Lung deposition predictions of airborne particles and the emergence of contemporary diseases - Part...
7
Introduction Since the onset of the industrial revolution some 150 years ago, people are exposed to ele- vated concentration of arbitrarily shaped ul- trafine particles along with the chemical by- products such as carbon monoxide (CO), nitric oxide (NO), semi-/volatile organic compounds (VOCs) of anthropogenic origin – mostly in the form of incomplete combusted by-products that leave stacks or tailpipes as macromolecular clusters. In addition, recent advances in nanotechnology, even more refined designed and engineered nanoparticles (in the range from 1 – 100 nm) are also being introduced in the form of scratch-proof paints, lotus-effect stained glass, suntan lotion, etc. Although their release into the environment is not intended in the first place, it will occur sooner rather than later, especially once wear and tear along with product degradation releases contained ultrafine particles into the environment where they easily can enter the food chain either via aerosolization or washing-out from dumping sites. Regardless of the particle‟s origin, the young research field of nano-toxicology deals with effects and potential risks of particle structures <1 μm in size. Yet, within these di- mensions, the well-known quote of Paracelsus “the dose makes the poison”, needs to be re- vised into “the dose determines the mechanism”. 1 This is particular true for nano-sized particles as the greater surface area per unit volume compared with their larger-sized siblings ren- ders them biologically more active. 2 The abil- ity of these particles to cross cell barriers and to interact with intracellular structures is well established, and has yielded the various path- ways leading to oxidative stress effects. Here in particular insoluble ultrafine particles can extend their multiple adverse effects even fur- ther when redistributed from one line of de- fence to the next as metabolites or cellular debris are released into the interstitial upon cell death. In continuation to Part-I, 3 this short review aims to provide an overview in the un- derstanding of the hazardous effects relevant to humans and at the same time to promote a better understanding of how most contempo- rary diseases are related to ultrafine particle exposure. Lung deposition predictions of airborne particles and the emergence of contemporary diseases - Part II Mankind has been exposed to airborne nanosized particles (<100 nm) for eons, yet mechanization and industrialization of societies has increased the overall load to which humans are exposed to. Ultrafine-particles (below 1 μm in diameter) can thus be incorporated via any organic surface structure and in particular when the area available is large enough – as is the case with the skin (approx. 1.5-2 m 2 ), the digestive tract (intestinal villi, approx. 200 m 2 ) or the lungs (approx. 140 m 2 ). Since aerosolised particles are readily inhaled rather than ingested, the lungs represent an ideal gateway with high penetration efficiency rates. If seen from a toxicological rather than from a therapeutic point of view, deposited xenobiotic particles that interact with biological tissues do so first on a cellular level where they are readily translocated into the cell to interfere with metabolic pathways and eventually induce inflammatory cellular responses. At an organismic level and in response to long-term exposure, these particles become redistributed via the lymphatic or the blood circulatory system to reach sensitive organs or tissues such as the central nervous system, bone marrow, lymph nodes, spleen, and heart. At this organismic level, the persistent particle exposure may trigger or even modulate the severity of chronic diseases. Madl P 1 , Hussain M 1,2 1 Division of Physics and Biophysics, Department of Materials Research and Physics, University of Salzburg, Austria, 2 Higher Education Commission, Islamabad, Pakistan theHealth 2011; 2(3): 101-107 Correspondence Pierre Madl Division of Physics and Biophysics, Department of Materials Research and Physics, University of Salzburg, Hellbrunnerstrasse 34, A-5020 Salzburg, Austria E-mail: [email protected] Keywords: Nanoparticle deposition, Bioreactivity, Lung Disease, Chronic Disease, Epigenetics Funding This work was funded in part by EU contract no. 516483 (Alpha Risk) and Higher Education Commission of Pakistan under the scholarschip program (Overseas Scholarships for Pakistani Nationals) Competing Interest None declared. Received: March 30, 2011 Accepted: August 9, 2011 Abstract ISSN (print): 2218-3299 ISSN (online): 2219-8083 Review theHealth | Volume 2 | Issue 3 | 101
Transcript of Lung deposition predictions of airborne particles and the emergence of contemporary diseases - Part...
Introduction
Since the onset of the industrial revolution some
150 years ago, people are exposed to ele-
vated concentration of arbitrarily shaped ul-
trafine particles along with the chemical by-
products such as carbon monoxide (CO), nitric
oxide (NO), semi-/volatile organic compounds
(VOCs) of anthropogenic origin – mostly in the
form of incomplete combusted by-products that
leave stacks or tailpipes as macromolecular
clusters. In addition, recent advances in
nanotechnology, even more refined designed
and engineered nanoparticles (in the range
from 1 – 100 nm) are also being introduced in
the form of scratch-proof paints, lotus-effect
stained glass, suntan lotion, etc. Although their
release into the environment is not intended in
the first place, it will occur sooner rather than
later, especially once wear and tear along
with product degradation releases contained
ultrafine particles into the environment where
they easily can enter the food chain either via
aerosolization or washing-out from dumping
sites. Regardless of the particle‟s origin, the
young research field of nano-toxicology deals
with effects and potential risks of particle
structures <1 μm in size. Yet, within these di-
mensions, the well-known quote of Paracelsus
“the dose makes the poison”, needs to be re-
vised into “the dose determines the mechanism”. 1 This is particular true for nano-sized particles
as the greater surface area per unit volume
compared with their larger-sized siblings ren-
ders them biologically more active. 2 The abil-
ity of these particles to cross cell barriers and
to interact with intracellular structures is well
established, and has yielded the various path-
ways leading to oxidative stress effects. Here
in particular insoluble ultrafine particles can
extend their multiple adverse effects even fur-
ther when redistributed from one line of de-
fence to the next as metabolites or cellular
debris are released into the interstitial upon
cell death. In continuation to Part-I, 3 this short
review aims to provide an overview in the un-
derstanding of the hazardous effects relevant
to humans and at the same time to promote a
better understanding of how most contempo-
rary diseases are related to ultrafine particle
exposure.
