hemolytic anemia
185
PDF generated using the open source mwlib toolkit. See http://code.pediapress.com/ for more information. PDF generated at: Sun, 31 Aug 2014 12:50:17 UTC Hemolytic anemia
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of hemolytic anemia

PDF generated using the open source mwlib toolkit. See http://code.pediapress.com/ for more information.PDF generated at: Sun, 31 Aug 2014 12:50:17 UTC
Hemolytic anemia

ContentsArticlesMain topic 1
Anemia 1Hemolysis 12Hemolytic anemia 16Acquired hemolytic anemia 20Congenital hemolytic anemia 22
Related articles 23
Blood 23Blood transfusion 40Blood vessel 55Bone marrow 58Erythropoietin 64Erythropoiesis 73Gallstone 76Haematopoiesis 84Hemoglobin 89Jaundice 105Malaria 112Pulmonary hypertension 129Red blood cell 138Spleen 149Sickle-cell disease 155Thalassemia 168
ReferencesArticle Sources and Contributors 174Image Sources, Licenses and Contributors 180
Article LicensesLicense 183

1
Main topic
AnemiaFor other uses, see Anemia (disambiguation).Contributors [1]
AnemiaClassification and external resources
Human blood from a case of iron-deficiency anemia
ICD-10 D50 [2]-D64 [3]
ICD-9 280 [4]-285 [5]
DiseasesDB 663 [6]
MedlinePlus 000560 [7]
eMedicine med/132 [8] emerg/808 [9] emerg/734 [10]
MeSH D000740 [11]
Anemia or anaemia (/əˈniːmiə/; also spelled anæmia) is usually defined as a decrease in amount of red blood cells(RBCs) or the amount of hemoglobin in the blood. It can also be defined as a lowered ability of the blood to carryoxygen. When anemia comes on slowly the symptoms are often vague and may include: feeling tired, weakness,shortness of breath or a poor ability to exercise. Anemia that comes on quickly often has greater symptoms whichmay include: confusion, feeling like one is going to pass out, and an increased desire to drink fluids. There needs tobe significant anemia before a person becomes noticeably pale. There may be additional symptoms depending on theunderlying cause.There are three main types of anemia, that due to blood loss, that due to decreased red blood cell production, and that due to increased red blood cell breakdown. Causes of blood loss include trauma and gastrointestinal bleeding among others. Causes of decreased production include iron deficiency, a lack of vitamin B12, thalassemia and a number of neoplasms of the bone marrow among others. Causes of increased breakdown include a number of genetic conditions such as sickle cell anemia, infections like malaria and some autoimmune diseases among others. It can also be classified based on the size of red blood cells and amount of hemoglobin in each cell. If the cells are small it is microcytic anemia, if they are large it is macrocytic anemia and if they are normal sized it is normocytic anemia.

Anemia 2
Diagnosis in men is based on a hemoglobin of less than 130 to 140 g/L (13 to 14 g/dL) while in women it must beless 120 to 130 g/L (12 to 13 g/dL). Further testing is then required to determine the cause.Certain groups of individuals, such as pregnant people, benefit from the use of iron pills for prevention. Dietarysupplementation, without determining the specific cause, is not recommended. The use of blood transfusions istypically based on a persons signs and symptoms. In those without symptoms they are not recommended unlesshemoglobin levels are less than 60 to 80 g/L (6 to 8 g/dL). These recommendations may also apply to some peoplewith acute bleeding. Erythropoiesis-stimulating medications are only recommended in those with severe anemia.Anemia is the most common disorder of the blood with it affecting about a quarter of people globally.Iron-deficiency anemia affects nearly 1 billion. It is more common in females than males among children, duringpregnancy and in the elderly. Anemia increases costs of medical care and lowers a person's productivity through adecreased ability to work. The name is derived from Ancient Greek: ἀναιμία anaimia, meaning "lack of blood",from ἀν- an-, "not" + αἷμα haima, "blood".
Signs and symptoms
Main symptoms that may appear in anemia[12]
Anemia goes undetected in many people, and symptomscan be minor or vague. The signs and symptoms can berelated to the underlying cause or the anemia itself. Mostcommonly, people with anemia report feelings ofweakness, or fatigue, general malaise, and sometimespoor concentration. They may also report dyspnea(shortness of breath) on exertion. In very severe anemia,the body may compensate for the lack of oxygen-carryingcapability of the blood by increasing cardiac output. Thepatient may have symptoms related to this, such aspalpitations, angina (if pre-existing heart disease ispresent), intermittent claudication of the legs, andsymptoms of heart failure. On examination, the signsexhibited may include pallor (pale skin, lining mucosa,conjunctiva and nail beds), but this is not a reliable sign.There may be signs of specific causes of anemia, e.g.,koilonychia (in iron deficiency), jaundice (when anemia results from abnormal break down of red blood cells — inhemolytic anemia), bone deformities (found in thalassemia major) or leg ulcers (seen in sickle-cell disease). Insevere anemia, there may be signs of a hyperdynamic circulation: tachycardia (a fast heart rate), bounding pulse,flow murmurs, and cardiac ventricular hypertrophy (enlargement). There may be signs of heart failure. Pica, theconsumption of non-food items such as ice, but also paper, wax, or grass, and even hair or dirt, may be a symptom ofiron deficiency, although it occurs often in those who have normal levels of hemoglobin. Chronic anemia may resultin behavioral disturbances in children as a direct result of impaired neurological development in infants, and reducedscholastic performance in children of school age. Restless legs syndrome is more common in those withiron-deficiency anemia

Anemia 3
CausesBroadly, causes of anemia may be classified as impaired red blood cell (RBC) production, increased RBCdestruction (hemolytic anemias), blood loss and fluid overload (hypervolemia). Several of these may interplay tocause anemia eventually. Indeed, the most common cause of anemia is blood loss, but this usually does not causeany lasting symptoms unless a relatively impaired RBC production develops, in turn most commonly by irondeficiency.[13] (See Iron deficiency anemia)
Impaired production•• Disturbance of proliferation and differentiation of stem cells
• Pure red cell aplasia[14]
• Aplastic anemia affects all kinds of blood cells. Fanconi anemia is a hereditary disorder or defect featuringaplastic anemia and various other abnormalities.
• Anemia of renal failure by insufficient erythropoietin production• Anemia of endocrine disorders
• Disturbance of proliferation and maturation of erythroblasts• Pernicious anemia is a form of megaloblastic anemia due to vitamin B12 deficiency dependent on impaired
absorption of vitamin B12. Lack of dietary B12 causes non-pernicious megaloblastic anemia• Anemia of folic acid deficiency, as with vitamin B12, causes megaloblastic anemia• Anemia of prematurity, by diminished erythropoietin response to declining hematocrit levels, combined with
blood loss from laboratory testing, generally occurs in premature infants at two to six weeks of age.• Iron deficiency anemia, resulting in deficient heme synthesis• Thalassemias, causing deficient globin synthesis• Congenital dyserythropoietic anemias, causing ineffective erythropoiesis• Anemia of renal failure (also causing stem cell dysfunction)
•• Other mechanisms of impaired RBC production• Myelophthisic anemia or myelophthisis is a severe type of anemia resulting from the replacement of bone
marrow by other materials, such as malignant tumors or granulomas.•• Myelodysplastic syndrome• anemia of chronic inflammation
Increased destructionFurther information: Hemolytic anemiaAnemias of increased red blood cell destruction are generally classified as hemolytic anemias. These are generallyfeaturing jaundice and elevated lactate dehydrogenase levels.• Intrinsic (intracorpuscular) abnormalities cause premature destruction. All of these, except paroxysmal nocturnal
hemoglobinuria, are hereditary genetic disorders.[15]
• Hereditary spherocytosis is a hereditary defect that results in defects in the RBC cell membrane, causing theerythrocytes to be sequestered and destroyed by the spleen.
• Hereditary elliptocytosis is another defect in membrane skeleton proteins.• Abetalipoproteinemia, causing defects in membrane lipids•• Enzyme deficiencies
• Pyruvate kinase and hexokinase deficiencies, causing defect glycolysis• Glucose-6-phosphate dehydrogenase deficiency and glutathione synthetase deficiency, causing increased
oxidative stress•• Hemoglobinopathies

Anemia 4
•• Sickle cell anemia•• Hemoglobinopathies causing unstable hemoglobins
•• Paroxysmal nocturnal hemoglobinuria•• Extrinsic (extracorpuscular) abnormalities
• Antibody-mediated• Warm autoimmune hemolytic anemia is caused by autoimmune attack against red blood cells, primarily by
IgG. It is the most common of the autoimmune hemolytic diseases. It can be idiopathic, that is, without anyknown cause, drug-associated or secondary to another disease such as systemic lupus erythematosus, or amalignancy, such as chronic lymphocytic leukemia.[]
• Cold agglutinin hemolytic anemia is primarily mediated by IgM. It can be idiopathic or result from anunderlying condition.
• Rh disease, one of the causes of hemolytic disease of the newborn• Transfusion reaction to blood transfusions
•• Mechanical trauma to red cells• Microangiopathic hemolytic anemias, including thrombotic thrombocytopenic purpura and disseminated
intravascular coagulation• Infections, including malaria•• Heart surgery•• Haemodialysis
Blood loss• Anemia of prematurity from frequent blood sampling for laboratory testing, combined with insufficient RBC
production• Trauma or surgery, causing acute blood loss• Gastrointestinal tract lesions, causing either acute bleeds (e.g. variceal lesions, peptic ulcers or chronic blood loss
(e.g. angiodysplasia)•• Gynecologic disturbances, also generally causing chronic blood loss• From menstruation, mostly among young women or older women who have fibroids• Infection by intestinal nematodes feeding on blood, such as hookworms and the whipworm Trichuris trichiura.

Anemia 5
Fluid overloadFluid overload (hypervolemia) causes decreased hemoglobin concentration and apparent anemia:• General causes of hypervolemia include excessive sodium or fluid intake, sodium or water retention and fluid
shift into the intravascular space.[16]
• Anemia of pregnancy is induced by blood volume expansion experienced in pregnancy.
Diagnosis
Peripheral blood smear microscopy of a patientwith iron-deficiency anemia
Anemia is typically diagnosed on a complete blood count. Apart fromreporting the number of red blood cells and the hemoglobin level, theautomatic counters also measure the size of the red blood cells by flowcytometry, which is an important tool in distinguishing between thecauses of anemia. Examination of a stained blood smear using amicroscope can also be helpful, and it is sometimes a necessity inregions of the world where automated analysis is less accessible. Inmodern counters, four parameters (RBC count, hemoglobinconcentration, MCV and RDW) are measured, allowing others(hematocrit, MCH and MCHC) to be calculated, and compared tovalues adjusted for age and sex. Some counters estimate hematocritfrom direct measurements.
WHO's Hemoglobin thresholds used to define anemia
Age or gender group Hb threshold (g/dl) Hb threshold (mmol/l)
Children (0.5–5.0 yrs) 11.0 6.8
Children (5–12 yrs) 11.5 7.1
Teens (12–15 yrs) 12.0 7.4
Women, non-pregnant (>15yrs) 12.0 7.4
Women, pregnant 11.0 6.8
Men (>15yrs) 13.0 8.1
Reticulocyte counts, and the "kinetic" approach to anemia, have become more common than in the past in the large medical centers of the United States and some other wealthy nations, in part because some automatic counters now have the capacity to include reticulocyte counts. A reticulocyte count is a quantitative measure of the bone marrow's production of new red blood cells. The reticulocyte production index is a calculation of the ratio between the level of anemia and the extent to which the reticulocyte count has risen in response. If the degree of anemia is significant, even a "normal" reticulocyte count actually may reflect an inadequate response. If an automated count is not available, a reticulocyte count can be done manually following special staining of the blood film. In manual examination, activity of the bone marrow can also be gauged qualitatively by subtle changes in the numbers and the morphology of young RBCs by examination under a microscope. Newly formed RBCs are usually slightly larger than older RBCs and show polychromasia. Even where the source of blood loss is obvious, evaluation of erythropoiesis can help assess whether the bone marrow will be able to compensate for the loss, and at what rate. When the cause is not obvious, clinicians use other tests, such as: ESR, ferritin, serum iron, transferrin, RBC folate level, serum vitamin B12, hemoglobin electrophoresis, renal function tests (e.g. serum creatinine) although the tests will depend on the clinical hypothesis that is being investigated. When the diagnosis remains difficult, a bone marrow examination allows direct examination of the precursors to red cells, although is rarely used as is painful,

Anemia 6
invasive and is hence reserved for cases where severe pathology needs to be determined or excluded.
Red blood cell sizeIn the morphological approach, anemia is classified by the size of red blood cells; this is either done automatically oron microscopic examination of a peripheral blood smear. The size is reflected in the mean corpuscular volume(MCV). If the cells are smaller than normal (under 80 fl), the anemia is said to be microcytic; if they are normal size(80–100 fl), normocytic; and if they are larger than normal (over 100 fl), the anemia is classified as macrocytic. Thisscheme quickly exposes some of the most common causes of anemia; for instance, a microcytic anemia is often theresult of iron deficiency. In clinical workup, the MCV will be one of the first pieces of information available, so evenamong clinicians who consider the "kinetic" approach more useful philosophically, morphology will remain animportant element of classification and diagnosis. Limitations of MCV include cases where the underlying cause isdue to a combination of factors - such as iron deficiency (a cause of microcytosis) and vitamin B12 deficiency (acause of macrocytosis) where the net result can be normocytic cells.
Production vs. destruction or lossThe "kinetic" approach to anemia yields arguably the most clinically relevant classification of anemia. Thisclassification depends on evaluation of several hematological parameters, particularly the blood reticulocyte(precursor of mature RBCs) count. This then yields the classification of defects by decreased RBC production versusincreased RBC destruction and/or loss. Clinical signs of loss or destruction include abnormal peripheral blood smearwith signs of hemolysis; elevated LDH suggesting cell destruction; or clinical signs of bleeding, such asguaiac-positive stool, radiographic findings, or frank bleeding. The following is a simplified schematic of thisapproach:<tr style="height: 1px; text-align: center;"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Anemia<td rowspan="2"colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><tr style="height: 1px; text-align: center;"><tr style="height: 1px; text-align: center;"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2">

Anemia 7
<td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Reticulocyte production indexshows inadequate production response to anemia.<td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Reticulocyte production indexshows appropriate response to anemia = ongoing hemolysis or blood loss without RBC production problem.<tdrowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><tr style="height: 1px; text-align: center;"><tr style="height: 1px; text-align: center;"><td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">No clinical findings consistentwith hemolysis or blood loss: pure disorder of production.<td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Clinical findings and abnormalMCV: hemolysis or loss and chronic disorder of production*.<td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Clinical findings and normalMCV= acute hemolysis or loss without adequate time for bone marrow production to compensate**.<tdrowspan="2" colspan="2"><tr style="height: 1px; text-align: center;"><tr style="height: 1px; text-align: center;"><td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Macrocytic anemia(MCV>100)<td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Normocytic anemia(80<MCV<100)<td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td colspan="6" rowspan="2" style="border: 2px solid black; padding: 0.2em; ; ">Microcytic anemia (MCV<80)<tdrowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><td rowspan="2" colspan="2"><tr style="height: 1px; text-align: center;"> * For instance, sickle cell anemia with superimposed iron deficiency;chronic gastric bleeding with B12 and folate deficiency; and other instances of anemia with more than one cause.** Confirm by repeating reticulocyte count: ongoing combination of low reticulocyte production index, normal MCVand hemolysis or loss may be seen in bone marrow failure or anemia of chronic disease, with superimposed orrelated hemolysis or blood loss. Here is a schematic representation of how to consider anemia with MCV as thestarting point:

Anemia 8
Anemia
Macrocytic anemia(MCV>100)
Normocytic anemia (MCV80–100)
Microcytic anemia(MCV<80)
High reticulocytecount
Low reticulocytecount
Other characteristics visible on the peripheral smear may provide valuable clues about a more specific diagnosis; forexample, abnormal white blood cells may point to a cause in the bone marrow.
Microcytic
Main article: Microcytic anemiaMicrocytic anemia is primarily a result of hemoglobin synthesis failure/insufficiency, which could be caused byseveral etiologies:• Heme synthesis defect
• Iron deficiency anemia (microcytosis is not always present)• Anemia of chronic disease (more commonly presenting as normocytic anemia)
• Globin synthesis defect• Alpha-, and beta-thalassemia•• HbE syndrome•• HbC syndrome•• Various other unstable hemoglobin diseases
• Sideroblastic defect•• Hereditary sideroblastic anemia• Acquired sideroblastic anemia, including lead toxicity•• Reversible sideroblastic anemia
Iron deficiency anemia is the most common type of anemia overall and it has many causes. RBCs often appearhypochromic (paler than usual) and microcytic (smaller than usual) when viewed with a microscope.• Iron deficiency anemia is due to insufficient dietary intake or absorption of iron to meet the body's needs. Infants,
toddlers, and pregnant women have higher than average needs. Increased iron intake is also needed to offset bloodlosses due to digestive tract issues, frequent blood donations, or heavy menstrual periods.[17] Iron is an essentialpart of hemoglobin, and low iron levels result in decreased incorporation of hemoglobin into red blood cells. Inthe United States, 12% of all women of childbearing age have iron deficiency, compared with only 2% of adultmen. The incidence is as high as 20% among African American and Mexican American women. Studies haveshown iron deficiency without anemia causes poor school performance and lower IQ in teenage girls, althoughthis may be due to socioeconomic factors. Iron deficiency is the most prevalent deficiency state on a worldwidebasis. It is sometimes the cause of abnormal fissuring of the angular (corner) sections of the lips (angularstomatitis).
• In the United States, the most common cause of iron deficiency is bleeding or blood loss, usually from thegastrointestinal tract. Fecal occult blood testing, upper endoscopy and lower endoscopy should be performed toidentify bleeding lesions. In older men and women, the chances are higher that bleeding from the gastrointestinaltract could be due to colon polyps or colorectal cancer.
• Worldwide, the most common cause of iron deficiency anemia is parasitic infestation (hookworms, amebiasis,schistosomiasis and whipworms).

Anemia 9
The Mentzer index (mean cell volume divided by the RBC count) predicts whether microcytic anaemia may be dueto iron deficiency or thallasemia, although it requires confirmation.Wikipedia:Citation needed
Macrocytic
Main article: Macrocytic anemia• Megaloblastic anemia, the most common cause of macrocytic anemia, is due to a deficiency of either vitamin B12,
folic acid, or both. Deficiency in folate and/or vitamin B12 can be due either to inadequate intake or insufficientabsorption. Folate deficiency normally does not produce neurological symptoms, while B12 deficiency does.• Pernicious anemia is caused by a lack of intrinsic factor, which is required to absorb vitamin B12 from food. A
lack of intrinsic factor may arise from an autoimmune condition targeting the parietal cells (atrophic gastritis)that produce intrinsic factor or against intrinsic factor itself. These lead to poor absorption of vitamin B12.
• Macrocytic anemia can also be caused by removal of the functional portion of the stomach, such as duringgastric bypass surgery, leading to reduced vitamin B12/folate absorption. Therefore, one must always be awareof anemia following this procedure.
•• Hypothyroidism• Alcoholism commonly causes a macrocytosis, although not specifically anemia. Other types of liver disease can
also cause macrocytosis.• Drugs such as Methotrexate, zidovudine, and other substances may inhibit DNA replication such as heavy metals
(e.g. Lead)Macrocytic anemia can be further divided into "megaloblastic anemia" or "nonmegaloblastic macrocytic anemia".The cause of megaloblastic anemia is primarily a failure of DNA synthesis with preserved RNA synthesis, whichresults in restricted cell division of the progenitor cells. The megaloblastic anemias often present with neutrophilhypersegmentation (six to 10 lobes). The nonmegaloblastic macrocytic anemias have different etiologies (i.e.unimpaired DNA globin synthesis,) which occur, for example, in alcoholism. In addition to the nonspecificsymptoms of anemia, specific features of vitamin B12 deficiency include peripheral neuropathy and subacutecombined degeneration of the cord with resulting balance difficulties from posterior column spinal cordpathology.[18] Other features may include a smooth, red tongue and glossitis. The treatment for vitamin B12-deficientanemia was first devised by William Murphy, who bled dogs to make them anemic, and then fed them varioussubstances to see what (if anything) would make them healthy again. He discovered that ingesting large amounts ofliver seemed to cure the disease. George Minot and George Whipple then set about to isolate the curative substancechemically and ultimately were able to isolate the vitamin B12 from the liver. All three shared the 1934 Nobel Prizein Medicine.
Normocytic
Main article: Normocytic anemiaNormocytic anemia occurs when the overall hemoglobin levels are decreased, but the red blood cell size (meancorpuscular volume) remains normal. Causes include:• Acute blood loss•• Anemia of chronic disease• Aplastic anemia (bone marrow failure)•• Hemolytic anemia

Anemia 10
Dimorphic
A dimorphic appearance on a peripheral blood smear occurs when there are two simultaneous populations of redblood cells, typically of different size and hemoglobin content (this last feature affecting the color of the red bloodcell on a stained peripheral blood smear). For example, a person recently transfused for iron deficiency would havesmall, pale, iron deficient red blood cells (RBCs) and the donor RBCs of normal size and color. Similarly, a persontransfused for severe folate or vitamin B12 deficiency would have two cell populations, but, in this case, the patient'sRBCs would be larger and paler than the donor's RBCs. A person with sideroblastic anemia (a defect in hemesynthesis, commonly caused by alcoholism, but also drugs/toxins, nutritional deficiencies, a few acquired and rarecongenital diseases) can have a dimorphic smear from the sideroblastic anemia alone. Evidence for multiple causesappears with an elevated RBC distribution width (RDW), indicating a wider-than-normal range of red cell sizes, alsoseen in common nutritional anemia.
Heinz body anemia
Heinz bodies form in the cytoplasm of RBCs and appear as small dark dots under the microscope. Heinz bodyanemia has many causes, and some forms can be drug-induced. It is triggered in cats by eating onions oracetaminophen (paracetamol). It can be triggered in dogs by ingesting onions or zinc, and in horses by ingesting dryred maple leaves.
HyperanemiaHyperanemia is a severe form of anemia, in which the hematocrit is below 10%.
Refractory anemiaRefractory anemia, an anemia which does not respond to treatment, is often seen secondary to myelodysplasticsyndromes. Iron deficiency anemia may also be refractory as a clinical manifestation of gastrointestinal problemswhich disrupt iron absorption or cause occult bleeding.
TreatmentsTreatments for anemia depend on cause and severity. Vitamin supplements given orally (folic acid or vitamin B12) orintramuscularly (vitamin B12) will replace specific deficiencies.
Oral ironNutritional iron deficiency is common in developing nations. An estimated two-thirds of children and of women ofchildbearing age in most developing nations are estimated to suffer from iron deficiency; one-third of them have themore severe form of the disorder, anemia. Iron deficiency from nutritional causes is rare in men and postmenopausalwomen. The diagnosis of iron deficiency mandates a search for potential sources of loss, such as gastrointestinalbleeding from ulcers or colon cancer. Mild to moderate iron-deficiency anemia is treated by oral ironsupplementation with ferrous sulfate, ferrous fumarate, or ferrous gluconate. When taking iron supplements, stomachupset and/or darkening of the feces are commonly experienced. The stomach upset can be alleviated by taking theiron with food; however, this decreases the amount of iron absorbed. Vitamin C aids in the body's ability to absorbiron, so taking oral iron supplements with orange juice is of benefit.In anemias of chronic disease, associated with chemotherapy, or associated with renal disease, some cliniciansprescribe recombinant erythropoietin or epoetin alfa, to stimulate RBC production, although since there is alsoconcurrent iron deficiency and inflammation present, parenteral iron is advised to be taken concurrently.[19]

Anemia 11
Injectable ironIn cases where oral iron has either proven ineffective, would be too slow (for example, pre-operatively) or whereabsorption is impeded (for example in cases of inflammation), parenteral iron can be used. The body can absorb upto 6 mg iron daily from the gastrointestinal tract. In many cases the patient has a deficit of over 1,000 mg of ironwhich would require several months to replace. This can be given concurrently with erythropoietin to ensuresufficient iron for increased rates of erythropoiesis.
Blood transfusionsBlood transfusions in those without symptoms is not recommended until the hemoglobin is below 60 to 80 g/L (6 to8 g/dL). In those with coronary artery disease who are not actively bleeding transfusions are only recommendedwhen the hemoglobin is below 70 to 80g/L (7 to 8 g/dL). Transfusing earlier does not improve survival.Transfusions otherwise should only be undertaken in cases of cardiovascular instability.
Erythropoiesis-stimulating agentThe motive for the administration of an erythropoiesis-stimulating agent (ESA) is to maintain hemoglobin at thelowest level that both minimizes transfusions and meets the individual persons needs. They should not be used formild or moderate anemia. They are not recommended in people with chronic kidney disease unless hemoglobinlevels are less than 10 g/dL or they have symptoms of anemia. Their use should be along with parenteral iron.
Hyperbaric oxygenTreatment of exceptional blood loss (anemia) is recognized as an indication for hyperbaric oxygen (HBO) by theUndersea and Hyperbaric Medical Society. The use of HBO is indicated when oxygen delivery to tissue is notsufficient in patients who cannot be given blood transfusions for medical or religious reasons. HBO may be used formedical reasons when threat of blood product incompatibility or concern for transmissible disease are factors. Thebeliefs of some religions (ex: Jehovah's Witnesses) may require they use the HBO method. A 2005 review of the useof HBO in severe anemia found all publications reported positive results.
EpidemiologyA moderate degree of iron-deficiency anemia affected approximately 610 million people worldwide or 8.8% of thepopulation. It is slightly more common in female (9.9%) than males (7.8%). Mild iron deficiency anemia affectsanother 375 million.
HistoryEvidence of anemia goes back more than 4000 years.
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Anemia[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D50[3] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D64[4] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=280[5] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=285[6] http:/ / www. diseasesdatabase. com/ ddb663. htm[7] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000560. htm[8] http:/ / www. emedicine. com/ med/ topic132. htm[9] http:/ / www. emedicine. com/ emerg/ topic808. htm#[10] http:/ / www. emedicine. com/ emerg/ topic734. htm#[11] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D000740

Anemia 12
[12] eMedicineHealth > anemia article (http:/ / www. emedicinehealth. com/ anemia/ page3_em. htm) Author: Saimak T. Nabili, MD, MPH.Editor: Melissa Conrad Stöppler, MD. Last Editorial Review: 12/9/2008. Retrieved on 4 April 2009
[13] National Heart Lung and Blood Institute > What Causes Anemia? (http:/ / www. nhlbi. nih. gov/ health/ dci/ Diseases/ anemia/anemia_causes. html) Retrieved on June 9, 2010
[14][14] Table 12-1 in: 8th edition.[15] Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; & Mitchell, Richard N. (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. p.
432 ISBN 978-1-4160-2973-1[16][16] Page 62 (Fluid imbalances) in:[17] Recommendations to Prevent and Control Iron Deficiency in the United States (http:/ / www. cdc. gov/ nccdphp/ dnpa/ nutrition/
nutrition_for_everyone/ iron_deficiency/ index. htm) MMWR 1998;47 (No. RR-3) p. 5[18] eMedicine – Vitamin B-12 Associated Neurological Diseases : Article by Niranjan N Singh, MD, DM, DNB (http:/ / www. emedicine. com/
NEURO/ topic439. htm) July 18, 2006[19] http:/ / guidance. nice. org. uk/ CG114/ Guidance/ pdf/ English
External links• National Anemia Action Council (http:/ / www. anemia. org/ ) (USA)• Anemia (http:/ / labtestsonline. org/ understanding/ conditions/ anemia/ ) - Lab Tests Online
HemolysisThis article is about medical aspects of hemolysis. For hemolysis in the culture of microorgranisms, see Hemolysis(microbiology)."Laking" redirects here. For other uses, see Laking (disambiguation).Hemolysis (or haemolysis)—from the Greek αἷμα (aima, haema, hemo-) meaning "blood" and λύσις (lusis, lysis,-lysis) meaning a "loosing", "setting free" or "releasing"[1]—is the rupturing of erythrocytes (red blood cells) and therelease of their contents (cytoplasm) into surrounding fluid (e.g., blood plasma). Hemolysis may occur in vivo or invitro (inside or outside the body).
In vivo (inside the body)In vivo hemolysis can be caused by a large number of medical conditions, including many Gram-positive bacteria(e.g., Streptococcus, Enterococcus, and Staphylococcus), some parasites (e.g., Plasmodium), some autoimmunedisorders (e.g., drug-induced hemolytic anemia), some genetic disorders (e.g., Sickle-cell disease or G6PDdeficiency), or blood with too low a solute concentration (hypotonic to cells).
Streptococcus
Main article: StreptococcusMany species of the genus Streptococcus cause hemolysis. Streptococcal bacteria species are classified according totheir hemolytic properties.• Alpha-hemolytic species, including S. pneumoniae, Streptococcus mitis, S. mutans, and S. salivarius, oxidize the
iron in the hemoglobin (turning it dark green in culture).• Beta-hemolytic species, including S. pyogenes and S. agalactiae, completely rupture the red blood cells (visible as
a halo in culture).•• Gamma-hemolytic, or non-hemolytic, species do not cause hemolysis and rarely cause illness.

Hemolysis 13
Enterococcus
Main article: EnterococcusThe genus Enterococcus includes lactic acid bacteria formerly classified as gamma-hemolytic Group D in the genusstreptococcus (see above), including E. faecilis (S. faecalis), E. faecium (S. faecium), E. durans (S. durans), and E.avium (S. avium).
Staphylococcus
Main article: StaphylococcusStaphylococcus is another Gram-positive cocci. S. aureus, the most common cause of "staph" infections, isfrequently hemolytic on BA.[2]
Parasitic hemolysisBecause the feeding process of the Plasmodium parasites damages red blood cells, malaria is sometimes called"parasitic hemolysis" in medical literature.
Hemolytic disease of the newbornMain article: Hemolytic disease of the newbornHemolytic disease of the newborn is an autoimmune disease resulting from the mother's antibodies crossing theplacenta to the fetus.
Hemolytic anemiaMain article: Hemolytic anemiaBecause in vivo hemolysis destroys the red blood cells, in uncontrolled chronic or severe cases it can lead tohemolytic anemia.
Hemolytic crisisA hemolytic crisis, or hyperhemolytic crisis, is characterized by an accelerated rate of red blood cell destructionleading to anemia, jaundice, and reticulocytosis.[3] Hemolytic crises are a major concern with sickle-cell disease andG6PD deficiency.

Hemolysis 14
In vitro (outside the body)
Hemolysis of blood samples. Red blood cells without(left and middle) and with (right) hemolysis. If as little
as 0.5% of the red blood cells are hemolyzed, thereleased hemoglobin will cause the serum or plasma toappear pale red or cherry red in color.[4] Note that thehemolyzed sample is transparent, because there are no
cells to scatter light.
In vitro hemolysis can be caused by improper technique duringcollection of blood specimens, by the effects of mechanicalprocessing of blood, or by bacterial action in cultured bloodspecimens.
From specimen collection
Most causes of in vitro hemolysis are related to specimencollection. Difficult collections, unsecure line connections,contamination, and incorrect needle size, as well as improper tubemixing and incorrectly filled tubes are all frequent causes ofhemolysis. Excessive suction can cause the red blood cells to besmashed on their way through the hypodermic needle owing toturbulence and physical forces. Such hemolysis is more likely tooccur when a patient's veins are difficult to find or when theycollapse when blood is removed by a syringe or a modern vacuumtube. Experience and proper technique are key for anyphlebotomist or nurse to prevent hemolysis.
In vitro hemolysis during specimen collection can cause inaccurate laboratory test results by contaminating thesurrounding plasma with the contents of hemolyzed red blood cells. For example, the concentration of potassiuminside red blood cells is much higher than in the plasma and so an elevated potassium level is usually found inbiochemistry tests of hemolyzed blood.
In vitro hemolysis can also occur in a blood sample because of prolonged storage or storage in incorrect conditions(i.e., too hot or too cold).
From mechanical blood processing during surgeryIn some surgical procedures (especially some heart operations) where substantial blood loss is expected, machineryis used for intraoperative blood salvage. A centrifuge process takes blood from the patient, washes the red bloodcells with normal saline, and returns them to the patient's blood circulation. Hemolysis may occur if the centrifugerotates too quickly (generally greater than 500 rpm)—essentially this is hemolysis occurring outside of the body.Unfortunately, increased hemolysis occurs with massive amounts of sudden blood loss, because the process ofreturning a patient's cells must be done at a correspondingly higher speed to prevent hypotension, pH imbalance, anda number of other hemodynamic and blood level factors.
Hemolysis 15
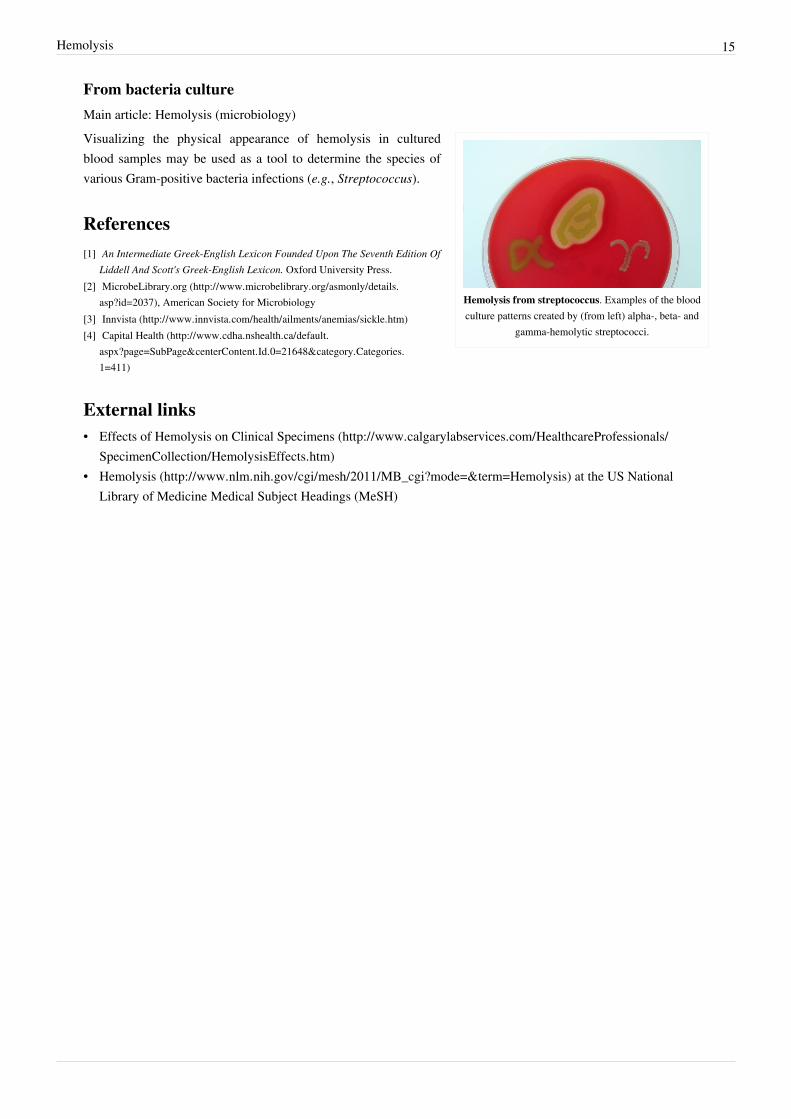
From bacteria cultureMain article: Hemolysis (microbiology)
Hemolysis from streptococcus. Examples of the bloodculture patterns created by (from left) alpha-, beta- and
gamma-hemolytic streptococci.
Visualizing the physical appearance of hemolysis in culturedblood samples may be used as a tool to determine the species ofvarious Gram-positive bacteria infections (e.g., Streptococcus).
References[1] An Intermediate Greek-English Lexicon Founded Upon The Seventh Edition Of
Liddell And Scott's Greek-English Lexicon. Oxford University Press.[2] MicrobeLibrary.org (http:/ / www. microbelibrary. org/ asmonly/ details.
asp?id=2037), American Society for Microbiology[3] Innvista (http:/ / www. innvista. com/ health/ ailments/ anemias/ sickle. htm)[4] Capital Health (http:/ / www. cdha. nshealth. ca/ default.
aspx?page=SubPage& centerContent. Id. 0=21648& category. Categories.1=411)
External links• Effects of Hemolysis on Clinical Specimens (http:/ / www. calgarylabservices. com/ HealthcareProfessionals/
SpecimenCollection/ HemolysisEffects. htm)• Hemolysis (http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?mode=& term=Hemolysis) at the US National
Library of Medicine Medical Subject Headings (MeSH)

Hemolytic anemia 16
Hemolytic anemiaContributors [1]
Hemolytic anemiaClassification and external resources
ICD-10 D55 [2]-D59 [3]
ICD-9 282 [4], 283 [5], 773 [6]
DiseasesDB 5534 [7]
MedlinePlus 000571 [8]
eMedicine med/979 [9]
MeSH D000743 [10]
Hemolytic anemia is a form of anemia due to hemolysis, the abnormal breakdown of red blood cells (RBCs), eitherin the blood vessels (intravascular hemolysis) or elsewhere in the human body (extravascular). It has numerouspossible causes, ranging from relatively harmless to life-threatening. The general classification of hemolytic anemiais either inherited or acquired. Treatment depends on the cause and nature of the breakdown.Symptoms of hemolytic anemia are similar to other forms of anemia (fatigue and shortness of breath), but inaddition, the breakdown of red cells leads to jaundice and increases the risk of particular long-term complications,such as gallstones and pulmonary hypertension.
Basic featuresHemolytic anemia involves the following:1.1. Abnormal and accelerated destruction of red cells and, in some anemias, their precursors2.2. Increased breakdown of hemoglobin, which may result in:
1. increased bilirubin level (mainly indirect-reacting) with jaundice2. increased fecal and urinary urobilinogen3. Hemoglobinemia, methemalbuminemia, hemoglobinuria and hemosiderinuria (where there is significant
intravascular hemolysis).3.3. Bone marrow compensatory reaction:
1. Erythroid hyperplasia with accelerated production of red cells, reflected by reticulocytosis, and slightmacrocytosis in peripheral blood
2.2. Expansion of bone marrow in infants and children with severe chronic hemolysis - changes in boneconfiguration visible on X-ray
4.4. The balance between red cell destruction and marrow compensation determines the severity of anemias.

Hemolytic anemia 17
Signs and symptomsIn general, signs of anemia (pallor, fatigue, shortness of breath, and potential for heart failure) are present. In smallchildren, failure to thrive may occur in any form of anemia. Certain aspects of the medical history can suggest acause for hemolysis, such as drugs, consumption of fava beans due to Favism, the presence of prosthetic heart valve,or other medical illness.Chronic hemolysis leads to an increased excretion of bilirubin into the biliary tract, which in turn may lead togallstones. The continuous release of free hemoglobin has been linked with the development of pulmonaryhypertension (increased pressure over the pulmonary artery); this, in turn, leads to episodes of syncope (fainting),chest pain, and progressive breathlessness. Pulmonary hypertension eventually causes right ventricular heart failure,the symptoms of which are peripheral edema (fluid accumulation in the skin of the legs) and ascites (fluidaccumulation in the abdominal cavity).
CausesMain articles: Congenital hemolytic anemia and Acquired hemolytic anemiaThey may be classified according to the means of hemolysis, being either intrinsic in cases where the cause is relatedto the red blood cell (RBC) itself, or extrinsic in cases where factors external to the RBC dominate.[11] Intrinsiceffects may include problems with RBC proteins or oxidative stress handling, whereas external factors includeimmune attack and microvascular angiopathies (RBCs are mechanically damaged in circulation).
Intrinsic causesHereditary (inherited) hemolytic anemia can be due to :• Defects of red blood cell membrane production (as in hereditary spherocytosis and hereditary elliptocytosis)• Defects in hemoglobin production (as in thalassemia, sickle-cell disease and congenital dyserythropoietic anemia)• Defective red cell metabolism (as in glucose-6-phosphate dehydrogenase deficiency and pyruvate kinase
deficiency)
Extrinsic causesAcquired hemolytic anemia may be caused by immune-mediated causes, drugs and other miscellaneous causes.• Immune-mediated causes could include transient factors as in Mycoplasma pneumoniae infection (cold agglutinin
disease) or permanent factors as in autoimmune diseases like autoimmune hemolytic anemia (itself more commonin diseases such as systemic lupus erythematosus, rheumatoid arthritis, Hodgkin's lymphoma, and chroniclymphocytic leukemia).
• Paroxysmal nocturnal hemoglobinuria (PNH), sometimes referred to as Marchiafava-Micheli syndrome, is a rare,acquired, potentially life-threatening disease of the blood characterized by complement-induced intravascularhemolytic anemia.
• Any of the causes of hypersplenism (increased activity of the spleen), such as portal hypertension.• Acquired hemolytic anemia is also encountered in burns and as a result of certain infections.• Lead poisoning resulting from the environment causes non-immune hemolytic anemia.• Runners can suffer hemolytic anemia due to "footstrike hemolysis", owing to the destruction of red blood cells in
feet at foot impact.•• Low-grade hemolytic anemia occurs in 70% of prosthetic heart valve recipients, and severe hemolytic anemia
occurs in 3%.

Hemolytic anemia 18
PathophysiologyIn a healthy person, a red blood cell survives 90 to 120 days in the circulation, so about 1% of human red blood cellsbreak down each day. The spleen (part of the reticulo-endothelial system) is the main organ that removes old anddamaged RBCs from the circulation. In healthy individuals, the breakdown and removal of RBCs from thecirculation is matched by the production of new RBCs in the bone marrow.In conditions where the rate of RBC breakdown is increased, the body initially compensates by producing moreRBCs; however, breakdown of RBCs can exceed the rate that the body can make RBCs, and so anemia can develop.Bilirubin, a breakdown product of hemoglobin, can accumulate in the blood, causing jaundice, and be excreted in theurine causing the urine to become a dark brown color.In general, hemolytic anemia occurs as a modification of the RBC life cycle. That is, instead of being collected at theend of its useful life and disposed of normally, the RBC disintegrates in a manner allowing free iron-containingmolecules to reach the blood. It is perhaps then helpful to understand the physiology of the RBC and things that cango wrong to cause it to "die" prematurely. With their complete lack of mitochondria, RBCs rely on glycolysis for thematerials needed to reduce oxidative damage. Any limitations of glycolysis can result in more susceptibility tooxidative damage and a short or abnormal lifecycle. If the cell is unable to signal to the reticuloendothelialphagocytes by externalizing phosphatidylserine, it is likely to lyse through uncontrolled means. Dogs and cats differslightly from humans in some details of their RBC composition and have altered susceptibility to damage, notably,increased susceptibility to oxidative damage from onion or garlic.The distinguishing feature of intravascular hemolysis is the release of RBC contents into the blood stream. Themetabolism and elimination of these products, largely iron-containing compounds capable of doing damage throughFenton reactions, is an important part of the condition. Several reference texts exist on the elimination pathways, forexample.[12][13] Free hemoglobin can bind to haptoglobin, or it may oxidize and release the heme group that is ableto bind to either albumin or hemopexin. The heme is ultimately converted to bilirubin and removed in stool andurine. Hemoglobin may be cleared directly by the kidneys resulting in fast clearance of free hemoglobin but causingthe continued loss of hemosiderin loaded renal tubular cells for many days.Additional effects of free hemoglobin seem to be due to specific reactions with NO.
Diagnosis• Peripheral blood smear microscopy:
• fragments of the red blood cells ("schistocytes") can be present• some red blood cells may appear smaller and rounder than usual (spherocytes)• Reticulocytes are present in elevated numbers. This may be overlooked if a special stain is not used.• Bite cells may be present due to Heinz body removal by the spleen in G6PD deficiency.
•• The level of unconjugated bilirubin in the blood is elevated. This may lead to jaundice.• The level of lactate dehydrogenase (LDH) in the blood is elevated•• Haptoglobin levels are decreased• If the direct Coombs test is positive, hemolysis is caused by an immune process (e.g. autoimmune hemolytic
anemia).• Hemosiderin in the urine indicates chronic intravascular hemolysis. There is also urobilinogen in the urine.• Haemaglobinuria in the morning is suggestive of paroxysmal nocturnal haemoglobinuria.

Hemolytic anemia 19
TreatmentDefinitive therapy depends on the cause:• Symptomatic treatment can be given by blood transfusion, if there is marked anemia.• In severe immune-related hemolytic anemia, steroid therapy is sometimes necessary.• Sometimes splenectomy can be helpful where extravascular hemolysis, or hereditary spherocytosis, is
predominant (i.e. most of the red blood cells are being removed by the spleen).
Veterinary casesHemolytic anemia affects nonhuman species as well as humans. It has been found, in a number of animal species, toresult from specific triggers.[14]
Some notable cases include hemolytic anemia found in black rhinos kept in captivity, with the disease, in oneinstance, affecting 20% of captive rhinos at a specific facility.[15][16][17] The disease is also found in wild rhinos.[18]
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Hemolytic_anemia[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D55[3] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D59[4] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=282[5] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=283[6] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=773[7] http:/ / www. diseasesdatabase. com/ ddb5534. htm[8] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000571. htm[9] http:/ / www. emedicine. com/ med/ topic979. htm[10] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D000743[11] Current Medical Diagnosis and Treatment 2009 By Stephen J. McPhee, Maxine A. Papadakis page 436 http:/ / books. google. com/
books?id=zQlH4mXSziYC& pg=PT454& dq=hemoglobin+ hemosiderin+ hemolysis+ bilirubin&ei=Z2P_SuzwA6D2ygT9vOz3Dg#v=onepage& q=hemoglobin%20hemosiderin%20hemolysis%20bilirubin& f=false
[12] Hematology in clinical practice: a guide to diagnosis and management By Robert S. Hillman, Kenneth A. Ault, Henry M. Rinder page136-139 http:/ / books. google. com/ books?id=NJs1VpA8SEoC& pg=PA138& dq=hemoglobin+ hemosiderin+ hemolysis+ bilirubin&ei=Z2P_SuzwA6D2ygT9vOz3Dg#v=onepage& q=hemoglobin%20hemosiderin%20hemolysis%20bilirubin& f=false
[13] Wintrobe's Clinical Hematology, Volume 1 By John P. Greer http:/ / books. google. com/ books?id=68enzUD7BVgC& pg=PA161&dq=hemoglobin+ hemosiderin+ hemolysis+ bilirubin& ei=Z2P_SuzwA6D2ygT9vOz3Dg#v=onepage&q=hemoglobin%20hemosiderin%20hemolysis%20bilirubin& f=false page 160
[14] Mary Anna Thrall, Dale C. Baker, E. Duane Lassen, Veterinary hematology and clinical chemistry, ISBN 0-7817-6850-0, 2004.[15] Edward F. Gibbons, Barbara Susan Durrant, Jack Demarest, Conservation of endangered species in captivity: an interdisciplinary approach,
page 324, 2005, ISBN 0-7914-1911-8[16] Oliver A. Ryder, Zoological Society of San Diego, Rhinoceros biology and conservation, Zoological Society of San Diego, 1993, page 312,
335.[17] Texas Monthly, Oct 1992, Vol. 20, No. 10, ISSN 0148-7736, page 98-100.[18] Jutta Meister, ed. Catharine E. Bell, Encyclopedia of the world's zoos, Volume 3, page 1008, ISBN 1-57958-174-9, 2001.
Acquired hemolytic anemia 20
Acquired hemolytic anemiaContributors [1]
Acquired hemolyticanemia
Classification and external resources
ICD-10 D59 [3]
ICD-9 283 [5]
Acquired hemolytic anemia can be divided into immune and non-immune mediated forms of hemolytic anemia.
ImmuneImmune mediated hemolytic anemia (direct Coombs test is positive)•• Autoimmune hemolytic anemia
•• Warm antibody autoimmune hemolytic anemia•• Idiopathic• Systemic lupus erythematosus (SLE)• Evans' syndrome (antiplatelet antibodies and hemolytic antibodies)
•• Cold antibody autoimmune hemolytic anemia•• Idiopathic cold hemagglutinin syndrome• Infectious mononucleosis and mycoplasma (atypical) pneumonia• Paroxysmal cold hemoglobinuria (rare)
• Alloimmune hemolytic anemia• Hemolytic disease of the newborn (HDN)
• Rh disease (Rh D)•• ABO hemolytic disease of the newborn•• Anti-Kell hemolytic disease of the newborn•• Rhesus c hemolytic disease of the newborn•• Rhesus E hemolytic disease of the newborn• Other blood group incompatibility (RhC, Rhe, Kidd, Duffy, MN, P and others)
• Alloimmune hemolytic blood transfusion reactions (i.e. from a non-compatible blood type)•• Drug induced immune mediated hemolytic anemia
• Penicillin (high dose)•• Methyldopa

Acquired hemolytic anemia 21
Non-immuneNon-immune mediated hemolytic anemia (direct Coombs test is negative)• Drugs (i.e., some drugs and other ingested substances lead to hemolysis by direct action on RBCs, e.g. ribavirin )• Toxins (e.g., snake venom; plant poisons such as aesculin)•• Trauma
• Mechanical (from heart valves, extensive vascular surgery, microvascular disease, repeated mechanicalvascular trauma)
• Microangiopathic hemolytic anemia (a specific subtype with causes such as TTP, HUS, DIC and HELLPsyndrome)
•• Infections (Note: Direct Coombs test is sometimes positive in hemolytic anemia due to infection)•• Malaria•• Babesiosis•• Septicemia
•• Membrane disorders• Paroxysmal nocturnal hemoglobinuria (rare acquired clonal disorder of red blood cell surface proteins)•• Liver disease
Drug induced hemolysisDrug induced hemolysis has large clinical relevance. It occurs when drugs actively provoke red blood celldestruction. It can be divided in the following manner:•• Drug-induced autoimmune hemolytic anemia•• Drug-induced nonautoimmune hemolytic anemiaA total of four mechanisms are usually described, but there is some evidence that these mechanisms may overlap.
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Acquired_hemolytic_anemia

Congenital hemolytic anemia 22
Congenital hemolytic anemiaContributors [1]
Congenital hemolyticanemia
Classification and external resources
ICD-10 D55 [2]-D58 [2]
ICD-9 282 [4]
MeSH D000745 [3]
Congenital hemolytic anemia (or hereditary hemolytic anemia) refers to hemolytic anemia which is primarily dueto congenital disorders.
TypesBasically classified by causative mechanism, types of congenital hemolytic anemia include:•• Genetic conditions of RBC Membrane
•• Hereditary spherocytosis•• Hereditary elliptocytosis
• Genetic conditions of RBC metabolism (enzyme defects). This group is sometimes called congenitalnonspherocytic (hemolytic) anemia, which is a term for a congenital hemolytic anemia without spherocytosis, andusually excluding hemoglobin abdormalities as well, but rather encompassing defects of glycolysis in theerythrocyte.[4]
• Glucose-6-phosphate dehydrogenase deficiency (G6PD or favism)•• Pyruvate kinase deficiency•• Aldolase A deficiency
• Hemoglobinopathies/genetic conditions of hemoglobin•• Sickle cell anemia•• Congenital dyserythropoietic anemia•• Thalassemia
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on&
page=Congenital_hemolytic_anemia[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D58[3] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D000745[4] medconditions.net > Hemolytic Congenital, Nonspherocytic Anemia Definition (http:/ / medconditions. net/
hemolytic-congenital-nonspherocytic-anemia. html) Retrieved April 15, 2011

23
Related articles
BloodFor other uses, see Blood (disambiguation).
Human blood smear:a – erythrocytes; b – neutrophil;c – eosinophil; d – lymphocyte.
A scanning electron microscope (SEM) image ofa normal red blood cell, a platelet, and a white
blood cell.
Blood is a bodily fluid in animals thatdelivers necessary substances such asnutrients and oxygen to the cells andtransports metabolic waste products awayfrom those same cells.
In vertebrates, it is composed of blood cellssuspended in blood plasma. Plasma, whichconstitutes 55% of blood fluid, is mostlywater (92% by volume), and containsdissipated proteins, glucose, mineral ions,hormones, carbon dioxide (plasma being themain medium for excretory producttransportation), and blood cells themselves.Albumin is the main protein in plasma, andit functions to regulate the colloidal osmoticpressure of blood. The blood cells aremainly red blood cells (also called RBCs orerythrocytes) and white blood cells,including leukocytes and platelets. The mostabundant cells in vertebrate blood are redblood cells. These contain hemoglobin, aniron-containing protein, which facilitatestransportation of oxygen by reversiblybinding to this respiratory gas and greatlyincreasing its solubility in blood. In contrast,carbon dioxide is almost entirely transportedextracellularly dissolved in plasma asbicarbonate ion.
Vertebrate blood is bright red when its hemoglobin is oxygenated. Some animals, such as crustaceans and mollusks,use hemocyanin to carry oxygen, instead of hemoglobin. Insects and some mollusks use a fluid called hemolymphinstead of blood, the difference being that hemolymph is not contained in a closed circulatory system. In

Blood 24
Human blood fractioned by centrifugation.Plasma (upper layer), buffy coat (middle, whitecolored layer) and erytrocite layer (bottom) can
be seen.
Blood circulation:Red = oxygenated
Blue = deoxygenated
most insects, this "blood" does not contain oxygen-carrying moleculessuch as hemoglobin because their bodies are small enough for theirtracheal system to suffice for supplying oxygen.
Jawed vertebrates have an adaptive immune system, based largely onwhite blood cells. White blood cells help to resist infections andparasites. Platelets are important in the clotting of blood. Arthropods,using hemolymph, have hemocytes as part of their immune system.
Blood is circulated around the body through blood vessels by thepumping action of the heart. In animals with lungs, arterial bloodcarries oxygen from inhaled air to the tissues of the body, and venousblood carries carbon dioxide, a waste product of metabolism producedby cells, from the tissues to the lungs to be exhaled.
Medical terms related to blood often begin with hemo- or hemato-(also spelled haemo- and haemato-) from the Greek word αἷμα(haima) for "blood". In terms of anatomy and histology, blood isconsidered a specialized form of connective tissue, given its origin inthe bones and the presence of potential molecular fibers in the form offibrinogen.

Blood 25
Human blood magnified 600 times
Frog blood magnified 600 times
Fish blood magnified 600 times

Blood 26
Functions
Haemoglobin, a globular proteingreen = haem groups
red & blue = protein subunits
Heme
Blood performs many important functions within the body including:• Supply of oxygen to tissues (bound to hemoglobin, which is carried
in red cells)• Supply of nutrients such as glucose, amino acids, and fatty acids
(dissolved in the blood or bound to plasma proteins (e.g., bloodlipids))
• Removal of waste such as carbon dioxide, urea, and lactic acid• Immunological functions, including circulation of white blood cells,
and detection of foreign material by antibodies• Coagulation, the response to a broken blood vessel, the conversion
of blood from a liquid to a semi-solid gel to stop bleeding.• Messenger functions, including the transport of hormones and the
signaling of tissue damage• Regulation of body pH• Regulation of core body temperature• Hydraulic functions
Constituents of human blood
Illustration depicting formed elements of blood.
See also: Reference ranges for common blood tests

Blood 27
Two tubes of EDTA-anticoagulatedblood.
Left tube: after standing, the RBCshave settled at the bottom of the tube.
Right tube: contains freshly drawnblood.
Blood accounts for 7% of the human body weight, with an average density ofapproximately 1060 kg/m3, very close to pure water's density of 1000 kg/m3. Theaverage adult has a blood volume of roughly 5 liters (1.3 gal), which is composedof plasma and several kinds of cells. These blood cells (which are also calledcorpuscles or "formed elements") consist of erythrocytes (red blood cells,RBCs), leukocytes (white blood cells), and thrombocytes (platelets). By volume,the red blood cells constitute about 45% of whole blood, the plasma about54.3%, and white cells about 0.7%.
Whole blood (plasma and cells) exhibits non-Newtonian fluid dynamics; its flowproperties are adapted to flow effectively through tiny capillary blood vesselswith less resistance than plasma by itself. In addition, if all human hemoglobinwere free in the plasma rather than being contained in RBCs, the circulatory fluidwould be too viscous for the cardiovascular system to function effectively.
Cells
Further information: Complete blood countOne microliter of blood contains:• 4.7 to 6.1 million (male), 4.2 to 5.4 million (female) erythrocytes: Red blood cells contain the blood's
hemoglobin and distribute oxygen. Mature red blood cells lack a nucleus and organelles in mammals. The redblood cells (together with endothelial vessel cells and other cells) are also marked by glycoproteins that define thedifferent blood types. The proportion of blood occupied by red blood cells is referred to as the hematocrit, and isnormally about 45%. The combined surface area of all red blood cells of the human body would be roughly 2,000times as great as the body's exterior surface.
• 4,000–11,000 leukocytes: White blood cells are part of the body's immune system; they destroy and remove oldor aberrant cells and cellular debris, as well as attack infectious agents (pathogens) and foreign substances. Thecancer of leukocytes is called leukemia.
• 200,000–500,000 thrombocytes: Also called platelets, they take part in blood clotting (coagulation). Fibrin fromthe coagulation cascade creates a mesh over the platelet plug.
Constitution of normal blood
Parameter Value
Hematocrit 45 ± 7 (38–52%) for males42 ± 5 (37–47%) for females
pH 7.35–7.45
base excess −3 to +3
PO2 10–13 kPa (80–100 mm Hg)
PCO2 4.8–5.8 kPa (35–45 mm Hg)
HCO3− 21–27 mM
Oxygen saturation Oxygenated: 98–99%Deoxygenated: 75%
Blood 28
PlasmaMain article: Blood plasmaAbout 55% of blood is blood plasma, a fluid that is the blood's liquid medium, which by itself is straw-yellow incolor. The blood plasma volume totals of 2.7–3.0 liters (2.8–3.2 quarts) in an average human. It is essentially anaqueous solution containing 92% water, 8% blood plasma proteins, and trace amounts of other materials. Plasmacirculates dissolved nutrients, such as glucose, amino acids, and fatty acids (dissolved in the blood or bound toplasma proteins), and removes waste products, such as carbon dioxide, urea, and lactic acid.Other important components include:•• Serum albumin• Blood-clotting factors (to facilitate coagulation)• Immunoglobulins (antibodies)• lipoprotein particles• Various other proteins• Various electrolytes (mainly sodium and chloride)The term serum refers to plasma from which the clotting proteins have been removed. Most of the proteinsremaining are albumin and immunoglobulins.
Narrow range of pH valuesSee also: Acid-base homeostasisBlood pH is regulated to stay within the narrow range of 7.35 to 7.45, making it slightly basic. Blood that has a pHbelow 7.35 is too acidic, whereas blood pH above 7.45 is too basic. Blood pH, partial pressure of oxygen (pO2),partial pressure of carbon dioxide (pCO2), and HCO3
− are carefully regulated by a number of homeostaticmechanisms, which exert their influence principally through the respiratory system and the urinary system in order tocontrol the acid-base balance and respiration. An arterial blood gas test will measure these. Plasma also circulateshormones transmitting their messages to various tissues. The list of normal reference ranges for various bloodelectrolytes is extensive.
Blood in non-mammalian vertebratesHuman blood is typical of that of mammals, although the precise details concerning cell numbers, size, proteinstructure, and so on, vary somewhat between species. In non-mammalian vertebrates, however, there are some keydifferences:•• Red blood cells of non-mammalian vertebrates are flattened and ovoid in form, and retain their cell nuclei•• There is considerable variation in the types and proportions of white blood cells; for example, acidophils are
generally more common than in humans• Platelets are unique to mammals; in other vertebrates, small nucleated, spindle cells called thrombocytes are
responsible for blood clotting instead
Blood 29
Physiology
Cardiovascular system
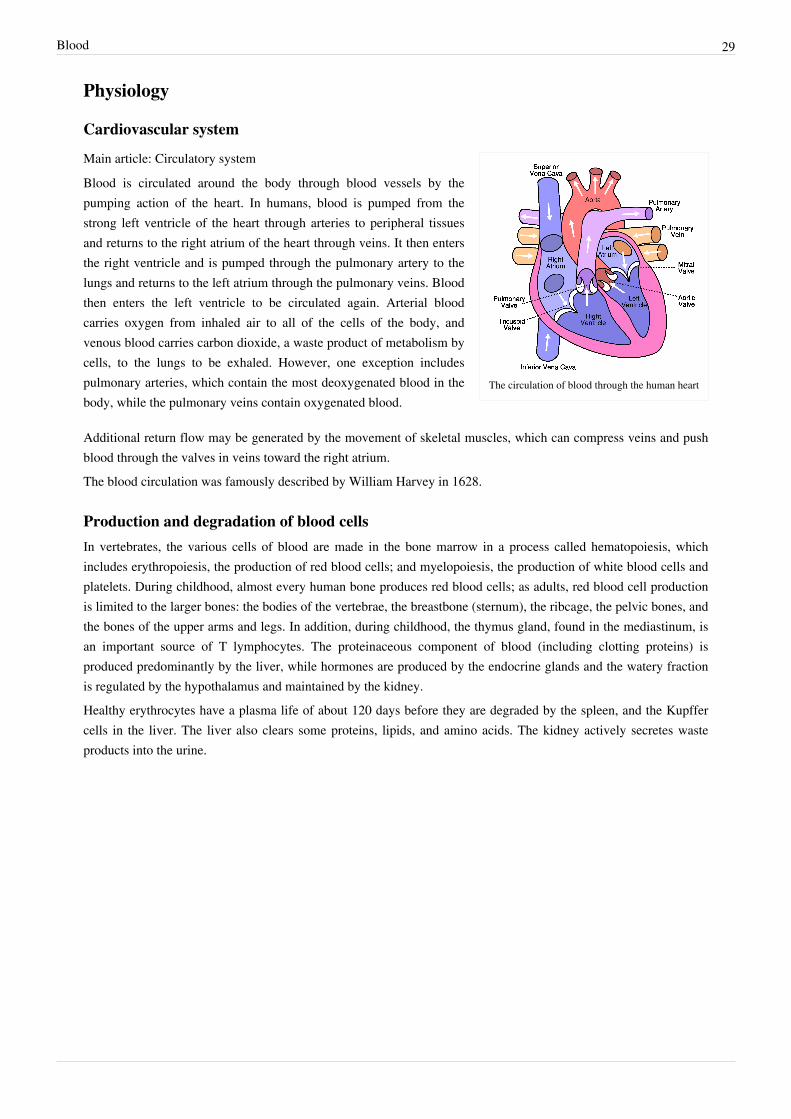
The circulation of blood through the human heart
Main article: Circulatory systemBlood is circulated around the body through blood vessels by thepumping action of the heart. In humans, blood is pumped from thestrong left ventricle of the heart through arteries to peripheral tissuesand returns to the right atrium of the heart through veins. It then entersthe right ventricle and is pumped through the pulmonary artery to thelungs and returns to the left atrium through the pulmonary veins. Bloodthen enters the left ventricle to be circulated again. Arterial bloodcarries oxygen from inhaled air to all of the cells of the body, andvenous blood carries carbon dioxide, a waste product of metabolism bycells, to the lungs to be exhaled. However, one exception includespulmonary arteries, which contain the most deoxygenated blood in thebody, while the pulmonary veins contain oxygenated blood.
Additional return flow may be generated by the movement of skeletal muscles, which can compress veins and pushblood through the valves in veins toward the right atrium.The blood circulation was famously described by William Harvey in 1628.
Production and degradation of blood cellsIn vertebrates, the various cells of blood are made in the bone marrow in a process called hematopoiesis, whichincludes erythropoiesis, the production of red blood cells; and myelopoiesis, the production of white blood cells andplatelets. During childhood, almost every human bone produces red blood cells; as adults, red blood cell productionis limited to the larger bones: the bodies of the vertebrae, the breastbone (sternum), the ribcage, the pelvic bones, andthe bones of the upper arms and legs. In addition, during childhood, the thymus gland, found in the mediastinum, isan important source of T lymphocytes. The proteinaceous component of blood (including clotting proteins) isproduced predominantly by the liver, while hormones are produced by the endocrine glands and the watery fractionis regulated by the hypothalamus and maintained by the kidney.Healthy erythrocytes have a plasma life of about 120 days before they are degraded by the spleen, and the Kupffercells in the liver. The liver also clears some proteins, lipids, and amino acids. The kidney actively secretes wasteproducts into the urine.

Blood 30
Oxygen transport
Basic hemoglobin saturation curve. It is moved tothe right in higher acidity (more dissolved carbon
dioxide) and to the left in lower acidity (lessdissolved carbon dioxide)
About 98.5% of the oxygen in a sample of arterial blood in a healthyhuman breathing air at sea-level pressure is chemically combined withthe Hgb. About 1.5% is physically dissolved in the other blood liquidsand not connected to Hgb. The hemoglobin molecule is the primarytransporter of oxygen in mammals and many other species (forexceptions, see below). Hemoglobin has an oxygen binding capacity ofbetween 1.36 and 1.37 ml O2 per gram hemoglobin, which increasesthe total blood oxygen capacity seventyfold, compared to if oxygensolely were carried by its solubility of 0.03 ml O2 per liter blood permm Hg partial pressure of oxygen (approximately 100 mm Hg inarteries).
With the exception of pulmonary and umbilical arteries and theircorresponding veins, arteries carry oxygenated blood away from theheart and deliver it to the body via arterioles and capillaries, where theoxygen is consumed; afterwards, venules, and veins carrydeoxygenated blood back to the heart.
Under normal conditions in adult humans at rest; hemoglobin in blood leaving the lungs is about 98–99% saturatedwith oxygen, achieving an oxygen delivery of between 950 and 1150 ml/min[1] to the body. In a healthy adult at rest,oxygen consumption is approximately 200 - 250 ml/min, and deoxygenated blood returning to the lungs is stillapproximately 75%[2][3] (70 to 78%) saturated. Increased oxygen consumption during sustained exercise reduces theoxygen saturation of venous blood, which can reach less than 15% in a trained athlete; although breathing rate andblood flow increase to compensate, oxygen saturation in arterial blood can drop to 95% or less under theseconditions. Oxygen saturation this low is considered dangerous in an individual at rest (for instance, during surgeryunder anesthesia). Sustained hypoxia (oxygenation of less than 90%), is dangerous to health, and severe hypoxia(saturations of less than 30%) may be rapidly fatal.[4]
A fetus, receiving oxygen via the placenta, is exposed to much lower oxygen pressures (about 21% of the level foundin an adult's lungs), and, so, fetuses produce another form of hemoglobin with a much higher affinity for oxygen(hemoglobin F) in order to function under these conditions.[5]
Carbon dioxide transportCO2 is carried in blood in three different ways. (The exact percentages vary depending whether it is arterial orvenous blood). Most of it (about 70%) is converted to bicarbonate ions HCO−3 by the enzyme carbonic anhydrase in the red blood cells by the reaction CO2 + H2O → H2CO3 → H+ + HCO−3; about 7% is dissolved in the plasma; and about 23% is bound to hemoglobin as carbamino compounds.Hemoglobin, the main oxygen-carrying molecule in red blood cells, carries both oxygen and carbon dioxide.However, the CO2 bound to hemoglobin does not bind to the same site as oxygen. Instead, it combines with theN-terminal groups on the four globin chains. However, because of allosteric effects on the hemoglobin molecule, thebinding of CO2 decreases the amount of oxygen that is bound for a given partial pressure of oxygen. The decreasedbinding to carbon dioxide in the blood due to increased oxygen levels is known as the Haldane effect, and isimportant in the transport of carbon dioxide from the tissues to the lungs. A rise in the partial pressure of CO2 or alower pH will cause offloading of oxygen from hemoglobin, which is known as the Bohr effect.
Blood 31
Transport of hydrogen ionsSome oxyhemoglobin loses oxygen and becomes deoxyhemoglobin. Deoxyhemoglobin binds most of the hydrogenions as it has a much greater affinity for more hydrogen than does oxyhemoglobin.
Lymphatic systemMain article: Lymphatic systemIn mammals, blood is in equilibrium with lymph, which is continuously formed in tissues from blood by capillaryultrafiltration. Lymph is collected by a system of small lymphatic vessels and directed to the thoracic duct, whichdrains into the left subclavian vein where lymph rejoins the systemic blood circulation.
ThermoregulationBlood circulation transports heat throughout the body, and adjustments to this flow are an important part ofthermoregulation. Increasing blood flow to the surface (e.g., during warm weather or strenuous exercise) causeswarmer skin, resulting in faster heat loss. In contrast, when the external temperature is low, blood flow to theextremities and surface of the skin is reduced and to prevent heat loss and is circulated to the important organs of thebody, preferentially.
Hydraulic functionsThe restriction of blood flow can also be used in specialized tissues to cause engorgement, resulting in an erection ofthat tissue; examples are the erectile tissue in the penis and clitoris.Another example of a hydraulic function is the jumping spider, in which blood forced into the legs under pressurecauses them to straighten for a powerful jump, without the need for bulky muscular legs.
InvertebratesIn insects, the blood (more properly called hemolymph) is not involved in the transport of oxygen. (Openings calledtracheae allow oxygen from the air to diffuse directly to the tissues). Insect blood moves nutrients to the tissues andremoves waste products in an open system.Other invertebrates use respiratory proteins to increase the oxygen-carrying capacity. Hemoglobin is the mostcommon respiratory protein found in nature. Hemocyanin (blue) contains copper and is found in crustaceans andmollusks. It is thought that tunicates (sea squirts) might use vanabins (proteins containing vanadium) for respiratorypigment (bright-green, blue, or orange).In many invertebrates, these oxygen-carrying proteins are freely soluble in the blood; in vertebrates they arecontained in specialized red blood cells, allowing for a higher concentration of respiratory pigments withoutincreasing viscosity or damaging blood filtering organs like the kidneys.Giant tube worms have unusual hemoglobins that allow them to live in extraordinary environments. Thesehemoglobins also carry sulfides normally fatal in other animals.

Blood 32
ColorThe coloring matter of blood (hemochrome) is largely due to the protein in the blood responsible for oxygentransport. Different groups of organisms use different proteins.
HemoglobinMain article: Hemoglobin
Capillary blood from a bleeding finger
Venous blood collected during blood donation
Hemoglobin is the principal determinant of the color of blood invertebrates. Each molecule has four heme groups, and their interactionwith various molecules alters the exact color. In vertebrates and otherhemoglobin-using creatures, arterial blood and capillary blood arebright red, as oxygen imparts a strong red color to the heme group.Deoxygenated blood is a darker shade of red; this is present in veins,and can be seen during blood donation and when venous blood samplesare taken. This is because the spectrum of light absorbed byhemoglobin differs between the oxygenated and deoxygenated states.
Blood in carbon monoxide poisoning is bright red, because carbonmonoxide causes the formation of carboxyhemoglobin. In cyanidepoisoning, the body cannot utilize oxygen, so the venous bloodremains oxygenated, increasing the redness. There are some conditionsaffecting the heme groups present in hemoglobin that can make theskin appear blue—a symptom called cyanosis. If the heme is oxidized,methaemoglobin, which is more brownish and cannot transportoxygen, is formed. In the rare condition sulfhemoglobinemia, arterialhemoglobin is partially oxygenated, and appears dark red with a bluishhue.
Veins close to the surface of the skin appear blue for a variety ofreasons. However, the factors that contribute to this alteration of color perception are related to the light-scatteringproperties of the skin and the processing of visual input by the visual cortex, rather than the actual color of thevenous blood.
Skinks in the genus Prasinohaema have green blood due to a buildup of the waste product biliverdin.
HemocyaninMain article: HemocyaninThe blood of most mollusks – including cephalopods and gastropods – as well as some arthropods, such ashorseshoe crabs, is blue, as it contains the copper-containing protein hemocyanin at concentrations of about50 grams per liter. Hemocyanin is colorless when deoxygenated and dark blue when oxygenated. The blood in thecirculation of these creatures, which generally live in cold environments with low oxygen tensions, is grey-white topale yellow, and it turns dark blue when exposed to the oxygen in the air, as seen when they bleed. This is due tochange in color of hemocyanin when it is oxidized. Hemocyanin carries oxygen in extracellular fluid, which is incontrast to the intracellular oxygen transport in mammals by hemoglobin in RBCs.

