
Cybertherapy 2005 - DTIC
313
AD Award Number: W81XWH-05-1-0393 TITLE: Cybertherapy 2005: A Decade of VR PRINCIPAL INVESTIGATOR: Brenda K. Wiederhold, Ph.D. CONTRACTING ORGANIZATION: Interactive Media Institute San Diego, CA 92124 REPORT DATE: July 2005 TYPE OF REPORT: Final Proceedings PREPARED FOR: U.S. Army Medical Research and Materiel Command Fort Detrick, Maryland 21702-5012 DISTRIBUTION STATEMENT: Approved for Public Release; Distribution Unlimited The views, opinions and/or findings contained in this report are those of the author(s) and should not be construed as an official Department of the Army position, policy or decision unless so designated by other documentation. 20050802 015
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Cybertherapy 2005 - DTIC
AD
Award Number: W81XWH-05-1-0393
TITLE: Cybertherapy 2005: A Decade of VR
PRINCIPAL INVESTIGATOR: Brenda K. Wiederhold, Ph.D.
CONTRACTING ORGANIZATION: Interactive Media InstituteSan Diego, CA 92124
REPORT DATE: July 2005
TYPE OF REPORT: Final Proceedings
PREPARED FOR: U.S. Army Medical Research and Materiel CommandFort Detrick, Maryland 21702-5012
DISTRIBUTION STATEMENT: Approved for Public Release; Distribution Unlimited
The views, opinions and/or findings contained in this report are those of the author(s) andshould not be construed as an official Department of the Army position, policy or decisionunless so designated by other documentation.
20050802 015
Annual Review ofCyberTherapy and Telemedicine
Editors:Brenda K. Wiederhold, Ph.D., MBA, BCIA
Giuseppe Riva, Ph.D., M.S., M.A.Alex H. Bullinger, M.D., MBA
Publisher: Interactive Media Institute,a 501c3 non profit organization
httD: //ww-wv.cvbertheranvreview.com
. . Form Approved•REPORT DOCUMENTA1ION AGE O 0MB No. 0704-0188
Public reporting burden for this collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources gathering and maintaining thedata needed, and cbmpleting and reviewing this collection of information. Send comments regarding this burden estimate or any other aspect of this collection of infornation, including suggestions for reducingthis burden to Department of Defense, Washingtorl Headquarters Services, Directorate for Information Operations and Reports (0704-0188), 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302. Respondents should be aware that notwithsitanding any other provision of law, no person shalt be subject to any penalty for failing to comply with a collection of information if it does not display a currentlyvalid OMB control number. PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ADDRESS.1. REPORT DATE (DD-MM-YYYY) 2. REPORT TYPE 3. DATES COVERED (From - To)01-07-2005 Final Proceedings 6 Jun 05- 10 Jun 05
4. TITLE AND SUBTITLE 5a. CONTRACT NUMBERCybertherapy 2005: A Decade of VR _ _.. .. _"
5b. GRANT NUMBERW81XWH-05-1-03935c. PROGRAM ELEMENT NUMBER
6. AUTHOR(S) 5d. PROJECT NUMBERBrenda K. Wiederhold, Ph.D.
5e. TASK NUMBER
St WORK UNIT NUMBER
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) 8. PERFORMING ORGANIZATION REPORTNUMBER
Interactive Media InstituteSan Diego, CA 92124
E-Mail: [email protected]. SPONSORING I MONITORING AGENCY NAME(S) AND ADDRESS(ES) 10. SPONSOR/MONITOR'S ACRONYM(S)U.S. Army Medical Research and Materiel CommandFort Detrick, Maryland 21702-5012
11. SPONSORIMONITOR'S REPORT
NUMBER(S)
12. DISTRIBUTION I AVAILABILITY STATEMENTApproved for Public Release; Distribution tTnlimited.
13. SUPPLEMENTARY NOTES
14. ABSTRACT
No abstract provided.
//
15. SUBJECT TERMSNo subject terms provided.
16. SECURITY CLASSIFICATION OF: 17. LIMITATION 18. NUMBER 19a. NAME OF RESPONSIBLE PERSONOF ABSTRACT OF PAGES
a. REPORT b. ABSTRACT c. THIS PAGE 19b. TELEPHONE NUMBER (include areaU U U UU 315 code)
Standard Form 298 (Rev. 8-98)Prescribed by ANSI Std. Z39.18
Annual Review of CyberTherapy and Telemedicine
Interactive Media in Training and Therapeutic Interventions
Editors-in-Chief
Brenda K. Wiederhold, PhD, MBA, BCIAInteractive Media Institute, San Diego, CA, USA
Giuseppe Riva, PhD, MS, MAIstituto Auxologico Italiano, Verbania, Italy
Alex H. Bullinger, MD, MBACOAT-Basel, Basel, Switzerland
Interactive Media Institute
Annual Review of CyberTherapy and Telemedicine
Copyright © 2005 Interactive Media Institute6160 Cornerstone Court EastSan Diego, CA 92121
ISBN: 0-9724074-7-2ISSN: 1554-8716
All rights reserved.Printed in the United States of America
Interactive Media Institute Website: www.interactivemediainstitute.com
LEGAL NOTICEThe publisher is not responsible for the use which might be made of the following information.
Editors-in-Chief
Brenda K. Wiederhold, Ph.D., MBA, BCIAInteractive Media Institute
Giuseppe Riva, Ph.D., M.S., M.A.Applied Technology for Neuro-Psychology Laboratory
Istituto Auxologico Italiano
Alex H. Bullinger, M.D., MBACenter of Applied Technologies in Neuroscience (COAT-Basel)
University of Basel
Assistant Editors
Stephane Bouchard, Ph.D.Universite du Quebec en Outavais
Mark D. Wiederhold, M.D., Ph.D., FACPVirtual Reality Medical Center
Editorial Assistant
Kira SchabramInteractive Media Institute
Editorial Board
Mariano Alcahiz Raya, Ph.D. Gabriele Optale, M.D.Universidad Politecnica de Valencia Association of Medical Psychotherapists
Cristina Botella, Ph.D. Albert "Skip" Rizzo, Ph.D.Universitat Jaume I University of Southern California
Ken Graap, M.Ed. Professor Paul SharkeyVirtually Better, Inc. University of Reading
Walter Greenleaf, Ph.D. Mel Slater, DSc.Greenleaf Medical University College London
Hunter Hoffman, Ph.D. Erik Viirre, M.D., Ph.D.University of Washington University of California, San Diego
Sun I. Kim, Ph.D. David Walshe, Ph.D.Hanyang University University College Cork
General Information
Annual Review of CyberTherapy and Telemedicine (ARCTT - ISSN: 1554-8716) is published an-nually (once per year) by the Interactive Media Institute (IMI), a 501c3 non profit organization, dedi-cated to incorporating interdisciplinary researchers from around the world to create, test, and developclinical protocols for the medical and psychological community. IMI realizes that the mind and bodywork in concert to affect quality of life in individuals and works to develop technology that can be ef-fectively used to improve the standards and reduce the cost of healthcare delivery.
Interactive Media Institute, 6160 Cornerstone Court East, Suite 161, San Diego, CA, USA.
Telephone: (858) 642-0267, Fax: (858) 642-0285, E-mail: cybertherapyvyrphobia.comIMI Web site: hthti://www.interactivemediainstitute.com
Copyright © 2004 by Interactive Media Institute. Printed in the United States of America
About the journalARCTT is a peer-reviewed all-purpose journal covering a wide variety of topics of interest to the men-tal health, neuroscience, and rehabilitation communities. The mission of ARCTT is to provide system-atic, periodic examinations of scholarly advances in the field of CyberTherapy and Telemedi-cine through original investigations in the telemedicine and cybertherapy areas, novel experimentalclinical studies, and critical authoritative reviews.
It is directed to healthcare providers and researchers who are interested in the applications of ad-vanced media for improving the delivery and efficacy of mental healthcare and rehabilitative services.
Manuscript Proposal and Submission
Because Annual Review papers examine either novel therapeutic methods and trials or a specificclinical application in depth, they are written by experienced researchers upon invitation from our Edi-torial Board. The editors nevertheless welcome suggestions from our readers. Questions or com-ments about editorial content or policies should be directed to the editors only.
Manuscript PreparationManuscripts should be submitted in electronic format on CD-Rom or floppy disks as well as on 8% x11-in. paper (three copies), double-spaced format. Authors should prepare manuscripts according tothe Publication Manual of the American Psychological Association (5 Ed.).
Original, camera-ready artwork for figures is required. Original color figures can be printed in color atthe editors' discretion and provided the author agrees to pay in full the associated production costs;an estimate of these costs is available from the ARCTT production office on request.
ARCTT policy prohibits an author from submitting the same manuscript for concurrent consideration bytwo or more publications. Authors have an obligation to consult journal editors concerning prior publica-tion of any data upon which their article depends. As this journal is a primary journal that publishesoriginal material only, ARCHT policy prohibits as well publication of any manuscript that has alreadybeen published in whole or substantial part elsewhere, unless authorized by the journal editors.
DisclaimerAll the published papers, editorial news and comments, opinions, findings, conclusions, or recom-mendations in ARCH" are those of the author(s), and do not necessarily reflects or constitute theopinions of the Journal, its Publisher, and its editorial staff.
Table of Contents
Editorials 9B.K. Wiederhold, G. Riva, A.H. Bullinger
CRITICAL REVIEWS
Motivational Training Tool to Promote Healthy Life Styles 13N. Fernandez, E. del Hoyo Barbolla, C. Ramirez, R. de las Heras, M. T. Arredondo
Real Time Changing Virtual Environments: A New Tool for Virtual Therapy 19M. Alcahiz, B. Rey, J. Montesa, J. A. Lozano, M. C. Juan
Towards a Neuropsychological Basis of Presence 25W. lJsselsteijn
Virtual Reality in Everyday Memory Assessment and Rehabilitation: Progress 31to Date and Future PotentialP.R. Penn, F.D. Rose, B.M. Brooks
Virtual Reality in the Treatment of Eating Disorders and Obesity: State of the 39Art and Future ChallengesG. Riva
Virtual Technologies for Extreme Environment Effect Mitigation 47E. Gaia
EVALUATION STUDIES
A Computational Model of Emotion and Personality: Applications to 51Psychotherapy Research and PracticeE. Hudlicka
Building Biologically Based Immune System Simulations for Education 59and TrainingK. Howell
General Training of Spatial Abilities by Geometry Education in 65Augmented RealityH. Kaufmann, K. SteinbCjgl, A. Djnser, J. GlIck
The Gedanken Experiment of Human Dynamics 77Y. Cai, J. Klein-Seetharaman
The Recording of Observational Behaviors in Virtual Immersion: A New 85Research and Clinical Tool to Address the Problem of Sexual Preferenceswith ParaphiliacsP. Renaud, J. Proulx, J. L. Rouleau, S. Bouchard, G. Madrigrano, J. Bradford, P. Fedoroff

, , I I I I I I I1 1 I I I I I I I I ý
Treating Acrophobia in a Virtual Environment 93A. H. Bullinger, I. Angehm, B. K. Wliederhold, F. Mueller-Spahn, R. Mager
Virtual Environments to Address Autistic Social Deficits 101C. Y. Trepagnier, M. M. Sebrechts, A. Finkelmeyer, M. Coleman, W. Stewart,Jr., M. Werner-Adler,
VR for Blood-Injection-Injury Phobia 109B. K. Wiederhold, M. Mendoza, T. Nakatani, A. H. Bullinger, M. D. Wiederhold
Working Things Out: A Therapeutic Interactive CD-Rom Containing the 117Stories of Young People Dealing with Depression and Other MentalHealth Problems
E. Brosnan, J. Sharry, C. Fitzpatrick
ORIGINAL RESEARCH
Assessment of Emotional Reactivity Produced by Exposure to Virtual 123Environments in Patients with Eating DisorderM. Ferrer-Garcia, J. Gutierrez-Maldonado
Investigation of Social Anxiety of Patients with Schizophrenia Using 129Virtual AvatarH. J. Jang, J. Ku, S. H. Park, S. Y. Kim, I. Y. Kim, C-H. Kim, J-J. Kim, S. I. Kim
Investigation of Social Cue Perception in Schizophrenia using Virtual Reality 135K. Kim, J-J. Kim, J. Kim, D-E. Park, J. Ku, H. J. Jang, S. H. Park, S. Y. Kim, C. H. Kim,J. H. Lee, I. Y. Kim, S. I. Kim
Relationship between Social Response to Virtual Avatar and Symptom 143Severity of Patients with SchizophreniaJ. Ku, J. J. Kim, H. J. Jang, S. H. Park, S. Y. Kim, C-H. Kim, K. U. Kim, J. H. Kim,J. H. Lee, In Y. Kim, S. I. Kim
Spatial Ability and Navigation Learning in a Virtual City 151J-H. Lee, R. Mraz, K. K. Zakzanis, S. E. Black, P. J. Snyder, S. I. Kim, S. J. Graham
Telepsychiatry: Psychiatric Consultation through Videoconference 159Clinical ResultsC. De las Cuevas
Training Blind Children to Develop Mathematics Skills Through Audio 165J. Sbnchez, H. Flores
Virtual War PTSD - a Methodological Thread 173P. Gamito, J. Pacheco, C. Ribeiro, C. Pablo, T. Saraiva

CLINICAL OBSERVATIONS
A Progress Report of Long-Term Robot Assisted Activity at a Health 179Service Facility for the AgedK. Wada, T. Shibata, T. Saito, K. Sakamoto, K. Tanie
Subjective and Physiologic Reactions of Flight Phobics during VR 185Exposure and Treatment Outcome: What Adds Motion Simulation?A. Muhlberger, G. Wiedemann, P. Pauli
The Virtual Mall: A Functional Virtual Environment for Stroke Rehabilitation 193D. Rand, N. Katz, M. Shahar, R. Kizony, P. L. Weiss
The Virtual Reality Mirror: Mental Practice with Augmented Reality for 199Post-Stroke RehabilitationA. Gaggioli, F. Morganti, A. Meneghini, M. Alcaniz, J. A. Lozano, J. Montesa,J. M. Martinez Saez, R. Walker, I. Lorusso, G. Riva
Use, Understanding and Learning in Virtual Environments by 207Adolescents With Autistic Spectrum DisordersS. Parsons
Abstracts from CyberTherapy 2005, June 6-10, 2005, Basel, Switzerland 217

Editorials
Welcome to the third volume of Annual Review of CyberTherapy and Telemedicine. A decade ago,CyberTherapy, then still in its infancy, only existed as a specialized Virtual Reality and BehavioralHealthcare Symposium at the Medicine Meets Virtual Reality (MMVR) Conference. At that first ses-sion, Dr. Ralph Lamson presented a small study on virtual reality (VR) exposure for treatment of ac-rophobia in ten participants. It is now clear that in 1996, we had only begun to realize what promisemight lie ahead for both VR technology and the CyberTherapy Conference.
Much has changed over the past ten years and we have now tapped further into VR's potential thanmany of us could have ever imagined. Today, researchers from around the world are busy complet-ing hundreds of trials, applying VR for such varied disorders as Anxiety, Eating Disorders and Obe-sity, Addictions, Erectile Dysfunction, Autism and Schizophrenia. In addition, VR for Neurorehabilita-tion and Physical Rehabilitation has shown definite success, as has VR for other such diverse areasas Pain Distraction (both acute and chronic), Education, Training, and Physical Disabilities.
I am proud to report that as VR's use in Behavioral Healthcare has grown, so has the CyberTherapyConference. What began as a specialized symposium at MMVR concerned mainly with conceptualmatters, has now grown into the largest program on controlled clinical trials of VR and other ad-vanced technologies in the areas of behavioral healthcare, rehabilitation, disabilities, education, andtraining.
Along with my colleagues in the VR community, the conference's focus has expanded from simplyVR to now include such cutting-edge technologies as robotics, non-invasive physiological monitoring,videogames, E-health, and adaptive displays. CyberTherapy 2005 (CT05) represents a group of out-standing international researchers and clinicians working tirelessly to improve our understanding ofhow advanced technologies can improve 2 1st century healthcare. In addition to bringing together thebest clinicians and researchers from various disciplines, it is our specific intention to also facilitatetheir introduction to representatives from funding agencies interested in providing support for ad-vanced technologies and healthcare.
In celebration of a decade of CyberTherapy, this year's Annual Review encompasses a state-of-the-art collection of clinical trials with an eye on the future of advanced technologies for health care. Inthis way, I hope that this collection can serve as a catalyst to improve the quality of life of the patientswe seek to serve, and ultimately allow society to benefit from the remarkable technological revolutionthat is occurring.
I hope you find this volume to be both an exciting and useful addition to your bookshelf.
Sincerely,
Brenda K. Wiederhold, Ph.D., MBA, BCIACo-Editor-in-Chief
9
Editorials
Since 1986, when Jaron Lamier used the term for the first time, virtual reality (VR) has been usuallydescribed as a collection of technological devices: a computer capable of interactive three-dimensional (3D) visualization, a head-mounted display, and data gloves equipped with one or moreposition trackers. The trackers sense the position and orientation of the user, and report that informa-tion to the computer that updates (in real time) the images for display.
In medicine many researchers share this vision: VR is a collection of technologies that allow peopleto interact efficiently with 3D computerized databases in real time using their natural senses andskills.
However, if we shift our attention to behavioral sciences, we find a different vision: VR is describedas an advanced form of human-computer interface that allows the user to interact with, and becomeimmersed in a computer-generated environment in a naturalistic fashion.
In fact, psychologists use specialized technologies - head-mounted displays, tracking systems, ear-phones, gloves, and sometimes haptic feedback - to develop and provide a new human-computerinteraction paradigm. In VR, patients are no longer simply external observers of images on a com-puter screen, but are active participants within a computer-generated 3D virtual world. This approachis clearly detailed in many papers of this issue: VR is used as an advanced communication interfacebased on interactive 3D visualization, able to collect and integrate different inputs and data sets in asingle real-like experience.
This point underlines the importance of the therapeutical relationship for the efficacy of most of theapproached presented: VR is a tool augmenting the possibility of relation and interaction between thetherapist and the patient. However, many psychotherapists still think that in technology supportedtreatments, and in particular in VR therapy, there is no place for a therapeutic relationship.
To allow a widespread diffusion of communication technologies real clinical practice is critical both tocounter this prejudice, and to offer training courses helping therapists in understanding how to inte-grate technologies in their own approach and methods.
Giuseppe Riva, Ph.D., M.S., M.A.Co-Editor-in-Chief
Editorials
In 2005, It has been my pleasure not only to co-organize the first of what promises to be a long lineof internationally held CyberTherapy Conferences here in Basel, Switzerland, but also to help cele-brate the conference's tenth anniversary! Once again, I would like to use this opportunity to I extenda warm welcome, or as we say here in Switzerland, a warm "Grizi", to all attendants.
As co-organizer of this year's meeting, it has also been my pleasure to serve as one of the AnnualReview of Cybertherapy and Telemedicine's esteemed board of editors. This year's Cybertherapywas organized as a joint conference together with the 1st International Conference on Applied Tech-nologies in Medicine and Neuroscience and I expect a fruitful interdisciplinary gathering of many in-terested researchers, clinicians and engineers alike. I do believe that the change in venue for themeeting has served to attract an even more diverse number of researchers from around the worldand led to a most impressive number of submissions for this year's Annual Review.
I would like to thank especially Brenda K. Wiederhold and the Interactive Media Institute for makingthis joint conference possible. Thanks also to Stephane Bouchard who with utmost efficiency organ-ized the workshops. And finally, a special thanks goes to all those who submitted papers and post-ers, to all participants as well as to the members of the program committee.
We all hope for an exciting conference that all of you will enjoy attending!
Sincerely,
Dr. Alex H. Bullinger, MBACo-Editor-in-Chief
11

12

Annual Review of CyberTherapy and Telemedicine
Critical Reviews
Motivational Training Tool to Promote Healthy Life Styles
N. Fernandez M.Sc., E. del Hoyo Barbolla M.Sc., C. Ramirez M.Sc., R. de las HerasM.Sc., M. T. Arredondo F.P., Ph.D.
Life Supporting Technologies, Telecommunication Engineering School, Technical Universityof Madrid, Spain
Abstract: The aim of the project is to apply augmented-reality technology to teach motor skills topatients suffering from stroke. To achieve this goal the project adopts an innovative approach basedon the use of so-called "motor imagery." Recent studies in neuroscience have provided convergingevidence that "imagining" a motor action involves the same brain areas involved in performing theaction. This supports the idea - already exploited by sports trainers - that training with motor imagery(mental practice) could be effective in learning new motor skills or in promoting motor recovery afterdamage to the central nervous system. Previous clinical studies have shown that the rehabilitation ofpost-stroke hemiplegic patients can be made more effective by combining physical practice withmental practice. However, for many patients who suffer from damage to the central nervous system,mental simulation of movements can be difficult, even when the relevant neural circuitry has not beeninjured. Starting from these premises, we have designed and developed an augmented-reality work-bench (called "VR Mirror') to help post-stroke hemiplegic patients evoking motor images. First, themovement is acquired by the system from the healthy arm. Second, the movement is being mirroredand displayed so that the patient can observe and see as if the impaired arm is performing the move-ment. Third, the patient is instructed to rehearse in his/her imagination the movement he/she has justobserved. Last, the patient has to perform the movement with the affected arm. In this article, we de-scribe preliminary results of a pilot clinical study, which has evaluated the feasibility of using technol-ogy-supported mental simulation as an adjunct in the rehabilitation of the upper limb following stroke.DESIGN: Single-case study. SETTING: Physical Rehabilitation Unit of Padua Teaching Hospital, Pa-dua, Italy. SUBJECTS: A 46-year-old man with stable motor deficit of the upper right limb followingstroke. INTERVENTION: The patient underwent a single-case design, with four weeks intervention.The intervention consisted of 3 practice sessions per week at the hospital using the VR-Mirror, in ad-dition to usual therapy (Bobath method). This intervention was followed by 1-month home-rehabilitation program using a portable device. MAIN OUTCOME MEASURES: The patient wasevaluated for level of impairment and disability. Pre-treatment and post treatment measures included:the upper-extremity scale of the Fugl-Meyer Assessment of Sensorimotor Impairment and the ActionResearch Arm Test. RESULTS: The patient showed improvement in upper limb score as measuredby the two scales. CONCLUSIONS: The improvement observed in the patient is encouraging andwarrants further study.
INTRODUCTION
One of the main challenges that developed so- major cause of death and disability worldwide,cieties face is the prevention of non- and increasingly affect people from countries allcommunicable diseases such as diabetes or over the world.6
obesity. These diseases are responsible for60% of the registered global deaths and for Guidelines on diet, physical activity and health45% of the global burden of disease. A few, serve two important purposes: to guide policylargely preventable, risk factors account for makers and to educate consumers, aboutmost of the world's disease burden. These are healthful lifestyles. In order to promote preven-high cholesterol, high blood pressure, obesity, tion and create motivation and adherence to thesmoking and alcohol. Chronic diseases are the prevention programmes it is highly recom-
13
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
mended to stress the importance of lifestyle- VRML or JSP (Java Server Technology). Thesehealth relationship. And it is also essential to technologies have been chosen taking into ac-analyse in depth how to formulate these pro- count the interactive, portable, visual and inte-grammes and what the process and information grative identified requirements for the tool. Fur-they should convey. The strategies drafted by thermore, these technologies allow the possibil-the international institutions competent in this ity of introducing some kind of intelligence to thematter stress the importance to increase the tool behind the interface in order to obtain aoverall awareness and understanding of the system that could respond to the individual userinfluences of diet and physical activity on health needs and preferences.and of the positive impact of preventive inter-ventions. The complete process has been divided into
four different stages. Therefore, in each step, aThe work presented in this paper contributes group of technologies has been selected topartially to solve this situation by using one of achieve the required functionalities for thethe most effective strategies: the prevention, whole system. These stages are: Profiling, Stor-through the procedure of education. In this age, Personalisation & Management. The nextsense, providing users with personalised infor- paragraphs describe these four stages:mation is key to be able to adhere them to theprevention strategy. More than that, the new The Profiling stage helps to acquire individualhealthcare delivery process models tend to be user information, to structure it and hence, tocitizen/patient centred, that are respectful of the define what the user needs are. The system isindividual preferences, needs and values and designed to be accessed through the Internet.place information and training at the heart of the The registration and the questionnaires abouthealthcare delivery strategies. 2 nutritional, statistical, physical activity and moti-
vational data have been developed with JSP.An interactive and visual tool based on virtual The goal of these questions is to define a user3D technologies for the Internet,5 using X3D, a profile and to discover his motivation status ac-powerful and extensible open file format stan- cording to the "States of Change" methodology. 3
dard for 3D visual effects, has been developed The methodology sets the characteristics to beand integrated in an e-learning system that of- classified in each state of change and the moti-fers personalised information about healthy life- vational techniques to be used for citizens.styles.
The Storage stage responds to the need ofMATERIALS AND METHODS storing the user profiles and the information to
be shown in the system. Each profile is storedThe tool implemented intends to give answers as an XML file in the native database. The sce-to the situation referred above by offering the narios have been developed in X3D. This allowsusers personalised information for their own describing a virtual world in XML by means ofself-care and moreover, motivating them to predefined tags representing objects. The sce-make use of this information and take control narios are virtual worlds that simulate the "realover their decisions regarding their lifestyle, world" and daily activities. However, as the X3DPersonalised information makes users more plug-in was not compliant with the X3D stan-independent, makes them conscious of the pos- dard at the development time, the display of thesible results due to their behaviour and facili- sessions is performed by using VRML (an X3Dtates them to take care of their own health. In antecedent). Translations between the two lan-this sense, the development of a virtual reality guages are made by applying a style sheet totool helps to motivate the user and also im- the X3D files in their XML format.proves the e-learning process.1
The Management stage is necessary in orderThe main contribution of the implemented sys- to maintain the static information used by thetem is the delivery of personalised information system.in an adapted environment. This goal has beenachieved by the integration of several technolo- Finally, the Personalisation stage carries outgies such as XML, native databases, X3D, the process of adapting the system to the users.
14
FERNANDEZ ET AL.
At the time the user profile is created or modi- ther starting their training session or modifyingfled (either by the user or by the intelligence their data.added to the system), the scenarios are person-alised to meet the user preferences and are The personalisation of the scenarios involvescompleted with the information that suits the presenting different information (links, articles,user needs most and they are stored in the sys- recipes, sport videos, etc.) to each user profile.tem. These tasks involve reading and writing In order to perform the personalisation, the sys-XML files by means of a XML parser. It is used tem accesses the database and extracts thea SAX (Simple API for XML) parser because of model files stored in. The user session "world"its speed and straightforward features. Once the is then created from this pattern and is filled inpersonalised worlds have been created, they according to the user needs. Adapting the infor-are stored. mation includes not only the content but also
the form (i.e. tone in which it is presented, waysRESULTS in which the information is shown to the user).
This depends strongly on the user motivationThe tool implemented has been developed to state 4 to follow advice and to adopt changes topresent the following features: a healthier lifestyle which was identified in the
profiling stage. In this sense, only the relevant
"* To offer personalised information in information in the appropriate mode (direct, indi-form and content rect, soft, etc.) is delivered to the user through a
"* To be visual and interactive scenario personalised accordingly (avatar, col-ours, links, etc.).
"* To be integrated in an e-learning sys-
tem The database has been hierarchically structuredin three collections (similar to directories): pro-
In this sense, a training activity in the system files, patterns and information. The most impor-consists of an Internet multimedia session that tant is the first of them and it is due to be dy-shows personalised information by means of an namically changed every time a new user ac-attractive visual interface. The session starts by cesses the system by storing the user profilechoosing the users a login and a password for and creating a user collection under it. In theidentification and introducing their data. The user user collection, called as the user login, the per-profiles are created the first time the user ac- sonalised scenarios are stored. In this way, ifcesses the system by filling in a structured ques- the user has not introduced any change in theirtionnaire about nutritional, statistical, motivational data from the previous session, the system ac-and physical exercise. Each group of questions cesses the adapted scenarios and displayshas a specific objective: the statistical questions them to the user, thus, saving time and re-try to classify the users per age, gender, health sources. The other collections, patterns andstatus, ICT knowledge or profession. Nutritional information, contain static data such as scenar-questions try to enquire if the users are vegetar- ios models or information to be shown to theian or if it is common that they often eat out in user. The pattern collection stores the scenariosorder to prepare a customised diet. Motivational models files. Each of these files contains thequestions are related to the importance the users common information, which is shared betweengive to their self-care through the lifestyle all the users in a specific scenario, such as im-adopted up to the moment or the intentions to ages or help links. The second collectionincorporate healthier attitudes in the future (i.e., (information) stores data related to health careintention to lose weight, to practise any sport, in different modes, depending on the needs theetc). user has. The corresponding information will be
selected during the personalisation stage de-In subsequent accesses the users must enter pending on the user needs and motivation.the login and password to be recognised by thesystem as registered users and this way, skip- The files stored in these collections can beping the questionnaires and be led directly to modified by the administrator in order to im-the welcome page where they can choose ei- prove the system quality, by adding new infor-
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
mation or modifying the existing one; adding interesting research line due to the increase ofnew features to the scenarios or readapting the e-learning systems and the importance of hav-ones stored in previous sessions. It is important ing access to quality information related toto notice that changes to the data and scenarios health. Joining both in the same system pro-will not affect the users due to the models us- vides citizens with a way to obtain information toage to generate the personalised worlds. In this possible them to be responsible for their ownway, the next session the users establish with health. People should have better access tothe system, the scenarios ("worlds") shown to trusted sources for the information they need,them will include the changes performed and tailored to their individual requirements. In thisthe new added or modified information if it is way, the implemented tool goes further by add-relevant to them. ing a motivational feature with the aim of mak-
ing users feel taking control of their own self-The tool is completely developed and personal- care.ization features are included, a process westarted working together with healthcare profes- To conclude, the tool developed provides certi-sionals. Different users' profiles have been fled information and achieves personalisation byidentified. considering different dimensions of people's
lifestyle and filtering the information accordingThe tool has been tested with a number of us- to:ers to check whether the tool and the informa-tion provided suited the users' needs. A survey * Who the user is: a Healthcare professional,was handed out for completion after the first a Citizen, etc.training session in order to measure their satis-faction with the system. The survey is structured o What the user nes deenin different parts which are related to the or servicesthe user mayneedadaptability of the contents, the appropriateness e Where the user is: considering different sce-of the relation between the scenarios and the narios, including "on the move"information showed in each of them, the choice * How the user needs the service: consider-of Virtual Reality as the interface and the usabil- ing different type of devicesity of the global tool. Statistical data were alsocollected, such as the age, the job or the com- However, the tool has strong requirements toputer knowledge level, perform in an acceptable way. In this sense, it
may be a solution to try to adopt more dynamicThe results of the survey indicate that Virtual software in order to be able to include it in otherReality is an unknown technology yet although it devices such as mobile phones or PDAs thatpresents high potential for the implementation of facilitate the information access in active life-e-learning systems. Elderly people value it quite styles.negatively opposed to the students and techni-cal professionals. A similar answer is also given ACKNOWLEDGMENTSto the usability of the global tool due to thestrong dependence this aspect has with the We appreciate the information provided by Dr.ability of handling Virtual Reality. However, the Claudia Duarte and Joy Ngo de la Cruz fromusers state that the relation between the sce- GRNC (Group de Regerca de Nutrici6 Comuni-narios developed and the information provided taria) for their time and advice to make our sys-in each of them was tailored to their needs and tem more complete and qualified.the contents were marked as a good educa-tional tool to adopt a healthy lifestyle. REFERENCES
CONCLUSIONS Gutierrez, J., 2002. Aplicaciones de la realidadvirtual en Psicologia clinica. Aula medica
An interactive and visual tool has been devel- psiquiatria, 4 (2), 92-126.oped and integrated in an e-learning systemthat offers personalised information about NHS, 2004. Department of Health. Better infor-healthy lifestyles. We consider that this is a very mation, better choices, better health. Putting
16
FERNANDEZ ET AL.
information at the centre of health.
R. Prochaska, J.O., & DiClemente, C.C. (1982).Transtheoretical therapy toward a more in-tegrative model of change. Psychotherapy:Theory, Research and Practice, 19(3), 276-287.
UCLA Center for Human Nutrition. SampleScripts for Stages of Change httplwwwcellinteractive.com/ucl/phhscian ed/scripts for change.htmL%201996.
Web 3C Consortium. http://!,vww.web3d~org.
WHO (2004) Guidelines on diet, physical activ-ity and nutrition. ht. ://wwjvwho.int/b/ebwha/pdf files/WHA57/A57 R17-enpdf.
CONTACT
Natatia FernandezE.T.S.l.Telecomunicaci6n. Ciudad UniversitariaUniversidad Politecnica de MadridPhone: +34 91 549 57 00 ext. 332Fax: +34 91 336 68 28Email: [email protected]

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
18

Annual Review of CyberTherapy and Telemedicine
Real Time Changing Virtual Environments:A New Tool for Virtual Therapy
M. Alcariz, Ph.D., B. Rey, M.Sc., J. Montesa, M.Sc., J. A. Lozano, Ph.D., M. C. Juan, Ph.D.
Medical Image Computing Laboratory (MedICLab), Technical University of Valencia
Abstract: Environments used up to now for therapeutic applications are invariable ones whose con-tent cannot be changed by the therapist or by the patient. However, this is a technical issue that canbe solved with current technology. In this paper, we describe a virtual environment that has been de-veloped taking into account this factor. The main technical feature of the environment is that its as-pect can be controlled and modified by the therapist that conducts the clinical sessions depending onthe emotions that the patient is feeling at each moment.
The applications of these dynamic changes are not limited to the field of clinical psychology. Theyopen a new arena of possibilities for many other kinds of applications including industry, architecture,medicine etc. The virtual environment that is described in this paper is a step towards a truly adaptivedisplay.
INTRODUCTION
The concept of "adaptive displays" has been Since this initial study, this technique has beenconsidered for many years. It is the use of tech- used for the treatment of different phobias. Wenical devices that adapt to the requirements of can point out the environments designed forthe user, rather than having the users adapt to acrophobia treatment, 3-5 aoraphobia, '7 spiderthe device. The term "adaptive display" has re- phobia 8 or flying phobia. 010 Its effectivenessferred to displays that change their contents has been analyzed for the fight against otherdepending only on situational content rather psychological problems: obsessive-compulsivethan on any awareness of the user.1 These disorders, attention deficit disorders, post-adaptive displays can be used in many different traumatic stress and eating disorders.11
,1 2
applications such as medicine, industry, archi- However, environments used up to now fortecture, and psychology, therapeutic applications are invariable ones
whose content allows for only minor changes.In the field of clinical psychology, virtual reality As a result, no modification can be made in thehas in recent years been applied to the treat- contents of the virtual environment even whenment of psychological disorders. This idea was high emotional responses can be obtained fromfirst voiced in November 1992 in the Human- the user. It is our claim, that the psychologistComputer Interaction Group of the Clark Atlanta should have a greater control over the aspect ofUniversity. The first experiment was a pilot the virtual environment that is shown to thestudy with a 32-years-old woman who suffered user.from flying phobia. She was treated using avirtual environment 2 in which she followed eight In the environment that we are presenting inthirty-minute sessions. At the beginning of each this paper, the psychologist can make changessession, the subject had a high level of anxiety, in the aspect of the environment depending onwhich was decreasing gradually after remaining the reactions of the patient to different parts ofin the situation for several minutes. This effect the therapy session. This work has been con-also was transferred from the virtual to the real ducted inside the EMMA Project (IST-2001-world. 39192).
19
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
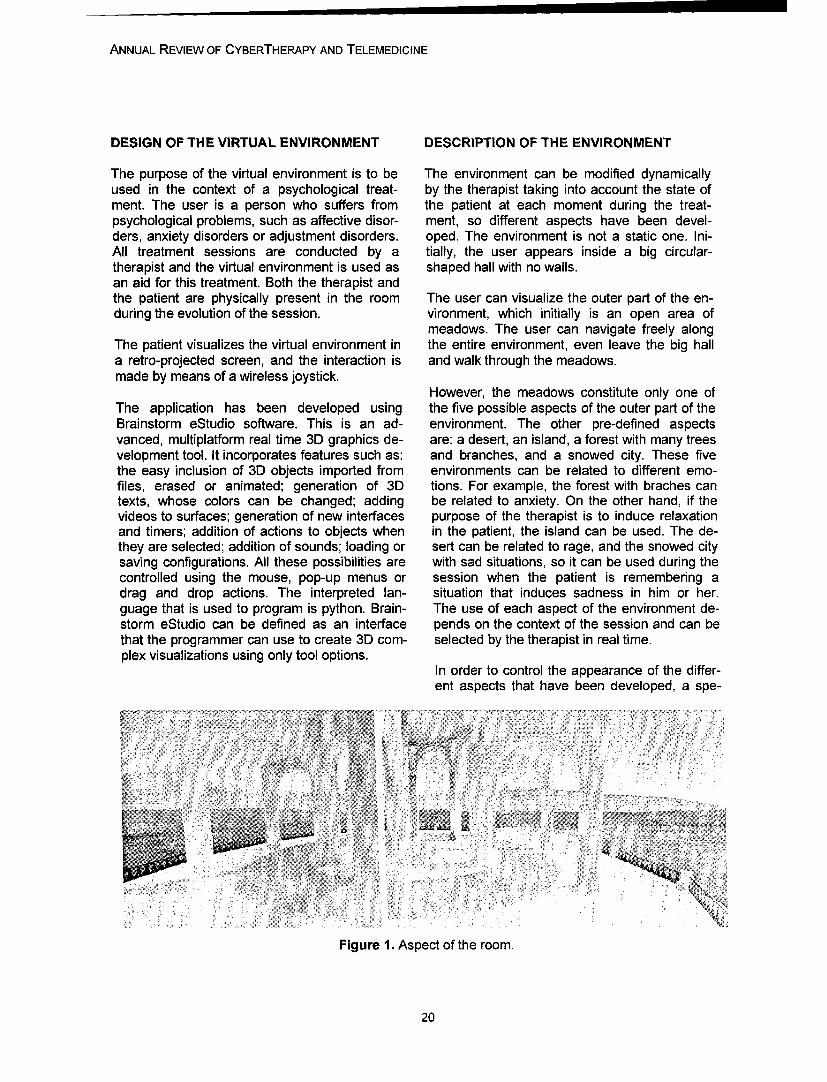
DESIGN OF THE VIRTUAL ENVIRONMENT DESCRIPTION OF THE ENVIRONMENT
The purpose of the virtual environment is to be The environment can be modified dynamicallyused in the context of a psychological treat- by the therapist taking into account the state ofment. The user is a person who suffers from the patient at each moment during the treat-psychological problems, such as affective disor- ment, so different aspects have been devel-ders, anxiety disorders or adjustment disorders. oped. The environment is not a static one. Ini-All treatment sessions are conducted by a tially, the user appears inside a big circular-therapist and the virtual environment is used as shaped hall with no walls.an aid for this treatment. Both the therapist andthe patient are physically present in the room The user can visualize the outer part of the en-during the evolution of the session. vironment, which initially is an open area of
meadows. The user can navigate freely alongThe patient visualizes the virtual environment in the entire environment, even leave the big halla retro-projected screen, and the interaction is and walk through the meadows.made by means of a wireless joystick.
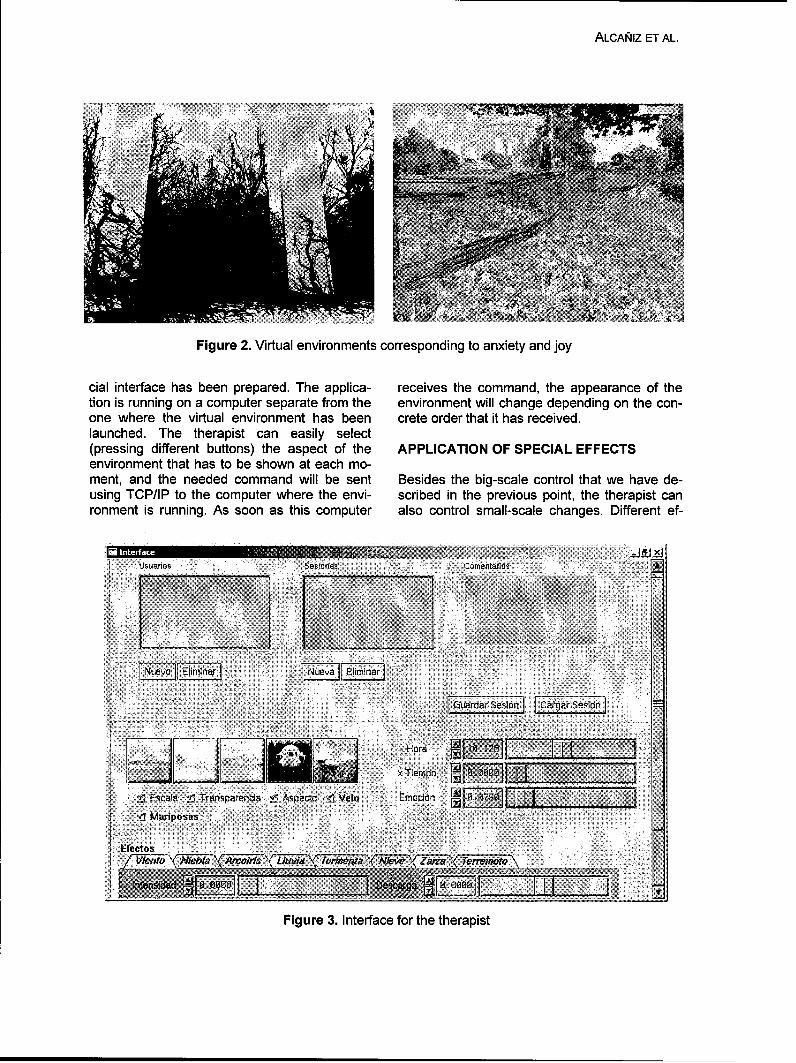
However, the meadows constitute only one ofThe application has been developed using the five possible aspects of the outer part of theBrainstorm eStudio software. This is an ad- environment. The other pre-defined aspectsvanced, multiplatform real time 3D graphics de- are: a desert, an island, a forest with many treesvelopment tool. It incorporates features such as: and branches, and a snowed city. These fivethe easy inclusion of 3D objects imported from environments can be related to different emo-files, erased or animated; generation of 3D tions. For example, the forest with braches cantexts, whose colors can be changed; adding be related to anxiety. On the other hand, if thevideos to surfaces; generation of new interfaces purpose of the therapist is to induce relaxationand timers; addition of actions to objects when in the patient, the island can be used. The de-they are selected; addition of sounds; loading or sert can be related to rage, and the snowed citysaving configurations. All these possibilities are with sad situations, so it can be used during thecontrolled using the mouse, pop-up menus or session when the patient is remembering adrag and drop actions. The interpreted lan- situation that induces sadness in him or her.guage that is used to program is python. Brain- The use of each aspect of the environment de-storm eStudio can be defined as an interface pends on the context of the session and can bethat the programmer can use to create 3D com- selected by the therapist in real time.plex visualizations using only tool options.
In order to control the appearance of the differ-ent aspects that have been developed, a spe-
Figure 1. Aspect of the room.
20
ALCANI1Z ET AL.
Figure 2. Virtual environments corresponding to anxiety and joy
cial interface has been prepared. The applica- receives the command, the appearance of thetion is running on a computer separate from the environment will change depending on the con-one where the virtual environment has been crete order that it has received.launched. The therapist can easily select(pressing different buttons) the aspect of the APPLICATION OF SPECIAL EFFECTSenvironment that has to be shown at each mo-ment, and the needed command will be sent Besides the big-scale control that we have de-using TCP/IP to the computer where the envi- scribed in the previous point, the therapist canronment is running. As soon as this computer also control small-scale changes. Different ef-
IFFnf Iuv j lmT&Nueva Elimina
Gýuardar Sesion CaarSso
Hora ~ 9 1 8
_1 d x Fiemnpo .9
ZEscala , Transpzvarenda • Aspect f Velo Emcclojn 6.i79
Efectos47i7v_ 77r--nrtto Awoir/ Lkrza (7 iiwer(mmoly)
Figure 3. Interface for the therapist

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Figure 4. The sad environment snowing and with a storm.
fects can be applied to the environment: a rain- the associated sound or video will be repro-bow can appear, it can start raining, snowing, duced. This can be used as a way to personal-an earthquake can be generated, and the illumi- ize the environment. These object holders cannation can change to the one corresponding to serve as a mixer tool to combine several ele-different hours of the day and the night. ments to form a new complex element. This is
achieved if different elements from differentAll these effects are also launched from the categories are copied to the same object holder.same interface that controls the big-scale There are some special object holders that arechanges. The therapist can control by means of placed in a balcony of the room. The patient cana slider the moment when the effect is launched modify the size of the objects that are placed onand its intensity, them by means of the loudness of the voice.
They will be used as a discharge area whereOTHER INTERACTIONS the patient can give free rein to his/her feelings.
A system has been programmed that detectsBut it is not only the therapist who can control the loudness of the input sounds and modifiesthe personalization of the environment. The accordingly the size of the objects placed onuser can also play an active role on this task. those special object holders.
The big hall that is present in any of the possi- The living book is a special object where theble aspects of the virtual environment is com- patient can place icons that represent the ele-posed by different systems that interoperate ments from the database. These icons can beand allow the patient to express ideas using classified in different chapters. It is the instru-different items (videos, images, sounds, colors ment that the patient will use to put in order theand 3D objects) that can be selected from a contents that have been used during the clinicaldatabase. session with the therapist.
Distributed along the environment, there are Finally, the drain can be used to destroy anyseveral places (object holders) where the pa- element that is not needed anymore.tient can locate an item from the database, sothe 3D aspect of the element will be shown, or
22
ALCANIZ ET AL.
Figure 5. The living book and the drain.
CONCLUSIONS
Using this new technical approach, different 5. Rothbaum B., Hodges L., Kooper R., Opdykeenvironments can be developed to treat differ- D., Williford M., North M. Virtual reality gradedent kinds of psychological problems. The possi- exposure in the treatment of acrophobia: A casebility of dynamically changing the aspect of the report. Behavior Therapy 1995; 26: 547-554.environment, which is the main improvement ofthis system from the technical point of view, 6. North M., North S. Virtual environments andopens a new area and new possibilities for psychological disorders. Electric Journal of Vir-treating psychological disorders. tual Culture 1994; 2: 25-34.
Besides, this system constitutes a step forward 7. North M., North S., Coble J.R. Effectivenesstowards a true adaptive display. The ultimate of virtual environment desensitization in thepurpose would be that the system itself would treatment of agoraphobia. Presence 1996; 5(3):be able to detect the emotional state of the user 346-352.and adapt its contents to this state without anyintervention from the therapist. 8. Carlin A., Hoffman H., Weghorst S. Virtual
reality and tactile augmentation in the treatmentREFERENCES of spider phobia: A case report. Behavior Re-
search and Therapy 1997; 35: 153-158.1. Schmeisser, E.T. Dream of a Display thatPays Attention to the Viewer. CyberPsychology 9. Rothbaum B., Hodges L, North M., Weghorst& Behavior 2004; 7(6): 607-609. S. Overcoming phobias by virtual exposure.
Communications of the ACM 1997; 40: 34-392. North, M.M., North, S.M. y Coble, J.R. Virtualenvironment psychotherapy: a case study of 10. Bahos R., Botella C., Perpifi6 C. (2000). Elfear of flying disorder. Presence: Teleoperators abordaje de la fobia a volar mediante realidadand Virtual Environments 1997; 6 (1): 127-132. virtual (Approach to flying phobia by virtual real-
ity). Communication presented at the IX Meet-3. North M., North S. Virtual reality psychother- ing of the Psychiatric Association of the Comu-apy. The Journal of Medicine and Virtual Reality nidad Valenciana, Castell6n, Spain.1996; 1: 28-32.
11. Riva G., Baccheta M., Cesa G., Conti S.,4. Rothbaum, B., Hodges L., Kooper R., Op- Molinari E. (2001) Virtual Reality and Telemedi-dyke D., Williford M., North M. Effectiveness of cine Based Experiential Cognitive Therapy: Ra-computer-generated (virtual reality) graded ex- tionale and Clinical Protocol. In: Fiva G, Galim-posure in the treatment of acrophobia. Ameri- berti C., eds. Towards CyberPsychology: Mind,can Journal of Psychiatry 1995; 152: 626-628.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Cognitions and Society in the Internet Age. Am-sterdam: lOS Press.
12. PerpiM6 C., Botella C., Bahos R., MarcoJ.H., Alcahiz M., Quero S. Body Image and vir-tual reality in eating disorders: Is exposure byvirtual reality more effective than the classicalbody image treatment? Cyberpsychology andBehavior 1999; 2: 149-159.
CONTACT
Mariano Alcahiz, Ph.D.Medical Image Computing Laboratory(MedICLab)Technical University of ValenciaCamino Vera s/n46022 Valencia (Spain)e-mail: alvcanizsdegi.p esTelephone: +34 96 387 75 17Fax: +34 96 387 95 10
24

Annual Review of CyberTherapy and Telemedicine
Towards a Neuropsychological Basis of Presence
W. IJsselsteijn, Ph.D.
Human-Technology Interaction Group, Eindhoven University of Technology, Eindhoven, The Netherlands
Abstract: Presence research studies the experience of being in a place or being with someone as itis mediated through technology. The experience of presence appears to be a complex perception,formed through an interplay of raw multisensory data, spatial perception, attention, cognition, andmotor action, all coupled through a constant dynamic loop of sensorimotor correspondence. The factthat technology can start working as a transparent extension of our own bodies is critically dependenton (i) intuitive interaction devices which are 'invisible-in-use', seamlessly matched to our sensorimo-tor abilities, and (ii) the highly plastic nature of our brain, which is continuously able and prone toadapt to altered sensorimotor contingencies. The perception of ourselves as part of an environment,virtual or real, critically depends on the ability to actively explore the environment, allowing the per-ceptual systems to construct a spatial map based on sensorimotor dependencies. Provided the real-time, reliable correlations between motor actions and multisensory inputs remain intact, the integra-tion of telepresence technologies into our ongoing perceptual-motor loop can be usefully understoodas a change in body image perception - a phenomenal extension of the self.
INTRODUCTION
Interactive systems that allow users to control objects within it, virtual environments (VEs) allowand manipulate real-world objects within a re- users to interact with synthetic or computer-mote real environment are known as teleopera- generated environments. In its most well-knowntor systems. Remote-controlled manipulators incarnation, VEs are presented to the user via a(e.g., robot arms) and vehicles (e.g., NASA's head-mounted display (HMD) where visual infor-Mars Exploration Rovers) are being employed to mation is presented to the eyes via small CRTsenable human work in hazardous or challenging or LCDs, and auditory information can be pre-environments such as space exploration, under- sented using headphones. Importantly, the HMDsea operations, or hazardous waste clean-up, is fitted with a position tracking device which pro-They also allow for transforming the temporal vides the necessary information for the computerand spatial scale of operation, as is the case to calculate and render the appropriate visualwith for instance minimally invasive surgery. In and auditory perspective, congruent with theteleoperation, the human operator directly and user's head and body movements. Haptic infor-continuously guides and causes each change in mation, although not yet usually included in pre-the remote manipulator. Sensors at the remote sent-day VEs, can be added through the use ofsite (e.g., a stereoscopic camera, force sensors) for instance an exoskeletal glove or arm, actingprovide continuous feedback about the slave's both as sensor and actuator.position in relation to the remote object, therebyclosing the continuous perception-action loop Telepresence (in relation to teleoperation) andthat involves the operator, the master system virtual presence (in relation to VEs) both addresswith which she interacts locally, and the remote the psychological phenomenon of presence -slave system. In the context of telerobotics, the sense of 'being there' in a mediated environ-telepresence is closely associated to the sense ment, or a "perceptual illusion of non-mediation"of distal attribution,1 the externalisation of the as Lombard and Ditton 2 defined it. Perceivedself to include remote tools that phenomenologi- transparency of the medium is crucial, i.e. acally become extensions of one's own body, sense of direct perceptual stimulation and poten-even if they are not physically part of it. tial for action, without an awareness of the re-
moteness in time or space of the simulated orWhereas teleoperation systems enable the ma- reproduced realities.nipulation of remote real-world environments and
25

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
MEDIA CHARACTERISTICS INFLUENCING mum is unattainable, which elements are mostPRESENCE critical to the experience of presence. It appears,
for instance, that pictorial realism contributesSince the early 1990s onwards, presence has less to the experience of presence in VEs than,been empirically studied in relation to various for instance, interactivity of viewpoint.6 Asmedia, most notably VEs. A large number of fac- Heeter7 noted, "the alchemy of presence in VR istors that may potentially influence the sense of in part a science of tradeoffs." It is not clear atpresence have already been suggested in the present how much each feature or perceptualliterature. Depending on the levels of appropri- cue contributes to eliciting a sense of presenceate, rich, and consistent sensory stimulation, for the participant (i.e., the relative weighting),varying levels of presence can be produced. nor is it clear how these cues interact with eachSheridan 3 proposed three categories of determi- other. A model of multisensory information inte-nants of presence: gration and interaction for presence - a presence
equation, if you like - will be a valuable theoreti-The extent of sensory information presented to cal and practical contribution. Ellis 6 has argued
the participant, i.e. the amount of salient that an equation relating presence to its contrib-sensory information presented in a consis- uting factors should allow for iso-presencetent manner to the appropriate senses of equivalence classes to be established, that is,the user. maintaining the same level of measured pres-
The level of control the participant has over the ence, whilst trading off contributing factorsvarious sensor and interface mechanisms against each other. However, testing such a(tracked HMD, dataglove, etc.). This refers model's empirical validity will critically depend onto the various sensorimotor contingencies, sufficiently reliable, valid, and sensitive meas-i.e. the mapping or correlation between the ures of presence which are currently being re-users actions and the perceptible spatio- searched (for an overview see van Baren &temporal effects of those actions. IJsselsteijn, 2004;9), but can not yet be said to
The participant's ability to modify the environ- exist at this point in time.ment, i.e., the ability to interact with the vir-tual or remote environment and to affect a ESTABLISHING SENSORIMOTOR DEPEND-change within that environment. ENCIES THROUGH ACTIVE EXPLORATION
The extent of sensory information is similar to Perception serves the individual's need to con-Steuer's4 notion of vividness. Level of control trol relevant moment-to-moment behaviour orover sensors and effectors, and the ability to action within a changing environment. The de-modify the environment correspond to Steuer's 4 velopment of visual perception of object shapenotion of interactivity. These three factors all and environmental layout is strongly dependentrefer to the media form, that is, to the physical, on consistent correlations between vision andobjective properties of the media technology, input from other sensory systems (mainly touchImportantly, presence research is about relating and kinesthetics) through active exploratorythose media form variables to the human re- behaviour of the environment, establishing asponse. In principle, Slater's5 contention that one stable yet flexible multisensory representationshould try to keep content variables out of the of space.presence equation as much as possible isadopted here. According to Slater,5 "presence is In a classic study, Held 10 convincingly demon-about form, the extent to which the unification of strated the relation between locomotor experi-simulated sensory data and perceptual process- ence and the understanding of spatial relations.ing produces a coherent 'place' that you are 'in' He designed an experiment using a 'kitten car-and in which there may be the potential for you ousel' in which kittens, who were raised fromto act." birth in total darkness, were placed in pairs.
One kitten pulled the carousel, thus using itsIt is of clear theoretical and practical value to movement to determine what it saw. The otherestablish what the optimal mix of cues might be kitten was placed in a basket at the other end offor different application contexts, or, if the opti- the carousel, which was controlled by the first
26
IJSSELSTEIJN
kitten. In this way, the second kitten received trolled the movements of a remote cameraidentical visual stimulation to the first kitten, yet (generating movement parallax), over passivewithout the ability to control the visual input, observers, who received identical visual inputBetween these sessions of visual exposure, the (i.e. motion parallax), yet without the ability tokittens were returned to the dark. After 42 days actively change the viewpoint. This is in lineof 3 hour sessions, the effects of active versus with results found in relation to virtual environ-passive movement became strikingly apparent ments, where Welch et al.15 showed that partici-when the kittens were tested on a visual cliff pants who had active control over a simulatedsurface. The kittens who had been active in the environment indicated higher levels of presencecarousel shied away from the cliff and appropri- than participants who were passively exposedately stretched out their legs to land on the to the same environment.lower surface. The passive kittens showednone of that behaviour, thereby providing sup- BRAIN PLASTICITY AND OUR NEGOTIABLEport for the view that the development of per- BODY-IMAGEception is action-dependent. Observations inhumans have led to similar conclusions. For The fact that technology can start working as ainstance, Verkuyl11 indicated that so-called Sof- transparent extension of our own bodies is criti-ten on children, who do not possess upper ex- cally dependent on the highly plastic nature oftremities due to the use of a sleeping drug in our brain, which is continuously able and pronethe early stages of the mother's pregnancy, had to adapt to altered sensorimotor contingencies,severe problems in 3D-perception. as the studies on adaptation to prismatic dis-
placement and tele-systems already illustrated.Studies of adaptation to prismatic displace- This fact finds its basis in the significant evolu-ments provide further support for the impor- tionary benefit of having a negotiable body im-tance of establishing reliable sensorimotor cor- age to accommodate lifetime development andrelation maps through actively negotiating the change, which requires a continuous re-physical environment. Held & Hein 12 studied mapping of bodily boundaries. Although body-prismatic displacements in humans under three image adaptations across the lifespan can af-conditions: active arm movement, passive arm ford to take their time, it is the relative speed ofmovement, and no arm movement. In the active these sensorimotor adaptations that enables usarm movement condition the subject swung her to experience man-made technology as, quitearm back and forth in the frontal plane, in the literally, part of ourselves - be they a blind per-passive condition it was transported in the son's cane or an advanced telerobotic arm.same manner by means of a moving cradle towhich it was strapped. Results, as measured in Further evidence of the high-speed plasticity ofterms of visual-motor negative after-effects, the body image is provided by the amazing ad-showed that adaptation was only produced in aptation processes that may occur in the body-the active movement condition and not in the image of people with an amputated limb.passive or no-movement conditions. Another Ramachandran, Rogers-Ramachandran andclassic experiment on visual displacement 13 Cobb 16 had (amputated) phantom limb patientsused lenses that turn the world upside-down. view their intact arm in a mirror, such that theirThe study showed that full adaptation to this amputated arm appeared to be resurrected.situation (i.e., seeing the world right side up Several subjects reported feeling their phantomagain) occurred after a few days only when limb touched when they viewed the mirror im-subjects were allowed to actively explore a age of their intact arm being touched - see alsocomplex world. When a subject was simply Ramachandran & Blakeslee. 17
pushed around in a wheelchair, he did not showthis perceptual adaptation to the lenses. Botvinick and Cohen18 provided a first descrip-
tion of the 'rubber hand illusion'. This crossmo-Similarly, telemanipulation experiments using dal perceptual illusion occurred when partici-the Delft Virtual Window System14 demon- pants' left hand was placed out of view and astrated a significant perceptual advantage of life-size rubber model was placed in front ofactive observers, whose head movements con- them. Subsequently, both the rubber hand and

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
participants' left hand were gently stroked by maps, thus allowing for higher order perceptiontwo small paintbrushes, synchronizing timing as and categorisation of objects and environ-closely as possible. In line with the ments. 22 The ensuing body image is most use-Ramachandran et al.16 results, subjects re- fully conceptualised as a temporary constructported feeling a sense of ownership of the rub- which is remarkably flexible, and may includeber hand, as if it was actually their own. non-biological artefacts as an integral part of it.Ramachandran, Hirstein and Rogers-Ramachandran 19 further extended this work, FROM FAR TO NEAR: REMAPPING SPACEshowing that this illusion also works when IN TELEPRESENCEphysical similarity is absent. Instead of using arubber hand, they simply stroked and tapped In general, the space that surrounds the userthe tabletop for about a minute. In this case, can be meaningfully segmented into a number ofsubjects also reported sensations arising from ranges, usually three or four, based on principlesthe tabletop. They argue that the illusion mainly of human perception and action. Several modelsarises "from the 'Bayesian logic' of all percep- have been proposed,23' 24 all of which distinguishtion; the brain's remarkable ability to detect sta- between a peripersonal space (the immediatetistical correlations in sensory inputs in con- behavioural space surrounding the person) andstructing useful perceptual representations of a far or extrapersonal space. Referring to hapticthe world - including one's body."(p. 1500). In space, the peripersonal space corresponds toa further study, Armel and Ramachandran 20 what Lederman, Klatzky, Collins & Wardell refershowed that when the physical integrity of the to as the manipulatory space, i.e., within hand'srubber hand was threatened (bending a finger reach, whereas the extrapersonal realm wouldbackwards to seem painful), a clear skin con- be regarded as ambulatory space, requiring ex-ductance response was generated, and that the ploration by movements of the body, or throughillusion could even be projected to anatomically the use of a tool which extends the bodily reach.impossible locations. Using the rubber hand Animal and human brain studies have confirmedillusion, Ehrsson, Spence, and Passingham 21 this distinction between peripersonal and ex-have recently studied the neuronal counterparts trapersonal space, showing that space is not
25,26of the feeling of body ownership. On fMRI homogeneously represented in the brain.measures of brain activity, they found that ar-eas in the premotor cortex reflected the feeling Telepresence technologies can be viewed asof ownership of the rubber hand, indicating that attempts to overcome the boundaries of spatialthe multisensory integration in this region pro- segmentation. Their success in doing so is evi-vides a mechanism for bodily self-attribution. denced by a clinical case, described by Berti and
27Frassinetti, where a patient (P.P.), after a rightThe results on perceptual adaptation described hemisphere stroke, showed a dissociation be-in the previous paragraph, as well as the rubber tween near and far spaces in the manifestationhand illusion, both seem to suggest that what of severe visuo-spatial neglect. Using a line bi-matters most is a closely and continuously cor- section task, the neglect was apparent in nearrelated loop of sensory input, neural com- space, but not in far space when bisection in themands, and motor action. Thus, modality- far space was performed with a projection lightspecific feature maps appear to project onto pen. However, neglect appeared in the far spaceone another through re-entrant connections, as well when the line bisection task was per-which allows disjunctive feature characteristics formed with a stick (used by the patient to reach(e.g., visual and haptic properties of a stimulus) the line) and it was as severe as neglect in theto be connected in the responses of higher- near space. Thus, this study provides evidenceorder networks. Sensorimotor correlations will that an artificial extension of a person's body (theinitially be driven by the temporally ongoing par- stick) causes a remapping of far space as nearallel signalling between primary cortical areas space - essentially telepresence.receiving the sense data associated with stimu-lus objects at a given time and place. Next, sta- CONCLUSIONble feature correlations establish reciprocal con-nections between previously disjunct feature The same sensorimotor and brain systems re-
sponsible for our sense of bodily boundaries and
28
IJSSELSTEIJN
our sense of spatial location are also remarkably 3. Sheridan, T. B. (1992). Musings onadaptable to include non-biological elements telepresence and virtual presence. Presence:within the perceptual-motor loop, provided reli- Teleoperators and Virtual Environments 1, 120-able, real-time sensorimotor correlations can be 126.established. When we interact with virtual or re- 4. Steuer, J. (1992). Defining virtualmote environments using intuitive interaction reality: Dimensions determining telepresence.devices, isomorphic to our sensorimotor abilities, Journal of Communication 42(4), 73-93.the real-time, reliable and persistent chain of 5. Slater, M. (2003). A note on pres-user action and system feedback will effectively ence terminology. Presence-Connect 3, Janu-integrate the technology as a phenomenal exten- ary 2003.sion of the self. This fluid integration of technol- 6. lJsselsteijn, W.A. & de Kort, Y.A.W.ogy into the perceptual-motor loop eventually (in preparation). Rethinking realism: A tale ofmay blur the boundary between our 'unmediated' two paradoxes.self and the 'mediating' technology. 7. Heeter, C. (1992). Being There: The
Subjective Experience of Presence. Presence:Naive definitions of 'self as everything contained Teleoperators and Virtual Environments 1, 262-within our bodily boundaries, and 'non-self as 271.the world outside our own bodies become much 8. Ellis, S. (1996). Presence of mind: Aless obvious when we regard the intimate de- reaction to Thomas Sheridan's 'Further mus-pendencies and co-adaptation we can experi- ings on the psychophysics of presence'. Pres-ence when technology starts working as a trans- ence: Teleoperators and Virtual Environmentsparent extension of our own bodies and minds. 5, 247-259.As cognitive scientist Andy Clark convincingly 9. lJsselsteijn, W.A. (2004). Presenceargues in his wonderful book 'Natural Born Cy- in Depth. Eindhoven University of Technologyborgs' , what 'T' am is not defined by the outer 10. Held, R. (1965). Plasticity in sen-limits of the 'biological skin-bag'. He states: "For sory-motor systems. Scientific American 213,our sense of self, of what we know and of who 84-94.and what we are, is surprisingly plastic and re- 11. Stassen, H. & Smets, G. (1995).flects not some rigid preset biological boundary Telemanipulation and telepresence. In: T.so much as our ongoing experience of thinking, Sheridan (ed.) Analysis, Design and Evaluationreasoning, and acting within whatever potent of Man-Machine Systems. Amsterdam: Elsevierweb of technology and cognitive scaffolding we Science, pp 13-23.happen currently to inhabit" (p.45).28 Thus we 12. Held, R., & Hein, A. (1958). Adapta-learn that our relationship with technology is a tion to disarranged hand-eye coordination con-two-way adaptive process - we adapt the tech- tingent upon reafferent stimulation. Perceptualnologies to fit our needs and abilities (a process and Motor Skills 8, 87-90.also known as user-centred design), but at the 13. Hein, A. (1980). The developmentsame time, our brain adapts itself to the technol- of visually-guided behavior. In: C. Harris (ed.)ogy, so that the technology becomes part of our Visual Coding and Adaptability. Lawrenceextended self - the biological self and all non- Erlbaum.biological tools and toys we employ to enhance 14. Smets, J., Overbeeke, C., & Strat-our performance and pleasure. mann, H. (1987). Depth on a flat screen. Per-
ceptual and Motor Skills 64, 1023-1034.REFERENCES 15. Welch, R., Blackmon, T., Liu, A.,
Mellers, B., & Stark, L. (1996). The effects of1. Loomis, J. (1992). Distal attribution pictorial realism, delay of visual feedback, and
and presence. Presence: Teleoperators & Vir- observer interactivity on the subjective sense oftual Environments 1, 113-119. presence. Presence: Teleoperators and Virtual
2. Lombard, M., & Ditton, T.B. (1997). Environments 5, 263-273.At the heart of it all: The concept of presence. 16. Ramachandran, V.S., Rogers-Journal of Computer-Mediated Communication Ramachandran, D., & Cobb, S. (1995). Touch-3(2). [Online: http:llwww.ascusc.org/jcmc/vol3/ ing the phantom limb. Nature 377, 489-490.issue2/ lombard.html] 17. Ramachandran, V.S. & Blakeslee,
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
S. (1998). Phantoms in the Brain. New York: Department of Technology ManagementHarper Collins. Eindhoven University of Technology
18. Botvinick, M. & Cohen, J. (1998). Eindhoven, The NetherlandsRubber hands 'feel' touch that eyes see. Nature Phone: +31 40 2474455391,756. Fax: +31 40 2449875
19. Ramachandran, V.S., Hirstein, W., Email: W.A. lJsselsteijn@tue. nI& Rogers-Ramachandran, D. (1998). Phantomlimbs, body image, and neural plasticity. Int.Brain. Res. Org. News 26 (1), 10-11.
20. Armel, K.C. & Ramachandran, V.S.(2003). Projecting sensations to external ob-jects: Evidence from skin conductance re-sponse. Proceedings of the Royal Society ofLondon B 270, 1499-1506.
21. Ehrsson, H.H., Spence, C., & Pass-ingham, R.E. (2004). That's my hand! Activity inthe premotor cortex reflects feeling of owner-ship of a limb. Science 305, 875-877.
22. Edelman, G. (1987). Neural Darwin-ism: The Theory of Neuronal Group Selection.New York: Basic Books.
23. Grusser, O.-J. (1983). Multimodalstructure of the extrapersonal space. In: Hein,A. & Jeannerod, M. (eds.), Spatially OrientedBehavior. New York: Springer-Verlag, 327-352.
24. Rizzolatti, G. & Camarda, R.(1987). Neural circuits for spatial attention andunilateral neglect. In: Jeannerod, M. (ed.), Neu-rophysiological and Neuropsychological As-pects of Spatial Neglect. Amsterdam: ElsevierScience, pp. 289-313.
25. Rizzolatti, G., Fadiga, L., Fogassi,L. & Gallese, V. (1997). The space around us.Science 277, 190-191.
26. Previc, F.H.. (1998). The neuropsy-chology of 3-D space. Psychological Bulletin124,123-164.
27. Berti, A. & Frassinetti, F. (2000).When far becomes near: Remapping of spaceby tool use. Journal of Cognitive Neuroscience12,1215-420.
28. Clark, A. (2003). Natural Born Cy-borgs. Minds, Technologies, and the Future ofHuman Intelligence. Oxford: Oxford UniversityPress.
Contact
Wijnand lJsselsteijn, Ph.D.Human-Technology Interaction Group
30

PENN ET AL.
Virtual Reality in Everyday Memory Assessment and Rehabilitation:Progress to Date and Future Potential
P.R.Penn, F.D.Rose, B.M. Brooks
School of Psychology, University of East London
Abstract: Memory impairments are one of the most disabling consequences of brain injury. Theycan be problematical to assess and rehabilitate, as conventional "paper and pencil" neuropsychologi-cal assessments and rehabilitation strategies are often criticised as lacking in relevance to the use ofmemory in the real world i.e., "ecological validity." Conventional neuropsychological memory assess-ments and rehabilitation strategies also often fail to cover important aspects of 'everyday memory,'such as prospective memory (remembering to perform actions in the future) and incidental memory(the encoding and recall of information without any instructions from a third party). Unfortunately, itcan be very difficult to achieve the ecological validity necessary to assess everyday memory withoutcompromising experimental control. Similarly, it is often difficult to devise rehabilitation strategies thatinvolve real life scenarios owing to practical constraints. Virtual reality (VR) provides an elegant solu-tion to these problems and is, therefore, an ideal tool with which to study everyday memory. This pa-per briefly summarises the current state of research on the applications of VR to everyday memoryassessment and rehabilitation, with reference to some seminal VR work within the domains of spa-tial, incidental and prospective memory. Some directions for future research are suggested, and is-sues associated with turning empirical findings into real benefits for patients considered.
INTRODUCTION
Over the last decade, the potential of virtual tablishing whether a patient has memory im-reality (VR) has, at last, begun to be realised. In pairments is a crucial aspect of cognitive as-the early to mid-nineties, the aspirations for the sessment and addressing any such impairment,technology far exceeded its capacity to deliver a crucial aspect of cognitive rehabilitation.on its potentiall. 1 However, massive advancesin the sophistication of the hardware that under- 1.1. Reconciling ecological validity and reliabil-pins VR and significant reductions in the cost of ity: VR and everyday memory.such hardware have taken VR "out of the realmof expensive toy and into that of functional tech- There are numerous "paper and pencil" neuro-nology" (p3).2 psychological tests of memory, e.g. the
Wechsler Memory Scale - Revised,11 the AdultThe incorporation of VR into neuropsychologi- Memory and Information Processing test, 12 thecal assessment and rehabilitation has possibly Recognition Memory Test,1 3 and the Doors andattracted the greatest expansion of interest People Test.14 However, conventional neuro-from researchers in recent times. Many authors psychological tests have been heavily criticizedhave argued that the assets of VR are espe- as lacking "ecological validity" or, put anothercially well suited to this field.3 5 VR has been way, relevance to memory under conditionsapplied to a number of domains of cognitive other than the laboratory/rehabilitation ward.15
assessment and rehabilitation, such as: execu- Indeed, it was the poor correlations betweentive functioning; 6 attention ;7 and spatial trans- laboratory tests and 'everyday memory' assess-formation. 8 However, as Brooks et al.9 point ments found by Sunderland, Harris andout, the application of VR to memory impair- Baddeley1 6 that prompted the development ofments has been of particular interest, as mem- the Rivermead Behavioural Memory Testory disorders are one of the most disabling con- (RBMT), which is designed to assess everydaysequences of brain damage.10 Therefore, es- memory. However, it has been argued that the
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
cost of introducing ecological validity into con- experiments that, though methodologically de-ventional neuropsychological assessment has sirable, would not be practical in the real world.been a loss of strict control over the test situa- This is particularly true for research into spatialtion.17 memory. A good example would be the VR ad-
aptation of the Morris Water Task, an exp~eri-The problem of balancing the demands of eco- mental paradigm that had proved highly infor-logical validity with sufficiently rigorous control is mative in investigating spatial ability in rodents,also apparent in rehabilitation. Doubts have to research into human spatial ability. The taskbeen raised as to whether rehabilitation strate- involves finding a platform, which is submergedgies that lack ecological validity will transfer to in water, purely by using memory of its positionthe real world 18 and whether training behaviours relative to external environmental cues. A desk-in the absence of any change in the environ- top VR variant of this paradigm has proved use-ment, or task demands, fosters sufficient intel- ful in assessing spatial learning decrements inlectual flexibility and creativity to be useful in TBI patients, which corresponded to self- re-everyday life. 19 Therefore, of all the assets of ported frequency of place learning problems inVR for assessment and rehabilitation (see everyday life.2 °Rizzo, Schultheis, Kerns and Mateer,3 for acomprehensive review) it is perhaps VR's ca- Using the control and ecological validity af-pacity to generate environments that are satisfy- forded by VR together with fMRI generatesing from an ecological standpoint, without com- unique and exciting insights into the neurologi-promising on experimenter/therapist control, cal correlates of everyday memory, which wouldthat is most exciting for memory assessment not be possible in the real world owing to port-and rehabilitation research. This capacity brings ability issues inherent in fMRI equipment. Forwith it exciting opportunities to study everyday example, Morris et al.2 1 and Paslow et al.22 usedmemory phenomena. Indeed, applications of a PC-based virtual reality set up in conjunctionVR to memory research to date have predomi- with fMRI in order to examine the brain corre-nantly focused on three domains of everyday lates of egocentric memory (spatial knowledgememory, which have proved particularly prob- relative to the observer) and allocentric memorylematical for conventional assessment and re- (spatial knowledge relative to cues independenthabilitation: i.e., spatial memory, incidental of the observer) in patients with anoxic hippo-memory and prospective memory. The following campal damage and normal controls. The re-provides an illustration of how the assets of VR suits from these studies provided an in vivohave contributed to our understanding of the demonstration of how anoxic brain damage canabove domains of everyday memory, with refer- affect hippocampal function.ence to some significant VR research.
In addition to overcoming practical difficultiesVR AND SPATIAL MEMORY with implementing a desired methodology or
permitting the incorporation of relatively inac-A good deal of the developing literature on eve- cessible medical technology, a brief look at theryday memory assessment and rehabilitation in use of VR in the rehabilitation of spatial memoryVR to date has been directed at spatial mem- reveals that it can also directly facilitate the re-ory, arguably for two reasons. Firstly, as Brooks organisation of memory ability. Research haset al.9 state, adequate spatial memory is a pre- shown that procedural memory for motor tasksrequisite for independent living. Secondly, VR can often remain relatively intact, even in indi-spatial memory tasks are particularly amenable viduals who exhibit profound impairments into being orientated to utilise users' procedural other aspects of memory- as in the widely re-memory for motor tasks e.g., simulated naviga- ported case of HM. 23 Research has also indi-tion between waypoints. This has significant cated that one can utilize intact proceduralimplications for the reorganisation of memory memory to aid or replace damaged memoryfunction in individuals who have suffered brain systems.2426 Unfortunately, conducting spatialdamage, which will be elaborated on below, navigation tasks involving more than one room,
or in an environment relevant to the patient'sOne of the primary assets of VR in everyday everyday life, can be highly problematical in thememory assessment is the capacity to perform real world. This problem is easily rectified within
32

PENN ET AL.
VR, the question was: is a simulation of a motor advantage of using VR in everyday memory as-activity sufficient to tap into spared procedural sessment; that the spatial memory of physicallymemory in an amnesic patient? Brooks et al.28 disabled participants can be assessed using VRused a desktop VR system to train an amnesic in some situations where other forms of assess-patient (MT) to independently navigate between ment might not be possible.locations within her hospital's rehabilitation unit.When the training was extended to encompass VR AND INCIDENTAL MEMORYreal world and VR based training of routes(matched for complexity) within the ward, it tran- Incidental memory is, perhaps, the type of mem-spired that MT learned the route practised in ory most relevant to everyday life as, unlike inVR, but not the route practised in the real world. conventional memory tests, often in day-to-dayA number of features of the VR rehabilitation life individuals are not made explicitly aware thatmay have been responsible for this outcome. they will be required to remember a particularFor example, MT could perform the route very stimulus prior to having reason to recall it. Thisquickly in VR resulting in more repetitions of the scenario is difficult to achieve in a laboratory, asVR route than the route practised in the real an everyday environment is usually an integralunit. The rehabilitation strategy of backwards part of the task. However, VR is ideally suited totraining was easier to implement in VR than in conducting incidental memory assessments, as itthe real world. Finally, extraneous distractions can easily mimic real-life environments andwere easily controlled in VR. A follow up study tasks, and participants can then be incidentally
28reported in Rose et al. provides further sup- tested on items encountered during their per-port for the use of VR for route training in amne- formance of the tasks. Despite this, the use ofsic patients. VR in incidental memory studies is still rare.
Researchers have also shown interest in VR as a Andrews et al.32 conducted a pioneering study ofmeans to encourage the development of spatial incidental memory for objects in VR. Participantsmemory in children whose physical disabilities examined a series of objects in one of five condi-restrict their mobility. For example, Stanton et tions: during interaction with a four-room virtualal;29 Stanton et a130 have conducted experiments environment; in four static displays without anyfeaturing a VR model of a real school, which context; in the same four static displays, butphysically disabled children were asked to inde- where the participants were required to move apendently explore with a view to determining cursor over each object in turn; in four static pic-whether VR-based spatial memory training trans- tures of virtual rooms; and using the same fourlates into improvements in performance in the pictures, but where the participants were re-real environment on which the virtual environ- quired to move a cursor over each of the fourment was modelled. Subsequent testing of the objects in turn. Subsequent object recognitionchildren on their spatial knowledge of the real tests revealed that the poorest recognition per-school indicated that they performed better at formance occurred in the condition where partici-pointing tasks and showed better route knowl- pants encountered the objects in the virtual envi-edge than undergraduate students who had not ronment. Andrews et al. concluded that partici-used the virtual environment. Similarly, Wilson et pants were being distracted by their interactional.31 conducted an experiment, which featured a with the virtual environment and that incidentalvirtual reality reproduction of two floors of the memory is particularly susceptible to distraction.Astley Clarke building at the University of Leices- However, they cautioned that the virtual interac-ter, UK. The children were asked to activate fire tion condition was most representative of partici-equipment and open a fire door to escape from pants' real-world memory ability.the building in VR. Subsequent assessment in-volved asking the children to identify items of fire Rose et al.33 conducted an experiment to investi-equipment that would not have been visible from gate incidental spatial and incidental object rec-their vantage points and the identification of the ognition memory in vascular brain injury patientsshortest route to the fire exit. The children out- and controls. This experiment involved the pres-performed a control group of undergraduate stu- entation of a four room virtual bungalow that par-dents who had not been exposed to the virtual ticipants were asked to search, ostensibly for aenvironment. These studies highlight another

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
toy car. A yoked-control design was used, in based tasks (an action is required before or afterwhich half of each group of participants were performing an activity).assigned to an 'active' condition, which entailedcontrolling movement through the bungalow via a Based on this classification, Brooks et al. 9 de-joystick. The other half were assigned to a vised and conducted a desktop VR prospective'passive' condition, which entailed watching the memory test on patients from a stroke rehabilita-active participant's progress on a second monitor tion unit and age-matched controls. The virtualin an adjoining cubicle. Participants were as- environment used in the test was a four-roomsessed via a spatial layout recognition test, in bungalow. The test involved participants perform-which they were required to assemble 2-D maps ing a furniture removal task, in which they wereof the virtual environment by choosing room required to instruct the experimenter to moveshapes and the positions of entry and exit door- furniture and items from the virtual bungalow toways from an array of possibilities. Active experi- the appropriate room (out of a possible eight) ofence of the virtual environment was found to im- a new house, one piece at a time. This consti-prove incidental spatial recognition memory of tuted the background task. Before performingthe layout of the four-room building for both pa- this task, they were asked to remember to in-tients and controls. Conversely, passive observa- struct the experimenter to put "Fragile" notices ontion was found to improve controls' performance five glass items (the event-based prospectivein the object recognition test, but not patients' memory task); to keep the kitchen door closed toperformance. Using the same procedure Pugnetti keep the cat in (the activity-based prospectiveet al.4 and Rose et al.35 replicated these findings memory task); and to return to a clock in the hallwith multiple sclerosis patients and people with at five-minute intervals and press a button, sup-learning disabilities, respectively. Pugnetti et al. 4 posedly to let removal men in (the time-basedalso found that the above finding with MS pa- prospective memory task). It transpired that 14 oftients could not be accounted for via standard the 36 stroke patients and 2 of the 22 controlpencil & paper memory assessment tools. Thus, participants were unable to recall all three of thethere is evidence that, in addition to providing an prospective memory task instructions immedi-experimental tool more amenable to the study of ately after they had finished the furniture removalincidental memory per se, VR may also provide a task, even though they had been able to recallmore sensitive test of incidental memory, particu- them immediately prior to beginning the task. Alarly in impaired populations. comparison of the results of the remaining stroke
patients and controls, who were able to recall allVR AND PROSPECTIVE MEMORY three prospective memory tasks, indicated that
the stroke patients were severely impaired rela-Impaired prospective memory is a particularly tive to controls at the event and activity baseddisabling form of memory impairment, and poten- tasks, but only marginally impaired at the time-tially the most hazardous, as often in everyday based task. These results were surprising as,life actions that one needs to remember to per- based on Craik's37 theory of age-related decre-form at some point in the future are inherently ments in memory, which proposes that self-important, e.g. remembering to attend a meeting, initiated processing becomes more difficult foror turn off the cooker. Consequently, the need for the elderly, it was envisaged that impairments ina comprehensive assessment of prospective stoke patients would be more apparent in time-memory as part of a cognitive rehabilitation pro- based tasks (which involve self-initiated retrieval)gramme is self-evident. However, performing an than in event or activity-based tasks (which fea-ecologically valid, yet rigorously controlled as- ture external cues). If, as these results of thissessment of prospective memory ability in a re- study indicate, self-initiated retrieval does nothabilitation setting is problematical. Kvavilashvili become much more difficult for stroke patients,and Ellise classified prospective memory accord- their failure to remember to perform tasks in theing to the type of cue the particular task to be future in this study may be attributable to a differ-remembered entailed, i.e. event-based tasks (an ent impairment, perhaps an inability to multi-task.action is required to be performed in response toa cue); time-based tasks (an action is required at Brooks et al's. 9 exploratory study indicates thata previously specified future time); or activity- VR can provide a more comprehensive and con-
trolled assessment of prospective memory ability
34
PENN ET AL.
than would be possible using standard memory The implications of active vs. passive explorationassessment. This contributes to our understand- of virtual environments for incidental spatial lay-ing of the neuropsychological consequences of out and object recognition are interesting andstroke. It also enables rehabilitation to be more potentially very significant.3 3 The impact, positiveeffectively directed towards the specific impair- or otherwise, of active and passive explorationments of individual patients. appears to be contingent on the stimuli and task
demands. Rose et al. speculated that active ex-DIRECTIONS FOR FUTURE RESEARCH AND ploration promoted the activation of proceduralISSUES ASSOCIATED WITH TURNING VR'S memory in the active participants, thereby en-POTENTIAL INTO BENEFITS FOR PATIENTS hancing their spatial memory of the layout of the
virtual environment compared to the passive par-The literature on VR and spatial memory pro- ticipants. The active participants' advantage didvides a glimpse of the exciting potential of using not extend to enhanced recall of the objects inVR in conjunction with fMRI in order to examine the virtual environment because active partici-the neurological correlates of different forms of pants did not interact with the virtual objects.everyday memory.22 Future studies could utilize However, it should be noted that the degree ofthis procedure to elucidate the relationship be- interaction afforded by VR in memory assess-tween the area of the brain affected by stroke, ment and rehabilitation is something of a double-traumatic brain injury (TBI), or dementia and im- edged sword. Increased interaction can have apaired everyday memory ability. Quite apart from deleterious effect on memory assessment andbeing theoretically significant, such data would rehabilitation, as amnesic patients can have diffi-permit therapists to more accurately predict and culty explicitly distinguishing between correct andrehabilitate the particular memory impairments incorrect responses/actions 38 and freedom tothat a patient would be likely to experience on examine a virtual environment can prove asthe basis of their fMRI scan. much of a distraction as an advantage. 2329 Thus,
experimenters/therapists must be careful to en-VR has demonstrated utility in assisting people sure that the range of interaction offered by awith memory impairments by utilizing intact pro- virtual environment does not detract from thecedural memory 9 this learning has translated to purpose of the exercise by providing careful cue-improved performance in the real world. How- ing or adopting error free learning approaches,ever, it is probably true to say that spatial mem- such as that employed by.29
ory tasks are particularly amenable to being bro-ken down into a series of steps that tap into pro- VR has been shown to provide a more compre-cedural memory.9 The task of researchers and hensive, ecologically valid, and controlled as-therapists is now to ascertain whether this use of sessment of prospective memory ability than isVR can be successfully applied to other everyday currently possible using standard memory as-tasks, and whether it can be used to negate sessment tests. However, some questions re-some of the other disorientation, disorganization main from Brooks et al. 9 Firstly, it is not entirelyand repetition disabilities which result from differ- clear whether the lack of impairment in the time-ent forms of memory impairment. Researchers based prospective memory task in stroke pa-will also have to be creative in providing ways of tients relative to controls may have been an arti-overcoming the lack of conscious awareness of fact of the interval between each retrieval occa-learned knowledge common in patients with am- sion being too short. Thus, this aspect of the re-nesia who have learned new motor skills. 14 suits may have been due to the time-based taskBrooks et al also identified numerous reasons for not being sufficiently representative of an every-the greater efficacy of VR training relative to real day time-based prospective memory task, asworld training, e.g., less distraction, more fre- opposed to a genuine reflection on preservedquent repetition, greater amenability of VR train- prospective memory capacity. Further research,ing to the errorless learning paradigm etc. It utilizing different time intervals in the time-basedwould be useful for the design of future memory task, is planned to investigate this effect.rehabilitation strategies in VR to have some dataon the relative importance of each of these as- Brooks et al. also revealed that motivation is im-sets in contributing to rehabilitation outcomes. portant in prospective memory performance, es-

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
pecially for stroke patients. During this study, Washington D.C.: National Academy of Scienceparticipants were also given two real world based Press.prospective memory tasks i.e. remember to ask 2. Schultheis, M.T., Himelstein, J., & Rizzo, A.A.the experimenter to return a personal belonging (2002) Virtual reality and neuropsychology: Up-at the end of the study, and ask for a written ex- grading the current tools. Journal of Headplanation of the study. Results indicated that par- Trauma Rehabilitation, 17:5, 379-394.ticipants were significantly more likely to remem- 3. Rizzo, A., Schultheis, M., Kerns, K., &ber the former task, probably because they were Mateer, C. (2004). Analysis of Assets for Virtualmore motivated to ask for the return of their prop- Reality Applications in Neuropsychology.erty than for the written explanation. If rehabilita- Neuropsychological Rehabilitation.14 (1/2), 207-tion strategies can encourage stroke patients to 239.be more motivated to remember, it seems logical 4. Rizzo, A., Buckwalter, J.G., & van der Zaag,and reasonable to assume that their prospective C (2002), Virtual environment applications inmemory abilities would improve. VR is particu- clinical neuropsychology. In The Handbook oflarly well suited to improving motivation in reha- Virtual Environments, (Stanney, K Ed.), Erl-bilitation by, for example, introducing gaming baum Publishing, New York, 1027-1064elements into rehabilitation strategies. Re- 5. Rose, F.D., Brooks, B.M. & Rizzo, A. (2004)search is currently underway to determine Virtual Reality in Brain Damage Rehabilitation.whether manipulation of the salience of the differ- CyberPsychology and Behaviour. (In press).ent types of prospective memory tasks (e.g., 6. Elkind, J.S., Rubin, E., Rosenthal, S., Skoff,time, event and activity based) can influence pa- B. & Prather, P. (2001) A simulated reality sce-tients' capacity to remember to perform them. nario compared with the computerized Wincon-This may be particularly useful for the patients sin Card Sorting test: An analysis of preliminary(and controls) in Brooks et al. who were unable results. CyberPsychology and Behaviour, 4,even to remember what the prospective memory 489-496.tasks were. 7. Rizzo, A., Pryor, L., Matheis, R., Schultheis,
M., Ghahremani, K., & Sey, A. (2004) MemoryCONCLUSION assessment using graphics-based and pano-
ramic video virtual environments. Proc, 5th In-The work conducted to date clearly indicates ternational Conf. on Disability, Virtual Realitythat VR has very significant potential in the as- and Associated Technologies, in Sharkey,sessment and rehabilitation of everyday mem- McCrindle & Brown (Eds.) 331-338. Oxford, UK,ory in individuals that have suffered brain injury. 20-22 Sept, 2004.Further work is needed to establish whether VR 8. Rizzo, A. A., Buckwalter, J. G., Neumann, U.,can be used in the reorganization of everyday Kesselman, C., Thiebaux, M., Larson, P., & vanmemory tasks other than simple navigation.2 8 Rooyan, A. (1998b). The virtual reality mentalResearch is also needed to further elucidate the rotation/spatial skills project: Preliminary find-implications of active vs. passive exploration of ings. CyberPsychology and Behavior, 1(2), 107-virtual environments and the relative contribu- 113.tion of the other assets of VR to everyday mem- 9. Brooks, B.M., Rose, F.D., Potter, J., Attree,ory assessment and rehabilitation scenarios. E.A., Jayawardena, S., & Morling, A. (2002)Additional work involving VR used in conjunc- Assessing stroke patients' ability to remembertion with fMRI is clearly warranted to provide to perform actions in the future using virtual re-new and exciting insights into the neurological ality, Proceedings of the 4th International Con-correlates of everyday memory and gain a ference on Disability, Virtual Reality and Associ-greater understanding of how damage to differ- ated Technologies, Hungary, 239-245.ent regions of the brain impacts upon everyday 10. Schacter, D.L., Glisky, E.L., & McGlynn,memory performance. S.M. (1990) Impact of memory disorders on
everyday life: awareness of deficits and returnREFERENCES to work, in: The Neuropsychology of Everyday
Life: Assessment and Basic Competencies,1. Durlach, N.I., and Mayor, A (1995). Virtual D.E. Tupper and K.D. Cicerone, eds., KluwerReality: Scientific and Technological Chal- Academic Publishers, Massachusetts, 1990,lenges, Durlach, N.I., and Mavor, A. (Eds), 231-257.
36
PENN ET AL.
11. Wechsler, D. Wechsler Memory Scale - Re- Andrew, C., Goparlen, N., Vythelingum, N.,vised. Psychological Corporation, San Antonio, Loannou, G., Simmons, A., & Morris, R.G.1987. (2004). Allocentric spatial memory activation12. Coughlan, A.K & Hollows, S.E. The Adult of the hippocampal formation measured usingMemory and Information Processing Battery, fMRI. Neuropsychology. 18 (3) 450-461A.K. Coughlan, St. James's Hospital, Leeds, 23. Milner, B., Corkin, S. & Treuber, H.L.1985. (1968), Further analysis of the hippocampal13. Warrington, E.K. Recognition Memory Test, amnesic syndrome: 14-year follow-up of HM,NFER-Nelson, Windsor, (1984). Neuropsychologia, 6, 215-234.Baddeley, A., Emslie, H., & Nimmo-Smith, I. 24. Glisky, E.L. (1995) Acquisition and transfer ofThe Doors and People Test, Thames Valley word processing skill by an amnesic patient,Test Co., Bury St Edmunds, Suffolk, 1994. Neuropsychological Rehabilitation, 5, 299-318.14. Baddeley, A.D. (1990) Human Memory: 25. Glisky, E.L., and Schacter, D.L. (1988) Long-Theory and Practice, Psychology Press, Hove, term retention of computer learning by patientsUK, 1990. with memory disorders, Neuropsychologia, 26,15. Neisser, U. (1978) Memory: What are the 173-178.important questions? in: Practical Aspects of 26. Glisky, E.L., & Schacter, D.L. (1986) Learn-Memory, Gruneberg, M. M., Morris, P.E. and ing and retention of computer-related vocabularySykes, R.N. eds., Academic Press, London, in amnesic patients: Method of vanishing cues,1978, 3-24. Journal of Clinical and Experimental Neuropsy-16. Sunderland, A., Harris, J.E., & Baddeley, chology, 8, 292-312.A.D. (1983) Do laboratory tests predict every- 27. Brooks, B.M., McNeil, J.E., Rose, F.D.,day memory? Journal of Verbal Learning and Greenwood, R.J., Attree, E.A., & Leadbetter,Verbal Behavior, 22, 341-357. A.G. (1999) Route learning in a case of amne-17. Banaji, M.R., & Crowder, R.G. (1989) The sia: A preliminary investigation into the efficacybankruptcy of everyday memory, American Psy- of training in a virtual environment, Neuropsy-chologist, 44,1185-1193. chological Rehabilitation 9, 63-76.18. O'Conner, M., & Cermack, L. S. (1987). Re- 28. Rose, F.D., Attree, E.A., Brooks, B.M., &habilitation of organic memory disorders. In M. Andrews, T.K. (2001) Learning and memory inJ. Meier, A. L. Benton, & L. Diller (Eds.) virtual environments: A role in neurorehabilita-Neuropsychological rehabilitation. New York: tion? Questions (and occasional answers) fromGuilford. the University of East London, Presence 10,19. Kirsch, N.L., Levine, S. P. Lajiness-O'neill, 345-358.R., & Schnyder, M. (1992). Computer-assisted 29. Stanton, D., Wilson, P., Duffy, H., and Fore-interactive task guidance: Facilitating the per- man, N. (2000) Virtual environments as spatialformance of a simulated vocational task. Jour- training aids for children and adults with physi-nal of Head Trauma Rehabilitation, 7 (3), 13-25. cal disabilities. 3rd International Conference on20. Skelton, R.W., Bukach, C.M., Laurance, Disability, Virtual Reality and Associated Tech-H.E., Thomas, K.G., Jacobs, J.W. (2000) Hu- nologies. Sardinia, 23rd-25th September.mans with traumatic brain injuries show place- 30. Stanton, D, Foreman, N., Wilson, P., Duffy,learning deficits in computer-generated virtual H. & Parnell, R. (2002) Use of virtual environ-space. Journal of Clinical Experimental Neuro- ments to acquire spatial understanding of real-psychology, 22, 157-75. world multi-level environments. Proceedings of21. Morris, R.G., Parslow, D., Fleminger, S., the 4th International Conference on Disability,Brooks, B., Brammer, M. & Rose, D. (2002) Virtual Reality and Associated technologies,Functional magnetic resonance imagining in- Hungary, 2002,13-18vestigation of allocentric spatial memory tested 31. Wilson, B.A. and Evans, J.J. (1996) Error-using virtual reality in patients with anoxic hip- free learning in the rehabilitation of people withpocampal damage, Proceedings of the 4th In- memory impairments, Journal of Head Traumaternational Conference on Disability, Virtual Re- Rehabilitation, 11, 54-64.ality and Associated Technologies, Hungary, 32. Andrews, T.K., Rose, F.D., Leadbetter,87-92 A.G., Attree, E.A. & Painter, J. (1995) The use22. Parslow, D.M., Rose, F.D., Brooks, B.M., of virtual reality in the assessment of cognitiveFleminger, S., Gray, J.A., Giampietro, V.,Brammer, M.J., Williams, S.C.R. Gasston, D.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ability, in: Proceedings of the 2nd TIDE Con- Contactgress, I. Placencia Porrero and R. Puig de laBellacasa, eds., lOS Press, Amsterdam, 1995, Paul Penn PhD276-279. School of Psychology.33. Rose, F.D., Brooks, B.M., Attree, E.A., University of East London. UK.Parslow, D.M., Leadbetter, A.G., McNeil, J.E., Telephone: +44(0) 208 223 [44241442514500]Jayawardena, S., Greenwood, R. & Potter, J. E-mail: [email protected](1999) A preliminary investigation into the useof virtual environments in memory retrainingafter vascular brain injury: Indications for futurestrategy? Disability and Rehabilitation, 21, 548-554.34. Pugnetti, L., Mendozzi, L., Brooks, B.M.,Attree, E.A., Barbieri, E., Alpini, D., Motta, A., &Rose, F.D. (1998) Active versus passive explo-ration of virtual environments modulates spatialmemory in MS patients: a yoked control study.The Italian Journal of Neurological Sciences 19,424-430.35. Rose, F.D., Brooks, B.M., & Attree, E.A.(2002) An exploratory investigation into the us-ability and usefulness of training people withlearning disabilities in a virtual environment,Disability and Rehabilitation, 24, 627-633.36. Kvavilashvili, L., & Ellis, J. Varieties of in-tention: Some distinctions and classifications(1996) in: Prospective Memory: Theory and Ap-plications, Brandimonte, M., Einstein, G.O. andMcDaniel, M.A. eds., Lawrence Erlbaum, NewJersey, 23-51.37. Craik, F.I.M. (1986) A functional account ofage differences in memory, in: Human Memoryand Cognitive Capabilities, Mechanisms andPerformances, Klix, F. and Hagendorf, H. eds.,Elsevier, Amsterdam, 1986, 409-422.38. Wilson, P.N., Foreman, N. & Tlauka, M.Transfer of spatial information from a virtual to areal environment in physically disabled children.(1996) Disability and Rehabilitation 18, 633-637.39. Rizzo, A., Klimchuk, D., Mitura, R., Bowerly,T., Shahabi, C., & Buckwalter, J.G. (2004). Di-agnosing Attention Disorders in a Virtual Class-room. IEEE Computer. 37 (5), 87-89.40. Deutsch, J., Latonio, J., Burdea, G., &Boian, R. (2001) Rehabilitation of Muscu-loskeletal Injuries Using the Rutgers Ankle Hap-tic Interface: Three Case Reports, EurohapticsConference, Birmingham UK, July 1-4, 2001
38

