
Detection and genotyping by microarray of Human Papillomavirus in tissue of bladder and bladder...
15
In: Bladder Cancer: Etymology, Diagnosis, and Treatments ISBN: 978-1-61728-002-3 Editor: William E. Nilsson © 2009 Nova Science Publishers, Inc. Chapter 8 DETECTION AND GENOTYPING BY MICROARRAY OF HUMAN P APILLOMAVIRUS IN TISSUE OF BLADDER AND BLADDER CARCINOMA BIOPSY Antonio Sorlózano a , Ana Isabel Moraga b , Manuel Pareja c , Enrique Villegas a , María Luisa Villahermosa b , José Antonio Carrillo a and Jose Gutiérrez a+* a Department of Microbiology, School of Medicine, University of Granada, and + Service of Microbiology, University Hospital Virgen de las Nieves, Granada, Spain b GENOMICA, ZELTIA Group, Coslada, Spain c Department of Urology, University Hospital San Cecilio, Granada, Spain ABSTRACT Background Several studies have analyzed the association between bladder cancer (BC) and Human Papillomavirus (HPV) infection using various direct and indirect diagnostic techniques. However, even though there may be evidence of such association, the debate on whether it is sheer coincidence or on whether a relationship of causality exists remains open due, amongst other factors, to the lack of a high sensitivity standardized procedure that can detect the virus. Thus, the aim of this work was to develop a technique with appropriate sensitivity that may allow the detection of HPV DNA both in tumour tissue biopsies as well as in healthy vesical tissue biopsies, while, at the same time, allowing the detection of the genotype in question. * Corresponding author: Departamento de Microbiologia, Facultad de Medicina, Avda de Madrid 11, E-18012 Granada, Spain. E-mail: [email protected]
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Detection and genotyping by microarray of Human Papillomavirus in tissue of bladder and bladder...

In: Bladder Cancer: Etymology, Diagnosis, and Treatments ISBN: 978-1-61728-002-3
Editor: William E. Nilsson © 2009 Nova Science Publishers, Inc.
Chapter 8
DETECTION AND GENOTYPING BY MICROARRAY OF
HUMAN PAPILLOMAVIRUS IN TISSUE OF BLADDER
AND BLADDER CARCINOMA BIOPSY
Antonio Sorlózanoa, Ana Isabel Moraga
b, Manuel Pareja
c,
Enrique Villegasa, María Luisa Villahermosa
b,
José Antonio Carrilloa and Jose Gutiérrez
a+*
aDepartment of Microbiology, School of Medicine, University of Granada,
and +Service of Microbiology, University Hospital Virgen de las Nieves, Granada, Spain
bGENOMICA, ZELTIA Group, Coslada, Spain
cDepartment of Urology, University Hospital San Cecilio, Granada, Spain
ABSTRACT
Background
Several studies have analyzed the association between bladder cancer (BC) and
Human Papillomavirus (HPV) infection using various direct and indirect diagnostic
techniques. However, even though there may be evidence of such association, the debate
on whether it is sheer coincidence or on whether a relationship of causality exists remains
open due, amongst other factors, to the lack of a high sensitivity standardized procedure
that can detect the virus. Thus, the aim of this work was to develop a technique with
appropriate sensitivity that may allow the detection of HPV DNA both in tumour tissue
biopsies as well as in healthy vesical tissue biopsies, while, at the same time, allowing the
detection of the genotype in question.
* Corresponding author: Departamento de Microbiologia, Facultad de Medicina, Avda de Madrid 11, E-18012
Granada, Spain. E-mail: [email protected]

Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 2
Material and Methods
Eighty-five biopsies of vesical tissue were obtained from patients operated upon at
the Urology Unit of Hospital San Cecilio in Granada, Spain: 34 bladder cancer and 51
healthy vesical tissue biopsies. Initially, the CLART®HPV (GENOMICA, ZELTIA
Group) system was used in all samples. This technique amplifies a fragment of the L1
region of HPV and identifies the genotype through microarray. With the aim of
increasing the sensitivity in HPV DNA detection, a nested-PCR specific for each of the
genotypes with greater oncogenic risk were designed.
Results
HPV DNA was detected in 5.9% of the biopsies (2 samples with genotype 16 and
3 with genotype 82) through CLART®HPV detection. HPV DNA was however detected
in 17.6% of the samples analyzed (1 with genotype 35, 2 with 51, 3 with 52, 2 with 58, 5
with 82 and 2 with two concomitant genotypes) through nested-PCR. Nested-PCR
increased the sensitivity in the detection of genotypes 18, 33, 51 and 82 by two 10-fold
serial diluted in relation with the CLART®HPV system, and in the detection of
genotypes 52 and 58, by one 10-fold serial diluted, although the same sensitivity was
maintained in both techniques in the detection of genotypes 35 and 39.
Conclusion
The development of an ultrasensitive technique in the future for detecting HPV DNA
in bladder cancer and in vesical healthy tissue biopsies will allow the determination of a
causal relationship between HPV infection and bladder carcinoma.
INTRODUCTION
Bladder carcinoma (BC), often considered as only one type of neoplasia, comprises a
heterogeneous group of processes which encompasses lesions of very different
biopathological behaviour. Various clinical observations have shown that, notwithstanding
(high grade) in situ carcinoma, BC comprises of two main clinicopathological groups:
superficial and deep or musculo-invasive. Each of them has a different natural history and,
maybe also different risk factors in their development [1]. The mechanisms associated to the
appearance and progression of these tumours, as well as the possible risk factors involved,
continue being subject to study to date [1-7].
On the other hand the oncogenic potential of the human papillomavirus (HPV) has been
clearly proven [8] and, although most studies have centred on tumours of the female genital
tract, specially those of the neck of the uterus, the study of its participation in other urogenital
tumours, amongst them, BC, has also been promoted [9-11]. In this sense, various authors
have tried to establish the relationship between HPV infection and BC, mainly with
transitional cell tumours [12], a possible relationship based on the virus epithelial tropism and
on the anatomic proximity of the urogenital area.
A meta-analysis carried out by our team shows how the results obtained from the
44 studies analyzing said relations (all published before June 2005) are contradictory [13]. In
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 3
39 studies, the researchers determined the presence of HPV DNA and found a prevalence of
between 0% [14-22] and 100% [23]; pooled estimation of the presence of the infection was
16.0% (95% CI 12.8 to 19.1) and pooled Odds Ratio (OR) estimation was 2.3 (95% CI 1.3 to
4.1). Seven studies analyzed HPV infection by detecting the antigen or antibodies and the
prevalence found was between 14% [24] and 60% [22,25]. Pooled estimation of the
prevalence of infection was 32.4% (95% CI 17.0 to 47.8) while pooled OR estimation was 2.9
(95% CI 1.7 to 5.3).
Globally considered, then, although most of the studies show the presence of the
infection, however there is a significant dispersion of the results, it may be because the
methodologies employed in such studies varied, were badly standardized (in some cases
control groups were absent) and/or scarcely explicit, thus making it difficult for totally valid
conclusions to be obtained. In spite of all the research work, therefore, it is impossible to
obtain definite conclusions that may indicate the participation of HPV in the development of
vesical neoplasia [13].