Lung deposition predictions of airborne particles and the emergence of contemporary diseases - Part II
Mankind has been exposed to airborne nanosized particles (<100 nm) for eons, yet
mechanization and industrialization of societies has increased the overall load to which humans
are exposed to. Ultrafine-particles (below 1 µm in diameter) can thus be incorporated via any
organic surface structure and in particular when the area available is large enough – as is the
case with the skin (approx. 1.5-2 m2), the digestive tract (intestinal villi, approx. 200 m2) or the
lungs (approx. 140 m2). Since aerosolised particles are readily inhaled rather than ingested, the
lungs represent an ideal gateway with high penetration efficiency rates. If seen from a
toxicological rather than from a therapeutic point of view, deposited xenobiotic particles that
interact with biological tissues do so first on a cellular level where they are readily translocated
into the cell to interfere with metabolic pathways and eventually induce inflammatory cellular
responses. At an organismic level and in response to long-term exposure, these particles become
redistributed via the lymphatic or the blood circulatory system to reach sensitive organs or tissues
such as the central nervous system, bone marrow, lymph nodes, spleen, and heart. At this
organismic level, the persistent particle exposure may trigger or even modulate the severity of
chronic diseases.
Madl P1, Hussain M1,2 1Division of Physics and Biophysics, Department of Materials Research and Physics, University of Salzburg, Austria, 2Higher Education Commission, Islamabad, Pakistan
theHealth 2011; 2(3): 101-107
Correspondence
Pierre Madl
Division of Physics and
Biophysics, Department of
Materials Research and Physics,
University of Salzburg,
Hellbrunnerstrasse 34, A-5020
Salzburg, Austria
E-mail:
Keywords:
Nanoparticle deposition,
Bioreactivity, Lung Disease,
Chronic Disease, Epigenetics
Funding
This work was funded in part
by EU contract no. 516483
(Alpha Risk) and Higher
Education Commission of
Pakistan under the scholarschip
program (Overseas
Scholarships for Pakistani
Nationals)
Competing Interest
None declared.
Received: March 30, 2011
Accepted: August 9, 2011
Abstract
ISSN (print): 2218-3299
ISSN (online): 2219-8083
Review
theHealth | Volume 2 | Issue 3 | 101
Potential health effects
Experimental investigations have shown that size and the
associated surface area indeed do make a difference,
thereby significantly extending the retention time of inhaled
nanosized compared with larger particles in alveolar macro-
phages. 1, 2 Although macrophages is the most important de-
fense mechanism in the alveolar region for fine and coarse
particles, this mechanism is impaired in the case of inhaled
ultrafine particles as they are not efficiently phagocytized.
Animal studies have revealed that bronchio-alveolar lavage
after aerosol exposure reveal that only about 20% of nano-
sized particle fraction (15 - 20 nm) can be flushed out along
with the macrophages, whereas lavage-efficiency increased
to approximately 80% in particles >0.5 μm in size. 1, 2 As
demonstrated in Figure 4 (see part-I), 3 removal of these par-
ticles then can only occur via redistribution into the lymphatic
or blood stream. With regards to the coarser particle frac-
tion, the larger numbers of ultrafine siblings leads to particle
dispersion into other tissues and organs to ultimately burden
the entire organism (compare with Figure 2). Due to their
