Contracting Non governmental Organizations to Combat HIV/AIDS
Background paper prepared fo
Education for All Global Monitoring
Literacy for Life
Education and HIV
Matthew Jukes and Kamal D2005
This paper was commissioned by the Education for All Gbackground information to assist in drafting the 2006 report.team. The views and opinions expressed in this paper are thosebe attributed to the EFA Global Monitoring Report or to UNEwith the following reference: “Paper commissioned for the E2006, Literacy for Life”. For further information, please contac
2006/ED/EFA/MRT/PI/46
r the
Report 2006
/AIDS
esai
lobal Monitoring Report as It has not been edited by the of the author(s) and should not SCO. The papers can be cited FA Global Monitoring Report t [email protected]
1

Education and HIV/AIDS
A report prepared for the UNESCO Global Monitoring Report 2005 by Matthew
Jukes and Kamal Desai.
Section 1 – The relationship between Education and HIV prevalence
As the HIV epidemic shows few signs of slowing in Africa, and threatens to gather
momentum in much of Asia and Eastern Europe, an effective prevention response is
desperately sought. An educated population may be an important foundation for this
response. This paper examines the relationship between schooling, sexual behaviour
and HIV prevalence and investigates the role expanded primary school access and
increased literacy can play in tackling the HIV epidemic. The following sections
consider the relationship between literacy and HIV at the national level and then
examines data concerning sexual behaviour and HIV infections and its relationship
with education.
National level associations between Education and HIV.
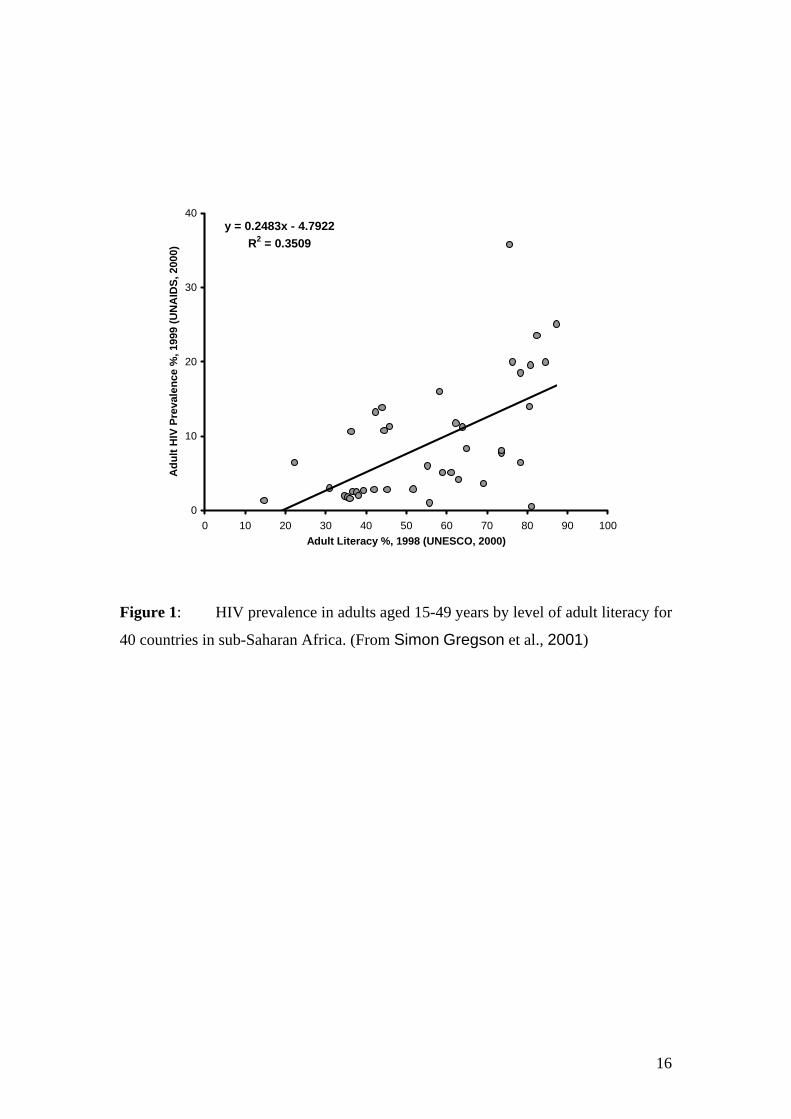
At the national level in Africa there is a positive relationship between literacy rates
and HIV infection rates (Figure 1)1: More literate countries have higher rates of HIV
infection. More literate African countries tend to be the most developed on the
continent and they share a number of features that make them vulnerable to high rates
of HIV infection. First the most developed countries often have the largest income
disparities between men and women, a factor associated with HIV infection rates
(World Bank, 1997). Similarly, employment in the formal sector is associated with
HIV infection (Barongo, Borgdorff, Mosha, Nicoll, & al., 1992; Serwadda et al.,
1992). Second, increased migration and improved transport infrastructure can
facilitate the spread of HIV (Caldwell & Caldwell, 1993). Similarly, urban residence
is associated with higher levels of HIV infection (Barongo et al., 1992; Boerma,
Urassa, Senkoro, Klokke, & Ng'weshemi, 1999; Fylkesnes et al., 1997;
1 Permission not yet sought for reproduction of graphs.
2

Serwadda et al., 1992). Finally, as discussed below, higher levels of education per
se are associated with higher infection rates.
Although various demographic and socioeconomic conditions put the educated at
greater risk of HIV infection it has been hypothesized (Simon Gregson, Waddell, &
Chandiwana, 2001; Over & Piot, 1993) that they will be more likely to change their
behaviour in response to information about the epidemic. One way in which this trend
may manifest itself at the national level is in the weakening of the relationship
between literacy and HIV infection rates as the epidemic matures. In the early stages
of the epidemic the most educated will be at great risk and a strong relationship will
be expected between literacy and HIV infection rates. In later stages of the epidemic,
when information is available about prevention methods and education campaigns
have begun, the educated are more likely, it is argued, to change their behaviour and
this mitigates against socioeconomic factors putting them at greater risk of infection.
We would therefore expect the relationship between national HIV infection and
literacy to be weaker in later stages of the epidemic. This hypothesis has been tested
(Simon Gregson et al., 2001) by comparing the relationship between adult HIV
prevalence in 1999 and adult literacy in 1998 in three different regions of sub-Saharan
African. In two regions the epidemic is more mature and the relationship between
HIV prevalence and literacy is relatively weak. In West and Central Africa, a 1%
increase in national literacy rates is associated with a 0.077% rise in national HIV
prevalence; in East Africa a 1% rise in literacy rates is associated with a 0.033% rise
in HIV prevalence. For example, the literacy rates in Kenya (~80%) were much
greater than in Ethiopia (~40%) in 1998 but HIV prevalence estimates at the time
were similar for the two countries (~12% and ~10% respectively). This stands in
contrast with the relatively recent epidemic in Southern Africa where a 1% rise in
literacy rates is associated with a 0.35% rise in HIV prevalence. For example,
Zimbabwe has a higher literacy rate (~85%) than Malawi (~60%) and similarly
Zimbabwe has one of the highest prevalences in region (~23%) and Malawi one of
the lowest (~17%).
Thus, the evidence suggests that there is a strong relationship between education and
HIV prevalence in the early stages of an epidemic, but a weaker relationship or no
relationship in more mature epidemics. This analysis is consistent with the hypothesis
that education prepares individuals better to mount a response to the HIV/AIDS
3

epidemic but for a more fine-grained assessment of the hypothesis we look at the
relationship between HIV infection and education at the level of the individual.
Education and HIV at the level of the individual
Education and sexual behaviour
As with the picture at the national level, an individual level analysis suggests that
educated individuals should be at greater risk of infection at the early stages of an
HIV epidemic but should be better equipped to change their sexual behaviour when
faced with the facts of HIV transmission. There are a number of aspects of the sexual
behaviour of more education individuals that initially puts them at great risk of
infection. More educated individuals change partners more rapidly, in part because
they are more mobile and because they have greater control over their own sexual
behaviour (A. Blanc, 2000). The higher socioeconomic status of more educated men
gives them a greater disposable income, increase leisure time, increased ability to
travel and to use commercial sex partners (Berkley et al., 1989; Dallabetta et al.,
1993; Quigley et al., 1997). In addition, more educated women start having sex later
but delayed marriage to an even great extent. This leads to them being single and
sexually active for a longer period of time and thus to them having a greater number
of sexual partners (A. K. Blanc & Way, 1998). Choice of contraceptives may also be
influenced by education. Although educated people may be more likely to use
contraception overall, they are also more likely to choose methods, such as the
contraceptive pill, which do not protect against sexually transmitted diseases such as
HIV. Taken together, and in the absence of any response to an epidemic, these factors
increase the vulnerability of more educated individuals to HIV infection in the early
stages of an epidemic.
However, evidence and theory suggest that educated people should be more likely to
adopt safe sexual practices in response to health promotion (Fylkesnes et al., 1997)
or from other sources of information about HIV/AIDS. Social cognitive models point
to several key determinants of sexual behaviour. In all theories, knowledge and
understanding of a behaviour and its consequences is a necessary but not sufficient
condition for performing the behaviour and underpins the perception of (Rosentock,
1990) and attitudes (I Ajzen, 1985) towards that behaviour. In the context of HIV,
4

understanding transmission routes and methods to block them are essential for the
adoption of safe sexual behaviour. More educated people are more likely to be
exposed to such information as part of formal schooling and also through the media
(S. Gregson, Zhuwau, Anderson, & Chandiwana, 1998). For example, a study in 32
countries found that literate women were three times more likely than illiterate
women to know that a healthy looking person can have HIV, and four times more
likely to know the main way s to avoid AIDS (Vandemoortele & Delamonica, 2000).
Greater levels of education may also provide a framework of biological knowledge
and understanding of causality into which HIV prevention messages can be
assimilated. For example, children with a deeper understanding of the biological
mechanisms of viruses are more resistant to myths about HIV transmission
(Keselman, Kaufman, & Patel, 2004). A second key determinant of behaviour is the
perceived control one has over the behaviour. This includes self-efficacy, one’s belief
in one’s capabilities to perform a specific action required to attain a desired outcome
(Bandura, 1977), the perceived personal power one has over the behaviour (I Ajzen,
1985) and the actual personal power one has over a behaviour (I. Ajzen, 2002).
Evidence suggests that education is associated with increased self-efficacy in general
(Bandura, 1977) and in the context of the HIV epidemic in sub-Saharan Africa in
particular (Lindan et al., 1991). In addition, more educated people are more likely to
believe they have control over their own behaviour, rather than another individual or
fate, and they are more likely to have actual control over their own behaviour. For
example, educated women are more able to negotiate safe sex with a partner (GCE,
2004).
This analysis suggests that education should lead to a greater adoption of safe sexual
behaviour in response to the HIV epidemic. Data from Demographic and Health
Surveys (DHS) in 11 countries (GCE, 2004) showed that women with primary school
education were more likely than those with no education to report using a condom at
last sex. In nine of these countries, secondary education was associated with a further
increase likelihood of using a condom at last sex. Another study in Zimbabwe
(Simon Gregson et al., 2001) found that women with secondary education were less
likely to report having had unprotected casual sex. A study in the four African cities
of Cotonou in Benin, Ndola in Zambia, Yaoundé in Cameroon, and Kisumu in Kenya
found that education led to less risky sexual behaviour. Condom use was more
common amongst more educated individuals in all four cities (Lagarde et al., 2001).
5