Several other articles were published after said meta-analysis, and until September 2009;
again, however, while some state that HPV does not seem to play a role in the pathogenesis of
either type of bladder cancer [26,27], others state that HPV might play a causative role in BC
[11,12,28]. Notwithstanding, these analyses, like the previous ones, are lacking in sufficient
methodological information, so that they do not allow us to establish a definite conclusion.
In the last few years the microbiological tests used to detect HPV infection have
undergone changes. Today it is most common to use PCR but this should not detract from
other techniques that rely on host response or that detect the virus in situ, the sensitivity and
reliability of which have been compared. In support of this fact is the satisfactory relationship
between the results obtained by Ludwig et al [29], who used direct and indirect results to
detect infection.
Our retrospective study of the published results of HPV involvement in bladder cancer
[13] leads to some interesting conclusions. One of the conclusions is that comparisons among
studies can be complicated by various factors: 1) the different populations studied may have
different risk factors, such as genetics, geography and life-style, of which any might affect
carcinoma development in the bladder epithelium; 2) different researchers often use different
techniques with varying specificity and sensitivity; 3) technical mistakes made by the
laboratory researcher or even the choice of the right primer can affect the experimental
results. Thus, current diagnostic methods such as biopsy specimens may well provide low
numbers of HPV genomes and they are often inconclusive for identifying the specific HPV
strain, encouraging researchers to further examine universal detection methods using DNA.
The less valid results of our study could be due to a lack of HPV test sensitivity. For this
reason, it is the intention of HPV experts and the WHO to establish international biological
standard materials for the diagnosis and therapy of human disease. The availability of
international HPV DNA standards would contribute to the field of HPV prevention, diagnosis
and treatment [30,31].
Thus, the aim of our study was to develop a technique for detecting HPV DNA in
biopsies of BC and of healthy vesical tissues, with adequate sensitivity and which may also
allow the detection of the genotype in question.
Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 4
MATERIAL AND METHOD
Study Design and Tissue Samples
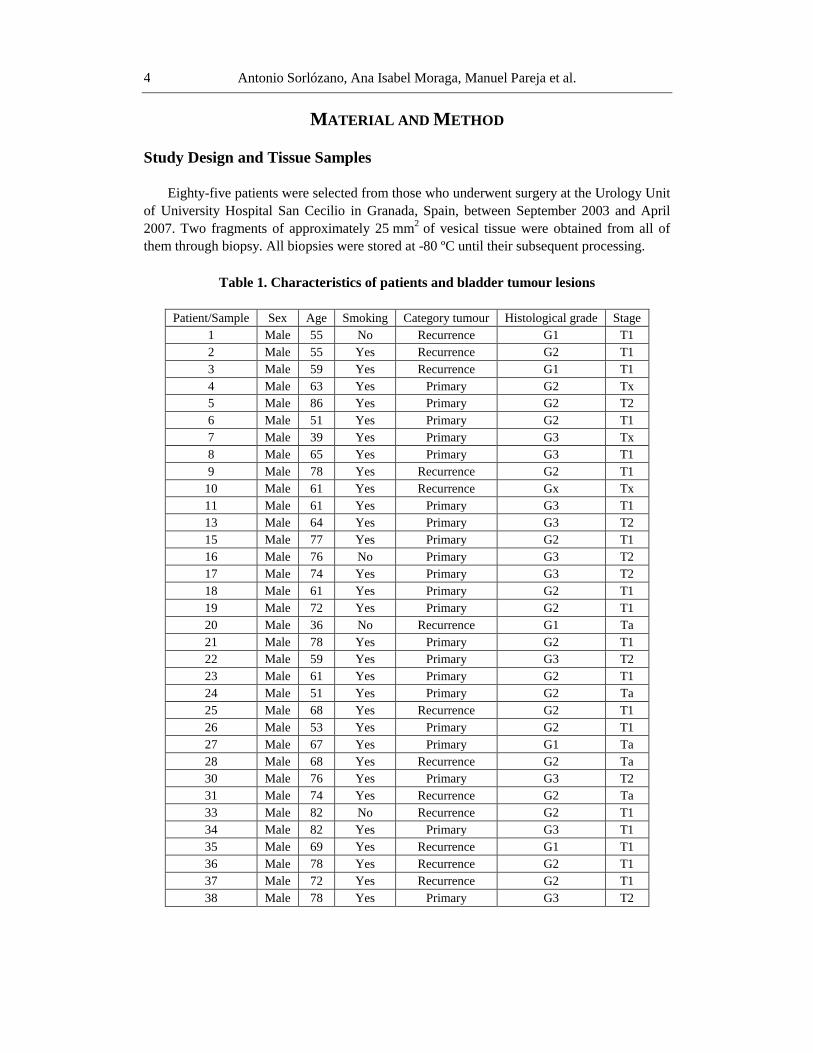
Eighty-five patients were selected from those who underwent surgery at the Urology Unit
of University Hospital San Cecilio in Granada, Spain, between September 2003 and April
2007. Two fragments of approximately 25 mm2
of vesical tissue were obtained from all of
them through biopsy. All biopsies were stored at -80 ºC until their subsequent processing.
Table 1. Characteristics of patients and bladder tumour lesions
Patient/Sample Sex Age Smoking Category tumour Histological grade Stage
1 Male 55 No Recurrence G1 T1
2 Male 55 Yes Recurrence G2 T1
3 Male 59 Yes Recurrence G1 T1
4 Male 63 Yes Primary G2 Tx
5 Male 86 Yes Primary G2 T2
6 Male 51 Yes Primary G2 T1
7 Male 39 Yes Primary G3 Tx
8 Male 65 Yes Primary G3 T1
9 Male 78 Yes Recurrence G2 T1
10 Male 61 Yes Recurrence Gx Tx
11 Male 61 Yes Primary G3 T1
13 Male 64 Yes Primary G3 T2
15 Male 77 Yes Primary G2 T1
16 Male 76 No Primary G3 T2
17 Male 74 Yes Primary G3 T2
18 Male 61 Yes Primary G2 T1
19 Male 72 Yes Primary G2 T1
20 Male 36 No Recurrence G1 Ta
21 Male 78 Yes Primary G2 T1
22 Male 59 Yes Primary G3 T2
23 Male 61 Yes Primary G2 T1
24 Male 51 Yes Primary G2 Ta
25 Male 68 Yes Recurrence G2 T1
26 Male 53 Yes Primary G2 T1
27 Male 67 Yes Primary G1 Ta
28 Male 68 Yes Recurrence G2 Ta
30 Male 76 Yes Primary G3 T2
31 Male 74 Yes Recurrence G2 Ta
33 Male 82 No Recurrence G2 T1
34 Male 82 Yes Primary G3 T1
35 Male 69 Yes Recurrence G1 T1
36 Male 78 Yes Recurrence G2 T1
37 Male 72 Yes Recurrence G2 T1
38 Male 78 Yes Primary G3 T2
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 5
In 34 patients (Table 1) the biopsy was obtained from the vesical tumour lesion after
undergoing transurethral resection (TUR). All of them were male. The mean age of the group
was 66 years, with a range of 36 to 86 years. 88.2% were, or had been, smokers. Of the
vesicle lesions resected, 61.8% were primary tumours while the rest were recurrent. 9.5% of
the primary tumours were Ta, 47.6% were T1 and 33.3% were T2. Assessing the histological
grade, we discovered that within the primary tumours 4.8% were G1, while 47.6% were G2
and also G3. Of the recurrent, 30.8% were G1 and 61.6% were G2; in said cases, 23.1% were
Ta and 69.2% were T1.
