing through a tackle. The difference is that the pyramid and the running back are “robust” to perturbations—they both continue or quickly resume their previous behavior despite significant per-turbations. Therefore, a reasonable way to quantify the stability of a system is to quantify perturbations and determine whether the system in question remains stable. Systems that remain stable in the face of large perturbations may then be thought of as “more stable” than systems which become unstable when challenged by lesser perturbations (Figure 1).
Systems With “Small Feet”
In the case of a rigid object, such as the pyramid, the physical size of the base of support is relevant to the magnitude of perturbation the system can receive and still remain stable. The greater the size of the base of support the easier it is to keep the center of mass over it and the more robust the system. Conversely, a very small base of support for a rigid object, as in the case of the salt shaker balanced on edge, renders the system minimally robust to perturbations. However, in the case of the human balancing on one foot, the flex-
Table 1 The Effect of Neuropathy on Measures of Balance
Balance Task PN subjects Control SignificanceBipedal StanceForce platform measured center of pressure excursion (in cm)37 Eyes open: 550 ± 50* 350 ± 20* p < 0.05 Eyes closed: 1100 ± 100* 600 ± 50* p < 0.01Center of pressure excursion (in cm)32 Eyes open: 35 ± 12* 20 ± 8* p < 0.01 Eyes closed: 55 ± 18* 30 ± 10* p < 0.01Unipedal StanceBalancing 3 seconds on command (success rate)24 0.12 0.58 P = 0.021Subject controlled (sec)24 3.8 ± 3.5 32.2 ± 17.7 P = < 0.001Perturbed Unipedal StanceSuccess rate recovering from a tilting surface2 Eyes open: 0.47 0.75 P = 0.036 Eyes closed: 0.02 0.21 Lateral LeansSubjects recovering successfully for a given % foot width10 5% lean, 0/6 5% lean, 3/6 P = 0.068 10% lean, 0/6 10% lean, 1/6
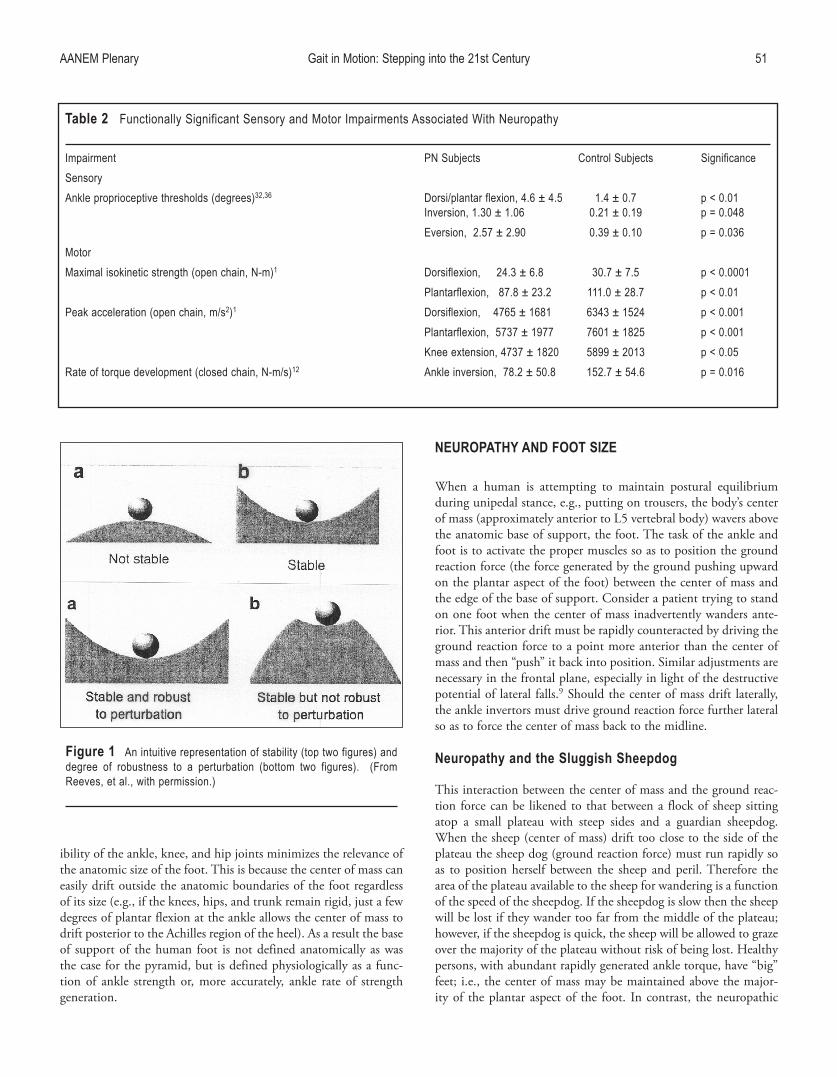
AANEM Plenary Gait in Motion: Stepping into the 21st Century 51
ibility of the ankle, knee, and hip joints minimizes the relevance of the anatomic size of the foot. This is because the center of mass can easily drift outside the anatomic boundaries of the foot regardless of its size (e.g., if the knees, hips, and trunk remain rigid, just a few degrees of plantar flexion at the ankle allows the center of mass to drift posterior to the Achilles region of the heel). As a result the base of support of the human foot is not defined anatomically as was the case for the pyramid, but is defined physiologically as a func-tion of ankle strength or, more accurately, ankle rate of strength generation.
