
Diagnosing and Characterizing Neuropathic Pain in Dogs with ...
77
Diagnosing and Characterizing Neuropathic Pain in Dogs with Spinal Cord Injury Thesis Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the Graduate School of The Ohio State University By Austin Kerns, DVM Graduate Program in Comparative and Veterinary Medicine The Ohio State University 2018 Thesis Committee Members: Dr. Sarah Moore, Advisor Dr. Ronaldo da Costa Dr. Laurie Cook Dr. Nina Kieves
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Diagnosing and Characterizing Neuropathic Pain in Dogs with ...

Diagnosing and Characterizing Neuropathic Pain in Dogs with Spinal Cord Injury
Thesis
Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the
Graduate School of The Ohio State University
By
Austin Kerns, DVM
Graduate Program in Comparative and Veterinary Medicine
The Ohio State University
2018
Thesis Committee Members:
Dr. Sarah Moore, Advisor
Dr. Ronaldo da Costa
Dr. Laurie Cook
Dr. Nina Kieves

Copyright by Austin Kerns
2018

i
Abstract
Electronic von Frey anesthesiometry (VFA) has been previously reported by our
laboratory and others as a useful method of mechanical quantitative sensory testing (QST) for
evaluating neuropathic pain in dogs. Intraobserver agreement has been previously shown to be
good to excellent; however, interobserver agreement has not been evaluated and is vital to the
use of this technique in multicenter veterinary clinical trials in neuropathic pain. The goal of this
study was to evaluate the interobserver agreement of sensory thresholds obtained using
electronic VFA in a group of normal small breed dogs.
Twenty healthy dogs (< 20kg) were recruited from the general practice population at the
Ohio State University Veterinary Medical Center. Three novice evaluators used an electronic
von Frey device (IITC Life Science; Woodlands, CA) to measure mechanical sensory threshold
(ST) after a brief standardized training session conducted by an expert evaluator. Each dog was
evaluated by all three investigators on the same day with both evaluator and limb test order
randomized and testing sessions separated by five minutes.
Mean ST values were averaged for all four limbs to produce a single value per dog for
comparison between evaluators. Agreement between evaluators was determined using the intra-
class correlation coefficient (ICC; two-way model for consistency, single measures). ICC across
all three evaluators was 0.48, indicating moderate agreement. Moderate interobserver agreement
is not sufficient to support the use of this technique in multi-center clinical trials, and our results
underscore the importance of using a single evaluator for this QST technique in canine
neuropathic pain studies.
ii
VFA was then used to objectively measure mechanical ST in 21 dogs with acute spinal
cord injury (SCI) caused by spontaneous thoracolumbar intervertebral disc extrusion (IVDE) at
10 days, 30 days, and 90 days after decompressive hemilaminectomy. ST values were compared
over time and correlated with locomotor scores.
There was no significant change in ST in the thoracic limbs over the 90 day recovery
period. Pelvic limb ST were highest at 10 days consistent with hypoalgesia and declined over
time, though the decline from 30 to 90 days was not statistically significant (means ± standard
error of the mean ST for pelvic limbs at 10 days = 209.2 ± 14.1 g, at 30 days = 173.8 ± 11.1 g,
and at 90 days = 162.6 ± 12.3 g). A significant difference was identified in the pelvic limbs when
comparing ST at 10 and 30 days (mean difference 35.4 g; P=0.01) and at 10 and 90 days (mean
difference 46.7 g; P=0.001), but not at 30 and 90 days (mean difference 11.2 g; P=0.93). There
was an inverse correlation between locomotor score and pelvic limb ST over time (r = -0.5; P =
0.03). These findings are suggestive of recovery of sensorimotor spinal cord function, and
potentially the development of hyperesthesia indicative of neuropathic pain. This is the first
study to evaluate ST over an extended period of time to evaluate for chronic neuropathic pain in
dogs and results suggest the need for further longitudinal studies related to neuropathic pain in
dogs after SCI.
iii
Acknowledgements
I would like to thank my advisor and mentor, Dr. Sarah Moore for her guidance and
support throughout this process. I would also like to thank my examination committee for their
input and advice. I would like to thank Amanda Disher, Heather Anderson, Dr. Daniella
Vansteenkiste, and Dr. Ashley Hechler for their assistance with data collection. I would like to
thank Dr. Laurie Cook and Dr. Nina Kieves for their participation. Additionally, I would like to
thank the entire Neurology and Surgery service for their help in case recruitment.

iv
Vita
May 2005....................................................... El Camino High School
May 2009....................................................... B.S. Neurobiology, Physiology, & Behavior, UC
Davis
June 2013....................................................... D.V.M., UC Davis
2013 to 2014.................................................. Intern, University of Georgia
2014-2015...................................................... Neurology Intern, Veterinary Specialty Hospital of
San Diego
2015 to present .............................................. Residency in Neurology and Neurosurgery,
Veterinary Medical Center, The Ohio State
University
Publications
1. Kerns A, Brakel K, Premanandan C, Saffire A, Moore A. Extranodal non-B, non-T-cell
lymphoma with bilateral tympanic bulla involvement in a cat. J Fel Med Surg Open Rep.
2018: 1-5.
2. Kerns A, Kieves N, Cook L, Moore S. Interobserver Agreement of Mechanical Sensory
Thresholds in Normal Dogs. Intended for submission to The Veterinary Journal.
3. Kerns A, Cook L, da Costa R, Moore S. von Frey anesthesiometry to diagnose chronic
neuropathic pain after acute spinal cord injury caused by thoracolumbar intervertebral disc
extrusion in dogs. Intended for submission to The Veterinary Journal.

v
Fields of Study
Major Field: Comparative and Veterinary Medicine
vi
Table of Contents
Abstract……………………………………………………………………… …………………...i
Acknowledgements………………………………………………………………………....……iii
Vita……………………………...……………………………………………….………….…….iv
Publications………………………………………………………………………….………....…iv
Fields of Study……………………………………………………………………..………....…...v
Table of Contents………………………………………………………………………....………vi
List of Tables……………………………………………………………………..…………..…viii
List of Figures…………………………………………………………………...……………..…ix
Chapter 1: Introduction……………….………………………………………….………………..1
Chapter 2: Literature review…………………………………….…………………….………..…4
2.1 Pain syndromes after spinal cord injury…………………....………………………..……..4
2.1.1 Pain taxonomy…………………..…………………...………………………..…..……4
2.1.2 Neuropathic pain after spinal cord injury…………………….………..…………….....5
2.1.3 Pathophysiology of neuropathic pain after spinal cord injury…….…………….…......6
2.2 Von Frey anesthesiometry………………………...……………………………….……...12
2.3 Treatment of neuropathic pain after spinal cord injury…………………....……………...14
Chapter 3: Interobserver agreement of mechanical sensory thresholds in normal dogs ………...21
3.1 Abstract……………………………………...………………………………………........20
3.2 Introduction………………...………………………………………………………….….21
3.3 Materials and methods…………………...……………………………………….……….22
3.4 Results……………………………………………………………...………….………….24
3.5 Discussion………………………………………………………………..……………….25

vii
3.6 Conclusions…………………………………………………………………..…………...28
3.7 Conflict of interest statement…………………………………………..…………………28
3.8 Acknowledgements………………………………………………..………………….…..28
3.9 References…………………………………………………………..………….…………28
Chapter 4: von Frey anesthesiometry to diagnose chronic neuropathic pain after acute spinal cord
injury caused by thoracolumbar intervertebral disc extrusion in dog…………...….……………35
4.1 Abstract……………………………………………...…………………………………....35
4.2 Introduction……………………………………………………………...……….……….35
4.3 Materials and methods…………………...……………………………...………….…….37
4.4 Results………………………………………………………………….………...……….38
4.5 Discussion…………………………………………………………………………..…….41
4.6 Conclusions………………………………………………………………………..……...44
4.7 Conflict of interest statement……………………………………………………..………45
4.8 Acknowledgements………………………………………………………………...……..45
4.9 References………………………………………………………………………...………45
Chapter 5: Conclusions and future directions……………....……..……………………....…..…52
References………………………………………………………………………………………..55

viii
List of Tables
Table 1: List of drugs commonly used for treatment of neuropathic pain……….....……………15
Table 2: Comparison of mean sensory threshold for each observer for each dog. Sensory
threshold values from all four limbs in each dog are averaged to provide a mean sensory
threshold for each observer………………….…………………………………………………...32
Table 3: Intraclass correlation coefficient for each pair of observers and average for all observers
combined………………………………………………………………………….……………...33
Table 4: Summary of oral medications at day 10. No dogs were receiving medication at 30 or 90
days……………………………………………………………………………………………....48
Table 5: Mean sensory threshold for each limb across three testing sessions over 90 days…….49

ix
List of Figures
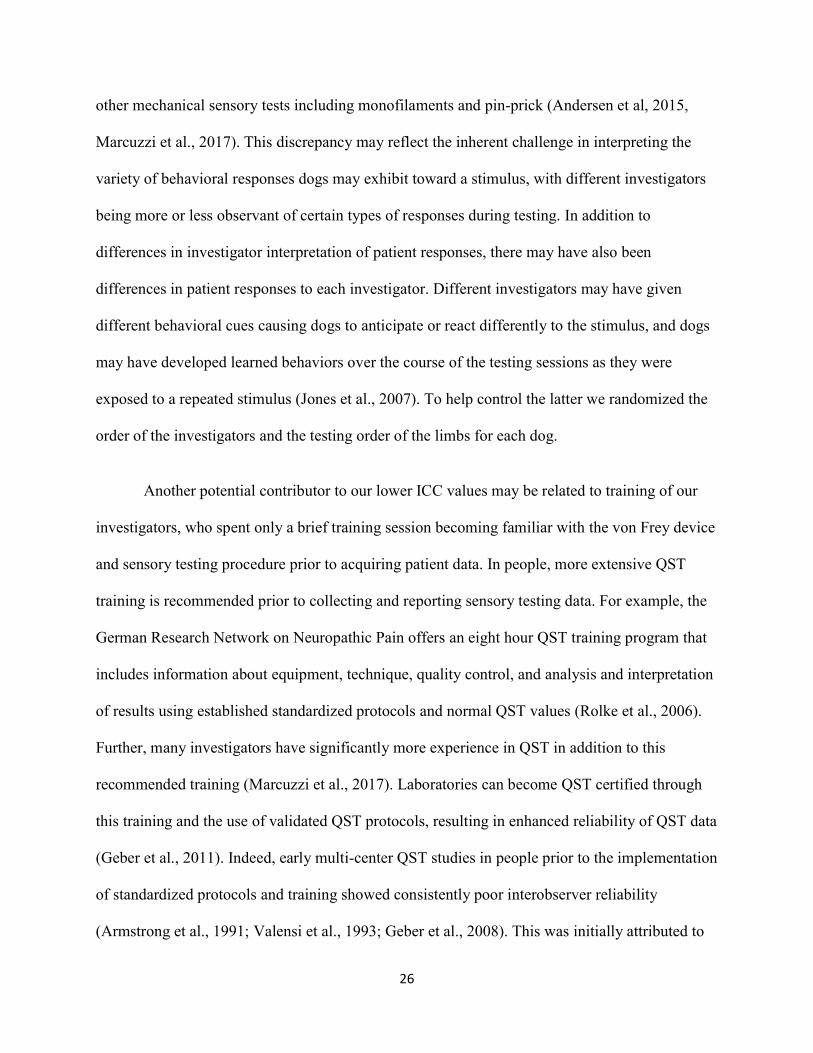
Figure 1: The electronic von Frey device and patient positioning for mechanical quantitative
sensory testing in dogs. The device consists of a load cell (A), handle (B), recording device (C),
and tip (D). The system measures and displays the amount of pressure applied to a subject, from
0.1 to 1000 g……………………………....………………………………………………..……33
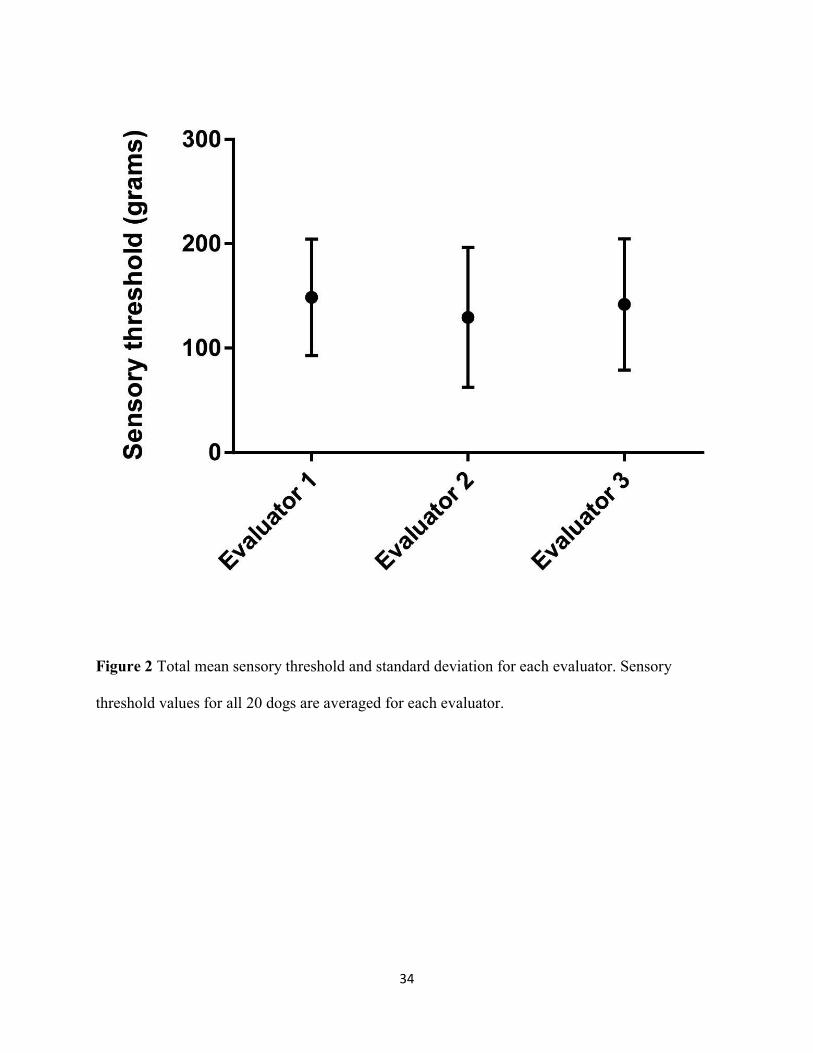
Figure 2: Total mean sensory threshold and standard deviation for each evaluator. Sensory
threshold values for all 20 dogs are averaged for each evaluator...…………………....……...…34
Figure 3: Mean ± SEM for combined thoracic limb and combined pelvic limb ST values at each
time point ……………………………………………………....………………………………..51

1
Chapter 1
Introduction
Spinal cord injury (SCI) is a common condition in both domestic animals and people. An
estimated 276,000 people in the United States currently live with disabilities from SCI, with
approximately 17,000 new cases of SCI reported each year (National Spinal Cord Injury
Statistical Center [NSCISC], 2016). Causes of SCI in dogs include intervertebral disc extrusion,
spinal fracture, and fibrocartilaginous embolism. Intervertebral disc extrusion (IVDE) is by far
the most common cause of acute SCI in dogs, affecting approximately 3.5% of dogs under the
age of 12 (Bergknut et al., 2012), and comprising 2% of all veterinary hospital visits (Brisson et
al., 2010; Webb et al., 2010; Levine et al., 2011). SCI results in permanent changes in sensory
and motor function, and the life-altering and life-limiting consequences after injury are
appreciated across species. The most common and most debilitating of these are impaired
mobility and development of neuropathic pain (Sjolund et al., 2002; Kloos et al., 2005; NSCISC
2016).
Neuropathic pain is a type of pain caused by damage to or dysfunction of nervous tissue
and is generated by the subsequent changes in formation and modulation of nociceptive signaling
(Treede et al., 2008). This pain persists long after resolution of the initial injury and is often
associated with burning, stabbing, and tingling sensations (Merskey et al., 2002). Neuropathic
pain syndromes are characterized by allodynia (pain associated with a non-painful stimulus) and
hyperesthesia (heightened sensitivity to a painful stimulus). This is distinguished from
nociceptive pain which is caused by damage to non-nervous tissue and inflammation resulting in

2
stimulation of nociceptors. Nociceptive pain is often described as a sharp or throbbing pain that
decreases with resolution of the primary insult.
Up to 90% of people report chronic neuropathic pain after SCI (Boldt et al., 2014), which
is severe and disabling in up to 63% of cases (Turner et al., 2001). Estimates of the prevalence of
neuropathic pain have increased dramatically over the past decade as better methods for
detecting such pain have been developed (Freynhagen et al., 2006). Despite the fact that
neuropathic pain syndromes are well documented in humans with SCI, there is limited
information regarding its existence in dogs (Moore et al., 2013). This is likely because the
presence of neuropathic pain in people is typically self-reported and this is not possible in
veterinary patients. Further, sensory testing in dogs with SCI has been historically limited to
testing for the presence or absence of a behavioral response to pinching the toes, which is
interpreted as presence or absence of nociception, also referred to in the literature as deep pain
perception (Lascelles et al., 2013). While this relatively crude method is useful and important in
the clinical setting for determination of prognosis for recovery after SCI, it does not allow for
identification and quantification of neuropathic pain.
Given the prevalence of neuropathic pain in patients with SCI and its negative impact on
quality of life, further investigation into objective methods for sensory testing in veterinary
patients is of immense importance. Methods for quantitative sensory testing (QST) have been
developed for use in rodent models of SCI to test neuropathic pain and have also been employed
in the human clinical setting. Mechanical methods of QST typically test an objective value called
sensory threshold (ST), defined as the minimum amount of a particular stimulus (e.g. pin-prick,

3
light touch) that can be detected or is considered painful. QST allows objective evaluation of
allodynia and hyperesthesia, manifest as a decrease in ST (Felix et al., 2009; Walk et al., 2009).
Von Frey anesthesiometry (VFA) is a technique used for QST that tests ST for a
mechanical stimulus (a plastic pressure probe applied to the skin). Variations of this technique
have been applied in rodent models, dogs, and human patients (Detloff et al., 2012; Tena et al.,
2012; Lascelles et al., 2013). Patients with diminished sensation (hypoesthesia) have a higher
than normal ST, whereas patients with hyperesthesia and allodynia have a lower than normal ST
(Hoschouer et al., 2010). VFA has recently been shown to be a valuable technique to evaluate ST
in both normal dogs and dogs with SCI caused by IVDE (Moore et al., 2013; Song et al., 2016).
Not only does this offer an objective and reliable way to identify neuropathic pain in veterinary
patients, but also allows the use of dogs with SCI due to IVDE as a naturally-occurring model of
SCI and neuropathic pain. This is important for outcome assessment where therapeutic
interventions are intended for human clinical translation (Felix et al., 2009; Lascelles et al.,
2013).

