
CLINICAL- END6CRINOLOGY & METABOLISM
53
THE JOURNAt OF CLINICAL- END6CRINOLOGY & METABOLISM %\ PUBLISHED MONTHLY BY * " THE ENDOCRINE SOCIETY In this issue: Neuroendocrine-metabolic dysregulation in polycystic ovary syndrome in the absence of the confound- ing influence of obesity may be viewed as the pathophysi- ology underlying the "authentic syndrome," and obesity constitutes a modifier of the syndrome. (See page 2854.) lume 81 umber 8 Downloaded from https://academic.oup.com/jcem/issue/81/8 by guest on 16 April 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of CLINICAL- END6CRINOLOGY & METABOLISM

THE JOURNAt OF
CLINICAL-END6CRINOLOGY& METABOLISM
%\ PUBLISHED MONTHLY BY* " THE ENDOCRINE SOCIETY
In this issue: Neuroendocrine-metabolic dysregulation inpolycystic ovary syndrome in the absence of the confound-ing influence of obesity may be viewed as the pathophysi-ology underlying the "authentic syndrome," and obesityconstitutes a modifier of the syndrome. (See page 2854.)
lume 81
umber 8
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Bri
ef S
um
mar
y (f
or f
ull
pre
scri
bin
g i
nfo
rmat
ion
see
pac
kag
e ci
rcul
ar.)
SYN
TH
RO
ID®
(Lev
oth
yro
xin
e S
od
ium
, U
SP
)S
YN
THR
OID
Tab
lets
- f
or o
ral a
dmin
istra
tion
SY
NTH
RO
ID In
ject
ion
- f
or p
aren
tera
l adm
inis
tratio
nC
ON
TR
AIN
DIC
AT
ION
S: S
YN
THR
OID
is c
ontra
indi
cate
d in
pat
ient
s w
ith u
ntre
ated
thyr
otox
icos
is o
f an
y et
iolo
gy o
r an
app
aren
t hy
pers
ensi
tivity
to
thyr
oid
horm
ones
or
any
of t
he in
activ
e pr
oduc
t con
stitu
ents
. (Th
e 50
meg
tabl
et is
form
ulat
ed w
ithou
t col
orad
ditiv
es fo
r pa
tient
s w
ho a
re se
nsiti
ve to
dye
s.) T
here
is n
o w
ell-d
ocum
ente
d ev
iden
ceof
true
alle
rgic
or
idio
sync
ratic
rea
ctio
ns to
thyr
oid
horm
one.
SY
NTH
RO
ID is
als
o co
n-tr
aind
icat
ed i
n pa
tient
s w
ith u
ncor
rect
ed a
dren
al i
nsuf
ficie
ncy,
as
thyr
oid
horm
ones
incr
ease
tiss
ue d
eman
ds fo
r ad
reno
corti
cal
horm
ones
and
may
ther
eby
prec
ipita
te a
cute
adre
nal c
risis
(see
PR
EC
AU
TIO
NS)
.W
AR
NIN
GS:
Thy
roid
hor
mon
es, e
ither
alo
ne o
r to
geth
er w
ith o
ther
the
rape
utic
agen
ts, s
houl
d no
t be
used
for
the
trea
tmen
t of
obe
sity
. In
euth
yroi
d pa
tient
s, d
oses
with
in th
e ra
nge
of d
aily
hor
mon
al re
quir
emen
ts a
re in
effe
ctiv
e fo
r wei
ght r
educ
tion.
Lar
ger d
oses
may
pro
duce
ser
ious
or e
ven
life-
thre
aten
ing
man
ifest
atio
ns o
f tox
icity
,pa
rticu
larly
whe
n gi
ven
in a
ssoc
iatio
n w
ith s
ympa
thom
imet
ic a
min
es s
uch
as th
ose
used
for
thei
r ano
rect
ic e
ffect
s.T
he u
se o
f SY
NTH
RO
ID in
the
trea
tmen
t of
obe
sity
, eith
er a
lone
or
in c
ombi
natio
nw
ith o
ther
dru
gs, i
s un
just
ified
. T
he u
se o
f SY
NTH
RO
ID is
als
o un
just
ified
in
the
trea
t-m
ent
of m
ale
or f
emal
e in
ferti
lity
unle
ss t
his
cond
ition
is
asso
ciat
ed w
ith h
ypot
hy-
roid
ism
.PR
ECA
UTI
ON
S: G
ener
al: S
YN
THR
OID
sho
uld
be u
sed
with
cau
tion
in p
atie
nts
with
card
iova
scul
ar d
isor
ders
, inc
ludi
ng a
ngin
a, c
oron
ary
arte
ry d
isea
se, a
nd h
yper
tens
ion,
and
in th
e el
derly
who
hav
e a
grea
ter
likel
ihoo
d of
occ
ult c
ardi
ac d
isea
se. C
onco
mita
ntad
min
istra
tion
of th
yroi
d ho
rmon
e an
d sy
mpa
thom
imet
ic a
gent
s to
pat
ient
s w
ith c
oro-
nary
art
ery
dise
ase
may
incr
ease
the
risk
of c
oron
ary
insu
ffici
ency
.U
se o
f SY
NT
HR
OID
in
pati
ents
wit
h co
ncom
itant
dia
bete
s m
ellit
us,
diab
etes
insi
pidu
s or
adr
enal
cor
tical
ins
uffic
ienc
y m
ay a
ggra
vate
the
int
ensi
ty o
f th
eir
sym
p-to
ms.
App
ropr
iate
adj
ustm
ents
of
the
vari
ous
ther
apeu
tic m
easu
res
dire
cted
at
thes
eco
ncom
itant
end
ocri
ne d
isea
ses
may
the
refo
re b
e re
quir
ed.
Tre
atm
ent
of m
yxed
ema
com
a m
ay r
equi
re s
imul
tane
ous
adm
inis
trat
ion
of g
luco
corti
coid
s (s
ee D
OSA
GE
AN
DA
DM
INIS
TR
AT
ION
).T 4
enh
ance
s th
e re
spon
se to
ant
icoa
gula
nt t
hera
py. P
roth
rom
bin
time
shou
ld b
e cl
ose-
ly m
onito
red
in p
atie
nts
taki
ng b
oth
SYN
THR
OID
and
ora
l an
ticoa
gula
nts,
and
the
dosa
ge o
f ant
icoa
gula
nt a
djus
ted
acco
rdin
gly.
Seiz
ures
hav
e be
en r
epor
ted
rare
ly in
ass
ocia
tion
with
the
initi
atio
n of
levo
thyr
oxin
eso
dium
ther
apy,
and
may
be
rela
ted
to th
e ef
fect
of
thyr
oid
horm
one
on s
eizu
re th
resh
-ol
d. Lith
ium
blo
cks
the
TSH
-med
iate
d re
leas
e of
T4
and
T 3. T
hyro
id f
unct
ion
shou
ld th
ere-
fore
be
care
fully
mon
itore
d du
ring
lith
ium
ini
tiatio
n, s
tabi
lizat
ion,
and
mai
nten
ance
. If
hypo
thyr
oidi
sm o
ccur
s du
ring
lith
ium
tre
atm
ent,
a hi
gher
tha
n us
ual
SYN
THR
OID
dose
may
be
requ
ired
.L
abor
ator
y T
ests
: Tre
atm
ent
of p
atie
nts
with
SY
NTH
RO
ID r
equi
res
perio
dic
asse
ss-
men
t of
thyr
oid
stat
us b
y ap
prop
riat
e la
bora
tory
test
s an
d cl
inic
al e
valu
atio
n. S
elec
tion
of a
ppro
pria
te te
sts
for
the
diag
nosi
s an
d m
anag
emen
t of
thyr
oid
diso
rder
s de
pend
s on
patie
nt v
aria
bles
suc
h as
pre
sent
ing
sign
s an
d sy
mpt
oms,
pre
gnan
cy, a
nd c
onco
mita
ntm
edic
atio
ns. A
com
bina
tion
of s
ensi
tive
TSH
ass
ay a
nd f
ree
T, e
stim
ate
(free
T4 i
ndex
,FT
4I) a
re re
com
men
ded
to c
onfir
m a
dia
gnos
is o
f th
yroi
d di
seas
e. T
SH a
lone
or i
nitia
llym
ay b
e us
eful
for
thy
roid
dis
ease
scr
eeni
ng a
nd f
or m
onito
ring
ther
apy
for
prim
ary
hypo
thyr
oidi
sm,
as a
line
ar i
nver
se c
orre
latio
n ex
ists
bet
wee
n se
rum
TSH
and
fre
e T 4
.M
easu
rem
ent
of to
tal
seru
m T
4 and
Tv
resi
n T 3
upt
ake,
and
fre
e T 3
con
cent
ratio
ns m
ayal
so b
e us
eful
. A
ntith
yroi
d m
icro
som
al a
ntib
odie
s ar
e an
indi
cato
r of
aut
oim
mun
e th
y-ro
id d
isea
se. T
he c
ombi
natio
n of
an
incr
ease
d TS
H a
nd p
ositi
ve m
icro
som
al a
ntib
odie
sin
an
euth
yroi
d pa
tient
is
a m
ajor
ris
k fa
ctor
for
the
fut
ure
deve
lopm
ent
of c
linic
alhy
poth
yroi
dism
. A
n el
evat
ed s
erum
TSH
in th
e pr
esen
ce o
f a
norm
al T
, may
indi
cate
subc
linic
al h
ypot
hyro
idis
m.
Intra
cellu
lar
resi
stan
ce t
o th
yroi
d ho
rmon
e is
qui
te r
are,
and
is s
ugge
sted
by
clin
ical
sig
ns a
nd s
ympt
oms
of h
ypot
hyro
idis
m i
n th
e pr
esen
ce o
fhi
gh s
erum
T4
leve
ls. A
dequ
acy
of S
YN
THR
OID
ther
apy
for
hypo
thyr
oidi
sm o
f pi
tu-
itary
or
hypo
thal
amic
orig
in s
houl
d be
ass
esse
d by
mea
suri
ng F
T 4I,
whi
ch s
houl
d be
mai
ntai
ned
in th
e up
per
half
of th
e no
rmal
ran
ge. M
easu
rem
ent o
f TSH
is n
ot a
relia
ble
indi
cato
r of
resp
onse
to th
erap
y fo
r th
is c
ondi
tion.
Dru
g In
tera
ctio
ns: T
he m
agni
tude
and
rel
ativ
e cl
inic
al im
port
ance
of
the
pote
ntia
l int
er-
actio
ns b
etw
een
SYN
THR
OID
and
oth
er d
rugs
are
like
ly to
be
patie
nt-s
peci
fic a
nd m
ayva
ry b
y su
ch f
acto
rs a
s ag
e, g
ende
r, r
ace,
int
ercu
rren
t ill
ness
es, d
ose
of e
ither
age
nt,
addi
tiona
l co
ncom
itant
med
icat
ions
, and
tim
ing
of d
rug
adm
inis
trat
ion.
Any
age
nt th
atal
ters
thyr
oid
horm
one
synt
hesi
s, s
ecre
tion,
dis
trib
utio
n, e
ffect
on
targ
et ti
ssue
s, m
etab
-ol
ism
, or e
limin
atio
n m
ay a
lter
the
optim
al t
hera
peut
ic d
ose
of S
YN
THR
OID
./W
rew
corfi
coirf
s-M
etab
olic
cle
aran
ce o
f ad
reno
cort
icoi
ds i
s de
crea
sed
in h
ypot
hyro
idpa
tient
s an
d in
crea
sed
in h
yper
thyr
oid
patie
nts,
and
may
the
refo
re c
hang
e w
ith c
hang
-in
g th
yroi
d st
atus
./4
m/o
t/aro
ne-A
mio
daro
ne t
hera
py a
lone
can
cau
se h
ypot
hyro
idis
m o
r hy
pert
hy-
roid
ism
.A
ntic
oagu
lant
s (o
ral)
-The
hyp
opro
thro
mbi
nem
ic e
ffec
t of
ant
icoa
gula
nts
may
be
pote
ntia
ted,
app
aren
tly b
y in
crea
sed
cata
bolis
m o
f vi
tam
in K
-dep
ende
nt c
lotti
ng f
ac-
tors
.A
ntid
iabe
tic
agen
ts (
insu
lin, s
u//b
ny/u
rajs
)-R
equi
rem
ents
for
ins
ulin
or
oral
ant
idia
betic
agen
ts m
ay b
e re
duce
d in
hyp
othy
roid
pat
ient
s w
ith d
iabe
tes
mel
litus
, and
may
sub
se-
quen
tly in
crea
se w
ith th
e in
itiat
ion
of th
yroi
d ho
rmon
e re
plac
emen
t th
erap
y.$-
adre
nerg
ic b
lock
ing
agen
ts-A
ctio
ns o
f so
me
beta
-blo
ckin
g ag
ents
may
be
impa
ired
whe
n hy
poth
yroi
d pa
tient
s be
com
e eu
thyr
oid.
Cyt
okin
es (
inte
rfer
on,
inte
rleu
kin)
-Cyt
okin
es h
ave
been
rep
orte
d to
indu
ce b
oth
hype
r-th
yroi
dism
and
hyp
othy
roid
ism
.D
igit
alis
g/y
cos/
des-
The
rape
utic
effe
cts
of d
igita
lis g
lyco
side
s m
ay b
e re
duce
d. S
erum
digi
talis
lev
els
may
be
decr
ease
d in
hyp
erth
yroi
dism
or
whe
n a
hypo
thyr
oid
patie
ntbe
com
es e
uthy
roid
.K
etam
ine-
Mar
ked
hype
rten
sion
and
tac
hyca
rdia
hav
e be
en r
epor
ted
in a
ssoc
iatio
nw
ith c
onco
mita
nt a
dmin
istr
atio
n of
levo
thyr
oxin
e so
dium
and
ket
amin
e.M
apro
tili
ne-R
isk
of c
ardi
ac a
rrhy
thm
ias
may
incr
ease
.So
dium
iod
ide
('"l
and
'"I)
, so
dium
per
tech
neta
te T
c99r
a-U
ptak
e of
rad
iola
bele
d io
ns m
aybe
dec
reas
ed.
Som
atre
m/s
omat
ropi
n—E
xces
sive
con
curr
ent
use
of t
hyro
id h
orm
one
may
acc
eler
ate
epip
hyse
al c
losu
re. U
ntre
ated
hyp
othy
roid
ism
may
int
erfe
re w
ith t
he g
row
th r
espo
nse
to so
mat
rem
or s
omat
ropi
n.T
heop
hyll
ine—
The
ophy
lline
cle
aran
ce m
ay d
ecre
ase
in h
ypot
hyro
id p
atie
nts
and
retu
rn to
war
d no
rmal
whe
n a
euth
yroi
d st
ate
is a
chie
ved.
Tri
cycl
ic a
ntid
epre
ssan
ts—
Con
curr
ent
use
may
inc
reas
e th
e th
erap
euti
c an
d to
xic
effe
cts
of b
oth
drug
s, p
ossi
bly
due
to i
ncre
ased
cat
echo
lam
ine
sens
itivi
ty. O
nset
of
actio
n of
tric
yclic
s m
ay b
e ac
cele
rate
d.Sy
mpa
thom
imet
ic a
gent
s—Po
ssib
le i
ncre
ased
ris
k of
cor
onar
y in
suff
icie
ncy
in p
atie
nts
with
cor
onar
y ar
tery
dis
ease
.L
abor
ator
y T
est
Inte
ract
ions
: A n
umbe
r of
dru
gs o
r m
oiet
ies
are
know
n to
alte
r se
rum
leve
ls o
f TSH
, T4
and
T3
and
may
ther
eby
influ
ence
the
inte
rpre
tatio
n of
labo
rato
ry t
ests
of th
yroi
d fu
nctio
n (s
ee D
rug
Inte
ract
ions
).1.
Cha
nges
in T
BG c
once
ntra
tion
shou
ld b
e ta
ken
into
con
side
ratio
n w
hen
inte
rpre
t-in
g T
4and
T, v
alue
s. D
rugs
suc
h as
es
trog
ens
and
estr
ogen
-con
tain
ing
oral
con
trac
ep-
tives
incr
ease
TBG
con
cent
ratio
ns.
TBG
con
cent
ratio
ns m
ay a
lso
be in
crea
sed,
dur
ing
preg
nanc
y an
d in
infe
ctio
us h
epat
itis.
Dec
reas
es in
TB
G c
once
ntra
tions
are
obs
erve
d in
neph
rosi
s, a
crom
egal
y, a
nd a
fter
andr
ogen
or
corti
cost
eroi
d th
erap
y. F
amili
al h
yper
- or
hypo
-thy
roxi
ne-b
indi
ng-g
lobu
linem
ias
have
bee
n de
scri
bed.
The
inci
denc
e of
TB
G d
efi-
cien
cy is
app
roxi
mat
ely
1 in
900
0. C
erta
in d
rugs
suc
h as
sal
icyl
ates
inh
ibit
the
prot
ein-
bind
ing
of T
4. In
suc
h ca
ses,
the
unb
ound
(fr
ee)
horm
one
shou
ld b
e m
easu
red.
Alte
rnat
ivel
y, a
n in
dire
ct m
easu
re o
f fre
e th
yrox
ine,
such
as
the
FTJ
may
be
used
.2.
Med
icin
al o
r di
etar
y io
dine
inte
rfer
es w
ith i
n vi
vo te
sts
of r
adio
iodi
ne u
ptak
e, p
ro-
duci
ng lo
w u
ptak
es w
hich
may
not
indi
cate
a tr
ue d
ecre
ase
in h
orm
one
synt
hesi
s.3.
Per
sist
ent
clin
ical
and
lab
orat
ory
evid
ence
of
hypo
thyr
oidi
sm d
espi
te a
n ad
equa
tere
plac
emen
t do
se s
ugge
sts
eith
er p
oor
patie
nt c
ompl
ianc
e, i
mpa
ired
abs
orpt
ion,
dru
gin
tera
ctio
ns, o
r dec
reas
ed p
oten
cy o
f th
e pr
epar
atio
n du
e to
impr
oper
sto
rage
.C
arci
noge
nesi
s, M
utag
enes
is, a
nd I
mpa
irm
ent
of F
ertil
ity: A
lthou
gh a
nim
al s
tudi
es to
dete
rmin
e th
e m
utag
enic
or
carc
inog
enic
pot
entia
l of
thy
roid
hor
mon
es h
ave
not b
een
perf
orm
ed,
synt
hetic
T4
is i
dent
ical
to
that
pro
duce
d by
the
hum
an t
hyro
id g
land
. Are
port
ed a
ssoc
iatio
n be
twee
n pr
olon
ged
thyr
oid
horm
one
ther
apy
and
brea
st c
ance
r ha
sno
t bee
n co
nfirm
ed a
nd p
atie
nts
rece
ivin
g le
voth
yrox
ine
sodi
um f
or e
stab
lishe
d in
dica
-tio
ns sh
ould
not
dis
cont
inue
ther
apy.
Preg
nanc
y: P
regn
ancy
Cat
egor
y A
. Stu
dies
in
preg
nant
wom
en h
ave
not
show
n th
atle
voth
yrox
ine
sodi
um i
ncre
ases
the
ris
k of
fet
al a
bnor
mal
ities
if
adm
inis
tere
d du
ring
preg
nanc
y. I
f le
voth
yrox
ine
sodi
um i
s us
ed d
urin
g pr
egna
ncy,
the
pos
sibi
lity
of f
etal
harm
app
ears
rem
ote.
Bec
ause
stu
dies
can
not
rule
out
the
pos
sibi
lity
of h
arm
, le
voth
y-ro
xine
sod
ium
sho
uld
be u
sed
duri
ng p
regn
ancy
onl
y if
clea
rly
need
ed.
Thy
roid
hor
mon
es c
ross
the
pla
cent
al b
arri
er t
o so
me
exte
nt.
T4
leve
ls i
n th
e co
rdbl
ood
of a
thyr
oid
fetu
ses
have
bee
n sh
own
to b
e ab
out
one-
thir
d of
mat
erna
l le
vels
.N
ever
thel
ess,
mat
erna
l-fe
tal
tran
sfer
of T
4 m
ay n
ot p
reve
nt in
ute
ro h
ypot
hyro
idis
m.
Hyp
othy
roid
ism
dur
ing
preg
nanc
y is
ass
ocia
ted
with
a h
ighe
r ra
te o
f co
mpl
icat
ions
,in
clud
ing
spon
tane
ous
abor
tion
and
pree
clam
psia
, an
d ha
s be
en r
epor
ted
to h
ave
anad
vers
e ef
fect
on
feta
l an
d ch
ildho
od d
evel
opm
ent.
On
the
basi
s of
cur
rent
kno
wle
dge,
SYN
TH
RO
ID s
houl
d th
eref
ore
not
be d
isco
ntin
ued
duri
ng p
regn
ancy
, an
d hy
poth
y-ro
idis
m d
iagn
osed
dur
ing
preg
nanc
y sh
ould
be
trea
ted.
Stu
dies
hav
e sh
own
that
dur
-in
g pr
egna
ncy
T 4 c
once
ntra
tions
may
dec
reas
e an
d TS
H c
once
ntra
tions
may
inc
reas
e to
valu
es o
utsi
de n
orm
al r
ange
s.
Post
part
um v
alue
s ar
e si
mila
r to
pre
conc
eptio
n va
lues
.E
leva
tions
in T
SH m
ay o
ccur
as
earl
y as
4 w
eeks
ges
tatio
n.Pr
egna
nt w
omen
whe
are
mai
ntai
ned
on S
YN
THR
OID
sho
uld
have
the
ir T
SH m
ea-
sure
d pe
riod
ical
ly. A
n el
evat
ed T
SH s
houl
d be
cor
rect
ed b
y an
incr
ease
in S
YN
TH
RO
IDdo
se.
Afte
r pr
egna
ncy,
the
dose
can
be
decr
ease
d to
the
optim
al p
reco
ncep
tion
dose
.N
ursi
ng M
othe
rs: M
inim
al a
mou
nts
of t
hyro
id h
orm
ones
are
exc
rete
d in
hum
an m
ilk.
Thy
roid
hor
mon
es a
re n
ot a
ssoc
iate
d w
ith s
erio
us a
dver
se r
eact
ions
and
do
not
have
know
n tu
mor
igen
ic p
oten
tial.
Whi
le c
autio
n sh
ould
be
exer
cise
d w
hen
SYN
TH
RO
ID is
adm
inis
tere
d to
a n
ursi
ng w
oman
, ade
quat
e re
plac
emen
t do
ses
of l
evot
hyro
xine
sod
i-um
are
gen
eral
ly n
eede
d to
mai
ntai
n no
rmal
lac
tatio
n.Pe
diat
ric
Use
: The
inci
denc
e of
con
geni
tal
hypo
thyr
oidi
sm i
s re
lativ
ely
high
(1
in 4
,000
).R
outin
e de
term
inat
ions
of
seru
m T
4 an
d/or
TSH
are
the
refo
re s
tron
gly
advi
sed
inne
onat
es in
vie
w o
f th
e de
lete
riou
s ef
fect
s of
thyr
oid
defic
ienc
y on
gro
wth
and
dev
elop
-m
ent.
Tre
atm
ent
shou
ld b
e in
itiat
ed i
mm
edia
tely
upo
n di
agno
sis
and
gene
rally
mai
ntai
ned
for
life.
If,
how
ever
, tr
ansi
ent
hypo
thyr
oidi
sm i
s su
spec
ted,
the
rapy
may
be
inte
rrup
ted
for
30 d
ays
afte
r th
e ag
e of
3 y
ears
to re
asse
ss th
e co
nditi
on.
If T 4
is lo
w a
nd T
SH is
ele
-va
ted
afte
r th
at t
ime,
per
man
ent
hypo
thyr
oidi
sm i
s co
nfirm
ed a
nd t
hera
py s
houl
d be
rein
stitu
ted.
If
the
T 4 a
nd T
SH r
emai
n in
the
nor
mal
ran
ge, a
pre
limin
ary
diag
nosi
s of
tran
sien
t hy
poth
yroi
dism
can
be
mad
e. N
ever
thel
ess,
con
tinue
d cl
ose
obse
rvat
ion
with
peri
odic
thyr
oid
func
tion
test
ing
is w
arra
nted
.
AD
VE
RSE
RE
AC
TIO
NS:
Adv
erse
rea
ctio
ns o
ther
tha
n th
ose
indi
cativ
e of
thy
roto
xico
-si
s as
a r
esul
t of
ther
apeu
tic o
verd
osag
e, e
ither
initi
ally
or
duri
ng t
he m
aint
enan
ce p
eri-
ods,
are
rar
e (s
ee O
VE
RD
OSA
GE
). C
rani
osyn
osto
sis
has
been
ass
ocia
ted
with
iat
ro-
geni
c hy
pert
hyro
idis
m i
n in
fant
s re
ceiv
ing
thyr
oid
horm
one
repl
acem
ent
ther
apy.
Inad
equa
te d
oses
of
SYN
THR
OID
may
pro
duce
or
fail
to r
esol
ve s
ympt
oms
of h
ypot
hy-
roid
ism
. Hyp
erse
nsiti
vity
rea
ctio
ns to
the
prod
uct e
xcip
ient
s, s
uch
as r
ash
and
urtic
aria
,m
ay o
ccur
. Par
tial h
air
loss
may
occ
ur d
urin
g th
e in
itial
mon
ths
of th
erap
y, b
ut is
gen
er-
ally
tra
nsie
nt.
The
inc
iden
ce o
f co
ntin
ued
hair
los
s is
unk
now
n. P
seud
otum
or c
ereb
riha
s be
en r
epor
ted
in p
edia
tric
pat
ient
s re
ceiv
ing
thyr
oid
horm
one
repl
acem
ent
ther
apy.
OV
ER
DO
SAG
E:
Sig
ns a
nd S
ympt
oms:
Exc
essi
ve d
oses
of
SYN
TH
RO
ID r
esul
t in
ahy
perm
etab
olic
sta
te i
ndis
tingu
isha
ble
from
thy
roto
xico
sis
of e
ndog
enou
s or
igin
. Sig
nsan
d sy
mpt
oms
of t
hyro
toxi
cosi
s in
clud
e w
eigh
t lo
ss, i
ncre
ased
app
etit
e, p
alpi
tati
ons,
nerv
ousn
ess,
dia
rrhe
a, a
bdom
inal
cra
mps
, sw
eatin
g, t
achy
card
ia,
incr
ease
d pu
lse
and
bloo
d pr
essu
re,
card
iac
arrh
ythm
ias,
tre
mor
s, i
nsom
nia,
hea
t in
tole
ranc
e, f
ever
, an
dm
enst
rual
irr
egul
ariti
es. S
ympt
oms
are
not a
lway
s ev
iden
t or
may
not
app
ear
until
sev
-er
al d
ays
afte
r in
gest
ion.
CA
UT
ION
: Fed
eral
(USA
) law
pro
hibi
ts d
ispe
nsin
g w
ithou
t a p
resc
ript
ion.
See
Full
Pres
crib
ing
Info
rmat
ion.
Tab
lets
Man
ufac
ture
d by
In
ject
ion
Man
ufac
ture
d by
BA
SF P
harm
aceu
tical
s B
en V
enue
Lab
orat
orie
s, In
c.A
Uni
t of
BA
SF
Bed
ford
, Ohi
o 44
146
USA
Jayu
ya, P
uert
o R
ico
0066
4Fo
rK
noll
Phar
mac
eutic
al C
ompa
nyM
ount
Oliv
e, N
J 078
28 U
SA79
20-0
7
8/95
©
1995
Kno
ll Ph
arm
aceu
tical
Com
pany
All
righ
ts r
eser
ved.
Pri
nted
in
USA
Kno
O P
ttan
nsc
Gu
tics
l C
om
pa
ny
30
00
Con
tinen
tal D
rive
No
rth
Ma
rt O
&V
B.N
J 07
828-
1234
Rev
. 05/
24/9
5
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

IN
TH
YR
OID
H
OR
MO
NE
RE
PL
AC
EM
EN
T..
.
SYN
THR
OID
-TH
E ST
ANDA
RD B
Y W
HICH
ALL
OTH
ERS
ARE
MEA
SURE
D
THE
NAME
YOU
TRU
ST...
as th
e ben
chm
ark
in th
yroi
dho
rmon
e re
plac
emen
t
THE
QUAL
ITY
YOU
EXPE
CT
M T
HE P
RECI
SION
YOU
NEE
D..
.from
ove
r 3 d
ecad
es of
man
ufac
turin
g ..
.pat
ient
to p
atie
nt, d
ose t
o do
sean
d re
sear
chin
g th
yroi
d ho
rmon
e rep
lacem
ent
The
Mea
sure
of E
xcel
lenc
e
SY
NTH
RO
ID(L
evot
hyro
xine
Sodi
um Ta
blets,
USP
)
25
50
75
88
10
0 1
12
125
15
0 17
5 2
00
30
0
meg
m
eg
meg
m
eg
mig
m
eg
meg
m
eg
meg
m
eg
mtg
The
Tru
sted
Sta
ndar
d in
Thy
roid
Hor
mon
e R
epla
cem
ent
Plea
se s
et' b
rief
sum
mar
y of
pre
scri
bing
inf
orm
atio
n on
adj
acen
t pa
ge.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