NeUroPATHy AND FooT SIZe
When a human is attempting to maintain postural equilibrium during unipedal stance, e.g., putting on trousers, the body’s center of mass (approximately anterior to L5 vertebral body) wavers above the anatomic base of support, the foot. The task of the ankle and foot is to activate the proper muscles so as to position the ground reaction force (the force generated by the ground pushing upward on the plantar aspect of the foot) between the center of mass and the edge of the base of support. Consider a patient trying to stand on one foot when the center of mass inadvertently wanders ante-rior. This anterior drift must be rapidly counteracted by driving the ground reaction force to a point more anterior than the center of mass and then “push” it back into position. Similar adjustments are necessary in the frontal plane, especially in light of the destructive potential of lateral falls.9 Should the center of mass drift laterally, the ankle invertors must drive ground reaction force further lateral so as to force the center of mass back to the midline.
Neuropathy and the Sluggish Sheepdog
This interaction between the center of mass and the ground reac-tion force can be likened to that between a flock of sheep sitting atop a small plateau with steep sides and a guardian sheepdog. When the sheep (center of mass) drift too close to the side of the plateau the sheep dog (ground reaction force) must run rapidly so as to position herself between the sheep and peril. Therefore the area of the plateau available to the sheep for wandering is a function of the speed of the sheepdog. If the sheepdog is slow then the sheep will be lost if they wander too far from the middle of the plateau; however, if the sheepdog is quick, the sheep will be allowed to graze over the majority of the plateau without risk of being lost. Healthy persons, with abundant rapidly generated ankle torque, have “big” feet; i.e., the center of mass may be maintained above the major-ity of the plantar aspect of the foot. In contrast, the neuropathic
Table 2 Functionally Significant Sensory and Motor Impairments Associated With Neuropathy
Impairment PN Subjects Control Subjects SignificanceSensoryAnkle proprioceptive thresholds (degrees)32,36 Dorsi/plantar flexion, 4.6 ± 4.5 1.4 ± 0.7 p < 0.01 Inversion, 1.30 ± 1.06 0.21 ± 0.19 p = 0.048 Eversion, 2.57 ± 2.90 0.39 ± 0.10 p = 0.036MotorMaximal isokinetic strength (open chain, N-m)1 Dorsiflexion, 24.3 ± 6.8 30.7 ± 7.5 p < 0.0001 Plantarflexion, 87.8 ± 23.2 111.0 ± 28.7 p < 0.01Peak acceleration (open chain, m/s2)1 Dorsiflexion, 4765 ± 1681 6343 ± 1524 p < 0.001 Plantarflexion, 5737 ± 1977 7601 ± 1825 p < 0.001 Knee extension, 4737 ± 1820 5899 ± 2013 p < 0.05Rate of torque development (closed chain, N-m/s)12 Ankle inversion, 78.2 ± 50.8 152.7 ± 54.6 p = 0.016
Figure 1 An intuitive representation of stability (top two figures) and degree of robustness to a perturbation (bottom two figures). (From Reeves, et al., with permission.)

52 The Sluggish Sheepdog and the Incredible Shrinking Foot AANEM Plenary
patient with diminished ankle torque generation must maintain the center of mass over a small portion of the plantar aspect of the foot, giving such patients “small” feet.
Afferent Dysfunction at the Ankle
The afferent impairments associated with neuropathy act synergis-tically with the efferent impairments in the rate of strength genera-tion to further impair one-legged balance. The afferent impairment delays the rapid perception of a perturbation occurring during single stance. This delay further prolongs the initiation of the appropriate ankle torque generation necessary to counteract the perturbation. In terms of the sheepdog analogy, the afferent impairment associ-ated with neuropathy is the equivalent of a drowsy sheepdog that is delayed in perceiving the dangerous wanderings of the sheep and so has a late start, while the efferent impairment ensures that the sheepdog is slow once it begins traveling. In terms of motor control theory, the afferent and efferent impairments both contribute to feedback delay which in turn coarsens motor control.