minute size, these particles are routed through the interstitial
compartment between cells or straight through the cells via
caveolae - openings of around 40 nm in diameter that engulf
these particles, forming vesicles that are thought to function
as transport vehicles for macromolecules across the cells. A
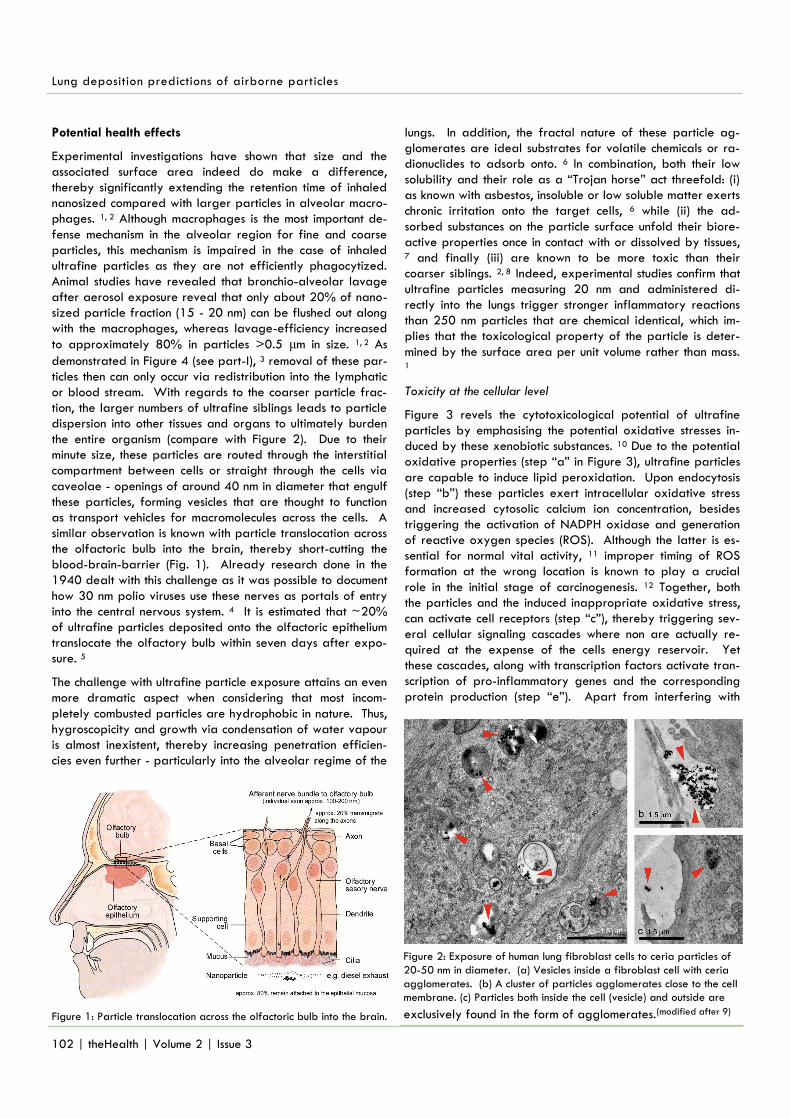
similar observation is known with particle translocation across
the olfactoric bulb into the brain, thereby short-cutting the
blood-brain-barrier (Fig. 1). Already research done in the
1940 dealt with this challenge as it was possible to document
how 30 nm polio viruses use these nerves as portals of entry
into the central nervous system. 4 It is estimated that ~20%
of ultrafine particles deposited onto the olfactoric epithelium
translocate the olfactory bulb within seven days after expo-
sure. 5
The challenge with ultrafine particle exposure attains an even
more dramatic aspect when considering that most incom-
pletely combusted particles are hydrophobic in nature. Thus,
hygroscopicity and growth via condensation of water vapour
is almost inexistent, thereby increasing penetration efficien-
cies even further - particularly into the alveolar regime of the
lungs. In addition, the fractal nature of these particle ag-
glomerates are ideal substrates for volatile chemicals or ra-
dionuclides to adsorb onto. 6 In combination, both their low
solubility and their role as a “Trojan horse” act threefold: (i)
as known with asbestos, insoluble or low soluble matter exerts
chronic irritation onto the target cells, 6 while (ii) the ad-
sorbed substances on the particle surface unfold their biore-
active properties once in contact with or dissolved by tissues,
7 and finally (iii) are known to be more toxic than their
coarser siblings. 2, 8 Indeed, experimental studies confirm that
ultrafine particles measuring 20 nm and administered di-
rectly into the lungs trigger stronger inflammatory reactions
than 250 nm particles that are chemical identical, which im-
plies that the toxicological property of the particle is deter-
mined by the surface area per unit volume rather than mass. 1
Toxicity at the cellular level
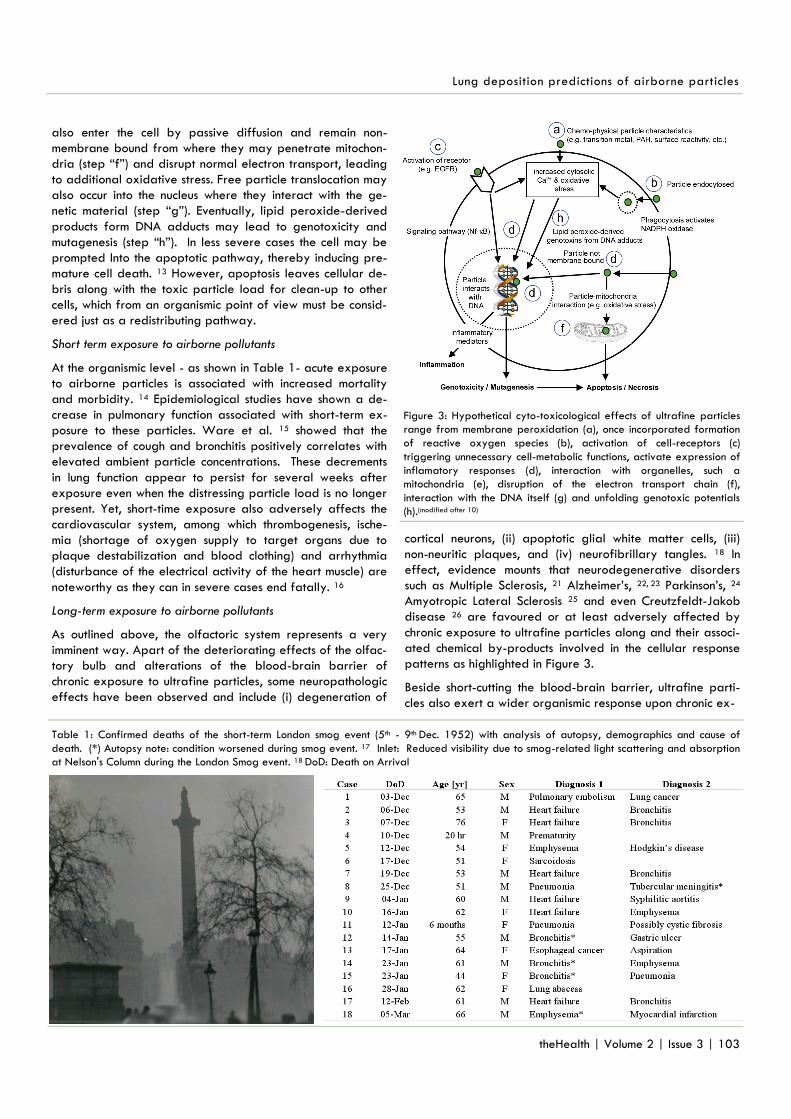
Figure 3 revels the cytotoxicological potential of ultrafine
particles by emphasising the potential oxidative stresses in-
duced by these xenobiotic substances. 10 Due to the potential
oxidative properties (step “a” in Figure 3), ultrafine particles
are capable to induce lipid peroxidation. Upon endocytosis
(step “b”) these particles exert intracellular oxidative stress
and increased cytosolic calcium ion concentration, besides
triggering the activation of NADPH oxidase and generation
of reactive oxygen species (ROS). Although the latter is es-
sential for normal vital activity, 11 improper timing of ROS
formation at the wrong location is known to play a crucial
role in the initial stage of carcinogenesis. 12 Together, both
the particles and the induced inappropriate oxidative stress,
can activate cell receptors (step “c”), thereby triggering sev-
eral cellular signaling cascades where non are actually re-
quired at the expense of the cells energy reservoir. Yet
these cascades, along with transcription factors activate tran-
scription of pro-inflammatory genes and the corresponding
protein production (step “e”). Apart from interfering with
102 | theHealth | Volume 2 | Issue 3
Lung deposition predictions of airborne particles
Figure 1: Particle translocation across the olfactoric bulb into the brain.
