Diseases associated with calcium pyrophosphate deposition disease
15
Diseases Associated With Calcium Pyrophosphate Deposition Disease By Adrian C. Jones, Alexis J. Chuck, Eleanor A. Arie, Desmond J. Green, and Michael Doherty Although many metabolic and endocrine dis- eases have been reported to predispose to cal- cium pyrophosphate dihydrate crystal deposi- tion, the validity of many of these associations remains unclear. A critical review of the litera- ture relating to these associations, with illustra- tive cases and data derived from the authors’ own experience, is presented. It is concluded that there is good evidence to associate hy- pophosphatasia, hypomagnesemia, and hyper- parathyroidism with chondrocalcinosis and acute attacks of “pseudogout.” Meta-analysis also sug- gests a small but significant association be- tween hypothyroidism and chondrocalcinosis. D EPOSITION OF calcium pyrophosphate dihydrate (CPPD) crystals within hyaline cartilage and fibrocartilage, “chondrocalcinosis” (CC), may be asymptomatic or associated with acute crystal synovitis or chronic arthropathy.1-5 The formation of CPPD crystals involves both the “seed” (the product of calcium and inor- ganic pyrophosphate [PPi]) and the “soil” (the matrix in which the crystals form and grow).h Both components could be affected by many factors, including metabolic and endocrine dis- ease, and a number of such diseases have been associated with CPPD crystal deposition. How- ever, CPPD deposition is also associated with gender,’ structural damage,8-10 and osteoarthri- tis (OA),’ and isolated CPPD deposition is a From the Rheumatology Unit, City Hospital, Nottingham, England; the Drybum Hospital, Durham, England; and the Royal Hospital and Home, Putney, England. Supported in part by the Arthritis and Rheumatism Council. Adrian C. Jones, MRCP: Research Fellow, Rheumatology Unit, City Hospital, Nottingham; Alexis J. Chuck, MRCP: Consultant Rheumatologist, Dryburn Hospital, Durham; Eleanor A. Arie, MRCP: Consultant Rheumatologist, Royal Hospital and Home, Putney; Desmond J. Green, FRCR: Consultant Radiologist, City Hospital, Nottingham; Michael Doherty, MD: Senior Lecturer, Rheumatology Unit, City Hospital, Nottingham. Address reprint requests to Adrian C. Jones, MRCP, Rheumo- tology Unit, City Hospital, Nottingham NG5 IPB, England. Copyright 0 1992 by U! B. Saunders Company 0049.0172/9212203-0006$5.OOlO Hemochromatosis stands alone in clearly associ- ating not only with chondrocalcinosis but also with structural change and chronic arthropathy. The biochemical mechanisms that may produce these various associations are discussed. Recom- mendations are made concerning appropriate screening for metabolic and endocrine disease in patients with chondrocalcinosis. Copyright 0 1992 by W. B. Saunders Company INDEX WORDS: Chondrocalcinosis; calcium py- rophosphate dihydrate; endocrine disease; met- abolic disease. common finding in aging but otherwise normal joint tissues. 2,7~11~12 Therefore, distinguishing true from spurious associations is difficult.“-” Two approaches may be used to determine associations between diseases. For common diseases, case-control studies or large popula- tion surveys with complete ascertainment of the two diseases are necessary.‘” For less common diseases, unusual features such as young age of onset or severity may suffice. This review will consider the prevalence of CC in the general population, consider the evidence for metabolic and endocrine disease associations, and discuss the various etiopatho- genetic mechanisms that have been proposed. Because terminology of CPPD-related dis- eases is not yet standardized, we shall adopt the following conventions: chondrocalcinosis, radio- graphic or histological calcification of fibrocarti- lage or hyaline cartilage; pseudogout, acute CPPD crystal-associated synovitis; andpyrophos- phate arthropathy (PA), structural arthropathy associated with intraarticular CPPD crystal dep- osition (with or without associated CC). NORMAL POPULATIONS A number of techniques have been used in an attempt to determine the frequency of CC in the general population. These include postmor- tem studies,4.‘2.17 examination of joint tissue removed at surgery,i8xr9 and radiographic sur- 188 Seminars in Arthritis and Rheumatism, Vol22, No 3 (December), 1992: pp 188-202
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Diseases associated with calcium pyrophosphate deposition disease

Diseases Associated With Calcium Pyrophosphate Deposition Disease
By Adrian C. Jones, Alexis J. Chuck, Eleanor A. Arie, Desmond J. Green,
and Michael Doherty
Although many metabolic and endocrine dis- eases have been reported to predispose to cal- cium pyrophosphate dihydrate crystal deposi- tion, the validity of many of these associations remains unclear. A critical review of the litera- ture relating to these associations, with illustra- tive cases and data derived from the authors’ own experience, is presented. It is concluded that there is good evidence to associate hy- pophosphatasia, hypomagnesemia, and hyper- parathyroidism with chondrocalcinosis and acute attacks of “pseudogout.” Meta-analysis also sug- gests a small but significant association be- tween hypothyroidism and chondrocalcinosis.
D EPOSITION OF calcium pyrophosphate dihydrate (CPPD) crystals within hyaline
cartilage and fibrocartilage, “chondrocalcinosis” (CC), may be asymptomatic or associated with acute crystal synovitis or chronic arthropathy.1-5 The formation of CPPD crystals involves both the “seed” (the product of calcium and inor- ganic pyrophosphate [PPi]) and the “soil” (the matrix in which the crystals form and grow).h Both components could be affected by many factors, including metabolic and endocrine dis- ease, and a number of such diseases have been associated with CPPD crystal deposition. How- ever, CPPD deposition is also associated with gender,’ structural damage,8-10 and osteoarthri- tis (OA),’ and isolated CPPD deposition is a
From the Rheumatology Unit, City Hospital, Nottingham, England; the Drybum Hospital, Durham, England; and the Royal Hospital and Home, Putney, England.
Supported in part by the Arthritis and Rheumatism Council. Adrian C. Jones, MRCP: Research Fellow, Rheumatology
Unit, City Hospital, Nottingham; Alexis J. Chuck, MRCP:
Consultant Rheumatologist, Dryburn Hospital, Durham; Eleanor A. Arie, MRCP: Consultant Rheumatologist, Royal Hospital and Home, Putney; Desmond J. Green, FRCR:
Consultant Radiologist, City Hospital, Nottingham; Michael
Doherty, MD: Senior Lecturer, Rheumatology Unit, City Hospital, Nottingham.
Address reprint requests to Adrian C. Jones, MRCP, Rheumo- tology Unit, City Hospital, Nottingham NG5 IPB, England.
Copyright 0 1992 by U! B. Saunders Company 0049.0172/9212203-0006$5.OOlO
Hemochromatosis stands alone in clearly associ- ating not only with chondrocalcinosis but also with structural change and chronic arthropathy. The biochemical mechanisms that may produce these various associations are discussed. Recom- mendations are made concerning appropriate screening for metabolic and endocrine disease in patients with chondrocalcinosis. Copyright 0 1992 by W. B. Saunders Company
INDEX WORDS: Chondrocalcinosis; calcium py- rophosphate dihydrate; endocrine disease; met- abolic disease.
common finding in aging but otherwise normal joint tissues. 2,7~11~12 Therefore, distinguishing true from spurious associations is difficult.“-”
Two approaches may be used to determine associations between diseases. For common diseases, case-control studies or large popula- tion surveys with complete ascertainment of the two diseases are necessary.‘” For less common diseases, unusual features such as young age of onset or severity may suffice.
This review will consider the prevalence of CC in the general population, consider the evidence for metabolic and endocrine disease associations, and discuss the various etiopatho- genetic mechanisms that have been proposed.
Because terminology of CPPD-related dis- eases is not yet standardized, we shall adopt the following conventions: chondrocalcinosis, radio- graphic or histological calcification of fibrocarti- lage or hyaline cartilage; pseudogout, acute CPPD crystal-associated synovitis; andpyrophos- phate arthropathy (PA), structural arthropathy associated with intraarticular CPPD crystal dep- osition (with or without associated CC).
NORMAL POPULATIONS
A number of techniques have been used in an attempt to determine the frequency of CC in the general population. These include postmor- tem studies,4.‘2.17 examination of joint tissue removed at surgery,i8xr9 and radiographic sur-
188 Seminars in Arthritis and Rheumatism, Vol22, No 3 (December), 1992: pp 188-202
DISEASES ASSOCIATED WITH CPPD CRYSTALS 189
veys.7,11,13,20-44 1 n Nottingham, we have con- ducted two random radiographic surveys of patients, including (1) 138 patients attending general medical clinics and (2) 96 geriatric inpatients. In both studies, patients with inflam- matory joint disease, diabetes mellitus, current corticosteroid therapy, or neoplasia were ex- cluded. The findings of these surveys are shown in Table 1.
Comparisons between surveys are hampered by differences in radiographic technique,16,20- 22,45 patient selection differences,21~22~25 small sample size,7 and choice of joints examined.16~21~22 Despite these difficulties, there is broad agree- ment in the data.
CC occurs in approximately 5% to 10% of adults (7% in the Nottingham 138-patient sur- vey). CC shows a marked increase with age, with a prevalence as high as 30% in those older than 75 years7 (32% in the Nottingham inpatient survey). It is apparent therefore that age must be accounted for as a confounding factor in any study relating to CC.
Conflicting evidence is available concerning predisposition of gender. Most studies suggest a female preponderance, although there have been exceptions. Such contradictory results may arise from differences in sample selection; it has been suggested that males are more likely to have pseudogout. 21,37,46 However, the best pres- ently available data confirm a female preponder- ance,7,40,47 with an estimated relative risk of 1.33 (95% confidence interval [CI], 0.93 to 1.92).7
The proposed association between CC and OA has now been confirmed by a large popula- tion study.7 However, relative risk is small (1.52 [95% CI, 1.03 to 3.17]),7 and causality is uncer- tain.7,19 Local joint damage may also predispose
Table 1: Prevalence of Chondrocalcinosis of the Knees in the Two Nottingham Surveys
Age (vr)
Clinic Patients (n = 138)
Inpatients (n = 98)
Overall (n = 234)
l/8 (13%) 30/88 (34%) 31/96 (32%)
NOTE. Data represent number of patients with chondrocalcino-
sis/total number of patients sampled.
to local CPPD deposition,s-10 trauma appearing to induce premature CC in otherwise predis- posed individuals.8 The inverse relationship be- tween rheumatoid arthritis (RA) and CC sug- gests that factors other than joint damage per se, for example the OA process, are also impor- tant.42148
Knowledge of ethnic variation in predisposi- tion to CC is limited. Apart from an increased prevalence in Tunisian Muslims compared with Tunisian Jews,43 direct comparisons are lacking. Familial cases are well described,2,34,49-54 with HLA linkage demonstrated in some34,54 but not all pedigrees. 50-53 The role of genetic factors in sporadic CC is unknown.
PUTATIVE METABOLIC AND ENDOCRINE DISEASE ASSOCIATIONS
Hypomagnesemia
Numerous case reports provide convincing evidence for an association between chronic hypomagnesemia and CC.15,s5-65 Reported cases occur in young patients (mean age, 40 years; range, 15 to 59 years), often show florid polyar- titular CC, and are associated with multiple episodes of pseudogout. Interestingly, PA does not seem to be a feature. The two cases re- ported here, assessed in our unit, are similar to previously reported cases. Both were associated with renal wasting of magnesium, in one case with associated renal potassium wasting.
Case 1. A 50-year-old woman had a l-year history of recurrent episodes of pseudogout of the right knee, confirmed by identification of synovial fluid CPPD crystals. There was. no accompanying structural arthropathy, and radio- graphs showed florid, polyarticular CC. Investi- gation showed persistent hypomagnesemia (0.5 to 0.65 mmol/L, normal range, 0.7 to 1.0 mmol/L) and hypokalemia (2.4 to 3.1 mmol/L; normal range, 3.5 to 5.3 mmol/L). Results of screening for other metabolic or endocrine abnormalities were unremarkable, and there was no familial predisposition. Further studies were consistent with Bartter’s syndrome in show- ing renal leakage of magnesium and potassium, hyperreninism, and normal serum aldosterone levels.56 Her recurrent pseudogout, hypokale- mia, and hypomagnesemia all resolved with indomethacin, 75 mg daily, and oral magnesium supplements.