Exchange of money for sex was less likely amongst educated women in all four cities
and amongst more educated men in Yaoundé. Non-marital sex without a condom was
less prevalent among more educated women in all four cities and among more
educated men in Cotonou and Kisumu. In Yaoundé, more educated men and women
were less likely to have sex with a casual partner on the day of meeting, and in Ndola,
for both men and women, not knowing a partner’s age was much more common
among those with little schooling (Glynn et al., 2004).
Other behaviours that reduce HIV infection are also more common among the
educated. For example, more educated people are more likely to seek treatment for
other sexually transmitted diseases which would otherwise increase their chances of
becoming infected with HIV (A. Blanc, 2000). Overall, the evidence suggests that
more educated people are at a greater risk of HIV infection in the early stages of an
epidemic but tend to adopt less risky sexual behaviours in response to the epidemic.
How is this reflected in empirical data on HIV prevalence and its relationship with
education?
Education and HIV prevalence
The majority of studies investigating this issue have found a positive relationship
between education and HIV infection. That is, HIV prevalence is higher among
educated individuals. This was found at the population level in data from Rakai,
Uganda in 1990 and 1992 (Kirunga & Ntozi, 1997; Smith et al., 1999); from Mwanza,
Tanzania in 1991-1996 (Grosskurth et al., 1995; Quigley et al., 1997; Senkoro et al.,
2000) and amongst women attending ante-natal clinics in Fort Portal, Uganda in
1991-4 (Kilian et al., 1999) and in Zambia in 1994 and 1998 (Fylkesnes et al., 2001;
Fylkesnes, Ndhlovu, Kasumba, Musonda, & Sichone, 1998). In all cases, the
relationship was adjusted for age, sex and setting (urban or rural). Five population
based studies found the opposite trend. Education had a protective effect against HIV
among young women of Manicaland, Zimbabwe from 1998-2000 (Simon Gregson
et al., 2001), among men and women in Masaka district in Uganda in 2000 but not in
1990 (De Walque, 2002), among women in Youndé, Cameroon and men in Cotonou,
Benin (Glynn et al., 2004) and against HIV-2 infection in the Gambia (Wilkins et al.,
1991). Two Ethiopian studies focusing on sub-populations found opposing trends.
Education was related to lower HIV prevalence amongst sugar estate workers
6

(Fontanet et al., 2000), but higher HIV prevalence in male army recruits in rural areas
(Abebe et al., 2003). Several large studies of HIV prevalence among 21-year old Thai
army recruits found that those with more years of education had lower levels of HIV
infection (Carr et al., 1994; Mason et al., 1998; Mason et al., 1995; Nelson et al.,
1993; Sirisopana et al., 1996) although no relationship between HIV and education
was found in studies from Northern Thailand where the prevalence is highest
(Celentano et al., 1996; Dobbins et al., 1999; Nopkesorn et al., 1993). Several other
studies found that HIV prevalence and education were not statistically related,
including studies in Zimbabwe (S. Gregson et al., 2001), in Ndola, Zambia and
Kisumu, Kenya (Glynn et al., 2004) and in 7 of the 27 studies reported in a review
(Hargreaves & Glynn, 2002).
There is no consistent pattern in these results. This inconsistency may represent the
combination of two opposing trends in the data: the initial increased vulnerability of
educated individuals to HIV infection followed by their more rapid behavioural
change once informed about the epidemic. The studies reported do allow us several
opportunities to try and pick apart these two trends from their data by analyzing the
evolution of these trends with epidemic maturity.
Changing relationship between HIV and education with epidemic maturity
It is notable that the majority of studies conducted in Africa until the mid 1990s found
higher HIV prevalence among the more educated whereas later studies were more
likely to find the opposite. This is consistent with the view that educated Africans
were more at risk of HIV infection initially and were only equipped with the
information required to mount a response to the epidemic years later. In Thailand the
picture is different. The HIV epidemic was monitored by existing mechanisms and
was initially confined to high-risk groups. This allowed the spread of information
about the epidemic before the spread of the disease to the general population. This is
perhaps why the most educated individuals are protected from HIV from the early
1990s.
More direct evidence addresses the hypothesis that the relationship between HIV and
education evolves as the epidemic matures. The clearest evidence comes from a serial
7

cross-sectional survey in the rural areas of Masaka district, Uganda (De Walque,
2002). The national prevalence of HIV in the adult population declined from its peak
of 14% in the early 1990s to around 5%, largely due to a strong prevention campaign
(Stoneburner & Low-Beer, 2004). As illustrated in Figure 2, the rate of decline in
prevalence was greater for those with secondary education and those with primary
education showed faster decline in prevalence than those with no education. The
chances of contracting HIV infection during this period was reduced by 6.7% for each
year spent in education (De Walque, 2002) and those with no education were 2.2
times more likely to become infected than those who had completed primary
education. These analyses were restricted to those born after 1971 most of whom
would have become sexually active after the beginning of the information campaigns
(in 1986). For older Ugandans, the more educated were actually more likely than less
educated people to become infected during the period of the study, suggesting that
population behaviour change is driven by young people. On the basis of these figures,
the Global Campaign for Education argue that less educated young adults will
experience a disproportionately large number of new infections. They estimate that
the 36% of young adults in low-income countries without a complete primary
education will experience 55% of new infections – 1.3 million of the total of 5 million
new infections in the whole population every year. The estimates imply that achieving
Universal Primary Education could reduce the number of new infections in this group
by 700,000 a year (GCE, 2004).
The data from Uganda demonstrate the importance of schooling in an individual’s
response to a prevention campaign. It also demonstrates the evolving nature of the
relationship between HIV and education. In 1990 there was no relationship between
HIV prevalence and education. In 2000, having completed primary education was
associated with a 5.1% reduction in the risk of HIV infection and secondary education
was associated with an 8.8% reduction in risk. This relationship between HIV and
education was found for women but not men. Similarly, in Rakai, Uganda, HIV
infection was associated with increased levels of education in 1990 and 1992 but not
by 1994 (Kelly et al., 1999; Smith et al., 1999).
These finding supports the thesis that more educated individuals are better able to
mount a response to the HIV epidemic. However, the reversal of the epidemic in
Uganda is not typical of African countries. What evidence is there that education
8

protects against HIV in the absence of a successful national prevention campaign? In
fact, data from a number of countries show a similar evolution in the relationship
between HIV and education. In the following studies, this evolution is evident in
comparisons between younger and older age groups at one time point, and in
comparisons between similar populations over time. In a population-based study in
Zimbabwe, men and women aged 17-19 were at a lower risk of HIV infection if they
had secondary education. The benefit of education was less for those aged 20-24 and
there was little or no protective benefit for those aged 25 and over (Simon Gregson
et al., 2001). In Fort Portal, HIV prevalence amongst women aged 15-49 attending an
antenatal clinic was highest for those with secondary education in 1991-1994 but by
1995-97 older illiterate women had the highest prevalence (Kilian et al., 1999).
Prevalence reduced to the greatest extent amongst women with secondary education
and among young women. Similarly, there was a positive association between
education and HIV infection amongst women attending an antenatal clinic in 1994 but
not by 1998 (Fylkesnes et al., 1997; Fylkesnes et al., 2001). Again, largest
reductions were seen amongst younger more educated women. Similar patterns were
seen in northern Malawi (Crampin et al., 2003) but there was no evidence of a
changing association between HIV and education in Blantyre, Malawi (Taha et al.,
1998) or in Kagera, Tanzania (Kwesigabo et al., 1998).
The data presented so far have been concerned with the static relationship between
HIV and education. An important policy question concerns the impact of increasing
levels of education on the epidemic. There is no experimental evidence addressing
this issue, but one study has estimated this relationship by analysing longitudinal data
from 20 regions in Tanzania over 8 years (Brent, 2005). This study estimated that an
increase of 1% in female primary school enrolment would be responsible for a 0.15%
reduction in HIV prevalence in this group, corresponding to 1,408 infections in the
period 1994-2001. A further analysis of these data suggest that the investment in
increased school enrolment is justified by the averted cases of HIV and the earning
potential of these individuals, with a cost-benefit ratio of between 1.3 and 2.9.
Urban-rural differences in the HIV-education relationship
9

Three studies have collected comparable data from urban and rural areas on the
relationship between HIV infection and education. The finding from all three is that
education is a greater risk factor for infection in rural areas compared to urban areas.
In Kagera, Tanzania (Kwesigabo et al., 1998), secondary educated individuals were
3.3 times more likely than those with no education to be infected with HIV in rural
areas. Conversely, in urban areas secondary education was associated with a reduction
in HIV risk. In Zambia in 1994 (Fylkesnes et al., 1997), having more than 10 years
of education was associated with an increased risk of being HIV infection, compared
to those with less than 4 years of education, in both rural and urban areas. However,
the increased risk was greater in rural areas (odds ratio of 4.2) than in urban areas
(odd ratio of 2.5). By 1999 figures from Zambia (Fylkesnes et al., 2001) showed that
education was now associated with a decrease in HIV prevalence in urban areas but
there was no relationship between education and infection in rural areas. A similar
pattern of results was found in Rakai, Uganda, in 1990 (Smith et al., 1999). Increased
education was associated with an increased risk of HIV in rural villages but there was
no relationship in roadside trading centres or in trading villages. Similarly, in
Mwanza, Tanzania, in 1991-2, HIV infection was positively associated with education
levels in rural villages and in roadside trading villages but not in urban centres.
All studies show a stronger relationship between HIV infection and education in rural
areas compared to urban areas. This should be considered with the finding that urban
residence is associated with a higher risk of HIV infection overall (Barongo et al.,
1992; Boerma et al., 1999; Fylkesnes et al., 1997; Serwadda et al., 1992). Taken
together these findings suggest that, at least in the early stages of the epidemic,
educated individuals were similarly at risk of infection in urban and rural areas. The
less educated were at a lower risk of HIV infection in urban areas and to a greater
extent in rural areas (Fylkesnes et al., 1997).
Sex differences in the HIV-education relationship
Data on sex differences are limited by the common use of infection rates in women
visiting ante-natal clinics as a proxy for population infection rates. Nevertheless, four
studies have looked at gender differences in the HIV-education relationship (Barongo
et al., 1992; Fylkesnes et al., 2001; Grosskurth et al., 1995; Smith et al., 1999). In all
four studies the increased risk of HIV infection associated with education was very
10

similar for men and women, suggesting there are no sex differences in the relationship
between HIV and education.
Sex differences in the HIV-education relationship are complicated by consideration of
the partner’s education. Evidence shows that a women’s risk of HIV infection is
increased with higher levels of education in their partner (Allen et al., 1991;
Dallabetta et al., 1993).
Considering evidence from education interventions, where sex differences are found
they consistently suggest that HIV-related knowledge is more strongly associated with
sexual behaviour in women, compared to men (Jukes, in preparation). Therefore,
although there is no evidence of sex differences in the HIV-education association at
present, we might expect more educated women to change their behaviour more
rapidly than men in response to the HIV epidemic.
Education and social capital
Studies in Uganda show how more educated people are more likely to change their
behaviour in response to an HIV prevention education campaign. One study in
Manicaland, Zimbabwe shows how more educated women are also able to benefit
more from other protective measures. This study looked at membership of social
groups related to, among others, churches or political parties. Women who were
members of a well-functioning social group were 1.3 times more likely to avoid HIV
infection than those who were not in such groups or who were in groups with which
they were dissatisfied. Education played a key role in the protective effect of the
social groups. Women with secondary education were more likely to belong to such
groups and among women with secondary education, those who were members of
well functioning groups were 1.5 times less likely to be infected with HIV, whereas
women with no education received no such benefits from group membership (S.
Gregson, Terceira, Mushati, Nyamukapa, & Campbell, 2004).
Explaining the relationship between HIV and education
In trying to understand the relationship between HIV and education two questions are
of interest. What is it about educated people that enables them to change their
behaviour in response to the epidemic? And, what aspects of behaviour change are
11

responsible for the reduction in HIV prevalence in this group? Few studies have
addressed these questions directly. In response to the first question, analyses from
Uganda (De Walque, 2002) and elsewhere (Vandemoortele & Delamonica, 2000)
suggest that parental and individual income are not explanatory factors. This supports
the view that the increased knowledge, understanding or self-efficacy that comes with
education is responsible for behaviour change.
One study in Zimbabwe addresses the question of which behaviours change amongst
educated individuals. The finding was that the secondary educated women acquired
HIV infection at a slower rate and have both a later sexual debut and less unprotected
casual sex (Simon Gregson et al., 2001). Subsequent analyses suggest that the
delayed age of sexual debut is primarily responsible for the relationship between
education and HIV infection (James Lewis, pers. comm.). This relationship may result
from the impact of sexual behaviour on girls’ education (through pregnant young
women dropping out of school) as well as the impact of education on sexual
behaviour.
Conclusion
Overall there is convincing evidence that education better equips individuals to
respond to the HIV epidemic. Although education is associated with higher HIV
prevalence in the early stages of an epidemic, in the later stages more educated
individuals have less risky sexual behaviour and are less likely to be HIV positive.
This is true in many settings but is particularly evident in Uganda, where a national
prevention campaign has successfully reduced HIV prevalence. There have been few
estimates of the likely impact of increasing primary school completion on the HIV
epidemic. One analysis based on the Uganda data suggests that universal primary
education could save 700,000 young adults from HIV infection. Another analysis
from Tanzania suggests that investments in expanded school enrolment for girls is
cost effective purely in terms of the effect this increased enrolment will have on the
HIV epidemic. Taken together, there is a strong case for making expanded primary
education and improved literacy a central part of the global response to the HIV/AIDS
epidemic.
12