Figure 2: Exposure of human lung fibroblast cells to ceria particles of
20-50 nm in diameter. (a) Vesicles inside a fibroblast cell with ceria
agglomerates. (b) A cluster of particles agglomerates close to the cell
membrane. (c) Particles both inside the cell (vesicle) and outside are
exclusively found in the form of agglomerates.(modified after 9)
also enter the cell by passive diffusion and remain non-
membrane bound from where they may penetrate mitochon-
dria (step “f”) and disrupt normal electron transport, leading
to additional oxidative stress. Free particle translocation may
also occur into the nucleus where they interact with the ge-
netic material (step “g”). Eventually, lipid peroxide-derived
products form DNA adducts may lead to genotoxicity and
mutagenesis (step “h”). In less severe cases the cell may be
prompted Into the apoptotic pathway, thereby inducing pre-
mature cell death. 13 However, apoptosis leaves cellular de-
bris along with the toxic particle load for clean-up to other
cells, which from an organismic point of view must be consid-
ered just as a redistributing pathway.
Short term exposure to airborne pollutants
At the organismic level - as shown in Table 1- acute exposure
to airborne particles is associated with increased mortality
and morbidity. 14 Epidemiological studies have shown a de-
crease in pulmonary function associated with short-term ex-
posure to these particles. Ware et al. 15 showed that the
prevalence of cough and bronchitis positively correlates with
elevated ambient particle concentrations. These decrements
in lung function appear to persist for several weeks after
exposure even when the distressing particle load is no longer
present. Yet, short-time exposure also adversely affects the
cardiovascular system, among which thrombogenesis, ische-
mia (shortage of oxygen supply to target organs due to
plaque destabilization and blood clothing) and arrhythmia
(disturbance of the electrical activity of the heart muscle) are
noteworthy as they can in severe cases end fatally. 16
Long-term exposure to airborne pollutants
As outlined above, the olfactoric system represents a very
imminent way. Apart of the deteriorating effects of the olfac-
tory bulb and alterations of the blood-brain barrier of
chronic exposure to ultrafine particles, some neuropathologic
effects have been observed and include (i) degeneration of
cortical neurons, (ii) apoptotic glial white matter cells, (iii)
non-neuritic plaques, and (iv) neurofibrillary tangles. 18 In
effect, evidence mounts that neurodegenerative disorders
such as Multiple Sclerosis, 21 Alzheimer‟s, 22, 23 Parkinson‟s, 24
Amyotropic Lateral Sclerosis 25 and even Creutzfeldt-Jakob
disease 26 are favoured or at least adversely affected by
chronic exposure to ultrafine particles along and their associ-
ated chemical by-products involved in the cellular response
patterns as highlighted in Figure 3.
Beside short-cutting the blood-brain barrier, ultrafine parti-
cles also exert a wider organismic response upon chronic ex-
theHealth | Volume 2 | Issue 3 | 103
Lung deposition predictions of airborne particles
Figure 3: Hypothetical cyto-toxicological effects of ultrafine particles
range from membrane peroxidation (a), once incorporated formation
of reactive oxygen species (b), activation of cell-receptors (c)
triggering unnecessary cell-metabolic functions, activate expression of
inflamatory responses (d), interaction with organelles, such a
mitochondria (e), disruption of the electron transport chain (f),
interaction with the DNA itself (g) and unfolding genotoxic potentials
(h).(modified after 10)
Table 1: Confirmed deaths of the short-term London smog event (5th - 9th Dec. 1952) with analysis of autopsy, demographics and cause of
death. (*) Autopsy note: condition worsened during smog event. 17 Inlet: Reduced visibility due to smog-related light scattering and absorption
at Nelson's Column during the London Smog event. 18 DoD: Death on Arrival
exposure that extends far beyond respiratory ailments men-
tioned above. The ability of these particles to translocate
from their portal of entry to secondary target tissues is high-
lighted by some investigations. These wider organismic ef-
fects involve structurally higher hierarchic levels such as or-
gans and ultimately the entire organism. At these levels, im-
munological and inflammatory effects decrease the overall
stress-tolerance and pave the way for cascades of events
that culminate into the commonly known chronic disease pat-
tern - viewed at a first glance - seem to be decoupled from
exposure to particles and their chemical associates. Aside
from a few experimental studies focusing on the eco-
toxicological effects, 1, 27 little effort has been made to study
the collateral effects on organs other than the lungs, in par-
ticular studies that highlight for example the conditioning
effect of airborne pollutants onto the immune system. 28 A
particular set of epidemiological studies even focus on the
combined effect of administered chemicals and the environ-
mental setting the organism is embedded in. Here it was
observed that patients have become so ingrained that the
mere sight of a given location was enough to trigger a de-
crease in immune activity without even exposing them to
imuno-suppressing agents - a phenomenon known as immune
conditioning. 29 Investigations of this kind emphasize the fact
that suppression of the immune system is a controlled process
underlying the subconscious regime of our mind. In this re-
gard, the animal study of Sepolsky et al. 30 is quite interest-
ing as they could show how the continuous activation of the
acute phase response pattern eventually can lead to a state
of chronic inflammation, in which “sickness behavior” becomes
a way of life. In the context of aerosol exposure, the com-
plex interaction of various regulatory layers with different
hierarchical preferences makes it very difficult to assign a
single toxic agent (i.e. ultrafine particle) the full adverse po-
tential. It‟s important to keep in mind that in most cases the
cocktail of distressing influences of various kinds synergisti-
cally act on the exposed organism. To shed just some light on
this intrinsically interwoven network, synergism between two
types of aerosols shall be demonstrated – the combined ef-
fect of carbonaceous ultrafine particles and pollen allergens.
