NSP AIDS 2011 2015
73
MALAYSIA National Strategy Plan on 2011 – 2015 2011 – 2015 MINISTRY OF HEALTH 2011 National Strategic Plan on HIV and AIDS
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of NSP AIDS 2011 2015

MALAYSIA
National Strategy Plan on HIV and AIDS 2011 – 2015
National Strategy Plan onHIV and AIDS2011 – 2015
MINISTRY OF HEALTH 2011
National Strategic Plan onHIV and AIDS
i
MALAYSIA
National Strategy on HIV and AIDS 2011 – 2015
Acknowledgement: We acknowledge with gratitude and sincere thanks the significant inputs of MOH technical staff at Sector HIV/STI, State and District Level as well as to the UN family in Malaysia for their endless contribution. We are deeply indebted to officials of Government of Malaysia particularly the Ministry of Health, other government agencies such as Ministry of Women, Family and Community Development, Malaysia Department of Islamic Development (JAKIM), National Anti-Narcotic Agency, Royal Police of Malaysia, Legal Advisor, Ministry of Higher Learning, Ministry of Education, Ministry of Human Resource, Ministry of Defence, Ministry of Home Affairs and many others; and all Non-Government Organizations particularly Malaysia AIDS Council and its Partner Organizations, Academia and individuals for their views and valuable advice.
We greatly admire the dedication of all sectors, both government and non-government for their countless support.
i
National Strategic Plan on HIV and AIDS
ii
Table of Contents Acknowledgement
Table of Contents
…………………………………………………………………………..……
.................................................................................…
I
ii
Forward by the Director General of Health ………………………………………………………………………………… iii
List of Figures and Tables ………………………………………………………………………………………………………… iv
Acronyms and abbreviations ……………………………………………………………………………………………………….. v
Glossary of terms and definition used in this document …………………………………………………………. vi
Executive Summary ……………………………………………………………………………………………………………………… 1
Chapter 1: Introduction …………………………………………………………………………………………………………… 3
1.1 Background
1.2 Rationale
1.3 Developing the National Strategy on HIV and AIDS 2011 – 2015
Chapter 2: The Malaysian HIV Epidemic: Situation, response and challenges ………………….. 6
2.1 The HIV situation in the country
2.2 The national response
2.3 Issues and challenges
Chapter 3: The National Strategic Plan on HIV and AIDS 2011 – 2015 ………………………………. 17
3.1 Guiding principles
3.2 Goal and specific objectives
3.3 Strategic targets
3.4 Strategies
Chapter 4: Coordination and Implementation ………………………………………………………………………. 24
Chapter 5: Resource Mobilisation …………………………………………………………………………….…………… 28
Chapter 6: Monitoring and Evaluation …………………………………………………………………………………. 30
Annex 1: Framework of the National Strategic Plan on HIV and AIDS 2011 – 2015 ………. 37
Annex 2: National Action Plan on HIV and AIDS 2011 – 2015 ………………………………………….. 43
Annex 3: Target Proposal …………………………………………………………………………………………………… 54
Annex 4: Performance Indicators for the National Strategic Plan on HIV and AIDS 2011 – 2015
………. 57
Annex 5: Technical Team …………………………………………………………………………………………………… 64
ii
National Strategic Plan on HIV and AIDS2011 – 2015

iii
FFOREWORD
HIV/AIDS was first diagnosed in Malaysia in 1986. By the end of 2010, there was a cumulative figure of 91,362 HIV cases reported to the Ministry of Health out of which 77,064 people living with HIV. The epidemic peaked in 2002 with the rate of 28.5 per 100,000 population. Since then, there has been a steady decline and achieved at 12.8 per 100,000 population in 2010. The Government aims to reduce to 11.0 per 100,000 population by 2015.
With this NSP 2011-2015, we envisage that this target will be reached within the next couple of years and we aim to see a more significant decline by 2015. On reaching this target, it is important that comprehensive HIV prevention, treatment, care and support towards HIV/AIDS should be in place through strong political will, comprehensive policies and participation of the community.
The Government is confident that the new NSP 2011 – 2015 will be able to guide Malaysia towards fulfilling the objectives of the Millennium Development Goals (MDG), UNGASS and Universal Access (UA) targets. It is also intended to reflect the country’s participation in fulfilling these international commitments.
In spite of significant achievements over the years, yet there is even more critical work ahead for all of us and Malaysia is committed to the United Nations pledge ‘Getting to Zero’ - zero new HIV infections, zero discrimination and zero AIDS-related deaths. Indeed, there is an urgent and greater need for a more concerted and coordinated effort between the multiple sectors concerned.
Thank you.
DATO’ SRI DR. HASAN ABDUL RAHMAN
Director General of Health Malaysia
iii
National Strategic Plan on HIV and AIDS2011 – 2015