4
Chapter 2
Literature Review
2.1 Pain syndromes after SCI
2.1.1 Pain Taxonomy
Specific types of pain syndromes are associated with SCI. A three-tier pain taxonomy has
been developed by the SCI Pain Task Force of the International Association for the Study of Pain
(IASP), which has assisted with standardization in description of pain in the human clinical
setting (Bryce et al., 2012). The first tier divides pain into the broad categories of nociceptive
and neuropathic pain. The second tier sub-divides these categories into organ systems:
Nociceptive pain can be visceral or musculoskeletal, while neuropathic pain is described in
reference to the level of SCI (at-level, above-level, or below-level). The third tier identifies
specific anatomical structures or etiologies as the source of pain (e.g. myocardial infarction for
visceral nociceptive pain, cauda equina compression for at-level neuropathic pain). An additional
pain category includes those syndromes that do not fit well into either nociceptive or neuropathic
pain, including fibromyalgia and complex regional pain syndrome. While these conditions have
characteristics of neuropathic, nociceptive, and mixed pain, unlike these causes of pain there is
no original tissue damage, and the source of pain appears to be functional in origin (Arnold et al.,
2016). Depending on the cause of SCI, several different nervous and non-nervous tissues can be
affected resulting in multiple concurrent pain syndromes.
The International Spinal Cord Injury Basic Pain Data Set was developed to aid in the
consistent collection and reporting of pain in the human SCI population (Widerstrom-Noga et al.,
2008, 2014). The data set contains clinically relevant core questions concerning SCI-related pain.

5
Questions cover the type, location, intensity, frequency, and duration of pain. The data set also
addresses the impact of pain on physical, emotional, and social function, and sleep. The basic
pain data set is intended to be used by health-care professionals in daily clinical practice and
provides a framework for standardized evaluation of pain in clinical studies.
2.1.2 Neuropathic pain after SCI
Neuropathic pain after SCI can be spontaneous without a peripheral stimulus, or evoked
due to an innocuous (allodynia) or noxious (hyperalgesia) stimulus (Baron et al., 2006).
Development of neuropathic pain is typically delayed weeks to months after SCI, and in rare
instances longer than a year (Tasker et al., 1992). Pain syndromes after SCI are classified as
central neuropathic pain because lesions affect the central nervous system. In the human clinical
setting, central neuropathic pain is diagnosed based on patient history and clinical sensory
examination. Clinical criteria include the presence of hyperalgesia, allodynia, or loss of
sensation, distribution of affected dermatomes, and an identified underlying cause (Treede et al.,
2008). There are three major distributions of chronic neuropathic pain with SCI. Above-level
pain occurs in dermatomes cranial to the site of injury, at-level pain occurs in dermatomes at the
site of injury, and below-level neuropathic pain occurs in dermatomes caudal to the neurological
lesion (Hulsebosch et al., 2009). These are described based on somatosensory mapping using
mechanical and thermal sensory testing (Vogel et al., 2016).
At-level pain can be present at the time of injury, or can develop directly afterward. This
pain is described as shooting, tingling, burning, pins and needles, and electric, and is associated
with allodynia and hyperesthesia (Widerstrom-Noga et al., 2008). At-level pain requires a lesion
in the spinal cord or nerve roots, and in many cases nerve root injury results in spontaneous pain
6
(Yezierski et al., 2000). A potential complication of SCI is syringomyelia, where a syrinx forms
at the site of SCI and expands with time resulting in further spinal cord damage. Syringomyelia
is implicated when new symptoms develop, particularly at-level neuropathic pain, months to
years after SCI (Tasker et al., 1992; Brodbelt et al., 2003).
Below-level pain is the most common central pain syndrome after SCI and is the most
difficult to treat (Turner et al., 2001). This pain is typically associated with a burning sensation
and can be spontaneous or evoked by different auditory stimuli or movements (Widerstrom-
Noga et al., 2008). Various regions of the limbs, hands/feet, and digits are commonly reported
sites of below-level pain (Soler et al., 2010). At-level hypersensitivity, determined by QST, after
complete SCI has been associated with below-level pain (Vogel et al., 2016). Injuries that affect
spinothalamic tracts are associated with below-level pain, where changes in neuronal excitability
of residual spinothalamic afferents are suspected to play a role (Finnerup et al., 2014).
Above-level pain develops reliably in rodents with a variety of SCI, typically manifested
as forelimb hyperalgesia after thoracic SCI (Mills et al., 2001; Wang et al., 2008; Carlton et al.,
2009; Densmore et al., 2010). However, the limited QST data in humans and primates suggests
that above-level pain is uncommon (Defrin et al., 1999; Finnerup et al., 2003; Masri et al., 2012),
which may implicate important species differences in neuropathic mechanisms for above-level
pain.
2.1.3 Pathophysiology of neuropathic pain after SCI
In its functional state, pain serves a protective role to prevent or minimize tissue damage.
It provides an important defense mechanism by alerting the body to noxious stimuli including
mechanical, thermal, and chemical insults. When pain persists without potential or actual tissue

7
damage it is maladaptive, and becomes the disease itself. The generation of pain in response to a
noxious stimulus involves four basic steps: 1. Transduction of the noxious stimulus into a
nociceptive signal, 2. Transmission of the nociceptive signal from the site of injury to the central
nervous system via Aẟ and C fibers, 3. Modulation of the signal by ascending, descending, and
local facilitation and inhibition, and 4. Perception of pain manifested as cognitive and emotional
responses that are a key component of clinical pain (Cohen et al., 2014). In the physiologic state
these steps are well regulated, but in the pathophysiologic state after neurotrauma (e.g. after SCI)
there is dysregulation resulting in neuropathic pain.
The four steps for generation of pain described previously allow for accurate coding of
external stimuli as noxious or non-noxious. Specifically, dorsal horn neurons along the spinal
cord are a key component of the nociceptive apparatus to correctly characterize external stimuli
(Thalhammer et al., 1994). Alteration of dorsal horn neuronal function results in loss of accurate
sensory perception and abnormal sensory recognition, and may ultimately lead to the perception
of non-noxious input as noxious (allodynia) or enhance noxious input (hyperesthesia) (Drew et
al., 2004; Hains et al., 2005; Gwak et al., 2008). For this reason, a primary cause of neuropathic
pain after SCI is hyperexcitability of dorsal horn neurons for which a variety of underlying
mechanisms have been identified including peripheral sensitization, reorganization of synaptic
circuits, altered intracellular pathways, disinhibition, and activation of glial cells (Hulsebosch et
al., 2009; Gwak et al., 2011; Cohen et al., 2014). These mechanisms are further discussed here.
Peripheral sensitization occurs when there is a decreased threshold for firing of
nociceptors and/or increased frequency of firing in response to stimulation. Electrophysiological
study of peripheral nociceptors after SCI has revealed peripheral sensitization with both
8
enhanced activity to evoked stimuli (mechanical and thermal) and increased spontaneous activity
in the absence of external stimuli (Carlton et al., 2009). This chronic spontaneous activity in
primary peripheral nociceptors after SCI has been shown to result in pain-related behavior (Bedi
et al., 2010). Dorsal root ganglion neurons also play an important role in peripheral sensitization.
There are a variety of isoforms of voltage-gated sodium channels (the Nav family) in dorsal root
ganglion neurons, classified as either tetrodotoxin sensitive (TTX-S) or tetrodotoxin resistant
(TTX-R) (Goldin et al., 2000; Yin et al., 2016). After SCI, there are dramatic changes in
expression of some of these sodium channels, with an increase in expression of TTX-S isoforms
and decrease in expression of TTX-R isoforms in affected dorsal root ganglion neurons (Yin et
al., 2016). This altered transcription of Nav genes may result in abnormal action potential firing
and contribute to spontaneous pain.
Further support for the role of sodium channels in the development and maintenance of
neuropathic pain is that a particular TTX-S isoform, Nav1.3, which is normally not expressed in
dorsal root ganglion neurons, is expressed after peripheral nerve injury (Black et al., 1999).
Recent evidence has shown that inhibition of Nav1.3 in injured dorsal root ganglia diminishes
allodynia (Samad et al., 2013; Tan et al., 2015). Dorsal root ganglion neurons appear to
contribute to below-level pain after SCI as demonstrated by systemic, but not intrathecal,
administration of sodium-channel blockers resulting in diminished allodynia and hyperalgesia
(Weston et al., 2009; Hama et al., 2010).
In addition to peripheral sensitization, primary changes in the function and distribution of
dorsal horn neurons after SCI contribute to neuropathic pain. Dorsal horn neurons are
categorized as low threshold (which respond primarily to non-noxious stimuli), high threshold

9
(which respond primarily to noxious stimuli), and wide dynamic range neurons (which respond
to several stimuli but maximally to noxious stimuli) (Maixner et al., 1986; Chung et al., 1986;
Leem et al., 2010). Normally, low threshold neurons are found in the deep dorsal horn where
non-noxious information is received from the periphery. High threshold neurons are found in the
superficial dorsal horn where noxious information is received predominantly from Aẟ and C
fibers. Wide dynamic range neurons are found throughout the dorsal horn (Menetrey et al.,
1977). In vivo electrophysiological data has shown that there is increased excitability in all three
types of dorsal horn neurons after SCI over the course of a month compared to controls (Gwak et
al., 2011). Not only do dorsal horn neurons become more excitable, but their proportions change
as well, with the proportion of low threshold neurons decreasing in the deep dorsal horn and
proportion of wide dynamic range neurons increasing in all areas of the dorsal horn after injury
(Hao et al., 2004; Gwak et al., 2011).
The mechanism underlying this altered distribution is unknown, but one possible
explanation is a dorsal horn neuronal phenotypic switch: After nerve injury there are significant
changes in gene expression that can result in changes in excitability, transduction, and
transmission. Ultimately, this can result in a change in the phenotype of neurons, where certain
genes are now upregulated or downregulated allowing a neuron to take on different functional
characteristics. This has been demonstrated in injured nerves where non-nociceptive fibers begin
expressing neuromodulators normally expressed by C fibers such as calcitonin gene related
peptide or substance P (Ueda et al., 2006). In the case of dorsal horn neurons this may, for
example, result in low threshold neurons that normally receive and transmit non-nociceptive
signals taking on the characteristics of wide dynamic range neurons, which could result in
allodynia.

10
Once dorsal horn neuronal hyperexcitability develops it continues for months, and
persists after injury. One possible explanation for continued hyperexcitability is reorganization of
synaptic circuits in the dorsal horn after SCI. SCI results in damage to ascending and descending
pathways in the spinal cord. After the primary injury, secondary injury occurs that results in
further disruption of synaptic circuits with continued neuronal death (Wasner et al., 2008).
Following injury, surviving neurons and microglia produce neurotrophic factors such as nerve
growth factor, which promotes regeneration and axon sprouting of primary afferent fibers and
subsequent newly formed synaptic circuits in the dorsal horn (Christensen et al., 1997).
Normally, primary afferents carrying non-noxious information would terminate in the deep
dorsal horn and those carrying noxious information would terminate in the superficial dorsal
horn. However, expression of nerve growth factor by primary afferent fibers after SCI results in
atypical axonal sprouting and inappropriate synapse formation. As a result, deep dorsal horn
neurons receive nociceptive signals and superficial dorsal horn neurons receive non-nociceptive
signals. This results in neuronal hyperexcitability and abnormal neuronal response properties
(Braz et al., 2009). When treated with anti-nerve growth factor after SCI, there is reduced
primary afferent sprouting, decreased dorsal horn excitability, and decreased neuropathic pain
(Christensen et al., 1997; Romero et al., 2000). Together, changes in the dorsal horn neuronal
populations and synaptic circuits offer an explanation for the permanent changes seen in dorsal
horn neuronal hyperexcitability and subsequent chronic central neuropathic pain.
Another mechanism for post-SCI dorsal horn neuron hyperexcitability and neuropathic
pain is altered intracellular pathways. SCI results in large increases in extracellular glutamate
concentrations (McAdoo et al., 1999), which then leads to receptor activation and increased

11
intracellular calcium levels (Tator et al., 1991). These changes lead to activation of various
protein kinases and downstream transcriptional factor pathways that result in central sensitization
(Crown et al., 2006). For example, it has been shown that a number of mitogen-activated protein
kinases (MAPKs) are activated after SCI, which then phosphorylate and activate transcription
factors (Crown et al., 2006). One of these transcription factors, cyclic AMP response element
binding protein (CREB), has been highlighted for its role in nociception (Ji et al., 2003). In a rat
model of SCI, both MAPKs and CREB had increased activity in microglia, astrocytes, and dorsal
horn neurons in rats that went on to develop at-level allodynia, compared to normal activity in
rats that did not develop neuropathic pain (Crown et al., 2006, 2008). Further, use of a MAPK
inhibitor after SCI resulted in dose-dependent attenuation of allodynia and decreased dorsal horn
neuronal hyperexcitability (Crown et al., 2008).
In addition to activation of certain intracellular pathways, disinhibition also plays an
important role in the development of neuropathic pain. Gamma-amino butyric acid (GABA) acts
to inhibit dorsal horn cells via GABA receptors distributed in presynaptic and postsynaptic
neurons and glial cells (Malcangio et al., 1996). After SCI there is altered ratios of apoptotic and
antiapoptotic factors resulting in death of GABAergic neurons (Rafati et al., 2008). Furthermore,
there is proinflammatory cytokine activation of caspases that result in apoptosis of GABA
interneurons in the dorsal horn (Meisner et al., 2010). There is increasing evidence that this loss
of GABAergic tone after SCI contributes to the development and maintenance of central
neuropathic pain. Several SCI models have shown good correlation between loss of GABA
function, dorsal horn hyperexcitability, and neuropathic pain (Hao et al., 1991; Gwak et al.,
2008). When GABAergic tone is returned by a variety of mechanisms, there is decreased

12
neuronal hyperexcitability, allodynia, and hyperesthesia (Liu et al., 2004; Eaton et al., 2007; Kim
et al., 2010).
2.2 Von Frey anesthesiometry
Quantitative sensory testing (QST) analyzes the response to a quantified external
stimulus, typically applied to the skin. A variety of external stimuli can be used, the most
common being touch, vibration, pin-prick and thermal (cold, warmth, burning) stimuli.
Assessment of mechanical stimuli can be used to assess large fiber and dorsal column function,
while thermal and pain thresholds can be used to assess small fiber (Aẟ and C fibers) and
spinothalamic tract function (Nathan et al., 1986). Methods for QST have long been developed
for use in rodent models of SCI and in the human clinical setting. QST has been promoted for
more accurate evaluation of somatosensory dysfunction in neuropathic pain populations
(Greenspan et al., 2001), and standardized protocols and normal values have been published
(Rolke 2006). Many of these methods test an objective value called sensory threshold (ST),
defined as the minimum amount of a particular stimulus that can be detected or is considered
painful. However, when performing QST in animals, they cannot communicate verbally and thus
ST is by convention defined as the strength of stimulus required to produce a conscious
behavioral response to that stimulus (Mills et al., 2001; Detloff et al., 2012; Moore et al., 2013).
Use of QST and ST allows for evaluation of somatosensory hypofunction and hyperfunction,
both of which are common after SCI.
Von Frey Anesthesiometry (VFA) is one method of QST that has primarily been used in
rodent models and human clinical setting. This technique, first described by Max von Frey in
1895, tests ST by applying a mechanical stimulus to the skin, allowing for assessment of

13
mechanical hyperesthesia. Von Frey monofilaments have been used historically and are still used
today, but the more recent electronic VFA has simplified the procedure. Electronic VFA uses a
plastic probe to apply a punctate mechanical stimulus, with the pressure at which ST is achieved
being automatically recorded. Variations of this technique have been applied in rodent models,
dogs, and human patients (Detloff et al., 2012; Tena et al., 2012; Lascelles et al., 2013). Patients
with diminished sensation have a higher than normal ST because they require a larger stimulus
for detection, while patients with hyperesthesia or allodynia have a lower than normal ST
(Hoschouer et al., 2010). The use of electronic VFA has allowed for more rapid and reproducible
results in the human clinical setting (Tena et al., 2012).
VFA has shown promise in veterinary medicine as a useful clinical and research
tool. VFA has been used in dogs to assess the pharmacodynamics and anti-nociceptive effects of
a variety of medications (KuKanich et al., 2005, 2011, 2016; Abimussi et al., 2014), identify
sensory abnormalities in dogs with orthopedic disease (Brydges et al., 2012; Tomas et al., 2014),
and quantify postoperative pain with different surgery techniques for ovariohysterectomy (Case
et al., 2011). Recently, a modified dorsal technique for VFA in dogs has been shown to be a
reliable method for QST in normal dogs and in dogs with SCI due to IVDE, and has shown a
difference in ST between normal and SCI dogs (Moore et al., 2013; Song et al., 2016). Chronic
neuropathic pain after SCI has yet to be investigated in dogs. Spontaneous SCI is common in
dogs (Levine et al., 2011), and results in similar histologic and structural changes in the spinal
cord as humans (Smith et al., 2006; Bock et al., 2013). Not only does VFA offer an objective and
reliable way to identify neuropathic pain in veterinary patients, but also allows the use of dogs
with SCI due to IVDE as a naturally-occurring model of SCI and neuropathic pain. This is

