
BYC, an atypical aspartic endopeptidase from Rhipicephalus (Boophilus) microplus eggs
Upload
independentCategory
view
0download
0
American Journal of TransplantationWiley Periodicals Inc.
C! Copyright 2012 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2012.04252.x
Eculizumab for Atypical Hemolytic Uremic SyndromeRecurrence in Renal Transplantation
J. Zubera,*, M. Le Quintrecb, S. Kridc,C. Bertoyed, V. Gueutine, A. Lahochef, N. Heyneg,G. Ardissinoh, V. Chateleti, L.-H. Noeld,M. Hourmantj, P. Niaudetc, V. Fremeaux-Bacchik,E. Rondeaul, C. Legendrea, and C. Loiratm for theFrench Study Group for atypical HUS
aAssistance Publique-Hopitaux de Paris, Hopital Necker;Universite Paris Descartes, Sorbonne Paris Cite;Department of Renal Transplantation, Paris, FrancebService de Nephrologie et Transplantation Renale,Hopital Foch, SuresnescAssistance Publique-Hopitaux de Paris, Hopital Necker;Universite Paris Descartes, Sorbonne Paris Cite;Department of Pediatric Nephrology, Paris, FrancedAssistance Publique-Hopitaux de Paris, Hopital Necker;Department of Renal Pathology, Paris, FranceeAssistance Publique-Hopitaux de Paris, HopitalPitie-Salpetriere; Universite Paris VI; Department of RenalTransplantation, Paris, FrancefService de Nephrologie et Transplantation RenalePediatrique, CHU Lille, Lille, FrancegSection of Nephrology and Hypertension, UniversityHospital Tuebingen, Tuebingen, GermanyhCenter for HUS control, Fondazione IRCCS Ca’ GrandaOspedale Maggiore Policlinico, Milan, ItalyiService de Nephrologie et Transplantation Renale, CHUCaen, FrancejService de Nephrologie et Immunologie Clinique, CHUNantes, FrancekAssistance Publique-Hopitaux de Paris, Hopital EuropeenGeorges Pompidou; Universite Paris Descartes, SorbonneParis Cite; Department of Immunology, Paris, FrancelAssistance Publique-Hopitaux de Paris, Hopital Tenon;Universite Paris VI; Department of Renal Transplantation,Paris, FrancemAssistance Publique-Hopitaux de Paris, HopitalRobert-Debre; Universite Paris VII; Department ofPediatric Nephrology, Paris, France*Corresponding author: Julien Zuber,[email protected]
[Correction made after online publication September 7,2012: the author listing has been updated.]
Eculizumab (anti-C5) has been sporadically reportedas an efficient therapy for atypical hemolytic uremicsyndrome (aHUS). However, the lack of series pre-cludes any firm conclusion about the optimal use ofanti-C5 for preventing or treating aHUS posttrans-plant aHUS recurrence. We thoroughly studied 22 re-nal transplant recipients with aHUS who received off-label therapy with anti-C5, including 12 cases, whichhave not been reported yet. Nine patients, all car-
rying a complement genetic abnormality associatedwith a high risk of aHUS recurrence, received pro-phylactic anti-C5 therapy to prevent posttransplantrecurrence. Eight of them had a successful recurrence-free posttransplant course and achieved a satisfac-tory graft function, while the remaining patient expe-rienced early arterial thrombosis of the graft. Thirteenrenal transplant recipients were given anti-C5 for post-transplant aHUS recurrence. A complete reversal ofaHUS activity was obtained in all of them. Importantly,the delay of anti-C5 initiation after the onset of theaHUS episode inversely correlated with the degree ofrenal function improvement. Three patients in whomanti-C5 was subsequently stopped experienced a re-lapse. Altogether these data suggest that long-termeculizumab is highly effective for preventing and treat-ing posttransplant aHUS recurrence. Our study alsoindicates that anti-C5 should be promptly started if arecurrence occurs.
Key words: Atypical hemolytic uremic syndrome,eculizumab, renal transplant recipient
Abbreviations: aHUS, atypical hemolytic uremic syn-drome; C3, complement component 3; C5, comple-ment component 5; CFB, complement factor B; CFH,complement factor H; CFHR1, CFH-related protein 1;CFI, complement factor I; SCR, short consensus repeatdomain.
Received 02 April 2012, revised 05 July 2012 andaccepted for publication 23 July 2012
Introduction
The interest in developing complement inhibitors hasstemmed from the growing implication of complement ac-tivation in many pathological conditions, including atypicalhemolytic uremic syndrome (aHUS) (1,2). Genetically de-termined or acquired uncontrolled activation of the com-plement alternative pathway has been found in up to70% of patients with aHUS, in whom this constitutesa strong susceptibility factor for thrombotic microangio-pathic processes triggered by endothelial cell damage(1,2). Eculizumab (anticomplement component 5 (C5)), arecombinant, fully humanized monoclonal antibody, is thefirst complement inhibitor licensed for clinical use (3). Byspecifically targeting the human C5, anti-C5 inhibits thegeneration of the proinflammatory mediator C5a and pre-vents the formation of the membrane attack complex (3).Anti-C5 has become a breakthrough therapy for parox-ysmal nocturnal hemoglobinuria, a chronic and disabling

Zuber et al.
disease, whose symptoms are dominated by complement-dependent hemolytic anemia and related vascularthrombosis (4).
Since 2009, anti-C5 has been successfully used in off-trialpatients with aHUS, involving either native or transplantedkidneys (5–14). Four recent reports also indicated that anti-C5 could be efficiently used as prophylaxis to prevent post-transplant aHUS recurrence in patients in whom a highrecurrence risk could be predicted from identified geneticabnormalities (15–18). In addition, anti-C5 was used withsuccess in two cases of de novo posttransplant aHUS, oc-curring in simultaneous pancreas kidney transplant recip-ients (19,20). This is reminiscent of the finding that com-plement dysregulation may contribute to the pathogenesisof de novo posttransplant HUS as well (21). This prelimi-nary experience based on anti-C5 off-label use was in linewith the early results of two prospective phase II trials,reported in 2010 and 2011 at the congresses of the Amer-ican Societies of Nephrology and Hematology, highlightingthe safety profile and efficacy of anti-C5 in treating aHUS.These studies enrolled 37 patients with aHUS involvingnative or transplant kidneys. These patients had a plasma-resistant aHUS (n = 17) (22–24) or were on chronic plasmatherapy (n = 20) (25–27). Anti-C5 succeeded in controllingthe disease in most cases, as evidenced by normalizationof hemolytic markers and thrombocytopenia and improve-ment of renal function (22–27).
However, accurate information regarding the use of anti-C5 in posttransplant settings, according to individualizedrecurrence risk assessment, is critically lacking. In an at-tempt to provide clues to optimize the chance for recoveryof renal function with anti-C5 treatment and to draw thefirst lessons from the still limited experience in the set-tings of renal transplantation, we thoroughly studied 22renal transplant recipients with aHUS who had receivedoff-label anti-C5 therapy.
Patients and Methods
This was a retrospective multicenter study describing renal transplants re-cipients, who were given anti-C5 (eculizumab Soliris R!, Alexion Pharmaceu-ticals, Cheshire, CT, USA) for preventing or treating posttransplant aHUSrecurrence. French adult and pediatric renal transplant centers were inter-viewed to know whether any of the patients followed in their institutionshad been provided anti-C5 for preventing or treating posttransplant aHUSrecurrence. Eleven patients were identified including two cases, which havealready been reported (6,18,28). In addition, all authors having reported theuse of eculizumab in the prevention or treatment of aHUS recurrence inpeer-reviewed journals (n = 8) (5,7,9,11,13,15–17), and congress abstracts(n = 3) (29–31) were contacted by C. Loirat and invited to share their expe-rience. Altogether, 13 patients, identified in nine centers, including seven inFrance, one in Italy and one in Germany, were included in the study. Clinicaland genetic data were obtained from medical records. Because the studypopulation size was limited, we performed a pooled analysis of data fromthese 13 cases and from 9 other cases, already reported as case reports.When corresponding authors agreed to provide updated data, regardinglate outcome of their patients, this was mentioned in Tables 1 and 2 as(personal communication, name of the corresponding author, date).
The schedule of the anti-C5 regimen is well defined in adults heavierthan 40 kg, while doses and intervals should be adapted in patientswith weight of less than 40 kg (Soliris R! US prescribing information pro-vided by Alexion Pharmaceuticals, Inc. 2011 at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/125166s172lbl.pdf).
Complement assays and genetic screeningAll patients enrolled in the study from the French aHUS cohort underwenta complete complement work-up in the reference laboratory for comple-ment assessment at the Georges Pompidou European Hospital in Paris,France, after having provided informed written consent for gene screen-ing. Screening for anticomplement factor H (CFH) antibodies and completeexon sequencing of the genes encoding for CFH, membrane cofactor pro-tein (MCP), complement factor I (CFI), complement component 3 (C3),complement factor B (CFB) and thrombomodulin (THBD) was performedas previously described. Patients were screened for a CFH/CFHR1 hybridgene and CFHR1 deletion using multiplex ligation-dependent probe ampli-fication (MLPA).
In the reference laboratory for complement assessment, the extent of C5blockade is measured with the CH50 assay (complement hemolytic assay).This lytic assay uses antibody-sensitized sheep erythrocytes as the acti-vator of the classical complement pathway. The proteins of the terminalpathway, from C5 to C9, are involved in the formation of the C5b-9 lyticcomplex. Various dilutions of the test plasma are used to determine theamount required to induce 50% of lysis. The CH50 test is therefore anindirect measure of residual functional C5 activity. Patients with hereditaryhomozygous C5 deficiency exhibit a CH50 lower than 10%. Titration hasshown that a CH50 activity below the detection level (<10%), indicates aC5 activity lower than 1% of the normal value.
Immunostaining on graft biopsiesC5b-9 staining was performed in biopsies of four patients, for which frozensamples were available. C5b-9 staining was studied using a mouse antihu-man C5b-9 monoclonal antibody (clone aE11, Dako) by indirect immunoflu-orescence on slides obtained from frozen specimen. C4d staining was stud-ied using a rabbit antihuman C4d monoclonal antibody (DB107, clone A24-T,DB Biotech) by immunohistochemistry on slides obtained from AFA-fixedspecimen.