190 JONES ET AL
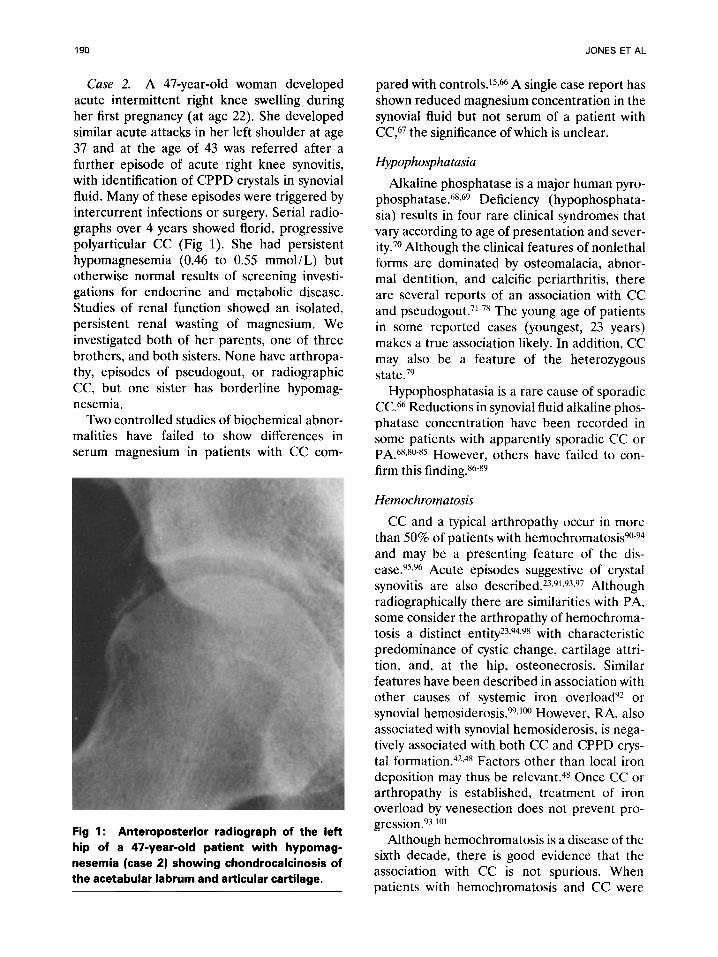
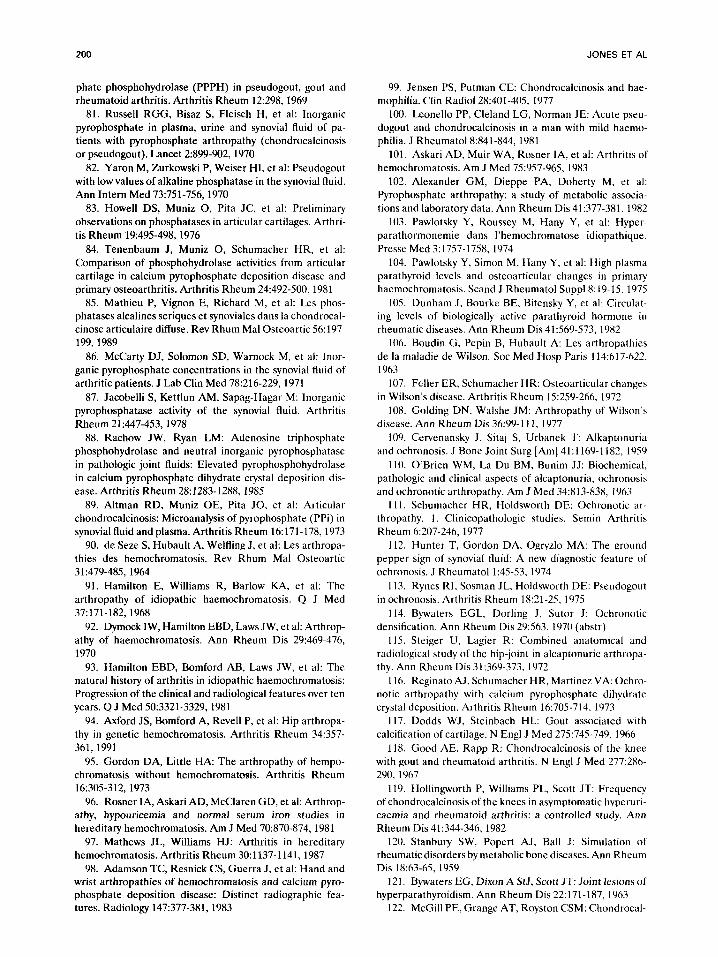
Case 2. A 47-year-old woman developed acute intermittent right knee swelling during her first pregnancy (at age 22). She developed similar acute attacks in her left shoulder at age 37 and at the age of 43 was referred after a further episode of acute right knee synovitis, with identification of CPPD crystals in synovial fluid. Many of these episodes were triggered by intercurrent infections or surgery. Serial radio- graphs over 4 years showed florid, progressive polyarticular CC (Fig 1). She had persistent hypomagnesemia (0.46 to 0.55 mmol/L) but otherwise normal results of screening investi- gations for endocrine and metabolic disease. Studies of renal function showed an isolated, persistent renal wasting of magnesium. We investigated both of her parents, one of three brothers, and both sisters. None have arthropa- thy, episodes of pseudogout, or radiographic CC, but one sister has borderline hypomag- nesemia.
Two controlled studies of biochemical abnor- malities have failed to show differences in serum magnesium in patients with CC com-
Fig 1: Anteroposterior radiograph of the left
hip of a 47-year-old patient with hypomag- nesemia (case 2) showing chondrocalcinosis of the acetabular labrum and articular cartilage.
pared with controls.‘5*66 A single case report has shown reduced magnesium concentration in the synovial fluid but not serum of a patient with CC6’ the significance of which is unclear.
Hypophosphatasia
Alkaline phosphatase is a major human pyro- phosphatase.68,69 Deficiency (hypophosphata- sia) results in four rare clinical syndromes that vary according to age of presentation and sever- ity.‘O Although the clinical features of nonlethal forms are dominated by osteomalacia, abnor- mal dentition, and calcific periarthritis, there are several reports of an association with CC and pseudogout.71-7R The young age of patients in some reported cases (youngest, 23 years) makes a true association likely. In addition, CC may also be a feature of the heterozygous state.79
Hypophosphatasia is a rare cause of sporadic CC.h6 Reductions in synovial fluid alkaline phos- phatase concentration have been recorded in some patients with apparently sporadic CC or PA.h8.80-85 However, others have failed to con- firm this finding.86-89
Hemochromatosis
CC and a typical arthropathy occur in more than 50% of patients with hemochromatosis90-94 and may be a presenting feature of the dis- ease.95,96 Acute episodes suggestive of crystal synovitis are also described.2”~91~9”~97 Although radiographically there are similarities with PA, some consider the arthropathy of hemochroma- tosis a distinct entity23,94s98 with characteristic predominance of cystic change, cartilage attri- tion, and, at the hip, osteonecrosis. Similar features have been described in association with other causes of systemic iron overload’? or synovial hemosiderosis. 99,100 However, RA, also associated with synovial hemosiderosis, is nega- tively associated with both CC and CPPD crys- tal formation.42,48 Factors other than local iron deposition may thus be relevant.4x Once CC or arthropathy is established, treatment of iron overload by venesection does not prevent pro- gression.9X,1D1
Although hemochromatosis is a disease of the sixth decade, there is good evidence that the association with CC is not spurious. When patients with hemochromatosis and CC were
DISEASES ASSOCIATED WITH CPPD CRYSTALS 191
compared with those with sporadic CC, a younger mean age and a marked male prepon- derance was noted.23 Similarly, a study compar- ing patients with known cases of hemochromato- sis, patients with hyperparathyroidism, and rheumatology outpatient controls (without overt arthropathy) found a similar overall prevalence of CC in the three groups but a younger age of onset in those with hemochromatosis.41 These data must be treated with caution because not all patients with hemochromatosis were studied by radiography, and the control population was highly selected. Overall, however, there is strong evidence that hemochromatosis is associated with premature CC.
With one exception,15 most surveys have failed to show an increased prevalence of hemochro- matosis among patients with sporadic CC,U,37,66JM suggesting that hemochromatosis is an unusual cause of sporadic CC. However, a few studies have found elevated levels of immunoreac- tivelo3J04 and bioactivelo5 parathyroid hormone (PTH) in hemochromatosis. The relevance of these findings to idiopathic and hemochroma- totic CC remains unclear.
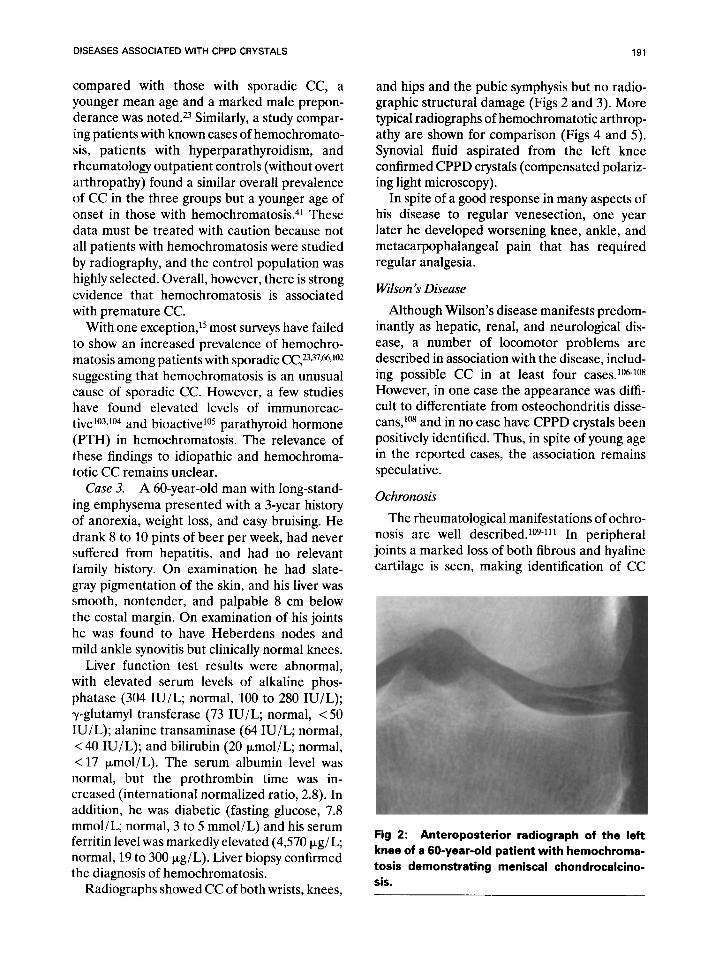
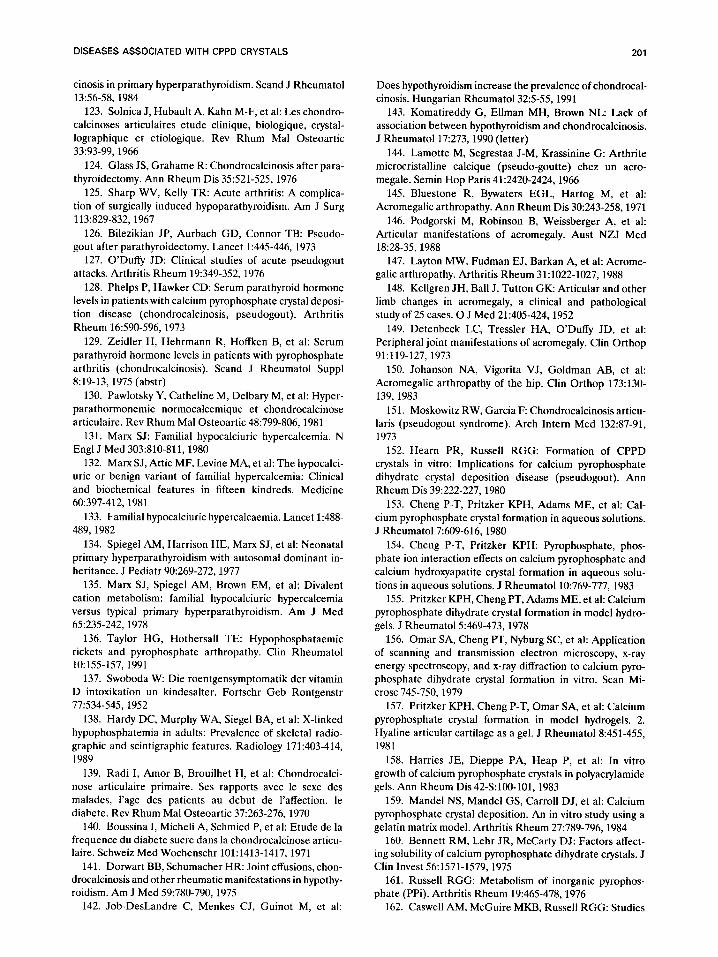
Case 3. A 60-year-old man with long-stand- ing emphysema presented with a 3-year history of anorexia, weight loss, and easy bruising. He drank 8 to 10 pints of beer per week, had never suffered from hepatitis, and had no relevant family history. On examination he had slate- gray pigmentation of the skin, and his liver was smooth, nontender, and palpable 8 cm below the costal margin. On examination of his joints he was found to have Heberdens nodes and mild ankle synovitis but clinically normal knees.
