
Identification of Novel Genetic Alterations in Samples of Malignant Glioma Patients
Upload
independentCategory
view
1download
0
Acta neuropath. (Berl.) 30, 243--249 (1974) �9 by Springer-u 1974
Diffuse Periventricular and Meningeal Glioma
D e v i n d e r B h r a n y , Michae l G. M u r p h y , S i m o n H o r e n s t e i n ,
a n d Sh i r l ey W. S i lbe r t
Departments of Pathology (Neuropathology), :Neurosurgery, and :Neurology St. Louis University Medical School
R~ceived July 15, 1974; Accepted September 10, 1974
Summary. Diffuse periventricular and meningeal gliomatosis occurring together in one patient without underlying definite infiltrative mass is a rare occurrence. A 46 year old woman suffered severe recurrent headaches for the last 18 months of her life. An acute confusional illness with increased intracranial pressure appeared 4 months before death and was followed by progressive mental deterioration, multiple cranial nerve palsies, weakness, muscle atrophy, sensory loss involving all four extremities and loss of bowel and bladder control. Postmortem diffuse glioma was fmmd to involve the periventrieular regions of the 3rd and 4th ventricles and the subaraehnoid space throughout the cerebrospinal axis, along and around the cranial and spinal nerves. I t is suggested in this case that the primary neoplastic change occurred in the subependymal glia with subsequent seeding of tumor cells throughout the subarachnoid space via cerebrospinal fluid pathways.
Key words: Glioma -- Periventricular -- Meningeal -- Subependymal Glia.
Introduction
Diffuse p e r i v e n t r i c u l a r a n d m e n i n g e a l g l i o m a t o s i s occu r r ing t o g e t h e r in 1
p a t i e n t w i t h o u t u n d e r l y i n g i n f i l t r a t i v e g r o w t h is a r a r e occur rence . I n a n e x t e n s i v e
r e v i e w o f t h e l i t e r a t u r e we h a v e b e e n u n a b l e to f ind a s imi l a r case. T h e p u r p o s e o f
th i s r e p o r t is t o e m p h a s i z e t h e d i t e m m a wh ich c l in ic ians m a y face in t h e m a n a g e -
m e n t o f such a p a t i e n t a n d r e c o r d t h e u n u s u a l p o s t m o r t e m findings.
Case R e p o r t
A 46 year old woman suffered severe recurrent headaches for one year. She woke one morning confused and soon had a generalized convulsion. She was admitted to a local hospital where for two weeks her confusion and lethargy progressed. The patient was then transferred t o the Firmin Desloge Hospital of St. Louis University.
On examination she was found to be lethargic and responded to various questions in- appropriately. The neck was stiff and resisted displacement in all directions. Fundi showed bilateral papilledema estimated to be 1.5--2D. The pupils were small and reacted sluggishly %o light and upon accomodation. She did not abduct her left eye. Spontaneous movements in the lower extremities were diminished. Except for an absent left knee jerk, all tendon -reflexes were symmetrical though sluggish. Plantar stimulation produced no response. Sensory examinat ion revealed loss of pinprick sensation over the left lower leg. Her gait was wide based. She was incontinent of urine.
A right retrograde brachial arteriogram was normal. The spinal fluid pressure was 430ram. 'The fluid was xanthochromic and the protein 1060 mg~ Sugar was 49 rag~ No white blood cells were seen but there were 84 RBC/mm ~. Gram stain of the spinal fluid showed no organisms and a cell block disclosed some inflammatory but no tumor cells. A ventriculo- g ram showed moderate dilatation of the ventricular system. Ventricular fluid was "under :pressure". I t was clear and contained 55 RBCs/mm 3 and 40 rag~ protein. A myelogram
244 D. Bhrany et at.
of the spinal axis below the foramen magnum showed no abnormality. In the next two weeks repeated spinal fluid examinations including cultures for bacteria, fungi and viruses were. unrevealing. During this period, she developed a sucking reflex, loss of upward gaze, and loss of the stretch reflexes in both upper and lower extremities. A ventriculoperitoneal shunt was emplaced at the end of the 4th week of illness. A brain biopsy obtained from the right occipital area at the time of the shunt procedure was unremarkable. Postoperatively there was no improvement in her neurological status and she was discharged to a nursing home.
The patient was readmitted 8 weeks later with progressive neurological deterioration. Her speech was inappropriate and dysarthric. Doll's head eye movements were present. The neck was stiff. She was unable to swallow. The muscles of both upper and lower extremities were weak and wasted. She was incontinent of urine and feces and had multiple decubitus ulcers over her back, sacrum and ankles. Her sensorium continued to deteriorate and she died two weeks later. Extensive laboratory investigation disclosed only diffuse slowing of the electroencephalogram.