List of Figures and Tables Figures
Figure 1: Reported AIDS-related deaths, Malaysia 1985 - 2010 16 Figure 2: Reported HIV cases in Malaysia 16 Figure 3: HIV Prevalence (%) among key at-risk populations 18 Figure 4: National HIV and AIDS Policy Framework 32 Figure 5: Stakeholders in the Malaysian HIV response 34 Figure 6: Monitoring and Evaluation Process 39 Figure 7: Monitoring and Evaluation Reporting Structure 41 Tables
Table 1: Overview of the Malaysian HIV Epidemic (as of Dec 2010) 15 Table 2: Findings from bio-behavioural studies conducted in 2009 18 Table 3: Estimates of the Malaysian HIV Epidemic 2010 19 Table 4: Source of approximate AIDS expenditure 2008 – 2010 37 Table 5: Programme coverage targets (2011 & 2015) 38
iv
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategic Plan on HIV and AIDS2011 – 2015
Acronyms and abbreviations AIDS Acquired Immune Deficiency Syndrome ART Anti-Retroviral Therapy CBO Community-based Organisation DIC Drop-In Centre DRC Drug Rehabilitation Centre FBO Faith based organisation HAART Highly Active Anti-Retroviral Therapy HIV Human Immunodeficiency Virus IDU Injecting Drug Use/User IBBS Integrated Bio-Behavioural Surveillance MAC Malaysian AIDS Council MARPs Most At Risk Populations M&E Monitoring and Evaluation MDGs Millennium Development Goals MMT Methadone Maintenance Therapy MOH Ministry of Health MSM Men who have sex with men NGO Non-governmental organisation PTCT Parent-to-child transmission MWFCD Ministry of Women, Family and Community Development NADA National Anti Drug Agency NAP National AIDS Programme NGO Non-Government Organisation NSEP Needle and Syringe Exchange Programme NSP National Strategic Plan on HIV/AIDS PITC Provider Initiated Testing and Counselling PLHIV People Living With HIV PMTCT Prevention of Mother-to-Child Transmission SRH Sexual Reproductive Health STI Sexually Transmitted Infection SW Sex Worker TB Tuberculosis TG Transgender Person UA Universal Access UNAIDS Joint United Nations Programme on HIV/AIDS UNDP United Nations Development Programme UNICEF United Nations Children’s Fund UNFPA United Nations Population Fund UNGASS United Nations General Assembly Special Session UNHCR United Nations High Commissioner for Refugees UNTG United Nations Theme Group on HIV VCT Voluntary Counselling and Testing WHO World Health Organisation
v
National Strategic Plan on HIV and AIDS2011 – 2015
i
Glossary of terms and definitions used in this document Civil society refers to NGOs and informal groups (may include People Living with HIV (PLHIV), MARPs, vulnerable populations, women’s organisations, faith-based organisations and advocacy groups) usually apolitical. Cost estimates are financial estimations of how much is envisaged to be spent for a particular programme, usually not be considered as detailed budgets. (Detailed budgets are prepared for usually for Annual Work Plans itemising details of the budget). Coverage is a measure of whether a programme is working in the right places and reaching its target population. For a programme to have a maximum impact on HIV prevention among most-at-risk populations, it must do both. Evaluation is a rigorous, scientifically-based collection of information about programme activities, characteristics, and outcomes that determine the merit or worth of a specific programme. Evaluation studies are used to improve programmes and inform decisions about future resource allocations. Impact evaluation looks at the rise and fall of disease incidence and prevalence as a function of HIV/AIDS programmes. The effects (impact) on entire populations can seldom be attributed to a single programme or even several programmes, therefore, evaluations of impact on populations usually entail a rigorous evaluation design that includes the combined effects of a number of programmes for at-risk populations. Input indicators are used to monitor the amount and level of resources made available to the implementation of the National Strategic Plan on HIV and AIDS. These can be sourced from public, private and international sources. This indicator is critical in evaluating the sustainability of programmes and interventions. Impact mitigation refers to programmes and activities which work towards decreasing the negative impact and direct consequences of HIV on MARPs, vulnerable persons and People Living with HIV such as illness, loss of employment, discrimination and death. Impact indicators are used to evaluate the impact of programmes and interventions to the overall epidemic. These are measured using HIV prevalence amongst MARPs as well as the general population. Incidence is defined as new infections per population at risk in a specified period of time. Injecting drug users (IDU) refers to drug users who inject drugs and use drug equipment. Intervention is a set of activities implemented by a project and that are often provided at the community level. Men who have Sex with Men (MSM). Many men who have sex with men (MSM) engage in anal sex and often have multiple sexual partners; male-to-male sexual transmission is an issue of great importance to HIV prevention. Monitoring is the routine tracking of key elements of a programme or project and its intended outcomes. It usually includes information from record keeping and surveys – both population and client-based.
vi
Outcome indicators are used to measure the effectiveness of implemented programmes in changing risk behaviours among most at risk populations, encourage prevention, treatment, care and support seeking behaviours. This indicator is critical to evaluate the effectiveness of programmes. Output indicators are linked closely to the coverage of programmes of MARPs. This is often measured by the coverage achieved through behavioural change communication programmes, harm reduction interventions such as access to needles, syringes and condoms, utilisation of VCT, treatment, care and support services. This indicator is critical to evaluate the development and implementation of programmes. Outreach services are those which take health information and services into the communities where most-at-risk populations live, or place where they congregate (such as back lanes where injecting drug use occurs or where pickups for transactional sex occur). Prevalence is defined as the total number of cases of HIV at a point in time per base population. Programme refers to an overarching national or subnational response to a disease and generally includes a number of projects. Project refers to a mix of interventions with activities supported by resources and that often operates at the community level. Transgender persons are refers to persons whose gender identity, expression, or behavior differs from the norms expected from their birth sex. The term “mak nyah” is commonly used within the Malaysian context to refer to persons of this category. Universal Access refers to the global commitment to scale up access to HIV treatment, prevention, care and support which all governments agreed to when they adopted the Political Declaration on HIV/AIDS at the UN General Assembly in 2006. This involves the setting up of ambitious national targets set against key outcome areas – such as ART coverage, prevention of mother to child transmission, coverage of prevention programmes for most at risk groups and testing coverage. Young person/ people refer to individuals within the ages of 15 – 24 years old.
vii
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
1
Executive Summary
The National Strategic Plan on HIV and AIDS 2011 – 2015 (NSP) runs parallel and is harmonised with the aims and objectives of the 10th Malaysian Plan (10MP) for 2011 – 2015. This NSP will continue to place strong emphasis on strengthening the multi-sectoral collaboration undertaken under the previous strategic plans. The HIV epidemic in Malaysia is driven by injecting drug use and sexual transmission occurring among most at risk populations such as drug users, sex workers, men who have sex with men and transgender persons. Operational research have shown that overlapping of injecting drug use and high risk sexual behaviour is occurring resulting in HIV infection between different segments of the populations. Studies and consensus discussions among experts have concluded that HIV in Malaysia is predicted to be increasingly spread through sexual transmission, though the infections acquired through injecting drug use (and other means e.g. vertical transmission) need to be monitored as well.
The review of the first National Strategic Plan on HIV and AIDS formulated in 1998 was done in 2001. The development of the National Strategic Plan on HIV/AIDS 2006 – 2010 in 2005 led to its implementation and use over the past five years, whilst this document (NSP 2011 – 2015) replaces the latter strategic document.
The lessons learnt and experience gained in the implementation and monitoring of the previous NSPs have shown that there are still a lot of opportunities to strengthen the commitment of all stakeholders. Various opportunities need to be enhanced to achieve greater harmonisation, coordination and alignment; maintain and sustain high levels of funding; achieve greater programme coverage, effectiveness, and efficiency; and to continue the provision of affordable treatment to those who need it. The NSP 2011–2015 intends to build upon the achievements and progress made during implementation of the previous strategic framework as well as address emerging issues and challenges. The National Strategy on HIV and AIDS 2011 – 2015 comprises three main components: 1. The National Strategic Plan on HIV and AIDS 2011 - 2015 2. The National Action Plan on HIV and AIDS 2011 – 2015 3. The national monitoring and evaluation framework
The goals of the Malaysian NSP 2011 - 2015, are:- 1. To prevent and reduce the risk and spread of HIV infection 2. Improve the quality of life of People Living with HIV 3. Reduce the social and economic impact resulting from HIV and AIDS on the individual, family and
society.
1
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
2
The specific objectives of the NSP2011-2015 are:- 1. To further reduce by 50% the number of new HIV infections by scaling up, improving upon and
initiating new and current targeted and evidence based comprehensive prevention interventions
2. To increase coverage and quality of care, treatment and support for People Living with HIV and those affected
3. To alleviate the socioeconomic and human impact of AIDS on the individual, family, community and society.
4. To create and maintain a conducive and enabling environment for government and civil society to play meaningful and active roles in decreasing stigma and discrimination.
5. To further increase general awareness and knowledge of HIV, and reduce risk behaviour for at risk and vulnerable populations.
These objectives can only be meaningfully achieved and sustained under the commitments to UA and MDG after programmes worked towards achieving 80% service coverage among most at risk populations where 60% practice safe behaviours. To achieve these objectives, the NSP has adopted the following multisectoral strategies which provided an appropriate balance between prevention, treatment, care and support, namely:
Strategy 1 Improving the quality and coverage of prevention programmes among most at risk
and vulnerable populations
Strategy 2 Improving the quality and coverage of testing and treatment
Strategy 3 Increasing the access and availability of care, support and social impact mitigation programmes for People Living with HIV and those affected.
Strategy 4 Maintaining and improving an enabling environment for HIV prevention, treatment, care and support.
Strategy 5 Increasing the availability and quality of strategic information and its use by policy makers and programme planners through monitoring, evaluation and research.
The execution and fulfilment of the following strategies will require renewed and strengthened commitment and multisectoral partnership of government, civil society and private sector stakeholders to work together in the spirit of consultation and collaboration under the 1Malaysia initiative.
2
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
3
CHAPTER 1 Introduction
1.1 Background It is estimated that 34 million people currently live with HIV globally, and each year, it is estimated that 2.7 million more people become infected with HIV and 2 million die of AIDS. The 2009 Commission on AIDS in Asia Report stated that more than 5 million Asians currently live with HIV, and approximately 440,000 become infected each year. Yearly, about 300,000 persons die of AIDS-related diseases. The report indicates that the pandemic in Asia is entering its second growth phase, which is expected to result in increasing HIV prevalence and nearly 10 million Asians infected if prevention efforts are not expanded or fully implemented. The Government of Malaysia is concerned by the continued spread of HIV in the country, particularly amongst most at risk populations (MARPs) identified mainly as injecting drug users (IDUs), sex workers (SW), transgender persons (TG) and men who have sex with men (MSM). The National Strategic Plan on HIV/AIDS (NSP) 2006-2010, which was developed by the Government and drafted with the involvement of key civil society representatives in 2005 / 2006, incorporated a multi-sectoral strategy covering issues from young people’s vulnerability to the delivery of healthcare services and antiretroviral treatment. Through this strategy, the Malaysia has made much progress in HIV prevention, particularly utilising the harm reduction approach which has begun to yield results in reducing the spread of the HIV epidemic. People living with HIV and in need of treatment are able to access first line treatment at no cost whilst the second line regimes at heavily subsidised as well. While NSP 2006 – 2010 has made the promotion and implementation of harm reduction and the intervention with injecting drug users as the focus of its HIV prevention interventions, the NSP 2011 - 2015 will need to deal with a variety of new challenges, among which are expected higher incidences of sexual transmission of HIV/AIDS to be detected and the focus of concentrated epidemic that Malaysia is being classified with the emergence of populations at risk. 1.2 Rationale Over the past five years, increased levels and additional sources of funding have made it possible to expand or upscale the support of HIV and AIDS interventions in the region, giving Malaysia avenues to accelerate the national response to the epidemic. Nevertheless, there remain gaps and opportunities for improvement in certain identified programmes. The 2008 and 2010 UNGASS Country Progress Reports identified certain challenges in the national response to HIV and AIDS. These reports have also recognised the significant progress and positive
3
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
4
developments which have occurred in the last few years in Malaysia for example i.e. harm reduction interventions, the affordable treatment for PLHIVs, and the wide availability voluntary counselling and testing services. The government and the key stakeholders have agreed that the next National Strategy on HIV should be able to sustain and upscale the abovementioned achievements and commitments, while at the same time be able to address concerns and identified gaps as well as respond more effectively to the needs of its stakeholders, especially those of civil society and most at risk communities. The lessons learnt and experience gained in the implementation and monitoring of NSP 2006 – 2010 have also shown that there are opportunities could be tapped upon, namely to strengthen political commitment, to achieve greater harmonisation, coordination and alignment; maintain and sustain high levels of funding; and to continue the provision of affordable treatment to those who need it. The new strategic plan should achieve greater programme coverage amongst MARPs with high impact results, effectiveness, and efficiency. The NSP 2011–2015 intends to build upon the achievements and progress made during implementation of the previous strategic framework as well as address emerging issues and challenges which threaten the sustainability of the abovementioned gains. It is also intended to guide Malaysia towards achieving the Millennium Development Goals, UNGASS and Universal Access targets. 1.3 Developing the National Strategy on HIV and AIDS 2011 – 2015
1.3.1 The Ministry of Health initiated the process of multisectoral consultation in preparation of the NSP in May 2010. It was a matter of priority and concern for all key stakeholders that this National Strategy on HIV and AIDS would be able to capture as much of the issues, progress and challenges experienced by both Government and civil society stakeholders in the response to HIV in Malaysia.
1.3.2 An orientation and preparatory briefing on the NSP development process was organised by the Ministry of Health on 21 June 2010 for Government, civil society stakeholders and UN agencies. The intention was to ensure that all partners understood the process and were also able to participate and contribute to the substance and overall development of the National Strategy. The meeting also provided guidance for the consultations which would happen independently amongst the different MARPs communities.
1.3.3 Six technical working groups (TWG) consisting of government and NGO stakeholders, discussed and recommended key areas for response under the new National Strategy on HIV and AIDS; identified gaps in current interventions, technical skills, capacity building and financial requirements under the existing NSP; and provided input in identifying priority areas, programmes and targets for the next 5 years. Issue papers were submitted in the following areas: HIV prevention amongst IDUs; MSM, transgender persons, sex workers, intimate partners; prevention amongst other populations (at risk youth, migrants, refugees); Treatment and PLHIV; Impact mitigation through care and support; and enabling environment (advocacy, policy, strategic information, research and surveillance). The findings of the TWGs were presented, consolidated and integrated into the strategic framework at the first national consultative workshop with stakeholders.
4
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
5
1.3.4 The first and second consultative meetings to develop the national strategic framework and the national action plan took place on 5-6 August and 20-21 September respectively and were attended by various government bodies and representative of MARPS.
1.3.5 A costing and budgeting workshop was organised as 11-12 October to ensure that the cost of the proposed interventions and activities contained within the national action framework was able to be properly estimated. A cost standardisation exercise was also conducted on 19 October. A monitoring and evaluation workshop was also convened on 1-2 November to develop a common understanding of monitoring and evaluation and to discuss the development of a common framework for use of government and civil society stakeholders to monitor, evaluate and manage AIDS programme, the results of which would be used for managing the AIDS response, improving performance and revising the national strategy and action plan.
1.3.6 The completed drafts of the individual components of the National Strategy on HIV and AIDS 2011 - 2015, consisting of the National Strategic Plan on HIV and AIDS, National Action Plan 2011 – 2015 and the national monitoring and evaluation framework were presented during a national workshop on 10 November.
The approach utilising information sharing, inclusivity and consensus building for the development of the National Strategy on HIV and AIDS has enabled many of the new developments in the Malaysian national AIDS programme to be properly reflected in the strategic document. The setting of clear, prioritized and evidence-driven national priorities which respond to the evolving dynamics of the Malaysian HIV epidemic was dependent on much of the strategic information and research data which became available over the past two years. Much of the research data utilised for priority originated from the efforts and work of civil society and community based organisations, working in partnership with Government agencies and academic institutions. Though obtaining data remains a continuing challenge, the inputs from government and civil society stakeholders have been critical in improving the understanding and response to the epidemic and form the backbone of the new strategy. The National Strategy on HIV and AIDS 2011 – 2015 was developed and prepared by the AIDS/STI Sector of the Disease Control Division, Ministry of Health. Technical support in the formulation and preparation of the consultation process, consolidation of inputs and drafting of the document was provided by the United Nations Theme Group on HIV and AIDS.
5
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
6
CHAPTER 2 The Malaysian HIV Epidemic: Situation, response and challenges
2.1 The HIV situation in the country The present As of December 2010, an estimated 80,922 people (Estimation & Projection Model – EPP) are currently living with HIV. By the end of 2010, Malaysia had a cumulative figure of 91,362 of HIV cases, 16,352 AIDS cases and 14,298 deaths, thus giving reported people living with HIV (PLHIV) of 77,064.
The annual number of reported new HIV cases by the Ministry of Health has been on a steady decline from a peak of 6,978 in 2002. In 2010, there were 3,652 new cases reported to the Ministry of Health, approximately halve of what was reported in 2002. The notification rate of HIV also continues to experience a decrease from 27.0 in 2003 to 23.4 in 2005 and to 12.8 cases per 100,000 population in 2010. Currently, there are 10 new reported cases of HIV each day with a ratio of 2 females for every 8 males reported. In 2010, an average of 5 persons acquired HIV through injecting drugs while 5 others were infected sexually.
Table 1: Overview of the Malaysian HIV Epidemic (as of Dec 2010)
Cumulative number of reported HIV infections since 1986 91 362
Cumulative number of reported AIDS related deaths since 1986 14 298
Estimated number of people living with HIV (EPP & Spectrum model 2010) 80 922
Reported number of people living with HIV 77 064
Cumulative number of women reported with HIV 8 759
Cumulative number of children under 13 with HIV 909
New HIV infections detected in 2010 3 652
AIDS related deaths in 2010 904
Number of PLHIV currently on ART in 2010 13 981
Estimated PLHIV needing ART (CD4 <350) (EPP & Spectrum model 2010) 30 600
Estimated adult (aged 15-49 years) HIV prevalence (EPP & Spectrum model 2010)
0.42%
Notification rate of HIV (per 100 000) 12.6 Source: Ministry of Health, 2011
6
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
7
The decline in the number of AIDS related deaths has been directly attributed to the introduction of more affordable and accessible first and second line antiretroviral (ARV) treatment. It has been estimated that by end of 2015, Malaysia will have an estimated 81,946 people living with HIV. Male continue to represent the majority (90%) of cumulative HIV cases in Malaysia. About 35% of reported infections are amongst young people between the ages 13-29 years old. Most reported infections occur among young heterosexual males, between the ages of 20 – 39 who inject drugs. However, in 2010 HIV infection through sexual transmission has exceeded the infection through injecting drug use. Children aged 13 years below consistently comprised 1% of cumulative total of HIV infections from 1986 to December 2010.
Figure 1: Reported HIV and AIDS-related deaths, Malaysia 1985 – 2010 Source: Ministry of Health, 2011
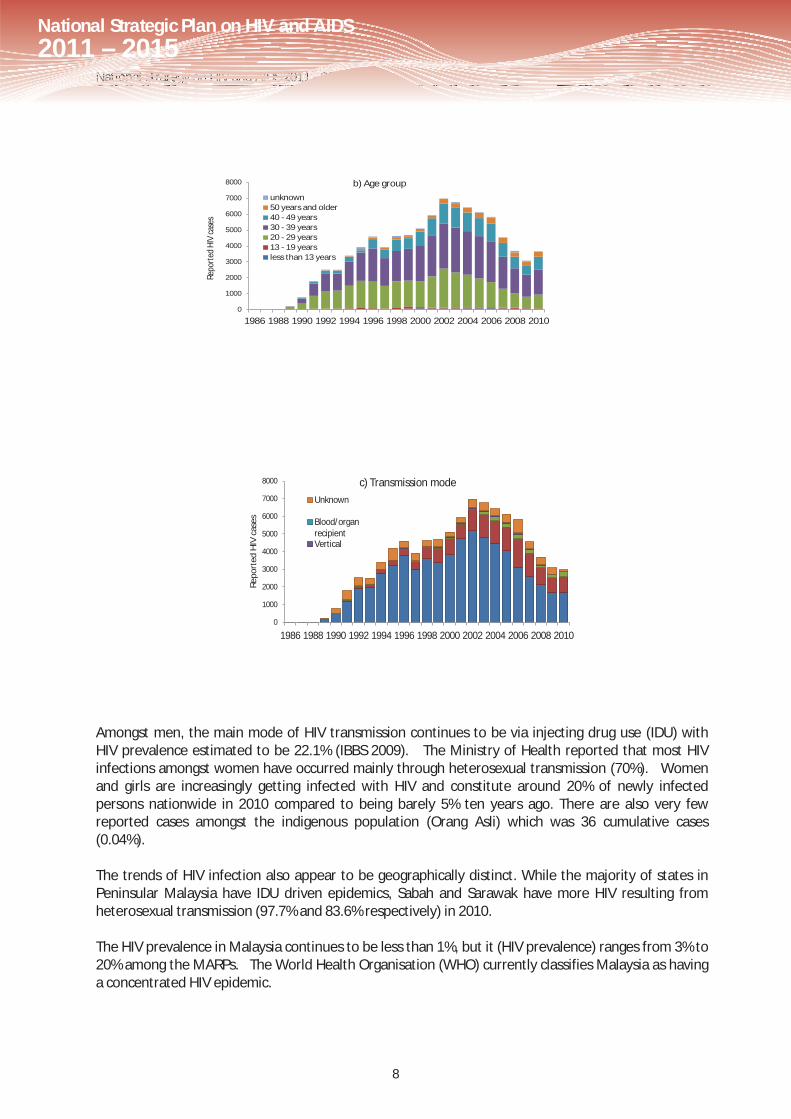
Figure 2: Reported new HIV cases in Malaysia, 1986 – 2010, disaggregated by sex, age group and transmission mode.
Source: Ministry of Health, 2011
7
National Strategic Plan on HIV and AIDS2011 – 2015
National Strategy on HIV and AIDS 2011 - 2015
8
0
1000
2000
3000
4000
5000
6000
7000
8000
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Repo
rted
HIV
case
s
b) Age group
unknown50 years and older40 - 49 years30 - 39 years20 - 29 years13 - 19 yearsless than 13 years
0
1000
2000
3000
4000
5000
6000
7000
8000
1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Repo
rted
HIV
cas
es
c) Transmission modeUnknown
Blood/organ recipientVertical
Amongst men, the main mode of HIV transmission continues to be via injecting drug use (IDU) with HIV prevalence estimated to be 22.1% (IBBS 2009). The Ministry of Health reported that most HIV infections amongst women have occurred mainly through heterosexual transmission (70%). Women and girls are increasingly getting infected with HIV and constitute around 20% of newly infected persons nationwide in 2010 compared to being barely 5% ten years ago. There are also very few reported cases amongst the indigenous population (Orang Asli) which was 36 cumulative cases (0.04%). The trends of HIV infection also appear to be geographically distinct. While the majority of states in Peninsular Malaysia have IDU driven epidemics, Sabah and Sarawak have more HIV resulting from heterosexual transmission (97.7% and 83.6% respectively) in 2010. The HIV prevalence in Malaysia continues to be less than 1%, but it (HIV prevalence) ranges from 3% to 20% among the MARPs. The World Health Organisation (WHO) currently classifies Malaysia as having a concentrated HIV epidemic.
8
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
9
Most at risk populations The HIV epidemic in Malaysia was initially driven by transmission among injecting drug users in the 1990s. During that period, up to 83% of annual newly detected HIV cases were attributed to injecting drug use. Cumulative reported cases of HIV transmission was predominantly among injecting drug use (70.6%), followed by heterosexual intercourse (16.9%) and homosexual contact (2.0%)., However, 2010 data indicates that 47.6% of new reported HIV cases for that year were attributed to injecting drugs while 48.5% was through sexual transmission (heterosexual and homosexual).
In 2002, it was decided that the existing HIV surveillance system, based on notification of newly diagnosed HIV infection and screening in sub-populations, needed further strengthening, especially to predict the course of the epidemic. The Ministry of Health decided to incorporate the use of behavioural surveillance studies into the existing system. Through discussions and consensus meetings among local experts, it was recommended that monitoring HIV risk behaviour could play a vital role in determining the future direction in the spread of HIV within the different most-at-risk populations. Behavioural Surveillance Surveys were adapted for this purpose beginning in 2004 which was later followed by the use of Integrated Bio-Behavioural Surveillance (IBBS) studies.
Figure 3: HIV Prevalence (%) among key at-risk populations (EPP estimates 2011)
Most-At-Risk Populations (MARPs) refers to specific people or populations whose practices or behaviours put them at greater risk of HIV infection include high rates of unprotected sexual partnerships, unprotected anal sex with multiple partners, and injecting drugs with shared equipment. Thus in Malaysia, the population groups where these behaviours are concentrated include: injecting drug users (IDUs); female sex workers (FSWs), clients of FSWs; men who have sex with men (MSM); and transgender persons (TG). Included within this category, are partners, and spouses of the abovementioned populations as well as any group documented or projected to have HIV prevalence over 5%. Vulnerable populations refer to persons subject to factors or conditions which increase the possibility of them engaging in risky behaviours. A person vulnerable to HIV can be defined as one who is susceptible to, or unable to protect themselves from, significant harm or exploitation linked with HIV infection. Vulnerable populations include various categories of young people (e.g. out of school youth, children of sex workers and injecting drug users, street children, young people in incarcerated settings, foster care and other institutional settings), migrant workers and refugee populations, and other undocumented persons.
TG (8.3%)
IDU (23.2%)
MSM (3.6%)
FSW (10.3%)
Client (1.5%)
IBBS IDU (22.1%)
IBBS FSW (10.5%)
IBBS TG (9.7%)
IBBS MSM (3.9%)
9
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
10
Table 2: Findings from bio-behavioural studies conducted in 2009
Source: Ministry of Health (2010). HIV Epidemic in Malaysia. Powerpoint presentation presented by Dr. Shaari Ngadiman, at 1st Consolidation and Consultation Workshop, 5-6 August 2010. Figure 4 above shows the HIV epidemic in Malaysia is driven by injecting drug use and sexual transmission occurring among MARPs. There is also clear evidence based on operational research that overlapping of injecting drug use and high risk sexual behaviour is occurring resulting in HIV infection between the different populations. Based on the evidence, the government has taken steps towards targeting increasing existing coverage of IDUs under the NSEP programmes. Relevant government healthcare facilities in recent years have also been upscaled the NSEP and MMT programmes thus eventually bringing down the costs of existing IDU related intervention programmes and activities. The future Based on recent HIV estimations and projections modelling conducted by the Ministry of Health, sexual transmission of HIV in Malaysia is predicted to be on the rise, while the newer cases of HIV infection through IDU are expected to plateau. The proportion of reported cases attributed to MSM and heterosexual route of transmission is slowly increasing which is consistent with the results of the HIV estimation and projections model for Malaysia, which was tabulated in 2011.
10
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
11
Table 3: Estimates of the Malaysian HIV Epidemic (EPP 2010)
2010 2015
Total People Living With HIV 80,922 81,946 Male 65,669 (81.1%) 62,898 (76.8%) Female 14,739 (18.9%) 19,048 (23.2%)
Total new infections/ year 7,516 6,699 Male 5,751 4,692 Female 1,766 2,007
Total AIDS related deaths/ year 6,741 6,335 Male 5,698 5,137 Female 1,042 1,199
Source: National Consensus Workshop on Estimation and Projection of the Malaysian HIV Epidemic (2011) The key findings from the estimation and projection 2011 (EPP) workshops are as follows:- 1 Since 2008, the estimated number of new HIV infections among IDUs appears stabilized.
2 For every single male detected with HIV, there are two other male cases which would go undetected.
3 The number of AIDS related deaths is expected to decrease in the next 3-5 years, as accessibility to antiretroviral treatment and preventive activities increased.
4 The number of women living with HIV is higher than previously thought. It estimated that there is 1 female newly infected with HIV for every 3 males infected.
5 Revised needs and coverage estimates based on the adoption of WHO’s recommended criteria of CD4<350 for ARV treatment initiation, indicate a higher financial allocation is needed for the provision of ARV.
It is expected that the evolving phenomena of the HIV epidemic (particularly that of sexual transmission of the disease), will pose newer challenges for HIV programming taking into consideration Malaysia’s cultural and religious context and sensitivities. 2.2 The national policy and programmatic response The Malaysian HIV response over the past five years has been guided by the National Strategic Plan on HIV/AIDS 2006 – 2010 which was drafted via multi-sectoral approach incooperating issues ranging from young people’s vulnerability to the delivery of healthcare services and ARV treatment. This framework provided a common ground and emphasis on an integrated and comprehensive approach addressing the needs of prevention, treatment, care and support. As a result of many of the progress and accomplishments made by Malaysia in the duration of the NSP 2006-2010, the country is well on its mark to achieve the sixth goal of the MDG (Millennium Development Goals) within the next five years. There are however, still many challenges which lay ahead, thus maintaining the political support and further up-scaling financial resources are indeed crucial.
11
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
12
2.2.1 Strengthening the national commitment and supporting the NSP 2006 – 2010.
The Cabinet Committee on AIDS (CCA) was restructured in 2009, and being replaced by the National Coordinating Committee on AIDS Intervention (NCCAI) chaired by the Minister of Health. Civil society is also being represented on this new committee.
The increase in proportion of female HIV cases in Malaysia over the past five years has made the government to revive the Taskforce on Women, Girls and HIV/AIDS. This taskforce is currently chaired by the Ministry of Women, Family and Community Development (MWFCD), mandated to guide the actions of the Government in its response to addressing the behavioural and socioeconomic factors on the sexual transmission of HIV. 2.2.2 Multi-sectoral engagement in the HIV response Malaysia has taken the multi-sectoral approach when addressing the issues and challenges on HIV/AIDS. Non-health sectors i.e. the Ministry of Women, Family and Community Development, National Anti Drug Agency (Home Affairs Ministry) Department of Orang Asli (Indigenous People) Affairs, the Department of Islamic Development (JAKIM), the Prison’s Department, and the Information Ministry now form part of the key stakeholders in the country involved in the national HIV prevention and control programmes. The Ministry of Women, Family and Community Development has been instrumental in improving the overall response especially on matters pertaining to care and support services for PLHIV and those affected. 2.2.3 ARV treatment, resource mobilisation and funding support The Government has provided an allocation of RM 500 million (USD 143 million) for a period of 5 years during the NSP 2006-2010. This translates to RM 100 million (approximately USD 28 million) yearly which goes towards funding of Government and non-government HIV prevention, care and support programmes. A bulk of the funds also provides for the provision of ARV treatment for almost 10,000 people living with HIV. During the NSP 2006-2010, two significant achievements have accomplished, firstly, the availability and provision of first line ARV treatment at no cost for those who need it and secondly, the availability of ARV treatment for incarcerated populations specifically for HIV+ prisoners as well as inmates in drug rehabilitation centres. Currently, the second line regime is also heavily subsidised by the government. 2.2.4 The harm reduction programme The harm reduction programme, comprising the Needle Syringe Exchange Programme (NSEP) and the Methadone Maintenance Therapy (MMT,) remains the cornerstone of the Malaysian Government’s HIV prevention strategy. This programme is currently being implemented in partnership with non-governmental organisations (NGOs), community based organisations (CBOs) and private health practitioners. Significant successes which have been attributed with increased sites and clients over the last few years have made this one of the programmes which has managed to get worldwide attention. A number of innovative strategies have been introduced lately i.e. the introduction of the
12
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
13
MMT at National Anti Drug Agency service centres and incarcerated settings specifically prisons. More than 40,000 injecting drug users have been beneficiaries of this programme so far. 2.2.5 PMTCT programme The prevention of mother-to-child transmission (PMTCT) (prevention of vertical transmission) programme in Malaysia introduced in 1998 is based strongly around ARV prophylaxis for the child, safer delivery and infant feeding practices. It is also depended on detection of HIV infection during the mother’s antenatal period. The programme is implemented nationwide since 1998 at government health clinics and hospitals, and incorporates HIV screening utilising an opt-out approach. Although it covers only women receiving antenatal care at these government facilities, it is estimated that over 70% of total antenatal mothers nationwide utilise public antenatal facilities. Antenatal HIV cases from the private sector are also referred to the government medical system. 2.2.6 Mobilisation and involvement of MARPs and civil society Involvement of key civil society stakeholders in national level policy and programme development continues to be dependent on issues of capacity and relevance. Civil society is being represented at the National Coordinating Committee on AIDS Intervention and the Country Coordinating Mechanism. In the former, civil society is represented by the Malaysian AIDS Council while in the later several representatives (e.g. sex workers, PLHIV and transgender) have been elected onto the CCM by their respective communities. 2.2.7 Engagement with religious leaders The engagement with and involvement of religious leaders, especially Muslim religious leaders has increased significantly over the past few years. A lot of advocacy and investment in programming was done to mobilise and harness the support of Islamic religious leaders for HIV prevention and the provision of care and support. Muslim religious leaders have been actively involved in the implementation of HIV awareness programmes and also proactively established care and support facilities from financial and welfare assistance to shelters for Muslim PLHIV. The past 2 years in particular have seen the remarkable development of programmes by the Department of Islamic Development which involve a number of religious bodies engaging most-at-risk populations such as female sex workers and transgender persons through the availability of religious classes. 2.2.8 Increased availability and improvement of quality strategic information Much progress has been made in understanding the Malaysian HIV epidemic and most at risk populations (MARPs), particularly vulnerability to HIV and STI infection and the need for specific essential services. Much improvement has been achieved in the reporting of UNGASS country progress indicator data as a result of a number of surveys and research studies conducted in the past two years by a number of NGOs working with the Ministry of Health, such as the Malaysian AIDS Council (MAC), PT Foundation (PTF) and Federation of Reproductive Health Associations Malaysia (FRHAM) as well as the involvement of research bodies such as the Centre for Excellence on Research
13
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
14
in AIDS (CERIA). The involvements of these NGOs have complemented the efforts made by the government bodies to produce quality data. Detailed gender disaggregated data has also recently become available as a result of a revision of the national HIV reporting system and the National AIDS Registry by the Ministry of Health. Analysis of this data is critical to ensure a better understanding of how men and women are vulnerable to HIV infection in Malaysia. 2.3 Key challenges As a result of the progress made in the NSP, expectations on both Government and civil society have become significantly higher. Much of the challenges are related to sustaining the results of existing HIV prevention, treatment, care and support programmes both financially and programmatically. 2.3.1 The rise in sexual transmission The rise in sexual transmission would require a further strengthening of commitment from the Government to undertake and improve upon programmes which specifically address the issue of sexual reproductive health, especially among young people. Policy-makers will need to be better informed about the importance of adolescent health and sexual reproductive health, particularly within the context of HIV. As issues relating to sexuality and young people are often contentious and linked to public morality, thus, making it more essential to further consult and engage religious leaders and other community leaders. The upholding of social and religious values and rulings should take into consideration the realities of an epidemic which is increasingly spread through sexual transmission. 2.3.2 Sustainability of human, financial and infrastructure resources Concern has been expressed as to whether many of the achievements made in the past few years are financially sustainable due to the sole reliance on public funding. Reaching out to these populations also remains a significant challenge. Over the last decade, the vast majority of prevention programmes involving MARPs by CBOs and NGOs have been heavily funded by the government. As a result, interventions programmes are sometimes confined to certain geographical locations and communities to get the maximum coverage and impact. Sustainability of funding, and human capacity enhancement in HIV/AIDS prevention programmes especially among the civil society therefore is one of the major concerns for Malaysia and NSP 2011-2015. 2.3.3 Financial cost of providing increased ARV treatment coverage Revised needs and coverage estimates based on the 2009 adoption of WHO’s recommended criteria of CD4<350 for ARV treatment initiation, indicate an increased burden in the provision of ART. This revision of treatment protocol has significantly increased the number of persons estimated to be in
14
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
15
need of treatment. Of major concern for the Government on this issue, is the large financial cost of providing this increased coverage which is expected to cost an estimated RM 60 million annually. 2.3.4 Engaging religious leaders The engagement of religious leaders from all faiths is expected to play a continued, expanding and critical role over the years in providing complementary care and support services for PLHIV and those affected as well as prevention of sexual HIV transmission. The Government is currently making an effort to expand this engagement to those from non-Muslim faiths. Some of the religious departments e.g. Selangor and Pahang have provision in their enactment to provide deserving PLHIVs zakat (tithes). The next few years will probably see more shelter homes being built by the religious departments. 2.3.5 Mobilising MARPs and vulnerable populations to access public HIV healthcare services Mobilising MARPs, vulnerable populations and related civil society organisations to access and utilise the many available public HIV related healthcare facilities and service points remains an ongoing challenge. Perceived as well as actual occurrences of stigma and discrimination by these communities may act as deterrents and obstacles for them to utilise these facilities. There is also a need for NGOs to be able to work with these public facilities to provide services for vulnerable populations such as former prisoners and drug rehabilitation centres inmates who have been released from such institutions. One of the greatest challenges to date would definitely have to be adhering to ARV treatment. 2.3.6 Stigma and discrimination Stigma and discrimination continues to be an issue, however it has lessen now. Nevertheless, it not only affects PLHIV but to those around them, and also affect the progress and successful implementation of HIV prevention, treatment, care and support programmes. Vulnerable populations and MARPs may encounter incidences of discriminatory practices in public and private workspaces as well as during the implementation of HIV programmes, which inevitably might complicate the outcomes of impact of such programmes. 2.3.7 Structural challenges The Ministry of Health and its civil society partners face many challenges in responding to AIDS in the country, some of which are structural in nature. These may affect the implementation of the harm reduction programme as well as interventions with sex workers, transgender persons and MSM programmes. However, in dealing with these issues, government officials and their civil society counterparts have been encouraged to work together. Frequent dialogues and discussions have been held either at the local or national levels to address some of these challenges. A lot more needs to be done to overcome some of these challenges.
15
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
16
2.3.8 More research and studies needed Strategic information such as behavioural data necessary to plan and implement a comprehensive response to HIV was previously quite limited. Data for these populations on HIV prevalence, profiles of risk behaviour and vulnerabilities were often anecdotal, limited or simply not available. The availability of relevant strategic information has improved tremendously since 2009. Though there continues to be limited research concerning most-at-risk populations and HIV, the past few years have seen the implementation of a number of behavioural studies and research with these communities. These are still limited in certain geographical locations and must be further expanded to other parts of Malaysia.
16
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
17
CHAPTER 3 The National Strategic Plan on HIV and AIDS 2011 - 2015
The National Strategic Plan on HIV and AIDS 2011 – 2015 runs parallel and is harmonised with the aims and objectives of the 10th Malaysian Plan (10MP) for 2011 – 2015 which guides the development of Malaysia for the next five years as well as the policies outlined under the 1Malaysia initiative related to healthcare. 3.1 Guiding Principles for the National Strategic Plan on HIV and AIDS 2011 – 2015 Malaysia’s national multisectoral response to HIV and AIDS is built and guided by the following guiding principles: 3.1.1 The spread of HIV is a challenge to the national development of Malaysia and is a concern to
be addressed under the 10th Malaysian Plan and the 1Malaysia initiative.
3.1.2 The HIV and AIDS response will be based on evidence and prioritise interventions among most at risk populations (MARPs) and will also include other populations made vulnerable to HIV infection due to risk behaviours and environment.
3.1.3 The HIV and AIDS response will be comprehensive and focus on promoting healthy practices, disease prevention, as well as treatment, care and support for People Living with HIV and people affected by HIV and AIDS.
3.1.4 The response to HIV and AIDS should take into consideration cultural, religious and societal values.
3.1.5 Government, civil society and private sector stakeholders will work together in multisectoral partnership to respond to the spread of HIV and AIDS in the country. Working in consultation and collaboration with relevant stakeholders, the Government will provide policy direction, HIV treatment for those in need, and financial resources in support of this effort. Civil society, including non-government organisations, community groups, People Living With HIV and those affected by HIV and AIDS, will support and complement the Government in the prevention of HIV, as well as care and support for those living with HIV and those affected.
3.1.6 All stakeholders will work together to create a conducive and enabling environment to ensure the effectiveness of interventions under the HIV response which respect human dignity, gender and sexuality.
3.1.7 Active and meaningful participation of key populations including most at risk communities, People Living with HIV and those affected will be integral to the development, implementation, monitoring and evaluation of all interventions.
17
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
18
3.2 Goal and Specific Objectives 3.2.1 Goal The National Strategic Plan on HIV and AIDS 2011 – 2015 aims to prevent and reduce the risk and spread of HIV infection, improve the quality of life of People Living with HIV, and reduce the social and economic impact resulting from HIV and AIDS on the individual, family and society. 3.2.2 Specific Objectives a) To further reduce by 50% the number of new HIV infections (i.e. notification rate of HIV) by scaling
up, improving upon and initiating new and current targeted and evidence based comprehensive prevention interventions
b) To increase coverage and quality of care, treatment and support for People Living with HIV and those affected
c) To alleviate the socioeconomic and human impact of AIDS on the individual, family, community and society.
d) To create and maintain a conducive and enabling environment for government and civil society to play meaningful and active roles in decreasing stigma and discrimination.
e) To further increase general awareness and knowledge of HIV, and reduce risk behaviour for at risk and vulnerable populations.
These objectives can only be meaningfully achieved and sustained under the commitments to Universal Access and the Millennium Development Goals after programmes have achieved 80% service coverage among MARPs where 60% of those covered practice safe behaviours. 3.3 Strategic Targets It is aimed that by the end of 2015, a 50% reduction of new infections able to be prevented and averted is achieved. Malaysia is currently able to provide Universal Access coverage on a number of limited services related to treatment of HIV and AIDS. However, the National Strategic Plan on HIV and AIDS 2011 – 2015 strives to sustain the progress and achievements made over the past National Strategic Plans on HIV and AIDS. To do so, this National Strategic Plan on HIV and AIDS targets to achieve the following: a) Comprehensive HIV prevention programmes are able to effectively cover 80% of most at risk
populations.
b) 60% of most at risk populations use condoms consistently.
c) 60% of most at risk populations, who are also injecting drug users, use clean injecting equipment.
d) All cases of vertical HIV transmission are able to be prevented with all HIV positive pregnant mothers receiving treatment and children born receive ARV prophylaxis.
e) Provision and access to comprehensive services for at least 80% of People Living with HIV who are eligible for ARV treatment, care and support which are non-discriminatory and professional.
18
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
19
3.4 Strategies The National Strategic Plan on HIV and AIDS 2011 – 2015 is both a continuation and is as a result of the efforts of the previous National Strategic Plan 2006 – 2010. It is a response to the improved understanding and increase in behavioural and surveillance data availability amongst most at risk populations. This National Strategic Plan on HIV and AIDS is also a response to the increasing challenges and issues faced in the Malaysian HIV epidemic. It is intended to be a component within the 1Malaysia framework related to healthcare. There will be 5 main strategies to be undertaken under this plan, namely: a) Improving the quality and coverage of prevention programmes among most at risk and vulnerable
populations
b) Improving the quality and coverage of testing and treatment
c) Increasing the access and availability of care, support and social impact mitigation programmes for People Living with HIV and those affected.
d) Maintaining and improving an enabling environment for HIV prevention, treatment, care and support.
e) Increasing the availability and quality of strategic information and its use by policy makers and programme planners through monitoring, evaluation and research.
The key stakeholders of the National Strategic Plan will continue to support the government, policy makes and the Ministry of Health in advocating the multisectoral approach on HIV and AIDS issues. For the execution and fulfilment of the strategies to be implemented fully, the commitment and partnership of government, civil society and private sector stakeholders working together in the spirit of consultation and collaboration are crucial. 3.4.1 Strategy 1: Improving the quality and coverage of prevention programmes among
most at risk and vulnerable populations HIV prevention efforts in 2011 – 2015 will focus on addressing the three primary prongs of HIV transmission in Malaysia, namely the sharing of needles and syringes through injecting drug use, unprotected sexual intercourse, amongst most at risk and vulnerable populations and advocacy amongst the most-at-risk youth populations Strategy 1.1: Prevention of HIV transmission through the sharing of needles and syringes The primary mode of transmission in Malaysia continues to be through injecting drug use. Sustaining and scaling up of existing comprehensive prevention interventions which includes the harm reduction (needle syringe exchange and methadone maintenance therapy) programme continues to be needed and their coverage increased to include other identified populations. Key Activities: a. Build an enabling environment for HIV prevention with IDUs and their partners by mobilizing key
stakeholders, including, health care providers, community networks, NGOs, local authorities, and law enforcement.
19
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
20
b. Develop other innovative strategies to address challenges for the delivery of HIV prevention with IDUs.
c. Implement targeted behaviour change approaches for male and female IDUs which emphasize risk reduction and promote safer sexual and risk reduction behaviours.
d. Implement national scale up of HIV prevention with IDUs and their partners including needle and syringe exchange programmes and opioid substitution therapy.
e. Strengthen mechanisms to manage HIV prevention among drug users in prisons and other detention facilities and drug rehabilitation centres.
Strategy 1.2: Prevention of HIV transmission through unprotected sex Under this strategy addressing sexual transmission of HIV, coverage of interventions is improved upon to encourage barrier methods (e.g. condom use) among MARPs and vulnerable populations; provision of sexual reproductive health (SRH) education and other essential SRH services; encourage behavioural change among MARPs towards safer sexual practices; implementation of programmes which address intimate partner transmission of HIV; encouraging HIV testing through voluntary testing and counselling; and promotion of information and awareness of HIV and STIs through media. Key Activities: a. Review existing strategies including awareness programmes and activities to encourage and
facilitate behavioural change among MARPs.
b. Build an enabling environment for behavioural change through economic, welfare and religious aid.
c. Raise awareness and build knowledge and awareness on HIV and other diseases (e.g. TB and STIs), among MARPs, married and unmarried couples, and members of most at risk youth and their sexual partners.
d. Improve and strengthen VCT, STI and SRH services to all MARPs, including counselling for married and unmarried couples.
e. Raise awareness and understanding of HIV and STIs, support and promote the appropriate use of condoms and lubricants when engaged in sexual activities, particularly among MARPs, their partners and/or clients.
f. Develop and scale up services on sexual reproductive health, counselling and treatment related to STIs, HIV and AIDS to ensure universal coverage.
g. Expand and scale up HIV prevention programming incorporating a comprehensive package of services for men who have sex with men (MSM) and transgender persons.
h. Strengthen the participation of national and local partners in the provision of HIV prevention programmes targeting migrant workers and refugees.
i. Implement targeted behaviour change communication interventions to promote safer sexual behaviour, address negative gender values, and promote male responsibility for positive health.
j. Develop strategies to address barriers and challenges which prevent the efficient and effective delivery of HIV prevention services to MARPs especially MSM, SW and TGs
20
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
21
Strategy 1.3: Prevention of mother to child transmission The Prevention of Mother To Child Transmission (PMTCT) programme in government healthcare facilities should be continued including screening, providing treatment, care and support for pregnant women with HIV and their partners/ spouses. More pregnant women will be screened for HIV through integration of PMTCT in antenatal services at public and private health facilities with improved linkages between existing SRH and HIV programmes. The goal would be to eliminate vertical transmission by 2015. Key Activities: a. Maintain the provision of quality, comprehensive national PPTCT services, in line with the WHO
recommended four pronged strategy, to reach pregnant women, their partners and their infants, including most at risk populations.
b. Strengthen community awareness of HIV to increase enrolment in the PMTCT programme and other related antenatal, family planning, sexual and reproductive health, voluntary confidential counselling and testing services, particularly among most at risk populations.
c. Ensure all HIV-infected pregnant women and their HIV-exposed infants under the PMTCT programme receive ARV treatment/ prophylaxis and breastfeeding education to reduce mother-to-child transmission of HIV.
d. Ensure the availability of PMTCT in all ANC facilities including private health care facilities 3.4.2 Strategy 2: Improving the quality and coverage of testing and treatment The Government continues to support a decentralised approach to health services which includes community-based and primary health care through to hospital-based care. It provides psychosocial support including voluntary, counselling and testing (VCT), nutritional support and treatment for common opportunistic infections. Malaysia already provides and is committed to affordable access to clinical care through the public health system, including free or subsidized access to ART. People Living with HIV (PLHIV) in closed settings and those living outside the major cities are of particularly concern and will need to be covered under existing programmes. Stronger linkages and referral systems between HIV and related services such as VCT, tuberculosis (TB), opportunistic infections (OIs), SRH, opioid substitution therapy (OST) and PMTCT will be encouraged. There is also a need to ensure and maintain the quality and sustainability of treatment, care and support services for PLHIV. Positive prevention should also be promoted among those living with HIV. Key Activities: a. Ensure adequate number and training of healthcare workers to deliver VCT and ARV and related
services.
b. Strengthen priority health services through increased integration of HIV service delivery.
c. Improve coverage and early access to and quality of HIV testing, care and treatment, sexual reproductive health and STI services for most at risk populations and their partners.
d. Increase access and quality of HIV testing and counselling services in the public and private sectors to identify those in need of HIV treatment.
e. Strengthen capacity of VCT related staff.
21
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
22
f. Improve adherence to treatment and detection of treatment failure.
g. Expand routine PICT for pregnant women, TB and STI patients and strengthen linkages from prevention to care and treatment.
h. Develop and scale up care and treatment with anti-retroviral drugs and TB treatment for drug users in prisons and other detention centres.
3.4.3 Strategy 3: Increasing the access and availability of care, support and social impact mitigation programmes for People Living with HIV and those affected.
Increasing access and availability of care and support programmes for People Living with HIV (PLHIV) and those affected which address physical, mental, social, spiritual, religious and economical aspects. Key Activities: a. Improve coordination, linkages and referral among social, health and community based services at
the community level.
b. Strengthen the quality and impact of PLHIV and MARPs support groups and networks.
c. Link PLHIV and their families to existing social support programmes to ensure access to essential services.
d. Increase visibility and meaningful participation and decision making of PLHIV and MARPs in impact mitigation programmes.
e. Provide quality emotional, religious and spiritual support to PLHIV and their families.
3.4.5 Strategy 4: Maintaining and improving an enabling environment for HIV prevention, treatment, care and support.
Prevention and treatment programmes are more effective when operating in an enabling environment which does not stigmatise and discriminate against those most at risk and those affected. Creating and maintaining a better understanding of HIV to reduce risk taking as well as stigma and discrimination are therefore essential. It is necessary to establish and maintain an enabling public policy and structural environment which will help to reduce HIV stigma and discrimination, respects human dignity, gender and sexuality and is supportive to HIV programmes and interventions. Key Activities: a. Ensure HIV issues are mainstreamed into national social development plans and the necessary
financial and technical resources are mobilised to support development and implementation of HIV and AIDS plans and programmes.
b. Strengthen capacity of key ministries and other government and civil society stakeholders at the national and local levels to develop and implement targeted evidence-based interventions.
c. Engage law enforcement, healthcare service providers, relevant public officials and civil society stakeholders, to assess and mitigate complications to the national HIV response.
22
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
23
d. Improve the representation, involvement and capacity of civil society, community based organizations and affected population networks in dialogue and decision-making, towards achieving Universal Access and strengthening the national response.
e. Strengthen the work of the private sector among local businesses to promote corporate social responsibility and to establish workplace-based HIV prevention programmes and to address stigma and discrimination in the private sector.
f. Intensify public understanding and awareness of HIV and AIDS through focused communications and integration into community-based HIV education messages.
3.4.6 Strategy 5: Increasing the availability and quality of strategic information and its use
by policy makers and programme planners through monitoring, evaluation and research.
There is a continuous need to improve upon the availability of research, surveillance and bio-behavioural data, and analysis of monitoring and evaluation of HIV programmes to guide and determine policy and programme frameworks for prevention, treatment, care and support. Key Activities: a. Develop and strengthen partnerships to plan, coordinate and manage the national monitoring and
evaluation, research and surveillance systems.
b. Produce and disseminate timely and high quality data from research, integrated biological behavioural surveillance (IBBS), population size estimations and other studies.
c. Promote the production, dissemination and effective use of strategic information to inform and guide programme and policy decision making.
d. Consolidate and streamline mechanism for data collection from both private and public HC facilities for future planning
23
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
24
CHAPTER 4 Coordination and Implementation
It is necessary to ensure that the implementation of the National Strategic Plan on HIV and AIDS is structured and managed accordingly to facilitate the participation and involvement of relevant stakeholders from government, civil society, the private sector and development partners, and to ensure output of the intended results from the many interventions. Strong governance and coordination of the National AIDS Programme by the Ministry of Health will ensure harmonisation and alignment of all stakeholders involved in the Malaysian AIDS response. The overarching principle in management of the National Strategic Plan is the Three Ones Principle of one national multisectoral strategy, one national coordination platform with a multisectoral mandate and one monitoring and evaluation framework. 4.1 Coordination NCCAI and NATCA In 2009, the HIV policy and decision making structure was revised with the intention of streamlining the functions of the different entities involved in HIV policy development.
Under this new revision, the Cabinet Committee on AIDS was restructured and is now known as the National Coordinating Committee on AIDS Intervention (NCCAI) chaired by the Minister of Health. The NCCAI functions as the highest decision-making body on HIV and AIDS related policies. Its membership includes all the Secretary Generals of the relevant ministries and agencies listed in the NSP as well as civil society representatives, including the Malaysian AIDS Council.
Figure 4: National HIV and AIDS Policy Framework
Source: Ministry of Health (2009)
24
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
25
The National Advisory and Technical Committee on AIDS (NATCA), is actually a merging of the two bodies present in the previous framework namely, the National Advisory Committee on AIDS and the Technical Committee on AIDS. This committee, which is chaired by the Director General of Health, acts as a high level advisory body to the NCCAI. It provides a forum for discussion of policy issues relevant to increasing the success of Malaysia’s response to the HIV epidemic as well as to review progress against the annual work plans and budgets. The membership of the NATCA is made up of key Ministry officials, subject matter experts, NGO and community representatives and the Director Generals and HIV Focal Points of the Ministries. It meets and reports to the NCCAI. National AIDS Programme Secretariat The responsibility for the overall coordination of Malaysia’s HIV and AIDS responses is currently tasked to the AIDS/STI Sector of the Disease Control Division, Ministry of Health located in Putrajaya, the Federal Administrative capital of Malaysia. The AIDS/STI Sector is currently functioning as the National AIDS Programme (NAP) Secretariat. The Secretariat interacts and engages the other institutions within the Federal Government (and the civil society) through HIV Focal Points who are present in each of the relevant Ministries. The NAP Secretariat will be strengthened with sufficient resources and capacity to the implementation of the National Strategy on HIV and AIDS 2011 – 2015. It will be responsible for overall coordination, monitoring, evaluation and reporting. This secretariat will continue to strengthen and maintain linkages with state and district authorities through the respective State AIDS Officers build capacity of ministerial AIDS focal points and facilitate information sharing among the different national level committees. The work of the National AIDS Programme Secretariat is supported by the State AIDS Officers whose tasks are to plan, coordinate, implement and evaluate HIV interventions. The AIDS Officers and the NAP Secretariat are also instrumental and critical in ensuring that HIV prevention, care and support programmes carried out by NGOs, who are recipients of public funds, are harmonised and in line with the identified priorities under the National Strategy on HIV and AIDS. Country Coordinating Mechanism (CCM) The Country Coordinating Mechanism, chaired by the Deputy Minister of Health, provides governance for all programmes and activities related to the Global Fund for AIDS, Tuberculosis and Malaria (GFATM) in Malaysia. This mechanism operates concurrently and complements the work of the NATCA. Taskforce on Women, Girls and HIV/AIDS The Government established the Taskforce on Women, Girls and HIV/AIDS as a response to the increase in the number of female HIV cases and in incidences of sexual HIV transmission. This taskforce is spearheaded by the Ministry of Women, Family and Community Development and is tasked to guide the actions of the Government in its response to
25
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
26
addressing the abovementioned situation as well as the behavioural and socioeconomic factors behind the sexual transmission of HIV.
Figure 5: Stakeholders in the Malaysian HIV response
Civil society The Malaysian AIDS Council (MAC) was initially established in 1992 by the Ministry of Health and serves as an umbrella organisation to support and coordinate the efforts of partner organisations working on HIV and AIDS issues in Malaysia. In partnership with government agencies, private sectors and international organisations, MAC works towards ensuring a committed and effective response by NGOs working on HIV and AIDS issues. Most of the public funds for use by non-governmental organisations working on HIV and AIDS projects are channelled through and coordinated by the MAC. The MAC facilitates the collaboration with civil society organisations in the implementation of the National Strategy on HIV and AIDS. Consultative mechanisms such as CSO stakeholder meetings at the national level will be established in an effort to seek a wide variety of viewpoints from the different at risk and vulnerable communities which would help streamline Malaysia’s response to HIV and provide input towards the implementation and evaluation of the National Strategy on HIV and AIDS.
4.2 Implementing the National Strategic Plan Priority Setting Priority setting is a key task in the management of the National Strategy on HIV and AIDS and will be guided by further improvements in the availability and use of strategic information. The priorities set in the National Strategy on HIV and AIDS will be reviewed regularly, as part of the monitoring and evaluation arrangements described in Chapter 6.
26
National Strategic Plan on HIV and AIDS2011 – 2015
Government Stakeholders Civil society stakeholders
National AIDS ProgrammeSecretariat
Ministry of Health (MOH)
Ministry of Health
State AIDS Officers
Ministry of Women,Family andCommunity
Development
Ministry ofEducation
Ministry of HigherEducation
Ministry of HumanResources
Ministry of HomeAffairs
Taskforce onWomen, Girls and
HIV
PLHIV and thoseaffected
VulnerablePopulations
Private Sectorclinics/ hospitals
Internationalorganisations
Local communitynetworks
Private laboratories
NCCAI
NATCAMalaysia AIDS Council (MAC)
Non-NSEP, NGOs
CBOs
MARPs
Academia
Universities
United Nations
Regional communitynetworks
NGOs FBOs
NSEP NGOs
CountryCoordinatingMechanism
Ministry of HomeAffairs
National Anti DrugAgency
Police
JAKIM

