
PREVENTING HIV/AIDS IN YOUNG PEOPLE
357
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of PREVENTING HIV/AIDS IN YOUNG PEOPLE


The World Health Organization was established in 1948 as a specialized agency ofthe United Nations serving as the directing and coordinating authority for internationalhealth matters and public health. One of WHO’s constitutional functions is to provideobjective and reliable information and advice in the field of human health, a respon-sibility that it fulfils in part through its extensive programme of publications. TheOrganization seeks through its publications to support national health strategies andaddress the most pressing public health concerns of populations around the world.To respond to the needs of Member States at all levels of development, WHO pub-lishes practical manuals, handbooks and training material for specific categories ofhealth workers; internationally applicable guidelines and standards; reviews and anal-yses of health policies, programmes and research; and state-of-the-art consensusreports that offer technical advice and recommendations for decision-makers. Thesebooks are closely tied to the Organization’s priority activities, encompassing diseaseprevention and control, the development of equitable health systems based on pri-mary health care, and health promotion for individuals and communities. Progresstowards better health for all also demands the global dissemination and exchange ofinformation that draws on the knowledge and experience of all WHO’s Member coun-tries and the collaboration of world leaders in public health and the biomedicalsciences. To ensure the widest possible availability of authoritative information andguidance on health matters, WHO secures the broad international distribution of itspublications and encourages their translation and adaptation. By helping to promoteand protect health and prevent and control disease throughout the world, WHO’sbooks contribute to achieving the Organization’s principal objective — the attainmentby all people of the highest possible level of health.
The WHO Technical Report Series makes available the findings of various interna-tional groups of experts that provide WHO with the latest scientific and technicaladvice on a broad range of medical and public health subjects. Members of suchexpert groups serve without remuneration in their personal capacities rather than asrepresentatives of governments or other bodies; their views do not necessarily reflectthe decisions or the stated policy of WHO. An annual subscription to this series,comprising about six such reports, costs CHF 168.00/US$ 106.00 (CHF 128.40/US$ 115.00 in developing countries). For further information, please contact: WHOPress, World Health Organization, 20 avenue Appia, 1211 Geneva 27, Switzerland(tel. +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]; order online: http://www.who.int/bookorders).
92-4-120938-0_FM_a

92-4-120938-0_FM_b

WHO Technical Report Series938
PREVENTING HIV/AIDSIN YOUNG PEOPLE
A SYSTEMATIC REVIEW OF THEEVIDENCE FROM DEVELOPING COUNTRIES
UNAIDS Inter-agency Task Team on Young People
Edited byDavid A. Ross, Bruce Dick & Jane Ferguson
92-4-120938-0_FM_i

WHO Library Cataloguing-in-Publication Data
Preventing HIV/AIDS in young people : a systematic review of the evidence from developing countries :UNAIDS interagency task team on HIV and young people / editors: David Ross, Bruce Dick, Jane Ferguson.
(WHO technical report series ; no. 938)
1.HIV infections - prevention and control. 2.Acquired immunodeficiency syndrome- prevention and control. 3.Adolescent. 4.Sex education. 5.Program evaluation.6.Developing countries. I.Ross, David A. II.Dick, Bruce. III.Ferguson, Jane. IV.WorldHealth Organization. V.Series.
ISBN 92 4 120938 0 (NLM classification: WC 503.6)ISBN 978 92 4 120938 0ISSN 0512-3054
© World Health Organization 2006
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, WorldHealth Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 7914857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications –whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address(fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expressionof any opinion whatsoever on the part of the World Health Organization concerning the legal status of anycountry, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsedor recommended by the World Health Organization in preference to others of a similar nature that are notmentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initialcapital letters.
All reasonable precautions have been taken by the World Health Organization to verify the informationcontained in this publication. However, the published material is being distributed without warranty of any kind,either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader.In no event shall the World Health Organization be liable for damages arising from its use.
The named authors alone are responsible for the views expressed in this publication.
Typeset in IndiaPrinted in Geneva
92-4-120938-0_FM_ii

Table of contents
1. Introduction and rationaleBruce Dick, Jane Ferguson, & David A. Ross1.1 Background 1.2 Young people, HIV/AIDS and the global goals 1.3 Priorities for action 1.4 Objectives and limitations 1.5 Process and methodology 1.6 Scope and limitations of the data 1.7 Challenges in interpreting the findings and follow up
2. Young people: the centre of the HIV epidemicRoeland Monasch & Mary Mahy2.1 Introduction 2.2 Data and methods 2.3 Types of epidemics 2.4 Progress towards UNGASS commitments 2.5 Limitations of the data 2.6 Conclusions
3. Overview of effective and promising interventions to preventHIV infectionJudith D. Auerbach, Richard J. Hayes, & Sonia M. Kandathil3.1 Introduction 3.2 Interventions to change behaviour 3.3 Biomedical interventions: evaluating technologies 3.4 Social interventions 3.5 Behavioural and social issues in developing and
implementing interventions 3.6 Conclusion
4. The weight of evidence: a method for assessing thestrength of evidence on the effectiveness of HIV preventioninterventions among young peopleDavid A. Ross, Danny Wight, Gary Dowsett, Anne Buvé, &Angela I.N. Obasi4.1 Introduction 4.2 Types of interventions and evidence on effectiveness 4.3 Thresholds for strength of evidence needed for widespread
implementation 4.4 What information do policy-makers need? 4.5 Assessing the quality of an intervention 4.6 Types of evidence and their relative weight 4.7 Conclusion
1124579
10
15161717243435
4343445158
6163
798081
8488919298
iii
92-4-120938-0_FM_iii

5. The effectiveness of sex education and HIV educationinterventions in schools in developing countriesDouglas Kirby, Angela Obasi, & B.A. Laris5.1 Introduction and background 5.2 Methods 5.3 Findings 5.4 Discussion and recommendations
6. Review of the evidence for interventions to increase youngpeople’s use of health services in developing countriesBruce Dick, Jane Ferguson, Venkatraman Chandra-Mouli,Loretta Brabin, Subidita Chatterjee, & David A. Ross6.1 Introduction 6.2 Methods 6.3 Findings 6.4 Discussion 6.5 Conclusions
7. The effectiveness of mass media in changing HIV/AIDS-related behaviour among young people in developingcountriesJane T. Bertrand & Rebecca Anhang7.1 Introduction 7.2 Methods 7.3 Findings 7.4 Discussion
8. The effectiveness of community interventions targeting HIVand AIDS prevention at young people in developingcountriesEleanor Maticka-Tyndale & Chris Brouillard-Coyle8.1 Introduction 8.2 Methods 8.3 Findings 8.4 Go, ready, steady, do not go 8.5 Conclusions
9. Achieving the global goals on HIV among young people mostat risk in developing countries: young sex workers, injectingdrug users and men who have sex with menOliver Hoffmann, Tania Boler, & Bruce Dick9.1 Introduction 9.2 Methods 9.3 Findings 9.4 Discussion
103104111117142
151152153158191199
205206207226236
243244244247276281
287288289293306
iv
92-4-120938-0_FM_iv

10. Conclusions and recommendationsJane Ferguson, Bruce Dick, & David A. Ross10.1 Introduction 10.2 The road to “Steady, Ready, Go” 10.3 Results 10.4 Discussion 10.5 Recommendations
Glossary
Acknowledgements
317317319322328335
343
347
v
92-4-120938-0_FM_v

92-4-120938-0_FM_vi

1. Introduction and rationaleBruce Dick,a Jane Ferguson,a & David A. Rossb
1.1 Background
In 1995, WHO in collaboration with UNFPA and UNICEF convened a studygroup on programming for adolescent health and development. One of theproducts of this group was a joint technical report publication on Program-ming for adolescent health and development (1). The report synthesized theevidence for the effectiveness of interventions for adolescent health and de-velopment, and it set the direction and provided the conceptual frameworkfor much of the programming for young people’s health and developmentthat has taken place since its publication (2–6).
The challenges posed by HIV have progressed inexorably during the pastdecade, especially for young people in developing countries. (Young peopleare defined in this report as those aged 10–24 years; this group combinesadolescents – aged 10–19 years – and youth – aged 15–24 years). At the sametime, many lessons have been learnt about developing and implementingprogrammes for young people’s health and development, including pro-grammes to prevent the spread of HIV. In 2004, the UNAIDS Inter-AgencyTask Team on Young People decided that it was time to review the progressthat had been made and to look again at the evidence for the effectiveness ofinterventions, focusing explicitly on interventions to prevent the spread ofHIV among young people in developing countries.
This report is an attempt to rise to the challenge by providing systematicreviews of the evidence for policies and programmes to decrease HIV preva-lence among young people, as a contribution towards achieving universalaccess to prevention, treatment and care (7) and attaining the MillenniumDevelopment Goal on AIDS (8).
a Department of Child and Adolescent Health and Development, WHO, Geneva, Switzerland.Correspondence should be sent to Bruce Dick (email: [email protected]).
b Infectious Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine,London, England.
1
92-4-120938-0_CH01_1

1.2 Young people, HIV/AIDS and the global goals
During the past 20 years, and despite the continued lack of an effective vac-cine, the armamentarium for preventing the transmission and decreasing theimpact of HIV and AIDS has slowly grown (9, 10) (see also chapter 3).
HIV/AIDS has its roots in a range of problems that undermine people’s healthand human rights, such as inequity and discrimination, poverty, social unrestand migration, exploitation and abuse. Changing these structural and con-textual determinants (11) will be fundamental to making the prevention ofHIV sustainable. However, there have been growing experiences with a rangeof shorter-term interventions that have been directed towards encouragingpeople to avoid the behaviours that underlie the transmission of HIV or toreduce the risk associated with these behaviours (9).
To achieve widespread implementation of these preventive interventionsmany things will need to be done through many sectors and by many actors.At the same time, it will be important to ensure that the interventions reachthose people who are vulnerable and most at risk of becoming infected withHIV, both in terms of where the virus is and where the virus is going, as thepandemic develops and matures.
Young people make up a segment of the population that is particularly vul-nerable to HIV. Altogether, 50% of HIV transmission takes place amongthose aged 15–24, and 5 000–6 000 young people become infected every day(12, 13). The second decade of life is a period of experimentation and risk,and many factors increase young people’s vulnerability to HIV during theseyears of rapid physical and psychosocial development. These factors includea lack of knowledge about HIV/AIDS, lack of education and life skills, pooraccess to health services and commodities, early sexual debut, early marriage,sexual coercion and violence, trafficking and growing up without parents orother forms of protection from exploitation and abuse.
In recognition of young people’s vulnerability to HIV/AIDS, the UnitedNations General Assembly Special Session on HIV/AIDS (14) (UNGASS onHIV/AIDS) outlined a number of goals and targets focusing on young peopleaged 15–24. These are based on the core elements of the joint WHO/UNFPA/UNICEF document Action for adolescent health: towards a commonagenda (2). The goals of UNGASS on HIV/AIDS build on and are reflectedin the commitments made at a range of other global fora (Box 1.1), includingthe International Conference on Population and Development’s programmeof action (known as ICPD+5) (15) and the United Nations Special Sessionon Children (16). The goals and targets endorsed during the UNGASS onHIV/AIDS not only focus on decreasing HIV prevalence among young peo-ple but also on promoting the core elements of the programme framework
2
92-4-120938-0_CH01_2

that was developed during the 1995 study group – that is, they focus onproviding access to information, skills and services as well as decreasingvulnerability.
The UNGASS on HIV/AIDS goals and targets help to unpack the prevalencegoal, and provide both light and heat for all people working to decrease thetransmission and impact of HIV and AIDS among young people. Achievingthese goals and targets will make an important contribution towards achievingthe goal of universal access to prevention, treatment and care, and this will
Box 1.1
Highlights of important goals for young people’s health and development, witha focus on HIV/AIDS
The UN General Assembly Special Session on Children (17)
Develop and implement national health policies and programmes foradolescents, including goals and indicators, to promote their physicaland mental health
The Millennium Development Goal on HIV/AIDS (7)
By 2015 halt and begin to reverse the spread of HIV/AIDS (using theprevalence of HIV among pregnant 15–24 year olds as an indicator)
The UN General Assembly Special Session on HIV/AIDS (14)
By 2005, ensure that at least 90% (and by 2010 that 95%) of youngpeople have access to the information they need to reduce their vul-nerability to HIV
By 2005, ensure that at least 90% (and by 2010 that 95%) of youngpeople have access to the skills they need to reduce their vulnera-bility to HIV
By 2005, ensure that at least 90% (and by 2010 that 95%) of youngpeople have access to the services they need to reduce their vul-nerability to HIV
By 2003, develop and/or strengthen strategies, policies and pro-grammes which reduce the vulnerability of children and youngpeople
By 2005 HIV prevalence among young people (15–24 years)reduced by 25% in the most affected countries, and by 2010 reduceprevalence by 25% globally
3
92-4-120938-0_CH01_3

be necessary, if not sufficient, to achieve the Millennium Development Goalthat aims to halt and begin to reverse the spread of HIV/AIDS.
1.3 Priorities for action
Now that there are global goals and targets, and a growing number of inter-ventions that may contribute to their achievement, it is important to synthesizethe evidence base for these interventions in ways that assist the decision-making of policy-makers and programme planners. Research findings needto help them decide how to most effectively allocate resources in differentepidemic settings and for different groups of young people. With 5 000–6 000 young people becoming infected with HIV every day, these are clearlydecisions that need to be taken today, despite the fact that the evidence maybe less than complete. We know that there is no magic bullet, and that a rangeof interventions will need to be implemented. We also know that many thingswill influence the choices made about which interventions to focus on, in-cluding moral opinions and political expediency. But the evidence of effec-tiveness needs to be one of them.
The decisions that need to be taken are made all the more difficult by the factthat evidence from multiple interventions is needed; the evidence for manyinterventions is weak; and most evidence comes from developed countries.In addition, it is not always clear what different groups – for example, re-searchers, programme managers and policy-makers – understand by the termevidence. And it is often not clear what they have used as evidence: random-ized controlled trials, quasi-experimental trial designs, recommendations ofbest practice, or anecdotes. So there is not only a need to be clear about theevidence but also to be more systematic, transparent and consistent about howthe available evidence is reviewed and assessed.
There is now wide consensus about the main settings through which youngpeople can be reached with preventive interventions; these include schools,health services, the mass media and through communities and outreach pro-grammes targeting the young people who are most at risk of HIV. Further-more, although the evidence of the effectiveness of interventions remainsincomplete for many of these settings, there is a growing research base fromwhich to draw, and this includes research from developing countries. In ad-dition, the global goals provide a range of outcomes that can be used to reviewthe evidence: decreased prevalence, decreased vulnerability and increasedaccess to relevant information, skills and services.
4
92-4-120938-0_CH01_4

1.4 Objectives and limitations
1.4.1 Objectives
The various chapters in this report focus on ways of meeting the global goalson young people and HIV. They also emphasize the sense of urgency thatshould accompany the drive to achieve these goals, as well as the need for aspecific emphasis on prevention, and within that, a focus on the young peoplewho remain at the centre of the HIV pandemic. The chapters also explore theneed to have a better understanding of the evidence base for making decisionsabout the allocation of resources, and they particularly focus on developingcountries.
This report has three specific objectives:
1. first, to clarify our collective understanding of the term “evidence” incomplex areas of programme development and delivery – such as theprevention of HIV among young people – and to develop a transparentmethodology for reviewing the effectiveness of different types of inter-ventions in different settings – such as schools, health services, the massmedia, within geographically defined communities and for services tar-geting the young people most at risk of HIV infection;
2. second, to provide a comprehensive review of the evidence on the effec-tiveness of interventions to prevent HIV among young people in devel-oping countries;
3. third, to inform the choices of policy-makers, people responsible forprogramme development and delivery, and researchers about interven-tions to achieve the global goals on HIV and young people that wereendorsed during the UNGASS on HIV/AIDS. The report also seeks toprovide decision-makers with guidance on which interventions they cansupport with confidence, which interventions need to be implementedmore cautiously along with careful evaluation of their impact on key healthoutcomes, which interventions require further development and demon-stration of effectiveness before they can be recommended for widespreadimplementation, and which interventions should not be implemented be-cause there is sufficient evidence of their lack of effectiveness.
The chapters in this report are divided into three sections.
Chapters 1, 2 and 3 provide an outline of the aims and objectives of thesubsequent chapters, a synthesis of the epidemiological data that describethe epidemic among young people and an overview of what is known aboutthe effectiveness of prevention interventions in general.
5
92-4-120938-0_CH01_5

Chapters 4, 5, 6, 7, 8 and 9 explain the methods used to review the evidenceand provides detailed reviews of the evidence from each of the key settingsthrough which young people can be reached by interventions for the pre-vention of HIV.
Chapter 10 contains the overall conclusions from the reviews of the evi-dence, including recommendations for policy-makers, programme devel-opment and delivery staff, and researchers.
1.4.2 Limitations
It is hoped that this report will make an important contribution to discussionsand decisions about priorities for action, by providing a snapshot of theknowledge base for the effectiveness of different interventions. It is alsoanticipated that this report will contribute to increasing the transparency ofhow the evidence for effectiveness is assessed. However, it is important tobe clear from the outset about some of the limitations of the scope and aimsof this report.
First, in order to limit the scope of each chapter, the authors have focused oninterventions that were primarily intended to prevent HIV transmission. Theyhave not dealt with studies that focused on providing treatment, care or sup-port for young people living with HIV and AIDS. This does not in any wayimply that treatment is unimportant or that treatment does not have the po-tential to make important contributions to prevention. Rapidly increasingaccess to effective HIV treatment is likely to provide many opportunities tostrengthen HIV prevention efforts as well as mitigate the impact of AIDS.These chapters have also not dealt with interventions designed to mitigate theimpact of HIV, for example interventions with orphans and other young peo-ple affected and made vulnerable by HIV and AIDS.
Second, chapters do not review structural interventions that primarily aim toprevent HIV by decreasing young people’s vulnerability, for example bydecreasing poverty, marginalization, stigma or discrimination. Many youngpeople are vulnerable to HIV as a result of belonging to a group or subcultureor living in a particular setting, because of the poor quality and coverage ofservices and other programmes available to them, or as a result of broadersocietal and environmental influences, including behavioural norms. Butagain this is not to imply that interventions that aim to alleviate these vul-nerabilities are unimportant. The decision not to focus on these types ofinterventions was based on preliminary work that indicated that althoughthere have been some successes, such as increasing the enrolment of adoles-cent girls in school, it is not always clear what can be done to change thedeterminants of vulnerability, and for those interventions that have been
6
92-4-120938-0_CH01_6

implemented the mechanisms of action are not clear and the evidence for theireffectiveness remains weak.
Third, the chapters have not reviewed evidence for the effectiveness ofinterventions in all settings where they could possibly be delivered. In par-ticular, they have not reviewed the evidence for the effectiveness of inter-ventions in the political environment – those delivered, for example, throughactivism, political commitment and policies that create a supportive envi-ronment to enable specific interventions to be implemented. Few rigorousstudies have looked at the effectiveness of actions to create a favourableenvironment for intervention delivery. Although a chapter reviewing suchinterventions was originally foreseen, a preliminary assessment indicated thatthere were insufficient studies to carry out a review using the methods appliedto the other settings included in this report.
Fourth, we have not reviewed the evidence for the effectiveness of interven-tions among all groups who are particularly at risk of HIV. For example, whilethere has been an explicit focus on young injecting drug users, young sexworkers and young men who have sex with men; young prisoners and youngmigrant workers have not received specific attention.
Finally, although the primary focus of this report is to examine interventionsaffecting young people in developing countries, we have had to refer to find-ings from developed countries in order to place the evidence in a widercontext. In some of the chapters, studies have also been included in whichthe interventions were directed towards populations that included young peo-ple but that did not disaggregate data by age.
1.5 Process and methodology
This report has been developed over a 2-year period. The process started inMay 2004, when a meeting was organized in Talloires, France. This meetingbrought together policy-makers, people who make decisions about pro-gramme development and delivery, and researchers who have an interest andexpertise in interventions to prevent HIV among young people. At this time,the participants reviewed a set of background papers that had been speciallyprepared for the meeting, and they made recommendations for improving thepapers and the methods used to review the evidence, and for developing ad-ditional papers.
Following this meeting the papers were re-drafted and additional paperswere developed. An information brief was prepared based on the outcome ofthe meeting (17), and presentations were made in different fora to assesswhether the approach that was being developed was useful to people makingdecisions about priorities for action. It was clear that the comprehensive
7
92-4-120938-0_CH01_7

and transparent approach, and the classification of the interventions as“Steady”, “Ready” and “Go”, resonated with policy-makers and programmedevelopers alike.
A second meeting was held in Gex, France, in March 2005. This meetingincluded the authors of the chapters and selected external advisers who alsoprovided further peer review and suggestions for refining the papers. Thiswas followed in June 2005 by a meeting in Chavannes, Switzerland, whichinvolved the editors of this report and reviewers from different regions whohad not previously been involved in the process. These reviewers were invitedto provide external review of the papers and to assist with developing theconclusions and recommendations. Final changes were made to the papersduring the second half of 2005, prior to the papers going through furtherexternal peer review and editorial review processes.
As described in more detail in the first paper in section 2, the authors ofchapters 5 to 9 in section 2 were asked to use the following approach to reviewthe evidence for the effectiveness of the interventions in their respectivesettings.
1. First, the interventions provided through each of the settings were to beclassified into different types of interventions based on common charac-teristics and the choices policy-makers and programme developers needto make in deciding what to do.
2. Second, the authors were asked to assess the strength of evidence (theevidence threshold) needed to recommend the widespread implementa-tion of the different types of interventions.
3. Third, authors were asked to assess the strength of the empirical evidenceavailable from the studies for each of the different types of interventions,in terms of specific outcomes as defined by the UNGASS goals on youngpeople, by grading the evidence using standard criteria.
4. Finally, this evidence was to be compared with the threshold of evidencerequired to recommend a particular type of intervention for widespreaduse and a decision made as to whether the threshold had been fully met,partially met, not met but had encouraging characteristics, or if there wasevidence of a lack of effectiveness.
Based on the categorizations in point number 4 each type of intervention wasclassified as “Do not go”, “Steady”, “Ready” and “Go”, as shown in Box 1.2.
For each of the settings, the authors have attempted to review the evidencein relation to the UNGASS goals and targets for young people and HIV/AIDS, to assess whether the interventions are effective in terms of increasingyoung people’s access to information, skills and services, decreasing their
8
92-4-120938-0_CH01_8

vulnerability to HIV and decreasing HIV prevalence. In some settings, theoutcome that has been the focus of the studies reviewed has been more lim-ited, for example the UNGASS goal on providing access to services for thehealth services setting. And in some cases, behavioural outcomes, such asdelaying sexual debut, decreasing the number of sexual partners, and in-creasing the consistent and correct use of condoms, have been used as proxyindicators for decreased prevalence. The assumption is that all of these be-haviours are important in preventing the spread of HIV and that the balancebetween them is likely to vary depending on the specific groups of youngpeople under consideration and the contexts in which they live.
1.6 Scope and limitations of the data
A number of factors need to be considered when reviewing and interpretingthe findings of the chapters in this report. First, in general the findings showthat despite the importance of young people in the HIV/AIDS pandemic,surveillance and monitoring data are often unavailable for them; data that arecollected are frequently not disaggregated by age; and many important indi-cators are not routinely collected (18). These issues have their roots in a much
Box 1.2
Categorization of types of interventions
Category CriteriaGo Evidence threshold met
Sufficient evidence to recommend widespreadimplementation on large scale now, as long as there iscareful monitoring of coverage, quality and cost, andoperations research is implemented to better understandthe mechanisms of action
Ready Evidence threshold partially metEvidence suggests interventions are effective but large-scale implementation must be accompanied by furtherevaluation and operations research to clarify impact andmechanisms of action
Steady Evidence threshold not metSome of the evidence is promising but furtherdevelopment, pilot-testing and evaluation are neededbefore it can be determined whether these interventionsshould move into the “Ready” category or “Do not go”
Do not go Strong enough evidence of lack of effectiveness or of harmNot the way to go
9
92-4-120938-0_CH01_9

more widespread problem: good research on young people in developingcountries remains scarce.
Second, there is wide variability in the research that is available in differentsettings, with schools, for example, having a much more extensive evidencebase than interventions to reach the young people who are most at risk. Thisreflects a number of factors, from the ease with which research can be carriedout in different settings to the priorities of researchers and the people whofund research.
Third, despite extensive efforts by the authors to identify relevant researchstudies and programme reports, there is never enough time to access all eval-uations, particularly those published in the grey literature and in differentlanguages. Linked to this is the much more general problem of reporting biaswith which all authors had to contend: negative evaluations are generallymuch less likely to be published.
Fourth, few studies have included any costing data, and this has importantimplications for decision-makers as they try to use the evidence to chooseinterventions. However, attempts have been made to take this into consider-ation when assessing the threshold of evidence required to categorize thevarious types of interventions.
Finally, it is clear that much is going on that is not evaluated. So it is importantto remember that just because an intervention has not been evaluated scien-tifically or an evaluation has not been made accessible in the publishedliterature it does not necessarily mean that it is not effective.
1.7 Challenges in interpreting the findings and follow up
This report is timely, especially in view of the attention that is being paid tothe challenge of achieving universal access to HIV prevention interventions,treatment and care. While young people are at the centre of the epidemic’stransmission and impact, they are certainly not at the centre of the resources,and have been pushed even farther away as a result of the growing focus ontreatment.
One of the most important issues that will affect the interpretation and useof the findings in this report is context. Contextual factors are important notonly in terms of the transmission and impact of HIV but also in relation tothe implementation of interventions, which is affected by the availabilityof resources and the broader socioeconomic environment. The context isalso important because HIV touches on many issues that are sensitive in arange of cultural, religious and political settings. This is particularly anissue for young people because sex is at the heart of most HIV transmission,albeit frequently coerced sex, and because many of the groups who are most
10
92-4-120938-0_CH01_10

seriously affected are already suffering from marginalization, discriminationand stigma. Young people are not all alike and the epidemic itself is differentin different countries, even between different subgroups within a specificcountry. This is likely to have important repercussions that need to be con-sidered when deciding on the intervention mix.
For all of the settings, it was frequently impossible for authors to find suffi-cient details of the interventions and the outcomes from published reports ofthe original studies. These problems were compounded by the challenge ofinterpreting the findings of interventions that contained a number of differentcomponents.
The intention of this report was to focus on HIV. However, HIV and AIDSare associated with other problems that undermine young people’s health anddevelopment, that grow from common roots and that frequently are linked interms of cause and effect, for example alcohol and drug use, gender-basedviolence, sexually transmitted infections and pregnancy. Making the linksbetween the evidence base for interventions to prevent HIV among youngpeople and that from other issues facing young people will clearly be impor-tant both in interpreting and building on the findings in this report.
In the Conclusion and recommendations chapter there are clear messagesfor policy-makers, programme developers and researchers about how tomove interventions from “Ready” to “Go” and from “Steady” to “Ready” or,depending on the evidence, to “Do not go”. However, all of the authors real-ize that their reviews will not answer all the questions that policy-makers,programme developers and researchers might have after reading the reportand that decisions will still be difficult. Challenges that will need to be facedinclude addressing issues of replicability, adaptation, cost and sustainability;ensuring the quality of the interventions as they are scaled-up; understandingthe individual components of complex interventions and how they interact;determining the suitability of different interventions and intervention mixesfor different phases of the epidemic; achieving clarity about what is effec-tive “in the laboratory” and what is known about implementing effectiveinterventions in the real world; being able to more clearly define the contentof information, skills and services for different groups in different cul-tures; and knowing more about the “how” of interventions in addition tothe “what”.
This report provides one perspective on defining priorities for action, and theauthors hope that it will contribute to ongoing discussions and debates andwill be enriched by other methods of assessing the evidence. If we are toengage the people responsible for policies, programmes, and resource allo-cation in order to give young people the attention that they warrant and toaccelerate action for achieving the global goals, it will be necessary to make
11
92-4-120938-0_CH01_11

a compelling case for action, be clear about what needs to be done (based onthe evidence) and demonstrate that what needs to be done is doable on areasonable scale in a reasonably sustainable way. This report focuses partic-ularly on the first and second of these issues and has prepared the foundationsfor the third. The challenge for a report in 2015 will be to demonstrate thatwhat needs to be done, has be done.
References
1. WHO. Programming for adolescent health and development: report of a WHO/UNFPA/UNICEF study group. Geneva, WHO, 1999 (Technical Report SeriesNo. 886).
2. WHO. Action for adolescent health: towards a common agenda.Recommendations from a joint study group. Geneva, WHO, 1997.
3. Pathfinder International, Focus on Young Adults. Advancing young adultreproductive health: actions for the next decade, 2001 (http://www.pathfind.org/pf/pubs/focus/pubs/eop_report.pdf).
4. Family Health International. YouthNet: partners in reproductive health and HIVprevention, 2005 (http://www.fhi.org/en/Youth/YouthNet/About/index.htm).
5. African Youth Alliance. What is AYA?, 2005 (http://www.ayaonline.org/overview.htm).
6. EU/UNFPA Reproductive Health Initiative for Youth in Asia. What is RHIYA?,2006 (http://www.asia-initiative.org/rhiya_in_brief_what.html).
7. UNAIDS. The road towards universal access: scaling up access to HIVprevention, treatment, care and support, 2006 (http://data.unaids.org/pub/Periodical/2006/Universal_Access_bulletin_8_en.pdf?preview=true).
8. United Nations. What are the Millennium Development Goals?,(http://www.un.org/millenniumgoals/).
9. Global HIV Prevention Working Group. Global mobilization for HIV prevention,a blueprint for action, 2002 (http://www.kff.org/hivaids/loader.cfm?url=/commonspot/security/getfile.cfm&PageID=14190).
10. UNAIDS. Intensifying HIV prevention: a UNAIDS policy position paper. Geneva,UNAIDS, 2005.
11. UNAIDS. Sex and youth: contextual factors affecting risk for HIV. Geneva,UNAIDS, 1999.
12. UNICEF, UNAIDS, WHO. Young people and HIV/AIDS – opportunity in crisis.New York, UNICEF, 2002.
13. UNAIDS, WHO. AIDS epidemic update: December 2005,(http://data.unaids.org/Publications/IRC-pub06/epi_update2005_en.pdf).
14. United Nations. Declaration of commitment on HIV/AIDS. United NationsGeneral Assembly Special Session on HIV/AIDS, 2001 (http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html).
15. United Nations. Key actions for the further implementation of the Programmeof Action of the International Conference on Population and Development:report of the Ad Hoc Committee of the Whole of the Twenty First SpecialSession of the General Assembly. New York, United Nations, 1999.
12
92-4-120938-0_CH01_12

16. United Nations. A world fit for children. United Nations Special Session onChildren, 2002 (http://www.unicef.org/specialsession/wffc).
17. WHO. “Steady, Ready, GO!”: an information brief on the global consultation toreview the evidence for policies and programmes to achieve the global goalson young people and HIV/AIDS, 2004 (http://www.who.int/child-adolescent-health/publications/ADH/IB_SRG.htm).
18. WHO. National AIDS programmes: a guide to indicators for monitoring andevaluating national HIV/AIDS prevention programmes for young people.Geneva, WHO, 2004.
13
92-4-120938-0_CH01_13

92-4-120938-0_CH01_14

2. Young people: the centre of the HIVepidemicRoeland Monascha & Mary Mahyb
Objectives This chapter reviews data on the situation of young people andHIV/AIDS. It assesses whether young people have access to the information,skills and services required to reduce their vulnerability and whether therehas been any reduction in HIV prevalence among 15—24-year-olds.
Methods We reviewed the data on knowledge, behaviour, life skills, accessto services and HIV prevalence among young people from nationally repre-sentative household surveys, antenatal care surveillance reports, behaviouralsurveillance surveys, a global coverage survey and other special studies.
Findings In countries where HIV is concentrated among sex workers, in-jecting drug users or men who have sex with men, high-risk behaviourcommences for most during adolescence, and large proportions of these high-risk populations are younger than 25 years. In countries with generalizedepidemics, the epidemic is also driven by young people. Half of all new in-fections in sub-Saharan Africa occur among this group. Many young peopledo not have the basic knowledge and skills to prevent themselves from be-coming infected with HIV. Young people continue to have insufficient accessto information, counselling, testing, condoms, harm-reduction strategies andtreatment and care for sexually transmitted infections. Other socioeconomicfactors beyond the control of individuals need to be addressed. Countries thathave reported a decline in HIV prevalence have recorded the biggest changesin behaviour and prevalence among younger age groups.
Conclusions The epidemic varies greatly in different regions of the world,but in each of these epidemics young people are at the centre, both in termsof new infections as well as being the greatest potential force for change ifthey can be reached with the right interventions.
a United Nations Children’s Fund, 6 Fairbridge Avenue, Belgravia, Harare, Zimbabwe.Correspondence should be sent to Dr Monasch (email: [email protected]).
b UNICEF, New York, NY, USA.
15
92-4-120938-0_CH02_15

2.1 Introduction
Globally, an estimated 40 million people were living with HIV/AIDS at theend of 2005 (1). More than 10 million of them are young people aged 15–24years. Half of the 4.2 million new infections in adults in 2005 occurred in thisage group. Each day 5 000–6 000 new infections occur among young people.Sub-Saharan Africa contains almost two thirds of all young people living withHIV or AIDS (6.2 million); 76% of them are female (Figure 2.1). The regionwith the second highest prevalence is Asia, which has an estimated 2.2 millionyoung people who are living with the virus. The regions where young peopleaccount for the biggest share of the overall number of infections are easternEurope and Central Asia, where nearly half of adults living with HIV or AIDS(600 000/1.3 million) are younger than 25 years; most of them are male.
A clear understanding of the situation of young people and their needs isrequired to design and successfully implement interventions to stem the tideof infections among young people. Without this information, the scale of theresponse required and the focus and relative urgency of the interventionsremain unknown. Governments must strategically target their resources tointerventions that respond to the specific situation in each individual country.
This information also allows governments to measure how well they aremoving towards reaching the goals that have been agreed as being necessary
Figure 2.1Worldwide prevalence of HIV among young women and men aged 15–24 years. (Thesize of the pie chart indicates the size of the population affected)
70%30%
24%
76%
40%
60%
South and South East Asia1.8 million
High IncomeCountries188,000
68%
32%
Middle East & North Africa118,000
Central Asia and Eastern Europe
630,000
East Asia & Pacific351,000
Sub-Saharan Africa6.2 million
28%72%
38%62%
Latin America610,000
31% 69%
Caribbean125,000
29%71%
Source: UNAIDS, UNICEF 2004 (Updated from reference (70))
16
92-4-120938-0_CH02_16

to slow the epidemic and that were defined in the Millennium DevelopmentGoals. During the UN General Assembly Special Session on HIV/AIDS(UNGASS), 189 governments committed themselves to meeting specificgoals in the fight against the HIV/AIDS pandemic; these goals included spe-cific targets for young people (2). This paper reviews the data on the situationof young people in relation to the UNGASS goals and looks specifically atwhether young people have access to the information, skills and services thatthey need to reduce their vulnerability and whether there has been any re-duction in HIV prevalence among 15–24 year olds.
2.2 Data and methods
Data on knowledge, sexual behaviour and life skills among the general pop-ulation of young people were tabulated from nationally representative house-hold surveys, such as the Demographic and Health Surveys (3) and theMultiple Indicator Cluster Surveys (4). These surveys use similar methodsand instruments to ensure that data are comparable between survey roundsand between countries (5). Data on vulnerable groups with high risk be-haviour come mainly from Behavioral Surveillance Surveys and other specialstudies. Information on access to services comes from a 2003 coveragesurvey implemented by the Policy Project (6). HIV prevalence data are prin-cipally based on information from country surveillance reports and theepidemiological fact sheets available from UNAIDS, WHO and UNICEF(7). In addition, data were used from EuroHIV (8), which collects routinelyreported data from countries in Europe and Central Asia, but, because theyare based on HIV diagnoses reported through the health system, they maysubstantially underestimate the true population prevalence.
2.3 Types of epidemics
Young people are exposed to HIV infection in different ways depending onthe type of epidemic present in the country in which they live. In this section,the situation of young people living in countries with a low-level epidemic,a concentrated epidemic or a generalized epidemic is reviewed. In low-levelepidemics HIV may have been recorded for many years, but prevalence hasnever consistently exceeded 5% in any subpopulation. In concentrated epi-demics, HIV is well established in subpopulations with behaviours known toput them at high risk, such as injecting drug users, sex workers or men whohave sex with men. In concentrated epidemics, HIV prevalence consistentlyexceeds 5% in at least one of these groups, but there is no sign of substantialspread beyond these groups. Countries where HIV has spread to the generalpopulation – with more than 1% HIV prevalence among pregnant women –are said to have generalized epidemics (9). These exact values do not preciselydelineate where a concentrated epidemic ends and a generalized epidemic
17
92-4-120938-0_CH02_17

begins. However, these classifications are useful for understanding the trans-mission routes that drive epidemics and are critical for developing appropriateresponses.
2.3.1 Concentrated epidemics
2.3.1.1 Injecting drug users
Sharing needles and syringes with an infected person is the most efficientmeans of transmitting HIV. People who share injecting equipment are there-fore at high risk of contracting HIV. In eastern Europe and many Asiancountries, most of the reported HIV infections are linked to drug injecting.Data on known sources of infection in this region show that more than 55%are the result of intravenous drug use (Table 2.1). An estimated 60–70% ofreported HIV infections in China occur among injecting drug users (10). In-jecting drug users also often engage in other high-risk activities that exposethem and their partners to an increased risk of heterosexual transmission (1).
There has been a marked growth in the use of injected drugs in eastern Europesince 1990 (11). In the Russian Federation an estimated 1–2% of the adultpopulation injects drugs (12), and the use of injected drugs has become par-ticularly widespread among young people, especially young men. Accordingto the Ministry of Health in Russia, since 1991 the number of teenage drugusers has grown 18-fold. A survey of adolescents in Moscow found that 8%of young people overall, and 12% of young males, had injected drugs (13).
Data from a number of countries in eastern Europe and Asia confirm that drugabuse often begins during adolescence (14). A review of studies suggestedthat at least half of injecting drug users in Russia are aged 25 years or youngerand that on average they inject drugs for about 3–4 years. Most studies esti-mate that the average age at first use of injected drugs is between 18 and 20years, although some suggest that the average age at first use may be falling(14). In Saint Petersburg, Russia, almost one third of injecting drug users areyounger than 19 years. In Ukraine, 20% of injecting drug users are adoles-cents (15). In a study in five cities in India, 24% of respondents reported thatthey started injecting drugs before the age of 20 (16). In Indonesia, 70% ofinjecting drug users were younger than 25 years (17).
The combination of being an injecting drug user and being young potentiallyincreases the risk of becoming infected with HIV. For example, in Kaza-khstan, where 54% of injecting drug users are younger than 25, young peoplewere more likely to share needles and inject in a group than older drug users(18). Limited age-specific data on HIV infection among injecting drug usersshows that large proportions of young injecting drug users are infected. Inthe city of Togliatti in Russia, 65% of all injecting drug users were younger
18
92-4-120938-0_CH02_18

than 20, and 55% of injecting drug users aged 20–24 years were HIV positive(14). In Santos, Brazil, 56% of injecting drug users who were younger than25 years were HIV positive (19).
Data from Central Asia show that 48% of people diagnosed with HIV andsuspected of having become infected through the use of injected drugs wereaged 15–24 years. In eastern Europe, 40% of newly diagnosed HIV infectionsamong injecting drug users were estimated to occur among those aged 15–24 years. Young people in Belarus have been particularly affected: 60% ofthose living with HIV are aged between 15 and 24 years (20). In westernEurope this ratio is lower, but still significant at 19% (Table 2.1).
2.3.1.2 Sex workers
Sex workers are at an increased risk of HIV because they engage frequentlyin sexual acts with multiple partners; and their clients are also at an increasedrisk. HIV prevalence among female sex workers is therefore much higherthan among the general population. In Myanmar, HIV prevalence among sexworkers in 2004 was estimated to be 27% compared with 1.8% among preg-nant women (21). A study in Ghana found prevalences of HIV among sexworkers as high as 40% , while the prevalence among the general populationwas only 3% (22). And in Ecuador, sex workers had an HIV prevalence of11%, while among the general population it was estimated to be 0.3% (23).
Data from behavioural surveillance surveys of female sex workers show thata large majority are younger than 25 years of age. For example, in Cambodia
Table 2.1Percentage of HIV diagnoses among young people aged 15–24 years by risk group,Europe and Central Asia, 1993-2003
Risk group
Region Injectingdrug usersa
Homosexualor bisexual
Heterosexual Other Total
WesternEurope
19 (19 093) 10 (54 742) 13 (49 628) 10 (53 138) 12 (176 601)
CentralEurope
40 (5 740) 14 (2 033) 15 (2 977) 11 (10 355) 19 (21 105)
CentralAsia
48 (180 612) 21 (1 176) 33 (26 195) 52 (116 125) 48 (324 108)
Source: Data provided by EuroHIV 2004 (8)a Values are percentages (numbers) of infections. Percentages are weighted by the number of
infections in the region.
19
92-4-120938-0_CH02_19

(24), China (10), Lao People’s Democratic Republic (25), Myanmar (26), theRussia Federation (27) and Viet Nam (28), between 60% and 70% of sexworkers were younger than 25 years of age. Estimates of the absolute numberof young people involved in sex work are limited and range widely. In Thai-land it is estimated that between 27 500 and 35 000 children (younger than18) are engaged in sex work (29).
Sex work often starts at an early age. A rapid assessment in 74 establishmentsin four urban areas in Viet Nam found that 37% were children (< 18 years)at the time of the survey (30). In Jamaica, 50% of female sex workers reportedthat they had begun sex work by their 18th birthday (31). In Djibouti, 63%of female sex workers reported that they were younger than 20 when theyfirst had sex, with about 14% reporting that they were younger than 16 (32).
Evidence from surveys suggests that these young sex workers are at high riskof acquiring HIV. In Eritrea, a survey found that 12% of female sex workersaged 15–19 years and 24% of those aged 20–24 years were HIV positive(33). In Myanmar, 41% of female sex workers aged 15–19 years and 20–24years were HIV positive (34). However, evidence from Cambodia suggeststhat young sex workers may also benefit most rapidly from effective inter-ventions. Cambodia is one of the rare countries where HIV/AIDS preventionefforts have led to a decline in HIV prevalence among both high-risk groupsand the general population. HIV prevalence in Cambodia, while still thehighest in Asia, has dropped among the general population, from 3% in 1997to 1.9% in 2003, and among female brothel-based sex workers, from 43% in1998 to 21% in 2003 (35). HIV prevalences have declined most dramaticallyamong younger sex workers (36). A decline in prevalence among female sexworkers has also been reported in Benin and Côte d’Ivoire (37, 38).
Many clients of sex workers are also young. Data from behavioural surveysin India (39) and Nepal (40) show that between 17% and 70% of clients areyoung people, with the majority aged 20–24 years. In Kosovo, 18% of clientssurveyed were younger than 20 years, and 20% were aged 20–24 years (41).
Clients who are younger than 25 are more likely to use condoms consistently(an important factor in reducing the prevalence among sex workers) (42). Astudy in the Dominican Republic also found that men who were younger than25 were more likely to consistently use a condom compared with older men(43). The success of Thailand’s “100% condom” programme, which man-dated the use of condoms in brothels, has been well documented (44). Lesswell known is the success of the country’s efforts to alter long-establishednorms regarding male patronage of commercial sex businesses. Between1990 and 1993, the percentage of men who reported having visited brothelsduring the prior 12 months fell dramatically. The decline was especially no-table among young men aged 20–24 years (45).
20
92-4-120938-0_CH02_20

2.3.1.3 Men who have sex with men
Sexual transmission of HIV between men, which occurs principally duringanal sex, is an important factor driving the epidemic not only in the industri-alized world but also in a number of countries in Latin America and in somecountries in Asia. Men who have unprotected anal sex with other men are atincreased risk of HIV infection (46). In Argentina 14% of men who hadsex with men were HIV positive, and in El Salvador 18% of men who hadsex with men were HIV positive compared with 0.7% of the general popu-lation (47).
A substantial proportion of men who have sex with men are younger than 25.In behavioural studies among this group in five countries in Central America,carried out at places where men meet other men, such as gay bars, discos andother public areas, 20% of those surveyed were found to be younger than 20,and 34% were aged 20–24 years (48). In a study in Lima, Peru, conductedamong men who have sex with men 50% were younger than 25, and 18% ofthe men (of all ages) were HIV positive. In Central Asia and eastern Europe,14–20% of new diagnoses attributed to transmission by men having sex withmen have been reported to occur among young people aged 15–24 years; inwestern Europe this proportion was 10% (Table 2.1). Unfortunately, fewstudies have reported data disaggregated by age, which makes it difficult tocompare the behaviour of and prevalence among young men and older men.
Evidence from Cambodia suggests that young men who have sex with mentend to start having sex at an earlier age than young men who have sex withwomen. In Cambodia the reported mean age at first sexual intercourse was17.7 years among men having sex with men, whereas the average age amongthe general population of males in Cambodia was 22 years (49). Additionally,young people may be disproportionately represented among male sexworkers. In a study in Moscow, 40% of male commercial sex workers wereaged 19 years or younger, with another 45% being between the ages of 20and 24 (50).
2.3.1.4 Bridging to the general population
Transmission of HIV from groups with high prevalence to other groups islikely, and the future occurrence of a generalized epidemic in countries cur-rently experiencing concentrated epidemics cannot be ruled out (51). Youngpeople will be an important bridge between different population groups. Forexample, young injecting drug users are likely to be sexually active, whichmay put their partners at increased risk of HIV in addition to the risks posedby the high rates of sexually transmitted infections (STIs) and hepatitis thathave been documented among injecting drug users (52). In India, a survey ofinjecting drug users found that more than one quarter were currently married
21
92-4-120938-0_CH02_21

and living with their spouse (16). In a study in Cambodia, one fifth of menwho said they had had sex with men during the 6 months before the studyreported also having had sex with one or more women (49).
A study among male injecting drug users (63% of whom were younger than25) in three Indonesian cities found that 35% had had unprotected commercialsex and 29% had had sex with a casual female partner in the 12 months priorto the survey (53). In Russia a survey among young female sex workers foundthat 93% had injected drugs during the past 12 months, with the median ageat first use of injecting drugs being 18.7 years; one third of adolescent sexworkers were HIV positive. Altogether, 63% of the sex workers were aged20–24 years (54).
Mobile populations and migrants are important “bridging populations” thattake HIV to the general population (55). Studies on highly mobile groupshave identified travel and migration as important factors related to infectionas the mobile groups come into contact with networks of high-risk groups(56–58). For example, in Kenya a survey showed that men who slept awayfrom their house five or more times in the 12 months prior to the survey hadthree times the risk of being infected with HIV than did men who did notsleep away from home (59). In one community in Nepal, HIV prevalence was8 times higher among migrants than non-migrants (60). Young people areoften involved in migration because they have the most to gain economicallyby starting out in a new setting. A study in Myanmar found that the majorityof migrants were aged 14 to 18 years, and that most were migrating for eco-nomic reasons (61). In Estonia a survey found that 17% of young people (aged17–27 years) had already worked abroad (62).
2.3.2 Generalized epidemics
In generalized epidemics the main mode of HIV transmission is through pen-etrative heterosexual sex in the general population. Such epidemics arecurrently found mainly in sub-Saharan Africa and in some countries in theCaribbean. Generalized epidemics are also driven by young people: half ofall new infections in sub-Saharan Africa are estimated to occur among thosebetween the ages of 15 and 24 years (23). In sub-Saharan Africa HIV preva-lence varies considerably across the continent, ranging from less than 1% inSenegal to 40% in Swaziland (among young pregnant women aged 15–24years attending antenatal clinics). Although political instability in severalcountries in central Africa makes it difficult to assess their current situation,Cameroon may have the highest HIV prevalence levels in this subregion,reporting a median prevalence of 11.9% among pregnant women aged 15–24 years in 27 sentinel sites. HIV prevalence in western Africa varies from< 1% in countries in the Sahelian belt to 5–6% in Côte d’Ivoire and Nigeria.
22
92-4-120938-0_CH02_22

Southern Africa is the most seriously affected subregion. In Botswana,Lesotho, South Africa, Swaziland and Zambia, more than 20% of pregnantwomen aged 15–24 years attending antenatal clinics are HIV positive. Basedon data from women attending antenatal clinics in capital cities, the epidemicin eastern Africa seems to be slowly declining. However, the prevalenceof HIV infection in most urban antenatal clinics remains between 10% and15% (63).
A country that has seen well documented reductions in HIV prevalence isUganda. A declining HIV prevalence over the past 10 to 15 years has beenobserved, especially among young women aged 15–24 years attending ante-natal clinics. For example, at Nsambya hospital in Kampala, HIV infectionrates among women aged 15–19 years attending antenatal clinics declinedfrom 29% in 1991 to 9% in 1998 and further to 5% in 2002.
In generalized epidemics, HIV prevalence among young women is consid-erably higher than among young men. In 11 countries with nationally repre-sentative surveys of HIV prevalence, young women aged 15–24 years werebetween 1.3 times and 12 times more likely to be infected than young men(Figure 2.2). Adolescent girls are especially vulnerable to HIV infection.About two thirds of newly infected young people aged 15–19 years in sub-Saharan Africa are female (63).
Figure 2.2HIV prevalence among young men and women aged 15–24 years, selected countries,2001–2003
0
5
10
15
20
Do
min
ica
n
Re
pu
blic
20
02
Nig
er 2
00
2
Gh
an
a 2
00
3
Bu
rkin
a F
aso
20
03
Ma
li 20
01
Bu
run
di 2
00
2
Ta
nza
nia
20
03
Ke
nya
20
03
Za
mb
ia 2
00
1
So
uth
Afric
a
20
03
Zim
ba
bw
e 2
00
1
% H
IV-p
os
itiv
e
Male
Female
Source: Demographic and Health Surveys (3) and WHO Regional Office for Africa, 2002 (63)
23
92-4-120938-0_CH02_23

The social reasons why young women have higher HIV prevalence and in-cidence than young men include the fact that many women are younger,sometimes considerably younger, than their male sexual partners. Studiesfrom several countries show that the prevalence of HIV among young womenwho reported having had sex with older men is significantly higher than theprevalence among those who had sex only with partners their own age (64).In a survey among young women aged 15–19 in rural Zimbabwe, the risk ofHIV infection was significantly associated with the age of their most recentsexual partner. HIV prevalence among women aged 21–24 whose last partnerwas less than 5 years older than they were was 16%, whereas among youngwomen with partners 10 or more years older, the prevalence was twice ashigh (65). In Kisumu, Kenya, similar trends were found: no woman who wasyounger than 20 and was married to a man less than 4 years older than herselfwas infected with HIV compared with 38% of those who had husbands 10 ormore years older (66). Sexual relationships between young women and oldermen, whether inside marriage or outside, have the potential to drive the spreadof HIV in high-prevalence generalized epidemics.
Other STIs play a large part in the spread of HIV in many populations (67).For example, a study in South Africa showed that young men infected withherpes simplex virus–type 2 (HSV-2) were 5 times more likely to be HIVpositive than sexually active people who were not infected with HSV-2.Young women with HSV-2 were 8 times more likely to be infected with HIV(68). WHO estimates that more than 100 million STIs, excluding HIV, occureach year among people younger than 25 (69). Treatment of STIs has provento be an effective method of preventing HIV (see chapter 3).
In summary, it is clear that, although there are many different HIV epidemicsacross the world, young people are at their centre in all cases.
2.4 Progress towards UNGASS commitments
The previous section highlighted the fact that young people in low-level,concentrated and generalized epidemics represent a large proportion of thosebecoming infected. The Declaration of Commitment signed at the UNGASSdedicated governments to meeting specific goals to fight HIV/AIDS amongyoung people. They agreed to:
ensure that at least 95 per cent of young men and women aged 15 to 24 haveaccess to the information, education, including peer education and youth-specific HIV education, and services necessary to develop the life skillsrequired to reduce their vulnerability to HIV infection by 2010 (2).
This section reviews the response to these goals.
24
92-4-120938-0_CH02_24

2.4.1 Information
An important, but not sufficient, foundation for any prevention effort aimedat young people is to provide them with basic information on how to protectthemselves and their partners from acquiring the virus. Although significantprogress has been achieved during the past decade, surveys suggest that de-spite the fact that the majority of young people have heard of AIDS, manystill do not know how to prevent transmission. Furthermore, misconceptionsabout HIV and AIDS are widespread. They vary from one culture to another,and specific rumours gain credibility in some populations, both on how HIVis spread (by mosquito bites or witchcraft, for example) (70) and on how itcan be avoided (for example, by eating a certain fish or having sex with avirgin).
In 17 countries surveyed between 1999 and 2003, the average proportion ofyoung people aged 15–24 years deemed to have “sufficient knowledge” aboutHIV/AIDS was 24% among young women and 29% among young men (5)(Table 2.2). (Sufficient knowledge was defined as the percentage of youngmen and women aged 15–24 who both correctly identified two ways of pre-venting the sexual transmission of HIV and rejected three major misconcep-tions about HIV.)
These surveys showed that, in countries with generalized HIV epidemics,such as Burkina Faso, Haiti, Mozambique and Nigeria, more than 80% ofyoung women aged 15–24 still did not have sufficient knowledge about HIV.(Because the indicator has five components, one might not expect a score of100% even if knowledge levels were high.) The simple question “Can ahealthy looking person have the AIDS virus” has been asked of young womenin repeated surveys in more than 25 countries. The data generally show animprovement in knowledge in responses to this question in recent years (Fig-ure 2.3). The most seriously affected countries in southern Africa havereached levels where around 80% of participants respond correctly. However,in nearly all countries one fifth or more of young women in this age groupremain uncertain about the response to this question.
2.4.2 Education
HIV/AIDS information and life-skills education can be provided to youngpeople in a number of ways, including through peer education or counselling,community activities that include parents, and through the mass media andschool-based education programmes. Often, these interventions are dispersedacross many organizations and community groups and their effects are dif-ficult to measure and evaluate consistently. However, schools are a keysetting for providing information and teaching adolescents the life skills nec-essary to prevent HIV/AIDS; they have therefore been used as a proxy for
25
92-4-120938-0_CH02_25

Tab
le 2
.2K
no
wle
dg
e o
f H
IV/A
IDS
an
d s
exu
al b
ehav
iou
r am
on
g y
ou
ng
men
an
d w
om
en a
ged
15–
24 y
ears
fo
r se
lect
ed c
ou
ntr
ies,
199
9–20
03(3
, 4).
(V
alu
es a
re p
erce
nta
ges
)
Fem
ales
Mal
es
Co
un
trya
Kn
ow
that
ah
ealt
hy-
loo
kin
gp
erso
nca
n h
ave
AID
S
Co
mp
reh
ensi
veco
rrec
tkn
ow
led
ge
abo
ut
AID
S
Sex
bef
ore
age
15b
Hig
her
risk
sex
in t
he
last
year
Co
nd
om
use
d a
tla
sth
igh
erri
skse
x
Kn
ow
that
ah
ealt
hy-
loo
kin
gp
erso
nca
n h
ave
AID
S
Co
mp
reh
ensi
veco
rrec
tkn
ow
led
ge
abo
ut
AID
S
Sex
bef
ore
age
15b
Hig
her
risk
sex
in t
he
last
year
Co
nd
om
use
dat
last
hig
her
risk
sex
Eas
tern
an
d S
ou
ther
n A
fric
aB
otsw
ana
8140
NA
cN
A75
7933
NA
NA
88E
thio
pia
39N
A14
717
54N
A5
6430
Ken
ya83
3415
3025
8647
3184
47M
alaw
i84
3417
1732
8941
2971
38M
ozam
biqu
e65
20N
A37
2982
33N
A83
33N
amib
ia82
3110
8048
8741
3185
69R
wan
da64
233
1023
6920
NA
4255
Uni
ted
Rep
ublic
of T
anza
nia
7444
1036
4278
4911
8147
Uga
nda
7628
1422
4483
4016
5962
Zam
bia
7431
1830
3373
3327
8642
Zim
babw
e74
NA
320
4283
NA
682
69W
est
Afr
ica
Ben
in56
816
3619
6914
2490
34
26
92-4-120938-0_CH02_26

Bur
kina
Fas
o56
1521
2354
6123
1478
67G
hana
7838
750
3383
444
8352
Gui
nea
60N
A27
2317
56N
A20
9232
Mal
i46
926
1814
5915
1185
30N
iger
ia52
1820
2924
6521
878
46C
arib
bea
nD
omin
ican
Rep
ublic
92N
A13
2929
89N
A18
8352
Hai
ti68
1512
5919
7828
2893
30C
om
mo
nw
ealt
h o
f In
dep
end
ent
Sta
tes
Arm
enia
537
10
NA
488
169
44K
azak
hsta
n63
NA
127
3273
NA
678
65U
zbek
ista
n55
80
1N
A58
7N
A45
50W
eig
hte
dav
erag
e67
2312
2833
7329
1677
49
aC
ount
ries
incl
uded
in th
is ta
ble
are
only
thos
e fo
r w
hich
ther
e ar
e da
ta b
oth
for
fem
ales
and
mal
es a
nd d
ata
colle
cted
with
in th
e pa
st 5
yea
rs.
b A
mon
g yo
ung
peop
le a
ged
15–1
9 ye
ars.
c NA
= n
ot a
vaila
ble.
27
92-4-120938-0_CH02_27

educational prevention efforts in some countries. For example, 57% of ado-lescent boys in Zimbabwe reported that their only source of sex education onHIV/AIDS was school (71). In many countries, especially in west Africa andsome parts of Asia, large proportions of children do not attend school (72).
The region where general HIV prevention through school is likely to havethe most impact is sub-Saharan Africa. In 2003, 36 countries in sub-SaharanAfrica had a generalized epidemic; 30 of these countries reported to the globalcoverage survey on selected services for HIV/AIDS prevention, care andsupport; and 11 of these indicated that AIDS education was not part of theircurriculum in primary school (6). Additionally, in six countries, AIDS edu-cation was not part of the curriculum in secondary school. Overall it wasestimated that only 58% of primary school students and 64% of secondaryschool students were exposed to AIDS-related education through the educa-tion system in sub-Saharan Africa. These numbers are likely to overestimatethe proportion of students receiving effective AIDS-related education sincemany teachers either have not learnt the appropriate skills or do not feel com-fortable teaching topics related to HIV/AIDS and sexuality (73, 74) (seechapter 5). Furthermore, the quality of the interventions is also an issue. In astudy among students in South Africa, less than one quarter of the respondents
Figure 2.3Proportion of young women aged 15–24 years who know that a healthy lookingperson can have the AIDS virus, by region with data from early-to-mid 1990scompared with data from early 2000 (3, 4)
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100
Period: early/mid 1990s
Pe
rio
d:
ea
rly
20
00
s
West AfricaEastern & Southern AfricaLatin America & CaribbeanAsiaEastern Europe
Increased
Decreased
Y=X, no change in
knowledge level
28
92-4-120938-0_CH02_28

recalled having discussed all eight core life-skills topics of the curriculumduring their last year of school (75).
2.4.3 Services
Providing access to youth-friendly health services is an integral part of anynational prevention programme. The main services necessary to prevent HIVand other STIs include providing access to information, condoms and harmreduction (where injecting drug use is prevalent) and access to diagnosis(testing), treatment and care for STIs and HIV/AIDS. Access to services re-mains insufficient (76). In most countries, young people’s access to effectivehealth services is lower than older people’s, and this is particularly true foradolescents (70). The types of interventions that have been used in developingcountries to try to improve young people’s access to health services, and theireffectiveness, are described in chapter 6.
2.4.3.1 Condoms
Globally, the number of condoms available has increased (6). However theavailability of condoms does not ensure that condoms are used. In addition,there are still significant proportions of young men in countries with gener-alized epidemics who do not know where to obtain condoms (Figure 2.4).
Figure 2.4Proportion of young people who knew where to obtain condoms, by age group,selected countries in sub-Saharan Africa, 1999–2004 (3)
0
10
20
30
40
50
60
70
80
90
100
Gh
an
a (2
00
3)
Ke
ny
a (2
00
3)
Ma
law
i (20
00
)
Na
mib
ia (2
00
0)
Ta
nza
nia
(20
03
-04
)
Za
mb
ia (2
00
1-0
2)
Zim
ba
bw
e (1
99
9)
% k
no
w a
so
urc
e
15-19 years
20-24 years
29
92-4-120938-0_CH02_29

2.4.3.2 Voluntary counselling and testing
As antiretroviral therapy becomes more widely available, the demand forcounselling and testing will increase. In order for young people to use testingservices they need to have access to such services. Many different factorsaffect access, but knowing where testing and counselling are offered is clearlyan essential first step. Surveys have shown that many young people do notknow where to obtain these services. In 25 of 39 countries surveyed, less than50% of young women aged 15–24 knew where they could go to be tested forHIV. Women with higher levels of education were more likely to know wherethey could go (77).
2.4.3.3 STI treatment
Adolescents are less likely to seek treatment for STIs than people aged 20–24 and older adults, despite having higher rates of STIs and the strong asso-ciation between STIs and HIV (Figure 2.5). Even when adolescents suspectthat they have an infection, they often do not seek medical care because theymay be too embarrassed or feel too guilty or fear that their privacy will notbe respected. Additionally, services may be inaccessible because clinics arefar away or have limited or inconvenient opening hours (78). Health providers
Figure 2.5Proportion of women who reported having a sexually transmitted infection withinthe past 12 months and sought treatment for it, by age group for selected countries,1999–2003 (3)
0
10
20
30
40
50
60
70
80
90
100
Bu
rkin
a F
aso
(20
03
)
Gh
an
a (2
00
3)
Gu
ine
a (1
99
9)
Ma
law
i (20
00
)
Ma
li (20
01
)
Mo
za
mb
iqu
e (2
00
3)
Ug
an
da
(20
01
)
Za
mb
ia (2
00
2)
Arm
en
ia (2
00
0)
Do
min
ica
n
Re
pu
blic
(20
02
)
Ha
iti (20
00
)
Pe
ru (2
00
0)
% s
ee
kin
g t
rea
tme
nt
15-19
20-24
25-49
30
92-4-120938-0_CH02_30

may be reluctant to serve adolescents, and when services are located in ma-ternal and child health centres, they are unlikely to be used by young men (70).
2.4.3.4 Harm reduction for injecting drug users
Among the six countries in eastern Europe that reported to the global coveragesurvey in 2003 on the number of injecting drug users that received needle andsyringe exchange services, it is estimated that 70 000 of an estimated 2.5million injecting drug users (2.8%) were reached (6). In the Middle East,north Africa, and south-east Asia, it was estimated that 4–5% of injectingdrug users were reached with harm reduction services. All other regions hadlower coverage. Although the information was not disaggregated by age, wecan assume from these numbers that the majority of young people are notbeing reached. While there is relatively little information available about theutilization of health services by the general population of young people,data are more scarce on the extent to which services reach vulnerable youngpeople engaged in behaviours that put them at high risk of acquiring HIV(see chapter 9).
2.4.3.5 Special services for sex workers and men who have sex with men
In 2003, global access to prevention interventions for men who have sex withmen was reported to be 11%, and for sex workers it was reported to be 16%(6). The region with the highest coverage for both of these high-risk groupswas Latin America and the Caribbean, where 31% of men who have sex withmen and 25% of sex workers were estimated to be reached. Again, no infor-mation had been disaggregated by age, but since many sex workers and menwho have sex with men are aged 15–24 (see above), we can assume that themajority of young people in these two high-risk groups are not being reached.
2.4.4 Life skills
Information, education, and access to services should contribute to the de-velopment of life skills that can help reduce a young person’s vulnerabilityto HIV infection. However, there is no standardized internationally compa-rable method for assessing directly whether young people have developedsufficient adaptive and positive behaviours to enable them to deal effectivelywith the demands of everyday life (79). As a proxy indicator, “reported be-haviours” can be used (5). The assumption is that regardless of high levels ofknowledge about prevention strategies, young people may engage in unpro-tected sex because they lack the skills to negotiate abstinence, reduce thenumber of partners that they have or use condoms. If young peoplepossess adequate life skills, levels of risky behaviour should be lower. (This
31
92-4-120938-0_CH02_31

assumption obviously ignores the fact that certain risk behaviours may bebeyond the control of the individual, such as forced sex.)
Young people may be fearful or embarrassed to talk with a partner about sexor may simply not be aware of their individual risk. Data from Demographicand Health Surveys in Burkina Faso, Nigeria and the United Republic ofTanzania showed that the proportion of young unmarried boys who reportedthey did not use a condom at last sexual intercourse was substantial. Themajority who did not use a condom felt that they were not at risk. In Nigeria,93% of men aged 15–24 years perceived their risk of getting AIDS to beminimal or non-existent; in Burkina Faso the figure was 77% and in theUnited Republic of Tanzania the proportion was 53%.
2.4.4.1 Age at first sex
Delaying the age at which young people first engage in sexual intercoursecan protect them from infection. Adolescents who begin sexual activity earlyare at a higher risk of becoming infected with HIV; research in differentcountries has shown that adolescents who start sexual activity early are morelikely to have sex with high-risk partners or multiple partners and are lesslikely to use condoms (80, 81). Sexual activity begins in adolescence for themajority of people, and in some countries it starts for young women beforethey are 15 years old. Table 2.2 shows that in the 20 countries for which thereare recent data, in 10 countries more than 1 in 7 girls aged 15–19 reportedhaving had sex before the age of 15. Among young men aged 15–19 years inHaiti, Kenya, Malawi, Namibia and Zambia, more than one quarter reportedhaving had sex before they were 15 years old.
2.4.4.2 Condom use
When young people become sexually active, they must have the skills topractise safe sex. This means either being faithful to one faithful partneror consistently using a condom properly. Data from household surveysshow that the proportion of young people using condoms is still quite loweven when they have sex with people who are not their regular partner(Table 2.2). In Malawi, where 1 out of 6 people aged 15–49 is infected withHIV, only 32% of young women and 38% of young men reported using acondom the last time they had had sex with a non-cohabiting partner. In manycountries, the reported use of a condom is higher among young men thanyoung women. In Zimbabwe, for example, where approximately one quarterof all people are infected, 69% of young men aged 15–24 years reported usinga condom during their last episode of sex with a high-risk partner while only42% of young women reported using a condom during their last episode ofsex with a high-risk partner.
32
92-4-120938-0_CH02_32

2.4.5 Vulnerability
A person’s ability to avoid HIV infection depends only partly on their ownindividual knowledge and skills. There are other social and economic factorsthat are beyond the individual’s control and that can put young people athigher or lower risk of infection (82). Such factors include social norms, thestatus of women in society and the socioeconomic environment (83). Thesecontextual factors often result in young people having less power to reducetheir risk of HIV than adults.
2.4.5.1 Social norms
There are norms and values in communities that increase or reduce the riskof HIV infection. Parents and other family members have an important rolein providing information and skills to their children. However, open com-munication about sexuality remains a challenge in many cultures and soci-eties. Boys and girls may be embarrassed to discuss issues related to sex;parents may be unwilling to talk about sex or be uncomfortable doing so, bothof which may result in young people having limited knowledge and skillsabout prevention. Demographic and Health Surveys have asked men andwomen whether they feel that children aged 12–14 years should be taughtabout using a condom to avoid AIDS. Out of five countries surveyed in east-ern and southern Africa, the proportion of respondents who agreed thatchildren should be taught this skill varied from just over 40% among men inUganda to over 80% among women in Namibia.
Among men having sex with men, social taboos and stigma may increasetheir risks of contracting HIV. These men may hide their sexuality and con-sequently not have access to the information or support that they need toreduce risky behaviour.
2.4.5.2 Gender inequality
When the status of women within sexual relationships is low they are at anincreased risk of contracting HIV (82, 84). For example, for many girls andyoung women the onset of sexual activity does not occur by choice. In Ja-maica 12% of young women aged 15–19 and 10% of this group in SouthAfrica reported they were unwilling or coerced during their first sexual ex-perience (81, 85). In a study among secondary school students in Swaziland,18% of female students reported being coerced during their first sexual en-counter (86). In Zambia, 1 in 8 young women aged 15–19 years reportedhaving been forced to have sex by a man in the 12 months prior to a generalpopulation-based survey (87). In Zimbabwe, more than 1 in 5 women aged15–29 years reported ever having been forced to have sex by a man (71).In many societies people turn a blind eye to sexual abuse against young
33
92-4-120938-0_CH02_33

women, and to gender-based violence more generally, both of which haveimportant implications for HIV transmission.
2.4.5.3 Socioeconomic environment
The socioeconomic situation in which young people live can have both pos-itive and negative impacts on their vulnerability to HIV infection. Forexample, in the United Republic of Tanzania young women aged 15–24 yearsin the highest wealth quintile were more likely to engage in higher risk sexualactivities (such as having sex with a non-marital non-cohabiting partner) thanwomen in the lowest quintile (48% in the highest quintile versus 30% in thelowest quintile). To a large extent this can be explained by the fact that womenin the lowest quintile were more likely to be married. However, the youngwomen in the highest income quintile were more than twice as likely to haveused a condom during their last episode of higher risk sexual activity than theyoung women in the lowest quintile (58% highest quintile versus 23% lowestquintile) (88). Lower socioeconomic status may result in lower educationalattainment, which may result in gaining less information and skills to protectoneself from HIV (89). Lower socioeconomic status may also provide a rea-son for engaging in sexual relationships in exchange for financial compen-sation or support.
Young people with lower socioeconomic status have been reported to expe-rience more physical abuse and sexual coercion within relationships (82). Anincreasing number of young people who do not grow up in a protective en-vironment in which they have parental support, as a result of adult mortalityfrom AIDS, may be increasingly vulnerable to infection. A study in ruralZimbabwe found that among women aged 15–18 years, young people whosemother had died and young women with an infected parent had a significantlyhigher prevalence of HIV than other young women, and they also had moreSTI symptoms and were more likely to become pregnant (90).
Another example of a socioeconomic situation that is inherently unsafe foryoung people, provides no protection for them and puts them at an increasedrisk of HIV, is people trafficking. Children are increasingly being taken fromtheir usual environments by means of threat, force or other abuses of powerfor the purpose of sexual exploitation. Studies commissioned by the Interna-tional Labour Organization in eastern Europe, Asia and west Africa foundthat most young people involved in prostitution have been forced into thework (91–93).
2.5 Limitations of the data
Most surveys of young people are targeted at those aged 15 years and older.In many situations, however, a significant proportion of 15-year-olds have
34
92-4-120938-0_CH02_34

already begun to have sex or are involved in other risky behaviours. There isa need to collect systematically more data from younger adolescents – thatis, those aged 10–14 years. However, there remains uncertainty about theappropriateness of questions, the reliability of responses, parental consentand other ethical issues (6). These will need to be addressed before data fromthis age group will be improved.
Most research among injecting drug users, sex workers and men who havesex with men, analyse data using an epidemiological lens and do not considerthe data in terms of HIV prevention programmes. As a result data in reportsare rarely disaggregated by the age and sex of the respondent for groups athigh risk of becoming infected with HIV. For example, 16-year-old girls whoinject drugs and are involved in sex work are likely to have different needsand require a different response from a prevention programme than olderinjecting drug users who have been injecting for a long time. BehavioralSurveillance Surveys need to be analysed with a stronger focus on their im-plications for programmes.
A number of the tables and figures in this chapter compare two variables, forexample age and knowledge or behaviour. The analysis has been madewithout controlling for other variables, such as household wealth or the par-ticipant’s education level. A regression analysis would clarify whether dif-ferences are related to the age of the participant or to other variables that mightalso affect knowledge or behaviour, but it was not possible to conduct suchan analysis for this broad review of HIV among young people. The findingsin this chapter suggest areas in which further research and analysis are needed.
2.6 Conclusions
This chapter shows that young people are at the centre of the global AIDSepidemic, both in terms of new infections and opportunities for halting thetransmission of HIV. The epidemic varies greatly among the different regionsof the world, but in each of these epidemics young people are potentially thegreatest force for change if they can be reached with the right interventions(as outlined in the UNGASS goals). There is increasing evidence from severalcountries that where HIV prevalence is decreasing it is young people who arereversing the trends. Young people are much more likely to adopt and main-tain safe behaviours, and it is therefore important to implement interventionsearly.
While there have been a number of efforts to scale-up interventions aimed atyoung people, large numbers of young people continue to lack the basic in-formation and skills they need to protect themselves. The majority of youngpeople start sexual activity during adolescence, and this review suggests thatin all regions large proportions of young people still know little about HIV
35
92-4-120938-0_CH02_35

transmission and prevention; they continue to have serious misconceptions;and access to effective health services, such as treatment for STIs and vol-untary counselling and testing, remains inadequate.
Given that about half of all new infections occur among those aged 15–24,and that young people account for a substantial proportion of the groups whoare at particularly high risk of acquiring HIV – such as injecting drug users,sex workers and men who have sex with men – there is a clear need to focusprevention activities on these behaviours and the populations that engage inthem and to ensure that those interventions for which there is strong evidenceof effectiveness are rapidly and intensively scaled-up. Efforts to increaseyoung people’s knowledge, life skills and access to services need to be in-tensified. These efforts must consider the different needs of young men andyoung women and the different age groups among those aged 10–24 years.In addition, societal–contextual issues should be addressed to ensure thatyoung people grow up in a safe and protective environment that reduces theirvulnerability.
Each year new cohorts will be added to the large numbers of young men andwomen (115 million) (94) reaching the stage in their life where they will needto be prepared and supported to make the right choices in order to minimizetheir risk of HIV infection and thus turn the epidemic around. Without thisfocus on young people, the global HIV-related goals that have been agreedby 189 nations are not likely to be met, and the number of new infectionscould even increase before 2010.
References
1. UNAIDS. AIDS epidemic update 2005. Geneva, UNAIDS, WHO, 2005.
2. United Nations. Declaration of commitment on HIV/AIDS. United NationsGeneral Assembly Special Session on HIV/AIDS, 2001 (available athttp://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html).
3. Demographic and Health Surveys. Tools (http://www.measuredhs.com/accesssurveys/tools.cfm).
4. UNICEF. End decade assessment: multiple indicator cluster survey,(http://www.childinfo.org/MICS2/Gj99306m.htm).
5. UNAIDS, UNICEF, WHO. National AIDS programmes: a guide to indicators formonitoring and evaluating national HIV/AIDS prevention programmes for youngpeople. Geneva, UNAIDS, 2004.
6. USAID, UNAIDS, WHO, UNICEF, Policy Project. Coverage of selected servicesfor HIV/AIDS prevention, care and support in low and middle income countriesin 2003. Washington, DC, Policy Project, 2004.
7. WHO. Global health atlas, 2004 (http://www.who.int/GlobalAtlas/predefinedReports/EFS2004/index.asp).
8. EuroHIV. HIV/AIDS surveillance in Europe, (http://www.eurohiv.org/).
36
92-4-120938-0_CH02_36

9. UNAIDS/WHO. Second generation surveillance for HIV: the next decade.Geneva, UNAIDS, 2000.
10. Kong-lai Zhang, Shao-Jun Ma. Epidemiology of HIV in China: intravenous drugusers, sex workers, and large mobile populations are high risk groups. BMJ,2002, 324:803-804.
11. Dehne K et al. The HIV/AIDS epidemic in eastern Europe: recent patterns andtrends and their implications for policy-making. AIDS 1999, 13:741-749.
12. Dehne K, Kobyshcha Y. The HIV epidemic in central and eastern Europe:update 2000. Geneva, UNAIDS, 2000.
13. Médecins Sans Frontières. Knowledge and attitude of ‘safe sex’ in Moscow.Moscow, MSF, 2000.
14. Rhodes T et al. Review: HIV transmission and HIV prevention associated withinjecting drug use in the Russian Federation. International Journal of DrugPolicy, 2004, 15:1-16.
15. Kelly JA, Amirkhanian YA. The newest epidemic: a review of HIV/AIDS incentral and eastern Europe. International Journal of STD and AIDS, 2003,14:361-371.
16. National AIDS Control Organisation. National baseline high risk and bridgepopulation behavioural surveillance survey (2002) report. Part II: men who havesex with men and injecting drug users. New Delhi, Ministry of Health and FamilyWelfare, Government of India, 2002.
17. Indonesia Ministry of Health and Central Bureau of Statistics. Behaviouralsurveillance in 13 provinces 2002-2003. Jakarta, Ministry of Health, 2004.
18. Zhusupov B, Behavioural surveillance among injecting drug users in nine citiesof Kazakhstan (Almaty, Pavllodar, Shymkent, Karaganda, Temiirtau, Astana,Petropavllovsk, Urallsk, Ust Kamenogorsk) within the framework of HIVepidemiological surveillance. Almaty, Center on Research of Public Opinion(CRPO), 2002.
19. Mesquita F et al. Trends of HIV infection among injection drug users in Brazilin the 1990s: the impact of changes in patterns of drug use. Journal of AcquiredImmune Deficiency Syndromes, 2001, 28:298-302.
20. UNAIDS. HIV/AIDS Belarus epidemic update. Minsk, UNAIDS, 2000.
21. Myanmar AIDS Prevention and Control Project, Department of Health. Sentinelsurveillance data for March-April 2004. Yangon, AIDS Prevention and ControlProject, 2004.
22. Asamoah-Adu C et al. HIV infection among sex workers in Accra: need to targetnew recruits entering the trade. Journal of Acquired Immune DeficiencySyndromes, 2001, 28:358-366.
23. UNAIDS. 2004 report on the global HIV/AIDS epidemic: 4th global report.Geneva, UNAIDS, 2004.
24. Cambodia, National Center for HIV/AIDS, Dermatology and STIs (NCHADS).HIV sentinel surveillance in Cambodia. Phnom Penh, NCHADS, 2002.(Unpublished report.)
25. Lao People’s Democratic Republic, National Committee for the Control of AIDSBureau, , Family Health International. Behavioral surveillance survey in LaoPeople’s Democratic Republic, 2000-2001. Lao PDR; 2003.
37
92-4-120938-0_CH02_37

26. Myanmar AIDS Prevention and Control Project, Department of Health. Sentinelsurveillance data for March-April 2000, Yangon, AIDS Prevention and ControlProject, 2000.
27. Population Services International Russia. Study of sexual behavior amongfemale commercial sex works in Saratov Oblast. Moscow, Population ServicesInternational, 2000.
28. Viet Nam, National AIDS Standing Bureau, Family Health International. HIV/AIDS behavioral surveillance survey in Vietnam, 2000. Hanoi, National AIDSStanding Bureau, 2001.
29. Steinfatt T. Working at the bars: sex work and health communication inThailand. New Haven, CT, Greenwood, 2002.
30. Duong LB. Children in prostitution in Hanoi, Hai Phong, Ho Chi Minh City andCan Tho: a rapid assessment. Bangkok, International Labour Organization,International Programme on the Elimination of Child Labour, 2002.
31. Family Health international. HIV/AIDS behavioral surveillance survey Jamaica1999-2000: female sex workers. Kingston, IMPACT/FHI/UNAIDS, 2002.
32. Michael T, Ahmed M, Lemma W. HIV/AIDS behavioral surveillance survey(BSS): round one. Djibouti, Ministry of Health, 2003. (Draft report.)
33. Eritrea Ministry of Health, CTMRE Consultancy Service. HIV/AIDS risk groupsand risk behaviours identification survey. Eritrea, Ministry of Health, CTMREConsultancy Service, 2001.
34. Myanmar AIDS Prevention and Control Project, Department of Health. Sentinelsurveillance data for 1989-2003. Yangon, AIDS Prevention and Control Project,2004
35. Cambodia, National Center for HIV/AIDS, Dermatology and STIs (NCHADS).HIV sentinel surveillance (HSS) 2003: trends results, and estimates. PhnomPenh, NCHADS, 2004.
36. Cambodia, National Center for HIV/AIDS, Dermatology and STDs. CambodiaHIV sentinel surveillance 2000. Phom Penh, NCHADS, 2000.
37. Alary M et al. Decline in the prevalence of HIV and sexually transmitted diseasesamong female sex workers in Cotonou, Benin, 1993-1999. AIDS, 2002,16:463-470.
38. Ghys PD et al. Increase in condom use and decline in HIV and sexuallytransmitted diseases among female sex workers in Abidjan, Cote d’Ivoire.AIDS, 2003, 17:1691-1694.
39. National AIDS Control Organisation. National baseline high risk and bridgepopulation behavioural surveillance survey (2001) report. Part I: female sexworkers and their clients. New Delhi, Ministry of Health and Family Welfare,Government of India, 2002.
40. Family Health international. Behavioral surveillance survey of female sexworkers and clients in Kathmandu valley: round 1. Kathmandu, 2003.
41. Population Services International. The study of knowledge, attitude andpractices related to HIV/AIDS and antenatal care. Kosovo, PSI, 2001.
42. Alary M, Lowndes CM. The central role of clients of female sex workers in thedynamics of heterosexual HIV transmission in sub-Saharan Africa. AIDS, 2004,18:945-947.
38
92-4-120938-0_CH02_38

43. Kerrigan D et al. Environmental-structural factors significantly associated withconsistent condom use among female sex workers in the Dominican Republic.AIDS, 2003, 17:415-423.
44. AIDS Division, Department of Communicable Disease Control, Thailand. 2002report on HIV/AIDS and STI in Thailand. Bangkok, Ministry of Public Health,2003.
45. Thongthai V, Guest P. Thai sexual attitudes and behaviour: results from a recentnational survey. Canberra, Australian National University, 1995. (Unpublisheddata presented at conference on Gender and sexuality in modern Thailand.)
46. UNAIDS. AIDS and men who have sex with men: UNAIDS points of view.Geneva, UNAIDS, 1998.
47. De los Angeles Pando M et al. High human immunodeficiency virus type 1seroprevalence in men who have sex with men in Buenos Aires, Argentina: riskfactors for infection. Journal of Epidemiology, 2003, 32:735-740.
48. Latin American Institute of Prevention and Education in Health. Baseline studyfor condom use promotion in Central American cities. Washington, DC,Population Services International, 1997.
49. Girault P et al. Sexual behaviour, STIs and HIV among men who have sex withmen in Phnom Penh, Cambodia 2000. Phnom Penh, Family HealthInternational, 2002.
50. Population Services International. The study of sexual behaviour of maleCSW’s in Moscow. Moscow, PSI Russia, 1999.
51. Wiessing L, Kretzschmar M. Can HIV epidemics among IDUs ‘trigger’ ageneralised epidemic? International Journal of Drug Policy, 2003, 14:99-102.
52. Kelly JA, Amirkhanian YA. The newest epidemic: a review of HIV/AIDS incentral and eastern Europe. International Journal of STD and AIDS, 2003,14:361-371.
53. Pisani E et al. Sexual behavior among injection drug users in 3 Indonesian citiescarries a high potential for HIV spread to non-injectors. Journal of AcquiredImmune Deficiency Syndromes, 2003, 34:403-406.
54. Smolskaya T et al. Sentinel sero-epidemiological and behavioural surveillanceamong female sex workers. St Petersburg, Russian Federation, St PetersburgPasteur Institute, 2003.
55. UNAIDS. Population mobility and AIDS: UNAIDS technical update. Geneva,UNAIDS, 2001.
56. UNDP, South East Asia HIV and Development Programme. The impacts ofmapping assessments on population movement and HIV vulnerability in SouthEast Asia. Bangkok, UNOPS,UNDP, 2001.
57. Lurie MN et al. Who infects whom? HIV-1 concordance and discordance amongmigrant and non-migrant couples in South Africa. AIDS, 2003, 17:2245-2252.
58. Lydie N et al. Mobility, sexual behavior, and HIV Infection in an urban populationin Cameroon. Journal of Acquired Immune Deficiency Syndromes, 2004,35:67-74.
59. Kenya Central Bureau of Statistics, Ministry of Health and ORC Macro. Kenyademographic and health survey 2003. Calverton, MD, ORC Macro, 2004.
39
92-4-120938-0_CH02_39

60. New ERA/ STD/AIDS Counseling and Training Service, Family HealthInternational. HIV/STD prevalence and risk factors among migrant and non-migrant males of Achham District in far-western Nepal. Kathmandu, New ERA/SACTS, FHI, 2002.
61. Dorning K. Reducing migration among young people, 2005 (http://tilz.tearfund.org/Publications/Footsteps+51-60/Footsteps+55/Reducing+migration+among+young+people.htm). (Tearfund International LearningZone.)
62. Kruusvall J, Tomson L. [Estonian youth on the way to the European Union].Tallinn, Estonia, Estonian Youth Institute and Department of Sociology, TallinnPedagogical University, 2004. (In Estonian.)
63. WHO Regional Office for Africa. HIV/AIDS epidemiological surveillance updatefor the WHO African Region: 2002. Harare, WHO Regional Office for Africa,2003.
64. Kelly RJ et al. Age differences in sexual partners and risk of HIV-1 infection inrural Uganda. Journal of Acquired Immune Deficiency Syndromes, 2003,32:446-451.
65. Gregson S et al. Sexual mixing patterns and sex-differentials in teenageexposure to HIV infection in rural Zimbabwe. Lancet, 2002, 359:1896-1903.
66. Glynn J, Caraël M, Auvert B. Why do young women have a much higherprevalence of HIV than young men? A study in Kisumu, Kenya, and Ndola,Zambia. AIDS 2001, 15 Supplement 4: S51-60.
67. Weiss HA et al. The epidemiology of HSV-2 infection and its association withHIV infection in four urban African populations. AIDS, 2001, 15 Suppl 4:S97-108
68. Auvert B et al. HIV infection among youth in a South African mining town isassociated with herpes simplex virus-2 seropositivity and sexual behaviour.AIDS, 2001, 15:885-898.
69. WHO. Global prevalence and incidence of selected curable sexuallytransmitted diseases: overview and estimates. Geneva, WHO, 2001.
70. UNICEF, UNAIDS, WHO. Young people and HIV/AIDS – opportunity in crisis.New York, UNICEF, 2002.
71. Ministry of Health and Child Welfare, Zimbabwe. The Zimbabwe young adultsurvey, 2001-2002. Harare, Ministry of Health and Child Welfare, 2004.
72. UNICEF. The state of the world’s children 2005. New York, UNICEF, 2004.
73. Schenker II. Nyirenda JM. Preventing HIV/AIDS in schools. Paris, UNESCO,2002. (Education Practices Series – 9.)
74. Chen J, Zhao D, Dunne MP. HIV/AIDS prevention: knowledge, attitudes andeducation practices of secondary school health personnel in 14 cities of China.Asia Pacific Journal of Public Health, 2004, 16:9-14.
75. Rutenberg N et al. Transitions to adulthood in the context of AIDS in SouthAfrica: report of wave I. Washington, DC, Population Council, 2001.
76. WHO, UNAIDS, UNFPA, UNODC, YouthNet. Protecting young people fromHIV/AIDS: the role of health services. Geneva, WHO, 2004.
77. UNICEF. Girls, HIV/AIDS and education. New York, UNICEF, 2004.
40
92-4-120938-0_CH02_40

78. UNAIDS. HIV voluntary counseling and testing: gateway to prevention and care.Five case studies related to prevention of mother-to-child transmission of HIV,tuberculosis, young people, and reaching general population groups. Geneva,UNAIDS, 2002.
79. WHO. Skills for health. Skills-based health education including life skills: animportant component of a child-friendly/health-promoting school. Geneva,WHO, 2003. (WHO Information Series on School Health No. 9.)
80. Pettifor AE et al. Early age of first sex: a risk factor for HIV infection amongwomen in Zimbabwe. AIDS, 2004, 18:1435-1442.
81. Manzini N. Sexual initiation and childbearing among adolescent girls inKwaZulu Natal, South Africa. Reproductive Health Matters, 2001, 9:44-52.
82. Eaton L, Flisher AJ, Aaro LE. Unsafe sexual behaviour in South African youth.Social Science and Medicine, 2003, 56:149-165.
83. The World Bank. Confronting AIDS: public priorities in a global epidemic.Revised edition. Washington, DC, World Bank, 1999.
84. Ng’weshemi J et al. HIV prevention and AIDS care in Africa: a district levelapproach. Amsterdam, Royal Tropical Institute, 1997.
85. Hope Enterprises. Report of the adolescent condom survey Jamaica, 2001.Kingston, , Hope Enterprises, 2001.
86. Buseh AG. Patterns of sexual behaviour among secondary school students inSwaziland, southern Africa. Culture, Health and Sexuality, 2004, 4:355-367.
87. Central Statistical Office, Zambia. Zambia Demographic and Health Survey2001-2002. Calverton, MD, Central Statistical Office, Central Board of Health,ORC Macro, 2003.
88. Tanzania Commission for AIDS. Tanzania 2003 AIDS indicator survey finalreport. Dar es Salaam, Commission for AIDS, National Bureau of Statistics,ORC Macro, Calverton, MD, 2003.
89. Taffa N et al. STD and sexual risk behaviour of Ethiopian youths. SexuallyTransmitted Diseases, 2002, 29:828-833
90. Gregson S et al. HIV infection and reproductive health care in teenage womenorphaned and made vulnerable by AIDS in Zimbabwe. AIDS Care 2005,17:785-794.
91. International Labour Organization International Programme on the Eliminationof Child Labour. Rapid assessment of trafficking in children for labour andsexual exploitation in Romania. Bucharest, ILO, 2003.
92. International Labour Organization International Programme on the Eliminationof Child Labour. Rapid assessment on trafficking in children for exploitativeemployment in Bangladesh. Geneva, ILO, 2002.
93. Amorim A, Murray U, Bland J. Girl child labour in agriculture, domestic work andsexual exploitation. Rapid assessments on the cases of the Philippines, Ghanaand Ecuador. Geneva, ILO, 2004.
94. Population Division of the Department of Economic and Social Affairs, UnitedNations Secretariat. World population prospects: the 2004 revision. New York,United Nations, 2005.
41
92-4-120938-0_CH02_41

92-4-120938-0_CH02_42

3. Overview of effective and promisinginterventions to prevent HIVinfectionJudith D. Auerbach,a Richard J. Hayes,b & Sonia M.Kandathila
Objective To review the evidence for the effectiveness of a variety ofapproaches to preventing HIV infection.
Methods We reviewed what is known about the efficacy and effectivenessof a range of prevention approaches that are at various stages of research.These interventions attempt to induce behavioural change, apply technolo-gies or modify social environments. Our intention was not to provide anexhaustive review of all types of HIV prevention strategies but rather to il-lustrate the landscape of interventions that have been developed and evaluatedin different settings and that have the potential for widespread applicationamong both adults and young people.
Findings There is a large quantity of evidence from experimental and ob-servational research as well as from practical real-world experience in bothdeveloped and developing countries. This evidence supports the implemen-tation and scale-up of a number of interventions and strategies. At the sametime, there is a need to continue to develop new and more effective interven-tions while attending to a number of behavioural and social issues that cutacross virtually all interventions designed to prevent the spread of HIV.
Conclusion We caution against confusing lack of implementation with lackof effectiveness and call for continual improvement in the quality and quantityof evidence. We have also identified a number of important directions forfuture HIV prevention research.
3.1 Introduction
In the face of increasing rates of HIV infection around the world, there arethose who doubt that HIV prevention strategies work, despite extensive ev-idence of the effectiveness of several interventions (1–4). In large part, thisdoubt is due either to a lack of understanding that prevention strategies maybe working even when HIV infection rates are high or increasing (see
a The Foundation for AIDS Research (amfAR), 1150 17th Street NW, Washington, DC, 20036,USA. Correspondence should be sent to Dr Auerbach (email: [email protected]).
b London School of Hygiene and Tropical Medicine, University of London, London, England.
43
92-4-120938-0_CH03_43

chapter 2) or to a belief that only certain kinds of data constitute valid evidenceof effectiveness (see chapter 4). Perceptions that HIV prevention “doesn’twork” may also be a function of confusing the efficacy of interventions withnot having taken effective interventions to scale.
Despite these challenges the field of HIV prevention is alive and well. In thecourse of the past 20 years, many approaches for stemming the spread of HIVhave been developed, tested and evaluated (although relatively few have beenevaluated systematically and rigorously) in different populations and settings,and a number have been widely adopted. The following is a brief review ofwhat is known about the effectiveness of a range of interventions at variousstages of research that attempt to induce behavioural change, apply tech-nologies or modify social environments in order to prevent the spread of HIV.Some of these interventions have involved young people, and some inter-ventions are more appropriate for young people than are others. Our intentionis not to provide an exhaustive review of all types of HIV prevention strate-gies, nor to systematically evaluate the strength of evidence for them, butrather to illustrate the landscape of interventions that have the potential forwidespread application among both adults and young people. Our reviewincludes evidence from experimental studies (including quasi-experimentalstudies) and observational studies and related analyses that have used a rangeof designs and evaluation methods. The merits of different study designs, aswell as criteria for assessing their quality and evaluating their evidence ofeffectiveness, are described in detail in chapter 4. Other chapters elaborateon the evidence for particular types of youth-focused interventions imple-mented in different settings.
3.2 Interventions to change behaviour
The goal of interventions aimed at changing behaviours is to reduce the riskof HIV-related sexual and drug-use behaviours. Behavioural change inter-ventions seek to delay the onset of sexual intercourse, reduce the number ofsexual partners a person has and reduce the incidence of unprotected sex byincreasing condom use. Behavioural change interventions also target druguse and seek to reduce or eliminate the incidence of drug injecting and theincidence of sharing needles, syringes and other drug-use equipment. Truereductions in such behavioural risks would reduce the transmission and ac-quisition of HIV infection.
Interventions aimed at changing behaviours focus on counselling individuals,couples and small groups (and these interventions sometimes include HIVtesting) and running workshops and other programmes that provide infor-mation and skills (including, for example, sex education, instructions on howto use condoms and other harm reduction strategies). These interventions may
44
92-4-120938-0_CH03_44

also aim to change social norms by seeking the involvement of opinion lead-ers or they may be peer-based, use social networks or be targeted at thecommunity. Additionally, they may include social marketing, communica-tions and mass media campaigns (2–6). These interventions are based onpsychological and social science theories that emphasize the importance ofknowing about the risks of HIV transmission, instilling motivation to protectoneself and others, changing expectations of outcomes, developing skills forengaging in protective behaviours and the ability to maintain protective be-haviours, and providing social support for protective actions (5, 6). Evalua-tion designs have included experimental and observational studies.
Behavioural change interventions have been tested in a range of social set-tings, including health-care systems, HIV/AIDS service organizations,schools, churches, community centres, commercial establishments, work-places, correctional facilities, the military and in homes. Outcomes related toHIV/AIDS that were assessed in these interventions generally fall into threecategories:
psychosocial (such as self-efficacy, perceived risk, personal or interper-sonal skills, HIV/AIDS knowledge, intentions to adopt risk-reductionbehaviours, communication with partners)
behavioural (such as the safe use of injected drugs, reducing the incidenceof sharing drug paraphernalia, encouraging the use of male or female con-doms, reducing the number of partners and frequency of unprotected sexualactivity and encouraging HIV testing), and
biological (such as the incidence or prevalence of HIV or other sexuallytransmitted infections [STIs], hepatitis and, sometimes, pregnancy, par-ticularly in studies with young people) (5, 6).
In fact, most behavioural interventions target a number of risk reductionoutcomes.
Hundreds of studies of behavioural change interventions have been con-ducted since the early 1980s, both in the developed and the developing world.Until recently, these have almost entirely targeted people who are not infectedwith HIV, although there is a growing body of studies of interventionsfocusing on people who are HIV positive (7). Several systematic reviews andmeta-analyses have summarized findings from these studies (5–18).
Most meta-analyses have included only experimental studies, and so haveonly reported on a subset of all studies of behavioural interventions, most ofwhich have been conducted in North America and western Europe. Studiesin these meta-analyses and systematic reviews of experimentally designedbehavioural interventions have focused on HIV-negative heterosexual adults
45
92-4-120938-0_CH03_45

and adolescents, injecting drug users and men who have sex with men. Theyhave found that such interventions can result in as little as no reduction inrisk behaviours to as much as a 40% reduction in risk behaviours amongdifferent population groups and exposure categories over periods that gen-erally have ranged from 3 months to 2 years. Of those interventions that haveshown efficacy in reducing risk, most have had small to moderate effect sizes(not all of which are statistically significant) (5, 7–13, 19, 20), although sub-stantial effect sizes were found in some studies included in reviews ofinterventions among men who have sex with men (14, 18). Within the overallcategory of behavioural change interventions, those considered to work bestin reducing sexual risk include small-group cognitive behavioural interven-tions, educational interventions and face-to-face counselling and skill-building programmes (for example, teaching proper condom use, negotiationand refusal skills). Those that work best for reducing risks from drug useinclude outreach programmes, needle exchange activities, addiction treat-ment programmes and face-to-face counselling (21).
Beyond these meta-analyses, other reviews have provided additional evi-dence of the efficacy and effectiveness of behavioural interventions in re-ducing the risk of HIV infection in developing countries among commercialsex workers, adolescents, injecting drug users and men who have sex withmen (14–16, 18, 22, 23).
There are some important caveats to meta-analyses and the behavioural in-terventions they assess. First, most behavioural intervention studies measuremultiple outcomes and many report a composite risk-reduction outcome soone would have to tease out the data for each outcome from each study toknow exactly what had been achieved, and this has often not been done.Indeed, it is possible that published studies tend to emphasize the one outcomethat is significant, leading to reporting bias. Second, behavioural outcomesare not operationalized or measured consistently across studies. For example,condom use is measured as “never, sometimes, always used”, “number ofunprotected acts of intercourse” or “condom used at last act of intercourse”,to name just a few. So we cannot be certain that like outcomes have beenpooled.
Additionally, most studies of behavioural intervention are population-specific, with the reference group being defined variously by age, sex of theparticipant, sexual orientation, ethnicity, cultural community, geographicalsetting or exposure category. Thus, most summary reviews of behaviouralinterventions are specific to these particular social groups (7, 8, 10–19).Consequently, it takes careful sifting to determine which of the effectiveinterventions ought to and could be replicated and scaled-up for differentpopulations and settings.
46
92-4-120938-0_CH03_46

