Cardiac Resynchronization Therapy: Long-Term Alternative to Cardiac Transplantation?
Upload
univ-bpclermontCategory
view
0download
0
Effects of chronic administration of clenbuterol on function and metabolismof adult rat cardiac muscle
Gopal K. R. Soppa,1 Ryszard T. Smolenski,1 Najma Latif,1 Ada H. Y. Yuen,1 Aalya Malik,1
Joanna Karbowska,2 Zdzislaw Kochan,2 Cesare M. N. Terracciano,1 and Magdi H. Yacoub1
1Imperial College London, National Heart and Lung Institute, Harefield Heart Science Centre,Harefield, Middlesex, United Kingdom; and 2Department of Biochemistry, Medical University of Gdansk, Gdansk, Poland
Submitted 23 June 2004; accepted in final form 31 October 2004
Soppa, Gopal K. R., Ryszard. T. Smolenski, Najma Latif, AdaH. Y. Yuen, Aalya Malik, Joanna Karbowska, Zdzislaw Kochan,Cesare M. N. Terracciano, and Magdi H. Yacoub. Effects ofchronic administration of clenbuterol on function and metabolism ofadult rat cardiac muscle. Am J Physiol Heart Circ Physiol 288:H1468–H1476, 2005. First published November 4, 2004; doi:10.1152/ajpheart.00624.2004.—Clenbuterol (Clen), a �2-agonist, isknown to produce skeletal and myocardial hypertrophy. This com-pound has recently been used in combination with left ventricularassist devices for the treatment of end-stage heart failure to reverse orprevent the adverse effects of unloading-induced myocardial atrophy.However, the mechanisms of action of Clen on myocardial cells havenot been fully elucidated. In an attempt to clarify this issue, weexamined the effects of chronic administration of Clen on Ca2�
handling and substrate preference in cardiac muscle. Rats were treatedwith either 2 mg �kg�1 �day�1 Clen or saline (Sal) for 4 wk with theuse of osmotic minipumps. Ventricular myocytes were enzymaticallydissociated. Cells were field stimulated at 0.5, 1, and 2 Hz, andcytoplasmic Ca2� transients were monitored with the use of thefluorescent indicator indo-1 acetoxymethyl ester. Two-dimensionalsurface area and action potentials in current clamp were also mea-sured. We found that in the Clen group there was significant hyper-trophy at the organ and cellular levels compared with Sal. In Clenmyocytes, the amplitude of the indo-1 ratio transients was signifi-cantly increased. Sarcoplasmic reticulum Ca2� content, estimated byrapid application of 20 mM caffeine, was significantly increased in theClen group. The action potential was prolonged in the Clen groupcompared with Sal. Carbohydrate contribution to the tricarboxyliccycle (Krebs cycle) flux was increased several times in the Clengroup. This increase was associated with decreased expression ofperoxisome proliferator-activated receptor-�. This study shows thatchronic administration of Clen induces cellular hypertrophy andincreases oxidative carbohydrate utilization together with an increasein sarcoplasmic reticulum Ca2� content, which results in increasedamplitude of the Ca2� transients. These effects could be importantwhen Clen is used in conjunction with left ventricular assist devicestreatment.
sarcoplasmic reticulum Ca2� content; tricarboxylic cycle; left ven-tricular assist devices
LONG-TERM LEFT VENTRICULAR (LV) assist device (LVAD) sup-port has been shown to improve survival and quality of life inpatients with advanced heart failure and contraindications tocardiac transplantation (22). LVAD support is also routinelyused as a bridge to transplantation in patients with end-stageheart failure. In a number of patients, with the use of this
strategy in association with pharmacological therapy (combi-nation therapy), a significant improvement in myocardial per-formance has been observed. In some cases the mechanicaldevice could be explanted without resorting to heart transplan-tation (“bridge to recovery”) (11–13, 27, 40).
LVAD support results in profound and complex changes inthe structure and function of the myocardium, which include“reverse remodeling,” paving the way to recovery and explan-tation and others, such as “atrophy,” possibly counteractingrecovery (8–10, 17, 18, 21, 32, 33, 41). Strategies aimed tohelp improve myocardial function together with prevent orreverse adverse consequences of unloading could increase thefrequency and reliability of recovery.
The �2-agonist clenbuterol (Clen) has been used clinically toprevent and/or reverse the potentially harmful changes in themyocardium (40). We have recently studied the effects of thistreatment associated with LVAD and pharmacological therapyon cardiomyocyte properties in patients with severe heartfailure. Terracciano et al. (28) found that sarcoplasmic reticu-lum (SR) Ca2� content was increased and action potentialprolonged when clinical recovery was obtained with this strat-egy. However, the mechanisms of action of Clen alone at themolecular and cellular level have not been adequately investi-gated. In this study, we chronically treated male Lewis ratswith Clen and found that this treatment induces 1) developmentof organ and cellular hypertrophy, 2) increased Ca2� transientsand SR Ca2� content without changes in the rate of Ca2�
decline in isolated ventricular myocytes, and 3) increasedoxidative carbohydrate utilization in the heart. These resultssuggest that Clen may have beneficial effects on Ca2� regula-tion and energy substrate preference while inducing mildhypertrophy with preserved ventricular function. This could bebeneficial in counteracting possible disuse atrophy in com-pletely unloaded hearts.