National Strategy on HIV and AIDS 2011 - 2015
27
Effective resource tracking system will be put in place to provide information and feedback concerning the alignment of resource allocations to agreed priorities. The collection, storage and sharing of strategic information and the need for a resource tracking system is addressed under Strategy 5. Development of the 2011 – 2012 and 2013 – 2015 workplans Two set of workplans based on clear and evidence driven national priorities will be developed to guide the implementation of the National Action Plan on HIV and AIDS 2011 – 2015 and will cover the periods of 2011 – 2012 and 2013 – 2015. These workplans will be used to detail the activities to be conducted and to guide decision making in resource allocation of public funds. These activities must be clear, action and results oriented, and targeted which will translate strategic priorities to operational realities. The development of the 2013 – 2015 workplan will also be guided by the outputs from the mid-term review of the NSP. The workplans of other individual stakeholders involved in the HIV response will be complementary to those mentioned above. Given its role in monitoring and evaluation as well as resource tracking, the National AIDS Programme Secretariat will play a central role in priority setting and the development of the workplans. The Secretariat will facilitate this process through the supporting of relevant partnership and stakeholder forums and technical working groups. It will collect, analyse and provide the strategic programmatic and financial information that is needed to inform the priority setting process. For specific components of the National Action Plan on HIV and AIDS, relevant Ministries and organisations will collaborate through technical working groups established for specific issues and population groups. The work of the individual Ministries and organisations will contribute towards the implementation of components of the National Strategic Plan and towards the achievement of agreed expected results and targets.
27
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
28
CHAPTER 5 Resource Mobilisation
Over the next five years, it will be important to advocate for sustained domestic commitment to fund the national response to HIV and AIDS. Resource allocations will need to be aligned to the priority areas and programmes identified in the National Strategic Plan on HIV and AIDS and National Action Plan on HIV and AIDS. The National AIDS Programme Secretariat will track the variety and amount of resources allocated to the National Strategy which will provide crucial information on whether the existing allocation of funding is aligned with agreed national priorities. Such a system will highlight areas where insufficient resources are being allocated and experiencing gaps in funding. The provision of necessary and adequate resources and technical assistance will be needed for the next five years to further strengthen organisational and human capacity for HIV programmes to be sustained and to build upon the progress and results obtained from the previous National Strategic Plan. 5.1 Estimating the resources needed The resources required to achieve the NSP coverage and impact goals needs to be calculated from estimates of the number of people receiving each service and the cost per person. Service estimates are based on the population in need of the service or programme and the coverage level to be achieved. Coverage is assumed to increase from the baseline levels to the planned targets by 2015. The unit costs for these services are based on existing interventions currently being implemented by agencies and organisations. A number of assumptions have been made, which the cost estimates are based on i.e.:- a) Population sizes: The population sizes are estimated based on size estimation studies. Particular
populations such as MSM and clients of sex workers are extremely difficult to reach and therefore to estimate their sizes.
b) Target setting: Targets to be reached are based on perceived implementation capacity which varies according to the different implementing partners.
c) Unit costs: these are the main assumptions for calculation of total costs; As the same programme and interventions might have several unit costs depending on the geographical location, the unit costs indicated are the average value.
d) Overhead and management costs: these costs are not fully represented in the unit costs as they differ according to the programmes and activities involved.
28
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
29
5.2 Sources of funding A bulk of the allocation from the previous NSPs was spent on the provision of HIV treatment and involved funding of HIV NGO prevention programmes which were small scale and with limited coverage. A three-fold increase in this allocation, now totalling RM 100 million (approximately USD 32 million) per annum, was made available to both government agencies and civil society organisations for the past five years (2006 – 2010) in support of implementation of the NSP. With an annual budget of RM 100 million allocated to it, the allocation provided by the Government utilising public funds to the national HIV programme currently translates to approximately RM 3.1 (USD 1) per capita. In 2008, total AIDS expenditure was approximately RM 86.6 million, 96.95% was financed by Government funding and 3.05% by the private sector and international sources. In 2009, expenditure increased by RM 8.6 million. Regarding sources of financing for HIV programmes, as indicated in the table below, in 2008 and 2009, the domestic public funding from the Government shouldered most of the AIDS related expenditure, whereas international and private sector contributions resources contributed to less than 3%.
Table 4: Source of approximate AIDS expenditure 2008 – 2009
Source of Funding Year 2008
(RM) %
Year 2009 (RM)
%
Domestic Public 83 993 000 96.95 92 661 000 96.71 Domestic Private 1 619 000 1.87 1 629 000 1.70 International 1 020 000 1.18 1 520 000 1.59
Total 86 632 000 100.0 95 810 000 100.0 Source: UNGASS Country Progress Report (Malaysia) 2008 & 2010
Government funding is channelled from the Ministry of Finance to the Ministry of Health which disburses the funds to other government ministries and departments. The other Ministries are also able to provide funding for their own HIV related programmes utilising their individual budgets. The government is committed to subsidise ARV for PLHIV either in institutionalised settings or otherwise, HIV screening programmes and activities either at the Primary Care Levels (VCT, PPCT, pre-marital HIV screening, STI patients) or secondary levels. In the case of NGO related programmes, the MOH uses the Malaysian AIDS Council as a conduit for channelling the necessary public funds to the individual NGOs. Currently, a lot of HIV prevention and control programmes and activities are channelled to MAC namely the NSEP for IDUs and intervention programmes for MARPs (sex workers, MSM, transgender).
29
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
30
CHAPTER 6 Monitoring and Evaluation
In line with the Three Ones Principle, implementation of the National Strategic Plan will be monitored and evaluated through the national HIV monitoring and evaluation framework, which is coordinated by the National AIDS Programme Secretariat. Information gathered from national monitoring and evaluation of HIV and AIDS programmes will be used to: a) Ensure HIV and AIDS prevention programmes achieve high levels of accountability and efficiency
b) Inform and help determine whether programme up scaling or expansion is required
c) Allow corrective or remedial action to be taken
d) Provide information and data which is beneficial for the implementation of the programme and serve as input for the design of future programmes.
e) For the purpose of reporting on international commitments such as UNGASS reporting, Universal Access and the MDGs.
Partners involved in the implementation of the National Strategic Plan will continue to operate their own systems for programme monitoring and evaluation. The national monitoring and evaluation framework system (M&E), as outlined by the NSP 2011-2015 will consolidate information that is generated by the government and other key stakeholders. Expected results and targets will be monitored and evaluated periodically. 6.1 Programme Coverage It is aimed that by 2015, coverage of programmes reaching out to most at risk populations will be at 80%. To achieve the targets of Universal Access by that year, as shown in Table 5, the programme coverage targets are determined accordingly to ensure that MARPs and PLHIVs are able to access prevention, treatment, care and support services needed.
Therefore, in general by 2015, it is aimed that 80% of injecting drug users are able to be reached by the harm reduction programme (MMT and NSEP) of which 60% of them would consistently not be sharing needles; 60% of key most at risk populations would consistently be using condoms; 60% of all PLHIV in need of and eligible for treatment are able to access ARV.
30
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
31
Table 5: Programme coverage targets (2010 & 2015)
Population Est. no. (as of 2010)
Baseline 2010 2011 2012 2013 2014 2015 Actual % No. % No. % No. % No. % No. %
IDU 170 0001 21 559 13% 34 000 20% 51 000 30% 85 000 50% 119 000 70% 136 000 80% Female sex workers 60 0002 18 000 30% 25 200 40% 31 500 50% 37 800 60% 44 100 70% 50 400 80% Transgender persons 5 0003 1 500 30% 2100 40% 2 625 50% 3 150 60% 3 675 70% 4 200 80% MSM 173 0004 6 000 3.5% 36 330 20% 54 495 30% 90 825 50% 127 155 70% 145 320 80% Clients of sex workers
845 0005 - - 17 745 2% 44 363 5% 88 725 10% 133 088 15% 177 450 20%
Intimate partners of at risk populations*
Data not available.
To be estimated
- - TBD 5% TBD 10% TBD 15% TBD 20% TBD 30%
Mothers needing PMTCT
4106 171 42% 450 100% 450 100% 460 100% 470 100% 490 100%
PLHIV (Eligible: CD4 <350 )
26 7227 9 962 37% 15 567 50% 21 794 70% 24 907 80% 28 021 90% 31 134 100%
*Estimation exercise to be conducted
6.2 Monitoring and Evaluation Process Monitoring and evaluation will be utilising a process which is able to capture and evaluate various levels of programme implementation, from input, activities, output to impact. All stakeholders involved in the response to HIV in Malaysia are contributors to the various indicators and are equally responsible to ensure that they are regularly monitored and utilised to measure progress. The National AIDS Programme Secretariat is given the responsibility to monitor and evaluate the overall HIV/AIDS framework. The NAP Secretariat is also empowered to ensure that all relevant stakeholders report to the Secretariat on specific indicators as necessary.
1 Malaysian AIDS Council (2010) Integrated Bio-Behavioural Surveillance (IBBS) survey with IDUs, SW, TG. Powerpoint presentation. Presented on 11 March 20102 Lim Hock Eam, Ang Chooi Leng and Teh Yik Koon (2010). Size Estimation for Local Responses in Malaysia for HIV Prevention in Sex Work. UNFPA Project3 Malaysian AIDS Council (2010) Integrated Bio-Behavioural Surveillance (IBBS) survey with IDUs, SW, TG. Powerpoint presentation. Presented on 11 March 20104 Kanter J, Koh C, Kiew R, Tai R, Izenberg J, Razali K and Kamarulzaman A (2009). Abstract: Risk Behaviour and HIV Prevalence among MSM in a Predominantly Muslim and Multi-Ethnic Society: A Venue-Based Study in Kuala Lumpur, Malaysia.5 Ministry of Health and World Health Organisation (2009). National Consensus Workshop on Estimation and Projection of the Malaysian HIV Epidemic. Revised version 20th March 2011.6 Ibid7 Ibid
31
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
32
Figure 7: Monitoring and Evaluation Process
Adapted from ‘Rugg et al (2004). Global advances in HIV/AIDS monitoring and evaluation. New directions for Evaluation. Referenced within ‘UNAIDS (2007). A Framework for Monitoring and Evaluating HIV Prevention Programmes for Most-At-Risk Populations. ’, page 13
The overall monitoring and evaluation framework for the National Strategic Plan on HIV and AIDS can be found in Annex 3, and provides a detailed account of the various indicators, method of measurement and the stakeholder responsible for each individual indicator. This process of information and data gathering for monitoring and evaluation is best illustrated in Figure 7 above. 6.3 Data Collection The NAP Secretariat will work with Ministries in the Government and civil society organisations to conduct national monitoring and evaluation. Utilising strategic information gained from the framework, the NAP Secretariat will be able to evaluate the existing response as well as determine areas needing improvement or change. 6.3.1 Surveillance The responsibility of HIV surveillance is with the AIDS/STI Sector of the Ministry of Health. A number of surveillance related activities will be needed, namely:
(a) HIV sentinel surveillance The Ministry of Health conducts ongoing sentinel surveillance covering different populations including injecting drug users, sex workers, pregnant women, and many others.
(b) National AIDS Registry The Ministry of Health established the National AIDS Registry (NAR) in 2009. Intended to replace the existing surveillance system, the Internet-based registry is designed to function as a more streamlined and effective national HIV programme monitoring mechanism able to capture detailed disaggregated data systematically. The Registry captures data on each HIV
Situational assessment & planning
Situational and epidemiological analysis Response analysis Stakeholder needs
Input
Staff Financial resources Material Facilities
Activities
Behavioural change communication Trainings Prevention programmes Treatment, etc
Output
Trained personnel MARPs reached Clients served Needles distributed Condoms distributed Tests conducted
Results/ Outcome
Risk behaviour Users accessing services Clinical results Quality of life
Impact
HIV incidence & prevalence STI incidence & prevalence AIDS morbidity and mortality Economic impact
Programme Development Data
Programme Data Population-based biological, behavioural and social data
32
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
33
patient relating to their socioeconomic background, status of HIV treatment and background information
(c) Integrated bio-behavioural surveillance (IBBS)
Periodic IBBS will be conducted with most at risk populations in different states as needed.
(d) Other strategic information needed Other strategic information needed and currently being developed are the ARV resistance surveillance, estimation of MARPs, PLHIVs, etc. Such information will to be developed with the universities, institutions and international agencies to have a more meaningful data collection and future projections.
Other data sources:
Mapping of Most-At-Risk Populations Monitoring of programme coverage Monitoring of prevention services Monitoring of behavioural change communication programmes Monitoring of treatment services Monitoring of impact mitigation services Various researches, especially operational research needed to increase the effectiveness of prevention, treatment, care and support programmes.
6.4 Monitoring and Reporting Structure Horizontal working relationships between government and non-government agencies at the state level are critical to ensure that there is appropriate programme monitoring at both operational programme and national levels. The National HIV and AIDS Monitoring, Evaluation and Reporting Guidelines that will be produced and used as the basis for monitoring and evaluation in respect of the implementation of the National Strategic Plan on HIV and AIDS 2011 – 2015. These guidelines will kept as simple and practical as possible so as to allow monitoring, evaluation and reporting to be properly carried out. The dissemination of these guidelines, and the provision of training on how they should be used, will be initiated so that monitoring, evaluation and reporting will be optimized at all levels. A Technical Working Group on Monitoring and Evaluation (TWG-M&E) chaired by the Monitoring and Evaluation Unit of the National AIDS Programme Secretariat is proposed to lead on the HIV programme performance reviews conducted at the National level. This provides an opportunity for a strengthening of the Secretariat’s own technical capacity as well as those of the relevant and involved ministries and civil society organisations.
33
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
34
Figure 8: Monitoring and Evaluation Reporting Structure
6.5 Progress Monitoring and Evaluation Progress monitoring and evaluation are conducted utilising a joint government and civil society periodic performance review which should be conducted at both state and national levels. The intention of the performance reviews is to evaluate progress based on coverage, effectiveness and sustainability of programmes. 6.5.1 HIV programme performance review (State level) The frequency of the state level HIV programme review should be every 4 months with the State AIDS Officers and the State Health Department taking the lead. The review will be conducted with government and civil society organisations responding to HIV at the state level. 6.5.2 Annual Progress Report The National AIDS Programme Secretariat will coordinate and facilitate the preparation of annual progress reports and the Work Plans through the national HIV programme performance review, which will be discussed and finalised as part of the annual joint stakeholder meeting held in October. The inputs of the annual progress reports will also be based on the HIV programme performance review conducted at the State level.
34
National Strategic Plan on HIV and AIDS2011 – 2015
Line Ministries andAgencies (MWFCD,NADA, JAKIM, etc)
National AIDS Programme SecretariatMinistry of Health (MOH)
TWG on Monitoring andEvaluation
State AIDS OfficersDistrict Health
Office
Malaysia AIDSCouncil (MAC)
MMTDrug Rehabilitation
CentresPrisons
Research/surveyNon-NSEP,
NGOs
NGO working on:- MSM- SW- TG- Vulnerable people
•IBBS•VDTS•Population based survey•Health facility survey•Sentinel surveillance
- PLHIVNGO working onIDU
NSEPNGOsGovt Healthcare
Facilities
Private HealthcareFacilities
National Monitoring and Evaluation Reporting Flow