Influence of Afferent/efferent Ankle Function on Unipedal Balance
In previous work in older diabetic women with and without neuropathy, it was found that ankle rate of strength generation ex-plained 57.5% of the variability in unipedal balance time10 (Figure 2). Similarly, older subjects who fell during an experimental trip were unable to arrest the angular momentum of the fall due to an inability to rapidly generate plantar flexion torque.19 The data are consistent with the concept that subjects with greater ankle rate of strength development had a larger functional base of support which allowed greater center of mass excursions without loss of balance. There is also experimental evidence to support the impact of impaired afferent ankle function on balance. A group of 25 older persons was studied, 12 with neuropathy and 13 matched healthy older control subjects, and it was found that combined ankle inver-sion and eversion proprioceptive thresholds explained 51.4% of the subjects’ unipedal balance times.33 Taken together, these findings suggest that when the afferent impairment is severe enough the center of mass drifts, unperceived, beyond the area over which the ankle muscles can drive the ground reaction force and unipedal stance becomes unreliable—a near universal finding in patients with functionally significant neuropathy.
“Small Feet” Lead to Falls and Increased Gait Variability
Falls
Small feet, due to neuropathic impairments, lead to a system (patient) that is not robust to perturbations. As a consequence, patients with neuropathy have a markedly increased rate of falls and injury due to falls. Moreover, clinical experience and the only pro-spective study of falls exclusively in neuropathic patients6 indicate that they almost invariably fall as the result of surface irregularity.
Increased Gait Variability
Gait variability is increasingly recognized as a quantifiable sign of dynamic disequilibrium; i.e., a sign that the system (the patient) is not robust to perturbation. (The reader is directed to excellent works by Jeffrey M. Haursdorff, PhD and colleagues that found increased gait variability, both temporally and spatially, to be associated with mobility function, falls, and a variety of diseases.12) Although the precise biomechanical advantage, or necessity, of in-creased gait variability has not been definitively identified, it seems likely that when a patient who is not robust to perturbations during single limb stance is challenged, they will rapidly place the swing limb onto the ground. Rapid, urgent placement of the swing limb in response to perceived instability likely occurs in an intermittent fashion, both temporally and spatially, and in aggregate leads to measurably increased gait variability, particularly on an irregular surface. In support of this, strong negative correlations have been found between step length on an irregular surface and the degree of shortening of step length on an irregular surface as compared to a smooth surface, and step time variability on an irregular surface (-0.433; p = 0.005 and -0.656; p < 0.001 for step length and change in step length, respectively; Richardson, unpublished data, 2007).
Gait variability is disproportionately accentuated on an irregular surface. Measures of gait variability determined on an irregular surface—which serves as a repetitive source of perturbation—appear to provide superior resolution in detecting groups of clinical interest. For example, increased step time variability on an irregular, but not smooth, surface differentiates between older women with and without neuropathy28 (Figure 3a); older neuropathic patients with and without a history of falling29 (Figure 3b); and older
Figure 2 The relationship between ankle rate of torque generation (RTD, in Newton-meters/second) and unipedal balance time in seconds in a group of 12 older diabetic women, 6 of whom have neuropathy.
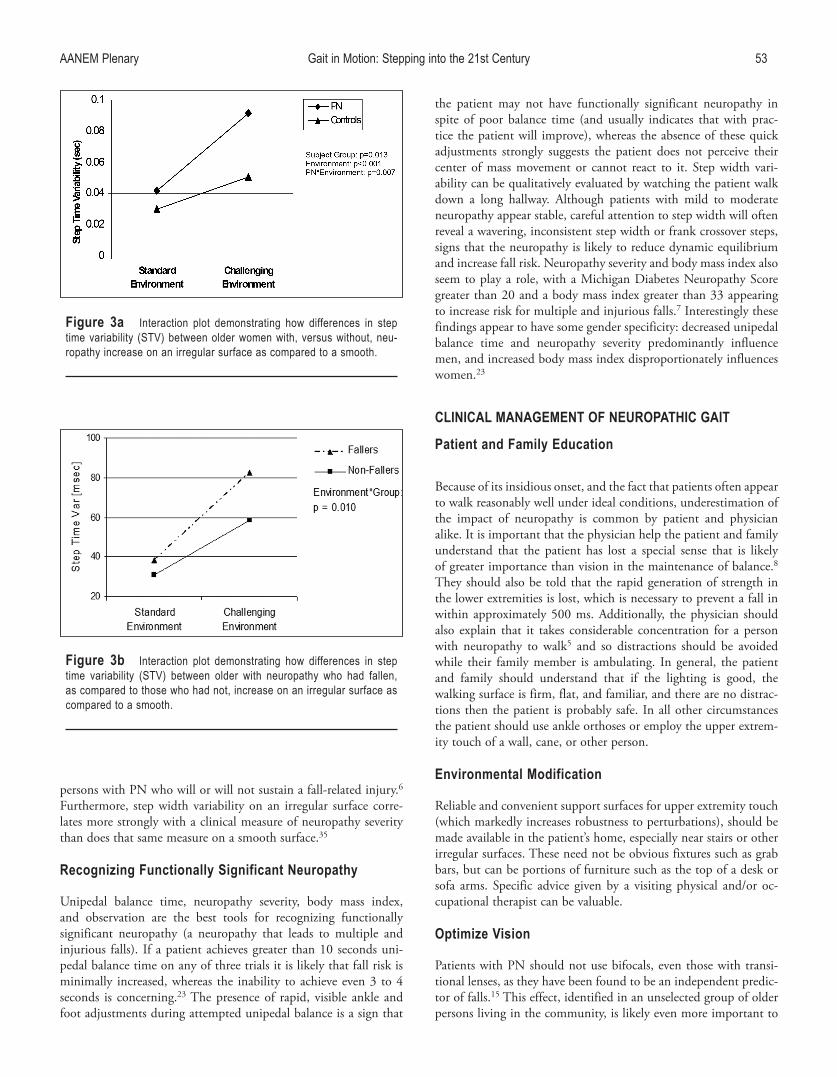
AANEM Plenary Gait in Motion: Stepping into the 21st Century 53
persons with PN who will or will not sustain a fall-related injury.6 Furthermore, step width variability on an irregular surface corre-lates more strongly with a clinical measure of neuropathy severity than does that same measure on a smooth surface.35