RIVA
Virtual Reality in the Treatment of Eating Disorders and Obesity:State of the Art and Future Challenges
G. Riva, Ph.D.
ATN-P Lab., Istituto Auxologico Italiano, Milan, Italy
Abstract: Virtual Reality (VR) is an advanced human-computer interface that allows the user to inter-act with and become immersed in a computer-generated environment in a naturalistic fashion.
Different clinical data suggest that VR can help in addressing two key features of eating disordersand obesity not always adequately addressed by existing approaches: body experience disturbancesand self-efficacy.
In fact, performance-based methods are the most effective in producing therapeutic change acrossbehavioral, cognitive, and affective modalities. The experiential approach allowed by VR helps pa-tients in discovering that difficulties can be defeated, so improving their cognitive and behavioralskills for coping with stressful situations. On the downside, the cost of this technology remains rela-tively high, its availability is still limited and some patients (1-2%) may experience simulation sick-ness.
The paper discusses the pros and cons of this approach presenting the results coming from the lastcontrolled clinical trials.
INTRODUCTION
Different new technologies have been intro- This feature of VR has been extensively used induced over the last few years that are increas- different clinical psychology treatments - fromingly finding application in health care delivery phobias to sexual disorders - and it is expectedfor patients with eating disorders and obesity. to increase in the future.5,6 In particular, an areaThese include self-help (supervised and unsu- in which VR may offer a competitive advantagepervised), telemedicine, telephone therapy, e- is the treatment of eating disorders and obesity.mail, Internet, computer software, CD-ROMs,portable computers, and virtual reality tech- Different clinical data suggest that VR can helpniques.1 One of the most promising is virtual in addressing two key features of eating disor-reality (VR), an advanced form of human- ders and obesity not always adequately ad-computer interface that allows the user to inter- dressed by existing approaches: body experi-act with and become immersed in a computer- ence disturbances and self-efficacy.7
generated environment in a naturalistic fash-ion.2 The paper discusses the pros and cons of this
approach presenting the results coming fromIn fact, therapists are using VR to provide a the last controlled clinical trials.new human-computer interaction paradigm inwhich users are active participants within a RATIONALE AND CLINICAL DATAcomputer-generated three-dimensional virtual3world. Using VR in this way, the patient is Distorted body image, negative emotions andmore likely not only to gain an awareness of lack of faith in the therapy are typical featureshis/her need to do something to create change of these disturbances and are the most difficultbut also to experience a greater sense of per- characteristics to change. One innovative ap-sonal efficacy.4 proach to their treatment is to enhance tradi-
39

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Hardware Graphic Workstation with high-end graphic card
Head Mounted Display or 3D shutter glasses
Tracking System (Head and Hands)
VR Gloves
Software VR environment
Table 1: VR Components
tional cognitive-behavioral therap (CBT) with cognitive-behavioral methods (see Table 1):the use of a virtual environment.h1e3X Countering, Alternative Interpretation, Label
Shifting, Deactivating the Illness Belief andA first approach is the one offered by the Inte- Temptation Exposure with Response Pre-grated Experiential Therapy (lET). Developed vention. 15'16
by Giuseppe Riva and his group inside the * the body experience of the subject. ToVREPAR and VEPSY Updated European reach this goal, the virtual environment inte-funded projects (http://www.cybertherapy.info) grated the therapeutic methods used byis a relatively short-term, patient oriented ap- Butter & Cash17 and Wooley & Wooley.18 Inproach that focuses on individual discovery.,t 012 particular in VREDIM the virtual environ-lET shares with CBT the use of a combination ment is used in the same way as guidedof cognitive and behavioral procedures to help imagery19 is used by the cognitive and vis-the patient identify and change the maintaining ual/motorial approach. Moreover, in termsmechanisms. However it is different for: of learning theory, repeated and prolonged
exposure with the conditioned stimulus"* Its use of Virtual Reality (VR): 10 VR ses- "seeing one's own body" is supposed to
sions. induce decreases in the conditioned nega-"* Its focus on the negative emotions related to tive reactivity by preventing negative rein-
the body, a major reason patients want to lose forcement, e.g., avoidance.2
weight. The VR sessions (see Figure 1) approximate"* Its focus on supporting the empowerment natural settings, providing an alternative for ex-
process. VR has the right features to support posure and desensitization exercises as well asempowerment process, since it is a special, a more general enhancement to therapy. Spe-sheltered setting where patients can start to cifically, VR is believed to increase motivationexplore and act without feeling threatened. by allowing individuals to virtually witness
changes in their behavior and shape and reachFor the virtual reality sessions, the Virtual Real- their own conclusions based on actual experi-
ity for Eating Disorders Modification - VREDIM -
is used. VREDIM is an enhanced version of the ence. During a typical VR sessions, patients areis ued.VREIM s a enhnce vesio ofthe asked to wear a head mounted VR display sys-original Virtual Reality for Body Image Modifica- ter An aroachesimouided imay s
tion(VEIM) mmesiv virualenvionmnt, tern. An approach similar to guided imagery istion (VEBIM) immersive virtual environment, used to lead the subject through various zones
previously used in different preliminary studies over the cue of te sons. Stimul thaton non-clinical subjects 13,14 over the course of ten sessions. Stimuli that
contribute to abnormal eating behaviors are
identified and associated anxiety and body ex-VREDIM is composed by 14 Virtual environ- p re c saet r ee o oii ai nments, used by the therapist during a 50-minutesession with the patient. 1 After a first assess- Subjects are also asked to identify figures thatment session, the next 9 sessions are used to most closely resemble their current and idealassess and modify: body sizes. They are also confronted with a
photograph of their actual body.* the symptoms of anxiety related to food ex-
posure. This is done by integrating different
40
RIVA
This approach was validated through different likely to report increased self-efficacy and moti-case studies 21 and trials. In the first one, uncon- vation to change.trolled, three groups of patients were used2 2 :patients with Binge Eating Disorders (BED), In a second one, the same randomized ap-patients with Eating Disorders Not Otherwise proach was used with a sample of 36 womenSpecified (EDNOS), and obese patients with a with BED. 12 The results showed that 77% of thebody mass index higher than 35. All patients ECT group quit binging after 6 months versusparticipated in five biweekly sessions of the 56% for the CBT sample and 22% for the nutri-therapy. All the groups showed improvements in tional group sample. Moreover, the ECT sampleoverall body satisfaction, disordered eating, and reported better scores in most psychometricrelated social behaviors, although these tests including EDI-2 and body image scores.changes were less noticeable in the EDNOS In the final one, recently presented in the Medi-group. cine Meets Virtual Reality Conference 2005, lET
was compared with nutritional and cognitive-More recently, the approach was tested in dif- behavioral treatments, using a randomized con-ferent controlled studies. The first one involved trolled trial, in a sample of 211 female obesetwenty women with BED who were seeking resi- patients. Both lET and CBT produced a betterdential treatment.11 The sample was assigned weight loss than NT after a 6-month follow-up.randomly to lET or to CBT based nutritional However, lET was able to significantly improve,therapy. Both groups were prescribed a 1,200- over CBT and NT, both body image satisfactioncalorie per day diet and minimal physical activ- and self-efficacy. This change produced a re-ity. Analyses revealed that although both groups duction in the number of avoidance behaviorswere binge free at 1-month follow-up, lET was as well as an improvement in adaptive behav-significantly better at increasing body satisfac- iors.tion. In addition, lET participants were more
Figure 1: A patient is trying the Integrated Experiential Therapy
41
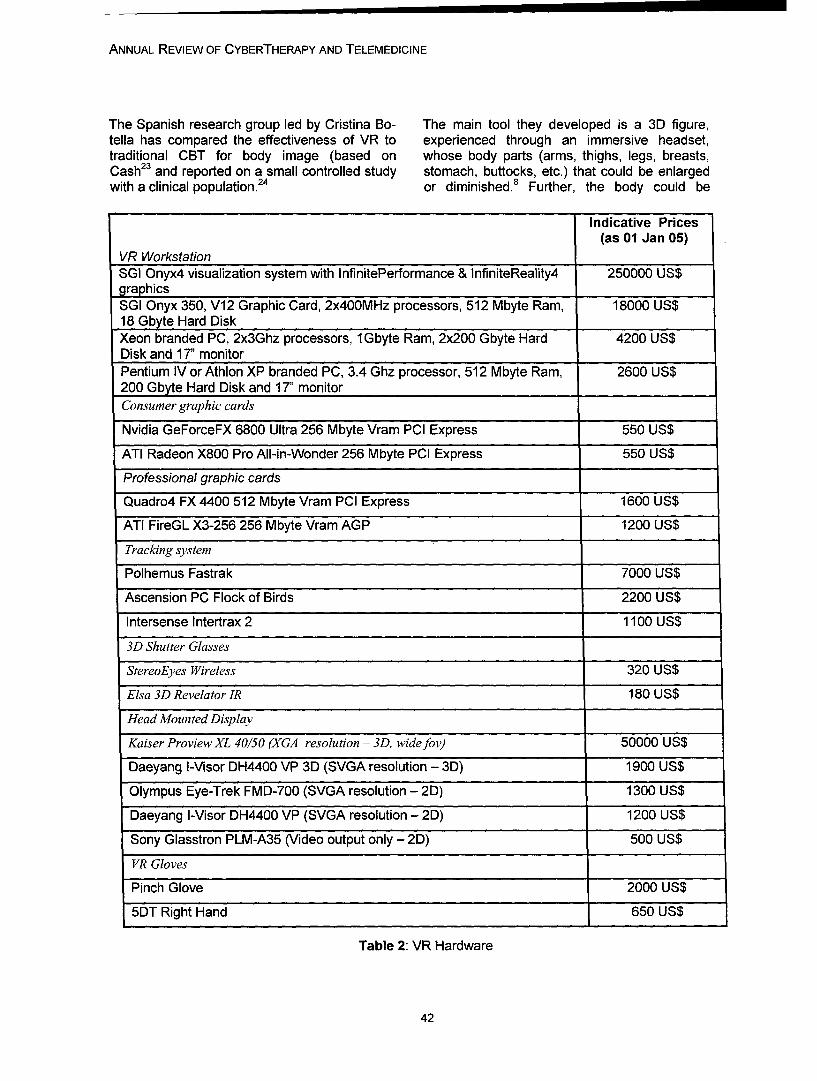
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
The Spanish research group led by Cristina Bo- The main tool they developed is a 3D figure,tella has compared the effectiveness of VR to experienced through an immersive headset,traditional CBT for body image (based on whose body parts (arms, thighs, legs, breasts,Cash23 and reported on a small controlled study stomach, buttocks, etc.) that could be enlargedwith a clinical population.24 or diminished.8 Further, the body could be
Indicative Prices(as 01 Jan 05)
VR WorkstationSGI Onyx4 visualization system with InfinitePerformance & InfiniteReality4 250000 US$graphicsSGI Onyx 350, V12 Graphic Card, 2x400MHz processors, 512 Mbyte Ram, 18000 US$18 Gbyte Hard DiskXeon branded PC, 2x3Ghz processors, 1Gbyte Ram, 2x200 Gbyte Hard 4200 US$Disk and 17" monitorPentium IV or Athlon XP branded PC, 3.4 Ghz processor, 512 Mbyte Ram, 2600 US$200 Gbyte Hard Disk and 17" monitorConsumer graphic cards
Nvidia GeForceFX 6800 Ultra 256 Mbyte Vram PCI Express 550 US$
ATI Radeon X800 Pro All-in-Wonder 256 Mbyte PCI Express 550 US$
Professional graphic cards
Quadro4 FX 4400 512 Mbyte Vram PCI Express 1600 US$
ATI FireGL X3-256 256 Mbyte Vram AGP 1200 US$
Tracking system
Polhemus Fastrak 7000 US$
Ascension PC Flock of Birds 2200 US$
Intersense Intertrax 2 1100 US$
3D Shutter Glasses
StereoEyes Wireless 320 US$
Elsa 3D Revelator IR 180 US$
Head Mounted Display
Kaiser Proview XL 40/50 (XGA resolution - 3D, wide fov) 50000 US$
Daeyang I-Visor DH4400 VP 3D (SVGA resolution - 3D) 190.0 US$
Olympus Eye-Trek FMD-700 (SVGA resolution - 2D) 1300 US$
Daeyang I-Visor DH4400 VP (SVGA resolution - 2D) 1200 US$
Sony Glasstron PLM-A35 (Video output only - 2D) 500 US$
VR Gloves
Pinch Glove 2000 US$
5DT Right Hand 650 US$
Table 2: VR Hardware
42
RIVA
evaluated wholly or in parts and placed in differ- relatively high (see Table 1) and availability isent contexts (for instance, in the kitchen, before still limited: a typical VR system as the one usedeating, after eating, facing attractive persons, in the studies discussed before costs betweenetc.). 15000 and 25000 euro (hardware 10000-15000
euro; software: 5000-10000 euro).Within the published study, five patients - 3 withAnorexia Nervosa and 2 with Bulimia Nervosa Finally, communication networks have the po-completed the traditional treatment and 8 - 4 tential to transform VEs into shared worlds inwith Anorexia Nervosa and 4 with Bulimia Ner- which individuals, objects, and processes inter-vosa - completed the VR condition. act without regard to their location. In the next
five years, such networks will probably mergeAlthough both groups showed improvements on VR and telemedicine applications allowing us togeneral ED measures, there were no significant use VR for such purposes as distance learning,between-group differences. However, the VR distributed training, and e-therapy.group did show greater improvement on meas-ures of body image, dysphoria, and anxiety, ACKNOWLEDGMENTSleading the authors to conclude that VR targetsdisturbances in body image better than stan- The present work was partially supported by thedard CBT. On a 10-point scale, patients rated Italian MIUR FIRB programme (Projec "Neurotivthe realism of VR from 7 to 9. Since then, the Managed care basata su telepresenzagroup has also developed a VR simulator of immersiva virtuale per /'assessment efood and eating 25 actually under evaluation with riabilitazione in neuro-psicologia e psicologiapatients. clinica" - RBNEO1W8WH- hthxll
www.neurotivyorg - and Project "Realta virtualeCONCLUSIONS come strumento di valutazione e trattamento in
psicologia clinica: aspetti tecnologici,In summary, the published data suggest that VR ergonomici e clinici" - RBAU014JE5).can help in addressing two key features of eat-ing disorders and obesity not always adequately REFERENCESaddressed by existing approaches: body experi-ence disturbances and self-efficacy. VR tech- 1. Myers, T. C., Swan-Kremeier, L., Wonderlich,nology offers an innovative approach to the S., Lancaster, K., & Mitchell, J. E.treatment of body image disturbance, a difficult (2004). The use of alternative deliveryconcept to address in therapy. Previously, cog- systems and new technologies in thenitive-behavioral and feminist approaches have treatment of patients with eating disor-been the standard interventions, although in our ders. International Journal of Eatingexperience, it seems that many patients con- Disorders, 36(2), 123-143.tinue to struggle with negative body image post- 2. Riva, G., Botella, C., Legeron, P., & Optale,treatment. G. (Eds.). (2004b). Cybertherapy: Inter-
net and virtual reality as assessmentAs emphasized by social cognitive theory, per- and rehabilitation tools for clinical psy-formance-based methods are the most effective chology and neuroscience. Amsterdam:in producing therapeutic change across behav- lOS Press; Online: http:IIioral, cognitive, and affective modalities.2 6'27 The www.cvbertherapyrinfo/paqes!proposed experiential approach could help pa- book3.htm.tients in discovering that difficulties can be de- 3. Rizzo, A., Schultheis, M. T., Kerns, K., &feated, so improving their cognitive and behav- Mateer, C. (2004). Analysis of assetsioral skills for coping with stressful situations. for virtual reality applications in
neuropsychology. NeuropsychologicalOn the downside, a limited number of patients Rehabilitation, 14(1-2), 207-239.(less than 2%) experienced simulator sickness, 4. Riva, G., & Gamberini, L. (2000). Virtual real-which consists of nausea, disorientation, and ity as telemedicine tool: Technology,eye strain or blurred vision during and after use. ergonomics and actual applications.In addition, the cost of this technology remains Technology and Health Care, 8(2), 113-
43
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
127. 14. Riva, G. (1998a). Modifications of body im-5. Botella, C., Quero, S., Banos, R. M., Perpina, age induced by virtual reality. Percep-
C., Garcia Palacios, A., & Riva, G. tual and Motor Skills, 86, 163-170.(2004). Virtual reality and 15. Riva, G. (1998b). Virtual reality vs. Virtualpsychotherapy. Stud Health Technol body: The use of virtual environments inInform, 99, 37-54. the treatment of body experience distur-
6. Riva, G. (Ed.). (1997b). Virtual reality in bances. CyberPsychology & Behavior,neuro-psycho-physiology: Cognitive, 1(2), 129-137.clinical and methodological issues in 16. Schlundt, D. G., & Johnson, W. G. (1990).assessment and rehabilitation. Amster- Eating disorders: Assessment anddam: lOS Press. Online: http:// treatment. Needham Heights, MA: Allynwww.cvberthera v.info/paaes! and Bacon.bookl.htm. 17. Butters, J. W., & Cash, T. F. (1987). Cogni-
7. Riva, G., Bacchetta, M., Cesa, G., Conti, S., tive-behavioral treatment of women's& Molinari, E. (2004a). The use of VR in body image satisfaction: A controlledthe treatment of eating disorders. outcome-study. Journal of ConsultingStudies in Health Technology and and Clinical Psychology, 55, 889-897.Informatics, 99, 121-163. 18. Wooley, S. C., & Wooley, 0. W. (1985). In-
8. Perpifia, C., Botella, C., & Bahos, R. M. tensive out-patient and residential trat-(2003). Virtual reality in eating disor- ment for bulimia. In D. M. Garner & P.ders. European Eating Disorders E. Garfinkel (Eds.), Handbook of psy-Review, 11(3), 261-278. chotherapy for anorexia and bulimia
9. Riva, G., Bacchetta, M., Cesa, G., Conti, S., (pp. 120-132). New York: Guilford& Molinari, E. (2002b). E-health in Press.eating disorders: Virtual reality and 19. Leuner, H. (1969). Guided affective im-telemedicine in assessment and agery: A method of intensive psycho-treatment. Stud Health Technol Inform, therapy. American Journal of Psycho-85, 402-408. therapy, 23, 4-21.
10. Riva, G., Bacchetta, M., Baruffi, M., & 20. Hilbert, A., Tuschen-Caffier, B., & Vogele,Molinari, E. (2001). Virtual reality-based C. (2002). Effects of prolonged and re-multidimensional therapy for the peated body image exposure in binge-treatment of body image disturbances eating disorder. Journal ofin obesity: A controlled study. Psychosomatic Research, 52(3), 137-Cyberpsychology and Behavior, 4(4), 144.511-526. 21. Riva, G., Bacchetta, M., Baruffi, M., Rinaldi,
11. Riva, G., Bacchetta, M., Baruffi, M., & S., & Molinari, E. (1999). Virtual realityMolinari, E. (2002a). Virtual-reality- based experiential cognitive treatmentbased multidimensional therapy for the of anorexia nervosa. Journal oftreatment of body image disturbances Behavioral Therapy and Experimentalin binge eating disorders: A preliminary Psychiatry, 30(3), 221-230.controlled study. IEEE Transactions on 22. Riva, G., Bacchetta, M., Baruffi, M., Rinaldi,Information Technology in Biomedicine, S., Vincelli, F., & Molinari, E. (2000).6(3), 224-234. Virtual reality based experiential
12. Riva, G., Bacchetta, M., Cesa, G., Conti, S., cognitive treatment of obesity and& Molinari, E. (2003). Six-month follow- binge-eating disorders. Clinicalup of in-patient experiential-cognitive Psychology and Psychotherapy, 7(3),therapy for binge eating disorders. 209-219.CyberPsychology & Behavior, 6(3), 23. Cash, T. F. (1996). The treatment of body251-258. image disturbances. In J. K. Thompson
13. Riva, G. (1997a). The virtual environment (Ed.), Body image, eating disorders andfor body-image modification (vebim): obesity (pp. 83-107). Washington, DC:Development and preliminary evalua- APA - American Psychological Associa-tion. Presence, Teleoperators, and Vir- tion.tual Environments, 6(1), 106-117. 24. Perpifia, C., Botella, C., Bathos, R. M.,
44
RIVA
Marco, J. H., Alcahiz, M., & Quero, S.(1999). Body image and virtual reality ineating disorders: Exposure by virtualreality is more effective than the classi-cal body image treatment? CyberPsy-chology & Behavior, 3(2), 149-159.
25. Lozano, J. A., Alcaniz, M., Gil, J. A., Moser-rat, C., Juan, M. C., Grau, V., et al.(2002). Virtual food in virtual environ-ments for the treatment of eating disor-ders. Stud Health Technol Inform, 85,268-273.
26. Alcahiz, M., Bahos, R., Botella, C., & Rey,B. (2003). The emma project: Emotions as adeterminant of presence. PsychNology Journal,1(2), 141-150. On-line: http:IIwww. psychnologyo. rg/article204. htm.27. Bandura, A. (1985). Social foundation of
thought and action: A social cognitivetheory. Englewood Cliffs, NJ: Prentice-Hall.
Contact
Giuseppe RivaApplied Technology for Neuro-Psychology LabIstituto Auxologico ItalianoEmail: [email protected]
45

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
46
Annual Review of CyberTherapy and Telemedicine
Virtual Technologies for Extreme Environment Effect Mitigation
E. Gaia, Dr. Ing
Alenia Spazio S.p.A., Torino Italy
Abstract: This paper examines the demands of a manned system operating in an extreme environ-ment, where there is the need to enhance or at least maintain crew health, team spirit and cohesion,and how nouvelles techniques based on Virtual Reality technologies can provide some answers. Atypical example is a manned mission to Mars with a crew of 4-8 astronauts where it is mandatory tomaintain their psychological health for a mission that is envisaged to last from two to three years.They will have to work and live in an artificial environment with limited resources (for example com-munication capability with ground, due to the distances involved, cannot be a direct two way system)and living volumes. The paper proposes some possible fields of investigation. It will also consider thefact of how these innovative technologies based on Virtual Reality will have to be developed andtested.
INTRODUCTION
In the next 25 years we can expect to see two possible support, and it is expected that VR/ARthings. First human beings will be installed in techniques will be widely employed to providevarious extreme environments of which one can this support, augmenting crew capability in con-be the Moon or even Mars. On the other hand trolling the overall system, robots and handlingmany new Virtual Reality (VR) applications will communications. It would not be surprising, forbe available to augment our capabilities in vari- example, if VR/AR based training techniquesous areas from entertainment to medicine and were employed both on ground in preparing theengineering, but it is also possible to envisage mission and in orbit to handle the unexpected.that VR or AR (Augmented Reality) may be es- But there is another area where VR/AR may bepecially employed where the human being is employed, that is in the maintenance of thefacing highly demanding challenges. In this pa- crew's psychical well-being and in maintainingper what might be used in future manned space the team's positive attitude and cohesion.missions is discussed with a special emphasison the possible utilisation of VR/AR to supportthe maintenance of on-board crew well-being. TYPICAL MISSION: EXPLORATION SPIRAL
3/LUNAR BASE AND MARS TESTBEDIDENTIFICATION OF THE PROBLEM
From NASA Requirements Document "ESMD-The future Moon and Mars exploration missions RQ-0013". "Exploration Spiral 3 will establishforesee, after some pilot missions to the Moon, the capability to conduct routine human long-a series of long missions with human perma- duration missions at a lunar base to test outnence on board. These range from perma- technologies and operational techniques fornence on the Moon surface of one year (the trip expanding the human presence to Mars andof 3-4 days to the Moon is negligible compared beyond. Missions in Spiral 3 will extend up toto the permanence) to a mission to Mars of several months in duration at the lunar poles orthree years of which up to one may be spent in equatorial region in order to serve as an opera-travelling to and fro. The envisaged size of the tional analog of future Mars missions. Spiral 3crew ranges from 4 to 8 people, each of whom will require the development and deployment ofis highly motivated and knowledgeable. The habitats and surface power systems. ... Oncecrew will certainly be specifically selected and the surface systems are in place, successivelyhighly trained. In addition, they will receive all longer missions will be conducted to increase
47
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
the understanding of system technical perform- o Eating, sleeping and hygieneance (including health and human systems), Free time.and to provide increasing levels of operationalautonomy capabilities that will be necessary for Identified issues:future human Mars exploration missions."
Related Main Mission Characteristics: Communications: although the distancebetween the Moon and the Earth is relatively"small, communication delay is of approximately
* Crew: 4 Astronauts. 6 seconds each leg. This will require a different"* Gravity: 1/6 of the gravity of the Earth concept of control for all used automated sys-"* Mission Duration: tems. Now most of the controls are performed
on ground by the flight control personnel. Forvoice communication it might be only a nui-
o 6 days travel from Earth to Moon; sance but its effects on the crew over a longo 42 to 600 days permanence on the sur- period are unknown. In case of Mars mission
face; the communication delay can be up to 20 min-o 7.5 days from Moon back to Earth. utes each leg: this will sharply increase the
communication problem.
* Habitation Facilities:* Safety & Isolation: the handling of emer-gencies during these exploration missions is
o Transportation phases Crew Exploration completely innovative with respect to the ap-Vehicle (CEV) plus Mission Module proach taken for the Space Station where anapprox. 14 m3 volume available for the injured or ill crew member can be back on thecrew; Earth in approximately 12-16 hours. Starting
o Up to 200 m3 gross volume available for from the Moon surface it would take as a mini-the crew for habitability and working areas. mum 5-6 days and from Mars up to 6 months toThis volume may be increased with an return to Earth, so most of the emergenciesadditional logistic cargo module that can must be handled there.be connected to the main habitation andlaboratory module. 0 Group dynamics and roles of each astro-
naut: this is one of the keys to mission suc-* Surface Crew working and related Activi- cess, which means being able to maintain -
ties: throughout the mission and despite any prob-lem that may arise - a positive attitude of each
"o It is expected that in one year there will be single component of the team as well as of the
more than 200 Extra Vehicular Sorties with team itself.
two people in each one; POSSIBLE ROLE OF VR
"o Control the extensive utilization of robotsand automated Rovers for exploration Most probably there will be quite ample applica-
"o Other activities foreseen are system main- tions of VR/AR techniques to improve the qual-tenance and performance of experiments ity of the working environment on board duringto prepare for Mars missions. these long exploration missions. These applica-
tions can be envisaged in the field of:* Surface Crew off-duty and related Activities:
* Communications between Moon base and
the Earth or between the exploring astronauts"o Housekeeping and the Moon Base."o Exercise & health maintenance * Training (on the job)
* Automatics and Robotics command/control
48
GAlA
* Support to procedure implementation, * Communication system: How to overcomeLeisure i.e. movies and scenery display (some the time lag constraint maintaining a level ofstudents have conceived a relaxation room with "quality" and "effectiveness" in communication?VR) - especially if it is used as a keystone for well-
being maintenance.All these applications are up to now perceived 0 Psychological Health maintenance: Howas single pieces of application, each developed and when can VR/AR be used to support theto handle a specific need but not linked one to Crew's Psychological Health?the other. What has been missing up to now is 0 Psychological Health monitoring system:an integrated system that can perform all that How can the psychological well-being of thehas been mentioned before, but beyond that singular member and of the group be moni-will be able to take care of the maintenance of tored?the psychological well-being of the astronautsboth at individual level as well as at team level. f Training and other VR/AR applications usedThis system shall be capable to move from pre- for crew s ortriAR are r s candi-sent applications of VR techniques aimed at date techniques for training as well as to pro-restoring people's well-being by, for example, vide information and control capability to a crewtreating the fear of flying like the VR technique member but can this VR/AR system be ex-described in reference 2 to a nouvelle application ploited to the level required without overloadingof monitoring and maintaining the human be- the human being?ing's well being. 0 Human VR interfaces: New interfaces are
being developed including the BCI: how canAn integrated system based on VR/AR tech- these be used without violating ethical rules?nique of exchange of information and controlwith the crew also with the use of nouvelle tech- If such a system can be developed and ac-niques of Brain Computer Interface (BCI) can cepted for utilisation would it be possible to re-be developed. This integrated system can not fer to it as VR/AR system or must we use a newonly give the crew an effective support both in word like an enhanced reality system?working and non-working activities but, since itcan be envisaged that it would be capable of CONCLUSIONmonitoring their health, it can also intervene bytaking actions to reduce/control potentially dan- This paper was not aimed at giving solutionsgerous situations. but more at collecting questions and doubts.
Nevertheless two positive issues can be gath-DISCUSSION ered from what was presented before:
Clearly a system such as the one proposed is 0 First how extreme environments can benot available in the short term and it will take a used as technological trend identification andwell coordinated effort to develop; on the other then can become valid test beds for researchhand, there are some issues - some simple but and development of new techniquessome others much more complex involving eth- How a user centred approach is more and moreics - that it is better to start discussing now. needed in order not to be overcome by theThe following are the issues to be investigated technological push especially in new areas likein order to set the requirements capable to de- VR/AR.scribe a system to be produced that respectsthe ethics of the human being but on the other REFERENCEShand is capable of guaranteeing the missionsuccess: [1] Exploration Crew Transportation System
Requirements Document (Spiral 3) Version Pre-* Private experiences vs. common experi- liminary - Revision D 22 Feb 2005 (ESMD-RQ-ence (screen vs. helmet or both): How can the 0013) - htt_://exploration.nasa•,ov/documents/group dynamics be supported? documents~html

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
[2] The Treatment of Fear of flying: A ControlledStudy of Imaginal and Virtual Reality GradedExposure Therapy: Brenda K. Wiederhold, etall. - IEEE Transactions on Information Tech-nology in Biomedicine, Vol. 6, NO. 3, Septem-ber 2002.
Contact
Enrico GaiaAlenia Spazio S.p.A.Torino, ItalyPhone: +39 011 7180742Email: Enrico.Gaiat-Mleniasnazio.it
50

Annual Review of CyberTherapy and Telemedicine
EvaluationStu s
A Computational Model of Emotion and Personality:
Applications to Psychotherapy Research and Practice
E. Hudlicka, Ph.D.
Psychometrix Associates, Inc. Blacksburg, Virginia
Abstract: VR applications in psychotherapy are gaining prominence in the research community andacceptance among practitioners, with particular successes in the area of phobia treatments. How-ever, a promising technology remains unexplored: computational models of cognition and emotion.Cognitive models (also termed cognitive- or agent-architectures) aim to emulate cognitive processingsuch as attention, perception, and decision-making, and are used by cognitive scientists to advanceunderstanding of the mechanisms and structures mediating cognition. These models are also used inapplied settings to improve the realism of training and assessment environments, and to improvehuman-computer interaction and system design. Recently, architectures have been developed thatexplicitly represent emotions: both emotion appraisal processes, and effects of emotions on cogni-tion. Such computational models of cognition and emotion have two types of applications in cy-bertherapy. First, they can enhance the realism of a synthetic agents used in VR assessment andtreatment environments (e.g., avatars used in social phobia treatment). Second, they have the poten-tial to advance our understanding of the etiology and treatment of a variety of affective disorders, byenabling the modeling of the mechanisms of cognitive-affective interactions that play central role inthese disorders, and in their treatments. In this paper I first describe a cognitive-affective architec-ture capable of modeling the dynamic generation of emotions (affect appraisal), and selected effectsof emotion on cognition. I then describe possible applications of this architecture to psychotherapypractice and research.
INTRODUCTION
VR applications in psychotherapy are gaining While a number of researchers are advocatingprominence in the research community and ac- the use of avatars in VR therapy environ-ceptance among practitioners. Significant suc- ments,10 and promising research efforts exist,1"cess has been achieved with VR therapies little work has been done in coupling syntheticaimed at a variety of phobias and PTSD (e.g., avatars with cognitive-affective architectures.http://www~virtuallybetter.com/). 1 However, a Thus, the potential of cognitive architectures,promising technology remains unexplored: com- and associated computational modeling re-putational models of cognition and emotion. search methods, have not been explored in psy-Cognitive models (also termed cognitive- or chotherapy research and practice. The primaryagent-architectures) aim to emulate cognitive purpose of this paper is to introduce computa-processing such as attention, perception, learn- tional cognitive-affective architectures to theing, problem-solving, planning and decision- cybertherapy community, and describe exam-making, and are used by cognitive scientists to pies of possible applications in psychotherapyadvance understanding of the mechanisms and research and practice. These include the en-structures mediating cognition.2 These models hancement of synthetic avatars in VR treatmentare also used in applied settings to improve and assessment environments (e.g., distinct3training and human-system design. Recently, avatars could be defined to support dynamic,architectures have been developed that explic- adaptive interaction during social phobia treat-itly represent emotions: both emotion appraisal ment, each with different behavioral characteris-processes, and effects of emotions on cogni- tics to practice particular situations), and thetion.49 development of computational models aimed at
51
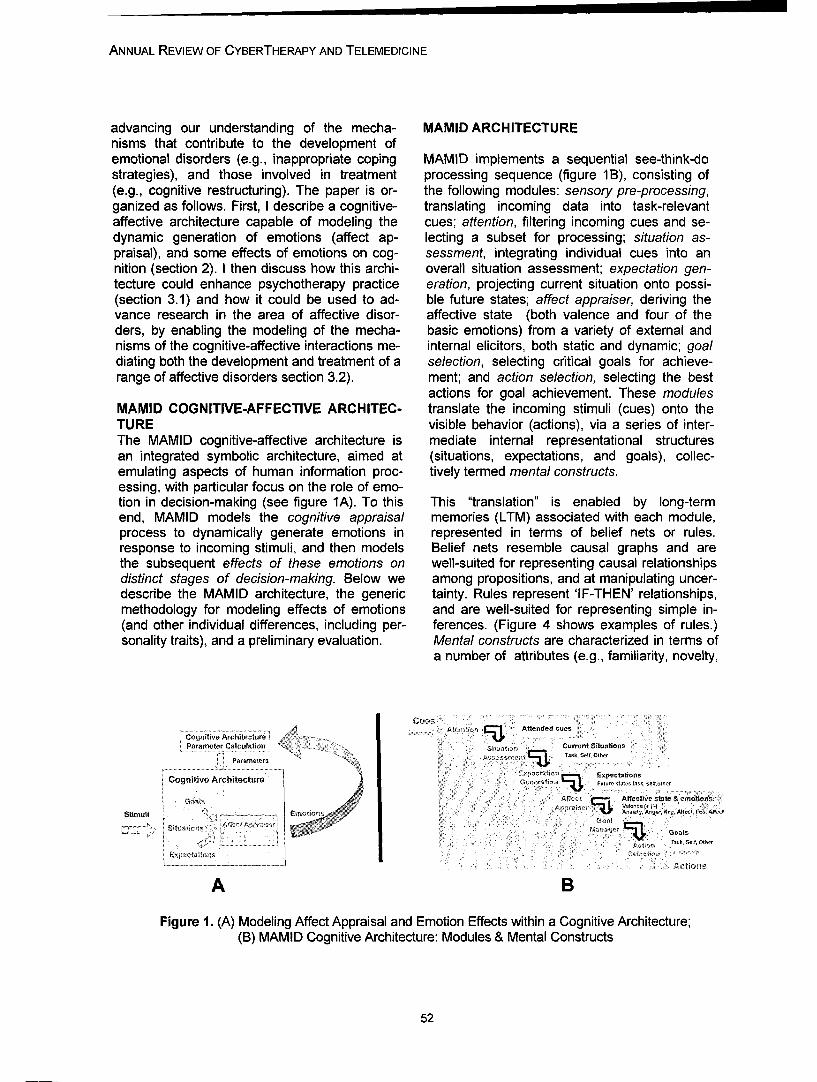
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
advancing our understanding of the mecha- MAMID ARCHITECTUREnisms that contribute to the development ofemotional disorders (e.g., inappropriate coping MAMID implements a sequential see-think-dostrategies), and those involved in treatment processing sequence (figure 1B), consisting of(e.g., cognitive restructuring). The paper is or- the following modules: sensory pre-processing,ganized as follows. First, I describe a cognitive- translating incoming data into task-relevantaffective architecture capable of modeling the cues; attention, filtering incoming cues and se-dynamic generation of emotions (affect ap- lecting a subset for processing; situation as-praisal), and some effects of emotions on cog- sessment, integrating individual cues into annition (section 2). I then discuss how this archi- overall situation assessment; expectation gen-tecture could enhance psychotherapy practice eration, projecting current situation onto possi-(section 3.1) and how it could be used to ad- ble future states; affect appraiser, deriving thevance research in the area of affective disor- affective state (both valence and four of theders, by enabling the modeling of the mecha- basic emotions) from a variety of external andnisms of the cognitive-affective interactions me- internal elicitors, both static and dynamic; goaldiating both the development and treatment of a selection, selecting critical goals for achieve-range of affective disorders section 3.2). ment; and action selection, selecting the best
actions for goal achievement. These modulesMAMID COGNITIVE-AFFECTIVE ARCHITEC- translate the incoming stimuli (cues) onto theTURE visible behavior (actions), via a series of inter-The MAMID cognitive-affective architecture is mediate internal representational structuresan integrated symbolic architecture, aimed at (situations, expectations, and goals), collec-emulating aspects of human information proc- tively termed mental constructs.essing, with particular focus on the role of emo-tion in decision-making (see figure 1A). To this This "translation" is enabled by long-termend, MAMID models the cognitive appraisal memories (LTM) associated with each module,process to dynamically generate emotions in represented in terms of belief nets or rules.response to incoming stimuli, and then models Belief nets resemble causal graphs and arethe subsequent effects of these emotions on well-suited for representing causal relationshipsdistinct stages of decision-making. Below we among propositions, and at manipulating uncer-describe the MAMID architecture, the generic tainty. Rules represent 'IF-THEN' relationships,methodology for modeling effects of emotions and are well-suited for representing simple in-(and other individual differences, including per- ferences. (Figure 4 shows examples of rules.)sonality traits), and a preliminary evaluation. Mental constructs are characterized in terms of
a number of attributes (e.g., familiarity, novelty,
Cognitive Architecture i tT i l-J, A n c.esParameter Calculation ! Current S:tU ,tn :
Parameters s, at055
.......... ............. .: : . ..Cognitivv Architecture F;t
Goal) t AffectMveestate & emotiuse-l
Stimuli Emotions,5
1.0k, Salt, Other
Expcxfntior,
A B
Figure 1. (A) Modeling Affect Appraisal and Emotion Effects within a Cognitive Architecture;(B) MAMID Cognitive Architecture: Modules & Mental Constructs
52
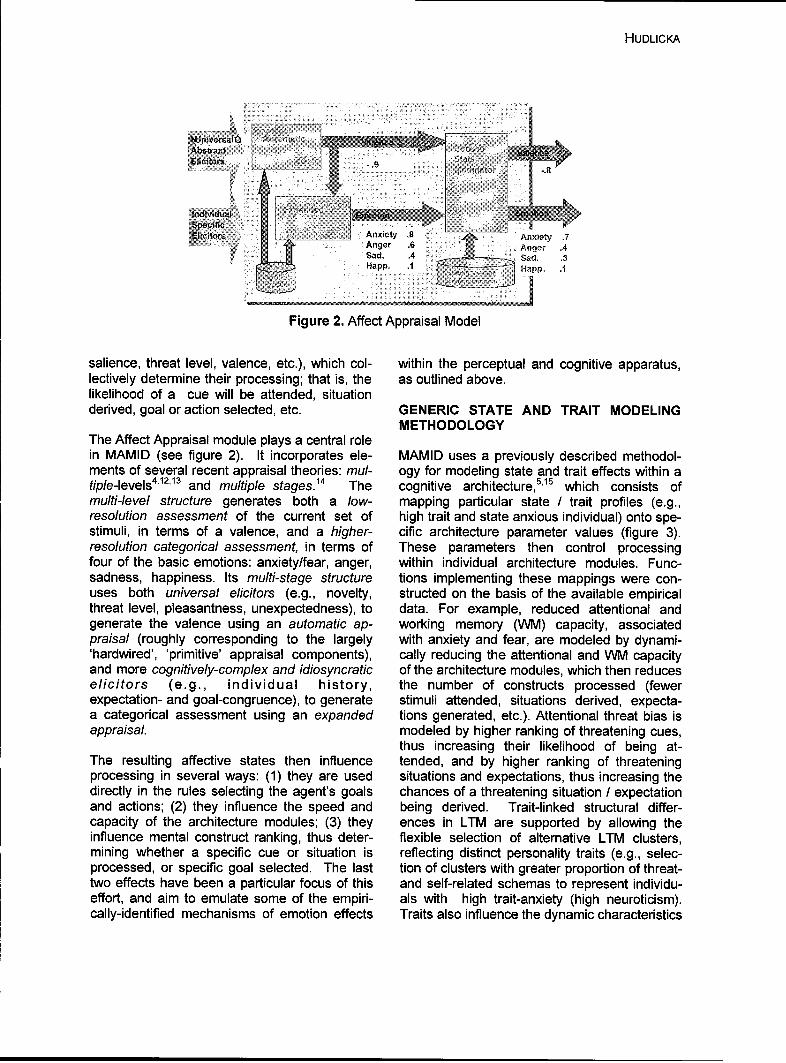
HUDLICKA
E I Anxiety 87Ane .6 An~ger .4Sasd. .4 a, .
Figure 2. Affect Appraisal Model
salience, threat level, valence, etc.), which col- within the perceptual and cognitive apparatus,lectively determine their processing; that is, the as outlined above.likelihood of a cue will be attended, situationderived, goal or action selected, etc. GENERIC STATE AND TRAIT MODELING
METHODOLOGYThe Affect Appraisal module plays a central rolein MAMID (see figure 2). It incorporates ele- MAMID uses a previously described methodol-ments of several recent appraisal theories: mul- ogy for modeling state and trait effects within atiple-levels4'12'13 and multiple stages. 14 The cognitive architecture5,1'5 which consists ofmulti-level structure generates both a low- mapping particular state / trait profiles (e.g.,resolution assessment of the current set of high trait and state anxious individual) onto spe-stimuli, in terms of a valence, and a higher- cific architecture parameter values (figure 3).resolution categorical assessment, in terms of These parameters then control processingfour of the basic emotions: anxiety/fear, anger, within individual architecture modules. Func-sadness, happiness. Its multi-stage structure tions implementing these mappings were con-uses both universal elicitors (e.g., novelty, structed on the basis of the available empiricalthreat level, pleasantness, unexpectedness), to data. For example, reduced attentional andgenerate the valence using an automatic ap- working memory (WM) capacity, associatedpraisal (roughly corresponding to the largely with anxiety and fear, are modeled by dynami-
'hardwired', 'primitive' appraisal components), cally reducing the attentional and WM capacityand more cognitively-complex and idiosyncratic of the architecture modules, which then reduceselicitors (e.g., individual history, the number of constructs processed (fewer
expectation- and goal-congruence), to generate stimuli attended, situations derived, expecta-a categorical assessment using an expanded tions generated, etc.). Attentional threat bias isappraisalF modeled by higher ranking of threatening cues,
thus increasing their likelihood of being at-The resulting affective states then influence tended, and by higher ranking of threateningprocessing in several ways: (1) they are used situations and expectations, thus increasing thedirectly in the rules selecting the agent's goals chances of a threatening situation / expectation
and actions; (2) they influence the speed and being derived. Trait-linked structural differ-capacity of the architecture modules; (3) they ences in LTM are supported by allowing theinfluence mental construct ranking, thus deter- flexible selection of alternative LTM clusters,mining whether a specific cue or situation is reflecting distinct personality traits (e.g., selec-processed, or spe cific goal selected. The last tion of clusters with greater proportion of threat-two effects have been a particular focus of this and self-related schemas to represent individu-effort, and aim to emulate some of the empiri- als with high trait-anxiety (high neuroticism).cally-identified mechanisms of emotion effects Traits also influence the dynamic characteristics
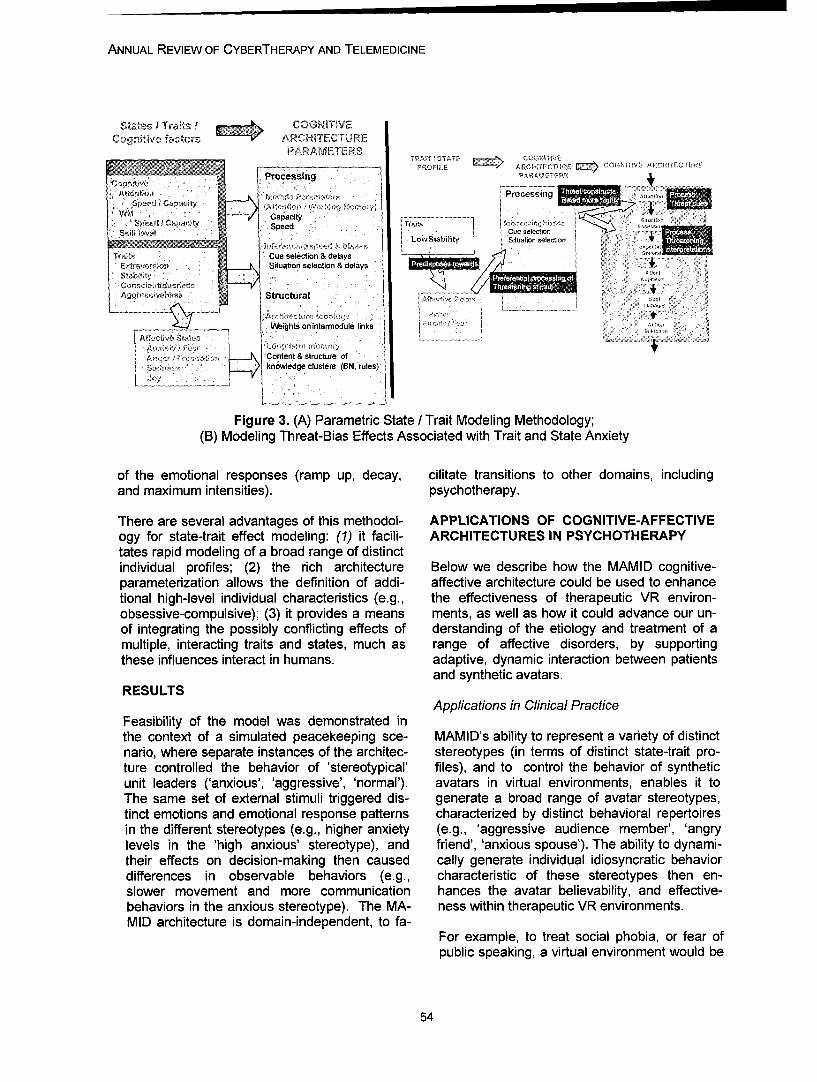
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
SII tesI Traits I 1 COGNITIVECognitive factors- ARCHITECTURE
PARAAMETERS7~ 1AIT 1 ST YEII IJ~" •'~~~ R W U ,ý A•pO F L A RrO M T E C T rU R E C O G :-N M V E A lR H I r M JCT R E
Processing
Sp d Capacity ...... ......a,,l o~,• Speed 'Tr.. ,=ooi,
L.oStab~litSituation selectionTrait• :Cue selection & delays
Situation selection & delays
A e I Structural
Weights onintermodule links
SsContent tructure ofknowledge clusters (BN, rules)
Figure 3. (A) Parametric State / Trait Modeling Methodology;(B) Modeling Threat-Bias Effects Associated with Trait and State Anxiety
of the emotional responses (ramp up, decay, cilitate transitions to other domains, includingand maximum intensities), psychotherapy.
There are several advantages of this methodol- APPLICATIONS OF COGNITIVE-AFFECTIVEogy for state-trait effect modeling: (1) it facili- ARCHITECTURES IN PSYCHOTHERAPYtates rapid modeling of a broad range of distinctindividual profiles; (2) the rich architecture Below we describe how the MAMID cognitive-parameterization allows the definition of addi- affective architecture could be used to enhancetional high-level individual characteristics (e.g., the effectiveness of therapeutic VR environ-obsessive-compulsive); (3) it provides a means ments, as well as how it could advance our un-of integrating the possibly conflicting effects of derstanding of the etiology and treatment of amultiple, interacting traits and states, much as range of affective disorders, by supportingthese influences interact in humans. adaptive, dynamic interaction between patients
and synthetic avatars.RESULTS
Applications in Clinical PracticeFeasibility of the model was demonstrated inthe context of a simulated peacekeeping sce- MAMID's ability to represent a variety of distinctnario, where separate instances of the architec- stereotypes (in terms of distinct state-trait pro-ture controlled the behavior of 'stereotypical' files), and to control the behavior of syntheticunit leaders ('anxious', 'aggressive', 'normal'). avatars in virtual environments, enables it toThe same set of external stimuli triggered dis- generate a broad range of avatar stereotypes,tinct emotions and emotional response patterns characterized by distinct behavioral repertoiresin the different stereotypes (e.g., higher anxiety (e.g., 'aggressive audience member', 'angrylevels in the 'high anxious' stereotype), and friend', 'anxious spouse'). The ability to dynami-their effects on decision-making then caused cally generate individual idiosyncratic behaviordifferences in observable behaviors (e.g., characteristic of these stereotypes then en-slower movement and more communication hances the avatar believability, and effective-behaviors in the anxious stereotype). The MA- ness within therapeutic VR environments.MID architecture is domain-independent, to fa-
For example, to treat social phobia, or fear ofpublic speaking, a virtual environment would be
54

HUDLICKA
RuleIF (Situation = Speaker talking)
IWSupportive6AudienceMember Avatar THEN
(Action = Facial expression: smile)(Action = Head movement: nod)(Action = Utterance: !Thatc& righto)
Rule
Aggressive Audience IF (Situation = Speaker talking)
Member Avatar THEN(Action = Facial expression: frown)(Action = Head movement: shake)(Action = Utterance: l' don()think soC>)
Figure 4. Examples of MAMID Rules Controlling Action Selection in Two Distinct Stereo-types, Controlling Avatars in a "Fear of Public Speaking" Application
populated by synthetic avatars displaying par- tions, the MAMID architecture also provides aticular characteristics that trigger undesirable tool for modeling the etiology and treatment of asymptoms (e.g., aggressive individuals would variety of disorders, as well as the systematicbe defined for patients exhibiting fear of public development of targeted assessment and treat-speaking symptoms when confronted with criti- ment protocols. In this case MAMID would becal or aggressive remarks). The avatars would used to model specific cognitive-affective proc-then generate aggressive or critical behaviors esses characteristic of a particular disorder. For(e.g., frown while producing utterances critical example, the positive feedback cycle amongof the speaker-patient). Figure 4 shows exam- symptoms and behaviors characterizing gener-pies of two rules that would define distinct be- alized anxiety disorders and phobias could behavior sequences for distinct audience member modeled by representing the increasing pre-avatars. The 'optimal' behaviors triggering the dominance of anxiety-related schemas in theundesirable symptoms would be identified em- patient's long-term memory, increased sensitiv-pirically, so that the avatar behavior could be ity to anxiety-producing stimuli, and generaliza-customized to produce the desired level of anxi- tion across previously neutral stimuli, as theety in the patient. Once identified, the patient disorder becomes established, all contributingwould be exposed to these behaviors to imple- to increasingly avoidant behaviors and with-ment the desired therapeutic protocol (e.g., ex- drawal, characteristic of generalized anxiety.posure therapy, systematic desensitization). Results of therapeutic interventions could thenThe patient would be able to interact with the be modeled by 'exposing' the MAMID architec-avatars (e.g., defend himself against a verbal ture patient model to repeated simulated inputs,attack, take time to implement a coping strat- representing particular therapeutic interventionsegy), and the avatar's ability to dynamically re- (e.g., cognitive restructuring, systematic desen-spond to these interactions (e.g., back off vs. sitization), as well as changing social and envi-persist) would then provide a degree of realism ronmental contexts. This would then result inand customization that are not currently possi- the gradual emergence of more adaptive mem-ble in VR treatment environments. The use of ory schemas and interpretations (in the case ofsuch avatars, embedded within simulated situa- cognitive restructuring aimed at teaching spe-tions, would also enhance assessment. cific anxiety-coping strategies), and diminished
sensitivity and reactiveness to previously anxi-ADVANCING PSYCHOTHERAPY RESEARCH ety-producing stimuli (in the case of systematicTHROUGH COGNITIVE-AFFECTIVE MODEL- desensitization and exposure protocols). Im-ING proved understanding of these processes would
provide opportunities for more finely-tuned as-By enabling the construction of computational sessment and treatment protocols. Computa-causal models of cognitive-affective interac-

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
tional models support the development of more ducing a range of 'stereotypical' behaviors,refined theories and the generation of specific which would resemble real humans and en-experimental hypotheses aimed at validating a hance VR treatment protocols requiring socialparticular theoretical model. interaction. The computational modeling meth-
ods are also well suited for advancing researchSUMMARY AND CONCLUSIONS in clinical psychology, by allowing the develop-
ment of models of particular disorders, and ex-While much progress has been made in virtual ploring the different effects of alternative treat-reality treatment environments, the use of cog- ment protocols.nitive models to control synthetic avatar behav-ior has not been explored. In this paper I sug- Research programs combining empirical stud-gest that the incorporation of such models ies with computational modeling are becomingwould greatly enhance the effectiveness of more common in cognitive science. I believethese environments, by enhancing the believ- that the modeling methods have matured to theability and effectiveness of synthetic avatars, point where similar applications in psychother-and by supporting the development of custom- apy research can be of great benefit.ized treatment and assessment protocols.
REFERENCESI described a cognitive-affective computationalarchitecture (MAMID), capable of controlling the 1. Zimand, E., Anderson, P., Gershon, G.,behavior of such adaptive avatars. MAMID Graap, K., Hodges, L. & Rothbaum, B.models affect appraisal processes and the ef- (2003). Virtual Reality Therapy: Innovativefects of several emotions on distinct aspects of Treatment for Anxiety Disorders. Primarydecision-making, thereby enabling the definition Psychiatry, 9 (7), 51-54.of a variety of 'stereotypes', capable of exhibit- 2. Anderson, J. (1990). The adaptive charactering distinct patterns of behavior within the VR of thought. Hillsdale, NJ: LEA. htjpIenvironments. I provided examples of how the act.Psv.cmu.edu.MAMID architecture could be used to enhance 3. Pew, R.W. and Mayor, A.S. (1998). Repre-
senting Human Behavior in Military Simula-believability of synthetic avatars, and thereby tions. Washington, DC. National Academyenable the construction of customized VR treat- Press.ment and assessment environments. I also dis- 4. Sloman, A. (2003). How many separatelycussed how a computational model of cogni- evolved emotional beasties live within us? Intive-affective interactions, and their role in per- Emotions in Humans and Artifacts, R.Trappl,ception and decision-making (including situation P. Petta, & S. Payr (Eds.). Cambridge, MA:assessment, expectation generation and goal MITmanagement), could be used to advance our 5. Hudlicka, E. (2002). This time with feeling:understanding of the role of these mechanisms Integrated Model of Trait and State Effects onin the etiology, maintenance and treatment of a Cognition and Behavior. Applied Artificial In-variety of affective disorders. To this end, I de- telligence, 16:1-31.scribed an example of how MAMID could be 6. Hudlicka, E. (2003). Modeling Effects of Be-used to model a patient suffering from a particu- havior Moderators on Performance: Evalua-lar set of symptoms, and how specific interven- tion of the MAMID Methodology and Architec-tions could be simulated and represented within ture, In Proceedings of BRIMS-12, Phoenix,the MAMID model. AZ, May.
7. Hudlicka, E. (2004). Two Sides of Appraisal:The development of cognitive architecture in Implementing Appraisal and Its Conse-general, and cognitive-affective architectures in quences within a Cognitive Architecture. Inparticular, is an active research area. Much pro- Proceedings of the AAAI Spring Symposium
gress has been made in modeling specific cog- 2004, Architectures for Modeling Emotion, TR
nitive processing (e.g., acquisition of particular SS-04-02. Menlo Park, CA: AAAI Press.
arithmetic skill, perception). While currently 8. Gratch, J. and Marsella, S. (2004). A Do-
there is no validated architecture of cognition, main-independent Framework for Modelingtherexistino Emotion. Journal of Cognitive Systems Re-the existing architectures are capable of pro- search, 5, 269-306.
56
HUDLICKA
9. Hudlicka, E. and Canamero, L. (2004) (eds.)Architectures for Modeling Emotion, TR SS-04-02. Menlo Park, CA: AAAI Press.
10. Gaggioli, A., Mantovani, F., Castelnuovo,G., Wiederhold, B., and Riva, G. (2003). Ava-tars in Clinical Psychology: A Framework forthe Clinical Use of Virtual Humans. CyberP-sychology & Behavior, 6(2).
11. Pertaub, D.P., Slater, M. & Barker, C.(2002). An experiment on public speakinganxiety in response to three different types ofvirtual audience. Presence- Teleoperators andVirtual Environments 11, 68-78.
12. Leventhal, H. and Scherer, K.R. (1987). Therelationship of emotion to cognition. Cognitionand Emotion, 1, 3-28.
13. Smith, C.A. and Kirby, L.D. (2001). TowardDelivering on the Promise of Appraisal The-ory. In Appraisal Processes in Emotion. K.R.Scherer, A.Schorr, T. Johnstone (Eds.). NY:Oxford.
14. Scherer, K.R. (2001). Appraisal Consideredas a Process of Multilevel Sequential Check-ing. In Appraisal Processes in Emotion. InAppraisal Processes in Emotion. K.R.Scherer, A.Schorr, T. Johnstone (Eds.). NY:Oxford.
15. Hudlicka, E. (1998). Modeling Emotion inSymbolic Cognitive Architectures. AAAI FallSymposium Series, TR FS-98-03. MenloPark, CA: AAAI Press.
Contact
Eva Hudlicka, Ph.D.Psychometrix Associates, Inc.Blacksburg, VA, USA
Tel: (01) 540 552 4803Email: [email protected]

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
58

Annual Review of CyberTherapy and Telemedicine
Immune Attack: Building Biologically Based Immune System Simula-tions for Education and Training
K. Howell, B.A., MBA
Federation of American Scientists, Washington, DC
Abstract: A growing literature suggests that simulation, visualization and gaming can play an impor-tant role in deepening understanding of difficult concepts in mathematics, engineering, and science.Learning sciences research suggests that learning by doing with understanding produces bettertransfer than mere doing alone. 1,2 Challenge-based simulations can provide students opportunities toreceive feedback and revise their thinking, a critical part of the learning process.3'4 Immune Attack isa simulation game to teach biological concepts related to immunology and wound infection, allowingthe student to explore the internal compartments and cells of the human body and visualize immu-nological processes. Simulations of biological functions at a variety of levels, from subcellular to or-gan systems, that are easily navigable by instructors and students with a range of backgrounds willprovide a rich exploratory environment for learning immunology.
BACKGROUND
Immune Attack is a simulation game to teach vances in cognitive science point to new strate-biological concepts related to immunology and gies for increasing the productivity and depth ofwound infection, allowing the student to explore learning if the learner is continuously given chal-the internal compartments and cells of the hu- lenges whose solution depends on masteringman body and visualize immunological proc- the material. 2 The game-based simulations thatesses, including pathology. The game com- are integral to the gameplay will let learners ap-bines three-dimensional visualizations of bio- ply their knowledge immediately in an attempt tological structure and function with advanced defeat a variety of diseases, from simple infec-educational technologies to provide an introduc- tions to more challenging infections. The stu-tion to basic concepts in immunology for high dent's success in designing an immune strategyschool students. Immune Attack is intended to capable of overcoming an array of infectiousbe as fun and compelling as the computer agents will provide a much richer measure ofgames currently played by many adolescents understanding than standardized tests. Learn-and young adults. Students are motivated with a ing is further enhanced if the students are soseries of progressively more difficult challenges motivated to meet the challenges that they arein a gaming environment in which success de- eager to ask questions that can help them - andpends on increasingly sophisticated grasp of if they are able to get timely, accurate answersconcepts in immunology. The learning experi- tailored to the student and the context of theences are individualized by use of context- question.5sensitive help and dialogues and continuousassessment techniques to determine when the METHODITOOLSlearner is ready to move to a new level. Theproject is funded by a National Science Founda- The biological models for the game were devel-tion Information Technology Research grant. oped working closely with prominent immunol-
ogy researchers and educators. ExperiencedThe goal of this research is to test the hypothe- video game developers are developing thesis that visualization of, and immersion in realis- game and assisting in integrating the learningtic depictions of human biology will be highly tools. The learning objectives and instructionalengaging to high school students and hold their strategies are being developed in consultationinterest long enough for learning to occur. Ad- with biology teachers, at both the high school
59

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
LEARNING OBJECTIVES GAME DESIGNIPLAY
General
The student will comprehend the basic Simple rules govern the stylized but accurate behaviors of a varietystrategies of major pathogens of bacteria, viruses, and toxins.The student will be able to identify and The player must master the rules that govern the behavior of macro-understand role of key components of the phages, neutrophils, mast cells, NK cells, T and B cells and will beimmune system including innate responses, able to guide these cells by following key signals, such as proteins.inflammatory responses, and secondaryresponse systems
The student will have knowledge of how Pop up tutorials, a health status bar, and visualizations of the patientthe immune systems and its component provide clinical information to alert the player as to the patient'sresults clinical symptoms physiologic condition and introduce medical termiinolou,.
The student will be knowledge about de- Allergies, autoimmune disease, AIDS are included to show the howfects in the immune system the disease progression changes in individuals with compromised
immune systems.
Table 1. Example Learning Objectives
and college freshmen levels, and with learning cal system work?" While the details of the im-research scientists. plementation may be captured in complex equa-
tions, the vocabulary, rules represented, andDevelopment of valid educational content cou- terms used to describe inputs and outputs arepled with simulations of biological components all easily understandable in biological terms.and their processes and interactions is a keycomponent of the project. We have worked Our formalism is based on the Universal Model-closely with leading immunologists and the ing Language (UML).6 UML tools were used toteachers participating in the evaluation of the build a formal map of knowledge about the im-game to develop an instructional plan for the mune system that includes named variablesgame based on introductory curricula, including and formal relationships (that should be coveredimmunology content, determination of educa- by the ontology), information about rules andtional objectives, strategy for integration of equations describing behavior, clear Englishlearning tools into the game, and evaluation of descriptions of what is being represented avail-the game. Particular emphasis was placed on able through some kind of introspection, thedetermination of appropriate levels of content referenced source of the information encapsu-for the target audience. A sample of the learn- lated, and mechanisms for maintaining versioning objectives is shown in Table 1. control. The structures extend the structures of
the ontology to ensure consistent inheritance ofA major challenge of the project was to define both fields and functions. For example, a com-the learning content so that it would be easily ponent representing the essential elements of aaccessible and understandable both by the bi- cell can be extended to represent a ge-ologists who need to ensure that it is correct neric leukocyte that can in turn be extended toand the software engineers who will need to represent a generic lymphocyte and then a spe-instantiate it in code. One of the great chal- cific B cell. Such structures provide a seamlesslenges in developing reusable software objects connection between ontologies and the frame-is that they are often so difficult to understand work of software objects. It provides a way tothat it is easier to build from scratch rather than ensure that functionality and updated data atrisk misinterpreting often sparse instructions the root of an object tree are accurately propa-about how to use legacy objects. We have de- gated.veloped formalisms that minimize the differencebetween the question "how does this object op- The central challenge of the game is to teacherate?" and the question "how does the biologi- rules to a set of players that represent all the
60
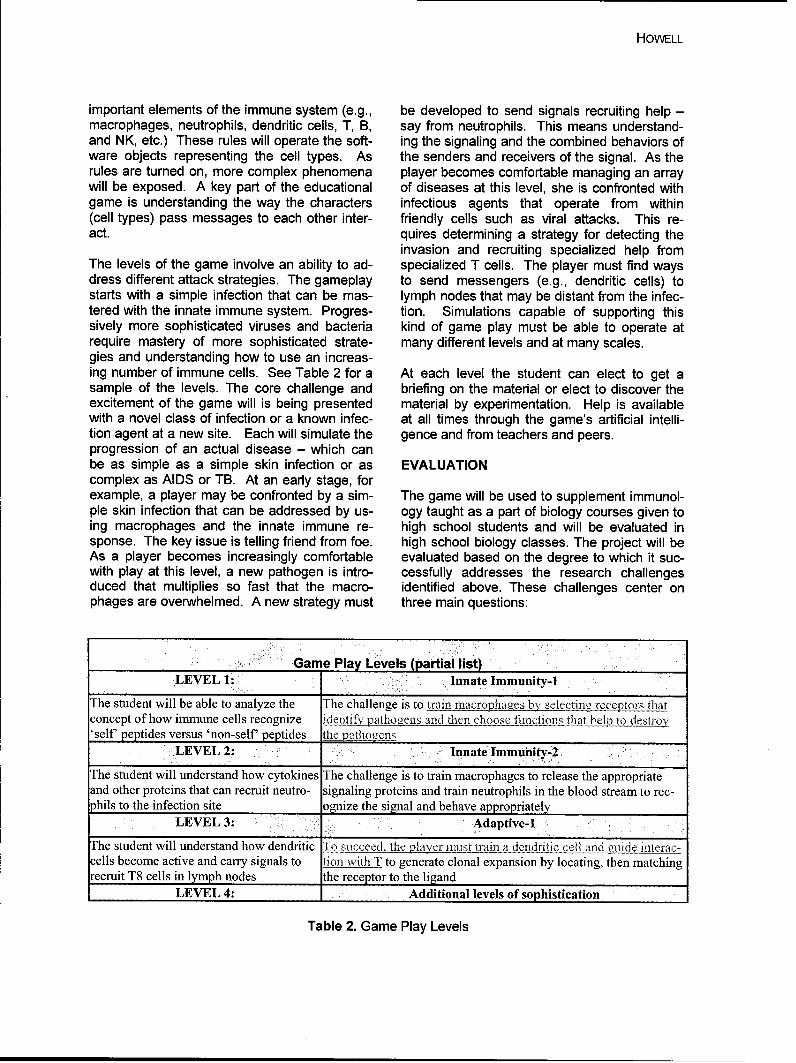
HOWELL
important elements of the immune system (e.g., be developed to send signals recruiting help -macrophages, neutrophils, dendritic cells, T, B, say from neutrophils. This means understand-and NK, etc.) These rules will operate the soft- ing the signaling and the combined behaviors ofware objects representing the cell types. As the senders and receivers of the signal. As therules are turned on, more complex phenomena player becomes comfortable managing an arraywill be exposed. A key part of the educational of diseases at this level, she is confronted withgame is understanding the way the characters infectious agents that operate from within(cell types) pass messages to each other inter- friendly cells such as viral attacks. This re-act. quires determining a strategy for detecting the
invasion and recruiting specialized help fromThe levels of the game involve an ability to ad- specialized T cells. The player must find waysdress different attack strategies. The gameplay to send messengers (e.g., dendritic cells) tostarts with a simple infection that can be mas- lymph nodes that may be distant from the infec-tered with the innate immune system. Progres- tion. Simulations capable of supporting thissively more sophisticated viruses and bacteria kind of game play must be able to operate atrequire mastery of more sophisticated strate- many different levels and at many scales.gies and understanding how to use an increas-ing number of immune cells. See Table 2 for a At each level the student can elect to get asample of the levels. The core challenge and briefing on the material or elect to discover theexcitement of the game will is being presented material by experimentation. Help is availablewith a novel class of infection or a known infec- at all times through the game's artificial intelli-tion agent at a new site. Each will simulate the gence and from teachers and peers.progression of an actual disease - which canbe as simple as a simple skin infection or as EVALUATIONcomplex as AIDS or TB. At an early stage, forexample, a player may be confronted by a sim- The game will be used to supplement immunol-pie skin infection that can be addressed by us- ogy taught as a part of biology courses given toing macrophages and the innate immune re- high school students and will be evaluated insponse. The key issue is telling friend from foe. high school biology classes. The project will beAs a player becomes increasingly comfortable evaluated based on the degree to which it suc-with play at this level, a new pathogen is intro- cessfully addresses the research challengesduced that multiplies so fast that the macro- identified above. These challenges center onphages are overwhelmed. A new strategy must three main questions:
Game Play Levels (partial list)LEVEL 1: Innate Immunity-1
The student will be able to analyze the The challenge is to train macrophages by selectina receptors thatconcept of how immune cells recognize identify pathogens and then choose functions that help to destroy'self` peptides versus 'non-self peptides Lhe pathocens
LEVEL 2: Innate Immunity-2
The student will understand how cytokines The challenge is to train macrophages to release the appropriateand other proteins that can recruit neutro- signaling proteins and train neutrophils in the blood stream to rec-phils to the infection site ognize the signal and behave appropriately
LEVEL 3: Adaptive-I
The student will understand how dendritic To succeed, the player must train a dendritic cell and guide interac-cells become active and carry signals to tion with T to generate clonal expansion by locating, then matchingrecruit T8 cells in lymph nodes the receptor to the ligand
LEVEL 4: 1 Additional levels of sophistication
Table 2. Game Play Levels
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
"* Has the project developed biologically cor- with other users (in web-based games), therect, visually compelling simulations of the story or context in which the game is couched,immune system that can be easily navi- or some other feature is an important part ofgated by people without specialized techni- this research project. Exploiting the inherentcal proficiency? motivational aspects of games and simulations
"* Do the simulations effectively incorporate for education and training must be based on astate-of-the-art open architectures and in- sound understanding of which features of theseteroperability frameworks that will both fa- systems are important for learning and why.cilitate revisions and augmentations for avariety of purposes and encourage use of The instructional game will be used to supple-simulation components in the work of oth- ment immunology taught as a part of introduc-ers? tory biology courses given to high school stu-
* Can the simulations be used in conjunction dents. The research will provide the basis forwith existing instructional tools to develop a building engaging simulations that teachers canprototype instructional system that incorpo- use to convey subtle concepts in the immunerates a variety of assessment, feedback, system and infection control. It should improveand augmentation tools? biology education by presenting educational
materials in a way that is engaging and usefulFor the first two research challenges, assess- to people with a variety of interests and back-ments will be conducted through workshops grounds. A student motivated to learn the com-that are planned annually for each year of the plexities of the immune system can also haveproject. A panel of experts will be convened as the basis for understanding a wide range of bio-part of the workshops to assess the biological logical concepts. The interest generated by theaccuracy of the simulations at various stages of game could encourage students from manydesign and development and the interoperability different backgrounds to enter a scientific orframeworks. The panel will consist of biologists, medical profession. While the initial target audi-immunologists, computational biologists, and ence will be senior high school and first-yearmedical professionals. The evaluation plan for college students, we expect that the system willthe instructional game will be developed with facilitate learning for a broad class of learners,advice by the Education Advisory Panel. The including the many professionals that need toevaluation will focus on four key questions: master elementary concepts in infection and
infection control - such as people who nowmust be trained to deal with potential biological
1. Does use of the instructional game improve attacks. The research will result in tools that canthe performance of students on tests now assist people to improve their own health caregiven by instructors in applicable courses? by presenting difficult concepts in ways that a
2. Does the system improve understanding in typical patient can understand. It is also likelyareas of immunology that are particularly to help research specialists get a clear, visualdifficult to master? understanding of the way their research special-
3. Does the system increase student interest ties fit into the extravagantly complex network ofin science and their interest in a career in operations that combine to make the immunescience? system.
4. Does the effect of 1-3 depend significantlyon sex, ethnicity, or other characteristics of REFERENCESthe learners?
1. Barron, B.J., D.L. Schwartz, N.J.; Vye, A.NOVELTY/DISCUSSION Moore, A. Petrosino, I. Zech, J.D. Bransford, and
the Cognitive and Technology Group at Vander-Computer games hold special interest to a gen- bilt. Doing with Understanding: Lessons fromeration who has grown up with them, and as research on problem and project-based learning.such, they show promise as educational tools. Journal of Learning Sciences 7 (3 and 4): 271-Whether this is due to the inherent challenge 312.built into game play, the richness of graphics 2. John D. Bransford, Sean Brophy, and Susanpresented to the user, the opportunity to interact Williams. "When computer technologies meet the
62
HOWELL
learning sciences: Issues and opportunities" inJournal of Applied Developmental Psychology,21 (1) pp. 59-84.3. Black, P., and William D. 1998. Assessmentand classroom learning. In Assessment andEducation. Special issue of Assessment inEducation: Principles, policy and practice 5(1):7-75. Carfax Pub. Co.4. Vye, N.J. , D.L. Schwartz, J.D. Bransford,B.J. Barron, L. Zech, and Cognition TechnologyGroup at Vanderbilt, 1998. SMART environ-ments that support monitoring, reflection, andrevision. In Metacognition in Educational The-ory and Practice, D. Hacker, J. Dunlosku, andA. Graesser, eds. Mahwah, NJ: Erbaum.5. Graesser, A. C., VanLehn, K., Rose, C.,Jordan, P., & Harter, D. (2001). Intelligenttutoring systems with conversational dialogue.Al Magazine, 22, 39-51.6. Booch, G., Rumbaugh, J., & Jacobson, I.(1999). The unified modeling language userguide. Reading, MA: Addison-Wesley.
Contact
H. Kay Howell, B.A., MBAFederation of American Scientists1717 K. St., NWSuite 209Washington, DC 20036Ph: 202.454.4685 Fax: 202.6751010khowell5fas.org

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
64

Annual Review of CyberTherapy and Telemedicine
General Training of Spatial Abilitiesby Geometry Education in Augmented Reality
H. Kaufmann1 , K. Steinb{igl 1, A. Dunser2, J. GI0ck 2
1 Institute of Software Technology and Interactive Systems, Vienna University of Technology2 Institute of Psychology, University of Vienna
Abstract: Geometry education has proven as one powerful means of improving spatial abilities, animportant component of human intelligence. In the first part of this paper we summarize our develop-ment of a system that uses collaborative augmented reality as a medium for teaching, and uses 3Ddynamic geometry to facilitate mathematics and geometry education. Our immersive collaborativeeducational application, specifically developed for geometry education, serves as the basis of a com-prehensive evaluation study regarding its efficacy in training spatial abilities. The main contribution isthe description of evaluation design including the test instruments, learning tasks and practical ex-periences with using our system for actual training of high school students. Results of a pre-studywith spatial ability tests in high schools are presented. They point to interesting gender-specific differ-ences of strategies when solving spatial ability tests, which have not been reported in literature be-fore.
INTRODUCTION
Spatial abilities present an important component hensive evaluation study will be conducted inof human intelligence. Many studies have order to study the general and differential ef-shown that spatial abilities can be improved by fects of the training on several components ofwell-designed trainings.32 Geometry education spatial ability.has proven as one powerful means of improvingthese skills;10 recently, a number of training In this paper, we briefly describe our experi-studies have shown the usefulness of virtual ences in developing and using Construct3D inreality (VR) in training spatial ability. 9,29 How- high school geometry education. To provide aever, little to no work has been done towards natural face-to-face setting for teachers andsystematic development of VR applications for students, this system uses an immersive setup,practical education purposes in this field. more specifically a collaborative augmented
reality (AR) setup, based on see-through head-"* No VR/AR application for actual use in high mounted displays (HMD). The main advantage
school or higher education has ever been of using AR is that students actually see threedeveloped with the main purpose of improv- dimensional objects which they until now had toing spatial skills. calculate and construct with traditional - mostly
"* Hardly any evaluations can be found in lit- pen and paper - methods (Figure 1). The face-erature which give hints to the actual learn- to-face setting allows for traditional pedagogicing transfer from a VR/AR learning environ- communication.ment to the real world.
It is important to note that while geometry edu-The authors initiated a national research project cation software shares many aspects with con-which addresses these two key issues by devel- ventional computer aided design software at aoping a prototype AR system for geometry edu- first glance, its aims and goals are fundamen-cation. As a pilot study for this proposal, a three tally different. Geometry education software isdimensional geometric construction tool called not intended for generating polished results, butConstruct3D 1- has been developed that puts an emphasis on the construction processserves as a platform for our work. A compre- itself. While relatively simple geometric primi-
tives and operations will suffice for the intended
65

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
[2.Transfer of the training effect to more dis-tant spatial tasks;
3. Effect of the training on strategy use in cen-tral and distant spatial tasks;
4. Aptitude-treatment interactions: Depend-ence of individual training effects on pretest
$ a spatial ability, verbal ability, and reasoningability;
5. Gender differences in training effects.
RELATED WORK
For the development of any educational VRIARapplication, technological, domain specific,pedagogical and psychological aspects are ofimportance. Accordingly, literature from different
S...and diverse research areas relates to our work:VR/AR collaborative distributed systems, desk-top 3D modeling, immersive modeling, educa-tional 2D/3D applications, dynamic 2D geome-try, parametric CAD, pedagogic theories suchas constructivism or activity theory and psycho-logical literature from the field of spatial abilityresearch. We will briefly mention work related totraining and psychological aspects of this paper.For a comprehensive overview of related work
Figure 1. Students are working in 3D space we refer to.16
with Construct3D.Educational VR Applications
audience of age 10 to 20 (especially 10 to 14), Since the early 1990th researchers have beenthe user interface must be both intuitive and working on virtual reality applications for purelyinstructive in terms of the provided visualiza- educational use.1'5'22 In the area of mathematicstions and tools. Commercial CAD software of- education the most recent and most advancedfers an overwhelming variety of complex fea- project is CyberMath. 34 CyberMath is an avatar-tures and often has a steep learning curve. In based shared virtual environment aimed at im-contrast, geometry educators are interested in proving mathematics education. It is suitable forsimple construction tools that expose the under- exploring and teaching mathematics in situa-lying spatial process in a comprehensive way. tions where both the teacher and the studentsThe interface might be restricted to their stu- are co-present and physically separated. A verydents needs. In accordance to that our aim with good summary of educational and training appli-Construct3D was not to create a professional cations is given by Mantovani. 25
3D modeling package but a simple and intuitive3D construction (not animation) tool in an im- Training Spatial Abilities in VRmersive environment for educational purposes.The main part of our work concentrates on our Training of spatial abilities in VR is of strongevaluation study - the test instruments, partici- interest in application areas such as surgery,"pants and the study design. We intend to ad- navigation and way finding, 8 for rehabilitation ofdress the following research questions in our patients with psychiatric illnesses such as trau-evaluation study: matic stress disorder, schizophrenia, and Alz-
heimer's disease2•2 or for pre-fligh space tan1. Effect of the training on performance in ing.
tasks central to the training;
66

KAUFMANN ET AL.
A recent article by Durlach et al.9 gives a very reduce spatial information to an essentially non-good overview of work that has already been spatial, serial format. For example, a route candone in the area of enhancing spatial skills be represented as a list of landmarks, and thewithin virtual environments but mainly identifies spatial relations among the patterns on a cubethe indispensable need for comprehensive fu- can be represented as a list of relations amongture research in this area. pairs of patterns. Thus, the complexity of spatial
information is reduced, and the focus is on partsSpatial Cognition of the object or the environment rather than on
the object as a whole. Compared to holisticPsychological literature on spatial cognition strategies, analytic strategies usually take moreranges from studies on the way people process time, but less mental effort, as the informationsimple spatial objects to studies about how peo- represented is less complex. Note that analyticpie orient themselves in real environments. In and holistic strategies should not be viewed asthe following, we give a brief introduction into mutually exclusive categories.spatial cognition with references to related work.Several authors 6'13'23'33 suggested how spatial Gender differences in strategy use have fre-ability can be structured into sub domains. Most quently been found in studies of environmentalof the proposed structures focus on relation- orientation and navigation. Men more often ac-ships and similarities among spatial tests and quire map-like knowledge about their environ-were developed through analysis of test inter- ment, use Euclidean information, and are awarecorrelations. The results of structural analyses of relative directions, whereas women more of-of spatial ability are highly convergent. In addi- ten rely on landmarks and represent routes astion to some simple, basic performance as- lists of landmarks. These gender differencespects, at least two factors are consistently re- have been found in self-reported strategy use inported: "Spatial Relations" (as labeled by Loh- new environments 21 and in use of landmarksman 23), that is, speeded mental rotation, and and Euclidean information in learning routes"Visualization", which includes all complex, from maps and giving directions.4 With respectmulti-step spatial tasks. Tasks involving three- to spatial tests, gender differences in strategydimensional mental rotation are somewhat inter- use have not been studied much, but at leastmediate and have been grouped into each of one" found that men more often used holisticthese two factors. Tasks requiring participants strategies than women, and women more oftento imagine different perspectives either form a used analytic and mixed strategies than men inthird factor or are grouped into Spatial Rela- two different spatial tests.tions.
A different approach to thinking about spatialcognition is by analyzing the processes peopleactually use to solve spatial tasks. Basically, allspatial tasks can be solved in different ways,and the more complex a task is, the more differ-ent strategies can be used to solve it (overviewin24 ). People differ in the strategies they use,and people shift their strategies within a task ifnecessary. A basic distinction is between holis-tic and analytic strategies.11 Holistic strategiesinvolve representing and manipulating spatialinformation "in a spatial way", that is, mentallyusing information about spatial relations be-tween elements in the mental representation. Aperson using holistic strategies imagines, forexample, how a stimulus figure is rotated, or Figure 2. Two students collaborate in our stan-how a two-dimensional shape can be folded into dard lab setup, wearing an HMD, holding aa three-dimensional object. Analytic strategies wireless pen and panel. All devices are optically
tracked.

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
CONSTRUCT3D defining elements such as corner points of arigid body. It can be seen what parts of a con-
Construct3D is based on the Studierstube AR struction change and which remain the same.system30 and uses augmented reality to provide The histories of constructions as well as de-a natural setting for face-to-face collaboration of pendencies between geometric objects areteachers and students. maintained. Experiencing what happens under
movement allows better insight into a particularHardware Setup construction and geometry in general.
In our standard Studierstube setup, we have 2 At its start Construct3D initializes a 3D windowcollaborating users wearing HMDs for a shared which has maximum size to cover the "whole"virtual space, and holding fully tracked interac- virtual space. The user interface is initialized,tion props in their hands. One dedicated host the menu system is mapped to a hand-heldwith 2 graphic ports renders stereoscopic views tracked panel called the personal interactionfor both users. We are using this setup for dem- panel (PIP). The PIP allows the straightforwardonstrations and evaluations. Other setups for integration of conventional 20 interface ele-educational use have been reported in.16 ments like buttons, sliders, dials etc. as well as
novel 3D interaction widgets. Haptic feedbackSoftware Design from the physical props guides the user when
interacting with the PIP, while the overlaidThe current version of Construct3D offers func- graphics allows the props to be used as multi-tions for the construction of points, two- functional tools.dimensional geometric primitives and three-dimensional geometric objects. It provides func- All construction steps are carried out via directtionality for planar and spatial geometric opera- manipulation in 3D using a stylus tracked withtions on these objects, allows measurements, six degrees of freedom. In order to generate afeatures structuring of elements into layers and new point the user clicks with his pen exactly atoffers basic system functions. the location in 3D space where the point should
appear. Users can easily switch between pointConstruct3D promotes and supports exploratory mode (for setting new points) and selectionbehavior through dynamic geometry. A funda- mode (for selecting 3D objects). We omit a de-mental property of dynamic geometry software tailed description of the user interface in thisis that dynamic behavior of a construction can context.be explored by interactively moving individual
Figure 3. Left: Surface of revolution with the tangential plane in a surface point. Right: Two studentsare collaborating to solve the problem. Vienna is marked on the globe and a geostationary satellite
(in the equatorial plane) is given too.
68
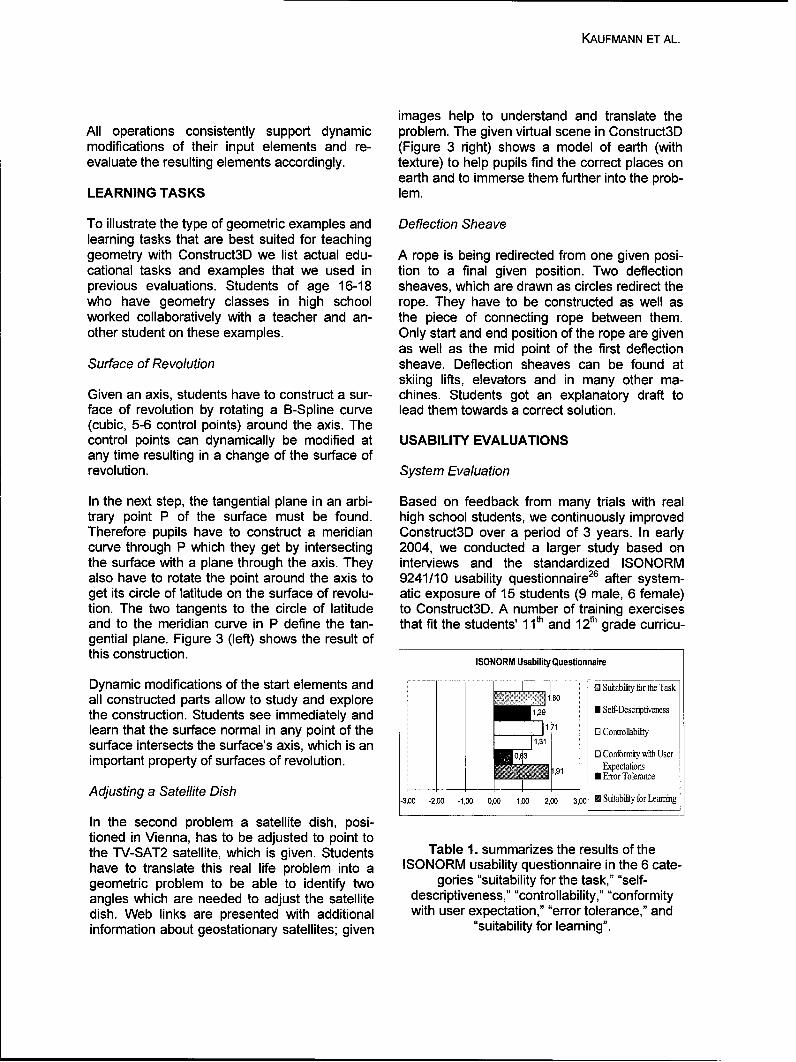
KAUFMANN ET AL.
images help to understand and translate theAll operations consistently support dynamic problem. The given virtual scene in Construct3Dmodifications of their input elements and re- (Figure 3 right) shows a model of earth (withevaluate the resulting elements accordingly. texture) to help pupils find the correct places on
earth and to immerse them further into the prob-LEARNING TASKS lem.
To illustrate the type of geometric examples and Deflection Sheavelearning tasks that are best suited for teachinggeometry with Construct3D we list actual edu- A rope is being redirected from one given posi-cational tasks and examples that we used in tion to a final given position. Two deflectionprevious evaluations. Students of age 16-18 sheaves, which are drawn as circles redirect thewho have geometry classes in high school rope. They have to be constructed as well asworked collaboratively with a teacher and an- the piece of connecting rope between them.other student on these examples. Only start and end position of the rope are given
as well as the mid point of the first deflectionSurface of Revolution sheave. Deflection sheaves can be found at
skiing lifts, elevators and in many other ma-Given an axis, students have to construct a sur- chines. Students got an explanatory draft toface of revolution by rotating a B-Spline curve lead them towards a correct solution.(cubic, 5-6 control points) around the axis. Thecontrol points can dynamically be modified at USABILITY EVALUATIONSany time resulting in a change of the surface ofrevolution. System Evaluation
In the next step, the tangential plane in an arbi- Based on feedback from many trials with realtrary point P of the surface must be found. high school students, we continuously improvedTherefore pupils have to construct a meridian Construct3D over a period of 3 years. In earlycurve through P which they get by intersecting 2004, we conducted a larger study based onthe surface with a plane through the axis. They interviews and the standardized ISONORMalso have to rotate the point around the axis to 9241/10 usability questionnaire 26 after system-get its circle of latitude on the surface of revolu- atic exposure of 15 students (9 male, 6 female)tion. The two tangents to the circle of latitude to Construct3D. A number of training exercisesand to the meridian curve in P define the tan- that fit the students' 1 1th and 12th grade curricu-gential plane. Figure 3 (left) shows the result ofthis construction. ISONORM Usability Questionnaire
Dynamic modifications of the start elements and . . Suitability for the Taskall constructed parts allow to study and explore 1.80
the construction. Students see immediately and 1,29 •Self-Descriptiveness
learn that the surface normal in any point of the 1D Controllability
surface intersects the surface's axis, which is an 131
important property of surfaces of revolution. 0 Ectatons1,9 Expectations
0 Error ToleranceAdjusting a Satellite Dish __ __ _
-3,00 -2,00 -1,00 0,00 1,00 2,00 3,00 M Suitability for Learning
In the second problem a satellite dish, posi-tioned in Vienna, has to be adjusted to point tothe TV-SAT2 satellite, which is given. Students Table 1. summarizes the results of thehave to translate this real life problem into a ISONORM usability questionnaire in the 6 cate-geometric problem to be able to identify two gories "suitability for the task," "self-angles which are needed to adjust the satellite descriptiveness," "controllability," "conformitydish. Web links are presented with additional with user expectation," "error tolerance," andinformation about geostationary satellites; given "suitability for learning".