METHODS
Insertion of Osmotic Minipumps
Male Lewis rats (Charles River) 210–310 g (260.4 � 7.57 g) weretreated with eith Clen (2 mg/kg body wt, Sigma) or with vehicle only[0.9% saline (Sal), 154 mM Na�, and 154 mM Cl�] using continuousinfusion by osmotic minipumps (model-2ML4, Alzet). All animalswere anesthetized with an intraperitoneal injection of fentanyl �fluanisone (Hypnorm) and midazolam (Hypnovel). Under asepticconditions, the scruff of the neck was shaved and skin incised. Theskin was then dissected from the muscle layer by blunt dissection to
Address for reprint requests and other correspondence: C. M. N. Terracciano,Imperial College London, National Heart and Lung Institute, Harefield HeartScience Centre, Laboratory of Cellular Electrophysiology, Harefield Hospital,Harefield, Middlesex UB9 6JH, UK (E-mail: [email protected]).
The costs of publication of this article were defrayed in part by the paymentof page charges. The article must therefore be hereby marked “advertisement”in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Am J Physiol Heart Circ Physiol 288: H1468–H1476, 2005.First published November 4, 2004; doi:10.1152/ajpheart.00624.2004.
0363-6135/05 $8.00 Copyright © 2005 the American Physiological Society http://www.ajpheart.orgH1468

create a subcutaneous pocket into which the osmotic minipump wasplaced. The skin was closed with interrupted sutures and a single doseof antibiotic (amoxycillin) given. All the animals were monitoreddaily and weighed weekly. At the end of 4 wk, Clen levels in theblood were measured using liquid chromatography-tandem massspectrometry followed by blood extraction using a methanol-zincsulfate procedure. The sample was separated on a 2 mm � 15 cmchromatographic column packed with 3 �m BDS Hypersil. The massdetector was operated in a selective reaction-monitoring mode. Thisnew procedure has been validated for linearity, specificity, and recov-ery with satisfactory results. Using this procedure in blood samplescollected at the end of the experiments, we found that the Clen levelwas maintained between 0.1 and 0.2 �M. All animal procedures werein compliance with the Home Office UK regulations.
Assessment of Hypertrophy and LV Function
After 4 wk of treatment, the animals were anesthetized and under-went transthoracic echocardiography (Sequoia 512, Siemens and 15MHz probe) for assessment of hypertrophy and cardiac function.M-mode images were acquired and used for calculation of chamberdimensions and LV function using calculation procedures provided bythe manufacturer. The chest was then opened, and the heart wasexcised and weighed after being blotted on paper. Left tibial lengthwas measured with the use of a caliper. The heart weight-to-bodyweight ratio and the heart weight-to-tibial length ratio were calculated.
Cardiomyocyte Studies
Cell isolation. Cells were isolated using a method described indetail elsewhere (30). Briefly, LV myocytes were enzymaticallydissociated using hyaluronidase (0.5 mg/ml, Sigma) and collagenase(0.75 mg/ml, Worthington). The cells were filtered, centrifuged,resuspended, and then stored in enzyme solution (in mM: 120 NaCl,5.4 KCl, 5 MgSO4, 5 sodium pyruvate, 20 glucose, 20 taurine, 10HEPES, and 200 �l of 1 mM CaCl2; pH 6.96) at room temperature.After isolation, 75–90% myocytes were rod shaped and Ca2� tolerant.
Cell size measurements. Cells were selected as randomly as pos-sible, and digital images were recorded using a video camera. Theimages were analyzed offline to assess cell dimensions (cell area,width, and length) using Image J software (NIH).
Functional measurements. Cells were placed on a superfusingchamber (volume, �60 �l) positioned on the stage of an inverted
microscope (Nikon TE200). A thin coating of laminin (Sigma) wasapplied to the bottom of the chamber to improve cell adhesion. Cellswere superfused at 37°C with normal Tyrode solution (in mM: 140NaCl, 6 KCl, 1 MgCl2, 2 CaCl2, 10 glucose, and 10 HEPES, pH to 7.4with 2 M NaOH) at a rate of 1–2 ml/min. Stimulation of the cells wasachieved with either field stimulation using a pair of platinum wires orvia the microelectrode.
Action potential measurements. The electrophysiological experi-ments were performed with the use of an Axoclamp-2B system (AxonInstruments). To avoid dialysis of the cells and to minimize the effectsof changing the intracellular environment, high-resistance (15–30M) microelectrodes were used. The microelectrode filling solutioncontained 2 M KCl, 0.1 mM EGTA, and 5 mM HEPES (pH 7.2).Action potentials were elicited by a 1.2-nA current pulse (5 msduration) at 1 Hz and measured in current clamp mode.
Monitoring of cytoplasmic [Ca2�]. Cytoplasmic [Ca2�] was de-termined using the Ca2�-sensitive, single-excitation, dual-emissionfluorescent dye indo-1. Cells were loaded with 10 �M of the AM formof the indicator (indo-1 AM, Molecular Probes) for 20 min at roomtemperature. The supernatant was then discarded and replaced byfresh ES solution. Cells were stored in the dark at room temperatureand used within 6–7 h. Myocytes were field stimulated at differentfrequencies. For the assessment of SR Ca2� content, cells were fieldstimulated to a steady-state contraction, stimulation was stopped, and20 mM caffeine in Na�-free/Ca2�-free solution (in mM: 140 LiCl, 6KOH, 1 MgCl, 10 glucose, 10 HEPES, 0.1 EGTA; pH to 7.4 with 1M LiOH) was rapidly applied for 5 s as previously described (29).