recognizing Functionally Significant Neuropathy
Unipedal balance time, neuropathy severity, body mass index, and observation are the best tools for recognizing functionally significant neuropathy (a neuropathy that leads to multiple and injurious falls). If a patient achieves greater than 10 seconds uni-pedal balance time on any of three trials it is likely that fall risk is minimally increased, whereas the inability to achieve even 3 to 4 seconds is concerning.23 The presence of rapid, visible ankle and foot adjustments during attempted unipedal balance is a sign that
the patient may not have functionally significant neuropathy in spite of poor balance time (and usually indicates that with prac-tice the patient will improve), whereas the absence of these quick adjustments strongly suggests the patient does not perceive their center of mass movement or cannot react to it. Step width vari-ability can be qualitatively evaluated by watching the patient walk down a long hallway. Although patients with mild to moderate neuropathy appear stable, careful attention to step width will often reveal a wavering, inconsistent step width or frank crossover steps, signs that the neuropathy is likely to reduce dynamic equilibrium and increase fall risk. Neuropathy severity and body mass index also seem to play a role, with a Michigan Diabetes Neuropathy Score greater than 20 and a body mass index greater than 33 appearing to increase risk for multiple and injurious falls.7 Interestingly these findings appear to have some gender specificity: decreased unipedal balance time and neuropathy severity predominantly influence men, and increased body mass index disproportionately influences women.23
cLINIcAL MANAGeMeNT oF NeUroPATHIc GAIT
Patient and Family education
Because of its insidious onset, and the fact that patients often appear to walk reasonably well under ideal conditions, underestimation of the impact of neuropathy is common by patient and physician alike. It is important that the physician help the patient and family understand that the patient has lost a special sense that is likely of greater importance than vision in the maintenance of balance.8 They should also be told that the rapid generation of strength in the lower extremities is lost, which is necessary to prevent a fall in within approximately 500 ms. Additionally, the physician should also explain that it takes considerable concentration for a person with neuropathy to walk5 and so distractions should be avoided while their family member is ambulating. In general, the patient and family should understand that if the lighting is good, the walking surface is firm, flat, and familiar, and there are no distrac-tions then the patient is probably safe. In all other circumstances the patient should use ankle orthoses or employ the upper extrem-ity touch of a wall, cane, or other person.
environmental Modification
Reliable and convenient support surfaces for upper extremity touch (which markedly increases robustness to perturbations), should be made available in the patient’s home, especially near stairs or other irregular surfaces. These need not be obvious fixtures such as grab bars, but can be portions of furniture such as the top of a desk or sofa arms. Specific advice given by a visiting physical and/or oc-cupational therapist can be valuable.
optimize Vision
Patients with PN should not use bifocals, even those with transi-tional lenses, as they have been found to be an independent predic-tor of falls.15 This effect, identified in an unselected group of older persons living in the community, is likely even more important to
Figure 3b Interaction plot demonstrating how differences in step time variability (STV) between older with neuropathy who had fallen, as compared to those who had not, increase on an irregular surface as compared to a smooth.
Figure 3a Interaction plot demonstrating how differences in step time variability (STV) between older women with, versus without, neu-ropathy increase on an irregular surface as compared to a smooth.

54 The Sluggish Sheepdog and the Incredible Shrinking Foot AANEM Plenary
neuropathic patients who are heavily reliant upon vision. Therefore it is recommended that patients have reading and “walking” glasses that are used separately.