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
lum were designed by us and then worked simply too long for continuous work with anthrough by students from two high schools with HMD. Since negative side effects are a generalthe aid of their teachers. All students attended problem when working with HMDs and influenceto geometry classes (descriptive geometry) the user's subjective experience of a VR/ARsince the beginning of grade 11. Each of them environment considerably they are relevant toparticipated in 5 training sessions lasting 6 all VR/AR applications that use HMDs. We iden-hours. Our main objective was to at least infor- tified some possible reasons of cybersicknessmally assess the usability and potential of our that may be relevant to our virtual environmentsystem and method for real high school work. such as accommodation problems, low frame
rate, lag or bad fitting helmets. In the meantimeConstruct3D Usability Results we already reduced some of these negative
side effects (using light weight bicycle helmetsAt the end of all training sessions students had and increasing frame rate).to answer an ISONORM usability questionnaire.Two questions regarding self-descriptiveness of We must stress that we designed Construct3Dthe application had to be removed since they to be a valuable addition to traditional or com-were related to desktop applications only. After- puter aided geometry education and not a sub-wards students answered general questions stitute of it. A very reasonable time for workingregarding user acceptance, user behaviour, and teaching with Construct3D during a class istechnical requirements and organisational as- about 20-30 minutes. According to our observa-pects. tions, this would guarantee that less than 5% of
all students feel any negative side effects suchA closer look at the data reveals that the cate- as eyestrain or even headache. Of course itgories "suitability for learning" and "suitability for would be desirable to find the exact reasons oftask" received the highest grading which is very cybersickness and ways to avoid it - as pointedimportant in this context. In our opinion the high- out by other researchers.20est priorities for an educational application thatcomplies with pedagogic theories such as con- EVALUATION DESIGN ON TRAINING SPA-structivism are that it (1) is easy to use and re- TIAL ABILITIESquires little time to learn, (2) encourages learn-ers to try new functions and (3) can be used The presented system serves as a base of fur-consistently and is designed in a way that things ther research and allows to do more in depthyou learned once are memorized well. These evaluations of various aspects regarding VR/ARare exactly the items that students rated very learning that have not been studied before.high. Nearly all students reported that they canimagine using the current version of Con- Currently we focus on the largest evaluationstruct3D in high school or university education. with Construct3D yet, involving over 250 stu-The categories "self-descriptiveness" and dents. It concentrates on 5 main questions"conformity with user expectations" got lower about training and improving spatial abilities asgrades than the rest. The self-descriptiveness of mentioned in the introduction.Construct3D is currently improved by addingbetter labeling and tool tips to widgets on our Test Groupspanel in order to explain all menu items. We arealso restructuring the menu system to give a We will conduct a pre-/post-test experiment withbetter overview of the functionality, four different training groups and one untrained
control group. At pre-test, all participants will beSome of the students reported negative side presented with a battery of spatial testseffects after working in the virtual environment. (including strategy assessments) and tests ofOne female student reported headache and verbal and reasoning ability. Then, each partici-eyestrain after 20 minutes of work in the virtual pant will be randomly assigned to one of fiveenvironment but did not stop working and groups:wanted to use Construct3D again (in total sheworked for 3 hours with the system). In retro- a. Untrained control group: Participates in thespect we know that our one hour lessons were
70
KAUFMANN ET AL.
pre- and post-test but does not receive any (PSVT:R 12): shortform: mental rotation com-training; bined with visualization.
b.Traditional school group: Participates in the 9 Mental Cutting Test (MCT7): shortform: visu-pre- and post-test, but is taught geometry in alization.their normal school classes between pre- * Differential Aptitude Test: Space Relationsand post-test with traditional paper & pencil (DAT:SR 12): shortform: visualization.methods; * Spatial Orientation Test (SOT19); mental
c. Modern instruction/school group: Partici- rotation - large scalepates in the pre- and post-test, but is taught * Judgement of Line Orientation Test (JLO3);geometry in their normal school classes visuospatial perception and processing.between pre- and post-test on the computerusing CAD software; Reasoning and Verbal Ability Tests:
d. Individual tutoring group: works with a tutorusing standard teaching methods without e "Letter Sequence": subtest from the Ger-Construct3D; man intelligence test battery "Wilde Intelli-
e. Construct3D group: works with Con- genz Test" (WIT) by:14 shortformstruct3D. * "Verbal analogies": subtest from the Ger-
f" man intelligence test battery "Berliner Intelli-The reason we use an individual tutoring group genzstruktur Test" (BIS)15
is that this condition is probably "harder to beat" 9 "Vocabulary" ("Wortschatztest" WST):31
than standard class-wise Descriptive Geometry shortform(DG) instruction. Tutors are likely to use handdrawing and sketching as teaching methods, Strategy Questionnaire: Assessment of differentthus, they will provide a "hands-on" experience aspects of holistic vs. analytic strategies, the
that has proven to be particularly effective in most important ones are "Visualization Imagi-
other training studies. However, we expect the nation" vs. "Non-visual Reasoning I Thinking"
Construct3D tutorial to lead to broader transfer and "Focus on the object as a whole" vs. "Focus
of training gains than the tutoring. As women on details".
more often than men use analytic strategies on
spatial tests, the Construct3D training, which These tests have also been used at two prelimi-focuses on visualization, might have different nary studies that we did in Austrian higheffects on female than on male participants. It is schools. In the first study 42 students (39certainly interesting to see how different types males, 3 females; aged 17-19 years, 11t grade)of training affect such differences. participated, in the second bigger one there
were 79 students (44 females, 33 males, 2 un-Between pre- and post-tests five training ses- known; aged 16-19, 1 1m and i2t grade). Due tosions will be conducted. Participants will be stu- time restrition in sh we develope to
dent inthei 11h ad 12h yar f scoolng, time restrictions in schools, we developed twodents in their 11th and 12th year of schooling, short versions of each test except the MRTattending secondary schools in Vienna. Austria which was used in its full length. We split thehas several different secondary-education cur- tests (PSVT:R, MCT, DAT:SR) into halves byricula, some of which have a focus on the natu- simply assigning all odd items to test version Aral sciences, including Descriptive Geometry and all even ones to test version B. In order to(DG). DG classes start in the 11lth form. eliminate obvious inequalities, we thereafter
Instruments exchanged some items or assigned some itemsto both test versions. The final test forms con-
The following instruments will be presented to sisted of 15 (MCT and PSVT:R) respectively 25particoipang instprume-andpo-test. w b attey tof (DAT:SR) items. The time limits set for the testsparticipants at pre- and post-test. A battery of were calculated based on the regular test ver-spatial tests as listed below will be used: sions and the number of problems selected for
the short versions and were therefore 12.5 min-v Mental Rotations Test (MRT 3 ), German utes for the PSVT:R, 12 minutes for the MCTversion by:27 speeded mental rotation. and 12.5 minutes for the DAT:SR. Our short test
e Purdue Spatial Visualization Test: Rotations

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
versions had reliability coefficients (Cronbach's factors could be identified: spatial ability (withalphas) ranging form 0.66 to 0.90. loadings of the 4 spatial ability tests as well as a
lower loading of non-verbal reasoning tests),PRELIMINARY STUDY reasoning ability (with loadings of both reason-
ing tests), and vocabulary. There were positiveThe purpose of the preliminary study was to significant correlations between the DAT:SRexamine some frequently employed spatial tests and the PSVT:R on one hand and the non-that contain different kinds of tasks and are sup- verbal reasoning test on the other hand. Thisposed to affect different aspects of spatial ability finding goes together with the one from the pre-in regard to performance, strategy use and the study indicating that DAT:SR and PSVT:Rrelation between these two variables. More pre- scores are not a pure measure of "real" spatialcisely, we aimed to find answers to the following (holistic / visualization) ability but confounded byquestions: reasoning abilities.
a. How do performances in different spatial Analyses of the strategy use questions revealability tests correlate with each other and that, on the one hand, there are differences inwhat is the nature of the relationship to cog- strategy use on an inter-individual level: Signifi-nitive tests measuring analytical abilities cant positive correlations over the tests indicate(reasoning and verbal abilities)? that subjects tend to certain strategies that are
b.Are there intra-individual differences in rather independent from the kind of spatial task.strategy use across tests? Do different spa- On the other hand, these personal strategy ten-tial tests evoke different strategies? dencies are not completely unaffected by the
c. Are there inter-individual differences in the nature of the spatial test: The use of holisticuse of strategies? Do participants show a strategies is significantly higher for the MRT astendency to use holistic or analytic strate- for the other three spatial tests.gies irrespective of the nature of the task?
d. How are performance and strategy use as- When drawing the conjunction between per-sociated with each other? formance and strategy use, we found that there
were no correlation between performance andRESULTS strategy regarding the DAT:SR, the PSVT:R,
and the MCT, i.e., subjects using mainly holisticThe first study (39 males, 3 females; aged 17- strategies could not achieve higher scores than19 years, 1 1h grade) aimed to examine associa- subjects using mainly analytic scores. However,tions and intra- and inter-individual differences there was a significant correlation betweenbetween several spatial ability tests regarding strategy use and performance in the MRT, indi-performance and strategy use and to make con- cating that "holistic" subjects scored slightly bet-nections between performance and strategy ter than "analytic" subjects.use. The spatial ability tests used were theMRT, the PSVT:R, the DAT:SR and the MCT Considering these results, it seems that thetogether with reasoning (verbal and non-verbal) MRT stands out from the other three spatialand verbal ability (vocabulary) tests. tests we used in this study: It is processed more
holistic than the other tests and the use of holis-In an explorative pre-study subjects were asked tic strategies has more (positive) influence onto solve problems of these tests by thinking the performance compared to the DAT:SR, thealoud. The findings of this pre-study suggest PSVT:R and the MCT.that a major part of these problems (especiallyPSVT:R and DAT:SR problems) can be suc- Altogether, our findings give some evidence thatcessfully solved not only in a spatial (holistic) spatial ability tests - in particular the PSVT:Rway but also by using analytic non-spatial and the DAT:SR - can be successfully solvedstrategies. The way the MCT was solved indi- not only with "real" spatial (holistic) strategiescates that (geometry) knowledge may also be but also with analytical strategies - at least asan important factor. long the time limit set is ample enough as these
analytical strategies are generally more time-Applying a factor analysis on the test scores 3 consuming than holistic processing. Results
72
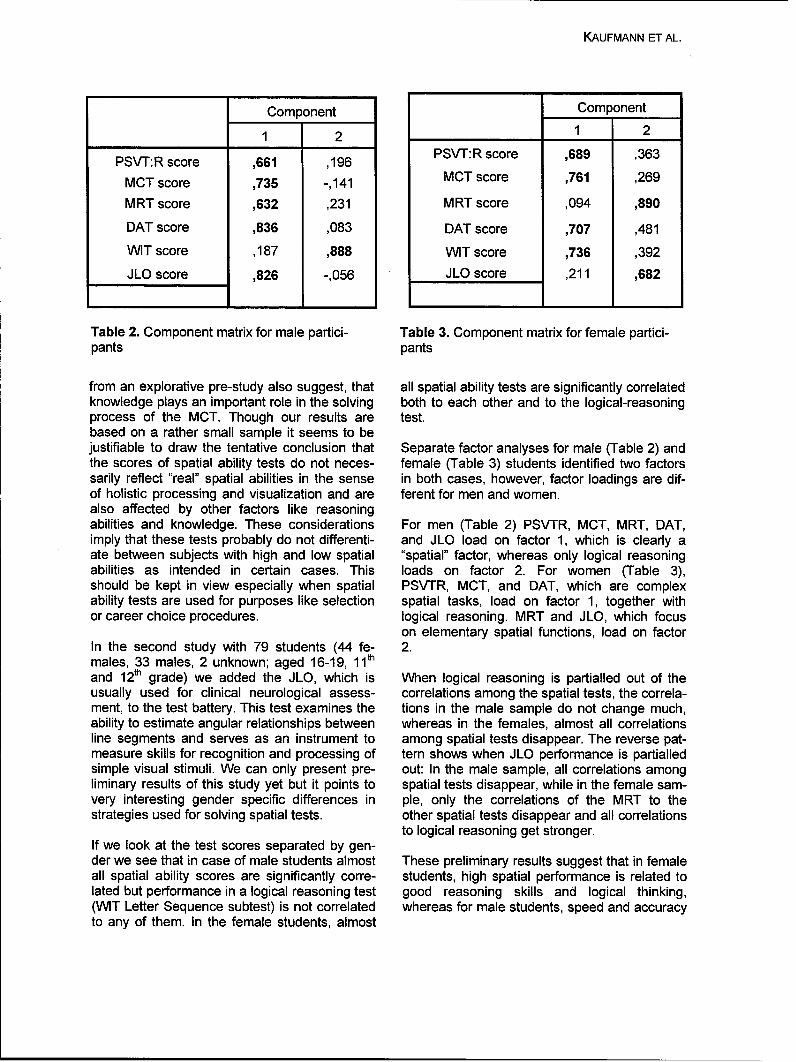
KAUFMANN ET AL.
Component Component
1 2 1 2
PSVT:R score 661 196 PSVT:R score ,689 ,363
MCT score ,735 -,141 MCT score ,761 269
MRT score ,632 ,231 MRT score ,094 ,890
DAT score ,836 ,083 DAT score ,707 ,481
WIT score ,187 ,888 WIT score ,736 ,392
JLO score ,826 -,056 JLO score ,211 ,682
Table 2. Component matrix for male partici- Table 3. Component matrix for female partici-pants pants
from an explorative pre-study also suggest, that all spatial ability tests are significantly correlatedknowledge plays an important role in the solving both to each other and to the logical-reasoningprocess of the MCT. Though our results are test.based on a rather small sample it seems to bejustifiable to draw the tentative conclusion that Separate factor analyses for male (Table 2) andthe scores of spatial ability tests do not neces- female (Table 3) students identified two factorssarily reflect "real" spatial abilities in the sense in both cases, however, factor loadings are dif-of holistic processing and visualization and are ferent for men and women.also affected by other factors like reasoningabilities and knowledge. These considerations For men (Table 2) PSVTR, MCT, MRT, DAT,imply that these tests probably do not differenti- and JLO load on factor 1, which is clearly aate between subjects with high and low spatial "spatial" factor, whereas only logical reasoningabilities as intended in certain cases. This loads on factor 2. For women (Table 3),should be kept in view especially when spatial PSVTR, MCT, and DAT, which are complexability tests are used for purposes like selection spatial tasks, load on factor 1, together withor career choice procedures. logical reasoning. MRT and JLO, which focus
on elementary spatial functions, load on factorIn the second study with 79 students (44 fe- 2.males, 33 males, 2 unknown; aged 16-19, 11thand 12th grade) we added the JLO, which is When logical reasoning is partialled out of theusually used for clinical neurological assess- correlations among the spatial tests, the correla-ment, to the test battery. This test examines the tions in the male sample do not change much,ability to estimate angular relationships between whereas in the females, almost all correlationsline segments and serves as an instrument to among spatial tests disappear. The reverse pat-measure skills for recognition and processing of tern shows when JLO performance is partialledsimple visual stimuli. We can only present pre- out: In the male sample, all correlations amongliminary results of this study yet but it points to spatial tests disappear, while in the female sam-very interesting gender specific differences in pie, only the correlations of the MRT to thestrategies used for solving spatial tests. other spatial tests disappear and all correlations
to logical reasoning get stronger.If we look at the test scores separated by gen-der we see that in case of male students almost These preliminary results suggest that in femaleall spatial ability scores are significantly corre- students, high spatial performance is related tolated but performance in a logical reasoning test good reasoning skills and logical thinking,(WIT Letter Sequence subtest) is not correlated whereas for male students, speed and accuracyto any of them. In the female students, almost
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
of basic spatial processes are the best predictor strategy use for route information: A "map-of spatial test performance. present" direction-giving paradigm," Envi-
ronment and Behavior, vol. 30, pp. 123-FUTURE WORK 143,1998.
[5] C. Byrne, "Water on Tap: The Use of VirtualWithin the next few months our evaluation re- Reality as an Educational Tool," Universitygarding spatial intelligence, as described in pre- of Washington, College of Engineering,vious sections, will be conducted. In the future Washington 1996.we plan to study general improvements of spa- [6] J. B. Carroll, Human cognitive abilities. Atial ability in contrast to task specific improve- survey of factor-analytic studies. Cam-ments in detail. We want to seek for an answer bridge, UK: Cambridge University Press,to the question if direct manipulation as used in 1993.Construct3D and explorative interaction is suffi- [7] CEEB College Entrance Examinationcient to improve spatial understanding and last Board, "Special Aptitude Test in Spatialbut not least if training of spatial intelligence in a Relations MCT," CEEB College Entrancevirtual environment is more "efficient" than in a Examination Board, 1939.real environment. [8] R. P. Darken, T. Allard, and L. Achille,
"Spatial Orientation and Wayfinding inFurther, we plan to utilize Construct3D as a tool Large-Scale Virtual Spaces: An Introduc-for evaluating various aspects in virtual environ- tion," Presence: Teleoperators & Virtualments in our future research. For example a Environments, vol. 7, pp. 101-107, 1998.comprehensive pedagogic evaluation, evaluat- [9] N. Durlach, G. Allen, R. Darken, R. L. Gar-ing e.g. teaching styles or transfer of learning in nett, J. Loomis, J. Templeman, and T. E.educational VRIAR applications would be inter- von Wiegand, "Virtual environments and theesting. enhancement of spatial behavior: Towards
a comprehensive research agenda," PRES-ACKNOWLEDGEMENTS ENCE - Teleoperators and Virtual Environ-
ments, vol. 9, pp. 593-615, 2000.The authors thank Istvan Barakonyi for his help [101 G. Gittler and J. GI0ck, "Differential Trans-during the evaluation studies. We thank all par- fer of Learning: Effects of Instruction in De-ticipants of evaluations as well as other teach- scriptive Geometry on Spatial Test Perform-ers and students for testing and giving useful ance," Journal of Geometry and Graphics,feedback. Part of this research was funded by vol. 2, pp. 71-84, 1998.the Austrian Science Fund (FWF) contract no. [11] J. GlOck and S. Fitting, "Spatial strategyP14470, P16803 and Y193 and by the EU IST selection: Interesting incremental informa-project Lab@Future (IST-2001-34204). tion," International Journal of Testing, vol. in
press, 2003.REFERENCES [12] R. B. Guay, "Purdue Spatial Visualization
Test: Rotations," Purdue Research Founda-[1] J. T. Bell and H. S. Fogler, "The Investiga- tion, West Lafayette, IN 1977.
tion and Application of Virtual Reality as an [13] R. E. Guttman, E. Epstein, M. Amir, and L.Educational Tool," American Society for Guttman, "A structural theory of spatialEngineering Education 1995 Annual Con- abilities," Applied Psychological Measure-ference, 1995. ment, vol. 14, pp. 217-236, 1990.
[2] G. K. Benett, H. G. Seashore, and A. G. [14] 0. A. Ja§ger and K. Althoff, Der WILDE-Wesman, "Differential Aptitude Tests, Intelligenz-Test. (WIT); e.Forms S and T." New York: The Psycho- Strukturdiagostikum; Handanweisung.logical Corporation, 1973. G6ttingen: Hogrefe, Verlag fOr Psychologie,
[3] A. L. Benton, K. Hamsher, N. R. Varney, 1994.and 0. Spreen, Contributions to neurologi- [15] 0. A. Jager, H.-M. SCI1, and A. Beauducell,cal assessment: A clinical manual. New "Berliner lntelligenzstruktur-Test."York: Oxford, 1983. Gottingen: Hogrefe, Verlag fOr Psychologie,
[4] L. N. Brown, C. J. Lahar, and J. L. Mosley, 1997."Age and gender-related differences in
74
KAUFMANN ET AL.
[16] H. Kaufmann, "Geometry Education with Ergonomie '97, R. Liskowsky, Ed. Stuttgart,Augmented Reality.," in Ph.D. Thesis. Vi- 1997.enna: Vienna University of Technology, [27] C. Quaiser-Pohl and W. Lehmann, "Der2004, pp. 179. Mental-Rotation-Test," Swets Test Ser-
[17] H. Kaufmann and D. Schmalstieg, vices, Frankfurt/Main 2002."Mathematics and geometry education with [28] A. A. Rizzo, J. G. Buckwalter, J. S. MCGee,collaborative augmented reality," Com- T. Bowerly, C. van der Zaag, U. Neumann,puters & Graphics, vol. 27, pp. 339-345, M. Thiebaux, L. Kim, L. Pair, and C. Chua,2003. "Virtual environments for assessing and
[18] H. Kaufmann, D. Schmalstieg, and M. Wag- rehabilitating cognitive/functional perform-ner, "Construct3D: a virtual reality applica- ance," Presence - Teleoperators and Virtualtion for mathematics and geometry educa- Environments, vol. 10, pp. 359-374, 2001.tion," Education and Information Technolo- [29] A. A. Rizzo, J. G. Buckwalter, U. Neumann,gies, vol. 5, pp. 263-276, 2000. C. Kesselman, M. Thiebaux, P. Larson, and
[19] M. Kozhevnikov and M. Hegarty, "A disso- A. Van Rooyen, "The Virtual Reality Mentalciation between object manipulation, spatial Rotation Spatial Skills Project," CyberPsy-ability and spatial orientation ability," Mem- chology and Behavior, vol. 1, pp. 113-120,ory & Cognition, vol. 29, pp. 745-756, 2001. 1998.
[20] J. J. LaViola Jr., "A discussion of cybersick- [30] D. Schmalstieg, A. Fuhrmann, G. Hesina,ness in virtual environments," ACM SIGCHI Z. S. Szalavari, L. M. Encarnacao, M. Ger-Bulletin, vol. 32, pp. 47-56, 2000. vautz, and W. Purgathofer, "The Studier-
[21] C. A. Lawton, "Gender differences in way- stube augmented reality project," Presencefinding strategies: Relationship to spatial - Teleoperators and Virtual Environments,ability and spatial strategies," Sex Roles, vol. 11, pp. 33-54, 2002.vol. 30, pp. 765-779, 1994. [31] K.-H. Schmidt and P. Metzler,
[22] B. Loftin, M. Engelberg, and R. Benedetti, Wortschatztest. Weinheim: Belz, 1992."Applying virtual reality in education: A pro- [32] E. Souvignier, "Training raiumlichertotypical virtual physics laboratory," in Pro- Fahigkeiten. [Training spatial abilities.]," inceedings of the IEEE 1993 Symposium on Handbuch Kognitives Training, K. J. Klauer,Research Frontiers in Virtual Reality. Los Ed. Gottingen: Hogrefe, 2001, pp. 293-319.Alamitos, CA: IEEE Computer Society [33] H. Stumpf and J. Eliot, "A structural analy-Press, 1993, pp. 67-74. sis of visual spatial ability in academically
[23] D. F. Lohman, "Spatial ability: A review and talented students," Learning and Individualreanalysis of the correlational literature," Differences, vol. 11, pp. 137-151, 1999.Stanford University School of Education, [34] G. Taxen and A. Naeve, "CyberMath: Ex-Aptitude Research Project, Stanford, CA ploring Open Issues in VR-Based Learn-Tech. Rep. No. 8,1979. ing," SIGGRAPH 2001 Educators Program,
[24] D. F. Lohman and P. C. Kyllonen, vol. SIGGRAPH 2001 Conference Ab-"Individual differences in solution strategy stracts and Applications, pp. 49-51, 2001.on spatial tasks," in Individual differences in [35] F. Tendick, M. Downes, T. Goktekin, M. C.cognition, D. F. Dillon and R. R. Schmeck, Cavusoglu, D. Feygin, X. Wu, R. Eyal, M.Eds. New York: Academic Press, 1983, pp. Hegarty, and L. W. Way, "A Virtual Environ-105-135. ment Testbed for Training Laparoscopic
[25] F. Mantovani, 'yR Learning: Potential and Surgical Skills," Presence, vol. 9, pp. 236-Challenges for the Use of 3D Environments 255, 2000.in Education and Training," in Towards Cy- [36] S. G. Vandenberg and A. R. Kuse, "MentalberPsychology: Mind, Cognitions and Soci- Rotations: a group test of three-dimensionalety in the Internet Age, G. Riva and C. spatial visualization," Perceptual and MotorGalimberti, Eds. Amsterdam: lOS Press, Skills, vol. 47, pp. 599-604,1978.2001.
[26] J. Primper, "Der BenutzungsfragebogenISONORM 9241/10: Ergebnisse ZurReliabilitat und Validitit," in Software-
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Contact
Hannes KaufmannInstitute of Software Technology and InteractiveSystemsVienna University of TechnologyFavoritenstr. 9-11/188-2,A-1040 Vienna, AustriaEmail: [email protected]
76

Annual Review of CyberTherapy and Telemedicine
The Gedanken Experiment of Human Dynamics
Y. Cail and J. Klein-Seetharaman1'21CyLab, Carnegie Mellon University, Pittsburgh
2 Department of Pharmacology, University of Pittsburgh Medical School, Pittsburgh
Abstract: Understanding human dynamics is an important step in clinical therapies, such as bloodglucose management or weight control. It requires insight into the complex interactions between thecomponents of biomedical systems. This is challenging because of the enormous amount of dataand knowledge in this domain. Gedanken Experiment is an intuitive, qualitative thinking process,which have been used by physicists for decades. Our goal is to enable an interactive game-like envi-ronment for users with any background, while remaining sufficiently flexible to target medical prob-lems at a level of abstraction, from the conformational changes of a protein to the interaction of thevarious biochemical pathways in our body. Here, we present an interactive and visual problem-solving environment for the biomedical domain. We designed a biological world model, in which us-ers can explore biological interactions by role-playing "characters" such as cells and molecules or asan observer in a "shielded vessel", both with the option of networked collaboration between simulta-neous users. The system architecture of these "characters" contains four main components:1 Bio-behavior is modeled using cellular automata.2 Bio-rnorphin 9 uses vision-based shape tracking tech-niques to learn from recordings of real biological dynamics. Bio-sensing is based on molecular prin-ciples of recognition to identify objects, environmental conditions and progression in a process.4 Bio-dynamics implements mathematical models of cell growth and fluid-dynamic properties of biologicalsolutions. The principles are implemented in a simple world model of the human vascular system anda biomedical problem that involves an infection by Neisseria meningitides where the biological char-acters are white and red blood cells and Neisseria cells. Our case studies show that the system canbe used for public health education, biomedical simulation and creative problem solving.
INTRODUCTION
Understanding human dynamics is an important tive. More interaction is provided in the "Virtualstep in clinical therapies, such as blood glucose Cell", a virtual environment in which question-management or weight control. It requires in- based assignments are given to users in asight into the complex interactions between the simulated laboratory.7 A submarine is launchedcomponents of biomedical systems. This is that immerses the user in the virtual environ-challenging because of the enormous amount of ment of the cell populated by sub-cellular com-data and knowledge in this domain. Gedanken ponents which the user can investigate. With aExperiment (GE) is an intuitive, qualitative think- toolbox, various cellular processes can be in-ing process, which have been used by physi- vestigated experimentally. The results of thesecists for decades. Novel approaches are being investigations and experimentations allow usersdeveloped, for example a storytelling system to solve the assignments at their own pace andhas been presented to fertilize multidisciplinary through their own motivation. It was shown thatbiomedical problem solving.5 Furthermore, mod- this approach significantly improves authenticern biomedical education makes extensive use learning, in particular for large enrollment gen-of visualization of biomedical processes and eral biology classes.8 At the other end of theconcepts, for example the publication of the hu- spectrum, realistic, fully interactive virtual labo-man genome sequence was accompanied by a ratories have been developed to simulateCD-ROM that presented genome background chemical, 9 biomedical, 10 and recentlyas well as DNA sequencing techniques in an- nanoscience11 laboratory experiments. How-imations.6 However, these visualization tools ever, in their present form, these systems wereare mostly designed to complement traditional not designed to be integrated GEs becauseteaching techniques and are not very interac- they are targeted to students and researchers
77
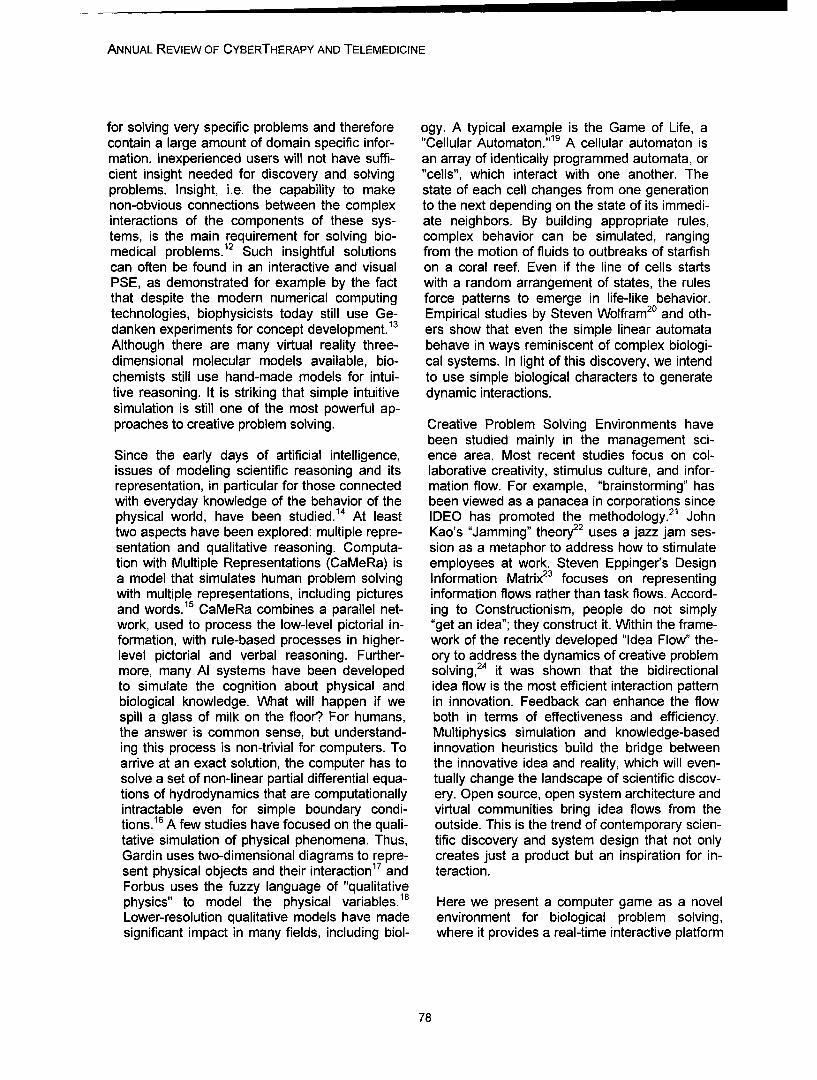
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
for solving very specific problems and therefore ogy. A typical example is the Game of Life, acontain a large amount of domain specific infor- "Cellular Automaton."19 A cellular automaton ismation. Inexperienced users will not have suffi- an array of identically programmed automata, orcient insight needed for discovery and solving "cells", which interact with one another. Theproblems. Insight, i.e. the capability to make state of each cell changes from one generationnon-obvious connections between the complex to the next depending on the state of its immedi-interactions of the components of these sys- ate neighbors. By building appropriate rules,tems, is the main requirement for solving bio- complex behavior can be simulated, rangingmedical problems.12 Such insightful solutions from the motion of fluids to outbreaks of starfishcan often be found in an interactive and visual on a coral reef. Even if the line of cells startsPSE, as demonstrated for example by the fact with a random arrangement of states, the rulesthat despite the modern numerical computing force patterns to emerge in life-like behavior.technologies, biophysicists today still use Ge- Empirical studies by Steven Wolfram 20 and oth-danken experiments for concept development. 13 ers show that even the simple linear automataAlthough there are many virtual reality three- behave in ways reminiscent of complex biologi-dimensional molecular models available, bio- cal systems. In light of this discovery, we intendchemists still use hand-made models for intui- to use simple biological characters to generatetive reasoning. It is striking that simple intuitive dynamic interactions.simulation is still one of the most powerful ap-proaches to creative problem solving. Creative Problem Solving Environments have
been studied mainly in the management sci-Since the early days of artificial intelligence, ence area. Most recent studies focus on col-issues of modeling scientific reasoning and its laborative creativity, stimulus culture, and infor-representation, in particular for those connected mation flow. For example, "brainstorming" haswith everyday knowledge of the behavior of the been viewed as a panacea in corporations sincephysical world, have been studied.14 At least IDEO has promoted the methodology.21 Johntwo aspects have been explored: multiple repre- Kao's "Jamming" theory22 uses a jazz jam ses-sentation and qualitative reasoning. Computa- sion as a metaphor to address how to stimulatetion with Multiple Representations (CaMeRa) is employees at work. Steven Eppinger's Designa model that simulates human problem solving Information Matrix 23 focuses on representingwith multiple representations, including pictures information flows rather than task flows. Accord-and words.15 CaMeRa combines a parallel net- ing to Constructionism, people do not simplywork, used to process the low-level pictorial in- "get an idea"; they construct it. Within the frame-formation, with rule-based processes in higher- work of the recently developed "Idea Flow" the-level pictorial and verbal reasoning. Further- ory to address the dynamics of creative problemmore, many Al systems have been developed solving,24 it was shown that the bidirectionalto simulate the cognition about physical and idea flow is the most efficient interaction patternbiological knowledge. What will happen if we in innovation. Feedback can enhance the flowspill a glass of milk on the floor? For humans, both in terms of effectiveness and efficiency.the answer is common sense, but understand- Multiphysics simulation and knowledge-baseding this process is non-trivial for computers. To innovation heuristics build the bridge betweenarrive at an exact solution, the computer has to the innovative idea and reality, which will even-solve a set of non-linear partial differential equa- tually change the landscape of scientific discov-tions of hydrodynamics that are computationally ery. Open source, open system architecture andintractable even for simple boundary condi- virtual communities bring idea flows from thetions. 16 A few studies have focused on the quali- outside. This is the trend of contemporary scien-tative simulation of physical phenomena. Thus, tific discovery and system design that not onlyGardin uses two-dimensional diagrams to repre- creates just a product but an inspiration for in-sent physical objects and their interaction17 and teraction.Forbus uses the fuzzy language of "qualitativephysics" to model the physical variables.18 Here we present a computer game as a novelLower-resolution qualitative models have made environment for biological problem solving,significant impact in many fields, including biol- where it provides a real-time interactive platform
78

CAI ET AL.
Figure 1. World model and biological characters implemented in the game. A. Wireframe model ofthe vascular system world model. B. 3-D photorealistic model showing arteries and capillaries. C.The Macrophage (white blood cell) is inside the blood stream with red blood cells. D. After activelymoving out of the blood stream, the macrophage approaches bacteria that infected human body tis-sue.
for users. The goal of this study is to develop a to develop an interactive interface modeled aftergame-based PSE for users to explore multi- traditional game engines that teaches users with-modal interactions inside a biological system. It out background in biology the understanding ofincludes essential biological simulation models this research problem ranging in hierarchy fromfor the immune system and the blood system. It atomic to macroscopic scales (Fig. 1). In this hi-allows users to manipulate and to participate in erarchy, the macroscopic level is that of infectionthe interactions among the components of the of a human body with Neisseria. Fighting the in-system. The biological characters are simulated fection requires a molecular level understandingby software agents. of the processes involved. The goal is to provide
the user with the necessary insight to creativelyPROTOTYPE generate and test possible approaches to solving
this problem using the simulator.As a test bed for the development of a game-based Gedanken experiment system for bio- BioSim version 1.0 is a rapid prototype for thismedical science, we designed a scientific prob- system. It is a two-stage game that simulateslem that is derived from our ongoing research the journey of red blood cells and white bloodprojects. By applying computational language cells (macrophages). The goal is to introducetechnologies to the large amounts of whole ge- the basic concepts of cellular interaction and thenome sequence data publicly available, we have human immune system. The game begins withidentified "genome signatures" that may provide an animated scene of a blood stream with rednovel approaches to the development of vac- and white cells moving passively with the heart-cines against 2pathogenic microorganisms such beat. Using a mouse and the arrow keys, theas Neisseria.2 The biomedical problem to be player can take the role of a biological charac-explored here is to find treatment for fatal menin- ter, for example a macrophage, and navigategitis. The new idea for the biomedical simulator is

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
inside the blood stream. The user can actively SYSTEM ARCHITECTUREmove to tissue that is infected by bacterial cells,which multiply at a certain speed. Screen shots The PSE contains three interaction modes: role-of these processes are shown in Fig. 2. play, voyage and networked problem solving.
BioSim 1.0 is implemented on PC. Photorealis- Role-Play. The system allows the user to be atic 3D models of components of the system biological character in the game. Cognition Sci-were created with 3D Studio Max and exported ence shows that role-play is an important way toto Game Studio 3D (an example is shown in stimulate creative ideas. It enables the user toFig. 3). The 3D Modeler of GameStudio 3D was have an intimate connection to the character.used to create the game scenes, biomorphed Also, personalization of a biological charactercharacters and the integration of the world/ makes a game more interactive.character dynamics and interactions. C-script, aC-style language, was used to encode the bio- Voyage. The user can navigate through the bio-dynamics and bio-sensing behaviors. Game logical system in the game, either as a character,Studio is run under the Windows operation sys- or using a 'ship', supporting different view angles,tem. It provides capability for either single user e.g. traveling through capillaries and tissues.or multiple users across the Internet. Voyage allows exploration at the user's chosen
leisure, accommodating users with various back-BIOLOGICAL "WORLD MODEL" grounds.
In game design, "world models" are similar to Distributed Problem Solving. The game en-the theatre stage or film scene with which actors gine allows users to play the game over the Inter-and characters interact. A world model is often net so that large problems can be solved collabo-static and large in size. In this project, we devel- ratively or antagonistically, e.g. some users canoped a comprehensive world model that in- play macrophages and others can play bacteria.cludes the vascular system with artery, veins The distributed problem solving enables diverseand capillaries, as well as tissues (Fig. 1 A,B). game strategies and more excitement of theIn this world, the user can fly, walk or run game. The user can also choose between twothrough as one of the biological characters (Fig. aims, rather than playing the role of a single bio-1 C,D). In the prototype BioSim 1.0, we have logical component only. The user can assumedeveloped two scenes: inside and outside of the the roles of multiple biological characters, thuscapillary. The transition of the scenes is possi- studying their individual influence on a particularble by "squeezing" a character actively from the aim. These aims are to induce an infection withblood stream to the tissue in the capillary re- Neisseria and ensure its successful propagationgions. in the human body or to fight the Neisseria infec-
tion.BIOLOGICAL CHARACTERS
BIOLOGICAL CHARACTER LIBRARYWe have defined the following 3D animatedcharacters that simulate biological behavior: A biological character is defined as an entitybacteria, macrophages, and red blood cells. To that includes functions, forms, behaviors anddefine interactions among characters and be- interfaces. For example, some of the functionstween the characters and the world model, we of a macrophage are to locate and destroy bac-use collision detection (section 2.4.3 below). For teria (see below), while the function of a bacte-the stand-alone characters, we apply bio- rium is to divide and spread. A given charactermorphing to assign key frames to them (section has a sequence of forms in correspondence to2.4.2 below). Bio-morphing is accomplished by its dynamic behaviors. An interface to interactdigitizing deformed shapes from microscopic with other entities or the environment is de-images of organisms, building wire frames and signed.attaching texture and color skins.
Example Macrophage:Functions = locate bacteria I destroy bacteria
80
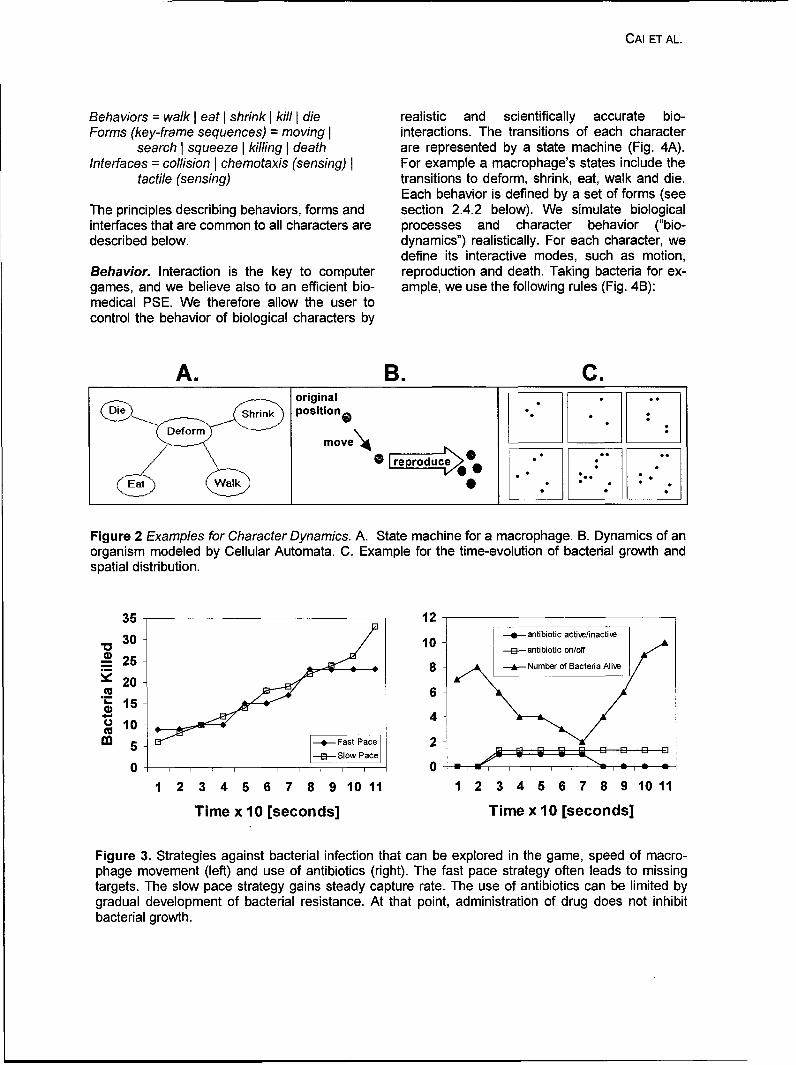
CAI ET AL.
Behaviors = walk I eat I shrink I kill I die realistic and scientifically accurate bio-Forms (key-frame sequences) = moving I interactions. The transitions of each character
search I squeeze I killing I death are represented by a state machine (Fig. 4A).Interfaces = collision I chemotaxis (sensing) I For example a macrophage's states include the
tactile (sensing) transitions to deform, shrink, eat, walk and die.Each behavior is defined by a set of forms (see
The principles describing behaviors, forms and section 2.4.2 below). We simulate biologicalinterfaces that are common to all characters are processes and character behavior ("bio-described below. dynamics") realistically. For each character, we
define its interactive modes, such as motion,Behavior. Interaction is the key to computer reproduction and death. Taking bacteria for ex-games, and we believe also to an efficient bio- ample, we use the following rules (Fig. 4B):medical PSE. We therefore allow the user tocontrol the behavior of biological characters by
A. B. C.original
Shrink position"
move\•4
Figure 2 Examples for Character Dynamics. A. State machine for a macrophage. B. Dynamics of anorganism modeled by Cellular Automata. C. Example for the time-evolution of bacterial growth andspatial distribution.
35 -1230 102- antibiotic active/inactiwe
3310 --- antibiotic on/off
25 8 Number of Bacteria A28-S20
6"15
o10S5 - Fast Pace 2
-E-- Slow Pace 3 E El
0 II0
1 2 3 4 5 6 7 8 9 10 11 1 2 3 4 5 6 7 8 9 10 11
Time x 10 [seconds] Time x 10 [seconds]
Figure 3. Strategies against bacterial infection that can be explored in the game, speed of macro-phage movement (left) and use of antibiotics (right). The fast pace strategy often leads to missingtargets. The slow pace strategy gains steady capture rate. The use of antibiotics can be limited bygradual development of bacterial resistance. At that point, administration of drug does not inhibitbacterial growth.
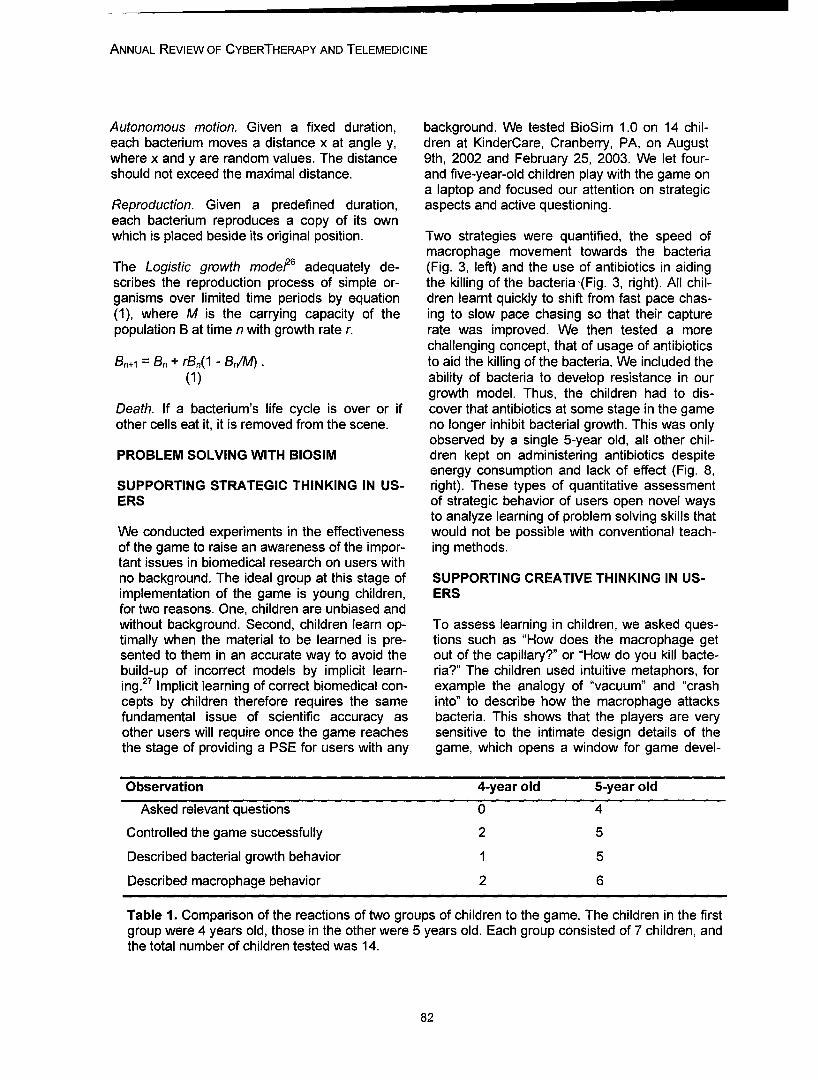
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Autonomous motion. Given a fixed duration, background. We tested BioSim 1.0 on 14 chil-each bacterium moves a distance x at angle y, dren at KinderCare, Cranberry, PA, on Augustwhere x and y are random values. The distance 9th, 2002 and February 25, 2003. We let four-should not exceed the maximal distance. and five-year-old children play with the game on
a laptop and focused our attention on strategicReproduction. Given a predefined duration, aspects and active questioning.each bacterium reproduces a copy of its ownwhich is placed beside its original position. Two strategies were quantified, the speed of
macrophage movement towards the bacteriaThe Logistic growth modef 6 adequately de- (Fig. 3, left) and the use of antibiotics in aidingscribes the reproduction process of simple or- the killing of the bacteria (Fig. 3, right). All chil-ganisms over limited time periods by equation dren learnt quickly to shift from fast pace chas-(1), where M is the carrying capacity of the ing to slow pace chasing so that their capturepopulation B at time n with growth rate r. rate was improved. We then tested a more
challenging concept, that of usage of antibioticsBn+1 = B, + rBn(1 - B'A4). to aid the killing of the bacteria. We included the
(1) ability of bacteria to develop resistance in ourgrowth model. Thus, the children had to dis-
Death. If a bacterium's life cycle is over or if cover that antibiotics at some stage in the gameother cells eat it, it is removed from the scene. no longer inhibit bacterial growth. This was only
observed by a single 5-year old, all other chil-PROBLEM SOLVING WITH BIOSIM dren kept on administering antibiotics despite
energy consumption and lack of effect (Fig. 8,SUPPORTING STRATEGIC THINKING IN US- right). These types of quantitative assessmentERS of strategic behavior of users open novel ways
to analyze learning of problem solving skills thatWe conducted experiments in the effectiveness would not be possible with conventional teach-of the game to raise an awareness of the impor- ing methods.tant issues in biomedical research on users withno background. The ideal group at this stage of SUPPORTING CREATIVE THINKING IN US-implementation of the game is young children, ERSfor two reasons. One, children are unbiased andwithout background. Second, children learn op- To assess learning in children, we asked ques-timally when the material to be learned is pre- tions such as "How does the macrophage getsented to them in an accurate way to avoid the out of the capillary?" or "How do you kill bacte-build-up of incorrect models by implicit learn- ria?" The children used intuitive metaphors, foring. 27 Implicit learning of correct biomedical con- example the analogy of "vacuum" and "crashcepts by children therefore requires the same into" to describe how the macrophage attacksfundamental issue of scientific accuracy as bacteria. This shows that the players are veryother users will require once the game reaches sensitive to the intimate design details of thethe stage of providing a PSE for users with any game, which opens a window for game devel-
Observation 4-year old 5-year old
Asked relevant questions 0 4
Controlled the game successfully 2 5
Described bacterial growth behavior 1 5
Described macrophage behavior 2 6
Table 1. Comparison of the reactions of two groups of children to the game. The children in the firstgroup were 4 years old, those in the other were 5 years old. Each group consisted of 7 children, andthe total number of children tested was 14.
82

CAI ET AL.
opers to encode very subtle knowledge about ACKNOWLEDGMENTScomplex biological interactions. Finally, wetested the game-induced stimulation of ques- This work was supported by the Alexander vontioning and creative thinking in the children. The Humboldt-Foundation and Zukunftsinvestition-results are summarized in Table 1. The five- sprogramm der Bundesregierung, Germany.year-old children asked several meaningfulquestions, for example: "Are bacteria germs?" REFERENCES"Where do the white cells go?" "What's a redcell?" "Where do the bacteria live?" "Is the Altshuller, G., The Innovation Algorithm. 2000:macrophage good or bad?" Overall, four-year- Technical Innovation Center.old children asked fewer questions, and most of Sullivan, J.A., Chemotaxis of Human Neutro-their questions were not relevant, for example, phils: Charlottesville, VA, USA. p. 8 min."Do you have other games?" "I don't want my Kass, M., A.P. Witkin, and D. Terzopoulos,head eaten off." These observations suggest Snakes: Active Contour Models. Int. J.that there may be a turning point between ages Computer Vision, 1988. 1(4): p. 321-331.4 and 5 where a PSE can become effective. Roco, M.C. and W.S. Bainbridge, Overview:
Converging Technologies for Improving Hu-SUMMARY man Performance: Nanotechnology, Bio-
technology, Information Technology, andFuture biomedical problem solving is beyond Cognitive Science (NBIC), in Convergingtraditional means because of the existing chal- Technologies for Improving Human Per-lenges in cross-disciplinary communication and formance, M.C. Roco and W.S. Bainbridge,interpretation and utilization of vast quantities of Editors. 2002, Kluwer Academic Publishers:available biomedical data. We want to build a Arlington. p. 1-23.virtual PSE that combines advanced computer Kuchinsky, A., K. Graham, D. Moh, A. Adler, K.graphics, computer vision, artificial intelligence Babaria, and M.L. Creech. Biological Story-technologies and creative instruction technolo- telling: A Software Tool for Biological Infor-gies. In this PSE, cross-disciplinary education mation Organization Based Upon Narrativewill be on-demand, entertaining and interactive. Structure. in AVI. 2002.This will allow focus on discovery and creativity www.sciencemag.org.rather than one-way tutoring. Towards this long- White, A.R., P.E. McClean, and B.M. Slator.term goal, here, we have presented a game- The Virtual Cell: An Interactive, Virtual Envi-based PSE, where users can explore complex ronment for Cell Biology. in Wold Confer-biological interactions with navigation, role-play, ence on Educational Media, Hypermediaand networked collaboration. The study investi- and Telecommunications. 1999. Seattle,gates the system architecture of the biological WA.game, bio-morphing characters, and bio- McClean, P.E., B. Saini-Eidukat, D. Schwert,interactions with bio-sensing and bio-dynamics. B.M. Slator, and A.R. White. Virtual WorldsThe game is based on realistic biological mod- in Large Enrollment Science Classes Sig-els, such as logistic growth models of simple nificantly Improve Authentic Learning. inorganism reproduction and immigration models 12th Intl. Conf. on College Teaching andof cell movements. The prototype has been im- Learning. 2001. Jacksonville, FL: Center forplemented on PC and tested in a preschool en- the Advancement of Teaching and Learn-vironment where users have little knowledge in ing.biology. The experiment shows that the game ir.chem.cmu.edulirprojectlapplets/virtuallab/.greatly inspired users both in concept learning http://www.biointeractive.org/.and entertainment. It supports strategic thinking, Guggisberg, M., P. Fornaro, T. Gyalog, and H.creative thinking, as well as professional inno- Burkhart, An Interdisciplinary Virtual Labo-vative problem solving. Our study suggests that ratory on Nanoscience. Future Generationthe game-based PSE helps users to learn bio- Computer Systems, 2003. 19: p. 133-141.system dynamics and multiple object interac- Cai, Y., Pictorial Thinking. Journal of Cognitiontions. Science, 1986.
Hayden, T., The Inner Einstein, in US News.2002.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
McCarthy, J. and P.J. Hayes, Some Philosophi-cal Problems from the Standpoint of Artifi-cial Intelligence, in Machine Intelligence, D.Michie, Editor. 1969, Edinburgh UniversityPress: Edinburgh.
Simon, H., Models of Thought. Vol. I1. 1989,Yale: Yale Press.
Feynman, R., The Feynman Lectures on Phys-ics. 1963, Reading, Massachusetts: Addi-son-Wesley.
Gardin, F. and B. Meltzer, Analogical Represen-tations of Naive Physics. Artificial Intelli-gence, 1989. 38: p. 139-159.
Forbus, K.D., Qualitative Process Theory. Artifi-cial Intelligence, 1994. 24: p. 85-168.
Gardner, M., Mathematical Games: The Fantas-tic Combinations of John Conway's NewSolitaire Game "Life". Scientific American,1970. 223: p. 120-123.
Wolfram, S., A New Kind of Science. 2002:Wolfram Publishing.
Schrage, M., Serious Play: How the World'sBest Companies Simulate to Innovate.2000, Boston: Harvard Business SchoolPress.
Kao, J., Jamming. 1997: HarperBusiness.Eppinger, S.D., Innovation at the Speed of Infor-
mation. Harvard Business Review, 2001. 79(1): p. 149-158.
Cai, Y. Idea Flow. in International Conf. of De-sign and Management. 2001. Boston.
Ganapathiraju, M., D. Weisser, R. Rosenfeld, J.Carbonell, R. Reddy, and J. Klein-Seetharaman. Comparative N-Gram Analy-sis of Whole-Genome Protein Sequences.in Human Language Technologies. 2002.San Diego.
Guyton, A.C. and J.E. Hall, Textbook of MedicalPhysiology. 1997, Philadelphia: W.B. Saun-ders Co.
Perrig, P. and W.J. Perrig, Implicit and ExplicitMemory in Mentally Retarded, Learning Dis-abled, and Normal Children. Swiss J. ofPsychology, 1995. 54(2): p. 77-86.
Contact
Yang CaiCarnegie Mellon UniversityEmail: [email protected]
84

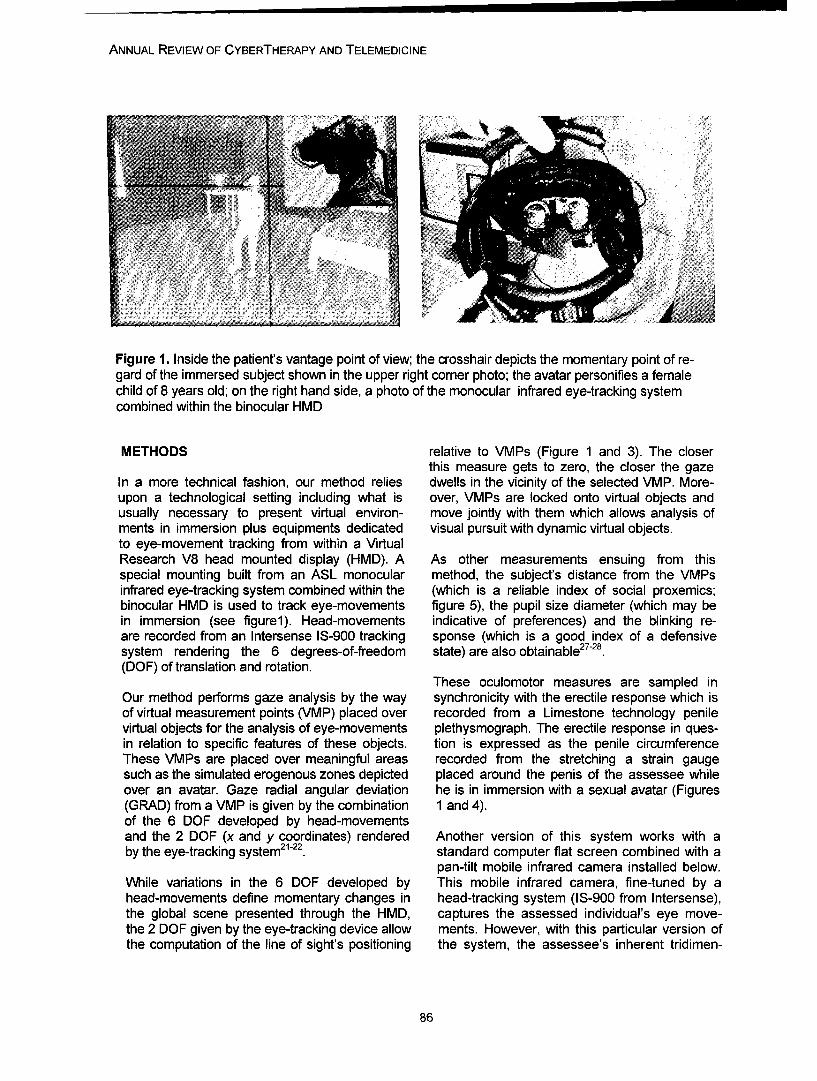
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Figure 1. Inside the patient's vantage point of view; the crosshair depicts the momentary point of re-gard of the immersed subject shown in the upper right corner photo; the avatar personifies a femalechild of 8 years old; on the right hand side, a photo of the monocular infrared eye-tracking systemcombined within the binocular HMD
METHODS relative to VMPs (Figure 1 and 3). The closerthis measure gets to zero, the closer the gaze
In a more technical fashion, our method relies dwells in the vicinity of the selected VMP. More-upon a technological setting including what is over, VMPs are locked onto virtual objects andusually necessary to present virtual environ- move jointly with them which allows analysis ofments in immersion plus equipments dedicated visual pursuit with dynamic virtual objects.to eye-movement tracking from within a VirtualResearch V8 head mounted display (HMD). A As other measurements ensuing from thisspecial mounting built from an ASL monocular method, the subject's distance from the VMPsinfrared eye-tracking system combined within the (which is a reliable index of social proxemics;binocular HMD is used to track eye-movements figure 5), the pupil size diameter (which may bein immersion (see figurel). Head-movements indicative of preferences) and the blinking re-are recorded from an Intersense IS-900 tracking sponse (which is a good index of a defensivesystem rendering the 6 degrees-of-freedom state) are also obtainable27 -2a.(DOF) of translation and rotation.
These oculomotor measures are sampled inOur method performs gaze analysis by the way synchronicity with the erectile response which isof virtual measurement points (VMP) placed over recorded from a Limestone technology penilevirtual objects for the analysis of eye-movements plethysmograph. The erectile response in ques-in relation to specific features of these objects. tion is expressed as the penile circumferenceThese VMPs are placed over meaningful areas recorded from the stretching a strain gaugesuch as the simulated erogenous zones depicted placed around the penis of the assessee whileover an avatar. Gaze radial angular deviation he is in immersion with a sexual avatar (Figures(GRAD) from a VMP is given by the combination 1 and 4).of the 6 DOF developed by head-movementsand the 2 DOF (x and y coordinates) rendered Another version of this system works with aby the eye-tracking system21-22. standard computer flat screen combined with a
pan-tilt mobile infrared camera installed below.While variations in the 6 DOF developed by This mobile infrared camera, fine-tuned by ahead-movements define momentary changes in head-tracking system (IS-900 from Intersense),the global scene presented through the HMD, captures the assessed individual's eye move-the 2 DOF given by the eye-tracking device allow ments. However, with this particular version ofthe computation of the line of sight's positioning the system, the assessee's inherent tridimen-
86

RENAUD ET AL.
Figure 2 Ocular saccades (lines) and fixations (dots) patterns as superimposed over a male adult ava-tar (right) and a female adult avatar (left); 2 minutes data sampling coming from one male heterosexualsubject.
sional visual perspective is not grasped as suchlike with full immersive video-oculography as The virtual stimuli that we use to prompt sexualdescribed above. With this pan-tilt mobile infra- attraction and arousal are animated naked ava-red camera method, measurements are limited tars. These have been designed, developed andto the recording of eye movements as ex- validated in order to make sure that they wouldpressed by ocular saccades and fixations be perceived as representing the required sexualmapped over a 2D plane. Saccades are the properties to assess sexual preference with pe-most common eye movements, they involve dophile patients 23'18. Other paraphilias will ofrapid jumps of the eyes from one position to course require the development of other specificanother while fixation, i.e. the steady gaze hold- virtual environments and avatars. See section 3ing over stationary objects, can be considered for statistical results.as a special case of visual pursuit in which thetarget is at zero velocity; fixation time ranges You can get access to online video and Powerfrom 150ms to 600ms with an average of point documents presenting this method as well300ms; jumps observed in major saccadic eye as the avatars that we developed (hftp-.//movements are usually larger than 1.2 de- w3,u o.ca/cyberpsv/atsa2OO4vid.avi; http.;gree 8. Figure 2 presents two examples of ocu- w3.u o.ca/cvbernsv/atsa2OO4pdf.pdf; 18lar saccades (lines) and fixations (dots) pat-terns as superimposed over a male adult avatar(right) and a female adult avatar (left).
C:÷aze dewia~tion £dceg•
90
20
1 00(.0 2000 31)0. 4I'i0l Si7)110 6(hW(FrlTi- "f, FI-I)
Figure 3. Gazing response as expressed in angular deviation from a virtual measurement point(VMP) marking out the avatar's head; 2 minutes data sampling coming from one subject (expressedin degree).
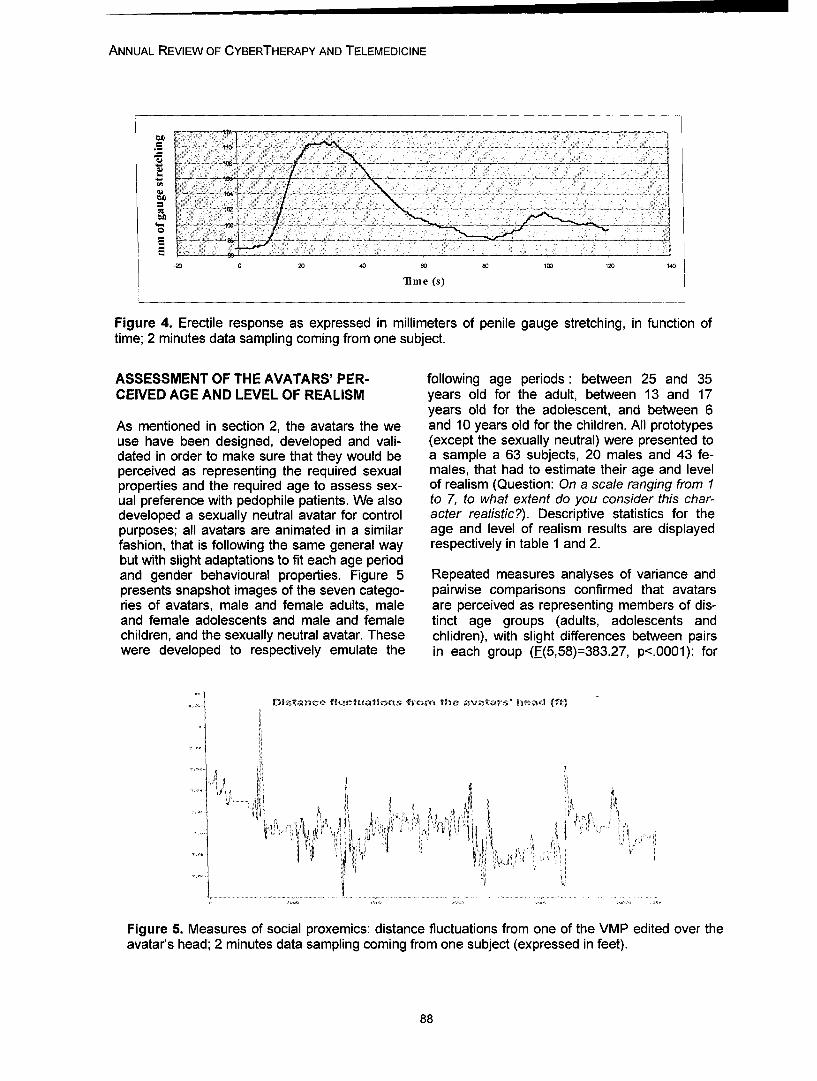
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
-2 0 20 40 60 80 100 120 140
Time (s)
Figure 4. Erectile response as expressed in millimeters of penile gauge stretching, in function oftime; 2 minutes data sampling coming from one subject.
ASSESSMENT OF THE AVATARS' PER- following age periods: between 25 and 35CEIVED AGE AND LEVEL OF REALISM years old for the adult, between 13 and 17
years old for the adolescent, and between 6As mentioned in section 2, the avatars the we and 10 years old for the children. All prototypesuse have been designed, developed and vali- (except the sexually neutral) were presented todated in order to make sure that they would be a sample a 63 subjects, 20 males and 43 fe-perceived as representing the required sexual males, that had to estimate their age and levelproperties and the required age to assess sex- of realism (Question: On a scale ranging from Iual preference with pedophile patients. We also to 7, to what extent do you consider this char-developed a sexually neutral avatar for control acter realistic?). Descriptive statistics for thepurposes; all avatars are animated in a similar age and level of realism results are displayedfashion, that is following the same general way respectively in table 1 and 2.but with slight adaptations to fit each age periodand gender behavioural properties. Figure 5 Repeated measures analyses of variance andpresents snapshot images of the seven catego- pairwise comparisons confirmed that avatarsries of avatars, male and female adults, male are perceived as representing members of dis-and female adolescents and male and female tinct age groups (adults, adolescents andchildren, and the sexually neutral avatar. These chlidren), with slight differences between pairswere developed to respectively emulate the in each group (F(5,58)=383.27, p<.0001): for
Distartc& fiuctuations trom trt avatars'tiow (ft)
Figure 5. Measures of social proxemics: distance fluctuations from one of the VMP edited over theavatar's head; 2 minutes data sampling coming from one subject (expressed in feet).
88
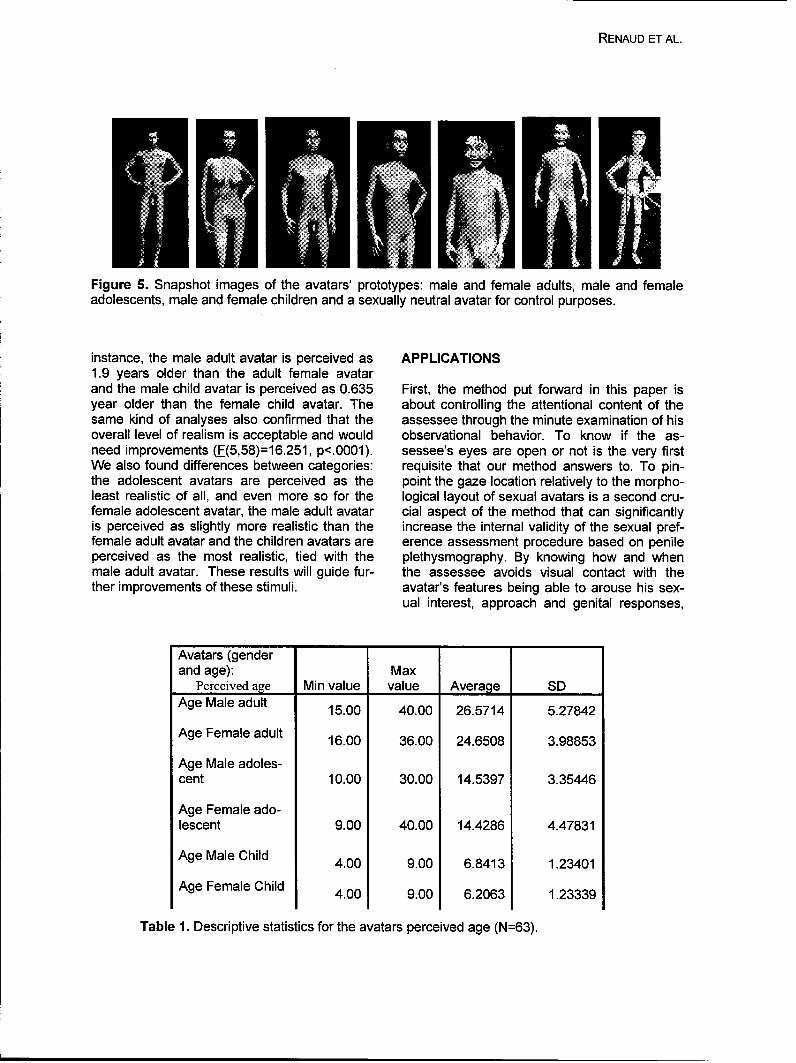
RENAUD ET AL.
441
Figure 5. Snapshot images of the avatars' prototypes: male and female adults, male and femaleadolescents, male and female children and a sexually neutral avatar for control purposes.
instance, the male adult avatar is perceived as APPLICATIONS1.9 years older than the adult female avatarand the male child avatar is perceived as 0.635 First, the method put forward in this paper isyear older than the female child avatar. The about controlling the attentional content of thesame kind of analyses also confirmed that the assessee through the minute examination of hisoverall level of realism is acceptable and would observational behavior. To know if the as-need improvements (F(5,58)=16.251, p<.0001). sessee's eyes are open or not is the very firstWe also found differences between categories: requisite that our method answers to. To pin-the adolescent avatars are perceived as the point the gaze location relatively to the morpho-least realistic of all, and even more so for the logical layout of sexual avatars is a second cru-female adolescent avatar, the male adult avatar cial aspect of the method that can significantlyis perceived as slightly more realistic than the increase the internal validity of the sexual pref-female adult avatar and the children avatars are erence assessment procedure based on penileperceived as the most realistic, tied with the plethysmography. By knowing how and whenmale adult avatar. These results will guide fur- the assessee avoids visual contact with thether improvements of these stimuli, avatar's features being able to arouse his sex-
ual interest, approach and genital responses,
Avatars (genderand age): Max
Perceived age Min value value Average SDAge Male adult 15.00 40.00 26.5714 5.27842
Age Female adult 16.00 36.00 24.6508 3.98853
Age Male adoles-cent 10.00 30.00 14.5397 3.35446
Age Female ado-lescent 9.00 40.00 14.4286 4.47831
Age Male Child 4.00 9.00 6.8413 1.23401
Age Female Child 4.00 9.00 6.2063 1.23339
Table 1. Descriptive statistics for the avatars perceived age (N=63).
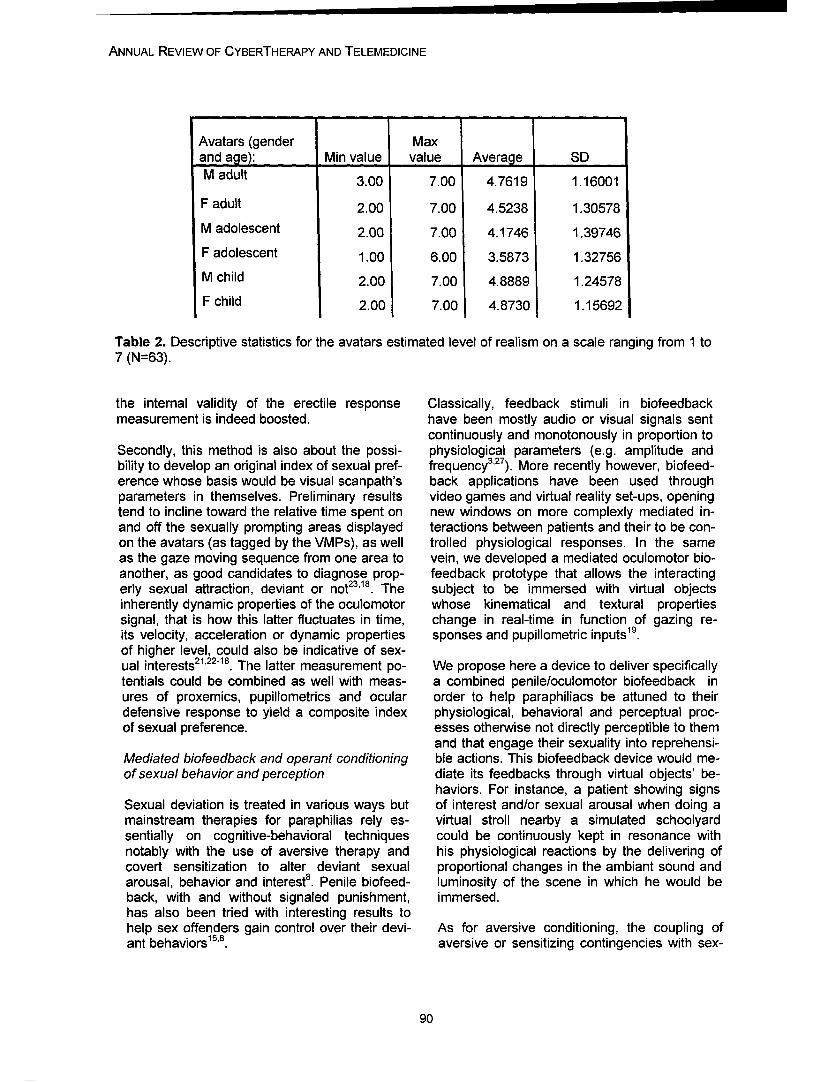
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Avatars (gender Maxand age): Min value value Average SDM adult 3.00 7.00 4.7619 1.16001
F adult 2.00 7.00 4.5238 1.30578
M adolescent 2.00 7.00 4.1746 1.39746
F adolescent 1.00 6.00 3.5873 1.32756
M child 2.00 7.00 4.8889 1.24578
F child 2.00 7.00 4.8730 1.15692
Table 2. Descriptive statistics for the avatars estimated level of realism on a scale ranging from 1 to7 (N=63).
the internal validity of the erectile response Classically, feedback stimuli in biofeedbackmeasurement is indeed boosted. have been mostly audio or visual signals sent
continuously and monotonously in proportion toSecondly, this method is also about the possi- physiological parameters (e.g. amplitude andbility to develop an original index of sexual pref- frequency3 '27 ). More recently however, biofeed-erence whose basis would be visual scanpath's back applications have been used throughparameters in themselves. Preliminary results video games and virtual reality set-ups, openingtend to incline toward the relative time spent on new windows on more complexly mediated in-and off the sexually prompting areas displayed teractions between patients and their to be con-on the avatars (as tagged by the VMPs), as well trolled physiological responses. In the sameas the gaze moving sequence from one area to vein, we developed a mediated oculomotor bio-another, as good candidates to diagnose prop- feedback prototype that allows the interactingerly sexual attraction, deviant or not23 18. The subject to be immersed with virtual objectsinherently dynamic properties of the oculomotor whose kinematical and textural propertiessignal, that is how this latter fluctuates in time, change in real-time in function of gazing re-its velocity, acceleration or dynamic properties sponses and pupillometric inputs19.of higher level, could also be indicative of sex-ual interests2 1 22 '. The latter measurement po- We propose here a device to deliver specificallytentials could be combined as well with meas- a combined penile/oculomotor biofeedback inures of proxemics, pupillometrics and ocular order to help paraphiliacs be attuned to theirdefensive response to yield a composite index physiological, behavioral and perceptual proc-of sexual preference. esses otherwise not directly perceptible to them
and that engage their sexuality into reprehensi-Mediated biofeedback and operant conditioning ble actions. This biofeedback device would me-of sexual behavior and perception diate its feedbacks through virtual objects' be-
haviors. For instance, a patient showing signsSexual deviation is treated in various ways but of interest and/or sexual arousal when doing amainstream therapies for paraphilias rely es- virtual stroll nearby a simulated schoolyardsentially on cognitive-behavioral techniques could be continuously kept in resonance withnotably with the use of aversive therapy and his physiological reactions by the delivering ofcovert sensitization to alter deviant sexual proportional changes in the ambiant sound andarousal, behavior and interest8. Penile biofeed- luminosity of the scene in which he would beback, with and without signaled punishment, immersed.has also been tried with interesting results tohelp sex offenders gain control over their devi- As for aversive conditioning, the coupling ofant behaviors'. aversive or sensitizing contingencies with sex-
90

RENAUD ET AL.
ual responses could be done automatically, in a search and Therapy, 34, 389-394.discrete fashion, when a preset criterion would 6. Harris, G. T., Rice, M. E., Quinsey, V. L., &be reached. For instance, a patient exceeding a Chaplin, T. C. (1999). Dissimulation in phal-preset criterion equivalent to 10% of his maxi- lometric testing of rapists' sexual preferences.mum erectile response and displaying at the Archives of sexual behavior, 34, 223-232.same time a critical visual sampling pattern with 7. Kalmus, E., & Beech, A.R. (2005). Forensicregard to potential simulated victims would see assessment of sexual interest: A review. Ag-himself provided with an aversive or sensitizing gression and Violent Behavior, 10, 193-217.stimulus that could take the form of a virtual 8. Laws, D.R. (2001). Olfactory aversion: Notespoliceman entering the precinct; alternatively, on procedure, with speculations on its mecha-the stimulus could be purely and simply a dras- nism of effect. Sexual Abuse: A Journal of Re-tic removal from the scene to an other environ- search and Treatment, 13, 275-287.ment designed to be aversive, eg: a virtual cell 9. Marshall, W. L., & Fernandez, Y. M. (2000).or a virtual arrest situation or any event that Phallometric testing with sexual offenders:would be particularly aversive to that individual. Limits to its value. Clinical Psychology Review,
20, 807-822.CONCLUSION 10. Palsson, O.S., & Pope, A.T. (1999). Stress
counter-response training of pilots via instru-Concrete applications of virtual reality in mental ment functionality feedback. Abstract, Proceed-health are becoming more and more common. ings of the 1999 Association for Applied Psy-However, virtual reality applications for forensic chophysiology and Biofeedback Meeting, Van-science and correctional rehabilitation are still couver, Canada.not very numerous. With the method put for- 11. Palsson, O.S., Pope, A.T., Ball, J.D.,ward in this paper we tried to bring solutions to Turner, M.J., Nevin, S., & DeBeus, R. (2001).real and important psychological and social Neurofeedback videogame ADHD technology:problems by using the immersive properties of Results of the first concept study. Proceedingsvirtual reality together with the analytical poten- of the 2001 Association for Applied Psycho-tial of eye-tracking technologies, physiology and Biofeedback Meeting, Raleigh-
Durham, NC.REFERENCES 12. Palsson, O.S., & Pope, A.T. (2002). Morph-
ing Beyond Recognition: The Future of Biofeed-1. Abel, G.G., Huffman, J., Warberg, B.W., & back Technologies. Biofeedback, 30 (1), 14-18.Holland, C.L. (1998). Visual reaction time and 13. Proulx, J., Cote, G., & Achille, F.J. (1993).plethysmography as measures of sexual Prevention of Voluntary Control of Penileinterest in child molesters. Sexual Abuse: A Response in Homosexual Pedophiles DuringJournal of Research and Treatment, 10, 81-95. Phallometric Testing. The Journal of Sex2. Abel, G.G., Lawry, S.S., Karlstrom, E.M., Research, 30,140-147.Osborn, C.A. and Gillespie, C.F. (1994). 14. Quinsey, V.L., & Chaplin, T.C. (1988b). Pre-Screening tests for pedophilia. Criminal Justice venting faking in phallometric assessments ofand Behavior, 21(1), 115-131. sexual preference. In R. Prentky and V.L.3. Basmajian, J. V. (1989). Biofeedback: Princi- Quinsey (Eds.), Human sexual aggression: Cur-pies and Practice for Clinicians (3rd ed.), Wil- rent perspectives (pp. 49-58). Annals of the Newliam & Wilkins, Baltimore. York Academy of Sciences, Vol. 528.4. Cho, B. H., Jang, D. P., Lee, J. M., Kim, J. 15. Quinsey, V.L., Chaplin, T.C., & Carrigan,S., Kim, S. I., Ku, J. H., Kim, I. Y., & Lee J. H. W.F. (1980). Biofeedback and signaled punish-(2002). Attention Enhancement System using ment in the modification of inappropriate sexualVirtual Reality and EEG Biofeedback. IEEE Vir- age preferences. Behavior therapy, 11, 567-576.tual Reality Conference 2002, March 24-28, 16. Quinsey, V.L., & Lalumiere, M. (1992). The2002, Orlando, Florida. assessment of sexual offenders against children.5. Harris, G.T., Rice, M.E., Quinsey, V.L. & The APSAC study guide. California: Sage.Chaplin, T.C. (1996). Viewing time as a meas- 17. Renaud, P. (2004). Moving assessment ofure of sexual interest among child molesters sexual interest into the 2 1 st century : the poten-and normal heterosexual men. Behaviour Re- tial of new information technology. Invited
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
speaker at The 2 3 rd Annual Research and In Seguin, M., Leblanc, L. (Eds.), La relationTreatment Conference (Association for the d'aide (pp 251-282). Montreal : EditionsTreatment of Sexual Abusers), Albuquerque, Logiques.27-30 October 2004. 26. Singer, B. (1984). Conceptualizing sexual18. Renaud, P., Albert, G., Sauve, L., Renaud, arousal and attraction. The Journal of Sex Re-L., D6carie, J., & Bouchard, S. (2004). search, 20 (3), 230-240.Assessing perceptual learning dynamics during 27. Schwartz G.E., & Beatty J. (1977).visual search in virtual immersion using eye- Biofeedback: Theory And Research, Academictracking technologies. Proceedings of the IADIS press, New York.International Conference on Cognition and 28. Stern, J.A, Walrath, L.C., & Goldstein R.Exploratory Learning in Digital Age, Lisbon, (1984). The endogenous eyeblink.Portugal: IADIS Press, pp. 413-418. Psychophysiology, 21, 22-33.19. Renaud, P., Bernier, S., Decarie, J., Gourd, 29. Stern, J.A. & Dunham, D.N. (1990). TheS.-P., & Bouchard, S., (2003a). Oculomotor ocular system. In Caccioppo, J.T. & Tassinary,biofeedback mediated in virtual immersion. Pro- L.G. (eds.), Principles ofceedings of the Ninth International Conference psychophysiology:physical, social andon Virtual Systems and Multimedia : Hybrid Re- inferential elements (pp. 513-553). Cambridge,ality : Art, Technology and the Human Factor U.K.: Cambridge University Press.2003 (VSMM), Montreal, pp. 732-740.20. Renaud, P., Bouchard, S., & Proulx, R.(2002a). Behavioral avoidance dynamics in the Contactpresence of a virtual spider. IEEE (Institute ofElectrical and Electronics Engineers). Transac- Patrice Renaud, Ph.D.tions in Information Technology and Bio- Laboratoire de cyberpsychologiemedecine, 6 (3), 235-243. Departement de psychoeducation et de21. Renaud, P., Cusson, J.-F., Bernier, S., psychologieD6carie, J., Gourd, S.-P., & Bouchard, S. Universite du Quebec en Outaouais(2002b). Extracting perceptual and motor invari- Institut Philippe-Pinel de Montrealants using eye-tracking technologies in virtual C.P. 1250, Succ. Bimmersions. Proceedings of HAVE'2002-1EEE Gatineau (Quebec) Canada, J8X 3X7(Institute of Electrical and Electronics Engi- patrice.renaudLc-Duqo~caneers) International Workshop on Haptic Virtual T. : 819 595 3900Environments and their Applications, Ottawa,pp. 73-78.22. Renaud, P., Ddcarie, J., Gourd, S.-P.,Paquin, L.-C., & Bouchard, S. (2003b). Eye-tracking in immersive environments : a generalmethodology to analyze affordance-based inter-actions from oculomotor dynamics. Cyberpsy-chology and Behavior, 6 (5), 519-526.
23. Renaud, P., Rouleau, J.-L.,Granger, L., Barsetti, I., & Bouchard, S.(2002c). Measuring sexual preferences invirtual reality: A pilot sudy. Cyberpsychologyand Behavior, 5 (1), 1-10.24. Renaud, P., Singer, G., & Proulx, R. (2001).Head-tracking fractal dynamics in visually pur-suing virtual objects. In Sulis W., Trofimova I.(Eds.), Nonlinear Dynamics in Life and SocialSciences (NATO Science series, Vol. 320), In-stitute of Science Press (lOS Press), Amster-dam, pp 333-346.25. Rouleau, J.-L., Renaud, P., & Barsetti, I.(2001). Le traitement des agresseurs sexuels.
92

Annual Review of CyberTherapy and Telemedicine
Treating Acrophobia in a Virtual Environment
A. H. Bullinger1, I. Angehrn1, B. K. Wiederhold 2,3, F. Mueller-Spahn1 , R. Mager1
'COAT-Basel / UPK (Center of Applied Technologies in Neuroscience), University of Basel, Switzerland2 Interactive Media Institute, San Diego, USA
3 Virtual Reality Medical Center, San Diego, USA
Abstract: Specific phobias are one of the most frequent mental health problems and can lead toyears of personal suffering. The most effective treatment is exposure therapy. Our aim was to proofthe feasibility and efficacy of virtual environments in treating acrophobia patients using a manuallyguided exposure therapy. Our pilot study was designed as a crossover intervention with a waiting listcondition as a control group. After treatment, our results show that exposure in virtual environmentsis a feasible technique can provoke anxiety, and leads to a therapeutic effect.
INTRODUCTION
Anxiety disorders appear with a lifetime preva- ing virtual environments as an exposure plat-lence of about 25% (12). Chronic processes form there will also be a great success in thehave been observed up to a percentage of 50% investigation of the biological basis of specificin agoraphobic, specifically phobic and socio- phobias: Because the environments generatedphobic cases (24). Among these, specific pho- by the computer are always represented com-bias are the most widespread disorders (11, pletely unmodified and exactly corresponding to16). Currently, the internationally accepted the preceding and succeeding sequences, theytreatment strategy is behavior therapy with ex- are very suitable for studying the psycho-posure (20, 21). Many trials have been con- physiological stimulus-reaction conditions andducted to substitute situations of exposure us- for examining the therapeutic effects on theseing computer-based simulations. Today one psycho-physiological reactions (23).can say that the attempts to develop computer-based psychotherapy programs have not been PILOT STUDYvery successful.
METHODSBut, the early 1990s saw a change, broughtabout by the introduction of virtual reality (VR) Study Designsystems in research at universities. Three-dimensional virtual environments are computer- At first, three test persons were exposed to alti-generated interactive visualizations, in which tude in VR while the other three test personsthe user is able to experience spatial and tem- were supervised in a waiting list conditionporal correlations. Data helmets or specially (WLC). WLC means that the test persons coulddesigned presentation media, based on func- perform self-selected computer games concur-tion units composed of screens and appropriate rently to the exposure therapy. After a break ofprojectors, are used to produce the three- three months the test persons in the WLC diddimensional effects. In the last years, virtual the VR exposure, and the group that had al-environments have often been used by several ready been exposed to altitude played on theresearch teams in Europe and the USA, to re- computer.search, for example, acrophobia (3, 8), claus-trophobia (4), arachnophobia (5) and fear of In a preliminary talk the therapeutic rationaleflying (9,26,27,28). This technique is also used was discussed with the test persons. All of theto study addictions (cue exposure) (15). Fur- six treatments (each with three exposures)thermore, expectations are raised that by apply- were carried out by a therapist with many years
93