Metabolic Studies
Analysis of the rate of cardiac carbohydrate utilization was per-formed as previously described (19) except that rats were keptanesthetized during the experiment and that tandem mass spectrom-etry was applied for identification of 13C enrichments. [1-13C]glucosewas infused as a 20% solution at the rate of 2 mg �kg�1 �min�1 for 180min. After 3 h of glucose infusion, rats were connected to a ventilationsystem, the chest was opened, and the hearts were freeze clamped insitu. Perchloric acid extracts were prepared as previously described(25), and the extracts were analyzed by liquid chromatography massspectrometry. Separation procedure followed ion-pairing method fornonderivatized amino acids described previously (Petritis, 2002 1168/id) using a LCQ Deca XP ion-trap tandem mass detector linked to thesurveyor chromatography system. Mass detection was carried out infragmentation mode (Tandem MS), and 13C isotopic enrichment offragments containing C3 of alanine or C4 of glutamate was monitored.Carbohydrate contribution to the tricarboxylic cycle (Krebs cycle)was calculated from the ratio of glutamate to alanine after correctionfor natural abundance of 13C. This is a simplified approach that doesnot take into account the anaplerotic entry into the Krebs cycle orsecondary labeling of the other cardiac substrates, such as lactate, thatcould reach as much as 50% of glucose enrichment (37). Our resultstherefore represent carbohydrate contribution rather than glucosecontribution to the Krebs cycle flux. During infusion of [1-13C]glu-cose, blood samples were collected for measurement of free fatty acid,
Table 1. Echocardiographic measurements
Sal (n 8) Clen (n 9) P Value
LVAWd, �m 0.19�0.009 0.22�0.011 �0.05LVAWs, �m 0.31�0.02 0.37�0.02 NSLVPWd, �m 0.19�0.01 0.22�0.01 �0.05LVPWs, �m 0.32�0.01 0.34�0.01 NSLVEDD, �m 0.76�0.03 0.76�0.02 NSLVESD, �m 0.35�0.04 0.31�0.03 NSLVAW% thickening 69.5�8.8 68.04�5.07 NSLVPW% thickening 70.04�10.1 54.98�8.95 NS%FS 54.73�4.12 59.63�2.48 NSLVAW/LVPW 0.995�0.077 1�0.08 NSLV mass, �g 1.44�0.04 1.69�0.05 �0.01LVEF (M-mode), % 87.73�2.62 91.69�1.4 NS
Values are means � SE; n, number of rats. Sal, saline; Clen, clenbuterol;LVAWd, left ventricular (LV) anterior wall thickness in diastole; LVAWs, LVanterior wall thickness in systole; LVPWd, LV posterior wall thickness indiastole; LVPWs, LV posterior wall thickness in systole; LVEDD, LV end-diastolic diameter; LVESD, LV end-systolic diameter; LVAW% thickening,LV anterior wall percent thickening; LVPW% thickening, LV posterior wallpercent thickening; %FS, percent fractional shortening; LVAW/LVPW, ratioof LV anterior and posterior wall thickness; LVEF, LV ejection fraction; NS,not significant.
Table 2. Morphometric measurements
Sal (n 8) Clen (n 10) P Value
Heart weight, g 1.13�0.04 1.37�0.04 �0.001Body weight, g 367�4 427�4 �0.001Tibial length, mm 45�0.18 45�0.1 NSHeart weight/body weight
(g/g � 1,000) 3.1�0.1 3.2�0.08 NSHeart weight/tibial length,
g/mm 0.025�0.0008 0.03�0.0008 �0.001
Values are means � SE; n, number of rats.
H1469CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

glucose, and lactate concentrations at hourly intervals. Analysis hasbeen performed with enzymatic methods using diagnostic kits fromWako Chemicals according to manufacturer recommendations.
RNA Analysis
Peroxisome proliferator-activated receptor-� (PPAR-�) and mus-cle carnitine palmitoyl transferase-1 (MCPT-1) mRNA expressionwere quantified by real-time RT-PCR using the iCycler iQ Real Time
Detection System (Bio-Rad). Total RNA was extracted from thefrozen tissue specimens using the Qiagen RNeasy minicolumn pro-cedure according to the manufacturer’s instructions (Hilden, Ger-many). RNA quality and quantity was assessed by agarose gelelectrophoresis and by relative absorbance at 260 versus 280 nm.Primers were designed with sequence analysis software package(Informagen) from gene sequences obtained from Ensembl GenomeBrowser (www.ensembl.org). A BLAST (2) search for each primer
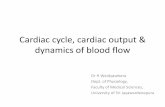
Fig. 1. Morphometric assessment of isolated cardiac myocytes from the left ventricle showed increased cell area and cell width in the clenbuterol (Clen)-treatedgroup compared with control. Top: examples of Clen-treated myocytes; middle: control myocytes; bottom: despite variability in cell dimension in both groups,in the Clen-treated myocytes larger dimensions were more frequent than in the control group, suggesting cellular hypertrophy. No difference was found in celllength between the groups. *P � 0.05 vs. saline; NS, not significant.
Fig. 2. Left: action potentials recorded fromcardiac myocytes isolated from Clen-treatedand control animals (saline). Cells werestimulated at 1 Hz using a pulse of 1.2 nAcurrent (5 ms). Action potentials were re-corded using high-resistance microelec-trodes in current clamp. Right: action poten-tial duration was increased in myocytes fromthe Clen-treated group.