National Strategy on HIV and AIDS 2011 - 2015
35
The annual progress report will provide information on the progress made in implementing the Work Plan. Based on programme monitoring data that is routinely collected by the National AIDS Programme Secretariat and the Malaysian AIDS Council, an assessment is made whether planned activities have been implemented and whether planned outputs and expected results have been achieved. The annual progress report will also be based on the indicators and targets agreed in the M&E framework, which includes core indicators (see Annex 3). Based on data collected by the National AIDS Programme Secretariat and the Malaysian AIDS Council, and stored in a centralised database, an analysis will be made concerning the progress made in achieving the agreed targets for these core indicators. Finally, the annual progress report will include an analysis of most recent surveillance data as well as data from other recent surveys in order to assess changing and emerging epidemiological trends. Based on the results and findings of the assessments presented in the annual progress report, the National AIDS Programme Secretariat, in close consultation with its partners, will prepare or revise the Work Plan for the coming years. 6.5.3 Mid Term Review A mid-term review of the implementation of the National Strategic Plan is planned to take place in 2013. It will review progress made in the first two years of the NSP. The review will be discussed in a joint stakeholder meeting, with the aim of reaching consensus on: (a) Progress made in the implementation of the national response as agreed in the current National
Strategic Plan
(b) The direction and scope of future implementation of the response to HIV and AIDS. 6.5.4 Final Review and Impact Evaluation A final evaluation of the National Strategic Plan will take place in the second half of 2015. The final evaluation will assess whether expected results and targets have been achieved, through the analysis of available data to measure outcome and impact and a comparison with baselines values for these core indicators. The final evaluation will not only assess effectiveness of individual programmes and of the overall national response, but will also take into consideration the quality and efficiency of programmes and interventions. 6.5.5 HIV and AIDS Research Monitoring and evaluation of the National Strategic Plan will also require data collected through research, including regular surveys. Research, as indicated in Strategy 5 of the National Strategic Plan on HIV and AIDS, compliments monitoring and evaluation by building a knowledge base which will guide the national response. Thematic research will be needed in order to better understand
35
National Strategic Plan on HIV and AIDS2011 – 2015

National Strategy on HIV and AIDS 2011 - 2015
36
underlying causes, dynamics and impacts of the epidemic, such as epidemiological trends, new and emerging areas of concern and a better understanding of vulnerability and long-term consequences of the epidemic. It is therefore envisaged that:
(a) Appropriate research is conducted which is clear and current to support the broader picture of AIDS alleviation, amongst the various MARPs and vulnerable populations.
(b) There is better access to and resource mobilisation of funding for research.
(c) There is a systematic management and sharing of research data put into place to ensure that findings are used to improve the response to the HIV epidemic.
36
National Strategic Plan on HIV and AIDS2011 – 2015

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Ann
ex 1
:
Fr
amew
ork
for t
he N
atio
nal S
trat
egic
Pla
n on
HIV
and
AID
S 20
11 –
201
5
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
Stra
tegy
1:
Impr
ovin
g th
e qu
ality
and
cov
erag
e of
pre
vent
ion
prog
ram
mes
am
ong
mos
t at r
isk
and
vuln
erab
le
popu
latio
ns
Mos
t at r
isk
and
vuln
erab
le
popu
latio
ns
HIV
pre
vent
ion
effo
rts
in 2
011
– 20
15 w
ill fo
cus
on tw
o pr
imar
y pr
ongs
of H
IV tr
ansm
issi
on:
Shar
ing
of n
eedl
es a
nd s
yrin
ges
thro
ugh
inje
ctin
g dr
ug u
se
Unp
rote
cted
sex
ual i
nter
cour
se
1.1
Prev
entio
n of
HIV
tran
smis
sion
th
roug
h th
e sh
arin
g of
nee
dles
an
d sy
ringe
s
IDU
s Pr
imar
y m
ode
of tr
ansm
issi
on in
Mal
aysi
a co
ntin
ues
to b
e th
roug
h in
ject
ing
drug
use
. Su
stai
ning
and
sca
ling
up o
f a m
ore
com
preh
ensi
ve p
rogr
amm
e co
verin
g th
e ha
rm
redu
ctio
n (n
eedl
e sy
ringe
exc
hang
e an
d m
etha
done
mai
nten
ance
ther
apy)
pro
gram
me
cont
inue
s to
be
need
ed. I
ncre
ased
cov
erag
e to
in
clud
e:
Fish
erm
en a
nd o
ther
mob
ile p
opul
atio
ns
Popu
latio
ns in
clo
sed
sett
ings
At
risk
you
th
Wom
en a
nd tr
ansg
ende
r per
sons
Build
an
enab
ling
envi
ronm
ent f
or H
IV p
reve
ntio
n w
ith ID
Us
and
thei
r par
tner
s by
mob
ilizi
ng k
ey
stak
ehol
ders
, inc
ludi
ng, h
ealth
car
e pr
ovid
ers,
co
mm
unity
net
wor
ks, N
GO
s, lo
cal a
utho
ritie
s, a
nd
law
enf
orce
men
t
Dev
elop
str
ateg
ies
to a
ddre
ss b
arrie
rs a
nd c
halle
nges
w
hich
pre
vent
the
effic
ient
and
eff
ectiv
e de
liver
y of
H
IV p
reve
ntio
n w
ith ID
Us.
Impl
emen
t tar
gete
d be
havi
our c
hang
e ap
proa
ches
fo
r mal
e an
d fe
mal
e ID
Us
whi
ch e
mph
asiz
e ris
k re
duct
ion
and
prom
ote
safe
r sex
ual a
nd ri
sk
redu
ctio
n be
havi
ours
.
Impl
emen
t nat
iona
l sca
le u
p of
HIV
pre
vent
ion
with
ID
Us
and
thei
r par
tner
s in
clud
ing
need
le a
nd s
yrin
ge
exch
ange
pro
gram
mes
and
opi
oid
subs
titut
ion
ther
apy.
Stre
ngth
en m
echa
nism
s to
man
age
HIV
pre
vent
ion
amon
g dr
ug u
sers
in p
rison
s an
d ot
her d
eten
tion
cent
res.
37

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
1.2
Prev
entio
n of
HIV
tran
smis
sion
th
roug
h un
prot
ecte
d se
x
Sex
wor
kers
, at r
isk
yout
h, m
en w
ho
have
sex
with
men
, m
igra
nts,
refu
gees
, se
xual
par
tner
s of
ID
Us,
fem
ale
sexu
al
part
ners
of M
SM,
clie
nts
of s
ex
wor
kers
, tra
nsge
nder
pe
rson
s Se
xual
par
tner
s of
M
ARPs
Impr
ovin
g co
vera
ge o
f int
erve
ntio
ns w
hich
: En
cour
age
beha
viou
ral c
hang
e am
ong
MAR
Ps
enco
urag
e co
ndom
use
am
ong
MAR
Ps
prov
ide
sexu
al re
prod
uctiv
e he
alth
ed
ucat
ion
and
othe
r SRH
ser
vice
s
addr
ess
intim
ate
part
ner t
rans
mis
sion
of
HIV
enco
urag
e H
IV te
stin
g th
roug
h VC
T
prom
ote
info
rmat
ion
and
awar
enes
s of
HIV
an
d ST
I thr
ough
med
ia a
nd m
eans
whi
ch a
re
acce
ssib
le a
nd fr
iend
ly to
mos
t at r
isk
popu
latio
ns.
By 2
015,
ach
ieve
d 80
% s
ervi
ce c
over
age
amon
g m
ost a
t ris
k po
pula
tions
whe
re 6
0% o
f tho
se
cove
red
prac
tice
safe
beh
avio
urs.
Revi
ew e
xist
ing
stra
tegi
es in
clud
ing
awar
enes
s pr
ogra
mm
es a
nd a
ctiv
ities
to e
ncou
rage
and
fa
cilit
ate
beha
viou
ral c
hang
e am
ong
MAR
Ps.
Bu
ild a
n en
ablin
g en
viro
nmen
t for
beh
avio
ural
ch
ange
thro
ugh
econ
omic
, wel
fare
and
relig
ious
aid
.
Rais
e aw
aren
ess
and
build
kno
wle
dge
and
awar
enes
s on
HIV
and
oth
er d
isea
ses
(e.g
. TB
and
STIs
), am
ong
MAR
Ps, m
arrie
d an
d un
mar
ried
coup
les,
and
m
embe
rs o
f mos
t at r
isk
yout
h an
d th
eir s
exua
l pa
rtne
rs.
Impr
ove
and
stre
ngth
en V
CT, S
TI a
nd S
RH s
ervi
ces
to
all M
ARPs
, inc
ludi
ng c
ouns
ellin
g fo
r mar
ried
and
unm
arrie
d co
uple
s.
Rais
e aw
aren
ess
and
unde
rsta
ndin
g of
HIV
and
STI
s,
supp
ort a
nd p
rom
ote
the
appr
opria
te u
se o
f co
ndom
s an
d lu
bric
ants
whe
n en
gage
d in
sex
ual
activ
ities
, par
ticul
arly
am
ong
MAR
Ps, t
heir
part
ners
an
d/ o
r the
ir cl
ient
s.
Dev
elop
and
sca
le u
p se
rvic
es o
n se
xual
repr
oduc
tive
heal
th, c
ouns
ellin
g an
d tr
eatm
ent r
elat
ed to
STI
s, H
IV
and
AID
S to
ens
ure
univ
ersa
l cov
erag
e.
Expa
nd a
nd s
cale
up
HIV
pre
vent
ion
prog
ram
min
g in
corp
orat
ing
a co
mpr
ehen
sive
pac
kage
of s
ervi
ces
for m
en w
ho h
ave
sex
with
men
(MSM
) and
tr
ansg
ende
r per
sons
.
Stre
ngth
en th
e pa
rtic
ipat
ion
of n
atio
nal a
nd lo
cal
part
ners
in th
e pr
ovis
ion
of H
IV p
reve
ntio
n pr
ogra
mm
es ta
rget
ing
fore
ign
mig
rant
wor
kers
and
re
fuge
es.
Impl
emen
t tar
gete
d be
havi
our c
hang
e co
mm
unic
atio
n in
terv
entio
ns to
pro
mot
e sa
fer
38

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
sexu
al b
ehav
iour
, add
ress
neg
ativ
e ge
nder
val
ues,
an
d pr
omot
e m
ale
resp
onsi
bilit
y fo
r pos
itive
hea
lth.
Revi
ew e
xist
ing
polic
ies
and
deve
lop
stra
tegi
es to
ad
dres
s ba
rrie
rs a
nd c
halle
nges
whi
ch p
reve
nt th
e ef
ficie
nt a
nd e
ffec
tive
deliv
ery
of H
IV p
reve
ntio
n se
rvic
es to
MAR
Ps e
spec
ially
MSM
, SW
and
TG
s.
1.3
Prev
entio
n of
par
ent t
o ch
ild
tran
smis
sion
(PPT
CT)
Mar
ried
and
unm
arrie
d pr
egna
nt
mot
hers
, wom
en o
f re
prod
uctiv
e ag
e
The
PPTC
T pr
ogra
mm
e in
gov
ernm
ent
heal
thca
re fa
cilit
ies
cont
inue
s to
be
need
ed to
sc
reen
and
pro
vide
trea
tmen
t, ca
re a
nd s
uppo
rt
for p
regn
ant w
omen
with
HIV
and
thei
r pa
rtne
rs/
spou
ses.
Mor
e pr
egna
nt w
omen
will
be
scr
eene
d fo
r HIV
thro
ugh
inte
grat
ion
of
PPTC
T in
ant
enat
al s
ervi
ces
at p
ublic
and
priv
ate
heal
th fa
cilit
ies
with
impr
oved
link
ages
bet
wee
n ex
istin
g SR
H a
nd H
IV p
rogr
amm
es.
The
goal
wou
ld b
e to
elim
inat
e in
cide
nces
of
vert
ical
tran
smis
sion
by
2015
.
Mai
ntai
n th
e pr
ovis
ion
of q
ualit
y, c
ompr
ehen
sive
na
tiona
l PPT
CT s
ervi
ces,
in li
ne w
ith th
e W
HO
re
com
men
ded
four
pro
nged
str
ateg
y, to
reac
h pr
egna
nt w
omen
, the
ir pa
rtne
rs a
nd th
eir i
nfan
ts,
incl
udin
g m
ost a
t ris
k po
pula
tions
.
Stre
ngth
en c
omm
unity
aw
aren
ess
of H
IV to
incr
ease
en
rolm
ent i
n th
e PP
TCT
prog
ram
me
and
othe
r re
late
d an
tena
tal,
fam
ily p
lann
ing,
sex
ual a
nd
repr
oduc
tive
heal
th, v
olun
tary
con
fiden
tial
coun
selli
ng a
nd te
stin
g se
rvic
es, p
artic
ular
ly a
mon
g m
ost a
t ris
k po
pula
tions
.
Ensu
re a
ll H
IV-in
fect
ed p
regn
ant w
omen
and
thei
r H
IV-e
xpos
ed in
fant
s un
der t
he P
PTCT
pro
gram
me
rece
ive
ARV
trea
tmen
t/ p
roph
ylax
is a
nd
brea
stfe
edin
g ed
ucat
ion
to re
duce
mot
her-
to-c
hild
tr
ansm
issi
on o
f HIV
.
Ensu
re th
e av
aila
bilit
y of
PPT
CT in
all
ANC
faci
litie
s in
clud
ing
priv
ate
heal
th c
are
faci
litie
s
St
rate
gy 2
: Im
prov
ing
the
qual
ity a
nd c
over
age
of te
stin
g an
d tr
eatm
ent.
PLH
IV (a
dults
and
ch
ildre
n) a
nd th
ose
affe
cted
The
Gov
ernm
ent c
ontin
ues
to s
uppo
rt a
de
cent
ralis
ed a
ppro
ach
to h
ealth
ser
vice
s w
hich
in
clud
es c
omm
unity
-bas
ed a
nd p
rimar
y he
alth
ca
re th
roug
h to
hos
pita
l-bas
ed c
are.
It p
rovi
des
psyc
hoso
cial
sup
port
incl
udin
g VC
T, n
utrit
iona
l su
ppor
t and
trea
tmen
t for
com
mon
Ensu
re a
dequ
ate
num
ber a
nd tr
aini
ng o
f hea
lthca
re
wor
kers
to d
eliv
er V
CT a
nd A
RV a
nd re
late
d se
rvic
es
Stre
ngth
en p
riorit
y he
alth
ser
vice
s th
roug
h in
crea
sed
inte
grat
ion
of H
IV s
ervi
ce d
eliv
ery.
Impr
ove
cove
rage
and
ear
ly a
cces
s to
and
qua
lity
of
39

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
oppo
rtun
istic
infe
ctio
ns.
Mal
aysi
a al
read
y pr
ovid
es a
nd is
com
mitt
ed to
af
ford
able
acc
ess
to c
linic
al c
are
thro
ugh
the
publ
ic h
ealth
sys
tem
, inc
ludi
ng fr
ee o
r su
bsid
ized
acc
ess
to A
RT.
Peop
le L
ivin
g w
ith H
IV in
clo
sed
sett
ings
and
th
ose
livin
g ou
tsid
e th
e m
ajor
citi
es a
re o
f pa
rtic
ular
ly c
once
rn. S
tron
ger l
inka
ges
and
refe
rral
sys
tem
s be
twee
n H
IV a
nd re
late
d se
rvic
es s
uch
as V
CT, T
B, O
I, SR
H, O
ST a
nd P
PTCT
w
ill b
e ne
eded
. The
re is
als
o a
need
to e
nsur
e an
d m
aint
ain
the
qual
ity a
nd s
usta
inab
ility
of
trea
tmen
t, ca
re a
nd s
uppo
rt s
ervi
ces
for P
LHIV
. Po
sitiv
e pr
even
tion
shou
ld a
lso
be p
rom
oted
am
ong
thos
e liv
ing
with
HIV
Se
rvic
e co
vera
ge is
aim
ed to
be
80%
of t
hose
es
timat
ed to
be
elig
ible
for t
reat
men
t.
HIV
test
ing,
car
e an
d tr
eatm
ent,
sexu
al re
prod
uctiv
e he
alth
and
STI
ser
vice
s fo
r mos
t at r
isk
popu
latio
ns
and
thei
r par
tner
s.
Incr
ease
acc
ess
and
qual
ity o
f HIV
test
ing
and
coun
selli
ng s
ervi
ces
in th
e pu
blic
and
priv
ate
sect
ors
to id
entif
y th
ose
in n
eed
of H
IV tr
eatm
ent
Stre
ngth
en c
apac
ity o
f VCT
rela
ted
staf
f.
Impr
ove
adhe
renc
e to
trea
tmen
t and
det
ectio
n of
lin
e tr
eatm
ent f
ailu
re
Expa
nd ro
utin
e PI
CT fo
r pre
gnan
t wom
en, T
B an
d ST
I pa
tient
s an
d st
reng
then
link
ages
from
pre
vent
ion
to
care
and
trea
tmen
t.
Dev
elop
and
sca
le u
p ca
re a
nd tr
eatm
ent w
ith a
nti-
retr
ovira
l dru
gs a
nd T
B tr
eatm
ent f
or d
rug
user
s in
pr
ison
s an
d ot
her d
eten
tion
cent
res.
Stra
tegy
3:
Incr
easi
ng th
e ac
cess
and
ava
ilabi
lity
of c
are,
sup
port
and
soc
ial i
mpa
ct
miti
gati
on p
rogr
amm
es fo
r Peo
ple
Livi
ng w
ith H
IV a
nd th
ose
affe
cted
.
PLH
IV (a
dults
and
ch
ildre
n) a
nd th
ose
affe
cted
Incr
easi
ng a
cces
s an
d av
aila
bilit
y of
car
e an
d su
ppor
t pro
gram
mes
for P
eopl
e Li
ving
with
HIV
an
d th
ose
affe
cted
whi
ch a
ddre
ss p
hysi
cal,
men
tal,
soci
al, s
pirit
ual,
relig
ious
and
ec
onom
ical
asp
ects
.
Impr
ove
coor
dina
tion,
link
ages
and
refe
rral
am
ong
soci
al, h
ealth
and
com
mun
ity b
ased
ser
vice
s at
the
com
mun
ity le
vel.
Stre
ngth
en th
e qu
ality
and
impa
ct o
f PLH
IV a
nd
MAR
Ps s
uppo
rt g
roup
s an
d ne
twor
ks.
Link
PLH
IV a
nd th
eir f
amili
es to
exi
stin
g so
cial
pr
otec
tion
prog
ram
mes
to e
nsur
e ac
cess
to e
ssen
tial
serv
ices
.
Incr
ease
vis
ibili
ty a
nd m
eani
ngfu
l par
ticip
atio
n an
d de
cisi
on m
akin
g of
PLH
IV a
nd M
ARPs
in im
pact
m
itiga
tion
prog
ram
mes
.
40

