Reduced creatine kinase as a central and peripheral biomarker in Huntington's disease

Clinica Chimica Acta 304 (2001) 65–74www.elsevier.com/ locate /clinchim
Cardiac troponins and creatine kinase content of striated muscle incommon laboratory animals
a , a a b*Salim Fredericks , Gurcharan K. Merton , Maria J. Lerena , Peter Heining ,c aNicholas D. Carter , David W. Holt
aAnalytical Unit, Cardiological Sciences, St George’s Hospital Medical School, London SW17 0RE, UKbToxicology /Pathology, Novartis Pharma AG, Basel, CH-4002 Basel, Switzerland
cMedical Genetics, St. George’s Hospital Medical School, London SW17 0RE, UK
Received 13 June 2000; received in revised form 11 October 2000; accepted 21 October 2000
Abstract
Animal models are important for the investigation of human heart pathology, novel treatments, and medical or surgicalinterventions for disease. Serum markers of myocardial damage may also be important tools within this field of research. Inorder to assess the cardiac specificity of widely utilised serum markers, we measured the cardiac troponins and creatinekinase (CK) isoenzymes in cardiac and skeletal muscle samples taken from dog, monkey, pig and rat. These samples werealso analysed by immunoblotting for cardiac troponin I (cTnI) and cardiac troponin T (cTnT). The content of cTnI and cTnTin skeletal muscle was below 0.6% of that found in heart for all animal species studied. This low immunoreactivity inskeletal muscle was confirmed by immunoblot analysis. The content of CK was higher in skeletal muscle than in heartmuscle for all species. The CK-MB/total CK ratio was lower in skeletal muscle than in cardiac muscle for all species. Thedifferences in CK-MB content of skeletal muscle and heart muscle were much less pronounced than the tissue differences inthe amounts of the cardiac troponins. The cardiac troponins are potentially useful serum markers of myocardial damage, withhigh specificity for myocardial muscle in these common laboratory animals. Creatine kinase-MB is much less cardiac-specific. 2001 Elsevier Science B.V. All rights reserved.
Keywords: Cardiac troponin; Creatine kinase; Markers of myocardial damage; Animal models; Cardiac specificity
1. Introduction played a significant role in the diagnosis of myocar-dial infarction. Serum markers have more recently
Specific markers of myocardial damage have been used to investigate less severe myocardialdamage as a result of surgery [1], myopathies [2],exercise [3,4], myocarditis [5,6] and a variety ofAbbreviations: cTnI, cardiac troponin I; cTnT, cardiac troponin
T; SDS, sodium dodecyl sulfate; PAGE, polyacrylamide gel other medical interventions, such as angioplastyelectrophoresis; CK-MM, creatine kinase MM isoform; CK-MB, [7,8], radiofrequency catheter ablation [9] and elec-creatine kinase MB isoform; CK-BB, creatine kinase BB isoform; trical cardioversion of arrhythmias [10]. Many ofMAb, monoclonal antibody
these conditions and procedures may be investigated*Corresponding author. Tel.: 144-20-8725-5345; fax: 144-20-using animal-model experiments.8767-9687.
E-mail address: [email protected] (S. Fredericks). There is increasing interest in the specific de-
0009-8981/01/$ – see front matter 2001 Elsevier Science B.V. All rights reserved.PI I : S0009-8981( 00 )00409-5

66 S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74
tection of myocardial damage in nonhuman species 2. Materials and methods[11–14]. In addition to basic research involvinganimal models of human pathology, and the in- 2.1. Animals and tissuesvestigation of medical and surgical interventions, thisinterest stems from toxicological studies for the Cardiac and skeletal muscle taken from a beaglepharmaceutical industry. Some of the limitations of dog (n52), cynomologus monkey (n52), Wistar ratthe non-biochemical techniques used clinically to (n54) and mini-pig (n52) were studied. Muscleevaluate pharmacological cardiotoxicity have been samples were removed from sacrificed animals andreviewed [11,12]. There exists a need to rule-out the immediately frozen in liquid nitrogen and stored atpotential for myocardial damage of new candidate 2808C until analysis. Prior to sacrifice, all animalsdrugs at an early stage in their development. De- showed no apparent signs of cardiac