But perhaps the most important limitation of studies of behavioural inter-ventions is that virtually all behavioural outcomes are self-reported, whichraises questions about their veracity and validity. It is both difficult and oftenundesirable to directly observe and measure HIV risk and protective be-haviours related to sexual intercourse and drug use, so we must rely chieflyon the indirect measures of self-reporting (24–26). Given the sensitivity ofthese behaviours, there is the possibility that people will consciously or sub-consciously misreport them in ways they consider to be socially desirable.This has been demonstrated by studies that have compared self-reported dataand biological markers; and it may be especially severe in studies of adoles-cents and young people. For example, a study of adolescents in the UnitedRepublic of Tanzania found substantial discrepancies in reported behaviourusing five different methods of data collection. On self-completed question-naires or during structured interviews, most young women denied havingengaged in any sexual activity but many had biological markers of activity(such as pregnancy or an STI), and during in-depth interviews most admittedto engaging in sexual activity (26). Also, reporting bias may differ betweenthe intervention and control arms of a study or between those exposed orunexposed to the intervention in an observational study, thereby distortingthe effects of the intervention. Thus although there have been significant ad-vances in developing techniques to optimize the validity of self-reports (suchas through the use of computer-assisted survey instruments and carefully de-signed questionnaires), questions remain about the validity of study resultsbased exclusively on self-reported behaviours. This has led to the increasinginterest in including biological outcomes (such as STI or HIV incidence) instudies of behavioural interventions as complementary measures and some-times as primary endpoints.
There are only a few published experimental studies testing the effectivenessof an intervention to reduce behavioural risk using both behavioural andbiomedical endpoints (incidence of STIs or HIV, or both), and these havefound mixed results. For example, two multisite intervention studies amongheterosexual men and women in the United States found significant positiveeffects both on outcomes of behavioural change and STI incidence (27, 28).As a result, one of the protocols (Project RESPECT) has been widelyreplicated in the United States. But a study in London among men who havesex with men found only modest positive change in reported behaviours andan unexpectedly higher rate of STI acquisition among the intervention groupthan the control group, although this difference attenuated over time (29). Alarge multisite behavioural intervention trial in the United States among menwho have sex with men, and which included HIV incidence as an outcomemeasure, found an 18.2% lower rate of HIV infection (15.7% after adjustmentfor baseline covariates) in the intervention group compared with the controlgroup and a 20.5% lower incidence of unprotected receptive anal intercourse
47
92-4-120938-0_CH03_47

with partners who were HIV positive or of unknown serostatus in the inter-vention group compared with the control group. Although the behaviouraloutcome was statistically significant, the HIV incidence outcome was not(30). A randomized community trial of a multicomponent adolescent sexualhealth programme in rural Mwanza, United Republic of Tanzania, assessedboth behavioural and biological outcomes, including HIV incidence and STIprevalence. The intervention had a significant impact on knowledge aboutHIV, reported attitudes towards HIV and some reported behaviours, withvariations occurring by the sex of the participant, but it did not have a con-sistent impact in either direction on STI outcomes (31, 32). Finally, inMasaka, Uganda, the effects of a community-wide behavioural intervention,with and without improved STI treatment services, were assessed in a three-arm community-randomized trial. Comparison of the behavioural interven-tion and control arms showed an increase in condom use with casual partners,but there was no significant impact on HIV incidence, possibly because thetrial was carried out at a time when incidence was already falling as a resultof larger changes toward safer behaviour in Uganda (33).
In addition to experimental data, surveillance and other observational dataprovide evidence of behavioural change at the population level that is plau-sibly related to behavioural interventions, including information and educa-tion provided by nongovernmental organizations, social institutions, peersand the media. However, if we look at the observational data from countriesand communities that have documented behavioural change, it is difficult toascertain exactly what produced the change; this is especially true for specificbehavioural interventions. This leaves us in a quandary and makes it difficultto determine what really works and how it might be replicated elsewhere. Forexample, documented declines in HIV prevalence in Uganda have been at-tributed to the promotion of a strategy known as “ABC”: “abstain” (chieflyaimed at delaying sexual debut among young people); “be faithful” (aimedchiefly at reducing the number of partners); and “use condoms” (chieflyaimed at use with non-regular partners). But the actual interventions (scien-tifically tested or otherwise) that produced these behavioural changeshave not been specified (34). In the absence of clear data, a controversyemerged – and continues – about the relative importance of delayed sexualdebut, partner reduction and condom use in influencing the dynamics of theepidemic in Uganda (35). Similarly, a population-based study in Zimbabwehas shown evidence of a decline in HIV prevalence, particularly among youngpeople, that was accompanied by changes in reported sexual behaviour. Againit is not possible to attribute this change to specific interventions (36).
Attribution issues notwithstanding, observational data from these and othercountries provide evidence that delaying sexual debut, reducing the numberof sexual partners and increasing the use of condoms has been achieved
48
92-4-120938-0_CH03_48

through the implementation of various behavioural change interventions –both formal and informal – and that these behavioural changes appear to havecontributed to 50–90% reductions in HIV incidence and prevalence in anumber of populations in the 1990s, as measured by epidemiological surveil-lance (37–42). Most analysts have concluded that it was the combination ofbehavioural intervention strategies and involvement by high-level politicaland community leaders that produced significant behavioural changes and,as a result, reductions in HIV incidence and prevalence in these countries(3, 4, 34, 36, 42).
Some of the observed trends in HIV incidence and prevalence may be due tothe natural dynamics of the epidemic, including an “exhaustion of suscepti-bles” and people modifying their behaviour in the light of knowing otherswho have AIDS; and behavioural trends may reverse over time, erasing someof the gains made in earlier years. An analysis by researchers leading theRakai cohort study in Uganda illustrates these possibilities. HIV prevalence,reported age at first sexual intercourse, reported number of sexual partnersand condom use had probably all improved in this cohort in the late 1980sand early 1990s, as they had in other areas of southern Uganda. However,although HIV prevalence declined by 6.2% between 1994 and 2003, most ofthis decline (about 5%) was attributable to HIV-related mortality. In thiscommunity, between 1995 and 2002 the age at first sexual intercourse actu-ally dropped among both males and females, and from 1994 to 2003 theproportion of adolescent girls aged 15–19 reporting having had two or morenon-marital sexual partners increased significantly. But despite these be-havioural changes, HIV incidence remained stable, which the study authorsattributed to an increase in condom use with casual partners occurring amongboth males and females (43).
These observations underscore the need for, and the usefulness of, combiningepidemiological and behavioural data for the same time periods. They alsoemphasize the usefulness of prevalence data for young people, which can beused as a marker of recent change and lead to a better understanding of whatis really occurring in terms of HIV transmission and prevention and to whatbehavioural changes epidemiological outcomes may be attributed (36, 44).
3.2.1 Voluntary counselling and testing
The establishment of voluntary counselling and testing programmes has beena feature of national HIV prevention strategies in a number of countries. Thekey goals of these programmes are to provide people with the opportunity tolearn their HIV status, to counsel people about how to avoid becoming in-fected or spreading HIV and to refer people to appropriate medical and psy-chosocial care. A number of studies in developed and developing countries
49
92-4-120938-0_CH03_49

have been undertaken to determine if, in addition to its diagnostic and referralbenefits, voluntary counselling and testing may lead to reductions in riskybehaviours and reductions in HIV infection rates (45). Overall, data fromrandomized controlled trials and observational studies show mixed results inthis regard (46). For example, in a randomized trial of an intervention forcouples, which was conducted in Kenya, Trinidad and the United Republicof Tanzania, both male and female participants who had counselling and weretested were significantly more likely to report a reduction in the incidence ofunprotected intercourse with a non-primary partner than those in the controlgroup, who received only basic health information. Among those in the in-tervention group, HIV-positive men were more likely than HIV-negative mento report a reduction in the incidence of unprotected intercourse with bothprimary and non-primary partners (47). (This study also looked at STI end-points, but it was underpowered and the effect was non-significant.) Otherresearch from sub-Saharan Africa has found that behavioural changes in-duced by voluntary counselling and testing programmes among coupleswhose HIV status is discordant (that is, one partner is HIV positive and oneis not) varied by the sex of the participant: condom use within these coupleswas more frequent and consistent when men were the HIV-negative partners(48–50). Thus, it appears that the effectiveness of these programmes in pre-venting HIV infection is limited to certain individuals and couples.
Additionally, utilization of voluntary counselling and testing remains low inmost communities with a high prevalence of HIV, chiefly because access toservices is often limited and stigma and discrimination continue to surroundHIV infection. To address this situation, a large community-randomized in-tervention study of voluntary counselling and testing is under way in SouthAfrica, Thailand, the United Republic of Tanzania and Zimbabwe. The in-tervention aims to increase the availability of services in community settings,to engage communities through outreach and to provide post-test support –all of which are intended to change community norms, mitigate stigma andreduce the risk of HIV infection among all community members regardlessof whether they participate directly in the intervention (51).
3.2.2 Treatment for drug addiction
Numerous studies have shown that substance abuse treatment programmescan have a significant effect on HIV transmission among injecting drug users(52, 53), although few of these studies are experimental and most have oc-curred in the United States. These drug treatment programmes usually involveboth opiate substitution (particularly with methadone) and the provision ofbehavioural counselling; they generally attempt to help injecting drug usersdecrease the number and frequency of injections or to cease injecting alto-gether. Reducing drug-related risk behaviours leads to fewer potential
50
92-4-120938-0_CH03_50

exposures to HIV. Some of the earliest data demonstrating the efficacy ofdrug treatment programmes to prevent the spread of HIV came from an ob-servational study in the United States of in-treatment and out-of-treatmentintravenous opiate users randomly recruited from a methadone maintenanceprogramme and its surrounding neighbourhood in Philadelphia, Pennsylvania.At follow up at 18 months, 3.5% of the methadone maintenance patients whohad been in treatment continuously were HIV positive compared with 22%of out-of-treatment injecting drug users, representing a 6-fold difference inthe rate of seroconversion (54). Another prospective study showed that at36 months 8% of injecting drug users in treatment had become infected com-pared with 30% of those not in treatment (55). Although these data come fromobservational studies rather than experimental studies, the large differencesobserved suggest that such interventions can be effective. But the availabilityof methadone maintenance programmes is limited throughout the world, notleast because drug substitution is illegal or highly regulated in many coun-tries, including those with HIV epidemics strongly associated with the use ofinjected drugs.
3.3 Biomedical interventions: evaluating technologies
Research into biomedical interventions to prevent HIV infection involvestesting the effectiveness of physical and chemical technologies to prevent thetransmission or acquisition of HIV. The goal of such interventions is to mod-erate the influence of biological or physiological factors that may increaseinfectiousness or susceptibility to HIV or to prevent infection from progress-ing after actual exposure. Some biomedical strategies have been well testedand implemented; others are still at the early stages of development. Althoughmost studies of biomedical interventions assess outcomes at the individuallevel, some have been designed to effect community-level change.
3.3.1 Reducing iatrogenic transmission
As soon as it was understood that AIDS was caused by a bloodbornepathogen, the importance of the health services taking steps to avoidparenteral iatrogenic transmission became apparent. Beginning in themid-1980s, several strategies were introduced to reduce the likelihood ofpatients acquiring HIV infection from blood transfusions both in developedand developing countries; these included the widespread use of diagnosticassays for detecting HIV in blood and imposing restrictions on donorsknown to be at risk of HIV infection (56–59). Other strategies that have beenused to reduce iatrogenic transmission include educating the public aboutthe risks of engaging in non-sterile medical practices, such as sharing needles,and demonstrating to patients that the medical care they are receiving issafe by taking a new auto-disable syringe out of a sealed package and using
51
92-4-120938-0_CH03_51

single-dose phials (60). Although rigorous studies testing the effectivenessof these interventions are lacking, implementing such practices in developedcountries has been effective in virtually eliminating HIV transmissionthrough blood donation and medical practices (61, 62). However, some epi-demiologists continue to argue that unsafe injection practices account for agreater proportion of HIV transmissions in resource-poor settings than sexualintercourse does (63). But this has been countered by a thorough assessmentof the epidemiological data from across sub-Saharan Africa and by a cohortstudy in rural Zimbabwe both of which unequivocally concluded that sexualinteraction and not unsafe injections remains the primary mode of HIV trans-mission in that region (64, 65). Despite these conflicting perspectives, allagree that there is a need to effectively monitor injection practices at healthfacilities and to ensure the scale-up of safe procedures.
3.3.2 Managing STIs
A large body of evidence accumulated from epidemiological and clinicalstudies has shown that the risk of sexual transmission of HIV is substantiallyincreased in the presence of other STIs (66). The evidence shows thatSTIs – particularly those associated with genital ulceration – can enhance theinfectiousness of people who are HIV positive as well as the susceptibility ofpeople who are HIV negative. STI prevalence is high in many countries withsubstantial HIV epidemics, and this is often due at least partly to poor STItreatment services. Therefore, the diagnosis and treatment of STIs have thepotential to be effective prevention strategies by reducing STI prevalence incouples whose HIV status is discordant. Three large randomized trials havemeasured the effects of community-wide STI treatment interventions in dif-ferent populations living close to Lake Victoria in east Africa. The first,conducted in the Mwanza region of the United Republic of Tanzania, showedthat improved STI treatment services, using syndromic management and de-livered through government-run primary health-care units, reduced HIVincidence in the general adult population by an estimated 38% (67, 68). Thesecond, conducted in the Rakai district of Uganda, evaluated the effect ofperiodic mass treatment of STIs. All adults living in intervention communitieswere treated for STIs at 10-monthly intervals, whether or not they reportedSTI symptoms. After 20 months of follow up, this intervention showed nosignificant effect on HIV incidence (69). The third trial, conducted in theMasaka district of Uganda, evaluated whether a combined behavioural andSTI syndromic management intervention was more effective than a be-havioural intervention alone in reducing HIV transmission; it found nosignificant difference in HIV incidence between study arms after 3.6 yearsof follow up (33). All three trials reported some significant reductions in theincidence and prevalence of STIs.
52
92-4-120938-0_CH03_52

The contrasting results of these studies call for careful analysis and interpre-tation. A synthesis of data from these trials concluded that differences in thestudy populations – with respect to sexual risk behaviour and STI rates aswell as the stage of the HIV epidemic – and not differences in interventionstrategy, were the key determinants of the contrasting HIV outcomes in thethree locations (70, 71). The investigators concluded that using STI controlmeasures to prevent the spread of HIV is likely to be most effective in pop-ulations with sexually transmitted epidemics that are early and concentratedand in populations with a high prevalence of STIs and sexual risk behaviours.The results of the Mwanza trial have led to widespread implementation ofsyndromic STI management in many countries.
It has been recognized that infection with herpes simplex virus type 2(HSV-2) plays a particularly important role in HIV transmission. A system-atic review and a meta-analysis summarized evidence from observationalstudies (72, 73). The more recent review found that prevalent HSV-2 infectionwas associated with a 3-fold increase in the risk of HIV acquisition both inmen and women in studies in the general population; weaker effects wereseen in studies of at-risk groups, possibly because such groups also have ahigh prevalence of other STIs (73). It is likely that HSV-2 infection alsoincreases the infectiousness of people who are HIV positive. Data from arandomized controlled trial of valacyclovir in Burkina Faso showed that sup-pressive therapy administered during a 3-month period reduced genitalshedding of HSV-2 and HIV and also reduced HIV plasma load (74). Basedon these observational data, and strengthened by the findings of the study inBurkina Faso, a number of phase III randomized trials are under way in Peru,South Africa, the United Republic of Tanzania, the United States, Zambiaand Zimbabwe to measure the effects of episodic or suppressive antiviraltherapy in people who are infected with HSV-2 on HIV acquisition or trans-mission (75).
3.3.3 Antiretrovirals to prevent HIV infection
3.3.3.1 Preventing mother to child transmission
One of the most significant developments in HIV prevention was the findingthat certain antiretroviral drugs could be administered to pregnant women andtheir newborns in such a way as to significantly reduce the likelihood of HIVbeing passed from mother to child before, during and after delivery. Threekey randomized controlled trials provided the proof. The first, conducted inthe United States, involved a three-part regimen of zidovudine given to themother and her newborn; it reduced HIV transmission by two thirds (76). Thesecond, conducted in Thailand and Côte d’Ivoire, involved a shorter regimenof zidovudine, and it reduced transmission by 44–50% (77, 78). The third
53
92-4-120938-0_CH03_53

trial, conducted in Uganda, demonstrated that a single dose of nevirapineadministered to the mother at the onset of labour and to the infant soon afterbirth reduced HIV transmission by nearly 50% (79). Together these studiesdemonstrate that long-course and short-course zidovudine and single-dosenevirapine are effective interventions for reducing mother to child transmis-sion of HIV (80). Several studies are under way in resource-poor settings toassess the effects of using highly active antiretroviral treatment (HAART)during pregnancy (that is, treating the woman for her own infection) on thesubsequent incidence of mother to child transmission. Preliminary resultsfrom one study conducted in Côte d’Ivoire showed the HIV transmission rateamong pregnant women on HAART was 1.45% compared with 3.89% forthose on a standard short-course antiretroviral regimen (81).
Interventions to reduce the incidence of HIV transmission that occurs throughbreastfeeding have also been tested. Where feasible and acceptable, the useof breast-milk substitutes has been shown to significantly reduce infectionamong infants (82, 83). Where implemented fully, antiretroviral treatmentand breastfeeding interventions have had a remarkable effect: in the UnitedStates, for example, the number of children who acquired HIV perinatallydecreased by 89% between 1992 and 2001 (84).
3.3.3.2 Antiretrovirals for post-exposure prophylaxis
In some countries health-care workers and prison officers have had access totreatment with antiretroviral drugs following assumed (chiefly parenteral)exposure to HIV infection in the workplace. A retrospective study of occu-pational post-exposure prophylaxis concluded that zidovudine monotherapy(administered within 24 hours of exposure and over the course of 28 days)reduced occupational HIV transmission (chiefly through needle-stick in-juries) by approximately 81% (85). In more recent years, this approach hasbeen extended to become a medical strategy for coping with non-occupational exposures, such as sexual assault or condom breakage, and itappears to be effective (86, 87). However, studies have not included data onuntreated individuals, so these findings should be interpreted with caution.Also, adherence to the full regimen of post-exposure prophylaxis is difficultto achieve but it is likely to be important. In a programme in San Francisco,40% of all eligible survivors of sexual abuse initiated post-exposure prophy-laxis regimens but less than 10% completed them (88). Lack of completeadherence might compromise the effectiveness of using antiretrovirals forpost-exposure prevention, as has been shown for incomplete adherence inHIV treatment.
54
92-4-120938-0_CH03_54

3.3.3.3 Antiretrovirals for preventing sexual transmission
A key benefit of using HAART for treatment of HIV disease is that it reducesplasma viral load. Strict adherence to HAART regimens contributes to thesustained suppression of virus. Some data indicate that the risk of HIV trans-mission is directly associated with the infected individual’s viral load (89).These findings have led many experts and laypeople to believe that thewidespread use of HAART could have important effects on the sexual trans-mission of HIV. There are no prospective data yet to prove this, although amultisite randomized controlled trial is under way to determine whether an-tiretroviral treatment can prevent sexual transmission of HIV-1 in serodis-cordant couples (90, 91). The primary data establishing the relationshipbetween lower plasma viral load and reduced sexual transmission of HIVcome from a cohort in Rakai, Uganda, who were not taking HAART (92).
It is making a significant leap to assume that the effects of HAART at theindividual level will translate into similar effects at the population level.Mathematical models have demonstrated that at the population level the ben-eficial effect of HAART on reducing sexual transmission of HIV could beoffset by an increase in the circulation of drug-resistant strains of HIV andincreases in risky sexual behaviour that might occur if people believe HIVtransmission is unlikely or if HIV infection becomes less feared becausetreatment is available (93, 94). Furthermore, because HAART extends sur-vival time, where it is widely used there is a larger pool of HIV-positiveindividuals who have the potential to spread the infection over a longer periodof time. The net effect of all these competing factors is, therefore, difficult topredict. However, an observational study in Taiwan, China, concluded thatthe estimated HIV transmission rate in the country declined by 53% after theintroduction of free access to HAART in 1997, while no significant be-havioural change occurred. The researchers were careful to note that thewidespread use of HAART can be an effective measure to control HIV epi-demics in countries with a low prevalence, but may not be as effective, ormay not be effective at all, in settings with an already high prevalence ofinfection, for a number of reasons having to do with the exponential courseof HIV epidemics (95).
Considering these data together – data from studies in animals, of post-exposure prophylaxis, of preventing mother to child transmission and datafrom Rakai on lower viral loads and lowered rates of transmission – has ledto an interest in exploring the possibility of using antiretroviral treatment forpre-exposure prophylaxis. Randomized trials are planned or under way inBotswana, Ghana, Peru, Thailand and the United States to test the hypothesisthat administering antiretroviral treatment (specifically tenofovir) to peoplewho are HIV negative but at high risk will reduce HIV acquisition amongthem (96).
55
92-4-120938-0_CH03_55

3.3.4 Male circumcision
Numerous studies have found evidence that uncircumcised men have higherrates of HIV infection than their circumcised counterparts (97). It has beenhypothesized that male circumcision protects against HIV infection chieflybecause the foreskin, which contains a high density of HIV-specific cellulartargets, has been removed (98). In the Rakai STI trial in Uganda, no HIV-negative male partner of an HIV-positive female acquired HIV if he had beencircumcised, even when the female had a high viral load (99). Two meta-analyses of observational studies (reviewing 37 and 25 studies, respectively)found that the prevalence of HIV among circumcised men was about half thatof uncircumcised men (100, 101), and this finding has been reinforced by acohort study in India (98). The association was even stronger in the 15 studiesthat adjusted for potential confounders; and it was stronger among men athigher risk of HIV infection than those in the general population (100, 101).
Results from the first randomized controlled trial testing the efficacy of malecircumcision as an intervention to prevent HIV infection confirmed findingsfrom earlier observational studies. This trial, conducted in Orange Farm,South Africa, involved more than 3 000 uncircumcised, HIV-negative menaged 18–24 years. At interim analysis, results indicated that circumcision(which was performed by physicians under sterile conditions) conferred 70%protection against HIV infection (102). This remarkable result caused thestudy to be halted and the intervention to be offered to participants in thecontrol group. Additional trials of male circumcision, including one that willassess protection from male-to-female transmission, are ongoing in Kenyaand Uganda to determine whether the results from South Africa can bereplicated. Meanwhile, discussions of the public health implications ofmale circumcision interventions already have begun, including the possibil-ities of circumcision occurring under non-sterile conditions and “riskcompensation” (that is, circumcised men may engage in riskier behaviourbecause they think they are protected against infection) (103).
3.3.5 Vaccines
There is general consensus that the HIV prevention strategy with the potentialto have the greatest impact would be an HIV vaccine. Unfortunately, no ef-fective vaccine exists, nor is one expected for many years. The complexityof HIV, the multiplicity of its variants, the ability of the virus to mutate, thelack of validated correlates of protection – not to mention the costs andlogistics of mounting large-scale clinical trials – have made it extremelydifficult to develop and test candidate vaccines. Moreover, there is little ex-pectation that any vaccine that emerges in the near future will be close to100% effective. More than 30 products or combinations of products have
56
92-4-120938-0_CH03_56

been tested in more than 50 phase I and phase II trials, but only oneproduct (AIDSVAX gp120) so far has completed phase III testing – in theNetherlands, Thailand and the United States – and it showed no efficacy(104). Another phase III trial is under way at several sites in Thailand; it istesting two vaccine candidates, ALVAC-HIV vCP1521 and AIDSVAXgp120 B/E (105).
3.3.6 Microbicides
A microbicide is a chemical compound designed to block the sexual trans-mission of HIV by killing or inactivating the virus, blocking the entry of thevirus into target cells or interrupting the viral life cycle once it has enteredtarget cells. Microbicides are being developed chiefly for vaginal use, al-though research on products for rectal use is also under way. The drive behindmicrobicide development is the urge to provide women with an HIV preven-tion technology that does not depend on male cooperation to the same extentas the male, or even the female, condom. The earliest randomized trials wereconducted with nonoxynol-9, which has been used as a spermicide but hasalso shown anti-HIV activity in vitro. Altogether there were five rigorousrandomized controlled trials conducted in a number of countries, chieflyamong female commercial sex workers; these studies found no evidence thatnonoxynol-9 protects against vaginal acquisition of HIV infection (106,107). There was some evidence that it may, in fact, cause harm by increasinggenital lesions. For example, the large multisite study of COL-1492 vaginalgel, which contains nonoxynol-9, found a significant increase in HIV inci-dence among female sex workers who used the gel compared with those whodid not (106, 107).
There are more than 60 products in preclinical and clinical development, tar-geting a number of different mechanisms of action and different phases ofthe HIV life-cycle (108). In early 2006, there were about 10 compounds inphase I trials, 6 in phase II trials, and 4 in phase III trials (109). The difficultiesof developing and testing microbicides are similar to those of vaccines, in-cluding scientific uncertainties, the complexity of trial designs and the costs(3). Also, as in the case of vaccines, it is unlikely that any microbicide willbe 100% effective. Yet, it is estimated that the introduction of even a partiallyeffective microbicide could prevent as many as 2.5 million new HIV infec-tions over 3 years (110).
3.3.7 Cervical barrier methods
In addition to microbicides, which function as a chemical barrier, interest hasgrown in examining other female-initiated barrier methods that may offersome physical protection against the transmission and acquisition of HIV
57
92-4-120938-0_CH03_57

infection. The female condom is a lubricated polyurethane sheath with a ringon either end that is inserted into the vagina before sexual intercourse. It hasbeen studied primarily for its effectiveness in preventing pregnancy and STIsother than HIV. Laboratory studies and clinical trials have shown that thefemale condom provides an effective barrier to organisms smaller than thosethat cause most STIs, and it is at least equivalent to male condoms in termsof preventing gonorrhoea, trichomoniasis and chlamydia (111). There havebeen no clinical trials specifically assessing the efficacy or effectiveness ofthe female condom in preventing HIV infection. However, based on studiesin which STI prevention and pregnancy prevention were assessed, it is esti-mated that the female condom is 94–97% effective in reducing the risk ofHIV infection if used correctly and consistently (111). The female condommay be a more attractive choice than male condoms for some women becauseit resists breaks and tears and covers both the internal and external genitals,which are primary sites of STI lesions (112–114).
Findings from basic and clinical research indicate that HIV susceptibility maynot be equally distributed across the epithelial surfaces in the vagina and thatthe cervix may be particularly vulnerable to HIV and STI transmission(115, 116). This has led to an interest in the risk-reduction potential of cervicalbarrier methods, such as the diaphragm and cervical cap. These barriers aremade of soft latex or silicone and are used with spermicidal cream or jellyand then inserted into the vagina to fit over the cervix. Several observationalstudies have indicated that when the diaphragm is used in conjunction withspermicide it may offer protection against some STIs and their associatedsequelae (117–121). As of March 2006, seven clinical trials at various stages(phase I to phase III) were under way to examine the diaphragm’s effective-ness in preventing STIs (122). Of these studies, the furthest along is theMethods for Improving Reproductive Health in Africa Trial, a phase III trialthat will measure the effectiveness of the diaphragm when used with Replenslubricant gel in preventing heterosexual acquisition of HIV infection amongwomen in South Africa and Zimbabwe (123).
3.3.8 Summary
There are a number of biomedical technologies under development that showpromise for preventing the spread of HIV. Unfortunately, for some of theseinterventions, the scientific, logistical and ethical complexities inherent inrunning large-scale trials of effectiveness mean that it may be many yearsbefore this promise is realized.
3.4 Social interventions
Social arrangements, institutions, laws, policies and customs can influencegreatly the ability of individuals to engage in protective behaviours and to
58
92-4-120938-0_CH03_58

use biomedical technologies to avoid becoming infected with HIV. In recentyears, increased attention has been paid to the possibilities of modifying so-cial arrangements that affect HIV prevention. Whether they are called “socialstrategies” (2), “structural interventions” (124–127) or “environmental in-terventions” (125), efforts to create social conditions that facilitate healthpromotion and risk reduction have proven to be effective in a number oflocales, although there are few examples of rigorously tested approaches.
3.4.1 100% condom use
Perhaps the most notable example of a social intervention aimed at preventingthe spread of HIV is the Thai “100% condom” use programme, which madecondom use mandatory in all brothels, even while prostitution remainedtechnically illegal. The promotion of condom use was coupled with an em-phasis on decreasing visits to sex workers and other non-regular partners,particularly among Thai military recruits. But the Thai national response, likethat in Uganda, also included national sentinel surveillance, mass mediacampaigns, community mobilization and interaction between nongovern-mental organizations, community-based organizations and industry, as wellas strong public statements and resource commitments made by politicalleaders at the highest levels (128). As a result of this comprehensive socialstrategy, the rate of Thai military recruits having sex with commercial sexworkers decreased from 57.1% in 1991 to 23.8% in 1995; of those who con-tinued to have sex with commercial sex workers, the proportion that usedcondoms increased from 61% in 1991 to 92.6% in 1995. Between 1991 and1993 the rate of HIV incidence among military conscripts fell from 3/100person-years to 0.3/100 person-years (42, 129, 130).
A cohort study of repeat blood donors in the northern provinces in Thailandfound similar results: HIV incidence decreased from 1.7/100 person-years in1989 to 0.5/100 person-years in 1994 (42). As a result of the success of theThai programme, a number of other Asian nations have implemented similarprogrammes, which have involved making policy changes in order to workaround the continued illegality of prostitution. Data from these countries in-dicate that there have been increases in the use of condoms and decreases inthe incidence of STIs (131). In Cambodia, declining HIV rates between 1996and 2000 have been attributed to the 100% condom use programme and im-provements in STI care (131).
3.4.2 Access to syringes
Perhaps the most studied social intervention is that of increasing access tosterile syringes for those who use injected drugs. Although such drug use isillegal nearly everywhere in the world, many countries have adopted harm
59
92-4-120938-0_CH03_59

reduction policies that allow, if not provide, for access to sterile injectingequipment for those who continue to inject. The implementation of needle/syringe-exchange programmes, in particular, has resulted in decreased nee-dle-sharing and related practices, and reduced HIV incidence and prevalencein numerous locales (124, 132–136). A review of data from 81 cities acrossEurope, Asia, and North America with and without syringe-exchange pro-grammes found that, on average, HIV prevalence among injecting drug usersincreased by 5.9% per year in the 52 cities without exchange programmesand decreased by 5.8% per year in the 29 cities with exchange programmes.Thus the average annual change in prevalence was 11% lower in cities withexchange programmes (132). But political resistance to strategies that maybe construed as condoning drug use has prevented many countries andcities from implementing exchange programmes and other harm reductioninterventions.
3.4.3 Economic empowerment interventions for women
The increasingly disproportionate impact of HIV and AIDS on women andgirls throughout the world (see chapter 2) has implicated gender inequity asa driver of the epidemic. The cultural construction and social organization ofgender have disempowered women and girls in many settings, making themparticularly vulnerable to HIV infection and its consequences. These socialfactors operate in a number of ways, including through low educational at-tainment, early marriage, fertility expectations and sexual violence and alsothrough economic inequities, such as lower wages and unpaid care work anda lack of property and inheritance rights. As a result of such arrangements,many women and girls do not have basic information about their bodies, sexor sexuality, and do not know how to prevent HIV and other STIs; they cannotdemand that male partners use condoms; they cannot refuse sex; they areoften forced to sell sex; and if they inject drugs they often are given a dirtyneedle to use after their male partner.
In response to these situations, interest has been growing in implementingincome-generation interventions, such as microfinance projects – anotherform of social or structural intervention – as a means of empowering womenin their relationships and reducing their material dependence on men. Severalstudies of micro-credit interventions targeting women and their fertility out-comes (pregnancy rates and contraceptive use) indicated that economicempowerment translated into increased self-esteem, improved social net-works, increased control over household decision-making, increased bar-gaining power and increased contraceptive use (137). Micro-financing hasonly recently been applied to HIV prevention, so few empirical examples ofinterventions exist. One large-scale community-level randomized controlledtrial in South Africa of an integrated, comprehensive intervention that
60
92-4-120938-0_CH03_60

simultaneously provided micro-credit to women and HIV/AIDS education tothe whole community has been completed. The study assessed intermediateattitudinal and behavioural outcomes and HIV incidence (138). In this struc-tural intervention, eight communities were matched and randomly allocatedto receive the intervention at onset of the study or after 3 years. There was noevidence of an effect on community-level HIV incidence or risky sexual be-haviour in the short-term, although there was a significant reduction inphysical and sexual abuse among intervention participants (139).
Although the need for more social interventions has been recognized, thereare a number of obstacles to evaluating their effectiveness. Chief among theseis the fact that it can be exceedingly difficult to fit social-level analysis andinterventions into an experimental study design (127). Essentially, the prob-lem is that complex social phenomena – such as gender, poverty, economicinequality and violence – cannot be reduced to a few variables that can easilybe modified or controlled for testing in experimental designs; and the attri-bution of effects to such interventions is often difficult without suitablecomparison groups.
3.5 Behavioural and social issues in developing and implementinginterventions
There are a number of interrelated issues that cut across virtually all inter-ventions designed to prevent the spread of HIV, and these must be attendedto in developing and implementing such interventions. Space limitations donot allow us to discuss these in detail, but they are important to mention.
3.5.1 Recruitment to and retention in studies
The requirements of rigorous randomized controlled trials, the range andnumber of HIV prevention technologies under study, and HIV incidence lev-els necessary to enable researchers to detect true effects from an interventionmean that large numbers of people must be recruited and retained in multisitestudies over many years. This is logistically challenging and also expensive(127, 140, 141).
3.5.2 Adherence to prevention protocol
Once recruited and retained, it is essential that study participants adhere tothe prevention protocol if the full effectiveness of the intervention is to becaptured. For some technologies and in some social and familial circum-stances, this may prove impossible for study participants. If significantnumbers of participants have less than optimal adherence, the study and itsoutcomes may be compromised. Counselling about the importance of
61
92-4-120938-0_CH03_61

adherence is an essential but labour-intensive and costly component of HIVprevention trials (142, 143).
3.5.3 Behavioural disinhibition (risk compensation)
As discussed in the context of circumcision and pre-exposure prophylaxis, itis possible that when people perceive that a particular HIV prevention methodis effective (even if it is only partially effective), they may stray from usingother methods that are already known to be equally or more effective (forexample, using male condoms, delaying their first experience of sexual in-tercourse and reducing their number of sexual partners). Such behaviouraldisinhibition (or risk compensation) may slow the progress of new interven-tions in reducing HIV infection rates at the individual level and the populationlevel (43, 144). This concern is relevant to all prevention modalities – be-havioural, biomedical and social – and for those who are participating instudies and those who are not (145). However, we must not let fears overdisinhibition impede efforts to develop and implement interventions becausewe need as many effective tools as possible to tackle the HIV/AIDS epidemic.It is essential that service providers diligently promote behavioural changeand communicate the need to continue to engage in risk reduction or avoid-ance even as new prevention methods emerge.
3.5.4 Partial efficacy and partial effectiveness
No single prevention method is 100% effective. Even sexual abstinence,which may be theoretically effective, is imperfectly practised. The most ef-fective prevention technology is the male latex condom, which has anestimated 80–90% level of expected risk reduction with correct and consistentuse. Based on the outcomes of the first randomized controlled trial of malecircumcision, that intervention appears to have the next highest level of ef-ficacy, at 65–70% for a single procedure (102). Additional methods understudy (such as vaccines, microbicides, pre-exposure antiretroviral prophy-laxis) are estimated to have only a 25–50% level of effectiveness using currentstudy-design calculations and are methods that require repeated administra-tion (145, 146). This means that researchers, service providers, programmemanagers, policy-makers and community advocates must not promise toomuch for any particular method; they must be clear about the need to use acombined approach to preventing the spread of HIV; and they must empha-size the importance of adherence to behavioural changes.
3.5.5 Engaging communities in research
The question of how best to facilitate the involvement of affected communi-ties in research has been present since the beginning of the epidemic. Much
62
92-4-120938-0_CH03_62

has been written about culture clashes between scientists and community ad-vocates. Recently, this conflict has affected the inauguration of HIV preven-tion trials, particularly pre-exposure antiretroviral prophylaxis trials (usingtenofovir), in a number of developing countries (147, 148).
Although researchers may feel they are abiding by ethical standards in theconduct of trials and consulting with community leaders and representatives,community advocates continue to raise questions about the adequacy of HIVprevention counselling, informed consent, provision of treatment for peoplewho acquire HIV infection during the time they are participating in studiesand the limited involvement of communities in designing studies. These ten-sions must be resolved because most researchers and advocates believe thatHIV prevention studies should go forward as long as they are ethically con-ducted and are done with, rather than on, communities (147, 148).
3.6 Conclusion
This review of the landscape of HIV prevention strategies tells us a numberof things. First, we have a great deal of evidence from research studies – bothexperimental and observational – and from practical real-world experienceto make the case for the effectiveness – and potential effectiveness – of anumber of interventions to prevent the spread of HIV. (See Table 3.1 for asummary of the evidence reviewed in this chapter.) Although not all researchhas been rigorous, and not all interventions have shown significant results,we do know that reductions in risk and rates of HIV infection can be achievedthrough behavioural, biomedical and social strategies, particularly when theyoccur together. Principles derived from infectious disease epidemiology andbehavioural and social theory can be incorporated into rigorous interventiondesigns and real-world practices that are relevant and appropriate in differentsettings. These may yield different effects as a result of such things as havingto vary the intervention to fit different contexts (including local culture andsocial structure), variations in the quality of implementation, and variationsin underlying HIV and STI epidemiology (as in the case of the STI manage-ment trials in Rakai and Masaka in Uganda and Mwanza in the UnitedRepublic of Tanzania, described above). No intervention will be 100% ef-fective, but implementing many that have been shown to work, and doing soin different combinations in different places as befits the local situation, willyield important prevention outcomes at a population level.
63
92-4-120938-0_CH03_63

Tab
le 3
.1S
um
mar
y o
f ev
iden
ce a
nd
key
ref
eren
ces
for
beh
avio
ura
l, b
iom
edic
al a
nd
so
cial
inte
rven
tio
ns
to p
reve
nt
HIV
infe
ctio
n
Typ
e o
f in
terv
enti
on
Co
mm
ents
on
th
e ev
iden
ceK
ey r
efer
ence
s
Beh
avio
ura
lIn
terv
entio
ns a
imed
at r
educ
ing
sexu
al r
isks
and
ris
ksas
soci
ated
with
inje
ctin
g dr
ug u
se th
at in
volv
e co
unse
lling
for
indi
vidu
als,
cou
ples
or s
mal
l gro
ups;
wor
ksho
ps; s
kill-
build
ing
prog
ram
mes
; use
of p
opul
ar o
pini
on le
ader
s, p
eer-
base
d,ne
twor
ks, c
omm
unity
mem
ber;
mas
s m
edia
inte
rven
tions
Sys
tem
atic
rev
iew
s an
d m
eta-
anal
yses
con
duct
ed a
mon
g:
H
eter
osex
uals
In
ject
ing
drug
use
rs
M
en w
ho h
ave
sex
with
men
Y
oung
peo
ple
H
IV-p
ositi
ve p
eopl
e
• M
uch
evid
ence
from
man
y R
CT
sa in
dev
elop
ed a
ndde
velo
ping
cou
ntrie
s•
Num
erou
s sy
stem
atic
rev
iew
s an
d m
eta-
anal
yses
• G
ener
ally
indi
cate
sm
all t
o m
oder
ate
effe
ct s
izes
ove
r lim
ited
follo
w-u
p pe
riods
• T
arge
ted
at s
peci
fic p
opul
atio
ns o
r gr
oups
• B
ehav
iour
al o
utco
mes
are
chi
efly
sel
f-re
port
ed; s
ome
ST
Ib
and
HIV
out
com
es• S
ome
obse
rvat
iona
l evi
denc
e fo
r im
pact
of b
ehav
iour
cha
nge
on H
IV in
cide
nce
and
prev
alen
ce a
t cou
ntry
leve
l
• W
eak
to m
oder
ate
effe
cts
for
redu
ctio
ns in
sex
ual r
isk
and
ST
I out
com
es•
Mod
erat
e ef
fect
s on
sex
ual r
isk
redu
ctio
n; w
eak
to s
tron
gef
fect
s on
redu
ctio
n of
risk
s as
soci
ated
with
dru
g us
e an
d H
IVou
tcom
es•
Mod
erat
e to
str
ong
effe
cts
on s
exua
l ris
k re
duct
ion;
wea
k to
stro
ng e
ffect
s on
ST
I and
HIV
out
com
es•
Wea
k to
mod
erat
e ef
fect
s on
sex
ual r
isk
redu
ctio
n•
Mod
erat
e to
str
ong
effe
cts
on s
exua
l ris
k re
duct
ion
and
ST
Iou
tcom
es
5–21
, 27–
32
8–10
13, 1
7, 1
9
11, 1
4, 1
8
12, 1
5, 1
67
64
92-4-120938-0_CH03_64

Vol
unta
ry c
ouns
ellin
g an
d te
stin
g•
Few
RC
Ts
and
obse
rvat
iona
l stu
dies
in d
evel
oped
and
deve
lopi
ng c
ount
ries
• 1
syst
emat
ic r
evie
w•
Mix
ed r
esul
ts fo
r se
xual
ris
k be
havi
ours
and
HIV
inci
denc
e•
Effe
cts
of in
terv
entio
ns v
arie
d by
sex
of p
artic
ipan
t and
sero
stat
us
45–4
7
Tre
atm
ent f
or d
rug
addi
ctio
n (m
etha
done
mai
nten
ance
)•
Obs
erva
tiona
l stu
dies
in d
evel
oped
cou
ntrie
s su
gges
tsi
gnifi
cant
effe
ctiv
enes
s in
red
ucin
g H
IV in
cide
nce
(3.7
-fol
dto
6-f
old
diffe
renc
e in
ser
ocon
vers
ion
betw
een
thos
e in
trea
tmen
t and
thos
e ou
t of t
reat
men
t)
52, 5
4, 5
5
Bio
med
ical
Iatr
ogen
ic tr
ansm
issi
on•
Few
rig
orou
s st
udie
s ei
ther
in d
evel
oped
or
deve
lopi
ngco
untr
ies
• R
estr
ictin
g bl
ood
dono
rs a
nd r
educ
ing
unsa
fe in
ject
ing
prac
tices
hav
e be
en e
ffect
ive
in r
educ
ing
iatr
ogen
ictr
ansm
issi
on
56–6
0
61, 6
2
Man
agem
ent o
f ST
Is
Com
mun
ity tr
ials
H
SV
-2c i
nfec
tion
• F
ew R
CT
s in
dev
elop
ed a
nd d
evel
opin
g co
untr
ies.
Tria
lsfo
und
mix
ed r
esul
ts fo
r re
duci
ng S
TD
and
HIV
inci
denc
e.E
ffect
s of
inte
rven
tion
varie
d by
stu
dy p
opul
atio
ns w
ithre
spec
t to
sexu
al r
isk
beha
viou
r, S
TI r
ates
and
sta
ge o
f HIV
epid
emic
• 2
met
a-an
alys
es a
sses
sing
cor
rela
tion
betw
een
HS
V-2
and
prev
alen
ce o
f HIV
• 1
RC
T c
ompl
eted
and
oth
ers
unde
r way
mea
surin
g ef
fect
s of
supp
ress
ive
HS
V-2
ther
apy
on H
IV tr
ansm
issi
on o
rac
quis
ition
67–7
1
72, 7
3
74, 7
5
65
92-4-120938-0_CH03_65

Typ
e o
f in
terv
enti
on
Co
mm
ents
on
th
e ev
iden
ceK
ey r
efer
ence
s
Ant
iretr
ovira
ls fo
r pr
even
ting
HIV
infe
ctio
n
Pre
vent
ing
mot
her
to c
hild
tran
smis
sion
P
ost-
expo
sure
pro
phyl
axis
A
ntire
trov
irals
for
prev
entin
g se
xual
tran
smis
sion
• R
CT
s an
d sy
stem
atic
rev
iew
in d
evel
oped
and
dev
elop
ing
coun
trie
s sh
ow s
tron
g ef
ficac
y of
ant
iretr
ovira
l the
rapy
bef
ore,
durin
g an
d af
ter
deliv
ery
for
prev
entin
g m
othe
r to
chi
ldtr
ansm
issi
on•
RC
Ts
show
effi
cacy
of b
reas
tfeed
ing
inte
rven
tions
• O
bser
vatio
nal s
tudi
es in
dev
elop
ed a
nd d
evel
opin
g co
untr
ies
indi
cate
effi
cacy
of p
ost-
expo
sure
pro
phyl
axis
• N
o R
CT
s co
mpl
eted
but
one
und
er w
ay in
bot
h de
velo
ping
and
deve
lope
d co
untr
ies
to e
xam
ine
rela
tions
hip
betw
een
low
erpl
asm
a vi
ral l
oad
due
to H
AA
RT
d and
redu
ced
sexu
al tr
ansm
issi
onof
HIV
• 1
obse
rvat
iona
l stu
dy in
dica
ted
decl
ine
in H
IV tr
ansm
issi
on ra
te a
tco
untr
y le
vel s
ince
intr
oduc
tion
of H
AA
RT
• R
CT
s un
der
way
in d
evel
oped
and
dev
elop
ing
coun
trie
s to
exam
ine
usin
g an
tiret
rovi
ral t
hera
py a
s pr
e-ex
posu
re p
roph
ylax
isam
ong
unin
fect
ed p
eopl
e
76–8
1
82 85–8
8
90 95 96, 1
47
Mal
e ci
rcum
cisi
on•
Obs
erva
tiona
l dat
a fr
om d
evel
opin
g co
untr
ies
sugg
est p
rote
ctiv
eef
fect
of c
ircum
cisi
on a
gain
st m
ale
acqu
isiti
on o
f HIV
infe
ctio
n fr
omfe
mal
es•
1 R
CT
in d
evel
opin
g co
untr
y co
nfirm
s fin
ding
s fr
om o
bser
vatio
nal
stud
ies;
sho
ws
stro
ng e
ffica
cy (
65–7
0% r
educ
tion
in r
isk)
• A
dditi
onal
RC
Ts
unde
r w
ay in
dev
elop
ing
coun
trie
s to
con
firm
100,
101
102
103
Vac
cine
s•
Onl
y 1
com
plet
ed p
hase
III R
CT
in d
evel
oped
and
dev
elop
ing
coun
trie
s; s
how
ed n
o ef
ficac
y•
Sec
ond
phas
e III
RC
T in
dev
elop
ing
coun
try
unde
r w
ay
104
105
66
92-4-120938-0_CH03_66

Mic
robi
cide
s•
RC
Ts
in d
evel
opin
g co
untr
ies
of n
onox
ynol
-9 p
rodu
cts
show
ed n
oef
ficac
y an
d po
ssib
le h
arm
• 4
cand
idat
es ta
rget
ing
diffe
rent
mec
hani
sms
of a
ctio
n in
pha
se II
Itr
ials
106,
107
109
Cer
vica
l bar
rier
met
hods
• Bas
ed o
n S
TI a
nd p
regn
ancy
dat
a, fe
mal
e co
ndom
s ar
e es
timat
edto
be
94%
to 9
7% e
ffect
ive
in r
educ
ing
risk
of H
IV in
fect
ion
• 7
RC
Ts
unde
r w
ay to
exa
min
e ef
fect
iven
ess
of d
iaph
ragm
inpr
even
ting
HIV
and
ST
I
111
122
So
cial
100%
con
dom
use
pro
gram
me
• O
bser
vatio
nal d
ata
show
dec
reas
ed v
isits
to s
ex w
orke
rs,
incr
ease
d co
ndom
use
and
dec
reas
ed H
IV in
cide
nce
amon
g T
hai
mal
e m
ilita
ry c
onsc
ripts
in 4
- ye
ar p
erio
d
128–
130
Syr
inge
acc
ess,
incl
udin
g ne
edle
or
syrin
ge e
xcha
nge
• O
bser
vatio
nal d
ata
from
dev
elop
ed c
ount
ries
show
ed s
tron
gev
iden
ce o
f effe
ctiv
enes
s of
syr
inge
acc
ess
prog
ram
mes
in te
rms
of d
ecre
ased
nee
dle
shar
ing
and
othe
r un
safe
dru
g us
e pr
actic
esas
wel
l as
posi
tive
effe
cts
on H
IV in
cide
nce
and
prev
alen
ce
132–
135
Eco
nom
ic e
mpo
wer
men
t int
erve
ntio
ns ta
rget
ing
wom
en•
Evi
denc
e fr
om 1
RC
T o
f mic
rocr
edit
prog
ram
me
in d
evel
opin
gco
untr
y in
dica
tes
no e
ffect
on
com
mun
ity-le
vel H
IV in
cide
nce
orre
duct
ion
in s
exua
l ris
k bu
t sig
nific
ant r
educ
tion
in p
hysi
cal a
ndse
xual
abu
se
138,
139
a R
CT
s =
ran
dom
ized
con
trol
led
tria
ls.
b S
TI =
sex
ually
tran
smitt
ed in
fect
ion.
c HS
V-2
= h
erpe
s si
mpl
ex v
irus-
type
2.
d H
AA
RT
= h
ighl
y ac
tive
antir
etro
vira
l the
rapy
.
67
92-4-120938-0_CH03_67

Second, we must not confuse a lack of implementation with a lack of effec-tiveness. Those who quickly dismiss HIV prevention interventions as “notworking” usually do not take into account the fact that most interventionswith proven effectiveness have not been implemented on a large scale normade available to a high proportion of the people in need of them, even amongthe populations where they have been implemented. Based on data fromUNAIDS, the Global HIV Prevention Working Group estimates that the pro-portion of individuals at risk of acquiring or transmitting HIV infection andwho have access to selected key prevention interventions is as follows: 5%have access to care to prevent mother to child transmission; 12% have accessto voluntary counselling and testing; 19% to harm reduction strategies; 24%to AIDS education; and 42% to condoms (149).
Of course, providing access to interventions is not the same as ensuring thequality of the intervention, so scale-up must include a quality assurance com-ponent. Moreover, where financial, political, social and individual commit-ments to HIV prevention wane, we can expect to see the erosion of preventionsuccess, as appears to be the case in such places as Thailand and Uganda.Prevention only works if it is sustained over time by individuals practisingrisk reduction or avoidance and by societies making commitments of humanand financial resources to facilitate and support prevention efforts for the longhaul.
Third, given that there is no perfect method for ascertaining the true effec-tiveness of interventions, we should accept different levels and types ofevidence (as described in chapter 4) that taken together are appropriate forguiding public health policy and practice. This means that for cases in whichwe do not have sufficient evidence from rigorous experimental studies, wemust use observational data; and our interpretation of the strength of evidencemust take into account the methodological strengths and weaknesses of dif-ferent data sources. Yet, as we commit to implementing and scaling-up thoseinterventions that we know work, we must also continually strive to improvethe quality and quantity of evidence on the effectiveness of HIV preventionstrategies, which means we must continue to push for more rigorous research.
In this regard we can identify a number of important directions for HIV pre-vention research. First, we must develop and test more behavioural interven-tions that target people who are HIV positive since the psychosocial bases ofthese interventions may be slightly different from those directed at peoplewho are HIV negative. And we must develop and test more social interven-tions to address many of the factors underlying vulnerability to HIV infectionamong specific groups of people. Second, we can improve and expand ourresearch methods. This should include developing more rigorously conductedintervention trials and observational (plausibility) studies, making better use
68
92-4-120938-0_CH03_68

of observational data, recording and analysing data on time trends in be-haviour and infection rates in settings with different mixes and intensities ofinterventions, using statistical modelling with study results and other data togain a better understanding of interventions’ effects and determiningappropriate outcome indicators for social-level interventions. Third, we mustcollect and provide more data on the costs, as well as the effectiveness, ofinterventions in order to make a more compelling case to policy-makers.Fourth, we must continue to invest in the prevention technologies that havethe greatest potential for bringing about population-level effects. Finally, wemust be more explicit and specific with the public and with policy-makersabout HIV prevention successes (and failures) and the evidence behind them.
Acknowledgements
The authors are grateful to the World Health Organization and UNAIDS, inparticular Bruce Dick and Jane Ferguson from the WHO Department of Childand Adolescent Health and Development, for inviting us to prepare thischapter and for convening meetings with the authors of other chapters andreviewers to discuss and improve its content. We owe particular thanks toDavid Ross from the London School of Hygiene and Tropical Medicine forhis excellent comments and editorial suggestions. JA and SK thank amfARfor providing the work environment and organizational resources that facil-itated our research and writing.
References
1. Stover J et al. Can we reverse the HIV/AIDS pandemic with an expandedresponse? Lancet, 2002, 360:73-77.
2. Auerbach JD, Coates TJ. HIV prevention research: accomplishments andchallenges for the third decade of AIDS. American Journal of Public Health,2000, 90:1029-1032.
3. Global HIV Prevention Working Group. Global mobilization for HIV prevention:a blueprint for action, 2002 (http://www.gatesfoundation.org/nr/downloads/globalhealth/aids/HIVprevreport_final.pdf).
4. Valdiserri RO, Ogden LL, McCray E. Accomplishments in HIV preventionscience: implications for stemming the epidemic. Nature Medicine, 2003,9:881-886.
5. Semaan S et al. A profile of U.S.-based trials of behavioural and socialinterventions for HIV risk reduction. Journal of Acquired Immune DeficiencySyndromes, 2002, 30 Suppl:S30-50.
6. Kelly JA, Kalichman SC. Behavioural research in HIV/AIDS primary andsecondary prevention: recent advances and future directions. Journal ofConsulting and Clinical Psychology, 2002, 70:626-639.
7. Crepaz N et al. Do prevention interventions reduce HIV risk behaviours amongpeople living with HIV? A meta-analytic review of controlled trials. AIDS, 2006,20:143-157
69
92-4-120938-0_CH03_69

8. Neumann MS et al. Review and meta-analysis of HIV prevention interventionresearch for heterosexual adult populations in the United States. Journal ofAcquired Immune Deficiency Syndromes, 2002, 30 Suppl 1:S106-117.
9. Kalichman S, Carey M, Johnson B. Prevention of sexually transmitted HIVinfection: a meta-analytic review of the behavioural outcome literature. Annalsof Behavioral Medicine, 1996, 18:6-15.
10. Elwy R et al. Effectiveness of interventions to prevent sexually transmittedinfections and human immunodeficiency virus in heterosexual men. Archivesof Internal Medicine, 2002, 162:1818-1830.
11. Johnson WD, Hedges LV, Diaz RM. Interventions to modify sexual riskbehaviors for preventing HIV infection in men who have sex with men. CochraneDatabase of Systematic Reviews, 2004, 1:CD001230
12. Mullen PD et al. Meta-analysis of the effects of behavioral HIV preventioninterventions on the sexual risk behavior of sexually experienced adolescentsin controlled studies in the United States. Journal of Acquired ImmuneDeficiency Syndromes, 2002, 30 Suppl 1:S94-105.
13. Prendergast M, Urada D, Podus D. Meta-analysis of HIV risk-reductioninterventions within drug abuse treatment programs. Journal of Consulting andClinical Psychology, 2001, 69:389-405.
14. Herbst JH et al. A meta-analytic review of HIV behavioral interventions forreducing sexual risk behavior of men who have sex with men. Journal ofAcquired Immune Deficiency Syndromes, 2005, 39:228-241.
15. Gallant M, Maticka-Tyndale E. School-based HIV prevention programmes forAfrican youth. Social Science and Medicine, 2004, 58:1337-1351.
16. Speizer IS, Magnani RJ, Colvin CE. The effectiveness of adolescentreproductive health interventions in developing countries: a review of theevidence. Journal of Adolescent Health, 2003, 33:324-348.
17. Semaan S et al. A meta-analysis of the effect of HIV prevention interventionson the sex behaviors of drug users in the United States. Journal of AcquiredImmune Deficiency Syndromes, 2002, 30 Suppl 1:S73-93.
18. Johnson WD et al. HIV intervention research for men who have sex with men:a 7-year update. AIDS Education and Prevention, 2005, 17:568-589.
19. Gibson DR, Flynn NM, Perales D. Effectiveness of syringe exchange programsin reducing HIV risk behavior and HIV seroconversion among injecting drugusers. AIDS, 2001,15
20. Ellis S et al. HIV prevention: a review of reviews assessing the effectiveness ofinterventions to reduce the sexual risk of HIV transmission, Health DevelopmentAgency, National Institute for Health and Clinical Excellence, 2003 (http://www.publichealth.nice.org.uk/page.aspx?o=502573, accessed 11 May 2004).
21. National Institutes of Health Consensus Development Program. Interventionsto prevent HIV risk behaviors, 1997 (http://consensus.nih.gov/1997/1997PreventHIVRisk104html.htm, accessed 15 May 2004).
22. Rosenfield A, Myer L, Merson M. The HIV/AIDS pandemic: the case forprevention, (http://www.kff.org/hivaids/upload/Fact-Sheet-The-HIV-AIDS-Pandemic-The-Case-for-Prevention.pdf, accessed 25 May 2005).
23. Merson MH, Dayton JM, O’Reilly K. Effectiveness of HIV preventioninterventions in developing countries. AIDS, 2000, 14 Suppl 2:S68-84.
70
92-4-120938-0_CH03_70

24. Catania JA et al. Methodological problems in AIDS behavioral research:influences on measurement error and participation bias in studies of sexualbehavior. Psychological Bulletin, 1990, 108:339-362.
25. Weinhardt LS et al. Reliability and validity of self-report measures of HIV-relatedsexual behavior: progress since 1990 and recommendations for research andpractice. Archives of Sexual Behavior, 1998, 27:155-180.
26. Plummer ML et al. “A bit more truthful”: the validity of adolescent sexualbehaviour data collected in rural northern Tanzania using five methods.Sexually Transmitted Infections, 2004, 80 Suppl 2:S49-56.
27. Kamb ML et al. Efficacy of risk-reduction counseling to prevent humanimmunodeficiency virus and sexually transmitted diseases: a randomizedcontrolled trial. Journal of the American Medical Association, 1998,280:1161-1167.( Project RESPECT Study Group.)
28. National Institute of Mental Health (NIMH) Multisite HIV Prevention Trial Group.The NIMH Multisite HIV Prevention Trial: reducing HIV sexual risk behavior.Science, 1998, 280:1889-1894.
29. Imrie J et al. A cognitive behavioural intervention to reduce sexually transmittedinfections among gay men: randomised trial. BMJ, 2001, 322:1451-1456.
30. Koblin B, Chesney M, Coates T. Effects of a behavioural intervention to reduceacquisition of HIV infection among men who have sex with men: the EXPLORErandomised controlled study. Lancet, 2004, 364:41-50.
31. Hayes RJ et al. The MEMA kwa Vijana project: design of a community-randomised trial of an innovative adolescent sexual health intervention in ruralTanzania. Contemporary Clinical Trials, 2005, 26:430-442
32. Ross DA et al. Community randomised trial of an innovative adolescent sexualhealth interventin programme in rural Tanzania: the MEMA kwa Vijana trial.(Unpublished data.)
33. Kamali A et al. Syndromic management of sexually-transmitted infections andbehaviour change interventions on transmission of HIV-1 in rural Uganda: acommunity randomised trial. Lancet, 2003, 361:645-652.
34. Stoneburner RL, Low-Beer D. Population-level HIV declines and behavioral riskavoidance in Uganda. Science, 2004, 304:714-718.
35. Halperin DT et al. The time has come for common ground on preventing sexualtransmission of HIV. Lancet, 2004, 364:1913-1915.
36. Gregson S et al. HIV decline associated with behavior change in easternZimbabwe. Science, 2006, 311:664-666.
37. Nelson KE et al. Changes in sexual behavior and a decline in HIV infectionamong young men in Thailand. New England Journal of Medicine, 1996,335:297-303.
38. Asiimwe-Okiror G et al. Change in sexual behaviour and decline in HIV infectionamong young pregnant women in urban Uganda. AIDS, 1997, 11:1757-1763.
39. Bessinger R, Akwara P, Helperin D. Sexual behvior, HIV and fertility trends: acomparative analysis of six countries, (http://www.cpc.unc.edu/measure/publications/pdf/sr-03-21b.pdf).
40. Shelton JD et al. Partner reduction is crucial for balanced “ABC” approach toHIV prevention. BMJ, 2004, 328:891-893.
71
92-4-120938-0_CH03_71

41. Serwadda D. Monitoring and evaluation of national HIV prevention, AIDS careand STD control programs: Uganda case study. (Unpublished data presentedat Towards Improved Monitoring and Evaluation of HIV Prevention, AIDS Careand STD Control Programs, 17–20 November 1999.)
42. Phoolcharoen W. HIV/AIDS prevention in Thailand: success and challenges.Science, 1998, 280:1873-1874.43.
43. Wawer M et al. Declines in HIV prevalence in Uganda: not as simple as ABC.(Unpublished data presented at 12th Conference on Retroviruses andOpportunistic Infections, Boston, MA, 22–25 February 2005.)
44. Hayes R, Weiss H. Epidemiology: understanding HIV epidemic trends in Africa.Science, 2006, 311:620-621.
45. Painter TM. Voluntary counselling and testing for couples: a high-leverageintervention for HIV/AIDS prevention in sub-Saharan Africa. Social Science andMedicine, 2001, 53:1397-1411.
46. Weinhardt LS et al. Effects of HIV counseling and testing on sexual riskbehavior: a meta-analytic review of published research, 1985-1997. AmericanJournal of Public Health, 1999, 89:1397-1405.
47. Coates TJP et al. Efficacy of voluntary HIV-1 counselling and testing inindividuals and couples in Kenya, Tanzania, and Trinidad: a randomised trial.Lancet, 2000, 356:103-111.
48. Maposhere C et al. General political issues raised in HIV counseling of 200couples in Zimbabwe (Unpublished data presented at XI InternationalConference on AIDS, Vancouver, 7–12 July 1996.)
49. Serwadda D et al. Gender specific HIV transmission/prevention in discordantcouples in rural Uganda. (Unpublished data presented at X InternationalConference on AIDS, Yokohama, 7–12 August 1994.)
50. Van der Straten A et al. Couple communication, sexual coercion and HIV riskreduction in Kigali, Rwanda. AIDS, 1995, 9:935-944.
51. NIMH Project Accept: A phase III randomized trial of community mobilization,mobile testing, same-day results, and post-test support for HIV in Sub-SaharanAfrica and Thailand (http://www.cbvct.med.ucla.edu/overview.html)
52. Gibson DR, Flynn NM, McCarthy JJ. Effectiveness of methadone treatment inreducing HIV risk behavior and HIV seroconversion among injecting drug users.AIDS, 1999, 13:1807-1818.
53. Institute of Medicine. No time to lose: getting more from HIV prevention.Washington, DC, National Academy Press, 2001.
54. Metzger DS et al. Human immunodeficiency virus seroconversion amongintravenous drug users in- and out-of-treatment: an 18-month prospectivefollow-up. Journal of Acquired Immune Deficiency Syndromes, 1993,6:1049-1056.
55. McLellan AT et al. Evaluating the effectiveness of addiction treatments:reasonable expectations, appropriate comparisons. Milbank Quarterly, 1996,74:51-85.
56. Mundee Y et al. Infectious disease markers in blood donors in northernThailand. Transfusion, 1995, 35:264-267.
72
92-4-120938-0_CH03_72

57. Chattopadhya D, Riley LW, Kumari S. Behavioural risk factors for acquisitionof HIV infection and knowledge about AIDS among male professional blooddonors in Delhi. Bulletin of the World Health Organization, 1991, 69:319-323.
58. Lackritz EM et al. Blood transfusion practices and blood-banking services in aKenyan hospital. AIDS, 1993, 7:995-999.
59. Schutz R et al. Excluding blood donors at high risk of HIV infection in a westAfrican city. BMJ, 1993, 307:1517-1519.
60. Gisselquist D et al. Four policies to reduce HIV transmission through unsterilehealth care. International Journal of STD and AIDS, 2003, 14:717-722.
61. Sloand EM, Pitt E, Klein HG. Safety of the blood supply. Journal of the AmericanMedical Association, 1995, 274:1368-1373.
62. Wong ES et al. Are universal precautions effective in reducing the number ofoccupational exposures among health care workers? A prospective study ofphysicians on a medical service. Journal of the American MedicalAssociation, 1991, 265:1123-1128.
63. Gisselquist D et al. Does selected ecological evidence give a true picture of HIVtransmission in Africa? International Journal of STD and AIDS, 2004,15:434-439.
64. Schmid GP et al. Transmission of HIV-1 infection in sub-Saharan Africa andeffect of elimination of unsafe injections. Lancet, 2004, 363:482-488.
65. Lopman BA et al. Individual level injection history: a lack of association with HIVincidence in rural Zimbabwe. PLoS Medicine, [Online journal] 2005, 2:e37.(http://medicine.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.0020037)
66. Fleming DT, Wasserheit JN. From epidemiological synergy to public healthpolicy and practice: the contribution of other sexually transmitted diseases tosexual transmission of HIV infection. Sexually Transmitted Infections, 1999,75:3-17.
67. Grosskurth H et al. A community trial of the impact of improved sexuallytransmitted disease treatment on the HIV epidemic in rural Tanzania. 2:baseline survey results. AIDS, 1995, 9:927-934.
68. Mayaud P et al. Improved treatment services significantly reduce theprevalence of sexually transmitted diseases in rural Tanzania: results of arandomized controlled trial. AIDS, 1997, 11:1873-1880.
69. Wawer MJ et al. Control of sexually transmitted diseases for AIDS preventionin Uganda: a randomised community trial. Lancet, 1999, 353:525-535. (RakaiProject Study Group.)
70. Orroth KK et al. Higher risk behaviour and rates of sexually transmitted diseasesin Mwanza compared to Uganda may help explain HIV prevention trialoutcomes. AIDS, 2003, 17:2653-2660.
71. Korenromp EL et al. Determinants of the impact of sexually transmitted infectiontreatment on prevention of HIV infection: a synthesis of evidence from theMwanza, Rakai, and Masaka intervention trials. Journal of InfectiousDiseases, 2005, 191 Suppl 1:S168-178.
72. Wald A, Link K. Risk of human immunodeficiency virus infection in herpessimplex virus type 2-seropositive persons: a meta-analysis. Journal ofInfectious Diseases, 2002, 185:45-52.
73
92-4-120938-0_CH03_73

73. Freeman EE et al. Herpes simplex virus 2 infection increases HIV acquisitionin men and women: systematic review and meta-analysis of longitudinalstudies. AIDS, 2006, 20:173-183
74. Nagot et al. Effect of HSV-2 suppressive therapy on HIV-1 genital shedding andplasma viral load: a proof of concept randomized double-blind placebocontrolled trial (ANRS 1285 trial). (Unpublished data presented at 13thConference on Retroviruses and Opportunistic Infections, Denver, CO, 5–8February 2006.)
75. Celum CM. Herpes simplex and the global epidemiology of HIV. (Unpublisheddata presented at the 11th Conference on Retroviruses and OpportunisticInfections, San Francisco, 8–11 February 2004.)
76. Connor EM et al. Reduction of maternal-infant transmission of humanimmunodeficiency virus type 1 with zidovudine treatment. New England Journalof Medicine, 1994, 331:1173-1180. (Pediatric AIDS Clinical Trials GroupProtocol 076 Study Group.)
77. Shaffer N et al. Short-course zidovudine for perinatal HIV-1 transmission inBangkok, Thailand: a randomised controlled trial. Lancet, 1999, 353:773-780.(Bangkok Collaborative Perinatal HIV Transmission Study Group.)
78. Wiktor SZ et al. Short-course oral zidovudine for prevention of mother-to-childtransmission of HIV-1 in Abidjan, Cote d’Ivoire: a randomised trial. Lancet,1999, 353:781-785.
79. Guay LA et al. Intrapartum and neonatal single-dose nevirapine compared withzidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala,Uganda: HIVNET 012 randomised trial. Lancet, 1999, 354:795-802.
80. Brocklehurst P. Interventions aimed at decreasing the risk of mother-to-childtransmission of HIV infection. Cochrane Database of Systematic Reviews,2004, 2:CD000102.
81. Tonwe-Gold B. Management of pregnant women in the MTCT plus program,(http://www.mtctplus.org/pdf/Maputo%202005/Pregnant%20Women/Cote%20dIvoire%20Experience_Tonwe-Gold.pdf).
82. Nduati R et al. Effect of breastfeeding and formula feeding on transmission ofHIV-1: a randomized clinical trial. Journal of the American MedicalAssociation, 2000, 283:1167-1174.
83. Amornwichet P et al. Preventing mother-to-child HIV transmission: the first yearof Thailand’s national program. Journal of the American Medical Association,2002, 288:245-248.
84. Cooper ER et al. Combination antiretroviral strategies for the treatment ofpregnant HIV-1-infected women and prevention of perinatal HIV-1transmission. Journal of Acquired Immune Deficiency Syndromes, 2002,29:484-494.
85. Cardo DM et al. A case-control study of HIV seroconversion in health careworkers after percutaneous exposure. New England Journal of Medicne, 1997,337:1485-1490. (Centers for Disease Control and Prevention NeedlestickSurveillance Group.)
86. Wulfsohn A. Post-exposure prophylaxis for HIV after sexual assault in SouthAfrica. (Unpublished data presented at the 2003 National HIV PreventionConference, Atlanta, GA, 27–30 July 2003.)
74
92-4-120938-0_CH03_74

87. Roland ME et al. Seroconversion following nonoccupational postexposureprophylaxis against HIV. Clinical Infectious Diseases, 2005, 41:1507-1513.
88. Bamberger J. HIV post-exposure prophylaxis after sexual assault and otherunprotected non-occupational exposures. (Unpublished data presented at the2003 National HIV Prevention Conference, Atlanta, GA, 27–30 July 2003).
89. Quinn TC et al. Viral load and heterosexual transmission of humanimmunodeficiency virus type 1. New England Journal of Medicine, 2000,342:921-929. (Rakai Project Study Group.)
90. HIV Prevention Trials Network. HPTN 052: a randomized trial to evaluate theeffectiveness of antiretroviral therapy plus HIV primary care versus HIV primarycare alone to prevent the sexual transmission of HIV-1 in serodiscordantcouples, (http://www.hptn.org/research_studies/hptn052.asp).
91. Cohen M. HIV prevention rsearch: new advances, continued challenges.(Unpublished data presented at the 13th Conference on Retroviruses andOpportunistic infections, Denver, CO, 5–8 February 2006.)
92. Gray R et al. Probability of HIV-1 transmission per coital act in monogamous,heterosexual, HIV-1-discordant couples in Rakai, Uganda. Lancet, 2001,357:1149-1153.
93. Blower S et al. Predicting the impact of antiretrovirals in resource-poor settings:preventing HIV infections whilst controlling drug resistance. Current DrugTargets. Infectious Disorders, 2003, 3:345-353.
94. Velasco-Hernandez JX, Gershengorn HB, Blower SM. Could widespread useof combination antiretroviral therapy eradicate HIV epidemics? LancetInfectious Diseases, 2002, 2:487-493.
95. Fang CT et al. Decreased HIV transmission after a policy of providing freeaccess to highly active antiretroviral therapy in Taiwan. Journal of InfectiousDiseases, 2004, 190:879-885.
96. Centers for Disease Control and Prevention. CDC’s clinical studies of daily oraltenofovir for HIV prevention, 2005 (http://www.cdc.gov/hiv/pubs/faq/Tenofovir_Q&A.pdf).
97. Cameron DW et al. Female to male transmission of human immunodeficiencyvirus type 1: risk factors for seroconversion in men. Lancet, 1989, 2:403-407.
98. Reynolds SJ et al. Male circumcision and risk of HIV-1 and other sexuallytransmitted infections in India. Lancet, 2004, 363:1039-1040.
99. Gray RH et al. Male circumcision and HIV acquisition and transmission: cohortstudies in Rakai, Uganda. AIDS, 2000, 14:2371-2381. (Rakai Project Team.)
100. Weiss HA, Quigley MA, Hayes RJ. Male circumcision and risk of HIV infectionin sub-Saharan Africa: a systematic review and meta-analysis. AIDS, 2000,14:2361-2370.
101. Siegfried N et al. HIV and male circumcision – a systematic review withassessment of the quality of studies. Lancet Infectious Diseases, 2005,5:165-173.
102. Auvert B et al. Randomized, controlled intervention trial of male circumcisionfor reduction of HIV infection risk: the ANRS 1265 trial. PLoS Medicine, [Onlinejournal] 2005, 2:e298. (http://medicine.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.0020298)
75
92-4-120938-0_CH03_75

103. UNAIDS. UNAIDS statement on South African trial findings regarding malecircumcision and HIV, 2005 (http://www.who.int/mediacentre/news/releases/2005/pr32/en/).
104. AIDS Vaccine Advocacy Coalition. AIDS vaccine fails to show efficacy in Thaitrial, (http://www.avac.org/AIDSVAXthai.htm).
105. International AIDS Vaccine Initiative. Ongoing trials of preventive AIDSvaccines, (http://www.iavireport.org/specials/OngoingTrialsofPreventiveHIVVaccines.pdf).
106. Wilkinson D et al. Nonoxynol-9 for preventing vaginal acquisition of HIVinfection by women from men. Cochrane Database of Systematic Reviews,2002, 4:CD003936.
107. Van Damme L et al. Effectiveness of COL-1492, a nonoxynol-9 vaginal gel, onHIV-1 transmission in female sex workers: a randomised controlled trial.Lancet, 2002, 360:971-977.
108. Alliance for Microbicide Development. Microbiciodes and clinical trials, (http://www.microbicide.org/microbicideinfo/reference/clinical.trials.factsheet.pdf).
109. Alliance for Microbicide Development. Microbicide Research and DevelopmentDatabase (MRDD), (http://www.microbicide.org/microbicideinfo/reference/TMQvol2no12004.pdf).
110. Rockefeller Foundation. The public health benefits of microbicides in lower-income countries: model projections. New York, Rockefeller Foundation, 2002.
111. Trussell J et al. Comparative contraceptive efficacy of the female condom andother barrier methods. Family Planning Perspectives, 1994, 26:66-72
112. Gollub EL, Stein ZA.The new female condom–item 1 on a women’s AIDSprevention agenda. American Journal of Public Health, 1993, 83:498-500.
113. Gollub EL. The female condom: STD protection in the hands of women.American Journal of Gynecologic Health, 1993, 7:91-92.
114. Leeper MA. Preliminary evaluation of reality, a condom for women. AIDSCare, 1990, 2:287-290.
115. Moench TR, Chipato T, Padian NS. Preventing disease by protecting the cervix:the unexplored promise of internal vaginal barrier devices. AIDS, 2001,15:1595-1602.
116. Howell AL et al. Human immunodeficiency virus type 1 infection of cells andtissues from the upper and lower human female reproductive tract. Journal ofVirology, 1997, 71:3498-3506.
117. Magder LS et al. Factors related to genital Chlamydia trachomatis and itsdiagnosis by culture in a sexually transmitted disease clinic. American Journalof Epidemiology, 1988, 128:298-308.
118. Rosenberg MJ et al. Barrier contraceptives and sexually transmitted diseasesin women: a comparison of female-dependent methods and condoms.American Journal of Public Health, 1992, 82:669-674.
119. Kelaghan J et al. Barrier-method contraceptives and pelvic inflammatorydisease. Journal of the American Medical Association, 1982, 248:184-187.
120. Austin H, Louv WC, Alexander WJ. A case-control study of spermicides andgonorrhea. Journal of the American Medical Association, 1984, 251:2822-2824.
76
92-4-120938-0_CH03_76

121. Becker TM et al. Sexually transmitted diseases and other risk factors for cervicaldysplasia among southwestern Hispanic and non-Hispanic white women.Journal of the American Medical Association, 1994, 271:1181-1188.
122. Matthews J, personal communication, 2006.
123. Cervical Barrier Advancement Society. can diaphragms protect women fromHIV: an update on the mira trial. Cervical Barrier Advancement SocietyNewsletter, 2005, 2:1.
124. Sumartojo E. Structural factors in HIV prevention: concepts, examples, andimplications for research. AIDS, 2000, 14 Suppl 1:S3-10.
125. Sweat MD, Denison JA. Reducing HIV incidence in developing countries withstructural and environmental interventions. AIDS, 1995, 9 Suppl A:S251-257.
126. Blankenship KM, Bray SJ, Merson MH. Structural interventions in public health.AIDS, 2000, 14 Suppl 1:S11-21.
127. Blankenship KM et al. Structural interventions: concepts, challenges andopportunities for research. Journal of Urban Health: Bulletin of the New YorkAcademy of Medicine, 2006, 1-14.
128. Phoolcharoen W et al. Thailand: lessons from a strong national response toHIV/AIDS. AIDS, 1998, 12 Suppl B:S123-135.
129. Hanenberg RS et al. Impact of Thailand’s HIV-control programme as indicatedby the decline of sexually transmitted diseases. Lancet, 1994, 344:243-245.
130. Celentano DD et al. Decreasing incidence of HIV and sexually transmitteddiseases in young Thai men: evidence for success of the HIV/AIDS control andprevention program. AIDS, 1998, 12 Suppl F:S29-36.
131. WHO Regional Office for the Western Pacific. Meeting on the 100% CondomUse Programme For Prevention of HIV/AIDS and STI. (Unpublished data frommeeting in Vientiane, Lao People’s Democratic Republic, 18–21 August 2003.)
132. Hurley SF, Jolley DJ, Kaldor JM. Effectiveness of needle-exchangeprogrammes for prevention of HIV infection. Lancet, 1997, 349:1797-1800.
133. Des Jarlais DC et al. Maintaining low HIV seroprevalence in populations ofinjecting drug users. Journal of the American Medical Association, 1995,274:1226-1231.
134. Ksobiech K. A meta-analysis of needle sharing, lending, and borrowingbehaviors of needle exchange program attenders. AIDS Education andPrevention, 2003, 15:257-268.
135. Satcher D-SG. Evidence-based findings on the efficacy of syringe exchangeprograms: an analysis of the scientific research completed since April 1998.Washington, DC, U.S. Department of Health and Human Services, 2000.
136. National Research Council. Preventing HIV transmission: the role of sterileneedles and bleach. Washington, DC, National Academy Press, 1995.
137. Pitt MM et al. Credit programs for the poor and reproductive behavior in low-income countries: are the reported causal relationships the result ofheterogeneity bias? Demography, 1999, 36:1-21.
138. Hargreaves J et al. Social interventions for HIV/AIDs: intervention with micro-finance for AIDS and gender equity, (http://www.sarpn.org.za/mitigation_of_HIV_AIDS/m0025/index.php).
77
92-4-120938-0_CH03_77

139. Pronyk P, Hargreaves J, personal communication, 2006.
140. Newman PA et al.. Challenges for HIV vaccine dissemination and clinical trialrecruitment: if we build it, will they come? AIDS Patient Care and STDS, 2004,18:691-701.
141. AIDS Vaccine Advocacy Coalition. AIDS vaccines trials: getting the globalhouse in order. New York, AIDS Vaccine Advocacy Coalition, 2004.
142. Mantell JE et al. Microbicide acceptability research: current approaches andfuture directions. Social Science and Medicine, 2005, 60:319-330
143. Fleming TR, Richardson BA. Some design issues in trials of microbicides forthe prevention of HIV infection. Journal of Infectious Diseases, 2004,190:666-674.
144. Blower S. Modeling the potential public health impact of imperfect HIV vaccines.Journal of Infectious Diseases, 2005, 192:1494-1495. (Author reply:1495-1496.)
145. Cassell MM et al. Risk compensation: the Achilles’ heel of innovations in HIVprevention? BMJ, 2006, 332:605-607.
146. Cates W. Future HIV prevention trials: sexual transmission.(Unpublished datapresented at the 3rd International AIDS Society Conference, Rio de Janeiro,26 July 2005.)
147. AIDS Vaccine Advocacy Coalition. Will a pill a day prevent HIV? New York,AIDS Vaccine Advocacy Coalition, 2005:9.
148. Community HIV/AIDS Mobilization Project, AIDS Vaccine Advocacy Coalition,Gay Men’s Health Crisis, Group TA. A statement of support for HIV preventionresearch on pre-exposure prophylaxis. New York, Community AIDS/HIVMobilization Project, 2006.
149. Global HIV Prevention Working Group. Access to HIV prevention: closing thegap, (http://www.kff.org/hivaids/200305-index.cfm).
78
92-4-120938-0_CH03_78

4. The weight of evidence: a methodfor assessing the strength ofevidence on the effectiveness ofHIV prevention interventions amongyoung peopleDavid A Ross,a Danny Wight,b Gary Dowsett,c Anne Buvé,d
& Angela I N Obasie
Objectives To design a method for assessing the strength of evidence on theeffectiveness of different interventions to prevent the spread of HIV that willbe the basis for the reviews in this series.
Methods The literature on the evaluation of public health interventions wasreviewed, and a method was developed in consultation with colleagues in-volved in this series of reviews and others.
Findings The method involves the following steps. First, define the key typesof intervention that policy-makers need to choose between in the populationsetting under consideration. Second, define the strength of evidence thatwould be needed to justify widespread implementation of the intervention.Third, develop explicit inclusion and exclusion criteria for the studies underreview. Fourth, critically review all eligible studies and their findings, byintervention type. Fifth, summarize the strength of the evidence on the ef-fectiveness of each type of intervention. Sixth, compare the strength of theevidence provided by the studies against the threshold of evidence that wouldbe needed to recommend widespread implementation. Seventh, from thiscomparison, derive evidence-based recommendations related to the imple-mentation of each type of intervention in the setting or population group.
a Infectious Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine,Keppel Street, London WC1E 7HT, England. Correspondence should be sent to Dr Ross(email: [email protected]).
b MRC Social and Public Health Sciences Research Unit, Glasgow, Scotland.c Australian Research Centre in Sex, Health and Society, La Trobe University, Melbourne,
Australia.d STD/HIV Research and Intervention Unit, Institute of Tropical Medicine, Antwerp, Belgium.e Liverpool School of Tropical Medicine, Liverpool, England.
79
92-4-120938-0_CH04_79

Conclusions The method proposed here provides a systematic, rigorous andtransparent approach to reviewing evidence on the effectiveness of interven-tions of different types and in different population settings in order to generaterecommendations for policy-makers.
4.1 Introduction
The AIDS epidemic is a major public health emergency, and young peopleare bearing the main brunt of new infections worldwide. There is an urgentneed to work towards a consensus on what should be done in order to meetthe internationally accepted goals for the prevention of HIV among youngpeople that were defined at the United Nations General Assembly SpecialSession on HIV/AIDS (UNGASS) in 2001 (1). These global goals are pre-sented and discussed in chapter 1, but in sum they give specific targets forimproving access to information, skills and services; reducing vulnerability;and reducing HIV prevalence.
In an area as important as preventing the spread of HIV among young peoplein developing countries, difficult choices have to be made by policy-makersand programme developers irrespective of whether the evidence that is avail-able to guide these decisions is weak or strong. Although evidence on theeffectiveness of interventions will be only one of the factors that policy-makers use when deciding in which programmes to invest, a systematicreview of the evidence related to all the options will be more useful to themthan piecemeal reviews using different criteria and weights for different typesof evidence. As in most areas of social policy, gaining consensus on the rel-ative weights that should be given to different types of evidence has beendifficult, but for policy decisions to be rational and transparent, reaching suchconsensus is crucially important. Furthermore, the lack of any explicit policyor programme is in fact a policy decision. And, finally, because of the com-plexity of the interventions, the evidence for and against any interventionstrategy is likely also to be complex, requiring the synthesis of multiple typesof evidence of varying quality and weight. Evaluation researchers shouldprovide evidence that is as valid as possible to policy-makers and ensure thatit is synthesized and presented in a way that will make it relevant, accessibleand easy to interpret and act on.
While recognizing that there are major obstacles to rational evidence-baseddecision-making in this field, this chapter aims to indicate a way forward bypresenting a structure within which researchers, advisers and policy-makerscan assess the strength of the evidence for each of the interventions discussedin subsequent chapters in this series. In this chapter we are concerned withthe broad principles involved in assessing the evidence. Later chapters in theseries will address how these principles apply to specific interventions. The
80
92-4-120938-0_CH04_80

criteria that we propose for assessing the evidence draw on recent debates onthe relative merits and limitations of randomized controlled trials (2–7), andsuggestions for approaches to the evaluation of evidence on public healthinterventions (6, 8–10), and to the presentation and systematic review of studyresults (11–15).
4.2 Types of interventions and evidence on effectiveness
Most of the programmes that have been introduced or advocated to reducethe prevalence of HIV among adolescents are complex, often comprisingcombinations of components, such as:
in-school teacher-led sex and/or life skills education;
in-school peer education and/or mentoring or counselling;
specific interventions (such as peer education) for out-of-school youths(including those who would be expected to be in school but are not), forspecific groups of youths (for example, groups affiliated with religiousorganizations) and for groups at high risk of HIV (such as intravenous drugusers, commercial sex workers or men who have sex with men);
condom promotion and improved access to condoms (for example, throughsocial marketing, health-worker training, providing supplies or reorganiz-ing clinical services);
youth-friendly health services;
access to counselling and voluntary HIV testing;
access to care, support and treatment for people who are HIV positive;
community development approaches to modifying sexual and socialnorms;
mass media approaches to changing social values, norms and behaviours;
legislative changes.
These components may be targeted at different levels, including the individ-ual (for example, by providing life skills training), the family (for example,by improving intrafamily communication about sexuality) and the commu-nity (for example, by providing access to youth-friendly health services, massmedia campaigns aimed at changing norms in society regarding gender rolesor interventions directed towards men to decrease girls’ vulnerability). Fur-thermore, many of these specific components are, in themselves, complex in-terventions. To be effective, most would involve bringing about profound socialand behavioural changes among both the implementers (for example, who
81
92-4-120938-0_CH04_81

must respect confidences and understand and empathize with young people’sconcerns) and the potential target groups; however, evaluating such outcomesis notoriously difficult. Finally, when a programme is made up of severalinterventions, often with a different emphasis given to each, it is difficult toassess the relative effectiveness of each component.
The key policy questions are:
which interventions should be selected?
in which contexts are they appropriate?
what proportion of the available resources should be allocated to each?
The complexity of the interventions and the inadequacy of evaluations ofthem mean that policy decisions will often need to be based only on partialor imperfect evidence. Some of the reasons for this imperfect evidence aresummarised in Box 4.1.
Box 4.1
Obstacles to obtaining perfect evidence
HIV prevention interventions are complex
There are numerous interventions and strategies to choose from.
The content and quality of interventions may differ substantially from oneanother, and interventions may be implemented in different ways by dif-ferent people. For example, two life-skills programmes in secondaryschools that have different content and theoretical bases and are deliv-ered in different ways are likely to have different impacts.
The interventions needed to address the five UNGASS goals (seechapter 1) will be social interventions of varying and often substantialdegrees of complexity. This will necessarily complicate their evaluation.
The mechanisms by which these strategies are meant to work arediverse, complex and poorly understood. In contrast to the biologicalmechanisms by which therapeutic drugs work, there is far less con-sensus on the workings of the social world in and through whichbehavioural interventions operate (16).
Lack of understanding of the mechanisms raises the added problemthat purported intermediate outcomes may or may not be valid. Forexample, an increase in the skills needed to avoid HIV infection maynot necessarily result in a reduction in HIV prevalence amongadolescents.
82
92-4-120938-0_CH04_82

Specific interventions may be synergistic or even antagonistic, and yetmost programmes will combine several intervention strategies, makingevaluation of the effects of specific interventions or components withinthe programme package difficult or impossible to disentangle.
Evaluating interventions targeting young people is difficult
Measuring the ultimate goal of reducing HIV prevalence among youngpeople requires that substantial numbers of young people are followedup for several years at considerable cost.
The validity of surrogate outcome measures, such as reported sexualbehaviour, may be particularly problematic among young people be-cause of the effects of social desirability biases, age differencesbetween researchers and respondents, etc. (17).
This age group is particularly mobile and therefore difficult to followthrough longitudinal research.
Evaluation strategies cannot be standardized
It is intrinsically easier to evaluate the effectiveness of some interven-tions (such as those targeted at individuals) than others (such as thosetargeted at whole communities or nations).
The timescales in which the various interventions might work varywidely. For example, condom promotion and supply or treatment of othersexually transmitted infections may produce measurable outcomes in arelatively short time, while other approaches, such as changing the so-cioeconomic status of women, may be expected to have a substantialimpact on HIV prevalence among adolescents only in the longer term.Furthermore, some interventions may have longer lasting effects thanothers.
Evaluation results are not always generalizable
The impact of an intervention may vary substantially according to thesetting in which it is delivered and the broader context. For instance, theeffectiveness of a life-skills programme may differ according to the de-gree of control young women have over their sexuality in that culture.
Furthermore, the impact of an intervention within a tightly controlledevaluation setting may be different from that within a routine programme.
The contested nature of evidence itself
Different people accord different weight to different types of evidence.This often reflects their disciplinary background, and sterile debates be-tween “positivists” and “interpretivists” or “relativists” have been at leastas common as constructive discussions in this field (18).
83
92-4-120938-0_CH04_83

The need to make decisions using imperfect evidence is the norm when for-mulating social policy. In fact, within the field of HIV prevention, theevidence available to enable us to make rational policy decisions, and theconsensus among researchers and policy-makers, may be greater than it is inmany other areas of social policy (19). One reason for this relative consensushas been the fact that explicit theoretical models for how interventions arepostulated to work exist for most, if not all, of the major interventions thathave been proposed for inclusion in programmes to reduce HIV prevalencein adolescents. These models are often imperfect, and empirical evidence forthe causal chain within any given model is often weak and sometimes missing,but plausible models usually do exist, often based on social or psychologicaltheory, though also occasionally on biological theory (such as the potentialeffectiveness of condoms if used correctly).
4.3 Thresholds for strength of evidence needed for widespreadimplementation
Some types of interventions need stronger evidence than others in order tobe recommended for widespread implementation. The strength of the evi-dence needed depends on their feasibility (including cost), potential foradverse outcomes, acceptability, potential size of effect and potential for otherhealth or social benefits.
The more feasible the intervention, the lower the threshold of evidenceneeded. Key areas in this domain include the logistics, cost and humanresources required for its implementation. The question is: can it be im-plemented on a large scale in a way that will be sustainable?
The lower the potential for adverse outcomes, the lower the threshold ofevidence needed. For example, is there any evidence that the interventioncould actually lead to increased HIV incidence or to violations of humanrights (20) or could it put individuals at an increased risk of domesticviolence? Ideally, the assessment of potential adverse outcomes should notbe limited to short-term outcomes among the specific individuals targetedbut should also include longer-term outcomes within the wider community.For example, in evaluating male circumcision, the assessment should notrestrict itself to the impact on the young men who are circumcised. It shouldalso consider the possibility that encouraging male circumcision might leadto more circumcisions being performed in informal non-sterile circum-stances, that appearing to endorse “circumcision” might lead to increasedfemale genital cutting, and that it might increase sexual risk-taking becausethose circumcised may think they are “immune” from HIV and other sex-ually transmitted infections.
84
92-4-120938-0_CH04_84

The more acceptable the intervention, the lower the threshold of evidenceof effectiveness required. The intervention’s acceptability needs to be as-sessed not only among the target group but also among implementers,politicians, donors, religious and other community leaders, and within thewider community. A controversial intervention will require stronger evi-dence than a well accepted intervention simply because of the greaterreluctance that policy-makers will have to introduce it because of the riskof opposition or protest from key stakeholders. For example, in most con-texts policy-makers are likely to be reluctant to introduce active condompromotion and provision within primary schools and more likely to allowthe provision of basic information about what HIV is and how it is spread.
The greater the potential size of the effect, the lower the required evidencethreshold. Not surprisingly, given the complexity described above, mostinterventions do not have empirical evidence of their impact on key out-comes such as HIV prevalence. In the absence of this, however, it mightbe possible to make a plausible assessment of maximum potential impactbased on theoretical grounds, process evaluation data or data on interme-diate outcomes. Policy-makers might be more willing to gamble on anintervention that has the potential to bring about a major beneficial impact(as long as its cost and potential for adverse outcomes are low and its ac-ceptability and potential sustainability are high) than on another interven-tion that may have only a marginally beneficial impact. A related issue isthe time required to achieve a measurable effect: the longer the timeneeded, the higher the evidence threshold.
Some interventions, such as increased access to schooling for girls, mayreceive additional justification because they are associated with otherhealth or social benefits. If so, policy-makers might reasonably have alower threshold for the strength of evidence of the intervention’s impacton HIV risk.
Subsequent papers in this series review the evidence on interventions in fivedifferent “settings”: schools, health services, geographically definedcommunities, specific population groups at high risk of HIV infection, andinterventions delivered through the mass media. The grid in Box 4.2 has beenused in the “settings” papers in this series to decide what threshold of evidencea particular type of intervention requires in order for it to be recommendedfor widespread implementation in developing countries. The decision on thestrength of evidence needed for widespread implementation should be takenprior to considering the actual evidence that is available for a particular typeof intervention. The examples in Box 4.3 illustrate why some interventionsrequire stronger evidence (that is, have a higher evidence threshold) thanothers.
85
92-4-120938-0_CH04_85

Box
4.2
Th
resh
old
of
evid
ence
nee
ded
to
rec
om
men
d w
ides
pre
ad im
ple
men
tati
on
in a
dev
elo
pin
g c
ou
ntr
y, b
ased
on
fiv
e ke
y at
trib
ute
s o
f th
ein
terv
enti
on
Th
resh
old
of
evid
ence
nee
ded
Att
rib
ute
s o
f th
e in
terv
enti
on
Fea
sib
leL
ow
ris
k o
f ad
vers
eo
utc
om
esA
ccep
tab
le (
to t
arg
etp
op
ula
tio
n, p
ract
itio
ner
s,g
atek
eep
ers)
Lar
ge
po
ten
tial
eff
ect
size
Oth
er h
ealt
h o
r so
cial
ben
efit
s
Low
DD
Med
ium
DD
DH
igh
XX
XX
X
Key =
nec
essa
ryD
= d
esira
ble
X =
not
nec
essa
ry
86
92-4-120938-0_CH04_86

Box
4.3
Exa
mp
les
of
inte
rven
tio
ns
and
th
resh
old
s o
f ev
iden
ce n
eed
ed t
o r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n
Inte
rven
tio
nF
easi
ble
Lo
w r
isk
of
adve
rse
ou
tco
mes
Acc
epta
ble
(to
tar
get
po
pu
lati
on
,p
ract
itio
ner
s,g
atek
eep
ers)
Lar
ge
po
ten
tial
effe
ct s
ize
Oth
er h
ealt
h o
r so
cial
ben
efit
sT
hre
sho
ld o
fev
iden
ce
Info
rmat
iona
Yes
Yes
Yes
Pro
babl
y no
tY
es (
cont
race
ptio
n m
aybe
use
d, p
reva
lenc
e of
ST
Iscm
ay b
e re
duce
d)
Low
Con
dom
s in
sch
ools
bY
esP
erce
ived
pot
entia
l to
incr
ease
pro
mis
cuity
(alth
ough
ther
e is
evid
ence
that
this
rare
ly, i
f eve
r, o
ccur
s)
No
(esp
ecia
lly a
mon
gte
ache
rs a
ndga
teke
eper
s)
Yes
Yes
(pr
ovid
esco
ntra
cept
ion,
prev
alen
ce o
f ST
Is m
aybe
red
uced
)
Hig
h
a F
or e
xam
ple,
pro
visi
on o
f bas
ic in
form
atio
n on
the
caus
e of
AID
S, h
ow it
can
be
tran
smitt
ed, a
nd h
ow it
can
be
avoi
ded,
esp
ecia
lly e
arly
inan
epi
dem
ic.
b F
or e
xam
ple,
pro
mot
ion
of th
e us
e of
con
dom
s an
d pr
ovis
ion
of c
ondo
ms
with
in s
choo
ls.
c ST
Is =
sex
ually
tran
smitt
ed in
fect
ions
.
87
92-4-120938-0_CH04_87

For each type of intervention, the recommendations relating to whether aparticular intervention should be implemented depend on the pre-definedthreshold of evidence needed and the degree to which the evidence meets thatthreshold. Four kinds of recommendation are found in the papers: widespreadimplementation now (categorized as “Go”), widespread implementation withcareful evaluation in terms both of outcomes and processes (“Ready”), im-plementation within specific evaluation studies but not yet in large-scaleroutine intervention programmes (“Steady”), or do not implement becausethere is strong evidence of a lack of effectiveness or there is evidence ofharmful effects (“Do not go”) (see also chapter 1). In this series of papers,the guidelines in Box 4.4 were developed to assist authors in reaching deci-sions about which recommendation should be made for each intervention.
4.4 What information do policy-makers need?
Ideally, detailed and clear information is needed on all of the following as-pects of any intervention under consideration:
a detailed description of the characteristics of the most promising ap-proaches or strategies for implementing a particular intervention, includingits content, delivery setting, intensity of implementation (for example, thenumber of hours of training or education involved) and the human, finan-cial and other resource requirements;
the theoretical mechanism by which the intervention is postulated to leadto a reduction in HIV prevalence in young people. Ideally, as well as therebeing a plausible mechanism, there should also be empirical evidence thatthe intervention actually works through this mechanism and evidence thatrelevant changes can occur through this mechanism. As will be discussedin the next section, this evidence need not necessarily come from the spe-cific field of HIV prevention in young people or even HIV prevention atall. It could equally well be drawn from evaluations of interventions usingthe same mechanism to achieve other outcomes. For example, evidence ofthe effectiveness of mass media as a mechanism for influencing behaviourcould come from interventions related to, for instance, drug abuse, health-ier eating, safer driving or the use of seat-belts (18, 19);
the feasibility and cost of its implementation, including its sustainabilityand acceptability to different stakeholders. For instance, there is little valuein implementing an intervention that would be too expensive to disseminatewidely, would require skills or knowledge that the implementers do nothave or could be trained in readily, or that is resisted by the professionalsthat are meant to implement it. Clearly, taking practitioners’ views intoaccount is likely to be critical in assessing feasibility;
88
92-4-120938-0_CH04_88

Box
4.4
Gu
idel
ines
fo
r m
akin
g r
eco
mm
end
atio
ns
of
“Ste
ady”
, “R
ead
y”, “
Go
” o
r “D
o n
ot
go
”
Min
imu
m c
rite
ria
to r
eco
mm
end
Inte
rven
tio
ns
nee
din
g a
hig
hth
resh
old
of
evid
ence
to
be
reac
hed
Inte
rven
tio
ns
nee
din
g a
tle
ast
a lo
wth
resh
old
of
evid
ence
tob
e re
ach
edG
oR
ead
yS
tead
yD
o n
ot
go
Go
Rea
dy
Ste
ady
Do
no
t g
oQ
ual
ity
of
inte
rven
tio
n
Ide
ntifi
ed m
echa
nism
of a
ctio
nN
NN
Na
NA
NN
NN
aN
A
Exp
erie
ntia
l bas
e
Ade
quat
e in
tens
ity, d
urat
ion
and
com
plet
enes
sN
Na
NN
a
Qu
alit
y o
f ev
iden
ce f
or
po
siti
ve o
utc
om
es
Car
eful
pilo
t or
info
rmed
judg
emen
tN
AN
A(N
eg)
NA
NA
(Neg
)
Evi
denc
e of
ass
ocia
tions
NA
NA
NN
a(N
eg)
NA
NN
a(N
eg)
P
laus
ibili
ty e
vide
nceb
NA
NN
aN
egN
Na
NN
(Neg
)
Pro
babi
lity
evid
ence
cN
Na
NN
Neg
NN
NN
NN
Neg
Evi
den
ce
Pro
babl
e si
ze o
f pos
itive
effe
ctd
MS
aN
AN
egS
aS
aS
Neg
P
ositi
ve e
ffect
is in
the
cultu
ral c
onte
xt b
eing
pro
pose
dN
Na
NN
aN
egN
Na
NN
aN
eg
Con
sist
ency
of f
indi
ngs
in >
1 s
tudy
NN
aN
egN
Na
Neg
a A
reas
whe
re fu
rthe
r re
sear
ch s
houl
d co
ncen
trat
e.b
Cas
es in
whi
ch o
ther
pot
entia
l exp
lana
tions
hav
e be
en la
rgel
y di
scou
nted
.c E
vide
nce
from
ran
dom
ized
con
trol
led
tria
ls.
d T
his
is b
ased
on
the
stat
istic
al e
ffect
siz
e pl
us th
e “r
each
” of
the
inte
rven
tion.
= n
eces
sary
con
ditio
nN
N =
not
a n
eces
sary
con
ditio
nN
A =
not
app
licab
leN
eg =
neg
ativ
e (h
arm
ful)
effe
ct is
suf
ficie
nt c
ondi
tion
for
“Do
not g
o”(N
eg)
= s
uffic
ient
con
ditio
n to
rec
omm
end
“Do
not g
o” if
lack
of e
ffect
iven
ess
or h
arm
ful e
ffect
s fo
und
in s
ever
al s
tudi
es fo
r th
is ty
pe o
f int
erve
ntio
nS
= p
roba
ble
size
of b
enef
icia
l effe
ct is
at l
east
sm
all
M =
pro
babl
e si
ze o
f ben
efic
ial e
ffect
is a
t lea
st m
oder
ate.
89
92-4-120938-0_CH04_89

in evaluating the strength of evidence provided by a particular study, it isessential to have detailed evidence on the actual process of delivery of theintervention that establishes the extent and quality of delivery as well asevidence on intermediate indicators that support the theoretical mechanismof the intervention (16). For example, for an intervention based on in-school teaching sessions, process information might include data on thenumber and quality of sessions taught, attendance rates at these sessionsand a qualitative assessment by the participants of the sessions’ usefulness,appropriateness and relevance. The evidence collected by implementers orpractitioners in their daily work can be valuable in offering insights intothe daily operations of an intervention and into the kinds of evidence prac-titioners draw on in their work. Evidence and evaluations at the level ofdaily practice or through “learning by doing” are often needed to framefuture policy. Yet evaluators sometimes do not take into account the keyfact that – to be effective when it is scaled-up from a pilot project to thenational scale – interventions are likely to need further modifications. Ad-ditionally, issues such as political commitment, feasibility, cost and ac-ceptability to implementers and gatekeepers will increase in importance;
the degree to which the intervention’s effectiveness is dependent on thespecific context in which it is being implemented, for instance the setting,the local and national sociocultural contexts and the specific time periodor specific group involved. Information on the context will elucidate fac-tors that may have been necessary preconditions for the intervention tohave had the effects observed. Conversely, such evidence will help policy-makers decide on its likely generalizability to other settings or populations.If an intervention has been shown to be highly effective in multipledifferent, but relevant, contexts, this increases the likelihood that it mayalso be effective in a new context (21);
the effectiveness of the intervention in achieving each of the five keyUNGASS goals (1) described in the introductory chapter using appropriateoutcomes. These goals are:
Goal 1 – provide appropriate information to young people and evidenceof improvements in their resulting knowledge.Goal 2 – provide appropriate skills training to young people and evi-dence of their ability to demonstrate these skills, and, if possible,evidence that they have actually used these skills to decrease their riskof becoming infected.Goal 3 – provide appropriate skills-based training, equipment and sup-plies to health-workers and evidence of this resulting in increaseddelivery of effective, high quality health services to young people. Inthis context, the health services that are particularly important include
90
92-4-120938-0_CH04_90

providing advice, counselling on the sexual health (and other concerns)of young people, condoms, treatment for sexually transmitted infec-tions, HIV counselling and testing, and family planning. Clean needles,and other medical instruments and uninfected blood products are es-sential (see chapter 6).Goal 4 – provide evidence of decreased vulnerability to HIV amongyoung people, such as changes in the attitudes and behaviours of adultcommunity members, fewer girls having to resort to “survival sex”, andreductions in HIV prevalence among young people’s potential sexualpartners.Goal 5 – provide evidence of a reduction in HIV prevalence amongyoung people that can be attributed to the intervention.
Policy-makers will also need to know many other things: the scale, trendsand likely future course of the epidemic in their region, country or districtand within specific subgroups of the population (for example, among youngpeople as a whole – that is, those aged 10–24 years, adolescents – those aged10–19 years – and youths – aged 15–24 years, married and unmarried youngpeople, rural and urban young people, injecting drug users, commercial sexworkers and men who have sex with men). Furthermore, policy-makers arelikely to put much more weight on some outcomes, such as a decrease inincidence or prevalence of HIV, than on other outcomes, such as those relatedto the global goals on knowledge, skills, services and vulnerability.
4.5 Assessing the quality of an intervention
Results from a high quality evaluation of a poor quality intervention (that is,an intervention that is badly conceived or badly implemented) merit lessweight than those from a high quality evaluation of a good quality interven-tion. For example, only low weight should be given to the outcome results ofa rigorous evaluation of an intervention in schools in which only 20% of thesessions were actually taught. On the other hand, a process evaluation thatseeks to explain why this intervention was not delivered effectively in thisparticular context might be of great value for future attempts to develop aneffective delivery strategy for this intervention.
Some criteria that may be used to assess the quality and appropriateness ofan intervention are listed below.
Relevance: How relevant is the intervention to HIV prevention amongyoung people? Are the main objectives relevant? Is the intervention rele-vant to this context? For example, in contexts where most HIV infectionis transmitted through injecting drug use, an intervention that ignores thismode of transmission will be of only limited relevance.
91
92-4-120938-0_CH04_91