Section 3. Education and Antiretroviral Therapy
Treatment adherence is a critical issue in the promotion of antiretroviral therapy in
developing countries. Poor adherence is associated with reduced viral suppression
(Bangsberg et al., 2000; McNabb et al., 2001; Paterson et al., 2000), progression to
AIDS (Bangsberg et al., 2001), the development of multidrug resistance and death
(Hogg et al., 2002; Stephenson, 1999). Adherence is perceived as a significant barrier
to the delivery of ART in sub-Saharan Africa in particular (Harries, Nyangulu,
Hargreaves, Kaluwa, & Salaniponi, 2001). Poor education is often implied as a reason
why adherence is unlikely to be high in sub-Saharan Africa. A spokesman for USAID
is quoted as saying ‘Ask Africans to take their drugs at a certain time of day and they
do not know what you are talking about’ (cited in Orrell, Bangsberg, Badri, & Wood,
2003). Here we review the evidence that education and literacy are related to
treatment adherence.
Treatment adherence in Africa.
Initial studies of treatment adherence in Africa have allayed some fears of poor
adherence on the continent. A study in South Africa looked at adherence in a poor
HIV-positive cohort receiving ART through a public sector hospital (Orrell et al.,
2003). Adherence of the cohort was 93.5%. A composite measure of socioeconomic
status, including education and income, was not related to adherence. Those speaking
English at home were more than twice as likely to adhere to the treatment regimen.
Older patients and those required to take fewer doses were also more likely to adhere
to their regimen.
One study in Uganda looked at adherence in 304 HIV-infected individuals on a self-
financed regimen of antiretroviral therapy. The study population was relatively well
educated and wealthy. Monthly income was greater than $250 for 87.8% of the
sample and 63.2% had post-secondary education. Those with a monthly income of
less than $50 were 2.8 times more likely to miss 5% or more of doses. Seventy five
percent gave lack of money to buy drugs as a reason for lapses in adherence. Those
who were single (never married) were 2.9 times as likely to miss 5% or more of
doses. There was no significant relationship between adherence and post-secondary
13

education. An analysis by years of education was not reported (Byakika-Tusiime et
al., 2005).
A relationship between education and adherence was found in a study of 109 patients
attending private clinics in Botswana (Weiser et al., 2003). However, the relationship
was in the unexpected direction. Those who had not completed secondary education
were 3.9 times as likely to adhere to their treatment as those with higher education. In
this study, those who perceived cost or side effects as a barrier to treatment were less
likely to adhere to treatment; those who had disclosed their HIV status to others were
more likely to adhere to their treatment.
Treatment adherence in resource rich settings.
Studies in the West show that more educated individuals are more likely to adhere to
treatment with combination ART (Chesney, 2000; Chesney, Ickovics, Hecht, Sikipa,
& Rabkin, 1999). For example, in one study in America, high school completion was
associated with a 5.5% increase in adherence to a regimen of combined anti-retroviral
therapy (Golin et al., 2002). However, education does not emerge as a major
determinant of treatment adherence in the West. Alcohol and drug abuse are the key
patient characteristics affecting adherence. Other factors include depression, anxiety,
extreme pain, low self-efficacy and being young, male, or from an ethnic minority
(Chesney, 2000).
In a review of adherence to highly active antiretroviral therapy (HAART) similar
factors emerged as key determinants of adherence. In 14 studies that assessed the
relationship between education and adherence, 10 found no relationship and 4 found
higher levels of adherence amongst the more educated. This relationship disappeared
when controlling for other demographic factors in all 4 studies (Ammassari et al.,
2002).
Other studies show a relationship between adherence and knowledge, beliefs and
other cognitive factors of the patient that may be related to their level of education. A
patient's beliefs about their illness and the effectiveness of medication are predictive
of adherence. A patient's level of knowledge about HIV disease (Eldred, Wu,
Chaisson, & Moore, 1995; Eraker, Kirscht, & Becker, 1984; Morse, Simon, &
14

Walker, 1995) a belief that HAART is effective (Klosinski & Brooks, 1998;
Wenger, Gifford, Liu, Chesney, & Golin, 1999) and prolongs life (Stone et al.,
1998), and a recognition that poor adherence may equal viral resistance and treatment
failure (Wenger et al., 1999) all impact favourably upon a patients ability to adhere.
Conversely, a lack of interest in becoming knowledgeable about HIV (Kammann,
Williams, Chesney, & Currier, 1999) and a belief that HAART may in fact cause
harm, impede adherence (Brigido et al., 1998; Horne, Pearson, Leake, Fisher, &
Weinman, 1999; Johnston, Ahmad, Smith, & Rose, 1998).
Conclusion
There is insufficient evidence to make strong conclusions about the relationship
between education and ART treatment adherence in low-income countries. Of the
three studies conducted so far, only one was with relatively poor patients in a public
hospital. This found that those speaking English at home were more likely to adhere
to their treatment. It is possible this relationship was mediated through improved
education or literacy of those receiving treatment. The other two studies were
conducted with more wealthy individuals paying for their own treatment. These
studies found either no associated between adherence and education or found that
more education was associated with poorer adherence. However, these studies
compared those with or without complete secondary education and their findings may
not be relevant to questions of basic education and literacy. Findings from the West
suggest that there is a link between education and literacy. It seems that improving
education levels in developing countries is likely only to improve ART treatment
adherence and, perhaps more importantly, greater education levels may serve to allay
widespread fears amongst policy makers about the problems of adherence in Africa.
15
y = 0.2483x - 4.7922R2 = 0.3509
0
10
20
30
40
0 10 20 30 40 50 60 70 80 90 100Adult Literacy %, 1998 (UNESCO, 2000)
Adu
lt H
IV P
reva
lenc
e %
, 199
9 (U
NA
IDS,
200
0)
Figure 1: HIV prevalence in adults aged 15-49 years by level of adult literacy for
40 countries in sub-Saharan Africa. (From Simon Gregson et al., 2001)
16

Figure 2. HIV prevalence by education category, Rural Uganda,
1990-2001. Individuals aged 18-29. (De Walque 2002).
17

1
Education and HIV/AIDS
A report prepared for the UNESCO Global Monitoring Report 2005 by Kamal Desai
and Matthew Jukes
Section 2 – What is the evidence of impact of HIV/AIDS on education systems in
Africa?
The debate:
The HIV/AIDS epidemic is having a significant impact on service provision in many
high prevalence countries. Although this is widely recognised, there is a lack of
precision in estimating the extent of the impact, due primarily to inadequate primary
data and methodological limitations (Boler, 2003). Two categories of evidence exist:
data based evidence on teacher mortality comes from school-based surveys and
educational personnel records while projection models provide a second independent
source of estimates. However, the two approaches, to date, have not produced
agreement on the likely impact of HIV/AIDS on education systems (Bennell, 2005a;
Bennell, 2005b, Bundy, 2004). While the debate continues, two fundamental and
pressing questions remain unanswered : How big is the impact of HIV/AIDS to
educators and education systems and how seriously do governments and other
stakeholders need to take this issue?
Focussing on educators in sub-Saharan Africa, we attempt to ground some of the
tensions between the adherents of the primary data and the believers in projection
modelling by explaining their respective strengths and weaknesses. Also by reviewing
the available data and complementing them with our original analyses from 5
countries we demonstrate that the two approaches actually reflect the same probable
epidemiological and financial impact of HIV/AIDS on education systems, within the
bounds of uncertainty that we are forced to accept. Last, we explain why we believe
this issue must be taken seriously.
What are the strengths and weaknesses of existing primary data?

2
The most common form of data-based evidence of the impact of HIV/AIDS on
teachers comes from mortality rates taken from Education and Management
Information Systems, which also include personnel and payroll records. These
information systems are attractive sources of data as they are not resource-intensive in
many sub-Saharan countries and can contain a wealth of information about the
mortality and demographic characteristics of teachers. However, these valuable
sources have important limitations for three reasons: (i) they tend to measure only in-
service mortality and therefore miss AIDS related post-service mortality as teachers
leave on medical grounds or claim early retirement. In the private sector in South
Africa, up to 50% of mortality due to long illnesses occurs after leaving work when
the employee status is no longer on record (Badcock-Walters et al., 2003); (ii) such
information systems do not indicate AIDS specifically as cause of death, but instead
frequently report long-term illness; (iii) not all education information systems record
accurate and complete information on deaths, profession, residence, age or sex.
A second source of primary data comes from school-based surveys in which randomly
selected head teachers and professional staff in Ministries of Education (MoE) are
asked to respond to questionnaires about teacher absenteeism and mortality. This
method is resource-intensive and is characterised by high levels of non-response
particularly on the question of teacher mortality. Also, this approach is potentially
biased by the ‘healthy-worker’ effect. Like information systems, it does not indicate
AIDS as cause of death. This approach has been carried out in a number of high-
prevalence countries including Uganda, Malawi, Botswana, Kenya, Zimbabwe,
Tanzania, South Africa, Namibia and Zambia (Boler, 2003).
For the reasons above, neither the information systems nor the school-based surveys
are likely to capture the full-extent of teacher mortality, and so it should not be
surprising if such sources do underestimate AIDS-related morbidity and mortality in
teachers. Not all studies to date have reported included confidence intervals for
mortality estimates. Nevertheless, they remain a relevant and necessary source of
information.
What are the strengths and weaknesses of projection models?
3
Projection models are an important tool for estimating present and future impact of
HIV/AIDS on the basis of observed historical HIV prevalence from sentinel
surveillance data. Projection models offer a way to estimate likely impact on AIDS-
related teacher mortality which can be compared to field data for mutual validation
purposes. Models additionally provide information which is impracticable to obtain
otherwise, such as estimates of teacher seroprevalence and future death rates.
Projection studies are ideally done by experienced modellers and require a certain
level of sophistication. Projection modelling work to date has exhibited the following
shortcomings : (i) teachers are assumed to be a homogenous group thereby neglecting
age, sex and other demographic variables which are relevant to the force of HIV
infection; (ii) education sector professionals are assumed, possibly incorrectly, to have
similar infection rates as found for the general population in sentinel surveillance
data; (iii) model-based analyses have not reflected uncertainty in their mortality
estimates; (iv) future projections do not consider the benefits of antiretroviral therapy
or the adoption of protective sexual behaviours; (v) reported mortality estimates do
not reflect that uncertainty analyses were performed.
Projection models, like primary data, are essential for independently quantifying the
potential impact of HIV/AIDS. Moreover, the two are required to mutually strengthen
the body of evidence and refine impact estimates.
What is the available evidence from all sources and can their discrepancies be
reconciled?
The best reviews of available evidence on the impact of HIV/AIDS on teachers from
primary data and projection studies are contained in Bennell (Bennell, 2005a) and
Grant et al (Grant et al.,2004). Where there is debate, it is essentially due to the
discrepancy between data-based and projection-based estimates on AIDS-related
mortality in educator populations. Tables 1 and 2, from Grant et al., summarise the
available impacts on teacher mortality from data and from projections.
Projections, if correct, would suggest that in some high prevalence countries AIDS-
related deaths could add a substantial 4% - 5% to annual staff attrition rates in the
absence of behavioral change or antiretroviral intervention, while in low prevalence