or skeletaltection of myocardial damage in animals may also be muscle disease. In addition to these samples, humanof use in the diagnosis and treatment of pathological samples of explanted myocardium and intercostalconditions affecting the hearts of agricultural or muscle were taken during surgery from a recipient ofdomestic animals. With animal subjects, special a heart transplant. Approval was obtained from theconsideration has to be given to inter-species differ- local research ethics committee of St George’sences in metabolism, tissue location and specificity. Hospital.The complications associated with the coexistence ofskeletal muscle and cardiac muscle injury, as seen 2.2. Preparation of crude muscle extractswith humans [15], are further exacerbated withanimals. Issues of excess handling, restraints and Cytosolic and myofibrillar fractions were preparedinjections, which may lead to skeletal muscle dam- from both heart and skeletal muscles from all of theage, are all factors that have limited relevance to the above-mentioned animal species. Approximately 30study of humans. In addition, underlying myopathies mg of cardiac or skeletal muscle tissue weremay go undetected in animals in the absence of homogenised in 3 ml of 0.05 mol / l Tris buffer, pHthorough, regular, medical examinations, as seen 7.4, using an Ultra-Turrax homogeniser. Thewith humans. The choice of anaesthetics and muscle homogenate was incubated for 1 h at 48C andrelaxants usually differs from those used with centrifuged at 100,000 g for 1 h. The supernatanthumans, and these drugs may have less well docu- was retained. The pellet was then resuspended in 3mented toxicological profiles. ml of 0.05 mol / l Tris buffer. This process was
Some of the conventional analytes used in clin- repeated on two more occasions to produce a cyto-ical medicine to detect myocardial damage are solic fraction. The three aliquots containing theapplicable for use with samples of non-human or- cytosolic fraction were then pooled, aliquoted andigin. Thus, measurement of the enzymatic activity stored at 2808C until the analyses for CK, CK-of creatine kinase and its isoenzymes, the iso- isoenzymes, cTnT, cTnI and total protein wereenzymes of lactate dehydrogenase, or of a-hydroxy- performed. The pellet remaining after the last cen-butyrate dehydrogenase, are all feasible, but they trifugation (containing the myofibrillar proteins) waslack both specificity and sensitivity for myocardial resuspended in 3 ml of 0.05 mol / l Tris buffer, pHinjury [13,16]. 8.0, containing 8 mol / l urea (Merck), 1 mmol / l
In an effort to characterise the performance of the CaCl (Merck) and 15 mmol / l b-mercaptoethanol2
clinical assays for cardiac troponin I (cTnI) and (Sigma). This suspension was incubated for 1 h atcardiac troponin T (cTnT), these troponins were room temperature and then centrifuged at 20,000 gmeasured in heart and skeletal muscle from several for 30 min. The supernatant was retained. The pelletspecies of laboratory mammals and compared with was then resuspended in 3 ml of the same buffer.measurements of total creatine kinase (CK; EC This process was repeated two more times, to extract2.7.3.2) and the isoenzymes of CK and the isoforms the myofibrillar fraction. The three aliquots ofof CK-MB and CK-MM. myofibrillar fraction were pooled. Urea was then
S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74 67
removed from this fraction using gel exclusion human serum, donated by a healthy volunteer, to achromatography, eluting with Tris buffer minus urea. concentration within the range of the calibrators forThis was achieved by loading 2.5 ml of sample onto each assay. cTnI was measured on an Access ana-a Sephadex G-25 (PD-10) sample preparation car- lyser (Beckman Instruments) and cTnT on an E5300tridge (Amersham Pharmacia Biotech) and collecting analyser (Roche Diagnostics /Boehringer, Mann-the second 3 ml fraction after sample application. heim). Total protein was analysed using the BradfordThis fraction was then used for analysis of cTnT, method [18].cTnI and total protein concentrations. The effect of using samples in a Tris buffer
matrix, rather than serum, on the two auto-analysers2.3. Measurement of CK isoenzymes and CK-MB (ES300 and the Access) was investigated. Samplesisoforms of sera from patients with confirmed recent acute
