Exercise capacity and quadriceps muscle metabolism following training in subjects with COPD
9
Respiratory Medicine (2006) 100, 1817–1825 Exercise capacity and quadriceps muscle metabolism following training in subjects with COPD Zoe J. McKeough a,b, , Jennifer A. Alison a,b , Peter T.P. Bye a , Michael I. Trenell c , Toos Sachinwalla d , Campbell H. Thompson e , Graham J. Kemp f a Department of Respiratory Medicine, Level 11 West, Building 75, Royal Prince Alfred Hospital, Missenden Rd, Camperdown, NSW, Australia 2050 b School of Physiotherapy, Faculty of Health Sciences, Sydney University, PO Box 170, Lidcombe, NSW, Australia 1825 c Woolcock Institute for Medical Research, Missenden Rd, Camperdown, NSW, Australia 2050 d Rayscan Imaging, 41–43 Goulburn St, Liverpool, Australia 2170 e Department of General Medicine, Flinders University, Adelaide, Australia 5042 f Division of Metabolic & Cellular Medicine, University of Liverpool, L69 3GA, UK Received 16 September 2005; accepted 23 January 2006 KEYWORDS Chronic obstructive pulmonary disease; Exercise training; Magnetic resonance imaging; Magnetic resonance spectroscopy; Muscle function Summary The aim of the study was to determine whether 16 sessions of exercise training, completed twice weekly, alters exercise capacity, quadriceps muscle metabolism, cross-sectional area (CSA) and strength in subjects with chronic obstructive pulmonary disease (COPD). We studied (a) 10 COPD subjects (mean age7SEM ¼ 7172 years; FEV 1 ¼ 0.9970.1 L) before and after 16 sessions of exercise training, and (b) 10 healthy subjects (age ¼ 6873 years). The COPD subjects underwent an incremental peak exercise test using a cycle ergometer and a 6-min walk test: both improved following exercise training (Po0:05). Magnetic resonance spectroscopy measurements, in quadriceps muscle, of post-exercise phosphocrea- tinine (PCr) recovery kinetics were used to assess mitochondrial function in vivo: in the COPD subjects pre-training this was 1978% lower than in healthy subjects (P ¼ 0:03), but a 38712% increase was seen in the COPD subjects following training (P ¼ 0:003). Magnetic resonance imaging was used to assess quadriceps CSA: after training in the COPD subjects this showed a 772% increase (P ¼ 0:03). Quadriceps strength, measured by the best of five maximum voluntary contractions, also showed a 32711% increase in the COPD subjects (P ¼ 0:007). Sixteen sessions of exercise ARTICLE IN PRESS 0954-6111/$ - see front matter & 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.rmed.2006.01.017 Corresponding author. School of Physiotherapy, Faculty of Health Sciences, Sydney University, PO Box 170, Lidcombe, NSW, Australia 1825. Tel.: +61 2 9351 9269; fax: +61 2 9351 9278. E-mail address: [email protected] (Z.J. McKeough).
Transcript of Exercise capacity and quadriceps muscle metabolism following training in subjects with COPD

ARTICLE IN PRESS
Respiratory Medicine (2006) 100, 1817–1825
0954-6111/$ - sdoi:10.1016/j.r
�CorrespondiAustralia 1825.
E-mail addr
Exercise capacity and quadriceps musclemetabolism following training in subjectswith COPD
Zoe J. McKeougha,b,�, Jennifer A. Alisona,b, Peter T.P. Byea,Michael I. Trenellc, Toos Sachinwallad, Campbell H. Thompsone,Graham J. Kempf
aDepartment of Respiratory Medicine, Level 11 West, Building 75, Royal Prince Alfred Hospital,Missenden Rd, Camperdown, NSW, Australia 2050bSchool of Physiotherapy, Faculty of Health Sciences, Sydney University, PO Box 170, Lidcombe,NSW, Australia 1825cWoolcock Institute for Medical Research, Missenden Rd, Camperdown, NSW, Australia 2050dRayscan Imaging, 41–43 Goulburn St, Liverpool, Australia 2170eDepartment of General Medicine, Flinders University, Adelaide, Australia 5042fDivision of Metabolic & Cellular Medicine, University of Liverpool, L69 3GA, UK
Received 16 September 2005; accepted 23 January 2006
KEYWORDSChronic obstructivepulmonary disease;Exercise training;Magnetic resonanceimaging;Magnetic resonancespectroscopy;Muscle function
ee front matter & 2006med.2006.01.017
ng author. School of PTel.: +61 2 9351 9269; fess: [email protected]
Summary The aim of the study was to determine whether 16 sessions of exercisetraining, completed twice weekly, alters exercise capacity, quadriceps musclemetabolism, cross-sectional area (CSA) and strength in subjects with chronicobstructive pulmonary disease (COPD). We studied (a) 10 COPD subjects (meanage7SEM ¼ 7172 years; FEV1 ¼ 0.9970.1 L) before and after 16 sessions of exercisetraining, and (b) 10 healthy subjects (age ¼ 6873 years). The COPD subjectsunderwent an incremental peak exercise test using a cycle ergometer and a 6-minwalk test: both improved following exercise training (Po0:05). Magnetic resonancespectroscopy measurements, in quadriceps muscle, of post-exercise phosphocrea-tinine (PCr) recovery kinetics were used to assess mitochondrial function in vivo: inthe COPD subjects pre-training this was 1978% lower than in healthy subjects(P ¼ 0:03), but a 38712% increase was seen in the COPD subjects following training(P ¼ 0:003). Magnetic resonance imaging was used to assess quadriceps CSA: aftertraining in the COPD subjects this showed a 772% increase (P ¼ 0:03). Quadricepsstrength, measured by the best of five maximum voluntary contractions, also showeda 32711% increase in the COPD subjects (P ¼ 0:007). Sixteen sessions of exercise
Elsevier Ltd. All rights reserved.
hysiotherapy, Faculty of Health Sciences, Sydney University, PO Box 170, Lidcombe, NSW,ax: +61 2 9351 9278.syd.edu.au (Z.J. McKeough).