4
countries deaths are likely to have more limited effect on attrition and staff capacity
when compared to other causes (Grant et al., 2004). An apparently less-serious picture
would emerge from data-based estimates. Data suggests that in countries, including
Botswana, Namibia and South Africa where rollout of antiretrovirals is substantial,
annual mortality rates (for all causes) between 1999 and 2002 would lie between 0.2%
and 3.2%. Therefore, in certain settings, mortality rates are below projected levels
while in others they are consonant and may be as high as 2.5% to 3% (Bennell, 2005).
Tables 1 and 2 indicate that for 6 countries, both data-based estimates and model-
based estimates were available. For 2 of the 6 (Zambia and Namibia), mortality
estimates for years 1999 - 2002, if taken at face value, are not dissimilar. For Rwanda
and South Africa, model based and data based estimates of teacher mortality differ by
not more than 0.5%, which is not sufficient reason for debate. If there is to be debate
it would therefore have to focus on the remaining 2 countries, Botswana and
Zimbabwe, where the average discrepancy is 1.5% between the higher model based
estimates and data-based estimates, if taken at face value. It is worth noting that
UNAIDS estimates of prevalence in many high prevalence countries have been
revised downwards since 2003, and so early projections which were based on
UNAIDS methods may be intrinsically too high.
Given that overall teacher attrition for all causes ranges between ~1.5 - 4.0%, this
magnitude of discrepancy (~1.5%) for annual teacher mortality is important, but we
suggest it is within the bounds of uncertainty that we must accept. We illustrate this
by presenting new results from 5 sub-Saharan countries which explicitly factor in
uncertainty analyses to illustrate the plausible range of AIDS-related teacher
mortality.
New results from 5 sub-Saharan countries
To this body of knowledge, we add new impact estimates for 5 sub-Saharan countries:
Eritrea, Kenya, Mozambique, Tanzania and Zambia. Details of our analysis are in
Annex 1.
5
Our modeling approach is consistent with UNAIDS methodology. Rather than assume
teachers are representative of the general population, we allow teacher infection rates
to vary in our model from one half to double the infection rate in the general
population. We also vary baseline population-level HIV prevalence between the upper
and lower end of the most recent UNAIDS estimates. Where independent estimates
were available, we found our low-high range of AIDS-related teacher mortality to
include the independent estimates.
In the best case scenario, Zambia, Tanzania and Kenya will each lose 600 teachers to
AIDS in 2005 alone. Mozambique will lose over 300. This is the result of ~0.5%
annual AIDS mortality, the least plausible annual AIDS mortality in teachers in these
countries (Table 3).
In the worst case scenario, Zambia, Tanzania and Kenya will each lose between 1500
and 3000 teachers to AIDS in 2005 alone. Mozambique will lose over 1100. This is
the result of up to 3.1% annual mortality, the highest plausible rate in these countries
(Table 3).
Table 3 further shows that in any given country, including low-prevalence Eritrea,
annual AIDS mortality in teachers estimates lie within a ~1.5% range (difference
between lowest and highest estimate for a given country). Note that this is also the
range of discrepancy between the data-based estimates of teacher mortality and
previous projection models.
Absenteeism is a significant rising problem in several service sectors, but data-based
research cannot clearly quantify or ascribe any absenteeism to AIDS only (Grant et
al., 2004, World Bank, 2004). In surveys of head teachers in southern Africa, one in
five saw absenteeism as a serious problem for quality of education, with 47% of
absenteeism attributed to attending funerals and 30% due to sickness. Reliable data on
absenteeism due to HIV/AIDS are scarce, not least because of the stigmatization and
loss of benefits resulting form declaring status.
Our model provides estimates of AIDS-related absenteeism (Table 3). In a best case
scenario between 600-700 teacher-years of absenteeism for personal illness due to

6
HIV/AIDS will be felt by educators in Kenya, Tanzania and Zambia in 2005 alone.
Mozambique will experience a lost of almost 400 teacher-years. In a worst case these
countries will experience 1200-3000 teacher years of absenteeism.
Financial impacts of HIV/AIDS felt by MoE were possible to estimate for
Mozambique and Zambia. In Mozambique, AIDS-related teacher absenteeism for
personal illnesses will likely cost $3.3 million USD in 2005 alone plus another $300
000 USD for increased teacher training costs. In a worst case scenario this will rise to
total $6.0 million, and the figure will be approximately 10 times this over next 10
years, in absence of any behavioural intervention or antiretroviral drugs.
In Zambia, these figures are $1.7 million USD for absenteeism and $700 000 USD for
teacher training in 2005 alone. In a worst case scenario, the total cost to MoE will
reach $3.4 million this year.
Projection data consistently indicate that the cost of absenteeism to employers is
substantially greater than the cost of training and recruitment to replace staff lost
through AIDS: absenteeism is variously estimated at 24% to 89% of the total
HIV/AIDS costs to employers, and training and recruitment at 17% to 24% (Grant et
al., 2004, Grassly et al., 2003).
Are female teachers differentially affected by HIV/AIDS compared to male teachers?
Relatively little empirical data exists at present to clearly indicate whether HIV/AIDS
affects male and female teachers differentially, and generalizations are not possible to
answer this question. However, an ongoing longitudinal household-based survey
study conducted in Manicaland, Zimbabwe between 1998-2000 reported 19% HIV
seroprevalence in males compared to 29% in females for respondents employed in
education sector, and these respondents are almost exclusively teachers or
administrators (personal communication: James Lewis and Constance Ny, Dept
Infectious Disease Epidemiology, Imperial College London). On the other hand,
Bennell (Bennell, 2005a) reports lower mortality rates in female primary school
teachers compared males (0.76% – females,1.21% - males) in Botswana in 1999-
2000. Similarly in Tanzania female teachers had lower mortality rates (0.58% -
7
females, 1.10% - males). However, female primary school teachers in Malawi had
higher mortality than males (2.49% - females, 1.96% - males), while in Uganda male
and female teachers had equivalent mortality rates (0.92% - female, 0.97% - male).
However, these mortality rates arise from all causes and cannot be attributed to
HIV/AIDS alone.
Projection models which are based on UNAIDS methodology are likely to suggest
that HIV infection rates in female teachers will be higher than in male teachers if the
recruitment of new teachers includes a significant proportion of young female women
in countries with established epidemics. This is because the projection models assume
a similar pattern of age- and sex- stratified HIV prevalence as that observed in many
sub-Saharan countries (Glynn et al., 2000; Wawer et al., 1997; Fylkesnes et al., 2001).
However, concluding higher infection rates in female teachers based on mathematical
models is sensible only if the initial assumption of the age- and sex- distribution of
HIV prevalence is correct to apply to the teaching population.
What is the evidence of impact of HIV/AIDS on orphans and vulnerable children?
There are two main sources of data which are used to estimate the impact of
HIV/AIDS on children. These are Demographic and Health Surveys and cluster
surveys which are representative samples of rural and urban households undertaken
every 4-5 years in many sub-Saharan countries. These focus on all orphans rather than
AIDS orphans specifically. Another source is based on country-specific demographic
models which incorporate HIV/AIDS epidemiology to give current and projected
numbers of orphans disaggregating between AIDS and non-AIDS causes. The best
reviews of recent DHS and cluster surveys are contained in Ainsworth and Filmer
(Ainsworth and Filmer, 2002) and Monasch and Boerma (Monasch and Boerma,
2004), while the key resource based on demographic models is the well-known
Children on the Brink publication (Hunter and Williamson, 2004). To date, these
sources only allow to quantify numbers of orphans or seek to correlate characteristics
of the orphan to school enrolment.
Ainsworth and Filmer analyzed the relationship between orphan status, household
wealth and school enrolment in 22 sub-Saharan African countries. Their findings are

8
quite revealing on the diversity and complexity of orphanhood characteristics and
school enrolment such that generalizations are not possible. In terms of frequency of
orphans, paternal-only orphans were more prevalent than maternal-only orphans and
two-parent orphans. Also Eastern and Southern African countries had somewhat
greater prevalence than West African countries. For example, West African countries
had between 5-10% of children who were paternal orphans compared to 6-13% in
Eastern and Southern African countries. In terms of the relationship between
orphanhood characteristics and school enrolment, there was no strong evidence of
enrolment gaps between boys and girls who were orphaned compared to non-
orphans. Although 16 of 22 countries indicated lower-enrolment for at least one type
of orphan (maternal-, paternal- or two-parent orphans), they state that it is not
orphanhood status but household wealth which is the main determinant of a child’s
enrollment in school. Monasch and Boerma suggest that participation in school was
somewhat lower for orphans compared to non-orphans in 30 of 31 countries studied,
but attendance levels among orphans are nevertheless still fairly high. However, they
find that two-parent orphans are more disadvantaged in terms of school enrolment
compared to maternal- or paternal-only orphans. They reiterate the result from
Ainsworth that sex of the orphan has not clear association with school enrolment.
The Children on the Brink publication add an interesting dimension to orphan
numbers in that they indicate the percentage of all orphans who are likely to be
paternal-, maternal-, or two-parent orphans. Unsurprisingly the share of orphans due
to HIV/AIDS corresponds with the severity of the epidemic in a given country. For
example, in Eastern and Southern African countries which are often characterized by
high prevalence, 31-77% of all orphans are AIDS orphans. This is in contrast with the
rest of Africa where the share of orphans due to AIDS is 4-39%. The calculations
agree with DHS data in that paternal- orphans generally outnumber maternal- and
two-parent orphans for AIDS and non-AIDS orphans combined. For AIDS orphans
however this order is reversed: it is the maternal orphans who outnumber the paternal
orphans. Although the impact of HIV/AIDS on children is somewhat less
controversial than the impact on teachers, Bennell (Bennell, 2005b) points out that in
terms of total numbers of orphans, the demographic projection figures are 30-50%
higher than that obtained through DHS.