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
Prov
ide
qual
ity e
mot
iona
l, re
ligio
us a
nd s
pirit
ual
supp
ort t
o PL
HIV
and
thei
r fam
ilies
.
Stre
ngth
en th
e ro
le o
f com
mun
ity a
nd h
ome
base
d ca
re to
sup
port
pos
itive
pre
vent
ion
and
linka
ges
to
TB a
nd S
RH s
ervi
ces.
Stra
tegy
4:
Mai
ntai
ning
and
impr
ovin
g an
en
ablin
g en
viro
nmen
t for
HIV
pr
even
tion,
trea
tmen
t, c
are
and
supp
ort.
All
Prev
entio
n an
d tr
eatm
ent p
rogr
amm
es a
re
mor
e ef
fect
ive
whe
n op
erat
ing
in a
n en
ablin
g en
viro
nmen
t tha
t doe
s no
t stig
mat
ise
and
disc
rimin
ate
agai
nst t
hose
mos
t at r
isk
and
thos
e af
fect
ed. C
reat
ing
and
mai
ntai
ning
a
bett
er u
nder
stan
ding
of H
IV to
redu
ce s
tigm
a an
d di
scrim
inat
ion.
Es
tabl
ish
and
mai
ntai
n an
ena
blin
g pu
blic
pol
icy
and
lega
l env
ironm
ent t
hat w
ill h
elp
to re
duce
H
IV s
tigm
a an
d di
scrim
inat
ion
and
is s
uppo
rtiv
e to
HIV
pro
gram
mes
and
inte
rven
tions
resp
ectin
g hu
man
dig
nity
, gen
der a
nd s
exua
lity
Ensu
re H
IV is
sues
are
mai
nstr
eam
ed in
to n
atio
nal
soci
al d
evel
opm
ent p
lans
and
the
nece
ssar
y fin
anci
al
and
tech
nica
l res
ourc
es a
re m
obili
sed
to s
uppo
rt
deve
lopm
ent a
nd im
plem
enta
tion
of H
IV a
nd A
IDS
plan
s an
d pr
ogra
mm
es.
Stre
ngth
en c
apac
ity o
f key
min
istr
ies
and
othe
r go
vern
men
t and
civ
il so
ciet
y st
akeh
olde
rs a
t the
na
tiona
l and
loca
l lev
els
to d
evel
op a
nd im
plem
ent
targ
eted
evi
denc
e-ba
sed
inte
rven
tions
.
Enga
ge la
w e
nfor
cem
ent,
heal
thca
re s
ervi
ce
prov
ider
s, re
leva
nt p
ublic
off
icia
ls a
nd c
ivil
soci
ety
stak
ehol
ders
, to
asse
ss a
nd m
itiga
te c
ompl
icat
ions
to
the
natio
nal H
IV re
spon
se.
Impr
ove
the
repr
esen
tatio
n, in
volv
emen
t and
ca
paci
ty o
f civ
il so
ciet
y, c
omm
unity
bas
ed
orga
niza
tions
and
aff
ecte
d po
pula
tion
netw
orks
in
dial
ogue
and
dec
isio
n-m
akin
g, to
war
ds a
chie
ving
U
nive
rsal
Acc
ess
and
stre
ngth
enin
g th
e na
tiona
l re
spon
se.
Stre
ngth
en th
e w
ork
of th
e pr
ivat
e se
ctor
am
ong
loca
l bus
ines
ses
to p
rom
ote
corp
orat
e so
cial
re
spon
sibi
lity
and
to e
stab
lish
wor
kpla
ce-b
ased
HIV
pr
even
tion
prog
ram
mes
and
to a
ddre
ss s
tigm
a an
d di
scrim
inat
ion
in th
e pr
ivat
e se
ctor
.
Inte
nsify
pub
lic u
nder
stan
ding
and
aw
aren
ess
of H
IV
and
AID
S th
roug
h fo
cuse
d co
mm
unic
atio
ns a
nd
41

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Stra
tegi
es
Targ
et P
opul
atio
ns
Ratio
nale
Ke
y A
ctiv
ity
inte
grat
ion
into
com
mun
ity-b
ased
HIV
edu
catio
n m
essa
ges.
Stra
tegy
5:
Incr
easi
ng th
e av
aila
bilit
y an
d qu
ality
of
str
ateg
ic in
form
atio
n an
d its
use
by
pol
icy
mak
ers
and
prog
ram
me
plan
ners
thro
ugh
mon
itori
ng,
eval
uatio
n an
d re
sear
ch.
All
The
avai
labi
lity
of re
sear
ch, s
urve
illan
ce a
nd b
io-
beha
viou
ral d
ata,
and
ana
lysi
s of
mon
itorin
g an
d ev
alua
tion
of H
IV p
rogr
amm
es is
impr
oved
upo
n an
d us
ed to
gui
de a
nd d
eter
min
e po
licy
and
prog
ram
me
fram
ewor
ks fo
r pre
vent
ion,
tr
eatm
ent,
care
and
sup
port
.
Dev
elop
and
str
engt
hen
part
ners
hips
to p
lan,
co
ordi
nate
and
man
age
the
natio
nal m
onito
ring
and
eval
uatio
n, re
sear
ch a
nd s
urve
illan
ce s
yste
ms.
Prod
uce
and
diss
emin
ate
timel
y an
d hi
gh q
ualit
y da
ta fr
om re
sear
ch, i
nteg
rate
d bi
olog
ical
be
havi
oura
l sur
veill
ance
(IBB
S), p
opul
atio
n si
ze
estim
atio
ns a
nd o
ther
stu
dies
.
Pr
omot
e th
e pr
oduc
tion,
dis
sem
inat
ion
and
effe
ctiv
e us
e of
str
ateg
ic in
form
atio
n to
info
rm a
nd
guid
e pr
ogra
mm
e an
d po
licy
deci
sion
mak
ing.
Cons
olid
ate
and
stre
amlin
e m
echa
nism
s fo
r dat
a co
llect
ion
from
bot
h pr
ivat
e an
d pu
blic
HC
faci
litie
s fo
r fut
ure
plan
ning
42

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Ann
ex 2
:
Nat
iona
l Act
ion
Plan
on
HIV
and
AID
S 20
11 –
201
5
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
Stra
tegy
1:
Impr
ovin
g th
e qu
ality
and
cov
erag
e of
pre
vent
ion
prog
ram
mes
am
ong
mos
t at r
isk
and
vuln
erab
le p
opul
atio
ns
1.1
Prev
entio
n of
HIV
tran
smis
sion
thro
ugh
the
shar
ing
of n
eedl
es a
nd s
yrin
ges
Build
an
enab
ling
envi
ronm
ent f
or H
IV
prev
entio
n w
ith ID
Us
and
thei
r par
tner
s by
mob
ilizi
ng k
ey s
take
hold
ers,
incl
udin
g,
heal
th c
are
prov
ider
s, c
omm
unity
ne
twor
ks, N
GO
s, lo
cal a
utho
ritie
s, a
nd
law
enf
orce
men
t
PDRM
, AAD
K, M
OH
, JAK
IM,
MAC
,
All d
istr
icts
whi
ch im
plem
ent h
arm
redu
ctio
n pr
ogra
mm
es w
ill h
ave
harm
redu
ctio
n co
mm
ittee
s in
volv
ing
law
enf
orce
men
t of
ficer
s.
Sust
ain
ongo
ing
advo
cacy
with
gov
ernm
ent b
odie
s an
d ci
vil s
ocie
ty o
rgan
isat
ions
at s
tate
and
nat
iona
l le
vels
Enga
gem
ent w
ith p
rint a
nd e
lect
roni
c m
ass
med
ia
on ID
U is
sues
.
Dev
elop
str
ateg
ies
to a
ddre
ss b
arrie
rs
and
chal
leng
es w
hich
pre
vent
the
effic
ient
and
eff
ectiv
e de
liver
y of
HIV
pr
even
tion
with
IDU
s.
PDRM
, AAD
K, M
OH
, JAK
IM,
MAC
Iden
tifie
d ba
rrie
rs a
nd c
halle
nges
hav
e be
en
sign
ifica
ntly
redu
ced
or re
mov
ed.
Enga
ge d
ecis
ion
and
polic
y m
aker
s, c
omm
unity
gr
oups
and
med
ia o
n ID
U re
late
d is
sues
incl
udin
g ne
edle
syr
inge
exc
hang
e, tr
eatm
ent,
reha
bilit
atio
n an
d co
mm
unity
sup
port
.
Im
plem
ent t
arge
ted
beha
viou
r cha
nge
appr
oach
es fo
r mal
e an
d fe
mal
e ID
Us
whi
ch e
mph
asiz
e ris
k re
duct
ion
and
prom
ote
safe
r sex
ual a
nd ri
sk re
duct
ion
beha
viou
rs.
AAD
K, D
istr
ict H
ealth
Off
ices
, Re
ligio
us D
epar
tmen
t
60%
of m
ale
and
fem
ale
IDU
s re
port
not
sh
arin
g in
ject
ing
equi
pmen
t.
60
% o
f sex
ually
act
ive
mal
e an
d fe
mal
e ID
Us
adop
t saf
er s
ex b
ehav
iour
(i.e
. usi
ng
cond
oms)
Ups
cale
cov
erag
e of
exi
stin
g ID
U a
nd S
RH
prog
ram
mes
to a
chie
ve im
prov
emen
t in
HIV
kn
owle
dge
and
unde
rsta
ndin
g, ri
sk a
sses
smen
t and
ab
ility
to a
cces
s se
rvic
es s
uch
as N
SEP,
MM
T,
cond
oms
and
lubr
ican
ts a
s w
ell a
s in
form
atio
n fo
r H
IV p
reve
ntio
n of
IDU
s an
d th
eir p
artn
ers.
Impl
emen
t nat
iona
l sca
le u
p of
HIV
pr
even
tion
with
IDU
s an
d th
eir p
artn
ers
incl
udin
g ne
edle
and
syr
inge
exc
hang
e pr
ogra
mm
es a
nd o
pioi
d su
bstit
utio
n th
erap
y.
MO
H, A
ADK,
MAC
, Priv
ate
Dru
g Re
hab
Cent
res
Each
dis
tric
t gov
ernm
ent h
ealth
clin
ic is
abl
e to
pro
vide
har
m re
duct
ion
serv
ices
.
Incr
ease
in th
e nu
mbe
r of N
GO
s ab
le to
pr
ovid
e N
SEP
serv
ices
.
Ups
cale
cov
erag
e of
exi
stin
g N
SEP
and
MM
T pr
ogra
mm
es w
ith g
over
nmen
t hea
lthca
re c
linic
s an
d N
GO
s.
In
crea
se th
e nu
mbe
r of a
cces
s po
ints
for M
MT
with
priv
ate
heal
thca
re s
ervi
ces.
.
43

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
Wai
ting
list s
houl
d no
t be
mor
e th
an o
ne
mon
th.
Stre
ngth
en m
echa
nism
s to
man
age
HIV
pr
even
tion
amon
g dr
ug u
sers
in p
rison
s an
d ot
her d
eten
tion
cent
res.
PUSP
EN,
Pris
ons
Dep
artm
ent,
PDRM
M
MT
is a
vaila
ble
in 1
8 pr
ison
s an
d 24
dru
g re
habi
litat
ion
cent
res
(PU
SPEN
).
Ups
cale
exi
stin
g M
MT
prog
ram
me
cove
ring
inca
rcer
ated
set
tings
.
Link
age
of fo
rmer
det
aine
es w
ith p
ost-
rele
ase
serv
ices
(cou
nsel
ling,
MM
T, tr
eatm
ent a
nd s
uppo
rt
grou
ps)
1.
2Pr
even
tion
of H
IV tr
ansm
issi
on th
roug
h un
prot
ecte
d se
x Re
view
exi
stin
g st
rate
gies
incl
udin
g aw
aren
ess
prog
ram
mes
and
act
iviti
es to
en
cour
age
and
faci
litat
e be
havi
oura
l ch
ange
am
ong
MAR
Ps.
MO
H, r
elev
ant M
inis
trie
s,
MAC
, NG
Os
Revi
ew a
nd re
form
s of
HIV
pro
gram
mes
and
ot
her r
elev
ant i
nter
vent
ions
hav
e be
en
cond
ucte
d.
Esta
blis
h na
tiona
l mul
ti st
akeh
olde
r Wor
king
G
roup
with
a m
anda
te to
revi
ew e
xist
ing
HIV
pr
ogra
mm
es a
nd p
rovi
de re
com
men
datio
ns fo
r re
form
.
Iden
tify
and
inte
grat
e be
st p
ract
ices
for H
IV
prev
entio
n pr
ogra
mm
es w
ith s
ex w
orke
rs, t
heir
part
ners
and
clie
nts.
Build
an
enab
ling
envi
ronm
ent f
or
beha
viou
ral c
hang
e th
roug
h ec
onom
ic,
wel
fare
and
relig
ious
ass
ista
nce.
KPW
KM, J
AKIM
, KKL
W, M
AC
Prog
ram
mes
are
ava
ilabl
e to
add
ress
vu
lner
abili
ties
linke
d to
soc
ioec
onom
ic
fact
ors
and
gend
er (e
.g. p
over
ty a
nd s
ingl
e m
othe
rs)
Esta
blis
h liv
elih
ood,
life
ski
lls a
nd w
elfa
re
com
mun
ity p
rogr
amm
es to
add
ress
pov
erty
and
th
e ne
eds
of lo
w in
com
e po
pula
tions
.
Esta
blis
h pa
rtne
rshi
p w
ith g
over
nmen
t and
civ
il so
ciet
y st
akeh
olde
rs o
n th
e is
sues
of
soci
oeco
nom
ic d
ispa
rity,
gen
der a
nd H
IV.
Ra
ise
awar
enes
s an
d bu
ild k
now
ledg
e of
H
IV a
nd o
ther
dis
ease
s (e
.g T
B an
d ST
Is),
amon
g M
ARPs
, mar
ried
and
unm
arrie
d co
uple
s, a
nd m
embe
rs o
f mos
t at r
isk
yout
h an
d th
eir s
exua
l par
tner
s.
MO
H, K
PWKM
, MAC
, NG
Os,
M
edia
Map
ping
, siz
e es
timat
e an
d so
ciob
ehav
iour
al
stud
ies
for e
ach
MAR
Ps h
ave
been
don
e at
le
ast o
nce.
Cond
uct m
appi
ng, s
ize
estim
atio
n an
d IB
BS
exer
cise
s w
ith e
ach
MAR
Ps a
nd id
entif
ied
vuln
erab
le p
opul
atio
ns.
D
isse
min
ate
findi
ngs
from
HIV
stu
dies
to re
leva
nt
gove
rnm
ent a
nd c
ivil
soci
ety
stak
ehol
ders
to a
ssis
t
44
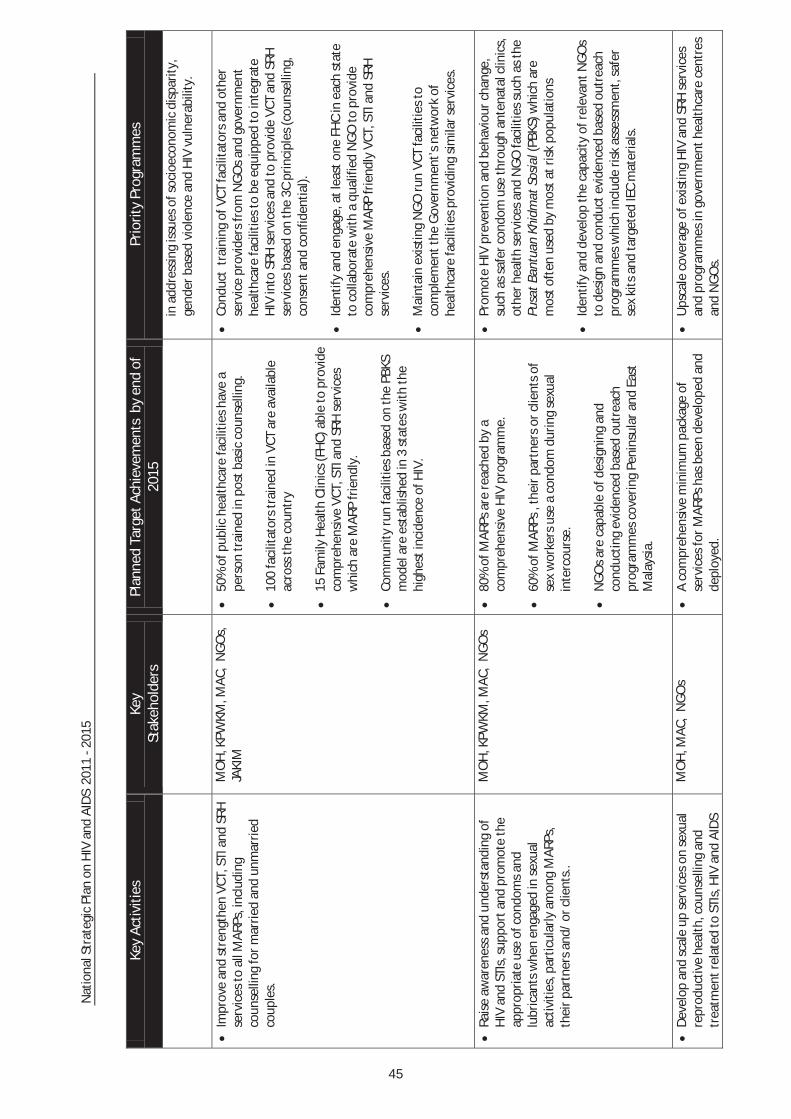
Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
in a
ddre
ssin
g is
sues
of s
ocio
econ
omic
dis
parit
y,
gend
er b
ased
vio
lenc
e an
d H
IV v
ulne
rabi
lity.
Impr
ove
and
stre
ngth
en V
CT, S
TI a
nd S
RH
serv
ices
to a
ll M
ARPs
, inc
ludi
ng
coun
selli
ng fo
r mar
ried
and
unm
arrie
d co
uple
s.
MO
H, K
PWKM
, MAC
, N
GO
s,
JAKI
M
50%
of p
ublic
hea
lthca
re fa
cilit
ies
have
a
pers
on tr
aine
d in
pos
t bas
ic c
ouns
ellin
g.
10
0 fa
cilit
ator
s tr
aine
d in
VCT
are
ava
ilabl
e ac
ross
the
coun
try
15 F
amily
Hea
lth C
linic
s (F
HC)
abl
e to
pro
vide
co
mpr
ehen
sive
VCT
, STI
and
SRH
ser
vice
s w
hich
are
MAR
P fr
iend
ly.
Co
mm
unity
run
faci
litie
s ba
sed
on th
e PB
KS
mod
el a
re e
stab
lishe
d in
3 s
tate
s w
ith th
e hi
ghes
t inc
iden
ce o
f HIV
.
Cond
uct
trai
ning
of V
CT fa
cilit
ator
s an
d ot
her
serv
ice
prov
ider
s fr
om N
GO
s an
d go
vern
men
t he
alth
care
faci
litie
s to
be
equi
pped
to in
tegr
ate
HIV
into
SRH
ser
vice
s an
d to
pro
vide
VCT
and
SRH
se
rvic
es b
ased
on
the
3C p
rinci
ples
(cou
nsel
ling,
co
nsen
t and
con
fiden
tial).
Iden
tify
and
enga
ge, a
t lea
st o
ne F
HC
in e
ach
stat
e to
col
labo
rate
with
a q
ualif
ied
NG
O to
pro
vide
co
mpr
ehen
sive
MAR
P fr
iend
ly V
CT, S
TI a
nd S
RH
serv
ices
.
Mai
ntai
n ex
istin
g N
GO
run
VCT
faci
litie
s to
co
mpl
emen
t the
Gov
ernm
ent’s
net
wor
k of
he
alth
care
faci
litie
s pr
ovid
ing
sim
ilar s
ervi
ces.
Rais
e aw
aren
ess
and
unde
rsta
ndin
g of
H
IV a
nd S
TIs,
sup
port
and
pro
mot
e th
e ap
prop
riate
use
of c
ondo
ms
and
lubr
ican
ts w
hen
enga
ged
in s
exua
l ac
tiviti
es, p
artic
ular
ly a
mon
g M
ARPs
, th
eir p
artn
ers
and/
or c
lient
s..
MO
H, K
PWKM
, MAC
, N
GO
s 80
% o
f MAR
Ps a
re re
ache
d by
a
com
preh
ensi
ve H
IV p
rogr
amm
e.
60
% o
f MAR
Ps ,
thei
r par
tner
s or
clie
nts
of
sex
wor
kers
use
a c
ondo
m d
urin
g se
xual
in
terc
ours
e.
N
GO
s ar
e ca
pabl
e of
des
igni
ng a
nd
cond
uctin
g ev
iden
ced
base
d ou
trea
ch
prog
ram
mes
cov
erin
g Pe
nins
ular
and
Eas
t M
alay
sia.
Prom
ote
HIV
pre
vent
ion
and
beha
viou
r cha
nge,
su
ch a
s sa
fer c
ondo
m u
se th
roug
h an
tena
tal c
linic
s,
othe
r hea
lth s
ervi
ces
and
NG
O fa
cilit
ies
such
as
the
Pusa
t Ban
tuan
Khi
dmat
Sos
ial (
PBKS
) whi
ch a
re
mos
t oft
en u
sed
by m
ost a
t ris
k po
pula
tions
Iden
tify
and
deve
lop
the
capa
city
of r
elev
ant N
GO
s to
des
ign
and
cond
uct e
vide
nced
bas
ed o
utre
ach
prog
ram
mes
whi
ch in
clud
e ris
k as
sess
men
t, sa
fer
sex
kits
and
targ
eted
IEC
mat
eria
ls.
Dev
elop
and
sca
le u
p se
rvic
es o
n se
xual
re
prod
uctiv
e he
alth
, cou
nsel
ling
and
trea
tmen
t rel
ated
to S
TIs,
HIV
and
AID
S
MO
H, M
AC,
NG
Os
A co
mpr
ehen
sive
min
imum
pac
kage
of
serv
ices
for M
ARPs
has
bee
n de
velo
ped
and
depl
oyed
.
Ups
cale
cov
erag
e of
exi
stin
g H
IV a
nd S
RH s
ervi
ces
and
prog
ram
mes
in g
over
nmen
t hea
lthca
re c
entr
es
and
NG
Os.
45