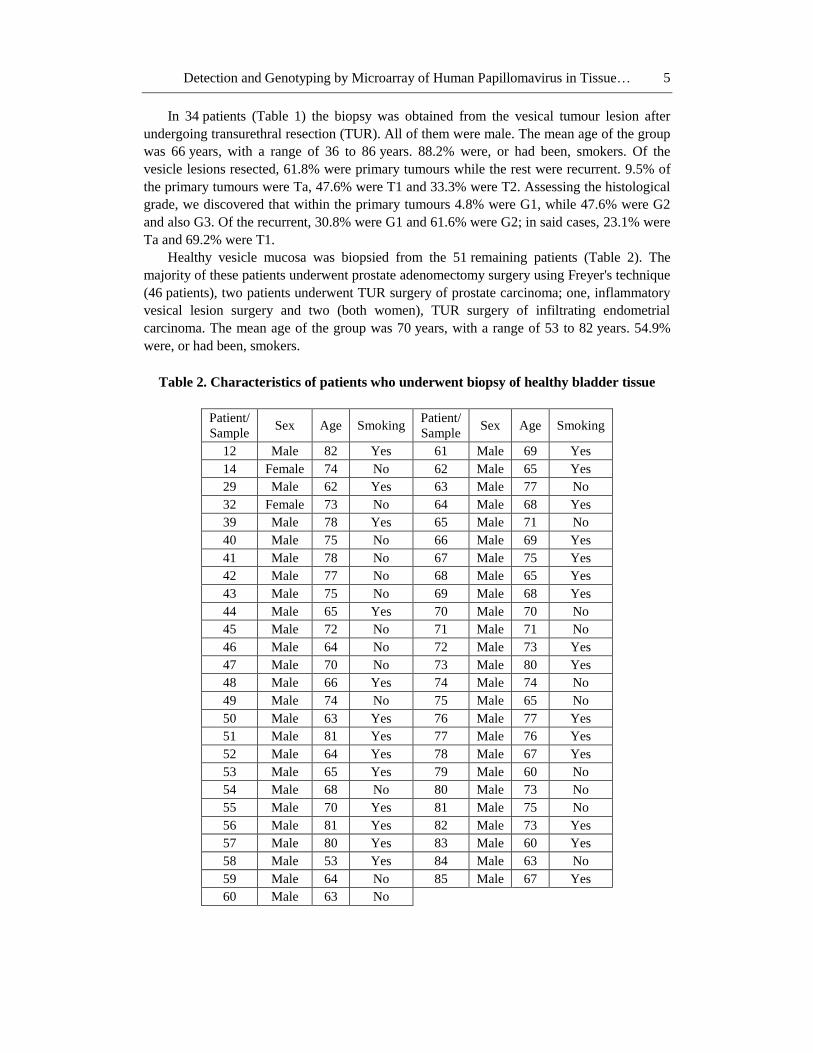
Healthy vesicle mucosa was biopsied from the 51 remaining patients (Table 2). The
majority of these patients underwent prostate adenomectomy surgery using Freyer's technique
(46 patients), two patients underwent TUR surgery of prostate carcinoma; one, inflammatory
vesical lesion surgery and two (both women), TUR surgery of infiltrating endometrial
carcinoma. The mean age of the group was 70 years, with a range of 53 to 82 years. 54.9%
were, or had been, smokers.
Table 2. Characteristics of patients who underwent biopsy of healthy bladder tissue
Patient/
Sample Sex Age Smoking
Patient/
Sample Sex Age Smoking
12 Male 82 Yes 61 Male 69 Yes
14 Female 74 No 62 Male 65 Yes
29 Male 62 Yes 63 Male 77 No
32 Female 73 No 64 Male 68 Yes
39 Male 78 Yes 65 Male 71 No
40 Male 75 No 66 Male 69 Yes
41 Male 78 No 67 Male 75 Yes
42 Male 77 No 68 Male 65 Yes
43 Male 75 No 69 Male 68 Yes
44 Male 65 Yes 70 Male 70 No
45 Male 72 No 71 Male 71 No
46 Male 64 No 72 Male 73 Yes
47 Male 70 No 73 Male 80 Yes
48 Male 66 Yes 74 Male 74 No
49 Male 74 No 75 Male 65 No
50 Male 63 Yes 76 Male 77 Yes
51 Male 81 Yes 77 Male 76 Yes
52 Male 64 Yes 78 Male 67 Yes
53 Male 65 Yes 79 Male 60 No
54 Male 68 No 80 Male 73 No
55 Male 70 Yes 81 Male 75 No
56 Male 81 Yes 82 Male 73 Yes
57 Male 80 Yes 83 Male 60 Yes
58 Male 53 Yes 84 Male 63 No
59 Male 64 No 85 Male 67 Yes
60 Male 63 No

Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 6
Preliminary Detection of HPV DNA in Bladder Biopsies through
CLART®HPV
Genotyping of eighty-five bladder biopsies was performed with CLART®HPV
(GENOMICA, ZELTIA Group, Coslada, Spain) [32], This CE labelled kit comprises a
multiplex-amplification of L1 conserved region which is performed using biotin-labeled
primers, and a hybridization of the amplicon (450 bp) on a low-density tube array containing
HPV type-specific probes. HPV types genotyped with the kit included high-risk (HR)
genotypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82; low-risk (LR)
genotypes 6, 11, 40, 42, 43, 44, 54, 61, 66, 70, 72, 81 and 89 and genotypes with probable
high-risk (PHR) 53 and 66. The amplified fragment contain highly conserved regions used as
PCR targets for the amplification of different types of HPV virus, but shows enough
variations as to allow the differentiation of each type of virus using specific probes.
The amplified product is visualized through a tube microarray (ArrayTube, AT), a system
that basically consists of the inclusion of a microarray in the lower part of an Eppendorf-type
test tube. This type of technology allows the simultaneous detection of multiple molecular
markers of diagnostic utility, in this case, as stated, a fragment of the L1 region of 35 different
types of HPV, and the controls necessary to guarantee the reliability of the results obtained.
The amplified fragments obtained through PCR were hybridized with their respective
specific probes immobilized in specific and known areas of the AT tube; then they were
incubated with a conjugate of streptavidin-peroxidase. This binds to the biotin present in the
amplified products through streptavidin and the peroxidase activity provokes the appearance
of a product that is insoluble with 3,3',5,5'-tetramethylbenzidine (TMB), and thus its
precipitation takes place in the areas of the AT tube where hybridization occurs.