Experiential base: To what extent was the intervention developed in thelight of existing experience with similar interventions either by drawingon the literature or practitioners’ experience?
Theoretical basis: Is there an explicit and plausible theoretical mechanismby which the intervention is postulated to contribute to a reduction in HIVprevalence among young people? Added weight should be given to thiscriterion if there is evidence that a particular mechanism has worked inother contexts or for other outcomes. For example, if the intervention in-volves peer education, what is the evidence that peer education has workedin other contexts, such as among older adults or in high-income countries,or for other outcomes, for example programmes directed at preventing do-mestic violence or decreasing the consumption of alcohol, tobacco andother drugs?
Careful pilot testing: Has the intervention undergone successful pilottesting in the relevant target group? Has it been appropriately evaluatedand modified?
Feasibility: Is the intervention logistically viable, acceptable to the rele-vant stakeholders, and can it be widely disseminated and sustained givenexisting and projected funds and human resources?
Quality and completeness of implementation: Has the intervention beenimplemented to a high standard?
Other chapters in this series will address the extent to which specific inter-ventions to achieve the global UNGASS goals meet these criteria.
4.6 Types of evidence and their relative weight
There is a wide array of types of evidence that can be used to guide policy.These range from informed judgements based on experience without any ob-jective evidence of impact on the indicators of the five UNGASS goalsthrough to evidence that is based on more rigorous qualitative and quantitativeevaluations of the processes, implementation and outcomes of interventions.One can distinguish between criteria by which to assess the methodologicalquality or soundness of evidence in its own right and criteria by which moreor less weight might be given to findings from different types of evaluationresearch of equally high quality.
4.6.1 Assessing the methodological quality of evidence
The criteria for good evaluation evidence are largely the same as those forresearch evidence in general, and they can be found in numerous research
92
92-4-120938-0_CH04_92

methodology textbooks (22, 23). Some of the main criteria that apply to bothqualitative and quantitative research are summarized below.
Transparency: How clear are all aspects of the research design, the the-oretical framework for the study and the literature base? Are the aims andobjectives explicit? Is there a clear description of the data collection meth-ods and how the data were analysed? Is the completeness of the data clear(such as, refusals to participate, partial participation, losses to follow-up)?Are possible biases of the researchers made explicit?
Representativeness of the data: Can the findings be assumed to apply tothe whole population or group that they are purported to apply to?
Data presentation: Are sufficient data included to mediate between thedata and the interpretation?
Analysis: Does the analysis take account of all relevant data?
Validity: Is there an objective assessment of the internal and external va-lidity of the indicators used?
Plausibility: Is a plausible argument made as to why alternative potentialexplanations for the findings are unlikely or at least less likely than that thefindings were due to the intervention itself?
4.6.2 Criteria for attaching weight to different kinds of evidence
Given interventions (section 4.5) and evaluations of equally high quality(section 4.6), policy-makers should place different values or weights on dif-ferent types of evidence. Criteria that can be used to assess the weight thatshould be placed on evidence include the repeatability of the findings insimilar and/or different contexts. Also, evidence based on multiple evalua-tions with consistent findings should receive more weight than evidence froma single evaluation. If a programme is to be implemented in a similar contextto where the evaluations were done, the key issue will be the repeatability ofthe results from evaluations done in that context. However, for a new or dif-ferent context, the key issues will be the repeatability of the results fromevaluations done in as many different contexts as possible.
In terms of evidence related to the impact of interventions on health and socialoutcomes, a useful framework for categorising evidence from summativeevaluations has been proposed by Victora, Habicht and colleagues (8, 9). Thisframework proposes three levels of evidence:
adequacy evidence. (This is the term used by Victora, Habicht and col-leagues (8, 9) though “supportive” might be a better term). For this level
93
92-4-120938-0_CH04_93

of evidence, all that needs to be shown is that an intervention was imple-mented and the expected changes occurred;
plausibility evidence. Here, in addition to the expected changes occurring,it needs to be shown that the effects related to the programme were greaterthan could be explained by any other external influences;
probability evidence. In addition to plausibility evidence, it needs to beshown there was only a small statistical probability that the programme’sobserved effects would have occurred by chance. This type of evidencecan come only from randomized controlled trials.
It is important to note that plausibility evaluations must include an adequacycomponent, and that probability evaluations benefit from assessing adequacyand plausibility at the same time (for example, through careful process eval-uation and through comparisons of the effects among those who actuallyreceived the intervention, sometimes known as “compliers”, versus those inthe group that was allocated to the intervention but did not receive it, some-times known as “non-compliers”).
This hierarchical typology of evaluation evidence is demonstrated by theexample given in Box 4.5. In this framework, evidence may come either fromexperimental studies (randomized controlled trials or quasi-experimentalstudies) or from observational studies, such as cross-sectional, case–controlor cohort studies. Quasi-experimental studies are those in which individualsor groups are deliberately and prospectively allocated to intervention orcomparison groups, but this allocation is not done randomly. The advantagesand disadvantages of randomized controlled trials for evaluating behaviouralinterventions have been discussed in detail elsewhere (2–9, 24). Assumingthat both the design and implementation of the intervention and evaluationare of high quality, and that there is evidence of ethical practice andgeneralizability, the hierarchy of evidence used in this series of papers willbe as follows. The greatest weight will be put on evidence from “probabilityevaluations” (that is, randomized controlled trials) that potentially providevery strong evidence. Next in the hierarchy will be quasi-experimental eval-uations that have one or more contemporaneous comparison groups thatpotentially provide strong evidence. These will be followed by before-and-after or time-series evaluation studies in individuals or groups of individuals(all of whom receive the intervention) that potentially provide weak-to-moderate evidence depending on the degree to which other potential causesof any observed effects have been ruled out. The least weight will be givento reports of anecdotal or experiential evidence or informed judgement, whichpotentially provide very weak to weak evidence depending on the degree towhich other potential causes of any observed effects have been ruled out.
94
92-4-120938-0_CH04_94

Box 4.5
Examples of evaluations providing supportive (adequacy), plausibility, andprobability evidence
Example: A condom promotion programme is initiated amongyoung people throughout a developing country using mass mediaand social marketing approaches.
Key outcome evaluated: Use of condoms
Supportive (adequacy) evaluation: The number of condomsrecorded as having been distributed to young people and the pro-portion of sexually active young people who reported having useda condom during their last sexual intercourse were substantial afterthe introduction of the intervention.
Plausibility evaluation: In addition to supportive (adequacy) evi-dence, there is well documented evidence that both the condomsdistributed and the proportion of young people using condoms weresubstantially greater than before the programme was launched. Thiscould be demonstrated from before–after or time-series studies.There is also evidence that the impact was proportional to the in-tensity of the intervention in various geographical areas or amongvarious population groups, and the impact was substantially greaterin areas that received the intervention when compared with areasthat did not. This is best demonstrated through quasi-experimentalmethods using a control group that is similar to the interventiongroup. Finally, there is documented evidence that no other activitiesor background (secular) changes could explain the effects seen. Itis therefore plausible that the programme was responsible for theincreases that were observed.
Probability evaluation: In addition to plausibility evidence, a suf-ficient number of individuals (or, where relevant, clusters of indi-viduals) were randomly allocated to receive the new programme.For example, the programme was phased in and during the initialevaluation phase 12 regions were randomly allocated to receive theprogramme immediately, while the other 12 received the pro-gramme after the probability evaluation (randomized controlledtrial) period.
95
92-4-120938-0_CH04_95

Two important caveats should be emphasized. First, there is an importantdistinction between evaluations of efficacy and effectiveness. Efficacy stud-ies aim to measure the impact of an intervention when delivered in a mannerthat is as close as possible to the ideal; effectiveness studies measure impactwhen the intervention is delivered through routine real-life channels. Usuallythe efficacy of an intervention will be greater than its effectiveness whenimplemented on a large scale through routine channels. The second caveat isthe importance of considering context (for example, delivery setting, culture,country or timing) in evaluating all such evidence. The fact that there may bestrong evidence from a well conducted plausibility or probability evaluationthat a particular intervention has the intended effects, does not necessarilymean that it will bring similar benefits if implemented in a different context.For instance, bar-based HIV peer education for gay men was effective in theUnited States of America in the early 1990s (25) but not in Scotland a decadelater, probably because of different cultural norms and the fact that the in-tervention was implemented at a different stage in the epidemic (26). It isimportant, therefore, to include at least an adequacy or plausibility evaluationwhen an intervention that has been found to be efficacious or effective in onecontext is implemented in a substantially different context.
For simplicity, in this series the policy recommendations (“Do not go”,“Steady”, “Ready” or “Go”) will be made for developing countries as a whole.However, policy-makers should review these in the light of local contexts toensure that the interventions are important and relevant to their context. Forexample, the priority given to interventions among intravenous drug userswill obviously depend on the frequency of intravenous drug use; equally wellthe likely effectiveness of interventions in schools will depend on, amongother things, the proportion of young people in the relevant age group whoattend school.
Information that comes from informed judgment – that is, the consideredassessments, decisions and opinions of experienced practitioners or keyinformants – constitutes a different kind of evidence. This might ordinarilybe thought of as being less objective in scientific terms and may not alwaysfit directly into the three-part model discussed above. Nevertheless, suchevidence can offer important guidance to policy-makers in the absence ofevidence of adequacy, plausibility or probability from formal evaluations ofa programme’s impact. It can also be useful for triangulation with other datato provide extra certainty in terms of indicators of a programme’s operationsand effects when aspects of programmes are not documented in ways that areeasily accessed by other methods of data collection. Informed judgement andexpert-generated evidence (sometimes called evidence of best practice) canbe gathered by methods such as interviewing key informants and Delphi scans(27). Each of these methods may have different levels of theoretical
96
92-4-120938-0_CH04_96

sophistication and methodological rigour depending on the design and re-sources deployed. Such techniques gain strength with repetition over time(for example, repeated interviews with key informants used as a part of aprocess evaluation) and can be particularly valuable in contextualizinginterventions.
Ideally all the different types and sources of evidence for and against the likelyeffectiveness of an intervention should be appraised in the assessment ofwhether that intervention should be adopted. The decision should be takenafter careful appraisal of the quality of the intervention (see 4.5), the qualityof each piece of evidence (see 4.6.1), assignment of weights based on boththe evidence threshold for that type of intervention (see 4.3) and the strengthof the evidence available (see 4.6.2). To some extent this follows Tones’argument for the use of a “judicial review” in deciding on interventions(28) but, unlike us, he avoids weighting one kind of evidence over anotherand simply calls for triangulation.
Common situations faced by policy-makers include that of having differenttypes of evidence for different interventions or a situation in which the evi-dence for one intervention is more comprehensive than that for another. Inthese situations it will be important to carefully assess the evidence and beexplicit about what weight is assigned to the different types of evidence. Thiscan be illustrated by comparing the evidence available for the “SteppingStones” community-wide intervention in the Gambia (29) with the evidenceavailable from a recent trial of a complex package of interventions largelytargeted directly at young people within the “MEMA kwa Vijana” project inthe United Republic of Tanzania (30). Put simplistically, there is now a lotof evidence from relatively small-scale programmes that the Stepping Stonesapproach is feasible to implement (if expensive per person involved) and isassociated with changes in knowledge, reported attitudes and reported sexualbehaviours (31). However, no evaluation has yet reported on the impact ofthe Stepping Stones community-wide interventions on HIV incidence orprevalence or on other biological markers of sexual behaviour. The relativelylarge-scale MEMA kwa Vijana project showed that the package of interven-tions tested within this rigorous community-based randomized trial resultedin substantial improvements in knowledge, reported attitudes and somereported sexual behaviours. However, this trial also evaluated the impact onHIV and other biological markers of sexual risk behaviour, and showed that,at least within a 3-year follow-up period, there was no consistent impact onthese biological outcomes (32, 33). Policy-makers may be tempted to choosethe Stepping Stones intervention because there is no discouraging, short-termbiological outcome data but this would be illogical.
97
92-4-120938-0_CH04_97

Policy-makers must beware of equating evidence from high quality, rigorousevaluations with evidence from less rigorous evaluations. Although a recentsystematic review comparing effect sizes in randomized and non-randomizedstudies did not find a consistent difference (34), for interventions of equalquality and effectiveness, the less rigorous the evaluation the more likely itis to give encouraging results (35, 36). This has been demonstrated in a reviewof pregnancy prevention among adolescents (37) and presents a real threat toevidence-based decision-making when rigorous evaluations are not available.
4.7 Conclusion
This chapter has proposed a method for reviewing evidence on the effective-ness of interventions that aim to contribute towards achieving the global goalsrelated to HIV prevention among young people in developing countries (im-proving access to information, skills and services; reducing vulnerability; andreducing HIV prevalence). This method has been used in the five chaptersthat follow, each of which reviews the evidence for the effectiveness of in-terventions in a key prevention setting or population group (in schools, healthservices, geographically-defined communities or groups at high risk of HIV,and through the mass media).
The method involves the following key steps.
1. Define the key types of intervention that policy-makers need to choosebetween in the population setting under consideration (for example,schools).
2. Define the strength of evidence that would be needed to justify thewidespread implementation of this type of intervention (“the evidencethreshold”).
3. Describe explicit inclusion and exclusion criteria for the studies that willreviewed.
4. Critically review all studies that meet the inclusion criteria and their find-ings, by type of intervention. This review should include a criticalappraisal of:
the quality of the intervention. In particular, is it feasible and does ithave a clearly identified mechanism by which it operates in order for itto be effective?the data on the process of implementation. Is there evidence that inter-mediate outcomes predicted by the theoretical mechanism of action areachievable?the context. Is the context in which the evaluation evidence was gen-erated relevant to the context in which the intervention is now proposed?
98
92-4-120938-0_CH04_98

the quality. What was the quality of the outcome evaluations, and whatwere their findings?
5. Summarize the strength of the evidence for the effectiveness of each typeof intervention in making progress towards each of the global goals.
6. Compare the strength of the evidence provided by the studies against thethreshold of evidence needed to recommend widespread implementation.
7. From this comparison, derive evidence-based recommendations relatedto implementation of each type of intervention in this setting or populationgroup, putting each type of intervention into one of the “Do not go”,“Steady”, “Ready” or “Go” categories.
It is important not to be misguided by positive results from poor research. Weargue that it is preferable to roll-out a well evaluated programme with goodevidence of modest impact than to roll-out a poorly evaluated programmewith weak evidence of a larger impact.
The evidence on which we have to make decisions about interventions toprevent the spread of HIV is extremely complex, being about different kindsof interventions, most of which are themselves complex, and arising fromdiverse evaluation methods. Furthermore, the evidence is imperfect, partic-ularly due to the scarcity of rigorous evaluations of outcomes. Anothercomplication in assessing the evidence is that the very existence of evidencefor some interventions and not for others does not occur for reasons that areneutral, but is often the result of past policy preferences, the intrinsic ease ofconducting either the intervention or its evaluation, or because the interven-tion has been seen as controversial. In spite of these difficulties,policy-makers must strive to apply rigour and logic to the selection of inter-vention strategies, resisting political and other pressures that fly in the faceof the evidence.
Finally, even if the evidence that is available leads policy-makers to investin a particular intervention, this does not mean that there is sufficient evidenceabout that intervention. Rather, we should always be building on and refiningthe evidence in the course of implementing public health interventions. Fur-thermore, evaluators should strive to provide as much detail as possible aboutthe actual intervention, process indicators of the coverage and quality of itsimplementation, and its costs and effectiveness.
Acknowledgements
We thank Jane Ferguson, Bruce Dick and Ties Boerma of WHO; MarkPetticrew of the MRC Social and Public Health Sciences Unit, Glasgow;Cesar Victora of the University of Pelotas, Brazil; and the participants at
99
92-4-120938-0_CH04_99

several meetings including Talloires (May 2004), Gex (March 2005) andBogis-de-Chavannes (June 2005) for their stimulating comments and sug-gestions on earlier versions of this paper.
References
1. United Nations. Declaration of commitment on HIV/AIDS. United NationsGeneral Assembly Special Session on HIV/AIDS. Geneva, United Nations,2001 (also available from http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html).
2. Kippax S, van de Ven P. An epidemic of orthodoxy? Design and methodologyin the evaluation of the effectiveness of HIV health promotion. Critical PublicHealth, 1998, 8:371-386.
3. Kippax S. Sexual health interventions are unsuitable for experimentalevaluation. In: Stephenson JM, Imrie J, Bonell C, eds. Effective sexual healthinterventions: issues in experimental evaluation. Oxford, Oxford UniversityPress, 2003:17-34.
4. Klein R. From evidence-based medicine to evidence-based policy? Journal ofHealth Services Research and Policy, 2000, 5:65-66.
5. Heller RF, Page J. A population perspective to evidence based medicine:“evidence for population health”. Journal of Epidemiology and CommunityHealth, 2002, 56:45-47.
6. Rychetnik L et al. Criteria for evaluating evidence on public health interventions.Journal of Epidemiology and Community Health, 2002, 56:119-127.
7. Ross DA, Wight D. The role of randomized controlled trials in assessing sexualhealth interventions. In: Stephenson JM, Imrie J, Bonell C, eds. Effective sexualhealth interventions: issues in experimental evaluation. Oxford, OxfordUniversity Press, 2003: 35-48.
8. Victora C, Habicht J-P, Bryce J. Evidence-based public health: moving beyondrandomized trials. American Journal of Public Health, 2004, 94:400-405.
9. Habicht JP, Victora CG, Vaughan JP. Evaluation designs for adequacy,plausibility and probability of public health programme performance and impact.International Journal of Epidemiology, 1999, 28:10-18.
10. Briss PA et al. Developing an evidence-based guide to community preventiveservices: methods. American Journal of Preventive Medicine, 2000, 18 Suppl1:S35-43.
11. Moher D et al. The CONSORT statement: revised recommendations forimproving the quality of parallel group randomized trials. Lancet, 2001,357:1191-1194.
12. Campbell MK, Elbourne DR, Altman DG. CONSORT statement: extension tocluster randomised trials. BMJ, 2004, 328:702- 708.
13. Campbell C et al. Framework for design and evaluation of complex interventionsto improve health. BMJ, 2000, 321:694-696.
14. Des Jarlais DC et al. Improving the reporting quality of non-randomizedevaluations: the TREND statement. American Journal of Public Health, 2004,94:361-366.
100
92-4-120938-0_CH04_100

15. Cochrane Collaboration. Preparing, maintaining and promoting the accessibilityof systematic reviews of the effects of health care interventions (http://www.update-software.com/Cochrane).
16. Wight D, Obasi A. Unpacking the black box: the importance of process data toexplain outcomes. In: Stephenson J, Imrie J, Bonell C, eds. Effective sexualhealth interventions: issues in experimental evaluation. Oxford, OxfordUniversity Press, 2003.
17. Plummer ML et al. “A bit more truthful”: the validity of adolescent sexualbehaviour data collected in rural northern Tanzania using five methods.Sexually Transmitted Infections, 2004, 80 Suppl II:S49-56.
18. Pawson R, Tilley N. Realistic evaluation. London, Sage, 1997.
19. Pawson R. Evidence-based policy: The promise of ‘realist synthesis’.Evaluation, 2002, 8:340-358.
20. Human Rights Watch. The less they know, the better: abstinence-only HIV/AIDS programs in Uganda. Human Rights Watch, 2005, 17(4):1-79.
21. Victora CG et al. Context matters: interpreting impact findings in child survivalevaluations. Health Policy and Planning, 2005, 20 Suppl i:S18-31.
22. Bowling A. Research methods in health. Maidenhead, Open University Press,2002.
23. Bryman A. Social research methods. Oxford, Oxford University Press, 2004.
24. Stephenson JM, Imrie J, Bonell C, eds. Effective sexual health interventions:issues in experimental evaluation. Oxford, Oxford University Press, 2003.
25. Kelly JA et al. Outcomes of a randomized controlled community-level HIVprevention intervention: effects on behaviour amongst at-risk gay men in smallUS cities. Lancet, 1997, 350:1500-1505.
26. Flowers P et al. Does bar-based, peer-led sexual health promotion have acommunity-level effect amongst gay men in Scotland? International Journal ofSTD and AIDS, 2002, 13;102-108.
27. Sarantakos S. Social research. 3rd edition. Melbourne, Palgrave Macmillan,2004.
28. Tones K. Beyond the RCT: a case for “judicial review”. Health EducationResearch Theory and Practice, 1997, 12:i-iv.
29. Welbourn A. Gender, sex and HIV: how to address issues that no-one wants tohear about. In: Tant qu’on a la Santé. Geneva, DDC, 1999:195-227. (Chapterin English.)
30. Hayes RJ et al. The MEMA kwa Vijana project: design of a community-randomised trial of an innovative adolescent sexual health intervention in ruralTanzania. Contemporary Clinical Trials, 2005, 26:430-442.
31. Paine K et al. ‘Before we were sleeping, now we are awake’: preliminaryevaluation of the Stepping Stones sexual health programme in the Gambia.African Journal of AIDS Research, 2002, 1:39-50.
32. Ross DA et al. MEMA kwa Vijana, a randomised controlled trial of an adolescentsexual and reproductive health intervention programme in rural Mwanza,Tanzania. 3. Results: knowledge, attitudes and behaviour. In: InternationalSociety for Sexually Transmitted Diseases Research 15th biennialconference. Ottawa, ISSTDR, 2003. (Abstract No. 0698.).
101
92-4-120938-0_CH04_101

33. Changalucha J et al. MEMA kwa Vijana, a randomised controlled trial of anadolescent sexual and reproductive health intervention programme in ruralMwanza, Tanzania. 4. Results: biomedical outcomes. In: International Societyfor Sexually Transmitted Diseases Research 15th biennial conference. Ottawa,ISSTDR, 2003:253. (Abstract No. 0699.)
34. MacLehose RR et al. A systematic review of comparisons of effect sizes derivedfrom randomized and non-randomized studies. Health Technology Assessment(Winchester), 2000, 4:1-154.
35. Rossi P. The iron law of evaluation and other metallic rules. Research in SocialProblems and Public Policy, 1987, 4:3-20.
36. Schulz K et al. Empirical evidence of bias dimensions of methodological qualityassociated with estimates of treatment effects in controlled trials. Journal of theAmerican Medical Association, 1995, 273:408-412.
37. Guyatt GH et al. Randomized trials versus observational studies in adolescentpregnancy prevention. Journal of Clinical Epidemiology, 2000, 53:167-174.
102
92-4-120938-0_CH04_102

5. The effectiveness of sex educationand HIV education interventions inschools in developing countriesDouglas Kirby,a Angela Obasi,b & B.A Larisa
Objective To review the impact of sex education and HIV education inter-ventions in schools in developing countries on both risk behaviours for HIVand the psychosocial factors that affect them.
Methods We conducted a systematic review. Searches identified studies indeveloping countries that evaluated interventions using either experimentalor strong quasi-experimental designs and measured the impact of the inter-vention on sexual risk behaviours. Each study was summarized and coded,and the results were tabulated by type of intervention.
Findings Twenty-two intervention evaluations met the inclusion criteria: 17were based on a curriculum and 5 were not, and 19 were implemented pri-marily by adults and 3 by peers. These 22 interventions significantly im-proved 21 out of 55 sexual behaviours measured. Only one of theinterventions (a non-curriculum-based peer-led intervention) increased anymeasure of reported sexual intercourse; 7 interventions delayed the reportedonset of sex; 3 reduced the reported number of sexual partners; and 1 reducedthe reported frequency of sexual activity. Furthermore, 16 of the 22 inter-ventions significantly delayed sex, reduced the frequency of sex, decreasedthe number of sexual partners, increased the use of condoms or contraceptivesor reduced the incidence of unprotected sex. Of the 17 curriculum-based in-terventions, 13 had most of the characteristics believed to be importantaccording to research in developed and developing countries and were taughtby adults. Of these 13 studies, 11 significantly improved one or more reportedsexual behaviours, and the remaining 2 showed non-significant improve-ments in reported sexual behaviour. Among these 13 studies, interventionsled by both teachers and other adults had strong evidence of positive im-pact on reported behaviour. Of the 5 non-curriculum-based interventions, 2of 4 adult-led and the 1 peer-led intervention improved one or more sexualbehaviours.
a ETR Associates 4 Carbonero Way, Scotts Valley, CA 95061, USA. Correspondence shouldbe sent to Dr Kirby (email: [email protected]).
b Liverpool School of Tropical Medicine, Pembroke Place Liverpool, L3 5QA England.
103
92-4-120938-0_CH05_103

Conclusions A large majority of school-based sex education and HIV edu-cation interventions reduced reported risky sexual behaviours in developingcountries. The curriculum-based interventions having the characteristics ofeffective interventions in the developed and developing world should beimplemented more widely. All types of school-based interventions need ad-ditional rigorous evaluation, and more rigorous evaluations of peer-led andnon-curriculum-based interventions are necessary before they can be widelyrecommended.
5.1 Introduction and background
In many respects, schools are well placed to achieve the ultimate goal ofdecreasing HIV prevalence among youths. In many societies they are the oneinstitution that is regularly attended by most young people. Of those youthswho attend school, most do so before they begin having sexual intercourse,and many are enrolled in school when they actually initiate sex. Thus, schoolsprovide an opportunity for interventions to achieve high coverage of youngpeople before or around the time they become sexually active; they also offerthe opportunity to encourage young people to delay the onset of sexual ac-tivity and increase their use of condoms and contraceptives after sexualinitiation. Of course, school-based interventions are less useful where manyor most adolescents are no longer in school.
This chapter will examine school-based interventions in relation to the globalgoals of the United Nations General Assembly Special Session on HIV/AIDSfor young people (UNGASS) (1). Briefly, these goals are to provide youngpeople with access to information (goal 1), with skills to avoid becominginfected with HIV (goal 2), with access to services (goal 3) and to decreasetheir vulnerability to infection (goal 4) as well as decrease the prevalence ofHIV among young people (goal 5).
Numerous, well-conducted studies have demonstrated the effectiveness ofschool-based programmes in producing improvements in knowledge abouthow to avoid HIV infection in developing countries (2–4). However, the ev-idence is much less clear about the effectiveness of schools in meeting theremaining goals. This is partly due to difficulty in formulating and measuringoutcomes such as skills, vulnerability and HIV prevalence (5). It may also bebecause refusal, negotiation and condom-use skills require teaching tech-niques or cultures that are often unfamiliar to school environments in thedeveloping world (6–9). However, in order to truly affect HIV prevalence,schools in the developing world must move beyond making an impact onknowledge alone to demonstrating significant and sustained improvementsin sexual risk behaviours and addressing the more complex affective factors
104
92-4-120938-0_CH05_104

influencing them, such as the values, attitudes and perceived norms about sexand condom use (8, 10).
There have been a few reviews of studies that examined school-based inter-ventions in the developing world and that examined their impact on be-haviour. However, they have been limited by a focus on a particulargeographical area (2) or by the strengths of the evaluations, and they havenot examined the characteristics of interventions in developing countriesworldwide (4, 11, 12).
One review has identified key characteristics of curriculum-based interven-tions shown to be effective in changing behaviours in both developed anddeveloping countries in the settings of schools, clinics and other communityorganizations (12). However, similar analyses are needed of all school-basedprogrammes in developing countries if schools are to fulfil their potential forcombating HIV among youths.
5.1.1 Objectives
This article reviews the literature on the effects of school-based sex educationand HIV education interventions on sexual risk behaviours among youngpeople in all developing countries. This review builds on previous work(2–4, 7, 8, 11–14) by (i) focusing specifically on studies that examine anintervention’s impact on sexual behaviour, (ii) including more interven-tion studies that measure the impact on behaviour than previous reviews,(iii) assessing the strength of the evaluation design of different study strate-gies and (iv) assessing the characteristics of effective interventions.
5.1.2 Schools and their interventions
For the purposes of this review, schools are defined as any formal educationalestablishment providing training or education to youths who are youngerthan 25 years of age. As the field of HIV prevention evolves, schools areincreasingly being included as part of multicomponent HIV interventions.This review evaluates such interventions only if the specific impact of theschool intervention has been separately evaluated or if the school componentrepresents the major part of the overall intervention and a substantial partof the overall impact of the intervention could be attributed to the schoolintervention.
A large number of sex education and HIV education interventions are beingimplemented in schools worldwide. They vary widely in terms of objectives,structure, length, content, implementation strategy and other characteristics(4, 12, 13). In practice, however, the choice and implementation of interven-tions in schools in developing countries is constrained by the availability of
105
92-4-120938-0_CH05_105

teachers and curricular materials as well as teacher training; access to otherfinancial, material and technical resources; and the culture and norms of boththe local communities and the schools themselves (9, 15). Inadequate levelsof training and the prevalence of didactic teaching methods may mean thatteachers are sometimes unable to use the participatory, student-centred tech-niques that are often necessary for effective skill building (6, 9). Furthermore,in many societies, resistance among teachers to discussing sexual behaviourwith adolescents or issues such as age, sex and status differentials may meanthat pupils or teachers, or both, feel uncomfortable discussing sexual mattersin the classroom (8, 16). Resistance to discussing the use of condoms is par-ticularly widespread in schools (2, 9); authors have reported that sometimes,where discussions of condoms are included in an intervention, the informa-tion communicated to pupils about condoms has been mostly negative inorder to discourage condom use and encourage abstinence (17).
In order to overcome some of these obstacles to school-based interventions,programme developers and staff have provided structured curricula to guideactivities, have trained teachers, and have involved trained individuals otherthan teachers in delivering the interventions. Curriculum is defined here asan organized set of activities or exercises designed to convey specific knowl-edge, skills or experiences in an ordered or incremental fashion. Suchactivities may be implemented either in the classroom during the school dayor after school.
5.1.3 Categories of interventions
School-based interventions can be categorized according to at least three dif-ferent dimensions. These are described below. (In reviews of school-basedinterventions, whether the school was primary, secondary or post-secondarymight be considered important. However, in this review, all of the studies ofinterventions in primary schools were conducted in Africa and the age rangeof the youths who participated – 10 to 18 years – was within the age range ofyouths in secondary schools in other developing countries – 10 to 25 years.Thus, studies were not grouped by school level in this review.)
5.1.3.1 Curriculum-based versus non-curriculum-based
Curriculum-based interventions are often more intensive and more structuredthan non-curriculum-based interventions. In addition, curriculum-based in-terventions are more likely to be based on theory and previous research andmay have been extensively pilot-tested and sanctioned by the appropriateauthorities. The curricula serve to guide and inform the educators, and theiruse may overcome or ameliorate some of the educators’ personal prejudices
106
92-4-120938-0_CH05_106

or limitations in teaching skills. These characteristics may enhance the ef-fectiveness of these interventions.
Non-curriculum-based interventions include a variety of activities such asone-on-one spontaneous or opportunistic counselling about sexual activityand HIV while the student is on school grounds, school health fairs, dramasthat present stories about HIV during school assemblies, the use of posters orleaflets, or combinations of these. Some of these activities may be easier toimplement in schools, at least initially, because they may not require thatteachers be trained. In addition, some people have argued that spontaneousone-on-one interaction between educators and youths may be more effective,given the personal nature of sexual behaviour. However, such interactionsrequire a degree of sensitivity, skill and empathy that may be beyond thescope of many implementers or may necessitate a high level of training.
5.1.3.2 Interventions with and without characteristics of effective curriculum-basedinterventions
There are a variety of other characteristics of interventions, especiallycurriculum-based interventions, that may affect their effectiveness (for ex-ample, the focus of the activities, the information provided and the instruc-tional methods implemented).
In developed countries, there have been at least 65 evaluations of curriculum-based sex education and HIV education interventions, and there have alsobeen additional studies of non-curriculum-based interventions. Reviews ofthese studies have identified some of the characteristics of interventions be-lieved to be important in producing behavioural change (12, 14, 17–21).
While these characteristics of effective interventions have not been derivedfrom interventions used primarily in developing countries, they neverthelessprovide a potential set of guidelines that can be used to assess these inter-ventions in developing countries. The most recent set of characteristicsidentified by Kirby et al. (12) is based on the greatest number of studies andincludes some studies from developing countries. That review identified 17characteristics that appear to distinguish effective programmes and that de-scribe programme development, the curricula and programme implementa-tion. These characteristics are described in Box 5.1.
107
92-4-120938-0_CH05_107

Box
5.1
Ch
arac
teri
stic
s o
f ef
fect
ive
curr
icu
lum
-bas
ed p
rog
ram
mes
Dev
elo
pin
g t
he
curr
icu
lum
Co
nte
nt
Imp
lem
enta
tio
n1.
Invo
lve
mul
tiple
peo
ple
with
diff
eren
tba
ckgr
ound
s in
theo
ry, r
esea
rch
and
sex/
HIV
edu
catio
n.
Cu
rric
ulu
m g
oal
s an
d o
bje
ctiv
es1.
Foc
us o
n cl
ear
heal
th g
oals
, suc
h as
thep
reve
ntio
n of
ST
Isa
and
HIV
and
/or
preg
nanc
y.
1. S
ecur
e at
leas
t min
imal
sup
port
from
appr
opria
te a
utho
ritie
s, s
uch
asm
inis
trie
s of
hea
lth, s
choo
l dis
tric
ts o
rco
mm
unity
org
aniz
atio
ns.
2. A
sses
s re
leva
nt n
eeds
and
ass
ets
ofta
rget
gro
up.
2. F
ocus
nar
row
ly o
n sp
ecifi
c be
havi
ours
lead
ing
to th
ese
heal
th g
oals
(su
ch a
sab
stai
ning
from
sex
or
usin
g co
ndom
sor
oth
er c
ontr
acep
tives
); g
ive
clea
rm
essa
ges
abou
t the
se b
ehav
iour
s;an
d ad
dres
s si
tuat
ions
that
mig
ht le
adto
them
and
how
to a
void
them
.
2. S
elec
t edu
cato
rs w
ith d
esire
dch
arac
teris
tics,
trai
n th
em a
nd p
rovi
dem
onito
ring,
sup
ervi
sion
and
sup
port
.
3. U
se a
logi
c m
odel
app
roac
h to
deve
lop
the
curr
icul
um th
at s
peci
fies
the
heal
th g
oals
, the
beh
avio
urs
affe
ctin
g th
ose
heal
th g
oals
, the
ris
kan
d pr
otec
tive
fact
ors
affe
ctin
g th
ose
beha
viou
rs, a
nd th
e ac
tiviti
esad
dres
sing
thos
e ris
k an
d pr
otec
tive
fact
ors.
3. A
ddre
ss m
ultip
le s
exua
l–ps
ycho
soci
alris
k an
d pr
otec
tive
fact
ors
affe
ctin
gse
xual
beh
avio
urs
(suc
h as
know
ledg
e, p
erce
ived
ris
ks, v
alue
s,at
titud
es, p
erce
ived
nor
ms
and
self-
effic
acy)
.
3. If
nee
ded,
impl
emen
t act
iviti
es to
recr
uit a
nd r
etai
n yo
uths
and
over
com
e ba
rrie
rs to
thei
r inv
olve
men
t(f
or e
xam
ple,
pub
liciz
e th
epr
ogra
mm
e, o
ffer
food
or
obta
inco
nsen
t fro
m y
outh
s or
par
ents
).
4. D
esig
n ac
tiviti
es c
onsi
sten
t with
com
mun
ity v
alue
s an
d av
aila
ble
reso
urce
s (s
uch
as s
taff
time,
sta
ffsk
ills,
faci
lity
spac
e an
d su
pplie
s).
Act
ivit
ies
and
tea
chin
g m
eth
od
s4.
Cre
ate
a sa
fe s
ocia
l env
ironm
ent i
nw
hich
you
ths
can
part
icip
ate.
4. Im
plem
ent v
irtua
lly a
ll ac
tiviti
es a
sde
sign
ed.
108
92-4-120938-0_CH05_108

5. P
ilot-
test
the
prog
ram
.5.
Incl
ude
mul
tiple
act
iviti
es to
cha
nge
each
of t
he ta
rget
ed ri
sk a
nd p
rote
ctiv
efa
ctor
s.6.
Use
inst
ruct
iona
lly s
ound
teac
hing
met
hods
that
act
ivel
y in
volv
epa
rtic
ipan
ts, t
hat h
elp
part
icip
ants
pers
onal
ize
the
info
rmat
ion
and
that
are
desi
gned
to c
hang
e ea
ch g
roup
of
risk
and
prot
ectiv
e fa
ctor
s.7.
Use
act
iviti
es, i
nstr
uctio
nal m
etho
dsan
d be
havi
oura
l mes
sage
s th
at a
reap
prop
riate
to th
e cu
lture
,de
velo
pmen
tal a
ge a
nd s
exua
lex
perie
nce
of th
e pa
rtic
ipan
ts.
8. C
over
topi
cs in
a lo
gica
l seq
uenc
e.
Sou
rce:
Kirb
y D
, Lar
is B
A, R
olle
ri L.
The
impa
ct o
f sex
and
HIV
edu
catio
n pr
ogra
ms
in s
choo
ls a
nd c
omm
uniti
es o
n se
xual
beh
avio
rsam
ong
youn
g ad
ults
. Was
hing
ton,
DC
, Fam
ily H
ealth
Inte
rnat
iona
l, 20
06.
a S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
109
92-4-120938-0_CH05_109

5.1.3.3 Adult-led versus peer-led interventions
The choice of educator also represents a balance among pedagogy, pre-vailing culture and infrastructure capacity. Adults most commonly imple-ment curriculum-based interventions because typically they have more ofthe experience, knowledge and skills needed. The adults who implement aparticular curriculum may include both schoolteachers and others, such ashealth-workers.
Teacher-led interventions are logistically the easiest to implement in schoolsonce teachers have been adequately trained. Such interventions are alsohighly replicable. However these benefits may be offset by the limitations ofteachers discussed above, including their status in relation to pupils or theirdiscomfort in using interactive teaching methods and discussing sensitivetopics such as adolescents’ sexual behaviour.
Because of these limitations, people in some communities favour usinghealth-workers or other local experts to teach these curricula. These expertsmay be more knowledgeable about the sexual topics covered, more comfort-able discussing these topics and more comfortable using interactive learningmethods. In addition, using health-workers or other trained adults to discusssensitive matters, such as condoms, in schools may help teachers avoid theinternal conflicts mentioned above and may allay fears of community cen-sure. However, limited infrastructure, transportation, time and other re-sources may prevent health-workers from teaching intensive and lengthycurricula to many students in many schools.
Peer educators have been widely advocated as alternatives or adjuncts toteachers or other adults (22). Many believe that peer educators may be ableto relate more closely to other young adults than older adults can. However,peers are less likely to be knowledgeable about these topics and less likely tohave the skills needed to teach curriculum activities (23). Furthermore, theinevitable annual student turnover and subsequent requirements for recurringtraining and supervision raise doubts about the sustainability and cost effec-tiveness of using peer educators (11).
In order to provide a discussion that is helpful to programme developers, wehave categorized all 22 interventions studied according to whether they arebased on a curriculum, whether they incorporate most of the characteristicsin Box 5.1 and whether they are taught by adults or peers. These three di-mensions produced the following six categories with one or more studies percategory:
curriculum-based interventions that incorporate most of the 17 character-istics and are led by adults;
110
92-4-120938-0_CH05_110

curriculum-based interventions that incorporate most of the 17 character-istics and are led by peers;
curriculum-based interventions that lack several of the 17 characteristicsand are led by adults;
curriculum-based interventions that lack several of the 17 characteristicsand are led by peers;
non-curriculum-based interventions that incorporate several of the 17 char-acteristics and are led by adults;
non-curriculum-based interventions that lack several of the 17 character-istics and are led by peers.
5.2 Methods
5.2.1 Identification of studies
For this review, we sought to identify and retrieve studies meeting the criteriain Table 5.1. For the most part, the review is limited to studies that measuredan intervention’s impact on behaviour for two reasons: first, because it is wellestablished that school-based sex education and HIV education interventionscan increase knowledge (all studies that measured impact on knowledgefound a positive impact) and second because changes in knowledge, skillsand other mediating factors will not lead to a decrease in HIV prevalenceunless behaviour also changes.
In order to identify and retrieve as many of the studies from developingcountries as possible we:
1. reviewed the results of a previous search for studies undertaken by ETRAssociates and the University of Minnesota and identified those studiesmeeting the criteria specified above;
2. reviewed studies already summarized in previous reviews of theseinterventions;
3. reviewed multiple computerized list-serves for studies meeting the crite-ria (including PubMed, PsycINFO, POPLINE, Sociological Abstracts,Psychological Abstracts, Bireme, Dissertation Abstracts Online, ERIC, Com-bined Health Information Database – CHID, and Biological Abstracts);
4. contacted researchers in the process of completing studies and obtainedresults (sometimes preliminary) whenever appropriate and possible;
5. attended professional meetings, scanned abstracts, spoke with authors andobtained studies whenever possible;
111
92-4-120938-0_CH05_111

6. scanned each issue from 1990 to 2005 of 12 journals in which relevantstudies might appear;
7. reviewed reports of intervention development, training materials, andprocess evaluation reports.
5.2.2 Threshold of evidence needed for widespread implementation
Overall, because of the potential ability of school-based interventions to beimplemented broadly and to reach large proportions of young people, theseinterventions should require low-to-moderate thresholds of evidence beforebeing recommended for widespread implementation. However, because thediscussion of sexual activity, especially condom use, in schools may be con-troversial, the threshold varies somewhat according to the community, the
Table 5.1Inclusion and exclusion criteria used to identify studies for review
Inclusion criteria Exclusion criteria
Characteristics of the programmeProgramme was implemented in adeveloping country
Programme was implemented in developedcountry
Programme implemented in primary,secondary or post-secondary schools (forexample, night schools or universities)Focused on young people aged 24 years Focused on a cross-section of age groups
that included some young people but did notinclude a sample with at least 80% ofparticipants aged < 25 years
Characteristics of the studyWas published in EnglishUsed a reasonably strong experimental orquasi-experimental design with bothintervention and comparison groups andbaseline and follow-up data
Lacked a comparison group or baseline andfollow-up data
Had a minimum sample size of 100Measured the impact of the programme onone or more reported sexual behaviours(initiation of sexual intercourse, frequency ofsexual intercourse or number of sexualpartners), reported use of condoms orcontraception, pregnancy rates, birth ratesand STIa rates
Measured impact only on knowledge,values, attitudes or intentions and notbehaviour
Was completed or published betweenJanuary 1990 and June 2005
a STI = sexually transmitted infection.
112
92-4-120938-0_CH05_112

grade level in which the intervention is designed to take place and the inter-vention’s content, targeted behaviour and implementer. Conclusions made inthis review are based on the consideration of these issues and thresholds(Table 5.2).
5.2.3 Review of studies
All studies were summarized in a template by one of this review’s authors(BL) and then reviewed by a second author (DK). The summaries were thensent to the author of the original study for verification. Changes were madeas appropriate. The complete version of these summaries is available on theweb (www.who.int/child-adolescent-health/).
For this review, all reported outcomes (for example, effects on behaviour)were considered significant if they were statistically significant at the 0.05level and this significance was based either on the total sample or a subsamplethat was roughly one third of the total sample or larger (for example, eithermales or females, youths younger or older than a certain age, or sexuallyexperienced or sexually inexperienced youths). Some studies found signifi-cant effects for important subgroups but not for the entire sample.
Studies sometimes reported results for multiple measures of each behaviour,for different time periods, for different subgroups or for combinations ofthese. Thus, some studies reported only one or a small number of significantpositive effects on behaviour as well as a large majority of results that werenot significant. To avoid presenting only the positive results and to providea more balanced overview, the following rules for summarizing results wereadopted. First, for different measures of the same outcome behaviour: allmeasures across all the studies were rank-ordered according to their probableimpact on prevalence. For example, the use of condoms over a long periodof time was ranked higher than condom use at first sexual intercourse. Onlythe results from the highest ranked measure reported in each study were in-cluded in the tables. Second, because short-term effects on behaviour wouldhave little impact on HIV prevalence, only those results reported for periodsof 3 months or longer were included in the tables. In addition, because studieswere not likely to have sufficient statistical power to measure the impact onthose behaviours or outcomes that change slowly (that is, initiation of sex,pregnancy rates or rates of sexually transmitted infections [STIs]), onlythose results measuring impact on these outcomes for at least 6 months wereincluded.
113
92-4-120938-0_CH05_113

Tab
le 5
.2T
hre
sho
ld o
f ev
iden
ce n
eed
ed t
o r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n o
f ea
ch t
ype
of
inte
rven
tio
n
Inte
rven
tio
n t
ype
Cri
teri
on
aO
vera
llT
hre
sho
ldC
om
men
ts
Feasibility
Lack of poten-tial for adverse
outcomes
Acceptability
Potentialsize of effect
Other health orsocial benefits
By
bro
ad in
terv
enti
on
typ
eC
urric
ulum
-bas
ed+
++
++
++
+Lo
wC
urric
ulum
-bas
ed in
terv
entio
ns p
rovi
de c
onsi
dera
ble
guid
ance
toth
e ed
ucat
or a
bout
impl
emen
ting
the
inte
rven
tion
and
may
hav
ebe
en p
revi
ousl
y ev
alua
ted.
Thu
s, th
ey h
ave
less
pot
entia
l for
adve
rse
outc
omes
and
a g
reat
er p
oten
tial e
ffect
siz
e th
anin
terv
entio
ns th
at a
re n
ot c
urric
ulum
-bas
ed.
Not
cur
ricul
um-b
ased
++
+-
++
+Lo
wIn
terv
entio
ns th
at a
re n
ot c
urric
ulum
-bas
ed m
ay b
e ea
sier
toim
plem
ent a
nd m
ay n
ot re
quire
as
muc
h cl
assr
oom
tim
e or
as
muc
htr
aini
ng o
f as
man
y ed
ucat
ors
as c
urric
ulum
-bas
ed in
terv
entio
ns.
By
char
acte
rist
ics
of
the
inte
rven
tio
nb
With
cha
ract
eris
tics
ofef
fect
ive
inte
rven
tions
++
++
++
++
Low
Cha
ract
eris
tics
of e
ffect
ive
inte
rven
tions
req
uire
that
the
inte
rven
tion
focu
s on
HIV
, oth
er S
TIs
c an
d pr
egna
ncy,
the
risk
and
prot
ectiv
e be
havi
ours
affe
ctin
g th
em a
nd th
at th
ey u
se in
tera
ctiv
eac
tiviti
es to
cha
nge
beha
viou
rs. T
hese
cha
ract
eris
tics
mig
ht m
ake
the
inte
rven
tion
mor
e di
fficu
lt to
impl
emen
t and
less
acc
epta
ble
toth
ose
who
pre
fer
not t
o fo
cus
on s
exua
l beh
avio
ur. H
owev
er, t
hey
grea
tly in
crea
se th
e po
tent
ial s
ize
of th
e ef
fect
.W
ithou
t cha
ract
eris
tics
of e
ffect
ive
inte
rven
tions
++
++
++
++
Low
Inte
rven
tions
with
out e
ffect
ive
char
acte
ristic
s m
ay b
e ea
sier
toim
plem
ent a
nd m
ore
acce
ptab
le. H
owev
er, t
heir
estim
ated
effe
ctsi
ze is
sm
alle
r.
114
92-4-120938-0_CH05_114

By
typ
e o
f ed
uca
tor
Adu
lt-le
d (t
each
er)
++
-+
++
+Lo
wT
each
ers
may
hav
e to
be
trai
ned
both
to d
iscu
ss s
exua
l top
ics
and
to u
se in
tera
ctiv
e te
achi
ng m
etho
ds. O
nce
trai
ned,
they
can
impl
emen
t the
inte
rven
tion
durin
g sc
hool
at r
elat
ivel
y lit
tle c
ost.
The
re is
the
poss
ibili
ty o
f mal
e te
ache
rs ta
king
adv
anta
ge o
fdi
scus
sion
s of
sex
ualit
y to
pre
ssur
e fe
mal
e st
uden
ts to
hav
e se
xual
rela
tions
.A
dult-
led
(oth
er a
dult)
++
++
++
++
Low
Oth
er a
dults
(su
ch a
s co
mm
unity
hea
lth p
erso
nnel
) m
ay b
e m
ore
accu
stom
ed to
dis
cuss
ing
sexu
al to
pics
and
may
hav
e le
arnt
how
to u
se in
tera
ctiv
e te
achi
ng m
etho
ds. H
owev
er, o
ngoi
ng r
esou
rces
are
need
ed to
allo
w th
em to
trav
el to
sch
ools
and
impl
emen
tin
terv
entio
ns.
Pee
r-le
d+
++
++
++
Low
Pee
rs m
ay r
equi
re c
onsi
dera
ble
trai
ning
bef
ore
they
hav
e th
ekn
owle
dge
and
skill
s to
impl
emen
t an
inte
rven
tion.
The
y m
ayre
quire
res
ourc
es to
trav
el to
the
scho
ols,
and
they
will
mat
ure
and
ceas
e be
ing
peer
s af
ter
a fe
w y
ears
ther
eby
crea
ting
a ne
ed fo
ron
goin
g re
crui
tmen
t and
trai
ning
.P
eers
may
lear
n im
port
ant s
kills
as
peer
edu
cato
rs.
By
sch
oo
llev
elP
rimar
y sc
hool
++
--
++
Mod
erat
eT
he p
ossi
bilit
y of
mal
e te
ache
rs ta
king
adv
anta
ge o
f the
ir po
wer
and
the
disc
ussi
on o
f sex
ualit
y to
pre
ssur
e fe
mal
e st
uden
ts to
hav
ese
xual
rela
tions
is m
ost l
ikel
y in
prim
ary
scho
ol o
r sec
onda
ry s
choo
l.T
he d
iscu
ssio
n of
con
dom
s in
prim
ary
scho
ol m
ay b
e le
ssac
cept
able
initi
ally
to s
ome
adul
ts in
the
com
mun
ity. A
bstin
ence
-on
ly in
terv
entio
ns m
ay b
e m
ore
acce
ptab
le, b
ut m
ay h
ave
less
impa
ct (
or a
neg
ativ
e im
pact
) on
con
dom
use
.In
terv
entio
ns m
ay h
ave
a gr
eate
r im
pact
on
dela
ying
sex
ual
rela
tions
am
ong
prim
ary
and
seco
ndar
y sc
hool
stu
dent
s, a
t a ti
me
befo
re m
ost y
oung
peo
ple
have
sex
ual r
elat
ions
, tha
n in
pos
t-se
cond
ary
scho
ol w
hen
mos
t stu
dent
s ha
ve a
lread
y ha
d se
xual
rela
tions
.
115
92-4-120938-0_CH05_115

Inte
rven
tio
nty
pe
Cri
teri
on
aO
vera
llT
hre
sho
ldC
om
men
ts
Feasibility
Lack of poten-tial for adverse
outcomes
Acceptability
Potentialsize of effect
Other health orsocial benefits
Sec
onda
rysc
hool
++
-+
++
+M
oder
ate
The
pos
sibi
lity
of m
ale
teac
hers
taki
ng a
dvan
tage
of t
heir
pow
er a
ndth
e di
scus
sion
of s
exua
lity
to p
ress
ure
fem
ale
stud
ents
to h
ave
sexu
alre
latio
ns is
mos
t lik
ely
in p
rimar
y sc
hool
or
seco
ndar
y sc
hool
.In
terv
entio
ns m
ay h
ave
a gr
eate
r im
pact
on
dela
ying
sex
ual r
elat
ions
amon
g pr
imar
y an
d se
cond
ary
scho
ol s
tude
nts,
at a
tim
e be
fore
mos
tyo
ung
peop
le h
ave
sexu
al r
elat
ions
, tha
n in
pos
t-se
cond
ary
scho
ol w
hen
mos
t stu
dent
s ha
ve a
lread
y ha
d se
xual
rel
atio
ns.
Pos
t sec
onda
rysc
hool
s+
++
++
++
Low
Inte
rven
tions
may
hav
e a
grea
ter
impa
ct o
n de
layi
ng s
exua
l rel
atio
nsam
ong
prim
ary
and
seco
ndar
y sc
hool
stu
dent
s at
a ti
me
befo
re m
ost
youn
g pe
ople
hav
e se
xual
rel
atio
ns th
an in
pos
t-se
cond
ary
scho
ol w
hen
mos
t stu
dent
s ha
ve a
lread
y ha
d se
xual
rel
atio
ns b
ut in
terv
entio
n in
pos
tse
cond
ary
scho
ol m
ay s
till h
ave
an im
pact
on
cond
om u
se.
a D
egre
e of
des
irabi
lity
is in
dica
ted
with
a m
axim
um o
f 3 “
+”
sign
s. D
egre
e of
und
esira
bilit
y is
indi
cate
d w
ith a
max
imum
of 3
“-”
sig
ns.
b S
ee B
ox 5
.1 a
nd th
e te
xt fo
r fu
ll de
scrip
tion
of th
ese
char
acte
ristic
s.c S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
116
92-4-120938-0_CH05_116

Even these rules for summarizing the results may have provided a more pos-itive picture than an analysis of all the results from all studies. However, thisprobable positive bias was offset by a different negative bias: many resultspresented in the studies were based on samples with insufficient power. Thus,interventions may have produced programmatically meaningful results thatwere found to be not significant. (Insufficient statistical power is further dis-cussed in the section below.)
5.3 Findings
Our search identified 22 studies (16, 17, 24–44) meeting the inclusion criteria.The characteristics of the 22 interventions and their respective evaluationsare summarized in Table 5.3 and Table 5.4, respectively. The impact of allthese interventions on specified behaviours is summarized in Table 5.5 aswell as in Table 5.4a and Table 5.4b.
5.3.1 Characteristics of interventions
Of the 22 studies and respective interventions, 17 were curriculum-based and5 were non-curriculum based. Of the 17 curriculum-based interventions, 14incorporated at least four fifths of the characteristics described in Box 5.1.Altogether, 15 of the 17 were taught primarily by adults and 2 were taughtsolely by peers. Of the 15 taught by adults, 10 were taught by the schools’teachers and the remaining 5 were taught by other adults, such as health-workers, trained counsellors and facilitators, and young adult volunteers.However, of the 15 interventions led by adults, 2 also involved peer educatorsin significant ways. Of the five non-curriculum-based interventions, fourwere primarily led by teachers or other adults and one by peers.
A total of 16 of the interventions evaluated had been implemented in sec-ondary schools; five had been implemented in primary schools; and three hadbeen implemented in night schools or teacher-training colleges. (The sumexceeds 22 because one intervention was implemented in both primary andsecondary schools and another in both secondary and night schools.)
Finally, only three of the interventions were abstinence-only interventions;the remainder of the interventions encouraged abstinence but also discussedor promoted the use of condoms or contraception for young people who choseto be sexually active.
5.3.2 Characteristics of the studies
Eight of these studies used an experimental design, while the remaining 14used a quasi-experimental design. In order to be included in the review, all
117
92-4-120938-0_CH05_117

Tab
le 5
.3D
escr
ipti
on
s o
f th
e in
terv
enti
on
s b
y st
ud
y
Stu
dy,
loca
tio
n a
nd
pro
gra
mm
eT
arg
et p
op
ula
tio
n a
nd
pri
mar
yo
bje
ctiv
esD
escr
ipti
on
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
(te
ach
ers)
A –
Tha
iland
,T
eens
on
Sm
art S
ex (
16)
• Y
outh
s ag
ed 1
8–21
yea
rs in
urba
n ar
eas
• T
arge
ted
sexu
al in
itiat
ion,
num
ber
of p
artn
ers
and
cond
omus
e
• 16
hou
rs•
Add
ress
ed is
sues
of l
ove,
atti
tude
s to
war
d H
IV a
nd s
exua
lity,
livi
ng w
ith H
IV/A
IDS
, HIV
and
pre
gnan
cy p
reve
ntio
n, h
ealth
ser
vice
s•
Pra
ctic
ed n
egot
iatin
g sk
ills
B –
Chi
le,
Tee
n S
tar
(24)
• Y
outh
s ag
ed 1
5–16
yea
rs in
urba
n ar
eas
• P
regn
ancy
pre
vent
ion
• M
inim
um 1
0.5
hour
s in
volv
ing
part
icip
ants
in g
roup
dis
cuss
ions
,br
ains
torm
ing
• T
ackl
ed is
sues
suc
h as
gen
der,
pre
judi
ce, a
nato
my,
pub
erty
, fer
tility
,em
otio
ns, m
edia
, sel
f-as
sura
nce,
dec
isio
n-m
akin
g, m
arria
ge a
nd fa
mily
,fa
mily
pla
nnin
g m
etho
ds, p
regn
ancy
and
birt
h•
Use
d cl
ass
disc
ussi
ons,
fert
ility
aw
aren
ess
activ
ities
, rol
e-pl
ayin
g an
dho
mew
ork
C –
Uni
ted
Rep
ublic
of T
anza
nia,
“Nga
o” (
25)
• Y
outh
s ag
ed 1
0–16
yea
rs in
urba
n an
d ru
ral a
reas
• T
arge
ted
sexu
al in
itiat
ion
• 20
hou
rs o
ver
2–3
mon
ths
• C
over
ed tr
ansm
issi
on o
f AID
S, p
erso
nal H
IV r
isk,
ref
usal
ski
lls,
com
mun
icat
ion
with
par
ents
and
com
mun
ity•
Use
d le
ctur
es, p
oste
rs, s
ongw
ritin
g, d
iscu
ssio
n, r
ole-
play
ing,
etc
.D
– K
enya
,P
rimar
y sc
hool
act
ion
for
bette
rhe
alth
(17
)•
You
ths
aged
11–
17 y
ears
inur
ban
and
rura
l are
as•
Tar
gete
d se
xual
initi
atio
n
• T
ackl
ed is
sues
suc
h as
abs
tinen
ce, c
ondo
m u
se, s
choo
l pla
nnin
g,gu
idan
ce, t
rans
mis
sion
and
pre
vent
ion
of S
TIs
,a HIV
and
AID
S; l
ife s
kills
;he
alth
, sex
ualit
y, H
IV m
anag
emen
t•
Use
d pa
rtic
ipat
ory
met
hods
• S
et u
p sc
hool
hea
lth c
lubs
E –
Mex
ico,
Pla
nead
o tu
Vid
a (2
6)• Y
outh
s w
ith m
ean
age
14.4
yea
rs•
Tar
gete
d se
xual
initi
atio
n an
dco
ntra
cept
ive
use
• D
iscu
ssed
rel
atio
nshi
ps, s
exua
lity,
ana
tom
y, p
hysi
olog
y, r
epro
duct
ion,
ST
Is, c
ontr
acep
tion,
dec
isio
n-m
akin
g, c
onse
quen
ces,
sel
f-es
teem
,va
lues
, com
mun
icat
ion,
ass
ertiv
enes
s•
Use
d ro
le-p
lays
and
writ
ing
exer
cise
s
118
92-4-120938-0_CH05_118

F –
Sou
th A
fric
a,Li
fe s
kills
(27
, 28)
• Y
outh
s ag
ed 1
2–21
yea
rs in
urba
n an
d ru
ral a
reas
• T
arge
ted
freq
uenc
y of
sex
ual
activ
ity, c
ondo
m u
se, n
umbe
r of
part
ners
• 16
hou
rs•
Cov
ered
HIV
/AID
S, i
mm
une
syst
em, s
elf-
este
em, s
elf-
awar
enes
s,re
latio
nshi
ps, v
alue
s, s
exua
lity,
abs
tinen
ce, c
ondo
m u
se, r
ape/
abus
e,de
cisi
on-m
akin
g, c
onfli
ct r
esol
utio
n, e
tc.
• U
sed
inte
ract
ive
and
dida
ctic
met
hods
, inc
ludi
ng g
roup
wor
k an
d ro
le-
play
sG
– U
nite
d R
epub
lic o
f Tan
zani
a,M
EM
A k
wa
Vija
na (
Goo
d th
ings
for
youn
g pe
ople
) (2
9)
• You
ths
aged
12–
19 y
ears
in ru
ral
area
s•
Tar
gete
d se
xual
initi
atio
n,co
ndom
use
, num
ber
ofpa
rtne
rs, S
TIs
, pre
gnan
cy
• In
-sch
ool p
rogr
amm
e w
as te
ache
r-le
d, a
lso
peer
-ass
iste
d•
Cov
ered
ref
usal
, sel
f-ef
ficac
y, s
elf-
este
em, S
TI/H
IV, s
exua
lity,
cont
race
ptio
n, a
bstin
ence
, acc
ess
to r
epro
duct
ive
care
and
cont
race
ptio
n, s
ocia
l val
ues,
res
pect
, gen
der
• U
sed
dram
a, s
torie
s, g
ames
• A
lso
deve
lope
d m
ore
yout
h-fr
iend
ly h
ealth
ser
vice
sH
– C
hile
,T
een
ST
AR
cam
paig
n (3
0)• Y
outh
s w
ith m
ean
age
15.8
yea
rsin
urb
an a
reas
• T
arge
ted
sexu
al in
itiat
ion
• 18
uni
ts•
Dis
cuss
ed m
ale
and
fem
ale
fert
ility
, men
stru
al c
ycle
, psy
chos
exua
lde
velo
pmen
t, se
xual
res
pons
ibili
ty, r
elat
ions
hips
, con
trac
eptio
n, S
TIS
• U
sed
expe
rient
ial l
earn
ing
met
hods
to e
xplo
re fe
elin
gs, v
alue
s an
dat
titud
esA
du
lt-l
ed (
oth
er t
han
tea
cher
s)I –
Bra
zil,
Sex
ualit
y, R
epro
duct
ion
and
AID
S P
reve
ntio
n (3
1)
• Y
outh
s ag
ed 1
8–25
yea
rs in
urba
n ar
eas
• T
arge
ted
sexu
al in
itiat
ion,
cond
om u
se, f
requ
ency
of s
ex,
num
ber
of p
artn
ers,
type
of
part
ners
, unp
rote
cted
sex
• 12
hou
rs•
Cov
ered
AID
S s
ymbo
lism
, kno
wle
dge
and
impa
ct o
f AID
S, r
isk
perc
eptio
n, s
exua
l nor
ms,
repr
oduc
tion
and
sexu
al p
leas
ure,
con
dom
use
nego
tiatio
n•
Use
d di
scus
sion
s, r
ole-
play
s, g
roup
dyn
amic
s, m
odel
s, d
emon
stra
tions
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
J –
Jam
aica
,G
rade
7 p
roje
ct (
32)
• Y
outh
s ag
ed 1
1–14
yea
rs in
urba
n an
d ru
ral a
reas
• T
arge
ted
sexu
al in
itiat
ion,
cont
race
ptiv
e us
e
• 27
hou
rs•
Cov
ered
rep
rodu
ctiv
e an
atom
y an
d ph
ysio
logy
, ST
Is, c
ontr
acep
tive
met
hods
and
myt
hs, r
isks
and
con
sequ
ence
s of
sex
and
pre
gnan
cy,
med
ia, n
orm
s•
Use
d cl
assr
oom
lect
ures
, vis
ual a
ids,
que
stio
n an
d an
swer
ses
sion
s,sm
all g
roup
dis
cuss
ions
119
92-4-120938-0_CH05_119

Stu
dy,
loca
tio
n a
nd
pro
gra
mm
eT
arg
et p
op
ula
tio
n a
nd
pri
mar
yo
bje
ctiv
esD
escr
ipti
on
K –
Nig
eria
, Sch
ool-b
ased
AID
Sed
ucat
ion
(33)
• Y
outh
s w
ith m
ean
age
17.7
inur
ban
area
s•
Tar
gete
d se
xual
initi
atio
n,co
ntra
cept
ive
use,
num
ber
ofpa
rtne
rs, S
TIs
• 12
–36
hour
s• C
over
ed tr
ansm
issi
on a
nd p
reve
ntio
n of
AID
S, a
ttitu
des
tow
ards
HIV
/A
IDS
, sex
ual p
ract
ices
, con
trac
eptiv
e us
e•
Use
d le
ctur
es, f
ilms,
rol
e-pl
ays,
sto
ries,
son
gs, d
ebat
es, e
ssay
s,co
ndom
use
dem
onst
ratio
nsL
– M
exic
o, H
IV p
reve
ntio
nw
orks
hop
and
cond
omdi
strib
utio
n (3
4)
• Y
outh
s w
ith m
ean
age
17.6
yea
rsin
urb
an a
reas
• T
arge
ted
sexu
al in
itiat
ion,
freq
uenc
y of
sex
ual i
nter
cour
se,
unpr
otec
ted
sex
• 3
hour
s•
Cov
ered
HIV
atti
tude
s, m
yths
, fac
ts a
nd r
isk,
effe
cts
of A
IDS
, HIV
tran
smis
sion
and
pre
vent
ion,
livi
ng w
ith H
IV, c
ondo
m u
se a
ndne
gotia
tion
skill
s•
Use
d dr
amas
, gam
es, r
ole-
play
s, v
ideo
s, H
IV-p
ositi
ve s
peak
er,
disc
ussi
ons,
con
dom
use
dem
onst
ratio
nM
– N
amib
ia, M
y fu
ture
is m
ych
oice
(35
)•
You
ths
aged
9–1
1 ye
ars
in u
rban
and
rura
l are
as•
Tar
gete
d se
xual
initi
atio
n, n
umbe
rof
par
tner
s, c
ondo
m u
se,
freq
uenc
y of
sex
ual a
ctiv
ity
• 28
hou
rs•
Dis
cuss
ed r
epro
duct
ive
biol
ogy
and
HIV
/AID
S, r
isk
beha
viou
rs,
com
mun
icat
ion
skill
s, fr
amew
ork
for
deci
sion
-mak
ing
• U
sed
narr
ativ
es, g
ames
, fac
ts, e
xerc
ises
, que
stio
ns a
nd d
iscu
ssio
ns
Pee
r-le
dN
– B
eliz
e,P
roje
ct L
ight
(36
)•
You
ths
aged
13–
17 y
ears
in u
rban
area
s•
Tar
gete
d se
xual
initi
atio
n, n
umbe
rof
par
tner
s, c
ondo
m u
se
• 14
hou
rs•
Cov
ered
HIV
tran
smis
sion
and
pre
vent
ion,
bar
riers
and
sol
utio
ns to
avoi
ding
sex
or
usin
g co
ndom
s, p
eer
pres
sure
, con
dom
use
,co
mm
unic
atio
n•
Use
d ro
le-p
lays
, exe
rcis
es, s
kill-
build
ing
activ
ities
, pee
r ro
le-m
odel
test
imon
ials
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
ho
ut
char
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
(te
ach
ers)
O –
Mex
ico,
A T
eam
Aga
inst
AID
S (
37)
• Y
outh
s ag
ed 1
3–23
yea
rs in
urb
anar
eas
• T
arge
ted
sexu
al in
itiat
ion,
con
dom
use
• 25
hou
rs•
Cov
ered
sex
ualit
y, a
nato
my
and
phys
iolo
gy, v
alue
s, H
IV/A
IDS
tran
smis
sion
, myt
hs, p
reve
ntio
n, r
isk
perc
eptio
n, s
afer
sex
,ab
stin
ence
, ass
ertiv
enes
s, s
elf-
este
em, e
tc.
120
92-4-120938-0_CH05_120

P –
Chi
le,
Ado
lesc
ence
, a ti
me
ofde
cisi
on-m
akin
g (3
8)
• U
rban
you
ths
• T
arge
ted
sexu
al in
itiat
ion,
cont
race
ptiv
e us
e
• D
urat
ion
of 2
yea
rs•
Cov
ered
rel
atio
nshi
ps, p
aren
t–ch
ild c
omm
unic
atio
n, g
oals
,re
prod
uctiv
e ph
ysio
logy
, pos
tpon
ing
sex,
ST
Is, g
ende
r, r
isk
beha
viou
rs•
Use
d sm
all g
roup
dis
cuss
ions
, par
ticip
ator
y ed
ucat
iona
l mod
ules
Pee
r-le
dQ
– Z
ambi
a,T
he Z
ambi
a P
eer
Sex
ual H
ealth
Inte
rven
tion
(39)
• Y
outh
s ag
ed 1
4–23
in u
rban
are
as•
Tar
gete
d ab
stin
ence
, con
dom
use
• 1.
75 h
ours
• C
over
ed H
IV tr
ansm
issi
on a
nd p
reve
ntio
n, a
bstin
ence
, con
dom
use
,S
TIs
, asy
mpt
omat
ic p
hase
s, r
efus
al s
kills
• U
sed
disc
ussi
on, s
kits
, con
dom
dem
onst
ratio
n an
d a
leaf
let
ST
I - W
hy s
houl
d I w
orry
?N
on
-cu
rric
ulu
m-b
ased
inte
rven
tio
ns
Ad
ult
-led
R –
Sou
th A
fric
a,D
ram
Aid
e (4
0)•
You
ths
aged
13–
29 y
ears
in u
rban
and
rura
l are
as•
Tar
gete
d se
xual
initi
atio
n, n
umbe
rof
par
tner
s, c
ondo
m u
se, S
TIs
• C
over
ed H
IV/A
IDS
tran
smis
sion
, pre
vent
ion
and
mis
conc
eptio
ns;
pers
onal
sus
cept
ibili
ty a
nd th
reat
; atti
tude
s to
war
ds p
eopl
e w
ith A
IDS
• U
sed
part
icip
ator
y pr
oces
s of
lear
ning
and
then
pre
sent
ing
info
rmat
ion
usin
g dr
ama
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
S –
Zim
babw
e,IE
C h
ealth
edu
catio
n (4
1)•
You
ths
age
10–1
9 ye
ars
in u
rban
and
rura
l are
as•
Tar
gete
d se
xual
initi
atio
n
• C
over
ed r
epro
duct
ion,
AID
S/S
TIs
, sex
ualit
y, p
regn
ancy
pre
vent
ion,
impa
ct o
f unp
lann
ed p
regn
ancy
• Use
d he
alth
edu
catio
n, in
form
atio
n an
d co
unse
lling
; lea
flets
, pos
ters
,an
d pa
mph
lets
T –
Nig
eria
,S
TD
inte
rven
tion
(42)
• Y
outh
s ag
ed 1
2–21
yea
rs in
urb
anar
eas
• T
arge
ted
cond
om u
se a
nd S
TIs
• C
over
ed S
TI p
reve
ntio
n an
d tr
eatm
ent
• U
sed
repr
oduc
tive
heal
th c
lubs
and
pee
r ed
ucat
ors
to p
rovi
deco
unse
lling
and
ref
erra
lsU
– U
gand
a,S
choo
l hea
lth e
duca
tion
prog
ram
me
(43)
• Y
outh
s ag
ed 9
–22
year
s in
urb
anar
eas
• T
arge
ted
sexu
al in
itiat
ion,
freq
uenc
y of
sex
ual a
ctiv
ity,
num
ber
of p
artn
ers
• C
over
ed h
ealth
y se
xual
dec
isio
n-m
akin
g, p
eer
inte
ract
ions
, AID
S,
sexu
ality
, hea
lth•
Use
d hi
ghly
inte
ract
ive,
chi
ld-t
o-ch
ild c
ompe
titio
n in
pla
ys, e
ssay
s,po
ems
and
song
s, q
uest
ion
box
121
92-4-120938-0_CH05_121

Stu
dy,
loca
tio
n a
nd
pro
gra
mm
eT
arg
et p
op
ula
tio
n a
nd
pri
mar
yo
bje
ctiv
esD
escr
ipti
on
Pee
r-le
dV
– G
hana
and
Nig
eria
,W
est A
fric
an Y
outh
Initi
ativ
e (4
4)
• U
rban
you
ths
• T
arge
ted
freq
uenc
y of
sex
ual
activ
ity, c
ontr
acep
tive
use
• C
over
ed r
epro
duct
ive
heal
th, p
regn
ancy
, ST
Is, H
IV, c
ontr
acep
tion,
com
mun
icat
ion
• U
sed
peer
lead
ers
to p
rovi
de in
form
atio
n, e
duca
tion
and
coun
selli
ngon
rep
rodu
ctiv
e he
alth
and
ref
erra
ls
a S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
122
92-4-120938-0_CH05_122

Tab
le 5
.4D
escr
ipti
on
of
ou
tco
me
eval
uat
ion
s b
y st
ud
y
Stu
dy
Des
ign
an
d s
amp
le s
izea
Eva
luat
ion
res
ult
sbA
llM
ales
Fem
ales
Fac
tors
aff
ecti
ng
str
eng
th o
f ev
iden
ce
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
pro
gra
mm
es (
teac
her
s)A
(16)
D
esig
n: q
uasi
-exp
erim
enta
l(c
ohor
t by
scho
ol)
Sam
ple
size
: 245
0ba
selin
e, 1
786
last
follo
w u
p•
3 in
terv
entio
n, 3
com
paris
onsc
hool
s•
Mat
ched
pre
-tes
t and
pos
t-te
stsu
rvey
s•
Bas
elin
e, 4
and
8 m
onth
follo
wup
All
resu
lts fo
r fo
llow
up
at 4
and
8 m
onth
s
• In
itiat
ion
of s
ex (
4 an
d 8
mon
th)
• C
onsi
sten
t con
dom
use
• N
umbe
r se
xual
par
tner
s
0 0
0 0
0 0
0 0
+ 0 0 0
Str
engt
hs: l
arge
sam
ple
size
Lim
itatio
ns: b
iase
d by
hig
h re
fusa
l rat
e;co
ntro
l gro
up s
igni
fican
tly y
oung
er a
nd m
ore
likel
y to
be
livin
g w
ith fa
mily
; ana
lysi
s di
d no
tco
mpa
re c
hang
e ov
er ti
me
betw
een
grou
ps
B (
24)
Des
ign:
exp
erim
enta
l (co
hort
by
clas
s)S
ampl
e si
ze: 1
259
base
line,
1259
at l
ast f
ollo
w u
p•
One
sch
ool w
ith in
terv
entio
nan
d co
ntro
l gro
ups
• M
atch
ed c
linic
al d
ata
• B
asel
ine,
4 y
ear
follo
w u
p
• B
irths
/spo
ntan
eous
abor
tion
+S
tren
gths
: lar
ge s
ampl
e si
ze; l
ong-
term
follo
w u
p; la
rge
effe
ct s
ize
Lim
itatio
ns: r
epor
ting
of p
regn
ancy
unc
lear
;on
e sc
hool
onl
y
123
92-4-120938-0_CH05_123

Stu
dy
Des
ign
an
d s
amp
le s
izea
Eva
luat
ion
res
ult
sbA
llM
ales
Fem
ales
Fac
tors
aff
ecti
ng
str
eng
th o
f ev
iden
ce
C (
25)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y sc
hool
)S
ampl
e si
ze: 2
026
base
line,
814
at la
st fo
llow
up
• 6
inte
rven
tion
, 12
com
paris
on s
choo
ls•
Cro
ss-s
ectio
nal s
urve
ys•
Bas
elin
e, 6
, and
12
mon
thfo
llow
up
• In
itiat
ion
of s
exua
l rel
atio
ns0
00
Str
engt
hs: l
arge
sam
ple
size
; wel
l con
duct
edco
mm
unity
tria
l; al
l sch
ools
incl
uded
Lim
itatio
ns: B
asel
ine
sam
ple
of s
exua
llyin
expe
rienc
ed y
outh
und
erpo
wer
edN
ote:
larg
e de
sire
d ef
fect
siz
e; 1
7 vs
7%
initi
ated
but
P =
0.1
9.
D (
17)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y sc
hool
)S
ampl
e si
ze: 9
036
base
line,
1344
1 at
last
follo
w u
p•
120
inte
rven
tion,
100
com
paris
on s
choo
ls•
Cro
ss-s
ectio
nal s
urve
ys•
Bas
elin
e, 2
4 (o
r 15
)m
onth
s
• In
itiat
ion
of s
exua
l rel
atio
ns
• C
ondo
m u
sed
at la
st s
ex
+ 0
+ +
Str
engt
hs: v
ery
stro
ng tr
ial w
ith a
larg
e sa
mpl
esi
ze a
nd lo
ng-t
erm
follo
w u
pN
ote:
var
ious
inte
rven
tions
in c
ompa
rison
scho
ols
E (
26)
Des
ign:
exp
erim
enta
l(c
ohor
t by
clas
sroo
m)
Sam
ple
size
: 491
bas
elin
e,41
6 at
last
follo
w u
p•
6 sc
hool
s w
ith in
terv
entio
nan
d co
ntro
l gro
ups
• Mat
ched
pre
-tes
t and
pos
t-te
st s
urve
ys•
Bas
elin
e,6
wee
ks, 4
and
8m
onth
s fo
llow
up
• S
exua
l int
erco
urse
• C
ontr
acep
tive
use
at fi
rst
sexu
al in
terc
ours
e
0 +
Lim
itatio
ns: m
oder
ate
sam
ple
size
; sho
rt fo
llow
up
124
92-4-120938-0_CH05_124

Sam
ple
size
: 114
1 ba
selin
e,64
6 at
last
follo
w u
p•
11 in
terv
entio
n an
d 11
com
paris
on s
choo
ls• M
atch
ed p
re-t
est a
nd p
ost-
test
sur
veys
• B
asel
ine,
6 a
nd 1
0 m
onth
follo
w u
p
• F
requ
ency
of s
exua
lin
terc
ours
e•
Con
dom
use
• N
umbe
r of
sex
ual p
artn
ers
+ 0 0
did
not c
ompa
re th
e ch
ange
ove
r tim
e be
twee
ntr
ial g
roup
s
G (
29)
Des
ign:
exp
erim
enta
l(c
ohor
t by
com
mun
ity)
Sam
ple
size
: 964
5 ba
selin
e,70
40 a
t las
t fol
low
up
• 10
inte
rven
tion
com
mun
ities
with
62
scho
ols
and
10 c
ontr
olco
mm
uniti
es w
ith 6
3sc
hool
s• M
atch
ed p
re-t
est a
nd p
ost-
test
sur
veys
• B
asel
ine,
18,
and
36
mon
ths
follo
w u
p
• In
itiat
ion
of s
exua
lin
terc
ours
e•
> 1
par
tner
in p
ast 1
2m
onth
s•
Con
dom
use
: at l
ast s
exua
lin
terc
ours
e/ev
er•
ST
Id
0 +
+ /
+
0
0 0
0 / + -
Str
engt
hs: v
ery
stro
ng R
CT
c eva
luat
ion
with
ala
rge
sam
ple
size
and
long
-ter
m fo
llow
-up;
use
of b
iolo
gica
l out
com
es
H (
30)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y cl
assr
oom
s)S
ampl
e si
ze: 3
05 b
asel
ine,
243
at la
st fo
llow
up
• 5
scho
ols
with
inte
rven
tion
and
cont
rol g
roup
s• M
atch
ed p
re-t
est a
nd p
ost-
test
sur
veys
• B
asel
ine
and
12 m
onth
sfo
llow
up
• In
itiat
ion
of s
exua
lin
terc
ours
e+
Lim
itatio
ns: b
iase
d by
teac
her s
elec
tion
of s
tudy
grou
ps; s
mal
l sam
ple
size
125
F (
27,2
8)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y sc
hool
)•
Initi
atio
n of
sex
ual
inte
rcou
rse
00
0Li
mita
tions
: non
-ran
dom
ass
ignm
ent o
f sch
ools
;sh
ort f
ollo
w u
p; h
igh
loss
es to
follo
w u
p; a
naly
sis
92-4-120938-0_CH05_125

Stu
dy
Des
ign
an
d s
amp
le s
izea
Eva
luat
ion
res
ult
sbA
llM
ales
Fem
ales
Fac
tors
aff
ecti
ng
str
eng
th o
f ev
iden
ce
Ad
ult
-led
pro
gra
mm
es (
oth
er t
han
tea
cher
s)I (
31)
Des
ign:
exp
erim
enta
l (co
hort
by s
choo
l)S
ampl
e si
ze: 3
94 b
asel
ine,
198
at la
st fo
llow
up
• 2
inte
rven
tion
and
2 co
ntro
lsc
hool
s•
Mat
ched
pre
-tes
t and
pos
t-te
st s
urve
ys•
Bas
elin
e, 6
, and
12
mon
ths
follo
w u
p
• In
itiat
ion
of s
exua
lin
terc
ours
e/se
xual
act
ivity
durin
g pa
st6
mon
ths
• C
ondo
m u
se•
Unp
rote
cted
sex
ual
inte
rcou
rse
with
ste
ady
part
ner
• U
npro
tect
ed s
exua
lin
terc
ours
e w
ith c
asua
l/non
-m
onog
amou
s pa
rtne
r
0/0 0 0 0/0
0/0 0 0 0 /+
Lim
itatio
ns: s
mal
l sam
ple
size
; hig
h dr
op-o
utra
te b
y 12
mon
ths
desp
ite tr
acki
ng a
ttem
pts
J (3
2)D
esig
n: q
uasi
-exp
erim
enta
l(c
ohor
t by
scho
ol)
Sam
ple
size
: 945
bas
elin
e,71
8 at
last
follo
w u
p•
5 in
terv
entio
n an
d 5
com
paris
on s
choo
ls•
Mat
ched
pre
-tes
t and
pos
t-te
st s
urve
ys•
Bas
elin
e, 9
, and
21
mon
ths
follo
w u
p
All
resu
lts fo
r fo
llow
up
at 9
and
21 m
onth
s•
Initi
atio
n of
sex
ual
inte
rcou
rse
• C
ontr
acep
tion
use
at fi
rst
sexu
al in
terc
ours
e
0 0
0 0
Str
engt
hs: s
choo
ls s
elec
ted
to b
ere
pres
enta
tive;
larg
e sa
mpl
e si
ze; l
ong-
term
follo
w u
pLi
mita
tions
: com
paris
on s
choo
ls r
ecei
ved
varie
d cu
rric
ula
K (
33)
Des
ign:
exp
erim
enta
l (co
hort
by s
choo
l)S
ampl
e si
ze: 4
50 b
asel
ine,
433
at la
st fo
llow
up
• 2
inte
rven
tion
and
2 co
ntro
lsc
hool
s•
Cro
ss-s
ectio
nal s
urve
ys
• In
itiat
ion
of s
ex•
Num
ber
of s
exua
l par
tner
s•
Con
dom
: use
at l
ast s
ex/
cons
iste
nt u
se•
ST
I
+ +0
/ 0 0
Lim
itatio
ns: m
oder
ate
sam
ple
size
; cha
nge
scor
es o
ver
time
for
each
exp
erim
enta
l gro
upw
ere
not c
alcu
late
d an
d co
mpa
red
126
• B
asel
ine
and
6 m
onth
sfo
llow
up
92-4-120938-0_CH05_126
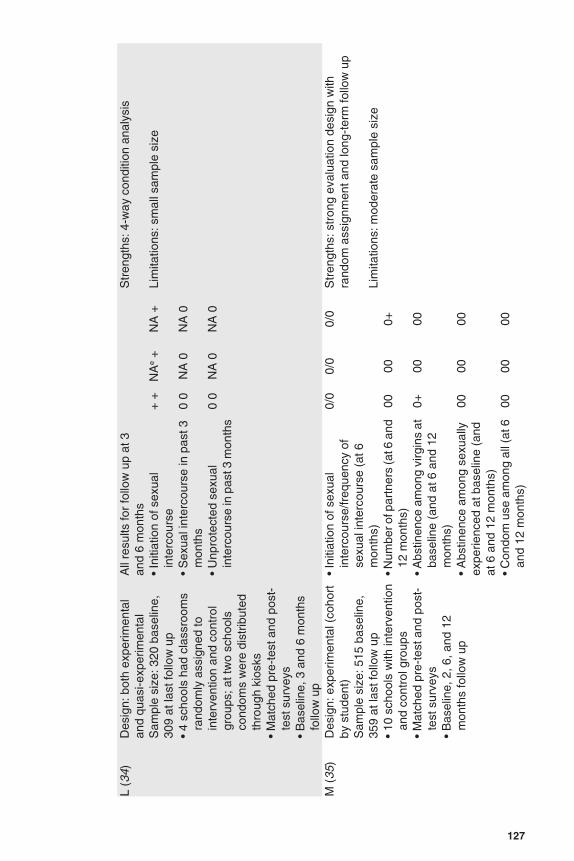
L (3
4)D
esig
n: b
oth
expe
rimen
tal
and
quas
i-exp
erim
enta
lS
ampl
e si
ze: 3
20 b
asel
ine,
309
at la
st fo
llow
up
• 4
scho
ols
had
clas
sroo
ms
rand
omly
ass
igne
d to
inte
rven
tion
and
cont
rol
grou
ps; a
t tw
o sc
hool
sco
ndom
s w
ere
dist
ribut
edth
roug
h ki
osks
• M
atch
ed p
re-t
est a
nd p
ost-
test
sur
veys
• B
asel
ine,
3 a
nd 6
mon
ths
follo
w u
p
All
resu
lts fo
r fo
llow
up
at 3
and
6 m
onth
s•
Initi
atio
n of
sex
ual
inte
rcou
rse
• S
exua
l int
erco
urse
in p
ast 3
mon
ths
• U
npro
tect
ed s
exua
lin
terc
ours
e in
pas
t 3 m
onth
s
+ + 0 0
0 0
NA
e +
NA
0
NA
0
NA
+
NA
0
NA
0
Str
engt
hs: 4
-way
con
ditio
n an
alys
is
Lim
itatio
ns: s
mal
l sam
ple
size
M (
35)
Des
ign:
exp
erim
enta
l (co
hort
by s
tude
nt)
Sam
ple
size
: 515
bas
elin
e,35
9 at
last
follo
w u
p•
10 s
choo
ls w
ith in
terv
entio
nan
d co
ntro
l gro
ups
• M
atch
ed p
re-t
est a
nd p
ost-
test
sur
veys
• B
asel
ine,
2, 6
, and
12
mon
ths
follo
w u
p
• In
itiat
ion
of s
exua
lin
terc
ours
e/fr
eque
ncy
ofse
xual
inte
rcou
rse
(at 6
mon
ths)
• Num
ber o
f par
tner
s (a
t 6 a
nd12
mon
ths)
• A
bstin
ence
am
ong
virg
ins
atba
selin
e (a
nd a
t 6 a
nd 1
2m
onth
s)•
Abs
tinen
ce a
mon
g se
xual
lyex
perie
nced
at b
asel
ine
(and
at 6
and
12
mon
ths)
• C
ondo
m u
se a
mon
g al
l (at
6an
d 12
mon
ths)
0/0
00 0+ 00 00
0/0
00 00 00 00
0/0
0+ 00 00 00
Str
engt
hs: s
tron
g ev
alua
tion
desi
gn w
ithra
ndom
ass
ignm
ent a
nd lo
ng-t
erm
follo
w u
p
Lim
itatio
ns: m
oder
ate
sam
ple
size
127
92-4-120938-0_CH05_127

Stu
dy
Des
ign
an
d s
amp
le s
izea
Eva
luat
ion
res
ult
sbA
llM
ales
Fem
ales
Fac
tors
aff
ecti
ng
str
eng
th o
f ev
iden
ce
Pee
r-le
d p
rog
ram
mes
N (
36)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort)
Sam
ple
size
: 150
bas
elin
e, 1
50at
last
follo
w u
p•
3 in
terv
entio
n an
d 3
com
paris
on s
choo
ls•
Mat
ched
pre
-tes
t and
pos
t-te
stsu
rvey
s• B
asel
ine
and
4 m
onth
follo
w u
p
• C
ondo
m u
se +
Lim
itatio
ns: b
iase
d sc
hool
sel
ectio
n; s
mal
lsa
mpl
e si
ze; s
hort
follo
w u
p
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
wit
ho
ut
char
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
(tea
cher
s)O
(37
)D
esig
n: q
uasi
-exp
erim
enta
l(c
ohor
t by
scho
ol)
Sam
ple
size
: 206
4 ba
selin
e,94
6 at
last
follo
w u
p•
2 in
terv
entio
n an
d 2
com
paris
on s
choo
ls•
Mat
ched
pre
-tes
t and
pos
t-te
stsu
rvey
s•
Bas
elin
e, 4
, and
10
mon
thfo
llow
up
• In
itiat
ion
of s
exua
lin
terc
ours
e•
Con
dom
use
0 0
Lim
itatio
ns: c
hang
e sc
ores
ove
r tim
e fo
r ea
chex
perim
enta
l gro
up w
ere
not c
alcu
late
d an
dco
mpa
red
P (
38)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y sc
hool
)sa
mpl
e si
ze: 4
238
base
line,
4135
at l
ast f
ollo
w u
p•
2 in
terv
entio
n an
d 3
com
paris
on s
choo
ls
• In
itiat
ion
of s
exua
lin
terc
ours
e•
Con
trac
eptiv
e us
e,ev
er•
Con
trac
eptiv
e us
e,la
st s
exua
lin
terc
ours
e
+ 0 0
+ + 0
Str
engt
hs: l
arge
sam
ple
size
; lon
g te
rm fo
llow
up Lim
itatio
ns: n
on-r
ando
m a
ssig
nmen
t of
scho
ols;
adj
ustm
ent f
or e
xpos
ure
toin
terv
entio
n m
ay o
vere
stim
ate
effe
ct
128
92-4-120938-0_CH05_128

• M
atch
ed p
re-t
est a
nd p
ost-
test
surv
eys
• B
asel
ine,
8, 2
0, a
nd 3
2 m
onth
follo
w u
pP
eer-
led
pro
gra
mm
esQ
(39
)D
esig
n: e
xper
imen
tal (
coho
rt b
ysc
hool
)•
3 in
terv
entio
n an
d 2
com
paris
on s
choo
ls•
Mat
ched
pre
-tes
t and
pos
t-te
stsu
rvey
s• B
asel
ine
and
6 m
onth
follo
w u
p
• M
ultip
le r
egul
arpa
rtne
rs•
Dis
cuss
con
dom
use/
abst
ain
with
regu
lar
part
ner
• C
ondo
m u
se w
ithre
gula
r pa
rtne
r:ev
er/la
st ti
me
• C
asua
l par
tner
0 0/0
0/0 0
Lim
itatio
ns: m
oder
ate
sam
ple
size
; diff
eren
ces
betw
een
inte
rven
tion
and
cont
rol g
roup
s lik
ely
to fa
vour
inte
rven
tion
No
n-c
urr
icu
lum
-bas
ed in
terv
enti
on
s w
ith
ou
t ch
arac
teri
stic
s o
f ef
fect
ive
pro
gra
mm
esA
du
lt-l
edR
(40
)D
esig
n: e
xper
imen
tal (
coho
rt b
ysc
hool
) us
ing
adul
ts n
otaf
filia
ted
with
the
scho
olS
ampl
e si
ze: 1
080
base
line,
699
at la
st fo
llow
up
• 10
inte
rven
tion
and
10 c
ontr
olsc
hool
s•
Mat
ched
pre
-tes
t and
pos
t-te
stsu
rvey
s•
Bas
elin
e an
d 18
mon
th fo
llow
up
• In
itiat
ion
of s
exua
lin
terc
ours
e•
Con
dom
use
• N
umbe
r of
par
tner
s•
ST
I in
past
6m
onth
s
0 0 0 0
Str
engt
hs: l
arge
-sca
le e
valu
atio
n in
are
pres
enta
tive
sam
ple;
long
-ter
m fo
llow
up
Lim
itatio
ns: h
igh
drop
-out
rat
e; n
umbe
r of
scho
ols
not r
epor
ted
129
92-4-120938-0_CH05_129

Stu
dy
Des
ign
an
d s
amp
le s
izea
Eva
luat
ion
res
ult
sbA
llM
ales
Fem
ales
Fac
tors
aff
ecti
ng
str
eng
th o
f ev
iden
ce
S (
41)
Des
ign:
exp
erim
enta
l (co
hort
by
scho
ol);
teac
her-
led
Sam
ple
size
: 168
9 ba
selin
e, 1
605
at la
st fo
llow
up
• In
terv
entio
n sc
hool
s: n
ot r
epor
ted
and
3 co
ntro
l sch
ools
• M
atch
ed p
re-t
est a
nd p
ost-
test
surv
eys
• B
asel
ine
and
5 m
onth
follo
w u
p
• In
itiat
ion
of s
exua
lin
terc
ours
e0
Str
engt
hs: l
arge
-sca
le r
epre
sent
ativ
e sa
mpl
e
Lim
itatio
ns: l
imite
d in
form
atio
n ab
out t
he s
tatis
tical
anal
ysis
; sho
rt fo
llow
up
T (
42)
Des
ign:
qua
si-e
xper
imen
tal
(coh
ort b
y sc
hool
); p
eer-
led
with
heal
th w
orke
rS
ampl
e si
ze: 1
886
base
line,
1801
at f
ollo
w u
p•
4 in
terv
entio
n an
d 8
com
paris
onsc
hool
s•
Cro
ss-s
ectio
nal s
urve
ys•
Bas
elin
e an
d 11
mon
th fo
llow
up
• C
ondo
m u
se•
ST
I+ +
0+
Str
engt
hs: l
arge
sam
ple
size
U (
43)
Des
ign:
qua
si-e
xper
imen
tal (
coho
rtby
sch
ool a
nd s
tude
nt);
impr
oved
scho
ol h
ealth
inst
ruct
ion
Sam
ple
size
: 400
- ba
selin
e, 4
00 a
tfo
llow
up
• 38
inte
rven
tion
scho
ols
and
com
paris
on s
choo
ls•
Cro
ss-s
ectio
nal s
urve
ys•
Bas
elin
e an
d 32
mon
th fo
llow
up
• In
itiat
ion
of s
exua
lin
terc
ours
e•
Sex
ual i
nter
cour
se in
the
past
mon
th•
Life
time
num
ber
ofpa
rtne
rs
+ 0 0
++
Str
engt
hs: l
ong-
term
follo
w u
p
Lim
itatio
ns: r
epor
ted
sexu
al a
ctiv
ity a
mon
g m
ales
diffe
rent
at b
asel
ine
130
92-4-120938-0_CH05_130

Pee
r-le
d p
rog
ram
mes
V (
44)
Des
ign:
qua
si-e
xper
imen
tal (
coho
rtby
sch
ool a
nd c
omm
unity
)S
ampl
e si
ze: 1
784
base
line,
1801
at l
ast f
ollo
w u
p•
6 in
terv
entio
n sc
hool
s an
d 2
inte
rven
tion
com
mun
ities
,co
mpa
rison
com
mun
ities
not
repo
rted
• C
ross
-sec
tiona
l sur
veys
• B
asel
ine
and
18-2
6 m
onth
follo
wup
• E
ver
had
sexu
alin
terc
ours
e•
Use
mod
ern
cont
race
ptiv
es
– +
Str
engt
hs: l
arge
-sca
le in
mul
tiple
set
tings
; lon
g-te
rm fo
llow
up
Lim
itatio
ns: n
on-r
ando
m a
ssig
nmen
t; la
ck o
fm
ultiv
aria
te s
tatis
tical
dat
a fo
r be
havi
oura
lou
tcom
es
a E
xper
imen
tal i
s de
fined
as
rand
omiz
ed a
lloca
tion
of p
artic
ipan
ts, s
choo
ls o
r co
mm
uniti
es in
to in
terv
entio
n or
con
trol
gro
ups.
b R
esul
ts r
epor
ted
are
for
last
follo
w u
p un
less
oth
erw
ise
indi
cate
d. R
esul
ts c
ateg
oriz
ed a
s: “
0” fo
r no
sig
nific
ant c
hang
e, “
+”
for
sign
ifica
nt d
esira
ble
chan
ge, “
-” f
or s
igni
fican
t und
esira
ble
chan
ge.
c RC
T =
ran
dom
ized
con
trol
led
tria
l.d
ST
I = s
exua
lly tr
ansm
itted
infe
ctio
n.e
NA
= n
ot a
pplic
able
.
131
92-4-120938-0_CH05_131

Tab
le 5
.4a
Su
mm
ary
of
effe
cts
of
sch
oo
l-b
ased
inte
rven
tio
ns1
Typ
e o
fin
terv
enti
on
NIn
itia
tio
n o
f se
xF
req
uen
cy o
f sex
Nu
mb
er o
fp
artn
ers
Co
nd
om
use
Bir
th c
on
tro
lu
seU
np
rote
cted
sex
An
y b
ehav
ior
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
Cu
rric
ulu
m-b
ased
Wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
130
75
03
10
22
05
30
11
01
10
211
Pee
r-le
d o
nly
10
00
00
00
00
00
10
00
00
00
01
Wit
ho
ut
char
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Ad
ult
-led
20
11
00
00
00
01
00
01
00
00
11
Pee
r-le
d o
nly
10
00
00
00
10
01
00
00
00
00
10
No
n-c
urr
icu
lum
-bas
edW
ith
ou
t ch
arac
teri
stic
s o
f ef
fect
ive
pro
gra
mm
esA
du
lt-l
ed4
02
10
10
02
00
11
00
00
00
02
2P
eer-
led
on
ly1
10
00
00
00
10
01
00
10
00
00
1T
ota
l22
110
70
41
05
30
86
01
30
11
06
16
1 “-
” m
eans
an
incr
ease
in r
isk
in te
rms
of H
IV, e
.g.,
a ha
sten
ing
of th
e in
itiat
ion
of s
ex, m
ore
sexu
al p
artn
ers
or le
ss c
ondo
m u
se.
“NS
” m
eans
not
sig
nific
ant.
“+”
mea
ns a
red
uctio
n in
ris
k in
term
s of
HIV
, e.g
., a
dela
y in
the
initi
atio
n of
sex
, few
er s
exua
l par
tner
s, o
r gr
eate
r co
ndom
use
.
132
92-4-120938-0_CH05_132

Tab
le 5
.4b
Su
mm
ary
of
effe
cts
for
adu
lt-l
ed c
urr
icu
lum
-bas
ed s
cho
ol i
nte
rven
tio
ns2
NIn
itia
tio
n o
fse
xN
um
ber
of
par
tner
sF
req
uen
cy o
fse
xC
on
do
m u
seB
irth
co
ntr
ol
use
Un
pro
tect
ed s
exA
ny
beh
avio
r
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
-N
S+
To
tal
130
84
02
20
32
04
30
11
01
111
Sch
oo
l set
tin
gP
rimar
y33
02
10
01
nana
na0
02
nana
nana
nana
01
2S
econ
dary
28
04
30
11
02
10
40
01
10
10
01
7C
olle
ge/N
ight
sch
ool
30
21
01
00
10
01
1na
nana
00
10
03
Pro
gra
m e
du
cato
rsT
each
ers
80
52
02
10
01
01
30
01
nana
na0
17
Oth
er A
dults
50
23
00
10
30
04
00
10
01
10
14
Par
tici
pan
ts s
ex4
Mal
es6
05
10
11
02
00
41
00
00
10
04
2F
emal
es6
04
20
20
02
00
23
00
00
10
02
4T
ype
of
eval
uat
ion
des
ign
Qua
si-e
xper
imen
tal
60
33
03
00
11
02
20
10
01
00
15
Exp
erim
enta
l7
04
20
02
02
00
31
00
10
01
01
6
2 T
his
is th
e gr
oup
of in
terv
entio
ns g
iven
a “
Go”
rec
omm
enda
tion.
“-”
mea
ns a
n in
crea
se in
ris
k in
term
s of
HIV
, e.g
., a
hast
enin
g of
the
initi
atio
n of
sex
, mor
e se
xual
par
tner
s or
less
con
dom
or
cont
race
ptiv
e us
e.“N
S”
mea
ns n
ot s
igni
fican
t.“+
” m
eans
a r
educ
tion
in r
isk
in te
rms
of H
IV, e
.g.,
a de
lay
in th
e in
itiat
ion
of s
ex, f
ewer
sex
ual p
artn
ers,
or
grea
ter
cond
om u
se.
“na”
mea
ns n
o st
udy
in th
is g
roup
mea
sure
d th
is o
utco
me.
3 O
ne s
tudy
incl
uded
bot
h pr
imar
y an
d se
cond
ary
scho
ols
and
its r
esul
ts a
re in
clud
ed in
bot
h ca
tego
ries.
4 O
nly
6 of
the
13 s
tudi
es p
rovi
ded
sepa
rate
res
ults
for
each
sex
. The
se 6
stu
dies
pro
vide
d re
sults
for
both
mal
es a
nd fe
mal
es.
133
92-4-120938-0_CH05_133

Tab
le 5
.5S
tren
gth
of
evid
ence
of
effe
ctiv
enes
s fo
r ea
ch in
terv
enti
on
typ
e an
d r
eco
mm
end
atio
ns
for
pro
gra
mm
es
Eva
luat
ion
des
ign
Po
siti
ve e
ffec
tN
o s
ign
ific
ant
effe
ctN
egat
ive
effe
ctS
tren
gth
of
evid
ence
and
rec
om
men
dat
ion
Cu
rric
ulu
m-b
ased
inte
rven
tio
ns
Wit
h c
har
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Adu
lt-le
d
Qua
si-e
xper
imen
tal
A, D
, F,H
JV
ery
stro
ng
RC
Ta
(< 6
clu
ster
s pe
r gr
oup)
I, K
Go
R
CT
( 6
clu
ster
s pe
r gr
oup)
B, E
, G, L
, MC
Pee
r-le
dW
eak
Q
uasi
-exp
erim
enta
lN
Ste
ady
Wit
ho
ut
char
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Adu
lt-le
dW
eak
Q
uasi
-exp
erim
enta
lP
OS
tead
yP
eer-
led
Wea
k
RC
T (
< 6
clu
ster
s pe
r gr
oup)
QS
tead
yN
on
-cu
rric
ulu
m-b
ased
inte
rven
tio
ns
Wit
ho
ut
char
acte
rist
ics
of
effe
ctiv
e p
rog
ram
mes
Adu
lt-le
dW
eak
Q
uasi
-exp
erim
enta
lT
, US
tead
y
RC
T (
< 6
clu
ster
s pe
r gr
oup)
R, S
Pee
r-le
dbE
quiv
ocal
Q
uasi
-exp
erim
enta
lV
VS
tead
ya
RC
T =
ran
dom
ized
con
trol
led
tria
l.b T
here
was
onl
y on
e st
udy
of a
non
-cur
ricul
um-b
ased
onl
y pe
er-le
d pr
ogra
mm
e. It
had
a s
tatis
tical
ly s
igni
fican
t neg
ativ
e im
pact
on
initi
atio
n of
sex
and
sta
tistic
ally
si
gnifi
cant
pos
itive
effe
cts
on th
e nu
mbe
r of
sex
ual p
artn
ers
and
the
use
of c
ondo
ms
and
cont
race
ptiv
es. T
hus,
it is
cou
nted
twic
e in
the
tabl
e, b
oth
as h
avin
g
a ne
gativ
e im
pact
and
a p
ositi
ve im
pact
.
134
92-4-120938-0_CH05_134

quasi-experimental designs had to have both intervention and comparisongroups and both pre-test and follow-up data.
Of the 22 studies, nine clearly lacked sufficient statistical power to detectprogrammatically meaningful effects on behaviour. For example, if an inter-vention reduced the percentage of young people who initiated sexual activity(or who had sexual intercourse without a condom) from 30% to 20%, thisreduction would be programmatically meaningful. However, to have an 80%chance of finding an absolute change of 10 percentage points in a dichoto-mous outcome and to achieve significance at the 0.05 level, a completed pre-test follow-up sample size of close to 600 would be needed. The smallestmatched baseline and follow-up sample was 150. This study and eight othersclearly lacked statistical power.
However, the problem of insufficient power was greatly aggravated by thefact that studies typically had to divide their samples into sexually inexperi-enced youths at baseline in order to measure initiation of sex and sexuallyexperienced youths at follow up to measure impact on condom and contra-ceptive use among those who did have sex. Some studies further divided theirsample into males and females because prior studies had found that resultssometimes differed according to the sex of the participant. This further in-creased the problem of statistical power.
Although many studies lacked sufficient statistical power, they are includedin the results because some of them produced statistically significant results.Nevertheless, their inclusion biases the results and may suggest that inter-ventions were less effective than they actually were. This may offset some ofthe positive biases discussed above. When two studies produced large pro-grammatically important results that were not significant, they were codedin the tables as not having an impact but their possible impact is noted inthe text.
The statistical analyses in the studies ranged from marginally acceptable torigorous. For example, a few studies compared whether the intervention andcomparison groups were statistically different at baseline and then also useda separate test to determine whether they were significantly different at followup instead of comparing the change over time in the intervention group withthe change over time in the comparison group. Some failed to statisticallycontrol for background characteristics that may have been related to outcomebehaviours. And still others assigned entire schools to intervention groupsbut failed to control for clustering. It is difficult to assess the net impact ofthese limitations in the statistical analyses. Fortunately, a few studies usedrigorous statistical analyses.
135
92-4-120938-0_CH05_135