Physical Training
At the University of Michigan, 20 older subjects with neuropathy were randomized to a 3-week balance and ankle strengthening program or a 3-week sham exercise program.27 Subjects who per-formed the intervention program showed significant improvements in unipedal balance time, functional reach, and tandem stance. The trial was small and single-blind; firm conclusions cannot be drawn. However, the exercises were tolerated well and are reasonable to consider. In addition, strengthening of the hip abductor/adductor groups and trunk musculature is intuitively appealing as techniques that may minimize excessive lateral trunk shift during gait. This author has seen clinical improvement in the gait of patients with neuropathy who have followed such programs. Finally, in a second-ary analysis of gait data previously obtained30 we found that active ankle frontal plane range of motion (ankle inversion/eversion) was a significant predictor of step width variability (R = -0.344; p = 0.032) and range (R = -0.386; p = 0.015) during neuropathic gait on a smooth surface (Richardson, unpublished data, 2007). Multivariate analysis showed that this effect was independent of neuropathy severity and other variables. Therefore, although cause and effect were not confirmed by this work, the data suggest that increasing ankle eversion and inversion range of motion may allow improved frontal plane control during neuropathic gait. Finally, strengthening of the upper extremities so that 25%-30% of body weight can be supported on a cane may be beneficial for reasons to be described.
external Devices
Patient use of a cane was studied in two separate protocols and found that it appears to improve balance on both occasions. In the first, a cane was found to markedly improve the ability of older neuropathic subjects to maintain unipedal balance for 3 seconds when challenged with an inverting or everting perturbation.2 Two findings were of clear clinical significance: (1) subjects performed equally well whether the perturbation was toward or away from the cane, and (2) up to 25%-30% of patient body weight was placed on the cane during this simulated emergent recovery of balance. In a separate study, 43 older neuropathic subjects underwent gait analy-sis on an irregular surface in low light conditions (Figure 4a) with and without three interventions: a cane, ankle orthoses (Figure 4b), and touch of a vertical surface.30 The interventions were chosen to improve frontal plane control given the injury potential of lateral falls. Step width variability and step time variability were chosen as outcomes given the work supporting the former as a marker of dynamic frontal plane control,16 and the association between the latter and falls.12 Each of the three interventions significantly decreased step width and step time variability, as compared to the
baseline condition, and did so after the subject was given just 5 minutes of practice with each intervention. It seems likely that the interventions made the subjects more robust to perturbations during single stance which, in turn, allowed for a more controlled placement of the swing limb.
Accentuating Plantar Surface Sensation
Older persons with decreased plantar sensation demonstrated more rapid responses to frontal plane perturbations when standing
Figure 4a Schematic of irregular surface (randomly oriented trian-gular prisms are shown beneath the carpet surface) and placement of optoelectronic markers on the body for calculation of step width, step length and velocity.

AANEM Plenary Gait in Motion: Stepping into the 21st Century 55
on small (1 mm) ball bearings.17 In addition, a similar group of patients showed diminished standing sway when insoles provided vibratory noise to the plantar surface of the feet.20 The effect of these interventions on the gait of patients with neuropathy under standard and challenging conditions is not yet known.
reFereNceS
1. Andersen H, Poulsen PL, Mogensen CE, Jakobsen J. Isokinetic muscle strength in long-term IDDM patients in relation to diabetic complications. Diabetes 1996;45:440-445.
2. Ashton-Miller JA, Yeh MWL, Richardson JK, Galloway T. A cane reduces loss of balance in patients with peripheral neuropathy: results from a challenging unipedal balance test. Arch Phys Med Rehabil 1996;77:446-452.
3. Berg WP, Alessio HM, Mills EM, Tong C. Circumstances and con-sequences of falls in independent community-dwelling older adults. Age and Aging 1997;6:261-268.
4. Cavanagh PR, Derr JA, Ulbrecht JS, Maser RE, Orchard TJ. Problems with gait and posture in neuropathic patients with insulin-dependent diabetes mellitus. Diabetes Med 1992;9:469-474.
5. Courtemanche R, Teasdale N, Boucher P, Fleury M, Lajoi Y, Bard C. Gait problems in diabetic neourpathic patients. Arch Phys Med Rehabil 1996;77:849-855.
6. DeMott TK, Richardson JK, Thies SB, Ashton-Miller JA. Falls and gait characteristics among older persons with peripheral neuropathy. Am J Phys Med Rehabil 2007;86:125-132.
7. Feldman EL, Stevens MJ, Thomas PK, Brown MB, Canal N, Greene DA. A practical two-step quantitative clinical and electrophysiologi-cal assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care 1994;17:1281-1289.
8. Fitzpatrick R, McCloskey DI. Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. J Physiol 1994;478:173-186.
9. Greenspan SL, Meyers ER, Maitland LA, Resnick NJ, Hayes WC. Fall severity and bone mineral density as risk factors for hip fracture in ambulatory elderly. JAMA 1994;271:128-133.
10. Gutierrez MS, Helber MB, Dealva D, Ashton-Miller, Richardson JK. Mild diabetic neuropathy affects ankle motor function. Clin Biomech 2001;16:522-528.
11. Hakim AA, Petrovitch H, Burchfiel CM, Ross GW, Rodriguez BL, White LR, Yano K, Curb JD, Abbott RD. Effects of walking on mortality among nonsmoking retired men. N Engl J Med 1998;338:94-99.