The Endocrine Society's ClinicalEndocrinology Update: 1996
(formerly The Postgraduate Assembly)
October 6-9, 1996, Palmer House Hilton, Chicago, Illinois
J Larry Jameson, MD, PhD, Program DirectorMark E Molitch, MD, Co-Program Director
CEU '96 offers the most comprehensive update available to practicing endocrinologists, internists,and clinicians. The focus is on diagnosis and management of all major facets of contemporary en-
docrinology. Seven topic areas will be covered: pituitary/neuroendocrinology, reproductive endocrinol-ogy, calcium & bone, diabetes, thyroid, adrenal, and obesity/lipids.
Sunday, October 6
PITUITARY & NEUROENDOCRINOLOGYSECTION
Hypopltuitarism, Clinically Nonfunctionlng PituitaryTumors. Cushing's Syndrome Grand Rounds, SIADH,Alternatives to Bromocriptine in Management of Pro-lactinomas, Prolactin & Pregnancy, Cushing's Dis-ease, Acromegaly, Cost-effective Evaluation ofPituitary Masses
REPRODUCTIVE ENDOCRINOLOGYSECTION
Newer Therapeutic Options in the Male, PolycysticOvarian Disease, Menopausal Replacement Therapy,Amenorrhea, Hlrsutism, Gynecomastla, Hypogo-nadotropism
Monday, October 7
CALCIUM & BONE SECTION
Osteoporosis Therapy, Clinical Importance of the Cal-cium Receptor, Paget's Disease, Osteoporosis,Hypoparathyroldism and Hypocalcemia,Nonosteoporotic Metabolic Bone Disease, MEN Syn-dromes, Hypercalcemla
CEU '96 is supported by educational grants fromSandoz Pharmaceuticals, Eli Lilly and Company,Parke-Davis Pharmaceuticals, Knoll Pharmaceu-tical Company, Ferring Laboratories, and Wyeth-Ayerst Laboratories
DIABETES SECTION
NIDDM Treatment Strategies, Cost-effective DiabetesManagement Pregnancy in Diabetes, Practical Man-agement of NIDDM, Intensive Insulin Therapy, Ado-lescents & Diabetes, The Diabetic Foot, Prevention ofDiabetic Nephropathy
Tuesday, October 8
THYROID SECTION
Subclinical Thyroid Dysfunction, Thyrotoxicosis,Management of Thyroid Cancers, Thyroid FunctionTest Abnormalities, Amiodarone-induced Thyrotoxi-cosis, Graves' Orbitopathy, Expanding Goiter in anElderly Woman, Hypothyroidism in a Patient withUnstable Angina, Thyroid Nodule with IndeterminateCytopathologic Findings
ADRENAL SECTION
MEN II, Pheochromocytoma, Adrenal Masses GrandRounds
Wednesday, October 9
OBESITY/LIPIDS SECTION
CHD Clinical Trials, Biology of CHD Regression, Biol-ogy of Obesity, Diabetic Dyslipidemia, Hyper-triglyceridemia, Lipid Disorders in Children,Cholesterol Lowering, Management of Obesity, Man-agement of Hypercholesterolemia in Women & Elderly
To receive a brochure listing topics andspeakers, contact The Endocrine SocietyMeetings Department at 301-941-0220
(phone)! 301-941-0259 {fax)
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Q
^^k 1 25 meg^ ^ P M 0.025 mg
50 meg0.05 mg
75 meg0 075 mg
t
88 meg0 088mg
100 meg0.1 mg
112 meg0.112mg
125 meg0125mg
137 mcq0 137mg
^
150 meg0.150 mg
175 meg0175mg
200 meg0.2 mg
300 meg0.3 mg
No wider range of LT4dosages availablefor optimal managementof all yourhypothyroid patients
Remember, Forest/UAD offers Levothroid 137...a notable addition to your LT4 dosing options
Rx: Levothroid(levothyroxine sodium tablets, USP)
Forest/UAD: Dedicated to you, your patients and your practices FOREST PHARMACEUTICALS, INC.
' UAD LABORATORIESSt. Louis. Missouri 63045
lijcibo sot; brief summary of prescribing information on adjacent page.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Brief Summary (for full prescribing Information and patient Information, see package circular)
Levothroid® Tablets (levothyroxine sodium tablets, USP)
DESCRIPTION: LEVOTHROID* TABLETS (levothyroxine sodium tablets, USP) provide crystalline sodium levothyroxine (T4),a potent thyroid hormone, in twelve different strengths to permit easy, convenient dosage adjustment.INDICATIONS AND USAGE: Levothroid Tablets are indicated as replacement or substitution therapy for diminished or absentthyroid function (e.g., cretinism, myxedema, non-toxic goiter or hypothyroidism generally, including the hypothyroid state inchildren, in pregnancy and in the elderly) resulting from functional deficiency, primary atrophy, from partial or completeabsence of the gland or from the effects of surgery, radiation or antithyroid agents. Therapy must be maintained continuous-ly to control the symptoms of hypothyroidism. It may also be used to suppress the secretion of thyrotropin (TSH). actionwhich may be beneficial in simple nonendemic goiter and in chronic lymphocytic thyroiditis. This may cause a reduction inthe goiter size. Thyroid hormone drugs are indicated as a diagnostic agent in suppression tests to differentiate suspectedmild hyperthyroidism or thyroid gland autonomy. Thyroid hormones may also be used with antithyroid drugs to treat thyro-toxicosis. This combination has been used to prevent goitrogenesis and hypothyroidism.CONTRAINDICATIONS: Levothroid Tablets administration is contraindicated in untreated thyrotoxicosis and in acutemyocardial infarction. Levothroid Tablets are contraindicated in the presence of uncorrec'ted adrenal insufficiency becauseit increases the tissue demands for adrenocortical hormones and may cause an acute adrenal crisis in such patients.(See PRECAUTIONS).
WARNINGSDrugs with thyroid hormone activity, alone or together with other therapeutic agents, have been used for the treatmentof obesity. In euthyroid patients, doses within the range of daily hormonal requirements are ineffective for weightreduction. Larger doses may produce serious or even life-threatening manifestations of toxicity, particularly whengiven in association with sympathomimetic amines such as those used for their anorectic effects.
The use of thyroid hormones in the therapy of obesity, alone or combined with other drugs, is unjustified and has beenshown to be ineffective. Neither is their use justified for the treatment of male or female infertility unless this condition isaccompanied by hypothyroidism.PRECAUTIONS: GENERAL: Levothroid Tablets should be used with caution in patients with cardiovascular disease, includinghypertension. The development of chest pain or other aggravation of cardiovascular disease will require a decrease in dosage.Thyroid hormone therapy in patients with concomitant diabetes mellitus or diabetes insipidus or adrenal cortical insufficiencyaggravates the intensity of their symptoms. Appropriate adjustments of the various therapeutic measures directed at theseconcomitant endocrine diseases are required. The therapy of myxedema coma requires simultaneous administration ofglucocorticoids (See DOSAGE AND ADMINISTRATION).
In infants, excessive doses of thyroid hormone preparations may produce craniosynostosis.Information for the Patient: For full prescribing information, see package circular.
Laboratory Tests: The patient's response to thyroid replacement may be followed by laboratory tests such as serumthyroxine (T4), serum triiodothyronine (T3). free thyroxine index and thyroid stimulating hormone (TSH) blood levels.Drug Interactions: In patients with diabetes mellitus, addition of thyroid hormone therapy may cause an increase in therequired dosage of insulin or oral hypoglycemic agents. Conversely, decreasing the dose of thyroid hormone may possiblycause hypoglycemic reactions if the dosage of insulin or oral hypoglycemic agents is not adjusted.Thyroid replacement may potentiate anticoagulant effects with agents such as warfarin or bishydroxycoumarin and reductionof one-third of anticoagulant dosage should be undertaken upon initiation of Levothroid Tablets therapy. Subsequent anti-coagulant dosage adjustment should be made on the basis of frequent prothrombin determinations.Injection of epinephrine in patients with coronary artery disease may precipitate an episode of coronary insufficiency. Thismay be enhanced in patients receiving thyroid preparations. Careful observation is required if catecholamines are admin-istered lo patients in this category.
Cholestyramine or colestipol binds both T4 and T3 in the intestine, thus impairing absorption of these thyroid hormones.In vitro studies indicate that the binding is not easily removed. Therefore, four to five hours should elapse between admin-istration of cholestyramine or colestipol and thyroid hormones.Estrogens tend to increase serum thyroxine-binding globulin (TBg). In a patient with a non-functioning thyroid gland whois receiving thyroid replacement therapy, free levothyroxine may be decreased when estrogens are started thus increasingthyroid requirements. However, if the patient's thyroid gland has sufficient function the decreased free thyroxine will result ina compensatory increase in thyroxine output by the thyroid. Therefore, patients without a functioning thyroid gland who areon thyroid replacement therapy may need to increase their thyroid dose if estrogens or estrogen-containing oral contracep-tives are given.Drug/Laboratory Test Interactions: The following drugs or moieties are known to interfere with laboratory tests performedin patients on thyroid hormone therapy: androgens, corticosteroids, estrogens, oral contraceptives containing estrogens,iodine-containing preparations, and the numerous preparations containing salicylates.Carcinogenesis, Mutagenesis, and Impairment of Fertility: A reportedly apparent association between prolonged thyroidtherapy and breast cancer has not been confirmed and patients on thyroid for established indications should not discontinuetherapy. No confirmatory long-term studies in animals have been performed to evaluate carcinogenic potential, mutagenicity,or impairment of fertility in either males or females.Pregnancy-Category A: Thyroid hormones do not readily cross the placental barrier. The clinical experience to date doesnot indicate any adverse effect on fetuses when thyroid hormones are administered to pregnant women. On the basis ofcurrent knowledge, thyroid replacement therapy to hypothyroid women should not be discontinued during pregnancy.Nursing Mothers: Minimal amounts of thyroid hormones are excreted in human milk. Thyroid is not associated with seriousadverse reactions and does not have a known tumorigenic potential. However, caution should be exercised when thyroid isadministered to a nursing woman.
Pedlatric Use: The diagnosis and institution of therapy for cretinism should be done as soon after birth as feasible to preventdevelopmental deficiency. Screening tests lor serum T4 and TSH will identify this group of newborn patients.ADVERSE REACTIONS: Patients who are sensitive to lactose may show intolerance to Levothroid Tablets since thissubstance is used in the manufacture of the product.
Adverse reactions other than those indicative of hyperthyroidism because of therapeutic overdosage, either initially or duringthe maintenance period, are rare (See OVERDOSAGE).OVERDOSAGE: Excessive dosage of thyroid medication may result in symptoms of hyperthyroidism. Since, however, theeffects do not appear at once, the symptoms may not appear for one to three weeks after the dosage regimen is begun. Themost common signs and symptoms of overdosage are weight loss, palpitation, nervousness, diarrhea or abdominal cramps,sweating, tachycardia, cardiac arrhythmias, angina pectoris. tremors, headache, insomnia, intolerance to heat and fever. Ifsymptoms of overdosage appear, discontinue medication (or several days and reinstitute treatment at a lower dosage level.Laboratory tests such as serum T4 and serum T3 and the free thyroxine index will be elevated during the period of over-dosage. Complications as a result of the induced hypermetabolic state may include cardiac failure and death due toarrhythmia or failure.Treatment ol Overdosage: Dosage should be reduced or therapy temporarily discontinued if signs and symptoms of over-dosage appear. Treatment may be reinstituted at a lower dosage. In normal individuals, normal hypothalamic-pituitary-thyroid axis function is restored in 6 to 8 weeks after thyroid suppression.Treatment of acute massive thyroid hormone overdosage is aimed at reducing gastrointestinal absorption of the drugs andcounteracting central and peripheral effects, mainly those of increased sympathetic activity. Vomiting may be induced initial-ly if further gastrointestinal absorption can reasonably be prevented and barring contraindications such as coma, convul-sions, or loss of the gagging reflex. Treatment is symptomatic and supportive. Oxygen may be administered and ventilationmaintained. Cardiac glycosides may be indicated if congestive heart failure develops. Measures to control fever, hypoglycemiaor fluid loss should be instituted if needed. Antiadrenergic agents, particularly propranolol, have been used advantageouslyin the treatment of increased sympathetic activity. Propranolol may be administered intravenously at a dosage of 1 to 3 mgover a tO-minute period or orally, 80 to 160 mg/day, initially, especially when no contraindications exist for its use. Otheradjunctive measures may include administration of cholestyramine to interfere with thyroxine absorption, and glucocorticoidsto inhibit conversion of T4 to T3.DOSAGE AND ADMINISTRATION: The goal of therapy should be restoration of euthyroidism as judged by clinical responseand confirmed by appropriate laboratory values. In adults with no complicating endocrine or cardiovascular disease, thepredicted full maintenance dose may be achieved immediately with adjustments made as indicated by clinical evaluation:The usual maintenance dose of Levothroid Tablets is 100 to 200 meg.In patients with known complications or in case of doubt, individual dose titration at 2- to 4-week intervals is recommended.The usual starting dose is 50 meg with increases of 50 meg at 2- to 4-week intervals until the patient is euthyroid or symp-toms ensue which preclude further dose increase.In adult myxedema or hypothyroid patients with angina, the starting dose should be 25 meg with increases at 2- to 4-weekintervals of 25 lo 50 meg as determined by clinical response.
CAUTION: Federal law prohibits dispensing without prescription.
Dist. by: Forest Pharmaceuticals, Inc.A Subsidiary of Forest Laboratories. Inc.St. Louis, MO 63045
I FOREST PHARMACEUTICALS, INC.' UAD LABORATORIES
Rev. 9/9481100994
O D D
ENDOCRINE REVIEWSMONOGRAPHS
SERIES EDITORANDRES NEGRO-VILAR, M.D., Ph.D.
3. Clinical and MolecularAspects of Diseases of the
ThyroidGUEST EDITORS
LEWIS E. BRAVERMAN, M.D.SAMUEL REFETOFF, M.D.
Clinical and Molecular Aspects ofDiseases of the Thyroid
Guest Editors: Lewis E. Braverman, M.D.and Samuel Refetoff, M.D.
Endocrine Reviews Monograph Series Editor:
Andres Negro-Vilar, M.D., Ph.D.Clinical and Molecular Aspects of Diseases of
the Thyroid, the third volume in the well-receivedEndocrine Reviews Monograph Series, presents the
clinician, researcher, and student with anoutstanding and up-to-date sequence of reviewarticles on this complex topic. Thesecomprehens.ive and authoritative articles providethoughtful discussion, enhanced by up-to-datebibliographies, making them invaluable forteaching or further study.
ISBN 1-879225-17-4, 414 pages, paper-bound, 1994. $45.00 (Members), $55.00 (Non-members). Add $15.00 for international air mail.
Order by mail, fax, or phone, from:The Endocrine Society Press,
c/o Nations Bank,
P.O. Box 630331, Baltimore, MD 21263
Fax: (301)941-0259 • Telephone: (301)941-0240
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Introducingthe new wave ingrowth hormone
therapy ^ *
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

THELIQ
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

May improvedosing accuracy
Eliminatesreconstitution
Reduces4 product waste
Leading the wayin growth hormone
therapy
NewNutropinN[somatropin (rDNA origin) injection]
Indicated for the long-term treatment of children with growth failure dueto a lack of adequate endogenous growth hormone secretion and thetreatment of children who have growth failure associated with chronicrenal insufficiency up to the time of renal transplantation.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Nutropin \Q[somatropin (rDNA origin) injection]DESCRIPTIONNutropin AQ™ [somatropin (rONA origin) injection) is a human growth hormone (hGH)produced by recombinant DNA technology. Nutropin AQ has 191 amino acid residues and amolecular might of 22,125 daltons. The amino acid sequence of the product is identicalto that of pituitary-derived human growth hormone. The protein is synthesized by aspecific laboratory strain of £. coli as a precursor consisting of the rhGH moleculepreceded by the secretion signal from an £. coli protein. This precursor is directed to theplasma membrane of the cell. The signal sequence is removed and the native protein issecreted into the periplasm so that the protein is folded appropriately as it is synthesized.Nutropin AQ is a highly purified preparation. Biological potency is determined bymeasuring the increase in body weight induced in hypophysectomized rats. Nutropin AQmay contain not more than fifteen percent deamidated growth hormone at expiration.The deamidated form of growth hormone has been extensively characterized and hasbeen shown to be safe and fully active.
Nutropin AQ is a sterile liquid intended for subcutaneous administration. The product isnearly isotonic at a concentration of 5 mg of growth hormone per mL and has a pH ofapproximately 6.0.Each 2 m l vial contains 10 mg (approximately 30IU) somatropin, formulated in 17.4mg sodium chloride, 5 mg phenol, 4 mg polysorbate 20, and 10 mM sodium citrate.
CLINICAL PHARMACOLOGY
GeneralIn vitro, preclinical, and clinical testing have demonstrated that Nutropin AQ istherapeutically equivalent to pituitary-derived human growth hormone. Treatment ofchildren who lack adequate endogenous growth hormone secretion with Nutropin AQresulted in an increase in growth rate and an increase in insulin-like growth factor-llevels similar to that seen with pituitary-derived human growth hormone.Actions that have been demonstrated for Nutropin AQ, somatropin, somatrem and/orpituitary-derived human growth hormone include:A. fitsue Growth—1) Skeletal Growth: Nutropin AQ stimulates skeletal growth in
children with growth failure due to a lack of adequate secretion of endogenousgrowth hormone. Skeletal growth is accomplished at the epiphyseal plates at theends of a growing bone. Growth and metabolism of epiphyseal plate cells are directlystimulated by growth hormone and one of its mediators, insulin-like growth factor-l.Serum levels of insulin-like growth factor-l are low in children and adolescents whoare growth hormone inadequate, but increase during treatment with Nutropin AQ.New bone is formed at the epiphyses in response to growth hormone. This results inlinear growth until these growth plates fuse at the end of puberty. 2) Cell Growth:Treatment with pituitary-derived human growth hormone results in an increase inboth the number and the size of skeletal muscle cells. 3) Organ Growth: Growthhormone of human pituitary origin influences the size of internal organs, includingkidneys, and increases red cell mass. Treatment of hypophysectomized or geneticdwarf rats with somatropin results in organ growth that is proportional to the overallbody growth. In normal rats subjected to nephrectomy-induced uremia, somatropinpromoted skeletal and body growth.
8. Protein Metabolism— Linear growth is facilitated in part by growthhormone-stimulated protein synthesis. This is reflected by nitrogen retention asdemonstrated by a decline in urinary nitrogen excretion and blood urea nitrogenconcentration during growth hormone therapy.
C Carbohydrate Metabolism—Growth hormone is a modulator of carbohydratemetabolism. For example, children with inadequate secretion of growth hormonesometimes experience fasting hypoglycemia that is improved by treatment withgrowth hormone. Administration of somatropin to normal adults, patients withchronic renal insufficiency, and patients who lack adequate secretion of endogenousgrowth hormone resulted in increases in mean serum fasting and postprandialinsulin levels. There were no clinically significant persistent abnormalities in any ofthese measurements of glucose regulation that were related to growth hormonetreatment. Mean values remained well within the normal range.
D. Upld Metabolism—Acute administration of pituitary-derived human growth hormoneto humans results in lipid mobilization. Nonesterified fatty acids increased in plasmawithin two hours of pituitary-derived human growth hormone administration. Ingrowth hormone inadequate patients, long-term growth hormone administration oftendecreases body fat. Mean cholesterol levels decreased in patients treated withNutropin AQ.
f. Mineral Metabolism—The retention of total body potassium in response to growthhormone administration apparently results from cellular growth. Serum levels ofinorganic phosphorus may increase slightly in patients with inadequate secretion ofendogenous growth hormone or chronic renal insufficiency after growth hormonetherapy due to metabolic activity associated with bone growth as well as increasedtubular reabsorption of phosphate by the kidney. Serum calcium is not significantlyaltered in these patients. Sodium retention also occurs. (See PRECAUTIONS:Laboratory Tests.)
f. Connective Tissue Metabolism—Growth hormone stimulates the synthesis ofchondroitin sulfate and collagen as well as the urinary excretion of hydroxyproline.
Pharmacok ine t i csSubcutaneous absorption - The absolute bioavailability of rhGH after subcutaneousadministration in healthy adult males has been determined to be 81 ± 20 %. The meanterminal t i n after subcutaneous administration is significantly longer than that seenafter intravenous administration (2.3 ± 0.42 hrs vs.19.5 ± 3.1 min) indicating that thesubcutaneous absorption of the compound is slow and rate-limiting.Distribution - Animal studies with rhGH showed that growth hormone localizes to highlyperfused organs, particularly the liver and kidney. The volume of distribution at steadystate for rhGH in healthy adult males is about 50 mL/kg body weight, approximating theserum volume.Mstabolism - Both the liver and kidney have been shown to be important metabolizingorgans for pituitary-derived human growth hormone. Animal studies suggest that thekidney is the dominant organ of clearance. Growth hormone is filtered at the glomerulusand reabsorbed in the proximal tubules. It is then cleaved within renal cells into itsconstituent amino acids, which return to the systemic circulation.Elimination - The mean terminal t m after intravenous administration of rhGH inhealthy adult males is estimated to be 19.5 ± 3.1 minutes. Clearance of rhGH afterintravenous administration in healthy adults and children is reported to be in the rangeof 116-174 mL/hr/kg.Bioequivatence of Formulations - Nutropin AQ has been determined to be bioequivalentto Nutropin8 Isomatropin (rDNA origin) for injection] based on the statistical evaluationof AUC and Cm a x .Special PopulationsPediatric - Available literature data suggest that rhGH clearances are similar in adultsand children.Gender - No data are available for rhGH. Available data for methionyl recombinantgrowth hormone and pituitary-derived human growth hormone suggest no consistentgender-based differences in rhGH clearance.Race • No data are available.Growth Hormone Insufficiency (GHI) - Reported values for clearance of rhGH in adultsand children with GHI range from 138-245 mL/hr/kg and are similar to those observedin healthy adults and children. Mean terminal t m values following intravenous andsubcutaneous administration in adult and pediatric GHI patients are also similar tothose observed in healthy adult males.
Renal Insufficiency - Children and adults with chronic renal failure (CRF) tend to havedecreased clearance as compared to normals. However, no rhGH accumulation has beenreported in children with CRF or end-stage renal disease (ESRD) dosed with currentregimens.Hepatic Insufficiency - A reduction in rhGH clearance has been noted in patients withsevere liver dysfunction. The clinical significance of this decrease is unknown.Effects of Nutropin8 [somatropin (rDNA origin) for injection] on Growth Failure Dueto Chronic Renal Insufficiency (CRI)Two multicenter, randomized, controlled clinical trials were conducted to determinewhether treatment with Nutropin prior to renal transplantation in children with chronicrenal insufficiency could improve their growth rates and height deficits. One study wasa double-blinded, placebo-controlled trial and the other was an open-label, randomizedtrial. The dose of Nutropin in both controlled studies was 0.05 mg/kg/day (0.35mg/kg/wk) administered daily by subcutaneous injection. Combining the data fromthose patients completing two years in the two controlled studies results in 62 childrentreated with Nutropin and 28 children in the control groups (either placebo-treated oruntreated). The mean first year growth rate was 10.8 cm/yr for Nutropin-treatedpatients, compared with a mean growth rate of 6.5 cm/yr for placebo/untreated controls(p<0.00005). The mean second year growth rate was 7.8 cm/yr for the Nutropin-treatedgroup, compared with 5.5 cm/yr for controls (p<0.00005). There was a significantincrease in mean height standard deviation score in the Nutropin group (-2.9 atbaseline to -1.5 at Month 24, n=62) but no significant change in the controls (-2.8 atbaseline to -2.9 at Month 24, n=28). The mean third year growth rate of 7.6 cm/yr inthe Nutropin-treated patients (n=27) suggests that Nutropin stimulates growth beyondtwo years. However, there are no control data for the third year because control patientscrossed over to growth hormone treatment after two years of participation. The gains inheight were accompanied by appropriate advancement of skeletal age. These datademonstrate that Nutropin therapy improves growth rate and corrects the acquiredheight deficit associated with chronic renal insufficiency. Currently there are insufficientdata regarding the benefit of treatment beyond three years. Although predicted finalheight was improved during Nutrooin therapy, the effect of Mutropin on final adultheight remains to be determined.Post-Transplant GrowthThe North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) hasreported data for growth post-transplant in children who did not receive growthhormone. The average change in height SD score during the initial two yearspost-transplant was 0.18 (n=300, J Ped 1993; 122:397-402).Controlled studies of growth hormone treatment for the short stature associated withCRI were not designed to compare the growth of treated or untreated patients after theyreceived renal transplants. However, growth data are available from a small number ofpatients who have been followed for at least 11 months. Of the 7 control patients, 4increased their height SD score and 3 had either no significant change or a decrease inheight SD score. The 13 patients treated with Nutropin prior to transplant had either nosignificant change or an increase in height SD score after transplantation, indicatingthat the individual gains achieved with growth hormone therapy prior to transplant weremaintained after transplantation. The differences in the height deficit narrowed betweenthe treated and untreated groups in the post-transplant period.
INDICATIONS AND USAGENutropin AQm [somatropin (rDNA origin) injection] is indicated for the long-termtreatment of children who have growth failure due to a lack of adequate endogenousgrowth hormone secretion.Nutropin AQ is also indicated for the treatment of children who have growth failureassociated with chronic renal insufficiency up to the time of renal transplantation.Nutropin AQ therapy should be used in conjunction with optimal management of chronicrenal insufficiency.
CONTRAINDICATIONSNutropin AQ should not be used in subjects with closed epiphyses.Nutropin AQ should not be used in patients with active neoplasia. Growth hormonetherapy should be discontinued if evidence of neoplasia develops.WARNINGSNone.PRECAUTIONSGeneral: Nutropin AQ should be prescribed by physicians experienced in the diagnosisand management of patients with CRI or growth failure. No studies have beenperformed of Nutropin AQ in children who have received renal transplants. Currently,treatment of patients with functioning renal allografts is not indicated.Because Nutropin AQ may induce a state of insulin resistance, patients should be ,monitored for evidence of glucose intolerance.Patients with a history of an intracranial lesion taking somatropin and/or somatropinliquid should be examined frequently for progression or recurrence of the lesion.Patients with growth failure secondary to CRI should be examined periodically for evidenceof progression of renal osteodystrophy. Slipped capital femoral epiphysis or avascularnecrosis of the femoral head may be seen in children with advanced renal osteodystrophy,and it is uncertain whether these problems are affected by growth hormone therapy. X-raysof the hips should be obtained prior to initiating therapy for CRI patients.Slipped capital femoral epiphysis may also occur more frequently in patients withendocrine disorders or in patients undergoing rapid growth. Therefore, physicians andparents should be alert to the development of a limp or complaints of hip or knee painin GHI or CRI patients treated with Nutropin AQ.Progression of scoliosis can occur in children who experience rapid growth. Becausegrowth hormone increases growth rate, patients with a history of scoliosis who aretreated with growth hormone should be monitored for progression of scoliosis. Growthhormone has not been shown to increase the incidence of scoliosis.Intracranial hypertension (IH) with papilledema, visual changes, headache, nauseaand/or vomiting has been reported in a small number of patients treated with growthhormone products. Symptoms usually occurred within the first eight (8) weeks of theinitiation of growth hormone therapy. In all reported cases, IH-associated signs andsymptoms resolved after termination of therapy or a reduction of the growth hormonedose. Funduscopic examination of patients is recommended at the initiation andperiodically during the course of growth hormone therapy.As for any protein, local or systemic allergic reactions may occur. Parents/Patient shouldbe informed that such reactions are possible and that prompt medical attention shouldbe sought if allergic reactions occur.Laboratory Tests: Serum levels of inorganic phosphorus, alkaline phosphatase, andparathyroid hormone (PTH) may increase with Nutropin AQ therapy. Changes in thyroidhormone laboratory measurements may develop during Nutropin AQ treatment in childrenwho lack adequate endogenous growth hormone secretion. Untreated hypothyroidismprevents optimal response to Nutropin AQ. Therefore, patients should have periodicthyroid function tests and should be treated with thyroid hormone when indicated.Drug Interaction: The use of Nutropin AQ in patients with CRI receiving glucocorticoidtherapy has not been evaluated. Concomitant glucocorticoid therapy may inhibit thegrowth promoting effect of Nutropin AQ. If glucocorticoid replacement is required, thedose should be carefully adjusted.There was no evidence in the controlled studies of somatropin's interaction with drugscommonly used in chronic renal insufficiency patients. However, formal drug interactionstudies have not been conducted.Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity, mutagenicity andreproduction studies have not been conducted with Nutropin AQ.Pregnancy: Pregnancy (Category C). Animal reproduction studies have not beenconducted with Nutropin AQ. It is also not known whether Nutropin AQ can cause fetalharm when administered to a pregnant woman or can affect reproduction capacity.Nutropin AQ should be given to a pregnant woman only if clearly needed.
Nursing Mothers: It is not known whether Nutropin AQ'" [somatropin (rDNA origin)injection] is excreted in human milk. Because many drugs are excreted in human milk,caution should be exercised when Nutropin AQ is administered to a nursing mother.Information for Patients: Patients being treated with growth hormone and/or their parentsshould be informed of the potential benefits and risks associated with treatment. If homeuse is determined to be desirable by the physician, instructions on appropriate use shouldbe given, including a review of the contents of the Patient Information Insert. Thisinformation is intended to aid in the safe and effective administration of the medication.It is not a disclosure of all possible adverse or intended effects.If home use is prescribed, a puncture resistant container for the disposal of usedsyringes and needles should be recommended to the patient. Patients and/or parentsshould be thoroughly instructed in the importance of proper disposal and cautionedagainst any reuse of needles and syringes (see Patient Information Insert).
ADVERSE REACTIONSAs with all protein Pharmaceuticals, a small percentage of patients may developantibodies to the protein. Growth hormone antibody binding capacities below 2 mg/Lhave not been associated with growth attenuation. In some cases when binding capacityexceeds 2 mg/L, growth attenuation has been observed. In clinical studies of patientsthat were treated with Nutropin® [somatropin (rDNA origin) for injection] for the firsttime, 0/107 growth hormone inadequate (GHI) patients and 0/125 CRI patients screenedfor antibody production developed antibodies with binding capacities 22 mg/L at sixmonths. In a clinical study of patients that were treated with Nutropin AQ for the firsttime, 0/38 GHI patients screened for antibody production, for up to 15 months,developed antibodies with binding capacities 22 mg/L.Additional short-term immunologic and renal function studies were carried out in agroup of patients with chronic renal insufficiency after approximately one year oftreatment to detect other potential adverse effects of antibodies to growth hormone.Testing included measurements of Clq, C3, C4, rheumatoid factor, creatinine, creatinineclearance and BUN. No adverse effects of growth hormone antibodies were noted.In addition to an evaluation of compliance with the prescribed treatment program andthyroid status, testing for antibodies to human growth hormone should be carried out inany patient who fails to respond to therapy.In studies in children treated with somatropin, injection site pain was reportedinfrequently.Leukemia has been reported in a small number of growth hormone deficient patientstreated with growth hormone. It is uncertain whether this increased risk is related to thepathology of growth hormone deficiency itself, growth hormone therapy, or otherassociated treatments such as radiation therapy for intracranial tumors. On the basis ofcurrent evidence, experts cannot conclude that growth hormone therapy is responsiblefor these occurrences. There have been no reports of leukemia in CRI patients treatedwith growth hormone. The risk to GHI and CRI patients, if any, remains to beestablished.Other adverse drug reactions that have been reported in growth hormone-treatedpatients include the following: 1) Metabolic: Infrequent, mild and transient peripheraledema. 2) Musculoskeletal: Rare carpal tunnel syndrome. 3) Skin: Rare increased growthof pre-existing nevi. Malignant nevi transformation has not been reported.4) Endocrine: Rare gynecomastia. Rare pancreatitis.
OVERDOSAGEThe recommended dosage for GHI is 0.30 mg/kg (approximately 0.90 Ill/kg) of bodyweight weekly. The recommended dosage for CRI is 0.35 mg/kg (approximately 1.05lU/kg) of body weight weekly. Long-term overdosage could result in signs and symptomsof gigantism and/or acromegaly consistent with the known effects of excess humangrowth hormone.DOSAGE AND ADMINISTRATION
Growth Hormone Inadequacy (GHI)A weekly dosage of 0.30 mg/kg (approximately 0.90 lU/kg) of body weight administeredby daily subcutaneous injection is recommended.The Nutropin AQ dosage and administration schedule for GHI should be individualizedfor each patient. Therapy should not be continued if final height is achieved orepiphyseal fusion occurs. Patients who fail to respond adequately while on Nutropin AQshould be evaluated to determine the cause of unresponsiveness.
Chronic Rena l Insuf f i c iency (CRI)A weekly dosage of 0.35 mg/kg (approximately 1.05 lU/kg) of body weight administeredby daily subcutaneous injection is recommended.The duration of Nutropin AQ therapy for CRI should be individualized for each patient.Nutropin AQ therapy may be continued up to the time of renal transplantation. Therapyshould not be continued if final height is achieved or epiphyseal fusion occurs. Patientswho fail to respond adequately while on Nutropin AQ therapy should be evaluated todetermine the cause of unresponsiveness.In order to optimize therapy for patients who require dialysis, the following guidelines forinjection schedule are recommended:1. Hemodialysis patients should receive their injection at night just prior to going to
sleep or at least 3-4 hours after their hemodialysis to prevent hematoma formationdue to the heparin.
2. Chronic Cycling Peritoneal Dialysis (CCPD) patients should receive their injection inthe morning after they have completed dialysis.
3. Chronic Ambulatory Peritoneal Dialysis (CAPD) patients should receive their injectionin the evening at the time of the overnight exchange.
The solution should be clear immediately after removal from the refrigerator.Occasionally, after refrigeration, you may notice that small colorless particles of proteinare present in the solution. This is not unusual for solutions containing proteins. Allowthe vial to come to room temperature and gentry swirl. If the solution is cloudy thecontents MUST NOT be injected.Before needle insertion, wipe the septum of the Nutropin AQ vial with rubbing alcohol oran antiseptic solution to prevent contamination of the contents by microorganisms thatmay be introduced by repeated needle insertions. It is recommended that Nutropin AQ beadministered using sterile, disposable syringes and needles. The syringes should be ofsmall enough volume that the prescribed dose can be drawn from the vial withreasonable accuracy.STABILITY AND STORAGEVial contents are stable for 28 days after initial use when stored at 2-8°C/36-46°F(under refrigeration). Avoid freezing the vial of Nutropin AQ.
HOW SUPPLIEDNutropin AQ is supplied as 10 mg (approximately 30 IU) of sterile liquid somatropin pervial.Each carton contains six single vial cartons containing one 2 mL vial of Nutropin AQ(5 mg/mL).NDC 50242-114-11
Nutropin AO™ [somatropin (rDNA origin) injection]Manufactured by:
Genentech, Inc.460 Pt San Bruno BlvdSo San Francisco, CA 94080-4990
©1996 Genentech, Inc.
G7O8O7-RO(G48109-R0)
LF108January 1996
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Therapeutic regimens requiring reconstitution are more complicated, which may lead to dosing errors that may go undetected untila patient's follow-up visit to his or her physician.
• By eliminating reconstitution, Nutropin AQ greatly simplifies the preparation of growth hormone, which in turn may reducetraining time.
Nutropin AQ can be used for 28 days after initial vial entry, compared to 14 days for reconstituted lyophilized growth hormone,resulting in less product waste for some patients.
• Genentech has made a long-term commitment to offer the latest advances in growth management products and programs to thepediatric endocrinology and nephrology communities. Nutropin AQ is the most recent example of our commitment.
Patients being treated with this and other growth hormone products, and/or their parents, should be informed of thepotential benefits and risks associated with growth hormone therapy.• Intracranial hypertension (with papilledema, visual changes, headache, nausea, and/or vomiting) has been reported
in a small number of patients treated with growth hormone.• Patients should be advised to seek prompt medical attention if allergic reactions occur.• Testing for antibodies to human growth hormone should be carried out in any patient who fails to respond to therapy.• Patients should be encouraged to report the development of a limp or complaints of hip or knee pain.• Leukemia has been reported in a small number of growth hormone-deficient patients treated with growth hormone;
however, experts cannot conclude that growth hormone therapy is responsible for these occurrences. The risk, if any, remainsto be established.
• Growth hormone should not be used insubjects with closed epiphyses or inpatients with active neopiasia.
ytropinA®
For more information on Nutropin AQ,please contact your Genentech salesrepresentative.
Nutropin[somatropin (rDNA origin) injection]
Genentech, Inc.
© 1996 Genentech, Inc. All Rights Reserved. G70824-R0 LF0149 277-V2-287-95 Printed in U.S.A. May 1996 Please see Nutropin AQ full prescribing information on back page.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

May improvedosing accuracy
Eliminatesreconstitution
ReducesA product waste
Leading the wayin growth hormone
il A therapy
«,
NewNutropinAi[somatropin (rDNA origin) injection]
Indicated for the long-term treatment of children with growth failure dueto a lack of adequate endogenous growth hormone secretion and thetreatment of children who have growth failure associated with chronicrenal insufficiency up to the time of renal transplantation.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