Results
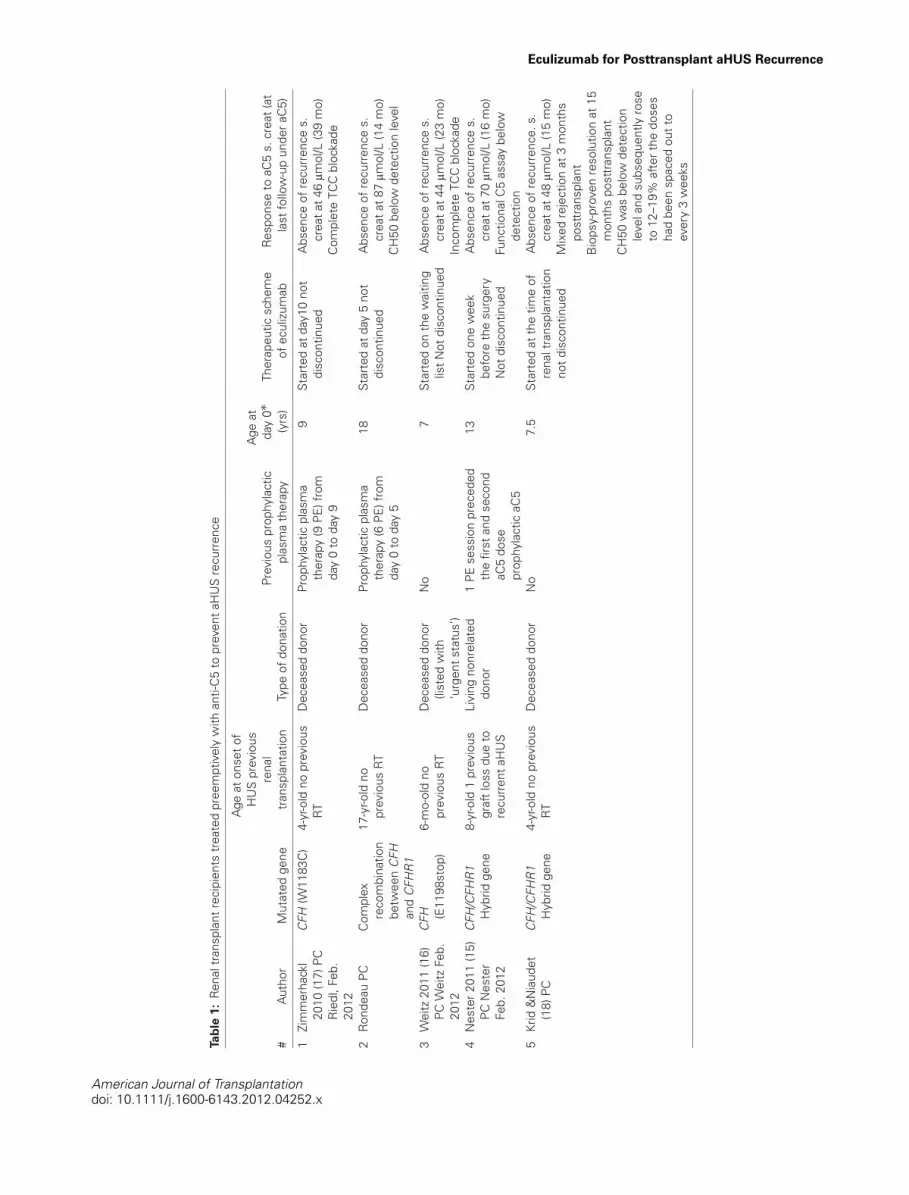
Characteristics of 9 aHUS patients given prophylacticanti-C5Six patients from our cohort had received prophylactic anti-C5 to prevent posttransplant aHUS recurrence (18), in ad-dition to three other cases already reported in the literature(Table 1) (15–17). All but one cases had a child-onset aHUShistory with a median age of 4 years old [range, 0.5–33]at diagnosis. They all harbored a genetic abnormality asso-ciated with a high risk of recurrence. Five patients carrieda heterozygous mutation in C-terminus of CFH, locatedin the SCR20 (n = 4) or SCR19 (n = 1), and three oth-ers had a large nonhomologous genomic rearrangementbetween the CFH and CFHR1 genes. The remaining pa-tient displayed a gain-of-function mutation in the C3 gene.Three patients had previously received four renal trans-plants, which had been lost from early aHUS recurrence(cases 4, 8 and 9). The median age at the time of thepresent renal transplantation was 9 years (range, 6.4–41).
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x
Eculizumab for Posttransplant aHUS Recurrence
Tabl
e1:
Ren
altr
ansp
lant
reci
pien
tstr
eate
dpr
eem
ptiv
ely
with
anti-
C5
topr
even
taH
US
recu
rren
ce
#A
utho
rM
utat
edge
ne
Age
aton
seto
fH
US
prev
ious
rena
ltr
ansp
lant
atio
nTy
peof
dona
tion
Prev
ious
prop
hyla
ctic
plas
ma
ther
apy
Age
atda
y0"
(yrs
)Th
erap
eutic
sche
me
ofec
uliz
umab
Res
pons
eto
aC5
s.cr
eat(
atla
stfo
llow
-up
unde
raC
5)
1Zi
mm
erha
ckl
2010
(17)
PCR
iedl
,Feb
.20
12
CFH
(W11
83C
)4-
yr-o
ldno
prev
ious
RT
Dec
ease
ddo
nor
Prop
hyla
ctic
plas
ma
ther
apy
(9PE
)fro
mda
y0
toda
y9
9St
arte
dat
day1
0no
tdi
scon
tinue
dA
bsen
ceof
recu
rren
ces.
crea
tat4
6lm
ol/L
(39
mo)
Com
plet
eTC
Cbl
ocka
de
2R
onde
auPC
Com
plex
reco
mbi
natio
nbe
twee
nC
FHan
dC
FHR
1
17-y
r-old
nopr
evio
usR
TD
ecea
sed
dono
rPr
ophy
lact
icpl
asm
ath
erap
y(6
PE)f
rom
day
0to
day
5
18St
arte
dat
day
5no
tdi
scon
tinue
dA
bsen
ceof
recu
rren
ces.
crea
tat8
7lm
ol/L
(14
mo)
CH
50be
low
dete
ctio
nle
vel
3W
eitz
2011
(16)
PCW
eitz
Feb.
2012
CFH (E
1198
stop
)6-
mo-
old
nopr
evio
usR
TD
ecea
sed
dono
r(li
sted
with
‘urg
ents
tatu
s’)
No
7St
arte
don
the
wai
ting
listN
otdi
scon
tinue
dA
bsen
ceof
recu
rren
ces.
crea
tat4
4lm
ol/L
(23
mo)
Inco
mpl
ete
TCC
bloc
kade
4N
este
r201
1(1
5)PC
Nes
ter
Feb.
2012
CFH
/CFH
R1
Hyb
ridge
ne8-
yr-o
ld1
prev
ious
graf
tlos
sdu
eto
recu
rren
taH
US
Livi
ngno
nrel
ated
dono
r1
PEse
ssio
npr
eced
edth
efir
stan
dse
cond
aC5
dose
prop
hyla
ctic
aC5
13St
arte
don
ew
eek
befo
reth
esu
rger
yN
otdi
scon
tinue
d
Abs
ence
ofre
curr
ence
s.cr
eata
t70
lmol
/L(1
6m
o)Fu
nctio
nalC
5as
say
belo
wde
tect
ion
5Kr
id&
Nia
udet
(18)
PCC
FH/C
FHR
1H
ybrid
gene
4-yr
-old
nopr
evio
usR
TD
ecea
sed
dono
rN
o7.
5St
arte
dat
the
time
ofre
nalt
rans
plan
tatio
nno
tdis
cont
inue
d
Abs
ence
ofre
curr
ence
.s.
crea
tat4
8lm
ol/L
(15
mo)
Mix
edre
ject
ion
at3
mon
ths
post
tran
spla
ntB
iops
y-pr
oven
reso
lutio
nat
15m
onth
spo
sttr
ansp
lant
CH
50w
asbe
low
dete
ctio
nle
vela
ndsu
bseq
uent
lyro
seto
12–1
9%af
tert
hedo
ses
had
been
spac
edou
tto
ever
y3
wee
ks
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x
Zuber et al.
Tabl
e1:
Con
tinue
d.
#A
utho
rM
utat
edge
ne
Age
aton
seto
fH
US
prev
ious
rena
ltr
ansp
lant
atio
nTy
peof
dona
tion
Prev
ious
prop
hyla
ctic
plas
ma
ther
apy
Age
atda
y0"
(yrs
)Th
erap
eutic
sche
me
ofec
uliz
umab
Res
pons
eto
aC5
s.cr
eat(
atla
stfo
llow
-up
unde
raC
5)
6La
hoch
ePC
C3
(Arg
161T
ryp)
10-m
o-ol
dno
prev
ious
RT
Dec
ease
ddo
nor
No
6.4
Star
ted
atth
etim
eof
rena
ltra
nspl
anta
tion
Not
disc
ontin
ued
Abs
ence
ofre
curr
ence
.s.
crea
tat4
4lm
ol/L
(4.5
mon
ths)
CH
50be
low
dete
ctio
nle
vel
7Kr
id&
Nia
udet
PCC
FH(Q
1137
X)1-
yr-o
ldno
prev
ious
RT
Dec
ease
ddo
nor
No
9St
arte
dat
the
time
ofre
nalt
rans
plan
tatio
nno
tdis
cont
inue
d
Abs
ence
ofre
curr
ence
.s.
crea
tat5
8lm
ol/L
CH
50be
low
dete
ctio
nle
vel
upon
ever
ytw
ow
eeks
mai
nten
ance
regi
men
(4m
onth
s)8
Hou
rman
tPC
CFH
(S11
91L)
3-yr
-old
1pr
evio
usgr
aftl
oss
due
tore
curr
enta
HU
SR
elap
sing
aHU
Sdu
ring
the
dial
ysis
perio
d
Dec
ease
ddo
nor
1PE
sess
ion
prec
eded
the
first
aC5
dose
Prop
hyla
ctic
aC5
18St
arte
dat
the
time
ofre
nalt
rans
plan
tatio
nEa
rlyar
teria
lthr
ombo
sis
ofth
egr
afta
tday
1.Tr
ansp
lant
neph
rect
omy
atda
y3.
9Zu
ber&
Lege
ndre
PCC
FH(p
.Y11
77C
)33
-yr-o
ld2
prev
ious
graf
tlos
ses
due
tore
curr
enta
HU
S
Dec
ease
ddo
nor
No
41St
arte
dat
the
time
ofre
nalt
rans
plan
tatio
nno
tdis
cont
inue
d
Abs
ence
ofre
curr
ence
s.cr
eata
t176
lmol
/lM
ixed
reje
ctio
nat
6w
eeks
post
tran
spla
nt.
Bio
psy-
prov
enre
solu
tion
15da
ysla
terC
H50
belo
wde
tect
ion
leve
l(2
mon
ths)
aC5
=an
ticom
plem
entc
ompo
nent
5an
tibod
y;aH
US
=at
ypic
alhe
mol
ytic
urem
icsy
ndro
me;
mo
=m
onth
s;N
D=
notd
isco
ntin
ued;
PC=
pers
onal
com
mun
icat
ion;
PE=
plas
ma
exch
ange
;RT
=re
nalt
rans
plan
tatio
n;TC
C=
term
inal
com
plem
entc
ompl
ex;w
k=
wee
k;yr
=ye
ar.
" Ref
ers
toth
est
arto
fant
i-C5
ther
apy.