In such cases it was found that exposure to carbonaceous
particles before allergen challenge exerts strong adjuvant
effects on the manifestation of allergic airway inflammation. 31 Hence, allergen-sensitized individuals are more susceptible
to the detrimental health effects of ultrafine aerosol expo-
sure. Similar experiments investigating the conditioning ef-
fects of soot particles with adsorbed volatile organics on the
immune system confirm the proallergic potential. This implies
a crucial role of airborne pollutants for an allergic break-
through in atopic individuals, who have not developed an
allergic disease yet. 32 In this regard it is crucial to stress, that
the conditioning effects of the immune system can occur within
short periods of time. It is sufficient that the triggering event
is a coordinated with a immuno-suppressive eposode of the
exposed individual, thereby the extra stress excerted by the
aerosol burden induces - as emphasized further below in
Figure 3-a distressing response pattern.
On the other hand, extended exposure without synergistic
agents likewise induce adverse health effects. Such well-
investigated aerosols regard vaporized heavy metals that
tend to bioaccumulate if inhaled over longer time. Lead tox-
icity, for example is associated with deficits in central nervous
system functioning especially in younger ages. Absorption
into blood from lung can cause high blood pressure and
damage to renal function. 33 Inhalation of Cadmium fumes is
identified as a potential human carcinogen, causing lung
104 | theHealth | Volume 2 | Issue 3
Lung deposition predictions of airborne particles
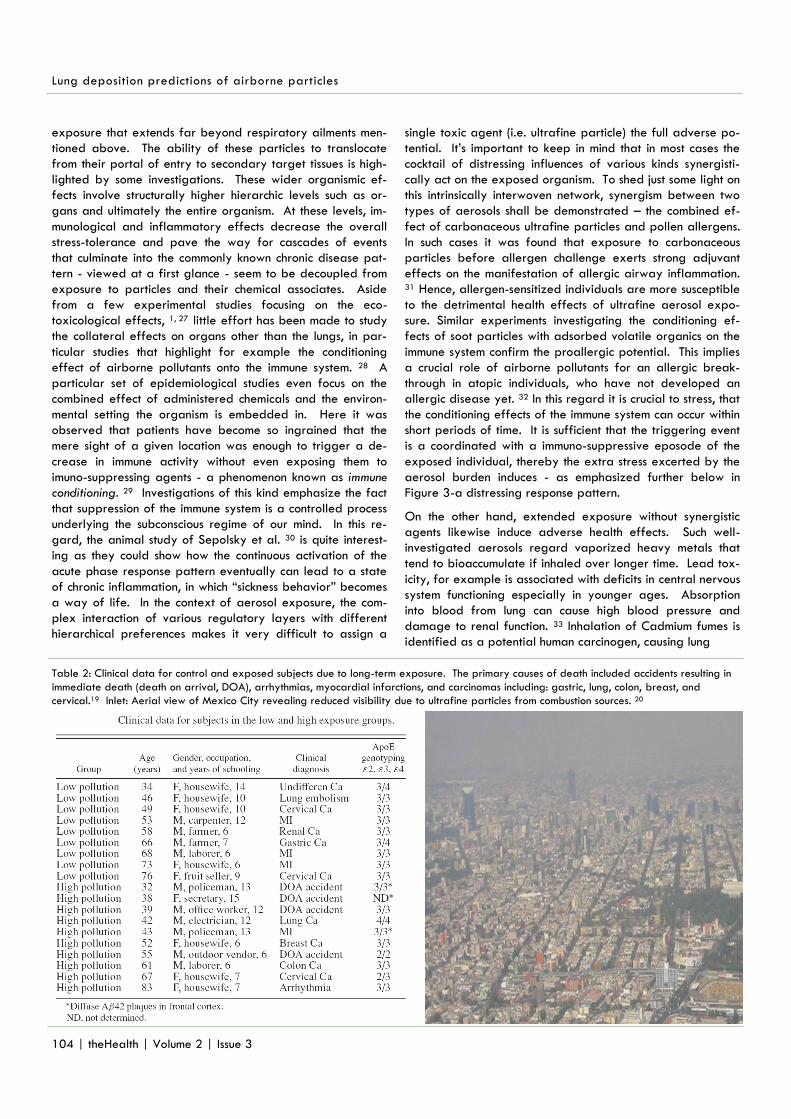
Table 2: Clinical data for control and exposed subjects due to long-term exposure. The primary causes of death included accidents resulting in
immediate death (death on arrival, DOA), arrhythmias, myocardial infarctions, and carcinomas including: gastric, lung, colon, breast, and
cervical.19 Inlet: Aerial view of Mexico City revealing reduced visibility due to ultrafine particles from combustion sources. 20
cancer. Breathing lower levels for years leads to a build-up
of cadmium in the kidneys that can cause kidney disease.
Other effects that may occur after breathing cadmium for a
long time are lung damage and fragile bones. 33 It is difficult
to distinguish mercury toxicity symptoms from those of some
bronchial irritation and pneumonitis (see also Table 1). 33 In
the field of occupational exposure, where threshold-levels
are generally higher, inhalation for example to arsenic
fumes, is causally associated with lung cancer. 34 Other com-
mon ailments however acute exposure to mercury (e.g. in the
organo-metallic form of methyl-mercury) has shown adverse
effects on the central nervous system, kidneys and thyroid.
Yet, long term low level exposure to mercury, as a byproduct
of coal combustion, is known to cause Having made the tran-
sition from milder to more severe, chronic disease patterns, it
is not difficult to understand that genotoxic properties of
long-term aerosol exposure replaces the acute symptoms by
unfolding the full pathogenic spectrum and include even can-
cer cases. Table 2 summarizes some of the major findings of
the epidemiological investigation made in Mexico City,
known for its notorious pollutant laden air. 19 Although the list
is not extensive, the high occurrence of various types of can-
cers is striking. Just by considering the fact that only about
5-10% of cancer and cardiovascular cases can be attributed
to heredity, it becomes obvious that 90-95% are controlled
by our lifestyles. 35 Hence, malignancies are derived from
environmentally-induced epigenetic alterations and not de-
fective genes. 36, 37, 38 While genetic factors determine the
tendency towards malignancy, environmental factors largely
contributes to cardiovascular diseases, cancers, and other
major causes of mortality. 35 Environmental factors are repre-
sented by one‟ lifestyle and includes diet, exposure to biore-
active toxins as well as psychic stress.