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
of clinical experience in psychiatry and training DSM IV (1) were excluded. Especially any psy-in cognitive behavior therapy. On the basis of chotic disorder, suicide attempts in the anamne-empirical and theoretical models the origin, trig- sis, disorders caused by using psychotropicgering factors and the perpetuating factors of substances like addiction, delirium and appar-the specific phobia were explained. Also the ent physical disorders (especially considerablycorrelation of cognitive, affective and vegetative impaired vision or defective hearing) were crite-symptoms of anxiety with situational character- ria for exclusion.istics was described. The model of a dysfunc-tional interaction (also known as "vicious circle") The therapeutic effect was measured by meansof intrapersonal and external stimuli was well of self-evaluation on a 4-point-scale at 5 pointsunderstood by the concerned people because in time: 4 of them were before and after expo-of their own experience. Besides, the negative sure/waiting list (respectively waiting list/impact of anxiety-avoidance on the process of exposure) and one interview was conducted 6the disorder was emphasized. The program months later (figure la). We asked the test per-sequence and the expectations of the test per- sons about the subjective evaluation of theirson were clarified. The expectations were, at discomfort (scale "comfort/discomfort") and theirfirst, very skeptical and affected by frustration of contentment (scale "contentment") and alsomany years, but after the medical education the about the dimension of phobic avoidance (scaleattitude changed regularly into a rather hopeful "avoidance"). These 3 scales measured from "Ione. The test persons were encouraged to fre- feel very good" (point 1) to "I feel veryquent autonomously, in the period between the bad" (point 4).sessions, situations which they had avoided so Furthermore, the concept of the Subjectivefar. All test persons were physically examined Units of Discomfort (SUD (7)) was explained toby a medical doctor. Therefore, somatic dis- the test persons. It refers to an individuallyeases sometimes related to anxiety syndromes "calibrated" rating of the actual anxiety andcould be excluded. In doing so, a psychiatric stress on a scale of 0-100. During the later ex-and medical anamnesis was made. posure, the test person was asked, in intervals
of 5 min, about the level of his anxiety/stress onThe diagnosis of a specific phobia (acrophobia) a scale of 0 (conveniently balanced feeling) towas made by the Composite International Diag- 100 (maximal anxiety). The purpose of thatnostic Interview (CIDI (25)). Other phobias or was, on the one hand, to identify potential cog-comorbid disorders according to ICD-10 and nitive avoidance-strategies and on the other
100 25D
Q -' 20D
70-
60 15
110
"I Z 3 4 5 6 7 l 9 10 9 11121314 151e17 19 2T2222J~i22 30 3214ISS•9
Figure 1. First exposure treatment of test person No. 5. The horizontal axis shows 39 intervals of 5minutes. The left vertical axis indicates the dimension of anxiety (black line with squares) between 0and 100, the right vertical axis indicates the altitude of the elevator in meters (maximal 220m,dashed line with lozenges)
94
BULLINGER ET AL.
hand to survey the impact of the virtual environ- son made during the therapy was discussed.ment on the stress of the test persons. Further- The person was again encouraged to continuemore, the test persons were asked to give their confronting himself with situations he hadsubjective evaluation regarding the dimension avoided so far.of the "worst" anxiety situation. The scale"maximal anxiety" was divided in 10 stages to The first of three confrontations was dominatedsimplify an adaptation to the 100 scale points of by the cognition of anxiety. The test personthe SUDs. should, if possible, experience maximal occur-
rence of anxiety cognitions, anxiety feelings andThe Virtual Environment anxiety physiology. Every session lasted 2-4
hours. During the exposure the test person wasThe computer-based program is generated by asked every 5 min about the level of his anxi-True Space, TCL (the software can be bought) ety/stress measured on a scale ranging from 0-and by Lightning (virtual interaction- and anima- 100 (SUDs). After having surpassed the point oftion software especially created for our applica- culmination of the emotional-vegetative reac-tion, ICIDO Ltd., Stuttgart, Deutschland). The tion, the exposure continued until the test per-virtual environment is visualized by a Silicon son showed a significant subjective easeGraphics (SGI) Onyx2 Deskside System. For (scale: <30).data transfer a Head Mounted Display (V8, Vir-tual Research), a Tracking System (Flock of The test person was instructed to verbalizeBirds, Ascension) and an interaction medium clearly his perception. The therapist was em-(Space Mike, ICIDO Ltd.), also especially cre- pathic-supporting and motivated the test personated for our application, were used. to endure the situation. In principle, the decision
to drop out or to continue the exposure was notThe Exposure made by the therapist. If the test person wanted
to drop out, the therapist was supposed to en-The gradual exposure in VR was made by courage him to continue. An "emergency-stopmeans of the aforementioned technique, alti- procedure" has been arranged individually (i.e.tude "situations" generated by the computer verbal signs as "Stop, it is enough").served to elicit anxiety. A manual was used and(13) served to assure standardization of the Test Personstherapy process; the virtual environment wasalways generated homogenously by the com- The test persons were people from the Ger-puter. man-speaking area around Basel. There was
an advertisement in the newspaper and in theThe manual consisted of an introduction to the period from February 2000 to January 2001, 38technique and information about specific pho- persons answered the advertisement. Twentybias as well as a therapy schedule. of them could be excluded already on the
phone, because either they did not have acro-
* In session 1, in addition to the diagnosis via phobia or they had some other symptoms asthe CIDI and the medical examination, a behav- i.e. eating disorders, alcohol addiction, and ago-ioral analyses (problem definition, analyses of raphobia. Eighteen people were invited to a
condition and function, developing an individual preliminary talk, but 4 of them cancelled it be-
phobia hierarchy) was made. The identification forehand. After the 14 preliminary talks, 2 per-
of further problem areas completed the data sons withdrew their consent for the treatment. 6
acquisition. of the remained 12 persons were selected via a
* In the second session the therapy rationale, random generator and were accepted for the
the schedule and the expectations were dis- pilot study.
cussed. The test person received instructions All 6 test persons were male and did not sufferfor practicing in-between the sessions. from a further somatic mental disorder. They* In session 3 to 5, the test person was con- were socially well-integrated and employed.fronted with the virtual environment. The mean age was 37.8 years.In a final session the experience of the test per-
95
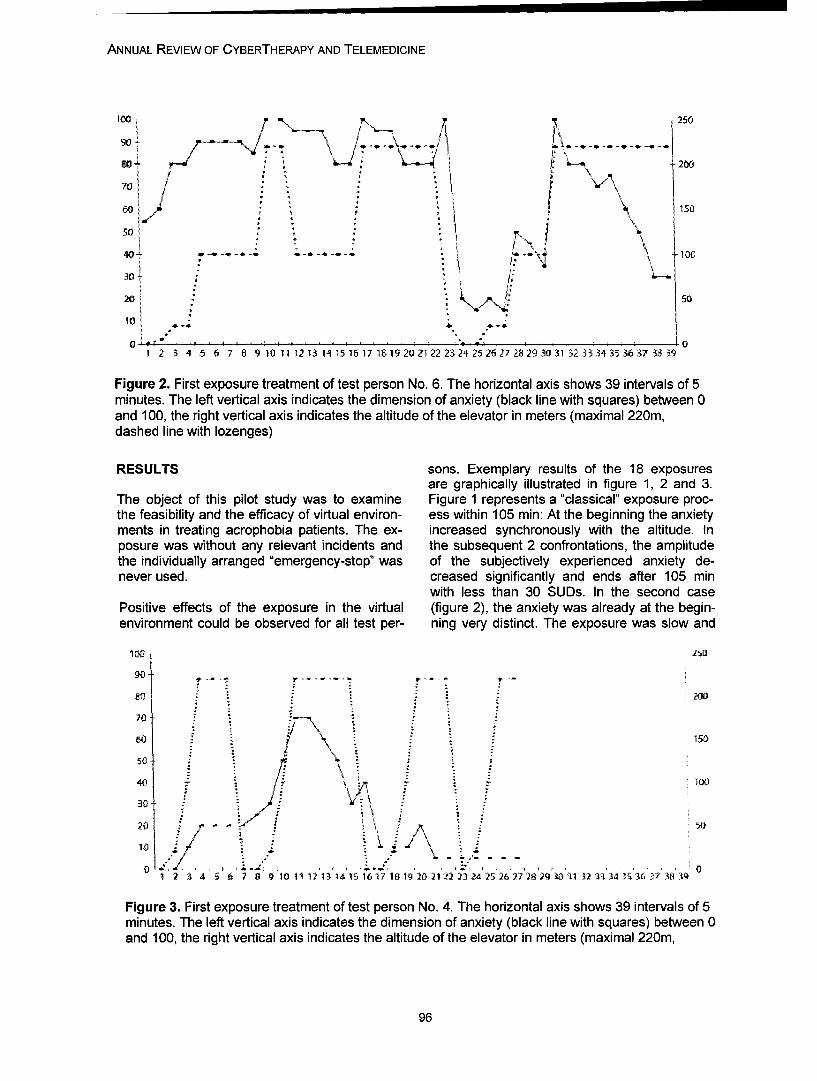
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
'250
go
510
*103~0
201 \R~5
10 .
Figure 2. First exposure treatment of test person No. 6. The horizontal axis shows 39 intervals of 5minutes. The left vertical axis indicates the dimension of anxiety (black line with squares) between 0and 100, the right vertical axis indicates the altitude of the elevator in meters (maximal 220m,dashed line with lozenges)
RESULTS sons. Exemplary results of the 18 exposuresare graphically illustrated in figure 1, 2 and 3.
The object of this pilot study was to examine Figure 1 represents a "classical" exposure proc-the feasibility and the efficacy of virtual environ- ess within 105 min: At the beginning the anxietyments in treating acrophobia patients. The ex- increased synchronously with the altitude. Inposure was without any relevant incidents and the subsequent 2 confrontations, the amplitudethe individually arranged "emergency-stop" was of the subjectively experienced anxiety de-never used. creased significantly and ends after 105 min
with less than 30 SUDs. In the second casePositive effects of the exposure in the virtual (figure 2), the anxiety was already at the begin-environment could be observed for all test per- ning very distinct. The exposure was slow and
400 100J
200
10 Z
: " 150
50
1 56 7 10001 231 S16711 022 32 2 62 8J3 1323 43 63 83III
Figure 3. First exposure treatment of test person No. 4. The horizontal axis shows 39 intervals of 5minutes. The left vertical axis indicates the dimension of anxiety (black line with squares) between 0and 100, the right vertical axis indicates the altitude of the elevator in meters (maximal 220m,
96
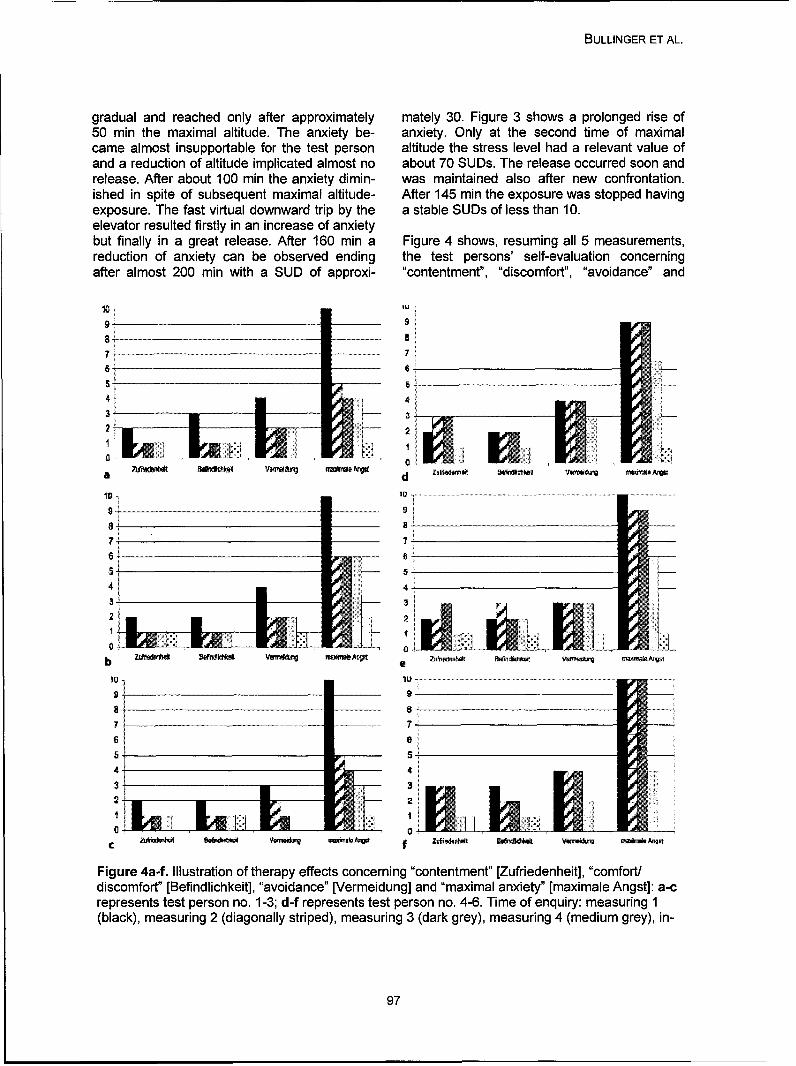
BULLINGER ET AL.
gradual and reached only after approximately mately 30. Figure 3 shows a prolonged rise of50 min the maximal altitude. The anxiety be- anxiety. Only at the second time of maximalcame almost insupportable for the test person altitude the stress level had a relevant value ofand a reduction of altitude implicated almost no about 70 SUDs. The release occurred soon andrelease. After about 100 min the anxiety dimin- was maintained also after new confrontation.ished in spite of subsequent maximal altitude- After 145 min the exposure was stopped havingexposure. The fast virtual downward trip by the a stable SUDs of less than 10.elevator resulted firstly in an increase of anxietybut finally in a great release. After 160 min a Figure 4 shows, resuming all 5 measurements,reduction of anxiety can be observed ending the test persons' self-evaluation concerningafter almost 200 min with a SUD of approxi- "contentment", "discomfort", "avoidance" and
10 NU9- 9
a- d
6
4t,I ;
o o
dicmot [Bfnlihet, aodac"[eredng n maxma Bandity [m-axim -ale kAngst]a-
10-
represents test person no. 1-3; d-f represents test person no. 4-6. Time of enquiry: measuring 1(black), measuring 2 (diagonally striped), measuring 3 (dark grey), measuring 4 (medium grey), in-
97

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
maximal anxiety in single situations. One can gency-stop even if they often talked about doingsee that all test persons experienced the ther- it. In a real exposure such moments are veryapy as successful. This estimation was stable critical because the avoidance is easy to do.for 6 months: The subjectively felt comfort in- Drop-out is known as a common strategy and iscreased and previously avoided situations were almost automated. The very different way of thefrequented more and more and were experi- virtual environment could be a cesura in thisenced with decreasing anxiety. Discontent, dis- automation. These experiences have to be in-comfort and the degree of avoidance were terpreted with caution. The test persons wereevaluated by the test persons on a scale rang- typical for specific phobic disorders insofar asing from 0 (no problem) to 4 (every altitude with the beginning of the disorder was in early adult-more than 5 m was avoided). The evaluations hood and was chronically restricting. Among allwere to be explicitly subjective and general. In the healing attempts there were psychothera-terms of "discontent" the test person was asked peutic treatments of "school psychology", so-to what extent he was discontent because of his called alternative intervention and even esotericphobia. With regard to "comfort/discomfort" he practices. Some of our test persons also triedwas asked how much the phobia affects his sporadically to reduce their anxiety in takingphysical and mental orientation. An occurrence "benzodiazepines" or alcohol.of 2 and 3 improved to 0-1. "Avoidance" meantthe avoidance of being in altitude. This avoid- Because of using self-evaluation-scales there isance was at the beginning 3-4 and after 6 another limitation of the data. This process ismonths only 0-1. The occurrence of anxiety was common in therapeutic terms, but leads to diffi-also quantified by a 0-100-scale. All test per- culties in the evaluation of the data and in itssons experienced values of 90 or even more comparability. The technique of the VR couldbefore they underwent the therapy. After 6 be a great advantage because of its standardi-months the Subjective Units of Discomfort were zation. During exposure, additional physiologi-only around 10. cal parameters (23) could be measured forming
the objective of the so far only subjective aspectDISCUSSION of anxiety. In this case, the investigation of the
biological basis of the specific phobias is auspi-The pilot study shows that an exposure in a cious by means of using virtual environmentsvirtual environment is possible and evokes anxi- as an exposure platform. Because the com-ety among patients suffering from a specific puter-generated environments are always rep-phobia and has therapeutic effects. It has not resented completely unmodified compared tobeen clarified so far to what extent habituation- the preceding and succeeding processes, theyprocesses and to what extent cognitive restruc- are suitable for the study of the psycho-turings took place. physiological stimulus-reaction conditions and
for the examination of the therapeutic effectsPossible side effects of virtual environments are resulting from these psycho-physiological reac-sickness in the simulator (2) or impaired vision tions.after the exposure (18). According to our inquirynone of the 6 test persons experienced such or CONCLUSIONother side effects. The experience was domi-nated by anxiety symptoms as i.e. sweating, Our pilot study showed an improvement in allgastrospasms, nervousness and sometimes the measured domains (contentment, comfort/even "panic" anxiety. The pressure of the data discomfort, anxiety occurrence, avoidance).helmet on the head, vertigo, sickness or further The occurrence of the test person's anxiety di-disturbances were not said to be disagreeable. minished significantly during exposure. Situa-It can be supposed that because of the subjec- tions previously avoided were frequented. Gen-tive threat of the virtual altitude such further dis- eral life-contentment and comfort rose. The im-agreeable feeling have been suppressed. Coin- provement after the therapy is very evidentpared to exposures in vivo, the test persons among the test persons. The waiting conditionshowed -in vitro- very similar reaction patterns. "computer games" changed nothing. After 6It is remarkable that nobody used the emer- months the positive results could still be ob-
98
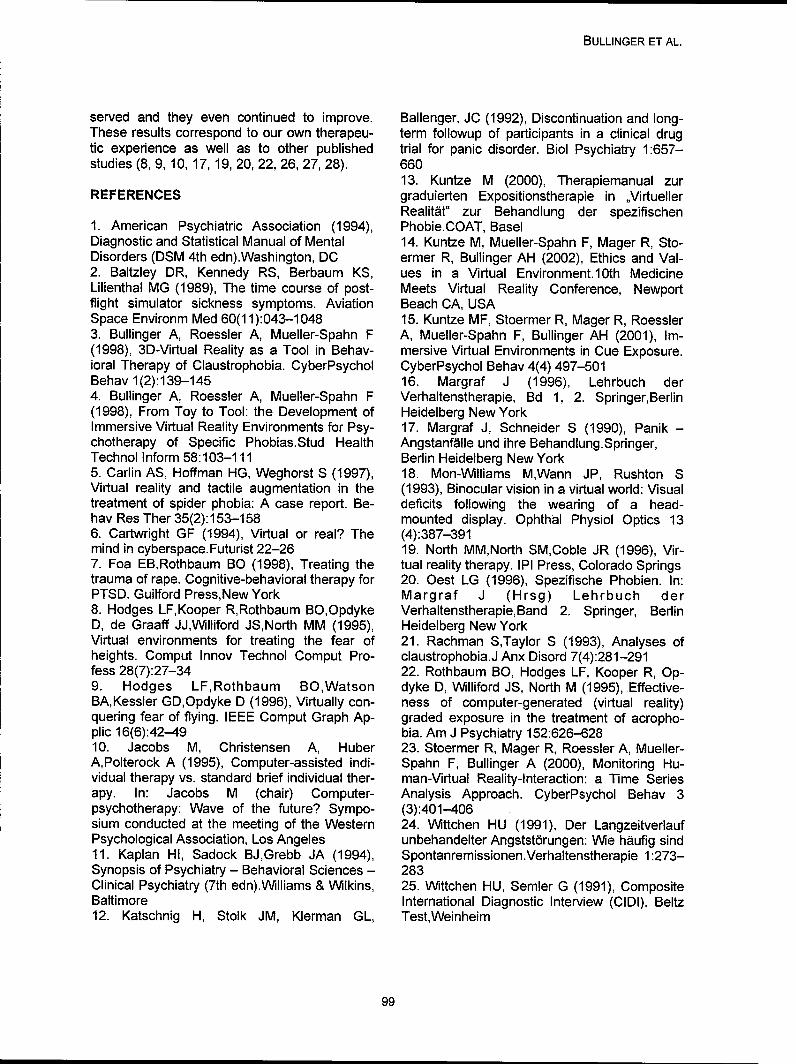
BULLINGER ET AL.
served and they even continued to improve. Ballenger, JC (1992), Discontinuation and long-These results correspond to our own therapeu- term followup of participants in a clinical drugtic experience as well as to other published trial for panic disorder. Biol Psychiatry 1:657-studies (8, 9, 10, 17, 19, 20, 22, 26, 27, 28). 660
13. Kuntze M (2000), Therapiemanual zurREFERENCES graduierten Expositionstherapie in ,,Virtueller
Realitat" zur Behandlung der spezifischen1. American Psychiatric Association (1994), Phobie.COAT, BaselDiagnostic and Statistical Manual of Mental 14. Kuntze M, Mueller-Spahn F, Mager R, Sto-Disorders (DSM 4th edn).Washington, DC ermer R, Bullinger AH (2002), Ethics and Val-2. Baltzley DR, Kennedy RS, Berbaum KS, ues in a Virtual Environment. 10th MedicineLilienthal MG (1989), The time course of post- Meets Virtual Reality Conference, Newportflight simulator sickness symptoms. Aviation Beach CA, USASpace Environm Med 60(11):043-1048 15. Kuntze MF, Stoermer R, Mager R, Roessler3. Bullinger A, Roessler A, Mueller-Spahn F A, Mueller-Spahn F, Bullinger AH (2001), Im-(1998), 3D-Virtual Reality as a Tool in Behav- mersive Virtual Environments in Cue Exposure.ioral Therapy of Claustrophobia. CyberPsychol CyberPsychol Behav 4(4) 497-501Behav 1(2):139-145 16. Margraf J (1996), Lehrbuch der4. Bullinger A, Roessler A, Mueller-Spahn F Verhaltenstherapie, Bd 1, 2. Springer,Berlin(1998), From Toy to Tool: the Development of Heidelberg New YorkImmersive Virtual Reality Environments for Psy- 17. Margraf J, Schneider S (1990), Panik -chotherapy of Specific Phobias.Stud Health Angstanfalle und ihre Behandlung.Springer,Technol Inform 58:103-111 Berlin Heidelberg New York5. Carlin AS, Hoffman HG, Weghorst S (1997), 18. Mon-Williams M,Wann JP, Rushton SVirtual reality and tactile augmentation in the (1993), Binocular vision in a virtual world: Visualtreatment of spider phobia: A case report. Be- deficits following the wearing of a head-hav Res Ther 35(2):153-158 mounted display. Ophthal Physiol Optics 136. Cartwright GF (1994), Virtual or real? The (4):387-391mind in cyberspace.Futurist 22-26 19. North MM,North SM,Coble JR (1996), Vir-7. Foa EB,Rothbaum BO (1998), Treating the tual reality therapy. IPI Press, Colorado Springstrauma of rape. Cognitive-behavioral therapy for 20. Oest LG (1996), Spezifische Phobien. In:PTSD. Guilford Press,New York Margraf J (Hrsg) Lehrbuch der8. Hodges LF,Kooper R,Rothbaum BO,Opdyke Verhaltenstherapie, Band 2. Springer, BerlinD, de Graaff JJ,Williford JS,North MM (1995), Heidelberg New YorkVirtual environments for treating the fear of 21. Rachman STaylor S (1993), Analyses ofheights. Comput Innov Technol Comput Pro- claustrophobia.J Anx Disord 7(4):281-291fess 28(7):27-34 22. Rothbaum BO, Hodges LF, Kooper R, Op-9. Hodges LF,Rothbaum BO,Watson dyke D, Williford JS, North M (1995), Effective-BA,Kessler GD,Opdyke D (1996), Virtually con- ness of computer-generated (virtual reality)quering fear of flying. IEEE Comput Graph Ap- graded exposure in the treatment of acropho-plic 16(6):42-49 bia. Am J Psychiatry 152:626-62810. Jacobs M, Christensen A, Huber 23. Stoermer R, Mager R, Roessler A, Mueller-A,Polterock A (1995), Computer-assisted indi- Spahn F, Bullinger A (2000), Monitoring Hu-vidual therapy vs. standard brief individual ther- man-Virtual Reality-Interaction: a Time Seriesapy. In: Jacobs M (chair) Computer- Analysis Approach. CyberPsychol Behav 3psychotherapy: Wave of the future? Sympo- (3):401-406sium conducted at the meeting of the Western 24. Wittchen HU (1991), Der LangzeitverlaufPsychological Association, Los Angeles unbehandelter Angstst6rungen: We hiufig sind11. Kaplan HI, Sadock BJ,Grebb JA (1994), Spontanremissionen.Verhaltenstherapie 1:273-Synopsis of Psychiatry - Behavioral Sciences - 283Clinical Psychiatry (7th edn).Williams & Wilkins, 25. Wittchen HU, Semler G (1991), CompositeBaltimore International Diagnostic Interview (ClDI). Beltz12. Katschnig H, Stolk JM, Klerman GL, Test,Weinheim
99
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
26. Wiederhold, B.K. (1999). "A comparison ofimaginal exposure and virtual reality exposurefor the treatment of fear of flying" [doctoral dis-sertation]. California School of ProfessionalPsychology.27. Wiederhold, B.K. & Wiederhold, M.D.(2000). "Lessons Learned From 600 Virtual Re-ality Sessions." CyberPsycholoqy & Behavior. 3(3): 393-400.28. Wiederhold, B.K., Wiederhold, M.D.,(2005). Virtual Reality Therapy for Anxiety Dis-orders- Advances in Evaluation and Treatment.Washington, DC: American Psychological As-sociation.
Contact:
Alex H. BullingerCOAT-Basel / UPKWilhelm Klein - Str- 274025 Basel, Switzerlandbua~u)coat-basel.corn
100

Annual Review of CyberTherapy and Telemedicine
Virtual Environments to Address Autistic Social Deficits
C. Y. Trepagnier, Ph.D., M. M. Sebrechts, A. Finkelmeyer, M. Coleman, W. Stewart,Jr., M. Werner-Adler,
The Catholic University of America, Washington, DC
Abstract: Background: Autistic Disorder is defined by social and communicative impairments andrestricted, narrow interests. Impaired motivation is also common. Several investigators have devel-oped computer-based and virtual environment tools to address various issues in autism(I-5). Fourprojects at CUA address the social impairment.
Method/Tools: Face Processing. The prediction that autistic face processing impairment involvesgaze differences was tested in an eye tracking study using a VR display. A replication in progressuses a monitor. Early Intervention. A virtual environment, with kiddie-ride, monitor display and eyetracker, is being tested. The goal is to induce young children with autism to attend to faces. SocialNavigation. A joystick-navigable, first-person-perspective shopping mall is presented on a monitor.To locate objects, the user must move either between or around social and non-social obstacles.Data include user comments and path records. Training in Social Conversation. SIMmersion LLCTMare collaborating with us to develop a social conversation module for adults with Asperger's Disor-der. A virtual character remembers the conversation and responds as would an actual interlocutor tothe user's speech.
Results: Face Processing. Preliminary results (with headset) confirmed gaze differences(6). The rep-lication is in progress. Early intervention. Reliability-testing is being completed. Social Navigation.Controls describe their avatar's actions in the first person, and refrain from walking between con-versing characters. Data collection with persons with autism has begun. Training in Social Conversa-tion. Development is in progress.
Discussion: The projects described above derive from the hypothesis that failure to establish spe-cies-typical face attention and processing itself undermines cognitive development(7). Accordinglyface processing is targeted in young children, and compensatory training is addressed with olderindividuals. The challenge is to make the technology not only effective, but adequately entertainingto overcome autistic motivational barriers.
INTRODUCTION
Autism Spectrum Disorder (ASD) is character- people's behavior. During adolescence andized by impairment in verbal and nonverbal young adulthood some individuals with ASDcommunication skills and social interaction, and develop enough insight to become aware thatthe presence of repetitive behavior and narrow, they are different from their peers, and experi-obsessive interests, according to the standard ence loneliness and sadness.diagnostic criteria used in research over thepast decade.1 While ASD can be diagnosed as Once thought to be rare, ASD and related dis-early as 18 months, and most individuals are orders are now being identified in large num-diagnosed by or near the start of their educa- bers. Prevalence estimates range from 15 to 60tional career, some are not identified until later per 10,000 individuals. 2,3 The symptoms of au-childhood or even adulthood. tism can be mitigated and quality of life im-
proved thanks to evidence-based treatmentsFacial expressions and gestures often hold little such as intensive, autism-specific interventionmeaning for individuals with ASD. As a result it in early childhood,4 '5 and psychopharmacologi-can be very difficult for them to make sense of cal interventions.7' 8 Despite the popular percep-
101

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
tion of autism as a disorder of childhood, most toms of anxiety and depression in individualsindividuals with ASD are adults. with ASD,21 findings that continue to be con-
firmed in more recent studies (e.g., face proc-In summary, there is a large population of chil- essing impairment22' 23; psychiatric comorbid-dren and older individuals who have severe ity2 5-2). It was hypothesized that infant onset ofdeficits in their ability to interpret facial expres- symptoms of anxiety and depressive disordersions and other nonverbal behavior; and could disrupt face attention, with the conse-equivalent lacks in their ability to transmit com- quence that the bases of face processing wouldmunication through these channels. The ASD not be established during the period when thesyndrome results in a variety of social impair- infant is most apt, biologically, neurologicallyments that constitute major obstacles to the and behaviorally, for face processing to takeindividual's possibilities of achieving independ- root.29 Following is a brief description of fourence and sustained employment, and having projects at CUA that address autistic social im-friends and intimate relationships. pairments: Face Gace, Early Intervention, the
Virtual Mall, and development of a Simulation toInterventions to modify the young child's devel- Train Conversational Interactionopmental course, or to teach older individualsskills that were not acquired naturally in child- FACE GAZEhood cannot approach in duration or intensitythe on-going, unavoidable social instruction that These studies addressed the hypothesis thatis experienced by typically developing individu- autistic differences in face processing wouldals. The most intensive autism intervention pro- have correlates in gaze behavior, specificallygrams are offered primarily to young children that people with ASD would not look at the(generally aged two to four), and these pro- same locations on the face as controls. Bygrams target a range of skills, among which means of a VR headset in which an eye track-social interaction is not an important focus. In- ing camera was installed significant differencestensive programs in social skill acquisition for were found between groups: while typically de-older children are rare; for adolescents and veloping participants looked at the interior of theadults with ASD they are largely unavailable, face, persons with ASD showed a greater ten-and the majority of such programs are not dency to look at the periphery.2 9 Since use ofbased on scientific evidence, the headset excluded many potential partici-
pants, a replication using a monitor and desk-Virtual environments have been shown to be top eye tracker was next undertaken. Prelimi-clinically useful for distraction from pain 8'9 and nary analysis of these data has found a signifi-in the treatment of phobias10 -13 and are being cant correlation between gaze at the eye areainvestigated for their applicability to a number of and lesser impairment on the social componentother medical and psychiatric problems. Sev- of the Autism Diagnostic Interview- Revisederal investigators have developed computer- (ADI-R),30 an instrument that focuses primarilybased and virtual environment tools to examine on the individual's behavior at age four. Thissocial behavior in autism14-16 and to improve finding suggests that deficits in early social de-face processing, emotion recognition, and so- velopment may have a lasting effect on howcial problem solving.17-19 The Autism Research these individuals look at faces. Since foveal andGroup at The Catholic University of America perifoveal vision are restricted to a narrow an-shares this focus on exploiting computer and gle, gaze directed at the facial periphery29 or atvirtual reality technology to develop techniques the mouth32 fails to take in with adequate acuityto improve the social competence of individuals the information necessary for interpreting facialwith autism. expression.
Our motivation for approaching autism mitiga- EARLY INTERVENTIONtion through the social deficits grew out of therecognition of the centrality of the social deficit An outgrowth of this project has been to pro-in autism,2° and observation and review of face pose an intervention to teach young childrenprocessing impairments and presence of symp- with autism to direct their gaze to the eye area
102
TREPAGNIER ET AL.
of the face, and to convey that attention to the cord of their navigation paths. Participants toeye area has inherent functional benefits. The date have been 4 females and 4 males (onegoal of this project, therefore, is to develop and with an ASD diagnosis), 7 of whom were Cau-pilot a technique to induce children with ASD casian and one African-American, ranging inaged 24 to 54 months to attend to the meaning- age from 19-27 (Mean age 20.9).ful areas of faces, and to make use of the infor-mation transmitted by them. In order to accom- Virtual activities were defined in detail for theplish this it is critical to attract and sustain the human factors trials in order to assure that allchild's participation, in addition to differentially participants experienced all of the challenges ofrewarding the target gaze behaviors, as sensed the mall, including virtual humans and inani-by a desktop eye tracker. The rewards available mate objects, situated at locations that requirefor this purpose include a wide range of videos, participants to navigate through or around themand 'rides' in the 'kiddie' helicopter in which the in order to reach their target. Placement andmonitor and tracker are installed. Current test- orientation of the virtual humans creates situa-ing addresses the validity of our 'semi- tions that are identical in terms of spatial prop-automatic' calibration technique for children, erties (e.g. space between humans and walls,and adjustments to the positioning of a child or between obstacles and walls) but differ im-car-seat and head-rest for head stabilization portantly in social implications (e.g., passingadequate for reliable eye tracking. A pre-pilot between a person and a store window to whichstudy beginning in May will assess the feasibil- her back is turned, versus passing between twoity of the training schedule for children and their characters facing each other at a conversa-families. tional distance vs. passing between two adver-
tising signs). Choice of path and distance be-VIRTUAL MALL tween the operator's avatar and obstacles
(other humans, inanimate objects and walls)Young children with autism may exhibit a vari- are interpreted as relating to participants' ex-ety of reactions to finding themselves in large, perience of the ecological validity of this envi-busy environments such as airports and shop- ronment. To the extent users' verbal descrip-ping malls. Among the reactions particularly tions, comments and navigational decisionsdisconcerting for parents can be an apparent suggest adequate ecological validity, the envi-insensitivity to the presence of other people, ronment is considered to have potential as atreating them as mildly inconvenient obstacles tool for use in assessing and intervening withthat will give way on approach or even contact. individuals with social impairments, includingAs adolescents and adults, some people with autism.ASD still seem unaware of social spatial con-ventions, walking between two people engaged The controller used was a joystick with minimalin conversation with each other, or passing be- displacement, that moved the avatar in the di-tween a person and a display window at which rection that force was applied. Participants wereshe is looking. The Virtual Mall is being devel- trained in the operation of the controls by fol-oped with the participation of non-disabled and lowing__,a path through large virtual mall corri-ASD adults through an iterative design process, dors, during which they were instructed to avoidusing standardized tasks to draw the user to collision with walls and obstacles. Next theyexplore the environment and encounter its so- were familiarized with the layout of the mall bycial navigational challenges. The long-term goal following experimenter instructions to navigateis the development and evaluation of a clinically to each of the individual stores. The target loca-practical and ecologically valid assessment of tion task entailed navigating to four differentsocial cognition, and a rehabilitation modality to stores to locate in each a box containing a col-improve the ability of individuals with ASD to ored, numbered sphere. The experimenterfunction in everyday environments, named the store in which the next target could
be found, and the participant's task was to lo-Data has been compiled from 8 participants' cate the box, which opened once s/he wascomments during and after performance of the within range, and to read out the number andtasks, as well as an automatically acquired re- name the color. Participants performed two
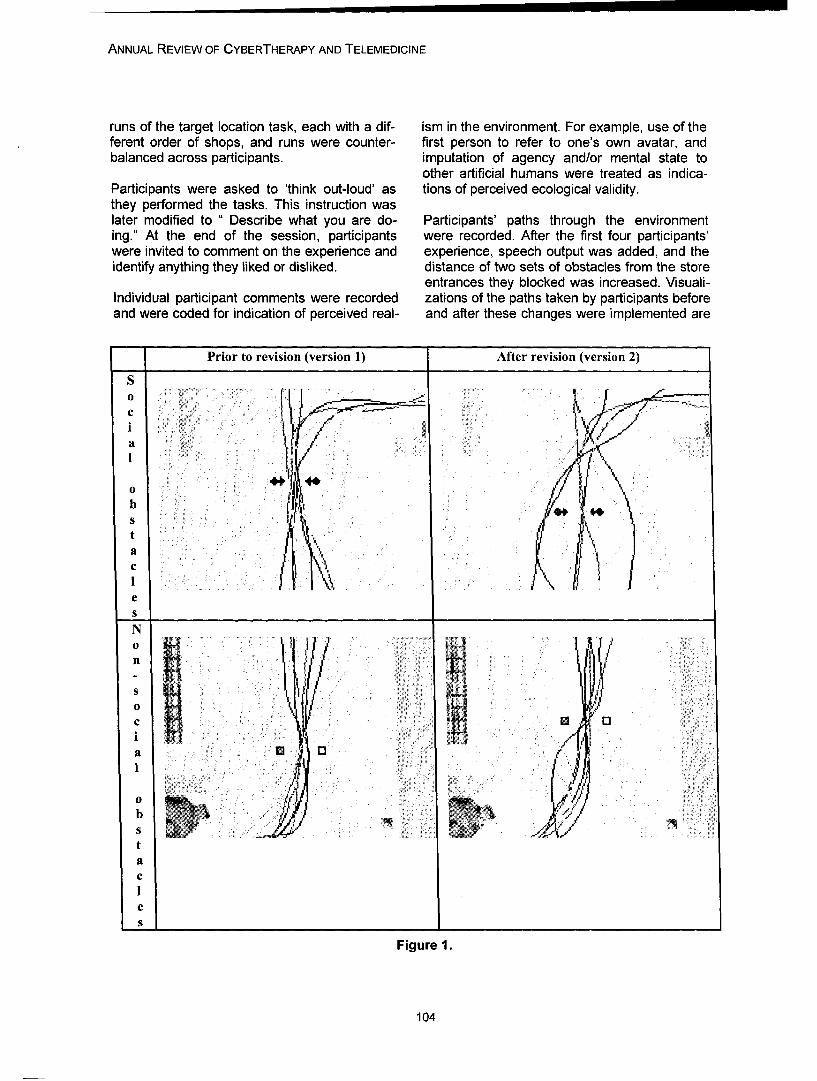
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
runs of the target location task, each with a dif- ism in the environment. For example, use of theferent order of shops, and runs were counter- first person to refer to one's own avatar, andbalanced across participants. imputation of agency and/or mental state to
other artificial humans were treated as indica-Participants were asked to 'think out-loud' as tions of perceived ecological validity.they performed the tasks. This instruction waslater modified to " Describe what you are do- Participants' paths through the environmenting." At the end of the session, participants were recorded. After the first four participants'were invited to comment on the experience and experience, speech output was added, and theidentify anything they liked or disliked, distance of two sets of obstacles from the store
entrances they blocked was increased. Visuali-Individual participant comments were recorded zations of the paths taken by participants beforeand were coded for indication of perceived real- and after these changes were implemented are
Prior to revision (version 1) After revision (version 2)
S
akKo *
00
b ~4S
eS
N
0
a M. 0
b
taC
S
Figure 1.
104
TREPAGNIER ET AL.
shown in Figure 1. All four participants using SIMULATION TO TRAIN CONVERSATIONALVersion 1 (no speech) walked between the two INTERACTIONcharacters who were facing each other, both onentering and exiting the store, and., similarly, Lack of success in initiating and, especially, inwalked between the two inanimate objects. In maintaining a conversation is a hallmark ofcontrast, participants who used the Version 2 of ASD. The impoverished opportunities and poorthe mall, to which speech had been added, success rate of peer interaction persists intowere more likely to walk around the now audibly older adolescence and adulthood, presentingconversing characters, rather than between an obstacle to the casual social interaction thatthem, while all navigated between the inani- is a part of much of human activity. Participatingmate objects, despite the increased ease of in a conversation involves, among other things,circumnavigating both pairs of obstacles, turn-taking, gaining awareness of the topic of
the conversation, interpreting the partner's non-Figure 1: Paths taken in the vicinity of social verbal as well as verbal cues and knowing(virtual humans) vs. non-social (objects) obsta- when and how it is appropriate to change thecles, by participants experiencing Versions 1 topic.and 2 of the Virtual Mall. Arrows indicate thedirection the virtual humans are facing. In Ver- The Autism Research Group is collaboratingsion 2 the two people facing each other can be with SIMmersion LLCTM to develop an interac-heard to converse. In addition, in Version 2, tive social conversation simulation for adultsboth the pair of people and the pair of objects with high-functioning ASD.have been moved farther from the door, so thatit is easier to go around both rather than pass- In this system, the simulated charactering between the two members of the pair. (represented by a data-base of video clips per-
formed by an actor) remembers the conversa-Participants were able to learn rapidly to navi- tion history and responds as would an actualgate the mall, and locate the targets. Review of interlocutor to the user's speech.participants' paths and their verbal commentsduring and after participation suggest that their Structure is provided by the responses offerednavigational decisions reflect their awareness of for the user's choice. The simulated character'ssocial constraints. They used the first person in verbal and nonverbal responses, and his will-describing their avatar's movement and inten- ingness to continue the interaction provide in-tions, irrespective of whether they experienced trinsic feedback.. At the same time, cues area first-person or a third-person perspective, available from a help agent in a separate win-They tended to ascribe agency and even men- dow who enthusiastically applauds when thetal states to the virtual humans. One participant, user chooses an appropriate question, and cov-passing near a virtual human, said "Excuse ers her face with both hands when the user'sme!" response choice is inappropriate. Each play of
the simulation is different, the interaction isIn addition, they tended to refrain from walking compelling, and there is the possibility of im-between characters who were facing each proving one's score each time. These game-likeother, when the characters were audibly con- aspects of the simulation are expected to helpversing. The gain in eliciting socially appropriate motivate the user to play the simulation repeat-responses from addition of speech is a promis- edly and thus build his/her conversation skills.ing indication for further development of themall as an evaluative and training tool. Addi- The goal is to provide the individual with in-tional design trials are planned with younger creasingly successful experience, supported, toindividuals with ASD and controls matched for the extent s/he chooses, with simplified instruc-nonverbal mental age. tion and reviewing of parts or all of the past
conversation, that can be pursued in a non-threatening environment, in order to develop abase of conversational skills.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
DISCUSSION Swiezy N, Kohn A, Scahill L, MartinA, Koenig K, Volkmar F, Carroll D, Lancor A,
Individuals with ASD have missed out on much Tierney E, Ghuman J, Gonzalez NM,of the experience required for social and cogni- Grados M, Vitiello B, Ritz L, Davies M,tive development, possibly because of disrup- Robinson J, McMahon D. (2002). Risperidonetion to their development in infancy as a result in children with autism and serious behavioralof heavy genetic liability to anxiety/depressive problems. N Engl J Med. 347(5):314-21.disorders leading to very early onset of symp- 8. Steele E, Grimmer K, Thomas B, Mulley B,toms of these genetically related disorders Fulton I, Hoffman H. (2003). Virtual reality as a(Trepagnier, 1996). These individuals require pediatric pain modulation technique: a casetraining appropriate to their developmental level study. Cyberpsychol Behav. 6(6):633-8.to improve the success of their social interac- 9. Gershon J, Zimand E, Pickering M,tions, thereby raising the likelihood that they will Rothbaum BO, Hodges (2004). A pilot and fea-become more integrated into their community. sibility study of virtual reality as a distraction forComputerized and virtual reality technologies children with cancer. J Am Acad Child Adolescenormously broaden the scope of possible in- Psychiatry. 43(10):1243-9.terventions. The dual challenge is to make tech- 10. Garcia-Palacios A, Hoffman H, Carlin A,nology-based interventions both efficacious in Furness TA 3rd, Botella C. (2002). Virtual real-inculcating gains in social skills and entertaining ity in the treatment of spider phobia: a con-enough to overcome autistic motivational barri- trolled study. Behav Res Ther. 2002 Sep;40ers, so that consumers and their families, edu- (9):983-93.cators and clinicians will use and benefit from 11. Wiederhold BK, Jang DP, Gevirtz RG, Kimthem. SI, Kim IY, Wiederhold MD (2002). The treat-
ment of fear of flying: a controlled study ofREFERENCES imaginal and virtual reality graded exposure
therapy. IEEE Trans Inf Technol Biomed. 61.American Psychiatric Association (1994). Di- (3):218-23.agnostic and Statistical Manual - Revised. 12. Wiederhold BK, Wiederhold MD. (2003).Washington, DC: author. Three-year follow-up for virtual reality exposure2. Fombonne E. (2003). Epidemiological sur- for fear of flying. Cyberpsychol Behav. (4):441-veys of autisma and other pervasive develop- 5.mental disorders: an update. J Autism Dev Dis- 13. Vincelli F, Anolli L, Bouchard S, Wiederholdord. 33(4): 365-82. BK, Zurloni V, Riva G. (2003). Experiential cog-3. Lauritsen MB, Pedersen CB, Mortensen PB. nitive therapy in the treatment of panic disor-(2004) The incidence and prevalence of perva- ders withsive developmental disorders: a Danish popula- agoraphobia: a controlled study. Cyberpsycholtion-based study. Psychol Med. 34(7):1339-46. Behav. 6(3):321-8.4. Smith T, Groen AD, Wynn JW (2000). Ran- 14. Parsons S, Mitchell P. (2002). The potentialdomized trial of intensive early intervention for of virtual reality in social skills training for peo-children with pervasive developmental disorder. pie with autistic spectrum disorders. J IntellectAm J Ment Retard. 105(4):269-85. Disabil Res. 46(Pt 5):430-43.5. Eikseth S, Smith T, Jahr E, Eldevik S. (2002). 15. Parsons S, Mitchell P, Leonard A. (2004).Intensive behavioral treatment at school for 4- The use and understanding of virtual environ-to 7-year-old children with autism. A 1-year ments by adolescents with autistic spectrumcomparison controlled study.Behav Modif. 2002 disorders. J Autism Dev Disord. 34(4):449-66.Jan;26(1):49-68. 16. Parsons S, Mitchell P, Leonard A. (2005).6. Hollander E, Phillips AT, Yeh CC. (2003). Do adolescents with autistic spectrum disordersTargeted treatments for symptom domains in adhere to social conventions in virtual environ-child and adolescent autism. Lancet 30;362 ments? Autism. 9(1):95-117.(9385):732-4. 17. Silver M, Oakes P.(2001). Evaluation of a7. McCracken JT, McGough J, Shah B, Cronin new computer intervention to teach people withP, Hong D, Aman MG, Arnold LE, Lindsay autism or Asperger syndrome to recognize andR, Nash P, Hollway J, McDougle CJ, Posey D, predict emotions in others. Autism. 5(3):299-
106
TREPAGNIER ET AL.
316. 29. Trepagnier C, Sebrechts MM, Peterson R.18. Bolte S, Feineis-Matthews S, Leber S, (2002). Atypical face gaze in autism.Dierks T, Hubl D, Poustka F. (2002). The devel- Cyberpsychol Behav. 5(3):213-7.opment and evaluation of a computer-based 30. Lord C, Rutter M & Le Couteur A. (1994).program to test and to teach the recognition of Autism Diagnostic Interview-Revised: a revisedfacial affect. : Int J Circumpolar Health. 61 version of a diagnostic interview for caregiversSuppl 2:61-8. of individuals with possible pervasive19. Bernard-Opitz V, Sriram N, Nakhoda- developmental disorders.J Autism Dev Disord.Sapuan S. (2001). Enhancing social problem 24(5):659-85.solving in children with autism and normal chil- 31. Klin A, Jones W, Schultz R, Volkmar F, &dren through computer-assisted instruction. J Cohen D. (2002). Visual fixation patterns duringAutism Dev Disord. 31(4):377-84. viewing of naturalistic social situations as20. Fein D, Pennington B, Markowitz P, predictors of social competence in individualsBraverman M, Waterhouse L.Toward a neuro- with autism. Arch Gen Psychiatry 59(9):809-16psychological model of infantile autism: are the 32. Orsmond GI, Krauss MW, & Seltzer MM.social deficits primary? (1986). Am Acad Child (2004). Peer relationships and social and rec-Psychiatry. (2):198-212. reational activities among adolescent s and21. Trepagnier C. (1996). A Possible Origin for adults with autism. Journal of Autism and De-the Social and Communicative Deficits of Au- velopmental Disorders 34:245-55.tism. Focus on Autism and Other Developmen-tal Disabilities. 11(3): 170-82.22. Gross TF. (2004). The perception of four Contactbasic emotions in human and nonhuman facesby children Cheryl Y. Trepagnier, Ph.D.,with autism and other developmental disabili- The Catholic University of America,ties. J Abnorm Child Psychol. 32(5):469-80. Washington, DC23. Dawson G, Webb SJ, Carver L, USAPanagiotides H, McPartland J.(2004). Young 1 (202) 319-5780 (voice)children with autism show atypical brain re- 1 (202) 319-6162 (fax)sponses to fearful versus neutral facial expres- trepaqnier6,cua.edusions of emotion. Dev Sci.7(3):340-59.24. Grelotti DJ, Klin AJ, Gauthier I, SkudlarskiP, Cohen DJ, Gore JC, Volkmar FR, SchultzRT. (2005). fMRI activation of the fusiformgyrus and amygdala to cartoon characters butnot to faces in a boy with autism. : Neuropsy-chologia. 43(3):373-85.25. Ghaziuddin M, Ghaziuddin N, Greden J(2002). Depression in persons with autism: im-plications for research and clinical care J Au-tism Dev Disord. 32(4):299-306.26. Gillott A, Furniss F, Walter A. (2001). Anxi-ety in high-functioning children with autism. Au-tism. 5(3):277-86.27. Ghaziuddin M, Weidmer-Mikhail E,Ghaziuddin N. (1998). Comorbidity of Aspergersyndrome: a preliminary report. J Intellect Dis-abil Res. 1998 Aug;42 ( Pt 4):279-83.28. Gadow KD, DeVincent CJ, Pomeroy J,Azizian A. (2004). Psychiatric symptoms in pre-school children with PDD and clinic and com-parisonsamples. J Autism Dev Disord .34(4):379-93

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
108

Annual Review of CyberTherapy and Telemedicine
VR for Blood-Injection-Injury Phobia
B. K. Wiederhold1'2 , M. Mendoza 1 , T. Nakatanil, A. H. Bullinger3, M. D. Wiederhold'
1 Virtual Reality Medical Center, San Diego, California2 Interactive Media Institute, San Diego, California
3COAT-BaseI/UPKBS, University of Basel, Switzerland, Department of Psychiatry
Abstract: Virtual reality (VR) exposure therapy has been shown to be successful in treating manytypes of specific phobias which are mostly visual in nature. However, limited research has beencompleted on the use of VR therapy for Blood Injection-Injury (BII) phobias, one of the subtypes ofSpecific Phobia listed in the DSM-IV TR. Since B11 phobia may operate by some tactile component,it may respond differently to VR therapy compared to other categories of specific phobias that arelargely visually activated. This paper discusses initial development and results from a study on bothsubjective and objective arousal elicited by a prototype virtual world which has been developed totreat those with BII phobia. The present study evaluated the responses of 20 healthy, non-phobicmale and female participants to VR blood and injection stimuli. Initial results are positive and showthat the VR world delivers appropriate cues to elicit physiological and self-reported arousal whenexposed to the injection scenarios. Correlations between self-reported anxiety and physiologicalarousal confirm that individuals experiencing greater symptoms of fear in conditions involving bloodor injections will exhibit more intense arousal from the virtual stimuli than those who experience re-duced symptoms. Findings suggest that the virtual world is an effective method of cue exposure forindividuals who experience anxiety in situations related to blood and injections. Future research onthe use of VR exposure therapy in the treatment of B11 phobia is warranted.
INTRODUCTION
The DSM-IV TR classifies phobias into three differ from other specific phobias in how it willgroups: 1) Agoraphobia, 2) Social Phobia, and respond to VR. In the previous injection study,3) Specific Phobias. The further subdivision it was found that VR could be used to success-within Specific Phobias is: 1) Blood-Injection- fully elicit subjective (measured with SubjectiveInjury (BII), 2) Animal, 3) Natural Environment, Units of Distress (SUDs ratings) and physiologi-4) Situational, and 5) "Other". 1 Although VR cal arousal (measured with heart rate (HR)) inexposure therapy has been used successfully those with needle phobia, however, the resultsfor more than a decade to treat phobias; includ- indicated that the addition of tactile stimuliing specific phobias, panic disorder and agora- would have proven to be more advantageous.phobia, and social phobia (4-13); only one study In addition, the previous study presented thehas attempted VR usage for injection phobia.2 VR environment via a desktop display instead
of a more immersive head-mounted displayThose who suffer from BII phobias may fear (HMD). 2 The present study, therefore, soughteither the sight or the pain of the injection and to investigate elicitation of arousal via a HMDoften begin avoidance of any situation which VR system to be used in treating those with BIImay cause exposure to an injection, such as phobias. As an initial first step, however, wedonating blood or going to the doctor. In ex- have sought to establish a baseline with thosetreme cases, the phobic may even begin to fear who do not meet the DSM-IV TR criteria for adriving past a hospital.3 Because BII phobia BII phobia in order to use this arousal level as ainvolves not only visual stimuli which elicit the baseline comparison for phobic participantsphobic response, but also tactile stimuli; it may exposed to the VR world.
109

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
MATERIALS AND METHODS Design
Participants Ten (10) participants were randomly assigned,using a random numbers table, to Group A and
Twenty healthy, non-phobic participants (13 10 were randomly assigned to Group B. Groupfemales and 7 males) from the San Diego area A was verbally instructed to navigate throughwere recruited for this study. Their mean age the virtual clinic to a specified exam roomwas 27 ± 10, ranging from 20 to 54 years of where they would be seated but was not in-age. formed that they would be "receiving an injec-
tion". Group B was given the same instructions,Virtual World but was also notified that they would receive an
injection. Outcome measures were analyzedThe low cost VR system was developed to be between groups to determine effect of instruc-used on a personal computer (PC) platform with tions on anxiety (e.g. anticipatory anxiety).a HMD and tracking system so that the partici-pant could explore the world via head tracking All 20 participants provided consent beforeas well as navigation provided via a joystick. completing the pre-test questionnaires. All par-The virtual world was modeled after an outpa- ticipants completed a 3 minute baseline duringtient clinic in La Jolla, CA and is almost an ex- which physiological measures were continu-act replica of the real life structure. Participants ously collected. After baseline, participantscan navigate through the clinic's entrance, completed the S-BISS and each group (A andlobby, waiting room and exam rooms. Exam B) received their respective instructions. Par-rooms are filled with typical phlebotomy lab ticipants navigated the virtual world for 3 min-paraphernalia, including vials of blood. In one utes and physiological data was collectedof the exam rooms, the participant may sit down throughout. During VR exposure, investigatorsand have a "nurse avatar" administer an injec- recorded time markers, indicating when the in-tion. This is viewed in first person, as if the par- jection was received by each participant. Afterticipant is seated in the exam room chair and VR exposure, participants completed the post-viewing his arm while receiving the injection, test questionnaires and subjective feedback
was collected by investigators.Measurements
RESULTSObjective physiological measures and subjec-tive self-report data were collected from each Physiological data from both conditions (A andparticipant. Physiological data consisted of B) was averaged and differences betweenheart rate and multiple respiration measures baseline and VR were compared using a pairedcollected using VivoMetric's wireless Lifeshirt t-test (a = 0.05). Analyses indicated a signifi-system; and heart rate, skin conductance and cant increase in skin conductance (df = 1, 17; pperipheral skin temperature data collected us- = 0.018) and respiration rate (df = 1, 18; p =ing J & J Engineering's C2 device. Physiologi- 0.0003) during VR. Temperature also in-cal data was collected at baseline and continu- creased during VR, but the difference was notously in real-time throughout exposure to the statistically significant (df = 1, 18; p = 0.089).virtual world. Self-report data consisted of a Combined group data exhibited a decrease inFear Questionnaire, a Blood Injection Symp- HRV (df = 1, 18; p = 0.057) and LF (df = 1, 18;toms Scale (BISS), a State Blood Injection p = 0.099) during VR, but neither difference wasSymptoms Scale (S-BISS), and a Post- statistically significant. T-tests determined thatExperience Questionnaire. The Fear Question- differences in heart rate (df=l, 18; p=0.631),naire and BISS were administered before base- VLF (df = 1, 18; p = 0.672) and HF (df = 1, 18; pline, the S-BISS was administered pre- and = 0.0442) measurements were not significant.post-VR exposure, and the Post-ExperienceQuestionnaire, which included questions on Combined group data from VR exposure waspresence and simulator sickness, was adminis- averaged into three distinct segments and ana-tered after VR exposure. lyzed; period before injection (VR1), injection
110
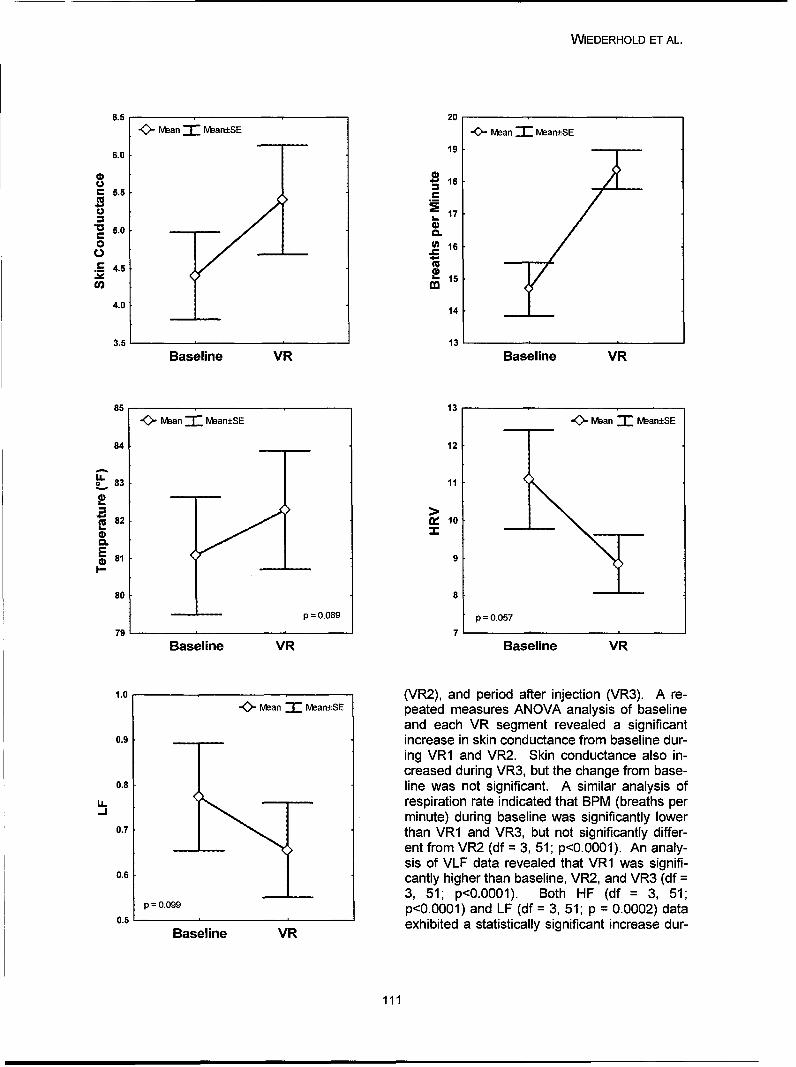
WIEDERHOLD ET AL.
6.5 20w" Mean -17 Mban±SE w Mean "-an+SE
6.0 19
185.5 C
17
5.0 0)
o () 16
S4.5"Cn • 15
4.0 14
3.5 13'
Baseline VR Baseline VR
85 13-0- man 1 Nean±SE w- Man 1- Mean±SE
84 12
LL.o 83 1
82 10
0.
E 81 9
80 8
p = 0.089 p = 0.057
79 7 1 1
Baseline VR Baseline VR
1.0 (VR2), and period after injection (VR3). A re-K>an- an:SE peated measures ANOVA analysis of baseline
and each VR segment revealed a significant0.9 increase in skin conductance from baseline dur-
ing VR1 and VR2. Skin conductance also in-creased during VR3, but the change from base-
0.8 line was not significant. A similar analysis ofU. respiration rate indicated that BPM (breaths per"minute) during baseline was significantly lower
0.7 than VR1 and VR3, but not significantly differ-
ent from VR2 (df = 3, 51; p<0.0001). An analy-sis of VLF data revealed that VR1 was signifi-
0.6 cantly higher than baseline, VR2, and VR3 (df =3, 51; p<0.0001). Both HF (df = 3, 51;
p=0.099 p<0.0001) and LF (df = 3, 51; p = 0.0002) data0.5 B l , exhibited a statistically significant increase dur-
Baseline VR
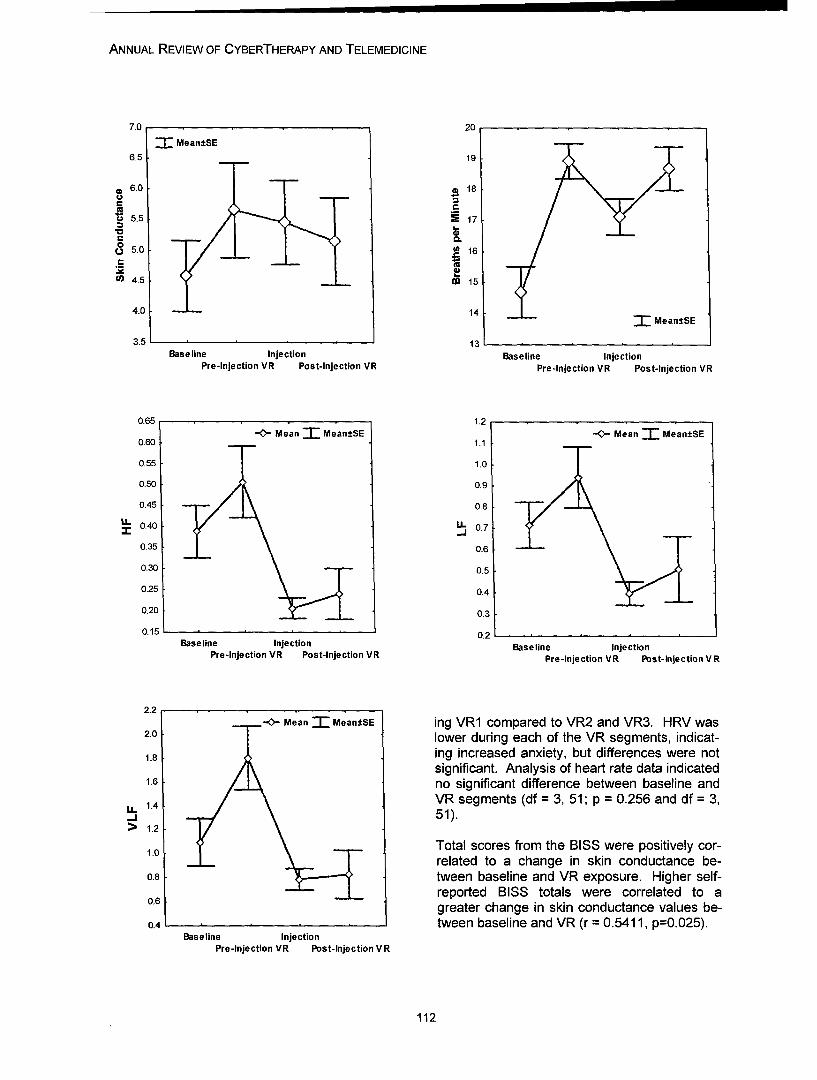
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
7.0 20
- Mean±SE6.5 19
a 6.0 . 18
S5.5 i 17
00o 5.0 } 16
(4 4.5 00 15
4.0 14 TMean±SE
3.5 13,Baseline Injection Baseline Injection
Pre-injection VR Post-Injection VR Pre-injection VR Post-Injection VR
0.65 1.2
-0,- Mean' Mean±SE 1.- MeanT Mean±SE0.60 1.1
0.55 1.0
0.50 0.9
0.45 0.8
IU. 0.40 IU 0.7
0.35 0.6
0,30 0.5
0.25 0.4
0.20 0.3
0.15 . 0.2.Baseline Injection Baseline Injection
Pre-injection VR Post-Injection VR Pre-injection VR Post-Injection VR
2.2-0- Mean Mean±SE ing VR1 compared to VR2 and VR3. HRV was
2.0 lower during each of the VR segments, indicat-
1.8 ing increased anxiety, but differences were notsignificant. Analysis of heart rate data indicated
1.6 no significant difference between baseline and
1.4 VR segments (df = 3, 51; p = 0.256 and df = 3,.J 51).
> 1.2
1.0 Total scores from the BISS were positively cor-related to a change in skin conductance be-0.8 tween baseline and VR exposure. Higher self-0.6 reported BISS totals were correlated to a
greater change in skin conductance values be-0.4 tween baseline and VR (r = 0.5411, p=0.025).
Baseline InjectionPre-injection VR Post-Injection VR
112
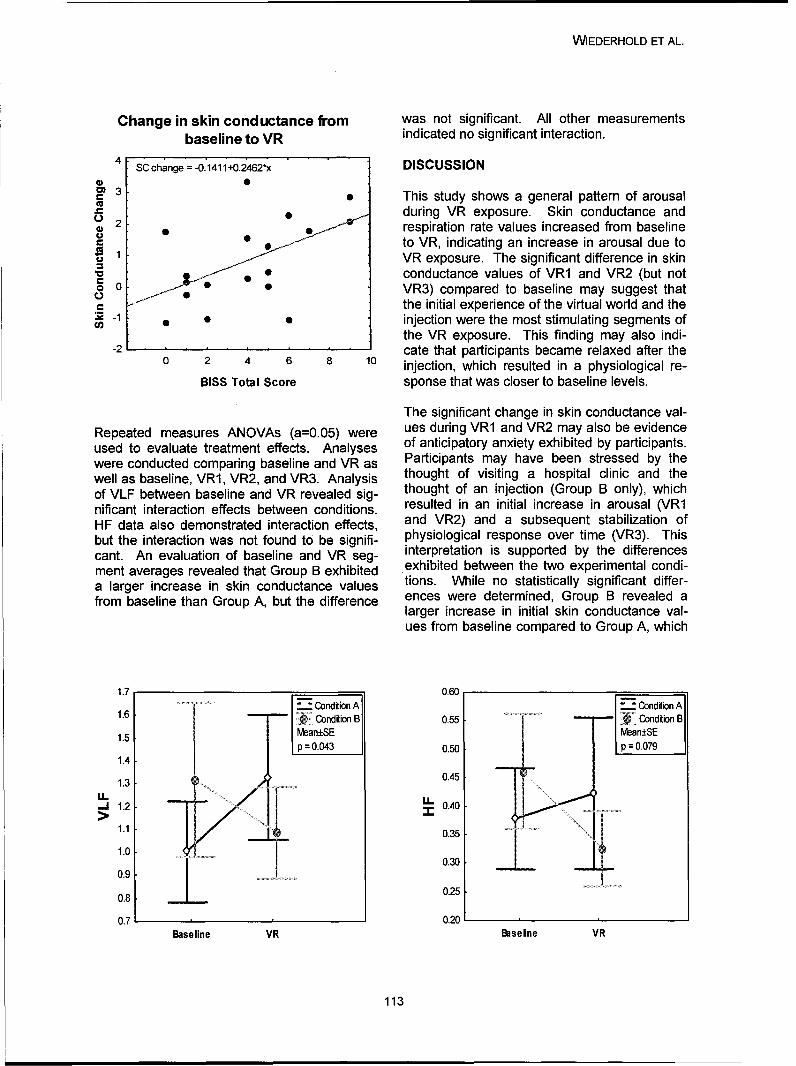
WIEDERHOLD ET AL.
Change in skin conductance from was not significant. All other measurementsbaseline to VR indicated no significant interaction.
4 SC change = -0.41411+0.2"462*x DISCUSSION4)CD 3This study shows a general pattern of arousal0 2 during VR exposure. Skin conductance and
respiration rate values increased from baselineto VR, indicating an increase in arousal due to
S1 VR exposure. The significant difference in skinV0 conductance values of VR1 and VR2 (but noto 0 VR3) compared to baseline may suggest that
the initial experience of the virtual world and the• -1 ••injection were the most stimulating segments of
the VR exposure. This finding may also indi--2 cate that participants became relaxed after the
0 2 4 6 8 10 injection, which resulted in a physiological re-
BISS Total Score sponse that was closer to baseline levels.
The significant change in skin conductance val-Repeated measures ANOVAs (a=0.05) were ues during VR1 and VR2 may also be evidenceused to evaluate treatment effects. Analyses of anticipatory anxiety exhibited by participants.were conducted comparing baseline and VR as Participants may have been stressed by thewell as baseline, VR1, VR2, and VR3. Analysis thought of visiting a hospital clinic and theof VLF between baseline and VR revealed sig- thought of an injection (Group B only), whichnificant interaction effects between conditions. resulted in an initial increase in arousal (VR1HF data also demonstrated interaction effects, and VR2) and a subsequent stabilization ofbut the interaction was not found to be signifi- physiological response over time (VR3). Thiscant. An evaluation of baseline and VR seg- interpretation is supported by the differencesment averages revealed that Group B exhibited exhibited between the two experimental condi-a larger increase in skin conductance values tions. While no statistically significant differ-from baseline than Group A, but the difference ences were determined, Group B revealed a
larger increase in initial skin conductance val-ues from baseline compared to Group A, which
1.7 0.60-. ondition A Condition A1.6 -- - '• iCondition~ B 0.5 ........... ..... " " - /• iConditin B
1.5 rv'ean±SE/ vean+SEp=0.043 0.50 P0.079
1.4
0.451.3
.. 1.2 0.40
1.1 • ~ ~~0.35 ..........
1.0 ii30.9 0.25
0.8
0.7 0.20Baseline VR Baseline VR
113
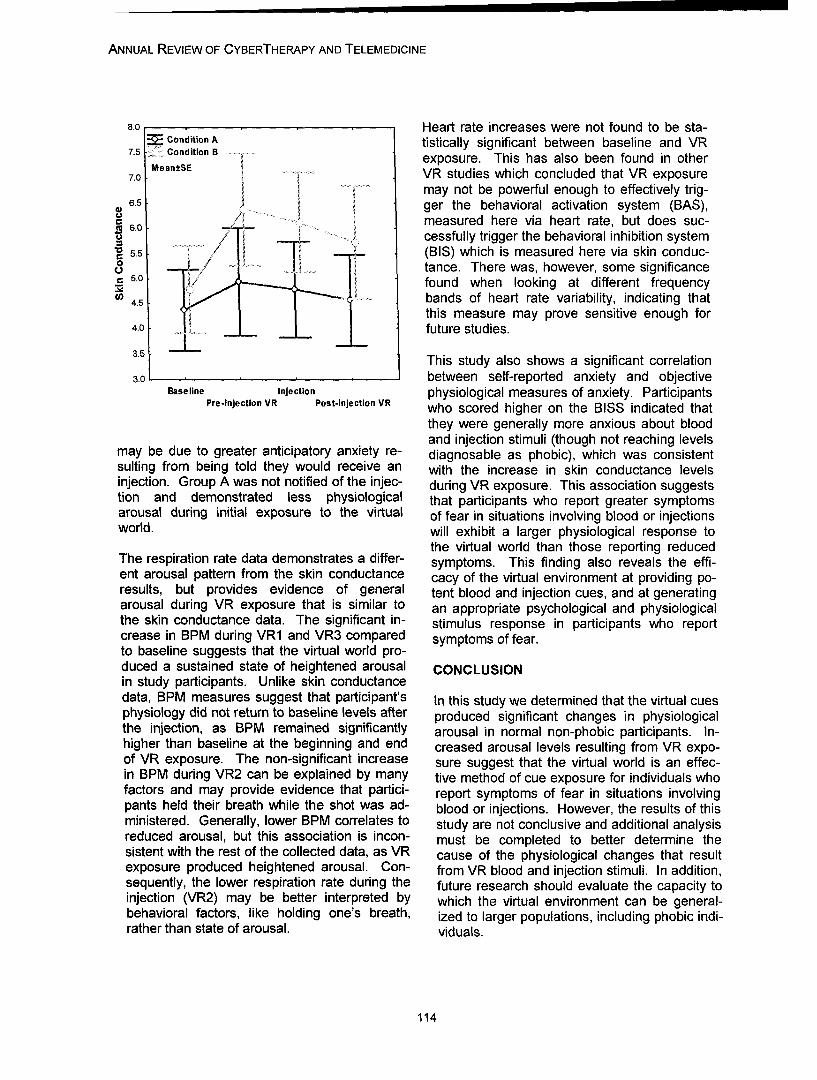
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
8.0 Heart rate increases were not found to be sta-SCondition A tistically significant between baseline and VR
7.5. Conditon B exposure. This has also been found in other7.0. VR studies which concluded that VR exposure
may not be powerful enough to effectively trig-6.5 •ger the behavioral activation system (BAS),6.0 _. measured here via heart rate, but does suc-
"�cessfully trigger the behavioral inhibition system5.5 (BIS) which is measured here via skin conduc-
- .... tance. There was, however, some significanceS5.0 ./ found when looking at different frequency4. bands of heart rate variability, indicating that
this measure may prove sensitive enough for4.0 future studies.
3.5 This study also shows a significant correlation3.0 between self-reported anxiety and objective
Baseline Injst-injephysiological measures of anxiety. ParticipantsPre-lnjection VR Post-injection VR who scored higher on the BISS indicated that
they were generally more anxious about bloodand injection stimuli (though not reaching levels
may be due to greater anticipatory anxiety re- diagnosable as phobic), which was consistentsuiting from being told they would receive an with the increase in skin conductance levelsinjection. Group A was not notified of the injec- during VR exposure. This association suggeststion and demonstrated less physiological that participants who report greater symptomsarousal during initial exposure to the virtual of fear in situations involving blood or injectionsworld. will exhibit a larger physiological response to
the virtual world than those reporting reducedThe respiration rate data demonstrates a differ- symptoms. This finding also reveals the effi-ent arousal pattern from the skin conductance cacy of the virtual environment at providing po-results, but provides evidence of general tent blood and injection cues, and at generatingarousal during VR exposure that is similar to an appropriate psychological and physiologicalthe skin conductance data. The significant in- stimulus response in participants who reportcrease in BPM during VR1 and VR3 compared symptoms of fear.to baseline suggests that the virtual world pro-duced a sustained state of heightened arousal CONCLUSIONin study participants. Unlike skin conductancedata, BPM measures suggest that participant's In this study we determined that the virtual cuesphysiology did not return to baseline levels after produced significant changes in physiologicalthe injection, as BPM remained significantly arousal in normal non-phobic participants. In-higher than baseline at the beginning and end creased arousal levels resulting from VR expo-of VR exposure. The non-significant increase sure suggest that the virtual world is an effec-in BPM during VR2 can be explained by many tive method of cue exposure for individuals whofactors and may provide evidence that partici- report symptoms of fear in situations involvingpants held their breath while the shot was ad- blood or injections. However, the results of thisministered. Generally, lower BPM correlates to study are not conclusive and additional analysisreduced arousal, but this association is incon- must be completed to better determine thesistent with the rest of the collected data, as VR cause of the physiological changes that resultexposure produced heightened arousal. Con- from VR blood and injection stimuli. In addition,sequently, the lower respiration rate during the future research should evaluate the capacity toinjection (VR2) may be better interpreted by which the virtual environment can be general-behavioral factors, like holding one's breath, ized to larger populations, including phobic indi-rather than state of arousal. viduals.
114
WIEDERHOLD ET AL.
FUTURE WORK 7. Vincelli, F., Anolli, L., Bouchard, S.,Wiederhold, B.K., Zurloni, V., & Riva, G. (2003).
Future studies should include the presentation "Experiential Cognitive Therapy in theof the current VR world to those who meet Treatment of Panic Disorders withDSM-IV TR criteria for BiI phobia. In addition, Agoraphobia: A Controlled Study."comparison studies should include presentation CyberPsychology & Behavior. 6(3): 321-328.via both a flat screen and a HMD to determine ifindeed the more immersive HMD increases 8. Vincelli, F., Choi, Y.H., Molinari, E.,presence, immersion, and arousal. A compari- Wiederhold, B.K., & Riva, G. (2001). "A Multi-son study should also be included to determine Center Study for the Treatment of Panic Disor-if tactile feedback done in reality which corre- der with Agoraphobia: The Experiential-sponds to the VR visual stimuli would increase dernithvAgoraphobIa Th Experieal-initial arousal and possibly result in a more effi- Cognitive Therapy." In T. Scrimali & L. Grimaldicient method of treatment. Finally, given ad- (Eds). Cognitive Psychotherapy toward a Newvances in wireless technology for physiological Millenium, Kluwer Academic/Plenum Publisher:monitoring, it would be interesting to test partici-pants in both the actual real world setting and 9. Walshe, D.G., Lewis, E.J., Kim S.I.,compare results to those elicited in VR expo- O'Sullivan, K., Wiederhold, B.K. (2003).sure. "Exploring the Use of Computer Games and
REFERENCES Virtual Reality in Exposure Therapy for Fear ofDriving Following a Motor Vehicle Accident".
1. American Psychiatric Association: APA. CyberPsycholoqy & Behavior. 6 (3): 329-334.
(2000). Diagnostic and Statistical Manual ofMental Disorders Fourth Edition Text Revision. 10. Wiederhold, B.K. (1999). "A comparison ofWashington, DC: American Psychiatric Asso- imaginal exposure and virtual reality exposureciation. for the treatment of fear of flying" [doctoral dis-
2. Hamza, S., Jones, N., Lesaoana, M., Blake, sertation]. California School of Professional
E., & Strauss, R. (2000). A first study of virtual Psychology.
reality exposure therapy in needle phobia. The- 1 V~iederhold, B.K. (2001). Overview of Vir-sis Report: October 2000. tual Reality Therapy." Proceedings of the 9t
3. Marks, l.M. (1969). Fears and Phobias. Annual Medicine Meets Virtual Reality Confer-ence. January 24-27, 2001, Newport Beach,
William Heinemann Medical Books Ltd.: Lon- cania.don. California.
4. Bullinger, A.H., Roessler, A, Mueller-Span, 12. Wiederhold, B.K. & Wiederhold, M.D.F, (1998). "Three Dimensional Virtual Reality as (2000). "Lessons Learned From 600 Virtual Re-a Tool in Cognitive-Behavioral Therapy of ality Sessions." CLberPsnchologr & Behavior. 3Claustrophobic Patients", Cyberpsychology and (3): 393-400.Behavior, 1 (2): 139-145.
5. James, LK., Lin, CY, Steed, A, Swapp, D, 13. Wiederhold, B.K., Wiederhold, M.D.,Slater, M (2003). "Social Anxiety in Virtual Envi- (2005). Virtual Reality Therapy for Anxiety Dis-
ronments: Results of A Pilot Study." CyberPsy- orders- Advances in Evaluation and Treatment.
chology & Behavior. 6(3): 237-243. Washington, DC: American Psychological As-sociation.
6. Pertaub, D-P., Slater M., Barker, C. (2001)."An Experiment on Fear of Public Speaking in 14. Wilhelm, F.H., Pfaltz, M.C., Gross, J.J.,Virtual Reality." Medicine Meets Virtual Reality Mauss, I.B., Kim, S.I., and Wiederhold, B.K.2001, J.D. Westwood et al. (Eds.), OS Press, (2005, in press). "Mechanisms of Virtual Real-2001. ity Exposure Therapy: The Role of the Behav-
115
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ioral Activation and Behavioral Inhibition Sys-tems". Applied Psychophysiology and Biofeed-back Journal.
Contact
Brenda K. WiederholdInteractive Media Institute6160 Cornerstone Court East, Suite 161San Diego, CA 92121Ph: (866) 822-8762Fax: (858) 642-0285
116

BROSNAN ET AL.
Working Things Out:A Therapeutic Interactive CD-Rom Containing the Stories of YoungPeople Dealing with Depression and other Mental Health Problems
E. Brosnan, Dr. J. Sharry, Prof. C. Fitzpatrick
University College Dublin/ Mater Hospital
Abstract: It is widely accepted that children and young people enjoy using computers. Seymour Pa-pert' suggests that 'it is timely for school counsellors and child therapists to bridge the digital genera-tion gap and innovate with computers in their work with children of the digital age. ' Working ThingsOut (WTO) was developed in response to the growing need for computer-based resources for ado-lescents in therapy. It is an interactive CD ROM/DVD developed as a means of engaging adoles-cents about mental health issues by giving them information in the form of animated personal storiestold by other young people dealing with problems such as depression, bullying, eating problems andself-harm. The CD-ROM/DVD is accompanied by a manual for professionals on how to use the re-source.
With the help of therapists, and in collaboration with graphic designers, animators and multimediaprofessionals, the 11 young people who participated in the project told their stories, narrated in theirown voice and illustrated by graphics and animation. 'Working Things Out' is currently being used asan educational and therapeutic tool with other adolescents at risk of mental health problems, both asa way of engaging young people to reflect about mental health issues and as a means of invitingthem to tell their own story. The paper describes the background and development of the 'WorkingThings Out' project, including samples from the stories and a description of how the CD-ROM/DVDcan be used in psychotherapy.
ACKNOWLEDGEMENTS
In developing this project we would like to ac- great meaning to the storytellers as well as theknowledge the work of Bernie McCarthy, Ciara listeners in that the act of telling the story canDevine, Pilar Valencia, Hugh O'Neill, Peter shape and define their lives.McCormack and John Stapleton from the pro-duction team. As a result psychotherapists are very interested
in personal stories. Psychotherapy can be con-THERAPEUTIC STORY TELLING AND DIGI- ceived as process of inviting clients to tell andTAL MEDIA retell their life story from a variety of perspec-
tives with the aim of reaching a coherent andTelling and listening to stories is a fundamental meaningful narrative at the end.2 Within ahuman activity, both as a means of entertain- strengths-based approach to psychotherapy thement and communicating information. Whether process can be conceived as helping clientswe are listening to a personal anecdote, reading shift from initially self-limiting and problem-a novel or watching a soap opera, a 'good story' focused accounts of their lives to more positiveholds much greater appeal than a series of facts and strengths-oriented accounts that are morealone and is much more likely to engage our liberating and empowering.3 4 For example, aimagination and hold our attention. Personal person may begin psychotherapy by telling thestories that relate real-life accounts of peoples story of how he became depressed and howlives, and which have the mark of authenticity this damages his life and end therapy with acan hold a particular appeal to an audience, 'new' story of how he has coped with the de-allowing special identification with the character pression and how this leads to new possibilitiesand context. Further, personal stories can have in his life. This is not simply a semantic differ-
117

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ence: the act of retelling your story to an em- tive study8 engaged a smaller group of youngpathic listener, in a way that identifies new people to share their stories of how they werestrengths-based 'plot lines' and that incorpo- coping and dealing with depression and otherrates supportive 'characters' more centrally to difficult life experiences. A key finding of thethe story, is in itself beneficial and transforming studies was the fact many young people in theto ones personal identity. community who suffered from depression did
not access traditional professional mentalComputers and digital media health services.
Computers and digital media provide therapists The WTO project grew out of a desire to createwith new means to engage clients and assist an accessible means of providing mental healththem in telling their life stories. Narrative struc- information as well as a means of engagingtures and storylines are widely employed in young people in professional services and psy-many different types of digital media, including chotherapy. To ensure this was relevant tovideo game design, web-design, and e- young people, participants from the study werelearning. By including a narrative structure, this invited to contribute to the making of the CD-can increase the appeal for users and offer a ROM/DVD and to share their personal stories ofcontext for creating meaning, thereby deepen- dealing with a difficult life experience duringing their experiences of the information being adolescence. The inclusion of real young peo-presented. Abbe Don in an article entitled pie's experiences in a story format makes the"Narrative and the Interface" argues that com- material much more real and relevant. A multi-puters can play in modern society the role of media interactive CD-Rom was chosen as thethe storyteller of oral cultures.5 '6 The computer format for the collection of stories as this moti-becomes the processor of the "told" information, vated the young people tell their story, (manythe user/viewer takes on the information and were keen to gain experience of creatively us-interprets it in a way that is meaningful to them. ing digital media creatively) and also provided
an engaging 'youth centred' format for futureDigital storytelling techniques are particularly users.relevant in the context of psychotherapy. Thecomputer provides novel means of both ex- The project was developed as a partnershippressing and listening to therapeutic stories, between the Department of Child and familyThe computer facilitates the expression of the Psychiatry in the Mater Hospital, the charitytherapeutic story by allowing the incorporation Parents Plus (which will distribute the CD-Rom)of sound, image, animation as well as text and and the Therapeutic Technologies Group inverbal communication in the telling. Equally the Media Lab Europe.computer facilitates the listening to the story, byproviding interactive interfaces and databases Developmentthat allow the listener to pace the story to theirown need and to make choices about what is Young people aged 13 to 16 who attended therelevant. The Working Things Out project aimed Mater Child and Adolescent Mental Health Ser-to build on these twin key potentials that are vice and/ or who participated in the Challengingafforded by digital media in therapeutic storytel- Times research study above were invited toling. participate in the project. Specifically, they were
asked to share their experience and stories inWTO PROJECT RATIONALE AND BACK- order to make a CD-ROM to help young peopleGROUND overcome problems in their lives. The altruistic
nature of the project appealed to many of them,The idea for the WTO project emerged during as much as the possibility of working with multi-the 'Challenging Times' research study6 which media to tell their stories. After a series of gen-looked at the incidence of depression and other eral focus groups, eleven young people weremental health difficulties amongst the12-15 year selected to take part. The problems the youngold population in secondary schools in the people were dealing with ranged from moreNorth Dublin City area. A subsequent qualita- 'everyday' issues such as bullying, conflict with
118
BROSNAN ET AL.
parents and school problems to more specialist have gone away but the way we understandproblems such as self-harm, bereavement, ob- and deal with them has changed. While wesessive-compulsive disorder, and eating prob- don't have all the answers, we might havelems. some useful messages and information.
To develop a 'script' for the stories, each young In developing the project we were keen to en-person attended a series of individual meetings sure that the final accounts were confidentialwith a therapist who through a process of listen- meaning that we would not use any identifyinging and clarifying helped the young people be- material such as pictures or real names. Thus,gin to tell their story in a structured format. This in order to maintain the authenticity of the pro-structure focused not only on their experience ject, the young people themselves provided theof having a problem, but also how they coped 'voice over' recording to a script that had beenand what supports and resources helped them. co-written with the therapists. The final produc-The final scripts for the short movies were co- tion includes ten mini-movies of the young peo-authored by therapist and young person. Some pies' stories and one recorded song written byyoung people were able to write the majority of one participant who preferred to share his ex-the script themselves and others needed more periences in lyrics and music.support (e.g. the therapist would transcribe themain points from a recorded interview and re- Case Example - Michelle's Storyread to the young person for approval).
To illustrate the content and purpose of WTOThe young people were also involved in the we reproduce below the opening text for Mi-creative aspects of the production. Some were chelle's story who had been referred to an ado-involved in the storyboarding of the scenes, the lescent mental health service due to her eatingdevelopment of the graphics and the choice of problems.images. Alongside the individual sessions, sev-eral workshops were conducted with the young 'Shocked Into Reality' - Other kids at schoolpeople on animation, graphics, photography were calling me fat.and digital audio. This helped each young per- Other kids at school were calling me fat. I wasson take ownership of his/her story both in its only ten at the time. I started feeling fat andscript and in how it would be animated and rep- paranoid and thought everybody was looking atresented. A key aspect of this project was to me. Like if I went shopping with the other girlsensure that the stories are personal and mean- in my class and one of them said to another "ingful to the participating adolescents and their oh those jeans would fit you" I would think itfamilies. The introduction to the stories was was directed at me like, that she meant theywritten in conjunction with the young people wouldn't fit me. I used to think that commentsand is as follows: like that were aimed at me, though they would-
n't be in reality. I started skipping breakfastWelcome to 'Working Things Out' the stories of purposefully and would try not to eat much at11 young people who have gone through some lunch. Like I'd eat half a cracker at break anddifficult fife experiences. By sharing our stories, the other half at lunch. I used to think that if Iour feelings and our ways of coping with our ate any more I'd get fat. Then I started exercis-problems, we hope that others who might be ing, doing sit ups and making a big effort in PEgoing through a similar hard time will be re- so I'd be thinner.minded that they are not alone and that thereare many different things you can do to make This was going on for a few months and mythings better. Mam noticed I was losing weight.
Telling our stories definitely made us feel better, She took me to the doctor. The doctor talked toit was good to get stuff off our chests. We hope me about my food intake and told me I shouldthat the very real experiences you hear will be a be eating more. My Main and my sister weresource of support and learning for you. Our telling me the same thing but I didn't listen tostories are ongoing and not all our problems any of them. I still wanted to be thinner. I didn't
119
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
think I was losing weight myself. When I'd look with the story teller helping them feel 'not alone'in the mirror I used to see myself as bigger than if similar issues affect them. In addition, viewingI actually was. My friends started saying I was the story could provide an important focal pointtoo skinny but I didn't believe them either. I for discussion and also engage the adolescentwould feel the hunger in my stomach but I ig- to open up and share their own experience ifnored it because I was determined not to eat that is appropriate.and I'd feel the cold even when it was sunnyout. The final version of the CD-ROM contains an
introduction and a panoramic interface (fig 2),Michelle's story is played as a movie and illus- representing a street, which they can scrolltrated with line graphics that support her narra- across left and right to view the silhouette oftion (fig 1). In later parts of the story she goes eleven young people whose pseudonyms areon to say how she and her mother finally sought given along with a title of their story. Selecting ahelp for her difficulties. A turning point comes story allows it to be played in a linear fashionwhen in her own words she is 'shocked into from beginning to the end, with the options ofreality' by a medical report which highlights just pause, fast forward and rewind. The stories arehow underweight and undernourished she is. At illustrated by graphics and animation and nar-the end of the story she relays how she cur- rated by the personal voice of the young per-rently maintains her eating and health. son. In addition, each story is punctuated by
several 'information points' which provide aUSING WTO AS AN EDUCATIONAL GUIDE commentary on some of the key points raised inWITH YOUNG PEOPLE the story as well as some sample questions for
professionals to use to promote reflection andAs well as being beneficial to the participants, to facilitate the personalisation of the material.the WTO CD ROM has been designed as an For example, the opening information point foreducational guide for young people (and their Michelle's story above is as followsfamilies) who are experiencing similar prob-lems. The current version of "Working Things Pressure to be thinOut" is designed to be used in a facilitated way Like Michelle, many young people fee/ self-by professionals working with young people conscious about their appearance and bodyeither individually or with a small group of ado- shape and fee/ under pressure to look a certainlescents, in either a mental health or school way and to be a certain weight. For Michelle itsetting. The aim is that on viewing the stories became a problem and she began to see her-adolescents may feel a resonance or empathy self as 'bigger than she actually was, and she
J7
12
S.. .. . . .. .. .. . .. .. .. .. .. . . ... .. .. .. .. .. ... . .. : '" •" • • .i. . .. .. .. . ........ . . ... . .. .. .. .. • "•' °• .. . . .. . .. , . .... ......... .. ...... .. .
_fC,• ' Figure..... Graphics from.Michelle's +Story
/G120
BROSNAN ET AL.
Figure 2. Panoramic Opening Interface
started controlling her food intake to the point Professionals who have used the stories withwhere she ignored the hunger and cold. Like young people have found it a useful engage-many people, Michelle was using control over ment tool with young people, inviting them tofood to cover up the upset, loneliness and sad- begin to talk about their own experience, par-ness she was feeling. However, when a young ticularly when the viewed story resonates withperson begins to ignore the reality of his/ her the particular experience of the adolescent. Ini-weight loss and discomfort and get obsessed tial cautions are to ensure that the story shownabout limiting food intake he/she is in danger of is relevant to the young persons concerns anddeveloping a serious eating disorder. context.
Questions It is our experience that computers and multi-How real are the pressures on young people media can positively engage young people into diet so as to be thin? coming to therapy. There is anecdotal evidenceIf you were a friend of Michelle's what could to suggest that the initial 'resistance' to comingyou do to help her? to therapy often expressed by adolescents dis-
sipates when the computer is used as an en-DISCUSSION AND EVALUATION gagement tool.
Following completion of the Working Things Out FUTURE DEVELOPMENTSProject the young people who participated in ittook part in an evaluation of the process. They A further project has now developed out of theall reported it as a beneficial experience. Aside Working Things Out research. As part of thefrom it being therapeutic for them to tell their Therapeutic Technologies Research Groupstory in a creative form, it has also provided (University College Dublin/Mater Hospital) wethem with the opportunity to learn new skills are current developing "Transforming Stories"and to use multimedia. For many, participation which is a database driven multimedia storytel-has also had positive impacts on their families. ling tool delivered both online and on standWhen parents have reviewed their children's alone platform. The software currently beingstory it has often opened up family communica- developed will allow the user to choose a storytion. One mother described how proud she was template and build up the story plot using cus-of what her daughter had achieved and review- tomisable characters and background scenesing the story became a special moment of con- adding in their own voiceover and animation.nection for them both. Finally, participation in The user has a drag and drop facility for placingthe CD Rom has copper-fastened, for many of story objects and further features such as posi-the young people, their coping skills and sur- tioning tools, playback and story editing. Othervival strategies. They have moved from being options include building from seed stories'recipients' of mental health information to being where they can change the plotline and add in'teachers' and those who provide it. their own characters and dialogue. In the
method, the therapist introduces the idea ofThe Working Things Out CD-Rom/DVD and making a story and shows examples of what isResource Manual was launched in February possible using the software. It can be a story2005. The package was field tested with young tailored to a problem that needs resolution or apeople attending the Mater Hospital both indi- general story that brings about some positivevidually and in small groups. change in the storyline. A key therapeutic fea-
ture is a notebook facility where the child and
121