Blood 33
ChlorocruorinMain article: ChlorocruorinThe blood of most annelid worms and some marine polychaetes use chlorocruorin to transport oxygen. It is green incolor in dilute solutions.[6]
HemerythrinMain article: HemerythrinHemerythrin is used for oxygen transport in the marine invertebrates sipunculids, priapulids, brachiopods, and theannelid worm, magelona. Hemerythrin is violet-pink when oxygenated.
HemovanadinMain article: HemovanadinThe blood of some species of ascidians and tunicates, also known as sea squirts, contains proteins called vanabins.These proteins are based on vanadium, and give the creatures a concentration of vanadium in their bodies 100 timeshigher than the surrounding sea water. It is not clear whether these vanabins actually carry oxygen. When exposed tooxygen, however, vanabins turn a mustard yellow.
Pathology
General medical disorders•• Disorders of volume
• Injury can cause blood loss through bleeding. A healthy adult can lose almost 20% of blood volume (1 L)before the first symptom, restlessness, begins, and 40% of volume (2 L) before shock sets in. Thrombocytesare important for blood coagulation and the formation of blood clots, which can stop bleeding. Trauma to theinternal organs or bones can cause internal bleeding, which can sometimes be severe.
• Dehydration can reduce the blood volume by reducing the water content of the blood. This would rarely resultin shock (apart from the very severe cases) but may result in orthostatic hypotension and fainting.
•• Disorders of circulation• Shock is the ineffective perfusion of tissues, and can be caused by a variety of conditions including blood loss,
infection, poor cardiac output.• Atherosclerosis reduces the flow of blood through arteries, because atheroma lines arteries and narrows them.
Atheroma tends to increase with age, and its progression can be compounded by many causes includingsmoking, high blood pressure, excess circulating lipids (hyperlipidemia), and diabetes mellitus.
• Coagulation can form a thrombosis, which can obstruct vessels.• Problems with blood composition, the pumping action of the heart, or narrowing of blood vessels can have
many consequences including hypoxia (lack of oxygen) of the tissues supplied. The term ischemia refers totissue that is inadequately perfused with blood, and infarction refers to tissue death (necrosis), which can occurwhen the blood supply has been blocked (or is very inadequate)

Blood 34
Hematological disordersSee also: Hematology•• Anemia
• Insufficient red cell mass (anemia) can be the result of bleeding, blood disorders like thalassemia, or nutritionaldeficiencies; and may require blood transfusion. Several countries have blood banks to fill the demand fortransfusable blood. A person receiving a blood transfusion must have a blood type compatible with that of thedonor.
•• Sickle-cell anemia•• Disorders of cell proliferation
• Leukemia is a group of cancers of the blood-forming tissues and cells.• Non-cancerous overproduction of red cells (polycythemia vera) or platelets (essential thrombocytosis) may be
premalignant.• Myelodysplastic syndromes involve ineffective production of one or more cell lines.
•• Disorders of coagulation• Hemophilia is a genetic illness that causes dysfunction in one of the blood's clotting mechanisms. This can
allow otherwise inconsequential wounds to be life-threatening, but more commonly results in hemarthrosis, orbleeding into joint spaces, which can be crippling.
• Ineffective or insufficient platelets can also result in coagulopathy (bleeding disorders).• Hypercoagulable state (thrombophilia) results from defects in regulation of platelet or clotting factor function,
and can cause thrombosis.•• Infectious disorders of blood
• Blood is an important vector of infection. HIV, the virus that causes AIDS, is transmitted through contact withblood, semen or other body secretions of an infected person. Hepatitis B and C are transmitted primarilythrough blood contact. Owing to blood-borne infections, bloodstained objects are treated as a biohazard.
• Bacterial infection of the blood is bacteremia or sepsis. Viral Infection is viremia. Malaria and trypanosomiasisare blood-borne parasitic infections.
Carbon monoxide poisoningMain article: Carbon monoxide poisoningSubstances other than oxygen can bind to hemoglobin; in some cases this can cause irreversible damage to the body.Carbon monoxide, for example, is extremely dangerous when carried to the blood via the lungs by inhalation,because carbon monoxide irreversibly binds to hemoglobin to form carboxyhemoglobin, so that less hemoglobin isfree to bind oxygen, and fewer oxygen molecules can be transported throughout the blood. This can causesuffocation insidiously. A fire burning in an enclosed room with poor ventilation presents a very dangerous hazard,since it can create a build-up of carbon monoxide in the air. Some carbon monoxide binds to hemoglobin whensmoking tobacco.Wikipedia:Citation needed
Medical treatments
Blood productsFurther information: Blood transfusionBlood for transfusion is obtained from human donors by blood donation and stored in a blood bank. There are manydifferent blood types in humans, the ABO blood group system, and the Rhesus blood group system being the mostimportant. Transfusion of blood of an incompatible blood group may cause severe, often fatal, complications, socrossmatching is done to ensure that a compatible blood product is transfused.

Blood 35
Other blood products administered intravenously are platelets, blood plasma, cryoprecipitate, and specificcoagulation factor concentrates.
Intravenous administrationMany forms of medication (from antibiotics to chemotherapy) are administered intravenously, as they are not readilyor adequately absorbed by the digestive tract.After severe acute blood loss, liquid preparations, generically known as plasma expanders, can be givenintravenously, either solutions of salts (NaCl, KCl, CaCl2 etc.) at physiological concentrations, or colloidal solutions,such as dextrans, human serum albumin, or fresh frozen plasma. In these emergency situations, a plasma expander isa more effective life-saving procedure than a blood transfusion, because the metabolism of transfused red blood cellsdoes not restart immediately after a transfusion.
BloodlettingMain article: bloodlettingIn modern evidence-based medicine, bloodletting is used in management of a few rare diseases, includinghemochromatosis and polycythemia. However, bloodletting and leeching were common unvalidated interventionsused until the 19th century, as many diseases were incorrectly thought to be due to an excess of blood, according toHippocratic medicine.
HistoryAccording to the Oxford English Dictionary, the word "blood" dates to the oldest English, circa 1000 AD. The wordis derived from Middle English, which is derived from the Old English word blôd, which is akin to the Old HighGerman word bluot, meaning blood. The modern German word is (das) Blut.
Classical Greek medicineIn classical Greek medicine, blood was associated with air, with Springtime, and with a merry and gluttonous(sanguine) personality. It was also believed to be produced exclusively by the liver.
Hippocratic medicineIn Hippocratic medicine, blood was considered to be one of the four humors, the others being phlegm, yellow bile,and black bile.
Human bloodThe ABO blood group system was discovered in the year 1900 by Karl Landsteiner. Jan Janský published his workin 1907. In 1907 the first successful blood transfusion was performed. The first non-direct transfusion was performedon March 27, 1914. The Rhesus factor was discovered in 1937.
Cultural and religious beliefsSee also: Blood libelDue to its importance to life, blood is associated with a large number of beliefs. One of the most basic is the use ofblood as a symbol for family relationships through birth/parentage; to be "related by blood" is to be related byancestry or descendance, rather than marriage. This bears closely to bloodlines, and sayings such as "blood is thickerthan water" and "bad blood", as well as "Blood brother".

Blood 36
Blood is given particular emphasis in the Jewish and Christian religions, because Leviticus 17:11 says "the life of acreature is in the blood." This phrase is part of the Levitical law forbidding the drinking of blood or eating meat withthe blood still intact instead of being poured off.Mythic references to blood can sometimes be connected to the life-giving nature of blood, seen in such events aschildbirth, as contrasted with the blood of injury or death.
Indigenous AustraliansIn many indigenous Australian Aboriginal peoples' traditions, ochre (particularly red) and blood, both high in ironcontent and considered Maban, are applied to the bodies of dancers for ritual. As Lawlor states:
In many Aboriginal rituals and ceremonies, red ochre is rubbed all over the naked bodies of the dancers.In secret, sacred male ceremonies, blood extracted from the veins of the participant's arms is exchangedand rubbed on their bodies. Red ochre is used in similar ways in less-secret ceremonies. Blood is alsoused to fasten the feathers of birds onto people's bodies. Bird feathers contain a protein that is highlymagnetically sensitive.
Lawlor comments that blood employed in this fashion is held by these peoples to attune the dancers to the invisibleenergetic realm of the Dreamtime. Lawlor then connects these invisible energetic realms and magnetic fields,because iron is magnetic.
European paganismAmong the Germanic tribes (such as the Anglo-Saxons and the Norsemen), blood was used during their sacrifices;the Blóts. The blood was considered to have the power of its originator, and, after the butchering, the blood wassprinkled on the walls, on the statues of the gods, and on the participants themselves. This act of sprinkling bloodwas called blóedsian in Old English, and the terminology was borrowed by the Roman Catholic Church becoming tobless and blessing. The Hittite word for blood, ishar was a cognate to words for "oath" and "bond", see Ishara. TheAncient Greeks believed that the blood of the gods, ichor, was a substance that was poisonous to mortals.As a relic of Germanic Law the cruentation, an ordeal where the corpse of the victim was supposed to start bleedingin the presence of the murderer was used until the early 17th century.
ChristianityIn Genesis 9:4, God prohibited Noah and his sons from eating blood (see Noahide Law). This command continued tobe observed by the Eastern Orthodox.It is also found in the Bible that when the Angel of Death came around to the Hebrew house that the first-born childwould not die if the angel saw lamb's blood wiped across the doorway.At the Council of Jerusalem, the apostles prohibited certain Christians from consuming blood—this is documented inActs 15:20 and 29. This chapter specifies a reason (especially in verses 19-21): It was to avoid offending Jews whohad become Christians, because the Mosaic Law Code prohibited the practice.Christ's blood is the means for the atonement of sins. Also, ″… the blood of Jesus Christ his [God] Son cleanseth usfrom all sin." (1 John 1:7), “… Unto him [God] that loved us, and washed us from our sins in his own blood."(Revelation 1:5), and "And they overcame him (Satan) by the blood of the Lamb [Jesus the Christ], and by the wordof their testimony …” (Revelation 12:11).Some Christian churches, including Roman Catholicism, Eastern Orthodoxy, Oriental Orthodoxy, and the Assyrian Church of the East teach that, when consecrated, the Eucharistic wine actually becomes the blood of Jesus for worshippers to drink. Thus in the consecrated wine, Jesus becomes spiritually and physically present. This teaching is rooted in the Last Supper, as written in the four gospels of the Bible, in which Jesus stated to his disciples that the bread that they ate was his body, and the wine was his blood. "This cup is the new testament in my blood, which is

Blood 37
shed for you." (Luke 22:20).Most forms of Protestantism, especially those of a Wesleyan or Presbyterian lineage, teach that the wine is no morethan a symbol of the blood of Christ, who is spiritually but not physically present. Lutheran theology teaches that thebody and blood is present together "in, with, and under" the bread and wine of the Eucharistic feast.
JudaismIn Judaism, animal blood may not be consumed even in the smallest quantity (Leviticus 3:17 and elsewhere); this isreflected in Jewish dietary laws (Kashrut). Blood is purged from meat by rinsing and soaking in water (to loosenclots), salting and then rinsing with water again several times.[7] Eggs must also be checked and any blood spotsremoved before consumption.[8] Although blood from fish is Biblically kosher, it is rabbinically forbidden toconsume fish blood to avoid the appearance of breaking the Biblical prohibition.[9]
Another ritual involving blood involves the covering of the blood of fowl and game after slaughtering (Leviticus17:13); the reason given by the Torah is: "Because the life of the animal is [in] its blood" (ibid 17:14). In relation tohuman beings, Kabbalah expounds on this verse that the animal soul of a person is in the blood, and that physicaldesires stem from it.Likewise, the mystical reason for salting temple sacrifices and slaughtered meat is to remove the blood ofanimal-like passions from the person. By removing the animal's blood, the animal energies and life-force containedin the blood are removed, making the meat fit for human consumption.[10]
IslamConsumption of food containing blood is forbidden by Islamic dietary laws. This is derived from the statement in theQur'an, sura Al-Ma'ida (5:3): "Forbidden to you (for food) are: dead meat, blood, the flesh of swine, and that onwhich has been invoked the name of other than Allah."Blood is considered as unclean and in Islam cleanliness is part of the faith, hence there are specific methods to obtainphysical and ritual status of cleanliness once bleeding has occurred. Specific rules and prohibitions apply tomenstruation, postnatal bleeding and irregular vaginal bleeding. But Islam does not forbid blood transfusion as longas it is done to save lives.
Jehovah's WitnessesMain article: Jehovah's Witnesses and bloodBased on their interpretation of scriptures such as Acts 15:28, 29 ("Keep abstaining...from blood."), Jehovah'sWitnesses neither consume blood nor accept transfusions of whole blood or its major components: red blood cells,white blood cells, platelets (thrombocytes), and plasma. Members may personally decide whether they will acceptmedical procedures that involve their own blood or substances that are further fractionated from the four majorcomponents.[11]
East Asian cultureIn south East Asian popular culture, it is often said that if a man's nose produces a small flow of blood, he isexperiencing sexual desire. This often appears in Chinese-language and Hong Kong films as well as in Japanese andKorean culture parodied in anime, manga, and drama. Characters, mostly males, will often be shown with anosebleed if they have just seen someone nude or in little clothing, or if they have had an erotic thought or fantasy;this is based on the idea that a male's blood pressure will spike dramatically when aroused.[12]Wikipedia:Identifyingreliable sources

Blood 38
Vampire legendsMain article: VampireVampires are mythical creatures that drink blood directly for sustenance, usually with a preference for human blood.Cultures all over the world have myths of this kind; for example the 'Nosferatu' legend, a human who achievesdamnation and immortality by drinking the blood of others, originates from Eastern European folklore. Ticks,leeches, female mosquitoes, vampire bats, and an assortment of other natural creatures do consume the blood ofother animals, but only bats are associated with vampires. This has no relation to vampire bats, which are new worldcreatures discovered well after the origins of the European myths.
Applications
In the applied sciencesBlood residue can help forensic investigators identify weapons, reconstruct a criminal action, and link suspects to thecrime. Through bloodstain pattern analysis, forensic information can also be gained from the spatial distribution ofbloodstains.Blood residue analysis is also a technique used in archeology.
In artBlood is one of the body fluids that has been used in art.[13] In particular, the performances of Viennese ActionistHermann Nitsch, Istvan Kantor, Franko B, Lennie Lee, Ron Athey, Yang Zhichao, Lucas Abela and Kira O' Reilly,along with the photography of Andres Serrano, have incorporated blood as a prominent visual element. Marc Quinnhas made sculptures using frozen blood, including a cast of his own head made using his own blood.
In genealogy and family historyThe term blood is used in genealogical circles to refer to one's ancestry, origins, and ethnic background as in theword bloodline. Other terms where blood is used in a family history sense are blue-blood, royal blood, mixed-bloodand blood relative.
References[1] Edwards Lifesciences LLC - Normal Hemodynamic Parameters – Adult (http:/ / www. edwards. com/ SiteCollectionImages/ edwards/
products/ presep/ ar04313hemodynpocketcard. pdf) 2009[2] Ventilation and Endurance Performance (https:/ / web. archive. org/ web/ 20100323054138/ http:/ / home. hia. no/ ~stephens/ ventphys. htm)[3] Transplant Support- Lung, Heart/Lung, Heart (https:/ / web. archive. org/ web/ 20040224085741/ http:/ / groups. msn. com/
TransplantSupportLungHeartLungHeart/ oxygen2. msnw) MSN groups[4] The 'St George' Guide To Pulmonary Artery Catheterisation (https:/ / web. archive. org/ web/ 20100925053056/ http:/ / manbit. com/ PAC/
chapters/ P30. cfm)[5] Oxygen Carriage in Blood - High Altitude (https:/ / web. archive. org/ web/ 19990502195422/ http:/ / members. aol. com/ Bio50/ LecNotes/
lecnot20. html)[6] Carnegie Library of Pittsburgh, The Handy Science Answer Book, p. 465, Visible Ink Press, 2011 ISBN 1578593212.[7] Koshering Meat. (http:/ / www. chabad. org/ library/ article_cdo/ aid/ 82678/ jewish/ Koshering-Meat. htm) Chabad.org.[8] Removing the Blood. (http:/ / www. chabad. org/ library/ howto/ wizard_cdo/ aid/ 113470/ jewish/ Removing-the-Blood. htm) Chabad.org.[9] Citron, R. Aryeh. All About Kosher Fish. (http:/ / www. chabad. org/ library/ article_cdo/ aid/ 1182104/ jewish/ All-About-Kosher-Fish. htm)
Chabad.org.[10] Schneerson, R. Menachem M. Igrot Kodesh, vol. vii, p. 270.[11] The Watchtower 15 June 2004, page 22, "Be Guided by the Living God"[12] Law of Anime No. 40 aka Law of Nasal Sanguination at ABCB.com (http:/ / www. abcb. com/ laws/ index. htm), The Anime Cafe.[13] "Nostalgia" (http:/ / artscad. com/ A. nsf/ Opra/ SRVV-6MDNX5) Artwork in blood

Blood 39
External links
Wikiquote has quotations related to: Blood
Look up blood in Wiktionary, the free dictionary.
Wikimedia Commons has media related to Blood.
• Blood Groups and Red Cell Antigens. (http:/ / www. ncbi. nlm. nih. gov/ books/ NBK2261) Free online book atNCBI Bookshelf ID: NBK2261
• Blood (http:/ / www. bbc. co. uk/ programmes/ p00548ym) on In Our Time at the BBC. ( listen now (http:/ /www. bbc. co. uk/ iplayer/ console/ p00548ym/ In_Our_Time_Blood))

Blood transfusion 40
Blood transfusion
Blood transfusionIntervention
Plastic bag with 0.5 - 0.7 liters containing packed red blood cells in citrate, phosphate, dextrose, and adenine (CPDA) solution
ICD-9-CM 99.0
MeSH D001803 [1]
OPS-301 code: 8-80 [2]
MedlinePlus 000431 [3]
Blood transfusion is generally the process of receiving blood products into one's circulation intravenously.Transfusions are used for various medical conditions to replace lost components of the blood. Early transfusionsused whole blood, but modern medical practice commonly uses only components of the blood, such as red bloodcells, white blood cells, plasma, clotting factors, and platelets.
Medical usesUnits of packed red blood cells are typically only recommended when either a patient's hemoglobin level falls below10 g/dL or hematocrit falls below 30%. Because each unit of blood given carries risks, a trigger level lower than thatat 7-8 g/dL is increasingly being used and has been shown to have better patient outcomes. The administration of asingle unit of blood is the standard for hospitalized people who are not bleeding, with this treatment then followedwith re-assessment and consideration of symptoms and hemoglobin concentration. Patients with poor oxygensaturation may need more blood. The caution in avoiding the transfusion of too much blood is in part due to theincreasing evidence that there are cases where patients have worse outcomes when transfused. One may considertransfusion for people with symptoms of cardiovascular disease such as chest pain or shortness of breath. In caseswhere patients have low levels of hemoglobin but are cardiovascularly stable, parenteral iron is increasingly apreferred option based on both efficacy and safety. Other blood products are given where appropriate, such asclotting deficiencies.

Blood transfusion 41
Procedure
Illustration depicting intravenous bloodtransfusion
Before a blood transfusion is given, there are many steps taken toensure quality of the blood products, compatibility, and safety to therecipient. In 2012, a national blood policy was in place in 70% ofcountries and 62% of countries had specific legislation that covers thesafety and quality of blood transfusion.
Blood donation
Main article: Blood donationBlood transfusions typically use sources of blood: one's own(autologous transfusion), or someone else's (allogeneic or homologoustransfusion). The latter is much more common than the former. Usinganother's blood must first start with donation of blood. Blood is mostcommonly donated as whole blood intravenously and collecting it withan anticoagulant. In developed countries, donations are usuallyanonymous to the recipient, but products in a blood bank are always individually traceable through the whole cycleof donation, testing, separation into components, storage, and administration to the recipient. This enablesmanagement and investigation of any suspected transfusion related disease transmission or transfusion reaction. Indeveloping countries the donor is sometimes specifically recruited by or for the recipient, typically a family member,and the donation occurs immediately before the transfusion.
Processing and testing
A bag containing one unit of fresh frozen plasma
Donated blood is usually subjected to processing after it is collected, tomake it suitable for use in specific patient populations. Collected bloodis then separated into blood components by centrifugation: red bloodcells, plasma, platelets, albumin protein, clotting factor concentrates,cryoprecipitate, fibrinogen concentrate, and immunoglobulins(antibodies). Red cells, plasma and platelets can also be donatedindividually via a more complex process called apheresis.
• All donated blood is tested for infections.Wikipedia:Citation neededThe current protocol tests donated blood for HIV-1, HIV-2,HTLV-1, HTLV-2, Hepatitis B, Hepatitis C, Syphilis (Treponemapallidum), Chagas disease (Trypanosoma cruzi), and West NileVirus. In addition, platelet products are also tested for bacterialinfections due to its higher inclination for contamination due tostorage at room temperature. Presence of Cytomegalovirus (CMV)is also tested because of risk to certain immunocompromisedrecipients if given, such as those with organ transplant or HIV.However, not all blood is tested for CMV because only a certain amount of CMV-negative blood needs to beavailable to supply patient needs. Other than positivity for CMV, any products tested positive for infections arenot used.
•• All donated blood is also tested for ABO and Rh groups, along with the presence of any red blood cell antibodies.• Leukoreduction is the removal of white blood cells by filtration. Leukoreduced blood products are less likely to
cause HLA alloimmunization (development of antibodies against specific blood types), febrile non-hemolytic

Blood transfusion 42
transfusion reaction, cytomegalovirus infection, and platelet-transfusion refractoriness.• Pathogen Reduction treatment that involves, for example, the addition of riboflavin with subsequent exposure to
UV light has been shown to be effective in inactivating pathogens (viruses, bacteria, parasites and white bloodcells) in blood products. By inactivating white blood cells in donated blood products, riboflavin and UV lighttreatment can also replace gamma-irradiation as a method to prevent graft-versus-host disease (TA-GvHD).
Compatibility testing
Illustration of labeled blood bag.
Main articles: ABO blood group system and Rh blood group systemBefore a recipient receives a transfusion, compatibility testing betweendonor and recipient blood must be done. The first step before atransfusion is given is to Type and Screen the recipient's blood. Typingof recipient's blood determines the ABO and Rh status. The sample isthen Screened for any alloantibodies that may react with donorblood.[4] It takes about 45 minutes to complete (depending on themethod used). The blood bank scientist also checks for specialrequirements of the patient (e.g. need for washed, irradiated or CMVnegative blood) and the history of the patient to see if they have apreviously identified antibodies and any other serological anomalies;.
A positive screen warrants an antibody panel/investigation todetermine if it is clinically significant. An antibody panel consists ofcommercially prepared group O red cell suspensions from donors that have been phenotyped for antigens thatcorrespond to commonly encountered and clinically significant alloantibodies. Donor cells may have homozygous(e.g. K+k-), heterozygous (K+k+) expression or no expression of various antigens (K-k-). The phenotypes of all thedonor cells being tested are shown in a chart. The patient's serum is tested against the various donor cells. Based onthe reactions of the patient's serum against the donor cells, a pattern will emerge to confirm the presence of one ormore antibodies. Not all antibodies are clinically significant (i.e. cause transfusion reactions, HDN, etc.). Once thepatient has developed a clinically significant antibody it is vital that the patient receive antigen-negative red bloodcells to prevent future transfusion reactions. A direct antiglobulin test (Coombs test) is also performed as part of theantibody investigation.
If there is no antibody present, an immediate spin crossmatch or computer assisted crossmatch is performed wherethe recipient serum and donor rbc are incubated. In the immediate spin method, two drops of patient serum are testedagainst a drop of 3-5% suspension of donor cells in a test tube and spun in a serofuge. Agglutination or hemolysis(i.e., positive Coombs test) in the test tube is a positive reaction and the unit should not be transfused.If an antibody is suspected, potential donor units must first be screened for the corresponding antigen byphenotyping them. Antigen negative units are then tested against the patient plasma using an antiglobulin/indirectcrossmatch technique at 37 degrees Celsius to enhance reactivity and make the test easier to read.In urgent cases where crossmatching cannot be completed, and the risk of dropping hemoglobin outweighs the risktransfusing uncrossmatched blood, O-negative blood is used, followed by crossmatch as soon as possible. O-negativeis also used for children and women of childbearing age. It is preferable for the laboratory to obtain a pre-transfusionsample in these cases so a type and screen can be performed to determine the actual blood group of the patient and tocheck for alloantibodies.

Blood transfusion 43
Adverse effectsIn the same way that the safety of pharmaceutical products are overseen by pharmacovigalence, the safety of bloodand blood products are overseen by Haemovigilance. This is defined by the World Health Organization (WHO) as asystem "...to identify and prevent occurrence or recurrence of transfusion related unwanted events, to increase thesafety, efficacy and efficiency of blood transfusion, covering all activities of the transfusion chain from donor torecipient." The system should include monitoring, identification, reporting, investigation and analysis of adverseevents near-misses and reactions related to transfusion and manufacturing. In the UK this data is collected by anindependent organisation called SHOT (Serious Hazards Of Transfusion).Transfusions of blood products are associated with several complications, many of which can be grouped asimmunological or infectious. There is also increasing focus (and controversy) on complications arising directly orindirectly from potential quality degradation during storage.[5] Overall, adverse events from transfusions in the USaccount for about $17 Billion - and in effect add more to the cost of each transfusion than acquisition and procedurecosts combined. While some complication risks depend on patient status or specific transfusion quantity involved, abaseline risk of complications simply increases in direct proportion to the frequency and volume of transfusion.
Immunologic reaction• Acute hemolytic reactions occur with transfusion of red blood cells, and occurs in about 0.016 percent of
transfusions, with about 0.003 percent being fatal.Wikipedia:Citation needed This is due to destruction of donorred blood cells by preformed recipient antibodies. Most often this occurs due to clerical errors or improper ABOblood typing and crossmatching resulting in a mismatch in ABO blood type between the donor and the recipient.Symptoms include fever, chills, chest pain, back pain, hemorrhage, increased heart rate, shortness of breath, andrapid drop in blood pressure. When suspected, transfusion should be stopped immediately, and blood sent for teststo evaluate for presence of hemolysis. Treatment is supportive. Kidney injury may occur due to the effects of thehemolytic reaction (pigment nephropathy).
• Delayed hemolytic reactions occur more frequently (about 0.025 percent of transfusions) and are due to the samemechanism as in acute hemolytic reactions. However, the consequences are generally mild and a great proportionof patients may not have symptoms. However, evidence of hemolysis and falling hemoglobin levels may stilloccur. Treatment is generally not needed, but due to the presence of recipient antibodies, future compatibility maybe affected.
• Febrile nonhemolytic reactions are the most common type of blood transfusion reaction and occur due to therelease of inflammatory chemical signals released by white blood cells in stored donor blood. This type ofreaction occurs in about 7% of transfusions. Fever is generally short lived and is treated with antipyretics, andtransfusions may be finished as long as an acute hemolytic reaction is excluded. This is a reason for thenow-widespread use of leukoreduction - the filtration of donor white cells from red cell product units.
• Allergic reactions may occur when the recipient has preformed antibodies to certain chemicals in the donor blood,and does not require prior exposure to transfusions. Symptoms include hives, itching, low blood pressure, andrespiratory distress which may lead to anaphylactic shock. Treatment is the same as for any other type 1hypersensitivity reactions and includes administering intramuscular epinephrine, glucocorticoids, antihistamines,medications to keep the blood pressure from dropping, and mechanical ventilation if needed. A small population(0.13%) of patients are deficient in the immunoglobulin IgA, and upon exposure to IgA-containing blood, maydevelop an anaphylactic reaction.
• Posttransfusion purpura is a rare complication that occurs after transfusion containing platelets that express asurface protein HPA-1a. Recipients who lack this protein develop sensitization to this protein from priortransfusions, and develop thrombocytopenia about 7–10 days after subsequent transfusions. Treatment is withintravenous immunoglobulin, and recipients should only receive future transfusions with washed cells or HPA-1anegative cells.

Blood transfusion 44
• Transfusion-associated acute lung injury (TRALI) is an increasingly recognized adverse event associated withblood transfusion. TRALI is a syndrome of acute respiratory distress, often associated with fever, non-cardiogenicpulmonary edema, and hypotension, which may occur as often as 1 in 2000 transfusions. Symptoms can rangefrom mild to life-threatening, but most patients recover fully within 96 hours, and the mortality rate from thiscondition is less than 10%. Although the cause of TRALI is not clear, it has been consistently associated withanti-HLA antibodies. Because these types of antibodies are commonly formed during pregnancy, severaltransfusion organisations have decided to use only plasma from men for transfusion. TRALI is typicallyassociated with plasma components rather than packed red blood cells (RBCs), though there is some residualplasma in RBC units.
InfectionThe use of greater amount of red blood cells is associated with a high risk of infections. In those who were given redblood only with significant anemia infection rates were 12% while in those who were given red blood at milderlevels of anemia infection rates were 17%.On rare occasion, blood products are contaminated with bacteria. This can result in life-threatening infection, alsoknown as transfusion-transmitted bacterial infection. The risk of severe bacterial infection is estimated, as of 2002, atabout 1 in 50,000 platelet transfusions, and 1 in 500,000 red blood cell transfusions. Blood product contamination,while rare, is still more common than actual infection. The reason platelets are more often contaminated than otherblood products is that they are stored at room temperature for short periods of time. Contamination is also morecommon with longer duration of storage, especially when exceeding 5 days. Sources of contaminants include thedonor's blood, donor's skin, phlebotomist's skin, and from containers. Contaminating organisms vary greatly, andinclude skin flora, gut flora, or environmental organisms. There are many strategies in place at blood donationcenters and laboratories to reduce the risk of contamination. A definite diagnosis of transfusion-transmitted bacterialinfection includes the identification of a positive culture in the recipient (without an alternative diagnosis) as well asthe identification of the same organism in the donor blood.Since the advent of HIV testing of donor blood in the 1980s, the transmission of HIV during transfusion has droppeddramatically. Prior testing of donor blood only included testing for antibodies to HIV. However, due to latentinfection (the "window period" in which an individual is infectious, but has not had time to develop antibodies),many cases of HIV seropositive blood were missed. The development of a nucleic acid test for the HIV-1 RNA hasdramatically lowered the rate of donor blood seropositivity to about 1 in 3 million units. As transmittance of HIVdoes not necessarily mean HIV infection, the latter could still occur, at an even lower rate.The transmission of hepatitis C via transfusion currently stands at a rate of about 1 in 2 million units. As with HIV,this low rate has been attributed to the ability to screen for both antibodies as well as viral RNA nucleic acid testingin donor blood.Other rare transmissible infections include hepatitis B, syphilis, Chagas disease, cytomegalovirus infections (inimmunocompromised recipients), HTLV, and Babesia.

Blood transfusion 45
InefficacyTransfusion inefficacy or insufficient efficacy of a given unit(s) of blood product, while not itself a "complication"per se, can nonetheless indirectly lead to complications - in addition to causing a transfusion to fully or partly fail toachieve its clinical purpose. This can be especially significant for certain patient groups such as critical-care orneonatals.For red blood cells (RBC), by far the most commonly transfused product, poor transfusion efficacy can result fromunits damaged by the so-called storage lesion - a range of biochemical and biomechanical changes that occur duringstorage. With red cells, this can decrease viability and ability for tissue oxygenation. Although some of thebiochemical changes are reversible after the blood is transfused, the biomechanical changes are less so, andrejuvenation products are not yet able to adequately reverse this phenomenon. There has been increasing controversyabout whether a given product unit's age is a factor in transfusion efficacy, specifically about whether "older" blooddirectly or indirectly increases risks of complications. Studies have not been consistent on answering this question,with some showing that older blood is indeed less effective but with others showing no such difference; thesedevelopments are being closely followed by hospital blood bankers - who are the physicians, typically pathologists,who collect and manage inventories of tranfusable blood units.Certain regulatory measures are in place to minimize RBC storage lesion - including a maximum shelf life (currently42 days), a maximum auto-hemolysis threshold (currently 1% in the US, 0.8% in Europe), and a minimum level ofpost-transfusion RBC survival in vivo (currently 75% after 24 hours). However, all of these criteria are applied in auniversal manner that does not account for differences among units of product. For example, testing for thepost-transfusion RBC survival in vivo is done on a sample of healthy volunteers, and then compliance is presumedfor all RBC units based on universal (GMP) processing standards (of course, RBC survival by itself does notguarantee efficacy, but it is a necessary prerequisite for cell function, and hence serves as a regulatory proxy).Opinions vary as to the "best" way to determine transfusion efficacy in a patient in vivo. In general, there are not yetany in vitro tests to assess quality or predict efficacy for specific units of RBC blood product prior to theirtransfusion, though there is exploration of potentially relevant tests based on RBC membrane properties such aserythrocyte deformability and erythrocyte fragility (mechanical).Many physicians have adopted a so-called "restrictive protocol" - whereby transfusion is held to a minimum - due inpart to the noted uncertainties surrounding storage lesion, in addition to the very high direct and indirect costs oftransfusions, along with the increasing view that many transfusions are inappropriate or use too many RBC units. Ofcourse, restrictive protocol is not an option with some especially vulnerable patients who may require the bestpossible efforts to rapidly restore tissue oxygenation.Although tranfusions of platelets are far less numerous (relative to RBC), platelet storage lesion and resultingefficacy loss is also a concern.
Other•• Transfusion-associated volume overload is a common complication simply due to the fact that blood products
have a certain amount of volume. This is especially the case in recipients with underlying cardiac or kidneydisease. Red cell transfusions can lead to volume overload when they must be repeated due to insufficient efficacy(see above). Plasma transfusion is especially prone to causing volume overload due to its hypertonicity.
•• Hypothermia can occur with transfusions with large quantities of blood products which normally are stored atcold temperatures. Core body temperature can go down as low as 32 °C and can produce physiologicdisturbances. Prevention should be done with warming the blood to ambient temperature prior to transfusions.
•• Transfusions with large amounts of red blood cells, whether due to severe hemorrhaging and/or transfusioninefficacy (see above), can lead to an inclination for bleeding. The mechanism is thought to be due todisseminated intravascular coagulation, along with dilution of recipient platelets and coagulation factors. Close

Blood transfusion 46
monitoring and transfusions with platelets and plasma is indicated when necessary.•• Metabolic alkalosis can occur with massive blood transfusions due to the breakdown of citrate stored in blood
into bicarbonate.•• Hypocalcemia can also occur with massive blood transfusions due to the complex of citrate with serum calcium.• Blood doping is often used by athletes, drug addicts or military personnel for reasons such as to increase physical
stamina, to fake a drug detection test or simply to remain active and alert during the duty-times respectively.However a lack of knowledge and insufficient experience can turn a blood transfusion into a sudden death. Forexample, when individuals run the frozen blood sample directly in their veins this cold blood rapidly reaches theheart, where it disturbs the heart's original pace leading to cardiac arrest and sudden death.
Frequency of useGlobally around 85 million units of red blood cells are transfused in a given year.In the United States, blood transfusions were performed nearly 3 million times during hospitalizations in 2011,making it the most common procedure performed. The rate of hospitalizations with a blood transfusion nearlydoubled from 1997, from a rate of 40 stays to 95 stays per 10,000 population. It was the most common procedureperformed for patients 45 years of age and older in 2011, and among the top five most common for patients betweenthe ages of 1 and 44 years.[6]
According to the New York Times: "Changes in medicine have eliminated the need for millions of bloodtransfusions, which is good news for patients getting procedures like coronary bypasses and other procedures thatonce required a lot of blood." And, "Blood bank revenue is falling, and the decline may reach $1.5 billion a year thisyear [2014] from a high of $5 billion in 2008." Job losses will reach as high as 12,000 within the next three to fiveyears, roughly a quarter of the total in the industry, according to the Red Cross.
HistoryBeginning with William Harvey's experiments on the circulation of blood, research into blood transfusion began inthe 17th century, with successful experiments in transfusion between animals. However, successive attempts byphysicians to transfuse animal blood into humans gave variable, often fatal, results.Pope Innocent VIII is sometimes said to have been given the world's first blood transfusion by his Jewish physicianGiacomo di San Genesio, who had him drink (by mouth) the blood of three 10-year old boys. The boys subsequentlydied. The evidence for this story, however, is unreliable and may have been motivated by anti-semitism.[7]

Blood transfusion 47
Early attempts
Animal blood
Richard Lower pioneered the first bloodtransfusion from animal to human in 1665 at the
Royal Society.
Working at the Royal Society in the 1660s, the physician RichardLower began examining the effects of changes in blood volume oncirculatory function and developed methods for cross-circulatory studyin animals, obviating clotting by closed arteriovenous connections. Thenew instruments he was able to devise enabled him to perform the firstreliably documented successful transfusion of blood in front of hisdistinguished colleagues from the Royal Society.
According to Lower's account, "...towards the end of February 1665 [I]selected one dog of medium size, opened its jugular vein, and drew offblood, until ... its strength was nearly gone. Then, to make up for thegreat loss of this dog by the blood of a second, I introduced blood fromthe cervical artery of a fairly large mastiff, which had been fastenedalongside the first, until this latter animal showed ... it was overfilled ...by the inflowing blood." After he "sewed up the jugular veins," theanimal recovered "with no sign of discomfort or of displeasure."Lower had performed the first blood transfusion between animals. Hewas then "requested by the Honorable [Robert] Boyle ... to acquaint theRoyal Society with the procedure for the whole experiment," which hedid in December 1665 in the Society's Philosophical Transactions.
The first blood transfusion from animal to human was administered by Dr. Jean-Baptiste Denys, eminent physicianto King Louis XIV of France, on June 15, 1667. He transfused the blood of a sheep into a 15-year-old boy, whosurvived the transfusion. Denys performed another transfusion into a labourer, who also survived. Both instanceswere likely due to the small amount of blood that was actually transfused into these people. This allowed them towithstand the allergic reaction.
Denys' third patient to undergo a blood transfusion was Swedish Baron Gustaf Bonde. He received two transfusions.After the second transfusion Bonde died. In the winter of 1667, Denys performed several transfusions on AntoineMauroy with calf's blood, who on the third account died.[8]
Six months later in London, Lower performed the first human transfusion of animal blood in Britain, where he"superintended the introduction in [a patient's] arm at various times of some ounces of sheep's blood at a meeting ofthe Royal Society, and without any inconvenience to him." The recipient was Arthur Coga, "the subject of aharmless form of insanity." Sheep's blood was used because of speculation about the value of blood exchangebetween species; it had been suggested that blood from a gentle lamb might quiet the tempestuous spirit of anagitated person and that the shy might be made outgoing by blood from more sociable creatures.Lower went on to pioneer new devices for the precise control of blood flow and the transfusion of blood; his designswere substantially the same as modern syringes and catheters. Shortly after, Lower moved to London, where hisgrowing practice soon led him to abandon research.These early experiments with animal blood provoked a heated controversy in Britain and France. Finally, in 1668,the Royal Society and the French government both banned the procedure. The Vatican condemned these experimentsin 1670. Blood transfusions fell into obscurity for the next 150 years.

Blood transfusion 48
Human blood
James Blundell, successfully transfused humanblood in 1818.
The science of blood transfusion dates to the first decade of the 20thcentury, with the discovery of distinct blood types leading to thepractice of mixing some blood from the donor and the receiver beforethe transfusion (an early form of cross-matching).
In the early 19th century, British obstetrician Dr. James Blundell madeefforts to treat hemorrhage by transfusion of human blood using asyringe. In 1818 following experiments with animals, he performed thefirst successful transfusion of human blood to treat postpartumhemorrhage. Blundell used the patient's husband as a donor, andextracted four ounces of blood from his arm to transfuse into his wife.During the years 1825 and 1830, Blundell performed 10 transfusions,five of which were beneficial, and published his results. He alsoinvented a number of instruments for the transfusion of blood.[9] Hemade a substantial amount of money from this endeavour, roughly $2million ($50 million real dollars).Wikipedia:Citation needed
In 1840, at St George's Hospital Medical School in London, SamuelArmstrong Lane, aided by Dr. Blundell, performed the first successful whole blood transfusion to treat haemophilia.
However, early transfusions were risky and many resulted in the death of the patient. By the late 19th century, bloodtransfusion was regarded as a risky and dubious procedure, and was largely shunned by the medical establishment.
Modern eraIt was not until 1901, when the Austrian Karl Landsteiner discovered human blood groups, that blood transfusionwas put onto a scientific basis and became safer.Mixing blood from two incompatible individuals can lead to an immune response, and the destruction of red bloodcells releases free hemoglobin into the bloodstream, which can have fatal consequences. Karl Landsteiner discoveredthat when incompatible types are mixed, the red blood cells clump, and that this immunological reaction occurswhen the receiver of a blood transfusion has antibodies against the donor blood cells. His work made it possible todetermine blood type and allowed a way for blood transfusions to be carried out much more safely. For thisdiscovery he was awarded the Nobel Prize in Physiology and Medicine in 1930, and many other blood groups havebeen discovered since.Jan Janský also discovered the human blood groups in which he classified blood into four groups I, II, III, IV.William Lorenzo Moss's blood typing technique was widely used throughout the world until World War II.[10]
George Washington Crile is credited with performing the first surgery using a direct blood transfusion in 1906 at St.Alexis Hospital in Cleveland while a professor of surgery at Case Western Reserve University.Wikipedia:Manual ofStyle/Dates and numbers#Chronological items

Blood transfusion 49
Blood banks in WW1
Main article: Blood bank
Dr. Luis Agote (2nd from right) overseeing oneof the first safe and effective blood transfusions
in 1914
While the first transfusions had to be made directly from donor toreceiver before coagulation, it was discovered that by addinganticoagulant and refrigerating the blood it was possible to store it forsome days, thus opening the way for the development of blood banks.John Braxton Hicks was the first to experiment with chemical methodsto prevent the coagulation of blood at St Mary's Hospital, London inthe late 19th century. His attempts, using phosphate of soda, however,were unsuccessful.
The first non-direct transfusion was performed on March 27, 1914 bythe Belgian doctor Albert Hustin, though this was a diluted solution ofblood. The Argentine doctor Luis Agote used a much less dilutedsolution in November of the same year. Both used sodium citrate as an anticoagulant.
The First World War acted as a catalyst for the rapid development of blood banks and transfusion techniques.Canadian Lieutenant Lawrence Bruce Robertson was instrumental in persuading the Royal Army Medical Corps toadopt the use of blood tranfusion at the Casualty Clearing Stations for the wounded. In October 1915, Robertsonperformed his first wartime transfusion with a syringe to a patient suffering from multiple shrapnel wounds. Hefollowed this up with four subsequent transfusions in the following months and his success was reported to SirWalter Morley Fletcher, director of the Medical Research Committee.
World War II Russian syringe for directinter-human blood transfusion.
Robertson published his findings in the British Medical Journal in1916 and, with the help of a few like minded individuals (including theeminent physician Edward William Archibald who introduced thecitrate anticoagulant method), was able to persuade the Britishauthorities of the merits of blood transfusion. Robertson went on toestablish the first blood transfusion apparatus at a Casualty ClearingStation on the Western Front in the spring of 1917.
Oswald Hope Robertson, a medical researcher and U.S. Army officerwas attached to the RAMC in 1917, where he was instrumental inestablishing the first blood banks, in preparation for the anticipatedThird Battle of Ypres. He used sodium citrate as the anticoagulant andthe blood was extracted from punctures in the vein and was stored inbottles at British and American Casualty Clearing Stations along theFront. He also experimented with preserving separated red blood cells
in iced bottles. Geoffrey Keynes, a British surgeon, developed a portable machine that could store blood to enabletransfusions to be carried out more easily.

Blood transfusion 50
Expansion
Alexander Bogdanov established a scientificinstitute to research the effects of blood
transfusion in Moscow, 1925.
The world's first blood donor service was established in 1921 by thesecretary of the British Red Cross, Percy Oliver. In that year, Oliverwas contacted by King's College Hospital, where they were in urgentneed of a blood donor. After providing a donor, Oliver set aboutorganizing a system for the voluntary registration of blood donors atclinics around London, with Sir Geoffrey Keynes appointed as amedical adviser. Volunteers were subjected to a series of physical teststo establish their blood group. The London Blood Transfusion Servicewas free of charge and expanded rapidly in its first few years ofoperation. By 1925, it was providing services for almost 500 patientsand it was incorporated into the structure of the British Red Cross in1926. Similar systems were established in other cities includingSheffield, Manchester and Norwich, and the service's work began toattract international attention. Similar services were established inFrance, Germany, Austria, Belgium, Australia and Japan.
An academic institution devoted to the science of blood transfusionwas founded by Alexander Bogdanov in Moscow in 1925. Bogdanovwas motivated, at least in part, by a search for eternal youth, andremarked with satisfaction on the improvement of his eyesight,suspension of balding, and other positive symptoms after receiving 11 transfusions of whole blood. Bogdanov diedin 1928 as a result of one of his experiments, when the blood of a student suffering from malaria and tuberculosiswas given to him in a transfusion.[11] Following Bogdanov's lead, Vladimir Shamov and Sergei Yudin in the USSRpioneered the transfusion of cadaveric blood from recently deceased donors. Yudin performed such a transfusionsuccessfully for the first time on March 23, 1930 and reported his first seven clinical transfusions with cadavericblood at the Fourth Congress of Ukrainian Surgeons at Kharkiv in September. However, this method was never usedwidely, even in Russia.

Blood transfusion 51
British poster encouraging people to donate bloodfor the war effort.
One of the earliest blood banks was established by Federico DuranJorda during the Spanish Civil War in 1936. Duran joined theTransfusion Service at the Barcelona Hospital at the start of theconflict, but the hospital was soon overwhelmed by the demand forblood and the paucity of available donors. With support from theDepartment of Health of the Spanish Republican Army, Duranestablished a blood bank for the use of wounded soldiers and civilians.The 300-400 ml of extracted blood was mixed with 10% citratesolution in a modified Duran Erlenmeyer flask. The blood was storedin a sterile glass enclosed under pressure at 2 °C. During 30 months ofwork, the Transfusion Service of Barcelona registered almost 30,000donors, and processed 9,000 liters of blood.
In 1937 Bernard Fantus, director of therapeutics at the Cook CountyHospital in Chicago, established the first hospital blood bank in theUnited States. In creating a hospital laboratory that preserved,refrigerated and stored donor blood, Fantus originated the term "bloodbank". Within a few years, hospital and community blood banks wereestablished across the United States.
Federico Duran Jorda fled to Britain in 1938, and worked with Dr JanetVaughan at the Royal Postgraduate Medical School at Hammersmith Hospital to create a system of national bloodbanks in London. With the outbreak of war looking imminent in 1938, the War Office created the Army BloodSupply Depot (ABSD) in Bristol headed by Lionel Whitby and in control of four large blood depots around thecountry. British policy through the war was to supply military personnel with blood from centralized depots, incontrast to the approach taken by the Americans and Germans where troops at the front were bled to providerequired blood. The British method proved to be more successful at adequately meeting all requirements and over700,000 donors were bled over the course of the war. This system evolved into the National Blood TransfusionService established in 1946, the first national service to be implemented.
Medical advances
Wounded soldier is given blood plasma in Sicily,1943.
A blood collection program was initiated in the US in 1940 and EdwinCohn pioneered the process of blood fractionation. He worked out thetechniques for isolating the serum albumin fraction of blood plasma,which is essential for maintaining the osmotic pressure in the bloodvessels, preventing their collapse.
The use of blood plasma as a substitute for whole blood and fortransfusion purposes was proposed as early as 1918, in thecorrespondence columns of the British Medical Journal, by Gordon R.Ward. At the onset of World War II, liquid plasma was used in Britain.A large project, known as 'Blood for Britain' began in August 1940 tocollect blood in New York City hospitals for the export of plasma toBritain. A dried plasma package was developed, which reducedbreakage and made the transportation, packaging, and storage much simpler.[12]

Blood transfusion 52
Charles R. Drew oversaw the production of bloodplasma for shipping to Britain during WW2.
The resulting dried plasma package came in two tin cans containing400 cc bottles. One bottle contained enough distilled water toreconstitute the dried plasma contained within the other bottle. In aboutthree minutes, the plasma would be ready to use and could stay freshfor around four hours.[13] Dr. Charles R. Drew was appointed medicalsupervisor, and he was able to transform the test tube methods into thefirst successful technique for mass production.
Another important breakthrough came in 1939-40 when KarlLandsteiner, Alex Wiener, Philip Levine, and R.E. Stetson discoveredthe Rhesus blood group system, which was found to be the cause of themajority of transfusion reactions up to that time. Three years later, theintroduction by J.F. Loutit and Patrick L. Mollison ofacid-citrate-dextrose (ACD) solution, which reduced the volume ofanticoagulant, permitted transfusions of greater volumes of blood andallowed longer term storage.
Carl Walter and W.P. Murphy, Jr. introduced the plastic bag for bloodcollection in 1950. Replacing breakable glass bottles with durable
plastic bags allowed for the evolution of a collection system capable of safe and easy preparation of multiple bloodcomponents from a single unit of whole blood.
In the field of cancer surgery replacement of massive blood loss became a major problem. The cardiac arrest rate washigh. In 1963, C. Paul Boyan and William S. Howland discovered that the temperature of the blood and the rate ofinfusion greatly affected survival rates, and introduced blood warming to surgery.Further extending the shelf life of stored blood was an anticoagulant preservative, CPDA-1, introduced in 1979,which increased the blood supply and facilitated resource-sharing among blood banks.As of 2006, there were about 15 million units of blood products transfused per year in the United States.
Special populations
Neonatal transfusionTo ensure the safety of blood transfusion to pediatric patients, hospitals are taking additional precaution to avoidinfection and prefer to use specially tested pediatric blood units that are guaranteed negative for Cytomegalovirus.Most guidelines recommend the provision of CMV-negative blood components and not simply leukoreducedcomponents for newborns or low birthweight infants in whom the immune system is not fully developed. Thesespecific requirements place additional restrictions on blood donors who can donate for neonatal use. vnv Neonataltransfusions typically fall into one of two categories:•• "Top-up" transfusions, to replace losses due to investigational losses and correction of anemia.• Exchange (or partial exchange) transfusions are done for removal of bilirubin, removal of antibodies and
replacement of red cells (e.g., for anemia secondary to thalassemias and other hemoglobinopathies).

Blood transfusion 53
Persons with massive traumaA massive transfusion protocol is used for massive trauma resuscitation, when more than ten units of blood areneeded. Packed red blood cells, fresh frozen plasma, and platelets are administered in lieu of crystalloids or wholeblood. Typically higher ratios of fresh frozen plasma and platelets are given relative to packed red blood cells.
Persons with unknown blood typeBecause blood type O negative is compatible with anyone, O negative blood is often overused and consequently isalways in short supply.[14] The use of this blood should be restricted to persons with O negative blood, as nothingelse is compatible with them, and women who might be pregnant and for whom it would be impossible to do bloodgroup testing before giving them emergency treatment. Whenever possible, O negative blood is to be conserved byusing blood type testing to identify a less scarce alternative.
People with religious objectionsSee also: Jehovah's Witnesses and blood transfusionsObjections to blood transfusions may arise for personal, medical, or religious reasons. For example, Jehovah'sWitnesses object to blood transfusion primarily on religious grounds—they believe that blood is sacred, as the Biblesays "abstain from blood" (Acts 15:28,29). They have also highlighted complications associated with transfusion.[15]
Research into alternativesSee also: Blood substitutesAlthough there are clinical situations where transfusion with red blood cells is the only clinically appropriate option,increasingly clinicians are looking at alternatives. This can be due to several reasons, such as patient safety,economic burden or scarcity of blood. Increasingly guidelines recommend blood transfusions should be reserved forpatients with or at risk of cardiovascular instability due to the degree of their anaemia. In these cases parenteral ironis recommended.Thus far, there are no available oxygen-carrying blood substitutes, which is the typical objective of a blood (RBC)transfusion; however, there are widely available non-blood volume expanders for cases where only volumerestoration is required. These are helping doctors and surgeons avoid the risks of disease transmission and immunesuppression, address the chronic blood donor shortage, and address the concerns of Jehovah's Witnesses and otherswho have religious objections to receiving transfused blood.A number of blood substitutes have been explored (and still are), but thus far they all suffer from many challenges.Most attempts to find a suitable alternative to blood thus far have concentrated on cell-free hemoglobin solutions.Blood substitutes could make transfusions more readily available in emergency medicine and in pre-hospital EMScare. If successful, such a blood substitute could save many lives, particularly in trauma where massive blood lossresults. Hemopure, a hemoglobin-based therapy, is approved for use in South Africa.
Veterinary useMain article: Blood type (non-human)Veterinarians also administer transfusions to other animals. Various species require different levels of testing toensure a compatible match. For example, cats have 3 known blood types, cattle have 11, dogs have 12, pigs 16 andhorses have 34. However, in many species (especially horses and dogs), cross matching is not required before thefirst transfusion, as antibodies against non-self cell surface antigens are not expressed constitutively - i.e. the animalhas to be sensitized before it will mount an immune response against the transfused blood.The rare and experimental practice of inter-species blood transfusions is a form of xenograft.

Blood transfusion 54
References[1] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?field=uid& term=D001803[2] http:/ / ops. icd-code. de/ ops/ code/ 8-80. html[3] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000431. htm[4] Blood Processing. University of Utah. Available at: (http:/ / library. med. utah. edu/ WebPath/ TUTORIAL/ BLDBANK/ BBPROC. html).
Accessed on: December 15, 2006.[5][5] Wang SS. What's the Shelf Life of Blood? Focus on Whether Older Donations Impair Recovery of Transfusion Recipients. The Wall Street
Journal. 2009 Dec. 1.[6] Pfuntner A., Wier L.M., Stocks C. Most Frequent Procedures Performed in U.S. Hospitals, 2011. HCUP Statistical Brief #165. October 2013.
Agency for Healthcare Research and Quality, Rockville, MD. (http:/ / www. hcup-us. ahrq. gov/ reports/ statbriefs/ sb165. jsp).[7] Jacalyn Duffin, History of Medicine: A scandalously short introduction, University of Toronto Press, 1999, p. 171.[8][8] p. 406.[9] Ellis, H. Surgical Anniversaries: James Blundell, pioneer of blood transfusion (http:/ / www. bjhm. co. uk/ cgi-bin/ go. pl/ library/ article.
cgi?uid=24500;article=hm_68_8_447) British Journal of Hospital Medicine, August 2007, Vol 68, No 8.[10] Dr. William Lorenzo Moss (http:/ / onlineathens. com/ stories/ 090501/ ath_drmoss. shtml)[11] Bernice Glatzer Rosenthal. New Myth, New World: From Nietzsche to Stalinism, Pennsylvania State University, 2002, ISBN 0-271-02533-6,
pp. 161-162.[12] Transfusion before World War I (http:/ / history. amedd. army. mil/ booksdocs/ wwii/ blood/ chapter1. htm)[13] Plasma Equipment and Packaging, and Transfusion Equipment (http:/ / history. amedd. army. mil/ booksdocs/ wwii/ blood/ chapter7. htm)[14][14] , which cites[15] http:/ / www. jw. org/ en/ publications/ books/ blood/ how-can-blood-save-your-life/
External links
Wikimedia Commons has media related to Blood transfusion.
• Transfusion, ISSN: 1537-2995 (electronic) 0041-1132 (paper) (http:/ / www. blackwell-synergy. com/ loi/ trf)• Patient Blood Management (http:/ / www. transfusesolutions. com)• Blood Groups and Red Cell Antigens. (http:/ / www. ncbi. nlm. nih. gov/ books/ NBK2261) Free online book at
NCBI Bookshelf ID: NBK2261• Blood Transfusion Indications (http:/ / mahasbtc. aarogya. com/ index. php/ history-of-blood-transfusion/
transfusion-indications-), information provide by Maharashtra State Blood Transfusion Council.• Five Myths on Blood Transfusions (http:/ / www. cec. health. nsw. gov. au/ programs/ blood-watch/ myths#1), an
information campaign by the New South Wales Government.• The Dangers of Illegal Blood Trade (http:/ / healthopine. com/ legal-issues/
red-alert-illegal-blood-trade-thrives-in-india)• Cochrane Injuries Group (http:/ / injuries. cochrane. org/ ), publishes systematic reviews of interventions for
traumatic injury, which include evaluations of blood and blood substitute transfusions
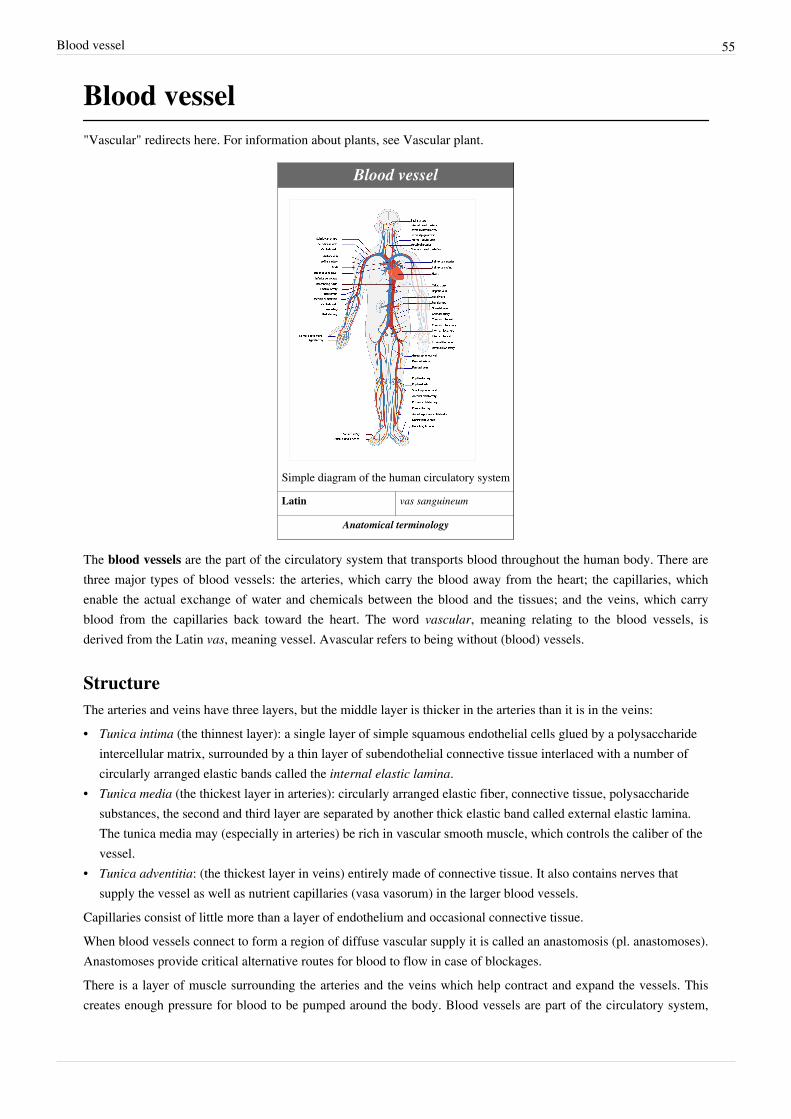
Blood vessel 55
Blood vessel"Vascular" redirects here. For information about plants, see Vascular plant.
Blood vessel
Simple diagram of the human circulatory system
Latin vas sanguineum
Anatomical terminology
The blood vessels are the part of the circulatory system that transports blood throughout the human body. There arethree major types of blood vessels: the arteries, which carry the blood away from the heart; the capillaries, whichenable the actual exchange of water and chemicals between the blood and the tissues; and the veins, which carryblood from the capillaries back toward the heart. The word vascular, meaning relating to the blood vessels, isderived from the Latin vas, meaning vessel. Avascular refers to being without (blood) vessels.
StructureThe arteries and veins have three layers, but the middle layer is thicker in the arteries than it is in the veins:• Tunica intima (the thinnest layer): a single layer of simple squamous endothelial cells glued by a polysaccharide
intercellular matrix, surrounded by a thin layer of subendothelial connective tissue interlaced with a number ofcircularly arranged elastic bands called the internal elastic lamina.
• Tunica media (the thickest layer in arteries): circularly arranged elastic fiber, connective tissue, polysaccharidesubstances, the second and third layer are separated by another thick elastic band called external elastic lamina.The tunica media may (especially in arteries) be rich in vascular smooth muscle, which controls the caliber of thevessel.
• Tunica adventitia: (the thickest layer in veins) entirely made of connective tissue. It also contains nerves thatsupply the vessel as well as nutrient capillaries (vasa vasorum) in the larger blood vessels.
Capillaries consist of little more than a layer of endothelium and occasional connective tissue.When blood vessels connect to form a region of diffuse vascular supply it is called an anastomosis (pl. anastomoses).Anastomoses provide critical alternative routes for blood to flow in case of blockages.There is a layer of muscle surrounding the arteries and the veins which help contract and expand the vessels. Thiscreates enough pressure for blood to be pumped around the body. Blood vessels are part of the circulatory system,

Blood vessel 56
together with the heart and the blood.
Types
Blood vessel with an erythrocyte (red blood cell,E) within its lumen, endothelial cells forming itstunica intima (inner layer), and pericytes forming
its tunica adventitia (outer layer)
There are various kinds of blood vessels:•• Arteries
• Aorta (the largest artery, carries blood out of the heart)• Branches of the aorta, such as the carotid artery, the subclavian
artery, the celiac trunk, the mesenteric arteries, the renal arteryand the iliac artery.
• Arterioles• Capillaries (the smallest blood vessels)• Venules• Veins
• Large collecting vessels, such as the subclavian vein, the jugularvein, the renal vein and the iliac vein.
• Venae cavae (the two largest veins, carry blood into the heart).They are roughly grouped as arterial and venous, determined bywhether the blood in it is flowing away from (arterial) or toward(venous) the heart. The term "arterial blood" is nevertheless used to indicate blood high in oxygen, although thepulmonary artery carries "venous blood" and blood flowing in the pulmonary vein is rich in oxygen. This is becausethey are carrying the blood to and from the lungs, respectively, to be oxygenated.

Blood vessel 57
PhysiologyBlood vessels do not actively engage in the transport of blood (they have no appreciable peristalsis), butarteries—and veins to a degree—can regulate their inner diameter by contraction of the muscular layer. This changesthe blood flow to downstream organs, and is determined by the autonomic nervous system. Vasodilation andvasoconstriction are also used antagonistically as methods of thermoregulation.Oxygen (bound to hemoglobin in red blood cells) is the most critical nutrient carried by the blood. In all arteriesapart from the pulmonary artery, hemoglobin is highly saturated (95-100%) with oxygen. In all veins apart from thepulmonary vein, the hemoglobin is desaturated at about 75%. (The values are reversed in the pulmonary circulation.)The blood pressure in blood vessels is traditionally expressed in millimetres of mercury (1 mmHg = 133 Pa). In thearterial system, this is usually around 120 mmHg systolic (high pressure wave due to contraction of the heart) and 80mmHg diastolic (low pressure wave). In contrast, pressures in the venous system are constant and rarely exceed 10mmHg.Vasoconstriction is the constriction of blood vessels (narrowing, becoming smaller in cross-sectional area) bycontracting the vascular smooth muscle in the vessel walls. It is regulated by vasoconstrictors (agents that causevasoconstriction). These include paracrine factors (e.g. prostaglandins), a number of hormones (e.g. vasopressin andangiotensin) and neurotransmitters (e.g. epinephrine) from the nervous system.Vasodilation is a similar process mediated by antagonistically acting mediators. The most prominent vasodilator isnitric oxide (termed endothelium-derived relaxing factor for this reason).Permeability of the endothelium is pivotal in the release of nutrients to the tissue. It is also increased in inflammationin response to histamine, prostaglandins and interleukins, which leads to most of the symptoms of inflammation(swelling, redness, warmth and pain).
DiseaseMain article: Vascular diseaseBlood vessels play a huge role in virtually every medical condition. Cancer, for example, cannot progress unless thetumor causes angiogenesis (formation of new blood vessels) to supply the malignant cells' metabolic demand.Atherosclerosis, the formation of lipid lumps (atheromas) in the blood vessel wall, is the most commoncardiovascular disease, the main cause of death in the Western world.Blood vessel permeability is increased in inflammation. Damage, due to trauma or spontaneously, may lead tohemorrhage due to mechanical damage to the vessel endothelium. In contrast, occlusion of the blood vessel byatherosclerotic plaque, by an embolised blood clot or a foreign body leads to downstream ischemia (insufficientblood supply) and possibly necrosis. Vessel occlusion tends to be a positive feedback system; an occluded vesselcreates eddies in the normally laminar flow or plug flow blood currents. These eddies create abnormal fluid velocitygradients which push blood elements such as cholesterol or chylomicron bodies to the endothelium. These depositonto the arterial walls which are already partially occluded and build upon the blockage.[1]
Vasculitis is inflammation of the vessel wall, due to autoimmune disease or infection.

Blood vessel 58
References[1][1] Multiphase Flow and Fluidization, Gidaspow et al., Academic Press, 1992
Wikimedia Commons has media related to Blood vessels.
Bone marrowThis article is about the medical aspects of bone marrow in humans. For use of animal bone marrow in cuisine, seeBone marrow (food).
Bone marrow
A simplified illustration of cells in bone marrow
Latin Medulla ossium
MeSH Bone+Marrow [1]
TA A13.1.01.001 [2]
FMA FMA:9608 [3]
Anatomical terminology
Bone marrow is the flexible tissue in the interior of bones. In humans, red blood cells are produced by cores of bonemarrow in the heads of long bones in a process known as hematopoiesis. On average, bone marrow constitutes 4% ofthe total body mass of humans; in an adult weighing 65 kilograms (143 lb), bone marrow typically accounts forapproximately 2.6 kilograms (5.7 lb). The hematopoietic component of bone marrow produces approximately 500billion blood cells per day, which use the bone marrow vasculature as a conduit to the body's systemic circulation.Bone marrow is also a key component of the lymphatic system, producing the lymphocytes that support the body'simmune system.[4]
Bone marrow transplants can be conducted to treat severe diseases of the bone marrow, including certain forms ofcancer. Additionally, bone marrow stem cells have been successfully transformed into functional neural cells, andcan also potentially be used to treat illnesses such as inflammatory bowel disease.

Bone marrow 59
Marrow types
A femoral head with a cortex of cortical bone andmedulla of trabecular bone. Both red bonemarrow and a central focus of yellow bone
marrow are visible.
The two types of bone marrow are medulla ossium rubra (red marrow),which consists mainly of hematopoietic tissue, and medulla ossiumflava (yellow marrow), which is mainly made up of fat cells. Redblood cells, platelets, and most white blood cells arise in red marrow.Both types of bone marrow contain numerous blood vessels andcapillaries. At birth, all bone marrow is red. With age, more and moreof it is converted to the yellow type; only around half of adult bonemarrow is red. Red marrow is found mainly in the flat bones, such asthe pelvis, sternum, cranium, ribs, vertebrae and scapulae, and in thecancellous ("spongy") material at the epiphyseal ends of long bonessuch as the femur and humerus. Yellow marrow is found in themedullary cavity, the hollow interior of the middle portion of longbones. In cases of severe blood loss, the body can convert yellow marrow back to red marrow to increase blood cellproduction.
Stroma
The stroma of the bone marrow is all tissue not directly involved in the marrow's primary function of hematopoiesis.Yellow bone marrow makes up the majority of bone marrow stroma, in addition to smaller concentrations of stromalcells located in the red bone marrow. Though not as active as parenchymal red marrow, stroma is indirectly involvedin hematopoiesis, since it provides the hematopoietic microenvironment that facilitates hematopoiesis by theparenchymal cells. For instance, they generate colony stimulating factors, which have a significant effect onhematopoiesis. Cell types that constitute the bone marrow stroma include:
• fibroblasts (reticular connective tissue)• macrophages, which contribute especially to red blood cell production, as they deliver iron for hemoglobin
production.•• adipocytes•• osteoblasts•• osteoclasts• endothelial cells, which form the sinusoids. These derive from endothelial stem cells, which are also present in the
bone marrow.
Bone marrow barrierThe blood vessels of the bone marrow constitute a barrier, inhibiting immature blood cells from leaving the marrow.Only mature blood cells contain the membrane proteins required to attach to and pass the blood vessel endothelium.Hematopoietic stem cells may also cross the bone marrow barrier, and may thus be harvested from blood.
Mesenchymal stem cellsMain article: Mesenchymal stem cellThe bone marrow stroma contains mesenchymal stem cells (MSCs), also known as marrow stromal cells. These aremultipotent stem cells that can differentiate into a variety of cell types. MSCs have been shown to differentiate, invitro or in vivo, into osteoblasts, chondrocytes, myocytes, adipocytes and beta-pancreatic islets cells.

Bone marrow 60
Red marrow parenchyma
Cellular components
Hematopoietic precursor cells: promyelocyte in the center, twometamyelocytes next to it and band cells from a bone marrow
aspirate.
Cellular constitution of the red bone marrow parenchyma[5]
Group Cell type Averagefraction
Referencerange
Myelopoieticcells
Myeloblasts 0.9% 0.2-1.5
Promyelocytes 3.3% 2.1-4.1
Neutrophilic myelocytes 12.7% 8.2-15.7
Eosinophilic myelocytes 0.8% 0.2-1.3
Neutrophilic metamyelocytes 15.9% 9.6-24.6
Eosinophilic metamyelocytes 1.2% 0.4-2.2
Neutrophilic band cells 12.4% 9.5-15.3
Eosinophilic band cells 0.9% 0.2-2.4
Segmented neutrophils 7.4% 6.0-12.0
Segmented eosinophils 0.5% 0.0-1.3
Segmented basophils and mast cells 0.1% 0.0-0.2
Erythropoieticcells
Pronormoblasts 0.6% 0.2-1.3
Basophilic normoblasts 1.4% 0.5-2.4
Polychromatic normoblasts 21.6% 17.9-29.2
Orthochromatic normoblast 2.0% 0.4-4.6
Other celltypes
Megakaryocytes < 0.1% 0.0-0.4
Plasma cells 1.3% 0.4-3.9
Reticular cells 0.3% 0.0-0.9
Lymphocytes 16.2% 11.1-23.2
Monocytes 0.3% 0.0-0.8

Bone marrow 61
In addition, the bone marrow contains hematopoietic stem cells, which give rise to the three classes of blood cellsthat are found in the circulation: white blood cells (leukocytes), red blood cells (erythrocytes), and platelets(thrombocytes).
CompartmentalizationBiological compartmentalization is evident within the bone marrow, in that certain cell types tend to aggregate inspecific areas. For instance, erythrocytes, macrophages, and their precursors tend to gather around blood vessels,while granulocytes gather at the borders of the bone marrow.
Lymphatic roleThe red bone marrow is a key element of the lymphatic system, being one of the primary lymphoid organs thatgenerate lymphocytes from immature hematopoietic progenitor cells. The bone marrow and thymus constitute theprimary lymphoid tissues involved in the production and early selection of lymphocytes. Furthermore, bone marrowperforms a valve-like function to prevent the backflow of lymphatic fluid in the lymphatic system.
Diseases of the bone marrowThe normal bone marrow architecture can be damaged or displaced by aplastic anemia, malignancies such asmultiple myeloma, or infections such as tuberculosis, leading to a decrease in the production of blood cells and bloodplatelets. The bone marrow can also be affected by various forms of leukemia, which attacks its hematologicprogenitor cells. Furthermore, exposure to radiation or chemotherapy will kill many of the rapidly dividing cells ofthe bone marrow, and will therefore result in a depressed immune system. Many of the symptoms of radiationpoisoning are due to damage sustained by the bone marrow cells.To diagnose diseases involving the bone marrow, a bone marrow aspiration is sometimes performed. This typicallyinvolves using a hollow needle to acquire a sample of red bone marrow from the crest of the ilium under general orlocal anesthesia.
ExaminationMain article: Bone marrow examination
A Wright's-stained bone marrow aspiratesmear from a patient with leukemia.
Bone marrow examination is the pathologic analysis of samples of bonemarrow obtained via biopsy and bone marrow aspiration. Bone marrowexamination is used in the diagnosis of a number of conditions, includingleukemia, multiple myeloma, anemia, and pancytopenia. The bone marrowproduces the cellular elements of the blood, including platelets, red bloodcells and white blood cells. While much information can be gleaned bytesting the blood itself (drawn from a vein by phlebotomy), it is sometimesnecessary to examine the source of the blood cells in the bone marrow toobtain more information on hematopoiesis; this is the role of bone marrowaspiration and biopsy.
The ratio between myeloid series and erythroid cells is relevant to bonemarrow function, and also to diseases of the bone marrow and peripheralblood, such as leukemia and anemia. The normal myeloid-to-erythroid ratio is
around 3:1; this ratio may increase in myelogenous leukemias, decrease in polycythemias, and reverse in cases ofthalassemia.

Bone marrow 62
Donation and transplantationMain article: Hematopoietic stem cell transplantation
A bone marrow harvest in progress.
In a bone marrow transplant, hematopoietic stem cells are removedfrom a person and infused into another person (allogenic) or into thesame person at a later time (autologous). If the donor and recipient arecompatible, these infused cells will then travel to the bone marrow andinitiate blood cell production. Transplantation from one person toanother is conducted for the treatment of severe bone marrow diseases,such as congenital defects, autoimmune diseases or malignancies. Thepatient's own marrow is first killed off with drugs or radiation, and thenthe new stem cells are introduced. Before radiation therapy orchemotherapy in cases of cancer, some of the patient's hematopoieticstem cells are sometimes harvested and later infused back when the therapy is finished to restore the immune system.
Bone marrow stem cells can be induced to become neural cells to treat neurological illnesses, and can alsopotentially be used for the treatment of other illnesses, such as inflammatory bowel disease. In 2013, following aclinical trial, scientists proposed that bone marrow transplantation could be used to treat HIV in conjunction withantiretroviral drugs; however, it was later found that HIV remained in the bodies of the test subjects.
HarvestingThe stem cells are typically harvested directly from the red marrow in the iliac crest, often under general anesthesia.The procedure is minimally invasive and does not require stitches afterwards. Depending on the donor's health andreaction to the procedure, the actual harvesting can be an outpatient procedure, or can require 1–2 days of recoveryin the hospital.[6]
Another option is to administer certain drugs that stimulate the release of stem cells from the bone marrow intocirculating blood.[7] An IV is inserted into the donor's arm, and the stem cells are filtered out of the blood. Thisprocedure is similar to that used in blood or platelet donation. In adults, bone marrow may also be taken from thesternum, while the tibia is often used when taking samples from infants. In newborns, stem cells may be retrievedfrom the umbilical cord.
References[1] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?mode=& term=Bone+ Marrow[2] http:/ / www. unifr. ch/ ifaa/ Public/ EntryPage/ TA98%20Tree/ Entity%20TA98%20EN/ 13. 1. 01. 001%20Entity%20TA98%20EN. htm[3] http:/ / fme. biostr. washington. edu/ FME/ index. jsp?fmaid=9608[4] The Lymphatic System (http:/ / allonhealth. com/ health-news/ par-lymphatic-system. htm). Allonhealth.com. Retrieved 5 December 2011.[5] Appendix A:IV (http:/ / www. msd. com. mx/ secure/ ebooks/ WintrobesClinicalHematology/ sid4266054. html) in Wintrobe's clinical
hematology (9th edition). Philadelphia: Lea & Febiger (1993).[6] National Marrow Donor Program Donor Guide (http:/ / www. marrow. org/ DONOR/ When_You_re_Asked_to_Donate_fo/ index. html).
Marrow.org. Retrieved 5 November 2012.[7] Mayo Clinic: Bone marrow donation: What to expect when you donate (http:/ / www. mayoclinic. com/ health/ bone-marrow/ CA00047).
Mayo Clinic. Retrieved 16 February 2013.