SYNTHROID®, $22.7(?
LEVOXYL™
IF YOU'RE STILLPRESCRIBING SYNTHROID,
HERE'S A DOSE OF REALITY.At less than half the cost of Synthroid, it's no surprise Levoxyl (Levothyroxine Sodium
Tablets, USP) is the fastest growing name brand levothyroxine preparation on the markettoday. With precise dosing and consistent therapeutic effectiveness, Levoxyl is trusted bypatients, pharmacists and physicians alike.
So trusted, Levoxyl is the second most dispensed brand name levothyroxine preparation—and the 64th* most often dispensed medication in America.
For your patients' sake, prescribe Levoxyl. It boasts a spotless recall record. No small featthese days. But seeing as we've manufactured and tested Levoxyl in the same facility for overa decade, we've earned it.
Levoxyl. Take a closer look. You'll be shocked at the difference it means for your patient.
Formerly Levoxine8
(Levothyroxine SodiumTablets, USP)Synthroid" is a registered trademark of Knoll Pharmaceutical Company. nOO meg (0.1 mg), 100's each. AWP DATA, MEDI-SPAN* Sept. 1995. * American Druggist, Feb. 1996.
;g 75 meg 88 meg 100 meg 112 meg 125 meg 137 meg 150 meg 175 meg 200 meg 300 meg(0.025 mg) (0.05mg) (0.075mg) (0.088mg) (0.1 mg) (0.112 nig) (0.125 ing) (0.137mg) (0.150mg) (0.175mg) (0.2 mg) (0.3 mg)
DANIELS PHARMACEUTICALS, INC. PliTHRSlSURG, FLORIDA X,7\VMB
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
BRIEF SUMMARY. BEFORE PRESCRIBING, PLEASE CONSULT PACKAGE INSERT.
LevoxyfFormerly I£ixmne +JFormerly Levoxine
FOR ORAL ADMINISTRATIONINDICATIONS AND USAGE: LEVOXYL (L-thyroxine) tablets are indicated:1. As replacement or supplemental therapy lor diminished or absent thyroid (unction (e.g., cretinism, myxedema, nontoxic goiteror hypothyroidism generally, including the hypothyroid state in children, in pregnancy and in the elderly) resulting from functionaldeficiency, primary atrophy, from partial or complete absence ol the gland or from the effects of surgery, radiation or antithyroidagents. Therapy must be maintained continuously to control the symptoms of hypothyroidism.2. As a pituitary TSH suppressant, in the treatment or prevention of various types of euthyroid goiters, including thyroid nodules,subacute or chronic lymphocytic thyroiditis (Hashimoto's), multinodular goiter, and in the management ol thyroid cancer.3. As a diagnostic agent in suppression tests to aid in the diagnosis of suspected mild hyperthyroidism or thyroid gland autonomy.CONTRAINDjCATIONS: L-thyroxine therapy is contraindicated in thyrotoxicosis, acute myocaidial infarction and uncorrectedadrenal insufficiency.
WARNINGS:
Drugs with thyroid hormone activity, alone or together with other therapeutic agents, have been used for the treatment of obesity.In euthyroid patients, doses within the range of daily hormonal requirements are ineffective for weight reduction. Larger dosesmay produce serious or even life-threatening manifestations of toxicity, particularly when given is association with sympathomimeticamines such as those used for their anorectic effects.
PRECAUTIONS: Qtnaral • Caution must be exercised in the administration of this drug to patients with cardiovasculardisease. Development of chest pain or other aggravation ol the cardiovascular disease requires a reduction of dosage.Information For Th« Patient - Patients on thyroid preparations and parents of children on thyroid therapy should be informedthat:1. Replacement therapy is to be taken essentially for life, with the exception of cases of transient hypothyroidism, usually associatedwith thyroiditis, and in those patients receiving a therapeutic trial of the drug.2. They should immediately report during the course of therapy any signs or symptoms of thyroid hormone toxicity, e.g., chestpain, increased pulse rate, palpitations, excessive sweating, heat intolerance, nervousness, or any other unusual event.3. In case of concomitant diabetes mellitus, the daily dosage of antidiabetic medication may need readjustment as thyroid hormonereplacement is achieved. II thyroid medication is stopped, a downward readjustment of the dosage of insulin or oral hypoglycemicagent may be necessary to avoid hypoglycemia. At all times, close monitoring of urinary or blood glucose levels is mandatory insuch patients.4. In case of concomitant oral anticoagulant therapy, the prothrombin time should be measured frequently to determine il thedosage of oral anticoagulants is to be readjusted.5. Partial loss ol hair may be experienced by children in the first few months of thyroid therapy, but this is usually a transientphenomenon and later recovery is usually the rule.Drug I n u n c t i o n s - In patients with diabetes mellitus, addition of thyroid hormone therapy may cause an increase in requireddosage of insulin or oral hypoglycemic agents. Therefore, patients with diabetes mellitus should be observed closely for possiblechanges in antidiabetic drug dosage requirements.Patients stabilized on oral anticoagulants who are found to require thyroid replacement therapy should be watched very closelywhen therapy is started. If a patient is truly hypothyroid, it is likely that a reduction in anticoagulant dosage will be required. Nospecial precautions appear to be necessary when oral anticoagulant therapy is begun in a patient already stabilized on maintenancethyroid replacement therapy.Cholestyramine binds both Tt and T3 in the intestine, thus impairing absorption of these thyroid hormones. In vitro studies indicatethat the binding is not easily removed. Therefore, four to five hours should elapse between administration ol cholestyramine andthyroid hormones.Estrogens tend to increase serum thyroxine-binding globulin (TBG). In a patient with a non-functioning thyroid gland who is receivingthyroid replacement therapy, free thyroxine may be decreased when estrogens are started thus increasing thyroid requirements.However, if the patient's thyroid gland has sufficient function the decreased free thyroxine will result in a compensatory increase inthyroxine output by the thyroid. Therefore, patients without a functioning thyroid gland who are on thyroid replacement therapy mayneed to increase their thyroid dose il estrogens or estrogen containing oral contraceptives are given.Drug/Laboratory Tost Interactions -The following drugs or moieties are known to interfere with laboratory tests performed onpatients taking thyroid hormone: androgens, corticosteroids, estrogens, oral contraceptives containing estrogens, iodine-containingpreparations, and the numerous preparations containing salicylates.1. Changes in TBG concentration should be taken into consideration in the interpretation of T4 and T3 values. In such cases, theunbound (Tree) hormone should be measured. Pregnancy, estrogens, and estrogen-containing oral contraceptives increase TBGconcentrations. TBG may also be increased during infectious hepatitis. Decreases in TBG concentrations are observed in nephrosis,acromegaly, and after androgen or corticosteroid therapy. Familial hyper-or hypo-thyroxine-binding-globulinemias have beendescribed. The incidence of TBG deficiency approximates 1 in 9000. The binding of thyroxine by thyroid-binding pre-albumin(TBPA) is inhibited by salicylates.2. Medical or dietary iodine interferes with all in vivo tests of radio-iodine uptake, producing low uptakes which may not bereflective of a true decrease in hormone synthesis.3. The persistence of clinical and laboratory evidence of hypothyroidism in spite ol adequate dosage replacement indicateseither poor patient compliance, poor absorption, excessive fecal loss, or inactivity of the preparation. Tntracellular resistance tothyroid hormone is quite rare.CarclnogoMsIs, MutageiMtls, And Impairment Of Fertility - A reportedly apparent association between prolongedthyroid therapy and breast cancer has not been confirmed and patients on thyroid for established indications should not discontinuetherapy. No confirmatory long-term studies in animals have been performed to evaluate carcinogenic potential, mutagenicity, orimpairment of fertility in either males or females.Pregnancy • Category A • Thyroid hormones do not readily cross the placental barrier. The clinical experience to date does notindicate any adverse effect on fetuses when thyroid hormones are administered to pregnant women. On the basis of current knowledge,thyroid replacement therapy to hypothyroid women should not be discontinued during pregnancy.Nursing Mothers - Minimal amounts of thyroid hormones are excreted in human milk. Thyroid is not associated with seriousadverse reactions and does not have a known tumorigenic potential. However, caution should be exercised when thyroid isadministered to a nursing woman.Pediatric Use • Pregnant mothers provide little or no thyroid hormone to the fetus. The incidence of congenital hypothyroidism isrelatively high (1:4,000) and the hypothyroid fetus would not derive any benefit from the small amounts of hormone crossing theplacental barrier. Routine determinations or serum (TJ and/or TSH is strongly advised in neonates in view of the deleterious effectsof thyroid deficiency on growth and development.Treatment should be initiated immediately upon diagnosis, and maintained for life, unless transient hypothyroidism is suspected: inwhich case, therapy may be interrupted for 2 to 8 weeks after the age of 3 years to reassess the condition. Cessation of therapy isjustified in patients who have maintained a normal TSH during those 2 to 8 weeks.ADVERSE REACTIONS: Adverse reactions are due to overdosage and are those of induced hyperthyroidism.OVERDOSE • Excessive dosage of thyroid medication may result in symptoms of hyperthyroidism. Since, however, the effects donot appear at once, the symptoms may not appear for one to three weeks after the dosage regimen is begun. The most commonsigns and symptoms of overdosage are weight loss, palpitation, nervousness, diarrhea or abdominal cramps, sweating, tachycardia,cardiac arrhythmias, angina pectoris, tremors, headache, insomnia, intolerance to heat and fever. If symptoms of overdosageappear, discontinue medication for several days and reinstate treatment at a lower dosage level.Laboratory test such as serum T serum T, and the free thyroxine index will be elevated during the period ol overdosage.Complications as a result of the induced hypermetabolic state may include cardiac failure and death due to arrhythmia or failure.TREATMENT OF OVERDOSE • Dosage should be reduced or therapy temporarily discontinued if signs and symptoms ofoverdosage appear. Treatment may be reinstituted at a lower dosage. In normal individuals, normal hypothalamic pituitary-thyroidaxis function is restored in 6 to 8 weeks after thyroid suppression.Treatment of acute massive thyroid hormone overdosage is aimed at reducing gastrointestinal absorption of the drugs andcounteracting central and peripheral effects, mainly those ol increased sympathetic activity. Vomiting may be induced initially ilfurther gastrointestinal absorption can reasonably be prevented and barring contraindications such as coma, convulsions, or loss olthe gagging reflex. Treatment is symptomatic and supportive. Oxygen may be administered and ventilation maintained. Cardiacglycosides may be indicated il congestive heart failure develops. Measures to control fever, hypoglycemia, or fluid loss should beinstituted if needed. Antiadrenergic agents, particularly propranolol, have been used advantageously in the treatment ol increasedsympathetic activity. Propranolol maybe administered intravenously at a dosage ol 1 to 3 mg over a 10 minute period or orally, 80 to160 mg/day, especially when no contraindications exist for its use.
(JANIEISPHARMACEUTICALS, INC.2517 25th Avenue North • St. Petersburg, Florida 33713Revised December 1995
r a m ; r»RECENT PROGRESS
IN HORMONE RESEARCHCONFERENCE PROCEEDINGS,
VOLUME 51(Formerly The Laurentian Hormone Conference)
Edited by P. Michael ConnThe pre-eminence of the contributors and the significance
of their topics make this Proceedings volume of the new Recent
Progress in Hormone Research Conference especially
noteworthy. Now under the auspices of The Endocrine Society,
the meeting, formerly known as The Laurentian Hormone
Conference, was characterized by the communication of
significant new and emerging topics in endocrinology and allied
areas of biochemistry, molecular biology, and neuroscience. So
stellar is the line-up of speakers that the phrase "the Super Bowl
of Endocrinology" has been aptly applied to the meeting.
CONTENTS
Conference Speaker Correspondence Information
Preface1. Genetic Analysis of Thyroid Hormone Receptors in Development
and Disease2. The Gonadotropin Genes: Evolution of Distinct Mechanisms for
Hormonal Control3. A Nuclear Matrix Acceptor Site for the Progesterone Receptor in
the Avian c-myc Gene Promoter4. Resistance to Thyrotropin and Other Abnormalities of the
Thyrotropin Receptor5. Transgenic Models to Study the Roles of Inhibins and Activins in
Reproduction, Oncogenesis, and Development6. Estrogen Receptor Gene Disruption: Molecular Characterization
and Experimental and Clinical Phenotypes7. IGF-I Receptor Signalling: Lessons from the Somatotroph8. Transcriptional Control of Cell Phenotypes in the Neuroendocrine
System9. The Gene Responsible for Adrenal Hypoplasia Congenita, DAX-1,
Encodes a Nuclear Hormone Receptor That Defines a New ClassWithin the Superfamily
10. Modulation of Pulsatile GH Release Through a Novel Receptor inHypothalamus and Pituitary Gland
11. The Melanocortin Receptors: Agonists, Antagonists, and theHormonal Control of Pigmentation
12. Desensitization of G Protein-Coupled Receptors13. Modulator and Messenger Functions of Cyclic ADP-Ribose in
Calcium Signaling14. The JAK-STAT Pathway: Summary of Initial Studies and Recent
Advances15. Protein Tyrosine Phosphatases: Their Roles in Signal
Transduction16. Extracellular Matrix Signaling from the Cellular Membrane
Skeleton to the Nuclear Skeleton: A Model of Gene Regulation17.Gonadal Cell Apoptosis18. The Biochemistry and Molecular Biology of Glucocorticoid-
Induced Apoptosis in the Immune System19. Programmed Cell Death in Human Breast Cancer Cells
Index
ISBN: 1-879225-22-0. Hardcover, 522 pages. $105.00Add $15.00 per book for airmail shipment outside the United States
The Endocrine Society
4350 East West Highway, Suite 500
Bethesda MD 20814-4410
Telephone: (301)941-0240
Fax:(301)941-0259
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

The current treatment algorithm foracromegaly recommends surgery as first-line therapy. While initial success is ashigh as 80%, surgery may be contraindi-cated in some patients or may fail tonormalize hormone levels*'' Radiation,which is usually second-line therapy, maytake years to become fully effective' andis associated with significant sideeffects:' This suggests that other med-ical therapies may play a critical role inthe treatment of some patients.
RADIATION THERAPY
Conventional radiation halts tumor growthand shrinks most tumors; however, growthhormone (GH) levels decline slowly over time.'In fact, circulating GH and insulin-like growth
factor-1 (IGF-1) levels continue to be elevated,often taking more than 2 to 20 years beforenormal values are achieved.' During this time,the acromegalic patient is exposed to elevatedGH levels, which are associated with disfigure-ment, as well as many serious metabolic,endocrine, respiratory, and cardiovasculardisorders. Excessive GH secretion has alsobeen linked to increased mortality, reducinglife expectancy by about 10 years.3
In addition, radiation therapy is associatedwith a number of side effects, including hypo-pituitarism, which occurs in more than 50% ofall patients." Side effects such as hair loss,cranial nerve palsy, and brain necrosis occur fre-quently despite modern facilities and methods.Brain tumors, infertility, loss of vision, lethargy,and impaired memory have also been associat-ed with radiation therapy.'56
Di. is and Localization
mZph°Ad"n™an
Surgery ,
T H E CURRENT ACROMEGALYTREATMENT ALGORITHM'1
GH <2 no/ml ' GH >2 ng/ml1 ,
r Irradiation ,
GH <2 ng/ml1 GH >2 ng/ml1 1
I Parlodel* ,I (bromocriptine mesylate) \
GH<2 ng/mL1 GH >2 ng/mL' ,
I SANDOSTATIN" .| (octreotide acetate) \
Adapted with perm,ssion from Melmed. GH<2 ng/mL1 GH>2 ng/mL1 ,
Indocrinologisl 1991;1:334. SANDOSTATIN
'After oral glucose tolerance test a n d p » r l o d 8 1
o
PHARMACOLOGICTHERAPY
Although bromocriptine mesylate isrecommended as the first-line pharmacologicoption, the effectiveness of this therapy islimited by its ability to normalize GH levelsin only 12% of patients/
However, one pharmacologic therapymay demonstrate an ability to reduce hormonelevels when other therapies have failed.SANDOSTATIN® (octreotide acetate), atdosages of 100 meg t.i.d., has been shownto reduce serum GH to within normal ranges*in 50% of patients and to reduce IGF-1 towithin normal ranges in 50% to 60% ofpatients after 2 weeks of therapy.''
The primary goal of long-term therapyis to reduce GH and IGF-1 levels to withinnormal ranges.* In a long-term study of 103acromegalic patients, SANDOSTATIN signif-icantly reduced mean GH levels (30.9 ng/mLto 5.7 ng/mL) and normalized IGF-1 levels inthe majority of patients for up to 30 monthsof therapy."
Gastrointestinal effects such as diar-rhea, loose stools, nausea, and abdominaldiscomfort were each seen in 30% to 58%of acromegalic patients in US studiesalthough only 2% of patients discontinuedtherapy because of these symptoms.'
Given the potential risks associated withlong-term GH and IGF-1 hypersecretion, med-ical therapy may be an effective choice whileawaiting the effectiveness of radiation therapy,or in cases where radiation is inappropriate.
Sandostatinoctreotide acetate I SANDOZ
INJECTION
Do you have a question related to SANDOSTATIN? For insurance or reimbursement information,call 1-800-772-7556. For medical or technical information, call 1-800-732-8096.
Please see references and brief summary of prescribing information on following page.
"Normal GH: <5 ng/mL; Normal IGF-1: Males <1.9 U/mL, Females <2.2 U/mL—using a radioimmunoassay from the Nichols Institute.1 The long-term effects of SANDOSTATIN* loctreotide acetate) on morbidity and mortality have not been evaluated in clinical trials. Adverse reactions associated with SANDOSTATIN therapy includegallstones (27%), biliary sludge without stones (22%). biliary duct dilatation (3%), and bradycardia |21%|. Patients should be observed upon introduction of SANDOSTATIN therapy for symptomaticevidence of hyperglycemia (15%) and hypoglycemia (3%), which may necessitate dosage changes in insulin therapy. Hypothyroidism has been demonstrated in some patients (12%).
©1996 Sandoz Pharmaceuticals Corporation 4/96 Printed in USA SDS-1195-01
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Sandostatin'octiwlide acetate ISANDOZ
INJECTIONCAUTION: Federal law prohibits dispensing without a prescription.
BRIEF SUMMARY: Please see package insert for full prescribing information.
INDICATIONS AND USAGE
Acromegaly: Sandostatin® (octreotide acetate) is indicated to reduce blood levels of growth hormoneand IGF-I (somatomedin C) in acromegaly patients who have had inadequate response to or cannot betreated with surgical resection, pituitary irradiation, and bromocriptine mesylate at maximally tolerateddoses. The goal is to achieve normalization of growth hormone and IGF-I (somatomedin C) levels(See DOSAGE AND ADMINISTRATION in the full prescribing information). In patients with acromegaly,Sandostatin® (octreotide acetate) reduces growth hormone to within normal ranges in 50% of patientsand reduces IGF-I (somatomedin C) to within normal ranges in 50%-60% of patients. Since the effectsof pituitary irradiation may not become maximal for several years, adjunctive therapy with Sandostatin®(octreotide acetate) to reduce blood levels of growth hormone and IGF-I (somatomedin C) offers poten-tial benefit before the effects of irradiation are manifested.
Improvement in clinical signs and symptoms or reduction in tumor size or rate of growth were notshown in clinical trials performed with Sandostatin® (octreotide acetate); these trials were not optimallydesigned to detect such effects.
Carclnold Tumors: Sandostatin® (octreotide acetate) is indicated for the symptomatic treatment ofpatients with metastatic carcinoid tumors where it suppresses or inhibits the severe diarrhea andflushing episodes associated with the disease.
Sandostatin® (octreotide acetate) studies were not designed to show an effect on the size, rate of growthor development of metastases.
Vasoactlve Intestinal Peptide Tumors (VIPomas): Sandostatin® (octreotide acetate) is indicated for thetreatment of the profuse watery diarrhea associated with VIP-secreting tumors. Sandostatin® (octreotideacetate) studies were not designed to show an effect on the size, rate of growth or development ofmetastases.
CONTRAINDICATIONSSensitivity to this drug or any of its components.
WARNINGSSingle doses of Sandostatin® (octreotide acetate) have been shown to inhibit gallbladder contractilityand decrease bile secretion in normal volunteers. In clinical trials (primarily patients with acromegaly orpsoriasis), the incidence of biliary tract abnormalities was 63% (27% gallstones, 24% sludge withoutstones, 12% biliary duct dilatation). The incidence of stones or sludge in patients who receivedSandostatin® (octreotide acetate) for 12 months or longer was 52%. Less than 2% of patients treatedwith Sandostatin® (octreotide acetate) for 1 month or less developed gallstones. The incidence ofgallstones did not appear related to age, sex or dose. Like patients without gallbladder abnormalities,the majority of patients developing gallbladder abnormalities on ultrasound had gastrointestinal symptoms.The symptoms were not specific for gallbladder disease. A few patients developed'acute cholecystitis,ascending cholangitis, biliary obstruction, cholestatic hepatitis, or pancreatitis during Sandostatin®(octreotide acetate) therapy or following its withdrawal. One patient developed ascending cholangitisduring Sandostatin® (octreotide acetate) therapy and died.
PRECAUTIONS
General: Sandostatin® (octreotide acetate) alters the balance between the counter-regulatory hormones,insulin, glucagon and growth hormone, which may result in hypoglycemia or hyperglycemia. Sandostatin®(octreotide acetate) also suppresses secretion of thyroid stimulating hormone, which may result inhypothyroidism. Cardiac conduction abnormalities have also occurred during treatment with Sandostatin®(octreotide acetate). However, the incidence of these adverse events during long-term therapy wasdetermined vigorously only in acromegaly patients who, due to their underlying disease and/or the sub-sequent treatment they receive, are at an increased risk for the development of diabetes mellitus, hypo-thyroidism, and cardiovascular disease. Although the degree to which these abnormalities are related toSandostatin® (octreotide acetate) therapy is not clear, new abnormalities of glycemic control, thyroidfunction and ECG developed during Sandostatin® (octreotide acetate) therapy as described below.The hypoglycemia or hyperglycemia which occurs during Sandostatin® (octreotide acetate) therapy isusually mild, but may result in overt diabetes mellitus or necessitate dose changes in insulin or otherhypoglycemic agents. Hypoglycemia and hyperglycemia occurred on Sandostatin® (octreotide acetate)In 3% and 16% of acromegalic patients, respectively. Severe hyperglycemia, subsequent pneumonia,and death following initiation of Sandostatin® (octreotide acetate) therapy was reported in one patientwith no history of hyperglycemia.
In acromegalic patients, 12% developed biochemical hypothyroidism only, 8% developed goiter, and4% required initiation of thyroid replacement therapy while receiving Sandostatin® (octreotide acetate).Baseline and periodic assessment of thyroid function (TSH, total and/or free T4) is recommended duringchronic therapy.
In acromegalics, bradycardia (<50 bpm) developed in 25%; conduction abnormalities occurred in 10%and arrhythmias occurred in 9% of patients during Sandostatin® (octreotide acetate) therapy. Other EKGchanges observed included QT prolongation, axis shifts, early repolarization, low voltage, R/S transition,and early R wave progression. These ECG changes are not uncommon in acromegalic patients. Doseadjustments in drugs such as beta-blockers that have bradycardia effects may be necessary. In oneacromegalic patient with severe congestive heart failure, initiation of Sandostatin® (octreotide acetate)therapy resulted in worsening of CHF with improvement when drug was discontinued. Confirmation ofa drug effect was obtained with a positive rechallenge.
Several cases of pancreatitis have been reported in patients receiving Sandostatin® (octreotide acetate)
therapy.
Sandostatin® (octreotide acetate) may alter absorption of dietary fats in some patients.
In patients with severe renal failure requiring dialysis, the half-life of Sandostatin® (octreotide acetate)may be increased, necessitating adjustment of the maintenance dosage.Depressed vitamin B,2 levels and abnormal Schilling's tests have been observed in some patients receivingSandostatin® (octreotide acetate) therapy, and monitoring of vitamin B|2 levels is recommended duringchronic Sandostatin® (octreotide acetate) therapy.
Information lor Patients: Careful instruction in sterile subcutaneous injection technique should be givento the patients and to other persons who may administer Sandostatin® (octreotide acetate) Injection.
Laboratory Tests: Laboratory tests that may be helpful as biochemical markers in determining andfollowing patient response depend on the specific tumor. Based on diagnosis, measurement of thefollowing substances may be useful in monitoring the progress of therapy:
Acromegaly: Growth Hormone, IGF-I (somatomedin C)
Responsiveness to Sandostatin® (octreotide acetate) may be evaluated by determininggrowth hormone levels at 1-4 hour intervals for 8-12 hours post dose. Alternatively,a single measurement of IGF-I (somatomedin C) level may be made two weeks afterdrug initiation'or dosage change.
Carcinoid: 5-HIAA (urinary 5-hydroxyindole acetic acid), plasma serotonin, plasma Substance P
VIPoma: VIP (plasma vasoactive intestinal peptide)
Baseline and periodic total and/or free T< measurements should be performed during chronic therapy(see PRECAUTIONS — General).
Drug Interactions: Sandostatin® (octreotide acetate) has been associated with alterations in nutrientabsorption, so it may have an effect on absorption of orally administered drugs. Concomitant adminis-tration of Sandostatin® (octreotide acetate) with cyclosporine may decrease blood levels of cyclosporineand result in transplant rejection.
Patients receiving insulin, oral hypoglycemic agents, beta blockers, calcium channel blockers, or agentsto control fluid arid electrolyte balance, may require dose adjustments of these therapeutic agents.
Drug Laboratory Test Interactions: No known interference exists with clinical laboratory tests, includingamine or peptide determinations.
Carclnogenesis/Mutagenesls/lmpairment of FertilityStudies in laboratory animals have demonstrated no mutagenic potential of Sandostatin® (octreotideacetate).
No carcinogenic potential was demonstrated in mice treated subcutaneously for 85-99 weeks at doses upto 2000 mcg/kg/day (8x the human exposure based on body surface area). In a 116-week subcutaneousstudy in rats, a 27% and 12% incidence of injection site sarcomas or squamous cell carcinomas wasobserved in males and females, respectively, at the highest dose level of 1250 mcg/kg/day (10x the humanexposure based on body surface area) compared to an incidence of 8%-10% in the vehicle control groups.The increased incidence of injection site tumors was most probably caused by irritation and the highsensitivity of the rat to repeated subcutaneous injections at the same site. Rotating injection sites wouldprevent chronic irritation in humans. There have been no reports of injection site tumors in patients treatedwith Sandostatin® (octreotide acetate) for up to 5 years. There was also a 15% incidence of uterineadenocarcinomas in the 1250 mcg/kg/day females compared to 7% in the saline control females and 0%in the vehicle control females. The presence of endometritis coupled with the absence of corpora lutea,the reduction in mammary fibroadenomas, and the presence of uterine dilatation suggest that the uterinetumors were associated with estrogen dominance in the aged female rats which does not occur in humaps.Sandostatin® (octreotide acetate) did not impair fertility in rats at doses up to 1000 mcg/kg/day, whichrepresents 7x the human exposure based on body surface area.
Pregnancy Category B: Reproduction studies have been performed in rats and rabbits at doses up to16 times the highest human dose based on body surface area and have revealed no evidence of impairedfertility or harm to the fetus due to Sandostatin® (octreotide acetate). There are, however, no adequateand well-controlled studies in pregnant women. Because animal reproduction studies are not alwayspredictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers: It is not known whether this drug is excreted in human milk. Because many drugs areexcreted in milk, caution should be exercised when Sandostatin® (octreotide acetate) is administered toa nursing woman.
Pediatric Use: Experience with Sandostatin® (octreotide acetate) in the pediatric population is limited.The youngest patient to receive the drug was 1 month old. Doses of 1-10 mcg/kg body weight were welltolerated in the young patients. A single case of an infant (nesidioblastosis) was complicated by a seizurethought to be independent of Sandostatin® (octreotide acetate) therapy.
ADVERSE REACTIONS
Gallbladder Abnormalities: Gallbladder abnormalities, especially stones and/or biliary sludge, frequentlydevelop in patients on chronic Sandostatin® (octreotide acetate) therapy (See WARNINGS).
Cardiac: In acromegalics, sinus bradycardia (<50 bpm) developed in 25%; conduction abnormalitiesoccurred in 10% and arrhythmias developed in 9% of patients during Sandostatin® (octreotide acetate)therapy (See PRECAUTIONS — General).
Gastrointestinal: Diarrhea, loose stools, nausea and abdominal discomfort were each seen in 34%-61%of acromegalic patients in US studies although only 2.6% of the patients discontinued therapy due tothese symptoms. These symptoms were seen in 5%-10% of patients with other disorders.The frequency of these symptoms was not dose-related, but diarrhea and abdominal discomfort generallyresolved more quickly in patients treated with 300 meg/day than in those treated with 750 meg/day.Vomiting, flatulence, abnormal stools, abdominal distention, and constipation were each seen in lessthan 10% of patients.
Hypo/Hyperglycemia: Hypoglycemia and hyperglycemia occurred in 3% and 16% of acromegalicpatients, respectively, but only in about 1.5% of other patients. Symptoms of hypoglycemia were notedin approximately 2% of patients.
Hypothyroidism: In acromegalics, biochemical hypothyroidism alone occurred in 12% while goiteroccurred in 6% during Sandostatin® (octreotide acetate) therapy (See PRECAUTIONS — General).In patients without acromegaly, hypothyroidism has only been reported in several isolated patients andgoiter has not been reported.
Other Adverse Events: Pain on injection was reported in 7.7%, headache in 6% and dizziness in 5%.
Other Adverse Events 1%-4%: Other events (relationship to drug not established), each observed in1%-4% of patients, included fatigue, weakness, pruritus, joint pain, backache, urinary tract infection,cold symptoms, flu symptoms, injection site hematoma, bruise, edema, flushing, blurred vision,pollakiuria, fat malabsorption, hair loss, visual disturbance and depression.
Other Adverse Events <1%: Events reported in less than 1 % of patients and for which relationship to drugis not established are listed: Gastrointestinal: hepatitis, jaundice, increase in liver enzymes, Gl bleeding,hemorrhoids, appendicitis, gastric/peptic ulcer, gallbladder polyp; Integumentary: rash, celluiitis, petechiae,urticaria, basal cell carcinoma; Musculoskeletal: arthritis, joint effusion, muscle pain, Raynaud's phenome-non; Cardiovascular: chest pain, shortness of breath, thrombophlebitis, ischemia, congestive heart failure,hypertension, hypertensive reaction, palpitations, orthostatic BP decrease, tachycardia; C/vS: anxiety,libido decrease, syncope, tremor, seizure, vertigo, Bell's Palsy, paranoia, pituitary apoplexy, increasedintraocular pressure, amnesia, hearing loss, neuritis; Respiratory: pneumonia, pulmonary nodule, statusasthmaticus; Endocrine: galactorrhea, hypoadrenalism, diabetes insipidus, gynecomastia, amenorrhea,polymenqrrhea, oligomenorrhea, vaginitis; Urogenital: nephrolithiasis, hematuria; Hematologic: anemia,iron deficiency, epistaxis; Miscellaneous: otitis, allergic reaction, increased CK, weight loss.Evaluation of 20 patients treated for at least 6 months has failed to demonstrate titers of antibodiesexceeding background levels. However, antibody titers to Sandostatin® (octreotide acetate) were sub-sequently reported in three patients and resulted in prolonged duration of drug action in two patients.Anaphylactoid reactions, including anaphylactic shock, have been reported in several patients receivingSandostatin® (octreotide acetate).
Storage: For prolonged storage, Sandostatin® (octreotide acetate) ampuls and multi-dose vials shouldbe stored at refrigerated temperatures 2'-8'C (36"-46*F) and protected from light. At room temperature,(20*-30"C or 7O'-86'F), Sandostatin® (octreotide acetate) is stable for 14 days if protected from light.The solution can be allowed to come to room temperature prior to administration. Do not warm artificially.After initial use, multiple dose vials should be discarded within 14 days. Ampuls should be opened justprior to administration and the unused portion discarded.
The ampuls are manufactured by SANDOZ PHARMA LTD., Basle, SwitzerlandforSANDOZ PHARMACEUTICALS CORPORATION, East Hanover, New Jersey 07936
The multi-dose vials are manufactured by SCHERING-PLOUGH PRODUCTS, INC., Manati, Puerto RicoforSANDOZ PHARMACEUTICALS CORPORATION, East Hanover, New Jersey 07936
Sandoz Pharmaceuticals Corporation, East Hanover, New Jersey 07936
REV: DECEMBER 1995 P30283902
References: 1. Melmed S. Management choices in acromegaly. Endocrinologist. 1991:1:331-335. 2. MelmedS,Dowling RH, Frohman L, et al. Consensus statement: benefits versus risks of medical therapy for acromegaly. AmJMed. 1994:97:468-473. 3. Rajasoorya C, Holdaway IM, Wrightson P, et al. Determinants of clinical outcome andsurvival in acromegaly. Clin Endocrinol. 1994:41:95-102. 4. Snyder PJ, Fowble BF, Schatz NJ. et al.Hypopituitarism following radiation therapy of pituitary adenomas. Am JMed. 1986:81:457-462. 5. MelmedS.Acromegaly. N Engl J Med. 1990:322:966-977. 6. Molitch ME. Management of persistent or recurrent functionalpituitary adenomas following pituitary adenoma surgery. Endocrinologist. 1995:5:451-456. 7. Ezzat S, Snyder PJ,Young WF. et al. Octreotide treatment of acromegaly: a randomized, multicenter study. Ann Intern Med.1992;117:711-718. 8. Newman CB, Melmed S, Snyder PJ, et al. Safety and efficacy of long-term octreotide therapyof acromegaly: results of a multicenter trial in 103 patients — a clinical research center study. J Clin EndocrinolMetab. 1995:80:2768-2775.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