Liver function test results were abnormal, with elevated serum levels of alkaline phos- phatase (304 IU/L; normal, 100 to 280 IU/L); y-glutamyl transferase (73 IU/L, normal, <50 IU/L); alanine transaminase (64 III/L, normal, < 40 IU/L); and bilirubin (20 pmol/L, normal, < 17 umol/L). The serum albumin level was normal, but the prothrombin time was in- creased (international normalized ratio, 2.8). In addition, he was diabetic (fasting glucose, 7.8 mmol/L; normal, 3 to 5 mmol/L) and his serum ferritin level was markedly elevated (4,570 pg/L; normal, 19 to 300 kg/L). Liver biopsy confirmed the diagnosis of hemochromatosis.
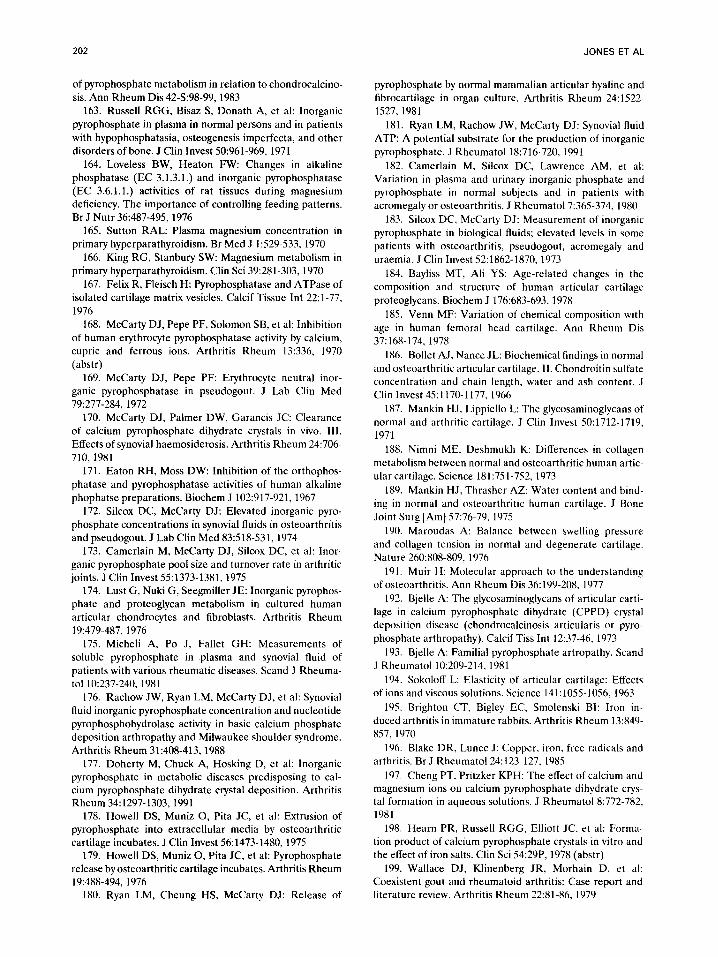
Radiographs showed CC of both wrists, knees,
and hips and the pubic symphysis but no radio- graphic structural damage (Figs 2 and 3). More typical radiographs of hemochromatotic arthrop- athy are shown for comparison (Figs 4 and 5). Synovial fluid aspirated from the left knee confirmed CPPD crystals (compensated polariz- ing light microscopy).
In spite of a good response in many aspects of his disease to regular venesection, one year later he developed worsening knee, ankle, and metacarpophalangeal pain that has required regular analgesia.
Wilson ‘s Disease
Although Wilson’s disease manifests predom- inantly as hepatic, renal, and neurological dis- ease, a number of locomotor problems are described in association with the disease, includ- ing possible CC in at least four cases.106-108 However, in one case the appearance was diffi- cult to differentiate from osteochondritis disse- cans,lo8 and in no case have CPPD crystals been positively identified. Thus, in spite of young age in the reported cases, the association remains speculative.
Ochronosis
The rheumatological manifestations of ochro- nosis are well described.109-111 In peripheral joints a marked loss of both fibrous and hyaline cartilage is seen, making identification of CC
Fig 2: Anteroposterior radiograph of the left knee of a 60-year-old patient with hemochroma-
tosis demonstrating meniscal chondrocalcino- sis.
192 JONES ET AL
include 84 patients with hyperuricemia, only 1 additional case of CC was noted.“” Analysis of these results cannot determine whether CC is associated with hyperuricemia per se or only with those patients who form crystals, ie, pa- tients with gout. The latter association may be attributable to promotion of the formation of one type of crystal by another (epitaxy), com- mon factors that promote general crystal forma- tion, or an indirect result of gout-associated joint damage.
Hyperparathyroidism
Although hyperparathyroidism is strongly as- sociated with both CC120,121 and pseudogout,” much of the evidence results from case series. Few studies have addressed the incidence of hyperparathyriodism, pseudogout, and CC in a controlled fashion.
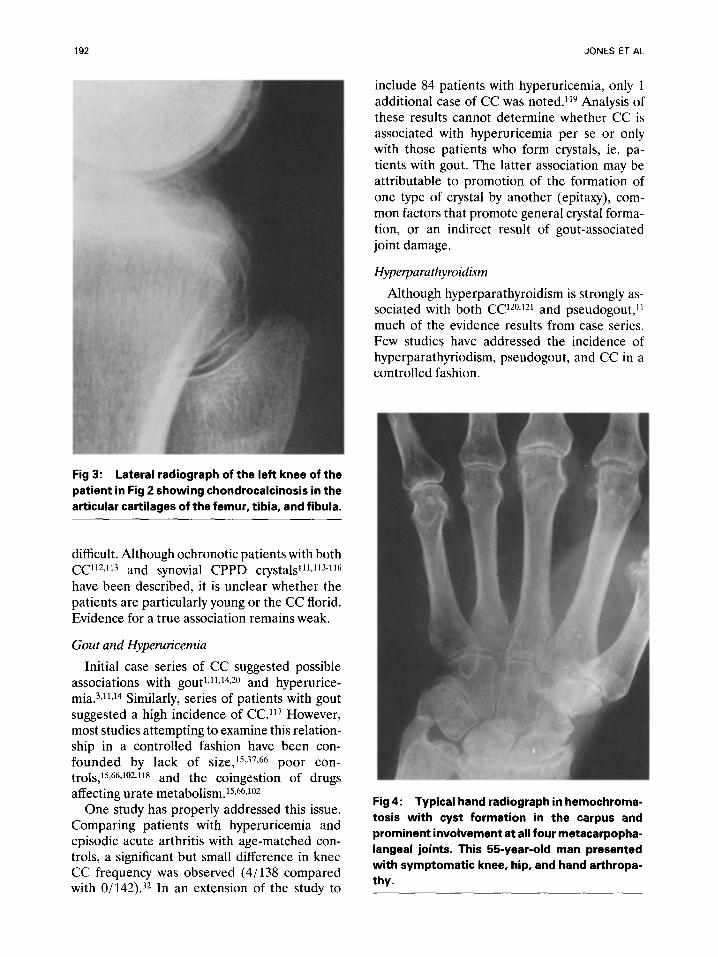
Fig 3: Lateral radiograph of the left knee of the
patient in Fig 2 showing chondrocalcinosis in the
articular cartilages of the femur, tibia, and fibula.
difficult. Although ochronotic patients with both CC”*,“” and synovial CPPD crystals111J1-7-116 have been described, it is unclear whether the patients are particularly young or the CC florid. Evidence for a true association remains weak.
Gout and Hyperuricemia
Initial case series of CC suggested possible associations with gout1J1J4,20 and hyperurice- mia.3J1J4 Similarly, series of patients with gout suggested a high incidence of CC.“’ However, most studies attempting to examine this relation- ship in a controlled fashion have been con- founded by lack of size,15,37,66 poor con- trols,15,66J02J18 and the coingestion of drugs affecting urate metabolism.15~66J02
One study has properly addressed this issue. Comparing patients with hyperuricemia and episodic acute arthritis with age-matched con- trols, a significant but small difference in knee CC frequency was observed (4/138 compared with O/142).32 In an extension of the study to
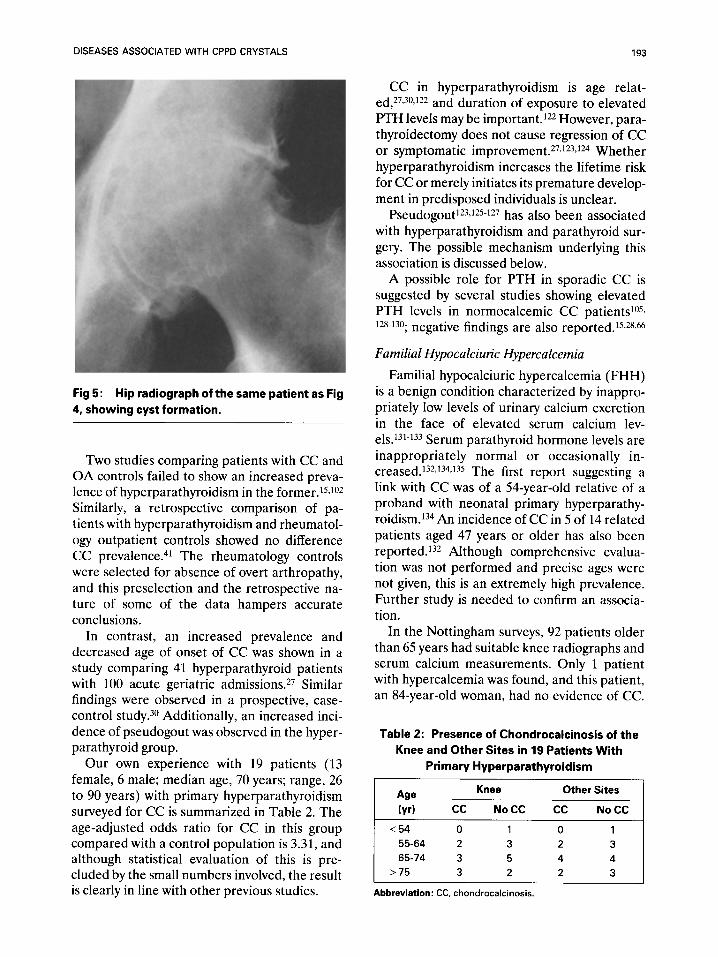
Fig 4: Typical hand radiograph in hemochroma-
tosis with cyst formation in the carpus and prominent involvement at all four metacarpopha-
langeal joints. This 5byear-old man presented with symptomatic knee, hip, and hand arthropa- thy.