Bone marrow 63
Further reading
Wikimedia Commons has media related to Bone marrow.
• Nature Bone Marrow Transplantation (http:/ / www. nature. com/ bmt/ index. html) (Nature Publishing Group) –specialist scientific journal with articles on bone marrow biology and clinical uses.
• Cooper, B (2011). "The origins of bone marrow as the seedbed of our blood: from antiquity to the time of Osler"(http:/ / baylorhealth. edu/ proceedings/ 24_2/ 24_2_Cooper. pdf). Baylor University Medical Center Proceedings24 (2): 115–8. PMC 3069519 (http:/ / www. ncbi. nlm. nih. gov/ pmc/ articles/ PMC3069519). PMID 21566758(http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 21566758).

Erythropoietin 64
Erythropoietin
Erythropoietin
Available structures
PDB Ortholog search: PDBe [1], RCSB [2]
List of PDB id codes
1BUY [3], 1CN4 [4], 1EER [5]
Identifiers
Symbols EPO [6] ; EP; MVCD2
External IDs OMIM: 133170 [7] MGI: 95407 [8] HomoloGene: 624 [9] ChEMBL: 5837 [10] GeneCards: EPO Gene [11]

Erythropoietin 65
Gene ontology
Molecular function • erythropoietin receptor binding [12]
• hormone activity [13]
• protein binding [14]
• protein kinase activator activity [15]
Cellular component • extracellular region [16]
• extracellular space [17]
• cell surface [18]
Biological process • apoptotic process [19]
• signal transduction [20]
• embryo implantation [21]
• aging [22]
• blood circulation [23]
• positive regulation of cell proliferation [24]
• response to salt stress [25]
• negative regulation of calcium ion transport into cytosol [26]
• peptidyl-serine phosphorylation [27]
• response to lipopolysaccharide [28]
• response to vitamin A [29]
• response to testosterone [30]
• positive regulation of tyrosine phosphorylation of Stat5 protein [31]
• hemoglobin biosynthetic process [32]
• erythrocyte maturation [33]
• response to estrogen [34]
• positive regulation of neuron differentiation [35]
• positive regulation of DNA replication [36]
• positive regulation of protein kinase activity [37]
• positive regulation of transcription, DNA-templated [38]
• positive regulation of Ras protein signal transduction [39]
• response to axon injury [40]
• response to electrical stimulus [41]
• response to hyperoxia [42]
• regulation of transcription from RNA polymerase II promoter in response to hypoxia [43]
• response to interleukin-1 [44]
• cellular response to hypoxia [45]
• cellular hyperosmotic response [46]
• negative regulation of intrinsic apoptotic signaling pathway in response to osmotic stress[47]
• negative regulation of erythrocyte apoptotic process [48]
• negative regulation of cation channel activity [49]
Sources: Amigo [50] / QuickGO [51]
RNA expression pattern

Erythropoietin 66
More reference expression data [52]
Orthologs
Species Human Mouse
Entrez 2056 [53] 13856 [54]
Ensembl ENSG00000130427 [55] ENSMUSG00000029711 [56]
UniProt P01588 [57] P07321 [58]
RefSeq (mRNA) NM_000799 [59] NM_007942 [60]
RefSeq (protein) NP_000790 [61] NP_031968 [62]
Location (UCSC) Chr 7:100.32 – 100.32 Mb [63]
Chr 5:137.48 – 137.53 Mb [64]
PubMed search [65] [66]
This box:•• view•• talk• edit [67]
Erythropoietin, (/ɨˌrɪθrɵˈpɔɪ.ɨtɨn/) also known as EPO, is a glycoprotein hormone that controls erythropoiesis, or redblood cell production. It is a cytokine (protein signaling molecule) for erythrocyte (red blood cell) precursors in thebone marrow. Human EPO has a molecular weight of 34 kDa.Also called hematopoietin or hemopoietin, it is produced by interstitial fibroblasts in the kidney in close associationwith peritubular capillary and tubular epithelial tubule. It is also produced in perisinusoidal cells in the liver. Whileliver production predominates in the fetal and perinatal period, renal production is predominant during adulthood. Inaddition to erythropoiesis, erythropoietin also has other known biological functions. For example, it plays animportant role in the brain's response to neuronal injury. EPO is also involved in the wound healing process.Exogenous erythropoietin is produced by recombinant DNA technology in cell culture. Several differentpharmaceutical agents are available with a variety of glycosylation patterns, and are collectively callederythropoiesis-stimulating agents (ESA). The specific details for labelled use vary between the package inserts, butESAs have been used in the treatment of anemia in chronic kidney disease, anemia in myelodysplasia, and in anemiafrom cancer chemotherapy. Boxed warnings include a risk of death, myocardial infarction, stroke, venousthromboembolism, and tumor recurrence. Exogenous erythropoietin has been used illicitly as aperformance-enhancing drug; it can often be detected in blood, due to slight differences from the endogenousprotein, for example, in features of posttranslational modification.

Erythropoietin 67
Function
Red blood cell productionThe primary role of erythropoietin is an essential hormone for red cell production. Without it, definitiveerythropoiesis does not take place. Under hypoxic conditions, the kidney will produce and secrete erythropoietin toincrease the production of red blood cells by targeting CFU-E, proerythroblast and basophilic erythroblast subsets inthe differentiation. Erythropoietin has its primary effect on red blood cell progenitors and precursors (which arefound in the bone marrow in humans) by promoting their survival through protecting these cells from apoptosis.Erythropoietin is the primary erythropoietic factor that cooperates with various other growth factors (e.g., IL-3, IL-6,glucocorticoids, and SCF) involved in the development of erythroid lineage from multipotent progenitors. Theburst-forming unit-erythroid (BFU-E) cells start erythropoietin receptor expression and are sensitive toerythropoietin. Subsequent stage, the colony-forming unit-erythroid (CFU-E), expresses maximal erythropoietinreceptor density and is completely dependent on erythropoietin for further differentiation. Precursors of red cells, theproerythroblasts and basophilic erythroblasts also express erythropoietin receptor and are therefore affected by it.
Nonhematopoietic rolesErythropoietin has a range of actions including vasoconstriction-dependent hypertension, stimulating angiogenesis,and inducing proliferation of smooth muscle fibers. It can increase iron absorption by suppressing the hormonehepcidin.EPO levels of 100 times the baseline have been detected in brain tissue as a natural response to hypoxic damage. Inrats, pretreatment with erythropietin was associated with neuronal protection during induced cerebral hypoxia. Trialsin humans have not been reported.Multiple studies have suggested that EPO improves memory. This effect is independent of its effect on hematocrit.Rather, it is associated with an increase in hippocampal response and effects on synaptic connectivity, neuronalplasticity, and memory-related neural networks. EPO may have effects on mood.
Mechanism of actionErythropoietin has been shown to exert its effects by binding to the erythropoietin receptor (EpoR).EPO is highly glycosylated (40% of total molecular weight), with half-life in blood around five hours. EPO'shalf-life may vary between endogenous and various recombinant versions. Additional glycosylation or otheralterations of EPO via recombinant technology have led to the increase of EPO's stability in blood (thus requiringless frequent injections). EPO binds to the erythropoietin receptor on the red cell progenitor surface and activates aJAK2 signaling cascade. Erythropoietin receptor expression is found in a number of tissues, such as bone marrowand peripheral/central nervous tissue. In the bloodstream, red cells themselves do not express erythropoietin receptor,so cannot respond to EPO. However, indirect dependence of red cell longevity in the blood on plasma erythropoietinlevels has been reported, a process termed neocytolysis.
Synthesis and regulationErythropoietin levels in blood are quite low in the absence of anemia, at around 10 mU/ml. However, in hypoxicstress, EPO production may increase 1000-fold, reaching 10,000 mU/ml of blood. EPO is produced mainly byperitubular capillary lining cells of the renal cortex, which are highly specialized, epithelial-like cells. It issynthesized by renal peritubular cells in adults, with a small amount being produced in the liver. Regulation isbelieved to rely on a feedback mechanism measuring blood oxygenation. Constitutively synthesized transcriptionfactors for EPO, known as hypoxia-inducible factors, are hydroxylated and proteosomally digested in the presence ofoxygen.

Erythropoietin 68
Medical usesErythropoietins available for use as therapeutic agents are produced by recombinant DNA technology in cell culture,and include Epogen/Procrit (epoetin alfa) and Aranesp (darbepoetin alfa); they are used in treating anemia resultingfrom chronic kidney disease, inflammatory bowel disease (Crohn's disease and ulcer colitis) and myelodysplasiafrom the treatment of cancer (chemotherapy and radiation). The package inserts include boxed warnings of increasedrisk of death, myocardial infarction, stroke, venous thromboembolism, and tumor recurrence, particularly when usedto increase the hemoglobin levels to more than 11 to 12 g/dl.
Available formsRecombinant erythropoietin has a variety of glycosylation patterns giving rise to alfa, beta, delta, and omega forms:
• epoetin alfa:
• Darbepoetin (Aranesp)•• Epocept (Lupin pharma)•• Nanokine (Nanogen Pharmaceutical biotechnology, Vietnam•• Epofit (Intas pharma)• Epogen, made by Amgen•• Epogin• Eprex, made by Janssen-Cilag• Binocrit, made by Sandoz•• Procrit
• epoetin beta:
• NeoRecormon, made by Hoffmann–La Roche•• Recormon• Methoxy polyethylene glycol-epoetin beta (Mircera) by Roche
• epoetin delta:
• Dynepo trademark name for an erythropoiesis stimulatingprotein, by Shire plc
• epoetin omega:
•• Epomax
• epoetin zeta (biosimilar forms for epoetin alpha):
•• Silapo (Stada)•• Retacrit (Hospira)
•• Miscellaneous:
• Epocept, made by Lupin Pharmaceuticals•• EPOTrust, made by Panacea Biotec Ltd•• Erypro Safe, made by Biocon Ltd.• Repoitin, made by Serum Institute of India Limited• Vintor, made by Emcure Pharmaceuticals•• Epofit, made by Intas pharma•• Erykine, made by Intas Biopharmaceutica•• Wepox, made by Wockhardt Biotech•• Espogen, made by LG life sciences.•• ReliPoietin, made by Reliance Life Sciences•• Shanpoietin, made by Shantha Biotechnics Ltd•• Zyrop, made by Cadila Healthcare Ltd.•• EPIAO (rHuEPO), made by Shenyang Sunshine Pharmaceutical
Co.. LTD. China•• Cinnapoietin, made by CinnaGen biopharmaceutical Iran.
Darbepoetin alfa, which early literature during its development often termed as novel erythropoiesis-stimulatingprotein (NESP), is a form created by five substitutions (Asn-57, Thr-59, Val-114, Asn-115 and Thr-117) that createtwo new N-glycosylation sites. This glycoprotein has a longer terminal half-life, meaning it may be possible toadminister it less frequently.
Blood dopingErythropoiesis-stimulating agents (ESAs) have a history of use as blood doping agents in endurance sports, such as horseracing, boxing, cycling, rowing, distance running, race walking, snowshoeing, cross country skiing, biathlon, and triathlon. The overall oxygen delivery system (blood oxygen levels, as well as heart stroke volume, vascularization, and lung function) is one of the major limiting factors to muscles' ability to perform endurance exercise. Therefore, the primary reason athletes may use ESAs is to improve oxygen delivery to muscles, which directly improves their endurance capacity. With the advent of recombinant erythropoietin in the 1990s, the practice of autologous and homologous blood transfusion has been partially replaced by injecting erythropoietin such that the body naturally produces its own red cells. ESAs increase hematocrit (% of blood volume that is red cell mass) and total red cell mass in the body, providing a good advantage in sports where such practice is banned. In addition to ethical considerations in sports, providing an increased red cell mass beyond the natural levels reduces blood flow due to increased viscosity, and increases the likelihood of thrombosis and stroke. Due to dangers associated with using ESAs, their use should be limited to the clinic where anemic patients are boosted back to normal hemoglobin

Erythropoietin 69
levels (as opposed to going above the normal levels for performance advantage, leading to an increased risk ofdeath).Though EPO was believed to be widely used in the 1990s in certain sports, there was no way at the time to directlytest for it, until in 2000, when a test developed by scientists at the French national antidoping laboratory (LNDD) andendorsed by the World Anti-Doping Agency (WADA) was introduced to detect pharmaceutical EPO bydistinguishing it from the nearly identical natural hormone normally present in an athlete's urine. The firstEPO-doping cases were found by the Swiss Laboratory for Doping Analyses.[68]
In 2002, at the Winter Olympic Games in Salt Lake City, Dr. Don Catlin, the founder and then-director of the UCLAOlympic Analytical Lab, reported finding darbepoetin alfa, a form of erythropoietin, in a test sample for the firsttime in sports. At the 2012 Summer Olympics in London, Alex Schwazer, the gold medalist in the 50-kilometer racewalk in the 2008 Summer Olympics in Beijing, tested positive for EPO and was disqualified.[69]
Since 2002, EPO tests performed by US sports authorities have consisted of only a urine or "direct" test. From2000–2006, EPO tests at the Olympics were conducted on both blood and urine. However, several compounds havebeen identified that can be taken orally to stimulate endogenous EPO production. Most of the compounds stabilizethe hypoxia-inducible transcription factors which activate the EPO gene. The compounds include oxo-glutaratecompetitors, but also simple ions such as cobalt(II) chloride.[70]
Inhalation of a xenon/oxygen mixture activates production of the transcription factor HIF-1-alpha, which leads toincreased production of erythropoietin and improved performance. It has been used for this purpose in Russia sinceat least 2004.
CyclingSynthetic EPO is believed to have come into use in cycling about 1990. In theory, EPO use can increase VO2max bya significant amount, making it useful for endurance sports like cycling. Italian antidoping advocate Sandro Donatihas claimed that the history of doping in cycling can be traced to the Italian Dr Francesco Conconi at the Universityof Ferrara. Conconi had worked on the idea of giving athletes tranfusions of their own blood in the 1980s. Donati feltthis work "opened the road to EPO . . . because blood doping was a trial to understand the role of EPO".Dr Michele Ferrari, a former student and mentee of Conconi, had a controversial interview mentioning the drug in1994, just after his Gewiss-Ballan team had a remarkable performance in the La Flèche Wallonne race. Ferrari toldl'Equipe journalist Jean-Michel Rouet that EPO had no "fundamental" effect on performance and that if his ridersused it, it wouldn't "scandalize" himself. After the journalist pointed out several riders were suspected of dying fromEPO, Ferrari said EPO was not dangerous, and only abuse of it was dangerous, saying, "It's also dangerous to drink10 liters of orange juice." The 'orange juice' comment has been widely misquoted.[71] Ferrari was fired shortly after,but continued to work in the industry with top riders that allegedly included Lance Armstrong.[72] That same year,Sandro Donati, working for the Italian National Olympic Committee, presented a report accusing Conconi of beinglinked to the use of EPO in the sport.In 1997, the Union Cycliste Internationale (UCI) instituted a new rule that riders testing above 50% haematocritwere not allowed to race. Robert Millar, former racer, later wrote for Cycling News that the 50% limit was "an openinvitation to dope to that level", pointing out that normally haematocrit levels would start "around 40-42%" and dropduring the course of a "grand tour", but after EPO, they were staying at 50% for "weeks at a time". By 1998, EPOuse had become widespread, and the Festina affair tarnished the 1998 Tour de France. One manager offered a270,000-franc-per-month raise to Christophe Bassons if he would use EPO, but Bassons refused.In the 1998 Tour de France Stuart O'Grady won one stage, held the Tour de France yellow jersey for three days, and came second in the points classification with the assistance of EPO. In 2010, Floyd Landis admitted to using performance-enhancing drugs, including EPO, throughout his career as a professional cyclist. In 2012, the USADA released a report on its investigation into the US Postal Service cycling team and blood doping. The report contained affidavits from numerous riders on the team, including Frankie Andreu, Tyler Hamilton, George Hincapie, Floyd

Erythropoietin 70
Landis, Levi Leipheimer, and others, outlining that they, and Lance Armstrong, used a cocktail ofperformance-enhancing substances for the Tour de France, most notably EPO, during the 1999 tour. Armstrong waslater stripped of his seven tour wins by USADA, and the UCI concurred with the decision, even though several of hiswins occurred outside of the 8 year statute of limitations. Tour organizers have removed Armstrong's name andresults from the race's history. These severe penalties are a direct result of the findings outlined in USADAs"Reasoned Decision" which goes beyond Armstrong's personal cheating to outline how he and team manager, JohanBruyneel, forced other cyclists to dope as well. The document goes to the root of their doping network, also targetingthe shadowy, doctors and back room enablers who helped cyclists procure and administer drugs and highly placedexecutives who helped to avoid doping controls and hide positive test results.[73]
Witnesses testified that code words used for EPO included "Edgar", "Poe", "Edgar Allen Poe", and "Zumo" (Spanishfor 'juice').
HistoryIn 1905, Paul Carnot, a professor of medicine in Paris, and his assistant, Clotilde Deflandre, proposed the idea thathormones regulate the production of red blood cells. After conducting experiments on rabbits subject to bloodletting,Carnot and Deflandre attributed an increase in red blood cells in rabbit subjects to a hemotropic factor calledhemopoietin. Eva Bonsdorff and Eeva Jalavisto continued to study red cell production and later called thehemopoietic substance 'erythropoietin'. Further studies investigating the existence of EPO by K.R. Reissman(unknown location) and Allan J. Erslev (Thomas Jefferson Medical College) demonstrated that a certain substance,circulated in the blood, is able to stimulate red blood cell production and increase hematocrit. This substance wasfinally purified and confirmed as erythropoietin, opening doors to therapeutic uses for EPO in diseases such asanemia.Haematologist John Adamson and nephrologist Joseph W. Eschbach looked at various forms of renal failure and therole of the natural hormone EPO in the formation of red blood cells. Studying sheep and other animals in the 1970s,the two scientists helped establish that EPO stimulates the production of red cells in bone marrow and could lead to atreatment for anemia in humans. In 1968, Goldwasser and Kung began work to purify human EPO, and managed topurify milligram quantities of over 95% pure material by 1977. Pure EPO allowed the amino acid sequence to bepartially identified and the gene to be isolated. Later, an NIH-funded researcher at Columbia University discovered away to synthesize EPO. Columbia University patented the technique, and licensed it to Amgen. Controversy hasensued over the fairness of the rewards that Amgen reaped from NIH-funded work, and Goldwasser was neverfinancially rewarded for his work.In the 1980s, Adamson, Joseph W. Eschbach, Joan C. Egrie, Michael R. Downing and Jeffrey K. Browne conducteda clinical trial at the Northwest Kidney Centers for a synthetic form of the hormone, Epogen, produced by Amgen.The trial was successful, and the results were published in the New England Journal of Medicine in January 1987.In 1985, Lin et al isolated the human erythropoietin gene from a genomic phage library and were able to characterizeit for research and production. Their research demonstrated the gene for erythropoietin encoded the production ofEPO in mammalian cells that is biologically active in vitro and in vivo. The industrial production of recombinanthuman erythropoietin (RhEpo) for treating anemia patients would begin soon after.In 1989, the US Food and Drug Administration approved the hormone Epogen, which remains in use today.

Erythropoietin 71
References[1] http:/ / www. ebi. ac. uk/ pdbe/ searchResults. html?display=both&
term=P01588%20or%20P33707%20or%20P48617%20or%20P07321%20or%20Q0VED9%20or%20P29676%20or%20B1N8Y1[2] http:/ / www. rcsb. org/ pdb/ search/ smartSubquery. do?smartSearchSubtype=UpAccessionIdQuery&
accessionIdList=P01588,P33707,P48617,P07321,Q0VED9,P29676,B1N8Y1[3] http:/ / www. rcsb. org/ pdb/ cgi/ explore. cgi?pdbId=1BUY[4] http:/ / www. rcsb. org/ pdb/ cgi/ explore. cgi?pdbId=1CN4[5] http:/ / www. rcsb. org/ pdb/ cgi/ explore. cgi?pdbId=1EER[6] http:/ / www. genenames. org/ cgi-bin/ gene_symbol_report?hgnc_id=3415[7] http:/ / omim. org/ entry/ 133170[8] http:/ / www. informatics. jax. org/ marker/ MGI:95407[9] http:/ / www. ncbi. nlm. nih. gov/ entrez/ query. fcgi?cmd=Retrieve& db=homologene& dopt=HomoloGene& list_uids=624[10] https:/ / www. ebi. ac. uk/ chembldb/ index. php/ target/ inspect/ CHEMBL5837[11] http:/ / www. genecards. org/ cgi-bin/ carddisp. pl?id_type=entrezgene& id=2056[12] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0005128[13] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0005179[14] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0005515[15] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0030295[16] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0005576[17] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0005615[18] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0009986[19] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0006915[20] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0007165[21] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0007566[22] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0007568[23] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0008015[24] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0008284[25] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0009651[26] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0010523[27] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0018105[28] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0032496[29] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0033189[30] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0033574[31] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0042523[32] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0042541[33] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0043249[34] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0043627[35] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0045666[36] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0045740[37] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0045860[38] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0045893[39] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0046579[40] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0048678[41] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0051602[42] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0055093[43] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0061418[44] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0070555[45] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0071456[46] http:/ / amigo. geneontology. org/ amigo/ term/ GO:0071474[47] http:/ / amigo. geneontology. org/ amigo/ term/ GO:1902219[48] http:/ / amigo. geneontology. org/ amigo/ term/ GO:1902251[49] http:/ / amigo. geneontology. org/ amigo/ term/ GO:2001258[50] http:/ / amigo. geneontology. org/ cgi-bin/ amigo/ gp-assoc. cgi?gp=UniProtKB:P01588[51] http:/ / www. ebi. ac. uk/ QuickGO/ GProtein?ac=P01588[52] http:/ / biogps. org/ gene/ 2056/[53] http:/ / www. ncbi. nlm. nih. gov/ entrez/ query. fcgi?db=gene& cmd=retrieve& dopt=default& list_uids=2056& rn=1[54] http:/ / www. ncbi. nlm. nih. gov/ entrez/ query. fcgi?db=gene& cmd=retrieve& dopt=default& list_uids=13856& rn=1[55] http:/ / www. ensembl. org/ Homo_sapiens/ geneview?gene=ENSG00000130427;db=core

Erythropoietin 72
[56] http:/ / www. ensembl. org/ Mus_musculus/ geneview?gene=ENSMUSG00000029711;db=core[57] http:/ / www. uniprot. org/ uniprot/ P01588[58] http:/ / www. uniprot. org/ uniprot/ P07321[59] http:/ / www. ncbi. nlm. nih. gov/ entrez/ viewer. fcgi?val=NM_000799[60] http:/ / www. ncbi. nlm. nih. gov/ entrez/ viewer. fcgi?val=NM_007942[61] http:/ / www. ncbi. nlm. nih. gov/ entrez/ viewer. fcgi?val=NP_000790[62] http:/ / www. ncbi. nlm. nih. gov/ entrez/ viewer. fcgi?val=NP_031968[63] http:/ / genome. ucsc. edu/ cgi-bin/ hgTracks?org=Human& db=hg19& position=chr7:100318423-100321323[64] http:/ / genome. ucsc. edu/ cgi-bin/ hgTracks?org=Mouse& db=mm10& position=chr5:137483020-137533242[65] http:/ / www. ncbi. nlm. nih. gov/ sites/ entrez?db=gene& cmd=Link& LinkName=gene_pubmed& from_uid=2056[66] http:/ / www. ncbi. nlm. nih. gov/ sites/ entrez?db=gene& cmd=Link& LinkName=gene_pubmed& from_uid=13856[67] http:/ / en. wikipedia. org/ w/ index. php?title=Template:PBB/ 2056& action=edit[68] History of the Swiss Laboratory for Doping Analyses (http:/ / www. doping. chuv. ch/ en/ lad_home/ lad-qui-sommes-nous/
lad-qui-sommes-nous-historique. htm), www.doping.chuv.ch (page visited on 11 June 2014).[69] "Ousted Olympic race walk champion says he bought EPO in Turkey, hid it in refrigerator at home" (http:/ / www. washingtonpost. com/
sports/ olympics/ 2008-olympic-race-walk-champ-i-bought-epo-in-turkey-hid-doping-from-kostner-im-destroyed/ 2012/ 08/ 29/5c7b3c7a-e14d-11e1-89f7-76e23a982d06_story. html) Associated Press story in the Washington Post (August 8, 2012)
[70] W. Jelkmann: The disparate roles of cobalt in erythropoiesis, and doping relevance. Open Journal of Hematology, 2012, 3-6. http:/ /rossscience. org/ ojhmt/ 2075-907X-3-6. php
[71] 10 liters of orange juice: see the article on Water intoxication, for example.[72][72] Juliet Macur: Cycle of Lies: The Fall of Lance Armstrong[73][73] "A lifetime ban: Does the time fit the crime?" Velo News, 12/16/13
Further reading• Takeuchi M, Kobata A (1992). "Structures and functional roles of the sugar chains of human erythropoietins".
Glycobiology 1 (4): 337–46. doi: 10.1093/glycob/1.4.337 (http:/ / dx. doi. org/ 10. 1093/ glycob/ 1. 4. 337).PMID 1820196 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 1820196).
• Semba RD, Juul SE (2002). "Erythropoietin in human milk: physiology and role in infant health". Journal ofhuman lactation : official journal of International Lactation Consultant Association 18 (3): 252–61. PMID 12192960 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 12192960).
• Ratcliffe PJ (2003). "From erythropoietin to oxygen: hypoxia-inducible factor hydroxylases and the hypoxiasignal pathway". Blood Purif. 20 (5): 445–50. doi: 10.1159/000065201 (http:/ / dx. doi. org/ 10. 1159/000065201). PMID 12207089 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 12207089).
• Westenfelder C (2002). "Unexpected renal actions of erythropoietin". Exp. Nephrol. 10 (5–6): 294–8. doi:10.1159/000065304 (http:/ / dx. doi. org/ 10. 1159/ 000065304). PMID 12381912 (http:/ / www. ncbi. nlm. nih.gov/ pubmed/ 12381912).
• Becerra SP, Amaral J (2002). "Erythropoietin--an endogenous retinal survival factor". N. Engl. J. Med. 347 (24):1968–70. doi: 10.1056/NEJMcibr022629 (http:/ / dx. doi. org/ 10. 1056/ NEJMcibr022629). PMID 12477950(http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 12477950).
• Genc S, Koroglu TF, Genc K (2004). "Erythropoietin and the nervous system". Brain Res. 1000 (1–2): 19–31.doi: 10.1016/j.brainres.2003.12.037 (http:/ / dx. doi. org/ 10. 1016/ j. brainres. 2003. 12. 037). PMID 15053948(http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 15053948).
• Fandrey J (2004). "Oxygen-dependent and tissue-specific regulation of erythropoietin gene expression". Am. J.Physiol. Regul. Integr. Comp. Physiol. 286 (6): R977–88. doi: 10.1152/ajpregu.00577.2003 (http:/ / dx. doi. org/10. 1152/ ajpregu. 00577. 2003). PMID 15142852 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 15142852).
• Juul S (2004). "Recombinant erythropoietin as a neuroprotective treatment: in vitro and in vivo models". Clinicsin perinatology 31 (1): 129–42. doi: 10.1016/j.clp.2004.03.004 (http:/ / dx. doi. org/ 10. 1016/ j. clp. 2004. 03.004). PMID 15183662 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 15183662).
• Buemi M, Caccamo C, Nostro L, Cavallaro E, Floccari F, Grasso G (2005). "Brain and cancer: the protective roleof erythropoietin". Med Res Rev 25 (2): 245–59. doi: 10.1002/med.20012 (http:/ / dx. doi. org/ 10. 1002/ med.20012). PMID 15389732 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 15389732).

Erythropoietin 73
• Sytkowski AJ (2007). "Does erythropoietin have a dark side? Epo signaling and cancer cells". Sci. STKE 2007(395): e38. doi: 10.1126/stke.3952007pe38 (http:/ / dx. doi. org/ 10. 1126/ stke. 3952007pe38). PMID 17636183(http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 17636183).
•• Goldwasser, Eugene. A Bloody Long Journey: Erythropoietin and the Person Who Isolated It. Xlibris, 2011.ISBN 978-1-4568-5737-0
External links• NYT - 1987 announcement of Epogen's clinical success (http:/ / query. nytimes. com/ gst/ fullpage.
html?res=9B0DE2D81138F93BA35752C0A961948260& sec=& spon=& partner=permalink&exprod=permalink)
Erythropoiesis
Haematopoiesis
Erythropoiesis (from Greek 'erythro'meaning "red" and 'poiesis' meaning"to make") is the process whichproduces red blood cells(erythrocytes). It is stimulated bydecreased O2 in circulation, which isdetected by the kidneys, which thensecrete the hormone erythropoietin.[1]
This hormone stimulates proliferationand differentiation of red cellprecursors, which activates increasederythropoiesis in the hemopoietictissues, ultimately producing red bloodcells. In postnatal birds and mammals(including humans), this usually occurswithin the red bone marrow. In theearly fetus, erythropoiesis takes placein the mesodermal cells of the yolk sac. By the third or fourth month, erythropoiesis moves to the liver. After sevenmonths, erythropoiesis occurs in the bone marrow. Increased level of physical activity can cause an increase inerythropoiesis. However, in humans with certain diseases and in some animals, erythropoiesis also occurs outside thebone marrow, within the spleen or liver. This is termed extramedullary erythropoiesis.
The bone marrow of essentially all the bones produces red blood cells until a person is around five years old. Thetibia and femur cease to be important sites of hematopoiesis by about age 25; the vertebrae, sternum, pelvis and ribs,and cranial bones continue to produce red blood cells throughout life.

Erythropoiesis 74
Erythrocyte differentiationIn the process of red blood cell maturation, a cell undergoes a series of differentiations. The following stages ofdevelopment all occur within the bone marrow:1. A Hemocytoblast, a multipotent hematopoietic stem cell, becomes2. a common myeloid progenitor or a multipotent stem cell, and then3.3. a unipotent stem cell, then4. a pronormoblast, also commonly called an proerythroblast or a rubriblast.5.5. This becomes a basophilic or early normoblast, also commonly called an erythroblast, then6.6. a polychromatophilic or intermediate normoblast, then7.7. an orthochromatic or late normoblast. At this stage the nucleus is expelled before the cell becomes8. a reticulocyte.The cell is released from the bone marrow after Stage 7, and so in newly circulating red blood cells there are about1% reticulocytes. After one to two days, these ultimately become "erythrocytes" or mature red blood cells.These stages correspond to specific appearances of the cell when stained with Wright's stain and examined by lightmicroscopy, and correspond to other biochemical changes.In the process of maturation, a basophilic pronormoblast is converted from a cell with a large nucleus and a volumeof 900 fL to an enucleated disc with a volume of 95 fL. By the reticulocyte stage, the cell has extruded its nucleus,but is still capable of producing hemoglobin.Essential for the maturation of red blood cells are Vitamin B12 (cobalamin) and Vitamin B9 (Folic acid). Lack ofeither causes maturation failure in the process of erythropoiesis, which manifests clinically as reticulocytopenia, anabnormally low amount of reticulocytes.
Characteristics seen in erythrocytes during erythropoiesisAs they mature, a number of erythrocyte characteristics change: The size of the cell is reduced and the cytoplasmicmatrix increases in amount, and the staining reaction of the cytoplasm changes from blue to pinkish red because ofthe decrease in the amount of RNA and DNA. Initially, the nucleus is large in size and contains open chromatin. Butas red blood cells mature the size of the nucleus decreases and finally disappears with the condensation of thechromatin material.[2]
Regulation of erythropoiesisA feedback loop involving erythropoietin helps regulate the process of erythropoiesis so that, in non-disease states,the production of red blood cells is equal to the destruction of red blood cells and the red blood cell number issufficient to sustain adequate tissue oxygen levels but not so high as to cause sludging, thrombosis, or stroke.Erythropoietin is produced in the kidney and liver in response to low oxygen levels. In addition, erythropoietin isbound by circulating red blood cells; low circulating numbers lead to a relatively high level of unbounderythropoietin, which stimulates production in the bone marrow.Recent studies have also shown that the peptide hormone hepcidin may play a role in the regulation of hemoglobinproduction, and thus affect erythropoiesis. The liver produces hepcidin. Hepcidin controls iron absorption in thegastrointestinal tract and iron release from reticuloendothelial tissue. Iron must be released from macrophages in thebone marrow to be incorporated into the heme group of hemoglobin in erythrocytes. There are colony forming unitsthat the cells follow during their formation. These cells are referred to as the committed cells including thegranulocyte monocyte colony forming unitsLoss of function of the erythropoietin receptor or JAK2 in mice cells causes failure in erythropoiesis, so productionof red blood cells in embryos and growth is disrupted. If there is no feedback inhibition, such as suppressors of

Erythropoiesis 75
cytokine signaling proteins in the system, that would cause giantism in mice.
References[1] Sherwood, L, Klansman, H, Yancey, P: Animal Physiology, Brooks/Cole, Cengage Learning, 2005.[2][2] Textbook of Physiology by Dr. A. K. Jain reprint 2006-2007 3rd edition.
External links• Microscopic Hematology (http:/ / www. healthsystem. virginia. edu/ internet/ hematology/ HessIDB/ home.
cfm)Wikipedia:Link rot• More information on erythropoiesis (http:/ / www. ndsu. nodak. edu/ instruct/ tcolvill/ 435/ erythrocytes.
htm)Wikipedia:Link rot

Gallstone 76
GallstoneContributors [1]
GallstoneClassification and external resources
Numerous small gallstones made up largely of cholesterol.
ICD-10 K80 [2]
ICD-9 574 [3]
OMIM 600803 [4]
DiseasesDB 2533 [5]
MedlinePlus 000273 [6]
eMedicine emerg/97 [7]
MeSH D042882 [8]
A gallstone (also called cholelithiasis) is a crystalline concretion formed within the gallbladder by accretion of bilecomponents. These calculi are formed in the gallbladder but may distally pass into other parts of the biliary tractsuch as the cystic duct, common bile duct, pancreatic duct or the ampulla of Vater. Rarely, in cases of severeinflammation, gallstones may erode through the gallbladder into adherent bowel potentially causing an obstructiontermed gallstone ileus.Presence of gallstones in the gallbladder may lead to acute cholecystitis,[9] an inflammatory condition characterizedby retention of bile in the gallbladder and often secondary infection by intestinal microorganisms, predominantlyEscherichia coli, Klebsiella, Enterobacter and Bacteroides species.[10] Presence of gallstones in other parts of thebiliary tract can cause obstruction of the bile ducts, which can lead to serious conditions such as ascendingcholangitis or pancreatitis. Either of these two conditions can be life-threatening and are therefore considered to bemedical emergencies.

Gallstone 77
DefinitionsPresence of stones in the gallbladder is referred to as cholelithiasis, from the Greek chol- (bile) + lith- (stone) +iasis- (process). If gallstones migrate into the ducts of the biliary tract, the condition is referred to ascholedocholithiasis, from the Greek chol- (bile) + docho- (duct) + lith- (stone) + iasis- (process).Choledocholithiasis is frequently associated with obstruction of the biliary tree, which in turn can lead to acuteascending cholangitis, from the Greek: chol- (bile) + ang- (vessel) + itis- (inflammation), a serious infection of thebile ducts. Gallstones within the ampulla of Vater can obstruct the exocrine system of the pancreas, which in turn canresult in pancreatitis.
Characteristics and composition
Images of a CT of gallstones
Gallstones can vary in size and shape from as small as a grain of sandto as large as a golf ball.[11] The gallbladder may contain a single largestone or many smaller ones. Pseudoliths, sometimes referred to assludge, are thick secretions that may be present within the gallbladder,either alone or in conjunction with fully formed gallstones. The clinicalpresentation is similar to that of cholelithiasis.Wikipedia:Citationneeded The composition of gallstones is affected by age, diet andethnicity. On the basis of their composition, gallstones can be dividedinto the following types:
Cholesterol stonesCholesterol stones vary from light yellow to dark green or brown and are oval, between 2 and 3 cm long, each oftenhaving a tiny, dark, central spot. To be classified as such, they must be at least 80% cholesterol by weight (or 70%,according to the Japanese- classification system).
Pigment stones

Gallstone 78
Large gallstone
Pigment stones are small and dark and comprise bilirubin and calciumsalts that are found in bile. They contain less than 20% of cholesterol(or 30%, according to the Japanese-classification system).
Mixed stones
Mixed gallstones typically contain 20–80% cholesterol (or 30–70%, according to the Japanese- classificationsystem). Other common constituents are calcium carbonate, palmitate phosphate, bilirubin and other bile pigments.Because of their calcium content, they are often radiographically visible.
Gallbladder opened to show numerous small cholesterol gallstones µCT of agallstone.
Imageacquisitiondone using"CT Alpha"by "Procon
X-RayGmbH",Garbsen,Germany.
Visualizationdone with
"VG StudioMax 2.0" by
"VolumeGraphics",Heidelberg,Germany

Gallstone 79
Cholelithiasis
SymptomsGallstones may be asymptomatic, even for years. These gallstones are called "silent stones" and do not requiretreatment. The size and number of gallstones present does not appear to influence whether or not patients aresymptomatic or asymptomatic. A characteristic symptom of gallstones is a "gallstone attack", in which a person mayexperience intense pain in the upper-right side of the abdomen, often accompanied by nausea and vomiting, thatsteadily increases for approximately 30 minutes to several hours. A patient may also experience referred painbetween the shoulder blades or below the right shoulder. These symptoms may resemble those of a "kidney stoneattack". Often, attacks occur after a particularly fatty meal and almost always happen at night, and after drink.A positive Murphy's sign is a common finding on physical examination.
CausesGallstone risk increases for females (especially before menopause) and for people near or above 40 years; thecondition is more prevalent among both North and South Americans and among those of European descent thanamong other ethnicities. A lack of melatonin could significantly contribute to gallbladder stones, as melatonininhibits cholesterol secretion from the gallbladder, enhances the conversion of cholesterol to bile, and is anantioxidant, which is able to reduce oxidative stress to the gallbladder. Researchers believe that gallstones may becaused by a combination of factors, including inherited body chemistry, body weight, gallbladder motility(movement), and low calorie diet.[12] The absence of such risk factors does not, however, preclude the formation ofgallstones.No clear relationship has been proved between diet and gallstone formation; however, low-fiber and high-cholesteroldiets have been suggested as contributing to gallstone formation.Wikipedia:Citation needed Other nutritional factorsthat may increase risk of gallstones include rapid weight loss; constipation; eating fewer meals per day; and lowintake of the nutrients folate, magnesium, calcium, and vitamin C. On the other hand, wine and whole-grained breadmay decrease the risk of gallstones. Pigment gallstones are most commonly seen in the developing world. Riskfactors for pigment stones include hemolytic anemias (such as sickle-cell disease and hereditary spherocytosis),cirrhosis, and biliary tract infections. People with erythropoietic protoporphyria (EPP) are at increased risk todevelop gallstones. Additionally, prolonged use of proton pump inhibitors has been shown to decrease gallbladderfunction, potentially leading to gallstone formation.
PathophysiologyCholesterol gallstones develop when bile contains too much cholesterol and not enough bile salts. Besides a highconcentration of cholesterol, two other factors are important in causing gallstones. The first is how often and howwell the gallbladder contracts; incomplete and infrequent emptying of the gallbladder may cause the bile to becomeoverconcentrated and contribute to gallstone formation. This can be caused by high resistance to the flow of bile outof the gallbladder due to the complicated internal geometry of the cystic duct.[13] The second factor is the presenceof proteins in the liver and bile that either promote or inhibit cholesterol crystallization into gallstones. In addition,increased levels of the hormone estrogen, as a result of pregnancy or hormone therapy, or the use of combined(estrogen-containing) forms of hormonal contraception, may increase cholesterol levels in bile and also decreasegallbladder movement, resulting in gallstone formation.

Gallstone 80
Diagnosis
A 1.9 cm gallstone impacted in the neck of thegallbladder and leading to cholecystitis as seen on
ultrasound. Note the 4 mm gall bladder wallthickening.
Gallstones as seen on plain Xray.
Diagnosis can be made using ultrasound
Treatment
MedicalCholesterol gallstones can sometimes be dissolved by oralursodeoxycholic acid, but it may be necessary for the patient to takethis medication for up to two years. Gallstones may recur, however,once the drug is stopped. Obstruction of the common bile duct withgallstones can sometimes be relieved by endoscopic retrogradesphincterotomy (ERS) following endoscopic retrogradecholangiopancreatography (ERCP). Gallstones can be broken up usinga procedure called extracorporeal shock wave lithotripsy (often simplycalled "lithotripsy"), which is a method of concentrating ultrasonicshock waves onto the stones to break them into tiny pieces. They arethen passed safely in the feces. However, this form of treatment issuitable only when there is a small number of gallstones.
SurgicalCholecystectomy (gallbladder removal) has a 99% chance ofeliminating the recurrence of cholelithiasis. Surgery is only indicatedin symptomatic patients. The lack of a gallbladder may have nonegative consequences in many people. However, there is a portion ofthe population — between 10 and 15% — who develop a conditioncalled postcholecystectomy syndrome which may causegastrointestinal distress and persistent pain in the upper-right abdomen,as well as a 10% risk of developing chronic diarrhea.
There are two surgical options for cholecystectomy:• Open cholecystectomy is performed via an abdomenal incision (laparotomy) below the lower right ribs. Recovery
typically requires 3–5 days of hospitalization, with a return to normal diet a week after release and to normalactivity several weeks after release.
• Laparoscopic cholecystectomy, introduced in the 1980s, is performed via three to four small puncture holes for acamera and instruments. Post-operative care typically includes a same-day release or a one night hospital stay,followed by a few days of home rest and pain medication. Laparoscopic cholecystectomy patients can, in general,resume normal diet and light activity a week after release, with some decreased energy level and minor residualpain continuing for a month or two. Studies have shown that this procedure is as effective as the more invasiveopen cholecystectomy, provided the stones are accurately located by cholangiogram prior to the procedure so thatthey can all be removed.Wikipedia:Citation needed

Gallstone 81
Choledocholithiasis
Choledocholithiasis is the presence of gallstones in the common bile duct. This condition causes jaundice and livercell damage, and requires treatment by cholecystectomy and/or ERCP.
Signs and symptomsMurphy's sign is commonly negative on physical examination in choledocholithiasis, helping to distinguish it fromcholecystitis. Jaundice of the skin or eyes is an important physical finding in biliary obstruction. Jaundice and/orclay-colored stool may raise suspicion of choledocholithiasis or even gallstone pancreatitis. If the above symptomscoincide with fever and chills, the diagnosis of ascending cholangitis may also be considered.Greater than 70% of people with gallstones are asymptomatic and are found incidentally on ultrasound. Studies haveshown that 10% of those people will develop symptoms within five years of diagnosis and 20% within 20 years.

Gallstone 82
CausesWhile stones can frequently pass through the common bile duct (CBD) into the duodenum, some stones may be toolarge to pass through the CBD and may cause an obstruction. One risk factor for this is duodenal diverticulum.
PathophysiologyThis obstruction may lead to jaundice, elevation in alkaline phosphatase, increase in conjugated bilirubin in theblood and increase in cholesterol in the blood. It can also cause acute pancreatitis and ascending cholangitis.
Diagnosis
Choledocholithiasis (stones in common bile duct) is one of the complications of cholelithiasis (gallstones), so theinitial step is to confirm the diagnosis of cholelithiasis. Patients with cholelithiasis typically present with pain in theright-upper quadrant of the abdomen with the associated symptoms of nausea and vomiting, especially after a fattymeal. The physician can confirm the diagnosis of cholelithiasis with an abdominal ultrasound that shows theultrasonic shadows of the stones in the gallbladder.The diagnosis of choledocholithiasis is suggested when the liver function blood test shows an elevation in bilirubinand serum transaminases. Other indicators include raised indicators of ampulla of vater (pancreatic duct obstruction)such as lipases and amylases. In prolonged cases the INR may change due to a decrease in vitamin K absorption. (Itis the decreased bile flow which reduces fat breakdown and therefore absorption of fat soluble vitamins). Thediagnosis is confirmed with either an MRCP (magnetic resonance cholangiopancreatography), an ERCP, or anintraoperative cholangiogram. If the patient must have the gallbladder removed for gallstones, the surgeon maychoose to proceed with the surgery, and obtain a cholangiogram during the surgery. If the cholangiogram shows astone in the bile duct, the surgeon may attempt to treat the problem by flushing the stone into the intestine or retrievethe stone back through the cystic duct.On a different pathway, the physician may choose to proceed with ERCP before surgery. The benefit of ERCP is thatit can be utilized not just to diagnose, but also to treat the problem. During ERCP the endoscopist may surgically

Gallstone 83
widen the opening into the bile duct and remove the stone through that opening. ERCP, however, is an invasiveprocedure and has its own potential complications. Thus, if the suspicion is low, the physician may choose toconfirm the diagnosis with MRCP, a non-invasive imaging technique, before proceeding with ERCP or surgery.
Treatment
Fluoroscopic image taken during ERCP. Multiplegallstones are present in the gallbladder and
cystic duct. The common bile duct and pancreaticduct appear to be patent.
Treatment involves an operation called a choledocholithotomy, whichis the removal of the gallstone from the bile duct using ERCP, althoughsurgeons are now increasingly using laparoscopy withcholangiography. In this procedure, tiny incisions are made in theabdomen and then in the cystic duct that connects the gallbladder to thebile duct, and a thin tube is introduced to perform a cholangiography.If stones are identified, the surgeon inserts a tube with an inflatableballoon to widen the duct and the stones are usually removed usingeither a balloon or tiny basket.
If laparoscopy is unsuccessful, an open choledocholithotomy isperformed. This procedure may be used in the case of large stones,when the duct anatomy is complex, during or after some gallbladderoperations when stones are detected, or when ERCP or laparoscopicprocedures are not available.Typically, the gallbladder is then removed, an operation calledcholecystectomy, to prevent a future occurrence of common bile duct obstruction or other complications.[14]
Other animals
Gallstones are a valuable by-product of animals butchered for meat because their use as a purported antipyretic andantidote in the folk remedies of some cultures, in particular, in China. The finest gallstones tend to be sourced fromold dairy cows, which are called Niu-Huang (yellow thing of cattle) in Chinese. Much as in the manner of diamondmines, slaughterhouses carefully scrutinize workers for gallstone theft.
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Gallstone[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ K80[3] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=574[4] http:/ / omim. org/ entry/ 600803[5] http:/ / www. diseasesdatabase. com/ ddb2533. htm[6] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000273. htm[7] http:/ / www. emedicine. com/ emerg/ topic97. htm[8] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D042882[9][9] Available on: April 26, 2013.[10][10] Simultaneous bacteriologic assessment of bile from gallbladder and common bile duct in control subjects and patients with gallstones and
common duct stones, Csendes A, Burdiles P, Maluenda F, Diaz JC, Csendes P, Mitru N, Arch Surg. 1996;131(4):389.[11] Gallstones - Cholelithiasis; Gallbladder attack; Biliary colic; Gallstone attack; Bile calculus; Biliary calculus (http:/ / www. ncbi. nlm. nih.
gov/ pubmedhealth/ PMH0001318) Last reviewed: July 6, 2009. Reviewed by: George F. Longstreth. Also reviewed by David Zieve[12] http:/ / www. nhs. uk/ Livewell/ loseweight/ Pages/ should-you-lose-weight-fast. aspx[13] Experimental investigation of the flow of bile in patient specific cystic duct models M Al-Atabi, SB Chin… - Journal of biomechanical
engineering, 2010[14] Vivian McAlister, Eric Davenport, and Elizabeth Renouf. "Cholecystectomy Deferral in Patients with Endoscopic Sphincterotomy.
Cochrane Database of Systematic Reviews .4 (2007): CD006233. Available at: (http:/ / ir. lib. uwo. ca/ cgi/ viewcontent. cgi?article=1026&context=surgerypub)

Gallstone 84
• Beers, MH; Porter, RS; Jones, TV, eds. (2006). Merck Manual of Diagnosis and Therapy (18th ed.). WhitehouseStation, New Jersey: Merck Sharp & Dohme Corporation. ISBN 978-0-911910-18-6.
• National Library of Medicine (2010). "Gallstones" (http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/000273. htm). Bethesda, Maryland: United States National Library of Medicine, National Institutes of Health,United States Department of Health and Human Services. Retrieved 2010-11-06.
External links
Wikimedia Commons has media related to Gallstones.
• Public domain NIH/NIDDK e-pub on gallstones (http:/ / www. pueblo. gsa. gov/ cic_text/ health/ gallstones/gallstns. htm)
• MedlinePlus Encyclopedia Gallbladder removal (http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/100021_1. htm)
• 5-Minute Clinical Consult Cholelithiasis (http:/ / www. unboundmedicine. com/ 5minute/ ub/ view/5-Minute-Clinical-Consult/ 116129/ all/ Cholelithiasis)
• cholelithiasis US (http:/ / rad. usuhs. edu/ medpix/ cow_image. html?imageid=29001) Classic gallstone withshadow and cholecystitis
• Symptoms Of Gallstones (http:/ / www. gallbladdersymptoms. gallbladderpain. co) 57 Gallstone Indicators
Haematopoiesis
Diagram showing the development of different blood cells from haematopoietic stem cellto mature cells
Haematopoiesis (from Greek αἷμα,"blood" and ποιεῖν "to make"; alsohematopoiesis in American English;sometimes also haemopoiesis orhemopoiesis) is the formation of bloodcellular components. All cellular bloodcomponents are derived fromhaematopoietic stem cells. In a healthyadult person, approximately 1011–1012
new blood cells are produced daily inorder to maintain steady state levels inthe peripheral circulation.[1]
Haematopoietic stem cells(HSCs)
Haematopoietic stem cells (HSCs) reside in the medulla of the bone (bone marrow) and have the unique ability togive rise to all of the different mature blood cell types and tissues. HSCs are self-renewing cells: when theyproliferate, at least some of their daughter cells remain as HSCs, so the pool of stem cells does not becomedepleted.This phenomenon is called asymmetric division. The other daughters of HSCs (myeloid and lymphoidprogenitor cells), however can commit to any of the alternative differentiation pathways that lead to the production
of one or more specific types of blood cells, but cannot self-renew. The pool of progenitors is heterogeneous and can be divided into two groups, long-term self-renewing HSC and only transiently self-renewing HSC, also called

Haematopoiesis 85
short-terms. This is one of the main vital processes in the body.All blood cells are divided into three lineages.• Erythroid cells are the oxygen carrying red blood cells. Both reticulocytes and erythrocytes are functional and are
released into the blood. In fact, a reticulocyte count estimates the rate of erythropoiesis.• Lymphocytes are the cornerstone of the adaptive immune system. They are derived from common lymphoid
progenitors. The lymphoid lineage is primarily composed of T-cells and B-cells (types of white blood cells). Thisis lymphopoiesis.
• Myelocytes, which include granulocytes, megakaryocytes and macrophages and are derived from commonmyeloid progenitors, are involved in such diverse roles as innate immunity, adaptive immunity, and bloodclotting. This is myelopoiesis.
Granulopoiesis (or granulocytopoiesis) is haematopoiesis of granulocytes.Megakaryocytopoiesis is haematopoiesis of megakaryocytes.
Locations
Sites of haematopoesis (human) in pre- and postnatal periods
In developing embryos, bloodformation occurs in aggregates ofblood cells in the yolk sac, calledblood islands. As developmentprogresses, blood formation occurs inthe spleen, liver and lymph nodes.When bone marrow develops, iteventually assumes the task of formingmost of the blood cells for the entireorganism. However, maturation,activation, and some proliferation oflymphoid cells occurs in secondarylymphoid organs (spleen, thymus, and lymph nodes). In children, haematopoiesis occurs in the marrow of the longbones such as the femur and tibia. In adults, it occurs mainly in the pelvis, cranium, vertebrae, and sternum.
ExtramedullaryIn some cases, the liver, thymus, and spleen may resume their haematopoietic function, if necessary. This is calledextramedullary haematopoiesis. It may cause these organs to increase in size substantially. During fetaldevelopment, since bones and thus the bone marrow develop later, the liver functions as the main haematopoeticorgan. Therefore, the liver is enlarged during development.
Other vertebratesIn some vertebrates, haematopoiesis can occur wherever there is a loose stroma of connective tissue and slow bloodsupply, such as the gut, spleen or kidney.

Haematopoiesis 86
MaturationAs a stem cell matures it undergoes changes in gene expression that limit the cell types that it can become and movesit closer to a specific cell type. These changes can often be tracked by monitoring the presence of proteins on thesurface of the cell. Each successive change moves the cell closer to the final cell type and further limits its potentialto become a different cell type.
DeterminationThere are two points of view. For the stem cells and other undifferentiated blood cells in the bone marrow, thedetermination is generally explained by the determinism theory of haematopoiesis, saying that colony stimulatingfactors and other factors of the haematopoietic microenvironment determine the cells to follow a certain path of celldifferentiation. This is the classical way of describing haematopoiesis. The other point of view is stochastic theory:Undifferentiated blood cells are determined to specific cell types by randomness. The haematopoieticmicroenvironment prevails upon some of the cells to survive and some, on the other hand, to perform apoptosis anddie. By regulating this balance between different cell types, the bone marrow can alter the quantity of different cellsto ultimately be produced.
Haematopoietic growth factors
Diagram including some of the important cytokines that determine which type of bloodcell will be created. SCF= Stem Cell Factor Tpo= Thrombopoietin IL= Interleukin
GM-CSF= Granulocyte Macrophage-colony stimulating factor Epo= ErythropoietinM-CSF= Macrophage-colony stimulating factor G-CSF= Granulocyte-colony stimulatingfactor SDF-1= Stromal cell-derived factor-1 FLT-3 ligand= FMS-like tyrosine kinase 3ligand TNF-a = Tumour necrosis factor-alpha TGFβ = Transforming growth factor beta
[2]
Red and white blood cell production isregulated with great precision inhealthy humans, and the production ofleukocytes is rapidly increased duringinfection. The proliferation andself-renewal of these cells depend onGrowth factors. One of the key playerin self-renewal and development ofhaematopoietics cells is stem cellfactor (SCF). Absence of this factor islethal. But there are other importantGlycoprotein growth factors, whichregulate the proliferation andmaturation, these are for exampleIL-2,3,6,7. There are three moreexamples of factors that stimulate theproduction of committed stem cells. Socalled colony-stimulating factors(CSFs) and includegranulocyte-macrophage CSF(GM-CSF), granulocyte CSF (G-CSF)and macrophage CSF (M-CSF). Thesestimulate granulocyte formation andare active on either progenitor cells orend product cells.
Erythropoietin is required for a myeloid progenitor cell to become an erythrocyte.[] On the other hand,thrombopoietin makes myeloid progenitor cells differentiate to megakaryocytes (thrombocyte-forming cells).Examples of cytokines and the blood cells they give rise to, is shown in the picture to the right.

Haematopoiesis 87
Transcription factors in hematopoiesisGrowth factors initiate signal transduction pathways, which leads to activation of transcription factors. Signal, whichis received by cells, is not digital. It means that cells can distinguish time, amount, and frequency. For examplelong-term expression of PU.1 resulted in myeloid commitment, short-term induction of PU.1 activity led to theformation of immature eosinophils. Recently, it was reported that transcription factors such as NF-κB could beregulated by microRNAs (e.g., miR-125b) in hematopoiesis.First key player of differentiation from HSC to multipotent progenitor (MPP) is transcription factorCCAAT-enhancer binding protein alfa (C/EBP alfa). Mutations in C/EBP alfa are associated with acute myeloidleukaemia. Than the way is divided to Erythroid-megakaryocyte lineage or lymphoid and myeloid lineage, whichhave common progenitor, called lymphoid-primed multipotent progenitor. There are two main transcription factors.Pu.1 for Erythroid-megakaryocyte lineage and GATA-1 lead to lymphoid-primed multipotent progenitor.Among other factors are Ikaros, Gfi1 or IRF8. What is of greater significance is the occurrence of the same factorsmultiple times in the haematopoiesis tree. For example, CEBP alfa in neutrophil development or Pu.1. in monocytesand dendritic cells development. It is important to note that processes are not unidirectional.As example I would like to introduce PAX5 factor. It was Known, that it is important factor in B-cell developmentand thus associated with lymphomas. But It has been big surprise, when pax5 conditional knock out in mouseallowed peripheral mature B cells dedifferentiate to early bone marrow progenitors. So it completely change point ofview on transcription regulation, because now we are looking on transcription factors as a care keepers ofdifferentiation level and not as only the iniciators.Mutations in transtription factors are tightly connected to blood cancers, as acute myeloid leukaemia or acutelymphoblastic leukemia (All). For example Ikaros is known to be regulator of numerous biological events. Mice withno Ikaros lack B cells, Natural killer and T cells. Ikaros has six zinc fingers domains, four are conservedDNA-binding domain and two are for dimerization. Very important finding is, that different zinc fingers areinvolved in binding to different place in DNA and this is the reason for pleiotropic effect of Ikaros and differentinvolvement in cancer, but mainly are mutations associated with BCR-Abl patients and it is bad prognostic marker.
The myeloid-based modelFor a decade now, the evidence is growing that HSC maturation follows a myeloid-based model instead of the'classical' schoolbook dichotomy model. In the latter model, the HSC first generates a common myeloid-erythroidprogenitor (CMEP) and a common lymphoid progenitor (CLP). The CLP produces only T or B cells. Themyeloid-based model postulates that HSCs first diverge into the CMEP and a common myelo-lymphoid progenitor(CMLP), which generates T and B cell progenitors through a bipotential myeloid-T progenitor and a myeloid-Bprogenitor stage. The main difference is that in this new model, all erythroid, T and B lineage branches retain thepotential to generate myeloid cells (even after the segregation of T and B cell lineages). The model proposes the ideaof erythroid, T and B cells as specialized types of a prototypic myeloid HSC. Read more in Kawamoto et al. 2010.[3]

Haematopoiesis 88
References[1][1] Semester 4 medical lectures at Uppsala University 2008 by Leif Jansson
• For the growth factors also mentioned in previous version File:Hematopoiesis (human) cytokines.jpg: Molecular cell biology. Lodish,Harvey F. 5. ed. : - New York : W. H. Freeman and Co., 2003, 973 s. b ill. ISBN 0-7167-4366-3
•• The rest:[3][3] Kawamoto, Wada, Katsura. A revised scheme for developmental pathways of haematopoietic cells: the myeloid-based model. International
Immunology 2010.
Further reading• Godin, Isabelle & Cumano, Ana, ed. (2006). Hematopoietic stem cell development (http:/ / books. google. com/
books?id=tUsSmZwW_9MC). Springer. ISBN 978-0-306-47872-7.
External links• Granulopoiesis from tulane.edu (http:/ / www. som. tulane. edu/ classware/ pathology/ Krause/ Blood/ GP. html)

Hemoglobin 89
Hemoglobin
hemoglobin(heterotetramer, (αβ)2)
Structure of human hemoglobin. The proteins' α and β subunits are in red and blue, and the iron-containing heme groups in green. From PDB 1GZX [1]Proteopedia Hemoglobin [2]
-
Protein type metalloprotein, globulin
Function oxygen-transport
Cofactor(s) heme (4)
-
SubunitName
Gene ChromosomalLocus
Hb-α1 HBA1 Chr. 16 p13.3 [3]
Hb-α2 HBA2 Chr. 16 p13.3 [3]
Hb-β HBB Chr. 11 p15.5 [4]
Hemoglobin (/ˈhiːməˌɡloʊbɪn/); also spelled haemoglobin and abbreviated Hb or Hgb, is the iron-containingoxygen-transport metalloprotein in the red blood cells of all vertebrates (with the exception of the fish familyChannichthyidae) as well as the tissues of some invertebrates. Hemoglobin in the blood carries oxygen from therespiratory organs (lungs or gills) to the rest of the body (i.e. the tissues) where it releases the oxygen to burnnutrients to provide energy to power the functions of the organism in the process called metabolism.In mammals, the protein makes up about 96% of the red blood cells' dry content (by weight), and around 35% of thetotal content (including water). Hemoglobin has an oxygen-binding capacity of 1.34 mL O2 per gram of hemoglobin,which increases the total blood oxygen capacity seventy-fold compared to dissolved oxygen in blood. Themammalian hemoglobin molecule can bind (carry) up to four oxygen molecules.Hemoglobin is involved in the transport of other gases: It carries some of the body's respiratory carbon dioxide(about 10% of the total) as carbaminohemoglobin, in which CO2 is bound to the globin protein. The molecule alsocarries the important regulatory molecule nitric oxide bound to a globin protein thiol group, releasing it at the sametime as oxygen.Hemoglobin is also found outside red blood cells and their progenitor lines. Other cells that contain hemoglobininclude the A9 dopaminergic neurons in the substantia nigra, macrophages, alveolar cells, and mesangial cells in thekidney. In these tissues, hemoglobin has a non-oxygen-carrying function as an antioxidant and a regulator of ironmetabolism.

Hemoglobin 90
Hemoglobin and hemoglobin-like molecules are also found in many invertebrates, fungi, and plants. In theseorganisms, hemoglobins may carry oxygen, or they may act to transport and regulate other things such as carbondioxide, nitric oxide, hydrogen sulfide and sulfide. A variant of the molecule, called leghemoglobin, is used toscavenge oxygen away from anaerobic systems, such as the nitrogen-fixing nodules of leguminous plants, before theoxygen can poison the system.
Research historyIn 1825 J.F. Engelhard discovered that the ratio of Fe to protein is identical in the hemoglobins of several species.From the known atomic mass of iron he calculated the molecular mass of hemoglobin to n × 16000 (n = number ofirons per hemoglobin, now known to be 4), the first determination of a protein's molecular mass. This "hastyconclusion" drew a lot of ridicule at the time from scientists who could not believe that any molecule could be thatbig. Gilbert Smithson Adair confirmed Engelhard's results in 1925 by measuring the osmotic pressure of hemoglobinsolutions.The oxygen-carrying protein hemoglobin was discovered by Hünefeld in 1840. In 1851, German physiologist OttoFunke published a series of articles in which he described growing hemoglobin crystals by successively diluting redblood cells with a solvent such as pure water, alcohol or ether, followed by slow evaporation of the solvent from theresulting protein solution. Hemoglobin's reversible oxygenation was described a few years later by FelixHoppe-Seyler.In 1959, Max Perutz determined the molecular structure of myoglobin (similar to hemoglobin) by X-raycrystallography. This work resulted in his sharing with John Kendrew the 1962 Nobel Prize in Chemistry.The role of hemoglobin in the blood was elucidated by French physiologist Claude Bernard. The name hemoglobinis derived from the words heme and globin, reflecting the fact that each subunit of hemoglobin is a globular proteinwith an embedded heme group. Each heme group contains one iron atom, that can bind one oxygen moleculethrough ion-induced dipole forces. The most common type of hemoglobin in mammals contains four such subunits.
GeneticsHemoglobin consists mostly of protein subunits (the "globin" molecules), and these proteins, in turn, are foldedchains of a large number of different amino acids called polypeptides. The amino acid sequence of any polypeptidecreated by a cell is in turn determined by the stretches of DNA called genes. In all proteins, it is the amino acidsequence that determines the protein's chemical properties and function.There is more than one hemoglobin gene. The amino acid sequences of the globin proteins in hemoglobins usuallydiffer between species. These differences grow with evolutionary distance between species. For example, the mostcommon hemoglobin sequences in humans and chimpanzees are nearly identical, differing by only one amino acid inboth the alpha and the beta globin protein chains. These differences grow larger between less closely related species.Even within a species, different variants of hemoglobin always exist, although one sequence is usually a "mostcommon" one in each species. Mutations in the genes for the hemoglobin protein in a species result in hemoglobinvariants.[5][6] Many of these mutant forms of hemoglobin cause no disease. Some of these mutant forms ofhemoglobin, however, cause a group of hereditary diseases termed the hemoglobinopathies. The best knownhemoglobinopathy is sickle-cell disease, which was the first human disease whose mechanism was understood at themolecular level. A (mostly) separate set of diseases called thalassemias involves underproduction of normal andsometimes abnormal hemoglobins, through problems and mutations in globin gene regulation. All these diseasesproduce anemia.