GLUCOPHAGE(METFORMIN HYDROCHLORIDE TABLETS)soo me
BOUND FOR EFFICACYAND SECONDARY BENEFITS
Please see brief summary of prescribinginformation, including the boxedWARNING regarding Lactic Acidosis,on the last page of this advertisement.
Bristol-Myers Squibb Company
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

BENEFITS BEYOND GLUCOSE CONTROLIN TYPE II DIABETES
GLUCOPHAGEimproves insulinsensitivityNo effect on pancreatic beta cellsor insulin secretion.
GLUCOPHAGE ishighly effective first-linedrug therapy1
Significantly decreases fastingplasma glucose (FPG) when usedas an adjunct to diet.
Mean difference inFPG comparedwith placebo
GLUCOPHAGEvs placebo
PO.00I
Study I : Results of a double-blind, placebo-controlled, multicenter trial over 29 weeks. 286randomized type II patients: GLUCOPHAGE,n = l4l;placebo,n=l45. Average dosage ofGLUCOPHAGE was 1,980 mg/day.12
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

GLUCOPHAGEdelivers four importantsecondary benef i
1. Does not cause hyperinsulinemia
2. Does not produce hypoglycemia
3. Helps keep weight from increasing
4. Has modest, favorable effectson lipids
GLUCOPHAGEoffers unique synergyin combination1
Combining GLUCOPHAGEand a sulfonylurea with dietlowers FPG significantly morethan monotherapy.1
Mean difference inFPG comparedwith monotherapy
GLUCOPHAGEplus glyburidevs glyburide alone PO.00I
Study 2: Results of a double-blind, placebo-controlled,parallel-group, multicenter trial comparing GLUCOPHAGE(n=210), glyburide (n=209),and the combination (n=2l3)over 29 weeks. 632 randomized type II patients in whomglyburide monotherapy (20 mg/day) plus dietary interventionhad failed to provide adequate control. Average dosage ofGLUCOPHAGE was 2,050 mg/day as monotherapy and1,894 mg/day in combination.1-1
W I T H D I E T — A L O N E O R W I T H A S U L F O N Y L U R E A
GLUCOPHAGE(METFORMIN HYDROCHLORIDE TABLETS)™ mgBOUND FOR EFFICACY AND SECONDARY BENEFITS
Please see brief summary of prescribing information, including the boxedWARNING regarding Lactic Acidosis, on the last page of this advertisement.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

IN TYPE II DIABETES
ESTABLISHED SAFETY AND BID DOSING
established inmillions of patient-yearsof experience3
Mild and transient Gl side effects are mostcommon.
Diarrhea, nausea, vomiting, bloating, orflatulence may occur, especially duringinitiation of GLUCOPHAGE.• Approximately 30% more frequent than with
placebo.• Only ~ 4% of patients discontinue therapy due
to Gl reactions.
Rare occurrence of lacticacidosis, a serious conditionApproximately 0.03 cases per 1,000patient-years reported worldwide.• If cases occur, up to half may be fatal.• Seen primarily in patients with renal
insufficiency.• Patient Package Insert lists symptoms to be
discussed with patients.
The UGDP study suggested increased cardio-vascular risk with oral antidiabetics.
Appropriate patientselection is keyContraindicated in patients with renaldisease or renal dysfunction and inpatients with metabolic acidosis.
Temporarily withhold in patients receivingiodinated contrast materials for radiologicstudies.
Avoid in patients with impaired hepaticfunction or excessive alcohol intake (acuteor chronic).
Not recommended for children orpregnant women.
Titrate to effective dosagerange (ISOO-25OO mg/day)Recommended starting dosage:500 mg BID with meals.
Increase dosage by one 500 mg tableteach week.
Minimize Gl side effects: Administrationwith meals helps.• Occasionally, temporary dose reduction may
be useful.
Individualize dosage based on effectivenessand tolerance up to a maximum of 2500 mgadministered on aTlD schedule.
W I T H D I E T — A L O N E O R W I T H A S U L F O N Y L U R E A
GLUCOPHAGE(METFORMIN HYDROCHLORIDE TABLETS)soo mg
BOUND FOR EFFICACY AND SECONDARY BENEFITS
References: I . Data on file. Bristol-Myers Squibb Company. 2. DeFronzo RA, Goodman A, and the Multicenter Metformin Study Group: Efficacy ofmetformin in patients with non-insulin-dependent diabetes mellitus. N Englj Med 333(9):541 -549.1995. 3.Sirtori CR, Pasik C: Re-evaluation of abiguanide, metformin: mechanism of action and tolerability. Pharmacol Res 30(3): 187-228,1994.
Please see brief summary of prescribing information, including theboxed WARNING regarding Lactic Acidosis, on the last pageof this advertisement.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

GLUCOPHAGE* (METFORMIN HYDROCHLORIDE TABLETS) 500 mgCONTRAINDICATIONS: GLUCOPHAGE is contraindicated in patients with: 1. Renal disease or renal dysfunction(e.g., as suggested by serum creatinine levels 21.5 mg/dL [males], £1.4 mg/dL [females] or abnormal creatinineclearance) which may also result from conditions such as cardiovascular collapse (shock), acute myocardialinfarction, and septicemia (see WARNINGS and PRECAUTIONS). 2. GLUCOPHAGE should be temporarily withheldin patients undergoing radiologic studies involving parenteral administration of iodinated contrast materials,because use of such products may result in acute alteration of renal function. (See also PRECAUTIONS). 3. Knownhypersensitlvity to metformin hydrochloride. 4. Acute or chronic metabolic acidosis, including diabetic ketoacido-sis, with or without coma. Diabetic ketoacidosis should be treated with insulin.
WARNINGS: Lactic Acidosis: Lactic acidosis Is a rare, but serious, metabolic complication that can occur due tometformin accumulation during treatment with GLUCOPHAGE; when it occurs, it is fatal in approximately 50% ofcases. Lactic acidosis may also occur In association with a number of pathophyslologlc conditions, Including dia-betes mellitus, and whenever there Is significant tissue hypoperfuslon and hypoxemia. Lactic acidosis is charac-terized by elevated blood lactate levels (>5 mmol/L), decreased blood pH, electrolyte disturbances with anIncreased anlon gap, and an Increased lactate/pyruvate ratio. When metformin is implicated as the cause of lac-tic acidosis, metformin plasma levels > 5 ug/mL are generally found. The reported incidence of lactic acidosis inpatients receiving metformin hydrochloride Is very low (approximately 0.03 cases/1,000 patient-years, withapproximately 0.015 latal cases/1,000 patient-years). Reported cases have occurred primarily in diabeticpatients with significant renal Insufficiency, Including both intrinsic renal disease and renal hypoperfuslon, oftenIn the setting of multiple concomitant medical/surgical problems and multiple concomitant medications. The riskof lactic acidosis Increases with the degree of renal dysfunction and the patient's age. The risk of lactic acidosismay, therelore, be significantly decreased by regular monitoring of renal function in patients takingGLUCOPHAGE and by use of the minimum effective dose of GLUCOPHAGE. In addition, GLUCOPHAGE should bepromptly withheld In the presence of any condition associated with hypoxemia or dehydration. Because impairedhepatic function may significantly limit the ability to clear lactate, GLUCOPHAGE should generally be avoided inpatients with clinical or laboratory evidence of hepatic disease. Patients should be cautioned against excessivealcohol Intake, either acute or chronic, when taking GLUCOPHAGE, since alcohol potentiates the effects of met-formin hydrochloride on lactate metabolism. In addition, GLUCOPHAGE should be temporarily discontinued priorto any intravascular radiocontrast study and for any surgical procedure (see also PRECAUTIONS). The onset oflactic acidosis often Is subtle, and accompanied only by nonspecific symptoms such as malaise, myalgias, res-piratory distress, Increasing somnolence and nonspecific abdominal distress. There may be associatedhypothermia, hypotension and resistant bradyarrhythmlas with more marked acidosis. The patient and thepatient's physician must be aware of the possible Importance of such symptoms and the patient should beInstructed to notify the physician immediately If they occur (see also PRECAUTIONS). GLUCOPHAGE should bewithdrawn until the situation Is clarified. Serum electrolytes, ketones, blood glucose and, if Indicated, blood pH,lactate levels and even blood metformin levels may be useful. Once a patient is stabilized on any dose level ofGLUCOPHAGE, gastrointestinal symptoms, which are common during initiation of therapy, are unlikely to be drugrelated. Later occurrence of gastrointestinal symptoms could be due to lactic acidosis or other serious disease.Levels of fasting venous plasma lactate above the upper limit of normal but less than 5 mmol/L In patients takingGLUCOPHAGE do not necessarily indicate impending lactic acidosis and may be explainable by other mecha-nisms, such as poorly controlled diabetes or obesity, vigorous physical activity or technical problems In samplehandling. (See also PRECAUTIONS.) Lactic acidosis should be suspected in any diabetic patient with metabolicacidosis lacking evidence of ketoacidosis (ketonurfa and ketonemla). Lactic acidosis Is a medical emergencythat must be treated In a hospital setting. In a patient with lactic acidosis who is taking GLUCOPHAGE, the drugshould be discontinued immediately and general supportive measures promptly instituted. Because metforminhydrochloride Is dlalyzable (with a clearance of up to 170 mL/mln under good hemodynamic conditions), prompthemodialysls Is recommended to correct the acidosis and remove the accumulated metformin. Suchmanagement often results In prompt reversal of symptoms and recovery. (See also CONTRAINDICATIONS andPRECAUTIONS).
SPECIAL WARNING ON INCREASED RISK OF CARDIOVASCULAR MORTALITY: The administration of oral antJdiabetJcdrugs has been reported to be associated with Increased cardiovascular mortality as compared to treatment withdiet alone or diet plus Insulin.PRECAUTIONS: General: Monitoring of renal function—GLUCOPHAGE is known to be substantially excreted by thekidney, and the risk of metformin accumulation and lactic acidosis increases with the degree of impairment of renalfunction. Thus, patients with serum creatinine levels above the upper limit of normal for their age should not receiveGLUCOPHAGE. In patients with advanced age, GLUCOPHAGE should be carefully titrated to establish the minimumdose tor adequate glycemic effect, because aging is associated with reduced renal function. In elderly patients, renalfunction should be monitored regularly and, generally, GLUCOPHAGE should not be titrated to the maximum dose (seeDOSAGE AND ADMINISTRATION). Before initiation of GLUCOPHAGE therapy and at least annually thereafter, renalfunction should be assessed and verified as normal. In patients in whom development of renal dysfunction isanticipated, renal function should be assessed more frequently and GLUCOPHAGE discontinued if evidence of renalimpairment is present.—Use of concomitant medications that may affect renal function or metformin disposition—Concomitant medicationfs) that may affect renal function or result in significant hemodynamic change or may inter-fere with the disposition of GLUCOPHAGE, such as cationic drugs that are eliminated by renal tubular secretion (SeeDrug Interactions), should be used with caution.—Radiologic studies Involving the use of iodinated contrast mate-rials (for example, Intravenous urogram, Intravenous cholanglography, anglography, and scans with contrastmaterials)—Parenteral contrast studies with iodinated materials can lead to acute renal failure and have been asso-ciated with lactic acidosis in patients receiving GLUCOPHAGE (see CONTRAINDICATIONS). Therefore, in patients inwhom any such study is planned, GLUCOPHAGE should be withheld for at least 48 hours prior to, and 48 hourssubsequent to, the procedure and reinstituted only after renal function has been re-evaluated and found to be normal.— Hypoxlc states—Cardiovascular collapse (shock) from whatever cause, acute congestive heart failure, acutemyocardial infarction and other conditions characterized by hypoxemia have been associated with lactic acidosis andmay also cause prerenal azotemia. When such events occur in patients on GLUCOPHAGE therapy, the drug should bepromptly discontinued. — Surgical procedures—GLUCOPHAGE therapy should be temporarily suspended for anysurgical procedure (except minor procedures not associated with restricted intake of food and fluids) and should notbe restarted until the patient's oral intake has resumed and renal function has been evaluated as normal.—AlcoholIntake —Alcohol is known to potentiate the effect of metformin on lactate metabolism. Patients, therefore, should bewarned against excessive alcohol intake, acute or chronic, while receiving GLUCOPHAGE.—Impaired hepatic func-tion—Since impaired hepatic function has been associated with some cases of lactic acidosis, GLUCOPHAGE shouldgenerally be avoided In patients with clinical or laboratory evidence of hepatic disease. — Vitamin B» levels—Adecrease to subnormal levels of previously normal serum vitamin B,2 levels, without clinical manifestations, isobserved in approximately 7% of patients receiving GLUCOPHAGE in controlled clinical trials of 29 weeks duration.Such decrease, possibly due to interference with Bl? absorption from the B,2-intrinsic factor complex, is, however, veryrarely associated with anemia and appears to be rapidly reversible with discontinuation of GLUCOPHAGE or vitamin B,,supplementation. Measurement of nematologic parameters on an annual basis is advised in patients on GLUCOPHAGEand any apparent abnormalities should be appropriately investigated and managed (see Laboratory Tests). CertainIndividuals (those with inadequate vitamin B12 or calcium intake or absorption) appear to be predisposed to developingsubnormal vitamin B,2 levels. In these patients, routine serum vitamin B,, measurements at two- to three-year inter-vals may be useful.—Changelnclinlcalstatusotpreviouslycontrolledalabetic—M\zM\z patient previously wellcontrolled on GLUCOPHAGE who develops laboratory abnormalities or clinical illness (especially vague and poorlydefined illness) should be evaluated promptly for evidence of ketoacidosis or lactic acidosis. Evaluation should includeserum electrolytes and ketones, blood glucose and, if indicated, blood pH, lactate, pyruvate and metformin levels. Ifacidosis of either form occurs, GLUCOPHAGE must be stopped immediately and other appropriate correctivemeasures initiated (see also WARNINGS). — Hypoglycemia—Hypoglycemia does not occur in patients receivingGLUCOPHAGE alone under usual circumstances of use, but could occur when caloric intake is deficient, when strenu-ous exercise is not compensated by caloric supplementation, or during concomitant use with other glucose-loweringagents (such as sulfonylureas) or ethanol. Elderly, debilitated or malnourished patients, and those with adrenal orpituitary insufficiency or alcohol intoxication are particularly susceptible to hypoglycemic effects. Hypoglycemia maybe difficult to recognize in the elderly, and in people who are taking beta-adrenergic blocking drugs.—Loss of controlofbloodglucose—\Nhet\ a patient stabilized on any diabetic regimen is exposed to stress such as fever, trauma, infec-tion, or surgery, a temporary loss of glycemic control may occur. At such times, it may be necessary to withholdGLUCOPHAGE and temporarily administer insulin. GLUCOPHAGE may be reinstituted after the acute episode isresolved. The effectiveness of oral antidiabetic drugs in lowering blood glucose to a targeted level decreases in manypatients over a period of time. This phenomenon, which may be due to progression of the underlying disease or todiminished responsiveness to the drug, is known as secondary failure, to distinguish it from primary failure in whichthe drug is ineffective during initial therapy. Should secondary failure occur with GLUCOPHAGE or sulfonylureamonotherapy, combined therapy with GLUCOPHAGEand sulfonylurea may result inaresponse. Should secondary fail-ure occur with combined GLUCOPHAGE/sulfonylurea therapy, it may be necessary to initiate insulin therapy.—Information for Patients: Patients should be informed of the potential risks and advantages of GLUCOPHAGE andof alternative modes of therapy. They should also be informed about the importance of adherence to dietary instruc-tions, of a regular exercise program, and of regular testing of blood glucose, glycosylated hemoglobin, renal functionand hematologic parameters. The risks of lactic acidosis, its symptoms, and conditions that predispose to its develop-
ment, as noted in the WARNINGS and PRECAUTIONS sections should be explained to patients. Patients should beadvised to discontinue GLUCOPHAGE9 (metformin hydrochloride tablets) immediately and to promptly notify their healthpractitioner if unexplained hyperventilation, myalgia, malaise, unusual somnolence or other nonspecific symptomsoccur.Once a patient is stabilized on any dose level of GLUCOPHAGE, gastrointestinal symptoms, which are commonduring initiation of therapy, are unlikely to be drug related. Later occurrence of gastrointestinal symptoms could bedue to lactic acidosis or other serious disease. Patients should be counselled against excessive alcohol intake, eitheracute or chronic, while receiving GLUCOPHAGE. GLUCOPHAGE alone does not usually cause hypoglycemia, althoughit may occur when GLUCOPHAGE is used in conjunction with oral sulfonylureas. When initiating combination therapy,the risks of hypoglycemia, its symptoms and treatment, and conditions that predispose to its development should beexplained to patients. (See Patient Package Insert.)—Laboratory Tests: Response to all diabetic therapies should bemonitored by periodic measurements of fasting blood glucose and glycosylated hemoglobin levels, with a goal ofdecreasing these levels toward the normal range. During initial dose titration, fasting glucose can be used to determinethe therapeutic response. Thereafter, both glucose and glycosylated hemoglobin should be monitored. Measurementsof glycosylated hemoglobin may be especially useful for evaluating long-term control (see also DOSAGE AND ADMIN-ISTRATION). Initial and periodic monitoring of hematologic parameters (e.g., hemoglobin/hematocrit and red blood cellindices) and renal function (serum creatinine) should be performed, at least on an annual basis. While megaloblasticanemia has rarely been seen with GLUCOPHAGE therapy, if this is suspected, vitamin B,2 deficiency should be excluded.— Drug Interactions: Glyburide— In a single-dose interaction study in NIDDM subjects, co-administration ofmetformin and glyburide did not result in any changes in either metformin pharmacokinetics or pharmacodynamics.Decreases in glyburide AUC and Cm^were observed, but were highly variable. The single-dose nature of this study andthe lack of correlation between glyburide blood levels and pharmacodynamic effects, makes the clinical significance ofthis interaction uncertain (see DOSAGE AND ADMINISTRATION, Concomitant Glucophage and Oral SulfonylureaTherapy).—Furosemide—A single-dose, metformin-furosemide drug interaction study in healthy subjects demon-strated that pharmacokinetic parameters of both compounds were affected by co-administration. Furosemideincreased the metformin plasma and blood Cm^by 22% and blood AUC by 15%, without any significant change inmetformin renal clearance. When administered with metformin, the Cm™ and AUC of furosemide were 31 % and 12%smaller, respectively, than when administered alone, and the terminalnalf-life was decreased by 32%, without anysignificant change in furosemide renal clearance. No information Is available about the interaction of metformin andfurosemide when co-administered chronically.—Nifedlpine—A single-dose, metformin-nifedipine drug interactionstudy in normal healthy volunteers demonstrated that co-administration of nifedipine increased plasma metforminC m » and AUC by 20% and 9%, respectively, and increased the amount excreted in the urine. Tm3|< and half-life wereunaffected. Nifedipine appears to enhance the absorption of metformin. Metformin had minimal effects on nifedipine.— Cationic drugs—Cationic drugs (e.g., amiloride, digoxin, morphine, procainamide, quinidine, quinine, ranitidine,tn'amterene, trimethoprim, and vancomycin) that are eliminated by renal tubular secretion theoretically have the poten-tial for interaction with metformin by competing for common renal tubular transport systems. Such Interactionbetween metformin and oral cimetidine has been observed in normal healthy volunteers in both single- and multiple-dose, metformin-cimetidine drug interaction studies, with a 60% increase in peak metformin plasma and whole bloodconcentrations and a 40% increase in plasma and whole blood metformin AUC. There was no change In eliminationhalf-life in the single-dose study. Metformin had no effect on cimetidine pharmacokinetics. Although such interactionsremain theoretical (except for cimetidine), careful patient monitoring and dose adjustment of GLUCOPHAGE and/or theinterfering drug is recommended in patients who are taking cationic medications that are excreted via the proximal renaltubular secretory system.—Other—Certain drugs tend to produce hyperglycemia and may lead to loss of glycemiccontrol. These drugs include thiazide and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens,
adequate glycemic control. In healthy volunteers, the pharmacokinetics of metformin and propranolol and metforminand ibuprofen were not affected when co-administered in single-dose interaction studies. Metformin is negligibly boundto plasma proteins and is, therefore, less likely to interact with highly protein-bound drugs such as salicylates, sulfon-amides, chloramphenicol, and probenecid, as compared to the sulfonylureas, which are extensively bound to serumproteins. — Carcinogenesls, Mutagenesls, Impairment of Fertility: Long-term carcinogenicity studies have beenperformed in rats (dosing duration of 104 weeks) and mice (dosing duration of 91 weeks) at doses up to and including900 mg/kg/day and 1500 mg/kg/day, respectively. These doses are both approximately three times the maximum rec-ommended human daily dose on a body surface area basis. No evidence of carcinogenicity with metformin was found ineither male or female mice. Similarly, there was no tumorigenic potential observed with metformin in male rats. However,an increased incidence of benign stromal uterine polyps was seen in female rats treated with 900 mg/kg/day. No evidenceof a mutagenic potential of metformin was found in the Ames test (S. typhimurium), gene mutation test (mouse lymphomacells), chromosomal aberrations test (human lymphocytes), or in-vivo micronuclei formation test (mouse bonemarrow). Fertility of male or female rats was unaffected by metformin administration at doses as high as 600 mg/kg/day,or approximately two times the maximum recommended human dailydoseonabody surface area basis.—Pregnancy:Teratogenlc effects—Pregnancy Category B. Safety in pregnant women has not been established. Metformin wasnot teratogenic in rats and rabbits at doses up to 600 mg/kg/day, or about two times the maximum recommendedhuman daily dose on a body surface area basis. Determination of fetal concentrations demonstrated a partial placenta!barrier to metformin. Because animal reproduction studies are not always predictive of human response, any decisionto use this drug should be balanced against the benefits and risks. Because recent information suggests that abnormalblood glucose levels during pregnancy are associated with a higher incidence of congenital abnormalities, there is aconsensus among experts that insulin be used during pregnancy to maintain blood glucose levels as close to normalas possible.—Nursing Mothers: Studies in lactating rats show that metformin is excreted into milk and reaches levelscomparable to those in plasma. Similar studies have not been conducted in nursing mothers, but caution should beexercised in such patients, and a decision should be made whether to discontinue nursing or to discontinue the drug,taking into account the importance of the drug to the mother.—Pediatric Use: Safety and effectiveness in children havenot been established. Studies in maturity-onset diabetes of theyoung (MODY) have not been conducted.—Geriatric Use:Controlled clinical studies of GLUCOPHAGE did not include sufficient numbers of elderly patients to determine whetherthey respond differently from younger patients, although other reported clinical experience has not identified differencesin responses between the elderly and younger patients. GLUCOPHAGE is known to be substantially excreted by the kidneyand because the risk of serious adverse reactions to tfie drug is greater in patients with impaired renal function, it should onlybe used in patients with normal renal function (see CONTRAINDICATIONS, CLINICAL PHARMACOLOGY, Pharmacoki-netics). Because aging is associated with reduced renal function, GLUCOPHAGE should be used with caution as ageincreases. Care should be taken in dose selection and should be based on careful and regular monitoring of renalfunction. Generally, elderly patients should not be titrated to the maximum dose of GLUCOPHAGE (see also DOSAGEAND ADMINISTRATION).ADVERSE REACTIONS: Lactic Acidosis: See WARNINGS, PRECAUTIONS and OVERDOSAGE Sections. — Gastroin-testinal Reactions: Gastrointestinal symptoms (diarrhea, nausea, vomiting, abdominal bloating, flatulence, andanorexia) are the most common reactions to GLUCOPHAGE and are approximately 30% more frequent in patients onGLUCOPHAGE monotherapy than in placebo-treated patients, particularly during initiation of GLUCOPHAGE therapy.These symptoms are generally transient and resolve spontaneously during continued treatment. Occasionally, tempo-rary dose reduction may be useful. In controlled trials, GLUCOPHAGE was discontinued due to gastrointestinal reac-tions in approximately 4% of patients. Because gastrointestinal symptoms during therapy initiation appear to bedose-related, they may be decreased by gradual dose escalation and by having patients take GLUCOPHAGE with meals(see DOSAGE AND ADMINISTRATION). Because significant diarrhea and/or vomiting may cause dehydration and pre-renal azotemia, under such circumstances, GLUCOPHAGE should be temporarily discontinued. For patients who havebeen stabilized on GLUCOPHAGE, nonspecific gastrointestinal symptoms should not be attributed to therapy unlessintercurrent illness or lactic acidosis have been excluded.—Special Senses: During initiation of GLUCOPHAGE ther-apy, approximately 3% of patients may complain of an unpleasant or metallic taste, which usually resolves sponta-neously. —Dermatologlc Reactions: The incidence of rash/dermatitis in controlled clinical trials was comparable toplacebo forGLUCOPHAGE monotherapy and to sulfonylurea forGLUCOPHAGE/sulfonylurea therapy.—Hematologic:(See also PRECAUTIONS). During controlled clinical trials of 29 weeks duration, approximately 9% of patients onGLUCOPHAGE monotherapy and 6% of patients on GLUCOPHAGE/sulfonylurea therapy developed asymptomaticsubnormal serum vitamin B.2 levels; serum folic acid levels did not decrease significantly. However, only five cases ofmegaloblastic anemia have been reported with metformin administration (none during U.S. clinical studies) and noincreased incidence of neuropathy has been observed. Therefore, serum B12 levels should be appropriately monitoredor periodic parenteral B12 supplementation considered.OVERDOSAGE: Hypoglycemia has not been seen even with ingestion of up to 85 grams of GLUCOPHAGE, althoughlactic acidosis has occurred in such circumstances (see WARNINGS). Metformin is dialyzable with a clearance ofup to 170 mL/min under good hemodynamic conditions. Therefore, hemodiarysis may be useful for removal ofaccumulated drug from patients in whom metformin overdosage is suspected.(tensultpackageinsertbeforeprescrtbingGLUCOPHAGE(metformlnhydrochloridetablets). F5-B001A 1/95GLUCOPHAGE is a registered trademark of LIPHA s.a.Licensed to Bristol-Myers Squibb Company.
| MEDWatch 1 -800-332-1088 available to report serious adverse events for any drug. |
© 1996 Bristol-Myers Squibb Company, Princeton, NJ F5-K022 Issued: May 1996
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

For many patients -with established postmenopausal osteoporosis'
MIACALCIN® Nasal Spray:(calcitonin-salmon)
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Efficacy Made Simple forthe Complex PatientDependable Absorption for Dependable Efficacy
One Spray per Day Increases Bone Mineral Density• Significantly increases lumbar vertebral bone mineral density (BMD)
• 76% of patients receiving MIACALCIN® (calcitonin-salmon) Nasal Spraygained BMD, in a recent study+1
Anytime -Anywhere Convenience Helps Ensure Success• Well suited for patients receiving multiple medications
• No dosing restrictions—absorption is independent of foods, liquids,and medications
• Convenient for older patients with rigid lifestyles
• No contraindications/labeling precautions for patients with esophagealdisorders, other GI problems, or renal impairment
Rhinitis, other nasal symptoms,1 back pain, arthralgia, epistaxis, and headache were the most commonadverse events. Because calcitonin-salmon is a protein, the potential for an allergic reaction exists,although no such reactions have been reported with MIACALCIN Nasal Spray.8 In rare cases, nasalulcerations have been reported, which required temporary discontinuation until healing occurred."
For more information, call 1-800-239-4917.
• MIACALCIN Nasal Spray is indicated for the treatment of postmenopausal osteoporosis in femalesgreater than 5 years postmenopause with low bone mass who refuse or cannot tolerate estrogens, or inwhom estrogens are contraindicated. Patients should ensure adequate calcium and vitamin D intake.
* A subanalysis of die results of a 2-year, randomized, double-blind,placebo-con trolled, parallel-group, dose-ranging study to evaluate theresponse to therapy with MIACALCIN Nasal Spray (200 lU/day) pluscalcium compared with placebo plus calcium among a total of 208women 5 or more veal's postmenopause with established osteoporosis.Seventy-six percent (31/41) of patients receiving MIACALCIN NasalSpray therapy (200 IU/day) plus calcium achieved statistically significantincreases in lumbar vertebral BMD (P< .05) compared to thirty-eightpercent (15/40) receiving placebo plus calcium.
* Nasal symptoms include nasal crusts, dryness, redness, nasal sores,irritation, itching, thick feeling, soreness, pallor, infection, stenosis,runny /blocked, small wound, bleeding wound, tenderness, uncomfort-able feeling, and sore across bridge of nose.
s Anaphylactic reactions have occurred with injectable calcitonin.MIACALCIN* (calcitonin-salmon) Nasal Spray is contraindicated inpatients who are allergic to calcitonin.
11 Please see accompanying brief summary of prescribing information.
Reference: 1. Overgaard K, Lindsay R, Christiansen C. Patient responsive-ness to calcitonin salmon nasal spray: a subanalysis of a2-year study. Cliri Tktr. 1995:17:680-685.
MiacalcirfNASAL S P RAY
(calcitonin-salmon) Nasal Solution
S I M P L Y B U I L D S B O N E M A S S
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