DISEASES ASSOCIATED WITH CPPD CRYSTALS
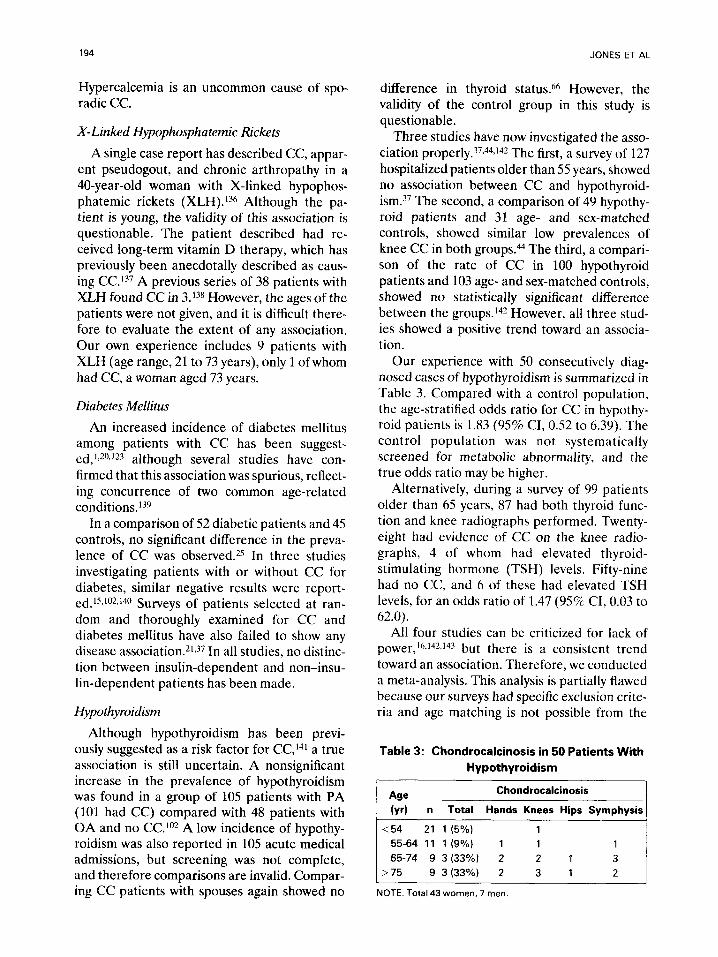
Fig 5: Hip radiograph of the same patient as Fig
4, showing cyst formation.
Two studies comparing patients with CC and OA controls failed to show an increased preva- lence of hyperparathyroidism in the former.15s102 Similarly, a retrospective comparison of pa- tients with hyperparathyroidism and rheumatol- ogy outpatient controls showed no difference CC prevalence.41 The rheumatology controls were selected for absence of overt arthropathy, and this preselection and the retrospective na- ture of some of the data hampers accurate conclusions.
In contrast, an increased prevalence and decreased age of onset of CC was shown in a study comparing 41 hyperparathyroid patients with 100 acute geriatric admissions.27 Similar findings were observed in a prospective, case- control study. 3o Additionally, an increased inci- dence of pseudogout was observed in the hyper- parathyroid group.
Our own experience with 19 patients (13 female, 6 male; median age, 70 years; range, 26 to 90 years) with primary hyperparathyroidism surveyed for CC is summarized in Table 2. The age-adjusted odds ratio for CC in this group compared with a control population is 3.31, and although statistical evaluation of this is pre- cluded by the small numbers involved, the result is clearly in line with other previous studies.
193
CC in hyperparathyroidism is age relat- ed,27,30J22 and duration of exposure to elevated PTH levels may be important.122 However, para- thyroidectomy does not cause regression of CC or symptomatic improvement.27J23J24 Whether hyperparathyroidism increases the lifetime risk for CC or merely initiates its premature develop- ment in predisposed individuals is unclear.
Pseudogout123J25-127 has also been associated with hyperparathyroidism and parathyroid sur- gery. The possible mechanism underlying this association is discussed below.
A possible role for PTH in sporadic CC is suggested by several studies showing elevated PTH levels in normocalcemic CC patientsio5, 128-130; negative findings are also reported.15J8s66
Familial Hypocalciutic Hypercalcemia
Familial hypocalciuric hypercalcemia (FHH) is a benign condition characterized by inappro- priately low levels of urinary calcium excretion in the face of elevated serum calcium lev- e1s.131-133 Serum parathyroid hormone levels are inappropriately normal or occasionally in- creased.132,134J35 The first report suggesting a link with CC was of a 54-year-old relative of a proband with neonatal primary hyperparathy- roidism.134 An incidence of CC in 5 of 14 related patients aged 47 years or older has also been reported. 132 Although comprehensive evalua- tion was not performed and precise ages were not given, this is an extremely high prevalence. Further study is needed to confirm an associa- tion.
In the Nottingham surveys, 92 patients older than 65 years had suitable knee radiographs and serum calcium measurements. Only 1 patient with hypercalcemia was found, and this patient, an 84-year-old woman, had no evidence of CC.
Table 2: Presence of Chondrocalcinosis of the
Knee and Other Sites in 19 Patients With
Primary Hyperparathyroidism
Age Knee Other Sites
WI CC NoCC CC No CC
<54 0 1 0 1
55-64 2 3 2 3
65-74 3 5 4 4
>75 3 2 2 3
Abbreviation: CC, chondrocalcinosis.
194
Hypercalcemia is an uncommon cause of spo- radic CC.
X-Linked Hypophosphatemic Rickets
A single case report has described CC, appar- ent pseudogout, and chronic arthropathy in a 40-year-old woman with X-linked hypophos- phatemic rickets (XLH).136 Although the pa- tient is young, the validity of this association is questionable. The patient described had re- ceived long-term vitamin D therapy, which has previously been anecdotally described as caus- ing CC.“’ A previous series of 38 patients with XLH found CC in 3.138 However, the ages of the patients were not given, and it is difficult there- fore to evaluate the extent of any association. Our own experience includes 9 patients with XLH (age range, 21 to 73 years), only 1 of whom had CC, a woman aged 73 years.
Diabetes Mellitus
An increased incidence of diabetes mellitus among patients with CC has been suggest- ed,1,20J23 although several studies have con- firmed that this association was spurious, reflect- ing concurrence of two common age-related conditions.13y
In a comparison of 52 diabetic patients and 45 controls, no significant difference in the preva- lence of CC was observed.25 In three studies investigating patients with or without CC for diabetes, similar negative results were report- ed.15J02J40 Surveys of patients selected at ran- dom and thoroughly examined for CC and diabetes mellitus have also failed to show any disease association.21s37 In all studies, no distinc- tion between insulin-dependent and non-insu- lin-dependent patients has been made.
Hypothyroidism
Although hypothyroidism has been previ- ously suggested as a risk factor for CC,14’ a true association is still uncertain. A nonsignificant increase in the prevalence of hypothyroidism was found in a group of 105 patients with PA (101 had CC) compared with 48 patients with OA and no CC.‘02 A low incidence of hypothy- roidism was also reported in 105 acute medical admissions, but screening was not complete, and therefore comparisons are invalid. Compar- ing CC patients with spouses again showed no
JONES ET AL
difference in thyroid status.66 However, the validity of the control group in this study is questionable.
Three studies have now investigated the asso- ciation properly.37,44J42 The first, a survey of 127 hospitalized patients older than 55 years, showed no association between CC and hypothyroid- ism.37 The second, a comparison of 49 hypothy- roid patients and 31 age- and sex-matched controls, showed similar low prevalences of knee CC in both groups .44 The third, a compari- son of the rate of CC in 100 hypothyroid patients and 103 age- and sex-matched controls, showed no statistically significant difference between the groups. ‘42 However, all three stud- ies showed a positive trend toward an associa- tion.
Our experience with 50 consecutively diag- nosed cases of hypothyroidism is summarized in Table 3. Compared with a control population, the age-stratified odds ratio for CC in hypothy- roid patients is 1.83 (95% CI, 0.52 to 6.39). The control population was not systematically screened for metabolic abnormality, and the true odds ratio may be higher.
Alternatively, during a survey of 99 patients older than 65 years, 87 had both thyroid func- tion and knee radiographs performed. Twenty- eight had evidence of CC on the knee radio- graphs, 4 of whom had elevated thyroid- stimulating hormone (TSH) levels. Fifty-nine had no CC, and 6 of these had elevated TSH levels, for an odds ratio of 1.47 (95% CI, 0.03 to 62.0).
All four studies can be criticized for lack of power,‘hJ42J43 but there is a consistent trend toward an association. Therefore, we conducted a meta-analysis. This analysis is partially flawed because our surveys had specific exclusion crite- ria and age matching is not possible from the
Table 3: Chondrocalcinosis in 50 Patients With
Hypothyroidism
be Chondrocalcinosis
(vr) n Total Hands Knees Hips Symphysis
<54 21 1 (5%) 1
55-64 11 1(9%) 1 1 1
65-74 9 3 (33%) 2 2 1 3
>75 9 3 (33%) 2 3 1 2
NOTE. Total 43 women, 7 men

DISEASES ASSOCIATED WITH CPPD CRYSTALS 195
published data from the Australian survey.37 However, with these caveats, the calculated odds ratio from the four surveys is 1.94 (95% CI, 1.06 to 3.53).
Combining two studies in which there was random testing of an elderly population (ours and that of Gordon et a13’) produces an odds ratio of 1.96 (95% CI, 0.40 to 9.72). A significant but small association between the two condi- tions seems likely.
Acromegaly
In 1966, a 53-year-old male acromegalic with recurrent attacks of apparent pseudogout of the right knee was reported.lM Crystals were seen in synovial fluid but were not positively identified. Although other case series of acromegalic ar- thropathy have commented on CC,145-147 the evidence for an association is slight. Five sur- veys totaling 314 acromegalics comment on only 2 cases of CC,146-150 neither of which is described in sufficient detail to allow comment on age of onset. Conversely, only one case of acromegaly has been noted in case series of CC.15’ There- fore, an association seems unlikely.
MECHANISMS OF PREDISPOSITION
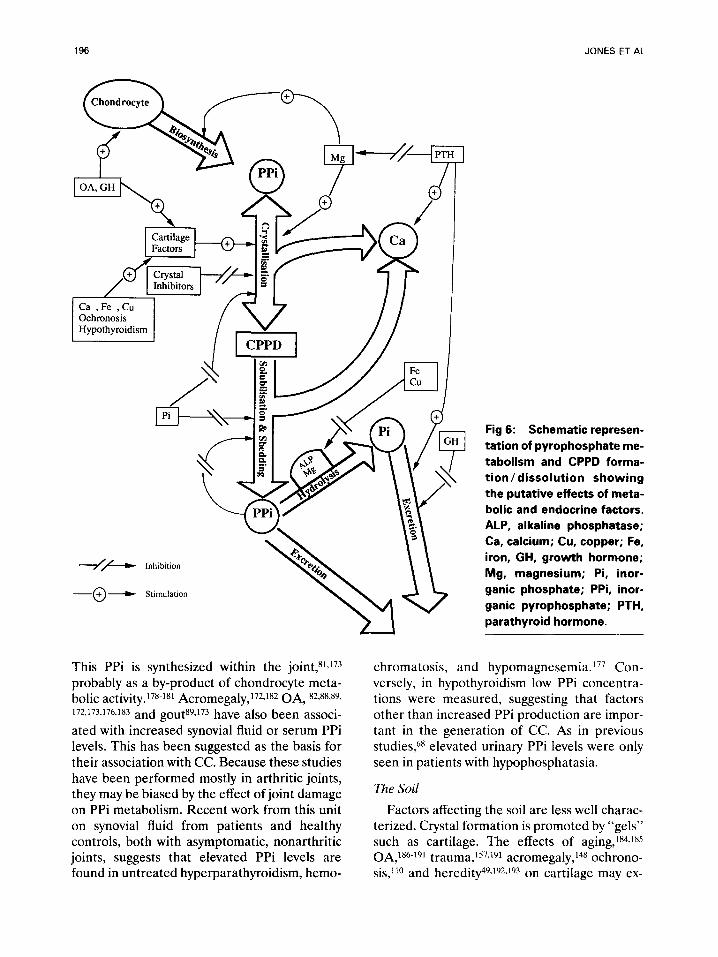
Various mechanisms have been postulated to explain the association between metabolic and endocrine diseases and CC, as summarized in Fig 6. CPPD crystal formation is difficult to study in vivo, and knowledge of parameters affecting it derive from in vitro work.ls2-ls9 Several parameters appear to be important: the “seed” (the calcium and inorganic pyrophos- phate (PPi) that are available for combination) and the “soil” (the matrix within which the crystals form as well as tissue factors that promote or inhibit this crystal formation).