Hemoglobin 91
Protein alignment of human hemoglobin proteins, alpha, beta, and delta subunitsrespectively. The alignments were created using Uniprot's alignment tool available
online.
Variations in hemoglobin amino acidsequences, as with other proteins, may beadaptive. For example, recent studies havesuggested genetic variants in deer mice thathelp explain how deer mice that live in themountains are able to survive in the thin airthat accompanies high altitudes. Aresearcher from the University ofNebraska-Lincoln found mutations in fourdifferent genes that can account fordifferences between deer mice that live in lowland prairies versus the mountains. After examining wild micecaptured from both highlands and lowlands, it was found that: the genes of the two breeds are "virtuallyidentical–except for those that govern the oxygen-carrying capacity of their hemoglobin". "The genetic differenceenables highland mice to make more efficient use of their oxygen", since less is available at higher altitudes, such asthose in the mountains.[7] Mammoth hemoglobin featured mutations that allowed for oxygen delivery at lowertemperatures, thus enabling mammoths to migrate to higher latitudes during the Pleistocene.
SynthesisHemoglobin (Hb) is synthesized in a complex series of steps. The heme part is synthesized in a series of steps in themitochondria and the cytosol of immature red blood cells, while the globin protein parts are synthesized byribosomes in the cytosol. Production of Hb continues in the cell throughout its early development from theproerythroblast to the reticulocyte in the bone marrow. At this point, the nucleus is lost in mammalian red bloodcells, but not in birds and many other species. Even after the loss of the nucleus in mammals, residual ribosomalRNA allows further synthesis of Hb until the reticulocyte loses its RNA soon after entering the vasculature (thishemoglobin-synthetic RNA in fact gives the reticulocyte its reticulated appearance and name).Wikipedia:Citationneeded
Structure
Heme b group
Hemoglobin has a quaternary structure characteristic of manymulti-subunit globular proteins.[8] Most of the amino acids inhemoglobin form alpha helices, connected by short non-helicalsegments. Hydrogen bonds stabilize the helical sections inside thisprotein, causing attractions within the molecule, folding eachpolypeptide chain into a specific shape.[9] Hemoglobin's quaternarystructure comes from its four subunits in roughly a tetrahedralarrangement.
In most vertebrates, the hemoglobin molecule is an assembly of fourglobular protein subunits. Each subunit is composed of a protein chaintightly associated with a non-protein heme group. Each protein chainarranges into a set of alpha-helix structural segments connectedtogether in a globin fold arrangement, so called because thisarrangement is the same folding motif used in other heme/globinproteins such as myoglobin. This folding pattern contains a pocket that strongly binds the heme group.
A heme group consists of an iron (Fe) ion (charged atom) held in a heterocyclic ring, known as a porphyrin. This porphyrin ring consists of four pyrrole molecules cyclically linked together (by methine bridges) with the iron ion

Hemoglobin 92
bound in the center.[10] The iron ion, which is the site of oxygen binding, coordinates with the four nitrogens in thecenter of the ring, which all lie in one plane. The iron is bound strongly (covalently) to the globular protein via theimidazole ring of F8 histidine residue (also known as the proximal histidine) below the porphyrin ring. A sixthposition can reversibly bind oxygen by a coordinate covalent bond,[11] completing the octahedral group of sixligands. Oxygen binds in an "end-on bent" geometry where one oxygen atom binds Fe and the other protrudes at anangle. When oxygen is not bound, a very weakly bonded water molecule fills the site, forming a distortedoctahedron.Even though carbon dioxide is carried by hemoglobin, it does not compete with oxygen for the iron-bindingpositions but is bound to the protein chains of the structure.The iron ion may be either in the Fe2+ or in the Fe3+ state, but ferrihemoglobin (methemoglobin) (Fe3+) cannot bindoxygen. In binding, oxygen temporarily and reversibly oxidizes (Fe2+) to (Fe3+) while oxygen temporarily turns intosuperoxide, thus iron must exist in the +2 oxidation state to bind oxygen. If superoxide ion associated to Fe3+ isprotonated, the hemoglobin iron will remain oxidized and incapable of binding oxygen. In such cases, the enzymemethemoglobin reductase will be able to eventually reactivate methemoglobin by reducing the iron center.In adult humans, the most common hemoglobin type is a tetramer (which contains 4 subunit proteins) calledhemoglobin A, consisting of two α and two β subunits non-covalently bound, each made of 141 and 146 amino acidresidues, respectively. This is denoted as α2β2. The subunits are structurally similar and about the same size. Eachsubunit has a molecular weight of about 16,000 daltons,[12] for a total molecular weight of the tetramer of about64,000 daltons (64,458 g/mol). Thus, 1 g/dL = 0.01551 mmol/L. Hemoglobin A is the most intensively studied of thehemoglobin molecules.In human infants, the hemoglobin molecule is made up of 2 α chains and 2 γ chains. The gamma chains aregradually replaced by β chains as the infant grows.[13]
The four polypeptide chains are bound to each other by salt bridges, hydrogen bonds, and the hydrophobic effect.
Oxygen saturationIn general, hemoglobin can be saturated with oxygen molecules (oxyhemoglobin), or desaturated with oxygenmolecules (deoxyhemoglobin).[14]
Oxyhemoglobin
Oxyhemoglobin is formed during physiological respiration when oxygen binds to the heme component of the proteinhemoglobin in red blood cells. This process occurs in the pulmonary capillaries adjacent to the alveoli of the lungs.The oxygen then travels through the blood stream to be dropped off at cells where it is utilized as a terminal electronacceptor in the production of ATP by the process of oxidative phosphorylation. It does not, however, help tocounteract a decrease in blood pH. Ventilation, or breathing, may reverse this condition by removal of carbondioxide, thus causing a shift up in pH.Hemoglobin exists in two forms, a taut (tense) form (T) and a relaxed form (R). Various factors such as low pH, highCO2 and high 2,3 BPG at the level of the tissues favor the taut form, which has low oxygen affinity and releasesoxygen in the tissues. Conversely, a high pH, low CO2, or low 2,3 BPG favors the relaxed form, which can betterbind oxygen. The partial pressure of the system also affects O2 affinity where, at high partial pressures of oxygen(such as those present in the alveoli), the relaxed (high affinity, R) state is favoured. Inversely, at low partialpressures (such as those present in respiring tissues), the (low affinity, T) tense state is favoured.[15] Additionally, thebinding of oxygen to the Iron-II heme pulls the iron into the plane of the porphyrin ring, causing a slightconformational shift. The shift encourages oxygen to bind to the three remaining hemes within hemoglobin (thus,oxygen binding is cooperative).
Hemoglobin 93
Deoxygenated hemoglobin
Deoxygenated hemoglobin is the form of hemoglobin without the bound oxygen. The absorption spectra ofoxyhemoglobin and deoxyhemoglobin differ. The oxyhemoglobin has significantly lower absorption of the 660 nmwavelength than deoxyhemoglobin, while at 940 nm its absorption is slightly higher. This difference is used formeasurement of the amount of oxygen in patient's blood by an instrument called pulse oximeter. This difference alsoaccounts for the presentation of cyanosis, the blue to purplish color that tissues develop during hypoxia.
Iron's oxidation state in oxyhemoglobinAssigning oxygenated hemoglobin's oxidation state is difficult because oxyhemoglobin (Hb-O2), by experimentalmeasurement, is diamagnetic (no net unpaired electrons), yet the low-energy electron configurations in both oxygenand iron are paramagnetic (suggesting at least one unpaired electron in the complex). The lowest-energy form ofoxygen, and the lowest energy forms of the relevant oxidation states of iron, are these:• Triplet oxygen, the lowest-energy molecular oxygen species, has two unpaired electrons in antibonding π*
molecular orbitals.• Iron(II) tends to exist in a high-spin configuration where unpaired electrons exist in Eg antibonding orbitals.•• Iron(III) has an odd number of electrons, and thus must have one or more unpaired electrons, in any energy state.All of these structures are paramagnetic (have unpaired electrons), not diamagnetic. Thus, a non-intuitive (e.g., ahigher-energy for at least one species) distribution of electrons in the combination of iron and oxygen must exist, inorder to explain the observed diamagnetism and no unpaired electrons.The three logical possibilities to produce diamagnetic (no net spin) Hb-O2 are:1. Low-spin Fe2+ binds to singlet oxygen. Both low-spin iron and singlet oxygen are diamagnetic. However, the
singlet form of oxygen is the higher-energy form of the molecule.2. Low-spin Fe3+ binds to .O2
- (the superoxide ion) and the two unpaired electrons couple antiferromagnetically,giving diamagnetic properties.
3. Low-spin Fe4+ binds to peroxide, O22-. Both are diamagnetic.
Direct experimental data:
• X-ray photoelectron spectroscopy suggests iron has an oxidation state of approximately 3.2• Infrared vibrational frequencies of the O-O bond suggests a bond length fitting with superoxide (a bond order of
about 1.6, with superoxide being 1.5).• X-ray Absorption Near Edge Structures at the iron K-edge. The energy shift of 5 eV between Deoxyhemoglobin
and Oxyhemoglobin, as for all the Methemoglobin species, strongly suggests an actual local charge closer to Fe3+
than Fe2+.Thus, the nearest formal oxidation state of iron in Hb-O2 is the +3 state, with oxygen in the −1 state (as superoxide.O2
-). The diamagnetism in this configuration arises from the single unpaired electron on superoxide aligningantiferromagnetically from the single unpaired electron on iron, to give no net spin to the entire configuration, inaccordance with diamagnetic oxyhemoglobin from experiment.The second choice of the three logical possibilities above for diamagnetic oxyhemoglobin being found correct byexperiment, is not surprising: singlet oxygen (possibility #1) and large separations of charge (possibility #3) are bothunfavorably high-energy states. Iron's shift to a higher oxidation state in Hb-O2 decreases the atom's size, and allowsit into the plane of the porphyrin ring, pulling on the coordinated histidine residue and initiating the allostericchanges seen in the globulins.Early postulates by bio-inorganic chemists claimed that possibility #1 (above) was correct and that iron should exist in oxidation state II. This conclusion seemed likely, since the iron oxidation state III as methemoglobin, when not accompanied by superoxide .O2
- to "hold" the oxidation electron, was known to render hemoglobin incapable of binding normal triplet O2 as it occurs in the air. It was thus assumed that iron remained as Fe(II) when oxygen gas

Hemoglobin 94
was bound in the lungs. The iron chemistry in this previous classical model was elegant, but the required presence ofthe required diamagnetic high-energy singlet oxygen was never explained. It was classically argued that the bindingof an oxygen molecule placed high-spin iron(II) in an octahedral field of strong-field ligands; this change in fieldwould increase the crystal field splitting energy, causing iron's electrons to pair into the low-spin configuration,which would be diamagnetic in Fe(II). This forced low-spin pairing is indeed thought to happen in iron when oxygenbinds, but is not enough to explain iron's change in size. Extraction of an additional electron from iron by oxygen isrequired to explain both iron's smaller size and observed increased oxidation state, and oxygen's weaker bond.The assignment of a whole-number oxidation state is a formalism, as the covalent bonds are not required to haveperfect bond orders involving whole electron transfer. Thus, all three models for paramagnetic Hb-O2 may contributeto some small degree (by resonance) to the actual electronic configuration of Hb-O2. However, the model of iron inHb-O2 being Fe(III) is more correct than the classical idea that it remains Fe(II).
Cooperativity
A schematic visual model of oxygen-bindingprocess, showing all four monomers and hemes,and protein chains only as diagramatic coils, to
facilitate visualization into the molecule. Oxygenis not shown in this model, but, for each of the
iron atoms, it binds to the iron (red sphere) in theflat heme. For example, in the upper-left of the
four hemes shown, oxygen binds at the left of theiron atom shown in the upper-left of diagram.
This causes the iron atom to move backward intothe heme that holds it (the iron moves upward asit binds oxygen, in this illustration), tugging thehistidine residue (modeled as a red pentagon onthe right of the iron) closer, as it does. This, in
turn, pulls on the protein chain holding thehistidine.
When oxygen binds to the iron complex, it causes the iron atom tomove back toward the center of the plane of the porphyrin ring (seemoving diagram). At the same time, the imidazole side-chain of thehistidine residue interacting at the other pole of the iron is pulledtoward the porphyrin ring. This interaction forces the plane of the ringsideways toward the outside of the tetramer, and also induces a strainin the protein helix containing the histidine as it moves nearer to theiron atom. This strain is transmitted to the remaining three monomersin the tetramer, where it induces a similar conformational change in theother heme sites such that binding of oxygen to these sites becomeseasier.In the tetrameric form of normal adult hemoglobin, the binding ofoxygen is, thus, a cooperative process. The binding affinity ofhemoglobin for oxygen is increased by the oxygen saturation of themolecule, with the first oxygens bound influencing the shape of thebinding sites for the next oxygens, in a way favorable for binding. Thispositive cooperative binding is achieved through steric conformationalchanges of the hemoglobin protein complex as discussed above; i.e.,when one subunit protein in hemoglobin becomes oxygenated, aconformational or structural change in the whole complex is initiated,causing the other subunits to gain an increased affinity for oxygen. Asa consequence, the oxygen binding curve of hemoglobin is sigmoidal,or S-shaped, as opposed to the normal hyperbolic curve associated withnoncooperative binding.
The dynamic mechanism of the cooperativity in hemoglobin and its relation with the low-frequency resonance hasbeen discussed.
Binding for ligands other than oxygenBesides the oxygen ligand, which binds to hemoglobin in a cooperative manner, hemoglobin ligands also include competitive inhibitors such as carbon monoxide (CO) and allosteric ligands such as carbon dioxide (CO2) and nitric oxide (NO). The carbon dioxide is bound to amino groups of the globin proteins as carbaminohemoglobin, and is thought to account for about 10% of carbon dioxide transport in mammals. Nitric oxide is bound to specific thiol

Hemoglobin 95
groups in the globin protein to form an S-nitrosothiol, which dissociates into free nitric oxide and thiol again, as thehemoglobin releases oxygen from its heme site. This nitric oxide transport to peripheral tissues is hypothesized toassist oxygen transport in tissues, by releasing vasodilatory nitric oxide to tissues in which oxygen levels are low.
CompetitiveThe binding of oxygen is affected by molecules such as carbon monoxide (CO) (for example, from tobacco smoking,car exhaust, and incomplete combustion in furnaces). CO competes with oxygen at the heme binding site.Hemoglobin binding affinity for CO is 250 times greater than its affinity for oxygen, meaning that small amounts ofCO dramatically reduce hemoglobin's ability to transport oxygen. Since carbon monoxide is a colorless, odorless andtasteless gas, and poses a potentially fatal threat, detectors have become commercially available to warn ofdangerous levels in residences. When hemoglobin combines with CO, it forms a very bright red compound calledcarboxyhemoglobin, which may cause the skin of CO poisoning victims to appear pink in death, instead of white orblue. When inspired air contains CO levels as low as 0.02%, headache and nausea occur; if the CO concentration isincreased to 0.1%, unconsciousness will follow. In heavy smokers, up to 20% of the oxygen-active sites can beblocked by CO.In similar fashion, hemoglobin also has competitive binding affinity for cyanide (CN−), sulfur monoxide (SO), nitricoxide (NO), and sulfide (S2−), including hydrogen sulfide (H2S). All of these bind to iron in heme without changingits oxidation state, but they nevertheless inhibit oxygen-binding, causing grave toxicity.The iron atom in the heme group must initially be in the ferrous (Fe2+) oxidation state to support oxygen and othergases' binding and transport (it temporarily switches to ferric during the time oxygen is bound, as explained above).Initial oxidation to the ferric (Fe3+) state without oxygen converts hemoglobin into "hemiglobin" or methemoglobin(pronounced "MET-hemoglobin"), which cannot bind oxygen. Hemoglobin in normal red blood cells is protected bya reduction system to keep this from happening. Nitric oxide is capable of converting a small fraction of hemoglobinto methemoglobin in red blood cells. The latter reaction is a remnant activity of the more ancient nitric oxidedioxygenase function of globins.
AllostericFurther information: Oxygen-hemoglobin dissociation curveCarbon dioxide occupies a different binding site on the hemoglobin. Carbon dioxide is more readily dissolved indeoxygenated blood, facilitating its removal from the body after the oxygen has been released to tissues undergoingmetabolism. This increased affinity for carbon dioxide by the venous blood is known as the Haldane effect. Throughthe enzyme carbonic anhydrase, carbon dioxide reacts with water to give carbonic acid, which decomposes intobicarbonate and protons:
CO2 + H2O → H2CO3 → HCO3- + H+

Hemoglobin 96
The sigmoidal shape of hemoglobin's oxygen-dissociation curve resultsfrom cooperative binding of oxygen to hemoglobin.
Hence, blood with high carbon dioxide levels isalso lower in pH (more acidic). Hemoglobin canbind protons and carbon dioxide, which causes aconformational change in the protein and facilitatesthe release of oxygen. Protons bind at variousplaces on the protein, while carbon dioxide bindsat the α-amino group.[16] Carbon dioxide binds tohemoglobin and forms carbaminohemoglobin. Thisdecrease in hemoglobin's affinity for oxygen by thebinding of carbon dioxide and acid is known as theBohr effect (shifts the O2-saturation curve to theright). Conversely, when the carbon dioxide levelsin the blood decrease (i.e., in the lung capillaries),carbon dioxide and protons are released fromhemoglobin, increasing the oxygen affinity of theprotein. A reduction in the total binding capacity ofhemoglobin to oxygen (i.e. shifting the curve
down, not just to the right) due to reduced pH is called the root effect. This is seen in bony fish.
It is necessary for hemoglobin to release the oxygen that it binds; if not, there is no point in binding it. The sigmoidalcurve of hemoglobin makes it efficient in binding (taking up O2 in lungs), and efficient in unloading (unloading O2in tissues).
In people acclimated to high altitudes, the concentration of 2,3-Bisphosphoglycerate (2,3-BPG) in the blood isincreased, which allows these individuals to deliver a larger amount of oxygen to tissues under conditions of loweroxygen tension. This phenomenon, where molecule Y affects the binding of molecule X to a transport molecule Z, iscalled a heterotropic allosteric effect.Animals other than humans use different molecules to bind to hemoglobin and change its O2 affinity underunfavorable conditions. Fish use both ATP and GTP. These bind to a phosphate "pocket" on the fish hemoglobinmolecule, which stabilizes the tense state and therefore decreases oxygen affinity. GTP reduces hemoglobin oxygenaffinity much more than ATP, which is thought to be due to an extra hydrogen bond formed that further stabilizes thetense state. Under hypoxic conditions, the concentration of both ATP and GTP is reduced in fish red blood cells toincrease oxygen affinity.A variant hemoglobin, called fetal hemoglobin (HbF, α2γ2), is found in the developing fetus, and binds oxygen withgreater affinity than adult hemoglobin. This means that the oxygen binding curve for fetal hemoglobin is left-shifted(i.e., a higher percentage of hemoglobin has oxygen bound to it at lower oxygen tension), in comparison to that ofadult hemoglobin. As a result, fetal blood in the placenta is able to take oxygen from maternal blood.Hemoglobin also carries nitric oxide in the globin part of the molecule. This improves oxygen delivery in theperiphery and contributes to the control of respiration. NO binds reversibly to a specific cysteine residue in globin;the binding depends on the state (R or T) of the hemoglobin. The resulting S-nitrosylated hemoglobin influencesvarious NO-related activities such as the control of vascular resistance, blood pressure and respiration. NO is notreleased in the cytoplasm of erythrocytes but transported by an anion exchanger called AE1 out of them.A study was performed to examine the influence of the form of hemoglobin (Hb) on the partitioning of inhaledvolatile organic compounds (VOCs) into [human and animal] blood. Benzene was the prototypic VOC used in theinvestigations for this research due to the similar properties it shares with many other VOCs. To be specific, thisstudy analyses the influence of the water solubility of Hb on the partitioning coefficient (PC) of a VOC as comparedto the influence of the "species" or form of Hb. The different forms of blood used include: human hemoglobin

Hemoglobin 97
(HbA), rat Hb, and sickle-cell hemoglobin (HbS). Rat Hb contains little water and is in a quasi-crystalline form,found inside the red blood cells (RBC), meaning they are more hydrophobic than human Hb, which arewater-soluble. Sickle-cell hemoglobin (HbS) is water-soluble, however it can become water-insoluble, forminghydrophobic polymers, when deoxygenated. The findings state that the benzene PC for rat Hb was much higher thanhuman that for Hb; however, the tests that measured the PCs of the oxygenated and deoxygenated forms of HbA andHbS did not differ, indicating that the affinity of benzene was not affected by the water solubility of Hb.
Types in humansHemoglobin variants are a part of the normal embryonic and fetal development, but may also be pathologic mutantforms of hemoglobin in a population, caused by variations in genetics. Some well-known hemoglobin variants suchas sickle-cell anemia are responsible for diseases, and are considered hemoglobinopathies. Other variants cause nodetectable pathology, and are thus considered non-pathological variants.In the embryo:• Gower 1 (ζ2ε2)• Gower 2 (α2ε2) (PDB 1A9W [17])• Hemoglobin Portland I (ζ2γ2)• Hemoglobin Portland II (ζ2β2).In the fetus:• Hemoglobin F (α2γ2) (PDB 1FDH [18]).In postnatal people:• Hemoglobin A (α2β2) (PDB 1BZ0 [19]) – The most common with a normal amount over 95%• Hemoglobin A2 (α2δ2) – δ chain synthesis begins late in the third trimester and, in adults, it has a normal range of
1.5–3.5%• Hemoglobin F (α2γ2) – In adults Hemoglobin F is restricted to a limited population of red cells called F-cells.
However, the level of Hb F can be elevated in persons with sickle-cell disease and beta-thalassemia.
Gene expression of hemoglobin before and after birth. Also identifies the types ofcells and organs in which the gene expression (data on Wood W.G., (1976). Br.
Med. Bull. 32, 282.)
Variant forms that cause disease:• Hemoglobin D-Punjab – (α2βD
2) – Avariant form of hemoglobin.
• Hemoglobin H (β4) – A variant form ofhemoglobin, formed by a tetramer of βchains, which may be present in variantsof α thalassemia.
• Hemoglobin Barts (γ4) – A variant formof hemoglobin, formed by a tetramer of γchains, which may be present in variantsof α thalassemia.
• Hemoglobin S (α2βS2) – A variant form
of hemoglobin found in people withsickle cell disease. There is a variation inthe β-chain gene, causing a change in theproperties of hemoglobin, which resultsin sickling of red blood cells.
• Hemoglobin C (α2βC2) – Another variant due to a variation in the β-chain gene. This variant causes a mild
chronic hemolytic anemia.

Hemoglobin 98
• Hemoglobin E (α2βE2) – Another variant due to a variation in the β-chain gene. This variant causes a mild
chronic hemolytic anemia.• Hemoglobin AS – A heterozygous form causing Sickle cell trait with one adult gene and one sickle cell disease
gene• Hemoglobin SC disease – A compound heterozygous form with one sickle gene and another encoding
Hemoglobin C.
Degradation in vertebrate animalsWhen red cells reach the end of their life due to aging or defects, they are broken down in spleen. The hemoglobinmolecule is broken up, and the iron gets recycled. This process also produces one molecule of carbon monoxide forevery molecule of heme degraded. Heme degradation is one of the few natural sources of carbon monoxide in thehuman body, and is responsible for the normal blood levels of carbon monoxide even in people breathing pure air.The other major final product of heme degradation is bilirubin. Increased levels of this chemical are detected in theblood if red cells are being destroyed more rapidly than usual. Improperly degraded hemoglobin protein orhemoglobin that has been released from the blood cells too rapidly can clog small blood vessels, especially thedelicate blood filtering vessels of the kidneys, causing kidney damage. Iron is removed from heme and salvaged forlater use, it is stored as hemosiderin or ferritin in tissues and transported in plasma by beta globulins as transferins.When the porphyrin ring is broken up, the fragments are normally secreted as a yellow pigment called bilirubin,which is secreted into the intestines as bile. Intestines metabolise bilirubin into urobilinogen. Urobilinogen leaves thebody in faeces, in a pigment called stercobilin. Globulin is metabolised into amino acids that are then released intocirculation.
Role in diseaseHemoglobin deficiency can be caused either by decreased amount of hemoglobin molecules, as in anemia, or bydecreased ability of each molecule to bind oxygen at the same partial pressure of oxygen. Hemoglobinopathies(genetic defects resulting in abnormal structure of the hemoglobin molecule) may cause both. In any case,hemoglobin deficiency decreases blood oxygen-carrying capacity. Hemoglobin deficiency is, in general, strictlydistinguished from hypoxemia, defined as decreased partial pressure of oxygen in blood,[20][21] although both arecauses of hypoxia (insufficient oxygen supply to tissues).Other common causes of low hemoglobin include loss of blood, nutritional deficiency, bone marrow problems,chemotherapy, kidney failure, or abnormal hemoglobin (such as that of sickle-cell disease).High hemoglobin levels may be caused by exposure to high altitudes, smoking, dehydration, or tumors.The ability of each hemoglobin molecule to carry oxygen is normally modified by altered blood pH or CO2, causingan altered oxygen–hemoglobin dissociation curve. However, it can also be pathologically altered in, e.g., carbonmonoxide poisoning.Decrease of hemoglobin, with or without an absolute decrease of red blood cells, leads to symptoms of anemia.Anemia has many different causes, although iron deficiency and its resultant iron deficiency anemia are the mostcommon causes in the Western world. As absence of iron decreases heme synthesis, red blood cells in irondeficiency anemia are hypochromic (lacking the red hemoglobin pigment) and microcytic (smaller than normal).Other anemias are rarer. In hemolysis (accelerated breakdown of red blood cells), associated jaundice is caused bythe hemoglobin metabolite bilirubin, and the circulating hemoglobin can cause renal failure.Some mutations in the globin chain are associated with the hemoglobinopathies, such as sickle-cell disease andthalassemia. Other mutations, as discussed at the beginning of the article, are benign and are referred to merely ashemoglobin variants.

Hemoglobin 99
There is a group of genetic disorders, known as the porphyrias that are characterized by errors in metabolic pathwaysof heme synthesis. King George III of the United Kingdom was probably the most famous porphyria sufferer.To a small extent, hemoglobin A slowly combines with glucose at the terminal valine (an alpha aminoacid) of each βchain. The resulting molecule is often referred to as Hb A1c. As the concentration of glucose in the blood increases,the percentage of Hb A that turns into Hb A1c increases. In diabetics whose glucose usually runs high, the percent HbA1c also runs high. Because of the slow rate of Hb A combination with glucose, the Hb A1c percentage isrepresentative of glucose level in the blood averaged over a longer time (the half-life of red blood cells, which istypically 50–55 days).Glycosylated hemoglobin is the form of hemoglobin to which glucose is bound. The binding of glucose to aminoacids in the hemoglobin takes place spontaneously (without the help of an enzyme) in many proteins, and is notknown to serve a useful purpose. However, the binding to hemoglobin does serve as a record for average bloodglucose levels over the lifetime of red cells, which is approximately 120 days. The levels of glycosylated hemoglobinare therefore measured in order to monitor the long-term control of the chronic disease of type 2 diabetes mellitus(T2DM). Poor control of T2DM results in high levels of glycosylated hemoglobin in the red blood cells. The normalreference range is approximately 4–5.9 %. Though difficult to obtain, values less than 7% are recommended forpeople with T2DM. Levels greater than 9% are associated with poor control of the glycosylated hemoglobin, andlevels greater than 12% are associated with very poor control. Diabetics who keep their glycosylated hemoglobinlevels close to 7% have a much better chance of avoiding the complications that may accompany diabetes (thanthose whose levels are 8% or higher).[22] In addition, increased glycosylation of hemoglobin increases its affinity foroxygen, therefore preventing its release at the tissue and inducing a level of hypoxia in extreme cases.Elevated levels of hemoglobin are associated with increased numbers or sizes of red blood cells, calledpolycythemia. This elevation may be caused by congenital heart disease, cor pulmonale, pulmonary fibrosis, toomuch erythropoietin, or polycythemia vera.[23]
A recent study done in Pondicherry, India, shows its importance in coronary artery disease.

Hemoglobin 100
Diagnostic usesMain article: Hemoglobinometer
A Hemoglobin concentration measurement beingadministered before a blood donation at the
American Red Cross Boston Blood DonationCenter.
Hemoglobin concentration measurement is among the most commonlyperformed blood tests, usually as part of a complete blood count. Forexample it is typically tested before or after blood donation. Results arereported in g/L, g/dL or mol/L. 1 g/dL equals about 0.6206 mmol/L,although the latter units are not used as often due to uncertaintyregarding the polymeric state of the molecule.[24] This conversionfactor, using the single globin unit molecular weight of 16,000 Da, ismore common for hemoglobin concentration in blood. For MCHC(mean corpuscular hemoglobin concentration) the conversion factor0.155, which uses the tetramer weight of 64,500 Da, is morecommon.[25] Normal levels are:
•• Men: 13.8 to 18.0 g/dL (138 to 180 g/L, or 8.56 to 11.17 mmol/L)•• Women: 12.1 to 15.1 g/dL (121 to 151 g/L, or 7.51 to 9.37 mmol/L)•• Children: 11 to 16 g/dL (111 to 160 g/L, or 6.83 to 9.93 mmol/L)• Pregnant women: 11 to 14 g/dL (110 to 140 g/L, or 6.83 to
8.69 mmol/L)[26][27]
Normal values of hemoglobin in the 1st and 3rd trimesters of pregnantwomen must be at least 11 g/dL and at least 10.5 g/dL during the 2ndtrimester.[28]
Dehydration or hyperhydration can greatly influence measured hemoglobin levels. Albumin can indicate hydrationstatus.If the concentration is below normal, this is called anemia. Anemias are classified by the size of red blood cells, thecells that contain hemoglobin in vertebrates. The anemia is called "microcytic" if red cells are small, "macrocytic" ifthey are large, and "normocytic" otherwise.Hematocrit, the proportion of blood volume occupied by red blood cells, is typically about three times thehemoglobin concentration measured in g/dL. For example, if the hemoglobin is measured at 17 g/dL, that compareswith a hematocrit of 51%.Laboratory hemoglobin test methods require a blood sample (arterial, venous, or capillary) and analysis onhematology analyzer and CO-oximeter. Additionally, a new noninvasive hemoglobin (SpHb) test method calledPulse CO-Oximetry is also available with comparable accuracy to invasive methods.Concentrations of oxy- and deoxyhemoglobin can be measured continuously, regionally and noninvasively usingNIRS. NIRS can be used both on the head as on muscles. This technique is often used for research in e.g. elite sportstraining, ergonomics, rehabilition, patient monitoring, neonatal research, functional brain monitoring, brain computerinterface, urology (bladder contraction), neurology (Neurovascular coupling) and more.Long-term control of blood sugar concentration can be measured by the concentration of Hb A1c. Measuring itdirectly would require many samples because blood sugar levels vary widely through the day. Hb A1c is the productof the irreversible reaction of hemoglobin A with glucose. A higher glucose concentration results in more Hb A1c.Because the reaction is slow, the Hb A1c proportion represents glucose level in blood averaged over the half-life ofred blood cells, is typically 50–55 days. An Hb A1c proportion of 6.0% or less show good long-term glucose control,while values above 7.0% are elevated. This test is especially useful for diabetics.[29]
The functional magnetic resonance imaging (fMRI) machine uses the signal from deoxyhemoglobin, which is sensitive to magnetic fields since it is paramagnetic. Combined measurement with NIRS shows good correlation

Hemoglobin 101
with both the oxy- and deoxyhemoglobin signal compared to the BOLD signal.
Analogues in non-vertebrate organismsA variety of oxygen-transport and -binding proteins exist in organisms throughout the animal and plant kingdoms.Organisms including bacteria, protozoans, and fungi all have hemoglobin-like proteins whose known and predictedroles include the reversible binding of gaseous ligands. Since many of these proteins contain globins and the hememoiety (iron in a flat porphyrin support), they are often called hemoglobins, even if their overall tertiary structure isvery different from that of vertebrate hemoglobin. In particular, the distinction of "myoglobin" and hemoglobin inlower animals is often impossible, because some of these organisms do not contain muscles. Or, they may have arecognizable separate circulatory system but not one that deals with oxygen transport (for example, many insects andother arthropods). In all these groups, heme/globin-containing molecules (even monomeric globin ones) that dealwith gas-binding are referred to as oxyhemoglobins. In addition to dealing with transport and sensing of oxygen,they may also deal with NO, CO2, sulfide compounds, and even O2 scavenging in environments that must beanaerobic. They may even deal with detoxification of chlorinated materials in a way analogous to heme-containingP450 enzymes and peroxidases.
The giant tube worm Riftia pachyptila showingred hemoglobin-containing plumes
The structure of hemoglobins varies across species. Hemoglobinoccurs in all kingdoms of organisms, but not in all organisms.Primitive species such as bacteria, protozoa, algae, and plants oftenhave single-globin hemoglobins. Many nematode worms, molluscs,and crustaceans contain very large multisubunit molecules, muchlarger than those in vertebrates. In particular, chimeric hemoglobinsfound in fungi and giant annelids may contain both globin and othertypes of proteins.
One of the most striking occurrences and uses of hemoglobin inorganisms is in the giant tube worm (Riftia pachyptila, also calledVestimentifera), which can reach 2.4 meters length and populates ocean volcanic vents. Instead of a digestive tract,these worms contain a population of bacteria constituting half the organism's weight. The bacteria react with H2Sfrom the vent and O2 from the water to produce energy to make food from H2O and CO2. The worms end with adeep-red fan-like structure ("plume"), which extends into the water and absorbs H2S and O2 for the bacteria, andCO2 for use as synthetic raw material similar to photosynthetic plants. The structures are bright-red due to theircontaining several extraordinarily complex hemoglobins that have up to 144 globin chains, each including associatedheme structures. These hemoglobins are remarkable for being able to carry oxygen in the presence of sulfide, andeven to carry sulfide, without being completely "poisoned" or inhibited by it as hemoglobins in most other speciesare.
Other oxygen-binding proteinsMyoglobin
Found in the muscle tissue of many vertebrates, including humans, it gives muscle tissue a distinct red or darkgray color. It is very similar to hemoglobin in structure and sequence, but is not a tetramer; instead, it is amonomer that lacks cooperative binding. It is used to store oxygen rather than transport it.
HemocyaninThe second most common oxygen-transporting protein found in nature, it is found in the blood of manyarthropods and molluscs. Uses copper prosthetic groups instead of iron heme groups and is blue in color whenoxygenated.
Hemerythrin

Hemoglobin 102
Some marine invertebrates and a few species of annelid use this iron-containing non-heme protein to carryoxygen in their blood. Appears pink/violet when oxygenated, clear when not.
ChlorocruorinFound in many annelids, it is very similar to erythrocruorin, but the heme group is significantly different instructure. Appears green when deoxygenated and red when oxygenated.
VanabinsAlso known as vanadium chromagens, they are found in the blood of sea squirts. There were oncehypothesized to use the rare metal vanadium as an oxygen binding prosthetic group. However, although theydo contain vanadium by preference, they apparently bind little oxygen, and thus have some other function,which has not been elucidated (sea squirts also contain some hemoglobin). They may act as toxins.
ErythrocruorinFound in many annelids, including earthworms, it is a giant free-floating blood protein containing manydozens—possibly hundreds—of iron- and heme-bearing protein subunits bound together into a single proteincomplex with a molecular mass greater than 3.5 million daltons.
PinnaglobinOnly seen in the mollusc Pinna squamosa. Brown manganese-based porphyrin protein.
LeghemoglobinIn leguminous plants, such as alfalfa or soybeans, the nitrogen fixing bacteria in the roots are protected fromoxygen by this iron heme containing oxygen-binding protein. The specific enzyme protected is nitrogenase,which is unable to reduce nitrogen gas in the presence of free oxygen.
CoboglobinA synthetic cobalt-based porphyrin. Coboprotein would appear colorless when oxygenated, but yellow whenin veins.
Presence in nonerythroid cellsSome nonerythroid cells (i.e., cells other than the red blood cell line) contain hemoglobin. In the brain, these includethe A9 dopaminergic neurons in the substantia nigra, astrocytes in the cerebral cortex and hippocampus, and in allmature oligodendrocytes. It has been suggested that brain hemoglobin in these cells may enable the "storage ofoxygen to provide a homeostatic mechanism in anoxic conditions, which is especially important for A9 DA neuronsthat have an elevated metabolism with a high requirement for energy production". It has been noted further that "A9dopaminergic neurons may be at particular risk since in addition to their high mitochondrial activity they are underintense oxidative stress caused by the production of hydrogen peroxide via autoxidation and/or monoamine oxidase(MAO)-mediated deamination of dopamine and the subsequent reaction of accessible ferrous iron to generate highlytoxic hydroxyl radicals". This may explain the risk of these cells for degeneration in Parkinson's disease. Thehemoglobin-derived iron in these cells is not the cause of the post-mortem darkness of these cells (origin of the Latinname, substantia nigra), but rather is due to neuromelanin.Outside the brain, hemoglobin has non-oxygen-carrying functions as an antioxidant and a regulator of ironmetabolism in macrophages, alveolar cells, and mesangial cells in the kidney.

Hemoglobin 103
In history, art and music
Heart of Steel (Hemoglobin) (2005) by JulianVoss-Andreae. The images show the 5-foot
(1.60 m) tall sculpture right after installation,after 10 days, and after several months of
exposure to the elements.
Historically, an association between the color of blood and rust occursin the association of the planet Mars, with the Roman god of war, sincethe planet is an orange-red, which reminded the ancients of blood.Although the color of the planet is due to iron compounds incombination with oxygen in the Martian soil, it is a commonmisconception that the iron in hemoglobin and its oxides gives bloodits red color. The color is actually due to the porphyrin moiety ofhemoglobin to which the iron is bound, not the iron itself, although theligation and redox state of the iron can influence the pi to pi* or n topi* electronic transitions of the porphyrin and hence its opticalcharacteristics.
Artist Julian Voss-Andreae created a sculpture called "Heart of Steel (Hemoglobin)" in 2005, based on the protein'sbackbone. The sculpture was made from glass and weathering steel. The intentional rusting of the initially shinywork of art mirrors hemoglobin's fundamental chemical reaction of oxygen binding to iron.
Rock band Placebo recorded a song called "Haemoglobin" with the lyrics "Haemoglobin is the key to a healthyheartbeat".Wikipedia:Citation needed French rap artist MC Solaar also had a successful single titled "La Concubinede l'hémoglobine" in 1994.Wikipedia:Citation needed
References[1] http:/ / www. rcsb. org/ pdb/ explore/ explore. do?structureId=1GZX[2] http:/ / www. proteopedia. org/ wiki/ index. php/ Hemoglobin[3] http:/ / www. ncbi. nlm. nih. gov/ Omim/ getmap. cgi?chromosome=16p13. 3[4] http:/ / www. ncbi. nlm. nih. gov/ Omim/ getmap. cgi?chromosome=11p15. 5[5] A Syllabus of Human Hemoglobin Variants (1996) (http:/ / globin. cse. psu. edu/ html/ huisman/ variants/ ). Globin.cse.psu.edu. Retrieved on
2013-09-05.[6] Hemoglobin Variants (http:/ / www. labtestsonline. org/ understanding/ analytes/ hemoglobin_var/ glance-3. html). Labtestsonline.org.
Retrieved on 2013-09-05.[7][7] Reed, Leslie. "Adaptation found in mouse genes." Omaha World-Herald 11 Aug. 2009: EBSCO. Web. 30 Oct. 2009.[8] van Kessel et al. (2003) "2.4 Proteins – Natural Polyamides." Chemistry 12. Toronto: Nelson, p. 122.[9] "Hemoglobin Tutorial." (http:/ / www. umass. edu/ molvis/ tutorials/ hemoglobin/ index. htm) University of Massachusetts Amherst. Web. 23
Oct. 2009.[10] "Hemoglobin." (http:/ / www. chm. bris. ac. uk/ motm/ hemoglobin/ hemoglobjm. htm) School of Chemistry – Bristol University – UK.
Web. 12 Oct. 2009.[11] WikiPremed > Coordination Chemistry (http:/ / wikipremed. com/ interdisciplinary_course. php?code=0213000100000000) Retrieved on
July 2, 2009[12] Hemoglobin (http:/ / www. worthington-biochem. com/ HB/ cat. html). Worthington-biochem.com. Retrieved on 2013-09-05.[13] "Hemoglobin." (http:/ / www. medicinenet. com/ hemoglobin/ article. htm) MedicineNet. Web. 12 Oct. 2009.[14] "Hemoglobin Home." (http:/ / www. bio. davidson. edu/ Courses/ Molbio/ MolStudents/ spring2005/ Heiner/ hemoglobin. html) Biology @
Davidson. Web. 12 Oct. 2009.[15] Voet, D. (2008) Fundamentals of Biochemistry, 3rd. ed., Fig. 07_06, John Wiley & Sons[16] Nelson, D. L.; Cox, M. M. (2000). Lehninger Principles of Biochemistry, 3rd ed. New York, NY: Worth Publishers. p. 217, ISBN
1572599316.[17] http:/ / www. rcsb. org/ pdb/ explore/ explore. do?structureId=1A9W[18] http:/ / www. rcsb. org/ pdb/ explore/ explore. do?structureId=1FDH[19] http:/ / www. rcsb. org/ pdb/ explore/ explore. do?structureId=1BZ0[20] hypoxemia (http:/ / www. britannica. com/ EBchecked/ topic/ 280141/ hypoxemia). Encyclopædia Britannica, stating hypoxemia (reduced
oxygen tension in the blood).[21] Biology-Online.org --> Dictionary » H » Hypoxemia (http:/ / www. biology-online. org/ dictionary/ Hypoxemia) last modified 29 December
2008[22] "Definition of Glycosylated Hemoglobin." (http:/ / www. medterms. com/ script/ main/ art. asp?articlekey=16295) Medicine Net. Web. 12
Oct. 2009.

Hemoglobin 104
[23] Hemoglobin (http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 003645. htm#What abnormal results mean) at Medline Plus[24] Society for Biomedical Diabetes Research. SI Unit Conversion Calculator (http:/ / www. soc-bdr. org/ rds/ authors/
unit_tables_conversions_and_genetic_dictionaries/ e5196/ index_en. html).[25] Handin, Robert I.; Lux, Samuel E. and StosselBlood, Thomas P. (2003). Blood: Principles & Practice of Hematology. Lippincott Williams
& Wilkins, ISBN 0781719933[26] Hemoglobin Level Test (http:/ / ibdcrohns. about. com/ od/ diagnostictesting/ p/ testhemo. htm). Ibdcrohns.about.com (2013-08-16).
Retrieved on 2013-09-05.[27] Although other sources can have slightly differing values, such as haemoglobin (reference range) (http:/ / www. gpnotebook. co. uk/
simplepage. cfm?ID=1026883654). gpnotebook.co.uk[28] Murray S.S. & McKinney E.S. (2006). Foundations of Maternal-Newborn Nursing. 4th ed., p. 919. Philadelphia: Saunders Elsevier[29] This Hb A1c level is only useful in individuals who have red blood cells (RBCs) with normal survivals (i.e., normal half-life). In individuals
with abnormal RBCs, whether due to abnormal hemoglobin molecules (such as Hemoglobin S in Sickle Cell Anemia) or RBC membranedefects – or other problems, the RBC half-life is frequently shortened. In these individuals, an alternative test called "fructosamine level" canbe used. It measures the degree of glycation (glucose binding) to albumin, the most common blood protein, and reflects average blood glucoselevels over the previous 18–21 days, which is the half-life of albumin molecules in the circulation.
Further reading• Campbell, MK (1999). Biochemistry (third ed.). Harcourt. ISBN 0-03-024426-9.• Eshaghian, S; Horwich, TB; Fonarow, GC (2006). "An unexpected inverse relationship between HbA1c levels
and mortality in patients with diabetes and advanced systolic heart failure". Am Heart J 151 (1): 91. doi:10.1016/j.ahj.2005.10.008 (http:/ / dx. doi. org/ 10. 1016/ j. ahj. 2005. 10. 008). PMID 16368297 (http:/ / www.ncbi. nlm. nih. gov/ pubmed/ 16368297).
• Ganong, WF (2003). Review of Medical Physiology (21st ed.). Lange. ISBN 0-07-140236-5.• Hager, T (1995). Force of Nature: The Life of Linus Pauling. Simon and Schuster. ISBN 0-684-80909-5.• Kneipp J, Balakrishnan G, Chen R, Shen TJ, Sahu SC, Ho NT, Giovannelli JL, Simplaceanu V, Ho C, Spiro T
(2005). "Dynamics of allostery in hemoglobin: roles of the penultimate tyrosine H bonds". J Mol Biol 356 (2):335–53. doi: 10.1016/j.jmb.2005.11.006 (http:/ / dx. doi. org/ 10. 1016/ j. jmb. 2005. 11. 006). PMID 16368110(http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 16368110).
External links• Proteopedia Hemoglobin (http:/ / www. proteopedia. org/ wiki/ index. php/ Hemoglobin)• National Anemia Action Council (http:/ / www. anemia. org/ ) – anemia.org• New hemoglobin type causes mock diagnosis with pulse oxymeters (http:/ / www. life-of-science. net/ medicine/
news/ new-hemoglobin-type-discovered-causing-mock-diagnosis-of-cardiac-insufficiency. html)• Animation of hemoglobin: from deoxy to oxy form (https:/ / vimeo. com/ 92241783)

Jaundice 105
Jaundice"Yellowing" redirects here. For the plant disease, see lethal yellowing. For paper degradation, see foxing. For theCharles Dickens character Jarndyce, see Jarndyce."Icterus" and "icteric" redirect here. For the physiological event, see Ictal. For the songbird Icteria, seeYellow-breasted Chat.
Jaundice
Jaundice of the skin caused by hepatic failure.
ICD-10 R17 [1]
ICD-9 782.4 [2]
DiseasesDB 7038 [3]
MedlinePlus 003243 [4]
MeSH D007565 [5]
Jaundice (also known as icterus, from the Greek word ίκτερος; adjectival form, icteric) is a yellowish pigmentationof the skin, the conjunctival membranes over the sclerae (whites of the eyes), and other mucous membranes causedby hyperbilirubinemia (increased levels of bilirubin in the blood). This hyperbilirubinemia subsequently causesincreased levels of bilirubin in the extracellular fluid. Concentration of bilirubin in blood plasma is normally below1.2 mg/dL (<25µmol/L). A concentration higher than approx. 3 mg/dL (>50µmol/L) leads to jaundice. The termjaundice comes from the French word jaune, meaning yellow.Jaundice is often seen in liver disease such as hepatitis or liver cancer. It may also indicate leptospirosis orobstruction of the biliary tract, for example by gallstones or pancreatic cancer, or less commonly be congenital inorigin (e.g., biliary atresia).Yellow discoloration of the skin, especially on the palms and the soles, but not of the sclera and mucous membranes(i.e. oral cavity) is due to carotenemia—a harmless condition[6] important to differentiate from jaundice.

Jaundice 106
Signs and symptoms
A 4-year-old boy with icteric (jaundiced) sclerawhich later proved to be a manifestation ofhemolytic anemia due to G6PD deficiency
following fava bean consumption.
The main symptom of jaundice is a yellow discoloration of the whitepart of the eyes (sclera) and of the skin.The conjunctiva of the eye are one of the first tissues to change coloras bilirubin levels rise in jaundice. This is sometimes referred to asscleral icterus. However, the sclera themselves are not "icteric"(stained with bile pigment) but rather the conjunctival membranes thatoverlie them. The yellowing of the "white of the eye" is thus moreproperly termed conjunctival icterus. The term "icterus" itself issometimes incorrectly used to refer to jaundice that is noted in thesclera of the eyes, however its more common and more correctmeaning is entirely synonymous with jaundice.[7]
Differential diagnosis
When a pathological process interferes with the normal functioning ofthe metabolism and excretion of bilirubin just described, jaundice maybe the result. Jaundice is classified into three categories, depending onwhich part of the physiological mechanism the pathology affects. The three categories are:
Types of jaundice
Category Definition
Pre-hepatic/ hemolytic The pathology is occurring prior to the liver.
Hepatic/ hepatocellular The pathology is located within the liver.
Post-Hepatic/ cholestatic The pathology is located after the conjugation of bilirubin in the liver.
Pre-hepaticPre-hepatic jaundice is caused by anything which causes an increased rate of hemolysis (breakdown of red bloodcells). In tropical countries, malaria can cause jaundice in this manner. Certain genetic diseases, such as sickle cellanemia, spherocytosis, thalassemia and glucose 6-phosphate dehydrogenase deficiency can lead to increased red celllysis and therefore hemolytic jaundice. Commonly, diseases of the kidney, such as hemolytic uremic syndrome, canalso lead to coloration. Defects in bilirubin metabolism also present as jaundice, as in Gilbert's syndrome (a geneticdisorder of bilirubin metabolism which can result in mild jaundice, which is found in about 5% of the population)and Crigler-Najjar syndrome, Type I and II.In jaundice secondary to hemolysis, the increased production of bilirubin leads to the increased production ofurine-urobilinogen. Bilirubin is not usually found in the urine because unconjugated bilirubin is not water-soluble,so, the combination of increased urine-urobilinogen with no bilirubin (since, unconjugated) in urine is suggestive ofhemolytic jaundice.

Jaundice 107
Laboratory findings include:• Urine: no bilirubin present, urobilinogen > 2 units (i.e., hemolytic anemia causes increased heme metabolism;
exception: infants where gut flora has not developed).•• Serum: increased unconjugated bilirubin.• Kernicterus is associated with increased unconjugated bilirubin; neonates are especially vulnerable to this due to
increase permeability of the blood brain barrier.
HepatocellularHepatocellular (hepatic) jaundice can be caused by acute or chronic hepatitis, hepatotoxicity, cirrhosis, drug inducedhepatitis and alcoholic liver disease. Cell necrosis reduces the liver's ability to metabolize and excrete bilirubinleading to a buildup of unconjugated bilirubin in the blood. Other causes include primary biliary cirrhosis leading toan increase in plasma conjugated bilirubin because there is impairment of excretion of conjugated bilirubin into thebile. The blood contains an abnormally raised amount of conjugated bilirubin and bile salts which are excreted in theurine. Jaundice seen in the newborn, known as neonatal jaundice, is common in newborns as hepatic machinery forthe conjugation and excretion of bilirubin does not fully mature until approximately two weeks of age. Rat fever(leptospirosis) can also cause hepatic jaundice. In hepatic jaundice, there is invariably cholestasis.Laboratory findings depend on the cause of jaundice.• Urine: Conjugated bilirubin present, urobilirubin > 2 units but variable (except in children). Kernicterus is a
condition not associated with increased conjugated bilirubin.•• Plasma protein show characteristic changes.•• Plasma albumin level is low but plasma globulins are raised due to an increased formation of antibodies.Bilirubin transport across the hepatocyte may be impaired at any point between the uptake of unconjugated bilirubininto the cell and transport of conjugated bilirubin into biliary canaliculi. In addition, swelling of cells and oedemadue to inflammation cause mechanical obstruction of intrahepatic biliary tree. Hence in hepatocellular jaundice,concentration of both unconjugated and conjugated bilirubin rises in the blood. In hepatocellular disease, there isusually interference in all major steps of bilirubin metabolism—uptake, conjugation and excretion. However,excretion is the rate-limiting step, and usually impaired to the greatest extent. As a result, conjugatedhyperbilirubinaemia predominates.[8]
The unconjugated bilirubin still enters the liver cells and becomes conjugated in the usual way. This conjugatedbilirubin is then returned to the blood, probably by rupture of the congested bile canaliculi and direct emptying of thebile into the lymph leaving the liver. Thus, most of the bilirubin in the plasma becomes the conjugated type ratherthan the unconjugated type, and this conjugated bilirubin which did not go to intestine to become urobilinogen givesthe urine the dark color.[9]
Post-hepaticPost-hepatic jaundice, also called obstructive jaundice, is caused by an interruption to the drainage of bile in thebiliary system. The most common causes are gallstones in the common bile duct, and pancreatic cancer in the headof the pancreas. Also, a group of parasites known as "liver flukes" can live in the common bile duct, causingobstructive jaundice. Other causes include strictures of the common bile duct, biliary atresia, cholangiocarcinoma,pancreatitis and pancreatic pseudocysts. A rare cause of obstructive jaundice is Mirizzi's syndrome.In complete obstruction of the bile duct, no urobilinogen is found in the urine, since bilirubin has no access to theintestine and it is in the intestine that bilirubin gets converted to urobilinogen to be later released into the generalcirculation. In this case, presence of bilirubin (conjugated) in the urine without urine-urobilinogen suggestsobstructive jaundice, either intra-hepatic or post-hepatic.

Jaundice 108
The presence of pale stools and dark urine suggests an obstructive or post-hepatic cause as normal feces get theircolor from bile pigments. However, although pale stools and dark urine are a feature of biliary obstruction, they canoccur in many intra-hepatic illnesses and are therefore not a reliable clinical feature to distinguish obstruction fromhepatic causes of jaundice.Patients also can present with elevated serum cholesterol, and often complain of severe itching or "pruritus" becauseof the deposition of bile salts.No single test can differentiate between various classifications of jaundice. A combination of liver function tests isessential to arrive at a diagnosis.
Table of diagnostic tests[10]
Function test Pre-hepaticJaundice
Hepatic Jaundice Post-hepatic Jaundice
Total bilirubin Normal / Increased Increased
Conjugated bilirubin Normal Increased Increased
Unconjugated bilirubin Normal / Increased Increased Normal
Urobilinogen Normal / Increased Decreased Decreased / Negative
Urine Color Normal Dark (urobilinogen + conjugatedbilirubin)
Dark (conjugatedbilirubin)
Stool Color Normal Normal/Pale Pale
Alkaline phosphatase levels Normal Increased
Alanine transferase and Aspartate transferaselevels
Increased
Conjugated Bilirubin in Urine Not Present Present
Splenomegaly Present Present Absent
Neonatal jaundiceMain article: Neonatal jaundiceNeonatal jaundice is usually harmless: this condition is often seen in infants around the second day after birth,lasting until day 8 in normal births, or to around day 14 in premature births. Typical causes for neonatal jaundiceinclude normal physiologic jaundice, jaundice due to formula supplementation, and hemolytic disorders that includehereditary spherocytosis, glucose-6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency, ABO/Rhblood type autoantibodies, or infantile pyknocytosis. Serum bilirubin normally drops to a low level without anyintervention required. In cases where bilirubin rises higher, a brain-damaging condition known as kernicterus canoccur, leading to significant disability. This condition has been rising in recent years due to less time spent outdoors.A Bili light is often the tool used for early treatment, which often consists of exposing the baby to intensivephototherapy. Sunbathing is effective treatment, and has the advantage of ultra-violet-B, which promotes Vitamin Dproduction. Bilirubin count is lowered through bowel movements and urination, so frequent and effective feedingsare especially important.

Jaundice 109
PathophysiologyJaundice itself is not a disease, but rather a sign of one of many possible underlying pathological processes that occurat some point along the normal physiological pathway of the metabolism of bilirubin in blood.When red blood cells have completed their life span of approximately 120 days, or when they are damaged, theirmembranes become fragile and prone to rupture. As each red blood cell traverses through the reticuloendothelialsystem, its cell membrane ruptures when its membrane is fragile enough to allow this. Cellular contents, includinghemoglobin, are subsequently released into the blood. The hemoglobin is phagocytosed by macrophages, and splitinto its heme and globin portions. The globin portion, a protein, is degraded into amino acids and plays no role injaundice. Two reactions then take place with the heme molecule. The first oxidation reaction is catalyzed by themicrosomal enzyme heme oxygenase and results in biliverdin (green color pigment), iron and carbon monoxide. Thenext step is the reduction of biliverdin to a yellow color tetrapyrol pigment called bilirubin by cytosolic enzymebiliverdin reductase. This bilirubin is "unconjugated," "free" or "indirect" bilirubin. Approximately 4 mg of bilirubinper kg of blood is produced each day. The majority of this bilirubin comes from the breakdown of heme fromexpired red blood cells in the process just described. However approximately 20 percent comes from other hemesources, including ineffective erythropoiesis, and the breakdown of other heme-containing proteins, such as musclemyoglobin and cytochromes.
Hepatic eventsThe unconjugated bilirubin then travels to the liver through the bloodstream. Because this bilirubin is not soluble,however, it is transported through the blood bound to serum albumin. Once it arrives at the liver, it is conjugatedwith glucuronic acid (to form bilirubin diglucuronide, or just "conjugated bilirubin") to become more water soluble.The reaction is catalyzed by the enzyme UDP-glucuronyl transferase.This conjugated bilirubin is excreted from the liver into the biliary and cystic ducts as part of bile. Intestinal bacteriaconvert the bilirubin into urobilinogen. From here urobilinogen can take two pathways. It can either be furtherconverted into stercobilinogen, which is then oxidized to stercobilin and passed out in the feces, or it can bereabsorbed by the intestinal cells, transported in the blood to the kidneys, and passed out in the urine as the oxidisedproduct urobilin. Stercobilin and urobilin are the products responsible for the coloration of feces and urine,respectively.

Jaundice 110
Diagnostic approach
Biliary tract dilation due to obstruction as seen onCAT scan
Biliary tract dilation due to obstruction
Most patients presenting with jaundice will have various predictablepatterns of liver panel abnormalities, though significant variation doesexist. The typical liver panel will include blood levels of enzymesfound primarily from the liver, such as the aminotransferases (ALT,AST), and alkaline phosphatase (ALP); bilirubin (which causes thejaundice); and protein levels, specifically, total protein and albumin.Other primary lab tests for liver function include gamma glutamyltranspeptidase (GGT) and prothrombin time (PT).
Some bone and heart disorders can lead to an increase in ALP and theaminotransferases, so the first step in differentiating these from liverproblems is to compare the levels of GGT, which will only be elevatedin liver-specific conditions. The second step is distinguishing frombiliary (cholestatic) or liver (hepatic) causes of jaundice and alteredlaboratory results. The former typically indicates a surgical response,while the latter typically leans toward a medical response. ALP andGGT levels will typically rise with one pattern while aspartateaminotransferase (AST) and alanine aminotransferase (ALT) rise in aseparate pattern. If the ALP (10–45 IU/L) and GGT (18–85) levels riseproportionately about as high as the AST (12–38 IU/L) and ALT(10–45 IU/L) levels, this indicates a cholestatic problem. On the otherhand, if the AST and ALT rise is significantly higher than the ALP andGGT rise, this indicates an hepatic problem. Finally, distinguishingbetween hepatic causes of jaundice, comparing levels of AST and ALTcan prove useful. AST levels will typically be higher than ALT. Thisremains the case in most hepatic disorders except for hepatitis (viral orhepatotoxic). Alcoholic liver damage may see fairly normal ALTlevels, with AST 10x higher than ALT. On the other hand, if ALT ishigher than AST, this is indicative of hepatitis. Levels of ALT andAST are not well correlated to the extent of liver damage, althoughrapid drops in these levels from very high levels can indicate severenecrosis. Low levels of albumin tend to indicate a chronic condition, while it is normal in hepatitis and cholestasis.
Lab results for liver panels are frequently compared by the magnitude of their differences, not the pure number, aswell as by their ratios. The AST:ALT ratio can be a good indicator of whether the disorder is alcoholic liver damage(above 10), some other form of liver damage (above 1), or hepatitis (less than 1). Bilirubin levels greater than 10xnormal could indicate neoplastic or intrahepatic cholestasis. Levels lower than this tend to indicate hepatocellularcauses. AST levels greater than 15x tends to indicate acute hepatocellular damage. Less than this tend to indicateobstructive causes. ALP levels greater than 5x normal tend to indicate obstruction, while levels greater than 10xnormal can indicate drug (toxic) induced cholestatic hepatitis or Cytomegalovirus. Both of these conditions can alsohave ALT and AST greater than 20× normal. GGT levels greater than 10x normal typically indicate cholestasis.Levels 5–10× tend to indicate viral hepatitis. Levels less than 5× normal tend to indicate drug toxicity. Acutehepatitis will typically have ALT and AST levels rising 20–30× normal (above 1000), and may remain significantlyelevated for several weeks. Acetaminophen toxicity can result in ALT and AST levels greater than 50x normal.

Jaundice 111
ComplicationsComplications of jaundice include sepsis especially cholangitis, biliary cirrhosis, pancreatitis, coagulopathy, renaland liver failure. Other complications are related to the underlying disease and the procedures employed in thediagnosis and management of individual diseases. Cholangitis, especially the suppurative type (Charcot’s triad orReynolds' pentad), is usually secondary to choledocholithiasis. It may also complicate procedures like ERCP.Treatment should include correction of coagulopathy, fluid/electrolyte anomaly, antibiotics and biliary drainage withERCP where available or trans-hepatic drainage or surgery.
References[1] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ R17[2] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=782. 4[3] http:/ / www. diseasesdatabase. com/ ddb7038. htm[4] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 003243. htm[5] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2009/ MB_cgi?field=uid& term=D007565[6] Schwartz, Robert A. Carotenemia (http:/ / emedicine. medscape. com/ article/ 1104368-overview#showall). emedicine.medscape.com[7] Icterus | Define Icterus at Dictionary.com (http:/ / dictionary. reference. com/ browse/ icterus). Dictionary.reference.com. Retrieved on
2013-12-23.[8] Mathew K.G. (2008) Medicine: Prep Manual for Undergraduates, 3/e, Elsevier India, ISBN 8131211541, pp. 296–297[9] Hall, John Edward and Guyton, Arthur C. (2011) Textbook of Medical Physiology, Saunders/Elsevier, p. 841, ISBN 1416045740[10] Goljan, Edward F. (2007) Rapid Review Pathology, 2nd ed., Elsevier Health Sciences, pp. 368–369, ISBN 032304414X.
External links• The dictionary definition of jaundice at Wiktionary• Media related to Jaundice at Wikimedia Commons

Malaria 112
MalariaContributors [1]
MalariaClassification and external resources
A Plasmodium from the saliva of a female mosquito moving across a mosquito cell.
ICD-10 B50 [2]-B54 [3]
ICD-9 084 [4]
OMIM 248310 [5]
DiseasesDB 7728 [6]
MedlinePlus 000621 [7]
eMedicine med/1385 [8] emerg/305 [9] ped/1357 [10]
MeSH C03.752.250.552 [11]
Malaria is a mosquito-borne infectious disease of humans and other animals caused by parasitic protozoans (a typeof single cell microorganism) of the Plasmodium type. Malaria causes symptoms that typically include fever, fatigue,vomiting and headaches. In severe cases it can cause yellow skin, seizures, coma or death. These symptom usuallybegin ten to fifteen days after being bitten. In those who have not been appropriately treated disease may recurmonths later. In those who have recently survived an infection, re-infection typically causes milder symptoms. Thispartial resistance disappears over months to years if there is no ongoing exposure to malaria.Commonly, the disease is transmitted by the bite of an infected female Anopheles mosquito. This bite introduces theparasites from the mosquito's saliva into a person's blood. The parasites then travel to the liver where they matureand reproduce. Five species of Plasmodium can infect and be spread by humans. Most deaths are caused byP. falciparum because P. vivax, P. ovale, and P. malariae generally cause a milder form of malaria. The speciesP. knowlesi rarely causes disease in humans. Malaria is typically diagnosed by the microscopic examination of bloodusing blood films, or with antigen-based rapid diagnostic tests. Methods that use the polymerase chain reaction todetect the parasite's DNA have been developed, but are not widely used in areas where malaria is common due totheir cost and complexity.

Malaria 113
The risk of disease can be reduced by preventing mosquito bites by using mosquito nets and insect repellents, or withmosquito-control measures such as spraying insecticides and draining standing water. Several medications areavailable to prevent malaria in travellers to areas where the disease is common. Occasional doses of the medicationsulfadoxine/pyrimethamine are recommended in infants and after the first trimester of pregnancy in areas with highrates of malaria. Despite a need, no effective vaccine exists, although efforts to develop one are ongoing. Therecommended treatment for malaria is a combination of antimalarial medications that includes an artemisinin. Thesecond medication may be either mefloquine, lumefantrine, or sulfadoxine/pyrimethamine. Quinine along withdoxycycline may be used if an artemisinin is not available. It is recommended that in areas where the disease iscommon, malaria is confirmed if possible before treatment is started due to concerns of increasing drug resistance.Resistance has developed to several antimalarial medications; for example, chloroquine-resistant P. falciparum hasspread to most malarial areas, and resistance to artemisinin has become a problem in some parts of Southeast Asia.The disease is widespread in tropical and subtropical regions which are present in a broad band around the equator.This includes much of Sub-Saharan Africa, Asia, and Latin America. The World Health Organization estimates thatin 2012, there were 207 million cases of malaria. That year, the disease is estimated to have killed between 473,000and 789,000 people, many of whom were children in Africa. Malaria is commonly associated with poverty and has amajor negative effect on economic development. In Africa it is estimated to result in losses of $12 billion USD ayear due to increased healthcare costs, lost ability to work and effects on tourism.
Signs and symptoms
Main symptoms of malaria
The signs and symptoms of malaria typically begin8–25 days following infection; however, symptomsmay occur later in those who have taken antimalarialmedications as prevention. Initial manifestations of thedisease—common to all malaria species—are similar toflu-like symptoms, and can resemble other conditionssuch as septicemia, gastroenteritis, and viral diseases.The presentation may include headache, fever,shivering, joint pain, vomiting, hemolytic anemia,jaundice, hemoglobin in the urine, retinal damage, andconvulsions.
The classic symptom of malaria is paroxysm—acyclical occurrence of sudden coldness followed byshivering and then fever and sweating, occurring everytwo days (tertian fever) in P. vivax and P. ovaleinfections, and every three days (quartan fever) forP. malariae. P. falciparum infection can causerecurrent fever every 36–48 hours or a less pronouncedand almost continuous fever.
Severe malaria is usually caused by P. falciparum (often referred to as falciparum malaria). Symptoms of falciparummalaria arise 9–30 days after infection. Individuals with cerebral malaria frequently exhibit neurological symptoms,including abnormal posturing, nystagmus, conjugate gaze palsy (failure of the eyes to turn together in the samedirection), opisthotonus, seizures, or coma.

Malaria 114
ComplicationsThere are several serious complications of malaria. Among these is the development of respiratory distress, whichoccurs in up to 25% of adults and 40% of children with severe P. falciparum malaria. Possible causes includerespiratory compensation of metabolic acidosis, noncardiogenic pulmonary oedema, concomitant pneumonia, andsevere anaemia. Although rare in young children with severe malaria, acute respiratory distress syndrome occurs in5–25% of adults and up to 29% of pregnant women. Coinfection of HIV with malaria increases mortality. Renalfailure is a feature of blackwater fever, where hemoglobin from lysed red blood cells leaks into the urine.Infection with P. falciparum may result in cerebral malaria, a form of severe malaria that involves encephalopathy. Itis associated with retinal whitening, which may be a useful clinical sign in distinguishing malaria from other causesof fever. Splenomegaly, severe headache, hepatomegaly (enlarged liver), hypoglycemia, and hemoglobinuria withrenal failure may occur.Malaria in pregnant women is an important cause of stillbirths, infant mortality and low birth weight, particularly inP. falciparum infection, but also with P. vivax.
CauseMalaria parasites belong to the genus Plasmodium (phylum Apicomplexa). In humans, malaria is caused byP. falciparum, P. malariae, P. ovale, P. vivax and P. knowlesi. Among those infected, P. falciparum is the mostcommon species identified (~75%) followed by P. vivax (~20%). Although P. falciparum traditionally accounts forthe majority of deaths, recent evidence suggests that P. vivax malaria is associated with potentially life-threateningconditions about as often as with a diagnosis of P. falciparum infection. P. vivax proportionally is more commonoutside of Africa. There have been documented human infections with several species of Plasmodium from higherapes; however, with the exception of P. knowlesi—a zoonotic species that causes malaria in macaques—these aremostly of limited public health importance.Climate change is likely to affect malaria transmission, but the severity and geographic distribution of such effects iscurrently uncertain.

Malaria 115
Life cycle
The life cycle of malaria parasites. A mosquito causes an infection by a bite. First,sporozoites enter the bloodstream, and migrate to the liver. They infect liver cells, wherethey multiply into merozoites, rupture the liver cells, and return to the bloodstream. Then,
the merozoites infect red blood cells, where they develop into ring forms, trophozoitesand schizonts that in turn produce further merozoites. Sexual forms are also produced,
which, if taken up by a mosquito, will infect the insect and continue the life cycle.
In the life cycle of Plasmodium, afemale Anopheles mosquito (thedefinitive host) transmits a motileinfective form (called the sporozoite)to a vertebrate host such as a human(the secondary host), thus acting as atransmission vector. A sporozoitetravels through the blood vessels toliver cells (hepatocytes), where itreproduces asexually (tissueschizogony), producing thousands ofmerozoites. These infect new red bloodcells and initiate a series of asexualmultiplication cycles (bloodschizogony) that produce 8 to 24 newinfective merozoites, at which pointthe cells burst and the infective cyclebegins anew.
Other merozoites develop intoimmature gametocytes, which are theprecursors of male and femalegametes. When a fertilised mosquitobites an infected person, gametocytesare taken up with the blood and maturein the mosquito gut. The male andfemale gametocytes fuse and form a ookinete—a fertilized, motile zygote. Ookinetes develop into new sporozoitesthat migrate to the insect's salivary glands, ready to infect a new vertebrate host. The sporozoites are injected into theskin, in the saliva, when the mosquito takes a subsequent blood meal.
Only female mosquitoes feed on blood; male mosquitoes feed on plant nectar, and thus do not transmit the disease.The females of the Anopheles genus of mosquito prefer to feed at night. They usually start searching for a meal atdusk, and will continue throughout the night until taking a meal. Malaria parasites can also be transmitted by bloodtransfusions, although this is rare.
Recurrent malariaSymptoms of malaria can recur after varying symptom-free periods. Depending upon the cause, recurrence can be classified as either recrudescence, relapse, or reinfection. Recrudescence is when symptoms return after a symptom-free period. It is caused by parasites surviving in the blood as a result of inadequate or ineffective treatment. Relapse is when symptoms reappear after the parasites have been eliminated from blood but persist as dormant hypnozoites in liver cells. Relapse commonly occurs between 8–24 weeks and is commonly seen with P. vivax and P. ovale infections. P. vivax malaria cases in temperate areas often involve overwintering by hypnozoites, with relapses beginning the year after the mosquito bite. Reinfection means the parasite that caused the past infection was eliminated from the body but a new parasite was introduced. Reinfection cannot readily be distinguished from recrudescence, although recurrence of infection within two weeks of treatment for the initial infection is typically attributed to treatment failure. People may develop some immunity when exposed to frequent

Malaria 116
infections.
PathophysiologyFurther information: Plasmodium falciparum biology
Micrograph of a placenta from a stillbirth due tomaternal malaria. H&E stain. Red blood cells are
anuclear; blue/black staining in bright redstructures (red blood cells) indicate foreign nuclei
from the parasites.
Malaria infection develops via two phases: one that involves the liver(exoerythrocytic phase), and one that involves red blood cells, orerythrocytes (erythrocytic phase). When an infected mosquito pierces aperson's skin to take a blood meal, sporozoites in the mosquito's salivaenter the bloodstream and migrate to the liver where they infecthepatocytes, multiplying asexually and asymptomatically for a periodof 8–30 days.
After a potential dormant period in the liver, these organismsdifferentiate to yield thousands of merozoites, which, following ruptureof their host cells, escape into the blood and infect red blood cells tobegin the erythrocytic stage of the life cycle. The parasite escapes fromthe liver undetected by wrapping itself in the cell membrane of theinfected host liver cell.
Within the red blood cells, the parasites multiply further, again asexually, periodically breaking out of their host cellsto invade fresh red blood cells. Several such amplification cycles occur. Thus, classical descriptions of waves offever arise from simultaneous waves of merozoites escaping and infecting red blood cells.Some P. vivax sporozoites do not immediately develop into exoerythrocytic-phase merozoites, but instead producehypnozoites that remain dormant for periods ranging from several months (7–10 months is typical) to several years.After a period of dormancy, they reactivate and produce merozoites. Hypnozoites are responsible for long incubationand late relapses in P. vivax infections, although their existence in P. ovale is uncertain.
The parasite is relatively protected from attack by the body's immune system because for most of its human life cycleit resides within the liver and blood cells and is relatively invisible to immune surveillance. However, circulatinginfected blood cells are destroyed in the spleen. To avoid this fate, the P. falciparum parasite displays adhesiveproteins on the surface of the infected blood cells, causing the blood cells to stick to the walls of small blood vessels,thereby sequestering the parasite from passage through the general circulation and the spleen. The blockage of themicrovasculature causes symptoms such as in placental malaria. Sequestered red blood cells can breach theblood–brain barrier and cause cerebral malaria.
Genetic resistanceMain article: Genetic resistance to malariaAccording to a 2005 review, due to the high levels of mortality and morbidity caused by malaria—especially theP. falciparum species—it has placed the greatest selective pressure on the human genome in recent history. Severalgenetic factors provide some resistance to it including sickle cell trait, thalassaemia traits, glucose-6-phosphatedehydrogenase deficiency, and the absence of Duffy antigens on red blood cells.The impact of sickle cell trait on malaria immunity illustrates some of the evolutionary trade-offs that have occurred because of endemic malaria. Sickle cell trait causes a defect in the hemoglobin molecule in the blood. Instead of retaining the biconcave shape of a normal red blood cell, the modified hemoglobin S molecule causes the cell to sickle or distort into a curved shape. Due to the sickle shape, the molecule is not as effective in taking or releasing oxygen. Infection causes red cells to sickle more, and so they are removed from circulation sooner. This reduces the frequency with which malaria parasites complete their life cycle in the cell. Individuals who are homozygous (with two copies of the abnormal hemoglobin beta allele) have sickle-cell anaemia, while those who are heterozygous

Malaria 117
(with one abnormal allele and one normal allele) experience resistance to malaria. Although the shorter lifeexpectancy for those with the homozygous condition would not sustain the trait's survival, the trait is preservedbecause of the benefits provided by the heterozygous form.
Liver dysfunctionLiver dysfunction as a result of malaria is uncommon and usually only occurs in those with other liver conditionsuch as viral hepatitis or chronic liver disease. The syndrome is sometimes called malarial hepatitis. While it hasbeen considered a rare occurrence, malarial hepatopathy has seen an increase, particularly in Southeast Asia andIndia. Liver compromise in people with malaria correlates with a greater likelihood of complications and death.
DiagnosisMain article: Diagnosis of malaria
The blood film is the gold standard for malariadiagnosis.
Ring-forms and gametocytes of Plasmodiumfalciparum in human blood
Owing to the non-specific nature of the presentation of symptoms,diagnosis of malaria in non-endemic areas requires a high degree ofsuspicion, which might be elicited by any of the following: recenttravel history, enlarged spleen, fever, low number of platelets in theblood, and higher-than-normal levels of bilirubin in the bloodcombined with a normal level of white blood cells.
Malaria is usually confirmed by the microscopic examination of bloodfilms or by antigen-based rapid diagnostic tests (RDT). Microscopy isthe most commonly used method to detect the malarial parasite—about165 million blood films were examined for malaria in 2010. Despite itswidespread usage, diagnosis by microscopy suffers from two maindrawbacks: many settings (especially rural) are not equipped toperform the test, and the accuracy of the results depends on both theskill of the person examining the blood film and the levels of theparasite in the blood. The sensitivity of blood films ranges from75–90% in optimum conditions, to as low as 50%. Commerciallyavailable RDTs are often more accurate than blood films at predictingthe presence of malaria parasites, but they are widely variable indiagnostic sensitivity and specificity depending on manufacturer, andare unable to tell how many parasites are present.
In regions where laboratory tests are readily available, malaria shouldbe suspected, and tested for, in any unwell person who has been in anarea where malaria is endemic. In areas that cannot afford laboratorydiagnostic tests, it has become common to use only a history of feveras the indication to treat for malaria—thus the common teaching "fever equals malaria unless proven otherwise". Adrawback of this practice is overdiagnosis of malaria and mismanagement of non-malarial fever, which wasteslimited resources, erodes confidence in the health care system, and contributes to drug resistance. Althoughpolymerase chain reaction-based tests have been developed, they are not widely used in areas where malaria iscommon as of 2012, due to their complexity.

Malaria 118
ClassificationMalaria is classified into either "severe" or "uncomplicated" by the World Health Organization (WHO). It is deemedsevere when any of the following criteria are present, otherwise it is considered uncomplicated.•• Decreased consciousness•• Significant weakness such that the person is unable to walk•• Inability to feed• Two or more convulsions• Low blood pressure (less than 70 mmHg in adults and 50 mmHg in children)•• Breathing problems•• Circulatory shock• Kidney failure or hemoglobin in the urine•• Bleeding problems, or hemoglobin less than 50 g/L (5 g/dL)•• Pulmonary oedema• Blood glucose less than 2.2 mmol/L (40 mg/dL)• Acidosis or lactate levels of greater than 5 mmol/L• A parasite level in the blood of greater than 100,000 per microlitre (µL) in low-intensity transmission areas, or
250,000 per µL in high-intensity transmission areasCerebral malaria is defined as a severe P. falciparum-malaria presenting with neurological symptoms, includingcoma (with a Glasgow coma scale less than 11, or a Blantyre coma scale greater than 3), or with a coma that lastslonger than 30 minutes after a seizure.
Prevention
An Anopheles stephensi mosquito shortly afterobtaining blood from a human (the droplet of
blood is expelled as a surplus). This mosquito is avector of malaria, and mosquito control is an
effective way of reducing its incidence.
Methods used to prevent malaria include medications, mosquitoelimination and the prevention of bites. There is no vaccine formalaria. The presence of malaria in an area requires a combination ofhigh human population density, high anopheles mosquito populationdensity and high rates of transmission from humans to mosquitoes andfrom mosquitoes to humans. If any of these is lowered sufficiently, theparasite will eventually disappear from that area, as happened in NorthAmerica, Europe and parts of the Middle East. However, unless theparasite is eliminated from the whole world, it could becomere-established if conditions revert to a combination that favours theparasite's reproduction. Furthermore, the cost per person of eliminatinganopheles mosquitoes rises with decreasing population density, makingit economically unfeasible in some areas.
Prevention of malaria may be more cost-effective than treatment of the disease in the long run, but the initial costsrequired are out of reach of many of the world's poorest people. There is a wide difference in the costs of control (i.e.maintenance of low endemicity) and elimination programs between countries. For example, in China—whosegovernment in 2010 announced a strategy to pursue malaria elimination in the Chinese provinces—the requiredinvestment is a small proportion of public expenditure on health. In contrast, a similar program in Tanzania wouldcost an estimated one-fifth of the public health budget.

Malaria 119
Mosquito controlFurther information: Mosquito control
Man spraying kerosene oil in standing water,Panama Canal Zone 1912
Walls where indoor residual spraying of DDT hasbeen applied. The mosquitoes remain on the wall
until they fall down dead on the floor.
Vector control refers to methods used to decrease malaria by reducingthe levels of transmission by mosquitoes. For individual protection, themost effective insect repellents are based on DEET or picaridin.Insecticide-treated mosquito nets (ITNs) and indoor residual spraying(IRS) have been shown to be highly effective in preventing malariaamong children in areas where malaria is common. Prompt treatmentof confirmed cases with artemisinin-based combination therapies(ACTs) may also reduce transmission.
Mosquito nets create a protective barrier againstmalaria-carrying mosquitoes that bite at night.
Mosquito nets help keep mosquitoes away from people and reduceinfection rates and transmission of malaria. Nets are not a perfectbarrier and are often treated with an insecticide designed to kill themosquito before it has time to find a way past the net.Insecticide-treated nets are estimated to be twice as effective asuntreated nets and offer greater than 70% protection compared with nonet. Between 2000 and 2008, the use of ITNs saved the lives of anestimated 250,000 infants in Sub-Saharan Africa. About 13% ofhouseholds in Sub-Saharan countries own ITNs. In 2000, 1.7 million(1.8%) African children living in stable malaria-endemic conditionswere protected by an ITN. That number increased to 20.3 million(18.5%) African children using ITNs in 2007, leaving 89.6 million
children unprotected. An increased percentage of African households (31%) are estimated to own at least one ITN in 2008. Most nets are impregnated with pyrethroids, a class of insecticides with low toxicity. A recommended practice

Malaria 120
for usage is to hang a large "bed net" above the center of a bed to drape over it completely with the edges tucked in.Pyrethroid-treated nets and long-lasting insecticide-treated nets offer the best protection, and are most effective whenused from dusk to dawn.Indoor residual spraying is the spraying of insecticides on the walls inside a home. After feeding, many mosquitoesrest on a nearby surface while digesting the bloodmeal, so if the walls of houses have been coated with insecticides,the resting mosquitoes can be killed before they can bite another person and transfer the malaria parasite. As of 2006,the World Health Organization recommends 12 insecticides in IRS operations, including DDT and the pyrethroidscyfluthrin and deltamethrin. This public health use of small amounts of DDT is permitted under the StockholmConvention, which prohibits its agricultural use. One problem with all forms of IRS is insecticide resistance.Mosquitoes affected by IRS tend to rest and live indoors, and due to the irritation caused by spraying, theirdescendants tend to rest and live outdoors, meaning that they are less affected by the IRS.There are a number of other methods to reduce mosquito bites and slow the spread of malaria. Efforts to decreasemosquito larva by decreasing the availability of open water in which they develop or by adding substances todecrease their development is effective in some locations. Electronic mosquito repellent devices which make veryhigh frequency sounds that are supposed to keep female mosquitoes away, do not have supporting evidence.
Other methodsCommunity participation and health education strategies promoting awareness of malaria and the importance ofcontrol measures have been successfully used to reduce the incidence of malaria in some areas of the developingworld. Recognizing the disease in the early stages can stop the disease from becoming fatal. Education can alsoinform people to cover over areas of stagnant, still water, such as water tanks that are ideal breeding grounds for theparasite and mosquito, thus cutting down the risk of the transmission between people. This is generally used in urbanareas where there are large centers of population in a confined space and transmission would be most likely in theseareas. Intermittent preventive therapy is another intervention that has been used successfully to control malaria inpregnant women and infants, and in preschool children where transmission is seasonal.June has been marked as Anti-malaria month by National Vector Borne Disease Control Programme (NVBDCP) ofIndia with an objective to increase multisectoral collaboration and community involvement in malaria control.
MedicationsMain article: Malaria prophylaxisThere are a number of drugs that can help prevent malaria while travelling in areas where it exists. Most of thesedrugs are also sometimes used in treatment. Chloroquine may be used where the parasite is still sensitive. Becausemost Plasmodium is resistant to one or more medications, one of three medications—mefloquine (Lariam),doxycycline (available generically), or the combination of atovaquone and proguanil hydrochloride (Malarone)—isfrequently needed. Doxycycline and the atovaquone and proguanil combination are the best tolerated; mefloquine isassociated with death, suicide, and neurological and psychiatric symptoms.The protective effect does not begin immediately, and people visiting areas where malaria exists usually start takingthe drugs one to two weeks before arriving and continue taking them for four weeks after leaving (with the exceptionof atovaquone/proguanil, which only needs to be started two days before and continued for seven days afterward).The use of preventative drugs is seldom practical for those who reside in areas where malaria exists, and their use isusually only in short-term visitors and travellers. This is due to the cost of the drugs, side effects from long-term use,and the difficulty in obtaining anti-malarial drugs outside of wealthy nations. The use of preventative drugs wheremalaria-bearing mosquitoes are present may encourage the development of partial resistance.