(calcitonin-salmon) Nasal SprayCaution: Federal law prohibits dispensing without prescription.
BRIEF SUMMARY: Please see package Insert for full prescribing Information.
INDICATION AND USAGEPostrmnopausal Osteoporosis - Miacalcin® (calcitonin-salmon) Nasal Spray is indicated for thetreatment of postmenopausal osteoporosis in females greater than 5 years postmenopause with lowbone mass relative to healthy premenopausal females. Miacalcin® (calcitonin-salmon) Nasal Sprayshould be reserved for patients who refuse or cannot tolerate estrogens or in whom estrogens arecontraindicated. Use of Miacalcin® (calcitonin-salmon) Nasal Spray is recommended in conjunctionwith an adequate calcium (at least 1000 mg elemental calcium per day) and vitamin D (400 I.U. perday) intake to retard the progressive loss of bone mass. The evidence of efficacy is based on increasesin spinal bone mineral density observed in clinical trials.Two randomized, placebo controlled trials were conducted in 325 postmenopausalfemales [227 Miacalcin® (calcitonin-salmon) Nasal Spray treated and98 placebo treated] with spinal, forearm or femoral bone mineral density(BMD) at least one standard deviation below normal for healthy premeno-pausal females. These studies conducted over two years demonstratedthat 200 I.U. daily of Miacalcin® (calcitonin-salmon) Nasal Spray increaseslumbar vertebral BMD relative to baseline and relative to placebo inosteoporotic females who were greater than 5 years postmenopause.Miacalcin® (calcitonin-salmon) Nasal Spray produced statistically signifi-cant increases in lumbar vertebral BMD compared to placebo as early as sixmonths after initiation of therapy with persistance of this level for up to2 years of observation.No effects of Miacalcin® (calcitonin-salmon) Nasal Spray on cortical bone ofthe forearm or hip were demonstrated. However, in one study, BMD of the hipshowed a statistically significant increase compared with placebo in a regioncomposed of predominantly trabecular bone after one year of treatment changingto a trend at 2 years that was no longer statistically significant.
CONTRAINDICATIONS . , - . . . . . . . , , . . .Clinical allergy to calcitonin-salmon. -,,"' '[••'','.•.-• •''•-' "..
Allergic ReactionsBecause calcitonin is a polypeptide, the possibility of a systemic allergic reaction exists.In clinical trials with Miacalcin® (calcitonin-salmon) Nasal Spray and foreign marketing experience,no serious allergic-type adverse reactions have been reported. However, with injectable calcitonin-salmon there have been a few reports of serious allergic-type reactions (e.g., bronchospasm, swellingof the tongue or throat, anaphylactic shock, and in one case death attributed to anaphylaxis). Theusual provisions should be made for the emergency treatment of such a reaction should it occur.Allergic reactions should be differentiated from generalized flushing and hypotension.Skin testing should be considered prior to treatment with nasal calcitonin for patients with suspectedsensitivity to calcitonin. The following procedure is suggested: Prepare a dilution of 10 I.U. per mL bywithdrawing 1/20 mL (0.05 mL) of injectable calcitonin-salmon in a tuberculin syringe and filling it to1.0 mL with Sodium Chloride Injection, USP. Mix well, discard 0.9 mL and inject intracutaneously0.1 mL (approximately 1 I.U.) on the inner aspect of the forearm. Observe the injection site 15 min-utes after injection. The appearance of more than mild erythema or wheal constitutes a positiveresponse.
PRECAUTIONS1. Drug Interactions
Formal studies designed to evaluate drug interactions with calcitonin-salmon have not been done.No drug interaction studies have been performed with Miacalcin® (calcitonin-salmon) NasalSpray ingredients.Currently, no drug interactions with calcitonin-salmon have been observed. The effects of prioruse of diphosphonates in postmenopausal osteoporosis patients have not been assessed;however, in patients with Paget's Disease prior diphosphonate use appears to reduce the anti-resorptive response to Miacalcin® (calcitonin-salmon) Nasal Spray.
2. Periodic Nasal ExaminationsPeriodic nasal examinations with visualization of the nasal mucosa, turbinates, septum andmucosal blood vessel status are recommended.The development of mucosal alterations or transient nasal conditions occurred in up to 9% ofpatients who received Miacalcin® (calcitonin-salmon) Nasal Spray and in up to 12% of patientswho received placebo nasal spray in studies in postmenopausal females. The majority of patients(approximately 90%) in whom nasal abnormalities were noted also reported nasally relatedcomplaints/symptoms as adverse events. Therefore, a nasal examination should be performedprior to start of treatment with nasal calcitonin and at any time nasal complaints occur.In all postmenopausal patients treated with Miacalcin® (calcitonin-salmon) Nasal Spray, the mostcommonly reported nasal adverse events included rhinitis (12%), epistaxis (3.5%), and sinusitis(2.3%). Smoking was shown not to have any contributory effect on the occurrence of nasal adverseevents. One patient (0.3%) treated with Miacalcin® (calcitonin-salmon) Nasal Spray who wasreceiving 400 I.U. daily developed a small nasal wound. In clinical trials in another disorder(Paget's Disease), 2.8% of patients developed nasal ulcerations.
If severe ulceration of the nasal mucosa occurs, as indicated by ulcers greater than 1.5 mm indiameter or penetrating below the mucosa, or those associated with heavy bleeding, Miacalcin®(calcitonin-salmon) Nasal Spray should be discontinued. Although smaller ulcers often heal with-out withdrawal of Miacalcin® (calcitonin-salmon) Nasal Spray, medication should be discontinuedtemporarily until healing occurs.
3. Information for PatientsCareful instructions on pump assembly, priming of the pump and nasal introduction ofMiacalcin® (calcitonin-salmon) Nasal Spray should be given to the patient. Although instructionsfor patients are supplied with individual bottles, procedures for use should be demonstrated toeach patient. Patients should notify their physician if they develop significant nasal irritation.
4. Carcinogenlcity, Mutagenicity, and Impairment of FertilityAn increased incidence of non-functioning pituitary adenomas has been observed in one-yeartoxicity studies in Sprague-Dawley and Fischer 344 Rats administered (subcutaneously)calcitonin-salmon at dosages of 80 I.U. per kilogram per day (16-19 times the recommendedhuman parenteral dose and about 130-160 times the human intranasal dose based on body sur-face area). The findings suggest that calcitonin-salmon reduced the latency period for develop-ment of pituitary adenomas that do not produce hormones, probably through the perturbation ofphysiologic processes involved in the evolution of this commonly occurring endocrine lesion inthe rat. Although administration of calcitonin-salmon reduces the latency period of the develop-ment of non-functional proliferative lesions In rats, it did not induce the hyperplastic/neoplasticprocess.Calcitonin-salmon was tested for mutagenicity using Salmonella typhimurium (5 strains) andEscherlchia coli (2 strains), with and without rat liver metabolic activation, and found to be non-mutagenic. The drug was also not mutagenic in a chromosome aberration test in mammalianV79 cells of the Chinese Hamster in vitro.
5. Laboratory TestsUrine sediment abnormalities have not been reported in ambulatory volunteers treated withMiacalcin® (calcitonin-salmon) Nasal Spray. Coarse granular casts containing renal tubular epi-thelial cells were reported in young adult volunteers at bed rest who were given injectablecalcitonin-salmon to study the effect of immobilization on osteoporosis. There was no evidence ofrenal abnormality and the urine sediment became normal after calcitonin was stopped. Periodicexaminations of urine sediment should be considered.
6. PregnancyTeratogenic EffectsCategory CCalcitonin-salmon has been shown to cause a decrease in fetal birth weights in rabbits whengiven by injection in doses 8-33 times the parenteral dose and 70-278 times the intranasal doserecommended for human use based on body surface area.Since calcitonin does not cross the placental barrier, this finding may be due to metabolic effectson the pregnant animal. There are no adequate and well controlled studies in pregnant womenwith calcitonin-salmon. Miacalcin® (calcitonin-salmon) Nasal Spray is not indicated for use inpregnancy.
7. Nursing MothersIt is not known whether this drug is excreted in human milk. As a general rule, nursing should
not be undertaken while a patient is on this drug since many drugs are excreted in humanmilk. Calcitonin has been shown to inhibit lactation in animals.
Geriatric UseClinical trials using Miacalcin® (calcitonin-salmon) Nasal Spray have included post-menopausal patients up to 77 years of age. No unusual adverse events or Increasedincidence of common adverse events have been noted in patients over 65 yearsof age.
9. Pediatric UseThere are no data to support the use of Miacalcin® (calcitonin-salmon) NasalSpray in children. Disorders of bone in children referred to as idiopathicjuvenile osteoporosis have been reported rarely. The relationship of these
disorders to postmenopausal osteoporosis has not been established andexperience with the use of calcitonin in these disorders is very limited.
ADVERSE REACTIONSThe incidence of adverse reactions reported in studies involvingpostmenopausal osteoporotic patients chronically exposed toMiacalcin® (calcitonin-salmon) Nasal Spray (N=341) and to placebonasal spray (N=131) and reported in greater than 3% of Miacalcin®(calcitonin-salmon) Nasal Spray treated patients are presented below in
the following table. Most adverse reactions were mild to moderate in severity.Nasal adverse events were most common with 70% mild, 25% moderate, and 5%
severe in nature (placebo rates were 71% mild, 27% moderate, and 2% severe).
Adverse Reactions Occurring in at Least 3%of Postmenopausal Patients Treated Chronically
Adverse ReactionRhinitisSymptom of NosefBack PainArthralgiaEpistaxisHeadache
Miacalcin® (calcitonin-salmon)Nasal Spray
N=341% of Patients
12.010.65.03.83.53.2
PlaceboN=131
% of Patients6.9
16.02.35.34.64.6
tSymptom of nose includes: nasal crusts, dryness, redness or erythema, nasal sores, irritation,itching, thick feeling, soreness, pallor, infection, stenosis, runny/blocked, small wound, bleedingwound, tenderness, uncomfortable feeling and sore across bridge of nose.
In addition, the following adverse events were reported in fewer than 3% of patients during chronictherapy with Miacalcin® (calcitonin-salmon) Nasal Spray. Adverse events reported in 1%-3% ofpatients are identified with an asterisk)*). The remainder occurred in less than 1% of patients. Otherthan flushing, nausea, possible allergic reactions, and possible local irritative effects in the respiratorytract, a relationship to Miacalcin® (calcitonin-salmon) Nasal Spray has not been established.Body as a whole - General Disorders: influenza-like symptoms', fatigue*, periorbital edema, feverIntegumentary:erythematous rash", skin ulceration, eczema, alopecia, pruritus, increased sweatingMusculoskeletal/Collagen: aftbmsis", myalgia*, arthritis, polymyalgia rheumatica, stiffnessRespiratory/Special Senses: sinusitis*, upper respiratory tract infection*, bronchospasm",pharyngitis, bronchitis, pneumonia, coughing, dyspnea, taste perversion, parosmiaCardiovascular: hypertension*, angina pectoris*. tachycardia, palpitation, bundle branch block,myocardial infarctionGastrointestinal:dyspepsia*, constipation*, abdominal pain*, nausea*, diarrhea*, vomiting,flatulence, increased appetite, gastritis, dry mouthLiter/Metabolic: cholelithiasis, hepatitis, thirst, weight increaseEndocrine: goiter, hyperthyroidism
Urinary System: cystitis*, pyelonephritis, hematuria, renal calculusCentral and Peripheral Nervous System: dizziness*, paresthesia*, vertigo, migraine, neuralgia,agitationHearing/Vestlbular: tinnitus, hearing loss, earacheVision: abnormal lacrimation*, conjunctivitis", blurred vision, vitreous floaterVascular: flushing, cerebrovascular accident, thrombophlebitisHematologic/Reslstame Mechanisms: lymphadenopathy*. infection*, anemiaPsychiatric: depression*, insomnia, anxiety, anorexia
Common adverse reactions associated with the use of injectable calcitonin-salmon occurred lessfrequently In patients treated with Miacalcin® (calcitonin-salmon) Nasal Spray than in those patientstreated with injectable calcitonin. Nausea, with or without vomiting, which occurred in 1.8% ofpatients treated with the nasal spray (and 1.5% of those receiving placebo nasal spray) occursin about 10% of patients who take injectable calcitonin-salmon. Flushing, which occurred in lessthan 1% of patients treated with the Nasal Spray, occurs in 2%-5% of patients treated with inject-able calcitonin-salmon. Although the administered dosages of injectable and nasal spraycalcitonin-salmon are comparable (50-100 units daily of injectable versus 200 units daily of nasalspray), the nasal dosage form has a mean bioavailability of about 3% (range 0.3%-30.6%) andtherefore provides less drug to the systemic circulation, possibly accounting for the decrease in fre-quency of adverse reactions.The collective foreign marketing experience with Miacalcin® (calcitonin-salmon) Nasal Spray doesnot show evidence of any notable difference in the incidence profile of reported adverse reactionswhen compared with that seen in the clinical trials.Sandoz Pharmaceuticals CorporationEast Hanover, New Jersey 07936SEPTEMBER 1995 P30367901
©1996 Sandoz Pharmaceuticals Corporation MN&O59&O1-A Printed in U.SA.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

NDRCJDERMTestosrerone Transdermal System
Restores male hormonalbalance to physiologic levels
Mimics the natural diurnal testosterone cycle1
Serum testosterone concentrations during Androderm therapy (N=29)*'
400-200-
A ModemCZ=I Natural Diurnal Range
V—•0
10m4
2M8
6M12
10lMHow
162m
206 PM
241 0 PM
*Mean±S.D.
APPROACHING THE PHYSIOLOGIC IDEALPlease see brief summary of prescribing information on adjacent page.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Significant reductionin risk parameters vs
IM therapyMean PSA levels reduced significantly
compared to prior IM therapy*1
PSA levels remained well below recognizedcutoff point for early detection of prostate cancer'23
Week 12
Androderm
Week 24
Androdeim
O Safety demonstrated in patients treated up to 48 months1
O Geriatric patients treated with androgens may be at anincreased risk for the development of prostatic hyperplasiaand prostatic carcinoma
O Androgens are contraindicated in men with carcinoma of thebreast or known or suspected carcinoma of the prostate
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

ANDR<5DERMTestosterone Transdermal SgstemFewer above-normal hematocrit values with
Androderm than with IM therapy'
Range of hematocrit levels over 6 months of treatment11
65 1 • IM Therapy (N=32) • Androderm (N=26)
60
55
50
45
35
30
• • # • — — if-4^- —
2Lnil Mil
Standard Reference Ronge
12Weeb
16 20 24
'Data are from a 12-month study of 29 testosterone-deficient patients previously treated with IM therapyfor 3 months or more who were switched to Androderm.
'Data are from a 24-week study of 58 testosterone-deficient patients who were randomly assigned to IMor Androdtrm therapy.
APPROACHING THE PHYSIOLOGIC IDEALPlease see brief summary of prescribing information on adjacent page.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Significantly relievessymptoms of testosteronedeficiency, while providing
long-term benefits
Complaints of decreased libido4
00%
80%
60V
40V
20%
ov
2 1 % *• •1 ^^^BLPrevious
IM Therapy
79%
|
No Therapy
7%*JHHH
Androderm
•/"sO.05 vsno therapy
Complaints of fatigue4
79%
PreviousIM Therapy
No Therapy Androderm
'PsO.05 vs no therapy.
Complaints of erectile dysfunction4
100%
PreviousIM Therapy
No Therapy Andtodeim
•PsO.05 vs no therapy.
Complaints of depressed mood4
100S
80%
j 60%
; 40%
20%
0%Previous
IM Therapy
14%"
No Therapy Androdeim
SPsO.05 vs no therapy.!|N.S. vs no therapy.
Symptom relief data are from a study of 29 testosterone-deficient patients who served as their own controls.'Data were collected by questionnaire during 3 weeks of IM therapy, an 8-week washout period and 12 monthsof Androderm therapy.4
APPROACHING THE PHYSIOLOGIC IDEALPlease see brief summary of prescribing information on adjacent page.AD9898
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

NDRCJDERMTestosterone Transdermal Sqsrem
Applied every evening at bedtime1
O Apply two (2) patches, rotating placement on theupper arms, thighs, back or abdomen1
O Eliminates the peaks and troughs of IM injection15 whilemimicking the natural diurnal cycle
O Mean PSA11 and hematocrit" levels reduced significantlycompared to prior IM therapy1
O Improves libido, erectile function, energy and mood4
O The most common adverse event is transient skin irritation**1
'Data are from a 12-month study of 29 testosterone-deficient patients previouslytreated with IM therapy for 3 months or more who were switched to Androderm.Data are from a 24-week study in which 26 testosterone-deficient patients previouslytreated with IM therapy for 3 months or more were switched to Androderm.
** While 53% of patients experienced application site reactions at some time duringtreatment, only 5% discontinued treatment due to chronic irritation, and 4% dueto allergic contact dermatitis.
ANDRODERM®TESTOSTERONE TRANSDERMAL SYSTEMBrief summary. See complete prescribing information in SmlthKline Beecham Pharma-ceuticals literature.INDICATIONS AND USAGE: Androderm is indicated for testosterone replacement therapy in menfor conditions associated with a deficiency or absence of endogenous testosterone:—primary hypogonadism (congenital or acquired)—testicular failure due to cryptorchidism, bilateral
torsion, orchitis, vanishing testis syndrome, or orchidectomy, Klinefelter's syndrome, chemother-apy, or toxic damage from alcohol or heavy metals.
—secondary, i.e.,- hypogonadotropic hypogonadism (congenital or acquired)—idiopathic gonado-tropin or LHRH deficiency, or pituitary-hypothalamic injury from tumors, trauma, or radiation.
CONTRAINDICATIONS: Androderm is contraindicated in men with carcinoma of the breast, menwith known or suspected carcinoma of the prostate, or those with known hypersensitivity to any ofits components. Androderm must not be used in women. Testosterone may cause fetal harm.WARNINGSPeliosis hepatis, cholestatic jaundice and hepatic neoplasms, including hepatocellular carcinoma,may develop following prolonged use of high doses of orally active 17-alpha-alkyl androgens (e.g.,methyltestosterone). Peliosis hepatis can be life-threatening or fatal. Testosterone is not known toproduce these adverse effects.Geriatric patients treated with androgens may be at an increased risk for the development of prosta-tic hyperplasia.Geriatric patients and other patients with clinical or demographic characteristics that are recognizedto be associated with an increased risk of prostate cancer should be evaluated for the presence ofsubclinical or clinical prostate cancer prior to initiation of testosterone replacement therapy, becausetestosterone therapy may promote the growth of existing subclinical foci of prostate cancer.In men receiving testosterone replacement therapy, surveillance for prostate cancer should beconsistent with current practices for eugonadal men.Edema, with or without congestive heart failure, may be a serious complication of androgen treat-ment in patients with preexisting cardiac, renal, or hepatic disease. In addition to discontinuation ofandrogens, diuretic therapy may be required. Gynecomastia frequently develops and occasionallypersists in patients being treated for hypogonadism.PRECAUTIONSInstruct patients to report too frequent or persistent erections of the penis, nausea, vomiting,jaundice, or ankle swelling, as well as signs of virilization of the female sexual partner, such aschanges in body hair distribution or significant increase in acne. Androderm should not be applied tothe scrotum, or over bony prominences or on parts of the body that could be subject to prolongedpressure during sleep or sitting. Application to these sites has been associated with burn-like blisterreactions.Laboratory TestsCheck hemoglobin and hematocrit to detect polycythemia in patients receiving androgentherapy. Also periodically check liver function, prostate specific antigen, total cholesterol and HDLcholesterol.Drug InteractionsAnticoagulants: CM substituted derivatives of testosterone, such as methandrostenolone, maydecrease the anticoagulant requirements of patients receiving oral anticoagulants. Monitor suchpatients closely, especially when starting or stopping androgen therapy.Oxyphenbutazone: Concurrent administration of oxyphenbutazone and androgens may elevateoxyphenbutazone serum levels.Insulin: Metabolic effects of androgens may decrease blood glucose and insulin requirements ofdiabetic patients.Drug/Laboratory Test InterferencesAndrogens may decrease levels of thyroxine-binding globulin, resulting in decreased total T4 serumlevels and increased resin uptake of T3 and T<. Free thyroid hormone levels remain unchanged; thereis no clinical evidence of thyroid dysfunction.Carcinogenesis, Mutagenesls, Impairment of FertilityAnimal Data: Testosterone has been tested by subcutaneous injection and implantation in mice andrats. The implant induced cervical-uterine tumors in mice, which metastasized in some cases. Thereis suggestion that injection of testosterone into some strains of female mice increases their sus-ceptibility to hepatoma. Testosterone is also known to increase the number of tumors and decreasethe degree of differentiation of chemically induced carcinomas of the liver in rats.Human Data: There are rare reports of hepatocellular carcinoma in patients receiving long-termtherapy with high-dose androgens. Withdrawal of drugs did not lead to regression of the tumors inall cases.See WARNINGS for patients at increased risk for prostatic hyperplasia and/or prostate cancer.Pregnancy Category X: (See Contraindications.)Teratogenlc Effects: Androderm must not be used in women.Nursing Mothers: Androderm must not be used in women.Pediatric Use: Androderm has not been evaluated clinically in males under 15 years of age.ADVERSE REACTIONSIn clinical studies in 122 patients, the most common adverse events reported were skin reactions atthe site of system application. Transient mild to moderate erythema was observed at the applicationsite in the majority of patients at some time during treatment. Adverse reactions reported by morethan 1 % of patients, with the % of patients reporting the event in parentheses, were: pruritus atapplication site (37%); burn-like blister reaction under system (12%); erythema at application site(7%); vesicles at application site (6%); prostate abnormalities (5%); headache (4%); allergic contact
Patient rotatesplacement of
two (2) patches
dermatitis to the system (4%); burning at application site (3%); induration at application site (3%);depression (3%); rash (2%); gastrointestinal bleeding (2%). The following reactions occurred in lessthan 1% of patients: fatigue; body pain; pelvic pain; hypertension; peripheral vascular disease;increased appetite; accelerated growth; anxiety; confusion; decreased libido; paresthesia; thinkingabnormalities; vertigo; acne; bullae at application site; mechanical irritation at application site; rash atapplication site; contamination of application site; prostate carcinoma; dysuria; hematuria; impo-tence; urinary incontinence; urinary tract infection; testicular abnormalities.Three types of application site reactions occurred; irritation which included mild to moderateerythema, induration or burning; allergic contact dermatitis; and burn-like blister reactions.Chronic skin irritation caused 5% of patients to discontinue treatment. Mild skin irritation may beameliorated by treatment of affected skin with over-the-counter topical hydrocortisone cream ortopical antihistamine products.Five patients (4%) developed allergic contact dermatitis after 3 to 8 weeks treatment that requireddiscontinuation. These reactions were characterized by pruritus, erythema, induration and in someinstances vesicles or bullae, which recurred with each system application. Rechallenge with com-ponents of the system showed ethanol sensitization in 4 patients. One patient's reaction wasattributed to testosterone. None of these patients had adverse sequelae related to oral alcoholingestion or to injectable testosterone use. Older patients may be more prone to develop allergiccontact dermatitis.Fourteen patients (12%) had burn-like blister reactions that involved bullae, epidermal necrosis orthe development of ulcerated lesions. These reactions typically occurred once, at a single applica-tion site; 5 patients experience a single recurrence. None withdrew from the clinical trials. Thesereactions occurred at a rate of approximately 1 in 6,500 system applications (1 in 3,250 treatmentdays). The majority of these lesions were associated with system application over bony promi-nences or on parts of the body that may have been subject to prolonged pressure during sleep orsitting (e.g., over the deltoid region of the upper arm, -the greater trochanter of the femur, or theischial tuberosity). The more severe lesions healed over several weeks with scarring in some cases.Such lesions should be treated as burns.Adverse Events Associated with Injection or Oral TreatmentsSkin and Appendages: Hirsutism, male pattern of baldness, seborrhea, acne. Endocrine andUrogenital: Gynecomastia, excessive frequency and duration of penile erections. Oligospermia mayoccur at high dosages. Fluid and Electrolyte Disturbances: Retention of sodium, chloride, water,potassium, calcium, inorganic phosphates. Gastrointestinal: Nausea, cholestatic jaundice, alter-ations in liver function tests. Rare instances of hepatocellular neoplasms and peliosis hepatis.Hematologic: Suppression of clotting factors II, V, VII, and X, bleeding in patients on concomitantanticoagulant therapy, polycythemia. Nervous System: Increased or decreased libido, headache,anxiety, depression, generalized paresthesia. Metabolic: Increased serum cholesterol. Miscell-aneous: Rarely, anaphylactoid reactions.DRUG ABUSE AND DEPENDENCE: Androderm is a Schedule III controlled substance under theAnabolic Steroids Control Act. Oral consumption of the system or its gel contents will not result inclinically significant serum testosterone concentrations in target organs due to extensive first-passmetabolism.OVERDOSAGE: One report of acute overdosage with testosterone enanthate injection with testos-terone levels up to 11,400 ng/dL was implicated in a cerebrovascular accident.DOSAGE AND ADMINISTRATION: The usual starting dose is two Androderm systems appliednightly to the back, abdomen, upper arms, or thighs for 24 hours, providing a total dose of 5 mg/day.Avoid application over bony prominences or on a part of the body that may be subject to pro-longed pressure during sleep or sitting (e.g., the deltoid region of the upper arm, the greatertrochanter of the femur, and the ischial tuberosity). DO NOT APPLY TO THE SCROTUM. Rotateapplication sites, with 7 days between applications to the same site. To ensure proper dosing, mea-sure morning serum testosterone concentration the morning following system application the pre-vious evening. If the serum concentration is outside the normal range, repeat the sampling afterchecking the system was properly applied at the appropriate time. Confirmed serum concentrationsoutside the normal range may require increasing the dosing regimen to 3 systems, or decreasingthe regimen to 1 system, while maintaining nightly application. Use the same laboratory for all anal-yses. Androderm therapy for non-virilized patients may be initiated with one system applied nightly.BRS-AD:L3
References:1. Data on file, SmithKline Beecham Pharmaceuticals. 2. Meikle AW, Arver S, Dobs AS,et al. Comparison of the Androderm™ Testosterone Transdermal System and testosterone-enanthate injections for the treatment of male hypogonadism: pharmacokinetics, efficacyand safety. Program of the 77th annual meeting of the Endocrine Society; June 14-17, 1995;Washington, DC. Abstract P2-120. 3. Catalona W], Smith DS, Ratliff TL, et al. Measurementof prostate-specific antigen in serum as a screening test for prostate cancer. N Engl ] Med.1991;321:1156-1161. 4. Arver S, Dobs AS, Meikle AW, et al. Long-term efficacy and safetyof a permeation-enhanced testosterone transdermal system in hypogonadal men. Manuscripton file, SmithKline Beecham Pharmaceuticals. 5. Matsumoto AM. Clinical use and abuseof androgens and antiandrogens. In: Becker KL, ed. Principles and Practice of Endocrinologyand Metabolism. Philadelphia, Pa: JB Lippincott Co; 1990:991-1000. nm
SBPhiladelphia, PA 19101
SmithKline BeechamPharmaceuticals
© SmithKline Beecham, 1996
THERATECH
Developed and Manufacturedby TheraTech
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Neuroendocrine Tumor Case Review
Recurrent Carcinoid Tumor
Abdominal MRI indicated evidenceof recurrent disease...
Abdominal MRI indicating evidence of hepatic tumor.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

1OctreoScan imaging identified additional
metastases for surgical intervention
Patient History
This middle-aged male underwent resection of a pancreaticcarcinoid tumor four years ago. Subsequent 3 and 4 yearCT scans presented evidence of recurrent disease. The patientwas referred for OctreoScan imaging.
OctreoScan Scintigraphy
Five hepatic tumors and two periaortic nodal lesions wereclearly visible on the whole-body planar images. OctreoScanimaging enabled differentiation between a non-receptor-expressing cavernous hemangioma and receptor-positivecarcinoid metastases.
Clinical Course
Correlative MRI indicated disease, but some lesions wouldlikely have been missed without the benefit of OctreoScanscintigraphy. The patient underwent surgery to freeze all fivehepatic lesions identified by OctreoScan. Follow-up MRIand OctreoScan studies were planned to assess post-operativestatus.
Decisive Clinical Information
In patients who have a known or suspected neuroendocrinetumor, OctreoScan imaging often can be the differencebetween cautious uncertainty and decisive clinicalintervention. Contact your nuclear medicine specialist formore information.
OctreoScan whole-body images showing five hepaticlesions and two periaortic lesions.
&
OCTREOSCAN*Kit for the Preparation of Indium In-I i i Pentetreotide
Please see adjacent page for brief summary of prescribing information.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
OCTREOSCANTKit for the Preparation of Indium In-111 Pentetreotide
BRIEF SUMMARY OFPRESCRIBING INFORMATION
OctreoScan0 is a kit for the preparation ofindium ln-111 pentetreotide, a diagnostic radio-pharmaceutical. It is a kit consisting of twocomponents:
1) A 10-mL OctreoScan Reaction Vial whichcontains a lyophilized mixture of 10 ug pentetreotide.
2) A 10-mL vial of Indium ln-111 Chloride SterileSolution.
Indium ln-111 pentetreotide is prepared bycombining the two kit components.
INDICATIONS AND USAGE
Indium ln-111 pentetreotide is an agent for the scintigraphic localization of primary and metastatic neuroendocrinetumors bearing somatostatin receptors.
CONTRAINDICATIONS
None known.
WARNINGS
DO NOT ADMINISTER IN TOTAL PARENTERAL NUTRITION (TPN) ADMIXTURES OR INJECT INTO TPNINTRAVENOUS ADMINISTRATION LINES; IN THESE SOLUTIONS, A COMPLEX GLYCOSYL OCTREOTIDECONJUGATE MAY FORM.
The sensitivity of scintigraphy with indium ln-111 pentetreotide may be reduced in patients concurrently receivingtherapeutic doses of octreotide acetate. Consideration should be given to temporarily suspending octreotideacetate therapy before the administration of indium ln-111 pentetreotide and to monitoring the patient for any signsof withdrawal.
General
1. Therapy with octreotide acetate can produce severe hypoglycemia in patients with insulinomas. Sincepentetreotide is an analog of octreotide, an intravenous line is recommended in any patient suspected of having aninsulinoma. An intravenous solution containing glucose should be administered just before and duringadministration of indium ln-111 pentetreotide.
2. The contents of the two vials supplied with the kit are intended only for use in the preparation of indium ln-111pentetreotide and are NOT to be administered separately to the patient.
3. Since indium ln-111 pentetreotide is eliminated primarily by renal excretion, use in patients with impaired renalfunction should be carefully considered.
4. To help reduce the radiation dose to the thyroid, kidneys, bladder, and other target organs, patients should bewell hydrated before the administration of indium ln-111 pentetreotide. They should increase fluid intake and voidfrequently for one day after administration of this drug. In addition, it is recommended that patients be given a mildlaxative (e.g., bisacodyl or lactulose) before and after administration of indium ln-111 pentetreotide (see Dosageand Administration section).
5. Indium ln-111 pentetreotide should be tested for labeling yield of radioactivity prior to administration. The productmust be used within six hours of preparation.
6. Components of the kit are sterile and nonpyrogenic. To maintain sterility, it is essential that directions arefollowed carefully. Aseptic technique must be used during the preparation and administration of indium ln-111pentetreotide.
7. Octreotide acetate and the natural somatostatin hormone may be associated with cholelithiasis, presumably byaltering fat absorption and possibly by decreasing motility of the gallbladder. A single dose of indium ln-111pentetreotide is not expected to cause cholelithiasis.
8. As with any other radioactive material, appropriate shielding should be used to avoid unnecessary radiationexposure to the patient, occupational workers, and other persons.
9. Radiopharmaceuticals should be used only by physicians who are qualified by specific training in the safe useand handling of radionuclides.
Carcinoaenesis. Mutagenesis. Impairment of FertilityStudies have not been performed with indium ln-111 pentetreotide to evaluate carcinogenic potential or effects onfertility. Pentetreotide was evaluated for mutagenic potential in an in vitro mouse lymphoma forward mutation assayand an in vivo mouse micronucleus assay; evidence of mutagenicity was not found.
Pregnancy Category CAnimal reproduction studies have not been conducted with indium ln-111 pentetreotide. It is not known whetherindium ln-111 pentetreotide can cause fetal harm when administered to a pregnant woman or can affectreproduction capacity. Therefore, indium ln-111 pentetreotide should not be administered to a pregnant womanunless the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk,caution should be exercised when indium ln-111 pentetreotide is administered to a nursing woman.
Safety and effectiveness in children have not been established.
ADVERSE REACTIONS
The following adverse effects were observed in clinical trials at a frequency of less than 1% of 538 patients:dizziness, fever, flush, headache, hypotension, changes in liver enzymes, joint pain, nausea, sweating, andweakness. These adverse effects were transient. Also in clinical trials, there was one reported case of bradycardiaand one case of decreased hematocrit and hemoglobin.
Pentetreotide is derived from octreotide which is used as a therapeutic agent to control symptoms from certaintumors. The usual dose for indium ln-111 pentetreotide is approximately 5 to 20 times less than for octreotide andis subtherapeutic. The following adverse reactions have been associated with octreotide in 3% to 10% of patients:nausea, injection site pain, diarrhea, abdominal pain/discomfort, loose stools, and vomiting. Hypertension andhyper- and hypoglycemia have also been reported with the use of octreotide.
DOSAGE AND ADMINISTRATIONBefore administration, a patient should be well hydrated. After administration, the patient must be encouraged todrink fluids liberally. Elimination of extra fluid intake will help reduce the radiation dose by flushing out unbound,labelled pentetreotide by glomerular filtration. It is also recommended that a mild laxative (e.g., bisacodyl or
lactulose) be given to the patient starting the evening before the radioactive drug is administered, and continuing for48 hours. Ample fluid uptake is necessary during this period as a support both to renal elimination and the bowel-cleansing process. In a patient with an insulinoma, bowel-cleansing should be undertaken only after consultationwith an endocrinologist.
The recommended intravenous dose for planar imaging is 111 MBq (3.0 mCi) of indium ln-111 .pentetreotideprepared from an OctreoScan kit. The recommended intravenous dose for SPECT imaging is 222 MBq (6.0 mCi)of indium ln-111 pentetreotide.
The dose should be confirmed by a suitably calibrated radioactivity ionization chamber immediately beforeadministration.
As with all intravenously administered products, OctreoScan should be inspected visually for paniculate matter anddiscoloration prior to administration, whenever solution and container permit. Preparations containing particulatematter or discoloration should not be administered. They should be disposed of in a safe manner, in compliancewith applicable regulations.
Aseptic techniques and effective shielding should be employed in withdrawing doses for administration to patients.
Waterproof gloves should be worn during the administration procedure.
Do not administer OctreoScan in TPN solutions or through the same intravenous line.
Radiation Dosimetry
The estimated radiation doses' to the average adult (70 kg) from intravenous administration of 111 MBq (3 mCi)and 222 MBq (6 mCi) are presented below. These estimates were calculated by Oak Ridge Associated Universitiesusing the data published by Krenning, et al.!
Estimated Absorbed Radiation Doses after Intravenous Administrationof Indium ln-111 Pentetreotide3 to a 70 kg patient
Kidneys
Liver
Spleen
Uterus
Ovaries
Testes
Red Marrow
Urinary
Bladder Wall
Gl Tract
Stomach Wall
Small Intestine
Upper Large
Intestine
Lower Large
Intestine
Adrenals
Thyroid
Effective Dose4
Equivalent
5416
12.15
73.86
6.34
4.89
2.90
3.46
30.42
5.67
4.78
5.80
7.73
7.55
7.43
13.03
PLAhJAR
itllilSl542
1.22
7.39
0.63
0.49
0.29
0.35
3.04
0.57
0.48
0.58
0.77
0.76
0.74
^ , ^ m ? 3 l n ^ ^ ^
1.30
108.32
24.31
147.73
12.67
9.79
5.80
6.91
60.48
11.34
9.56
11.59
15.46
15.11
14.86
BmStiil^iq
26.06
SPECT I
10.83
2.43
14.77
1.27
0.98
0.58
0.69
6.05
1.13
0.96
1.16
1.55
1.51
1.49
JBBM
2.61
1. Values listed include a correction for a maximum of 0.1% indium ln-114m radiocontaminant at calibration.
2. E.P. Krenning, W.H. Bakker, P.P.M. Kooij, W.A.P. Breeman, H.Y.Oei, M. de Jong, J.C. Reubi, T.J. Visser, C.Bruns, D.J. Kwekkeboom, A.E.M. Reijs, P.M. van Hagen, J.W. Koper, and S.W.J. Lamberts, "Somatostatin ReceptorScintigraphy with lndium-111-DTPA-D-Phe-1-Octreotide in Man: Metabolism, Dosimetry and Comparison withIodine-123-Tyr-3-Octreotide," The Journal of Nuclear Medicine, Vol. 33, No. 5, May 1992, pp. 652-658.
3. Assumes 4.8 hour voiding interval and International Commission on Radiological Protection (ICRP) 30 model forthe gastrointestinal tract calculations.
4. Estimated according to ICRP Publication 53.
HOW SUPPLIEDThe OctreoScan kit, NDC 0019-9050-40, is supplied with the following components:
1. A10-mL OctreoScan Reaction Vial which contains a lyophilized mixture of:(i) 10 ug pentetreotide [N-(diethylenetriamine-N,N,N',N"-tetraaceticacid-N"-acetyl)-D-
phenylalanyl-L-hemicystyl-L-phenylalanyl-D-tryptophyl-L-lysyl-L-threonyl-L-hemicystyl-L-threoninol cyclic (2-7) disulfide], (also known as octreotide DTPA),
(ii) 2.0 mg gentisic acid [2,5-dihydroxybenzoic acid],(iii) 4.9 mg trisodium citrate, anhydrous,(iv) 0.37 mg citric acid, anhydrous, and(v) 10.0 mg inosttol.
Before lyophilization, sodium hydroxide or hydrochloric acid may have been added for pH adjustment. The vialcontents are sterile and nonpyrogenic. No bacteriostatic preservative is present.
2. A 10-mL vial of Indium ln-111 Chloride Sterile Solution, which contains 1.1 mL of 111 MBq/mL (3,0 mCi/mL)indium ln-111 chloride in 0.02 N HCI at time of calibration. The vial also contains ferric chloride at a concentrationof 3.5 ug/mL (ferric ion, 1.2 pg/mL). The vial contents are sterile and nonpyrogenic. No bacteriostatic preservativeis present.
In addition, the kit also contains the following items: (1) a 25 G x 5/8* needle (B-D, Monoject) used to transferIndium ln-111 Chloride Sterile Solution to the OctreoScan Reaction Vial, (2) a pressure sensitive label, and (3) apackage insert.
ALLINCKRODTI MEDICAL
Mallinckrodt Medical, Inc.,675 McDonnell Blvd.St. Louis, MO 63134
©1996 Mallinckrodt Medical, Inc. MI22600 3/96
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
Sl8i8996i£ll I
: <
:
^ • • 1
ff'tfijh
it aa
8
:<
k*
i
\i
DNIlinDHOd
33IOH3M3NV
|| 3dA) J0|M3N
Kit i
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