14
important for outcome assessment where therapeutic interventions are intended for human
clinical translation (Felix et al., 2009; Lascelles et al., 2013).
2.3 Treatment of neuropathic pain after spinal cord injury
SCI is common in people and domestic animal species. A large majority of people report
chronic neuropathic pain after SCI (Boldt et al., 2014), which is severe and disabling in many
cases (Turner et al., 2001). Neuropathic pain is also a common and reliable outcome in SCI
rodent models, but has not yet been thoroughly explored in veterinary medicine. While rodent
models have allowed elucidation of several potential mechanisms and treatment targets for
neuropathic pain, translation to effective treatment in people has not yet been borne out. Despite
significant improvement in managing other comorbidities after SCI (e.g. cardiorespiratory, skin,
bladder, and bowel complications), neuropathic pain has remained largely refractory to treatment
and continues to be the most debilitating problem that people face (Finnerup et al., 2003;
Cardenas et al., 2009). Clinical resolution of pain is often unrealistic, and modulation of pain
may be a more reasonable and achievable goal.
A variety of pharmacological interventions have been used to treat neuropathic pain after
SCI. These include anticonvulsants (gabapentin, pregabalin), antidepressants (amitriptyline,
trazodone), analgesics (lidocaine, ketamine, opioids), cannabinoids (tetrahydrocannabinol) and
antispasticity medications (baclofen, botulinum toxin) (Table 1). Treatment is generally long-
lasting and so the expected benefits and potential side effects should be carefully considered.
Two recent systematic reviews evaluated the evidence for more than twenty pharmacologic
agents after SCI. Both concluded that only gabapentin and pregabalin have strong evidence for
their ability to modulate neuropathic pain, and are now considered first-line treatment (Teasell et

15
al., 2010; Hagen et al., 2015). Amitriptyline, a tricyclic antidepressant, may have some effect on
certain types of neuropathic pain including pain associated with diabetic neuropathy and
postherpetic neuralgia (Moore et al., 2012). Injectable analgesics in general can help to decrease
neuropathic pain, but these only provide short-term relief and require the patient to be in the
hospital. In particular, opioids are commonly prescribed for both neuropathic and nociceptive
pain. After nerve injury, dorsal root ganglia have decreased expression of μ opioid receptors and
dorsal horn neurons become less responsive to opioids (Kohno et al., 2005). In contrast,
inflammation can increase expression and affinity of opioid receptors that enhances the efficacy
of opioids (Przewlocki et al., 2001). This may explain why patients with chronic neuropathic
pain require higher doses of opioids compared to those with nociceptive pain (Benedetti et al.,
1998). Unique to opioid exposure in people is opioid-induced hyperalgesia, characterized by a
paradoxical response where a patient receiving opioids to treat pain may actually become more
sensitive to that pain. While several mechanisms for opioid-induced hyperalgesia have been
proposed, none have been confirmed (Lee et al., 2011). The remainder of treatments show no
effect or inconclusive results (Teasell et al., 2010; Hagen et al., 2015).
Table 1 Medications used for neuropathic pain.
Analgesics Major Mechanism of Action Selected References (Human; Veterinary)
Anesthetics/Antiarrhythmics
Ketamine NMDA receptor antagonist Eide 1995; Kaka 2016
Lidocaine voltage-gated Na+ channel blocker Finnerup 2005; Kaka 2016
Mexiletine voltage-gated Na+ channel blocker Chiou-Tan 1996; Not evaluated
Opioids Alfentanil μ-opioid receptor agonist Eide 1995; Arndt
1986 Morphine μ-opioid receptor agonist Attal 2002; KuKanich

16
2005 Tramadol μ-opioid receptor agonist; SNRI Norbrink 2009;
Schutter 2017 Antidepressants
Amitriptyline SNRI Moore 2012; Cashmore 2009
Duloxetine SNRI; Na+ channel blocker Vranken 2011; Not evaluated
Lithium Unknown Yang 2012; Not evaluated
Trazodone serotonin receptor antagonist Davidoff 1987; Not evaluated
Antiepileptics Carbamazepine voltage-gated Na+ channel blocker Salinas 2012; Not
evaluated Gabapentin voltage-gated Ca++ channel blocker Levendoglu 2004;
Plessas 2015 Lamotrigine voltage-gated Na+ channel blocker Finnerup 2002; Not
evaluated Levetiracetam binds synaptic vesicle glycoprotein 2A Finnerup 2009; Not
evaluated Pregabalin voltage-gated Ca++ channel blocker Siddall 2006; Salazar
2009 Valproate voltage-gated Na+ channel blocker;
increases brain GABA levels Drewes 1994; Not evaluated
Cannabinoids Cannabis cannabinoid receptor agonist Wade 2003; Not
evaluated Dronabinol cannabinoid receptor agonist Rintala 2010; Not
evaluated Tetrahydrocannabinol cannabinoid receptor agonist Phillips 2010; Not
evaluated NMDA, N-methyl-D-aspartate ; SNRI, serotonin-norepinephrine reuptake inhibitor ; GABA, gamma-aminobutyric acid
Gabapentin was initially designed to mimic the structure and function of the inhibitory
neurotransmitter GABA, and thereby act as an anticonvulsant. While it is structurally similar to
GABA, it was subsequently discovered to be useful in the treatment of pain. Gabapentin appears
to act via binding the α2ẟ subunit of voltage gated calcium channels resulting in decreased
17
calcium influx and diminishing excitatory neurotransmitter release (Offord et al., 2015). One to 2
weeks after nerve injury, there is increased expression of calcium channels containing the α2ẟ
subunit in and around the dorsal root ganglia, which results in increased excitability (Luo et al.,
2001). Administration of gabapentin has been shown to decrease nociceptive signaling (Hendrich
et al., 2008), and provides adequate relief of neuropathic pain in about one third of patients
(Moore et al., 2014). While side effects are common, they are generally mild and well-tolerated.
The most common side effects seen are dizziness and somnolence, and severe effects were found
to be no more common than with placebo (Moore et al., 2014). Gabapentin is also commonly
prescribed for veterinary patients to alleviate pain, though its efficacy has not been established
for chronic neuropathic pain in animals. While gabapentin’s side effects have not been
thoroughly investigated in veterinary medicine, it appears to have a similar safety profile as in
people, perhaps with even more mild sedative effects at higher dosages.
There are limited clinical studies evaluating the analgesic effects of gabapentin in dogs.
In a study evaluating gabapentin as an adjunctive analgesic in dogs after mastectomy, dogs
receiving gabapentin required 44% less rescue analgesia with morphine compared to placebo,
despite no differences in pain scores (Crociolli et al., 2015). A similar study evaluated
gabapentin in dogs undergoing hemilaminectomy for IVDE, where gabapentin was started 12
hours prior to surgery, and no differences in pain score were found compared to placebo
(Aghighi et al., 2012). A study evaluating gabapentin in dogs undergoing forelimb amputation
also found no difference in pain scores postoperatively compared to placebo (Wagner et al.,
2010). Of note is that a gabapentin dose of 5-10 mg/kg given every 12 hours was used in these
studies. Based on available pharmacokinetic data in dogs, a dose of 10-20 mg/kg given every 8
hours may be necessary to maintain minimum effective plasma concentrations, and in some dogs

18
an even higher dose or frequency may be necessary (Kukanich et al., 2011). Further, as
previously discussed the primary molecular target for gabapentin is the α2ẟ subunit of voltage
gated calcium channels in the dorsal root ganglion and dorsal horn of the spinal cord, and
upgregulation of these calcium channels does not occur in the immediate postoperative period
(Luo et al., 2001). These studies are therefore likely evaluating the immediate postoperative
analgesic effects of gabapentin on nociceptive pain rather than a chronic pain state, which may
explain why no change in pain score was identified in dogs undergoing these various surgical
procedures. For this reason, the results of these studies are difficult to translate to dogs with
chronic neuropathic pain.
One study has evaluated the use of gabapentin at approximately 10 mg/kg given every 8
hours in dogs with Chiari-like malformation and syringomyelia, with clinical signs suggestive of
chronic neuropathic pain. No difference was found in the quality of life of these dogs when
gabapentin and carprofen were used compared to carprofen alone (Plessas et al., 2015). Even less
information about pregabalin exists in veterinary medicine. A pharmacokinetic study using a
single dose of 4 mg/kg in normal dogs resulted in plasma levels remaining above the reported
therapeutic minimum in people for slightly over 11 hours, suggesting that dosing pregabalin
every 12 hours may be adequate (Salazar et al., 2009). No clinical studies have evaluated the
efficacy of pregabalin in dogs, and the significantly higher cost of pregabalin compared to
gabapentin often precludes its use in the veterinary clinical setting, particularly for chronic
administration.
Given the significant impact of neuropathic pain on daily function and quality of life in
people, and the difficulty in treating neuropathic pain, further research is necessary to improve
19
our ability to diagnose and treat neuropathic pain in veterinary patients. This would not only
allow for better care and improved quality of life in veterinary patients, but also open an entire
field of inquiry to translate this information to the human clinical setting. One of the primary
methods for evaluating neuropathic pain in people is via quantitative sensory testing, which has
only just begun to be explored in the veterinary clinical setting. Further validation of mechanical
sensory testing in veterinary patients, including interobserver reliability, must be performed prior
to implementing this technique in multi-center trials allowing for large-scale pain studies in dogs.
Once validated, the prevalence and character of neuropathic pain in the veterinary population can
be detailed, and subsequently the efficacy of various treatments, including gabapentin, can be
explored. The aims of this project were to 1. Determine the interobserver reliability of VFA in
normal dogs, and 2. Use VFA to evaluate the existence and time course for development of
neuropathic pain in dogs with acute SCI due to IVDE.

20
Chapter 3
Interobserver Agreement of Mechanical Sensory Thresholds in Normal Dogs
3.1 Abstract
Electronic von Frey anesthesiometry (VFA) has been previously reported as a useful
method of mechanical quantitative sensory testing (QST) for evaluating neuropathic pain in
dogs. Intraobserver agreement has been previously shown to be good to excellent; however,
interobserver agreement has not been evaluated and is vital to the use of this technique in
multicenter veterinary clinical trials in neuropathic pain. The goal of this study was to evaluate
the interobserver agreement of sensory thresholds obtained using electronic VFA in a group of
normal small breed dogs.
Twenty healthy dogs (< 20kg) were recruited from the general practice population at the
Ohio State University Veterinary Medical Center. Three novice evaluators used an electronic
von Frey device (IITC Life Science; Woodlands, CA) to measure mechanical sensory threshold
(ST) after a standardized training session conducted by an expert evaluator. Each dog was
evaluated by all three investigators on the same day with both evaluator and limb test order
randomized and testing sessions separated by five minutes.
Mean ST values were averaged for all four limbs to produce a single value per dog for
comparison between evaluators. Agreement between evaluators was determined using the intra-
class correlation coefficient (ICC; two-way model for consistency, single measures). ICC across
all three evaluators was 0.48, indicating moderate agreement. Moderate interobserver agreement
is not sufficient to support the use of this technique in multi-center clinical trials, and our results

21
underscore the importance of using a single evaluator for this QST technique in canine
neuropathic pain studies.
3.2 Introduction
Neuropathic pain is generated by the changes in formation and modulation of nociceptive
signals in response to injury due to damage or dysfunction of nervous tissue (Treede et al.,
2008). Up to 90% of people report chronic neuropathic pain after spinal cord injury (SCI) (Boldt
et al., 2014), which is severe and disabling in up to 63% of cases (Turner et al., 2001). Despite
the fact that neuropathic pain syndromes are well documented in people with SCI, there is
limited information regarding its diagnosis and treatment in dogs with SCI (Moore et al., 2013).
Given the prevalence of neuropathic pain in people with SCI and its negative impact on
quality of life, further investigation into quantitative methods for assessing neuropathic pain in
veterinary patients is of immense importance. Methods for quantitative sensory testing (QST)
have been developed for use in rodent models of SCI and in the human clinical setting. These
methods test an objective value called sensory threshold (ST), defined as the minimum amount
of a particular stimulus (e.g. pinprick, light touch, temperature) that can be detected or is
considered painful. In veterinary patients specifically, mechanical ST has been defined as the
strength of mechanical stimulus required to produce a conscious behavioral response to that
stimulus (Moore et al., 2013). QST allows quantitative evaluation of hyperesthesia, which
manifests as a decrease in ST (Felix et al., 2009; Walk et al., 2009).
Von Frey anesthesiometry (VFA) is a technique used for QST that tests ST for a
mechanical stimulus (a plastic pressure probe applied to the skin). Variations of this technique
have been applied in rodent models, dogs, and people (Detloff et al., 2012; Tena et al., 2012;

22
Lascelles et al., 2013,). VFA has recently been shown to be a feasible technique to evaluate ST
in both normal dogs and dogs with SCI caused by intervertebral disc extrusion (IVDE) (Moore
2013 et al.; Song et al., 2016). While intraobserver reliability of the technique has been
established to be strong (Moore 2013 et al.; Knazovicky et al., 2017); interobserver agreement
using the technique has not been previously reported. Recently, there has been a surge of interest
in the use of dogs with IVDE as a clinical model of SCI (Smith et al., 2006; Levine et al., 2011;
Moore et al., 2017), therefore veterinary clinical trials assessing treatments to improve
neuropathic pain after SCI may provide important advances in translational pain management
strategies. An understanding of interobserver agreement related to measurements of QST is
necessary before multi-institutional veterinary pain studies can be undertaken and their findings
interpreted with confidence. The goal of this study was to evaluate the interobserver reliability of
one method of mechanical QST, electronic VFA, in normal dogs.
3.3 Materials and methods
Animals
This study was approved by the Institutional Animal Care and Use Committee (protocol
# 2015A00000054) and the Clinical Research Advisory Committee of The Ohio State
University Veterinary Medical Center (OSU VMC). Written informed consent was obtained
from owners of all dogs prior to enrollment. Healthy dogs were recruited from the general patient
population at the OSU VMC. All dogs enrolled were ≤20 kg, were reported by their owners to be
systemically healthy, had a normal physical and neurologic examination performed by a single
investigator (AK), had not received any medications during the month prior to study enrollment,
and had no owner-reported history of neurologic or orthopedic disease.
23
Evaluator training
To mirror the expected landscape of a multicenter veterinary clinical trial scenario, three
novice QST evaluators (one veterinary neurology resident, one board certified veterinary surgeon
specializing in orthopedics, and board certified veterinary neurologist) were recruited to
participate in the study. Each novice evaluator underwent a standardized training session prior to
initiation of the study which was led by an expert evaluator (SAM). The training session
consisted of a demonstration of proper VFA technique as described below using a normal,
cooperative dog and focused on method and location of probe application and evaluating
behavioral response to the stimulus. After demonstration, each evaluator performed the VFA
technique on the same normal dog with feedback from the expert evaluator until both the trainer
and the trainee felt comfortable with the technique being performed. Each evaluator had a single
training session which lasted 10-20 minutes depending on speed with which the evaluator
became comfortable with the technique.
Electronic von Frey device and technique
The device used and patient positioning are shown in Figure 1. An electronic von Frey
device (IITC Life Science; Woodlands, CA) with a 1000 g probe and rigid 0.8 mm diameter tip
was used for all measurements. Mechanical ST was measured in every dog by each of three
investigators using a technique previously published by our laboratory (Moore et al., 2013; Song
et al., 2016). After an acclimation period of 5 minutes, dogs were placed in lateral recumbency
and maintained there with minimal restraint. A testing session consisted of a single investigator
performing QST on each of the dog’s four limbs in a randomized order. Five measurements were
obtained in a blinded fashion from each limb, with the highest and lowest values excluded and
the middle three values averaged for a given limb to produce a mean ST for each limb. Dogs