The Seed
Elevation of either calcium or PPi concentra- tion could sufficiently increase the ionic product and thus promote CPPD crystal formation and growth. Calcium moves easily into and out of cartilage,15’ and extracellular free calcium con- centrations thus influence cartilage concentra- tion. Calcium concentration is tightly controlled by PTH levels, and elevation of calcium concen-
tration in hyperparathyroidism is an obvious mechanism to explain predisposition to CPPD formation in this condition. Once CPPD crys- tals are formed within cartilage, hypocalcemia would promote their solubilization and hence shedding into the synovial space. This sequence may explain the phenomenon of postparathy- roidectomy pseudogout.
PPi is a by-product of numerous biosynthetic reactions, particularly those using nucleoside triphosphates.161J’j2 PPi concentrations depend not only on rate of synthesis, but also on rate of hydrolyzation by pyrophosphatases, including alkaline phosphatase. 161 Absence of the latter in hypophosphatasia is associated with increased urinary and blood concentrations of PPi,68J63 providing a ready explanation for predisposition to CC in this condition. Relative reductions in synovial fluid alkaline phosphatase levels have been shown in some patients with sporadic CPPD,so-s5 suggesting that localized reductions in pyrophosphatase activity may be relevant in sporadic CPPD crystal formation.
Pyrophosphatases, including alkaline phos- phatase, are magnesium dependent. Hypomag- nesemia could thus be expected to promote CPPD formation via inhibition of PPi hydroly- sis, thus resulting in elevated PPi concentra- tions. In addition, hypomagnesemia may reduce total pyrophosphatase activity.164 Calcium and magnesium metabolism are closely interrelated, and the hypomagnesemia that may occur in hyperparathyroidism provides a further mecha- nism promoting CPPD formation in this con- text 165,166
Interestingly, FHH is associated with hyper- magnesemia.135 Although at first this appears paradoxical, high concentrations of magne- sium16’ and other divalent cations, including calcium, ferrous iron, and copper,83,84J68J69 in- hibit intracellular pyrophosphatases and thus impair CPPD crystal clearance.170
Orthophosphate (P04) has many effects on CPPD formation, including elevation of PPi levels by competitive inhibition of pyrophos- phatases,87J67J71 decreased solubility of formed CPPD crystalsg6 and inhibition of CPPD crystal growth.154 It is thus difficult to explain the possible association with XLH.
Elevated synovial fluid PPi levels occur in pa- tients with CPPD crystal deposition.81~86~89J72-177
196 JONES ET AL
-//L-) Inhibition
-_O-+ Stimulation
This PPi is synthesized within the joint,81J73 probably as a by-product of chondrocyte meta- bolic activity.178-181 Acromegaly,172~182 OA, 82,88,89, 172,173~176~183 and gout89,173 have also been associ- ated with increased synovial fluid or serum PPi levels. This has been suggested as the basis for their association with CC. Because these studies have been performed mostly in arthritic joints, they may be biased by the effect of joint damage on PPi metabolism. Recent work from this unit on synovial fluid from patients and healthy controls, both with asymptomatic, nonarthritic joints, suggests that elevated PPi levels are found in untreated hyperparathyroidism, hemo-
Fig 6: Schematic represen-
tation of pyrophosphate me-
tabolism and CPPD forma-
tion/dissolution showing
the putative effects of meta-
bolic and endocrine factors.
ALP, alkaline phosphatase;
Ca, calcium; Cu, copper; Fe,
iron, GH, growth hormone;
Mg, magnesium; Pi, inor-
ganic phosphate; PPi, inor-
ganic pyrophosphate; PTH,
parathyroid hormone.
chromatosis, and hypomagnesemia.“’ Con- versely, in hypothyroidism low PPi concentra- tions were measured, suggesting that factors other than increased PPi production are impor- tant in the generation of CC. As in previous studies6s elevated urinary PPi levels were only seen in patients with hypophosphatasia.
The Soil
Factors affecting the soil are less well charac- terized. Crystal formation is promoted by “gels” such as cartilage. The effects of aging,lS4.rS5 0A,186-‘91 trauma,‘57~191 acromegaly,148 ochrono- sis,llo and heredity49~192~193 on cartilage may ex-
DISEASES ASSOCIATED WITH CPPD CRYSTALS 197
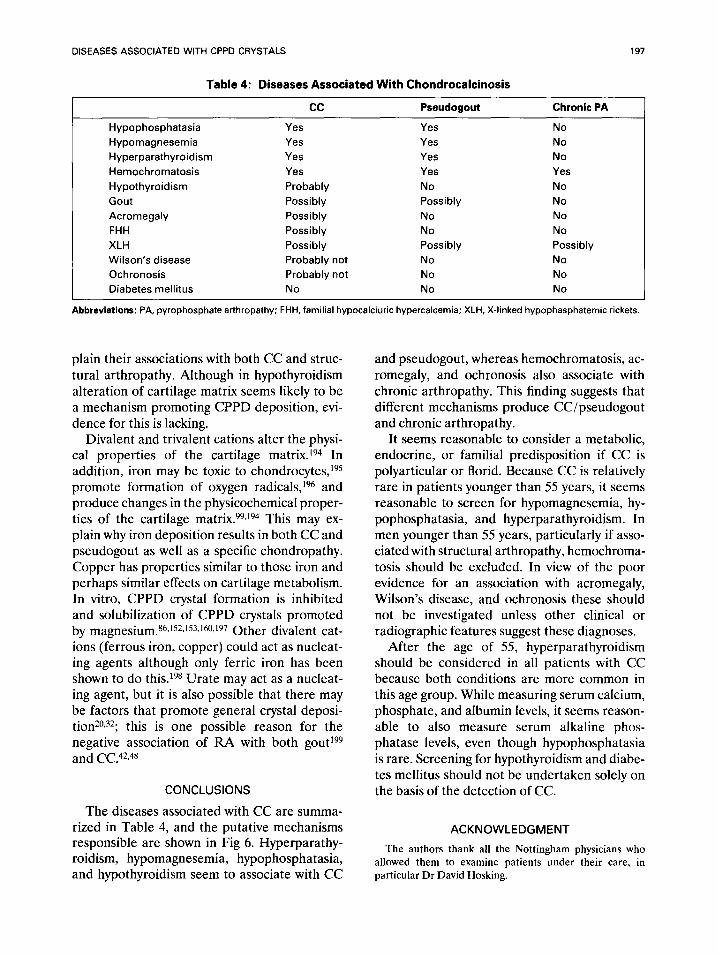
Table 4: Diseases Associated With Chondrocalcinosis
cc Pseudogout Chronic PA
Hypophosphatasia Yes Yes No
Hypomagnesemia Yes Yes No
Hyperparathyroidism Yes Yes No
Hemochromatosis Yes Yes Yes
Hypothyroidism Probably No No
Gout Possibly Possibly No
Acromegaly Possibly No No
FHH Possibly No No
XLH Possibly Possibly Possibly
Wilson’s disease Probably not No No
Ochronosis Probably not No No
Diabetes mellitus No No No
Abbreviations: PA, pyrophosphate arthropathy; FHH, familial hypocalciuric hypercalcemia; XLH, X-linked hypophasphatemic rickets.
plain their associations with both CC and struc- and pseudogout, whereas hemochromatosis, ac- tural arthropathy. Although in hypothyroidism romegaly, and ochronosis also associate with alteration of cartilage matrix seems likely to be chronic arthropathy. This finding suggests that a mechanism promoting CPPD deposition, evi- different mechanisms produce CC/pseudogout dence for this is lacking. and chronic arthropathy.
Divalent and trivalent cations alter the physi- cal properties of the cartilage matrix.194 In addition, iron may be toxic to chondrocytes,ig5 promote formation of oxygen radicals,196 and produce changes in the physicochemical proper- ties of the cartilage matrix.99J94 This may ex- plain why iron deposition results in both CC and pseudogout as well as a specific chondropathy. Copper has properties similar to those iron and perhaps similar effects on cartilage metabolism. In vitro, CPPD crystal formation is inhibited and solubilization of CPPD crystals promoted by magnesium.86J52J53J@J197 Other divalent cat- ions (ferrous iron, copper) could act as nucleat- ing agents although only ferric iron has been shown to do this.19* Urate may act as a nucleat- ing agent, but it is also possible that there may be factors that promote general crystal deposi- tion2092; this is one possible reason for the negative association of FM with both gout*99 and CC.42,48
It seems reasonable to consider a metabolic, endocrine, or familial predisposition if CC is polyarticular or florid. Because CC is relatively rare in patients younger than 55 years, it seems reasonable to screen for hypomagnesemia, hy- pophosphatasia, and hyperparathyroidism. In men younger than 55 years, particularly if asso- ciated with structural arthropathy, hemochroma- tosis should be excluded. In view of the poor evidence for an association with acromegaly, Wilson’s disease, and ochronosis these should not be investigated unless other clinical or radiographic features suggest these diagnoses.
CONCLUSIONS
After the age of 55, hyperparathyroidism should be considered in all patients with CC because both conditions are more common in this age group. While measuring serum calcium, phosphate, and albumin levels, it seems reason- able to also measure serum alkaline phos- phatase levels, even though hypophosphatasia is rare. Screening for hypothyroidism and diabe- tes mellitus should not be undertaken solely on the basis of the detection of CC.
The diseases associated with CC are summa- rized in Table 4, and the putative mechanisms responsible are shown in Fig 6. Hyperparathy- roidism, hypomagnesemia, hypophosphatasia, and hypothyroidism seem to associate with CC
ACKNOWLEDGMENT
The authors thank all the Nottingham physicians who
allowed them to examine patients under their care, in
particular Dr David Hosking.
198 JONES ET AL
REFERENCES
1. McCarty DJ, Kohn NN, Faires JS: The significance of
calcium phosphate crystals in the synovial fluid of arthritic
patients: the “pseudogout syndrome.” 1. Clinical aspects.
Ann Intern Med 56:711-737,1962
2. Zitnan D, Sitaj S, Valsik J, et al: Chondrocalcinosis
articularis. Ann Rheum Dis 22:142-170, 1963
3. McCarty DJ, Haskin ME: The roentgenographic as-
pects of pseudogout (articular chondrocalcinosis). AJR
90:1248-1257,1963
4. McCarty DJ, Hogan JM, Gatter RA, et al: Studies on
pathological calcifications in human cartilage. J Bone Joint
Surg [Am] 48:309-324, 1966
5. Doherty M, Dieppe P: Clinical aspects of calcium
pyrophosphate dihydrate crystal deposition. Rheum Dis
Clin North Am 14:305-414,1988
6. Mandel N, Mandel G: Calcium pyrophosphate crystal
deposition in model systems. Rheum Dis Clin North Am
14:321-340,1988
7. Felson DT, Anderson JJ, Naimark A, et al: The
prevalence of chondrocalcinosis in the elderly and its
association with knee osteoarthritis: The Framingham study.