Malaria 121
TreatmentMalaria is treated with antimalarial medications; the ones used depends on the type and severity of the disease.While medications against fever are commonly used, their effects on outcomes are not clear.Uncomplicated malaria may be treated with oral medications. The most effective treatment for P. falciparuminfection is the use of artemisinins in combination with other antimalarials (known as artemisinin-combinationtherapy, or ACT), which decreases resistance to any single drug component. These additional antimalarials include:amodiaquine, lumefantrine, mefloquine or sulfadoxine/pyrimethamine. Another recommended combination isdihydroartemisinin and piperaquine. ACT is about 90% effective when used to treat uncomplicated malaria. To treatmalaria during pregnancy, the WHO recommends the use of quinine plus clindamycin early in the pregnancy (1sttrimester), and ACT in later stages (2nd and 3rd trimesters). In the 2000s (decade), malaria with partial resistance toartemisins emerged in Southeast Asia.Infection with P. vivax, P. ovale or P. malariae is usually treated without the need for hospitalization. Treatment ofP. vivax requires both treatment of blood stages (with chloroquine or ACT) as well as clearance of liver forms withprimaquine.Recommended treatment for severe malaria is the intravenous use of antimalarial drugs. For severe malaria,artesunate is superior to quinine in both children and adults. Treatment of severe malaria involves supportivemeasures that are best done in a critical care unit. This includes the management of high fevers and the seizures thatmay result from it. It also includes monitoring for poor breathing effort, low blood sugar, and low blood potassium.
ResistanceDrug resistance poses a growing problem in 21st century malaria treatment. Resistance is now common against allclasses of antimalarial drugs save the artemisinins. Treatment of resistant strains became increasingly dependent onthis class of drugs. The cost of artemisinins limits their use in the developing world. Malaria strains found on theCambodia-Thailand border are resistant to combination therapies that include artemisinins, and may therefore beuntreatable. Exposure of the parasite population to artemisinin monotherapies in subtherapeutic doses for over 30years and the availability of substandard artemisinins likely drove the selection of the resistant phenotype. Resistanceto artemisinin has been detected in Cambodia, Myanmar, Thailand, Vietnam. and emerging resistance in Laos.[12]
Prognosis
Disability-adjusted life year for malaria per 100,000inhabitants in 2004
When properly treated, people with malaria can usually expecta complete recovery. However, severe malaria can progressextremely rapidly and cause death within hours or days. In themost severe cases of the disease, fatality rates can reach 20%,even with intensive care and treatment. Over the longer term,developmental impairments have been documented inchildren who have suffered episodes of severe malaria.Chronic infection without severe disease can occur in animmune-deficiency syndrome associated with a decreasedresponsiveness to Salmonella bacteria and the Epstein–Barr virus.
During childhood, malaria causes anemia during a period of rapid brain development, and also direct brain damageresulting from cerebral malaria. Some survivors of cerebral malaria have an increased risk of neurological andcognitive deficits, behavioural disorders, and epilepsy. Malaria prophylaxis was shown to improve cognitivefunction and school performance in clinical trials when compared to placebo groups.

Malaria 122
Epidemiology
Distribution of malaria in the world:♦ Elevatedoccurrence of chloroquine- or multi-resistant
malaria ♦ Occurrence of chloroquine-resistantmalaria
♦ No Plasmodium falciparum orchloroquine-resistance
♦ No malaria
The WHO estimates that in 2010 there were 219 million cases ofmalaria resulting in 660,000 deaths. Others have estimated the numberof cases at between 350 and 550 million for falciparum malaria anddeaths in 2010 at 1.24 million up from 1.0 million deaths in 1990. Themajority of cases (65%) occur in children under 15 years old. About125 million pregnant women are at risk of infection each year; inSub-Saharan Africa, maternal malaria is associated with up to 200,000estimated infant deaths yearly. There are about 10,000 malaria casesper year in Western Europe, and 1300–1500 in the United States.About 900 people died from the disease in Europe between 1993 and2003. Both the global incidence of disease and resulting mortality havedeclined in recent years. According to the WHO, deaths attributable tomalaria in 2010 were reduced by over a third from a 2000 estimate of
985,000, largely due to the widespread use of insecticide-treated nets and artemisinin-based combination therapies.
Malaria is presently endemic in a broad band around the equator, in areas of the Americas, many parts of Asia, andmuch of Africa; in Sub-Saharan Africa, 85–90% of malaria fatalities occur. An estimate for 2009 reported thatcountries with the highest death rate per 100,000 of population were Ivory Coast (86.15), Angola (56.93) andBurkina Faso (50.66). A 2010 estimate indicated the deadliest countries per population were Burkina Faso,Mozambique and Mali. The Malaria Atlas Project aims to map global endemic levels of malaria, providing a meanswith which to determine the global spatial limits of the disease and to assess disease burden. This effort led to thepublication of a map of P. falciparum endemicity in 2010. As of 2010, about 100 countries have endemic malaria.Every year, 125 million international travellers visit these countries, and more than 30,000 contract the disease.
The geographic distribution of malaria within large regions is complex, and malaria-afflicted and malaria-free areasare often found close to each other. Malaria is prevalent in tropical and subtropical regions because of rainfall,consistent high temperatures and high humidity, along with stagnant waters in which mosquito larvae readily mature,providing them with the environment they need for continuous breeding. In drier areas, outbreaks of malaria havebeen predicted with reasonable accuracy by mapping rainfall. Malaria is more common in rural areas than in cities.For example, several cities in the Greater Mekong Subregion of Southeast Asia are essentially malaria-free, but thedisease is prevalent in many rural regions, including along international borders and forest fringes. In contrast,malaria in Africa is present in both rural and urban areas, though the risk is lower in the larger cities.
HistoryMain articles: History of malaria and Mosquito-malaria theoryAlthough the parasite responsible for P. falciparum malaria has been in existence for 50,000–100,000 years, thepopulation size of the parasite did not increase until about 10,000 years ago, concurrently with advances inagriculture and the development of human settlements. Close relatives of the human malaria parasites remaincommon in chimpanzees. Some evidence suggests that the P. falciparum malaria may have originated in gorillas.References to the unique periodic fevers of malaria are found throughout recorded history, beginning in 2700 BC inChina. Malaria may have contributed to the decline of the Roman Empire, and was so pervasive in Rome that it wasknown as the "Roman fever". Several regions in ancient Rome were considered at-risk for the disease because of thefavourable conditions present for malaria vectors. This included areas such as southern Italy, the island of Sardinia,the Pontine Marshes, the lower regions of coastal Etruria and the city of Rome along the Tiber River. The presenceof stagnant water in these places was preferred by mosquitoes for breeding grounds. Irrigated gardens, swamp-likegrounds, runoff from agriculture, and drainage problems from road construction led to the increase of standing water.

Malaria 123
British doctor Ronald Ross received the NobelPrize for Physiology or Medicine in 1902 for his
work on malaria.
The term malaria originates from Medieval Italian: mala aria — "badair"; the disease was formerly called ague or marsh fever due to itsassociation with swamps and marshland. Malaria was once common inmost of Europe and North America, where it is no longer endemic,though imported cases do occur.
Scientific studies on malaria made their first significant advance in1880, when Charles Louis Alphonse Laveran—a French army doctorworking in the military hospital of Constantine in Algeria—observedparasites inside the red blood cells of infected people for the first time.He therefore proposed that malaria is caused by this organism, the firsttime a protist was identified as causing disease. For this and laterdiscoveries, he was awarded the 1907 Nobel Prize for Physiology orMedicine. A year later, Carlos Finlay, a Cuban doctor treating peoplewith yellow fever in Havana, provided strong evidence that mosquitoeswere transmitting disease to and from humans. This work followedearlier suggestions by Josiah C. Nott, and work by Sir Patrick Manson,the "father of tropical medicine", on the transmission of filariasis.
In April 1894, a Scottish physician Sir Ronald Ross visited Sir PatrickManson at his house on Queen Anne Street, London. This visit was the
start of four years of collaboration and fervent research that culminated in 1898 when Ross, who was working in thePresidency General Hospital in Calcutta, proved the complete life-cycle of the malaria parasite in mosquitoes. Hethus proved that the mosquito was the vector for malaria in humans by showing that certain mosquito speciestransmit malaria to birds. He isolated malaria parasites from the salivary glands of mosquitoes that had fed oninfected birds. For this work, Ross received the 1902 Nobel Prize in Medicine. After resigning from the IndianMedical Service, Ross worked at the newly established Liverpool School of Tropical Medicine and directedmalaria-control efforts in Egypt, Panama, Greece and Mauritius. The findings of Finlay and Ross were laterconfirmed by a medical board headed by Walter Reed in 1900. Its recommendations were implemented by WilliamC. Gorgas in the health measures undertaken during construction of the Panama Canal. This public-health worksaved the lives of thousands of workers and helped develop the methods used in future public-health campaignsagainst the disease.
The first effective treatment for malaria came from the bark of cinchona tree, which contains quinine. This treegrows on the slopes of the Andes, mainly in Peru. The indigenous peoples of Peru made a tincture of cinchona tocontrol fever. Its effectiveness against malaria was found and the Jesuits introduced the treatment to Europe around1640; by 1677, it was included in the London Pharmacopoeia as an antimalarial treatment. It was not until 1820 thatthe active ingredient, quinine, was extracted from the bark, isolated and named by the French chemists Pierre JosephPelletier and Joseph Bienaimé Caventou.

Malaria 124
Artemisia annua, source of the antimalarial drugartemisin
Quinine become the predominant malarial medication until the 1920s,when other medications began to be developed. In the 1940s,chloroquine replaced quinine as the treatment of both uncomplicatedand severe malaria until resistance supervened, first in Southeast Asiaand South America in the 1950s and then globally in the 1980s.Artemisinins, discovered by Chinese scientist Tu Youyou andcolleagues in the 1970s from the plant Artemisia annua, became therecommended treatment for P. falciparum malaria, administered incombination with other antimalarials as well as in severe disease.
Plasmodium vivax was used between 1917 and the 1940s for malariotherapy—deliberate injection of malariaparasites to induce fever to combat certain diseases such as tertiary syphilis. In 1917, the inventor of this technique,Julius Wagner-Jauregg, received the Nobel Prize in Physiology or Medicine for his discoveries. The technique wasdangerous, killing about 15% of patients, so it is no longer in use.The first pesticide used for indoor residual spraying was DDT. Although it was initially used exclusively to combatmalaria, its use quickly spread to agriculture. In time, pest control, rather than disease control, came to dominateDDT use, and this large-scale agricultural use led to the evolution of resistant mosquitoes in many regions. The DDTresistance shown by Anopheles mosquitoes can be compared to antibiotic resistance shown by bacteria. During the1960s, awareness of the negative consequences of its indiscriminate use increased, ultimately leading to bans onagricultural applications of DDT in many countries in the 1970s. Before DDT, malaria was successfully eliminatedor controlled in tropical areas like Brazil and Egypt by removing or poisoning the breeding grounds of themosquitoes or the aquatic habitats of the larva stages, for example by applying the highly toxic arsenic compoundParis Green to places with standing water.Malaria vaccines have been an elusive goal of research. The first promising studies demonstrating the potential for amalaria vaccine were performed in 1967 by immunizing mice with live, radiation-attenuated sporozoites, whichprovided significant protection to the mice upon subsequent injection with normal, viable sporozoites. Since the1970s, there has been a considerable effort to develop similar vaccination strategies within humans.
Society and cultureSee also: World Malaria Day
Economic impact
Malaria clinic in Tanzania
Malaria is not just a disease commonly associated with poverty: someevidence suggests that it is also a cause of poverty and a majorhindrance to economic development. Although tropical regions aremost affected, malaria's furthest influence reaches into some temperatezones that have extreme seasonal changes. The disease has beenassociated with major negative economic effects on regions where it iswidespread. During the late 19th and early 20th centuries, it was amajor factor in the slow economic development of the Americansouthern states.
A comparison of average per capita GDP in 1995, adjusted for parityof purchasing power, between countries with malaria and countries without malaria gives a fivefold difference($1,526 USD versus $8,268 USD). In the period 1965 to 1990, countries where malaria was common had an averageper capita GDP that increased only 0.4% per year, compared to 2.4% per year in other countries.

Malaria 125
Poverty can increase the risk of malaria, since those in poverty do not have the financial capacities to prevent or treatthe disease. In its entirety, the economic impact of malaria has been estimated to cost Africa $12 billion USD everyyear. The economic impact includes costs of health care, working days lost due to sickness, days lost in education,decreased productivity due to brain damage from cerebral malaria, and loss of investment and tourism. The diseasehas a heavy burden in some countries, where it may be responsible for 30–50% of hospital admissions, up to 50% ofoutpatient visits, and up to 40% of public health spending.Cerebral malaria is one of the leading causes of neurological disabilities in African children. Studies comparingcognitive functions before and after treatment for severe malarial illness continued to show significantly impairedschool performance and cognitive abilities even after recovery. Consequently, severe and cerebral malaria havefar-reaching socioeconomic consequences that extend beyond the immediate effects of the disease.
Counterfeit and substandard drugsSophisticated counterfeits have been found in several Asian countries such as Cambodia, China, Indonesia, Laos,Thailand, and Vietnam, and are an important cause of avoidable death in those countries. The WHO said that studiesindicate that up to 40% of artesunate-based malaria medications are counterfeit, especially in the Greater Mekongregion and have established a rapid alert system to enable information about counterfeit drugs to be rapidly reportedto the relevant authorities in participating countries. There is no reliable way for doctors or lay people to detectcounterfeit drugs without help from a laboratory. Companies are attempting to combat the persistence of counterfeitdrugs by using new technology to provide security from source to distribution.Another clinical and public health concern is the proliferation of substandard antimalarial medicines resulting frominappropriate concentration of ingredients, contamination with other drugs or toxic impurities, poor qualityingredients, poor stability and inadequate packaging. A 2012 study demonstrated that roughly one-third ofantimalarial medications in Southeast Asia and Sub-Saharan Africa failed chemical analysis, packaging analysis, orwere falsified.
War
World War II poster
Throughout history, the contraction of malaria has played a prominentrole in the fates of government rulers, nation-states, military personnel,and military actions. In 1910, Nobel Prize in Medicine-winner RonaldRoss (himself a malaria survivor), published a book titled ThePrevention of Malaria that included a chapter titled "The Prevention ofMalaria in War." The chapter's author, Colonel C. H. Melville,Professor of Hygiene at Royal Army Medical College in London,addressed the prominent role that malaria has historically playedduring wars: "The history of malaria in war might almost be taken tobe the history of war itself, certainly the history of war in the Christianera. ... It is probably the case that many of the so-called camp fevers,and probably also a considerable proportion of the camp dysentery, ofthe wars of the sixteenth, seventeenth and eighteenth centuries weremalarial in origin."
Malaria was the most important health hazard encountered by U.S.troops in the South Pacific during World War II, where about 500,000 men were infected. According to JosephPatrick Byrne, "Sixty thousand American soldiers died of malaria during the African and South Pacific campaigns."
Significant financial investments have been made to procure existing and create new anti-malarial agents. During World War I and World War II, inconsistent supplies of the natural anti-malaria drugs cinchona bark and quinine

Malaria 126
prompted substantial funding into research and development of other drugs and vaccines. American militaryorganizations conducting such research initiatives include the Navy Medical Research Center, Walter Reed ArmyInstitute of Research, and the U.S. Army Medical Research Institute of Infectious Diseases of the US Armed Forces.Additionally, initiatives have been founded such as Malaria Control in War Areas (MCWA), established in 1942,and its successor, the Communicable Disease Center (now known as the Centers for Disease Control and Prevention,or CDC) established in 1946. According to the CDC, MCWA "was established to control malaria around militarytraining bases in the southern United States and its territories, where malaria was still problematic".
Eradication effortsSeveral notable attempts are being made to eliminate the parasite from sections of the world, or to eradicate itworldwide. In 2006, the organization Malaria No More set a public goal of eliminating malaria from Africa by 2015,and the organization plans to dissolve if that goal is accomplished. Several malaria vaccines are in clinical trials,which are intended to provide protection for children in endemic areas and reduce the speed of transmission of thedisease. As of 2012[13], The Global Fund to Fight AIDS, Tuberculosis and Malaria has distributed 230 millioninsecticide-treated nets intended to stop mosquito-borne transmission of malaria. The U.S.-based Clinton Foundationhas worked to manage demand and stabilize prices in the artemisinin market. Other efforts, such as the Malaria AtlasProject, focus on analysing climate and weather information required to accurately predict the spread of malariabased on the availability of habitat of malaria-carrying parasites. The Malaria Policy Advisory Committee (MPAC)of the World Health Organization (WHO) was formed in 2012, "to provide strategic advice and technical input toWHO on all aspects of malaria control and elimination". In November 2013, WHO and the malaria vaccine fundersgroup set a goal to develop vaccines designed to interrupt malaria transmission with the long-term goal of malariaeradication.Malaria has been successfully eliminated or greatly reduced in certain areas. Malaria was once common in theUnited States and southern Europe, but vector control programs, in conjunction with the monitoring and treatment ofinfected humans, eliminated it from those regions. Several factors contributed, such as the draining of wetlandbreeding grounds for agriculture and other changes in water management practices, and advances in sanitation,including greater use of glass windows and screens in dwellings. Malaria was eliminated from most parts of the USAin the early 20th century by such methods, and the use of the pesticide DDT and other means eliminated it from theremaining pockets in the South in the 1950s. (see National Malaria Eradication Program) In Suriname, the diseasehas been cleared from its capital city and coastal areas through a three-pronged approach initiated by the GlobalMalaria Eradication program in 1955, involving: vector control through the use of DDT and IRS; regular collectionof blood smears from the population to identify existing malaria cases; and providing chemotherapy to all affectedindividuals. Bhutan is pursuing an aggressive malaria elimination strategy, and has achieved a 98.7% decline inmicroscopy-confirmed cases from 1994 to 2010. In addition to vector control techniques such as IRS in high-riskareas and thorough distribution of long-lasting ITNs, factors such as economic development and increasing access tohealth services have contributed to Bhutan's successes in reducing malaria incidence.
ResearchSee also: Malaria vaccineImmunity (or, more accurately, tolerance) to P. falciparum malaria does occur naturally, but only in response to years of repeated infection. An individual can be protected from a P. falciparum infection if they receive about a thousand bites from mosquitoes that carry a version of the parasite rendered non-infective by a dose of X-ray irradiation. An effective vaccine is not yet available for malaria, although several are under development. The highly polymorphic nature of many P. falciparum proteins results in significant challenges to vaccine design. Vaccine candidates that target antigens on gametes, zygotes, or ookinetes in the mosquito midgut aim to block the transmission of malaria. These transmission-blocking vaccines induce antibodies in the human blood; when a

Malaria 127
mosquito takes a blood meal from a protected individual, these antibodies prevent the parasite from completing itsdevelopment in the mosquito. Other vaccine candidates, targeting the blood-stage of the parasite's life cycle, havebeen inadequate on their own. For example, SPf66 was tested extensively in endemic areas in the 1990s, but clinicaltrials showed it to be insufficiently effective. Several potential vaccines targeting the pre-erythrocytic stage of theparasite's life cycle are being developed, with RTS,S as the leading candidate; it is expected to be licensed in 2015. AUS biotech company, Sanaria, is developing a pre-erythrocytic attenuated vaccine called PfSPZ that uses wholesporozoites to induce an immune response. In 2006, the Malaria Vaccine Advisory Committee to the WHO outlineda "Malaria Vaccine Technology Roadmap" that has as one of its landmark objectives to "develop and license afirst-generation malaria vaccine that has a protective efficacy of more than 50% against severe disease and death andlasts longer than one year" by 2015.Malaria parasites contain apicoplasts, organelles usually found in plants, complete with their own genomes. Theseapicoplasts are thought to have originated through the endosymbiosis of algae and play a crucial role in variousaspects of parasite metabolism, such as fatty acid biosynthesis. Over 400 proteins have been found to be produced byapicoplasts and these are now being investigated as possible targets for novel anti-malarial drugs.With the onset of drug-resistant Plasmodium parasites, new strategies are being developed to combat the widespreaddisease. One such approach lies in the introduction of synthetic pyridoxal-amino acid adducts, which are taken up bythe parasite and ultimately interfere with its ability to create several essential B vitamins. Antimalarial drugs usingsynthetic metal-based complexes are attracting research interest.A non-chemical vector control strategy involves genetic manipulation of malaria mosquitoes. Advances in geneticengineering technologies make it possible to introduce foreign DNA into the mosquito genome and either decreasethe lifespan of the mosquito, or make it more resistant to the malaria parasite. Sterile insect technique is a geneticcontrol method whereby large numbers of sterile males mosquitoes are reared and released. Mating with wildfemales reduces the wild population in the subsequent generation; repeated releases eventually eliminate the targetpopulation.Genomics is now central to malaria research. With the sequencing of P. falciparum, one of its vectors Anophelesgambiae, and the human genome, the genetics of all three organisms in the malaria lifecycle can be studied. Anothernew application of genetic technology is the ability to produce genetically modified mosquitoes that do not transmitmalaria, potentially allowing biological control of malaria transmission.Researchers are encouraged by the findings of a study that commenced in 2002 involving the monitoring of the livesof 1,000 Tanzanian children. The study is one of many being explored in 2014 in the race to find a malaria vaccine.
Other animalsNearly 200 parasitic Plasmodium species have been identified that infect birds, reptiles, and other mammals, andabout 30 species naturally infect non-human primates. Some of the malaria parasites that affect non-human primates(NHP) serve as model organisms for human malarial parasites, such as P. coatneyi (a model for P. falciparum) andP. cynomolgi (P. vivax). Diagnostic techniques used to detect parasites in NHP are similar to those employed forhumans. Malaria parasites that infect rodents are widely used as models in research, such as P. berghei. Avianmalaria primarily affects species of the order Passeriformes, and poses a substantial threat to birds of Hawaii, theGalapagos, and other archipelagoes. The parasite P. relictum is known to play a role in limiting the distribution andabundance of endemic Hawaiian birds. Global warming is expected to increase the prevalence and globaldistribution of avian malaria, as elevated temperatures provide optimal conditions for parasite reproduction.

Malaria 128
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Malaria[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ B50[3] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ B54[4] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=084[5] http:/ / omim. org/ entry/ 248310[6] http:/ / www. diseasesdatabase. com/ ddb7728. htm[7] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000621. htm[8] http:/ / www. emedicine. com/ med/ topic1385. htm[9] http:/ / www. emedicine. com/ emerg/ topic305. htm#[10] http:/ / www. emedicine. com/ ped/ topic1357. htm#[11] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?mode=& term=Malaria& field=entry#TreeC03. 752. 250. 552[12] Briggs, Helen (30 July 2014) Call for 'radical action' on drug-resistant malaria (http:/ / www. bbc. co. uk/ news/ health-28569966) BBC
News, health, Retrieved 30 July 2013[13] http:/ / en. wikipedia. org/ w/ index. php?title=Malaria& action=edit
Cited literature• WHO (2010) (PDF). Guidelines for the Treatment of Malaria (http:/ / whqlibdoc. who. int/ publications/ 2010/
9789241547925_eng. pdf) (Report) (2nd ed.). World Health Organization. ISBN 978-9-2415-4792-5.• Schlagenhauf-Lawlor P (2008). Travelers' Malaria (http:/ / books. google. com/ books?id=54Dza0UHyngC).
PMPH-USA. ISBN 978-1-55009-336-0.
Further reading• Packard RM (2007). The Making of a Tropical Disease: A Short History of Malaria (http:/ / books. google. com/
books?id=B_V1Xj6wH7IC). Johns Hopkins Biographies of Disease. JHU Press. ISBN 978-0-8018-8712-3.• Shah S (2010). The Fever: How Malaria Has Ruled Humankind for 500,000 Years (http:/ / books. google. com/
books?id=4jUjPh64X9UC). Macmillan. ISBN 978-0-374-23001-2. excerpt and text search (http:/ / www.amazon. com/ Fever-Malaria-Ruled-Humankind-Years/ dp/ 0374230013/ )
• Bynum WF, Overy C (1998). The Beast in the Mosquito: The Correspondence of Ronald Ross and PatrickManson (http:/ / books. google. com/ books?id=5BXbsSJLaToC). Wellcome Institute Series in The History ofMedicine. Rodopi. ISBN 978-90-420-0721-5.
External links
Wikimedia Commons has media related to Malaria.
Wikivoyage has a travel guide for Malaria.
Look up malaria in Wiktionary, the free dictionary.
• Malaria (http:/ / www. dmoz. org/ Health/ Conditions_and_Diseases/ Infectious_Diseases/ Parasitic/ Malaria) atDMOZ
• WHO site on malaria (http:/ / www. emro. who. int/ entity/ malaria-control-and-elimination/ )• UNHCO site on malaria (http:/ / www. unhco. org/ malaria/ )• Global Malaria Action Plan (http:/ / www. rollbackmalaria. org/ gmap/ ) (2008)• Doctors Without Borders/Médecins Sans Frontières – Malaria (http:/ / doctorswithoutborders. org/ news/ issue.
cfm?id=2395) information pages

Malaria 129
• Who/TDR Malaria Database (http:/ / www. wehi. edu. au/ other_domains/ MalDB/ who. html)• Anti malaria and sustainable development (http:/ / www. antimalariaomd. org/ en/ index. php)• Worldwide Antimalarial Resistance Network (WWARN) (http:/ / www. wwarn. org)
Pulmonary hypertensionContributors [1]
Pulmonary arterial hypertensionClassification and external resources
Micrograph showing a plexiform lesion of the lung, as seen in irreversible pulmonary hypertension. H&E stain.
ICD-10 I27.0 [2], I27.2 [3]
ICD-9 416.0 [4]
DiseasesDB 10998 [5]
MedlinePlus 000112 [6]
eMedicine med/1962 [7]
MeSH D006976 [8]
Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary vein, orpulmonary capillaries, together known as the lung vasculature, leading to shortness of breath, dizziness, fainting, legswelling and other symptoms. Pulmonary hypertension can be a severe disease with a markedly decreased exercisetolerance and heart failure. It was first identified by Ernst von Romberg in 1891. According to the most recentclassification, it can be one of six different types (see below).
Signs and symptomsBecause symptoms may develop very gradually, patients may delay seeing a physician for years. Commonsymptoms are shortness of breath, fatigue, non-productive cough, angina pectoris, fainting or syncope, peripheraledema (swelling around the ankles and feet), and rarely hemoptysis (coughing up blood).Pulmonary venous hypertension typically presents with shortness of breath while lying flat or sleeping (orthopnea orparoxysmal nocturnal dyspnea), while pulmonary arterial hypertension (PAH) typically does not.A detailed family history is established to determine whether the disease might be familial. A history of exposure to drugs such as cocaine, methamphetamine, alcohol leading to cirrhosis, and tobacco leading to emphysema are

Pulmonary hypertension 130
considered significant. A physical examination is performed to look for typical signs of pulmonary hypertension,including a loud S2 (pulmonic valve closure sound), (para)sternal heave, jugular venous distension, pedal edema,ascites, hepatojugular reflux, clubbing etc. Evidence of tricuspid insufficiency is also sought and, if present, isconsistent with the presence of pulmonary hypertension.
Causes and classificationA 1973 meeting organized by the World Health Organization was the first to attempt classification of pulmonaryhypertension. A distinction was made between primary and secondary PH, and primary PH was divided in the"arterial plexiform", "veno-occlusive" and "thromboembolic" forms. A second conference in 1998 at Évian-les-Bainsalso addressed the causes of secondary PH (i.e. those due to other medical conditions), and in 2008, the 4th WorldSymposium on Pulmonary Arterial Hypertension was convened in Dana Point to modify the classification based onnew understandings of disease mechanisms. The revised system developed by this group provides the currentframework for understanding pulmonary hypertension. The system includes several improvements over the former2004 Venice Classification system.The Dana Point 2008 Updated Clinical Classification system can be summarized as follows:•• WHO Group I - Pulmonary arterial hypertension (PAH)
• Idiopathic PAH•• Heritable
•• BMPR2• ALK1, endoglin (with or without hereditary hemorrhagic telangiectasia)•• Unknown
•• Drug- and toxin-induced•• Associated with
•• Connective tissue disease•• HIV infection•• Portal hypertension• Congenital heart diseases•• Schistosomiasis• Chronic hemolytic anemia (including sickle cell disease)
• Persistent pulmonary hypertension of the newborn• WHO Group I' - Pulmonary veno-occlusive disease (PVOD) and/or pulmonary capillary hemangiomatosis
(PCH)• WHO Group II - Pulmonary hypertension owing to left heart disease
•• Systolic dysfunction•• Diastolic dysfunction•• Valvular heart disease
• WHO Group III - Pulmonary hypertension owing to lung disease and/or hypoxia•• Chronic obstructive pulmonary disease•• Interstitial lung disease• Other pulmonary diseases with mixed restrictive and obstructive pattern•• Sleep-disordered breathing• Alveolar hypoventilation disorders•• Chronic exposure to high altitude•• Developmental abnormalities
• WHO Group IV - Chronic thromboembolic pulmonary hypertension (CTEPH)

Pulmonary hypertension 131
• WHO Group V - Pulmonary hypertension with unclear multifactorial mechanisms• Hematologic diseases: myeloproliferative disease, splenectomy• Systemic diseases: sarcoidosis, pulmonary Langerhans cell histiocytosis: lymphangioleiomyomatosis,
neurofibromatosis, vasculitis• Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid diseases• Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on dialysis
PathogenesisWhatever the initial cause, pulmonary arterial hypertension (WHO Group I) involves the vasoconstriction ortightening of blood vessels connected to and within the lungs. This makes it harder for the heart to pump bloodthrough the lungs, much as it is harder to make water flow through a narrow pipe as opposed to a wide one. Overtime, the affected blood vessels become both stiffer and thicker, in a process known as fibrosis. This furtherincreases the blood pressure within the lungs and impairs their blood flow. In common with other types ofpulmonary hypertension, the increased workload of the heart causes hypertrophy of the right ventricle, making theheart less able to pump blood through the lungs, ultimately causing right heart failure (a condition known as corpulmonale). The right ventricle is normally part of a low pressure system, with pressures that are around one-sixth ofthose that the left ventricle has to deal with. As such, the right ventricle is much less able to cope as pressure rises,and although hypertrophy of the heart muscle helps initially, it ultimately leads to a situation where the rightventricular muscle cannot get enough oxygen to meet its needs and right heart failure follows. As the blood flowingthrough the lungs decreases, the left side of the heart receives less blood. This blood may also carry less oxygen thannormal. Therefore it becomes harder and harder for the left side of the heart to pump to supply sufficient oxygen tothe rest of the body, especially during physical activity.Pathogenesis in pulmonary hypertension owing to left heart disease (WHO Group II) is completely different in thatconstriction or damage to the pulmonary blood vessels is not the issue. Instead, the left heart fails to pump bloodefficiently, leading to pooling of blood in the lungs and back pressure within the pulmonary system. This causespulmonary edema and pleural effusions.In hypoxic pulmonary hypertension (WHO Group III), the low levels of oxygen are thought to causevasoconstriction or tightening of pulmonary arteries. This phenomenon is called hypoxic pulmonary vasoconstrictionand it is initially a protective response designed to stop too much blood flowing to areas of the lung that are damagedand do not contain oxygen. When the damage is widespread and prolonged, this hypoxia-mediated vasoconstrictionoccurs across a large portion of the pulmonary vascular bed and becomes a very real issue.In chronic thromboembolic pulmonary hypertension (WHO Group IV), the blood vessels are blocked or narrowedwith recurrent blood clots, and these clots can lead to release of substances that cause the blood vessels to constrict.This combination of blocked or narrowed vessels and vasoconstriction once again increases the resistance to bloodflow and so the pressure within the system rises.
Molecular pathologyThe molecular mechanism of pulmonary arterial hypertension (PAH) is not known yet, but it is believed that theendothelial dysfunction results in a decrease in the synthesis of endothelium-derived vasodilators such as nitric oxideand prostacyclin. Moreover, there’s a stimulation of the synthesis of vasoconstrictors such as thromboxane andvascular endothelial growth factor (VEGF). These results in a severe vasoconstriction and smooth muscle andadventitial hypertrophy characteristic of patients with PAH.[9]
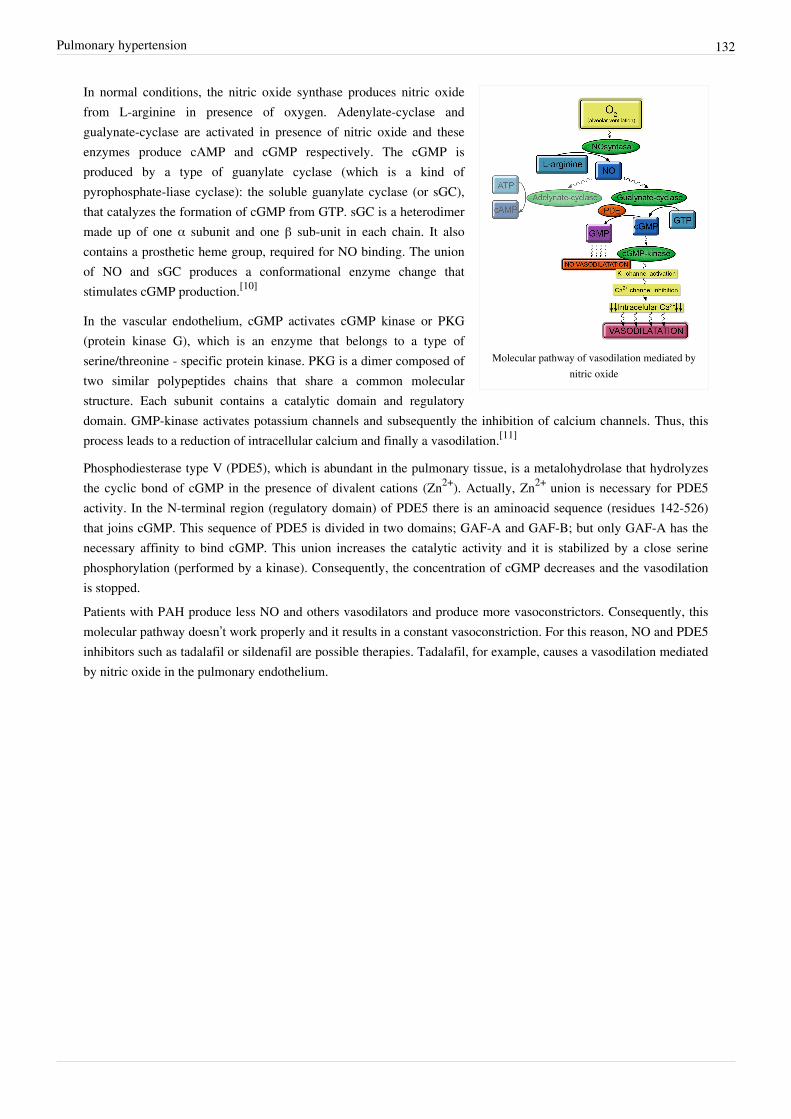
Pulmonary hypertension 132
Molecular pathway of vasodilation mediated bynitric oxide
In normal conditions, the nitric oxide synthase produces nitric oxidefrom L-arginine in presence of oxygen. Adenylate-cyclase andgualynate-cyclase are activated in presence of nitric oxide and theseenzymes produce cAMP and cGMP respectively. The cGMP isproduced by a type of guanylate cyclase (which is a kind ofpyrophosphate-liase cyclase): the soluble guanylate cyclase (or sGC),that catalyzes the formation of cGMP from GTP. sGC is a heterodimermade up of one α subunit and one β sub-unit in each chain. It alsocontains a prosthetic heme group, required for NO binding. The unionof NO and sGC produces a conformational enzyme change thatstimulates cGMP production.[10]
In the vascular endothelium, cGMP activates cGMP kinase or PKG(protein kinase G), which is an enzyme that belongs to a type ofserine/threonine - specific protein kinase. PKG is a dimer composed oftwo similar polypeptides chains that share a common molecularstructure. Each subunit contains a catalytic domain and regulatorydomain. GMP-kinase activates potassium channels and subsequently the inhibition of calcium channels. Thus, thisprocess leads to a reduction of intracellular calcium and finally a vasodilation.[11]
Phosphodiesterase type V (PDE5), which is abundant in the pulmonary tissue, is a metalohydrolase that hydrolyzesthe cyclic bond of cGMP in the presence of divalent cations (Zn2+). Actually, Zn2+ union is necessary for PDE5activity. In the N-terminal region (regulatory domain) of PDE5 there is an aminoacid sequence (residues 142-526)that joins cGMP. This sequence of PDE5 is divided in two domains; GAF-A and GAF-B; but only GAF-A has thenecessary affinity to bind cGMP. This union increases the catalytic activity and it is stabilized by a close serinephosphorylation (performed by a kinase). Consequently, the concentration of cGMP decreases and the vasodilationis stopped.Patients with PAH produce less NO and others vasodilators and produce more vasoconstrictors. Consequently, thismolecular pathway doesn’t work properly and it results in a constant vasoconstriction. For this reason, NO and PDE5inhibitors such as tadalafil or sildenafil are possible therapies. Tadalafil, for example, causes a vasodilation mediatedby nitric oxide in the pulmonary endothelium.
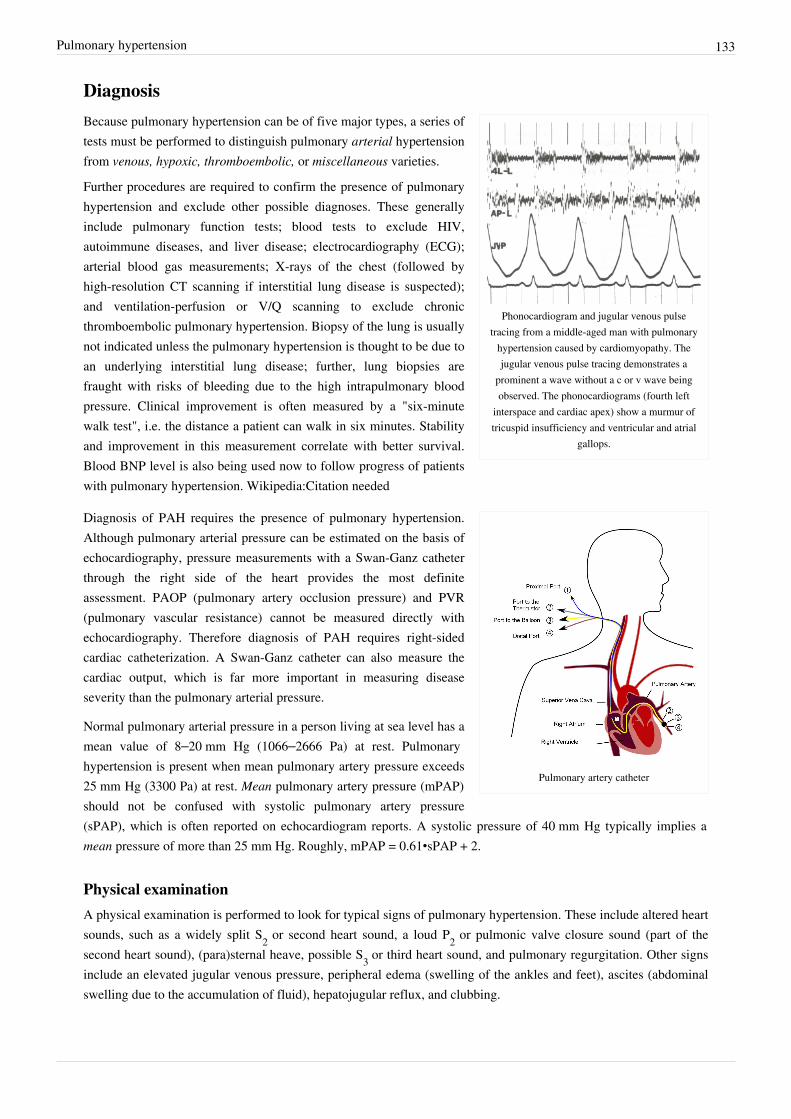
Pulmonary hypertension 133
Diagnosis
Phonocardiogram and jugular venous pulsetracing from a middle-aged man with pulmonary
hypertension caused by cardiomyopathy. Thejugular venous pulse tracing demonstrates a
prominent a wave without a c or v wave beingobserved. The phonocardiograms (fourth left
interspace and cardiac apex) show a murmur oftricuspid insufficiency and ventricular and atrial
gallops.
Because pulmonary hypertension can be of five major types, a series oftests must be performed to distinguish pulmonary arterial hypertensionfrom venous, hypoxic, thromboembolic, or miscellaneous varieties.
Further procedures are required to confirm the presence of pulmonaryhypertension and exclude other possible diagnoses. These generallyinclude pulmonary function tests; blood tests to exclude HIV,autoimmune diseases, and liver disease; electrocardiography (ECG);arterial blood gas measurements; X-rays of the chest (followed byhigh-resolution CT scanning if interstitial lung disease is suspected);and ventilation-perfusion or V/Q scanning to exclude chronicthromboembolic pulmonary hypertension. Biopsy of the lung is usuallynot indicated unless the pulmonary hypertension is thought to be due toan underlying interstitial lung disease; further, lung biopsies arefraught with risks of bleeding due to the high intrapulmonary bloodpressure. Clinical improvement is often measured by a "six-minutewalk test", i.e. the distance a patient can walk in six minutes. Stabilityand improvement in this measurement correlate with better survival.Blood BNP level is also being used now to follow progress of patientswith pulmonary hypertension. Wikipedia:Citation needed
Pulmonary artery catheter
Diagnosis of PAH requires the presence of pulmonary hypertension.Although pulmonary arterial pressure can be estimated on the basis ofechocardiography, pressure measurements with a Swan-Ganz catheterthrough the right side of the heart provides the most definiteassessment. PAOP (pulmonary artery occlusion pressure) and PVR(pulmonary vascular resistance) cannot be measured directly withechocardiography. Therefore diagnosis of PAH requires right-sidedcardiac catheterization. A Swan-Ganz catheter can also measure thecardiac output, which is far more important in measuring diseaseseverity than the pulmonary arterial pressure.
Normal pulmonary arterial pressure in a person living at sea level has amean value of 8–20 mm Hg (1066–2666 Pa) at rest. Pulmonaryhypertension is present when mean pulmonary artery pressure exceeds25 mm Hg (3300 Pa) at rest. Mean pulmonary artery pressure (mPAP)should not be confused with systolic pulmonary artery pressure(sPAP), which is often reported on echocardiogram reports. A systolic pressure of 40 mm Hg typically implies amean pressure of more than 25 mm Hg. Roughly, mPAP = 0.61•sPAP + 2.
Physical examinationA physical examination is performed to look for typical signs of pulmonary hypertension. These include altered heartsounds, such as a widely split S2 or second heart sound, a loud P2 or pulmonic valve closure sound (part of thesecond heart sound), (para)sternal heave, possible S3 or third heart sound, and pulmonary regurgitation. Other signsinclude an elevated jugular venous pressure, peripheral edema (swelling of the ankles and feet), ascites (abdominalswelling due to the accumulation of fluid), hepatojugular reflux, and clubbing.

Pulmonary hypertension 134
EchocardiographyA meta-analysis of Doppler echocardiography for predicting right heart catheterization reported a sensitivity andspecificity of 88% and 56%, respectively.
TreatmentTreatment is determined by whether the PH is arterial, venous, hypoxic, thromboembolic, or miscellaneous. Sincepulmonary venous hypertension is synonymous with congestive heart failure, the treatment is to optimize leftventricular function by the use of diuretics, beta blockers, ACE inhibitors etc., or to repair/replace the mitral valve oraortic valve.Patients with left heart failure or hypoxemic lung diseases (groups II or III pulmonary hypertension) should notroutinely be treated with vasoactive agents including prostanoids, phosphodiesterase inhibitors, or endothelinantagonists, as these are approved for the different condition called pulmonary arterial hypertension.[12] To make thedistinction, doctors at a minimum will conduct cardiac catheterization of the right heart, echocardiography, chest CT,a six-minute walk test, and pulmonary function testing. Using treatments for other kinds of pulmonary hypertensionin patients with these conditions can harm the patient and wastes substantial medical resources.In PAH, lifestyle changes, digoxin, diuretics, oral anticoagulants, and oxygen therapy are considered conventionaltherapy, but have never been proven to be beneficial in a randomized, prospective manner.Wikipedia:CitationneededHigh dose calcium channel blockers are useful in only 5% of IPAH patients who are vasoreactive by Swan-Ganzcatheter. Unfortunately, calcium channel blockers have been largely misused, being prescribed to many patients withnon-vasoreactive PAH, leading to excess morbidity and mortality. The criteria for vasoreactivity have changed. Onlythose patients whose mean pulmonary artery pressure falls by more than 10 mm Hg to less than 40 mm Hg with anunchanged or increased cardiac output when challenged with adenosine, epoprostenol, or nitric oxide are consideredvasoreactive. Of these, only half of the patients are responsive to calcium channel blockers in the long term.A number of agents have recently been introduced for primary and secondary PAH. The trials supporting the use ofthese agents have been relatively small, and the only measure consistently used to compare their effectivity is the "6minute walk test". Many have no data on mortality benefit or time to progression.
Vasoactive substancesMany pathways are involved in the abnormal proliferation and contraction of the smooth muscle cells of thepulmonary arteries in patients with pulmonary arterial hypertension. Three of these pathways are important sincethey have been targeted with drugs — endothelin receptor antagonists, phosphodiesterase type 5 (PDE-5) inhibitors,and prostacyclin derivatives.Because inexpensive generic drugs for this disease are not widely available, the World Health Organization does notinclude them in its model list of essential medicines.
Prostaglandins
Prostacyclin (prostaglandin I2) is commonly considered the most effective treatment for PAH. Epoprostenol (synthetic prostacyclin, marketed as Flolan) is given via continuous infusion that requires a semi-permanent central venous catheter. This delivery system can cause sepsis and thrombosis. Prostacyclin is unstable, and therefore has to be kept on ice during administration. Since it has a half-life of 3 to 5 minutes, the infusion has to be continuous (24/7), and interruption can be fatal. Other prostanoids have therefore been developed. Treprostinil (Remodulin) can be given intravenously or subcutaneously, but the subcutaneous form can be very painful. An increased risk of sepsis with intravenous Remodulin has been reported by the CDC. Iloprost (Ilomedin) is also used in Europe intravenously and has a longer half life. Iloprost (marketed as Ventavis) was the only inhaled form of prostacyclin approved for use

Pulmonary hypertension 135
in the US and Europe, until the inhaled form of treprostinil was approved by the FDA in July 2009 and is marketedunder the trade name Tyvaso. The inhaled form of administration has the advantage of selective deposition in thelungs with less systemic side effects, however coughing and throat irritation commonly occur. Oral and inhaledforms of Remodulin are under development. Beraprost is an oral prostanoid available in South Korea and Japan.
Endothelin receptor antagonists
The dual (ETA and ETB) endothelin receptor antagonist bosentan (marketed as Tracleer) was approved in 2001.Sitaxentan (Thelin), a selective endothelin receptor antagonist that blocks only the action of ETA, was approved foruse in Canada, Australia, and the European Union. but not in the United States. In 2010, Pfizer withdrew Thelinworldwide because of fatal liver complications. A similar drug, ambrisentan is marketed as Letairis in U.S. by GileadSciences. In addition, another dual/nonselective endothelin antagonist, Actelion-1, from the makers of Tracleer, willenter clinical trials in 2008.
Phosphodiesterase type 5 inhibitors
The U.S. FDA approved Sildenafil, a selective inhibitor of cGMP specific phosphodiesterase type 5 (PDE5), for thetreatment of PAH in 2005. It is marketed for PAH as Revatio. In 2009, they also approved Tadalafil, another PDE5inhibitor, marketed under the name Adcirca. PDE5 inhibitors are believed to increase pulmonary artery vasodilation,and inhibit vascular remodeling, thus lowering pulmonary arterial pressure and pulmonary vascularresistance.Wikipedia:Citation neededTadalafil is taken orally, as well as sildenafil, and it is rapidly absorbed (serum levels are detectable at 20 minutes).The recommended dose is 40 mg in one single dose per day and the T1/2 (biological half-life) hovers around 17.5hours in healthy subjects.[13] Moreover, if we consider pharmacoeconomic implications, patients that take tadalafilwould pay ⅔ of the cost of sildenafil therapy.[14] However, there are some adverse effects of this drug such asheadache, diarrhea, nausea, back pain, dyspepsia, flushing and myalgia.[15]
Activators of soluble guanylate cyclase
Soluble guanylate cyclase (sGC) is the intracellular receptor for NO. As of April 2009[16], the sGC activatorscinaciguat and riociguat were undergoing clinical trials for the treatment of PAH. In October 2013, riociguat(Adempas), was FDA approved for the treatment of PAH. It is the first of its class.
SurgicalAtrial septostomy is a surgical procedure that creates a communication between the right and left atria. It relievespressure on the right side of the heart, but at the cost of lower oxygen levels in blood (hypoxia).Lung transplantation cures pulmonary arterial hypertension, but leaves the patient with the complications oftransplantation, and a post-surgical median survival of just over five years.Pulmonary thromboendarterectomy (PTE) is a surgical procedure that is used for chronic thromboembolicpulmonary hypertension. It is the surgical removal of an organized thrombus (clot) along with the lining of thepulmonary artery; it is a very difficult, major procedure that is currently performed in a few select centers. Caseseries show remarkable success in most patients.Wikipedia:Citation neededTreatment regimens for hypoxic and miscellaneous varieties of pulmonary hypertension have not been established.However, studies of several agents are currently enrolling patients. Many physicians will treat these diseases with thesame medications as for PAH, until better options become available. Such treatment is called off-label use.

Pulmonary hypertension 136
MonitoringPatients are normally monitored through commonly available tests such as:•• pulse oximetry• arterial blood gas tests• chest X-rays• serial ECG tests• serial echocardiography• spirometry or more advanced lung function studies
PrognosisThe NIH IPAH registry from the 1980s showed an untreated median survival of 2–3 years from time of diagnosis,with the cause of death usually being right ventricular failure (cor pulmonale).Wikipedia:Citation needed A recentoutcome study of those patients who had started treatment with bosentan (Tracleer) showed that 89% patients werealive at 2 years. With new therapies, survival rates are increasing. For 2,635 patients enrolled in The Registry toEvaluate Early and Long-term Pulmonary Arterial Hypertension Disease Management (REVEAL Registry) fromMarch 2006 to December 2009, 1-, 3-, 5-, and 7-year survival rates were 85%, 68%, 57%, and 49%, respectively.For patients with idiopathic/familial PAH, survival rates were 91%, 74%, 65%, and 59%.[17]
Levels of mortality are very high in pregnant women with severe pulmonary hypertension. Pregnancy is sometimesdescribed as contraindicated in these women.[18]
EpidemiologyIdiopathic pulmonary arterial hypertension is a rare disease with an incidence of about 2-3 cases per million per yearand a prevalence of about 15 per million. Adult females are almost three times as likely to present with IPAH thanadult males. The presentation of IPAH within children is more evenly split along gender lines.Other forms of PAH are far more common. In scleroderma the incidence has been estimated to be 6 to 60% of allpatients, in rheumatoid arthritis up to 21%, in systemic lupus erythematosus 4 to 14%, in portal hypertensionbetween 2 to 5%, in HIV about 0.5%, and in sickle cell disease ranging from 20 to 40%.Diet pills such as Fen-Phen produced an annual incidence of 25-50 per million per year.Pulmonary venous hypertension is exceedingly common, since it occurs in most patients symptomatic withcongestive heart failure.Up to 4% of people who suffer a pulmonary embolism go on to develop chronic thromboembolic disease includingpulmonary hypertension.Only about 1.1% of patients with COPD develop pulmonary hypertension with no other disease to explain the highpressure. Sleep apnea is usually associated with only very mild pulmonary hypertension, typically below the level ofdetection. On the other hand Pickwickian syndrome (obesity-hypoventilation syndrome) is very commonlyassociated with right heart failure due to pulmonary hypertension.

Pulmonary hypertension 137
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Pulmonary_hypertension[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ I27. 0[3] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ I27. 2[4] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=416. 0[5] http:/ / www. diseasesdatabase. com/ ddb10998. htm[6] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000112. htm[7] http:/ / www. emedicine. com/ med/ topic1962. htm[8] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D006976[9] Budhiraja R, Tuder RM, Hassoun. PM. Endothelial dysfunction in pulmonary hypertension. Circulation. 2004;109:159–165.[10] Fosfodiesterasas del AMPc y del GMPc en el cerebro: Expresión en procesos neuroinflamatorios y neurodegenerativos. URL: http:/ / www.
tesisenred. net/ bitstream/ handle/ 10803/ 891/ 03. ERI_METODOS. pdf?sequence=4. Viewed 3 November 2012.[11] Ghofrani HA, Pepke-Zaba J, Barbera JA, et al. Nitric oxide pathway and phosphodiesterase inhibitors in pulmonary arterial hypertension. J
Am Coll Cardiol. 2004;43:68S–72S.[12][12] , which cites[13] Forgue ST, Patterson BE, Bedding. AW, et al. Tadalafil pharmacokinetics in healthy subjects. Br J Clin Pharmacol. 2005;61:280–288.[14] Sally A. Arif, PharmD, BCPS (Department of Pharmacy Practice, Chicago College of Pharmacy, Midwestern University, Downers Grove,
Illinois, and Department of Pharmacy, Rush University Medical Center, Chicago, Illinois); and Henry Poon, PharmD, BCPS (Department ofPharmacy, James J. Peters VA Medical Center, Bronx, New York). Tadalafil: A Long-Acting Phosphodiesterase-5 Inhibitor for the Treatmentof Pulmonary Arterial Hypertension. 2011;33:993–1004
[15] Galié N, Brundage BH, Ghofrani HA, et al. Tadalafil therapy for pulmonary arterial hypertension. Circulation. 2009;119:2894–2903.[16] http:/ / en. wikipedia. org/ w/ index. php?title=Pulmonary_hypertension& action=edit[17][17] [FREE][18] British Journal of Anaesthesia: "Primary pulmonary hypertension in pregnancy; a role for novel vasodilators" (http:/ / bja. oxfordjournals.
org/ content/ 87/ 2/ 295. full) March 19, 2011
Sources• Rubin LJ, Badesch DB (2005). "Evaluation and management of the patient with pulmonary arterial hypertension"
(http:/ / www. annals. org/ cgi/ reprint/ 143/ 4/ 282). Ann. Intern. Med. 143 (4): 282–92. doi:10.7326/0003-4819-143-4-200508160-00009 (http:/ / dx. doi. org/ 10. 7326/0003-4819-143-4-200508160-00009). PMID 16103472 (http:/ / www. ncbi. nlm. nih. gov/ pubmed/ 16103472).
External links
Wikimedia Commons has media related to Pulmonary hypertension.
• The Merck Manual Home Edition: Pulmonary Hypertension (http:/ / www. merckmanuals. com/ home/lung_and_airway_disorders/ pulmonary_hypertension/ pulmonary_hypertension. html#v727742)
• Pulmonary Arterial Hypertension database (http:/ / bioinfo. mc. vanderbilt. edu/ PAHKB/ )• Pulmonary Hypertension Association (http:/ / www. phassociation. org/ Page. aspx?pid=197)• PH Central - the internet resource for Pulmonary Arterial Hypertension (http:/ / www. phcentral. org/ )• Facts About Primary Pulmonary Hypertension (http:/ / www. nhlbi. nih. gov/ health/ dci/ Diseases/ pah/
pah_what. html) from the National Heart, Lung, and Blood Institute (NHLBI)• Webcast: The Changing World of Pulmonary Arterial Hypertension Therapies - American College of CHEST
Physicians (http:/ / www. cirquemeded. com/ ACCP/ CHEST2005/ CoTherix/ player. html)• GeneReviews/NCBI/NIH/UW entry on Heritable Pulmonary Arterial Hypertension (http:/ / www. ncbi. nlm. nih.
gov/ books/ NBK1485/ )• OMIM entries on Heritable Pulmonary Arterial Hypertension (http:/ / www. ncbi. nlm. nih. gov/ omim/
178600,600799,178600,600799)

Red blood cell 138
Red blood cell
Scanning electron micrograph of humanred blood cells (ca. 6–8 μm in diameter;
artificial colors)
Red blood cells (RBCs), also called erythrocytes, are the most commontype of blood cell and the vertebrate organism's principal means ofdelivering oxygen (O2) to the body tissues via the blood flow through thecirculatory system. They take up oxygen in the lungs or gills and release itinto tissues while squeezing through the body's capillaries.
The cytoplasm of erythrocytes is rich in hemoglobin, an iron-containingbiomolecule that can bind oxygen and is responsible for the red color of thecells. The cell membrane is composed of proteins and lipids, and thisstructure provides properties essential for physiological cell function such asdeformability and stability while traversing the circulatory system andspecifically the capillary network.
In humans, mature red blood cells are flexible and oval biconcave disks.They lack a cell nucleus and most organelles, in order to accommodatemaximum space for hemoglobin. Approximately 2.4 million newerythrocytes are produced per second.[1] The cells develop in the bone marrow and circulate for about 100–120 daysin the body before their components are recycled by macrophages. Each circulation takes about 20 seconds.Approximately a quarter of the cells in the human body are red blood cells.[2]
Red blood cells are also known as RBCs, red cells, red blood corpuscles (an archaic term), haematids, erythroidcells or erythrocytes (from Greek erythros for "red" and kytos for "hollow vessel", with -cyte translated as "cell" inmodern usage). Packed red blood cells (pRBC) are red blood cells that have been donated, processed, and stored in ablood bank for blood transfusion.
HistoryThe first person to describe red blood cells was the young Dutch biologist Jan Swammerdam, who had used an earlymicroscope in 1658 to study the blood of a frog.[3] Unaware of this work, Anton van Leeuwenhoek provided anothermicroscopic description in 1674, this time providing a more precise description of red blood cells, evenapproximating their size, "25,000 times smaller than a fine grain of sand".In 1901, Karl Landsteiner published his discovery of the three main blood groups—A, B, and C (which he laterrenamed to O). Landsteiner described the regular patterns in which reactions occurred when serum was mixed withred blood cells, thus identifying compatible and conflicting combinations between these blood groups. A year laterAlfred von Decastello and Adriano Sturli, two colleagues of Landsteiner, identified a fourth blood group—AB.In 1959, by use of X-ray crystallography, Dr. Max Perutz was able to unravel the structure of hemoglobin, the redblood cell protein that carries oxygen.The oldest intact red blood cells ever discovered were found in Ötzi the Iceman, a natural mummy of a man whodied around 3255 BCE. These cells were discovered in May 2012.

Red blood cell 139
Vertebrate erythrocytes
There is an immense size variation in vertebrateerythrocytes, as well as a correlation between cell andnucleus size. Mammalian erythrocytes, which do notcontain nuclei, are considerably smaller than those of
most other vertebrates.
Erythrocytes consist mainly of hemoglobin, a complexmetalloprotein containing heme groups whose iron atomstemporarily bind to oxygen molecules (O2) in the lungs or gillsand release them throughout the body. Oxygen can easily diffusethrough the red blood cell's cell membrane. Hemoglobin in theerythrocytes also carries some of the waste product carbon dioxideback from the tissues; most waste carbon dioxide, however, istransported back to the pulmonary capillaries of the lungs asbicarbonate (HCO3
-) dissolved in the blood plasma. Myoglobin, acompound related to hemoglobin, acts to store oxygen in musclecells.
The color of erythrocytes is due to the heme group of hemoglobin.The blood plasma alone is straw-colored, but the red blood cellschange color depending on the state of the hemoglobin: whencombined with oxygen the resulting oxyhemoglobin is scarlet, andwhen oxygen has been released the resulting deoxyhemoglobin isof a dark red burgundy color, appearing bluish through the vesselwall and skin. Pulse oximetry takes advantage of this color changeto directly measure the arterial blood oxygen saturation usingcolorimetric techniques. Hemoglobin also has a very high affinityfor carbon monoxide, forming carboxyhaemoglobin which is avery bright red in color. Flushed, confused patients with asaturation reading of 100% on pulse oximetry are sometimesfound to be suffering from carbon monoxide poisoning.
The sequestration of oxygen-carrying proteins inside specializedcells (as opposed to oxygen carriers being dissolved in body fluid)was an important step in the evolution of vertebrates as it allows for less viscous blood, higher concentrations ofoxygen, and better diffusion of oxygen from the blood to the tissues. The size of erythrocytes varies widely amongvertebrate species; erythrocyte width is on average about 25% larger than capillary diameter, and it has beenhypothesized that this improves the oxygen transfer from erythrocytes to tissues.
The only known vertebrates without erythrocytes are the crocodile icefishes (family Channichthyidae); they live invery oxygen-rich cold water and transport oxygen freely dissolved in their blood. While they do not use hemoglobinanymore, remnants of hemoglobin genes can be found in their genome.
NucleusErythrocytes in mammals are anucleate when mature, meaning that they lack a cell nucleus. In comparison, theerythrocytes of other vertebrates have nuclei; the only known exceptions are salamanders of the Batrachoseps genusand fish of the Maurolicus genus with closely related species.The elimination of the nucleus in vertebrate erythrocytes has been offered as an explanation for the subsequentaccumulation of non-coding DNA in the genome. The argument runs as follows: Efficient gas transport requireserythrocytes to pass through very narrow capillaries, and this constrains their size. In the absence of nuclearelimination, the accumulation of repeat sequences is constrained by the volume occupied by the nucleus, whichincreases with genome size.

Red blood cell 140
Secondary functionsWhen erythrocytes undergo shear stress in constricted vessels, they release ATP, which causes the vessel walls torelax and dilate so as to promote normal blood flow.When their hemoglobin molecules are deoxygenated, erythrocytes release S-nitrosothiols, which also act to dilateblood vessels, thus directing more blood to areas of the body depleted of oxygen.It has been recently demonstrated that erythrocytes can also synthesize nitric oxide enzymatically, using L-arginineas substrate, as do endothelial cells. Exposure of erythrocytes to physiological levels of shear stress activates nitricoxide synthase and export of nitric oxide, which may contribute to the regulation of vascular tonus.Erythrocytes can also produce hydrogen sulfide, a signalling gas that acts to relax vessel walls. It is believed that thecardioprotective effects of garlic are due to erythrocytes converting its sulfur compounds into hydrogen sulfide.Erythrocytes also play a part in the body's immune response: when lysed by pathogens such as bacteria, theirhemoglobin releases free radicals, which break down the pathogen's cell wall and membrane, killing it.
Mammalian erythrocytes
Typical mammalian erythrocytes: (a) seen from surface; (b) in profile, formingrouleaux; (c) rendered spherical by water; (d) rendered crenate by salt. (c) and (d)
do not normally occur in the body.
Mammalian erythrocytes are unique amongthe vertebrates as they are non-nucleatedcells in their mature form. These cells havenuclei during early phases of erythropoiesis,but extrude them during development asthey mature in order to provide more spacefor hemoglobin. In mammals, erythrocytesalso lose all other cellular organelles such astheir mitochondria, Golgi apparatus andendoplasmic reticulum.
As a result of not containing mitochondria,these cells use none of the oxygen theytransport; instead they produce the energycarrier ATP by the glycolysis of glucose andlactic acid fermentation on the resultingpyruvate.
Because of the lack of nuclei and organelles, mature red blood cells do not contain DNA and cannot synthesize anyRNA, and consequently cannot divide and have limited repair capabilities. This also ensures that no virus can evolveto target mammalian red blood cells.
Mammalian erythrocytes are typically shaped as biconcave disks: flattened and depressed in the center, with a dumbbell-shaped cross section, and a torus-shaped rim on the edge of the disk. This distinctive biconcave shape optimises the flow properties of blood in the large vessels, such as maximization of laminar flow and minimization of platelet scatter, which suppresses their atherogenic activity in those large vessels. However, there are some exceptions concerning shape in the artiodactyl order (even-toed ungulates including cattle, deer, and their relatives), which displays a wide variety of bizarre erythrocyte morphologies: small and highly ovaloid cells in llamas and camels (family Camelidae), tiny spherical cells in mouse deer (family Tragulidae), and cells which assume fusiform, lanceolate, crescentic, and irregularly polygonal and other angular forms in red deer and wapiti (family Cervidae). Members of this order have clearly evolved a mode of red blood cell development substantially different from the mammalian norm. Overall, mammalian erythrocytes are remarkably flexible and deformable so as to squeeze through tiny capillaries, as well as to maximize their apposing surface by assuming a cigar shape, where they

Red blood cell 141
efficiently release their oxygen load.In large blood vessels, red blood cells sometimes occur as a stack, flat side next to flat side. This is known asrouleaux formation, and it occurs more often if the levels of certain serum proteins are elevated, as for instanceduring inflammation.The spleen acts as a reservoir of red blood cells, but this effect is somewhat limited in humans. In some othermammals such as dogs and horses, the spleen sequesters large numbers of red blood cells which are dumped into theblood during times of exertion stress, yielding a higher oxygen transport capacity.
Scanning electron micrograph of blood cells. From leftto right: human erythrocyte, thrombocyte (platelet),
leukocyte.
Human erythrocytes
Two drops of blood are shown with a bright redoxygenated drop on the left and a deoxygenated drop
on the right.
A typical human erythrocyte has a disk diameter of approximately6.2–8.2 µm and a thickness at the thickest point of 2–2.5 µm and aminimum thickness in the centre of 0.8–1 µm, being much smallerthan most other human cells. These cells have an average volumeof about 90 fL with a surface of about 136 μm2, and can swell upto a sphere shape containing 150 fL, without membrane distension.
Adult humans have roughly 2–3 × 1013 (20–30 trillion) red bloodcells at any given time, comprising approximately one quarter ofthe total human body cell number (women have about 4 to 5million erythrocytes per microliter (cubic millimeter) of blood andmen about 5 to 6 million; people living at high altitudes with low oxygen tension will have more). Red blood cellsare thus much more common than the other blood particles: there are about 4,000–11,000 white blood cells andabout 150,000–400,000 platelets in each microliter of human blood.
Human red blood cells take on average 20 seconds to complete one cycle of circulation.As red blood cells contain no nucleus, protein biosynthesis is currently assumed to be absent in these cells, althougha recent study indicates the presence of all the necessary biomachinery in the cells to do so.

Red blood cell 142
An animation of a typical human red blood cell cyclein the circulatory system. This animation occurs at realtime (20 seconds of cycle) and shows the red blood cell
deform as it enters capillaries, as well as changingcolor as it alternates in states of oxygenation along the
circulatory system.
The blood's red color is due to the spectral properties of the hemiciron ions in hemoglobin. Each human red blood cell containsapproximately 270 million of these hemoglobin biomolecules,each carrying four heme groups; hemoglobin comprises about athird of the total cell volume. This protein is responsible for thetransport of more than 98% of the oxygen (the remaining oxygenis carried dissolved in the blood plasma). The red blood cells of anaverage adult human male store collectively about 2.5 grams ofiron, representing about 65% of the total iron contained in thebody.[4][5] (See Human iron metabolism.)
Life cycleHuman erythrocytes are produced through a process named erythropoiesis, developing from committed stem cells tomature erythrocytes in about 7 days. When matured, in a healthy individual these cells live in blood circulation forabout 100 to 120 days (and 80 to 90 days in a full term infant). At the end of their lifespan, they become senescent,and are removed from circulation. In many chronic diseases, the lifespan of the erythrocytes is markedly reduced(e.g. patients requiring haemodialysis).
Erythropoiesis
Erythropoiesis is the development process by which new erythrocytes are produced; it lasts about 7 days. Throughthis process erythrocytes are continuously produced in the red bone marrow of large bones, at a rate of about 2million per second in a healthy adult. (In the embryo, the liver is the main site of red blood cell production.) Theproduction can be stimulated by the hormone erythropoietin (EPO), synthesised by the kidney. Just before and afterleaving the bone marrow, the developing cells are known as reticulocytes; these comprise about 1% of circulatingred blood cells.
Functional lifetime
The functional lifetime of an erythrocyte is about 100–120 days, during which time the erythrocytes are continuallymoved by the blood flow push (in arteries), pull (in veins) and a combination of the two as they squeeze throughmicrovessels such as capillaries.
Senescence
The aging erythrocyte undergoes changes in its plasma membrane, making it susceptible to selective recognition by macrophages and subsequent phagocytosis in the mononuclear phagocyte system (spleen, liver and lymph nodes), thus removing old and defective cells and continually purging the blood. This process is termed eryptosis, erythrocyte programmed cell death. This process normally occurs at the same rate of production by erythropoiesis, balancing the total circulating red blood cell count. Eryptosis is increased in a wide variety of diseases including sepsis, haemolytic uremic syndrome, malaria, sickle cell anemia, beta-thalassemia, glucose-6-phosphate dehydrogenase deficiency, phosphate depletion, iron deficiency and Wilson's disease. Eryptosis can be elicited by osmotic shock, oxidative stress, energy depletion as well as a wide variety of endogenous mediators and xenobiotics. Excessive eryptosis is observed in erythrocytes lacking the cGMP-dependent protein kinase type I or the

Red blood cell 143
AMP-activated protein kinase AMPK. Inhibitors of eryptosis include erythropoietin, nitric oxide, catecholaminesand high concentrations of urea.Much of the resulting breakdown products are recirculated in the body. The heme constituent of hemoglobin arebroken down into Fe3+ and biliverdin. The biliverdin is reduced to bilirubin, which is released into the plasma andrecirculated to the liver bound to albumin. The iron is released into the plasma to be recirculated by a carrier proteincalled transferrin. Almost all erythrocytes are removed in this manner from the circulation before they are oldenough to hemolyze. Hemolyzed hemoglobin is bound to a protein in plasma called haptoglobin, which is notexcreted by the kidney.
Membrane compositionThe membrane of the red blood cell plays many roles that aid in regulating their surface deformability, flexibility,adhesion to other cells and immune recognition. These functions are highly dependent on its composition, whichdefines its properties. The red blood cell membrane is composed of 3 layers: the glycocalyx on the exterior, which isrich in carbohydrates; the lipid bilayer which contains many transmembrane proteins, besides its lipidic mainconstituents; and the membrane skeleton, a structural network of proteins located on the inner surface of the lipidbilayer. Half of the membrane mass in human and most mammalian erythrocytes are proteins. The other half arelipids, namely phospholipids and cholesterol.
Membrane lipids
The most common erythrocyte cell membrane lipids, schematicallydisposed as they are distributed on the bilayer. Relative abundances
are not at scale.
The erythrocyte cell membrane comprises a typicallipid bilayer, similar to what can be found in virtuallyall human cells. Simply put, this lipid bilayer iscomposed of cholesterol and phospholipids in equalproportions by weight. The lipid composition isimportant as it defines many physical properties such asmembrane permeability and fluidity. Additionally, theactivity of many membrane proteins is regulated byinteractions with lipids in the bilayer.
Unlike cholesterol, which is evenly distributed betweenthe inner and outer leaflets, the 5 major phospholipidsare asymmetrically disposed, as shown below:Outer monolayer
• Phosphatidylcholine (PC);• Sphingomyelin (SM).Inner monolayer
• Phosphatidylethanolamine (PE);• Phosphoinositol (PI) (small amounts).• Phosphatidylserine (PS);This asymmetric phospholipid distribution among thebilayer is the result of the function of severalenergy-dependent and energy-independentphospholipid transport proteins. Proteins called“Flippases” move phospholipids from the outer to the
inner monolayer, while others called “floppases” do the opposite operation, against a concentration gradient in an energy dependent manner. Additionally, there are also “scramblase” proteins that move phospholipids in both

Red blood cell 144
directions at the same time, down their concentration gradients in an energy independent manner. There is stillconsiderable debate ongoing regarding the identity of these membrane maintenance proteins in the red cellmembrane.The maintenance of an asymmetric phospholipid distribution in the bilayer (such as an exclusive localization of PSand PIs in the inner monolayer) is critical for the cell integrity and function due to several reasons:• Macrophages recognize and phagocytose red cells that expose PS at their outer surface. Thus the confinement of
PS in the inner monolayer is essential if the cell is to survive its frequent encounters with macrophages of thereticuloendothelial system, especially in the spleen.
• Premature destruction of thallassemic and sickle red cells has been linked to disruptions of lipid asymmetryleading to exposure of PS on the outer monolayer.
•• An exposure of PS can potentiate adhesion of red cells to vascular endothelial cells, effectively preventing normaltransit through the microvasculature. Thus it is important that PS is maintained only in the inner leaflet of thebilayer to ensure normal blood flow in microcirculation.
• Both PS and phosphatidylinositol-4,5-bisphosphate (PIP2) can regulate membrane mechanical function, due totheir interactions with skeletal proteins such as spectrin and protein 4.1R. Recent studies have shown that bindingof spectrin to PS promotes membrane mechanical stability. PIP2 enhances the binding of protein band 4.1R toglycophorin C but decreases its interaction with protein band 3, and thereby may modulate the linkage of thebilayer to the membrane skeleton.
The presence of specialized structures named "lipid rafts" in the erythrocyte membrane have been described byrecent studies. These are structures enriched in cholesterol and sphingolipids associated with specific membraneproteins, namely flotillins, stomatins (band 7), G-proteins, and β-adrenergic receptors. Lipid rafts that have beenimplicated in cell signaling events in nonerythroid cells have been shown in erythroid cells to mediate β2-adregenicreceptor signaling and increase cAMP levels, and thus regulating entry of malarial parasites into normal red cells.
Membrane proteins
Red blood cell membrane proteins separated bySDS-Page and silverstained
The proteins of the membrane skeleton are responsible for thedeformability, flexibility and durability of the red blood cell, enablingit to squeeze through capillaries less than half the diameter of theerythrocyte (7–8 μm) and recovering the discoid shape as soon as thesecells stop receiving compressive forces, in a similar fashion to anobject made of rubber.
There are currently more than 50 known membrane proteins, whichcan exist in a few hundred up to a million copies per erythrocyte.Approximately 25 of these membrane proteins carry the various bloodgroup antigens, such as the A, B and Rh antigens, among many others.These membrane proteins can perform a wide diversity of functions,such as transporting ions and molecules across the red cell membrane,adhesion and interaction with other cells such as endothelial cells, assignaling receptors, as well as other currently unknown functions. Theblood types of humans are due to variations in surface glycoproteins oferythrocytes. Disorders of the proteins in these membranes areassociated with many disorders, such as hereditary spherocytosis, hereditary elliptocytosis, hereditarystomatocytosis, and paroxysmal nocturnal hemoglobinuria.
The red blood cell membrane proteins organized according to their function:

Red blood cell 145
Red Blood Cell membrane major proteins
Transport
• Band 3 – Anion transporter, also an important structural componentof the erythrocyte cell membrane, makes up to 25% of the cellmembrane surface, each red cell contains approximately one millioncopies. Defines the Diego Blood Group;
• Aquaporin 1 – water transporter, defines the Colton Blood Group;• Glut1 – glucose and L-dehydroascorbic acid transporter;• Kidd antigen protein – urea transporter;• RhAG – gas transporter, probably of carbon dioxide, defines Rh
Blood Group and the associated unusual blood group phenotype Rhnull;• Na+/K+ – ATPase;• Ca2+ – ATPase;• Na+ K+ 2Cl- – cotransporter;• Na+-Cl- – cotransporter;• Na-H exchanger;• K-Cl – cotransporter;• Gardos Channel.Cell adhesion
• ICAM-4 – interacts with integrins;• BCAM – a glycoprotein that defines the Lutheran blood group and also known as Lu or laminin-binding protein.Structural role – The following membrane proteins establish linkages with skeletal proteins and may play animportant role in regulating cohesion between the lipid bilayer and membrane skeleton, likely enabling the red cell tomaintain its favorable membrane surface area by preventing the membrane from collapsing (vesiculating).• Ankyrin-based macromolecular complex – proteins linking the bilayer to the membrane skeleton through the
interaction of their cytoplasmic domains with Ankyrin.• Band 3 – also assembles various glycolytic enzymes, the presumptive CO2 transporter, and carbonic anhydrase
into a macromolecular complex termed a "metabolon," which may play a key role in regulating red cellmetabolism and ion and gas transport function);
• RhAG – also involved in transport, defines associated unusual blood group phenotype Rhmod.• Protein 4.1R-based macromolecular complex – proteins interacting with Protein 4.1R.
• Protein 4.1R – weak expression of Gerbich antigens;• Glycophorin C and D – glycoprotein, defines Gerbich Blood Group;• XK – defines the Kell Blood Group and the Mcleod unusual phenotype (lack of Kx antigen and greatly
reduced expression of Kell antigens);• RhD/RhCE – defines Rh Blood Group and the associated unusual blood group phenotype Rhnull;• Duffy protein – has been proposed to be associated with chemokine clearance;• Adducin – interaction with band 3;• Dematin- interaction with the Glut1 glucose transporter.