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
Tabl
e2:
Ren
altr
ansp
lant
reci
pien
tstr
eate
dw
ithan
ti-C
5to
trea
taH
US
recu
rren
ce
#A
utho
rM
utat
edge
ne
Age
aton
seto
faH
US
prev
ious
rena
ltr
ansp
lant
atio
n
TIbe
twee
nR
Tan
daH
US
recu
rren
ce
Res
pons
eto
plas
ma
ofth
ecu
rren
tepi
sode
TIbe
twee
nep
isod
eon
seta
ndaC
5
Age
[s.c
reat
]at
day
0"(l
mol
/L)
Ther
apeu
ticsc
hem
eof
aC5
Res
pons
eto
aC5
s.cr
eat
(atl
astf
/uun
dera
C5)
10C
hate
let&
Hur
ault
deLi
gny
(6)
PC,
Cha
tele
tFe
b20
12
C3 (R
570Q
)30
-yr-o
ld1
prev
ious
graf
tlos
sco
nsec
utiv
eto
recu
rren
taH
US
4m
oPl
asm
ade
pend
ent
14m
o42
[320
]C
ompl
ete
adul
tpr
otoc
ol.
Mai
nten
ance
dose
inte
rval
has
been
incr
ease
dto
3w
ksfo
rthe
last
6m
o(N
D)
CR
ofaH
US;
2re
laps
esoc
curr
edaf
tera
C5
dose
sha
dbe
ende
laye
dfr
om6
to8
days
s.cr
eat
at23
0lm
ol/L
(43
mo)
CH
50be
low
the
dete
ctio
nth
resh
old
11D
avin
2010
(7)P
C,
Dav
inFe
b20
12
CFH (S
1191
L)3-
yr-o
ld2
prev
ious
graf
tlos
ses
cons
ecut
ive
tore
curr
enta
HU
S
4m
oPl
asm
ade
pend
ent
(rela
pse
whe
nPE
wer
esp
aced
ata
freq
uenc
ylo
wer
than
2/w
k
6m
o18
[131
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
CR
ofaH
US
s.cr
eata
t120
lmol
/L(4
9m
o)
12N
urnb
erge
r20
09(1
1)PC
,N
urnb
erge
rA
p.20
10
CFH (Y
475S
)25
-yr-o
ld1
prev
ious
graf
tlos
sco
nsec
utiv
eto
recu
rren
taH
US
6w
ksPl
asm
are
sist
ant4
daily
PE5
days
37[1
32]
One
sing
le60
0m
gdo
seC
Rof
aHU
Ss.
crea
tat9
7lm
ol/L
rela
pse
at21
mo
retu
rnto
HD
(22
mo)
13La
rrea
2010
(9)P
C,
Loza
noJa
n.20
11
NI
20-y
r-old
No
prev
ious
RT
12da
ys(tr
igge
red
byfe
brile
diar
rhea
)
Plas
ma
resi
stan
t5da
ilyPE
9da
ys22
[415
]O
nesi
ngle
600
mg
dose
CR
ofaH
US
s.cr
eata
t70
lmol
/LR
elap
seat
11m
oaC
5w
asre
sum
edbu
tgra
ftdy
sfun
ctio
npe
rsis
ted
(s.c
reat
at17
5lm
ol/L
).Pr
ogre
ssio
nto
war
dES
RD
afte
rces
satio
nof
aC5
4m
ola
ter
14Le
gaul
t200
9(3
1)N
SN
SN
opr
evio
usR
T1
mo
Inco
mpl
ete
resp
onse
topl
asm
a(3
PE/w
k)
8m
o34
[321
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
CR
ofaH
US
s.cr
eata
t238
lmol
/L(6
mo)
.R
enal
sequ
elae
(pro
tein
uria
)15
Al-A
kash
2010
(5)
PC,
Al-A
kash
Feb.
2012
C3 (R
570W
)16
-mo-
old
2pr
evio
usgr
aft
loss
esco
nsec
utiv
eto
recu
rren
taH
US
9w
ks(tr
igge
red
byin
fluen
zaA
infe
ctio
n)
Inco
mpl
ete
resp
onse
topl
asm
a(1
0PE
sess
ions
)
3w
ks15
[202
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
CR
ofaH
US
s.cr
eata
t115
lmol
/L(3
0m
o)N
oTM
Ale
sion
ona
12-m
opr
otoc
olbi
opsy
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.Ta
ble
2:C
ontin
ued.
#A
utho
rM
utat
edge
ne
Age
aton
seto
faH
US
prev
ious
rena
ltr
ansp
lant
atio
n
TIbe
twee
nR
Tan
daH
US
recu
rren
ce
Res
pons
eto
plas
ma
ofth
ecu
rren
tepi
sode
TIbe
twee
nep
isod
eon
seta
ndaC
5
Age
[s.c
reat
]at
day
0"(l
mol
/L)
Ther
apeu
ticsc
hem
eof
aC5
Res
pons
eto
aC5
s.cr
eat
(atl
astf
/uun
dera
C5)
16A
rdis
sino
2010
(29)
PC
CFH
11-m
o-ol
dN
opr
evio
usR
T2
mo
Plas
ma
resi
stan
t2da
ilyPE
2da
ys6
[442
]St
arte
dat
600
mg/
wee
kan
dth
en60
0m
gev
ery
3w
eeks
(ND
)
CR
ofaH
US
s.cr
eata
t48
lmol
/L(2
5m
o)
17Zu
ber&
Lege
ndre
PC
CFH (S
1191
LV1
197A
)
3-yr
-old
1pr
evio
usgr
aftl
oss
cons
ecut
ive
tore
curr
enta
HU
S
3da
ysPl
asm
are
sist
ant
(pro
phyl
actic
plas
ma
ther
apy)
FFP
atda
y0,
1an
d2,
then
3da
ilyPE
3da
ys23
[627
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
CR
ofaH
US
s.cr
eata
t65
lmol
/L(1
7m
o)N
oTM
Ale
sion
ona
12-m
opr
otoc
olbi
opsy
CH
50be
low
the
dete
ctio
nth
resh
old
18Zu
ber&
Lege
ndre
PC
CFH
-C
FHR
1H
ybrid
gene
1-yr
-old
4pr
evio
usR
T,in
clud
ing
2lo
sses
byre
curr
ence
and
2lo
sses
byea
rlygr
aftv
esse
lth
rom
bosi
s
3da
ys(p
ersi
sten
tan
emia
,TH
Cat 60
000/
mm
3)
Inco
mpl
ete
resp
onse
topr
ophy
lact
icpl
asm
ath
erap
y(2
0PE
and
8FF
Pin
fusi
ons
durin
gth
efir
stm
onth
)
1m
o27
[237
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
Ris
ein
Hb
and
stab
iliza
tion
arou
nd11
g/dL
,s.c
reat
at20
4lm
ol/L
(14
mo)
Low
hapt
oglo
bin
leve
lbe
twee
n6
and
12w
ksan
dfr
esh
TMA
lesi
ons
ona
rena
lbio
psy
3m
onth
saf
tert
heon
set
ofaC
5C
H50
belo
wth
ede
tect
ion
thre
shol
d19
Zube
r&Le
gend
rePC
Ant
i-FH
anti-
body
!
CFH
R1/
3
6-yr
-old
4pr
evio
usR
T,in
clud
ing
3lo
sses
byre
curr
ence
A5-
yr-p
ost-R
Tgr
aftb
iops
y(s
light
decr
ease
inre
nalf
unct
ion)
disc
lose
dfr
esh
TMA
lesi
ons
Inco
mpl
ete
resp
onse
topr
ophy
lact
icpl
asm
ath
erap
y(1
PEev
ery
6w
ksas
mai
nten
ance
plas
ma
ther
apy)
3m
o41
[89]
Com
plet
ead
ult
prot
ocol
(ND
)St
abili
zatio
nof
s.cr
eata
t80
lmol
/L(9
mo)
CH
50be
low
the
dete
ctio
nth
resh
old
20G
ueut
inPC
CFI (G
101R
)27
-yr-o
ld1
prev
ious
graf
tlos
sco
nsec
utiv
eto
recu
rren
taH
US
15m
oC
urat
ive
plas
ma
exch
ange
sw
ere
perf
orm
edan
dpr
ogre
ssiv
ely
tape
red
over
8m
onth
s,an
dsu
bseq
uent
lyst
oppe
d.
Thirt
een
mon
ths
afte
rces
satio
nof
plas
ma
ther
apy,
aris
ein
s.cr
eat.
Ass
ocia
ted
with
THC
led
togr
aft
biop
syw
hich
disc
lose
dfr
esh
lesi
ons
ofTM
A.
PEse
ssio
nsw
ere
resu
med
but
faile
dto
impr
ove
rena
lfun
ctio
n(n
=7)
9w
ks43
[190
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
Incr
ease
inpl
atel
etco
unt
upto
134,
000/
mm
3.A
dela
yof
7da
ysin
the
fifth
infu
sion
ofaC
5le
dto
am
ildre
laps
e(ri
sein
s.cr
eata
ndLD
Hle
vels
).Pa
tient
subs
eque
ntly
reco
vere
dba
selin
ere
nal
func
tion
(aro
und
156
lmol
/L)f
ollo
win
gre
-initi
atio
nof
trea
tmen
t(4
.5m
o)
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
Tabl
e2:
Con
tinue
d.
#A
utho
rM
utat
edge
ne
Age
aton
seto
faH
US
prev
ious
rena
ltr
ansp
lant
atio
n
TIbe
twee
nR
Tan
daH
US
recu
rren
ce
Res
pons
eto
plas
ma
ofth
ecu
rren
tepi
sode
TIbe
twee
nep
isod
eon
seta
ndaC
5
Age
[s.c
reat
]at
day
0"(l
mol
/L)
Ther
apeu
ticsc
hem
eof
aC5
Res
pons
eto
aC5
s.cr
eat
(atl
astf
/uun
dera
C5)
21D
uran
2012
(13)
PC,
Cam
pist
olFe
b.20
12
CFH (Q
1172
X)28
-yr-o
ldN
opr
evio
usR
T2.
5m
o(tr
igge
red
byco
cain
eco
nsum
ptio
n)
Part
ialr
espo
nse
to8
ever
yot
herd
ayPE
sess
ions
,fr
ank
rela
pse
1m
ola
ter
1m
o32
[HD
]C
ompl
ete
adul
tpr
otoc
ol(N
D)
Nor
mal
izat
ion
ofpl
atel
etco
unta
ndha
ptog
lobi
nle
vel
Rec
over
yfr
omhe
mod
ialy
sis
ther
apy.