Two internal controls were also added to the CLART®HPV. On the one hand, a fragment
of 892-bp of human CFTR (Cystic Fibrosis Transmembrane Regulator) gene is amplified and
serves as control of the human DNA present in the sample and, on the other, all the tubes also
contain a modified plasmid that serves as inhibition control for the amplification reaction.
This internal control is amplified with the same primers as the human CFTR gene, but the
size of the amplified part is different (1202-bp). Both controls are amplified simultaneously
with HPV in a single reaction tube.
The DNA was extracted from all biopsied vesical tissue samples and purified following
the manufacturer instructions. Five microliters of DNA were amplified in a final volume of
50 l. Amplification conditions consisted of 95 °C for 9 min; 45 cycles of consecutive
denaturation, annealing, and DNA extension (94 °C for 30 sec, 55 °C for 1 min, and 72 °C for
90 sec, respectively) and final extension for 8 min at 72 °C. All PCR tubes for CLART®HPV
have the reagents necessary for amplifying a fragment of the L1 region of the 35 HPV
genotypes (buffer, MgCl2, dNTPs, taq polymerase, primers specific for amplifying HPV
DNA and primers for both controls, at the appropriate levels).
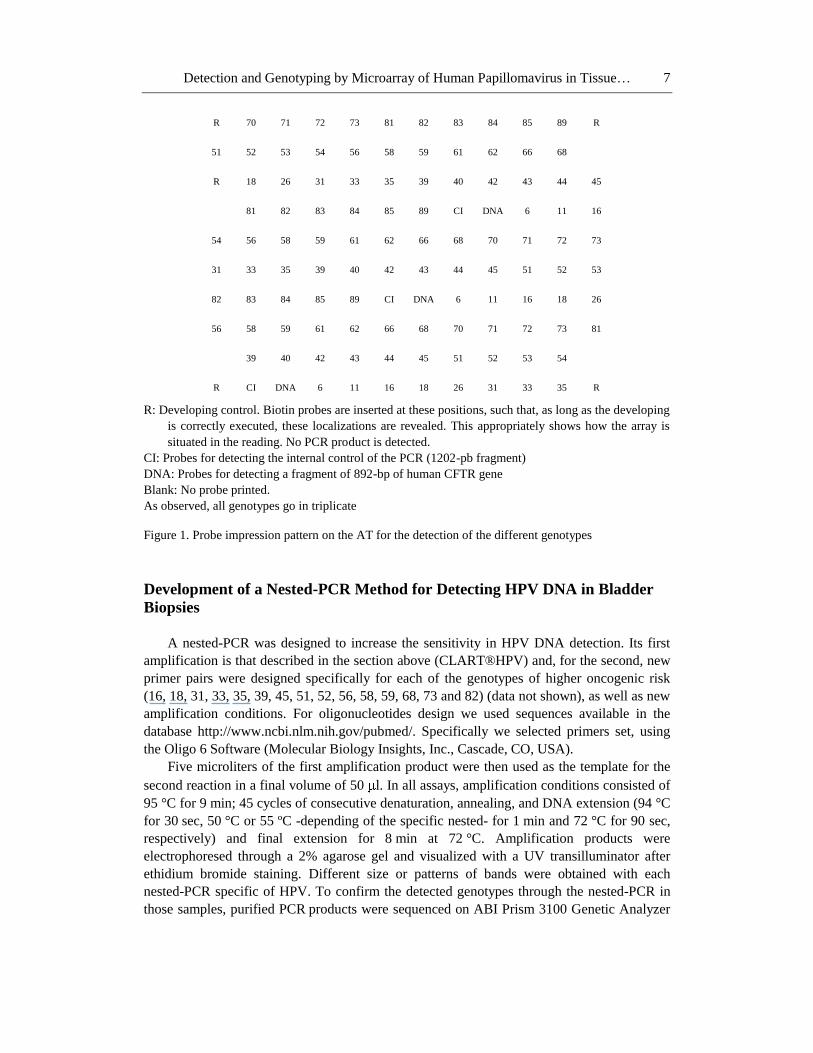
Amplification products were also subsequently hybridized using the AT system with the
aim of determining the genotype. The image obtained in the visualization of the microarray
corresponds to the probe imprint pattern observed in Figure 1 (each genotype is detected three
times).
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 7
R 70 71 72 73 81 82 83 84 85 89 R
51 52 53 54 56 58 59 61 62 66 68
R 18 26 31 33 35 39 40 42 43 44 45
81 82 83 84 85 89 CI DNA 6 11 16
54 56 58 59 61 62 66 68 70 71 72 73
31 33 35 39 40 42 43 44 45 51 52 53
82 83 84 85 89 CI DNA 6 11 16 18 26
56 58 59 61 62 66 68 70 71 72 73 81
39 40 42 43 44 45 51 52 53 54
R CI DNA 6 11 16 18 26 31 33 35 R
R: Developing control. Biotin probes are inserted at these positions, such that, as long as the developing
is correctly executed, these localizations are revealed. This appropriately shows how the array is
situated in the reading. No PCR product is detected.
CI: Probes for detecting the internal control of the PCR (1202-pb fragment)
DNA: Probes for detecting a fragment of 892-bp of human CFTR gene
Blank: No probe printed.
As observed, all genotypes go in triplicate
Figure 1. Probe impression pattern on the AT for the detection of the different genotypes
Development of a Nested-PCR Method for Detecting HPV DNA in Bladder
Biopsies
A nested-PCR was designed to increase the sensitivity in HPV DNA detection. Its first
amplification is that described in the section above (CLART®HPV) and, for the second, new
primer pairs were designed specifically for each of the genotypes of higher oncogenic risk
(16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82) (data not shown), as well as new
amplification conditions. For oligonucleotides design we used sequences available in the
database http://www.ncbi.nlm.nih.gov/pubmed/. Specifically we selected primers set, using
the Oligo 6 Software (Molecular Biology Insights, Inc., Cascade, CO, USA).
Five microliters of the first amplification product were then used as the template for the
second reaction in a final volume of 50 l. In all assays, amplification conditions consisted of
95 °C for 9 min; 45 cycles of consecutive denaturation, annealing, and DNA extension (94 °C
for 30 sec, 50 °C or 55 ºC -depending of the specific nested- for 1 min and 72 °C for 90 sec,
respectively) and final extension for 8 min at 72 °C. Amplification products were
electrophoresed through a 2% agarose gel and visualized with a UV transilluminator after
ethidium bromide staining. Different size or patterns of bands were obtained with each
nested-PCR specific of HPV. To confirm the detected genotypes through the nested-PCR in
those samples, purified PCR products were sequenced on ABI Prism 3100 Genetic Analyzer

Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 8
(Applied Biosystems, Foster City, CA, USA). The sequences were submitted to
the
comparative sequence program BLAST (www.ncbi.nlm.nih.gov/blast/)
for searching
sequences with the highest degree of similarity to identify the genotype.