Epigenetics
With every breath, bite, and sip, we introduce countless ul-
trafine particles, viruses and bacteria into our body. Due to
the orchestrated surveillance and countermeasures carried
out by our immune system, the delicate balance between a
healthy and a diseased state is normally biased towards a
state of wellbeing (Figure 4). In order to maintain this ho-
meostasis, the immune system along with specialized white
blood cells have to track and phagocytose xenobiotic aero-
sols, harmful viruses and opportunistic bacteria before they
do any harm. In the process of such an organismic response,
every interaction of theses substances on a cellular level aids
in the fine-tuning of cell-metabolic pathways, thereby en-
training or conditioning each cell for an optimal response. If
chronic disturbances (multiple stress exposure on a cellular
level) favour down-turning developments, in that every tip-
ping point at a bifurcation unit (Figure 4) biases the system
towards a distressing path. If this series of distressing devel-
opments is not reversed, this eventually will lead to differen-
tiation of abnormal cell types (i.e. cancer precursor cells). On
the other hand, upon cessation or neutralization of one or
more distressing events and at any new bifurcation point in
time, the system can flip back to a more eustress-like equilib-
rium, with an improved response pattern when dealing with
individual stress burdens as a result of aerosol exposure. To
enable the immune system to differentiate between foreign
entities and “itself”, certain membrane markers are used to
facilitate dendritic cell recognition. During one‟s lifetime
these membrane markers are enriched by cellular experi-
ence; that is, exposure to pathogens triggers for example a
cellular response that utilizes the NF-κB signalling pathway in
which the resulting endproducts of the immuno-proteasome
activity are displayed along with the original ID-recognition
markers on the lipid bilayer. 40 In order to memorize this ex-
perience at a cellular level, the information has to pass on the
progeny cells. 41, 42 This is the moment where epigenetics
comes into effect. Cells can learn in predominantly two ways,
they either do it via “bookmarking” or via “paramutation”. 43,
44 The former transmits cellular memory in the pattern of
gene expression via mitosis to somatic progeny cells within
the same generation and kind (i.e. somatic liver stem-cells
divide into liver cells and not some other cell type). The lat-
ter on the other hand, regard the quasi “inheritance” of char-
acteristic of a gene that is "remembered" and seen in later
generations (e.g. via the germ cell linage), even if the
stressor that caused the epigenomic modification is no longer
present.
This rather new field in genomic research is about to unravel
- apart from the more rigid lower genome level - a second,
very plastic level of information processing that employs the
epigenome. Mounting evidence confirms that environmental
exposure to stressors are indeed able to modulate the epige-
nome in such a way that entire cell-lines – both somatic as
well as germ cells – can pass the stress-information in a re-
versible manner extending over three generations 42 before
theHealth | Volume 2 | Issue 3 | 105
Lung deposition predictions of airborne particles
Figure 4. Bifurcation patterns between health and disease: In case of
brief disturbances, homeostasis is restored once the disturbance
passes. However, if the disturbance is prolonged, a series of
irreversible distressing events force the organism to a new „steady
state‟. Inlet: the magnifying glass should highlight the sensitivity of the
tipping point of a bifurcation. At this moment in time, the system is so
sensitive to environmental stimuli that the slightest disturbance
determines the progression in the di- or eu-stress regime. (modified after 39)
it is lost again without altering the sequence of the DNA itself. 45, 46 This Lamarckian-type of inheritance is achieved via vari-
ous processes and involves in particular DNA-methylation,
histone modifications, mRNA silencing and other regulatory
interference mechanisms. 47, 48 Together these tools switch “on
or off” certain sections on the DNA, thereby enabling or in-
hibiting ribosomal activity to attain access to genetic informa-
tion. Modulating the epigenome implies that environmental
exposure (lifestyle, dietary preferences and distressing psy-
chological events – refer to Figure 5) are able to alter the
phenotypic appearance both on the cellular as well as on the
organismic level and are even passed on to future genera-
tions just in the same manner as DNA blueprints are passed
on via the double helix. 49 Studies employing both animals 50
as well as humans 51 underline the crucial role of epigenetic
modulation and the onset of chronic diseases. Although ex-
posure to ultrafine particles seem to be just one element in a
multidimensional stressphase relationship, a slight pressure
from one or the other side (e.g. via airborne pollutants) can
bring an apparently stable but labile equilibrium into a dy-
namic non-linear response pattern until a new metastable
equilibrium is reached. This also implies that diseases should
just be regarded as organismic proxy indicators in the at-
tempt to attain a new steady state. Hence, we can say that
extended environmental ultrafine particle exposure contain
distressing agents that, along with other stressors, shift the
constantly fluctuating homeostatic steady state into new fluc-
tuating instabilities. However, the difference between these
states lies in the fact that in the latter stages affected indi-
viduals increasingly feel physically less fit than in the former
from these have been kicked out of.
Exposure to anthropogenically released ultrafine particles
originating from incomplete combustion processes fully unfold
their toxicological potential – particularly in congested areas.
These particles have multitude ways to enter the body, which
include adsorption via the skin, the olfactoric nerve bundles
(inducing neurodegenerative diseases), deposition within the
respiratory tract (directly related to respiratory diseases),
ingestion of cleared particle laden mucus and redistribution
of the cellularly absorbed particle load throughout the or-
ganism - in combination with the former responsible of the
wider organismic health problems. Toxicity itself not only
depends on the nature of the particle (solubility, hydropho-
bicity, chemical properties) but also on the surface structure,
onto which volatile substances and radionuclides can adsorb.