9
Kinghorn and Kelly (Kinghorn and Kelly, 2005) correctly point out that the balance
of available evidence would indicate that orphans’ schooling is not as severely
affected as is often assumed. However, the HIV/AIDS orphans epidemic has served to
highlight that education goals are undermined by huge numbers of orphans and other
vulnerable children, independent of orphan status or cause of orphanhood. Lastly the
available statistics on impact of AIDS on schooling of orphans do not fully capture
important dimensions of schooling outcomes or assess impact of HIV/AIDS on school
participation in children caring for parents.
Conclusion
AIDS–related mortality in teachers, by whichever means it is estimated, is certain to
be at least 0.5% and probably as high as 4.0%. This, is in addition to other causes of
attrition, normally around 1.5-4.0%, depending on relative desirability of teaching
profession and other forces of labour markets. Thus, HIV/AIDS can considerably
exacerbate turnover rates and place considerable strain on MoE human resource
requirements. At the worst extreme, it doubles attrition rates.
The question of impact of HIV/AIDS on administrators in education sectors has been
posed. Current evidence, which comes from Education Management Information
Systems, school-based surveys and mathematical models, have not provided analyses
specific to administrators. However, our experience in several countries has shown
that many administrators in central or regional MoE offices themselves are former
teachers, are more senior than the in-service teaching population and are often urban
rather than rural based. We could conjecture therefore that the pattern of infection in
administrators may be similar to urban educated professionals not younger than 30
years from the same country, but this would need verification.
The evidence on impact in teachers and children is that data and projections are
actually more concordant than has been argued in some areas of the literature. Both
sources suggest that the impact in affected countries - and thus presumably the future
impact in countries with a rising epidemic – is serious. In the context of any
continuing disagreement, Kinghorn and Kelly (Kinghorn and Kelly, 2005) offer a
sound viewpoint: it is important not to give undue attention to details to the extent of
10
obscuring the larger picture. Discrepancies should instead call for fine-tuning of
estimates and a more nuanced understanding of the impacts that HIV/AIDS has on
teachers and children.
To confirm the degree of seriousness in individual countries (and their regions, for
AIDS is geographically diverse) there is a need for better sector-specific data on both
HIV prevalence and teacher mortality (Boler, 2003). Recent analysis by the World
bank has shown that only 45% of country education projects include specific
HIV/AIDS indicators. There is a need to strengthen education management
information systems and include HIV/AIDS indicators, and to include education
specific measures in DHS surveys. In the meantime, uncertainties in data are to be
expected, and we should learn to feel comfortable in our uncertainty in order to press
onward. Whatever the quality of current data, projections remain the only way to
explore the future impacts, and in particular to examine how teacher needs may
change in addressing the goal of EFA by 2015. This suggests a need for planners to
use EdSIDA and similar models in EFA projections of future teacher needs (World
Bank, 2002).
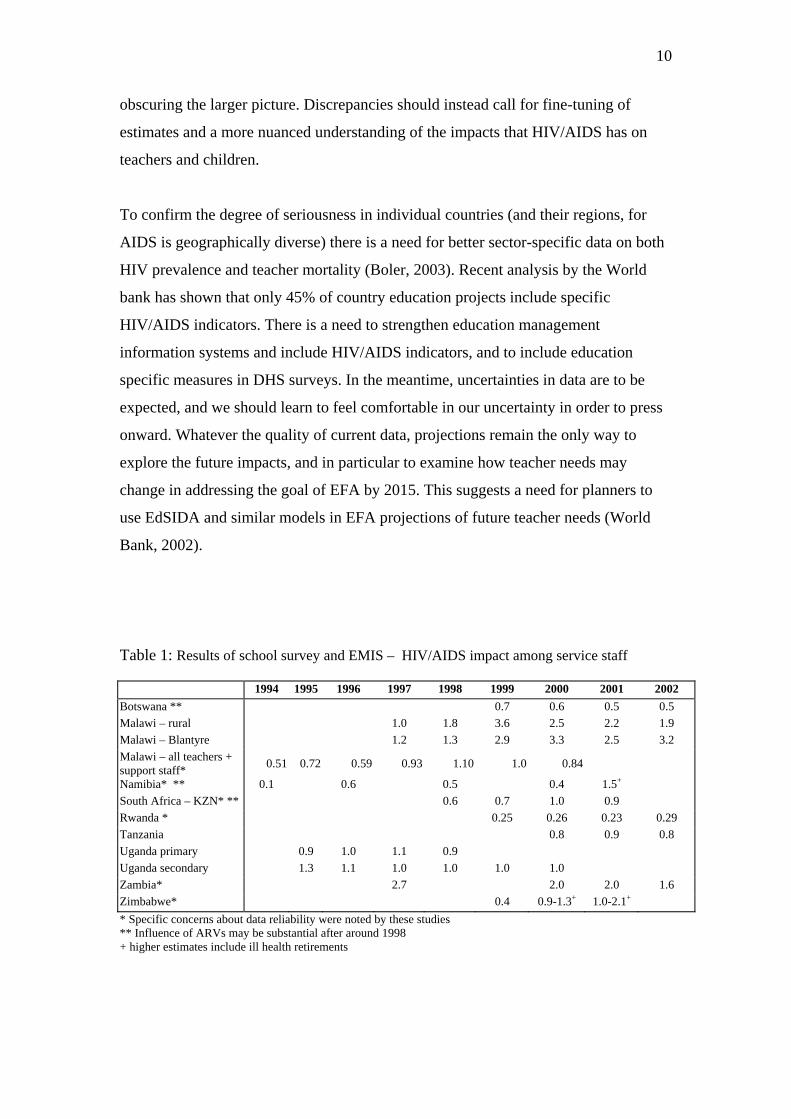
Table 1: Results of school survey and EMIS – HIV/AIDS impact among service staff
1994 1995 1996 1997 1998 1999 2000 2001 2002 Botswana ** 0.7 0.6 0.5 0.5 Malawi – rural 1.0 1.8 3.6 2.5 2.2 1.9 Malawi – Blantyre 1.2 1.3 2.9 3.3 2.5 3.2 Malawi – all teachers + support staff* 0.51 0.72 0.59 0.93 1.10 1.0 0.84
Namibia* ** 0.1 0.6 0.5 0.4 1.5+ South Africa – KZN* ** 0.6 0.7 1.0 0.9 Rwanda * 0.25 0.26 0.23 0.29 Tanzania 0.8 0.9 0.8 Uganda primary 0.9 1.0 1.1 0.9 Uganda secondary 1.3 1.1 1.0 1.0 1.0 1.0 Zambia* 2.7 2.0 2.0 1.6 Zimbabwe* 0.4 0.9-1.3+ 1.0-2.1+ * Specific concerns about data reliability were noted by these studies ** Influence of ARVs may be substantial after around 1998 + higher estimates include ill health retirements

11
Table 2: Results of projection studies – HIV/AIDS impact among service staff
Country Sector Estimated staff HIV
prevalence (%, year)
Projected Death rates
(%, year)
Projected Death rates with
ARVs*
(%, year)
Source
Botswana Education (teachers only)
45 (2000) 2.5 (2000) 5 (2005)
1.2-1.5 (2000) 1.5-2 (2005)
Abt Associates 2001
Botswana Health 32 (1999) 1.2 -1.5 (1999) 3.5(2005)
4 - 6 (2010)
-
Abt Associates 2000
Mozambique Education - 1.7 (2010) - Verde Azul 2002 Mozambique Customs 21 (2001) 0.8-1.1 (2000)
2.5- 3.2 (2010) 1 (2010) Abt Associates
2002 Namibia Education 15 (2002) 1.25 (2000)
3.3 (2010) 0.6 (2000) 1.4 (2010)
Abt Associates 2002
Rwanda Education 4-4.7 (2002)
6-8 (2005)
0.6-0.9 (2010) 0.3-0.45 (2010) HAD 2003
South Africa Education 12 (2000) 26 (2010)
0.5 (2000) 3.2(2010)
- Abt Associates 2001
Zambia Education 19-28 (2002)
1.2-2 (2000) 1.5-2.5 (2005)
1.1-1.25 (2008) SIAPAC, forthcoming
Zimbabwe Education 33 (2000) 3.6-3.9 (2000) 4 -4.4 (2010)
_ Abt Associates 2002
* Specific assumptions about levels of ARV coverage and effectiveness should be noted.

12
Table 3: Impact of HIV/AIDS on education in 5 sub-Saharan countries for year 2005 Eritrea medium low High Total teacher mortalities due to AIDS (% total attrition)
35 (12.4) 7 (2.1) 130 (30.9)
Annual teacher mortality due to AIDS 0.3 0.07 1.5 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
37 (0.4) 7 (0.1) 130(1.5)
Kenya medium low high Total teacher mortalities due to AIDS (% total attrition)
1620 (18.0) 700 (7.5) 3020 (29.6)
Annual teacher mortality due to AIDS 0.8 0.4 1.8 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1590 (0.8) 690 (0.4) 2930 (1.8)
Mozambique medium low high Total teacher mortalities due to AIDS (% total attrition)
675 (33.2) 340 (16.6) 1150 (43.1)
Annual teacher mortality due to AIDS 1.4 0.7 2.3 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
730 (1.5) 370 (0.8) 1240 (2.9)
Tanzania medium low high Total teacher mortalities due to AIDS (% total attrition)
1290 (19.9) 605 (9.3) 2010 (31.0)
Annual teacher mortality due to AIDS 1.1 0.5 1.9 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1290 (1.1) 610 (0.5) 2200 (2.3)
Zambia medium low high Total teacher mortalities due to AIDS (% total attrition)
1030 (40.4) 580 (23.3) 1500 (48.8)
Annual teacher mortality due to AIDS 2.1 1.2 3.1 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1090 (2.2) 605 (1.3) 1580 (3.9)

Supporting material only for Section 2.
Annexe – Methods, data sources and results for 5 country analysis
The Ed-Sida model, used for these projections, is a compartmental mathematical model which captures the dynamics of an age- and sex-stratified teacher population in terms of recruitment, retirement, attrition, HIV infection and death using difference equations with yearly time steps. The model was developed jointly by the World Bank, the Department for International Development UK and the Partnership for Child Development of Imperial College London and has been described extensively in Grassly et al [A-1] and by the World Bank publication [A-2]. The model takes as inputs the current and historical size of the teacher population by age and sex, annual teacher recruitment rates by age and sex and annual attrition by sex. This data was provided generously by the MoE or Teacher Training Colleges of the respective countries and are also available, though more crudely, from the UNESCO Institute for Statistics [A-3]. When relevant data were missing, values were sensibly imputed. For instance the most frequently missing information was annual recruitment, which was determined from the year over year increase in total teacher numbers less total annual attrition and in line with most recent recruitment trends. The incidence and prevalence of HIV amongst teachers by age and sex are derived using UNAIDS models EPP and SPECTRUM [A-4, 5] based on country-specific estimates of adult HIV prevalence from HIV sentinel surveillance sites [A-6]. In absence of teacher-specific data on HIV infection, it is assumed that teachers have HIV infection rates similar to the general population, but this assumption is varied in sensitivity analyses, where HIV infection can vary from half to double the infection rate in the general population. The model also takes as input projected the total school-aged population (usually ages 6-14) to year 2015 from UN Population Division medium variant projections [A-7] and gross enrolment rate. Model impacts are obtained by comparing total teacher numbers in a given year in presence of AIDS and the theoretical number in absence of AIDS-related mortality, number who are HIV-positive, AIDS mortality rate, HIV/AIDS-related absenteeism and pupil-teacher ratio in presence and absence of HIV/AIDS. AIDS-related absenteeism is directly related to the number of HIV-positive teachers and is based on the assumption that a HIV infected teacher will have 10-12 episodes of HIV-related illness each lasting 10 working days and is additional absent from work during the last 6 months of life during late AIDS disease [A-1]. A similar calculation has been adopted in the World Bank [A-8]. The pupil-teacher ratio is calculated according to total enrolled primary school population in given year divided by the total in-service teacher population but is not adjusted for double-shifting [A-9].
Sensitivity analysis was performed by varying national HIV prevalence estimates between high and low values in line with UNAIDS estimates [A-10], by assuming teachers have half to double the risk of HIV infection relative to general population, and non-AIDS attrition rates between 1.0 to 3.0%. The impacts reported here should be interpreted as those incurred ‘passively’ and therefore do not reflect interventions to minimise risk-behaviours in teachers or benefits of provision of anti-retroviral drugs. Anti-retroviral therapy is being rolled out successfully since 1998 in teacher populations in Botswana, Namibia and Kwazulu Natal [A-11]. Where possible and relevant we compare our results with data-based evidence from other survey and projection studies on HIV/AIDS impacts on sub-Saharan African education systems. Impact indicators For the five countries, Table 4 lists five HIV/AIDS impact indicators for year 2005 for medium, low and high epidemic scenarios: (i) The number of in-service HIV-positive teachers and percentage of all teachers (ii) Shortfall in teacher number due to AIDS. This is the theoretical decline in teacher numbers due to the cumulation of previous years’ AIDS-related attritions under same historical recruitment levels. (iii) Teacher mortalities due to AIDS and percentage of total attrition. (iv) AIDS mortality rate. (v) Absenteeism in teacher-years and percentage of total teacher years. Seroprevalence in Teachers Of the five countries considered, Zambia is projected to experience the greatest impact on teacher supply, having reached high adult seroprevalence levels (~15%) in 1990 and has since remained close to this level. Seroprevalence in Zambian teachers in 2005 is estimated by the model at 21.9% [range 12.5-38.8]. This is higher than general population seroprevalence (16.5%) given the high proportion of teachers between ages 25-34, the most afflicted age group in Eastern and Southern African countries. Given that HIV testing in teacher populations only rarely exists, it is not possible to validate these estimates against independently collected data. However, another projection study indicates prevalence of 19-28% in education sector service staff in Zambia [A-12]. A household survey conducted in Manicaland, Zimbabwe, also a high prevalence setting, indicated seroprevalence of 19% in adult males and 29% females amongst those employed in education sector [personal communication with James Lewis, Imperial College London]. Like Zambia, teachers in Kenya, Mozambique, Tanzania and Eritrea are found to have seroprevalences around ~2-3% higher than their national average, based on medium scenario assumptions. The uncertainty range for seroprevalence estimates for Eritrea are widest, given relatively insufficient data from few HIV sentinel surveillance site which were only recently established [A-10]. Here seroprevalence may range between 0.7-15.0%. Shortfall in teachers numbers