ARTICLE IN PRESS
Z.J. McKeough et al.1818
training, performed twice weekly, increased exercise capacity as well as quadricepsmitochondrial capacity, CSA and strength in the subjects with COPD.& 2006 Elsevier Ltd. All rights reserved.
Introduction
Skeletal muscle dysfunction has been proposed to bea primary determinant of reduced exercise capacityin subjects with chronic obstructive pulmonarydisease (COPD).1 A number of studies have shown areduction in muscle endurance,2–6 strength7–9 andmuscle atrophy3,10,11 in subjects with COPD.
The cause of skeletal muscle dysfunction and theextent to which it occurs in all COPD subjects iscurrently under debate. Physical inactivity andconsequent deconditioning may be an importantcause, and so exercise training may be an im-portant preventive and therapeutic strategy. Phy-siological benefits from moderate-to-high-intensityexercise training, performed 3–5 times weekly for8–12 weeks, have been shown in subjects withmoderate to severe COPD12–14 including an increasein muscle oxidative enzymes.13 No studies wereidentified that have examined both muscle meta-bolism and exercise capacity following twiceweekly, supervised exercise training.
Phosphorus magnetic resonance spectroscopy(31P-MRS) is a non-invasive method of assessingskeletal muscle metabolism at rest, during exerciseand in recovery. One study15 has used 31P-MRS toexamine the effect of cycle training performed fivetimes weekly for 8 weeks on quadriceps musclemetabolism in moderate COPD, reporting a longerthan normal half-time of post-exercise phospho-creatine recovery (PCr t1/2) in the COPD subjectsprior to training, suggestive of a defect of muscleoxidative capacity, which improved after training.
The primary aim of this study was to examine theeffect of 16 sessions of an endurance and strengthtraining program, performed twice weekly, onexercise capacity, quadriceps mitochondrial capacity,and quadriceps cross-sectional area (CSA) andstrength in subjects with COPD. The hypothesis wasthat the exercise training would increase exercisecapacity as well as quadriceps mitochondrial capa-city, CSA and strength in the subjects with COPD.
Methods
Subjects
Ten subjects diagnosed with COPD (6 male, 4female) were recruited from the pulmonary
rehabilitation program at Royal Prince AlfredHospital (RPAH), Australia. Subjects were includedif they had COPD Stage II and Stage III asclassified by the Global Initiative for ChronicObstructive Lung Disease (GOLD) standards16 andexcluded if they had previously undergonepulmonary rehabilitation, required oxygentherapy, were still smoking or suffered fromclaustrophobia.
Ten healthy, age-matched, control subjects(5 male, 5 female) were recruited from the generalcommunity. These subjects had no respiratoryhistory and were sedentary, assessed by thephysical activity questionnaire17 in which sedentaryphysical activity level was defined as expendingo10% of daily energy expenditure in the perfor-mance of moderate-to-high-intensity activities(i.e. a resting metabolic equivalent level 44METS).18
All subjects were questioned about their capacityto enter a magnetic field. Standard magneticresonance exclusions applied.
Informed, written consent was obtained from allsubjects, and the study was approved by the EthicsReview Committee (RPAH zone) of the Sydney SouthWest Area Health Service.
All COPD subjects had testing performed atbaseline and following 8 weeks exercise training.All healthy subjects had testing performed atbaseline only.
Muscle tests
Both magnetic resonance imaging (MRI) and 31P-MRS were performed. The same protocol was usedon all subjects. This protocol has been previouslydescribed by this group.19 Subjects lay prone on acustom-built rig positioned inside a Philips 1.5 TGyroscan Intera magnet (Philips Medical Systems,Best, The Netherlands). The right thigh wasstrapped to the rig (Fig. 1) with the P-100 pulse-receive coil (Philips Medical Systems, Best, TheNetherlands) positioned under the right quadricepsmuscle. The right knee was flexed to 301 with thelower leg positioned on a force platform whichwas equipped with an electronic load cell (PT-100PT electronics, Auckland NZ) to evaluate forceproduction.

ARTICLE IN PRESS
Figure 1 Schematic of leg positioning on the rig. (A)force platform, (B) lower leg, (C) straps, (D) thigh.
Exercise capacity and quadriceps metabolism in COPD 1819
Magnetic resonance imagingImages of the right quadriceps muscle were takento assess CSA. Two transverse stacks of T2 weightedimages (6mm thick–30mm gap) were collected.The area of the quadriceps muscle group wasanalysed manually using the Philips Easy Visionsoftware (Philips Medical Systems, Best, TheNetherlands). The CSA was taken as the maximaluncorrected area from review of all the singleimages from that subject.