24
were provided a five minute rest period between sessions, during which time they were allowed
to freely roam about the testing room. Each dog underwent a total of three testing sessions, one
with each investigator. Investigator test order was determined via a random number generator.
The total session time (in minutes) required for testing to be completed by each observer was
recorded.
Statistical analysis
For ease in statistical comparisons, mean ST for each of four limbs as determined by a
single investigator were averaged to produce a mean overall ST for each individual dog and
investigator. Agreement was compared between investigators by calculating an intra-class
correlation coefficient (ICC) using a two-way model for consistency of single measures and
where <0.2 was considered slight agreement, 0.21-0.40 was considered fair agreement, 0.41-0.60
was considered moderate agreement, 0.61-0.80 was considered substantial agreement, and 0.81-
1.00 was considered almost perfect agreement (Landis and Koch, 1977; Tena et al., 2012;
Andersen et al., 2015). Statistical analysis was performed using MedCalc software.
3.4 Results
A total of 20 normal dogs were enrolled. Dogs ranged in age from 1 to 11 years (median
5 years), and weighed between 3.6 and 15.3 kg (median 7.7 kg). There were 13 castrated males
and 7 spayed females. Breeds were as follows: 7 mixed breed dogs, 3 Border Terriers, 2
Dachshunds, 2 Terrier mixes, 1 Boston Terrier, 1 Pomeranian, 1 Silky Terrier, 1 Sealyham
Terrier, 1 Pug, and 1 Pembroke Welsh Corgi. Mean overall ST for all dogs, as determined by
each of three investigators, is shown in Figure 2.
25
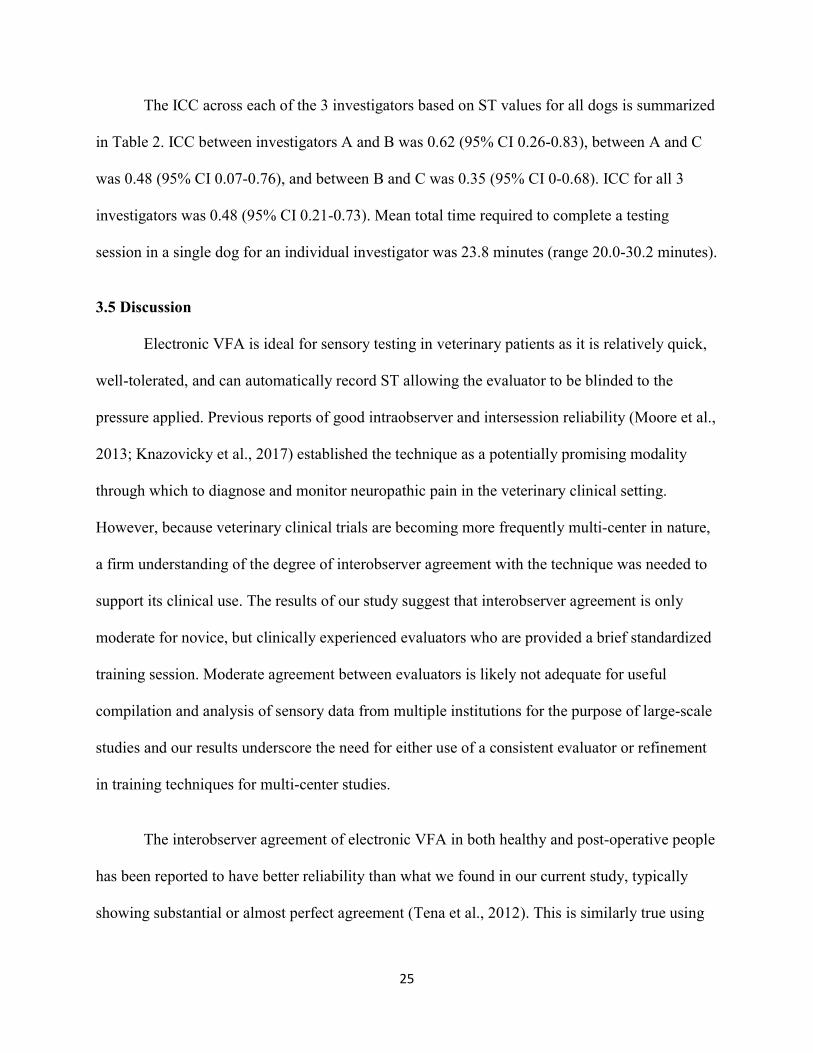
The ICC across each of the 3 investigators based on ST values for all dogs is summarized
in Table 2. ICC between investigators A and B was 0.62 (95% CI 0.26-0.83), between A and C
was 0.48 (95% CI 0.07-0.76), and between B and C was 0.35 (95% CI 0-0.68). ICC for all 3
investigators was 0.48 (95% CI 0.21-0.73). Mean total time required to complete a testing
session in a single dog for an individual investigator was 23.8 minutes (range 20.0-30.2 minutes).
3.5 Discussion
Electronic VFA is ideal for sensory testing in veterinary patients as it is relatively quick,
well-tolerated, and can automatically record ST allowing the evaluator to be blinded to the
pressure applied. Previous reports of good intraobserver and intersession reliability (Moore et al.,
2013; Knazovicky et al., 2017) established the technique as a potentially promising modality
through which to diagnose and monitor neuropathic pain in the veterinary clinical setting.
However, because veterinary clinical trials are becoming more frequently multi-center in nature,
a firm understanding of the degree of interobserver agreement with the technique was needed to
support its clinical use. The results of our study suggest that interobserver agreement is only
moderate for novice, but clinically experienced evaluators who are provided a brief standardized
training session. Moderate agreement between evaluators is likely not adequate for useful
compilation and analysis of sensory data from multiple institutions for the purpose of large-scale
studies and our results underscore the need for either use of a consistent evaluator or refinement
in training techniques for multi-center studies.
The interobserver agreement of electronic VFA in both healthy and post-operative people
has been reported to have better reliability than what we found in our current study, typically
showing substantial or almost perfect agreement (Tena et al., 2012). This is similarly true using
26
other mechanical sensory tests including monofilaments and pin-prick (Andersen et al, 2015,
Marcuzzi et al., 2017). This discrepancy may reflect the inherent challenge in interpreting the
variety of behavioral responses dogs may exhibit toward a stimulus, with different investigators
being more or less observant of certain types of responses during testing. In addition to
differences in investigator interpretation of patient responses, there may have also been
differences in patient responses to each investigator. Different investigators may have given
different behavioral cues causing dogs to anticipate or react differently to the stimulus, and dogs
may have developed learned behaviors over the course of the testing sessions as they were
exposed to a repeated stimulus (Jones et al., 2007). To help control the latter we randomized the
order of the investigators and the testing order of the limbs for each dog.
Another potential contributor to our lower ICC values may be related to training of our
investigators, who spent only a brief training session becoming familiar with the von Frey device
and sensory testing procedure prior to acquiring patient data. In people, more extensive QST
training is recommended prior to collecting and reporting sensory testing data. For example, the
German Research Network on Neuropathic Pain offers an eight hour QST training program that
includes information about equipment, technique, quality control, and analysis and interpretation
of results using established standardized protocols and normal QST values (Rolke et al., 2006).
Further, many investigators have significantly more experience in QST in addition to this
recommended training (Marcuzzi et al., 2017). Laboratories can become QST certified through
this training and the use of validated QST protocols, resulting in enhanced reliability of QST data
(Geber et al., 2011). Indeed, early multi-center QST studies in people prior to the implementation
of standardized protocols and training showed consistently poor interobserver reliability
(Armstrong et al., 1991; Valensi et al., 1993; Geber et al., 2008). This was initially attributed to

27
the effect of multiple observers, but improved substantially once more extensive training and
standardized protocols were implemented (Delaney et al., 1993; Geber et al., 2011). Rigorous
QST training programs do not currently exist for veterinarians, and in the present study we
designed our training protocol to mimic what would be feasible for novice evaluators in the
clinical setting; however, our results suggest that the development of standardized training and
QST protocols will likely be needed before undertaking multi-center veterinary pain studies
using QST as an outcome measure.
Several other factors have been identified that influence QST results in people. Circadian
rhythm may affect the stability of QST measures (Geber et al., 2011). Our testing was performed
on the same day and at the same time of day with just 5 minutes between testing sessions by all 3
investigators, which controlled for this in the present study. In people it has also been shown that
age and sex affect ST (Chesterton et al., 2007). Each patient acted as its own control in our study
with respect to age and sex, eliminating impact of signalment on sensory threshold as obtained
by any single investigator. The effect of time of day, age, and sex on QST in dogs has not been
previously reported and when implementing a multicenter approach it may be important to
standardize these aspects of study design. Further evaluation of the effects of environmental and
dog-specific factors on the results of QST are needed.
Our results suggest that interobserver reliability is not currently adequate to support the
use of electronic VFA to collect QST data in multi-institutional studies. However, QST as a
means to evaluate ST and document neuropathic pain has only recently been investigated in
veterinary medicine, and this study highlights the need for further research to better establish
standardized QST protocols, define normal reference values for sensory threshold, and develop

28
effective standardized training protocols for investigators using QST. This may allow for
improved interobserver reliability and ultimately large-scale multi-center veterinary pain studies,
as has occurred over the last few decades in human medicine.
3.6 Conclusions
The results of the present study suggest that a brief training session provided to
investigators with advanced clinical training, but no prior experience with VFA does not result in
sufficient interobserver reliability to support the use of the technique in multi-center veterinary
clinical studies. This, along with previous reports of good intraobserver reliability, suggests that
a single investigator should be used to collect data for mechanical QST studies in dogs,
especially when evaluating changes over time. However, refinement of investigator training may
enhance reliability of the technique and will be vital before multi-center pain studies can be
effectively undertaken.
3.7 Conflict of interest statement
None of the authors has any financial or personal relationships that could inappropriately
influence or bias the content of the paper.
3.8 Acknowledgements
The study was funded by the Gray Lady Foundation [grant number]. In addition to the
funding source, the authors gratefully acknowledge Mrs. Amanda Disher, Mrs. Heather
Anderson, and Dr. Ashley Hechler for their assistance with the study.
3.9 References
29
Andersen, K.G., Kehlet, H., Aasvang, E.K., 2015. Test-retest agreement and reliability of quantitative sensory testing 1 year after breast cancer surgery. Clinical Journal of Pain 31, 393-403. Armstrong, F.M., Bradbury, J.E., Ellis, S.H., Owens, D.R., Rosen, I., Sonksen, P., Sundkvist, G, 1991. A study of peripheral diabetic neuropathy. The application of age-related reference values. Diabetes Medicine 8, 94–99. Boldt, I., Eriks-Hoogland, I., Brinkhof, M.G., de Bie, R., Joggi, D., von Elm, E., 2014. Non-pharmacological interventions for chronic pain in people with spinal cord injury (Review). The Cochrane Collaboration, Issue 11. Delaney, G.A., McKee, A.C., 1993. Inter- and intra-rater reliability of the pressure threshold meter in measurement of myofascial trigger point sensitivity. American Journal of Physical Medicine & Rehabilitation 72, 136–139. Detloff, M.R., Fisher, L.C., Deibert, R.J., Basso, D.M., 2012. Acute and chronic tactile sensory testing after spinal cord injury in rats. Journal of Visualized Experiments 62, e3247. Felix, E.R., Widerstrom-Noga, E.G., 2009. Reliability and validity of quantitative sensory testing in persons with spinal cord injury and neuropathic pain. Journal of Rehabilitation Research and Development 46, 69–84. Geber, C., Magerl, W., Fondel, R., Fechir, M., Rolke, R., Vogt, T., Treede, R.D., Birklein, F., 2008 Numbness in clinical and experimental pain—a cross-sectional study exploring the mechanisms of reduced tactile function. Pain 139, 73–81. Geber, C., Klein, T., Azad, S., Birklein, F., Gierthmuhlen, J., Huge, D., Lauchart, M., Nitzche, D., Stengel, M., Valet, M., 2011. Test-retest and interobserver reliability of quantitative sensory testing according to the protocol of the German Research Network on Neuropathic Pain (DFNS): a multi-centre study. Pain 152, 548-556. Haas, M., 1991. Statistical methodology for reliability studies. Journal of Manipulative Physiology and Therapy 14, 119–132. Jones, D.H., Kilgour, R.D., Comtois, A.S., 2007. Test-retest reliability of pressure pain threshold measurements of the upper limb and torso in young healthy women. Pain 8, 650-656. Kalliomaki, M., Kieseritzky, J.V., Schmidt, R., Hagglof, B., Karlsten, R., Sjorgren, N., Albrecht, P., Gee, L., Rice, F., Wiig, M., Schmelz, M., Gordh, T., 2011. Structural and functional differences between neuropathy with and without pain? Experimental Neurology 231, 199-206. Knazovicky, D., Helgeson, E.S., Case, B, Thomson, A, Gruen, M.E., Maixner, W., Lascelles, B.D., 2017. Replicate effects and test-retest reliability of quantitative sensory threshold testing in dogs with and without chronic pain. Veterinary Anaesthesia and Analgesia 44, 615-624.

30
Landis, J.R., Koch, G.G., 1977. The measurement of observer agreement for categorical data. Biometrics 33, 159-174. Lascelles, B.D., 2013. Getting a sense of sensations. The Veterinary Journal 197, 115–117. Lee, K.M., Lee, J., Chung, C.Y., Ahn, S., Kim, T.W., Lee, H.J, Park, M.S., 2012. Pitfalls and important issues in testing reliability using intraclass correlation coefficients in orthopaedic research. Clinical Orthopedic Surgery 4, 149–155. Levine, J.M., Levine, G.J., Porter, B.F., Topp, K., Noble-Haeusslein, L.J., 2011. Naturally occurring disk herniation in dogs: An opportunity for pre-clinical spinal cord injury research. Journal of Neurotrauma 28, 675–688. Marcuzzi, A., Wrigley, P.J., Dean, C.M., Adams, R., Hush, J.M., 2017. The long-term reliability of static and dynamic quantitative sensory testing in healthy individuals. Pain 158, 1217-1223. Moore, S.A., Hettlich, B.F., Waln, A., 2013. The use of an electronic von Frey device for evaluation of ST in neurologically normal dogs and those with acute spinal cord injury. The Veterinary Journal 197, 216–219. Moore, S.A., Granger, N., Olby, N.J., Spitzbarth, I., Jeffery, N.D., Tipold, A., Nout-Lomas, Y.S., da Costa, R.C., Stein, V.M., Noble-Haeusslein, L.J., Blight, A.R., Grossman, R.G., Basso, D.M., Levine, J.M., 2017. Targeting Translational Successes through CANSORT-SCI: Using Pet Dogs To Identify Effective Treatments for Spinal Cord Injury. Journal of Neurotrauma 34, 2007-2018. Rolke, R., Baron, R., Maier, C, Tolle, T.R., Treede, R.D., Beyer, A., Binder, A., Birbaumer, N., Birklein, F., Botefur, I.C., et al., 2006. Quantitative Sensory Testing in the German Research Network on Neuropathic Pain (DFNS): Standardized Protocol and Reference Values. Pain 123, 231-243. Smith, P.M., Jeffery, N.D., 2006. Histological and ultrastructural analysis of white matter damage after naturally occurring spinal cord injury. Brain Pathology 16, 99–109. Song, R.B., Basso, D.M., da Costa, R.C., Fisher, L.C., Mo, X, Moore, S.A., 2016. von Frey anesthesiometry to assess sensory impairment after acute spinal cord injury caused by thoracolumbar intervertebral disc extrusion in dogs. The Veterinary Journal 209, 144-149. Tena, B., Escobar, B., Jose Arguis, M., Cantero, C., Rios, J., Gomar, C., 2012. Reproducibility of electronic von Frey and von Frey monofilaments testing. Clinical Journal of Pain 28, 318-323. Treede, R.D., Jensen, T.S., Campbell, J.N., Cruccu, G., Dostrovosky, J.O., Griffin, J.W., Hansson, H., Hughes, R., Nurmikko, T., Serra, J., 2008. Neuropathic pain: Redefinition and a grading system for clinical research purposes. Neurology 70, 1630-1635.

31
Turner, J.A., Cardenas, D.D., Warms, C.A., McClellan, C.B., 2001. Chronic pain associated with spinal cord injuries: A community survey. Archives of Physical Medicine and Rehabilitation 82, 501-508. Valensi, P., Attali, J.R., Gagant, S., 1993, Reproducibility of parameters for assessment of diabetic neuropathy. The French Group for Research and Study of Diabetic Neuropathy. Diabetes Medicine 10, 933–939. Walk, D., Sehgal, N., Moeller-Bertram, T., Edwards, R.R., Wasan, A., Wallace, M., Irving, G., Argoff, C., Backonja, M.M., 2009. Quantitative sensory testing and mapping – A review of nonautomated quantitative methods for examination of the patient with neuropathic pain. The Clinical Journal of Pain 25, 632–640.

32
Tables Table 2 Comparison of mean sensory threshold (ST) of clinically normal dogs for each observer for each dog. To aid in statistical comparison, sensory threshold values from all four limbs in each dog are averaged to provide a mean sensory threshold for each observer.
Mean Sensory Threshold (g)
Dog Observer 1 Observer 2 Observer 3
1 131.3 61.7 67.2
2 73.9 187.5 82.1
3 184.8 241.9 81.9
4 163.1 123.3 80.4
5 165.2 133.8 187.4
6 168.0 153.3 284.8
7 207.4 175.4 151.6
8 311.7 316.3 278.9
9 166.0 153.9 167.3
10 126.4 105.1 156.0
11 182.3 79.5 139.9
12 122.3 56.8 153.7
13 101.0 67.5 220.1
14 150.0 115.1 156.4
15 52.7 47.7 90.1
16 188.7 76.3 97.5
17 111.1 180.8 129.3
18 146.7 114.4 126.1
19 92.2 96.7 92.2
20 127.6 103.2 92.9
Total Mean ST 148.6 129.5 141.8
Std Deviation 55.7 67.0 62.9
33
Table 3 Intraclass correlation coefficient for each pair of observers and average for all observers
combined.
Observers Intraclass Correlation Coefficient (95% CI)a
Observers 1 & 2 0.62 (0.26-0.83)
Observers 1 & 3 0.49 (0.07-0.76)
Observers 2 & 3 0.35 (0.0-0.68)
Mean All Observers 0.48 (0.21-0.73)
a95% CI, 95% Confidence interval.
Figures
Figure 1 The electronic von Frey device and patient positioning for mechanical quantitative
sensory testing in dogs. The device consisted of a load cell (A), handle (B), recording device (C),
and tip (D). The system measures and displays the amount of pressure applied to a subject, from
0.1 to 1000 g. Figure originally published by Moore et al., 2013.
34
Figure 2 Total mean sensory threshold and standard deviation for each evaluator. Sensory
threshold values for all 20 dogs are averaged for each evaluator.