Because the shortfall in teacher numbers occurring in year 2005 is due to the cumulative effect of AIDS mortality during the preceding years, the countries which reached high prevalence levels earliest and maintained these levels since experience the greatest shortfall in teachers. Thus Zambia has a shortfall of 20.1% (range 11.8-33.4%) in teacher numbers relative to actual levels, while Tanzania and Kenya have shortfall of 11.9% (range 5.9-24.4%) and 8.9% (range 4.2-20.0%). Eventhough Mozambique has currently higher seroprevalence than Tanzania, it has a lower shortfall currently at 9.2% (range 4.7-17.6%) than Tanzania whose seroprevalence was greater during the period prior to 1996. Again Eritrea, having the lowest HIV prevalence currently and historically, has the lowest shortfall (3.4%, range 0.9-13.8%). Teacher mortality The most common form of data-based evidence of the impact of HIV/AIDS on teachers is based on mortality rates which can be observed from Education and Management Information Systems which include personnel and payroll records or from school-based surveys in which head teachers are asked to respond to questionnaires about teacher mortality [A-13,14]. The former source tends to measure only in-service mortality therefore missing AIDS-related post-service mortality. In South Africa, up to 50% of mortality due to illness in the private sector occurs after leaving work [A-15]. Also such information systems do not indicate AIDS specifically as cause of death. The latter source of information is characterised by high levels of non-response from head teachers and also do not indicate AIDS as cause of death. A review of available data on teacher mortality (for all causes) by Bennell [A-14] indicates mortality in Zambia at 2.7% in 1997 and declining to 1.6% in 2002, while Haacker [A-15] reports 2.8% AIDS-related mortality in public-sector servants in Zambia in 2003, Grant et al [A-11] report 1.5-2.5%, and a World Bank report indicates 1.7% [A-17]. These are consistent with our estimates for Zambia (2.1%, range 1.2-3.1%). In our projections, Zambia had the highest mortality, followed by Mozambique (1.4%, range 0.7-2.3%), Tanzania (1.1%, range 0.5-1.9%), Kenya (0.8%, range 0.4-1.8%) and Eritrea (0.3%, range 0.07-1.5%). These estimates are also consistent with other reports which indicate mortality of 1.4% for Kenya [A-17], 0.8% for Tanzania [14] in 2000-2002 and 1.7% projected in 2010 for Mozambique [A-11]. We did not find other independent estimates of AIDS-related mortality for Eritrea. Our projection also indicate that AIDS-related deaths in teachers can account for 40.4% (range 23.3-48.8%) of all annual attritions at one extreme and 12.4% (range 2.1-30.9%) at the other extreme in Eritrea. These figures assume that attritions due to non-AIDS causes vary between 1% and 3% depending on economic and social desirability of the teaching profession which if high will help retain teachers. From our experience, we find that many employees in higher managerial positions of MoE were former teachers. It is plausible therefore that AIDS-related deaths in MoE can be

filled by in-service teachers seeking better pay or work conditions. Anecdotal evidence also exists that teachers may leave their profession to take up positions in other sectors if teachers are considered a well-educated segment of the workforce. This is likely to occur in labour markets where supply of highly educated or skilled individuals is tight [A-16]. Absenteeism Empirical data on absenteeism is limited, and it is generally difficult to ascribe causes of absenteeism to HIV/AIDS. However, surveys in Namibia and Zimbabwe [A-11] indicate that only 1 out of 5 school head teachers saw absenteeism as a serious problem. Our projections indicate that absenteeism due to HIV/AIDS-related illness accounts for only ~1% or 2% of total teacher time annually even in high prevalence Zambia and Mozambique. If true it is not surprising that few head teachers consider absenteeism a major problem. However, our figures do not account for time away from the classroom to attend funerals for AIDS deaths in relatives or work colleagues which can potentially be as important as teacher absence due to illness [A-11]. It should be noted that while these are small percentages, they derive from the assumption that the HIV positive teacher may be ill 10% of the time. In terms of student learning, research by Das and Habyarimana [A-18] have indicated that a 5% increase in the teacher absence rate reduced student learning by 4-8 percent of the average yearly gains in Mathematics and English in Zambia. This implies that learners of HIV-positive educators may have on average lower achievement levels than other learners. Economic impacts A rapid assessment of the economic impact of HIV/AIDS from perspective of MoE was possible for Mozambique and Zambia. In 2001, World Bank estimates of average annual salaries in Mozambique for 2 categories of primary teacher were 4.6 and 3.1 times GDP per capita ($1050 USD). This corresponds annual salaries of $4830 USD and $3255 USD. According to MoE, the proportion of teachers per category were 46.0% and 54.0%. The double shift ratio of 1.2 combined with 60% salary premium for teachers teaching two classes raises the weighted average salary to $4457 USD. Applying these salary costs to the estimated teacher-years of AIDS related absenteeism for Mozambique in 2005 indicates a cost of $3 254 000 USD (range $1 649 000 – $5 527 000). Given the costs of teacher training are $479 USD per trainee, the training costs incurred to replace teachers dying of AIDS in 2005 is $323 000 USD (range $163 000 - $551 000). We previously performed an economic impact analysis from the perspective of the MoE of Zambia [A-1]. These figures are updated based on projections in this paper. Weighted average annual salary cost for teachers was $1548 USD based on salary scales from 2001 Collective Agreement between MoE and Primary School Teachers Union. Teacher training costs were on average $510 USD per teacher-trainee in a Teacher Training College. Death benefits were $176 USD per teacher mortality. Applying these figures to HIV/AIDS-related absenteeism and mortality, we find costs to be $1 687 000 (range $936 000 – $2 446 000) for absenteeism and $ 707 000 (range $398 000 – $1 029 000) for mortality in 2005.

Although it is generally difficult to compare economic analyses between different countries, two conclusions can be drawn. The current major cost component to MoE arises from teacher absenteeism eventhough studies indicate absenteeism is not perceived to be major problem. However, the most important cost component in future will be that associated with enrolling orphans and vulnerable children. World Bank uses unit cost of $50 USD to enrol one OVC for one year. Combining this figure with estimates of AIDS orphans of school-age numbering ~250 000 in Mozambique and ~340 000 in Zambia generates costs of $12.5 million and $17 million in these countries in 2005 alone. Further costs categories not discussed here include cost related to management responses to HIV/AIDS and adjustment of education programmes and curriculum to an HIV/AIDS context. Orphans With respect to demand, demographic methods have been developed to quantify the number of maternal, paternal and dual-orphans resulting from AIDS and non-AIDS causes [A-19]. These figures have been recently updated [A-20]. Such estimates complement empirical estimates from Demographic and Health Surveys. Ainsworth et al [A-21] has reviewed results of DHS from 28 sub-Saharan, Latin American and Caribbean countries and examined, in particular, patterns of primary school enrolment of orphans and children from low-income households. Their main finding is that enrolment patterns of orphans are not generalisable but are country-specific. For instance, orphans from Tanzania had higher enrolment than non-orphans. On the other hand only dual orphans from Zambia and Mozambique had lower enrolment rates and orphans of all types had lower enrolment in Kenya. Eritrea was not covered in the study. The strongest finding was that the enrolment gap was greatest between poor and rich households, irrespective of orphan status. Moreover, there no strong evidence of enrolment gaps between boys and girls who were orphaned. Responses
HIV/AIDS tends to exacerbate existing weaknesses in HR management and planning, and few affected countries have put in place processes to respond effectively to the additional stresses that the epidemic places on supply of services. Our work with the UNAIDS Inter Agency Task Team for Education and HIV/AIDS has established a working group that has worked with more than thirty countries to accelerate the education sector response to HIV/AIDS in Africa, including strengthening management and planning. Experience indicates that less than 5 of 30 Ministries of Education included HIV/AIDS indicators in the education management information system, and only a similar minority included AIDS impact projections in their models of future HR needs in planning for EFA. Similarly, of the initial 12 countries with education sector plans that had been endorsed by the EFA-FTI partnership, only 1 included this aspect of the AIDS response in its sector plan. Another frequent omission is a work place policy that mitigates the impact of HIV/AIDS and supports and strengthens the role of the workforce (for example, ensuring access to prevention, VCT, care, support and treatment for staff). In order to assist countries in addressing

these needs, the FTI has developed a partnership with the UNAIDS Inter Agency Task Force on Education to assist governments in strengthening their sector plans to respond effectively to HIV/AIDS.
Table 4: Impact of HIV/AIDS on education supply and pupil-teacher ratio in 5 sub-Saharan countries for year 2005 based on Ed-Sida projections Eritrea medium low high Number HIV positive teachers (% total teachers)
370 (3.5) 75 (0.7) 1325 (15.0)
Shortfall in teacher numbers (% of actual teacher numbers)
360 (3.4) 90 (0.9) 1230 (13.8)
Total teacher mortalities due to AIDS (% total attrition)
35 (12.4) 7 (2.1) 130 (30.9)
Annual teacher mortality due to AIDS 0.3 0.07 1.5 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
37 (0.4) 7 (0.1) 130(1.5)
Kenya medium low high Number HIV positive teachers (% total teachers)
15900 (7.8) 6900 (3.6) 29300 (17.7)
Shortfall in teacher numbers (% of actual teacher numbers)
18100 (8.9) 8000 (4.2) 33200 (20.0)
Total teacher mortalities due to AIDS (% total attrition)
1620 (18.0) 700 (7.5) 3020 (29.6)
Annual teacher mortality due to AIDS 0.8 0.4 1.8 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1590 (0.8) 690 (0.4) 2930 (1.8)
Mozambique Number HIV positive teachers (% total teachers)
7330 (14.9) 3670 (7.7) 12340 (29.0)
Shortfall in teacher numbers (% of actual teacher numbers)
4520 (9.2) 2250 (4.7) 7500 (17.6)
Total teacher mortalities due to AIDS (% total attrition)
675 (33.2) 340 (16.6) 1150 (43.1)
Annual teacher mortality due to AIDS 1.4 0.7 2.3 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
730 (1.5) 370 (0.8) 1240 (2.9)
Tanzania medium low high Number HIV positive teachers (% total teachers)
12900 (10.9) 6080 (5.4) 22000 (22.6)
Shortfall in teacher numbers (% of actual teacher numbers)
14000 (11.9) 6600 (5.9) 23700 (24.4)
Total teacher mortalities due to AIDS (% total attrition)
1290 (19.9) 605 (9.3) 2010 (31.0)
Annual teacher mortality due to AIDS 1.1 0.5 1.9 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1290 (1.1) 610 (0.5) 2200 (2.3)
Zambia medium low high Number HIV positive teachers 10800 (21.9) 6030 (12.5) 15800 (38.8)

(% total teachers) Shortfall in teacher numbers (% of actual teacher numbers)
9940 (20.1) 5700 (11.8) 13600 (33.4)
Total teacher mortalities due to AIDS (% total attrition)
1030 (40.4) 580 (23.3) 1500 (48.8)
Annual teacher mortality due to AIDS 2.1 1.2 3.1 Teacher-years of absenteeism due to AIDS (% of total teacher-years)
1090 (2.2) 605 (1.3) 1580 (3.9)
References for Annex [A-1] Grassly, N.C., Desai, K., Pegurri, E., Sikazwe, A., Malambo, I., Siamatowe, C. & Bundy, D.A.P. 2003 The economic impact of HIV/AIDS on the education sector in Zambia. AIDS 17, 1-6. [A-2] World Bank 2002. Education and HIV/AIDS: Modeling the impact of HIV/AIDS on education systems – A training manual. [A-3] Unesco Institute of Statistics website. http://www.uis.unesco.org [A-4] Estimation and Projection Package. UNAIDS Reference Group on Estimates, Models and Projections. http://www.futuresgroup.com [A-5] SPECTRUM Policy Modeling System. UNAIDS Reference Group on Estimates, Models and Projections. http://www.futuresgroup.com [A-6] HIV/AIDS Surveillance Database. U.S. Census Bureau, Population Division, Health Studies Branch http://www.census.gov/ipc/www/hivaidsn.html [A-7] United Nations Population Division. Dept of Economic and Social Affairs http://esa.un.org/unpp/ [A-8] World Bank 2001. Costs of scaling HIV program activities to a national level in sub-Saharan Africa: Methods and estimates. World Bank AIDS Campaign Team for Africa, Washington DC. [A-9] Unesco Institute of Statistics. Educational indicators – technical guidelines. http://www.uis.unesco.org/ [A-10] UNAIDS Country Factsheets. http://www.unaids.org/ [A-11] Grant, K.B, Gorgens, M. & Kinghorn, A. (2004) Mitigating the impact of HIV on service providers what has been attempted, what is working, what has not worked, where and why? A study commissioned by the DFID Service Delivery Team (Workstream on Capacity Development and Human Resources) in collaboration with USAID, May 2004. [A-12] Siapac to appear. From Grant et al.