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Act
iviti
esKe
y St
akeh
olde
rsPl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
to e
nsur
e un
iver
sal c
over
age.
80
% o
f MA
RPs
are
cove
red
by a
co
mpr
ehen
sive
HIV
pro
gram
me.
D
evel
op a
com
preh
ensi
ve m
inim
um p
acka
ge o
f se
rvic
es to
pro
vide
MA
RPS
wit
h th
e fo
llow
ing
com
pone
nts:
info
rmat
ion,
HIV
/STI
and
SRH
se
rvic
es, V
CT, c
ondo
ms
and
outr
each
ser
vice
s Ex
pand
and
sca
le u
p H
IV p
reve
ntio
n pr
ogra
mm
ing
inco
rpor
atin
g a
com
preh
ensi
ve p
acka
ge o
f ser
vice
s fo
r m
en w
ho h
ave
sex
with
men
(MSM
) and
tr
ansg
ende
r pe
rson
s
MO
H, M
AC,
NG
Os
80%
of M
SM a
nd T
G p
opul
atio
ns r
each
ed b
y H
IV p
reve
ntio
n pr
ogra
mm
es.
NG
Os
are
capa
ble
of d
eliv
erin
g a
com
preh
ensi
ve p
acka
ge o
f MSM
and
TG
HIV
pr
even
tion
serv
ices
cov
erin
g Pe
nins
ular
and
Ea
st M
alay
sia.
Dev
elop
a c
ompr
ehen
sive
pac
kage
of M
SM a
nd T
G
spec
ific
HIV
pre
vent
ion
serv
ices
bas
ed o
n be
st
prac
tices
.
Iden
tify
and
deve
lop
the
capa
city
of N
GO
s to
be
able
to d
eliv
er a
com
preh
ensi
ve p
acka
ge o
f HIV
pr
even
tion
serv
ices
focu
sing
MSM
and
TG
.
Stre
ngth
en th
e pa
rtic
ipat
ion
of n
atio
nal
and
loca
l par
tner
s in
the
prov
isio
n of
HIV
pr
even
tion
prog
ram
mes
targ
etin
g fo
reig
n m
igra
nt w
orke
rs a
nd r
efug
ees.
UN
HCR
H
IV p
reve
ntio
n pr
ogra
mm
es a
re a
vaila
ble
for
mig
rant
wor
kers
and
ref
ugee
s.
Redu
ctio
n of
60%
in th
e nu
mbe
r of
mig
rant
w
orke
rs fo
und
to b
e w
ith H
IV th
roug
h ro
utin
e an
nual
hea
lth s
cree
ning
.
80%
of r
efug
ees
reac
hed
by H
IV p
reve
ntio
n pr
ogra
mm
es a
nd 6
0% p
ract
ice
safe
r se
x be
havi
our.
Dev
elop
a m
inim
um s
tand
ard
pack
age
of H
IV
prev
entio
n se
rvic
es fo
r m
igra
nt w
orke
rs a
nd
refu
gees
.
Initi
ate
and
stre
ngth
en e
xist
ing
HIV
pro
gram
mes
fo
r m
igra
nt w
orke
rs a
nd r
efug
ees
utili
sing
the
min
imum
sta
ndar
d pa
ckag
e of
HIV
pre
vent
ion
serv
ices
.
Impl
emen
t tar
gete
d be
havi
our
chan
ge
com
mun
icat
ion
inte
rven
tions
to
prom
ote
safe
r se
xual
beh
avio
ur, a
ddre
ss n
egat
ive
gend
er v
alue
s, a
nd p
rom
ote
mal
e re
spon
sibi
lity
for
posi
tive
heal
th.
MO
H, M
AC,
NG
Os,
KPW
KM,
Min
istr
y of
Info
rmat
ion,
Co
mm
unic
atio
n an
d Cu
lture
, N
GO
s, M
edia
60%
of M
SM a
nd T
G r
each
ed b
y H
IV
prev
entio
n in
terv
entio
ns p
ract
ice
safe
r se
x be
havi
our
Dev
elop
a s
erie
s of
wor
ksho
ps fo
r yo
ung
MSM
and
TG
(18
– 24
yea
rs o
ld) w
hich
inte
grat
e liv
ing
skill
s,
gend
er a
nd s
exua
lity
with
saf
er s
ex k
now
ledg
e/
skill
s to
rei
nfor
ce s
afer
sex
beh
avio
ur.
Iden
tify
and
deve
lop
the
capa
city
of N
GO
s to
be
able
to c
ondu
ct th
ese
MSM
and
TG
wor
ksho
ps.
Dev
elop
str
ateg
ies
to a
ddre
ss b
arri
ers
and
chal
leng
es w
hich
pre
vent
the
MO
H, r
elev
ant g
over
nmen
t ag
enci
es, M
AC,
NG
Os.
Re
view
and
ref
orm
s of
str
ateg
ies
whi
ch h
ave
impa
ct o
n H
IV p
reve
ntio
n se
rvic
es h
ave
been
Es
tabl
ish
natio
nal m
ulti
stak
ehol
der
Wor
king
G
roup
with
a m
anda
te to
rev
iew
exi
stin
g po
licie
s to
46
Str
engt
hen
the
part
icip
atio
nof
natio
nal
and
loca
lpar
tner
sin
the
prov
isio
nof
HIV
prev
entio
npr
ogra
mm
esfo
rre
fuge
es.
UN
HCR
,MO
H
HIV
prev
entio
npr
ogra
mm
esar
eav
aila
ble
for
refu
gees
.
80
%of
refu
gees
reac
hed
byH
IVpr
even
tion
prog
ram
mes
and
60%
prac
tice
safe
rse
xbe
havi
our.
D
evel
opa
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
for
refu
gees
.
In
itiat
ean
dst
reng
then
exis
ting
HIV
prog
ram
mes
for
refu
gees
utili
sing
the
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
.
Str
engt
hen
the
part
icip
atio
nof
natio
nal
and
loca
lpar
tner
sin
the
prov
isio
nof
HIV
prev
entio
npr
ogra
mm
esfo
rre
fuge
es.
UN
HCR
,MO
H
HIV
prev
entio
npr
ogra
mm
esar
eav
aila
ble
for
refu
gees
.
80
%of
refu
gees
reac
hed
byH
IVpr
even
tion
prog
ram
mes
and
60%
prac
tice
safe
rse
xbe
havi
our.
D
evel
opa
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
for
refu
gees
.
In
itiat
ean
dst
reng
then
exis
ting
HIV
prog
ram
mes
for
refu
gees
utili
sing
the
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
.
Str
engt
hen
the
part
icip
atio
nof
natio
nal
and
loca
lpar
tner
sin
the
prov
isio
nof
HIV
prev
entio
npr
ogra
mm
esfo
rre
fuge
es.
UN
HCR
,MO
H
HIV
prev
entio
npr
ogra
mm
esar
eav
aila
ble
for
refu
gees
.
80
%of
refu
gees
reac
hed
byH
IVpr
even
tion
prog
ram
mes
and
60%
prac
tice
safe
rse
xbe
havi
our.
D
evel
opa
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
for
refu
gees
.
In
itiat
ean
dst
reng
then
exis
ting
HIV
prog
ram
mes
for
refu
gees
utili
sing
the
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
.
Str
engt
hen
the
part
icip
atio
nof
natio
nal
and
loca
lpar
tner
sin
the
prov
isio
nof
HIV
prev
entio
npr
ogra
mm
esfo
rre
fuge
es.
UN
HCR
,MO
H
HIV
prev
entio
npr
ogra
mm
esar
eav
aila
ble
for
refu
gees
.
80
%of
refu
gees
reac
hed
byH
IVpr
even
tion
prog
ram
mes
and
60%
prac
tice
safe
rse
xbe
havi
our.
D
evel
opa
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
for
refu
gees
.
In
itiat
ean
dst
reng
then
exis
ting
HIV
prog
ram
mes
for
refu
gees
utili
sing
the
min
imum
stan
dard
pack
age
ofH
IVpr
even
tion
serv
ices
.
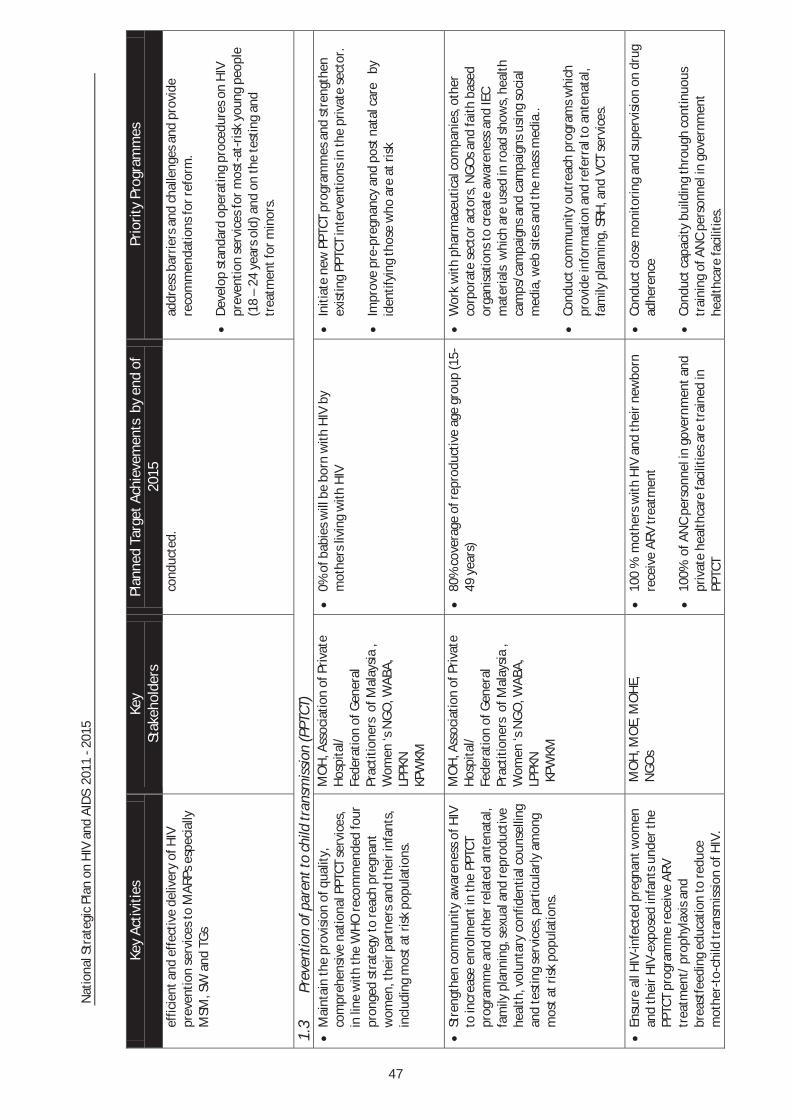
Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
effic
ient
and
eff
ectiv
e de
liver
y of
HIV
pr
even
tion
serv
ices
to M
ARPs
esp
ecia
lly
MSM
, SW
and
TG
s
cond
ucte
d.
addr
ess
barr
iers
and
cha
lleng
es a
nd p
rovi
de
reco
mm
enda
tions
for r
efor
m.
D
evel
op s
tand
ard
oper
atin
g pr
oced
ures
on
HIV
pr
even
tion
serv
ices
for m
ost-
at-r
isk
youn
g pe
ople
(1
8 –
24 y
ears
old
) and
on
the
test
ing
and
trea
tmen
t for
min
ors.
1.3
Prev
entio
n of
par
ent t
o ch
ild tr
ansm
issi
on (P
PTCT
) M
aint
ain
the
prov
isio
n of
qua
lity,
co
mpr
ehen
sive
nat
iona
l PPT
CT s
ervi
ces,
in
line
with
the
WH
O re
com
men
ded
four
pr
onge
d st
rate
gy to
reac
h pr
egna
nt
wom
en, t
heir
part
ners
and
thei
r inf
ants
, in
clud
ing
mos
t at r
isk
popu
latio
ns.
MO
H, A
ssoc
iatio
n of
Priv
ate
Hos
pita
l/
Fede
ratio
n of
Gen
eral
Pr
actit
ione
rs o
f Mal
aysi
a ,
Wom
en ‘s
NG
O, W
ABA,
LP
PKN
KP
WKM
0% o
f bab
ies
will
be
born
with
HIV
by
mot
hers
livi
ng w
ith H
IV
Initi
ate
new
PPT
CT p
rogr
amm
es a
nd s
tren
gthe
n ex
istin
g PP
TCT
inte
rven
tions
in th
e pr
ivat
e se
ctor
.
Impr
ove
pre-
preg
nanc
y an
d po
st n
atal
car
e b
y id
entif
ying
thos
e w
ho a
re a
t ris
k
Stre
ngth
en c
omm
unity
aw
aren
ess
of H
IV
to in
crea
se e
nrol
men
t in
the
PPTC
T pr
ogra
mm
e an
d ot
her r
elat
ed a
nten
atal
, fa
mily
pla
nnin
g, s
exua
l and
repr
oduc
tive
heal
th, v
olun
tary
con
fiden
tial c
ouns
ellin
g an
d te
stin
g se
rvic
es, p
artic
ular
ly a
mon
g m
ost a
t ris
k po
pula
tions
.
MO
H, A
ssoc
iatio
n of
Priv
ate
Hos
pita
l/
Fede
ratio
n of
Gen
eral
Pr
actit
ione
rs o
f Mal
aysi
a ,
Wom
en ‘s
NG
O, W
ABA,
LP
PKN
KP
WKM
80%
cov
erag
e of
repr
oduc
tive
age
grou
p (1
5-
49 y
ears
) W
ork
with
pha
rmac
eutic
al c
ompa
nies
, oth
er
corp
orat
e se
ctor
act
ors,
NG
Os
and
faith
bas
ed
orga
nisa
tions
to c
reat
e aw
aren
ess
and
IEC
mat
eria
ls w
hich
are
use
d in
road
sho
ws,
hea
lth
cam
ps/c
ampa
igns
and
cam
paig
ns u
sing
soc
ial
med
ia, w
eb s
ites
and
the
mas
s m
edia
..
Co
nduc
t com
mun
ity o
utre
ach
prog
ram
s w
hich
pr
ovid
e in
form
atio
n an
d re
ferr
al to
ant
enat
al,
fam
ily p
lann
ing,
SRH
, and
VCT
ser
vice
s.
En
sure
all
HIV
-infe
cted
pre
gnan
t wom
en
and
thei
r HIV
-exp
osed
infa
nts
unde
r the
PP
TCT
prog
ram
me
rece
ive
ARV
trea
tmen
t/ p
roph
ylax
is a
nd
brea
stfe
edin
g ed
ucat
ion
to re
duce
m
othe
r-to
-chi
ld tr
ansm
issi
on o
f HIV
.
MO
H, M
OE,
MO
HE,
N
GO
s
100
% m
othe
rs w
ith H
IV a
nd th
eir n
ewbo
rn
rece
ive
ARV
trea
tmen
t
100%
of A
NC
pers
onne
l in
gove
rnm
ent a
nd
priv
ate
heal
thca
re fa
cilit
ies
are
trai
ned
in
PPTC
T
Cond
uct c
lose
mon
itorin
g an
d su
perv
isio
n on
dru
g ad
here
nce
Cond
uct c
apac
ity b
uild
ing
thro
ugh
cont
inuo
us
trai
ning
of A
NC
pers
onne
l in
gove
rnm
ent
heal
thca
re fa
cilit
ies.
47

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
Ensu
re th
e av
aila
bilit
y of
PPT
CT in
all
ANC
faci
litie
s in
clud
ing
priv
ate
heal
th c
are
faci
litie
s.
Publ
ic a
nd P
rivat
e se
ctor
s
0% v
ertic
al tr
ansm
issi
on re
port
ed
Initi
ate
and
sust
ain
PPTC
T pr
ogra
mm
es a
nd
stre
ngth
en e
xist
ing
PPTC
T in
terv
entio
ns in
clud
ing
in th
e pr
ivat
e se
ctor
.
Stra
tegy
2:
Impr
ovin
g th
e qu
ality
and
cov
erag
e of
test
ing
and
trea
tmen
t. En
sure
ade
quat
e nu
mbe
r and
trai
ning
of
heal
thca
re w
orke
rs to
del
iver
ARV
and
re
late
d se
rvic
es
MO
H, M
AC, P
rivat
e M
edic
al
Prac
titio
ners
, civ
il so
ciet
y
Incr
ease
d nu
mbe
r of r
efer
rals
of A
RV/S
TI/
PLH
IV fr
om p
rivat
e he
alth
care
pra
ctiti
oner
s.
Furt
her d
evel
op, r
evis
e an
d en
sure
impl
emen
tatio
n of
trea
tmen
t rel
ated
pol
icie
s, s
trat
egie
s an
d gu
idel
ines
Trai
n ad
ditio
nal s
taff
and
furt
her s
tren
gthe
n ca
paci
ty o
f sta
ff in
volv
ed in
faci
lity
base
d ca
re
St
reng
then
prio
rity
heal
th s
ervi
ces
thro
ugh
incr
ease
d in
tegr
atio
n of
HIV
se
rvic
e de
liver
y.
MO
H, M
AC, c
ivil
soci
ety
Com
preh
ensi
ve a
nd C
SO in
tegr
ated
HIV
se
rvic
e su
ppor
t mod
el d
eplo
yed
in o
ne
desi
gnat
ed c
linic
per
sta
te
Dev
elop
com
preh
ensi
ve a
nd C
SO in
tegr
ated
HIV
re
late
d su
ppor
t ser
vice
s m
odel
Impr
ove
cove
rage
and
ear
ly a
cces
s to
and
qu
ality
of H
IV te
stin
g, c
are
and
trea
tmen
t, se
xual
repr
oduc
tive
heal
th
and
STI s
ervi
ces
for m
ost a
t ris
k po
pula
tions
and
thei
r par
tner
s.
MO
H, M
AC, c
ivil
soci
ety
60
% o
f MAR
Ps re
ache
d by
cur
rent
pr
ogra
mm
es re
port
kno
wle
dge
of o
r ac
cess
ing
a SR
H/S
TI/H
IV s
ervi
ce.
80
% o
f tho
se e
ligib
le fo
r tre
atm
ent r
ecei
ve
ARV
Stre
ngth
en li
nkag
es a
nd re
ferr
al b
etw
een
faci
lity
base
d pr
ivat
e an
d go
vern
men
t ser
vice
s (V
CT,
OI/
ART,
PPT
CT, T
B, S
TI, a
nd S
RH) a
nd N
GO
ser
vice
s.
M
aint
ain
the
avai
labi
lity
of A
RT fo
r adu
lt an
d pa
edia
tric
pat
ient
s in
all
maj
or g
over
nmen
t he
alth
care
faci
litie
s.
In
crea
se a
cces
s an
d qu
ality
of H
IV te
stin
g an
d co
unse
lling
ser
vice
s in
the
publ
ic a
nd
priv
ate
sect
ors
to id
entif
y th
ose
in n
eed
of H
IV tr
eatm
ent
MO
H, M
AC, c
ivil
soci
ety
60%
of M
ARPs
reac
hed
by c
urre
nt
prog
ram
mes
repo
rt k
now
ledg
e of
or
acce
ssin
g a
SRH
/STI
/HIV
ser
vice
.
Upd
ate
and
revi
sion
of S
tand
ard
Ope
ratin
g Pr
oced
ures
(SO
P) fo
r tes
ting.
Dep
loym
ent o
f rev
ised
SO
P th
roug
h tr
aini
ng o
f go
vern
men
t, pr
ivat
e an
d N
GO
hea
lthca
re w
orke
rs.
St
reng
then
cap
acity
of V
CT re
late
d st
aff.
M
OH
, MAC
, civ
il so
ciet
y 80
% o
f gov
ernm
ent h
ealth
care
wor
kers
and
N
GO
s in
volv
ed in
the
prov
isio
n of
VCT
hav
e un
derg
one
HIV
test
ing
rela
ted
trai
ning
Prov
ide
HIV
test
ing
rela
ted
trai
ning
for
gove
rnm
ent,
priv
ate
and
NG
O h
ealth
care
wor
kers
.
48

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
Impr
ove
adhe
renc
e to
trea
tmen
t and
de
tect
ion
of tr
eatm
ent f
ailu
re
MO
H, M
AC, c
ivil
soci
ety
50%
redu
ctio
n in
the
num
ber o
f cas
es o
f 1st
lin
e tr
eatm
ent f
ailu
re
Incr
ease
cap
acity
and
ava
ilabi
lity
of tr
aine
d re
leva
nt c
ouns
ello
rs a
nd p
eer s
uppo
rt s
ervi
ces,
and
of
rele
vant
hea
lthca
re p
ract
ition
ers
in th
e ar
ea o
f re
sist
ance
test
ing.
Prov
ide
sim
pler
opt
ions
for f
irst l
ine
trea
tmen
t re
gim
en (3
in 1
)
Expa
nd ro
utin
e PI
CT fo
r pre
gnan
t w
omen
, TB
and
STI p
atie
nts
and
stre
ngth
en li
nkag
es fr
om p
reve
ntio
n to
ca
re a
nd tr
eatm
ent.
MO
H, M
AC, p
rivat
e he
alth
care
faci
litie
s, c
ivil
soci
ety
80%
of
gove
rnm
ent a
nd p
rivat
e he
alth
care
fa
cilit
ies
are
able
to p
rovi
de P
ICT
to p
regn
ant
wom
en, T
B an
d ST
I pat
ient
s
Prov
ide
PICT
rela
ted
trai
ning
for r
elev
ant
gove
rnm
ent,
priv
ate
and
NG
O h
ealth
care
wor
kers
.
Dev
elop
and
sca
le u
p ca
re a
nd tr
eatm
ent
with
ant
i-ret
rovi
ral d
rugs
and
TB
trea
tmen
t for
dru
g us
ers
in p
rison
s an
d ot
her d
eten
tion
cent
res.
MO
H, M
inis
try
of H
ome
Affa
irs, P
rison
s D
epar
tmen
t, N
ADA,
MAC
, civ
il so
ciet
y
90%
of a
ll el
igib
le p
erso
ns in
clo
sed
sett
ings
ha
ve a
cces
s to
ART
and
/or T
B tr
eatm
ent.
Pr
ovid
e AR
T an
d TB
trea
tmen
t to
elig
ible
per
sons
in
pris
ons
and
drug
reha
bilit
atio
n ce
ntre
s.
Stra
tegy
3:
Incr
easi
ng th
e ac
cess
and
ava
ilabi
lity
of c
are,
sup
port
and
soc
ial i
mpa
ct m
itiga
tion
prog
ram
mes
for P
eopl
e Li
ving
with
HIV
and
thos
e af
fect
ed.
Impr
ove
coor
dina
tion,
link
ages
and
re
ferr
al a
mon
g so
cial
, hea
lth a
nd
com
mun
ity b
ased
ser
vice
s at
the
com
mun
ity le
vel.
MO
H, K
PWKM
, MAC
, civ
il so
ciet
y Ea
ch d
esig
nate
d in
fect
ious
dis
ease
clin
ic p
er
stat
e w
ill h
ave
an a
ccre
dite
d pe
er s
uppo
rt
grou
p.
Al
l pee
r sup
port
per
sonn
el in
thes
e gr
oups
ar
e tr
aine
d in
refe
rral
and
link
ages
of H
IV
rela
ted
serv
ices
and
rele
vant
soc
ial s
uppo
rt
prog
ram
mes
.
Esta
blis
h an
acc
redi
tatio
n sy
stem
for H
IV p
eer
supp
ort g
roup
s w
hich
is s
tand
ardi
zed
thro
ugho
ut
the
coun
try
Br
ief p
eer e
duca
tors
and
hos
pita
l cou
nsel
lors
on
avai
labl
e go
vern
men
t and
NG
O w
elfa
re a
nd s
ocia
l su
ppor
t pro
gram
mes
.
Stre
ngth
en th
e qu
ality
and
impa
ct o
f PL
HIV
and
MAR
Ps s
uppo
rt g
roup
s an
d ne
twor
ks.
MO
H, M
AC, K
PWKM
A
PLH
IV s
uppo
rt g
roup
in e
ach
stat
e an
d lin
ked
to a
nat
iona
l net
wor
k.
A
MAR
Ps s
uppo
rt g
roup
s in
des
igna
ted
stat
es.
Trai
ning
of P
LHIV
faci
litat
ors
Es
tabl
ish
PLH
IV s
uppo
rt g
roup
s in
eac
h st
ate
and
stre
ngth
en a
n ex
istin
g na
tiona
l PLH
IV n
etw
ork.
49