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
therapist keep a log of their thoughts on the Contactprocess and their analysis of the story. Thisallows for reflection and gives the therapist the Dr John Sharryopportunity to prompt new ideas for problem Dept. of child and family psychiatrysolving. Finally they can upload and share their Mater Hospitalstories to an online community. Over time it is Dublin 7 Ireland.hoped that a large database of stories will be Tel: +353 1 803 4793build up as a shared resource that can be made Email Eileen, [email protected] to young people struggling with prob- www.workincdhinqSoutielems as a source of support and reliable infor-mation.
REFERENCES
1. Papert, S. (1996) "The Connected Family:Bridging the Digital Generation Gap",Atlanta, USA: Longstreet Press.2. White, M., & Epston, D. (1990). Narrative
means to therapeutic ends. New York: Nor-ton.
3. Sharry, J. (2001). Solution Focused Group-work. London: Sage.
4. Sharry, J. (2004). Counselling children, ado-lescents and families: A strengths-basedcollaborative approach. London: Sage.
5. Ryan, T., & Walker, R. (1993). Life StoryWork. London: British Agencies for Fosteringand Adoption.
6. Ryan, M.-L. (2001). Beyond Myth and Meta-phor - The Case for Narrative in Digital Me-dia. The International Journal of ComputerGame Research, 1(1).
7. Lynch, F., Mills, C., Daly, I., & Fitzpatrick, C.(in press). Challenging Times: A Study ToDetect Irish Adolescents At Risk Of Psychi-atric Disorders And Suicidal Ideation. Jour-nal of Adolescence.
8. Fitzpatrick, C., & Sharry, J. (2004). Copingwith Depression in Young People - A Guidefor Parents. Chichester: Wiley.
Gardner, R. A. (1993). Story-telling in psycho-therapy with children. New Jersey: Aronson.
Philips, R., Brewer, D., & Stavrianoudakis, J.(1993). Gem of the First Water: An OralStory for Helping Teens Make Good Deci-sions.: Resource Publications
Schafer, C. E., & O'Connor, K. J. (Eds.). (1983).Handbook of play therapy. Toronto: Wiley
122
Annual Review of CyberTherapy and Telemedicine
Original Research
Assessment of Emotional Reactivity Produced by Exposure to Virtual
Environments in Patients with Eating Disorder
M. Ferrer-Garcia & J. Gutidrrez Maldonado, PhD.
University of Barcelona
Abstract: This paper describes the effectiveness of virtual environments to elicit emotional re-sponses in eating disordered patients. This study is part of a wider research project analysing theinfluence of the situation to which subjects are exposed on their performance on body image estima-tion tasks.
Though it seems self-evident that there is a close relation between eating disorders (ED) and alteredbody image, in the literature on the subject no clear association has in fact been established, and in-deed the results of the studies are often contradictory or inconclusive. A number of hypotheses havebeen proposed to account for these results. Some authors have stressed the fact that body image maybe to a certain extent more a state than a trait and may change according to situational or emotionalvariables. Several studies have analysed the possible impact of exposure to specific objects or situa-tions on the stability of the body image.
In this study we designed several virtual environments that were emotionally significant for subjectswith ED in order to generate different levels of anxiety and variations in mood. Unlike conventionalmethods (real exposure to the situation, exposure to photographs, exposure via guided imagination,and so on), virtual reality exposes subjects to interactive three-dimensional environments that simulatereal situation. These environments have ecological validity but also permit strict control over the vari-ables and the recording of data. Virtual reality offers many of the advantages of the conventional meth-ods mentioned above, and also overcomes many of their drawbacks.
Thirty female patients with eating disorders were exposed to six virtual environments: a living-room(neutral situation), a kitchen with high-calorie food, a kitchen with low-calorie food, a restaurant withhigh-calorie food, a restaurant with low-calorie food, and a swimming-pool. After exposure to eachenvironment the STAI-S (a measurement of state anxiety) and the CDB (a measurement of depres-sion) were administered to all subjects.
The results showed significantly higher levels of state anxiety in the kitchen with high-calorie food(F=13.120; p = 0.001), the restaurant with high-calorie food (F = 14, 954; p = 0.001) and the swim-ming-pool (F = 4.230; p = 0.049) than in the neutral environment. Analysing the scores for depres-sion obtained on the CDB, significant differences again appeared between the high-calorie food en-vironments (F = 7.187; p = 0.012 in the kitchen and F = 5.933; p = 0.021 in the restaurant) and theneutral environment. In the high-calorie food situations patients with ED showed a more depressedmood.
Virtual reality thus appears to be a valid instrument particularly useful for simulating everyday situa-tions that may provoke emotional reactions such as anxiety and depression, in patients with ED. Vir-tual environments in which subjects are obliged to ingest high-calorie food provoke the highest levelsof state anxiety and depression. Previous studies have shown the capacity of VR to elicit states ofanxiety in patients with other pathologies too.
123

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
INTRODUCTION graphs, exposure via guided imagination, andso on), and also overcomes many of their draw-
During the last four decades, body image distur- backs.bances have been considered one of the mainfeatures of eating disorders. Nevertheless, the It is accepted that patients with ED show anxietypublished literature has not established a clear on seeing high-calorie food and in situations inassociation between Eating Disorders (ED) and which their body is displayed or in which theyaltered body image, and found results have come into contact with other people 17 . In our de-been often contradictory or inconclusive. 2, 8,18,19, sign of the environments we incorporated these20 In order to explain these results some authors two variables in the following conditions: Pres-have stressed the fact that body image may be ence of food (No food, high-calorie food and low-considered more a state than a trait20 '21' 24 and calorie food) and presence of other people (Nomay change according to situational or emotional other people present and other people present).variables. Several studies have analysed the The combination of the two variables gives risepossible impact of exposure to specific objects or to a repeated measures design (2x3) with sixsituations on the stability of the body image. experimental conditions or virtual environments:1,3,6,7,9,10 These studies suggest that body image, The living-room or neutral environment (no foodor some of its components, can indeed be under- and no other people present), the kitchen withstood as a state. low-calorie food (low-calorie food and no other
people present), the kitchen with high-calorieFollowing the same research line, we want to food (high-calorie food and no other people pre-study whether exposure to virtual environments sent), the restaurant with low-calorie food (low-produces variations in the estimation of body calorie food and other people present), the res-image and whether anxiety exerts a mediating taurant with high-calorie food (high-calorie foodrole in this relation. With this aim, we designed and other people present) and the swimming-several virtual environments that were emotion- pool (no food and other people present).ally significant for subjects with ED in order togenerate different levels of anxiety and varia- This study aims to assess the effectiveness oftions in mood. This paper describes the first virtual environments to provoke emotionalstage of the project, in which we evaluate the reactions (anxiety and depressed mood) ineffectiveness of these virtual environments to patients with ED. The following hypotheses areelicit emotional responses in ED patients. considered: the first one, if food constitutes an
aversive, anxiety-provoking stimulus for peopleIn the area of eating disorders, virtual reality with ED, exposure to virtual situations in whichhas been used for the assessment and treat- subjects must eat different types of food (highment of body image disorders'-. Perpifia and or low calorie) will increase their level of anxietyco-workers (1999) compared the efficacy of a and depression; the second one, if subjectstraditional body image disorders treatment pro- with ED experience higher levels of stress ingram with the efficacy of a treatment program social situations and situations that involvethat included virtual exposure. Patients treated scrutiny by others, exposure to these types ofwith virtual reality showed a significantly major situation will increase their level of anxiety andrecovery in body image disorder and in depres- depression.sive and anxious sintomathology.
MATERIALS AND METHODSThese studies show virtual reality as a valuabletechnology for psychopathological assessment Procedureand treatment. One of the main advantages ofthis technology is its capability of simulating real In a first stage, all the subjects of the samplesituations (high ecological validity) and allowing filled two self-report questionnaires, the EDI-2a severe control of the variables, at the same (Eating Disorders Inventory) and the STAI-Ttime. So, virtual reality offers many of the ad- (Trait Anxiety Inventory). Each subject was thenvantages of the conventional methods (real ex- measured and weighed individually in order toposure to the situation, exposure to photo- calculate their body mass index (BMI). The
124

FERRER-GARCIA ET AL.
measurements were performed after the ques- Instrumentstionnaires were completed to avoid the possibleinfluence on the test scores of anxiety caused EDI-2 (Eating Disorders Inventory-2). D.M. Gar-by the measuring and weighing. Finally, a form ner. Spanish adaptation by S. Corral, M. Gon-was filled out for each subject specifying their zalez, J. Perefia & N. Seisdedos (1998): self-age, weight, height and BMI, type and course of report questionnaire for the evaluation of symp-the disorder and severity of symptoms. In a sec- toms that normally accompany anorexia ner-ond stage the six virtual environments were ran- vosa and bulimia nervosa. The questionnairedomly administered. In the interval between the offers scores on 11 scales: Drive for Thinness,presentation of each environment, the subject Bulimia, Body Dissatisfaction, Ineffectiveness,was administered the STAI-S (State Anxiety Perfectionism, Interpersonal Distrust, Interocep-Inventory) and the CDB (a depression scale). tive Awareness, Maturity Fears, Asceticism,Both tests were computerized using a program Impulse Regulation and Social Insecurity.that integrates them in the sequence of virtualenvironments, and records and saves the data. STAI (Stait-Trait Anxiety Inventory). C.D. Spiel-
berger, R.L. Gorsuch and R.E. Lushene. Span-Subjects ish adaptation by N. Seisdedos (1988): anxiety
questionnaire comprising two separate self-The sample comprised 30 women with a prior report scales that measure two independentdiagnosis of eating disorder (17 with anorexia concepts of anxiety, a) as a state and b) as anerviosa, 11 with bulimia nerviosa and 2 with trait.non-specific eating disorder) and with agesranging from 16 to 32 (mean = 20.57 and stan- CDB (The Barcelona Depressiondard deviation = 4.15). The patients were from Questionnaire). J. Guti~rrez-Maldonado and M.hospital centres and private clinics in Barce- Mora-Bello (2000): Self-report instrument forlona: the Hospital Germans Tries i Pujol, the measuring variations in depressed mood. ItHospital de Sant Juan de Deu, the Clinica La- comprises 23 items, each one with a visual-bor and the Centro ABB. analog scale with an adjective describing a
mood written at the top: subjects mark the linecorresponding to their experience of this mood,
40 ranging from "I don't feel like this at all now" to"I feel completely like this now". The items weretaken from the diagnostic criteria for major de-pression from the nosological classification ofthe DSM-IV and were presented in the ques-tionnaire in the same order as the criteria. All
30 the items are formulated in the same direction.
Virtual environments: six virtual environments(living-room, kitchen with low-calorie food,kitchen with high-calorie food, restaurant withlow-calorie food, restaurant with high-calorie
<- food, and swimming-pool) developed using theW 20 virtual reality software 3d Studio Max5.1 and
2 %. 6k k % programmed using the Lingo language with the%' " % : •. "- •'6• .Director software.
"RESULTS
Situations Using repeated measures analysis, we com-pared subjects' scores on the STAI-S and the
Figure 1. STAI-S scores obtained after visiting CDB after visiting each of the five experimentaleach virtual environment environments with the score obtained after visit-ing the neutral environment (the living-room).
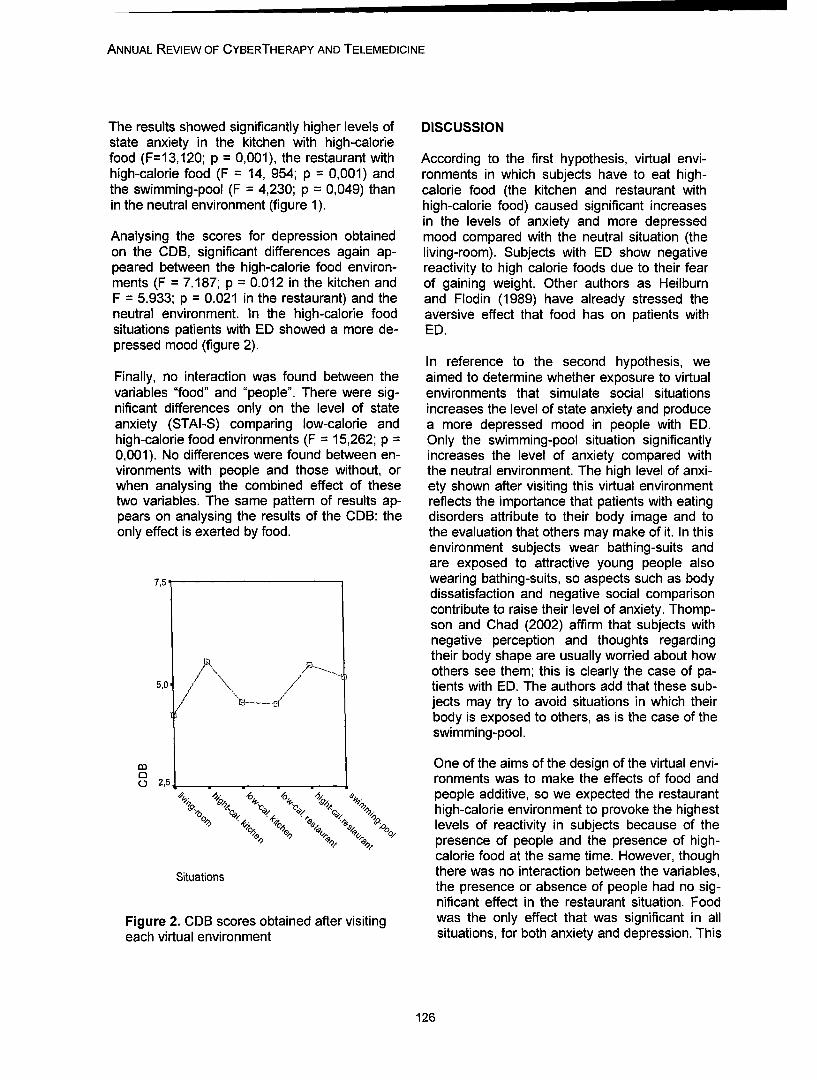
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
The results showed significantly higher levels of DISCUSSIONstate anxiety in the kitchen with high-caloriefood (F=13,120; p = 0,001), the restaurant with According to the first hypothesis, virtual envi-high-calorie food (F = 14, 954; p 0,001) and ronments in which subjects have to eat high-the swimming-pool (F = 4,230; p = 0,049) than calorie food (the kitchen and restaurant within the neutral environment (figure 1). high-calorie food) caused significant increases
in the levels of anxiety and more depressedAnalysing the scores for depression obtained mood compared with the neutral situation (theon the CDB, significant differences again ap- living-room). Subjects with ED show negativepeared between the high-calorie food environ- reactivity to high calorie foods due to their fearments (F = 7.187; p = 0.012 in the kitchen and of gaining weight. Other authors as HeilburnF = 5.933; p = 0.021 in the restaurant) and the and Flodin (1989) have already stressed theneutral environment. In the high-calorie food aversive effect that food has on patients withsituations patients with ED showed a more de- ED.pressed mood (figure 2).
In reference to the second hypothesis, weFinally, no interaction was found between the aimed to determine whether exposure to virtualvariables "food" and "people". There were sig- environments that simulate social situationsnificant differences only on the level of state increases the level of state anxiety and produceanxiety (STAI-S) comparing low-calorie and a more depressed mood in people with ED.high-calorie food environments (F = 15,262; p = Only the swimming-pool situation significantly0,001). No differences were found between en- increases the level of anxiety compared withvironments with people and those without, or the neutral environment. The high level of anxi-when analysing the combined effect of these ety shown after visiting this virtual environmenttwo variables. The same pattern of results ap- reflects the importance that patients with eatingpears on analysing the results of the CDB: the disorders attribute to their body image and toonly effect is exerted by food. the evaluation that others may make of it. In this
environment subjects wear bathing-suits andare exposed to attractive young people also
7,5 wearing bathing-suits, so aspects such as bodydissatisfaction and negative social comparisoncontribute to raise their level of anxiety. Thomp-son and Chad (2002) affirm that subjects withnegative perception and thoughts regardingtheir body shape are usually worried about howothers see them; this is clearly the case of pa-
5,0 tients with ED. The authors add that these sub-jects may try to avoid situations in which theirbody is exposed to others, as is the case of theswimming-pool.
m One of the aims of the design of the virtual envi-2,51 ronments was to make the effects of food and
/0 / . people additive, so we expected the restaurantI., high-calorie environment to provoke the highest
o,,. " '•*' 4Oo3. levels of reactivity in subjects because of the" % -% presence of people and the presence of high-
calorie food at the same time. However, thoughSituations there was no interaction between the variables,
the presence or absence of people had no sig-nificant effect in the restaurant situation. Food
Figure 2. CDB scores obtained after visiting was the only effect that was significant in alleach virtual environment situations, for both anxiety and depression. This
126

FERRER-GARCIA ET AL.
means that the subject's exposure to a situation and extend of body image disturbances in ano-with low or high calorie food does indeed pro- rexia nervosa and bulimia nervosa: a Meta-duce substantial changes in their level of anxi- analysis. International Journal of Eating Disor-ety and their mood, a finding that appears to ders, 22, 107-125.confirm our first hypothesis. Nevertheless, thesecond hypothesis is not verified. 3. Cash, T.F.; Cash, D.W. & Butters, J.W.
(1983). "Mirror, mirror, on the wall...?": ContrastThe results of this study confirm the utility of effects and self-evaluations of physical attrac-virtual environments as instruments capable of tiveness. Personality and Social Psychologyprovoking emotional reactions in patients with Bulletin, 9 (3), 351-358.eating disorders, but they show too that it isnecessary to introduce changes to improve the 4. Gardner, D.M. (1998). Eating Disorders In-effectiveness of some of the developed situa- ventory-2. Spanish adaptation: Corral, S.,tions. Particularly, the interaction with the appli- Gonzalez, M., Perefia, J. & Seisdedos, N.cation should be increased, especially with re- Barcelona: Ediciones TEA.gard to the avatars representing human figures.In contrast to the food stimuli, which the subject 5. Guti6rrez, J. & Mora, M. (2000). Cuestionariocan eat, in none of the environments was there de Depresi6n Barcelona. Not publishedany interaction between the subject and the manuscript. In B. P6rez, J. Gutierrez-other people present. This is probably why the Maldonado & M. Ferrer-Garcia. VII Europeanpresence or absence of other people has not Conference on Psychological Assessment.produced significant changes in the levels of Malaga (Spain), 1-4th April, 2004.emotional reactivity. 6. Haimovitz D.; Lansky L.M. & O'Reilly P.
(1993). Fluctuations in body satisfaction acrosssituations. International Journal of Eating Disor-
CONCLUSION ders, 3 (1), 77-84.
Virtual reality seems to be a valid instrument 7. Heilbrun, A.B. & Flodin, A. (1989). Food cuesparticularly useful for simulating everyday situa- and perceptual distortion of the female body:tions that may provoke emotional reactions implications for food avoidance in the early dy-such as anxiety and depression, in patients with namics of anorexia nervosa. Journal of ClinicalED. Virtual environments in which subjects are Psychology, 45 (6), 843-851.obliged to ingest high-calorie food provoke thehighest levels of state anxiety and depression. 8. Hsu, L.K.G. & Sobkiewick, T.A. (1991).BodyNonetheless, certain changes need to be intro- image disturbance: Time to abandon de con-duced in the environments in order to increase cept for eating disorders? International Journalthe impact that the presence of people has on of Eating Disorders, 10 (1), 15-30.the patients. These changes should aim princi-pally to add movement and sound to the ava- 9. Laberg, J.C.; Wilson G.T.; Eldredge K. &tars representing human figures and increase Nordby H. (1991). Effects of Mood on Heartthe degree of interactivity between the users Rate Reactivity in Bulimia Nervosa. Intema-and the virtual environments. tional Journal of Eating Disorders, 10 (2), 169-
178.
REFERENCES 10. McKenzie, S.J.; Williamson, D.A. & Cubic,B.A. (1993). Stable and reactive body image
1. Carter F.A., Bulick C.M., Lawson R.H., Sulli- disturbances in bulimia nervosa. Behavior Ther-van P.F. & Wilson J.S. (1996). Effect of mood apy, 24, 195-207.and food cues on body image in women withbulimia and controls. International journal of 11. Perpifa, C., Botella, C., & Bahos, R. (2003).eating disorders, 20 (1), 65-76. Virtual reality in Eating Disorders. European
Eating Disorders Review, 11 (3), 261-18.2. Cash, T.F. & Deagle, E.A. (1997). The nature
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
12. Perpifia, C.; Botella, C.; Bafios, R.; Marco, 21. Smeets, M.A.M. (1997).The rise and fall ofJ.H; Alcafiiz, M. & Quero, S. (1999). Body Im- body size estimation research in anorexia ner-age and Virtual Reality in Eating Disorders: Is vosa: a review and reconceptualization. Euro-Exposure to Virtual Reality More Effective than pean Eating Disorders, 5, 75-95.the Classical Body Image Treatment? CyberP-sychology & Behavior, 2(2), 149-155. 22. Spielberger, C.D., Gorsuch, R.L. &
Lushene, R.E. (1988). Spanish adaptation:13. Riva, G. (1997). Virtual reality as assess- Seisdedos, N. Barcelona: Ediciones TEA.ment tool in Psychology. In G. Riva (Ed.), Vir-tual Reality in Neuro-Psycho-Physiology. Am- 23. Thompson, A.M. & Chad, K.E. (2002). Thesterdam: lOS Press. relationship of social physique anxiety to risk for
developing an eating disorder in young females.Journal of Adolescent Health, 31, 183-189.
14. Riva, G. (1998a). Virtual environment forbody image modification: virtual reality system 24. Thompson, J.K. (1996). Body image, eatingfor treatment of body image disturbances. disorders and obesity. Washington, DC: Ameri-Computer in Human Behavior, 14 (3), 477-490. can Psychological Association.
15. Riva, G. (1998b). Virtual reality in Contactpsychological assessment: the Body ImageVirtual Reality Scale. CyberPsychology-and- Marta Ferrer-GarciaBehavior, 11(1), 37-44. Departamento de Personalidad
Evaluaci6n y Tratamientos Psicol6gicosFacultad de Psicologia.
16. Riva, G. Bacchetta, M.; Baruffi, M.; Rinaldi, Paseo Valle de Hebron, 171S. & Molinari, E. (1998). In G. Riva (Ed.), Virtual 08035 Barcelona, SpainEnvironments in Clinical Psychology and Tel: +34933125126Neuroscience. Amsterdam: lOS Press. Fax: +34934021362
E-mail: [email protected]: [email protected]
17. Saldafia, C.; Tomas, I. & Bach, L. (1997).Tkcnicas de intervenci6n en los trastornos delcomportamiento alimentario. Estr6s y Ansiedad,3 (2-3), 319-337.
18. Septilveda, A.R.; Botella, J. & Le6n, J.K.(2001). La alteraci6n de la imagen corporal enlos trastornos de la alimentaci6n: un meta-analisis. Psicothema, 13 (1), 7-16:
19. Skrzypek, S.; Wehmeier, P.M. &Remschmidt, H. (2001). Body image assess-ment using body size estimation in recent stud-ies on anorexia nervosa. A brief review. Euro-pean Child & Adolescent Psychiatry, 10, 215-221.
20. Slade, P.D. & Brodie, D. (1994). Body Im-age distortion and eating disorder: A reconcep-tualitation based on recent literature. EatingDisorders Review, 1 (2), 32-46.
128

Annual Review of CyberTherapy and Telemedicine
Investigation of Social Anxiety of Patients with Schizophrenia UsingVirtual Avatar
H. J. Jang1 B. A., J. Ku3 Ph.D.,S. H. Park1' 2M.S., S. Y. Kim 1 B. A., I. Y. Kim 3 M.D.,Ph.D., C-H. Kim 1'2M.D., Ph.D., J-J. Kim 1'2 M.D., Ph.D., S. I. Kim 3, Ph.D.
'Mind mapping laboratory, Institute of behavioral science in medicine,Yonsei University College of Medicine
2Department of Psychiatry, Yonsei University College of Medicine,Severance Mental Health Hospital, Gyunggi-do, Korea
3Dept. of Biomedical Engineering, Hanyang University, Seoul, Korea
Abstract: Backgrounds: Patients with schizophrenia show a tendency to avoid social interaction be-cause they feel great anxiety during their social interactions. As a result, they have trouble in makingsocial relationships. This trouble is largely due to the fact that these patients show emotional with-drawal as well as passive/apathetic social withdrawal. Social deficits of these patients have beenovercome through social skills training programs, which provide them opportunities to experiencevarious social situations by role play method. Objectives: This study was conducted in order to inves-tigate whether an interaction with a virtual avatar can evoke patient's social anxiety and the relation-ship between patient's symptom severity and social anxiety traits. Method/Tools: Fifteen patients withschizophrenia and fifteen controls were recruited. A male and a female avatar were generated.2x2x3 (group, avatar's gender and avatar's emotional expression) was used in this experiment. Eachavatar has three emotional expressions: are happy, neutral and angry. Subjects performed an intro-duction task in six conditions (gender x emotional expression) in random order. The task was com-posed of "approach", "listening to avatar's introduction" and "introduce oneself to the avatar". After allsix tasks were performed, subjects completed a State-Trait Anxiety Inventory (STAI) questionnaire.In addition, patients' symptom severity was evaluated using the Positive and Negative SyndromeScale (PANSS). Results: The social anxiety level to avatar's emotional representation was signifi-cantly different in the two group (p<.001). In the control group, the level was lowest when subjectscoped with an avatar expressing "happy," while the highest anxiety level was shown when they facedan avatar expressing "angry." However, in the patient group, the level difference was not significantbetween "neutral" and "happy" avatar. Patients only showed a significantly high anxiety level whenthey experience the "angry" avatar condition compared to other two conditions. In a correlation analy-sis between patient's anxiety level and their symptom severity, social anxiety for "happy" and"neutral" avatars was positively correlated with the negative syndrome of PANSS (happy : r=.539,p=.038, neutral: r=.533, p=.041). Particularly, the anxiety level for "happy" and "neutral" avatars waspositively correlated with two subscales (NI: blunted affect, N4: passive/apathetic social withdrawal)of the negative syndrome of PANSS (NI. happy: r=.549, p=.034/neutral: r=.536, p=.039) (N4. happy:r=.536, p=.039/ neutral: r=.658, p=.008). Conclusion: Through this study, we discovered that virtualavatar displaying emotional expression can cause social anxiety in patients with schizophrenia andthat a patient's symptom severity was correlated with social anxiety level. It could be said, from theseresults, that the more severe the negative symptoms a patient has, the greater social anxiety they willfeel. This might be due to their passive, apathetic and isolated trait. They may tend to recognize so-cially positive emotion as fearful stimuli. This inference could be supported by the relationship be-tween anxiety and subscales of negative symptom of PANSS. In this sense, we could say that a vir-tual avatar could provide an opportunity for patients to experience emotionally induced social situa-tion. In addition, it could be used for training patients to cope effectively by experiencing emotionsclose to reality as well as to find out the clinical characteristics related to patient's symptoms.
129

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
INTRODUCTION posure to an anxiety evoking situation (gradualconfrontation of feared event/situation) and to
Since it seriously affects higher mental func- learning coping strategies for a situationstions, such as thinking, feeling, and perceiving,1 through role-play (behavioral acting out). It isschizophrenia can be considered one of the very important that patients experience socialmost devastating psychiatric disorders. The anxiety in treatment or in evaluation session.clinical course of schizophrenic patients is char- However, the existing therapeutic programsacterized by higher rates of relapse, disability depend on patient's imagination ability. 12
and suicide when anxiety symptoms are con-currently experienced.2'3 Although social anxi- Therefore, virtual reality could be a powerfulety symptoms are common in patients with tool to provide patients with schizophrenia suf-schizophrenia,4 they often goes unrecognized, fering from social anxiety to be immersed in aor are considered to be part and parcel of the specific situation and feel and experienced so-schizophrenic symptomatology.5 cial anxiety. Accordingly, the aims of this study
were to develop a virtual avatar that could inter-In fact, many patients with schizophrenia suffer act with patients with schizophrenia, and tofrom anxiety symptoms. 3 As a result, they ac- evaluate whether a virtual avatar could evoketively avoid social interactions and appear to patient's social anxiety. In addition, this studyhave little motivation to develop social relation- was conducted in order to investigate the rela-ships. Social interaction is often very anxiety tionship between patient's symptom severityprovoking and leads to avoidance; patients of- and social anxiety traits.ten seek to escape from interactions initiated byothers.6 Existent research suggests that schizo- MATERIALS AND METHODSphrenic patients are particularly sensitive toconflict and criticism and will withdraw from po- Apparatus for this studytential conflict situations even when they arebeing taken advantage of or unjustly accused of The apparatus for this study was composed ofthings they have not done.7 a personal computer, a 6 DOF (Degrees of
Freedom) position sensor, an HMD (HeadIn order to treat these patients with schizophre- Mounted Display) and tracker. It could providenia, effective psychological treatment studies a user an immersive virtual environment. Thefor social anxiety have been developed and position sensor was composed of a transmitterevaluated. 8'9 A combined program including and receiver. The transmitter worked as an ori-exposure treatment together with cognitive ther- gin creating a surrounding magnetic around it,apy delivered in a group format has had signifi- in order for the receiver to detect its positioncant outcomes.10'1 Cognitive behavioral group and orientation from the transmitter by calculat-treatment (CBGT) for social anxiety in schizo- ing strength of the magnetic field. The receiverphrenia was demonstrated to be effective as an attached on the user's head could detect theadjunctive treatment12 The important factors in user's head position and orientation so that thethe established therapeutic techniques are ex-
Schizophrenia Normal
Age 28.69 ± 7.064 25.1 ± 1.553
Gender M : 10 F : 5 M:9/F:6
PANSSNegative Syndrome 18.85 ± 3.23
Positive Syndrome 19.78 ± 4.6638.21 ± 5.80
General Psychopathology .- _____
Table 1. Demographic data of participants
130
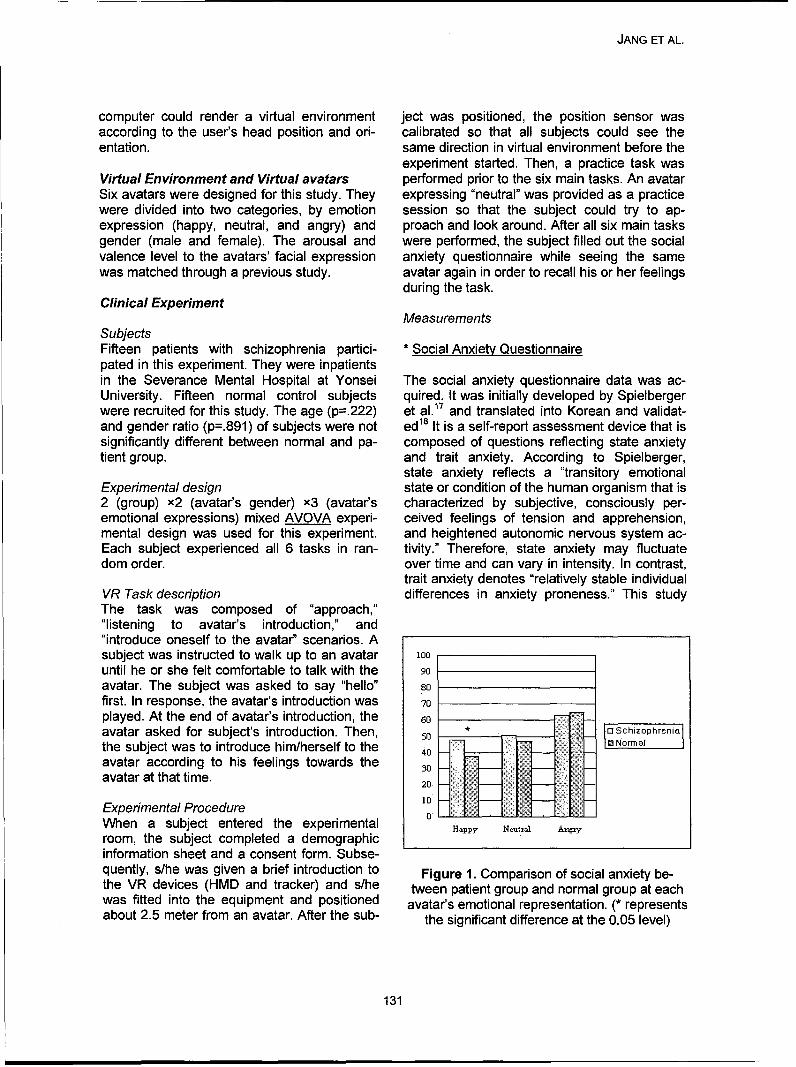
JANG ET AL.
computer could render a virtual environment ject was positioned, the position sensor wasaccording to the user's head position and ori- calibrated so that all subjects could see theentation. same direction in virtual environment before the
experiment started. Then, a practice task wasVirtual Environment and Virtual avatars performed prior to the six main tasks. An avatarSix avatars were designed for this study. They expressing "neutral" was provided as a practicewere divided into two categories, by emotion session so that the subject could try to ap-expression (happy, neutral, and angry) and proach and look around. After all six main tasksgender (male and female). The arousal and were performed, the subject filled out the socialvalence level to the avatars' facial expression anxiety questionnaire while seeing the samewas matched through a previous study. avatar again in order to recall his or her feelings
during the task.Clinical Experiment
MeasurementsSubjectsFifteen patients with schizophrenia partici- * Social Anxiety Questionnairepated in this experiment. They were inpatientsin the Severance Mental Hospital at Yonsei The social anxiety questionnaire data was ac-University. Fifteen normal control subjects quired. It was initially developed by Spielbergerwere recruited for this study. The age (p=.222) et al. 17 and translated into Korean and validat-and gender ratio (p=.891) of subjects were not ed18 It is a self-report assessment device that issignificantly different between normal and pa- composed of questions reflecting state anxietytient group. and trait anxiety. According to Spielberger,
state anxiety reflects a "transitory emotionalExperimental design state or condition of the human organism that is2 (group) x2 (avatar's gender) x3 (avatar's characterized by subjective, consciously per-emotional expressions) mixed AVOVA experi- ceived feelings of tension and apprehension,mental design was used for this experiment, and heightened autonomic nervous system ac-Each subject experienced all 6 tasks in ran- tivity." Therefore, state anxiety may fluctuatedom order. over time and can vary in intensity. In contrast,
trait anxiety denotes "relatively stable individualVR Task description differences in anxiety proneness." This studyThe task was composed of "approach,""listening to avatar's introduction," and"introduce oneself to the avatar" scenarios. Asubject was instructed to walk up to an avatar 100until he or she felt comfortable to talk with the 90avatar. The subject was asked to say "hello" 8ofirst. In response, the avatar's introduction wasplayed. At the end of avatar's introduction, the 60avatar asked for subject's introduction. Then, 50 a rSchizphreniathe subject was to introduce him/herself to the 40 0] Norma
avatar according to his feelings towards theavatar at that time. 20
Experimental Procedure 0When a subject entered the experimental Happy N0tr Ar,room, the subject completed a demographicinformation sheet and a consent form. Subse-quently, s/he was given a brief introduction to Figure 1. Comparison of social anxiety be-the VR devices (HMD and tracker) and s/he tween patient group and normal group at eachwas fitted into the equipment and positioned avatar's emotional representation. (* representsabout 2.5 meter from an avatar. After the sub- the significant difference at the 0.05 level)
131

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
excluded the measurement regarding the trait and their social anxiety level. As a result, theanxiety, because state anxiety would better rep- negative syndrome score of PANSS was posi-resent social anxiety induced by experiencing tively correlated with social anxiety on "happy"of emotional virtual environment which was of and "neutral" avatars (happy: r=.539, p=.038,interest in this study. neutral: r=.533, p=.041).
RESULTS In particular, a significant positive correlationwas found between the social anxiety level
The main effect of the avatar's emotional ex- evoked by "happy" and "neutral" avatars andpression was observed in both group (p<.001), two subscales (NI: blunted affect, N4: passive/while a main effect towards the avatar's gender apathetic social withdrawal) of the negativewas not observed, syndrome of PANSS (N1. happy: r=.549,
p=.034/ neutral: r=.536, p=.039 ; N4. happy:An interaction effect between avatar's express- r=.536, p=.039/ neutral: r=.658, p=.008), buting emotion and the subject group was ob- there were no correlations with other subscales,served (p=.007). It means that social anxiety such as positive syndrome and general psycho-level to avatar's expressing emotion showed a pathology score.significantly different pattern between the twogroups. In the control group, the level was the DISCUSSIONlowest when they faced an avatar expressing Schizophrenia is a multi-dimensional disorder"happy", and the highest when they met an ava- and necessitates a comprehensive treatmenttar expressing "angry". However, members of approach. 13 Social anxiety symptom are de-the patient group did not show any anxiety level scribed especially frequently by patients withdifference between "happy" and "neutral" ava- schizophrenia in their clinical course. 14 Patientstar. In addition, they only showed a significantly tend to avoid social interactions and appear tohigher social anxiety level when they experi- have little motivation to develop social relation-enced an avatar expressing "angry" compared ships because social interaction often is veryto other emotional conditions. anxiety provoking. 6 This study explored
whether an interaction with virtual avatar canIn short, normal control subjects felt less social provoke patient's social anxiety and investi-anxiety in happy and neutral condition than pa- gated the relationship between patient' symp-tients did (happy: p=.016/ neutral: p=.332), toms severity and social anxiety.while normal subjects felt more social anxiety inangry emotion than patients did (angry: The observed result of a variation of anxietyp=.490). level to a virtual avatar's emotional expression
shows that an interaction with a virtual avatarIn order to learn how a patient's symptom se- can induce social anxiety of patients withverity affects their social anxiety level, a corre- schizophrenia. It means that a virtual reality orlation analysis was performed between PANSS
Positive syndrome Negative syndrome GeneralPsychopathology
happy -.020 (p=.944) .539 (p=.038)* .591 (p=,020)*
neutral -.038 (p=.893) .533 (p=.041)* .474 (p=.074)
angry -.323 (p=.240) -.163 (p=.563) .013 (p=.964)
Table 2. The correlations between the social anxiety level to avatar's emotional representation(happy, neutral, angry) and PANSS
(: p-value,• : correlation is significant at the 0.05 level (2-tailed)
132
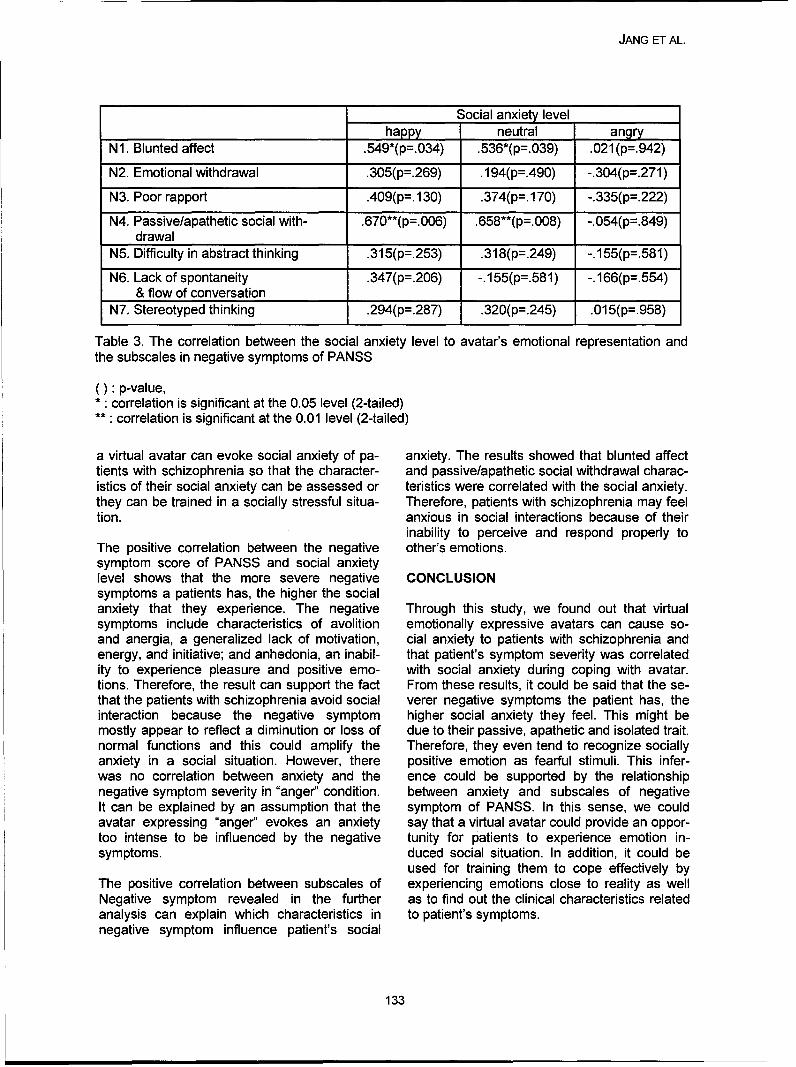
JANG ET AL.
Social anxiety levelhappy neutral angry
N1. Blunted affect .549*(p=.034) .536*(p=.039) .021(p=.942)
N2. Emotional withdrawal .305(p=.269) .194(p=.490) -.304(p=.271)
N3. Poor rapport .409(p=. 130) .374(p=. 170) -.335(p=.222)
N4. Passive/apathetic social with- .670**(p=.006) .658**(p=.008) -.054(p=.849)drawal
N5. Difficulty in abstract thinking .315(p=.253) .318(p=.249) -.155(p=.581)
N6. Lack of spontaneity .347(p=.206) -.155(p=.581) -.166(p=. 5 5 4)& flow of conversation
N7. Stereotyped thinking .294(p=.287) .320(p=.245) .015(p=.958)
Table 3. The correlation between the social anxiety level to avatar's emotional representation andthe subscales in negative symptoms of PANSS
(): p-value,correlation is significant at the 0.05 level (2-tailed)
**: correlation is significant at the 0.01 level (2-tailed)
a virtual avatar can evoke social anxiety of pa- anxiety. The results showed that blunted affecttients with schizophrenia so that the character- and passive/apathetic social withdrawal charac-istics of their social anxiety can be assessed or teristics were correlated with the social anxiety.they can be trained in a socially stressful situa- Therefore, patients with schizophrenia may feeltion. anxious in social interactions because of their
inability to perceive and respond properly toThe positive correlation between the negative other's emotions.symptom score of PANSS and social anxietylevel shows that the more severe negative CONCLUSIONsymptoms a patients has, the higher the socialanxiety that they experience. The negative Through this study, we found out that virtualsymptoms include characteristics of avolition emotionally expressive avatars can cause so-and anergia, a generalized lack of motivation, cial anxiety to patients with schizophrenia andenergy, and initiative; and anhedonia, an inabil- that patient's symptom severity was correlatedity to experience pleasure and positive emo- with social anxiety during coping with avatar.tions. Therefore, the result can support the fact From these results, it could be said that the se-that the patients with schizophrenia avoid social verer negative symptoms the patient has, theinteraction because the negative symptom higher social anxiety they feel. This might bemostly appear to reflect a diminution or loss of due to their passive, apathetic and isolated trait.normal functions and this could amplify the Therefore, they even tend to recognize sociallyanxiety in a social situation. However, there positive emotion as fearful stimuli. This infer-was no correlation between anxiety and the ence could be supported by the relationshipnegative symptom severity in "anger" condition. between anxiety and subscales of negativeIt can be explained by an assumption that the symptom of PANSS. In this sense, we couldavatar expressing "anger" evokes an anxiety say that a virtual avatar could provide an oppor-too intense to be influenced by the negative tunity for patients to experience emotion in-symptoms. duced social situation. In addition, it could be
used for training them to cope effectively byThe positive correlation between subscales of experiencing emotions close to reality as wellNegative symptom revealed in the further as to find out the clinical characteristics relatedanalysis can explain which characteristics in to patient's symptoms.negative symptom influence patient's social
133
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
REFERENCES phrenia: perspective in the era of atypicalantipsychotic agents. American Journal of
[1] Schults, S.K., Andreasen, N.C. (1999). Psychiatry. 157, 1379-1389.Schizophrenia, Lancet, vol. 353, 1425-30. [15] Andreasen, N.C. (1982). Negative symp-
[2] Hirsh, S.R., Jolley, A.G. (1989). The dys- toms in schizophrenia: Definition and reli-phoric syndrome in schizophrenia and its ability. Archives of General Psychiatry, 39,implications for relapse. British Journal of 784-788.Psychiatry. Supplement 155, 46-50. [16] Bellack, A.S., Blanchard, J.J., & Mueser,
[3] Roy, 1. (1989). Suicidal behavior in schizo- K.T. (1996). Cue availability and affect per-phrenics. In: Williams, R., Dalby, J.T. ception in schizophrenia. Schizophrenia(Eds.), Depression in Schizophrenics. Pie- Bulletin, 22, 535-544.num, New York, NY. [17] Spileberger, C. D., Gorsuch, R.L., & Lush-
[4] Cosoff SJ, Hafner J. (1998). The preva- ene, R.E. (1970). Manual for the State-Traitlence of comorbid anxiety in schizophrenia, Anxiety Inventory. Pal. Alto, CA: ConsultingAustralian and New Zealand Journal of Psychologist Press.Psychiatry, 33: 67-72. [18] Kim, J. T. (1978). The relationship of trait
[5] Walker EF. (1994) Developmentally moder- anxiety and sociality, M.A. Thesis of Koreaate expressions of the neuropathology un- University.derlying schizophrenia. Schizophrenia Bul-letin, 20: 453-480.
[6] Bellack, A.S, Mueser, K.T., Gingerich, S., Contactand Agresta, J. (1997). Social Skills Train-ing for Schizophrenia: A Step-by-Step Hee Jeong JangGuide. New York: The Guilford press, 3-9. Mind Mapping Laboratory
[7] Bellack, A.S, Mueser, K.T., Wade, J., Institute of Behavioral Science in MedicineSayers, S.L., and Morrison, R.L. (1992). Yonsei University College of MedicineThe ability of schizophrenics to perceive Email: [email protected] cope with negative affect. British Jour-nal of Psychiatry, vol. 160, 473-480.
[8] Gould, R.A., Buckminster, S., Pollack,M.H., Otto, M. W., Yap, L. (1997). Cogni-tive-behavioral and pharmacological treat-ment for social phobia: a meta-analysis.Clinical Psychology-Science and Practice5, 291-306.
[9] Van Dyck, R (1996). Non-drug treatmentfor social phobia. International Clinical Psy-chopharmacology 11, 65-70.
[10] Mattick, R.P., Peter, L., Clarke, J. C.,(1989). Exposure and cognitive restructur-ing for social phobia; a controlled study.Behavior Therapy 20, 3-23.
[111 Hope, D.A., Heimberg, R.G., Brunch,M.A.. (1995). Dismantling cognitive behav-ioral group therapy for social phobia. Be-havior research and Therapy 33, 637-650.
[12] Patrick Kingsep, Paula Nathan, DavidCastle. (2003). Cognitive behavioral grouptreatment for social anxiety in schizophre-nia. Schizophrenia Research 63, 121-129.
[13] Andreasen, N.C. (1995). Symptoms,signs, and diagnosis of schizophrenia. TheLancet 346, 477-481.
[14] Siris, S.G., (2000). Depression in schizo-
134

Investigation of Social Cue Perceptionin Schizophrenia using Virtual Reality
K. Kim, M.S.1 , J-J. Kim, M.D., Ph.D2, J. Kim, M.S.1 , D-E. Park, B.S.1 , J. Ku, Ph.D.', H. J.Jang, B.A.2 , S. H. Park, M.D.2 , S. Y. Kim, B.A.2 , C. H. Kim, M.D., Ph.D2 , J. H. Lee, Ph.D.',
I. Y. Kim, M.D., Ph.D.1 , and S. I. Kim, Ph.D'
1Department of Biomedical Engineering, Hanyang University, Seoul, Korea;2Institute of Behavioral Science in Medicine, Yonsei University Severance Mental Health Hospital, Seoul, Korea
Abstract: Background/Problem: An impairment in social skills is one of the few criteria that all indi-viduals diagnosed with schizophrenia must meet Successful social skills require the coordination ofmany abilities, including social perception, which involves the decoding and interpretation of socialcues from others. Previous studies on social perception in schizophrenia have focused on interpret-ing the emotions from facial expressions. There are some reports showing the potential of virtual re-ality (VR) in social skills training. This study developed VR for assessing the social perception includ-ing an interpretation of non-facial expressions. In addition, the suitability of VR for determining aschizophrenia patient's social perception ability was evaluated.
Method/Tools: For an effective social perception test, VR consisting various situations and contentsmay be needed. Therefore, the VR Behavior & Facial Data Base architecture (VRBFDB) was usedfor the easy and fast VR composition. The contents can be divided into two areas "interpretation ofthe relevant cue test" and "Emotion Recognition test." The "Interpretation of the relevant cue test" iscomposed of the recognition of a non-verbal social situation as well as the recognition of a verbalsocial situation, and the "Emotion Recognition test" is composed of happy, sad, angry and surprisefacial expression recognition.
There were 17 subjects (12 males and 5 females) and 17 controls (12 males and 5 females). Thisstudy obtained the data from the VR, a questionnaire, and the subject's symptoms. The VR data in-cluded the participant's response results, reaction time, presence and computer experience. Thequestionnaire data included age, education, gender, intelligence (K-WAIS) etc. The symptom datawas measured using the PANSS (Positive and Negative Syndrome Scales).
Results/Conclusion: According to the results, schizophrenia subjects perform significantly worse onthe VR test than normal subjects, and some parameters the correlated with previous clinical test.
INTRODUCTION
"Social skills" are interpersonal behaviors that Successful social competence is based on aare normative and/or socially sanctioned. They distinct set of component skills [3]. These com-include items such as dress and behavior ponents can be roughly divided into two broadcodes, rules about what to say and what not to sets: expressive skills (speech content, paralin-codeand stylistic guidelines about the expres- guistic features, and nonverbal behavior) andsay, asocial perception skills (interpretation of thesion of affect, social reinforcement, interper- relevant cues, emotion recognition). However,sonal distance etc [1]. Impairment in social skills regardless of the individual's ability to emit so-is one of the criteria that all individuals diag- cially skillful responses, he or she cannot benosed with schizophrenia must meet [21. These effective without an accurate social perceptiondeficits make it difficult for many clients to es- that involves the decoding and interpretation oftablish and maintain social relationships, fulfill various social cues in others [1]. Previous re-social roles or to have their needs met [1]. search on social perception in schizophrenia
135
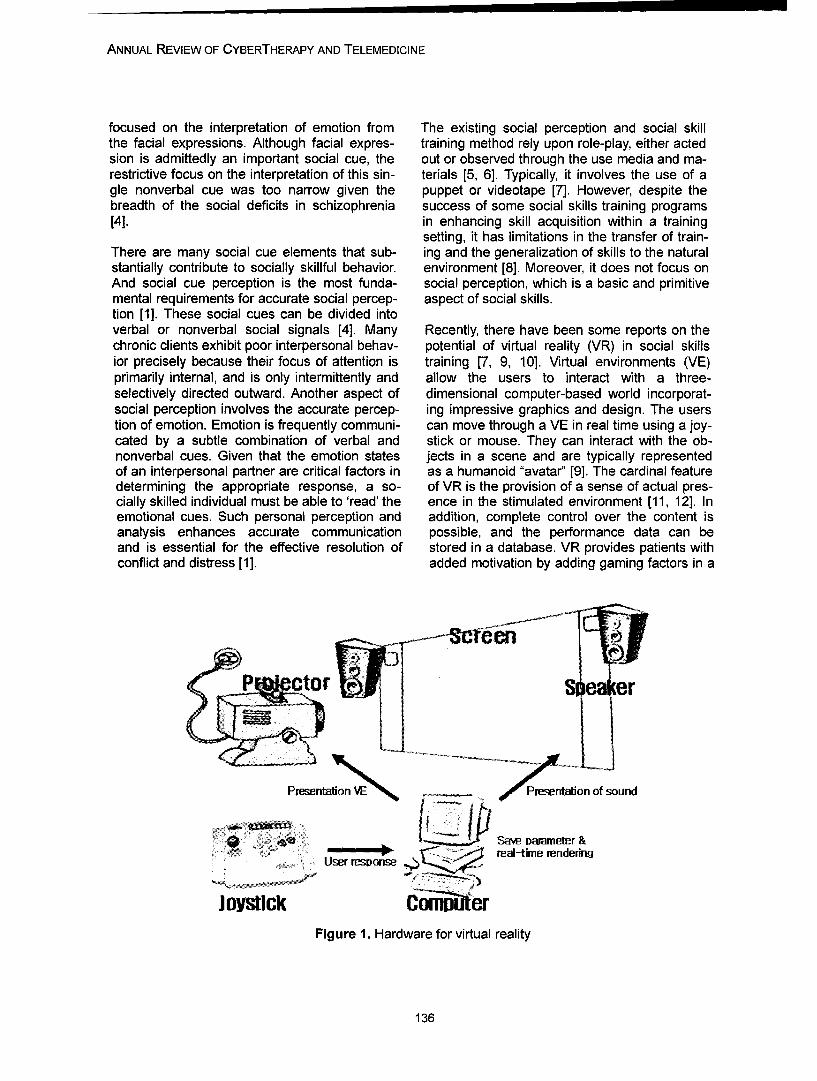
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
focused on the interpretation of emotion from The existing social perception and social skillthe facial expressions. Although facial expres- training method rely upon role-play, either actedsion is admittedly an important social cue, the out or observed through the use media and ma-restrictive focus on the interpretation of this sin- terials [5, 6]. Typically, it involves the use of agle nonverbal cue was too narrow given the puppet or videotape [7]. However, despite thebreadth of the social deficits in schizophrenia success of some social skills training programs[4]. in enhancing skill acquisition within a training
setting, it has limitations in the transfer of train-There are many social cue elements that sub- ing and the generalization of skills to the naturalstantially contribute to socially skillful behavior, environment [8]. Moreover, it does not focus onAnd social cue perception is the most funda- social perception, which is a basic and primitivemental requirements for accurate social percep- aspect of social skills.tion [1]. These social cues can be divided intoverbal or nonverbal social signals [4]. Many Recently, there have been some reports on thechronic clients exhibit poor interpersonal behav- potential of virtual reality (VR) in social skillsior precisely because their focus of attention is training [7, 9, 10]. Virtual environments (VE)primarily internal, and is only intermittently and allow the users to interact with a three-selectively directed outward. Another aspect of dimensional computer-based world incorporat-social perception involves the accurate percep- ing impressive graphics and design. The userstion of emotion. Emotion is frequently communi- can move through a VE in real time using a joy-cated by a subtle combination of verbal and stick or mouse. They can interact with the ob-nonverbal cues. Given that the emotion states jects in a scene and are typically representedof an interpersonal partner are critical factors in as a humanoid "avatar' [9]. The cardinal featuredetermining the appropriate response, a so- of VR is the provision of a sense of actual pres-cially skilled individual must be able to 'read' the ence in the stimulated environment [11, 12]. Inemotional cues. Such personal perception and addition, complete control over the content isanalysis enhances accurate communication possible, and the performance data can beand is essential for the effective resolution of stored in a database. VR provides patients withconflict and distress [1]. added motivation by adding gaming factors in a
P r Si leaer
Presentaion resentaton of sound
S• .. . •.• :::real-time renderingUser respionse
Joystick Ci0imIterFigure 1. Hardware for virtual reality
136
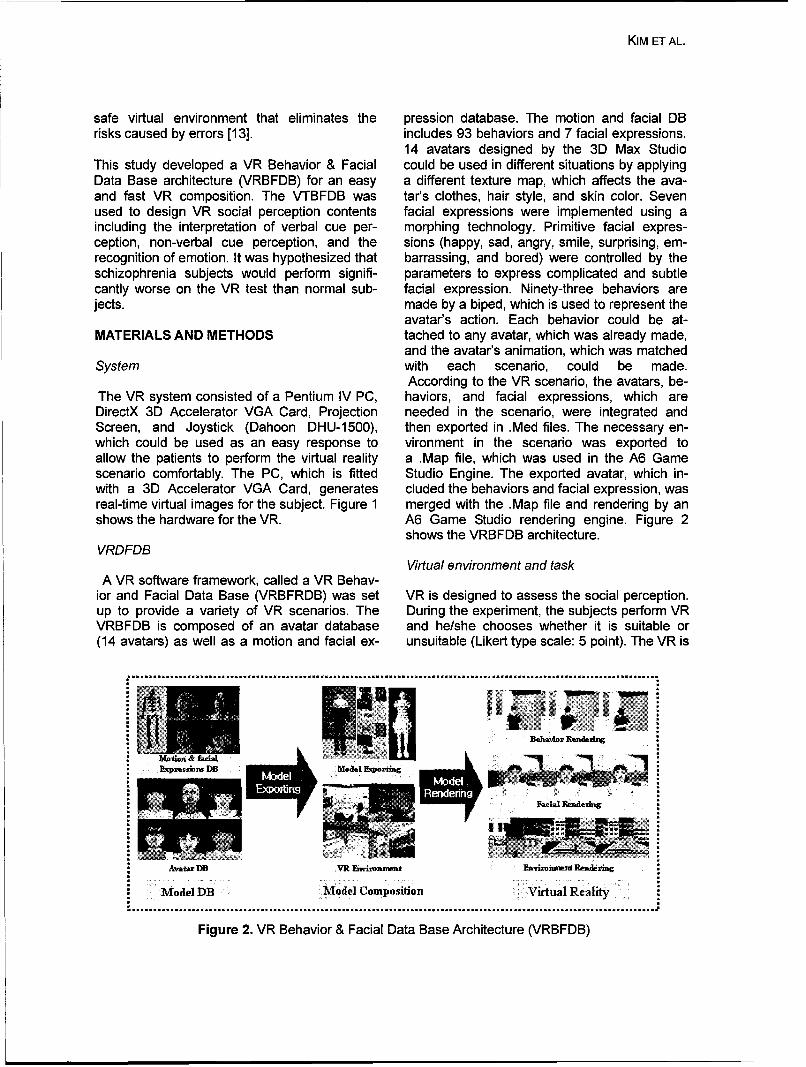
KIM ET AL.
safe virtual environment that eliminates the pression database. The motion and facial DBrisks caused by errors [13]. includes 93 behaviors and 7 facial expressions.
14 avatars designed by the 3D Max StudioThis study developed a VR Behavior & Facial could be used in different situations by applyingData Base architecture (VRBFDB) for an easy a different texture map, which affects the ava-and fast VR composition. The VTBFDB was tar's clothes, hair style, and skin color. Sevenused to design VR social perception contents facial expressions were implemented using aincluding the interpretation of verbal cue per- morphing technology. Primitive facial expres-ception, non-verbal cue perception, and the sions (happy, sad, angry, smile, surprising, em-recognition of emotion. It was hypothesized that barrassing, and bored) were controlled by theschizophrenia subjects would perform signifi- parameters to express complicated and subtlecantly worse on the VR test than normal sub- facial expression. Ninety-three behaviors arejects. made by a biped, which is used to represent the
avatar's action. Each behavior could be at-MATERIALS AND METHODS tached to any avatar, which was already made,
and the avatar's animation, which was matchedSystem with each scenario, could be made.
According to the VR scenario, the avatars, be-The VR system consisted of a Pentium IV PC, haviors, and facial expressions, which areDirectX 3D Accelerator VGA Card, Projection needed in the scenario, were integrated andScreen, and Joystick (Dahoon DHU-1500), then exported in .Med files. The necessary en-which could be used as an easy response to vironment in the scenario was exported toallow the patients to perform the virtual reality a .Map file, which was used in the A6 Gamescenario comfortably. The PC, which is fitted Studio Engine. The exported avatar, which in-with a 3D Accelerator VGA Card, generates cluded the behaviors and facial expression, wasreal-time virtual images for the subject. Figure 1 merged with the .Map file and rendering by anshows the hardware for the VR. A6 Game Studio rendering engine. Figure 2
shows the VRBFDB architecture.VRDFDB
Virtual environment and taskA VR software framework, called a VR Behav-
ior and Facial Data Base (VRBFRDB) was set VR is designed to assess the social perception.up to provide a variety of VR scenarios. The During the experiment, the subjects perform VRVRBFDB is composed of an avatar database and he/she chooses whether it is suitable or(14 avatars) as well as a motion and facial ex- unsuitable (Likert type scale: 5 point). The VR is
* Expresm~ni DB ::Model Exp~ortmg
: ... ......... ... ....... ..
Figure 2. VR Behavior & Facial Data Base Architecture (VRBFDB)
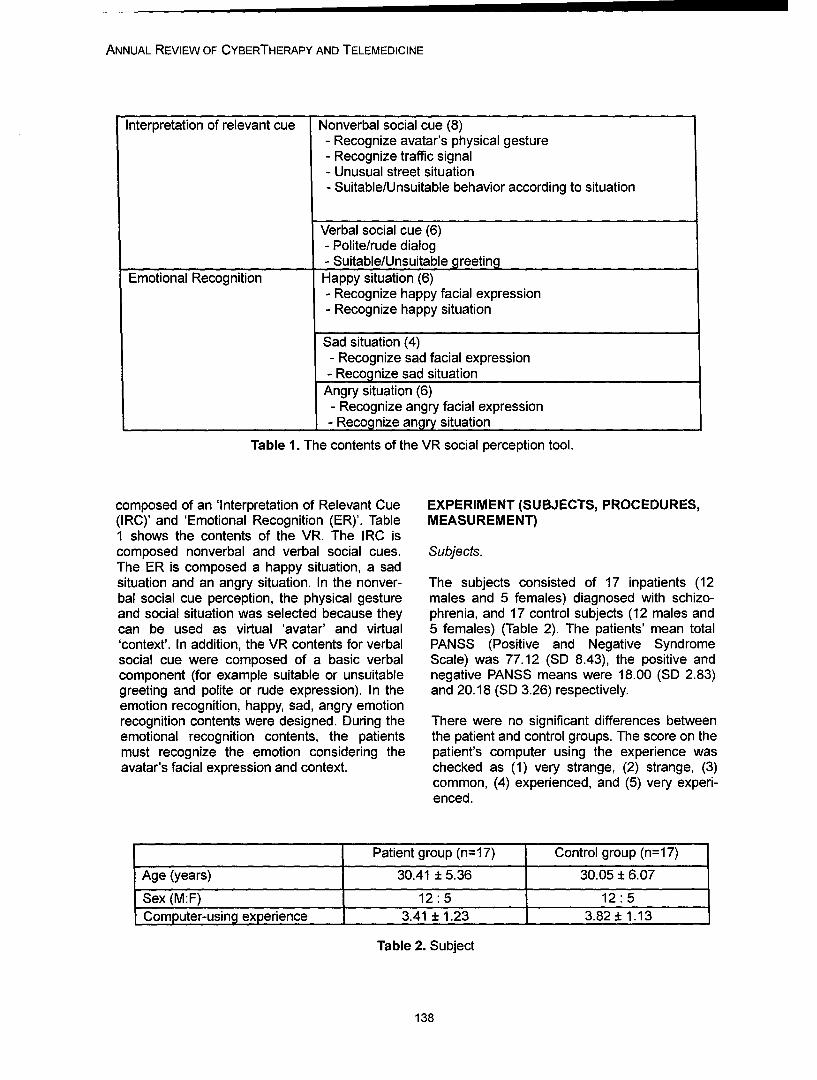
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Interpretation of relevant cue Nonverbal social cue (8)- Recognize avatar's physical gesture- Recognize traffic signal- Unusual street situation- Suitable/Unsuitable behavior according to situation
Verbal social cue (6)- Polite/rude dialog- Suitable/Unsuitable greeting
Emotional Recognition Happy situation (6)- Recognize happy facial expression- Recognize happy situation
Sad situation (4)- Recognize sad facial expression- Recognize sad situation
Angry situation (6)- Recognize angry facial expression- Recognize angry situation
Table 1. The contents of the VR social perception tool.
composed of an 'Interpretation of Relevant Cue EXPERIMENT (SUBJECTS, PROCEDURES,(IRC)' and 'Emotional Recognition (ER)'. Table MEASUREMENT)1 shows the contents of the VR. The IRC iscomposed nonverbal and verbal social cues. Subjects.The ER is composed a happy situation, a sadsituation and an angry situation. In the nonver- The subjects consisted of 17 inpatients (12bal social cue perception, the physical gesture males and 5 females) diagnosed with schizo-and social situation was selected because they phrenia, and 17 control subjects (12 males andcan be used as virtual 'avatar' and virtual 5 females) (Table 2). The patients' mean total'context'. In addition, the VR contents for verbal PANSS (Positive and Negative Syndromesocial cue were composed of a basic verbal Scale) was 77.12 (SD 8.43), the positive andcomponent (for example suitable or unsuitable negative PANSS means were 18.00 (SD 2.83)greeting and polite or rude expression). In the and 20.18 (SD 3.26) respectively.emotion recognition, happy, sad, angry emotionrecognition contents were designed. During the There were no significant differences betweenemotional recognition contents, the patients the patient and control groups. The score on themust recognize the emotion considering the patient's computer using the experience wasavatar's facial expression and context. checked as (1) very strange, (2) strange, (3)
common, (4) experienced, and (5) very experi-enced.
Patient group (n=17) Control group (n=17)
Age (years) 30.41 ± 5.36 30.05 ± 6.0
Sex (M:F) 12:5 12:5Computer-using experience 3.41 ± 1.23 3.82 ± 1.13
Table 2. Subject
138
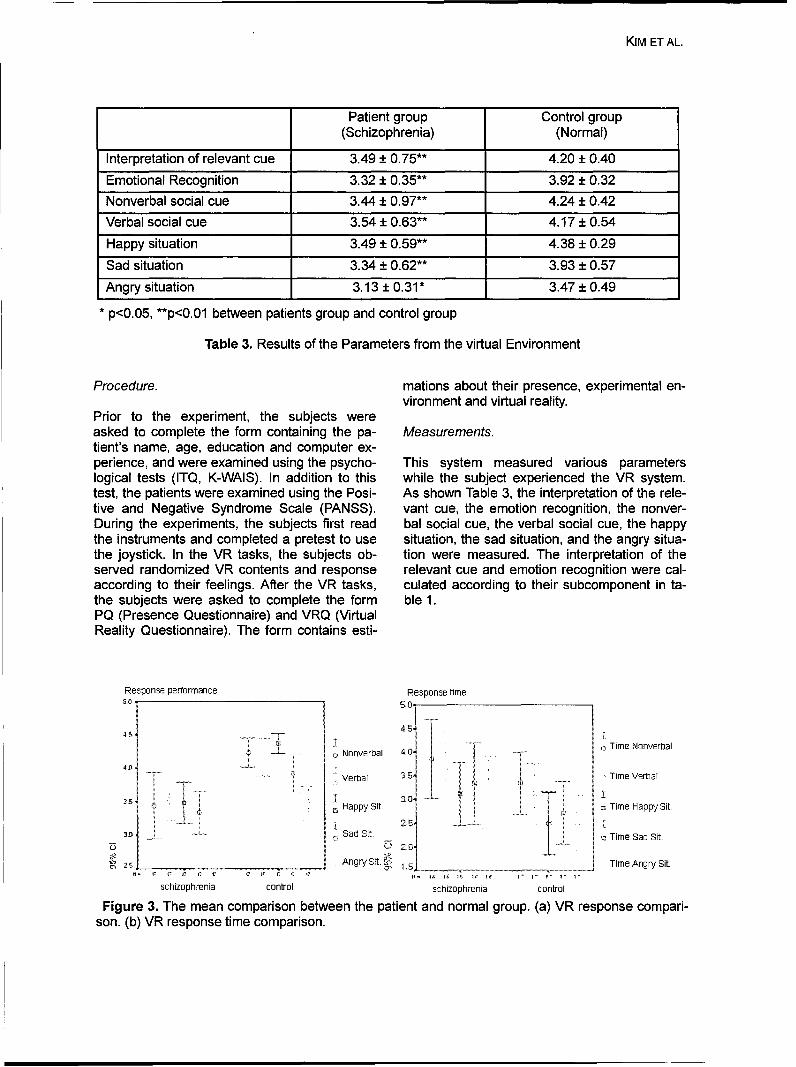
KIM ET AL.
Patient group Control group(Schizophrenia) (Normal)
Interpretation of relevant cue 3.49 ± 0.75** 4.20 ± 0.40
Emotional Recognition 3.32 ± 0.35** 3.92 ± 0.32
Nonverbal social cue 3.44 ± 0.97** 4.24 ± 0.42
Verbal social cue 3.54 ± 0.63** 4.17 ± 0.54
Happy situation 3.49 ± 0.59** 4.38 ± 0.29
Sad situation 3.34 ± 0.62** 3.93 ± 0.57
Angry situation 3.13 ± 0.31* 3.47 ± 0.49p<0.05, **p<0.01 between patients group and control group
Table 3. Results of the Parameters from the virtual Environment
Procedure. mations about their presence, experimental en-vironment and virtual reality.
Prior to the experiment, the subjects wereasked to complete the form containing the pa- Measurements.tient's name, age, education and computer ex-perience, and were examined using the psycho- This system measured various parameterslogical tests (ITQ, K-WAIS). In addition to this while the subject experienced the VR system.test, the patients were examined using the Posi- As shown Table 3, the interpretation of the rele-tive and Negative Syndrome Scale (PANSS). vant cue, the emotion recognition, the nonver-During the experiments, the subjects first read bal social cue, the verbal social cue, the happythe instruments and completed a pretest to use situation, the sad situation, and the angry situa-the joystick. In the VR tasks, the subjects ob- tion were measured. The interpretation of theserved randomized VR contents and response relevant cue and emotion recognition were cal-according to their feelings. After the VR tasks, culated according to their subcomponent in ta-the subjects were asked to complete the form ble 1.PQ (Presence Questionnaire) and VRQ (VirtualReality Questionnaire). The form contains esti-
Response performance Response time
45 71- -Nonverbal 4 Time Nonverbal
Verbal 3.Time V/erbaliiI •I
SHappy Sit. . Time Happy Sit.
.Sad Sit. Time Sad Sit.
U zoAngr Sit. X_ Time Angry Sit.
schizophrenia control schizophrenia control
Figure 3. The mean comparison between the patient and normal group. (a) VR response compari-son. (b) VR response time comparison.
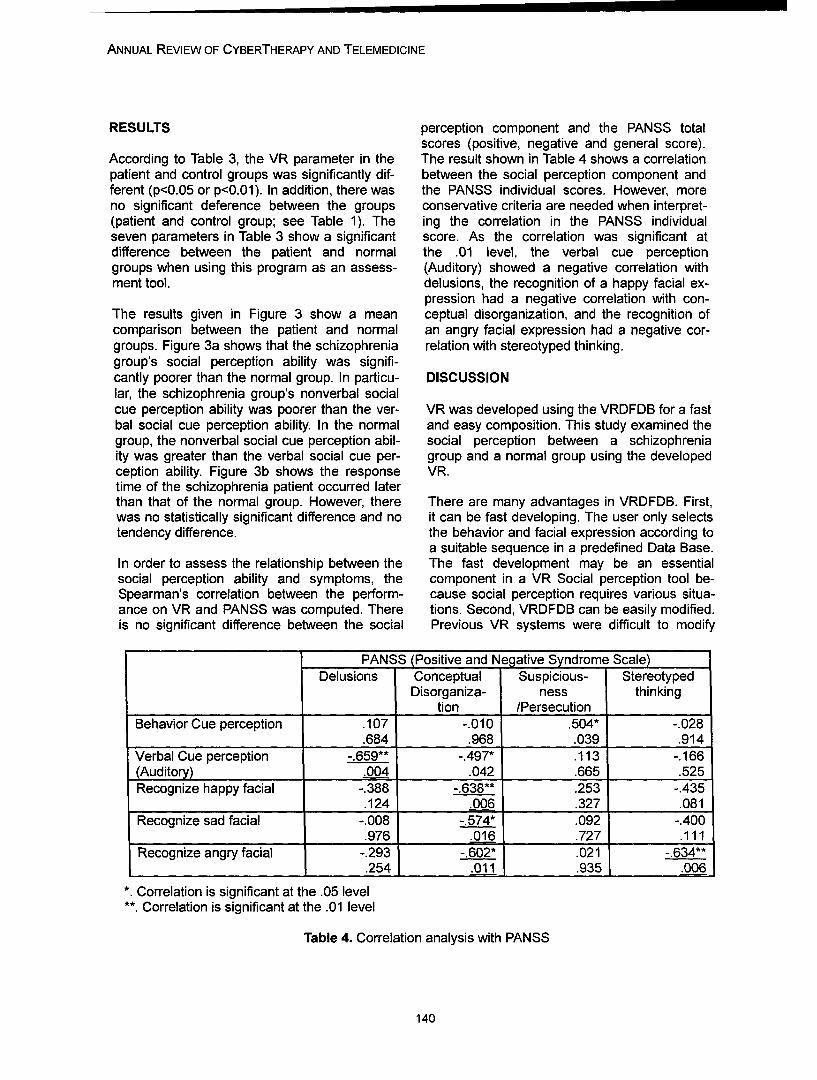
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
RESULTS perception component and the PANSS totalscores (positive, negative and general score).
According to Table 3, the VR parameter in the The result shown in Table 4 shows a correlation
patient and control groups was significantly dif- between the social perception component andferent (p<0.05 or p<0.01). In addition, there was the PANSS individual scores. However, moreno significant deference between the groups conservative criteria are needed when interpret-(patient and control group; see Table 1). The ing the correlation in the PANSS individualseven parameters in Table 3 show a significant score. As the correlation was significant atdifference between the patient and normal the .01 level, the verbal cue perceptiongroups when using this program as an assess- (Auditory) showed a negative correlation withment tool. delusions, the recognition of a happy facial ex-
pression had a negative correlation with con-
The results given in Figure 3 show a mean ceptual disorganization, and the recognition ofcomparison between the patient and normal an angry facial expression had a negative cor-groups. Figure 3a shows that the schizophrenia relation with stereotyped thinking.group's social perception ability was signifi-cantly poorer than the normal group. In particu- DISCUSSIONlar, the schizophrenia group's nonverbal socialcue perception ability was poorer than the ver- VR was developed using the VRDFDB for a fastbal social cue perception ability. In the normal and easy composition. This study examined thegroup, the nonverbal social cue perception abil- social perception between a schizophreniaity was greater than the verbal social cue per- group and a normal group using the developedception ability. Figure 3b shows the response VR.time of the schizophrenia patient occurred laterthan that of the normal group. However, there There are many advantages in VRDFDB. First,was no statistically significant difference and no it can be fast developing. The user only selectstendency difference, the behavior and facial expression according to
a suitable sequence in a predefined Data Base.In order to assess the relationship between the The fast development may be an essentialsocial perception ability and symptoms, the component in a VR Social perception tool be-Spearman's correlation between the perform- cause social perception requires various situa-ance on VR and PANSS was computed. There tions. Second, VRDFDB can be easily modified.is no significant difference between the social Previous VR systems were difficult to modify
PANSS (Positive and Negative Syndrom Scale)
Delusions Conceptual Suspicious- StereotypedDisorganiza- ness thinking
tion /PersecutionBehavior Cue perception .107 -.010 .504* -.028
.684 .968 .039 .914
Verbal Cue perception -.659** -.497* .113 -. 166(Auditory) .004 .042 .665 .525Recognize happy facial -.388 -.638** .253 -.435
.124 .006 .327 .081Recognize sad facial -.008 -.574* .092 -.400
.976 .016 .727 .111
Recognize angry facial -.293 -. 602* .021 -.634**.254 .011 .935 .006
* Correlation is significant at the .05 level
**. Correlation is significant at the .01 level
Table 4. Correlation analysis with PANSS
140
KIM ET AL.
during the developing period. However, REFERENCEVRDFDB can be modified easy by simply se-lecting another behavior and a facial change 1. Alan S. Bellack, Kim T. Mueser, Susan Gin-parameter. On the other hand, VRDFDB has gerich, & Jule Agresta (1997). Social Skill Train-some problem. First, it has limited behaviors ing for Schizophrenia. New York: The Guilfordand facial expressions. In a one time DB com- Press.position, there are 14 avatars with 93 behaviors 2. American Psychiatric Association (1994). Di-and 7 types of facial expressions. Despite this, agnostic and Statistical Manual of Mental Disor-there is still a large number. However, more ders (DSM-IV). 4 th ed.. Washington DC. Ameri-avatars and behaviors are needed for sufficient can Psychiatric Association.social perception content. Second, it is still a 3. Morrison R. L. (1990). Interpersonal dysfunc-programmer level architecture. Indeed, only tion. In A. S. Bellack, M. Hersen, & A. E. Kazdinprogrammer can develop VR using our archi- (Eds.), International handbook of behaviortecture. Ideally, everyone including clinicians modification and therapy (3rd ed., pp. 503-522).could make VR, but in view of current VR re- New York: Plenum Presssearch this is impossible until now. 4. Rosemary Toomey, David Schuldberg, Pat-
rick Corrigan & Michael F. Green (2002). Non-The results of the VR social perception tasks verbal social perception and symptomatology inrequire more research in clinical aspect. How- schizophrenia. Schizophrenia Research. 53:83-ever, some results are statistically significant or 91.concur with previous reports. First, according to 5. Cartlege. G., & Milburn J.A. (1978). The casethe result shown in figure 3 and table 3, the so- for teaching social skills in the classroom: A re-cial perception abilities in schizophrenia and view. Review of Education Research. 1:133-normal groups were significant different. This 155.result confirms the previous research using VR 6. Michelson L., & Wood R. (1980). Behavioralthat the schizophrenia patient's social percep- assessment and training of children' socialtion ability is worse than normal subjects [14]. skills. Progress in Behavior Modification. NewSecond, contrary to the tendency of a normal York: Academic Press.performance task between nonverbal and ver- 7. Howard S. Muscott & Timothy Gifford (1994).bal social perception, there was a reverse ten- Virtual Reality Applications for Teaching Socialdency within the schizophrenia patient group, Skills to Students with Emotional and Behav-which partially correlated with Toomey's re- ioral Disorders. 1994 VR Conference Proceed-search [15]. Third, although a correlation be- ings.tween Positive and Negative Syndrome Scale 8. Goldstein A.P. (1998). PREPARE: A prosocial(PANSS) and virtual reality parameters was curriculum for aggressive youth. In H.S. Mus-found, more research will be needed to confirm cott (Ed.), Prosocial skills training for childrenthe clinical significance. with emotional disturbances (ED) and behav-
ioral disorders (BD): The journey of 1,000 milesThis paper used VRDFDB for the fast and easy begins with the first few steps (Special issue).construction of a virtual environment, and Perception, 24(1): 20-25.tested the possibility of a social perception sys- 9. S. Parsons & P. Mitchell (2002). The potentialtem using VR. Although a more profound dis- of virtual reality in social skills training for peo-cussion about the virtual reality parameters will pie with autistic spectrum disorders. Journal ofbe needed to explain the clinical result, a VR Intellectual Disability Research, 46:430-443.system can be used to assess a schizophrenia 10. A. Leonard, P. Mitchell & S. Parsons (2002).patient's social cue perception ability by com- Finding a place to sit: a preliminary investiga-paring the performance between a normal and tion into the effectiveness of virtual environ-schizophrenia group in a given virtual reality ments for social skills training for people withtask. In future, VR will be used to train and as- autistic spectrum disorders, International Con-sess the social problem solving ability or social ference Disability Virtual Reality & Associatedskills on the whole. Technique. 249-258.
11. Witmer BG, Singer MJ. (1998). Measuringpresence in virtual environment: a presence
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
questionnaire. Presence. 7:225-4012. Kwanguk Kim, Jaehun Kim, Jeonghun Ku,Deongyoung Kim, Won Hyek Chang, Dong IkShin, Jang Han Lee, In Young Kim & Sun I. Kim(2004). A virtual reality assessment and trainingsystem for unilateral neglect. CyberPsychology& Behavior 7:742-749.13. Jang Han Lee, Jounghun Ku, WongeunCho, Wonyoung Hahn, In Y. Kim, Sang-minLee, Younjoo Kang, Deog Young Kim, TaewonYu, Breda K. Wiederhold, Bark D. Wiederhold,& Sun I. Kim (2003). A virtual reality system forthe assessment and rehabilitation of the activi-ties of daily living. CyberPsychology & Behav-ior. 6:383-388.14. David L. Penn, Mark Ritchie, Jennifer Fran-cis, Dannis Combs & James Martin (2002). So-cial perception in schizophrenia: the role of con-text. Psychiatry Research. 109: 149-159.15. Rosemary Toomey, Larry J. Seidman, Mi-chael J. Lyones, Stephen V. Faraone, & Ming T.Tsuang (1999). Poor perception of nonverbalsocial-emotional cues in relatives of schizophre-nia patients. Schizophrenia Research 40: 121-130.
Contact
Kwanguk Kim1 Department of Biomedical EngineeringHanyang UniversitySeoul, 133-605, KoreaPhone: +82-2-2290-0693Fax: +82-2-2296-5943Email: kwana6abmerhanyanQ.ac.kr
142

Annual Review of CyberTherapy and Telemedicine
Relationship between Social Response to Virtual Avatar and SymptomSeverity of Patients with Schizophrenia
1J. Ku, Ph.D., 2j. J. Kim, M.D., Ph.D., 2 H. J. Jang, B. A., 2S. H. Park, M.D., 2S. Y. Kim,B.A., 2C-H. Kim, M.D., Ph.D., 1K. U. Kim, M.S., 1Ja. H. Kim, M.S., 1J. H. Lee, Ph.D., 11. Y.
Kim, M.D., Ph.D. and 1S. I. Kim, Ph.D.
1Dept. of Biomedical Engineering, Hanyang University, Seoul, Korea2Department of Psychiatry, College of Medicine, Yonsei University, Severance Mental Health
Hospital, Gyunggi-do, Korea
Abstracts: A virtual avatar has been used for various applications that require communicationamong persons, or to train or educate people by demonstrating human-like behavior. Recently, muchresearch has shown an enhancement of virtual avatar technology, with the avatar perceived as a realperson. As a result, the technology could begin to be used for observing human behavior to a virtualavatar. This paper concerns whether a virtual avatar could acquire patients' behavioral characteris-tics during experiencing a virtual task which is composed of approaching and conducting a short con-versation. For this, we designed a virtual avatar that was standing in a virtual room, with elevenschizophrenic patients assigned the task of approaching the virtual avatar, initiating a conversation,and providing answers to the avatar's questions. To measure behavioral parameters in the virtualenvironment, we acquired the interpersonal distance and the verbal response time. In addition, werated patients on the Positive and Negative Syndrome Scale (PANSS) in order to investigate a rela-tionship between patients' symptomatic characteristic and behavioral parameters. Results of thisstudy revealed that the interpersonal distance was negatively correlated with the negative syndromescale, which is a subscale of PANSS (r-O0.687, p=0.02). By contrast, the verbal response time wasnot correlated with any other subscale of PANSS. However, after analyzing this variable with sub-items of the negative syndrome of PANSS, two positive correlations were found: one with bluntedaffect (r=.638, p=.035) and the other with poor rapport (r=.6 15, p=.044). The negative correlation be-tween the distance and negative symptom severity observed in this study is consistent with studiesthat investigated the relationship between schizophrenic patients' interpersonal distance and theirsymptoms. The positive correlation between the verbal response time acquired and subscales inPANSS in this study could be explained by the definition of these subscales. Therefore, this positivecorrelation means that the less a patient's emotional response, intimacy, and relationship makingwith a virtual avatar, the slower they answer the avatar's question. Inferring from these results, weconclude that the virtual avatar could be perceived as a real human by schizophrenic patients, theavatar could facilitate the schizophrenic patients' behavioral characteristics, and the avatar could beused as a tool for assessing the behavioral characteristics of patients with schizophrenia.
INTRODUCTION
Virtual Reality (VR) has the potential to provide to provide a realistic, interactive, immersive,a realistic three-dimensional world generated by and safe environment; this complements thecomputer graphics, with which the user can in- fact that it provides a flexible and controlled ex-teract, so that he or she can navigate within and perimental and therapeutic environment. It hasmanage the virtual world and obtain computer- been applied to several types of mental disor-ized objective scores. Due to its capacity to pro- ders such as illness,1 3 and attention deficit dis-vide realistic three-dimensional environments to orders (ADD)1' 4 for assessing patients' cognitiveusers, VR has already been applied to many functions5 and for providing training for strokefields such as industry, the military, entertain- patients' activities of daily living (ADL).6 VR hasment and medicine. In particular, many medical also been used to assess and investigate hu-applications have emerged because of its ability man characteristics in three-dimensional envi-
143

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ronments such as for navigation,7 and spatial tients' interpersonal behavior characteristicsmemory.8 during an interaction. The problems of those
methods for assessing the patient's behaviorMoreover, recent technological advances in concern the difficulty in establishing a controlledavatars enable computer-generated entities to experimental situation and observing behaviormimic both the appearance and behaviors of consistently.humans. Thus, Virtual Environments (VEs) canbe more realistic and social, because VEs can Due to these needs, in this study, we aimed tobe populated by representations of people as develop a method for assessing the interper-well as objects. Recent improvements in sonal behavioral characteristics of patients withgraphic and animation technology have made it schizophrenia using VR technology. VR tech-possible for the avatars used in these visual nology has many advantages in providing aimages to appear increasingly human-like, realistic environment, and allows us to investi-Studies have shown that people report feeling gate how schizophrenic patients perceive andsome level of presence in almost all mediated react to a virtual avatar. It also allows an inves-environments and even respond socially to tigation of whether interpersonal behavior to-computer-generated human-like entities.9 ward a virtual avatar is similar to behavior in
response to a human.In addition to these results, several studieshave shown that human behavioral characteris- For accomplishing the goal of this study, a vir-tics, such as proximity and social influence tual room, in which a virtual avatar is standing,could be investigated using a virtual avatar or a was designed and a short conversation tasksocial situation populated with several ava- was assigned to the patients. And, as objectivetars.10° 11 These studies support the hypothesis parameters from patients' virtual experience,that a VE populated with avatars could influ- the interpersonal distance and the verbal re-ence human behavior and emotion. sponse time were chosen because they are
representative factors to represent a relation-From these studies showing the capacity and ship between people and play an important rolepotential of VR, we can predict that VR could in conversation as well as social life.14 And,also be useful for investigating the interpersonal PANSS of the patients were also acquired inbehavior of patients with mental illness. In par- order to investigate the relationship betweenticular, we are interested in applications to their symptom and the behavioral parameters.schizophrenia because it is one of the most Through the investigation of the relationshipsdevastating psychiatric disorders, as it seriously among these parameters, we expected that theaffects the higher mental functions, such as patients react to the virtual avatar in the samethinking, feeling and perceiving.12 The Diagnos- way as to human and the virtual environmenttic and Statistical Manual of Mental Disorders, and the virtual avatar could be a tool for as-fourth edition (DSM-IV), states that schizophre- sessing the interpersonal behavior characteris-nia involves problems in one or more major ar- tics of the patients with schizophrenia.eas of functioning (e.g., interpersonal relations,work or self-care).1 3 It is also characterized by MATERIALS AND METHODsymptoms such as hallucinations or disorgan-ized thinking, the loss of goal-directed behav- Subjectsiors, and deterioration in social role functioning.Due to these deficits, patients with schizophre- We recruited 11 patients, 5 male and 6 female,nia have a negative effect on their partners in diagnosed with schizophrenia, for this experi-interpersonal or social interaction and they suf- ment. They were inpatients at the Severancefer when living with others. Although investigat- Mental Health Hospital in Korea and were ableing the interpersonal behavioral characteristics to perform a task and to control an interfaceof patients with schizophrenia is necessary to such as a joystick. Their mean age was 29.54 ±understand and treat them, currently only sub- 8.95 years (mean ± SD) and their PANSS scorejective materials such as videotaping or clinical were 21.81 ± 4.62 (mean ± SD) for negativeobservation are available for assessing pa- symptoms, 19.45 ±3.67 (mean ± SD) for posi-
144