Ren
alfu
nctio
npr
ogre
ssiv
ely
impr
oved
with
ala
stf/u
crea
tinin
ele
vela
t168
lmol
/L(1
6m
o)22
Hey
ne20
11(3
0)PC
NI
Post
-par
tum
1pr
evio
usgr
aft
loss
cons
ecut
ive
tore
curr
enta
HU
S
8da
ysaC
5w
asus
edas
first
-line
ther
apy
1da
y43
[176
]C
ompl
ete
adul
tpr
otoc
olun
til8
mon
thpo
st-R
Tw
hen
adm
inis
trat
ion
ofaC
5w
asta
pere
dof
fand
stop
ped
Nor
mal
izat
ion
ofhe
mat
olog
ical
para
met
ers
Ren
alfu
nctio
npr
ogre
ssiv
ely
impr
oved
with
acr
eatin
ine
nadi
rat
114
lmol
/LIn
fluen
zava
ccin
atio
ntr
igge
red
are
laps
e3
mon
ths
afte
raC
5ha
dbe
enst
oppe
daC
5w
asre
sum
edan
dsu
bseq
uent
lysp
aced
toev
ery
othe
rmon
thdo
sere
gim
enTh
ela
stf/u
crea
tinin
ele
vel
was
123
lmol
/L(1
4m
o)
aC5
=an
ti-co
mpl
emen
tco
mpo
nent
5an
tibod
y;aH
US
=at
ypic
alhe
mol
ytic
urem
icsy
ndro
me;
AR
F=
acut
ere
nal
failu
re;
AwR
T=
awai
ting
rena
ltr
ansp
lant
atio
n;B
P-TM
A=
biop
sy-p
rove
nTM
A;C
FH=
com
plem
ent
fact
orH
;CFI
=co
mpl
emen
tfa
ctor
I;C
3=
com
plem
ent
com
pone
nt3;
CN
S=
cent
raln
ervo
ussy
stem
;CR
=co
mpl
ete
rem
issi
on;H
b=
hem
oglo
bin
(g/d
L);
HD
=he
mod
ialy
sis;
HPN
=hy
pert
ensi
on;
mo
=m
onth
;ND
=no
tdi
scon
tinue
d;N
I=no
tid
entifi
ed;N
S=
not
spec
ified
;PC
=pe
rson
alco
mm
unic
atio
n;PE
=pl
asm
aex
chan
ge;
Prot
=pr
otei
nuria
;R
T=
rena
ltra
nspl
anta
tion;
SG=
scle
rotic
glom
erul
i;w
k=
wee
k;TH
C=
thro
mbo
cyto
peni
a;TI
=tim
ein
terv
al;
TMA
=th
rom
botic
mic
roan
giop
athy
;yr=
year
.
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
Figure 1: Prophylactic anti-C5 therapy. (A) The prophylactic eculizumab regimens depicted here represent those used to prevent aHUSrecurrence in the study population. (B) Light microscopy and immunofluorescence analysis of graft biopsies performed in case 5. Althoughan early 1-month biopsy displayed normal renal parenchyma (a), the 3-month posttransplant biopsy disclosed severe mixed acute rejection,following a prolonged discontinuation of mycophenolic acid due to neutropenia. The complete histological pattern included interstitialinflammation, tubulitis (c), endothelitis, and transmural necrosis of a small artery (e, white arrow), surrounded by perivascular infiltrate,associated with hallmark lesions of antibody-mediated rejection, including glomerular and peritubular capillaritis (d) and mild C4d staining(f, black arrow). The biopsy performed 12 months later demonstrated a complete recovery from severe rejection (g). Remarkably, none ofthese biopsies displayed any signs of thrombotic microangiopathy. Consistently, negative C5b-9 staining indicated efficient and sustainedin situ C5 blockade throughout the follow-up period (b, h). Anti-C5 = eculizumab; DD = deceased donor; LD = living donor; PE = plasmaexchanges.
Two cases (5 and 9) exhibited a preformed donor-specificantibody (DSA), with a low level titer (MFI <1000) at thetime of renal transplantation.
In all but one, the renal transplant was of deceased-donororigin. Basically three kinds of strategies were undertaken(Figure 1A). One of them consisted in sequential prophy-laxis by switching plasma exchanges started just beforetransplantation to eculizumab therapy (cases 1 and 2). Thefirst anti-C5 administration was thus postponed to days 10and 5 postsurgery in cases 1 and 2, respectively. Anotherstrategy relied on eculizumab-based prophylactic therapy,which was initiated 1 week or more before the transplan-tation, while the recipient was listed with urgent status for
deceased-donor renal transplantation (case 3) or awaitinga scheduled living nonrelated donor renal transplantation(case 4). Finally, the last and simplest strategy was basedon eculizumab therapy alone, started immediately beforetransplantation (cases 5–9). They all received the first doseof eculizumab treatment within the 24 h preceding thesurgery.
Notably, five patients (cases 5–9) were given two consecu-tive daily anti-C5 infusions at the time of the transplantationto circumvent the concern of high complement activationtriggered by ischemia reperfusion (17,32). Four patients re-ceived the starting dose a few hours before surgery andthe second dose within the next 24 h (cases 5, 6, 8 and
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
9). The remaining patient (case 7) had two doses beforesurgery at days #1 and 0.
Outcome of renal transplantation performed inpatients given prophylactic anti-C5Of the nine patients treated preemptively with eculizumab,eight experienced a successful recurrence-free posttrans-plant course after a median follow-up of 14.5 months(range, 2–39) (Table 1). The mean ± SD creatinine levelat last time point was 71.6 ± 44.8 lmol/L. Anti-C5 ther-apy was pursued in all patients except case 8, who losther graft from immediate arterial thrombosis, despite un-detectable CH50 activity. To confirm the full blockade of cir-culating C5, C5-dependent functional assay, terminal com-plement complex (TCC) dosing or CH50 were repeatedlymonitored just before dosing in all cases (Table 1). Theywere constantly measured below or around the detectionthreshold, suggesting an optimal circulating C5 blockade.In cases 1 and 5, the C5-dependent functional assay rosesignificantly when maintenance doses were spaced out toevery 3 weeks, instead of every 2 weeks. C5-dependentcomplement assay peaked two times in patient 3, con-comitantly with BK virus and upper respiratory tract infec-tions, respectively and once concurrently with Clostridiumdifficile infection in case 4. Notably, in this later, detec-tion of functional C5 coincided with a slight and transientdecrease in platelet count, which may indicate a mild re-activation of the aHUS process. In three patients (cases5, 7 and 9), C5b-9 staining was performed in biopsies(Figure 1B). In cases 5 and 7, a negative C5b-9 stain-ing revealed efficient and sustained in situ C5 blockade,while the two biospies performed in case 9, at 6 and 8weeks posttransplant, disclosed a mild granular mesangialstaining.
Cases 5 and 9 experienced a mixed rejection, includingtubulitis, endothelitis, and glomerular and peritubular cap-illaritis as well as diffuse C4d positive staining, at 6 and12 weeks posttransplant, respectively. Strikingly, none ofthese biopsies disclosed any lesions of TMA. Surprisingly,a de novo DSA, but not the preformed DSA, was readily de-tected in blood samples at the time of the rejection in bothcases. The treatment consisted of three pulses of methyl-prednisolone steroid, followed by high-dose oral steroidtherapy, with mycophenolate mofetil and tacrolimus, whileeculizumab was pursued. Graft function improved and re-turned to baseline values in both of these cases. Althoughlow-level DSA remained detectable throughout the follow-up, subsequent biopsies demonstrated a complete recov-ery from rejection in both patients. None of the other pa-tients treated prophylactically had any DSA or C4d-positivestaining on biopsy sections.
All of the patients were vaccinated against meningococcalinfection and all but one received daily antibioprophylaxisduring the treatment period. No significant infectious com-plications were reported.
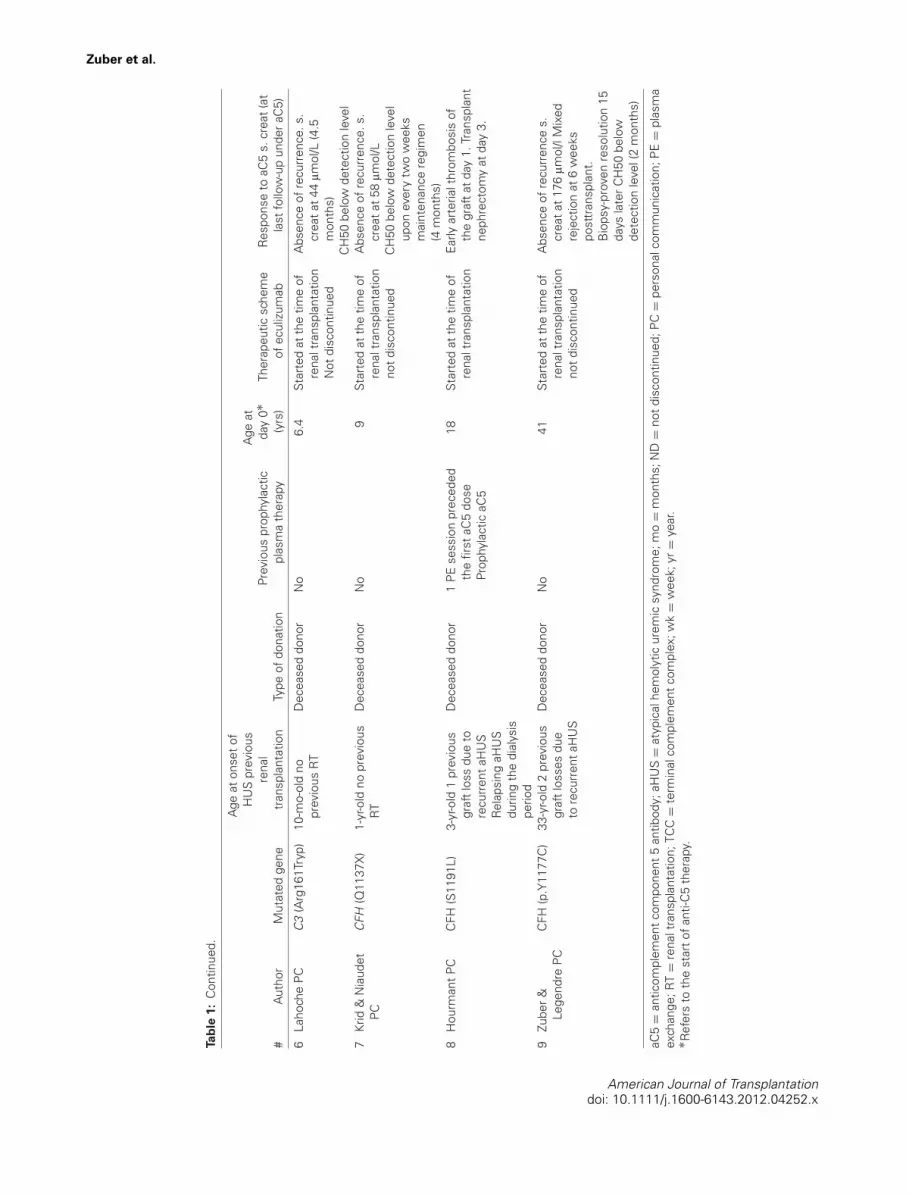
Characteristics of 13 renal transplant recipientstreated with anti-C5 for posttransplant aHUSrecurrenceSeven patients from our cohort received anti-C5 to treatposttransplant aHUS recurrence (6,28–30), as did six othercases reported in the literature (Table 2) (5,7,9,11,13,31).Two were switched from plasma therapy to anti-C5 for se-vere intolerance to plasma or for personal convenience,while being considered sensitive to, yet dependent on,plasma (cases 10 and 11). Ten others were switched forplasma-resistant forms of aHUS (cases 12 to 21). The re-maining received eculizumab as first-line therapy (case 22).The median age of aHUS onset was 6 years old (range,1–28 years). All but one was screened for mutations incomplement genes. Five, two and one had heterozygousmutations in the CFH, C3 and CFI genes, respectively.In addition, 10 of them were investigated by MLPA forgenomic rearrangements in the CFH-CFHR1–5 regions. Aharmful CFH/CFHR1 hybrid gene was identified in case18. Anti-CFH antibodies, associated with the polymorphicCFHR1-CFHR3 deletion, were detected in case 19. No mu-tation was identified in cases 13 and 22, but not all geneshave been studied. Nine of the 13 patients had previouslyreceived a total of 17 renal transplants, of which 14, 2 and 1had been lost by aHUS recurrence, graft vessels thrombo-sis and chronic rejection, respectively. The median time in-terval between the current renal transplantation and aHUSrecurrence was 2 months (range, 3 days to 5 years). Pa-tients underwent the current transplantation at a medianage of 32 years (range, 6–43 years) and received the firstdose of anti-C5 after a median delay of 30 days (range,1 day to 14 months) following the onset of posttransplantaHUS recurrence.