35
Chapter 4
von Frey anesthesiometry to diagnose chronic neuropathic pain after acute spinal cord
injury caused by thoracolumbar intervertebral disc extrusion in dogs
4.1 Abstract
Von Frey anesthesiometry (VFA) was used to objectively measure mechanical sensory
threshold (ST) in 21 dogs with acute SCI caused by spontaneous thoracolumbar intervertebral
disc extrusion (IVDE) at approximately 10 days, 30 days, and 90 days after decompressive
hemilaminectomy. ST values were compared over time and correlated with locomotor scores.
There was no significant change in ST in the thoracic limbs over the 90 day post-
operative period. Pelvic limb ST were highest at 10 days consistent with hypoalgesia and
declined over time, though the decline from 30 to 90 days was not statistically significant (means
± standard error of the mean ST for pelvic limbs at 10 days = 209.2 ± 14.1 g, at 30 days = 173.8
± 11.1 g, and at 90 days = 162.6 ± 12.3 g). A significant difference was identified in the pelvic
limbs when comparing ST at 10 and 30 days (mean difference 35.4 g; P=0.01) and at 10 and 90
days (mean difference 46.7 g; P=0.001), but not at 30 and 90 days (mean difference 11.2 g;
P=0.93). There was an inverse correlation between locomotor score and pelvic limb ST over
time (r = -0.5; P = 0.03). These findings are suggestive of recovery of sensorimotor spinal cord
function, and potentially the development of hyperesthesia indicative of neuropathic pain. This is
the first study to evaluate ST over an extended period of time to evaluate for chronic neuropathic
pain in dogs and results suggest the need for further longitudinal studies related to neuropathic
pain in dogs after SCI.
4.2 Introduction
36
Damage to or dysfunction of nervous tissue can result in neuropathic pain, which is
generated by changes in formation and modulation of nociceptive signals (Treede 2008). This
pain persists long after resolution of the initial injury and is often associated with burning,
stabbing, and tingling sensations (IASP 2002). Neuropathic pain syndromes are characterized by
allodynia (pain associated with a non-painful stimulus) and hyperesthesia (heightened sensitivity
to a painful stimulus). This is distinguished from nociceptive pain which is caused by
damage to non-nervous tissue and inflammation resulting in stimulation of nociceptors.
Von Frey anesthesiometry (VFA) is a technique used for quantitative sensory testing
(QST) that tests ST for a mechanical stimulus (a plastic pressure probe applied to the skin).
Variations of this technique have been applied in people, dogs, and rodent models (Detloff 2012,
Tena 2012, Lascelles 2013). Patients with diminished sensation have a higher than normal ST,
whereas patients with hyperesthesia and allodynia have a lower than normal ST (Hoschouer et
al., 2010). Up to 90% of people report chronic neuropathic pain after spinal cord injury (SCI)
(Boldt 2014), which in the majority of individuals is severe and debilitating (Turner 2001).
Despite the fact that neuropathic pain syndromes are well documented in people with SCI, the
presence of this phenomenon has been explored only in a limited fashion in dogs with SCI. Our
group and others have recently reported short-term results of mechanical and thermal
quantitative sensory testing (QST) in this veterinary patient population (Gorney et al. 2016; Song
et al., 2016), suggesting that sensory thresholds and thermal latencies are altered after SCI;
however, long term studies documenting the existence and time course for developing
neuropathic pain in dogs with SCI are lacking. Studies focusing on this phenomenon in dogs are
important, both for effective management of our veterinary patients and to facilitate translational
studies of neuropathic pain. The goal of the present study was to provide a longitudinal, long-

37
term assessment of mechanical QST in dogs with intervertebral disc extrusion (IVDE)-associated
SCI. Based on previous work, we hypothesized that ST would decline over time in SCI-affected
dogs, consistent with development of a neuropathic pain phenotype as dogs progressed to the
chronic injury state.
4.3 Materials and methods
Animals
This study was approved by the IACUC (protocol # 2015A00000054) and the Clinical
Research Advisory Committee of The Ohio State University Veterinary Medical Center (OSU
VMC). Written consent was obtained from the owner for all dogs prior to enrollment. Dogs
weighed ≤20 kg, had SCI due to IVDE in the T3-L3 region of the vertebral column, and were
determined to have intact pain sensation below the level of injury based on subjective response
to noxious stimuli in the pelvic limbs and tail at the time of initial evaluation by their attending
clinician. All dogs underwent routine decompressive hemilaminectomy after CT or MRI
confirmed the site of IVDE, and post-operative management was at the discretion of the
attending clinician.
Modified dorsal von Frey technique
An electronic von Frey device (IITC Life Science) with 1000 gram probe and rigid 0.8 m
diameter tip were used for evaluation of mechanical ST via a technique that has been recently
described by our laboratory. (Moore 2013, Song 2016). Briefly, dogs were introduced to a small
quiet room where the testing was performed and allowed to investigate the room for
approximately five minutes prior to the start of testing. Dogs were then placed in lateral
recumbency which was maintained with minimal restraint. Limb test order was randomized. The
38
probe tip was applied to the dorsal surface of the metacarpus in the thoracic limbs and metatarsus
in the pelvic limbs, seating the probe between the fourth and fifth digits. The pressure was then
gradually increased manually until a behavioral response was elicited, and this pressure was
recorded as the ST. The evaluator was blinded to the pressure recording until the patient elicited
a behavioral response. This method was repeated for a total of five pressure recordings for each
limb, waiting one minute between measurements to prevent windup and hypersensitization
(KuKanich 2005, Detloff 2010).
Testing schedule
Dogs were evaluated at approximately 10, 30, and 90 days after hemilaminectomy. At
each time point a neurologic exam was performed by a single evaluator (AK), and a locomotor
score was assigned using the Olby Spinal Cord Injury Scale (OSCIS) (Olby et al., 2001).
Statistical analysis
The highest and lowest ST values were excluded for each limb, and the remaining three
values were averaged to determine a ST for each limb. Sensory values are reported as means ±
standard error of the mean (SEM) for each limb. To ease statistical comparison, right and left
thoracic limb ST were combined to give a single thoracic limb value, and right and left pelvic
limb ST were combined to give a single pelvic limb value. A repeated measures ANOVA and
trend analysis were used to compare ST values over time. The relationship between ST and
OSCIS score was determined using a Pearson correlation. P values were corrected for multiple
comparisons using the Bonferroni method. For all statistical analyses, P ≤0.05 was considered
significant.
4.4 Results

39
Twenty-five dogs with IVDE-associated SCI were prospectively enrolled; however, four
dogs did not complete the study due to suspected (three dogs) or confirmed (one dog) recurrent
IVDE during the 90 day study period. One dog had a confirmed L4-L5 IVDE two months after
its L1-L2 hemilaminectomy, one dog had recurrent right pelvic limb paresis and lameness
similar to its original clinical signs caused by a L3-L4 IVDE 1.5 months earlier, one dog
presented with cervical pain 1.5 months after its T12-T13 hemilaminectomy, and one dog was
presented paraplegic with lack of nociception two months after its L3-L4 hemilaminectomy with
the suspected recurrent IVDE further cranial at the thoracolumbar junction based on discomfort
during palpation and the level of a cutaneous trunci cut-off. These four dogs were not included in
statistical analysis of ST at any time point. A total of 21 dogs completed the study. Ages ranged
from three to 11 years (median six years), and dogs weighed between 5.0 and 10.4 kg (median
6.4 kg). There were 10 spayed females, 10 neutered males, and one sexually intact male. With
respect to breed: there were 19 Dachshunds, one Shih Tzu, and one mixed breed.
Single or multi-site decompressive hemilaminectomy was performed between T10-T11
and L3-L4 intervertebral disc spaces in all dogs, with lateral disc fenestrations performed at one
or more sites based on imaging findings and the discretion of the surgeon. Post-operative pain
management was provided in all cases and drug selection was based on surgeon’s preference but
included combinations of a fentanyl constant rate infusion for 12 to 24 h, a fentanyl patch placed
immediately post-operatively and removed three to four days later, tramadol, and gabapentin. All
dogs were placed on a single post-operative anti-inflammatory medication based on surgeon
preference which included prednisone, carprofen, firocoxib, or deracoxib. Medication doses and
frequency were recorded at each testing session. Oral anti-inflammatory and analgesic
medications were continued for a minimum of seven days post-operatively in all dogs, with 16
40
dogs still receiving at least one of these oral medications at their initial 10 day recheck. A single
dog was also receiving trazodone to help control anxiety at the 10 day recheck. Medication doses
at the 10 day testing time are summarized in Table 4. No dogs were receiving any medication at
the 30 and 90 day testing times.
Mean ST values for each individual limb as well as combined thoracic limbs and
combined pelvic limbs at each of the three time points are listed in Table 2, and summary
statistics for combined thoracic limb and combined pelvic limb ST values at each time point are
compared in Figure 3. Mean ± SEM sensory threshold for the thoracic limbs at 10 days was
156.5 ± 15.8 g, at 30 days was 128.3 ± 12.1 g, and at 90 days was 136.3 ± 14.6 g. A significant
difference was not detected in the thoracic limbs when comparing ST at different time points
(P=0.22 between 10 and 30 days; P=0.39 between 10 and 90 days; P=1.0 between 30 and 90
days).
Mean ± SEM sensory threshold for pelvic limbs at 10 days was 209.2 ± 14.1 g, at 30 days
was 173.8 ± 11.1 g, and at 90 days was 162.6 ± 12.3 g. A significant difference was identified in
the pelvic limbs when comparing ST at 10 and 30 days (mean difference 35.4 g; P=0.01) and at
10 and 90 days (mean difference 46.7 g; P=0.001), but not at 30 and 90 days (mean difference
11.2 g; P=0.93).
Mean ± SEM OSCIS score at 10 days was 8.0 ± 0.5, at 30 days was 9.6 ± 0.4, and at 90
days was 11.4 ± 0.3. There were significant differences in OSCIS score when comparing all time
points, with scores increasing over time (mean difference in score at 10 and 30 days 1.6,
P<0.0001; 10 and 90 days 3.4, P<0.0001; 30 and 90 days 1.8, P<0.0001). There was a
significant inverse correlation between pelvic limb ST and OSCIS at 10 days (P=0.03) and 30

41
days (P=0.003), but not at 90 days (P=0.49). OSCIS was not significantly correlated with
thoracic limb ST at any time point.
4.5 Discussion
While a previous study assessed short-term alterations in ST in dogs with IVDE-
associated SCI (Song et al., 2016), the current study is the first to assess long-term alterations in
ST in this population. Another recent study assessed ST using thermal and mechanical sensory
testing in normal dogs and dogs with SCI caused by IVDE over the course of about two months,
though only a few dogs were tested beyond 30 days (Gorney et al., 2016). While thoracic limb
ST values did not change over the course of our study, pelvic limb ST values were significantly
lower at 30 and 90 days after surgery compared to 10 day post-operative values. This pattern is
consistent with initial hypoalgesia likely due to a combination of SCI and post-operative pain
medications, followed by gradual recovery of injured spinal cord sensory pathways, cessation of
pain medication, and potentially the development of neuropathic pain as ST continued to
decrease (Hoschouer et al., 2010). While ST values were decreased at both 30 and 90 days after
surgery, this finding achieved statistical significance only for the 30 day values. There was no
difference in thoracic limb ST over time, indicating that the decline in pelvic limb ST over time
is likely related to true alterations in sensory function and not simply discontinuation of post-
operative analgesics.
We chose a 90 day time frame for observation of ST based on literature from both the
human clinical setting as well as in animal models (Nakae et al., 2011). Development of
neuropathic pain is typically delayed weeks to months after SCI, and in rare instances longer
than a year (Tasker 1992). In a human study, approximately 34%, 55%, and 62% of people with
42
SCI developed neuropathic pain at 1 month, 6 months, and 12 months respectively (Finnerup et
al., 2014). Allodynia was reported by 78% of people at 2 weeks post-SCI (Siddall et al., 1999).
Based on the prevalence of neuropathic pain reported by people and detected in people and rats
over the first few months after SCI via sensory testing, we expected to capture evidence of the
development of neuropathic pain during the 3 month testing period. However, given that the
number of patients that develop neuropathic pain may continue to increase beyond 3 months,
future studies may need to extend the testing time frame.
There are three major distributions of chronic neuropathic pain with SCI. Above-level
pain occurs in dermatomes cranial to the site of injury, at-level pain occurs in dermatomes at the
site of injury, and below-level neuropathic pain occurs in dermatomes caudal to the neurological
lesion (Hulsebosch 2009). These are described based on somatosensory mapping using
mechanical and thermal sensory testing (Vogel 2017). We tested the metacarpal and metatarsal
region of the limbs in dogs with caudal thoracic and cranial lumbar SCI, and therefore tested for
above-level and below-level (but not at-level) pain.
Below-level pain is the most common central pain syndrome after SCI in people and
rodents, and is the most difficult to treat (Turner 2001). This pain is typically associated with a
burning sensation, and can be spontaneous or evoked by different auditory stimuli or movements
(Widerstrom-Noga 2008). Various aspects of the limbs, hands/feet, and digits are commonly
reported sites of below-level pain (Soler 2010). Injuries that affect spinothalamic tracts are
associated with below-level pain, where changes in neuronal excitability of residual
spinothalamic afferents are suspected to play a role (Finnerup 2014). In our study, the gradual
43
decrease in ST in the pelvic limbs over the course of three months may be consistent with the
development of below-level neuropathic pain (Hoschouer et al., 2010).
Above-level pain develops reliably in rodents with a variety of SCI, typically manifested
as forelimb hyperalgesia after thoracic SCI (Mills 2001, Wang 2008, Carlton 2009, Densmore
2010). However, the limited QST data in humans and other primates suggests that above-level
pain is uncommon (Defrin 1999, Finnerup 2003, Masri 2012), which may implicate important
species differences in neuropathic mechanisms for above-level pain. We did not find any change
in thoracic limb ST over time, suggesting a lack of development of above-level neuropathic pain.
Most of the dogs in our study were receiving an oral anti-inflammatory and/or analgesic
medication at the 10 day testing time, and one dog was receiving trazodone. The increased ST at
day 10, indicative of hypoalgesia, was likely due to a combination of disruption of sensory
pathways in the spinal cord as well as the effect of analgesic medications. Several of these drugs
have been shown to alter sensory testing results in animals (Lascelles et al., 1998; Wegner et al.,
2008; KuKanich and Papich, 2011; Kögel et al., 2014). While the magnitude and duration of
impact with each of these medications on ST has not been evaluated in dogs, the anticipated
result is that they increase ST while they are being administered and their effect on ST is
removed shortly after the drug is stopped and cleared. Ideally, a placebo-controlled study would
be performed to help determine the magnitude of impact of various medications on ST in dogs
with SCI, but withholding post-operative analgesia would be unethical for obvious reasons.
Alternatively, a placebo-controlled trial could be performed in normal dogs using these various
common analgesic and anti-inflammatory medications to help determine their impact on ST
using VFA. Given the lack of change in thoracic limb ST when the majority of dogs were
44
receiving medications at 10 days compared to later time points may suggest that these
medications likely had minimal effect on the 10 day ST, and that the change in ST over time in
the pelvic limbs primarily reflects alteration of sensory CNS pathways.
As expected for dogs with incomplete SCI caused by IVDE, there was a significant
improvement in pelvic limb locomotor scores over the course of the 3 month testing period,
indicating partial recovery of locomotor function. Locomotor score had a strong and significant
inverse correlation with ST at 10 days and 30 days. This relationship was also present at day 90
but was not statistically significant. This inverse correlation is consistent with improving
sensorimotor function over time, and is in agreement with recent reports showing similar
correlations (Gorney et al. 2016; Song et al., 2016).
A limitation of this study was the higher than expected dropout rate due to presumed or
confirmed recurrence of IVDE, which limited our statistical power. Four dogs out of the original
25 did not complete the study due to confirmed or suspected recurrent IVDE (of which three
were likely at a different site). These dogs were not included in data reporting or statistical
analysis, as repetitive SCI would be expected to alter sensory processing to an ever larger degree,
further increasing the chances of an individual developing neuropathic pain, and potentially
increasing the magnitude of pain beyond what would occur in our more routinely managed
canine SCI population. To our knowledge, no studies exist examining the occurrence and
character of neuropathic pain caused by recurrent SCI.
4.6 Conclusions
This is the first study to evaluate changes in ST over an extended period of time in dogs
with IVDE-associated SCI. Pelvic limb ST decreased over the course of three months after