5.3.3 Impact on prevalence and sexual behaviours
5.3.3.1 STI/HIV prevalence
Ideally, these studies would have measured the intervention’s impact on theincidence or prevalence of STIs or, preferably, HIV. However, only onestudy, the study with the largest sample size, measured impact on STI andHIV prevalence and even it was underpowered for some of these tests.
That one study was the randomized trial in Mwanza, United Republic ofTanzania (study G) (45). It found that the “MEMA kwa Vijana” (“Goodthings for young people”) intervention did not have a significant impact onthe prevalence of genital herpes, syphilis or chlamydia among either boysor girls. Furthermore, it did not have a significant impact on prevalence oftrichomoniasis among girls (it was not measured among boys) nor on gon-orrhoea among boys. However, it found a slight but significant negativeimpact on prevalence of gonorrhoea among girls.
This study was one of only two to attempt to measure an intervention’s impacton pregnancy or childbearing. It did not demonstrate an effect, but the otherstudy, a teacher-led curriculum-based intervention in Chile (study B) (24),demonstrated a marked decrease in reported births or miscarriages over a 4-year follow-up period. However, the authors noted that this outcome was nota true marker of pregnancy because of the likely bias caused by the illegalstatus of abortion in Chile.
5.3.3.2 Impact on behaviours
Because of the criteria used to select these studies, all of them measuredimpact on one or more reported sexual behaviours, which logically wouldaffect STI or HIV incidence or prevalence in the long term. Thus, those resultsare also presented.
Because the patterns of results are quite similar regardless of the type ofintervention or the type of evaluation design, they are first discussed as awhole and then the results for the group of interventions with the strongestevidence are further discussed.
5.3.3.3 Sexual activity
These studies present strong evidence that sex education and HIV educationinterventions do not increase sexual behaviour and that a substantial percent-age of interventions significantly decrease one or more types of sexualactivity.
136
92-4-120938-0_CH05_136

One important measure of sexual activity is the initiation of sex (having sex-ual intercourse for the first time). This was measured in 18 of the studies.Importantly, only one of these studies found a significantly greater increasein the reported initiation of sex among the intervention group than among thecomparison group (study V) (44). That intervention was a non-curriculum-based peer-led programme. (It should be noted that when 14 or more studiesare reviewed, there is a greater than even chance that one or more outcomeswill be found to be statistically significant by chance alone.) More impor-tantly, none of the remaining 17 interventions hastened the reported initiationof sex, and 7 significantly delayed reported initiation.
A second common measure of sexual activity is the reported frequency ofengaging in sex. This measure includes both the number of acts of sexualintercourse during a specified number of months prior to the survey andwhether respondents had sexual intercourse at all during that period: it thusmeasures the possible return to secondary abstinence. This measure is im-portant for the prevention of pregnancy and STIs and HIV. Only eight studiesmeasured the programmatic impact on the reported frequency of sexual ac-tivity. None of them found an increase, and three of them found a decreasein frequency.
A third measure of sexual activity is the reported number of sexual partners.This measure is especially important for preventing the transmission of STIsand HIV. Again, there were no increases in the reported number of sexualpartners, and 3 out of 8 interventions reported decreases in the number ofpartners.
5.3.3.4 Impact on use of condoms and contraceptives
Fourteen studies measured the impact on reported use of condoms; none ofthem found a decrease, and six found a significant increase in use. Althoughcontraceptives other than condoms do not markedly affect the transmissionof STIs or HIV, some of these interventions were sex education interventionsthat encouraged contraceptive use to prevent teen pregnancy as well as con-dom use to prevent STIs and HIV. Four studies measured the impact onreported contraceptive use, and three of them found significantly increasedreports of their use.
Two studies examined the impact on measures of unprotected sex that in-volved both the reported frequency of sexual activity or numbers of partnersand condom use. One of these two studies found a positive impact.
137
92-4-120938-0_CH05_137

5.3.3.5 Impact on one or more behaviours
Of the 22 interventions, 16 had a positive impact on one or more of the re-ported behaviours, and five had a positive impact on two or more behaviours.Only six had no significant impact on any reported behaviour. Overall, these22 interventions were found to have significantly improved 21 of 55 measuresof reported sexual behaviour across the studies.
5.3.4 Summary of behavioural effects
In sum, these studies present strong evidence that school-based sex educationand HIV education interventions did not increase sexual activity and somehad positive effects on each of the reported sexual and protective behavioursmeasured. It is possible for some school-based interventions to delay partic-ipants’ reported sexual activity, reduce their number of sexual partners,reduce their frequency reported of sexual activity or increase their use of con-doms or their use of contraception and thereby reduce their unprotected sex.
In addition, in all three categories of adult-led interventions at least half ofthe interventions had a positive impact on at least one of the reported sexualor protective behaviours. In addition, two of the three peer-led interventionshad a positive impact on one or more behaviours. These overall resultsdemonstrate that there is no single type of intervention that is effective: mosthave the potential to be effective in some situations.
However, it is also true that there are more studies and much stronger evidenceshowing that curriculum-based interventions that incorporated at least fourfifths of the characteristics described in Box 5.1 can change behaviour. Theseinterventions are discussed more fully below.
5.3.5 Impact on psychosocial factors affecting behaviour
5.3.5.1 Knowledge
Altogether, 10 of the 22 studies measured the intervention’s impact onknowledge, and all found that their respective interventions increased knowl-edge about one or more topics including STIs or HIV/AIDS and theirprevention. The interventions did not always increase knowledge about everyitem measured, perhaps because a particular curriculum may not have focusedon those specific facts. However, all of the interventions increased knowledgeabout one or more facts and increased overall knowledge.
This finding is consistent with 10 different studies from developing countriesthat did not measure an intervention’s impact on behaviour but did measurethe impact on knowledge (46–55). All of these studies found that their re-spective interventions significantly increased knowledge. This finding is also
138
92-4-120938-0_CH05_138

consistent with findings from developed countries that have repeatedly shownthat school-based sex education and HIV education interventions can increaseknowledge about sexuality, just as classes can increase knowledge aboutmaths, science and other topics. Sometimes they may be even more effectivein increasing students’ knowledge about various aspects of sexual behaviourbecause this is a topic that is often of greater interest and relevance to students’lives.
5.3.5.2 Reported values, attitudes, peer norms, skills, intentions and other risk andprotective behaviours
Skills, as identified in UNGASS goal 2, are one of a number of psychosocialfactors necessary to effectively change behaviour. Nineteen studies measuredintervention impact on sexual and psychosocial factors (such as personalvalues and perceptions of peer norms) or other behaviours (such as commu-nication about sex and condoms or use of alcohol) that are known to be relatedto sexual risk and protective behaviours. The results were not nearly as con-sistent as they were for knowledge.
The results indicate that interventions consistently did not negatively affectthese factors, and roughly half had positive effects. More specifically, one ormore studies found that their respective interventions improved reported val-ues about sex, values about pressuring someone to have sex, attitudes towardscondoms, attitudes towards people living with AIDS, perceptions of peernorms regarding condoms, self-efficacy to refuse to have sex, self-efficacyto obtain condoms and to use condoms, and intentions to discuss condom useor to use a condom. None of the three studies that measured intentions toabstain from sex or restrict the number of sexual partners found that the in-terventions increased these intentions. One study found that its interventiondecreased the use of alcohol or drugs; one study found the intervention helpedyouths avoid situations that might lead to sex; and a final study found that itsintervention increased the percentage of youths who reported having obtainedcondoms.
The results from these 22 studies measuring impact on reported behaviourare also supported by results from other studies that measured impacts onvalues, attitudes and norms but did not measure impact on behaviour. Sixsuch studies found that school-based interventions improved one or more ofthese reported values, attitudes, norms or intentions (46–48, 51, 54, 55).
5.3.6 Strength of evidence for curriculum-based adult-led interventions withthe characteristics in Box 5.1
The behavioural results for all six intervention types are summarized in Table5.5, as well as Table 5.4a and Table 5.4b. Although at least half of the studies
139
92-4-120938-0_CH05_139

in five of the six intervention types reported positive behavioural results, oneintervention type has particularly strong evidence for its impact on behaviour.Curriculum-based interventions that incorporated most of the characteristicsin Box 5.1 and that were led by adults have particularly strong evidence fortheir impact on behaviour. That evidence is strong for three reasons: there area large number of studies within that category; the strength of the evidencefor some of the individual studies is stronger than for the studies in othercategories; and the interventions more consistently had a positive impact onbehaviour.
Among the 13 interventions in that type:
5 out of 12 were successful in encouraging participants to delay the re-ported initiation of sex;
2 out 4 were successful in terms of participants reducing the reportednumber of sexual partners;
1 out of 4 were able to encourage participants to reduce the reported fre-quency of sexual relations;
3 out of 8 reported an increase in reported condom use;
1 out of 2 reported an increase in the reported use of contraceptives;
1 out of 2 reduced the reported frequency of unprotected sex as measuredin other ways; and
11 out of 13 significantly improved one or more reported sexual or pro-tective behaviours.
Notably, only 2 of the 13 interventions did not produce significant be-havioural changes. However, in the first of those two interventions, 17% ofthe control group initiated sex while only 7% of the intervention group didso (study C) (25). While this would have been programmatically meaningful,it was not statistically significant. Similarly, in the second study that did notreport significant results, the odds ratio for contraceptive use was 2.25 (P =0.08) (study J) (32). Thus, the only two studies that failed to report statisticallysignificant benefits may have produced programmatically meaningful resultsbut they lacked statistical power.
While the positive effects of some interventions lasted only a few months,the effects of other interventions lasted for years. For example, the MEMAkwa Vijana intervention found positive effects on reported behaviours overa 36-month period (study G) (45).
The positive effects of these interventions were remarkably robust (Table5.4b). In particular, roughly equal proportions of interventions were found to
140
92-4-120938-0_CH05_140

be effective regardless of whether they were implemented in primary or sec-ondary school or college or night school. Similar proportions of these cur-riculum-based interventions were effective regardless of whether they weretaught by teachers or other adults. They were also effective for both male andfemale students. It is encouraging that interventions may increase reports ofcondom use even among females who have less direct control over their use.And the interventions were equally likely to be effective regardless of whetherthey were evaluated with experimental or quasi-experimental designs.
In general, these patterns of findings are remarkably similar to those from theUnited States and other developed countries (12). Those studies also demon-strated that school-based interventions encouraging abstinence and condomuse do not increase sexual behaviour, and sometimes they delay participants’sexual activity, reduce participants’ frequency of sexual relations, reducetheir number of sexual partners and increase their use of condoms or contra-ceptives. Those studies also demonstrate that the positive effects of suchinterventions are quite robust (12, 14). This is encouraging and suggests thatthese interventions may be effective regardless of the level of economic de-velopment and prevalence of HIV.
5.3.6.1 Characteristics of curriculum-based adult-led interventions that changedbehaviour
As discussed above, this review coded each study according to the charac-teristics of interventions that have been found to be effective anywhere in theworld. This raises the important question: what are the characteristics of ef-fective school-based programmes in developing countries?
The results of coding revealed that these interventions had the same charac-teristics as effective curricula evaluated anywhere in the world. That is, mostof the effective programmes incorporated at least four-fifths of the charac-teristics described in Box 5.1. However, in part because of the limitations ofthe studies, we could not determine whether three particular characteristicshad been included. In particular, it was often difficult to determine whetherprogramme developers used a logic model to develop programmes, wheth-er curriculum activities had been pilot-tested before implementation orwhether educators created a safe environment for group discussions in theclassrooms.
5.3.7 Health services
Schools in the developing world may have an important role in achieving theUNGASS goal of improving access to health services for youths. However,full assessment of this question is beyond the scope of this chapter.
141
92-4-120938-0_CH05_141

5.3.8 Vulnerability
Schools in the developing world potentially also have a key role in addressingvulnerability among youths at several levels, for example, at the individuallevel, by improving their life chances through education and at the societallevel, by addressing adverse gender norms and contributing to incrementalchanges in norms and values. However, it is also true that schools themselvesmay contribute to adolescent vulnerability by subjecting young girls to sexualabuse by teachers (9, 56, 57) and by reinforcing adverse gender norms. How-ever, a review of all of these effects is also beyond the scope of this chapter.
5.4 Discussion and recommendations
Despite limitations in the documentation of interventions and in research re-sults, we reviewed school-based studies that were divided into six differentcategories, summarized the strength of evidence for each category and maderecommendations about each category (Table 5.5).
The recommendations used in this review are the same as those used in theintroduction and methods sections (chapter 1 and chapter 4) and elsewherein this report, namely:
“Go” – the evidence threshold has been met and there is sufficient evidenceto recommend widespread implementation on a large scale now with care-ful monitoring of coverage, quality and costs;
“Ready” – the evidence threshold has been partially met and the evidencesuggests these interventions are effective but large-scale implementationmust be accompanied by further evaluation to clarify their impact andmechanisms;
“Steady” – there is some encouraging evidence of effectiveness but thisevidence is still weak and further development, pilot testing and evaluationare urgently needed before they can move into the “Ready” category;
“Do not go” – there is strong enough evidence of a lack of effectiveness orof harm to indicate that this is not the type of intervention to pursue.
5.4.1 Knowledge
Given that these school-based interventions have a low-to-moderate thresh-old for evidence, given that all the studies that measured impact on knowledgefound a positive impact on knowledge, and given that innumerable studies ofschool-based interventions in developed countries have also found that theseinterventions increase knowledge, these interventions are clearly a “Go” forknowledge.
142
92-4-120938-0_CH05_142

5.4.2 Behaviour
Curriculum-based interventions incorporating most of the characteristics inBox 5.1 and led by adults had been evaluated by the greatest number of stud-ies, had the strongest evidence, and had the most consistent results demon-strating positive reports of behavioural change. These results are all based onreported behaviour with all of the limitations of self-reported sexual be-haviour, which include the potential for presentation bias, that may occur,especially within the context of interventions promoting specific behaviours.Thus, positive effects on actual STI or HIV prevalence are more credible.Nevertheless, the consistency of these positive results on reported sexual be-haviours is encouraging. Thus, these results warrant a “Go” for this type ofintervention. This does not mean that these interventions should not contin-ually be evaluated and improved, for they clearly should be, and theirimportant characteristics should be further refined.
Curriculum-based adult-led interventions without most of the characteristicsin Box 5.1 did not increase any measure of sexual risk behaviour but there islittle evidence that they decreased sexual risk behaviour. Studies of theseinterventions included only one with a quasi-experimental design that showeda positive impact and one study with the same design that showed no impact.Thus, this group of interventions warrants a “Steady” rating.
Some curricula are called “life-skills interventions”. These are quite popularthroughout the world but they constitute a heterogeneous group of interven-tions. Calling them “life skills” is not very descriptive. Some of theseinterventions focus on sexual behaviour and incorporate many or all of thecharacteristics in Box 5.1. These should be classified accordingly.
On the other hand, other life-skills interventions not studied in this reviewteach only general social skills, life-planning skills or other skills and do notfocus on sexual behaviour, do not provide a clear message about sexual be-haviour and do not incorporate some of the other characteristics described inBox 5.1. Few of these interventions have been evaluated. Thus, without muchinformation about them, these interventions would have to be classified“Steady”.
Only two curriculum-based interventions were implemented primarily bypeers. One of these incorporated many of the characteristics in Box 5.1 andincreased the use of condoms among participants, while the other did notincorporate these characteristics and did not significantly change any be-haviour. Thus, both of these types of peer-led interventions should also beclassified as “Steady”.
Results for non-curriculum-based interventions were not clear. Four out offive were adult-led and two of the four had a positive effect on one or more
143
92-4-120938-0_CH05_143

behaviours, while two did not. Of the four adult-led interventions, only onewas evaluated in a randomized trial and it failed to find an impact. Thus, thistype must be given a “Steady” rating both because of the small number ofstudies and the mixed results.
The fifth non-curriculum-based intervention was led by peers. While the re-sults indicate that it had important positive behavioural effects (fewer sexualpartners, increased condom use and increased use of contraception), the re-sults also include the only negative behavioural results, namely a hasteningof the initiation of sexual activity. Thus, this type must also be given a“Steady” rating.
All of these recommended ratings are affected by positive biases (as is thecase in the reporting of many results) and negative biases (for example, in-sufficient statistical power). They are limited by far too many weak evaluationdesigns that could either obscure or enhance effects and by reliance on re-ported behaviour instead of actual behaviour or measurement of STD or HIVrates. Finally, they are limited by inadequate descriptions of interventions, afew of which were only a couple of sentences long. This undoubtedly addederror to the categorization and coding of interventions.
5.4.3 HIV prevalence
Only one of the 22 interventions increased any measure of reported sexualbehaviour; the remaining 21 either had no impact on sexual behaviour ordelayed the onset of sexual activity, reduced the frequency of sexual activityor decreased the number of sexual partners. These results provide strong ev-idence that interventions focusing on sexual behaviour and its consequencesdo not lead to an increase in reported sexual behaviour. This conclusion isespecially strong and consistent for interventions taught by adults. Further-more, the majority of these interventions led to reductions in sexual activity,increased condom use or increases in contraceptive use. Given these changesin sexual behaviour, one could expect a reduction in both pregnancy and STIs.
However, only one study measured an intervention’s impact on STI rates andit did not find positive significant effects (study G) (45). This may be in partbecause sample sizes were too small to detect programmatically meaningfuleffects on HIV and bacterial STIs. However, the study was sufficiently wellpowered to estimate the effect of the intervention on rates of infection withherpes simplex virus–type 2 and pregnancy. Despite having strong evidencefor effects on reported sexual behaviours, this intervention had no impact onthese biomedical outcomes. Thus, greater understanding of this disarticula-tion between reported effects on behaviour and a lack of biomedical impactis clearly critical, and more studies need to measure an intervention’s impacton rates of STIs and pregnancy.
144
92-4-120938-0_CH05_144

5.4.4 Cost effectiveness
None of these studies included any cost–effectiveness analyses. This is animportant omission. Nevertheless, general experience in developing and im-plementing these types of programmes can provide some guidance.
If programmes are effective at reducing risky sexual behaviour, they have thepotential to be cost effective. Initially, effective curricula must be developedand teachers trained. This can be costly. Moreover, once teachers are trained,they must spend time in the classroom implementing programmes and thisclassroom time carries a cost. On the other hand, once effective curricula havebeen designed, training may be incorporated into the training of all newteachers. Furthermore, the length of these curricula is not long (28 hours isthe longest and most are much shorter) and thus the cost of classroom timeis relatively modest. Finally, relatively few materials are needed to implementthe programmes.
5.4.5 Conclusion
In terms of effectiveness in increasing knowledge, our review suggests a “Go”for most school-based sex education and HIV education interventions. Interms of changes in reported behaviour, our review suggests a “Go” forcurriculum-based interventions incorporating the characteristics described inBox 5.1 and led by adults. In part because of the limited number of studies,all other types warrant a “Steady” rating for reported behavioural change.These conclusions suggest a series of recommendations for different groups(Box 5.2).
It is encouraging that patterns of results were similar across both developingand developed countries. In general, interventions were just as likely to beeffective in developing countries as in developed countries (12). They wereeffective for different age groups and for both males and females. Thus, theyappear quite robust.
While studies have not yet demonstrated that these interventions in the de-veloping world significantly reduced the rates of STIs and HIV, many studiesdemonstrated that their intervention produced positive behavioural changesthat logically should lead to reductions in STIs and HIV. Thus, they may bean important component of larger, more comprehensive initiatives and shouldbe implemented more widely.
Funding: Financial support for this research was provided by the UnitedStates Agency for International Development (USAID) through the FamilyHealth International (FHI)/YouthNet Project, from WHO and from the Liv-erpool School of Tropical Medicine.
145
92-4-120938-0_CH05_145

References
1. United Nations. Declaration of commitment on HIV/AIDS. Geneva, UnitedNations, 2001 (available at (http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html).
Box 5.2
Recommendations for interventions in schools
For policy-makers
There is a sufficiently strong evidence base to support widespreadimplementation of school-based interventions that incorporate thecharacteristics of effective programmes that have been found to bepotentially important throughout the world (Box 5.1) and that areled by adults.
There is strong evidence that these programmes reduce sexual riskbehaviour.
Nearly all school-based programmes have strong evidence for in-creasing knowledge.
For programme development and delivery staff
To increase the chances of reducing sexual risk behaviour, school-based programmes should include as many of the characteristics ofeffective programmes as possible because these have been found tobe potentially important throughout the world (Box 5.1).
For researchers
More well designed studies of school-based programmes need to becompleted, particularly in rural areas in developing countries. Ifpossible, these studies should use randomized designs, have suffi-ciently large sample sizes and measure the impact on rates ofsexually transmitted infections, HIV and pregnancy.
Studies also need to examine more thoroughly the impact of pro-grammes on important mediating factors.
Improvements also need to be made in documenting and evaluatingintervention processes.
146
92-4-120938-0_CH05_146

2. Gallant M, Maticka-Tyndale E. School-based HIV prevention programmes forAfrican youth. Social Science and Medicine, 2004, 58:1337-1351.
3. Speizer IS, Magnani RJ, Colvin CE. The effectiveness of adolescentreproductive health interventions in developing countries: a review of theevidence. Journal of Adolescent Health, 2003, 33:324-348.
4. Grunseit A et al. Sexuality education and young people’s sexual behavior: areview of studies. Journal of Adolescent Research, 1997, 12:421-453.
5. MacPhail C, Campbell C. Evaluating HIV/STD interventions in developingcountries: do current indicators do justice to advances in interventionapproaches. South African Journal of Psychology, 1999, 29:149-165.
6. World Health Organization. Key issues in the implementation of adolescentsexual and reproductive health programmes. Geneva, Department of Child andAdolescent Health and Development, WHO, 2004.
7. Visser MJ, Schoeman JB, Perold JJ. Evaluation of HIV/AIDS prevention inSouth African schools. Journal of Health Psychology, 2004, 9:263-280.
8. Smith G et al. HIV/AIDS school-based education in selected Asia-Pacificcountries. Sex Education, 2003, 3-21.
9. James-Traore T et al. Teacher training: essential for school-based reproductivehealth and HIV/AIDS education: focus on sub-Saharan Africa. Arlington, VA,Family Health International, YouthNet Program, 2004.
10. Resnick MD et al. Protecting adolescents from harm: findings from the NationalLongitudinal Study on Adolescent Health. Journal of the American MedicalAssociation, 1997, 278:823-832.
11. James-Traore T et al. Intervention strategies that work for youth: summary ofFOCUS on young adults end of program report. Arlington, VA, Family HealthInternational, YouthNet Program, 2002.
12. Kirby D, Laris B, Rolleri L. Impact of sex and HIV education programs on sexualbehaviors of youth in developing and developed countries. Washington, DC,Family Health International, 2005:1-45.
13. Grunseit A. Impact of HIV and sexual health education on the sexual behaviourof young people: a review update. Geneva, UNAIDS, 1997
14. Kirby D. Emerging answers: research findings on programs to reduce teenpregnancy. Washington, DC, National Campaign to Prevent Teen Pregnancy,2001.
15. Oshi DC, Nakalema S, Oshi LL. Cultural and social aspects of HIV/AIDS sexeducation in secondary schools in Nigeria. Journal of Biosocial Science, 2005,37:175-183.
16. Baker S et al. Evaluation of a HIV/AIDS program for college students inThailand. Washington, DC, Population Council, 2003
17. Maticka-Tyndale E et al. Primary School Action for Better Health: 12-18 monthevaluation. Final Report on PSABH Evaluation in Nyanza and Rift Valley.Windsor, Ontario, University of Windsor, 2004.
18. Kirby DL, Ryan G. Sexual risk and protective factors – factors affecting teensexual behavior, pregnancy, childbearing and sexually transmitted disease:Which are important? Which can you change? Washington, DC, NationalCampaign to Prevent Teen Pregnancy, 2005.
147
92-4-120938-0_CH05_147

19. Pedlow CT, Carey MP. Developmentally appropriate sexual risk reductioninterventions for adolescents: rationale, review of interventions, andrecommendations for research and practice. Annals of Behavioral Medicine,2004, 27:172-184.
20. Robin LD et al. Behavior interventions to reduce incidence of HIV, STD, andpregnancy among adolescents: a decade in review. Journal of AdolescentHealth, 2004, 34:3-26.
21. Gallant M, Maticka-Tyndale E. School-based HIV prevention programmes forAfrican youth. Social Science and Medicine, 2004, 58:1337-1351.
22. UNAIDS. Peer education and HIV/AIDS: concepts, uses and challenges.Geneva, UNAIDS, 1999.
23. Irvin A. Taking steps of courage: teaching adolescents about sexuality andgender in Nigeria and Cameroon. New York, International Women’s HealthCoalition, 2000.
24. Cabezon C et al. Adolescent pregnancy prevention: An abstinence-centeredrandomized controlled intervention in a Chilean public high school. Journal ofAdolescent Health, 2005, 36:64-69.
25. Klepp KI et al. AIDS education in Tanzania: promoting risk reduction amongprimary school children. American Journal of Public Health, 1997,87:1931-1936.
26. Pick De Weiss S. Givaudan M, Givaudan S. Planeando tu vida: sex and familylife education. Fundamentals of development, implementation, and evaluation.International Journal of Adolescent Medicine and Health, 1993, 6:211-224.
27. Reddy P, James S, McCauley AP. Programming for HIV prevention in SouthAfrican schools: a report on program implementation. Cape Town, USAID andPopulation Council, 2003.
28. Reddy P, James S, McCauley AP. Programming for HIV prevention in SouthAfrican schools: horizons research summary. Washington, DC, PopulationCouncil, 2003
29. Ross DA et al. Community randomised trial of an innovative adolescent sexualhealth intervention programme in rural Tanzania: the MEMA kwa Vijana trial.(Unpublished data.)
30. Seidman M et al. Fertility awareness education in the schools: a pilot programin Santiago, Chile. San Diego, CA, American Public Health Association, 1995.(Unpublished data presented 31 October 1995.)
31. Antunes MC et al. Evaluating an AIDS sexual risk reduction program for youngadults in public night schools in Sao Paulo, Brazil. AIDS, 1997, 11 Suppl 1:S121-127.
32. Eggleston E et al. Evaluation of a sexuality education program for youngadolescents in Jamaica. Revista Panamericana Salud Pública, 2000,7:102-112.
33. Fawole IO et al. A school-based AIDS education programme for secondaryschool students in Nigeria: a review of effectiveness. Health EducationResearch, 1999, 14:675-683.
34. Martinez-Donate AP et al. Evaluation of two school-based HIV preventioninterventions in the border city of Tijuana, Mexico. Journal of Sex Research,2004, 41:267-278.
148
92-4-120938-0_CH05_148

35. Stanton BF et al. Increased protected sex and abstinence among Namibianyouth following a HIV risk-reduction intervention: a randomized, longitudinalstudy. AIDS, 1998, 12:2473-2480.
36. Kinsler J et al. Evaluation of a school-based intervention for HIV/AIDSprevention among Belizean adolescents. Health Education Research, 2004, 19:730-738.
37. McCauley AP. Programming for HIV prevention in Mexican schools.Washington, DC, Population Council, 2004.
38. Murray N et al. An evaluation of an integrated adolescent development programfor urban teenagers in Santiago, Chile. Futures Group International, Center forthe Reproductive Health of Adolescents , Johns Hopkins University, 2000.(Unpublished data.)
39. Agha S, Van Rossem R. Impact of a school-based peer sexual healthintervention on normative beliefs, risk perceptions, and sexual behavior ofZambian adolescents. Journal of Adolescent Health, 2004, 34:441-452.
40. Harvey B, Stuart J, Swan T. Evaluation of a drama-in-education programme toincrease AIDS awareness in South African high schools: a randomizedcommunity intervention trial. International Journal of STD and AIDS, 2000,11:105-111.
41. Mbizvo MT et al. Effects of a randomized health education intervention onaspects of reproductive health knowledge and reported behaviour amongadolescents in Zimbabwe. Social Science and Medicine, 1997, 44:573-577.
42. Okonofua FE et al. Impact of an intervention to improve treatment-seekingbehavior and prevent sexually transmitted diseases among Nigerian youths.International Journal of Infectious Diseases, 2003, 7:61-73.
43. Shuey DA et al. Increased sexual abstinence among in-school adolescents asa result of school health education in Soroti district, Uganda. Health EducationResearch, 1999, 14: 411-419.
44. Brieger WR et al. West African Youth Initiative: outcome of a reproductive healtheducation program. Journal of Adolescent Health, 2001, 29:436-446.
45. Changalucha J et al. MEMA kwa Vijana, a randomised controlled trial of anadolescent sexual and reproductive health intervention programme in ruralMwanza, Tanzania. 4. Results: biomedical outcomes. In: International Societyfor Sexually Transmitted Diseases Research 15th biennial conference. Ottawa,ISSTDR, 2003:253. (Abstract.)
46. Aplasca MA et al. Results of a model AIDS prevention program for high schoolstudents in the Philippines. AIDS, 1995, 9 Suppl 1:S1-13.
47. Caceres CF et al. Evaluating a school-based intervention for STD/AIDSprevention in Peru. Journal of Adolescent Health, 1994, 15:582-591.
48. Kuhn L, Steinberg M, Mathews C. Participation of the school community in AIDSeducation: an evaluation of a high school programme in South Africa. AIDSCARE, 1994, 6:161-171.
49. Munodawafa D, Marty PJ, Gwede C. Effectiveness of health instructionprovided by student nurses in rural secondary schools of Zimbabwe: a feasibilitystudy. International Journal of Nursing Studies, 1995, 32:27-38.
50. Perez F, Dabis F. HIV prevention in Latin America: reaching youth in Colombia.AIDS CARE, 2003, 15:77-87.
149
92-4-120938-0_CH05_149

51. Kim H. The effects of sex education programs on knowledge and attitude relatedto sex of elementary school high grade students. (Unpublished data presentedat 16th World Congress of Sexology 2005.)
52. Rusakaniko S et al., Trends in reproductive health knowledge following a healtheducation intervention among adolescents in Zimbabwe. Central AfricanJournal of Medicine, 1997, 43:1-6.
53. Samkaranarayan S et al. Impact of school-based HIV and AIDS education foradolescents in Bombay, India. AIDS Education in India, 1996, 27:692-695.
54. Singh S. Study of the effect of information, motivation and behavioural skills(IMB) intervention in changing AIDS risk behaviour in female universitystudents. AIDS CARE, 2003, 15:71-76.
55. Visser M. Evaluation of the First AIDS Kit: the AIDS lifestyle educationprogramme for teenagers. South African Journal of Psychology, 1996,26:103-113.
56. Gachuhi D. The impact of HIV/AIDS on education systems in the eastern andsouthern africa region and the response of education systems to HIV/AIDS:education/life skills programmes. Nairobi, UNICEF/East and Southern AfricaRegion,1999.
57. Schapink D, Hema J, Mujaya B. Youth and HIV/AIDS programmes. In:Ng’weshemi J et al, eds. HIV prevention and AIDS care in Africa: a district levelapproach. Amsterdam, Royal Tropical Institute, KIT Press, 1997:163-184.
150
92-4-120938-0_CH05_150

6. Review of the evidence forinterventions to increase youngpeople’s use of health services indeveloping countriesBruce Dick,a Jane Ferguson,a Venkatraman Chandra-Mouli,a
Loretta Brabin,b Subidita Chatterjee,c & David A. Rossd
Objective This chapter reviews the evidence base for interventions that aimto increase young people’s use of health services in developing countries.
Methods We identified published and unpublished studies and reports fromdeveloping countries that provided information about interventions designedto increase young people’s use of health services. The studies were classifiedinto six different types based on whether they included some or all of thefollowing characteristics: training for service providers and clinic staff; mak-ing efforts to improve the quality of the facilities; implementing communityactivities to generate demand and support for the services; and involvingother sectors, notably schools and the media. The levels of evidence requiredto make decisions about policies and programmes were defined for each ofthese types.
Findings Despite the lack of detailed descriptions of interventions in thestudies and difficulties interpreting the data reported in the evaluations, thestudies provided evidence of increased use of health services by young peoplefor those types of interventions that included training for service providers,making improvements to clinic facilities and implementing activities in thecommunity, with or without the involvement of other sectors.
Conclusion The evidence for the effectiveness of interventions to increaseyoung people’s use of health services was sufficient to recommend that in-terventions that include training for service providers, making improvements
a Department of Child and Adolescent Health and Development, WHO, Geneva, Switzerland.Correspondence should be sent to Dr Bruce Dick (email: [email protected]).
b Department of Obstetrics and Gynaecology, University of Manchester, Manchester, England.c Consultant in Reproductive Health, Geneva, Switzerland.d Infectious Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine,
London, England.
151
92-4-120938-0_CH06_151

to clinics and using activities in the community should be widely imple-mented with careful monitoring of quality and coverage and that those thatadditionally involve other sectors should also be widely but cautiously im-plemented, provided they include a strong evaluation component. Operationsresearch is also required to better understand the content of the interventionsand their mechanisms of action.
6.1 Introduction
During the past 10–15 years there has been growing awareness of the needto make health services more responsive to the specific needs of young people(1, 2). The HIV/AIDS epidemic has contributed to this increasing attention,and the United Nations General Assembly Special Session (UNGASS) onHIV/AIDS includes an explicit target related to ensuring young people’s ac-cess to health services (3, 4). Governments attending the special sessionagreed that by 2005, 90% of young people aged 15–24 years – and by 2010,95% of this age group – should have access to the services that they need todecrease their vulnerability to HIV.
In 2003, WHO and its partners organized a technical consultation in Montreux,Switzerland, to review the evidence base for a set of interventions that couldbe provided though health services and that would contribute to the preven-tion and care of HIV infection among young people (5). The package ofservices included providing reproductive health information and counselling;reducing risk by encouraging the use of condoms among sexually activeyoung people and the use of sterile injecting equipment and other harm re-duction interventions by young injecting drug users; and providing servicesto diagnose, treat and care for young people with sexually transmitted infec-tions (STIs) and HIV/AIDS. The evidence base for these and other interven-tions provided through health services is further elaborated in chapter 3.
The evidence-based package of interventions developed at Montreux needsto form the basis for the goal for services endorsed during UNGASS. Unfor-tunately, the data available to monitor these health service targets are gener-ally weak. Some data have been provided in chapter 2, and a major effort isbeing initiated by the Futures Group, Policy Project, using the triangulationof information obtained from interviews with key informants (6). Methodsthat use community surveys and health facility statistics are also being de-veloped (7). Although the data are scarce, what little data there are indicatethat we are far from achieving the global target on providing access to ser-vices, either for the general population of young people or for those who aremost at risk from HIV (8). (The evidence for interventions targeted towardsyoung people most at risk of HIV is reviewed in chapter 9.)
152
92-4-120938-0_CH06_152

The purpose of this paper is to review the evidence for interventions that aimto increase young people’s use of health services and to determine what it isthat needs to be done if we are to achieve the global goals on increasing youngpeople’s access to services.
6.2 Methods
This review has adopted a similar process to the other papers in this seriesin terms of assessing the evidence in a systematic and transparent way(chapter 4).
6.2.1 Inclusion and exclusion criteria
Details of the inclusion and exclusion criteria for the studies in this revieware outlined in Table 6.1. Several points require clarification.
First, it should be noted that the UNGASS target refers to young people’saccess to services. This review focuses on studies that have attempted to in-crease young people’s use of health services, which goes beyond merelyincreasing availability and includes elements of accessibility and acceptabil-ity. There was no attempt to explore “effectiveness coverage”, which not onlyanswers the question “were the services used” but also “did the services thatwere used make a difference?” (9). With one exception, a study from Nigeria(10), the data from studies included in this review were not sufficiently de-tailed to answer the second of these questions.
Second, studies were selected based on the contribution that the interventionmade specifically to the UNGASS target of increasing young people’s accessto services. Although health services may provide information to young peo-ple and help them develop skills, such as learning how to use a condom, theUNGASS targets that relate to information, skills and vulnerability were notincluded as outcomes in this review. The rationale for this was that generallythose studies that include data on changes in knowledge, skills, attitudes andbehaviour are multicomponent interventions, and it is difficult to tease outthe relative contribution of the health services’ component to any changesthat are reported. Those studies that include such data are indicated in thetables, although these data are not included in the analysis.
Third, studies were included if they had as their primary focus interventionsinvolving interactions between a young person (aged 10–24 years) and ahealth-care worker, such as a doctor, a nurse or a clinical officer. Studies werenot included if they had as their major focus interactions between adolescentsor youth and people who are not health-care workers, such as community-based condom distributors, peer educators, counsellors and other individualsand groups who provide information, education, counselling or supplies toyoung people.
153
92-4-120938-0_CH06_153

Table 6.1Inclusion and exclusion criteria used to identify studies for review
Inclusion criteria Exclusion criteria
Intervention studies and programmes orprojects carried out in developing countriesand where sufficient details given to allow thereader to know (at least in outline) of what theintervention consisted.
Intervention studies carried out indeveloped countries or where insufficientdetails given to allow the reader to be ableto know (at least in outline) of what theintervention consisted.
Intervention studies and programmes orprojects that attempted to increase utilizationof health services by adolescents (aged 10–19 years), young people (10– 24 years) oryouths (15–24 years) and that also tracked ordocumented utilization. Interventions thatshowed an increase in young people’s be-haviours that are related to service utilization(such as condom use) were also included.
Intervention studies and programmes orprojects that did not gather data showingutilization of health services byadolescents, young people or youths.
Intervention studies and programmes orprojects that provided health services for HIVprevention (including sexual andreproductive health), such as information,counselling, condom distribution, STIa
management and voluntary counselling andtesting in the context of an interactionbetween a health-service provider and ayoung person.
Intervention studies and programmes orprojects that provided information,counselling or condoms outside the contextof an interaction between a health-serviceprovider and a young person.
Intervention studies using the followingdesigns:• randomized controlled trials• quasi-experimental study designs• data collected before and after the study
(without data from comparison sites)• time-series data on service utilization after
the start of the intervention• Cross-sectional (that is, “after-only”) survey
data where service utilization data for youngpeople were presented either by their levelof exposure to the interventions orcompared with other clinics or services thatwere not exposed to the intervention.
Intervention studies that did not usedesigns that would enable the reader toevaluate the impact of the intervention or tomake inferences based on statistical tests.
Reports with interpretable quantitative dataon the use of health services by youngpeople.
Reports without interpretable quantitativedata on health service use by youngpeople.
a STI = sexually transmitted infection.
154
92-4-120938-0_CH06_154

Finally, studies were included if one of their primary aims was to increaseyoung people’s use of health facilities, including government clinics, privateclinics, stand-alone youth clinics or clinics that are included as a componentof multipurpose youth centres. Studies were not included if they did not havea health facility component, for example, if they focused primarily on otherfacilities where information and commodities are provided to young people,such as kiosks, pharmacies and youth centres that do not include a healthfacility (11, 12).
6.2.2 Identification of studies and reports
Studies were identified through different processes. This paper built on lit-erature reviews of adolescent-friendly health services that had been carriedout for previous WHO meetings that took place in 1995 (13), 2001 (14) and2002 (15). An additional search was undertaken for published papers usingelectronic reference databases (Medline, PubMed, EMBASE) and the Inter-net. In order to identify unpublished reports and evaluations, contact was alsomade with 24 agencies known to support programmes and projects in devel-oping countries that aim to make health services more responsive to the needsof adolescents and young people. A WHO collection of papers and reportson adolescent-friendly health services was also reviewed. The literature re-view focused primarily on articles and reports written in English.
Twenty one studies and projects were initially identified that met the inclusioncriteria. However, this number decreased to 16 following a more in-depthanalysis of the quality of the information provided in the studies in terms ofclarity about the interventions, the evaluation methods and results. The ninestudies that did not fully meet the inclusion criteria either had insufficientdata to allow an adequate assessment of the interventions or the evaluationdata were inadequate. Some of these excluded studies are referred to in thediscussion. In this paper the word “studies” has been used to describe bothstudies that were explicitly designed to explore the effectiveness of an inter-vention and projects where there were sufficient evaluation data to meet theinclusion and exclusion criteria.
6.2.3 Typology of studies
Once the studies had been identified, they were grouped into different typesbased on the specific activities that had been implemented. Strategies to in-crease young people’s use of services have generally included some combi-nation of the following: improving the knowledge and skills of serviceproviders and other clinic staff; making facilities more responsive to thespecific needs of young people, for example by changing the physical envi-ronment or opening hours; reaching out from the facility into the community
155
92-4-120938-0_CH06_155

to provide information, generate demand and create community support; andinvolving other sectors, such as schools and the media, to provide informationand mobilize community support.
The typology for this review was based on a combination of these differentcomponents, resulting in a 2 by 3 matrix of six types, as outlined in Box 6.1.
Type 1, type 3 and type 5 interventions (those included in the first row) ex-plicitly provided training to service providers, and sometimes other staff inthe health facility, on how to respond more appropriately to the health needsof young people. This training included improving their knowledge, skillsand attitudes in order to increase their capacity to provide information andtreat young people effectively, in a respectful and confidential manner.
Type 2, type 4 and type 6 interventions (those in the second row) includedtraining for service providers and other clinic staff and additionally containedexplicit actions that aimed to improve specific aspects of the health facility,such as changing the opening hours, decreasing the amount paid by youngpeople for services or commodities, changing the layout or other aspects ofthe physical environment to make it more appealing or to increase privacy,introducing recreational opportunities and involving peer educators in thefacility. Interventions were not placed in this row if a health facility had beenincluded in a multipurpose youth centre without some additional focus on theareas outlined above. Interventions were placed in this row only if there wasan indication that significant efforts had been made to improve the facility,so merely providing information materials in the facility would not havewarranted inclusion in this row.
Interventions allocated to the first column (types 1 and 2) included a rangeof activities that were conducted within the community. For example, theseactivities included having health-workers provide information outside thehealth facility, having young people provide information and counselling inthe community, holding meetings with gatekeepers and community leadersand providing information about the need for and availability of services,including putting up posters and distributing information materials, placingadvertisements in local newspapers and showing videos at communitygatherings.
Interventions allocated to the second column (types 3 and 4) involved othersectors, such as education or the media. Interventions were included in thistype if there were curriculum-based interventions, peer educators, healthclubs that linked or referred pupils to health services, or other activities thatrequired significant investment on the part of the education sector. For mediainterventions to be included, there had to be significant involvement ofthe print, radio or television media in terms of providing information or
156
92-4-120938-0_CH06_156

“edutainment”, generating debate and dialogue and encouraging youngpeople to use health services.
The interventions were classified based on the information contained in thestudies; this information was not always complete. Although every attempthas been made to ensure that decisions about classifying the interventionswere open and standardized, there was inevitably some level of interpretationthat occurred in allocating studies to the different types because it was notalways clear from the papers what had actually been done or with what in-tensity of effort.
6.2.4 Threshold of evidence required
Once the typology for the interventions had been defined, it was necessaryto make a decision about the threshold of evidence that would be required tocategorize the different intervention types as “Go”, “Ready”, “Steady” or Do
Box 6.1
Typology of interventions implemented to increase young people’s use ofhealth services
Interventionsin the healthfacility
Interventions outside the health facilityInterventionsin thecommunitya
Interventionswith othersectorsb
Interventionsin thecommunityand withother sectors
Trainingserviceproviders andclinic staff only
Type 1 Type 3 Type 5
Trainingserviceproviders andclinic staff plusinterventionsin the facility tomake it moreyouth-friendly
Type 2 Type 4 Type 6
a These may include the use of peer educators working in the communityor other forms of information and community sensitization about theavailability of services and the needs of adolescents.b The focus for these studies was the involvement of schools or the massmedia.
157
“
92-4-120938-0_CH06_157

not go” (see chapter 4). Table 6.2 provides an overview of the thresholds ofevidence required to recommend widespread implementation of the differenttypes of interventions.
For type 1 interventions (training health-workers and other clinic staff alongwith activities in the community) and type 2 interventions (training health-workers and other clinic staff along with taking action to improve facilitiesand implement activities in the community) only weak evidence for effec-tiveness is considered to be required to recommend interventions forwidespread implementation (“Go”). Once other sectors become involved,however, the design and implementation of the intervention is likely to be-come more complex, and coordination of the programme components andsustainability is likely to become more of a challenge (even if both the impactof the interventions and other possible health and social benefits may in-crease). It was therefore decided that in order to be able to recommend types3, 4, 5 and 6 as “Go”, they would require a moderate threshold of evidence.
6.3 Findings
Summaries of the analysis of the 16 papers are found in Table 6.3 andTables 6.4a–e. Table 6.3 synthesizes information about the interventions fromthe different studies, and Tables 6.4a–e summarizes the evaluation methodsand results, as well as assessing the strength of the evidence for an increasein the use of services by young people.
6.3.1 Characteristics of studies
There were 12 studies from Africa, 3 from Asia and 1 from Latin America.Most studies included here endeavoured to improve existing services, andmost frequently these were offered in public facilities. Only one study – inNigeria (10) – focused exclusively on private providers, although the fran-chised interventions in Madagascar (12) included both private and publicproviders. There were three studies that involved the creation of new facili-ties; these took place in China (19), Ghana (29) and Mongolia (23). Threestudies integrated clinical services into multipurpose youth centres; thesetook place in Ghana (29), Rwanda (12) and Zimbabwe (18). In Uganda (17)recreational activities were added to existing health facilities as a way ofattracting young people.
158
92-4-120938-0_CH06_158

Tab
le 6
.2.
Th
resh
old
of
evid
ence
nee
ded
to
rec
om
men
d w
ides
pre
ad im
ple
men
tati
on
of
each
typ
e o
f in
terv
enti
on
a
Inte
rven
tio
nty
pe
Fea
sib
ility
bL
ack
of
po
ten
tial
for
adve
rse
ou
tco
mes
c
Acc
epta
bili
tyfo
r ta
rget
gro
up
d
Acc
epta
bili
tyfo
r co
mm
un
ity
and
po
licy-
mak
erse
Po
ten
tial
size
of
effe
ctf
Oth
erh
ealt
h o
rso
cial
ben
efit
sg
Ove
rall
thre
sho
ldC
om
men
ts
1. In
terv
entio
nsw
ith s
ervi
cepr
ovid
ers
only
plus
inte
rven
tions
inth
e co
mm
unity
++
++
++
++
++
+Lo
wT
his
type
of
inte
rven
tion
is li
kely
tobe
eas
iest
and
mos
tac
cept
able
but t
o ha
ve le
ast
impa
ct b
ecau
se it
invo
lves
onl
yse
rvic
e pr
ovid
ers
with
out c
hang
es in
the
faci
litie
s2.
Inte
rven
tions
with
ser
vice
prov
ider
s an
d in
faci
litie
s pl
usin
terv
entio
ns in
the
com
mun
ity
++
++
++
++
++
++
Low
Incl
udin
g a
focu
s on
impr
ovin
g fa
cilit
ies
is li
kely
to in
crea
seth
e im
pact
with
out
sign
ifica
ntly
incr
easi
ng fe
asib
ility
or d
ecre
asin
gac
cept
abili
ty3.
Inte
rven
tions
with
ser
vice
++
++
++
++
Mod
erat
eW
ith th
e ad
ditio
n of
othe
r se
ctor
s th
ere
159
92-4-120938-0_CH06_159

Inte
rven
tio
n
typ
eF
easi
bili
tyb
Lac
k o
fp
ote
nti
alfo
r ad
vers
eo
utc
om
esc
Acc
epta
bili
tyfo
r ta
rget
gro
up
d
Acc
epta
bili
tyfo
r co
mm
un
ity
and
po
licy-
mak
erse
Po
ten
tial
size
of
effe
ctf
Oth
erh
ealt
h o
rso
cial
ben
efit
sg
Ove
rall
thre
sho
ldC
om
men
ts
prov
ider
s on
lypl
usin
terv
entio
nsw
ith o
ther
sect
ors
are
likel
y to
be
prob
lem
s of
acce
ptab
ility
by
scho
ols
and
poss
ibly
the
med
ia, a
nd th
ede
bate
is li
kely
to b
ew
ider
in th
eco
mm
unity
, whi
ch m
ayha
ve b
oth
posi
tive
and
nega
tive
impl
icat
ions
4. In
terv
entio
nsw
ith s
ervi
cepr
ovid
ers
and
infa
cilit
ies
plus
inte
rven
tions
with
oth
erse
ctor
s
++
++
++
++
++
Mod
erat
eA
s ab
ove
5. In
terv
entio
nsw
ith s
ervi
cepr
ovid
ers
plus
inte
rven
tions
inth
e co
mm
unity
and
with
oth
erse
ctor
s
++
++
++
++
+M
oder
ate
Invo
lvin
gco
mm
unity
outr
each
and
oth
erse
ctor
s is
likel
y to
incr
ease
som
e of
the
diffi
culti
es b
ut it
160
92-4-120938-0_CH06_160

may
als
o in
crea
seth
e im
pact
and
othe
r he
alth
and
soci
al b
enef
its6.
Inte
rven
tions
with
ser
vice
prov
ider
s an
d in
faci
litie
s pl
usin
terv
entio
ns in
the
com
mun
ityan
d w
ith o
ther
sect
ors
++
++
++
++
++
+M
oder
ate
As
abov
e
a D
egre
e of
des
irabi
lity
is in
dica
ted
with
a m
axim
um o
f 3 “
+”
sign
s. D
egre
e of
und
esira
bilit
y is
indi
cate
d w
ith a
max
imum
of 3
“-”
sig
ns.
b F
easi
bilit
y de
crea
ses
with
incr
easi
ng a
ctiv
ities
insi
de a
nd o
utsi
de th
e fa
cilit
y.c T
he p
oten
tial f
or a
dver
se o
utco
mes
incr
ease
s w
ith th
e in
volv
emen
t of o
ther
sec
tors
.d
Acc
epta
bilit
y lik
ely
to b
e in
crea
sed
if se
rvic
e pr
ovid
ers
and
faci
litie
s ar
e im
prov
ed; t
his
wor
ks s
imila
rly a
s in
terv
entio
ns o
utsi
de th
e fa
cilit
ies
are
incr
ease
d.e
Invo
lvin
g ot
her
sect
ors
is li
kely
to in
crea
se c
omm
unity
acc
epta
nce
but a
t the
sam
e tim
e in
crea
se c
halle
nges
for
polic
y-m
aker
s.f T
he m
ore
com
preh
ensi
ve th
e in
terv
entio
ns, t
he m
ore
likel
y th
ey a
re to
hav
e an
impa
ct.
g T
he m
ore
othe
r se
ctor
s ar
e in
volv
ed, t
he m
ore
likel
y it
is th
at p
rovi
ding
acc
ess
to s
ervi
ces
for
youn
g pe
ople
and
thei
r he
alth
and
dev
elop
men
t in
gene
ral w
illbe
com
e fo
cuse
s fo
r ad
voca
cy a
nd a
ctio
n.
161
92-4-120938-0_CH06_161

Tab
le 6
.3D
escr
ipti
on
of
the
inte
rven
tio
ns
by
stu
dy.
(T
her
e w
ere
no
stu
die
s o
f ty
pe
4 in
terv
enti
on
s.)
Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
Inte
rven
tio
n t
ype
1 (w
ith
ser
vice
pro
vid
ers
and
in t
he
com
mu
nit
y)C
– L
usak
a, Z
ambi
a:8
clin
ics
at 3
site
s (1
6)•
Ove
rall
obje
ctiv
e: to
impr
ove
the
heal
th a
ndw
ell-b
eing
of y
outh
s in
Lus
aka
• H
ealth
ser
vice
obj
ectiv
e: to
mak
e se
rvic
esm
ore
yout
h fr
iend
ly, f
or e
xam
ple,
dev
elop
ing
attr
ibut
es to
attr
act y
outh
s, m
eet t
heir
need
san
d re
tain
you
ng c
lient
s fo
r fo
llow
-up
visi
ts• T
arge
t gro
up: y
oung
peo
ple
aged
10–
24 y
ears
• 4-
year
stu
dy
• P
roje
ct c
linic
s se
lect
ed fr
om th
ose
alre
ady
prov
idin
g qu
ality
ser
vice
s or
rec
eptiv
e to
wor
king
with
you
ng p
eopl
e•
Tra
inin
g of
hea
lth-c
are
prov
ider
s an
d pe
ered
ucat
ors
to c
omm
unic
ate
abou
t ado
lesc
ent
sexu
al a
nd r
epro
duct
ive
heal
th; m
ajor
diffe
renc
e in
pro
ject
site
s w
as e
xten
t to
whi
chco
mm
unity
was
invo
lved
; par
ticip
ator
y“le
arni
ng fo
r act
ion”
exe
rcis
es u
sed
to s
ensi
tize
com
mun
ities
abo
ut a
dole
scen
t sex
ual a
ndre
prod
uctiv
e he
alth
.In
terv
enti
on
typ
e 2
(act
ion
s in
th
e cl
inic
, wit
h s
ervi
ce p
rovi
der
s an
d in
th
e co
mm
un
ity)
L –
Jinj
a di
stric
t, U
gand
a:4
heal
th c
entr
es w
ith c
atch
men
t pop
ulat
ion
of 1
00 0
00 p
eopl
e (1
7)
• T
o ev
alua
te th
e im
pact
of a
dole
scen
t frie
ndly
heal
th s
ervi
ces
pilo
ted
in J
inja
dis
tric
t, U
gand
ato
red
uce
ST
D, H
IV a
nd u
nwan
ted
preg
nanc
ies.
• T
arge
t gro
up: a
dole
scen
ts 1
0–19
yea
rs•
17-m
onth
stu
dy
• H
ealth
wor
kers
trai
ned
to c
omm
unic
ate
and
coun
sel a
dole
scen
ts (
4 he
alth
wor
kers
/cen
tre,
2 cl
inic
al o
ffice
rs, 1
3 nu
rses
/mid
wiv
es, 1
disp
ense
r); d
istr
ict h
ealth
team
trai
ned
to b
uild
capa
city
for
furt
her
trai
ning
and
sup
ervi
sion
,al
so tr
aine
d in
ado
lesc
ent s
exua
l and
repr
oduc
tive
heal
th, c
omm
unic
atio
n an
dco
unse
lling
• H
ealth
cen
tres
reo
rgan
ized
to c
ater
toad
oles
cent
s; g
ames
and
rec
reat
iona
l ser
vice
sin
trod
uced
at h
ealth
uni
ts•
Pro
vide
bas
ic s
uppl
ies
(ST
Ia tr
eatm
ent a
ndco
ntra
cept
ives
)
162
92-4-120938-0_CH06_162

• G
ames
and
recr
eatio
nal s
ervi
ces
intr
oduc
ed a
the
alth
uni
ts•
Dis
tric
t hea
lth te
am tr
aine
d to
bui
ld c
apac
ity fo
rfu
rthe
r tra
inin
g an
d su
perv
isio
n. A
lso
trai
ned
inad
oles
cent
sex
ual a
nd r
epro
duct
ive
heal
th,
com
mun
icat
ion,
and
cou
nsel
ling
• A
dole
scen
ts in
volv
ed in
des
ign
and
subs
eque
nt s
tage
s of
pro
ject
I – S
ongj
iang
dis
tric
t,S
hang
hai,
Chi
na:
1 to
wn
in S
ongj
iang
, 1 c
linic
and
net
wor
kof
loca
l fam
ily p
lann
ing
prov
ider
s (1
9)
• O
bjec
tive:
to b
uild
aw
aren
ess
and
offe
rco
unse
lling
and
ser
vice
s re
late
d to
sex
ualit
yan
d re
prod
uctio
n to
unm
arrie
d yo
uths
• S
peci
fic o
bjec
tives
: to
incr
ease
con
trac
eptiv
eus
e (c
ondo
m u
se)
amon
g un
mar
ried
yout
hsth
roug
h a
mul
tifac
eted
inte
rven
tion
prog
ram
me
prov
idin
g in
form
atio
n, s
kills
,co
unse
lling
and
ser
vice
s•
Tar
get g
roup
: you
ths
15–2
4 ye
ars
• 20
-mon
th in
terv
entio
n
• B
uild
ing
awar
enes
s: a
wid
e ra
nge
ofin
form
atio
n ac
tiviti
es fo
r yo
ung
peop
le c
arrie
dou
t in
the
inte
rven
tion
com
mun
ity; i
nfor
mat
ion
prov
ided
abo
ut s
exua
l and
rep
rodu
ctiv
e he
alth
and
the
avai
labi
lity
of s
ervi
ces
• C
ouns
ellin
g: a
you
th h
ealth
cou
nsel
ling
cent
rese
t up
in th
e in
terv
entio
n to
wn
prov
ided
rout
ine
and
tele
phon
e co
unse
lling
• T
rain
ing
of s
ervi
ce p
rovi
ders
(bu
ildin
gkn
owle
dge
and
skill
s ab
out a
dole
scen
t sex
ual
and
repr
oduc
tive
heal
th, s
ensi
tizin
g th
em to
inte
ract
with
you
ng p
eopl
e, te
achi
ng th
em h
owto
ass
ist y
oung
peo
ple
in d
ealin
g w
ith s
ex-
rela
ted
issu
es)
• D
istr
ibut
ing
free
con
trac
eptiv
e su
pplie
sN
– C
entr
e D
ushi
shoz
e, R
wan
da:
1 cl
inic
in B
utar
e (1
2)•
To
mot
ivat
e yo
ung
peop
le e
ither
to u
seco
ndom
s co
nsis
tent
ly o
r to
not
hav
e se
x, to
lear
n th
eir
HIV
sta
tus,
and
see
k to
trea
tmen
tfo
r ot
her
ST
Is•
Tar
get g
roup
: you
ths
15–2
4 ye
ars
• R
esul
ts a
fter
18 m
onth
s of
impl
emen
tatio
n of
4-ye
ar p
rogr
amm
e
• P
rovi
de s
ubsi
dize
d yo
uth-
frie
ndly
sex
ual a
ndre
prod
uctiv
e he
alth
ser
vice
s (in
clud
ing
volu
ntar
y co
unse
lling
and
test
ing
for
HIV
, ST
Itr
eatm
ent,
emer
genc
y co
ntra
cept
ion,
preg
nanc
y te
stin
g an
d re
prod
uctiv
e he
alth
coun
selli
ng)
alon
g w
ith s
kills
-bui
ldin
g an
dso
cial
act
iviti
es w
ithin
a p
urpo
se-b
uilt
cent
re;
163
92-4-120938-0_CH06_163

Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
serv
ices
pro
vide
d by
hea
lth-w
orke
rs a
nd fu
ll-tim
e pa
id p
eer
educ
ator
s; P
eer
educ
ator
s an
dhe
alth
-wor
kers
pro
vide
d sm
all-g
roup
and
indi
vidu
al c
ouns
ellin
g se
ssio
ns fo
r yo
uths
at
the
cent
re a
nd a
lso
in c
hurc
hes,
clu
bs, s
choo
lsan
d ru
ral c
omm
unity
cen
tres
• P
eer
educ
ator
s he
lped
iden
tify
and
prom
ote
yout
h-fr
iend
ly c
ondo
m s
elle
rs in
rur
al a
reas
0 –
Gw
eru,
Zim
babw
e (1
8)•
Cre
ate
a m
ore
favo
urab
le e
nviro
nmen
t for
the
prov
isio
n of
rep
rodu
ctiv
e he
alth
info
rmat
ion
and
serv
ices
for
yout
hs•
Incr
ease
util
izat
ion
of c
linic
al r
epro
duct
ive
heal
th s
ervi
ces
by y
outh
s by
20%
abo
veba
selin
e•
Incr
ease
kno
wle
dge
of s
elec
ted
sexu
ality
and
repr
oduc
tive
heal
th is
sues
am
ong
youn
gpe
ople
atte
ndin
g N
dhlo
vu Y
outh
Cen
tre
by20
%•
Inte
rven
tion
last
ed 1
1 m
onth
s
• R
aise
aw
aren
ess
of r
epro
duct
ive
heal
th n
eeds
of y
oung
peo
ple
thro
ugh
mee
tings
with
com
mun
ity le
ader
s, p
aren
ts, t
each
ers,
etc
• T
rain
clin
ic n
urse
s, d
evel
op “
yout
h co
rner
s” in
clin
ics,
trai
n pe
er e
duca
tors
to p
rovi
dein
form
atio
n an
d co
ntra
cept
ives
, and
est
ablis
ha
recr
eatio
nal y
outh
cen
tre
to s
uppo
rt th
epr
ovis
ion
of r
epro
duct
ive
heal
th s
ervi
ces
(Ndh
lovu
You
th C
entr
e)
Inte
rven
tio
n t
ype
3 (w
ith
ser
vice
pro
vid
ers
and
invo
lvem
ent
of
oth
er s
ecto
rs)
J –
Bah
ia s
tate
, Bra
zil:
10 r
efer
ence
clin
ics
paire
d w
ithse
cond
ary
scho
ols
(5 p
airs
inS
alva
dor,
5 in
inte
rior)
(20
)
• O
vera
ll ob
ject
ive:
to r
educ
e hi
gh p
regn
ancy
rate
s am
ong
adol
esce
nts
and
grow
ing
num
ber
of n
ew H
IV in
fect
ions
am
ong
youn
g ad
ults
• H
ealth
ser
vice
obj
ectiv
e: to
inte
grat
e sc
hool
base
d se
xual
and
rep
rodu
ctiv
e he
alth
educ
atio
n w
ith p
rovi
sion
in p
ublic
clin
ics
ofre
prod
uctiv
e he
alth
ser
vice
s ap
prop
riate
toad
oles
cent
s•
Tar
get g
roup
: you
ng p
eopl
e 10
–24
year
s•
Initi
ativ
e w
as u
nder
take
n ov
er a
2-y
ear
perio
d
• 30
0 se
rvic
e pr
ovid
ers
took
par
t in
19 tr
aini
ngse
ssio
ns in
rep
rodu
ctiv
e he
alth
ser
vice
s fo
rad
oles
cent
s ov
er 2
yea
r pe
riod
• A
t end
of t
his
time,
an
aver
age
of 3
.2 s
ervi
cepr
ovid
ers
per c
linic
had
bee
n tr
aine
d to
pro
vide
thes
e se
rvic
es in
a m
anne
r ap
prop
riate
for
adol
esce
nts;
no
desc
riptio
n of
con
tent
of
trai
ning
• S
exua
l and
rep
rodu
ctiv
e he
alth
cur
ricul
umin
trod
uced
in 1
0 “p
artn
er”
scho
ols
164
92-4-120938-0_CH06_164

• R
efer
rals
mad
e to
clin
ics
• C
onta
ct e
stab
lishe
d be
twee
n he
alth
ser
vice
and
educ
atio
nal s
taff
Inte
rven
tio
n t
ype
5 (w
ith
ser
vice
pro
vid
ers,
in t
he
com
mu
nit
y an
d in
volv
ing
oth
er s
ecto
rs)
D –
Zim
babw
e:5
pilo
t site
s (1
urb
an a
nd4
grow
th p
oint
s), 2
6 fa
mily
pla
nnin
g cl
inic
s(2
1)
• O
vera
ll ob
ject
ive:
to e
ncou
rage
you
ng p
eopl
eto
ado
pt b
ehav
iour
s th
at r
educ
e th
e ris
k of
preg
nanc
y an
d S
TIs
, inc
ludi
ng H
IV•
Hea
lth s
ervi
ce o
bjec
tive:
to e
ncou
rage
you
ngpe
ople
to u
se s
ervi
ces
• T
arge
t gro
up: y
oung
peo
ple
10–2
4 ye
ars
• M
ultim
edia
cam
paig
n fo
r 6
mon
ths;
inte
rven
tion
for
1 ye
ar
• C
ampa
ign
used
a v
arie
ty o
f cha
nnel
s in
clud
ing
post
ers,
leaf
lets
, new
slet
ters
, rad
iopr
ogra
mm
e, d
ram
a, c
omm
unity
eve
nts
and
hotli
nes;
som
e dr
amas
per
form
ed in
, and
prin
tm
ater
ial d
istr
ibut
ed th
roug
h, s
choo
ls b
ut n
osc
hool
-bas
ed c
urric
ulum
. Thr
ough
out
cam
paig
n pe
er e
duca
tors
, dra
ma
grou
ps a
ndpr
int m
ater
ials
refe
rred
you
ng p
eopl
e to
clin
ics.
• H
ealth
ser
vice
s: F
amily
pla
nnin
g pr
ovid
ers
wer
e tr
aine
d in
26
desi
gnat
ed c
linic
s in
com
mun
icat
ion
and
coun
selli
ng s
kills
dur
ing
a1-
wee
k co
urse
; exp
ecta
tion
that
atte
ndee
sw
ould
trai
n co
-wor
kers
in c
ouns
ellin
gG
– M
wan
za r
egio
n, U
nite
d R
epub
lic o
fT
anza
nia:
10
com
mun
ities
in 4
rur
al d
istr
icts
and
59 in
terv
entio
n sc
hool
s, 1
8 go
vern
men
the
alth
faci
litie
s (2
2)
• Hea
lth s
ervi
ce o
bjec
tive:
to in
crea
se a
cces
s to
(and
app
ropr
iate
util
izat
ion
of)
high
-qua
lity
sexu
al a
nd r
epro
duct
ive
heal
th s
ervi
ces
for
youn
g pe
ople
• Tar
get g
roup
: you
ng p
eopl
e ag
ed 1
2–24
yea
rsw
ith a
par
ticul
ar fo
cus
on th
ose
aged
12–
19ye
ars
• In
terv
entio
n ov
er 3
yea
rs
• Key
hea
lth w
orke
rs in
all
18 in
terv
entio
n an
d 21
com
paris
on h
ealth
faci
litie
s re
ceiv
ed e
ither
an
initi
al 1
-wee
k co
urse
or
1-w
eek
refr
eshe
rco
urse
in th
e sy
ndro
mic
man
agem
ent o
f ST
Is.
The
sam
e w
orke
rs fr
om th
e in
terv
entio
nfa
cilit
ies
rece
ived
a 1
-wee
k pa
rtic
ipat
ory
trai
ning
wor
ksho
p fo
cusi
ng o
n th
e ne
eds
ofyo
ung
peop
le a
nd m
etho
ds fo
r pro
vidi
ng s
exua
lan
d re
prod
uctiv
e he
alth
ser
vice
s fo
r th
em.
• A
ll 39
hea
lth fa
cilit
ies
rece
ived
4 s
uper
visi
onvi
sits
per
yea
r•
Add
ition
al in
terv
entio
ns in
clud
ed
165
92-4-120938-0_CH06_165

Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
In-s
choo
l sex
ual a
nd r
epro
duct
ive
heal
thed
ucat
ion
impl
emen
ted
thro
ugh
a te
ache
r-le
d, p
eer-
assi
sted
pro
gram
me
of p
artic
ipat
ory
less
ons
Com
mun
ity-b
ased
con
dom
pro
mot
ion
and
dist
ribut
ion,
for
and
by y
outh
s, u
sing
a s
ocia
lm
arke
ting
appr
oach
; mor
e th
an 3
000
cond
oms
per
year
wer
e di
strib
uted
by
yout
hco
ndom
pro
mot
ers
and
dist
ribut
ors
Com
mun
ity a
ctiv
ities
• T
he c
ost p
aper
sho
ws
that
68.
9% o
f ove
rall
impl
emen
tatio
n co
sts
wer
e fo
r th
e in
-sch
ool
com
pone
nt, 1
2.3%
for
the
com
mun
ity-b
ased
com
pone
nt, 1
0.1%
for
the
yout
h co
ndom
prom
oter
s an
d di
strib
utor
s, a
nd 8
.8%
for
the
yout
h-fr
iend
ly h
ealth
ser
vice
s co
mpo
nent
with
the
heal
th w
orke
rs a
nd c
linic
sIn
terv
enti
on
typ
e 6
(wit
h s
ervi
ce p
rovi
der
s, in
th
e co
mm
un
ity
and
invo
lvin
g o
ther
sec
tors
)A
– M
ongo
lia:
pilo
t of m
ultis
ecto
r pr
ojec
t (2
rura
l dis
tric
tsan
d 3
dist
ricts
in c
apita
l) (2
3)
• O
bjec
tive:
to in
crea
se a
dole
scen
ts’ a
cces
s to
qual
ity h
ealth
ser
vice
s•
Tar
get g
roup
: ado
lesc
ents
10–
19 y
ears
• A
sses
smen
t con
duct
ed a
fter
1 ye
ar o
f the
3-ye
ar p
roje
ct
• S
tand
ards
of q
ualit
y of
car
e fo
r ad
oles
cent
sw
ere
deve
lope
d•
Tra
inin
g st
aff i
n ad
oles
cent
hea
lth a
ndde
velo
pmen
t, in
clud
ing
teac
hing
new
ski
lls in
com
mun
icat
ion
and
coun
selli
ng, p
rovi
ding
basi
c eq
uipm
ent a
nd s
uppl
ies
to h
ealth
faci
litie
s (s
uch
as s
cale
s, c
ontr
acep
tives
),m
akin
g th
e fa
cilit
ies
mor
e at
trac
tive
to y
oung
peop
le, d
esig
ning
info
rmat
ion
and
educ
atio
nm
ater
ials
on
heal
th a
nd d
evel
opm
ent i
ssue
san
d di
strib
utin
g th
ese
mat
eria
ls to
ado
lesc
ents
,an
d de
velo
ping
pol
icie
s an
d pr
oced
ures
on
166
92-4-120938-0_CH06_166

conf
iden
tialit
y an
d ap
plyi
ng th
ese
atpa
rtic
ipat
ing
site
s•
Com
mun
ity m
obili
zatio
n at
eac
h si
te in
volv
edgo
vern
ors,
teac
hers
, hea
lth w
orke
rs, p
aren
tsan
d ad
oles
cent
s•
Ofte
n it
was
the
heal
th w
orke
rs w
ho tr
aine
dot
hers
• A
dole
scen
ts w
ere
part
of a
dole
scen
t boa
rds
and
invo
lved
in d
esig
n of
edu
catio
n m
ater
ials
and
advo
cacy
B –
Sou
th A
fric
a:na
tiona
l pro
gram
me
star
ted
in 1
999
and
linke
d w
ith “
love
Life
” m
ultim
edia
prog
ram
me
(24)
• O
vera
ll ob
ject
ive:
to c
ontr
ibut
e to
red
ucin
gpr
eval
ence
of H
IV, S
TIs
and
unw
ante
dpr
egna
ncie
s am
ong
Sou
th A
fric
an y
outh
s•
Hea
lth s
ervi
ce o
bjec
tives
: cat
alys
e an
adol
esce
nt-f
riend
ly e
thos
in a
ll go
vern
men
tcl
inic
s; p
rovi
de a
brid
ge b
etw
een
prev
entio
nan
d tr
eatm
ent t
hrou
gh im
prov
ed m
anag
emen
tsy
stem
s, in
fras
truc
ture
and
clin
ical
cap
acity
• Tar
get g
roup
: you
ng p
eopl
e ag
ed 1
0–24
yea
rs,
with
prim
ary
targ
et g
roup
age
d 12
–17
year
s•
Pro
gram
me
star
ted
in 1
999
Clin
ics
will
ing
to jo
in th
e in
itiat
ive
unde
rgo
the
follo
win
g st
eps:
• in
trod
uced
to id
ea o
f a Q
ualit
y Im
prov
emen
tT
eam
from
with
in th
e cl
inic
sta
ff an
d se
lect
sta
ffto
par
ticip
ate;
• un
derg
o a
base
line
asse
ssm
ent m
easu
red
agai
nst 1
0 na
tiona
l sta
ndar
ds;
• de
velo
p an
d im
plem
ent a
ctio
n pl
an a
gree
d by
Qua
lity
Impr
ovem
ent T
eam
;•
unde
rgo
exte
rnal
ass
essm
ent a
nd r
ecei
vera
ting
as a
n ad
oles
cent
-frie
ndly
clin
ic (
ratin
gva
lid fo
r 2
year
s);
• un
derg
o re
peat
ed e
xter
nal a
sses
smen
ts a
ndra
ting
ever
y 2
year
s•
Rea
sona
bly
high
pro
port
ion
of c
linic
s pr
ogre
ssto
acc
redi
tatio
n (v
ia e
xter
nal a
sses
smen
t); b
yD
ecem
ber
2004
, 65%
of c
linic
s in
volv
ed fo
r at
leas
t 12
mon
ths
had
been
acc
redi
ted
167
92-4-120938-0_CH06_167

Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
E –
nor
ther
n S
eneg
al:
“Fro
ntie
rs s
tudy
” (2
inte
rven
tion
arm
sin
volv
ing
com
mun
ities
, clin
ics
and
scho
ols)
(25
)
• O
vera
ll ob
ject
ive:
to im
prov
e re
prod
uctiv
ehe
alth
of y
oung
peo
ple
aged
10–
19 y
ears
• H
ealth
ser
vice
obj
ectiv
es: t
o de
term
ine
the
feas
ibili
ty, c
ost a
nd e
ffect
of i
mpr
ovin
g yo
uth-
frie
ndlin
ess
of s
ervi
ces
and
the
will
ingn
ess
and
abili
ty o
f ser
vice
pro
vide
rs to
offe
r qu
ality
coun
selli
ng a
nd s
ervi
ces
to y
outh
and
on
the
num
ber
of y
outh
s us
ing
thes
e se
rvic
es; t
ode
term
ine
whe
ther
ther
e is
an
addi
tiona
lco
ntrib
utio
n fr
om a
sch
ool-b
ased
inte
rven
tion
on th
e re
prod
uctiv
e he
alth
kno
wle
dge
ofyo
uths
, the
ir at
titud
es, s
exua
l beh
avio
ur a
ndus
e of
rep
rodu
ctiv
e he
alth
ser
vice
s•
Tar
get g
roup
: ado
lesc
ents
10–
19 y
ears
• 15
-mon
th in
terv
entio
n
• T
rain
ing
of h
ealth
-car
e pr
ovid
ers
and
peer
educ
ator
s in
8 c
linic
s; fi
ve s
choo
l hea
lth n
urse
sre
ceiv
ed th
e sa
me
trai
ning
• M
odifi
catio
n of
phy
sica
l lay
out o
f clin
ics
toim
prov
e pr
ivac
y fo
r ado
lesc
ents
(wai
ting
room
sfo
r ad
oles
cent
s an
d do
ors
to fa
cilit
ate
priv
ate
adol
esce
nt a
cces
s)•
Pee
r ed
ucat
ors
cond
ucte
d cl
asse
s in
the
com
mun
ity s
imila
r to
thos
e at
the
clin
ic•
Impl
emen
tatio
n co
sts
tota
lled
abou
tU
S$
100
000
over
2 y
ears
; com
mun
ity c
osts
wer
e U
S$
40 0
00; c
linic
inte
rven
tion
cost
s w
ere
US
$ 34
000
; and
sch
ool c
osts
wer
e U
S$
26 0
00•
Mos
t exp
endi
ture
s w
ere
for
plan
ning
and
trai
ning
at b
egin
ning
of i
nter
vent
ion
F –
Ban
glad
esh:
“Fro
ntie
rs”
stud
y (2
urb
an in
terv
entio
n ar
ms
invo
lvin
g co
mbi
natio
n of
com
mun
ity, c
linic
and
scho
ol)
(26)
• O
vera
ll ob
ject
ive
: to
dete
rmin
e th
e fe
asib
ility
and
effe
ctiv
enes
s of
a s
yste
mat
ic in
terv
entio
nto
fost
er a
sup
port
ive
envi
ronm
ent t
o ad
dres
sth
e pr
oble
ms
face
d by
ado
lesc
ents
by
mak
ing
heal
th s
ervi
ces
mor
e ac
cess
ible
and
pro
vidi
nged
ucat
ion
to e
nabl
e th
em to
man
age
thei
r ow
nre
prod
uctiv
e he
alth
• H
ealth
ser
vice
s ob
ject
ives
: to
impr
ove
the
repr
oduc
tive
heal
th o
f ado
lesc
ents
by
prov
idin
g in
form
atio
n an
d ad
oles
cent
-frie
ndly
serv
ices
to o
ut-o
f-sc
hool
and
in-s
choo
lad
oles
cent
s; to
ass
ess
the
effe
ct o
f an
educ
atio
n in
terv
entio
n on
ado
lesc
ents
’re
prod
uctiv
e he
alth
kno
wle
dge,
atti
tude
s an
dbe
havi
our,
incl
udin
g ut
iliza
tion
of s
ervi
ces;
to
• H
ealth
-car
e pr
ovid
ers
trai
ned
to b
e w
elco
min
gan
d m
aint
ain
non-
judg
emen
tal a
ttitu
de; o
ffer
min
imum
wai
ting
time,
priv
acy,
con
fiden
tialit
yan
d af
ford
able
ser
vice
s•
Non
-clin
ical
sta
ff tr
aine
d in
pro
vidi
ngre
prod
uctiv
e he
alth
car
e to
ado
lesc
ents
• A
dole
scen
ts w
ho a
ttend
ed e
duca
tion
sess
ions
rece
ived
a c
ard
allo
win
g th
em to
vis
it a
doct
orfr
ee fo
r 1
year
• C
linic
sta
ff vi
site
d th
e co
mm
unity
and
sch
ools
to m
onito
r ed
ucat
ion
sess
ions
and
info
rmad
oles
cent
s ab
out s
ervi
ces
• P
eer
educ
ator
s an
d te
ache
rs r
efer
red
adol
esce
nts
to s
ervi
ces
168
92-4-120938-0_CH06_168

dete
rmin
e w
heth
er a
n ad
ditio
nal c
ontr
ibut
ion
is m
ade
from
sch
ool-b
ased
inte
rven
tion
onre
prod
uctiv
e he
alth
and
atti
tude
s an
dut
iliza
tion
of s
ervi
ces
• T
arge
t gro
up: y
outh
s 13
–19
year
s•
Dur
atio
n of
inte
rven
tion:
20
mon
ths
• 2
year
stu
dy
• S
ervi
ces
prov
ided
bas
ed o
n go
vern
men
t-de
fined
ess
entia
l pac
kage
(fa
mily
pla
nnin
g,S
TI,
teta
nus
toxo
id v
acci
natio
n, a
nten
atal
and
post
nat
al s
ervi
ces)
• In
the
com
mun
ity, i
nfor
mat
ion
was
pro
vide
dth
roug
h te
leph
one
hotli
ne a
nd q
uest
ion
and
answ
er c
olum
ns in
loca
l new
spap
er; l
ette
rbo
xes
for r
espo
ndin
g to
ado
lesc
ents
’ que
stio
nsin
stal
led
outs
ide
clin
ics
• Tot
al c
ost o
f bot
h in
terv
entio
n si
tes
$US
41
388;
site
with
sch
ool-b
ased
inte
rven
tion
twic
e as
cost
ly (m
ajor
cos
t was
trai
ning
teac
hers
); c
osts
of c
omm
unity
and
sch
ool i
nter
vent
ions
abo
utU
S$
12 0
00 e
ach;
fina
ncia
l cos
ts o
f hea
lthse
rvic
e in
terv
entio
n (U
S$
2 35
3) w
ere
low
erbe
caus
e us
ed e
xist
ing
stru
ctur
es a
nd s
taff
(alth
ough
non
-fin
anci
al c
osts
, suc
h as
tim
esp
ent b
y st
aff i
n pl
anni
ng w
ere
note
d). T
rain
ing
cost
s lo
w in
clin
ics
due
to in
volv
emen
t of
inte
rnat
iona
l age
ncy
in s
tudy
(P
opul
atio
nC
ounc
il)H
– M
ozam
biqu
e:“G
eraç
ão B
iz”
prog
ram
me
(30
clin
ics
in 6
pro
vinc
es; 8
clin
ics
in M
aput
oci
ty e
valu
ated
) (2
7)
• O
vera
ll ob
ject
ive:
to im
prov
e ad
oles
cent
sexu
al a
nd r
epro
duct
ive
heal
th s
ervi
ces,
incr
ease
gen
der
awar
enes
s, r
educ
e th
ein
cide
nce
of u
npla
nned
pre
gnan
cies
and
decr
ease
vul
nera
bilit
y to
ST
Is, H
IV a
nd u
nsaf
eab
ortio
n•
Hea
lth s
ervi
ce o
bjec
tives
: to
esta
blis
h a
netw
ork
of q
ualit
y re
prod
uctiv
e he
alth
ser
vice
s
• 3 s
peci
aliz
ed a
dole
scen
t-on
ly c
linic
s in
2 u
rban
(Map
uto)
cen
tres
(1
in h
ospi
tal,
1 in
you
thce
ntre
, 1 in
cen
tre
offe
ring
voca
tiona
l ski
lls)
• C
entr
e in
hos
pita
l pro
vide
d pr
even
tive,
clin
ical
,co
unse
lling
and
con
trac
eptio
n se
rvic
es,
incl
udin
g em
erge
ncy
cont
race
ptio
n; a
lso
prov
ides
car
e fo
r S
TIs
and
pre
nata
l and
post
nata
l car
e; o
ffers
pos
t-ab
ortio
n
169
92-4-120938-0_CH06_169

Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
and
coun
selli
ng fo
r ad
oles
cent
s w
ithin
the
publ
ic h
ealth
sys
tem
and
at a
ltern
ativ
e si
tes
• T
arge
t gro
up: y
oung
peo
ple
10–2
4 ye
ars
• A
ctiv
ities
sta
rted
in N
ovem
ber
1999
, dat
a to
2001
coun
selli
ng; o
ffers
vol
unta
ry c
ouns
ellin
g an
dte
stin
g fo
r H
IV•
Ser
vice
s fr
ee e
xcep
t ST
I tre
atm
ent
• Clin
ics
refu
rbis
hed
and
equi
pped
to m
ake
them
yout
h-fr
iend
ly a
nd to
offe
r pr
ivac
y•
Tra
inin
g cu
rric
ulum
dev
elop
ed; p
rovi
ders
trai
ned;
spe
cial
ized
per
sonn
el r
ecru
ited,
info
rmat
ion
mat
eria
ls d
evel
oped
; dev
elop
edm
anag
emen
t inf
orm
atio
n sy
stem
for
clin
ic;
cond
ucte
d pe
riodi
c te
chni
cal m
eetin
gs fo
rse
rvic
e pr
ovid
ers
to e
xcha
nge
info
rmat
ion
• P
eer
activ
ists
situ
ated
in w
aitin
g ar
eas
tow
elco
me
and
educ
ate
clie
nts
M –
Mad
agas
car:
1 pr
ovin
ce w
ith “
fran
chis
ed”
clin
ics
(12)
• O
vera
ll ob
ject
ive:
to p
reve
nt H
IV/A
IDS
and
unpl
anne
d pr
egna
ncie
s by
mot
ivat
ing
sexu
ally
activ
e yo
uth
to b
e tr
eate
d fo
r S
TIs
; to
enco
urag
e th
em to
use
con
dom
s co
nsis
tent
lyor
not
hav
e se
x•
Tar
get g
roup
: you
ths
aged
15–
24 y
ears
• R
esul
ts a
fter
18 m
onth
s of
impl
emen
tatio
n of
4-ye
ar p
rogr
amm
e
• 13
for-
prof
it an
d 2
priv
ate
non-
prof
it cl
inic
s“f
ranc
hise
d” a
s a
netw
ork
of y
outh
-frie
ndly
clin
ics;
clin
ics
mee
t min
imum
sta
ndar
dsin
clud
ing
havi
ng w
ell-t
rain
ed n
on-ju
dgem
enta
lpr
ovid
ers,
flex
ible
hou
rs, w
elco
min
g de
cor a
nddi
scre
et p
hysi
cal l
ocat
ions
; ser
vice
s ar
esu
bsid
ized
(pric
e of
US
$ 1.
45 fo
r ST
I dia
gnos
isan
d ot
her
repr
oduc
tive
heal
th s
ervi
ces)
• S
pons
orin
g te
chni
cal o
rgan
izat
ion
prov
ided
trai
ning
, sup
ervi
sion
and
sup
port
to h
ealth
wor
kers
and
mat
eria
ls; d
urat
ion
and
cont
ent o
ftr
aini
ng n
ot s
peci
fied
• C
linic
s an
d he
alth
pro
mot
ion
activ
ities
are
adve
rtis
ed th
roug
h m
ass
med
ia a
nd fa
ce-t
o-fa
ce c
omm
unic
atio
n pr
ovid
ed b
y pa
id fu
ll-tim
epe
er e
duca
tors
who
con
duct
sm
all-g
roup
and
indi
vidu
al c
ouns
ellin
g se
ssio
ns a
t div
erse
170
92-4-120938-0_CH06_170

loca
tions
and
in m
obile
uni
ts. P
eer
educ
ator
sre
ceiv
ed in
itial
trai
ning
of 4
-5 d
ays.
• S
essi
ons
held
with
par
ents
and
rel
igio
usle
ader
s to
pro
mot
e ad
oles
cent
–par
ent
dial
ogue
on
repr
oduc
tive
heal
th is
sues
• T
rain
ed a
nd c
aref
ully
sup
ervi
sed
peer
educ
ator
s fa
cilit
ated
gro
up d
iscu
ssio
ns to
hel
pyo
ung
peop
le g
ain
conf
iden
ce a
nd s
kills
tone
gotia
te s
afer
sex
; ass
esse
d w
heth
er c
linic
sw
ere
adol
esce
nt-f
riend
ly;
P –
End
o, N
iger
ia (
10)
• Ove
rall
obje
ctiv
e: to
impr
ove
trea
tmen
t of S
TIs
amon
g ad
oles
cent
s• T
arge
t gro
up: y
oung
peo
ple
aged
14–
20 y
ears
atte
ndin
g sc
hool
• T
rain
ing
give
n to
ST
I tre
atm
ent p
rovi
ders
(priv
ate
prac
titio
ners
, pat
ent m
edic
ine
deal
ers,
phar
mac
ists
iden
tifie
d by
ado
lesc
ents
as
used
by y
outh
s in
the
neig
hbou
rhoo
d fo
r S
TI
trea
tmen
t)•
90%
(45
) of
pat
ent m
edic
ine
deal
ers
iden
tifie
dby
ado
lesc
ents
par
ticip
ated
in a
nd c
ompl
eted
trai
ning
as
did
81%
(29
) of
pha
rmac
ists
and
70%
(28)
of p
rivat
e pr
actit
ione
rs; a
ll w
ere
give
nce
rtifi
cate
of p
artic
ipat
ion;
priv
ate
prac
titio
ners
wer
e lis
ted
as a
dole
scen
t-fr
iend
ly c
linic
s an
dth
e lis
t was
pro
vide
d to
pee
r ed
ucat
ors
• D
iffer
ent c
ateg
orie
s of
hea
lth-w
orke
rs w
ere
trai
ned
sepa
rate
ly (
each
for
30 h
ours
) in
ST
Idi
agno
sis
and
trea
tmen
t usi
ng W
HO
syn
drom
icm
anag
emen
t gui
delin
es; d
iffer
ent a
lgor
ithm
sus
ed fo
r ea
ch g
roup
;•
Hea
lth-w
orke
rs tr
aine
d in
adv
ance
of
impl
emen
tatio
n of
sch
ool-b
ased
inte
rven
tions
171
92-4-120938-0_CH06_171

Stu
dy,
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
• H
ealth
clu
bs s
et u
p in
eac
h sc
hool
; hea
lthpr
ofes
sion
als
prov
ided
info
rmat
ion
abou
t ST
Ipr
even
tion
and
trea
tmen
t; di
strib
uted
info
rmat
ion;
org
aniz
ed d
iscu
ssio
ns a
nd fi
lms
• 10
pee
r ed
ucat
ors
trai
ned
over
4 w
eeks
abo
utS
TIs
; pee
r ed
ucat
ors
prov
ided
cou
nsel
ling
toot
her
in-s
choo
l ado
lesc
ents
on
indi
vidu
al a
ndgr
oup
basi
s, d
urin
g sc
hool
bre
aks
and
afte
rho
urs
K –
Gha
na:
“Inn
ovat
e” p
rogr
amm
e (2
9)•
Ove
rall
obje
ctiv
e: to
incr
ease
you
ng p
eopl
e’s
know
ledg
e ab
out a
nd a
cces
s to
rep
rodu
ctiv
ean
d se
xual
hea
lth s
ervi
ces
• Tar
get g
roup
: you
ng p
eopl
e ag
ed 1
0–24
yea
rs•
Dat
a co
llect
ed o
ver
8-m
onth
per
iod
• P
lann
ed P
aren
thoo
d in
Gha
na c
reat
ed th
e“Y
oung
and
Wis
e C
entr
e”, w
hich
incl
uded
acl
inic
(pro
vidi
ng S
TI t
estin
g an
d tr
eatm
ent,
HIV
test
ing
and
coun
selli
ng, p
regn
ancy
test
ing,
post
-abo
rtio
n ca
re a
nd fa
mily
pla
nnin
g), a
libra
ry a
nd c
ompu
ter
cent
re; i
t offe
red
a ra
nge
of e
duca
tiona
l, ar
tistic
and
ent
erta
inm
ent
activ
ities
• A
mul
timed
ia “
Be
Wis
e” c
ampa
ign
to p
rom
ote
the
cent
re in
clud
ed te
levi
sion
, rad
io, p
rint a
ndel
ectr
onic
med
ia•
Clin
ic h
ad y
outh
-frie
ndly
faci
litie
s, in
clud
ing
flexi
ble
open
ing
hour
s an
d pr
ivac
y po
licie
s as
wel
l as
deco
r at
trac
tive
to y
oung
peo
ple
a S
TI =
sex
ually
tran
smitt
ed in
fect
ion.
172
92-4-120938-0_CH06_172

Tab
le 6
.4a
Des
crip
tio
n o
f o
utc
om
e ev
alu
atio
ns
by
stu
dy
for
typ
e 1
inte
rven
tio
ns
(wit
h s
ervi
ce p
rovi
der
s an
d in
th
e co
mm
un
ity)
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
s (d
ata
are
esti
mat
es f
rom
gra
ph
s) 1
995-
1999
Str
eng
th o
f ev
iden
ce
C (
16)
Des
ign:
bef
ore–
afte
r stu
dy,
serv
ice
stat
istic
s fr
om 8
trea
tmen
t and
2 c
ontr
olcl
inic
s
Qu
arte
rly
nu
mb
er o
f fa
mily
pla
nn
ing
clie
nts
ag
ed 1
5–24
yea
rs
Inte
rven
tion
and
cont
rol
grou
ps (
No.
clin
ics)
Bas
elin
e(f
irst q
uart
er19
95)
Qua
rter
inte
rven
tion
star
ted
End
(th
irdqu
arte
r19
99)
Tim
e be
twee
nin
terv
entio
nan
d en
d
1 (2
)25
025
010
0021
mon
ths
2 (3
)0
5050
15 m
onth
s
3 (3
)25
017
5034
0015
mon
ths
Con
trol
(2)
250
–12
50–
Qu
arte
rly
nu
mb
er o
f cl
ien
ts f
or
ST
I ser
vice
s ag
ed 1
5–24
yea
rs
Inte
rven
tion
and
cont
rol
grou
ps (
No.
clin
ics)
Bas
elin
e(f
irst q
uart
er19
95)
Qua
rter
inte
rven
tion
star
ted
End
(th
irdqu
arte
r19
99)
Tim
e be
twee
nin
terv
entio
nan
d en
d
1 (2
)22
5050
040
0021
mon
ths
2 (3
)55
055
060
015
mon
ths
3 (3
)95
050
020
0015
mon
ths
Con
trol
(2)
400
–16
00–
Incr
ease
in u
se o
f ser
vice
s bu
tno
sta
tistic
al te
sts
perf
orm
edto
sho
w s
igni
fican
ce in
com
paris
on w
ith c
ontr
olcl
inic
s; d
ata
do n
ot in
dica
tesu
bsta
ntia
l or
cons
iste
ntdi
ffere
nces
in in
crea
se in
utili
zatio
n be
twee
nin
terv
entio
n an
d co
ntro
lcl
inic
s
Lim
itatio
ns: N
o st
atis
tical
test
s ca
rrie
d ou
t
Not
e: D
ata
colle
ctio
n al
soin
clud
ed c
lient
exi
t sur
veys
,fo
cus
grou
p di
scus
sion
s, in
-de
pth
inte
rvie
ws
prov
idin
gda
ta o
n re
latio
nshi
p be
twee
nse
rvic
e ut
iliza
tion,
com
mun
ityac
cept
ance
and
you
th-
frie
ndlin
ess
of c
linic
s
Wea
k ev
iden
ce o
f no
incr
ease
d us
e re
late
d to
the
inte
rven
tion
173
92-4-120938-0_CH06_173

Tab
le 6
.4b
Des
crip
tio
n o
f ou
tco
me
eval
uat
ion
s b
y st
ud
y fo
r typ
e 2
inte
rven
tio
ns
(act
ion
s in
the
clin
ic, w
ith
ser
vice
pro
vid
ers
and
in th
eco
mm
un
ity)
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
L (1
7)D
esig
n: q
uasi
-exp
erim
enta
l with
non-
equi
vale
nt c
ontr
ol g
roup
;kn
owle
dge–
attit
ude–
prac
tice
surv
eyof
ado
lesc
ents
(n=
128
) and
hea
lth-
wor
kers
(n
= 4
2) in
4 in
terv
entio
ncl
inic
s an
d 4
cont
rol c
linic
s; d
ata
colle
ctio
n al
so in
clud
ed s
ervi
cest
atis
tics,
focu
s gr
oup
disc
ussi
ons,
in-d
epth
inte
rvie
ws
Kno
wle
dge
• A
dole
scen
ts in
the
inte
rven
tion
site
s “h
ad in
crea
sed
know
ledg
e of
ado
lesc
ent h
ealth
pro
blem
s, p
redi
spos
ing
fact
ors,
fam
ily p
lann
ing,
HIV
and
ST
Is …
all
with
P<
0.0
001.
”(17
)%
ado
lesc
ents
usi
ng h
ealth
ser
vice
s ov
er 1
2 m
onth
s•
Out
patie
nt s
ervi
ces:
inte
rven
tion
grou
p= 4
9.3%
, con
trol
grou
p =
13.
1%, P
= 0
.000
1•
Fam
ily p
lann
ing
serv
ices
: int
erve
ntio
n gr
oup
= 6
9.4%
,co
ntro
l gro
up =
21.
1%, P
= 0
.000
1•
ST
Ia ser
vice
s: in
terv
entio
n gr
oup
= 6
5.5%
, con
trol
gro
up =
31.9
%, P
= 0
.000
1•
Labo
rato
ry s
ervi
ces:
inte
rven
tion
grou
p =
49.
8%, c
ontr
olgr
oup
= 4
.4%
, P=
0.0
001
Beh
avio
ur•
Cur
rent
ly u
sing
fam
ily p
lann
ing:
inte
rven
tion
grou
p =
65.6
%, c
ontr
ol g
roup
= 4
6.9%
, P=
0.0
06•
Eve
r us
ed fa
mily
pla
nnin
g : i
nter
vent
ion
grou
p =
68.
8%,
cont
rol g
roup
= 5
3.1%
, P=
0.0
20
Sta
tistic
ally
sig
nific
ant d
iffer
ence
s in
utili
zatio
n of
ser
vice
s am
ong
inte
rven
tion
and
cont
rol s
ites;
but
ther
e w
as a
non
-equ
ival
ent c
ontr
olgr
oup
and
aspe
cts
of s
tudy
des
ign
are
uncl
ear
Lim
itatio
ns: s
tatis
tical
ana
lysi
s do
esno
t tak
e ac
coun
t of c
lust
erin
g; n
ose
rvic
e st
atis
tics
on n
umbe
rs u
sing
heal
th u
nits
(on
ly “
prop
ortio
n of
adol
esce
nts
seek
ing
heal
thse
rvic
es”)
Wea
k ev
iden
ce fo
r in
crea
sed
use
ofse
rvic
es r
elat
ed to
the
inte
rven
tion
I (19
)D
esig
n: q
uasi
-exp
erim
enta
l(b
efor
e–af
ter)
with
1 in
terv
entio
nan
d 1
cont
rol c
omm
unity
Sam
ple
size
: int
erve
ntio
n gr
oup
=12
20, c
ontr
ol g
roup
= 1
007
unm
arrie
d yo
uths
(ag
ed 1
5– 2
4ye
ars)
Incr
ease
d “e
ver
cont
race
ptiv
e us
e”, “
regu
lar
cont
race
ptiv
eus
e” a
nd “
cond
om u
se”
at in
terv
entio
n si
tes,
P<
.001
Am
ong
thos
e w
ho b
ecam
e se
xual
ly a
ctiv
e du
ring
the
stud
ype
riod,
ther
e w
as in
crea
sed
use
of c
ontr
acep
tives
(P<
0.0
001)
and
incr
ease
d co
ndom
use
as
cont
race
ptiv
eof
cho
ice
(P<
0.0
5)
Use
d re
port
ed c
ondo
m u
se a
s a
prox
y fo
r se
rvic
e ut
iliza
tion;
stat
istic
ally
sig
nific
ant i
ncre
ase
inus
e of
ser
vice
s in
inte
rven
tion
site
s
Lim
itatio
ns: n
o ov
eral
l dat
a on
serv
ice
utili
zatio
n on
ly o
n re
port
ed
174
92-4-120938-0_CH06_174

Logi
stic
reg
ress
ion
anal
ysis
and
gen
eral
ized
est
imat
ing
equa
tions
ana
lysi
s of
dat
a fr
om s
exua
lly a
ctiv
e yo
ung
peop
le (n
= 6
44) i
ndic
ated
that
exp
osur
e to
the
inte
rven
tion
was
the
mos
t pow
erfu
l cor
rela
te o
f con
dom
use
(od
ds r
atio
= 1
4.54
, 95%
con
fiden
ce in
terv
al =
6.3
5–33
.30,
P>
0.0
001)
beha
viou
rs (
cond
om u
se)
that
cou
ldre
sult
from
ser
vice
util
izat
ion
Not
e: d
ata
also
ava
ilabl
e on
obst
acle
s to
con
trac
eptiv
e us
e an
d“jo
int d
ecis
ion
with
par
tner
”
Mod
erat
e ev
iden
ce fo
r inc
reas
ed u
seof
ser
vice
sN
(12
)D
esig
n: c
ross
-sec
tiona
l sur
vey
ofyo
uths
afte
r 18
mon
ths
ofin
terv
entio
n, w
ith s
ervi
ce u
seco
mpa
red
by le
vel o
f exp
osur
e to
inte
rven
tion;
200
2 ho
useh
old
surv
ey
Sur
vey
sam
ple
size
: 310
9un
mar
ried
youn
g pe
ople
age
d15
–24
year
s
Dat
a no
t pre
sent
ed o
n pr
e-ex
posu
re v
s po
st-e
xpos
ure
Dos
e–re
spon
se a
naly
sis
of:
Kno
wle
dge
• B
elie
f in
effe
ctiv
enes
s of
con
dom
s: m
ales
with
low
expo
sure
73%
, mal
es w
ith h
igh
expo
sure
92%
; fem
ales
with
low
exp
osur
e 64
%, f
emal
es w
ith h
igh
expo
sure
81%
Ski
lls•
Cor
rect
con
dom
use
: mal
es w
ith lo
w e
xpos
ure
17%
,m
ales
, with
hig
h ex
posu
re 3
0%•
Con
fiden
ce to
buy
con
dom
s: fe
mal
es w
ith lo
w e
xpos
ure
21%
, fem
ales
with
hig
h ex
posu
re 4
4%S
ervi
ces
• U
se o
f ser
vice
(H
IV te
st):
mal
es w
ith lo
w e
xpos
ure
2%,
mal
es w
ith h
igh
expo
sure
9%
; fem
ales
with
low
exp
osur
e2%
, fem
ales
with
hig
h ex
posu
re 7
%A
ll di
ffere
nces
sig
nific
ant a
t P<
0.0
5
Dat
a sh
ow s
tatis
tical
ly s
igni
fican
thi
gher
util
izat
ion
with
incr
ease
dex
posu
re to
the
inte
rven
tions
No
data
on
over
all u
tiliz
atio
n of
serv
ices
by
youn
g pe
ople
.
Lim
itatio
ns: P
re-in
terv
entio
n da
ta n
otpr
esen
ted;
no
over
all d
ata
pres
ente
dfo
r se
rvic
e ut
iliza
tion
Wea
k ev
iden
ce fo
r in
crea
sed
use
ofse
rvic
es in
thos
e w
ith h
igh
expo
sure
to th
e in
terv
entio
ns v
s. th
ose
with
low
expo
sure
O (
18)
Des
ign:
rev
iew
of c
linic
dat
a ov
er 1
year
afte
r the
sta
rt o
f the
inte
rven
tion
Man
y yo
uths
indi
cate
d th
at th
ey h
ad u
sed
the
You
th C
entr
e,bu
t onl
y 0.
2% o
f the
m s
aid
that
this
was
for
repr
oduc
tive
heal
th s
ervi
ces
A n
ew s
ervi
ce w
as p
rovi
ded
and
itw
as u
sed
by y
oung
peo
ple,
alth
ough
175
92-4-120938-0_CH06_175

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
A h
isto
gram
in th
e re
port
pro
vide
s th
e fo
llow
ing
data
on
the
num
ber
of c
lient
s w
ho u
sed
the
serv
ices
of 4
rep
rodu
ctiv
ehe
alth
clin
ics
(est
imat
ed fr
om h
isto
gram
)
Tim
eA
nten
atal
serv
ices
use
dby
fem
ales
aged
12–
18ye
ars
ST
I clin
icus
ed b
ym
ales
age
d12
–24
year
s
ST
I clin
icus
ed b
yfe
mal
es a
ged
12–2
4 ye
ars
4th
quar
ter
1998
02
3
1st q
uart
er19
9910
514
020
2
2nd
quar
ter
1999
6510
213
0
3rd
quar
ter
1999
5060
70
incr
ease
d ut
iliza
tion
decl
ined
in 2
ndan
d 3r
d qu
arte
rs o
f fol
low
up
Lim
itatio
ns: n
o co
mpa
rison
or c
ontr
olcl
inic
s; n
o st
atis
tical
test
s; n
ode
nom
inat
ors
Not
e: d
ata
also
ava
ilabl
e on
the
type
sof
ser
vice
s us
ed b
y yo
ung
peop
lean
d on
ris
k an
d pr
otec
tive
fact
ors,
know
ledg
e an
d be
havi
ours
from
abe
fore
and
afte
r st
udy
that
did
not
incl
ude
data
on
serv
ice
utili
zatio
n
Wea
k ev
iden
ce o
f inc
reas
ed u
se o
fse
rvic
es
a S
TI =
sex
ually
tran
smitt
ed in
fect
ion.
176
92-4-120938-0_CH06_176