H1470 CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

confirmed homologous binding to the desired mRNA. cDNA wassynthesized from 150 ng of total RNA with the use of AMV reversetranscriptase (Roche Molecular Biochemicals, Mannheim, Germany).Reactions were diluted to 100 �l. Two microliters of each RT reactionwere amplified in a 25-�l PCR mix containing 0.3 �M of each primerand QuantiTect SYBR Green PCR Master Mix. Samples were incu-bated for an initial denaturation and polymerase activation at 95°C for15 min, followed by 40 PCR cycles each consisting of 95°C for 30 s,55°C for 30 s, and 72°C for 90 s. The following oligonucleotideprimer pairs were used: PPAR-�, 5�-CAT CGA GTG TCG AAT ATGTGG-3� (sense) and 5�-GCA GTA CTG GCA TTT GTT CC-3�(antisense); MCPT-1, 5�-CAT GGT GAA CAG CAA CTA TTACG-3� (sense) and 5�-CAT CTG GTA GGA GCA CAT GG-3�(antisense); and 36B4, 5�-GCG ACC TGG AAG TCC AAC TAC-3�(sense) and 5�-TCT GCT GCA TCT GCT TGG-3� (antisense). SYBRgreen I fluorescence emission data were captured, and mRNA levelswere quantified using the critical threshold value. Analysis wasperformed with iCycler software. Controls without RT and with notemplate cDNA were performed with each assay, and all samples wererun in triplicate. To compensate for variations in input RNA amounts
and efficiency of RT, ribosomal protein 36B4 mRNA was quantified,and results were normalized to these values. Relative gene expressionlevels were obtained as previously described (36). Amplification ofspecific transcripts was further confirmed by obtaining melting curveprofiles and subjecting the amplification products to agarose gelelectrophoresis.
Western Blotting
Tissue samples were immediately frozen in liquid nitrogen andstored at �80°C. Samples were then homogenized in buffer contain-ing 10 mM Tris �HCl (pH 8.0), 0.3% Triton X-100, 1 mM EDTA, andprotease inhibitor mixture (Roche). Protein concentrations were as-sessed by using a Bradford assay, and 40 �g of total protein wereloaded per lane. Proteins were separated by 10% SDS-PAGE for mostproteins. The proteins were then blotted onto a nitrocellulose mem-brane (Hybond C-Super, Amersham). Membranes were blocked in3% (wt/vol) nonfat, dried milk in phosphate-buffered saline contain-ing 0.05% Tween 20 for 1 h. Blots were then incubated separately inprimary antibodies [1:500 sarco(endo)plasmic reticulum Ca2�-
Fig. 3. Top: Ca2� transient recorded using indo-1 fluorescence at 0.5, 1, and 2 Hz. Cells were field stimulated using a pair of platinum electrodes. In theClen-treated group, the amplitude of Ca2� transients was increased at all frequencies without changes in decline of fluorescence. Bottom: indo-1 ratio-frequencyrelationship was also unchanged. *P � 0.05 vs. saline; **P � 0.01 vs. saline; ***P � 0.001 vs. saline.
H1471CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

ATPase (SERCA2a), 1:20,000 phospholamban, 1:100 calsequestrin(Affinity Bioreagents), 1:500 Na�/Ca2� exchanger (Swant, Switzer-land), and 1:50 Ca channel V1.2 (�1C) (BD Biosciences)] against theabove proteins followed by exposure to horseradish peroxidase-conjugated, species-specific, secondary antibody (1:1,000; 1:5,000 forthe CaV-�1c subunit). Positivity was detected using enhanced chemi-luminescence (Amersham), and densitometry was performed usingGENE tools (Syngene) software. The level of expression of eachprotein was standardized to tubulin reactivity on the same blot.
Data Acquisition and Statistical Analysis
The data obtained from the epifluorescence apparatus and theAxoclamp-2B system were recorded on a computer using pCLAMP 8(Axon Instruments). The rate of sampling was between 0.5 and 3 kHz.Time to peak was measured between the point before the initialincrease of the trace and the peak of the signal. Time to 50% decay(T50) was measured between the peak of the signal and the point onthe declining phase corresponding to half of the total size of the Ca2�
transient. To assess statistical differences between means, the Stu-dent’s t-test was used. P � 0.05 was considered significant. Unlessotherwise specified, the results are expressed as means � SE. Incellular studies, n is the number of cells. Each set of experiments wasperform in cells isolated from a minimum of five different animals.
RESULTS
Clen Induces Hypertrophy Without Altering LV Function
Echocardiography was performed in Clen- and Sal-treatedanimals. Clen induced a significant increase in diastolic ante-rior and posterior wall thickness and LV mass compared withcontrol. However, the ejection fraction and fractional shorten-ing were unchanged, indicating preserved LV function. Theresults obtained are summarized in Table 1.
For a direct assessment of cardiac mass, we weighed theexcised hearts and normalized the values to body weight ortibial length because Clen affects skeletal muscle mass (23,34). Rats treated with Clen gained more body weight at the endof 4 wk compared with control (Sal) rats (weight change
between week 0 and week 4: Clen, 111 � 10.49 g; n 10; Sal,89.38 � 10.16 g; n 8; P � 0.0001). Total heart weight (Clen,1.37 � 0.123 g; n 10; Sal, 1.13 � 0.115 g; n 8; P �0.001) and heart weight-to-tibial length ratio (Clen, 0.031 �0.003 g/mm; n 10; Sal, 0.025 � 0.003 g/mm; n 8; P �0.001) were increased confirming cardiac hypertrophy (Table1). There was no change in the tibial length (Clen, 45.01 �0.325 mm; n 10; Sal, 45.08 � 0.512 mm; n 8; P notsignificant) between the two groups (Table 2).
LV myocytes from Clen-treated animals showed an increasein cell width (Clen, 39.972 � 1.098 �m; n 45; Sal, 37.23 �0.806 �m; n 40; P � 0.05) and surface area (Clen,3930.08 � 107.16 �m2; n 45; Sal, 3,607.78 � 108.72 �m2;n 40; P � 0.05) without any change in cell length (Clen,132.28 � 1.9 �m; n 45; Sal, 128.81 � 2.46 �m; n 40;P not significant) (Fig. 1).