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
Link
PLH
IV a
nd th
eir f
amili
es to
exi
stin
g so
cial
pro
tect
ion
prog
ram
mes
to e
nsur
e ac
cess
to e
ssen
tial s
ervi
ces.
MO
H, M
AC, K
PWKM
, Tas
k fo
rce
on W
oman
, Girl
s an
d H
IV, J
AKIM
A th
ird o
f all
PLH
IV s
uppo
rt g
roup
faci
litat
ors
(sta
te a
nd n
atio
nal)
are
wom
en.
In
crea
sed
refe
rral
cas
es b
y su
ppor
t gro
ups
to
soci
al p
rote
ctio
n (e
.g. w
elfa
re s
ervi
ces,
Ba
itulm
al, e
tc)
Trai
ning
of P
LHIV
wom
en fa
cilit
ator
s
Brie
f PLH
IV fa
cilit
ator
s on
ava
ilabl
e go
vern
men
t an
d N
GO
soc
ial p
rote
ctio
n pr
ogra
mm
es li
nked
to
gend
er b
ased
vio
lenc
e, s
ingl
e m
othe
rs a
s w
ell a
s w
elfa
re a
nd s
ocia
l sup
port
issu
es.
In
crea
se v
isib
ility
and
mea
ning
ful
part
icip
atio
n an
d de
cisi
on m
akin
g of
PL
HIV
and
MAR
Ps in
impa
ct m
itiga
tion
prog
ram
mes
.
MO
H, P
LHIV
org
aniz
atio
ns/
netw
orks
, rel
ated
gov
t or
gani
zatio
ns
PLH
IV a
nd M
ARPS
are
invo
lved
in th
e de
cisi
on m
akin
g pr
oces
s of
80%
of
prog
ram
mes
whi
ch in
volv
e th
em.
Incr
ease
cap
acity
and
cov
erag
e of
impa
ct
miti
gatio
n pr
ogra
mm
es to
cov
er a
ll PL
HIV
Incr
ease
opp
ortu
nity
for P
LHIV
and
MAR
PS t
o be
in
volv
ed in
the
plan
ning
, im
plem
enta
tion
and
eval
uatio
n of
impa
ct m
itiga
tion
prog
ram
mes
i.e.
tr
eatm
ent,
care
and
sup
port
pro
gram
mes
Prov
ide
qual
ity e
mot
iona
l, re
ligio
us a
nd
spiri
tual
sup
port
to P
LHIV
and
thei
r fa
mili
es.
Gov
ernm
ent a
nd N
GO
re
ligio
us b
odie
s, F
BOs,
JA
KIM
, MAC
, PLH
IV
orga
niza
tions
/net
wor
ks
Avai
labi
lity
of H
IV re
late
d pa
stor
al s
uppo
rt
by in
divi
dual
relig
ious
bel
iefs
in a
ll st
ates
and
w
ith a
ll re
ligio
ns.
Invo
lve
and
build
cap
acity
of f
aith
-bas
ed
orga
niza
tions
in p
rogr
amm
es in
volv
ing
PLH
IV/M
ARPs
Stre
ngth
en th
e ro
le o
f com
mun
ity a
nd
hom
e ba
sed
care
to s
uppo
rt p
ositi
ve
prev
entio
n an
d lin
kage
s to
TB
and
SRH
se
rvic
es
MO
H, M
AC, K
PWKM
, JAK
IM,
civi
l soc
iety
O
ne h
ome-
base
d ca
re p
rogr
amm
e es
tabl
ishe
d an
d pr
esen
t in
each
sta
te
Es
tabl
ishe
d re
ferr
al s
yste
m fo
r PLH
IV/M
ARPS
to
TB
and
SRH
ser
vice
s.
O
ne s
helte
r hom
e fo
r PLH
IV e
stab
lishe
d an
d op
erat
ing
in e
ach
stat
e.
Dev
elop
SO
P an
d pr
ovid
e tr
aini
ng fo
r hom
e-ba
sed
care
and
she
lter h
ome
prov
ider
s
Ensu
re th
at h
ome-
base
d ca
re a
nd s
helte
r hom
e pr
ovid
ers
are
know
ledg
eabl
e in
TB
and
SRH
re
ferr
als
Stra
tegy
4:
Mai
ntai
ning
and
impr
ovin
g an
ena
blin
g en
viro
nmen
t for
HIV
pre
vent
ion,
trea
tmen
t, c
are
and
supp
ort.
En
sure
HIV
issu
es a
re m
ains
trea
med
into
na
tiona
l soc
ial d
evel
opm
ent p
lans
and
th
e ne
cess
ary
finan
cial
and
tech
nica
l re
sour
ces
are
mob
ilise
d to
sup
port
NCC
AI, N
ATCA
, EPU
, MO
H,
MAC
, NG
Os
Incl
usio
n of
HIV
into
the
5 ye
ar M
alay
sian
Pl
an.
Th
e 5
year
Nat
iona
l Str
ateg
y on
HIV
and
AID
S
Stre
ngth
en th
e m
anag
emen
t and
cap
acity
of t
he
Nat
iona
l AID
S Pr
ogra
mm
e se
cret
aria
t (AI
DS/
STI
Sect
or a
nd th
e M
alay
sian
AID
S Co
unci
l) to
impr
ove
coor
dina
tion
and
man
agem
ent o
f the
nat
iona
l
50

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
deve
lopm
ent a
nd im
plem
enta
tion
of H
IV
and
AID
S pl
ans
and
prog
ram
mes
.
is fu
nded
and
sup
port
ed b
y ke
y st
akeh
olde
rs.
resp
onse
.
Cond
uct r
evie
w a
nd s
trea
mlin
ing
of e
xist
ing
polic
ies
and
stra
tegi
es.
St
reng
then
cap
acity
and
pla
ns o
f key
m
inis
trie
s, o
ther
gov
ernm
ent
stak
ehol
ders
and
civ
il so
ciet
y or
gani
satio
ns a
t the
nat
iona
l and
loca
l le
vels
to im
prov
e an
d st
reng
then
ta
rget
ed e
vide
nce-
base
d in
terv
entio
ns.
NCC
AI, N
ATCA
, MO
H, r
elev
ant
min
istr
ies,
MAC
Th
e N
atio
nal S
trat
egy
on H
IV a
nd A
IDS
2011
–
2015
is a
ble
to b
e ef
fect
ivel
y im
plem
ente
d,
mon
itore
d an
d ev
alua
ted
for i
mpa
ct.
Enga
ge k
ey m
inis
trie
s in
the
wor
k an
d de
cisi
on-
mak
ing
proc
esse
s of
the
Nat
iona
l Coo
rdin
atin
g Co
mm
ittee
on
AID
S In
terv
entio
n (N
CCAI
) and
N
atio
nal A
dvis
ory
and
Tech
nica
l Com
mitt
ee o
n AI
DS
(NAT
CA).
Bu
ild c
apac
ity o
f par
ticip
ants
who
rout
inel
y at
tend
Fe
dera
l, St
ate
and
Dis
tric
t lev
el H
IV p
rogr
amm
e m
eetin
gs.
Se
nsiti
se a
nd e
ngag
e la
w e
nfor
cem
ent,
heal
thca
re s
ervi
ce p
rovi
ders
, rel
evan
t pu
blic
off
icia
ls a
nd c
ivil
soci
ety
stak
ehol
ders
, to
asse
ss, p
reve
nt a
nd
miti
gate
any
neg
ativ
e co
nseq
uenc
es o
f la
ws
and
polic
ies
to th
e na
tiona
l HIV
re
spon
se
MO
H, M
embe
rs o
f Pa
rliam
ent,
law
enf
orce
men
t bo
dies
, MAC
, NG
Os.
Incr
ease
d ca
paci
ty o
f gov
ernm
ent a
nd c
ivil
stak
ehol
ders
to a
ddre
ss is
sues
of s
tigm
a an
d di
scrim
inat
ion
Build
cap
acity
of p
arlia
men
taria
ns, l
aw
enfo
rcem
ent o
ffic
ials
, and
key
pol
icy
and
deci
sion
m
aker
s on
HIV
rela
ted
issu
es.
Impr
ove
the
repr
esen
tatio
n, in
volv
emen
t an
d ca
paci
ty o
f civ
il so
ciet
y, c
omm
unity
ba
sed
orga
niza
tions
and
aff
ecte
d po
pula
tion
netw
orks
in p
olic
y di
alog
ue
and
deci
sion
-mak
ing,
tow
ards
ach
ievi
ng
Uni
vers
al A
cces
s an
d st
reng
then
ing
the
natio
nal r
espo
nse.
MAC
, NG
Os,
civ
il so
ciet
y ne
twor
ks
Incr
ease
d ca
paci
ty o
f civ
il so
ciet
y re
pres
enta
tives
in c
onsu
ltativ
e bo
dies
(e.g
. Co
untr
y Co
ordi
natin
g M
echa
nism
) and
pol
icy
disc
ussi
ons.
Build
cap
acity
of c
ivil
soci
ety
repr
esen
tativ
es to
en
able
them
to p
artic
ipat
e an
d co
ntrib
ute
in p
olic
y di
alog
ue a
nd d
ecis
ion
mak
ing.
Stre
ngth
en th
e w
ork
of th
e pr
ivat
e se
ctor
am
ong
loca
l bus
ines
ses
to p
rom
ote
corp
orat
e so
cial
resp
onsi
bilit
y an
d to
Min
istr
y of
Hum
an R
esou
rce,
M
AC, N
GO
s, p
rivat
e se
ctor
bo
dies
and
com
pani
es
30 p
rivat
e se
ctor
com
pani
es h
ave
adop
ted
eith
er th
e M
OH
R’s
HIV
in th
e W
orkp
lace
Po
licy,
the
Mal
aysi
an A
IDS
Char
ter o
r
Prom
ote
the
HIV
in th
e W
orkp
lace
Pol
icy
(MO
HR)
an
d th
e M
alay
sian
AID
S Ch
arte
r to
priv
ate
sect
or
com
pani
es a
nd o
rgan
isat
ions
.
51

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
esta
blis
h w
orkp
lace
-bas
ed H
IV
prev
entio
n pr
ogra
mm
es a
nd to
add
ress
st
igm
a an
d di
scrim
inat
ion
in th
e pr
ivat
e se
ctor
.
esta
blis
hed
som
e fo
rm o
f AID
S in
the
wor
kpla
ce p
olic
y.
Inte
nsify
pub
lic u
nder
stan
ding
and
aw
aren
ess
of H
IV a
nd A
IDS
thro
ugh
focu
sed
com
mun
icat
ions
and
inte
grat
ion
into
com
mun
ity-b
ased
HIV
edu
catio
n m
essa
ges.
MO
H, M
AC, N
GO
s, K
PWKM
, M
OE,
MO
HE,
Min
istr
y of
In
form
atio
n, C
omm
unic
atio
n an
d Cu
lture
, NG
Os,
Med
ia
60%
of y
oung
peo
ple
aged
15–
24 w
ho b
oth
corr
ectly
iden
tify
way
s of
pre
vent
ing
the
sexu
al tr
ansm
issi
on o
f HIV
and
who
reje
ct
maj
or m
isco
ncep
tions
abo
ut H
IV
tran
smis
sion
Prom
ote
com
preh
ensi
ve s
exua
l rep
rodu
ctiv
e he
alth
and
life
ski
lls b
ased
edu
catio
n an
d H
IV
awar
enes
s pr
ogra
mm
es a
mon
g yo
ung
peop
le a
ged
15-2
4.
Stra
tegy
5:
Incr
easi
ng th
e av
aila
bilit
y an
d qu
ality
of s
trat
egic
info
rmat
ion
and
its u
se b
y po
licy
mak
ers
and
prog
ram
me
plan
ners
thro
ugh
mon
itori
ng, e
valu
atio
n an
d re
sear
ch.
Dev
elop
and
str
engt
hen
part
ners
hips
to
plan
, coo
rdin
ate
and
man
age
the
natio
nal m
onito
ring
and
eval
uatio
n,
rese
arch
and
sur
veill
ance
sys
tem
s.
MO
H, M
AC,
Civi
l soc
iety
, rel
ated
go
vern
men
t age
ncie
s,
rese
arch
inst
itutio
ns
An in
tegr
ated
M&
E un
it ha
s be
en e
stab
lishe
d at
the
natio
nal l
evel
and
coo
rdin
ated
by
the
HIV
/STI
sec
tor.
Stre
ngth
en th
e ex
istin
g su
rvei
llanc
e sy
stem
by
deve
lopi
ng a
com
preh
ensi
ve n
atio
nal M
&E
fram
ewor
k
Prod
uce
and
diss
emin
ate
timel
y an
d hi
gh
qual
ity d
ata
from
rese
arch
, int
egra
ted
biol
ogic
al b
ehav
iour
al s
urve
illan
ce (I
BBS)
, po
pula
tion
size
est
imat
ions
and
oth
er
stud
ies.
MO
H, M
AC, M
ARPs
, res
earc
h in
stitu
tions
, re
gion
al &
inte
rnat
iona
l or
gani
satio
ns
Min
imum
of 1
rese
arch
per
MAR
P an
d ot
her
vuln
erab
le p
opul
atio
ns is
pro
duce
d an
d di
ssem
inat
ed w
ithin
6 m
onth
s of
rese
arch
All H
IV re
late
d re
sear
ch is
com
pile
d in
a
rese
arch
dire
ctor
y.
A
natio
nal M
&E
Fram
ewor
k an
d m
anua
l is
deve
lope
d an
d di
ssem
inat
ed to
all
stak
ehol
ders
Cond
uct s
ize
estim
atio
n an
d so
cial
rese
arch
on
MAR
PS/
othe
r det
erm
ined
vul
nera
ble
popu
latio
ns
with
indi
vidu
al re
sear
cher
s, in
stitu
tions
and
NG
Os.
at
nat
iona
l and
sta
te le
vel
Pr
oduc
e co
mpr
ehen
sive
and
hig
h qu
ality
rout
ine
prog
ram
me
mon
itorin
g da
ta b
y ha
rmon
izin
g an
d st
anda
rdis
ing
M&
E ef
fort
s in
clud
ing
alig
nmen
t of
mea
sure
able
indi
cato
rs w
hich
refle
ct a
ctua
l pr
ogra
mm
e ac
hiev
emen
t, in
dica
tor d
efin
ition
s,
data
col
lect
ion
tool
s, d
ata
man
agem
ent a
nd
repo
rtin
g pr
oced
ures
.
Prom
ote
the
prod
uctio
n, d
isse
min
atio
n an
d ef
fect
ive
use
of s
trat
egic
info
rmat
ion
to in
form
and
gui
de p
rogr
amm
e an
d
MO
H, r
elev
ant g
ovt a
genc
ies,
ci
vil s
ocie
ty, m
edia
A
min
imum
of 1
upd
ate
sess
ion
cond
ucte
d du
ring
NAT
CA.
Trai
n ex
pert
s in
writ
ing
evid
ence
bas
ed p
olic
y br
iefs
, ris
k co
mm
unic
atio
n m
ater
ial a
nd to
con
duct
m
edia
trai
ning
52

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Key
Activ
ities
Ke
y
Stak
ehol
ders
Pl
anne
d Ta
rget
Ach
ieve
men
ts b
y en
d of
20
15
Prio
rity
Prog
ram
mes
polic
y de
cisi
on m
akin
g.
60
% o
f new
s co
vera
ge o
n H
IV is
bas
ed o
n re
liabl
e da
ta a
nd fa
cts.
Dev
elop
sm
art p
artn
ersh
ip a
nd s
ensi
tisat
ion
prog
ram
mes
with
med
ia p
ract
ition
ers
on H
IV
rela
ted
issu
es.
D
evel
op m
echa
nism
for d
ata
colle
ctio
n fr
om b
oth
priv
ate
and
publ
ic h
ealth
care
fa
cilit
ies
for f
utur
e pl
anni
ng
MO
H, p
rivat
e he
alth
pr
actit
ione
rs, c
ivil
soci
ety
Fam
ily H
ealth
Div
isio
n an
d H
IV/S
TI e
stab
lish
an in
tegr
ated
and
con
solid
ated
dat
abas
e Es
tabl
ish
an a
gree
men
t bet
wee
n di
ffer
ent
stak
ehol
ders
(Gov
t, pr
ivat
e an
d BG
O) t
o sy
stem
atic
ally
and
con
sist
ently
con
trib
ute
rela
ted
HIV
dat
a
As
sess
and
upg
rade
exi
stin
g H
IV d
ata
colle
ctio
n sy
stem
s to
ena
ble
impr
oved
dat
a an
alys
is a
nd
acce
ssib
le to
MO
H a
nd N
GO
s.
53

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Ann
ex 3
:
Prop
osed
targ
et fo
r NSE
P un
der N
SP 2
011
– 20
15
STA
TE
TARG
ET O
F N
EW C
LIEN
T FO
R N
SEP
2011
20
12
2013
20
14
2015
Pe
rlis
248
392
494
530
587
Keda
h 1,
762
2,77
9 3,
502
3,76
3 4,
168
P. P
inan
g 2,
786
4,39
4 5,
538
5,94
9 6,
590
Pera
k 1,
583
2,49
7 3,
147
3,38
1 3,
745
W.P
. KL
3,69
0 5,
820
7,33
6 7,
882
8,73
0 Se
lang
or
3,14
1 4,
953
6,24
3 6,
708
7,43
0 N
. Sem
bila
n 1,
102
1,73
8 2,
190
2,35
4 2,
607
Mel
aka
603
950
1,19
9 1,
288
1,42
6 Jo
hor
2,55
0 4,
022
5,07
0 5,
447
6,03
3 Ke
lant
an
2,11
7 3,
339
4,20
8 4,
520
5,00
8 Te
reng
ganu
2,
208
3,48
2 4,
389
4,71
6 5,
223
Paha
ng
1,91
9 3,
027
3,81
5 4,
099
4,54
0 Sa
raw
ak
722
1,13
9 1,
436
1,54
3 1,
709
Saba
h 1,
438
2,26
8 2,
859
3,07
2 3,
403
TOTA
L 25
,869
40
,800
51
,425
55
,250
61
,200
54

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Pr
opos
ed ta
rget
for M
MT
unde
r NSP
201
1 –
2015
STA
TE
TARG
ET O
F N
EW C
LIEN
T FO
R M
MT
2011
20
12
2013
20
14
2015
Pe
rlis
202
270
438
548
742
Keda
h 1,
436
1,91
5 2,
963
3,89
1 5,
267
P. P
inan
g 2,
271
3,02
8 4,
685
6,15
1 8,
328
Pera
k 1,
291
1,72
1 2,
662
3,49
5 4,
744
W.P
. KL
3,00
9 3,
926
6,20
6 8,
149
11,0
33
Sela
ngor
2,
561
3,41
7 5,
282
6,93
5 9,
390
N. S
embi
lan
901
1,19
8 1,
854
2,53
4 3,
300
Mel
aka
492
655
1,03
5 1,
381
1,81
4 Jo
hor
2,07
8 2,
772
4,28
9 5,
632
7,62
5 Ke
lant
an
1,72
6 2,
301
3,56
0 4,
678
6,32
9 Te
reng
ganu
1,
800
2,40
0 3,
725
4,87
6 6,
329
Paha
ng
1,56
5 2,
086
3,22
7 4,
238
5,73
8 Sa
raw
ak
570
759
1,17
5 1,
543
2,08
9 Sa
bah
500
750
975
1,20
0 1,
800
TOTA
L 20
,400
27
,200
42
,075
55
,250
74
,800
55
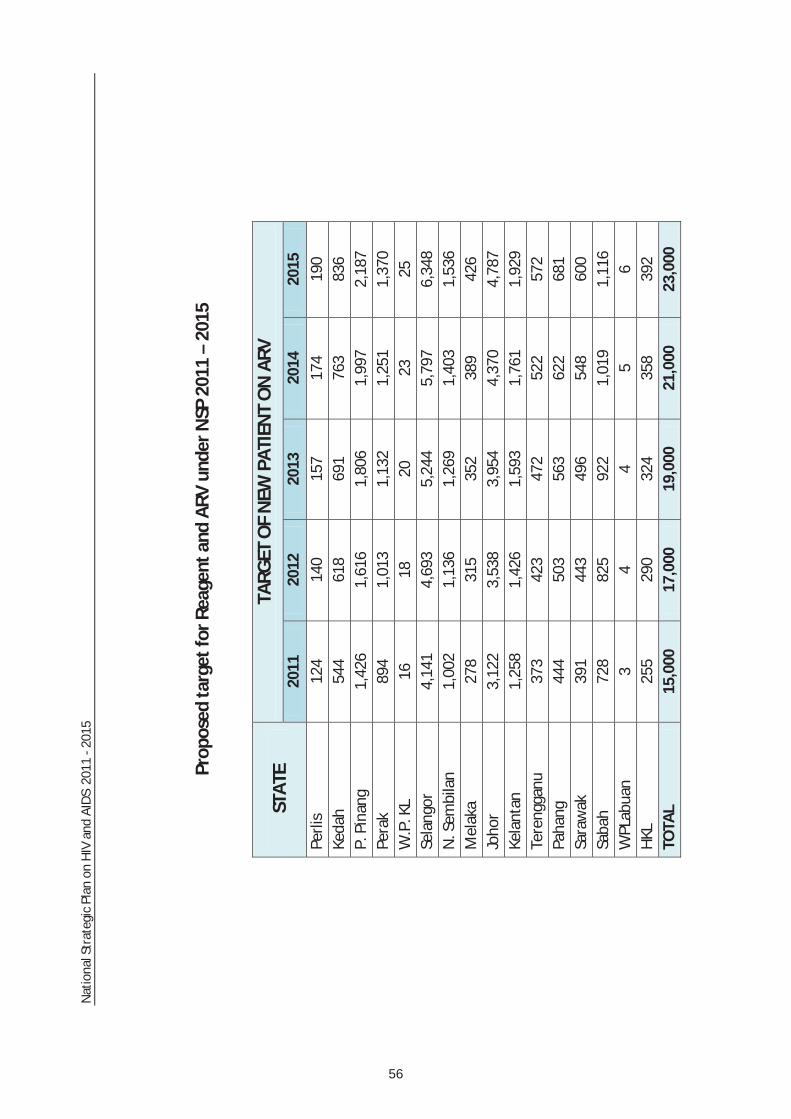
Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Pr
opos
ed ta
rget
for R
eage
nt a
nd A
RV u
nder
NSP
201
1 –
2015
STA
TE
TARG
ET O
F N
EW P
ATIE
NT
ON
ARV
20
11
2012
20
13
2014
20
15
Perli
s 12
4 14
0 15
7 17
4 19
0 Ke
dah
544
618
691
763
836
P. P
inan
g 1,
426
1,61
6 1,
806
1,99
7 2,
187
Pera
k 89
4 1,
013
1,13
2 1,
251
1,37
0 W
.P. K
L 16
18
20
23
25
Se
lang
or
4,14
1 4,
693
5,24
4 5,
797
6,34
8 N
. Sem
bila
n 1,
002
1,13
6 1,
269
1,40
3 1,
536
Mel
aka
278
315
352
389
426
Joho
r 3,
122
3,53
8 3,
954
4,37
0 4,
787
Kela
ntan
1,
258
1,42
6 1,
593
1,76
1 1,
929
Tere
ngga
nu
373
423
472
522
572
Paha
ng
444
503
563
622
681
Sara
wak
39
1 44
3 49
6 54
8 60
0 Sa
bah
728
825
922
1,01
9 1,
116
WPL
abua
n 3
4 4
5 6
HKL
25
5 29
0 32
4 35
8 39
2 TO
TAL
15,0
00
17,0
00
19,0
00
21,0
00
23,0
00
56