Red blood cell 146
Surface electrostatic potentialThe zeta potential is an electrochemical property of cell surfaces that is determined by the net electrical charge ofmolecules exposed at the surface of cell membranes of the cell. The normal zeta potential of the erythrocyte is−15.7 millivolts (mV).[6] Much of this potential appears to be contributed by the exposed sialic acid residues in themembrane: their removal results in zeta potential of −6.06 mV.
Clinical notes
Separation and blood dopingRed blood cells can be obtained from whole blood by centrifugation, which separates the cells from the blood plasmain a process known as blood fractionation. Packed red blood cells, which are made in this way from whole bloodwith the plasma removed, are used in transfusion medicine. During plasma donation, the red blood cells are pumpedback into the body right away and only the plasma is collected.Some athletes have tried to improve their performance by blood doping: first about 1 litre of their blood is extracted,then the red blood cells are isolated, frozen and stored, to be reinjected shortly before the competition. (Red bloodcells can be conserved for 5 weeks at −79 °C or −110 °F) This practice is hard to detect but may endanger the humancardiovascular system which is not equipped to deal with blood of the resulting higher viscosity. Another method ofblood doping involves injection with erythropoietin in order to stimulate production of red blood cells. Bothpractices are banned by the World Anti-Doping Agency.
Artificially grown red blood cellsIn 2008 it was reported that human embryonic stem cells had been successfully coaxed into becoming erythrocytesin the lab. The difficult step was to induce the cells to eject their nucleus; this was achieved by growing the cells onstromal cells from the bone marrow. It is hoped that these artificial erythrocytes can eventually be used for bloodtransfusions.[7]
Diseases and diagnostic tools
Affected by Sickle-cell disease, red bloodcells alter shape and threaten to damage
internal organs.
Blood diseases involving the red blood cells include:• Anemias (or anaemias) are diseases characterized by low oxygen
transport capacity of the blood, because of low red cell count or someabnormality of the red blood cells or the hemoglobin.
• Iron deficiency anemia is the most common anemia; it occurs whenthe dietary intake or absorption of iron is insufficient, and hemoglobin,which contains iron, cannot be formed
• Sickle-cell disease is a genetic disease that results in abnormalhemoglobin molecules. When these release their oxygen load in thetissues, they become insoluble, leading to mis-shaped red blood cells.These sickle shaped red cells are less deformable and viscoelasticmeaning that they have become rigid and can cause blood vesselblockage, pain, strokes, and other tissue damage.
• Thalassemia is a genetic disease that results in the production of anabnormal ratio of hemoglobin subunits.
• Hereditary spherocytosis syndromes are a group of inherited disorders characterized by defects in the red blood cell's cell membrane, causing the cells to be small, sphere-shaped, and fragile instead of donut-shaped and

Red blood cell 147
flexible. These abnormal red blood cells are destroyed by the spleen. Several other hereditary disorders of thered blood cell membrane are known.
• Pernicious anemia is an autoimmune disease wherein the body lacks intrinsic factor, required to absorb vitaminB12 from food. Vitamin B12 is needed for the production of hemoglobin.
• Aplastic anemia is caused by the inability of the bone marrow to produce blood cells.• Pure red cell aplasia is caused by the inability of the bone marrow to produce only red blood cells.
Effect of osmotic pressure on blood cells
Micrographs of the effects of osmotic pressure
• Hemolysis is the general term for excessive breakdown of red bloodcells. It can have several causes and can result in hemolytic anemia.
• The malaria parasite spends part of its life-cycle in red bloodcells, feeds on their hemoglobin and then breaks them apart,causing fever. Both sickle-cell disease and thalassemia are morecommon in malaria areas, because these mutations convey someprotection against the parasite.
• Polycythemias (or erythrocytoses) are diseases characterized by asurplus of red blood cells. The increased viscosity of the blood cancause a number of symptoms.
• In polycythemia vera the increased number of red blood cellsresults from an abnormality in the bone marrow.
• Several microangiopathic diseases, including disseminatedintravascular coagulation and thrombotic microangiopathies, presentwith pathognomonic (diagnostic) red blood cell fragments calledschistocytes. These pathologies generate fibrin strands that sever red blood cells as they try to move past athrombus.
• Hemolytic transfusion reaction is the destruction of donated red blood cells after a transfusion, mediated by hostantibodies, often as a result of a blood type mismatch.
Several blood tests involve red blood cells, including the RBC count (the number of red blood cells per volume ofblood), the hematocrit (percentage of blood volume occupied by red blood cells), and the erythrocyte sedimentationrate. Many diseases involving red blood cells are diagnosed with a blood film (or peripheral blood smear), where athin layer of blood is smeared on a microscope slide. The blood type needs to be determined to prepare for a bloodtransfusion or an organ transplantation.
References[1] Erich Sackmann, Biological Membranes Architecture and Function., Handbook of Biological Physics, (ed. R.Lipowsky and E.Sackmann,
vol.1, Elsevier, 1995[2] Laura Dean. Blood Groups and Red Cell Antigens (http:/ / www. ncbi. nlm. nih. gov/ books/ bv. fcgi?call=bv. View. . ShowTOC&
rid=rbcantigen. TOC& depth=2)[3] "Swammerdam, Jan (1637–1680)", McGraw Hill AccessScience, 2007. Accessed 27 December 2007.[4] Iron Metabolism (http:/ / www. med-ed. virginia. edu/ courses/ path/ innes/ nh/ iron. cfm), University of Virginia Pathology. Accessed 22
September 2007.[5] Iron Transport and Cellular Uptake (http:/ / sickle. bwh. harvard. edu/ iron_transport. html) by Kenneth R. Bridges, Information Center for
Sickle Cell and Thalassemic Disorders. Accessed 22 September 2007.[6] Tokumasu F, Ostera GR, Amaratunga C, Fairhurst RM (2012) Modifications in erythrocyte membrane zeta potential by Plasmodium
falciparum infection. Exp Parasitol[7] First red blood cells grown in the lab (http:/ / www. newscientist. com/ article/ dn14565-first-red-blood-cells-grown-in-the-lab. html), New
Scientist News, 19 August 2008

Red blood cell 148
External links
Wikimedia Commons has media related to Red blood cells.
• Blood Groups and Red Cell Antigens (http:/ / www. ncbi. nlm. nih. gov/ books/ bv. fcgi?call=bv. View. .ShowTOC& rid=rbcantigen. TOC& depth=2) by Laura Dean. Searchable and downloadable online textbook inthe public domain.
• Database of vertebrate erythrocyte sizes (http:/ / www. genomesize. com/ cellsize/ ).• Red Gold (http:/ / www. pbs. org/ wnet/ redgold), PBS site containing facts and history

Spleen 149
SpleenFor other uses, see Spleen (disambiguation).
Spleen
Spleen
Laparoscopic view of a horse's spleen (the purple and grey mottled organ)
Latin Lien
Greek splḗn–σπλήν[1]
Gray's p.1282 [2]
Artery Splenic artery
Vein Splenic vein
Nerve Splenic plexus
Precursor Mesenchyme of dorsal mesogastrium
MeSH Spleen [3]
Dorlands/Elsevier
Spleen [4]
Anatomical terminology

Spleen 150
The spleen (from Greek σπλήν—splḗn[5]) is an organ found in virtually all vertebrates. Similar in structure to a largelymph node, it acts primarily as a blood filter.It is possible to remove the spleen without jeopardizing life. The spleen plays important roles in regard to red bloodcells (also referred to as erythrocytes) and the immune system.[6] It removes old red blood cells and holds a reserveof blood, which can be valuable in case of hemorrhagic shock, and also recycles iron. As a part of the mononuclearphagocyte system, it metabolizes hemoglobin removed from senescent erythrocytes. The globin portion ofhemoglobin is degraded to its constitutive amino acids, and the heme portion is metabolized to bilirubin, which isremoved in the liver.The spleen synthesizes antibodies in its white pulp and removes antibody-coated bacteria and antibody-coated bloodcells by way of blood and lymph node circulation. A study published in 2009 using mice found that the spleencontains, in its reserve, half of the body's monocytes within the red pulp. These monocytes, upon moving to injuredtissue (such as the heart), turn into dendritic cells and macrophages while promoting tissue healing.[7] The spleen is acenter of activity of the mononuclear phagocyte system and can be considered analogous to a large lymph node, asits absence causes a predisposition to certain infections.In humans, the spleen is brownish in color and is located in the left upper quadrant of the abdomen.
StructureThe spleen, in healthy adult humans, is approximately 7 centimetres (2.8 in) to 14 centimetres (5.5 in) in length. Itusually weighs between 150 grams (5.3 oz)[8] and 200 grams (7.1 oz). An easy way to remember the anatomy of thespleen is the 1×3×5×7×9×11 rule. The spleen is 1" by 3" by 5", weighs approximately 7 oz, and lies between the 9thand 11th ribs on the left hand side.
Surfaces
Visceral surface of the spleen
The diaphragmatic surface of the spleen (or phrenic surface) isconvex, smooth, and is directed upward, backward, and to the left,except at its upper end, where it is directed slightly to the middle.It is in relation with the under surface of the diaphragm, whichseparates it from the ninth, tenth, and eleventh ribs of the left side,and the intervening lower border of the left lung and pleura.
The visceral surface of the spleen is divided by a ridge into tworegions: an anterior or gastric and a posterior or renal. The gastricsurface (facies gastrica) is directed forward, upward, and towardthe middle, is broad and concave, and is in contact with theposterior wall of the stomach. Below this it is in contact with thetail of the pancreas. Near to its mid-border is a long fissure, termedthe hilum. This is pierced by several irregular openings, for theentrance and exit of vessels and nerves. The renal surface (faciesrenalis) is directed medialward and downward. It is somewhatflattened, considerably narrower than the gastric surface, and is in
relation with the upper part of the anterior surface of the left kidney and occasionally with the left suprarenal gland.
Like the thymus, the spleen possesses only efferent lymphatic vessels. The spleen is part of the lymphatic system.Both the short gastric arteries and the splenic artery supply it with blood.The germinal centers are supplied by arterioles called penicilliary radicles.

Spleen 151
DevelopmentThe spleen is unique in respect to its development within the gut. While most of the gut viscera are endodermallyderived (with the exception of the neural-crest derived suprarenal gland), the spleen is derived from mesenchymaltissue. Specifically, the spleen forms within, and from, the dorsal mesentery. However, it still shares the same bloodsupply—the celiac trunk—as the foregut organs.
Function
Micrograph of splenic tissue showing the redpulp (red), white pulp (blue) and a thickened
inflamed capusule (mostly pink - top of image).H&E stain.
Area Function Composition
red pulp Mechanical filtration of red blood cells. In mice: Reserve ofmonocytes
• "sinuses" (or "sinusoids"), which are filled with blood• "splenic cords" of reticular fibers• "marginal zone" bordering on white pulp
whitepulp
Active immune response through humoral and cell-mediatedpathways.
Composed of nodules, called Malpighian corpuscles. These arecomposed of:
• "lymphoid follicles" (or "follicles"), rich in B-lymphocytes• "periarteriolar lymphoid sheaths" (PALS), rich in T-lymphocytes
Other functions of the spleen are less prominent, especially in the healthy adult:• Production of opsonins, properdin, and tuftsin.• Creation of red blood cells. While the bone marrow is the primary site of hematopoiesis in the adult, the spleen
has important hematopoietic functions up until the fifth month of gestation. After birth, erythropoietic functionscease, except in some hematologic disorders. As a major lymphoid organ and a central player in thereticuloendothelial system, the spleen retains the ability to produce lymphocytes and, as such, remains anhematopoietic organ.
• Storage of red blood cells, lymphocytes and other formed elements. In horses, roughly 30% of the red blood cellsare stored there. The red blood cells can be released when needed. In humans, up to a cup (236.5 ml) of red bloodcells can be held in the spleen and released in cases of hypovolemia. It can store platelets in case of an emergencyand also clears old platelets from the circulation. Up to a quarter of lymphocytes can be stored in the spleen at anyone time.

Spleen 152
Clinical significanceMain article: Splenic disease
Enlarged spleenMain article: splenomegalyDisorders include splenomegaly, where the spleen is enlarged for various reasons, such as cancer, specificallyblood-based leukemias, and asplenia, where the spleen is not present or functions abnormally.Traumas, such as a motor vehicle accident, can cause rupture of the spleen, which is a situation requiring immediatemedical attention.
Decreased functionSee also: Asplenia and HypospleniaAsplenia refers to a non-functioning spleen, which may be congenital or due to surgical removal. These may cause:• modest increases in circulating white blood cells and platelets,• diminished responsiveness to some vaccines,• increased susceptibility to infection by bacteria and protozoa; in particular, there is an increased risk of sepsis
from polysaccharide encapsulated bacteria. Encapsulated bacteria inhibit binding of complement or preventcomplement assembled on the capsule from interacting with macrophage receptors. Natural antibodies arerequired for phagocytosis, which are immunoglobulins that facilitate phagocytosis either directly or bycomplement deposition on the capsule. They are produced by IgM memory B cells in the marginal zone of thespleen. Splenectomy greatly diminishes the frequency of memory B cells.
A 28-year follow-up of 740 World War II veterans who had their spleens removed (splenectomy), on the battlefield,showed a significant increase in the usual death rate from pneumonia (6 rather than the expected 1.3) and an increasein the death rate from ischemic heart disease (4.1 rather than the expected 3) but not from other conditions.
Society and cultureThe word spleen comes from the Ancient Greek σπλήν (splḗn), and is the idiomatic equivalent of the heart inEnglish, i.e. to be good-spleened (εὔσπλαγχνος, eúsplankhnos) means to be good-hearted or compassionate.[9]
In English the word spleen was customary during the period of the 18th century. Authors like Richard Blackmore orGeorge Cheyne employed it to characterise the hypochondriacal and hysterical affections.[10][11] WilliamShakespeare, in Julius Caesar uses the spleen to describe Cassius' irritable nature.
Must I observe you? must I stand and crouchUnder your testy humour? By the godsYou shall digest the venom of your spleen,Though it do split you; for, from this day forth,I'll use you for my mirth, yea, for my laughter,When you are waspish.[12]
In French, "splénétique" refers to a state of pensive sadness or melancholy. It has been popularized by the poetCharles Baudelaire (1821–1867) but was already used before in particular to the Romantic literature (19th century).The word for the organ is "rate".The connection between spleen (the organ) and melancholy (the temperament) comes from the humoral medicine of the ancient Greeks. One of the humours (body fluid) was the black bile, secreted by the spleen organ and associated with melancholy. In contrast, the Talmud (tractate Berachoth 61b) refers to the spleen as the organ of laughter while

Spleen 153
possibly suggesting a link with the humoral view of the organ. In eighteenth- and nineteenth-century England,women in bad humor were said to be afflicted by the spleen, or the vapours of the spleen. In modern English, "tovent one's spleen" means to vent one's anger, e.g. by shouting, and can be applied to both males and females.Similarly, the English term "splenetic" is used to describe a person in a foul mood.
Other animalsIn cartilaginous and ray-finned fish it consists primarily of red pulp and is normally a somewhat elongated organ as itactually lies inside the serosal lining of the intestine. In many amphibians, especially frogs, it takes on the morerounded form and there is often a greater quantity of white pulp.In reptiles, birds, and mammals, white pulp is always relatively plentiful, and in the latter two groups, the spleen istypically rounded, although it adjusts its shape somewhat to the arrangement of the surrounding organs. In the greatmajority of vertebrates, the spleen continues to produce red blood cells throughout life; it is only in mammals thatthis function is lost in adults. Many mammals have tiny spleen-like structures known as haemal nodes throughoutthe body that are presumed to have the same function as the spleen. The spleens of aquatic mammals differ in someways from those of fully land-dwelling mammals. In general, they are bluish in colour. In cetaceans and manateesthey tend to be quite small, but in deep diving pinnipeds, they can be quite massive, due to their function of storingred blood cells.The only vertebrates lacking a spleen are the lampreys and hagfishes. Even in these animals, there is a diffuse layerof haematopoeitic tissue within the gut wall, which has a similar structure to red pulp and is presumed to behomologous with the spleen of higher vertebrates.In mice, the spleen stores half the body's monocytes so that upon injury they can migrate to the injured tissue andtransform into dendritic cells and macrophages and so assist wound healing.
Gallery
The celiac artery andits branch.
The celiac artery andits branches.
Horizontal disposition of theperitoneum in the upper part of
the abdomen.
Transverse section through themiddle of the first lumbar
vertebra.
The duodenum and pancreas. The visceralsurface of the
spleen.
Transverse section of thespleen, showing the
trabecular tissue and thesplenic vein and its
tributaries.
Transverse section of the humanspleen, showing the distribution
of the splenic artery and itsbranches.

Spleen 154
Section of the spleen, showingthe termination of the small
blood vessels.
Back of lumbarregion, showingsurface markings
for kidneys,ureters, and spleen.
Side ofthorax,
showingsurface
markingsfor bones,
lungs(purple),pleura
(blue), andspleen
(green).
Lymphaticsystem
Spleen Spleen (lien) Spleen
References[1] σπλήν (http:/ / www. perseus. tufts. edu/ hopper/ text?doc=Perseus:text:1999. 04. 0057:entry=splh/ n), Henry George Liddell, Robert Scott, A
Greek-English Lexicon, on Perseus Digital Library[2] http:/ / archive. org/ stream/ anatomyofhumanbo1918gray#page/ 1282/ mode/ 2up[3] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2011/ MB_cgi?mode=& term=Spleen[4] http:/ / www. mercksource. com/ pp/ us/ cns/ cns_hl_dorlands_split. jsp?pg=/ ppdocs/ us/ common/ dorlands/ dorland/ seven/ 000099557. htm[5] σπλήν (http:/ / www. perseus. tufts. edu/ hopper/ text?doc=Perseus:text:1999. 04. 0057:entry=splh/ n), Henry George Liddell, Robert Scott, A
Greek-English Lexicon, on Perseus Digital Library[6] Spleen (http:/ / www. daviddarling. info/ encyclopedia/ S/ spleen. html), Internet Encyclopedia of Science[7] Finally, the Spleen Gets Some Respect (http:/ / www. nytimes. com/ 2009/ 08/ 04/ science/ 04angier. html) By NATALIE ANGIER, The
New York Times, August 3, 2009[8] eMedicine > Splenomegaly (http:/ / emedicine. medscape. com/ article/ 206208-overview) Author: David J Draper. Coauthor(s): Ronald A
Sacher, Emmanuel N Dessypris, Lewis J Kaplan. Updated: Oct 4, 2009[9][9] Robertson's Word Pictures of the New Testament, commentary on 1 Peter 3:8[10] Cheyne, George: The English Malady; or, A Treatise of Nervous Diseases of All Kinds, as Spleen, Vapours, Lowness of Spirits,
Hypochondriacal and Hysterical Distempers with the Author's own Case at large, Dublin, 1733. Facsimile ed., ed. Eric T. Carlson, M.D.,1976, Scholars' Facsimiles & Reprints, ISBN 978-0-8201-1281-7;
[11] Blackmore, Richard: Treatise of the spleen and vapors. London, 1725[12] σπλήν (http:/ / www. perseus. tufts. edu/ hopper/ text?doc=Perseus:text:1999. 04. 0057:entry=splh/ n), Henry George Liddell, Robert Scott,
A Greek-English Lexicon, on Perseus Digital Library
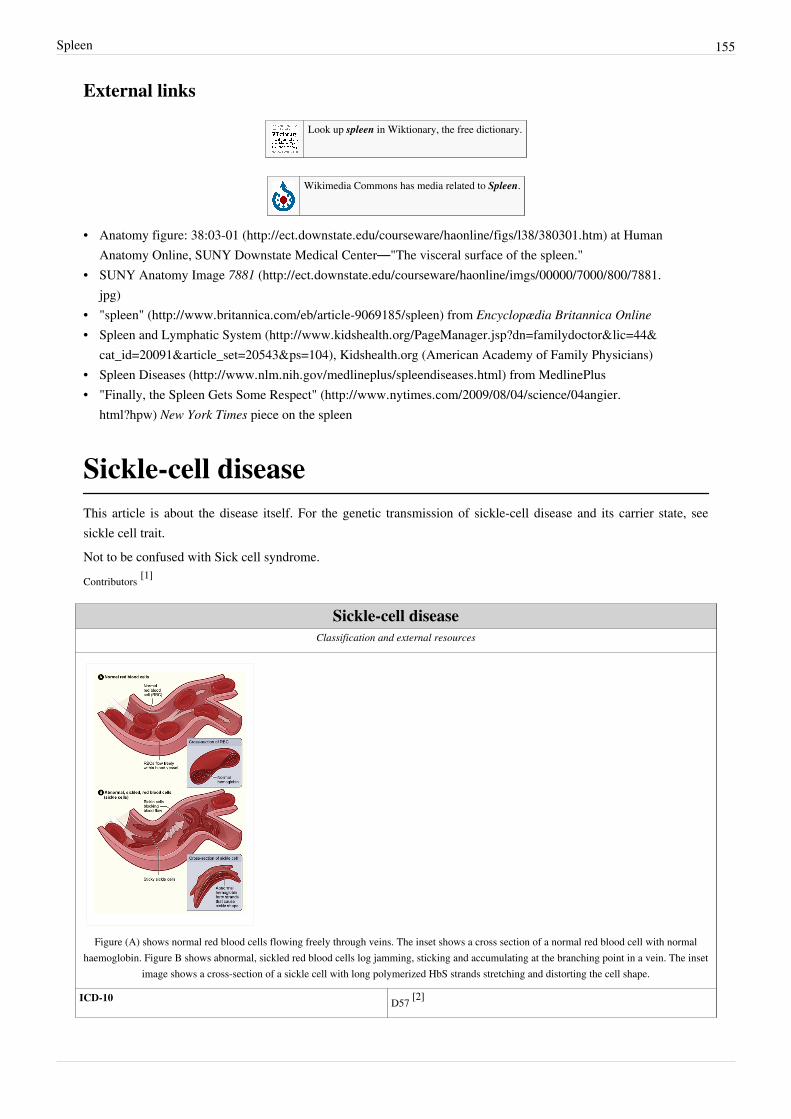
Spleen 155
External links
Look up spleen in Wiktionary, the free dictionary.
Wikimedia Commons has media related to Spleen.
• Anatomy figure: 38:03-01 (http:/ / ect. downstate. edu/ courseware/ haonline/ figs/ l38/ 380301. htm) at HumanAnatomy Online, SUNY Downstate Medical Center—"The visceral surface of the spleen."
• SUNY Anatomy Image 7881 (http:/ / ect. downstate. edu/ courseware/ haonline/ imgs/ 00000/ 7000/ 800/ 7881.jpg)
• "spleen" (http:/ / www. britannica. com/ eb/ article-9069185/ spleen) from Encyclopædia Britannica Online• Spleen and Lymphatic System (http:/ / www. kidshealth. org/ PageManager. jsp?dn=familydoctor& lic=44&
cat_id=20091& article_set=20543& ps=104), Kidshealth.org (American Academy of Family Physicians)• Spleen Diseases (http:/ / www. nlm. nih. gov/ medlineplus/ spleendiseases. html) from MedlinePlus• "Finally, the Spleen Gets Some Respect" (http:/ / www. nytimes. com/ 2009/ 08/ 04/ science/ 04angier.
html?hpw) New York Times piece on the spleen
Sickle-cell diseaseThis article is about the disease itself. For the genetic transmission of sickle-cell disease and its carrier state, seesickle cell trait.Not to be confused with Sick cell syndrome.Contributors [1]
Sickle-cell diseaseClassification and external resources
Figure (A) shows normal red blood cells flowing freely through veins. The inset shows a cross section of a normal red blood cell with normalhaemoglobin. Figure B shows abnormal, sickled red blood cells log jamming, sticking and accumulating at the branching point in a vein. The inset
image shows a cross-section of a sickle cell with long polymerized HbS strands stretching and distorting the cell shape.
ICD-10 D57 [2]

Sickle-cell disease 156
ICD-9 282.6 [3]
OMIM 603903 [4]
DiseasesDB 12069 [5]
MedlinePlus 000527 [6]
eMedicine med/2126 [7] oph/490 [8] ped/2096 [9] emerg/26 [10] emerg/406 [11]
MeSH C15.378.071.141.150.150 [12]
GeneReviews • Sickle-cell disease [13]
Sickle-cell disease (SCD), or sickle-cell anaemia (SCA) or drepanocytosis, is a hereditary blood disorder,characterized by red blood cells that assume an abnormal, rigid, sickle shape. Sickling decreases the cells' flexibilityand results in a risk of various life-threatening complications. This sickling occurs because of a mutation in thehaemoglobin gene. Individuals with one copy of the mutant gene produce a mixture of both normal and abnormalhaemoglobin. This is an example of codominance.Life expectancy is shortened. In 1994, in the US, the average life expectancy of persons with this condition wasestimated to be 42 years in males and 48 years in females, but today, thanks to better management of the disease,patients can live into their 70s or beyond.[14]
Sickle-cell disease occurs more commonly among people whose ancestors lived in tropical and sub-tropicalsub-Saharan regions where malaria is or was common. Where malaria is common, carrying a single sickle-cell allele(sickle cell trait) confers a selective advantage—in other words, being a heterozygote is advantageous. Specifically,humans with one of the two alleles of sickle-cell disease show less severe symptoms when infected with malaria.Sickle-cell anaemia is a form of sickle-cell disease in which there is homozygosity for the mutation that causes HbS.Sickle-cell anaemia is also referred to as "HbSS", "SS disease", "haemoglobin S" or permutations of those names. Inheterozygous people, that is, those who have only one sickle gene and one normal adult haemoglobin gene, thecondition is referred to as "HbAS" or "sickle cell trait". Other, rarer forms of sickle-cell disease are compoundheterozygous states in which the person has only one copy of the mutation that causes HbS and one copy of anotherabnormal haemoglobin allele. They include sickle-haemoglobin C disease (HbSC), sickle beta-plus-thalassaemia(HbS/β+) and sickle beta-zero-thalassaemia (HbS/β0).The term disease is applied because the inherited abnormality causes a pathological condition that can lead to deathand severe complications. Not all inherited variants of haemoglobin are detrimental, a concept known as geneticpolymorphism.

Sickle-cell disease 157
Signs and symptoms
Sickle cells in human blood: both normal redblood cells and sickle-shaped cells are present
Normal blood cells next to a sickle-blood cell.Colored scanning electron microscope image.
Sickle-cell disease may lead to various acute and chroniccomplications, several of which have a high mortality rate.
Sickle cell crisis
The terms "sickle cell crisis" or "sickling crisis" may be used todescribe several independent acute conditions occurring in patientswith sickle cell disease. Sickle cell disease results in anemia and crisesthat could be of many types including the vaso-occlusive crisis,aplastic crisis, sequestration crisis, haemolytic crisis and others. Mostepisodes of sickle cell crises last between five and seven days."Although infection, dehydration, and acidosis (all of which favorsickling) can act as triggers, in most instances no predisposing cause isidentified."[15]
Vaso-occlusive crisis
The vaso-occlusive crisis is caused by sickle-shaped red blood cellsthat obstruct capillaries and restrict blood flow to an organ resulting inischaemia, pain, necrosis and often organ damage. The frequency,severity, and duration of these crises vary considerably. Painful crisesare treated with hydration, analgesics, and blood transfusion; painmanagement requires opioid administration at regular intervals untilthe crisis has settled. For milder crises, a subgroup of patients manageon NSAIDs (such as diclofenac or naproxen). For more severe crises,most patients require inpatient management for intravenous opioids;patient-controlled analgesia (PCA) devices are commonly used in thissetting. Vaso-occlusive crisis involving organs such as the penis orlungs are considered an emergency and treated with red-blood cell transfusions. Incentive spirometry, a technique toencourage deep breathing to minimise the development of atelectasis, is recommended.
Splenic sequestration crisis
Because of its narrow vessels and function in clearing defective red blood cells, the spleen is frequently affected. It isusually infarcted before the end of childhood in individuals suffering from sickle-cell anemia. This autosplenectomyincreases the risk of infection from encapsulated organisms; preventive antibiotics and vaccinations arerecommended for those with such asplenia.Splenic sequestration crises are acute, painful enlargements of the spleen, caused by intrasplenic trapping of red cellsand resulting in a precipitous fall in hemoglobin levels with the potential for hypovolemic shock. Sequestrationcrises are considered an emergency. If not treated, patients may die within 1–2 hours due to circulatory failure.Management is supportive, sometimes with blood transfusion. These crises are transient, they continue for 3–4 hoursand may last for one day.

Sickle-cell disease 158
Acute chest syndrome ACSAcute chest syndrome (ACS) is defined by new pulmonary infiltrate with a manifestation of pulmonary symptomslike tachypnea and dyspnea. It is the second most common complication and it accounts for about 25% of death inpatients with SCD, majority of cases present with vaso occlusive crises then they develop ACS. Nevertheless, inDessap et al., 2007 study they reported that about 80% of patients has vaso occlusive crises during ACS.
Aplastic crisisAplastic crises are acute worsenings of the patient's baseline anaemia, producing pallor, tachycardia, and fatigue.This crisis is normally triggered by parvovirus B19, which directly affects production of red blood cells by invadingthe red cell precursors and multiplying in them and destroying them.[16] Parvovirus infection nearly completelyprevents red blood cell production for two to three days. In normal individuals, this is of little consequence, but theshortened red cell life of sickle-cell patients results in an abrupt, life-threatening situation. Reticulocyte counts dropdramatically during the disease (causing reticulocytopenia), and the rapid turnover of red cells leads to the drop inhaemoglobin. This crisis takes 4 days to one week to disappear. Most patients can be managed supportively; someneed blood transfusion.
Haemolytic crisisHaemolytic crises are acute accelerated drops in haemoglobin level. The red blood cells break down at a faster rate.This is particularly common in patients with co-existent G6PD deficiency. Management is supportive, sometimeswith blood transfusions.
OtherOne of the earliest clinical manifestations is dactylitis, presenting as early as six months of age, and may occur inchildren with sickle trait. The crisis can last up to a month.[17] Another recognised type of sickle crisis is the acutechest syndrome, a condition characterised by fever, chest pain, difficulty breathing, and pulmonary infiltrate on achest X-ray. Given that pneumonia and sickling in the lung can both produce these symptoms, the patient is treatedfor both conditions. It can be triggered by painful crisis, respiratory infection, bone-marrow embolisation, or possiblyby atelectasis, opiate administration, or surgery.
ComplicationsSickle-cell anaemia can lead to various complications, including:• Increased risk of severe bacterial infections due to loss of functioning spleen tissue (and comparable to the risk of
infections after having the spleen removed surgically). These infections are typically caused by encapsulatedorganisms such as Streptococcus pneumoniae and Haemophilus influenzae. Daily penicillin prophylaxis is themost commonly used treatment during childhood, with some haematologists continuing treatment indefinitely.Patients benefit today from routine vaccination for S. pneumoniae.
• Stroke, which can result from a progressive narrowing of blood vessels, preventing oxygen from reaching thebrain. Cerebral infarction occurs in children and cerebral haemorrhage in adults.
• Silent stroke is a stroke that causes no immediate symptoms but is associated with damage to the brain. Silentstroke is probably five times as common as symptomatic stroke. Approximately 10–15% of children with sicklecell disease suffer strokes, with silent strokes predominating in the younger patients.
• Cholelithiasis (gallstones) and cholecystitis, which may result from excessive bilirubin production andprecipitation due to prolonged haemolysis.
• Avascular necrosis (aseptic bone necrosis) of the hip and other major joints, which may occur as a result ofischaemia.
• Decreased immune reactions due to hyposplenism (malfunctioning of the spleen).

Sickle-cell disease 159
• Priapism and infarction of the penis.• Osteomyelitis (bacterial bone infection); the most common cause of osteomyelitis in sickle cell disease is
Salmonella (especially the non-typical serotypes Salmonella typhimurium, Salmonella enteritidis, Salmonellacholeraesuis and Salmonella paratyphi B), followed by Staphylococcus aureus and Gram-negative enteric bacilliperhaps because intravascular sickling of the bowel leads to patchy ischaemic infarction.
• Opioid tolerance, which can occur as a normal, physiologic response to the therapeutic use of opiates. Addictionto opiates occurs no more commonly among individuals with sickle-cell disease than among other individualstreated with opiates for other reasons.
• Acute papillary necrosis in the kidneys.•• Leg ulcers.•• In eyes, background retinopathy, proliferative retinopathy, vitreous haemorrhages and retinal detachments,
resulting in blindness. Regular annual eye checks are recommended.• During pregnancy, intrauterine growth retardation, spontaneous abortion, and pre-eclampsia.•• Chronic pain: Even in the absence of acute vaso-occlusive pain, many patients have chronic pain that is not
reported.• Pulmonary hypertension (increased pressure on the pulmonary artery), leading to strain on the right ventricle and
a risk of heart failure; typical symptoms are shortness of breath, decreased exercise tolerance and episodes ofsyncope.
• Chronic renal failure due to Sickle cell nephropathy—manifests itself with hypertension (high blood pressure),proteinuria (protein loss in the urine), haematuria (loss of red blood cells in urine) and worsened anaemia. If itprogresses to end-stage renal failure, it carries a poor prognosis.
HeterozygotesThe heterozygous form (sickle cell trait) is almost always asymptomatic, and the only usual significant manifestationis the renal concentrating defect presenting with isosthenuria.
Pathophysiology
Scanning Electron Micrograph showing amixture of red blood cells, some withround normal morphology, some withmild sickling showing elongation and
bending
Sickle-cell anaemia is caused by a point mutation in the β-globin chain ofhaemoglobin, causing the hydrophilic amino acid glutamic acid to be replacedwith the hydrophobic amino acid valine at the sixth position. The β-globingene is found on chromosome 11. The association of two wild-type α-globinsubunits with two mutant β-globin subunits forms haemoglobin S (HbS).Under low-oxygen conditions (being at high altitude, for example), theabsence of a polar amino acid at position six of the β-globin chain promotesthe non-covalent polymerisation (aggregation) of haemoglobin, which distortsred blood cells into a sickle shape and decreases their elasticity.
The loss of red blood cell elasticity is central to the pathophysiology ofsickle-cell disease. Normal red blood cells are quite elastic, which allows thecells to deform to pass through capillaries. In sickle-cell disease, low-oxygentension promotes red blood cell sickling and repeated episodes of sicklingdamage the cell membrane and decrease the cell's elasticity. These cells fail toreturn to normal shape when normal oxygen tension is restored. As aconsequence, these rigid blood cells are unable to deform as they pass
through narrow capillaries, leading to vessel occlusion and ischaemia.

Sickle-cell disease 160
The actual anaemia of the illness is caused by haemolysis, the destruction of the red cells, because of their misshape.Although the bone marrow attempts to compensate by creating new red cells, it does not match the rate ofdestruction. Healthy red blood cells typically live 90–120 days, but sickle cells only survive 10–20 days.
GeneticsNormally, humans have Haemoglobin A, which consists of two alpha and two beta chains, Haemoglobin A2, whichconsists of two alpha and two delta chains and Haemoglobin F, consisting of two alpha and two gamma chains intheir bodies. Of these, Haemoglobin A makes up around 96-97% of the normal haemoglobin in humans.Sickle-cell gene mutation probably arose spontaneously in different geographic areas, as suggested by restrictionendonuclease analysis. These variants are known as Cameroon, Senegal, Benin, Bantu and Saudi-Asian. Theirclinical importance springs from the fact that some of them are associated with higher HbF levels, e.g., Senegal andSaudi-Asian variants, and tend to have milder disease.In people heterozygous for HgbS (carriers of sickling haemoglobin), the polymerisation problems are minor, becausethe normal allele is able to produce over 50% of the haemoglobin. In people homozygous for HgbS, the presence oflong-chain polymers of HbS distort the shape of the red blood cell from a smooth doughnut-like shape to ragged andfull of spikes, making it fragile and susceptible to breaking within capillaries. Carriers have symptoms only if theyare deprived of oxygen (for example, while climbing a mountain) or while severely dehydrated. The sickle-celldisease occurs when the sixth amino acid, glutamic acid, is replaced by valine to change its structure and function; assuch, sickle cell anemia is also known as E6V. Valine is hydrophobic, causing the haemoglobin to collapse in onitself occasionally. The structure is not changed otherwise. When enough haemoglobin collapses in on itself the redblood cells become sickle-shaped.
Distribution of the sickle-cell trait shownin pink and purple
Historical distribution of malaria (nolonger endemic in Europe) shown in
green
The gene defect is a known mutation of a single nucleotide (seesingle-nucleotide polymorphism - SNP) (A to T) of the β-globin gene, whichresults in glutamic acid being substituted by valine at position 6.Haemoglobin S with this mutation is referred to as HbS, as opposed to thenormal adult HbA. The genetic disorder is due to the mutation of a singlenucleotide, from a CTC to CAC codon on the coding strand, which istranscribed from the template strand into a GUG codon. This is normally abenign mutation, causing no apparent effects on the secondary, tertiary, orquaternary structure of haemoglobin in conditions of normal oxygenconcentration. What it does allow for, under conditions of low oxygenconcentration, is the polymerization of the HbS itself. The deoxy form ofhaemoglobin exposes a hydrophobic patch on the protein between the E and Fhelices. The hydrophobic residues of the valine at position 6 of the beta chainin haemoglobin are able to associate with the hydrophobic patch, causinghaemoglobin S molecules to aggregate and form fibrous precipitates.
The allele responsible for sickle-cell anaemia can be found on the short armof chromosome 11. A person that receives the defective gene from both fatherand mother develops the disease; a person that receives one defective and onehealthy allele remains healthy, but can pass on the disease and is known as acarrier. If two parents who are carriers have a child, there is a 1-in-4 chance
of their child developing the disease and a 1-in-2 chance of their child being just a carrier. Heterozygotes are stillable to contract malaria, but their symptoms are generally less severe.

Sickle-cell disease 161
Modern distribution of malaria
Due to the adaptive advantage of the heterozygote, the disease is stillprevalent, especially among people with recent ancestry in malaria-strickenareas, such as Africa, the Mediterranean, India and the Middle East. Malariawas historically endemic to southern Europe, but it was declared eradicated inthe mid-20th century, with the exception of rare sporadic cases.
The malaria parasite has a complex life cycle and spends part of it in red blood cells. In a carrier, the presence of themalaria parasite causes the red blood cells with defective haemoglobin to rupture prematurely, making theplasmodium unable to reproduce. Further, the polymerization of Hb affects the ability of the parasite to digest Hb inthe first place. Therefore, in areas where malaria is a problem, people's chances of survival actually increase if theycarry sickle-cell trait (selection for the heterozygote).In the USA, where there is no endemic malaria, the prevalence of sickle-cell anaemia among blacks is lower (about0.25%) than in West Africa (about 4.0%) and is falling. Without endemic malaria, the sickle cell mutation is purelydisadvantageous and will tend to be selected out of the affected population via natural selection. However, theAfrican American community of the USA is known to be the result of significant admixture between several Africanand non-African ethnic groups, and also represents the descendants of survivors of the slavery and the slave trade.Thus, a lower degree of endogamy and, particularly, abnormally high health-selective pressure through slavery maybe the most plausible explanations for the lower prevalence of sickle-cell anaemia (and, possibly, other geneticdiseases) among African-Americans compared to Sub-Saharan Africans. Another factor limiting the spread ofsickle-cell genes in North America is the absence of cultural proclivities to polygamy, which allows affected malesto continue to seek unaffected children with multiple partners.
Sickle-cell disease is inherited in the autosomalrecessive pattern.
Inheritance
Sickle-cell conditions have an autosomal recessive pattern ofinheritance from parents.[18] The types of haemoglobin a personmakes in the red blood cells depend on what haemoglobin genesare inherited from her or his parents. If one parent has sickle-cellanaemia (SS) and the other has sickle-cell trait then there is a 50%chance of a child's having sickle-cell disease and a 50% chance ofa child's having sickle-cell trait. When both parents havesickle-cell trait a child has a 25% chance of sickle-cell disease,25% will not carry any sickle cell alleles, and 50% will have theheterozygous condition, as shown in the diagram.
Diagnosis
In HbSS, the full blood count reveals haemoglobin levels in therange of 6–8 g/dL with a high reticulocyte count (as the bonemarrow compensates for the destruction of sickle cells byproducing more red blood cells). In other forms of sickle-cell disease, Hb levels tend to be higher. A blood film mayshow features of hyposplenism (target cells and Howell-Jolly bodies).
Sickling of the red blood cells, on a blood film, can be induced by the addition of sodium metabisulfite. The presenceof sickle haemoglobin can also be demonstrated with the "sickle solubility test". A mixture of haemoglobin S (Hb S)in a reducing solution (such as sodium dithionite) gives a turbid appearance, whereas normal Hb gives a clearsolution.

Sickle-cell disease 162
Abnormal haemoglobin forms can be detected on haemoglobin electrophoresis, a form of gel electrophoresis onwhich the various types of haemoglobin move at varying speeds. Sickle-cell haemoglobin (HgbS) and haemoglobinC with sickling (HgbSC)—the two most common forms—can be identified from there. The diagnosis can beconfirmed with high-performance liquid chromatography (HPLC). Genetic testing is rarely performed, as otherinvestigations are highly specific for HbS and HbC.An acute sickle-cell crisis is often precipitated by infection. Therefore, a urinalysis to detect an occult urinary tractinfection, and chest X-ray to look for occult pneumonia should be routinely performed.People who are known carriers of the disease often undergo genetic counseling before they have a child. A test to seeif an unborn child has the disease takes either a blood sample from the fetus or a sample of amniotic fluid. Sincetaking a blood sample from a fetus has greater risks, the latter test is usually used. Neonatal screening provides notonly a method of early detection for individuals with sickle cell disease, but also allows for identification of thegroups of people that carry the sickle cell trait.[19]
After the mutation responsible for this disease was discovered in 1979, the U.S. Air Force required black applicantsto test for the mutation. It dismissed 143 applicants because they were carriers, even though none of them had thecondition. It eventually withdrew the requirement, but only after a trainee filed a lawsuit.
Management
Folic acid and penicillinChildren born with sickle-cell disease will undergo close observation by the pediatrician and will requiremanagement by a haematologist to assure they remain healthy. These patients will take a 1 mg dose of folic aciddaily for life. From birth to five years of age, they will also have to take penicillin daily due to the immature immunesystem that makes them more prone to early childhood illnesses.
Malaria chemoprophylaxisThe protective effect of sickle cell trait does not apply to people with sickle cell disease; in fact, they are uniquelyvulnerable to malaria, since the most common cause of painful crises in malarial countries is infection with malaria.It has therefore been recommended that people with sickle cell disease living in malarial countries should receiveanti-malarial chemoprophylaxis for life.
Vaso-occlusive crisesMost people with sickle-cell disease have intensely painful episodes called vaso-occlusive crises. The frequency,severity, and duration of these crises, however, vary tremendously. Painful crises are treated symptomatically withanalgesics; pain management requires opioid administration at regular intervals until the crisis has settled. For mildercrises, a subgroup of patients manage on NSAIDs (such as diclofenac or naproxen). For more severe crises, mostpatients require inpatient management for intravenous opioids; patient-controlled analgesia (PCA) devices arecommonly used in this setting. Diphenhydramine is also an effective agent that is frequently prescribed by doctors inorder to help control any itching associated with the use of opioids.
Acute chest crisisManagement is similar to vaso-occlusive crisis, with the addition of antibiotics (usually a quinolone or macrolide,since cell wall-deficient ["atypical"] bacteria are thought to contribute to the syndrome), oxygen supplementation forhypoxia, and close observation. Should the pulmonary infiltrate worsen or the oxygen requirements increase, simpleblood transfusion or exchange transfusion is indicated. The latter involves the exchange of a significant portion ofthe patients red cell mass for normal red cells, which decreases the percent of haemoglobin S in the patient's blood.

Sickle-cell disease 163
HydroxyureaThe first approved drug for the causative treatment of sickle-cell anaemia, hydroxyurea, was shown to decrease thenumber and severity of attacks in a study in 1995 (Charache et al.) and shown to possibly increase survival time in astudy in 2003 (Steinberg et al.). This is achieved, in part, by reactivating fetal haemoglobin production in place ofthe haemoglobin S that causes sickle-cell anaemia. Hydroxyurea had previously been used as a chemotherapy agent,and there is some concern that long-term use may be harmful, but this risk has been shown to be either absent or verysmall and it is likely that the benefits outweigh the risks.
Transfusion therapyBlood transfusions are often used in the management of sickle cell disease in acute cases and to preventcomplications by decreasing the number of red blood cells (RBC) that can sickle by adding normal red blood cells.In children prophylactic chronic red blood cell (RBC) transfusion therapy has been shown to be efficacious to acertain extent in reducing the risk of first stroke or silent stroke when transcranial Doppler (TCD) ultrasonographyshows abnormal increased cerebral blood flow velocities. In those who have sustained a prior stroke event it alsoreduces the risk of recurrent stroke and additional silent strokes.
Bone marrow transplantsBone marrow transplants have proven to be effective in children. Bone marrow transplants are the only known curefor SCD. However, bone marrow transplants are difficult to obtain because of the specific HLA typing necessary.Ideally, a twin family member (syngeneic) or close relative (allogeneic) would donate the bone marrow necessary fortransplantation.
PrognosisAbout 90% of patients survive to age 20, and close to 50% survive beyond the fifth decade.[20] In 2001, according toone study, the estimated mean survival for sickle cell patients was 53 years old for men and 58 years old for womenwith homozygous SCD.
EpidemiologyThe highest frequency of sickle cell disease is found in tropical regions, particularly sub-Saharan Africa, India andthe Middle-East. Migration of substantial populations from these high prevalence areas to low prevalence countriesin Europe has dramatically increased in recent decades and in some European countries sickle cell disease has nowovertaken more familiar genetic conditions such as haemophilia and cystic fibrosis. In 2010, there were about 29,000deaths attributed to sickle cell disease globally.
AfricaThree quarters of sickle-cell cases occur in Africa. A recent WHO report estimated that around 2% of newborns inNigeria were affected by sickle cell anaemia, giving a total of 150,000 affected children born every year in Nigeriaalone. The carrier frequency ranges between 10% and 40% across equatorial Africa, decreasing to 1–2% on the northAfrican coast and <1% in South Africa.
United StatesThe prevalence of the disease in the United States is approximately 1 in 5,000, mostly affecting Americans of Sub-Saharan African descent, according to the National Institutes of Health. In the United States, about 1 out of 500 African-American children and 1 in every 36,000 Hispanic-American children born will have sickle-cell anaemia. It is estimated that Sickle Cell Disease (SCD) affects 90,000 Americans. Most infants with SCD born in the United

Sickle-cell disease 164
States are now identified by routine neonatal screening. Forty-four states along with the District of Columbia, PuertoRico and the Virgin Islands currently provide universal neonatal screening for SCD. Sickle Cell trait occurs amongabout 1:12 African-Americans and 1:100 Hispanic-Americans. It is estimated that 2.5 million Americans areheterozygous carriers for the sickle cell trait.
FranceAs a result of population growth in African-Caribbean regions of overseas France and immigration from North andsub-Saharan Africa to mainland France, sickle cell disease has become a major health problem in France. SCD hasbecome the most common genetic disease in the country, with an overall birth prevalence of 1/2,415 in mainlandFrance, ahead of phenylketonuria (1/10,862), congenital hypothyroidism (1/3,132), congenital adrenal hyperplasia(1/19,008) and cystic fibrosis (1/5,014) for the same reference period. In 2010, 31.5% of all newborns in mainlandFrance (253,466 out of 805,958) were screened for SCD (this percentage was 19% in 2000). 341 newborns withSCD and 8,744 heterozygous carriers were found representing 1.1% of all newborns in mainland France. The Parismetropolitan district (Île-de-France) is the region that accounts for the largest number of newborns screened for SCD(60% in 2010). The second largest number of at-risk is in Provence-Alpes-Côte d'Azur at nearly 43.2% and thelowest number is in Brittany at 5.5%.[21]
United KingdomIn the United Kingdom, all babies receive a blood test to screen for this condition.[22]
Middle EastIn Saudi Arabia about 4.2% of the population carry the sickle-cell trait and 0.26% have sickle cell disease. Thehighest prevalence is in the Eastern province where approximately 17% of the population carry the gene and 1.2%have sickle cell disease. In 2005 in Saudi Arabia a mandatory pre-marital test including HB electrophoresis waslaunched and aimed to decrease the incidence of SCD and thalassemia.
IndiaSickle cell disease is common in many parts of India, where the prevalence has ranged from 9.4 to 22.2% in endemicareas.
Caribbean IslandsIn Jamaica, 10% of the population carries the sickle cell gene, making it the most prevalent genetic disorder in thecountry.
HistoryThe first report of sickle cell anaemia may have been in 1846 where the autopsy of an executed runaway slave wasdiscussed.[23] The author noted the curious absence of a spleen in this case.In 1910 a Chicago physician, James B. Herrick, reported the presence of sickle cells in the blood of an anaemicdental student, Walter Clement Noel.[24] These cells had first been observed by his intern Ernest Irons while theywere treating Noel in 1904.An association with pigmented gall stones was noted in 1911 by Washborn. A genetic basis for this disease was proposed in 1915 by Cook and Meyer. The disease was named sickle cell anaemia in 1922 by Verne Mason after several additional cases were reported. All the known cases had been reported in blacks and he concluded that this disease was confined to those of black African descent. The heterozygous condition was independently recognised in 1923 by Huck and Syndestrickler. Syndestrickler also was the first to note the splenic atrophy that occurs in this

Sickle-cell disease 165
condition. It was recognised as a Mendelian autosomal characteristic by Taliaffero and Huck also in 1923. Apredisposition to pneumonia was noted in 1924 by Graham. The concept of progressive splenic atrophy wasproposed by Hahn and Gilespie in 1927. Pneumococcal meningitis in this condition was first reported in 1928 byWollstein and Kriedel but it was not until 1966 that the association between splenic atrophy and infection was madeby Robinson and Watson.In 1927 Vernon Hahn and Elizabeth Biermann Gillespie showed that sickling of the red cells was related to lowoxygen. In some individuals this change occurs at partial pressures of O2 prevalent in the body, and produces anemia and other disorders, termed sickle-cell disease. In other personssickling occurs only at very low O2 partial pressures; these are asymptomatic sickle-cell trait carriers.The association with kidney and lung infarcts was noted in 1931 by Yater and Mollari and Baird in 1934respectively. The term sickle cell trait was coined by Samuel Diggs in Memphis in 1933 to distinguish heterozygotesfrom those with sickle cell anaemia. Diggs also reported the association with splenic fibrosis in 1935. Thepathological mechanism of vaso-occlusion was proposed by Ham and Castle in 1940.In 1946, E A Beet, a British medical officer stationed in Southern Rhodesia (Zimbabwe), observed that blood frommalaria patients who had sickle cell trait had fewer malarial parasites than blood from patients without the trait andsuggested that this might be a protective feature. In 1947 Beet published that the incidence of enlarged spleens insickle cell patients was much lower than in non sickle cell and suggested that this was due to recurrent thromboseswhich resulted in fibrosis and shrinkage of the spleen. In 1949 Lehmann and Raper published a map of Uganda andshowed that the presence of sickle cell anaemia correlated with the presence of malaria. In 1950 Singer et al. notedthe abrupt cessation of marrow activity that may occur and coined the term aplastic crisis. The role of parvovirus inaetiology of this condition was not recognised until 1981. P. Brain also while working in Northern Rhodesiaconfirmed the lower incidence of splenomegaly and suggested that while homozygotes for the sickle cell genesuffered from several problems heterozygotes might be protected against malaria.The modern phase of research on this disorder was initiated by the famous chemist Linus Pauling in 1949. Paulingpostulated that the hemoglobin (Hb) in sickle-cell disease is abnormal; when deoxygenated it polymerizes into long,thin, helical rods that distort the red cell into a sickle shape. In his laboratory, electrophoretic studies showed thatsickle-cell Hb (S) is indeed abnormal, having at physiological pH a lower negative charge than normal adult humanHb (A). In sickle-cell trait carriers there is a nearly equal amount of HbA and HbS, whereas in persons withsickle-cell disease nearly all the Hb is of the S type, apart from a small amount of fetal Hb. These observationsshowed that most patients with sickle-cell disease are homozygous for the gene encoding HbS, while trait carriersare heterozygous for this gene. Persons inheriting a sickle-cell gene and another mutant at the same locus, e.g. athalassemia gene, can also have a variant form of sickle-cell disease. Pauling also introduced the term "moleculardisease", which, together with molecular medicine, has become widely used.The next major advance was the discovery by Vernon Ingram in 1959 that HbS differs from HbA by only a singleamino-acid substitution in the β-polypeptide chain (β6Glu → Val). It was later established that this results from asubstitution of thymine for adenine in the DNA codon (GAG → GTG). This was the first example in any species ofthe effects of a mutation on a protein.This collection of clinical findings was unknown until the explanation of the sickle cells in 1910 by a Chicagocardiologist and professor of medicine James B. Herrick (1861–1954), whose intern Ernest Edward Irons(1877–1959) found "peculiar elongated and sickle-shaped" cells in the blood of Walter Clement Noel, a 20-year-oldfirst-year dental student from Grenada, after Noel was admitted to the Chicago Presbyterian Hospital in December1904 suffering from anaemia.[25]
Noel was readmitted several times over the next three years for "muscular rheumatism" and "bilious attacks". Noel completed his studies and returned to the capital of Grenada (St. George's) to practice dentistry. He died of pneumonia in 1916 and is buried in the Catholic cemetery at Sauteurs in the north of Grenada. Herrick's published

Sickle-cell disease 166
account included illustrations, but the earliest available slide showing sickle cells is that of a 1918 autopsy from asoldier with sickle trait, initially reviewed only 92 years later.The disease was named "sickle-cell anemia" by Verne Mason in 1922, then a medical resident at Johns HopkinsHospital. However, some elements of the disease had been recognized earlier: A paper in the Southern Journal ofMedical Pharmacology in 1846 described the absence of a spleen in the autopsy of a runaway slave. The Africanmedical literature reported this condition in the 1870s, when it was known locally as ogbanjes ("children who comeand go") because of the very high infant mortality rate caused by this condition. A history of the condition trackedreports back to 1670 in one Ghanaian family.[26]
Linus Pauling and colleagues were the first, in 1949, to demonstrate that sickle-cell disease occurs as a result of anabnormality in the haemoglobin molecule. This was the first time a genetic disease was linked to a mutation of aspecific protein, a milestone in the history of molecular biology, and it was published in their paper "Sickle CellAnemia, a Molecular Disease".
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Sickle-cell_disease[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D57[3] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=282. 6[4] http:/ / omim. org/ entry/ 603903[5] http:/ / www. diseasesdatabase. com/ ddb12069. htm[6] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000527. htm[7] http:/ / www. emedicine. com/ med/ topic2126. htm[8] http:/ / www. emedicine. com/ oph/ topic490. htm#[9] http:/ / www. emedicine. com/ ped/ topic2096. htm#[10] http:/ / www. emedicine. com/ emerg/ topic26. htm#[11] http:/ / www. emedicine. com/ emerg/ topic406. htm#[12] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?mode=& term=Sickle+ Cell+ anemia& field=entry#TreeC15. 378. 071. 141. 150. 150[13] http:/ / www. ncbi. nlm. nih. gov/ books/ n/ gene/ sickle/[14] http:/ / ericksontribune. com/ 2007/ 10/ mds-launch-network-to-treat-sickle-cell/[15][15] Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009-05-28). Robbins and Cotran Pathologic Basis of Disease, Professional
Edition: Expert Consult - Online (Robbins Pathology) (Kindle Locations 33498-33499). Elsevier Health. Kindle Edition.[16][16] Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009-05-28). Robbins and Cotran Pathologic Basis of Disease, Professional
Edition: Expert Consult - Online (Robbins Pathology) (Kindle Location 33329). Elsevier Health. Kindle Edition.[17] http:/ / www. ejbjs. org/ cgi/ content/ abstract/ 58/ 8/ 1161[18] http:/ / www. mayoclinic. com/ health/ sickle-cell-anemia/ DS00324/ DSECTION=causes[19] Lee, C., Davies, S.,& Dezatoux, C.(2000). Neonatal Screening for sickle cell disease. The Cochrane Collaboration. John Wiley & Sons, Ltd.[20][20] Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009-05-28). Robbins and Cotran Pathologic Basis of Disease, Professional
Edition: Expert Consult - Online (Robbins Pathology) (Kindle Locations 33530-33531). Elsevier Health. Kindle Edition.[21] Le dépistage néonatal de la drépanocytose en France. Numéro thématique. La drépanocytose en France : des données épidémiologiques pour
améliorer la prise en charge (http:/ / www. invs. sante. fr/ pmb/ invs/ (id)/ PMB_10831), Bardakdjian-Michau J, INVS, July 2012[22] http:/ / www. nhs. uk/ conditions/ sickle-cell-anaemia/ Pages/ Introduction. aspx[23][23] Lebby R (1846) Case of absence of the spleen. Southern J of Med Pharmacol 1: 481-483[24][24] ; Reprinted in[25][25] ; reprinted as[26][26] Konotey-Ahulu FID. Effect of environment on sickle cell disease in West Africa: epidemiologic and clinical considerations. In: Sickle Cell
Disease, Diagnosis, Management, Education and Research. Abramson H, Bertles JF, Wethers DL, eds. CV Mosby Co, St. Louis. 1973; 20;cited in

Sickle-cell disease 167
Further reading• Brown, Robert T., ed. (2006). Comprehensive handbook of childhood cancer and sickle cell disease: a
biopsychosocial approach (http:/ / books. google. com/ books?id=O2sq8EeKTdwC). Oxford University Press.ISBN 978-0-19-516985-0.
• Hill, Shirley A. (2003). Managing Sickle Cell Disease in Low-Income Families (http:/ / books. google. com/books?id=YG0Oi9mAaoQC). Temple University Press. ISBN 978-1-59213-195-2.
• Serjeant, Graham R. & Beryl E. (2001). Sickle Cell Disease (http:/ / books. google. com/books?id=SetrAAAAMAAJ). Oxford University Press. ISBN 978-0-19-263036-0.
• Tapper, Melbourne (1999). In the blood: sickle cell anemia and the politics of race (http:/ / books. google. com/books?id=YzM0oARlXvIC). University of Pennsylvania Press. ISBN 978-0-8122-3471-8.
External links
Wikimedia Commons has media related to Sickle-cell anemia.
• Sickle cell (http:/ / www. dmoz. org/ Health/ Conditions_and_Diseases/ Blood_Disorders/ Sickle_Cell) at DMOZ• Sickle Cell Anaemia OER Project (http:/ / www. sicklecellanaemia. org)

Thalassemia 168
ThalassemiaContributors [1]
ThalassemiaClassification and external resources
ICD-10 D56 [2]
ICD-9 282.4 [3]
OMIM 141800 [4] 141850 [5] 142310 [6] 604131 [7] 141800 [4] 141850 [5] 142310 [6] 604131 [7]
DiseasesDB 448 [8] 33334 [9] 33678 [10] 3087 [11]
MedlinePlus 000587 [12]
eMedicine article/958850 [13] article/206490 [14] article/955496 [15] article/396792 [16]
MeSH D013789 [17]
GeneReviews • Alpha-Thalassemia [18]
• Beta-Thalassemia [19]
Thalassemia (British English: thalassaemia) are forms of inherited autosomal recessive blood disorders thatoriginated in the Mediterranean region. In thalassemia, the disorder is caused by the weakening and destruction ofred blood cells. Thalassemia is caused by variant or missing genes that affect how the body makes hemoglobin.Hemoglobin is the protein in red blood cells that carries oxygen. People with thalassemia make less hemoglobin andhave fewer circulating red blood cells than normal, which results in mild or severe anemia. Thalassemia will bepresent as microcytic anemia.Thalassemia can cause significant complications, including iron overload, bone deformities and cardiovascularillness. However this same inherited disease of red blood cells may confer a degree of protection against malaria(specifically, malaria caused by the protozoan parasite Plasmodium falciparum), which is or was prevalent in theregions where the trait is common. This selective survival advantage of carriers (known as heterozygous advantage)may be responsible for perpetuating the mutation in populations. In that respect, the various thalassemias resembleanother genetic disorder affecting hemoglobin, sickle-cell disease.
Signs and symptoms• Iron overload: People with thalassemia can get an overload of iron in their bodies, either from the disease itself or
from frequent blood transfusions. Too much iron can result in damage to the heart, liver and endocrine system,which includes glands that produce hormones that regulate processes throughout the body. The damage ischaracterized by excessive deposits of iron. Without adequate iron chelation therapy, almost all patients withbeta-thalassemia will accumulate potentially fatal iron levels.
•• Infection: people with thalassemia have an increased risk of infection. This is especially true if the spleen hasbeen removed.
•• Bone deformities: Thalassemia can make the bone marrow expand, which causes bones to widen. This can resultin abnormal bone structure, especially in the face and skull. Bone marrow expansion also makes bones thin andbrittle, increasing the risk of broken bones.
• Enlarged spleen: the spleen aids in fighting infection and filters unwanted material, such as old or damaged blood cells. Thalassemia is often accompanied by the destruction of a large number of red blood cells and the task of removing these cells causes the spleen to enlarge. Splenomegaly can make anemia worse, and it can reduce the

Thalassemia 169
life of transfused red blood cells. Severe enlargement of the spleen may necessitate its removal.• Slowed growth rates: anemia can cause a child's growth to slow. Puberty also may be delayed in children with
thalassemia.•• Heart problems: such as congestive heart failure and abnormal heart rhythms (arrhythmias), may be associated
with severe thalassemia.
Cause
Thalassemia has an autosomal recessive patternof inheritance
Both α and β thalassemias are often inherited in an autosomal recessivemanner, although this is not always the case. Cases of dominantlyinherited α and β thalassemias have been reported, the first of whichwas in an Irish family with two deletions of 4 and 11 bp in exon 3interrupted by an insertion of 5 bp in the β-globin gene. For theautosomal recessive forms of the disease, both parents must be carriersin order for a child to be affected. If both parents carry ahemoglobinopathy trait, there is a 25% risk with each pregnancy for anaffected child. Genetic counseling and genetic testing is recommendedfor families that carry a thalassemia trait.
There are an estimated 60-80 million people in the world carrying thebeta thalassemia trait.Wikipedia:Citation needed This is a roughestimate; the actual number of those thalassemia major is unknown dueto the prevalence of thalassemia in less developedcountries.Wikipedia:Citation needed Countries such as Nepal,Bangladesh and Pakistan are seeing a large increase of thalassemiapatients due to lack of genetic counseling and screening.Wikipedia:Citation needed There is growing concern thatthalassemia may become a very serious problem in the next 50 years, one that will burden the world's blood banksupplies and the health system in general.Wikipedia:Citation needed There are an estimated 1,001 people living withthalassemia major in the United States and an unknown number of carriers.Wikipedia:Citation needed Because ofthe prevalence of the disease in countries with little knowledge of thalassemia, access to proper treatment anddiagnosis can be difficult.Wikipedia:Citation needed
EvolutionHaving a single gene for thalassemia may protect against malaria and thus be an advantage.People diagnosed with heterozygous (carrier) β thalassemia have some protection against coronary heart disease.
PathophysiologyNormally, the majority of adult hemoglobin (HbA) is composed of four protein chains, two α and two β globinchains arranged into a heterotetramer. In thalassemia, patients have defects in either the α or β globin chain causingproduction of abnormal red blood cells (In sickle-cell disease, the mutation is specific to β globin).The thalassemias are classified according to which chain of the hemoglobin molecule is affected. In α thalassemias,production of the α globin chain is affected, while in β thalassemia production of the β globin chain is affected.The β globin chains are encoded by a single gene on chromosome 11; α globin chains are encoded by two closely linked genes on chromosome 16.[20] Thus, in a normal person with two copies of each chromosome, there are two loci encoding the β chain, and four loci encoding the α chain. Deletion of one of the α loci has a high prevalence in people of African or Asian descent, making them more likely to develop α thalassemias. β Thalassemias are not only

Thalassemia 170
common in Africans, but also in Greeks and Italians.
Alpha (α) thalassemiasMain article: Alpha-thalassemiaThe α thalassemias involve the genes HBA1 and HBA2, inherited in a Mendelian recessive fashion. There are twogene loci and so four alleles. It is also connected to the deletion of the 16p chromosome. α Thalassemias result indecreased alpha-globin production, therefore fewer alpha-globin chains are produced, resulting in an excess of βchains in adults and excess γ chains in newborns. The excess β chains form unstable tetramers (called Hemoglobin Hor HbH of 4 beta chains), which have abnormal oxygen dissociation curves.
Beta (β) thalassemiaMain article: Beta-thalassemiaBeta thalassemias are due to mutations in the HBB gene on chromosome 11, also inherited in an autosomal-recessivefashion. The severity of the disease depends on the nature of the mutation. Mutations are characterized as either βo orβ thalassemia major if they prevent any formation of β chains, the most severe form of β thalassemia; as either β+ orβ thalassemia intermedia if they allow some β chain formation to occur; or as β thalassemia minor if only one of thefour β globin alleles contains a mutation, so that β chain production is not terribly compromised and patients may berelatively asymptomatic.
Delta (δ) thalassemiaMain article: Delta-thalassemiaAs well as alpha and beta chains present in hemoglobin, about 3% of adult hemoglobin is made of alpha and deltachains. Just as with beta thalassemia, mutations that affect the ability of this gene to produce delta chains canoccur.Wikipedia:Citation needed
Combination with other hemoglobinopathiesThalassemia can co-exist with other hemoglobinopathies. The most common of these are:• hemoglobin E/thalassemia: common in Cambodia, Thailand, and parts of India; clinically similar to β thalassemia
major or thalassemia intermedia.• hemoglobin S/thalassemia, common in African and Mediterranean populations; clinically similar to sickle cell
anemia, with the additional feature of splenomegaly• hemoglobin C/thalassemia: common in Mediterranean and African populations, hemoglobin C/βo thalassemia
causes a moderately severe hemolytic anemia with splenomegaly; hemoglobin C/β+ thalassemia produces amilder disease.
•• hemoglobin D/thalassemia, common in north west parts of India and Pakistan (Punjab region)
ManagementMain article: Management of thalassemiaMild thalassemia: people with thalassemia traits do not require medical or follow-up care after the initial diagnosis ismade. People with β-thalassemia trait should be warned that their condition can be misdiagnosed as the morecommon iron deficiency anemia. They should avoid routine use of iron supplements; yet iron deficiency can developduring pregnancy or from chronic bleeding. Counseling is indicated in all persons with genetic disorders, especiallywhen the family is at risk of a severe form of disease that may be prevented.