Clen Affects Excitation-Contraction Coupling
Functional studies performed on isolated myocytes fromClen-treated animals showed differences in action potentialmorphology and Ca2� regulation compared with control. Ac-tion potential duration was increased in the Clen myocytescompared with control (time to 90% repolarization, Clen:204 � 30 ms, n 11 Sal: 117 � 14 ms, n 7; P � 0.05) (Fig.2). Figure 3, top, shows that in Clen myocytes the amplitude ofthe indo-1 ratio transients was significantly increased com-pared with control at all frequencies (0.5 Hz: Clen, 1.18 �0.08, n 38; Sal, 0.8 � 0.04, n 36; P � 0.05; 1 Hz: Clen,1.14 � 0.08, n 38; Sal, 0.8 � 0.06, n 36; P � 0.05; 2 Hz:Clen, 0.9 � 0.07, n 38; Sal, 0.6 � 0.02, n 36; P � 0.01).However, indo-1 fluorescence decay (T50) was not statisticallydifferent. The indo-1 fluorescence-frequency relationship, nor-mally negative at these frequencies in rat myocardium, re-mained negative after the administration of Clen (Fig. 3).Finally, the SR Ca2� content assessed by rapid application of
Fig. 4. Sarcoplasmic reticulum (SR) Ca2�
content was monitored by changes in indo-1fluorescence induced by rapid applicationof 20 mM caffeine. Caffeine applicationwas preceded by a train of stimulation at 1Hz followed by 1-s rest. Caffeine wasapplied in Na�-free/Ca2� free solution tominimize Ca2� extrusion via the Na�/Ca2� exchanger. In the Clen-treated group,caffeine elicited a larger indo-1 transientsuggesting a larger SR Ca2� content com-pared with control. **P � 0.01 vs. saline.
H1472 CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

20 mM caffeine was significantly increased in Clen myocytescompared with control (indo-1 ratio Clen: 2.87 � 0.2, n 23;Sal: 1.88 � 0.2, n 20; P � 0.05) (Fig. 4).
Western blotting analysis showed that there was a signif-icant increase in SERCA2a (Clen: 0.11 � 0.02 OD units,n 10; Sal: 0.04 � 0.007 OD units; n 8; P � 0.02), inphospholamban (Clen: 2.14 � 0.18 OD units, n 10; Sal:0.6 � 0.1 OD units; n 8; P � 0.0001), and in Na�/Ca2�
exchanger (Clen: 0.68 � 0.11 OD units, n 10; Sal: 0.2 �0.03 OD units, n 8; P � 0.002) protein levels in the Clengroup compared with control. There was no change in theexpression of calsequestrin or the cardiac �-subunit of theCa2� channels (Fig. 5).
Clen Increases Carbohydrate Oxidation in Hearts
Analysis of the heart extracts for [13C]glutamate and[13C]alanine isotopomers after [1-13C]glucose infusion in-dicated that carbohydrate contribution to the Krebs cycleincreased in Clen-treated hearts compared with control.According to isotopomer ratio calculations for alanine andglutamate in heart extracts, carbohydrate contribution toKrebs cycle was 17.7 � 7.5% in control hearts, whereas inClen-treated hearts, it increased to 55.9 � 10.6% (Fig. 6).There were no differences in the levels of free fatty acid,lactate, and glucose between control and Clen groups at anytime point during the infusion of [1-13C]glucose. At the end
Fig. 5. Top: immunoblots for Ca2� handling proteins. Bottom: there was a 277% increase in sarco(endo)plasmic reticulum Ca2�-ATPase (SERCA2a), 357% inphospholamban, and 342% in Na�/Ca2� exchanger, protein levels in the Clen group compared with control. There was no change in the expression ofcalsequestrin. *P � 0.05 vs. saline; **P � 0.01 vs. saline; ***P � 0.001 vs. saline.
H1473CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

of the 3-h infusion, free fatty acid concentrations were498.8 � 73.4 and 509.4 � 103.8 �mol/l, glucose concen-trations were 6.15 � 0.48 and 6.89 � 0.97 mmol/l, andlactate concentrations were 535 � 86 and 521 � 93 �mol/lin Clen and control groups, respectively. To study potentialmechanism of metabolic switch in Clen-treated hearts, ex-pression of mRNA for PPAR-� and MCPT-1 was evaluated.PPAR-� mRNA expression decreased to about 60% of thecontrol value in the Clen group (Fig. 7A). Consistently withthis finding, expression of MCPT-1 decreased to 70% of thecontrol value in Clen group (Fig. 7B).
DISCUSSION
This study has shown that chronic administration of Cleninduces changes in Ca2� regulation and energy metabolism ofrat hearts that accompany organ and cellular hypertrophy.
Cardiac hypertrophy in Clen-treated rats was observed byechocardiography and confirmed by the presence of increasedheart weight. Heart weight was normalized to tibial length andto body weight. The ratio of heart weight to tibial lengthsignificantly increased in Clen-treated animals. However, theratio of heart weight to body weight did not change after Clenadministration, presumably because of the increase in bodyweight due to skeletal muscle hypertrophy (3, 7, 16). It couldbe argued that after the increase in body mass, a proportionalincrease in cardiac output and blood flow is expected; themyocyte hypertrophy observed could therefore be the conse-quence of pressure-volume overload rather than a direct effectof Clen. However, studies in cultured cardiomyocytes haveshown that Clen can directly induce hypertrophy (4). It istherefore likely that cardiac hypertrophy in our study is alsogenerated by a direct mechanism of induction of hypertrophymediated by Clen.
This study was designed to investigate the effects of chronic,rather than acute, Clen administration, and a single time point(4 wk) was chosen. However, studies designed to investigatedthe onset, the time course, and the reversibility of these effectsneed to be performed.
Ca2� Regulation in Cardiomyocytes FromClen-Treated Animals
We found that Clen induces several changes in Ca2� regu-lation. We observed increased Ca2� transient amplitude, in-creased SR Ca2� content, maintained rate of Ca2� removal,maintained indo-1 fluorescence-frequency relationship, and in-creased expression of SERCA2a, phospholamban, and Na�/Ca2� exchanger.