None of the patient exhibited preformed DSA. AtypicalHUS recurrence was demonstrated by biopsy in 10 outof the 13 patients. Importantly, only one of these initialbiopsies exhibited histological signs of antibody-mediatedrejection. In case 19, the diagnostic biopsy displayed C4dnegative glomerular and peritubular capillaritis, along withTMA lesions, associated with a low-level DSA. C4d stain-ing was performed on 7 biopsies at the time of diagnosisand was always negative.
Outcome of renal transplant in patients treated byanti-C5 for posttransplant aHUS recurrenceAll but three patients were given a complete anti-C5 pro-tocol, still ongoing at last follow-up. Strikingly, cases 12(11) and 13 (9) who received a single dose of anti-C5 ex-perienced a relapse after 21 and 11 months of a HUSremission, respectively (personal communication from J.Nurnberger (Apr 2010) and M. Lozano (Jan 2011) to C.Loirat, with permission). Anti-C5 retreatment failed to pre-vent evolution toward ESRD in the former and did not al-low complete recovery of renal function in the latter, whoultimately lost the graft from antibody-mediated rejectionafter anti-C5 had been withdrawn a second time owing to a
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
Figure 2: Early initiation of anti-C5 therapy is associated with better recovery of renal function. Left panel: Longitudinal follow-upof serum creatinine, including the values before aHUS recurrence, before anti-C5 (day 0) and the creatinine nadir achieved within thethree subsequent months. Red squares or black circles indicate patients in whom the treatment was administered before or after the firstmonth following the onset of aHUS episode, respectively. Right panel: Correlation of graft function recovery with the interval between theaHUS episode and the onset of anti-C5 treatment. The following formula was used to calculate the recovery of renal function after anti-C5therapy: graft function recovery = (day 0 creatinine level-–post-anti-C5 creatinine level)/(day 0 creatinine level-–pre-aHUS creatinine level)$ 100. Day 0 creatinine level indicates the value of creatinine on the first day of anti-C5 therapy. Post-anti-C5 creatinine level indicates thecreatinine nadir achieved within the 3 months following the onset of anti-C5. Pre-aHUS creatinine level indicates the baseline creatininelevel before the onset of the current aHUS episode.
severe pulmonary infection. In all 13 patients, hematologi-cal features of aHUS rapidly returned to or remained normalfollowing the onset of anti-C5 therapy, while mean creati-nine level (±SD) dropped from 295 ± 171 to 135 ± 69lmol/L (p = 0.002) during the three subsequent months.Importantly, in those with incomplete or no response toplasma, the longer the interval between the onset of theHUS episode and anti-C5 treatment initiation the lowerthe recovery of renal function (Figure 2). Typically, patientstreated with anti-C5 more than 28 days after the onset ofthe aHUS recurrence had a lower functional benefit fromanti-C5 than those treated earlier (Figure 2). Patient 17 illus-trates the case of a dramatic improvement of graft functionfollowing early onset anti-C5 therapy for a severe plasma-resistant form of aHUS recurrence (Figure 3A). Interest-ingly, on the biopsy performed 2 days after the first adminis-tration of anti-C5, while creatinine level was peaking, therewere mild thrombotic microangiopathic lesions, includinga fresh intraglomerular thrombosis, arterial wall edema andturgescent endothelial cells, while segmental C5 depositswere identified (Figure 3A). At 1-year posttransplant, theselesions as well as complement deposition had completelydisappeared (Figure 3A). Cases 10 and 11 were given anti-C5 while being dependent on plasma (6,33). Interestingly,both of them experienced a mild but clinically significantimprovement in renal function after switching to anti-C5,although aHUS was thought to be fully sensitive to plasma.The mean ± SD creatinine level at last follow-up was 140.6± 64.7 lmol/L in the 11 patients who were maintained oneculizumab and who were still off dialysis after a medianperiod of treatment of 16 months [range, 4.5–49].
Notably, in cases 10 and 20, a 6- to 8-day delay in anti-C5maintenance dose was three times associated with a mildaHUS relapse that was rapidly responsive to anti-C5 reini-tiation (Table 2, cases 10 and 20). Yet, maintenance doseswere eventually spaced again to every 3 weeks in case10, without further relapse while CH50 remained below oraround the detection level. In case 22, anti-C5 was suc-cessfully stopped for 3 months until a vaccine triggered amild relapse, easily controlled by anti-C5 reinitiation. Pro-gressive tapering of doses was undertaken again and de-tectable C5b-9 reflected incomplete C5 blockade underan every-other-month maintenance regimen. Notably, inthe cases 18 and 19, a graft biopsy performed 3 and 15months, respectively, after the onset of anti-C5 disclosedfresh lesions of thrombotic microangiopathy (TMA). Impor-tantly, these features suggestive of active thrombotic mi-croangiopathic processes coincided with tacrolimus over-exposure (trough levels were between 18 ng/mL and20 ng/mL) in the former and with persisting chronic activeAMR in the latter, which might have triggered endothelialinjury. In both of them, a CH50 activity below the detec-tion threshold argued in favor of an optimal drug expo-sure. However, a positive C5b-9 staining, coexisting withTMA lesions, was documented in case 18 but not in case19. Case 18 was switched back to plasma exchanges forthree daily sessions while tacrolimus exposure was signif-icantly reduced. Subsequently, anti-C5 was resumed. Thebiopsy performed 5 months later did not show any moreactive thrombotic microangiopathic lesions and barelydetected granular C5b-9 deposits within the glomeruli(Figure 3B).
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
Figure 3: Two aHUS patients treated with anti-C5 for overt aHUS posttransplant recurrence. (A) In case 16, daily preemptiveplasma therapy, including freshly frozen plasma infusions (green trapezium) and plasma exchanges (purple trapezium), failed to preventaHUS recurrence. She was switched to anti-C5 at day 6 and underwent a transplant biopsy at day 8, before experiencing a dramaticimprovement in graft function and complete clinical recovery from aHUS recurrence. (a–d) The day 8 graft biopsy disclosed a freshintraglomerular thrombosis (black arrow), arterial wall edema (star) turgescent endothelial cells (white arrow) and a mild yet positiveC5b-9 staining. (e, f) The 12-month protocol biopsy provided evidence that thrombomicroangiopathic lesions and C5b-9 depositions hadcompletely disappeared. (a, b) Jones’ staining; (c) Masson’s trichrome $ 250; (d, f) indirect immunofluorescence with anti-C5b-9; (e)Masson’s trichrome $100. (B) In case 17, daily preemptive plasma therapy undertaken for one month only partially prevented aHUSrecurrence, as suggested by low platelet counts at several times, persistent anemia and graft dysfunction. A biopsy performed at day 11posttransplant found ischemia-related lesions with significant C5b-9 deposition without C3 deposits in the glomeruli, but the biopsy wasdevoid of any thrombomicroangiopathic lesions. The patient was switched to anti-C5 at 1 month posttransplant. Three months later, abiopsy showed mesangiolysis and fresh intraglomerular thrombosis along with important C5b-9 deposition without C3 or C4d deposits.Notably, all these lesions had disappeared, while C5b-9 deposits were barely detected, in the latest biopsy at month 9 posttransplant.
All patients were vaccinated against meningococcal infec-tion and 5 of the 10 patients for whom information wasavailable received daily antibioprophylaxis. Cases 13 and19 each experienced a diffuse pulmonary infection by M.tuberculosis and H. influenza, respectively. Case 19 ex-hibited a profound hypogammaglobulinemia while she hadundergone splenectomy during the early childhood and hadreceived rituximab in an attempt to clear anti-CFH antibody.Her outcome was favorable with antibiotics. Weekly sub-cutaneous immunoglobulin supplementation successfullyprevented recurrence.
Discussion
We reported here the largest series of 22 renal transplantrecipients treated with anti-C5 for prevention or treatmentof aHUS recurrence.
Regarding prophylactic regimens, a first dose of anti-C5 was administered a few hours before surgery andan additional dose within the next 24 h (postopera-tive day 1) in three patients, as it has been proposedfor preventing antibody-mediated rejections (ClinicalTrials.gov: NCT01399593) (34) and catastrophic antiphospholipidsyndrome posttransplant recurrence (ClinicalTrials.gov:NCT01029587) (35). The day 1 infusion, incorporated inprophylactic protocols, stemmed from the finding thatcomplement products are dramatically released followinggraft reperfusion (17,32). This led to the idea that con-ventional protocols might not sufficiently block circulat-ing C5 during the early posttransplant course and that agreater anti-C5 exposure might be needed. Although nostudy has been designed to clarify whether this concernis clinically well grounded, this precaution seems to usquite reasonable. Among preemptively treated patients,anti-C5 treatment was started at least 1 week prior to
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
transplantation in two cases because either a living-donorrenal transplantation was scheduled or the patient waslisted with urgent status for deceased-donor renal trans-plantation (15,16). However, our study shows that an anti-C5 schedule started at day 0 with an additional dose in thefirst 24 h after surgery was remarkably effective at prevent-ing posttransplant recurrence and better accommodateswith most deceased-donor transplantation situations.
Given the limited size of the study population and the ab-sence of controls, one may nonetheless argue against ourability to firmly establish the efficacy of prophylactic anti-C5 therapy from these data. However, it is worth recallingthat all of these patients harbored a genetic abnormalityin complement genes associated with a very high recur-rence risk. In the French adult aHUS cohort, nonhomolo-gous recombinations of the 3% region of the CFH gene,loss-of-function mutations in SCR20 of the CFH gene, andgain of function mutations in the C3 gene have been as-sociated with a recurrence risk of 100, 100 and 80%, re-spectively (Le Quintrec, manuscript submitted). In addition,this is the subset of patients in whom prophylactic plasmatherapy was found to be the least effective at preventingaHUS recurrence (Le Quintrec, manuscript submitted), asillustrated here by case 17. Our data suggest that prophy-lactic anti-C5 therapy may be the most suitable strategy inaHUS patients in whom an identified genetic abnormalityin complement genes or a personal history of posttrans-plant recurrence predicts a very high risk of recurrence forthe current transplantation (Table 3).