45
injury, though the decline from 30 to 90 days was not statistically significant. There was an
inverse relationship between locomotor score and pelvic limb ST over time. These findings are
suggestive of recovery of sensorimotor spinal cord function, and potentially the development of
hyperesthesia indicative of neuropathic pain. The main limitation of this study was the relatively
small number of dogs which limited statistical power. However, our results suggest the need for
further studies with larger numbers of dogs and potentially over a longer period of time to help
confirm the existence of chronic neuropathic pain in dogs. Ultimately the goal of future
neuropathic pain studies in dogs would be to better identify and treat chronic pain in our patients
and to validate the use of a spontaneous acute SCI dog model of neuropathic pain for
translational therapeutic research.
4.7 Acknowledgements
The study was funded by The Ohio State University Canine Grant [No. 2015-22]. In
addition to the funding source, the authors gratefully acknowledge Mrs. Amanda Disher, Mrs.
Heather Anderson, Dr. Nina Kieves, Dr. Daniella Vansteenkiste, and Dr. Ashley Hechler for
their assistance with the study.
4.8 References
Boldt, I., Eriks-Hoogland, I., Brinkhof, M.G., de Bie, R., Joggi, D., von Elm, E., 2014. Non-pharmacological interventions for chronic pain in people with spinal cord injury (Review). The Cochrane Collaboration, Issue 11. Carlton, S.M., Junhui, D., Tan, H.Y., Nesic, O., Hargett, G.L., Bopp, A.C., Yamani, A., Lin, Q., Willis, W.D., Hulsebosch, C.E., 2009. Peripheral and central sensitization in remote spinal cord regions contribute to central neuropathic pain after spinal cord injury. Pain 147, 265–276.
Defrin, R., Ohry, A., Blumen, N., Urca, G., 1999. Acute pain threshold in subjects with chronic pain following spinal cord injury. Pain 83, 275–282.
46
Densmore, V.S., Kalous, A., Keast, J.R., Osborne, P.B., 2010. Above-level mechanical hyperalgesia in rats develops after incomplete spinal cord injury but not after cord transection, and is reversed by amitriptyline, morphine and gabapentin. Pain 151, 184–193.
Detloff, M.R., Fisher, L.C., Deibert, R.J., Basso, D.M., 2012. Acute and chronic tactile sensory testing after spinal cord injury in rats. Journal of Visualized Experiments 62, e3247. Finnerup, N.B., Johannesen, I.L., Bach, F.W., Jensen, T.S., 2003. Sensory function above lesion level in spinal cord injury patients with and without pain. Somatosensory & Motor Research 20, 71-76. Finnerup, N.B., Norrbrink, C., Trok, K., Piehl, F., Johannesen, I., Sørensen, J., Jensen, T.S., Werhageny, L., 2014. Phenotypes and predictors of pain following traumatic spinal cord injury: a prospective study. The Journal of Pain 15, 40-48 Gorney, A.M, Blau, S.R., Dohse, C.S., Griffith, E.H, Williams, K.D., Lim, J.H., Knazovicky, D., Lascelles, B.D.X., Olby, N.J., 2016. Mechanical and Thermal Sensory Testing in Normal Chondrodystrophoid Dogs and Dogs with Spinal Cord Injury caused by Thoracolumbar Intervertebral Disc Herniations. Journal of Veterinary Internal Medicine 30, 627-635.
Hoschouer, E.L., Basso, D.M., Jakeman, L.B., 2010. Aberrant sensory responses are dependent on lesion severity after spinal cord contusion injury in mice. Pain 148, 328–342.
Hulsebosch, C., Hains, B., Crown, E., Carlton, S., 2009. Mechanisms of chronic central neuropathic pain after spinal cord injury. Brain Research Reviews 60, 202-213.
Kögel, B., Terlinden, R., Schneider, J., 2014. Characterisation of tramadol, morphine and tapentadol in an acute pain model in Beagle dogs. Veterinary Anaesthesia and Analgesia 41, 297–304.
KuKanich, B., Papich, M.G., 2011. Pharmacokinetics and antinociceptive effects of oral tramadol hydrochloride administration in Greyhounds. American Journal of Veterinary Research 72, 256–262.
Lascelles, B.D., Cripps, P.J., Jones, A., Waterman-Pearson, A.E., 1998. Efficacy and kinetics of carprofen, administered preoperatively or postoperatively, for the prevention of pain in dogs undergoing ovariohysterectomy. Veterinary Surgery 27, 568–582.
Lascelles, B.D., 2013. Getting a sense of sensations. The Veterinary Journal 197, 115–117. Levine, G.J., Levine, J.M., Budke, C.M., Kerwin, S.C., Au, J., Vinayak, A., Hettlich, B.F., Slater, M.R., 2009. Description and repeatability of a newly developed spinal cord injury scale for dog. Preventive Veterinary Medicine 89, 121–127. Masri, R., Keller, A., 2012. Chronic pain following spinal cord injury. Advances in Experimental Medicine and Biology 760, 74-88.

47
Merskey, H., Bogduk, N. Classification of chronic pain: Descriptions of chronic pain syndromes and definitions of pain terms. 2nd ed. Seattle: IASP Press, 2002.
Mills, C.D., Hains, B.C., Johnson, K.M., Hulsebosch, C.E., 2001. Strain and model differences in behavioral outcomes after spinal cord injury in rat. Journal of Neurotrauma 18, 743-756. Nakae, A., Nakai, K., Yano, K., Hosokawa, K., Shibata, M., Mashimo, T., 2011. The Animal Model of Spinal Cord Injury as an Experimental Pain Model. Journal of Biomedicine and Biotechnology 2011, 1-11. Olby, N.J., De Risio, L., Muñana, K., Wosar, M.A., Skeen, T.M., Sharp, N.J., Keene, B.W., 2001. Development of a functional scoring system in dogs with acute spinal cord injuries. American Journal of Veterinary Research 62, 1624–1628. Siddall, P., Taylor, D., McClelland, J., Rutkowski, S., Cousins, M., 1999. Pain report and the relationship of pain to physical factors in the first 6 months following spinal cord injury. Pain 81, 187-197. Soler, M.D., Kumru, H., Vidal, J., Pelayo, R., Tormos, J.M., Fregni, F., Navarro, X., Pascual-Leone, A., 2010. Referred sensations and neuropathic pain following spinal cord injury. Pain 150, 192-198. Song, R.B., Basso, D.M., da Costa, R.C., Fisher, L.C., Mo, X, Moore, S.A., 2016. von Frey anesthesiometry to assess sensory impairment after acute spinal cord injury caused by thoracolumbar intervertebral disc extrusion in dogs. The Veterinary Journal 209, 144-149. Tasker, R.R., DeCarvalho, G., Dolan, E.J., 1992. Intractable pain of spinal cord origin: clinical features and implications for surgery. Journal of Neurosurgery 77, 373-378. Tena, B., Escobar, B., Jose Arguis, M., Cantero, C., Rios, J., Gomar, C., 2012. Reproducibility of electronic von Frey and von Frey monofilaments testing. Clinical Journal of Pain 28, 318-323. Treede, R.D., Jensen, T.S., Campbell, J.N., Cruccu, G., Dostrovosky, J.O., Griffin, J.W., Hansson, H., Hughes, R., Nurmikko, T., Serra, J., 2008. Neuropathic pain: Redefinition and a grading system for clinical research purposes. Neurology 70, 1630-1635. Turner, J.A., Cardenas, D.D., Warms, C.A., McClellan, C.B., 2001. Chronic pain associated with spinal cord injuries: A community survey. Archives of Physical Medicine and Rehabilitation 82, 501-508. Vogel, C., Rukwied, R., Stockinger, L., Schley, M., Schmelz, M., Schleinzer, W., Konrad, C., 2017. Functional characterization of at-level hypersensitivity in patients with spinal cord injury. Journal of Pain 18, 66-78.
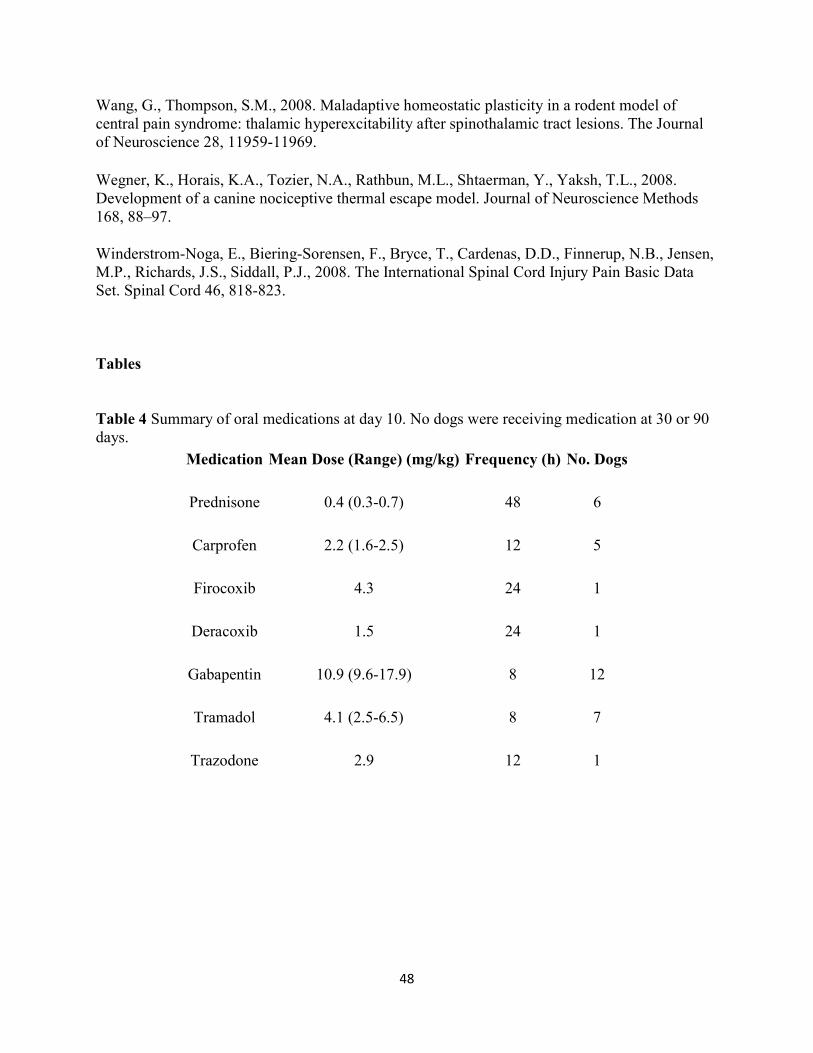
48
Wang, G., Thompson, S.M., 2008. Maladaptive homeostatic plasticity in a rodent model of central pain syndrome: thalamic hyperexcitability after spinothalamic tract lesions. The Journal of Neuroscience 28, 11959-11969. Wegner, K., Horais, K.A., Tozier, N.A., Rathbun, M.L., Shtaerman, Y., Yaksh, T.L., 2008. Development of a canine nociceptive thermal escape model. Journal of Neuroscience Methods 168, 88–97.
Winderstrom-Noga, E., Biering-Sorensen, F., Bryce, T., Cardenas, D.D., Finnerup, N.B., Jensen, M.P., Richards, J.S., Siddall, P.J., 2008. The International Spinal Cord Injury Pain Basic Data Set. Spinal Cord 46, 818-823.
Tables
Table 4 Summary of oral medications at day 10. No dogs were receiving medication at 30 or 90 days.
Medication Mean Dose (Range) (mg/kg) Frequency (h) No. Dogs
Prednisone 0.4 (0.3-0.7) 48 6
Carprofen 2.2 (1.6-2.5) 12 5
Firocoxib 4.3 24 1
Deracoxib 1.5 24 1
Gabapentin 10.9 (9.6-17.9) 8 12
Tramadol 4.1 (2.5-6.5) 8 7
Trazodone 2.9 12 1

49
Table 5 Mean sensory threshold for each limb in 21 dogs with acute spinal cord injury caused byintervertebral disc extrusion as measured at 10, 30, and 90 days after decompressive hemilaminectomy.
Mean Sensory Threshold (g)
Day 10
Day 30
Day 90
Dog LTL RTL LPL RPL LTL RTL LPL RPL LTL RTL LPL RPL
1 105.7 210.8 177.5 227.5 190.3 136.5 185.6 255.6 166.6 155.1 200.7 173.7
2 110.5 141.1 165.4 212.7 79.9 77.5 148.1 127.2 103.3 132.0 168.1 107.7
3 275.0 149.2 293.6 236.8 98.0 236.3 208.2 140.8 130.0 188.4 164.7 228.6
4 223.9 243.8 215.2 171.2 146.7 259.1 205.3 157.2 306.4 358.0 275.6 213.7
5 266.5 227.8 304.7 225.7 77.1 138.2 125.5 149.6 176.4 191.1 261.8 200.8
6 110.8 141.0 198.2 176.7 180.6 165.7 195.9 173.4 134.7 156.2 193.2 137.9
7 134.5 201.7 208.7 226.9 113.6 122.3 191.9 175.4 107.2 96.5 177.8 153.9
8 347.8 332.4 263.6 245.8 151.3 217.1 204.4 219.0 275.8 216.9 196.0 188.5
9 107.5 124.8 241.3 231.4 110.9 204.7 261.3 123.0 134.3 141.5 196.8 176.4
10 239.7 210.8 387.8 285.9 215.1 193.8 227.1 218.3 117.2 123.0 212.6 200.8
11 155.5 133.3 162.4 118.0 155.5 81.7 110.1 57.4 106.4 48.4 118.3 64.6
12 238.7 124.1 126.9 98.8 89.2 89.2 261.3 124.3 89.0 67.9 146.9 108.7
13 101.8 32.0 212.6 245.3 73.0 118.4 207.5 154.1 95.1 43.7 73.0 120.6
14 106.0 121.7 288.0 223.3 178.0 189.0 294.3 217.4 85.0 107.4 133.3 122.9
15 76.9 88.4 81.2 141.6 80.0 52.6 70.1 106.0 63.6 53.6 77.9 101.9
16 160.1 201.7 161.8 178.7 63.3 31.5 180.6 118.9 144.4 103.6 86.9 90.7
17 62.8 71.2 301.6 300.3 88.0 46.6 249.3 211.0 69.7 51.9 267.1 187.3
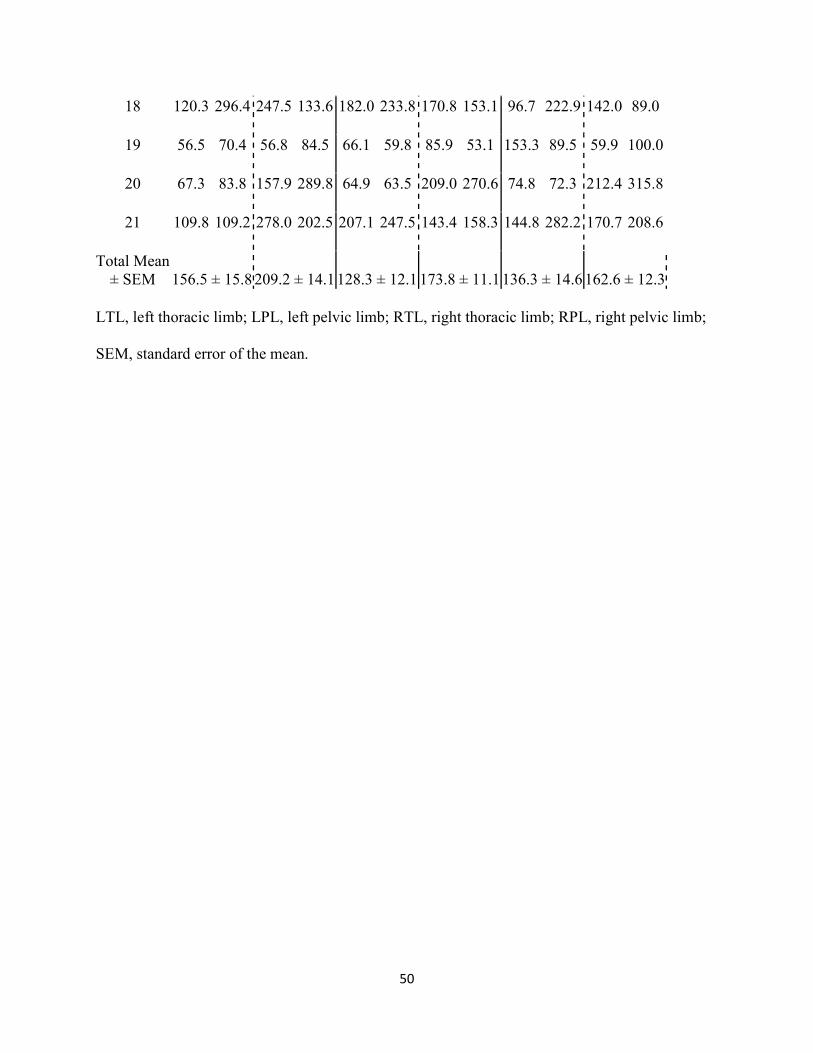
50
18 120.3 296.4 247.5 133.6 182.0 233.8 170.8 153.1 96.7 222.9 142.0 89.0
19 56.5 70.4 56.8 84.5 66.1 59.8 85.9 53.1 153.3 89.5 59.9 100.0
20 67.3 83.8 157.9 289.8 64.9 63.5 209.0 270.6 74.8 72.3 212.4 315.8
21 109.8 109.2 278.0 202.5 207.1 247.5 143.4 158.3 144.8 282.2 170.7 208.6
Total Mean ± SEM 156.5 ± 15.8 209.2 ± 14.1 128.3 ± 12.1 173.8 ± 11.1 136.3 ± 14.6 162.6 ± 12.3
LTL, left thoracic limb; LPL, left pelvic limb; RTL, right thoracic limb; RPL, right pelvic limb;
SEM, standard error of the mean.

51
Figures
Figure 3 Mean ± SEM for combined thoracic limb and combined pelvic limb ST values at each
time point in 21 dogs with acute spinal cord injury secondary to intervertebral disc extrusion.

52
Chapter 5
Conclusions and Future Directions
The primary goals of this study were to evaluate the interobserver reliability of VFA in
normal dogs and to use VFA to assess for evidence of chronic neuropathic pain in dogs after
acute SCI. VFA is ideal for sensory testing in veterinary patients as it is quick, well-tolerated,
and automatically records ST while allowing the evaluator to be blinded to the pressure applied.
In dogs with SCI, VFA was used to objectively measure ST as a means to follow sensory
function in all limbs throughout their recovery. The pattern of ST values over time could then be
used to determine if dogs with SCI develop neuropathic pain.
This was the first study to evaluate interobserver reliability of VFA in dogs. The results
of this study showed that while the average ST for each observer was similar across all dogs,
there was moderate agreement for any one individual dog. This is likely not enough agreement to
justify the use of VFA is multi-center pain studies in dogs, and highlights the shortcomings of
the brief training that was provided for the observers in this study. Interobserver reliability of
QST in people also was inadequate during its early stages in human medicine, but the
implementation of standardized testing protocols and more intensive training programs resulted
in strong interobserver reliability, allowing sensory testing data to be compiled and analyzed
from people with neuropathic pain from across the globe. For example, the German Research
Network on Neuropathic Pain, a leading organization in sensory testing and neuropathic pain,
offers in-depth QST training which allows researchers and clinicians to become comfortable and
familiar with equipment, technique, quality control, and analysis and interpretation of results
using established standardized protocols and normal QST values (Rolke et al., 2006).