Magnetic resonance spectroscopyAn adiabatic pulse sequence was used to collecteight unlocalised 31P spectra (TR ¼ 1500ms),summed to assess resting metabolic state. Spectrawere Fourier transformed and analysed for [PCr],adenosine triphosphate ([ATP]), adenosine dipho-sphate [ADP], and inorganic phosphate ([Pi]) usingthe Java-based magnetic resonance user interface(jMRUI version 2.0, EU Project).20 The chemicalshift between [PCr] and [Pi] was used to measuremuscle acidity (pH).21
Each subject performed five maximum voluntarycontractions of the right quadriceps muscle with15 s of rest between contractions, taking thehighest value as the maximum voluntary contrac-tion (MVC). The exercise protocol consisted ofpushing against the force platform at 60% MVC for3 s followed by 1 s relaxation. Visual force feedbackwas provided using a custom-built display unitcombined with a light metronome to ensure correcttiming of contraction and relaxation. The exercisecycle was repeated for 3min (45 cycles), afterwhich the subject was rested for 7min. Spectrawere collected every 4 s during exercise andrecovery, 150 in all (TR 4000ms), and analysed asfor the resting spectra. In the COPD subjects, thesame relative workload (i.e. 60% MVC) was usedpost-training following re-measurement of theMVC.
Muscle oxidative function was assessed from therecovery kinetics of PCr, fitting a least-squaresmonoexponential time-function to determine thehalftime (t1/2) and initial rate of PCr resynthesis.
The initial rate is a measure of the absolute end-exercise rate of oxidative ATP synthesis, and thehalftime is an inverse measure of mitochondrialcapacity (independent of the degree of PCr deple-tion), i.e. the maximum rate of oxidative ATPsynthesis22 if appropriate allowance is made for pHchange during exercise. We exploited the invariantnear-linear relationship between PCr t1/2 and end-exercise pH23,24 first to establish group differencesin mitochondrial function, and then to calculate foreach subject the ratio of the PCr t1/2 predictedfrom the end-exercise pH to that observed; this is arobust measure of the mitochondrial capacity in asubject relative to that on average in the controls.
Lung function tests
In the COPD subjects, measurements of spirometryand lung volumes were performed (SensormedicsVmax 20 and Sensormedics V6200 Autobox BodyPlethysmograph respectively; Sensormedics Cor-poration, CA) and compared to predicted normalvalues for spirometry25 and for lung volumes.26 Inthe healthy subjects, measurements of spirometrywere performed using a hot-wire anemometer(Minato Autospiro AS-500; Minato Medical Science,Osaka, Japan).
Exercise tests
Exercise tests were only performed in the COPDsubjects. An incremental symptom-limited cycletest was performed on an electrically brakedbicycle ergometer (Sensormedics 800 ComputerisedErgometer, Sensormedics Corporation, CA). Eachsubject breathed through a calibrated mass flowsensor with expired gas sampled on a breath-by-breath basis (Vmax 29 Cardiopulmonary ExerciseTesting Instrument; Sensormedics Corporation,California, USA) so that oxygen consumption VO2
,carbon dioxide production, minute ventilation (VE),tidal volume and breathing frequency could bedetermined. The peak VO2
and peak workload fromthis test were compared to the predicted normalvalues.27 Heart rate (HR) and percent oxygensaturation were obtained with a finger probeattached to a pulse oximeter (N200: Nellcor,Hayward CA). Each subject scored their dyspneaand rate of perceived exertion on a modified Borgscale reading 0 (‘‘nothing at all’’) to 10 (‘‘max-imal’’). Peak values were compared before andafter exercise training.
A 6min walk test was conducted in accordancewith a standardised protocol.28 All subjects com-pleted two walks separated by 30min rest. Each

ARTICLE IN PRESS
Z.J. McKeough et al.1820
subject was asked to walk as far as they could in6min up and down a 12m track which was markedout by tape. Standardised encouragement wasgiven throughout. The better 6min walk distance(6MWD) was used in the data analysis.
Table 1 Anthropometric and lung function datain the healthy control subjects (n ¼ 10) and in theCOPD subjects (n ¼ 10) before and after exercisetraining (ET)
Healthy COPD
Exercise training
Each session of exercise training consisted ofsupervised leg cycling, walking, and leg strengthtraining performed twice per week for 8 weeks.Sixteen sessions of exercise were required to becompleted prior to final testing. The intensity ofcycle exercise was set from the peak leg cycleexercise test. The cycle training initially con-sisted of a 5-min warm-up at 40% peak work,5–10min exercise at 60% peak work and a 5-mincool-down at 40% peak work. The intensity andduration of cycling was progressed as able.The intensity was increased up to 80% peak work-load by week 8 and the duration was progressed to20min by week 4 and to 30min by week 8. Theintensity of walking was set at 80% of the walkingspeed calculated from the initial 6min walk test,for 20min initially and progressed to 30min byweek 8.
Strength training for the quadriceps was per-formed on a leg extension machine. Trainingconsisted of two sets of 8–10 repetitions at 70% ofthe one repetition maximum (1RM). This wasprogressed, if able, up to three sets of 10repetitions by week 4 and up to three sets of 10repetitions at 80% of 1RM by week 8.
controlbaseline
Pre-ET Post-ET
Age (yr) 6873 7172 7172BMI (kg/m2) 2572 2671 2671FEV1 (L) 2.470.2 0.9970.1� 1.170.1% pred 10374 4275� 4476
FVC (L) 3.070.3 2.370.2� 2.370.1% pred 9374 6775� 6973
TLC (L) 6.370.5 6.570.5% pred 12076 12175
FRC (L) 4.570.4 4.570.4% pred 150714 150712
RV (L) 4.070.4 4.070.4% pred 188716 189715
Data are mean7SEM. BMI: body mass index; FEV1: forcedexpiratory volume in 1 s; FVC: forced vital capacity; TLC:total lung capacity; FRC: forced residual capacity; RV:residual volume.�Significantly different from healthy control group
(Po0:05).