With respect to curative protocols, several lessons couldbe drawn from this pioneer experience. First, a single-doseregimen was consistently associated with subsequentrelapses, with uncertainty about sequela-free recovery.Indeed, aside from the two renal transplant recipients re-ported here (9,11), two patients with aHUS involving nativekidneys experienced a relapse after a single dose of anti-C5 (10,36). Strikingly, anti-C5 reinitiation failed to preventevolution toward ESRD in three of them and achieved anincomplete functional recovery in the fourth one, who ul-timately also progressed to ESRD (2,9–11,36) (personalcommunication from M. Lozano [Jan 2011] and J. Nurn-berger [Apr 2010] to C. Loirat, with permission). Thus, asingle-dose regimen should not be recommended. Sec-ond, among the 11 patients who received anti-C5 for overtand uncontrolled aHUS recurrence, the interval betweenthe onset of the HUS episode and anti-C5 initiation criti-cally determined the extent of recovery of renal function.The earlier anti-C5 treatment was started following the on-set of HUS recurrence, the better the chances were forrecovering baseline renal function. It is likely that renalallografts, exposed to ischemia-prone conditions, includ-ing calcineurin inhibitor-related toxicity (2,37) and immune-mediated allograft vasculopathy (38), should be more pronethan native kidneys to rapidly develop ischemia-inducedgraft scarring in the settings of incomplete aHUS con-trol. Moreover, we recently provided evidence that cura-
tive plasma therapy failed to improve graft survival in pa-tients with posttransplant aHUS recurrence (Le Quintrec,submitted). Altogether, these data suggest that promptintroduction of anti-C5 should be recommended as a first-line therapy for the treatment of posttransplant aHUS re-currence. Third, aHUS renal transplant recipients underlong-term plasma therapy, considered sensitive to plasma,may experience an improvement in either renal functionor hemoglobin level after being switched to anti-C5 (cases9 and 10, Table 2). This finding is in line with other casesof aHUS involving native kidneys (39) and is reminiscentof the fact that mild and clinically truncated thromboticmicroangiopathic processes may continue to progress un-der long-term plasma therapy, as evidenced by case 19.Therefore, we recommend a liberal renal biopsy policy, es-pecially in the cases of slightly decreased renal function,appearance of de novo proteinuria, poorly explained ane-mia, increasing need of antihypertensive drugs. In this con-text, biopsy-proven TMA lesions would require a switch toanti-C5.
Antibody-mediated rejection (AMR) is the most commoncause of de novo posttransplant TMA (40). Interestingly,a recent case report described a renal transplant recipi-ent with severe AMR associated with TMA in whom thecomplete polymorphic deletion of CFHR3/1, but not theanti-CFH antibody, was identified (41). This finding raisedthe question of how genetic susceptibility factors may pre-dispose transplant recipients to develop de novo TMA inthe setting of AMR. This finding is further supported byour previous study, which identified mutations in the CFHand CFI genes in roughly one-third of renal transplant re-cipients with de novo posttransplant aHUS (21). We there-fore wondered whether antibody-mediated rejection mighthave triggered posttransplant aHUS recurrence, throughinitiation of endothelial insult. However, evidence of coex-isting AMR and TMA lesions at the time of the diagno-sis of aHUS recurrence was observed only in one patientunder long-term plasma therapy. Moreover, two patientstreated prophylactically with eculizumab remained free ofany aHUS recurrence, although they experienced a severe,yet steroid responsive, mixed rejection.
A 6- to 8-day delay in anti-C5 infusion has been associ-ated three times, in two patients, with a mild aHUS re-lapse that was rapidly responsive to anti-C5 re-initiation.This is consistent with the incomplete TCC blockade be-fore doses observed under every 3 week instead of every2-week regimens (17). Taken together, our data suggestthat the 14-day delay between two maintenance dosesshould not be spaced out in individuals who weigh morethan 10 kg or should be spaced out with extreme cautionin rare situations and under close monitoring of the com-plement assay. We also report evidence that active aHUSdisease may occur in patients treated with anti-C5 accord-ing to the recommended schedule. The transient increasein circulating C5 and TCC in patients with concurrent in-fections, including BK virus replication, upper respiratory
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
Tabl
e3:
Prom
ises
,unc
erta
intie
san
dch
alle
nges
fore
culiz
umab
inaH
US
recu
rren
cese
tting
s
Wor
king
hypo
thes
isPr
opos
als
Poss
ible
desi
gnof
futu
rest
udie
sKe
yen
dpo
ints
offu
ture
stud
ies
Prop
hyla
ctic
anti-
C5
ther
apy
Post
tran
spla
ntaH
US
recu
rren
ceis
ast
rong
pred
icto
rofe
arly
graf
tfa
ilure
.A
nti-C
5ef
ficie
ntly
prev
ents
aHU
Spo
sttr
ansp
lant
recu
rren
ces.
Prop
hyla
ctic
plas
ma
ther
apy
may
fail
topr
even
taH
US
recu
rren
ces
orm
aym
ask
subc
linic
al,y
etpr
ogre
ssiv
e,aH
US
recu
rren
ces
inth
esu
bgro
upof
patie
nts
with
high
-ris
km
utat
ions
.
We
prop
ose
tost
rati
fyre
nal
tran
spla
ntat
ion
cand
idat
esin
tori
skle
vels
ofre
curr
ence
byth
eirm
edic
alhi
stor
yan
dge
netic
back
grou
nd.
Patie
nts
athi
ghri
skof
recu
rren
cein
clud
eth
ose
who
have
alre
ady
expe
rienc
eda
recu
rren
cein
apr
evio
usgr
afta
ndth
ose
who
sem
utat
ions
are
asso
ciat
edw
itha
risk
ofre
curr
ence
grea
tert
han
80%
(mut
atio
nin
CFH
,CFH
-CFH
R1
hybr
idge
ne,g
ain
offu
nctio
nm
utat
ions
inC
3an
dC
FB)
Patie
nts
atm
oder
ate
risk
ofre
curr
ence
incl
ude
thos
ew
ithde
tect
edan
ti-C
FHan
tibod
y,is
olat
edm
utat
ions
inC
FI,
mut
atio
nsof
unkn
own
func
tiona
lsi
gnifi
canc
ean
dno
mut
atio
nid
entifi
ed.
Patie
nts
atlo
wri
skof
recu
rren
cein
clud
eth
ose
with
isol
ated
mut
atio
nsin
MC
Pan
dth
ose
inw
hom
anti-
CFH
antib
odie
sha
vebe
encl
eare
dfr
omci
rcul
atio
n.Pr
ophy
lact
icth
erap
ysh
ould
beun
dert
aken
inpa
tient
sw
ithhi
ghan
dm
oder
ate
risks
whi
leth
ose
atlo
wris
ksh
ould
only
bem
onito
red.
We
prop
ose
the
use
ofan
ti-C
5in
stea
dof
plas
ma
ther
apy
topr
even
tpos
ttran
spla
ntre
curr
ence
san
dto
atte
mpt
disc
ontin
uatio
nof
the
trea
tmen
tin
patie
nts
atm
oder
ate
risk.
Incl
usio
ncr
iter
ia:
Adu
ltaH
US
patie
nts
Can
dida
tes
forr
enal
tran
spla
ntat
ion
Com
plet
ion
ofth
orou
ghco
mpl
emen
tin
vest
igat
ions
Mod
erat
eto
high
risk
ofre
curr
ence
Loca
lava
ilabi
lity
ofda
ilypl
asm
aex
chan
ges
Excl
usio
ncr
iter
ia:
Seve
real
lerg
yto
one
ofth
eco
mpo
nent
sof
both
ther
apeu
ticar
ms
Ong
oing
men
ingo
cocc
alin
fect
ion
Con
trai
ndic
atio
nto
vacc
inat
ion
agai
nstN
.m
enin
gitid
isor
toda
ilyan
tibio
prop
hyla
xis
Des
ign:
Ara
ndom
ized
stud
yco
uld
com
pare
two
arm
sov
era
3-ye
arst
udy
perio
d:–
Prop
hyla
ctic
plas
ma
ther
apy"
–A
nti-C
5co
mpl
ete
prot
ocol
"",
incl
udin
gan
addi
tiona
ldos
e1
day
post
-sur
gery
.Pa
tient
sin
who
mth
ein
itial
trea
tmen
tw
ould
fail
topr
even
taH
US
recu
rren
cew
ould
besw
itche
dto
the
othe
rarm
.Pr
ophy
lact
icth
erap
yw
illbe
disc
ontin
ued
at1
year
post
-tran
spla
nton
lyin
the
subs
etof
patie
nts
with
am
oder
ate
risk
ofre
curr
ence
.Ant
i-C5
wou
ldbe
(re)-i
nitia
ted
ifaH
US
recu
rren
ceoc
curr
ed.
Prim
ary
Inci
denc
eof
aHU
Sre
curr
ence
at1
year
post
rena
ltra
nspl
ant
Seco
ndar
yIn
cide
nce
ofaH
US
recu
rren
ceat
the
end
ofth
est
udy
(3yr
s)Pe
riod
ofD
GF
Gra
ftsu
rviv
alO
ccur
renc
eof
aHU
Sre
curr
ence
afte
rdi
scon
tinua
tion
ofpr
ophy
laxi
s3-
and
12-m
onth
prot
ocol
biop
sies
12-,
24-a
nd36
-mon
theG
FRC
ost-e
ffect
iven
ess
anal
ysis
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
Tabl
e3:
Con
tinue
d.
Wor
king
hypo
thes
isPr
opos
als
Poss
ible
desi
gnof
futu
rest
udie
sKe
yen
dpo
ints
offu
ture
stud
ies
Cur
ativ
ean
ti-C
5th
erap
yPl
asm
ath
erap
yha
sfa
iled
toim
prov
egr
afts
urvi
vali
nre
nalt
rans
plan
trec
ipie
nts
with
aHU
Sre
curr
ence
The
earli
erth
ein
itiat
ion
ofan
ti-C
5af
tera
HU
Sre
curr
ence
the
grea
tert
here
cove
ryof
graf
tfun
ctio
n.
We
prop
ose
the
prom
ptin
itiat
ion
ofan
ti-C
5fo
rthe
trea
tmen
tofo
vert
post
tran
spla
ntaH
US
recu
rren
ce.
Full-
blow
nas
wel
las
inco
mpl
ete
pres
enta
tion
ofaH
US
shou
ldbe
trea
ted
ina
sim
ilarm
anne
ras
they
both
lead
tora
pid
irrev
ersi
ble
dam
ages
ofth
egr
aft.
Giv
enth
em
ultip
leen
doth
eliu
m-in
sulti
ngfa
ctor
sin
rena
ltra
nspl
antr
ecip
ient
s,w
ew
ould
notr
ecom
men
ddi
scon
tinua
tion
ofan
ti-C
5tr
eatm
enti
naH
US
patie
nts
who
have
expe
rienc
eda
post
tran
spla
ntre
curr
ence
inth
ecu
rren
tgra
ft.
Incl
usio
ncr
iter
ia:
Adu
ltre
nalt
rans
plan
trec
ipie
nts
with
aHU
Sre
curr
ence
Loca
lava
ilabi
lity
ofda
ilypl
asm
aex
chan
ges
Excl
usio
ncr
iter
iaSa
me
asfo
rthe
prop
hyla
ctic
prot
ocol
Des
ign:
The
stud
yco
uld
last
3ye
ars.
Two
rand
omiz
edar
ms: –C
urat
ive
plas
ma
ther
apy"
–A
nti-C
5co
mpl
ete
prot
ocol
""Pa
tient
s,in
who
mth
ein
itial
trea
tmen
twou
ldfa
ilto
obta
inpa
rtia
land
com
plet
ere
mis
sion
"""
ofaH
US
byda
y5
and
10,r
espe
ctiv
ely,
wou
ldbe
switc
hed
toth
eot
hera
rm.