53
Laboratories can become QST certified through this training and the use of validated QST
protocols, resulting in enhanced reliability of QST data (Geber et al., 2011). This process took
many years, but the limitations of multi-center trials were eventually overcome. Similar
standardized QST protocols and training programs will need to be further developed and
implemented in veterinary medicine to improve interobserver reliability and allow for large-scale
multi-center pain studies.
The next part of the study was the first to evaluate ST over an extended period of time to
evaluate for chronic neuropathic pain in dogs. Pelvic limb ST decreased over the course of three
months, though the decline from 30 to 90 days was not statistically significant. There was an
inverse relationship between locomotor score and pelvic limb ST over time. These findings are
suggestive of recovery of sensorimotor spinal cord function, and potentially the development of
allodynia indicative of neuropathic pain. The main limitation in this study was the relatively
small number of dogs which limited statistical power. However, the promising results in this
study indicate the need for further studies with larger numbers of dogs and potentially over a
longer period of time to help confirm the existence of chronic neuropathic pain in dogs.
Ultimately the goal of future neuropathic pain studies in dogs would be to better identify and
treat chronic pain in our patients and to validate the use of a spontaneous acute SCI dog model of
neuropathic pain for translational therapeutic research.
In addition to mechanical sensory testing such as VFA, the other primary form of QST
employed in the research and clinical setting is thermal sensory testing, which was not used in
this study. A recent study evaluated thermal sensory testing in normal dogs and dogs with SCI
caused by IVDE (Gorney et al., 2017). Thermal thresholds were tested using a handheld probe

54
set at 49°C (for heat) and 5°C (for cold) applied to the dorsal metatarsal region until a conscious
response was elicited. The thermal latency (time from applying the probe to the time of patient
response) was recorded. This study showed that thermal testing is feasible in dogs, that there was
moderate repeatability, and that there was a significant difference in latencies between normal
dogs and dogs with SCI. Thermal sensory testing is another testing modality that can be used
along with mechanical sensory testing to help evaluate for recovery and neuropathic pain in
veterinary patients, and similarly will require further research to help establish appropriate
veterinary protocols and training.
Future studies in dogs can evaluate the efficacy of various medications for the treatment
of neuropathic pain. Given that gabapentin has been shown to be one of the most effective drugs
for the treatment of neuropathic pain in people, is commonly prescribed in veterinary medicine,
and is very safe in dogs, this would be an ideal candidate for such a trial. Initially a placebo-
controlled cross-over study design could be implemented in normal dogs to evaluate how
gabapentin modulates ST. Normal dogs would be divided to receive either placebo or
gabapentin, VFA would then be performed, and after a wash-out period the treatment would be
switched and VFA repeated. If gabapentin was found to alter ST, this would lay the foundation
for further studies using gabapentin in dogs with SCI or other neuropathic conditions where there
is evidence of neuropathic pain. Once the QST data pool becomes robust in veterinary medicine,
this can also be translated to human clinical trials.

55
References
Abimussi, C., Menegheti, T., Wagatsuma, J., et al., 2014. Tumescent local anesthesia with ropivacaine in different concentrations in bitches undergoing mastectomy: plasma concentration and post-operative analgesia. Vet Anaesth Analg 41, 516-525. Aghighi, S.A., Tipold, A., Piechotta, M., Lewczuk, P., Kastner, S.B., 2012. Assessment of the effects of adjunctive gabapentin on postoperative pain after intervertebral disc surgery in dogs. Vet Anaesth Analg 39, 636–646. Andersen, K.G., Kehlet, H., Aasvang, E.K., 2015. Test-retest agreement and reliability of quantitative sensory testing 1 year after breast cancer surgery. Clinical Journal of Pain 31, 393-403. Armstrong, F.M., Bradbury, J.E., Ellis, S.H., Owens, D.R., Rosen, I., Sonksen, P., Sundkvist, G, 1991. A study of peripheral diabetic neuropathy. The application of age-related reference values. Diabetes Medicine 8, 94–99. Arndt, J.O., Bednarski, B., Parasher, C., 1986. Alfentanil’s analgesic, respiratory, and cardiovascular actions in relation to dose and plasma concentration in unanesthetized dogs. Anesthesiology 64, 345-352. Arnold, L., Choy, E., Clauw, D., et al, 2016. Fibromyalgia and Chronic Pain Syndromes. Clin J Pain 32, 737-736. Attal, N., Guirimand, F., Brasseur, L., Gaude, V., Chauvin, M., Bouhassira, D., 2002. Effects of IV morphine in central pain: a randomized placebo-controlled study. Neurology 58, 554–563. Baron, R., 2006. Mechanisms of Disease: neuropathic pain--a clinical perspective. Nature Clinical Practice (Neurology) 2, 95-106. Bedi, S.S., Yang, Q., Crook, R.J., et al., 2010, Chronic spontaneous activity generated in the somata of primary nociceptors is associated with pain-related behavior after spinal cord injury. J Neurosci 30, 14870-14882. Benedetti, F., Vighetti, S., Amanzio, M., Casadio, C., Oliaro, A., Bergamasco, B., et al., 1998. Dose-response relationship of opioids in nociceptive and neuropathic postoperative pain. Pain 74, 205-11. Bergknut, N., Egenvall, A., Hagman, R., et al., 2012. Incidence of intervertebral disk degeneration-related diseases and associated mortality rates in dogs. J Am Vet Med Assoc 240, 1300-1309. Black, J.A., Cummins, T.R., Plumpton, C., et al., 1999. Upregulation of a Silent Sodium Channel After Peripheral, but not Central, Nerve Injury in DRG Neurons. J Neurophysiol 5, 2776-2785.
56
Bock, P., Spitzbarth, I., Haist, V., Stein, V., et al., 2013. Spatio-Temporal Development of Axonopathy in Canine Intervertebral Disc Disease as a Translational Large Animal Model for Nonexperimental Spinal Cord Injury. Brain Pahtology 23, 82-99. Boldt, I., Eriks-Hoogland, I., Brinkhof, M.G., de Bie, R., Joggi, D., von Elm, E., 2014. Non-pharmacological interventions for chronic pain in people with spinal cord injury (Review). The Cochrane Collaboration, Issue 11. Braz, J., Basbaum, A., 2009. Triggering genetically-expressed transneuronal tracers by peripheral axotomy reveals convergent and segregated sensory neuron-spinal cord connectivity. Neuroscience 163, 1220-1232. Brisson, B.A., 2010 Intervertebral disc disease in dogs. Vet Clin Small Anim 40, 829-858. Brodbelt, A.R., Stoodley, M.A., 2003. Post-traumatic syringomyelia: A review. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 10, 401–408. Bryce, T.N., Biering-Sorensen, F., Finnerup, N.B., Cardenas, D.D., Defrin, R., Ivan, E. et al, 2012. International spinal cord injury pain (ISCIP) classification: part 2. Initial validation using vignettes. Spinal Cord 50, 404–412. Brydges, N.M., Argyle, D.J., Mosley, J.R., Duncan, J.C., Fleetwood-Walker, S., Clements, D.N., 2012. Clinical assessments of increased sensory sensitivity in dogs with cranial cruciate ligament rupture. Vet J 193, 545-550. Cardenas, D.D., Felix, E.R., 2009. Pain after spinal cord injury: a review of classification, treatment approaches, and treatment assessment. PM R 1, 1077–90. Carlton, S.M., Junhui, D., Tan, H.Y., Nesic, O., Hargett, G.L., Bopp, A.C., Yamani, A., Lin, Q., Willis, W.D., Hulsebosch, C.E., 2009. Peripheral and central sensitization in remote spinal cord regions contribute to central neuropathic pain after spinal cord injury. Pain 147, 265–276. Case, J., Marvel, S., Boscan, P., et al., 2011. Surgical time and severity of postoperative pain in dogs undergoing laparoscopic ovariectomy with one, two, or three instrument cannulas. J Am Vet Med Assoc 239, 203-208. Cashmore, R.G., Harcourt-Brown, T.R., Freeman, P.M., Jeffery, N.D., Granger, N., 2009. Clinical diagnosis and treatment of suspected neuropathic pain in three dogs. Aust Vet J 87, 45-50. Chiou-Tan, F.Y., Tuel, S.M., Johnson, J.C., Priebe, M.M., Hirsh, D.D., Strayer, J.R., 1996. Effect of mexiletine on spinal cord injury dysesthetic pain. Am J Phys Med Rehabil 75, 84–87.

57
Christensen, M.D., Hulsebosch, C.E., 1997. Spinal cord injury and anti-NGF treatment results in changes in CGRP density and distribution in the dorsal horn in the rat. Exp Neurol 147, 463–475. Chung, J., Sumeier, K., Lee, H., et al., 1986. Classification of Primate Spinothalamic and Somatosensory Thalamic Neurons Based on Cluster Analysis. J Neurophys 56, 308-327. Cohen, S., Mao, J., 2014. Neuropathic pain: mechanisms and their clinical implications. BMJ 348: f7656. Crociolli, G.C., Cassu, R.N., Barbero, R.C., Rocha, T.L., Gomes, D.R., Nicacio, G.M., 2015. Gabapentin as an adjuvant for postoperative pain management in dogs undergoing mastectomy. J Vet Med Sci 77, 1011. Crown, E.D., Ye, Z., Johnson, K.M., et al., 2006. Increases in the activated forms of ERK 1/2, p38 MAPK, and CREB are correlated with the expression of at-level mechanical allodynia following spinal cord injury. Exp Neurol 199, 397–407. Crown, E.D., Gwak, Y., Ye, Z., et al., 2008. Activation of p38 MAP Kinase is involved in central neuropathic pain following spinal cord injury. Exp Neurol 213, 257-267. Davidoff, G., Guarracini, M., Roth, E., Sliwa, J., Yarkony, G., 1987. Trazodone hydrochloride in the treatment of dysesthetic pain in traumatic myelopathy: a randomized, double-blind, placebo-controlled study. Pain 29, 151–161. Defrin, R., Ohry, A., Blumen, N., Urca, G., 1999. Acute pain threshold in subjects with chronic pain following spinal cord injury. Pain 83, 275–282. Delaney, G.A., McKee, A.C., 1993. Inter- and intra-rater reliability of the pressure threshold meter in measurement of myofascial trigger point sensitivity. American Journal of Physical Medicine & Rehabilitation 72, 136–139. Densmore, V.S., Kalous, A., Keast, J.R., Osborne, P.B., 2010. Above-level mechanical hyperalgesia in rats develops after incomplete spinal cord injury but not after cord transection, and is reversed by amitriptyline, morphine and gabapentin. Pain 151, 184–193. Detloff, M.R., Fisher, L.C., Deibert, R.J., Basso, D.M., 2012. Acute and chronic tactile sensory testing after spinal cord injury in rats. Journal of Visualized Experiments 62, e3247. Drew, G.M., Siddal, P.J., Duggan, A.W., 2004. Mechanical allodynia following contusion injury of the rat spinal cord is associated with loss of GABAergic inhibition in the dorsal horn. Pain 109, 379-388. Drewes, A.M., Andreasen, A., Poulsen, L.H., 1994. Valproate for treatment of chronic central pain after spinal cord injury. A double-blind cross-over study. Paraplegia 32, 565–569.

58
Eaton, M.J., Wolfe, S.Q., Martinez, M., et al., 2007. Subarachnoid transplant of a human neuronal cell line attenuates chronic allodynia and hyperalgesia after excitotoxic spinal cord injury in the rat. J Pain 8, 33–50. Eide, P.K., Stubhaug, A., Stenehjem, A.E., 1995. Central dysesthesia pain after traumatic spinal cord injury is dependent on N-methyl-D-aspartate receptor activation. Neurosurgery 37, 1080–1087. Felix, E.R., Widerstrom-Noga, E.G., 2009. Reliability and validity of quantitative sensory testing in persons with spinal cord injury and neuropathic pain. Journal of Rehabilitation Research and Development 46, 69–84. Finnerup, N.B., Sindrup, S.H., Bach, F.W., Johannesen, I.L., Jensen, T.S., 2002. Lamotrigine in spinal cord injury pain: a randomized controlled trial. Pain 96, 375–383. Finnerup, N.B., Johannesen, I.L., Bach, F.W., Jensen, T.S., 2003. Sensory function above lesion level in spinal cord injury patients with and without pain. Somatosensory & Motor Research 20, 71-76. Finnerup, N.B., Biering-Sorensen, F., Johannesen, I.L., Terkelsen, A.J., Juhl, G.I., Kristensen, A.D., et al., 2005. Intravenous lidocaine relieves spinal cord injury pain: a randomized controlled trial. Anesthesiology. 102, 1023–1030. Finnerup, N.B., Grydehoj, J., Bing, J., Johannesen, I.L., Biering-Sorensen, F., Sindrup, S.H., et al., 2009. Levetiracetam in spinal cord injury pain: a randomized controlled trial. Spinal Cord 47, 861–867. Finnerup, N.B., Norrbrink, C., Trok, K., Piehl, F., Johannesen, I., Sørensen, J., Jensen, T.S., Werhageny, L., 2014. Phenotypes and predictors of pain following traumatic spinal cord injury: a prospective study. The Journal of Pain 15, 40-48. Freynhagen, R., Baron, R., Ulrich, G., Tolle, T., 2006. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Current Medical Research and Opionion 22, 1911-1920. Geber, C., Magerl, W., Fondel, R., Fechir, M., Rolke, R., Vogt, T., Treede, R.D., Birklein, F., 2008 Numbness in clinical and experimental pain—a cross-sectional study exploring the mechanisms of reduced tactile function. Pain 139, 73–81. Geber, C., Klein, T., Azad, S., Birklein, F., Gierthmuhlen, J., Huge, D., Lauchart, M., Nitzche, D., Stengel, M., Valet, M., 2011. Test-retest and interobserver reliability of quantitative sensory testing according to the protocol of the German Research Network on Neuropathic Pain (DFNS): a multi-centre study. Pain 152, 548-556. Goldin, A.L., Barchi, R.L., Caldwell, J.H., et al., 2000. Nomenclature of voltage-gated sodium channels. Neuron 28, 365-368.

59
Gorney, A.M, Blau, S.R., Dohse, C.S., Griffith, E.H, Williams, K.D., Lim, J.H., Knazovicky, D., Lascelles, B.D.X., Olby, N.J., 2016. Mechanical and Thermal Sensory Testing in Normal Chondrodystrophoid Dogs and Dogs with Spinal Cord Injury caused by Thoracolumbar Intervertebral Disc Herniations. Journal of Veterinary Internal Medicine 30, 627-635. Greenspan, J.D., 2001. Quantitative assessment of neuropathic pain. Curr Pain Headache Rep 5, 107–113. Gwak, Y.S., Crown, E.D., Unabia, G.C., et al., 2008. Propentofylline attenuates allodynia, glial activation and modulates GABAergic tone after spinal cord injury in the rat. Pain 138, 410-422. Gwak, Y.S., Hulsebosch, C.E., 2011. Neuronal Hyperexcitability: A Substrate for Central Neuropathic Pain After Spinal Cord Injury. Curr Pain Headache Rep 15, 215-222. Haas, M., 1991. Statistical methodology for reliability studies. Journal of Manipulative Physiology and Therapy 14, 119–132. Hagen, E., Rekand, T., 2015. Management of Neuropathic Pain Associated with Spinal Cord Injury. Pain Ther 4, 51-65. Hains, B.C., Saab, C.Y., Waxmann, S.G., 2005. Changes in electrophysiological properties and sodium channel Nav1.3 expression in thalamic neurons after spinal cord injury. Brain 128, 2359-2371. Hama, A.T., Plum, A.W., Sagen, J., 2010. Antinociceptive effect of ambroxol in rats with neuropathic spinal cord injury pain. Pharmacol Biochem Behav 97, 249–255. Hao, J., Kupers, R., Xu, X., 2004. Response Characteristics of Spinal Cord Dorsal Horn Neurons in Chronic Allodynic Rats After Spinal Cord Injury. J Neurophysiol 92, 1391–1399. Hendrich, J., Van Minh, A., Heblich, F., et al., 2008. Pharmacological disruption of calcium channel trafficking by the alpha2delta ligand gabapentin. Proc Natl Acad Sci USA 105, 3628-3633. Hoschouer, E.L., Basso, D.M., Jakeman, L.B., 2010. Aberrant sensory responses are dependent on lesion severity after spinal cord contusion injury in mice. Pain 148, 328–342. Hulsebosch, C., Hains, B., Crown, E., Carlton, S., 2009. Mechanisms of chronic central neuropathic pain after spinal cord injury. Brain Research Reviews 60, 202-213. Ji, R., Kohno, T., Moore, K., et al., 2003. Central sensitization and LTP: do pain and memory share similar mechanisms? Trends in Neurosciences 26, 696-705. Jones, D.H., Kilgour, R.D., Comtois, A.S., 2007. Test-retest reliability of pressure pain threshold measurements of the upper limb and torso in young healthy women. Pain 8, 650-656.