Statistical analysis
Statistical analysis used StatView (Version 4.571992–1996, Abacus Concepts Inc., Berkeley, Cali-fornia) and StatsDirect (v. 2.4.1 http://www.statsdirect.com/). All data are presented asmean7standard error of the mean (SEM). Variableswere compared between groups using an unpairedt-test and within the COPD subjects from pre- topost-training using a paired t-test. Grouped linearregression was used to assess the relationship ofPCr t1/2 to end-exercise pH, and simple linearregression to back-predict PCr t1/2 using the pH-t1/2relationship in controls. Linear regression was usedto assess the relationship between change inexercise capacity and mitochondrial capacity inthe subjects with COPD. A P-value of o0.05 wastaken to be significant.
Results
Mean anthropometric data and lung function resultsare presented in Table 1. Lung function in the COPDsubjects was significantly reduced compared to thehealthy subjects. The mean time to complete 16sessions of exercise training in the COPD subjectswas 9.770.5 weeks. By the end of the 16 sessions,90% of subjects had achieved the required walkingprotocol, 30% had achieved the required cyclingprotocol (of the remainder: 40% of subjects werecycling for 20min at 60% peak work and 30% werecycling for 30min at 60% peak work), and allsubjects were performing strength training for 3sets of 10 repetitions at 70–80% 1RM.
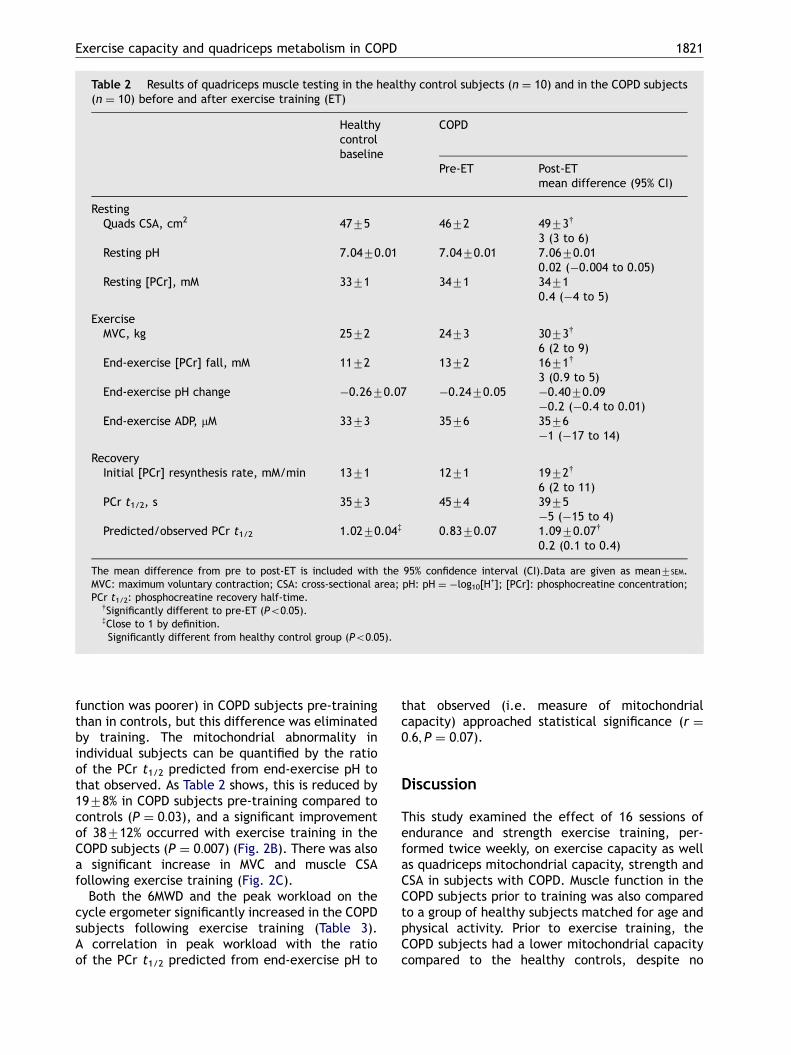
Results of quadriceps muscle testing are pre-sented in Table 2. There was a significant increasein the initial rate of PCr resynthesis from pre- topost-training in the COPD subjects. As PCr deple-tion was also significantly greater from pre- to post-training, the PCr t1/2 did not differ. The relation-ship between PCr t1/2 and end-exercise pH had astatistically indistinguishable slope in all threegroups, with a significant vertical separationbetween COPD subjects pre-training and controls,and between COPD subjects pre- and post-training(both Po0:01) (Fig. 2A). Thus for a given pHchange, PCr t1/2 was higher (i.e. mitochondrial
ARTICLE IN PRESS
Table 2 Results of quadriceps muscle testing in the healthy control subjects (n ¼ 10) and in the COPD subjects(n ¼ 10) before and after exercise training (ET)
Healthycontrolbaseline
COPD
Pre-ET Post-ETmean difference (95% CI)
RestingQuads CSA, cm2 4775 4672 4973y
3 (3 to 6)Resting pH 7.0470.01 7.0470.01 7.0670.01
0.02 (�0.004 to 0.05)Resting [PCr], mM 3371 3471 3471
0.4 (�4 to 5)
ExerciseMVC, kg 2572 2473 3073y
6 (2 to 9)End-exercise [PCr] fall, mM 1172 1372 1671y
3 (0.9 to 5)End-exercise pH change �0.2670.07 �0.2470.05 �0.4070.09
�0.2 (�0.4 to 0.01)End-exercise ADP, mM 3373 3576 3576
�1 (�17 to 14)
RecoveryInitial [PCr] resynthesis rate, mM/min 1371 1271 1972y
6 (2 to 11)PCr t1/2, s 3573 4574 3975
�5 (�15 to 4)Predicted/observed PCr t1/2 1.0270.04z 0.8370.07� 1.0970.07y
0.2 (0.1 to 0.4)
The mean difference from pre to post-ET is included with the 95% confidence interval (CI).Data are given as mean7SEM.MVC: maximum voluntary contraction; CSA: cross-sectional area; pH: pH ¼ �log10[H
+]; [PCr]: phosphocreatine concentration;PCr t1/2: phosphocreatine recovery half-time.ySignificantly different to pre-ET (Po0:05).zClose to 1 by definition.�Significantly different from healthy control group (Po0:05).