Transformation, Cloning and Sequencing of HPV DNA
In order to determine the sensitivity of detection of higher oncogenic risk HPV
genotypes, both through the CLART®HPV as well as through new nested-PCR, HPV DNA
samples with known genotypes were subjected to transformation, cloning and sequencing
procedures (Protocols and Plasmid Bank of GENOMICA).
To begin with, HPV DNA was amplified from the genotheque samples using primers
specific for each genotype. Amplified products were separated by agarose gel electrophoresis
and purified using a QIAquick Gel Extraction Kit (Qiagen, Valencia, CA, USA).
Purified DNA was cloned into the pGEM-T Easy Vector (Promega, Madison, WI, USA),
transformed into Escherichia coli novablue (Novagen Inc., Madison, WI, USA) competent
cells through the heat shock method and incubated overnight at 37°C with shaking.
Transformation was detected on LB agar plates supplemented with ampicillin / IPTG
(isopropyl-D-1-thiogalactopyranoside) / X-Gal (5-bromo-4-chloro-3-indolyl- -D-
galactopyranoside) by screening the blue-white colonies. A recombinant clone was identified
as the white colony on an X-Gal and IPTG plate.
The recombinant colonies were then screened by PCR with primers specific for the
cloning site of the vector, and those containing inserts of the expected size were grown
overnight in 10 ml of LB media supplemented with ampicillin. The plasmids of these colonies
were then extracted using the PureYield™ Plasmid Midiprep System (Promega) kit.
After purification, the insert DNA fragments were identified through sequencing using
automatic DNA sequencer (ABI Prism 3100 Genetic Analyzer). The DNA fragments were
spectrophotometrically quantified (SmartSpecTM Plus Spectrophotometer, Bio-Rad, Spain). A
theoretical number of plasmid copies and reaction efficiency were calculated considering the
molecular weight. The plasmid was 10-fold serial diluted (from 104 to 10
-1 plasmid copies/ l)
and stored at -20°C. Five microlitres of those dilutions were used to determine the sensitivity
of the CLART®HPV and for nested-PCR.
RESULTS
Detection of HPV DNA in Bladder Biopsies with CLART®HPV
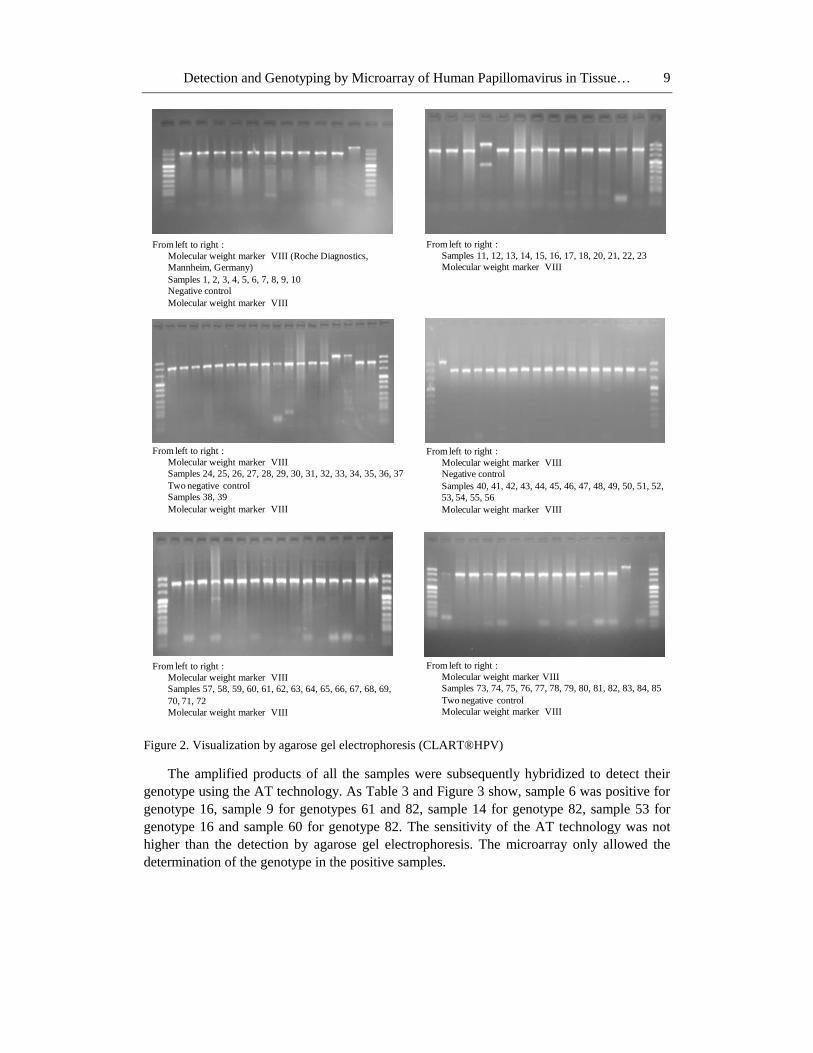
After DNA amplification of all samples and, subsequently, the visualization through
agarose gel electrophoresis, the results shown in Figure 2 were obtained. All samples showed
a fragment of 892-bp corresponding to the human CFTR gene, except for sample 14 where,
notwithstanding, the internal control was correctly amplified (1202-bp fragment). A fragment
of 450-bp was also observed in samples 6 and 9 (tumour tissue samples), 14, 53 and 60
(healthy vesical tissue samples). HPV DNA was thus detected in 5 of the 85 samples studied
(5.9%).
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 9
From left to right :
Molecular weight marker VIII (Roche Diagnostics,
Mannheim, Germany)
Samples 1, 2, 3, 4, 5, 6, 7, 8, 9, 10
Negative control
Molecular weight marker VIII
From left to right :
Samples 11, 12, 13, 14, 15, 16, 17, 18, 20, 21, 22, 23
Molecular weight marker VIII
From left to right :
Molecular weight marker VIII
Samples 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37
Two negative control
Samples 38, 39
Molecular weight marker VIII
From left to right :
Molecular weight marker VIII
Negative control
Samples 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52,
53, 54, 55, 56
Molecular weight marker VIII
From left to right :
Molecular weight marker VIII
Samples 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69,
70, 71, 72
Molecular weight marker VIII
From left to right :
Molecular weight marker VIII
Samples 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85
Two negative control
Molecular weight marker VIII
Figure 2. Visualization by agarose gel electrophoresis (CLART®HPV)
The amplified products of all the samples were subsequently hybridized to detect their
genotype using the AT technology. As Table 3 and Figure 3 show, sample 6 was positive for
genotype 16, sample 9 for genotypes 61 and 82, sample 14 for genotype 82, sample 53 for
genotype 16 and sample 60 for genotype 82. The sensitivity of the AT technology was not
higher than the detection by agarose gel electrophoresis. The microarray only allowed the
determination of the genotype in the positive samples.
Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 10
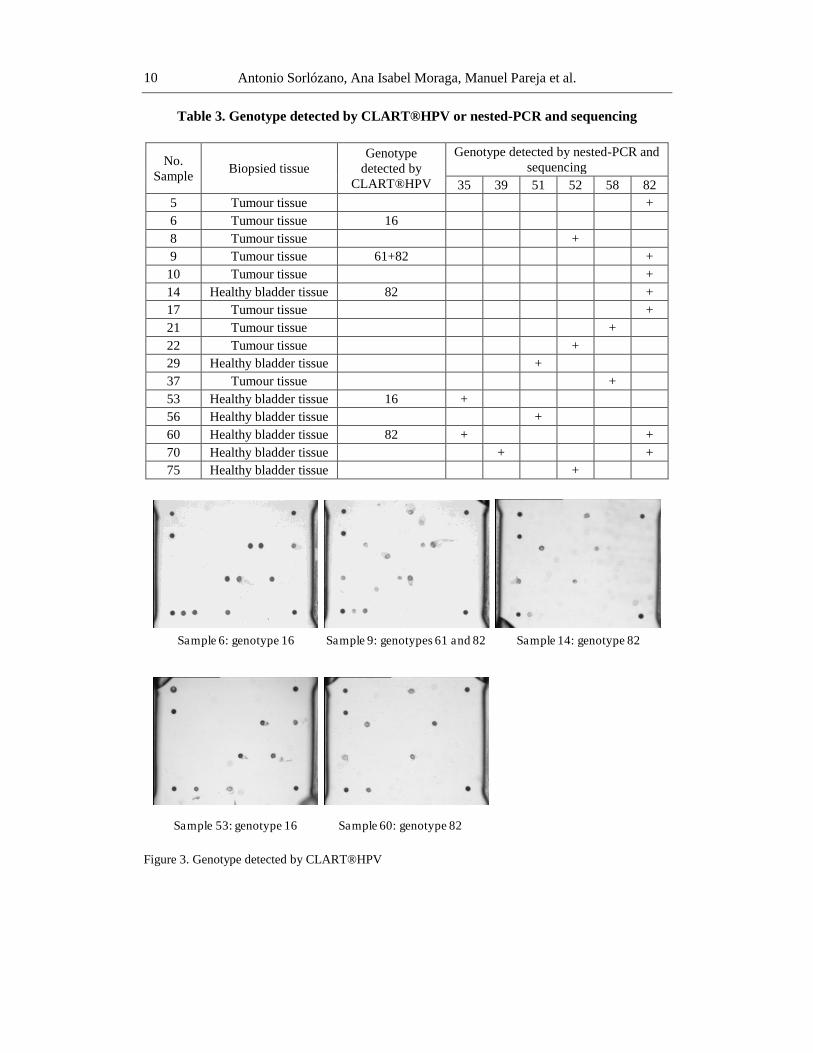
Table 3. Genotype detected by CLART®HPV or nested-PCR and sequencing
No.
Sample Biopsied tissue
Genotype
detected by
CLART®HPV
Genotype detected by nested-PCR and
sequencing
35 39 51 52 58 82
5 Tumour tissue +
6 Tumour tissue 16
8 Tumour tissue +
9 Tumour tissue 61+82 +
10 Tumour tissue +
14 Healthy bladder tissue 82 +
17 Tumour tissue +
21 Tumour tissue +
22 Tumour tissue +
29 Healthy bladder tissue +
37 Tumour tissue +
53 Healthy bladder tissue 16 +
56 Healthy bladder tissue +
60 Healthy bladder tissue 82 + +
70 Healthy bladder tissue + +
75 Healthy bladder tissue +
Sample 6: genotype 16 Sample 9: genotypes 61 and 82 Sample 14: genotype 82
Sample 53: genotype 16 Sample 60: genotype 82
Figure 3. Genotype detected by CLART®HPV
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 11
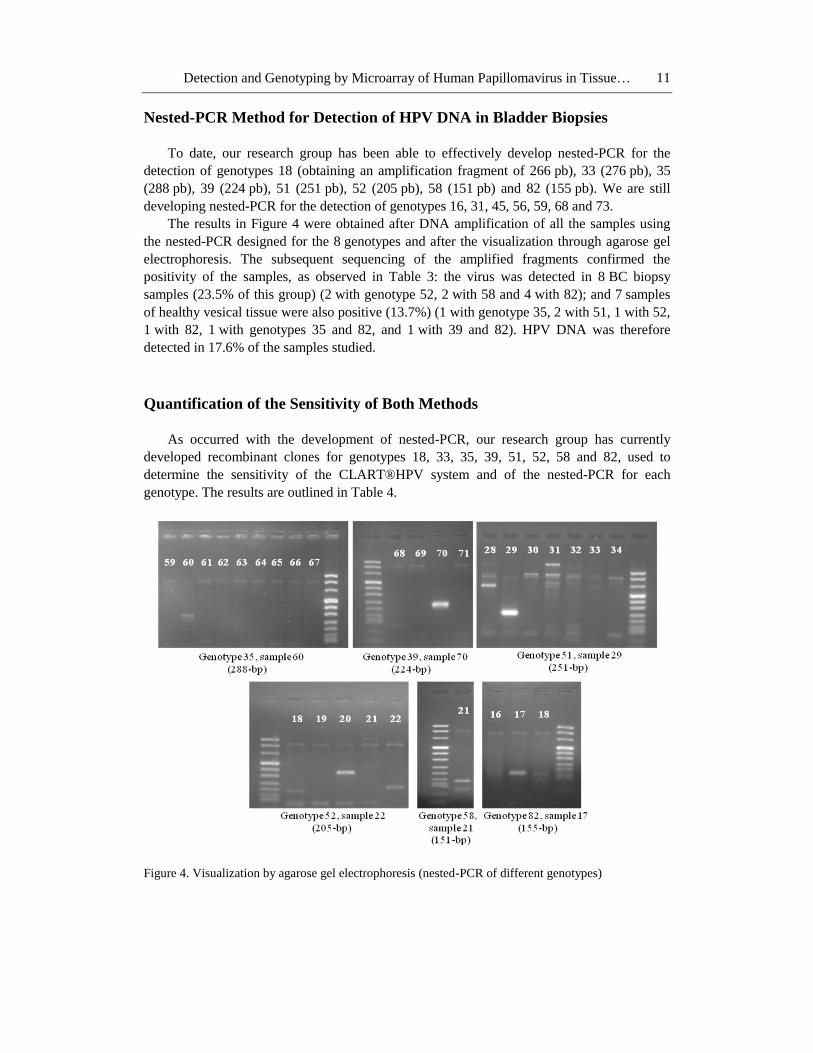
Nested-PCR Method for Detection of HPV DNA in Bladder Biopsies
To date, our research group has been able to effectively develop nested-PCR for the
detection of genotypes 18 (obtaining an amplification fragment of 266 pb), 33 (276 pb), 35
(288 pb), 39 (224 pb), 51 (251 pb), 52 (205 pb), 58 (151 pb) and 82 (155 pb). We are still
developing nested-PCR for the detection of genotypes 16, 31, 45, 56, 59, 68 and 73.