Since nano-sized particles exert more severe distressing ef-
fects on the cellular level than their coarser siblings, these
aerosols significantly contribute to chronic disease patterns
and epigenetic imprinting, which enables acquired lifestyle-
related stress-response patterns to be passed on to subse-
quent generations. Due to the fact that these particles access
secondary target organs along with their effects on the or-
ganismic level, they definitely will attain further toxico-
medical attention in the near future. The availability of more
and more products containing designed and engineered
nano-particles and fibers, adds to this dilemma as awareness
of associated risks and benefits have not yet lead to guide-
lines in order to limit side-effects of improper production
methods, inadequate usage and irresponsible disposal of
these materials. While the exact risk of aerosolized particles
is still hard to define, current scientific evidence already
stresses the adverse effects of long-term exposure as it tilts
the balance towards the emergence of so called “civil-
society-related” diseases that so far were either considered
harmless or not yet associated to these environmental stress-
ors. While it is not always possible to assign as a single det-
rimental aerosol with a particular disease, the evidence given
so far indicates that ultrafine xenobiotic particles are rather
promoters and modulators in the emergence of chronic dis-
eases that so far were scarcely known in the past. Since
these aerosols exert their effects not only on the cellular, or-
ganic and organismic level, but also interfere with the onto-
filogenetic patterns currently investigated in the field of epi-
genetics, their ever increasing presence will disproportianally
challenges our medicare system.
References
1. Oberdörster G, Oberdörster E, Oberdörster J. Nanotoxicology: an emerg-
ing discipline evolving from studies of ultrafine particles. Environ Health Per-
spect. 2005;113:823-39.
2. Geiser M, Kreyling WG. Deposition and biokinetics of inhaled nanoparticles.
Part Fibre Toxicol. 2010;7:1-17.
3. Hussain M, Pierre M, Khan A. Lung deposition predictors of airborne parti-
cles and the emergence of contemporary diseases, Part-I. theHealth.
2011;2:51-59.
4. Howe HA, Bodian D. Portals of entry of poliomyelitis virus in the chimpanzee.
Proc. Soc Exp Biol Med. 1940;43:718–21.
5. Oberdörster G, Sharp Z, Atudorei V, Elder A, Gelein R, et al. Translocation
of inhaled ultrafine particles to the brain. Inhal Toxicol. 2004;16:437-45.
6. Donaldson K, Li XY, MacNee W. Ultrafine (nanometre) particle mediated
lung injury. J Aerosol Sci. 1998;29:553-60.
7. Baron PA, Willeke K. (2nd edition). 2001. Aerosol Measurement-Principles,
Techniques, and Applications. p.781-2.
8. Oberdörster G., Oberdörster E., Oberdörster J. Nanotoxicology: An Emerg-
ing Discipline Evolving from Studies of Ultrafine Particles - Supplemental Web
Sections. Environ Health Perspect. 2005b;113:830-1. Available:
http://ehp.niehs.nih.gov/members/2005/7339/supplemental.pdf [Accessed
17 August 2011].
9. Limbach LK, Li Y, Grass RN, Brunner TJ, Hintermann MA, et al. Oxide nanop-
106 | theHealth | Volume 2 | Issue 3
Lung deposition predictions of airborne particles
Figure 5. Environmental influences, including nutrition, stress and
emotions, can epigenetically modify genes, without changing the
nucleotide sequence. The numbers above outline hierarchical
interdependences of eco-systemic relationship in which the organism is
embedded in.(modified after 49)

article uptake in human lung fibroblasts: effects of particle size, agglomera-
tion, and diffusion at low concentrations. Environ Sci Technol. 2005;39: 9370-6.
10. Oberdörster G, Stone V, Donaldson K. Toxicology of nanoparticles: A
historical perspective. Nanotoxicol. 2007;1:2-25.
11. Voeikov V. Reactive oxygen species, water, photons and life. Riv Biol.
2001;94:237-58.
12. DeNicola GM, Karreth FA, Humpton TJ, Gopinathan A, Wei C, et al. Onco-
gene-induced Nrf2 transcription promotes ROS detoxification and tumorigene-
sis. Nature. 2011;475:106-9.
13. Elder AC, Gelein R, Finkelstein JN, Cox C, Oberdörster G. Pulmonary
inflammatory response to inhaled ultrafine particles is modified by age, ozone
exposure, and bacterial toxin. Inhal Toxicol. 2000;12:227-46.
14. Dockery DW, Ware JH, Ferris BG Jr, Speizer FE, Cook NR, et al. Change
in pulmonary function in children associated with air pollution episodes. J Air
Pollut Control Assoc. 1982;32:937-42.
15. Ware JH, Ferris BG Jr, Dockery DW, Spengler JD, Stram DO, et al. Effects
of ambient sulfur oxides and suspended particles on respiratory health of
preadolescent children. Am Rev Respir Dis. 1986;133:834-42.
16. Mills NL, Donaldson K, Hadoke PW, Boon NA, MacNee W, et al. Adverse
cardiovascular effects of air pollution. Nat Clin Pract Cardiovasc Med.
2009;6:36-44.
17. Hunt A, Abraham JL, Judson B, Berry CL. Toxicologic and epidemiologic
clues from the characterization of the 1952 London smog fine particulate mat-
ter in archival autopsy lung tissues. Environ Health Perspect. 2003;111:1209-
14.
18. Wikipedia. London image. 2009. The Great Smog of 1952. Available:
http://en.wikipedia.org/wiki/Great_Smog_of_1952 [Accessed 17 August
2011].
19. Calderón-Garcidueñas L, Reed W, Maronpot RR, Henríquez-Roldán C,
Delgado-Chavez R, et al. Brain inflammation and Alzheimer's-Like pathology in
individuals exposed to severe air pollution. Toxicol Pathol. 2004;32:650-8.
20. Image Mexico City.
http://www.ucar.edu/news/releases/2006/images/mexico.jpg [Accessed 17
August 2011].
21. Bizzozero OA, DeJesus G, Bixler HA, Pastuszyn A. Evidence of nitrosative
damage in the brain white matter of patients with multiple sclerosis. Neurochem
Res. 2005;30:139-49.