Exercise capacity and quadriceps metabolism in COPD 1821
function was poorer) in COPD subjects pre-trainingthan in controls, but this difference was eliminatedby training. The mitochondrial abnormality inindividual subjects can be quantified by the ratioof the PCr t1/2 predicted from end-exercise pH tothat observed. As Table 2 shows, this is reduced by1978% in COPD subjects pre-training compared tocontrols (P ¼ 0:03), and a significant improvementof 38712% occurred with exercise training in theCOPD subjects (P ¼ 0:007) (Fig. 2B). There was alsoa significant increase in MVC and muscle CSAfollowing exercise training (Fig. 2C).
Both the 6MWD and the peak workload on thecycle ergometer significantly increased in the COPDsubjects following exercise training (Table 3).A correlation in peak workload with the ratioof the PCr t1/2 predicted from end-exercise pH to
that observed (i.e. measure of mitochondrialcapacity) approached statistical significance (r ¼0:6; P ¼ 0:07).
Discussion
This study examined the effect of 16 sessions ofendurance and strength exercise training, per-formed twice weekly, on exercise capacity as wellas quadriceps mitochondrial capacity, strength andCSA in subjects with COPD. Muscle function in theCOPD subjects prior to training was also comparedto a group of healthy subjects matched for age andphysical activity. Prior to exercise training, theCOPD subjects had a lower mitochondrial capacitycompared to the healthy controls, despite no

ARTICLE IN PRESS
0.0
0.2
0.4
0.6
0.8
1.0
-1.0 -0.5end-exercise pH change
PC
r re
cove
ry h
alft
ime
(min
)
COPD pre ET
COPD post ET
Healthy controls
COPD pre ET
COPD post ET
Control
(A)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Rel
ativ
e M
ito
cho
nd
rial
Cap
acit
y
COPD pre ET COPD post ET Controls Pre-post
0
10
20
30
40
50
60
70
CS
A (
cm2 )
(B) (C)
Figure 2 Results of muscle testing. (A) The relationship between PCr t1/2 and end-exercise pH change in the subjectswith COPD pre-exercise training (pre ET) and post-exercise training (post ET), and in the healthy control subjects: keyto symbols is in the panel. Lines are fitted by grouped linear regression (see Methods): that for COPD pre-exercisetraining is significantly vertically shifted (see Results). (B) The relative mitochondrial capacity (derived from data inFig. 2A: see Methods) in the subjects with COPD pre-exercise training (pre ET) and post-exercise training (post ET), andin the healthy control subjects: key to symbols is in the panel. Lines join pre- and post-exercise training data. Pre-exercise training mean in the subjects with COPD is significantly lower than control, and increases significantly pre-to post-exercise training (see Table 2). (C) Quadriceps CSA in the subjects with COPD pre-exercise training (pre ET) andpost-exercise training (post ET), and in the healthy control subjects: key to symbols is in the panel. Lines join pre- andpost-exercise training data. There was a significant increase from pre- to post-exercise training in the COPD subjects(see Table 2).
Z.J. McKeough et al.1822
difference between groups in the size of themuscle. Following exercise training in the COPDsubjects, exercise capacity as well as quadricepsmitochondrial capacity, CSA and strength all sig-nificantly increased.