myocardial infarctions were pooled and subjected toQuantitative measurement of total CK activity was the same procedure of gel exclusion chromatography
performed on a Cobas Mira (Roche Diagnostics) using a G-25 cartridge. A 2.5-ml volume of theauto analyser at 378C. CK isoenzymes were sepa- pooled serum sample, taken from patients withrated and quantified by agarose gel electrophoresis recent myocardial infarctions, was applied to theusing a rapid electrophoresis (REP) system (Helena column and eluted with Tris buffer. Four fractions (3Laboratories). Cytosolic fractions were diluted to an ml each) were then collected. The eluent fractions ofactivity of 500 U/ l prior to analysis on the REP. The diluted serum were then analysed, in the same bufferREP was also used to detect the isoforms of CK-MB medium, for cTnI and cTnT, using the Access andand CK-MM. ES300 instruments, respectively. Total protein was
also analysed. The original serum pool was also2.4. Conversion of the isoforms of CK-MB and assayed directly, without dilution, for these threeCK-MM analytes.
After release from the myocyte, the M subunit of 2.6. Gel electrophoresis and immunoblotting ofboth CK-MB and CK-MM is converted to a different troponin I and Tisoform by a circulating carboxyypeptidase [17]. Todemonstrate the in vitro conversion of the CK-MB Tissue homogenates were electrophoresed using‘tissue isoform’ (CK-MB2) to the ‘plasma isoform’ sodium dodecyl sulfate–polyacrylamide gel electro-(CK-MB1), and the conversion of CK-MM3 to CK- phoresis (SDS–PAGE). A 10-mg amount of totalMM2 and CK-MM1, tissue extracts were incubated protein for each sample was loaded onto 10% miniwith normal human serum. gels according to the Laemmli method [19], using
A serum sample was collected from a healthy the Xcell II system (Novex). Separated proteins werevolunteer. A 200-ml volume of cytosolic extract, then electrophoretically blotted onto nitrocellulosewith a CK activity of 500 U/ l, was incubated with membranes (Amersham Pharmacia Biotech). The100 ml of serum and incubated at 308C for 0, 2, 16 membranes were then blocked with 5% non-fat milkand 24 h. The reaction was stopped by the addition powder in phosphate-buffered saline (PBS) over-of 100 ml of 60 mmol / l EDTA solution. Samples night at 48C. The membranes were then incubatedfrom cardiac muscle for all animals at all four time with either mouse monoclonal antibody (MAb) anti-points were analysed for CK-MB and CK-MM cTnI antibody (Biogenisis) or mouse MAb anti-cTnTisoforms. antibodies M11-7 and M7 (Roche Diagnostics /
Boehringer-Mannheim). The concentration of all2.5. Tissue quantification of troponin-I and primary antibodies was 2 mg/ l.troponin-T Horseradish peroxidase conjugated to goat anti-
mouse IgG (Dako) was then used, at a dilution ofSamples were diluted in cTnI- and cTnT-free 1:1000, for the detection of specific binding anti-
68 S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74
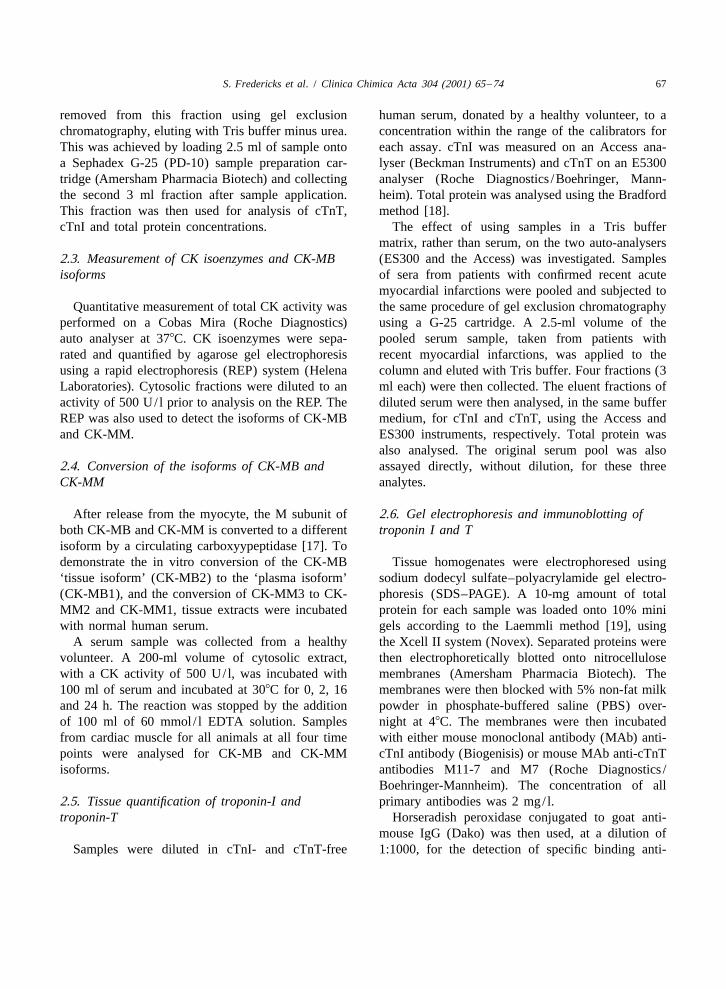
Table 2body. Immunoblots were developed using ECLPercent recovery of total protein, cTnI and cTnT from a pooledsubstrate (Amersham Pharmacia Biotech).serum sample eluted through a G-25 column. All samples wereanalysed in buffered medium
Protein (mg) cTnT (ng) cTnT (ng)3. ResultsOriginal 151.8 1.3 6.3Fraction 1 150.8 4.6 25.1Results are expressed as the amount of cTnI orFraction 2 4.1 2.8 12.7
cTnT relative to the total amount of protein for both Fraction 3 0.0 1.0 2.0muscles. The mean content of both cardiac troponins Fraction 4 0.0 0.3 0.1in skeletal muscle was less than 0.6% that of the Total collected 154.9 8.7 39.9
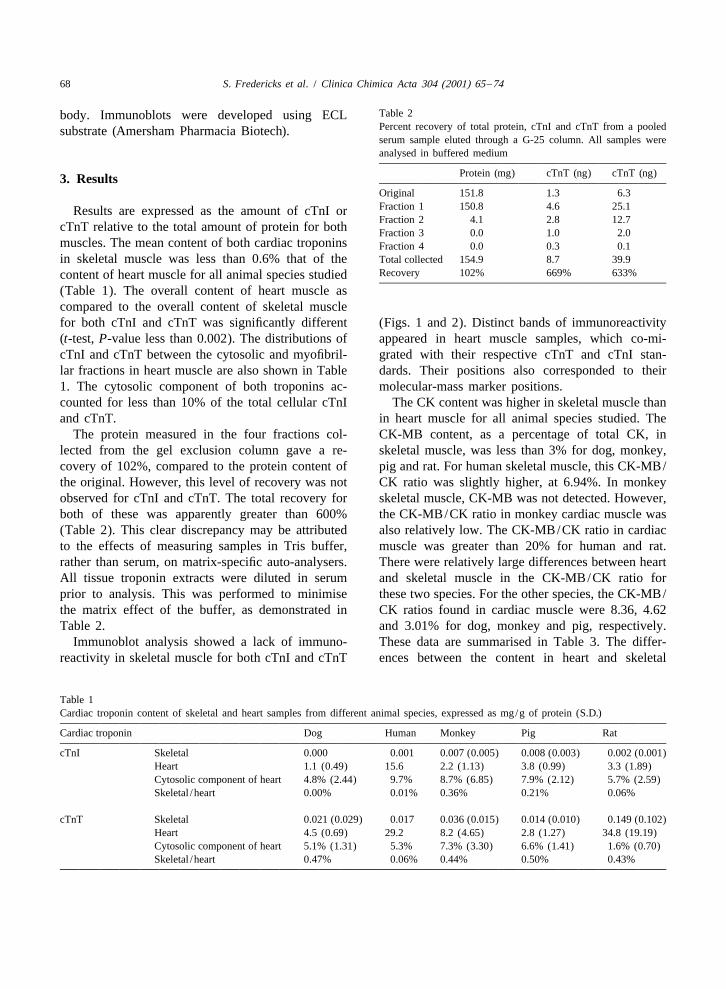
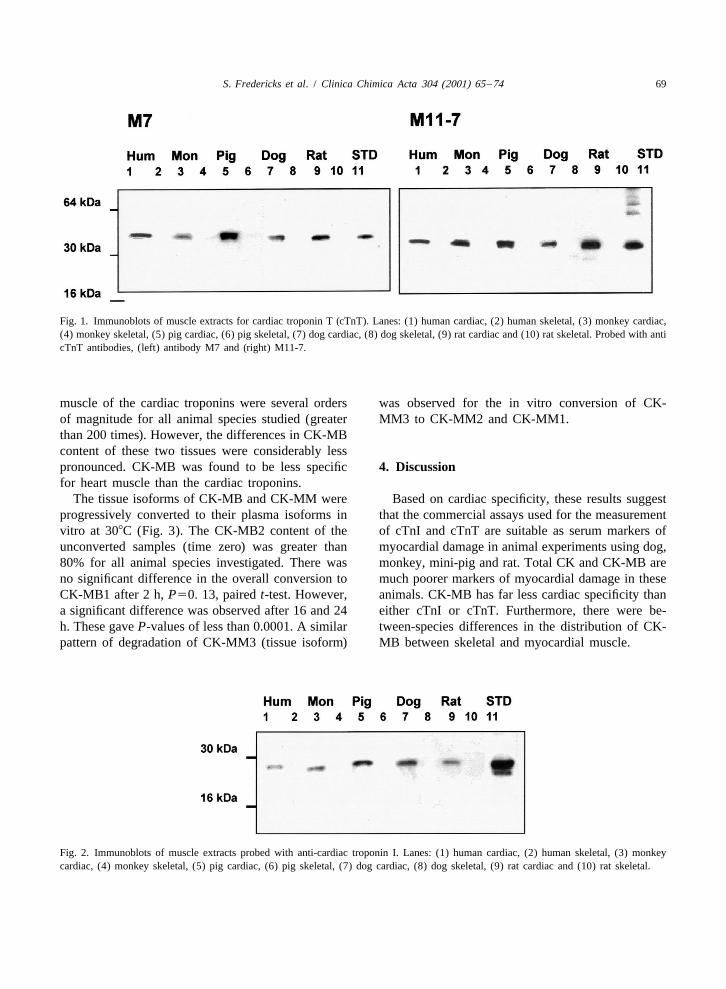
Recovery 102% 669% 633%content of heart muscle for all animal species studied(Table 1). The overall content of heart muscle ascompared to the overall content of skeletal musclefor both cTnI and cTnT was significantly different (Figs. 1 and 2). Distinct bands of immunoreactivity(t-test, P-value less than 0.002). The distributions of appeared in heart muscle samples, which co-mi-cTnI and cTnT between the cytosolic and myofibril- grated with their respective cTnT and cTnI stan-lar fractions in heart muscle are also shown in Table dards. Their positions also corresponded to their1. The cytosolic component of both troponins ac- molecular-mass marker positions.counted for less than 10% of the total cellular cTnI The CK content was higher in skeletal muscle thanand cTnT. in heart muscle for all animal species studied. The