Tab
le 6
.4c
Des
crip
tio
n o
f o
utc
om
e ev
alu
atio
ns
by
stu
dy
for
typ
e 3
inte
rven
tio
ns
(wit
h s
ervi
ce p
rovi
der
s an
d in
volv
emen
t o
f o
ther
sec
tors
)
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
J –
(20)
Des
ign:
qua
si-e
xper
imen
tal w
ith c
ontr
olgr
oup
of s
choo
ls a
nd c
linic
s in
the
sam
ear
ea; 3
rou
nds
of k
now
ledg
e–at
titud
es–
prac
tice
surv
eys
in in
terv
entio
n sc
hool
san
d 2
in c
ontr
ol s
choo
ls; s
ervi
ce s
tatis
tics
from
inte
rven
tion
and
cont
rol c
linic
s
Ave
rage
ann
ual n
umbe
r of
new
ado
lesc
ent
cont
race
ptiv
e us
ers
(all
met
hods
) at
6in
terv
entio
n cl
inic
s•
1997
(be
ginn
ing
of p
roje
ct):
390
• 19
99 (
end
of p
roje
ct):
500
Ave
rage
ann
ual n
umbe
r of
new
ado
lesc
ent
cont
race
ptiv
e us
ers
(all
met
hods
) at
258
cont
rol c
linic
s•
1997
(be
ginn
ing
of p
roje
ct):
110
• 19
99 (
end
of p
roje
ct):
200
No.
(%
) of
stu
dent
s re
ceiv
ing
info
rmat
ion
from
hea
lth-w
orke
r at
end
of p
roje
ct•
Mal
es: p
roje
ct s
choo
l – 5
88 (
13.7
%),
cont
rol s
choo
l – 6
86 (
10.1
%),
P<
0.0
5•
Fem
ales
: pro
ject
sch
ool –
104
8 (1
5.3%
),co
ntro
l sch
ool –
119
8 (1
2.5%
), P
< 0
.05
Ser
vice
sta
tistic
s in
dica
te n
o di
ffere
nce
amon
g in
terv
entio
n an
d co
ntro
l site
s, b
utno
sta
tistic
al te
sts
perf
orm
ed
Lim
itatio
ns: a
ll da
ta p
rovi
ded
as g
raph
s; n
ost
atis
tical
test
s fo
r se
rvic
e ut
iliza
tion
data
Not
e: d
ata
also
ava
ilabl
e on
qua
lity
stan
dard
s in
clud
ing
surv
ey o
f ser
vice
prov
ider
s (n
= 2
0, 1
00%
of p
rovi
ders
) an
dad
oles
cent
clie
nts
(n=
385
, 89%
of c
lient
s)in
4 r
efer
ence
clin
ics
(in S
alva
dor)
toas
sess
qua
lity
stan
dard
s
Wea
k ev
iden
ce o
f no
incr
ease
d us
e re
late
dto
the
inte
rven
tion
Wea
k ev
iden
ce o
f inc
reas
ed a
cces
s to
info
rmat
ion
rela
ted
to th
e in
terv
entio
n
177
92-4-120938-0_CH06_177

Tab
le 6
.4d
Des
crip
tio
n o
f o
utc
om
e ev
alu
atio
ns
by
stu
dy
for
typ
e 5
inte
rven
tio
ns
(wit
h s
ervi
ce p
rovi
der
s, in
th
e co
mm
un
ity
and
invo
lvin
g o
ther
sect
ors
)
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
D (
21)
Des
ign:
qua
si-e
xper
imen
tal b
efor
e–af
ter
stud
y w
ith c
ontr
ol g
roup
; com
mun
itysu
rvey
s of
mal
es a
nd fe
mal
es a
ged
10–2
4ye
ars
in in
terv
entio
n ar
ea a
nd 2
con
trol
com
mun
ities
Sam
ple
size
: 3 m
onth
pre
-inte
rven
tion
surv
ey =
142
6;1
year
pos
t-in
terv
entio
n =
140
0.
At e
nd-o
f-st
udy
surv
ey•
28.2
% o
f res
pond
ents
at i
nter
vent
ion
site
sre
port
ed to
hav
e so
ught
ser
vice
s at
hea
lthce
ntre
• 9.
5% o
f res
pond
ents
at c
ontr
ol s
ites
repo
rted
to h
ave
soug
ht s
ervi
ces
at h
ealth
cent
re•
OR
a =
4.7
, P<
0.0
01
Use
of m
oder
n co
ntra
cept
ives
incr
ease
d in
inte
rven
tion
site
s•
Inte
rven
tion
grou
p =
56%
at b
asel
ine,
67%
at e
nd o
f stu
dy, O
R =
1.7
, P<
0.0
5•
No
data
for
cont
rol s
ites
Res
pond
ents
at i
nter
vent
ion
vsco
ntro
l site
s•
Res
pond
ents
at i
nter
vent
ion
site
s m
ore
likel
y to
“st
ick
to o
ne p
artn
er”
than
thos
e in
cont
rol s
ites
(OR
= 2
6.1,
P<
0.0
01)
• R
espo
nden
ts a
t int
erve
ntio
n si
tes
likel
y to
star
t to
use
cond
oms
(OR
= 5
.7,
P =
0.0
5)•
Res
pond
ents
at i
nter
vent
ion
site
s m
ore
likel
y to
hav
e “s
aid
no to
sex
” (O
R =
2.5
,P
= 0
.000
1).
Sta
tistic
ally
sig
nific
ant d
iffer
ence
in in
crea
sein
ser
vice
util
izat
ion
in in
terv
entio
n si
tes
rela
tive
to c
ontr
ol s
ites
(how
ever
ther
e w
asco
ntam
inat
ion
of c
ontr
ol s
ites)
; sta
tistic
ally
sign
ifica
nt in
crea
se in
con
trac
eptiv
e us
e at
inte
rven
tion
site
s at
end
-of-
stud
y su
rvey
rela
tive
to b
asel
ine
surv
ey
Lim
itatio
ns: c
onta
min
atio
n at
con
trol
site
s;m
ajor
inte
rven
tion
in th
e st
udy
was
a m
edia
inte
rven
tion;
no
data
from
ser
vice
sta
tistic
spr
ovid
ed; n
o ba
selin
e da
ta fo
r se
rvic
e us
e;no
acc
ount
take
n of
clu
ster
ing
in s
tatis
tical
anal
ysis
Wea
k ev
iden
ce fo
r inc
reas
ed u
se o
f ser
vice
s
178
92-4-120938-0_CH06_178

G (
22)
Des
ign:
com
mun
ity-r
ando
miz
ed c
ontr
olle
dtr
ial w
ith fo
llow
-up
of a
coh
ort o
f 12–
24-
year
-old
s ov
er 3
yea
rs; d
ata
from
com
mun
ity s
urve
ys
Sur
vey
sam
ple
size
: Int
erve
ntio
n ar
ea –
10
com
mun
ities
(m
ales
= 2
076,
fem
ales
=14
48);
con
trol
are
a =
10
com
mun
ities
(mal
es =
202
4, fe
mal
es =
149
2)
Pro
port
ion
who
rep
orte
d go
ing
to a
hea
lthfa
cilit
y fo
r m
ost r
ecen
t ST
I sym
ptom
s w
ithin
the
last
12
mon
ths
• A
djus
ted
OR
(95
% c
onfid
ence
inte
rval
) fo
rin
terv
entio
n vs
cont
rol f
or m
ales
= 0
.84
(0.5
0–1.
41),
for
fem
ales
= 1
.02
(0.6
2–1.
70)
Pro
port
ion
who
rep
orte
d us
ing
cond
oms
atla
st s
exua
l int
erco
urse
• A
djus
ted
OR
(95
% c
onfid
ence
inte
rval
) fo
rin
terv
entio
n vs
cont
rol f
or m
ales
= 1
.47
(1.1
2–1.
93),
for
fem
ales
= 1
.12
(0.8
5–1.
48)
No
stat
istic
ally
sig
nific
ant i
ncre
ase
inre
port
ed u
se o
f ser
vice
s
Sta
tistic
ally
sig
nific
ant i
ncre
ase
in c
ondo
mus
e on
ly a
mon
g m
ales
but
like
ly to
be
mai
nly
due
to o
ther
com
pone
nts
of th
e in
terv
entio
n,su
ch a
s yo
uth
cond
om p
rom
oter
s an
ddi
strib
utio
n in
com
mun
ities
as
wel
l as
scho
ol-b
ased
inte
rven
tion.
Lim
itatio
ns: b
ased
on
repo
rted
util
izat
ion;
data
on
serv
ice
stat
istic
s no
t yet
pub
lishe
d
Mod
erat
e ev
iden
ce o
f no
effe
ct o
n se
rvic
eut
iliza
tion
a O
R =
odd
s ra
tio.
179
92-4-120938-0_CH06_179

Tab
le 6
.4e
Des
crip
tio
n o
f o
utc
om
e ev
alu
atio
ns
by
stu
dy
for
typ
e 6
inte
rven
tio
ns
(wit
h s
ervi
ce p
rovi
der
s, in
th
e co
mm
un
ity
and
invo
lvin
g o
ther
sect
ors
)
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
A (
23)
Des
ign:
qua
si-e
xper
imen
tal
desi
gn w
ith c
ompa
rison
of
serv
ice
utili
zatio
n da
ta in
inte
rven
tion
site
s (n
= 5
1,32
urb
an, 1
9 ru
ral)
and
con-
trol
site
s (n
= 2
8, 1
9 ur
ban,
9 ru
ral)
New
vis
itsin
terv
entio
n gr
oup
New
vis
itsco
ntro
l gro
upR
atio
inte
rven
tion:
cont
rol
Fol
low
-up
visi
tsin
terv
entio
n gr
oup
Fol
low
-up
visi
tsco
ntro
l gro
upR
atio
inte
rven
tion:
cont
rol
Tot
al v
isits
inte
rven
tion
grou
pT
otal
vis
itsco
ntro
l gro
upR
atio
inte
rven
tion:
cont
rol
Mal
es
430
296
1.5
P<
0.0
5
257
180
1.4
P<
0.0
5
617
384
1.6
P<
0.0
5
Fem
ales
577
299
1.9
P<
0.0
5
303
206
1.5
P<
0.0
5
770
420
1.8
P<
0.0
5
Tot
al
1007
595
1.7
560
386
1.5
1387
804
1.7
Sta
tistic
ally
sig
nific
antly
gre
ater
use
of s
ervi
ces
Alth
ough
Pva
lues
< 0
.05
thro
ugho
ut,
resu
lts a
re n
ot s
tand
ardi
zed
for
diffe
renc
es in
cat
chm
ent p
opul
atio
ns
Lim
itatio
ns: n
umbe
r of
atte
ndan
ces
com
pare
d am
ong
inte
rven
tion
and
cont
rol s
ites
with
no
atte
mpt
tost
anda
rdiz
e fo
r di
ffere
nces
in n
umbe
rof
ado
lesc
ents
in c
atch
men
t are
as,
desp
ite d
ata
indi
catin
g th
atad
oles
cent
pop
ulat
ion
was
1.4
tim
esgr
eate
r in
inte
rven
tion
area
s th
an in
cont
rol a
reas
; no
pre-
inte
rven
tion
data
pro
vide
d; ti
me-
serie
s in
inte
rven
tion
clin
ics
only
Wea
k ev
iden
ce fo
r sm
all i
ncre
ase
inut
iliza
tion
of s
ervi
ces
rela
tive
to th
ein
terv
entio
n
180
92-4-120938-0_CH06_180

B (
24)
Des
ign:
rev
iew
of c
linic
utili
zatio
n by
10–
19 y
ear
olds
in 3
2 cl
inic
s ta
king
par
tin
nat
iona
l pro
gram
me,
2002
–200
4A
vera
ge m
onth
ly c
linic
atte
ndan
ce20
0220
04
ST
Ia tr
eatm
ent v
isits
2002
2004
Vol
unta
ry c
ouns
ellin
g an
d te
stin
g20
0220
04
Pre
gnan
cy-r
elat
ed v
isits
2002
2004
Vis
its fo
r co
ntra
cept
ion
2002
2004
Tot
al
340
420
P<
0.0
5
30 48 P>
0.0
5
23 52 P<
0.0
01
48 54 P>
0.0
5
237
264
P>
0.0
5
Sta
tistic
ally
sig
nific
ant i
ncre
ase
inov
eral
l util
izat
ion
of s
ervi
ces
and
volu
ntar
y co
unse
lling
and
test
ing
serv
ices
(tim
e-se
ries
anal
ysis
),al
thou
gh th
e st
udy
lack
s co
ntro
l gro
up
Lim
itatio
ns: n
o da
ta p
rovi
ded
from
cont
rol c
linic
s
Not
e: d
ata
also
ava
ilabl
e on
qua
lity
ofse
rvic
es a
nd im
pact
on
info
rmat
ion,
skill
s an
d H
IV p
reva
lenc
e bu
t the
selik
ely
to b
e m
ainl
y re
late
d to
oth
erco
mpo
nent
s of
the
inte
rven
tion
Wea
k ev
iden
ce fo
r in
crea
sed
use
ofse
rvic
es r
elat
ed to
inte
rven
tion
181
92-4-120938-0_CH06_181

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
E (
25)
Des
ign:
qua
si-e
xper
imen
tal
pre-
test
and
pos
t-te
stde
sign
ass
essi
ng 2
diff
eren
tin
terv
entio
ns (s
ites
A a
nd B
)an
d a
cont
rol s
ite (
site
C)
thro
ugh
com
mun
ity s
urve
ys
Inte
rven
tion
site
AB
efor
eA
fter
Inte
rven
tion
site
BB
efor
eA
fter
Con
trol
site
CB
efor
eA
fter
Ado
lesc
ents
in in
terv
entio
n si
tes
mor
e fa
mili
ar w
ith th
e ex
iste
nce
ofse
rvic
es, a
nd m
ore
likel
y to
use
ser
vice
s•
Exp
osed
site
A:
• U
nexp
osed
site
A:
• E
xpos
ed s
ite B
:•
Une
xpos
ed s
iteB
:Boy
s10
–14
1% 7% (P<
0.0
5)
2% 9% (P<
0.0
5)
0 10%
(P<
0.0
5)
Boy
s15
–19
6% 7% 8% 13%
(P<
0.0
5)
9% 12%
(P<
0.0
5)
Girl
s10
–14
1% 7% (P<
0.0
5)
1% 4% 0 15%
(P<
0.0
5)
13%
7% 12%
5%
Girl
s15
–19
8% 18%
(P<
0.0
5)
12%
14%
8% 20%
(P<
0.0
5)
Sig
nific
ant i
ncre
ases
in r
epor
ted
use
of s
ervi
ces,
but
no
diffe
renc
es a
mon
gco
ntro
l and
inte
rven
tion
site
s(in
crea
ses
mos
t mar
ked
at c
ontr
olsi
tes)
; con
trol
site
con
tam
inat
ed
Lim
itatio
ns: p
oten
tial c
onta
min
atio
n of
cont
rol s
ite b
ecau
se o
fim
plem
enta
tion
of m
edia
inte
rven
tions
Not
e: d
ata
also
ava
ilabl
e on
know
ledg
e of
con
trac
eptiv
e m
etho
dsan
d kn
owle
dge
of a
vaila
bilit
y of
serv
ices
Wea
k ev
iden
ce o
f no
incr
ease
in u
seof
ser
vice
s as
a r
esul
t of t
hein
terv
entio
ns
F (
26)
Des
ign:
qua
si-e
xper
imen
tal
befo
re–a
fter
desi
gn b
ased
on c
olle
ctio
n of
ser
vice
stat
istic
s at
two
inte
rven
tion
site
s (A
and
B) a
nd a
con
trol
site
(C
)
Use
of s
ervi
ces
durin
g 6
mon
ths
Inte
rven
tion
site
AIn
terv
entio
n si
te B
Con
trol
site
C
Bef
ore
inte
rven
tion
135
84 271
Afte
rin
terv
entio
n
444
1216
232
Odd
s ra
tioIn
crea
se in
use
of s
ervi
ces
atin
terv
entio
n si
tes;
gre
ater
incr
ease
at
site
s th
at in
clud
ed a
n in
-sch
ool
com
pone
nt, a
lthou
gh n
o P
valu
esav
aila
ble
182
92-4-120938-0_CH06_182

Use
of s
ervi
ces
incr
ease
d in
the
inte
rven
tion
site
s•
Rat
io A
:C =
2:1
• R
atio
B:C
= 1
0:1
• R
atio
B:A
= 6
:1U
se o
f con
dom
at l
ast s
exua
l int
erco
urse
am
ong
unm
arrie
d m
ales
Inte
rven
tion
site
AIn
terv
entio
n si
te B
Con
trol
site
C
2.31
(P
< 0
. 1)
2.41
(P<
0. 1
)2.
0 (N
S)
No
incr
ease
in c
ondo
m u
se a
mon
gun
mar
ried
mal
es a
mon
g in
terv
entio
nan
d co
ntro
l site
s
Lim
itatio
ns: p
opul
atio
n-ba
sed
surv
eys
carr
ied
out i
n ca
tchm
ent
popu
latio
n bu
t did
not
incl
ude
info
rmat
ion
abou
t use
of s
ervi
ces
only
attit
udes
tow
ards
ser
vice
s; h
owev
erin
form
atio
n on
con
dom
use
obt
aine
d
Not
e: d
ata
also
ava
ilabl
e ab
out t
ypes
of s
ervi
ces
used
Wea
k ev
iden
ce o
f inc
reas
ed u
se o
fse
rvic
es r
elat
ed to
the
inte
rven
tion
M (
12)
Des
ign:
qua
si-e
xper
imen
tal
befo
re–a
fter
stud
y of
clin
icat
tend
ance
rec
ords
for
yout
hs a
ged
15–2
4 ov
er24
-mon
th in
terv
entio
npe
riod
in 1
5 cl
inic
s
• N
o. a
ttend
ing
clin
ic J
anua
ry–M
arch
200
1 =
138
mal
es, 3
89 fe
mal
es•
No.
atte
ndin
g O
ctob
er–D
ecem
ber
2002
= 2
50 m
ales
, 195
9 fe
mal
esS
ervi
ce s
tatis
tics
indi
cate
d in
crea
sed
utili
zatio
n by
mal
es a
nd fe
mal
es
Lim
itatio
ns: n
o co
ntro
l clin
ics;
no
stat
istic
al te
sts
Wea
k ev
iden
ce o
f inc
reas
ed u
se o
fse
rvic
esH
(27
)D
esig
n: b
efor
e–af
ter
com
paris
on o
f clin
icat
tend
ance
by
“you
ths”
ove
r3
year
s (1
999–
2002
);in
terv
entio
n be
gan
in 2
000
Tot
al a
ttend
ance
at t
he 8
inte
rven
tion
clin
ics
• 19
99 =
1 1
73•
2000
= 1
1 72
6•
2001
= 1
8 80
9
Ser
vice
dat
a in
dica
te in
crea
sed
use
by y
outh
Lim
itatio
ns: n
o co
ntro
l gro
up; n
ost
atis
tical
test
s; n
o de
nom
inat
ors;
only
par
tial d
ata
repo
rted
183
92-4-120938-0_CH06_183

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
Wea
k ev
iden
ce o
f inc
reas
edut
iliza
tion
of s
ervi
ces
Pro
port
ion
usin
gpr
ovid
erC
hang
efr
om p
re-
inte
rven
tion
to p
ost-
inte
rven
tion
Cha
nge
rela
tive
toco
ntro
l
P (
10)
Des
ign:
ran
dom
ized
cont
rolle
d tr
ial w
ith S
TI
trea
tmen
t pro
vide
rs c
lose
tosc
hool
s ra
ndom
ly a
lloca
ted
to in
terv
entio
n si
tes
(4sc
hool
s) a
nd 2
con
trol
site
s(4
sch
ools
eac
h); s
urve
ys in
the
scho
ols
befo
re a
nd a
fter
the
inte
rven
tions
Pro
port
ion
seek
ing
trea
tmen
tfr
om a
priv
ate
prov
ider
for
ST
Is
Inte
rven
tion
Con
trol
1
Con
trol
2
Rep
orte
d co
ndom
use
by m
ales
Inte
rven
tion
Con
trol
1
Bef
ore
17.5
%
19.0
%
24.0
%
Som
eco
ndom
use
30.8
%
32.1
%
Afte
r
40.7
%
29.1
%
30.4
%
Som
eco
ndom
use
40.5
%
36.1
%
OR
(95
%C
I)b
3.24
(1.8
4–5.
73)
1.75
(1.5
1–2.
03)
1.38
(0.7
5–2.
56)
1.5
(1.3
8–1.
69)
1.2
(1.0
7–1.
33)
OR
(95
%C
I)
… – 1.85
(1.0
6-3.
22)
2.35
(1.0
3-5.
17)
– 1.32
(0.9
7–1.
79)
Sta
tistic
ally
sig
nific
ant i
ncre
ase
and
diffe
renc
e am
ong
inte
rven
tion
and
cont
rol s
ites
in te
rms
of u
se o
fse
rvic
es fo
r bo
th m
ales
and
fem
ales
;fo
r fem
ales
am
ong
prox
y in
dica
tors
of
use
of s
ervi
ces
(con
dom
use
and
ST
Isy
mpt
om p
reva
lenc
e)
Lim
itatio
ns: s
tatis
tical
ana
lysi
s di
d no
tta
ke a
ccou
nt o
f clu
ster
ing
Not
e: d
ata
also
ava
ilabl
e on
know
ledg
e an
d sk
ills,
rep
orte
dsy
mpt
oms
of S
TI,
notif
icat
ion
ofpa
rtne
rs
Str
ong
evid
ence
of i
ncre
ased
use
of
serv
ices
184
92-4-120938-0_CH06_184

Con
trol
2R
epor
ted
cond
omus
e by
fem
ales
Inte
rven
tion
Con
trol
1
Con
trol
2
26.6
%
30.2
%
32.6
%
29.2
%
34.3
%
36.5
%
31.8
%
25.4
%
1.4
(1.0
9–2.
32)
1.3
(1.0
5–1.
72)
0.9
(0.7
8–1.
19)
0.8
(0.4
4–1.
59)
1.08
(0.6
0–1.
46)
– 1.82
(1.2
8–2.
60)
1.96
(0.9
4–4.
10)
K (
29)
Des
ign:
rev
iew
of c
linic
stat
istic
s ov
er 8
-mon
thpe
riod
afte
r in
trod
uctio
n of
yout
h ce
ntre
Man
y yo
ung
peop
le v
isite
d th
e ce
ntre
(re
port
ed a
ttend
ance
Jan
uary
=10
05, F
ebru
ary
= 2
685,
Mar
ch =
281
6, A
pril
= 2
993,
May
= 4
494,
Jun
e =
4379
, Jul
y =
253
4, A
ugus
t = 4
809)
but
onl
y 3.
3% o
f tho
se v
isiti
ng th
ece
ntre
use
d ei
ther
the
clin
ic o
r th
e co
unse
lling
ser
vice
s
Dur
ing
first
8 m
onth
s of
ope
ratio
n, th
e ce
ntre
pro
vide
d 18
995
mal
e an
d2
337
fem
ale
cond
oms;
ser
ved
2,64
6 cl
inic
clie
nts;
and
cou
nsel
led
102
yout
hs, w
ith a
n ad
ditio
nal 6
00–8
00 c
ouns
elle
d by
pho
ne. U
ncle
ar w
here
thes
e st
atis
tics
have
bee
n ob
tain
ed fr
om, a
nd th
ey d
o no
t cor
resp
ond
with
the
stat
istic
s in
the
eval
uatio
n. C
ondo
ms
and
coun
selli
ng p
rovi
ded
by o
ther
del
iver
y po
ints
in th
e ce
ntre
in a
dditi
on to
the
clin
ic
Diff
icul
t to
asse
ss tr
ends
ove
r th
e 8
mon
ths
beca
use
data
pre
sent
edso
met
imes
mon
thly
and
som
etim
es 3
-mon
thly
. No
obvi
ous
tren
ds in
num
bers
atte
ndin
g ce
ntre
as
a w
hole
. The
rep
ort s
tate
s: “
the
serv
ice
stat
istic
s in
dica
te th
e nu
mbe
r of
peo
ple
usin
g th
e cl
inic
ove
rall
has
incr
ease
d bu
t act
ual u
se o
f the
clin
ical
ser
vice
s av
aila
ble
is s
till l
imite
d”.
An
exam
ple
of s
tudy
that
look
s at
“a
serv
ice
was
pro
vide
d an
d so
me
youn
g pe
ople
use
d it”
Lim
itatio
ns: n
o co
ntro
l clin
ics;
it w
as a
new
cen
tre
so n
o be
fore
–afte
rst
atis
tics;
not
cle
ar h
ow m
any
clie
nts
wou
ld h
ave
atte
nded
an
alte
rnat
ive
clin
ic if
the
new
cen
tre
had
not
open
ed; n
ot p
ossi
ble
to u
se d
ata
toid
entif
y an
y tr
ends
ove
r tim
e; n
o te
sts
for
stat
istic
al s
igni
fican
ce
Wea
k ev
iden
ce o
f inc
reas
ed u
se o
fse
rvic
es
a S
TI =
sex
ually
tran
smitt
ed in
fect
ions
.b
OR
(95
% C
I) =
odd
s ra
tio (
95%
con
fiden
ce in
terv
al).
185
92-4-120938-0_CH06_185

Among the studies included in this review, the scale varied considerably. Tenof the studies involved fewer than 10 facilities; these took place in Bangladesh(26), Brazil (20), Ghana (29), Mozambique (27), Rwanda (12), Senegal(25), Uganda (17), Zambia (16) and Zimbabwe (18, 21). The remaining stud-ies looked at interventions occurring in larger numbers of facilities, from 15facilities in Madagascar (37) to 328 facilities in South Africa (24). Two stud-ies did not use facilities as the unit of analysis. In China (19) the unit wasnetworks of service providers, and in Nigeria (10) it was individual serviceproviders.
By virtue of their inclusion in this review, the health facilities in the studiesprovided one or several of the packages of services endorsed during theMontreux consultation (5). However, where data were available from thestudies, the Montreux package of services was often not the primary reasonwhy young people chose to use the health facilities. For example, in clin-ics in Gweru, Zimbabwe (18), 60% of adolescents sought curative (non-reproductive) services; in Senegal (25), 51% of services sought were forreasons other than reproductive health; and in 8 clinics in Maputo, Mozam-bique (27), counselling for unspecified issues was sought by 47% of youngclients.
6.3.2 Results by study
There was one study of a type 1 intervention, four of type 2 interventions,one of a type 3 intervention, none of a type 4 intervention, two of a type 5intervention and eight of type 6 interventions. All of the studies includedactions in the community, and all of the interventions that had activities aimedat improving health facilities also included training for service providers and,sometimes, other clinic staff.
The one study that examined a type 1 intervention was from Zambia (16); itreviewed baseline, start-up and end-of-study statistics on family planning andoutpatient attendances by 15–24-year-olds in eight participating clinics andtwo control sites. In the intervention clinics, service providers were trained,and peer educators also received training to work in the community servedby the clinic. Although there were increases in attendance during the studyperiod, these were not significantly greater than the increases seen in controlclinics during the same period.
The four studies of type 2 interventions were conducted in China (19),Rwanda (12), Uganda (17) and Zimbabwe (18). The findings from theRwanda study were based on a cross-sectional survey that assessed the impactof exposure to the interventions on the use of services by young people(12); this was one of only three studies that explored the dose–response effect
186
92-4-120938-0_CH06_186

of interventions. There was weak evidence of increased use of services, mostnotably voluntary counselling and testing, by those with high exposure to theintervention compared with those with low exposure. The Uganda study useda quasi-experimental design with a non-equivalent control group and demon-strated statistically significant increases in service use as a result of theinterventions (17). Although both these studies showed statistically signifi-cant differences in service utilization, aspects of the study designs were notclear, and they were therefore categorized as showing weak evidence of in-creased use of services.
The Zimbabwe study reviewed clinic data for a 1-year period following theimplementation of the interventions, and was one of several studies that didnot include any statistical tests but demonstrated that a service was providedand it was used (18). This was considered to be weak evidence of an increaseduse of services.
The study from China focused explicitly on increasing young people’s use ofcontraceptives, particularly condoms, which were provided by a range of fa-cilities. It was the only study included in the review that did not explicitlymeasure young people’s use of services, but had condom use as the outcomevariable (19). However, it was considered that condom use could be taken asa proxy indicator for service use in terms of how the study had been designed;there was moderate evidence for increased use from the quasi-experimentaldesign that included a before and after component and also included a con-trol site.
There was only one study that examined a type 3 intervention. This was fromBrazil (20) and was designed to strengthen links and referrals among schoolsand health facilities. Although no statistical tests were carried out, the quasi-experimental evaluation showed weak evidence for no increased use ofservices related to the intervention.
No studies of type 4 interventions were identified.
Two studies looked at the effect of type 5 interventions: one from Zimbabwe(21) and the other from the United Republic of Tanzania (22). The inter-vention in Zimbabwe was primarily a media campaign that also providedtraining for service providers in designated clinics in the project area. Thequasi-experimental design, which included a control site, showed statisticallysignificant increases in self-reported health service-seeking behaviours thatwere associated with increased exposure to the intervention. However, therewere no baseline data for these findings, and there was contamination of thecontrol site. This study was therefore designated as providing weak evidencefor an increased use of services, although in this study reported use of ser-vices, rather than actual use, was the outcome measured. The other type 5
187
92-4-120938-0_CH06_187

study, from the United Republic of Tanzania, was one of two randomizedcontrolled trials identified. The study did not show any statistically significantincrease in service provision despite the implementation of health-workertraining and interventions in communities and schools. It therefore providedmoderate evidence for no increased use of services.
Type 6 interventions were the subject of the largest number of studies; theseinterventions include training for service providers and activities in facilities,as well as actions in the community and with other sectors. There were eightstudies in the following countries: Bangladesh (26), Ghana (29), Madagascar(12), Mongolia (23), Mozambique (37), Nigeria (10), Senegal (25) and SouthAfrica (24). As outlined in Table 6.4e, six of these studies showed weakevidence for an increased use of services. The randomized controlled trialfrom Nigeria (10) showed strong evidence of an increase in the use of healthservices; the study from Senegal (25), which used a before and after designand a control site, showed increases in service utilization, but these increaseswere not statistically different from those at the control sites.
6.3.3 Results by intervention
Training health-service providers, and in some cases other clinic staff, wasthe most frequently implemented intervention used to increase service use byyoung people. However, descriptions of the content of the training were lim-ited. The most frequently mentioned topics were counselling and communi-cation skills in the studies in China (19), Mongolia (23), Mozambique (27),Uganda (17), Zambia (16) and Zimbabwe (21); clinical knowledge and skillsrelated to STIs in Madagascar (12), Mozambique (27), Nigeria (10), Senegal(25), South Africa (24) and the United Republic of Tanzania (22); clinicalknowledge and skills related to contraception in China (19), Senegal (25) andSouth Africa (24); and health-workers’ attitudes, particularly in relation toworking with young people and ensuring confidentiality, in Bangladesh(26), China (19) and Mongolia (23). The duration of the training was rarelyprovided, but where indicated it ranged from 30 hours (Nigeria) to 15 days(Mozambique) or 19 sessions (Brazil). In five studies, mention was made ofsupervising health-service providers to reinforce the knowledge and skillsdeveloped during training; this occurred in the studies in Madagascar,Mozambique, Uganda, South Africa and the United Republic of Tanzania.
Only one study explicitly set out to explore the relationship between differentaspects of quality in the facility, actions in the community and service uti-lization; this was conducted in Zambia (16). The analysis indicated that useof services was more strongly associated with levels of community accep-tance than with the “youth friendliness” of the services.
188
92-4-120938-0_CH06_188

Altogether, 11 of the 16 studies were multicomponent interventions that in-cluded involvement with other sectors. This reflects current thinking that acombination of interventions in different settings is likely to have the greatestimpact on young people’s behaviours and, subsequently, on HIV prevalence.In these multicomponent intervention studies, the aim of increasing youngpeople’s use of services was usually one of a number of objectives. Unfor-tunately, the actions implemented in the health services were often poorlydescribed, both those that were carried out in the health facility and those thatwere implemented in the community. Only one study – in Brazil (20) –specifically set out to measure the influence of actions in other sectors on theutilization of health services.
In the studies that included actions taken in health facilities mention was madeof reducing fees, subsidizing commodities and modifying the physical plantin order to improve privacy or make the facilities more appealing to youngpeople. The most frequently described community activities were holdingpublic meetings and advertising the facilities, for example by distributingposters and pamphlets.
Peer educators had a role in half of the studies, carrying out a range of activ-ities such as stimulating demand, referring young people to the facilities,ensuring that the facilities or services were welcoming, and providing infor-mation about sexual and reproductive health in clinics and in the community.This review indicates that merely placing a clinical service in a youth centre
(29) and Zimbabwe (18) where this was done, only a small proportion ofyoung people who used the centre used the clinics: 3.3% in Ghana and 0.2%in Zimbabwe.
The initiative in South Africa (24) was the most extensive in scale and rigour.It included the setting of national standards for delivering adolescent healthservices and the development of an accompanying internal quality improve-ment process that staff could carry out in their facilities, as well as an externalassessment that led to accreditation of the services as being adolescent-friendly. In Madagascar, standards for assessing the quality of servicesprovided to adolescents were part of the franchising approach to services thatwas implemented there (12), although the standards were not described indetail. National standards were also established in Mongolia (23). Elementscommon to the standards set in Mongolia and South Africa include standardsfor referral (for example, from schools to health services and from healthservices to other social services), for improving accessibility (for exampleby advertising the services), for creating an appealing physical environ-ment in the facilities, for instituting policies and procedures that ensure
189
does not ensure it will be used. In the studies reviewing interventions in Ghana
92-4-120938-0_CH06_189

confidentiality, for ensuring the technical competence of providers, ensuringadequate equipment and supplies, and generating community involvement.
Establishing standards for service delivery provides clear direction for actionand accountability through regular monitoring. Monitoring data were avail-able for South Africa but not for Madagascar. In Mongolia, assessments weremade through facility observation and surveys of clients and serviceproviders; these demonstrated that there were improvements in the physicalenvironment of the facilities, service providers’ competencies and attitudes,and in client satisfaction. Further analysis of client satisfaction data high-lighted the importance of basic amenities, such as toilets, in facilities in termsof adolescents’ perceptions of acceptability (30). In South Africa, the major-ity of the 72 clinics that were members of the National Adolescent FriendlyClinics Initiative that were assessed in 2004 complied with between 80% and90% of the initiative’s standards. In addition, the 11 clinics that were assessedannually showed statistically significant better performance on all but onestandard when compared with the control clinics.
Information about the costs of the interventions was provided in five of thestudies. Unfortunately the data do not make it possible to estimate the costsof increasing young people’s use of services. However, these data are usefulin indicating the relative costs of the different components of multisectorinterventions, including the costs of community engagement. In the studiesfrom Rwanda and Madagascar (12), the total in-country costs for all inter-ventions was US$ 1.1 million each. In addition, the costs for technicalassistance from the international nongovernmental organization supportingthese two projects, plus a third project in Cameroon that was excluded fromthis review (12), was US$ 1.7 million for the three countries over 4 years.Information from the Mwanza project in the United Republic of Tanzania(22) showed that 68.9% of overall implementation costs were for the in-school component, 12.3% for the community-based component, 10.1% forthe condom promoters and distributors, and 8.8% for the youth-friendlyhealth services component.
The studies in Senegal and Bangladesh (25, 26, 31) provided information onthe relative costs of making improvements in health services compared withother intervention components. In Senegal, implementation costs totalled ap-proximately US$ 100 000 over 2 years; the costs were shared betweencommunity interventions (US$ 40 000), clinic interventions (US$ 34 000)and school interventions (US$ 26 000). Most of the expenditures were forplanning and training at the beginning of the project. In Bangladesh, the totalcost for both intervention sites was US$ 41 388, with the site that includedschool-based interventions being twice as costly. The major additional costat this site was for teacher training. The costs of the community interventions
190
92-4-120938-0_CH06_190

and the school-based interventions were both approximately US$ 12 000each. The costs of interventions in the health services were lower, at US$ 2 353,because they used existing structures and staff (although non-financial costs,such as time spent by staff in planning, were said to be substantial). Anotherfactor that kept clinic costs low was that much of the training was carried outby the international agency involved in the study, and this was not includedin the costing.
6.4 Discussion
6.4.1 General
Providing young people with health services that will help prevent them be-coming infected with HIV and that will care for them if they do becomeinfected is a basic human right’s obligation (38), and all governments andcommunities need to ensure that these services are delivered. Providing theseservices to young people is also a key programme element for HIV preventionthat has been endorsed by governments in a range of international fora duringthe past decade (1, 3, 4). Policy-makers and programme managers, especiallythose working in resource-constrained settings, need to know which typesof interventions are most likely to increase young people’s use of healthservices.
Despite the fact that the evidence for the most part is weak, the majority ofstudies identified for inclusion in this review demonstrated an increased useof health services by young people as a result of the interventions. This isalso true for the additional studies that were identified but not included inthe review as a result of concerns about the details of the interventions or thequality of the data (32–36). This finding is encouraging because when thetechnical report on programming for adolescent health was published10 years ago (13), there was little evidence to indicate whether it was possibleto increase young people’s use of health services, even though a range ofservice delivery models had been described in the publication. Furthermore,many of the studies included in this review reflect the consensus around goodpractice that has been developing in discussions between researchers andpeople responsible for programme development and delivery during the pastdecade (2, 13, 28).
Table 6.5 summarizes the levels of evidence of effectiveness needed beforedifferent types of interventions can be recommended for widespread imple-mentation. The evidence for an increased use of services by young people iseither negative or equivocal for all types except types 2 and 6, which includeactivities that involve service providers and facilities and taking actions inthe community with or without the involvement of other sectors. For these
191
92-4-120938-0_CH06_191

two types there is weak evidence for an increased use of services. Type 2interventions require a weak level of evidence to recommend them as“Go” (Table 6.2); thus the evidence indicates that interventions that trainservice providers and other clinic staff, implement changes in clinics to makethem more responsive to the needs of young people and organize activitiesin the community should be taken to scale, with careful monitoring of cov-erage and quality. For type 6 interventions, with the weak evidence that isavailable it is possible to recommend them only as “Ready”. This means thatthey should be implemented widely and cautiously, but only if there is a strongevaluation component linked to implementation. These conclusions are sum-marized in Table 6.6. Intervention types that did not include components toimprove facilities or some type of community activity are categorized as“Steady” or “Do not go”. This emphasizes the importance of going beyondsimply training service providers if the aim is to increase service utilization:facilities also need to be improved and there needs to be outreach into thecommunity.
For many of these studies there were a number of unanswered questions aboutthe interventions and their mechanism of action. If interventions are to beimplemented, in addition to careful monitoring and evaluation, there is alsoa need for analytical case descriptions to clarify and document lessons learntand for operations research to specify and explain the content of the inter-ventions (that is, what is being done and why?) and to help answer some ofthe “how?” questions.
In general there is an ongoing need for research to tease out the relative im-portance of the various components of interventions in terms of their contri-bution to increasing the use of services by young people. For example, noneof the studies of type 6 interventions explored the relative contributions ofcommunity activities and the involvement of other sectors. Six of the eighttype 6 studies were multicomponent interventions that included schools andthe media. With one exception – in Brazil (20) – the activities in these sectorshad not been primarily developed to increase service utilization, although thiswas certainly one of their objectives. It will be important to better understandthe contributions that the involvement of schools and the media – as well asother sectors not included in this review, such as the workplace – make toincreasing the use of health services by young people. The question is: howmuch do they add to an effective community component? Also, it was clearfrom reviewing the studies that there was overlap between community ac-tivities and actions in other sectors. For example, it was not possible todisentangle the relative contribution made by health-workers providing in-formation in an ad hoc way to young people in schools and the implementa-tion of systematic curriculum-based programmes that provide pupils withrelevant information.
192
92-4-120938-0_CH06_192

Tab
le 6
.5S
tren
gth
of
evid
ence
of
effe
ctiv
enes
s fo
r ea
ch in
terv
enti
on
typ
e
Inte
rven
tio
n t
ype
and
stu
dy
des
ign
Po
siti
ve e
ffec
tN
o e
ffec
tE
vid
ence
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Typ
e 1
(wit
h s
ervi
ce p
rovi
der
s an
d in
th
e co
mm
un
ity)
Ane
cdot
alE
quiv
ocal
Qua
litat
ive
only
Cro
ss-s
ectio
nal (
no c
ompa
rison
gro
up)
Bef
ore–
afte
r (n
o co
mpa
rison
gro
up)
Qua
si-e
xper
imen
tal (
1 c
ompa
rison
gro
up)
CR
CT
a
Typ
e 2
(act
ion
s in
th
e cl
inic
, wit
h s
ervi
ce p
rovi
der
s an
d in
th
e co
mm
un
ity)
Ane
cdot
alW
eak
Qua
litat
ive
Onl
yO
Cro
ss-s
ectio
nal
NB
efor
e–af
ter
Qua
si-e
xper
imen
tal
L, I
RC
TT
ype
3 (w
ith
ser
vice
pro
vid
ers
and
invo
lvem
ent
of
oth
er s
ecto
rs)
Ane
cdot
alE
quiv
ocal
Qua
litat
ive
only
Cro
ss-s
ectio
nal
Bef
ore–
afte
rQ
uasi
-exp
erim
enta
lJ
RC
T
193
92-4-120938-0_CH06_193

Inte
rven
tio
n t
ype
and
stu
dy
des
ign
Po
siti
ve e
ffec
tN
o e
ffec
tE
vid
ence
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Typ
e 4
(wit
h s
ervi
ce p
rovi
der
s an
d in
th
e fa
cilit
y, in
volv
ing
oth
er s
ecto
rs)
No
stud
ies
of th
is ty
pe o
f int
erve
ntio
nT
ype
5 (w
ith
ser
vice
pro
vid
ers,
in t
he
com
mu
nit
y an
d in
volv
ing
oth
er s
ecto
rs)
Ane
cdot
alE
quiv
ocal
Qua
litat
ive
only
Cro
ss-s
ectio
nal
Bef
ore–
afte
rQ
uasi
-exp
erim
enta
lD
RC
TG
Typ
e 6
(wit
h s
ervi
ce p
rovi
der
s an
d in
th
e fa
cilit
y, in
th
e co
mm
un
ity
and
invo
lvin
g o
ther
sec
tors
)A
necd
otal
Wea
kQ
ualit
ativ
e on
lyB
, M, K
Cro
ss-s
ectio
nal
Bef
ore–
afte
rH
,Q
uasi
-exp
erim
enta
lA
FE
RC
TP
aR
CT
= r
ando
miz
ed c
ontr
olle
d tr
ial.
194
92-4-120938-0_CH06_194

Tab
le 6
.6R
eco
mm
end
atio
ns
on
th
e st
ren
gth
of
the
evid
ence
fo
r ef
fect
iven
ess
by
inte
rven
tio
n t
ype
Inte
rven
tio
n t
ype
Key
ch
arac
teri
stic
s o
f ef
fect
ive
inte
rven
tio
ns
Co
ncl
usi
on
Co
mm
ents
1. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
only
plu
s in
terv
entio
ns in
the
com
mun
ity
• A
dequ
ate
trai
ning
of s
ervi
ce p
rovi
ders
and
othe
r cl
inic
sta
ff•
Ade
quat
e in
terv
entio
ns in
the
com
mun
ity to
pro
vide
info
rmat
ion,
gene
rate
dem
and
and
ensu
reco
mm
unity
sup
port
Ste
ady
(or
Do
not g
o)T
hese
are
like
ly to
be
the
easi
est
inte
rven
tions
to im
plem
ent b
ut a
rele
ast l
ikel
y to
hav
e an
impa
ct; s
tudy
desi
gn w
as w
eak
and
the
resu
lts a
reeq
uivo
cal
2. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
and
in fa
cilit
ies
plus
inte
rven
tions
in th
e co
mm
unity
In a
dditi
on to
com
men
ts a
bout
type
1•
Cla
rity
abou
t whi
ch in
terv
entio
ns in
the
heal
th fa
cilit
ies
are
mos
t lik
ely
toco
ntrib
ute
to in
crea
sed
utili
zatio
n
Go
Alth
ough
the
stud
ies
wer
e no
t str
ong,
they
all
indi
cate
d an
incr
ease
d us
e of
serv
ices
by
youn
g pe
ople
Gre
ater
cla
rity
is r
equi
red
betw
een
type
2 a
nd ty
pe 6
inte
rven
tions
inte
rms
of th
e va
lue
adde
d by
the
“oth
erse
ctor
s” c
ompo
nent
3. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
only
plu
s in
terv
entio
ns w
ithot
her
sect
ors
In a
dditi
on to
com
men
ts a
bout
type
1•
Cla
rity
abou
t whi
ch s
peci
ficin
terv
entio
ns in
sch
ools
and
in th
em
edia
(an
d ot
her
sect
ors
such
as
the
empl
oym
ent s
ecto
r) a
re m
ost l
ikel
y to
cont
ribut
e to
incr
ease
d ut
iliza
tion
ofse
rvic
es
Ste
ady
(or
Do
not g
o)T
here
was
onl
y on
e st
udy
iden
tifie
d of
this
type
of i
nter
vent
ion
and
it sh
owed
no in
crea
se in
use
All
the
type
s th
at o
nly
focu
sed
ontr
aini
ng s
ervi
ce p
rovi
ders
with
out
mak
ing
chan
ges
in th
e cl
inic
sho
wed
varia
ble
resu
lts
195
92-4-120938-0_CH06_195

Inte
rven
tio
n t
ype
Key
ch
arac
teri
stic
s o
f ef
fect
ive
inte
rven
tio
ns
Co
ncl
usi
on
Co
mm
ents
4. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
and
in fa
cilit
ies
plus
inte
rven
tions
with
oth
er s
ecto
rs
No
data
5. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
plus
inte
rven
tions
in th
eco
mm
unity
and
with
oth
er s
ecto
rs
In a
dditi
on to
com
men
ts a
bout
type
3•
Cla
rity
abou
t whi
ch c
ombi
natio
n of
trai
ning
, com
mun
ity a
nd m
edia
inte
rven
tions
are
mos
t lik
ely
toin
crea
se u
tiliz
atio
n of
ser
vice
s
Ste
ady
(or
Do
not g
o)D
ata
wer
e eq
uivo
cal,
and
as w
ith ty
pe1
inte
rven
tions
, inc
reas
ed u
se o
fse
rvic
es is
unl
ikel
y w
ithou
t cha
nges
inth
e fa
cilit
ies
6. In
terv
entio
ns w
ith s
ervi
cepr
ovid
ers
and
in fa
cilit
ies
plus
inte
rven
tions
in th
e co
mm
unity
and
with
oth
er s
ecto
rs
In a
dditi
on to
com
men
ts a
bout
type
2•
Cla
rity
abou
t whi
ch c
ombi
natio
n of
inte
rven
tions
in th
e cl
inic
, and
inte
rven
tions
in th
e co
mm
unity
and
with
oth
er s
ecto
rs, a
re m
ost l
ikel
y to
incr
ease
ser
vice
use
by
youn
g pe
ople
Rea
dyT
hese
inte
rven
tions
are
mos
t lik
ely
toha
ve a
n im
pact
, and
eve
n th
ough
the
inte
rven
tions
wer
e no
t alw
ays
clea
ran
d m
ost o
f the
stu
dies
onl
y ha
d w
eak
evid
ence
for
a po
sitiv
e ef
fect
, all
but
one
of th
em h
ad a
pos
itive
effe
ct o
nse
rvic
e ut
iliza
tion
196
92-4-120938-0_CH06_196

There are a number of issues that need to be considered when interpretingthese data. First, although several studies did not show any evidence for ef-fectiveness, there is likely to be both reporting and publication bias – that is,researchers are more likely to report results and have them published if theyhave a positive result. There may also have been misclassification bias interms of the allocation of the studies to specific types of interventions.
Second, a range of studies is included in this review, from randomized con-trolled trials of specific interventions to reports that merely demonstrated thata service was provided and it was used by young people. The challenge ofinterpreting data from studies that merely showed an increase in use afterproviding a service is highlighted by the studies in Zambia (16) and Senegal(25). Both of these studies had a before and after design with a control site.In both of them there was an increase in young people’s use of services at theintervention sites but this was not different from the increase noted at thecontrol sites (and there was no indication that there had been contaminationof these control sites). Thus for these studies there was weak evidence of noeffect on utilization as a result of the intervention. However, if there had been
was used”, as was done in Ghana (29) for example, these interventions wouldhave been considered to have shown weak evidence for increased utilizationas a result of the interventions.
Third, it needs to be recognized that the levels of evidence – weak, moderateand strong – contain a spectrum of evidence. For some of the studies “veryweak” would have been a more appropriate description than “weak” whenthey were compared with some of the other studies also considered to showweak evidence for effectiveness.
6.4.2 Inclusion and exclusion criteria
Despite using detailed inclusion and exclusion criteria for the studies in thisreview, there was ongoing discussion among the authors about whether toinclude studies of the “we provided a service and young people used it” typebecause we recognized that there is a subtle difference between young peopleusing a newly created service (meeting a provision gap) and implementingspecific interventions to identify the most effective approaches to increaseyoung people’s use of services (evaluation research). An example of a “weprovided a service” paper that was excluded due to insufficient data was thereport of activities of the African Youth Alliance project in the United Re-public of Tanzania (35). In this study, the only service utilization data was acomment that there was a “17% increase in the use of the services” with nodenominator or statistics from before the intervention. Thus it is extremely
197
no control clinics in these studies, if they had simply “provided a service that
92-4-120938-0_CH06_197

difficult to know whether there was a statistically significant increase or noincrease.
In tightening the inclusion and exclusion criteria, some studies that focusedon providing information and commodities in the community may have beenexcluded both from this paper and from the paper in this series on geograph-ically defined communities (chapter 8). The social marketing of condoms isan obvious example of an intervention that would have been excluded(11, 12).
6.4.3 The typology
Two issues need to be mentioned in relation to the typology used for thisreview. First, it needs to be recognized that other typologies could have beendeveloped that would also have helped guide the decisions of policy-makersand programmers. For example, interventions could have been classified de-pending on whether services were provided through government facilities,stand-alone youth clinics or as part of multicomponent youth centres. Severaltypologies were developed and tried but either there were insufficient detailsin the papers to make it possible to allocate the studies or there were insuffi-cient studies in the majority of the types.
Even with the typology that was adopted it was still not always easy to allocatestudies to the different types, mainly due to the inadequacy of informationcontained in the studies. For example, the Uganda study (17) did not includean obvious community component but it was clear from the narrative thatsome efforts took place to make it possible for parents to come and see whatwas happening in the clinic. This was done because the baseline survey dis-covered that some parents were concerned about their children using theclinics. The parents who visited the health facilities then acted as advocatesfor the services in the community.
In placing studies in the different types it was noted that there was a spectrumof “interventions in the facility” and that in some cases the lack of clarity inthe descriptions of the interventions made classifying them difficult. For ex-ample, cases could be made for classifying the study in Zambia (16) as a type2 intervention and the study in Uganda (17) as a type 4. These changes wouldnot, however, have made any differences to the conclusions: weak evidencefor type 2 and type 6 would remain and the evidence for the other types wouldremain equivocal.
6.4.4 Interventions, outcomes and evaluations
This review has indicated the need for researchers and people responsible forprogramme development and delivery to be much clearer about what they
198
92-4-120938-0_CH06_198

do, what the mechanisms of action of the interventions are, what the intendedoutcomes are and how implementation and outcomes can be measured. Interms of intensity of effort, the studies from Gweru, Zimbabwe (18), andBrazil (20) provide some indication that as the intensity of the interventionwaned, there was a decrease in the use of services by young people; thisemphasizes the need to focus on interventions that can be realistically sus-tained over time. Conversely, the analysis of service statistics from both ofthe studies that explicitly developed and measured standards – in Mongolia(23) and South Africa (24) – showed a statistically significant increase in theuse of services as a result of attempts to maintain the quality of the services.
The UNGASS goal specifies that 95% of young people should have accessto services by 2010 (3). Planning for a target such as this requires some senseof the need for services, and this need can only be determined through de-mographic and epidemiological data. None of the studies in our reviewaddressed this issue: at best they provided service statistics (in 9/16 studies)indicative of “contact” coverage (the services were used) but they made noreference to the overall population of young people, the catchment area orother age groups served by the same facilities.
It is encouraging that several of the studies provided information on costs,although few conclusions can be derived. Data about costs are extremelyimportant in terms of the replication and sustainability of interventions, andthese are aspects of monitoring and evaluation that require further develop-ment. Attention should be paid not only to the relative costs of the variousactivities in the health services and in other sectors, but also to the establish-ment of baseline costs of existing services and to the additional costs ofimproving services (in order for the data to be useful to programme planners).
Finally, the context in which interventions are implemented is likely to be animportant consideration, and contextual factors that may have influenced thesuccess or failure of the interventions were mentioned in some of the studies.Again, this has important implications for replication, and contextual factorsthat may influence outcomes need to be a more central focus in futureresearch.
6.5 Conclusions
What do we know about the contribution that health services can make topreventing HIV transmission among young people? In order to answer thisquestion we need to know the following.
1. Have we identified a set of evidence-based interventions that can be pro-vided through health services?
199
92-4-120938-0_CH06_199

2. Do we know what to do to increase young people’s use of health services(the focus of the UNGASS health services target)?
3. Can we provide young people who use health services with the evidence-based package of interventions that have been defined?
4. And, finally, can we determine whether increasing young people’s use ofevidence-based interventions makes a difference to HIV prevalence orother health outcomes?
With the completion of this study, and building on the evidence from theMontreux meeting (5), we now have “yes” answers to questions 1 and 2. Thethird and fourth questions were not the focus of this review. Only one ofthe studies (10) attempted to answer these questions, and clearly these are thequestions for the future as we build the evidence base.
Despite the constraints imposed by the quality of the data from most of thestudies included in this review, if countries want to move towards achievingthe global goals on HIV and young people, there is sufficient evidence tosupport widespread implementation of interventions that include elements oftraining for service providers and other clinic staff, making improvements tofacilities, and informing and mobilizing communities to generate demand andcommunity support. These interventions will require careful planning andimplementation, and their coverage and quality will need to be monitored.Operations research will also be needed as will a better understanding of thecosts.
Interventions that additionally involve other sectors can also be recom-mended for widespread implementation provided that they are carefullyplanned, implemented and monitored and include an evaluation componentthat assesses their impact on service utilization. Again, there is a need foroperational research to be undertaken to better understand the mechanismsof action. It will be important to gain a better understanding of the interven-tions and to be much clearer about the relative merits of actions in thecommunity compared with actions in the community that are implementedalong with additional activities in other sectors.
Future research will be required to demonstrate that we not only have a pack-age of evidence-based interventions and know how to increase young peo-ple’s use of services but that we can also have an impact on young people’sbehaviours and health through interventions provided through health servicesin conjunction with interventions in other settings. Achieving the health ser-vices access goal that was endorsed during UNGASS will have significantimplications for the decisions and resource allocations made by policy-makers, programme managers and researchers. Recommendations for all ofthese actors, based on the findings of this review, are summarized in Box 6.2.
200
92-4-120938-0_CH06_200

Box 6.2
Recommendations for interventions to increase the use of health services byyoung people
For policy-makers
Interventions implemented through health services will be essential forachieving the global goals on HIV and young people, in particular for thetarget of increasing young people’s access to an evidence-based pack-age of services to prevent the spread of HIV.
The evidence is sufficient to support widespread implementation of in-terventions to increase young people’s use of health services. However,these interventions should be implemented only if they are carefullymonitored and evaluated.
Interventions to increase young people’s access to health servicesshould be linked to interventions in other settings that aim to improveyoung people’s knowledge, skills, attitudes and behaviours.
For programme development and delivery staff
In order to increase young people’s use of services it is necessary totrain service providers and other clinic staff, make facilities more acces-sible and acceptable to young people and work in the community togenerate demand and community support.
It will be important to better understand the key components of trainingprogrammes for services providers and other clinic staff, the most im-portant improvements to make in health facilities, and the most strategicactions to take in the community. This will require careful monitoring andlinks with researchers.
Interventions implemented through health services need to be carefullyplanned and monitored, and linked to actions in other sectors. In addi-tion, in order to ensure that these interventions have the desired impact,evaluation and operations research should be actively supported.
For researchers
Evaluation and operations research should be included as core ele-ments of any interventions aimed at increasing young people’s use ofhealth services.
Several research issues have been raised in this review, including theneed to better understand the content and duration of training, the rel-ative contribution that different interventions in the facilities make toincreasing the use of services and the benefit of involving other sectorsin relation to the increased effort required.
A number of specific issues have been highlighted in this review, in-cluding the need to tease out the relative contributions of the differentinterventions and for better costing data to be made available.
201
92-4-120938-0_CH06_201

Acknowledgements
We would like to thank Merlin Wilcox for his contribution to the early de-velopment of this paper. We would also like to thank the members of theHealth Services Working Group at the 2004 Talloires meeting for their ideasand support: Shanti Conly, Siobhan Crowley, Kim Dickson, JoannaNerquaye-Tetteh and Julitta Onabanjo.
References
1. United Nations Population Fund. Summary of the ICPD programme of action,2004 (http://www.unfpa.org/icpd/summary.htm).
2. WHO. Adolescent friendly health services: an agenda for change, 2003 (http://www.who.int/child-adolescent-health/publications).
3. United Nations. Declaration of commitment on HIV/AIDS. United NationsGeneral Assembly Special Session on HIV/AIDS, 2001 (http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html).
4. United Nations. A world fit for children. United Nations Special session onChildren, 2002 (http://www.unicef.org/specialsession/wffc).
5. WHO, UNFPA, UNAIDS. Achieving the global goals: access to services. GlobalConsultation Technical Report, 2003 (http://www.who.int/child-adolescent-health/publications/).
6. Tanahashi T. Health service coverage and its evaluation. Bulletin of the WorldHealth Organization, 1978, 56:295-303.
7. USAID, UNAIDS, UNFPA WHO, UNICEF, Policy Project. Coverage of selectedservices for HIV/AIDS prevention, care and support in low and middle incomecountries in 2003. Washington, DC, Futures Group, 2004.
8. WHO, Department of Child and Adolescent Health and Development.Conceptual overview: measuring coverage of interventions for young people.Geneva, WHO, 2004. (Unpublished report.)
9. UNAIDS. Report on the global AIDS epidemic: fourth global report. Geneva,UNAIDS, 2004.
10. Okonofua FE et al. Impact of an intervention to improve treatment-seekingbehavior and prevent sexually transmitted diseases among Nigerian youths.International Journal of Infectious Diseases, 2003, 7:61-73.
11. Townsend JW et al. Sex education and family planning services for youngadults: alternative urban strategies in Mexico. Studies in Family Planning, 1987,18:103-108.
12. Neukom J et al. Changing youth behaviour through social marketing: programexperiences and research findings from Cameroon, Madagascar, andRwanda. Washington, DC, Population Services International, PopulationReference Bureau, 2003.
13. WHO. Programming for adolescent health and development: report of a WHO/UNFPA/UNICEF study group on programming for adolescent health. Geneva,WHO, 1999.
202
92-4-120938-0_CH06_202

14. WHO, Department of Child and Adolescent Health and Development. Globalconsultation on adolescent friendly health services: a consensus statement.Geneva, WHO, 2001. (WHO/FCH/CAH/02.18.)
15. Brabin L. Adolescent friendly health services: an impact model to evaluate theireffectiveness and cost, 2002 (http://www.fhi.org/NR/rdonlyres/elwxby2675hwyyn7whpsj3om4n52wecgvunokzrqf5fn446dktcuo7fi3qufhfuelwm2zhjlcm3rkf/AFHSImpactModelfinalversion.pdf).
16. Mmari KN, Magnani RJ. Does making clinic-based reproductive health servicesmore youth-friendly increase service use by adolescents? Evidence fromLusaka, Zambia. Journal of Adolescent Health, 2003, 33:259-270.
17. Mbonye AK. Disease and health seeking patterns among adolescents inUganda. International Journal of Adolescent Medicine and Health, 2003,15:105-112.
18. Moyo I et al. Reproductive health antecedents, attitudes, and practices amongyouth in Gweru, Zimbabwe. Washington, D.C., Pathfinder International,FOCUS on Young Adults, June 2000.
19. Chao-Hua L et al. Effects of a community-based sex education and reproductivehealth service programme on contraceptive use of unmarried youths inShanghai. Journal of Adolescent Health, 2004, 34:433-440.
20. Magnani RJ et al. Impact of an integrated adolescent health program in Brazil.Studies in Family Planning, 2001, 32:230-243.
21. Kim YM et al. Promoting sexual responsibility among young people inZimbabwe. International Family Planning Perspectives, 2001, 27:11-19.
22. Hayes R et al. The MEMA kwa Vijana Project: design of a community-randomised trial of an innovative adolescent sexual health intervention in rualTanzania. Contemporary Clinical Trials, 2005, 26:430-442.
23. WHO, Ministry of Health Mongolia, UNFPA. Assessment of AFHS initiative inMongolia. Ulaanbaatar, 2003,. (Unpublished document.)
24. loveLife. loveLife 2004: report on activities and progress, Cape Town,Parklands, loveLife, 2004.
25. Diop NJ et al. Improving reproductive health of adolescents in Senegal.Washington, DC, Frontiers Reproductive Health Program, 2004. (Unpublisheddocument.)
26. Bhuiya I et al. Improving adolescent reproductive health in Bangladesh.Washington, DC, Frontiers Reproductive Health Program, 2004. (Unpublisheddocument.)
27. Hainsworth G. Providing sexual reproductive health and STI/HIV informationand services to this generation: insights from the Geracao Biz experience.Maputo, Ministry of Youth and Sports, Ministry of Education, Ministry of Health,AMODEFA and youth associates, UNFPA, Pathfinder International, 2002.
28. Moya C. Creating youth friendly sexual health services in sub-Saharan Africa,Advocates for Youth, 2002 (http://www.advocatesforyouth.org/publications/iag/youthfriendly.htm).
29. Solo J et al. Enjoy your youth, be wise: an evaluation of the Innovate project inGhana. London, International Planned Parenthood Federation, 2001.(Unpublished report.)
203
92-4-120938-0_CH06_203

30. Sovd T et al. Acceptability as a key determinant of client satisfaction: lessonsfrom an evaluation of adolescent friendly health services in Mongolia. Journalof Adolescent Health. (In press.)
31. Family Health International, YouthNet. New findings from intervention research:youth reproductive health and HIV prevention, 2003 (http://www.fhi.org/en/youth/youthnet/index.htm).
32. Askew I et al. A multi-sectoral approach to providing reproductive healthinformation and services to young people in western Kenya: Kenya adolescentreproductive health project Washington, DC, Frontiers Reproductive HealthProgram, 2003. (Unpublished document.)
33. Family Health International. Reaching out to bring young Haitians in: FHI helpstwo organizations work with youth in high-risk settings. Arlington, VA, FHI, 2004.
34. EC/UNFPA initiative for reproductive health in Asia. Learning from the RHIpartnerships 1998–2002. New York, UNFPA, 2003.
35. Senderowitz J. Partnering with African youth: Pathfinder International and theAfrican Youth Alliance experience. Watertown, MA, Pathfinder International,2004.
36. Naguru teenage and information centre: annual report. Kampala, Uganda,2003. (Unpublished report.) </unknown>
37. Correal D et al. Scaling up youth-friendly HIV and SRH services through multi-sectoral program in Mozambique. Bangkok, International AIDS Conference,2004. (Conference abstract WePeE6720.)
38. UN Office of the High Commissioner for Human Rights. Convention on the rightsof the child, 1989 (http://www.unhchr.ch/html/menu3/b/k2crc.htm).
204
92-4-120938-0_CH06_204

7. The effectiveness of mass media inchanging HIV/AIDS-relatedbehaviour among young people indeveloping countriesJane T. Bertranda & Rebecca Anhangb
Objectives To review the strength of the evidence for the effects of threetypes of mass media interventions (radio only, radio with supportingmedia, or radio and television with supporting media) on HIV/AIDS-relatedbehaviour among young people in developing countries and to assess whetherthese interventions reach the threshold of evidence needed to recommendwidespread implementation.
Methods We conducted a systematic review of studies that evaluated massmedia interventions and were published or released between 1990 and 2004.Studies were included if they evaluated a mass media campaign that had themain objective of providing information about HIV/AIDS or sexual health.To be eligible for inclusion studies had to use a pre-intervention versus post-intervention design or an intervention versus control design or analyse cross-sectional data comparing those who had been exposed to the campaign withthose who had not been exposed. Studies also had to comprehensively reportquantitative data for most outcomes.
Findings Of the 15 programmes identified, 11 were from Africa, 2 from LatinAmerica, 1 from Asia, and 1 from multiple countries. One programme usedradio only, six used radio with supporting media, and eight others used tele-vision and radio with supporting media. The data support the effectivenessof mass media interventions to increase the knowledge of HIV transmission,to improve self-efficacy in condom use, to influence some social norms, toincrease the amount of interpersonal communication, to increase condom useand to boost awareness of health providers. Fewer significant effects werefound for improving self-efficacy in terms of abstinence, delaying the age offirst sexual experience or decreasing the number of sexual partners.
Conclusions We found that mass media programmes can influence HIV-related outcomes among young people, although not on every variable or in
a Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs, 111Market Place, Suite 310, Baltimore, MD 21202, USA. Correspondence should be sent to JaneBertrand (email: [email protected]).
b Harvard University, Boston, MA, USA.
205
92-4-120938-0_CH07_205

every campaign. Campaigns that include television require the highest thresh-old of evidence, yet they also yield the strongest evidence of effects. Thissuggests that comprehensive mass media programmes are valuable.
7.1 Introduction
In countries worldwide, young people comprise a key audience for messagesabout preventing HIV/AIDS. Unless a young person acquired HIV in uteroor as an infant, almost all young people enter adolescence HIV-negative.Yet the very nature of adolescence – characterized by experimentation, risk-taking and a sense of immortality – make youths particularly vulnerable toHIV. Annually, 50% of all new HIV infections occur among young peopleaged 15–24 years (1).
Given the sheer number of young people and the critical importance of alert-ing them to the threat of HIV and AIDS, most governments have turned tothe mass media as a means of informing their population, shaping socialnorms and influencing behaviour associated with the transmission of HIV.
Given that adolescents are so attuned to mass media for information and cuesabout how to behave, the media have tremendous potential for reaching themwith messages about HIV and AIDS. Mass media campaigns may comple-ment other programmes (for example, the training of personnel or the distri-bution of condoms) designed to stop the spread of HIV.
Because the epidemic has continued to spread in many countries, it has beenconcluded that mass media interventions are not an effective means of pre-venting the spread of HIV (2). The evidence in the published literature on theeffectiveness of communication programmes is sparse but there have beenseveral rigorous studies that identified reported changes in HIV/AIDS-related behaviours, such as avoiding unprotected sex (3). A difficulty inarriving at an assessment of the potential effectiveness of communicationprogrammes is that relatively few countries have mounted full-scale, coor-dinated, comprehensive communication programmes aimed at combating thespread of HIV (4).
The mass media are an increasingly important component of interventionprogrammes when they are scaled-up. Thus, this review evaluates programmesthat have a mass media component although they may also have additionalcommunity or interpersonal components. We define mass media interven-tions as any programmes or other planned, time-limited efforts that have theexplicit goal of changing knowledge, attitudes and behaviours that are relatedto preventing the transmission of HIV and that disseminate messages amongan intended population through channels that reach a broad audience. For thepurposes of this review, these channels include radio, television, video, print
206
92-4-120938-0_CH07_206

media and the Internet; the programming may take a variety of forms, in-cluding variety shows, songs, advertisements or public service announce-ments, soap operas, music videos, films, pamphlets, billboards, posters andinteractive web sites. The review does not include certain media, such as streettheatre, puppetry or the work of itinerant singers, since these media are lessfrequently subject to evaluation, and the evaluation of such interventions mayoften be primarily of local relevance, rather than international.
This article reviews the literature evaluating the effects of mass media inter-ventions on the HIV/AIDS-related behaviour of young people in developingcountries in order to determine whether the evidence provides justificationfor recommending that these types of interventions be implemented morewidely in future.
7.2 Methods
The methods used in this review are similar to those used in other chaptersin this series (see chapter 4). First, we defined the most common types ofinterventions to prevent HIV transmission used in the mass media in devel-oping countries; we categorized them into radio only, radio with othersupporting media, and radio and television with other supporting media.These types were chosen to reflect the key decisions that programme devel-opment and delivery staff and policy-makers need to make when choosing inwhich mass media interventions to invest. The inclusion and exclusion cri-teria were then defined (Table 7.1). The authors, in discussion with the serieseditors, then decided on the strength of evidence needed to recommendwidespread implementation of each of these types of interventions taking intoaccount their feasibility, the potential for adverse outcomes, their acceptabil-ity, the potential size of the intervention effect and the potential for bringingabout other health or social benefits (Table 7.2). The literature was reviewed,and each of the eligible studies was summarized in a standard manner. Ad-ditional information is available on the web (www.who.int/child-adolescent-health/). Key aspects of the intervention, as well as the design of theevaluation study and results, were also summarized (Table 7.3 and Table 7.4).The overall conclusions on the strength of the evidence for the effectivenessof each of the three types of intervention were compared with the thresholdstrength of evidence needed to recommend widespread implementation(Table 7.2).
207
92-4-120938-0_CH07_207

Tab
le 7
.1In
clu
sio
n a
nd
exc
lusi
on
cri
teri
a u
sed
to
iden
tify
stu
die
s fo
r re
view
Incl
usi
on
cri
teri
aE
xclu
sio
n c
rite
ria
Eva
luat
ion
mus
t be
a st
udy
that
com
pare
s ou
tcom
es p
re-in
terv
entio
nve
rsus
pos
t-in
terv
entio
n or
inte
rven
tion
vers
us c
ontr
ol d
esig
n or
a c
ross
-se
ctio
nal d
esig
n co
mpa
ring
thos
e ex
pose
d to
the
cam
paig
n w
ith th
ose
unex
pose
d
Eva
luat
ion
desi
gn th
at d
oes
not c
ompa
re p
re-in
terv
entio
n ou
tcom
esw
ith p
ost-
inte
rven
tion
outc
omes
or
inte
rven
tion
vers
us c
ontr
ol o
rcr
oss-
sect
iona
l
Eva
luat
ion
resu
lts m
ust r
epor
t fin
ding
s co
mpr
ehen
sive
ly, w
hich
is d
efin
edas
incl
udin
g qu
antit
ativ
e an
d st
atis
tical
dat
a fo
r m
ost o
utco
mes
und
erst
udy
Inco
mpl
ete
repo
rtin
g of
find
ings
, inc
ludi
ng fa
ilure
to r
epor
tqu
antit
ativ
e or
sta
tistic
al s
igni
fican
ce fo
r mos
t out
com
es u
nder
stu
dy
Eva
luat
ion
mus
t hav
e be
en p
ublis
hed
or r
elea
sed
betw
een
1990
and
2004
Eva
luat
ions
pub
lishe
d be
fore
or
afte
r th
e de
sign
ated
tim
e fr
ame
Inte
rven
tion
mus
t be
a m
ass
med
ia p
rogr
amm
e, w
hich
is d
efin
ed a
s a
prog
ram
me
that
con
veys
mes
sage
s th
roug
h ch
anne
ls th
at re
ach
a br
oad
audi
ence
. Med
ia in
clud
e ra
dio,
tele
visi
on, v
ideo
, prin
t, an
d th
e In
tern
et;
the
prog
ram
mes
may
take
diff
eren
t for
ms,
suc
h as
rad
io v
arie
ty s
how
s,so
ngs,
adv
ertis
emen
ts o
r pu
blic
ser
vice
ann
ounc
emen
ts, s
oap
oper
as,
mus
ic v
ideo
s, fi
lms,
pam
phle
ts, b
illbo
ards
, pos
ters
and
inte
ract
ive
web
site
s
Inte
rven
tion
is c
omm
unity
-bas
ed, s
choo
l-bas
ed o
r in
terp
erso
nal b
utdo
es n
ot c
onta
in a
mas
s m
edia
com
pone
nt
Obj
ectiv
e of
inte
rven
tion
mus
t be
educ
atio
n ab
out H
IV/A
IDS
or
sexu
alhe
alth
or
risk
redu
ctio
nIn
terv
entio
ns w
hose
mai
n ou
tcom
es a
re n
ot e
xplic
itly
rela
ted
to H
IV/
AID
S, s
uch
as fa
mily
pla
nnin
gIn
terv
entio
n m
ust h
ave
take
n pl
ace
in a
dev
elop
ing
coun
try
Inte
rven
tions
taki
ng p
lace
in o
ther
par
ts o
f the
wor
ld
208
92-4-120938-0_CH07_208

Tab
le 7
.2T
hre
sho
ld o
f ev
iden
ce n
eed
ed t
o r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n o
f ea
ch t
ype
of
inte
rven
tio
n
Inte
rven
tio
nty
pe
Fea
sib
ility
Lac
k o
fp
ote
nti
al f
or
adve
rse
ou
tco
mes
Acc
ept-
abili
tyP
ote
nti
alsi
ze o
fef
fect
Oth
erh
ealt
h o
rso
cial
ben
efit
s
Ove
rall
thre
sho
ldC
om
men
ts
1. R
adio
-onl
y+
++
++
++
+M
oder
ate
Rad
io-o
nly
inte
rven
tions
targ
eted
at o
ther
hea
lthis
sues
hav
e be
en s
how
n to
hav
e su
bsta
ntia
l effe
cts.
2. R
adio
with
othe
r m
edia
++
++
++
++
+M
oder
ate
Sup
port
ing
med
ia o
ften
incl
ude
post
ers,
prin
tm
ater
ials
, lis
teni
ng g
roup
s an
d pr
omot
iona
lm
ater
ials
, suc
h as
T-s
hirt
s an
d ha
ts. S
uppl
emen
tary
inte
rven
tions
, suc
h as
sch
ool w
orks
hops
and
coun
selli
ng, p
rom
ote
awar
enes
s of
loca
l hea
lth a
ndso
cial
res
ourc
es.
3. R
adio
and
tele
visi
onw
ith o
ther
med
ia
++
++
++
+H
igh
Whi
le th
e br
oad
reac
h of
thes
e in
terv
entio
nsin
crea
ses
the
likel
ihoo
d an
d si
ze o
f the
ir ef
fect
s, th
eyar
e fe
asib
le o
nly
whe
n bu
dget
s pe
rmit,
whe
nte
levi
sion
is w
idel
y av
aila
ble
to th
e ta
rget
aud
ienc
e,an
d w
hen
ther
e is
a h
igh
leve
l of c
reat
ive
tale
nt a
ndpr
oduc
tion
faci
litie
s w
ithin
the
coun
try.
Imag
es a
ndst
orie
s in
crea
se th
e po
wer
of t
he m
essa
ges
but m
ayoc
casi
onal
ly c
ause
con
cern
for
loca
l rel
igio
us a
ndco
mm
unity
lead
ers;
how
ever
, with
suf
ficie
nt p
re-
test
ing
and
endo
rsem
ent f
rom
loca
l lea
ders
hip,
thes
e ca
mpa
igns
can
be
high
ly a
ccep
tabl
e
a D
egre
e of
des
irabi
lity
is in
dica
ted
with
a m
axim
um o
f 3 “
+”
sign
s. D
egre
e of
und
esira
bilit
y is
indi
cate
d w
ith a
max
imum
of 3
“-”
sig
ns.
209
92-4-120938-0_CH07_209

Tab
le 7
.3D
escr
ipti
on
of
the
inte
rven
tio
ns
by
stu
dy
Stu
dy,
loca
tio
n a
nd
cam
pai
gn
Tar
get
po
pu
lati
on
an
d p
rim
ary
ob
ject
ives
Des
crip
tio
na
Inte
rven
tio
n t
ype
1 (r
adio
on
ly)
A –
Sai
nt V
ince
nt a
nd th
eG
rena
dine
s, n
atio
nal c
ampa
ign
(5)
• P
aren
ts o
f ado
lesc
ents
, oth
er a
dults
, ado
lesc
ents
• E
ncou
rage
par
ents
to ta
lk to
ado
lesc
ents
abo
utsa
fer
sex
and
cond
om u
se
• R
adio
adv
ertis
ing
cam
paig
n•
Dur
atio
n: 2
mon
ths
Inte
rven
tio
n t
ype
2 (r
adio
wit
h o
ther
med
ia)
B –
Par
agua
y,A
rte
y P
arte
cam
paig
n (6
)•
Ado
lesc
ents
age
d 15
–19
year
s•
Incr
ease
kno
wle
dge
of s
exua
l and
rep
rodu
ctiv
ehe
alth
issu
es in
ord
er to
pro
mot
e re
spon
sibl
ese
xual
beh
avio
ur•
Impr
ove
com
mun
icat
ion
and
nego
tiatio
n sk
ills
• B
ookl
et, s
tree
t the
atre
ski
ts, r
adio
pro
gram
me
and
new
s fla
shes
, col
umns
in n
ewsp
aper
s an
d te
enm
agaz
ines
, sch
ool w
orks
hops
with
vid
eos
• R
each
: 44%
(%
exp
osed
to a
t lea
st o
ne c
ampa
ign
ac
tivity
or
prod
uct)
• D
urat
ion:
abo
ut 2
4–32
mon
ths
C –
Chi
na,
mul
tiple
mas
s m
edia
cam
paig
n in
east
ern
Chi
na (
7)
• Y
oung
adu
lts a
ged
18–3
0 ye
ars
• P
rom
ote
sexu
al a
bstin
ence
prio
r to
mar
riage
• Pro
mot
e us
e of
con
dom
s fo
r sex
ually
act
ive
peop
le,
rega
rdle
ss o
f mar
ital s
tatu
s
• W
ritte
n m
ater
ials
, vid
eos,
rad
io p
rogr
amm
e,w
orks
hops
, sm
all g
roup
dis
cuss
ions
, hom
e vi
sits
,pe
rson
al c
ouns
ellin
g, fr
ee c
ondo
ms
• D
urat
ion:
12
mon
ths
D –
Cam
eroo
n,H
oriz
on J
eune
s ad
oles
cent
repr
oduc
tive
heal
th p
rogr
amm
e(8
)
• Y
oung
peo
ple
(prim
ary
targ
et p
opul
atio
n); p
aren
ts,
teac
hers
, com
mun
ity le
ader
s (s
econ
dary
)•
Incr
ease
ado
lesc
ents
’ aw
aren
ess
and
use
ofre
prod
uctiv
e he
alth
pro
duct
s an
d se
rvic
es
• R
adio
spo
ts a
nd ta
lk s
how
s, b
roch
ures
, pos
ters
,di
scus
sion
s w
ith p
eer
educ
ator
s, v
ideo
bro
adca
sts,
cond
om d
emon
stra
tions
, pre
sen-
tatio
ns a
t soc
cer
gam
es, t
heat
re s
ketc
hes
• R
each
: 28%
eve
r in
volv
ed w
ith a
ctiv
ities
• D
urat
ion:
13
mon
ths
E –
Gui
nea,
PR
ISM
beh
avio
ur c
hang
e yo
uth
cam
paig
n in
Hau
te G
uine
a (9
)
• Y
oung
peo
ple
aged
15–
24 y
ears
• In
crea
se k
now
ledg
e an
d aw
aren
ess
of S
TIs
b an
dH
IV/A
IDS
• P
rom
ote
resp
onsi
ble
sexu
al p
ract
ices
, inc
ludi
ngde
lay
in s
exua
l deb
ut o
r (a
mon
g se
xual
ly a
ctiv
eyo
uth)
con
dom
use
• In
tera
ctiv
e ra
dio
show
s in
rur
al a
reas
, pos
ters
,br
ochu
res;
thea
tre
grou
ps p
rodu
ced
play
s, le
ddi
scus
sion
s•
Rea
ch: 8
3% o
f mal
es a
nd 6
3% o
f fem
ales
exp
osed
to a
ny c
ampa
ign
activ
ity•
Dur
atio
n: 1
2 m
onth
s
210
92-4-120938-0_CH07_210

F –
Zim
babw
e,pr
omot
ing
sexu
al r
espo
nsib
ility
amon
g yo
ung
peop
le (
10)
• Y
oung
peo
ple
aged
10–
24 y
ears
and
adu
lts•
Incr
ease
kno
wle
dge
of r
epro
duct
ive
heal
th a
ndco
ntra
cept
ion
• P
oste
rs, l
eafle
ts, n
ewsl
ette
r, r
adio
pro
gram
me,
laun
ch e
vent
s, d
ram
as, p
eer
educ
ator
s, h
otlin
e;tr
aini
ng fo
r fam
ily p
lann
ing
prov
ider
s, d
esig
natio
n of
yout
h-fr
iend
ly c
linic
s•
Rea
ch: 9
7% e
xpos
ure
to a
t lea
st o
ne c
ampa
ign
com
pone
nt•
Dur
atio
n: 6
mon
ths
G –
Bot
swan
a,T
sa B
anan
a ad
oles
cent
repr
oduc
tive
heal
th p
rogr
amm
e (1
1)
• A
dole
scen
ts (
prim
ary
targ
et p
opul
atio
n); p
aren
ts,
teac
hers
and
you
th c
omm
unity
lead
ers
(sec
onda
ry)
• P
ersu
ade
adol
esce
nts
that
rep
rodu
ctiv
e he
alth
serv
ices
exi
st fo
r th
em a
nd th
at th
ey s
houl
d us
eth
em
• R
adio
mes
sage
s, p
rinte
d m
edia
• R
each
: 71%
of m
ales
and
68%
fem
ales
exp
osed
toan
y ca
mpa
ign
activ
ity•
Dur
atio
n: 8
mon
ths
Inte
rven
tio
n t
ype
3 (r
adio
an
d t
elev
isio
n w
ith
oth
er m
edia
)H
– G
uine
a,ad
oles
cent
rep
rodu
ctiv
e he
alth
prog
ram
me
(12)
• A
dole
scen
ts a
nd y
oung
adu
lts•
Incr
ease
you
ng p
eopl
e’s
know
ledg
e of
ST
Is a
ndA
IDS
• Inc
reas
e kn
owle
dge
and
use
of c
ondo
ms
and
othe
rm
oder
n co
ntra
cept
ives
• D
elay
age
at s
exua
l deb
ut•
Enc
oura
ge s
exua
l abs
tinen
ce
• P
oste
rs, f
lyer
s, p
eer
educ
ator
dis
cuss
ions
;ca
mpa
ign
supp
lem
ente
d w
ith r
adio
and
tele
visi
onad
vert
isem
ents
for
spec
ific
cond
om b
rand
s•
Rea
ch: 3
9% o
f mal
es a
nd 1
5% o
f fem
ales
part
icip
ated
in p
rogr
amm
e•
Dur
atio
n: 8
-9 m
onth
s
I – Z
ambi
a,H
EA
RT
cam
paig
n (1
3)•
You
ng p
eopl
e ag
ed 1
5–19
yea
rs•
Cha
nge
soci
al n
orm
s an
d in
divi
dual
sex
ual
beha
viou
r, s
peci
fical
ly fo
cusi
ng o
n co
nsis
tent
cond
om u
se, c
ontin
uatio
n of
abs
tinen
ce,
know
ledg
e th
at p
eopl
e w
ho lo
ok h
ealth
y ca
n ha
veH
IV, b
elie
f tha
t con
dom
s an
d ab
stin
ence
are
hip
• T
elev
isio
n sp
ots,
rad
io s
pots
, son
gs, p
oste
rs,
stic
kers
, exe
rcis
e bo
oks,
mes
sage
s on
bus
es,
mus
ic v
ideo
s•
Dur
atio
n: 6
mon
ths
• R
each
: 52%
exp
osed
to a
t lea
st o
ne T
Vad
vert
isem
ent o
r pu
blic
ser
vice
ann
ounc
emen
t
211
92-4-120938-0_CH07_211

Stu
dy,
loca
tio
n a
nd
cam
pai
gn
Tar
get
po
pu
lati
on
an
d p
rim
ary
ob
ject
ives
Des
crip
tio
na
J –
Sou
th A
fric
a,lo
veLi
fe c
ampa
ign
(14,
15)
• Y
oung
peo
ple
aged
12–
17 y
ears
• R
educ
e th
e ra
te o
f HIV
infe
ctio
n, o
ther
ST
Is a
ndpr
egna
ncy
• P
rom
ote
posi
tive
choi
ces
arou
nd s
exua
lpa
rtne
rshi
ps, c
ondo
m u
se, s
exua
l deb
ut, t
reat
men
tse
ekin
g, H
IV r
isk
beha
viou
rs
• M
ultim
edia
cam
paig
n in
clud
ing
radi
o, te
levi
sion
, prin
tan
d bi
llboa
rds.
• D
urat
ion:
abo
ut 2
4 m
onth
s•
Rea
ch: 8
4% o
f you
th h
ad h
eard
of o
r se
en a
com
pone
nt o
f the
love
Life
cam
paig
n
K –
Côt
e d’
Ivoi
re,
PL.
U.S
pos
itive
dev
ianc
eca
mpa
ign
(16)
• Y
oung
fem
ales
age
d 13
–20
year
s (p
rimar
y ta
rget
popu
latio
n); m
ale
yout
h, p
aren
ts (
seco
ndar
y)•
Incr
ease
kno
wle
dge
and
prac
tice
of H
IV/A
IDS
prev
entio
n be
havi
ours
• In
crea
se u
se o
f rep
rodu
ctiv
e he
alth
ser
vice
s
• Tel
evis
ion
spot
s, c
omm
unity
radi
o va
riety
sho
w, a
udio
cass
ette
s of
pop
ular
son
gs, p
hoto
nove
lla, p
oste
rs,
leaf
lets
, adv
ocac
y br
ochu
re•
Dur
atio
n: 9
mon
ths
• Rea
ch: 7
0% o
f mal
es a
nd 6
4% o
f fem
ales
exp
osed
toat
leas
t one
cam
paig
n m
ater
ial o
r ac
tivity
L –
Sou
th A
fric
a,S
oul C
ity c
ampa
ign
(17–
19)
• P
revi
ousl
y di
sadv
anta
ged
“Afr
ican
” an
d “c
olou
red”
Sou
th A
fric
ans
(age
d 16
–65
year
s)•
Affe
ct a
war
enes
s of
and
kno
wle
dge
and
attit
udes
abou
t HIV
/AID
S•
Influ
ence
sub
ject
ive
soci
al n
orm
s, p
erce
ptio
n of
pers
onal
ris
k of
HIV
• In
crea
se s
elf-
effic
acy
with
reg
ard
to H
IV p
reve
ntio
nbe
havi
ours
• P
rom
ote
seek
ing
info
rmat
ion
and
supp
ort,
risk
redu
ctio
n
• T
elev
isio
n an
d ra
dio
dram
as, b
ookl
ets,
nat
iona
lad
voca
cy s
trat
egy
• S
oul B
uddy
z –
radi
o an
d bo
okle
ts d
esig
ned
to ta
rget
child
ren
aged
8–1
2 ye
ars
• R
each
: 82%
(an
y ca
mpa
ign
com
pone
nt)
M –
Sou
th A
fric
a,ad
oles
cent
rep
rodu
ctiv
e he
alth
prog
ram
me
(20)
• Y
oung
fem
ales
age
d 16
–20
year
s•
Edu
cate
ado
lesc
ents
abo
ut r
epro
duct
ive
heal
this
sues
• P
rom
ote
safe
r se
x
• R
adio
mes
sage
s, w
eekl
y ra
dio
talk
sho
ws,
docu
men
tary
sho
wn
on S
outh
Afr
ica
Bro
adca
stin
gC
orpo
ratio
n• D
urat
ion:
Rep
rodu
ctiv
e he
alth
cam
paig
n –
12 m
onth
s;so
cial
mar
ketin
g ca
mpa
ign
ongo
ing
4–5
year
spr
evio
usly
212
92-4-120938-0_CH07_212

N –
44
coun
trie
s w
orld
wid
e,S
tayi
ng A
live
MT
Vca
mpa
ign
(21)
• Y
oung
peo
ple
aged
16–
25 y
ears
• In
crea
se a
war
enes
s of
HIV
• E
ncou
rage
pre
vent
ion
• R
educ
e H
IV-r
elat
ed s
tigm
a an
d di
scrim
inat
ion
• T
elev
isio
n do
cum
enta
ry, p
rogr
amm
e fe
atur
ing
Bill
Clin
ton,
pub
lic s
ervi
ce a
nnou
ncem
ents
, glo
bal f
orum
,co
ncer
ts, w
eb s
ite.
• R
each
: Kat
hman
du: 1
2% e
xpos
ed to
at l
east
one
cam
paig
n m
ater
ial o
r act
ivity
; Sao
Pau
lo: 2
3%; D
akar
:82
%O
– G
hana
, Sto
p A
IDS
Love
Life
, pha
se 1
cam
paig
n (2
2)
• Y
oung
peo
ple
• In
crea
se k
now
ledg
e of
how
to a
void
AID
S a
ndpe
rcei
ved
pers
onal
ris
k of
HIV
infe
ctio
n•
Impr
ove
inte
rper
sona
l com
mun
icat
ion
abou
tH
IV/A
IDS
• In
crea
se p
erce
ptio
ns th
at s
ocia
l nor
ms
that
favo
urH
IV-p
rote
ctiv
e be
havi
ours
• In
crea
se u
se o
f saf
er s
exua
l beh
avio
urs
• La
unch
eve
nt, m
usic
vid
eo a
nd s
ong
perf
orm
ed b
yw
ell k
now
n lo
cal m
usic
ians
, tel
evis
ion
and
radi
osp
ots,
ser
ial d
ram
as, c
omm
unity
ral
lies,
van
s w
ithau
dio-
visu
al d
ispl
ays
• D
urat
ion:
17
mon
ths
• R
each
: 83%
mal
es a
nd 7
7% fe
mal
es o
f tho
se a
ged
15 to
45+
yea
rs e
xpos
ed to
any
cam
paig
n co
mpo
nent
a P
erce
ntag
es d
escr
ibin
g “r
each
” in
dica
te th
e pr
opor
tion
of th
e st
udy
popu
latio
n th
at r
epor
ted
bein
g ex
pose
d to
the
inte
rven
tion.
b S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
213
92-4-120938-0_CH07_213

Tab
le 7
.4D
escr
ipti
on
of
ou
tco
me
eval
uat
ion
s b
y st
ud
y
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
Inte
rven
tio
n t
ype
1 (r
adio
on
ly)
A (
5)D
esig
n: c
ross
-sec
tiona
l sur
vey
com
parin
gex
pose
d pa
rtic
ipan
ts w
ith u
nexp
osed
Sam
ple
size
: 297
(in
terv
entio
n gr
oup
= 2
13, c
ontr
ol g
roup
= 8
4)
No
stat
istic
al a
djus
tmen
ts m
ade
for
diffe
renc
es b
etw
een
expo
sed
and
unex
pose
d
Hea
lth s
ervi
ces
• H
eard
of A
IDS
hot
line
– si
gnifi
cant
Red
uctio
n in
vul
nera
bilit
y•
Frie
nds
use
cond
oms
– si
gnifi
cant
• P
artn
er s
ugge
sted
con
dom
use
– n
otsi
gnifi
cant
Red
uctio
n in
HIV
pre
vale
nce
• Eve
r or a
lway
s us
ed a
con
dom
or s
ugge
sted
cond
om u
se to
one
’s p
artn
er –
not
sign
ifica
nt
Sev
eral
mea
sure
s of
inte
rper
sona
lco
mm
unic
atio
n –
not s
igni
fican
t
Wea
k ev
iden
ce fo
r im
prov
ed p
erce
ptio
ns in
soci
al n
orm
s, in
terp
erso
nal c
omm
unic
atio
nan
d co
ndom
use
Str
ong
evid
ence
for i
ncre
ased
aw
aren
ess
ofA
IDS
hot
line
Inte
rven
tio
n t
ype
2 (r
adio
wit
h o
ther
med
ia)
B (
6)D
esig
n: s
urve
y pr
e-in
terv
entio
n an
d po
st-
inte
rven
tion
in th
ree
inte
rven
tion
citie
s.C
ross
-sec
tiona
l ana
lysi
s co
mpa
ring
expo
sed
with
une
xpos
ed
Sam
ple
size
: pre
-inte
rven
tion
= 9
47, p
ost-
inte
rven
tion
= 1
575
Kno
wle
dge
• 2/
2 ou
tcom
es –
not
sig
nific
ant
Red
uctio
n in
HIV
pre
vale
nce
• Had
sex
for t
he fi
rst t
ime,
con
dom
use
at f
irst
sexu
al r
elat
ions
hip
– no
t sig
nific
ant
• U
sed
a co
ndom
in la
st s
exua
l rel
atio
nshi
p –
not s
igni
fican
t
Wea
k ev
iden
ce fo
r im
prov
ed k
now
ledg
e;w
eak
evid
ence
for
impr
ovem
ents
inab
stin
ence
and
con
dom
-use
beh
avio
urs
C (
7)D
esig
n: e
xper
imen
tal r
ando
miz
edco
ntro
lled
tria
l with
pre
-inte
rven
tion
and
post
-inte
rven
tion
com
pone
nts
mat
chin
g
Kno
wle
dge
• 5/
5 ge
nera
l kno
wle
dge
outc
omes
–si
gnifi
cant
Str
ong
evid
ence
for
incr
easi
ng k
now
ledg
ean
d se
lf-ef
ficac
y to
neg
otia
te c
ondo
m u
se,
redu
cing
the
num
ber
of p
artn
ers
and
cond
om-u
se b
ehav
iour
s
214
92-4-120938-0_CH07_214

two
inte
rven
tion
villa
ges
and
two
cont
rol
villa
ges
Sam
ple
size
: pre
-inte
rven
tion
= 7
48, p
ost-
inte
rven
tion
= 7
10 (
366
in in
terv
entio
ngr
oup
and
344
in c
ontr
ol g
roup
)
• 10
/10
rout
es b
y w
hich
HIV
can
or c
anno
t be
tran
smitt
ed –
sig
nific
ant
Ski
lls•
Con
fiden
ce to
con
vinc
e pa
rtne
r to
use
cond
om –
sig
nific
ant
Red
uctio
n in
HIV
pre
vale
nce
• 3/
3 co
ndom
out
com
es –
sig
nific
ant
• 1/
1 ou
tcom
es r
egar
ding
num
ber o
f par
tner
s–
sign
ifica
ntD
(8)
Des
ign:
sep
arat
e sa
mpl
ing
pre-
inte
rven
tion
and
post
-inte
rven
tion
in o
nein
terv
entio
n ci
ty a
nd o
ne c
ontr
ol c
ity
Sam
ple
size
: pre
-inte
rven
tion
= 1
606,
post
-inte
rven
tion
= 1
633
(811
inin
terv
entio
n gr
oup
and
822
in c
ontr
ol)
Kno
wle
dge
• W
heth
er A
IDS
is a
void
able
– m
ixed
res
ults
Hea
lth s
ervi
ces
• E
ver
visi
ted
a he
alth
cen
tre
for
info
rmat
ion
abou
t con
trac
eptiv
es –
not
sig
nific
ant
Red
uctio
n in
vul
nera
bilit
y•
Sm
all t
o m
oder
ate
diffe
renc
es in
per
cept
ion
of b
eing
at h
igh
risk
for
ST
Ia or
AID
S –
sign
ifica
nt
Red
uctio
n in
HIV
pre
vale
nce
• 3/
6 A
BC
pro
gram
me
(Abs
tain
, Be
faith
ful,
use
Con
dom
s) o
utco
mes
– n
ot s
igni
fican
t•
Rem
aini
ng 3
out
com
es –
mix
ed r
esul
ts b
yse
x of
par
ticip
ant
Fre
quen
t dis
cuss
ion
of s
exua
lity
– si
gnifi
cant
Wea
k ev
iden
ce fo
r in
crea
ses
in k
now
ledg
e,pe
rcei
ved
pers
onal
risk
of H
IV a
nd in
crea
ses
in v
isits
to h
ealth
cen
tres
; wea
k ev
iden
ce o
fim
prov
emen
ts in
abs
tinen
ce, p
artn
erre
duct
ion
and
cond
om u
se
Mod
erat
e ev
iden
ce fo
r im
prov
emen
ts in
inte
rper
sona
l com
mun
icat
ion
215
92-4-120938-0_CH07_215

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
E (
9)D
esig
n: b
asel
ine
esta
blis
hed
by p
roxy
usin
g D
emog
raph
ic a
nd H
ealth
Sur
vey
data
; dat
a fo
r po
st-t
est c
olle
cted
from
rand
om s
ampl
e of
you
ths
in th
ein
terv
entio
n ar
ea a
nd a
redu
ced
sam
ple
inth
e co
mpa
rison
are
a
Sam
ple
size
: pre
-inte
rven
tion
= 4
17, p
ost-
inte
rven
tion
= 1
008
(908
in in
terv
entio
ngr
oup
and
100
in c
ontr
ol g
roup
)
Kno
wle
dge
• 1/
4 ou
tcom
es –
sig
nific
ant
Ski
lls•
Kno
wle
dge
of h
ow to
use
con
dom
s –
two
times
hig
her
for
mal
es a
nd n
early
thre
etim
es h
ighe
r fo
r fe
mal
es; s
igni
fican
t
Hea
lth s
ervi
ces
• K
now
s w
here
to g
et c
ondo
ms
– si
gnifi
cant
Red
uctio
n in
vul
nera
bilit
y•
Hig
h pe
rcei
ved
pers
onal
ris
k of
con
trac
ting
HIV
/AID
S –
not
sig
nific
ant
• Y
outh
who
rep
ort t
hat o
ther
s ar
e m
ore
open
to d
iscu
ssin
g re
prod
uctiv
e he
alth
que
stio
nsth
an o
ne y
ear
prio
r –
sign
ifica
nt
Red
uctio
n in
HIV
pre
vale
nce
• Eve
r use
a c
ondo
m, c
ondo
m u
se a
t las
t sex
,re
com
men
ding
con
dom
s to
oth
ers
–si
gnifi
cant
Wea
k ev
iden
ce o
f inc
reas
ed k
now
ledg
e an
dpe
rcep
tion
of p
erso
nal r
isk
Str
ong
evid
ence
for
impr
oved
con
dom
-use
skill
s, a
war
enes
s of
con
dom
ven
dors
as
wel
las
impr
ovem
ents
in s
ocia
l nor
ms,
con
dom
use
and
inte
rper
sona
l com
mun
icat
ion
F (
10)
Des
ign:
ran
dom
sam
ple
usin
g pr
e-in
terv
entio
n an
d po
st-in
terv
entio
n de
sign
with
cro
ss-s
ectio
nal a
sses
smen
tco
mpa
ring:
5 in
terv
entio
n an
d 2
com
paris
on s
ites
and
com
bini
ng d
ata
from
all s
ites
and
anal
ysin
g ou
tcom
es b
yex
posu
re to
inte
rven
tion
com
pone
nts
Sam
ple
size
: pre
-inte
rven
tion
= 1
426
(973
in in
terv
entio
n gr
oup
and
453
in c
ontr
ol),
Kno
wle
dge
• 1/
3 ou
tcom
es –
sig
nific
ant
Hea
lth s
ervi
ces
• Li
kelih
ood
of h
avin
g so
ught
ser
vice
s at
heal
th c
entr
e –
sign
ifica
ntly
hig
her
asnu
mbe
r of
cam
paig
n co
mpo
nent
s ex
pose
dto
incr
ease
s
Red
uctio
n in
HIV
pre
vale
nce
Wea
k ev
iden
ce fo
r in
crea
sing
kno
wle
dge
Str
ong
evid
ence
for
impr
ovem
ents
inse
ekin
g he
alth
ser
vice
s, a
bsta
inin
g fr
omse
x, r
educ
ing
num
ber
of p
artn
ers,
usi
ngco
ndom
s an
d in
terp
erso
nal c
omm
unic
atio
n
216
92-4-120938-0_CH07_216

post
-inte
rven
tion
= 1
400
(100
0 in
inte
rven
tion
grou
p an
d 40
0 in
con
trol
)
Sta
tistic
al a
djus
tmen
ts c
ondu
cted
for a
ge,
sex
of p
artic
ipan
t, ed
ucat
ion,
sex
ual
expe
rienc
e, m
arita
l sta
tus
and
urba
n vs
rura
l res
iden
ce
• Lik
elih
ood
of s
ayin
g no
to s
ex a
nd c
ontin
ued
abst
inen
ce –
sig
nific
antly
hig
her
amon
gin
terv
entio
n gr
oup
and
as n
umbe
r of
cam
paig
n co
mpo
nent
s ex
pose
d to
incr
ease
s•
6/7
outc
omes
reg
ardi
ng in
terp
erso
nal
com
mun
icat
ion
– si
gnifi
cant
G (
11)
Des
ign:
pre
-inte
rven
tion
and
post
-in
terv
entio
n co
mpo
nent
com
parin
g an
inte
rven
tion
city
with
a c
ontr
ol c
ity
Sam
ple
size
: pre
-inte
rven
tion
= 1
002,
post
-inte
rven
tion
= 2
396
(123
0 in
inte
rven
tion
grou
p an
d 11
66 in
con
trol
)
Kno
wle
dge
• 2/
2 ou
tcom
es –
not
sig
nific
ant
Red
uctio
n in
vul
nera
bilit
y•
Impr
ovem
ents
in b
oth
inte
rven
tion
and
com
paris
on g
roup
s fo
r st
atem
ent “
very
few
of m
y fr
iend
s us
e co
ndom
s” –
sig
nific
ant
Wea
k ev
iden
ce fo
r im
prov
ed k
now
ledg
ean
d im
prov
emen
ts in
soc
ial n
orm
s
Inte
rven
tio
n t
ype
3 (r
adio
an
d t
elev
isio
n w
ith
oth
er m
edia
)H
(12
)D
esig
n: p
re-in
terv
entio
n an
d po
st-
inte
rven
tion
surv
ey in
citi
es in
two
regi
ons;
inte
rven
tion
and
cont
rol g
roup
s w
ithin
each
city
Sam
ple
size
: pre
-inte
rven
tion
= 2
016,
post
-inte
rven
tion
= 2
005
(100
9 in
inte
rven
tion
grou
p an
d 99
6 in
con
trol
)
Sta
tistic
al a
djus
tmen
ts w
ere
mad
e fo
rdi
ffere
nces
in s
ex o
f par
ticip
ant,
age,
scho
ol e
nrol
men
t, sc
hool
type
,em
ploy
men
t sta
tus,
relig
ion,
mar
ital s
tatu
san
d nu
mbe
r of
chi
ldre
n
Kno
wle
dge
• K
now
ledg
e of
con
dom
as
mea
ns o
fpr
otec
ting
agai
nst A
IDS
– s
igni
fican
t
Hea
lth s
ervi
ces
• V
isiti
ng h
ealth
cen
tre
in th
e pa
st y
ear
–m
ixed
out
com
es b
y se
x of
par
ticip
ant
Red
uctio
n in
vul
nera
bilit
y•
Per
ceiv
ed p
erso
nal r
isk
of H
IV/A
IDS
– n
otsi
gnifi
cant
Wea
k ev
iden
ce fo
r im
prov
emen
ts in
seek
ing
heal
th s
ervi
ces,
per
ceiv
ed p
erso
nal
risk
and
AB
C b
ehav
iour
s (A
bsta
in, B
efa
ithfu
l, us
e C
ondo
ms)
Str
ong
evid
ence
for
impr
oved
kno
wle
dge
217
92-4-120938-0_CH07_217