Comparison of muscle function in COPD andhealth
As in other studies29–31 there were no significantabnormalities in resting [PCr] or pH in the subjectswith COPD. Thus the metabolic impairment in theCOPD subjects was not sufficiently severe as to beunequal to the metabolic demands of the restingmuscle. One way to further examine musclemitochondrial capacity is to exercise the muscle
sufficiently to cause [PCr] depletion and thenobserve the recovery of [PCr] once exercise stops.32
There are several ways of doing this: the moreintense the exercise the greater the PCr depletionachieved, and the better the precision of thecrucial measurement of PCr t1/2, but the associatedpH fall makes the interpretation more difficult, andruns the risk of ATP depletion. Alternative ap-proaches making use of the presumed causalrelationships between, for example, rates of PCrresynthesis and [ADP]32 are difficult when ADPchanges during exercise are relatively small, asthey tend to be when pH changes are large. Wehave chosen an exercise protocol that producesadequate PCr depletion in subjects without ex-cessive PCr depletion and ATP loss, and a method ofdata analysis that accounts for variable pH

ARTICLE IN PRESS
Table 3 Six minute walk distance and the peak exercise response on the cycle ergometer in the COPD subjects(n ¼ 10) before and after exercise training (ET)
Pre-ET Post-ET Mean difference (95%CI)
WorkWatts 4675 5374� 7 (2 to 12)% predicted 4175 4874� 7 (1 to 12)
VO2
L/min 0.8170.10 0.8570.04 0.04 (�0.07 to 0.1)ml/kg/min 11.270.8 11.970.5 0.7 (�0.9 to 2.3)% predicted 5977 6376 4 (�7 to 15)
VCO2(L/min) 0.8470.1 0.8870.1 0.05 (�0.1 to 0.2)
VE (L/min) 3273 3472 2 (�3 to 7)VE/MVV (%) 9879 9476 �4 (�15 to 7)Vt (L) 1.0470.1 1.0770.1 0.02 (�0.1 to 0.1)fb (brths/min) 3272 3372 2 (�1 to 4)SpO2 (%) 9172 9272 0.5 (�1 to 2)HR (bpm) 11778 11476 �2 (�9 to 4)HR (% pred) 7275 7074 �2 (�5 to 2)Dyspnea 771 771 �0.1 (�2 to 1)RPE 871 971 0.8 (�1 to 3)6MWD (m) 374717 451713� 77 (42 to 112)
Data are given as mean7SEM. VO2: oxygen consumption; VCO2
: carbon dioxide production; VE: minute ventilation; VE/MVV: ratioof minute ventilation to maximal voluntary ventilation; Vt: tidal volume; fb: breathing frequency; SpO2: oxygen saturation; HR:heart rate; RPE: rate of perceived exertion; 6MWD: six minute walk distance.�Significantly different to pre-ET (Po0:05).
Exercise capacity and quadriceps metabolism in COPD 1823
changes, and which can be used to quantitateabnormalities in functional mitochondrial capacityand changes produced by training.
Prior to exercise training in the COPD subjects,mitochondrial capacity was reduced compared tothe healthy subjects. Previous studies have indi-cated similar results with an increased PCr t1/2 inCOPD subjects compared to healthy sub-jects.15,30,31 However, two of these studies alsonoted a greater pH change with exercise in theCOPD subjects30,31 which makes the interpretationdifficult.29 In the present study, we allowed for pHchange in our calculation, and infer a defect inmitochondrial function similar to that in a recentstudy.15 In principle, this could be due to areduction in mitochondrial volume, intrinsic mito-chondrial defect or impaired oxygen supply be-cause of arterial hypoxaemia or reduced capillarynumber. A previous study has shown that leg oxygendelivery at a given power output was not signifi-cantly different between COPD subjects andhealthy subjects,33 suggesting that impaired oxy-gen supply was not a factor. Previous studies ofmuscle oxidative enzymes34–36 suggest that at leastpart of the functional defect is due to reducedmitochondrial number, volume or enzyme content.
The underlying aetiology for skeletal muscledysfunction in COPD subjects has not been con-clusively determined. Factors proposed to cause
skeletal muscle dysfunction in COPD subjectsinclude poor nutrition,37 corticosteroid use,38 sys-temic inflammatory processes,39 hypoxia,40 in-creased oxidative stress3 and disuse.41 Disuse isprobably one of the primary reasons for thereduced quadriceps mitochondrial capacity priorto exercise training in the COPD subjects. When thedisuse process was reversed by exercise training,quadriceps mitochondrial capacity improved. Thiswill be discussed in the next section.
Changes with exercise training in COPD
From PCr recovery kinetics we infer a 38712%increase in mitochondrial capacity from exercisetraining. Furthermore, quadriceps muscle CSA andMVC increased significantly (772% and 32711%,respectively) in the COPD subjects followingexercise training.
One other study has examined the effect of acontinuous exercise training protocol on musclemetabolism using 31P-MRS in COPD subjects.15 Theirresults showed a significant improvement in PCr t1/2following 8 weeks of leg cycle training achievingvalues similar to healthy subjects. In that study,with small pH changes, this amounts to a 48712%increase in mitochondrial capacity which is slightly,but probably not significantly, higher than in the

ARTICLE IN PRESS
Z.J. McKeough et al.1824
present work. One of the limitations of the work bySala and colleagues15 is that they recruited onlymale COPD subjects who had not had an exacerba-tion in the previous 6 months. This is not reflectiveof the usual COPD population attending pulmonaryrehabilitation. Furthermore, the study used atightly controlled training program of leg cycleexercise which differs from the comprehensiveexercise training programs often used. The resultsof the current study add to the findings by Sala andcolleagues15 that improvement in quadricepsmitochondrial capacity is also possible in a com-prehensive exercise training program for subjects(male and female) who attend pulmonaryrehabilitation.
Another finding of our study was the significantimprovement in 6MWD and peak work capacity on acycle ergometer following training performedtwice weekly. In contrast, Ringbaek et al.42 havesuggested that exercise training twice per weekwas not sufficient to show improvements in 6MWD.However, the description of the training componentused in their study was limited with intensity basedon dyspnea levels and the duration of endurancetraining (jogging and stair-climbing) not cited. Inour study, an extensive endurance training compo-nent was prescribed (30min of walking and20–30min of cycling by week 8) with intensitybased on the 6min walk test and cycle ergometertest. The trend towards a significant correlationbetween the increase in peak leg work capacity andthe improvement in mitochondrial function pro-vides some evidence that the improvement in peakexercise capacity was related to the physiologicalchanges at the skeletal muscle level after training.