J Rheumatol 16:1241-1245, 1989
8. Doherty M, Watt I, Dieppe PA: Localised chondrocal-
cinosis in post-meniscectomy knees. Lancet 1:1207-1210,
1982
9. De Lange EE, Keats TE: Localised chondrocalcinosis
in traumatized joints. Skeletal Radio1 14:249-256, 1985
10. Linden B, Nilssen BE: Chondrocalcinosis following
osteochondritis dissecans in the femur condyles. Clin Or-
thop 130:223-227, 1978
11. Currey HLF, Key JJ, Mason RM, et al: Significance
of radiological calcification of joint cartilage. Ann Rheum
Dis 25:295-306,1966
12. Mitrovic DR, Stankovic A, Iriarte-Borda 0, et al:
The prevalence of chondrocalcinosis in the human knee
joint. An autopsy survey. J Rheumatol 15:633-641,1988
13. Bother J, Mankin HJ, Berk RN, et al: Prevalence of
calcified meniscal cartilage in elderly persons. N Engl J Med
272:1093-1097,1965
14. Moskowitz RW, Katz D: Chondrocalcinosis and chon-
drocalsynovitis (pseudogout syndrome). Am J Med 43:322-
334,1967
15. McCarty DJ, Silcox DC, Coe F, et al: Diseases
associated with calcium pyrophosphate dihydrate crystal
deposition. a controlled study. Am J Med 56:704-714,1974
16. Smith MD: Lack of association between hypothyroid-
ism and chondrocalcinosis. J Rheumatol 17:272-273,199O
17. Lagier R, Baud C: Pathologic calcifications of the
locomotor system, in Milhaud R, Owen M, Blackwood HJJ
(eds): Rapports et communications au4symposium Euro-
pean des tissues calcifies, Bordeaux 1967. Paris, France,
Sedes, 1968, pp 109-113
18. Pritzker KPH, Renlund RC, Cheng PT: Which comes
first: Crystals or osteoarthritis? A study of surgically re-
moved femoral heads. J Rheumatol 10:38-39,1983 (suppl9)
19. Sokoloff L, Varma AA: Chondrocalcinosis in surgi-
cally resected joints. Arthritis Rheum 31:750-756, 1988
20. Serre H, Simon L, Sany J: Apropos de la chondrocal- cinose articulaire diffuse. Rev Rhum Ma1 Osteoartic 32:425-
430,1965
21. Ellman MH, Levin B: Chondrocalcinosis in elderly
persons. Arthritis Rheum 18:43-47, 1975
22. Trentham DE, Masi AT, Hamm RL: Roentgeno-
graphic prevalence of chondrocalcinosis. Arthritis Rheum
18:627-628, 1975
23. Atkins CJ, McIvor J, Smith PM, et al: Chondrocalci-
nosis and arthropathy: studies in haemochromatosis and in
idiopathic chondrocalcinosis. Q J Med 39:71-82,197O
24. Cabanel G, Phelip X, Verdier J-M, et al: Frequence
des calcifications meniscales et leur signification pathol-
ogique. Rhumatologie 22:255-262, 1970
25. Schmied P, van Rossum P, Gabay R, et al: Etude
radiologique sur la frequence de I’association autre la
condrocalcinose articulaire et le diabete. Schweiz Med
Wochenschr 101:272-276,197l
26. Delauche M-C, Stehle B, Cassou B, et al: Frequence
de la chondrocalcinose radiologique apres 80 ans. Rev
Rhum Ma1 Osteoartic 44:555-557. 1977
27. Pritchard MH, Jessop JD: Chondrocalcinosis in pri-
mary hyperparathyroidism. Ann Rheum Dis 36:146-151.
1977
28. Leonard A, Solnica J, Cauvin M, et al: La chondrocal-
cinose: Etude de sa frequence radiologique et des ses
rapports avec l’arthrose: Etude du taux de la parathormone.
Rev Rhum Mal Osteoartic 44559-564, 1977
29. Memin Y, Monville CI, Ryckewaert A: La chondrocal-
cinose articulaire apres 80 ans. Rev Rhum Ma1 Osteoartic
45:77-82, 1978
30. Rynes RI, Merzig EG: Calcium pyrophosphate crys-
tal deposition disease and hyperparathyroidism: A con-
trolled prospective study. J Rheumatol5:460-468,1978
31. Glimet T, Masse JP, Ryckewaert A: Etude ra-
diologique des genoux indolores des 50 femmes de plus de
65 ans. Rev Rhum Mal Osteoartic 46589-592, 1979
32. Stockman A, Darlington LG, Scott JT: Frequency of
chondrocalcinosis of the knee and avascular necrosis of the
femoral heads in gout: A controlled study. Ann Rheum Dis
39:7-11. 1980
33. Ellman MH, Brown NL, Levin B: Narrowing of knee
joint space in patients with pseudogout. Ann Rheum Dis
40:34-36, 1981
34. Megard M, Vignon E, Arcot M, et al: Etude chondro-
calcinose articulaire dans une population de 200 viellards.
Lyon Med 245:365-370, 1981
35. Megard M, Andre-Fouet E: La chondrocalcinose
chez les personnes ages. Rhumatologie 35:249-252, 1983
36. Wilkins E, Dieppe PA, Maddison P: Osteoarthritis
and articular chondrocalcinosis in the elderly. Ann Rheum
Dis 42:280-284, 1983
37. Gordon TP, Smith M. Ebert B, et al: Articular
chondrocalcinosis in a hospital population: An Australian
experience. Aust NZ J Med 14:655-659, 1984
38. Hochberg MC: Chondrocalcinosis articularis (CCA)
of the knee: Prevalence and association with osteoarthritis
(OA) of the knee. Arthritis Rheum 27:S-49, 1984 (suppl;
abstr)
39. Menkes CJ, Decraemere W, Postel M, et al: Chondro-
calcinosis and rapid destruction of the hip. J Rheumatol
12:130-133, 1985
40. Bergstrom G. Bjelle A, Sundh V, et al: Joint disorders
DISEASES ASSOCIATED WITH CPPD CRYSTALS 199
at ages 70, 75, and 79 years-A cross-sectional comparison. Br J Rheumatol25:333-341, 1986
41. Huaux JP, Geubel A, Koch MC, et al: The arthritis of hemochromatosis. A review of 25 cases with special refer- ence to chondrocalcinosis, and a comparison with patients with primary hyperparathyroidism and controls. Clin Rheu- matoI5:317-324.1986
42. Brasseur J-P, Huaux J-P, Devogelaer J-P: Articular chondrocalcinosis in seropositive rheumatoid arthritis. Com- parison with a control group. J Rheumatol 14:40-41, 1987
43. Hamza M, Elleach M, Sellami S, et al: Frequence de la chondrocalcinose articulaire dans deux groupes eth- niques. Press Med 18:493-494,1989
44. Komatireddy GR, Ellman MH, Brown NL: Lack of association between hypothyroidism and chondrocalcinosis. J Rheumatol 16:807-808, 1989
45. Parlee DE, Freundlich IM, McCarty DJ: A compara- tive study of roentgenographic techniques for detection of calcium pyrophosphate dihydrate deposits in human carti- lage. AJR 99:688-694, 1967
46. Dieppe PA, Alexander CJM, Jones HE, et al: Pyro- phosphate arthropathy: A clinical and radiological study of 105 cases. Ann Rheum Dis 41:371-376,1982
47. Bergstrom G, Bjelle A, Sorenson LB, et al: Preva- lence of rheumatoid arthritis, osteoarthritis, chondrocalcino- sis and gouty arthritis at age 79. J Rheumatol 13:527-534, 1986
48. Doherty M, Dieppe PA, Watt I: Low incidence of calcium pyrophosphate dihydrate crystal deposition in rheu- matoid arthritis with modification of radiographic features in coexistent disease. Arthritis Rheum 27:1002-1009,1984
49. Bjelle AO: Morphological study of articular cartilage in pyrophosphate arthropathy (chondrocalcinosis articu- Iaris or calcium pyrophosphate dihydrate crystal deposition disease). Ann Rheum Dis 31:449-456,1972
50. Gaucher A, Faure G, Netter P, et al: Hereditary diffuse articular chondrocalcinosis. Stand J Rheumatol 61217-221, 1977
51. Gaudreau A, Camerlain M, Pibarot M, et al: Familial articular chondrocalcinosis in Quebec. Arthritis Rheum 24:611-615, 1981
52. Richardson BC, Chafetz NI, Ferrell LD, et al: Hered- itary chondrocalcinosis in a Mexican-American family. Ar- thritis Rheum 26:1387-1396, 1983
53. Rodriguez-Valverde V, Zuniga M, Casaneuva B, et al: Hereditary articular chondrocalcinosis. Am J Med 84:101- 106,198s
54. Nyulassy S, Stefanovic J, Sitaj S, et al: HL-A system in articular chondrocalcinosis. Arthritis Rheum 19:391-393, 1976
55. Runeberg L, Collan Y, Jokinen EJ, et al: Hypomagne- saemia due to renal disease of unknown etiology. Am J Med 59:873-881, 1975
56. Schwarz HA, Weidmann P, Messerli FH, et al: Increased levels of renal venous and peripheral prostaglan- din E-like activity in Bartter’s syndrome. Miner Electrolyte Metab 1:288-294,1978
57. Bauer FM, Glasson PH, Vallotton MB, et al: Syn- drome de Bartter, chondrocalcinose at hypomagnesemie. Schweiz Med Wochenschr 109:1251-1256,1979
58. Goulon M, Raphael JC, de Rohan P: Syndrome de Bartter et chondrocalcinose. Presse Med 9:1291-1295, 1980
59. Hurault de Ligny B, Baumelou A, Bardin T, et al: Chondrocalcinose au tours du syndrome de Bartter. Presse Med 10:107,1981
60. Milazzo SC, Cleland LG, Ahern MJ: Calcium pyro- phosphate dihydrate deposition disease and familial hypo- magnesaemia. J Rheumatol8:767-771, 1981
61. Evans RA, Carter JN, George CRP: The congenital magnesium losing kidney. Q J Med 50:39-52, 1981
62. De Bruyne J, Chappel R, Mortier G, et al: Bartter’s syndrome en chondrocalcinose. J Belge Med Phys Rehabil 237-46, 1982
63. Resnick D, Rausch JM: Hypomagnesemia with chon- drocalcinosis. Can Assoc Radio1 J 35:214-216,1984
64. Mayoux-Benhamou MA, Clerc D, Ganeval D, et al: Chondrocalcinose articulaire et hypomagnesemie d’origine renale. Rev Rhum Ma1 Osteoartic 52:545-548, 1985
65. Salvarani C, Rossi F, Macchioni PL, et al: Bartter’s syndrome and chondrocalcinosis: a possible role for hypo- magnesemia in the deposition of calcium pyrophosphate dihydrate (CPPD) crystals. Clin Exp Rheumatol 7:415-420, 1989
66. Ellman MH, Brown NI, Porat AP: Laboratory investi- gations in pseudogout patients and controls. J Rheumatol 7:77-81, 1980
67. Cohen L, Kitzes R: Pseudogout with low values of magnesium and low alkaline phosphatase activity in synovial fluid. Isr J Med Sci 19:838-840, 1983
68. Russell RGG: Excretion of inorganic pyrophosphate in hypophosphatasia. Lancet 2:461-464,1965
69. Eaton RH, Moss DW: Alkaline orthophosphatase and inorganic pyrophosphatase activities in human serum. Nature 214:842-843, 1967
70. Whyte MP: Hypophosphatasia, in Striver CR, Beau- det AL, Sly WS, et al (eds): The Metabolic Basis of Inherited Disease, vol 2 (ed 6). New York, NY, McGraw- Hill, 1989, pp 2843-2856
71. Birtwell WM, Riggs BL, Peterson LFA, et al: Hy- pophosphatasia in an adult. Arch Intern Med 120:90-93, 1967
72. O’DutTy JP: Hypophosphatasia associated with cal- cium pyrophosphate dihydrate deposits in cartilage. Arthri- tis Rheum 13:381-388, 1970
73. Paologgi JB, Job C, Durignon M, et al: Hypophophata- sie de I’adulte a manifestations cliniques tardives. Presse Med 7:4285-4289,1978
74. Lindh J, Nylen 0: Hypofosfatasi hos en vuxen. Lakartidningen 77:131-132,198O
75. Eade AWT, Swannell AJ, Williamson N: Pyrophos- phate arthropathy in hypophosphatasia. Ann Rheum Dis 40:164-170, 1981
76. Whyte MP, Murphy WA, Fallon MD: Adult hy- pophosphatasia with chondrocalcinosis and arthropathy. Am J Med 72:631-641, 1982
77. Pinquier JL, Awada H, Delfieu F, et al: Chondrocal- cinose isolee relevant une hypophosphatasie de l’adulte. Rev Rhum Ma1 Osteoartic 54:501-504, 1987
78. Chuck AJ, Pattrick MG, Hamilton E, et al: Crystal deposition in hypophosphatasia: a reappraisal. Ann Rheum Dis 48:571-576, 1989
79. Macfarlane JD, Kroon HM, Cats A: Ectopic calcifica- tion in hypophosphatasia. Eur J Radio1 6:228-230, 1986
80. Good AE, Starkweather WH: Synovial fluid pyrophos-
200 JONES ET AL
phate phosphohydrolase (PPPH) in pseudogout, gout and
rheumatoid arthritis. Arthritis Rheum 12:298, 1969
81. Russell RGG, Bisaz S, Fleisch H, et al: Inorganic
pyrophosphate in plasma, urine and synovial fluid of pa-
tients with pyrophosphate arthropathy (chondrocalcinosis
or pseudogout). Lancet 2:899-902,197O
82. Yaron M, Zurkowski P, Weiser HI, et al: Pseudogout
with low values of alkaline phosphatase in the synovial fluid.