12. Hausdorff JM, Rios DA, Edelberg HK. Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch Phys Med Rehabil 2001;82:1050-1056.
13. Hu FB, Li TY, Colditz GA, Willett WC, Manson JE. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 2003;289:1785-1791.
14. LeMaster JW, Reiber GE, Smith DG, Heagerty PJ, Wallace C. Daily weight-bearing activity does not increase the risk of diabetic foot ulcers. Med Sci Sports Exerc 2003;35:1093-1099.
15. Lord SR, Dayhew J, Howland A. Multifocal glasses impair edge-contrast sensitivity and depth perception and increase the risk of falls in older people. J Am Geriatr Soc 2002;501:1760-1766.
16. MacKinnon CD, Winter DA. Control of whole body balance in the frontal plane during human walking. J Biomech 1993;26:633-644.
17. Maki BE, McIlroy WE. Postural control in the older adult. Clin Geriatr Med 1996;12:635-658.
18. Manson JE, Hu FB, Rich-Edwards JW, Colditz GA, Stampfer MJ, Willett WC, Speizer FE, Hennekens CH. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N Engl J Med 1999;341:650-658.
19. Pijnappels M, Bobbert MF, van Dieen JH. Push-off reactions in recovery after tripping discriminate young subjects, older non-fallers and older fallers. Gait Posture 2004;21:388-394.
20. Priplata AA, Niemi JB, Harry JD, Lipsitz LA, Collins JJ. Vibrating insoles and balance control in elderly people. Lancet 2003;362:2003-2004.
21. Reeves NP, Narenda KS, Cholewicki J. Spine stability: the six blind men and the elephant. Clin Biomech 2007;22:266-274.
22. Resnick HE, Vinik AI, Schwartz AV, Leveille SG, Brancati FL, Balfour J, Guralnik JM. Independent effects of peripheral nerve dysfunction on lower-extremity physical function in old age. Diabetes Care 2000;23:1642-1647.
23. Richardson JK. Factors associated with falls in older patients with diffuse polyneuropathy. J Amer Geriatr Soc 2002;50:1767-1773.
24. Richardson JK, Ashton-Miller JA, Lee SG, Jacobs K. Moderate pe-ripheral neuropathy impairs weight transfer and unipedal balance in the elderly. Arch Phys Med Rehabil 1996;77:1152-1156.
25. Richardson JK, Ching C, Hurvitz EA. The relationship between electromyographically documented peripheral neuropathy and falls. J Am Geriatr Soc 1992;40:1008-1012.
26. Richardson JK, Hurvitz EA. Peripheral neuropathy: a true risk factor for falls. J Gerontol A Biol Med Sci 1995;50A:M211-M215.
Figure 4b The ankle orthoses in place, with foam-lined shells on the medial and lateral aspects of the lower leg.

56 The Sluggish Sheepdog and the Incredible Shrinking Foot AANEM Plenary
27. Richardson JK, Sandman D, Vela S. A focused exercise regimen improves clinical measures of balance in patients with peripheral neuropathy. Arch Phys Med Rehabil 2001;82:205-209.
28. Richardson JK, Thies SB, DeMott TK, Ashton-Miller JA. A compar-ison of gait characteristics between older women with and without peripheral neuropathy in standard and challenging environments. J Amer Geriatr Soc 2004;52:1532-1537.
29. Richardson JK, Thies SB, DeMott TK, Ashton-Miller JA. Gait analy-sis in a challenging environment differentiates between fallers and non-fallers among older patients with peripheral neuropathy. Arch Phys Med Rehabil 2005;86:1539-1544.
30. Richardson JK, Thies S, DeMott T, Ashton-Miller JA. Interventions improve gait regularity in patients with peripheral neuropathy while walking on an irregular surface under low light. J Am Geriatr Soc 2004;52:510-515.
31. Simoneau GG, Derr JA, Ulbrecht JS, Becker MB, Cavanagh PR. Diabetic sensory neuropathy effect on ankle joint movement percep-tion. Arch Phys Med Rehabil 1996;77:453-460.
32. Simoneau GG, Ulbrecht JS, Derr JA, Becker MB, Cavanagh PR. Postural instability in patients with diabetic sensory neuropathy. Diabetes Care 1994;17:1411-1421.
33. Son J. Unipedal balance: biomechanical analyses of the effects of age and disease. PhD Dissertation, University of Michigan, Department of Mechanical Engineering, 2006.
34. Sorock GS, Labiner DM. Peripheral neuromuscular dysfunction and falls in an elderly cohort. Am J Epidemiol 1992:136:584-591.
35. Thies SB, Richardson JK, Demott T, Ashton-Miller JA. Influence of an irregular surface and low light on the step variability of pa-tients with peripheral neuropathy during level gait. Gait Posture 2005;22:40-45.