Prim
ary
Ach
ieve
men
tofc
ompl
ete
rem
issi
on(%
)Se
cond
ary
Rec
over
yof
rena
lfun
ctio
nN
umbe
rofd
ialy
sis
Gra
ftsu
rviv
alC
hang
esfr
omon
ear
mto
the
othe
r(%
)12
-mon
thpr
otoc
olbi
opsy
12,2
4an
d36
-mon
theG
FRC
ost-e
ffica
cyan
alys
is
This
tabl
esu
mm
ariz
esth
efin
ding
sof
the
pres
ent
stud
yan
dou
rpr
opos
als
for
the
prev
entio
nor
trea
tmen
tof
aHU
Sre
curr
ence
acco
rdin
gto
anin
divi
dual
ized
risk
asse
ssm
ent.
Aim
s,de
sign
and
endp
oint
sof
futu
rest
udie
sar
ebr
iefly
disc
usse
dto
addr
ess
the
pend
ing
ques
tions
rela
ted
toth
em
anag
emen
tofa
HU
Sre
curr
ence
.aH
US
=at
ypic
alhe
mol
ytic
urem
icsy
ndro
me;
DG
F=
dela
yed
graf
tfu
nctio
n;eG
FR=
estim
ated
glom
erul
arfil
trat
ion
rate
."Pl
ease
see
refe
renc
es46
–48,
""Pl
ease
,see
refe
renc
es43
and
45,"
""C
ompl
ete
rem
issi
onis
defin
edas
norm
aliz
atio
nof
plat
elet
coun
tand
LDH
leve
land
reco
very
ofba
selin
ere
nalf
unct
ion.
tract infection and infectious colitis (15,16), suggests thatan infection-related complement activation might inducetemporary underdosing in anti-C5, when treating with adose that is typically sufficient to block the complementassay at steady state. Notably, a significant decrease inplatelet count was noticed in the patient with detectableblood C5, concurrently with Clostridium difficile infection(15,16). Active TMA lesions were also observed in twocases, in which undetectable CH50 indicated a completedepletion of circulating C5 (below 1% of normal values).This finding suggests that TMA lesions may continue toprogress through complement-independent mechanismsin the setting of overwhelming and continuous endothe-lial damages. However, in one of these cases, biopsiesperformed 3 and 9 months after the onset of anti-C5 re-vealed C5b deposition coexisting with active TMA lesions,although the deposition was noticeably less in the latestbiopsy. As suggested by others, this may reflect a pro-longed half-life of pretreatment C5b deposits, rather thatinsufficient in situ C5 blockade (42). Taken together, thesefindings suggest that aHUS patients, regardless of thetreatment used, should be closely monitored when ex-posed to endothelium-insulting factors and/or to intercur-rent events associated with heightened activation or pro-duction of complement factors, including infections, vac-cines, CNI overexposure and antibody-mediated rejection.
The optimal duration of anti-C5 therapy in aHUS remains anelusive question, which has not been properly addressedso far. Life-long treatment has been approved in off-dialysisaHUS patients by the European agency (43). In the presentseries, anti-C5 was withdrawn in three cases, either af-ter a single dose in two of them or after 8 months oftreatment in another. They all subsequently experienced arelapse. However, in our opinion the duration of the treat-ment might be individualized based on genetic findings(Table 3). If complement genetic abnormalities are asso-ciated with a very high risk of posttransplant recurrence,i.e. mutations in CFH and gain of function mutations in C3and CFB, this suggests an overwhelming contribution ofgenetics over environmental triggers to aHUS pathogene-sis. In these patients, as well as in those patients treatedfor a recurrence in the current or a previous graft, long-term anti-C5 therapy should not be discontinued through-out the graft lifespan unless a combined liver–kidney trans-plantation is undertaken to definitively cure the disease.However, one should acknowledge that nobody can pre-dict the new posttransplant history of aHUS, now that aprophylactic treatment efficiently prevents the recurrenceduring the first months, associated with the highest risk of‘endothelial trigger’. Therefore, attempts to taper off anti-C5 therapy after a 12-month aHUS recurrence-free periodof full complement blockade might be a reasonable strat-egy, at least in those with a moderate risk of recurrence(Table 3). In this respect, prospective trials are criticallywarranted to address how long the treatment should becontinued according to an individual’s genetic backgroundand history of recurrence. These future studies will also be
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
Figure 4: Plasma exchange versus eculizumab costs model. (A) A detailed cost analysis of each procedure is provided in the leftpanel. Laboratory examinations include testing routine blood count and blood chemistry. (B) The schedule (doses and intervals) of anti-C5 regimen varies according to patient weight (46). The plasma exchange regimen used to model the cost is based on the currentrecommendations by Consensus Study Groups for aHUS (47–49). Briefly, each procedure should exchange 60 mL/kg body weight, usingvirus-inactivated pooled plasma fraction or individual units of fresh frozen plasma as replacement fluids. Plasma exchange should beperformed daily for 5 days, followed by five times a week for 2 weeks, then three times a week for 2 weeks and subsequently pursuedwith a maintenance regimen. (C) Cost difference between eculizumab—and plasma therapy-based therapies (cost of eculizumab-–cost ofplasma exchanges), according to the weight of individuals and the frequency of PE during the maintenance therapy (after the first monthof intensive therapy), for the treatment of an acute episode of aHUS over a 3-month period. This model is based on the assumption thatthe treatment is provided during a day-care hospitalization.
mandatory to definitively confirm the superiority of anti-C5-based therapy over plasma therapy (Table 3), to demon-strate the benefit of anti-C5-based prophylaxis in candi-dates for renal transplantation with a moderate to high riskof recurrence, and to establish that anti-C5 should be usedas first-line rather than as rescue therapy for the treat-ment of posttransplant recurrence (Table 3). However, forobvious ethical reasons, patients in whom the initial treat-ment would fail to prevent or fully resolve aHUS recurrenceshould be rapidly switched to the other arm.
The high cost of the drug may prompt clinicians to prema-turely discontinue the drug or to prefer initiating treatmentwith plasma therapy. To address this financial concern,
we compared the cost of both plasma and anti-C5-basedstrategies for a 3-month treatment of an acute episode (Fig-ure 4). This cost model was based on the assumption thatall procedures would be undertaken during day care hos-pitalizations. We postulated that most cases would havearteriovenous fistulas and did not take into account thecost of central venous catheter insertion and related com-plications. Our cost analysis indicates that the differencein cost between anti-C5 and plasma therapies varies sig-nificantly depending on the weight of the individual andthe frequency of maintenance plasma therapy (Figure 4).In addition, the over-cost related to a 3-month anti-C5treatment, particularly significant in patients heavier than40 kg, is on the same order of magnitude as the money
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
saved by rescuing a renal allograft from early failure (Fig-ure 4). A medico-economic study conducted by the FrenchHealth Authority (Hautes Autorites de Sante) and reportedin 2010 estimated the cost of 1 year spent on hemodialysisto be approximately 88 608 ! ($ 112 199), while the costof a first and subsequent years following renal transplan-tations were around 86 471 ! ($ 109 493) and 20 147 !($ 25 511), respectively (44). Therefore we believe thatshort-term anti-C5 therapy is the most cost-effective strat-egy to treat aHUS recurrence, although we agree thatthis issue should be more thoroughly addressed for long-term treatment. The duration of hospitalization stays, pe-riod of dialysis need, graft survival, vascular access-relatedcomplications, gain in health-related quality of life and thepreservation of satisfactory working ability would haveto be taken into considerations in a medico-econonomicstudy of long-term anti-C5 treatment in the subset of pa-tient with high risk of recurrence.
Finally, two of the 22 patients experienced a pulmonaryinfection, which could be explained in one case by thepatient’s profound hypogammaglobulinemia. However, nomeningococcal infection was reported. Although the inci-dence of meningococcal infection has been reported to beapproximately 4.2/1000 patient year in patients with parox-ysmal nocturnal hemoglobinuria treated with long-lastingeculizumab therapy (45), we are not aware of any infectionin patients receiving daily antibioprophylaxis. Importantly,to date serogroup B has not been covered by any vaccine,despite its status as the most frequent cause of invasivemeningococcal disease in both America and Europe. In ad-dition, the uncertainty surrounding the vaccine’s efficacyin immunocompromised patients further supports the useof daily antibioprohylaxis during the eculizumab treatmentperiod in renal transplant recipients.
In conclusion, anti-C5 therapy is highly effective for pre-venting and treating posttransplant aHUS recurrence. Ourstudy shows that a single-dose anti-C5 regimen should notbe used and that maintenance anti-C5 doses should notbe spaced out more than 14 days for patients heavier than10 kg. Despite the limitations of a small sample size, thisseries also emphasized that early anti-C5 initiation seemsto ensure better recovery of renal function. We also pro-vide the first evidence that in situ C5 deposition may beindicative of partial escape of C5 blockade in the setting ofexcessive endothelial damage triggered by environmentalfactors.
Acknowledgments
We wish to thank Ms. Laura Leboucher (Financial Administrator, NeckerHospital, Paris France) and Pr. Jean-Bernard Zuber (Laboratoire de PhysiqueTheorique et Hautes Energies, Universite Pierre et Marie Curie, Paris,France) for their invaluable help in performing the cost analysis study. The au-thors are also grateful to Dr. S. Al-Akash (Driscoll Children’s Hospital, Texas,USA), Dr. J.M. Campistol (Hospital Clinic, ICNU, University of Barcelona,
Barcelona, Spain), Dr. J.C Davin (Emma Children’s Hospital, Amsterdam,The Netherlands), Dr. M. Lozano (Hospital Clinic, IDIBAPS, University ofBarcelona, Barcelona, Spain), Dr. C. Nester (University of Iowa Hospitalsand Clinics, Iowa City, Iowa, USA), Dr. J. Nurnberger (University Duisburg-Essen, Essen, Germany), Dr. M. Riedl (Medical University Innsbruck, Inns-bruck, Austria), and Dr. Weitz (University Children’s Hospital Tuebingen,Tuebingen, Germany) for providing updated data on the late outcomes oftheir patients transplanted under eculizumab therapy. We would also like tothank all the members of the French Study Group for Atypical HUS who par-ticipated in fruitful and constructive discussions about this study, includingPr. M. Buchler (Tours, France), Pr. S. Burtey (Marseille, France), Dr. Y. Delmas(Bordeaux, France), Pr. G. Deschenes (Paris, France), Pr. F. Fakhouri (Nantes,France), Dr. A. Karras (Paris, France), Pr. B. Knebelmann (Paris, France), Pr.B. Moulin (Strasbourg, France), Pr. C. Pouteil-Noble (Lyon, France), Dr. F.Provost (Lille, France).
Disclosure
The authors have conflicts of interest to disclose as de-scribed by the American Journal of Transplantation. J.Z.,V.F.-B., C.L. and C.L. have received fees from Alexion Phar-maceuticals for invited lectures.
References
1. Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N EnglJ Med 2009; 17: 1676–1687.
2. Zuber J, Le Quintrec M, Sberro-Soussan R, et al. New insights intopostrenal transplant hemolytic uremic syndrome. Nat Rev Nephrol2011; 23–35.