[A-13] ] Boler, T. (2003) Approaches to examining the impact of HIV/AIDS on teachers. Policy and Research: series 1. UK Working Group on Education and HIV/AIDS. Save the Children and Actionaid International. pp 1-8. [A-14] Bennell, P. 2005. The Impact of the AIDS Epidemic on Teachers in Sub-Saharan Africa. The Journal of Development Studies, 41, pp 440-446. [A-15] Badcock-Walters, P., Desmond C., Wilson D, Heard W (2003). Educator mortality in-service in KwaZulu Natal – A consolidated study of HIV/AIDS impact and trends. Demographic and Socio-Economic Conference, Tropicana Hotel, Durban, March 2003. [A-16] Haacker M 2004. The impact of HIV/AIDS on government finance and the public sector. In The Macroeconomic of HIV/AIDS. International Monetary Fund. [A-17] Coombe C 2002. Mitigating the impact of HIV/AIDS on education supply, demand and quality. In AIDS, Public Policy and Child Well-Being. UNICEF Innocenti Research Centre. [A-18] Jishnu Das, Stefan Dercon, James Habyarimana, and Pramila Krishnan, "Teacher Shocks and Student Learning: Evidence from Zambia" (September 1, 2004). The Centre for the Study of African Economies Working Paper Series. Working Paper 226. http://www.bepress.com/csae/paper226 [A-19] Grassly NC & Timaeus IM 2003 Orphans and AIDS in sub-Saharan Africa. New York, UN Population Division UN/POP/MORT/2003/9, 2003. [A-20] UNAIDS, UNICEF and USAID 2004. Children on the Brink 2004: A joint report of new orphan estimates and a framework for action. [A-21] Ainsworth M, Filmer D (2002). Poverty, AIDS and Children’s Schooling: A Targeting Dilemma. World Bank Policy Research Working Paper 2885.

Abebe, Y., Ab, S., Mamo, G., Negussie, A., Darimo, B., Wolday, D., et al. (2003). HIV prevalence in 72 000 urban and rural male army recruits, Ethiopia. Aids, 17(12), 1835-1840.
Ainsworth, M., Filmer D. (2002). Poverty, AIDS and Children's Schooling: A Targetting Dilemma. World Bank Policy Research Working Paper 2885.
Ajzen, I. (1985). From intention to actions: a theory of planned behavior. In J. Kuhl & J. Beckam (Eds.), Action Control: from Cognitions to Behavior. (pp. 11-39). New York: Springer-Verlag.
Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32(4), 665-683.
Allen, S., Lindan, C., Serufilira, A., Vandeperre, P., Rundle, A. C., Nsengumuremyi, F., et al. (1991). Human-Immunodeficiency-Virus Infection in Urban Rwanda - Demographic and Behavioral-Correlates in a Representative Sample of Childbearing Women. Jama-Journal of the American Medical Association, 266(12), 1657-1663.
Ammassari, A., Trotta, M. P., Murri, R., Castelli, F., Narciso, P., Noto, P., et al. (2002). Correlates and predictors of adherence to highly active antiretroviral therapy: Overview of published literature. Jaids-Journal of Acquired Immune Deficiency Syndromes, 31, S123-S127.
Badcock-Walters, P., Desmond, C., Wilson, D., Heard, W. (2003). Educator mortality in-service in KwaZulu Natal -- A consolidated study of HIV/AIDS impact and trends. Demographic and Socio-Economic Conference, Durban, March 2003.
Bandura, A. (1977). Social learning theory: (1977). viii, 247pp. Bangsberg, D. R., Hecht, F. M., Charlebois, E. D., Zolopa, A. R., Holodniy, M.,
Sheiner, L., et al. (2000). Adherence to protease inhibitors, HIV-1 viral load, and development of drug resistance in an indigent population. Aids, 14(4), 357-366.
Bangsberg, D. R., Perry, S., Charlebois, E. D., Clark, R. A., Roberston, M., Zolopa, A. R., et al. (2001). Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. Aids, 15(9), 1181-1183.
Barongo, L., Borgdorff, M., Mosha, F., Nicoll, A., & al., e. (1992). The epidemiology of HIV-1 infection in urban areas, roadside settlements and rural villages in Mwanza Region, Tanzania. AIDS, 6(1521-1528).
Bennell, P. (2005a). The Impact of the AIDS Epidemic on Teachers in Sub-Saharan Africa. The Journal of Development Studies, 41(3), 440-466.
Bennell, P. (2005b). The Impact of the AIDS Epidemic on the Schooling of Orphans and Other Directly Affected Children in Sub-Saharan Africa. The Journal of Development Studies, 41(3), 467-488.
Berkley, S. F., Widywirski, R., Okware, S. I., Downing, R., Linnan, M. J., White, K. E., et al. (1989). Risk-Factors Associated with Hiv Infection in Uganda. Journal of Infectious Diseases, 160(1), 22-30.
Blanc, A. (2000). The relationship between sexual behaviour and level of education in developing countries. Geneva: UNAIDS.
Blanc, A. K., & Way, A. A. (1998). Sexual behavior and contraceptive knowledge and use among adolescents in developing countries. Studies in Family Planning, 29(2), 106-116.
Boerma, J., Urassa, M., Senkoro, K., Klokke, A., & Ng'weshemi, J. (1999). Spread of HIV infection ina rural area of Tanzania. AIDS, 13(10), 1233-1240.
1

Boler, T. (2003). Approaches to examining the impacts of HIV/AIDS on teachers. Policy and Research: Series 1. UK working Group on Education and HIV/AIDS. Save the Children and ActionAid International.
Brent, R. (2005). A cost-benefit analysis of female primary education as a means of reducting HIV/AIDS in Tanzania.Unpublished manuscript.
Brigido, L. F., Veiga, A. P., d'Ambrosio, A. C., Bueno, A., Casseb, J., & Galbitti, F. F. (1998). Low adherence in HAART users at Sao Paola, Brazil. Paper presented at the 12th World AIDS Conference, Geneva.
Bundy, D.A.P. (2004). Letter to Editor. Spectator, December 13, 2004. Byakika-Tusiime, J., Oyugi, J. H., Tumwikirize, W. A., Katabira, E. T., Mugyenyi, P.
N., & Bangsberg, D. R. (2005). Adherence to HIV antiretroviral therapy in HIV plus Ugandan patients purchasing therapy. International Journal of Std & Aids, 16(1), 38-41.
Caldwell, J., & Caldwell, P. (1993). The nature and limits of the sub-Saharan African AIDS epidemic: evidence from geographical and other patterns. Population and Development Review, 19(4), 817-848.
Carr, J. K., Sirisopana, N., Torugsa, K., Jugsudee, A., Supapongse, T., Chuenchitra, C., et al. (1994). Incidence of Hiv-1 Infection among Young Men in Thailand. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 7(12), 1270-1275.
Celentano, D. D., Nelson, K. E., Suprasert, S., Eiumtrakul, S., Tulvatana, S., Kuntolbutra, S., et al. (1996). Risk factors for HIV-1 seroconversion among young men in northern Thailand. Jama-Journal of the American Medical Association, 275(2), 122-127.
Chesney, M. A. (2000). Factors affecting adherence to antiretroviral therapy. Clinical Infectious Diseases, 30, S171-S176.
Chesney, M. A., Ickovics, J., Hecht, F. M., Sikipa, G., & Rabkin, J. (1999). Adherence: a necessity for successful HIV combination therapy. Aids, 13, S271-S278.
Crampin, A. C., Glynn, J. R., Ngwira, B. M. M., Mwaungulu, F. D., Ponnighaus, J. M., Warndorff, D. K., et al. (2003). Trends and measurement of HIV prevalence in northern Malawi. Aids, 17(12), 1817-1825.
Dallabetta, G. A., Miotti, P. G., Chiphangwi, J. D., Saah, A. J., Liomba, G., Odaka, N., et al. (1993). High Socioeconomic-Status Is a Risk Factor for Human- Immunodeficiency-Virus Type-1 (Hiv-1) Infection but Not for Sexually-Transmitted Diseases in Women in Malawi - Implications for Hiv-1 Control. Journal of Infectious Diseases, 167(1), 36-42.
De Walque, D. (2002). How does the impact of an HIV/AIDS Information Campaign Vary with Educational Attainment? Evidence from Rural Uganda. Washington, D. C.: World Bank, Development Research Group.
Dobbins, J. G., Mastro, T. D., Nopkesorn, T., Sangkharomya, S., Limpakarnjanarat, K., Weniger, B. G., et al. (1999). Herpes in the time of AIDS: A comparison of the epidemiology of HIV-1 and HSV-2 in young men in northern Thailand. Sexually Transmitted Diseases, 26(2), 67-74.
Eldred, L., Wu, A., Chaisson, R. E., & Moore, R. D. (1995). Medication adherence to long-term therapy in HIV disease. Paper presented at the 11th International AIDS Meeting, British Columbia: Vancouver.
Eraker, S. A., Kirscht, J. P., & Becker, M. H. (1984). Understanding and improving compliance. Annals of Internal Medicine, 100, 258-268.
2