The increased Ca2� transients support larger contractionsand can be explained by the increased SR Ca2� content. Themechanisms involved in the increased SR Ca2� content with-out increased diastolic [Ca2�] levels are unclear. IncreasedSERCA function associated with prolonged action potentials(31) may be responsible for this effect. Na�/Ca2� exchangerand phospholamban overexpression observed in Clen-treatedhearts can also be involved (24, 30, 42).
Increased Ca2� entry can be another reason for larger SRCa2� content. The L-type Ca2� current was not directly mea-sured. We did not observe changes in the expression of the�1c-subunit of the Ca2� channels. However, the Ca2� currentmay be increased on application of Clen because of a cAMP-
Fig. 6. Carbohydrate contribution to Krebs cycle in Clen-treated and controlhearts calculated according to glutamate-to-alanine 13C enrichements ratio inheart extracts following [1-13C]glucose infusion. Values are means � SE.*P � 0.05 vs. control.
Fig. 7. Expression of mRNA for peroxisome proliferator activated receptor-�(PPAR-�, A) and muscle carnitine palmitoyl transferase-1 (MCPT-1, B) incontrol hearts and following chronic treatment with Clen. Values are means �SE. *P � 0.05 vs. control.
H1474 CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

dependent activation of the channels, possibly via a stimulatoryG protein, as shown for other �2-adrenergic agonists (43).
Concomitant effects on the mechanisms involved in Ca2�
release from the SR may also be present but were not inves-tigated in this study. The maintained rate of Ca2� decline isconsistent with �2-adrenergic stimulation (39) and could beuseful to maintain diastolic function.
The increased contractility observed at a cellular level wasnot observed at organ level. This could be because an optimalcardiac performance, controlled by cardiac and extracardiacfactors, was already present in normal animals. Further studiesin diseased hearts (e.g., heart failure) are required to assesswhether cardiac function in vivo would be affected by Clenadministration.
In heart failure, Ca2� transients are reduced in size and havea slower decline, offering the basis for systolic and diastolicdysfunction (5). Restoring SR Ca2� content has been shown toreverse Ca2� dysregulation in heart failure (14). In this context,the findings from the present study suggest that the associationof Clen treatment with mechanical unloading in heart failurecould be beneficial.
It has been reported that administration of a single, largerdose of Clen (5 vs. 2 mg/kg used in this study) causes cardiacnecrosis in rats (6). We did not perform direct quantification ofcellular necrosis in our study, but we did not observe functionalimpairment of the heart nor was this observed in previousstudies where Clen was used chronically (38). This suggeststhat the extent of Clen-induced necrosis, if present in theconditions used in our study, is not relevant for cardiac func-tion.
Glucose Metabolism in Clen-Treated Hearts
In this study, we found changes in carbohydrate contributionto cardiac oxidative metabolism after chronic treatment withClen. Although our data could not provide exact details, suchas the relative contribution of glucose, pyruvate, and lactate,general finding of increased contribution of carbohydrates tocardiac energy metabolism is a solid and important observa-tion. This finding may represent a beneficial adaptive change toa different metabolic environment because both theoreticalconsideration and experimental data suggest that glucose orpyruvate are better substrates for cardiac cells under stress(26). The mechanism of this change could involve either directeffect of Clen on the regulation of enzymes or expression ofgenes related to substrate preference, e.g., increased expressionof glucose transporters and decrease of enzymes of fatty acidtransport and metabolism. PPAR-� is considered to be a majortranscriptional regulator of cardiac substrate preference (35).We provide evidence here that a possible mechanism involvesdownregulation of PPAR-� expression. In parallel to the de-creased PPAR-� mRNA level, we observed downregulation ofmuscle MCPT-1 mRNA–an enzyme that controls the rate ofcardiac fatty acid utilization and is transcriptionally regulatedby PPAR-�.
Relevance for Use of Clen in Patients With DilatedCardiomyopathy Undergoing LVAD Treatment
Although LVAD support could produce beneficial effects onthe myocardium (“reverse remodeling”), one potential problemis the consequent heart muscle atrophy (15, 20, 38, 40). This
could be an important impediment to the removal of the LVADwhen the reverse remodeling has been achieved, limiting theefficacy of the treatment. Pharmacological agents that preventatrophy or induce “physiological” hypertrophy, such as Clen,have been considered of value in this regard (40), but little isstill known about the effects of these drugs on cardiac function.This study shows that Clen induces cardiac hypertrophy with-out impaired cardiac function in vivo and with increased Catransient amplitude and carbohydrate utilization. These find-ings, together with the recent observation that �2-adrenergicagonists have beneficial effects in heart failure (1), support thehypothesis that Clen can be used in combination with LVADsto treat heart failure. However, the present study was carriedout in normal hearts, and further studies to test this hypothesisin the presence of both heart failure and mechanical unloadingneed to be performed. In addition, further studies to investigatethe time course of the observed effects are required.
In conclusion, chronic administration of Clen in rats inducescardiac hypertrophy without deterioration of function, in-creased Ca2� transient amplitude associated to increased SRCa2� content, expression of SERCA2a, phospholamban, andNa�/Ca2� exchanger, and increased carbohydrate over fattyacid utilization to provide energy. These findings suggest thatClen could have beneficial effects in preventing or reversingcardiac atrophy, but more studies, particularly using unloadedhearts with heart failure are required.
ACKNOWLEDGMENTS
We thank Dr. Jay Jayakumar for help in an early stage of this work.
GRANTS
We are grateful to the Wellcome Trust, the Magdi Yacoub Institute, and theBritish Heart Foundation for financial support.