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
Red
uctio
n in
HIV
pre
vale
nce
• B
eing
sex
ually
exp
erie
nced
– n
otsi
gnifi
cant
• H
avin
g 2
par
tner
s in
4 w
eeks
– n
otsi
gnifi
cant
• P
rote
ctin
g se
lf fr
om s
exua
l ris
ks b
y us
ing
cond
oms
– no
t sig
nific
ant
• O
nset
of s
exua
l act
ivity
by
age
15 y
ears
– m
ixed
out
com
es b
y se
x of
par
ticip
ant
• Usu
ally
use
s co
ndom
s –
mix
ed o
utco
mes
by s
ex o
f par
ticip
ant
• C
ondo
m u
se d
urin
g la
st s
ex –
sig
nific
ant
I (13
)D
esig
n: s
epar
ate
sam
ple
with
pre
-in
terv
entio
n an
d po
st-in
terv
entio
nco
mpo
nent
; cro
ss-s
ectio
nal a
naly
sis
com
parin
g pa
rtic
ipan
ts w
ho s
aw a
ll or
som
eof
the
tele
visi
on h
ealth
com
mun
icat
ion
spot
s an
d th
ose
who
saw
non
e
Sam
ple
size
: pre
-inte
rven
tion
= 9
01, p
ost-
inte
rven
tion
= 1
100;
vie
wer
s =
572
, non
-vi
ewer
s =
528
Sta
tistic
al a
djus
tmen
ts w
ere
mad
e fo
rdi
ffere
nces
in a
ge, e
duca
tion,
sex
of
part
icip
ant,
and
urba
n vs
rura
l res
iden
ce
Kno
wle
dge
• R
ecal
l abs
tinen
ce a
s a
way
to p
reve
ntH
IV –
sig
nific
ant
• R
ecal
ling
that
usi
ng c
ondo
ms
is a
way
topr
even
t HIV
– n
ot s
igni
fican
t
Ski
lls•
Sel
f-ef
ficac
y sc
ore
for
cond
om u
se –
sign
ifica
nt
Hea
lth s
ervi
ces
• A
war
enes
s of
vol
unta
ry c
ouns
ellin
g an
dte
stin
g –
sign
ifica
nt•
Aw
aren
ess
of p
lace
s to
pur
chas
eco
ndom
s –
sign
ifica
nt
Red
uctio
n in
vul
nera
bilit
y•
Per
ceiv
ed r
isk
of H
IV –
not
sig
nific
ant
Wea
k ev
iden
ce fo
r kn
owle
dge
of c
ondo
ms
Str
ong
evid
ence
for
incr
easi
ng k
now
ledg
eof
abs
tinen
ce, i
ncre
asin
g se
lf-ef
ficac
y in
use
of c
ondo
ms
and
impr
ovem
ents
inaw
aren
ess
of h
ealth
ser
vice
s, a
bstin
ence
and
cond
om-u
se b
ehav
iour
s
218
92-4-120938-0_CH07_218

Red
uctio
n in
HIV
pre
vale
nce
• 1/
1 ab
stin
ence
out
com
es –
sig
nific
ant
• 2/
2 co
ndom
-use
out
com
es –
sig
nific
ant
• M
ean
num
ber
of p
eopl
e w
ith w
hom
disc
usse
d ab
stin
ence
– s
igni
fican
tJ (1
4, 1
5)D
esig
n: r
ando
m s
ampl
e w
ith o
nly
post
-in
terv
entio
n cr
oss-
sect
iona
l ana
lysi
sco
mpa
ring
part
icip
ants
who
wer
e ex
pose
dto
the
inte
rven
tion
with
thos
e w
ho w
ere
not
Sam
ple
size
: 11
904
Ski
lls•
Eve
r te
sted
for
HIV
– s
igni
fican
t
Red
uctio
n in
HIV
pre
vale
nce
• P
reva
lenc
e of
HIV
am
ong
yout
h w
hopa
rtic
ipat
ed in
love
Life
pro
gram
mes
–fe
mal
es, a
djus
ted
odds
rat
io =
0.6
1(P
< 0
.01)
; mal
es: a
djus
ted
odds
rat
io=
0.6
0 (P
= 0
.01)
• E
ver
talk
ed to
par
ents
abo
ut H
IV –
sign
ifica
nt
Str
ong
evid
ence
for
impr
ovem
ents
inpa
rtic
ipat
ion
in H
IV te
stin
g, in
terp
erso
nal
com
mun
icat
ion
abou
t HIV
and
dec
reas
es in
HIV
infe
ctio
n ra
tes
K (
16)
Des
ign:
sep
arat
e sa
mpl
e pr
e-in
terv
entio
nan
d po
st-in
terv
entio
n
Sam
ple
size
: pre
-inte
rven
tion
= 2
681,
pos
t-in
terv
entio
n =
223
2
Ski
lls•
Sel
f-ef
ficac
y to
ref
use
sex
with
gift
-giv
ers
– si
gnifi
cant
• Sel
f-ef
ficac
y to
con
sist
ently
use
con
dom
s–
sign
ifica
nt
Red
uctio
n in
vul
nera
bilit
y•
Per
ceiv
ed p
eer
supp
ort f
or a
bstin
ence
–m
argi
nally
sig
nific
ant d
iffer
ence
Red
uctio
n in
HIV
pre
vale
nce
• C
onsi
sten
t con
dom
use
– m
argi
nally
sign
ifica
nt d
iffer
ence
s•
Dis
cuss
ion
abou
t abs
tinen
ce w
ithpa
rent
– s
igni
fican
t• E
ncou
ragi
ng s
omeo
ne to
use
con
dom
s in
the
past
12
mon
ths
– si
gnifi
cant
Wea
k ev
iden
ce fo
r in
crea
ses
in p
erce
ived
peer
sup
port
for
abst
inen
ce a
nd c
ondo
mus
e
Str
ong
evid
ence
for
incr
ease
s in
sel
f-ef
ficac
y an
d in
terp
erso
nal c
omm
unic
atio
n
219
92-4-120938-0_CH07_219

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
Lb –
stud
y 1
(17,
18)
;st
udy
2 (1
9)
Stu
dy 1
Des
ign:
ran
dom
sam
ple
with
pre
-in
terv
entio
n an
d po
st-in
terv
entio
nco
mpo
nent
, fol
low
ing
a pa
nel o
fre
spon
dent
s in
one
urb
an a
nd o
ne r
ural
site
; cro
ss-s
ectio
nal a
naly
sis
com
parin
gpa
rtic
ipan
ts w
ho w
ere
expo
sed
to th
ein
terv
entio
n to
thos
e w
ho w
ere
not
Sam
ple
size
: pre
-inte
rven
tion
= 2
000,
post
-inte
rven
tion
= 2
000
Stu
dy 2
Des
ign:
pre
-inte
rven
tion
and
post
-in
terv
entio
n tr
ial;
cros
s-se
ctio
nal
anal
ysis
com
parin
g pa
rtic
ipan
ts w
how
ere
expo
sed
to th
e in
terv
entio
n(in
terv
entio
n ar
m) t
o th
ose
who
wer
e no
tex
pose
d (c
ompa
rison
arm
), c
ontr
ollin
gfo
r ex
posu
re to
oth
er H
IV/A
IDS
prog
ram
mes
Sam
ple
size
: pre
-inte
rven
tion
= 4
21,
post
-inte
rven
tion
= 4
16
Kno
wle
dge
• D
isag
reem
ent w
ith id
ea th
at th
ere
is a
cure
for
AID
S –
sig
nific
ant d
iffer
ence
spr
e-in
terv
entio
n an
d po
st-in
terv
entio
n(2
1, 2
6)•
AID
S k
now
ledg
e in
dex
asso
ciat
ed w
ithex
posu
re to
Sou
l Bud
dyz
TV
and
rad
iopr
ogra
mm
ing
– si
gnifi
cant
ly lo
wer
(8)
Red
uctio
n in
vul
nera
bilit
y•
4/4
soci
al n
orm
out
com
es r
egar
ding
abst
inen
ce, c
ondo
ms
and
stig
ma
–si
gnifi
cant
(21
, 27)
Red
uctio
n in
HIV
pre
vale
nce
• A
lway
s us
e a
cond
om –
sig
nific
antly
high
er a
s ex
posu
re to
num
ber
of S
oul
City
med
ia in
crea
ses
• O
ften
talk
to s
omeo
ne c
lose
abo
ut H
IV/
AID
S –
sig
nific
antly
hig
her a
s ex
posu
re to
num
ber
of S
oul C
ity m
edia
incr
ease
s(2
1, 2
7)•
Hig
her
cons
iste
nt c
ondo
m u
se in
dex
–as
soci
ated
with
exp
osur
e to
Sou
l City
radi
o dr
ama
(8)
Mix
ed e
vide
nce
for
incr
ease
s in
know
ledg
e
Str
ong
evid
ence
for
impr
ovem
ents
inso
cial
nor
ms
rega
rdin
g ab
stin
ence
,co
ndom
s an
d st
igm
a, a
nd in
crea
ses
inco
ndom
use
and
inte
rper
sona
lco
mm
unic
atio
n
M (
20)
Des
ign:
ran
dom
sam
ple
with
pre
-in
terv
entio
n an
d po
st-in
terv
entio
nco
mpo
nent
s co
mpa
ring
two
purp
osiv
ely
sele
cted
com
mun
ities
Kno
wle
dge
• K
now
ledg
e th
at c
ondo
ms
are
the
best
way
to p
reve
nt H
IV/A
IDS
– s
igni
fican
t
Red
uctio
n in
HIV
pre
vale
nce
• E
ver
had
sex
– no
t sig
nific
ant
Wea
k ev
iden
ce fo
r in
crea
ses
in c
ondo
mus
e
Str
ong
evid
ence
for
incr
ease
s in
know
ledg
e ab
out c
ondo
ms
220
92-4-120938-0_CH07_220

Sam
ple
size
: pre
-inte
rven
tion
= 2
26,
(118
in in
terv
entio
n gr
oup
and
108
inco
ntro
l gro
up),
pos
t-in
terv
entio
n =
204
(no
data
on
inte
rven
tion
vs c
ontr
ol)
• E
ver
used
a c
ondo
m –
not
sig
nific
ant
• C
ondo
m u
sed
durin
g la
st s
ex a
ct –
not
sign
ifica
nt
N (
21)
Des
ign:
ran
dom
sam
ple
with
pre
-in
terv
entio
n an
d po
st-in
terv
entio
nco
mpo
nent
s us
ing
hous
ehol
d su
rvey
san
d po
pula
tion-
base
d su
rvey
s; c
ross
-se
ctio
nal a
naly
sis
com
parin
gpa
rtic
ipan
ts w
ho w
ere
expo
sed
to th
ein
terv
entio
n to
thos
e w
ho w
ere
not
expo
sed
in K
athm
andu
, Nep
al, S
aoP
aulo
, Bra
zil,
and
Dak
ar, S
eneg
al
Sam
ple
size
: pre
-inte
rven
tion
= 3
000
(100
0 pe
r si
te),
pos
t-in
terv
entio
n =
300
0(1
000
per
site
)
Red
uctio
n in
vul
nera
bilit
y•
Pos
itive
ass
ocia
tion
betw
een
cam
paig
nex
posu
re a
nd b
elie
fs a
bout
impo
rtan
ce o
fus
ing
cond
oms,
dis
cuss
ing
HIV
with
ase
xual
par
tner
, and
get
ting
test
ed fo
r HIV
• A
ssoc
iatio
n be
twee
n ex
posu
re a
ndeg
alita
rian
gend
er n
orm
s –
mix
ed r
esul
ts
Red
uctio
n in
HIV
pre
vale
nce
• Num
ber o
f diff
eren
t typ
es o
f peo
ple
talk
edto
in th
e pa
st m
onth
abo
ut H
IV/A
IDS
–si
gnifi
cant
Wea
k ev
iden
ce fo
r im
prov
emen
ts in
soc
ial
norm
s
Str
ong
evid
ence
for
incr
ease
s in
inte
rper
sona
l com
mun
icat
ion
O (
22)
Des
ign:
bas
elin
e es
tabl
ishe
d by
pro
xyus
ing
data
from
DH
S D
emog
raph
ic a
ndH
ealth
Sur
vey
and
the
Gha
na Y
outh
Sur
vey;
mid
-ter
m a
sses
smen
t use
d da
tafr
om th
e G
hana
Rep
rodu
ctiv
e H
ealth
and
Chi
ld S
urvi
val S
urve
y
Sam
ple
size
: Pre
-you
th s
urve
y =
135
5,po
st-y
outh
sur
vey
= 1
161
Sta
tistic
al a
djus
tmen
ts m
ade
for
diffe
renc
es in
age
, edu
catio
n, m
arita
lst
atus
, reg
ion,
urb
an v
sru
ral r
esid
ence
,re
ligio
n an
d m
edia
acc
ess
Ski
lls•
Sel
f-ef
ficac
y to
use
con
dom
s fo
r th
ose
expo
sed
with
hig
h ex
posu
re to
cam
paig
n–
sign
ifica
nt
Red
uctio
n in
vul
nera
bilit
y•
Per
ceiv
ed p
eer
appr
oval
for
abst
inen
cean
d co
ndom
use
– s
igni
fican
t
Red
uctio
n in
HIV
pre
vale
nce
• M
edia
n ag
e of
firs
t sex
– n
ot s
igni
fican
t
Wea
k ev
iden
ce fo
r in
crea
ses
in s
elf-
effic
acy
in te
rms
of a
bstin
ence
and
inab
stin
ence
and
par
tner
-red
uctio
nbe
havi
ours
Mod
erat
e ev
iden
ce fo
r in
crea
ses
in s
elf-
effic
acy
in th
e us
e of
con
dom
s
Str
ong
evid
ence
for i
ncre
ases
in p
erce
ived
peer
app
rova
l for
abs
tinen
ce a
nd c
ondo
mus
e, a
s w
ell a
s im
prov
emen
ts in
con
dom
use
and
inte
rper
sona
l com
mun
icat
ion
221
92-4-120938-0_CH07_221

Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
• N
umbe
r of
sex
ually
act
ive
resp
onde
nts
havi
ng s
ex w
ith m
ore
than
one
par
tner
in th
e pa
st 1
2m
onth
s –
not s
igni
fican
t•
Con
dom
use
at l
ast s
ex –
sig
nific
ant
• T
alki
ng a
bout
usi
ng c
ondo
ms
–si
gnifi
cant
• T
alki
ng a
bout
avo
idin
g or
del
ayin
gse
x in
the
past
yea
r –
sign
ifica
nt
a S
TI =
sex
ually
tran
smitt
ed in
fect
ion.
b T
he s
econ
d st
udy
liste
d fo
r th
e S
oul C
ity c
ampa
ign
(8)
eval
uate
s si
x ty
pes
of o
ngoi
ng H
IV p
reve
ntio
n ac
tiviti
es in
this
reg
ion
of S
outh
Afr
ica,
one
of w
hich
was
the
mas
s m
edia
cam
paig
n re
late
d to
Sou
l City
. The
aut
hors
trac
k ch
ange
s in
a s
erie
s of
out
com
e va
riabl
es o
ver
time,
to w
hich
the
six
type
s of
inte
rven
tions
colle
ctiv
ely
cont
ribut
ed. T
hus,
it is
not
pos
sibl
e to
iden
tify
the
exte
nt to
whi
ch a
giv
en in
terv
entio
n co
ntrib
uted
to th
e ob
serv
ed c
hang
e. T
he a
utho
rs c
reat
edin
dice
s fo
r kno
wle
dge
and
cons
iste
nt c
ondo
m u
se. M
ultip
le re
gres
sion
ana
lysi
s de
mon
stra
ted
that
exp
osur
e to
radi
o m
essa
ges
and
to th
e S
oul C
ity ra
dio
dram
aw
ere
posi
tivel
y lin
ked
to th
e co
nsis
tent
con
dom
use
inde
x bu
t not
to th
e A
IDS
kno
wle
dge
inde
x. S
ince
the
mul
tivar
iate
asp
ect o
f the
ana
lysi
s w
as th
e on
ly p
art
of th
e an
alys
is th
at a
llow
ed fo
r an
ass
essm
ent o
f the
effe
cts
of S
oul C
ity o
n th
e ou
tcom
es o
f int
eres
t, w
e re
port
onl
y th
ose
here
.
222
92-4-120938-0_CH07_222

The literature review for this paper took three forms. First, the authors par-ticipated in the mass media-intervention component of a WHO initiativeknown as “synthesizing intervention effectiveness”, which included an effortto locate all research published between 1990 and 2004 on the effects of massmedia interventions on HIV/AIDS-related behaviours (3). Another compo-nent summarized the findings of those papers that met certain criteria formethodological rigor. Studies were evaluated according to eight quality cri-teria (3) and were included in the review if they used either a pre-test versuspost-test design or a treatment versus comparison design. Of 25 studies thatperformed rigorous evaluations, four targeted young people and met the in-clusion criteria; these form part of the current review (5, 7, 10, 19).
Second, the Center for Communication Programs at Johns HopkinsBloomberg School of Public Health has conducted at least four studies on theimpact of mass media programmes on HIV/AIDS-related behaviours amongyoung people. All have been submitted for publication, but do not appear inthe previous WHO review because they were not published by 2004.
Third, we followed references from other published reviews (23, 24) andconsulted POPLINE, Medline, and the Communication Initiative web site(http://www.comminit.com) in an attempt to identify additional studies.
We included studies that evaluated the effectiveness of mass media cam-paigns in a developing country and that had the main objective of providingeducation on HIV/AIDS or sexual health. To be eligible for inclusion, studieshad to use a pre-intervention versus post-intervention design or an interven-tion versus control design or analyse cross-sectional data comparing thosewho had been exposed to the campaign with those who had not been exposed.They also had to comprehensively report quantitative and statistical data formost outcomes being studied (Table 7.1). We defined an interventioneffect as:
a significant change occurring from pre-intervention to post-intervention
a significant difference between the intervention and control groups, or
a significant association between exposure to a mass media campaign andthe outcome.
These types of studies yield results that allow “plausibility statements” to bemade when using the classification of scientific inference offered by Victoraet al. (25). Not surprisingly, we did not find any randomized controlled trialsthat randomized individuals because of the virtual impossibility of randomlyallocating participants to intervention and control groups in cases in whichthere is full coverage of a mass media intervention; one study did randomizeat the village level (7).
223
92-4-120938-0_CH07_223

There are several limitations to this study. The primary studies reviewed herevaried substantially in their rigor; several compared intervention and controlgroups without addressing baseline differences between groups. However,because they all met a minimum level of rigor, we did not attempt any furtherweighting of the evidence. Almost all of the studies relied on self-reportedmeasures of campaign exposure and outcomes; self-reporting is subject tostrong bias, especially in relation to sexual behaviour. Another limitationis the measurement of exposure to a given mass media intervention. Peoplealready performing a certain behaviour (for example, using condoms) may bemore likely to attend to and recall messages about condoms than those whoare not engaging in that behaviour. In addition, a given intervention classifi-cation (for example, television) may cover a wide range of highly variedprogramming and content – from a 30 second public service announcementto an hour long soap opera. Finally, most of the interventions that were studiedwere conducted in the context of multicomponent programmes offeringhealth services, peer counselling or other educational elements; however, theevaluations are largely unable to differentiate the effects of mass media fromthose of the other components of the intervention. These limitations are byno means trivial, nor are they unique to this set of evaluations of mass mediainterventions.
Additionally, few studies considered the costs and cost effectiveness of massmedia interventions, limiting donors’ ability to select programmes that offerthe most cost-effective interventions. Whereas mass media programming of-ten requires substantial investment in both production and diffusion, the costper person reached can be surprisingly low, as we know from evaluations ofprogrammes in other health sectors (26, 27). Further research examining thecost effectiveness of behaviour-change communication programmes is in thepipeline.
7.2.1 Outcomes of interest
We were interested in identifying outcomes that directly affect the globalgoals for preventing HIV/AIDS among young people as outlined in the Dec-laration of Commitment of the UN General Assembly Special Session onAIDS (28). To this end, we focused on the following outcomes as indicatorsof progress on the global goals:
increase awareness and knowledge of information on how to avoid HIVinfection, measured as
changes in knowledge (about modes of transmission, methods of pre-vention, how to tell if someone has HIV/AIDS);
increase access to the skills needed to avoid HIV infection, measured as
224
92-4-120938-0_CH07_224

self-efficacy (in abstinence, condom use);
increase access to the health services needed to avoid HIV infection, mea-sured as
awareness and utilization of health products and services;
decrease young people’s vulnerability to HIV, measured as
more accurate perceptions of personal riskchanges in social norms (friends’ approval of use of condoms orabstinence);
decrease HIV prevalence, measured by its proximate behavioural deter-minants, such as
abstinence (both intention and behaviour)a decrease in the number of sexual partners (intention and behaviour)the use of condoms (intention and behaviour)improvements in mediating factors, such as interpersonal communica-tion (about sexual health, HIV/AIDS, condoms).
The evaluations of most mass media campaigns do not measure directly thegoal of decreasing HIV prevalence but rather they measure its proximatedeterminants. The exception in this review is the “loveLife” campaign inSouth Africa, which did measure HIV prevalence (14). Interventions that aimto change behaviour are rarely subject to long-term evaluations of outcomes(such as prevalence) because change may be difficult to measure during thelife of the intervention, and factors outside the intervention may have a pow-erful influence on long-term outcomes. In the case of HIV/AIDS, a thirdfactor also comes into play: the logistical and ethical difficulty of measuringHIV prevalence as part of a programme evaluation. For these reasons, preva-lence is generally measured indirectly through reported behavioural deter-minants instead of directly through biological markers.
Within each of the outcome areas outlined above, the interventions underreview often measured a given concept in different ways (for example, con-dom use may have been measured as whether a participant ever used acondom, used one the last time he or she had sex or used one with a casualpartner). In this review, we combined different operational definitions into asingle category (for example, condom use). The lack of standardization ofindicators of outcome seriously limits the potential to perform a meta-analysison this topic.
225
92-4-120938-0_CH07_225

7.3 Findings
We found rigorous evaluation data for 15 mass media interventions address-ing HIV-related behaviours among young people: 11 examined interventionsin Africa, 2 in Latin America, 1 in Asia, and 1 examined a programme thattook place in 44 countries (Table 7.3). No studies of print-only materials metthe inclusion criteria. Intervention designs are summarized in Table 7.3. Onestudy evaluated a radio-only campaign (which we have designated a type 1intervention) (5). Six of the studies evaluated interventions using radio withother supporting media (for example, written materials, videos, posters, the-atre performances, school workshops); these are designated type 2 interven-tions (6–11). The remaining eight interventions involved television and radiowith other supporting media; these are designated type 3 interventions (12–22). One intervention (“Soul City” in South Africa) was evaluated in twostudies (17–19). All studies are described in detail on the web.
7.3.1 Additional outcomes
Additional outcomes are summarized in Table 7.4 and described below.
7.3.1.1 Access to information: changes in knowledge
Of the nine studies reporting data on knowledge of HIV transmission andprevention, four measured increased knowledge of modes of HIV/AIDStransmission. In China, study C (7) showed large, significant differences –measured both before and after the intervention – in knowledge of modes oftransmission, including sexual intercourse (77% before versus 95% after),having multiple sexual partners (69% before versus 93% after) and sharingneedles for drug use (67% before versus 95% after). Similarly large differ-ences were found for rejecting incorrect modes of transmission, and allknowledge measures were significantly different from the control group. The“Tsa Banana” campaign in Botswana (study G) (11) showed mixed resultson the item, “sexually active people risk getting infected with HIV,” withmales showing significant improvements in knowledge (adjusted oddsratio = 3.2) and females showing no significant improvement. In Guinea,study E (9) reported levels of knowledge of transmission of 90–96% amongthe control groups, leaving little room for improvement in the interventiongroup. One study of HIV programmes in South Africa (study L) (19) reporteda positive association between a low score on an AIDS knowledge index andexposure to “Soul Buddyz” (a programme within the Soul City interventionaimed at children aged 8–12 years) in South Africa.
The one study measuring knowledge of abstinence as a prevention technique,the “HEART” campaign in Zambia (study I) (13), showed significantlyhigher knowledge among those who had the seen the campaign compared
226
92-4-120938-0_CH07_226

with those who had not (66% of males exposed to the campaign versus53% of males not exposed; 65% for females exposed versus 55% forfemales not exposed). Three of the five studies measuring knowledge ofcondoms as a prevention method showed large and significant differencesbetween intervention and comparison groups (studies B, C and M) (6, 7, 20).The Soweto Adolescent Reproductive Health Programme (study M) (20)reported a significant jump in the knowledge that condoms can prevent HIVtransmission, from 60% pre-intervention to 85% post-intervention; study C(7), “HIV Prevention and Education in Rural China” also found a substantialimprovement in this type of knowledge (a change from 46% to 94% in theintervention group versus 44% to 49% for the control group) .
The one study measuring a response to the statement “there is a cure forAIDS” (study L in South Africa) (17) found significant increases indisagreement with the statement post-intervention (change from 79%pre-intervention to 89% post-intervention). Of five studies reporting on re-sponses to the statement that “you can tell someone has HIV/AIDS by theway that they look,” only study C (7) in China showed a significant improve-ment between intervention and control groups from pre-intervention topost-intervention.
7.3.1.2 Access to skills: self-efficacy to pursue preventive behaviours
Two evaluations measured young women’s self-efficacy in pursuing absti-nence or refusing to have sex with someone who offered gifts. Study K (16)in Côte d’Ivoire showed significant differences in self-efficacy across thosewith low levels of exposure to the campaign compared with those who hadhigh levels of exposure, while study O (22) in Ghana did not detect significantdifferences across levels of exposure. However, all four studies investigatingself-efficacy in using condoms or convincing a sexual partner to use condomsshowed significant differences between the intervention and comparisongroups (7, 13, 16, 22). Those who were highly exposed to the “Stop AIDSLove Life” campaign in Ghana (study O) (22) had significantly higher scoreson a scale of 1–6 measuring condom-related self-efficacy than those whowere not exposed to the campaign (3.9 for males exposed to the campaignversus 2.9 for males not exposed; 3.0 for females exposed versus 1.6 forfemales not exposed). Similarly, those who were exposed to a campaign inCôte d’Ivoire (study K) (16) were significantly more likely to report self-efficacy in terms of consistent condom use than those who were not exposed(58% of those with no exposure used condoms consistently versus 70% ofthose with low exposure versus 75% of those with high exposure). In studyC in China (7), both the intervention and the control groups showed increasesin their confidence about their abilities to convince sexual partners to usecondoms, but the increase for the intervention group was significantly larger
227
92-4-120938-0_CH07_227

(83% to 92% among the intervention group versus 78% to 84% among thecontrol group).
7.3.1.3 Access to health services: awareness and utilization
All four campaigns that measured awareness of a health product or serviceshowed significant positive differences between interventions and controls.Variables measured included awareness of an AIDS hotline in study A (5) inSaint Vincent and the Grenadines (91% of the intervention group versus 75%of the controls), and in study I (13) in Zambia the availability of voluntarycounselling and testing (79% for males in the intervention group versus 67%for male controls; 84% for females in the intervention group versus 64% forfemale controls) and places where condoms could be purchased (81% inter-vention versus 72% controls). Other variables measured included the locationof condom vendors in study E in Guinea (9) (86% for males in the interventiongroup versus 57% for male controls; 59% for females in the interventiongroup versus 22% for female controls). However, awareness did not neces-sarily translate into utilization; no significant differences were found in theuse of the AIDS hotline in Saint Vincent and the Grenadines (5), and studyD in Cameroon (8) reported no significant differences in visits to health cen-tres between the intervention and control groups. In Zimbabwe, study F(10) reported that members of intervention groups were significantly morelikely to attend health centres than controls (28% versus 10%) and more likelyto attend youth services (11% versus 2%). In South Africa, study J (14) re-ported that those exposed to the loveLife campaign were significantly morelikely than those who had not been exposed to have ever been tested for HIV(16% versus 10%).
7.3.1.4 Decreasing vulnerability
Perception of personal risk
None of the four evaluations reporting data on the perception of personal riskof HIV/AIDS showed a consistent and significant difference (studies D, E,H, I) (8, 9, 12, 13).
Social norms
Eight of the 15 studies reported measures of social norms; these measureswere highlighted especially by data for the broad-based media efforts of SoulCity in South Africa (study L) (17) and the global Staying Alive campaign(study N) (21). Evaluation of the Soul City programme (study L) (17, 18)found significant desirable changes in all norms tested before and after thecampaign, including disagreement with the expectation that a woman wouldhave sex with a man without using a condom (59% disagreed with the
228
92-4-120938-0_CH07_228

statement pre-intervention and 65% disagreed post-intervention). The Soulcity evaluation also found that participants disagreed with the idea that boysor men have the right to have sex with their girlfriends if they buy them gifts(65% pre-intervention versus 73% post-intervention) (17). The global Stay-ing Alive campaign reported more varied results; positive associations withcampaign exposure were shown for the importance of using a condom, dis-cussing HIV with a sexual partner and getting tested for HIV. However,norms regarding tolerance toward people living with HIV/AIDS did not showsimilar positive associations (21).
After the PRISM media campaign in Guinea, young people, parents, healthworkers, community leaders, religious leaders and members of establishedsocial networks were significantly more likely to report that their communitywas open to discussing young people’s reproductive health questions than theyear before campaign (study E) (9). In Cameroon, study D (8) reported thatthe proportion of youths that often discussed sexuality or contraceptives wassignificantly higher among the intervention group (0.897 versus 0.774). StudyK in Côte d’Ivoire (16) reported significantly higher perceptions of peer sup-port for abstinence among those who were highly exposed to the campaigncompared with those who were not exposed (62% versus 53%).
In study O in Ghana (22), the percentage of youths who believed that theirfriends approved of avoiding or delaying sexual activity decreased signifi-cantly from before the intervention to after the intervention (60% versus 42%for males; 61% versus 36% for females); however, those who had higherexposure to the Ghana Stop AIDS Love Life campaign were significantlymore likely to believe that their friends approved of delaying or avoiding sexthan those with no exposure (52% of males with high exposure versus 27%of males with no exposure; 47% of females with high exposure versus 26%of females with no exposure).
In study A (5) in Saint Vincent and the Grenadines, some measures of socialnorms showed improvement after a radio campaign while others did not.Although campaign listeners and non-listeners were equally likely to reportthat their friends, parents or most people important to them thought that theyshould use condoms, campaign listeners were significantly more likely thannon-listeners to report that their friends used condoms (46% for listenersversus 22% for non-listeners).
229
92-4-120938-0_CH07_229

7.3.1.5 Decreasing prevalence as measured by proximate behavioural determinants
Abstinence
The age of sexual debut or current or continued abstinence was evaluated forsix programmes. Two showed significant effects (10, 13); two did not (20,22); and two showed mixed results (8, 12). Study F (10) in Zimbabwe foundthat 53% of those in the intervention sites “said no to sex” compared with32% in the comparison sites; however no differences were found for partic-ipants’ responses to “stopped having sex due to the campaign”.
Number of sexual partners
Of the five studies reporting on whether the number of sexual partners wasreduced, four showed equivocal or null results (7, 8, 12, 22). However, studyF in Zimbabwe (10) showed a marked change, with 20% of respondents inthe intervention group reporting that they had had only one partner during therecall period compared with 2% of the control group.
Condom use
Twelve programmes reported on condom use, with eight reporting on condomuse during last sexual episode. Of these eight, five showed significant dif-ferences between intervention and comparison groups (7, 9, 12, 13, 22). Thelargest effects were reported by study O (22) in Ghana, which found that thosewho were highly exposed to the campaign were several times more likelythan those who were not exposed to report using a condom during the lasttime they had sex (males: 34% versus 10%; females: 22% versus 4%). StudyE (9) found similarly strong effects (males: 48% versus 24%; females: 27%versus 3%).
Of the five programmes reporting on whether condoms had ever been used,three found significant increases (8, 9, 13). Two separate evaluations of SoulCity in South Africa (study L) showed an association between consistentcondom use and exposure to the programme (17-19).
Mediating factors: interpersonal communication
Nine studies reported data on whether young people discussed HIV, absti-nence or condom use with peers, parents or partners. Study F (10) inZimbabwe showed a significant difference between intervention and controlgroups in participants having discussions with anyone about sexually trans-mitted infections or AIDS (78% of intervention group versus 67% of controlgroup). Significantly more youths who were exposed to the loveLife cam-paign in South Africa reported ever talking to their parents about HIV/AIDSthan youths who were not exposed to the campaign (90% versus 81%) (15).
230
92-4-120938-0_CH07_230

The Soul City campaign in South Africa (study L) also reported significantlymore frequent discussions with “someone close” among those with accessto more sources of Soul City media than among those with fewer sources(18, 19). The multicountry Staying Alive campaign (study N) calculated anetwork score, ranging from 0 to 6, for which respondents were assigned onepoint for each type of individual (parent, sibling, teacher or counsellor, doctoror nurse, sexual partner, friend or schoolmate) with whom they talked aboutHIV/AIDS during the previous month (21). In each of the three Staying Aliveevaluation sites, those exposed to the campaign scored significantly higherthan those who were unexposed (in Kathmandu: 2.26 points versus 1.30; inSao Paulo: 0.96 versus 0.65; in Dakar 1.48 versus 1.04).
In Zambia, abstinent youths who were exposed to the HEART campaign(study I) spoke to significantly more people about abstinence than those whowere not exposed (males: 2.9 for those exposed versus 2.3 for those not ex-posed; females: 3.8 for those exposed versus 2.2 for those not exposed)(13). Single females highly exposed to the “PL.U.S.” campaign in Côted’Ivoire (study K) were significantly more likely to discuss sexual abstinencewith a parent during the previous 12 months than those who were not (33%versus 15%) (16). The PL.U.S. campaign also showed significant gains indiscussions about condoms for both single males and single females: 90% ofsingle females who were highly exposed to the campaign encouraged some-one to use condoms during the previous 12 months compared with 56% ofthose who were not exposed to the campaign (16).
The PRISM campaign in Guinea (study E) and the Stop AIDS Love Lifecampaign in Ghana (study O) also showed significantly higher levels of dis-cussion about condoms among participants in the intervention group thanamong the control group. Those in the PRISM intervention group wereroughly twice as likely as controls to recommend condom use to someoneelse (males: 70% versus 31%; females: 31% versus 16%) (9). Study O, theStop AIDS Love Life campaign, also reported large and significant differ-ences between the proportion of participants who were highly exposed to thecampaign and the proportion of those who were not exposed in terms of dis-cussing the use of condoms to avoid AIDS and other sexually transmittedinfections during the past year (males: 57% versus 16%; females: 55% versus18%) (22). However, a radio campaign in Saint Vincent and the Grenadines(study A) did not show improvements in the proportion of adolescents andparents who discussed the use of condoms (5). Less than 2% of the sexuallyexperienced participants in the Zimbabwe study (study F) asked a partner touse a condom as a result of the campaign (10).
231
92-4-120938-0_CH07_231

HIV prevalence
Only one of the 15 studies recorded HIV prevalence (study J). The evaluationof study J in South Africa found that overall young people who participatedin the programme had an adjusted odds of being HIV positive of approxi-mately 0.60 compared with those who had not participated (15).
7.3.2 Summary of studies of effectiveness
The evidence supports the effectiveness of mass media interventions inincreasing the knowledge of HIV transmission and prevention, improvingself-efficacy in terms of condom use, influencing social norms about the ac-ceptability of young people discussing reproductive health, increasing inter-personal communication about HIV and prevention behaviours, increasingthe use of condoms, and boosting awareness of health providers. The studiesreviewed in this article did not tend to show significant effects with regard tocreating awareness that healthy looking people may have HIV/AIDS or im-proving self-efficacy in terms of abstinence. They also did not show signifi-cant effects in terms of increasing the proportion of adolescents who delaytheir first sexual experience or decreasing the number of sexual partners.
7.3.3 Relative effectiveness of different types of interventions
This section summarizes findings by intervention type (Table 7.5 and Table7.6). Although we highlight the results of the five goals of the UN Declarationand nine possible outcomes (see section 7.2.1), a given study usually reportedon only three or four of these outcomes. The summary below is based on thestudies that reported findings for the relevant variables.
7.3.3.1 Radio only
The one radio-only campaign (study A) showed mixed results: significantimprovements were achieved in awareness of an AIDS hotline but there wereno improvements in social norms, interpersonal communication about HIV/AIDS or in different measures of condom use (5).
7.3.3.2 Radio with other supporting media
There were six interventions of this type (6-11). All of the studies reportedsome measure of knowledge gain. With the notable exception of study C inChina (7), most results tended not to be significant. In contrast, more studiesthan not showed positive effects on skills, knowledge about health servicesand social norms.
232
92-4-120938-0_CH07_232

Tab
le 7
.5S
tren
gth
of e
vid
ence
of e
ffec
tive
nes
s fo
r eac
h in
terv
enti
on
typ
e b
y g
oal
as
ou
tlin
ed b
y th
e D
ecla
rati
on
of C
om
mit
men
t of t
he
UN
Gen
eral
Ass
emb
ly S
pec
ial S
essi
on
on
AID
S (
14)
Inte
rven
tio
n t
ype
and
stu
dy
des
ign
aIn
crea
sekn
ow
led
ge
Imp
rove
ski
llsIn
crea
se a
cces
s to
an
daw
aren
ess
of
hea
lth
serv
ices
Red
uce
vu
lner
abili
tyR
edu
ce H
IVp
reva
len
ce
Sb
Mix
edc
NS
dS
Mix
edN
SS
Mix
edN
SS
Mix
edN
SS
Mix
edN
S
Typ
e 1
(rad
io o
nly
)C
ross
-sec
tiona
lA
AA
Bef
ore–
afte
rIn
terv
entio
nvs
cont
rol
RC
Te
Typ
e 2
(rad
io w
ith
oth
er m
edia
)C
ross
-sec
tiona
lE
BE
E, F
EE
, FB
Bef
ore–
afte
rG
GIn
terv
entio
nvs
cont
rol
FD
DD
D, F
RC
TC
CC
Typ
e 3
(rad
io a
nd
tel
evis
ion
wit
h o
ther
med
ia)
Cro
ss-s
ectio
nal
KO
K, O
NK
OB
efor
e–af
ter
LL
LIn
terv
entio
nvs
cont
rol
MI
HI,
JH
, II,
JH
, MR
CT
a S
tudi
es a
re c
lass
ified
acc
ordi
ng to
the
type
of d
ata
they
rep
ort;
for
exam
ple,
a b
efor
e–af
ter
stud
y th
at u
ses
cros
s-se
ctio
nal d
ata
anal
ysis
may
app
ear
eith
er in
the
row
for
cros
s-se
ctio
nal s
tudy
or
the
row
for
befo
re–a
fter,
dep
endi
ng o
n w
hich
par
t of t
he s
tudy
the
findi
ngs
cam
e fr
om.
b S
= s
igni
fican
tc F
indi
ngs
are
desi
gnat
ed a
s “m
ixed
” if
they
wer
e si
gnifi
cant
for
som
e m
easu
res
but n
ot o
ther
s or
sig
nific
ant f
or o
ne s
ex b
ut n
ot th
e ot
her.
d N
S =
not
sig
nific
ant.
e R
CT
= r
ando
miz
ed c
ontr
olle
d tr
ial.
233
92-4-120938-0_CH07_233

Tab
le 7
.6R
eco
mm
end
atio
ns
on
th
e st
ren
gth
of
the
evid
ence
Inte
rven
tio
nty
pe
Co
ncl
usi
on
C
om
men
ts
1. R
adio
onl
yS
tead
y•
Impr
ove
know
ledg
e an
d sk
ills
– no
evi
denc
e (n
ot r
epor
ted)
• Im
prov
e ac
cess
to h
ealth
ser
vice
s –
stro
ng e
vide
nce
for
a sm
all i
ncre
ase
in a
war
enes
s of
ser
vice
s (A
IDS
hot
line)
but
only
wea
k ev
iden
ce fo
r in
crea
sing
rep
orte
d at
tend
ance
at t
hese
ser
vice
s•
Red
uce
vuln
erab
ility
–no
evi
denc
e of
impr
oved
per
cept
ions
in s
ocia
l nor
ms
• M
itiga
te v
ulne
rabi
lity/
risk
– no
evi
denc
e (n
ot r
epor
ted)
• R
educ
e H
IV p
reva
lenc
e (s
urro
gate
mea
sure
: con
dom
-use
beh
avio
urs)
– n
o ev
iden
ce o
f im
prov
emen
ts in
con
dom
use
• M
edia
ting
fact
ors
(inte
rper
sona
l com
mun
icat
ion
abou
t and
atti
tude
s to
war
ds c
ondo
ms)
– n
o ev
iden
ce o
f im
prov
emen
ts2.
Rad
iow
ith o
ther
med
ia
Go
• Im
prov
e kn
owle
dge
– w
eak
evid
ence
of i
mpr
oved
kno
wle
dge
• Im
prov
e sk
ills
– th
e tw
o st
udie
s re
port
ing
on th
is o
utco
me
show
ed s
tron
g ev
iden
ce fo
r in
crea
sed
self-
effic
acy
in u
sing
cond
oms
and
know
ledg
e of
how
to u
se c
ondo
ms
• Inc
reas
e us
e an
d aw
aren
ess
of h
ealth
ser
vice
s –
the
thre
e st
udie
s re
port
ing
on th
is o
utco
me
show
ed m
oder
ate
evid
ence
for
incr
ease
s in
thes
e va
riabl
es•
Red
uce
vuln
erab
ility
– 1
/1 s
tudy
foun
d im
prov
ed s
ocia
l nor
ms
• M
itiga
te v
ulne
rabi
lity/
risk
– no
evi
denc
e (n
ot r
epor
ted)
• R
educ
e H
IV p
reva
lenc
e –
Mod
erat
e to
str
ong
impr
ovem
ents
in A
BC
beh
avio
urs
(Abs
tain
, Be
faith
ful,
use
Con
dom
s)•
Med
iatin
g fa
ctor
s –
mod
erat
e to
str
ong
impr
ovem
ents
in in
terp
erso
nal c
omm
unic
atio
n an
d at
titud
es to
war
ds th
e A
BC
beha
viou
rs3.
Rad
ioan
dte
levi
sion
with
othe
r m
edia
Go
• Im
prov
e kn
owle
dge
– m
oder
ate-
to-s
tron
g ev
iden
ce, e
spec
ially
reg
ardi
ng c
ondo
ms
• Im
prov
e sk
ills
– m
oder
ate-
to-s
tron
g ev
iden
ce o
f im
prov
ed s
elf-
effic
acy
for
prev
entiv
e be
havi
ours
• In
crea
se a
war
enes
s of
hea
lth s
ervi
ces
– m
oder
ate-
to-s
tron
g ev
iden
ce fo
r in
crea
ses
• R
educ
e vu
lner
abili
ty –
no
evid
ence
to w
eak
evid
ence
of i
mpr
ovem
ents
in p
erce
ived
per
sona
l ris
k; m
oder
ate
evid
ence
of im
prov
ed s
ocia
l nor
ms
rega
rdin
g th
e A
BC
beh
avio
urs
• M
itiga
te v
ulne
rabi
lity/
risk
– no
evi
denc
e (n
ot r
epor
ted)
• Red
uce
HIV
pre
vale
nce
(sur
roga
te m
easu
re: A
BC
beh
avio
urs)
– w
eak
evid
ence
of i
ncre
ases
in a
bstin
ence
and
redu
ctio
nin
the
num
ber
of p
artn
ers;
str
ong
evid
ence
for i
mpr
ovem
ents
in c
ondo
m u
se. T
he o
ne s
tudy
mea
surin
g H
IV p
reva
lenc
efo
und
stro
ng e
vide
nce
of p
reva
lenc
e re
duct
ion
asso
ciat
ed w
ith p
artic
ipat
ion
in th
e in
terv
entio
n•
Med
iatin
g fa
ctor
s (in
terp
erso
nal c
omm
unic
atio
n) –
str
ong
evid
ence
of i
mpr
ovem
ent
234
92-4-120938-0_CH07_234

In terms of sexual behaviour, the findings were split fairly evenly betweensignificant and non-significant results related to abstinence and delay ofsexual debut. There was little evidence that interventions reduced partici-pants’ number of sexual partners. However, the weight of the evidence acrossstudies reporting condom use was strongly positive, and this type of pro-gramme had favourable effects on increasing interpersonal communicationwith others about HIV/AIDS. None of the studies of radio with supportingmedia included HIV prevalence as an outcome measure.
7.3.3.3 Television and radio with other supporting media
There were eight interventions of this type (12-22). Evaluations of this typeof intervention generally showed improvements in knowledge and skills re-lated to HIV/AIDS as well as knowledge about health services. The resultstended to be positive for social norms.
Evidence from the evaluations that measured abstinence or delay of sexualdebut varied but leaned towards having no effect. The findings of the fewstudies reporting a reduction in the number of sexual partners were also splitbut tended towards no effect. In contrast, data on different measures of con-dom use showed positive effects in the majority of studies. The only study toreport HIV prevalence (study J) (14, 15) found that programme participationwas associated with lower HIV prevalence. Finally, all studies reported apositive effect on interpersonal communication regarding HIV/AIDS.
7.3.4 Dose–response relationship
Dose–response theory suggests that if a campaign causes changes in an out-come, then higher levels of campaign exposure should yield larger changes(27). Four of the fifteen studies examined the dose–response question(10, 16, 17, 22); all four studies found significant differences between thosewith low exposure and those with high exposure to the campaigns, whensocioeconomic factors and access to media were controlled for.
In the programme in Ghana for example (study O), a dose–response rela-tionship was evident for 6 of 11 variables (22). In the intervention in Côted’Ivoire (study K), the proportion of single females who perceived that theyhad peer support to abstain from sex and the proportion of young people ofboth sexes who encouraged someone else to use condoms were significantlygreater among those with high exposure to the campaign (study K) thanamong those with low or no exposure (16). In the project in Zimbabwe (studyF), 9 out of 10 outcomes showed evidence of significant dose–response ef-fects. The likelihood of having had discussions with others about sexuallytransmitted infections or AIDS or of having sought care at a health centre or
235
92-4-120938-0_CH07_235

youth centre was significantly greater among those who had been exposed to5–8 components of the campaign than among those who had been exposedto 1–2 or 3–4 components (10). And in South Africa, study L reported thatthe frequency of talking to someone close about HIV/AIDS and always usinga condom were positively associated with exposure to more sources of thecampaign (17, 18).
7.4 Discussion
The purpose of this review was to identify methodologically rigorous studiesthat examined the effects of mass media interventions on HIV/AIDS-relatedbehaviours among young people in developing countries and to determinethe extent to which the evidence would justify future widespread implemen-tation of three types of mass media programmes (Box 7.1). Radio-onlyprogramming and radio programming with other media require a moderatethreshold of evidence to justify their expansion. In contrast, despite the factthat television and radio programming used with other media have the po-tential to reach millions of people it is a less feasible intervention primarilybecause of the financial and human resources needed to produce and broad-cast high quality programmes. Thus, the threshold of evidence needed torecommend future expansion of a comprehensive radio and television inter-vention with other media is high.
The lack of evidence for radio-only interventions indicates that most projectshave now moved beyond this single channel to offer more comprehensiveservices. Because we identified only one study of this intervention type, wecannot generalize about its effectiveness. The mixed results of that one studylead to our classifying this type of intervention as “Steady”.
The comparison of interest is between interventions that use radio togetherwith other media and those that use radio and television together with othermedia. For most outcomes, the two types of interventions showed a surpris-ingly similar pattern. First, both had positive effects on knowledge, skills,awareness and use of health services, use of condoms and interpersonal com-munication with others. Second, the two types of interventions yielded similarresults on social norms: they were generally positive though split or mixedwhen disaggregated by sex of the participant. The evidence was too limitedto make a comparison on mitigation of vulnerability or risk or on the preva-lence of HIV. Because of the consistently strong effects on multiple out-comes, we categorize both radio with other media and radio and televisionwith other media as interventions as “Go”. Although we required a higherlevel of evidence for radio and television than for radio alone with othermedia, we believe that both merit the endorsement of “Go” for the followingreason: the strong evidence of dose effect (that is, the greater the exposure
236
92-4-120938-0_CH07_236

via multiple channels, the stronger the effect) favours the use of a wider rangeof media, especially where access to television is high.
Box 7.1
Recommendations for mass media campaigns
For policy-makers
Mass media have the potential to reach millions of people with life-saving messages that can change behaviour.
Large-scale campaigns must be closely coordinated with other inter-ventions (such as those that are school-based or clinic-based) to max-imize their effects.
For programme development and delivery staff
To achieve large-scale effects, mass media programmes should be de-veloped and implemented through multiple channels with mutually re-inforcing messages.
Mass media interventions should be tailored for young people, andcampaign materials should be pre-tested among young people.
For researchers
Focus scarce evaluation resources on large-scale comprehensive com-munication programmes that have the potential to achieve population-based effects (rather than pilot studies or “boutique” programmes).
Recognize that randomized controlled trials are not the method of choicefor evaluating full-coverage mass media programmes. Instead, usestrong quasi-experimental designs and analytic approaches that build acase for inferring causality.
Work towards standardizing outcome indicators.
Conduct cost-effectiveness analyses for mass media programmes todetermine the cost per unit of effect.
It might be tempting to conclude that radio used with other media can producethe same results as radio and television used with other media. However, thispresupposes that the settings for the different mass media programmes arecomparable; this is a tenuous assumption. Our review of the findings providesprogramme developers and staff with a justification for using either type ofintervention. Given that television is generally more costly than radio – interms of both production and broadcast – this finding suggests that radio used
237
92-4-120938-0_CH07_237

with other media may be a valuable means of reaching young people whenbudgets are constrained. Another important factor in deciding between thetwo interventions relates to the intended audience. Radio without televisionmay work well where access to television is limited. However, among a pop-ulation where there is high access to television, it may be more difficult forradio-based interventions to capture the necessary attention. Thus, our find-ings do not lead to a hard and fast recommendation of one over the other.Rather, they point to the value of both, depending on the media habits andpreferences of the intended audience and the costs involved in programming.
7.4.1 Features of the most effective interventions
Given the nature of peer-reviewed journals, researchers often provide littledetail regarding the components of the communication intervention or theprocess of its development and monitoring. Thus we have relatively littleinformation on the interventions themselves even from published studies.Since this area of exploration is still in its infancy, it is premature to look tothe published literature to answer questions about which features of a cam-paign enhance its effectiveness.
7.4.2 Factors that facilitate or obstruct effective interventions
Although a list of all factors would be too lengthy to elaborate here, multiplefactors affect the development of effective media campaigns. Many are com-mon to other types of interventions: political will and adequate funding andpersonnel, among others. Two factors are particularly relevant to communi-cation programmes. They are described below.
7.4.2.1 Cultural sensitivities
Sexual behaviour is a taboo subject in many cultures, yet it lies at the heartof efforts to prevent the spread of HIV. Communicators must find ways to beas explicit as possible without crossing the fine line of cultural sensibility.
7.4.2.2 Availability of local talent
The use of “entertainment and education” together is one of the fastest grow-ing means of communication used to teach people about HIV/AIDS; it is alsopotentially one of the most effective because this type of programme engagesthe audience in compelling dramas about the lives of people to whom theycan relate. Maibach and Holtgrave dubbed entertainment and education pro-grammes “fun with a purpose” (29). However, for education and entertain-ment programmes on HIV/AIDS to compete with commercial programmes,they must have the same professional polish. Because many developingcountries do not have a sufficiently large pool of local talent experienced in
238
92-4-120938-0_CH07_238

scripting and producing this genre, communicators are faced with the specialchallenge of developing and producing materials. Nonetheless, a number ofhighly entertaining soap operas that touch on HIV/AIDS have emerged indeveloping countries (30).
7.4.3 Conclusions
Despite the millions of dollars that have been invested in communicationprogrammes to prevent the spread of HIV and AIDS, the number of pro-grammes that have undergone rigorous evaluation is limited. Results fromthe 15 studies reviewed here suggest that communication programmes canand do influence HIV-related outcomes among young people, although notfor every variable or in every campaign. The strongest evidence points tochanges in knowledge, interpersonal communication and condom use. How-ever, we need to continue to build the evidence base for the effectiveness ofmass media campaigns among youths and focus especially on comprehensiveprogrammes that go to scale with a combination of television, radio and othersupporting media.
Acknowledgements
The authors thank Michael Sweat, Kevin O’Reilly, and Julie Denison forinviting them to participate in the “synthesizing intervention effectiveness”initiative and for their assistance in identifying some of the articles used inthis review as part of that initiative.
References
1. World Health Organization. HIV/AIDS and adolescents. Child and AdolescentHealth and Development, WHO, Geneva, 200–2004 (http://www.who.int/child-adolescent-health/HIV/HIV_adolescents.htm, accessed 4 May 2004).
2. Scalway T, Deane J. Critical challenges in HIV communication. London, PanosInstitute, 2002.
3. Bertrand JT et al. Systematic review of the effectiveness of masscommunication programmes to change HIV/AIDS-related behaviors. HealthEducation and Behavior, 2006. In press.
4. McKee N, Bertrand JT, Becker-Benton A. Strategic communication in the HIV/AIDS epidemic. New Delhi, Sage Publications, 2004.
5. Middlestadt S et al. Evaluating the impact of a national AIDS prevention radiocampaign in St. Vincent and the Grenadines. Journal of Applied SocialPsychology, 1995, 25:21-34.
6. Magnani RJ et al. Impact of a health communications programme on adolescentreproductive health knowledge, attitudes and behaviors in three cities inParaguay. Washington, DC, Pathfinder International, 2001 (Focus on YoungAdults (FOCUS) Program Working Paper).
239
92-4-120938-0_CH07_239

7. Xiaoming S et al. Integrating HIV prevention education into existing familyplanning services: results of a controlled trial of a community-level interventionfor young adults in rural China. AIDS and Behavior, 2000, 4:103-110.
8. Van Rossem R, Meekers D. (1999b) An evaluation of the effectiveness oftargeted social marketing to promote adolescent reproductive health inCameroon. Washington, DC, Population Services International, ResearchDivision, 1999 (Working Paper No. 19).
9. Fonseca-Becker et al. HIV/AIDS prevention among youth in upper Guinea:impact evaluation report of a behavior change and community mobilizationcampaign. Baltimore, MD, Johns Hopkins University Bloomberg School ofPublic Health, Center for Communication Programs, 2003.
10. Kim et al. Promoting sexual responsibility among young people in Zimbabwe.International Family Planning Perspectives, 2001, 27:11-19.
11. Meekers D, Stallworthy G, Harris J. Changing adolescents’ beliefs aboutprotective sexual behavior: the Bostwana Tsa Banana programme.Washington, DC, Population Services International, Research Division, 1997(Working Paper No. 3).
12. Van Rossem R, Meekers D. (1999a). An evaluation of the effectiveness oftargeted social marketing to promote adolescent reproductive health inGuinea. Washington, DC, Population Services International, ResearchDivision, 1999 (Working Paper No. 23).
13. Underwood C et al. Reducing the risk of HIV transmission among adolescentsin Zambia: psychosocial and behavioural correlates of viewing a risk-reductionmedia campaign. Journal of Adolescent Health, 2006, 38:55e1-55e13(available from http://dx.doi.org/10.1016/j.jadohealth.2004.09.022).
14. Pettifor AE et al. Young people’s sexual health in South Africa: HIV prevalenceand sexual behaviors from a nationally representative household survey.AIDS, 2005, 19:1525-1534.
15. Pettifor AE et al. HIV and sexual behaviour among young South Africans: anational survey of 15-24 year olds. Johannesburg, Reproductive HealthResearch Unit, University of the Witwatersrand, 2004.
16. Babalola S, Ouedraogo D, Vondrasek C. Motivation for late sexual debut in Coted’Ivoire and Burkina Faso: a positive deviance inquiry. Journal of HIV/AIDSPrevention Education for Adolescents and Children, 2006. In press.
17. Goldstein S et al. Communicating HIV and AIDS, what works? A report on theimpact evaluation of Soul City’s fourth series. Journal of Health Communication,2005, 10:465-483.
18. Scheepers E et al. Evaluating health communication – a holistic overview of theimpact of Soul City IV. Australian Journal of Health Promotion, 2004,15:121-133.
19. Peltzer PT, Seoka P. Evaluation of HIV/AIDS prevention intervention messageson a rural sample of South African youths’ knowledge, attitudes, beliefs andbehaviours over a period of 15 months. Journal of Child and AdolescentMental Health 2004,16:93-102.
20. Meekers D. The effectiveness of targeted social marketing to promoteadolescent reproductive health: the case of Soweto, South Africa. Journal ofHIV/AIDS Prevention and Education for Adolescents and Children, 2000,3:73-92.
240
92-4-120938-0_CH07_240

21. Geary CW et al. Using global media to reach youth: the 2002 MTV Staying Alivecampaign. Arlington, VA, Family Health International, 2004.
22. Tweedie IM et al. Ghana Stop AIDS Love Life campaign, phase 1: February2000-June 2001 Evaluation Report. Baltimore, MD, Johns Hopkins University,Center for Communication Programs, 2002 (Technical Report).
23. Speizer IS, Magnani RJ, Colvin CE. The effectiveness of adolescentreproductive health interventions in developing countries: a review of theevidence. Journal of Adolescent Health, 2002, 33:324-348.
24. Family Health International. Intervention strategies that work for youth:summary of FOCUS on young adults: end of programme report. Arlington, VA,Family Health International, YouthNet Program, (2002).
25. Victora CG, Habicht JP, Bryce J. Evidence-based public health: moving beyondrandomized trials. American Journal of Public Health, 2004, 94:400-405.
26. Kincaid DL et al. Impact of a mass media vasectomy promotion campaign inBrazil. International Family Planning Perspectives, 1996, 4:169-175.
27. Piotrow PT et al. Health communication: lessons from family planning andreproductive health. Westport, CT, Praeger, 1997.
28. United Nations. Declaration of commitment on HIV/AIDS. United NationsGeneral Assembly Special Session on HIV/AIDS, 2001 (http://www.un.org/ga/aids/coverage/FinalDeclarationHIVAIDS.html, accessed 6 August 2004).
29. Maibach E, Holtgrave DR. Advances in public health communication. AnnualReview of Public Health, 1995, 16:219-238.
30. Piotrow PT, de Fossard E. Entertainment-education as a public healthintervention. In: Singhal A et al, eds. Entertainment-education and socialchange: history, research, and practice. Mahway, NJ, 2003.
241
92-4-120938-0_CH07_241

92-4-120938-0_CH07_242

8. The effectiveness of communityinterventions targeting HIV and AIDSprevention at young people indeveloping countriesEleanor Maticka-Tyndalea & Chris Brouillard-Coylea
Objective To identify successful HIV/AIDS prevention interventionstargeting youths and delivered in geographically bounded communities (forexample, rural villages, urban settlements or neighbourhoods) in developingcountries.
Methods A systematic review and synthesis of studies evaluating interven-tions that were published between January 1990 and December 2004 wasconducted. Using predetermined criteria, all interventions were summarizedinto multiple tables to facilitate comparison. Results of the evaluations ofeach of four types of intervention were reviewed using predetermined thresh-olds of evidence. The four types of interventions were classified as follows.Type 1 interventions were those targeting youths and delivered throughexisting organizations or centres that served youths. Type 2 were those tar-geting youths but not affiliated with existing organizations or centres. Type3 were those targeting all community members and delivered through tradi-tional kinship networks. Type 4 were those targeting communities as a wholeand delivered through community-wide events.
Findings Evaluations of 22 interventions were reviewed. Type 1 interven-tions produced primarily positive results at the required threshold of evidence.They are recommended for use in scaling-up projects but should be subjectto continued rigorous evaluations. Studies of all other intervention types pro-duced primarily positive results, but the evaluations were less rigorous soclear conclusions could not be drawn about their effectiveness. It is recom-mended that these interventions be continued and that priority should be givento implementing rigorous evaluations of these interventions.
Conclusions Considerable creativity, ingenuity and commitment is demon-strated in designing and delivering HIV interventions but there is a paucityof adequate evidence of their effectiveness. This precludes identification ofthe types of interventions that actually produce the targeted changes. It is
a Department of Sociology and Anthropology, University of Windsor, 401 Sunset Ave, Windsor,Ontario N9B 3P4, Canada. Correspondence should be sent to Dr Maticka-Tyndale(email: [email protected]).
243
92-4-120938-0_CH08_243

essential that governments and donor agencies invest in high quality processand outcome evaluations and cost–benefit analyses so that effective inter-ventions can be identified and promoted.
8.1 Introduction
There is increasing recognition that young people are at the centre of the AIDSpandemic regardless of whether they are living in countries with generalizedor concentrated epidemics. Not only are they carrying a disproportionatelyhigh burden of infection but they also consistently face conditions and cir-cumstances that make them vulnerable to new infection (see chapter 2). TheUnited Nations General Assembly Special Session on HIV/AIDS (UNGASS)(1) acknowledged the need to focus attention on young people by specifyinggoals for interventions targeting youths (see Paragraph 53). Reaching thesegoals requires that governments, organizations working with youth and donoragencies ensure that young people (those aged 15–24 years) have access toinformation about HIV and health services, to interventions that help thembuild skills to avoid becoming infected with HIV, and that the vulnerabilityto and prevalence of HIV infection among young people is decreased. Therehas been international acceptance of these goals. What remains is to identifythe best ways of achieving them.
Our objective is to strengthen the evidence base for interventions targetingyoung people in developing countries, particularly those interventions thatare delivered in geographically bounded communities. These communitiesmay be rural villages, urban settlements or neighbourhoods. What distin-guishes them in this case is that they are where young people live regardlessof whether they are in school or out of school, married or unmarried, em-ployed or unemployed. As such, interventions in these settings have thepotential to reach large numbers of people. The focus of this paper is onidentifying the types of interventions delivered in geographically boundedcommunities that have demonstrated success in achieving at least one of theUNGASS goals.
8.2 Methods
A systematic review of the literature was undertaken to locate interventionsdelivered in geographically bounded communities. We searched the follow-ing electronic databases: PsycINFO, AIDSLINE, Medline, POPLINE, ERIC,Sociological Abstracts, Social Sciences Abstracts and the Leeds HealthEducation Effectiveness Database. We also searched the reference sectionsof articles retrieved, conference proceedings, issues of journals that had pub-lished articles evaluating interventions and the web sites of organizationsinvolved in AIDS-related programmes and research (AEGiS, AVERT, the
244
92-4-120938-0_CH08_244

CORE Initiative, CAPS – the Center for AIDS Prevention Studies, Devel-opment Gateway, the United Kingdom Department for InternationalDevelopment, Europeer, Family Health International, the Pan AmericanHealth Organization, UNAIDS, UNFPA, UNESCO, UNICEF, WHO). Wealso sent requests to individuals knowledgeable about HIV prevention orworking for organizations involved in HIV prevention. Publications appear-ing in both peer-reviewed journals and grey literature were retrieved, andauthors or sponsoring organizations were contacted by email if additionalinformation was needed.
Inclusion criteria were set in consultation with the editors of this report.Articles and reports were reviewed by both authors to determine whether theymet the inclusion criteria outlined in Table 8.1. Studies that met the inclusioncriteria were summarized and put into a chart for comparison. Further detailon the studies is available on the web (www.who.int/child-adolescent-health).An iterative process of discussion and re-reading of documents was used toachieve consensus on categorizing the interventions.
Information on the shared characteristics of interventions was reviewed and,based on discussions with colleagues experienced in intervention research orprogramme delivery, interventions were divided into four types, whichdiffered in their target population and their mode of delivery. Type 1 inter-ventions and type 2 interventions target only young people (aged 15–24 years)and focus on providing information, building skills and changing behaviours.Type 1 interventions are affiliated with existing organizations or centres thatserve youths. Through this affiliation, the organization or centre’s acceptancewithin the community as well as their mechanisms for reaching young people,their infrastructure and mode of sustainability become available to the inter-vention. However, a suitable host organization must be found for theseinterventions and a working relationship with, placement of, and support forthe intervention must be negotiated; additionally, sensitive topics must beincluded in the intervention without challenging the position of the organi-zation in the community. Type 2 interventions create their own mechanismand infrastructure to deliver the intervention. While negotiating with anexisting organization is not necessary, this type of intervention must establishacceptance with gatekeepers, develop a mechanism to reach young people,as well as a sustainable method of delivery. A suitable location must also befound and infrastructure for delivering the intervention must be developed.
Type 3 interventions and type 4 interventions are delivered to the communityas a whole. Type 3 interventions use traditional kinship networks to deliverinterventions that have been designed to fit in with local traditions andcustoms for communicating about health and sexuality. These interventionsuse repeated one-on-one discussions or small, often family-based, group
245
92-4-120938-0_CH08_245

discussions in which a relationship is built among those delivering and thosereceiving the intervention. Since delivery of this type of intervention proceedsone individual or family at a time, these are the most labour-intensive type,and attention must be paid to the mechanism of delivery if large numbers of
Table 8.1Inclusion and exclusion criteria used to identify studies for review
Inclusion criteria Exclusion criteria
Some of the intervention content deals withHIV/AIDS
Intervention delivered exclusively to adults(aged > 24 years) or children (aged < 15years)
Youths (aged 15–24 years) included inpopulation targeted by intervention
Intervention delivered primarily throughschool, health facility or media
Description of intervention availableIntervention designed to be delivered ingeographically bounded community
Intervention targets youths living ininstitutional settings
Primary objectives are statedIntervention delivered in a developingcountry
Intervention delivered only in a developedcountry
One or more of the following outcomes isreported for youth: knowledge of HIV/AIDS,skills related to preventing sexualtransmission of HIV, behaviour related topreventing sexual transmission of HIV, HIVprevalence/incidence or outcomes relatedto community awareness of circumstancesand conditions contributing to youthvulnerability
Evaluation study has insufficient evidencefrom which to draw conclusions
Evaluation method described and includesjudgements based on project records orqualitative interviews with participants,cross-sectional surveys with or withoutcomparison groups, surveys conductedbefore and after the intervention with orwithout comparison groups, or randomizedcontrolled trials
No information about design of evaluationprovided
Results reported for youths aged 15–24years
No results reported for youths aged 15–24years
Report published between January 1990and December 2004
Intervention targets youths identified as“especially vulnerable” (for example,intravenous drug users, refugees, sexworkers)
Results published in English, French orSpanish
Results published only in a language otherthan English, French or Spanish
246
92-4-120938-0_CH08_246

people are to be reached. Type 4 interventions deliver their messages throughlarge-scale community activities, such as festivals, community theatre eventsor competitions. They have a broad reach and deliver a uniform message, butthere is little, if any, accommodation or response to individual concerns orcircumstances.
We identified 22 evaluated interventions that met the inclusion criteria. Theirdistribution across intervention types is shown in Figure 1.
8.3 Findings
8.3.1 Intervention types and threshold of evidence
Evidence-based decision-making typically requires the application of rigor-ous evaluation standards to support recommendations. However, as Ross etal. discuss in chapter 4, applying such standards is fraught with difficultywhen interventions targeting behaviour change and community norms arebeing evaluated. Thus, an alternative framework, based on establishing dif-ferent thresholds of evidence, is used here. The evidence required at eachthreshold is based on the typology presented by Habicht et al. (2) and de-scribed by Ross et al. In this framework, a threshold of evidence is set foreach type of intervention. This threshold takes into consideration the feasi-bility of delivering the intervention on a large scale, the acceptability of theintervention to participants and those who are implementing it, its risk ofproducing adverse outcomes, the potential size of the effect, and the presenceof other health and social benefits associated with delivery of the intervention.
Table 8.2 provides information on the criteria and threshold of evidenceneeded to recommend an intervention for each of the four intervention types
Fig. 1.Types of interventions
Intervention Types
In Geographical
Communities
Targeting
Youth
N=17
Targeting Entire
Communities
N=5
TYPE 1
Delivered using
existing
centres
N=11
TYPE 2
Created own system
and structure
for delivery
N=6
TYPE 3
Delivered through
traditional
networks
N=3
TYPE 4
Delivered through
community-
wide activities
N=2
247
92-4-120938-0_CH08_247

Tab
le 8
.2T
hre
sho
ld o
f ev
iden
ce n
eed
ed t
o r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n o
f ea
ch t
ype
of
inte
rven
tio
na
Inte
rven
tio
n
ty
pe
Fea
sib
ility
Lac
k o
fp
ote
nti
alfo
r ad
vers
eo
utc
om
es
Acc
epta
bili
tyP
ote
nti
alsi
ze o
fef
fect
Oth
erh
ealt
h o
rso
cial
ben
efit
s
Ove
rall
thre
sho
ldC
om
men
ts
1. T
arge
ts y
outh
s an
d is
deliv
ered
usi
ng e
xist
ing
orga
niza
tions
or
cent
res
serv
ing
yout
h
+ +
+-
-+
+ +
+ +
+ +
Mod
erat
eR
equi
res
an e
xist
ing
orga
niza
tion
or c
entr
e th
at is
acce
pted
by
the
com
mun
ity w
ithin
fras
truc
ture
to s
uppo
rtpr
ogra
mm
e. T
he e
ffect
siz
ede
pend
s on
the
reac
h of
the
orga
niza
tion
or c
entr
e2.
Tar
gets
you
ths
and
crea
tes
its o
wn
syst
em a
ndst
ruct
ure
for
deliv
ery
+-
++
+H
igh
Mus
t cre
ate
a sy
stem
of d
eliv
ery
acce
ptab
le to
the
com
mun
ity a
ndth
at a
dequ
atel
y pe
netr
ates
targ
etpo
pula
tion
3. C
omm
unity
-wid
ein
terv
entio
n de
liver
edth
roug
h ex
istin
gtr
aditi
onal
kin
ship
net
wor
ks
+ +
-+
++
++
+M
oder
ate
Mus
t add
ress
soc
ial n
orm
sas
soci
ated
with
com
mun
icat
ing
abou
t sex
ual m
atte
rs w
ithin
the
iden
tifie
d ne
twor
ks4.
Com
mun
ity-w
ide
inte
rven
tion
deliv
ered
thro
ugh
com
mun
ityw
ide
activ
ities
, (eg
. fes
tival
s)
+ +
+-
+ +
+ +
+ +
Mod
erat
eC
omm
unity
act
iviti
es p
rovi
de w
ide
reac
h if
the
appr
oach
isac
cept
able
and
mea
ning
ful t
oco
mm
unity
mem
bers
a D
egre
e of
des
irabi
lity
is in
dica
ted
with
a m
axim
um o
f 3 “
+”
sign
s. D
egre
e of
und
esira
bilit
y is
indi
cate
d w
ith a
max
imum
of 3
“-”
sig
ns.
248
92-4-120938-0_CH08_248

studied. All types of interventions must address the challenges posed by thepotential delivery of misinformation and community backlash. For example,misinformation may result from personal interpretation, lack of comprehen-sion, errors in recall or cultural norms associated with the information or itscommunication. Cultural resistance to the advocacy of condoms in much ofsub-Saharan Africa, for example, has at times resulted in schoolteachers,government officials, community leaders or religious leaders presenting in-formation about condoms in ways intended to discourage their use (3–5).Community backlash may occur if the content of an intervention is consideredinappropriate for young people (most typically this happens with interven-tions aimed at girls). While the challenge posed by misinformation andbacklash is evident, less obvious is the opportunity that these mishaps affordto open discussions of a community’s beliefs and norms and the potential forshifting such norms. This was the case for three interventions reviewed here(denoted as I, S and T in Table 8.3) (6–9). The threat posed by backlash andmisinformation are acknowledged in the negative rating given for potentialadverse effects for all intervention types. The greater potential for damageposed by a backlash to type 1 interventions, where it may threaten the ongoingwork of the host organization, is acknowledged in the more negative ratinggiven to this type of intervention.
Also common across intervention types is the possibility of producing otherhealth and social benefits by engaging participants in conscious considerationof their health, the possibility of changing their behaviour to protect theirhealth, and the adoption of attitudes favouring delayed gratification in orderto experience long-term health benefits. Each of these could extend beyondHIV to other areas of health and social life. As a result, all types of interven-tions received at least a small positive rating in the category assessing otherhealth and social benefits.
When considering the remaining threshold criteria, type 1 and type 4 inter-ventions benefit from their connection with existing community organiza-tions and events. The feasibility of the interventions as well as theiracceptability and reach may be enhanced by their association with and use ofthe infrastructures, facilities and delivery mechanisms of their host organi-zations. In addition, there is a potential synergy between the social benefitsand the health benefits provided by the host organization or event and theHIV interventions. Since type 4 interventions are delivered to an entire com-munity, their reach is especially wide; however, the personal relevance andspecificity of their message is limited, potentially weakening their effect.Based on these characteristics, intervention types 1 and 4 are judged to requirea moderate threshold of evidence before they can be recommended forinvestment and scaling-up – that is, evidence is needed at the level of plau-sibility. (See description of levels of evidence in chapter 4 and in Glossary).
249
92-4-120938-0_CH08_249

Tab
le 8
.3D
escr
ipti
on
of
the
inte
rven
tio
ns
by
stu
dy
Stu
dy,
loca
tio
n a
nd
dat
esT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
Inte
rven
tio
n t
ype
1 (t
arg
etin
g y
ou
ths
and
del
iver
ed u
sin
g e
xist
ing
yo
uth
org
aniz
atio
ns
or
cen
tres
)A
– C
amer
oon:
Nko
ngsa
mba
, 199
7–19
98 (
15)
• Y
outh
s ag
ed 1
2–25
yea
rs•
Incr
ease
con
trac
eptiv
e us
e•
Red
uce
inci
denc
e of
ST
Is,a
HIV
and
unin
tend
ed p
regn
anci
es
Car
eful
ly s
elec
ted
peer
edu
cato
rs w
ere
give
n1
wee
k of
trai
ning
(w
ith q
uart
erly
ret
rain
ing)
;th
ey h
ave
a hi
gh in
vest
men
t in
the
proj
ect a
ndde
liver
one
-on-
one
and
grou
p ac
tiviti
es th
atin
clud
e re
prod
uctiv
e he
alth
info
rmat
ion,
refe
rral
s an
d pr
omot
iona
l mat
eria
lsB
– C
amer
oon:
Mok
olo
neig
hbou
rhoo
d of
Yao
undé
(16
, 17)
• A
dole
scen
ts•
Impr
ove
repr
oduc
tive
heal
th k
now
ledg
eP
rom
ote
beha
viou
r ch
ange
usi
ng tr
aine
d pe
ered
ucat
ors
and
info
rmat
ion,
edu
catio
n an
dco
mm
unic
atio
n pu
blic
atio
ns
Car
eful
ly s
elec
ted
and
supe
rvis
ed p
eer
educ
ator
s de
liver
info
rmal
talk
s, o
ne-o
n-on
ese
ssio
ns, c
onfe
renc
es, r
ound
tabl
edi
scus
sion
s, c
ultu
ral a
nd a
thle
tic a
ctiv
ities
, as
wel
l as
a m
agaz
ine
cont
aini
ng r
epro
duct
ive
heal
th in
form
atio
nC
– N
iger
ia a
nd G
hana
,19
94–1
997
(28)
• Y
outh
s ag
ed 1
2–24
yea
rs, b
oth
in a
nd o
ut o
fsc
hool
• Im
prov
e kn
owle
dge
of s
exua
lity
and
repr
oduc
tive
heal
th is
sues
• P
rom
ote
safe
r se
x an
d co
ntra
cept
ive
use
amon
g th
ose
who
are
sex
ually
act
ive
8 yo
uth-
serv
ice
orga
niza
tions
in N
iger
ia, 2
inG
hana
trai
ned
staf
f to
deve
lop
prog
ram
me;
staf
f tra
ined
pee
r ed
ucat
ors
to d
eliv
er o
ne-o
n-on
e di
scus
sion
s an
d gr
oup
activ
ities
, to
dist
ribut
e m
ater
ial c
onta
inin
g ed
ucat
ion
abou
tan
d co
unse
lling
on
sexu
al a
nd r
epro
duct
ive
heal
th, r
efer
rals
to o
ther
ser
vice
sD
– B
ali:
Kut
a, U
bud,
Can
dida
sa a
nd L
ovin
a19
95–1
996
(13)
• B
ali a
ge-m
ate
(cul
tura
lly d
efin
ed c
ohor
ts)
grou
p m
embe
rs•
Util
ize
esta
blis
hed
Bal
ines
e yo
uth
grou
ps to
prov
ide
info
rmat
ion
on H
IV p
reve
ntio
n
Pee
r ed
ucat
ors
from
exi
stin
g ag
e-m
ate
(cul
tura
lly d
efin
ed c
ohor
t) g
roup
s to
whi
ch a
llyo
uth
belo
ng fr
om p
uber
ty to
mar
riage
rece
ived
3-d
ay tr
aini
ng to
del
iver
a s
ingl
e7-
hour
ses
sion
to a
ge-m
ate
grou
p co
ntai
ning
info
rmat
ion
on H
IV r
isk,
tran
smis
sion
and
prev
entio
n
250
92-4-120938-0_CH08_250

E –
Gha
na:
Fou
r pr
ojec
t are
as c
onne
cted
with
NG
Osb
begi
nnin
g in
199
8; m
ultic
ount
ry in
itiat
ive
(18)
• A
dole
scen
ts•
Rea
ch y
outh
s bo
th in
and
out
of s
choo
l with
info
rmat
ion
abou
t rep
rodu
ctiv
e he
alth
Pee
r ed
ucat
ors
trai
ned
peer
pro
mot
ers
who
recr
uit p
eer
cont
acts
and
del
iver
cou
nsel
ling,
disc
ussi
on g
roup
s, w
orks
hops
, dra
ma
and
mus
ic fo
cusi
ng o
n re
prod
uctiv
e he
alth
info
rmat
ion
and
serv
ices
, as
wel
l as
prov
idin
gno
n-pr
escr
iptio
n fa
mily
pla
nnin
g m
etho
dsF
– Z
ambi
a:4
NG
O-b
ased
pro
ject
s(d
ate
not r
epor
ted)
(19
)
• Y
outh
s ag
ed 1
4–25
yea
rs a
nd g
atek
eepe
rs•
Incr
ease
kno
wle
dge
of H
IV•
Pro
mot
e sa
fer
beha
viou
r• B
uild
cap
acity
to re
spon
d to
and
cop
e w
ith H
IV/
AID
S
Pee
r ed
ucat
or p
rogr
amm
es w
ere
part
of
over
all r
each
; pee
r ed
ucat
ors
with
reg
ular
lyup
date
d tr
aini
ng m
ater
ials
del
iver
dra
ma,
gam
es a
nd m
usic
that
focu
s on
ser
vice
s fo
ryo
uths
and
wom
en, c
ondo
m d
istr
ibut
ion,
life
-sk
ills
trai
ning
, gen
der
awar
enes
s an
dse
nsiti
zatio
nG
– M
alaw
i:m
id-1
997
to D
ec. 2
000
(12)
• Y
outh
s ag
ed 5
–20
year
s•
Com
pete
nce
and
life
skill
s to
pro
mot
esu
stai
ned
HIV
pre
vent
ion
amon
g ch
ildre
nag
ed 5
–14
year
s•
Red
uce
leve
ls o
f HIV
in y
outh
s ag
ed 1
5–20
year
s
You
th te
chni
cal s
ubco
mm
ittee
s tr
ain
club
mat
rons
and
pat
rons
, lin
k w
ith U
NIC
EF
, and
guid
e de
liver
y of
ser
vice
s th
at in
clud
e an
ti-A
IDS
clu
bs a
nd li
fe s
kills
edu
catio
n fo
r ou
t-of
-sc
hool
you
ths,
focu
sing
on
repr
oduc
tive
heal
thin
form
atio
n, s
ervi
ces
and
prom
otio
nal
mat
eria
lsH
– Z
ambi
a:tw
o pr
ovin
ces
in n
orth
ern
Zam
bia,
(da
te n
otre
port
ed)
(26)
• Y
outh
s in
sch
ool a
nd c
omm
unity
ant
i-AID
Scl
ubs
• T
rain
you
ths
to c
are
for
peop
le li
ving
with
HIV
/A
IDS
and
orp
hans
and
vul
nera
ble
child
ren
inho
pe o
f ins
pirin
g sa
fe b
ehav
iour
Hea
lth p
rofe
ssio
nals
trai
ned
yout
h ca
regi
vers
,w
ith fo
llow
up
afte
r 2
mon
ths
and
ongo
ing
trai
ning
eve
ry 3
mon
ths;
trai
ned
yout
hs p
rovi
deca
re to
peo
ple
livin
g w
ith H
IV/A
IDS
and
orph
ans
and
vuln
erab
le c
hild
ren;
pro
vide
repr
oduc
tive
heal
th in
form
atio
n, m
ater
ials
and
supp
ort
I – K
enya
:M
atha
re s
lum
, Nai
robi
,19
87, e
xpan
ded
in 1
992
to in
clud
e gi
rls (
6)
• A
dole
scen
ts a
ged
9–18
yea
rs•
Cre
ate
oppo
rtun
ities
for
yout
h de
velo
pmen
t•
Impa
rt H
IV/A
IDS
info
rmat
ion
as w
ell a
sm
otiv
atio
n to
sta
y sa
fe
Dev
elop
s lif
e sk
ills
thro
ugh
socc
er p
layi
ng,
com
mun
ity s
ervi
ces
and
info
rmal
conv
ersa
tions
am
ong
yout
hs; p
rogr
amm
e al
soof
fers
fina
ncia
l ass
ista
nce
for
educ
atio
n an
dH
IV in
form
atio
n pr
ovid
ed v
ia p
eer
educ
ator
s
251
92-4-120938-0_CH08_251

Stu
dy,
loca
tio
n a
nd
dat
esT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
J –
Nep
al:
Ter
ai d
istr
ict o
f Naw
alpa
rasi
and
Kaw
asot
i and
sub
urbs
of K
athm
andu
,(d
ate
not r
epor
ted)
(23
)
• A
dole
scen
ts a
nd a
dults
• U
se e
xist
ing
yout
h co
mm
unic
atio
n ne
twor
ks to
incr
ease
rep
rodu
ctiv
e he
alth
kno
wle
dge
Act
iviti
es d
esig
ned
and
impl
emen
ted
by lo
cal
yout
hs w
ho d
eliv
er a
dole
scen
t-fr
iend
ly h
ealth
serv
ices
and
pro
vide
a s
uppo
rt n
etw
ork
for
heal
th p
rofe
ssio
nals
; pee
r ed
ucat
ion
and
coun
selli
ng a
re a
lso
offe
red
as w
ell a
s ad
ult
educ
atio
n an
d dr
ama
addr
essi
ng H
IVin
form
atio
n an
d so
cial
nor
ms
K –
Ken
ya:
Nye
ri, 1
997–
2001
(24
)•
Unm
arrie
d yo
uths
age
d 10
–24
year
s an
din
fluen
tial a
dults
• D
elay
ons
et o
f sex
ual a
ctiv
ity•
Pre
vent
thos
e w
ho a
re s
exua
lly a
ctiv
e fr
omsu
fferin
g ne
gativ
e co
nseq
uenc
es o
f act
ivity
Car
eful
ly s
elec
ted
youn
g pa
rent
s de
liver
eded
ucat
iona
l act
iviti
es (
via
grou
p di
scus
sion
s,dr
ama
and
lect
ures
), c
ouns
ellin
g, r
efer
rals
for
heal
th s
ervi
ces
and
sens
itiza
tion
of a
dults
to th
esi
tuat
ions
and
nee
ds o
f you
ths
with
a fo
cus
onre
prod
uctiv
e he
alth
info
rmat
ion
Inte
rven
tio
n t
ype
2 (t
arg
etin
g y
ou
ths
and
cre
atin
g o
wn
sys
tem
an
d s
tru
ctu
re f
or
del
iver
y)L
– G
hana
:12
dis
tric
ts in
upp
er e
aste
rn a
nd n
orth
ern
Gha
na, 1
996
(29)
• Y
outh
s ag
ed 1
5–25
yea
rs•
Pro
mot
e H
IV/A
IDS
aw
aren
ess
and
know
ledg
ean
d sa
fer
sex
prac
tices
thro
ugh
peer
-to-
peer
educ
atio
n
You
th to
You
th is
one
of m
any
proj
ects
bei
ngru
n by
diff
eren
t loc
al o
rgan
izat
ions
; car
eful
lyse
lect
ed p
eer
educ
ator
s ar
e gi
ven
5-da
ytr
aini
ng, 3
-day
ref
resh
er c
ours
es, y
early
revi
ewm
eetin
g an
d tr
aini
ng o
f tra
iner
s w
orks
hop;
they
deliv
er w
eekl
y pe
er e
duca
tion
sess
ions
, gro
upac
tiviti
es c
onta
inin
g re
prod
uctiv
e he
alth
info
rmat
ion
and
cond
om d
emon
stra
tions
M –
Sri
Lank
a:lo
w in
com
e ur
ban
area
of K
andy
and
the
Uni
vers
ity o
f Per
aden
iya
(30)
(da
te n
otre
port
ed)
• U
rban
you
ths
aged
17–
27 y
ears
• Le
arn
sexu
al n
egot
iatio
n an
d de
cisi
on-m
akin
gsk
ills
nece
ssar
y to
avo
id r
isk,
suc
h as
saf
e se
xpr
actic
es
Pee
r ed
ucat
ors
recr
uite
d, s
uper
vise
d an
dte
chni
cally
ass
iste
d to
faci
litat
e gr
oup
sess
ions
that
incl
ude
fact
ual p
rese
ntat
ions
, writ
ten
activ
ities
, gro
up d
iscu
ssio
n an
d pr
oble
m-
solv
ing
arou
nd r
elat
ions
hips
, sex
ualit
y an
din
form
atio
n on
ST
Is, H
IV a
nd A
IDS
N –
Indi
a:G
ujar
at, 1
998
(20)
• Y
oung
men
age
d 15
–30
year
sO
utre
ach
wor
kers
trai
n pe
er e
duca
tors
and
wor
ker
educ
ator
s to
run
gro
up d
iscu
ssio
ns
252
92-4-120938-0_CH08_252

• Eng
age
mal
es in
repr
oduc
tive
heal
th e
duca
tion,
sexu
al ri
sk re
duct
ion
and
early
trea
tmen
t of H
IVan
d S
TIs
usin
g na
rrat
ive
inte
rven
tion
mod
el w
ithac
tiviti
es o
n se
men
loss
con
cern
s in
tegr
ated
into
HIV
and
ST
I edu
catio
n; th
is p
rogr
amm
eal
so in
clud
ed in
com
e ge
nera
tion,
sel
f-he
lpgr
oups
for
thos
e in
the
illeg
al li
quor
trad
e,co
uple
s’ c
lubs
and
3-d
ay h
ealth
fairs
how
ever
,th
ese
aspe
cts
of th
e pr
ogra
mm
e do
not
fall
with
in th
e sc
ope
of th
is p
aper
O–
Indi
a:14
/261
urb
an s
lum
s in
Luck
now
(25
) (d
ate
not r
epor
ted)
• A
dole
scen
t mal
es•
Incr
ease
aw
aren
ess
of S
TI r
isk
• E
xpan
d se
x ed
ucat
ion
to in
clud
e fo
rms
ofse
xual
ity o
ther
than
coi
tus
Ret
ired
psyc
hiat
rist a
nd 3
mal
e as
sist
ants
deliv
er p
rogr
amm
e in
clud
ing
a se
cure
box
for
anon
ymou
s qu
estio
ns fr
om p
artic
ipan
ts, t
aped
educ
atio
nal m
essa
ges,
lect
ures
and
ans
wer
ques
tions
focu
sing
on
repr
oduc
tive
heal
thin
form
atio
nP
– G
hana
:G
a M
ashi
e ar
ea o
f Acc
ra,
1998
(29
)
• Y
outh
s•
Pro
mot
e at
titud
inal
and
beh
avio
ural
cha
nges
rela
ted
to H
IV/A
IDS
and
oth
er S
TIs
am
ong
yout
hs b
oth
in a
nd o
ut o
f sch
ool
Sup
ervi
sed
peer
edu
cato
rs g
iven
5-d
ay tr
aini
ng(w
ith r
efre
sher
trai
ning
6 m
onth
s la
ter)
to r
ungr
oup
disc
ussi
ons,
rol
e pl
ay, d
ebat
es a
ndga
mes
with
rep
rodu
ctiv
e he
alth
info
rmat
ion;
prov
ide
acce
ss to
con
dom
s, h
ealth
ser
vice
san
d co
unse
lling
and
chi
ldca
re s
uppo
rt s
ervi
ces;
linke
d to
pro
gram
mes
run
by
othe
r N
GO
sta
rget
ing
yout
hs w
ho w
ere
in s
choo
l or
out o
fsc
hool
thes
e ar
e ot
her
aspe
cts
of th
epr
ogra
mm
e w
hich
are
not
par
t of t
he s
cope
of
this
pap
erQ
–N
epal
:T
him
i and
Bal
kot (
27)
(dat
e no
tre
port
ed)
• Y
outh
15-
24•
Ena
ble
beha
viou
ral c
hang
e to
pre
vent
HIV
/A
IDS
and
ST
I•
Incr
ease
acc
ess
to y
outh
-frie
ndly
hea
lth c
are
You
th A
ctio
n G
roup
s de
liver
trai
ning
in s
tree
tdr
ama,
lead
ersh
ip, H
IV in
form
atio
n, b
asic
coun
selli
ng a
nd tr
aini
ng-o
f-tr
aine
rs, w
ith fo
cus
on re
prod
uctiv
e he
alth
info
rmat
ion
and
serv
ices
Inte
rven
tio
n t
ype
3 (c
om
mu
nit
y-w
ide
inte
rven
tio
n d
eliv
ered
th
rou
gh
fam
ily n
etw
ork
s)R
–U
gand
a:2
Bag
anda
com
mun
ities
in r
ural
• A
dole
scen
t girl
s ag
ed 1
3–19
yea
rs w
ere
the
prim
ary
focu
s, b
ut “s
enga
s” a
cces
sibl
e to
ent
ire“S
enga
s” a
re g
iven
7 d
ays’
trai
ning
, mon
thly
mee
tings
and
6-m
onth
ly w
orks
hops
; the
y
253
92-4-120938-0_CH08_253

Stu
dy,
loca
tio
n a
nd
dat
esT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
Uga
nda
(21,
22)
(da
tes
and
exac
t loc
atio
nsno
t rep
orte
d)• c
omm
unity
(tra
ditio
nally
the
“sen
ga” o
r “fa
ther
’ssi
ster
” is
a c
hann
el o
f com
mun
icat
ion
abou
tse
xual
beh
avio
ur fo
r ad
oles
cent
girl
s)•
Use
trai
ned
“sen
gas”
to p
rovi
de a
dole
scen
tgi
rls w
ith in
form
atio
n on
rep
rodu
ctiv
e he
alth
deliv
er c
omm
unity
sup
port
ed o
ne-o
n-on
eac
tiviti
es a
nd d
istr
ibut
e co
ndom
s
S–
Bur
kina
Fas
o:4
villa
ges,
200
3 (7
)•
Mar
ried
and
unm
arrie
d ad
oles
cent
s•
Pro
vide
rep
rodu
ctiv
e he
alth
info
rmat
ion,
acce
ss to
birt
h co
ntro
l and
con
dom
s•
Wor
k to
influ
ence
com
mun
ity g
ende
r no
rms
30 m
arrie
d, a
dole
scen
t mot
hers
trai
ned
as p
eer
educ
ator
s pr
ovid
ed e
duca
tiona
l sup
port
kits
for
hom
e vi
sits
and
focu
sed
on o
ne-t
o-on
eco
unse
lling
and
pro
vidi
ng r
epro
duct
ive
heal
than
d H
IV p
reve
ntio
n in
form
atio
nT
–U
gand
a:M
pigi
and
Igan
ga, 1
992–
1994
(8, 9
)
• M
uslim
fam
ilies
in c
omm
unity
• U
se M
uslim
rel
igio
us s
truc
ture
to in
crea
sekn
owle
dge
of A
IDS
• Id
entif
y an
d m
odify
ris
ky p
ract
ices
Tra
ined
imam
s an
d fa
mily
AID
S w
orke
rs;
imam
s in
trod
uced
and
sup
port
ed A
IDS
wor
kers
in h
ouse
hold
-bas
ed e
duca
tion
focu
sing
on
HIV
and
AID
SIn
terv
enti
on
typ
e 4
(co
mm
un
ity-
wid
e in
terv
enti
on
del
iver
ed t
hro
ug
h c
om
mu
nit
y-b
ased
act
ivit
ies)
U–
Tha
iland
:A
ll 77
vill
ages
in S
uwan
naku
hadi
stric
t, N
ongb
ua L
amph
u pr
ovin
ce, n
orth
ern
Tha
iland
, Jul
y 19
95 (
14)
• C
omm
unity
mem
bers
age
d 15
–35
year
s•
Incr
ease
sel
f-ef
ficac
y, s
kills
and
con
fiden
ce in
cond
om u
se a
nd d
iscu
ssio
ns w
ith p
artn
er
Use
d tr
aini
ng-o
f-tr
aine
rs a
ppro
ach;
rec
ruite
dvi
llage
lead
ers
to p
artic
ipat
e in
con
dom
rel
ayra
ces
at v
illag
e, s
ubdi
stric
t and
dis
tric
t lev
el;
incl
uded
con
dom
dem
onst
ratio
ns a
nd a
focu
son
the
deve
lopm
ent o
f sel
f effi
cacy
inac
cess
ing,
dis
cuss
ing
and
usin
g co
ndom
sV
–U
nite
d R
epub
lic o
f Tan
zani
a:K
isar
awe,
Mus
oma,
Mas
asi,
Bag
amoy
odi
stric
ts (
10, 1
1) (
date
not
rep
orte
d)
• O
ut-o
f-sc
hool
you
ths
and
othe
r co
mm
unity
mem
bers
• E
nabl
e yo
uths
to r
educ
e th
eir
risk
of H
IVin
fect
ion
thro
ugh
popu
lar
thea
tre
You
ng a
rtis
ts tr
aine
d in
pop
ular
thea
tre
and
fact
s ab
out H
IV/A
IDS
del
iver
cas
cade
trai
ning
,au
dien
ce-d
irect
ed d
ram
as w
ith d
iscu
ssio
nsan
d w
orks
hops
focu
sing
on
HIV
/AID
Sin
form
atio
n an
d ex
plor
atio
n of
loca
l situ
atio
nsth
at m
ay in
crea
se th
e ris
k of
HIV
tran
smis
sion
a S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
b N
GO
s =
non
gove
rnm
enta
l org
aniz
atio
ns.
254
92-4-120938-0_CH08_254

Type 3 interventions, which work through traditional kinship networks, alsorequire a moderate threshold of evidence. Their feasibility and the potentialsize of their effect are weaker than for types 1 and 4 because they rely on alarger number of intervention leaders and are delivered on a one-on-one basisor on a family or household basis, thus they require greater effort to reach alarge number of community members. However, this intervention type has astronger potential to produce other social and health benefits because thepersonalized nature of the delivery makes it possible to incorporate otherbeneficial messages.
Intervention type 2 is judged to require a high threshold of evidence. Inter-ventions of this type must build their own delivery mechanism and infras-tructure, find a location for delivery and address issues of acceptabilitywithout forming an alliance with other already accepted community activitiesor organizations. This added effort and cost limits their feasibility, accept-ability and potential effect size as well as their ability to bring about otherhealth and social benefits.
None of the studies reviewed here provided any costing information. At most,there were comments about costs. For example, a participatory theatreapproach in the United Republic of Tanzania found that the cost of usingvideos of their productions to extend the reach of the intervention was pro-hibitive (study V in Table 8.3) (10, 11); in study G, the activities of anti-AIDSclubs that relied on sports and audiovisual equipment could not be sustainedbecause of the cost of maintaining, repairing and replacing damaged andstolen equipment (12). Without further information, the effect of costs on thefeasibility of interventions could not be judged for any of the interventiontypes.
8.3.2 Description of interventions
Table 8.3 briefly summarizes information about each intervention’s location,target population and primary objectives as well as giving a brief descriptionof the study. (Additional details are available on the web.)
8.3.2.1 Theoretical frameworks
Only three studies explicitly articulated a theoretical framework of behaviourchange. These frameworks included social influence theory (study D) (13),social learning theory (study U) (14), and theatre for change (study V) (10,11). Some type 1 and 2 studies commented on the assumptions on whichthey were based, with the most common set of assumptions those of theknowledge, attitudes and behaviour model – that is, that changes in knowl-edge and attitudes are necessary and potentially sufficient to change be-haviour (type 1:A, B, E, F; type 2: N) (15–20). However, not all of the
255
92-4-120938-0_CH08_255

knowledge, attitude and behaviour elements were necessarily measured inthe evaluations of these interventions, and no evaluations tested the associa-tion among knowledge, attitudes and behaviour. Some interventions sup-ported their use of peer educators with the claim that peers were better ableto effect change than adults (type 1: A, B, E) (15–18). However, only onestudy compared the difference in programme delivery between peers andadults (type 3: R) (21, 22), and none of the studies articulated a theory of howpeers influenced each other. Several intervention studies focused specificallyon cultural appropriateness either in the content or method of delivery (type1: F, J, K; type 2: N, O; type 3: R, T; type 4: U, V) (8–11, 14, 19–25). In thesestudies, cultural appropriateness was described as either a contributor toeffecting change or as being necessary to effect change. Mention was madeof the importance of building self-esteem and peer bonding around positivesocial behaviours (type 1: I) (6); in two studies there was also mention ofincreasing the perception among young people that “AIDS is real” byinvolving them in caring for people with HIV (type 1: H) (26). In the 10remaining studies, no mention was made of a theoretical framework or theassumptions on which a model of behaviour change was built.
Models of programme delivery were even less likely to be articulated. Threepeer-led interventions described the use of a cascade or step-down model ofdelivery in which training programmes were delivered through an everwidening circle of peer leaders as those who were originally trained went onto train others (type 1: E, F; type 2: Q) (18, 19, 27). One other study specif-ically described a model that linked organizations that were delivering theintervention with other organizations such as health centres that could providecounselling, testing and healthcare support (type 1: H) (26). Other interven-tion studies described methods used to train leaders and deliver programmesbut did not articulate the specific models or theoretical frameworks on whichthese were built.
8.3.2.2 Objectives
The objectives of most interventions were to convey information, build skillsneeded to establish or change targeted behaviours, and change sexualbehaviours that put young people at risk. In addition, most type 3 and 4interventions shared the objectives of raising awareness and changing com-munity norms that contributed to vulnerability. The objectives of the evalu-ations of two type 1 interventions also included testing the dispersal ofinformation from those directly involved in the intervention to all youth inthe community (studies C and G) (12, 28). Two others (studies E and J) (18,23) tested different forms of programme organization.
256
92-4-120938-0_CH08_256

8.3.2.3 Content
The most common information provided in all interventions was about thetransmission and prevention of HIV. In 14 of the 22 interventions this wasdone within the context of reproductive health (studies A, B, C, E, G, H, J,K, L, O, P, Q, R and S) (7, 12, 15–18, 21–29 ). Interventions that targetedskill building included both general life skills (studies C, D, J, Q, R, S) (7,13, 21–23, 27, 28,) and skills specific to avoiding HIV infection (studies C,D, L, P, R, U, V) (10, 11, 13, 14, 21, 22, 28, 29). Skills specific to preventingHIV were often restricted to locating and accessing condoms, condom self-efficacy and the proper use of condoms (studies D, L, P, U) (13, 14, 29). Skillsin communicating with partners were taught in four interventions (D, J, K,R) (13, 21– 24), and in two studies (T, V) (8–11) participants learnt to identifylocal situations and practices where there were heightened risks of becominginfected with HIV.
8.3.2.4 Providers and delivery
Interventions of all types (but not all interventions) were delivered by com-munity members. Thirteen of the 17 type 1 and 2 interventions used “peereducators”, “peer supporters” or “peer leaders” to deliver programmes.(There was no consistency in the terminology used or the definitions of theseroles.) The remaining four type 1 and 2 interventions used adult communitymembers as intervention leaders, but expected the youth who were partici-pating to become informal educators and role models for their peers (G, H,I, K) (6, 12, 24, 26). Two each of type 3 and 4 interventions used peer edu-cators either exclusively (S, V) (7, 10, 11) or with adult leaders (R, U) (14,21, 22 ). The remaining type 3 intervention (T) (8, 9) used trained adultcommunity members to deliver the programme.
8.3.3 Quality of the evidence
Only 9 of the 22 evaluations used experimental designs – that is,. designs thatmet the requirements for a moderate or high threshold of evidence. Threefrom type 1 used some form of random allocation to intervention and controlgroups (A, C, H) (15, 26, 28), and six from types 1, 2 and 3 used non-randomized comparisons (B, J, K, O, R, T) (8, 9, 16, 17, 21–25). Of theremaining studies, two each from types 1 and 2 and one from type 4 coulddemonstrate adequacy of the intervention either by using data collected beforeand after the intervention or by tracking the effects of the intervention usingproject records, field notes, interviews and materials produced by interven-tion participants (D, G, M, N, U) (12–14, 20, 30). The remaining eight (threetype 1, three type 2 and one each of types 3 and 4) provided evidence basedon the informed judgement of those responsible for the intervention (E, F, I,L, P, Q, S, V) (6, 7, 10, 11, 18, 19, 27, 29).
257
92-4-120938-0_CH08_257