INTRODUCING a new adjunct to diet and exercise
NEW 0 N C E - A - D A Y
Amarylgl imepjr ide TABLETS
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
INSULIN-SPARINGGLUCOSE CONTROL
i
^> A new sulfonylurea
^> Amaryl binds to a different part ofthe sulfonylurea receptor complex* -the clinical relevance of this mechanismhas not been established
^> Amaryl provides sustained bloodglucose control even in patients withhigher levels of HbA1c (glycosylatedhemoglobin)3
^> Amaryl is insulin sparing-controlsglucose without clinically meaningfulincreases in fasting insulin
^> Amaryl is indicated for both mono-therapy and second-line combination usewith insulin*
^> Favorable safety profile3—mostcommon adverse reactions (>!%)include dizziness (1.7%), asthenia(1.6%), headache (1.5%), nausea(1.1%), and hypoglycemia (0.9% to1.7%), as documented by glucose values<60 mg/dL
^> Proven 24-hour control with once-dailydosing
*Data derived from predinical animal model.The mechanism by which sulfonylureaslower blood glucose during long-term usehas not been clearly established.
^Combined use of Amaryl and insulin mayincrease the potential for hypoglycemia.
Please see brief summary of PrescribingInformation on last page of this advertisement.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
Amaryiglimepiride T A B L E T S1,2 , and 4 mgBrief SummaryDrug InteractionsThe hypoglycemic action of sulfonylureas may be potentiated by certain drugs, including nonsteroidalanti-inflammatory drugs and other drugs that are highly protein bound, such as salicylates, sulfonamides,chloramphenicol, coumarins, probenecid, monoamine oxidase inhibitors, and beta adrenergic blockingagents.
Certain drugs tend to produce hyperglycemia and may lead to loss of control. These drugs include thethiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oralcontraceptives, phenytoin, nicotinic acid, sympathomimetics, and isoniazid.
A potential interaction between oral miconazole and oral hypoglycemic agents leading to severehypoglycemia has been reported. Whether this interaction also occurs with the intravenous, topical, orvaginal preparations of miconazole is not known. Potential interactions of glimepiride with other drugsmetabolized by cytochrome P450 IIC9 also include phenytoin, diclofenac, ibuprofen, naproxen, andmefenamic acid.
Although no specific interaction studies were performed, pooled data from clinical trials showed noevidence of clinically significant adverse interactions with uncontrolled concurrent administration ofcalcium-channel blockers, estrogens, fibrates, NSAIOs, HMG CoA reductase inhibitors, sulfonamides,or thyroid hormone.INDICATIONS AND USAGEAMARYL is indicated as an adjunct to diet and exercise to lower the blood glucose in patients withnoninsulin-dependent (Type II) diabetes mellitus (NIDDM) whose hyperglycemia cannot be controlled bydiet and exercise alone.
AMARYL is also indicated for use in combination with insulin to lower blood glucose in patients whosehyperglycemia cannot be controlled by diet and exercise in conjunction with an oral hypoglycemic agent.Combined use of glimepiride and insulin may increase the potential for hypoglycemia.CONTRAINDICATIONSAMARYL is contraindicated in patients with
1. Known hypersensitivity to the drug.2. Diabetic ketoacidosis, with or without coma. This condition should be treated with insulin.
WARNINGS
SPECIAL WARNING ON INCREASED RISK OF CARDIOVASCULAR MORTALITYThe administration of oral hypoglycemic drugs has been reported to be associated with increasedcardiovascular mortality as compared to treatment with diet alone or diet plus insulin.PRECAUTIONSGeneral
Hypoglycemia: All sulfonylurea drugs are capable of producing severe hypoglycemia. Patients withimpaired renal function may be more sensitive to the glucose-lowering effect of AMARYL. A starting doseof 1 mg once daily followed by appropriate dose titration is recommended in those patients. Debilitated ormalnourished patients, and those with adrenal, pituitary, or hepatic insufficiency are particularlysusceptible to the hypoglycemic action of glucose-lowering drugs. Hypoglycemia is more likely to occurwhen caloric intake is deficient, after severe or prolonged exercise, when alcohol is ingested, or whenmore than one glucose-lowering drug is used.
Loss of control of blood glucose: When a patient stabilized on any diabetic regimen is exposed tostress such as fever, trauma, infection, or surgery, a loss of control may occur. At such times, it may benecessary to add insulin in combination with AMARYL or even use insulin monotherapy. Shouldsecondary failure occur with AMARYL monotherapy, AMARYL-insulin combination therapy may beinstituted. Combined use of glimepiride and insulin may increase the potential for hypoglycemia.Information lor PatientsPatients should be informed of the potential risks and advantages of AMARYL and of alternative modesof therapy. They should also be informed about the importance of adherence to dietary instructions, of aregular exercise program, and of regular testing of blood glucose.
The risks of hypoglycemia, its symptoms and treatment, and conditions that predispose to itsdevelopment should be explained to patients and responsible family members. The potential for primaryand secondary failure should also be explained.Laboratory TestsFasting blood glucose should be monitored periodically to determine therapeutic response. Glycosylatedhemoglobin should also be monitored, usually every 3 to 6 months, to more precisely assess long-termglycemic control.Canclnogenesls, Mutagenesls, and Impairment of FertilityStudies in rats at doses of up to 5000 ppm in complete feed (approximately 340 times the maximumrecommended human dose, based on surface area) for 30 months showed no evidence of carcinogenesis.In mice, administration of glimepiride for 24 months resulted in an increase in benign pancreatic adenomaformation which was dose related and is thought to be the result of chronic pancreatic stimulation. Theno-effect dose for adenoma formation in mice in this study was 320 ppm in complete feed, or 46-54 mg/kgbody weight/day. This is about 35 times the maximum human recommended dose of 8 mg once dailybased on surface area.
Glimepiride was non-mutagenic in a battery of in vitro and in vivo mutagenicity studies (Ames test,somatic cell mutation, chromosomal aberration, unscheduled DNA synthesis, mouse micronucleus test).
There was no effect of glimepiride on male mouse fertility in animals exposed up to 2500 mg/kg bodyweight (>1,700 times the maximum recommended human dose based on surface area). Glimepiride hadno effect on the fertility of male and female rats administered up to 4000 mg/kg body weight(approximately 4,000 times the maximum recommended human dose based on surface area).PregnancyTeratogenic EffectsPregnancy Category C. Glimepiride did not produce teratogenic effects in rats exposed orally up to 4000mg/kg body weight (approximately 4,000 times the maximum recommended human dose based onsurface area) or in rabbits exposed up to 32 mg/kg body weight (approximately 60 times the maximumrecommended human dose based on surface area). Glimepiride has been shown to be associated withintrauterine fetal death in rats when given in doses as low as 50 times the human dose based on surfacearea and in rabbits when given in doses as low as 0.1 times the human dose based on surface area. Thisfetotoxicity, observed only at doses inducing maternal hypoglycemia, has been similarly noted with othersulfonylureas, and is believed to be directly related to the pharmacologic (hypoglycemic) action ofglimepiride.
There are no adequate and well-controlled studies in pregnant women. On the basis of results fromanimal studies, AMARYL should not be used during pregnancy. Many experts recommend that insulin beused during pregnancy to maintain glucose levels as close to normal as possible.Nonteratogenic EffectsIn some studies in rats, offspring of dams exposed to high levels of glimepiride during pregnancy andlactation developed skeletal deformities consisting of shortening, thickening, and bending of the humerusduring the postnatal period. Significant concentrations of glimepiride were observed in the serum andbreast milk of the dams as well as in the serum of the pups. These skeletal deformations were determinedto be the result of nursing from mothers exposed to glimepiride.
Prolonged severe hypoglycemia (4 to 10 days) has been reported in neonates born to mothers who
were receiving a sulfonylurea drug at the time of delivery. This has been reported more frequently with theuse of agents with prolonged half-lives. Patients who are planning a pregnancy should consult theirphysician, and it is recommended that they change over to insulin for the entire course of pregnancy andlactation.Nursing MothersIn rat reproduction studies, significant concentrations of glimepiride were observed in the serum andbreast milk of the dams, as well as in the serum of the pups. Although it is not known whether AMARYLis excreted in human milk, other sulfonylureas are excreted in human milk. AMARYL should bediscontinued in nursing mothers. If AMARYL is discontinued, and if diet and exercise alone are .inadequate for controlling blood glucose, insulin therapy should be considered. (See above Pregnancy,Nonteratogenic Effects)Pedlatric UseSafety and effectiveness in pediatric patients have not been established.ADVERSE REACTIONSThe incidence of hypoglycemia with AMARYL, as documented by blood glucose values <60 mg/dL,ranged from 0.9-1.7% in two large, well-controlled, 1-year studies. (See WARNINGS and PRECAUTIONS)
AMARYL has been evaluated for safety in 2,013 patients in US controlled trials, and in 1,551 patients inforeign controlled trials. More than 1,650 of these patients were treated for at least 1 year.
Adverse events, other than hypoglycemia, considered to be possibly or probably related to study drugthat occurred in US placebo-controlled trials in more than 1 % of patients treated with AMARYL are shownbelow.
Adverse Events Occurring in > 1 % AMARYL PatientsAMARYL Placebo
Total TreatedDizzinessAstheniaHeadacheNausea
No.7461312118
%1001.71.61.51.1
No.294
1340
%1000.31.01.40.0
Gastrointestinal ReactionsVomiting, gastrointestinal pain, and diarrhea have been reported, but the incidence in placebo-controlledtrials was less than 1 % . Isolated transaminase elevations have been reported. Cholestatic jaundice hasbeen reported to occur rarely with sulfonylureas.Dermatologic ReactionsAllergic skin reactions, e.g., pruritus, erythema, urticaria, and morbilliform or maculopapujar eruptions,occur in less than 1 % of treated patients. These may be transient and may disappear despite continueduse of AMARYL; if skin reactions persist, the drug should be discontinued. Porphyria cutanea tarda andphotosensitivity reactions have been reported with sulfonylureas.Hematologic ReactionsLeukopenia, agranulocytosis, thrombocytopenia, hemolytic anemia, aplastic anemia, and pancytopeniahave been reported with sulfonylureas.Metabolic ReactionsHepatic porphyria reactions and disulfiram-like reactions have been reported with sulfonylureas; however,no cases have yet been reported with AMARYL. Cases of hyponatremia have been reported withglimepiride and all other sulfonylureas, most often in patients who are on other medications or havemedical conditions known to cause hyponatremia or increase release of antidiuretic hormone. Thesyndrome of inappropriate antidiuretic hormone (SIADH) secretion has been reported with certain othersulfonylureas, and it has been suggested that these sulfonylureas may augment the peripheral(antidiuretic) action of ADH and/or increase release of ADH.Other ReactionsChanges in accommodation and/or blurred vision may occur with the use of AMARYL. This is thought tobe due to changes in blood glucose, and may be more pronounced when treatment is initiated. Thiscondition is also seen in untreated diabetic patients, and may actually be reduced by treatment. Inplacebo-controlled trials of AMARYL, the incidence of blurred vision was placebo, 0.7%, and AMARYL, 0.4%.OVERDOSAGEOverdosage can produce hypoglycemia. Mild hypoglycemic symptoms without loss of consciousness orneurologic findings should be treated aggressively with oral glucose and adjustments in drug dosageand/or meal patterns. Close monitoring should continue until the physician is assured that the patient isout of danger. Severe hypoglycemic reactions with coma, seizure, or other neurological impairment occurinfrequently, but constitute medical emergencies requiring immediate hospitalization. If hypoglycemiccoma is diagnosed or suspected, the patient should be given a rapid intravenous injection of concentrated(50%) glucose solution. This should be followed by a continuous infusion of a more dilute (10%) glucosesolution at a rate that will maintain the blood glucose at a level above 100 mg/dL. Patients should beclosely monitored for a minimum of 24 to 48 hours, because hypoglycemia may recur after apparentclinical recovery.DOSAGE AND ADMINISTRATIONThere is no fixed dosage regimen for the management of diabetes mellitus with AMARYL or any otherhypoglycemic agent.Usual Starting DoseThe usual starting dose of AMARYL as initial therapy is 1-2 mg once daily, administered with breakfast orthe first main meal. Those patients who may be more sensitive to hypoglycemic drugs should be startedat 1 mg once daily, and should be titrated carefully. (See PRECAUTIONS Section for patients at increased risk).
No exact dosage relationship exists between AMARYL and the other oral hypoglycemic agents. Themaximum starting dose of AMARYL should be no more than 2 mg.
Failure to follow an appropriate dosage regimen may precipitate hypoglycemia. Patients who do notadhere to their prescribed dietary and drug regimen are more prone to exhibit unsatisfactory response totherapy.Usual Maintenance DoseThe usual maintenance dose is 1 to 4 mg once daily. The maximum recommended dose is 8 mg oncedaily. After reaching a dose of 2 mg, dosage increases should be made in increments of no more than 2mg at 1-2 week intervals based upon the patient's blood glucose response. Long-term efficacy should bemonitored by measurement of HbA1c levels, for example, every 3 to 6 months.AMARYL'-lnsulin Combination TherapyCombination therapy with AMARYL and insulin may be used in secondary failure patients. The fastingglucose level for instituting combination therapy is in the range of >150 mg/dL in plasma or serumdepending on the patient. The recommended AMARYL dose is 8 mg once daily administered with the firstmain meal. After starting with low-dose insulin, upward adjustments of insulin can be done approximatelyweekly as guided by frequent measurements of fasting blood glucose. Once stable, combination-therapypatients should monitor their capillary blood glucose on an ongoing basis, preferably daily. Periodicadjustments of insulin may also be necessary during maintenance as guided by glucose and HbA1c levels.Specific Patient PopulationsAMARYL is not recommended for use in pregnancy, nursing mothers, or children. In elderly, debilitated,or malnourished patients, or in patients with renal or hepatic insufficiency, the initial dosing, doseincrements, and maintenance dosage should be conservative to avoid hypoglycemic reactions (SeePRECAUTIONS, General).
" 1 HOECHST-ROUSSEL3N Pharmaceuticals IncorporatedA Somerville. NJ 08876-1258M HOECHST A3 922100-10/95
References: 1. Kramer W, Muller G, Cirbig F, et al. Differential interaction of glimepiride andglibendamide with the p-cell sulfonylurea receptor: II. photoaffinity labeling of a 65 kDa pro-tein by [3H]glimepiride. Biochim Biophys Ada. 1994,1191:278-290. 2. Muller G, Hartz D,Punter J, Okonomopulos R, Kramer W. Differential interaction of glimepiride and glibendamidewith the p-cell sulfonylurea receptor: I. binding characteristics. Biochim Biophys Ada. 1994;1191:267-277. 3. Data on file, Hoechst Marion Roussel.
1171-96687815 ©1996, Hoechst Marion Roussel, Inc. 0313B6
Hoechst Marion RousselHoechst Marion Roussel, Inc. • Kansas City, MO 64134A member of the Hoechst Group
Hoechst
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

NEW Testodernf With Adhesive
alzaPHARMACEUTICALS
MedicalInformation Line1-800-634-8977
Now with built-inadhesive strips
Give your patients all the benefits of Testoderm®:• Only one patch needed daily• Low irritation rate (2%)• Discreetly worn on highly permeable scrotal skin• Significantly improves mood, energy, libido, and sexual function1'2
• Physiologic testosterone levels—no peaks and troughs1"3
In clinical studies, the most common side effects were transientlocal itching (7%), discomfort (4%), and irritation (2%).
Restoring the Balance"
With Adhesive
TestodermTestosterone TransdermalSystem Q
6mg/daySee next page for brief summary of prescribing information.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Restoring the Balance
TestosteroneTransdermdlSystem4or6mg/day
Only one patch needed daily
Low irritation rate (2%)
Discreetly worn on highly permeable scrotal skin
In clinical studies, the most common side effectswere transient local itching (7%), discomfort(4%), and irritation (2%)
BRIEF SUMMARYINDICATIONS AND USAGETestoderm9 is indicated for replacement therapy in moles for conditions associated with a deficiency or absence of endogenoustestosterone:1. Primary hypogonadism (congenital or acquired)— testicular failure due to cryptorchidism, bilateral torsion, orchitis, vanish-ing testis syndrome, orchidectomy, Klinefelter's syndrome, chemotherapy, or toxic damage from alcohol or heavy metals.2. Hypogonadotropic hypogonadism (congenital or acquired)—idiopathic gonadotropin or IHRH deficiency or pituirary-hypotholo-mic injury. Testoderm9 is worn on the scrotum. Patients should start therapy with a 6 mg/d system applied daily; if scrotalarea is inadequate, a 4 mg/d system should be used (see Patient Information). The Testoderm® system should be worn22-24 hours.After 3-4 weeks of dairy system use, blood should be drawn 2-4 hours after system application for determination of serum totaltestosterone (see Laboratory Tests).If patients have not achieved desired results by the end of 6-8 weeks of therapy with the Testoderm® system, another formof testosterone replacement therapy should be considered.CONTRAINDICATIONSAndrogens are contraindicated in men with carcinoma of the breast or known or suspected carcinoma of the prostate.Testoderm® therapy has not been evaluated in women and must not be used in women. Testosterone may cause fetal harm.Testoderm® systems should not be used in patients with known hypersensitivity to any components of the system.WARNINGS
Prolonged use of high doses of orally active 17-alpho-alkyi androgens (eg, methyltestosterone) has been associated with seri-ous hepatic adverse effects (peliosis hepatitis, hepatic neoplasms, cholestatic hepatitis, and jaundice). Long-term therapywith testosterone enonthate, which elevates blood levels for prolonged periods, has produced multiple hepatic adenomas.Testosterone is not known to produce these adverse effects.Geriatric patients treated with androgens may be at an increased risk for the development of prostotic hyperplosia andprostatic carcinoma (see PRECAUTIONS: Carcinogenesis, Mutagenesis, Impairment of Fertility).Edema with or without congestive heart failure may be a serious complication in patients with preexisting cardiac, renal, orhepatic disease. In addition to discontinuation of the drug, diuretic therapy may be required.Gynecomastia frequently develops and occasionally persists in patients being treated for hypogonadism.PRECAUTIONSInformation for the Patient A booklet containing instructions for use of the Testoderm® system is available.The physician should instruct patients to report any of the following side effects of androgens:Too frequent or persistent erections of the penis.Any nausea, vomiting, changes in skin color or ankle swelling.Virilization of female partners has been reported with use of a topical testosterone solution. Changes in body hair distribu-tion or significant increase in acne of the female partner should be brought to the attention of a physician.Laboratory Tests1. Hemoglobin and hemotocrit levels should be checked periodically (to detect pofycythemia) in patients on long-term androgentherapy.2. liver function, prostatic acid phosphatase, prostatic specific antigen, cholesterol, and high density lipoproteins should bechecked periodically.Drug Interactions1. A n t i c o a g u l a n t s C-17 substituted derivatives of testosterone, such as methandrostenolone, have been reported to decreasethe anticoagulant requirements of patients receiving oral anticoagulants. Patients receiving oral anticoagulant therapy requireclose monitoring, especially when androgens are started or stopped.2 . Oxyphenbutozone Concurrent administration of oxyphenbutozone and androgens may result in elevated serum levelsof oxypnenbutazone.3 . Insulin In diabetic patients the metabolic effects of androgens may decrease blood glucose and, therefore, insulinrequirements.Drug/Laboratory Test Interactions Androgens moy decrease levels of ttiyroxin-binding globulin, resulting in decreasedtotal T4 serum levels and increased resin uptake of T3 ond T4. Free thyroid hormone levels remain unchanged, however, andthere is no clinical evidence of thyroid dysfunction.Cardnogenesis, Mutagenesis, Impairment of FertilityAnimal Data Testosterone has been tested by subcutaneous injection and implantation in mice and rats. In mice, the implantinduced cervical-uterine tumors, which metostosized in some coses. There is suggestive evidence that injection of testosterone
REFERENCES
1. Place VA, Atkinson L, Prattler DA, et al. Transdermal testosterone replacement through genital skin. In: Nieschlag E, BehreHM, eds. Testosterone: Action, Deficiency, Substitution. Berlin, Germany: Springer-Venog; 1990:165-181.
2. Data on file, ALZA Corporation, Palo Alto, CA.3. Findloy JC, Place V Snyder PJ. Treatment of primary hypogonadism in men by the transdermal administration of testos-
terone. J Gin Endocrinol Metob. 1989;68(2):369—373.
into some strains of female mice increases their susceptibility to hepatoma. Testosterone is olso known to increase the numberof rumors and decrease the degree of differentiation of chemically induced carcinomas of the liver in rats.Human Data There are rare reports of hepatocellular carcinoma in patients receiving long-term therapy with androgens inhigh doses. Withdrawal of the drugs did not lead to regression of the tumors in all cases.Geriatric Use Geriatric patients treated with androgens moy be at an increased risk for the development of prostatic hyperplosiaand prostatic carcinoma.Pregnancy Category X (See CONTRAINDICATIONS) Teratogenic Effects: Testoderm®, therapy must not be used in women.Nursing Mothers Testoderm® therapy must not be used in women.Pediatric Use Testoderm® therapy has not been evaluated clinically in males under 18 years of age.ADVERSE REACTIONS
Adverse Reactions with the Testoderm0 System In clinical studies of 104 patients treated with Testoderm®, the mostcommon adverse effects reported were local effects. In US clinical trials, most of the 72 patients filling out 0 dairy questionnairereported scrotal itching, discomfort, or irritation at some time during therapy. Of all the dairy questionnaire responses, /% reporteditching, 4% discomfort, and 2% irritation. All topical reactions decreased witri duration of use.The following adverse effects were reported in association with Testoderm® therapy in 104 patients using the product for up to threeyears; a causal relationship to Testoderm® treatment was not always determined. These effects are listed in decreasing order of occur-rence with the number o f patients reporting the effect in parentheses: Gynecomastia (51 acne (41 prostotitis/urinary tract infection(41 breast tenderness (3), stroke (2), memory loss (1), pupillary dilation (11 abnormal liver enzymes (11 scrotal cellulitis (1), deepvein phlebitis (1 } benign prostatic hyperplasio (11 rectal mucosal lesion over prostate (11 hematuria/blodder cancer (11 popillomoon scrotum (11 and congestive heart foilure (11See CLINICAL PHARMACOLOGY, Clinical Studies subsection, regarding effects on serum lipids.Adverse Reactions with Injection or Oral Androgen TherapySkin and Appendages Hirsufism, male pattern of baldness, seborrheo, and acne.Endocrine and Urogenital Gynecomastia and excessive frequency ond duration of penile erections. Oligospermia moyoccur at high dosoges (see CLINICAL PHARMACOLOGY).Fluid and Electrolyte Disturbances Retention of sodium, chloride, water, potassium, calcium, and inorganic phosphates.Gastrointestinal Nausea, cholestatic jaundice, alterations in liver function tests. Rare instances of hepatocellular neoplasmsand peliosis hepatitis have occurred (see WARNINGS). ,Hematologjc Suppression of dotting factors It V VII, and X, bleeding in patients on concomitant anticoagulant therapy, andporycythemia.Nervous System Increosed or decreased libido, headache, anxiety, depression, and generalized paresthesio.Metabolic Increosed serum cholesterol.Miscellaneous Rarely, anaphylactoid reactions.DRUG ABUSE AND DEPENDENCEControlled Substance Schedule III With oral administration, it is not possible to achieve clinically significant serum testos-terone concentrations in the target organs using the testosterone in Testoderm® due to extensive first pass metabolism. Thehalf-life of an IM injection of testosterone is about 10 minutes.Because scrotal skin is at least five times more permeable to testosterone than other skin sites, Testoderm® will notproduce adequate serum testosterone concentrations if it is applied to nongenirol skin.OVERDOSAGEThere is one report of acute overdosage with testosterone enanthate: testosterone levels of up to 11,400 ng/dL wereimplicated in 0 cerebrovascular accident.HOW SUPPLIEDTestoderm® systems are supplied as individually pouched systems, 30 per carton.Testoderm® 4 mg/d (Testosterone Transdermal System) • each 40 cm' system contains 10 mg testosterone USP for nominaldelivery of 4 mg for one day.Carton of 30 systems NDC17314-4608-3.Testoderm® 6 mg/d (Testosterone Transdermal System) • each 60 cm! system contains 15 mg testosterone USP for nominaldelivery of 6 mg for one day.Carton of 30 systems NDC 17314^609-3.Store at room temperature 15-30'C.Caution Federal law prohibits dispensing without prescription.ALZA Corporation, Palo Alto, California 94304 USAEdition: 6 / 94
©1996, ALZA Corporation. All rights reserved. Printed in U.S.A.
alzaPHARMACEUTICALS
A Division of ALZA CorporationPalo Alto, California 94304 USA
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

AUTHOR AND SUBSCRIPTION INFORMATIONAddress manuscripts and correspondence to:
MARIA I. NEW, M.D., Editor-in-ChiefJOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
The New York Hospital-Cornell Medical Center525 E. 68th Street, Box 164
New York, NY 10021Telephone: (212) 746-4970
Fax: (212) 746-4978
All business matters, including permission to reproduce ma-terial published in the journals, correspondence and remittancerelating to membership applications, member and nonmembersubscriptions, and back volumes, should be sent to The Endo-crine Society, 4350 East West Highway, Suite 500, Be-thesda, MD 20814-4410. Phone: (301) 941-0200; Fax: (301)941-0259. Copies will not be replaced without charge unless wereceive a request within 60 days of the mailing in the U.S. orwithin 90 days in all other countries. Inquiries and orders forreprints should be directed to Cadmus Journal Services, ReprintsDepartment, P.O. Box 751903; Charlotte, NC 28275-1903; Phone:(800) 407-9190 or (410) 819-3991; Fax: (410) 820-9765.
JOURNAL OF CLINICAL ENDOCRINOLOGY AND METAB-OLISM does not make the payment of page charges or otherassessments a condition for acceptance of a manuscript for pub-lication. However, authors will be assessed charges of $75 perprinted page at the time proofs are received. Furthermore, ad-ditional charges may be levied if the Editor-in-Chief finds the useof illustrative material to be excessive or unusual. In extraordi-nary cases, upon appeal by the author, the Publications Com-mittee may waive either or both of these assessments. Authorssubmitting color figures will be charged $950.00 per color figure.(Author color charges do no apply to authors of invited papers toThe Journal of Clinical Endocrinology & Metabolism.)
Bound copies of Volume No. 81 will be available in early 1997to subscribers only. The volumes will be hard bound in black
buckram, and the journal name, volume number, and year of issuewill be stamped in gold on the spine. The cost is $160.00 (plus anadditional $25.00 for orders outside the U.S.A). A $2.00 discountis given for advance payment. Orders must be received by thepublisher before December 1, 1996.
The appearance of advertisements in the journals of theEndocrine Society does not imply warranty, endorsement, or ap-proval of the products or services advertised or of their effective-ness, quality, or safety. The Society retains the prerogative toreject any advertisement it deems inappropriate and will acceptan advertisement only on the condition that the advertiser war-rants that the advertisement does not contravene legal require-ments on trade descriptions, medicines, race relations, or sexdiscrimination. No part may be duplicated or reproduced withoutpermission of The Endocrine Society. Advertising inquiriesshould be sent to Scherago International, Inc., 11 Penn Plaza,Suite 1003, New York, New York 10001. TEL (212) 643-1750, FAX(212) 643-1757. Authorization to photocopy items for internal orpersonal use, or the internal or personal use of specific clients, isgranted by The Endocrine Society, provided that the per copy feeof $3.00 is paid directly to Copyright Clearance Center, 222 Rose-wood Drive, Danvers MA 01923, USA. Payment should referencethe journal's ISSN.
CHANGE OF ADDRESS-Members and nonmembers notifyThe Endocrine Society 60 days in advance. When requesting achange, please include both the old and new addresses.
THE ENDOCRINE SOCIETY
P. MICHAEL CONN, PresidentDAVID N. ORTH, President-Elect
ROBERT B. JAFFE, Secretary-TreasurerD. LYNN LORIAUX, Past President
PUBLICATIONS COMMITTEE —CAROLE R. MENDELSON, Chair; LESLIE DEGROOT, RICHARD H. GOODMAN,MICHAEL D. GRISWOLD, ROBERT M. MACLEOD, WILLIAM ROSNER, JUDSON J. VAN WYK, ROBERT A. VIGERSKY, NANCYL. WEIGEL; P. MICHAEL CONN, ex-officio; ROBERT B. JAFFE, ex-officio; D. LYNN LORIAUX, ex-officio; DAVID N. ORTH,ex-officio; ROBERT M. CAREY, Council Liaison; PRISCILLA S. DANNIES, Council Liaison.
JOURNALS' STEERING COMMITTEE-CAROLE R. MENDELSON, Chair; MARC G. CARON, ANTHONY R. MEANS,SHLOMO MELMED, MARIA I. NEW; ROBERT M. CAREY, Council Liaison; PRISCILLA S. DANNIES, Council Liaison.
COUNCIL—ROBERT M. CAREY, PRISCILLA S. DANNIES, PAUL A. FITZGERALD, MARVIN C. GERSHENGORN, J. LARRYJAMESON, E. CHESTER RIDGWAY, JANET A. SCHLECHTE, MARGARET A. SHUPNIK, DEBORAH L. SEGALOFF.
SCOTT HUNT, Executive Director, 4350 East West Highway, Suite 500, Bethesda, Maryland 20814-4410.CINDY A. BODIN, Assistant Executive DirectorLENNE P. MILLER, Director of Journal Publications
28A
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