Ku ET AL.
tive symptoms and 40.91 ±5.54 (mean ± SD) the "talk" button then say "hello". After initiation,for the general psychopathology score. the avatar and the subject exchanged questions
and answers. In order to do this, we generatedApparatus a fixed simple scenario for a short conversation
and the clinician controlled the scenario accord-The apparatus for this experiment was com- ing to the subject's verbal response (for a de-posed of a personal computer (PC), a large tailed script, see Fig. 2).screen, a beam projector, and a joystick, whichwere used by the subjects to experience a VE. MeasurementsThe VE consisted of a room and a male-shapedvirtual avatar that had eye blink and breathing For VR-based measurements, we required themotions, but no facial expressions and no ges- interpersonal distance and the verbal responsetures. The VE and avatar were rendered on a time and saved them during the task. We de-PC using "3D Game Studio" (Conitec Datasys- fined former as a virtual distance between atems Corporation), which is a commercial 3D subject and the avatar at the moment that thegame engine, and projected onto a big screen subject approached and pressed the "talk" but-through a beam projector. This method was ton to initiate a conversation. It is reasonable forchosen because a patient with schizophrenia the distance to be regarded as the interpersonalmay feel discomfort when wearing a head distance, since the distance means the comfort-mounted display (HMD) and tracker. The sub- able distance for having a conversation with thejects moved forward and backward by pushing virtual avatar. We defined the verbal responseor pulling the lever on the joystick, and initiated time as the time elapsed following the momentconversation by pressing the talk button on the that the avatar asked the subject a questionjoystick. until the point that the subject commenced the
answer.Task Description
The PANSS, used to measure the severity ofWe designed the task so that the participant the patients' positive and negative symptoms,had to initiate and conduct a short conversation allowed assessment of the relationship betweenwith a virtual avatar. Therefore, a subject had to symptoms and behavioral characteristics. It isapproach a virtual avatar standing in front of the composed of three subscales: the negative syn-subject by pushing the lever of the joystick for- drome scale, positive syndrome scale, and gen-ward and try to talk to the virtual avatar by eral psychopathology scale. In more detail,pressing the talk button on the joystick. In order each subscale is determined by assessing sev-to initiate the conversation, subject had to press eral representative schizophrenic symptoms.
(a) (b)
Figure 1. Scene of an experiment (a) and a virtual avatar standing in a virtual room (b). A subject issitting on a chair, a screen is located in front of the subject and the subject controls a joystick tomove and respond.
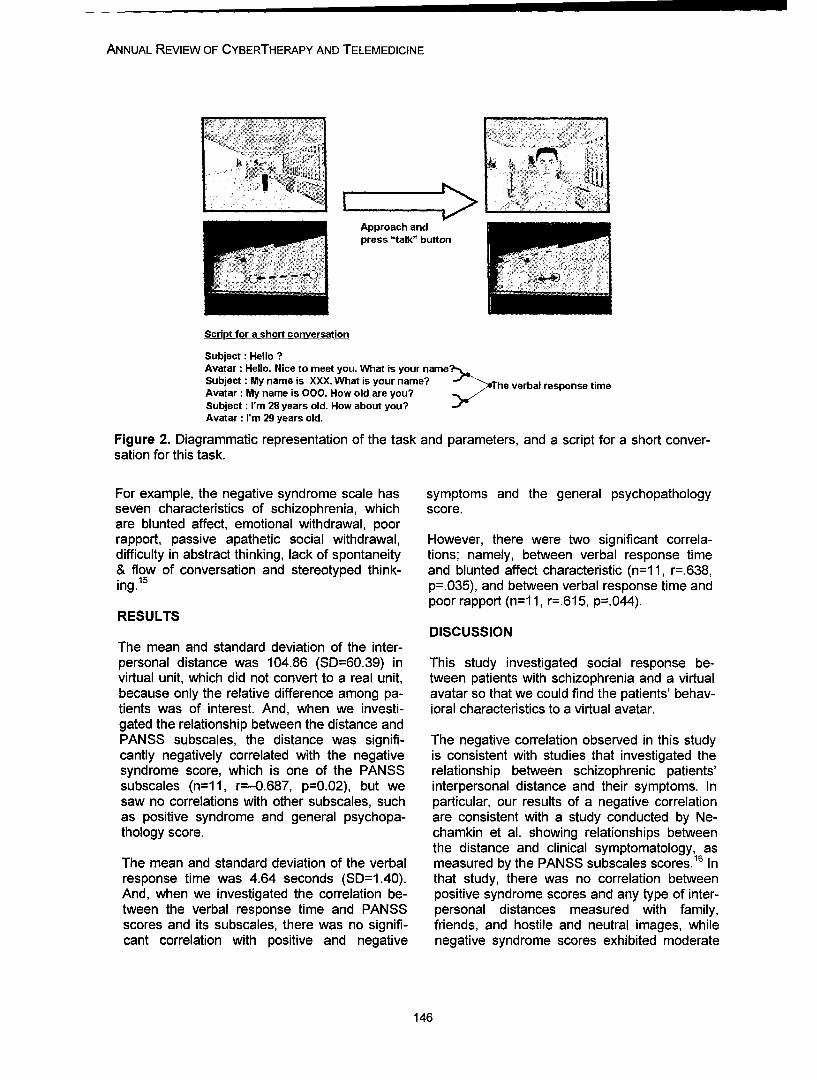
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Approach andpress "talk" button
Script for a short conversation
Subject: Hello ?Avatar: Hello. Nice to meet you. What is your name?Subject: My name is XXX. What is your name? >uýhe verbal response timeAvatar : My name is 000. How old are you?Subject : I'm 28 years old. How about you?Avatar: I'm 29 years old.
Figure 2. Diagrammatic representation of the task and parameters, and a script for a short conver-sation for this task.
For example, the negative syndrome scale has symptoms and the general psychopathologyseven characteristics of schizophrenia, which score.are blunted affect, emotional withdrawal, poorrapport, passive apathetic social withdrawal, However, there were two significant correla-difficulty in abstract thinking, lack of spontaneity tions; namely, between verbal response time& flow of conversation and stereotyped think- and blunted affect characteristic (n=1 1, r=.638,ing.1 p=.035), and between verbal response time and
poor rapport (n=1 1, r=.615, p=.044).RESULTS
DISCUSSIONThe mean and standard deviation of the inter-personal distance was 104.86 (SD=60.39) in This study investigated social response be-virtual unit, which did not convert to a real unit, tween patients with schizophrenia and a virtualbecause only the relative difference among pa- avatar so that we could find the patients' behav-tients was of interest. And, when we investi- ioral characteristics to a virtual avatar.gated the relationship between the distance andPANSS subscales, the distance was signifi- The negative correlation observed in this studycantly negatively correlated with the negative is consistent with studies that investigated thesyndrome score, which is one of the PANSS relationship between schizophrenic patients'subscales (n=1 1, r=-0.687, p=0.02), but we interpersonal distance and their symptoms. Insaw no correlations with other subscales, such particular, our results of a negative correlationas positive syndrome and general psychopa- are consistent with a study conducted by Ne-thology score. chamkin et al. showing relationships between
the distance and clinical symptomatology, asThe mean and standard deviation of the verbal measured by the PANSS subscales scores.16 Inresponse time was 4.64 seconds (SD=1.40). that study, there was no correlation betweenAnd, when we investigated the correlation be- positive syndrome scores and any type of inter-tween the verbal response time and PANSS personal distances measured with family,scores and its subscales, there was no signifi- friends, and hostile and neutral images, whilecant correlation with positive and negative negative syndrome scores exhibited moderate
146
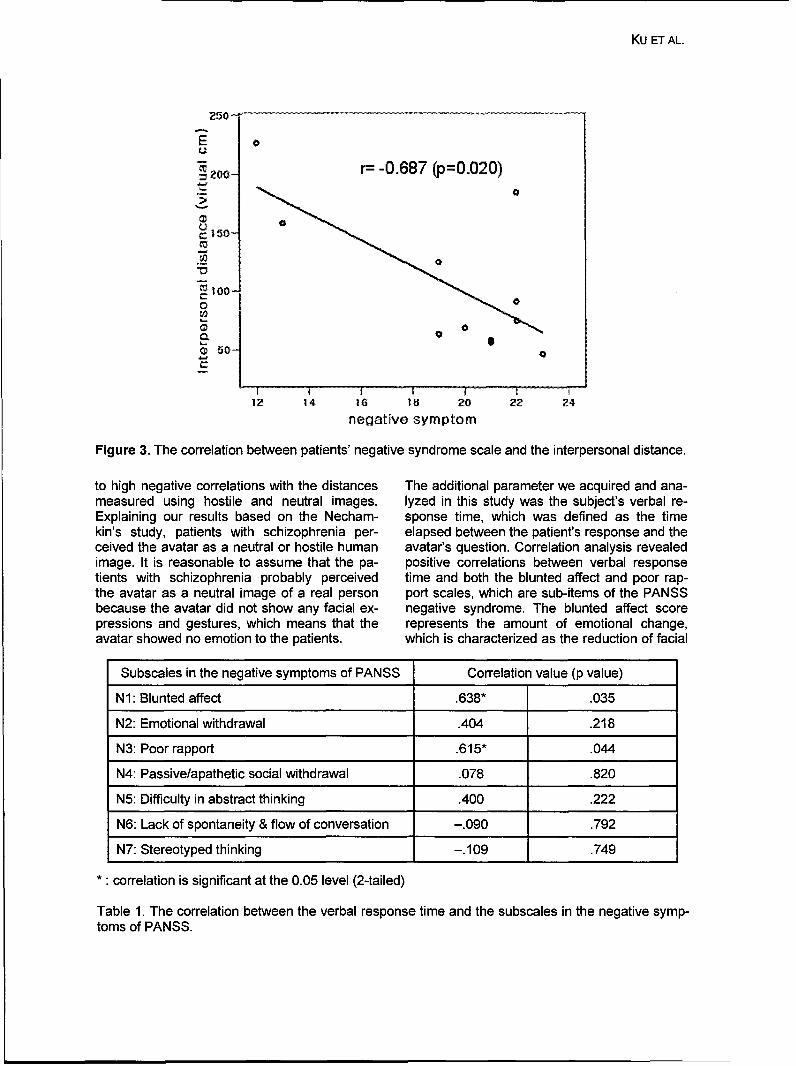
Ku ET AL.
250-
0
So r= -0.687 (p=0.020)2000
t 50-
.T
"100-
Q 50
1? 14 16 18 20 22 24negative symptom
Figure 3. The correlation between patients' negative syndrome scale and the interpersonal distance.
to high negative correlations with the distances The additional parameter we acquired and ana-measured using hostile and neutral images. lyzed in this study was the subject's verbal re-Explaining our results based on the Necham- sponse time, which was defined as the timekin's study, patients with schizophrenia per- elapsed between the patient's response and theceived the avatar as a neutral or hostile human avatar's question. Correlation analysis revealedimage. It is reasonable to assume that the pa- positive correlations between verbal responsetients with schizophrenia probably perceived time and both the blunted affect and poor rap-the avatar as a neutral image of a real person port scales, which are sub-items of the PANSSbecause the avatar did not show any facial ex- negative syndrome. The blunted affect scorepressions and gestures, which means that the represents the amount of emotional change,avatar showed no emotion to the patients. which is characterized as the reduction of facial
Subscales in the negative symptoms of PANSS Correlation value (p value)
N1: Blunted affect .638* .035
N2: Emotional withdrawal .404 .218
N3: Poor rapport .615" .044
N4: Passive/apathetic social withdrawal .078 .820
N5: Difficulty in abstract thinking .400 .222
N6: Lack of spontaneity & flow of conversation -. 090 .792
N7: Stereotyped thinking -. 109 .749
••correlation is significant at the 0.05 level (2-tailed)
Table 1. The correlation between the verbal response time and the subscales in the negative symp-toms of PANSS.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
expression, emotional modulation, and gesture REFERENCESduring communication. By contrast, the poorrapport score represents the amount of intimacy [1] D. P. Jang, J. Ku, Y. H. Choi, B. K.to an interviewer or the level of deficit in forming Wiederhold, S. W. Nam, I. Y. Kim, and S. I.a relationship, which is characterized as dis- Kim, "The development of virtual reality ther-tancing a human relationship and the reduction apy (VRT) system for the treatment of acro-of verbal and nonverbal communication. 15 phobia and therapeutic case," IEEE Trans Inf
Technol Biomed, vol. 6, pp. 213-7, 2002.The positive correlation between the verbal re- [2] B. 0. Rothbaum, L. F. Hodges, R.sponse time acquired and subscales in PANSS Kooper, D. Opdyke, J. S. Williford, and M.in this study could be explained by the definition North, "Effectiveness of computer-generatedof these subscales. Therefore, this correlation (virtual reality) graded exposure in the treat-means that the less a patient's emotional re- ment of acrophobia," Am J Psychiatry, vol.sponse, intimacy, and relationship making with 152, pp. 626-8, 1995.a virtual avatar, the slower they answer the ava- [3] B. K. Wiederhold, D. P. Jang, R. G.tar's question. When this fact is considered in Gevirtz, S. I. Kim, I. Y. Kim, and M. D.view of a virtual avatar, this could be additional Wiederhold, "The treatment of fear of flying: aevidence to show that a patient with schizo- controlled study of imaginal and virtual realityphrenia responds to a virtual avatar in the same graded exposure therapy," IEEE Trans Infway as to a real person. Technol Biomed, vol. 6, pp. 218-23, 2002.
[4] A. A. Rizzo, J. G. Buckwalter, L. Hum-CONCLUSIONS phrey, C. van der Zaag, T. Bowerly, C. Chua,
U. Neumann, C. Kyriakakis, A. van Rooyen,Our objective for this study was to investigate and D. Sisemore, "The Virtual Classroom: Awhether VR is a suitable tool for extracting and Virtual Environment for The Assessment andassessing the patient's behavioral characteris- Rehabilitation Of Attention Deficits," CyberP-tics. In order to do this, we investigated the be- sychology and Behavior, vol. 3, pp. 483-99,havioral and verbal response characteristics by 2000.observing the interpersonal distance between [5] J. Ku, W. Cho, J. J. Kim, A. Peled, B. K.the schizophrenic patients and a virtual avatar, Wiederhold, M. D. Wiederhold, I. Y. Kim, J. H.and the duration from the time the avatar asked Lee, and S. I. Kim, "A virtual environment fora question to the time the subject answered, investigating schizophrenic patients' charac-respectively, teristics: assessment of cognitive and naviga-
tion ability," Cyberpsychol Behav, vol. 6, pp.This study provided evidence supporting the 397-404, 2003.position that the patients respond to the virtual [61 J. H. Lee, J. Ku, W. Cho, W. Y. Hahn, I.avatar as if they were really standing near it and Y. Kim, S. M. Lee, Y. Kang, D. Y. Kim, T. Yu,conversing. It is also supported by data show- B. K. Wiederhold, M. D. Wiederhold, and S. I.ing that the patients' behavioral characteristics Kim, "A virtual reality system for the assess-to a virtual avatar vary in accordance with their ment and rehabilitation of the activities ofsymptoms, and these characteristics are the daily living," Cyberpsychol Behav, vol. 6, pp.same as those to a real person. This indicates 383-8, 2003.that virtual avatar could draw patient's social [7] M. Vidal, M. A. Amorim, and A. Ber-response in an objective manner. Therefore, thoz, "Navigating in a virtual three-this study could be meaningful because it may dimensional maze: how do egocentric andprovide the method and rationale for applying allocentric reference frames interact?" BrainVR techniques to training or assessing the be- Res Cogn Brain Res, vol. 19, pp. 244-58,havioral and/or cognitive characteristics of pa- 2004.tients with schizophrenia. [8] C. M. Oman, W. L. Shebilske, J. T.
Richards, T. C. Tubre, A. C. Beall, and A. Na-tapoff, "Three dimensional spatial memoryand learning in real and virtual environments,"Spat Cogn Comput, vol. 2, pp. 355-72, 2002.
148
KU ET AL.
[9] K. K. Nowak and F. Biocca, "The Effectof the Agency and Anthropomorphism onUser's Sense of Telepresence, Copresence,and Social Presence in Virtual Environments,"Presence: Teleoperators and Virtual Environ-ments, vol. 12, pp. 481-494, 2003.
[10] J. N. Bailenson, J. Blascovich, A. C.Beall, and J. M. Loomis, "Interpersonal dis-tance in immersive virtual environments,"Pers Soc Psychol Bull, vol. 29, pp. 819-33,2003.
[11] J. Blascovich, J. Loomis, A. Beall, K. R.Swinth, C. Hoyt, and J. N. Bailenson,"Immersive Virtual Environment Technologyas a Methodological Tool for Social Psychol-ogy," Psychological Inquiry, vol. 13, pp. 103-124, 2002.
[12] S. K. Schultz and N. C. Andreasen,"Schizophrenia," Lancet, vol. 353, pp. 1425-30,1999.
[13] "Diagnostic and statistical manual ofmental disorders, 4th edition (DSM-IV),"American Psychiatric Press, Washington, DC1994.
[14] H. C. Chien, C. H. Ku, R. B. Lu, H. Chu,Y. H. Tao, and K. R. Chou, "Effects of socialskills training on improving social skills of pa-tients with schizophrenia," Arch PsychiatrNurs, vol. 17, pp. 228-36, 2003.
[15] S. R. Kay, A. Fiszbein, and L. A. Opler,"The positive and negative syndrome scale(PANSS) for schizophrenia," Schizophr Bull,vol. 13, pp. 261-76, 1987.
[16] Y. Nechamkin, I. Salganik, I. Modai,and A. M. Ponizovsky, "Interpersonal distancein schizophrenic patients: relationship tonegative syndrome," Int J Soc Psychiatry, vol.49, pp. 166-74, 2003.
Contact
Jeonghun Ku133-605 Dept. of Biomedical Engineering,Hanyang UniversitySung Dong P.O. Box 55Seoul, KoreaTel: +82-2-2290-0693Fax: +82-2-2296-5943kuihcbbme.hanyanq.ac.kr

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
150
Annual Review of CyberTherapy and Telemedicine
Spatial Ability and Navigation Learning in a Virtual City
J-H. Lee, Ph.D.1 2 , R. Mraz, B.A.Sc.,P.Eng.2 , K. K. Zakzanis, Ph.D.3 ,S. E. Black, M.D.,Ph.D.4 , P. J. Snyder, Ph.D.6 , S. I. Kim, Ph.D.1 , and S. J.
Graham, Ph.D., P.Eng.2 '5
1 Department of Biomedical Engineering, Hanyang University, Seoul, Korea2 Imaging Research, Sunnybrook & Women's College Health Science Centre, Toronto, ON, Canada
3 Division of Life Sciences, 4 Department of Medicine-Neurology, and 5 Department of Medical Biophysics, Uni-versity of Toronto, ON, Canada6Pfizer Global Research & Development, Groton, CT, USA
Abstract: Background & Significance of the Problem: Virtual environments (VEs) can be used to as-sess spatial memory and navigation skills, although the behaviour elicited is inherently complex. Thepurpose of this study was to investigate the ecological validity and interrelationship between virtualnavigation tasks and several neuropsychological tests.
Methods/Tools: Forty-two participants (mean age: 70.42) took part in the study, of which eighteenwere recruited from the Cognitive Neurology Clinic at Sunnybrook & Women's College Health Sci-ences Centre (S&W) based on diagnosis of mild cognitive impairment (MCI). Subjects completed theGroton Maze Learning Test (GML T; a hidden maze task developed by one of the authors [P.J.S.)and several neuropsychological tests, including the MMSE, 1 the Rey Complex Figure Test,2 BentonVisual Retention test,3 Trail-Making Test (Forms A and B),4 and Digit Span.5 Sixteen of the partici-pants (9 normal, 7 MCI) also undertook a VE navigation task.6 Behaviour elicited by the VE task wascharacterized in terms of two components, as estimated by factor analysis: a VE memory index, anda VE movement index.
Results: The VE memory index was significantly associated with the results of a conventional mem-ory test (Rey Complex Figure), and the VE movement index was significantly associated with meas-ures of the Trail Making Test. Compared with normal participants, participants with mild cognitiveimpairment (MCI) showed a significant reduction in the memory-related measures in the PGRD MazeLearning Test and memory tests (particularly RCFT), and the MCI group deviated significantly fromthe correct route, particularly in novel environments. Performance in the VE navigation-learning taskwas significantly associated with measures of visual memory and the executive function in conven-tional neuropsychological tests.
Conclusion: The results of this study demonstrate that VE technology can be used to assess spatialmemory and navigation skills, and that measures of this behavior in a VE are related to those of con-ventional neuropsychological tests. Our results also demonstrate that the MCI group showed a sig-nificant reduction in memory-related measures in the GMLT and the neuropsychological tests. In par-ticular, differences between the groups were evident in the immediate and delayed recall in the ReyTest. However, because of the small sample size, statistically significant results were not found be-tween groups in the VE navigation task.
Novelty: The interrelationship between the VE task, the GMLT, and neuropsychological assessmentsis important for administration and interpretation of these computerized tests in the future.
151
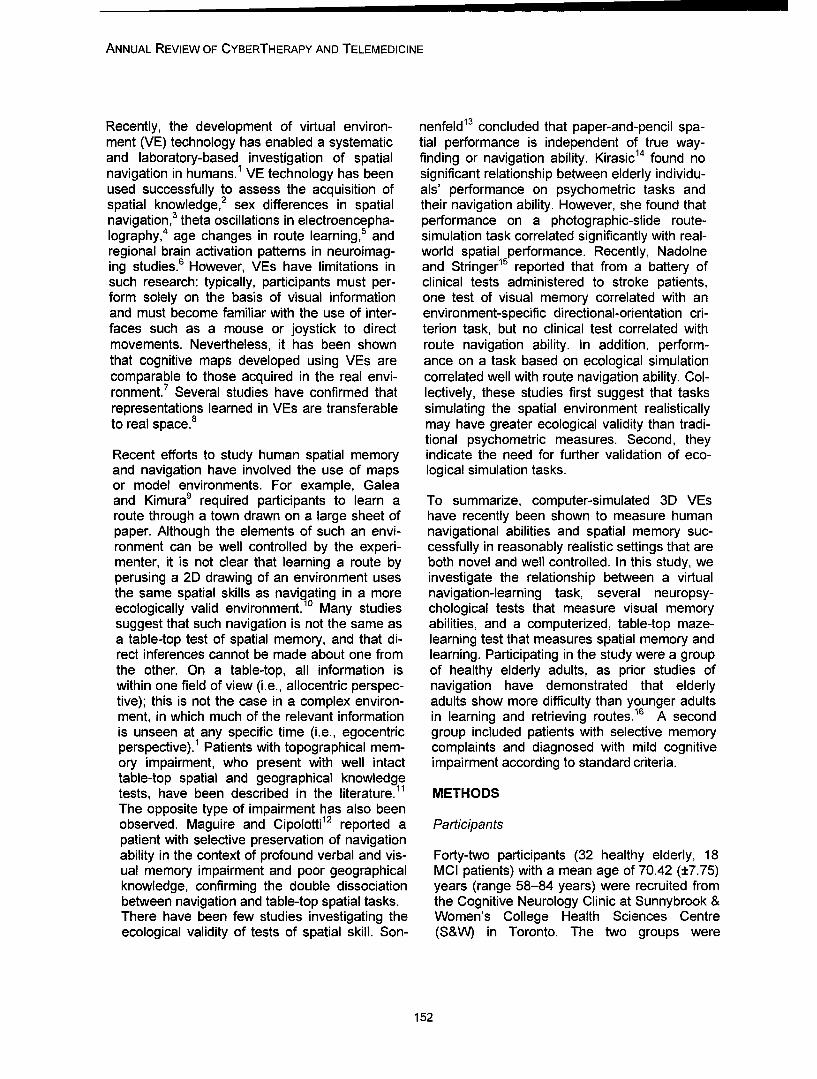
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Recently, the development of virtual environ- nenfeld 13 concluded that paper-and-pencil spa-ment (VE) technology has enabled a systematic tial performance is independent of true way-and laboratory-based investigation of spatial finding or navigation ability. Kirasic 14 found nonavigation in humans., VE technology has been significant relationship between elderly individu-used successfully to assess the acquisition of als' performance on psychometric tasks andspatial knowledge,2 sex differences in spatial their navigation ability. However, she found thatnavigation, 3 theta oscillations in electroencepha- performance on a photographic-slide route-lography,4 age changes in route learning,5 and simulation task correlated significantly with real-regional brain activation patterns in neuroimag- world spatial performance. Recently, Nadolneing studies.6 However, VEs have limitations in and Stringer15 reported that from a battery ofsuch research: typically, participants must per- clinical tests administered to stroke patients,form solely on the basis of visual information one test of visual memory correlated with anand must become familiar with the use of inter- environment-specific directional-orientation cri-faces such as a mouse or joystick to direct terion task, but no clinical test correlated withmovements. Nevertheless, it has been shown route navigation ability. In addition, perform-that cognitive maps developed using VEs are ance on a task based on ecological simulationcomparable to those acquired in the real envi- correlated well with route navigation ability. Col-ronment.7 Several studies have confirmed that lectively, these studies first suggest that tasksrepresentations learned in VEs are transferable simulating the spatial environment realisticallyto real space.8 may have greater ecological validity than tradi-
tional psychometric measures. Second, theyRecent efforts to study human spatial memory indicate the need for further validation of eco-and navigation have involved the use of maps logical simulation tasks.or model environments. For example, Galeaand Kimura 9 required participants to learn a To summarize, computer-simulated 3D VEsroute through a town drawn on a large sheet of have recently been shown to measure humanpaper. Although the elements of such an envi- navigational abilities and spatial memory suc-ronment can be well controlled by the experi- cessfully in reasonably realistic settings that arementer, it is not clear that learning a route by both novel and well controlled. In this study, weperusing a 2D drawing of an environment uses investigate the relationship between a virtualthe same spatial skills as navigating in a more navigation-learning task, several neuropsy-ecologically valid environment.10 Many studies chological tests that measure visual memorysuggest that such navigation is not the same as abilities, and a computerized, table-top maze-a table-top test of spatial memory, and that di- learning test that measures spatial memory andrect inferences cannot be made about one from learning. Participating in the study were a groupthe other. On a table-top, all information is of healthy elderly adults, as prior studies ofwithin one field of view (i.e., allocentric perspec- navigation have demonstrated that elderlytive); this is not the case in a complex environ- adults show more difficulty than younger adults16ment, in which much of the relevant information in learning and retrieving routes. A secondis unseen at any specific time (i.e., egocentric group included patients with selective memoryperspective).1 Patients with topographical mem- complaints and diagnosed with mild cognitiveory impairment, who present with well intact impairment according to standard criteria.table-top spatial and geographical knowledgetests, have been described in the literature.1 METHODSThe opposite type of impairment has also beenobserved. Maguire and Cipolotti12 reported a Participantspatient with selective preservation of navigationability in the context of profound verbal and vis- Forty-two participants (32 healthy elderly, 18ual memory impairment and poor geographical MCI patients) with a mean age of 70.42 (±7.75)knowledge, confirming the double dissociation years (range 58-84 years) were recruited frombetween navigation and table-top spatial tasks. the Cognitive Neurology Clinic at Sunnybrook &There have been few studies investigating the Women's College Health Sciences Centreecological validity of tests of spatial skill. Son- (S&W) in Toronto. The two groups were
152

LEE ET AL.
matched with respect to their scores on the the sidewalk, and to pay attention to where vari-Mini-Mental State Examination (MMSE), years ous objects in the city were located with respectof education, and age. All were paid US$50 for to each other. A set of three learning trials wasparticipating. Only a subset participated in the performed for one path (Path A), followed by oneVE task, and within this group the data for 14 learning trial for a second path (Path B). Shortparticipants were lost as a result of a computer delay (5 min.) and long delay (20 min.) recall tri-malfunction and withdrawals from the study be- als were also performed, during which Path Acause of nausea or dizziness induced by VE was navigated from memory.exposure. The final sample size for the naviga-tion trials in the VE was 16 (9 healthy elderly, 7 PROCEDURESMCI patients).
Informed consent was obtained from each par-Neuropsychological Tests ticipant, based on approval of the S&W Research
Ethics Board. Data collection for all participantsEach participant performed: the Rey-Osterieth occurred in the following order: (1) the CDR andComplex Figure Test (RCFT; copy, immediate the MMSE; (2) the neuropsychological tests; (3)recall, delayed recall); the Trail Making Test (A the PGRD Maze Learning Test (Trials 1 to 10,and B); the Digit Span subtest (forwards and delay, and reverse); (4) the VE navigation-backwards) from the Wechsler Adult Intelligence learning task followed by completion of the Simu-Scale-Revised; the Dementia Rating Scale lator Sickness Questionnaire2°. Statistical analy-(total, attention, initiation, construction, conceptu- sis was performed using commercial softwarealization, and memory components); and the (SPSS 11.0).Mini-Mental Status Examination.
RESULTSThe PGRD Maze Learning Test
An index of memory was estimated from theThe PGRD Maze Learning Test,17 a computer- neuropsychological tests by factor analysis:based neuropsychological measure of immedi- memory index=0.934xZ(Rey delayed recall)ate- and short-term retention of visuospatial infor- +0.904xZ(Rey immediate recall)+ 0.611xZmation, is based on the original work of Milner.18 (forward digit span)+0.530xZ(CDR memory).The goal is to learn over a series of trials how to Internal consistency of the memory index was a=navigate from table-top perspective through a 0.772. This memory index and the data fromhidden maze and capture a target. Participants learning tests were compared to determinepressed on a touch-screen to reveal the maze whether performance on paper-and-pencil testsunder a matrix of tiles. There were untimed and was similar to that on the computerized tests.timed components for either a 4 x 4 or a 10 x 10 Consistently high and significant correlationsChase Test. were found between the memory index and
measures of the PGRD Maze Learning Test. InVE Navigation-learning Task contrast, only two measures of the VE task were
significantly correlated with the memory index:A virtual city (adapted from Mraz et al. 19) was time to completion on Trial 1 and Long Delaycreated in which the user could navigate using a Recall. This initial finding was then used to per-projection screen, a 6-DOF head tracker, and a form an additional factor analysis providing anjoystick. Participants were initially trained to overall VE navigation index, consisting of a mem-move in virtual space by traversing an elemen- ory component and a movement component.tary maze consisting of 12 turns over a fixed dis- The VE movement index was composed oftance. Subsequently, participants were shown a measures in only Trial 1 (distance traveled andpath through the city with video playback in ego- wrong turn metrics, specifically excluding time)centric perspective, and alternately watched the because the other trials involved repeated expo-route or attempted to navigate it themselves, sure:They were instructed to navigate as accuratelyas possible without bumping into objects, to pay VE memory index = Z(Iong delay time) + Z(Trialattention to "the rules of the road" by staying on 1 time)
153
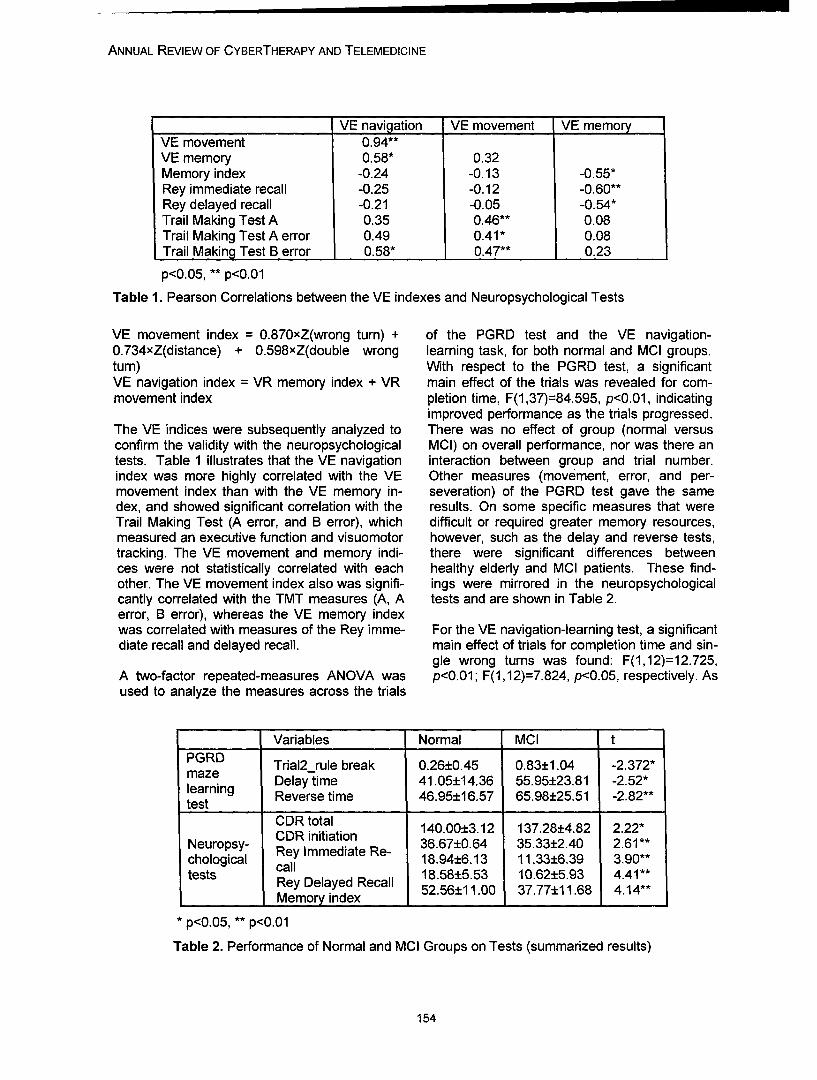
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
VE navilation VE movement VE memoryVE movement 0.94**VE memory 0.58* 0.32Memory index -0.24 -0.13 -0.55*Rey immediate recall -0.25 -0.12 -0.60**Rey delayed recall -0.21 -0.05 -0.54*Trail Making Test A 0.35 0.46** 0.08Trail Making Test A error 0.49 0.41* 0.08Trail Making Test B error 0.58* 0.47** 0.23
p<0.05, ** p<0.01
Table 1. Pearson Correlations between the VE indexes and Neuropsychological Tests
VE movement index = 0.870xZ(wrong turn) + of the PGRD test and the VE navigation-0.734xZ(distance) + 0.598xZ(double wrong learning task, for both normal and MCI groups.turn) With respect to the PGRD test, a significantVE navigation index = VR memory index + VR main effect of the trials was revealed for com-movement index pletion time, F(1,37)=84.595, p<0.01, indicating
improved performance as the trials progressed.The VE indices were subsequently analyzed to There was no effect of group (normal versusconfirm the validity with the neuropsychological MCI) on overall performance, nor was there antests. Table 1 illustrates that the VE navigation interaction between group and trial number.index was more highly correlated with the VE Other measures (movement, error, and per-movement index than with the VE memory in- severation) of the PGRD test gave the samedex, and showed significant correlation with the results. On some specific measures that wereTrail Making Test (A error, and B error), which difficult or required greater memory resources,measured an executive function and visuomotor however, such as the delay and reverse tests,tracking. The VE movement and memory indi- there were significant differences betweences were not statistically correlated with each healthy elderly and MCI patients. These find-other. The VE movement index also was signifi- ings were mirrored in the neuropsychologicalcantly correlated with the TMT measures (A, A tests and are shown in Table 2.error, B error), whereas the VE memory indexwas correlated with measures of the Rey imme- For the VE navigation-learning test, a significantdiate recall and delayed recall. main effect of trials for completion time and sin-
gle wrong turns was found: F(1,12)=12.725,A two-factor repeated-measures ANOVA was p<0.01; F(1,12)=7.824, p<0.05, respectively. Asused to analyze the measures across the trials
Variables Normal MCI t
PGRD Trial2_rule break 0.26±0.45 0.83±1.04 -2.372*maze Delay time 41.05±14.36 55.95±23.81 -2.52*learning Reverse time 46.95±16.57 65.98±25.51 -2.82**t e s t I
CDR total 140.00±3.12 137.28±4.82 2.22*
Neuropsy- CDR initiation 36.67±0.64 35.33±2.40 2.61**chological Rey Immediate Re- 18.94±6.13 11.33±6.39 390**tests call 18.58±5.53 10.62±5.93 4.41**Rey Delayed RecallMeo nydRex 52.56±11.00 37.77±11.68 4.14**Memory index
* p<0.05, ** p<0.01
Table 2. Performance of Normal and MCI Groups on Tests (summarized results)
154
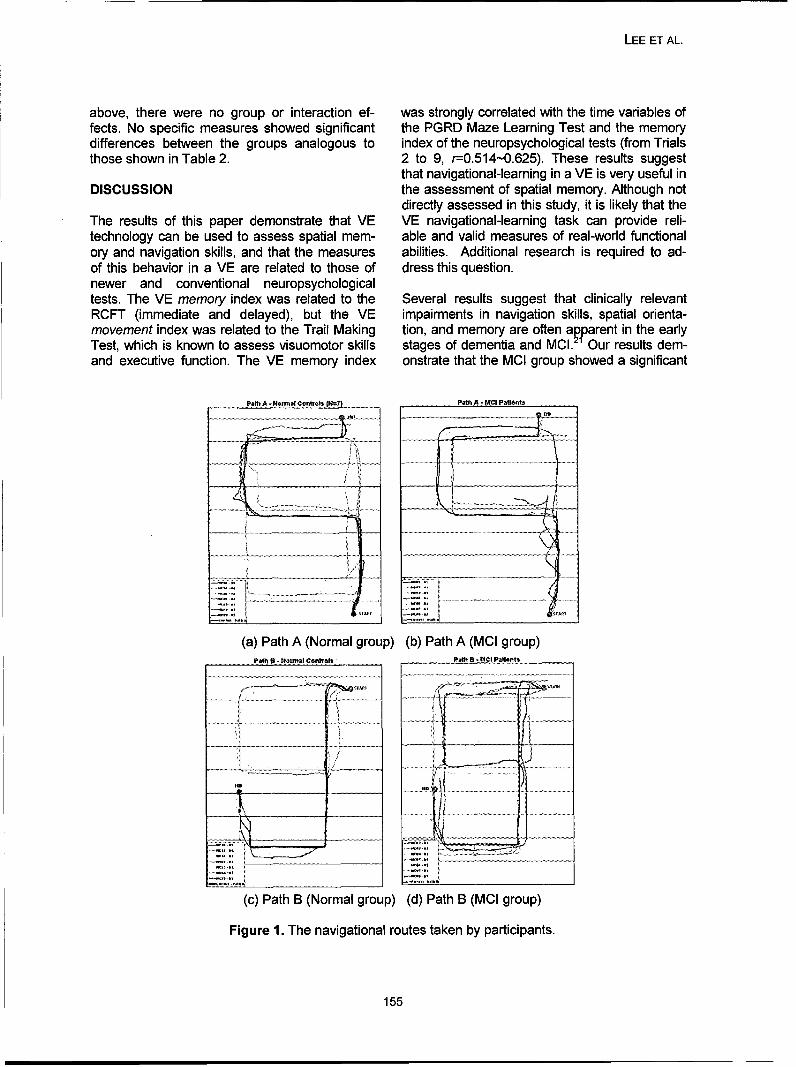
LEE ET AL.
above, there were no group or interaction ef- was strongly correlated with the time variables offects. No specific measures showed significant the PGRD Maze Learning Test and the memorydifferences between the groups analogous to index of the neuropsychological tests (from Trialsthose shown in Table 2. 2 to 9, r=0.514-0.625). These results suggest
that navigational-learning in a VE is very useful inDISCUSSION the assessment of spatial memory. Although not
directly assessed in this study, it is likely that theThe results of this paper demonstrate that VE VE navigational-learning task can provide reli-technology can be used to assess spatial mem- able and valid measures of real-world functionalory and navigation skills, and that the measures abilities. Additional research is required to ad-of this behavior in a VE are related to those of dress this question.newer and conventional neuropsychologicaltests. The VE memory index was related to the Several results suggest that clinically relevantRCFT (immediate and delayed), but the VE impairments in navigation skills, spatial orienta-movement index was related to the Trail Making tion, and memory are often apparent in the earlyTest, which is known to assess visuomotor skills stages of dementia and MCI. Our results dem-and executive function. The VE memory index onstrate that the MCI group showed a significant
PNth A - Namta tonfrots -N:7l Path A - MCI patMonts
............... . . . . ..... .............................. ................ ....... .................... ...................... ....................... .........................
S.....................•: ......... ............................... ;,•i .............. ........................... ........ ............... ...........................................................
S................... ...... .... ................................... ....... .........
(a) Path A (Normal group) (b) Path A (MCI group)Path a- Normalc Conols Path B MCI Pationh
S -............. ............._......_
. .............. ..... --.-.-......................
(c) Path B (Normal group) (d) Path B (MCI group)
Figure 1. The navigational routes taken by participants.
155
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
reduction in a subset of the memory-related 2. Gillner, S., & Mallot, H.A. (1998). Navigationmeasures in the PGRD Maze Learning Test and and acquisition of spatial knowledge in ain the neuropsychological tests. In particular, virtual maze. Journal of Cognitive Neurosci-differences between the groups were evident in ence 10:445-463.the immediate and delayed recall in the RCFT. 3. Astur, R.S., Ortiz, M.L., & Sutherland, R.J.These results were not observed for the VE navi- (1998). A characterization of performance bygation-learning task, which could be due to the men and women in a virtual Morris waterreduced sample size for this component of the task: a large and reliable sex difference. Be-study. It is also of interest to visualize the navi- havioural Brain Research 93:185-190.gational differences between the groups whenperforming the VE task (Figure 1). 4. Kahana, M.J., Sekuler, R., Caplan, J.B., Kir-
schen, M., & Madsen, J.R. (1999). Human
Although most of the normal group (except two theta oscillations exhibit task dependenceparticipants) did not deviate from the correct during virtual maze navigation. Nature
path, the MCI group tended to deviate from the 399:781-784.correct path, particularly Path B (Figure 4(d)). 5. Moffat, S.D., Zonderman, A.B., & Resnick,These results suggest that the MCI group en- S.M. (2001). Age differences in spatial mem-countered greater difficulty than the normal ory in a virtual environment navigation task.group in the novel environments. They also Neurobiology of Aging 22:787-796.highlight one of the recognized challenges in 6. Gron, G., Wunderlich, A.P., Spitzer, M.,the interpretation of behavior elicited in virtual Tomczak, R., & Riepe, M.W. (2000). Brainenvironments. Given that the behavior can be activation during human navigation: gender-complex, it is likely that characterizing behavior different neural networks as substrate of per-in terms of simple metrics such as time to com- formance. Nature Neuroscience 3:404-408.pletion fails to encapsulate the richness of thedata. 7. Ekstrom, A.D., Kahana, M.J., Caplan, J.B.,
Fields, T.A., Isham, E.A., Newman, E.L., &Although there are no differences in the effects Fried, I. (2003). Cellular networks underlyingof sex in the current study, studies with larger human spatial navigation. Nature 425sample sizes across the groups are needed (6954):184-188.before it can be definitively concluded that MCI 8. Regian, J.W., & Yadrick, R.M. (1994). As-groups have inferior spatial memory and navi- sessment of configurational knowledge ofgation skills irrespective of age and sex. Future naturally- and artificially-acquired large-scalestudies need to investigate how age, sex, and space. Journal of Environmental Psychologystrategy affect spatial memory and navigation 14:211-223.learning in normal, MCI, and Alzheimer pa- 9. Galea, L.A.M., & Kimura, D. (1992). Sex dif-tients. ferences in route-learning. Personality and
Individual Differences 14:53-65.ACKNOWLEDGMENTS 10. Sandstrom, N.J., Kaufman, J., & Huettel,
S.A. (1998). Males and females use differentThis work was supported through grants from dita cusi ita niomn aiaPfizr, nc.,theCandianFoudaton fr Ino- distal cues in a virtual environment naviga-Pfizer, Inc., the Canadian Foundation for Inno- tion task. Cognitive Brain Research 6:351-
vation, the Ontario Premier's Research Excel- 360.
lence Award, and the Ontario Research and
Development Challenge Fund. The authors 11. McCarthy, R.A., Evans, J.J., & Hodges, J.R.thank Le-Anh Ngo and Mark Boulos for their (1996). Topographic amnesia: spatial mem-assistance in testing the participants. ory disorder, perceptual dysfunction, or cate-References gory specific semantic memory impairment?1. Maguire, E. A., Burgess, N., & O'Keefe, J. Journal of Neurology Neurosurgery and Psy-
(1999). Human spatial navigation: cognitive chiatry 60:318-325.maps, sexual dimorphism, and neural sub- 12. Maguire, E.A., & Cipolotti, L. (1998). Thestrates. Current Opinion in Neurobiology selective sparing of topographical memory.9:171-177. Journal of Neurology Neurosurgery and Psy-
156
LEE ET AL.
chiatry 65:903-909. 2075 Bayview Ave.
13. Sonnenfeld, J. (1985). Tests of spatial skill: Toronto, ON, M4N 3M5 Canada
A validation problem. Man-Environment Sys- Email: [email protected]
tems 15:107-120.
14. Kirasic, K.C. (1988). Aging and spatial cog-nition: current status and new directions forexperimental researchers and cognitive neu-ropsychologists. In J.M. Williams & C.J.Long (eds.), Cognitive Approaches to Neuro-psychology. New York: Plenum.
15. Nadolne, M.J., & Stringer, A.Y. (2001). Eco-logic validity in neuropsychological assess-ment: prediction of wayfinding. Journal of theInternational Neuropsychological Society7:675-682.
16. Kirasic, K.C. (1991). Spatial cognition andbehavior in young and elderly adults: impli-cations for learning new environments. Psy-chological Aging 6(1): 10-18.
17. Peter J. Snyder (2001). PGRD Maze Learn-ing Test. Pfizer Inc.
18. Milner, B. (1965). Visually-guided mazelearning in man: Effects of bilateral hippo-campal, bilateral frontal, and unilateral cere-bral lesions. Neuropsychologia, 3, 317-338.
19. Mraz, R., Hong, J., Quintin, G., Staines,W.R., Mcllroy, W.E., Zakzanis, K.K., Gra-ham, S.J. (2003). A platform for combiningvirtual reality experiments with functionalmagnetic resonance imaging. CyberPsychol-ogy & Behavior 6(4):359-368.
20. Kennedy, R., Lane, N., Berbaum, N., &Lilienthal, M. (1993). A Simulator SicknessQuestionnaire (SSQ): A New Method forQuantifying Simulator Sickness. Interna-tional Journal of Aviation Psychology 3:203-220.
21. Passini, R., Rainville, C., Marchand, N., &Joanette, Y (1995). Wayfinding in dementiaof the Alzheimer type: planning abilities.Journal of Clinical and Experimental Neuro-psychology 17(6):820-832.
Contact
Simon J. Graham, Ph.D., P.Eng.S650-1maging ResearchSunnybrook & Women's College Health Sci-ences Center
157

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
158

Annual Review of CyberTherapy and Telemedicine
Telepsychiatry:Psychiatric Consultation through Videoconference Clinical Results
C. De las Cuevas PhD, MD
Department of Psychiatry. University of La LagunaCanary Islands Health Service
Abstract: Main Outcome Measures: Efficacy variables included scores on the Clinical Global Im-pressions-Severity of Illness (CGI-S) and -Improvement (CGI-l) scales as well as Global Indexes(GSI, PSDI and PST) from SCL-90R. Response was defined as a CGI-I score of I or 2. ReliableChange Indexes were computed in SCL-90R Global Indexes scores. A multivariate logistic regres-sion analysis was carried out to evaluate the effect of each factor associated with the success oftelepsychiatry.
Results: With respect to baseline severity of illness, the overall average Clinical Global Impression(CGI-S) score was between 4 (moderately ill) and 5 (markedly ill). Only 4 patients dropped-out pre-maturely the study. The patients' mean SCL-90-R Global Indexes scores decreased over time, indi-cating less psychiatric distress. Significant decreases from baseline to week 24 were obtained in psy-chiatric status. A significant proportion of patients showed clear clinical state improvement. Multivari-ate logistic regression analysis shows that telepsychiatry was effective independently of gender, age,educational level, ICD-10 diagnosis, initial severity of illness or the presence of antecedents of previ-ous psychiatric disorders and treatments.
Conclusion: Telepsychiatry showed to be an effective mean of delivering mental health services topsychiatric outpatients living in remote areas with limited resources.
INTRODUCTION
Telepsychiatry can be conceived as an inte- area. This new system of service delivery wasgrated system of mental health care delivery possible thanks to a research grant (EU QLRT-that employs telecommunications and comput- 2001-0167 - ISLANDS Project) from the Euro-erized information technology as an alternative pean Union. In order to investigate the effec-to face-to-face conventional modality. Video- tiveness of a routine telepsychiatry serviceconferencing is the central technology currently through videoconferencing a prospective cohortused in telepsychiatry, since it permit live, two- study of a sample of 70 psychiatric outpatientsway interactive, full-colour, video, audio and was carried out.data communication. Telepsychiatry, in theform of videoconferencing, has been well re- MATERIAL AND METHODSceived in terms of increasing access to careand user satisfaction. 1' 2 Questions persist, how- The telepsychiatry service provides psychiatricever, about its effectiveness since there are few consultations to individuals after referral from aclinical outcome studies and because there general practitioner. A patient living in La Gom-may also be a positive reporting bias in the lit- era with a mental health problem can chooseerature. 3 between joining the waiting list to see the visit-
ing psychiatrist, that travel every Monday fromThe Canary Islands Health Service developed Tenerife island, or being included in the telep-in 2003 a telepsychiatry programme to comple- sychiatry programme. Telepsychiatry sessionsment the mental health-care of the citizens liv- take place every Thursday from 9:00 to 13:00.ing on La Gomera island with the objectives of Emergency access is available from Monday toimproving access, reducing isolation and im- Friday (8:00 to 15:00). After the teleconsulta-proving the quality of mental health care in this tion, recommendations are provided directly to
159

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Table 1. Sociodemographic and clinical characteristics of the sample studied
Variable Category Number % of % 24 week % 24 week
I of cases sample CGI-Sev < 2 CGI- Imp < 2
Age
< 25 years 12 17.1 91.7 100
25-45 years 37 52.9 67.6 78.3
45-65 years 16 22.9 50 68.7
> 65 years 5 7.1 60 80
Gender
Male 22 31.4 72.7 86.4
Female 48 68.6 64.6 77.1
Educational level
Can read and write 11 15.8 63.6 81.8
Primary studies 33 47.1 95.6 78.8
College 13 18.6 46.1 69.2
University degree 13 18.6 92.3 92.3
ICD-10 Diagnosis *
F1 5 7.1 80 80
F2 5 7.1 80 80
F3 23 32.9 47.8 69.6
F4 31 44.3 77.4 83.9
F6 6 8.6 66.6 100
CGI - Severity of Illness
Moderatelly ill 8 11.4 62.5 62.5
Markedly ill 61 87.1 68.8 83.6
Severely ill 1 1.4 0 0
Total 70 100 67,2% 80%
I lCD-10 Diagnoses
(Fl): Mental and behavioural disorders due to psychoactive substance abuse(F2): Schizophrenia, schizotypal and delusional disorders(F3): Mood (affective) disorders(F4): Neurotic, stress-related and somatoform disorders(F6): Disorders of the adult personality and behaviour
% 24 week CGI - Sev 5 2: Proportion of patients with CGI Severity of Illness score < 2 (1= normal,not at all ill; 2=borderline, mentally ill) at week 24.% 24 week CGI - Imp < 2: Proportion of patients with CGI Global Improvement score < 2 (1= verymuch improved; 2= much improved) at week 24.
160
DE LAS CUEVAS ET AL.
the patient's GP via email. Telepsychiatry con- The Symptom Checklist-90 Revised is a stan-sultations use commercial videoconferencing dardized multidimensional 90-item self-reportequipment (Viewstation 512, Polycom®) con- symptom inventory covering various dimen-nected via ISDN lines at up to 512 kbit/s. sions of psychological distress. Each item is
rated on a 5-point scale of distress, rangingPATIENTS from not at all (0) to extremely (4). It utilizes
three global distress indexes: Global SeverityThe sample comprised 70 psychiatric outpa- Index (GSI), Positive Symptom Distress Indextients patients, with 66.3% female and 33.7% (PSDI) and Positive Symptom Total (PST). Themale, which were followed up through 24 GSI combines the number of symptoms re-
weeks. The mean age was 39.8±15 years ported and intensity of reported distress to yield(range 15-80). Women registered a higher the single best descriptor of current mentalmean age than men (42.9±15 vs. 33.2±12). Pa- health. The PSDI represents the average leveltients were diagnosed according to ICD-10 cri- of distress reported for symptoms endorsedteria. Anxiety disorders were the more prevalent and the PST reflects the total number of symp-diagnosis. Most of the patients (87.1%) in- toms reported regardless of symptom intensity.cluded were markedly ill at the beginning and Normative data for Canary Islands citizensthe majority of them (67.1%) have antecedents were available and were used to calculate reli-of previous psychiatric treatments in face-to- able changes indexes.face alternative. Of 70 patients included in thestudy, only 4 dropped-out prematurely. Other Clinical Global Impression is a three-item scalesocio-demographic and clinical characteristics used to assess treatment response in all cate-of the sample studied are shown in Table 1. gories of psychiatric patients. It was adminis-
tered by patient's psychiatrist and 2 minutes areTREATMENT enough to complete. The items are: Severity of
Illness; Global Improvement and Efficacy Index.The telepsychiatry treatment was conducted by Item 1 is rated on a seven-point scalevideoconference between the University Hospi- (1=normal to 7=extremely ill); item 2 on atal de la Candelaria in Santa Cruz de Tenerife seven-point scale (1=very much improved to(psychiatrist location) and the Mental Health 7=very much worse); and item 3 on a four-pointCare Health Centre of San Sebastian de la scale (from 'none' to 'outweighs therapeuticGomera. (Patients location). Treatment involves effect').at least 6 sessions lasting 30 minutes over the24 week study period. Additional treatment ses- PROCEDUREsions take place if clinically indicated. The treat-ment consists of pertinent psychotropic medica- In the same way that Jacobson and Truax,5 wetion plus cognitive-behavioural treatment and defined "reliable change" in terms of the reliabil-psychological evaluation concerning the dis- ity of the measurement instruments used. Weease, medications, and side effects. The mean considered that the error variance in a set ofnumber of psychoactive drugs prescribed was scores that is due to the unreliability of the1.76±0.84 (range 0-4). Antidepressants were scale is the standard error of measurement.the most prescribed drugs (74.3%), followed by Scales that are highly reliable will have a smallbenzodiazepine tranquillisers (72.9%) and an- standard error of measurement. If we know thetipsychotics (14.3%). reliability of the scale (typically measured as
Cronbach's alpha) and the standard deviationINSTRUMENTS of the raw scores on that scale we can find the
expected standard deviation of the variability ofThe efficacy of treatments received was meas- the error scores. The formula for the standardured by changes in the Symptom Checklist-90 error measurement is:Revised (SCL-90R)4 global distress indices andClinical Global Impression (CGI) (NIMH, 1970)ratings at weeks 0, 4, 8, 12, 16, 20 and 24. S& _o = IIIm = SD * - _. -11
Where SD = the standard deviation of themeasure, and rll= the reliability (typicallycoefficient alpha) of the measure.
161
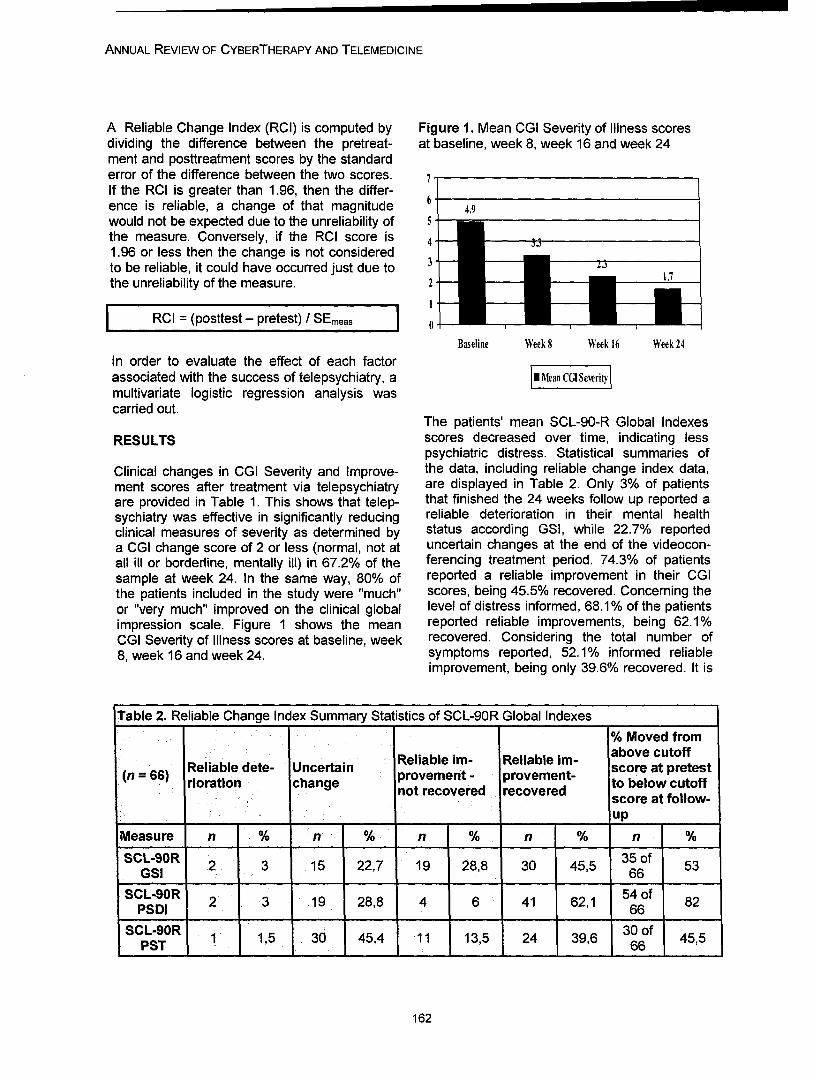
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
A Reliable Change Index (RCI) is computed by Figure 1. Mean CGI Severity of Illness scoresdividing the difference between the pretreat- at baseline, week 8, week 16 and week 24ment and posttreatment scores by the standarderror of the difference between the two scores. 7If the RCI is greater than 1.96, then the differ-ence is reliable, a change of that magnitude 6 4.9would not be expected due to the unreliability ofthe measure. Conversely, if the RCI score is 41.96 or less then the change is not consideredto be reliable, it could have occurred just due to 1.7the unreliability of the measure. 2
1
RCI = (posttest - pretest) / SEmeas 0
Baseline Week 8 Week 16 Week 24
In order to evaluate the effect of each factorassociated with the success of telepsychiatry, a I[| Mean CG Sevritymultivariate logistic regression analysis wascarried out.
The patients' mean SCL-90-R Global IndexesRESULTS scores decreased over time, indicating less
psychiatric distress. Statistical summaries of
Clinical changes in CGI Severity and Improve- the data, including reliable change index data,ment scores after treatment via telepsychiatry are displayed in Table 2. Only 3% of patientsare provided in Table 1. This shows that telep- that finished the 24 weeks follow up reported asychiatry was effective in significantly reducing reliable deterioration in their mental healthclinical measures of severity as determined by status according GSI, while 22.7% reporteda CGI change score of 2 or less (normal, not at uncertain changes at the end of the videocon-all ill or borderline, mentally ill) in 67.2% of the ferencing treatment period. 74.3% of patientssample at week 24. In the same way, 80% of reported a reliable improvement in their CGIthe patients included in the study were "much" scores, being 45.5% recovered. Concerning theor "very much" improved on the clinical global level of distress informed, 68.1% of the patientsimpression scale. Figure 1 shows the mean reported reliable improvements, being 62.1%CGI Severity of Illness scores at baseline, week recovered. Considering the total number of8, week 16 and week 24. symptoms reported, 52.1% informed reliable
improvement, being only 39.6% recovered. It is
Table 2. Reliable Change Index Summary Statistics of SCL-90R Global Indexes
% Moved from
Reliable dete- Uncertain Reliable im- Reliable im- above cutoff
(n = 66) provement - provement- tosbelowat prcutoffrioration change not recovered recovered toblwcof
score at follow-_ _up
Measure n % n % n % n % n %
SCL-90R 2 3 15 22,7 19 28,8 30 45,5 35of 53GSI ____ ___ ___66 _ __
SCL-90R 54 of 82PSDI 2 3 19 28,8 4 6 41 62,1 66
SCL-90R 1 1,5 30 45,4 11 13,5 24 39,6 3of 45,5PST 166
162
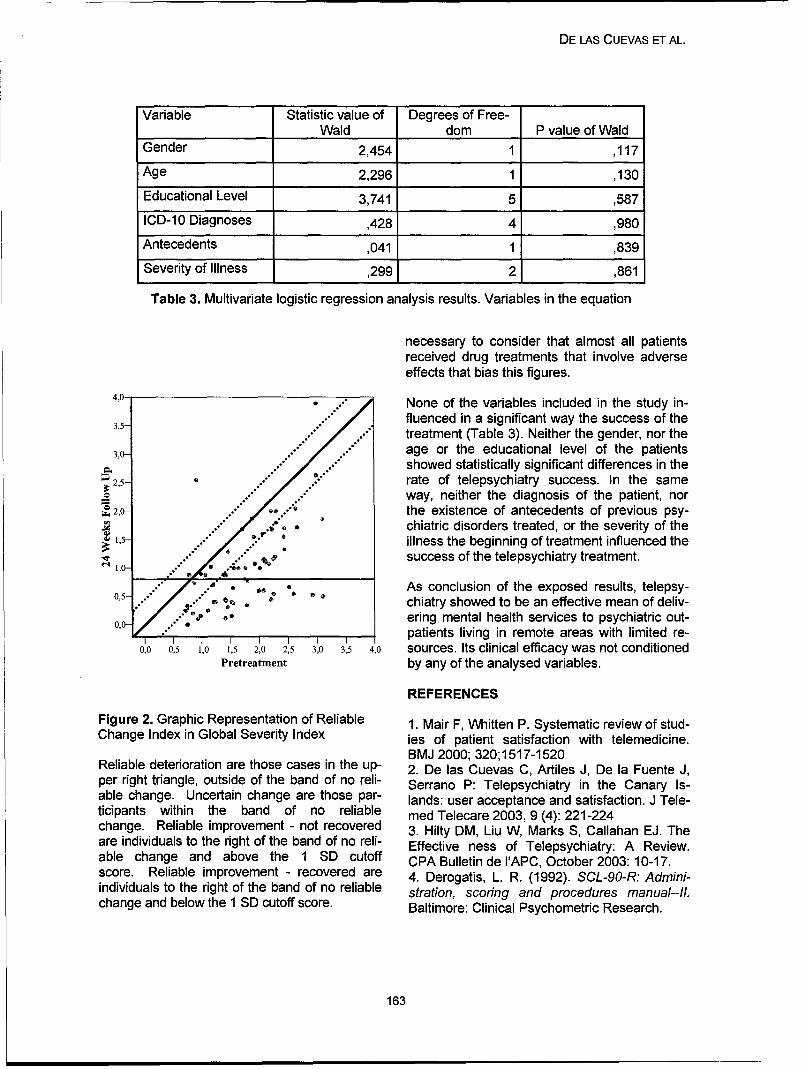
DE LAS CUEVAS ET AL.
Variable Statistic value of Degrees of Free-Wald dom P value of Wald
Gender 2,454 1 ,117
Age 2,296 1 ,130
Educational Level 3,741 5 ,587
ICD-10 Diagnoses ,428 4 ,980
Antecedents ,041 1 ,839
Severity of Illness ,299 2 ,861
Table 3. Multivariate logistic regression analysis results. Variables in the equation
necessary to consider that almost all patientsreceived drug treatments that involve adverseeffects that bias this figures.
4,0- * None of the variables included in the study in-
3,5- .fluenced in a significant way the success of thetreatment (Table 3). Neither the gender, nor the
3,0" age or the educational level of the patientsshowed statistically significant differences in the
2,5- rate of telepsychiatry success. In the sameway, neither the diagnosis of the patient, nor
S2,0- the existence of antecedents of previous psy-.. Y .chiatric disorders treated, or the severity of the
r ,-illness the beginning of treatment influenced the"success of the telepsychiatry treatment.
As conclusion of the exposed results, telepsy-0,5- •:.. a . chiatry showed to be an effective mean of deliv-
ering mental health services to psychiatric out-0,0-/ y-patients living in remote areas with limited re-I I I I I I I I
0,0 0,5 1,0 1,5 2,0 2,5 3,0 3,5 4,0 sources. Its clinical efficacy was not conditionedPretreatment by any of the analysed variables.
REFERENCES
Figure 2. Graphic Representation of Reliable 1. Mair F, Whitten P. Systematic review of stud-Change Index in Global Severity Index ies of patient satisfaction with telemedicine.
BMJ 2000; 320;1517-1520Reliable deterioration are those cases in the up- 2. De las Cuevas C, Artiles J, De la Fuente J,per right triangle, outside of the band of no reli- Serrano P: Telepsychiatry in the Canary Is-able change. Uncertain change are those par- lands: user acceptance and satisfaction. J Tele-ticipants within the band of no reliable med Telecare 2003, 9 (4): 221-224change. Reliable improvement - not recovered 3. Hilty DM, Liu W, Marks S, Callahan EJ. Theare individuals to the right of the band of no reli- Effective ness of Telepsychiatry: A Review.able change and above the 1 SD cutoff CPA Bulletin de I'APC, October 2003: 10-17.score. Reliable improvement - recovered are 4. Derogatis, L. R. (1992). SCL-90-R: Admini-individuals to the right of the band of no reliable stration, scoring and procedures manual--/I.change and below the 1 SD cutoff score. Baltimore: Clinical Psychometric Research.
163

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Figure 3. Graphic Representation of Reliable National Institute of Mental Health. CGI: ClinicalChange Index in Positive Symptom Distress Global Impressions. In: Guy W, Bonato RR,Index eds. Manual for the ECDEU Assessment Bat-
tery.2. Rev ed. Chevy Chase, Md: National In-stitute of Mental Health; 1970:12-1-12-6.
4,0- . 5. Jacobson N S, Truax P. Clinical significance:A statistical approach to defining meaningfulchange in psychotherapy research. Journal ofConsulting and Clinical Psychology 1991, 59,
." 12-19.
2,5- .b
=2,0 • Contact•2,0-.•, .'• -® ,
"1,5." -* Prof. Carlos De las Cuevas PhD MD.. ." Urbanizaci6n Las Cafias, 33
, • 38208 La Laguna, TenerifeCanary Islands, Spain
0,5- [email protected]
0,0-
0,0 0,5 1,0 1,5 2,0 2,5 3,0 3.5 4,0
Pretreatment
Figure 4. Graphic Representation of ReliableChange Index in Positive Symptom Total
90 .
8 3 ..
60""
350-70 . 3 D
*o .. •...,.."30-z .. 0 ... : , ..
20- .
0 10 20 30 40 50 60 70 80 90
Pretreatment
164
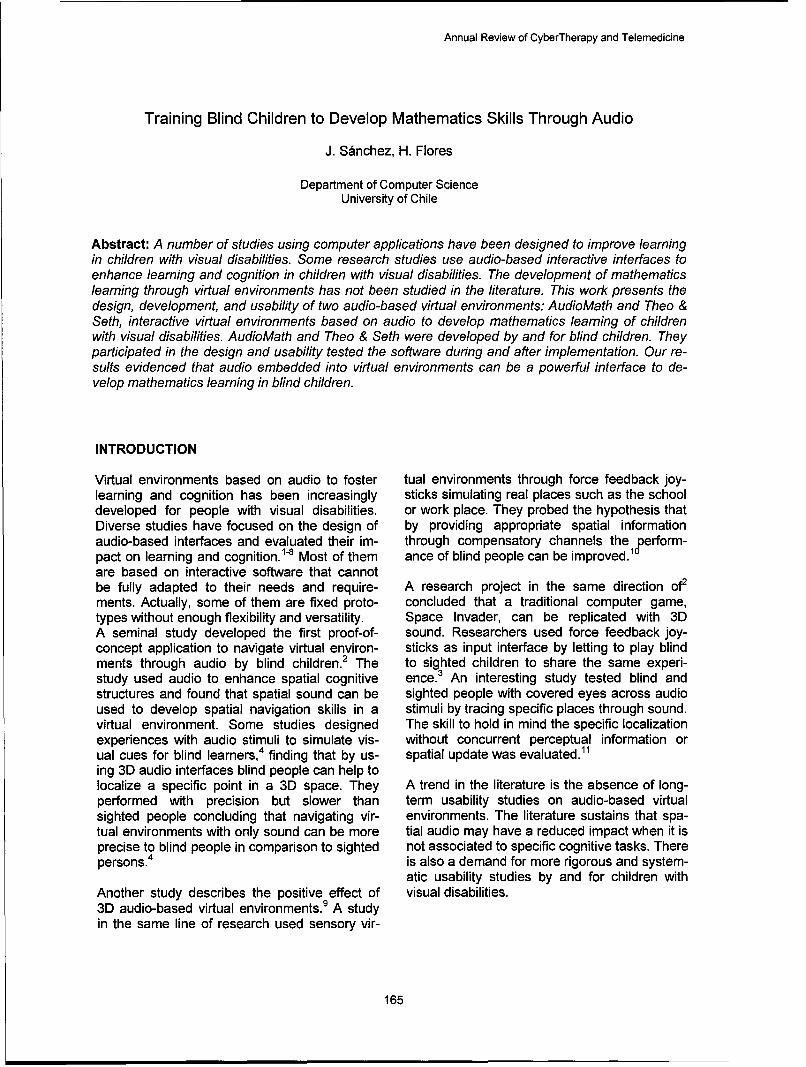
Annual Review of CyberTherapy and Telemedicine
Training Blind Children to Develop Mathematics Skills Through Audio
J. Sanchez, H. Flores
Department of Computer ScienceUniversity of Chile
Abstract: A number of studies using computer applications have been designed to improve learningin children with visual disabilities. Some research studies use audio-based interactive interfaces toenhance learning and cognition in children with visual disabilities. The development of mathematicslearning through virtual environments has not been studied in the literature. This work presents thedesign, development, and usability of two audio-based virtual environments: AudioMath and Theo &Seth, interactive virtual environments based on audio to develop mathematics learning of childrenwith visual disabilities. AudioMath and Theo & Seth were developed by and for blind children. Theyparticipated in the design and usability tested the software during and after implementation. Our re-sults evidenced that audio embedded into virtual environments can be a powerful interface to de-velop mathematics learning in blind children.
INTRODUCTION
Virtual environments based on audio to foster tual environments through force feedback joy-learning and cognition has been increasingly sticks simulating real places such as the schooldeveloped for people with visual disabilities, or work place. They probed the hypothesis thatDiverse studies have focused on the design of by providing appropriate spatial informationaudio-based interfaces and evaluated their im- through compensatory channels theloperform-pact on learning and cognition. 18 Most of them ance of blind people can be improved.are based on interactive software that cannotbe fully adapted to their needs and require- A research project in the same direction of2ments. Actually, some of them are fixed proto- concluded that a traditional computer game,types without enough flexibility and versatility. Space Invader, can be replicated with 3DA seminal study developed the first proof-of- sound. Researchers used force feedback joy-concept application to navigate virtual environ- sticks as input interface by letting to play blindments through audio by blind children. 2 The to sighted children to share the same experi-study used audio to enhance spatial cognitive ence.3 An interesting study tested blind andstructures and found that spatial sound can be sighted people with covered eyes across audioused to develop spatial navigation skills in a stimuli by tracing specific places through sound.virtual environment. Some studies designed The skill to hold in mind the specific localizationexperiences with audio stimuli to simulate vis- without concurrent perceptual information orual cues for blind learners, 4 finding that by us- spatial update was evaluated."ing 3D audio interfaces blind people can help tolocalize a specific point in a 3D space. They A trend in the literature is the absence of long-performed with precision but slower than term usability studies on audio-based virtualsighted people concluding that navigating vir- environments. The literature sustains that spa-tual environments with only sound can be more tial audio may have a reduced impact when it isprecise to blind people in comparison to sighted not associated to specific cognitive tasks. Therepersons.4 is also a demand for more rigorous and system-
atic usability studies by and for children withAnother study describes the positive effect of visual disabilities.3D audio-based virtual environments. 9 A studyin the same line of research used sensory vir-
165
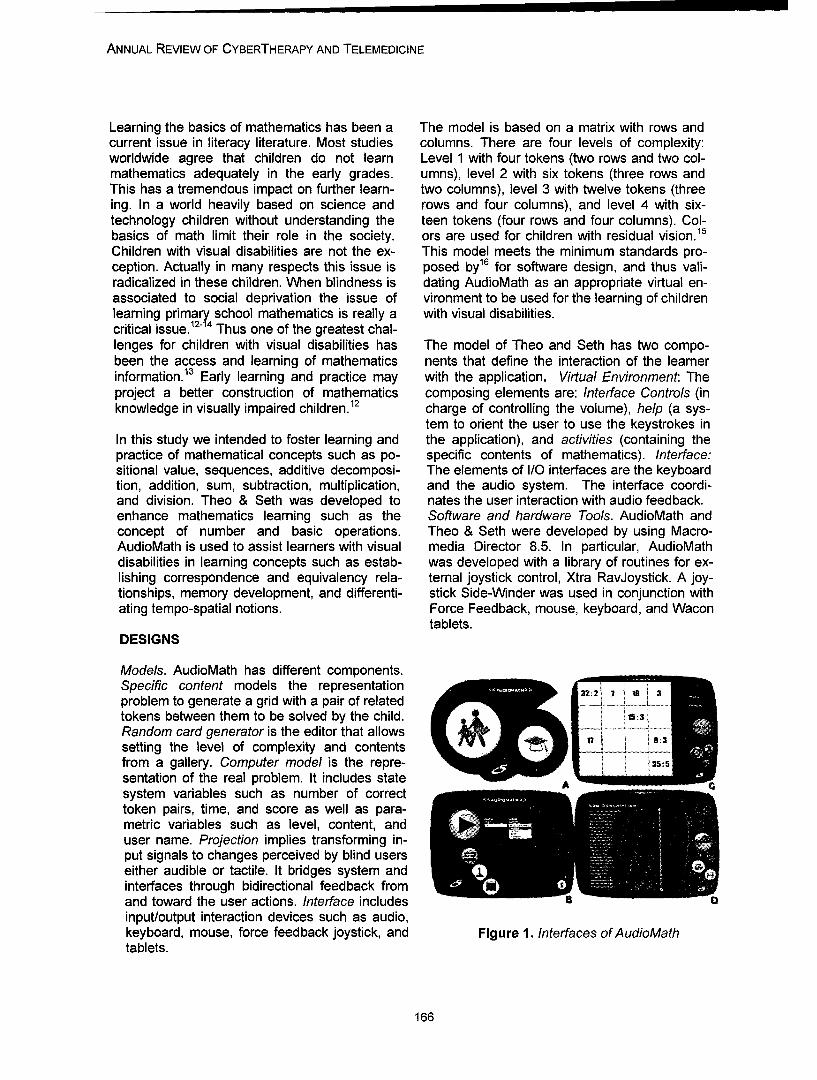
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Learning the basics of mathematics has been a The model is based on a matrix with rows andcurrent issue in literacy literature. Most studies columns. There are four levels of complexity:worldwide agree that children do not learn Level 1 with four tokens (two rows and two col-mathematics adequately in the early grades. umns), level 2 with six tokens (three rows andThis has a tremendous impact on further learn- two columns), level 3 with twelve tokens (threeing. In a world heavily based on science and rows and four columns), and level 4 with six-technology children without understanding the teen tokens (four rows and four columns). Col-basics of math limit their role in the society. ors are used for children with residual vision. 15
Children with visual disabilities are not the ex- This model meets the minimum standards pro-ception. Actually in many respects this issue is posed by16 for software design, and thus vali-radicalized in these children. When blindness is dating AudioMath as an appropriate virtual en-associated to social deprivation the issue of vironment to be used for the learning of childrenlearning primary school mathematics is really a with visual disabilities.critical issue.12"14 Thus one of the greatest chal-lenges for children with visual disabilities has The model of Theo and Seth has two compo-been the access and learning of mathematics nents that define the interaction of the learnerinformation.13 Early learning and practice may with the application. Virtual Environment: Theproject a better construction of mathematics composing elements are: Interface Controls (inknowledge in visually impaired children.12 charge of controlling the volume), help (a sys-
tem to orient the user to use the keystrokes inIn this study we intended to foster learning and the application), and activities (containing thepractice of mathematical concepts such as po- specific contents of mathematics). Interface:sitional value, sequences, additive decomposi- The elements of I/O interfaces are the keyboardtion, addition, sum, subtraction, multiplication, and the audio system. The interface coordi-and division. Theo & Seth was developed to nates the user interaction with audio feedback.enhance mathematics learning such as the Software and hardware Tools. AudioMath andconcept of number and basic operations. Theo & Seth were developed by using Macro-AudioMath is used to assist learners with visual media Director 8.5. In particular, AudioMathdisabilities in learning concepts such as estab- was developed with a library of routines for ex-lishing correspondence and equivalency rela- ternal joystick control, Xtra RavJoystick. A joy-tionships, memory development, and differenti- stick Side-Winder was used in conjunction withating tempo-spatial notions. Force Feedback, mouse, keyboard, and Wacon
tablets.DESIGNS
Models. AudioMath has different components.Specific content models the representation 3:2 1 ,i3problem to generate a grid with a pair of related -
tokens between them to be solved by the child.Random card generator is the editor that allowssetting the level of complexity and contentsfrom a gallery. Computer model is the repre- 135.5sentation of the real problem. It includes statesystem variables such as number of correcttoken pairs, time, and score as well as para-metric variables such as level, content, anduser name. Projection implies transforming in-put signals to changes perceived by blind userseither audible or tactile. It bridges system andinterfaces through bidirectional feedback fromand toward the user actions. Interface includesinput/output interaction devices such as audio,keyboard, mouse, force feedback joystick, and Figure 1. Interfaces of AudioMathtablets.
166
SANCHEZ ET AL.
Interfaces. The principal interfaces of Audio- action triggers an audio feedback and a highMath for children with residual vision are dis- visual contrast screen to be perceived by chil-played in Figure 1. For blind children interfaces dren with residual vision. The child has to moveare only audio-based. A is the identification through a grid and open the corresponding to-screen with two modes: facilitator or student ken. Each cell has associated music tones that(two buttons). B considers the level of complex- identify the position in the grid. Sound is lis-ity (list box), content (list box), and input device tened when moving through cells. When open a(buttons). Content can be filled, upgraded, and token the associated element is visible by trig-edited by using different media. C is the main gering an audio feedback. For example, if theinterface of AudioMath and includes options image is a car, a real traffic car sound is trig-such as the position of the card grid, accumu- gered. When open a correct token pair a feed-lated score, time elapsed (through speech), back is set. Finally, when all pairs are made therestart, register, and exit (through buttons). D time used, the final score, and feedback areincludes a logging actual use register (buttons) given.describing each game and movements.
AudioMath can be interacted through keyboard,Theo & Seth is game-based and includes inter- joystick, and tablets. A few keystrokes are usedesting mathematics learning activities with dif- with the keyboard. These devices have beenferent levels of complexity. The metaphor used used in different applications developed by theresembles a grange with two major virtual envi- research group after testing with children withronments: the kitchen and the henhouse. Two visual disabilities. The Microsoft SideWinderpersonages interact with the learner and exert joysticks in conjunction with Xtra RavJoystickactions during the game. The kitchen covers for Macromedia Director allow grading the usertwo topics: 1. The henhouse is a virtual space position in the grid and give direct feedbackwere learners learn how to do sum and rest with different forces. Counter forces to the(figure a), 2. Introduce ordinal numbers and to movement are generated per each token posi-
tion change as well as vibratory forces indicateS~to be near to the grid edge: up, down, left, and
A~ right. Force Feedback Joysticks allow direct4 46interaction with diverse degrees of freedom. A
plastic graphic grid is posed on the tablet defin-ing the position of each token. A pen is used topoint and select interface elements.
0 1 2 3 4 J 7 VIVM1 During interaction with Theo & Seth childrenwere exposed to cognitive tasks. They had tosolve diverse concrete tasks that complementand enrich the experience with the virtual envi-ronment. Tasks involved exercises by usingsimple concrete materials used in everyday life.The way children interact with the software is
Figure 2. Interfaces of Theo & Seth through keyboard and sound. All the interac-tion is thought in such a way that children cannavigate without assistance. To support this atthe very beginning there is a tutorial to learn
form soup of numbers (see figure b and c), and how to use the keyboard by orienting them3. Cardinality, including the number, the posi- about the localization of keystrokes necessarytion in the numerical straight line and informa- to navigate the virtual world. Once embedded intion about the antecessor and successor (figure the environment children can navigate freelyd). and autonomously by interacting with different
interfaces.Interaction. AudioMath allows interaction withavailable interface elements such as buttons AudioMath and Theo & Seth emphasize learn-and text screens through keyboard. Each inter- ing concepts such as establishing correspon-
167
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
dence and equivalency relationships, memory 8 years old learners with visual disabilities, fourdevelopment, and differentiating tempo-spatial totally blind and five with residual vision. All ofnotions. AudioMath were implemented by inte- them are legally blind. Testing was applied in agrating mathematics content based on the cur- school for blind children in Chile. We observedrent school curriculum. We embedded the soft- learners responses to both the use of only au-ware with mathematical concepts such as posi- die-based virtual environments and the interac-tional value, sequences, additive decomposi- tion with virtual environments and associatedtion, multiplication, division, subtraction. We cognitive tasks. Subjects were pre and postwanted to observe how audio-based virtual en- tested on mathematics learning.vironments can foster the construction ofmathematics learning in the mind of children Evaluation Instruments. Two measurementwith visual disabilities, tests were used to evaluate the impact of
AudioMath on learning and practice of mathe-METHODOLOGY matical concepts such as positional value, se-
quences, additive decomposition, multiplication,Participants. The study with AudioMath was and division: evaluation of mathematics knowl-developed with ten children ages 8 to 15 who edge test1 and a usability evaluation test forattend a school for blind children in Santiago, end-users. The evaluation of mathematicsChile. The sample was conformed of 5 girls and knowledge test measures: The capacity to un-5 boys. Most of them have also added deficits derstand numbers (oral and written), skills nec-such as diverse intellectual development: nor- essary to make oral and written calculations,mal, slow normal, border line, below to normal, skills to count numeric series and graphic ele-and with mental deficit. Four special education ments, and skills for mathematics reasoning.teachers also participated. All learners met thefollowing prerequisites: to be legally blind, to Two measurement tests were used to evaluateknow the natural numbers, to express se- the impact of Theo & Seth: 1. Precalculus Testquences orally, to order numbers, to decom- (by Neva Milicic and Sandra Schmidt) thatpose numbers through audio means, to men- evaluates the development of mathematics rea-tally estimate results of additions and subtrac- soning in students in early primary school; 2.tions, to mentally determine products and coef- Mathematics Knowledge Test (Benton and Lu-ficients, to mentally decompose numbers in ria), that evaluates the mathematics knowledgeadditions, to manipulate multiplication tables of first grade students. The Mathematics Knowl-efficiently, and to have notions of fractions. edge Test was adapted to the specific needs of
learners with visual disability.Theo & Seth was usability tested with nine 7 to
Figure 3-4. Children solving cognitive tasks with AudioMath and Theo & Seth
168
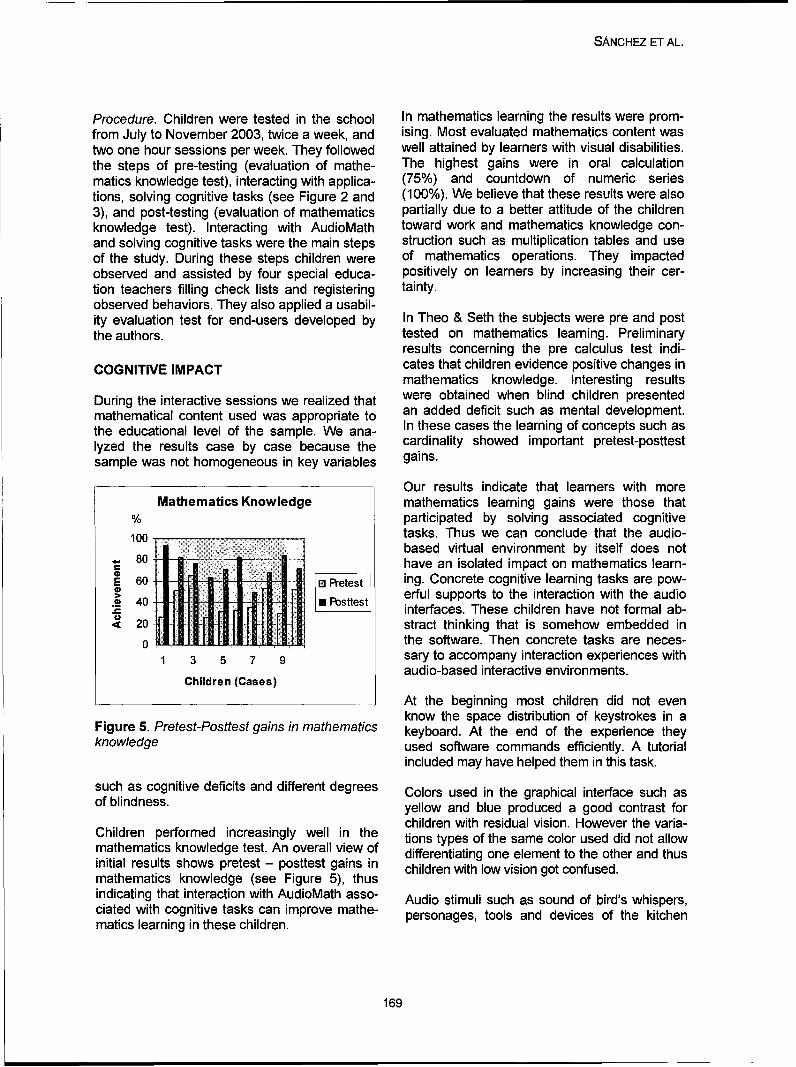
SANCHEZ ET AL.
Procedure. Children were tested in the school In mathematics learning the results were prom-from July to November 2003, twice a week, and ising. Most evaluated mathematics content wastwo one hour sessions per week. They followed well attained by learners with visual disabilities.the steps of pre-testing (evaluation of mathe- The highest gains were in oral calculationmatics knowledge test), interacting with applica- (75%) and countdown of numeric seriestions, solving cognitive tasks (see Figure 2 and (100%). We believe that these results were also3), and post-testing (evaluation of mathematics partially due to a better attitude of the childrenknowledge test). Interacting with AudioMath toward work and mathematics knowledge con-and solving cognitive tasks were the main steps struction such as multiplication tables and useof the study. During these steps children were of mathematics operations. They impactedobserved and assisted by four special educa- positively on learners by increasing their cer-tion teachers filling check lists and registering tainty.observed behaviors. They also applied a usabil-ity evaluation test for end-users developed by In Theo & Seth the subjects were pre and postthe authors. tested on mathematics learning. Preliminary
results concerning the pre calculus test indi-
COGNITIVE IMPACT cates that children evidence positive changes inmathematics knowledge. Interesting results
During the interactive sessions we realized that were obtained when blind children presentedmathematical content used was appropriate to an added deficit such as mental development.the educational level of the sample. We ana- In these cases the learning of concepts such aslyzed the results case by case because the cardinality showed important pretest-posttestsample was not homogeneous in key variables gains.
Our results indicate that learners with moreMathematics Knowledge mathematics learning gains were those that
% participated by solving associated cognitive100 tasks. Thus we can conclude that the audio-
based virtual environment by itself does not80 have an isolated impact on mathematics learn-
2 60 0 Pretest ing. Concrete cognitive learning tasks are pow-> 4erful supports to the interaction with the audio2Dl 40 0 bsttest interfaces. These children have not formal ab-
< 20 stract thinking that is somehow embedded in0 the software. Then concrete tasks are neces-
1 3 5 7 9 sary to accompany interaction experiences withaudio-based interactive environments.
Children (Cases)
At the beginning most children did not evenknow the space distribution of keystrokes in a
Figure 5. Pretest-Posttest gains in mathematics keyboard. At the end of the experience theyknowledge used software commands efficiently. A tutorial
included may have helped them in this task.
such as cognitive deficits and different degrees Colors used in the graphical interface such asof blindness. yellow and blue produced a good contrast for
children with residual vision. However the varia-Children performed increasingly well in the tions types of the same color used did not allow
mathematics knowledge test. An overall view of differentiating one element to the other and thus
initial results shows pretest - posttest gains in children with low vision got confused.
mathematics knowledge (see Figure 5), thus
indicating that interaction with AudioMath asso- Audio stimuli such as sound of bird's whispers,ciated with cognitive tasks can improve mathe- personages, tools and devices of the kitchenmatics learning in these children.
169
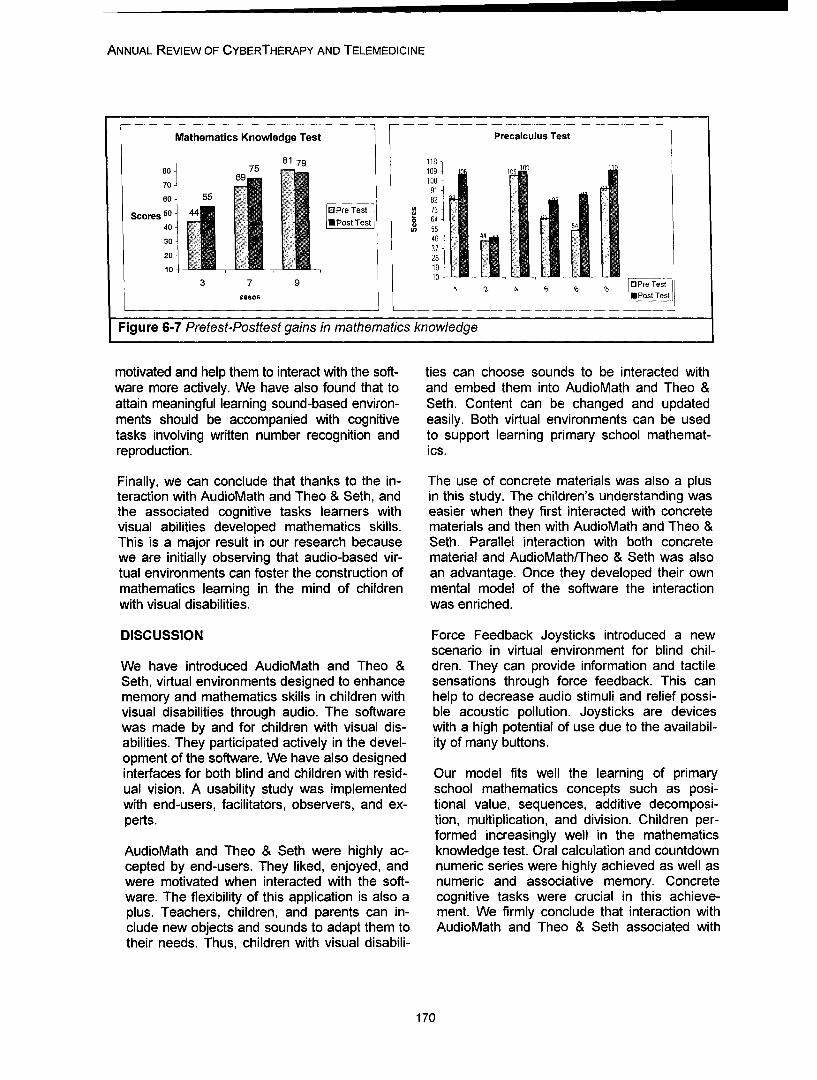
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Mathematics Knowledge Test Precalculus Test
81 791180 6975 -109 1 109
70 •10091
e60 55 582:t5
30 •46 4
3720 28 -10 L _ _19-
103 7 - O Pre Test
casos 0 Post Test
Figure 6-7 Pretest-Posttest gains in mathematics knowledge
motivated and help them to interact with the soft- ties can choose sounds to be interacted withware more actively. We have also found that to and embed them into AudioMath and Theo &attain meaningful learning sound-based environ- Seth. Content can be changed and updatedments should be accompanied with cognitive easily. Both virtual environments can be usedtasks involving written number recognition and to support learning primary school mathemat-reproduction. ics.
Finally, we can conclude that thanks to the in- The use of concrete materials was also a plusteraction with AudioMath and Theo & Seth, and in this study. The children's understanding wasthe associated cognitive tasks learners with easier when they first interacted with concretevisual abilities developed mathematics skills. materials and then with AudioMath and Theo &This is a major result in our research because Seth. Parallel interaction with both concretewe are initially observing that audio-based vir- material and AudioMath/Theo & Seth was alsotual environments can foster the construction of an advantage. Once they developed their ownmathematics learning in the mind of children mental model of the software the interactionwith visual disabilities, was enriched.
DISCUSSION Force Feedback Joysticks introduced a newscenario in virtual environment for blind chil-
We have introduced AudioMath and Theo & dren. They can provide information and tactileSeth, virtual environments designed to enhance sensations through force feedback. This canmemory and mathematics skills in children with help to decrease audio stimuli and relief possi-visual disabilities through audio. The software ble acoustic pollution. Joysticks are deviceswas made by and for children with visual dis- with a high potential of use due to the availabil-abilities. They participated actively in the devel- ity of many buttons.opment of the software. We have also designedinterfaces for both blind and children with resid- Our model fits well the learning of primaryual vision. A usability study was implemented school mathematics concepts such as posi-with end-users, facilitators, observers, and ex- tional value, sequences, additive decomposi-perts. tion, multiplication, and division. Children per-
formed increasingly well in the mathematicsAudioMath and Theo & Seth were highly ac- knowledge test. Oral calculation and countdowncepted by end-users. They liked, enjoyed, and numeric series were highly achieved as well aswere motivated when interacted with the soft- numeric and associative memory. Concreteware. The flexibility of this application is also a cognitive tasks were crucial in this achieve-plus. Teachers, children, and parents can in- ment. We firmly conclude that interaction withclude new objects and sounds to adapt them to AudioMath and Theo & Seth associated withtheir needs. Thus, children with visual disabili-
170
SANCHEZ ET AL.
cognitive tasks can help to improve mathematic tions of the ACM, 43(3). pp. 40-41.learning in these children. Winberg, F. and Helltrom, S. (2000). The quest
for auditory manipulation: the sonified Tow-More qualitative data are being analyzed. Most ers of Hanoi. In Proceedings of the Thirdof them are case study because each child with International Conference on Disability, Vir-visual disabilities is a whole case that deserves tual Reality and Associated Technologies,a deep analysis to construct meaning about the ICDVRAT 2000, Sardinia Italia, 23-25 Sep-role that can play audio-based devices in learn- tember, 2000. pp. 75-81.ing general and specific domain skills. Cooper, M. and Taylor, M. E. (1998). Ambisonic
sound in virtual environments and applica-Finally, we are convinced that further research tions for the blind people. In Proceedings ofstudies we are implementing right now concern- the Second European Conference on Dis-ing mathematic learning will reaffirm our hy- ability, Virtual Reality, and Associatedpothesis that audio-based virtual environment Technologies, ECDVRAT 1998, Skovde,can foster the construction of mathematics Sweden, 10-11 September, 1998. pp. 113-learning in the mind of children with visual dis- 118.abilities. Lahav 0. and Mioduser, D. (2000). Multisen-
sory virtual environment for supporting blindAcknowledgements: This report was funded persons' acquisition of spatial cognitiveby the Chilean National Fund of Science and mapping, orientation, and mobility skills. InTechnology, Fondecyt, Project 1030158. Proceedings of the Third International Con-
ference on Disability, Virtual Reality andREFERENCES Associated Technologies, ICDVRA T 2000,Baldis, J. (2001). Effects of spatial audio on Sardinia Italia, 23-25 September, 2000. pp.
memory, comprehension, and preference 53-58.during desktop conferences. In Proceeding Loomis, J., Lippa, Y., Klatzky, R. and Golledge,of the ACM CHI 2001, Seattle, Washington, R. (2002). Spatial updating of locationsUSA, March 31 - April 5, 2001. Vol 3, 1. pp. specified by 3-D sound and spatial lan-166-173. guage. Journal of Experimental Psychol-
Lumbreras, M. and Scnchez, J. (1998). 3D au- ogy: Learning, Memory, and Cognition, 28ral interactive hyperstories for blind chil- (2), pp. 335-345. 2002dren. International Journal of Virtual Reality Edwards, A. D. N. and Stevens, R. D. (1993).4(1. pp., 20-28. Mathematical representations: Graphs,
McCrindle, R. and Symons, D. (2000). Audio curves and formulas. In D. Burger and J. C.space invaders. In Proceedings of the Third Sperandio (ed.) Non-Visual Human-International Conference on Disability, Vir- Computer Interactions: Prospects for thetual Reality and Associated Technologies, visually handicapped. Paris: John LibbeyICDVRAT 2000, Sardinia Italia, 23-25 Sep- Eurotext, (1993), pp. 181-194.tember, 2000. pp. 59-65. Sahyun, S., Gardner, S. and Gardner, C.
Mereu, S. and Kazman, R. (1996). Audio en- (1998). Audio and Haptic Access to Mathhanced 3D interfaces for visually impaired and Science - Audio graphs, Triangle, theusers. Proceedings of CHI'96, ACM Press. MathPlus Toolbox, and the Tiger printer.(1996). Proceedings of the 15th IFIP World
Sinchez, J. (2000). 3D interactive games for Computer Congress, Vienna, Septemberblind children. In Proceedings of Technol- 1998, pp. 78-86.ogy and Persons with Disabilities, CSUN Scadden, L. (1996). Making mathematics and2000. Los Angeles, USA. science accessible to blind students
Scnchez, J. (2001). Interactive virtual acoustic through technology. Proceeding of Resnaenvironments for blind children. In Proceed- 96 Annual Conference, (1996), June 7-12,ings of ACM CHI '2001, pp. 23-25. Seattle, Salt Lake City, Utah, pp. 51-58.Washington, USA, March 31 - April 5, Rigden, C. (1999). The eye of the beholder-2001. designing for colour blind. British Telecom-
Tan, H. (2000). Haptic interfaces. Communica- munications Engineering, Vol. 17, January.
171
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Sanchez, J., Baloian, N. and Flores, H. (2004).A methodology for developing audio-basedinteractive environments for learners withvisual disabilities, Proceedings of the WorldConference on Educational Multimedia,Hypermedia & Telecommunications, ED-MEDIA 2004, Lugano, Switzerland, June21-26.
Chadwick, M. and Fuentes, M. (1980). Evalua-tion of Mathematics Knowledge (adaptationof Benton-Luria test). Santiago, 1980.
Contact
Jaime Sinchez, Ph D.Department of Computer ScienceUniversity of ChileBlanco Encalada 2120Santiago, Chile
172