The findings of this study were limited by factorswhich warrant some caution in data interpretation.The small sample size may have limited the abilityto distinguish between the COPD and healthysubjects particularly in regard to baseline musclestrength. We recognise that a number of studieshave detected differences in muscle strength andCSA between healthy and COPD subjects.3,11 How-ever, our healthy control group was sedentary andslightly older than subjects in these studies whichmay have minimised the differences between thehealthy and COPD subjects in our study. In addition,as there was no COPD control group, the effect ofexercise training on the muscle changes occurringin the COPD subjects will need to be confirmed in arandomised controlled trial.
In conclusion, 16 sessions of exercise training,performed twice weekly, significantly increased6MWD and peak leg work capacity in the subjectswith COPD. There was a significant improvement in[PCr] resynthesis kinetics of the quadriceps muscle
suggesting an improvement in the oxidative capa-city of the muscle. Quadriceps muscle mass andstrength also significantly increased following twiceweekly training.
Acknowledgements
The authors wish to thank Sing Kai Lo for statisticaladvice, Lissa Spencer and Tod Adams who assistedthe authors in running the exercise trainingprograms, and the radiographers (David Walton,Michelle Luong and Anita Kipf-Orr) at RayscanImaging for their technical expertise.
FundingThis study was supported financially by Commu-
nity Health and Tuberculosis Australia, the Austra-lian Physiotherapy Association’s PhysiotherapyResearch Foundation and the New South WalesPhysiotherapy Registration Board. These fundingsources were not involved in any aspect of thestudy design or interpretation.
Competing interest statementThe authors wish to declare no competing
interests with respect to this work.
References
1. American Thoracic Society. ATS statement: pulmonaryrehabilitation. Am J Respir Crit Care Med 1999;159:1666–82.
2. Serres I, Gautier V, Varray A, Prefaut C. Impaired skeletalmuscle endurance related to physical inactivity and alteredlung function in COPD patients. Chest 1998;113:900–5.
3. Couillard A, Maltais F, Saey D, et al. Exercise-inducedquadriceps muscle oxidative stress and peripheral muscledysfunction in patients with chronic obstructive pulmonarydisease. Am J Respir Crit Care Med 2003;167:1664–9.
4. Mador MJ, Deniz O, Aggarwal A, Kufel TJ. Quadricepsfatigability after single muscle exercise in patients withchronic obstructive pulmonary disease. Am J Respir CritCare Med 2003;168:102–8.
5. Coronell C, Orozco-Levi M, Mendez R, Ramirez-Sarmiento A,Galdiz JB, Gea J. Relevance of assessing quadricepsendurance in patients with COPD. Eur Respir J 2004;24:129–36.
6. Allaire J, Maltais F, Doyon J-F, et al. Peripheral muscleendurance and the oxidative profile of the quadriceps inpatients with COPD. Thorax 2004;59:673–8.
7. Clark CJ, Cochrane LM, Mackay E, Paton B. Skeletal musclestrength and endurance in patients with mild COPD and theeffects of weight training. Eur Respir J 2000;15:92–7.
8. Gosselink R, Troosters T, Decramer M. Peripheral muscleweakness contributes to exercise limitation in COPD. Am JRespir Crit Care Med 1996;153:976–80.
9. Hamilton AL, Killian KJ, Summers E, Jones NL. Musclestrength, symptom intensity, and exercise capacity inpatients with cardiorespiratory disorders. Am J Respir CritCare Med 1995;152:2021–31.

ARTICLE IN PRESS
Exercise capacity and quadriceps metabolism in COPD 1825
10. Bernard S, LeBlanc P, Whittom F, et al. Peripheral muscleweakness in patients with chronic obstructive pulmonarydisease. Am J Respir Crit Care Med 1998;158:629–34.
11. Debigare R, Matquis K, Cote CH, et al. Catabolic/anabolicbalance and muscle wasting in patients with COPD. Chest2003;124:83–9.
12. Maltais F, LeBlanc P, Jobin J, et al. Intensity of training andphysiologic adaptation in patients with chronic obstructivepulmonary disease. Am J Respir Crit Care Med1997;155:555–61.
13. Maltais F, LeBlanc P, Simard C, et al. Skeletal muscleadaptation to endurance training in patients with chronicobstructive pulmonary disease. Am J Respir Crit Care Med1996;154:442–7.
14. Casaburi R, Porszasz J, Burns MR, Carithers ER, Chang RS,Cooper CB. Physiologic benefits of exercise training inrehabilitation of patients with severe chronic obstructivepulmonary disease. Am J Respir Crit Care Med1997;155:1541–51.
15. Sala E, Roca J, Marrades RM, et al. Effects of endurancetraining on skeletal muscle bioenergetics in chronic ob-structive pulmonary disease. Am J Respir Crit Care Med1999;159:1726–34.
16. National Institutes of Health, National Heart Lung and BloodInstitute. Global initiative for chronic obstructive pulmonarydisease: Global strategy for the diagnosis, management, andprevention of chronic obstructive pulmonary disease (basedon 1998 NHLBI/WHO Workshop Report). Bethesda, MD;updated 2004.
17. Ainsworth BE, Haskell WL, Leon AS, et al. Compendium ofphysical activities: classification of energy costs of humanphysical activities. Med Sci Sports Exerc 1993;25:71–80.