The protein measured in the four fractions col- CK-MB content, as a percentage of total CK, inlected from the gel exclusion column gave a re- skeletal muscle, was less than 3% for dog, monkey,covery of 102%, compared to the protein content of pig and rat. For human skeletal muscle, this CK-MB/the original. However, this level of recovery was not CK ratio was slightly higher, at 6.94%. In monkeyobserved for cTnI and cTnT. The total recovery for skeletal muscle, CK-MB was not detected. However,both of these was apparently greater than 600% the CK-MB/CK ratio in monkey cardiac muscle was(Table 2). This clear discrepancy may be attributed also relatively low. The CK-MB/CK ratio in cardiacto the effects of measuring samples in Tris buffer, muscle was greater than 20% for human and rat.rather than serum, on matrix-specific auto-analysers. There were relatively large differences between heartAll tissue troponin extracts were diluted in serum and skeletal muscle in the CK-MB/CK ratio forprior to analysis. This was performed to minimise these two species. For the other species, the CK-MB/the matrix effect of the buffer, as demonstrated in CK ratios found in cardiac muscle were 8.36, 4.62Table 2. and 3.01% for dog, monkey and pig, respectively.
Immunoblot analysis showed a lack of immuno- These data are summarised in Table 3. The differ-reactivity in skeletal muscle for both cTnI and cTnT ences between the content in heart and skeletal
Table 1Cardiac troponin content of skeletal and heart samples from different animal species, expressed as mg/g of protein (S.D.)
Cardiac troponin Dog Human Monkey Pig Rat
cTnI Skeletal 0.000 0.001 0.007 (0.005) 0.008 (0.003) 0.002 (0.001)Heart 1.1 (0.49) 15.6 2.2 (1.13) 3.8 (0.99) 3.3 (1.89)Cytosolic component of heart 4.8% (2.44) 9.7% 8.7% (6.85) 7.9% (2.12) 5.7% (2.59)Skeletal /heart 0.00% 0.01% 0.36% 0.21% 0.06%
cTnT Skeletal 0.021 (0.029) 0.017 0.036 (0.015) 0.014 (0.010) 0.149 (0.102)Heart 4.5 (0.69) 29.2 8.2 (4.65) 2.8 (1.27) 34.8 (19.19)Cytosolic component of heart 5.1% (1.31) 5.3% 7.3% (3.30) 6.6% (1.41) 1.6% (0.70)Skeletal /heart 0.47% 0.06% 0.44% 0.50% 0.43%
S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74 69
Fig. 1. Immunoblots of muscle extracts for cardiac troponin T (cTnT). Lanes: (1) human cardiac, (2) human skeletal, (3) monkey cardiac,(4) monkey skeletal, (5) pig cardiac, (6) pig skeletal, (7) dog cardiac, (8) dog skeletal, (9) rat cardiac and (10) rat skeletal. Probed with anticTnT antibodies, (left) antibody M7 and (right) M11-7.
muscle of the cardiac troponins were several orders was observed for the in vitro conversion of CK-of magnitude for all animal species studied (greater MM3 to CK-MM2 and CK-MM1.than 200 times). However, the differences in CK-MBcontent of these two tissues were considerably lesspronounced. CK-MB was found to be less specific 4. Discussionfor heart muscle than the cardiac troponins.
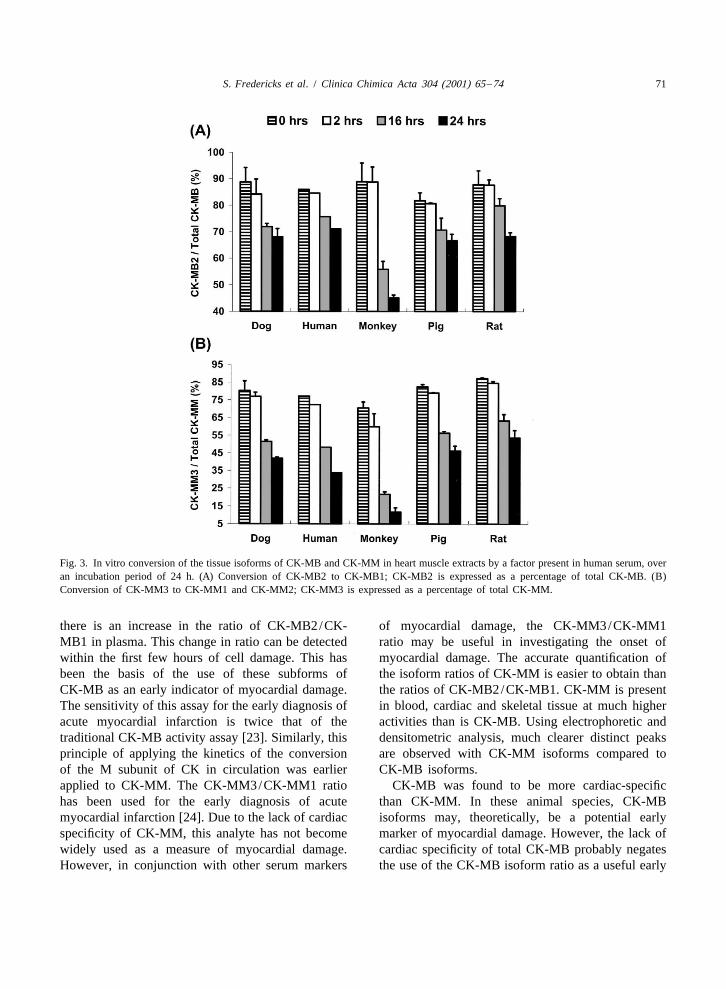
The tissue isoforms of CK-MB and CK-MM were Based on cardiac specificity, these results suggestprogressively converted to their plasma isoforms in that the commercial assays used for the measurementvitro at 308C (Fig. 3). The CK-MB2 content of the of cTnI and cTnT are suitable as serum markers ofunconverted samples (time zero) was greater than myocardial damage in animal experiments using dog,80% for all animal species investigated. There was monkey, mini-pig and rat. Total CK and CK-MB areno significant difference in the overall conversion to much poorer markers of myocardial damage in theseCK-MB1 after 2 h, P50. 13, paired t-test. However, animals. CK-MB has far less cardiac specificity thana significant difference was observed after 16 and 24 either cTnI or cTnT. Furthermore, there were be-h. These gave P-values of less than 0.0001. A similar tween-species differences in the distribution of CK-pattern of degradation of CK-MM3 (tissue isoform) MB between skeletal and myocardial muscle.