REFERENCES
1. Ahmet I, Krawczyk M, Heller P, Moon C, Lakatta EG, and Talan MI.Beneficial effects of chronic pharmacological manipulation of �-adreno-receptor subtype signaling in rodent dilated ischemic cardiomyopathy.Circulation 110: 1083–1090, 2004.
2. Altschul SF, Gish W, Miller W, Meyers EW, and Lipman DJ. Basiclocal alignment search tool. J Mol Biol 215: 403–410, 1990.
3. Babij P and Booth FW. Clenbuterol prevents or inhibits loss of specificmRNAs in atrophying rat skeletal muscle. Am J Physiol Cell Physiol 254:C657–C660, 1988.
4. Barton PJ, Bhavsar PK, Felkin LE, Sugden PH, and Yacoub MH.Morphological and molecular effects of clenbuterol on cardiac myocytes-role of IGF-1. J Heart Lung Transplant 2: S53, 2004.
5. Beuckelmann DJ, Nabauer M, and Erdmann E. Intracellular calciumhandling in isolated ventricular myocytes from patients with terminal heartfailure. Circulation 85: 1046–1055, 1992.
6. Burniston JG, Ng Y, Clark WA, Colyer J, Tan LB, and Goldspink DF.Myotoxic effects of clenbuterol in the rat heart and soleus muscle. J ApplPhysiol 93: 1824–1832, 2002.
7. Claeys MC, Mulvaney DR, McCarthy FD, Gore MT, Marple DN, andSartin JL. Skeletal muscle protein synthesis and growth hormone secre-tion in young lambs treated with clenbuterol. J Anim Sci 67: 2245–2254,1989.
8. Depre C, Shipley GL, Chen W, Han Q, Doenst T, Moore ML,Stepkowski S, Davies PJ, and Taegtmeyer H. Unloaded heart in vivoreplicates fetal gene expression of cardiac hypertrophy. Nat Med 4:1269–1275, 1998.
9. Dipla K, Mattiello JA, Jeevanandam V, Houser SR, and MarguliesKB. Myocyte recovery after mechanical circulatory support in humanswith end-stage heart failure. Circulation 97: 2316–2322, 1998.
10. Doenst T, Goodwin GW, Cedars AM, Wang M, Stepkowski S, andTaegtmeyer H. Load-induced changes in vivo alter substrate fluxes and
H1475CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org

insulin responsiveness of rat heart in vitro. Metabolism 50: 1083–1090,2001.
11. Farrar DJ, Holman WR, McBride LR, Kormos RL, Icenogle TB,Hendry PJ, Moore CH, Loisance DY, El Banayosy A, and Frazier H.Long-term follow-up of thoratec ventricular assist device bridge-to-recov-ery patients successfully removed from support after recovery of ventric-ular function. J Heart Lung Transplant 21: 516–521, 2002.
12. Frazier OH and Myers TJ. Left ventricular assist system as a bridge tomyocardial recovery. Ann Thorac Surg 68: 734–741, 1999.
13. Hetzer R, Muller J, Weng Y, Wallukat G, Spiegelsberger S, andLoebe M. Cardiac recovery in dilated cardiomyopathy by unloading witha left ventricular assist device. Ann Thorac Surg 68: 742–749, 1999.
14. Hobai IA and O’Rourke B. Decreased sarcoplasmic reticulum calciumcontent is responsible for defective excitation-contraction coupling incanine heart failure. Circulation 103: 1577–1584, 2001.
15. Hon JK, Steendijk P, Petrou M, Wong K, and Yacoub MH. Influenceof clenbuterol treatment during six weeks of chronic right ventricularpressure overload as studied with pressure-volume analysis. J ThoracCardiovasc Surg 122: 767–774, 2001.
16. Maltin CA, Delday MI, Hay SM, Smith FG, Lobley GE, and Reeds PJ.The effect of the anabolic agent, clenbuterol, on overloaded rat skeletalmuscle. Biosci Rep 7: 143–149, 1987.
17. Mann DL and Taegtmeyer H. Dynamic regulation of the extracellularmatrix after mechanical unloading of the failing human heart: recoveringthe missing link in left ventricular remodeling. Circulation 104: 1089–1091, 2001.
18. Margulies KB. Reversal mechanisms of left ventricular remodeling:Lessons from left ventricular assist device experiments. J Card Fail 8:S500–S505, 2002.
19. McNulty PH, Cline GW, Whiting JM, and Shulman GI. Regulation ofmyocardial [13C]glucose metabolism in conscious rats. Am J PhysiolHeart Circ Physiol 279: H375–H381, 2000.
20. Petrou M, Clarke S, Morrison K, Bowles C, Dunn M, and Yacoub M.Clenbuterol increases stroke power and contractile speed of skeletalmuscle for cardiac assist. Circulation 99: 713–720, 1999.
21. Razeghi P, Myers TJ, Frazier OH, and Taegtmeyer H. Reverseremodeling of the failing human heart with mechanical unloading. Car-diology 98: 167–174, 2002.
22. Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW,Dembitsky W, Long JW, Ascheim DD, Tierney AR, Levitan RG,Watson JT, Meier P, Ronan NS, Shapiro PA, Lazar RM, Miller LW,Gupta L, Frazier OH, Desvigne-Nickens P, Oz MC, and Poirier VL.Long-term mechanical left ventricular assistance for end-stage heart fail-ure. N Engl J Med 345: 1435–1443, 2001.
23. Rothwell NJ and Stock MJ. Increased body-weight gain and bodyprotein in castrated and adrenalectomized rats treated with clenbuterol.Br J Nutr 60: 355–360, 1988.
24. Sipido KR, Volders PG, Vos MA, and Verdonck F. Altered Na/Caexchange activity in cardiac hypertrophy and heart failure: a new target fortherapy? Cardiovasc Res 53: 782–805, 2002.