36. van den Bosch C, Gilsing MG, Lee SG, Richardson JK, Ashton-Miller JA. Peripheral neuropathy effect on ankle inversion and ever-sion detection thresholds. Arch Phys Med Rehabil 1995;76:850-856.
37. Uccioli L, Giacomini PG, Monticone G, Magrini A, Durola L, Bruno E, Parisi L, Di Girolamo S, Menzinger G. Body sway in diabetic neu-ropathy. Diabetes Care 1995;18:339-344.
38. Uccioli L, Gicomini PG, Pasqualetti P, DiGirolamo S, Ferrigno P, Monticone G, Bruno E, Boccasena P, Magrini A, Parisi L, Menzinger G, Rossini PM. Contribution of central neuropathy to postural insta-bility in IDDM patients with peripheral neuropathy. Diabetes Care 1997;20:929-934.
39. Visser M, Simonsick EM, Colbert LH, Brach J, Rubin SM, Kritchevsky SB, et al. Type and intensity of activity and risk of mobility limita-tion: the mediating role of muscle parameters. J Am Geriatr Soc 2005;53:762-70.
40. Yaffe K, Barnes D, Nevitt M, Lui LY, Covinsky K. A prospective study of physical activity and cognitive decline in elderly women: women who walk. Arch of Internal Med 2001;161:1703-1708

AANEM Plenary 57
AFTer coMPLeTIoN oF THIS AcTIVITyGAIT IN MoTIoN: STePPING INTo THe 21ST ceNTUry
AcTIVITy AND FAcULTy eVALUATIoNOn the Scantron Sheet provided rate how well you perceived the activity to have met your expectations using the following scale for questions 10-19. For questions 20 and beyond, use the scale provided under the question.
A. Extremely
B. Somewhat
C. Very Little
D. Not at all
This CME activity:
10. Addressed my most pressing questions.
11. Addressed competencies identified by my specialty.
12. Provided fair and balanced content.
13. Provided clear evidence to support content.
14. Included opportunities to learn interactively from faculty and participants.
15. Provided me with supporting materials or tools for my office (re-minders, patient materials, etc.).
16. Included opportunities to solve patient cases.
17. Translated trial data to patients I see in my practice.
18 Addressed barriers to my optimal patient management.
19. Improved my knowledge/ability in the objectives outlined?
20. Will you incorporate new elements presented in this educational session into your practice to improve patient care?A. Already do this.B. Yes.C. No.D. Not applicable to my patients.
21. After attending this session, do you expect your management strategies in this clinical area to change within the next 6 months?A. Definitely will change. B. Possibly will change. C. Definitely will not change.
Additional comments: See page 61
Fill
in an
swer
s here
Instructions for filling out
your parScore sheet
Using a #2 pencil, fill in your answers beginning with #10:
Leave the completed form at the table out-side your session.

58 Activity and Faculty Evaluation AANEM Plenary
22. How would you rate the quality of presentation received during Dr. Herbison’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
23. Did you perceive any commercial bias in Dr. Herbison’s presenta-tion?A. Yes.B. No.
24. How would you rate the quality of presentation received during Dr. Hallett’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
25. Did you perceive any commercial bias in Dr. Hallet’s presenta-tion?A. Yes.B. No.
26. How would you rate the quality of presentation received during Dr. Lomen-Hoerth’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
27. Did you perceive any commercial bias in Dr. Lomen-Hoerth’s presentation?A. Yes.B. No.
28. How would you rate the quality of presentation received during Dr. Graham’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
29. Did you perceive any commercial bias in Dr. Graham’s presenta-tion?A. Yes.B. No.
30. How would you rate the quality of presentation received during Dr. Kaufman’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
31. Did you perceive any commercial bias in Dr. Kaufman’s presenta-tion?A. Yes.B. No.
32. How would you rate the quality of presentation received during Dr. Richardson’s presentation?A. Best possible.B. Good.C. Average.D. Poor.E. Worst possible.
33. Did you perceive any commercial bias in Dr. Richardson’s presen-tation?A. Yes.B. No.

AANEM Plenary 59
34. Freezing of gait in Parkinson’s disease can be characterized by:A. Stiff legs.B. Lack of arm swing.C. Rapid stepping in place.D. Cold feet.
35. Walking backwards better than forwards can be seen with:A. Spasticity.B. Parkinson’s disease.C. Myoclonus.D. Dystonia.
36. If a patient stops walking in order to talk, this indicates:A. Good attentional capacity.B. A likely psychogenic gait disorder.C. A disposition to freezing.D. An increased risk of falling.
37. Normal pressure hydrocephalus is a cause of what type of gait disorder?A. Parkinsonian gait.B. Frontal gait disorder.C. Dystonic gait.D. Cerebellar gait.
38. Patients with essential tremor may exhibit what type of gait abnor-mality?A. Cerebellar gait.B. Parkinsonian gait.C. Bouncing gait.D. Dancing gait.