Fig. 2. Immunoblots of muscle extracts probed with anti-cardiac troponin I. Lanes: (1) human cardiac, (2) human skeletal, (3) monkeycardiac, (4) monkey skeletal, (5) pig cardiac, (6) pig skeletal, (7) dog cardiac, (8) dog skeletal, (9) rat cardiac and (10) rat skeletal.
70 S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74
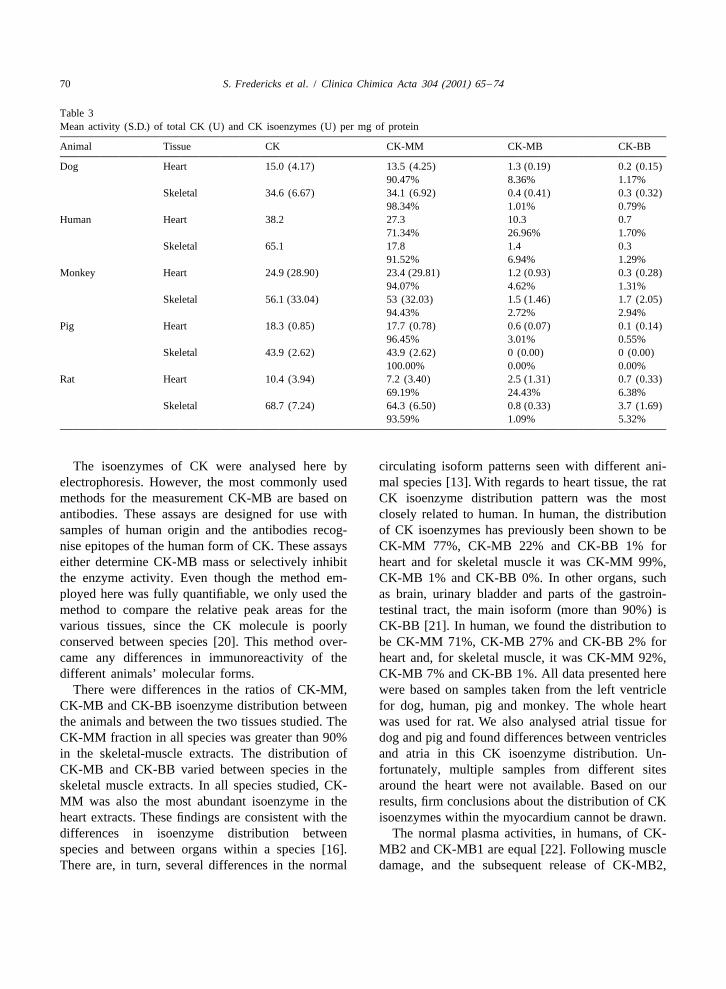
Table 3Mean activity (S.D.) of total CK (U) and CK isoenzymes (U) per mg of protein
Animal Tissue CK CK-MM CK-MB CK-BB
Dog Heart 15.0 (4.17) 13.5 (4.25) 1.3 (0.19) 0.2 (0.15)90.47% 8.36% 1.17%
Skeletal 34.6 (6.67) 34.1 (6.92) 0.4 (0.41) 0.3 (0.32)98.34% 1.01% 0.79%
Human Heart 38.2 27.3 10.3 0.771.34% 26.96% 1.70%
Skeletal 65.1 17.8 1.4 0.391.52% 6.94% 1.29%
Monkey Heart 24.9 (28.90) 23.4 (29.81) 1.2 (0.93) 0.3 (0.28)94.07% 4.62% 1.31%
Skeletal 56.1 (33.04) 53 (32.03) 1.5 (1.46) 1.7 (2.05)94.43% 2.72% 2.94%
Pig Heart 18.3 (0.85) 17.7 (0.78) 0.6 (0.07) 0.1 (0.14)96.45% 3.01% 0.55%
Skeletal 43.9 (2.62) 43.9 (2.62) 0 (0.00) 0 (0.00)100.00% 0.00% 0.00%
Rat Heart 10.4 (3.94) 7.2 (3.40) 2.5 (1.31) 0.7 (0.33)69.19% 24.43% 6.38%
Skeletal 68.7 (7.24) 64.3 (6.50) 0.8 (0.33) 3.7 (1.69)93.59% 1.09% 5.32%
The isoenzymes of CK were analysed here by circulating isoform patterns seen with different ani-electrophoresis. However, the most commonly used mal species [13]. With regards to heart tissue, the ratmethods for the measurement CK-MB are based on CK isoenzyme distribution pattern was the mostantibodies. These assays are designed for use with closely related to human. In human, the distributionsamples of human origin and the antibodies recog- of CK isoenzymes has previously been shown to benise epitopes of the human form of CK. These assays CK-MM 77%, CK-MB 22% and CK-BB 1% foreither determine CK-MB mass or selectively inhibit heart and for skeletal muscle it was CK-MM 99%,the enzyme activity. Even though the method em- CK-MB 1% and CK-BB 0%. In other organs, suchployed here was fully quantifiable, we only used the as brain, urinary bladder and parts of the gastroin-method to compare the relative peak areas for the testinal tract, the main isoform (more than 90%) isvarious tissues, since the CK molecule is poorly CK-BB [21]. In human, we found the distribution toconserved between species [20]. This method over- be CK-MM 71%, CK-MB 27% and CK-BB 2% forcame any differences in immunoreactivity of the heart and, for skeletal muscle, it was CK-MM 92%,different animals’ molecular forms. CK-MB 7% and CK-BB 1%. All data presented here
There were differences in the ratios of CK-MM, were based on samples taken from the left ventricleCK-MB and CK-BB isoenzyme distribution between for dog, human, pig and monkey. The whole heartthe animals and between the two tissues studied. The was used for rat. We also analysed atrial tissue forCK-MM fraction in all species was greater than 90% dog and pig and found differences between ventriclesin the skeletal-muscle extracts. The distribution of and atria in this CK isoenzyme distribution. Un-CK-MB and CK-BB varied between species in the fortunately, multiple samples from different sitesskeletal muscle extracts. In all species studied, CK- around the heart were not available. Based on ourMM was also the most abundant isoenzyme in the results, firm conclusions about the distribution of CKheart extracts. These findings are consistent with the isoenzymes within the myocardium cannot be drawn.differences in isoenzyme distribution between The normal plasma activities, in humans, of CK-species and between organs within a species [16]. MB2 and CK-MB1 are equal [22]. Following muscleThere are, in turn, several differences in the normal damage, and the subsequent release of CK-MB2,
S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74 71
Fig. 3. In vitro conversion of the tissue isoforms of CK-MB and CK-MM in heart muscle extracts by a factor present in human serum, overan incubation period of 24 h. (A) Conversion of CK-MB2 to CK-MB1; CK-MB2 is expressed as a percentage of total CK-MB. (B)Conversion of CK-MM3 to CK-MM1 and CK-MM2; CK-MM3 is expressed as a percentage of total CK-MM.
there is an increase in the ratio of CK-MB2/CK- of myocardial damage, the CK-MM3/CK-MM1MB1 in plasma. This change in ratio can be detected ratio may be useful in investigating the onset ofwithin the first few hours of cell damage. This has myocardial damage. The accurate quantification ofbeen the basis of the use of these subforms of the isoform ratios of CK-MM is easier to obtain thanCK-MB as an early indicator of myocardial damage. the ratios of CK-MB2/CK-MB1. CK-MM is presentThe sensitivity of this assay for the early diagnosis of in blood, cardiac and skeletal tissue at much higheracute myocardial infarction is twice that of the activities than is CK-MB. Using electrophoretic andtraditional CK-MB activity assay [23]. Similarly, this densitometric analysis, much clearer distinct peaksprinciple of applying the kinetics of the conversion are observed with CK-MM isoforms compared toof the M subunit of CK in circulation was earlier CK-MB isoforms.applied to CK-MM. The CK-MM3/CK-MM1 ratio CK-MB was found to be more cardiac-specifichas been used for the early diagnosis of acute than CK-MM. In these animal species, CK-MBmyocardial infarction [24]. Due to the lack of cardiac isoforms may, theoretically, be a potential earlyspecificity of CK-MM, this analyte has not become marker of myocardial damage. However, the lack ofwidely used as a measure of myocardial damage. cardiac specificity of total CK-MB probably negatesHowever, in conjunction with other serum markers the use of the CK-MB isoform ratio as a useful early