60
Kaka, U., Saifullah, B., Abubakar, A.A., et al., 2016. Serum concentration of ketamine and antinociceptive effects of ketamine and ketamine-lidocaine infusions in conscious dogs. BMC Vet Res 12, 198. Kalliomaki, M., Kieseritzky, J.V., Schmidt, R., Hagglof, B., Karlsten, R., Sjorgren, N., Albrecht, P., Gee, L., Rice, F., Wiig, M., Schmelz, M., Gordh, T., 2011. Structural and functional differences between neuropathy with and without pain? Experimental Neurology 231, 199-206. Kim, D.S., Jung, S.J., Nam, T.S., et al., 2010. Transplantation of GABAergic Neurons from ESCs Attenuates Tactile Hypersensitivity Following Spinal Cord Injury. Stem Cells 28, 2099–2108. Kloos, A.D., Fisher, L.C., Detloff, M.R., et al., 2005. Stepwise motor and all-or-none sensory recovery is associated with nonlinear sparing after incremental spinal cord injury in rats. Exp Neurol 191, 251-265. Kohno, T., Ji, R.R., Ito, N., Allchorne, A.J., Befort, K., Karchewski, L.A., et al., 2005. Peripheral axonal injury results in reduced mu opioid receptor pre- and post-synaptic action in the spinal cord. Pain 117,77-87. Knazovicky, D., Helgeson, E.S., Case, B, Thomson, A, Gruen, M.E., Maixner, W., Lascelles, B.D., 2017. Replicate effects and test-retest reliability of quantitative sensory threshold testing in dogs with and without chronic pain. Veterinary Anaesthesia and Analgesia 44, 615-624. KuKanich, B., Lascelles, B.D., Papich, M.G., 2005. Use of a von Frey device for evaluation of pharmacokinetics and pharmacodynamics of morphine after intravenous administration as an infusion or multiple doses in dogs. Am J Vet Res 66, 1968-1974. KuKanich, B., Papich, M.G., 2011. Pharmacokinetics and antinociceptive effects of oral tramadol hydrochloride administration in Greyhounds. Am J Vet Res 72, 256-262. KuKanich, B., 2016. Pharmacokinetics and pharmacodynamics of oral acetaminophen in combination with codeine in healthy Greyhound dogs. Vet Pharm Therap 39, 514-517. Landis, J.R., Koch, G.G., 1977. The measurement of observer agreement for categorical data. Biometrics 33, 159-174. Lascelles, B.D., 2013. Getting a sense of sensations. The Veterinary Journal 197, 115–117. Lee, K.M., Lee, J., Chung, C.Y., Ahn, S., Kim, T.W., Lee, H.J, Park, M.S., 2012. Pitfalls and important issues in testing reliability using intraclass correlation coefficients in orthopaedic research. Clinical Orthopedic Surgery 4, 149–155. Lee, M., Silverman, S.M., Hansen, H., et al., 2011. A comprehensive review of opioid-induced hyperalgesia. Pain Physician 14, 145-161.
61
Leem, J., Kim, H., Hulsebosch, C, Gwak, Y., 2010. Ionotropic glutamate receptors contribute to maintained neuronal hyperexcitability following spinal cord injury in rats. Exp Neurol 224, 321–324. Levendoglu, F., Ogun, C.O., Ozerbil, O., Ogun, T.C., Ugurlu, H., 2004. Gabapentin is a first line drug for the treatment of neuropathic pain in spinal cord injury. Spine 29, 743–751. Levine, J.M., Levine, G.J., Porter, B.F., Topp, K., Noble-Haeusslein, L.J., 2011. Naturally occurring disk herniation in dogs: An opportunity for pre-clinical spinal cord injury research. Journal of Neurotrauma 28, 675–688. Liu, J., Wolfe, D., Hao, S., et al., 2004. Peripherally delivered glutamic acid decarboxylase gene therapy for spinal cord injury pain. Mol Ther 10, 57–66. Luo, Z., Chaplan, S., Higuera, E., et al., 2001. Upregulation of dorsal root ganglion (alpha)2(delta) calcium channel subunit and its correlation with allodynia in spinal nerve-injured rats. J Neurosci 21, 1868-1875. Maixner, W., Dubner, R., Bushnell, M.C., et al., 1986. Wide-dynamic-range dorsal horn neurons participate in the encoding process by which monkeys perceive the intensity of noxious heat stimuli. Brain Res 374, 385–388. Malcangio, M., Bowery, N.G., 1996. GABA and its receptors in the spinal cord. Trends Pharmacol Sci 17, 457–462. Marcuzzi, A., Wrigley, P.J., Dean, C.M., Adams, R., Hush, J.M., 2017. The long-term reliability of static and dynamic quantitative sensory testing in healthy individuals. Pain 158, 1217-1223. Masri, R., Keller, A., 2012. Chronic pain following spinal cord injury. Advances in Experimental Medicine and Biology 760, 74-88. McAdoo, D.J., Xu, G.Y., Robak, G., Hughes, M.G., 1999. Changes in amino acid concentrations over time and space around an impact injury and their diffusion through the rat spinal cord. Exp Neurol 159, 538–544. Meisner, J.G., Marsh, A.D., Marsh, D.R., 2010. Loss of GABAergic interneurons in laminae I-III of the spinal cord dorsal horn contributes to reduced GABAergic tone and neuropathic pain after spinal cord injury. J Neurotrauma 27, 729–737. Menetrey, D., Giesler, G. J., Besson, J. M., 1977. An analysis of response properties of spinal cord dorsal horn neurones to nonnoxious and noxious stimuli in the spinal rat. Exp. Brain Res. 27, 15-33. Merskey, H., Bogduk, N. Classification of chronic pain: Descriptions of chronic pain syndromes and definitions of pain terms. 2nd ed. Seattle: IASP Press, 2002.

62
Mills, C.D., Hains, B.C., Johnson, K.M., Hulsebosch, C.E., 2001. Strain and model differences in behavioral outcomes after spinal cord injury in rat. Journal of Neurotrauma 18, 743-756. Moore, R.A., Derry, S., Aldington, D., et al., 2012. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev 12, CD008242. Moore, R.A., Wiffen, P., Derry, S., et al., 2014. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev 3, CD007938. Moore, S.A., Hettlich, B.F., Waln, A., 2013. The use of an electronic von Frey device for evaluation of ST in neurologically normal dogs and those with acute spinal cord injury. The Veterinary Journal 197, 216–219. Moore, S.A., Granger, N., Olby, N.J., Spitzbarth, I., Jeffery, N.D., Tipold, A., Nout-Lomas, Y.S., da Costa, R.C., Stein, V.M., Noble-Haeusslein, L.J., Blight, A.R., Grossman, R.G., Basso, D.M., Levine, J.M., 2017. Targeting Translational Successes through CANSORT-SCI: Using Pet Dogs to Identify Effective Treatments for Spinal Cord Injury. Journal of Neurotrauma 34, 2007-2018. Nakae, A., Nakai, K., Yano, K., Hosokawa, K., Shibata, M., Mashimo, T., 2011. The Animal Model of Spinal Cord Injury as an Experimental Pain Model. Journal of Biomedicine and Biotechnology 2011, 1-11. Nathan, P.W., Smith, M.C., Cook, A.W., 1986. Sensory effects in man of lesions of the posterior columns and of some other afferent pathways. Brain 109, 1003–1041. National Spinal Cord Injury Statistical Center, 2016. Facts and Figures at a Glance. Birmingham, AL: University of Alabama at Birmingham. Norrbrink, C., Lundeberg, T., 2009. Tramadol in neuropathic pain after spinal cord injury: a randomized, double-blind, placebo-controlled trial. Clin J Pain 25, 177–184. Offord, J., Isom, L., 2015. Drugging the undruggable: gabapentin, pregabalin and the calcium channel α2δ subunit. Crit Rev Biochem Mol Biol 51, 246-256. Olby, N.J., De Risio, L., Muñana, K., Wosar, M.A., Skeen, T.M., Sharp, N.J., Keene, B.W., 2001. Development of a functional scoring system in dogs with acute spinal cord injuries. American Journal of Veterinary Research 62, 1624–1628. Phillips, T.C., Cherry, C.L., Cox, S., Marshall, S.J., Rice, A.C., 2010. Pharmacological treatment of painful HIV-associated sensory neuropathy: a systematic review and meta-analysis of randomised controlled trials. PLoS One 5, e14433. Plessas, I.N., Volk, H.A., Rusbridge, C., Vanhaesebrouck, A.E., Jeffery, N.D., 2015. Comparison of gabapentin versus topiramate on clinically affected dogs with Chiari-like malformation and syringomyelia. Vet Rec 177, 288.

63
Przewłocki, R., Przewłocka, B., 2001. Opioids in chronic pain. Eur J Pharmacol 429, 79-91. Rafati, D.S., Geissler, K., Johnson, K., et al., 2008. Nuclear factor-kappaB decoy amelioration of spinal cord injury-induced inflammation and behavior outcomes. J Neurosci Res 86, 566–580. Rintala, D.H., Fiess, R.N., Tan, G., Holme,s S.A., Bruel, B.M., 2010. Effect of dronabinol on central neuropathic pain after spinal cord injury: a pilot study. Am J Phys Med Rehabil 89, 840–848. Rolke, R., Baron, R., Maier, C, Tolle, T.R., Treede, R.D., Beyer, A., Binder, A., Birbaumer, N., Birklein, F., Botefur, I.C., et al., 2006. Quantitative Sensory Testing in the German Research Network on Neuropathic Pain (DFNS): Standardized Protocol and Reference Values. Pain 123, 231-243. Romero, M.I., Rangappa, N., Li, L., et al., 2000. Extensive sprouting of sensory afferent and hyperalgesia induced by conditional expression of nerve growth factor in the adult spinal cord. J Neurosci 20, 4435–4445. Salazar, V., Dewey, C.W., Schwark, W., et al., 2009. Pharmacokinetics of single-dose oral pregabalin administration in normal dogs. Vet Anaesth Analg 36, 574–580. Salinas, F.A., Lugo, L.H., Garcia, H.I., 2012. Efficacy of early treatment with carbamazepine in prevention of neuropathic pain in patients with spinal cord injury. Am J Phys Med Rehabil 91, 1020–1027. Samad, O.A., Tan, A.M., Cheng, X., et al., 2013. Virus-mediated shRNA knockdown of Na(v)1.3 in rat dorsal root ganglion attenuates nerve injury-induced neuropathic pain. Mol Ther 21, 49–56. Schutter, A.F., Tunsmeyer, J., Kastner, S.R., 2017. Influence of tramadol on acute thermal and mechanical cutaneous nociception in dogs. Vet Anesth Analg 44, 309-316. Siddall, P., Taylor, D., McClelland, J., Rutkowski, S., Cousins, M., 1999. Pain report and the relationship of pain to physical factors in the first 6 months following spinal cord injury. Pain 81, 187-197. Siddall, P.J., Cousins, M.J., Otte, A., Griesing, T., Chambers, R., Murphy, T.K., 2006. Pregabalin in central neuropathic pain associated with spinal cord injury: a placebo-controlled trial. Neurology 67, 1792–1800. Sjolund, B.H., 2002. Pain and rehabilitation after spinal cord injury: the case of sensory spasticity? Brain Research Reviews 40, 250-256. Smith, P.M., Jeffery, N.D., 2006. Histological and ultrastructural analysis of white matter damage after naturally occurring spinal cord injury. Brain Pathology 16, 99–109.
64
Soler, M.D., Kumru, H., Vidal, J., Pelayo, R., Tormos, J.M., Fregni, F., Navarro, X., Pascual-Leone, A., 2010. Referred sensations and neuropathic pain following spinal cord injury. Pain 150, 192-198. Song, R.B., Basso, D.M., da Costa, R.C., Fisher, L.C., Mo, X, Moore, S.A., 2016. von Frey anesthesiometry to assess sensory impairment after acute spinal cord injury caused by thoracolumbar intervertebral disc extrusion in dogs. The Veterinary Journal 209, 144-149. Tan, A.M., Samad, A.S., Sulayman, D.H., et al., 2015. Virus-Mediated Knockdown of Nav1.3 in Dorsal Root Ganglia of STZ-Induced Diabetic Rats Alleviates Tactile Allodynia. Mol Med 21, 544-552. Tasker, R.R., DeCarvalho, G., Dolan, E.J., 1992. Intractable pain of spinal cord origin: clinical features and implications for surgery. Journal of Neurosurgery 77, 373-378. Tator, C.H., Fehlings, M.G., 1991. Review of the secondary injury theory of acute spinal cord trauma with emphasis on vascular mechanisms. J Neurosurg 75, 15–26. Teasell, R., Mehta, S., Aubut, J., et al., 2010. A Systematic Review of Pharmacological Treatments of Pain Following Spinal Cord Injury. Arch Phys Med Rehabil 91, 816-831. Tena, B., Escobar, B., Jose Arguis, M., Cantero, C., Rios, J., Gomar, C., 2012. Reproducibility of electronic von Frey and von Frey monofilaments testing. Clinical Journal of Pain 28, 318-323. Thalhammer, J.G., Raymond, S.A., Popitz-Bergez, F.A., et al., 1994. Modality-dependent modulation of conduction by impulse activity in functionally characterized single cutaneous afferents in the rat. Somatosens Mot Res 11, 243-257. Tomas, A., Marcellin-Little, D., Roe, S., et al., 2014. Relationship Between Mechanical Thresholds and Limb Use in Dogs with Coxofemoral Joint OA-Associated Pain and the Modulating Effects of Pain Alleviation From Total Hip Replacement on Mechanical Thresholds. Vet Surg 5, 542-548. Treede, R.D., Jensen, T.S., Campbell, J.N., Cruccu, G., Dostrovosky, J.O., Griffin, J.W., Hansson, H., Hughes, R., Nurmikko, T., Serra, J., 2008. Neuropathic pain: Redefinition and a grading system for clinical research purposes. Neurology 70, 1630-1635. Turner, J.A., Cardenas, D.D., Warms, C.A., McClellan, C.B., 2001. Chronic pain associated with spinal cord injuries: A community survey. Archives of Physical Medicine and Rehabilitation 82, 501-508. Ueda, H., 2006. Molecular mechanisms of neuropathic pain–phenotypic switch and initiation mechanisms. Pharmacology & Therapeutics 109, 57 – 77.

65
Valensi, P., Attali, J.R., Gagant, S., 1993, Reproducibility of parameters for assessment of diabetic neuropathy. The French Group for Research and Study of Diabetic Neuropathy. Diabetes Medicine 10, 933–939. Vogel, C., Rukwied, R., Stockinger, L., Schley, M., Schmelz, M., Schleinzer, W., Konrad, C., 2017. Functional characterization of at-level hypersensitivity in patients with spinal cord injury. Journal of Pain 18, 66-78. Vranken, J.H., Hollmann, M.W., van der Vegt, M.H., Kruis, M.R., Heesen, M., Vos, K., et al., 2011. Duloxetine in patients with central neuropathic pain caused by spinal cord injury or stroke: a randomized, double- blind, placebo-controlled trial. Pain 152, 267–273. Wade, D.T., Robson, P., House, H., Makela, P., Aram, J., 2003. A preliminary controlled study to determine whether whole-plant cannabis extracts can improve intractable neurogenic symptoms. Clin Rehabil 17, 21–29. Wagner, A.E., Mich, P.M., Uhrig, S.R., Hellyer, P.W., 2010. Clinical evaluation of perioperative administration of gabapentin as an adjunct for postoperative analgesia in dogs undergoing amputation of a forelimb. J Am Vet Med Assoc 236, 751–756. Walk, D., Sehgal, N., Moeller-Bertram, T., Edwards, R.R., Wasan, A., Wallace, M., Irving, G., Argoff, C., Backonja, M.M., 2009. Quantitative sensory testing and mapping – A review of nonautomated quantitative methods for examination of the patient with neuropathic pain. The Clinical Journal of Pain 25, 632–640. Wang, G., Thompson, S.M., 2008. Maladaptive homeostatic plasticity in a rodent model of central pain syndrome: thalamic hyperexcitability after spinothalamic tract lesions. The Journal Of Neuroscience 28, 11959-11969. Wasner, G., Lee, B.B., Engel, S., et al., 2008. Residual spinothalamic tract pathways predict development of central pain after spinal cord injury. Brain 131, 2387–2400. Webb, A.A., Ngan, S., Fowler, 2010. Spinal cord injury 1: a synopsis of the basic science. Can Vet J 51, 485-492. Wegner, K., Horais, K.A., Tozier, N.A., Rathbun, M.L., Shtaerman, Y., Yaksh, T.L., 2008. Development of a canine nociceptive thermal escape model. Journal of Neuroscience Methods 168, 88–97. Weston, R.M., Subasinghe, K.R., Staikopoulos, V., et al., 2009. Design and assessment of a potent sodium channel blocking derivative of mexiletine for minimizing experimental neuropathic pain in several rat models. Neurochem Res 34, 1816–1823. Winderstrom-Noga, E., Biering-Sorensen, F., Bryce, T., Cardenas, D.D., Finnerup, N.B., Jensen, M.P., Richards, J.S., Siddall, P.J., 2008. The International Spinal Cord Injury Pain Basic Data Set. Spinal Cord 46, 818-823.

66
Winderstrom-Noga, E., Biering-Sorensen, F., Bryce, T., Cardenas, D.D., Finnerup, N.B., Jensen, M.P., Richards, J.S., Siddall, P.J., 2014. The International Spinal Cord Injury Pain Basic Data Set (verson 2.0). Spinal Cord 52, 282-286. Yang, M.L., Li, J.J., So, K.F., Chen, J.Y., Cheng, W.S., Wu, J., et al., 2012. Efficacy and safety of lithium carbonate treatment of chronic spinal cord injuries: a double-blind, randomized, placebo-controlled clinical trial. Spinal Cord 50, 141–146. Yezierski, R., 2000. Pain following spinal cord injury: pathophysiology and central mechanisms. Progress in Brain Research 129, 429-449. Yin, R., Liu, D., Chhoa, M., et al., 2016. Voltage-gated sodium channel function and expression in injured and uninjured rat dorsal root ganglia neurons. Int J Neurosci 126, 182-192.




