The results in Figure 4 were obtained after DNA amplification of all the samples using
the nested-PCR designed for the 8 genotypes and after the visualization through agarose gel
electrophoresis. The subsequent sequencing of the amplified fragments confirmed the
positivity of the samples, as observed in Table 3: the virus was detected in 8 BC biopsy
samples (23.5% of this group) (2 with genotype 52, 2 with 58 and 4 with 82); and 7 samples
of healthy vesical tissue were also positive (13.7%) (1 with genotype 35, 2 with 51, 1 with 52,
1 with 82, 1 with genotypes 35 and 82, and 1 with 39 and 82). HPV DNA was therefore
detected in 17.6% of the samples studied.
Quantification of the Sensitivity of Both Methods
As occurred with the development of nested-PCR, our research group has currently
developed recombinant clones for genotypes 18, 33, 35, 39, 51, 52, 58 and 82, used to
determine the sensitivity of the CLART®HPV system and of the nested-PCR for each
genotype. The results are outlined in Table 4.
Figure 4. Visualization by agarose gel electrophoresis (nested-PCR of different genotypes)

Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 12
Table 4. Sensitivity (in plasmid copies/reaction) of CLART®HPV
and nested-PCR for detection of eight HPV genotypes
Genotype CLART®HPV Nested- PCR
5×104 5×103 5×102 5×101 5×100 5×10-1 5×104 5×103 5×102 5×101 5×100 5×10-1
18 + - - - - - + + + - - -
33 + + + - - - + + + + + -
35 + + + + - - + + + + - -
39 + + + + - - + + + + - -
51 + + + - - - + + + + + -
52 + + + - - - + + + + - -
58 + + + + - - + + + + + -
82 + + + + - - + + + + + +
As can be observed, nested-PCR increased the sensitivity in the detection of genotypes
18, 33, 51 and 82 by two 10-fold serial diluted; in the detection of genotypes 52 and 58 by
one 10-fold serial diluted; but the same sensitivity was maintained in both techniques in the
detection of genotypes 35 and 39. Specifically the nested-PCR is able to detect 500 copies of
genotype 18, 50 copies of genotypes 35, 39 and 52, 5 copies of genotypes 33, 51 and 58 and
only 1 copie of genotype 82.
DISCUSSION
HPV may not be cultured in vitro and serology studies have limited accuracy because of
their failure to distinguish between current and past infections [34]. That is why, if there is
need for a study on the relationship between the virus and any neoplasic process, whether
uterine neck carcinoma or, as in our case, bladder cancer, it is more appropriate to use HPV
DNA detection techniques [35]. In this sense, PCR is the technique with highest sensitivity,
confirmed in several publications [35-37]. However, considering that there are over a hundred
genotypes of the virus [35], of which 15 show high oncogenic risk [38], the use of a PCR
with primers specific for each genotype demands a lot of time and work and, in addition,
requires validation for each of them [36].
The originality of the CLART®HPV system lies in it being a single procedure, in two
phases, the first being the amplification of an region of the HPV genome which is conserved
in most of the genotypes, the L1 region, and the second to typify the virus present in the
sample through microarrays, with which, in addition to obtaining faster and objective results,
it allows for the concurrent detection of mixed infections in one sample.
However, to carry out a pathogenicity study in which we can establish the possibility of
causal relationship, in addition to establishing the existence (or lack thereof) of an
epidemiologic relationship between the viral infection and cancer, it would be necessary to
create a technique with the highest possible sensitivity, such as a nested-PCR. And that is
what happened in our research. Currently the nested-PCRs developed increased their
sensitivity in comparison with the CLART®HPV in up to 100-fold, thus allowing an increase
in the percentage of samples in which the virus was detected, 5.9% to 17.6%.
Nevertheless, our work is not yet finished. We are developing nested-PCR for genotypes
16, 31, 45, 56, 59, 68 and 73, to be later applied to the 85 samples of the assay. Our final

Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 13
objective would be to develop an ultra-sensitive technique that may allow the detection of
higher oncogenic risk genotypes in different tissue samples, in three steps. The first step
would still entail the amplification of the L1 region in the same conditions as presently done
by the CLART®HPV system; the second step would be a multiplex-nested-PCR in which the
amplification conditions would allow amplification of the DNA sequences specific for each
genotype, and a third step of microarray typification.
Finally, although we can not as yet reach any conclusions on the relationship between
bladder carcinoma and HPV infection, we believe that in a near future the current
development of this new technique will allow us to definitely determine whether or not said
relationship exists. Probably the development of multiple PCR techniques for the detection of
a high number of serotypes will improve the HPV detection and association to bladder cancer.
REFERENCES
[1] Mitra, AP; Cote, RJ. Molecular pathogenesis and diagnostics of bladder cancer. Annu.
Rev. Pathol., 2009, 4, 251-85.
[2] Augustine, A; Hebert, JR; Kabat, GC; Wynder, EL. Bladder cancer in relation to
cigarette smoking. Cancer Res., 1988, 48, 4405-8.
[3] Mostafa, MH; Sheweita, SA; O’Connor, PJ. Relationship between schistosomiasis and
bladder cancer. Clin. Microbiol. Rev., 1999, 12, 97-111.
[4] Villanueva, CM; Fernandez, F; Malats, N; Grimalt, JO; Kogevinas, M. Meta-analysis of
studies on individual consumption of chlorinated drinking water and bladder cancer. J.
Epidemiol. Community Health, 2003, 57, 166-73.
[5] Takkouche, B; Etminan, M; Montes-Martinez, A. Personal use of hair dyes and risk of
cancer: a meta-analysis. JAMA, 2005, 293, 2516-25.
[6] Bosetti, C; Pira, E; La Vecchia, C. Bladder cancer risk in painters: a review of the
epidemiological evidence, 1989-2004. Cancer Causes Control, 2005, 16, 997-1008.
[7] Friesen, MC; Demers, PA; Spinelli, JJ; Lorenzi, MF; Le, ND. Comparison of two
indices of exposure to polycyclic aromatic hydrocarbons in a retrospective aluminium
smelter cohort. Occup. Environ. Med., 2007, 64, 273-8.
[8] Morrison, EA. Natural history of cervical infection with human papillomaviruses. Clin.
Infect. Dis., 1994, 18, 172-80.
[9] Lopez-Beltran, A; Escudero, AL. Human papillomavirus and bladder cancer. Biomed.
Pharmacother., 1997, 51, 252-7.
[10] De Gaetani, C; Ferrari, G; Righi, E; Bettelli, S; Migaldi, M; Ferrari, P; et al. Detection
of human papillomavirus DNA in urinary bladder carcinoma by in situ hybridisation. J.
Clin. Pathol., 1999, 52, 103-6.
[11] Badawi, H; Ahmed, H; Ismail, A; Diab, M; Moubarak, M; Badawy, A; et al. Role of
human papillomavirus types 16, 18, and 52 in recurrent cystitis and urinary bladder
cancer among Egyptian patients. Medscape J. Med., 2008, 10, 232.