72 S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74
marker of myocardial damage. The electrophoretic We have confirmed that cTnI and cTnT, asactivity assays for the isoforms of CK-MB and determined by the Beckman Instruments and RocheCK-MM may have a role to play in investigating the Diagnostics /Boehringer-Mannheim assays, respec-early stages of skeletal muscle damage in animals. tively, are potentially suitable as serum markers of
Although we have demonstrated large differences myocardial damage in animal experiments. We havebetween the cTnI and cTnT content of heart and further confirmed that both the capture and detectionskeletal muscle, the absolute quantification of both antibodies used in the Roche Diagnostics /Boehring-cTnI and cTnT in this setting is open to a degree of er-Mannheim kit are highly specific for cardiacinaccuracy. Essentially, the assays used were de- troponin T by immunoblot analysis using tissue fromsigned to be performed on general-purpose auto- these laboratory animals. The combination of theanalysers. The primary function of these auto- antibodies M7 and M11-7 produced a cardiac-spe-analysers is to measure analytes in serum or plasma cific assay for cTnT for these animal species. Basedand not in buffered tissue extracts. These assays are on epitope studies performed on cTnT, this resultoptimised for serum. We minimised the matrix was to be expected. Malouf et al. [25] described aneffects by diluting the samples in cardiac, troponin- epitope conserved through several mammalianfree serum, taken from a young healthy volunteer. species and that was also found in chicken. Katus etThe manufacturers of the two kits provide a serum al. [26] demonstrated, by cyanogen-bromide cleav-diluent with their kits, comprising lyophilised age of the peptide fraction, that antibody M7 recog-troponin-free serum. We compared the diluents from nises PNLVPPKI. The same group later produced theboth manufacturers with a large serum pool that we antibody M11-7, which bound to an epitope that wascollected, using both assay platforms. We found no six amino-acid residues away from that of M7 [27].significant difference in the final results (data not The antibodies used in the first generation cTnTshown). Notwithstanding these limitations, these assay were found to react with cTnT from bovine,results demonstrate a huge difference in cTnI and pig, dog, rabbit, rat [26] and mouse origin [28]. ThecTnT content between skeletal muscle- and heart- cTnI MAb 11E12 has been shown to be directedmuscle extracts, which reflect insignificant amounts against a peptide sequence found in several animalof cardiac troponins in skeletal muscle. species [29]. The other MAb used in the cTnI assay,
This conclusion is further reinforced by the results 8E1, reacts with a peptide that differs from 11E12 byfrom a qualitative comparison of heart and skeletal one residue [30].muscle in terms of antibody binding, using immuno- There have been recent reports on the use of cTnIblotting. The same capture and detection antibodies and cTnT as markers of myocardial damage inthat are employed in the second generation cTnT various animal species. O’Brien et al. [31] comparedassay, M11-7 and M7, respectively, were used to the heart and skeletal muscle content of both cTnIprobe immunoblots of both heart- and skeletal and cTnT in a variety of animal species. Using themuscle extracts. These blots clearly demonstrated the Dade Stratus cTnI assay quantitatively and the Dadelack of immunoreactivity of the detection antibody antibodies 2B1.9 and 2F6.6 qualitatively, with im-with skeletal muscle extracts for all species tested. munoblots, they found cTnI to be more than 1000-These blots could not be probed with the Beckman fold higher in heart than in skeletal muscle in variousInstruments antibodies, 11E12 and 8E1, as the mammals [31]. The same group also quantified thecompany did not make these antibodies available. tissue content of cTnT for several species using bothThus, firm conclusions cannot be drawn here, based the first- and second-generation cTnT assays [32].on a qualitative assessment of the Beckman Instru- They found the first generation assay to have 10%ments’ antibodies. However, in an attempt to investi- cross-reactivity with skeletal and the second gene-gate the cardiac-specific expression of the cTnI ration to give 1% cross-reactivity. Using animalprotein, another source of anti-cTnI antibody was models of myocardial infarction and doxorubicin-used. This antibody demonstrated the cardiac-spe- induced cardiotoxicity, O’Brien et al. [33] havecific expression of cTnI. However, the exact anti- shown dramatic increases in serum concentrations ofbody-binding characteristics cannot necessarily be cTnT in response to various forms of cardiac dam-extrapolated to the Beckman Instruments assay. age. This was performed using dog, rat, mouse and