Thalassemia 171
Severe thalassemia: People with severe thalassemia require medical treatment. A blood transfusion regimen was thefirst measure effective in prolonging life.
MedicationsMultiple blood transfusions can result in iron overload. The iron overload related to thalassemia may be treated viachelation therapy with the medications deferoxamine, deferiprone or deferasirox. These treatments have resulted inimproved life expectancy in those with thalassemia major.Deferoxamine is only effective via daily injections which makes its long term use more difficult. It has the benefit ofbeing inexpensive and decent long term safety. Adverse effects are primary skin reactions around the injection siteand hearing loss.Deferasirox has the benefit of being an oral medication. Common side effects include: nausea, vomiting anddiarrhea. It however is not effective in everyone and is probably not suitable in those with significant cardiac issuesrelated to iron overload. The cost is also significant.Deferiprone is given as an oral medication. Nausea, vomiting and diarrhea is relatively common with its use. Whileavailable in Europe as of 2010 it is not available in North America. It appears to be the most effective agent when theheart is significantly involved.
Carrier detection• A screening policy exists in Cyprus to reduce the incidence of thalassemia, which since the program's
implementation in the 1970s (which also includes pre-natal screening and abortion) has reduced the number ofchildren born with the hereditary blood disease from 1 out of every 158 births to almost zero.
• In Iran as a premarital screening, the man's red cell indices are checked first, if he has microcytosis (mean cellhemoglobin < 27 pg or mean red cell volume < 80 fl), the woman is tested. When both are microcytic theirhemoglobin A2 concentrations are measured. If both have a concentration above 3.5% (diagnostic of thalassemiatrait) they are referred to the local designated health post for genetic counseling.
Bone marrow transplantBone marrow transplantation may offer the possibility of a cure in young people who have an HLA-matched donor.Success rates have been in the 80–90% range. Mortality from the procedure is about 3%.If the person does not have an HLA-matched compatible donor such as the first curative method requires, there isanother curative method called Bone Marrow Transplantation(BMT) from haploidentical mother to child(mismatched donor), in which the donor is the mother. It was invented in 2002 by Dr. Pietro Sodani. The results arethese: thalassemia-free survival rate 70%, rejection 23%, and mortality 7%. The best results are with very youngpatients.
EpidemiologyThe beta form of thalassemia is particularly prevalent among Mediterranean peoples and this geographicalassociation is responsible for its naming Wikipedia:Citation needed. Globally in 2010 it resulted in about 18,000deaths.In Europe, the highest concentrations of the disease are found in Greece, coastal regions in Turkey (particularly the Aegean Region such as Izmir, Balikesir, Aydin, Mugla, and Mediterranean Region such as Antalya, Adana, Mersin), in parts of Italy, particularly Southern Italy and the lower Po valley. The major Mediterranean islands (except the Balearics) such as Sicily, Sardinia, Malta, Corsica, Cyprus, and Crete are heavily affected in particular. Other Mediterranean people, as well as those in the vicinity of the Mediterranean, also have high rates of thalassemia, including people from West Asia and North Africa. Far from the Mediterranean, South Asians are also affected, with

Thalassemia 172
the world's highest concentration of carriers (16% of the population) being in the Maldives.Nowadays, it is found in populations living in Africa, the Americas and also, in Tharu people in the Terai region ofNepal and India. It is believed to account for much lower malaria sicknesses and deaths, accounting for the historicability of Tharus to survive in areas with heavy malaria infestation, where others could not. Thalassemias areparticularly associated with people of Mediterranean origin, Arabs (especially Palestinians and people of Palestiniandescent), and Asians.[21] The Maldives has the highest incidence of Thalassemia in the world with a carrier rate of18% of the population. The estimated prevalence is 16% in people from Cyprus, 1% in Thailand, and 3–8% inpopulations from Bangladesh, China, India, Malaysia and Pakistan. Thalassemias also occur in descendants ofpeople from Latin America and Mediterranean countries (e.g. Greece, Italy, Portugal, Spain, and others).
EtymologyThe name of this condition derives from the Greek Thalassa (θάλασσα), sea, and haema (αἷμα), blood. The termwas first used in 1932.
Society and cultureIn 2008, in Spain, a baby was selectively implanted in order to be a cure for his brother's thalassemia. The child wasborn from an embryo screened to be free of the disease before implantation with in vitro fertilization. The baby'ssupply of immunologically compatible cord blood was saved for transplantation to his brother. The transplantationwas considered successful.[22] In 2009, a group of doctors and specialists in Chennai and Coimbatore registered thesuccessful treatment of thalassemia in a child using an unaffected sibling's umbilical cord blood.[23]
References[1] http:/ / tools. wmflabs. org/ xtools/ articleinfo/ ?wikilang=en& wikifam=. wikipedia. org& grouped=on& page=Thalassemia[2] http:/ / apps. who. int/ classifications/ icd10/ browse/ 2010/ en#/ D56[3] http:/ / www. icd9data. com/ getICD9Code. ashx?icd9=282. 4[4] http:/ / omim. org/ entry/ 141800[5] http:/ / omim. org/ entry/ 141850[6] http:/ / omim. org/ entry/ 142310[7] http:/ / omim. org/ entry/ 604131[8] http:/ / www. diseasesdatabase. com/ ddb448. htm[9] http:/ / www. diseasesdatabase. com/ ddb33334. htm[10] http:/ / www. diseasesdatabase. com/ ddb33678. htm[11] http:/ / www. diseasesdatabase. com/ ddb3087. htm[12] http:/ / www. nlm. nih. gov/ medlineplus/ ency/ article/ 000587. htm[13] http:/ / emedicine. medscape. com/ article/ 958850-overview[14] http:/ / emedicine. medscape. com/ article/ 206490-overview[15] http:/ / emedicine. medscape. com/ article/ 955496-overview[16] http:/ / emedicine. medscape. com/ article/ 396792-overview[17] http:/ / www. nlm. nih. gov/ cgi/ mesh/ 2014/ MB_cgi?field=uid& term=D013789[18] http:/ / www. ncbi. nlm. nih. gov/ books/ NBK1435/[19] http:/ / www. ncbi. nlm. nih. gov/ books/ NBK1426/[20][20] Robbins Basic Pathology, Page No:428[21] E. Goljan, Pathology, 2nd ed. Mosby Elsevier, Rapid Review Series.[22] Spanish Baby Engineered To Cure Brother (http:/ / guanabee. com/ 2008/ 10/ baby-engineered-to-cure-brothe-1. php)[23] His sister's keeper: Brother's blood is boon of life (http:/ / timesofindia. indiatimes. com/ news/ city/ chennai/
His-sisters-keeper-Brothers-blood-is-boon-of-life/ articleshow/ 5020318. cms), Times of India, 17 September 2009

Thalassemia 173
External links• Thalassemia (http:/ / www. dmoz. org/ Health/ Conditions_and_Diseases/ Blood_Disorders/ Anemia/
Thalassemia/ ) at DMOZ• Information on Thalassemia (http:/ / www. thalassemia. co. uk)• Learning About Thalassemia (http:/ / www. genome. gov/ 10001221) published by the National Human Genome
Research Institute.• Cardiff Sickle Cell & Thalassaemia Centre (http:/ / www. cardiffandvaleuhb. wales. nhs. uk/
sickle-cell-thalassaemia-centre)

Article Sources and Contributors 174
Article Sources and ContributorsAnemia Source: http://en.wikipedia.org/w/index.php?oldid=623214622 Contributors: 12637man, 27 Juni, 4wajzkd02, AHIMS INDIA, ARA, Abune, Adam.J.W.C., Addshore, AdjustShift,Aechase1, Ahoerstemeier, Aidan Kehoe, Alansohn, Ale jrb, Alex.tan, Alison22, Allstarecho, Alpha Quadrant (alt), Alphius, AmiDaniel, Amorymeltzer, Andre Engels, Andy Dingley, Angr,Angrysockhop, Anir1uph, Anonymous Dissident, Antandrus, Anthonyhcole, Arcadian, Arctickinkajou, Arda Xi, Arripay, Arthur Albano, AtticusX, Auric, AussieJake, Avoided, AxelBoldt, Axl,Axxaer, B, BDE1982, Balaji Ravichandran, Bayushie, Belovedfreak, Ben Ben, Bender235, Benji2, BethNaught, Bgtuc84, Bigdumbdinosaur, Biosthmors, Bjb, Bluerasberry, Bobbis, Bobo192,Bodnotbod, Boghog, Booksrule9, Brandmeister (old), BritishWatcher, Brycechipmunk, CDrecche, CSZero, Cadwaladr, Caesarjbsquitti, Cakloss, Calmer Waters, Calvinchong, Camw, Can't sleep,clown will eat me, CanadianLinuxUser, Capricorn42, Caps tiki, Casey56, Causeandedit, Cenarium, Cereis, Cforrester101, Chaser, Cherubino, Chinesesurname, Choess, Choihei, Chris Fookes,Chris Roy, Chris the speller, Christian List, Chuunen Baka, Cleared as filed, Closedmouth, Coffee, ColdFusion650, CommonsDelinker, Comtebenoit, Cr299, Craigwwoods, CrazyGlu, CurbChain, Cvaneg, DMacks, DVD R W, DVMresearcher, DVdm, DabMachine, Dacheatcode, Daniel Bonniot de Ruisselet, Danilot, Davidiad, Davidone, Davidruben, Dddstone, Deadk82,DeborahDBartlett, Decltype, Deflective, Denisarona, DerHexer, Diberri, Dimboukas, Dimketr, Dina, Dinesh smita, Djsejpal, Dlohcierekim, Dmlevy 99, Dnepro86, Doc.mari, Dogdocdvm,DonnieJDube, Download, Dr.michael.benjamin, DrAlvi, Drgarden, Drparthnsy, Dysmorodrepanis, E. Sn0 =31337=, ESkog, EdwardLockhart, Egil, Eliz81, Elygra, Enzo Aquarius, Epbr123,Epicgenius, Erik9, Eshywiki, Everyking, Excirial, Fabiform, Falcon8765, Fieldday-sunday, Fleester, Flojesy, Flosseveryday, Flyer22, Fratrep, Fredrik, Freikorp, Friday, Furious Style, Fuzzbox,Fyrael, Gamer007, Ganesh Paudel, Geekchick77, Gene Hobbs, Generica, Gfirman en, Gigemag76, Gilliam, Gilvala, Ginkgo100, GlobeGores, Gobbleswoggler, Gobonobo, Gogo Dodo,GrahamColm, GreatWhiteNortherner, Green caterpillar, Gurch, Gwalla, Hadal, Hall4Life, Hallbrianh, Harold f, Hopping, Hoshin12, Hu12, HumanNaturOriginal, IceUnshattered, IdontHavaname, Immunize, Imran, Inferno, Lord of Penguins, Infrangible, Invocatus, Iridescent, Ixfd64, J.delanoy, JRHorse, JackLumber, Jaknouse, James Fryer, Jasonauk, Jclemens, Jeffhall318,JeffreyN, Jengod, Jfdwolff, Jfurr1981, Jh12, Jiang, Jkvandeusen, Jmh649, Jni, Jo Mengele, Joelloyd7, Joelmills, Joewright, John Cline, Johnnymadness, Jomunro, Jonathan.s.kt, Jossi, Jtdaugir,Juliancolton, KDS4444, Kalaiarasy, Kander, Kartano, Kateshortforbob, Kemfaye, Kendall35, Kimiko, King of Hearts, Kkailas, Knutux, Koavf, Koyaanis Qatsi, Kpjas, Kubra, Kungfuadam, Kuru,Kyouketsusha, LAAFan, LB48Steve03, LIC Habeeb, La Pianista, Landon1980, Larschan, Lass Lethe, Latka, LeaveSleaves, Lightmouse, Linzhoo2u, LittleOldMe, Lovepinkhore, Luboogers25,LuisEBenavente, Lycheeberries, MER-C, MK8, MONGO, Machn, Madhero88, Majkinetor, Mamemimomundem, Mandarax, Mandy Kaur, Mangoe, MarcDanilidou, MastCell, Matdrodes, Mato,Maypigeon of Liberty, McSly, Mean as custard, Meewam, Mentifisto, Mgmei, Mikael Häggström, Miniyazz, MithrandirAgain, Moe Epsilon, Moggie2002, Mogism, Mograi jamal, Moss S,MrBill3, Mycroft7, Mygerardromance, N5iln, Ndkartik, Neelix, Nephron, Neurolysis, Nick Number, Nick123, Nihiltres, Nikki Louladdl, Nmani77, Nmg20, NorthStarGirl, Notyoyoma, Novalia,Nubzor, Nunh-huh, Nuujinn, Ocdnctx, Ohnoitsjamie, Okunderground, Opelio, Oxymoron83, PMDrive1061, POVpushee, Papte, ParlerVousWiki, PatrikR, Peter Chastain, Peter.C, PhD Dre,Pharaoh of the Wizards, Philip Trueman, Piesquared93, Pigman, PinchasC, Pne, Poccil, Polemyx, Polihale, Postdlf, Pratha naik, Puckly, Pzrmd, Queerbubbles, Quentonamos, Quibik, RA0808,Rachelmk77, Raclemens, Radon210, Raul654, Ravensun, Redrecks, Redsox00002, Restepc, Reyps, Rich Farmbrough, Riley Huntley, Rjwilmsi, RobWBartel, Rodrigotorres, Romanm, Ronz,Rory 20 uk, RoshanMcG, Rsabbatini, RuM, SO-intO-yOuxX, SV Resolution, Saebjorn, Sarahj2107, Sassf, SchwarzeMelancholie, Scienceislife, Scientificone, Scohoust, ScottRaw,Seanconway21, Seaphoto, SeveredSpirit, Sgr927, Shadow4ARE, Shoeofdeath, Shuipzv3, SimonTrew, Sintesk7, Skizzik, Slgcat, Sliggy, Smettems, Smith2267, Smsarmad, Snowmanradio,Snoyes, Solon.KR, Some standardized rigour, Someone else, Sp00n17, SpNeo, SpaceFlight89, Spiritia, Spitfire, Statkit1, Stephenb, Stevenfruitsmaak, Still relentless, Storkk, Sunray, Suougibma,Supertouch, Supten, Sushmav, Syncategoremata, Synchronism, TBAmes, TK-P, Tapanhp, Taquittee, Tarquin, Taxman, Techman224, Template namespace initialisation script, The High FinSperm Whale, The Master of Mayhem, The Thing That Should Not Be, Thingg, Tiddly Tom, Tide rolls, Tom harrison, Tommy Bergin, Tommy2010, Tony K10, Touque, Tpbradbury, Trappistthe monk, Trevor Andersen, Tristanb, Troutbagel, Trsalmon, Truddle, Twaz, Twillisjr, Twsx, Uofhealth, Uriah923, VashiDonsk, Vldscore, Vrenator, Wael El Kabbany, Wavy, Wee Jimmy,WereSpielChequers, WhatamIdoing, WiHkibew, Wiki wiki1, Wikibofh, Wikipelli, Wikkipedia, Will314159, Windows.dll, Windweilder, Winston365, Wouterstomp, WriterHound, Xnyxx,Yamitoyume, Ynhockey, Yobol, Yonghokim, Yopogono, Yrsamama, Yudiweb, YuriSuassuna, Zackwhittaker, Zahid Abdassabur, Zerofenrir, Zujua, Zyxwv99, 1048 anonymous edits
Hemolysis Source: http://en.wikipedia.org/w/index.php?oldid=612764248 Contributors: AJim, AMMeier, AbinoamJr, Aeluwas, Altenmann, Andrew73, Anthonyhcole, Arcadian, Avitya,AxelBoldt, Baldhur, Beartenor1, Boleyn, C4dn, Chicocvenancio, Cit helper, Conti, Corpx, Cshell1187, Davidiad, DocWatson42, EnTerr, Eric119, Evanherk, Fish-Face, Gmelli, Hadal, Hellbus,Iridescent, Jfdwolff, Jmarchn, Julia W, Jvs, Karen Johnson, Kariandelos, Kelisi, KnightRider, Kubra, Kungtofumaster, Laurenbroadhurst1234, Li4kata, Lipothymia, LittleT889, Magnus Manske,MarcoTolo, Marj Tiefert, Mathwhiz 29, Mgmei, MightyWarrior, Naima.fatimi, Naniwako, Nihiltres, Nosbig, Nunh-huh, Oldlaptop321, Onco p53, Peskydan, Pieter Kuiper, PrincessCaitlai,Rayward, Robert the Devil, Rytyho usa, Sandbergja, Sbharris, Sgall, Shakespeare87, Sl, Snowmanradio, Some standardized rigour, Someone else, Tcbengals9, The Anome, Tristanb, Ubdodadd,WriterHound, Xwu, Y tambe, 95 anonymous edits
Hemolytic anemia Source: http://en.wikipedia.org/w/index.php?oldid=609259854 Contributors: AdjustShift, Aeluwas, AgentPeppermint, Alteripse, Apers0n, Arcadian, Autoerrant, CalmerWaters, Chris Capoccia, Cjmnyc, Clinical Cases, Copey23, Davidlwinkler, Drphilharmonic, Drsolomonvolg, Dysepsion, Exists, Flyaway214, Foobaz, Frood, Furrykef, Fuzbaby, Gongshow,Hydro, Immunize, JackFlareGun, JackWasey, Jeffrey Mall, Jfdwolff, Jonesey95, Katieh5584, Kochipoik, Kristenq, Lareine, Leszek Jańczuk, Madhero88, Mandarax, Mat8989, Mazerin,Mboverload, Mccready, Mikael Häggström, Mm40, Mr Bungle, Mr. Know-It-All, Nbauman, Nerdseeksblonde, Nihiltres, Nixpix99, Novangelis, Plumpurple, Possum, Rich Farmbrough,Sab3el3eish, Salwateama2008, Shadowjams, Shubinator, Smalljim, Snowmanradio, Some standardized rigour, That Guy, From That Show!, The Thing That Should Not Be, Thiseye, Tikiwont,Tjwatts, Tony K10, TopScholar, Typhoonchaser, Vectro, Vokes1, Whoop whoop pull up, Wikid77, Wouterstomp, 108 ,55דוד anonymous edits
Acquired hemolytic anemia Source: http://en.wikipedia.org/w/index.php?oldid=604984929 Contributors: Arcadian, Calmer Waters, Leszek Jańczuk, Mandarax, Mikael Häggström, MrBill3,Shadowjams, Some standardized rigour, 55דוד
Congenital hemolytic anemia Source: http://en.wikipedia.org/w/index.php?oldid=593844840 Contributors: Arcadian, Calmer Waters, ChrisGualtieri, Dmlevy 99, Jereiniger, MikaelHäggström, My Core Competency is Competency, Some standardized rigour
Blood Source: http://en.wikipedia.org/w/index.php?oldid=617218107 Contributors: ))ECB((, 1exec1, 2112 rush, 21655, 334a, 3idiot, 64ereye, A D 13, A8UDI, Abdoiu, Abductive, Abhinav, Abigail.Brooke.Carly, Academic Challenger, Acalamari, Accurizer, Ace of Spades, Achurch, Adamtenzer, Addshore, Adolfbatman, Adriaan, Advancedversion, Ahoerstemeier, Aish setia, Aitias, Ajaxkroon, Akanemoto, Akendall, Ala888, Alan012, Alansohn, Alasdair, Alchemist Jack, Aldocella, Alethe, Alex.muller, Alex19821982, AlexWangombe, Alexf, Aljasm, Allen3, Allstarecho, Altenmann, Anaxial, Anclation, Andres, AndrewHowse, Andy85719, Andycastille, Andycjp, Anger22, Angr, Anguzmalcolm, Animeronin, Aniten21, Anomalocaris, Ansell, Antandrus, Antelan, Anthonyhcole, Antiuser, AntonBryl, Anwar saadat, Apatterno, Apers0n, Arakunem, Arb, Arcadian, ArielGold, Arwalter, Asarelah, Aslaninnarnia, Astaines, Astral, Auno3, AussieLegend, Avg, Avoided, AxelBoldt, Axl, Ayvah, Azazel696, B15nes7, B9 hummingbird hovering, BD2412, Babykjwhat, Badmansamma, Bantam1983, BanyanTree, Bazonka, Bco2bq, Bdesham, Belovedfreak, Bem47, Ben-Zin, Benbest, Bender235, Bensaccount, Bento00, Benwd, BerserkerBen, Bertus, Bgold4, BigFatBuddha, Bignose, BillShurts, Binky, Biosthmors, BirgitteSB, Bjankuloski06, Bkonrad, Bloodstaind, Blue520, BlueLint, Blueguy2, Bob f it, Bob2653, Bob911911, Bobmalarky, Bobo192, Boccobrock, Bomac, Bongwarrior, Boofs, Borderline26, Borisblue, Brandmeister, Brazucs, Brian0918, Brianga, Brighterorange, Brilliantine, Bristow, Brownsgymbug777, Brtkrbzhnv, Bruce1ee, BruceBlaus, Bryan Derksen, Bubba hotep, Bunny14368, Burnoutfool, Bwthemoose, C45207, Cabletrain, Caknuck, Calair, Calatayudboy, Caltas, Cameron, Can't sleep, clown will eat me, CanisRufus, Carbon Caryatid, Caseydyck, Casper2k3, Catgut, CatherineMunro, Causa sui, Cazlo, Ce1984, Cek, Chaldor, CharlotteWebb, Charmonkey1337, Chavash, Checco, Chocolateman96, ChongDae, ChrisGualtieri, Chriskloos, Chrislk02, Christina Silverman, Church, ClassA, Cntras, CoJaBo, Cocytus, Coffee, ComfyKem, CommonsDelinker, Connormah, Conny, Conversion script, Coralmizu, Cordille3, Corinaw, Countincr, Courcelles, Cpl Syx, Cprompt, Cquan, Crazycomputers, Crecy99, Crystallina, Cureden, Cxz111, Czar, DARTH SIDIOUS 2, DCGeist, DELCHERD, DJ Clayworth, DMacks, DO11.10, Damo7644, Dana Montello, Dancter, Daniel C. Boyer, DanielDeibler, Darkcasualty54, Darker130, Darrendeng, Davewild, David Hedlund, David Stewart, Davidhorman, Davidiad, Davie4264, Dayewalker, Dbachmann, DeadEyeArrow, Deadlyfish, Dean Wormer, Deathawk, Delldot, Delta40, Demmy, Denaud, DennyColt, Dentalplanlisa, Deon, Deor, DerHexer, Derekmudd, Devmik18, Dgw, Diberri, Digitalme, Dimboukas, Dina, DinoPop, Dirkbb, Discospinster, Dispenser, Dlarmore, Doczilla, Doghover14, Dominus, Donarreiskoffer, DoubleBlue, Douchehole, Dougofborg, DougsTech, Dpeters11, Dpotter, Dpr, Dr. Blofeld, DrMacrophage, Dragana666, DragonflySixtyseven, Dreadstar, Drmies, Drphilharmonic, Drydom, Dungodung, Dwayne, E2e3v6, ERcheck, ESkog, Earthman990, Eatsaq, Echuck215, EcwNick, EdNeave, Edgar181, Eekerz, Ehalofan98, El137717, Eleassar777, Elembis, Elockid, Emperorbma, Enviroboy, Epbr123, Eric Kvaalen, Eridani, Erielhonan, Erik9, EronMain, EuroCarGT, Euryalus, Evercat, Excirial, Extransit, Exxon101, FF2010, FSwinton, Fabrício Kury, Fahadsadah, Fak119, Falcon8765, Farside, FastLizard4, Favonian, Fede.Campana, FelisLeo, Fennec, Fictitiouskies, Fieldday-sunday, Finlay McWalter, Finngall, Firien, Fish-Face, Fivetrees, Fl, Flume, Flyer22, Followship, Fourdee, Foxj, Fram, France3470, FrancoGG, Frankie1969, Freakofnurture, Fred Bradstadt, FreplySpang, Froakentoken, Frogfreak2000, Frostbite Q. Kelvin, FrozenMan, Fudgiebrownies, Funnyboy111, Fæ, Galoubet, Garagerockrival, Gareth Griffith-Jones, Garglebutt, Gecg, Gene Nygaard, Geneb1955, Gensanders, George Laffan, GeorgeStepanek, Gettysberg, Gfudrfu, Giants27, Giftlite, Gilgamesh, Gilliam, Gimboid13, GoShow, Godfinger, Godzillaisgay, Gogo Dodo, GoingBatty, Goldhawk7, Gontuzic, Googie man, Gouerouz, Gourami Watcher, Gracenotes, GraemeL, Graham87, GrahamColm, Grammarmonger, Graphium, GregorB, Gtamber, Gtstricky, Gurch, Gwernol, H Padleckas, HOMOSAPIEN294, HOUZI, Hachiko23, Hadal, Hairy Dude, Hallenrm, Halmstad, Handitems, HangingCurve, HappyFaces123, Harej, HarlandQPitt, Haseo9999, Hdt83, Heado, Heimstern, Heisenbergthechemist, Hellknowz, HenryLi, Herk1955, Heron, Hetar, HexaChord, Hibbity Dibbity, Hinata Huuya, Hipton45, Hires an editor, Hmrox, Hollz2k8blud, HonestPerson, Horoporo, Husky, Husond, Hydrargyrum, I am bubbles, IShadowed, IZAK, IamLeg3ndduh, Iapetus, Ignoscient, IiKkEe, Ijustam, Iketsi, Ikiroid, Ikmo, Illinois2011, Immunize, IndulgentReader, Inge-Lyubov, Insanity Incarnate, Invincible Ninja, Iridescent, IrisKawling, Ironcoremagma, Iste Praetor, J.delanoy, JForget, JHCaufield, JNW, JSharp, JaGa, JackLumber, Jackfork, Jahnavisatyan, Jakeathome, JamesTseng, Janarius, Jarble, Javierito92, Jayaguru-Shishya, Jeff Silvers, Jeffro77, Jeremyisstupid, Jfdwolff, Jfurr1981, Jjron, Jmh649, Jmundo, Jnestorius, Jni, Jnk, Joehall45, Johann Wolfgang, Johanneum, John, John Cardinal, John Elson, John(underscore)smith69, JohnCpalstringIII, Jonathunder, Jordan Yang, Joydeep, Joyous!, Jpark3909, Jprg1966, Jrtayloriv, Julio12324, Junglecat, Jusjih, JusticeGuy, Justinquigley, Jwissick, K6ka, KC Panchal, KC109, Kaare, Kaarel, Kaijura, Kaobear, Kariteh, Kat724, Katalaveno, Katanada, Katieh5584, Kaylabee28, Kdeepu442, Kehrbykid, Keilana, Kenm47, Kennycis9, Kevin Rector, Khalid Mahmood, Khazar2, Khukri, Kiensvay, Kiko4564, Kilo-Lima, Kingpin13, Kitty the Random, Kizor, Knighthawk7, KnowledgeOfSelf, Knutux, Konrad West, Kormoran, Kosebamse, Koveras, Kozmo81, Krakkos, Kralizec!, KristineElaine, Krun, Kuru, Kyle1278, Kylehogan90, L1ghtningDR, LOL, Lakshya (razor), Leapfrog314, LedgendGamer, Leebo, Leevclarke, LegitimateAndEvenCompelling, Lemon martini, Leništudent, Letatcestmoi94, LiSrt, Lieutenant of Melkor, LieutenantLatvia, Light current, Lightmouse, Lil Wes, Lilibomb24,

Article Sources and Contributors 175
Linnea11283, Lir, LoVe, Loadmaster, Logan, Lombroso, LongLiveMusic, Loonymonkey, Loren.wilton, Lotje, LovelyLillith, Lucifer(sc), Ludwigs2, Lugia2453, Luigifan, Luk, Lumpy3, LunaSantin, Lx Rogue, MER-C, MIT Trekkie, MKar, MPerel, MZMcBride, Mad Tinman, Madhav, Madhero88, Magnetic7, Majorly, Makemi, Malcolm Farmer, Mani1, Manisha Shetty, Manishearth,MarcM1098, Marek69, Mark Arsten, Mark v1.0, Marnanel, MarsRover, Martinl, Maryhannah, MastCell, Materialscientist, Matijap, Matticooper, MattieTK, Maureen101, Mavsfan101, McSly,Meekywiki, Megaman en m, Megametawolf, Megan1967, Melchoir, Menchi, Mentifisto, Meowington1337, Mercury, Merlion444, Meteor sandwich yum, Mets501, Mgiganteus1, MichaelDevore, Michael Hardy, Michael K. Edwards, Michi zh, MickWest, Midnightblaze, Mifter, Mikael Häggström, Mike Dill, Mike Rosoft, Mike1024, Mike2vil, MikeSammons007, Mindcry, MinnaSora no Shita, Minus198, Miscellaneous131, Mish meister, Mitch7677, Mitchzilla, MithrandirAgain, Modestbear, Mojo Hand, MonoAV, Montrealais, Moogwrench, Morqueozwald, Mr. Vernon,Mrtorr18, Mstroeck, Mugunth Kumar, Murdochious, Musashiaharon, N2X Dragon, N4nojohn, N5iln, NHRHS2010, NT1.0, NTox, Narutochic3000, Natalie Erin, Natural Cut, Nawazdaud,NawlinWiki, Nbansal4732, Ndteegarden, NeilN, NeoXenophon, Neverquick, NewEnglandYankee, Newmastermatt, Nibuod, Nicka7279, Nicki12dick, Nifky?, Nissan cube, Nivix, Njaard, Nlu,Nn123645, Nneonneo, NobelSturegatan 14, Nonpareility, Novangelis, Numbermaniac, Nunh-huh, Nurhafizah, Octopod, Oda Mari, Oden, OdentheGray, Ohnoitsjamie, Oliver202,Omicronpersei8, Optichan, Orinoco-w, Orphan Wiki, Otisjimmy1, Oulmaca, OverlordQ, Owen, Oxymoron83, Ozmaweezer, PFHLai, Pajz, Palica, Panoptical, Pass a Method, Patrick, Patxi lurra,Pavuman, Pax85, Pb30, Peace keeper, Penubag, Peter Karlsen, Peterisfun, Petrb, Phaedriel, Phantomsteve, Philip Trueman, Piano non troppo, Picaroon, Pinethicket, Piotrus, Pishogue, Platyna,Pne, Poeloq, PoeticVerse, Polskivinnik, PonyToast, Poofhaha, Poor Yorick, Porges, Possiblymad, Potters118, Preacherdoc, President Barrack Obama, Prodigaldruid, Psyche825, Ptudor,Pulaski123, Pumanhaladin, Qtea, Quantpole, Quebec99, QueenCake, Quintote, Qxz, R'n'B, RAWR I SCREW IT UP, RDBrown, RaLaMAMA, RachelBrown, RadiantRay, Radon210,Rajkiandris, Rajrajmarley, Ramses89, RandyGBrooks, RaseaC, Raxicoricofallapatorius, Rd232, Read-write-services, Realm of Shadows, Reaper Eternal, RebeccaJpriest, Recognizance, RedSunset, RetiredWikipedian789, Rettetast, RexNL, Rhys, Riana, Rich Farmbrough, RichG, Richard D. LeCour, Richhoncho, Rjwilmsi, Rlives16, Rmhermen, Roadrunner, Rob Hurt, RobertPrummel, Rocketpower12, Rocketrod1960, Rod57, RodC, Rodsan18, Romanm, Roscelese, Ross Monroe, RoyBoy, Rpresser, Rsabbatini, RunOrDie, Ryan032, RyanCross, Ryulong, SD5, SDY,Salix alba, Salsa Shark, Sam Hocevar, Samson1986, Samueljhun, Samwb123, Sandstein, Sara Neves, Satenus, Sbharris, Sc0ttkclark, Sceptre, SchfiftyThree, Schneelocke, SchuminWeb,Scottydude, Scwlong, Sean D Martin, Seaphoto, Seidenstud, Seungjin95, Shadow56121, Shannathe, ShawnD5th, Shinkolobwe, Shirik, Shizane, Shoessss, Shoshonna, SidP, Sidar, Silivrenion, SirVicious, Sitethief, Sjö, Sk8skanj, Skaterpunk17, Skier Dude, Skizzik, Skyintheeye, SlackerMom, SlightlyMad, Slightsmile, Smalljim, Smasher3kuk, SmilesALot, Smokizzy, Snisfrealaaa,Snowmanradio, Snowolf, Solarra, Solipsist, Some jerk on the Internet, Someone else, Sonett72, Sonjaaa, Sosthenes12, Soundoftoday, Spaully, Specs112, Spellcast, Spik33, Spinningspark,Spitfire, Stardust8212, Stemonitis, Stephen Gilbert, StephenWeber, Stephenb, Steven Zhang, Stevenfruitsmaak, Stewartadcock, Stfg, Stickee, Striver, Stroppolo, Stupid2, Subdolous, Suffusion ofYellow, Sun Ladder, Sunao shimomura, Sunrise, Superluser, Sven Manguard, Swerdnaneb, TCTony, TJDay, Tangentier, Tanvir Ahmmed, Tao of tyler, Tarawneh, Tartarus21, TastyCakes,Tbhotch, Tcncv, TedE, TedTschopp, Tedder, Tedius Zanarukando, Tellyaddict, Template namespace initialisation script, Tentinator, Terramite, TexasAndroid, Tgeairn, The Anome, TheRambling Man, The Subgenius, The Thing That Should Not Be, The elephantman, The sock that should not be, The undertow, The2belo, TheGreenMartian, Thejanker, Theovermind,Therock12345in, Therollingstones, Thingg, Think outside the box, Thinking of England, Tide rolls, Time for action, Tiptoety, Titodutta, TittleBit, Tkasmai, Toddst1, TomStar81, Tommy2010,TonySt, Torqueing, Transity, Travelbird, Traxs7, Tregoweth, Treypatton, Tristanb, Triwbe, Trounce, Trusilver, Truthflux, Tuor, Tuplanolla, Twerbrou, TwistOfCain, Twtje, Tyrol5,UberScienceNerd, Ucanlookitup, Ukuk, Uncle Dick, Unschool, UnstlthyNnja, Ute in DC, VMS Mosaic, VQuakr, Vacation9, Vadgt, Vainer2008, Valer, Vandal only and not only..., Vanderesch,Vanka5, Vary, Vdrakon, Veeven, Veltraum, Versageek, Vertigo315, Vibescom, Vic226, VictorianMutant, Vidhanm, Vineetcoolguy, Vipinhari, Viridae, Visium, Vsmith, Vsync, Vuo,WDavis1911, Wapcaplet, WatermelonPotion, Wavelength, Wayne Miller, Weatherbed, Welsh spud, Werdan7, West.andrew.g, What!?Why?Who?, WhatamIdoing, Where did all the money go?,Whitetiger224, Wiccan Quagga, Widr, Wiglaf, WikHead, Wiki alf, Wikieditor06, WikipedianMarlith, Wikipelli, Wikitumnus, Wikiwikiwiki123123123456, Willard, William Avery,Wilson44691, Wiltsher, Wimt, Winston365, Witan, Wknight94, Wouterstomp, Wsfgdrhj, Wtmitchell, Wysprgr2005, X1987x, X54fyqz1, Xiahou, XxKxXxDxX, Y, Yamamoto Ichiro, Yelyos,Yeyeimhot, Yintan, Yirzmo, Yourmumsbox, Youssefsan, YuriSuassuna, ZX81, Zenithos, Zerokitsune, Zinjixmaggir, ZooFari, Zyqqh, 2106 ,کاشف عقیل anonymous edits
Blood transfusion Source: http://en.wikipedia.org/w/index.php?oldid=622570128 Contributors: -df-, 28bytes, 88wipg99, AManWithNoPlan, AS, Aarongaming100, Abhay1998, Abtinb, Ackoz,Aitias, Akira1984, Alansohn, Alasdair Stuart, Aleksa Lukic, Alexian5, Aliljeho, Aloghar, AnakngAraw, Andre Engels, Angela, Angelito7, Apers0n, Arcadian, ArglebargleIV, Ario, Art LaPella,Asturnut, Auntof6, Avi8tor, Avoided, Avraham, Awien, Az1568, Az29, BD2412, Barista, Barney the barney barney, BartBenjamin, Baysolitude, Bdesham, Bencherlite, Bender235, Billposer,BjörnEF, Blakushmablob, Bluerasberry, BowlingKing37, Brandon, Bronsteijn, Bruce1ee, BruceBlaus, Bumm13, Butko, Calair, Calliopejen1, CambridgeBayWeather, Capricorn42,ChrisGualtieri, ChrisHodgesUK, CiaraBeth, Cjewell, Clayr21, Clngre, Contaldo80, Crd721, Crecy99, Cruccone, Crynix, Cyde, Cynicism addict, DMacks, DadaNeem, David Crawshaw,David.Mestel, Decibert, Deli nk, Delta x, Deltabeignet, Delusion23, Denis tarasov, DiverDave, Drappel, Drchriswilliams, Drdaveng, DuncanHill, ESkog, Earthbee24, Ed Poor, EdoDodo,Edward321, El C, Electron9, Elysianfields, Emersoni, Ennaear, Epbr123, Erianna, Erich gasboy, Estadje, Fallingmasonry, Fantumphool, FloNight, Frmorrison, Funandtrvl, Fuse809, Fuzbaby,Fuzheado, GB fan, Garagerockrival, Garik, George m, Geraki, Ghirlandajo, Gonzalo84, Graham87, GregorB, Gulfstorm75, Gurch, Hadal, Hair, Hans Dunkelberg, Hede2000, Hellbus, Hemanshu,Hibsch, Hires an editor, Hob, Horoporo, Howcheng, Hugo Dufort, Hv, Hyperionred, I dream of horses, IKWOWE, ITMM CWRU UH, IceDragon64, IiKkEe, InShaneee, Interested2, Interprof,Introvert, InvictaHOG, Irassassin, Iridescent, IronGargoyle, Ishrath h, Isnow, J.delanoy, JNW, JRSpriggs, Jaimeastorga2000, Japs 88, Jeffq, Jeffro77, Jfdwolff, Jimgeorge, Jimmy joe joeseph,Jmh649, Johanneum, John Entwistle, Jonathan Hall, Jonsg, Joseleo2002, Joseph Solis in Australia, Joy, Julesd, Junglecat, Jwbrother, Kablammo, Kalaiarasy, Karenblackhall, Karl Stas,Kenkoo1987, Kenmcl2, Kevin12622, Klemen Kocjancic, Knuckles, Kolbasz, Kyoko, Labrat97, Lambyte, Leafyplant, Leon7, Levineps, LilHelpa, Lotje, LuK3, Luceroanaicruz, Macronencer,Magioladitis, MagnusL, Manxruler, Mark v1.0, Mart H, Marvin Shilmer, MastCell, Materialscientist, Mav, Mean as custard, MelissaPeet, Mfhulskemper, Micah hainline, Michael Hardy,Michaelmas1957, MicroBio Hawk, Millstream3, Mimi8797, Miroku Sanna, Mogism, Moonriddengirl, Mortenoesterlundjoergensen, Mouchoir le Souris, MrBill3, MrOllie, Muon, MusikAnimal,MyVamp, Naddy, Naoki09, Nephron, Neøn, Nicolasmaek, Nivix, NobelSturegatan 14, Noodleki, Nosbig, Nummer29, Nunh-huh, O.Koslowski, Oda Mari, Ojigiri, Omulazimoglu, Oreo Priest,Oscarthecat, OttoMäkelä, Oyoyoy, PREMIS2010, Petrb, PicklePower, PierreAbbat, Pietro13, Piledhigheranddeeper, Pinethicket, Plindenbaum, Przepla, Puchiko, Qooth, Qtea, Quebec99,Rahul9890177973, RainbowOfLight, Rama, Ravn, Red bull43, RedWolf, Reigh, Richard D. LeCour, Richard cocks, Rjanag, Rjwilmsi, Roadrunner, Rocketrod1960, Rodejong, Rory 20 uk,Rrburke, Rsabbatini, SDY, ST47, Sam Hocevar, Sandstein, Sarayjuan, Scarian, SchreiberBike, Sci guy, Scientizzle, Scorpian ad, Seaphoto, Seraphim, Sgt. R.K. Blue, Shaolin md, Shimmerone,Shrena modi, Silvermask, Skizzik, Slashme, Smartsmith, Sminthopsis84, Smjg, Snowmanradio, Socialservice, Someone else, Sonianich, Sonjaaa, SpuriousQ, Srice13, SuatCoskun, Subcastrum,Subwayguy, Summer Song, Sun Creator, Szquirrel, TMSD, Talskiddy, Taragui, The Anome, The Thing That Should Not Be, The doctor23, The guy down the road, TheEgyptian, TheStarman,Theopolisme, Thue, Thumperward, Tigerhawkvok, Tim!, Titoxd, Tobby72, Toytoy, Treecko 09, Tslocum, TylerDurden8823, Ugodie25, Upholder, Valen8or, Valhalla, Vassilis78, Versus22,Victor Alexandrov, Vindigenous, Vipinhari, Vishnava, Vogon77, WLU, Wavelength, Wetman, WhatamIdoing, Whosasking, Whpq, Widr, Wik, Wikipelli, Williamsfreggie, Woodroar,Woohookitty, Wouterstomp, Zandperl, Zaphod Beeblebrox, Zeamays, Zidonuke, Zigger, Zugman, Zurishaddai, Zzuuzz, 544 ,2009 عبقري anonymous edits
Blood vessel Source: http://en.wikipedia.org/w/index.php?oldid=621935564 Contributors: 331dot, A930913, Abklassen, Air Bear, Alansohn, Alex Batt, Alex.tan, Alpha 4615, Alphachimp,Andre Engels, Andrew 1212, Aniten21, Annemo, Anonymous Dissident, Antandrus, Arcadian, Auxiliary Watchlist, BD2412, BarretB, Barzkar, Bcatt, Bensaccount, Beve, Bfigura's puppy,Biosthmors, Bomac, Bongat122, Brianga, CFCF, Chasingsol, ChrisGualtieri, Chromaticity, Closedmouth, CommonsDelinker, Coretheapple, Courcelles, Cremepuff222, Ctg4Rahat, DBigXray,DVdm, Darth Mike, DavidLeighEllis, Deor, DerHexer, Diderot's dreams, Discospinster, Dominiktesla, Donner60, Drgarden, Drmies, Dusti, ENGMED, Edgar181, ElinorD, Ellomate, Ellywa,EnSamulili, Eric-Wester, Everyking, Eyesnore, Faizan, Figma, Flyer22, Fritzpoll, Fromgermany, Fycafterpro, GTBacchus, Gggh, Gilliam, Ginsuloft, Goodvac, HD86, HOMOSAPIEN294,Hovea, Hydrargyrum, Ianthegecko, Insomniduck, Irving92, Ixfd64, Iztwoz, J.delanoy, JD0922, JForget, JSpung, JakobSteenberg, James086, Jason M Tilley, Jfdwolff, Joaquin008, Josh3580,Julesd, Jóna Þórunn, Keegan, Kelvinsong, Kerotan, KimChee, Kingjalis1, Knutux, Kosebamse, KoshVorlon, Kyle1278, LAX, LT910001, LadyofHats, Lahroo, Lambmeat, Lantay77, Leništudent,Liftarn, Lipothymia, Lova Falk, LucasVB, Lugia2453, Luna Santin, MAlvis, MER-C, Macy, Magioladitis, Magister Mathematicae, Malinaccier, Mamyles, Marcgal, Marek69, Mark Arsten,Master of Puppets, Materialscientist, Mcstrother, Mentifisto, Merube 89, Michael K. Edwards, Miketeelrox, Mintleaf, Mote, Neutrality, NickGorton, Njmagnusson, Nomad2u001, Nuno Tavares,Nurg, Orange Chicken7875, PFHLai, PhatRita, Philip Trueman, Pinethicket, Polyamorph, Qxz, Rabstar17, Reaper Eternal, RekishiEJ, Rob Hooft, Robert M. Hunt, RoyBoy, Rsvpair, RuM,Ruakh, Salvio giuliano, Sander123, SarekOfVulcan, Sasuke Sarutobi, Scarian, Shanes, Sigmamax, Sliggy, Smalljim, Smettems, Smithbrenon, Someone else, Sopoforic, Sunrise, SvetlanaMiljkovic, TLSuda, Tabletop, Taranet, Template namespace initialisation script, The Thing That Should Not Be, The Triple M, The man3001, TheEpTic, Thumperward, Tresiden, Troop350,Tuxide, Unschool, Utcursch, Van12Tiem, Vary, Vegaswikian, Vishnava, VvV, Wavelength, Why Other, Widr, Wikieditor06, Wikivmk, Wknight94, WojPob, Woohookitty, World, Wtwilson3,XJaM, Yamamoto Ichiro, Yintan, Youreviseforthebloodtest, Zack wadghiri, Žiga, आशीष भटनागर, 462 anonymous edits
Bone marrow Source: http://en.wikipedia.org/w/index.php?oldid=620102705 Contributors: AThing, Acdx, AdventurousSquirrel, Airplaneman, Aitias, Alansohn, Alex.tan, Alexwcovington, Allycat0527, Amroc, AnakngAraw, Angela, Angelito7, Angryshot, Arakunem, Arcadian, Ashadeofgrey, Ashcraft, Astanhope, Aveekbh, AxelBoldt, B9 hummingbird hovering, BMDP, Baylaurel, Before My Ken, Bejnar, Bender235, Biomed10, Bjb, Blanchardb, BlueDevil, Blueronin, Bme206timewasting, Bobjgalindo, Bobo192, Bogey97, Boing! said Zebedee, Borbrav, BullRangifer, Bz2, COMPFUNK2, CapitalLetterBeginning, CarsonTheGreatAndPowerful, CatherineMunro, Catongue, Cburnett, Ceclaeys, Ched, Cholerashot, Chris G, Clarkcj12, Cliff smith, CogitoErgoSum14, Connormah, Corti, Courcelles, Cpl Syx, Crystallina, Curb Chain, Cxz111, Cybermaniac sachit, Cyrus XIII, DARTH SIDIOUS 2, Danno uk, DavidLeighEllis, Deor, Diberri, Discospinster, DiverDave, Diyar se, Dr Aaron, Dr d12, Draalles, Dreadstar, Dreth, Drphilharmonic, Dysprosia, ERK, Eleassar, Enviroboy, Eras-mus, Erkcan, Erlenmayr, Everard Proudfoot, Excirial, Falcon8765, Fbarw, Fernando S. Aldado, Flowerpotman, Flyer22, Freekozak, Friginator, Funnyfarmofdoom, Fvasconcellos, G Clark, GT5162, Gadriel, Gaff, Gareth Griffith-Jones, Gargi Roy, Gaurav1146, GehfREE8, Germet, Giftlite, Gigemag76, Gilliam, Gimboid13, Ginsuloft, Glaisher, Glimz, Gongoozler123, Gregorius Pilosus, Gronky, Gsp8181, Gunkarta, Hadal, Hanacy, Haydnaston, HendrixEesti, HexaChord, Hi5kitty, Hobartimus, IRP, Ifrit, Igoldste, Immunize, Iph, Isfisk, Ish ishwar, IvanLanin, J.delanoy, JMD, Ja 62, Jack Greenmaven, Jack007, JackWasey, Jackfork, Jag123, Jasonasosa, Jauhienij, Jbergste, Jcbvsn, Jctcool1, Jean.artegui, Jengod, Jfdwolff, Jim1138, Jncraton, Joehall45, Joewright, Johan1298, John, JohnCD, Jordan117, Josh3580, Julesd, Jóna Þórunn, Kandar, Katalaveno, KateSelik, Keilana, Keith Lehwald, Kerowyn, Kim298, King Pickle, Kinotgell, Kukini, L Kensington, Larsobrien, Lateg, LeaveSleaves, Les boys, Lesgles, LiDaobing, Lightmouse, LindsayH, Linzhoo2u, Little Mountain 5, Lockesdonkey, Logan, LordCo Centre, LorenzoB, MER-C, Mad Max, Majorly, Malcolm Farmer, Malvineous, Maralia, Marek69, Marimberito, MarsRover, MastCell, Matthew Yeager, McSly, Michaelmas1957, Mikael Häggström, Mintleaf, Missionary, Monedula, Mononomic, Mr.Z-man, Mysid, Naddy, Nagy, Namayan, Natpowning, NellieBly, Newyowker, Niceguyedc, Nihiltres, Nono64, Notheruser, Nunh-huh, Occono, Oda Mari, Ohnoitsjamie, OliverHovmand, OohBunnies!, Optimist on the run, Otend, OverlordQ, Pacifist, Papercliper, Parent5446, Park3r, Pascal666, Patxi lurra, Persian Poet Gal, Peruvianllama, Phantomsteve, Pharaoh of the Wizards, Philip Trueman, Pinethicket, Polyamorph, Prashanthns, Pyrrhus16, RA0808, RJaguar3, Rachgia, Radon210, Raidon Kane, RandomAct, Registrar, Renato Caniatti, Res2216firestar, Rexbobo, Riccardo.Guidi87, Rklawton, Rkoiym, Roadmr, Robert M. Hunt, Rpm099, Russianplayer, Ryan032, SMC, Satarnion, Sceptre, Schrödinger's Cake, Scruffymmh, Seforadev, ShadowRangerRIT, Shadowjams, Shendar, SimonD, Sjones23, Slakr, Smartse, Smith11v, Socialmediarox, SohanDsouza, Sokching, SonicAD, Splatg, Stevencho, Stevenfruitsmaak, Svick, Syrthiss, TallNapoleon, Teles, Template

Article Sources and Contributors 176
namespace initialisation script, Tetracube, Tgeairn, Thane, Thatguyflint, The High Fin Sperm Whale, The Thing That Should Not Be, Theda, Thehelpfulone, Themfromspace, Thumperward, Tiderolls, Tired time, Tombliboo, Tombomp, Trusilver, U+003F, Uncle G, Venkatesh, Versus22, Vigyani, Vina, Vivio Testarossa, Vldscore, Vulturejoe, Wackjum, Waggers, Was a bee,Washburnmav, Wayiran, WhisperToMe, WhyBeNormal, Widr, Wiki13, Workster, Wouterstomp, Wtmitchell, Xxpor, Yidisheryid, Zack325, Zahakiel, Zenwhat, Zoe, Zuky79, Žiedas, ДаркоМаксимовић, 704 anonymous edits
Erythropoietin Source: http://en.wikipedia.org/w/index.php?oldid=616946647 Contributors: Alex.tan, Alteripse, Andrew Su, Angela, Anir1uph, Anrnusna, Anthonymhowarth, Anypodetos,Arcadian, Arcenciel, Asamudra, Asthapawar, AxelBoldt, BabbaQ, Badgettrg, Bejnar, Bemoeial, Bender235, BethNaught, Beyond My Ken, Bignoter, Bikeroo, BillpSea, BitQuirky, Blainster,Bluemoose, Boghog, Caliper, Can't sleep, clown will eat me, Captain-n00dle, Captainandrewwiggins, Charlie1995aza89r, Chaudeau, ChillyMD, Chirlu, Chowbok, Chris Roy, Chris the speller,Christian75, Chrysaor, Ciar, Clementine2009, Ctu2485, DGG, Dahoss, Dale Arnett, David D., David Santucci, David.Monniaux, Davidlwinkler, Decora, Deflective, Dekimasu, Delldot,Demantos, Dhara75, Dickandharry, Dinarabaggy, Doelleri, Dominantprefix, Dough34, Dr.michael.benjamin, DrComplement, DrGabriela, Drbobvan, Drphilharmonic, Duncan.france, Duncharris,E A S, EVula, Eamesa125, Edcolins, Egil, Einstein9073, Eklir, Elb2000, Ellis2ca, Equendil, Ericoides, Eug, Everything Is Numbers, Exercisephys, Facts707, FeatherPluma, FriendlyCaribou,Gak, Gareth Owen, Gene Nygaard, Gigemag76, Glotris173, Ground Zero, Habj, HaeB, Happily ever after, Hdt83, Hede2000, HenkvD, HighIntellectual, Hu12, ImperfectlyInformed, J.delanoy,Jackhammer111, Jackson Peebles, Jfdwolff, Job314, John R Rodgers, John Reaves, Julesd, Jytdog, KTo288, Kaiserkarl13, Katnap01, Kitkat21, Knowledge keen, Kpjas, Ktrenskow,Kwamikagami, L.tak, L509alumni, Lambiam, Law, Leafyplant, Leemorrison, Lensi, Lkinkade, Lurker27, Lvangundy, MBisanz, MEDICCGR, MER-C, Macdorman, Mahendern, Marycontrary,Materialscientist, Matt Gies, Medstudent29, Meewam, Mellery, Meodipt, Michael Devore, Mikael Häggström, Monkeyontheloose, Montgomery '39, MrOllie, MrTroy, MuZemike, NawlinWiki,Nbauman, Nephron, Nexus 215, Nyttend, Nyxos, Ocean57, Ost316, Paiamshadi, PaoloNapolitano, Patentpedant, Patrick-br, Peoplesunionpro, Philip Trueman, Philosopheratrest, Pne, Portillo,Pramanick, Quonston, Qwfp, RDBrown, Rcgy, Remedios44, Rewguy, Rich Farmbrough, Richard Arthur Norton (1958- ), RidinHood25, Riffle, Rjwilmsi, Rknrobin, Roboo.jack, S&W Sciences,SMC, Sballal, Scottalter, SeanMack, Serenity forest, Sk741, Slashme, Sliu2013, Smithbrenon, Some standardized rigour, Spaully, Spouima, Squids and Chips, StuffOfInterest, Sushbiotech,Svick, Tbuzz, Techelf, The Illusive Man, TheAMmollusc, Thirureddy, ThujaSol, Tide rolls, Timwhit, Tooto, Topnaman, Tpbradbury, Trekphiler, Tristanb, Unsweet Tea, VKemyss, Vanisheduser kijsdion3i4jf, VetPsychWars, Wavelength, Wayland, Wernher, Windwardside, Wingman4l7, Wiwaxia, Wmahan, Wolfgang Jelkmann, Woohookitty, Xmp, Xurei, Yeast2Hybrid, YoungPioneer, Zack wadghiri, ZayZayEM, Zeamays, Zoe, Роман Беккер, 381 ,خالقیان anonymous edits
Erythropoiesis Source: http://en.wikipedia.org/w/index.php?oldid=617551164 Contributors: Alonso49, Amkilpatrick, Andres, Arcadian, Arrowhead99, Ary29, Atit ghoda, Boghog, Dirac1933,Enz1, Equine.Scientist, Frederickjeanguerin, Gene Nygaard, Giddypenguin, Gihemm, Gustavocarra, H2ojulie, Hadal, Hodja Nasreddin, JNW, Jai20chand20, Jdcook, Jfdwolff, JimWae,Jimhsu77479, Kauczuk, Kdavidk, Linzhoo2u, Lucky 6.9, Markacohen, MedicShaft, MelbourneStar, MickiWiki, Mild Bill Hiccup, Mogism, Monkeyontheloose, Mudcake, Ncmvocalist,Niceguyedc, NickBush24, Nono64, Nunh-huh, Princess90ify, Qwfp, R'n'B, R. S. Shaw, Remotelysensed, Rjwilmsi, Saabisu, Sillyfolkboy, Smokin yall out, Snookerfran, Snowmanradio, Spiritia,Spudgun, Thestraycat57, ThingoeCRB, Tjmayerinsf, Topbanana, Triggtay, Uthbrian, Uwe Gille, Welsh, White Trillium, Yurik, 77 ,ابراهيم نصار anonymous edits
Gallstone Source: http://en.wikipedia.org/w/index.php?oldid=621042518 Contributors: 0Aldrin0, 2help, 90, Aaron Schulz, Acroterion, Afr77, Aleksa Lukic, Alex Khimich, Alex.tan,Anabela99, Anakin Lance Skywalker, Anam Gumnam, Anbu121, Ancjr, Animum, Antbring, Anthonyhcole, Aperium, Arcadian, Arthur Smart, Aviendah, AxelBoldt, B.d.mills, BD2412,Beetstra, Berlot7, Blancandrin, Bongwarrior, Bookandcoffee, BorgHunter, Burnte, Butterscotch, C557jem, CDN99, Calabe1992, Calidum, Calmargulis, Calton, Canihaveacookie, Cantor,Captain-n00dle, Carlsotr, Cathysus, Celique, Chaldor, ChanceTheGardener, Charivari, Charles Gaudette, Chaselby, Chaveso, Chris Capoccia, Clubmarx, Cmichael, Cminard, Coptic-orthodox,Coroebus, Countincr, Cuaxdon, Cyborg Ninja, DMacks, DadaNeem, Darekr, Daven200520, David Condrey, Delirium, DerHexer, Dgw, Diptanshu.D, Discospinster, DiverDave, DocWatson42,Dr.saran prakash, Draeco, Drphilharmonic, Duckycool124, Dwayne, Dysprosia, E3k, EKindig, Ebyabe, Edward321, EhJJ, Eliz81, Ellywa, Emeraude, Emmanuelm, Emmappleater, Epbr123,Eras-mus, Erebus Morgaine, Eugene CKG, Eukesh, EvilOverlordX, EvilResident, Excirial, Eyeresist, Fabiform, Falcon8765, Fconaway, FearTheDark0000, Feef, Flameeyes, Fraggle81, Francoisscience, Freestyle-69, Fæ, Gamer007, Gene Nygaard, GeoffGutha, Gimmetrow, Giraffedata, Gogo Dodo, Graham87, Grumpyoldgeek, Gzuckier, HPJoker, Hairy Dude, Halfalah, Herwigneefs,Hibsch, Hirohisat, Hnc, Hydrargyrum, I am One of Many, Iamozy, Igoldste, Iridescent, Ironwolf, J Di, J.delanoy, Jaardon, Jabronimus, Jacob.jose, James06108, Jamesmnduffy, Janke, Jerry,Jfdwolff, Jim1138, Jmarchn, Jmh649, Jmr30, Jmrowland, Jorgenplass, JoshuaZ, Julia W, Karada, Katalaveno, Kevin339, Kibzmungiz, King of Hearts, Kirinin, Kmukul1, Life.eXtreme.27,Lombroso, Lyrl, M-shit, MLRoach, Machn, Magioladitis, Mandarax, Maproom, MarcoTolo, MartinSpacek, Masiwiki, Materialscientist, Maxxicum, Meara, MeekMark, Menchi, Metta Bubble,Miguel Andrade, Mikael Häggström, Mike33, Moleyman1, MrBill3, MrOllie, Mushtakalatabi, Mustafarox, MyNameIsNotBob, N6, Nevit, New matt, NewEnglandYankee, Newone, Nickyus,Nixdorf, No Guru, Nono64, Northgrove, Nrsmoll, Nunh-huh, Ochib, OliverTwisted, Ombudsman, Origamite, Oshin99, Osm agha, OwenX, Oxymoron83, PaddyM, PassYourGallstones, Pedia07,Peter bertok, Phalgunadas, Pharmacyphil, Philip Trueman, Phlegat, Piast93, Pilotman6585, Pinethicket, Pkirk, Potato.battery, Ppntori, Predecess, Putnamehere3145, QuiescentWonder, RDBrown,RJASE1, Reagle, Redhill54, Redmarkviolinist, Renato Caniatti, RenderSeven, Rich Farmbrough, Ricky1222, Rjwilmsi, Rklawton, Robodoc.at, Rod5595678, Ronald.W.Martinez, Rose1018,Rotring, RoyBoy, Rr2009, Rrostrom, Rsabbatini, RslaterIII, Ruslik0, Sadcepa, Samir, Saraleerd, Sbakka, Sbmehta, Schwateacher, Seancolorado, SecretDisc, Seglea, Seventh Holy Scripture,Shadowfax0, Shinju, Simonxag, SineWave, Spellcast, Statenboxbox, SteveHargadon, Stismail, Strangerette, Su-steve, TJRC, TaintedZebra, Technopat, Teddpotts, TehBrandon, Templatenamespace initialisation script, Tghe-retford, The Haunted Angel, The RedBurn, The Thing That Should Not Be, TheLeopard, Thehusband, Tomj, Tommy2010, Tonytypoon, Toyokuni3,Transity, Typer 525, Una Smith, Uncle Dick, Utcursch, Vectro, Velella, Versageek, Vishnava, WadeSimMiser, Wasell, Wbm1058, Weeksgo, Weetoddid, Weird Bird, Wingman4l7, Wmahan,World wide wilson, Wouterstomp, Xaa, Xinit, Ykhwong, ZacJvR, Zad68, Zarius, Zgheng, 509 ,55דוד anonymous edits
Haematopoiesis Source: http://en.wikipedia.org/w/index.php?oldid=622490841 Contributors: .:Ajvol:., A. Rad, AThing, Aamer86, AdultSwim, AlphaEta, AndrewJD, Antibody2000, Aquatech,Arcadian, Ariostosilva, Auric, BarretB, BillC, Brazucs, Brim, Bryan Derksen, Buster79, Chrishmt0423, Christian75, Conversion script, Cquan, Ctrlaltdelete200390, Dcirovic, Diberri, DrGabriela,Draak grafula, Dthomsen8, Enchanter, Essent, Fallon Turner, Giftlite, Gikü, Glassneko, GoingBatty, Inferior Olive, Jag123, Jer ome, Jeyradan, Jfdwolff, John254, Kaobear, Kauczuk, Kipmaster,Lateg, Lbiscuit1980, Leptictidium, Linzhoo2u, Liveste, M.Komorniczak, Markacohen, Mccready, Mdhellman, Mesoderm, Mikael Häggström, NewEnglandYankee, Nina, Nina Gerlach,NottNott, Omnipaedista, Openlander, Pstragier, Qumsieh, R'n'B, Rakal87, Reedy, Rintrah, Rjwilmsi, Salwateama2008, SaminTietokirja, Schmiteye, SimonBorna, Snalwibma, Snek01,Snowmanradio, Some standardized rigour, Stephenb, Teesimhui, TheAMmollusc, Tkkoski, Vegaswikian, Vokesk, Wavelength, Wtmitchell, Yintan, 106 anonymous edits
Hemoglobin Source: http://en.wikipedia.org/w/index.php?oldid=619314989 Contributors: AWeenie, Abscissa, Achaemenes, Adrian J. Hunter, AdrianaW, AhMedRMaaty, Ahoerstemeier,Airconswitch, Aka ninja69, Alain.michalowicz, Alanl, Alansohn, Aldis90, Aleph Infinity, Alex.tan, Alison, Allens, Alsandro, Alvin Seville, Amb sib, Anatoly IVANOV, Andres, Andrewko,Aneurysmal, Anticipation of a New Lover's Arrival, The, Appraiser, Aragan Jarosalam, Arcadian, Arisa, Atlant, Atlantia, Avablass, AxelBoldt, Baron von Zandt, Beachbutt66, Becksdrake,Beepu, Belovedfreak, Benamies, Bender235, Bensaccount, BerserkerBen, BethNaught, Bhca, BiT, Bkell, Black Cat Claws, Blu3d, Bob Castle, Bobo192, Bogey97, Boghog, Bombhead,Boopoodoo, Braincricket, Brian Huffman, Bruce1ee, Bucephalus, CIreland, CS46, Cajolingwilhelm, Calm, CalumH93, CanadianJane, CanadianLinuxUser, Canderson7, Carlosisgay, Carstensen,Ccevo2010, Cek, Chad.burrus, Chairman S., Chaldor, Charles Brooking, ChrisGualtieri, Christian List, Christopherlin, ChunkySoup, ClockworkSoul, Cmcnicoll, Coasterlover1994, Codwiki,Commit charge, CommonsDelinker, Conversion script, Corinne68, Correctaboot, Cottingham, Crabula, Csv028, Cwtyler, D, DGaw, DRosenbach, DVD R W, Dan Gluck, Dan653, Dannyt101,Darklilac, Darthredpen, Darwinek, Davidfraser, Dawn Bard, Deflective, Dejvid, Dereck poliink, Deviceauthor1, Diberri, Difu Wu, Diptanshu.D, Discospinster, DmitTrix, Doc glasgow, Doc.mari,DocWatson42, Dodgeb2, Donarreiskoffer, Donner60, Doyley, Draeco, Drphilharmonic, Dungodung, Dusty777, Dwmyers, EMSPhydeaux, Edgar181, Edward Z. Yang, El piel, Eleassar, EmilTeofanov, Epbr123, Epingchris, Erik9, Escape Orbit, Ettrig, Eug, Excirial, Ezhuttukari, Fabrício Kury, Fallendarling, Fallon Turner, FisherQueen, Flyguy649, Forluvoft, Freakmighty,Fresheneesz, Friginator, Funkadan, Funnyfarmofdoom, Fvasconcellos, GPHemsley, Gak, Galoubet, Gator0929, Geoking66, Giftlite, Gilgamesh, Gilliam, Gladissk, GoShow, Gobonobo, GogoDodo, GorgeCustersSabre, Greatpatton, Green Giant, Guidemodel, Gurch, Gzkn, H Padleckas, Habj, Hairy Dude, Hamiltondaniel, Hans Dunkelberg, Hazmat2, Headleyp, Heathmoor, Heli1062,Helios87, Hellbus, Hellisp, HerbVick, Heron, HexaChord, Hitokirishinji, Hroychow, Hurricanefan24, IGeMiNix, Icek, Iepeulas, Immunize, Imnotminkus, InedibleHulk, Isaac.holeman, IvanBajlo, Ixfd64, J.delanoy, JGM73, JRamlow, JSquish, Jack B108, Jakec, Jaknouse, Jamessmith2011, Jared Wilmoth, Jay, Jebba, JesseAlanGordon, Jfdwolff, Jim1138, Jkl, Joeshmoe123123123,John of Reading, JohnArmagh, JohnCD, Jojocurler, Jonathan.s.kt, Jordanmif, Josve05a, Joyous!, Julesd, Julianva, Jusdafax, Jylothr, KGasso, Kalaiarasy, Kandar, Kbh3rd, KevM, Kinberg1, Kingof the Eagles, Kirika, Kisher07, Kittenono, Kku, Koavf, Kpjas, Kwamikagami, Kyoko, L Kensington, Lateg, LeadSongDog, LeeG, Lemchesvej, Lennert B, Lenov, Leonid 2, Lexoka,Lightmouse, LittleHow, LizardJr8, Loonymonkey, LostLucidity, Low-frequency internal, Luk, Lukas.S, Lunajurai, MER-C, Mac Davis, Macy, MadGuy7023, Madhero88, Magioladitis, MagnusManske, Mah131, Mahnifez, Man12345, Maralia, Mark Arsten, Mark Yen, Martin451, MartinezMD, Master of Pies, Master of Puppets, Master of darkness 666, Materialscientist, Matthias.hilty,Mattythefatty123, Mav, Maximaximax, Mean as custard, Mejoribus, Melman14, Mentifisto, Metalloid, Michaeldsuarez, Midorilily, Miguel Andrade, Mikael Häggström, Mike Rosoft, Mike2vil,MikeTheEditor104, Miranda, Mitch Ames, Mmoneypenny, Mogsmar5, Mojo Hand, Momo san, More.suraj33, MottyGlix, Moulder, Mstb42, Muzzypatmn, Mynameisnoted, Myxoma, Natisto,Natkeeran, Naturespace, NawlinWiki, Neptunecradle, New299, NewEnglandDr, NewEnglandYankee, Neøn, Nibuod, Nick Number, Nick04, Nieren, Nivix, Nixeagle, Nono64, Northfox, Notcart,Nuttycoconut, OmgItsTheSmartGuy, Onco p53, Opabinia regalis, Orangemarlin, Orphan Wiki, Ouishoebean, Oxymoron83, PDH, PKT, PaddyM, Pathew, Pdeitiker, Pedrora, Perditor,Perlygatekeeper, Persian Poet Gal, Peter morrell, Petergans, Peterl, Petiatil, Pgan002, Pgk, Ph.eyes, Philip Trueman, Phlegat, Phoenix2, Pinethicket, Pinot, Pinzo, Pmm530, Polypipe Wrangler,Prisonblues, Priyankadaga, Pseudo clever, Pseudomonas, Pwjb, Qaddosh, Quazgaa, Quercus solaris, Qworty, RJFJR, Rabend, Radagast83, Rainald62, Rainbowwrasse, Ramrajesh, Ramsus,ReallyNiceGuy, Reaper Eternal, RebootThalheimer, Recipe For Hate, Reyps, Rhiani-ani-on, Riana, Rich Farmbrough, Richthewitch, Rifleman 82, Rjwilmsi, Rmessenger, Robert K S, Rrenner,Rubicon, Sam Hocevar, Saravask, Savant13, Saxonwhittle, Sbharris, Sbmehta, Sceptre, Schzmo, Scientificone, Scottalter, Sephirothrr, Sercretions101, Shadowjams, Shanes, Sharksoup,Shawthorn, ShelfSkewed, Sherybatta, Shirik, Sietse Snel, Silivrenion, Silversink, Silversmith, Sir Vicious, Sitush, Sk741, Smodtactical, Smokefoot, Snek01, Snowmanradio, SoLando, Somestandardized rigour, SpuriousQ, Srnec, Staticd, Stemonitis, Stevertigo, SuperHamster, SwirlBoy39, TaintedMustard, Tarosan, Taucetiman, Taw, Taxman, Teh tennisman, Temporaluser,Tentinator, Testem, The Mysterious El Willstro, The Thing That Should Not Be, TheAlmightyEgg, TheTito, Three-quarter-ten, Tide rolls, Tillalb, TimVickers, Tjmayerinsf, Tobby72,Tommy2010, TonySt, Topbanana, Treisijs, Triacylglyceride, Triggtay, Tristanb, Twooars, Twsx, Uazikoff, Unixer, Vainamainien, Valpe, Vary, VasilievVV, VeryCrocker, Vgree 01, Vgriffeth,Vianello, Vivin, Vrenator, Wavelength, West Brom 4ever, WhatamIdoing, Whoisjohngalt, Wickey-nl, Widr, WikHead, WikipedianMarlith, Wikipelli, Will Beback Auto, Wimblecf, Winston365,Wouterblox, Wwallacee, Wywin, X!, Xiggelee, Yestefanov, Yikrazuul, Ym3, Yosaphbridge, Youssefsan, Ysangkok, Zaheer12a, ZarathustraD, ZenSaohu, Zephyris, Zfr, Ziggurat, Ziphon,Zzuuzz, 972 anonymous edits