25. Smolenski RT, Lachno DR, Ledingham SJ, and Yacoub MH. Deter-mination of sixteen nucleotides, nucleosides and bases using high-perfor-mance liquid chromatography and its application to the study of purinemetabolism in hearts for transplantation. J Chromatogr A 527: 414–420,1990.
26. Stanley WC and Chandler MP. Energy metabolism in the normal andfailing heart: potential for therapeutic interventions. Heart Fail Rev 7:115–130, 2002.
27. Sun BC, Catanese KA, Spanier TB, Flannery MR, Gardocki MT,Marcus LS, Levin HR, Rose EA, and Oz MC. 100 long-term implant-able left ventricular assist devices: the Columbia Presbyterian interimexperience. Ann Thorac Surg 68: 688–694, 1999.
28. Terracciano CM, Hardy J, Birks EJ, Khaghani A, Banner NR, andYacoub MH. Clinical recovery from end-stage heart failure using left-ventricular assist device and pharmacological therapy correlates withincreased sarcoplasmic reticulum calcium content but not with regressionof cellular hypertrophy. Circulation 109: 2263–2265, 2004.
29. Terracciano CM, Philipson KD, and MacLeod KT. Overexpression ofthe Na(�)/Ca(2�) exchanger and inhibition of the sarcoplasmic reticulumCa(2�)-ATPase in ventricular myocytes from transgenic mice. Cardio-vasc Res 49: 38–47, 2001.
30. Terracciano CMN, De Souza A, Philipson KD, and MacLeod KT.Na�/Ca2� exchange and sarcoplasmic reticular Ca2� regulation in ven-tricular myocytes from transgenic mice overexpressing the Na�/Ca2�
exchanger. J Physiol 512–513: 651–667, 1998.31. Terracciano CMN, Tweedie D, and MacLeod KT. The effects of
changes to action potential duration on the calcium content of the sarco-plasmic reticulum in isolated guinea-pig ventricular myocytes. PflugersArch 443: 542–544, 1997.
32. Torre-Amione G, Stetson SJ, Youker KA, Durand JB, RadovancevicB, Delgado RM, Frazier OH, Entman ML, and Noon GP. Decreasedexpression of tumor necrosis factor-alpha in failing human myocardiumafter mechanical circulatory support: a potential mechanism for cardiacrecovery. Circulation 100: 1189–1193, 1999.
33. Uray IP, Connelly JH, Frazier O, Taegtmeyer H, and Davies PJ.Altered expression of tyrosine kinase receptors Her2/neu and GP130following left ventricular assist device (LVAD) placement in patients withheart failure. J Heart Lung Transplant 20: 210, 2001.
34. Von Deutsch DA, Abukhalaf IK, Wineski LE, Aboul-Enein HY, PittsSA, Parks BA, Oster RA, Paulsen DF, and Potter DE. Beta-agonist-induced alterations in organ weights and protein content: comparison ofracemic clenbuterol and its enantiomers. Chirality 12: 637–648, 2000.
35. Watanabe K, Fujii H, Takahashi T, Kodama M, Aizawa Y, Ohta Y,Ono T, Hasegawa G, Naito M, Nakajima T, Kamijo Y, Gonzalez FJ,and Aoyama T. Constitutive regulation of cardiac fatty acid metabolismthrough peroxisome proliferator-activated receptor alpha associated withage-dependent cardiac toxicity. J Biol Chem 275: 22293–22299, 2000.
36. Winer J, Jung CK, Shackel I, and Williams PM. Development andvalidation of real-time quantitative reverse transcriptase-polymerase chainreaction for monitoring gene expression in cardiac myocytes in vitro. AnalBiochem 270, 41–49, 1999.
37. Wisneski JA, Gertz EW, Neese RA, Gruenke LD, Morris DL, andCraig JC. Metabolic fate of extracted glucose in normal human myocar-dium. J Clin Invest 76: 1819–1827, 1985.
38. Wong K, Boheler KR, Bishop J, Petrou M, and Yacoub MH. Clen-buterol induces cardiac hypertrophy with normal functional, morpholog-ical and molecular features. Cardiovasc Res 37: 115–122, 1998.
39. Xiao RP and Lakatta EG. Beta 1-adrenoceptor stimulation and beta2-adrenoceptor stimulation differ in their effects on contraction, cytosolicCa2�, and Ca2� current in single rat ventricular cells. Circ Res 73:286–300, 1993.
40. Yacoub MH. A novel strategy to maximize the efficacy of left ventricularassist devices as a bridge to recovery. Eur Heart J 22: 534–540, 2001.
41. Zafeiridis A, Jeevanandam V, Houser SR, and Margulies KB. Regres-sion of cellular hypertrophy after left ventricular assist device support.Circulation 98: 656–662, 1998.
42. Zhang XQ, Song J, Rothblum LI, Lun M, Wang X, Ding F, Dunn J,Lytton J, McDermott PJ, and Cheung JY. Overexpression of Na�/Ca2�
exchanger alters contractility and SR Ca2� content in adult rat myocytes.Am J Physiol Heart Circ Physiol 281: H2079–H2088, 2001.
43. Zhang ZS, Cheng HJ, Ukai T, Tachibana H, and Cheng CP. Enhancedcardiac L-type calcium current response to beta2-adrenergic stimulation inheart failure. J Pharmacol Exp Ther 298: 188–196, 2001.
H1476 CLENBUTEROL ON FUNCTION AND METABOLISM OF CARDIAC MUSCLE
AJP-Heart Circ Physiol • VOL 288 • MARCH 2005 • www.ajpheart.org
Copyright © 2022 FDOKUMEN