3. Wagner E, Frank MM. Therapeutic potential of complement mod-ulation. Nat Rev Drug Discov 2010; 1: 43–56.
4. McKeage, K. Eculizumab: A review of its use in paroxysmal noc-turnal haemoglobinuria. Drugs 2011; 17: 2327–2345.
5. Al-Akash SI, Almond PS, VH Savell, Jr., et al. Eculizumab induceslong-term remission in recurrent post-transplant HUS associatedwith C3 gene mutation. Pediatr Nephrol 2011; 4: 613–619.
6. Chatelet V, Fremeaux-Bacchi V, Lobbedez T, et al. Safety and long-term efficacy of eculizumab in a renal transplant patient with recur-rent atypical hemolytic-uremic syndrome. Am J Transplant 2009;11: 2644–2645.
7. Davin JC, Gracchi V, Bouts A, et al. Maintenance of kidneyfunction following treatment with eculizumab and discontinuationof plasma exchange after a third kidney transplant for atypicalhemolytic uremic syndrome associated with a CFH Mutation. AmJ Kidney Dis 2010; 55: 708–711.
8. Gruppo RA, Rother RP. Eculizumab for congenital atypicalhemolytic-uremic syndrome. N Engl J Med 2009; 5: 544–546.
9. Larrea CF, Cofan F, Oppenheimer F, et al. Efficacy of eculizumabin the treatment of recurrent atypical hemolytic-uremic syn-drome after renal transplantation. Transplantation 2010; 7: 903–904.
10. Mache CJ, Acham-Roschitz B, Fremeaux-Bacchi V, et al. Comple-ment inhibitor eculizumab in atypical hemolytic uremic syndrome.Clin J Am Soc Nephrol 2009; 8: 1312–1316.
11. Nurnberger J, Philipp T, Witzke O, et al. Eculizumab for atypicalhemolytic-uremic syndrome. N Engl J Med 2009; 5: 542–544.
12. Dorresteijn EM, van de Kar NC, Cransberg K. Eculizumab as res-cue therapy for atypical hemolytic uremic syndrome with normalplatelet count. Pediatr Nephrol 2012; 7: 1193–1195.
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Eculizumab for Posttransplant aHUS Recurrence
13. Duran CE, Blasco M, Maduell F, et al. Rescue therapy witheculizumab in a transient recipient with atypical haematologic-uraemic syndrome. Clin Kidney J 2012; 1: 28–30.
14. Kim JJ, Waller SC, Reid CJ. Eculizumab in atypical haemolytic-uraemic syndrome allows cessation of plasma exchange and dial-ysis. Clin Kidney J 2012; 1: 34–36.
15. Nester C, Stewart Z, Myers D, et al. Pre-emptive eculizumab andplasmapheresis for renal transplant in atypical hemolytic uremicsyndrome. Clin J Am Soc Nephrol 2011; 6: 1488–1494.
16. Weitz M, Amon O, Bassler D, et al. Prophylactic eculizumab priorto kidney transplantation for atypical hemolytic uremic syndrome.Pediatr Nephrol 2011; 8: 1325–1329.
17. Zimmerhackl LB, Hofer J, Cortina G, et al. Prophylactic eculizumabafter renal transplantation in atypical hemolytic-uremic syndrome.N Engl J Med 2010; 18: 1746–1748.
18. Krid S, Roumenina LT, Beury D, et al. Renal transplantation underprophylactic eculizumab in atypical hemolytic uremic syndromewith CFH/CFHR1 hybrid protein. Am J Transplant 2012; 12: 1938–1944.
19. Chandran S, Baxter-Lowe L, Olson JL, et al. Eculizumab for thetreatment of de novo thrombotic microangiopathy post simulta-neous pancreas-kidney transplantation—a case report. TransplantProc 2011; 5: 2097–2101.
20. Wilson CH, Brown AL, White SA, et al. Successful treatment of denovo posttransplant thrombotic microangiopathy with eculizumab.Transplantation 2011; 8: e42–e43.
21. Le Quintrec M, Lionet A, Kamar N, et al. Complement mutation-associated de novo thrombotic microangiopathy following kidneytransplantation. Am J Transplant 2008; 8: 1694–1701.
22. Greenbaum LA, Babu S, Furman RR, et al. Continued improvementin renal function with sustained eculizumab in patients with atyp-ical HUS resistant to plasma exchange/infusion. In: 44th AnnualMeeting of the American Society of Nephrology ; 2011, J.A.S.N.S.197A, Editor: Philadelphia, PA, USA.
23. Greenbaum LA, Babu S, Furman RR, et al. Eculizumab is an effec-tive long-term treatment in patients with atypical hemolytic uremicsyndrome resistant to plasma exchange/infusion: Results of an ex-tension study. In: 53th Annual Meeting of the American Societyof Hematology ; 2011: San Diego, CA, USA.
24. Legendre C, Babu S, RR Furman, et al. Safety and efficacy ofeculizumab in aHUS resistant to plasm therapy: Interim analysisfrom a phase II trial. In 43rd Annual Meeting of the AmericanSociety of Nephrology ; 2010, JASN (suppl): 93A, Editor: Denver,CO, USA.
25. Licht C, Muus P, Legendre C, et al. Eculizumab is an effectivelong-term treatment in patients with atypical haemolytic uremicsyndrome previously receiving chronic plasma exchange/infusion:Extension study results. In: 53th Annual Meeting of the AmericanSociety of Hematology; 2011: San Diego, CA, USA.
26. Licht C, Muus P, Legendre C, et al. Phase II study of eculizumabin patients with atypical HUS receiving chronic plasma ex-change/infusion. In: 44th Annual Meeting of the American Societyof Nephrology ; 2011 J Am Soc Nephrol 2011; 22(suppl): 197A:Philadelphia, PA, USA.
27. Muus P, Legendre C, Douglas K, et al. Safety and efficacy inaHUS patients on chronic plasma therapy: Interim analysis of aphase II trial. In: 43rd Annual Meeting of the American Societyof Nephrology ; 2010 JASN (suppl): 402A, Editor: Denver, CO,USA.
28. Chatelet V, Lobbedez T, Fremeaux-Bacchi V, et al. Eculizumab:Safety and efficacy after 17 months of treatment in a renal trans-plant patient with recurrent atypical hemolytic-uremic syndrome.Case report. Transplant Proc 2010; 10: 4353–4355.
29. Ardissino G, Testa S, Paglialonga F, et al. Remission of plasma-resistant atypical hemolytic uremic syndrome relapse on kidneygraft with eculizumab. In: 2nd International Conference on HUS-MPGN-PNH; 2010: Innsbruck, Austria. p. 17.
30. Heyne N, Terminal complement blockade by eculizumab effec-tively reverses recurrent atypical hemolytic uremic syndrome afterkidney transplantation. In: 44th Annual Meeting of the AmericanSociety of Nephrology ; 2011: Philadelphia, PA, USA.
31. Legault D, Boelkins M, Succesful treatment of aHUS recurrenceand arrest of plasma exchange resistant TMA post-renal transplan-tation with the terminal complement inhibitor eculizumab. In: 51stAnnual meeting of the American Society of Hematology ; 2009:Grand Rapids, MI. p. 2421.
32. Koskinen AR, Tukiainen E, Arola J, et al. Complement activationduring liver transplantation-special emphasis on patients with atyp-ical hemolytic uremic syndrome. Am J Transplant 2011; 9: 1885–1895.
33. Davin JC, Buter N, Groothoff J, et al. Prophylactic plasma exchangein CD46-associated atypical haemolytic uremic syndrome. PediatrNephrol 2009; 9: 1757–1760.
34. Stegall MD, Diwan T, Raghavaiah S, et al. Terminal comple-ment inhibition decreases antibody-mediated rejection in sensi-tized renal transplant recipients. Am J Transplant 2011; 11: 2405–2413.
35. Lonze BE, Singer AL, Montgomery RA. Eculizumab and renaltransplantation in a patient with CAPS. N Engl J Med 2010; 18:1744–1475.
36. Kose O, Zimmerhackl LB, Jungraithmayr T, et al. New treatmentoptions for atypical hemolytic uremic syndrome with the comple-ment inhibitor eculizumab. Semin Thrombosis Hemostasis 2010;6: 669–672.
37. English J, Evan A, Houghton DC, et al. Cyclosporine-induced acuterenal dysfunction in the rat. Evidence of arteriolar vasoconstric-tion with preservation of tubular function. Transplantation 1987; 1:135–141.
38. Loupy A, Suberbielle-Boissel C, Hill GS, et al. Outcome of sub-clinical antibody-mediated rejection in kidney transplant recipientswith preformed donor-specific antibodies. Am J Transplant 2009;11: 2561–2570.
39. Tschumi S, Gugger M, Bucher BS, et al. Eculizumab in atypicalhemolytic uremic syndrome: Long-term clinical course and histo-logical findings. Pediatr Nephrol 2011; 11: 2085–2088.
40. Satoskar AA, Pelletier R, Adams P, et al. De novo thrombotic mi-croangiopathy in renal allograft biopsies-role of antibody-mediatedrejection. Am J Transplant 2010; 8: 1804–18011.
41. Noone D, Al-Matrafi J, Tinckam K, et al. Antibody mediated re-jection associated with complement factor H-related protein 3/1deficiency successfully treated with eculizumab. Am J Transplant2012; 12: 2546–2553.
42. Herlitz LC, Bomback AS, Markowitz GS, et al. Pathology aftereculizumab in dense deposit disease and C3 GN. J Am SocNephrol 2012; 23: 1229–1237.
43. Summary of Product Characteristics, S., European Commis-sion Available at: http://www.medicines.org.uk/emc/medicine/19966/SPC/soliris./ Accessed November 29, 2011.
44. Sante, HAd. http://www.has-sante.fr/portail/jcms/c_995855/evalu-ation-medio-economique-des-strategies-de-prise-en-charge-de-linsuffisance-renale-en-france-note-de-cadrage. 2010;
45. Brodsky RA, de Castro C III, Schrezenmeier H, et al. Long termsafety and efficacy of sustained eculizumab treatment in patientswith paroxysmal nocturnal hemoglobinuria (PNH). In: 52nd AnnualMeeting of the American Society of Hematology : Orlando, FL,USA.
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x

Zuber et al.
46. Highlights of Prescribing Information, S., U.S. Food andDrug Administration. Available at: http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/125166s172lbl.pdf. Accessed September 23, 2011.
47. Ariceta G, Besbas N, Johnson S, et al. Guideline for the inves-tigation and initial therapy of diarrhea-negative hemolytic uremicsyndrome. Pediatr Nephrol 2009; 4: 687–696.
48. Saland JM, Ruggenenti P, and Remuzzi G. Liver-kidney transplan-tation to cure atypical hemolytic uremic syndrome. J Am SocNephrol 2009; 5: 940–949.
49. Taylor CM, Machin S, Wigmore SJ, et al. Clinical practice guide-lines for the management of atypical haemolytic uraemic syn-drome in the United Kingdom. Br J Haematol 2010; 1: 37–47.
American Journal of Transplantationdoi: 10.1111/j.1600-6143.2012.04252.x
Copyright © 2022 FDOKUMEN




