Ann Intern Med 73:751-756,197O
83. Howell DS, Muniz 0, Pita JC, et al: Preliminary
observations on phosphatases in articular cartilages. Arthri-
tis Rheum 19:495-498,1976
84. Tenenbaum J, Muniz 0, Schumacher HR, et al:
Comparison of phosphohydrolase activities from articular
cartilage in calcium pyrophosphate deposition disease and
primary osteoarthritis. Arthritis Rheum 24:492-500, 1981
85. Mathieu P, Vignon E, Richard M, et al: Les phos-
phatases alcalines seriques et synoviales dans la chondrocal-
cinose articulaire diffuse. Rev Rhum Mal Osteoartic 56:197-
199,1989
86. McCarty DJ, Solomon SD, Warnock M, et al: Inor-
ganic pyrophosphate concentrations in the synovial fluid of
arthritic patients. J Lab Clin Med 78:216-229, 1971
87. Jacobelli S, Kettlun AM, Sapag-Hagar M: Inorganic
pyrophosphatase activity of the synovial fluid. Arthritis
Rheum 211447-453, 1978
88. Rachow JW, Ryan LM: Adenosine triphosphate
phosphohydrolase and neutral inorganic pyrophosphatase
in pathologic joint fluids: Elevated pyrophosphohydrolase
in calcium pyrophosphate dihydrate crystal deposition dis-
ease. Arthritis Rheum 28:1283-1288, 1985
89. Altman RD, Muniz OE, Pita JO, et al: Articular
chondrocalcinosis: Microanalysis of pyrophosphate (PPi) in
synovial fluid and plasma. Arthritis Rheum 16:171-178,1973
90. de Seze S, Hubault A, Welfling J, et al: Les arthropa-
thies des hemochromatosis. Rev Rhum Mal Osteoartic
31:479-4851964
91. Hamilton E, Williams R, Barlow KA, et al: The
arthropathy of idiopathic haemochromatosis. Q J Med
37:171-182, 1968
92. Dymock IW, Hamilton EBD, Laws JW, et al: Arthrop-
athy of haemochromatosis. Ann Rheum Dis 29:469-476,
1970
93. Hamilton EBD, Bomford AB, Laws JW, et al: The
natural history of arthritis in idiopathic haemochromatosis:
Progression of the clinical and radiological features over ten
years. Q J Med 50:3321-3329,198l
94. Axford JS, Bomford A, Revel1 P, et al: Hip arthropa-
thy in genetic hemochromatosis. Arthritis Rheum 34:357-
361,199l
95. Gordon DA, Little HA: The arthropathy of hempo-
chromatosis without hemochromatosis. Arthritis Rheum
16:305-312, 1973
96. Rosner IA, Askari AD, McClaren GD, et al: Arthrop-
athy, hypouricemia and normal serum iron studies in
hereditary hemochromatosis. Am J Med 70:870-874,198l
97. Mathews JL, Williams HJ: Arthritis in hereditary
hemochromatosis. Arthritis Rheum 30:1137-1141, 1987
98. Adamson TC, Resnick CS, Guerra J, et al: Hand and
wrist arthropathies of hemochromatosis and calcium pyro- phosphate deposition disease: Distinct radiographic fea-
tures. Radiology 147:377-381, 1983
99. Jensen PS, Putman CE: Chondrocalcinosis and hae-
mophilia. Clin Radio1 28:401-405, 1977
100. Leonello PP, Cleland LG, Norman JE: Acute pseu-
dogout and chondrocalcinosis in a man with mild haemo-
philia. J Rheumatol8:841-844, 1981
101. Askari AD, Muir WA, Rosner IA, et al: Arthritis of
hemochromatosis. Am J Med 75:957-965, 1983
102. Alexander GM, Dieppe PA, Doherty M, et al:
Pyrophosphate arthropathy: a study of metabolic associa-
tions and laboratory data. Ann Rheum Dis 41:377-381. 1982
103. Pawlotsky Y, Roussey M. Hany Y, et al: Hyper-
parathormonemie dans I’hemochromatose idiopathique.
Presse Med 3:1757-1758, I974
104. Pawlotsky Y, Simon M, Hany Y, et al: High plasma
parathyroid levels and osteoarticular changes in primary
haemochromatosis. Stand J Rheumatol Suppl8:19-15, 1975
105. Dunham J, Bourke BE, Bitensky Y, et al: Circulat-
ing levels of biologically active parathyroid hormone in
rheumatic diseases. Ann Rheum Dis 41:569-573, 1982
106. Boudin G, Pepin B, Hubault A: Les arthropathies
de la maladie de Wilson. Sot Med Hosp Paris 114:617-622,
1963
107. Feller ER, Schumacher HR: Osteoarticular changes
in Wilson’s disease. Arthritis Rheum 15:259-266, 1972
108. Golding DN, Walshe JM: Arthropathy of Wilson’s
disease. Ann Rheum Dis 36:99-l 11, 1977
109. Cervenansky J, Sitaj S, Urbanek T: Alkaptonuria
and ochronosis. J Bone Joint Surg [Am] 41:1169-l 182, 1959
110. O’Brien WM, La Du BM, Bunim JJ: Biochemical,
pathologic and clinical aspects of alcaptonuria, ochronosis
and ochronotic arthropathy. Am J Med 34:813-838, 196.3
I I I. Schumacher HR, Holdsworth DE: Ochronotic ar-
thropathy. I. Clinicopathologic studies. Semin Arthritis
Rheum 6:207-246,1977
112. Hunter T, Gordon DA, Ogryzlo MA: The ground
pepper sign of synovial fluid: A new diagnostic feature of
ochronosis. J Rheumatol l:45-53, 1974
113. Rynes RI, Sosman JL, Holdsworth DE: Pseudogout
in ochronosis. Arthritis Rheum 182-25, 1975
114. Bywaters EGL. Dorling J, Sutor J: Ochronotic
densilication. Ann Rheum Dis 29563, 1970 (abstr)
115. Steiger U, Lagier R: Combined anatomical and
radiological study of the hip-joint in alcaptonuric arthropa-
thy. Ann Rheum Dis 31:369-373. 1972
116. Reginato AJ, Schumacher HR, Martinez VA: Ochro-
notic arthropathy with calcium pyrophosphate dihydrate
crystal deposition. Arthritis Rheum 16:705-714, 1973
117. Dodds WJ, Steinbach HL: Gout associated with
calcification of cartilage. N Engl J Med 275:745-749, 1966
118. Good AE. Rapp R: Chondrocalcinosis of the knee
with gout and rheumatoid arthritis. N Engl J Med 277:286-
290,1967
119. Hollingworth P, Williams PL, Scott JT: Frequency
of chondrocalcinosis of the knees in asymptomatic hyperuri-
caemia and rheumatoid arthritis: a controlled study. Ann
Rheum Dis 41:344-346, 1982
120. Stanbury SW, Popert AJ, Ball J: Simulation of
rheumatic disorders by metabolic bone diseases. Ann Rheum
Dis 1X:63-65, 1959
121. Bywaters EC, Dixon A StJ, Scott JT: Joint lesions of
hyperparathyroidism. Ann Rheum Dis 22:171-187, 1963
122. McGill PE, Grange AT, Royston CSM: Chondrocal-
DISEASES ASSOCIATED WITH CPPD CRYSTALS 201
cinosis in primary hyperparathyroidism. Stand J Rheumatol
13:56-58,1984
123. Solnica J, Hubault A, Kahn M-F, et al: Les chondro-
calcinoses articulaires etude clinique, biologique, crystal-
lographique et etiologique. Rev Rhum Mal Osteoartic
33:93-99, 1966
124. Glass JS, Grahame R: Chondrocalcinosis after para-
thyroidectomy. Ann Rheum Dis 35:521-525, 1976
125. Sharp WV, Kelly TR: Acute arthritis: A complica-
tion of surgically induced hypoparathyroidism. Am J Surg
113:829-832,1967
126. Bilezikian JP, Aurbach GD, Connor TB: Pseudo-
gout after parathyroidectomy. Lancet 1:445-446, 1973
127. O’Duffy JD: Clinical studies of acute pseudogout
attacks. Arthritis Rheum 19:349-352, 1976
128. Phelps P, Hawker CD: Serum parathyroid hormone
levels in patients with calcium pyrophosphate crystal deposi-
tion disease (chondrocalcinosis, pseudogout). Arthritis
Rheum 16:590-596, 1973
129. Zeidler H, Hehrmann R, Hoffken B, et al: Serum
parathyroid hormone levels in patients with pyrophosphate
arthritis (chondrocalcinosis). Stand J Rheumatol Suppl
8:19-13, 1975 (abstr)
130. Pawlotsky Y, Catheline M, Delbary M, et al: Hyper-
parathormonemie normocalcemique et chondrocalcinose
articulaire. Rev Rhum Mal Osteoartic 48:799-806, 1981
131. Marx SJ: Familial hypocalciuric hypercalcemia. N
Engl J Med 303:810-811, 1980
132. Marx SJ, Attie MF, Levine MA, et al: The hypocalci-
uric or benign variant of familial hypercalcemia: Clinical
and biochemical features in fifteen kindreds. Medicine
60:397-412,198l
133. Familial hypocalciuric hypercalcaemia. Lancet 1:488-
489,1982
134. Spiegel AM, Harrison HE, Marx SJ, et al: Neonatal
primary hyperparathyroidism with autosomal dominant in-
heritance. J Pediatr 90:269-272,1977
135. Marx SJ, Spiegel AM, Brown EM, et al: Divalent
cation metabolism: familial hypocalciuric hypercalcemia
versus typical primary hyperparathyroidism. Am J Med
651235-242, 1978
136. Taylor HG, Hothersall TE: Hypophosphataemic
rickets and pyrophosphate arthropathy. Clin Rheumatol
10:155-157, 1991
137. Swoboda W: Die roentgensymptomatik der vitamin
D intoxikation un kindesalter. Fortschr Geb Rontgenstr
771534-545, 1952
138. Hardy DC, Murphy WA, Siegel BA, et al: X-linked
hypophosphatemia in adults: Prevalence of skeletal radio-
graphic and scintigraphic features. Radiology 171:403-414,
1989
139. Radi I, Amor B, Brouilhet H, et al: Chondrocalci-
nose articulaire primaire. Ses rapports avec le sexe des
malades, I’age des patients au debut de l’affection. le
diabete. Rev Rhum Mal Osteoartic 37:263-276,197O
140. Boussina I, Micheli A, Schmied P, et al: Etude de la
frequence du diabete sucre dans la chondrocalcinose articu- laire. Schweiz Med Wochenschr 101:1413-1417, 1971
141. Dorwart BB, Schumacher HR: Joint effusions, chon-
drocalcinosis and other rheumatic manifestations in hypothy-
roidism. Am J Med 59:780-790,1975
142. Job-DesLandre C, Menkes CJ, Guinot M, et al:
Does hypothyroidism increase the prevalence of chondrocal-
cinosis. Hungarian Rheumatol32:5-55,199l
143. Komatireddy G, Ellman MH, Brown NL: Lack of
association between hypothyroidism and chondrocalcinosis.