S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74 73
ferret [33]. Increases in serum cTnT in response to Referencesdoxorubicin have also been confirmed in the sponta-
[1] Adams SE. Utility of cardiac troponins in patients withneously hypertensive rat [34]. Circulating cTnI andsuspected cardiac trauma or after cardiac surgery. Clin LabcTnT were both reported to be raised in response toMed 1997;17:613–23.orciprenaline-induced myocardial damage in rat [35].
[2] Braun SL, Pongratz DE, Bialk P et al. Discrepant results forThe cTnT and the Beckman Instruments cTnI assay cardiac troponin T and troponin I in chronic myopathy,have been validated in rats by using an isolated heart depending on instrument and assay generation. Clin Chem
1996;42:2039–41.model. cTnI and cTnT were found to be released in[3] Laslett L, Eisenbud E, Lind R. Evidence of myocardialparallel [36,37].
injury during prolonged strenuous exercise. Am J CardiolThe main criterion for an appropriate candidate 1996;78:488–90.
marker of myocardial damage is cardiac specificity [4] Siegel AJ, Sholar M, Yang J et al. Elevated serum cardiacmarkers in asymptomatic marathon runners after competi-[38]. However, there are several other factors thattion: is the myocardium stunned? Cardiology 1997;88:487–have to be taken into consideration, one of which is4891.the kinetics of the analytes once in the circulation. [5] Lauer B, Niederau C, Kuhl U et al. Cardiac troponin T in
The kinetics are, in turn, affected by factors such as patients with clinically suspected myocarditis. J Am CollCardiol 1997;30:1354–9.cellular compartmentalisation, post myocyte-release
[6] Franz WM, Remppis A, Kandolf R et al. Serum troponin T:degradation and elimination, binding to other mole-diagnostic marker for acute myocarditis. Clin Chemcules (e.g. calmodulin, binding to free cTnI) [39,40],1996;42:340–1.
and changes that occur in vitro after sample collec- [7] Genser N, Mair J, Talasz H et al. Cardiac troponin I totion [41]. In addition, there are issues such as cost diagnose percutaneous transluminal coronary angioplasty-
related myocardial injury. Clin Chim Acta 1997;265:207–17.and turn around times for assays that may affect the[8] Abbas SA, Glazier JJ, Wu Al-I et al. Factors associated withappropriateness of a particular assay. However, we
the release of cardiac troponin T following percutaneoushave confirmed that cTnI and cTnT are cardiac- transluminal coronary angioplasty. Clin Cardiolspecific markers of myocardial damage in certain 1996;19:782–6.
[9] Katritsis D, Hossein-Nia M, Anastasakis A et al. Use ofcommon laboratory animals. In recent years, thetroponin-T concentration and kinase isoforms for quantita-utility of serum markers of cardiac damage hastion of myocardial injury induced by radiofrequency catheterimproved dramatically, in terms of diagnosis, cardiac ablation. Eur Heart J 1997;18:1007–13.
risk stratification and as research tools. In humans, [10] Greaves K, Crake T. Cardiac troponin T does not increasethese improvements are the result of the development after electrical cardioversion for atrial fibrillation or atrial
flutter. Heart 1998;80:226–8.of automated assays for the measurement of the[11] Carrio I, Estorch M, Lopez-Pousa A. Assessing anthra-highly cardiac-specific cardiac troponins. Although
cycline cardiotoxicity in the 1990s. Eur J Nucl MedCK-MB has been shown to be adequate for the 1996;23:359–64.diagnosis of myocardial infarction in humans, its use [12] Ganz WI, Sridhar KS, Ganz SS et al. Review of tests foris limited in animals. In animals, the difference monitoring doxorubicin-induced cardiomyopathy. Oncology
1996;53:461–70.between CK-MB and the cardiac troponins in terms[13] Boyd JW. Serum enzymes in the diagnosis of disease in manof their cardiac specificity is at least as pronounced
and animals. J Comp Pathol 1988;98:381–404.as in humans. An increased use of these newer [14] Evans GO. Biochemical assessment of cardiac function andmarkers of myocardial damage in animals may damage in animal species. A review of the current approachsignificantly improve the quality of research in the of the academic, governmental and industrial institutions
represented by the animal clinical chemistry association. Jfield of drug development, agriculture and paradigmsAppl Toxicol 1991;11:15–21.of human pathology.