39. Reporting to the Department of Motor Vehicles by the physician is recommended for amyotrophic lateral sclerosis (ALS) patients:A. At the time of diagnosis.B. Once the patient is driving a wheelchair van.C. When one leg becomes weak.D. Whenever there is a concern about safety driving.
40. When a patient with ALS needs an electronic wheelchair:A. They must obtain a wheelchair van at the same time to trans-
port the chair.B. They must be unable to use a manual wheelchair indepen-
dently.C. They must have severe weakness of all 4 limbs.D. Their arms must strong enough to operate the controls on the
wheelchair.
41. An ALS diagnosis is considered when:A. The patient has upper and lower motor neuron findings.B. The weakness is progressive.C. Neuroimaging is normal.D. All of the above.
42. Spasticity in ALS can be managed:A. With botox.B. With a baclofen pump.C. With oral medications.D. All of the above.
43. Home physical therapy and occupational therapy:A. Must be paid for out of pocket by the patient in all cases.B. May perform a home safety assessment to guide remodeling.C. May be ordered and reimbursed by insurance at the time a
patient is undergoing outpatient physical therapy and occu-pational therapy.
D. Is not generally useful for ALS patients.
44. In children with cerebral palsy the most reliable classification is based on:A. Etiological factors: e.g., prematurity, maternal birth canal
infection, genetic central nervous system malformation, vascular event.
B. Movement disorder: e.g., spastic, dystonic, ataxic, or mixed.C. Topographical distribution: e.g., hemiplegia, diplegia, quad-
riplegia.D. Gross motor function: using the Gross Motor Function
Classification System (GMFCS).
Gait in Motion: Stepping into the 21st century
cMe SeLF-ASSeSSMeNT TeST
Select the oNe best answer for each question.

60 CME Self-Assessment Test AANEM Plenary
45. The GMFCS for children with cerebral palsy is predictive of long term gross motor function. A. True.B. False.
46. In gait analysis, kinematics are based on the measurement of ground reaction forces using force plates.A. True.B. False.
47. Physiological testing of children in the gait laboratory is a reliable measure of the overall efficiency of gait.A. True.B. False.
48. Dynamic electromyography provides a reliable measure of muscle power.A. True.B. False
49. Factors that increase fall risk among older persons with neuropathy include: 1. Increased body mass index. 2. More severe neuropathy. 3. Unipedal stance time less than 3 seconds. 4. The use of bifocal (or transitional) spectacle lenses.A. Only 1, 2, and 3 are correct.B. Only 1 and 3 are correct.C. Only 2 and 4 are correct.D. All are correct.
50. With increasingly severe neuropathy the functional base of support: A. Increases due to loss of foot intrinsic muscle strength and
“flattening” of the foot.B. Increases due to a compensatory increase in vestibular and
visual function.C. Decreases due to a decrease in rapidly availably strength at the
ankle.D. Decreases due to a decrement in arteriolar control in the distal
lower extremities.
51. Gait analysis on an irregular surface has been found to have improved resolution (likely because it involves repeated perturba-tions), as compared to gait analysis on a smooth surface, for the identification of: 1Patients with versus without neuropathy. 2. Older persons with neuropathy who fall versus those who
do not. 3. Older persons versus younger persons. 4. Neuropathy severity.A. Only 1, 2, and 3 are correct.B. Only 1 and 3 are correct.C. Only 2 and 4 are correct.D. All are correct.
52. With increasingly severe neuropathy: 1. Ankle proprioceptive thresholds increase (are less precise). 2. Ankle rate of strength generation increases. 3. Unipedal balance time decreases. 4. Gait variability decreases.A. Only 1, 2 and 3 are correct.B. Only 1 and 3 are correct.C. Only 2 and 4 are correct.D. All are correct.
53. Which one of the following is important when advising the families of patients with functionally significant neuropathy? A. Patients should be discouraged from touching stable
objects with their hands or fingertips as they may become “dependent” on such.
B. Patients should use their bifocals/transitional lenses so they can perceive their feet with greater clarity.
C. Families should keep talking with the patient while walking so that the “natural” gait rhythm is maintained.
D. Strengthening of the hip abductor/adductor muscle groups and weight loss may improve the patient’s stability.

coMMeNTS
Write out any additional comments about specific courses or the plenary session (please indicate which), and list suggestions for topics and speakers for future meetings. Leave at the AANEM Registration and Information Center or mail to the AANEM Executive Office at 2621 Superior Drive NW, Rochester, MN 55901.
AANEM Plenary 61

American Association of Neuromuscular & Electrodiagnostic Medicine
Advancing neuromuscular, musculoskeletal, & electrodiagnostic medicine
�����
ONLINEPodcasts
TeleconferencesCase Studies
Coding and BillingInvited Reviews
Practice Guidelines
PRINTCourse Handouts
Workshop Handouts
CD-ROMs
Case Reports
Videotapes
Brochures
Monographs
TPSAEs
OtherAANEM Learning
Opportunities
Copyright © 2022 FDOKUMEN