Materials and Methods The brain was fixed in 10~ buffered formalin. For light microscopy, the tissue was em-
bedded in paraffin, and sections stained with hematoxylin and eosin, phosphotungstic acid hematoxylin (PTAH), Wilder's retieulum, and Luxol fast blue-periodic acid Schiff stains. For electron microscopy, random small fragments of formalin fixed tissue from the surface of the medulla and spinal cord were washed with Millonig's phosphate buffer, post-fixed in 2~ osmium tetroxide, dehydrated through graded alcohols and propylene oxide, and embed- ded in epoxy resin. Ultra-thin sections were stained with uranyl acetate and lead citrate and examined with Philips 300 electron microscope.
Pathology
Autopsy Findings. The general autopsy disclosed severe aspiration pneumonia, an abscess of the right kidney and hemorrhagic cystitis. No systemic primary or secondary tumors were found.
a b~
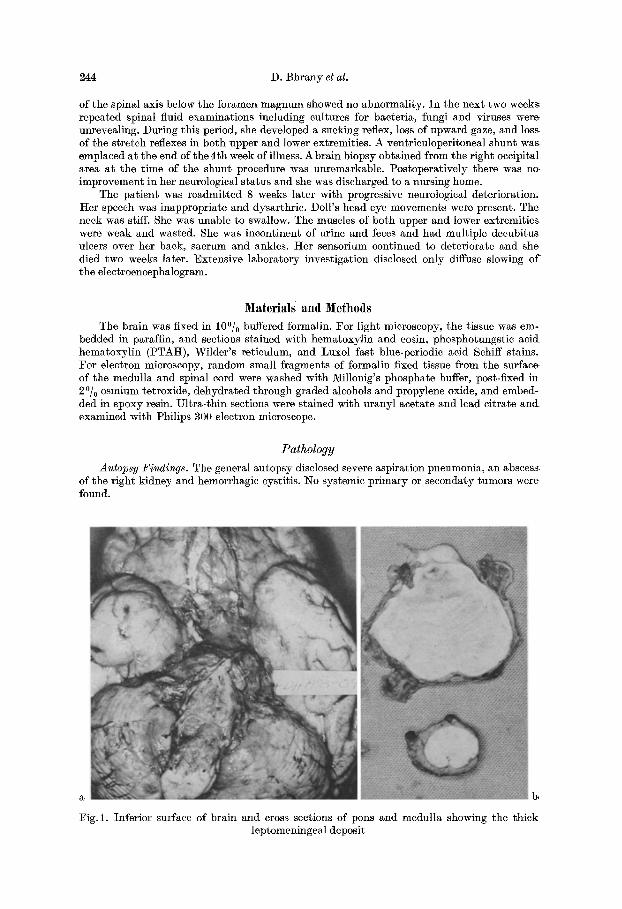
Fig. 1. Inferior surface of brain and cross sections of pons and medulla showing the thick leptomeningeal deposit

Diffuse Periventricular and Meningeal Glioma 245
b
a
Fig.2. (a) Fair ly uniform tumor cells fill the subarachnoid space over the cortex and spinal cord. The pia is in tac t with no parenehymal invasion ( • 65 H. E.)
(b and e) Higher magnification showing vesicular nuclei and delicate glial processes. No mitoses are seen. (b • 160 H. E.) (c • I60 PTAH)
Neuropathological Observations. Grossly the brain was edematous throughout bo th hemi- spheres. A tentorial groove was present on the r ight uneus 0.8 cm from the medial margin. The leptomeninges were clouded wi th diffuse pale gray to pale yellow infiltrate present over the convexities of the temporal and parietal lobes and the base of the brain where i t measured up to 2--3 ram thick. The infiltrate obli terated the landmarks along the ventra l surface of the brains tem and the c~reb~llum extending caudally along the entire circumference of the spinal cord (Fig. 1). A t the filum terminale the cauda equina was encased by a thick deposit which formed a mass 2.2 em in diameter. Coronal sections of the cerebral hemispheres showed congestion th roughout the gray and white matter . A subaraehnoid deposit of tissue up to 3 m m thick was present along the Sylvian fissure and the ventra l surface of the hypothalamus. The ventricIes were symmetrieMly narrowed. There were brown gray granular deposits along the ventr ieular surface most prominent in the 3rd and floor of the 4 th ventricles. Transverse

246 D. Bhrany et al.
Fig. 3. Third ventricle showing disruptions of the ependyma and shedding of tumor cells into the ventricular cavity ( • 16, H.-E.)