Article Sources and Contributors 177
Jaundice Source: http://en.wikipedia.org/w/index.php?oldid=620476270 Contributors: 4twenty42o, Accordionista, AchatesAVC, Adamshyde, Akaala, AlKing464, Ale jrb, Alex.tan,Alofferman, Alwaysanaggie, Amalthea, American Eagle, AnakngAraw, Andrejj, Angela, Anthony Appleyard, Anthonyhcole, Anthonyheadland6238, Apers0n, Arcadian, AshariMF, Astanhope,Atif.t2, Aude, Audionaut, Aunty didi, Aussie robinson, AxelBoldt, Basawala, Bgwhite, BiT, BillMasen, Black Falcon, Blue Elf, Bobaboon, Bobo192, BobtheWikiBuilder, Booyabazooka, Bubbahotep, Calabe1992, Caleiva, Can't sleep, clown will eat me, CanisRufus, Cannolis, Captain-n00dle, Cburnett, Charles Gaudette, Chiu frederick, Chrysaor, Civvi, Cliffb, ComfyKem,CommonsDelinker, Corinne68, Craig Pemberton, Crecy99, D, D.G.S.V.D. Gajasinghe, Daniel5127, Danielrajaiah, Darklilac, Darth Panda, DavidJ710, DavidOaks, Davidruben, Dbenbenn,Dcirovic, Dddstone, DeadEyeArrow, Dennbruce, Deodar, DerHexer, Dfoster617, Discospinster, Dlohcierekim, Doc*Craig*Adams, DocWatson42, Donner60, Dono, Download, Dr.PrabhuMD,Drbaker48, Drmithunsanil, DropDeadGorgias, ENeville, Edwin, Eleassar, Enigma55, Enviroboy, Epicgenius, Eras-mus, Everyking, Extransit, Facts707, Faizan, Frank Lofaro Jr.,Franklinjefferson, Freestyle-69, Gadget850, Gail, Gareth Griffith-Jones, Garion96, Gdr, Gfoley4, Glacialfox, Grafen, Grammarmonger, Gregfitzy, Gunnala, Habj, Hamdeo, Haoie, Headbomb,Hede2000, Hehkuviini, Hu12, IW.HG, Iced Kola, Imthatguy1010101, J.delanoy, JRmcannally, Jabronimus, JamesMoose, Javier Odom, Jeremykemp, Jfdwolff, Jfurr1981, Jhbuk, Jim1138, Jj137,Jmh649, Jnanadevm, JohnChrysostom, Jsbhavsar, Jtownsle, Jusdafax, Justinfr, Jwoodger, K kisses, Katieh5584, Kintetsubuffalo, Kitsune Misao, Knowledgeforever2, L Kensington, LT910001,Lambiam, Landon9720, Learnthesigns, Ledocteur86, Lights, LovesMacs, Madhero88, Maestozo, Magioladitis, Magog the Ogre, Malcolm Farmer, Martarius, Martin H., Martin8721, Mastac741,Mathewkurisummootil, Mattmazz3i, Mbryanton, Mccready, Mcstrother, Md10md, Menchi, Merope, Metafury, Metahacker, Mikael Häggström, Mild Bill Hiccup, Min.neel, Mmalik, Monty845,N5iln, NJA, Nandesuka, Ndkartik, Neelix, Nephron, Noah Salzman, Ohnoitsjamie, Omg ryan, Osmodiar, Paulrach, Peasantwarrior, Pevernagie, Philip Trueman, Quercus solaris, R500Mom,Rachel.truger, Rdrs, RetiredWikipedian789, Reytan, Rhombus, Riana, Rich2293, Ricky81682, Rjwilmsi, Rmky87, Roadrunner, RobertM525, Rod57, Rsabbatini, Rtyq2, Ruby Murray, Runeguy,RupertMillard, Rw362, Rytyho usa, SJP, Sab3el3eish, Sabar, Sbharris, Sbmehta, Schneelocke, Scottalter, Sean Jolly, SeanMack, Searchme, Sentineneve, Septilliard, Serrin, SewerCat, Shadiizadi, Shankaragarwal, SharkinthePool, Shiphead, Shorah, Slant, Some jerk on the Internet, Sonjaaa, Soodananachiketh, Spenc194, Stephenb, Stevenfruitsmaak, Strabismus, Sullivan.t.j, Sxoa,TTile, Tarif Ezaz, Tarnas, Tass-AJ, Tempshill, TenPoundHammer, Th4n3r, TheEgyptian, TheNewMessiah, Tide rolls, Tom harrison, Treisijs, Troytsm98, TylerDurden8823, Uncle Dick, V-pizz,Vanished User 4517, Versus22, Vilius Normantas, Vldscore, WadeSimMiser, Wesley, Wouterstomp, Wwwwolf, Yellsomething, Yogeesh, Zhohaq, Zigger, ZoRCoCuK, Роман Беккер, 644anonymous edits
Malaria Source: http://en.wikipedia.org/w/index.php?oldid=623492471 Contributors: .V., 100110100, 141.236.82.xxx, 62.253.64.xxx, 78.26, A4, AHeneen, ALloydFlanagan, Abanima,Abendroth85, Abhijeet Safai, Acalamari, AccursedOne, Acquisative, Adacus12, Adhib, AgadaUrbanit, Aherunar, Ahoerstemeier, Ajrodriguezm, Akamad, Alan.ca, Alex.tan, Alexius08,AlexiusHoratius, Alexsautographs, Alfie66, Algebraist, Allens, Allmightyduck, Alphax, AlwaysOnion, Amaraiel, Amit0108, Anclation, AndTheCrowdGoesWild, Andrew Benton, AndrewHartford, Andrew Levine, AndrewDressel, AndrewLeeson, Andrewman327, Andries, Andy tatem, Angus Lepper, Angusmclellan, Aniram21, Ankitsingh1708, Anna Frodesiak, Anne.rooney,Anonamouse77, Anrnusna, Antandrus, Anthonyhcole, Apha, Apliu, Applejack4180, Aprock, Arcadian, Arch dude, Archer3, Arcot, Aristiana, Art LaPella, Arthena, Ashnard, AubreyEllenShomo,AvicAWB, Avicennasis, Awolf002, AxelBoldt, Axl, Axlq, Azhyd, BJRD, Bachrach44, Baldyshaw, BanyanTree, Barak89, Basalisk, Basil II, Bassbonerocks, Bckirkup, Beaumont, Becksguy,Bejnar, Belovedfreak, Ben Ben, BenJWoodcroft, Bento00, Betacommand, BhagyaMani, Bibliomaniac15, BillC, Billjefferys, Billy64k, BillyGambela, Billypilgrim37, Biosthmors, BirgitteSB,Blago Tebi, Blathnaid, Bletch, Bluebasket, Bob Moffatt, Bobo192, Bogey97, Bongwarrior, Boris van Praag, Borisblue, Bossie20, Brady8, Brandmeister, Brian the Editor, Brian0918,BridgetEM2008, Brownie96, Brusegadi, Bschnitzel, Bskhaira55, Bunchofgrapes, C6541, CART fan, CDN99, CFCF, CO, Cacaman, Cactus.man, Calabe1992, Caliga10, Callanecc, Caltas, Can'tsleep, clown will eat me, CanOfWorms, CanadianCaesar, CanadianLinuxUser, Cantiorix, Capricorn42, Carey Evans, Carlymoy, Castaladin, CattleGirl, Ccevo2010, Cdc, Cessator, Chadud123,Charles Matthews, Charlesbridge, CheesusChrist, Chhandama, Chickenjock, Chowbok, Chris 73, Chris Capoccia, ChrisGualtieri, Christopher Parham, Chriswaterguy, Chun-hian, Cireshoe,Citanuleht, Ckl16, Clarkzz1234, Clemwang, Closetcloe, Cls micronerd, Colonel Warden, Colonies Chris, ComfyKem, CommonsDelinker, Conversion script, Coq Rouge, Corrector6879, Costyn,Courcelles, Cressmj, Ctbolt, Cteaton, Curps, Cwkmail, Cwolz, Cyberpower678, Cynical, Czyrko, D6, DBigXray, DO11.10, Damirgraffiti, Damonhater42, Danny, Darkwind, Davedash,Davemcarlson, David Edgar, David.scully93, Daviddragon96, Davidr222, Davidruben, Daygum, Dbtfz, Ddroar, DeadLeafEcho, Delldot, Demicx, Der Golem, DerHexer, Derekristow,Destroyer2000, DexDor, Diberri, Diderot, Diggerdude1993, Diptanshu.D, Dixonsej, Dksahu, Dmoskva, DocWatson42, Doctorfluffy, Dodo bird, Dominus, Dooblegoo, Doseiai2,Doubletrouble50, Download, Dr4chess, DrGaellon, DrMicro, DragonflySixtyseven, Drbaker48, Drmies, Drphilharmonic, Dsreyn, Dudewheresmywallet, Dupz, Dwa 21, ESkog, Ed Poor, EdGl,Edgar181, Eequor, Eleassar, Ellafb, Elliskev, Elyorvidal, Emperor Banh, Enock4seth, Epbr123, Erianna, Eric Kvaalen, Erina17, EryZ, Eugene van der Pijll, Euryalus, Evil Monkey, Ewlloyd, Exnihil, Excirial, Ezrakilty, Factsearch, Faithbco, Fan-1967, FarnersAR, Fartherred, Fconaway, FilippoSidoti, Finavon, Flatterworld, Fleester, Florentino floro, Flubbit, Folkrockprincess, Fram,Frankenpuppy, Frans Fowler, Freakofnurture, Fred Bauder, Fredbauder, Fresheneesz, Friedfish, Froid, Fvandrog, Fvasconcellos, Fæ, GT5162, Gabbe, Gaius Cornelius, Gak, Garrett.beisel,Gautier lebon, GeeSharpMinor, Geeteshgadkari, Gerbilfyed4, Giftlite, Gigemag76, Gil Gamesh, Gilliam, Ginkgo100, Glacialfury, Glass Sword, GlassLadyBug, Gogo Dodo, GoingBatty,Goodnightmush, GraemeL, Graham87, GrahamColm, Graphium, GrayFullbuster, GregorB, Gsarwa, Gtziavelis, Guanaco, Gurch, Gusicles, Gusman11, GuustFlater, Gwickwire, Gzuckier,Gökhan, HJ Mitchell, HLGallon, Hagerman, Hakufu Sonsaku, HalfShadow, Hashar, Hazard-SJ, Hcps-knachelsa, Headbomb, Hempelmann, HenkBouwman, Henrik, HenryLi, Heron, Hmains,Hmccann, Hmrox, Hockeytaav, Hoeale, Horoporo, Ht686rg90, Hu12, Hugo Merck, Hunter1084, Huntthetroll, Husond, Hydrargyrum, Hóra, I dream of horses, Ianavelon, Ianpigg95, IceHorse,Igno2, Imnotminkus, ImperatorExercitus, Indium, InnocentPikachu, InvictaHOG, Iridescent, IstvanWolf, Iwilker, Ixfd64, J.delanoy, JForget, JLM, JLaTondre, JMK, Jackferguson, Jackhynes,Jackingram, Jackovich at Central College, Jaganath, James logan, JamesBWatson, Jamietw, Janse, Jarbru, Jauhienij, JayJay, Jayarathina, Jeff G., Jennavecia, Jerry2112, Jesse V., Jfdwolff,Jhwang333, Jic, Jiggarman, Jim1138, Jimfbleak, Jimmy01, Jmh649, Jnoodle, JoanneB, JoeSmack, John Quiggin, JohnOwens, Johnson aj, Jojalozzo, JonHarder, Jons63, Josh Grosse, Josh ricePSU, Jpgordon, Jtgromis, Jtoomim, Julesd, Junglecat, JustinBlank, Jéské Couriano, KC Panchal, KVDP, KX36, Kaldari, Kandar, KarlM, Kazikameuk, Kazvorpal, Kcordina, Keilana, Kelapstick,Kerowyn, Kessy628, Kevin, Kevinz, Kip2001, Kipala, Kkre5074, Kmoksy, KnowledgeOfSelf, Knutknatter, Koavf, KojieroSaske, Komalsehgal12, Kosebamse, Kostisl, Kozuch, Kpjas, Kragen,Kralizec!, Krauss, Ksherin, Kungfuadam, Kurtrik, Kurykh, Kweedado eng, Kymacpherson, Kyoko, L Kensington, L33tminion, LADave, LOL, LT910001, La Pianista, LaggedOnUser,Lancethex, Larry R. Holmgren, Larry V, LarryBH, Latka, LeadSongDog, LearnedPingu, Lee, Leevanjackson, Legoktm, Leightonwalter, Lenticel, Leofer, Leon Byford, LeonardoRob0t, Leonxlin,Lexi Marie, Lgh, Liam Skoda, Lidiastarling, Lightdarkness, Lighthead, Lightmouse, Lights, LilHelpa, Lilonstitch, Linnell, Lisasmall, Litobro, LittleT889, Lollerskates, Lollipopisj, Lord British,Lord Emsworth, Lradrama, Lseidlein, Lucifer86, Lukas.S, Luna Santin, Lupin, Lvalero, Lycurgus, M.O.X, M.manary, M5a63, MC MasterChef, MER-C, MKar, MZMcBride, MaSt, Macrakis,Madscientist2212, Maelnuneb, Magioladitis, Malarial, Malariaman, Malcolm Farmer, Malleus Fatuorum, Malor, Mambuto omalley, Manifestation, Manum56, Marasama, Marco Krohn,MarcoTolo, Marcolop, Marj Tiefert, Mark Arsten, Mark-shea, Marknash, MarnetteD, Martinp, Martylunsford, Marvinandmilo, Massimo Macconi, Master of Puppets, Materialscientist,Mathonius, Matonen, Matt Crypto, MattEvans16, Mattbr, Matthewsimmons95, Mauler90, MaxSem, Maximecaffarel, Mayur, Mbc362, McDogm, Mdann52, Medicus quisnam, Megaman2700,Megfrey, Mesoderm, Metallion, Mets501, Metsavend, Mgiganteus1, Michael Devore, Michael Frind, Michael Hardy, Michael Zimmermann, Michael.burleigh, Mikael Häggström, Mike6271,Mikiemike, Mild Bill Hiccup, Millahnna, Mintleaf, Miradre, MistyMorn, Misza13, Mitchellp27, Mixer98, Mkpumphrey, Mogism, Mojoworker, Monteitho, Monty845, Mor, Mortense, Moumine,Mpradeep, Mr Adequate, Mr. Billion, Mradigan, Mrfish777, Mrh30, Mschel, Munita Prasad, Muntuwandi, Muon, Muxxa, Mytchill, Naddy, Naniwako, Nasnema, NawlinWiki, Nbauman, Ndiox,Neelix, Nephron, Neutrality, Nevillek1, NewEnglandYankee, Nhsnoboarder17, Nick C, Nick ostan, Nick.Herling, NickGorton, Nikitab, Nolelover, Nopetro, Northumbrian, Nouniquenames,Nunh-huh, Nunocordeiro, Nunquam Dormio, Nyq, O'Dea, OBIDOT, OVERM1ND, Obli, Ohnoitsjamie, Omicronpersei8, Omls2, Ondenc, Onkelschark, Onyambu, Optigan13, Orangemarlin,OrenBochman, Orenburg1, OscarK878, Osterluzei, Ottre, Ozzyorever, PDH, PMLawrence, Pahari Sahib, Paladin5555, PaleWhaleGail, Pangamini, Papa Lima Whiskey, Parkwells, Pascal.Tesson,Paul venter, Paulkappelle, Petekmit, Peter Shearan, Petersam, Pethr, Peulle, Pgan002, Pharos, Phfung, Phil Boswell, Phorteetoo, Piast93, Pibws001, Picaroon, Picstloup, PierreAbbat, Pigman,Pinethicket, Pingku, Pixma123, Plasticup, Plcoffey, Plumbago, PoliticalJunkie, Polkadot2479, Polmandc, Pracepig, Prashanthns, Precious Roy, PrestonH, PreventMalaria, Princeton wu,Procrastinator supreme, Prunesqualer, Psb313, Pseudomonas, Puffin, Pulsemeat, Q.manaan, Quadell, Quebec99, Quig, Qxz, R'n'B, RDBrown, RDT2, Radagast83, RandomP, Randywombat,Raph, RasputinAXP, Rbrwr, Rd232, Reaper Eternal, RedGav, Rees11, Res2216firestar, RexNL, Rexparry sydney, Rich Farmbrough, Richard Keatinge, Richard Taylor, Risker, Rivertorch,Rjensen, Rjm656s, Rjwellings, Rjwilmsi, Rmky87, Road Doc, Robert Merkel, RockMFR, Rockawares, Romanm, Ronns, Roothiepoothie, Rothorpe, RoyBoy, Rror, Rsabbatini, Rsheridan6,Rtyq2, Rui Gabriel Correia, Russianrevolutionary, Ryan Vesey, RyanGerbil10, Ryulong, S, SDY, SH84, ST47, SYTYCSM, Sagredo, Salamurai, Salseradoctora, Sangak, Santryl, Saravask,Sardar1875, Sasata, Sasquatch, Savedor, Sayden, Sbalfour, ScaldingHotSoup, ScarletLetterer, Scientist2, Scwlong, Sdicastro, Sean.hoyland, Seaphoto, Seb az86556, Seth Bresnett, Shadow007,Shadowjams, Shadwstalkr, Shaq141, Shardulkoza, Shotwell, Shrigley, Shureg, Shushruth, Shyamdash, SidP, Silent SAM, Silivrenion, SimDarthMaul, Simpsone4, Sionus, Siwardio, Skizzik,SkyrimHacker4579, Slothman32, Smarty12321, Smellyk, Snowmanradio, Solace098, SolomonHume, Some jerk on the Internet, Someguy1221, Sonicology, Sonicwave, Sophos II, Spark.1.4,Speakalotash, Spenceju, Spencer, SpuriousQ, Squandermania, Stemonitis, Steph100990, Stephen G. Brown, Stevenfruitsmaak, Stevieg143, Stink weasel, Studerby, SubContinentalGuru, Sudh2055, Sugarbat, Sunray, Supertommykniba, Sven Manguard, Svm2, Sw258, Swj1sfu, SylviaStanley, Syneil, TJAHorner, TK111, Tassedethe, TastyPoutine, Taxman, TedErnst, Teles, Tfcoates,Thanol, The Sanctuary Sparrow, The-G-Unit-Boss, TheArchitect, TheOneIsis, Thecathedral, Thecrampton, Theofenton, Theratedrsuperstar36, Thingg, This lousy T-shirt, Thisisbossi, ThoHug,Thomas Blomberg, Tide rolls, TimR, TimVickers, Timoluege, Timwi, Tkn20, Tlotoxl, Tobby72, Tomtefarbror, Topnaman, Touchatou, Tpbradbury, Trainthh, Traveliter, Treisijs, Tremblay,Trevor MacInnis, Trfasulo, Trojancowboy, Troy paulamalu, Trusilver, Ttlymate, Tunatunatunatuna, Twas Now, Twinkling, TyA, Tyrol5, Ulflarsen, Ultramarine, Umdreslifesuc, UnmitigatedSuccess, Unyoyega, Uruiamme, User27091, Uspn, VRCOutreach, Valerius Tygart, Vanderesch, Velella, Velterop, Vespertine27, Vgy7ujm, Viliyana89, Violask81976, Vmoses, Vrenator, WLU,WWARN, Wafulz, Wagon weel, Wainstead, Wantok, Wavelength, Wayne Slam, Wayward, Webclient101, Wechselstrom, Wednesday101, Werlop, Wertyyytrew, Wetman, Wharris65, Wiki13,WikiPuppies, Wikieditor06, Wikipelli, Wikiscribe, Wikita sss, Wildnox, William Avery, William.temperley, WillowW, Wimt, Wizardman, Wk muriithi, Wknight94, Wmahan, Woer$, Wolfrock,Woohookitty, World affairs, Wouterstomp, Wryandwatchful, Wtmitchell, XLerate, Xaosflux, Xenobiologista, Xompanthy, Xyzzyplugh, Yannako, YellowFives, Yersinia, Yilloslime, Yobol,Yom, ZL47, Zachary1555, Zad68, Zadcat, Zanhe, Zashaw, Zeamays, Zuhyc, Zyncodex, Ævar Arnfjörð Bjarmason, Јованвб, 551764 ,سچل ماڇي ,דוד anonymous edits
Pulmonary hypertension Source: http://en.wikipedia.org/w/index.php?oldid=622693684 Contributors: Alex.tan, Alexisd6, Alpha Quadrant, AndreaGoforth, Angelito7, Anypodetos, Aqadir149, Arcadian, Axl, BQmUB2012010, Badgettrg, Barek, BlaiseFEgan, Bluerasberry, Brighterorange, Bruinmed2017, C'est moi, Cbailey3765, Chaplain, Cheddar3210, Cholmes75, Chowbok, Chris the speller, Chuck-pharma, Chwats, Cornellrockey, Countincr, DVdm, DoctorEric, Drewsty, Eleassar, Fergua, Fvasconcellos, Fwiesbauer, G716, Gauss, Gaussgauss, Gawordcrafter, Gcgmd, Gilliam, Good Olfactory, Greg zimmerman, Ground Zero, HJA1234, Harry, Headbomb, Hehkuviini, Hertz1888, Humpath, Ibnyusuf 12, Ihmeidan, Inferior Olive, Infopharm, J04n, Jeremy68, Jfdwolff, Jim1138, Jmarchn, Johnsu01, Jonesey95, Jooe, Joseaperez, Jtorger1, Kaedus, Kander, Kellyschin, Kjtobo, Kmubarak, Ksheka, Kuru, Kyoko, Lacrimosa, Leonard Finger, Locusfr, MER-C, MarcoTolo, Mark viking, Mboverload, Mogism, MrDolomite, Nbauman, Nephron, Nevinc15, Nihiltres, Niteowlneils, Nono64, Novangelis, PFHLai, Painty99, Patapsco913, Philip Trueman, RDBrown, RainbowOfLight, RedSoxPrincess26, Reenus, RevDan, Riana, Rich Farmbrough, Richard Arthur Norton (1958- ), Richard Avery, Riemann Zeta, Rjwilmsi, Rlozano, RobP46, SRaemiA, Savorie, SchreiberBike, Skamecrazy123, Spiffulent, Squabblefish, Squids and Chips, Srice13, StaticGull, Stevenfruitsmaak, Superoxiddismutasa, THF, Tagishsimon, Tameamseo, Tdonoughue, The Asian Guy, TheBearPaw, Theodore Kloba, Tim1491625, Tlesher, Tlumok, Toby Douglass, ToothingLummox, Toyokuni3, Tsokota, TyrS,

Article Sources and Contributors 178
Unni3063, Vagus, Vedran12, Wawot1, WhatamIdoing, Whatever404, Whywhenwhohow, Woohookitty, Wouterstomp, Yobol, 214 ,55דוד anonymous edits
Red blood cell Source: http://en.wikipedia.org/w/index.php?oldid=623073998 Contributors: (jarbarf), -df-, 03lausmi, 28421u2232nfenfcenc, AJim, ASEEMASEEM, Academic Challenger,Adambro, Addshore, Adhib, AdjustShift, Adrian J. Hunter, Ahoerstemeier, Alansohn, Alec - U.K., Alfie66, Ali, Alksub, Alpha Quadrant, Amaher, Andre Engels, Andres, Andrew Delong,AndrewWTaylor, Andypandy.UK, Angelic Wraith, Angrycrustacean, Ann Stouter, Anoko moonlight, Anupam, Apers0n, Arcadian, Arisa, Arjun01, ArnoLagrange, Arvind0602, ArwinJ,Asparagirl, AssistantX, Atlantia, Aviad2001, Avoided, AxelBoldt, Baa, Bassbonerocks, Bbb2007, Beaumont, Bender235, Benjamin.friedrich, Bensaccount, Bfigura, Bidabadi, Bignoter,Bobblewik, Bobo192, Bomac, Bongwarrior, Borgx, Boud, Brantonli, Brianski, BrightStarSky, BruceBlaus, BryanD, Burek, CIreland, Caeruleancentaur, Caltas, Can't sleep, clown will eat me,Carturo222, Caseydyck, Causa sui, Ccvic2, Chaldor, Chanting Fox, ChongDae, Chris Capoccia, ClockworkSoul, Closedmouth, Corinne68, Corvus cornix, Countincr, Countmike, Cpl Syx,Crack98, Craig Pemberton, Craigmillar94, Crohnie, Cwmagee, DARTH SIDIOUS 2, DRosenbach, Dabomb87, Dan Gluck, Daniel5127, Danrudd, Darth Panda, Darthanakin, Davewild, DavidEppstein, DeadEyeArrow, Debresser, Deus Ex, Dictabeard, Dietzel65, Discospinster, Dogcow, Dogposter, Dominus, DoubleBlue, Download, Dr.Kane, DrMicro, Drmies, Dungodung, E Wing,ESkog, Eaefremov, Ed, Edcgooner, Egmontaz, Ego White Tray, Ekko, Ellywa, Emilyalbinoman, Epbr123, Estadje, Everyking, Excirial, Fafnir1, Ferkelparade, Fieldday-sunday, Fishyghost,Flamingspinach, Fr34k, Fraggle81, Franamax, Fratter, Fredil Yupigo, Fritzlein, Fryed-peach, Frymaster, Funnybunny, Fuzheado, Fvasconcellos, Gabbe, Gawaxay, Gene Nygaard, Giftlite,Gimboid13, Gobonobo, Golfandme, Gouerouz, Grafen, GraybeardBiochemist, Greentryst, GregorB, Grim23, Guest9999, Guy Peters, Hadal, HaeB, Haham hanuka, HalfShadow,HamburgerRadio, Harthacnut, Haza-w, Hellbus, Hempelmann, Hodja Nasreddin, Honette, Hu, Hunterd, Hydrogen Iodide, II MusLiM HyBRiD II, Ihope127, Immortal0king, ImplyingAuthority,Iridescent, J.delanoy, J04n, JNW, JSquish, JWSchmidt, JaGa, Jakejakejake1313, Jaknouse, James Crippen, JamesTseng, JamillyM, JediLofty, Jeffq, Jfdwolff, Jfurr1981, Jnquach, JoanneB,John254, Johnbrownsbody, Jon salisbury, JonLS, Jordell 000, JorisvS, Josh3580, Jossi, Jsfouche, Juju Power, Jusdafax, Jyril, KC0ZHQ, Kander, Kariteh, Kassal, Katimawan2005, KaySL,Kazrak, Kbir1, Kennycub, Kerfern, Killerkris88, Kineticman, KingTT, Kingpin13, KnowledgeOfSelf, Kpjas, Kriptyk, Krylonblue83, Kubra, Kusma, KyraVixen, L Kensington, L33th4x0rguy, Lagoutte de pluie, Lahiru k, Landon1980, Lars Washington, LeaveSleaves, Lectonar, Lightdarkness, Lilfti332, Linas, Linzhoo2u, Little Mountain 5, LittleOldMe old, LizardJr8, Looper5920, Lordof the Pit, Lotje, Luckydhaliwal, MC MasterChef, MZMcBride, Mad Max, Madhero88, Magister Mathematicae, Maias, Mailer diablo, Mailmindlin, Mandarax, Mangal.anukriti, Marek69,Markacohen, MartinGugino, Massimo Macconi, Masterjamie, Masur, Matt Deres, Mav, McSly, Mdw123, Meewam, Meteor sandwich yum, Mexinadian, Mfero, Michael Devore, MikaelHäggström, Mike2vil, Mindspillage, Minna Sora no Shita, Mintleaf, Miquonranger03, Moe Epsilon, Monkey.invasion, Mrfickle, Mwilso24, Nakon, Natty1991, NeilN, Nemesis of Reason,NewEnglandYankee, Niceguyedc, Nifky?, Nlu, Norman21, NotWith, Novalincoln, Nsaa, Nscheffey, Nunh-huh, Older and ... well older, Omnipaedista, Orkybash, Oscarthecat, Oxymoron83,PDH, Pablo-flores, Paul 012, Pb30, Peak, Perspeculum, Peter Karlsen, Phantomsteve, Philip Trueman, Piano non troppo, PierreAbbat, Pinethicket, Pinkadelica, Piperh, Policarp, Prari, Priyanath,Prolog, Prowster, Prvc, Pschwarzbaum, Puchiko, Quercus solaris, RUL3R, RainbowOfLight, Razimantv, Rcingham, Reaper X, Recognizance, Reconsider the static, RenamedUser01302013,Rettetast, Rgracesmyrna, Rhlozier, Riana, Rich Farmbrough, Rjwilmsi, Rob Maguire, Robo-rory, Rogeriopfm, Rory 20 uk, Roshan baladhanvi, Roux, Rrburke, Rsabbatini, Ryulong, SDY,SGGH, SJP, Saintrain, Sakkura, Salgueiro, Samuel, Samwb123, Santoshpath, Sceptre, Schoolscienceteacher, Scootdive, Scottalter, Scwlong, Ser Amantio di Nicolao, SetRochelewsad,Sfmammamia, Shadowjams, Shanel, Sheitan, Sheogorath, Shirik, Shoeofdeath, Shyamdash, Siegele, Sir Vicious, SkepticalRaptor, Sky Attacker, Slashme, Slowking Man, Smitz, Snowmanradio,Someone else, Spartan, Specs112, Spliffy, SquidSK, Squidnchips, StaticGull, Stephenb, Stevenfruitsmaak, Sundar, SuperHamster, SuperStingray, Sverdrup, SwammerBAM, THEN WHO WASPHONE?, TYelliot, Talu42, Tanthalas39, Tarquin, Taxman, Tchite, Template namespace initialisation script, Tempodivalse, The Bushranger, The Moose, The Rambling Man, The Thing ThatShould Not Be, TheEgyptian, Theroadislong, Tide rolls, TimVickers, Tiptoety, Torchwoodwho, Tosta Dojen, Traderjohn, Trevor Wennblom, Treygdor, Trojancowboy, Tsange, Turnstep, Tuspm,Tweetlebeetle367, Tyw7, Umheisman20, Uncle Dick, Valenciano, Vanished user uih38riiw4hjlsd, Vegfarandi, Vipinhari, Vrenator, WDM27, Wardface, Wars, Wavelength, Wayne Slam,Wayward, Wham Bam Rock II, WhatamIdoing, Whoop whoop pull up, Wiki alf, WikipedianMarlith, Willking1979, Wimt, Wisdom89, Wknight94, WolfmanSF, Woohookitty, Xenobiologista,Yamaguchi先 生, YetiSSM, Yuckfoo, Yurik, Zephyris, Zoomlines, 901 ,سمرقندی ,24.غامدي.أحمد anonymous edits
Spleen Source: http://en.wikipedia.org/w/index.php?oldid=623420778 Contributors: 16@r, 7179a, 72Dino, 777sms, A5, AMProSoft, Abklassen, AdamRoach, Ahoerstemeier, Ahpook,Alamosman10, Alansohn, Ale jrb, Alex.tan, AlexiusHoratius, Allens, Allsaints23, Allthingstoallpeople, Amatulic, Amcfreely, Amitch, Amr mohsen, AnakngAraw, Anatomist90, Anaxial, Anaxo,Andre Engels, Andrew c, Andrewpmk, Angela, Angr, Animum, Arcadian, Arisa, Arjun01, Arjun024, Ashcraft, Askeuhd, Asparagirl, Astral, Atlan, Avenue X at Cicero, Avernet, Axl, Bassetlvr,Beatle2102, Bender235, Bevo74, Biosthmors, Blaxthos, Blue Tie, Blue520, Bluezy, Bobsmith040689, Bogey97, Bookofjude, Brandon, Brian0918, BrightStarSky, Brim, BrokenSegue, Brownian,Bryan Derksen, Bubba hotep, Bubbachuck, CFCF, CIreland, Cacycle, Can't sleep, clown will eat me, Candice78, Canuck100, Capt Jim, Captain Courageous, Captain Spleen, Carmdot, Casliber,Catamorphism, Cdrum, Cecarr, Chamal N, Charitwo, ChaseAm, Chatool, Chrisbolt, CiciLinton, CityOfSilver, Clipjoint, Cocytus, Colonies Chris, Colt48, ComfyKem, Coneslayer,Confession0791, CountZepplin, Crabula, Crazyperson324, Criticalacclaim, Crosscountrycpjon, CryptoDerk, DBigXray, DJ1AM, DanielCD, Danierrr, Davidruben, Dawgystyle, Dcamp314,Delldot, Denisarona, Deor, Derbydave, DerekKiller, Dexter prog, Dffgd, Diberri, Discospinster, DocWatson42, Dolphin07, Dontforgettowipe, Dr. R, Draxfelton, DreamOfMirrors,Drphilharmonic, Drsaife, Dustin Dewynne, Dylan2106, ELApro, Edward, Efe, Egalitus, Ekko, Eliz81, Enteralite, Epbr123, Erutuon, EternaLEnVy, Eug, Euryalus, Everyking, Excirial, Factual,Falcon8765, Filip en, Fine, destroy my dreams!, Flowanda, Flyer22, Folajimi, Foolishgrunt, Fraggle81, Frammo, Freecat, Freekozak, FreplySpang, Fuzheado, GDonato, GIBBOUS3, Gadget850,Gareth Griffith-Jones, Garion96, Geeoharee, Gene Nygaard, Genjix, George100, Gershwinrb, Giftlite, Gilgamesh, Gilliam, Gimboid13, Glen, Glenn, Gogo Dodo, Goochelaar, Goodvac, Gozar,GrooveDog, Gscshoyru, Gumby55555, Gwib, Gzkn, Haegerman, Harpiegirl6, Harry lowis, HiDrNick, Huckfinne, Hydrargyrum, I do not exist, I.M.S., IW.HG, Ianbuchanan1, Ianeck, Id4abel,Iliveforcows, Immunize, Imnotminkus, Inferior Olive, Intubate, Iridescent, IronGargoyle, Iroony, Islaosh, IvanLanin, IxAmxJapan, Ixfd64, Iztwoz, J.delanoy, JForget, JFreeman, JNW, JackGreenmaven, Jakegissy, Jaknouse, Jakob Suckale, JakobSteenberg, James Maxx, Jampy1335, Jasonasosa, Jfdwolff, Jfournier, Jfurr1981, Jhenderson777, Jim1138, Jjalexand, Jken89, Jmarchn,Jmh649, Joelmills, John254, Johnakabean, Johnelson, Jonathan321, JorisvS, Jorybell, Josh3580, Juanlink, Julesd, Jóna Þórunn, K6ka, KJS77, KMan, Karl Dickman, Katefan0, Katiker, KeenanPepper, Keilana, Kenmcneil0, Killiondude, KirbyMaster14, Kjramesh, LT910001, Larseg, Latutcie, LearnAnatomy, LeaveSleaves, Lighthawk24, Linagh, Lissajous, LittleHow, Lk9984,Longhornsg, Looxix, Lovesick, Lugia2453, Luiscarlosrubino, Luna Santin, MDaisy, MECU, MJ94, Mac Davis, Macedonian, Magnus Manske, Malcolm Morley, Manop, Marco polo, Martpol,Materialscientist, MatheoDJ, MattieTK, Maxis ftw, Mdruyan, Meisterkoch, Michael Devore, Mikael Häggström, Mike V, Min.neel, Mindmatrix, Mister Morris, Mmoneypenny, Moeron,Montrealais, MrArifnajafov, Muguengue, MuncherOfSpleens, MusikAnimal, Mycroft007, NGPriest, NHRHS2010, Najibeltecle, Nakon, Naniwako, Nate Silva, Nbauman, Nburden,Needleboy007, Neelix, NellieBly, Neonblak, Nephron, Neuroschizl, NewEnglandYankee, Nick, Nihil, Nirmos, Nlu, NotWith, NuclearWarfare, Num1dgen, Oberonfitch, Okedem, Oldlaptop321,OllieFury, Omicronpersei8, Ontarioboy, Opelio, Oshwah, Osm agha, Oxymoron83, P-G-O, PFHLai, Pablo X, Patrick Berry, Patrick967, Patxi lurra, PaulWicks, Penarestel, Persian Poet Gal,Pgan002, Pgiii, Pharzo, PhilMacD, Philip Trueman, Piano non troppo, Pieguy67, PierreAbbat, Pit, Pratyya Ghosh, Princess Clown, Prolog, Proofreader77, Pscott22, Psychonaut, Ptschett,Purgatory Fubar, Quest for Truth, Quetzapretzel, Quintote, Qwertyytrewqqwerty, R'n'B, R'son-W, R. S. Shaw, Ram-Man, Randall Nortman, Recognizance, Recurve7, Redmarkviolinist,Remingtonhill1, Renaissanceboy, Renato Caniatti, RexNL, Rgoodermote, Riana, Rich Farmbrough, RinoaLnhrt, Rjwilmsi, Rkonert, Roadnottaken, Robbiesergent, Rokfaith, Roleplayer, RonRitzman, Ronz, Rrburke, Rsabbatini, Ryanin, Sahilm, Sannse, Sayeth, Scarian, Sceptre, SeanAhern, Seashorewiki, Seth3481, Sfahey, Shadowjams, Shoeofdeath, Shubblespleen, Signalhead,Slazenger, Smartiger, Snowmanradio, Snowolf, Someone else, Sortior, SpK, Spaully, Specter01010, Squids and Chips, Starwiz, Staticblast, Stevenfoley, Superbiggaylord99, Svick, Tagryn,Tassedethe, Taxman, Template namespace initialisation script, The Thing That Should Not Be, TheBlunderbuss, Therefore, Tide rolls, TigerDigm, Tomasboij, Tony K10, Tori2389, Tpbradbury,Tpemarshall, TreacherousWays, Trick man01, Tristanb, Troodon, TwoHundredNinety, TylerDurden8823, Uglinessman, Ulric1313, Unschool, Vadoff, Van helsing, Vectro, Vedran12, Versageek,Vijay20, WatermelonPotion, Wavetraced, WelshMatt, Whispering, Widders, Widr, WikiDao, Wikibudda89, Wikichanger1, Wikieditor06, Wikipelli, Wk muriithi, Woohookitty, Wouterstomp,Wtwilson3, Wwallacee, Xiaphias, Xinjin127, Yanks1020, Yasmeh, ZX81, Zashaw, Zdli005, Zerbey, Ziebell is gay, 司 徒 天, 937 anonymous edits
Sickle-cell disease Source: http://en.wikipedia.org/w/index.php?oldid=623242587 Contributors: -- April, 09hailj, 10metreh, 123ilikecheese, 28421u2232nfenfcenc, 4twenty42o, 54687o96542, 7mike5000, A.Ou, A520, A8UDI, ADEL67, AIZA123, AMON2000, AManWithNoPlan, ARUNKUMAR P.R, AVand, Abeg92, Acdx, Acesmitty121, Achowat, AddWittyNameHere, Addshore, Adedot, Adhib, Adler847, Adzz182, Aeolus91, Ahlalala 666, Ahoerstemeier, Airplaneman, Aj the vajayjay, Akriasas, Alansohn, Aldermanm, Ale jrb, AlecStewart, Alex.muller, AlexWaelde, Alnokta, AlphaEta, Alphax, Analogue Kid, Andonic, Andy M. Wang, Anetode, Animum, Anrnusna, Anthonyhcole, Anythingyouwant, Arcadian, Arcyqwerty, ArmadilloFromHell, Arthena, Ashmoo, AtheWeatherman, Atnorton, AtomicDragon, Atticus29, Austinlarson, Avnjay, AxelBoldt, Axl, Ayla, Ayrton Prost, B15nes7, BZTMPS, Backdbones, Bagatelle, Barndoorbarnes, Baryonic Being, Bcsilverman, Belovedfreak, Benjaminreid1, Beornas, BethNaught, Betswiki, Bhadani, Bill37212, Bill52270, Billybobsbushwhacker, Binary01, Bluewhale22, Bobbnext, Bobby joehanson, Bobo192, Boccobrock, Boghog, Boing! said Zebedee, Bongwarrior, BorgQueen, Borgx, BorisTM, Brain control, Braincricket, Brendan Moody, Brian0918, Brim, Bruce1ee, Bsadowski1, Bubbarachael, Bucketsofg, Bucksburg, Bueller 007, BullRangifer, Burntsauce, Buxbaum666, C'est moi, C628, CBM, CDN99, CFCF, CWY2190, Callmarcus, Caltas, Camahuetos, CambridgeBayWeather, Camw, Capricorn42, Capt. James T. Kirk, Caska, Cavoab, Cburnett, Cenarium, CensoredScribe, Cesium 133, Ceyockey, Cgingold, Chairman S., Chill doubt, Chinju, Chinyere130x, Chris 73, Chriso4444, Christopher Parham, Cipher42, Circeus, Cirt, Cjsmed, Ck lostsword, Clarince63, Clemwang, Closedmouth, Closenplay, Cmdrjameson, Cocokur, CodeWeasel, Coemgenus, Coffee, CommonsDelinker, Connormah, ContinueWithCaution, Conversion script, Cool Blue, CoolGuy202Cool, Corinne68, Corpx, Courcelles, Cprompt, Ct2288, CyberRaptor, CyborgTosser, D. Recorder, DARTH SIDIOUS 2, DRHagen, DabMachine, Dan653, Danim, DarkFalls, Darkdroom, Darklilac, Davehi1, Davewild, DavidLeighEllis, Davidaah, Davidruben, Dawn Bard, Dbrown123, Debresser, Declanowens, Dekisugi, Delicious carbuncle, Denisarona, Deor, DerHexer, Derumi, Dgunn11235, Dgw, Diberri, Diptanshu.D, Discospinster, Dmesoj, DocWatson42, Doctor Questionmark, Doctorsaif, Doctortomwiki, Donarreiskoffer, Dr.Suess, Dr.michael.benjamin, Dr.saptarshi, DrKIyer, DragonflySixtyseven, Dralwik, Drmed36, Drmies, Drphilharmonic, Dsr9996, Dumarest, Duncharris, E Wing, EGARCIA123, EJF, ESkog, Ed Poor, Edward Z. Yang, Edwy, Eeekster, Egmontaz, Ekwuah, ElHef, Eleassar, Elf, Ember of Light, Emeransid, Enginear, Epbr123, Eras-mus, Erebus Morgaine, Eric Shalov, Eric-Wester, Esparkhu, Esprit15d, Eteru, Everyking, Evlekis, Ewulp, Excirial, FF2010, Fail32, Falkonry, Faradayplank, Fend3r2k9, Firedrop, Fliassassin, Fniroanusi, Forever Dusk, Forteblast, Foxj, Francesca McKenna, Frankie0607, Frankj1978, Frecklefoot, Fritzpoll, Fuqmuffins, FuriousFreddy, Fvasconcellos, Fæ, GHe, Gadfium, Gaff, Gaia Octavia Agrippa, Garrettu12, Gavinatkinson, Gbilleter, Gene Hobbs, Giftlite, Gilderien, Gilliam, Ginsuloft, Gogo Dodo, GoingBatty, Gonzonoir, Goodvac, Goozemar, GraemeL, Grafen, Graham87, GrahamColm, Griffinofwales, Gscshoyru, Gymnastgurl814, Haham hanuka, Hairchrm, Haiti1804, HalfShadow, Hall Monitor, Hamamelis, Hammersoft, Hamtechperson, Hao2lian, Hasearch, Heloo15946, Hermione1980, Highb, Himyname isbob233, HisNHers2006, Hitokirishinji, Hockboy12, HolyBaloney, Hoo man, Hunt'in brooks, Icarntspel, IdleMindzMEG, Igoldste, Imdermie201, Imjustmatthew, Immunize, Inkerman, Insidiae, Ioverka, Ipatrol, Iridescent, IronJohnSr, Iselilja, Isoxyl, Itspancakes, J.delanoy, JCBug, JDG, JLaTondre, JRHorse, JSpung, JSquish, JTB55, JaGa, Jack Greenmaven, Jake Wartenberg, Jan1nad, Jclemens, Jd027, Jdrice8, Jesse Viviano, Jfdwolff, Jfire, Jim1138, JimCubb, Jimfbleak, Jjcobos, Jmh649, Jmundo, Joe2003k, Joehall45, Joel D. Reid, Joeygil, John Cline, JohnCD, JohnOwens, Johndheathcote, Johntex, Johnuniq, Jojhutton, Jordan.A.R., Josve05a, Jovianeye, Jpers36, Jpt1908, Jrodriguez2315, Jules991, Juliancolton, Jusdafax, Jwissick, Jwoodger, K1Bond007, KFP, Kaisershatner, Kalumba, Kazuhite, Kbdank71, Keesiewonder, Kehrbykid, Kesac, Ketyk, Kevjonesin, Khargas, Killiondude, King Modaddy Jr, King of Hearts, Kingmash, Kingpin13, Kishor kumar bhumi, Klilidiplomus, KlingonDoctor, Kosebamse, Kruglikov, Kukini,

Article Sources and Contributors 179
Kurowoofwoof111, Kws, Kyle1278, L Kensington, LSFenster, LaMenta3, Lamro, Lancevortex, Lartoven, Lazulilasher, Lcarscad, Leafyplant, Leapfrog314, LeaveSleaves, LedgendGamer,Leevanjackson, Legoktm, Leon7, Leszek Jańczuk, Leyo, Liaocyed, Lights, Lilbailey14, LinuxAngel, Linzhoo2u, LittleOldMe, Lizaweb, Lkc159, Londonsista, Lord Zoner, Lovemybooty1,Lowercase Sigma, Lugia2453, Luigi30, Lupin, M alhmmadi, MER-C, MONGO, Mackattack1991, Maddie!, Madeleine Price Ball, Madhero88, Maelin amelliasue, Magnus Manske, Magoo005,Malomeat, Mandarax, Manfi, Marek69, Mark Arsten, Martin451, MartinezMD, MastCell, Mattemerson, Mav, Max rspct, MaxBrains, McSly, MedicalCarpenter, Meekywiki, Meisterkoch,Melaen, Mentifisto, Mesoderm, Mgmei, Mhus, Michael Hardy, MichaelBillington, Micheal Lawrence, Mikael Häggström, Mike Rosoft, Mike2vil, Mikeo, Miniyazz, Minna Sora no Shita,Mjcdowling, Mman6357, Mmoneypenny, Mnavid, Mo0, Mogism, Montgomery '39, Morning277, MrBill3, Mswimmer11, Mtcv, Muchness, Mudassar Zia, Muenda, Muntuwandi, MusikAnimal,Muya, My Core Competency is Competency, Mygerardromance, NERIC-Security, Nanajoth, Naniwako, Nate gotlieb, Navy10760, NawlinWiki, Neighboursfiend14, NellieBly, Nephron,NerdyScienceDude, NetRolller 3D, Neutrality, Neverquick, NewEnglandYankee, NiceGuyAlberto, Nick Levine, Nicktownsend12, NicolasCruz, Nivix, No Guru, Nonagonal Spider, Noob1326,Novangelis, Nsigniacorp, Nthep, Nunh-huh, Nwbeeson, O, O.Koslowski, Octane, OhanaUnited, Oldsmobile, OllieFury, Omgitsrhys, Oneiros, Ouani, Ouishoebean, PAR, PCHS-NJROTC,PaleWhaleGail, Pamela jarmon, Pastir1100, Pathoschild, Paul A, PaulWicks, Pavel Vozenilek, Pengortm, PerfectStorm, Persian Poet Gal, Peter Chastain, Peyre, Pgan002, Pgcudahy,Phantomsteve, Pharaoh of the Wizards, Philip Trueman, Philippe, Pi, Pigman, Pinar, Pinethicket, Pjcotterill6445, Plm209, Poeloq, Polarscribe, Polly, Pratikmasti, Prestacious, Procrastinatorsupreme, Prolog, Psiphiorg, PurpleUrge, PwNeR3222, Pyfan, Qscanorg, Quintote, Quoth, Qxz, RA0808, RadicalBender, Ragesoss, RainbowOfLight, RaptorF22, Rayne Xalian, Rcej,Realtimemusic, Recognizance, Redmarkviolinist, Redvers, ResidentAnthropologist, Rettens2, Rettetast, RexNL, Rgoodermote, Rhinestone K, Rhyscox, Riana, Rich Farmbrough,Ringwarriorkayla, Rising*From*Ashes, Rjc34, Rjwilmsi, Roastfalcon3, Robert Foley, Roberticus, Rocketboy50, Rodney dez, Roland Kaufmann, Ronz, RoyBoy, Rror, SCEhardt, SILVERKNIGHT CYRIL, SJP, SMesser, ST47, Sab3el3eish, Saberclaw, SackYourMP, Sadalmelik, Saforrest, Salgueiro, Sam Hocevar, Sam Korn, Samiam08, Samuel Blanning, Satellizer, Sbalfour,Scarian, SchfiftyThree, Schmausschmaus, Scientizzle, Seandals, Seaphoto, Selket, Sephylight, Sertrel, Shanes, ShawntheGod, ShelfSkewed, Shlomke, Shoeofdeath, Sholom, Shopiapiapia,SiZors, Sicklecellanaemia, Sjjupadhyay, Sjzukrow, Skysmith, Slakr, Slrubenstein, Smartse, Smsarmad, Snigbrook, Soccerking9555, Sodaplayer, Sodium, Solindoc, Some jerk on the Internet,Some standardized rigour, Sophialive, Southern hippie, SpLoT, SpaceFlight89, Spangineer, Speyder66, Spock lone wolf, Springnuts, Stemonitis, Stephenb, Steven Zhang, Stomp stompclap,StonedChipmunk, Stwalkerster, Sugongchen, Suitrader, Superluser, Swagmaster420666, SwirlBoy39, Syndicate, TBAmes, THEN WHO WAS PHONE?, THF, Tapir Terrific, TastyPoutine,Taxman, TedE, Teddks, Teles, Tellyaddict, Template namespace initialisation script, Tempodivalse, Tentinator, Tequila11, The Rambling Man, The Thing That Should Not Be, The Utahraptor,TheArguer, TheRanger, Theda, Thestraycat57, Thingg, Thislove07, Thomasdelbert, Tiddly Tom, Tide rolls, Tkynerd, Tnoyce, Tnxman307, TorArne, Tozimbongo, Tpk5010, Traianus, Triwbe,Trlovejoy, Truddle, TubularWorld, Twigletmac, TylerDurden8823, UBeR, Ufwuct, Ulric1313, Uncle Dick, Urhixidur, Useight, Utcursch, Uwais98, Valenciano, Vanished userikijeirw34iuaeolaseriffic, Vanished188, Velella, Vengeful Cynic, Vicki Rosenzweig, VictorianMutant, Vipster, Viriditas, Visite fortuitement prolongée, Vrenator, WIKI, WLU, Wadood Parvez,Walterdavidsmith, Webclient101, WereSpielChequers, West Brom 4ever, Whirl, Whizo, Wickey-nl, Widr, WikHead, Wiki Doc, Wiki alf, WikiLaurent, Wikipelli, Wikiscribe, Wimt, Windchaser,Wizardman, Wizkid9005, Wknight94, WolfmanSF, Woohookitty, World, Wouterstomp, Xnyxx, Xris0, Yamamoto Ichiro, Yboord028, Yintan, Yobol, YuriSuassuna, Zad68, Zidane tribal,Zyryab, Zzuuzz, 55דוד, સતિષચંદ્ર, と あ る 白 い 猫, 2403 anonymous edits
Thalassemia Source: http://en.wikipedia.org/w/index.php?oldid=621013653 Contributors: (jarbarf), *drew, APerson, Addihockey10, Adyione, Aecis, Ahoerstemeier, Aisteco, Ajtmanansala,Alansohn, Alex.tan, Alexrazv2000, Alexrexpvt, AlmostReadytoFly, Alpha Quadrant (alt), Alyg8terz, Andrew73, Andrewman327, Anodyne, Anon423, Anoop v nachiket, Anrnusna, Apers0n,Aranel, Arcadian, Arthena, Ashnard, AsimAlsadeh, Autonomic111, Avg, AxelBoldt, Axl, Aziz1005, Baccyak4H, Balaji Ravichandran, Bayushie, Ben.yarmis, BerserkerBen, Bgpaulus,Bill37212, Bluefairyturnedred, Bobo192, Bobrayner, Boonshofter, Bunnyhop11, CIreland, CWii, Caiaffa, Cajolingwilhelm, Callmarcus, Can't sleep, clown will eat me, Capricorn42, Capsaicin,Captain dave86, Cburnett, Cetlan, ChangChienFu, Charles Matthews, Chris Capoccia, ChrisGualtieri, Chrisfow, Clappingsimon, CommonMed, Corvus cornix, Couchpotato99, Cprompt, Cutler,Cyferx, Danh10105, Danno uk, Dantadd, DerHexer, Derekawesome, Dewritech, Dfkeren, Dirkbb, Discospinster, Dolfrog, Donreed, Dr.michael.benjamin, Drphilharmonic, Dryke, Duinemerwen,Duncharris, ESkog, Ekem, Elennaro, Elipongo, Emayv, Epicgenius, Eric kws, Esparkhu, Eteq, EugenioLaMesa, Everyking, Falcon8765, Fang Aili, Fizzelo, Fluxtpe, Footprintx, FourBlades, FredBradstadt, Fuzheado, GK, Gadfium, Gak, Gakrivas, Gcgowans, Gfoley4, Gilliam, Glasszone33, Glowaurora, Gogo Dodo, Golbez, Graham87, Grauda1, GregorB, Habj, Haim Berman,Hamidnia101, Harken311, Harry, Hasseli, Helikophis, Hgrosser, Hhaithait, Hitokirishinji, Hlpavitt, HooXooH, Hpotter100, I dream of horses, Ibbn, InTheZone, Inferior Olive, Inkerman,Intoxicat, Ixfd64, J-beda, JForget, JaGa, Jakebarrington, Jfdwolff, Jmh649, Johan Burati, John254, Jojhutton, Jonomacdrones, Joshua, Jusdafax, JustPhil, JustinPS, Kander, KathrynLybarger,Katpjotr, KawasakiMan247, Kazem.fa, KeeganTheBrain, Kerotan, Kesac, Kjramesh, Kylu, Kyoko, LADave, Lancevortex, Lartoven, Learnthesigns, Lee, Legoktm, Leontios, Lights, Limac,M1ss1ontomars2k4, MASQUERAID, MK8, Magioladitis, Magister, Mainak, Malcolm Farmer, MaraNeo127, Maria Larsson, Marientina, MartinezMD, Mating panda, Matt641, Matttoothman,Mav, Mehdiakram, Mel Etitis, Menchi, Metzenberg, Michael Hardy, Michaelas10, Midoriko, Mifter, Mightyhansa, Mikael Häggström, Mike2vil, Mimihitam, Minimac, Mlaffs, Mlessard,Mogism, Mogren, Mountolive, MrBlueSky, Mvkulkarni23, NCurse, Neøn, NoWayRay, Noctibus, Nunh-huh, Obahliskh, Oleg Alexandrov, Onebravemonkey, Orange Suede Sofa, Ordibehesht22,Pak bahadur, Pandalf, Pascal.Tesson, Pascal666, Petersam, Pethr, Pigsonthewing, Pineappular, PlasmaTime, Plch, Pollinator, Posterweb, Preston.atteberry, Quantumor, Quaoarian, RDBrown,Ratznium, Rcej, Reswobslc, Rich Farmbrough, Ritesh7000, Rjwilmsi, Rmky87, Robth, Ronhjones, Rsabbatini, Rushbugled13, Sam Korn, Sanfedisti, Sasquatch, Saurabh523, Sbalfour, Sbharris,Sbmehta, Seans Potato Business, Serum21007, Shaddack, Shaedo, Shingra, SirJacobAstley, SolomonHume, Some standardized rigour, Someone else, Speciate, Spiff666, StephP, Sudhakarsr, SunCreator, Supersquid, Suvobroto, T0ms, TedlyW, Template namespace initialisation script, Temporaluser, Tennis Dynamite, Thalcare, Thingg, Tolly4bolly, Tornadowhiz, Triggtay, Tuur, Ufinne,Ujalm, Verybigfish86, Vicki Rosenzweig, Vogon77, Wachholder, Wareh, Wavelength, Widr, William Avery, Wingedsubmariner, Wouterstomp, Wwallacee, Yosri, ZimZalaBim, Zyryab, 55דוד,anonymous edits 628 ,ماني

Image Sources, Licenses and Contributors 180
Image Sources, Licenses and ContributorsFile:Iron deficiency anemia blood film.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Iron_deficiency_anemia_blood_film.jpg License: Creative Commons Attribution-Sharealike3.0 Contributors: User:GrahamColmFile:Symptoms of anemia.png Source: http://en.wikipedia.org/w/index.php?title=File:Symptoms_of_anemia.png License: Public Domain Contributors: Mikael HäggströmFile:Iron deficiency anemia.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Iron_deficiency_anemia.jpg License: Creative Commons Attribution-Sharealike 2.0 Contributors: E.Uthman, MDFile:Hemolysis.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Hemolysis.jpg License: Creative Commons Attribution-ShareAlike 3.0 Unported Contributors: Y tambeFile:Streptococcal hemolysis.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Streptococcal_hemolysis.jpg License: Creative Commons Attribution-Sharealike 2.5 Contributors: YtambeFile:Blood smear.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Blood_smear.jpg License: GNU Free Documentation License Contributors: Jacklee, Reytan, Santosga, Snek01, 1anonymous editsFile:Red White Blood cells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Red_White_Blood_cells.jpg License: Public Domain Contributors: Electron Microscopy Facility at TheNational Cancer Institute at Frederick (NCI-Frederick)File:Krew Frakcjonowana.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Krew_Frakcjonowana.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors:User:PlatynaFile:Blutkreislauf.png Source: http://en.wikipedia.org/w/index.php?title=File:Blutkreislauf.png License: Creative Commons Attribution-Sharealike 2.5 Contributors: Infrogmation, Jacklee,Mardetanha, Phrood, Str4nd, Wst, 10 anonymous editsImage:Humanbood600x.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Humanbood600x.jpg License: Creative Commons Attribution-Share Alike Contributors: John Alan ElsonImage:320frogblood600x2.jpg Source: http://en.wikipedia.org/w/index.php?title=File:320frogblood600x2.jpg License: Creative Commons Attribution-Share Alike Contributors: John AlanElsonImage:320fishblood600x2.jpg Source: http://en.wikipedia.org/w/index.php?title=File:320fishblood600x2.jpg License: Creative Commons Attribution-Share Alike Contributors: John AlanElsonFile:1GZX Haemoglobin.png Source: http://en.wikipedia.org/w/index.php?title=File:1GZX_Haemoglobin.png License: GNU Free Documentation License Contributors: Original uploaderwas Zephyris at en.wikipediaFile:Heme.svg Source: http://en.wikipedia.org/w/index.php?title=File:Heme.svg License: Public Domain Contributors: User:Lennert BFile:Blausen 0425 Formed Elements.png Source: http://en.wikipedia.org/w/index.php?title=File:Blausen_0425_Formed_Elements.png License: Creative Commons Attribution 3.0 Contributors: BruceBlaus, Hazmat2, Mikael HäggströmFile:Blut-EDTA.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Blut-EDTA.jpg License: GNU Free Documentation License Contributors: User:JHeuser, User:JHeuser,User:JHeuserFile:Diagram of the human heart (cropped).svg Source: http://en.wikipedia.org/w/index.php?title=File:Diagram_of_the_human_heart_(cropped).svg License: Creative CommonsAttribution-ShareAlike 3.0 Unported Contributors: User:YaddahFile:Oxyhaemoglobin dissociation curve.png Source: http://en.wikipedia.org/w/index.php?title=File:Oxyhaemoglobin_dissociation_curve.png License: Public Domain Contributors: Originaluploader was Ratznium at en.wikipedia Later versions were uploaded by Aaronsharpe at en.wikipedia.File:Bleeding finger.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Bleeding_finger.jpg License: Creative Commons Attribution 2.0 Contributors: Dodo, FlickreviewR, Grafite,Nilfanion, SouthgeistFile:Bloodbags.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Bloodbags.jpg License: Creative Commons Attribution-Sharealike 2.0 Contributors: User "montuno" on FlickrImage:Wikiquote-logo.svg Source: http://en.wikipedia.org/w/index.php?title=File:Wikiquote-logo.svg License: Public Domain Contributors: -xfi-, Dbc334, Doodledoo, Elian, Guillom, Jeffq,Krinkle, Maderibeyza, Majorly, Nishkid64, RedCoat, Rei-artur, Rocket000, 11 anonymous editsImage:Wiktionary-logo-en.svg Source: http://en.wikipedia.org/w/index.php?title=File:Wiktionary-logo-en.svg License: Public Domain Contributors: Vectorized by , based on original logotossed together by Brion VibberImage:Commons-logo.svg Source: http://en.wikipedia.org/w/index.php?title=File:Commons-logo.svg License: logo Contributors: AnomieFile:Erythrozytenkonzentrat neu.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Erythrozytenkonzentrat_neu.jpg License: Creative Commons Attribution-ShareAlike 3.0 Unported Contributors: Erythrozytenkonzentrat.jpg: Pflegewiki-User Würfel derivative work:MidnightsnackFile:Blausen 0087 Blood Transfusion.png Source: http://en.wikipedia.org/w/index.php?title=File:Blausen_0087_Blood_Transfusion.png License: Creative Commons Attribution 3.0 Contributors: BruceBlaus, Hazmat2, Mikael HäggströmFile:FreshFrozenPlasma.JPG Source: http://en.wikipedia.org/w/index.php?title=File:FreshFrozenPlasma.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: DiverDaveFile:Blausen 0086 Blood Bag.png Source: http://en.wikipedia.org/w/index.php?title=File:Blausen_0086_Blood_Bag.png License: Creative Commons Attribution 3.0 Contributors:BruceBlaus, Hazmat2, Mikael HäggströmFile:Richard Lower.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Richard_Lower.jpg License: Public Domain Contributors: User Magnus Manske on en.wikipediaFile:James Blundell (physician).jpg Source: http://en.wikipedia.org/w/index.php?title=File:James_Blundell_(physician).jpg License: Public Domain Contributors: Engraved by John Cochranafter Henry Room.File:Agote 1a transfusión.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Agote_1a_transfusión.jpg License: Public Domain Contributors: Barcex, Cambalachero, CsoliverezFile:Direct-blood-transfusion.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Direct-blood-transfusion.jpg License: GNU Free Documentation License Contributors: Originaluploader was Ravn at en.wikipediaFile:A A Bogdanov.jpg Source: http://en.wikipedia.org/w/index.php?title=File:A_A_Bogdanov.jpg License: Public Domain Contributors: INeverCry, LeuthaFile:Blood transfusion ww2 poster.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Blood_transfusion_ww2_poster.jpg License: Public Domain Contributors: UK government (Lifetime: na)File:Private Roy W. Humphrey of Toledo, Ohio is being given blood plasma after he was wounded by shrapnel in Sicily on 8-9-43 - NARA - 197268.jpg Source:http://en.wikipedia.org/w/index.php?title=File:Private_Roy_W._Humphrey_of_Toledo,_Ohio_is_being_given_blood_plasma_after_he_was_wounded_by_shrapnel_in_Sicily_on_8-9-43_-_NARA_-_197268.jpg License: Public Domain Contributors: Fæ, JustSomePics, TamboFile:Charles R Drew portrait.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Charles_R_Drew_portrait.jpg License: Public Domain Contributors: Original uploader was Darwinekat en.wikipediaFile:Circulatory System en.svg Source: http://en.wikipedia.org/w/index.php?title=File:Circulatory_System_en.svg License: Public Domain Contributors: LadyofHats, Mariana Ruiz VillarrealFile:Blood vessels.svg Source: http://en.wikipedia.org/w/index.php?title=File:Blood_vessels.svg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:KelvinsongFile:Microvessel.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Microvessel.jpg License: Creative Commons Attribution 3.0 Contributors: Robert M. HuntFile:Gray72-en.svg Source: http://en.wikipedia.org/w/index.php?title=File:Gray72-en.svg License: Public Domain Contributors: MysidImage:619 Red and Yellow Bone Marrow.jpg Source: http://en.wikipedia.org/w/index.php?title=File:619_Red_and_Yellow_Bone_Marrow.jpg License: Creative Commons Attribution 3.0 Contributors: CFCFFile:Bone marrow WBC.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Bone_marrow_WBC.JPG License: Creative Commons Attribution-Share Alike Contributors: BobjgalindoImage:acute leukemia-ALL.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Acute_leukemia-ALL.jpg License: GNU Free Documentation License Contributors: Original uploaderwas VashiDonsk at en.wikipediaImage:Bone marrow biopsy.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Bone_marrow_biopsy.jpg License: Public Domain Contributors: Photographer’s Mate 2nd Class ChadMcNeeleyFile:erythropoietin.png Source: http://en.wikipedia.org/w/index.php?title=File:Erythropoietin.png License: Public Domain Contributors: Cwbm (commons), Delwarl, E A S, Nagy, 4anonymous edits
Image Sources, Licenses and Contributors 181
File:PBB_GE_EPO_207257_at_tn.png Source: http://en.wikipedia.org/w/index.php?title=File:PBB_GE_EPO_207257_at_tn.png License: GNU Free Documentation License Contributors: -File:PBB_GE_EPO_217254_s_at_tn.png Source: http://en.wikipedia.org/w/index.php?title=File:PBB_GE_EPO_217254_s_at_tn.png License: GNU Free Documentation License Contributors: -Image:Illu blood cell lineage.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Illu_blood_cell_lineage.jpg License: Public Domain Contributors: Arcadian, Bestiasonica, Cristobalcarrasco, DO11.10, MichaelFrey, 6 anonymous editsFile:Gallensteine 2006 03 28.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Gallensteine_2006_03_28.JPG License: Public Domain Contributors: Geofrog, Moros, Stell98File:Gallstones.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Gallstones.jpg License: Creative Commons Attribution 3.0 Contributors: Emmanuelm at en.wikipedia (Original text :Emmanuelm (talk))File:Gallenstein FRONT.OGG Source: http://en.wikipedia.org/w/index.php?title=File:Gallenstein_FRONT.OGG License: Creative Commons Attribution-Sharealike 3.0 Contributors:SecretDiscFile:Big Gallstone.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Big_Gallstone.JPG License: Creative Commons Attribution 3.0 Contributors: User:HalfalahImage:Gallstones.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Gallstones.JPG License: Public Domain Contributors: Alex Khimich (talk). Original uploader was Alex Khimichat en.wikipediaImage:Gallstone µCT.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Gallstone_µCT.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: SecretDiscFile:Gallstones.PNG Source: http://en.wikipedia.org/w/index.php?title=File:Gallstones.PNG License: Creative Commons Attribution-Sharealike 3.0 Contributors: James Heilman, MDFile:StonesXray.PNG Source: http://en.wikipedia.org/w/index.php?title=File:StonesXray.PNG License: Creative Commons Attribution-Sharealike 3.0 Contributors: James Heilman, MDFile:CBD stones.JPG Source: http://en.wikipedia.org/w/index.php?title=File:CBD_stones.JPG License: Creative Commons Attribution-Sharealike 3.0,2.5,2.0,1.0 Contributors: Samir 04:04, 26September 2007 (UTC)File:Impacted ampulla.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Impacted_ampulla.jpg License: GNU Free Documentation License Contributors: User:Samir_(The_Scope)File:ERCP Roentgen.jpg Source: http://en.wikipedia.org/w/index.php?title=File:ERCP_Roentgen.jpg License: GNU Free Documentation License Contributors: J. Guntau at de.wikipediaFile:Hematopoiesis simple.svg Source: http://en.wikipedia.org/w/index.php?title=File:Hematopoiesis_simple.svg License: GNU Free Documentation License Contributors: Mikael Häggström(no attribution required), from original by A. Rad (requires attribution)Image:Hematopoesis EN.svg Source: http://en.wikipedia.org/w/index.php?title=File:Hematopoesis_EN.svg License: Creative Commons Attribution 3.0 Contributors: M.KomorniczakFile:Hematopoietic growth factors.png Source: http://en.wikipedia.org/w/index.php?title=File:Hematopoietic_growth_factors.png License: GNU Free Documentation License Contributors:User:Mikael Häggström and A. RadImage:1GZX Haemoglobin.png Source: http://en.wikipedia.org/w/index.php?title=File:1GZX_Haemoglobin.png License: GNU Free Documentation License Contributors: Original uploaderwas Zephyris at en.wikipediaFile:HemoglobinABDAlignment.png Source: http://en.wikipedia.org/w/index.php?title=File:HemoglobinABDAlignment.png License: Creative Commons Attribution Contributors:http://www.uniprot.org/Image:Heme b.svg Source: http://en.wikipedia.org/w/index.php?title=File:Heme_b.svg License: Public Domain Contributors: YikrazuulImage:Hemoglobin t-r state ani.gif Source: http://en.wikipedia.org/w/index.php?title=File:Hemoglobin_t-r_state_ani.gif License: GNU Free Documentation License Contributors:en:User:BerserkerBenImage:Hemoglobin saturation curve.svg Source: http://en.wikipedia.org/w/index.php?title=File:Hemoglobin_saturation_curve.svg License: Public Domain Contributors: Hazmat2File:Postnatal genetics en.svg Source: http://en.wikipedia.org/w/index.php?title=File:Postnatal_genetics_en.svg License: Creative Commons Attribution-Sharealike 3.0 Contributors:Postnatal_genetics.svg: original: Furfur, File:Haemoglobin-Ketten.svg, derivation/translation:Leonid 2 derivative work: Leonid 2 (talk)Image:Hemoglobin Test American Red Cross.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Hemoglobin_Test_American_Red_Cross.jpg License: GNU Free DocumentationLicense Contributors: WhoisjohngaltImage:Nur04505.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Nur04505.jpg License: Public Domain Contributors: Achim Raschka, Eugene van der Pijll, Liné1, Mithril,Royalbroil, Telim tor, TomCatX, 1 anonymous editsImage:Heart of Steel (Hemoglobin).jpg Source: http://en.wikipedia.org/w/index.php?title=File:Heart_of_Steel_(Hemoglobin).jpg License: GNU Free Documentation License Contributors:Photographer: Julian Voss-AndreaeImage:Jaundice08.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Jaundice08.jpg License: Creative Commons Attribution 3.0 Contributors: James Heilman, MDFile:Jaundice.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Jaundice.jpg License: Creative Commons Attribution 3.0 Contributors: Sab3el3eishFile:Jaundice-types.png Source: http://en.wikipedia.org/w/index.php?title=File:Jaundice-types.png License: GNU Free Documentation License Contributors: User:Enigma55File:Obstructivebiliarydilation.png Source: http://en.wikipedia.org/w/index.php?title=File:Obstructivebiliarydilation.png License: Creative Commons Attribution-Sharealike 3.0 Contributors:User:Jmh649File:Obstructivebiliarydilation2.png Source: http://en.wikipedia.org/w/index.php?title=File:Obstructivebiliarydilation2.png License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Jmh649file:Wiktionary-logo-en.svg Source: http://en.wikipedia.org/w/index.php?title=File:Wiktionary-logo-en.svg License: Public Domain Contributors: Vectorized by , based on original logo tossedtogether by Brion Vibberfile:Commons-logo.svg Source: http://en.wikipedia.org/w/index.php?title=File:Commons-logo.svg License: logo Contributors: AnomieFile:Malaria.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Malaria.jpg License: Creative Commons Attribution 2.5 Contributors: Abanima, CactusWriter, Cdc, ComputerHotline,Daniel Mietchen, Juliancolton, Masur, NeverDoING, Oks, Thuresson, Wlodzimierz, Überraschungsbilder, 3 anonymous editsFile:Symptoms of Malaria.png Source: http://en.wikipedia.org/w/index.php?title=File:Symptoms_of_Malaria.png License: Public Domain Contributors: Mikael Häggström, Stas1995, 1anonymous editsFile:Life Cycle of the Malaria Parasite.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Life_Cycle_of_the_Malaria_Parasite.jpg License: Public Domain Contributors: CFCF,Ruslik0Image:Maternal malaria placenta - cropped - very high mag.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Maternal_malaria_placenta_-_cropped_-_very_high_mag.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: NephronFile:5901 lores.jpg Source: http://en.wikipedia.org/w/index.php?title=File:5901_lores.jpg License: unknown Contributors: CDC/ Steven Glenn, Laboratory & Consultation DivisionFile:Plasmodium.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Plasmodium.jpg License: Public Domain Contributors: Original uploader was TimVickers at en.wikipediaFile:Anopheles stephensi.jpeg Source: http://en.wikipedia.org/w/index.php?title=File:Anopheles_stephensi.jpeg License: Public Domain Contributors: Jim GathanyFile:Mansprayingkeroseneoil.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Mansprayingkeroseneoil.jpg License: Public Domain Contributors: The Field Museum LibraryFile:Mosquitoes-Killedy-By-DDT-Lake-Victoria.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Mosquitoes-Killedy-By-DDT-Lake-Victoria.JPG License: Creative CommonsAttribution-Sharealike 3.0 Contributors: User:UspnFile:Midnight in Pediatric ICU.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Midnight_in_Pediatric_ICU.jpg License: Creative Commons Attribution 3.0 Contributors: MikeBlythImage:Malaria world map - DALY - WHO2004.svg Source: http://en.wikipedia.org/w/index.php?title=File:Malaria_world_map_-_DALY_-_WHO2004.svg License: Creative CommonsAttribution-Sharealike 2.5 Contributors: Lokal_ProfilFile:Paludisme.png Source: http://en.wikipedia.org/w/index.php?title=File:Paludisme.png License: Creative Commons Attribution-Sharealike 2.5 Contributors: PercherieFile:Ronald Ross.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Ronald_Ross.jpg License: Public Domain Contributors: PDH, Slomox, Tryphon, Väsk, Yelm, 竹 麦 魚(Searobin)File:Artemisia annua West Virginia.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Artemisia_annua_West_Virginia.jpg License: Public Domain Contributors: Jorge FerreiraFile:Saving Lives with SMS for Life.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Saving_Lives_with_SMS_for_Life.jpg License: Creative Commons Attribution 2.0 Contributors: Jeffrey Gluck from USAFile:"Don't go to Bed with Malaria Mosquito" - NARA - 514146.tif Source:http://en.wikipedia.org/w/index.php?title=File:"Don't_go_to_Bed_with_Malaria_Mosquito"_-_NARA_-_514146.tif License: Public Domain Contributors: Djembayz, Fæ, Michael Barera

Image Sources, Licenses and Contributors 182
Image:Wikivoyage-Logo-v3-icon.svg Source: http://en.wikipedia.org/w/index.php?title=File:Wikivoyage-Logo-v3-icon.svg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:AleXXwFile:Plexiform_lesion_-_Pulmonary_hypertension.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Plexiform_lesion_-_Pulmonary_hypertension.jpg License: Creative CommonsAttribution-Sharealike 2.0 Contributors: Image contributed by Bulent Celasun, MDFile:Molecular pathway of vasodilation mediated by cGMP.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Molecular_pathway_of_vasodilation_mediated_by_cGMP.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:BQmUB2012010File:Phonocardiogram.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Phonocardiogram.jpg License: Copyrighted free use Contributors: Butterworth PublishersFile:Pulmonary artery catheter english.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Pulmonary_artery_catheter_english.JPG License: Creative CommonsAttribution-Sharealike 3.0 Contributors: derivative work: Tariq Abdulla (talk) Pulmonary_artery_catheter_german.jpg: User:Chikumaya, modifizert von PhilippNPulmonary_arterial_catheter.svg: User:ChikumayaImage:redbloodcells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Redbloodcells.jpg License: Public domain Contributors: Dietzel65, Habj, Paul 012, Ranveig, Shizhao, SimonShek, Solon, Sundar, ThuressonImage:Erythrocytes in vertebrates.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Erythrocytes_in_vertebrates.jpg License: Public Domain Contributors: G Gulliver - Proceedingsof the Royal Society of LondonImage:Gray453.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray453.png License: Public Domain Contributors: Henry GrayImage:Red White Blood cells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Red_White_Blood_cells.jpg License: Public Domain Contributors: Electron Microscopy Facility atThe National Cancer Institute at Frederick (NCI-Frederick)Image:NIK 3232-Drops of blood medium.JPG Source: http://en.wikipedia.org/w/index.php?title=File:NIK_3232-Drops_of_blood_medium.JPG License: Creative Commons Attribution 3.0 Contributors: unknownImage:Erytrocyte deoxy to oxy v0.7.gif Source: http://en.wikipedia.org/w/index.php?title=File:Erytrocyte_deoxy_to_oxy_v0.7.gif License: Creative Commons Attribution-Sharealike 3.0 Contributors: RogeriopfmImage:Erythrocyte Membrane lipids.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Erythrocyte_Membrane_lipids.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: Cholesterol.svg: BorisTM Phosphatidylcholine.png: Likeitsmyjob Sphingomyelin.png: Original uploader was Jag123 at en.wikipedia Phosphatidyl-Inositol.png: Original uploaderwas Jag123 at en.wikipedia Phosphatidyl-Serine.png: Original uploader was Jag123 at en.wikipedia Phosphatidyl-Ethanolamine.png: Original uploader was Jag123 at en.wikipedia derivativework: Rogeriopfm (talk)File:RBC Membrane Proteins SDS-PAGE gel.jpg Source: http://en.wikipedia.org/w/index.php?title=File:RBC_Membrane_Proteins_SDS-PAGE_gel.jpg License: Creative Commons Zero Contributors: Ernst HempelmannFile:RBC membrane major proteins.png Source: http://en.wikipedia.org/w/index.php?title=File:RBC_membrane_major_proteins.png License: Public Domain Contributors:RBC_membrane_major_proteins.jpg: Author is Ernst Hempelmann derivative work: TimVickers (talk)Image:Sicklecells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Sicklecells.jpg License: Public Domain Contributors: NIDDKImage:Osmotic pressure on blood cells diagram.svg Source: http://en.wikipedia.org/w/index.php?title=File:Osmotic_pressure_on_blood_cells_diagram.svg License: Public Domain Contributors: LadyofHatsFile:Human Erythrocytes OsmoticPressure PhaseContrast Plain.svg Source: http://en.wikipedia.org/w/index.php?title=File:Human_Erythrocytes_OsmoticPressure_PhaseContrast_Plain.svg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:ZephyrisFile:Illu spleen.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Illu_spleen.jpg License: Public Domain Contributors: Arcadian, Grook Da Oger, 2 anonymous editsFile:Horse_spleen_laparoscopic.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Horse_spleen_laparoscopic.jpg License: GNU Free Documentation License Contributors: MalcolmMorley (my own image)File:Gray1188.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1188.png License: Public Domain Contributors: ArcadianImage:Spleen hyaloserositis - low mag.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Spleen_hyaloserositis_-_low_mag.jpg License: Creative Commons Attribution-Sharealike3.0 Contributors: NephronImage:Gray532.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray532.png License: Public Domain Contributors: Hellerhoff, SjoehestImage:Gray533.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray533.png License: Public Domain Contributors: Arcadian, Robert Weemeyer, 1 anonymous editsImage:Gray1039.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1039.png License: Public Domain Contributors: Arcadian, Magnus Manske, Quibik, Raimundo PastorImage:Gray1097.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1097.png License: Public Domain Contributors: Arcadian, Magnus Manske, Was a beeImage:Gray1098.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1098.png License: Public Domain Contributors: Arcadian, Magnus Manskeimage:Gray1188.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1188.png License: Public Domain Contributors: Arcadianimage:Gray1189.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1189.png License: Public Domain Contributors: Arcadianimage:Gray1190.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1190.png License: Public Domain Contributors: Arcadianimage:Gray1192.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1192.png License: Public Domain Contributors: Arcadian, Origamiemenschimage:Gray1226.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1226.png License: Public Domain Contributors: Arcadian, Grook Da Oger, Origamiemensch, Quibik, Was abeeimage:Gray1217.png Source: http://en.wikipedia.org/w/index.php?title=File:Gray1217.png License: Public Domain Contributors: Arcadian, Grook Da Oger, QuibikImage:Illu lymphatic system.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Illu_lymphatic_system.jpg License: Public Domain Contributors: Arcadian, AtonX, Cwbm(commons), M.Komorniczak, 3 anonymous editsFile:Slide2ii.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide2ii.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Lien 2.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Lien_2.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Slide10ffff.JPG Source: http://en.wikipedia.org/w/index.php?title=File:Slide10ffff.JPG License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:Anatomist90File:Sickle cell 01.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Sickle_cell_01.jpg License: Public Domain Contributors: The National Heart, Lung, and Blood Institute (NHLBI)File:Sickle cells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Sickle_cells.jpg License: Creative Commons Attribution-Sharealike 3.0 Contributors: User:GrahamColmFile:1911 Sickle Cells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:1911_Sickle_Cells.jpg License: Creative Commons Attribution 3.0 Contributors: OpenStax CollegeFile:Sicklecells.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Sicklecells.jpg License: Public Domain Contributors: NIDDKFile:Sickle cell distribution.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Sickle_cell_distribution.jpg License: GNU Free Documentation License Contributors: Original uploaderwas Muntuwandi at en.wikipediaFile:Malaria distribution.jpg Source: http://en.wikipedia.org/w/index.php?title=File:Malaria_distribution.jpg License: GNU Free Documentation License Contributors: Original uploader wasMuntuwandi at en.wikipediaFile:Paludisme - Frequence statistique.png Source: http://en.wikipedia.org/w/index.php?title=File:Paludisme_-_Frequence_statistique.png License: Creative Commons Attribution-Sharealike2.5 Contributors: PercherieFile:Autorecessive.svg Source: http://en.wikipedia.org/w/index.php?title=File:Autorecessive.svg License: Creative Commons Attribution-ShareAlike 3.0 Unported Contributors:en:User:CburnettImage:autorecessive.svg Source: http://en.wikipedia.org/w/index.php?title=File:Autorecessive.svg License: Creative Commons Attribution-ShareAlike 3.0 Unported Contributors:en:User:Cburnett

License 183
LicenseCreative Commons Attribution-Share Alike 3.0//creativecommons.org/licenses/by-sa/3.0/