18. Bernstein MS, Morabia A, Sloutskis D. Definition andprevalence of sedentarism in an urban population. Am JPublic Health 1999;89:862–7.
19. Trenell MI, Sue CM, Kemp GJ, Sachinwalla T, Thompson CH.Aerobic exercise and muscle metabolism in patients withmitchondrial myopathy. Muscle Nerve 2005 Published Online(21 December 2005).
20. Naressi A, Couturier C, Castang I, de Beer R, Graveron-Demilly D. Java-based graphical user interface for MRUI, asoftware package for quantitation of in vivo/medicalmagnetic resonance spectroscopy signals. Comput Biol Med2001;31:269–86.
21. Moon RB, Richards JH. Determination of intracellular pH by31P magnetic resonance. J Biol Chem 1973;248:7276–8.
22. Kemp GJ, Thompson CH, Taylor DJ, Hands LJ, Rajagopalan B,Radda GK. Quantitative analysis by 31P MRS of abnormalmitochondrial oxidation in skeletal muscle during recoveryfrom exercise. NMR Biomed 1993;6:302–10.
23. Bendahan D, Confort-Gouny S, Kozak-Reiss G, Cozzone P.Heterogeneity of metabolic response to muscular exercise inhumans. New criteria of invariance defined by in vivophosphorus-31 NMR spectroscopy. FEBS Lett 1990;272:155–8.
24. Iotti S, Lodi R, Frassineti C, Zaniol P, Barbiroli B. In vivoassessment of mitochondrial functionality in human gastro-cnemius muscle by 31P MRS. The role of pH in the evaluationof phosphocreatine and inorganic phosphate recoveries fromexercise. NMR Biomed 1993;6:248–53.
25. Crapo RO, Morris AH, Gardner RM. Reference spirometricvalues using techniques and equipment that meet ATSrecommendations. Am Rev Respir Dis 1981;123:659–64.
26. Goldman HI, Becklake MR. Respiratory function tests.Normal values at median altitudes and the prediction ofnormal results. Am Rev Tuberc 1959;79:457–67.
27. Jones NL. Clinical exercise testing, 3rd ed. Philadelphia:W.B. Saunders Company; 1988.
28. Butland RJA, Pang J, Gross ER, Woodcock AA, Geddes DM.Two-, six-, and twelve-minute walking tests in respiratorydisease. Br Med J 1982;284:1607–8.
29. Thompson CH, Davies RJO, Kemp GJ, Taylor DJ, Radda GK,Rajagopalan B. Skeletal muscle metabolism during exerciseand recovery in patients with respiratory failure. Thorax1993;48(5):486–90.
30. Wuyam B, Payen JF, Levy P, et al. Metabolism and aerobiccapacity of skeletal muscle in chronic respiratory failurerelated to chronic obstructive pulmonary disease. Eur RespirJ 1992;5:157–62.
31. Payen J-F, Wuyam B, Levy P, et al. Muscular metabolismduring oxygen supplementation in patients with chronichypoxemia. Am Rev Respir Dis 1993;147:592–8.
32. Kemp GJ, Taylor DJ, Radda GK. Control of phosphocreatineresynthesis during recovery from exercise in human skeletalmuscle. NMR Biomed 1993;6:66–72.
33. Maltais F, Jobin J, Sullivan MJ, et al. Lower limb metabolicand hemodynamic responses during exercise in normalsubjects and in COPD. J Appl Physiol 1998;84:1573–80.
34. Gosker HR, van Mameren H, van Dijk PJ, et al. Skeletalmuscle fibre-type shifting and metabolic profile in patientswith chronic obstructive pulmonary disease. Eur Respir J2002;19:617–25.
35. Jakobsson P, Jorfeldt L, Henriksson J. Metabolic enzymeactivity in the quadriceps femoris muscle in patients withsevere chronic obstructive pulmonary disease. Am J RespirCrit Care Med 1995;151:374–7.
36. Maltais F, Simard AA, Simard C, Jobin J, Desgagnes P, LeBlancP. Oxidative capacity of the skeletal muscle and lactic acidkinetics during exercise in normal subjects and in patientswith COPD. Am J Respir Crit Care Med 1996;153:288–93.
37. Schols AM, Soeters PB, Mostert R, Saris WH, Wouters EF.Energy balance in chronic obstructive pulmonary disease.Am Rev Respir Dis 1991;143:1248–52.
38. Decramer M, de Bock V, Dom R. Functional and histologicpicture of steriod-induced myopathy in chronic obstructivepulmonary disease. Am J Respir Crit Care Med 1996;153:1958–64.
39. Schols AM, Buurman WA, Staal-van den Brekel AJ, DentenerMA, Wouters EF. Evidence for a relation between metabolicderangements and increased levels of inflammatory media-tors in a subgroup of patients with chronic obstructivepulmonary disease. Thorax 1996;51:819–24.
40. Sauleda J, Garcia-Palmer F, Wiesner RJ, et al. Cytochromeoxidase activity and mitochondrial gene expression inskeletal muscle of patients with chronic obstructive pul-monary disease. Am J Respir Crit Care Med 1998;157:1413–7.
41. Jagoe RT, Engelen MPKJ. Muscle wasting and changes inmuscle protein metabolism in chronic obstructive pulmonarydisease. Eur Respir J 2003;22:52s–63s.
42. Ringbaek TJ, Broedum E, Hemmingsen L, et al. Rehabilita-tion of patients with chronic obstructive pulmonary disease.Exercise twice a week is not sufficient!. Respir Med2000;94:150–4.