[15] Lavomnne A, Hue G. Serum cardiac troponin I and T inearly posttraumatic rhabdomyolysis. Clin Chem1998;44:667–8.
Acknowledgements [16] Yasuda J, Teteyama K, Synto B et al. Lactate dehydrogenaseand creatine phosphokinase isoenzymes in tissues of labora-tory animals. Jpn J Vet Res 1990;38:19–29.This work was supported by Novartis Pharma. We
[17] Hendriks D, Soons J, Scharpe S et al. Identification of thewould like to thank Dr Klaus Hallermeyer of Roche carboxypeptidase responsible for the post-synthetic modi-Diagnostics /Boehringer-Mannheim for providing the fication of creatine kinase in human serum. Clin Chim Actaanti-cTnT antibodies M7 and M11-7 as a gift. 1988;172:253–60.
74 S. Fredericks et al. / Clinica Chimica Acta 304 (2001) 65 –74
[18] Bradford MM. A rapid and sensitive method for the quantifi- [30] Larue C, Calzolari C, Bertinchant JP et al. Cardiac-specificcation of microgram quantities of protein utilizing the immunoenzymatic assay of troponin I in the early phase ofprinciple of protein–dye binding. Anal Biochem acute myocardial infarction. Clin Chem 1993;39:972–9.1976;72:248–54. [31] O’Brien PJ, Landt Y, Ladenson JH. Differential reactivity of
[19] Laemmli UK. Cleavage of structural proteins during the cardiac and skeletal muscle from various species in a cardiacassembly of the head of bacteriophage T4. Nature troponin I immunoassay. Clin Chem 1997;43:2333–8.1970;227:680–5. [32] Dameron GW, Beck ML, Brandt M et al. Tissue species
[20] Holt DW. Pre-clinical applications of markers of myocardial specificity of two generations of cardiac troponin T immuno-damage. In: Kaski JC, Holt DW, editors, Myocardial dam- assays. [Abstract]. Clin Chem 1997;43:S192.age: early detection by novel biochemical markers, Dor- [33] O’Brien PJ, Dameron GW, Beck ML et al. Cardiac troponindricht: Kluwer Academic Publishers, 1998, pp. 59–72. T is a sensitive, specific biomarker of cardiac injury in
[21] Lott IA, Nemesanszky E. Creatine kinase. In: Lott JA, Wolf laboratory animals. Lab Anim Sci 1997;47:486–95.PL, editors, Clinical enzymology: a case-orientated ap- [34] Herman EH, Lipshultz SE, Rifai N et al. Use of cardiacproach, New York: Field and Rich/Yearbook, 1996, p. 166. troponin T levels as an indicator of doxorubicin-induced
[22] Puleo PP, Guadagno PA, Roberts R et al. Early diagnosis of cardiotoxicity. Cancer Res 1998;58:195–7.acute myocardial infarction based on assay for subforms of [35] Bertsch T, Bleuel H, Aufenanger J et al. Comparison ofcreatinine kinase MB. Circulation 1990;82:759–69. cardiac troponin T and cardiac troponin I concentrations in
[23] Puleo PR, Meyer D, Wathen C et al. Use of a rapid assay of peripheral blood during orciprenaline induced tachycardia insubforms of creatine kinase MB to diagnose or rule out acute rats. Exp Toxicol Pathol 1997;49:467–8.myocardial infarction. New England Journal of Medicine [36] Chocron S, Alwan K, Toubin G et al. Effects of myocardial1994;331:561–6. ischaemia on the release of cardiac troponin I in isolated rat
[24] Wu AHB, Gornet TG, Wu VH et al. Early diagnosis of acute hearts. J Thorac Cardiovasc Surg 1996;112:508–13.myocardial infarction by rapid analysis of creatine kinase [37] Vorderwinkler KP, Mair J, Puschendorf B et al. Cardiacisoenzyme-3 (CK-MM) subtypes. Clin Chem 1987;33:358– troponin I increases in parallel to cardiac troponin T, creatine62. kinase and lactate dehydrogenase in effluents from isolated
[25] Malouf NN, McMahon D, Oakeley AE et al. A cardiac perfused rat hearts after hypoxia–reoxygenation-inducedtroponin T epitope conserved across phyla. J Biol Chem myocardial injury. Clin Chim Acta 1996;251:113–7.1992;927:9269–74. [38] Bhayana V, Henderson AR. Biochemical markers of myocar-
[26] Katus HA, Looser S, Hallermayer K et al. Development and dial damage. Clin Biochem 1994;28:1–29.in vitro characterization of a new immunoassay of cardiac [39] Wu AH, Feng YJ, Moore R et al. Characterization of cardiactroponin T. Clin Chem 1992;38:386–93. troponin subunit release into serum after acute myocardial
[27] Muller-Bardorff M, Hallermayer K, Schroder A et al. infarction and comparison of assays for troponin T and I.Improved troponin T ELISA specific for cardiac troponin T Clin Chem 1998;44:1198–208.isoform: assay development and analytical and clinical [40] Shi Q, Mingfu L, Zhang M et al. Degradation of cardiacvalidation. Clin Chem 1997;43:458–66. troponin I in serum complicates comparisons of cardiac
[28] Bachrnaier K, Mair J, Ofther F et al. Serum cardiac troponin troponin I assays. Clin Chem 1999;45:1018–25.T and creatine kinase-MB elevations in murine autoimmune [41] Gerhardt W, Nordin G, Herbert AK et al. Troponin T and Imyocarditis. Circulation 1995;92:1927–32. assays show decreased concentrations in heparin plasma
[29] Larue C, Defacque-Lacquement H, Calzolari C et al. New compared with serum: lower recoveries in early than in latemonoclonal antibodies as probes for human cardiac troponin phases of myocardial injury. Clin Chem 2000;46:817–21.I: epitopic analysis with synthetic peptides. Mol Immunol1992;29:271–8.
Copyright © 2022 FDOKUMEN