[12] Barghi, MR; Hajimohammadmehdiarbab, A; Moghaddam, SM; Kazemi, B. Correlation
between human papillomavirus infection and bladder transitional cell carcinoma. BMC
Infect. Dis., 2005, 5, 102.
Antonio Sorlózano, Ana Isabel Moraga, Manuel Pareja et al. 14
[13] Gutierrez, J; Jimenez, A; de Dios Luna, J; Soto, MJ; Sorlozano, A. Meta-analysis of
studies analyzing the relationship between bladder cancer and infection by human
papillomavirus. J. Urol., 2006, 176, 2474-81.
[14] Knowles, MA. Human papillomavirus sequences are not detectable by Southern
blotting or general primer-mediated polymerase chain reaction in transitional cell
tumours of the bladder. Urol. Res., 1992, 20, 297-301.
[15] Saltzstein, DR; Orihuela, E; Kocurek, JN; Payne, DA; Chan, TS; Tyring, SK. Failure of
the polymerase chain reaction (PCR) to detect human papillomavirus (HPV) in
transitional cell carcinoma of the bladder. Anticancer Res., 1993, 13, 423-5.
[16] Chang, F; Lipponen, P; Tervahauta, A; Syrjanen, S; Syrjanen, K. Transitional cell
carcinoma of the bladder: failure to demonstrate human papillomavirus
deoxyribonucleic acid by in situ hybridization and polymerase chain reaction. J. Urol.,
1994, 152, 1429-33.
[17] Boucher, NR; Scholefield, JH; Anderson, JB. The aetiological significance of human
papillomavirus in bladder cancer. Br. J. Urol., 1996, 78, 866-9.
[18] Cooper, K; Haffajee, Z; Taylor, L. Human papillomavirus and schistosomiasis
associated bladder cancer. Mol. Pathol., 1997, 50, 145-8.
[19] Lu, QL; Lalani, el-N; Abel, P. Human papillomavirus 16 and 18 infection is absent in
urinary bladder carcinomas. Eur. Urol., 1997, 31, 428-32.
[20] Aynaud, O; Tranbaloc, P; Orth, G. Lack of evidence for a role of human
papillomaviruses in transitional cell carcinoma of the bladder. J. Urol., 1998, 159, 86-9.
[21] Westenend, PJ; Stoop, JA; Hendriks, JG. Human papillomaviruses 6/11, 16/18 and
31/33/51 are not associated with squamous cell carcinoma of the urinary bladder. BJU
Int., 2001, 88, 198-201.
[22] Youshya, S; Purdie, K; Breuer, J; Proby, C; Sheaf, MT; Oliver, RT; et al. Does human
papillomavirus play a role in the development of bladder transitional cell carcinoma? A
comparison of PCR and immunohistochemical analysis. J. Clin. Pathol., 2005, 58, 207-
10.
[23] Noel, JC; Peny, MO; Mat, O; Antoine, M; Firket, C; Detremmerie, O; et al. Human
papillomavirus type 16 associated with multifocal transitional cell carcinomas of the
bladder in two transplanted patients. Transpl. Int., 1994, 7, 340-3.
[24] Bryant, P; Skelly, J; Wilson, D. Demonstration of papillomavirus structural antigen in
human urinary bladder neoplasia. Br. J. Urol., 1987, 60, 405-9.
[25] Mantovani, G; Cermelli, C; Malagoli, M; Provvisionato, A; Ferrari, P; Castagnetti, M;
et al. IgG antibodies to papillomavirus genus-antigens in adult men with cancer of the
urinary bladder. New Microbiol., 1994, 17, 1-8.
[26] Helal Tel, A; Fadel, MT; El-Sayed, NK. Human papilloma virus and p53 expression in
bladder cancer in Egypt: relationship to schistosomiasis and clinicopathologic factors.
Pathol. Oncol. Res., 2006, 12, 173-8.
[27] Guo, CC; Fine, SW; Epstein, JI. Noninvasive squamous lesions in the urinary bladder: a
clinicopathologic analysis of 29 cases. Am. J. Surg. Pathol., 2006, 30, 883-91.
[28] Aggarwal, S; Arora, VK; Gupta, S; Singh, N; Bhatia, A. Koilocytosis: correlations with
high-risk HPV and its comparison on tissue sections and cytology, urothelial
carcinoma. Diagn. Cytopathol., 2009, 37, 174-7.
Detection and Genotyping by Microarray of Human Papillomavirus in Tissue… 15
[29] Ludwig, M; Kochel, HG; Fischer, C; Ringert, RH; Weidner, W. Human papillomavirus
in tissue of bladder and bladder carcinoma specimens. A preliminary study. Eur. Urol.,
1996, 30, 96-102.
[30] Stanley, M. The end for genital human papillomavirus infections? Lancet Oncol., 2005,
6, 256-7.
[31] Quint, WGV; Pagliusi, SR; Lelie, N; Villiers, EM; Wheeler, CM. World Health
Organization Human Papillomavirus DNA International Collaborative Study Group.
Results of the first World Heath Organization international collaborative study of
detection of human papillomavirus DNA. J. Clin. Microbiol., 2006, 44, 571-9.
[32] Garcia-Sierra, N; Martro, E; Castella, E; Llatjos, M; Tarrats, A; Bascuñana, E; et al.
Evaluation of an array-based method for Human Papillomavirus detection and
genotyping in comparison with conventional methods used in cervical cancer screening.
J. Clin. Microbiol., 2009, 47, 2165-9.
[33] Dunne, EF; Unger, ER; Sternberg, M; McQuillan, G; Swan, DC; Patel, SS; et al.
Prevalence of HPV infection among females in the United States. JAMA, 2007, 297,
813-9.
[34] Suarez, A; Esquivias, JL; Vidart, JA; Picazo, JJ. Detection and typing by molecular
biology of human papillomavirus in genital samples. Rev. Esp. Quimioterap., 2006, 19,
161-6.
[35] Molijn, A; Kleter, B; Quint, W; Doorn, LJ. Molecular diagnosis of human
papillomavirus (HPV) infections. J. Clin. Virol., 2005, 32, 43-51.
[36] Van Doorn, LJ; Kleter, B; Quint, WGV. Molecular detection and genotyping of human
papillomavirus. Expert. Rev. Mol. Diagn., 2001, 1, 394-402.
[37] Resnick, RM; Cornelissen, MT; Wright, DK; Eichinger, GH; Fox, HS; ter Schegget, J;
et al. Detection and typing of human papillomavirus in archival cancer specimens by
DNA amplification with consensus primers. J. Natl. Cancer Inst., 1990, 82, 1477-84.
[38] Muñoz, N; Bosch, FX; De Sanjose, S; Herrero, R; Castellsaqgue, X; Shan, KV; et al.
Epidemiologic classification of human papillomavirus types associated with cervical
cancer. N. Engl. J. Med., 2003, 348, 518-27.




