22. Hautot D, Pankhurst QA, Khan N, Dobson J. Preliminary evaluation of nano-
scale biogenic magnetite in Alzheimer's disease brain tissue. Proc Biol Sci.
2003;270:S62-4.
23. Sayre LM, Zelasko DA, Harris PL, Perry G, Salomon RG, et al. 4-
Hydroxynonenal-derived advanced lipid peroxidation end products are in-
creased in Alzheimer‟s disease. J Neurochem. 1997;68:2092-7.
24. Zhang J, Perry G, Smith MA, Robertson D, Olson SJ, et al. Parkinsons dis-
ease is associated with oxidative damage to cytoplasmic DNA and RNA in
substantia nigra neurons. Am J Pathol. 1999;154:1423-9.
25. Shibata N, Nagai R, Uchida K, Horiuchi S, Yamada S, et al. Morphological
evidence for lipid peroxidation and protein glycoxidation in spinal cords from
sporadic amyotrophic lateral sclerosis patients. Brain Res. 2001;917:97-104.
26. Oberdörster G, Utell MJ. Source specific health effects of fine/ultrafine
particles. Annual Progress Report, Rochester Particle Center. 2008. Available:
http://www2.envmed.rochester.edu/envmed/PMC/anrep08.pdf [Accessed 17
August 2011].
27. Donaldson K. The toxicology of nanoparticles. Nanotech Workshop.
Queens Medical Research Institute. University of Edinburgh - UK. 2009. Avail-
able: www.morst.govt.nz/Documents/work/nanotech/Ken-Donaldson--
Toxicology-of-Nanoparticles.pdf [Accessed 17 August 2011].
28. Vogt RF. Use of laboratory tests for immune biomarkers in environmental
health studies concerned with exposure to indoor air pollutants. Environ Health
Perspect. 1991;95:85-91.
29. Ader R, Cohen N. Behaviourally conditioned immunosuppression. Psychosom
Med. 1975;37:333-40.
30. Sapolsky RM, Alberts SC, Altmann J. Hypercortisolism associated with
social subordination or social isolation among wild baboons. Arch Gen Psychia-
try. 1997;54:1137-43.
31. Alessandirni F, Schulz H, Takenaka S, Lentner B, Karg E, et al. Effects of
ultrafine carbon particle inhalation on allergic inflammation of the lung. J Al-
lergy Clin Immunol. 2006;117:824-30.
32. Lubitz S, Schober W, Pusch G, Effner R, Klopp N, et al. Polycyclic aromatic
hydrocarbons from diesel emissions exert proallergic effects in birch pollen
allergic individuals through enhanced mediator release from basophils. Environ
Toxicol. 2010;25:188-97.
33. WHO (World Health Organization). Health risks of heavy metals from
long range transboundary air pollution. Report No. DK-2100. Copenhagen -
DK. 2007. Available:
http://www.euro.who.int/__data/assets/pdf_file/0007/78649/E91044.pdf
[Accessed 17 August 2011].
34. Alberg AJ, Samet JM. Epidemiology of lung cancer. Chest. 2003;123:
21S-49S.
35. Willett WC. Balancing life-style and genomics research for disease pre-
vention. Science. 2002;296:695-8.
36. Jones P.A. (2001). Death and methylation. Nature, Vol. 409: 141-144.
37. Seppa N. Silencing the BRCA1 gene spells trouble. Science News.
2000;247.
38. Baylin SB. Tying it all together: epigenetics, genetics, cell cycle, and cancer.
Science. 1997;277:1948-9.
39. Willeboordse FH. Chaos and Fractals, Faculty of Science, National Univer-
sity of Singapore. 2002. Available:
http://chaos.nus.edu.sg/teaching/GEM2505/indexlectures.html [Accessed 17
August 2011].
40. Meiners S, Ludwig A, Stangl V, Stangl K. Proteasome inhibitors: poisons
and remedies. Med Res Rev. 2008;28:309-27.
41. Stewart J. The Biology of Memory. Enaction Summer School, Laboratoire
d'Informatique en Image et Systèmes d'information. University of Lion. 2008.
Available: http://liris.cnrs.fr/enaction/docs/documents2008/stewart-2008-
text.pdf [Accessed 17 August 2011].
42. Jablonka E, Lamb MJ. The changing concept of epigenetics. Ann NY Aca
Sci. 2002;981:82-96.
43. Hollick JB, Dorweiler JE, Chandler VL. Paramutation and related allelic
interactions. Trends Genet. 1997;13:302-8.
44. Sarge KD, Park-Sarge OK. Gene bookmarking: keeping the pages open.
Trends Biochem Sci. 2005;30:605-10.
45. Nadeau K, McDonald-Hyman C, Noth EM, Pratt B, Hammond SK, et al.
Ambient air pollution impairs regulatory T-cell function in asthma. J Allergy Clin
Immunol. 2010;126:845-52.
46. Blum JL, Hoffman C, Xiong JQ, Zelikoff JT. Exposure of pregnant mice to
cadmium oxide (CdO) nanopartides (NP) poses a risk to the developing off-
spring. Biol Reprod. 2010;122:S115.
47. Allis CD, Jenuwein T, Reinberg D, (2006). Epigenetics. CSH Press, Cold
Spring Harbor, NY - USA; p.321-476.
48. Tost J. (2008). Epigenetics. Caister Academic Press, Norfolk - UK; p.303-
386.
49. Thaler DS, (1994). The evolution of genetic intelligence. Science, Vol. 264:
224-225.
50. Waterland RA, Jirtle RL. Transposable elements: targets for early nutri-
tional effects on epigenetic gene regulation. Mol Cell Biol .
2003;23:5293‑300.
51. Wong AH, Gottesman II, Petronis A. Phenotypic differences in genetically
identical organisms: the epigenetic perspective. Hum Mol Genet. 2005;14:
R11-8.
theHealth | Volume 2 | Issue 3 | 107
Lung deposition predictions of airborne particles