Fig.4. The spinal cord is surrounded by tumor cells which occasionally extend into the Vir- chow-Robin space (• 16, H.-E.)
sections of the brainstem showed the pons and medulla to be covered on their surfaces by a 2- -3 mm gray subarachnoid deposit. The aqueduct of Sylvius was patent. Sagittal sections of the cerebellum revealed a gray leptomeningeal infiltrate up to 1 mm thick. No discrete lesions were seen within the parenchyma of the central nervous system.
Microscopically the leptomeninges, subarachnoid space (Fig.2a--b), and the ventrieular system throughout the neuraxis were filled by rather uniform neoplastic astroeytes with pale vesicular nuclei and abundant delieate glial processes well demonstrated with the PTAH stain (Fig.2c), but negative for Wilder's reticulum stain. The leptomeningeal deposit was confined to the araehnoid and subaraehnoid space. I t did not breach the pial membrane, although occasional tumor cells were seen within the Virehow Robin spaces. Subependymal neoplastic proliferation was present diffusely along the walls and floor of the third and fourth ventricles. Small collections of tumor ceils caused nodular elevation of the ependyma and local disruption of its lining with streaming of tumor cells into the ventricular space (Fig. 3). The ehoroid plexus was free of tumor. However, neoplastic cells within the ventricle occasional- ly surrounded their villi. The aqueduct of Sylvius was patent without periaqueduetal tumor infiltrate. The cranial and spinal nerves, especially the roots of the eauda equina, were both surrounded and occasionally infiltrated by neoplastic astroeytes (Fig. 4) which also compressed the leptomeningeal vessels. Focal demyelination and vacuolization of lateral and anterior columns of the spinal cord were present beneath the thick meningeal infiltrate. No discrete tumor was found in multiple sections of the brain and spinal cord.
6
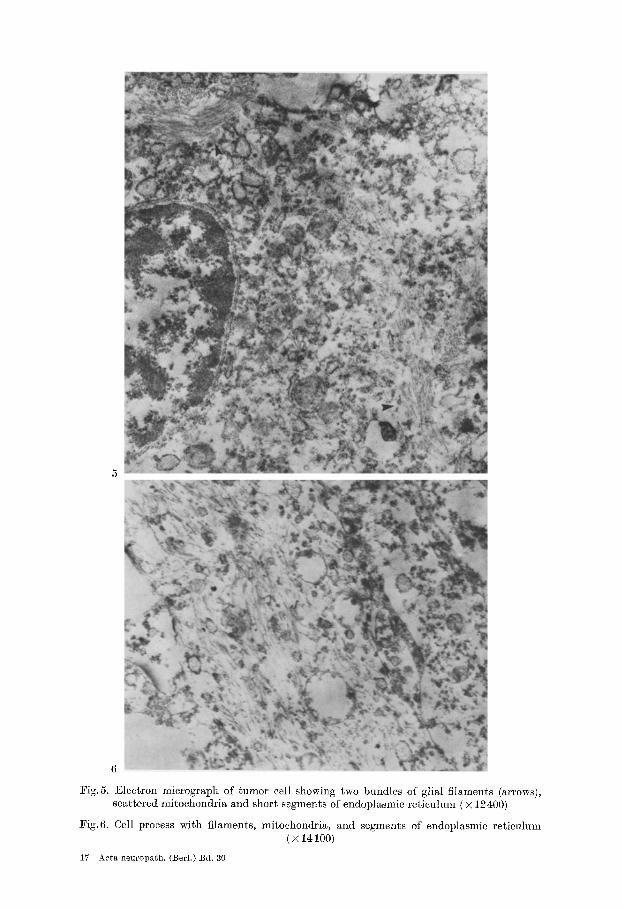
l~ig.5. Electron mierograph of tumor cell showing two bundles of glial filaments (arrows), scattered mitoehondria and short segments of endoplasmic reticulum ( • 12~00)
Fig.6. Cell process witch filaments, mitoehondria, and segments of endoplasmie reticulum ( • 14100)
17 Aeta neuropath. (Berl.) Bd. 30

248 D. Bhrany et al.
Electron microscopic examinatio;z showed the tumor cells to contain oval to round nuclei with moderate to small amounts of cytoplasm and occasional processes. The nuclei displayed focal margination of the chromatin along the nuclear membrane. Within the cytoplasm there were scattered free ribosomes, mitochondria, and short segments of rough endoplasmie reticu- lure. Occasional cisterns of Golgi complex were present. Small bundles of filaments similar to those seen in normal astrocytes were found within the cytoplasm (Fig.5). The processes contained longitudinally oriented filaments, mitochondria and segments of rough endoplasmic reticulum (Fig. 6). These features suggested the neoplastic cells to be astrocytic in origin.