Annual Review of CyberTherapy and Telemedicine
Virtual War PTSD - a Methodological Thread
P. Gamito1 , J. Pacheco 2, C. Ribeiro3, C. Pablo 2, T. Saraiva1
1 Psychology Department, University Lusofona de Humanidades e Tecnologias, Lisbon, Portugal2 J6lio de Matos Hospital, Lisbon, Portugal.
3 Military Academy, Lisbon, Portugal.
Abstract: In vivo exposure is a well-tested and effective treatment for anxious and phobic disorders.However, it is not viable to expose patients with War PTSD to real war environments. As virtual real-ity exposure (VRE) is currently the most approximate representation of a real war situation, we hy-pothesized that a treatments of War PTSD that included VRE along with Drug Treatment (DT) wouldbe better than DT alone. The clinical population of this ongoing research consists of male subjectswith the diagnostic of War PTSD according to DSM-IV-TR (APA, 2001) who looked for treatment atHospital J'lio de Matos in Lisbon, Portugal. The patients were distributed into 3 treatments groups(VRE; Drug treatment; VRE+Drug Treatment). The adequate therapeutic dosage of Sertraline(Zoloft, Pfeizer) will be administrated during 16 weeks to the Drug Treatment groups. VRE groupswill use a Head Mounted Device that enables fully immersive experience in the following war virtualscenarios: mine deflagration, mine deflagration + ambush, ambush and assisting casualties andwaiting for a rescue helicopter. These scenarios were developed using the most up-to-date videogame graphics engine. It is also a goal of this study to compare different measurement procedures.In this way, CAPS, BDI, STAI, SCL-90, MCM-11 for psychometric measures and TAS, DES, PQ,SUDS, heart rate and blood pressure, ECG, EEG and ACTH for physiological measures are theevaluation procedures selected for assessing the results.
INTRODUCTION
Studies published over the past thirty years minishing the gap between reality and imagina-show that exposure to phobic stimulus is a fun- tion.damental technique in helping patients get be-yond difficulties and minimizing the personal, Despite having established that VRE mayprofessional and social impact of many anxiety gather some advantages over traditional psy-disorders. Virtual reality exposure (VRE) hs chotherapeutic measures (namely, imaginationbeen used since 1992 to treat these disorders - exposure and in vivo exposure), studies aboutespecially acrophobia, fear of flying, fear of the application of VRE in anxiety disorders thatspeaking in public, fear of driving, etc. generally require the administration of psy-
chopharmacological procedures are lacking. 9
Virtual reality exposure (VRE) is more efficient Such is the case with war PTSD. As a disorderthan conventional imagination exposure (IE). with particularly profound effects on patient, his/For one, subjects can have difficulties in creat- her family structure and on society as a whole,ing or visualizing anxiety-invoking mental im- psychotherapeutic measures are usually notages. 1 4 Further, VRE allows for a more real sufficient to ease the distress caused by thereproduction1 '3-5 and is more immersive than memory of war episodes. More often than not,imagination exposure. VRE induces concen- such patients follow a therapy that includestration/attention augmentation to the phobic both psychotherapeutic procedures and thesituation and, during phobic stimulus exposure, administration of psychopharmacological drugsdiminishes the probability of distraction or cog- such as sertraline. This is the case of thou-nitive avoidance to the feared situation. In this sands of Portuguese males. Between 1961 andcontext, Vincelli3 states that virtual reality tech- 1974, the Portuguese fought a war on severalnology produces an experience capable of di- fronts (Mozambique, Angola and Guine Bis-
173
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
sau), the majority of them spending four years Huey helicopter flying over a virtual Vietnamon tour in the jungle. Without proper epidemiol- field and b) a clearing surrounded by jungle.ogical studies, authors estimate that 25.000 of The authors of said study write that therapiststhem still suffer from war PTSD. As in many found a reduction of PTSD symptoms in 34% ofcases a composed therapy of drugs and imagi- the subjects and a diminishing of PTSD symp-nation exposure doesn't show significant re- tomatology in 45% of them. These gains weresuits. We therefore hypothesized that the expo- maintained throughout 6 months of follow-up.sure to virtual war scenarios in addition to drug However, results of existent studies show thattreatment would provide a higher reduction on more research is still needed.PTSD symptomatology. Rothbaum et al.10 '11studied VRE as an alternative treatment to Another goal of the present ongoing research isimagination exposure (IE) in Vietnam war veter- to define which assessment methodologyans with PTSD, though no matching of VRE should be used for monitoring treatment effects.with drug treatment was made. The patients In most of the studies only psycometric meas-were exposed to two virtual scenarios: a) a ures were used. In fact, Wilhelm & Roth 12
41.
Picture 1a) Mine deflagration Picture 1 b) Ambush
Picture 2a) Mine deflagration + ambush Picture 2b) Facing fellow soldiers death/injurysituations and waiting for causalities evacuation
174

GAMITO ET AL.
stated that psycophysiological methods are not 0 Drug Treatment (DT)usual to evaluate the responses to a certain 0 Prescription will be executed by a psychia-aversive stimuli. Nevertheless, it is accepted trist with clinical experience who will indi-that self reports are not able to give the com- cate the adequate therapeutic doseplete picture of the reactions and modifications (initiating with 50 mg/day and after fixatingendured by the subject when exposed to the the doses in 100 or 200 mg/day, as re-stimuli. We therefore propose that besides psy- quired). Sertralina (Zoloft, Pfizer) will be thechometric measures like CAPS, BDI, STAI, drug treatment to be administered duringSCL-90, MCM-II, physiological procedures such 16 weeks.as, heart rate and blood pressure, ECG, EEG a Drug Treatment + Virtual Reality Exposureand ACTH, should be used to assess the expo- (DT+VRE)sure results. 0 Same clinical intervention concerning thera-
peutic relationship, techniques, frequencyMETHODOLOGY and duration of therapeutic sessions of
VRE and DT will be upheld. The differenceVR Model consists only on the exposure technique
administered.For the virtualization of traumatic scenes fromthe war of Portuguese ex-colonies in Africa VRE groups will receive psychoeducational in-(Guine Bissau, Angola, Mozambique), the formation about anxiety physiology and cogni-following scenarios were chosen (see picture tive-behavioral models of PTSD and anxiety1 a), 1 b), 2 a) and 2 b)): management techniques (diaphragmatic respi-
a) Mine deflagration; ration and relaxation) during the two first ses-b) Ambush; sions. Therapist will help the patient modify hisc) Mine deflagration + Ambush; dysfunctional thoughts and beliefs through cog-d) Facing fellow soldiers death/injury nitive restructuring.situations and waiting for causalitiesevacuation. To be included in DT and DT+VRE groups, all
subjects that are taking medication will have toThe scenarios were developed at the Psychol- pass a 15 day period of wash-out.ogy Computing Laboratory of University Luso-fona (Lisbon, Portugal) using a Half Life 2 Subjectsgraphic engine. For the immersive exposure alast generation fully immersive Head Mounted Inclusion criteria are male subjects with the di-Display HiRes 800 PC 3D with an Intertrax Iner- agnostic of War PTSD according to DSM-IV-TRtia Cube3 (3DOF) will be used. (APA, 2001) who attend a Lisbon central psy-
chiatric hospital (Hospital Julio de Matos). AnClinical Protocol independent technician will evaluate subjects
through a semi-structured clinical interview.Procedures Exclusion criteria are cardiovascular disease,
epilepsy, substance dependence (in the last90 selected subjects will be included, in se- year).quential order, in three groups (30 subjectseach): After complete description of the study to the
subjects, written informed consent will be ob-Virtual Reality Exposure (VRE) Treatment tained in accordance with Helsinki Declarationconsists in 30 minutes sessions for 14 of 1975, as revised in 1983. Patients that ac-weeks. Our option was presented by cept to participate in the study will be sequen-North.1 The VRE session will be interrupted tially distributed accordingly experimentalif a patient feels sick. During the session groups up to 30 persons for group.the patient will be sitting (per suggestion byNorth et al,1). The Patient will be instructedthat he may not speak about war experi-ences before beginning the session.
175
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Assessment also useful as a progress or outcomesmeasurement instrument.
There will be a pre-treatment evaluation periodand an evaluation at 1, 2, 4, 12 e 24 months. Personality
Pre -2 -4 - 6 -12 -24 months MCMI-11 - Millon Clinical Multiaxial Inven-tory-1181
Evaluating measures are: 175 true/false items grouped in 10 clinicalpersonality pattern scales, 3 severe person-
PTSD ality pathology scales, 6 clinical syndromescales, 3 modifier indices and 1 validity in-
* CAPS - Clinician-Administered PTSD dex. The MCMI-I1 instrument has been re-Scale 13 vised to correspond with DSM-IV criteria.A structured clinical interview that allowsfor the evaluation 17 symptoms (frequency VR reactionsand intensity) and 8 factors associated withsocial and professional functioning as well eTAS -Tellegen Absorption Scale 19
as clinical progress during treatment. The most commonly used measure of ab-• IES - Impact of Event Scale 14 sorption is the Tellegen Absorption Scale
A 15 items self-report questionnaire evalu- (TAS), a 34 true/false items that evaluateating experiences of avoidance and intru- subject involvement capacity on the task orsion giving current subjective distress re- environment. The TAS represents one oflated to a specific life event. 11 primary personality dimensions meas-
ured by the Multidimensional PersonalityPsychopathologic Comorbility Questionnaire (MPQ 19).
oDES - Dissociative Experiences Scale 20
"* BDI - Beck Depression Inventory15 It's a 28 item scale of self-report evaluatingA 21 questions survey presented in multiple dissociative experiences. It is the only dis-choice format which purports to measure sociative instrument that has been subjectpresence and degree of depression by as- to a number of replication studied by inde-sessing a specific symptom or attitude pendent investigators (Ross, Norton &"which appear(s) to be specific to de- Anderson, 1988).pressed patients, and which are consistent .PQ - Presence Questionnaires 21
with descriptions of the depression con- A subjective questionnaire in which subjectstained in the psychiatric literature."05 classify their experience to VR concerning
"* STAI - State-Trait Anxiety Inventory16 control, body sensations, distraction andA self-report inventory compose by two reality factors in a 7 points Likert scale.subscales developed to measure state and eSUDS - Subjective Units of Discomfort (0-100trait anxiety with 20 items each. - LB - 10 mn - 20 mn)
"* SCL-90 - Symptom-Check-List-90- This scale measure the degree in which theRevised1 7 subject is affected by VR by reporting theA brief, multidimensional self-report inven- anxiety level experienced during the expo-tory designed to screen for a broad range of sition session in regular intervals. Scorespsychological problems and symptoms of range from 0 to 100 (0 - no anxiety; 100 -psychopathology. It is composed by 9 symp- maximum anxiety/panic attack).tom scales - Somatization, Obsessive- *Verbal and motor behavior records, during theCompulsive, Interpersonal Sensitivity, De- session of VRE1
pression, Anxiety, Hostility, Phobic Anxiety, *Motivation and control sensation at the endParanoid Ideation and Psychoticism - and 3 of the VRE session1
global indices - Global Severity Index, Posi- *Physiological measurestive Symptom Distress Index and Positive Patients will be evaluated according to theirSymptom Total. The SCL-90-R instrument is medical history and to their records of heart
176
GAMITO ET AL.
rate and blood pressure, ECG e EEG and Psychiatry, 152: 626-628.ACTH, Cortisol and Prolactine analysis. 8. Wiederhold, B.K., Davis, R. & Wiederhold, M.
D. (1998) - ((The effects of immersiveness on3. FINAL CONSIDERATIONS physiology>) in G. Riva, B.K. Wedherhold & E.
Molinari (Eds.), Virtual Environments in ClinicalThe present paper continues the methodologi- Psychology and Neuroscience, los Press, Am-cal thread of the on-going research on the use sterdam.of virtual reality exposure (VRE) as a therapeu- 9. Wiederhold, B.K & Wiederhold, M. D (2005) -tic procedure on a clinical population of war (Virtual Reality Therapy for Anxiety Disorders:PTSD veterans. The study population is repre- Advances in Evaluation and Treatment>).sented by 90 subjects enrolled in the PTSD American Psychological Association.department of the Hospital Julio de Matos. It is 10. Rothbaum B., Hodges, L., Alarcon, R.,expected that VRE when associated with a psy- Ready, D., Shahar, F., Graap, K., Pair, J.,chopharmacological drug will reduce PTSD Hebert, P., Gotz, D., Wills, B., & Baltzell, D.symptomatology. Moreover, it is also expected (1999) -( Virtual reality exposure therapy forthat the application of physiological measures PTSD Vietnam veterans: A case study). J.will strengthen the assessment of VRE results. Traumatic Stress 12, 263-271.
11. Rothbaum, B., Hodges, L., Ready, D.,REFERENCES Graap, K. & Alarcon, R. (2001) - (Virtual reality
exposure therapy for Vietnam veterans with1. North, M.M., North, S.M. & Coble, J.R. posttraumatic stress disorderm. J. of Clinical(1998) - (Virtual Reality therapy: an effective Psychiatry 62, 617-622.treatment for psychological disorders)) in G. 12. Wilhelm, F.H., Roth, W.T., 2001 -( The so-Riva (Ed.), Virtual Reality in Neuro-Psycho- matic symptom paradox in DSMIV anxiety dis-Physiology, los Press, Amsterdam. orders: Suggestions for a clinical focus in psy-2. Riva, Wiederhold & Molinari, (1998) ((The chophysiology). Biological Psychology 57,Effects of Immersiveness on Physiology, Virtual 105-140.Environments in Clinical Psychology and Neu- 13. Blake, D, Weathers, F., Nagy, L., Kaloupek,roscience)), los Press, Amsterdam D., Klauminser, G., Charney, D. & Keane, T.3. Vincelli, F. (2001) - WVirtual Reality as a clini- (1990) - ((Clinician - Administered PTSD Scalecal tool: immersion and three-dimensionality in (CAPS))), National Center for PTSD, Boston.the relationship between patient and therapist. 14. Zilberg, N.J., Wiess, D.S. & Horowitz, M.J.Studies in Health Technology Informatics, 81: (1982) - ((Impact of Event Scale: a cross-551-553. validation study and some empirical evidence4. Vincelli, F. & Riva, G. (2002) - (Virtual Real- supporting a conceptual model of stress re-ity: a new tool for panic disorder therapy). Ex- sponse syndromes>). Journal of Consulting andpert Review of Neurotherapeutics 2(3): 89-95 Clinical Psychology, 50, 3: 407-414.5. Vincelli, F. & Molinari, E. (1998) - (Virtual 15. Beck, A.T., Ward, C.H., Mendelson, M.,Reality and imaginative techniques in clinical Mock, J. & Erbaugh,J. (1961) - ((An inventorypsychology)) in G. Riva, B.K. Wedherhold & E. for measuring depression)). Archives of GeneralMolinari (Eds.), Virtual Environments in Clinical Psychiatry, 4: 561-571.Psychology and Neuroscience, los Press, Am- 16. Spielberger, C.D. (1983). Manual for thesterdam. State-Trait Anxiety Inventory (Form Y-1). Palo6. Botella, C., Perpiria, C., Bahos, R.M. & Gar- Alto, CA: Consulting Psychologists Press.cia-Palacios, A. (1998) - ((Virtual Reality ther- 17. Derogatis, L. (1977) - ((SCL-90. Administra-apy: a clinical setting lab>) in G. Riva, B.K. tion, Scoring and Procedures. Manual-I for theWiedherhold & E. Molinari (Eds.), Virtual Envi- R (revised) Version and other instrument for theronments in Clinical Psychology and Neurosci- psychopathology rating scale series. John Hop-ence, los Press, Amsterdam. kins University Scool of Medicine, Chicago.7. Routhbaum, B.O., Hodges, L., Kooper, R., 18. Millon, T. (1987) - Millon Clinical MultiaxialOpdyke, D., Williford, J. & North, M.M. (1995) - Inventory manual I1. Minneapolis: National((Effectiveness of virtual graded exposure in the Computer Systems.treatment of acrophobia)), American Journal of 19. Tellegen, A. & Atkinson, G. (1974) -
177
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
((Openness to absorbing and self-altering ex-periences ("absorption"), a trait related to hyp-notic susceptibility)). Journal of Abnormal Psy-chology, 83: 268-277.20. Bernstein, E.M. e Putman, F.W. (1986).((Development, reliability and validity of a disso-ciation state>). Journal of the Nervous Systemand Mental disease, 178: 448-454.21. Witmer, B.G. & Singer, M.J. (1998) -((Measuring presence in virtual environments: APresence questionnaire)), Presence, 7:225-240.
Contact
Pedro Gamito, PhDUniversidade Lusofona de Humanidades eTecnologiasRua Prof. Barbosa Sueiro, 5 2B1600 Lisbon PortugalTel: +351966057132Email: edro.gamitoasappp
178

Annual Review of CyberTherapy and Telemedicine
Clinical Observations
A Progress Report of Long-Term Robot Assisted Activityat a Health Service Facility for the Aged
K. Wada*1, T. Shibata*13 , T. Saito*' K. Sakamoto*1 and K. Tanie.2
*'Intelligent Systems Research Institute, National Institute Advance Science and Technology (AIST)*2 National Institute Advance Science and Technology (AIST)
*3PERESTO, JST
Abstract: We have proposed Robot-Assisted Therapy and Activity since 1996, and have been devel-oping mental commit robots that provide psychological, physiological, and social effects to humanbeings through physical interaction 1)9). The appearances of these robots look like real animals suchas cat and seal. The seal robot, Paro, was developed especially for therapy. We have applied sealrobots to therapy of children at pediatric hospitals4) and to assisting activity of elderly people at a dayservice centert5)-7 . Recently, several research groups have tried robot assisted therapy and activity.Dautenhahn has used mobile robots and robotic dolls for therapy of autistic children . Besides, ro-bot-assisted activity that uses commercialized animal type robots (such as AIBO11 , NeCoRo, etc.)has been tried1 2 -14 . For example, Yokoyama used AIBO in a pediatrics ward, and observed the inter-action between children and pointed out that the initial stimulus received from AIBO was strong.However, the long term stability was quite weak, compared with living animals1 2). In this presentation,we will explain the results of the robot-assisted activity for elderly people at a health service facilityfor the aged for more than one year.
Method: In order to investigate the effects of seal robots to the elderly people, we evaluated moodsof elderly people by face scales 15) that express person's moods by illustration of person's faces,questionnaires of Geriatric Depression Scales (GDS)16). Seal robots were provided into the healthservice facility on two days per a week from Aug. 2003.
Results: The results of face scale and GDS showed that feelings and depression of elderly peoplewere improved by interaction with the seal robots, Paro. Regarding a case study, Hanako(pseudonym), aged 89, was sociable and comparatively independent. On the first day of the interac-tion with Paro, she looked a little nervous of the experiment. However, she soon came to like Paro.She treated Paro like her child or grandchild. Her face scale scores after interaction were alwayslower than before interaction after the first day. Unfortunately, she was hospitalized during Dec. 10 to26, 2003. When she met Paro for the first time after leaving hospital, she said to Paro "I was lonely,Paro. I wanted to see you again." Her GDS score then improved. To the present, she has continuedto join the activity and willingly interacted with Paro. Caregivers commented that interaction with Paromade the people laugh and become more active. For example, their facial expression changed, sof-tened, and brightened. In addition, Paro encouraged the people to communicate, both with eachother and caregivers, by becoming their common topic of conversation. Thus, the general atmos-phere became brighter.
Conclusions: We have used seal robots, Paro in RAA for elderly people at a health service facility forthe aged since August 2003. The results showed that interaction with Paro improved their moods anddepression, and then the effects showed up through more than one year. Consequently, the seal ro-bots, Paro were effective for therapy at health service facilities.
179
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
BACKGROUND In this paper, we discuss the application of theseal robots to assist elderly people at a health
Interaction with animals has long been known to service facility for the aged, observing their psy-be emotionally beneficial to people. The effects chological and social effects for more than oneof animals on humans have been applied to year. Chapter II describes a seal robot that wasmedical treatment. Especially in the United used for robot-assisted activity (RAA), and waysStates, animal-assisted therapy and activities of experiments. Chapter III explains the effects(AAT&AAA) are becoming widely used in hospi- of RAA on elderly people. Finally, chapter IVtals and nursing homes. 1 2 AAT has clear goals offers conclusions.set out in therapy programs designed by doc-tors, nurses or social workers, in cooperation METHODwith volunteers. In contrast, AAA refers to pa-tients interacting with animals without particular The robot and its major functions are shown intherapeutic goals, and depends on volunteers. Fig.l. Its appearance was designed using aAAT and AAA are expected to have 3 effects: baby harp seal as a model, and its surface was
covered with pure white fur. A newly-developed"* Psychological effect (e.g., relaxation, plane tactile sensor1 1 was inserted between the
motivation) hard inner skeleton and the fur to create a soft,"* Physiological effect (e.g., improvement of natural feel and to permit the measurement of
vital signs) human contact with the robot. The robot is"* Social effect (e.g., stimulation of communi- equipped with the four primary senses; sight
cation among inpatients and caregivers) (light sensor), audition (determination of soundsource direction and speech recognition), bal-
However, most hospitals and nursing homes, ance and the above-stated tactile sense. Itsespecially in Japan, do not accept animals, moving parts are as follows: vertical and hori-even though they admit the positive effects of zontal neck movements, front and rear paddleAAT and AAA. They are afraid of negative ef- movements and independent movement offects of animals on human beings, such as al- each eyelid, which is important for creating fa-lergy, infection, bites, and scratches. cial expressions. The robot operates by using
the 3 elements of its internal states, sensoryWe have proposed Robot-Assisted Therapy and information from its sensors and its own diurnalActivity (RAT and RAA) since 1996, and have rhythm (morning, daytime, and night) to carrybeen developing mental commit robots that pro- out various activities during its interaction withvide psychological, physiological, and social people.effects to human beings through physical inter-action. 3 11 The appearances of these robots look INSTRUCTIONS: The faces above range fromlike real animals such as cat and seal. The seal very happy at the left to very sad at the right.robot, Paro, was developed especially for ther-apy. We have applied seal robots to therapy ofchildren at pediatric hospitals 6 and to assistingactivity of elderly people at a day service cen-ter.7-9 Recently, several research groups havetried robot assisted therapy and activity. Dau-tenhahn has used mobile robots and roboticdolls for therapy of autistic children. 12 Besides,robot-assisted activity that uses commercializedanimal type robots (such as AIBO, 13 NeCoRo,etc.) has been tried.14-16 For example, Yoko-yama used AIBO in a pediatrics ward, and ob-served the interaction between children andpointed out that the initial stimulus receivedfrom AIBO was strong. However, the long termstability was quite weak, compared with livinganimals.14 Figure 1. Seal Robot "Paro"
180
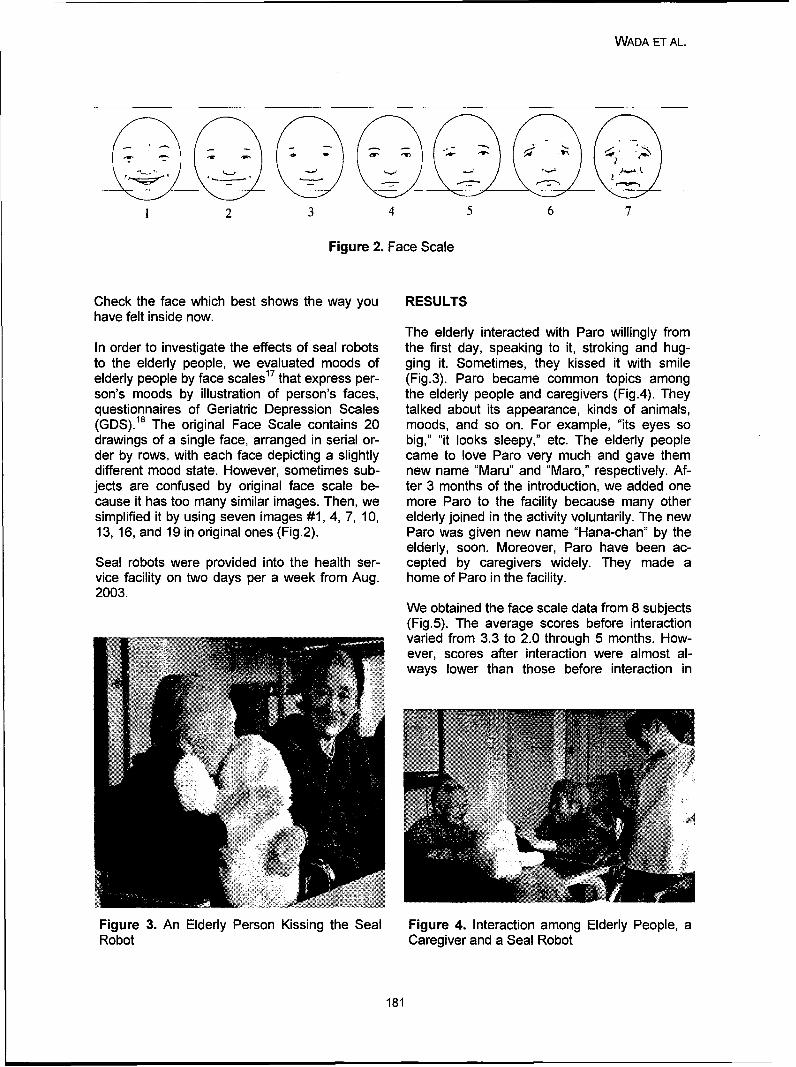
WADA ET AL.
1 2 3 4 5 6 7
Figure 2. Face Scale
Check the face which best shows the way you RESULTShave felt inside now.
The elderly interacted with Paro willingly fromIn order to investigate the effects of seal robots the first day, speaking to it, stroking and hug-to the elderly people, we evaluated moods of ging it. Sometimes, they kissed it with smileelderly people by face scales 17 that express per- (Fig.3). Paro became common topics amongson's moods by illustration of person's faces, the elderly people and caregivers (Fig.4). Theyquestionnaires of Geriatric Depression Scales talked about its appearance, kinds of animals,(GDS).18 The original Face Scale contains 20 moods, and so on. For example, "its eyes sodrawings of a single face, arranged in serial or- big," "it looks sleepy," etc. The elderly peopleder by rows, with each face depicting a slightly came to love Paro very much and gave themdifferent mood state. However, sometimes sub- new name "Maru" and "Maro," respectively. Af-jects are confused by original face scale be- ter 3 months of the introduction, we added onecause it has too many similar images. Then, we more Paro to the facility because many othersimplified it by using seven images #1, 4, 7, 10, elderly joined in the activity voluntarily. The new13, 16, and 19 in original ones (Fig.2). Paro was given new name "Hana-chan" by the
elderly, soon. Moreover, Paro have been ac-Seal robots were provided into the health ser- cepted by caregivers widely. They made avice facility on two days per a week from Aug. home of Paro in the facility.2003.
We obtained the face scale data from 8 subjects(Fig.5). The average scores before interactionvaried from 3.3 to 2.0 through 5 months. How-ever, scores after interaction were almost always lower than those before interaction in
Figure 3. An Elderly Person Kissing the Seal Figure 4. Interaction among Elderly People, aRobot Caregiver and a Seal Robot
181
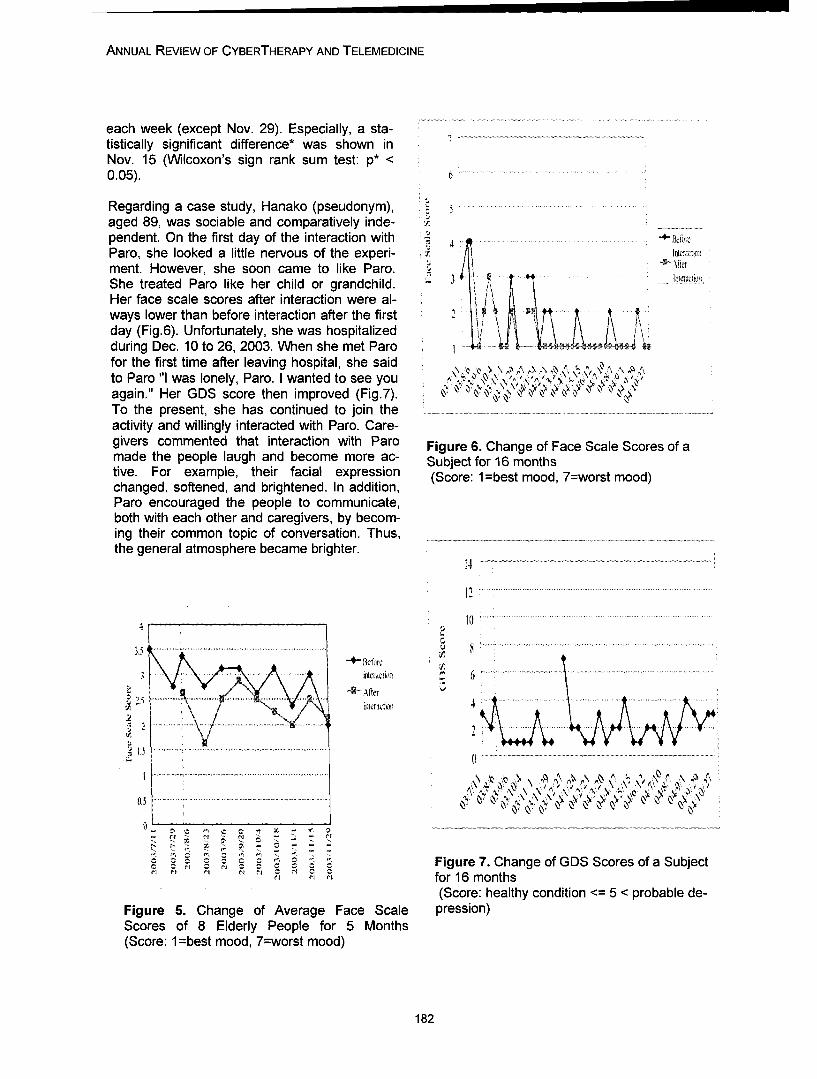
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
each week (except Nov. 29). Especially, a sta-tistically significant difference* was shown inNov. 15 (Wilcoxon's sign rank sum test: p* <0.05). 6
Regarding a case study, Hanako (pseudonym), .aged 89, was sociable and comparatively inde- .pendent. On the first day of the interaction with -4- lkhreParo, she looked a little nervous of the experi- • 'ni~c,,ment. However, she soon came to like Paro. .She treated Paro like her child or grandchild.Her face scale scores after interaction were al-ways lower than before interaction after the firstday (Fig.6). Unfortunately, she was hospitalizedduring Dec. 10 to 26, 2003. When she met Parofor the first time after leaving hospital, she saidto Paro "I was lonely, Paro. I wanted to see you " , , ,,.',again." Her GDS score then improved (Fig.7). ,To the present, she has continued to join theactivity and willingly interacted with Paro. Care-givers commented that interaction with Paro Figure 6. Change of Face Scale Scores of amade the people laugh and become more ac- Subject for 16 monthstive. For example, their facial expression (Score: 1 =best mood, 7=worst mood)changed, softened, and brightened. In addition,Paro encouraged the people to communicate,both with each other and caregivers, by becom-ing their common topic of conversation. Thus,the general atmosphere became brighter.
14
1.. .. ........... ...... ........
4 10 ............ ......... .....
......................
3 6
0.5~~~~~~~~~~~~~~~~ ~~~~~~~~ ....................................................................... ...•':• ; . . .... .......'• •........•
0 N
Figure 7. Change of GDS Scores of a Subject- • ',for 16 months
(Score: healthy condition <= 5 < probable de-Figure 5. Change of Average Face Scale pression)Scores of 8 Elderly People for 5 Months(Score: 1 =best mood, 7=worst mood)
182
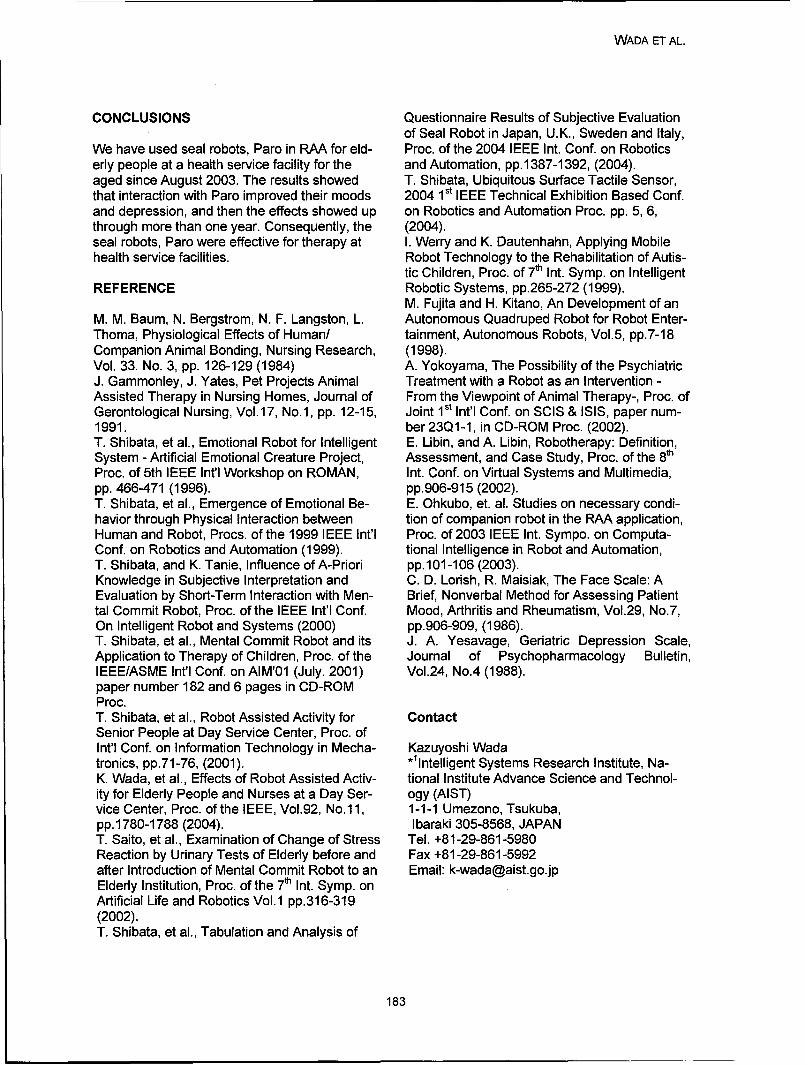
WADA ET AL.
CONCLUSIONS Questionnaire Results of Subjective Evaluationof Seal Robot in Japan, U.K., Sweden and Italy,
We have used seal robots, Paro in RAA for eld- Proc. of the 2004 IEEE Int. Conf. on Roboticserly people at a health service facility for the and Automation, pp. 1387-1392, (2004).aged since August 2003. The results showed T. Shibata, Ubiquitous Surface Tactile Sensor,that interaction with Paro improved their moods 2004 1 st IEEE Technical Exhibition Based Conf.and depression, and then the effects showed up on Robotics and Automation Proc. pp. 5, 6,through more than one year. Consequently, the (2004).seal robots, Paro were effective for therapy at I. Werry and K. Dautenhahn, Applying Mobilehealth service facilities. Robot Technology to the Rehabilitation of Autis-
tic Children, Proc. of 7th Int. Symp. on IntelligentREFERENCE Robotic Systems, pp.265-272 (1999).
M. Fujita and H. Kitano, An Development of anM. M. Baum, N. Bergstrom, N. F. Langston, L. Autonomous Quadruped Robot for Robot Enter-Thoma, Physiological Effects of Human/ tainment, Autonomous Robots, Vol.5, pp.7-18Companion Animal Bonding, Nursing Research, (1998).Vol. 33. No. 3, pp. 126-129 (1984) A. Yokoyama, The Possibility of the PsychiatricJ. Gammonley, J. Yates, Pet Projects Animal Treatment with a Robot as an Intervention -Assisted Therapy in Nursing Homes, Journal of From the Viewpoint of Animal Therapy-, Proc. ofGerontological Nursing, Vol.17, No.1, pp. 12-15, Joint 1st Int'l Conf. on SCIS & ISIS, paper num-1991. ber 23Q1-1, in CD-ROM Proc. (2002).T. Shibata, et al., Emotional Robot for Intelligent E. Libin, and A. Libin, Robotherapy: Definition,System - Artificial Emotional Creature Project, Assessment, and Case Study, Proc. of the 8thProc. of 5th IEEE Int'l Workshop on ROMAN, Int. Conf. on Virtual Systems and Multimedia,pp. 466-471 (1996). pp.906-915 (2002).T. Shibata, et al., Emergence of Emotional Be- E. Ohkubo, et. al. Studies on necessary condi-havior through Physical Interaction between tion of companion robot in the RAA application,Human and Robot, Procs. of the 1999 IEEE Int'l Proc. of 2003 IEEE Int. Sympo. on Computa-Conf. on Robotics and Automation (1999). tional Intelligence in Robot and Automation,T. Shibata, and K. Tanie, Influence of A-Priori pp.101-106 (2003).Knowledge in Subjective Interpretation and C. D. Lorish, R. Maisiak, The Face Scale: AEvaluation by Short-Term Interaction with Men- Brief, Nonverbal Method for Assessing Patienttal Commit Robot, Proc. of the IEEE Int'l Conf. Mood, Arthritis and Rheumatism, Vol.29, No.7,On Intelligent Robot and Systems (2000) pp.906-909, (1986).T. Shibata, et al., Mental Commit Robot and its J. A. Yesavage, Geriatric Depression Scale,Application to Therapy of Children, Proc. of the Journal of Psychopharmacology Bulletin,IEEE/ASME Int'l Conf. on AIM'01 (July. 2001) Vol.24, No.4 (1988).paper number 182 and 6 pages in CD-ROMProc.T. Shibata, et al., Robot Assisted Activity for ContactSenior People at Day Service Center, Proc. ofInt'l Conf. on Information Technology in Mecha- Kazuyoshi Wadatronics, pp.71-76, (2001). *Ilntelligent Systems Research Institute, Na-K. Wada, et al., Effects of Robot Assisted Activ- tional Institute Advance Science and Technol-ity for Elderly People and Nurses at a Day Ser- ogy (AIST)vice Center, Proc. of the IEEE, Vol.92, No.11, 1-1-1 Umezono, Tsukuba,pp. 1780-1788 (2004). Ibaraki 305-8568, JAPANT. Saito, et al., Examination of Change of Stress Tel. +81-29-861-5980Reaction by Urinary Tests of Elderly before and Fax +81-29-861-5992after Introduction of Mental Commit Robot to an Email: [email protected] Institution, Proc. of the 7th Int. Symp. onArtificial Life and Robotics Vol.1 pp.316-319(2002).T. Shibata, et al., Tabulation and Analysis of
183

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
184

Annual Review of CyberTherapy and Telemedicine
Subjective and Physiologic Reactions of Flight Phobics during VR Expo-sure and Treatment Outcome: What Adds Motion Simulation?
A. Muhlberger, Ph.D.1 , G. Wiedemann, MD2 , Paul Pauli, Ph.D.3
1Department of Psychology, Biological Psychology, Clinical Psychology, and Psychotherapy,University of WCirzburg, Germany
2University Hospital of Psychiatry and Psychotherapy, University of Frankfurt, Germany3 Department of Psychology, University of WMrzburg, Germany
Abstract: Background/problem: The efficacy of VR exposure for the treatment of fear of flying wasconfirmed in more than 8 controlled clinical trials. Important goals of future studies are the evalua-tion of underlying treatment processes and the identification of crucial treatment components, bothin order to optimize the treatment. The present study was designed to examine the effect of motionsimulation on subjective and physiological fear reactions as part of a VR exposure that also includedvisual and acoustic stimuli. Our hypotheses were that motion simulation results in stronger initialsubjective and physiological fear reactions, and as a consequence is associated with stronger ha-bituations of fear responses within VR flights and between VR flights. Furthermore, we assumedthat motion simulation enhances treatment efficacy as measured in the fear of flying scale (FFS).
Methods and tools: Twenty fife participants with flight phobia received a virtual reality exposuretreatment including written information about fear of flying and how to cope with it (information book-let), one hour of cognitive therapy, and VR exposure (four flights). However, VR exposure includedfor twelve participants motion simulation while thirteen participants received VR exposure withoutmotion simulation.
Virtual flights consisted out of a different flying phases (start, flying, turbulences, landing) and weresimulated using a head mounted display (HMD), a head tracking device and a motion platform tosimulate accelerations and provide proprioceptive stimuli.
Results: Overall, subjective fear ratings as well as skin conductance responses confirmed substan-tial fear of both groups during VR exposure. However, these responses were substantially strongerand habituated slower in the VR motion group compared to the VR no-motion group. Neverthelessand in contrast to network theories - which suggest that stronger activation of fear networks shouldresult in an enhanced treatment outcome - we found no differences between groups in treatmentoutcome. There was even no trend of a superior treatment outcome for the VR-motion compared tothe VR-no-motion group.
Conclusions and novelty: The present study helps to better understand VR exposure treatment andgives hints for future research to evaluate the treatment process. Based on our results it may bespeculated that treatment outcome is more related to the amount of habituation during exposurethan to the strength of the initial fear response.
ACKNOWLEDGEMENTSINTRODUCTION
Research was supported by the DeutscheAkademie for Flugmedizin (German Academy Many studies confirm the efficacy of Virtualfor Flight Medicine) with a grant to Drs. Pauli Reality (VR) exposure for the treatment of dif-and Wiedemann and by the German Research ferent psychiatric disorders, especially for spe-Foundation (DFG) with a stipend to Dr. A. cific phobia. 1' 2,3 The efficacy of VR exposureMuhlberger. The study was part of the disser- for the treatment of fear of flying was con-tation of Dr. A. Muhlberger. firmed in more than 8 controlled clinical trials.4 7
185

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Important goals of future studies are the VR flights and between VR flights. Based onevaluation of underlying treatment processes earlier results 4 we specifically expected heartand the identification of crucial treatment corn- rate to habituate mostly between flights andponents, both in order to optimize the treat- skin conductance levels to habituate especiallyment. VR exposure is an especially valuable strong within flights. Furthermore, we assumedtool to achieve this since it allows on the one that motion simulation enhances treatmenthand to control exposure settings and on the efficacy as measured in the fear of flying scaleother hand to create a wide range of experi- (FFS).mental manipulations.
METHODFor exposure therapy, a widely accepted theo-retical assumption is that the fear network has Participantsto be activated before it can be changed. Foaand Kozak9 further assumed that this activa- Participants were recruited through newspapertion has to be reflected in initial subjective as articles. Respondents completed a mailedwell as physiological fear responses. Following questionnaire package that included a socio-this initial activation, an effective exposure demographic and a medical history question-treatment should lead to a habituation of acti- naire, and several psychometric instrumentsvation both within and between repeated expo- which assessed fear of flying, trait anxiety, andsures.9 In line with this assumption, an asso- psychopathology. For a detailed description ofciation between strong initial heart rate reac- the selection procedure, the inclusion and ex-tions during exposure and superior treatment clusion criteria, the complete treatment pro-outcome was repeatedly found.10 gram and characteristics of the participants
see Muhlberger et al. 13 Written informed con-Network theories also predict that effective VR sent was obtained from all study participants.treatments must be able to induce substantial The presented analyses are based on 25 par-fear reactions. In flight phobics, such substan- ticipants with fear of flying with complete proc-tial fear reactions have been observed in VRs ess data: All participants received all treatmentincorporating visual, acoustic and motion components including written informationsimulation 4 or visual, acoustic and vibration about fear of flying and how to cope with itsimulation. 10 Variables that were discussed to (information booklet), one hour of cognitivemoderate the amount of fear elicited by VR therapy (CT), and VR exposure (four flights).exposure are the presence in MR11' 12 or the However, VR exposure included for twelvefeedback of physiological activation during participants motion simulation (VR-motionVR.7 An additional important variable modulat- group) while thirteen participants (VR-no-ing subjective and physiological fear reactions motion group) received VR exposure withoutwithin VR exposure might be the applied simu- motion simulation. For the presented evalua-lation modalities. tion of treatment outcome missing follow-up
data of two participants of the no-motion groupThe present study was designed to examine was completed by the group mean of all par-the effect of motion simulation on subjective ticipants who did not fly during follow-up pe-and physiological fear reactions as part of a riod.VR exposure that also included visual andacoustic stimuli. We considered this important Apparatussince motion simulation, on the one hand,might be important to trigger fear during virtual Virtual Reality (VR): The VR environment in-flights but, on the other hand, is rather expen- cluded visual, acoustic, and partly motionsive to add because it needs additional hard- simulations of a commercial flight. VR flightsware (motion chair). Our hypotheses were that lasted 18 min and included all important flightmotion simulation results in stronger initial phases (i.e., take-off, ascending, reachingsubjective and physiological fear reactions, flight altitude, two phases of air turbulence,and as a consequence is associated with descending, and landing).stronger habituations of fear responses within
186
MOHLBERGER ET AL.
The visual cues were presented by a head- Relevant Psychometric measures (for a com-mounted display (HMD; V6, Virtual Research plete list see Muhlberger et al., 2003).Corporation). The head position was moni-tored with an electro-magnetic tracking device Subjective Units of Discomfort (SUDs)14 ranging(Fast Track, Polhemus Corporation) in order to from 0 (no discomfort) to 100 (panic-like dis-adapt the field of view to head movements. A comfort) were used to assess fear responses.Reality Engine II Computer (Silicon Graphics Participants were trained to use this scale, andCorporation) with two processing units pro- ratings were requested at eight assessmentvided real-time texture mapping and imple- points per flight (before the start, directly aftermented the real-time rendering of the environ- the start, during quite flight, during two phasesment with respect to the head position. A high of turbulences, once again during quite flight,amount of details and a frame-rate of at least after landing and reaching the final parking po-12 frames per second were achieved by re- sition) via earphone instruction.nouncing stereoscopic rendering.
The Fear of Flying Scale (FFS15 )_consists of 21The three-dimensional environment consisted items describing situations representative for airof the inside of an airplane (Boeing 737) and travel (e.g., "The plane accelerates down thethe view through an airplane window runway and lifts off the ground"). The fear elic-(somewhat enlarged compared to reality). The ited by the described situations has to be ratedparticipant's position was a passenger com- on 5-point scales (not a all (0) to very muchpartment at the left window row in the middle (4)). A mean score was calculated. Cronbach'sof the plane. The seat at the right of the partici- a and 3 month retest reliability of the originalpant was taken by a virtual passenger. The FFS were .94 and .86, respectively.15 We con-participant was able to look out of the plane firmed these indices for our German translationthrough the window to the left. The outside in two studies:13 Cronbach's a were .90 (N=120)environment changed dependent on the flight and .98 (N=257); 3 month retest reliabilitiesphase (e. g., parking position, runway, airport- were .83 (N= 37) and .87 (N=43).tower, several airport-buildings at take-off orlanding, fields or clouds while flying). PROCEDURE
Sounds were presented by an Indigo Corn- For the evaluation of treatment outcome par-puter (Silicon Graphics Corporation) via ear- ticipants completed the FFS before and afterphone integrated in the HMD. The audio cues the VR exposure treatment and 6 month later.were original airplane sounds and flight an- For a detailed description of the completenouncements, both recorded and stored as treatment and the details of the outcome as-digital audio files. sessment see Muhlberger et al. 13
A motion base with 6 degrees of freedom Participants of both VR groups were accompa-(Symtech Corporation) was used to manipu- nied to the VR simulator after the same cogni-late the body position and to simulate motions. tive preparation. The VR devices were thenSimulations of speed accelerations, speed explained. Participants sat down on a cush-deceleration (during take-off or landing), and ioned seat mounted on a motion platform andair turbulence (during the flight) were imple- the HMD was put on. Before starting the VRmented. The motion data mirrored a flight that flights, participants were instructed not to sup-was performed by a real pilot in a professional press their fear during the VR flights, but toflight simulator. A special program ("Wash- experience the fear and its reduction with on-out") developed by the Fraunhofer-Institute for going exposure. Participants completed fourGraphical Data Processing (IGD) in Darmstadt successive VR flights of 18 min duration each;was used to transform the data for motion the VR-motion group with motion (includingbase use and to ensure an optimal and realis- vibration) simulation, the VR-non-motion grouptic perception of speed acceleration or speed without motion (and without vibration) simula-deceleration. tion. A break of 5 to 10 minutes separated the
second from the third flight.
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
=0.52), Phase (F(7,161)=12.0, p<.001, [fQ=0.34),Physiologqical data acquisition and data reduc- and Motion Group (F(j, 23)=5.5, p=.028, IPtion =0.19), and a significant Motion Group by
Phase (F(7,161)= 4.6, p=.005, I0=0.17) interac-Electrocardiogram (ECG) and skin conductance tion. Contrasts revealed a significant habitua-level (SCL) were registered continuously with a tion from flight to flight (F(1, 23)= 10.1; 32.5;sampling rate of 384 Hz with a Vitaport I system 32.1, p=.004; <.001; <.001, r] '=0.31; 0.59;(Becker Inc.). Skin conductance was recorded 0.58). The main effect of Phase can be tracedfrom two electrodes placed on the medial pha- back to enhanced fear during the start (F(1, 32)langes of the second and third finger of the non- =17.3, p<.001, [1Y=0.43) and the first flightdominant hand. The ECG was converted on- phase (F(1,23)=17.3, p<.001, [P= 0.17), andline to heart rate (HR) by an integrated R-wave reduced fear after landing (F(1, 23)=17.4, p<.001,detection algorithm. Phases of 60 s duration 00 =0.43), compared to the fear before thecorresponding to SUD ratings were extracted start of the flight. The motion group displayedand means for each phase and each flight were overall enhanced fear responses, which werecalculated. Then, differences to the pre-flights - as the interaction Motion Group by Phasebaseline measures were computed. Physiologi- indicated - stronger as the non-motion groupcal signals were pre-analyzed offline with the responses' during the first flight phase (F(1, 23)BrainVision Analyser Software of BrainProducts =5.9, p=.0 2 4 , F.=0.20) and both turbulenceInc. phases (F(1, 23)=4.1; p=.055, Lý=0.15; and F
(1,23)=6.5, p=.018, 113•=0.22).
Statistical data analysisHeart rate: The analysis returned significant
SUD, HR and skin conductance were ana- main effects of Flight (F(3,63)=9.2, p=.001, E]Llyzed with mixed ANOVAs with the between =0.30) and Phase (F(3, 63)=3.3, p=.023, 110factor Motion Group (with or without) and the =0.13), and significant Phase by Motion Groupwithin factors Flight (one to four) and Phase (8 (F(7,147)=4.3, p=.00 6 , 1Iý=0.17) and Flight byassessment points). Treatment outcome was Phase (F(21,441)=6.2, p<.001, E]i=0.23) interac-analyzed with mixed ANOVA with the between tions. Further analyses within groups returnedfactor Motion Group (with or without) and the no significant effects for the VR no-motionwithin factor Time (pre, post, follow-up). If ap- group. For the VR Motion group, the main ef-propriate, Greenhouse-Geisser corrections of fects Flight (F(3,3o)=8.9, p=.005, LI ý=0.47) anddegrees of freedom (df) were applied. Signifi- Phase (F(7,70)=5.4, p=.006, LI =0.35) and thecant effects were followed up with specific interaction Flight by Phase (F(21, 210)=5.1,ANOVAs or planed contrasts. p<.001, LI9=0.34) were significant. These ef-
fects are based on the strong initial heart rateRESULTS reaction during the start phase of flight one, a
smaller one during flight two (see Figure 2),Treatment process and no further reactions during flight tree and
four (not depicted).Fear reports (SUDs): Figure 1 depicts themean fear reports (SUDs) assessed during the Skin conductance level: The analysis yielded afour VR exposure flights separated for the significant main effect of Phase (F(7,154)=4.8,groups with (VR motion) and without motion p=.007, 0LI=0.18) and significant Flight by Mo-simulation (VR no-motion). Strongest fear re- tion Group (F(3,66)=5.9, p=.005, 11'=0. 2 1) andports were observed during the turbulence Phase by Flight by Motion Group (F(21,462)=4.5,phases of the first VR flight with a mean SUD p=.005, [1Y=0.17) interactions. A separateabove 40 in the VR motion group. A decrease ANOVA for the VR motion group revealed aof fear within VR exposure flights and across significant main effect of Flight (F(3,3o)=5.5,repeated VR flights is clearly visible. p=.017,1I0=0.36). Contrasts returned signifi-
cant habituations between the second and theThe overall analysis revealed significant main third flight (F(1,10)=5.9, p=.035,Lý=0.37) andeffects of Flight (F(3, 69)=24.7, p<.001, LI• between the third and the fourth flight (F(l0o)
188
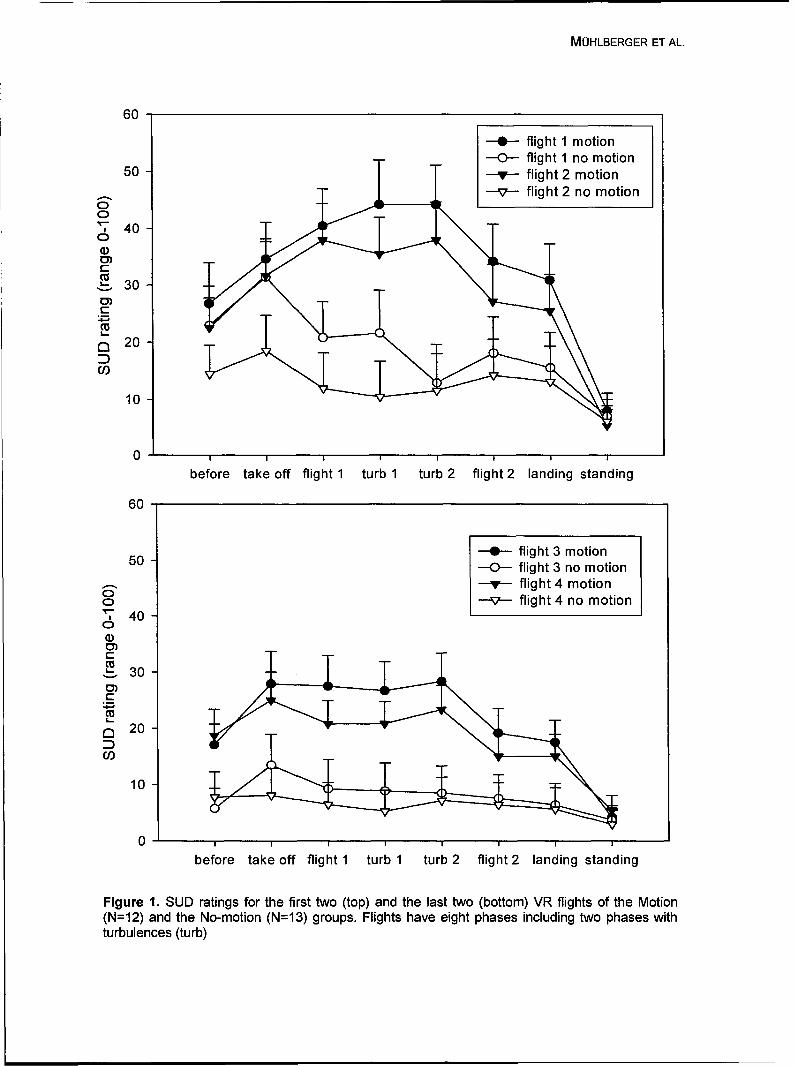
MOHLBERGER ET AL.
60
-0 flight 1 motion-0-- flight 1 no motion
50 - flight 2 motion
--v-- flight 2 no motion
40
W 400)C)
30
C) 2
CO
10-,
10
0 I I I I I I I
before take off flight 1 turb 1 turb 2 flight 2 landing standing
60
50 0- flight 3 motion-0-- flight 3 no motion-v-- flight 4 motion
40 -v- flight 4 no motion6• 40
30 -3
C21 20
10
before take off flight 1 turb 1 turb 2 flight 2 landing standing
Figure 1. SLID ratings for the first two (top) and the last two (bottom) VIR flights of the Motion(N=12) and the No-motion (N=13) groups. Flights have eight phases including two phases withturbulences (turb)
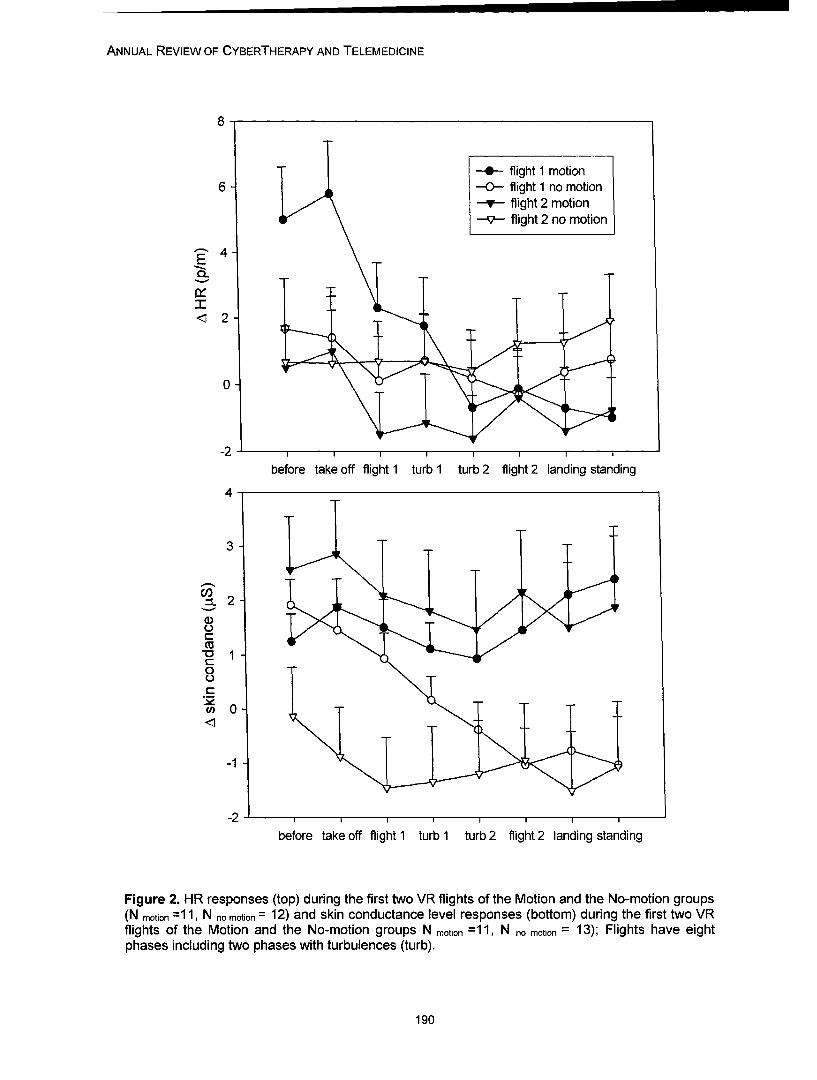
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
--- flight 1 motion6 --0- flight 1 no motion
-v-- flight 2 motion--v-- flight 2 no motion
4-
0-
- 2
0-
-2 I I I I I I
before take off flight 1 turb 1 turb 2 flight 2 landing standing
4-
3
.__
-01
-0C.
0-1
-2 I I I I I
before take off flight 1 turb 1 turb 2 flight 2 landing standing
Figure 2. HR responses (top) during the first two VR flights of the Motion and the No-motion groups(N motion =11, N no motion = 12) and skin conductance level responses (bottom) during the first two VRflights of the Motion and the No-motion groups N motion =11, N no motion = 13); Flights have eightphases including two phases with turbulences (turb).
190
MOHLBERGER ET AL.
=8.6, p=.015, 110=0.46) (not depicted). The groups did not differ in the strength of habitua-ANOVA for the VR no-motion group resulted in tion. As a consequence, fear responses at thea significant main effect of Phase (F(7,84)=3.6, end of the exposure of the VR-motion groupp=.041; 0L=0.23) and a significant Phase by were still higher than the responses of the VR-Flight (F(21,252)=4.0, p=.02 8 ; E1ý=0.25) interac- no-motion group, although both groups hadtion. As depicted in Figure 2, skin conductance widely diminished subjective fear responses.level of the VR no-motion group habituatedstrongly during the first flight and remained Fear associated heart rate responses couldconstant during the second flight, only be detected in the VR-motion group. Sig-
nificant HR accelerations were observed dur-Treatment outcome (FFS) ing the first flight's take off phase and - to aWithin the VR-motion group, the mean FFS weaker extend - during the second flight'sscore dropped from 2.7 pre treatment (sd = take off. During later flights, HR was habitu-0.4) to 1.9 post treatment (sd = 0.4) and 2.1 ated, and further significant reactions did notsix months later (sd = 0.7). The corresponding occur. The VR group without motion simulationscores for the VR-no-motion group were 2.5 at showed no significant HR reactions at all.pre treatment, (sd = 0.5), 1.7 post treatment(sd = 0.8) and 1.7 at follow-up (sd = 0. 9). Skin conductance level of the VR motionSignificant Time main effects (F(2,46)=18.6, group remained enhanced during the first andp<.001, r10=0.45) revealed an overall treat- second flights and habituated only afterwards.ment efficacy. The Motion Group by Time in- In contrast, the VR no-motion group displayedteraction was not significant (F(2,46)=0.5, enhanced SCL responses only during the takep=.489, If =0.02). Contrasts revealed that off phase of the first flight; SCL responsesfear of flying was effectively reduced from pre were habituated during later flight phases andto post treatment (F(1, 23)=39.7, p<.001, Df later flights.=0.63) and from pre-treatment to follow-up (F(1,23)=21. 6 , p<.001, ID0=0.49). Overall, subjective fear ratings as well as skin
conductance responses confirmed substantialDISCUSSION fear of both groups during VR exposure. How-
ever, these responses were substantiallyResults support prior investigations that found stronger and habituated slower in the VR mo-substantial subjective fear reactions of flight tion group compared to the VR no-motionphobics during virtual reality (VR) flights. How- group. Nevertheless and in contrast to networkever, the VR with motion simulation induced theories - which suggest that stronger activa-substantially stronger subjective fear over all tion of fear networks should result in an en-flights and all flight phases than the VR without hanced treatment outcome - we found no dif-motion simulation. Especially pronounced dif- ferences between groups in treatment out-ferences between the motion and the no- come. There was even no trend of a superiormotion groups were found during the first flight treatment outcome for the VR-motion com-before and during phases with intensive mo- pared to the VR-no-motion group. Both groupstion simulation, namely the phases with simu- also showed comparable habituation effects,lation of air turbulences. SUD ratings de- although the habituation within the VR-motioncreased immediately after the start phase in group took place at a higher level (subjectivethe group without motion simulation, while fear fear) or had a later onset (skin conductance).remained enhanced in the VR motion group Although these results are limited due to theuntil the phases with turbulences were com- small sample sizes, the present study helps topleted. better understand VR exposure treatment and
gives hints for future research to evaluate theBoth treatment groups displayed a habituation treatment process. Based on our results it mayof subjective fear responses from flight to be speculated that treatment outcome is moreflight. However, the expected association be- related to the amount of habituation duringtween strong initial fear reactions and strong exposure than to the strength of the initial fearhabituation effects was not confirmed. Both response. Furthermore, since activation and
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
habituation are highly related in exposure 11. Krijn, M., Emmelkamp, P.M., Biemond,therapies,1 6 the manipulation of distinct stimuli R., de Wilde de Ligny, C., Schuemie, M.J., &properties within VR exposure seems to be a van der Mast, C.A. (2004a). Treatment ofvaluable tool to clarify the active components acrophobia in virtual reality: the role ofof exposure treatments. immersion and presence. Behaviour
Research and Therapy, 42, 229-39.
REFERENCES 12. Regenbrecht, H., Schubert, T., & Fried-mann, F. (1998). Measuring the sense of
1. Anderson, P., Jacobs, C., & Rothbaum, presence and its relation to fear of heights invirtual environments. International Journal of
B.O. (2004). Computer-supported cognitive Human-Computer-Interaction, 10, 232-250.behavioral treatment of anxiety disorders. J 13. Mihlberger, A., Wiedemann, G., &Clin Psychol, 60, 253-67. Pauli, P. (2003). Efficacy of a one-session
2. Krijn, M., Emmelkamp, P.M., Olafsson, virtual reality exposure treatment for fear ofR.P., & Biemond, R. (2004b). Virtual reality flying. Psychotherapy Research, 13, 323-336.exposure therapy of anxiety disorders: A re- 14. Wolpe, J. (1973). The Practice of Be-view. Clinical Psychology Review, 24, 259-81. havior Therapy. (2nd ed.). New York: Perga-
3. Pull, C.B. (2005). Current status of virtual mon Press.reality exposure therapy in anxiety disorders. 15. Haug, T., Brenne, L., Johnsen, B.H.,Current Opinion in Psychiatry, 18, 7-14. Berntzen, D., & G6testam, K.-G. (1987). A
4. Mjhlberger, A., Herrmann, M.J., three-systems analysis of fear of flying: aWiedemann, G., Ellgring, H., & Pauli, P. comparison of a consonant vs a non-(2001). Repeated exposure of flight phobics consonant treatment method. Behaviourto flights in virtual reality. Behaviour Research Research and Therapy, 25, 187-194.and Therapy, 39, 1033-1050. 16. Muhlberger, A., Petrusek, S.,
5. Mu0hlberger, A. (2003). Herrmann, M.J., & Pauli, P. (2005).Flugangstfragebogen (FFS). In J. Hoyer & J. Biocyberpsychologie: Subjektive undMargraf (Eds.), Angstdiagnostik: Grundlagen physiologische Reaktionen von Flugphobikernund Testverfahren (pp. 431-434). Berlin: und Gesunden bei Exposition mit virtuellenSpringer. Flogen. Zeitschrift fOr Klinische Psychologie
6. Rothbaum, B.O., Hodges, L., Smith, S., und Psychotherapie, 34.& Lee, J.H. (2000). A controlled study of vir-tual reality exposure therapy for the fear offlying. Journal of Consulting and Clinical Psy- Contactchology, 68,1020-1026.
7. Wiederhold, B.K., & Wederhold, M.D. Andreas MQhlberger, Ph.D.(2003). Three-year follow-up for virtual reality Department of Psychology, Biological Psychol-exposure for fear of flying. CyberPsychology ogy, Clinical Psychology, and Psychotherapy& Behavior, 6, 441-5. University of Wirzburg
8. Foa, E.B., & Kozak, M.J. (1986). Emo- Marcusstr. 9-11tional processing of fear: exposure to correc- 97070 W{3rzburg, Germanytive information. Psychological Bulletin, 99, Tel.: +49 (0)931-31284320-35. Fax: +49 (0)931-312733
9. Lang, P.J., Cuthbert, B.N., & Bradley, E-mail: [email protected]. (1998). Measuring emotion in therapy: wuerzburg.deimagery, activation, and feeling. BehaviorTherapy, 29, 655-674.
10. Wiederhold, B.K., Jang, D.P., Kim, S.I.,& Wederhold, M.D. (2002). Physiologicalmonitoring as an objective tool in virtual real-ity therapy. CyberPsychology & Behavior, 5,77-82.
192

Annual Review of CyberTherapy and Telemedicine
The Virtual Mall: A Functional Virtual Environment for Stroke Rehabilitation
D. Rand M.Sc 1,3, N. Katz Ph.D2 , M. S. MBA 3,R. Kizony M.Sc 1,2, 3 and P. L. Weiss Ph.D 1' 3
1 Department of Occupational Therapy, University of Haifa,2 School of Occupational Therapy, Hadassah-Hebrew University, Jerusalem,
3 Laboratory for Innovations in Rehabilitation Technology, University of Haifa
Abstract: Patients who have had a stroke constitute a large population with significant needs for re-habilitation. Even after long, intensive and costly rehabilitation, these patients still suffer from manyimpairments leading to severe restrictions in participation in every day life. This is a result of limitedfunctional recovery of the upper extremity in addition to cognitive and meta-cognitive deficits. It isalso due to insufficient training of IADL functioning during rehabilitation, primarily since such trainingis both time consuming and technically difficult to implement. The use of VR for rehabilitation of indi-viduals with neurological impairments appears to be promising and its feasibility and effectivenesshave been demonstrated in a number of different studies. However, the VR-based interventions thathave been developed and reported in the literature used mainly desktop platforms, and the majorityof them did not include the stroke population. The aim of this paper is to present the development ofa virtual environment using a video capture VR system, which provides an opportunity to carry outtherapeutic intervention in a functional, natural and a motivating way. The results of a pilot study onpatients with stroke highlighted its many potential advantages. These results as well as future direc-tions will be discussed.
INTRODUCTION
Stroke is considered to be the third leading ciation of the patient's deficits, appears to because of death and the most important cause of time consuming and not suitable for the typicalsevere disability in old age. 1,2 Almost half of the clinical setting.?
patients suffering from stroke retain substantialdisability 3 affecting their performance of activi- The functional recovery of the upper extremityties of daily living. The main symptom following after stroke is considered to be exceptional instroke is paresis or paralysis to half of the body, most cases; the arm does not usually becomecontra lateral to the side of brain lesion. Addi- functional even after intensive and long-tional symptoms include sensory, perceptual, standing therapy.8 Most of patients quickly learncognitive and meta-cognitive deficits, which re- to cope by using only the unaffected arm, and,suit in a decreased ability to perform activities indeed, prefer to avoid failure by not using theof daily living. 4 Patients, who demonstrate diffi- affected arm at all. This phenomenon is knownculties functioning in activities of daily living of- as "learned non-use." 9 Recent research, usingten suffer from deficits in executive functions "Constraint Induced Movement Ther-despite being cognitively intact.5 ' 6 These pa- apy" (CIMT) has been shown to be very effec-tients present problems such as starting and tive1 ° due to the fact that patients use theirstopping activities, an inability to shift mental hands in a functional manner (and not as rou-processes and behavioral tasks, planning and tine exercises) many times a day (high repeti-monitoring deficits as well as keeping a goal in tion) which endeavors to stimulate healing proc-mind throughout a task.5 The assessment and ess associated with plasticity of the brain.1"rehabilitation of executive functions under non-natural conditions such as a research labora- The objective of rehabilitation is to decrease thetory or clinical facility is still very unsatisfactory, various motor, cognitive and meta-cognitiveand the evaluation of real life tasks, which has deficits described above, in order to promotethe advantage of giving a more accurate appre- the functional ability of basic and instrumental
193
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
activities daily living (BADL and IADL). To in need of lengthy rehabilitation and, in particu-date, most clinical settings rely on the use of lar, opportunities to practice instrumental activi-non-functional, routine exercises aimed at de- ties of daily living led us to develop the Virtualcreasing impairment, despite the fact that it Mall using the GX-VR system. The Virtual Mallwould appear to be much more relevant and (VMalI) was developed and designed to facili-motivating for patients to exercise while en- tate assessment and treatment whilst the pa-gaged in meaningful, purposeful tasks that are tient is engaged in a complex, everyday task ofrelated to real life interests and activities.1213 shopping. The aims of this paper are (1) to de-Unfortunately there are limited opportunities for scribe the development of a functional virtualimplementing purposeful activities within tradi- environment and it's usability for stroke patientstional clinical settings via conventional occupa- (2) to present the results of a pilot study withtional therapy. Therefore many stroke patients eight stroke patients.do not return to their premorbid functional level,especially in the more complex instrumental DEVELOPMENT OF THE VIRTUAL MALLactivities of daily living. 14 (VMALL)
Virtual Reality (VR) has the potential to be used The VMall aims to simulate a real shoppingas a novel modality in rehabilitation assessment mall consisting of different stores in order toand intervention due to its well known attrib- provide patients a functional and ecologicalutes.15• 16 To date, a few studies have examined valid environment which can be used to trainthe use of VR with a stroke population, and in motor, cognitive, and metacognitive skills asmost of these studies very small numbers of well as a shopping task itself.patients participated. Kizony et al. assessedthe sense of presence and whole body perform- The VMall was developed primarily for use withance in virtual games of patients with stroke. 17 neurological patients who suffer from motor,Piron et al used VR to train upper limb reaching cognitive and/or metacognitive deficits. The firstmovements18 and Broeren et al. developed a population tested was adults and elderly pa-VR haptic device for the assessment and train- tients who suffer from stroke and whose barri-ing of motor coordination 19 and Merians et al. ers for independence in daily living were de-used a force feedback glove to improve range scribed above. Thus it was important for theof motion, speed and strength of hand move- VMall to facilitate active movement and execu-ment.20 Safe street crossing which is a major tive functions while engaged in the shoppingconcern was trained with stroke patients who task. In addition, the consideration of rehabili-suffer unilateral neglect using a desktop VR tation principles including flexibility of the envi-system and found to be useful. ronment and the ability to adapt the task to suit
the patient's level of ability was also important.In order to encourage activation of a specificlimb, the GX system may be operated while To date, the VMall is a large supermarket con-users wear a red glove on one or both hands. If sisting of many different aisles. Photographs ofthe aim is to improve a user's weak upper ex- real grocery items were taken with a digitaltremity, the red glove will be worn only on the camera and rendered via 3-D graphic software.impaired hand thereby restricting responses These graphic files were then integrated intowithin the virtual environment to that specific the VMall virtual environment. Each aisle isbody part.10 composed of a maximum of 60 products lo-
cated on shelves, and sorted into different cate-To summarize, VR generally, and the GX VR gories such as baking goods, cleaning items,system especially, appear to have considerable and stationary products. The names of thepotential for assessing and treating executive aisles appear on a sign which also has an im-functions and the upper extremity motor func- age of the type of products located in that aisletion of patients with stroke. The importance in (see figure 1, right panel).developing additional intervention tools that aremotivating and challenging for patients with The products may be selected and sorted by astroke and other neurological disorders who are therapist thereby providing flexibility with regard
194
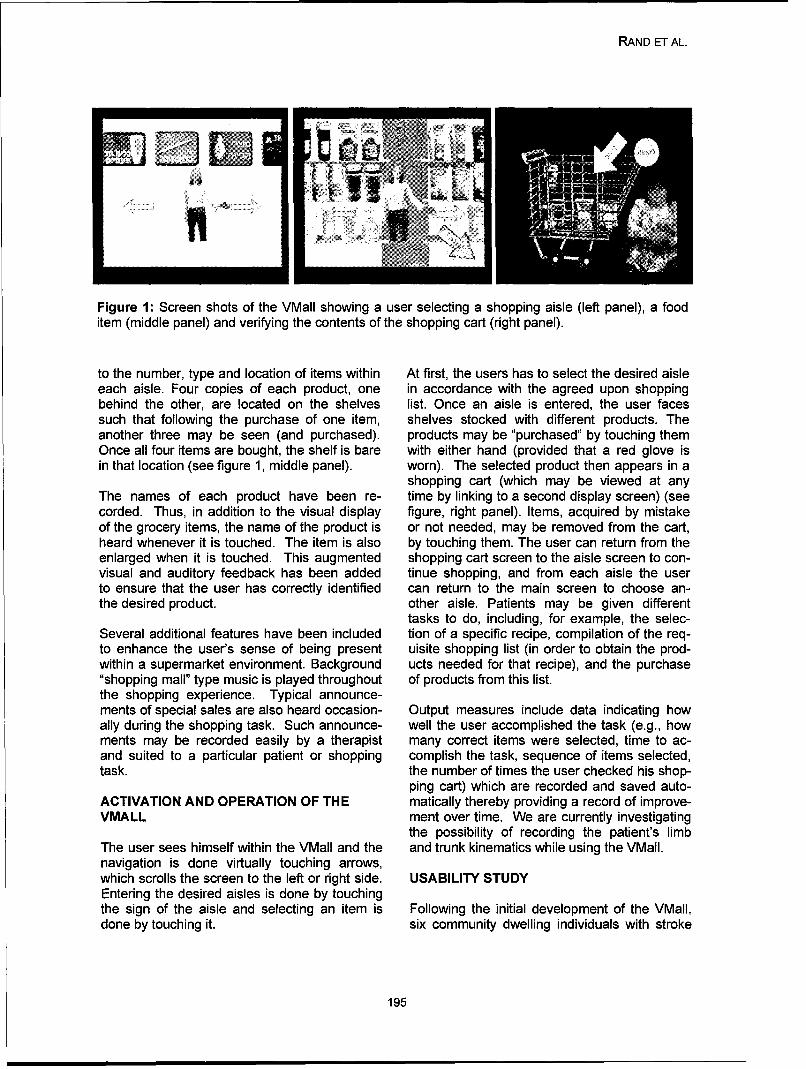
RAND ET AL.
Figure 1: Screen shots of the VWall showing a user selecting a shopping aisle (left panel), a fooditem (middle panel) and verifying the contents of the shopping cart (right panel).
to the number, type and location of items within At first, the users has to select the desired aisleeach aisle. Four copies of each product, one in accordance with the agreed upon shoppingbehind the other, are located on the shelves list. Once an aisle is entered, the user facessuch that following the purchase of one item, shelves stocked with different products. Theanother three may be seen (and purchased). products may be "purchased" by touching themOnce all four items are bought, the shelf is bare with either hand (provided that a red glove isin that location (see figure 1, middle panel). worn). The selected product then appears in a
shopping cart (which may be viewed at anyThe names of each product have been re- time by linking to a second display screen) (seecorded. Thus, in addition to the visual display figure, right panel). Items, acquired by mistakeof the grocery items, the name of the product is or not needed, may be removed from the cart,heard whenever it is touched. The item is also by touching them. The user can return from theenlarged when it is touched. This augmented shopping cart screen to the aisle screen to con-visual and auditory feedback has been added tinue shopping, and from each aisle the userto ensure that the user has correctly identified can return to the main screen to choose an-the desired product. other aisle. Patients may be given different
tasks to do, including, for example, the selec-Several additional features have been included tion of a specific recipe, compilation of the req-to enhance the user's sense of being present uisite shopping list (in order to obtain the prod-within a supermarket environment. Background ucts needed for that recipe), and the purchase".shopping mail" type music is played throughout of products from this list.the shopping experience, Typical announce-ments of special sales are also heard occasion- Output measures include data indicating howally during the shopping task. Such announce- well the user accomplished the task (e.g., howments may be recorded easily by a therapist many correct items were selected, time to ac-and suited to a particular patient or shopping complish the task, sequence of items selected,task. the number of times the user checked his shop-
ping cart) which are recorded and saved auto-ACTIVATION AND OPERATION OF THE matically thereby providing a record of improve-VMALL ment over time. We are currently investigating
the possibility of recording the patient's limbThe user sees himself within the VWall and the and trunk kinematics while using the W~all.navigation is done virtually touching arrows,which scrolls the screen to the left or right side. USABILITY STUDYEntering the desired aisles is done by touchingthe sign of the aisle and selecting an item is Following the initial development of the W~all,done by touching it. six community dwelling individuals with stroke
195

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
at a chronic stage were invited to experience During the usability study we encountered athe environment. The aim was to test its suit- few technical difficulties with the system whichability for the use with stroke patients and to have now been resolved. The requisite redreceive user-centered feedback prior to com- glove was difficult to put on the weak hand onpletion of the environment, some individuals, and it was therefore replaced
with a red mitten. One 72 year old patient com-Three males and three females, mean age 60.3 plained that the products were difficult to iden-± 9.5 (range 50-74 years), who sustained a tify, and the resolution of the 3D images hasright hemispheric stroke 1.5 to 5 years prior to now been improved. One female participanttesting, experienced the VMaIl. They all suf- said the task was not relevant for her since shefered from varying degrees of weakness in their never went shopping prior to her stroke, andaffected upper extremity but had no cognitive was not planning to do so in the future. Thisdeficits. Five patients were able to walk and point is crucial since relevance is a key objec-one was independently mobile in a wheel chair. tive in using the VMall as a therapeutic task.Four of them go shopping on a regular basis. We therefore now include an initial relevancy
question prior to usage: "Did you go shoppingThey experienced the VMall for approximately prior to your stroke?"ten minutes while receiving an explanationabout how to operate it. They then were given PILOT STUDYa six item shopping list and were asked to shopfor the items. When the task was completed Following these improvements, eight additionalthey filled in a feedback questionnaire (the Sce- patients with stroke experienced the VMalI.nario Feedback Questionnaire (SFQ)22 with They were all males and their ages ranged fromseveral additional questions related to VMall 38-73 years (mean 58.7± 13.3 years). Most ofusability (e.g., To what extent were the prod- them were during their sub-acute rehabilitationucts clear?). They were also asked to rate their (3-7 months post stroke) whilst one patient waslevel of perceived exertion (Borg's scale)26. A four years post stroke. Five patients had sus-short interview was done at the end. tained a right hemispheric stroke which caused
weakness to their left side of the body and theOverall the patients all enjoyed their virtual other two sustained a left hemispheric stroke.shopping experience very much and said they All patients used to shop alone or with a spousewould very much like to use it again. They all prior to the stroke. One patient (44 years old)found the task to be challenging and interest- was a butcher in a supermarket prior to hising, and commented that it had potential to use stroke. They did not have cognitive deficits (thein rehabilitation. The mean SFQ scores was mean Mini Mental State Examination (MMSE)25.6 ± 3.4 points (maximum 30 points) and the scores ranged from 26-30 points) but all suf-mean rated exertion was 13 ± 1.2 points which fered from a different degree of motor impair-indicates an easy level. It was interesting to ment of their upper extremity (upper extremityobserve that several patients decided to buy subtest of the Fugl-Meyer Motor assessmentitems that were not on the list because they (FMA) scores ranged from 7-58 points, meanneeded them at home! Others bought products 35.6 ± 17.5 points).that were on sale. From these responses welearn that the task appeared to be relevant and The protocol was identical except for the inter-realistic for the participants, and that they felt a view which was not conducted and extra detailshigh level of presence. After using the VMaIl, of the patient's impairments were collected.one male user remarked: "During the experi- This included the MMSE which was used as aence ones uses all of his senses, also his cognitive screening test (maximum score 30imagination and brain." A female user stated "It points) and FMA (maximum score 60 points) toforced me to straighten my fingers which I assess the affected arm's motor impairment.never do spontaneously." A second female usercommented "It made me feel as I was capable." RESULTS
The SFQ scores ranged from 19-28 points witha mean of 22.6± 3.2 points. For the first ques-
196
RAND ET AL.
tion "To what extent did you enjoy yourself?" tal lesioned head trauma patients performingthe mean score was 4.1 ± 0.99 points activities of daily living. Cortex, 39, 273-291.(maximum 5 points). The perceived exertion Chevignard, M., Pillon, B., Pradat-Diehl, P.,level was 13.2 ± 3.8 points (which ranged from Taillefer, C., Rousseau, S., Le Bras, C., &8-17 points on Borg's scale) and no side effects Dubois, S.B. (2000). An ecological approach towere reported. From these results it can be planning dysfunction: script execution. Cortex,seen that overall these stroke patients who 36, 649-669.were relatively a short time post stroke with dif- Brooks, J.G., Lankhorst, G.J., Rumping, K., &ferent degrees of motor impairments were able Prevo, A.J.H. (1999). The long term outcome ofto virtually shop for products using one or both arm function after stroke: results of a follow-up.of their hands. They too enjoyed the task and Disability and Rehabilitation, 21, 357-364.thought it to be relevant for their rehabilitation. Taub, E. (1980). Somatosensory deafferenta-
tion research with monkeys: Implications forrehabilitation medicine. Implications for Medical
CONCLUSIONS AND FUTURE DIRECTIONS Medicine: Clinical applications. Baltimore, Wil-liams & Wilkins.
The VMall seems to have great potential for the Taub, E., Miller, N.E., Novack., T.A., Cook,use with stroke patients during different rehabili- E.W., Fleming, W.C., Nepomuceno, C.S., Con-tation stages since it provides an interesting nell, J.S., & Crago, J.E. (1993). Technique toand motivating task which encourages active improve chronic motor deficit after stroke. Ar-movement especially of the weak upper extrem- chives of Physical Medicine and Rehabilitation,ity and facilitates the use of executive functions. 74, 347-354.Recently a protocol for intervention of stroke Liepert, J., Baunder, H., Wolfgang, H.R.,patients who suffer from motor and/or executive Miltner, W.H., Taub, E., & Weiller, C. (2000).functions deficits was developed and a study Treatment-induced cortical reorganization afterassessing the treatment efficacy has started. stroke in humans. Stroke, 31, 1210-1216.We also plan to use the VMall with different pa- Nelson D.L., & Perterson, C.Q. (1989). Pur-tient's population such as adolescents post poseful activity: A theoretic analysis. Topics instroke and patients suffering from traumatic Geriatric Rehabilitation, 4, 12-22.brain injury. Katz, N., Marcus, S., & Weiss, P. (1994).
Purposeful activity in physical rehabilitation.REFERENCES Critical reviews in physical and rehabilitation
medicine, 6, 199-218.Bonita, R. (1992). Epidemiology of stroke. The Pettersen, R., Dahl, T., & Wyller, T.B. (2002).lancet, 339, 342-344. Prediction of long term functional outcome afterDuncan, P. (1994). Stroke disability. Physical stroke. ClinicalRehabilitation, 16, 149-159.Therapy, 74, 399-407. Rizzo, A.A., & Kim (2005). A SWOT analysis ofStineman, M.G., & Granger, C.V. (1991). the field of virtual-reality rehabilitation and ther-Epidemiology of stroke-related disability and apy. Presence:teleoperators and Virtual Envi-rehabilitation outcome. Physical Medicine and ronments, 14.rehabilitation Clinics of North America, 2, 457- Riva, G. Rizzo, A., Alpini, D., Barbieri, E.,471. Bertella, L., Davies, R.C., Gamberini, L., Jo-Pedersen, P.M., Jorgesen, H.S., Nakayama, H., hansson, G., Katz, N., Marchi, S., Mendozzi, L.,Raaschov, H.O., & Olsen, T.S. (1996). Orienta- Molinari, E., Pugnetti, L., Weiss, P.L. (1999).tion in the acute and chronic stroke patient: im- Virtual environments in the diagnosis, preven-pact on ADL and social activities. The Copen- tion, and intervention of age-related diseases: Ahagen Stroke Study. Archives Physical Medi- review of VR scenarios proposed in the ECcine and Rehabilitation., 77, 336-339 VETERAN Project. CyberPsychology & Behav-Shallice, T., & Burgess, P.W. (1991a). Deficits ior, 2, 577-591.in strategy application following frontal lobe Kizony, R., Katz, N., Weingarden, H., & Weissdamage in man. Brain, 114, 727-741. P-L. (2002). Immersion without encumbrance:Fortin, S., Godbout, L., Braun, C.M.J. (2003). adapting a virtual reality system for the
Cognitive structure of executive deficits in fron- rehabilitation of individuals with stroke and
197
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
spinal cord injury. In P Sharkey, CS Lanyi, P ContactStanton (Eds); Proceeding of the 4thInternational Conference on Disability, Virtual Debbie Rand M.ScReality and Associated Technology, University Department of Occupational Therapyof Reading: Vresprem, Hungary, pp 55-61. University of HaifaPiron, L., Cenni, F., Tonin, P., & Dam, M. Tel.: +972 4 8240473(2001). Virtual Reality as an assessment tool Fax: +972 4 8249753for arm motor deficits after brain lesions. Stud- Email: drand(&univ.haifa.ac.ilies Health Technology Information, 81, 386-392.Broeren, J., Bjorkdahl, A., Pascher, R., &Rydmark, M. (2002). Virtual reality and hapticsas an assessment devise in the postacutephase after stroke. CyberPsychology andBehavior, 5, 207-211.Merians, A., Jack, D., Boian, R., Tremaine, M.,Burdea, G.C., Adamovich, S.V., Recce, M. &Poizner, H. (2002). Virtual reality- augmentedrehabilitation for patients following stroke.Phys. Ther. 82, 898-915.Weiss, P.L., Naveh, Y., & Katz, N. (2003).Design and testing of a virtual environment totrain CVA patients with unilateral spatial neglectto cross a street safely. Occupational TherapyInternational, 10, 39-55.Kizony, R., Katz, N., & Weiss, P.L. (2003).Adapting an immersive virtual reality systemfor rehabilitation. J.Visual. Comp. Anim. 14,261-268.www.irexonline.comSveistrup, H., McComas, J., Thornton, M., Mar-shal, S., Finestone, H., McCormick, A., Babulic,K., & Mayhew, A. (2003) Experimental studiesof virtual reality-delivered compared to conven-tional exercise programs for rehabilitation. CCyberPsvcholoqy & Behavior, 6:245-249.Weiss, P.L., Rand, D., Katz, N and Kizony, K.(2004).Video capture virtual reality as a flexibleand effective rehabilitation tool. Journal of Neu-roengineering and Rehabilitation, 1, 12.Borg, G. (1990). Psychophysical scaling withapplications in physical work and the perceptionof exertion. Scandinavian Journal of WorkHealth, 16, 55-58.
198