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Ann
ex 4
:
Perf
orm
ance
Indi
cato
rs fo
r the
Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
2011
– 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
GEN
ERA
L IN
DIC
ATO
RS (I
MPA
CT)
1 H
IV p
reva
lenc
e am
ong
popu
latio
n ag
ed
15-4
9 ye
ars
MO
H-P
roje
ctio
n of
the
Mal
aysi
a H
IV e
pide
mic
Ev
ery
2 ye
ars
0.50
%
N
SP
2 Pe
rcen
tage
of y
oung
wom
en a
nd m
en
aged
15–
24 w
ho a
re H
IV in
fect
ed.
Prog
ram
me
Mon
itorin
g (P
PTCT
Pro
gram
me)
Ev
ery
2 ye
ars
0.05
%
U
NG
ASS
22, M
DG
3 Pe
rcen
tage
of m
ost a
t- ri
sk p
opul
atio
ns
who
are
HIV
infe
cted
ID
U –
IBBS
Ev
ery
2 ye
ars
22.0
6% (2
009)
17
%
UN
GAS
S 23
SW –
IBBS
Ev
ery
2 ye
ars
10.5
3% (2
009)
7%
TG –
IBBS
Ev
ery
2 ye
ars
9.7%
(200
9)
6%
MSM
– V
DTS
Ev
ery
2 ye
ars
3.8
7% (2
009)
2%
4 Pe
rcen
tage
of a
dults
and
chi
ldre
n w
ith
HIV
kno
wn
to b
e on
trea
tmen
t 12
mon
ths
afte
r ini
tiatio
n of
ant
iretr
ovira
l th
erap
y
Nat
iona
l ART
Pro
gram
me
Mon
itorin
g Ev
ery
year
86
.9%
(200
9)
90%
U
NG
ASS
24, U
A
5 Pe
rcen
tage
of i
nfan
ts b
orn
to H
IV-
infe
cted
mot
hers
who
are
infe
cted
PMTC
T pr
ogra
m m
onito
ring
Ever
y ye
ar
2.67
% (2
009)
0%
U
NG
ASS
25
57

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
Stra
tegy
1: I
mpr
ovin
g th
e qu
ality
and
cov
erag
e of
pre
vent
ion
prog
ram
mes
am
ong
mos
t at r
isk
and
vuln
erab
le p
opul
atio
ns.
OU
TCO
ME
IND
ICA
TORS
6 Pe
rcen
tage
of y
oung
wom
en a
nd m
en
aged
15–
24 w
ho b
oth
corr
ectly
iden
tify
way
s of
pre
vent
ing
the
sexu
al
tran
smis
sion
of H
IV a
nd w
ho re
ject
m
ajor
mis
conc
eptio
ns a
bout
HIV
tr
ansm
issi
on
IBBS
Ev
ery
2 ye
ars
22.6
% (2
008)
50
%
UN
GAS
S 13
, UA
7 Pe
rcen
tage
of m
ost a
t- ri
sk p
opul
atio
ns
who
bot
h co
rrec
tly id
entif
y w
ays
of
prev
entin
g th
e se
xual
tran
smis
sion
of
HIV
and
who
reje
ct m
ajor
m
isco
ncep
tions
abo
ut H
IV tr
ansm
issi
on
IDU
– IB
BS (2
009)
Ev
ery
2 ye
ars
DU
: 49
.68%
60
%
UN
GAS
S 14
SW –
IBBS
(200
9)
Ever
y 2
year
s SW
: 38
.48%
60
%
TG –
IBBS
(200
9)
Ever
y 2
year
s TG
: 37%
60
%
MSM
– N
/A
Ever
y 2
year
s M
SM :
N/A
60
%
8 Pe
rcen
tage
of y
oung
wom
en a
nd m
en
who
hav
e ha
d se
xual
inte
rcou
rse
befo
re th
e ag
e of
15
Cros
s se
ctio
nal M
alay
sian
sc
hool
sur
vey
Ever
y 2
year
s 5.
38%
(200
6)
4%
UN
GAS
S 15
, UA
9 Pe
rcen
tage
of a
dults
age
d 15
–49
who
ha
ve h
ad s
exua
l int
erco
urse
with
mor
e th
an o
ne p
artn
er in
the
last
12
mon
ths
Popu
latio
n ba
sed
surv
ey
Ever
y 3-
5 ye
ars
N/A
UN
GAS
S 16
10
Perc
enta
ge o
f adu
lts a
ged
15–4
9 w
ho
had
mor
e th
an o
ne s
exua
l par
tner
in
the
past
12
mon
ths
who
repo
rt th
e us
e of
a c
ondo
m d
urin
g th
eir l
ast
inte
rcou
rse.
Popu
latio
n ba
sed
surv
ey
Ever
y 3-
5 ye
ars
N/A
UN
GAS
S 17
11
Perc
enta
ge o
f fem
ale
and
mal
e se
x w
orke
rs re
port
ing
the
use
of a
con
dom
w
ith th
eir m
ost r
ecen
t clie
nt
IBBS
Ev
ery
2 ye
ars
61.3
4%
(200
9-Fe
mal
e on
ly)
80%
U
NG
ASS
18
12
Perc
enta
ge o
f men
repo
rtin
g th
e us
e of
a
cond
om th
e la
st ti
me
they
had
ana
l se
x w
ith a
mal
e pa
rtne
r
MAC
Pro
gram
me
Mon
itorin
g
21
% (2
008)
60
%
UN
GAS
S 19
13
Perc
enta
ge o
f inj
ectin
g dr
ug u
sers
who
re
port
the
use
of a
con
dom
at l
ast
sexu
al in
terc
ours
e
IDU
– IB
BS
Ever
y 2
year
s 27
.8%
(200
9)
60%
U
NG
ASS
20
58

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
14
Perc
enta
ge o
f inj
ectin
g dr
ug u
sers
who
re
port
ed u
sing
ste
rile
inje
ctin
g eq
uipm
ent t
he la
st ti
me
they
inje
cted
IDU
– IB
BS
Ever
y 2
year
s 83
.49%
95
%
UN
GAS
S 21
OU
TPU
T IN
DIC
ATO
R
15
Perc
enta
ge o
f mos
t at-
risk
pop
ulat
ions
re
ache
d w
ith H
IV p
reve
ntio
n pr
ogra
mm
es d
isag
greg
ated
by
type
s of
M
ARPs
.
IDU
– IB
BS
Ever
y 2
year
s 27
% (2
009)
50
%
UN
GAS
S 9
SW –
IBBS
Ev
ery
2 ye
ars
12%
(200
9)
80%
TB –
IBBS
Ev
ery
2 ye
ars
65%
(200
9)
80%
MSM
– N
/A
Ever
y 2
year
s N
/A
80%
16
Num
ber o
f dis
tric
t gov
ernm
ent h
ealth
cl
inic
pro
vidi
ng N
SEP
serv
ices
MO
H
Ever
y ye
ar
73
800
NSP
17
Num
ber o
f NG
Os
prov
idin
g N
SEP
serv
ice
MO
H
Ever
y ye
ar
18
66
NSP
18
Perc
enta
ge o
f tar
gete
d cl
ient
s re
ceiv
ing
NSE
P ki
ts a
t NSE
P si
te
Prog
ram
mon
itorin
g (M
AC)
Ever
y ye
ar
N/A
10
0%
NSP
19
Num
ber o
f MM
T se
rvic
e av
aila
ble
disa
ggre
gate
d by
type
of c
entr
e.
MO
H
N
SP
Pris
on
Ever
y ye
ar
18 (2
010)
32
N
atio
nal A
nti-D
rug
Agen
cy
faci
litie
s Ev
ery
year
25
(201
0)
24
Gov
ernm
ent h
ealth
care
faci
lity
Ever
y ye
ar
174
(201
0)
800
20
Num
ber o
f com
preh
ensi
ve m
inim
um
pack
age
of s
ervi
ces
for M
ARPs
de
velo
ped
and
depl
oyed
.
MAC
Ev
ery
year
N
/A
5 N
SP
21
Num
ber o
f TW
G fo
r MAR
Ps to
mon
itor
com
preh
ensi
ve m
inim
um p
acka
ge o
f se
rvic
es e
stab
lishe
d
MAC
Ev
ery
year
N
/A
1
59

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
Stra
tegy
2:
Impr
ovin
g th
e qu
ality
and
cov
erag
e of
test
ing
and
trea
tmen
t.
OU
TCO
ME
IND
ICA
TORS
22
Perc
enta
ge o
f wom
en a
nd m
en a
ged
15-4
9 w
ho re
ceiv
ed a
n H
IV te
st in
the
last
12
mon
ths
and
who
kno
w th
e re
sults
(HIV
Pro
gram
me
Mon
itorin
g)
Ever
y ye
ar
98%
98
%
UN
GAS
S 7,
UA
23
Perc
enta
ge o
f MAR
Ps (M
ost a
t- ri
sk
popu
latio
ns) t
hat h
ave
rece
ived
an
HIV
te
st in
the
last
12
mon
ths
and
who
kn
ow th
e re
sults
.
IDU
– IB
BS
Ever
y 2
year
s ID
U :
33.0
%
(200
9)
60%
U
NG
ASS
8,
SW –
IBBS
Ev
ery
2 ye
ars
SW :
19.9
6%
(200
9)
90%
TG –
IBBS
Ev
ery
2 ye
ars
TG: 1
9%
(200
9)
90%
MSM
– N
/A
Ever
y 2
year
s M
SM :
N/A
60
%
OU
TPU
T ID
ICA
TORS
24
Perc
enta
ge o
f adu
lts a
nd c
hild
ren
with
ad
vanc
ed H
IV in
fect
ion
(CD
4 <3
50 o
r sh
owin
g si
gns
of A
IDS)
rece
ivin
g an
tiret
rovi
ral t
hera
py
Nat
iona
l AID
S Re
gist
ry
Ever
y ye
ar
37.3
%;
9,96
2 (2
009)
95
%
UN
GAS
S 4,
MD
G, U
A
25
Perc
enta
ge o
f hea
lth c
are
wor
ker
trai
ned
in H
IV re
late
d se
rvic
e de
liver
y di
sagg
rega
ted
by ty
pe o
f hea
lthca
re
wor
kers
:
MO
H /
MAC
NSP
Gov
ernm
ent h
ealth
care
wor
ker
Ever
y 2
year
s N
/A
85%
Priv
ate
heal
thca
re w
orke
r Ev
ery
2 ye
ars
N/A
85
%
26
Num
ber o
f des
igna
ted
clin
ic d
eplo
yed
com
preh
ensi
ve a
nd C
SO in
tegr
ated
H
IV s
ervi
ce s
uppo
rt m
odel
MO
H /
MAC
NSP
Gov
ernm
ent c
linic
Ev
ery
year
N
/A
14
Pr
ivat
e cl
inic
Ev
ery
year
N
/A
14
27
Perc
enta
ge o
f peo
ple
in e
nclo
sed
sett
ings
who
elig
ible
acc
essi
ng to
ART
an
d/or
TB
trea
tmen
t.
MO
H
Ever
y ye
ar
N/A
90
%
NSP
60

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
28
Perc
enta
ge o
f MAR
Ps re
ache
d by
cu
rren
t pro
gram
mes
repo
rt a
cces
sing
a
SRH
/STI
/HIV
ser
vice
s.
MAC
Ev
ery
2 ye
ars
IDU
: N
/A
60%
N
SP
Ever
y 2
year
s SW
: N
/A
60%
Ever
y 2
year
s M
SM :
N/A
60
%
Ever
y 2
year
s TG
: N/A
60
%
29
Perc
enta
ge o
f hea
lth c
are
faci
litie
s pr
ovid
ing
PICT
to p
regn
ant w
omen
, TB
and
STI p
atie
nts
disa
ggre
gate
d by
ty
pes
of h
ealth
car
e fa
cilit
ies.
MO
H
N
SP
Gov
ernm
ent h
ealth
faci
lity
Ever
y ye
ar
N/A
10
0%
Pr
ivat
e he
alth
faci
lity
Ever
y ye
ar
N/A
10
0%
Stra
tegy
3: I
ncre
asin
g th
e ac
cess
and
ava
ilabi
lity
of c
are,
sup
port
and
soc
ial i
mpa
ct m
itiga
tion
prog
ram
mes
for P
eopl
e Li
ving
with
HIV
and
thos
e af
fect
ed.
OU
TCO
ME
IND
ICA
TORS
30
Perc
enta
ge o
f pre
gnan
t wom
en w
ho
rece
ived
an
HIV
test
who
kno
w th
e re
sults
Prog
ram
mon
itorin
g (P
PTCT
) Ev
ery
year
N
/A
100%
N
SP
31
Perc
enta
ge o
f mal
e pa
rtne
rs o
f pos
itive
pr
egna
nt w
omen
att
endi
ng A
NC
who
kn
ow th
eir H
IV s
tatu
s
Prog
ram
mon
itorin
g (P
PTCT
) Ev
ery
year
N
/A
100%
N
SP
33
Perc
enta
ge o
f pos
itive
mal
e pa
rtne
rs o
f pr
egna
nt w
omen
use
con
dom
to
prot
ect P
PTCT
.
Prog
ram
mon
itorin
g (P
PTCT
) Ev
ery
year
N
/A
100%
N
SP
OU
TPU
T ID
ICA
TORS
33
Perc
enta
ge o
f HIV
pos
itive
pre
gnan
t w
omen
who
rece
ive
antir
etro
vira
l to
redu
ce th
e ris
k of
mot
her-
to-c
hild
tr
ansm
issi
on
Prog
ram
me
mon
itorin
g (P
PTCT
) Ev
ery
year
10
0% o
f 347
w
omen
rece
ived
AR
T ov
er th
e pa
st tw
o ye
ars
100%
U
NG
ASS
5, U
A
34
% o
f inf
ants
bor
n to
HIV
– In
fect
ed
wom
en re
ceiv
ing
any
ARV
prop
hyla
xis
for P
PTCT
Prog
ram
me
mon
itorin
g (P
PTCT
) Ev
ery
year
N
/A
100%
N
SP
61
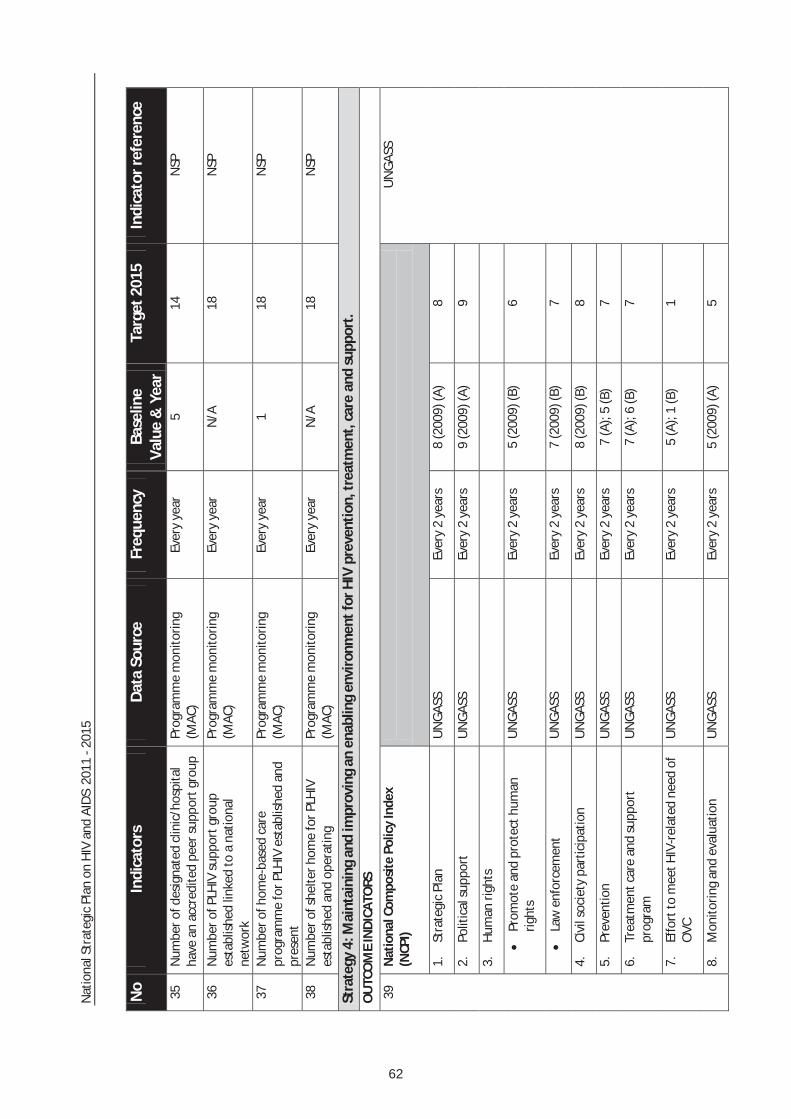
Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
35
Num
ber o
f des
igna
ted
clin
ic/h
ospi
tal
have
an
accr
edite
d pe
er s
uppo
rt g
roup
Pr
ogra
mm
e m
onito
ring
(MAC
) Ev
ery
year
5
14
NSP
36
Num
ber o
f PLH
IV s
uppo
rt g
roup
es
tabl
ishe
d lin
ked
to a
nat
iona
l ne
twor
k
Prog
ram
me
mon
itorin
g (M
AC)
Ever
y ye
ar
N/A
18
N
SP
37
Num
ber o
f hom
e-ba
sed
care
pr
ogra
mm
e fo
r PLH
IV e
stab
lishe
d an
d pr
esen
t
Prog
ram
me
mon
itorin
g (M
AC)
Ever
y ye
ar
1 18
N
SP
38
Num
ber o
f she
lter h
ome
for P
LHIV
es
tabl
ishe
d an
d op
erat
ing
Prog
ram
me
mon
itorin
g (M
AC)
Ever
y ye
ar
N/A
18
N
SP
Stra
tegy
4: M
aint
aini
ng a
nd im
prov
ing
an e
nabl
ing
envi
ronm
ent f
or H
IV p
reve
ntio
n, tr
eatm
ent,
car
e an
d su
ppor
t.
OU
TCO
ME
IND
ICA
TORS
39
Nat
iona
l Com
posi
te P
olic
y In
dex
(NCP
I)
UN
GAS
S
1.St
rate
gic
Plan
U
NG
ASS
Ev
ery
2 ye
ars
8 (2
009)
(A)
8
2.Po
litic
al s
uppo
rt
UN
GAS
S
Ever
y 2
year
s 9
(200
9) (A
) 9
3.H
uman
righ
ts
Prom
ote
and
prot
ect h
uman
rig
hts
UN
GAS
S
Ever
y 2
year
s 5
(200
9) (B
) 6
Law
enf
orce
men
t U
NG
ASS
Ev
ery
2 ye
ars
7 (2
009)
(B)
7
4.Ci
vil s
ocie
ty p
artic
ipat
ion
UN
GAS
S
Ever
y 2
year
s 8
(200
9) (B
) 8
5.Pr
even
tion
UN
GAS
S
Ever
y 2
year
s 7
(A);
5 (B
) 7
6.Tr
eatm
ent c
are
and
supp
ort
prog
ram
U
NG
ASS
Ev
ery
2 ye
ars
7 (A
); 6
(B)
7
7.Ef
fort
to m
eet H
IV-r
elat
ed n
eed
of
OVC
U
NG
ASS
Ev
ery
2 ye
ars
5 (A
); 1
(B)
1
8.M
onito
ring
and
eval
uatio
n U
NG
ASS
Ev
ery
2 ye
ars
5 (2
009)
(A)
5
62

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
No
Indi
cato
rs
Dat
a So
urce
Fr
eque
ncy
Base
line
Valu
e &
Yea
r Ta
rget
201
5 In
dica
tor r
efer
ence
Stra
tegy
5: I
ncre
asin
g th
e av
aila
bilit
y an
d qu
ality
of s
trat
egic
info
rmat
ion
and
its u
se b
y po
licy
mak
ers
and
prog
ram
me
plan
ners
thro
ugh
mon
itori
ng,
eval
uatio
n an
d re
sear
ch.
OU
TCO
ME
IND
ICA
TORS
40
Prog
ress
mad
e in
str
engt
heni
ng th
e M
&E
syst
em (a
sses
sed
thro
ugh
the
M
and
E Sy
stem
Str
engt
heni
ng to
ol)
1. A
n in
tegr
ated
M&
E U
nit h
as b
een
esta
blis
hed
at th
e na
tiona
l lev
el
coor
dina
ted
by H
IV/S
TI s
ecto
r
MO
H
Onc
e N
/A
Esta
blis
hed
2. A
ll H
IV re
late
d re
sear
ch is
com
pile
d in
a re
sear
ch d
irect
ory
MO
H
Ever
y 2
year
s N
/A
Com
plet
ed
3. M
inim
um o
f re
sear
ch p
er M
ARP
and
othe
r vul
nera
ble
popu
latio
ns is
co
nduc
ted
and
its re
port
is
diss
emin
ated
with
in 6
MO
H
Ever
y 2
year
s 4
(200
9)
Com
plet
ed
4. R
outin
e H
IV p
rogr
amm
e m
onito
ring
MO
H
Ever
y ye
ar
N/A
Co
mpl
eted
5. 6
0% o
f new
s co
vera
ge o
n H
IV is
ba
sed
on re
liabl
e da
ta a
nd fa
cts.
M
OH
Ev
ery
2 ye
ars
N/A
60
%
6. F
amily
Hea
lth D
ivis
ion
and
HIV
/STI
es
tabl
ish
an in
tegr
ated
and
co
nsol
idat
ed d
atab
ase
MO
H
Onc
e N
/A
Com
plet
ed
63

Nat
iona
l Str
ateg
ic P
lan
on H
IV a
nd A
IDS
201
1 - 2
015
Ann
ex 5
: Te
chni
cal T
eam
N
atio
nal A
dvis
or :
YB
hg. D
ato’
Sri
Dr H
asan
bin
Abd
ul R
ahm
an
Dire
ctor
Gen
eral
of H
ealth
Mal
aysi
a Te
chni
cal a
dvis
or :
D
r Lok
man
Hak
im b
in S
ulai
man
D
eput
y D
irect
or G
ener
al (P
ublic
Hea
lth)
Min
istr
y of
Hea
lth M
alay
sia
Dr C
hong
Che
e Kh
eong
D
irect
or o
f Dis
ease
Con
trol
Div
isio
n, M
inis
try
of H
ealth
Mal
aysi
a
Hea
d of
Tec
hnic
al T
eam
: D
r. Sh
a’ar
i Nga
dim
an,
Dep
uty
Dire
ctor
of D
isea
se C
ontr
ol a
nd H
ead
of A
IDS
Sect
ion,
M
inis
try
of H
ealth
Co
re M
embe
rs:
D
r. M
ohd
Nas
ir Ab
d Az
iz, A
IDS/
STI S
ecto
r, M
inis
try
of H
ealth
Dr.
Roha
ya A
bdul
Rah
man
, Pah
ang
Stat
e H
ealth
Dep
artm
ent
Dr.
Faz
idah
Yus
wan
, AID
S/ST
I Sec
tor,
Min
istr
y of
Hea
lth
Vass
undi
ra N
air,
Min
istr
y of
Wom
en, F
amily
and
Com
mun
ity D
evel
opm
ent
Prof
. Dr.
Teh
Yik
Koo
n, N
atio
nal D
efen
ce U
nive
rsity
of M
alay
sia
Prof
. Dr.
Ade
eba
Kam
aruz
aman
, Cen
tre
of E
xcel
lenc
e fo
r Res
earc
h in
AID
S (C
ERIA
), U
nive
rsiti
Mal
aya
Parim
elaz
haga
n El
lan,
Mal
aysi
an A
IDS
Coun
cil
Dr.
Zai
ton
Yahy
a, F
amily
Phy
sici
an, D
istr
ict H
ealth
Off
ice,
San
daka
n, S
abah
N
orle
la M
okht
ar, M
yPlu
s Az
rul M
ohd
Khal
ib, U
nite
d N
atio
ns M
alay
sia
64

HIV / STI SectionDisease Control Division
Level 4, Block E10, Complex E,Ministry of Health Malaysia,
Federal GovernmentAdministrative Centre
62590 Putrajaya, MALAYSIAwww.moh.gov.my