Among the 9 evaluations that used experimental designs, the net changefound before and after the interventions were tested in only two, both of whichwere type 1 interventions (A, H) (15, 26). Only one study with a non-randomized comparison (type 1: J) (23) controlled for potential confoundersother than sex of the participant; and only 8 of the 22 studies disaggregatedresults by the sex of the participant (A, B, H, J, K, M, T, U) (8, 9, 14–17,23, 24, 26, 30). All but one of these studies (study H) (26) found that resultswere conditional on the sex of the participant, raising the question of whetherresults in the remainder of studies would have been different had they beendisaggregated by the sex of the participant. None of the three evaluations thatused randomized cluster sampling took this into account in their data analysis(A, C, H) (15, 26, 28).
The generally poor quality of the design and data analyses must be consideredwhen weighing the evaluation outcomes.
8.3.4 Outcome measures
Four of the UNGASS goals were commonly set as objectives for the inter-ventions included here: increasing knowledge related to HIV, building skillsrelated to preventing HIV transmission or acquisition, decreasing vulnera-bility to HIV, and reducing the prevalence of HIV. Changing sexual be-haviour and increasing the use of condoms, which may be consideredantecedents to reducing prevalence, were also set as objectives in severalinterventions. Table 8.4 provides information on the design and outcomes ofthe evaluations. (More details about each intervention are available on theweb.) The results presented here are based primarily on evidence reported atthe 0.05 level of statistical significance and obtained in evaluations usingexperimental designs required for the probability (randomized comparisontrials) or plausibility (non-randomized comparison trials) levels of evidence.Results based on adequacy levels of evidence (produced by designs that in-cluded pre-intervention and post-intervention components with no controlcomparisons) or informed judgement (produced by qualitative assessmentwithout formal pre-intervention and post-intervention measures) are usedonly when they provide useful information, and they are identified as comingfrom less rigorously designed evaluations. When the net changes before andafter an intervention were not reported, results are considered to reflect gainsthat may be attributed to the intervention if there is a net gain of at least 10percentage points from baseline to post-intervention in the intervention groupwhen compared with the control group. The acceptance of the 0.05 level ofsignificance or a net change of 10 percentage points are liberal criteria thaterr on the side of inflating the chance of an alpha error in favour of reducingthe chance of a beta error. We felt this was justified since there is considerableurgency to identify interventions that might by useful.
258
92-4-120938-0_CH08_258

Tab
le 8
.4D
escr
ipti
on
of
ou
tco
me
eval
uat
ion
s b
y st
ud
ya
Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
Inte
rven
tio
n t
ype
1 (t
arg
etin
g y
ou
ths
and
del
iver
ed u
sin
g e
xist
ing
yo
uth
org
aniz
atio
ns
or
cen
tres
)A
– C
amer
oon
(15)
Des
ign:
Clu
ster
ran
dom
ized
tria
l usi
ngho
useh
old
clus
ters
;1
inte
rven
tion,
1 c
ontr
ol s
ite.
Pos
t-in
terv
entio
n da
ta c
olle
ctio
n to
ok p
lace
3m
onth
s af
ter
inte
rven
tion
com
plet
ion,
17
mon
ths
afte
r pr
e-in
terv
entio
n da
ta c
olle
ctio
nN
o. o
f par
ticip
ants
pre
-inte
rven
tion:
inte
rven
tion
grou
p =
402
, con
trol
= 4
00N
o. o
f par
ticip
ants
pos
t-in
terv
entio
n:in
terv
entio
n gr
oup
= 4
03, c
ontr
ol =
413
Lim
itatio
n: D
ata
anal
ysis
did
not
take
into
acco
unt c
lust
ered
sam
plin
g
Kno
wle
dge
• S
pont
aneo
us k
now
ledg
e of
ST
Isoc
curr
ing
in w
omen
Beh
avio
ur•
Eve
r ha
d se
x•
Had
sex
in la
st 3
mon
ths
• C
ondo
m u
sed
durin
g la
st s
exua
lep
isod
e (r
ecen
t sex
onl
y)
+N
Sb
+ +
+ -
Str
ong
evid
ence
for
gain
s in
know
ledg
e an
dse
xual
beh
avio
uran
d co
ndom
use
B –
Cam
eroo
n(1
6, 1
7)D
esig
n: N
on-r
ando
miz
ed tr
ial;
1 in
terv
entio
nan
d 1
cont
rol g
roup
sel
ecte
d us
ing
2-st
age
prob
abili
ty s
ampl
ing
Par
ticip
ants
: Maj
ority
wer
e se
cond
ary
scho
olst
uden
ts a
ged
15–1
9 ye
ars
No.
of p
artic
ipan
ts p
re-in
terv
entio
n:in
terv
entio
n gr
oup
= 1
248
(mal
es: 6
32;
fem
ales
: 616
), c
ontr
ol g
roup
= 1
256
(mal
es:
634;
fem
ales
: 622
)
Kno
wle
dge
• G
ener
al k
now
ledg
e of
HIV
/AID
S
Beh
avio
ur•
Sex
dur
ing
past
12
mon
ths
• 1
part
ner
durin
g pa
st 1
2 m
onth
s•
Rep
orte
d ab
stin
ence
• U
sed
cond
om d
urin
g la
st s
ex w
ithre
gula
r pa
rtne
r
NS
NS
NS
NS
+
NS + + NS
Str
ong
evid
ence
of n
o ga
ins
inkn
owle
dge
and
no g
ains
in y
oung
men
’s b
ehav
iour
but s
ome
gain
sfo
r yo
ung
wom
en’s
sex
ual
beha
viou
r
259
92-4-120938-0_CH08_259

260
Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
inte
rven
tion
grou
p =
123
8 (m
ales
: 604
;fe
mal
es: 6
34),
con
trol
= 1
226
(mal
es: 6
15;
fem
ales
: 611
)
Lim
itatio
n: A
noth
er s
imul
tane
ous
inte
rven
tion,
know
n as
“10
0% y
outh
” m
ay h
ave
influ
ence
dre
sults
• S
TI s
ympt
oms
durin
g pa
st 1
2m
onth
sN
SN
S
C –
Gha
naan
d N
iger
ia (
28)
Des
ign:
Clu
ster
ran
dom
ized
tria
l; 10
inte
rven
tion,
10
cont
rol s
ites;
dat
a co
llect
ion
also
incl
uded
in-d
epth
inte
rvie
ws,
focu
s gr
oup
disc
ussi
ons
and
proj
ect m
onito
ring
over
18
mon
ths
No.
of p
artic
ipan
ts p
re-in
terv
entio
n:in
terv
entio
n gr
oup
= 9
11, c
ontr
ol =
873
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
inte
rven
tion
grou
p =
908
, con
trol
= 8
93
Lim
itatio
n: R
esul
ts fo
r ent
ire c
omm
unity
with
out
cont
rol f
or p
rogr
amm
e pa
rtic
ipat
ion
Kno
wle
dge
• O
vera
ll kn
owle
dge
ofre
prod
uctiv
e he
alth
(ou
t-of
scho
ol y
outh
s)
Ski
lls (
mea
sure
d am
ong
out-
of-s
choo
l you
ths)
• C
ontr
acep
tive
self-
effic
acy
• W
illin
gnes
s to
buy
con
dom
s
Beh
avio
ur•
Sex
in p
ast 3
mon
ths
(all
yout
h)•
Use
of m
oder
nco
ntra
cept
ives
(out
-of-
scho
olyo
uth)
NS
NS
NS
NS
NS
Str
ong
evid
ence
for
lack
of s
prea
dfr
om ta
rget
edyo
uth
to y
outh
inge
nera
lco
mm
unity
92-4-120938-0_CH08_260

D –
Bal
i (13
)D
esig
n: B
efor
e an
d af
ter
surv
ey w
ith n
oco
ntro
l with
a to
tal o
f 12
“ban
jars
”, 3
sel
ecte
dfr
om e
ach
of 4
are
as; d
ata
colle
ctio
nin
clud
ed s
urve
ys, 6
focu
s gr
oup
disc
ussi
ons
No.
of p
artic
ipan
ts p
re-in
terv
entio
n: 3
75vo
lunt
eers
(m
ale:
218
; fem
ale:
157
)
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
97
part
icip
ants
(at
3 s
ites)
Lim
itatio
n: P
ost-
inte
rven
tion
surv
ey h
eld
durin
g to
uris
t sea
son
with
sub
stan
tial l
oss
ofpa
rtic
ipan
ts, r
educ
ing
stat
istic
al p
ower
Kno
wle
dge
• M
easu
red
onkn
owle
dge
scal
e
Ski
lls•
Tal
king
with
frie
nds/
adul
ts•
Per
ceiv
ed b
arrie
rs to
cond
om u
se•
Con
dom
sel
f-ef
ficac
y
+ + + +
Mod
erat
eev
iden
ce fo
rga
ins
inkn
owle
dge
and
skill
s
E –
Gha
na (
18)
Des
ign:
Qua
litat
ive
com
paris
on o
fst
ruct
ured
and
uns
truc
ture
d m
odel
s of
prog
ram
me
deliv
ery,
no
cont
rol g
roup
s; d
ata
colle
ctio
n fr
om s
urve
ys, f
ocus
gro
ups,
obse
rvat
ion
guid
es fo
r pe
er e
duca
tors
, and
in-d
epth
inte
rvie
ws
with
opi
nion
lead
ers
Str
uctu
red
mod
el: 8
7 pe
er e
duca
tors
(40
%tr
aine
d), 5
24 p
eer
prom
oter
s (5
8% tr
aine
d)
Uns
truc
ture
d m
odel
: 83
peer
edu
cato
rs(4
0% tr
aine
d), 3
78 p
eer
prom
oter
s (4
2%tr
aine
d)
Lim
itatio
ns: F
ield
wor
k co
inci
ded
with
firs
tna
tiona
l cen
sus;
res
pond
ents
not
alw
ays
coop
erat
ive
Kno
wle
dge
• P
rote
ctio
n ag
ains
tH
IV•
Ove
rall
know
ledg
eab
out H
IV•
Con
dom
use
know
ledg
e
Str
uct
ure
dp
rog
ram
me
+ + +
Un
stru
ctu
red
pro
gra
mm
e
+ NS
NS
Wea
k ev
iden
cefo
r ga
ins
inst
ruct
ured
inte
rven
tion
com
pare
dw
ith u
n-st
ruct
ured
261
92-4-120938-0_CH08_261

Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
F –
Zam
bia
(19)
Des
ign:
Qua
litat
ive
case
stu
dy w
ith v
aria
ble-
by-
varia
ble,
cro
ss-c
ase
anal
ysis
of o
pera
tiona
lizat
ion
ofpr
ojec
ts a
nd a
ctiv
ities
. Dat
a co
llect
ion
incl
uded
docu
men
t rev
iew
s, s
emi-s
truc
ture
d in
terv
iew
s an
dno
n-st
ruct
ured
inte
rvie
ws
with
key
info
rman
ts a
s w
ell
as o
n-si
te v
isits
to o
bser
ve p
eer
activ
ities
.
The
re w
as a
n im
pres
sion
istic
ass
essm
ent o
f pos
sibl
eim
pact
but
attr
ibut
able
cau
sal l
inks
cou
ld n
ot b
epr
oven
giv
en ti
me
cons
trai
nts
Kno
wle
dge
• G
ener
al k
now
ledg
e of
HIV
and
sym
ptom
s•
Mod
es o
f tra
nsm
issi
on
Beh
avio
ur•
Som
e ch
ange
of
beha
viou
r•
Red
uced
num
ber
ofpa
rtne
rs
+ + + NS
Wea
k ev
iden
ce fo
rga
ins
in k
now
ledg
ean
d so
me
beha
viou
r ch
ange
;no
cha
nge
innu
mbe
r of
par
tner
s
G –
Mal
awi (
12)
Des
ign:
Bef
ore
and
afte
r sur
vey
with
no
cont
rol g
roup
.D
ata
colle
ctio
n in
clud
ed n
arra
tive
rese
arch
and
annu
al fo
cus
grou
p di
scus
sion
s w
ith ta
rget
gro
ups,
info
rmat
ion
on S
TI a
nd H
IV p
reva
lenc
e, d
ocum
ent
revi
ews
and
site
vis
its.
Lim
itatio
ns: T
he g
roup
s m
easu
red
in th
e pr
e-kn
owle
dge,
atti
tude
s an
d be
havi
ours
stu
dy d
id n
otco
rres
pond
to th
e ta
rget
age
gro
up s
o co
uld
not b
eus
ed fo
r co
mpa
rison
Kno
wle
dge
• G
ener
al k
now
ledg
e an
daw
aren
ess
Tra
nsm
issi
on:
• S
entin
el s
urve
y
+ –
Wea
k ev
iden
ce fo
rga
ins
in k
now
ledg
ean
d so
me
evid
ence
for
nega
tive
effe
cton
HIV
inci
denc
e
H –
Zam
bia
(26)
Des
ign:
Clu
ster
ran
dom
ized
tria
l with
> 6
clu
ster
s; 1
6of
30
club
s se
lect
ed a
t ran
dom
in o
ne in
terv
entio
n,on
e co
mpa
rison
site
. Dat
a co
llect
ion
also
incl
uded
focu
s gr
oups
and
in-d
epth
inte
rvie
ws
with
car
egiv
ers,
patr
on o
r m
atro
ns, p
eopl
e liv
ing
with
AID
S a
nd th
eir
fam
ily m
embe
rs
Beh
avio
ur•
Eve
r ha
d se
x•
Had
sex
in th
e pa
st 3
mon
ths
• E
ver
used
a c
ondo
m:
• U
sed
cond
om d
urin
g la
stse
x
+ NS + NS
+ NS + NS
Str
ong
evid
ence
for
impr
ovem
ents
inso
me
sexu
albe
havi
ours
and
cond
om u
se
262
92-4-120938-0_CH08_262

No.
of p
artic
ipan
ts p
re-in
terv
entio
n: in
terv
entio
ngr
oup
mal
e =
200
, fem
ale
=16
5; c
ontr
ol g
roup
mal
e =
209
, fem
ale
= 2
22
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
inte
rven
tion
grou
p m
ale
= 2
80, f
emal
e =
216
; con
trol
gro
upm
ale
= 2
69, f
emal
e =
218
I – K
enya
(6)
Des
ign:
Ane
cdot
al r
epor
ts o
f pro
gram
me
activ
ities
Kno
wle
dge
• G
ener
al A
IDS
and
prev
entio
n
Ski
lls•
Abl
e to
del
iver
pee
red
ucat
ion
on H
IV/A
IDS
+
+
Wea
k ev
iden
ce fo
r ga
ins
inkn
owle
dge
and
skill
s
J –
Nep
al (
23)
Des
ign:
Non
-ran
dom
ized
tria
l; 2
inte
rven
tion
grou
ps w
ith m
atch
ed c
ontr
ol s
ites
(1 e
ach
urba
nan
d ru
ral);
sur
veys
and
qua
litat
ive
data
col
lect
ed;
part
icip
ator
y ap
proa
ch w
ith 9
act
iviti
es w
ith 4
–5gr
oups
eac
h in
pre
-inte
rven
tion,
and
5 a
ctiv
ities
with
20
grou
ps in
eac
h po
st-in
terv
entio
n.
No.
of p
artic
ipan
ts p
re-in
terv
entio
n: a
dole
scen
ts =
724,
adu
lts =
752
, ser
vice
pro
vide
rs =
59
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
ado
lesc
ents
=97
9, a
dults
= 6
54, s
ervi
ce p
rovi
ders
= 6
2; k
eyin
form
ant i
nter
view
s =
3; 1
4 in
-dep
th in
terv
iew
s; 1
0fo
cus
grou
ps; 2
31 fa
cilit
ator
rep
orts
; 48
mys
tery
clie
nt s
urve
ys; 6
7 co
mm
unity
gro
up a
sses
smen
tsat
mid
poin
t and
pos
t-in
terv
entio
n
Kno
wle
dge
• M
odes
of t
rans
mis
sion
(urb
an p
artic
ipan
ts)
• M
odes
of t
rans
mis
sion
(rur
al p
artic
ipan
ts)
Beh
avio
ur•
Eve
r ha
d se
x (u
nmar
ried
urba
n m
en o
nly)
• E
ver
had
sex
(unm
arrie
dru
ral m
en o
nly)
-
NS
- +
+
+
Str
ong
evid
ence
for g
ains
inyo
ung
wom
en’s
kno
wle
dge
and
redu
ctio
ns in
sex
ual
activ
ity a
mon
g ru
ral y
oung
men
Mod
erat
e ev
iden
ce fo
rne
gativ
e ef
fect
on
know
ledg
e of
rur
al y
oung
men
and
sex
ual b
ehav
iour
of u
rban
you
ng m
en
263
92-4-120938-0_CH08_263

Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
K –
Ken
ya (
24)
Des
ign:
Non
-ran
dom
ized
tria
l; 1
inte
rven
tion
and
1 co
ntro
l. D
ata
colle
ctio
n in
clud
edin
terv
iew
er-a
dmin
iste
red
and
self-
adm
inis
tere
d qu
estio
nnai
res
No.
of p
artic
ipan
ts p
re-in
terv
entio
n:in
terv
entio
n gr
oup
mal
e =
573
, fem
ale
= 5
23;
cont
rol g
roup
mal
e =
219
, fem
ale
= 2
29
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
inte
rven
tion
grou
p m
ale
= 7
11, f
emal
e =
697
;co
ntro
l gro
up m
ale
= 2
14, f
emal
e =
243
Ski
lls•
Com
mun
icat
ion
with
par
ent
Beh
avio
ur•
Sec
onda
ry a
bstin
ence
• >
3 p
artn
ers
durin
g pa
st 3
year
s•
Use
d co
ndom
last
tim
e ha
dse
x
+ NS
NS +
+ + + +
Str
ong
evid
ence
for
gain
s in
com
mun
i-ca
tion
with
pare
nts,
cha
nge
inco
ndom
use
and
in s
exua
lbe
havi
our
ofyo
ung
wom
en (n
otyo
ung
men
)
Inte
rven
tio
n t
ype
2 (t
arg
etin
g y
ou
ths
and
cre
atin
g o
wn
sys
tem
an
d s
tru
ctu
re f
or
del
iver
y)L
– G
hana
(29
)D
esig
n: Q
ualit
ativ
e st
udy;
pre
-inte
rven
tion
and
post
-inte
rven
tion
exer
cise
with
part
icip
ants
in p
eer
educ
atio
n se
ssio
ns; s
itevi
sits
; fee
dbac
k w
orks
hops
with
pee
red
ucat
ors,
out
reac
h st
aff a
nd m
anag
emen
tco
mm
ittee
. Dat
a co
llect
ion
incl
uded
obse
rvat
ions
, in-
dept
h in
terv
iew
s, fo
cus
grou
ps, r
evie
w o
f doc
umen
tatio
n an
d re
port
s,an
d vi
sits
to p
harm
acie
s. E
valu
atio
nsi
mul
tane
ous
with
stu
dy P
(18
)
Kno
wle
dge
• M
odes
of t
rans
mis
sion
and
AB
C p
rogr
amm
e (A
bsta
in,
Be
faith
ful,
use
Con
dom
s)as
pre
vent
ion
• S
TI k
now
ledg
e
Ski
lls•
Cou
ld d
emon
stra
te h
ow to
use
a co
ndom
Beh
avio
ur•
Abs
tain
• U
se c
ondo
ms
corr
ectly
and
cons
iste
ntly
+ - +
Som
e+S
ome+
Wea
k ev
iden
ce fo
rga
ins
in s
ome
know
ledg
e,co
ndom
use
ski
llsan
d se
xual
beha
viou
r an
dco
ndom
use
beha
viou
r
264
92-4-120938-0_CH08_264

M –
Sri
Lank
a (3
0)D
esig
n: B
efor
e an
d af
ter
inte
rven
tion,
no
cont
rol
No.
of p
artic
ipan
ts p
re-in
terv
entio
n an
d po
st-
inte
rven
tion:
615
you
ths
inte
rvie
wed
for
ethn
ogra
phic
rese
arch
; app
roxi
mat
ely
one
half
wer
e lo
w in
com
e, o
neha
lf w
ere
univ
ersi
ty s
tude
nts,
rou
ghly
sam
e nu
mbe
r of
mal
es a
nd fe
mal
es
Kno
wle
dge
• A
IDS
• C
ondo
ms
• S
exua
l ter
ms
NS
NS
NS
NS + +
Wea
k ev
iden
ce fo
r gai
nsin
kno
wle
dge
amon
gyo
ung
wom
en b
ut n
oef
fect
on
youn
g m
en
N –
Indi
a (2
0)D
esig
n: Q
ualit
ativ
e in
terv
entio
n w
ith p
re-in
terv
entio
nan
d po
st-in
terv
entio
n co
mpa
rison
of f
low
char
tspr
oduc
ed b
y pr
ogra
mm
e pa
rtic
ipan
ts. D
ata
also
colle
cted
thro
ugh
info
rmal
gro
ups
of m
en d
iscu
ssin
gm
astu
rbat
ion
and
noct
urna
l em
issi
ons
Flo
wch
arts
ana
lyse
d: p
re-in
terv
entio
n =
35,
pos
t-in
terv
entio
n =
16
No.
of p
artic
ipan
ts: 5
0 si
ngle
men
incl
udin
g 22
vill
ager
s,16
mig
rant
wor
kers
, 12
pris
on in
mat
es
Kno
wle
dge
• M
astu
rbat
ion
is s
afe
sex
Atti
tude
s• M
astu
rbat
ion
acce
ptab
le a
ndha
s po
sitiv
e co
nseq
uenc
es
+ +
Wea
k ev
iden
ce fo
r gai
nsin
kno
wle
dge
and
attit
ude
chan
ges
amon
gyo
ung
men
O –
Indi
a (2
5)D
esig
n: N
on-r
ando
miz
ed tr
ial;
14 in
terv
entio
n si
tes,
14
mat
ched
con
trol
site
s. D
ata
colle
cted
thro
ugh
surv
eys
and
part
icip
ator
y di
ssem
inat
ion
wor
ksho
ps
No.
of p
artic
ipan
ts p
re-in
terv
entio
n: in
terv
entio
n gr
oup
= 3
77, c
ontr
ol =
343
No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
inte
rven
tion
grou
p=
363
, con
trol
= 3
43
Kno
wle
dge
• T
ime
to s
ympt
oms
of H
IV•
Mul
tiple
pre
vent
ion
met
hods
+ +
Str
ong
evid
ence
for
gain
s in
kno
wle
dge
for
youn
g m
en
265
92-4-120938-0_CH08_265

Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
P –
Gha
na (
29)
Des
ign:
Ane
cdot
al e
vide
nce.
Dat
a co
llect
edfr
om s
ite v
isits
; fee
dbac
k w
orks
hops
and
repo
rts
from
pee
r ed
ucat
ors,
out
reac
h st
aff
and
man
agem
ent;
info
rmal
dis
cuss
ions
and
mee
tings
; in-
dept
h in
terv
iew
s an
d fo
cus
grou
ps w
ith p
eer
educ
ator
s an
d ta
rget
gro
upm
embe
rs. P
re-s
urve
y da
ta c
olle
cted
but
not
anal
ysed
unt
il 2
year
s la
ter.
Dat
a ev
alua
ted
sim
ulta
neou
sly
with
that
col
lect
ed in
stu
dy L
18
Kno
wle
dge
• K
now
s ab
out 2
or
mor
em
odes
of t
rans
mis
sion
and
prev
entio
n•
Info
rmat
ion
abou
t ST
Is
Ski
lls• D
emon
stra
te c
orre
ct c
ondo
mus
e (o
ut-o
f-sc
hool
you
th)
Beh
avio
ur•
Dem
and
for
cond
oms
and
cond
om u
se•
Fem
ale
cond
oms
purc
hase
d
+ - + + +
Wea
k ev
iden
ce fo
rga
ins
in s
ome
know
ledg
e, s
kills
,an
d co
ndom
acqu
isiti
on.
Q –
Nep
al (
27)
Des
ign:
Qua
litat
ive
stud
y. D
ata
colle
cted
from
disc
ussi
ons,
par
ticip
ator
y m
etho
ds a
nd 3
cas
est
udie
s; p
roje
ct d
ocum
ents
and
oth
er r
elev
ant
mat
eria
ls r
evie
wed
;
No.
of p
artic
ipan
ts: 1
62 m
embe
rs o
f 18
yout
hac
tion
grou
ps
Kno
wle
dge
• G
ener
al k
now
ledg
e of
HIV
/A
IDS
, ST
Is a
nd s
exua
lhe
alth
Ski
lls•
You
th h
ave
“sen
se o
f soc
ial
resp
onsi
bilit
y”
+W
eak
evid
ence
for
gain
s in
kno
wle
dge,
sens
e of
res
pons
i-bi
lity
and
sexu
albe
havi
ours
266
92-4-120938-0_CH08_266

Lim
itatio
ns: F
ew a
ctio
n gr
oup
mem
bers
or
loca
l rep
rese
ntat
ives
inte
rvie
wed
. How
ever
, all
actio
n gr
oup
coor
dina
tors
inte
rvie
wed
and
part
icip
ated
in d
ata
colle
ctio
n an
d an
alys
is
Beh
avio
ur•
Saf
er s
exua
l beh
avio
urs
• R
educ
ed p
erso
nal
vuln
erab
ility
+ + +In
terv
enti
on
typ
e 3
(co
mm
un
ity-
wid
e in
terv
enti
on
del
iver
ed t
hro
ug
h f
amily
net
wo
rks)
R –
Uga
nda
(21,
22)
Des
ign:
Non
-ran
dom
ized
tria
l; 2
inte
rven
tion,
1co
ntro
l com
mun
ity. I
nclu
ded
only
girl
s w
hopa
rtic
ipat
ed in
stu
dy fo
r fu
ll 12
mon
ths;
inte
rven
tion
grou
p w
as s
elf-
sele
cted
(83
girl
sliv
ed in
inte
rven
tion
com
mun
ities
, 30
inco
ntro
l); 8
focu
s gr
oups
(4 g
roup
s of
mal
es a
nd4
of fe
mal
es),
60
in-d
epth
inte
rvie
ws
with
adul
ts (
30 w
ith m
ales
and
30
with
fem
ales
).D
ata
colle
cted
from
wor
ksho
ps, c
omm
unity
focu
s gr
oups
and
in-d
epth
inte
rvie
ws
with
non
-ta
rget
adu
lts w
ho h
ad v
isite
d “s
enga
s” (w
omen
trai
ned
to p
rovi
de s
exua
l hea
lth in
form
atio
n in
the
man
ner
appr
opria
te to
trad
ition
al k
insh
ipne
twor
ks)
No.
of p
artic
ipan
ts: i
nter
vent
ion
grou
p =
71,
cont
rol =
24
Kno
wle
dge
• M
odes
of H
IV tr
ansm
issi
on
Ski
llsIf
sexu
ally
act
ive
• C
omm
unic
ate
with
par
tner
• C
omm
unic
ate
with
oth
erpe
ople
Beh
avio
ur (
amon
g se
xual
lyac
tive
girls
)•
Had
sym
ptom
s of
an
ST
I•
Rep
ort c
onsi
sten
t con
dom
use
+ NS
NS + +
Wea
k ev
iden
ce fo
rga
ins
in k
now
ledg
ean
d be
havi
our
chan
ge a
mon
gyo
ung
wom
en b
ut n
och
ange
in c
om-
mun
icat
ion
skill
s
267
92-4-120938-0_CH08_267

Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
S –
Bur
kina
Fas
o(7
)D
esig
n: Q
ualit
ativ
e st
udy.
Dat
a co
llect
ion
incl
uded
61
in-d
epth
inte
rvie
ws
with
pee
red
ucat
ors,
lead
ers,
spo
uses
c and
chi
efm
edic
al o
ffice
r; 1
7 fo
cus
grou
ps w
ith p
eer
educ
ator
s, m
othe
rs-in
-law
, mar
ried
adol
esce
nts
who
wer
e no
t pee
r ed
ucat
ors,
othe
r pr
ogra
mm
e be
nefic
iarie
s an
d m
embe
rsof
org
aniz
ing
com
mitt
ee. T
here
was
als
o a
revi
ew o
f pro
ject
doc
umen
tatio
n an
d 6
case
stud
ies
Kno
wle
dge
• O
f rep
rodu
ctiv
e he
alth
in th
eco
mm
unity
and
am
ong
peer
educ
ator
s
Beh
avio
ur•
Con
trac
eptiv
e us
e•
Cha
nge
in c
omm
unity
nor
ms
rela
ted
to w
omen
(fo
rex
ampl
e, m
ovem
ent a
bout
the
com
mun
ity, a
bilit
y to
talk
with
oth
ers
abou
t sex
ual
heal
th is
sues
, etc
)
+
Som
e+
+
Wea
k ev
iden
ce fo
rga
ins
in k
now
ledg
e,co
ntra
cept
ive
use
and
chan
ge in
com
mun
ity n
orm
sre
late
d to
you
ngw
omen
T –
Uga
nda
(8, 9
)D
esig
n: N
on-r
ando
miz
ed tr
ial;
2 co
mm
uniti
es.
Pre
-inte
rven
tion
part
icip
ants
div
ided
into
expo
sed
and
non-
expo
sed
grou
ps fo
r pr
e-in
terv
entio
n vs
–pos
t-in
terv
entio
n an
alys
is.
Non
-exp
osed
act
ed a
s co
ntro
l gro
up. D
ata
colle
ctio
n in
clud
ed s
urve
ys, f
ocus
gro
ups
(9w
ith a
bout
75
part
icip
ants
) an
d 25
inte
rvie
ws
with
key
info
rman
ts (
fam
ily A
IDS
wor
kers
,im
ams,
imam
’s a
ssis
tant
s, s
heik
hs)
No.
of p
artic
ipan
ts p
re-in
terv
entio
n: 1
907
Kno
wle
dge
• M
odes
of t
rans
mis
sion
and
prev
entio
n•
Ris
k pe
rcep
tion
Beh
avio
ur•
Dec
reas
e nu
mbe
r of
sex
ual
part
ners
• E
ver
use
cond
om (
Urb
anyo
uth:
+; R
ural
: NS
)+
+ +
+
Str
ong
evid
ence
of
gain
s in
kno
wle
dge
and
sexu
albe
havi
our
(am
ong
both
you
ng m
en a
ndw
omen
)
268
92-4-120938-0_CH08_268

No.
of p
artic
ipan
ts p
ost-
inte
rven
tion:
exp
osed
(inte
rven
tion
grou
p) =
126
0, n
on-e
xpos
ed(c
ontr
ol g
roup
) =
566
Lim
itatio
ns: n
atio
nal p
rogr
amm
es e
xist
, whi
chco
nfou
nd r
esul
ts; s
ampl
es in
clud
e w
ider
age
rang
e th
an “
yout
h”
Inte
rven
tio
n t
ype
4 (c
om
mu
nit
y-w
ide
inte
rven
tio
n d
eliv
ered
th
rou
gh
co
mm
un
ity-
bas
ed a
ctiv
itie
s)U
– T
haila
nd(1
4)D
esig
n: B
efor
e an
d af
ter
stud
y w
ith n
o co
ntro
lgr
oup;
sur
veye
d im
med
iate
ly b
efor
eco
mm
unity
-wid
e ra
ce, i
mm
edia
tely
afte
r ra
cean
d 6
wee
ks p
ost-
race
with
con
veni
ence
sam
ple;
29
villa
ges
used
in e
valu
atio
n
No.
of p
artic
ipan
ts p
re-r
ace
and
post
rac
e:w
omen
= 8
7, m
en =
77(
mem
bers
of f
irst t
eam
sfo
rmed
)
No.
of p
artic
ipan
ts in
con
veni
ence
cro
ss-s
ectio
n6
wee
ks a
fter
race
: men
= 7
9, w
omen
= 8
1
Lim
itatio
ns: H
ighl
y m
obile
targ
et g
roup
prec
lude
s m
easu
rem
ent o
f lon
g-te
rm e
ffect
Kno
wle
dge
• P
rope
r co
ndom
used
Ski
lls•
Con
dom
sel
f-ef
ficac
yd
Beh
avio
ur•
Pro
port
ion
acce
ssin
gco
ndom
s (p
ost-
inte
rven
tion
only
)
+ +
28%
+ +
Wea
k ev
iden
ce o
f gai
nsin
kno
wle
dge
and
skill
sre
late
d to
con
dom
use
V –
Uni
ted
Rep
ublic
of
Tan
zani
a(1
0, 1
1)
Des
ign:
Qua
litat
ive
data
col
lect
ion
by a
team
of
artis
ts w
ho k
ept n
oteb
ooks
of d
aily
obse
rvat
ions
; com
mun
ity m
embe
rs a
nd a
rtis
tsca
talo
gued
eco
nom
ic, s
ocia
l and
hea
lthpr
oble
ms
that
faci
litat
e th
e sp
read
of H
IV;
repo
rts
wer
e de
velo
ped
from
not
eboo
ks o
f the
grou
ps u
sed
to p
repa
re fo
r ne
xt p
hase
of
prog
ram
me
(tra
inin
g pe
er e
duca
tors
)
Kno
wle
dge
• C
ultu
ral p
ract
ices
cont
ribut
ing
toH
IV s
prea
d
+W
eak
evid
ence
of g
ains
in k
now
ledg
e an
d sk
ills,
chan
ges
in c
omm
unity
norm
s an
d co
mm
unity
taki
ng a
ctio
n
269
92-4-120938-0_CH08_269

Stu
dy
and
loca
tio
nD
esig
n
Ou
tco
mes
mea
sure
dM
ales
All
Fem
ales
Str
eng
th o
fev
iden
ce
Ski
lls•
Abl
e to
iden
tify
dang
erou
spr
actic
es u
npro
mpt
ed
Beh
avio
urs
• C
hang
es in
com
mun
ityno
rms
Com
mun
ity a
ctio
n•
Act
ion
take
n to
pro
tect
yout
h
+ + +
A “
+”
indi
cate
s th
at a
res
ult i
s st
atis
tical
ly s
igni
fican
t at l
east
at P
0.0
5 an
d in
the
desi
red
dire
ctio
n (f
or e
xam
ple,
an
incr
ease
in k
now
ledg
e, a
dec
reas
e in
sex
ual
activ
ity, o
r an
incr
ease
in c
ondo
m u
se).
A “-
” sig
n in
dica
tes
that
a re
sult
is s
tatis
tical
ly s
igni
fican
t at l
east
at P
0.0
5 an
d in
an
unde
sira
ble
dire
ctio
n (f
or e
xam
ple,
a de
crea
se in
kno
wle
dge,
an
incr
ease
in s
exua
l act
ivity
or
a de
crea
se in
con
dom
use
). F
or c
ases
in w
hich
no
appr
opria
te te
sts
of s
tatis
tical
sig
nific
ance
wer
eco
nduc
ted,
res
ults
are
rat
ed +
or
– if
the
net d
iffer
ence
betw
een
the
pre-
inte
rven
tion
and
post
-inte
rven
tion
resu
lts is
10
perc
enta
ge p
oint
s w
hen
com
pare
dw
ith c
ontr
ols.
For
stu
dies
that
use
d on
ly in
terv
entio
n gr
oups
, the
net
diff
eren
ce is
cal
cula
ted
betw
een
pre-
inte
rven
tion
and
post
-inte
rven
tion
cont
rols
and
mus
tbe
> 1
0 pe
rcen
tage
poi
nts.
For
qua
litat
ive
stud
ies,
resu
lts a
re ra
ted
+ o
r – b
ased
on
the
repo
rt; t
hese
are
iden
tifie
d as
wea
k re
sults
in th
e in
str
engt
h of
evi
denc
eco
lum
n.b
NS
= n
ot s
igni
fican
t.c W
ithin
this
cul
tura
l set
ting,
it w
as n
eces
sary
to g
et s
pous
al c
onfir
mat
ion
of in
form
atio
n pr
ovid
ed b
y fe
mal
e pe
er e
duca
tors
.d
Res
ults
dis
aggr
egat
ed b
y se
x pr
ovid
ed b
y th
e au
thor
s (O
ctob
er 2
005)
.
270
92-4-120938-0_CH08_270

8.3.4.1 Knowledge outcomes
Altogether, 20 of the 22 studies, representing all four intervention types,evaluated gains in knowledge related to HIV transmission and prevention.Seven produced evidence at the level of probability (type 1: A, C) (15, 28)or plausibility (type 1: B, J; type 2: O; type 3: R, T) (8, 9, 16, 17, 21–23,25). All but two of these found at least some gains in knowledge. Both of theinterventions that found no gains in knowledge were type 1 (B, C) (16, 17,28). However, one evaluation (study C) (28) tested the dispersal of an inter-vention from a sample of “out-of-school youths” to whom it was deliveredto all “out-of-school youths” in the community rather than the effect of theintervention on participating youths. Two of the three intervention studiesthat disaggregated knowledge effects by the sex of the participant demon-strated knowledge gains only for young women (type 1: J; type 2: M) (23, 30).
Specific gains were reported in knowledge related to modes of HIV trans-mission, including some distinctive cultural practices such as ablution of thedead or genital excision (type 3: T) (8, 9). Gains were also reported in knowl-edge of prevention behaviours, such as abstinence or condom use (type 2: A,B; type 3: T) (8, 9, 15–17), as well as in scores on summative knowledgescales (type 1: A, D; type 2: M; type 3: R) (13, 15, 21, 22, 30). Knowledgegains related to distinctive cultural practices were most often reported onlyat the level of adequacy or based on informed judgement. These included therecognition in a type 2 study that “semen loss” was not detrimental to healthand that masturbation could be used as an alternative to more risky sexualactivities (study N) (20) or that a variety of local practices increased vulner-ability to HIV infection (type 3: V) (10, 11).
8.3.4.2 Skills outcomes
Three interventions specifically taught skills in using condoms. The evalua-tion of a type 4 intervention (study U) (14) produced evidence at the level ofadequacy of gains in skills for both young men and women, with type 2intervention studies (L, P) (29) providing the informed judgement of inter-vention leaders that more young people demonstrated proper use of condoms.The evaluation of a type 1 intervention included measures of self-efficacy inusing condoms (study D) (13). Only the evaluation study of a type 4 interven-tion (study U) disaggregated results for skills by the sex of the participant (14).
Improvements in communication about sexuality and HIV/AIDS with peers,adults or sexual partners were assessed in three studies of type 1 interventions(studies D, J, K) (13, 23, 24) and one study of a type 3 intervention (study R)(21, 22). The three evaluations that provided plausibility evidence (type 1: J,K; type 3: R) (21–24) all demonstrated significant gains, although the onlyevaluation that tested for potential confounding effects found that commu-nication improved only among rural males and urban females (type 1: J)
271
92-4-120938-0_CH08_271

(23). Intervention leaders and case notes from several studies provided evi-dence at the level of informed judgement that girls had been empowered tospeak about sexual matters as a result of participating in the intervention (forexample, type 1: I; type 3: S) (6, 7).
8.3.4.3 Community norms, attitudes and actions
Interventions of all types provided evidence of increased awareness andpotential changes in community norms that could contribute to reducing vul-nerability to HIV. None, however, evaluated these outcomes above the levelof adequacy or extended their evaluations over a long enough period to drawconclusions about whether the changes had been realized.
Three interventions targeted local norms that made girls more vulnerable toHIV infection (type 1: I; type 3: S; type 4: V) (6, 7, 10, 11). Three targetedlocal beliefs and practices that contributed to HIV transmission or createdbarriers to preventing transmission (type 2: N; type 3: T; type 4: V) (8–11,20). Three targeted local communication norms that created barriers to pro-viding information about HIV to youths or to communication betweenpartners about risk and prevention (type 3: S; type 4: U, V) (7, 10, 11, 14).The evaluation studies documented ways in which communities were re-sponding to heightened awareness, including the actions being taken tochange local practices. For interventions targeting youths, some evaluationsalso documented shifts in personal norms and attitudes, but in only one eval-uation were data presented that suggested these may have led to less riskysexual behaviour (type 4: V) (10, 11).
8.3.4.4 HIV incidence
Changes in HIV incidence were used in only one evaluation (type 1: G)(12) This intervention included initiation of anti-AIDS clubs across Malawifollowing a national media campaign. Sentinel surveillance data demon-strated an increase in incidence over the period of this intervention. However,in the absence of an experimental design, it is not possible to determinewhether the change in HIV incidence was related to the intervention orwhether the intervention merely lacked the power to reverse the existing na-tional trend.
8.3.4.5 Sexual activity
Seven evaluations used experimental designs producing plausibility-level orprobability-level evidence to assess changes in sexual intercourse. Six weretype 1 interventions (studies A, B, C, H, J, K) (15–17, 23, 24, 26, 28) and onewas type 3 (study T) (8, 9).
272
92-4-120938-0_CH08_272

All evaluations of type 1 interventions found reductions in the proportion ofboth males and females reporting that they ever had sexual intercourse.Young women made positive gains in both of the studies that disaggregatedresults by sex (type 1: B, H) (16, 17, 26); young men made positive gainsonly in one (type 1: study H) (26). The other studies produced non-significantresults. However, reports of recent sexual activity (for example, occurringduring the past 3 months or past year) generally did not show statisticallysignificant changes, with the exception of two evaluations of type 1 inter-ventions. In young women, one found a decrease in reports of recent sexualactivity (type 1: B) (16, 17) and one an increase (type 1: A) (15); there wereno significant changes in young men’s reports. Women were more likely toreport a reduction in the number of partners (type 1: B, K; type 3: T) (8, 9,16, 17, 24). Only one study (type 3: T) (8, 9) found a decrease in the numberof partners for young men; two type 1 studies showed no change for youngmen (studies B, K) (16, 17, 24).
8.3.4.6 Condom use
Condom use was assessed using a variety of questions including whether acondom had ever been used (type 1: C; type 3: T) (8, 9, 28), had been usedduring the last sexual encounter (type 1: A, B, H, K) (15–17, 24, 26) andwhether condoms were used consistently (type 3: R) (21, 22). One study alsoasked about condom use with different types of partners (type 1: B) (16,17). All seven of these evaluations produced evidence at the level of plausi-bility or probability; four of them demonstrated gains in condom use. In thetwo studies that disaggregated results by sex of the participant (studies H andK) (24, 26) the gains were the same for both sexes. Both type 1 and type 3interventions demonstrated gains, with the level of evidence meeting or ex-ceeding the threshold requirement in each case.
8.3.4.7 Overview of outcomes
As is shown in Table 8.5, none of the studies produced strong, unequivocalevidence of positive effects. Most provided either mixed results or were eval-uated using designs that could produce conclusions only at the level ofplausibility or lower. However, in Table 8.4, when specific results are re-viewed relative to the threshold of evidence required for each interventiontype (see Table 8.2), it is evident that intervention types 1, 3 and 4 provideevidence at or above the required threshold for at least one, and most oftenseveral, of the UNGASS goals. The goal of reducing HIV prevalence, how-ever, was not met in the intervention in which incidence data were evaluated(12). In addition, the results suggest that changes in sexual behaviour, asantecedent conditions to reducing HIV prevalence, may require interventionsthat specifically target young people (type 1 interventions) or, if delivered toa broader age range in the community, may require delivery within a tradi-tional or family setting (type 3).
273
92-4-120938-0_CH08_273

Tab
le 8
.5S
tren
gth
of
evid
ence
of
effe
ctiv
enes
s fo
r ea
ch in
terv
enti
on
typ
e an
d r
eco
mm
end
atio
ns
for
pro
gra
mm
esa
Stu
dy
des
ign
Po
siti
ve e
ffec
tN
o s
ign
ific
ant
effe
ctN
egat
ive
effe
ctS
tren
gth
of
evid
ence
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Sta
tist
ical
lysi
gn
ific
ant
Inte
rven
tio
n t
ype
1 (t
arg
etin
g y
ou
ths
and
del
iver
ed u
sin
g e
xist
ing
yo
uth
org
aniz
atio
ns
or
cen
tres
)A
necd
otal
IE
quiv
ocal
Qua
litat
ive
E,F
Cro
ss-s
ectio
nal (
no c
ompa
rison
gro
up)
Bef
ore-
afte
r (n
o co
mpa
rison
gro
up)
D,G
GQ
uasi
-exp
erim
enta
l ( 1
com
paris
on g
roup
)B
,J,K
aB
,J,K
RC
Tb
(< 6
clu
ster
s)R
CT
( 6
clu
ster
s)A
,HC
,HIn
terv
enti
on
typ
e 2
(tar
get
ing
yo
uth
s an
d c
reat
ing
ow
n s
yste
m a
nd
str
uct
ure
fo
r d
eliv
ery)
Ane
cdot
alP
Wea
kQ
ualit
ativ
eL,
N,Q
Cro
ss-s
ectio
nal (
no c
ompa
rison
gro
up)
Bef
ore-
afte
r (n
o co
mpa
rison
gro
up)
MQ
uasi
-exp
erim
enta
l ( 1
com
paris
on g
roup
)O
RC
T (
<6
clus
ters
)R
CT
( 6
clu
ster
s)In
terv
enti
on
typ
e 3
(co
mm
un
ity-
wid
e in
terv
enti
on
del
iver
ed t
hro
ug
h f
amily
net
wo
rks)
Ane
cdot
alE
quiv
ocal
Qua
litat
ive
SC
ross
-sec
tiona
l (no
com
paris
on g
roup
)B
efor
e-af
ter
(no
com
paris
on g
roup
)Q
uasi
-exp
erim
enta
l ( 1
com
paris
on g
roup
)R
,TR
RC
T (
< 6
clu
ster
s)
274
92-4-120938-0_CH08_274

RC
T (
6 c
lust
ers)
Inte
rven
tio
n t
ype
4 (c
om
mu
nit
y-w
ide
inte
rven
tio
n d
eliv
ered
th
rou
gh
co
mm
un
ity-
bas
ed a
ctiv
itie
s)A
necd
otal
Wea
kQ
ualit
ativ
eV
Cro
ss-s
ectio
nal (
no c
ompa
rison
gro
up)
Bef
ore-
Afte
r (n
o co
mpa
rison
gro
up)
UQ
uasi
-exp
erim
enta
l ( 1
com
paris
on g
roup
)R
CT
(<
6 cl
uste
rs)
RC
T (
6 c
lust
ers)
a In
terv
entio
ns a
ppea
r in
mor
e th
an o
ne c
olum
n w
hen
they
had
mix
ed r
esul
ts. S
ee ta
ble
4 fo
r de
tails
.b
RC
T =
ran
dom
ized
con
trol
led
tria
l.
275
92-4-120938-0_CH08_275

8.4 Go, ready, steady, do not go
Table 8.6 presents recommendations for donors, governments and organiza-tions that work with or are concerned about youths based on the evidencereviewed in this paper. The criteria used for making these recommendationsare reviewed in chapter 4.
8.4.1 Go
The relatively weak study designs and incomplete information preclude giv-ing a “Go” recommendation to any of the intervention types.
8.4.2 Ready
Five of the 10 type 1 interventions were evaluated using designs that producedplausibility or probability evidence sufficient to meet the moderate thresholdset for this type. All of the studies that evaluated the effect of the interventionon knowledge, skills, age of sexual debut or condom use demonstrated sig-nificant gains. Gains were generally not obtained in changing the incidenceor frequency of recent sexual activity or number of partners. Given the di-versity within this type of intervention and the lack of adequate monitoringor process data that would provide a clear picture of the content or deliveryof these interventions, this type is not rated as “Go”, but is considered“Ready” for delivery on a large scale when this is accompanied by continuedevaluations of impact, particularly in different settings, and among differentpopulation subgroups; and with comprehensive monitoring of processes.
8.4.3 Steady
The remaining intervention types fall into the “Steady” category. While theygenerally produced positive results, the evaluation designs were too weak,conducted over too few interventions and over too short a time to support astronger recommendation. Only three of the 11 studies of types 2, 3 and 4interventions produced evidence at the level of plausibility (studies O, R, T)(8, 9, 21, 22, 25); the remainder had evidence either at the level of adequacy(studies M, U) (14, 30) or informed judgement (studies L, N, P, Q, S, V) (7,10, 11, 20, 27, 29). Each intervention type did, however, have unique char-acteristics that are likely to have contributed to their success. Type 2 inter-ventions often addressed unique local and cultural issues, and type 3 usedtraditional kinship networks of communication to convey information aboutmatters of sexuality. While the two type 4 interventions had the widest reachand involved large numbers of community members in participatory activitiesthat raised awareness and mobilized communities, the small number of in-terventions of this type and the weak study designs point to a need for furthertesting and verification of the results. Because of the generally positive results
276
92-4-120938-0_CH08_276

Tab
le 8
.6R
eco
mm
end
atio
ns
on
th
e st
ren
gth
of
the
evid
ence
by
inte
rven
tio
n t
ype
Inte
rven
tio
n t
ype
Key
ch
arac
teri
stic
sC
on
clu
sio
nC
om
men
ts
1. T
arge
ts y
outh
s an
dis
del
iver
ed u
sing
exi
stin
gor
gani
zatio
ns o
r ce
ntre
sth
at s
erve
you
ths
• Y
outh
org
aniz
atio
ns o
r ce
ntre
s al
read
y ac
cept
ed b
yco
mm
unity
; int
erve
ntio
n is
sus
tain
able
and
has
capa
city
to m
ove
into
HIV
/AID
S p
rogr
amm
ing
• S
ucce
ssfu
l neg
otia
tion
of e
ntra
nce
into
org
aniz
atio
n•
HIV
/AID
S e
duca
tion
mus
t hav
e lo
gica
l fit
with
orga
niza
tion
• P
eer
educ
ator
s sh
ould
be
chos
en u
sing
spe
cific
,re
leva
nt s
elec
tion
crite
ria; m
onito
ring
and
supp
ort
shou
ld b
e pr
ovid
ed
Rea
dyT
hese
inte
rven
tions
wer
e m
ost l
ikel
y to
have
dem
onst
rate
d su
stai
nabi
lity,
to h
ave
a st
rong
eva
luat
ion
desi
gn a
nd p
ositi
vere
sults
2. T
arge
ts y
outh
s an
dcr
eate
s its
ow
n sy
stem
and
stru
ctur
e
• S
ucce
ssfu
l neg
otia
tion
of e
ntra
nce
into
com
mun
ity•
Pre
limin
ary
cont
ext a
nd n
eeds
ass
essm
ent s
houl
d be
used
as
foun
datio
n fo
r th
e in
terv
entio
n•
Sen
sitiz
atio
n of
com
mun
ity a
nd/o
r ga
teke
eper
isne
cess
ary
• P
eer
educ
ator
s sh
ould
be
chos
en u
sing
spe
cific
,re
leva
nt s
elec
tion
crite
ria; m
onito
ring
and
supp
ort
shou
ld b
e pr
ovid
ed
Ste
ady
orD
o no
t go
All
eval
uatio
ns o
f the
se in
terv
entio
ns h
adw
eak
desi
gns
The
stu
dies
wer
e as
like
ly n
ot to
dem
onst
rate
sus
tain
abili
ty b
eyon
d th
ein
itial
test
pha
se a
s th
ey w
ere
tode
mon
stra
te s
usta
inab
ility
Spe
cific
pro
blem
s w
ith s
ome
inte
rven
tions
are
add
ress
ed in
the
disc
ussi
on o
f the
“D
o no
t go”
cat
egor
y3.
Com
mun
ity-w
ide
inte
rven
tion
deliv
ered
thro
ugh
exis
ting
trad
ition
alki
nshi
p ne
twor
ks
• S
ucce
ssfu
l neg
otia
tion
of e
ntra
nce
into
com
mun
ity•
Pre
limin
ary
cont
ext a
nd n
eeds
ass
essm
ent a
ndas
sess
men
t of m
ost a
ccep
tabl
e pe
er e
duca
tors
sho
uld
be u
sed
to b
uild
inte
rven
tion
• S
ensi
tizat
ion
of c
omm
unity
and
/or
gate
keep
er is
nece
ssar
y
Ste
ady
Onc
e th
e sy
stem
for
deliv
erin
g th
ein
terv
entio
n is
est
ablis
hed,
this
type
dem
onst
rate
d an
abi
lity
to c
over
a w
ide
rang
e of
issu
es; h
owev
er, f
ew o
f the
sein
terv
entio
ns w
ere
eval
uate
d
277
92-4-120938-0_CH08_277

Inte
rven
tio
n t
ype
Key
ch
arac
teri
stic
sC
on
clu
sio
nC
om
men
ts
• P
eer
educ
ator
s sh
ould
be
chos
en u
sing
spe
cific
,re
leva
nt s
elec
tion
crite
ria; m
onito
ring
and
supp
ort
shou
ld b
e pr
ovid
ed4.
Com
mun
ity-w
ide
inte
rven
tion
deliv
ered
thro
ugh
activ
ities
, suc
has
fest
ival
s
• Suc
cess
ful n
egot
iatio
n of
ent
ranc
e in
to c
omm
unity
• Pre
limin
ary
cont
ext a
nd n
eeds
ass
essm
ent s
houl
dbe
use
d as
a fo
unda
tion
for
the
inte
rven
tion
• S
ensi
tizat
ion
of c
omm
unity
and
/or
gate
keep
er is
nece
ssar
y• A
ppro
pria
te c
omm
unity
act
iviti
es m
ust b
e id
entif
ied
• P
eer
educ
ator
s sh
ould
be
chos
en u
sing
spe
cific
,re
leva
nt s
elec
tion
crite
ria; m
onito
ring
and
supp
ort
shou
ld b
e pr
ovid
ed
Ste
ady
The
se in
terv
entio
ns h
ave
the
wid
est r
each
and
are
mos
t suc
cess
ful i
n ad
dres
sing
com
mun
ity n
orm
san
d pr
oduc
ing
com
mun
ity-w
ide
resp
onse
s
The
stu
dies
eva
luat
ing
thes
e in
terv
entio
ns h
adw
eak
desi
gns
Diff
icul
t to
eval
uate
com
mun
ity-w
ide
resp
onse
s
278
92-4-120938-0_CH08_278

and the unique characteristics of many of these interventions, it is recom-mended that interventions of these types that are already in place shouldcontinue, but no new ones should be implemented until evaluations demon-strate their effectiveness at least at the level of plausibility.
One type 1 intervention has also been categorized as “Steady” (rather than“Ready”) based on promising results but a weak study design. The KenyanMathare Youth Sports Association’s intervention (study I) (6) is a type 1intervention that has received international awards for its work with youth.Its reach extends to thousands of youth, and its programming includes aninnovative approach to challenging the gender norms that heighten the vul-nerability of young girls. Education about HIV risks and risk avoidance isincorporated into small group activities. Considering the broader social ben-efits that this programme has brought to the community, it should continueto be supported at its current level but an evaluation to assess its effects onHIV-related knowledge, skills and behaviours should be undertaken.
8.4.4 Do not go
While no intervention type has been categorized as “Do not go”, lessons werelearnt from several interventions that led to the identification of approachesthat should be avoided. The evaluation of a type 2 programme in Nepaldemonstrated the need to monitor activities at all sites in multisite interven-tions to ensure the intervention is actually delivered and that the design isfeasible (study Q) (27) Multisite interventions that lack these characteristicsdo not warrant the financial investment of donor agencies or governments.
Also unsuitable for funding are interventions that have high resource needsand lack a mechanism to ensure their ongoing provision as well as interven-tions that do not provide training, structure, monitoring or support for peerleaders. The former is seen in an example of anti-AIDS clubs in Malawi (type1 intervention) that relied on videos, video equipment and sports equipment(study G) (12) The equipment was stolen or broken within 1–2 years, thuslimiting the ongoing activities of the clubs. In contrast, anti-AIDS clubs inZambia (also type 1 interventions) were able to replenish supplies in home-based care kits every 3 months by maintaining relationships with nongovern-mental organizations (NGOs) and health services (study H) (26) Theproblems of providing inadequate training, structure, monitoring or supportfor peer leaders is evidenced in the type 2 intervention in Nepal (study Q)(27) as well as the type 1 intervention in Ghana (study E) (18) that comparedresults of a structured intervention with those of an unstructured interventioninvolving peer leaders. Clearly, interventions that depend on a continuingsupply of materials and that do not have a long-term and sustainable sourceof supplies, or those that rely on peer leaders but do not provide them with
279
92-4-120938-0_CH08_279

the training, structure and support they need to do their job, should be cate-gorized as “Do not go”.
8.4.5 Requirements for success
From reviewing the materials brought together here, it is possible to identifykey characteristics that are required for interventions to succeed. It is essentialthat all types of interventions provide the following for the leaders of theinterventions, especially peer leaders.
A screening procedure should be used to select peer leaders to ensure theyare motivated and capable of taking on the required tasks.
Comprehensive training and refresher sessions in programme content andthe skills required for delivery should be provided.
Leaders should be assigned specific tasks and objectives, and their workmust be monitored and supported.
In addition, all intervention types should:
focus on gaining entry into the community and on developing strategies todeal with adverse reactions to programme components;
focus on participatory learning activities;
ensure there is a sustainable means of obtaining required programmesupplies;
build links between components of complex interventions (for example,referral systems and activities should operate across components).
Beyond the requirements common to all interventions, each type of inter-vention has its own requirements.
Those implementing type 1 interventions should:
ensure the intervention is incorporated into the activities of an existingorganization or centre that has demonstrated an ability to reach a largenumber of youths and also ensure it is sustainable and accepted by thecommunity;
ensure that the organization’s activities attract both males and females.
Those implementing intervention types 2, 3 or 4 need to develop a system ofoutreach to the target population that is sustainable and acceptable to com-munity members. Those implementing type 2 interventions need to developan infrastructure that can sustain the intervention over the long term.
Those implementing type 3 interventions need to:
280
92-4-120938-0_CH08_280

hold discussions with community leaders and gatekeepers to identify theappropriate traditional networks for delivering an intervention that dealswith sexual behaviour and to determine the best type of leaders to deliverthe intervention;
develop a method to ensure that appropriate material support and resourcesare available to programme leaders to compensate them for the sizablecommitment of time and to ensure they can reach the target population.
Those implementing type 4 interventions should:
identify activities that have wide community appeal;
choose the timing and location of the intervention to maximize its reachand community participation;
advertise the activities in a way that make them accessible to communitymembers.
Although using an established theoretical model of behaviour change hasoften been cited as a requirement for success (31), this conclusion is not sup-ported by the studies reviewed here. Few interventions were explicitly basedon a theoretical model, and neither the number nor the strength of outcomeswas influenced by the presence or absence of a theoretical framework. Thisfinding parallels that of Gallant and Maticka-Tyndale in their review ofschool-based programmes in sub-Saharan Africa (5).
8.5 Conclusions
In drawing conclusions about interventions implemented in specific geo-graphically bounded communities, the weakness of the study designs and dataanalyses and the paucity of evaluations for several intervention types cannotbe ignored. It is evident that the attention of NGOs involved in designing andimplementing interventions has most often been on the intervention itself andnot on its evaluation. This is understandable given the urgency of the AIDSepidemic and the mission of NGOs. Recognizing these priorities, this reporthas used a more liberal interpretation of the adequacy of the study designneeded to demonstrate the effectiveness of an intervention.
The most encouraging results in terms of outcomes and programme reach arefor intervention types 1, 3 and 4 in which AIDS programmes were linkedto existing youth-focused organizations, to traditional kinship networks orwere part of community-wide events. The stronger study designs and suc-cesses noted for type 1 interventions present a particular contrast with thoseassessing type 2 interventions, which differ from type 1 interventions only intheir lack of connection to existing organizations. Of the interventions tar-geting entire communities, type 3 interventions, which also used existing
281
92-4-120938-0_CH08_281

infrastructure, were most successful in demonstrating gains in knowledge andskills as well as behaviour change; they also provided some evidence of shiftsin community norms. Finally, while few in number, the success of the twotype 4 interventions in raising awareness and mobilizing communities to planaction that could reduce the vulnerability of young people suggests that type4 interventions are promising and more of them should be evaluated. Thechallenges encountered by type 2 interventions suggest that it may be easierto achieve success when attention can be focused on developing and deliv-ering the content of the intervention rather than also focusing attention ondeveloping an infrastructure for delivery.
While the publications reviewed for this paper provided evidence of a con-siderable amount of innovation and creativity, and there are several inter-ventions that may make substantial contributions to achieving the UNGASSgoals, it is clear that more attention needs to be paid and funding applied tothe evaluation of both processes and outcomes and particularly to the speci-fication of the conditionality of the effects of the intervention. Attention mustalso be paid to cost–benefit analyses or at least to the costing of interventions.Continued delivery of the best of these interventions is important. However,good quality evaluations of processes and outcomes that test the efficacy andeffectiveness of interventions and provide information on cost are essentialto providing the evidence base needed for future decision-making. To thisend, a summary of recommendations to guide the development, evaluationand delivery are contained in Box 8.1.
Box 8.1
Recommendations for interventions targeting youths that are delivered ingeographically defined communities
For policy-makers
There is a sufficiently strong evidence base to support widespreadimplementation of interventions to prevent HIV that are deliveredwithin the framework of existing youth-service organizations oryouth centres. However, these interventions should only be imple-mented if they are carefully evaluated.
In addition, there is also a sufficiently strong evidence base to sup-port the continued delivery of similar interventions when they arenot connected to existing youth-oriented organizations and to sup-port the continued delivery of interventions targeting both adultsand youths when they are delivered through traditional or familynetworks or when they are delivered through community-wide
282
92-4-120938-0_CH08_282

events, such as theatrical performances, health fairs or festivals andcompetitions. However, expansion of such interventions should nottake place until they have been more carefully evaluated.
For programme development and delivery staff
Interventions delivered within existing youth-oriented organiza-tions, centres or infrastructures (for example, through faith-basedorganizations, families or existing community festivals) are able tofocus greater attention on elements necessary for success than areinterventions that must also build their own infrastructure to supportdelivery. Attention should be paid to working with gatekeepers en-sure ongoing acceptance of and support for interventions; thereshould be careful selection, training and supervision of programmeleaders; the tasks and duties of intervention leaders should be iden-tified; mechanisms must be found to provide the necessary ongoingresources for intervention delivery; participatory learning activitiesshould be used; links should be established between institutions andorganizations involved in the delivery and support of multifacetedinterventions; and culturally appropriate leaders, content and deliv-ery methods should be identified.
For researchers
Evaluation and operations research should be core elements of anyintervention targeting either young people or communities as awhole for the purpose of increasing young people’s knowledge andskills and changing their behaviours related to HIV transmissionand infection. In particular, evaluation results should pay attentionto analyses that identify specific conditions for different levels ofsuccess (for example, gender differences, and differences betweenrural and urban areas) and should include an evaluation of the costof the intervention.
References
1. United National General Assembly Special Session on HIV/AIDS. Declarationof commitment on HIV/AIDS. Geneva: United Nations, 2001.
2. Habicht J, Victora C, Baughan J. Evaluation designs for adequacy, plausibilityand probability of public health programme performance and impact.International Journal of Epidemiology, 1999, 28:10–18.
3. Caldwell J. Rethinking the African AIDS epidemic. Population and DevelopmentReview, 2000, 26:117–135.
283
92-4-120938-0_CH08_283

4. Green E. Rethinking AIDS prevention. Westport, CT, Praeger, 2003.
5. Gallant, M., Maticka-Tyndale, E. School-based HIV prevention programmes forAfrican youth. Social Science and Medicine, 1994, 58:1337–1351.
6. Brady M, Bunu Khan A. Letting girls play: the Mathare Youth SportsAssociation’s football program for girls. New York, Population Council, 2002.
7. UNFPA. Rapport evaluation thematique du projet UNFPA: mobilisationcommunautaire, participation et renforcement de l’autonomie desadolescent(e)s [Thematic evaluation report of UNFPA project: communitymobilization, participation and empowerment of adolescents]. Burkina Faso,UNFPA, 2004.
8. Kagimu M, Marum E, Serwadda D. Planning and evaluating strategies for AIDShealth education interventions in the Muslim community in Uganda. AIDSEducation and Prevention, 1995, 7:10–21.
9. Kagimu M et al. Evaluation of the effectiveness of AIDS health educationinterventions in the Muslim community in Uganda. AIDS Education andPrevention, 1998, 10:215–228.
10. Bagamoyo College of Arts et al Participatory action research on HIV/AIDSthrough a popular theatre approach in Tanzania. Evaluation and ProgramPlanning, 2002, 25:333–339.
11. Bagamoyo College of Arts. Report on participatory action research on HIV/AIDSthrough popular theatre approach in Temeke district. Dar Es Salaam, UnitedRepublic of Tanzania, UNICEF, 2001.
12. Reijer P, Chalimba M, Nakwagala A. Malawi goes to scale with anti-AIDS clubsand popular media. Evaluation and Program Planning, 2002, 25:357–363.
13. Merati TP et al. Traditional Balinese youth groups as a venue for prevention ofAIDS and other sexually transmitted diseases. AIDS, 1997, 11 Suppl1:S111–119.
14. Elkins D et al. Relaying the message of safer sex. Health EducationResearch, 1998, 13:357–370.
15. Speizer I, Oleko Tambashe B, Tegang SP. An Evaluation of the “Entre NousJeunes” peer educator program for adolescents in Cameroon. Studies in FamilyPlanning, 2001, 32:339–351.
16. Institut de Recherche et des Etudes des Comportements (IRESCO) [Instituteof Research and Studies of Behaviour].. Peer education as a strategy toincrease contraceptive prevalence and reduce the rate of STIs/HIV amongadolescents in Cameroon. Washington, DC, Population Council, 2002.(Frontiers Final Report.)
17. Population Council, Frontiers in Reproductive Health. Cameroon: peereducation and youth-friendly media reduce risky sexual behaviour. Washington,DC, Population Council, 2003. (Summary No. 37.)
18. Centre for Development and Population Activities (CEDPA). Using PEs toimprove adolescent reproductive health in Ghana. Washington, DC, CEDPA,2000.
19. Hughes-d’Aeth A. Evaluation of HIV/AIDS peer education projects in Zambia.Evaluation and Program Planning, 2002, 25:397–407.
20. Lakhani A, Ketan G, Collumbien M. Addressing semen loss concerns.Reproductive Health Matters, 2001, 9:49–59.
284
92-4-120938-0_CH08_284

21. Muyinda H et al. Traditional sex counselling and STI/HIV among young womenin rural Uganda. Culture, Health and Sexuality, 2001, 3:353–361.
22. Muyinda H et al. Harnessing the senga institution of adolescent sex educationfor the control of HIV and STDs in rural Uganda. AIDS Care, 2003, 15:159–167.
23. Mathur S, Malhotra A, Mehta M. Youth reproductive health in Nepal: isparticipation the answer? Washington, DC, International Centre for Researchon Women (ICRW) , EngenderHealth, 2001.
24. Erulkar A et al. Behaviour change evaluation of a culturally consistentreproductive health program for young Kenyans. International Family PlanningPerspectives, 2004, 30:58–67.
25. Awasthi S, Nichter M, Pande V. Developing an interactive STD-preventionprogramme for youth: lessons from a north Indian slum. Studies in FamilyPlanning, 2000, 31:138–150.
26. Esu-Williams E et al. Involving young people in the care and support of peopleliving with HIV and AIDS in Zambia. Washington, DC, Population Council, 2004.(Horizons Final Report.)
27. Sharma M. Youth for Each Other programme: rapid impact assessment. NepalRed Cross Society Junior/Youth Department HIV/AIDS PreventionProgramme. Nepal, Centre for Development and Population Activities, 2002.
28. Brieger W et al. West African Youth Initiative: outcome of a reproductive healtheducation program. Journal of Adolescent Health, 2001, 29:436–446.
29. UNICEF, Ghana. Evaluation of HIV/AIDS prevention through peer education,counselling, health care, training and urban refuges in Ghana. Evaluation andProgram Planning, 2002, 25:409–420.
30. Nastasi B et al. Community-based sexual risk prevention programme for SriLankan youth: influencing sexual-risk decision making. International Quarterlyof Community Health Education, 1998, 18:139–155.
31. Kirby D. Emerging answers: research findings on programs to reduce teenpregnancy. Washington, DC, National Campaign to Prevent Teen Pregnancy,2001.
285
92-4-120938-0_CH08_285

92-4-120938-0_CH08_286

9. Achieving the global goals on HIVamong young people most at risk indeveloping countries: young sexworkers, injecting drug users andmen who have sex with menOliver Hoffmann,a Tania Boler,a & Bruce Dickb
Objective To review evaluations of interventions in developing countriestargeting three groups most at risk of becoming infected with HIV: young sexworkers, young injecting drug users and young men who have sex with men.
Methods A systematic literature review was undertaken to identify pro-grammes in developing countries targeting young people in the three selectedgroups most at risk from HIV. We also identified programmes directed atyoung people in developed countries as well as programmes in developingcountries that targeted these three population groups but that did not differ-entiate between young people and adults.
Findings Young people 10 to 24 years of age represent a large proportion ofthe population most at risk of becoming infected with HIV in developingcountries. Despite this fact, well documented evaluations of interventions thattarget these groups are scarce. However, there is evidence of effectivenessfor programmes that are facility-based and use outreach to provide informa-tion and services to at-risk young people.
Conclusion There is growing evidence from developing countries of suc-cessful interventions that target groups most at risk from HIV, and theseprogrammes should be widely implemented provided that they are carefullyplanned and monitored and have a strong evaluation component. However,there is an urgent need to disaggregate data by age in order to determine howeffective these programmes are in reaching young people and to better un-derstand the specific needs of at-risk young people as opposed to older agegroups.
a Department of Epidemiology and Population Health, London School of Hygiene and TropicalMedicine, Keppel Street, London WC1E 7HT, England. Correspondence should be sent to DrHoffmann (email: [email protected]).
b Department of Child and Adolescent Health and Development, Family and Community Health,World Health Organization, Geneva, Switzerland.
287
92-4-120938-0_CH09_287

9.1 Introduction
Since the beginning of the AIDS pandemic it has been clear that not everyoneis equally at risk of becoming infected with HIV. This remains true in gen-eralized epidemics, concentrated epidemics and low-level epidemics. Pre-venting transmission of HIV to and from individuals and groups who are mostat risk will be crucial if governments are to contain the epidemic and achievethe Millennium Development Goal on AIDS. In low-level and concentratedepidemics, groups with an increased risk of becoming infected include in-jecting drug users, sex workers, men who have sex with men, and people whoare incarcerated or live in institutions. In addition, in generalized epidemics,young girls, men who have many sexual partners and the women who aremarried to them, mobile groups and groups living in relative poverty mayalso be particularly at risk.
With the exception of injecting drug use, the virus is transmitted the sameway among the groups most at risk and other groups in the population. Forthose most at risk, however, there are many factors that increase their chancesof becoming infected, and underlying these factors are structural determi-nants, such as inequity and discrimination, exploitation and abuse. Interven-tions that aim to change these determinants of vulnerability are outside thescope of this chapter.
Many young people are particularly at risk of becoming infected with HIVbecause of the situations in which they live, learn and earn and as a result ofbehaviours they adopt, or are forced to adopt, as a result of social, culturaland economic factors. The ultimate long-term challenge is to decrease thesecauses of vulnerability. In the short term, however, the groups most at risk ofHIV are particularly in need of the interventions outlined in the United Na-tions General Assembly Special Session on HIV/AIDS (UNGASS) goals andtargets for young people, notably the goals of providing them with access toinformation, skills and services. Achieving these goals will mitigate theirvulnerability and decrease their risk of HIV infection.
During the process of developing this series of papers that review the evidencefor policies and programmes to achieve the global goals on HIV and youngpeople, it was felt important to review the evidence for achieving these targetsamong young people aged 15–24 years who are most at risk of becominginfected. Many of these young people live on the fringes of society, and theyare unlikely to be reached by the majority of interventions outlined in thisseries, such as those implemented through schools, health services or themedia. To complicate matters, these groups frequently suffer from discrim-ination and marginalization, and their behaviours – such as drug use or sexwork – are often illegal, making it even harder for interventions deliveredthrough mainstream settings to reach them.
288
92-4-120938-0_CH09_288

What then do we know about the evidence for reaching the global goals onyoung people who are most at risk and most in need of the interventions thatgovernments endorsed during UNGASS? Clearly it is important to preventHIV infection in these groups, and national responses need to focus stronglyon these groups. They also need to receive explicit attention because it wouldbe possible for countries to achieve the UNGASS targets without ensuringcoverage of these groups, who are at the centre of the HIV epidemic.
This is not to imply that young injecting drug users necessarily require sep-arate or parallel services from those provided to adult drug users. And this isthe same for young sex workers, young men who have sex with men, youngprisoners or other groups of young people at high risk from HIV. It is likelyto be neither necessary nor practicable to provide separate services. However,it is clear that any assessment of interventions designed to achieve the globalgoals must not ignore these groups. It is important to review what we knowabout reaching these groups through the interventions outlined in the globalgoals. It is also important to clarify whether young people most at risk havespecific needs relative to older age groups and whether these needs requireexplicit attention from policies and programmes.
9.2 Methods
9.2.1 A focus for this paper
It was clearly not possible to include all groups of young people who mightbe at particular risk in all epidemic scenarios. It was therefore decided to focuson groups most at risk in areas of low-level and concentrated epidemics, sincemany of the groups of young people most at risk in generalized epidemicsare likely to have some access to information, skills and services throughexisting channels. Within low-level and concentrated epidemics it was de-cided to focus on young injecting drug users, young sex workers and youngmen who have sex with men, since data are more likely to be available forthese groups than other at-risk groups, such as mobile populations or prison-ers. However, it needs to be emphasized that there is significant overlapamong these groups. For example, young men who have sex with men maybe sex workers, and sex workers may be injecting drug users.
In addition to selecting specific groups for inclusion in this review, it wasalso necessary to have a process for assessing the evidence for the effective-ness of interventions. An initial search for studies focusing on at-risk youngpeople in developing countries indicated that there were relatively few data,either in the published literature or the grey literature. It was thereforedecided also to review studies of interventions directed at young people indeveloped countries as well as studies that had been undertaken within
289
92-4-120938-0_CH09_289

general populations of sex workers, injecting drug users and men who havesex with men in developing countries but that had not disaggregated their databy age.
This chapter therefore reviews studies and reports that:
1. quantify the number of young people most at risk of HIV and assesstheir specific needs compared with older age groups of at-risk populations;
2. focus on young people most at risk of HIV in developing countries;
3. focus on young people most at risk of HIV in developed countries;
4. focus on people most at risk of HIV in developing countries that do notdisaggregate data by age.
9.2.2 Inclusion and exclusion criteria
Inclusion and exclusion criteria are outlined in Table 9.1.
The main focus of this series is to review the evidence for policies and pro-grammes aiming to achieve the global goals and targets on HIV and youngpeople in developing countries. The inclusion and exclusion criteria for thisspecific component of the chapter have therefore been tighter and morealigned with other chapters in this series than the inclusion and exclusioncriteria for studies that have been included for the last two categories above(studies in developed countries and studies in developing countries that havenot disaggregated their data by age). These categories have been includedonly to provide a broader evidence context for assessing the effectiveness ofinterventions directed towards the groups who are the primary focus of theseries.
A systematic literature review was undertaken, including searches indatabases (PubMed, POPLINE, CAB Direct, Cochrane Library and Educa-tional Research Abstracts Online), recent issues of journals focusing onyoung people’s health and HIV prevention activities (AIDS, AIDS and Be-havior, AIDS Care, AIDS Education and Prevention, Archives of Pediatricsand Adolescent Medicine, Behavior Modification, Journal of AdolescentHealth, Journal of Adolescent Research, Journal of HIV/AIDS Preventionand Education for Adolescents and Children, Journal of Sex Education andTherapy), and finally on relevant web sites, such as WHO, UNAIDS,UNICEF, UNESCO, the United Kingdom Department for InternationalDevelopment (including the Safe Passages to Adulthood research pro-gramme), German Technical Cooperation (GTZ), Family Health Interna-tional (including YouthNet), Population Council, Pathfinder International,AIDS Education Global Information System (AEGiS), International Centre
290
92-4-120938-0_CH09_290

Table 9.1Inclusion and exclusion criteria used to identify studies for review. (Numbers inparentheses refer to categories listed in section 9.2.1)
Inclusion criteria Exclusion criteria
Interventions designed to mitigatevulnerability to HIV infection throughproviding increased access to information,skills and services (categories 1–4)
Interventions that aim to decreasevulnerability to HIV, such as structuralinterventions
Interventions implemented in developingcountries that aim to reduce the risk of HIVtransmission among injecting drug users,sex workers and men who have sex withmen by providing increased access toinformation, skills and services for HIVprevention (categories 1 and 4)Interventions in developing countries wereaimed at reducing the risk of HIVtransmission among young people aged 10–24 who are injecting drug users, sex workersor men who have sex with men by providingincreased access to information, skills andservices for HIV prevention (categories 1and 2)Interventions in developed countries thataimed to reduce the risk of HIV transmissionin young (10-24 years) injecting drug users,sex workers, and men who have sex withmen by providing increased access toinformation, skills and services for HIVprevention (category 3)Study provides a description of theintervention that enables a judgement to bemade about what was done (category 2)
Study provides inadequate descriptions ofthe content of the intervention, the design ofthe study or how data were collected andanalysed (category 2)
Study provides a description of theevaluation design and there were sufficientdata to make a judgement about the level ofevidence of effectiveness (category 2)Research and reports were publishedbetween 1990 and 2004
for Reproductive Health (ICRH), International Center for Research onWomen (ICRW), KIT (Royal Tropical Institute of the Netherlands) librarycatalogue, International Council on Management of Population Programmes(ICOMP), Johns Hopkins Bloomberg School of Public Health Center for
291
92-4-120938-0_CH09_291

Communication Programs, CAPS – the Center for AIDS Prevention Studies,Streetkids–SRH.org, and the Network of Sex Work Projects.
A number of review articles on HIV prevention interventions that focused onyoung people (1–6) and developing countries (7) were scanned for relevantstudies. All reference sections of peer-reviewed papers identified during thisliterature search were checked for additional articles of interest. Finally, 12experts working in the field were contacted to identify unpublished research.
A less extensive search was made for studies assessing the effectiveness ofinterventions in developing countries directed towards injecting drug users,sex workers and men who have sex with men but that did not disaggregatethe data by age and for studies of interventions targeted at young people mostat risk of HIV in developed countries, predominantly the United States.
No systematic search for studies reported in languages other than English wasundertaken.
9.2.3 Developing a typology
From the initial review of the literature it was clear that interventions aimedat groups considered to be most at risk included some mix of facility-basedinterventions with or without outreach and the provision of information withor without additional services. The typology that was developed was basedon these programme elements, and the interventions were categorized intothe following types.
Type 1: these interventions only provided information through an outreachprogramme.
Type 2: these interventions provided information and services through anoutreach programme.
Type 3: these interventions provided information and services through afacility-based programme.
Type 4: these interventions provided information and services through afacility-based programme that also included an outreach component.
Apart from distinguishing the place where the intervention was based, thistypology also differentiates between those programmes that only provide in-formation and those that also include services. A range of services wereprovided in the studies reviewed, including treatment for sexually transmittedinfections (STIs), strategies to reduce harm by providing needle exchange orsubstitution therapy, or both, as well as condoms, counselling and support.
292
92-4-120938-0_CH09_292

9.2.4 Threshold of evidence required to recommend widespreadimplementation
As with the other papers in this series, once the typology had been defined itwas necessary to determine the threshold of evidence that would be requiredto recommend widespread implementation of different types of interventions –that is, to allocate them to the “Steady”, “Ready”, “Go” and “Do not go”categories. Table 9.2 provides an overview of the threshold of evidence re-quired to recommend the four types of interventions. As the complexity ofthe interventions increases – for example, offering information plus services,or outreach plus facilities – the levels of evidence required become highersince the interventions become increasingly difficult to develop and sustain,even though they are likely to have a greater impact.
9.3 Findings
9.3.1 Studies quantifying the number of at-risk young people and assessingtheir needs
The literature indicates that people who are younger than 25 years representa significant proportion of the groups most at risk of HIV (see chapter 2). Inseveral south-east Asian countries, for example, the proportion of womenyounger than 25 who are working in high-risk environments, such as brothels,has been estimated to vary between 41% in Indonesia (8) and 76% in the LaoPeople’s Democratic Republic (9).
In Africa, a large proportion of female sex workers are young. For example,37% of 622 female sex workers in a study from Zambia were younger than20 (10), and in one region in the United Republic of Tanzania, womenyounger than 20 accounted for 23% of 983 women working in bars and similarestablishments (11).
Two longitudinal studies from west Africa indicate possible trends towardsyounger people becoming involved in sex work. In Benin, the number offemale sex workers younger than 25 rose from 17% in 1993 to 34% in 1998–1999, despite an ongoing HIV intervention directed towards female sexworkers (12). In Côte d’Ivoire, the median age of female sex workers attend-ing an STI clinic declined from 30 years in 1992 to 23 years in 1998 (13).
In Central Asia and eastern Europe, areas that are experiencing some of thefastest growing HIV epidemics in the world, the impact of economic andsocial transition has led to unparalleled proportions of young people injectingdrugs, which is the main mode of HIV transmission in those regions (14). Itis estimated that the average age of young people using injected drugs for thefirst time is between 16 years and 19 years (15), and 70% of all people in-jecting drugs are younger than 25 (14). A study in Irkutsk, Russia, showed
293
92-4-120938-0_CH09_293

Tab
le 9
.2T
hre
sho
ld o
f ev
iden
ce n
eed
ed t
o r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n o
f ea
ch t
ype
of
inte
rven
tio
na
Inte
rven
tio
nty
pe
Fea
sib
ility
Lac
k o
fp
ote
nti
alfo
rad
vers
eo
utc
om
es
Acc
epta
bili
tyfo
r ta
rget
gro
up
Acc
epta
bili
tyfo
rco
mm
un
ity
and
po
licy-
mak
ers
Po
ten
tial
size
of
effe
ct
Oth
erh
ealt
h o
rso
cial
ben
efit
s
Ove
rall
thre
sho
ldC
om
men
tsb
1. In
form
atio
non
ly p
rovi
ded
thro
ugh
outr
each
++
++
++
++
++
++
Low
Rel
ativ
ely
easy
to o
rgan
ize
and
impl
emen
t but
leas
t lik
ely
to h
ave
any
long
-last
ing
posi
tive
effe
cton
the
targ
et g
roup
2. In
form
atio
nan
d se
rvic
espr
ovid
edth
roug
hou
trea
ch
++
++
++
++
++
Mod
erat
eS
ervi
ces
are
mor
e lik
ely
toha
ve a
n ef
fect
than
info
rmat
ion
alon
e bu
t thi
s ty
pe m
ay b
edi
fficu
lt to
org
aniz
e, e
spec
ially
the
outr
each
com
pone
nt3.
Fac
ility
-ba
sed
info
rmat
ion
and
serv
ices
++
++
++
++
++
++
++
Low
Like
ly to
be
effe
ctiv
e on
ly if
the
targ
et g
roup
vis
its th
e fa
cilit
y bu
tot
herw
ise
easi
er to
org
aniz
eth
an o
utre
ach
4. O
utre
ach
and
faci
lity-
base
din
form
atio
nan
d se
rvic
es
++
++
++
++
++
++
Mod
erat
eM
ost d
iffic
ult t
o es
tabl
ish
and
sust
ain
but a
lso
mos
t lik
ely
to b
eef
fect
ive,
esp
ecia
lly if
out
reac
hen
cour
ages
the
targ
et g
roup
tom
ake
use
of th
e fa
cilit
ies
a D
egre
e of
des
irabi
lity
is in
dica
ted
with
a m
axim
um o
f 3 “
+”
sign
s. D
egre
e of
und
esira
bilit
y is
indi
cate
d w
ith a
max
imum
of 3
“-”
sig
ns.
b A
ll in
terv
entio
ns n
eed
to o
verc
ome
stig
mat
izat
ion
of th
e ta
rget
gro
up a
nd th
e ill
egal
ity o
f the
beh
avio
urs
in o
rder
to b
e su
cces
sful
294
92-4-120938-0_CH09_294

that 90% of injecting drug users were younger than 20 years, and 65% ofyoung people living on the street who were also injecting drugs were HIVpositive (16).
Not only do young people make up a significant proportion of injecting drugusers, but as this study from Irkutsk indicates they may also be particularlyvulnerable. In Bangladesh, sex workers who are younger than 25 were almosttwice as likely to report having been beaten or raped when compared withtheir older peers (17); in Myanmar national surveillance reports show thatsex workers and injecting drug users who are younger than 25 have a higherprevalence of infection with HIV than other age groups (18). A cross-sectional study from India found a significantly higher prevalence of HIVinfection among female sex workers who were younger than 20 comparedwith the prevalence among older age groups (P = 0.002, odds ratio [OR] =2.4, 95% confidence interval [CI] = 1.3–4.4) (19). A high prevalence of HIVamong young women was also reported from a cohort of female sex workersin the United Republic of Tanzania that reviewed HIV prevalence amongwomen aged 16–39 years: 46% of those who were younger than 20 were HIVpositive; 72% of women aged 20–24 were HIV positive; and 68% of thoseaged 25 years or older were HIV positive (20).
Not only do the data indicate that young people represent a significant pro-portion of the population most at risk of becoming infected, and that they maybe particularly vulnerable, but there is also some evidence that their needsdiffer from older people in at-risk groups.
For example, Tawil (21) cited a Moroccan programme targeting men whohave sex with men. This programme’s baseline survey found that only 28%of males aged 15–24 years reported using condoms regularly, while 57%of those aged 25 years or older reported using condoms regularly. Similarly,a Bolivian study conducted among female sex workers reported an increasedrisk of gonorrhoea, trichomoniasis and genital ulcer among those aged24 years or younger, without indicating behavioural reasons for this disparity(22). A study that compared drug users who were younger than 26 with olderdrug users found significant differences in risk-taking behaviours betweenthe two groups (23). Although younger drug users were less likely to injecttheir drugs compared with older drug users, the age at which users startedtaking drugs had dropped significantly among the younger drug users(16.2 years for younger users versus 17.9 years for older users, P < 0.001),and younger users were also less likely to be aware of their HIV status (41.8%for younger users versus 64.9% for older users, P < 0.001).
295
92-4-120938-0_CH09_295

9.3.2 Studies focusing on young people most at risk in developing countries
While there is a wealth of information from cross-sectional studies conductedamong at-risk young people, there are few published evaluations of inter-ventions targeting these groups in developing countries. No studies werefound in peer-reviewed journals, and the 11 studies that were identified wereall in programme reports or other grey literature. Three of these were fromAfrica, two from Asia and six were from Latin America. Target groups in-cluded sex workers (5 studies), men who have sex with men (1 study),injecting drug users (3 studies) and youths living on the street (2 studies).Unfortunately, only four of these studies met the inclusion criteria (Table 9.1).The studies that met the inclusion criteria came from Africa (1 study) andfrom Latin America (3 studies). One of the Latin American studies examinedinterventions directed to sex workers; one examined interventions targeted atmen who have sex with men; and two examined interventions targeted atstreet youths.
9.3.2.1 Sex workers
Interventions targeting young sex workers were identified in Brazil, Ethiopiaand Nicaragua (24). The Ethiopian programme, run by the Organisation forSocial Services for AIDS, and the Brazilian “Sidewalk Girls” programmeboth used older peer educators who met with younger sex workers in an at-tempt to teach them how to reduce their risk of becoming infected. Unfortu-nately, no evaluations of these interventions were found. A secondintervention by the Instituto Centroamericano de la Salud in Nicaragua pro-vided all sex workers in Managua with vouchers that entitled them to receivea standardized package of free sexual and reproductive health treatment(study D) (24, 25). The project started in 1996 and for eight years afterwardsdistributed more than 30 000 vouchers and provided more than 12 000 con-sultations, during which a large number of STIs were treated among femalesex workers (25). A substudy among 114 sex workers who also sniffed glueshowed decreases in the prevalence of gonorrhoea (13.7% to 8.6%, not sig-nificant), syphilis (15.6% to 8.0%, not significant) and trichomoniasis (22.1%to 12.4%, P < 0.01) (24).
9.3.2.2 Injecting drug users
Interventions for young injecting drug users were identified in Argentina,India and Kenya (24). The Kenyan centre trained 54 volunteers in counsellingand HIV prevention, and it provided counselling and detoxification servicesfor 20 young injecting drug users. In Argentina, HIV testing, safer sex work-shops and a drug users’ network were provided; in India a drop-in centreprovided counselling and HIV testing as well as support groups for more than
296
92-4-120938-0_CH09_296

4 000 drug users. Unfortunately, none of these interventions provided eval-uation data.
9.3.2.3 Men who have sex with men
Only one project was identified that specifically targeted men who have sexwith men who were also sex workers. “El Salon” in Costa Rica provided asafe place in the form of a home at which young male sex workers couldaccess counselling, education and support (study B) (24). The evaluation ofthe intervention showed an increased use of condoms and the formation ofsupport groups among the target group (24).
9.3.2.4 Street youths
Evaluations of interventions targeting youths living on the street were alsoincluded because this group frequently becomes involved in sex work anddrug use. Studies of interventions were identified in Brazil and Uganda (26,27). In Uganda, services provided information and counselling and increasedaccess to condoms (147 000 condoms distributed) and STI treatment (29 000adolescents treated for STIs from April 2002 to March 2004). Unfortunatelyno denominators were available (study C) (26). In Brazil, the interventionaimed to increase knowledge about HIV prevention through the use of videos,comic books and drama groups (study A) (27). Cross-sectional surveysamong 400 young people carried out before and after the interventionsdemonstrated significant changes, with the interventions resulting in in-creased levels of knowledge about HIV transmission and decreased levels ofmisconceptions about HIV/AIDS.
Table 9.3 summarizes the studies that met the inclusion criteria according totypology (whether the interventions were outreach-based and/or clinic-basedand whether they included information and/or services). Only one project thatmet the inclusion criteria was identified as a type 1 intervention (providingonly information through an outreach programme). No studies of type 2 in-terventions (information and services provided through an outreach pro-gramme) had sufficient details on either the content or the evaluation. Forinterventions based only in facilities, (type 3 interventions), one programmefor male sex workers was identified. Two studies of type 4 interventions wereidentified; these provided facility-based services as well as outreach activi-ties. One worked with street children and sex workers and the other workedonly with sex workers.
Table 9.3, Table 9.4 and Table 9.5 include studies focusing on the main targetgroup of this review, namely young people in developing countries who aremost at risk of becoming infected with HIV. Table 9.4 describes the evalua-tion designs for each of the studies, and Table 9.5 summarizes the studiesaccording to the level of evidence of effectiveness that could be derived fromthe studies.
297
92-4-120938-0_CH09_297

Tab
le 9
.3D
escr
ipti
on
of
the
inte
rven
tio
ns
by
stu
dy
Stu
dy
and
loca
tio
nT
arg
et p
op
ula
tio
n a
nd
pri
mar
y o
bje
ctiv
esD
escr
ipti
on
Inte
rven
tio
n t
ype
1 (i
nfo
rmat
ion
on
ly p
rovi
ded
th
rou
gh
ou
trea
ch p
rog
ram
me)
A –
Bra
zil (
27)
• P
rimar
y ob
ject
ives
: to
prev
ent H
IV/A
IDS
tran
smis
sion
in th
e ta
rget
gro
up•
Tar
get g
roup
s: Y
oung
wom
en v
ulne
rabl
e to
sexu
al v
iole
nce,
you
ths
livin
g on
the
stre
et
• M
ultic
ompo
nent
pro
gram
me
cons
istin
g of
edu
catio
n ab
out
sexu
ality
and
HIV
/AID
S; t
rain
ing
in H
IV/A
IDS
pre
vent
ion
skill
s;se
nsiti
zatio
n of
edu
cato
rs a
nd in
stitu
tiona
l dire
ctor
s to
the
need
tosu
ppor
t vul
nera
ble
yout
hs• A
fter f
orm
ativ
e re
sear
ch, e
duca
tors
wer
e tr
aine
d w
ith a
man
ual a
ndth
roug
h m
eetin
gs. T
he in
terv
entio
n pr
oduc
ed a
vid
eo a
nd a
com
icbo
ok th
at w
ere
dist
ribut
ed a
mon
g th
e ta
rget
gro
up a
nd s
tage
dgr
oup
disc
ussi
ons,
role
-pla
ys a
nd th
eatr
e ac
tiviti
es. S
essi
ons
wer
eco
nduc
ted
in 1
0 in
stitu
tiona
l set
tings
and
125
out
reac
h ac
tiviti
esw
ere
impl
emen
ted
• S
cale
of p
roje
ct: i
nfor
mat
ion
not a
vaila
ble
Inte
rven
tio
n t
ype
2 (i
nfo
rmat
ion
an
d s
ervi
ces
pro
vid
ed t
hro
ug
h a
n o
utr
each
pro
gra
mm
e)N
o st
udy
met
the
incl
usio
n cr
iteria
Inte
rven
tio
n t
ype
3 (f
acili
ty-b
ased
info
rmat
ion
an
d s
ervi
ces)
B –
Cos
ta R
ica
(24)
• P
rimar
y ob
ject
ive:
not
sta
ted
• T
arge
t gro
ups:
you
ng p
eopl
e in
volv
ed in
sex
wor
k, in
ject
ing
drug
use
and
/or
youn
g m
ale
sex
wor
kers
livi
ng o
n th
e st
reet
• M
ultic
ompo
nent
pro
gram
me
cons
istin
g of
a s
afe
plac
e to
spe
ndtim
e of
f the
str
eets
in p
roje
ct h
ouse
and
edu
catio
n ab
out H
IV/A
IDS
prev
entio
n•
Cou
nsel
ling
and
supp
ort p
rovi
ded
for
alco
hol-r
elat
ed a
nd d
rug-
rela
ted
prob
lem
s•
Thi
s in
terv
entio
n st
arte
d w
ith a
thor
ough
situ
atio
n an
alys
is•
Em
phas
is p
lace
d on
cre
atin
g a
safe
spa
ce fo
r vu
lner
able
you
ths
298
92-4-120938-0_CH09_298
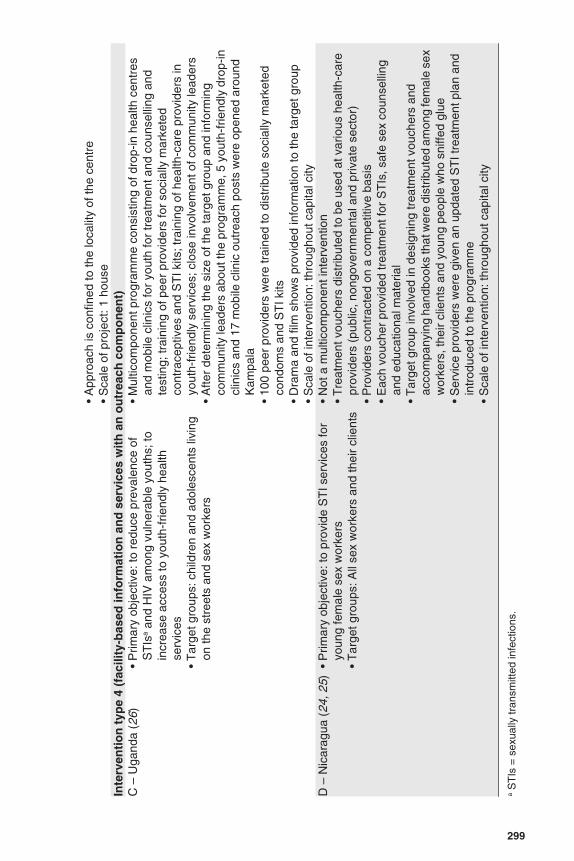
• A
ppro
ach
is c
onfin
ed to
the
loca
lity
of th
e ce
ntre
• S
cale
of p
roje
ct: 1
hou
seIn
terv
enti
on
typ
e 4
(fac
ility
-bas
ed in
form
atio
n a
nd
ser
vice
s w
ith
an
ou
trea
ch c
om
po
nen
t)C
– U
gand
a (2
6)•
Prim
ary
obje
ctiv
e: to
red
uce
prev
alen
ce o
fS
TIs
a an
d H
IV a
mon
g vu
lner
able
you
ths;
toin
crea
se a
cces
s to
you
th-f
riend
ly h
ealth
serv
ices
• T
arge
t gro
ups:
chi
ldre
n an
d ad
oles
cent
s liv
ing
on th
e st
reet
s an
d se
x w
orke
rs
• M
ultic
ompo
nent
pro
gram
me
cons
istin
g of
dro
p-in
hea
lth c
entr
esan
d m
obile
clin
ics
for
yout
h fo
r tr
eatm
ent a
nd c
ouns
ellin
g an
dte
stin
g; tr
aini
ng o
f pee
r pr
ovid
ers
for
soci
ally
mar
kete
dco
ntra
cept
ives
and
ST
I kits
; tra
inin
g of
hea
lth-c
are
prov
ider
s in
yout
h-fr
iend
ly s
ervi
ces;
clo
se in
volv
emen
t of c
omm
unity
lead
ers
• A
fter
dete
rmin
ing
the
size
of t
he ta
rget
gro
up a
nd in
form
ing
com
mun
ity le
ader
s ab
out t
he p
rogr
amm
e, 5
you
th-f
riend
ly d
rop-
incl
inic
s an
d 17
mob
ile c
linic
out
reac
h po
sts
wer
e op
ened
aro
und
Kam
pala
• 10
0 pe
er p
rovi
ders
wer
e tr
aine
d to
dis
trib
ute
soci
ally
mar
kete
dco
ndom
s an
d S
TI k
its•
Dra
ma
and
film
sho
ws
prov
ided
info
rmat
ion
to th
e ta
rget
gro
up•
Sca
le o
f int
erve
ntio
n: th
roug
hout
cap
ital c
ityD
– N
icar
agua
(24
, 25)
• P
rimar
y ob
ject
ive:
to p
rovi
de S
TI s
ervi
ces
for
youn
g fe
mal
e se
x w
orke
rs•
Tar
get g
roup
s: A
ll se
x w
orke
rs a
nd th
eir
clie
nts
• N
ot a
mul
ticom
pone
nt in
terv
entio
n•
Tre
atm
ent v
ouch
ers
dist
ribut
ed to
be
used
at v
ario
us h
ealth
-car
epr
ovid
ers
(pub
lic, n
ongo
vern
men
tal a
nd p
rivat
e se
ctor
)•
Pro
vide
rs c
ontr
acte
d on
a c
ompe
titiv
e ba
sis
• E
ach
vouc
her
prov
ided
trea
tmen
t for
ST
Is, s
afe
sex
coun
selli
ngan
d ed
ucat
iona
l mat
eria
l•
Tar
get g
roup
invo
lved
in d
esig
ning
trea
tmen
t vou
cher
s an
dac
com
pany
ing
hand
book
s th
at w
ere
dist
ribut
ed a
mon
g fe
mal
e se
xw
orke
rs, t
heir
clie
nts
and
youn
g pe
ople
who
sni
ffed
glue
• S
ervi
ce p
rovi
ders
wer
e gi
ven
an u
pdat
ed S
TI t
reat
men
t pla
n an
din
trod
uced
to th
e pr
ogra
mm
e•
Sca
le o
f int
erve
ntio
n: th
roug
hout
cap
ital c
ity
a S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
299
92-4-120938-0_CH09_299

Tab
le 9
.4D
escr
ipti
on
of
ou
tco
me
eval
uat
ion
s b
y st
ud
y
Stu
dy
Des
ign
an
d s
amp
le s
ize
Eva
luat
ion
res
ult
sS
tren
gth
of
evid
ence
fo
r ef
fect
Inte
rven
tio
n t
ype
1 (i
nfo
rmat
ion
pro
vid
ed o
nly
th
rou
gh
ou
trea
ch p
rog
ram
me)
A (
27)
Des
ign:
pre
-tes
t and
pos
t-te
stev
alua
tion;
no
com
paris
on g
roup
Sam
ple
size
: ran
dom
sam
ple
of 4
00 y
outh
sin
terv
iew
ed 1
0 m
onth
s ap
art
“Sig
nific
ant”
cha
nges
bot
h in
incr
ease
d le
vels
of
know
ledg
e ab
out H
IV tr
ansm
issi
on a
s w
ell a
s in
decr
ease
d le
vels
of m
isco
ncep
tions
Wea
kLi
mita
tions
: tes
ts fo
r st
atis
tical
sign
ifica
nce
not a
vaila
ble
Inte
rven
tio
n t
ype
2 (i
nfo
rmat
ion
an
d s
ervi
ces
pro
vid
ed t
hro
ug
h a
n o
utr
each
pro
gra
mm
e)N
o st
udy
met
the
incl
usio
n cr
iteria
Non
eIn
terv
enti
on
typ
e 3
(fac
ility
-bas
ed in
form
atio
n a
nd
ser
vice
s)B
(24
)D
esig
n: p
re-in
terv
entio
n an
d po
st-
inte
rven
tion
eval
uatio
n•
Incr
ease
in r
epor
ted
use
of c
ondo
ms
amon
gm
ale
sex
wor
kers
• In
crea
se in
num
ber
of s
uppo
rt g
roup
s
Wea
kLi
mita
tions
: no
com
paris
on g
roup
; no
deno
min
ator
Inte
rven
tio
n t
ype
4 (f
acili
ty-b
ased
info
rmat
ion
an
d s
ervi
ces
wit
h a
n o
utr
each
co
mp
on
ent)
C (
26)
Des
ign:
ser
vice
util
izat
ion
stat
istic
s•
29 5
64 tr
eatm
ents
pro
vide
d in
1½
yea
rs a
t6
369
drop
-in c
entr
es a
nd 2
3 19
5 ou
trea
ch s
ites
• 1
291
refe
rral
s (m
ainl
y fo
r bl
ood
test
s fo
rse
xual
ly tr
ansm
itted
infe
ctio
ns)
• 21
5 co
unse
lling
ses
sion
s pl
us te
stin
g pr
ovid
ed•
21 6
64 y
oung
peo
ple
rece
ived
con
dom
s(1
0 07
9 fe
mal
es a
nd 1
1 58
5 m
ales
)
Wea
kLi
mita
tions
: no
deno
min
ator
s pr
ovid
ed
D (
24, 2
5)D
esig
n: p
re-t
est a
nd p
ost-
test
eva
luat
ion
ina
subs
ampl
e of
targ
et p
opul
atio
n (f
emal
esw
ho s
niff
glue
)
• 15
000
vou
cher
s di
strib
uted
in 8
yea
rs, 4
0%le
adin
g to
med
ical
con
sulta
tions
• Gon
orrh
oea
prev
alen
ce re
duce
d fr
om 1
3.7%
to8.
6%•
Syp
hilis
pre
vale
nce
redu
ced
from
15.
6% to
8.0%
• T
richo
mon
iasi
s pr
eval
ence
red
uced
from
22.1
% to
12%
Wea
kLi
mita
tions
: no
com
paris
on g
roup
300
92-4-120938-0_CH09_300