INSTRUCTIONS TO AUTHORS
COPYRIGHT ASSIGNMENT
The Endocrine Society publishes papers describing theresults of original research in the field of endocrinology andmetabolism in the JOURNAL OF CLINICAL ENDOCRI-NOLOGY AND METABOLISM, ENDOCRINOLOGY, MO-LECULAR ENDOCRINOLOGY, and ENDOCRINE RE-VIEWS.
The JOURNAL OF CLINICAL ENDOCRINOLOGY ANDMETABOLISM publishes endocrine and metabolic studiesrelated to human and primate physiology and disease. EN-DOCRINOLOGY publishes nonprimate biochemical andphysiological studies, although work on material of primateorigin is not excluded. MOLECULAR ENDOCRINOLOGYpublishes studies of the effects of hormones and relatedsubstances on the molecular biology and genetic regulationof nonprimate and primate cells. ENDOCRINE REVIEWSpublishes bimonthly and features in-depth review articleson both experimental and clinical endocrinology. Authorsare invited to consult with the Editors concerning the mostappropriate journal to which to submit their manuscripts.
All authors submitting manuscripts for publication mustprovide assurance, on the form provided, or a copy thereof,that no substantial part of the work has been published oris being submitted or considered for publication elsewhere.When a portion of the results is to appear in another jour-nal, or in publications of congresses, symposia, workshops,etc., details should be supplied to the Editor, and a copy ofthe other paper(s) submitted, along with the expected dateof publication.
The Endocrine Society does not levy author manu-script submission fees. Page charges for acceptedmanuscripts are $75 per page. Page charges are notlevied for invited papers to The Journal of ClinicalEndocrinology & Metabolism, Molecular Endocrinol-ogy, or Endocrinology or for papers published in En-docrine Reviews. When authors submit the final versionof their manuscript, i.e. after it has gone through firstreview and returned to you for revision, the final manu-script must be submitted in both typewritten form and ona computer diskette that contains the complete, readabletext of the manuscript. (Most word processing languagesare acceptable; diskettes produced on IBM compatible com-puters are preferred; see "electronic editing" portion of fullInstructions to Authors in the January and July issues forcomplete specifications). For final, revised manuscriptsthat are not also submitted on a computer diskette, au-thors must then submit a processing fee of $100. Eitherthe diskette containing the complete and final text or theadditional $100 processing fee should be submitted to theeditorial office with the final manuscript. Failure to for-
ward either the diskette or the additional fee with your finalmanuscript will delay publication of your paper. If the final,revised manuscript is ultimately rejected, the diskette or$100 fee will be returned to the author. This fee must bepaid by check, money order, or MasterCard/VISA. Pur-chase Orders will not be accepted for payment of thisfee. If the processing fee is not paid by MasterCard/VISA,it must be paid in U.S. currency by check or money order,it must be made payable to the journal, and drawn on orpayable by a United States bank so that it will clear the U.S.Federal Reserve System without surcharge. Requirementsfor submission of manuscripts on computer diskettes donot apply to Rapid Communications since these are to besubmitted by authors in camera ready form. Please contactthe editorial office for the special forms on which to submitRapid Communications.
Authors submitting color photographs or illustrationsmust pay $950.00 per color figure for color separations andprinting if the manuscript is accepted for publication. Au-thors will receive verification of the total charges incurredwhen the manuscript is submitted to the printer for com-position, at which time authors must provide written ac-ceptance of the incurred charges before production can be-gin on the manuscript. (Author color charges do not applyto authors of invited papers to The Journal of ClinicalEndocrinology & Metabolism, provided the photographshave been approved by the Editor-in-Chief.)
The journals are copyrighted by The Endocrine Society toprotect the Society and authors from unauthorized use of itscontents. The Society grants to authors the royalty-freeright to reproduce material from their work published inEndocrine Society Journals in other works of which they arethe author or editor, subject only to formally requestingpermission to reprint from the Society and giving full at-tribution in the work to the original publication of thearticle by The Endocrine Society.
The following affidavit affirming originality and assign-ing copyright to The Endocrine Society must be submittedto the Editorial Office with all manuscripts. Separate copiesof this document may be submitted by authors currentlylocated at different institutions, but such copies must besubmitted with the manuscript. If the manuscript is notaccepted for publication, the copyright assignment on thereverse side has no legal effect and will be returned onrequest. A manuscript will not be considered for pub-lication until this affidavit is received.
(Please consult the latest January or July issue of thejournal for more detailed Instructions to Authors.)
29A
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Journal of Clinical Endocrinology and MetabolismAffirmation of Originality and Assignment of Copyright
Mail this form with the manuscript (in quadruplicate) to:Maria I. New, M.D., Editor-in-ChiefJournal of Clinical Endocrinology and MetabolismThe New York Hospital-Cornell Medical Center525 E. 68th Street, Box 164New York, NY 10021The author(s) hereby affirms that the manuscript entitled:
Manuscript No.:(If Known)
is original, that all statements asserted as facts are based on author(s) careful investigation and research foraccuracy, that the manuscript does not, in whole or part, infringe any copyright or violate any right of privacyor other personal or property right whatsoever, that it has not been published in total or in part and is not beingsubmitted or considered for publication in total or in part elsewhere, and that author(s) has full power andauthority to enter into this copyright assignment and to make the grants herein contained.
In signing this form, each author acknowledges that he/she participated in the work in a substantive way andis prepared to take public responsibility for the work. If the above statement cannot be certified, justification forduplicate publication and permission to republish copyrighted material must be included with the covering letter.
The author(s), in consideration of the acceptance of the above work for publication, does hereby assign and transferto The Endocrine Society all of the rights and interest in and to the copyright of the above titled work in its currentform and in any form subsequently revised for publication and/or electronic dissemination and does hereby appointthe Endocrine Society as the author(s)' attorney-in-fact to execute any written assignment or other document onthe author(s)' behalf necessary for The Endocrine Society to obtain all right, title, and interest to the copyrightfor the above titled work.A. All authors must sign. (If more than three authors, please copy this form. Please sign in the same order in
which authors' names are listed on title page.)Date Name (print) SignatureDate Name (print) SignatureDate . Name (print) Signature
B. The above work was written as part of the duties of our employee(s) or specially commissioned by employeras a "work made for hire." As an authorized agent of the employer, I hereby execute this copyright assignmenton behalf of employer.Date Employer's Name (print)
Authorized Agent'sName (print)Title (print)
signature
C. The above work has been written in the course of employment by the United States Government so that nocopyright exists, and thus there is no transfer of copyright.Date Name (print) SignatureDate Name (print) , Signature
In order to accommodate individuals who are unable to conveniently obtain U.S. funds, JCE & M is now able to acceptMasterCard/VISA. If after review the manuscript is accepted for publication, either a computer diskette of the full,revised paper or $100 must be submitted. If you wish to use Visa or MasterCard for payment of this fee, please supplythe information below. Please type all information, except signature.Ms. No.: Name of Contact Author:
Please circle: Visa MasterCard Name of Cardholder:
Acc't #: Expires:
Signature of Cardholder:By signing this form, you authorize JCE & M to bill your credit card for the processing fee of $100.
30A
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

JID Genotropin(somdtropin[rDNA origin]for injection)
w
From Pharmacia & Upjohn,a world leader in growthhormone research...
SimplifyingGrowth
HormoneTherapy
GENOTROPIN is indicated for the long-term treatment of childrenwho have growth failure due to an inadequate secretion of endogenousgrowth hormone.
Pharmacia& Upjohn
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
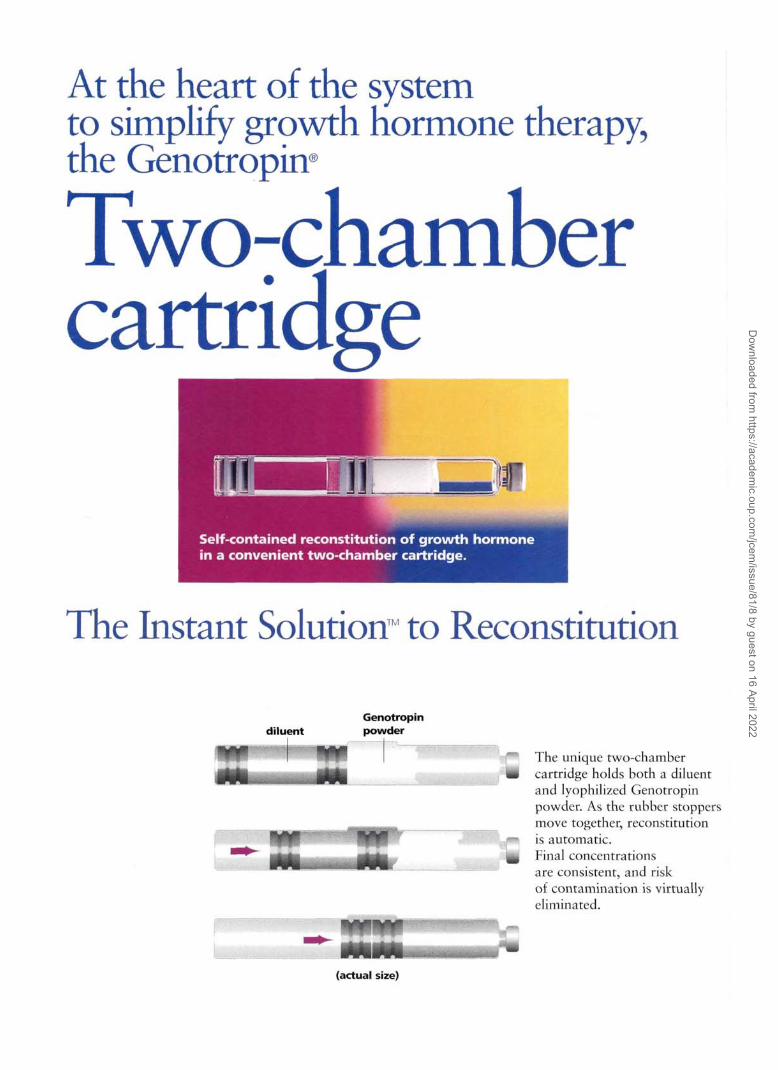
At the heart of the systemto simplify growth hormone therapy,the Genotropnr
Two:chambercartridge
The Instant Solution™ to Reconstitution
Genotropindiluent powder
The unique two-chambercartridge holds both a diluentand lyophilized Genotropinpowder. As the rubber stoppersmove together, reconstitutionis automatic.Final concentrationsare consistent, and riskof contamination is virtuallyeliminated.
(actual size)
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Threeinnovative devices for use withthe Genotropin® two-chamber cartridge:
Genotropln"(soflw(rojirnfrO«i»oWgin/fcr insertion) ^ ^s.gmq Intra-Mix" MM
Comprehensive support services simplify reimbursement and distribution
With a world of experience in growth hormone therapy, Pharmacia& Upjohn has made the Genotropin system as simple as it can be.A comprehensive support service stands ready to provide assistance.All it takes is a single phone call to simplify the complexities of growthhormone therapy. For more information, call 1-800-645-1280.
SimplifyingGrowth
HormoneTherapy
Special considerations
GENOTROPIN should not be used when there is any evidence of neoplastic activity,including intracranial lesions or tumors. Growth hormone should not be used in patientswith fused epiphyses, and used with caution in children with diabetes mellitus.
Physicians should be aware of the following precautions:intracranial hypertension(IH) reported in a small numberof patients; a higher incidence ofslipped capital femoral epiphyses(SCFE) reported in patients withendocrine disorders.
13.
Genotropin(smtropin[rDNA origin]for injection)
Please see full Prescribing Information on the next page.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

CenotropinDESCRIPTIONGENOTROPIN* (somatropin [rDNA origin] for injection) is a polypeptide hormone of recombinantDNA origin. It has 191 amino acid residues and a molecular weight of 22,124 daltons. The aminoacid sequence of the product is identical to that of human growth hormone of pituitary origin(somatropin). GENOTROPIN is synthesized in a strain of Escherichia coli that has been modified bythe addition of the gene for human growth hormone. GENOTROPIN is a sterile white lyophilizedpowder intended for subcutaneous injection. GENOTROPIN, 1.5 mg is dispensed in a two-chambercartridge. The front chamber contains recombinant somatropin 1.5 mg (approximately 4.5 IU),glycine 27.6 mg, sodium dihydrogen phosphate anhydrous 0.3 mg, disodium phosphate anhydrous0.3 mg; the rear chamber contains 1.13mL water for injection. GENOTROPIN, 5.8 mg is dispensedin a two-chamber cartridge. The front chamber contains recombinant somatropin 5.8 mg (approx-imately 17.4 IU), glycine 2.2 mg, mannitol 1.8 mg, sodium dihydrogen phosphate anhydrous 0.32mg and disodium phosphate anhydrous 0.31 mg; the rear chamber contains 0.3% m-Cresol (as apreservative) and mannitol 45 mg in 1.14mL water for injection. GENOTROPIN is a highly purifiedpreparation. The reconstituted recombinant somatropin solution has a concentration of either 1.3mg/mL (approximately 4 lU/mL), for GENOTROPIN 1.5 mg, or 5 mg/mL (approximately 15 lU/mL), forGENOTROPIN 5.8 mg, an osmolality of approximately 300 mosm/kg, and a pH of approximately 6.7.CLINICAL PHARMACOLOGYGENOTROPIN stimulates linear growth in children with growth hormone deficiency. In vitro, pre-clinical and clinical tests have demonstrated that GENOTROPIN is therapeutically equivalent tosomatropin and achieves similar pharmacokinetic profiles in normal adults. Treatment of growthhormone-deficient (GHD) children with GENOTROPIN produces increased growth rate and IGF-I(Insulin-like Growth Factor/Somatomedin-C) concentrations that are similar to those seen aftertherapy with somatropin.In addition, the following actions have been demonstrated for GENOTROPIN and/or somatropin.1. Tissue Growth
A. Skeletal Growth: GENOTROPIN stimulates skeletal growth in children with GHD. The mea-surable increase in body length after administration of either GENOTROPIN or somatropinresults from an effect on the epiphyseal plates of long bones. Concentrations of IGF-I, whichmay play a role in skeletal growth, are generally low in the serum of GHD children but tendto increase during treatment with GENOTROPIN. Elevations in mean serum alkaline phos-phatase concentration are also seen.
B. Cell Growth: It has been shown that there are fewer skeletal muscle cells in short-staturedchildren who lack endogenous growth hormone as compared with normal children.Treatment with somatropin results in an increase in both the number and size of musclecells.
2. Protein MetabolismLinear growth is facilitated in part by increased cellular protein synthesis. Nitrogen retention,as demonstrated by decreased urinary nitrogen excretion and serum urea nitrogen, follows theinitiation of therapy with somatropin. Treatment with GENOTROPIN results in similar decreases.
3. Carbohydrate MetabolismChildren with hypopituitarism sometimes experience fasting hypoglycemia that is improved bytreatment with GENOTROPIN. Large doses of human growth hormone may impair glucose tol-erance.
4. Lipid MetabolismIn GHD patients, administration of somatropin has resulted in lipid mobilization, reduction inbody fat stores, and increased plasma fatty acids.
5. Mineral MetabolismRetention of sodium, potassium, and phosphorus is induced by somatropin. Serum concentra-tions of inorganic phosphate are increased in patients with GHD after therapy withGENOTROPIN or somatropin. Serum calcium is not significantly altered by either GENOTROPINor somatropin. Growth hormone could increase calciuria.
PHARMACOKINETICSWhen compared to intravenous administration, approximately 80% of 1.5 mg GENOTROPIN wassystemically available following subcutaneous (SC) injection in the thigh in a study using healthymale subjects.In another study involving healthy male subjects following a SC injection dose of 0.033 mg/kg inthe thigh, the extent of absorption (AUC) for 5mg/mL GENOTROPIN was 35% greater than that for1.3 mg/mL GENOTROPIN. The mean (± standard deviation) peak (Cmax) serum levels were 35.5 (±14.5) ng/mL and 26.8 (± 14.2) ng/mL, respectively.In a study involving children with growth hormone deficiency, 5 mg/mL GENOTROPIN following aSC injection dose of 0.033 mg/kg in the thigh, had a mean AUC that was 17% greater than 1.3mg/mL GENOTROPIN. The mean (Cmax) levels were 32.4 ng/mL and 25.2 ng/mL, respectively.Mean (Cmax) levels were all achieved at approximately 3 to 4 hours and the apparent terminal half-life (T1/2) is approximately 2 hours following SC injection.INDICATION AND USAGEGENOTROPIN is indicated for the long-term treatment of children who have growth failure due toan inadequate secretion of endogenous growth hormone. Other causes of short stature should beexcluded.CONTRAINDICATIONSGENOTROPIN should not be used when there is any evidence of neoplastic activity. Intracraniallesions must be inactive and antitumor therapy complete prior to the institution of therapy.GENOTROPIN should be discontinued if there is evidence of tumor growth. Growth hormoneshould not be used in patients with fused epiphyses. Caution should be used if growth hormone isadministered to children with diabetes mellitus.WARNINGSThe 5.8 mg presentation of GENOTROPIN contains m-Cresol as a preservative. This product shouldnot be used by patients with a known sensitivity to this preservative. The 1.5 mg presentation ofGENOTROPIN is preservative-free. (See HOW SUPPLIED section).PRECAUTIONSGeneralTreatment with GENOTROPIN as with other growth hormone preparations, should be directed byphysicians who are experienced in the diagnosis and management of patients with GHD.Patients and caregivers who will administer GENOTROPIN in medically unsupervised situationsshould receive appropriate training and instruction on the proper use of GENOTROPIN from thephysician or other suitably qualified health professional.Patients with GHD secondary to an intracranial lesion should be examined frequently for progres-sion or recurrence of the underlying disease process. Because human growth hormone may inducea state of insulin resistance, patients should be observed for evidence of glucose intolerance.Concomitant glucocorticoid treatment may inhibit the growth promoting effect of human growthhormone. GHD patients with coexisting ACTH deficiency should have their glucocorticoid replace-ment dose carefully adjusted to avoid an inhibitory effect on growth.Hypothyroidism may develop during treatment with human growth hormone, and inadequatetreatment of hypothyroidism may prevent an optimal response to human growth hormone.Therefore, GHD patients should have periodic thyroid function tests and be treated with thyroidhormone when indicated.Patients with endocrine disorders, including GHD, have a higher incidence of slipped capitalfemoral epiphyses. Any child with the onset of a limp or complaints of hip or knee pain duringgrowth hormone therapy should be evaluated.Intracranial hypertension (IH) with papilledema, visual changes, headache, nausea and/or vomitinghas been reported in a small number of patients treated with growth hormone products.Symptoms usually occurred within the first eight (8) weeks of the initiation of growth hormonetherapy. In all reported cases, IH-associated signs and symptoms resolved after termination of ther-apy or a reduction of the growth hormone dose. Funduscopic examination of patients is recom-mended at the initiation, and periodically during the course of, growth hormone therapy.
Drug InteractionsConcomitant glucocorticoid treatment may inhibit the growth promoting effect of human growthhormone. GHD patients with coexisting ACTH deficiency should have their glucocorticoid replace-ment dose carefully adjusted to avoid an inhibitory effect on growth. See also PRECAUTIONS.Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenicity studies have not been conducted with rhGH. No potential mutagenicity of rhGHwas revealed in a battery of tests including the Ames test, induction of gene mutations in mam-malian cells (L5178Y) in vitro and in intact bone marrow cells (rats). See PREGNANCY section belowfor effect on fertility.Pregnancy: Pregnancy Category BReproduction studies carried out with GENOTROPIN at doses of 1, 3 and 10 lU/kg/day subcutaneouslyin the rat and 0.25, 1 and 4 lU/kg/day intramuscularly in the rabbit (highest doses approximately 24times and 19 times the recommended human therapeutic levels, respectively based on body surfacearea) showed decreased maternal body weight gains but were not teratogenic. In rats dosed subcu-taneously during gametogenesis and up to seven days of pregnancy, 10 lU/kg/day (approximately 24times human dose) produced a nest r us or extended estrus cycles in females and fewer and less motilesperm in males. When given to pregnant female rats (days 1-7 of gestation) at 10 lU/kg/day a veryslight increase in fetal deaths was observed. At 3 lU/kg/day (approximately 7 times human dose) ratsshowed slightly extended estrus cycles whereas at 1 lU/kg/day no effects were noted. Peri- andpost-natal studies in rats dosed with GENOTROPIN at doses of 1, 3 and 10 lU/kg/day produced growthpromoting effects in the dams but not in the fetuses. Young rats at the highest dose showedincreased weight gain during suckling but the effect was not apparent by 10 weeks of age.No adverse effects were observed on gestation, morphogenesis, parturition, lactation, post-nataldevelopment or reproductive capacity of the offsprings due to GENOTROPIN. There are, however, noadequate and well-controlled studies in pregnant women. Because animal reproduction studies are notalways predictive of human response, this drug should be used during pregnancy only if clearly needed.Nursing MothersThere have been no studies conducted with GENOTROPIN in nursing mothers. It is not knownwhether this drug is excreted in human milk. Because many drugs are excreted in human milk, cau-tion should be exercised when GENOTROPIN is administered to a nursing woman.ADVERSE REACTIONSAs with all protein drugs, a small number of patients may develop antibodies to the protein.Growth hormone antibody with binding lower than 2 mg/L has not been associated with growthattenuation. In some cases, when binding capacity is >2mg/L, interference with growth responsehas been observed.In 419 patients evaluated in clinical studies with GENOTROPIN, 244 had been treated previouslywith GENOTROPIN or other growth hormone preparations and 175 patients had received no pre-vious growth hormone therapy. Antibodies to growth hormone (anti-hGH antibodies), weTe pre-sent in 6 previously treated patients at baseline. Three of the six became negative for anti-hGHantibodies during 6 to 12 months of treatment with GENOTROPIN. Of the remaining 413, eight(1.9%) developed detectable anti-hGH antibodies during GENOTROPIN treatment, none had anantibody binding capacity > 2 mg/L. There was no evidence that the growth response toGENOTROPIN was affected in these antibody positive patients.GENOTROPIN preparations contain a small amount of periplasmic Escherichia coli peptides (PECP).Anti-PECP antibodies are found in a small number of patients treated with GENOTROPIN, but theseappear to be of no clinical significance.In clinical studies with GENOTROPIN, the following events were reported infrequently: injectionsite reactions, e.g., pain or burning associated with the injection, fibrosis, nodules, rash, inflamma-tion, pigmentation, bleeding; lipoatrophy; headache; hematuria; hypothyroidism; mild hyper-glycemia.Leukemia has been reported in a small number of children who have been treated with growthhormone, including growth hormone of pituitary origin and recombinant somatropin. The rela-tionship, if any, between leukemia and growth hormone therapy is uncertain.OVERDOSAGEThe recommended subcutaneous dosage of GENOTROPIN is 0.16 to 0.24 mg/kg body weight/weekgiven in 6 to 7 doses. There is little information on acute or chronic overdosage with GENOTROPIN.It is known that intravenously administered growth hormone has been shown to result in an acutedecrease in plasma glucose. Subsequently, hyperglycemia was seen. It is thought that the sameeffect might occur on rare occasions with high dosage of GENOTROPIN administered subcuta-neously. Long-term overdosage may result in signs and symptoms of acromegaly consistent withoverproduction of human growth hormone.DOSAGE AND ADMINISTRATIONGENOTROPIN dosage must be adjusted for the individual patient. Generally, a dose of 0.16 to 0.24mg/kg body weight/week is recommended. The weekly GENOTROPIN dose should be divided into6 to 7 subcutaneous injections. GENOTROPIN may be given in the thigh, buttocks or abdomen, thesite of s.c. injections should be rotated daily in an attempt to prevent lipoatrophy.GENOTROPIN must not be injected intravenously.GENOTROPIN is supplied as a powder, filled in a two-chamber cartridge with the active substancein the front chamber and the diluent in the rear chamber. A reconstitution device is used to co-mixthe diluent and the lyophilized powder. Gently tip the cartridge upside down a few times until thecontents are completely dissolved. Do not shake; this may cause denaturation of the activeingredient. For more specific information see directions accompanying the reconstitution device.All parenteral drug products should be inspected visually for paniculate matter and discolorationprior to administration, whenever solution and container permit. If the solution is cloudy, thecontents MUST NOT be injected.After using the reconstitution device, withdraw the GENOTROPIN solution using a 0.5 mL or 1.0 mLinsulin syringe with an attached needle.Patients and caregivers who will administer GENOTROPIN in medically unsupervised situationsshould receive appropriate training and instruction on the proper use of GENOTROPIN from thephysician or other suitably qualified health professional.STABILITY AND STORAGEGENOTROPIN should be stored under refrigeration 36° to 46"F (2°C to 8'C). (Do not freeze). Protectfrom light.The GENOTROPIN 1.5 mg cartridge reconstituted with diluent (without preservative) may be storedunder refrigeration for only up to 24 hours because it contains no antimicrobial agent. Use onceonly and discard any remaining solution.The GENOTROPIN 5.8 mg cartridge is reconstituted with a diluent containing a preservative. Thus,after reconstitution, it may be stored under refrigeration for up to 14 days.HOW SUPPLIEDGENOTROPIN (somatropin frDNA originl for injection) 1.5 mg. with a concentration of 1.3 mg/mL(approximately 4 lU/mL).NDC 0013-2606-94 GENOTROPIN 1.5 mg Intra-Mix two-chamber cartridge (without preservative)preassembled in a reconstitution device and co-packaged with a pressure release needle, packageof 5.GENOTROPIN (somatropin [rDNA oriqinl for injection) 5.8 mg. with a concentration of 5 ma/mL(approximately 15 lU/mL).NDC 0013-2616-94 GENOTROPIN 5.8 mg Intra-Mix two-chamber cartridge (with preservative) pre-assembled in a reconstitution device and co-packaged with a pressure release needle, package of 5.NDC 0013-2616-81 GENOTROPIN 5.8 mg Intra-Mix two-chamber cartridge (with preservative) pre-assembled in a reconstitution device and co-packaged with a pressure release needle, package of 1.NDC 0013-2626-94 GENOTROPIN 5.8 mg two-chamber cartridge (with preservative) for use withGENOTROPIN Pen 5 injection device,and/or the GENOTROPIN Mixer reconstitution device, package of 5.NDC 0013-2626-81 GENOTROPIN 5.8 mg two-chamber cartridge (with preservative) for use withGENOTROPIN Pen 5 injection device,and/or the GENOTROPIN Mixer reconstitution device, package of 1.Please see accompanying directions for use of the injection and/or reconstitution device.Caution: Federal law prohibits dispensing without prescription.
Pharmacia & UpjohnKalamazoo, Ml 49001, USA
© 1996, Pharmacia & Upjohn All Rights Reserved.121020496
April 4, 1996
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

1995SYLLABUS
The fastest way to get a complete update onclinical endocrinology -
CLINICAL ENDOCRINOLOGYUPDATE 1995 Syllabus(formerly Postgraduate Assembly Syllabus)San Diego, California, October 22-25, 1995Program Director: Wolfgang H. Dillmann, M.D.
EHDDCRIHOLOGYU P D R T E
'•?*-'• i ifl&ii*. ' *\V '•*:.'•"*;'>>.-
I'he Endocrine Society's CLINICAL ENDOCRINOLOGY UPDATE1995 Syllabus (formerly Postgraduate Assembly Syllabus) delivers inone convenient package the most useful information you can find on
the spectrum of clinical topics. Completely reformatted to allowconsistency of presentation, this summary of the lectures and workshopspresented at the 1995 CEU meeting is a convenient, accessible synopsisof all the major new developments in clinical endocrinology that youneed to know about. The CEU 1995 Syllabus design has beencompletely revamped. The book has been desk-top published fromauthor-supplied diskettes, in a uniform, two-column style. Figures andgraphs have been optically scanned and tables reset for consistency.
This new format allows for increased legibility and searchability. Workshop case study answers also now directly followthe questions.
The book is organized into the following sections:DIABETES • LIPIDS • THYROID • CALCIUM AND BONE• REPRODUCTIVE ENDOCRINOLOGY • ADRENAL • PITUITARY
Each section in this syllabus contains presentations written by leading physicians. The topics covered are those mostrequested by practicing endocrinologists, internists, and clinicians. The 363-page book is a bargain at $55.00.
YES! Send me Clinical Endocrinology Update1995 Syllabus at the price checked below!Order with payment by mail, The Endocrine Society Press,fax or phone from: c/o Nations Bank, PO Box 630331, Baltimore, MD 21263.Fax orders with credit card information to (301)941-0259; telephone orders with credit card information to (301)941-0240.
Clinical Endocrinology Update 1995 Syllabus(1995 ISBN 1-879225-20-4. 363 pages, 55 chapters Paperbound.)
$55.00 $15.00
Price includes postage and handling for U.S. and outside U.S. via surface mail (delivery 4-6 weeks). Add $15 per book forinternational air delivery. Prepaid only, no unpaid purchase orders. Telephone, fax, or mail credit card orders (American Express notaccepted); mail this order form for orders paid by check or money order. If paying by check, payment must be in U.S. funds only,drawn on a bank with a U.S. branch, made payable to The Endocrine Society. FEIN 73053 1256.
Name-Please print
Department
Address
City/State/Zip
D MasterCard • VISA Credit Card Number
Degree
Institution
Country
Expiration Date
Signature (for credit card purchase)
Total Remittance: $
Name on card
D Phone and/or • Fax Number
Date
FOR ES OFFICE USE ONLYBatch #:Check #:CC Auth:Ref Reas:CC Ref #:
Order #:CkDt:
Ref Amt:CC Batch #:
ID#:
CC Ref #:
Check issued by:Amount:
ESck#: 500-21502ES ck date:
JNLAD
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

LJO I ODH TG in Endocrinology and Diabetes
1916
is an official educational program of
The Endocrine Society
A New Approach to Medical Information
Physicians lack the time to spend hours researching questionssuch as establishing the cause of Cushing's syndrome or the roleof alendronate in osteoporosis. Relevant texts can be severalyears out of date, not organized to answer specific clinicalquestions, and often do not offer recommendations for therapy.UpToDate™ evolved from the need to get this essential informationquickly.
UpToDate™ is the revolutionary educational program on CD-ROMthat is redefining clinical practice in 60 countries. Described as a"welcome improvement over paperbound textbooks" (New EnglandJournal of Medicine), UpToDate™ provides authoritative, currentanswers to your common clinical questions. Accessing theinformation involves a simple three step process: A search term isentered. UpToDate™ produces a list of titles answering specificquestions related to the topic. After the desired title is chosen withthe click of a mouse, UpToDate™ provides a fully referenced,printable, in-depth discussion of the selected topic.
Features• An updated CD containing new and important information in all
areas is sent every four months.• The text is fully referenced with MedLine™ abstracts instantly
available. Specific recommendations are made.• Simple search technique with extensive cross-referencing.• Important data and major study results are illustrated in graphs
and tables. The program also incorporates radiographs anahistologic pictures.
• All of the material in UpToDate can be printed to put onpatients' charts or to send to referring physicians.
• Unlimited Category 1 CME credits From the AMA are availablefor every hour that you use UpToDate.
• On CD-ROM for Windows, Macintosh, and HP Palmtop.
The same CD contains complete sections in cardiology,nephrology, and hypertension, as well as developing sections in allof the other medical subspecialties (most of which are alsoendorsed by their major national society).
For More Information or to Subscribe:
UpToDate™P.O. Box 812098, Wellesley, MA 02181 USA
Toll Free: (800) 998-6374Voice: (617)237-4788Fax: (617)239-0391E-mail: [email protected]
Co-Editors
Jeffrey S. Flier, MDHarvard Medical School
Peter J. Snyder, MDUniversity of Pennsylvania School of Medicine
Section Editors
Adrenal DiseaseDavid N. Orth, MDVanderbilt UniversitySchool of Medicine
Bone DiseaseMichael Rosenblatt, MDHillel N. Rosen, MDHarvard Medical School
Diabetes MellitusDavid K. McCulloch, MDUniversity of WashingtonSchool of MedicineGroup Health Cooperativeof Puget Sound
Fluid and Electrolyte DisordersBurton D. Rose, MDHarvard Medical School
HypertensionNorman M. Kaplan, MDUniversity of Texas atSouthwestern Medical Center
Lipid DisordersRobert S. Rosenson, MDRush Medical College
Mineral MetabolismZalman S. Agus, MDUniversity of PennsylvaniaSchool of Medicine
Pituitary DiseasePeter J. Snyder, MDUniversity of PennsylvaniaSchool of Medicine
Reproductive EndocrinologyWilliam F. Crowley, MDHarvard Medical School
Eli Y. Adashi, MDUniversity of MarylandSchool of Medicine
Thyroid DiseaseDouglas S. Ross, MDHarvard Medical School
Editor-in-Chief of UpToDate™Burton D. Rose, MD
Harvard Medical School
Deputy EditorsZalman S. Agus, MD
University of Pennsylvania School of Medicine
Philip J. Podrid, MDBoston University School of Medicine
Systems DesignerJoseph M. Rush, MD
University of Florida School of Medicine
Prices:
Individual: for a single userTrainee: with proof of statusInstitution or NetworkCME Credits
$495 (for the first year)$245call for price$50
"The only software of its kind." JAMA
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