J Rheumatol 17:273,1990 (letter)
144. Lamotte M, Segrestaa J-M, Krassinine G: Arthrite
microcristalline calcique (pseudo-goutte) chez un acro-
megale. Semin Hop Paris 41:2420-2424,1966
145. Bluestone R, Bywaters EGL, Hartog M, et al:
Acromegalic arthropathy. Ann Rheum Dis 30:243-258,197l
146. Podgorski M, Robinson B, Weissberger A, et al:
Articular manifestations of acromegaly. Aust NZJ Med
18:28-35, 1988
147. Layton MW, Fudman EJ, Barkan A, et al: Acrome-
galic arthropathy. Arthritis Rheum 31:1022-1027, 1988
148. Kellgren JH, Ball J, Tutton GK: Articular and other
limb changes in acromegaly, a clinical and pathological
study of 25 cases. Q J Med 21:405-424,1952
149. Detenbeck LC, Tressler HA, O’Duffy JD, et al:
Peripheral joint manifestations of acromegaly. Clin Orthop
91:119-127, 1973
150. Johanson NA, Vigorita VJ, Goldman AB, et al:
Acromegalic arthropathy of the hip. Clin Orthop 173:130-
139,1983
151. Moskowitz RW, Garcia F: Chondrocalcinosis articu-
laris (pseudogout syndrome). Arch Intern Med 132:87-91,
1973
152. Hearn PR, Russell RGG: Formation of CPPD
crystals in vitro: Implications for calcium pyrophosphate
dihydrate crystal deposition disease (pseudogout). Ann
Rheum Dis 39:222-227, 1980
153. Cheng P-T, Pritzker KPH, Adams ME, et al: Cal-
cium pyrophosphate crystal formation in aqueous solutions.
J Rheumatol7:609-616,198O
154. Cheng P-T, Pritzker KPH: Pyrophosphate, phos-
phate ion interaction effects on calcium pyrophosphate and
calcium hydroxyapatite crystal formation in aqueous solu-
tions in aqueous solutions. J Rheumatol 10:769-777, 1983
155. Pritzker KPH, Cheng PT, Adams ME, et al: Calcium
pyrophosphate dihydrate crystal formation in model hydro-
gels. J Rheumatol5:469-473, 1978
156. Omar SA, Cheng PT, Nyburg SC, et al: Application
of scanning and transmission electron microscopy, x-ray
energy spectroscopy, and x-ray diffraction to calcium pyro-
phosphate dihydrate crystal formation in vitro. Scan Mi-
crosc 745-750, 1979
157. Pritzker KPH, Cheng P-T, Omar SA, et al: Calcium
pyrophosphate crystal formation in model hydrogels. 2.
Hyaline articular cartilage as a gel. J Rheumatol8:451-455,
1981
158. Harries JE, Dieppe PA, Heap P, et al: In vitro
growth of calcium pyrophosphate crystals in polyacrylamide
gels. Ann Rheum Dis 42-S:lOO-101,1983
159. Mandel NS, Mandel GS, Carroll DJ, et al: Calcium
pyrophosphate crystal deposition. An in vitro study using a
gelatin matrix model. Arthritis Rheum 27:789-796, 1984
160. Bennett RM, Lehr JR, McCarty DJ: Factors affect-
ing solubility of calcium pyrophosphate dihydrate crystals. J
Clin Invest 56:1571-1579,1975
161. Russell RGG: Metabolism of inorganic pyrophos-
phate (PPi). Arthritis Rheum 19:465-478,1976
162. Caswell AM, McGuire MKB, Russell RGG: Studies
202 JONES ET AL
of pyrophosphate metabolism in relation to chondrocalcino-
sis. Ann Rheum Dis 42-S:98-99, 1983
163. Russell RGG, Bisaz S, Donath A, et al: Inorganic
pyrophosphate in plasma in normal persons and in patients
with hypophosphatasia, osteogenesis imperfecta, and other
disorders of bone. J Clin Invest 50:961-969,197l
164. Loveless BW, Heaton FW: Changes in alkaline
phosphatase (EC 3.1.3.1.) and inorganic pyrophosphatase
(EC 3.6.1.1.) activities of rat tissues during magnesium
deficiency. The importance of controlling feeding patterns.
Br J Nutr 36:487-495, 1976 165. Sutton RAL: Plasma magnesium concentration in
primary hyperparathyroidism. Br Med J 1:529-533,197O
166. King RG, Stanbury SW: Magnesium metabolism in
primary hyperparathyroidism. Clin Sci 39:281-303, 1970
167. Felix R, Fleisch H: Pyrophosphatase and ATPase of
isolated cartilage matrix vesicles. Calcif Tissue Int 22:1-77,
1976
168. McCarty DJ, Pepe PF, Solomon SB, et al: Inhibition
of human erythrocyte pyrophosphatase activity by calcium,
cupric and ferrous ions. Arthritis Rheum 13:336, 1970
(abstr)
169. McCarty DJ, Pepe PF: Erythrocyte neutral inor-
ganic pyrophosphatase in pseudogout. J Lab Clin Med
791277-284, 1972
170. McCarty DJ, Palmer DW, Garancis JC: Clearance
of calcium pyrophosphate dihydrate crystals in vivo. III.
Effects of synovial haemosiderosis. Arthritis Rheum 24:706-
710, 1981
171. Eaton RH, Moss DW: Inhibition of the orthophos-
phatase and pyrophosphatase activities of human alkaline
phophatse preparations. Biochem J 102:917-921, 1967
172. Silcox DC, McCarty DJ: Elevated inorganic pyro-
phosphate concentrations in synovial fluids in osteoarthritis
and pseudogout. J Lab Clin Med 83:518-531,1974
173. Camerlain M, McCarty DJ, Silcox DC, et al: Inor-
ganic pyrophosphate pool size and turnover rate in arthritic
joints. J Clin Invest 55:1373-1381, 1975 174. Lust G, Nuki G, Seegmiller JE: Inorganic pyrophos-
phate and proteoglycan metabolism in cultured human
articular chondrocytes and fibroblasts. Arthritis Rheum
19:479-487, 1976
175. Micheli A, PO J, Fallet GH: Measurements of
soluble pyrophosphate in plasma and synovial Auid of
patients with various rheumatic diseases. Stand J Rheuma-
to1 10:237-240, 1981
176. Rachow JW, Ryan LM, McCarty DJ, et al: Synovial
fluid inorganic pyrophosphate concentration and nucleotide
pyrophosphohydrolase activity in basic calcium phosphate
deposition arthropathy and Milwaukee shoulder syndrome.
Arthritis Rheum 31:408-413,1988
177. Doherty M, Chuck A, Hosking D, et al: Inorganic
pyrophosphate in metabolic diseases predisposing to cal- cium pyrophosphate dihydrate crystal deposition. Arthritis
Rheum 34:1297-1303,199l
178. Howell DS, Muniz 0, Pita JC, et al: Extrusion of
pyrophosphate into extracellular media by osteoarthritic
cartilage incubates. J Clin Invest 56:1473-1480,1975 179. Howell DS, Muniz 0, Pita JC, et al: Pyrophosphate
release by osteoarthritic cartilage incubates. Arthritis Rheum
19:488-494, 1976 180. Ryan LM, Cheung HS, McCarty DJ: Release of
pyrophosphate by normal mammalian articular hyaline and
fibrocartilage in organ culture. Arthritis Rheum 24:1522-
1527,198l
181. Ryan LM, Rachow JW, McCarty DJ: Synovial fluid
ATP: A potential substrate for the production of inorganic
pyrophosphate. J Rheumatol 18:716-720, 1991
182. Camerlain M, Silcox DC, Lawrence AM, et al:
Variation in plasma and urinary inorganic phosphate and
pyrophosphate in normal subjects and in patients with
acromegaly or osteoarthritis. J Rheumatol7:365-374, 1980
183. Silcox DC, McCarty DJ: Measurement of inorganic
pyrophosphate in biological fluids; elevated levels in some
patients with osteoarthritis, pseudogout, acromegaly and
uraemia. J Clin Invest 52:1862-1870, 1973
184. Bayliss MT, Ah YS: Age-related changes in the
composition and structure of human articular cartilage
proteoglycans. Biochem J 176:683-693,197X
185. Venn MF: Variation of chemical composition with
age in human femoral head cartilage. Ann Rheum Dis
37:168-174, 1978
186. Ballet AJ, Nance JL: Biochemical findings in normal
and osteoarthritic articular cartilage. II. Chondroitin sulfate
concentration and chain length, water and ash content. J
Clin Invest 45:1170-1177, 1966
1X7. Mankin HJ, Lippiello L: The glycosaminoglycans of
normal and arthritic cartilage. J Clin Invest 50:1712-1719,
1971
188. Nimni ME, Deshmukh K: Differences in collagen
metabolism between normal and osteoarthritic human artic-
ular cartilage. Science 181:751-752, 1973
189. Mankin HJ, Thrasher AZ: Water content and bind-
ing in normal and osteoarthritic human cartilage. J Bone
Joint Surg [Am] 57:76-79. 1975
190. Maroudas A: Balance between swelling pressure
and collagen tension in normal and degenerate cartilage.
Nature 260:808-809, 1976
191. Muir H: Molecular approach to the understanding
of osteoarthritis. Ann Rheum Dis 36:199-208, 1977
192. Bjelle A: The glycosaminoglycans of articular carti-
lage in calcium pyrophosphate dihydrate (CPPD) crystal
deposition disease (chondrocalcinosis articularis or pyro-
phosphate arthropathy). Calcif Tiss Int 12:37-46, 1973
193. Bjelle A: Familial pyrophosphate artropathy. Stand
J Rheumatol 10:209-214, 1981
194. Sokoloff L: Elasticity of articular cartilage: Etfects
of ions and viscous solutions. Science 141:1055-1056, 1963
195. Brighton CT, Bigley EC. Smolenski BI: Iron in-
duced arthritis in immature rabbits. Arthritis Rheum 13:849-
857,197O
196. Blake DR, Lunec J: Copper, iron, free radicals and
arthritis. Br J Rheumatol24:123-127, 198.5
197. Cheng PT, Pritzker KPH: The effect of calcium and
magnesium ions on calcium pyrophosphate dihydrate crys-
tal formation in aqueous solutions. J Rheumatol 8:772-782. 1981
198. Hearn PR, Russell RGG, Elliott JC, et al: Forma-
tion product of calcium pyrophosphate crystals in vitro and
the effect of iron salts. Clin Sci 54:29P, 1978 (abstr)
199. Wallace DJ, Klinenberg JR, Morhain D, et al:
Coexistent gout and rheumatoid arthritis: Case report and
literature review. Arthritis Rheum 22:81-86, 1979