Tab
le 9
.5S
tren
gth
of
evid
ence
of
effe
ctiv
enes
s fo
r ea
ch in
terv
enti
on
typ
e
Inte
rven
tio
n t
ype
and
stu
dy
des
ign
Po
siti
ve e
ffec
tN
osi
gn
ific
ant
effe
ct
Neg
ativ
e ef
fect
Evi
den
ce
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Sta
tist
ical
lysi
gn
ific
ant
Sta
tist
ical
sig
nif
ican
cen
ot
kno
wn
Typ
e 1
(in
form
atio
n o
nly
pro
vid
ed t
hro
ug
h o
utr
each
)(1
eva
luat
ion)
Wea
k
Bef
ore–
afte
r (n
o co
mpa
rison
gro
up)
AT
ype
2 (i
nfo
rmat
ion
an
d s
ervi
ces
pro
vid
ed t
hro
ug
ho
utr
each
) (0
eva
luat
ions
)N
one
Typ
e 3
(fac
ility
bas
ed in
form
atio
n a
nd
ser
vice
s)(1
eva
luat
ion)
Wea
k
Bef
ore–
afte
r (n
o co
mpa
rison
gro
up)
BT
ype
4 (o
utr
each
an
d f
acili
ty-b
ased
info
rmat
ion
an
dse
rvic
es)
(2 e
valu
atio
ns)
Wea
k
Des
crip
tive
(ser
vice
sta
tistic
s)C
Bef
ore–
afte
r (n
o co
mpa
rison
gro
up)
D
301
92-4-120938-0_CH09_301

9.3.3 Studies focusing on at-risk young people in developed countries
Four evaluation studies from developed countries were reviewed to determinewhether they corroborated the findings from studies in developing countries.Two of these studies focused on interventions directed towards young menwho have sex with men (28, 29), and two focused on young injecting drugusers (30, 31). No studies of interventions directed towards young sex work-ers were identified.
Studies in Bulgaria and the Russian Federation targeted the leaders of previ-ously identified social networks of men who have sex with men and trainedthem as peer educators (28, 29). Risk surveys were administered to membersof their network and to members of a control network. Among members ofthe network in the intervention group, the frequency of unprotected inter-course dropped significantly as did the proportion of men engaging inunprotected intercourse with multiple partners (29).
A study in San Francisco (31) evaluated a needle and syringe exchange pro-gramme that targeted 15–25-year-old injecting drug users. The programmewas run by peers and targeted homeless injecting drug users, providing sterileinjecting equipment and educational materials. There was a significant re-duction in reported sharing and reusing of syringes among young peopleparticipating in the programme when compared with those in a control group.
9.3.4 Studies of interventions for at-risk populations in developing countriesthat did not disaggregate data by age
Thirty studies were identified that examined interventions directed towardsgeneral populations most at risk of becoming infected with HIV, of which 21were interventions directed towards sex workers, 5 towards injecting drugusers and 4 towards men who have sex with men. There were 16 studies fromAsia, 8 from Africa, and 6 from Latin America.
9.3.4.1 Sex workers
Studies of interventions with sex workers included several peer-reviewedarticles with data measured both pre-intervention and post-intervention, withor without control groups. Studies from the Asia–Pacific region included in-terventions in China (32), India (33–35), Indonesia (36–38), Papua NewGuinea (39) and Thailand (40–42). In Africa, studies from Benin (12), Côted’Ivoire (43), Ghana (44), Kenya (45, 46), Sierra Leone (47) and the Demo-cratic Republic of the Congo (48) were identified. In Latin America, threestudies were identified, one each from Bolivia, Honduras and Peru (22, 49,50). In addition, projects in Bangladesh, India and Papua New Guinea were
302
92-4-120938-0_CH09_302

documented in the UNAIDS case study Female sex worker HIV preventionprojects (51).
All of the interventions had information and education components, and mostoffered services either by providing free condoms (12 studies) or free STItreatment (6 studies). The majority of programmes were type 4 interventions.They operated in specially designed facilities (either STI clinics or commu-nity centres) where the education sessions or STI treatment took place, andthey engaged in outreach activities to attract clients to their facilities. A fewof the interventions had only outreach activities, although these sometimesincluded training peer educators at their workplaces.
The best documented intervention to reduce HIV transmission among sexworkers is the Thai government’s “100% condom” programme (40). Afterproving successful in Thailand, a similar approach was adopted by severalother Asian countries. Additional strategies have been tested in different lo-cations, mainly in Asia , including peer education, outreach education, groupeducation and the involvement of employers. Other measures tested widelyincluded distributing condoms and providing HIV counselling and testingand STI treatment. All programmes used more than one method to reduceHIV incidence, and therefore it was not possible to tease out the impact ofspecific interventions.
Other evaluation studies of interventions targeting sex workers in Asiancountries that showed positive changes in behaviour and knowledge included:peer education (increased AIDS and STI knowledge and decreased preva-lence of gonorrhoea, P = 0.05) (37) and combined educational activities andSTI treatment (increased knowledge about AIDS and STIs, P < 0.001;increased condom use, P = 0.01; and decreased prevalence of trichomoniasis,P < 0.001) (38).
In Côte d’Ivoire a randomized controlled trial among female sex workers wasconducted with 542 women who were given either a basic or intensive inter-vention (more frequent visits) consisting of information and education, freecondoms and STI treatment (type 4 interventions). Outcomes were measuredfor 225 women (42%) through self-reported behaviour and testing for STIs.When baseline data were compared with post-intervention data, the inter-vention was found to be significantly associated with increases in condomuse (from 40% to 82%) and decreases in the prevalence of gonorrhoea (from14% to 5%) and trichomoniasis (from 24% to 11%). In terms of HIV inci-dence, rates were lower among those who participated in the intensiveprogramme than among those in the basic programme, although these dif-ferences were not statistically significant (43).
303
92-4-120938-0_CH09_303

A longitudinal study of an intervention in the United Republic of Tanzaniainvolving 600 women at increased risk of becoming infected provided infor-mation sessions every 3 months on HIV and STIs and reproductive health,voluntary HIV counselling and testing, and clinical health check-ups includ-ing syndromic management of STIs. This intervention reduced HIV incidencefrom 13.9/100 person–years to 5.0/100 person–years over three consecutive9-month periods; the reduction was attributed to the combination of infor-mation and services, which describe a type 4 intervention (52).
Although the study in the United Republic of Tanzania demonstrated thatinterventions aimed at improving STI treatment can be successful in reducingHIV incidence among sex workers, monthly oral administration of 1g ofazithromycin among Kenyan sex workers in a randomized placebo-controlledtrial did not have this effect (46). Two studies – in Benin and Bolivia – triedto assess the impact of interventions through serial cross-sectional surveys(12, 22). Although both studies reported significant reductions in STI preva-lence that were achieved through treatment and educational activities, theresearch design is severely limited because it does not provide informationon any of the outcome measures for consecutive visits made by the sameperson, only for the group of sex workers as a whole. It also failed to documentthe level of participation in the programmes. The findings can at most, there-fore, show time trends for STI prevalence among a group of sex workers.
9.3.4.2 Injecting drug users
The vast majority of interventions for injecting drug users concentrate onmaking drug injecting safer (that is, they use a harm reduction approach). Akey component of this approach is needle and syringe exchange programmes,in which sterile injecting equipment is provided or exchanged for used equip-ment. Two evaluations of type 4 intervention exchange programmes werefound in Asia. An evaluation in Nepal interviewed 586 clients of a programmeduring a 4-year period and found that the median number of times participantsshared needles decreased from 14 to 2, and the median number of people theyshared injecting equipment with was reduced from 2 to 1 (53). An evaluationof an exchange intervention in Thailand reported significant reductions inrisk-taking behaviours, despite difficulties encountered by young injectingdrug users in accessing the programme (54).
Two type 2 outreach education interventions for adult injecting drug userswere also identified. The first was based in Chennai, India, and targeted menaged 18 years and older. An outreach team recruited injecting drug users andprovided various interventions at street level, including the distribution ofbleach. These combined interventions brought about safer injecting be-haviours (P = 0.01) without affecting sexual risk behaviour (55). The second
304
92-4-120938-0_CH09_304

intervention took place in Puerto Rico where outreach workers provided in-formation on HIV prevention to indigenous adults who were injecting drugusers. This intervention was associated with significant improvements inknowledge of HIV and a reduction in risky injecting behaviours (56).
A WHO multisite study that looked at injecting drug users and took place intwo cities in Brazil and one city in Thailand as well as nine cities in developedcountries (57), showed that the behavioural changes that occurred were sim-ilar in Bangkok and the cities in developed countries but different from thosein the Brazilian cities. The frequency of consistent condom use with casualpartners was lowest in Rio de Janeiro, whereas in Bangkok it was reported tobe higher than in most of the cities in developed countries. This highlightsthe challenge of comparing results from studies conducted in different de-veloping countries and between developed and developing countries.
In addition to the data from developing countries, evidence of successful HIVinterventions aimed at injecting drug users is available from a number ofliterature reviews (58). Consecutive HIV prevalence data from injecting drugusers in cities in the United States with and without needle-exchange pro-grammes were reviewed (59); there was significant evidence of a 5.8%decrease in seroprevalence among injecting drug users in the 29 cities thathad needle-exchange programmes compared with a 5.9% increase amongdrug users in the 52 cities without such programmes (P = 0.004) (59). ACochrane systematic review assessed the effect of oral substitution treatmentfor opioid-dependent injecting drug users on rates of HIV infection and high-risk behaviours and found significant associations between treatment andreductions in illicit opioid use, injecting use and the sharing of injectingequipment. Reductions in risk behaviours related to drug use also translatedinto reductions in the prevalence of HIV infection (60). In general, these weretype 4 interventions.
9.3.4.3 Men who have sex with men
Four interventions targeting men who have sex with men were identified fromBrazil (61), India and Morocco (both mentioned in Tawil) (21) and PuertoRico (62). The intervention in Morocco included 600 men and the interven-tion in India included 3 000 men reached through peer outreach programmesfocusing on safer sex messages, condom distribution and providing STI careat a drop-in centre (a type 4 intervention). Increased safer sex practices werereported in post-intervention analyses at both sites, with these effects beingstatistically significant in India but not in Morocco. The two interventions inLatin America identified participants though peer referral and focused on peereducation. The study in Brazil had a pre-intervention versus post-interventiondesign and included 227 men who have sex with men, who had a mean age
305
92-4-120938-0_CH09_305

of 29 years; in this study men were assigned either to an intensive series ofsafer sex workshops or a series of health education lectures. There were nosignificant differences in health outcomes between the two interventions, al-though comparisons between baseline and post-intervention surveys showedstatistically significant increases in knowledge and awareness and decreasesin self-reported risk behaviours. These differences were found to have beensustained at a 6-month follow-up survey.
In addition to these studies from developing countries, a meta-analysis of HIVbehavioural interventions aimed at reducing sexual risk behaviour among thisgroup of men included 33 studies from different parts of the world (63). Itdescribed significant decreases in the prevalence of unprotected anal inter-course (OR = 0.8, 95% CI = 0.7–0.9) and number of sexual partners (OR =0.85, 95% CI = 0.6–0.9) as well as a significant increase in condom use duringanal intercourse (OR = 1.6, 95% CI = 1.2–2.2). In this meta-analysis, suc-cessful programmes were those that were based on a theoretical model,included training in interpersonal skills, incorporated several delivery meth-ods and were delivered over multiple sessions spanning a minimum of 3weeks (63), thus providing evidence for the effectiveness of type 4interventions.
9.4 Discussion
The authors of the original papers that were commissioned for the meetingin Talloires in March 2004 that initiated the “Steady, Ready, Go!” processwere asked to give special consideration to young people who are most at riskof becoming infected with HIV. When the papers were reviewed during themeeting, participants recommended that a specific chapter be written focus-ing on these groups of young people. This is important for two reasons. First,interventions for young sex workers, men who have sex with men, and in-jecting drug users are likely to be key to decreasing the transmission of HIVin low-level and concentrated epidemics. Second, having the evidence of ef-fectiveness for these interventions is important because they are usuallysurrounded by controversy, the behaviours that this group participates in areoften illegal, and the groups themselves are marginalized and exposed todiscrimination.
However, there was uncertainty about whether enough data would be avail-able to allow the interventions to be analysed in the same manner used forother chapters in this series. There was also concern that the evidence foreffectiveness would be weak since programmes for groups most at risk oftenfocus more on taking action than finding out whether an action works. Thisproblem has already been described by Myers and colleagues (64) whosuggested that part of the reason for the difficulty in finding evaluations of
306
92-4-120938-0_CH09_306

interventions targeting these three groups is the fact that much of the literaturehas been produced by practitioners rather than researchers. While some ofthe reservations about writing this chapter were clearly justified, our reviewhas nonetheless enabled us to draw some conclusions and allowed us to iden-tify some important issues that require further attention.
This review set out to assess the level of evidence of effectiveness needed torecommend implementation of interventions targeting at-risk young peoplein developing countries, in order to achieve the global goals on preventingthe spread of HIV. Prior to reviewing the evidence, it was necessary to es-tablish whether young people were actually an important proportion of thegroup most at risk of becoming infected. Our findings support the conclusionsof Monasch and Mahy in chapter 2 that young people make up a significantproportion of the population most at risk from HIV. In addition, data indicatethat younger injecting drug users, sex workers and men who have sex withmen may be particularly vulnerable.
However, little is known about the specific needs of young people in thesegroups as opposed to older people. This issue needs to be emphasized in futureresearch, given the fact that a large number of the people most at risk areyoung, and it will be important to ensure that their needs are adequately metby any programmes that are implemented.
As anticipated, few studies were identified that explicitly focused on at-riskyoung people in developing countries. However, the fact that so few studieswere identified in either the published or the grey literature was surprising inview of the evidence from other areas of programming that young peoplerequire specific attention from policies and programmes, and that they maybe particularly vulnerable and have specific needs.
Not only was it difficult to identify relevant studies, but those that were iden-tified often did not provide adequate information to allow for comparisonamong studies or assessments of the studies themselves. In general, studiesdid not provide sufficient details about the interventions, did not clearly de-fine or measure expected outcomes, lacked information about the impact ofthe interventions and failed to provide adequate pre-test and post-test evalu-ations or control groups. Given that young people are at the centre of theepidemic in many developing countries, the lack of well evaluated interven-tions targeting them is a cause for concern.
Despite the comprehensive strategy used to identify relevant studies for thisreview, it is possible that studies may have been missed, for example if theywere reported only in conference abstracts or in internal programme reportsor other project documents. Furthermore, it must be recognized thatconducting research with these groups is challenging. Not only do many
307
92-4-120938-0_CH09_307

interventions not consider the specific needs of young people but data col-lected by studies are often not disaggregated by age. Additionally, research-ing and evaluating interventions for such marginalized groups may bedifficult for both methodological and ethical reasons.
In this review, we did not attempt to identify or analyse studies conductedamong the general population of people most at risk and that did not disag-gregate data by age with the same systematic rigour that had been used forstudies of interventions targeting young people. However, the studies we re-viewed provide consistently supportive evidence for the effectiveness ofinterventions targeting at-risk populations in developing countries in termsof changing knowledge and reported behaviours and even biological out-comes, such as reducing the prevalence of STIs.
Because of the lack of studies, this review did not really benefit from theoverall methodology that had been developed for chapters in this series. Inaddition, while the typology is likely to have some resonance with programmedevelopment and delivery staff, it is questionable whether these groups aresufficiently similar enough to warrant being combined, even if there is some-times overlap between them. It is therefore unrealistic to draw strong con-clusions from Table 9.5.
However, as indicated in Table 9.6, this does not mean that we do not haveevidence from which to recommend action. What it demonstrates is the needto see the evidence for young people in developing countries within the widercontext of evidence for the effectiveness of interventions in developing coun-tries that have been directed at adults and young people (where the data arenot disaggregated by age). When the evidence for effectiveness among youngpeople in developing countries is combined with the evidence for general at-risk populations in developing countries and the data from young people indeveloped countries, it becomes reasonable to move type 4 interventions from“Steady” to “Ready” or even to “Go”. The studies that focused on youngpeople in developed countries additionally demonstrate that good researchon at-risk young people is possible.
Young people who are at the centre of concentrated epidemics require inter-ventions urgently. Such interventions should be based on good practice (5)and should include facility and outreach components as well as a focus oninformation and services (Box 9.1); thus, they should be type 4 interventions.However, in recommending the widespread implementation of such inter-ventions it is important to include the caveat that they also should be carefullyplanned, monitored and evaluated and that an operations research componentshould be included to provide a better understanding of the mechanismsof action and the interactions between different parts of each intervention.
308
92-4-120938-0_CH09_308

Tab
le 9
.6.
Rec
om
men
dat
ion
s o
n t
he
stre
ng
th o
f th
e ev
iden
ce f
or
effe
ctiv
enes
s b
y in
terv
enti
on
typ
e
Inte
rven
tio
n t
ype
Key
ch
arac
teri
stic
sC
on
clu
sio
nC
om
men
ts
1. In
form
atio
n on
lypr
ovid
ed th
roug
hou
trea
ch
Tar
get g
roup
nee
ds to
be
iden
tifie
dan
d re
ache
d w
ith th
e in
form
atio
nS
tead
y•
Thi
s ty
pe o
f int
erve
ntio
n is
use
d w
idel
y an
d ai
ms
at im
prov
ing
info
rmat
ion
and
skill
s•
No
thor
ough
eva
luat
ions
hav
e be
en fo
und
• It
is q
uest
iona
ble
whe
ther
edu
catio
nal a
ctiv
ities
alo
ne c
an b
esu
cces
sful
in c
hang
ing
risk
beha
viou
r am
ong
vuln
erab
le g
roup
sw
ithou
t inc
ludi
ng s
ervi
ces
that
pro
vide
cond
oms,
ST
Ia tr
eatm
ent a
nd h
arm
-red
uctio
n in
terv
entio
ns2.
Info
rmat
ion
and
serv
ices
pro
vide
dth
roug
h ou
trea
ch
No
stud
y m
et th
e in
clus
ion
crite
riaN
one
• N
o in
terv
entio
n of
this
type
was
rev
iew
ed in
a s
tudy
that
met
the
incl
usio
n cr
iteria
3. F
acili
ty-b
ased
info
rmat
ion
and
serv
ices
Tar
get g
roup
mus
t kno
w a
bout
and
wan
t to
use
the
faci
lity,
whi
ch m
ust
be a
cces
sibl
e an
d pr
ovid
e a
conf
iden
tial s
ervi
ce
Ste
ady
• A
ll U
NG
AS
S g
oals
are
add
ress
ed b
y th
is in
terv
entio
n ty
pe:
info
rmat
ion,
ski
lls a
nd s
ervi
ces
are
prov
ided
in a
n at
tem
pt to
decr
ease
ris
k an
d ul
timat
ely
HIV
pre
vale
nce
• P
ossi
ble
stig
mat
izat
ion
mus
t be
over
com
e if
the
faci
lity-
base
dap
proa
ch is
to w
ork
• T
he o
ne s
tudy
cite
d pr
imar
ily p
rovi
des
safe
pla
ces
for
youn
g pe
ople
mos
t at r
isk
of H
IV, b
ut it
doe
s no
t inc
lude
spe
cific
ser
vice
s ai
med
at r
educ
ing
HIV
tran
smis
sion
(fo
r ex
ampl
e ne
edle
exc
hang
e)4.
Out
reac
h an
dfa
cilit
y-ba
sed
info
rmat
ion
and
serv
ices
Goo
d in
tegr
atio
n of
ser
vice
s in
outr
each
and
faci
lity-
base
d ac
tiviti
esne
cess
ary
Info
rmat
ion
abou
t ser
vice
s m
ust b
eco
nsis
tent
All
mem
bers
of t
arge
t gro
up m
ust
have
equ
al a
cces
s to
the
inte
rven
tion
Rea
dyb
• A
ll U
NG
AS
S g
oals
are
add
ress
ed b
y th
is in
terv
entio
n ty
pe:
info
rmat
ion,
ski
lls a
nd s
ervi
ces
are
prov
ided
in a
n at
tem
pt to
decr
ease
ris
k an
d ul
timat
ely
HIV
pre
vale
nce
• T
he o
utre
ach
com
pone
nt is
a c
ruci
al a
spec
t, he
lpin
g to
info
rm th
eta
rget
gro
up a
bout
faci
lity-
base
d se
rvic
es•
Bot
h st
udie
s in
this
cat
egor
y w
ere
succ
essf
ul in
incr
easi
ng k
now
l-ed
ge, i
mpr
ovin
g se
rvic
e ut
iliza
tion
and
redu
cing
pre
vale
nce
ST
Is
a S
TI =
sex
ually
tran
smitt
ed in
fect
ion.
b W
hen
taki
ng th
e ev
iden
ce fr
om a
dult
prog
ram
mes
in d
evel
opin
g co
untr
ies
into
acc
ount
.
309
92-4-120938-0_CH09_309

Box 9.1
Recommendations for interventions targeting young people most at risk
For policy-makers
Specific attention needs to be given to young people who are most atrisk from HIV, including young injecting drug users, sex workers andmen who have sex with men.
Urgent action must be taken if these young people are to benefit fromstrategies to meet the global goals on HIV/AIDS and the Millennium De-velopment Goal on AIDS.
Interventions should be widely implemented for these groups of youngpeople and more emphasis needs to be placed on identifying the specificneeds of young people compared with those of adults.
Interventions should include strong monitoring and evaluation compo-nents (an important message for donors as well).
Interventions to mitigate the vulnerability of young people need to beseen within the broader context of structural interventions being madeto decrease their vulnerability.
For programme development and delivery staff
When developing interventions for sex workers, injecting drug users,men who have sex with men and other groups at high risk from HIV, itis important to ensure that the specific needs of young people are givenadequate attention and that data are disaggregated by age and sex.
If the global goals on HIV and young people are to be achieved, at-riskyoung people will need to receive information, skills and servicesthrough facilities and outreach strategies.
Practitioners working with at-risk young people should monitor their in-terventions and collaborate more closely with researchers from the initialstages of project design in order to better assess the impact of theirprogrammes.
Researchers
There is an urgent need to strengthen the evaluation component of in-terventions for young people most at risk, in order to determine theimpact of the intervention and the mechanisms of action.
There is also a need to be clear about key indicators for monitoring andevaluating programmes to achieve the global goals on HIV among at-risk young people.
More research is needed to identify the special needs of young peoplemost at risk, compared with the needs of at-risk adults.
310
92-4-120938-0_CH09_310

Planning, monitoring and evaluating interventions will not only ensure thatthe evidence base for their effectiveness will be strengthened but it will alsocontribute to the collective ability to track the achievement of the global goalson HIV among these groups of at-risk young people.
Finally, it needs to be emphasized that stopping the spread of HIV among at-risk young people will depend on interventions that decrease their vulnera-bility to HIV not those that merely mitigate this vulnerability. Suchinterventions were beyond the scope of this review, although several studiesthat attempted to do this were identified (65, 66, 67). Unfortunately theirimpact is often difficult to assess.
Acknowledgements:
We would like to acknowledge the following people who contributed to theidentification of studies and reports of interventions directed to young peo-ple most at risk of HIV: Peter Aggleton, Andrew Ball, Gary Barker,Stacia Burnham, Catherine Campbell, John Howard, Carol Jenkins, RafaelMazin, Gabriele Riedner, Mary Jane Rotheram, Meindert Schaap andRichard Steen.
References:
1. Speizer IS, Magnani RJ, Colvin CE. The effectiveness of adolescentreproductive health interventions in developing countries: a review of theevidence. Journal of Adolescent Health, 2003, 33:324-348.
2. Robin L et al. Behavioral interventions to reduce incidence of HIV, STD, andpregnancy among adolescents: a decade in review. Journal of AdolescentHealth, 2004, 34:3-26.
3. Pedlow CT, Carey MP. HIV sexual risk-reduction interventions for youth: areview and methodological critique of randomized controlled trials. BehaviorModification, 2003, 27:135-190.
4. Rivers K, Aggleton P. Adolescent sexuality, gender and the HIV epidemic. NewYork, United Nations Development Programme, 1999.
5. Aggleton P, Rivers K. Interventions for adolescents. In: Gibney L, DiClementeD, Vermund S, eds. Preventing HIV in developing countries: biomedical andbehavioral approaches. New York, Plenum Publications, 1999:231-255.
6. Kim N et al. Effectiveness of the 40 adolescent AIDS-risk reductioninterventions: a quantitative review. Journal of Adolescent Health, 1997,20:204-215.
7. Merson MH, Dayton JM, O’Reilly K. Effectiveness of HIV preventioninterventions in developing countries. AIDS, 2000, 14 Suppl 2:S68-84.
8. Indonesia Ministry of Health. Behavioural surveillance among populations atrisk for HIV. Jakarta, Directorate of Communicable Disease Control andEnvironmental Health, Ministry of Health and Central Bureau of Statistics, 2002.
311
92-4-120938-0_CH09_311

9. Lao People’s Democratic Republic, National Committee for the Control of AIDSBureau, Family Health International. Behavioural surveillance survey in LaoPeople’s Democratic Republic, 2000-2001. Lao PDR, 2003.
10. National AIDS Council, Ministry of Health, Zambia, Family Health International.Behavioral and biologic surveillance survey: Zambia female sex workers.Zambia, Family Health International, 2004:67.
11. Hoffmann O et al. Methodological lessons from a cohort study of high riskwomen in Tanzania. Sexually Transmitted Infections, 2004, 80 Suppl 2:S69-73.
12. Alary M et al. Decline in the prevalence of HIV and sexually transmitted diseasesamong female sex workers in Cotonou, Benin, 1993-1999. AIDS, 2002,16:463-470.
13. Ghys PD et al. Increase in condom use and decline in HIV and sexuallytransmitted diseases among female sex workers in Abidjan, Cote d’Ivoire,1991-1998. AIDS, 2002, 16:251-258.
14. UNAIDS. 2004 report on the global HIV/AIDS epidemic: 4th global report.Geneva, UNAIDS, 2004.
15. Rhodes T et al. Drug injecting and sexual safety: cross-national comparisonsamong cocaine and opiod injectors. In: Stimson GV, Des Jarlais DC, Ball A,eds. Drug injecting and HIV infection: global dimensions and local responses.London, UCL Press, 1998.
16. Rhodes T. HIV transmission and HIV prevention asssociated with injecting druguse in the Russian Federation. International Journal of Drug Policy, 2004,15:1-15.
17. Bangladesh National AIDS/STD Programme. National HIV and behaviouralsurveillance 1999–2003. Bangladesh, Directorate General of Health Services,Ministry of Health and Family Welfare, 2004.
18. Myanmar AIDS Prevention and Control Project, Department of Health. Sentinelsurveillance data for 1989- 2003. Yangon, AIDS Prevention and Control Project,2004.
19. Sarkar K et al. Young age is a risk factor for HIV among female sex workers:an experience from India. Journal of Infection, 2005, Dec 26 [Epub ahead ofprint].
20. Riedner G et al. Baseline survey of sexually transmitted infections in a cohortof female bar workers in Mbeya Region, Tanzania. Sexually TransmittedInfections, 2003, 79:382-387.
21. Tawil O et al. HIV prevention among vulnerable populations: outreach in thedeveloping world. AIDS, 1999, 13 Suppl A:S239-247.
22. Levine WC et al. Decline in sexually transmitted disease prevalence in femaleBolivian sex workers: impact of an HIV prevention project. AIDS, 1998,12:1899-1906.
23. Welp E et al. HIV prevalence and risk behaviour in young drug users inAmsterdam. AIDS, 2002, 16:1279-1284.
24. Shaw C, Aggleton P. Preventing HIV/AIDS and promoting sexual health amongespecially vulnerable young people. Southampton, England, University ofSouthampton, Centre for Sexual Health Research, 2002.
25. World Bank. A guide to competitive vouchers in health. Washington, DC, WorldBank, 2004.
312
92-4-120938-0_CH09_312

26. Kasirye R. Empowering street and slum young people to prevent HIV/AIDS inKawempe division-Kampala city: a case study of Uganda youth developmentlink (UYDEL). Kampala, UYDEL, 2004:26.
27. Johns Hopkins Bloomberg School of Public Health. Reaching young peopleworldwide: reproductive health communication activities to date, 1986-1995.Baltimore, MD, Johns Hopkins Bloomberg School of Public Health, Center forCommunication Programs, 1995:110.
28. Kegeles SM, Hays RB, Coates TJ. The Mpowerment Project: a community-levelHIV prevention intervention for young gay men. American Journal of PublicHealth, 1996, 86:1129-1136.
29. Amirkhanian YA et al. A randomized social network HIV prevention trial withyoung men who have sex with men in Russia and Bulgaria. AIDS, 2005,19:1897-1905.
30. Gleghorn A et al. The impact of intensive outreach on HIV prevention activitiesof homeless, runaway, and street youth in San Francisco: the AIDS Evaluationof Street Outreach Project (AESOP). AIDS and Behavior, 1997, 1:261-271.
31. Sears C et al. Investigation of a secondary syring exchange programme forhomeless young adult injection drug users in San Francisco, California, USA.Journal of Acquired Immune Deficiency Syndromes, 2001, 27:193-201.
32. Ma S et al. Decreasing STD incidence and increasing condom use amongChinese sex workers following a short term intervention: a prospective cohortstudy. Sexually Transmitted Infections, 2002, 78:110-114.
33. Jana S et al. The Sonagachi project: a sustainable community interventionprogram. AIDS Education and Prevention, 2004, 16:405-414.
34. Bhave G et al. Impact of an intervention on HIV, sexually transmitted diseases,and condom use among sex workers in Bombay, India. AIDS, 1995, 9 Suppl1:S21-30.
35. Singh YN, Malaviya AN. Experience of HIV prevention interventions amongfemale sex workers in Delhi, India. International Journal of STD and AIDS, 1994,5:56-57.
36. Ford K et al. Behavioral interventions for reduction of sexually transmitteddisease/HIV transmission among female commercial sex workers and clientsin Bali, Indonesia. AIDS, 1996, 10:213-222.
37. Ford K et al. Evaluation of a peer education programme for female sex workersin Bali, Indonesia. International Journal of STD and AIDS, 2000, 11:731-733.
38. Ford K et al. The Bali STD/AIDS study: evaluation of an intervention for sexworkers. Sexually Transmitted Diseases, 2002, 29:50-58.
39. Elly J et al. Papua New Guinea: an innovative strategy to raise self-esteem ofsex workers in Port Moresby, Papua New Guinea, and to promote safer sexpractices with clients. Pacific AIDS Alert Bulletin, 2000, 19:17.
40. Hanenberg RS et al. Impact of Thailand’s HIV-control programme as indicatedby the decline of sexually transmitted diseases. Lancet, 1994, 344:243-5.
41. Van Griensven GJ et al. Evaluation of a targeted HIV prevention programmeamong female commercial sex workers in the south of Thailand. SexuallyTransmitted Infections, 1998, 74:54-58.
313
92-4-120938-0_CH09_313

42. Ford NJ, Koetsawang S. Narrative explorations and self-esteem: research,intervention and policy for HIV prevention in the sex industry in Thailand.International Journal of Population Geography, 1999, 5:213-233.
43. Ghys PD et al. Effect of interventions to control sexually transmitted disease onthe incidence of HIV infection in female sex workers. AIDS, 2001,15:1421-1431.
44. Asamoah-Adu A et al. Evaluation of a targeted AIDS prevention intervention toincrease condom use among prostitutes in Ghana. AIDS, 1994, 8:239-246.
45. Ngugi EN et al. Prevention of transmission of human immunodeficiency virusin Africa: effectiveness of condom promotion and health education amongprostitutes. Lancet, 1988, 2:887-890.
46. Kaul R et al. Monthly antibiotic chemoprophylaxis and incidence of sexuallytransmitted infections and HIV-1 infection in Kenyan sex workers. Journal of theAmerican Medical Association, 2004, 291:2555-2562.
47. Larsen MM et al. Changes in HIV/AIDS/STI knowledge, attitudes and practicesamong commercial sex workers and military forces in Port Loko, Sierra Leone.Disasters, 2004, 28:239-254.
48. Laga M et al. Condom promotion, sexually transmitted diseases treatment, anddeclining incidence of HIV-1 infection in female Zairian sex workers. Lancet,344:246-248.
49. Sanchez J et al. Prevention of sexually transmitted diseases (STDs) in femalesex workers: prospective evaluation of condom promotion and strengthenedSTD services. Sexually Transmitted Diseases, 2003, 30:273-279.
50. Fox LJ et al. Condom use among high-risk women in Honduras: evaluation ofan AIDS prevention program. AIDS Education and Prevention, 1993, 5:1-10.
51. UNAIDS. Female sex worker HIV prevention projects: lessons learnt fromPapua New Guinea, India and Bangladesh. Geneva, UNAIDS, 2000:127.
52. Riedner G et al. Decline in sexually transmitted infection prevalence and HIVincidence in female barworkers attending prevention and care services inMbeya Region, Tanzania. AIDS, 2006, 20:609-615.
53. Peak A et al. Declining risk for HIV among injecting drug users in Kathmandu,Nepal: the impact of a harm reduction programme. AIDS, 1995, 9:1067-1070.
54. Gray J. Harm reduction in the hills of northern Thailand. Journal of SubstanceUse and Misuse, 1998, 33:1075-1091.
55. Kumar MS, Mudaliar S, Daniels D. Community-based outreach HIV interventionfor street-recruited drug users in Madras, India. Public Health Reports, 1998,113 Suppl 1:S58-66.
56. Birkel RC et al. Findings from the Horizontes Acquired Immune DeficiencySyndrome Education Project: the impact of indigenous outreach workers aschange agents for injection drug users. Health Education Quarterly, 1993,20:523-538.
57. Stimson GV, Des Jarlais DC, Ball A. Drug injecting and HIV infection: globaldimensions and local responses. London, UCL Press, 1998.
58. Dolan KA and Niven H. A review of HIV prevention among young injecting drugusers: A guide for researchers. Harm Reduction Journal, 2005, 2:5
314
92-4-120938-0_CH09_314

59. Hurley SF, Jolley DJ, Kaldor JM. Effectiveness of needle-exchangeprogrammes for prevention of HIV infection. Lancet, 1997, 349:1797-1800.
60. Gowing L et al. Substitution treatment of injecting opioid users for prevention ofHIV infection. Cochrane Database of Systematic Reviews, 2004 (4):CD004145.
61. Sampaio M et al. Reducing AIDS risk among men who have sex with men inSalvador, Brazil. AIDS and Behavior, 2002, 6:173-181.
62. Toro-Alfonso J, Varas-Diaz N, Andujar-Bello I. Evaluation of an HIV/AIDSprevention intervention targeting Latino gay men and men who have sex withmen in Puerto Rico. AIDS Education and Prevention, 2002, 14:445-456.
63. Herbst JH et al. A meta-analytic review of HIV behavioral interventions forreducing sexual risk behavior of men who have sex with men. Journal ofAcquired Immune Deficiency Syndromes, 2005, 39:228-41. (HIV/AIDSPrevention Research Synthesis Team.)
64. Myers T, Aggleton P, Kippax S. Perspectives on harm reduction: editorialintroduction. Critical Public Health, 2004, 14:325-328.
65. UNAIDS. Reducing girls’ vulnerability to HIV/AIDS: the Thai approach. Geneva,UNAIDS, 1999:57.
66. UNAIDS. Innovative approaches to HIV prevention: selected case studies.Geneva, UNAIDS, 2000:15.
67. UNAIDS. Summary booklet of best practices. Issue 1. Geneva, UNAIDS,1999:221.
315
92-4-120938-0_CH09_315

92-4-120938-0_CH09_316

Conclusions and recommendations Jane Ferguson,a Bruce Dick,a & David A Rossb
10.1 Introduction
An estimated 40 million people were living with HIV at the end of 2005 (1).More than one quarter of this total are young people aged 15–24 years, andabout 2 million young people are newly infected each year. Almost 25 yearsafter the first cases of AIDS were recognized, the HIV pandemic continuesto pose unprecedented challenges to individuals, families, communities andgovernments around the world, especially in developing countries, whichbear the greatest burden. Young people are particularly affected in terms oftransmission, vulnerability and impact. (see chapter 2).
In addition to HIV being a focus of the Millennium Development Goals,global goals were also endorsed during the UN General Assembly SpecialSession on HIV/AIDS. Some of the goals and targets that were agreed areexplicitly directed towards young people (see chapter 1). Achieving thesetargets will require national governments, civil society and funding agenciesto expend far greater resources and make stronger efforts to prevent HIVamong young people. There are many programmes and activities competingfor limited HIV resources in all countries, including the growing demand foreffective treatment. In terms of the resources that are directed towards pre-venting infection among young people, it is not just a question of increasingthe resources but also of ensuring that the resources are used effectively. Soit is important not only to be able to make a compelling case for focusing onyoung people but also to be clear about what needs to be done. Although thereis broad consensus about the key interventions necessary to prevent HIVamong young people in developing countries (2–4) and there have been re-views of the effectiveness of several of these (5, 6), no systematic review ofa comprehensive set of interventions for young people has been undertaken,although one other effort is in development (7).
a Department of Child and Adolescent Health and Development, WHO, Geneva, Switzerland.Correspondence should be sent to Jane Ferguson (email: [email protected]).
b Infectious Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine,London, England.
317
10.
92-4-120938-0_CH10_317

Encouragingly, there has recently been an increase in the spending allocatedto tackling the epidemic (1, 8), and additional resources are likely to be gen-erated by recent calls for universal access to prevention, treatment and care(9). It has been estimated that US$ 6.1 billion was available for AIDS activ-ities from all sources in 2004. For 2005, 2006 and 2007, projections havebeen made, based on past trends and known pledges and commitments, thatamount to US$ 8.3 billion, US$ 8.9 billion and US$ 10 billion, respectively.Unfortunately, much of this spending has not been allocated according to theevidence of effectiveness. Many factors influence which programmes arefunded and implemented, and there is rarely a simple linear progression fromresearch evidence to policy and practice (10). Decision-makers are morelikely to make evidence-informed choices about the use of resources if theyare provided with evidence that has been synthesized and is presented in areadily understandable way that facilitates the transformation of informationto knowledge.
The authors of the chapters in this report have reviewed the evidence for theeffectiveness of interventions to achieve the global goals on preventing HIV/AIDS among young people in developing countries. They have explicitlyendeavoured to do this in ways that will be useful not only to researchers andother specialists in the field but also to programme managers and policy-makers. While the authors have applied rigorous research methods to sys-tematically review the evidence, they have also aimed to directly address thekey choices that policy-makers and programme managers in developingcountries need to make when deciding how to allocate funds for HIV pre-vention among young people.
Based on the major settings through which interventions are provided toyoung people (schools, health services, mass media, geographically-definedcommunities, and outreach to young people who are most at risk), the chaptershave teased out the different types of interventions provided in each setting.The interventions aimed to achieve a variety of outcomes (Box 10.1). Clearguidance has been provided about which types of interventions are suitablefor wide implementation, based on the evidence, in order to make the bestuse of resources to achieve the global goals and targets.
This chapter summarizes the main findings of the systematic reviews. Itdraws overall conclusions and makes recommendations from the whole seriesin terms of the “Do not go, Steady, Ready, Go” continuum (Box 10.2 andchapter 4). It has benefited from a meeting that was held in June 2005 inChavannes, Switzerland, that involved a number of external experts fromdifferent geographical regions who reviewed earlier versions of the chaptersand assisted the editors in identifying key conclusions and recommendationsfrom the papers.
318
92-4-120938-0_CH10_318

10.2 The road to “Steady, Ready, Go”
Although the scope of this report has been limited to a review of the evidenceon the effectiveness of interventions that have aimed to prevent HIV amongyoung people in developing countries, the task has not been easy. It has en-compassed different types of interventions of varying complexity and scalethat have taken place among different population groups, settings and con-texts and that have used a range of study designs. The iterative process bywhich the chapters in this report were written and revised has been describedin chapter 1. While this process has been relatively time consuming, it hasensured that all chapters have been extensively reviewed and revised in thelight of comments from a range of researchers, programme managers andpolicy-makers. It has also helped to ensure that the five reviews – despitespanning evidence from different types of interventions implemented in dif-ferent settings – all used the same methods and have the same structure. Thishas allowed the strength of the evidence for each type of intervention in eachsetting to be evaluated on a level playing field. The five systematic reviews
Box 10.1
Summary of intervention outcomes
Intervention setting Outcomes measuredSchools Knowledge, skills (personal values,
perceptions of peer norms, communicationabout sex), sexual behaviour (sexualinitiation, condom use, number of partners,use of contraceptives)
Health services Increased utilization of health servicesMass media Knowledge, skills (self-efficacy in terms of
abstinence or condom use), sexualbehaviour (condom use, numbers ofpartners, abstinence), communication(parents, others), social norms, awarenessand use of health services
Communities Knowledge, skills (communication withpeers, parents, partners, condom use),sexual behaviour (ever having sex,number of partners), community norms
Young people most at risk Increased access to information andservices (harm reduction interventions andSTIa treatment)
a STI = sexually transmitted infection.
319
92-4-120938-0_CH10_319

included in this technical report each followed the same seven key steps out-lined in Box 10.3 and described in greater detail in chapter 4.
The typologies that have been developed for the interventions used in differ-ent settings aimed to reflect the key choices that decision-makers need tomake when selecting, developing and implementing interventions. Beingclear about these different types of interventions makes the results of thereviews more transparent and useful to policy-makers and programme man-agers. For example, within the health services setting, rather than simplydiscussing “youth-friendly health services” the authors have discussed dif-ferent types of interventions that were defined according to their specificcomponents, such as training service providers and other clinic staff, chang-ing the structure or functioning of the health facility itself, providing outreachfrom the facility to the community and involving other sectors.
Some systematic reviews exclude evidence from studies that are not ran-domized controlled trials. A key concept in this report is that different typesof interventions require different strengths of evidence in order for them tobe recommended for widespread implementation. The strength of evidence
Box 10.2
The “Steady, Ready, Go” continuum for recommending interventions
Recommendation CriteriaGo Evidence threshold met
Sufficient evidence to recommend widespreadimplementation on large scale now, ideally withcareful monitoring of coverage, quality and cost,and operations research to better understand themechanisms of action
Ready Evidence threshold partially metEvidence suggests interventions are effective butlarge-scale implementation must be accompaniedby further evaluation and operations research toclarify impact and mechanisms of action
Steady Evidence threshold not metSome of the evidence is promising but furtherdevelopment, pilot-testing and evaluation ofprocesses and outcomes are needed before it canbe determined whether these interventions shouldmove into the “Ready” category or “Do not go”
Do not go Strong enough evidence of lack of effectivenessor of harmNot the way to go
320
92-4-120938-0_CH10_320

required depends on the feasibility of the intervention (including its likelycost), its potential risk of adverse outcomes, its acceptability, the potentialeffect size and the time needed for that effect to be achieved, as well as itspotential to bring about other benefits (see chapter 4). Where appropriate,therefore, the reviews have included evidence on effectiveness from quasi-experimental study designs, designs that included before-intervention andafter-intervention measurements, and other observational studies.
A key aim of the process used in these reviews was transparency. So althoughreaders may not necessarily agree with the conclusions reached by the authorsof each of the chapters, the transparency of the methods used make it easierto see where the disagreement lies. The authors have inevitably had to makevalue judgements in assessing the evidence, but the standardized method usedenables readers to be clear about the judgements that have been made. Thisstandard method includes creating a typology for the interventions, assigningthe threshold of evidence required to recommend widespread implementa-tion, weighing the strength of evidence from the different studies for eachintervention type and finally, making recommendations using the “Do NotGo, Steady, Ready, Go” continuum.
Box 10.3
Steps followed in the systematic reviews in this report
Step Description1. Define the key types of interventions that policy-makers need to
choose between in the setting under consideration2. Define the strength of evidence that would be needed to justify
widespread implementation of the intervention3. Develop explicit inclusion and exclusion criteria for the studies
under review4. Critically review all eligible studies and their findings, by
intervention type5. Summarize the strength of the evidence on the effectiveness of
each type of intervention6. Compare the strength of the evidence provided by the studies
against the threshold of evidence needed to recommendwidespread implementation
7. From this comparison, derive evidence-basedrecommendations related to the implementation of each type ofintervention in the setting or population group
321
92-4-120938-0_CH10_321

10.3 Results
Chapter 2 clearly demonstrates that young people (those aged 10–24 years)are at the centre of the HIV epidemic in developing countries, and it assertsthat they should be at the centre of prevention efforts. They are the age groupwith the highest incidence of HIV and they are disproportionately representedamong the population subgroups most at risk of becoming infected. Fortu-nately, they are also the age group where HIV prevention interventions mayhave the greatest potential for reversing the epidemic (11). Unless HIV is keptfrom spreading among young people, and especially among young womenliving in areas with generalized epidemics, future generations will be con-demned to suffer not only from HIV itself but also from the enormouseconomic and social costs of sustained HIV treatment and care services.
Chapter 3 provides an overview of the public health interventions that havebeen used to prevent HIV transmission. These include interventions aimed atchanging behaviours, including those that attempt to reduce sexual risk be-haviours and injecting drug use; biomedical interventions, such as managingsexually transmitted infections (STIs), providing antiretroviral treatment andcircumcision; and social or environmental interventions, including increasingaccess to sterile syringes and needles for those who inject drugs and usingmicrofinance initiatives aimed at women. This chapter does not specificallyfocus on young people but it clearly shows that there is a range of interven-tions, and that they have widely differing costs and logistical and humanresource implications, as well as varying evidence of their effectiveness. Thechapter concludes that there is a large and expanding armamentarium of pre-vention interventions available to policy-makers and programme managers,but it also cautions against confusing a lack of implementation with a lack ofefficacy (12, 13).
The key results of the systematic reviews of the different types of inter-ventions in the five settings – presented in chapters 5 to 9 – are shown inTable 10.1. This table summarizes the number of studies of each type ofintervention that met the inclusion criteria, the threshold of evidence neededto recommend widespread implementation, the strength of evidence for apositive impact provided by the studies reviewed and, finally, the overallrecommendation.
Altogether, 23 different types of interventions were defined, and a total of 85studies were identified that could be used to assess their effectiveness. Fiveof these studies contributed evidence to two intervention settings (14–18).
322
92-4-120938-0_CH10_322

323
Tab
le 1
0.1
Su
mm
ary
of f
ind
ing
s an
d r
eco
mm
end
atio
ns
fro
m th
e sy
stem
atic
rev
iew
s o
f in
terv
enti
on
s to
ach
ieve
the
glo
bal
go
als
on
HIV
an
d y
ou
ng
peo
ple
in f
ive
del
iver
y se
ttin
gs
Set
tin
gT
ype
of
inte
rven
tio
nN
o. o
fst
ud
ies
mee
tin
gin
clu
sio
ncr
iter
ia
Th
resh
old
of
evid
ence
nee
ded
to r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n
Str
eng
tho
fev
iden
cefo
r a
ben
efic
ial
imp
act
Rec
om
men
dat
ion
Sch
oo
lsC
urric
ulum
-bas
ed in
terv
entio
ns w
ith c
hara
cter
istic
sth
at h
ave
been
foun
d to
be
effe
ctiv
e in
dev
elop
edco
untr
ies
and
are
led
by a
dults
13Lo
wV
ery
stro
ngG
o
Cur
ricul
um-b
ased
with
cha
ract
eris
tics
foun
d to
be
effe
ctiv
e in
dev
elop
ed c
ount
ries
and
that
are
led
bype
ers
1Lo
wW
eak
Ste
ady
Cur
ricul
um-b
ased
with
out t
he c
hara
cter
istic
s fo
und
tobe
effe
ctiv
e in
dev
elop
ed c
ount
ries
and
that
are
led
byad
ults
2Lo
wW
eak
Ste
ady
Cur
ricul
um-b
ased
with
out t
he c
hara
cter
istic
s fo
und
to b
e ef
fect
ive
in d
evel
oped
cou
ntrie
s an
d le
d by
pee
rs1
Low
Wea
kS
tead
y
Non
-cur
ricul
um b
ased
with
out c
hara
cter
istic
s fo
und
tobe
effe
ctiv
e in
dev
elop
ed c
ount
ries
and
led
by a
dults
4Lo
wW
eak
Ste
ady
Non
-cur
ricul
um b
ased
with
out c
hara
cter
istic
s fo
und
tobe
effe
ctiv
e in
dev
elop
ed c
ount
ries
and
led
by p
eers
1Lo
wE
quiv
ocal
Ste
ady
Hea
lth
ser
vice
sIn
terv
entio
ns w
ith s
ervi
ce p
rovi
ders
and
in th
eco
mm
unity
1Lo
wE
quiv
ocal
Ste
ady
(or
Do
not
go)
Inte
rven
tions
with
ser
vice
pro
vide
rs a
nd in
faci
litie
s an
dth
e co
mm
unity
4Lo
wW
eak
Go
Inte
rven
tions
with
ser
vice
pro
vide
rs a
nd in
volv
ing
othe
rse
ctor
s1
Mod
erat
eE
quiv
ocal
Ste
ady
(or
Do
not
go)
92-4-120938-0_CH10_323

324
Set
tin
gT
ype
of
inte
rven
tio
nN
o. o
fst
ud
ies
mee
tin
gin
clu
sio
ncr
iter
ia
Th
resh
old
of
evid
ence
nee
ded
to r
eco
mm
end
wid
esp
read
imp
lem
enta
tio
n
Str
eng
tho
fev
iden
cefo
r a
ben
efic
ial
imp
act
Rec
om
men
dat
ion
Inte
rven
tions
with
ser
vice
pro
vide
rs a
nd in
faci
litie
s an
din
volv
ing
othe
r se
ctor
s0
Mod
erat
eN
o da
taN
o da
ta
Inte
rven
tions
with
ser
vice
pro
vide
rs a
nd in
the
com
mun
ity a
nd in
volv
ing
othe
r se
ctor
s2
Mod
erat
eE
quiv
ocal
Ste
ady
(or
Do
not
go)
Inte
rven
tions
with
ser
vice
pro
vide
rs a
nd in
faci
litie
s an
dth
e co
mm
unity
and
invo
lvin
g ot
her
sect
ors
8M
oder
ate
Wea
kR
eady
Mas
s m
edia
Rad
io o
nly
1M
oder
ate
Equ
ivoc
alS
tead
yR
adio
with
oth
er m
edia
(ex
clud
ing
tele
visi
on)
6M
oder
ate
Med
ium
Go
Rad
io a
nd te
levi
sion
with
oth
er m
edia
8H
igh
Str
ong
Go
Geo
gra
ph
ical
lyd
efin
ed c
om
mu
nit
ies
Tar
getin
g yo
uths
thro
ugh
exis
ting
yout
hs-s
ervi
ceor
gani
zatio
ns11
Mod
erat
eE
quiv
ocal
Rea
dy
Tar
getin
g yo
uths
thro
ugh
new
str
uctu
res
6H
igh
Wea
kS
tead
y (o
r D
o no
tgo
)T
arge
ting
the
com
mun
ity th
roug
h tr
aditi
onal
net
wor
ks3
Mod
erat
eE
quiv
ocal
Ste
ady
Tar
getin
g th
e co
mm
unity
thro
ugh
com
mun
ity e
vent
s2
Mod
erat
eW
eak
Ste
ady
Yo
un
g p
eop
le m
ost
at r
isk
Info
rmat
ion
only
pro
vide
d th
roug
h ou
trea
ch1
Mod
erat
eW
eak
Ste
ady
Info
rmat
ion
and
serv
ices
pro
vide
d th
roug
h ou
trea
ch0
Hig
hN
o da
taN
o da
taF
acili
ty-b
ased
info
rmat
ion
and
serv
ices
1Lo
wW
eak
Ste
ady
Out
reac
h an
d fa
cilit
y -
base
d in
form
atio
n an
d se
rvic
es2
Mod
erat
eW
eak
Ste
ady
(but
Rea
dyif
evid
ence
from
deve
lopi
ngco
untr
ies
amon
gal
l age
sco
nsid
ered
)
92-4-120938-0_CH10_324

There were six types of school-based interventions. These were classifiedon the basis of the content and quality of the interventions, whether theywere curriculum based and according to who delivered the intervention(teachers or peers).
There were also six types of health service interventions. These were clas-sified according to whether they provided training to clinic staff with orwithout implementing changes in the structure or functioning of the facilityitself and whether there were also information and sensitization activitiesheld in the community with or without the involvement of other sectors.
The three types of mass media interventions were classified according todistinctions between the delivery channels used to target young people:radio only, or some combination of radio, television and other media (suchas print).
Interventions in geographically defined communities were divided intofour types. The first distinction made was whether the target group wasyoung people or the entire community. The youth-only interventions werefurther subdivided according to whether they were delivered through a pre-existing youth-service organization or a new institutional structure; theinterventions targeting the entire community were subdivided accordingto the delivery channels used, namely traditional networks or communityevents.
The four types of interventions targeting young people most at risk of be-coming infected with HIV were classified based on the site of delivery ofthe interventions (within facilities, through outreach, or both) and the con-tent of the intervention (provision of information only or both informationand services).
The thresholds of evidence needed to recommend widespread implementa-tion of different interventions varied (Table 10.1). Nine types of interventionswere judged to require only weak evidence (a low threshold) (that is, therehad to be at least some evidence from adequacy studies and plausibility stud-ies), 11 to require at least moderately strong evidence (that is, at least someevidence from strong plausibility studies), and 3 to require strong evidence(a high threshold) (that is, substantial evidence from strong plausibility orprobability studies or both) (19). Interventions deemed to require a highthreshold of evidence were placed in that category because there were chal-lenges inherent in the feasibility of implementation that related to the com-plexity and likely costs of delivery.
Despite the fact that many of the studies included in the reviews had un-clear descriptions of the interventions and weak study designs, 23 of the 80studies were considered to show strong evidence of effectiveness or lack of
325
92-4-120938-0_CH10_325

effectiveness. These were distributed across the settings, with the exceptionof interventions targeting young people who were most at risk, for which theevidence was consistently weak.
Overall, however, the evidence for most intervention types was not strong(Table 10.1). Studies related to 11 types of interventions were considered tohave weak evidence (4 in schools, 2 in health services, 2 in geographicallydefined communities, 3 targeting the most at-risk young people). Studies ofan additional 7 intervention types were judged to have only equivocal evi-dence of effectiveness (1 in schools, 3 in health services, 1 in the mass media,2 in geographically defined communities). Authors used the term “equivocal”to describe those studies for which the quality of the evidence or the results,or both, made it difficult to definitively assess the impact of the intervention.The studies considered under one type of intervention type (mass media) wereconsidered to have moderately strong evidence. Only studies included underone of the intervention types for schools and one intervention type for massmedia were thought to have strong evidence.
All authors sought out studies of interventions that would lead towards achiev-ing the global goals – that is, by increasing access to information, skills andservices; reducing vulnerability to HIV infection and reducing HIV preva-lence. In the schools, mass media and communities settings (chapters 5, 7and 8), there was evidence of changes in knowledge as well as in reported atti-tudes, behaviours and skills, indicating that interventions delivered in thesesettings offer opportunities to increase access to information and skills. The ev-idence on the effectiveness of interventions in health services focused almostexclusively on their impact in increasing young people’s access to and use ofthe services themselves (chapter 6). The studies reviewed did not examinethe degree to which the health services could become a venue for providingeffective information or for improving skills, with the notable exception ofself-efficacy for condom use. Similarly, the focus of studies on interventionsfor the young people most at risk of HIV was on increasing access to infor-mation and services. Overall, there were few studies that provided evidenceon the prevalence of HIV or other biological outcomes, such as other STIs orpregnancy. And there were not many studies that addressed vulnerability.
The recommendations made for the different interventions are describedbelow.
“Go” – There were four types of interventions for which the authors con-cluded that the evidence threshold had been met. Thus there was sufficientpositive evidence to be able to recommend widespread implementation ofthese interventions on a large scale as long as coverage and quality weremonitored: there was one intervention in schools, one in health services andtwo in the mass media (Box 10.4).
326
92-4-120938-0_CH10_326

“Ready” – There were three types of interventions for which it was concludedthat the evidence threshold had been partially met. Thus there was sufficientlystrong positive evidence to recommend large-scale implementation but onlyif this were to be accompanied by further outcome evaluations and operationsresearch to clarify the impact of the intervention and the mechanisms of ac-tion. This applied to one intervention type in health services, one in geo-graphically defined communities, and one implemented among young peopleconsidered to be most at risk (but only when the evidence from interven-tions in developing countries targeting all ages was also taken into account)(Box 10.5).
“Steady” – The remaining interventions (14 in total) were given a “Steady”recommendation. There were five types of interventions in schools, three inhealth services, three in geographically defined communities, two interven-tion types targeting young people most at risk and one delivered through themass media (Box 10.6). For these types of interventions, some of the evidenceis promising but further development, pilot-testing and evaluation are neededbefore it can be determined whether they should move into the “Ready” cat-egory or the “Do not go” category.
Box 10.4
Interventions recommended to “Go” (widespread implementation now)
Setting Intervention typeSchools Curriculum-based interventions with
characteristics that have been found tobe effective in developed countries andare led by adults
Health services Interventions with service providers thatinclude making changes either to thestructure or functioning of the facilitiesthemselves and are linked tointerventions in the community topromote the health services for youngpeople
Mass media Interventions with messages deliveredthrough the radio and other media(forexample, print media), except televisionInterventions with messages deliveredthrough the radio and television andother media (for example, print media)
Geographically definedcommunities
No interventions met the criteria
Young people most at risk No interventions met the criteria
327
92-4-120938-0_CH10_327

“Do not go” – In four of the “Steady” interventions, the authors consideredthat there was some evidence, at least under certain circumstances, that thistype of intervention might have no beneficial impact on preventing the spreadof HIV. These four types of interventions included three in the health services(the types that did not include making any changes to facilities) and one ingeographically defined communities (interventions that used new deliverystructures).
10.4 Discussion
The choices that face policy-makers and programme managers are complex.Not only do they need to consider different settings and population groups,but also within each of these settings they need to choose between severaldifferent types of interventions. It is hoped that these reviews will go someway towards facilitating these difficult decisions.
We know that there is no magic bullet that will decrease HIV prevalenceamong young people, so programmes need to include a range of interventions.Fortunately, the global goals themselves assist with such decisions, since theyhelp us move beyond a simplistic focus linking specific interventions withdecreases in HIV prevalence towards a more realistic approach that linksspecific interventions with intermediate outcomes that are points on the pathto decreasing prevalence: these outcomes are to increase knowledge andskills, increase access to services and to decrease vulnerability.
Although we consider that the reviews included in this report will make animportant contribution to making decisions about the allocation of resources
Box 10.5
Interventions recommended as “Ready” (widespread implementation accom-panied by further evaluation and operations research)
Setting Intervention typeSchools No interventions met this criteriaHealth services Interventions with service providers and
in health facilities and in the communitythat involve other sectors
Mass media No interventions met the criteriaGeographically definedcommunities
Interventions targeting youths usingexisting youth-service organizations
Young people most at risk Facility based programmes that alsohave outreach and provide informationand services
328
92-4-120938-0_CH10_328

to different interventions, there were several important limitations. First, notall interventions for all groups of young people in all delivery settings havebeen included. Three groups of young people who are most at risk of HIVwere the focus of the studies included in chapter 9, namely young sex workers,young injecting drug users and young men who have sex with men. However,there are obviously other groups of young people who are also vulnerable and
Box 10.6
Interventions recommended as “Steady” (interventions that require further de-velopment, pilot-testing and evaluation before widespread implementation canbe recommended)
Setting Intervention typeSchools Curriculum-based with characteristics found
to be effective in developed countries and thatare led by peersCurriculum-based without the characteristicsfound to be effective in developed countriesand that are led by adultsCurriculum-based without the characteristicsfound to be effective in developed countriesand led by peersNon-curriculum based without characteristicsfound to be effective in developed countriesand led by adultsNon-curriculum based without characteristicsfound to be effective in developed countriesand led by peers
Health services Interventions with service providers and in thecommunityInterventions with service providers andinvolving other sectorsInterventions with service providers and infacilities and involving other sectorsInterventions with service providers and in thecommunity and involving other sectors
Mass media Radio onlyGeographicallydefined communities
Interventions targeting youths through newstructuresInterventions targeting the entire communitythrough traditional networksInterventions targeting the entire communitythrough community events
Young people mostat risk
Outreach only interventions providinginformation and services
329
92-4-120938-0_CH10_329

at increased risk, such as young migrant workers, young prisoners, and youngpeople in the uniformed services. For practical reasons these groups werenot included in order to limit the scope of the reviews and because data onthe effectiveness of interventions directed towards these groups are scarce.In addition to the absence of some groups from this review, some interven-tions have “fallen between the cracks” of the settings that were defined. Forexample, folk media, such as traditional theatre, songs and puppetry, fall be-tween interventions delivered through the media and those delivered throughthe community, and the social marketing of condoms falls among interven-tions delivered through the media, health services and the community.
Second, there was no attempt to review the evidence for the effectiveness ofinterventions directed towards underlying determinants of behaviour (some-times known as “upstream”, “structural” or “environmental” factors), suchas decreasing poverty, improving education or providing vocational training.In general, the focus of these chapters has been on mitigating vulnerabilityrather than preventing it. The decision not to include interventions directedtowards decreasing vulnerability was taken in order to limit the scope of thereview and because an initial search of the literature identified few studiesthat were likely to meet the inclusion criteria or would be amenable tothe methods that were used for reviewing evidence. As noted in chapter 3,evaluating such interventions remains a major challenge. However, the factthat such interventions were not included should not in any way be seen asimplying that they are unimportant. Clearly, changing these underlying de-terminants will be central to any long-term response to HIV and AIDS.Mitigating young people’s vulnerability is, however, likely to make importantcontributions in the short term, as will greater commitments to, and compli-ance with, the obligations of governments outlined in the Convention on therights of the child and other human rights instruments.
Third, none of the chapters has explicitly reviewed interventions in the po-litical environment that may contribute to achieving the global goals. (Thepolitical environment includes a number of different components, such aspolitical leadership, activism, policies and legislation. Policies and legislationare often a reflection of the other two components, since they are tangibleevidence of political commitment, providing both vision and the means forachieving specific outcomes). Such interventions have an impact both di-rectly – because they influence budget allocations and expressed prioritiesfor action – and indirectly – because they provide the basis for policies andlegislation, which subsequently facilitate or impede the implementation ofinterventions provided through other settings, such as schools and healthservices.
330
92-4-120938-0_CH10_330

Efforts were made at the start of this process to develop a chapter that wouldreview the evidence for a range of interventions in the political environmenton specific outcome measures related to HIV prevention (20). These effortsincluded exploring the links between political commitment and HIV/AIDSprevention, examining case studies on adolescent sexual and reproductivehealth policies in developing countries (case studies from 11 countries wereidentified) (21, 22), and conducting a preliminary analysis of the YouthNetdatabase on sexual and reproductive health policies for adolescents in 40countries that explicitly promoted behaviour-change communication or ac-tion to reduce STIs among adolescents (23). Preliminary conclusions fromthese efforts supported the likely relationship between the policy environmentand HIV interventions for young people, but it was not possible to apply themethods that had been used to assess the evidence for interventions in othersettings because there was insufficient information on the interventions. Al-ternative forms of analysis were beyond the scope of this project.
Some of the evidence that emerged from this initial review emphasized thepolitical nature of policy-making, the importance of credible data and re-search evidence to be used for advocacy and the value of assessing the“political palatability” of interventions – that is, whether they are technicallyfeasible, cost effective, simple to understand and pose minimal threats topolitical positions or yield political dividends. These issues are reflected inthe judgements made by the authors of the settings papers (chapters 5 to 9)when they established the thresholds of evidence that would be needed inorder to recommend widespread implementation.
In addition to developing specific policies and laws, there are a number ofother activities that are important in creating a supportive environment foreffective responses to HIV prevention; these are frequently included in “bestpractice” publications but often have not been systematically evaluated. Suchinterventions are particularly important when considering interventions di-rected towards young people’s sexuality and interventions targeting groupsthat are already subject to marginalization and discrimination, such as in-jecting drug users. The fact that we often do not have rigorous evaluations ofsuch activities is likely to be more a reflection of the difficulties of evaluatingthem than a lack of effectiveness.
Fourth, the reviews focused on HIV prevention and did not include treatment,care or support for young people living with HIV and AIDS, nor did theyprovide an explicit focus on “positive prevention”. This should in no way beseen as implying that these are unimportant components of national responsesto preventing the spread of HIV among young people. Although many clinicaldecisions are likely to be similar for adolescents and children or adults, andthe basic preventive interventions are likely to be the same whether or not a
331
92-4-120938-0_CH10_331

person is infected with HIV, there are a range of issues related to care andsupport that are likely to be of particular importance to young people livingwith HIV and AIDS; these include issues of sexuality, fertility, disclosure,living with a chronic disease, adhering to treatment regimens and dealing withstigma and discrimination. Testing, treatment and care are likely to provideimportant entry points for preventing HIV among young people.
With the growing focus on universal access, and as experiences are gainedin providing care and support for young people living with HIV and AIDS,a similar review may be warranted to assess the evidence for the effectivenessof interventions that aim to provide care and support. At the same time, asaccess to HIV testing and treatment expands it will be important to carefullymonitor the resources allocated to prevention and treatment. It will also beimportant to monitor and evaluate the impact of greater awareness about theavailability of treatment and greater community knowledge about the extentof HIV infection in the community on young people’s behaviours and on thecommunity’s values and norms, including stigma and discrimination.
In addition to the limitations that result from what we did not plan to include,there are also a number of limitations relating to the interventions and studiesthat actually were reviewed. First, although the authors of the five systematicreviews made every effort to ensure that all studies that met their inclusioncriteria were included, inevitably some will have been missed. For example,while computerized searches can locate the majority of articles appearing inpeer-reviewed journals, they do not identify books or chapters in books orgrey literature, such as unpublished project reports. There was also a languagebias towards English in the search criteria of most of the chapters. In addition,there are likely to be biases in the kind of evaluations that are published. Abias towards publishing positive results has been well documented as has thefact that expensive interventions are more likely to be evaluated more thor-oughly than less costly interventions (24, 25); this may reflect positively onmedia interventions but negatively on interventions delivered through com-munity settings.
Second, with the exception of the review of mass media approaches, the ma-jority of the studies reviewed were of local interventions and so they shedlimited light on the likely effectiveness of interventions implemented on alarger scale. It is possible that the effectiveness (and cost effectiveness) mightbe greater because of the economies of scale and the potential for changingsocial norms to the degree where a tipping point is reached. On the other hand,the quality and intensity of an intervention may be lower when it is imple-mented on a large scale.
Third, with a few notable exceptions, such as the “MEMA kwa Vijana”project in the United Republic of Tanzania (26), little data could be found on
332
92-4-120938-0_CH10_332

the costs of the interventions. Yet given that per capita annual spending onall health care in the least developed countries was estimated at US$ 11.00in 2000 (27), cost will obviously be a key factor in deciding which interven-tions to choose.
Fourth, few studies provided adequate information about the contextual fea-tures that were probably necessary to achieve the documented outcomes(28). The importance of context cannot be underestimated, and although thefocus of this review was on developing countries it is clear that there is a widerange of contexts within this broad categorization. For example, the effec-tiveness of interventions may well differ between Asia, Latin America andAfrica and between middle-income and low-income countries within one re-gion. Furthermore, the evidence for the effectiveness of interventions indeveloping countries needs to be viewed within the wider evidence base fromdeveloped countries. This wider evidence base informed the authors’ thinkingand is referred to in the reviews. As interventions classified as “Go” and“Ready” are introduced in new contexts it will be important to conduct carefulevaluations to ensure that they remain effective.
Fifth, there are well known measurement problems inherent in the reportingof attitudes and behaviours (29), and these may well be greater among youngpeople (30). For example, interventions may well bias reported behaviourstowards more socially desirable behaviours. However, few studies in anysetting included biological outcomes, and most relied on reported behavioursas surrogates for changes in HIV incidence or prevalence.
Sixth, a key finding of this series of reviews was that there are other seriouslimitations to many of the studies that provided the evidence. A number ofstudies that were initially identified did not meet even the minimum levels ofintervention specification required for inclusion. Furthermore, many of thereports of the interventions that did meet these minimum criteria were farfrom ideal in terms of the information they provided; at least some of the timethis reflected poor underlying design of the intervention and the evaluation,poor implementation, or some combination of these. Frequently, the specificsof the intervention were not described in detail, and this problem was oftencompounded either by a lack of evaluation of the process or the results notbeing reported. Many of the studies did not report the methods used in suf-ficient detail, and this often made assessing the quality of the evaluationdifficult.
In general, there was much more detail in studies of interventions conductedin schools and through the mass media than in the other settings. This reflectsthe greater effort that has gone into defining interventions in these settings,and makes it much easier to be clear about the characteristics of interventionsthat are related to their effectiveness in achieving health outcomes. Defining
333
92-4-120938-0_CH10_333

these characteristics remains a challenge in other settings, such as in the healthservices and for interventions in geographically defined communities andamong young people who are most at risk.
This had a number of implications for the programmatic recommendationsthat were made for different interventions by comparing evaluation data withthe predefined threshold of evidence needed to recommend widespread im-plementation. A number of value judgements had to be made by the authorsbased on their assessment of the quality of the intervention and of its evalu-ation in each study; less weight was placed on evidence from studies whereeither of these were poor. The benefits of the methods adopted for this revieware that the facts on which such judgements were based are summarized inthe tables in the printed version of the report and can be found in greater detailin the web versions of each of the five systematic reviews (www.who.int/child-adolescent-health/). Readers may not agree with all the judgementsmade, but the aim was to ensure that the basis for these judgements was asclear as possible, thus guaranteeing that they can act as a point of departurefor further debate and dialogue.
A final challenge in interpreting the data was the fact that a number of thestudies included multiple interventions, and it was difficult or often impos-sible to tease out the relative contributions of the different components. Giventhe importance of combining interventions in multiple settings, it is criticalto know which individual interventions should be included in a multicom-ponent package. It is also important to have a better understanding of howthe relative and absolute contributions of each component might differ if theyare used in different combinations.
Despite these many qualifications, this overview of the evidence does lead toa set of clear recommendations for policy-makers, programme developersand researchers. Some of the caveats arise because of the pragmatic natureof this endeavour. As many as 5 000–6 000 young people become infectedwith HIV every day, and governments, donors and nongovernmental orga-nizations are already allocating large amounts of money to prevent the spreadof HIV among young people. Even though the evidence is not perfect it isimportant that these funds are spent on interventions that are likely to haveas much impact as possible and that decisions are influenced by the evidenceon effectiveness. There would have been fewer caveats had the evidence beenmore rigorously reviewed – for example, if it had been restricted to random-ized controlled trials and, perhaps, quasi-experimental studies. However, thiswould likely have led to the conclusion that the data are not sufficient to makeany recommendations, which would neither help advocates for this importantaspect of national responses nor help policy-makers and programme man-agers move beyond such generic questions as “does prevention work?” It
334
92-4-120938-0_CH10_334

would also not have ensured that funds are spent on those interventions thathave the best evidence, even if it is incomplete.
There is clearly a great deal to do. The evidence is much clearer after thisreview but so are the challenges. First, interventions categorized as “Go” mustbe widely implemented on a large scale together with adequate monitoringand operations research. From this review, it is clear that these interventionsare effective in contributing to the global goals for increasing knowledge andskills and access to health services, and they will ultimately contribute toreducing the prevalence of HIV among young people. Second, interventionscategorized as “Ready” should be implemented together with adequate out-come and process evaluations to establish whether they should move into the“Go” category. Third, improvements in intervention design and piloting andevaluation should be accelerated for interventions in the “Steady” categoryto determine whether they should be moved into the “Ready” or the “Do notgo” categories.
Accomplishing all this will be a challenge for intervention developers andevaluators and for those who support and fund programmes. It should be ofconcern that 25 years into the epidemic we do not have enough evidence torecommend as “Go” any interventions targeting the young people who aremost at risk or any community interventions.
10.5 Recommendations
The key recommendations are summarized in Box 10.7, Box 10.8 andBox 10.9. As can be seen from these boxes, this series of reviews providesnumerous challenges for policy-makers, people responsible for programmedevelopment and delivery, and researchers. Policy-makers and programmemanagers should make every effort to ensure that “Go” interventions arewidely implemented now: requests for additional reviews and synthesis ofthe evidence for these types of interventions risk becoming an apology for alack of action and thus a form of denial, in the face of the challenge posed bythe need to ensure that we can demonstrate effectiveness and impact by takingsuch interventions to scale and ensuring their quality. Of course there will bean ongoing need to better understand different strategies for implementingthese interventions, for operations research and for more detailed informationabout costs and cost effectiveness. But this should not prevent us from actingnow to implement “Go” recommendations.
335
92-4-120938-0_CH10_335

Box
10.
7
Rec
om
men
dat
ion
s fo
r p
olic
y-m
aker
s
Set
tin
gR
eco
mm
end
atio
ns
Gen
eral
• Y
oung
peo
ple
are
at th
e ce
ntre
of t
he H
IV p
ande
mic
and
ther
e ar
e a
rang
e of
inte
rven
tions
that
hav
ean
ade
quat
e ev
iden
ce b
ase
to r
ecom
men
d th
em to
be
wid
ely
impl
emen
ted
to a
chie
ve th
e gl
obal
goa
lson
HIV
and
you
ng p
eopl
e as
long
as
ther
e is
car
eful
mon
itorin
g, e
valu
atio
n an
d op
erat
ions
res
earc
h•
Pre
vent
ion
can
wor
kS
cho
ols
• S
choo
l-bas
ed in
terv
entio
ns th
at in
corp
orat
e ch
arac
teris
tics
prev
ious
ly s
how
n to
be
rela
ted
toef
fect
iven
ess
in d
evel
oped
cou
ntrie
s an
d th
at a
re le
d by
adu
lts c
an r
educ
e se
xual
ris
k be
havi
our
and
incr
ease
kno
wle
dge
Hea
lth
ser
vice
s•
Tra
inin
g he
alth
-car
e pr
ovid
ers,
mak
ing
chan
ges
in fa
cilit
ies
and
unde
rtak
ing
activ
ities
to o
btai
nco
mm
unity
sup
port
can
incr
ease
you
ng p
eopl
e’s
use
of h
ealth
ser
vice
s th
at p
rovi
de tr
eatm
ent f
orS
TIs
a , c
ouns
ellin
g, te
stin
g an
d co
ndom
s•
Acc
ess
to h
ealth
ser
vice
s w
ill b
e en
hanc
ed b
y in
terv
entio
ns in
oth
er s
ecto
rs d
irect
ed a
t you
ng p
eopl
e’s
know
ledg
e, s
kills
, atti
tude
s an
d be
havi
ours
Mas
s m
edia
• M
ass
med
ia p
rogr
amm
es, p
artic
ular
ly w
hen
coor
dina
ted
with
inte
rven
tions
in o
ther
sec
tors
, can
rea
chm
any
youn
g pe
ople
with
impo
rtan
t pre
vent
ion
info
rmat
ion
on H
IV/A
IDS
as
wel
l as
help
to r
educ
ere
port
ed s
exua
l ris
k be
havi
our
Geo
gra
ph
ical
lyd
efin
ed c
om
mu
nit
ies
• E
stab
lishe
d co
mm
unity
org
aniz
atio
ns s
ervi
ng y
oung
peo
ple
can
influ
ence
thei
r kn
owle
dge,
atti
tude
san
d re
port
ed s
exua
l beh
avio
urs
to h
elp
prev
ent t
he s
prea
d of
HIV
Yo
un
g p
eop
lem
ost
at
risk
• Y
oung
peo
ple
who
are
mos
t at r
isk
of H
IV (
in th
is r
evie
w th
e gr
oups
con
side
red
wer
e in
ject
ing
drug
user
s, s
ex w
orke
rs, a
nd m
en w
ho h
ave
sex
with
men
) re
quire
urg
ent a
ctio
n•
Gre
ater
atte
ntio
n to
spe
cify
ing
the
need
s of
you
ng p
eopl
e in
ord
er to
tailo
r in
terv
entio
ns k
now
n to
be
effe
ctiv
e to
them
is r
equi
red
a S
TIs
= s
exua
lly tr
ansm
itted
infe
ctio
ns.
336
92-4-120938-0_CH10_336

337
Box
10.
8
Rec
om
men
dat
ion
s fo
r p
rog
ram
me
dev
elo
pm
ent
and
del
iver
y st
aff
Set
tin
gR
eco
mm
end
atio
ns
Gen
eral
• In
terv
entio
ns, a
nd th
eir
repo
rts,
sho
uld
be c
lear
abo
ut w
hat i
s be
ing
done
and
wha
t the
exp
ecte
dou
tcom
es a
re•
The
y sh
ould
als
o pr
ovid
e re
sults
dis
aggr
egat
ed b
y ag
e an
d se
x of
the
part
icip
ants
• The
impl
emen
tatio
n of
all
inte
rven
tions
sho
uld
be a
ccom
pani
ed b
y ca
refu
l mon
itorin
g an
d by
eva
luat
ion
appr
opria
te to
the
leve
l of e
xist
ing
evid
ence
• G
reat
er c
olla
bora
tion
is n
eede
d be
twee
n pr
ogra
mm
e m
anag
ers
and
rese
arch
ers
to fa
cilit
ate
effe
ctiv
em
onito
ring
and
eval
uatio
n de
sign
Sch
oo
ls•
Pro
gram
mes
sho
uld
be c
urric
ulum
-bas
ed a
nd d
esig
ned
and
impl
emen
ted
usin
g th
e ch
arac
teris
tics
show
n to
be
asso
ciat
ed w
ith e
ffect
iven
ess
Hea
lth
ser
vice
s•
In o
rder
to in
crea
se y
oung
peo
ple’
s us
e of
ser
vice
s it
is n
eces
sary
to tr
ain
serv
ice
prov
ider
s an
d ot
her
clin
ic s
taff
in h
ow to
pro
vide
hig
h qu
ality
hea
lth s
ervi
ces
for
youn
g pe
ople
• F
acili
ties
shou
ld b
e m
ade
mor
e ac
cess
ible
and
acc
epta
ble
to y
oung
peo
ple
• Wor
k al
so n
eeds
to b
e do
ne in
the
com
mun
ity to
gen
erat
e de
man
d an
d su
ppor
t for
the
serv
ices
targ
etin
gyo
ung
peop
le•
Oth
er s
ecto
rs, i
n pa
rtic
ular
sch
ools
and
the
med
ia, c
an a
ssis
t in
crea
ting
dem
and
by im
prov
ing
youn
gpe
ople
’s o
vera
ll kn
owle
dge
abou
t HIV
/AID
S a
nd e
ncou
ragi
ng h
ealth
-see
king
beh
avio
urs
Mas
s m
edia
• T
o ac
hiev
e th
e be
st r
esul
ts, m
ass
med
ia p
rogr
amm
es m
ust b
e ta
ilore
d sp
ecifi
cally
to y
oung
peo
ple
• T
hey
need
to p
rovi
de m
utua
lly r
einf
orci
ng m
essa
ges
thro
ugh
mul
tiple
cha
nnel
sG
eog
rap
hic
ally
def
ined
co
mm
un
itie
s•
Initi
ativ
es s
houl
d la
rgel
y fo
cus
on w
orki
ng w
ith e
xist
ing
yout
h-se
rvic
e or
gani
zatio
ns, w
here
car
eful
atte
ntio
n sh
ould
be
paid
to s
elec
ting,
trai
ning
and
spe
cify
ing
cultu
rally
app
ropr
iate
inte
rven
tions
and
task
s fo
r pr
ogra
mm
e st
aff
• S
taff
shou
ld b
enef
it fr
om o
ngoi
ng s
uper
visi
on•
Org
aniz
atio
n le
ader
s ne
ed to
be
vigi
lant
in m
aint
aini
ng o
vera
ll co
mm
unity
sup
port
and
res
ourc
em
obili
zatio
nY
ou
ng
peo
ple
mo
st a
t ri
sk•
The
se y
oung
peo
ple
shou
ld b
e pr
ovid
ed w
ith in
form
atio
n, s
kills
and
ser
vice
s th
roug
h fa
cilit
ies
and
thro
ugh
outr
each
str
ateg
ies
• T
heir
spec
ific
need
s sh
ould
be
give
n in
crea
sed
atte
ntio
n.•
Car
eful
eva
luat
ion
of th
e im
pact
and
pro
cess
es o
f int
erve
ntio
ns is
ess
entia
l to
incr
ease
kno
wle
dge
ofw
hat i
s ef
fect
ive
amon
g th
is g
roup
of y
oung
peo
ple
92-4-120938-0_CH10_337
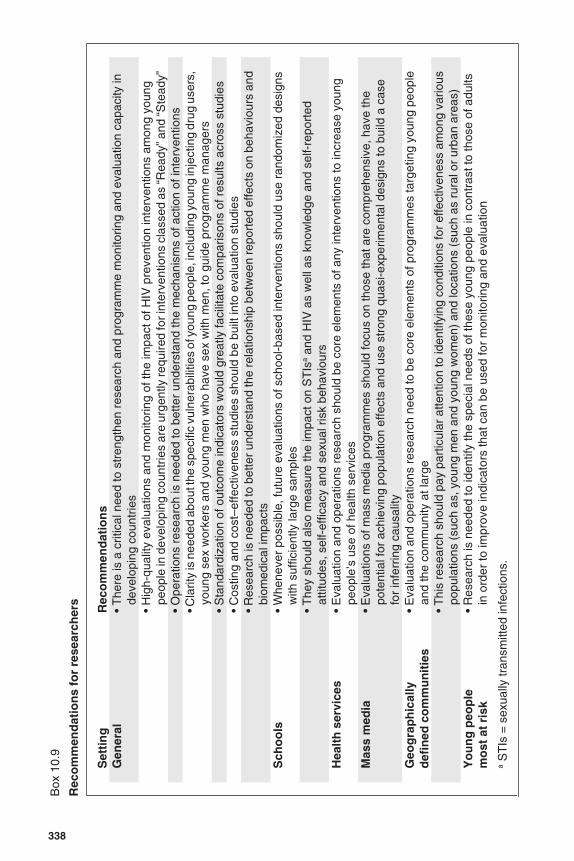
338
Box
10.
9
Rec
om
men
dat
ion
s fo
r re
sear
cher
s
Set
tin
gR
eco
mm
end
atio
ns
Gen
eral
• T
here
is a
crit
ical
nee
d to
str
engt
hen
rese
arch
and
pro
gram
me
mon
itorin
g an
d ev
alua
tion
capa
city
inde
velo
ping
cou
ntrie
s•
Hig
h-qu
ality
eva
luat
ions
and
mon
itorin
g of
the
impa
ct o
f HIV
pre
vent
ion
inte
rven
tions
am
ong
youn
gpe
ople
in d
evel
opin
g co
untr
ies
are
urge
ntly
requ
ired
for i
nter
vent
ions
cla
ssed
as
“Rea
dy” a
nd “S
tead
y”•
Ope
ratio
ns r
esea
rch
is n
eede
d to
bet
ter
unde
rsta
nd th
e m
echa
nism
s of
act
ion
of in
terv
entio
ns• C
larit
y is
nee
ded
abou
t the
spe
cific
vul
nera
bilit
ies
of y
oung
peo
ple,
incl
udin
g yo
ung
inje
ctin
g dr
ug u
sers
,yo
ung
sex
wor
kers
and
you
ng m
en w
ho h
ave
sex
with
men
, to
guid
e pr
ogra
mm
e m
anag
ers
• S
tand
ardi
zatio
n of
out
com
e in
dica
tors
wou
ld g
reat
ly fa
cilit
ate
com
paris
ons
of r
esul
ts a
cros
s st
udie
s•
Cos
ting
and
cost
–effe
ctiv
enes
s st
udie
s sh
ould
be
built
into
eva
luat
ion
stud
ies
• R
esea
rch
is n
eede
d to
bet
ter
unde
rsta
nd th
e re
latio
nshi
p be
twee
n re
port
ed e
ffect
s on
beh
avio
urs
and
biom
edic
al im
pact
sS
cho
ols
• W
hene
ver
poss
ible
, fut
ure
eval
uatio
ns o
f sch
ool-b
ased
inte
rven
tions
sho
uld
use
rand
omiz
ed d
esig
nsw
ith s
uffic
ient
ly la
rge
sam
ples
• T
hey
shou
ld a
lso
mea
sure
the
impa
ct o
n S
TIs
a an
d H
IV a
s w
ell a
s kn
owle
dge
and
self-
repo
rted
attit
udes
, sel
f-ef
ficac
y an
d se
xual
ris
k be
havi
ours
Hea
lth
ser
vice
s•
Eva
luat
ion
and
oper
atio
ns r
esea
rch
shou
ld b
e co
re e
lem
ents
of a
ny in
terv
entio
ns to
incr
ease
you
ngpe
ople
’s u
se o
f hea
lth s
ervi
ces
Mas
s m
edia
• E
valu
atio
ns o
f mas
s m
edia
pro
gram
mes
sho
uld
focu
s on
thos
e th
at a
re c
ompr
ehen
sive
, hav
e th
epo
tent
ial f
or a
chie
ving
pop
ulat
ion
effe
cts
and
use
stro
ng q
uasi
-exp
erim
enta
l des
igns
to b
uild
a c
ase
for
infe
rrin
g ca
usal
ityG
eog
rap
hic
ally
def
ined
co
mm
un
itie
s•
Eva
luat
ion
and
oper
atio
ns r
esea
rch
need
to b
e co
re e
lem
ents
of p
rogr
amm
es ta
rget
ing
youn
g pe
ople
and
the
com
mun
ity a
t lar
ge•
Thi
s re
sear
ch s
houl
d pa
y pa
rtic
ular
atte
ntio
n to
iden
tifyi
ng c
ondi
tions
for
effe
ctiv
enes
s am
ong
vario
uspo
pula
tions
(su
ch a
s, y
oung
men
and
you
ng w
omen
) an
d lo
catio
ns (
such
as
rura
l or
urba
n ar
eas)
Yo
un
g p
eop
lem
ost
at
risk
• R
esea
rch
is n
eede
d to
iden
tify
the
spec
ial n
eeds
of t
hese
you
ng p
eopl
e in
con
tras
t to
thos
e of
adu
ltsin
ord
er to
impr
ove
indi
cato
rs th
at c
an b
e us
ed fo
r m
onito
ring
and
eval
uatio
na
ST
Is =
sex
ually
tran
smitt
ed in
fect
ions
.
92-4-120938-0_CH10_338

Interventions classified as “Ready” also need to be widely implemented butat the same time supported by carefully conducted evaluations and monitor-ing, and operations research. Programme developers and researchers need towork together to achieve these aims, and this collaboration will ensure thatyoung people benefit from these interventions and, at the same time, that theirimplementation contributes to the evidence base so that others can learn fromthese experiences. For interventions classified as “Go” and “Ready” the re-views in this series have emphasized the need for much greater clarity aboutexpected outcomes and about what is being done and how it is being done.However, the challenge is to accelerate action towards the global goals, andincreased resources are only likely to become available if there is wide con-sensus about what needs to be done and if collectively we can demonstratethat it is doable on a large scale in a sustainable way.
The future research agenda is substantial. However, many of the priorityquestions that need to be answered are now much clearer. Our hope is that ifa similar exercise were to be conducted in 5 years’ time, a much greaternumber of interventions would either be in the “Go” or “Do not go” cate-gories. This would provide implementers with clearer evidence-based guid-ance to inform their decisions, and would also ensure that resources availablefor prevention are used effectively.
Acting on the recommendations of this review will have a significant impacton preventing the transmission of HIV among young people, which in turnwill have wide-ranging implications for the health and development of indi-viduals, families, communities and countries around the world.
Acknowledgements
We would particularly like to thank Danny Wight for his helpful commentson an earlier draft of this paper, and to thank him and the other participantsof the June 2005 Chavannes meeting for their contributions to identifying andrefining the conclusions and recommendations from the reviews included inthis report. Those people are: Carlos Cáceres, Michel Carael, Kim Dickson,Ashok Dylachand, Mahesh Mahalingam, Elizabeth Mason, Jotham Musin-guzi, Zhenzhen Zheng.
References
1. UNAIDS. AIDS epidemic update 2005. Geneva, UNAIDS, WHO, 2005.
2. UNICEF, UNAIDS, WHO. Young people and HIV/AIDS – opportunity in crisis.New York, UNICEF, 2002.
3. National Research Council, Institute of Medicine. Growing up global: thechanging transitions to adulthood in developing countries. Washington, DC,National Academy Press, 2005.
339
92-4-120938-0_CH10_339

4. Aggleton P, Rivers K. Preventing HIV: behavioural interventions with youngpeople, 1997 (http://www.id21.org/insights/insights22/insights-iss22-art05.html).
5. Kirby D, Laris BA, Rolleri L. Impact of sex and HIV education programs onsexual behavior in developed and developing countries. Research TrianglePark, NC, Family Health International YouthNet Program, 2005. (YouthResearch Working Paper No. 2.)
6. WHO, UNFPA, UNAIDS. Achieving the global goals: access to services., 2003(http://www.who.int/child-adolescent-health/publications/ADH/ISBN_92_4_159132_3.htm)
7. Peersman G, Grimley Evans J. Interventions for preventing HIV infection inyoung people in developing countries. Cochrane Database of SystematicReviews, 2002, (2):CD003649. (Protocol.)
8. UNAIDS. Resource needs for an expanded response to AIDS in low- andmiddle-income countries, 2005 (http://data.unaids.org/Publications/IRC-pub06/ResourceNeedsReport_en.pdf).
9. UNAIDS. The road towards universal access (http://www.unaids.org/en/Coordination/Initiatives/default.asp).
10. Weiss C. Research and policy-making: a limited partnership. In: Heller F, ed.The use and abuse of social science. London, Sage, 1986.
11. Gregson S et al. HIV decline associated with behavior change in easternZimbabwe. Science, 2006, 311:664-666.
12. Global Campaign for Education. Deadly inertia: a cross-country study ofeducational responses to HIV/AIDS, 2005 (http://www.campaignforeducation.org/resources/Nov2005/ENGLISHdeadlyinertia.pdf).
13. Global HIV Prevention Working Group. Access to HIV prevention: closing thegap, 2003 (http://www.gatesfoundation.org/nr/downloads/globalhealth/aids/PWGFundingReport.pdf).
14. Hayes RJ et al. The MEMA kwa Vijana project: design of a community-randomised trial of an innovative adolescent sexual health intervention in ruralTanzania. Contemporary Clinical Trials, 2005, 26:430-442.
15. Okonofua FE et al. Impact of an intervention to improve treatment-seekingbehavior and prevent sexually transmitted diseases among Nigerian youths.International Journal of Infectious Diseases, 2003, 7:61-73.
16. Kim YM et al. Promoting sexual responsibility among young people inZimbabwe. International Family Planning Perspectives, 2001, 27:11-19.
17. loveLife. loveLife 2004: report on activities and progress. Cape Town,Parklands, loveLife, 2004.
18. Brieger W et al. West African Youth Initiative: outcome of a reproductive healtheducation program. Journal of Adolescent Health, 2001, 29:436-446.
19. Habicht JP et al Evaluation designs for adequacy, plausibility and probability ofpublic health programme performance and impact. International Journal ofEpidemiology, 1999, 28:10-18
20. Buse K. Political environment, policies and outcomes related to HIV/AIDS andyoung people, 2005 (unpublished data presented at the Evidence for Policiesand Programmes to Achieve the Global Goals on HIV/AIDS and Young People
340
92-4-120938-0_CH10_340

meeting: 8-11 March 2005), available from WHO Department of Child andAdolescent Health and Development.
21. Greene ME, Houvras I. Policy development supporting adolescent and youthsexual and reproductive health: nine countries’ experiences and collaborationswith UNFPA, 2004. (Unpublished document). (Available [email protected].)
22. Rosen JE. Formulating and implementing national youth policy: lessons fromBolivia and Dominican Republic. Washington, DC, Focus on Young Adults,2000.
23. Youth-policy.com. Youth reproductive health policy database (http://www.youth-policy.com/compendium.cfm).
24. Schulz K et al. Empirical evidence of bias dimensions of methodological qualityassociated with estimates of treatment effects in controlled trials. Journal of theAmerican Medical Association, 1995, 273:408-412.
25. Guyatt GH et al. Randomized trials versus observational studies in adolescentpregnancy prevention. Journal of Clinical Epidemiology, 2000, 53:167-174.
26. Terris-Prestholt F et al. From trial intervention to scale-up: costs of anadolescent sexual health program in Mwanza, Tanzania. Sexually TransmittedDiseases (in press).
27. Organisation for Economic Co-operation and Development. Policy brief:poverty and health in developing countries: key actions, 2003 (http://www.oecd.org/LongAbstract/0,2546,en_2649_201185_18514160_1_1_1_1,00.html).
28. Pawson R, Tilley N. Realistic evaluation. London, Sage, 1997.
29. Catania JA et al. Methodological problems in AIDS behavioral research:influences on measurement error and participation bias in studies of sexualbehavior. Psychological Bulletin, 1990, 108:339-362.
30. Plummer ML et al. “A bit more truthful”: the validity of adolescent sexualbehaviour data collected in rural northern Tanzania using five methods.Sexually Transmitted Infections, 2004, 80 Suppl 2:S49-56.
341
92-4-120938-0_CH10_341

92-4-120938-0_CH10_342

Glossary
Adolescents10-19 year olds.
Before-after studyAn intervention study design in which one or more outcomes of interest aremeasured in a population before and after the introduction of an interven-tion. This intervention study design does not include a control populationwho do not receive the intervention.
Case-Control StudyAn observational study design that starts with the identification of individ-uals with the outcome of interest, such as a disease (cases), and individualswithout the outcome of interest (controls). The frequencies of exposures topotential risk or protective factors for the outcome of interest are comparedin cases and controls.
Cluster randomized trial (CRT)A specific type of randomized controlled trial in which groups of individ-uals, such as whole communities, are randomly allocated to the interven-tion and comparison (control) arms of the trial.
Cohort studyAn observational study in which individuals who do not have the outcomeof interest are identified as either being exposed or not being exposed to apossible risk or protective factor for the outcome of interest, and are thenfollowed up over time to measure the incidence of the outcome of interest,such as the development of a disease.
Cross-sectional studyAn observational study in which the frequency of one or more outcomes ofinterest (and/or exposures) is measured in a population at one point in time.
InterventionA defined set of activities that are implemented to achieve specified outcomesin a target population. Examples could include trained teachers delivering aseries of classes on sexual and reproductive heath to students, or a series of
343
92-4-120938-0_GLOSSARY_343

television “spots” to promote abstinence and/or condom use among youngpeople.
Intervention studyA study in which an intervention is assigned to individuals or to clusters ofindividuals and the frequency of the outcome(s) of interest is measured toassess the effect of the intervention. Examples of intervention study designsinclude before-after, time series, quasi-experimental, and randomizedcontrolled trials (including cluster randomized trials)
Intervention typeA group of interventions sharing common characteristics. In the systematicreviews in this report, similar interventions have been grouped into these“intervention types” based on key choices that policy makers and programmemanagers need to make. Examples include:
1. Curriculum-based interventions in schools, with characteristics thathave been found to be effective in developed country settings, and thatwere adult-led
2. Mass media interventions with messages delivered through the radio,television and through other media (eg. print media)
Observational studyA study design in which the distribution of both exposures and outcomes ofinterest are measured without the investigator attempting to influence them.
ProgrammeA set of interventions implemented on a large scale, such as a national ado-lescent health programme or a national AIDS control programme.
ProjectThe implementation of a particular intervention or interventions in a specificlocal setting.
Quasi-experimental studyAn intervention study design in which an intervention is assigned to someindividuals or clusters of individuals (intervention group) and not to others(comparison or control group) in a non-random manner. The frequency of theoutcome(s) of interest is measured in both intervention and control groups inorder to assess the effect of the intervention. Quasi-experimental studies in-clude studies where data are collected after an intervention has been imple-mented, before and after an intervention has been introduced, or at severalpoints in time after an intervention has been introduced. The key issue is thatsimilar data on the outcome(s) of interest are collected in both interventionand control groups, but that the individuals or clusters of individuals have
344
92-4-120938-0_GLOSSARY_344
been assigned to either receive or not receive the intervention in a non-randommanner.
Randomized controlled trial (RCT)An intervention study design in which individuals or groups of individuals(see cluster randomized trial) are randomly allocated either to receive(intervention arm) or not to receive (control or comparison arm) the inter-vention(s) under evaluation.
SettingThe situation in or through which the intervention is delivered, such as inschools, health services, geographically-defined communities, through massmedia, or among groups most at risk of HIV.
Strength of evidenceEach study of the effectiveness of an intervention contributes evidence. Inthis report, the strength of evidence that a study contributes has been definedas depending on a combination of the quality of the intervention, the evalu-ation design and its implementation. The evaluation designs have beenweighted, with increasing weight being assigned to study designs on a hier-archy from adequacy, to plausibility and probability.
Structural interventionAn intervention that aims to change underlying determinants of risk, vul-nerability or disease, such as interventions that aim to decrease poverty,improve education, or increase employment. Such interventions are some-times known as ‘upstream’, or ‘environmental’ interventions.
Time series studyAn intervention study design in which one or more outcomes of interest aremeasured at several points in time in a population receiving an interven-tion. This design of intervention study does not include a control populationwho do not receive the intervention.
Threshold of evidence for widespread implementationThe minimum strength of evidence needed to be able to recommendwidespread implementation of a specific intervention type within a partic-ular intervention setting. The threshold of evidence depends on the feasibility(including cost), potential for adverse outcomes, acceptability, potential sizeof effect and potential for other health or social benefits of that interventiontype.
Young people10-24 year-olds.
Youth15-24 year-olds.
345
92-4-120938-0_GLOSSARY_345

92-4-120938-0_GLOSSARY_346

ACKNOWLEDGEMENTS:
The authors of the chapters in this report have acknowledged those peoplewho made specific contributions to their respective chapters. In addition theeditors would like to thank the following people who, along with the authorsof specific chapters, have contributed to this report by reviewing and com-menting on drafts of the chapters, providing ideas and support for the overallSteady, Ready, GO project, or participating in the preparatory meetings(Talloires, France, May 2004; Gex, France, March 2005; Chavannes,Switzerland, June 2005): Professor Peter Aggleton, University of London,United Kingdom; Dr John D. Berman, AIDSMark, Population Services In-ternational, USA; Dr Ann Biddlecom, The Alan Guttmacher Institute, USA;Dr Anthony Bloome, Leadership Program in AIDS, World Bank, USA;Dr Katherine Bond, The Rockefeller Foundation, Thailand; Dr HeatherBoonstra, The Alan Guttmacher Institute, USA; Dr Kent Buse, LSHTM,United Kingdom; Dr Carlos F. Cáceres, Universidad Peruana CayetanoHeredia, Peru; Dr Ward Cates, Family Health International, USA; Ms ShantiConly, U.S. Agency for International Development, USA; Dr FrancesCowan, University of Zimbabwe, Zimbabwe; Dr Siobhan Crowley, WHO,Switzerland; Dr Mehboob Dada, UNESCO, France; Mr Paul de Lay,UNAIDS, Switzerland; Dr Kim Eva Dickson, WHO, Switzerland; Dr A.Dyalchand, Institute of Health Management Pachod (IHMP), India; Mr BillFinger, Family Health International, USA; Dr Annette Gabriel, GTZ,Germany; Dr Anna C. Gorter, Instituto CentroAmericano de la Salud,Nicaragua; Dr Catherine Hankins, UNAIDS, Switzerland; Mr DavidHarrison, loveLife, South Africa; Dr. John Howard, Ted Noffs Foundation,Australia; Dr Myat Htoo Razak, WHO, Thailand; Professor Anne M.Johnson, University College London, United Kingdom; Professor Knut-IngeKlepp, University of Oslo, Norway; Dr Marie Laga, Institute of TropicalMedicine, Belgium; Dr Erma Manoncourt, UNICEF, Egypt; Mr MaheshMahalingam, UNAIDS, Switzerland; Dr Rafael Mazin, PAHO, USA;Dr Kristin Mmari, Johns Hopkins University, USA; Ms Claire Mulanga,ILO, Switzerland; Dr Joanna Nerquaye-Tetteh, Planned ParenthoodAssociation of Ghana, Ghana; Mr Rick Olson, UNICEF, USA; Dr JulittaOnabanjo, UNFPA, USA; Dr Audrey Pettifor, University of North Carolina,
347
92-4-120938-0_ACKNOWLEDGEMENT_347

USA; Dr Arletty Pinel, UNFPA, USA; Dr Elizabeth Pisani, LSHTM, UnitedKingdom; Dr Leah Robin, CDC, USA; Professor John Santelli, ColumbiaUniversity, USA; Ms Sharifah Tahir, YouthNet/FHI, USA; Dr RichardSteen, WHO, Switzerland; Dr C. Johannes van Dam, Population Council,USA; Professor Cesar G Victora, Universidade Federal de Pelotas, Brazil;Dr Merlin L Wilcox, Liverpool School of Tropical Medicine, UnitedKingdom; Professor Zhenzhen Zheng, Chinese Academy of Social Sciences,China.
The editors would like to make special mention of the following people whomade substantial intellectual contributions throughout the preparation ofthis report: Professor Michel Carael, Free University of Brussels, Belgium;Professor Richard Hayes, LSHTM, United Kingdom; Ms Jane Hughes, ThePopulation Council, Vietnam; Ms Aurorita Mendoza, UNAIDS, Nepal;Dr Jotham Musinguzi, Ministry of Finance, Planning & Economic Develop-ment, Uganda; Dr Danny Wight, Medical Research Council Social & PublicHealth Sciences Unit, Scotland.
The work would not have been accomplished without the conscientious ad-ministrative assistance of Ms Anita Blavo of the Department of Child andAdolescent Health and Development (CAH), World Health Organization,and the support of Dr Hans Troedsson and Dr Elizabeth Mason of CAH.
Special thanks to colleagues in the Department of Knowledge Managementand Sharing (KMS), WHO: Dr Laragh Gollogly, Ms Kaylene Selleck andMr David Bramley who made the final arrangements for this report possible,and to Ms Miriam Pinchuk for her careful technical editing of the manuscripts.
Grateful acknowledgment is given to the UNAIDS Inter-agency Task Teamon HIV/AIDS and Young People for initiating the preparation of this report,and to the financial contributions from the Canadian International Develop-ment Agency, UNAIDS, UNFPA, UNICEF, and the United States Agencyfor International Development, as well as core support provided by WHO.
348
92-4-120938-0_ACKNOWLEDGEMENT_348




