Fontanet, A. L., Woldemichael, T., Sahlu, T., van Dam, G. J., Messele, T., de Wit, T. R., et al. (2000). Epidemiology of HIV and Schistosoma mansoni infections among sugar-estate residents in Ethiopia. Annals of Tropical Medicine and Parasitology, 94(2), 145-155.
Fylkesnes, K., Mubanga Musonda, R., Kasumba, K., Ndhlovu, Z., Mluanda, F., Kaetano, L., et al. (1997). The HIV epidemic in Zambia: socio-demographic prevalence patterns and indication trends among childbearing wormen. AIDS, 11(3), 339-346.
Fylkesnes, K., Musonda, R. M., Sichone, M., Ndhlovu, Z., Tembo, F., & Monze, M. (2001). Declining HIV prevalence and risk behaviours in Zambia: evidence from surveillance and population-based surveys. Aids, 15(7), 907-916.
Fylkesnes, K., Ndhlovu, Z., Kasumba, K., Musonda, R. M., & Sichone, M. (1998). Studying dynamics of the HIV epidemic: population-based data compared with sentinel surveillance in Zambia. Aids, 12(10), 1227-1234.
GCE. (2004). Learning to survive: How education for all would save millions of young from HIV/AIDS. Brussels, Belgium: Global Campaign for Education.
Glynn, J. R., Buve, A., Carael, M. et al. (2000). Factors influencing the difference in HIV prevalence between antenatal clinic and general population in sub-Saharan Africa. AIDS, 11, 1717-1725.
Glynn, J. R., Carael, M., Buve, A., Anagonou, S., Zekeng, L., Kahindo, M., et al. (2004). Does increased general schooling protect against HIV infection? A study in four African cities. Tropical Medicine & International Health, 9(1), 4-14.
Golin, C. E., Liu, H. H., Hays, R. D., Miller, L. G., Beck, C. K., Ickovics, J., et al. (2002). A prospective study of predictors of adherence to combination antiretroviral medication. Journal of General Internal Medicine, 17(10), 756-765.
Grant, K. B., Gorgens, M., Kinghorn A. (2004). Mitigating the impact on HIV on service providers: What has been attempted, what is working, what has not worked, where and why? A study commissioned by DfID Service Delivery Team in collaboration with USAID, May 2004.
Grassly, N. C., Desai, K., Pegurri E., et al. (2003). The economic impact of HIV/AIDS on the education sector in Zambia. AIDS. 17, 1-6.
Gregson, S., Mason, P. R., Garnett, G. P., Zhuwau, T., Nyamukapa, C. A., Anderson, R. M., et al. (2001). A rural HIV epidemic in Zimbabwe? Findings from a population- based survey. International Journal of Std & Aids, 12(3), 189-196.
Gregson, S., Terceira, N., Mushati, P., Nyamukapa, C., & Campbell, C. (2004). Community group participation: Can it help young women to avoid HIV? An exploratory study of social capital and school education in rural Zimbabwe. Social Science & Medicine, 58(11), 2119-2132.
Gregson, S., Waddell, H., & Chandiwana, S. (2001). School Education and HIV Control in Sub-Saharan Africa: From Discord to Harmony. Journal of Internationl Development, 13, 467-485.
Gregson, S., Zhuwau, T., Anderson, R. M., & Chandiwana, S. K. (1998). Is there evidence for behaviour change in response to AIDS in rural Zimbabwe? Social Science & Medicine, 46(3), 321-330.
Grosskurth, H., Mosha, F., Todd, J., Senkoro, K., Newell, J., Klokke, A., et al. (1995). A Community Trial of the Impact of Improved Sexually- Transmitted Disease Treatment on the Hiv Epidemic in Rural Tanzania .2. Base-Line Survey Results. Aids, 9(8), 927-934.
3
Hargreaves, J. R., & Glynn, J. R. (2002). Educational attainment and HIV-1 infection in developing countries: a systematic review. Tropical Medicine & International Health, 7(6), 489-498.
Harries, A. D., Nyangulu, D. S., Hargreaves, N. J., Kaluwa, O., & Salaniponi, F. M. (2001). Preventing antiretroviral anarchy in sub-Saharan Africa. Lancet, 358(9279), 410-414.
Hogg, R. S., Heath, K., Bangsberg, D., Yip, B., Press, N., O'Shaughnessy, M. V., et al. (2002). Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. Aids, 16(7), 1051-1058.
Horne, R., Pearson, S., Leake, H., Fisher, M., & Weinman, J. (1999). Patients beliefs about HAART influences adherence to HAART therapy. Paper presented at the 39th Interscience Conference on Antimicrobial Agents and Chemotherapy, San Francisco.
Hunter, S., Williamson J. (2004). Children on the Brink 2004 : A Joint Report of New Orphan Estimates and a Framework for Action.
Johnston, B. E., Ahmad, K., Smith, C., & Rose, D. N. (1998). Adherence to HAART among HIV-infected patients of the inner city. Paper presented at the 12th World AIDS Conference, Geneva. UNAIDS, UNICEF and USAID, July 2004.
Jukes, M. C. e. a. (in preparation). HIV Knowledge associated with sexual behaviour in girls but not boys: A study in school-age children of Western Kenya.
Kammann, E., Williams, P., Chesney, M. A., & Currier, J. (1999). Predictors of adherence to azithromycin prophylaxis for prevention of mycobacterium avium complex (MAC) disease. Paper presented at the 6th Conference on Retroviruses and Opportunistic Infections, Chicago.
Kelly, R., Kiwanuka, N., Wawer, M. J., Serwadda, D., Sewankambo, N. K., Wabwire-Mangen, F., et al. (1999). Age of male circumcision and risk of prevalent HIV infection in rural Uganda. Aids, 13(3), 399-405.
Keselman, A., Kaufman, D. R., & Patel, V. L. (2004). "You can exercise your way out of HIV" and other stories: The role of biological knowledge in adolescents' evaluation of myths. Science Education, 88(4), 548-573.
Kilian, A. H. D., Gregson, S., Ndyanabangi, B., Walusaga, K., Kipp, W., Sahlmuller, G., et al. (1999). Reductions in risk behaviour provide the most consistent explanation for declining HIV-1 prevalence in Uganda. Aids, 13(3), 391-398.
Kinghorn, A., Kelly, M.J. (2005). The impact of the AIDS Epidemic Articles by Paul Bennell: Some Comments. The Journal of Development Studies, 41(3), 489-499.
Kirunga, C., & Ntozi, J. (1997). Socio-economic determinants of HIV serostatus: a study in Rakai District, Uganda. Health Transition Review, 7 (Supplement), 175-188.
Klosinski, L. E., & Brooks, R. N. (1998). Predictors of non-adherence to HIV combination therapies. Paper presented at the 12th Worlds AIDS Conference, Geneva.
Kwesigabo, G., Killewo, J., Godoy, C., Urassa, W., Mbena, E., Mhalu, F., et al. (1998). Decline in the prevalence of HIV-1 infection in young women in the Kagera region of Tanzania. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 17(3), 262-268.
4

Lagarde, E., Carael, M., Glynn, J. R., Kanhonou, L., Abega, S. C., Kahindo, M., et al. (2001). Educational level is associated with condom use within non- spousal partnerships in four cities of sub-Saharan Africa. Aids, 15(11), 1399-1408.
Lindan, C., Allen, S., Carael, M., Nsengumuremyi, F., Vandeperre, P., Serufilira, A., et al. (1991). Knowledge, Attitudes, and Perceived Risk of Aids among Urban Rwandan Women - Relationship to Hiv-Infection and Behavior- Change. Aids, 5(8), 993-1002.
Mason, C. J., Kitsiripornchai, S., Markowitz, L. E., Chanbancherd, P., Supapongse, T., Jugsudee, A., et al. (1998). Nationwide surveillance of HIV-1 prevalence and subtype in young Thai men. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 19(2), 165-173.
Mason, C. J., Markowitz, L. E., Kitsiripornchai, S., Jugsudee, A., Sirisopana, N., Torugsa, K., et al. (1995). Declining Prevalence of Hiv-1 Infection in Young Thai Men. Aids, 9(9), 1061-1065.
McNabb, J., Ross, J. W., Abriola, K., Turley, C., Nightingale, C. H., & Nicolau, D. P. (2001). Adherence to highly active antiretroviral therapy predicts virologic outcome at an inner-city human immunodeficiency virus clinic. Clinical Infectious Diseases, 33(5), 700-705.
Monasch, R., Boerma, J.T. (2004). Orphanhood and childcare patterns in sub-Saharan Africa: an analysis of national surveys from 40 countries. AIDS, 18(suppl 2), S55-S65.
Morse, E. V., Simon, P. M., & Walker, J. (1995). Issues of recruitment, retention and compliance in community-based clinical trials with traditionally underserved populations. Applied Nursing Research, 8(1), 8-14.
Nelson, K. E., Celentano, D. D., Suprasert, S., Wright, N., Eiumtrakul, S., Tulvatana, S., et al. (1993). Risk-Factors for Hiv-Infection among Young-Adult Men in Northern Thailand. Jama-Journal of the American Medical Association, 270(8), 955-960.
Nopkesorn, T., Mastro, T. D., Sangkharomya, S., Sweat, M., Singharaj, P., Limpakarnjanarat, K., et al. (1993). Hiv-1 Infection in Young Men in Northern Thailand. Aids, 7(9), 1233-1239.
Orrell, C., Bangsberg, D. R., Badri, M., & Wood, R. (2003). Adherence is not a barrier to successful antiretroviral therapy in South Africa. Aids, 17(9), 1369-1375.
Over, M., & Piot, P. (1993). HIV infection and sexually transmitted diseases. In Jamison DT, W. Mosley, A. Measham & J. Bobadilla (Eds.), DIsease Control Priorities in Developing Counties. New York: Oxford University.
Paterson, D. L., Swindells, S., Mohr, J., Brester, M., Vergis, E. N., Squier, C., et al. (2000). Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Annals of Internal Medicine, 133(1), 21-30.
Quigley, M., Munguti, K., Grosskurth, H., Todd, J., Mosha, F., Senkoro, K., et al. (1997). Sexual behaviour patterns and other risk factors for HIV infection in rural Tanzania: A case-control study. Aids, 11(2), 237-248.
Rosentock, I. (1990). The Health Belief Model: Explaining health behavior through expectancies. In K. Glanz, F. Lewis & B. Rimmer (Eds.), Health Behaviour and Health Education (pp. 39-62). San Francisco: Jossey-Bass.
Senkoro, K. P., Boerma, J. T., Klokke, A. H., Ng'weshemi, J. Z. L., Muro, A. S., Gabone, R., et al. (2000). HIV incidence and HIV-associated mortality in a
5

cohort of factory workers and their spouses in Tanzania, 1991 through 1996. Journal of Acquired Immune Deficiency Syndromes, 23(2), 194-202.
Serwadda, D., Wawer, M., Musgrave, S., Sewankambo, N., Kaplan, J., & Gray, R. (1992). HIV risk factors in three geographical strata of rural Rakai District, Uganda. AIDS, 6, 983-989.
Sirisopana, N., Torugsa, K., Mason, C. J., Markowitz, L. E., Jugsudee, A., Supapongse, T., et al. (1996). Correlates of HIV-1 seropositivity among young men in Thailand. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 11(5), 492-498.
Smith, J., Nalagoda, F., Wawer, M. J., Serwadda, D., Sewankambo, N., Konde-Lule, J., et al. (1999). Education attainment as a predictor of HIV risk in rural Uganda: results from a population-based study. International Journal of Std & Aids, 10(7), 452-459.
Stephenson, J. (1999). AIDS researchers target poor adherence. Jama-Journal of the American Medical Association, 281(12), 1069-1069.
Stone, V. E., Adelson-Mitty, J., Duefield, C. A., Steger, K. A., Stein, M. D., & Mayer, K. H. (1998). Adherence to protease inhibitor therapy in clinical practice: Usefulness of demographics, attitudes, and knowledge as predictors. Paper presented at the 12th World AIDS Conference, Geneva.
Stoneburner, R. L., & Low-Beer, D. (2004). Population-level HIV declines and behavioral risk avoidance in Uganda. Science, 304(5671), 714-718.
Taha, T. E., Dallabetta, G. A., Hoover, D. R., Chiphangwi, J. D., Mtimavalye, L. A. R., Liomba, G. N., et al. (1998). Trends of HIV-1 and sexually transmitted diseases among pregnant and postpartum women in urban Malawi. Aids, 12(2), 197-203.
Vandemoortele, J., & Delamonica, E. (2000). Education "vaccine" against HIV/AIDS. Current Issues in Comparative Education, 3(1).
Wawer, M.J., Serwadda, D., Gray, R. (1997). Trends in HIV-1 prevalence may not reflect trends in incidence in mature epidemics: data from the Rakai population-based cohort, Uganda. AIDS, 11, 1023-1030.
Weiser, S., Wolfe, W., Bangsberg, D., Thior, I., Gilbert, P., Makhema, J., et al. (2003). Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. Jaids-Journal of Acquired Immune Deficiency Syndromes, 34(3), 281-288.
Wenger, N., Gifford, A., Liu, H., Chesney, M., & Golin, C. (1999). Patient characteristics and attitudes associated with HAART adherence. Paper presented at the 6th Conference on Retroviruses and Opportunistic, Inecyions, Chicago.
Wilkins, A., Hayes, R., Alonso, P., Baldeh, S., Berry, N., Cham, K., et al. (1991). Risk-Factors for Hiv-2 Infection in the Gambia. Aids, 5(9), 1127-1132.
World Bank. (1997). Confronting AIDS: Public Priorities in a Global Epidemic. In. Oxford: Oxford University Press.
6
Copyright © 2022 FDOKUMEN