BRIEF SUMMARY
F O S A M A X (Alendronate Sodium Tablets)INDICATIONS AND USAGE: FOSAMAX is indicated for the treatment of: Osteoporosis in Postmenopausal Women:Osteoporosis may be confirmed by the finding of low bone mass (for example, at least 2 standard deviations belowthe premenopausal mean) or by the presence or history of osteoporotic fracture; Paget's Disease of Bone: Treatmentis indicated in patients with Paget's disease of bone having alkaline phosphatase at least two times the upper limit ofnormal, or those who are symptomatic, or those at risk for future complications from their disease.
CONTRAINDICATIONS: Abnormalities of the esophagus which delay esophageal emptying such as strictureor achalasia; inability to stand or sit upright for at least 30 minutes; hypersensitivity to any component of thisproduct; hypocalcemia (See PRECAUTIONS, General).
WARNINGS: FOSAMAX, like other bisphosphonates, may cause local irritation of the upper gastrointestinal mucosa.Esophageal adverse experiences, such as esophagitis, esophageal ulcers and esophageal erosions have been
reported in patients receiving treatment with FOSAMAX. In some cases these have been severe and required hospi-talization. Physicians should therefore be alert to any signs or symptoms signaling a possible esophageal reaction andpatients should be instructed to discontinue FOSAMAX and seek medical attention if they develop dysphagia,odynophagia or retrosternal pain.
The risk of severe esophageal adverse experiences appears to be greater in patients who lie down after takingFOSAMAX and/or who fail to swallow it with a full glass (6-8 oz.) of water, and/or who continue to take FOSAMAXafter developing symptoms suggestive of esophageal irritation. Therefore, it is very important that the full dosinginstructions are provided to, and understood by, the patient (see DOSING AND ADMINISTRATION).
Because of possible irritant effects of FOSAMAX on the upper gastrointestinal mucosa, caution should be usedwhen FOSAMAX is given to patients with active upper gastrointestinal problems, such as dysphagia, esophageal dis-eases, gastritis, duodenitis, or ulcers.
PRECAUTIONS: General: FOSAMAX is not recommended for patients with renal insufficiency (creatinine clearance <35mL/min). (See DOSAGE AND ADMINISTRATION.)
Causes of osteoporosis other than estrogen deficiency and aging should be considered.Hypocalcemia must be corrected before initiating therapy with FOSAMAX (see CONTRAINDICATIONS). Other dis-
turbances of mineral metabolism (such as vitamin D deficiency) should also be effectively treated. Presumably due tothe effects of FOSAMAX on increasing bone mineral, small, asymptomatic decreases in serum calcium and phosphatemay occur, especially in patients with Paget's disease, in whom the pretreatment rate of bone turnover may be greatlyelevated. Adequate calcium and vitamin D intake should be ensured to provide for these enhanced needs.
Information for Patients: Patients should be instructed that the expected benefits of FOSAMAX may only be obtainedwhen each tablet is swallowed with plain water the first thing upon arising for the day at least 30 minutes before thefirst food, beverage, or medication of the day. Even dosing with orange juice or coffee has been shown to markedlyreduce the absorption of FOSAMAX.
To facilitate delivery to the stomach and thus reduce the potential for esophageal irritation, patients shouldbe instructed to swallow FOSAMAX with a full glass of water (6-8 oz.) and not to lie down for at least 30 minutes anduntil after their first food of the day. Patients should not chew or suck on the tablet. Patients should bespecifically instructed not to take FOSAMAX at bedtime or before arising for the day. Patients should beinformed that failure to follow these instructions may increase their risk of esophageal problems. Patientsshould be instructed that if they develop symptoms of esophageal disease (such as difficulty or pain uponswallowing, retrosternal pain or new or worsening heartburn) they should stop taking FOSAMAX and con-sult their physician.
Patients should be instructed to take supplemental calcium and vitamin D, if daily dietary intake is inadequate.Weight-bearing exercise should be considered along with the modification of certain behavioral factors, such as exces-sive cigarette smoking, and/or alcohol consumption, if these factors exist.
Physicians should instruct their patients to read the patient package insert before starting therapy with FOSAMAXand to reread it each time the prescription is renewed.
Drug Interactions: Estrogen: A small number of postmenopausal women in the osteoporosis trials received estrogen(intravaginal, transdermal, or oral) while taking FOSAMAX. No adverse experiences attributable to their concomitantuse were identified.
Concomitant use of hormone replacement therapy and FOSAMAX in the treatment of osteoporosis in post-menopausal women is not recommended because of lack of clinical experience.
Calcium Supplements/Antacids: It is likely that calcium supplements, antacids, and some oral medications will inter-fere with absorption of FOSAMAX. Therefore, patients must wait at least one-half hour after taking FOSAMAX beforetaking any other drug.
NSAIDS/Aspirirr. In clinical studies, the incidence of upper gastrointestinal adverse events was increased in patientsreceiving concomitant therapy with doses of FOSAMAX greater than 10 mg/day and aspirin-containing compounds.
Other Although specific interaction studies were not performed, FOSAMAX 10 mg/day was used in postmenopausalosteoporosis studies with a wide range of commonly prescribed drugs without evidence of clinical adverse interactions.These included antacids, anticholinergics, aspirin-containing compounds, benzodiazepines, beta blockers, calcium-chan-nel blockers, diuretics, gastric acid secretion inhibitors, glucocorticoids, nonsteroidal antiinflammatory drugs (NSAIDs),sedative hypnotics, thiazides, thyroid hormones, vasoconstrictors, and vasodilators.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Harderian gland (a retroorbital gland not present inhumans) adenomas were increased in high-dose female mice (p=0.003) in a 92-week carcinogenicity study at dosesof alendronate of 1,3, and 10 mg/kg/day (males) or 1,2, and 5 mg/kg/day (females). These doses are equivalent to0.5 to 4 times the 10 mg human dose based on surface area, mg/nf.
Parafollicular cell (thyroid) adenomas were increased in high-dose male rats (p=0.003) in a 2-year carcinogenicitystudy at doses of 1 and 3.75 mg/kg body weight. These doses are equivalent to 1 and 3 times the 10 mg human dosebased on surface area.
Alendronate was not genotoxic in the in vitro microbiaj mutagenesis assay with and without metabolic activation, inan in vitro mammalian cell mutagenesis assay, in an in vitro alkaline elution assay in rat hepatocytes, and in an in mochromosomal aberration assay in mice. In an in vitro chromosomal aberration assay in Chinese hamster ovary cells,however, alendronate was weakly positive at concentrations >5 mM in the presence of cytotoxicity.
Alendronate had no effect on fertility (male or female) in rats at oral doses up to 5 mg/kg/day (four times the 10 mghuman dose based on surface area).
Pregnancy: Pregnancy Category C: Reproduction studies in rats showed decreased postimplantation survival at 2mg/kg/day and decreased body weight gain in normal pups at 1 mg/kg/day. Sites of incomplete fetal ossification werestatistically significantly increased in rats beginning at 10 mg/kg/day in vertebral (cervical, thoracic, and lumbar), skull,and sternebral bones. The above doses ranged from 1 times (1 mg/kg) to 9 times (10 mg/kg) the 10 mg human dosebased on surface area, mg/m'. No similar fetal effects were seen when pregnant rabbits were treated at doses up to35 mg/kg/day (50 times the 10 mg human dose based on surface area, mg/m').
Both total and ionized calcium decreased in pregnant rats at 15 mg/kg/day (13 times the 10 mg human dose basedon surface area) resulting in delays and failures of delivery. Protracted parturition due to maternal hypocalcemiaoccurred in rats at doses as low as 0.5 mg/kg/day (0.5 times the recommended human dose) when rats were treatedfrom before mating through gestation. Maternotoxicity (late pregnancy deaths) occurred in the female rats treated with15 mg/kg/day for varying periods of time ranging from treatment onjy during pre-mating to treatment only during early,middle, or late gestation; these deaths were lessened but not eliminated by cessation of treatment. Calcium supple-mentation either in the drinking water or by minipump could not ameliorate the hypocalcemia or prevent maternal andneonatal deaths due to delays in delivery; calcium supplementation IV prevented maternal, but not fetal deaths.
There are no studies in pregnant women. FOSAMAX should be used during pregnancy only if the potential benefitjustifies the potential risk to the mother and fetus.
Nursing Mothers: Alendronate was secreted in the milk of rats after an IV dose. It is not known whether alendronateis excreted in human milk. FOSAMAX has not been studied in nursing women and should not be given to them.
Pediatric Use: Safety and effectiveness in pediatric patients have not been established.Use in the Elderly: Of the patients receiving FOSAMAX in the two large osteoporosis studies and Paget's disease stud-
ies, 45% and 70%, respectively, were 65 years of age or over. No overall differences in efficacy or safety were observedbetween these patients and younger patients but greater sensitivity of some older individuals cannot be ruled out.
Use in Men: Safety and effectiveness in male osteoporosis have not been established.
ADVERSE REACTIONS: Clinical Studies: In clinical studies adverse experiences associated with FOSAMAX9
(alendronate sodium tablets) usually were mild, and generally did not require discontinuation of therapy.Osteoporosis in Postmenopausal Women: FOSAMAX has been evaluated for safety in clinical studies in more than
1800 postmenopausal patients. In two large, three-year, placebo-controlled, double-blind, multicenter studies (UnitedStates and Multinational), discontinuation of therapy due to any clinical adverse experience occurred in 4 .1% of 196patients treated with FOSAMAX 10 mg/day and 6.0% of 397 patients treated with placebo. Adverse experiences report-ed by the investigators as possibly, probably, or definitely drug related in >1 % of patients treated with either FOSAMAX10 mg/day or placebo are presented in the following table.
Drug-Related* Adverse Experiences Reported in > 1 % of Patients
FOSAMAX10 mg/day Placebo%(n=196) %(n=397)
Gastrointestinal abdominal pain -nauseadyspepsiaconstipationdiarrheaflatulenceacid regurgitationesophageal ulcervomitingdysphagia
6.63.63.63.13.12.62.01.51.01.0
abdominal distention 1.0
4.03.51.81.80.54.30.01.50.00.8
Musculoskeletal
Nervous System/Psychiatric
Special Senses
gastritismusculoskeletal painmuscle cramp
headachedizziness
taste perversion
0.54.10.0
2.60.0
0.5
1.32.51.0
1.51.0
1.0
'Considered possibly, probably, or definitely drug related as assessed by the investigatorsRarely, rash and erythema have occurred.One patient treated with FOSAMAX (10 mg/day), who had a history of peptic ulcer disease and gastrectomy and
who was taking concomitant aspirin developed an anastomotic ulcer with mild hemorrhage, which was considereddrug related. Aspirin and FOSAMAX were discontinued and the patient recovered.
The adverse experience profile was similar for the 401 patients treated with either 5 or 20 mg doses of FOSAMAXin the United States and Multinational studies.
Paget's Disease: In clinical studies (osteoporosis and Paget's disease), adverse experiences reported in 175 patientstaking FOSAMAX 40 mg/day for 3-12 months were similar to those in postmenopausal women treated with FOSAMAX10 mg/day. However, there was an apparent increased incidence of upper gastrointestinal adverse experiences inpatients taking FOSAMAX 40 mg/day (17.7% FOSAMAX vs. 10.2% placebo). One case of esophagitis and two casesof gastritis resulted in discontinuation of treatment.
Additionally, musculoskeletal pain, which has been described in patients with Paget's disease treated with other bis-phosphonates, was reported by the investigators as possibly, probably, or definitely drug related in approximately 6%of patients treated with FOSAMAX 40 mg/day versus approximately 1 % of patients treated with placebo, but rarelyresulted in discontinuation of therapy. Discontinuation of therapy due to any clinical adverse experience occurred in6.4% of patients with Paget's disease treated with FOSAMAX 40 mg/day and 2.4% of patients treated with placebo.
Laboratory Test Findings: In double-blind, multicenter, controlled studies, asymptomatic, mild, and transientdecreases in serum calcium and phosphate were observed in approximately 18% and 10%, respectively, of patientstaking FOSAMAX versus approximately 12% and 3% of those taking placebo. However, the incidences of decreasesin serum calcium to <8.0 mg/dL (2.0 mM) and serum phosphate to <2.0 mg/dL (0.65 mM) were similar in both treat-ment groups.
Postmarketing Experience. The following adverse reactions have been reported in postmarketing use: esophagitis,esophageal erosions and esophageal ulcers (see WARNINGS and DOSAGE AND ADMINISTRATION).
OVERDOSAGE: Significant lethality after single oral doses was seen in female rats and mice at 552 mg/kg (3256mg/m') and 966 mg/kg (2898 mg/m!), respectively. In males, these values were slightly higher, 626 and 1280 mg/kg,respectively. There was no lethality in dogs at oral doses up to 200 mg/kg (4000 mg/m!).
No specific information is available on the treatment of overdosage with FOSAMAX. Hypocalcemia, hypophos-phatemia, and upper gastrointestinal adverse events, such as upset stomach, heartburn, esophagitis, gastritis, or ulcer,may result from oral overdosage. Milk or antacids should be given to bind alendronate. Due to the risk of esophagealirritation, vomiting should not be induced and the patient should remain fully upright.
Dialysis would not be beneficial.
DOSAGE AND ADMINISTRATION: FOSAMAX must be taken at least one-half hour before the first food, beverage, ormedication of the day with plain water only (see PRECAUTIONS, Information for Patients). Other beverages (includingmineral water), food, and some medications are likely to reduce the absorption of FOSAMAX (see PRECAUTIONS, DrugInteractions). Waiting less than 30 minutes, or taking FOSAMAX with food, beverages (other than plain water), or othermedications will lessen the effect of FOSAMAX by decreasing its absorption into the body.
To facilitate delivery to the stomach and thus reduce the potential for esophageal irritation, FOSAMAX should onlybe swallowed upon arising for the day with a full glass of water (6-8 oz.) and patients should not lie down for at least30 minutes and until after their first food of the day. FOSAMAX should not be taken at bedtime or beforearising for the day. Failure to follow these instructions may increase the risk of esophageal adverse expe-riences (see WARNINGS).
Patients with osteoporosis or Paget's disease should receive supplemental calcium and vitamin D, if dietary intakeis inadequate (see PRECAUTIONS, General).
No dosage adjustment is necessary for the elderly or for patients with mild-to-moderate renal insufficiency (creati-nine clearance 35 to 60 mL/min). FOSAMAX is not recommended for patients with more severe renal insufficiency(creatinine clearance <35 mL/min) due to lack of experience.
Osteoporosis in Postmenopausal Women: The recommended dosage is 10 mg once a day.Safety of treatment with FOSAMAX for longer than four years has not been studied; extension studies are ongoing.Paget's Disease of Bone: The recommended treatment regimen is 40 mg once a day for six months.Retreatment of Paget's Disease: In clinical studies in which patients were followed every six months, relapses dur-
ing the 12 months following therapy occurred in 9% (3 out of 32) of patients who responded to treatment withFOSAMAX. Specific retreatment data are not available, although responses to FOSAMAX were similar in patients whohad received prior bisphosphonate therapy and those who had not. Retreatment with FOSAMAX may be considered,following a six-month posttreatment evaluation period in patients who have relapsed, based on increases in serumalkaline phosphatase, which should be measured periodically. Retreatment may also be considered in those who failedto normalize their serum alkaline phosphatase.
MERCKFor more detailed information, consult your Merck Representative or see Prescribing Information, Merck & Co., Inc.,
West Point, PA 19486.
Copyright © 1996 by Merck & Co., Inc. All rights reserved.J6F010A(01) PRINTED IN U.S.A. CONTAINS 5 0 % RECYCLED MATERIAL i
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

TEOPOROSISJN POSTMENOPAUSAL
THE FIRSTAND ONLY>NHORMONAL^THERAPY
In clinical
U ILTBDR
1jre results based on pooled data in clinical studies. While stfidies i
ire not^signed with fracture risk as the primary ehdpointjarede-/^fined analyses support that FOSAMAX reduced vertebral fradiire
FQSAMAX is contraindicated in patients with esophage./aonormalities which delay esophageal emptying (e.g., sjfricture/or achalasia) and in patients unable to stand or sit upr^ht f o r /at least 30 minutes. FOSAMAX is contraindicated in patients /with hypersensitivity to any component of this product a n d /in patients with hypocal0mia (see PRECAUTIONS). FOSAMA& Jlike other bisphosphopiates, may cause local irritation of theupper gastrointestinal mucosa. For complete details aboutcontraindications, warnings, precautions, adverse reactions,and dosage and administration, please read the Brief /Summary of Jhe Prescribing Information oriihefollowing page.
Ik
(alendronatesodium tablets)
Watch for dramaticdata on fracture reduction from
the vertebral arm of the landmarkFRACTURE INTERVENTION TRIAL
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

SOmg, 100 mg
* Non-insulin-dependent diabetes mellitus (type II),
(acarbose tablets)NIDDM management from the first bite.
f
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

Lowers Blood Glucose as an Adjunct to Diet - Alone orWith a Sulfonylurea* When Glycemic Control Cannot Be Achieved
®PrecoseThe First Alpha-Glucosidase Inhibitor
Features a Unique, Nonsystemic Mode of Action1
1 Works locally in the small intestine to slow carbohydratedigestion and delay glucose absorption
1 Treats NIDDM without drug-induced hypoglycemia,hyperinsulinemia, lactic acidosis, or weight gain2
Manages Postprandial Glucose Peaks to ImproveGlycemic Control, Reducing HbAlc Levels to HelpPrevent Diabetes Complications, eg, Retinopathy,Neuropathy, and Nephropathy134 'h
' Majority of side effects in clinical trials were GI in nature (abdominal pain,diarrhea, and flatulence), related to the mode of action, and generally diminishedafter 4 to 8 weeks due to adaptation of small intestine enzyme activity5
1 Precose is not recommended in patients with significant renal dysfunction(serum creatinine > 2.0 mg/dL). Precose is contraindicated in patients withdiabetic ketoacidosis, cirrhosis, inflammatory bowel disease, cotonic ulceration,or partial intestinal obstruction JHMP
1 Because efficacy is similar across dosages > 100 mg tid, and dosages > 100 mg tidmay be associated with an increased risk of elevated serum transaminase levels,dosages > 100 mg tid are not recommended
Diet and exercise always should be emphasized as primary methods forNIDDM management
* Precose itself does not cause hypoglycemia. When used in combination withsulfonylureas, it may increase their hypoglycemic potential. Oral glucose, whoseabsorption is not inhibited by Precose, should be used instead of sucrose in thetreatment of mild to moderate hypoglycemia.
Please see brief summary of Prescribing Information on the last page of this advertisement.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022
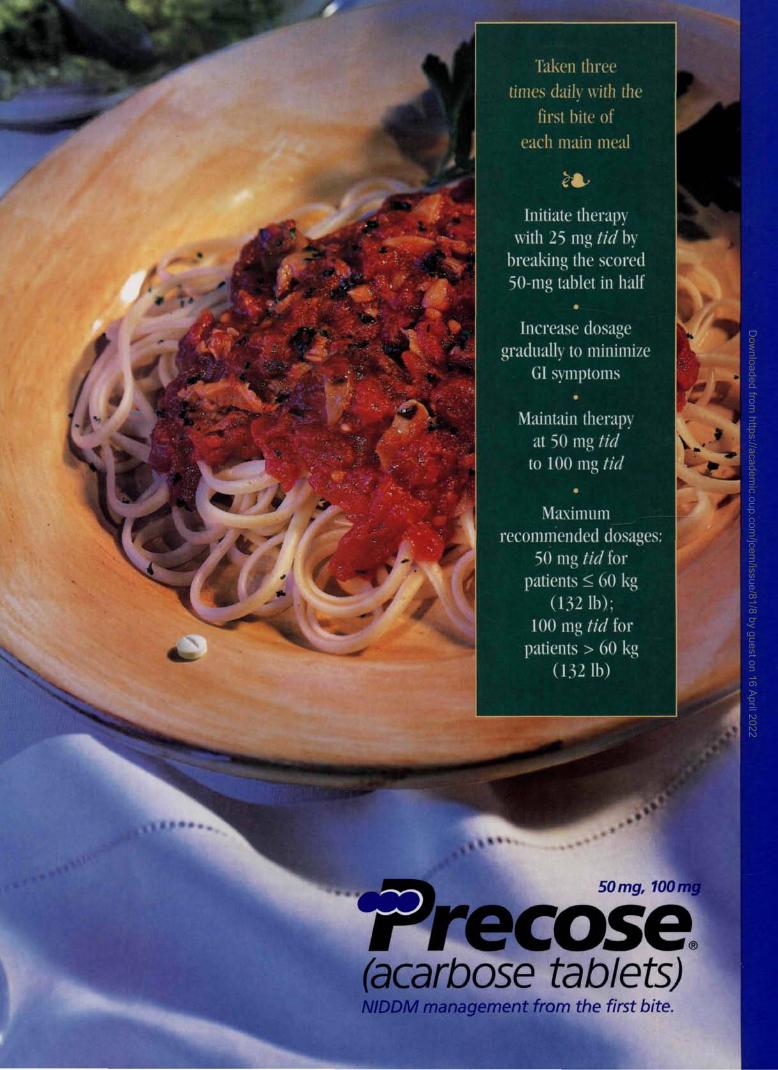
Taken threetimes daily with the
first bite ofeach main meal
*•#>•
Initiate therapywith 25 mg tid by
breaking the scored50-mg tablet in half
•Increase dosage
gradually to minimizeGI symptoms
Maintain therapyat 50 mg tidto 100 mg tid
•
Maximumrecommended dosages:
50 nig tid forpatients < 60 kg
(132 1b);100 mg tid for
patients > 60 kg(132 1b)
50 mg, 100 mg
(acarbose tablets)NIDDM management from the first bite.
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022

_ g 50 mg, 100 me
Trecose(acarbose tablets)
BRIEF SUMMARYCONSULT PACKAGE INSERT FOR FULL PRESCRIBING INFORMATION
PZ500036BS 4/96
INDICATIONS AND USAGEPRECOSE®, as monotherapy, is indicated as an adjunct to diet to lower blood glucose inpatients with non-insulin-dependent diabetes mellitus (NIDDM) whose hyperglycemia cannotbe managed on diet alone. PRECOSE® may also be used in combination with a sulfonylureawhen diet plus either PRECOSE® or a sulfonylurea do not result in adequate glycemic control.The effect of PRECOSE® to enhance glycemic control is additive to that of sulfonylureas whenused in combination, presumably because its mechanism of action is different.In initiating treatment for NIDDM, diet should be emphasized as the primary form of treatment.Caloric restriction and weight loss are essential in the obese diabetic patient. Proper dietarymanagement alone may be effective in controlling blood glucose and symptoms of hyper-glycemia. The importance of regular physical activity when appropriate should also bestressed. If this treatment program fails to result in adequate glycemic control, the use ofPRECOSE® should be considered. The use of PRECOSE® must be viewed by both the physi-cian and patient as a treatment in addition to diet, and not as a substitute for diet or as a con-venient mechanism for avoiding dietary restraint.
CONTRAINDICATIONSPRECOSE® is contraindicated in patients with known hypersensitivity to the drug and inpatients with diabetic ketoacidosis or cirrhosis. PRECOSE® is also contraindicated in patientswith inflammatory bowel disease, colonic ulceration, partial intestinal obstruction or inpatients predisposed to intestinal obstruction. In addition, PRECOSE® is contraindicated inpatients who have chronic intestinal diseases associated with marked disorders of digestion orabsorption and in patients who have conditions that may deteriorate as a result of increasedgas formation in the intestine.
PRECAUTIONSGeneralHypoglycemia: Because of its mechanism of action, PRECOSE® when administered aloneshould not cause hypoglycemia in the fasted or postprandial state. Sulfonylurea agents maycause hypoglycemia. Because PRECOSE® given in combination with a sulfonylurea will causea further lowering of blood glucose, it may increase the hypoglycemic potential of the sulfony-lurea. Oral glucose (dextrose), whose absorption is not inhibited by PRECOSE®, should beused instead of sucrose (cane sugar) in the treatment of mild to moderate hypoglycemia.Sucrose, whose hydrolysis to glucose and fructose is inhibited by PRECOSE®, is unsuitablefor the rapid correction of hypoglycemia. Severe hypoglycemia may require the use of eitherintravenous glucose infusion or glucagon injection.
Elevated Serum Transaminase Levels: In clinical trials, at doses of 50 mg t.i.d. and 100 mgt.i.d., the incidence of serum transaminase elevations with PRECOSE® was the same as withplacebo. In long-term studies (up to 12 months, and including PRECOSE® doses up to 300 mgt.i.d.) conducted in the United States, treatment-emergent elevations of serum transaminases(AST and/or ALT) occurred in 15% of PRECOSE®-treated patients as compared to 7% ofplacebo-treated patients. These serum transaminase elevations appear to be dose related. Atdoses greater than 100 mg t.i.d., the incidence of serum transaminase elevations greater thanthree times the upper limit of normal was two to three times higher in the PRECOSE® groupthan in the placebo group. These elevations were asymptomatic, reversible, more common infemales, and, in general, were not associated with other evidence of liver dysfunction.In international post-marketing experience with PRECOSE® in over 500,000 patients, 19 casesof serum transaminase elevations > 500 IU/L (12 of which were associated with jaundice)have been reported. Fifteen of these 19 cases received treatment with 100 mg t.i.d. or greaterand 13 of 16 patients for whom weight was reported weighed < 60 kg. In the 18 cases wherefollow-up was recorded, hepatic abnormalities improved or resolved upon discontinuation ofPRECOSE®.
Loss of Control of Blood Glucose: When diabetic patients are exposed to stress such as fever,trauma, infection, or surgery, a temporary loss of control of blood glucose may occur. At suchtimes, temporary insulin therapy may be necessary.
Information for Patients: Patients should be told to take PRECOSE® orally three times a day atthe start (with the first bite) of each main meal. It is important that patients continue to adhereto dietary instructions, a regular exercise program, and regular testing of urine and/or bloodglucose.PRECOSE® itself does not cause hypoglycemia even when administered to patients in the fast-ed state. Sulfonylurea drugs and insulin, however, can lower blood sugar levels enough tocause symptoms or sometimes life-threatening hypoglycemia. Because PRECOSE® given incombination with a sulfonylurea or insulin will cause a further lowering of blood sugar, it mayincrease the hypoglycemic potential of these agents. The risk of hypoglycemia, its symptomsand treatment, and conditions that predispose to its development should be well understoodby patients and responsible family members. Because PRECOSE® prevents the breakdown oftable sugar, patients should have a readily available source of glucose (dextrose, D-glucose) totreat symptoms of low blood sugar when taking PRECOSE® in combination with a sulfony-lurea or insulin.
If side effects occur with PRECOSE®, they usually develop during the first few weeks of thera-py. They are most commonly mild-to-moderate gastrointestinal effects, such as flatulence,diarrhea, or abdominal discomfort and generally diminish in frequency and intensity with time.Laboratory Tests: Therapeutic response to PRECOSE® should be monitored by periodic bloodglucose tests. Measurement of glycosylated hemoglobin levels is recommended for the moni-toring of long-term glycemic control.
PRECOSE®, particularly at doses in excess of 50 mg t.i.d., may give rise to elevations ofserum transaminases and, in rare instances, hyperbilirubinemia. It is recommended thatserum transaminase levels be checked every 3 months during the first year of treatment withPRECOSE® and periodically thereafter. If elevated transaminases are observed, a reduction indosage or withdrawal of therapy may be indicated, particularly if the elevations persist.Renal Impairment: Plasma concentrations of PRECOSE® in renally impaired volunteers wereproportionally increased relative to the degree of renal dysfunction. Long-term clinical trials indiabetic patients with significant renal dysfunction (serum creatinine >2.0 mg/dL) have notbeen conducted. Therefore, treatment of these patients with PRECOSE® is not recommended.Drug Interactions: Certain drugs tend to produce hyperglycemia and may lead to loss of bloodglucose control. These drugs include the thiazides and other diuretics, corticosteroids, phe-nothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sym-pathomimetics, calcium channel-blocking drugs, and isoniazid. When such drugs are adminis-tered to a patient receiving PRECOSE®, the patient should be closely observed for loss of
blood glucose control. When such drugs are withdrawn from patients receiving PRECOSE® incombination with sulfonylureas or insulin, patients should be observed closely for any evi-dence of hypoglycemia.
Intestinal adsorbents (e.g., charcoal) and digestive enzyme preparations containing carbohy-drate-splitting enzymes (e.g., amylase, pancreatin) may reduce the effect of PRECOSE® andshould not be taken concomitantly.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Nine chronic toxicity/carcino-genicity studies were conducted in three animal species (rat, hamster, dog) including two ratstrains (Sprague-Oawley and Wistar).
In the first rat study, Sprague-Dawley rats received acarbose in feed at high doses (up toapproximately 500 mg/kg body weight) for 104 weeks. Acarbose treatment resulted in a signif-icant increase in the incidence of renal tumors (adenomas and adenocarcinomas) and benignLeydig cell tumors. This study was repeated with a similar outcome. Further studies were per-formed to separate direct carcinogenic effects of acarbose from indirect effects resulting fromthe carbohydrate malnutrition induced by the large doses of acarbose employed in the studies.In one study using Sprague-Dawley rats, acarbose was mixed with feed but carbohydratedeprivation was prevented by the addition of glucose to the diet. In a 26-month study ofSprague-Dawley rats, acarbose was administered by daily postprandial gavage so as to avoidthe pharmacologic effects of the drug. In both of these studies, the increased incidence ofrenal tumors found in the original studies did not occur. Acarbose was also given in food andby postprandial gavage in two separate studies in Wistar rats. No increased incidence of renaltumors was found in either of these Wistar rat studies. In two feeding studies of hamsters,with and without glucose supplementation, there was also no evidence of carcinogenicity.Acarbose showed no mutagenic activity when tested in six In vitro and three In vivo assays.Fertility studies conducted in rats after oral administration produced no untoward effect on fer-tility or on the overall capability to reproduce.Pregnancy:
Teratogenic Effects: Pregnancy Category B. The safety of PRECOSE® in pregnant women hasnot been established. Reproduction studies have been performed in rats at doses up to 480mg/kg (corresponding to 9 times the exposure in humans, based on drug blood levels) andhave revealed no evidence of impaired fertility or harm to the fetus due to acarbose. In rabbits,reduced maternal body weight gain, probably the result of the pharmacodynamic activity ofhigh doses of acarbose in the intestines, may have been responsible for a slight increase in thenumber of embryonic losses. However, rabbits given 160 mg/kg acarbose (corresponding to10 times the dose in man, based on body surface area) showed no evidence of embryotoxicityand there was no evidence of teratogenicity at a dose 32 times the dose in man (based onbody surface area). There are, however, no adequate and well-controlled studies of PRECOSE®in pregnant women. Because animal reproduction studies are not always predictive of thehuman response, this drug should be used during pregnancy only if clearly needed. Becausecurrent information strongly suggests that abnormal blood glucose levels during pregnancyare associated with a higher incidence of congenital anomalies as well as increased neonatalmorbidity and mortality, most experts recommend that insulin be used during pregnancy tomaintain blood glucose levels as close to normal as possible.Nursing Mothers: A small amount of radioactivity has been found in the milk of lactating ratsafter administration of radiolabeled acarbose. It is not known whether this drug is excreted inhuman milk. Because many drugs are excreted in human milk, PRECOSE® should not beadministered to a nursing woman.Pediatric Use: Safety and effectiveness of PRECOSE® in pediatric patients have not beenestablished.
ADVERSE REACTIONSDigestive Tract: Gastrointestinal symptoms are the most common reactions to PRECOSE®. InU.S. placebo-controlled trials, the incidences of abdominal pain, diarrhea, and flatulence were21%, 33%, and 77% respectively in 1075 patients treated with PRECOSE® 50-300 mg t.i.d.,whereas the corresponding incidences were 9%, 12%, and 32% in 818 placebo-treatedpatients. Abdominaj pain and diarrhea tended to return to pretreatment levels over time, andthe frequency and intensity of flatulence tended to abate with time. The increased gastroin-testinal tract symptoms in patients treated with PRECOSE® is a manifestation of the mecha-nism of action of PRECOSE® and is related to the presence of undigested carbohydrate in thelower Gl tract. Rarely, these gastrointestinal events may be severe and might be confused withparalytic ileus.
Elevated Serum Transaminase Levels: See PRECAUTIONS.Other Abnormal Laboratory Findings: Small reductions in hematocrit occurred more often inPRECOSE®-treated patients than in placebo-treated patients but were not associated withreductions in hemoglobin. Low serum calcium and low plasma vitamin E levels were associat-ed with PRECOSE® therapy but were thought to be either spurious or of no clinical significance.
Caution: Federal law prohibits dispensing without a prescription.
PZ500036BS 4/96© 1996 Bayer Corporation
Bay g 54216160
PRECOSE®/5202/0/8/USA-1Printed in U.S.A.
References1. Precose* (acarbose tablets) Package Insert.2. Coniff RF, Shapiro JA, Robbins D, et al. Reduction of glycosylated hemoglobin and postprandial
hyperglycemia by acarbose in patients with NIDDM. Diabetes Care. 1995; 18(6) :817-824.3. Coniff RF, Shapiro JA, Seaton TB, Bray GA. Multicenter, placebo-controlled trial comparing
acarbose (BAY g 5421) with placebo, tolbutamide, and tolbutamide-plus-acarbose innon-insulin-dependent diabetes mellitus. AmJMed. 1995;98:443-451.
4. American Diabetes Association. Implications of the Diabetes Control and Complications Trial.Diabetes Care. 1993;l6(ll):1517-1520.
5. Hanefeld M. Acarbose efficacy review. Practical Diabetes Suppl. 1993; 10(6) :S21-S27.
BayerPharmaceuticalDivision
© May 1996 Bayer CorporationAll Rights Reserved. Printed in USA. AO9536
Dow
nloaded from https://academ
ic.oup.com/jcem
/issue/81/8 by guest on 16 April 2022




