Discussion
The clinical illness of this pat ient suggested a diffuse process involving the whole cerebrospinal axis such as a neoplasm or chronic inflammatory disease. Of the neoplastic processes, carcinomatous meningitis was considered very likely in view of the known involvement of the brain, spinal cord, cranial and spinal nerve roots in that disease state (Olson et al., 1971). A similar clinical picture may be seen with meningeal gliomatosis and pr imary leptomeningeal gliomas. Polmeteer et al. (1947) and Payan et al. (1968) described a total of 43 examples of meningeal gliomatosis. All of them, however, and in contrast to our patient, had a definite focal mass lesion. Pr imary leptomeningeal gliomas were believed by Bailey (1936) and Cooper and Kernohan (1951) to arise from hcterotopic glial nests in the lepto- meninges. These tumors are either entirely extracerebral with no connection with the underlying ncuraxis or may grow mainly in the subarachnoid space with bridges to the superficial layers of the adjacent cortex (Sumi et al., 1968). No ven- tricular involvement has been recorded.
We are aware of no case pathologically similar to ours, in which there was concomitant neoplastic involvement of the pcriventricular region and the lepto- meninges of the cerebrospinal axis. We suggest tha t the pr imary neoplastic trans- formation occurred in the glial cells of the subependymal plate owing to the mas- sive involvement of the ventricular wall. The subependymal cell plate contains immature cells which persist throughout postnatal life. Globus et al. (1944) de- scribed 9 brain tumors arising from these cells and Boykin et al. (1954) postulated subependymal glomerate astrocytomas to arise from these cells. Lantos (1972) produced periventricular gliomas in the offspring of pregnant female BD- IX rats by intravenous injection of N-ethyl-N-nitrosourea on the 15 day of gestation. The source of these gliomas was postulated to be the subependymal cell plate. Patho- logical findings in our ease suggest the possibility of an initial diffuse proliferation in the subependymal region of the 3rd and 4th ventricles. From the subependymal region, the tumor cells might then have infiltrated the ependymal lining and been shed into the ventricular system where they were carried into the subarachnoid space seeding throughout the cerebrospinal axis. Metastasis of glial tumor through- out the central nervous system by way of the CSF pathways is a well known event and has been described by Rubinstein (1972) and Best (1963). This sequence of events in evolution and spread of the tumor correlates very well with the clinical picture of our patient.
References Bailey, O. T. : Relation of glioma of the leptomeninges to neuroglia nests: Report of a case
of astrocytoma of the leptomeninges. Arch. Path. 21, 584--600 (1936)
Diffuse Periventrieular and Meningeal Glioma 249
Best, P. V. : Intracranial oligodendrogliomatosis. J. Neurol. Neurosurg. Psychiat. 26, 249--256 (1963)
]3oykin, F. C., Cowen, D., Iannucci, C. A. J., Wolf, A. : Subependymal glomerate astrocytomas J. Neuropath. exp. Neurol. 13, 30--49 (1954)
Cooper, I. S., Kernohan, J. W.: Heterotopic glial nests in the subarachnoid space: Histo- pathologic characteristics mode of origin and relation to meningeal gliomas. J. Neuropath. exp. Neurol. 10, 16--29 (1951)
Globus, J. H., Kuhlenbeek, H.: The subependymal cell plate (matrix) and its relationship to brain tumors of the ependymal type. J. Nenropath. exp. Neurol. 8, 1--35 (1944)
Lantos, P. L.: The fine structure of periventricular pleomorphic gliomas induced transpla- eentally by N-ethyl-N-nitrosourea in ]3D-IX rats. J. neurol. Sci. 17, 443--460 (1972)
Olson, M.E., Chernik, N.L., Posner, J. ]3.: Leptomeningeal metastasis from systemic cancer. A report of 47 eases. Trans. Amer. neurol. Ass. 96, 291 --293 (1971)
Payan, H., Toga, M., Berard, IV[., Hassoun, g.: Gliomatose m6ning6e d~ffuse du n6vraxe. Ann. Anat. path. 18, 253--262 (1968)
Polmeteer, F. E., Kernohan, J. W. : Meningeal gliomatosis. A study of 42 cases. Arch. Neurol. Psychiat. (Chic.) 57, 593--616 (1947)
Rubinstein, L. J. : Tumors of the central nervous system, Fascicle 6, Armed Forces Institute of Pathology, Washington, D. C. (1972)
Sumi, S. M., Leffman, It. : Primary intraeranial leptomeningeal glioma with persistent hy- poglycorrhachia. J. Neurol. Neurosurg. Psychiat. 81, 190--194 (1968)
Shirley W. Silbert, ~ . D. Department of Neuropathology St. Louis University School of Medicine 1402 South Grand Boulevard St. Louis, Missouri 63104 U.S.A.
1 7 "
Copyright © 2022 FDOKUMEN




