Annual Review of CyberTherapy and Telemedicine
The Virtual Reality Mirror: Mental Practice with Augmented Reality forPost-Stroke Rehabilitation
A. Gaggioli1 ; F. Morganti1 ; A. Meneghini2; M. Alcaniz3; J. A. Lozano3 ; J. Montesa3 ; J.M. Martinez S~ez 3; R. Walker4; I. Lorusso4; G. Riva 1.
1Applied Technology for Neuro-Psychology Lab, Istituto Auxologico Italiano, Milan, Italy2 Azienda Ospedaliera dell'Universit6 di Padova, UnitA Operativa di Riabilitazione, Italy
3 MediCLab, Universidad Politecnica of Valencia, Spain4 Telecom Italia Learning Services, Rome, Italy
Abstract The aim of the project is to apply augmented-reality technology to teach motor skills to pa-tients suffering from stroke. To achieve this goal the project adopts an innovative approach based onthe use of so-called "motor imagery." Recent studies in neuroscience have provided converging evi-dence that "imagining" a motor action involves the same brain areas involved in performing the ac-tion. This supports the idea - already exploited by sports trainers - that training with motor imagery(mental practice) could be effective in leaming new motor skills or in promoting motor recovery afterdamage to the central nervous system. Previous clinical studies have shown that the rehabilitation ofpost-stroke hemiplegic patients can be made more effective by combining physical practice withmental practice. However, for many patients who suffer from damage to the central nervous system,mental simulation of movements can be difficult, even when the relevant neural circuitry has not beeninjured. Starting from these premises, we have designed and developed an augmented-reality work-bench (called "VR Mirror') to help post-stroke hemiplegic patients evoking motor images. First, themovement is acquired by the system from the healthy arm. Second, the movement is being mirroredand displayed so that the patient can observe and see as if the impaired arm is performing the move-ment. Third, the patient is instructed to rehearse in his/her imagination the movement he/she has justobserved. Last, the patient has to perform the movement with the affected arm. In this article, we de-scribe preliminary results of a pilot clinical study, which has evaluated the feasibility of using technol-ogy-supported mental simulation as an adjunct in the rehabilitation of the upper limb following stroke.DESIGN: Single-case study. SETTING: Physical Rehabilitation Unit of Padua Teaching Hospital, Pa-dua, Italy. SUBJECTS: A 46-year-old man with stable motor deficit of the upper right limb followingstroke. INTERVENTION: The patient underwent a single-case design, with four weeks intervention.The intervention consisted of 3 practice sessions per week at the hospital using the VR-Mirror, in ad-dition to usual therapy (Bobath method). This intervention was followed by 1-month home-rehabilitation program using a portable device. MAIN OUTCOME MEASURES: The patient wasevaluated for level of impairment and disability. Pretreatment and posttreatment measures included:the upper-extremity scale of the Fugl-Meyer Assessment of Sensorimotor Impairment and the ActionResearch Arm Test. RESULTS: The patient showed improvement in upper limb score as measuredby the two scales. CONCLUSIONS: The improvement observed in the patient is encouraging andwarrants further study.
INTRODUCTION
Hemiplegia is total paralysis of the arm, leg, and control. Hemiplegia can be caused by damagetrunk on one side of the body. The paralysis pre- to a variety of structures including primary sen-sents as weakness that may be associated with sorimotor areas, supplementary motor, premo-abnormal muscle tone (e.g., rigidity or spastic- tor, and parietal cortices, basal ganglia and/ority). The most common cause is stroke, which the thalamus.1 Traditional rehabilitation afteroccurs when a rupture or blood clot reduces stroke focuses on passive (non-specific) move-blood flow to a specific area of the brain, killing ment or on compensatory training of the non-cells and disrupting the abilities or functions they paretic arm. However, only a small percentage
199
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
(5-52%) of patients regain functional recovery of motor imagery. The rehabilitation protocol con-the upper extremity.2 This observation may be sists of an inpatient and an outpatient phase,related to the limited effectiveness of current combining physical and mental practice. In thetherapy techniques used for improving upper inpatient phase, patient was trained in a labora-limb function, and the very small percentage of tory setting, using a custom-made augmented-the patient's day actually spent in upper limb reality workbench (VR-Mirror). At the end of thisintervention. 2 Clinical research has demon- phase, the patient used a portable display devicestrated that intensive, repetitive practice of active to guide mental and physical practice at hisfunctional tasks shows more positive outcomes home.for upper limb rehabilitation (Langhorne et al,1996). It has been suggested that these METHODSchanges occur by modifying neural reorganiza-tion of the cerebral cortex.3 In particular, there is Recruitmentevidence that the reorganization of the cortexmay be stimulated not only by physical practice Upon an appeal by the researcher to individualsof the task, but also by mental practice of the who had been discharged from the rehabilitationtask without any accompanying movement.4 setting, VP was the first volunteer who satisfied
inclusion criteria for participation in the pilot ex-Mental practice, also called symbolic rehearsal periment. VP was a 46-year-old man hospital-or motor rehearsal, is a training technique in ized from early November 2003 until end of Feb-which the subjects repeatedly "rehearse" a motor ruary 2004 after an ischemic stroke with rightact in working memory, without producing any hemiplegia.overt motor output.5 '6 In recent years, severalclinical studies have described the contribution Comparison between our observations at initialof motor imagery practice for improving upper screening and medical records, discharge sum-limb motor function after stroke.7 11 From a maries, therapist observations, and physiatristneuropsychological point of view, the benefit of observations suggested that the patient's af-mental practice would be to repetitively activate fected limb function had not improved since thecerebral and cerebellar sensorimotor structures time of discharge from the hospital. Before start-damaged by a stroke, thereby engaging com- ing the intervention, VP signed an informed con-pensatory networks to promote motor rehabilita- sent statement, in accordance with the guide-tion.4' 1 ' Recent neuroimaging experiments using lines of the institutional ethical review board, out-positron emission tomography (PET) and func- lining his rights as a subject.tional magnetic resonance imaging (fMRI) haveshown that imagining a motor act is a cognitive Neuropsychological assessmenttask that engages parts of the executive motorsystem: in particular the supplementary motor VP was shown to have normal communicationarea, premotor area, superior parietal lobule, and cognitive skills, as measured by the Folsteinand cerebellum. 4 Efferent discharges produced Mini-Mental State Examination,1 4 with his scoreduring imagery may also activate descending of 28/30 falling within the normal range. The Minimotor pathways. Motor imagery increases spinal Mental State Examination is a widely used stan-reflex excitability at a level only slightly weaker dardized method by which to grade cognitivethan during movement, and corticospinal excit- mental status. It assesses orientation, attention,ability is similar during imagery and movement. 12 immediate and short-term recall, language, andHowever, for many patients with damage to the the ability to follow simple verbal and writtencentral nervous system, mental simulation of commands. The patient's ability to image men-movements can be difficult, even when the rele- tally was measured using the Vividness of Visualvant neural circuitry has been spared.1 3 The goal Imagery Questionnaire.1 In the WIQ patient isof this project was thus to develop technology asked to imagine different scenarios and rate thetools to assist patients in creating motor imagery. vividness of the images generated. The re-In the following section, we describe a pilot clini- sponses to all the questions can be summed tocal study, which has evaluated the feasibility of provide an overall score. VP scored 75/80 on theusing technology to assist patients in creating WIQ, showing good visual imagery ability. This
200
GAGGIOLI ET AL.
result was confirmed by the positive perform- 2=completes test but takes abnormally long timeance on the Shepard-Metzler Mental Rotation or has great difficulty, 3=performs test normally)Test, which measures the ability to mentally ro- and a total possible score of 60.tate three-dimensional objects.' The Vividnessof Movement Imagery Questionnaire17 (VMIQ) Interventionwhich is extensively used in sports, was used totest VP's ability to imagine prior to his engage- Based on VP's responses to the VMIQ, we de-ment in motor imagery intervention. The VMIQ termined that he was able to use both kinestheticwas constructed specifically to test kinaesthetic and visual forms of imagery equally well. There-imagery ability (the ability to "visualize" and "feel" fore, internal as well as external imagery scenesmovement) and contains 24-item scale consist- were applied in his intervention protocol. Theing of movements that the subject is requested intervention focused on the amelioration of spe-to imagine. The questionnaire incorporates a cific impairments and on improving speed andvariety of relatively simple upper-extremity, precision. All inpatient practice sessions werelower-extremity, and whole-body movements, conducted by the same medical professionals.The best attainable score is 120, and the worst The coordinator of the practice session is aobtainable score is 24. VP scored 120 on the physiatrist, specialized in Orthopedics and Trau-VMIQ, showing good movement imagery skills. matology, with over 25 years of clinical exper-Further neuropsychological examination ex- ence.cluded motor apraxia, ideomotor apraxia, andideational apraxia. Inpatient phase: the Virtual Reality Mirror
Testing of motor abilities The inpatient intervention consists of one dailysession, three days a week, for four consecutive
VP was tested 5 times: (1) 2 weeks before the weeks. This time frame was chosen becausefirst practice session (baseline assessment); (2) according to available literature the majority ofat the beginning of the intervention period; (3) upper extremity rehabilitation programs last 4 to1,5 weeks after starting MI practice (midterm 6 weeks and because substantial improvementevaluation); (4) at the end of the intervention has been demonstrated after 4 weeks of im-period; (5) 1 month after hospital practice termi- agery practice. 12 Each therapeutic session in-nation. Further follow-up evaluations are sched- cluded /2 hour of traditional physiotherapyuled 12 and 24 weeks after practice termination. (muscle stretching and Bobath neuro-motor re-VP was evaluated for level of impairment and habilitation) plus 1/2 hour of VR-Mirror treatment.disability. Pretreatment and posttreatment meas- The treatment focused on the following motorures were the Fugl-Meyer Assessment of Sen- exercises: 1) flexion/extension of the wrist; 2)sorimotor Impairment (Fugl-Meyer Scale), and prono-supination of the forearm; 3) flexion/the Action Research Arm Test (ARA). The Fugl- extension of the elbow with (assisted) stabiliza-Meyer Scale1 8 has been used extensively as a tion of the shoulder. The apparatus used by themeasure of impairment in studies measuring patients consists of a movement tracking systemfunctional recovery in patients with strokes. Its and a custom-designed visualization workbenchprimary value is the 100-point motor domain, that we call the Virtual Reality Mirror.21 The VRwhich has received the most extensive evalua- mirror displays a 3D electronic image of thetion.19 The specific items in the upper-extremity movement performed by the patient's healthysubsections were derived from the Brunnstrom limb. This is viewed from an first-person per-stages of poststroke motor recovery. The upper- spective, which is supposed to facilitate the gen-extremity motor component, which consists of 66 eration of kinesthetic motor imagery.22 Eachpoints, was used in this study. The Action Re- practice session with the VR-mirror was com-search Arm Test2 ° is an outcome measure de- posed of four phases.signed specifically for use with patients withstrokes. The test is divided into 4 categories 1. During the pre-training phase the patient re-(grasp, grip, pinch, and gross movement), with ceives instructions, which explain how the treat-each item graded on a 4-point scale (0=can per- ment works, encouraging the patient to relaxform no part of the test, 1 =performs test partially, and reducing performance anxiety.
201
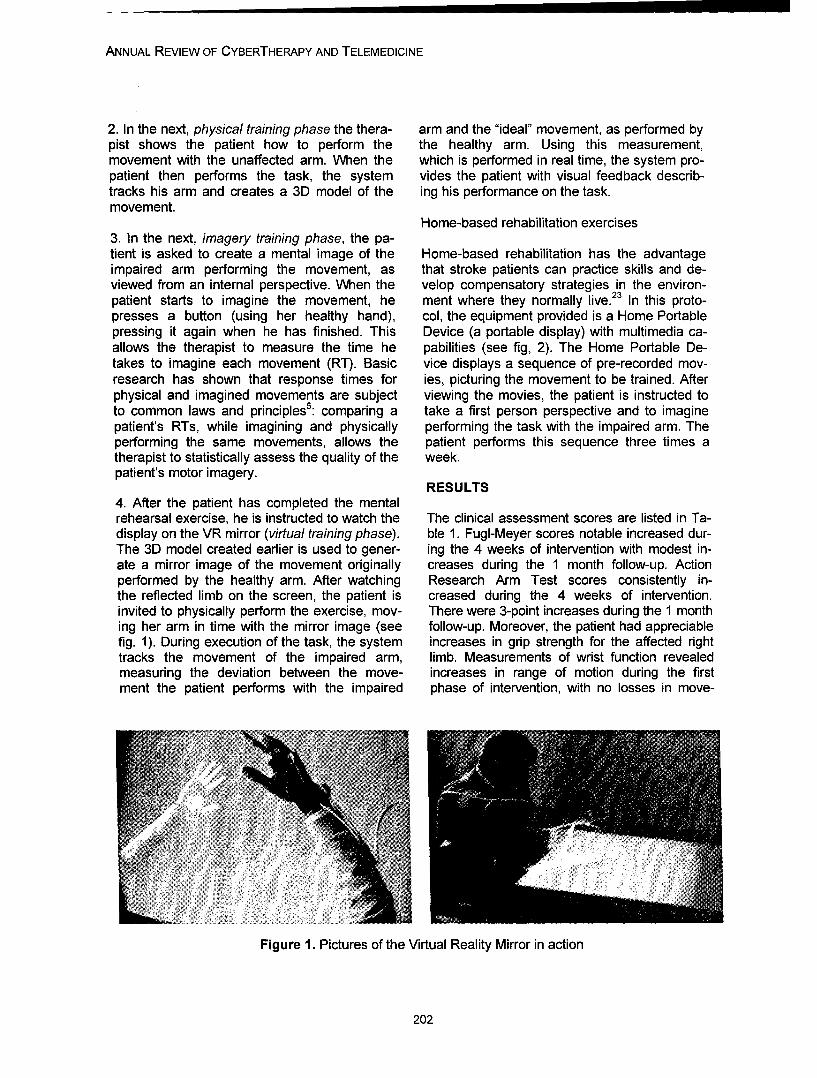
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
2. In the next, physical training phase the thera- arm and the "ideal" movement, as performed bypist shows the patient how to perform the the healthy arm. Using this measurement,movement with the unaffected arm. When the which is performed in real time, the system pro-patient then performs the task, the system vides the patient with visual feedback describ-tracks his arm and creates a 3D model of the ing his performance on the task.movement.
Home-based rehabilitation exercises3. In the next, imagery training phase, the pa-tient is asked to create a mental image of the Home-based rehabilitation has the advantageimpaired arm performing the movement, as that stroke patients can practice skills and de-viewed from an internal perspective. When the velop compensatory strategies in the environ-patient starts to imagine the movement, he ment where they normally live.23 In this proto-presses a button (using her healthy hand), col, the equipment provided is a Home Portablepressing it again when he has finished. This Device (a portable display) with multimedia ca-allows the therapist to measure the time he pabilities (see fig, 2). The Home Portable De-takes to imagine each movement (RT). Basic vice displays a sequence of pre-recorded mov-research has shown that response times for ies, picturing the movement to be trained. Afterphysical and imagined movements are subject viewing the movies, the patient is instructed toto common laws and principles5 : comparing a take a first person perspective and to imaginepatient's RTs, while imagining and physically performing the task with the impaired arm. Theperforming the same movements, allows the patient performs this sequence three times atherapist to statistically assess the quality of the week.patient's motor imagery.
RESULTS4. After the patient has completed the mentalrehearsal exercise, he is instructed to watch the The clinical assessment scores are listed in Ta-display on the VR mirror (virtual training phase). ble 1. Fugl-Meyer scores notable increased dur-The 3D model created earlier is used to gener- ing the 4 weeks of intervention with modest in-ate a mirror image of the movement originally creases during the 1 month follow-up. Actionperformed by the healthy arm. After watching Research Arm Test scores consistently in-the reflected limb on the screen, the patient is creased during the 4 weeks of intervention.invited to physically perform the exercise, mov- There were 3-point increases during the 1 monthing her arm in time with the mirror image (see follow-up. Moreover, the patient had appreciablefig. 1). During execution of the task, the system increases in grip strength for the affected righttracks the movement of the impaired arm, limb. Measurements of wrist function revealedmeasuring the deviation between the move- increases in range of motion during the firstment the patient performs with the impaired phase of intervention, with no losses in move-
Figure 1. Pictures of the Virtual Reality Mirror in action
202
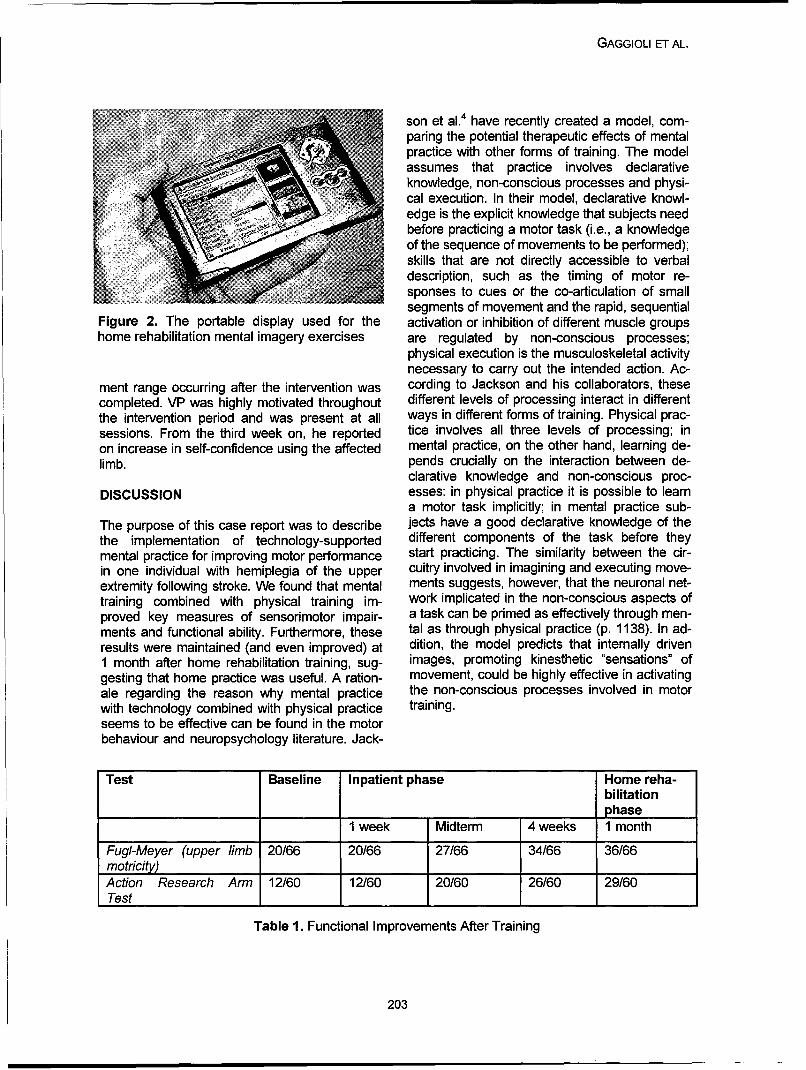
GAGGIOLI ET AL.
son et al.4 have recently created a model, com-paring the potential therapeutic effects of mentalpractice with other forms of training. The modelassumes that practice involves declarativeknowledge, non-conscious processes and physi-cal execution. In their model, declarative knowl-edge is the explicit knowledge that subjects needbefore practicing a motor task (i.e., a knowledgeof the sequence of movements to be performed);skills that are not directly accessible to verbaldescription, such as the timing of motor re-sponses to cues or the co-articulation of smallsegments of movement and the rapid, sequential
Figure 2. The portable display used for the activation or inhibition of different muscle groupshome rehabilitation mental imagery exercises are regulated by non-conscious processes;
physical execution is the musculoskeletal activitynecessary to carry out the intended action. Ac-
ment range occurring after the intervention was cording to Jackson and his collaborators, thesecompleted. VP was highly motivated throughout different levels of processing interact in differentthe intervention period and was present at all ways in different forms of training. Physical prac-sessions. From the third week on, he reported tice involves all three levels of processing; inon increase in self-confidence using the affected mental practice, on the other hand, learning de-limb. pends crucially on the interaction between de-
clarative knowledge and non-conscious proc-DISCUSSION esses: in physical practice it is possible to learn
a motor task implicitly; in mental practice sub-The purpose of this case report was to describe jects have a good declarative knowledge of thethe implementation of technology-supported different components of the task before theymental practice for improving motor performance start practicing. The similarity between the cir-in one individual with hemiplegia of the upper cuitry involved in imagining and executing move-extremity following stroke. We found that mental ments suggests, however, that the neuronal net-training combined with physical training im- work implicated in the non-conscious aspects ofproved key measures of sensorimotor impair- a task can be primed as effectively through men-ments and functional ability. Furthermore, these tal as through physical practice (p. 1138). In ad-results were maintained (and even improved) at dition, the model predicts that internally driven1 month after home rehabilitation training, sug- images, promoting kinesthetic "sensations" ofgesting that home practice was useful. A ration- movement, could be highly effective in activatingale regarding the reason why mental practice the non-conscious processes involved in motorwith technology combined with physical practice training.seems to be effective can be found in the motorbehaviour and neuropsychology literature. Jack-
Test Baseline Inpatient phase Home reha-bilitationphase
1 week Midterm 4 weeks 1 month
Fugl-Meyer (upper limb 20/66 20/66 27/66 34/66 36/66motricity) I I IAction Research Arm 12/60 12/60 20/60 26/60 29/60Test I I
Table 1. Functional Improvements After Training
203
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
According to Jackson and his colleagues, this zation after stroke. A brain stimulation study withwould explain why kinesthetic imagery is more focal magnetic pulses. Stroke 1997; 28(1):110-7.effective than purely visual imagery. Their model 4. Jackson, P. L., M. F. Lafleur, et al. Potentialproposes to conceptualize mental practice with role of mental practice using motor imagery inmotor imagery as a means to access the other- neurologic rehabilitation. Arch Phys Medical Re-wise non-conscious learning processes involved habilitation 2001; 82(8): 1133-41.in a task. They recognize, however, that the ab- 5. Decety, J. and M. Jeannerod Mentally simu-sence of direct feedback from physical execution lated movements in virtual reality: does Fitts'smakes mental practice on its own a less effective law hold in motor imagery? Behaviour Brain Re-training method than physical practice. search 1995; 72(1-2): 127-34.
6. Annett J. Motor imagery: perception or action?In conclusion, results of this pilot study indicate Neuropsychologia 1995; 33:1395-417.that the stimulation of mental practice through 7. Crosbie JH, McDonough SM, Gilmore DH,the use of advanced visualization technology, Wiggam MI. The adjunctive role of mental prac-combined with physical practice, leaded to func- tice in the rehabilitation of the upper limb aftertional gains in the paretic upper extremity of a hemiplegic stroke: a pilot study. Clinical Rehabili-patient with stable motor deficit of the upper right tation 2004; Feb; 18(1):60-8.limb following stroke. Although a single-case 8. Dijkerman HC, Letswaart M, Johnston M,study does not allow us to determine precisely MacWalter RS. Does motor imagery training im-the contribute of mental practice and which pa- prove hand function in chronic stroke patients? Arameters of the training are most useful, a future pilot study. Clinical Rehabilitation 2004; Aug;18goal is to systematically define the most effica- (5):538-49.cious protocol for each patient. Finally, random- 9. Page, S. J., P. Levine, et al. A randomizedized clinical studies are needed to assess efficacy and feasibility study of imagery in acutewhether this experimental protocol durably im- stroke.proves upper extremity motor function in hemi- Clinical Rehabilitation 2001; 15(3): 233-40.plegic patients and how these functional motor 10. Stevens, J. A. and M. E. Stoykov. Using mo-adaptations are mediated by central neural tor imagery in the rehabilitation of hemiparesis.mechanisms. Arch
Phys Med Rehabilitation 2003; 84(7): 1090-2.ACKNOWLEDGEMENT 11. Johnson, S.H. Stimulation through simula-
tion? Motor imagery and functional reorganiza-The present work was supported by the Coin- tion in hemiplegic stroke patients. Brain & Cogni-mission of the European Communities (CEC), tion 2004; 55(2):328-31.in particular by the IST programme (Project I- 12. Lacourse MG, Turner JA, Randolph-Orr E,Learning, IST 2001-38861) and by the Italian Schandler SL, Cohen MJ. Cerebral andMinistry of University and Research (MIUR) cerebellarwithin the project FIRB-NEUROTIV. sensorimotor plasticity following motor imagery-
based mental practice of a sequential move-REFERENCES ment. Journal of
Rehabilitation Research Dev. 2004 Jul; 411. Johnson, S. H., G. Sprehn, et al. Intact motor (4):505-24.imagery in chronic upper limb hemiplegics: evi- 13. Goldenberg, G The Ability of Patients withdence for activity-independent action representa- Brain Damage to Generate Mental Visual Im-tions. Journal of Cognitive Neuroscience 2002; ages.14(6): 841-52. Brain 1989; 112: 305-325.2. Whitall, J., S. McCombe Waller, et al. Repeti- 14. Folstein MF, Folstein, SE, McHugh PR Mini-tive bilateral arm training with rhythmic auditory Mental State: A practical method for grading thecueing improves motor function in chronic hemi- state of patients for the clinician, Journal of Psy-paretic stroke. Stroke 2000; 31(10): 2390-5. chiatric Research 1975; 12: 189-198.3. Traversa R, Cicinelli P, Bassi A, Rossini PM, 15. Marks, D.F. Visual imagery differences in theBemardi G. Mapping of motor cortical reorgani- recall of pictures. British Journal of Psychology
1973;
204
GAGGIOLI ET AL.
64,17.16. Metzler, J. and Shepard, R. N. Mental rota-tion of three-dimensional objects. Science 1971;171,1-32.17. Isaac, A., Marks, D., Russell, D. An instru-ment for assessing imagery of movement: Thevividness of movement imagery questionnaire(VMIQ). Journal of Mental Imagery 1986; 10, 23-30.18. Fugl-Meyer AR, Jaasko L, Leyman I, et al.The post-stroke hemiplegic patient, I: a methodforevaluation of physical performance. Scand JRehabil Med 1975; :13-31.19. Gladstone DJ, Danells CJ, Black SE. Thefugl-meyer assessment of motor recovery afterstroke: acritical review of its measurement properties,Neurorehabil Neural Repair 2002; 16(3):232-40.20. Lyle RC. A performance test for assessmentof upper limb function in physical rehabilitationtreatment and research. Int Jouranla Rehabilita-tion Research 1981; 4:483-492.21. Gaggioli, A, Morganti, F, Walker, R,Meneghini, A, et al. Training with Computer-SupportedMotor Imagery in Post-Stroke Rehabilitation,Cyberpsychology and Behavior 2004; 7(3), 327-332.22. Naito E, Kochiyama T, Kitada R, NakamuraS, Matsumura, M, Yonekura Y, Sadato N. Inter-nallySimulated Movement Sensations during MotorImagery Activate Cortical Motor Areas and theCerebellum.The Journal of Neuroscience, 2002; 22(9):3683-3691.23. Disler, PB, Wade DT "Should all stroke reha-bilitation be home based?" American Journal ofPhys Med Rehabilitation 2003; 82(9): 733-5.
Contact
Andrea Gaggioli, Ph.DApplied Technology for Neuro-Psychology LabIstituto Auxologico Italiano, Via Pelizza daVolpedo 41Milan, ItalyPh./Fax +39-02-619112892Email: [email protected]
205

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
206

Annual Review of CyberTherapy and Telemedicine
Use, Understanding and Learning in Virtual Environments By Adoles-cents With Autistic Spectrum Disorders
Sarah Parsons
School of Education, University of Birmingham
Abstract: There has been increasing interest over recent years in the application of virtual realitytechnology to facilitating skills and understanding for children with autistic spectrum disorders(ASDs). This paper presents a summary of a series of studies that sought to investigate three mainresearch questions; would adolescents with ASDs be able to: (1) Use Virtual environments (VEs)appropriately? (2) Understand them as representational devices? (3) Learn new information fromVEs about social skills? Overall findings suggest that some adolescents with ASDs can use, under-stand and learn social skills/conventions presented in VEs although some students with lower verbalIQ and weak executive skills benefited less from this kind of intervention. An important considerationfor future research is the role of the facilitator in 'scaffolding' participants' use of the VEs. If the aim isto provide effective educational support, to what extent is it useful to try to separate the effect of theVE from the role of a facilitator?
INTRODUCTION
At the time of writing, even a cursory search on ments in the target behaviours or learning ob-the Internet for "Autism and Virtual Reality" re- jectives for children with autism 4' 10' 13,22' 2 whichveals a wealth of hits reflecting the growing in- suggests that virtual reality could be a usefulterest in the application of advanced technology addition to any educational ICT toolkit. Doubtsto the educational realm of children with autistic about the usefulness of VR for people withspectrum disorders (ASDs). According to the ASDs arise though when considering a particu-National Autistic Society (NAS) in the UK this is lar aspect of the disorder: the difficulty in under-part of a trend that has recognised the benefits standing people's behaviour and intentions inof computers more generally for people diag- the real world, let alone within the realms of anosed with the disorder, which is characterised virtual one19. It perhaps seems counterintuitiveby severe social and communicative deficits: to facilitate social understanding or communica-
tion in the real world by immersing people in a"Because computers offer a context-free virtual one!environment in which many people withautism feel comfortable, therapists and However, the optimism for using VEs with peo-teachers are increasingly using virtual real- pie with ASDs is based on an important prem-ity tools to teach life skills, such as crossing ise which is that interactions or experiences in athe road, and social skills, such as recog- virtual world may be less threatening for peoplenising emotions in other people"15 with ASDs compared to the real world because
many of the inputs of real world interactionHowever, despite the burgeoning number of (which people with ASDs often find very confus-Internet hits, there has actually been little in the ing) can be directly controlled or manipulated.way of published, peer-reviewed, systematic This potentially allows a forum where behav-research investigating the usability and poten- iours and responses can be practised and built-tial of virtual environments (VEs) specifically for upon in a context that shares some similaritiespeople with ASDs. There are good reasons for with the real world, thereby offering greater po-wanting to know more about this topic though tential for generalisation. As the NAS notebecause there are ostensible pros and cons to though, the most important feature of VR isthe approach. On the plus side, there is growing safety: "Above all, VR offers a safe learningevidence that computer-based educational ap- environment in which the individual may makeplications have resulted in significant improve-
207
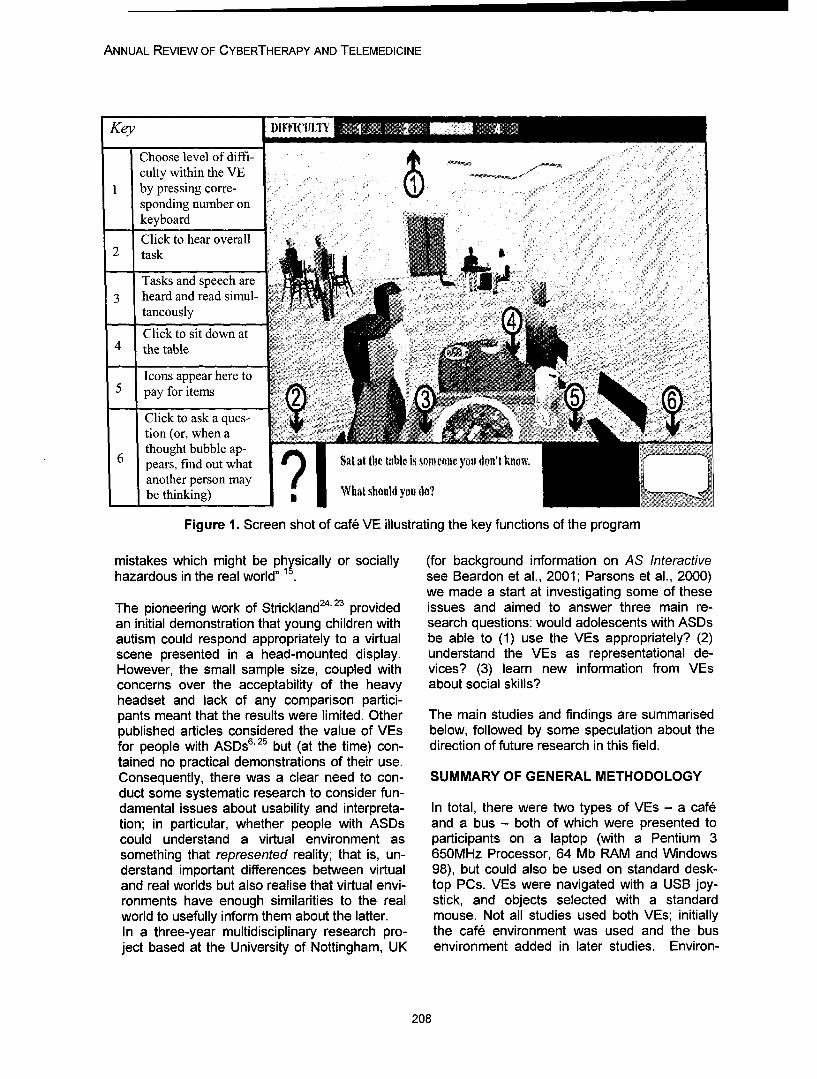
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Key I)IF!lITY
Choose level of diffi-culty within the VE .
I by pressing corre-sponding number onkeyboard
Click to hear overall2 task
Tasks and speech are3 heard and read simul-
taneously
Click to sit down at4 the table
Icons appear here to5 pay for items
Click to ask a ques-tion (or, when a Athought bubble ap-
6 pears, find out what Sat at the table i' soneone you don't knoiianother person maybe thinking) ?'W lhat should you do?
Figure 1. Screen shot of cafe VE illustrating the key functions of the program
mistakes which might be physically or socially (for background information on AS Interactivehazardous in the real world" 1 see Beardon et al., 2001; Parsons et al., 2000)
we made a start at investigating some of theseThe pioneering work of Strickland 24, 23 provided issues and aimed to answer three main re-an initial demonstration that young children with search questions: would adolescents with ASDsautism could respond appropriately to a virtual be able to (1) use the VEs appropriately? (2)scene presented in a head-mounted display. understand the VEs as representational de-However, the small sample size, coupled with vices? (3) learn new information from VEsconcerns over the acceptability of the heavy about social skills?headset and lack of any comparison partici-pants meant that the results were limited. Other The main studies and findings are summarisedpublished articles considered the value of VEs below, followed by some speculation about thefor people with ASDs 6'25 but (at the time) con- direction of future research in this field.tained no practical demonstrations of their use.Consequently, there was a clear need to con- SUMMARY OF GENERAL METHODOLOGYduct some systematic research to consider fun-damental issues about usability and interpreta- In total, there were two types of VEs - a cafetion; in particular, whether people with ASDs and a bus - both of which were presented tocould understand a virtual environment as participants on a laptop (with a Pentium 3something that represented reality; that is, un- 650MHz Processor, 64 Mb RAM and Windowsderstand important differences between virtual 98), but could also be used on standard desk-and real worlds but also realise that virtual envi- top PCs. VEs were navigated with a USB joy-ronments have enough similarities to the real stick, and objects selected with a standardworld to usefully inform them about the latter. mouse. Not all studies used both VEs; initiallyIn a three-year multidisciplinary research pro- the cafe environment was used and the busject based at the University of Nottingham, UK environment added in later studies. Environ-
208
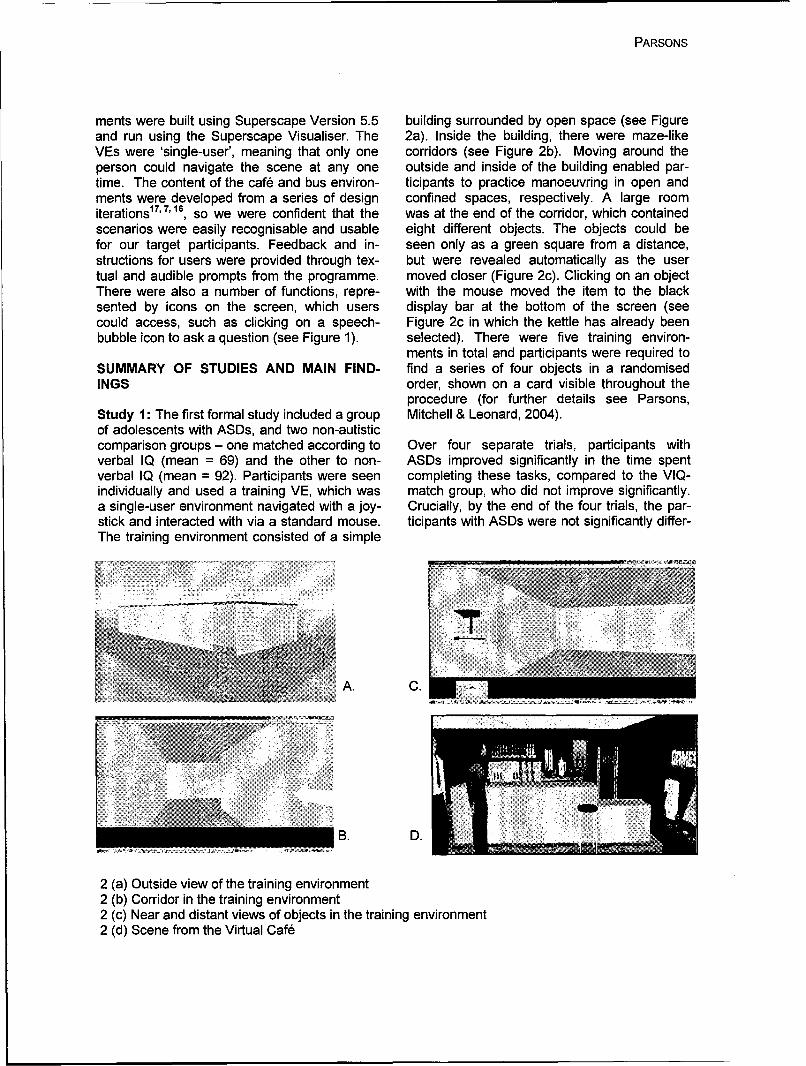
PARSONS
ments were built using Superscape Version 5.5 building surrounded by open space (see Figureand run using the Superscape Visualiser. The 2a). Inside the building, there were maze-likeVEs were 'single-user', meaning that only one corridors (see Figure 2b). Moving around theperson could navigate the scene at any one outside and inside of the building enabled par-time. The content of the cafe and bus environ- ticipants to practice manoeuvring in open andments were developed from a series of design confined spaces, respectively. A large roomiterations 17,7' 16, so we were confident that the was at the end of the corridor, which containedscenarios were easily recognisable and usable eight different objects. The objects could befor our target participants. Feedback and in- seen only as a green square from a distance,structions for users were provided through tex- but were revealed automatically as the usertual and audible prompts from the programme. moved closer (Figure 2c). Clicking on an objectThere were also a number of functions, repre- with the mouse moved the item to the blacksented by icons on the screen, which users display bar at the bottom of the screen (seecould access, such as clicking on a speech- Figure 2c in which the kettle has already beenbubble icon to ask a question (see Figure 1). selected). There were five training environ-
ments in total and participants were required toSUMMARY OF STUDIES AND MAIN FIND- find a series of four objects in a randomisedINGS order, shown on a card visible throughout the
procedure (for further details see Parsons,Study 1: The first formal study included a group Mitchell & Leonard, 2004).of adolescents with ASDs, and two non-autisticcomparison groups - one matched according to Over four separate trials, participants withverbal IQ (mean = 69) and the other to non- ASDs improved significantly in the time spentverbal IQ (mean = 92). Participants were seen completing these tasks, compared to the VIQ-individually and used a training VE, which was match group, who did not improve significantly.a single-user environment navigated with a joy- Crucially, by the end of the four trials, the par-stick and interacted with via a standard mouse. ticipants with ASDs were not significantly differ-The training environment consisted of a simple
ANS9'
A. C.
B. D.
2 (a) Outside view of the training environment2 (b) Corridor in the training environment2 (c) Near and distant views of objects in the training environment2 (d) Scene from the Virtual Caf6

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
A. B. C.
Figure 3(a) starting point; 3(b) approaching the caf6; 3(c) approaching the counter
ent from the PIQ-match group in time taken to couple stood at the bar, compared to both thecomplete the tasks. VIQ- and PIQ-matched groups. This behavior
seems socially inappropriate, especially asIn addition, all participants were required to there was a large empty space at the bar, to thecomplete a number of tasks in a virtual caf& (an right of the couple (see Figure 2d).After rulingearlier version to that depicted in Figure 1 taken out a number of explanations, such as weakfrom Brown et al., 1999), such as find some- navigational and executive skills (behaviourswhere to sit, order and pay for some food, and involved in sequencing, planning and impulsemove to the counter to order a drink. Partici- control), it seemed possible that the participantspants were also asked to make links, as well as with ASDs might struggle more than others withsuggest differences, between virtual scenes understanding the importance of personalencountered in the virtual cafe as well as a space in social situations (at least as depictedsimilar videoed scene including real people in a in a virtual environment), despite understandingreal bar. A video representation is different from the appropriate representational character ofvirtual reality in the sense that it is a photo- VEs.realistic representation, which is familiar to peo-ple through the use of television and other vid- Study 2: A second study21 explored whethereos. A virtual environment, by contrast, is less participants with ASDs adhered to social con-familiar to many people and is a more abstract ventions generally in VEs, such as avoidingform of representation. Comparing these repre- walking across a neighbour's garden and re-sentations enabled us to see whether partici- specting the personal space of people ostensi-pants interpreted them in similar ways. The ma- bly engaged in conversation (see Figure 3).jority of participants with ASDs understood theVE as something that represented, but was not The majority of participants with ASDs behavedidentical to, reality. That is, they said that virtual in a similar way to non-autistic comparisonpeople in the scene were talking to each other groups by treating the VE like a game in mostor to the barman even though they were not situations. That is, they often walked betweenactually talking, but were oriented towards each the two virtual people en route to a counter in aother in such a way that suggested interper- virtual cafe, however members of the ASDsonal interaction. In addition, the majority of group were less likely to remark that this wasparticipants with ASDs also acknowledged im- socially unacceptable than students in the com-portant differences between the VE and the parison groups. Students with ASDs were alsovideo; that the people in the VE were not real more likely to walk across a neighbour's gardenbut the people in the video were. compared to the PIQ-match group, and a third
of the ASD group (4 out of 12) showed substan-Most participants also completed the tasks in tial 'off-task' behaviour. This involved themthe virtual cafM successfully, but the groups dif- walking around the caf&, sometimes even be-fered significantly in one important respect. hind the bar, and navigating up to other peopleWhen approaching the counter to buy a drink, in the scene. This behaviour was shown by stu-the participants with ASDs were judged (by na- dents with low VIQ and weak executive abilities"ive observers) as significantly more likely to (as assessed by the Behavioural Assessmentmove very close to, or walk between a virtual of the Dysexecutive Syndrome; BADS 26), and
210
PARSONS
only by a subset within the ASD group. People In particular, there was evidence to suggest thatin this subset were also unable/unwilling to they were on a par with typically-developingcomment on the links between the VE and 'real counterparts in their ability to use the VEs, andworld' behaviour, even when compared to the understood the scenes as appropriately repre-VIQ-match group. Thus, it is possible that a mi- sentational. By contrast, the main weaknessesnority of students with ASDs may struggle es- for participants with ASDs seemed to be in thepecially with understanding how the VE can social domain - reinforcing the view that VEsinform them about reality, could offer some support in this area by pre-
senting scenes and ideas that were not alreadyBy contrast, many of the comparison partici- well within the grasp of most students withpants, but none in the ASD group, reflected on ASDs. Thus, a remaining crucial question wasthe fact that they would behave differently in whether participants with ASDs could learn spe-real life because it was not socially appropriate cific social conventions using the technology.to walk through people's gardens, or betweenpeople having a conversation, for example: Study 3: This was addressed in a third study12,
which included a group of six adolescents with'In real life, I wouldn't go though the middle, ASDs. Participants used a new version of thebut because it's VR you treat it differently - virtual cafe with the learning objectives of find-you know it's not real. [I was] just interested ing an appropriate place to sit, and asking ap-in the completion of the task' - PIQ-match propriate questions (Figure 1). Specifically, thestudent. aim was to help students understand that if
there is a completely empty table available in aInterestingly, although in the minority, some caf6 then it is more appropriate to sit at it thanparticipants who avoided walking between the with strangers, but if there are no completelytwo people en route to the counter were very empty tables free then it is appropriate to ask asensitive to the social relevance of the virtual question before sitting down (e.g.'Is it OK if I sitcafe (including some of the ASD students), for here?). The virtual caf6 incorporated four differ-example: ent levels of difficulty as the user progressed;
the caf6 became increasingly busy and noisy,if there were two people facing each with fewer choices of appropriate seating. Par-
other, it looked like they were having a con- ticipants used the VE, with the support of a fa-versation. It would not be very good to walk cilitator (the researcher in this case) over athrough. If they had their backs to each number of sessions. They were also asked toother it would not make much difference make judgments about where they wouldwhich way I was going'- ASD student. choose to sit, and why, in video clips of real
cafes. The video clips, whilst not ideal, servedThus, some of the participants with ASDs as approximations to judgements about the realshowed a good understanding of particular so- world. These were presented to participants forcial conventions in the VE - namely, not walk- comment before and after VE use and na'fveing across neighbours' gardens and not walking coders were asked to rate the explanations forbetween people having a conversation. Never- social appropriateness.theless, these individuals were in the minoritywithin the group - with the remainder unwilling Results showed that four of the six participantsto respond to questions or seemingly unaware improved in their awareness of social conven-of the real world implications of their behaviour. tions, both in terms of performance in the virtualThis was in contrast to the VIQ- and PIQ- cafe and in judgments and comments made inmatched groups, who seemed more willing to relation to the video clips. That is, a majority ofuse the path/pavement at the start of the task participants were judged as providing more so-and more aware of how their behaviour in the cially appropriate and insightful commentsVE related to real world social conventions, about where they would sit and why in relationTaken together, the first two studies provided to the video scenes, specifically following a ses-some in-depth information about how a group of sion with the VE. An example of high-scoringadolescents with ASDs use and interpret VEs. reasoning was: "because no-one's sitting there,

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
I won't be in anyone's way", and of low-scoring CONCLUSIONSreasoning: "so I can look at the windows".
Whilst anecdotal, comments like the one in-The design of the study allowed us to pinpoint cluded above are extremely encouraging andthe improvement in understanding to the spe- add to our growing body of knowledge aboutcific time of VE use, and not to general im- whether, and how, people with ASDs can use,provement in understanding over time. This understand and learn from VEs depicting socialwas because whilst all participants received the situations. Overwhelmingly, the emerging pic-same tasks, they were completed in a different ture from the four studies summarised here is aorder; for example, half the participants had positive one, which can continue to be builtsessions with the VE between the video meas- upon in any future work. This is especially en-ures at Time 1 and Time 2, whilst the remainder couraging in the context of fairly limited func-had their VE sessions between the video meas- tionality in the VE and the rather unconvincingures at Time 2 and Time 3. Gains in under- representations of people in the scene, whichstanding should be apparent directly following were blocky and cartoon-like in appearance.VE but not necessarily during testing sessions Despite such limitations, many of the partici-that did not directly follow the VE. Importantly, pants assigned representational qualities to thethe facilitator played a crucial role in the suc- scene (being like reality in some respects butcess of this approach, by helping the user to not identical to it) and enjoyed using the VEs.interpret, understand and discuss the social An important point to note too is that the VEsscenes depicted in the VE. and learning objectives were designed with the
input of teachers working with the participantsStudy 4: Finally, after demonstrating successful and so were based on clearly identified needs.outcomes in terms of use, understanding and This was an essential part of the project andlearning in the first three studies, it was impor- ensured that the research put the needs of par-tant to highlight the views of people with ASDs ticipants first rather than pursuing worthy butdirectly to gain a sense of how they viewed the perhaps esoteric agendas of the research team!VEs and whether they thought VEs could be Virtual environments and programming exper-useful to them in any way. Therefore, in the fi- tise can now accommodate far more sophisti-nal study we adopted a case study approach cated levels of representation as well as morewith two adolescent males with an ASD and finely tuned aspects of interpersonal behavioursought their opinions and comments over a including direction of gaze and conversation.number of sessions with the VEs, and during an Recent work from David Moore and his stu-informal interview18. Both students learned the dents in the UK, for example, has utilised col-target social conventions (these were the same laborative virtual environments (CVEs) for in-as the third study) over the period of VE use, vestigating the usefulness of emotionally ex-with the aid of rich discussions with the facilita- pressive avatars in communicative contexts fortor about social aspects of behaviour and what children with autism9 as well as consideringother people (in the virtual scene) could be aspects of gender, personal space and anxiety,thinking. In addition, both students commented which could eventually be useful for childrenon how the VE could be relevant to their lives, with autism14. The use of CVEs allows greatand one student excitedly remarked how he potential for developing social and communica-had used the information he had learned from tive skills in more dynamic (yet safe) environ-the VE in a real life situation. He was travelling ments than has hitherto been possible, thuson a busy train in the summer break and there offering greater potential for learning skills thatwere few empty seats, so he asked a man if the are likely to be of use in the real world.seat beside him was free. The student said thathe felt proud about asking the question be- It is an exciting time for researchers becausecause this was not something he would have the potential for creating really beneficial out-usually done. In addition, he said how much the comes for children with ASDs is a distinct possi-VE had helped him "Cause it could help me bility, although of course there is still a greatlearn what polite and sensible things to do in deal to be done in research terms. There is alsopublic places" (student with ASD, aged 14). a need for researchers to be clear about their
212

PARSONS
aims and why participants with clinical diagno- searchers' minds as they contemplate how toses (including autism) are involved in studies; it take this work forward. This may mean adoptingcould be too easy to pursue a line of investiga- research approaches that take into account thetion because it seems timely and interesting but importance of context and interaction aroundultimately of limited benefit to participants. the computer when considering whether andThere are essentially three main potential foci how learning takes place. The challenge of thisfor 'Autism and Virtual Reality' research: what became most apparent for me in discussionsparticipants with autism can tell us about VR; about the role of a facilitator in the use of thewhat VR can tell us about autism and what VR VEs; that is, someone who sat alongside thecan offer people with autism in terms of educa- participant and guided them verbally throughtional/learning needs. the social situations depicted, perhaps asking
the participant to clarify why they took that routeIn terms of what participants with autism can tell or talking through the motive or reasoning forus about VR, there are substantial ethical con- other people behaving in a particular way (seecerns about including people with clinical disor- Parsons et al., in press and Mitchell et al., sub-ders in research where the technology rather mitted).than the people is the primary focus. For exam-ple, the unique perspective that people with Quite clearly, from an experimental researchASDs may have on the (real) world could tell us point of view, it becomes impossible to saysomething interesting about the nature of VEs what was really helping to do the job of learn-themselves, but is it ethically justifiable to pur- ing; was it the 'experiential' nature of the VEsue such a question by itself? Similarly, there is and the opportunity to practice the behavioura query about what VR stands to tell us about repeatedly, or the interpretation andthe condition of autism per se? Despite sub- 'scaffolding' offered by the facilitator, or a com-stantial research on how non-autistic members bination of both? I would argue that, for me atof the population use, interpret and understand least, it doesn't really matter all that much be-VEs, the links between virtual and real world cause learning coincided with use of the VEbehaviours are still not properly understood, and so there was something about the contextincluding when and why people choose to apply that was useful and important (Mitchell et al.,real world conventions to virtual contexts and submitted). Moreover, as Crook (1991) argues,when they do not. Do we know enough about the context of learning (e.g. within a classroom)the use of VEs more generally to draw many should be a central consideration to the designconclusions about how or why participants with and use of ICT resources because it is alwaysASDs might respond in virtual contexts and how within such a context that we would expect thethat links to real world understanding? Of real world outputs of our research to be used tocourse, answers to these questions may arise (hopefully) beneficial effect:in the context of a project with a more educa-tional focus (and this was certainly the case for "In order to expose where and how computersthe AS Interactive project) and would be inter- are proving potent, the design of evaluationsesting to know, but I would question using the must be sensitive to events that are takingabove two foci as starting points. Instead, they place in the 'periphery' of the individual learner-could be questions that are tackled en route to computer interaction. In particular, evaluationa more outcome focused research approach, should be amenable to the idea that propertieswhich provides something (however imperfect of any computer application include the charac-and limited) back to the relevant participant ter of social processes that it supports duringgroups. the circumstances of use" 8
The main point is that the potential of VEs for Separating out, or attempting to narrow down,providing powerful learning contexts for people the specific factors that promote learning maywho would really benefit from them should be only be relevant if we are interested in claimingthe primary aim and driving force of research in that VEs are better than other formats/tools/this area. The question of 'what's in it for the contexts for facilitating learning and I wouldparticipants?' should be at the forefront of re- question the usefulness of such a claim or pur-
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
suit of one. For if we are in the business of put- 8. Crook, C. (1991). Computers in the zone ofting the needs of participants first and pursuing proximal development: implications for evalua-a research agenda that could be of substantial tion. Computers & Education, 17, 81-91.educational benefit to people with ASDs, then I 9. Fabri, M & Moore, D. (2005). The use of emo-think that VEs as an option amongst many for tionally expressive avatars in Collaborative Vir-the promotion of learning is not only good * tual Environments. Paper presented at AISBenough but also appropriate and desirable. This 2005. http://aisb2O05.feis.herts.ac.uk/index.htmiwill help to ensure that teachers, parents and 10. Heimann, M., Nelson, K., Tjus, T., Gilberg, C.therapists can be equipped with a toolkit of pos- (1995). Increasing reading and communicationsibilities that could be used where appropriate skills in children with autism through an interac-with different children with very different needs. tive multimedia computer program. Journal ofUltimately, the children benefit if there are a Autism and Developmental Disorders, 25, 459-range of stimuli and contexts in which learning 480.takes place and that should be 'what's in it for 11. Kerr, S.J. (2002). Scaffolding - Design is-them'! sues in single and collaborative virtual environ-
ments for social skills learning. Proc. 8thEGVE.REFERENCES In W. Sturzlinger, S Muller (Eds), 81-91 Barce-
lona, 2 9 th- 3 0 th May 2002.1. Beardon, L., Parsons, S. & Neale, H. (2001). 12. Mitchell, P., Parsons, S. & Leonard, A.An inter-disciplinary approach to investigating (under review). Using virtual environments forthe use of virtual reality environments for people teaching social understanding to adolescentswith Asperger Syndrome. Educational and Child with autistic spectrum disorders. UnpublishedPsychology, 18, 53-62. manuscript, University of Nottingham, UK.2. Bemard-Opitz, V., Sriram, N. & Nakhoda- 13. Moore, M. & Calvert, S. (2000). Brief report:Sapuan, S. (2001). Enhancing social problem Vocabulary acquisition for children with autism:solving in children with autism and normal chil- teacher or computer instruction. Journal of Au-dren through computer-assisted instruction. tism and Developmental Disorders, 30, 359-Journal of Autism and Developmental Disorders, 362.31, 377-384. 14. Nassiri, N., Powell, N. & Moore, D (2005).3. Brown, D.J., Neale, H.R., Cobb, S.V.G. and Avatar gender and personal space invasionReynolds, H. (1999). Development and evalua- anxiety level in desktop collaborative virtual en-tion of the virtual city. International Journal of vironments. Virtual Reality, published onlineVirtual Reality, 4, 28-41. 15th January 2005.4. Chen, S. H. A. & Bernard-Opitz, V. (1993). 15. National Autistic Society (UK) (2001). Coin-Comparison of personal and computer-assisted puter applications for people with autism. Ac-instruction for children with autism. Mental Retar- cessed online at www.nas.orq.uk (March 2005).
aigon, 31, 368-376. 16. Neale, H.R., Cobb, S.V. and Wilson, J.R.5. Cheng, Y. (2005). An avatar representation of (2002). A front-ended approach to the user-emotion in Collaborative Virtual Environments centred design of Virtual Environments. Proc.(CVE) technology for people with autism. Unpub- IEEEVR 2002, 24th-28th March, 191-198.lished PhD thesis, School of Computing, Leeds 17. Parsons, S., Beardon, L., Neale, H. R.,Metropolitan University, UK. Reynard, G., Eastgate, R., Wilson, J. R., Cobb,6. Clancy, H. (1996). Medical field prescribes S. V., Benford, S., Mitchell, P., & Hopkins, E.virtual reality for rehabilitation therapy. Computer (2000). Development of social skills amongstReseller News, 698, p.76. adults with Asperger's Syndrome using virtual7. Cobb, S., Beardon,L., Eastgate, R., Glover, T., environments: The AS Interactive project. Pro-Kerr, S., Neale, H., Parsons, S., Benford, S., ceedings of the 3 rd International Conference onHopkins, E., Mitchell, P., Reynard, G. and WIl- Disability, Virtual Reality and Associated Tech-son, J.R. (2002).Applied Virtual Environments to nologies, Sardinia, 2 3 -2 5 n September, 2000,support learning of Social Interaction Skills in pp. 163-170.users with Asperger's Syndrome. Digital Creativ- 18. Parsons, S., Leonard, A. & Mitchell, P. (inity,13,11-22 press). Virtual environments for social skills
training: comments from two adolescents with
214
PARSONS
autistic spectrum disorder. Computers & Educa-tion.19. Parsons, S. & Mitchell, P. (2002). The po-tential of virtual reality in social skills training forpeople with autistic spectrum disorders. Journalof Intellectual Disability Research, 46, 430-443.20. Parsons, S., Mitchell, P., & Leonard, A.(2004). The use and understanding of virtualenvironments by adolescents with autistic spec-trum disorders. Journal of Autism and Develop-mental Disorders. 34(4), 449-46621. Parsons, S., Mitchell, P., & Leonard, A.(2005). Do adolescents with autistic spectrumdisorders adhere to social conventions in virtualenvironments? Autism 9, 95-117.22. Silver, M. & Oakes, P. (2001). Evaluation ofa new computer intervention to teach peoplewith autism or Asperger syndrome to recognizeand predict emotions in others. Autism, 5, 299-316.23. Strickland, D. (1996). A virtual reality applica-tion with autistic children. Presence: Teleopera-tors and Virtual Environments, 5, 319-329.24. Strickland, D., Marcus, L.M., Mesibov, G.B.& Hogan, K. (1996). Brief report: Two casestudies using virtual reality as a learning tool forautistic children. Journal of Autism and Devel-opmental Disorders, 26, 651-659.25. Trepagnier, C.G. (1999). Virtual environ-ments for the investigation and rehabilitation ofcognitive and perceptual impairments. Neu-roRehabilitation, 12, 63-72.26. Wilson, B.A., Alderman, N., Burgess, P.W.,Emslie, H.C. and Evans, J.J. (1986). BehaviouralAssessment of the Dysexecutive Syndrome.Thames Valley Test Company: Flempton, BurySt. Edmunds.
ContactSarah ParsonsSchool of EducationUniversity of BirminghamEdgbaston, Birmingham, B15 2TT, UKEmail: s.i.parsonsobham.ac.uk

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
216
Annual Review of CyberTherapy and Telemedicine
Abstracts from CyberTherapy 2005, June 6-10, 2005, Basel, Switzerland
Presenter: Mariano Alcafiiz PhD THE TREATMENT OF ARACHNOPHO-BIA
REAL TIME CHANGING VIRTUAL EN-VIRONMENTS: A NEW TOOL FOR Juan, M.C. 1, Botella, C. 2, Baios, R.3,VIRTUAL THERAPY Guerrero, B. 3, Alcarhiz, M. 1, Rey, B.1, Gil, J.
A.1
M. Alcaiiz, Ph. D., Beatriz Rey, M.Sc.;Javier Montesa, M.Sc.; Jos6 Antonio 1 MedICLab (Universidad Polit6cnica de Valencia)Lozano, Ph.D.; M. Carmen Juan, Ph. D. 2 Departamento de Psicologia Bsica y
Psicobiologia (UJI)
Medical Image Computing Laboratory 3 Universidad de Valencia
(MedICLab), Valencia, Spain Spider phobia could be a great problem for
Research Status: Complete. people who suffer from this kind of phobia
and they have to visit or to stay in places
Environments used up to now for therapeu- where these insects could appear. Exposuretic applications are invariable ones whose therapies and Virtual Reality applicationscontent cannot be changed by the therapist have proved to be effective, but till now Aug-
or by the patient. However, this is a techni- mented Reality (AR) has not been used incal issue that can be solved with current this kind of treatments. We have developed
technology. In this paper, we describe a the first AR system for the treatment ofvirtual environment that has been devel- arachnophobia. Our AR system was devel-
oped taking into account this factor. The oped using ARToolKit software. We have
main technical feature of the environment is modelled three different types of spiders.
that its aspect can be controlled and modi- These spiders move their legs. Both the
fled by the therapist that conducts the clini- model and the basic movements have beencal sessions depending on the emotions modelled using 3DStudio Max. Textures are
that the patient is feeling at each moment. created using Adobe Photoshop 7.0. Objects
The applications of these dynamic changes have been exported to VRML format. GLUIare not limited to the field of clinical psychol- Library has been used to develop theogy. They open a new arena of possibilities Graphic User Interface. To include sounds,for many other kinds of applications includ- OpenAL Library has been used. When the
ing industry, architecture, medicine, etc. patient or the therapist kills a spider using aThe virtual environment that is described in flyswatter, the system plays a squishing
this paper is a step towards a truly adaptive sound like when you kill a real spider. If the
display. patient or the therapist uses an insecticide,the system plays the sound of a spray canlike when you use a real insecticide. The
Contact: user can choose that one or more spidersMariano Alcahiiz, PhD appear/disappear. Spiders can appear/
Medical Image Computing Laboratory disappear in increments of 3 or 20. When(MedICLab) more spiders have to appear, they appearTechnical University of Valencia randomly and half of them are close to theCamino Vera s/n center and they can move towards the out-46022 Valencia (Spain) side of the image. The rest of the spiders aremalcaniztdeggi.u v.es far away as possible from the center and
Ph: +34 963877517 they can move towards the center. Four pa-
Fax: +3496 3879510 tients have been treated with the system.They met DSM-IV criteria for phobia to smallanimals specifically, fear of spiders. Three of
Presenter: Mariano Alcafliz PhD them were females and one male. The expo-sure directives of Ost were followed in order
ARSPIDERS. A NEW SYSTEM FOR to carry out the exposure session. The ses-sions were about one hour. Subjective unitsof discomfort scale (SUDS) (0=no anxiety,
217

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
10=high anxiety) was used to measure the pists. Videoconferencing could be use todegree of anxiety during the AR exposure. increase the accessibility of validated treat-The anxiety level in some moment of the ex- ment (i.e., CBT) to reach patients. It is im-posure sessions arrived to 10 and decreased portant to determine is videoconferencingtill 0. So, the system stimulated anxiety level can be efficient to give a psychological treat-of patients. Before the exposure session, pa- ment. The aim of the study is to compare thetients had to enter to a room where a spider effectiveness of a validated treatment deliv-was inside a box. None of them were able to ered through videoconferencing and face-to-interact with the alive spider. After the AR face.session, patients were able to interact and tokill by themselves real spiders. So, our sys- Method/Toolstem has helped four people to overcome theirspider phobia in one hour of AR exposure For the study, 30 participants (15 = conditionsession. We are going to test our system with face-to-face; 15 = videoconferencing) weremore patients. Patients also answered three SClD-diagnosed in a face-to-face interviews.questions related to the degree of presence All participants were referrals to a mental clinicexperienced in the AR session. All patients in Montreal (remote site 180 km distance fromscored more than 7 (0-10 scale) in all ques- the local site) or in Gatineau (local site). Thetions. These scores reflect the high sense of selection criteria were: 1) principal diagnosispresence and reality judgment that the pa- of panic disorder with agoraphobia; 2) dura-tients experienced. This first system and its tion of illness for more than 6 months; 3) notfirst results demonstrate that AR can be suc- receiving concurrent psychotherapy; 4) nocessfully applied to psychological treatments. comorbid diagnosis invalidating the study. AllWe hope that new AR applications would be participants received 12 individual weekly ses-developed in future to treat other kind of pho- sions of cognitive-behavior therapy. The effi-bias. cacy measures were completed at pre- and
post-treatment and included the Panic andContact: Agoraphobia Scales and the AgoraphobicMariano Alcariz, PhD Cognitions Questionnaire.Medical Image Computing Laboratory(MedICLab) ResultsTechnical University of ValenciaCamino Vera s/n For all the measures, the results demon-46022 Valencia (Spain) strated significant improvement (p<.05) for [email protected] the participants in both conditions (face-to-Ph: +34 963877517 face and videoconferencing).Fax: +3496 3879510
Conclusion
Presenter: Micheline Allard PhD These results of the study show the effective-ness of the cognitive-behavioral therapy de-
EFFECTIVENESS OF CBT DELIVERED livered through face-to-face and via video-THROUGH VIDEOCONFERENCING conferencing. Those results may have an
AND FACE-TO-FACE FOR PANIC DIS- impact on the availability and the distribution
ORDER WITH AGORAPHOBIA of mental health services for panic disorderwith agoraphobia and other anxiety disor-
Micheline Allard, PhD Candidate & Stephane ders.
Bouchard, PhD Contact:
University of Quebec in Outaouais Cyberpsychol- Micheline Allard, Ph.D. Candidateogy Lab [email protected]
Phone: (819) 771-7761 ext.8419Cognitive-behavior therapy is a well validated Fax: (819) 776-8098psychological treatment for anxiety disorders.However, less than 15% of people sufferingfrom an anxiety disorder receive CBT or effec- Presenter: Angelos Amditis PhDtive medication. One possible explanation isthat patients don't have access to CBT thera- THE ISLANDS SYSTEM: A MODULAR
218

CYBERTHERAPY 2005 ABSTRACTS
NON-CONVENTIONAL E-MENTAL tablishing e-mental health and their re-HEALTH SYSTEM TO SUPPORT SER- quirements in relation to the existingVICES TO REMOTE AREAS equipment in the area of telemedicine in
general.Dr. Angelos Amditis 1, Ms. Zoi Lentziou1, Dr. 0 Cost efficiency issues.Euangelos Bekiaris 2, Dr. Maria Fernanda • Liability.Cabrera3, Dr. Alex Bullinger 4 0 Risk analysis
1 Institute of Communication and Computer Sys- The User (i.e. General Practitioner, Patienttems (ICCS) and/or relative) can have access through the2Center for Research and Technology Hellas/ Hel- network (i.e. Internet) to the ISLANDS Multi-lenic Institute of Transport (CERTH/HIT) Access Center. The IMAC has the potentials3 Telecommunication Engineering School, Techni- to allow users to access the remote servicescal University of Madrid (UPM) whatever access terminal or combination of4Center of Applied Technologies in Mental Health termals t eymay os t o ue(COAT) terminals they may choose to use.
IMAC consists of four parts mainly:
This paper is the output of the work performedin all multidisciplinary tasks of the WP, while + the ISLANDS databasefocusing on defining the technical specifica- + the ISLANDS routertions and operative scenarios for the IS- + the ISLANDS tools andLANDS system in order to develop services to * the Knowledge Management Organ-provide modular, non-conventional, remote iserpsychiatric and psychotherapeutic assistancefor remote areas. It is self evident that in most of the cases the
data transmission urgency should be takenThe ISLANDS project basically aims at: into consideration. This means that since the"* Improving the quality of life of the users, service delivery frequency is dependent on"* Enhancing the quality of mental health the type of the content, the format and the
care and the economic strength of the importance of the transmitted medical dataregion were identified and therefore the technology
"* Overweighting the costs of implementa- that should be used was defined to cover thetion and service support. application needs. For instance, screening a
"• Reducing inequalities in mental health patient, which can be considered as a lowservices and status among European re- importance service delivery, can be sup-gions. ported by text. The technology that can be
used in that case is possibly the mail. On theBuilding a complicated system like the IS- other hand, providing guided therapy to theLANDS system was a time consuming and patient, which is a case of high significancecomplicated task, since the combination of and importance, require the transmission ofboth the delivery of three different services video (audio and visual contact with the doc-(i.e. screening, counselling and therapy) to tor). This leads to the conclusion that thethree different target groups (i.e. general prac- technology that could be used to apply thistitioners, patients and their carers) and the situation is Videoconference or Computercompatibility between the standards and the conference.situation that exists in three different Euro-pean areas (Spain, Greece and France) isrequired. This is the reason why a thorough Presenter: Rosa Maria Banos PhDanalysis regarding the specifications and therequirements of the various components and USING "TRADITIONAL" STRATEGIESthe peripheral devices of the overall system IN A "VIRTUAL WORLD" FOR THEhas taken place and an elaborate study for TREATMENT OF PATHOLOGICALthe design of the system architecture has GRIEFbeen carried out.Primarily, the architecture of the ISLANDS Baftos, R. 2, Botella, C. 1, Garcia-Palacios, A.system takes the following parameters into 1, Quero, S. 1, Lasso de la Vega, N. 1account: Guill6n, V. 2 & Osma, J.* The various current technical ways of es-
219

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
1 Universitat Jaume I Castellon. (Spain). Presenter: Rosa Maria Banos PhD2 Universidad de Valencia (Spain).
THE ROLE OF PRESENCE AND RE-During the last decade notable advances in ALITY JUDGMENT IN VIRTUAL ENVI-the psychological treatments field have been RONMENTS IN CLINICAL PSYCHOL-produced. At this moment an important OGYamount of effective treatments or "based onevidence" treatments (Task Force on Promo- Banos, R.M., Quero, S2. Salvador, S1. &tion and Dissemination of Psychological Pro- Banos, C 2cedures, 1995) are available. The cognitive Botella, C2.model has had a notable contribution for this 'Universidad de Valencia (Spain).important advance to be achieved, however, 2Universitat Jaume I. Castellon (Spain).from a therapy perspective, this model is stillfar away from understanding and controlling Presence and Reality Judgment are two im-the human change processes. These insuffi- portant variables to take into account in theciencies come from the theoretical shortcom- Virtual Reality (VR) field. So far, scientificings, that is, there exist discrepancies be- literature has paid attention to the constructtween the lineal logic of many of the cognitive of presence, and several assessment meas-perspectives and the complexity of human ures are available. However, the concept offunctioning. Within these insufficiencies is Reality Judgment has received less attention,worth to point out the scarce attention that and usually, it has been subsumed into thehas been paid to emotions in therapy for a concept of presence. No too much effort haslong time. been dedicated to test whether or not both
constructs refer to the same domain. In aOne of the objectives of the European project previous work, our team developed a 78-itemEMMA (Engaging Media for Mental Health) is self-report questionnaire that assesses bothto examine the possibility of using new tech- constructs: sense of presence and realitynologies (virtual reality) with the aim of treat- judgment (Banos et al., 2000). This was ap-ing emotions from a different perspective than plied to 124 undergraduate students from thethe traditional one. In the EMMA project we University Jaume I of Castell6n (Spain) andhave developed a series of emotional devices the University of Washington (Seattle). Awhich can be customized so they can be full three factor solution was obtained: a realityof meaning and contain the fundamental ele- judgment factor, an interaction/external cor-ments that the person has to cope with. That respondence factor and an attention/is, our objective is to try to show in a physical absorption factor. While the reality judgementway the personal meanings and the emotions items grouped in a single factor, items con-associated to those meanings and to examine cerning presence were watered down amongto which extent this strategy helps the person the three obtained factors. We believe thatin the process of change. The purpose is to the sample employed had influenced re-create a series of "experiences" in therapy markably on the results. The scenariosthat can be used to activate, correct, struc- where the participants were immersed didture, and restructure previous life experiences not stimulate any type of emotion (those par-that can serve as cognitive-emotional struc- ticipants that could have had the slightesttural frames from which a new way of proc- problem in any of the environments wereessing and integrating present, past, and fu- excluded), and this fact prevented any emo-ture experiences can be structured. In this tional involvement or internal correspon-work we present the EMMA environment and dence factors from showing up. The followingthe clinical treatment protocol for pathological task was to apply the questionnaire to clinicalgrief in a case study. samples to elucidate whether the same or
different factors emerged. Preliminary resultsContact: obtained with clinical and subclinical partici-Rosa Maria Banos, PhD pants belonging also to Spanish and NorthUniversidad de Valencia. Spain American samples showed that in VR [email protected] cations for Clinical Psychology emotion wasPhone +34 963864412 playing an important role in the sense ofFax: +34 963864669 presence and the reality attribution of users
(Banos et al., 2001). In this case, the virtualenvironments were able to elicit emotions in
220
CYBERTHERAPY 2005 ABSTRACTS
the participants, so items related to emotions online, Israeli emotional support service forand sensations were the most important. suicidal and highly distressed people whoHowever, an important shortcoming of this had experienced various negative conditions,study was the small size of the sample including those related to rape and sexual(N=112). Therefore, the aim of the present abuse, eating disorders, depression, socialwork is to apply the Presence and Reality anxiety, drinking and drug use, homosexual-Judgement Questionnaire to a larger clinical ity, and domestic violence. Study 1 comparedand subclinical sample. 40 successful conversations (as indicated by
clients at the termination stage of session)References executed through instant messaging and
chat tools with 40 other conversations (notBathos, R.M., Botella, C., Garcia-Palacios, A., indicated as successful by clients), using ex-
Villa, H., Perpifia, C.& Alcahiz. M. (2000). pert judgments, on session-impact dimen-Presence and reality judgment in virtual sions as well as objective word count for tex-environments: A unitary construct?. tual variables. Study 2 examined correlationsCyberPsychology and Behavior, 3 (3), between helpers' evaluation of the sessions'327-335, contribution to clients in 60 (other) support
Bahos, R. M., Botella, C., Garcia Palacios, A., conversations and session impact factorsPerpifia, C., Quero, S. & Gallardo, M. and textual dimensions. The findings of(2001). The Role of Reality Judgment and Study 1 showed that all four impact dimen-Presence in Virtual Environments for sions, as well as expression of negative emo-Clinical Psychology. World Congress of tions, significantly differentiated between suc-Behavioral and Cognitive Therapies. Van- cessful and unsuccessful conversations. Incouver. July 17-21. Study 2, the results showed that all four im-
pact dimensions positively correlated withContact: helpers' evaluations (yielding multiple R=.54),Rosa Maria Banos, PhD as well as the length of helper's and client'sUniversidad de Valencia. Spain writing. The implication of these studies arebanos(@uv.es that similar to offline counselling sessions,Phone +34 963864412 deep, smooth conversations that yield posi-Fax: +34 963864669 tive responses and arouse clients' emotions
in online support are more successful thanshallow, bumbling conversations that leave
Presenter: Azy Barak PhD clients emotionally indifferent. Ventilatingnegative feelings and more expression in
FACTORS RELATED TO SUCCESS OF writing, by both helpers and clients, seem toHELPING HIGHLY DISTRESSED INDI- be important factors, as well.VIDUALS THROUGH EMOTIONALSUPPORT ONLINE CHAT Contact:
Azy Barak, PhDAzy Barak, PhD Department of Education
University of HaifaUniversity of Haifa Haifa, Israel 31905
Phone: +972-4-8249374The purpose of the study was to examine the Fax: +972-4-8240911contribution made by dimensions of session Email: azv_ construct.haifa.ac.ilimpact (experts' evaluation of session proc-ess, that includes factors of depth andsmoothness, and experts' evaluation of post- Presenter: Mihaela loana Baritz PhDsession factors of client's mood, that includespositivity and emotional arousal) and of sev- THE IMPROVEMENT OF THE AUDIO-eral textual variables (positive and negative VIDEO TECHNIQUES AND VIRTUALemotional expressions; helper's and client's ENVIRONMENT USED FOR INVESTI-writing length) to the success of emotional GATION METHODS AND ASSISTEDsupport conversations carried out by trained, PEOPLE WITH DISABILITIESparaprofessional helpers on an Internet chatwith highly distressed individuals. Two studies Mihaela loana Baritz PhDwere conducted at SAHAR, an exclusively
221

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
University of Transylvania Brasov important advance to be achieved, however,from a therapy perspective; this model is still
In this paper we propose an improvement far away from understanding and controllingmethod of audio video techniques and smart the human change processes. These insuffi-environment for optimization and objective ciencies come from the theoretical shortcom-methods of investigation in the bio-systems ings, that is, there exist discrepancies be-and for the disadvantage people assisting. tween the lineal logic of many of the cognitiveTaking in account the necessity for develop- perspectives and the complexity of humanment, the new facilities and services it is pro- functioning. Within these insufficiencies it isposed the accomplish a modulated infrastruc- worth to point out the scarce attention thatture which can generate the optimum systems has been paid to emotions in therapy for afor different investigations of the health prob- long time.lems, the creation of the smart environmentsfor the medical assistance, the generation of One of the objectives of the European projectnew methods-virtual reality- to prevent the EMMA (Engaging Media for Mental Health) isdeficiencies installation to the children and to examine the possibility of using new tech-adults. The most important objectives of the nologies (virtual reality) with the aim of treat-researches are: the implementation of this ing emotions from a different perspectivehealth investigation, assisting and information than the traditional one. In the EMMA projectstructure into public service by e-Health sys- we have developed a series of emotionaltems, the evaluation of the research impact devices which can be customized so theyon the assurance of the compatibilities de- can be full of meaning and contain the funda-mands for Romania integration in European mental elements that the person has to copesystem, and also the using of the methods with. That is, our objective is to try to show inlike virtual reality and biotelemetry, for devel- a physical way the personal meanings andoping of the news way to assist the people. the emotions associated to those meanings
and to examine to which extent this strategyContact: helps the person in the process of change.Mihaela loana Baritz PhD The purpose is to create a series ofUniversity of Transylvania Brasov "experiences" in therapy that can be used toB-ul EROILOR nr. 29, activate, correct, structure, and restructureBrasov, 2200 previous life experiences that can serve asR 0 M A N I A cognitive-emotional structural frames fromP h o n e: 0040. 268.416352 which a new way of processing and integrat-Email: [email protected] ing present, past, and future experiences can
be structured. In this work we present thePresenter: Cristina Botella PhD EMMA environment and the clinical treat-
ment protocol for posttraumatic stress disor-THE TREATMENT OF EMOTIONS IN A der in a case study.VIRTUAL WORLD. APPLICATION IN ACASE OF POSTTRAUMATIC STRESS References
DISORDER American Psychological Association Task
Botella, C., Ph.D.1 , Garcia-Palacios, A. Ph.D., force on Psychological Intervention Guide-1, Banos, R., Ph.D., 2, Guillen, V.1, Quero,S lines (1995). Template for developing guide-Ph.D. 1, Lasso de Ia Vega, N. 1 & Osma, S ., lines: Interventions for mental disorders and
psychological aspects of physical disorders.
1 Universitat Jaume I Castellon. (Spain). Washington, D. C.: American Psychological2 Universidad de Valencia (Spain). Association.
During the last decade notable advances in Contact:the psychological treatments field have been Botella, C., Ph. D.produced. At this moment an important Universitat Jaume 1. Castellon. Spainamount of effective treatments or "based on botellaapsb.uii.esevidence" treatments (Task Force on Promo- Phone: +34 964728881tion and Dissemination of Psychological Pro- Fax: +34 964729267cedures, 1995) are available. The cognitivemodel has had a notable contribution for this
222

CYBERTHERAPY 2005 ABSTRACTS
Presenter: Cristina Botella PhDPresenter: Stephane Bouchard PhD
MIXING REALITIES? AN AUGMENTEDREALITY SYSTEM FOR THE TREAT- RELIABILITY AND VALIDITY OF AMENT OF SPIDERS AND COCK- SINGLE-ITEM MEASURE OF PRES-ROACHES PHOBIA ENCE IN VR
Botella, C. 1, Bafos, R. 2 Guerrero, B. 1, Juan, Stephane Bouchard, Genevieve Robillard,M. C. & Alcafiz, M., Ph. D. 3 Julie St-Jacques, Stephanie Dumoulin, Marie-
Josee Patry & Patrice Renaud' Universitat Jaume I Castellon. (Spain).2 Universidad de Valencia (Spain). Universit6 du Quebec en Outaouais3 Medical Image Computing Laboratory(MediCLab). Technical University of Valencia Research Status: Completed.(Spain)
Measuring the subjective feeling of presence inAugmentel Realementsinty e ( r) a c onsiss of in c virtual environments usually relies on question-ing virtual elements in the real world. That is, naires. These instruments are long and, whilethe person is seeing an image conformed by many items are useful to tap the diverse subtletiesa visualization of the real world and by a se- and dimensions of a construct, it poses a signifi-ries of virtual elements that are over-imposed cant challenge if a researcher wants to measurein the real world. The main aspect of AR is presence during a VR immersion. This presenta-that virtual elements provide relevant and tion will document the validation process of a
useful information to the person that does not single-item measure of presence. The question
exist in the real world. AR has a high potential (<To which extend do you feel present in the vir-
and has been already used in several fields: tual environment, as if you wee re inally there» was
medicine, army, training, engineering, design, subjected to: a content and face validity study,
robotic, etc. Up to now AR has not been used st-retest reliabil ity studi oin te pychlogial reament ara. ow- two test-retest reliability studies, a convergentin the psychological treatments area. How- and divergent validity study, and two sensitivity
ever, AR presents several advantages. Like in stddies.
the classic virtual reality systems, it is possi- studies.
ble to have a total control over the virtual ele- Content and face validityments over-imposed in the real world and howto interact with them. But, AR has and addi- The goal of the first study was to ascertaintional advantage: it facilitates the person's that the single-item presence is well under-sense of presence (the sense of being there) stood by the general population. A commu-and reality judgment (to judge the experience nity sample of 49 adults (mostly low to mod-as real). This is possible because the environ- erate socio-economic status and not highlyment where the person is placed and what the educated) were immersed for 7 minutes in aperson is seeing are, in fact, "the reality". In virtual environment in a shopping mall. Afterthis work the data of a series of case studies the immersion, participants rated on a scalein which AR has been used for the treatment from 0 to 10 how well they understood theof specific phobia (spiders and cockroaches meaning of the item, as well as the meaningphobia) are presented. Results are very prom- of control items (including items from otherising. The patients showed a high degree of popular presence measure). The resultsfear and avoidance in the behavioural avoid- showed that the question was very well un-ance test at pre-test and, these scores not derstood. The clarity if the question was asonly decreased after treatment, but the pa- good as controlled items drawn from a psy-tients were able to approach, interact and kill chological test validated for adults with thealive insects. reading ability of a grade-five population. The
clarity was statistically better than the controlContact: items that were designed to be difficult toBotella, C., Ph. D. understand (e.g., items with double-Universitat Jaume I. Castellon. Spain negatives).botella(psb.uii.esPhone: +34 964728881 Test-retestFax: +34 964729267
A sample of 31 university students completed
223

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
the presence question on two occasions dur-ing a 7 minutes VR immersion, and another Eileen Brosnan, Research Fellow1, Dr. Johnsample of 26 adults completed the presence Sharry2, Richard Boyle 1, Prof Carol Fitz-question after two different VR immersions. patrick3
The test-retest coefficients were very high(.21 and .83, respectively). 1Media Lab Europe2Mater Hospital, DublinConvergent and divergent validity 3University College Dublin
The single-item measure of presence corre- Backgroundlates significantly with the Presence Question-naire, and much less with Perceived Realism In child and adolescent therapy, multimediaand the Immersive Tendencies Questionnaire. is most commonly used where the child and
therapist use professionally made CD-ROM'sSensitivity of interactive stories, computer games, or
internet resources to access information andTwo studies were devised to assess the sen- facilitate communication. This involves listen-sitivity of the item to experimental manipula- ing, watching, and reading. The interactivetions. In the first study, 33 participants were elements allow users a degree of controlimmersed twice in the same virtual under a over the narrative and direction of a story.condition that maximise presence and under a This is mainly passive. "Transforming Sto-condition that hinder presence. In a second ries" takes it a step further by using multime-study, 29 snake phobics were subjected to dia in therapy in a constructive way, allowingpsychological manipulations where anxiety the child to build their own story. In his re-was induced or not by leading them to believe search in the field of education Papert (1996)that the virtual environment could contain highlighted the importance of children makingdangerous hidden snakes. In both studies, the their own artifacts, something that is a realrepeated measures ANOVA confirmed the reaction to their world. This premise can alsosensitivity of our measure. be applied to the therapeutic process.
Conclusion and novelty MethodlTools
Item-response theory would recommend to be Transforming Stories is a database drivencareful in using only one item to measure a multimedia storytelling tool delivered bothconstruct, while practical factors such as dis- online and on stand alone platform. The soft-traction would militates in favour of using the ware currently being developed will allow theleast intrusive measure as possible. The vali- users to choose a story template and builddation process confirmed that a single-item up the story plot using customisable charac-measure of the subjective feeling of presence ters and background scenes, adding in theiris well understood, reliable and valid. These own voiceover and animation. The authoringresults will be very useful for any researcher timeline is presented in an immediate wayinterested in measuring presence while users using a drag and drop facility for placing storyare immersed in a virtual environment. The objects and further features such as position-presentation of the results of each study ing tools, playback and story editing. There isshould also be of interest to the audience. also a text tool allowing them to integrate
their own captions. Other options includeContact: building from seed stories where they canSt~phane Bouchard change the plotline and add in their ownUniversit6 du Quebec en Outaouais characters and dialogue. Finally they canSte•_haneboLuchard(uaoca upload and share their stories to an online
community.
Presenter: Eileen Brosnan In the method, the therapist introduces theidea of making a story and shows examples
TRANSFORMING STORIES: A MULTI- of what is possible using the software. It can
MEDIA TOOL FOR THERAPEUTIC be a story tailored to a problem that needsresolution or a general story that brings aboutST AORY ULDING ITH Csome positive change in the storyline. A keyAND ADOLESCENTS
224
CYBERTHERAPY 2005 ABSTRACTS
therapeutic feature is a notebook facility Mater Hospitalwhere the child and therapist keep a log of Dublin 7, Irelandtheir thoughts on the process and their analy- Tel: 00353 1 803 4793sis of the story. This allows for reflection and Email: eileen.brosnanftcd.iegives the therapist the opportunity to promptnew ideas for problem solving.
Presenter: Eileen BrosnanEvaluation
'WORKING THINGS OUT' A THERA-The current research focuses on evaluating PEUTIC INTERACTIVE CD-ROM CON-the therapeutic use of multimedia authoring TAINING THE STORIES OF YOUNGtools now being widely used in the classroom PEOPLE DEALING WITH DEPRES-setting. This research is based on case study SION AND OTHER MENTAL HEALTHexamination of the benefits of using these PROBLEMStools in engaging adolescents and progress-ing the therapeutic relationship in a small Dr. John Sharry', Eileen Brosnan, Researchsample of adolescents attending the Mater Fellow2, Prof Carol Fitzpatrick 3
Child and Adolescent Psychiatry Service,Dublin, Ireland. 2Media Lab Europe
1Mater Hospital, DublinThe second stage of the research will involve 3University College Dublithe initial testing of "Transforming Stories"across a range of client groups and profes- Acknowledgementssional disciplines including Psychotherapy,Social Work, Psychology, and Psychiatry. In developing this project we would like toThis testing will involve a qualitative study. acknowledge the work of Bernie McCarthy,
Ciara Devine, Pilar Valencia, Hugh O'Neill,Novelty/Discussion Peter McCormack and John Stapleton from
the production team."Transforming Stories" is an innovative new
approach to eliciting stories in child and ado- It is widely accepted that children and younglescent therapy. Over time the online forum people enjoy using computers. Seymour Pa-will provide an expanding database of story pert (1996) suggests that 'it is timely forbuilding material to be drawn from. The school counsellors and child therapists toplanned integration of drawing tools and other bridge the digital generation gap and inno-authoring features will give increase the crea- vate with computers in their work with chil-tive dimension and allow the users to create dren of the digital age.' Working Things Outuniquely designed work. (WTO) was developed in response to the
growing need for computer-based resourcesReferences for adolescents in therapy. It is an interactive
CD ROM/DVD developed as a means of en-Schafer, C. (1999). "Innovative Psychother- gaging adolescents about mental health is-apy Techniques in Child and adolescent Ther- sues by giving them information in the formapy." USA: Wiley & Son. of animated personal stories told by otherPapert, S. (1996) "The Connected Family: young people dealing with problems such asBridging the Digital Generation Gap", Atlanta, depression, bullying, eating problems, andUSA: Longstreet Press. self-harm. The CD-ROM/DVD is accompa-Goss, S., Anthony, K. (2003) "Technology in nied by a manual for professionals on how toCounselling and Psychotherapy: A Practitio- use the resource.ner's Guide" New York: Palgrave Macmillan.Hsiung, R.C. (2002) "e-Therapy: Case Stud- With the help of therapists, and in collabora-ies, Guiding Principles, and the Clinical Po- tion with graphic designers, animators, andtential of the Internet", New York: W.W. Nor- multimedia professionals, the 11 young peo-ton & Company. pIe who participated in the project told their
stories, narrated in their own voice, and illus-Contact: trated by graphics and animation. 'WorkingEileen Brosnan Things Out' is currently being used as anDepartment of Child and Family Psychiatry educational and therapeutic tool with other
225
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
adolescents at risk of mental health problems, desktop 3-D displays will begin in earnestboth as a way of engaging young people to opening up a vast number of potential appli-reflect about mental health issues and as a cations not only for scientist, engineers andmeans of inviting them to tell their own story. IT specialists but literally for everybody.The paper describes the background and de-velopment of the 'Working Things Out' project, Contact:including samples from the stories and a de- Alex H. Bullingerscription of how the CD-ROM/DVD can be COAT-Basel / UPKused in psychotherapy. Wilhelm Klein - Str- 27
4025 Basel, SwitzerlandReferences bua(&coat-basel.com
1. Offer, D., Howard, K.I., Schonert, K.A.,Ostrov, E., To whom do adolescents turn for Presenter: Alex H. Bullinger MD MBAhelp? Differences between disturbed and non-disturbed adolescents. J. AM. Acad Child TREATING ACROPHOBIA IN A VIR-Adolescence Psychiatry, 30:623-630, (1991). TUAL ENVIRONMENT2. US Department of Health and HumanServices, Mental Health: A Report of the Sur- Alex H. Bullinger1 , Isabelle Angenendt1 ,geon General, Rockville, MD: US Department Brenda K. Wederhold 2, Franz Mueller-of Health and Human Services, (1999) Spahn1 , Ralph Mager1
Sharry, J., Counselling Children, Adolescentsand Families. Sage, London, (2004). 'COAT-Basel I UPK (Center of Applied Technolo-gies in Neuroscience), University of Basel, Swit-zerlandContact: 2 IMI and VRMC, San Diego, USA
Dr John SharryDept of child and family psychiatry Specific phobias are one of the most frequentMater Hospital mental health problems and can lead toDublin 7 Ireland years of personal suffering. The most effec-Tel: +353 1 803 4793 tive treatment is exposure therapy. Our aimEmai: [email protected] was to proof the feasibility and efficacy of
virtual environments in treating acrophobiapatients using a manually guided exposure
Presenter: Alex H. Bullinger MD MBA therapy. Our pilot study was designed as acrossover intervention with a waiting list con-
NEXT GENERATION IMMERSIVE VISU- dition as a control group. After treatment, ourALIZATION SYSTEMS results show that exposure in virtual environ-
ments is a feasible technique can provokeAlex H. Bullinger1 anxiety, and leads to a therapeutic effect.
1 COAT-Basel / UPK (Center of Applied Technolo- Contact:gies in Neuroscience), University of Basel, Switzer- Alex H. Bullingerland COAT-Basel / UPK
Wilhelm Klein - Str- 27This paper deals with the ongoing develop- 4025 Basel, Switzerlandments towards immersive 3-D displays that bua5coat-basel.comrequire no special eyewear like shutterglasses anymore. Once these devices willhave penetrated the market to a larger scale Presenter: Maria Fernanda Cabrera PhDthey could easily mark the end to the era ofhuge rear projection - based installations E-MENT@L HE@LTH. THE ISLANDSsuch as Powerwalls or CAVE - systems. At PROJECT AS A CHALLENGE FORpresent only a handful of these 3-D display THE FUTUREdevices are on the market, most of them stillpromising more than what they are able tofulfill in the end. But technology development Maria Fernanda Cabrera PhDin this sector is moving with utmost velocity Universidad Politecnica de Madridand ferocity. By the end of 2005 marketing of
226

CYBERTHERAPY 2005 ABSTRACTS
and the Spanish western Canary Islands.It has been already accepted that the im-provement in medical care cannot be made Over the past 24 months, the ISLANDS con-merely by adding professionals to healthcare sortium has focused in the development andsystems, but in addition require restructuring deployment of feasible tools for diagnostic,the patterns of health-care delivery. The incor- counseling, and therapy purposes. Accordingporation into medical practice of relevant tech- to the preliminary results of a questionnairenological innovations is an essential part of survey, users' acceptance of and satisfactionthis reorganisation. This innovation is produc- with the technology were high. Ninety per-ing a promising field - e-mental health - whose cent of the patients considered that they re-focus is the use of communication and infor- ceived the follow-up care they required.mation technologies to improve the mentalhealth care processes. This area has devel- We can conclude that the development of aoped rapidly, accumulating knowledge and knowledge-based expert tool to guide theproposing innovative affirmations. This is a relevant services application aims to avertmultidisciplinary field that requires the coop- erroneous application of such services, byeration among different professionals. The inexperienced medical personnel or the us-results of this collaboration are represented ers themselves and their relatives.by the ISLANDS project, an attempt to de-velop and comprehend the potential of e- The project will, it is hoped, provide leader-mental health, which specific goal was to de- ship, enhance information about mentalvelop services to provide modular, non- health problems, and undertake research inconventional, remote psychiatric and psycho- cost-effective policies to improve the mentaltherapeutic assistance for remote areas. disorders addressed.The project started with a literature review ofthe state of the art on remote therapeutic psy- Contact:chiatric and psychotherapeutic interventions, Maria Fernanda Cabrera PhDcomplemented by field work with the realiza- Universidad Politecnica de Madridtion of questionnaires to patients, families and Madrid 28040doctors, and an international workshop, to Spainresult in appropriate service delivery scenar- Phone: +34915495700 ext. 332ios. Fax: +34913366828
Email: [email protected] scenarios specified, the different usergroup needs and the epidemiological findingsled to the definition of different remote service Presenter: Maria Fernanda Cabrera PhDcategories (diagnosis, counseling, and ther-apy) for patients, informal careers, and pro- OPEN MOBILE PLATFORM FORfessionals, as well as an overall service lay- EMERGENCY HEALTHCARE APPLI-out. These services are supported by interac- CATIONStive and user-friendly tools for service contentpresentation, namely: an interactive web chat Maria Fernanda Cabrera PhDtool, a database of reference case studies, anexpert tool for therapy guidance, a tool for Universidad Politecnica de Madridservice confidentiality, and the necessarycommunication tools and service delivery plat- In the new society, mobility has become aforms. All the above developments are inte- necessity and a competitive advantage, bothgrated into modular service typologies, taking for citizens and the human capital of compa-into account relevant security, legal and ethi- nies. Its next step is clearly to become acal issues. Four typical case studies of psy- complete product. In order to become a com-chological problems have been selected that modity for European society, mobile solutionscan be found quite often in normal popula- must provide five main characteristics: ubiq-tions and are of specific interest: post- uity, transparency, fundamentality, universal-traumatic stress disorder, depression, prob- ity, and value governance. As the new 3Glems of alcohol abuse, and psychotic disor- technology is "around the corner," suitableders. The proposed services are being tested platforms that make possible an interestingin three pilot sites: the French Overseas De- business model to access Pan-Europeanpartments, the Greek Southern Sporades, mobile services is a "must" that hasn't been
227
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
resolved, yet. Facing this reality, the Euro- fact that all user groups were in all cases andpean Union funded XMOB, an IST project that in both pilot sites positively oriented towardsjoined research groups, phone operators, the developed system. Nevertheless, itconsultancy companies, industry, and emer- should be remarked that all EMS do not needgency medical services (EMS) to build a plat- the same functionalities in their pre-hospitalform aimed to host mobile applications. The emergency management due to specificity ofbenefits and outputs of the platform were vali- environments (rural/urban, medical/dated through the development of a vertical paramedic) so that the main achievement ofapplication for the health emergency manage- this platform is to provide a widely open inte-ment. grated solution. This will enable any citizen to
benefit from the same quality of care, any-The mobile emergency services developed where, in pre-hospital emergencies domain.focused on the following main challenges:- Necessity to cover a broad set of de- The benefits of a seamless infrastructure arevices and channels the foundational components of this platform- Need to integrate a complex range of that improve the efficiency and efficacy of theinvolved actors (e.g., insurance call centers, EMS. This translates into lives saved andpublic emergency assistance, patients' histori- morbidity reduced.cal medical records repositories, hospitals,etc.) Contact:- Provision of complete, customized, and Maria Fernanda Cabrera PhDtimely assistance in emergency situations Universidad Politecnica de Madridbased on instant and secure mobile access to Madrid 28040standardized patients medical records Spain- Existence of emergency situations that Phone: +34915495700 ext. 332require the coordination between different Fax: +34913366828countries to provide an accurate attention to Email: [email protected] patient
The methodological approach consisted of Presenter: Yang Cai PhDtwo steps: to build a reusable horizontal plat-form and then, following an ASP model, todevelop vertical mobile applications for health GEDANKEN EXPERIMENT OF HUMANemergency management. These applications DYNAMICSwere made of several tools that help theemergency staff and the other actors involved Yang Caiin accessing critical data of patients. Carnegie Mellon University
The platform was validated in real life situa-tions and cost-effectiveness and patients' Understanding human dynamics is an impor-benefits analysis were conducted. The trials tant step in clinical therapies, such as bloodwere carried out in Madrid and Genoa cities glucose management or weight control. Itand lasted two months. requires insight into the complex interactionsbetween the components of biomedical sys-
The opinion of the users consisted of a self- tems. This is challenging because of the
evaluation with a questionnaire distributed to enormous amount of data and knowledge in
different staff categories. The questionnaires this domain. Gedanken Experiment is an in-
contained closed-ended questions and re- tuitive, qualitative thinking process, which
spondents were provided space to add written have been used by physicists for decades.
comments. The results were evaluated in Our goal is to enable an interactive game-like
scores on two scales, the "Usefulness" scale environment for users with any background,
denoting potential use of the system, and the while remaining sufficiently flexible to target
"Satisfying" scale reflecting pleasantness. The medical problems at a level of abstraction,patient's privacy and respect issues were cov- from the conformational changes of a protein
ered. to the interaction ofthe various biochemical pathways in our
The most important conclusion, which can be body. Here, we present an interactive and
derived from the pilots' comparisons, is the visual problem-solving environment for the
228
CYBERTHERAPY 2005 ABSTRACTS
biomedical domain. We designed a biological ent limitations related to costs of typical be-world model, in which users can explore bio- havioral procedures or difficulty with cognitivelogical interactions by role-playing techniques. Virtual Reality has already"characters" such as cells and molecules or shown its possible utility in enhancing theas an observer in a "shielded vessel," both CBT for different mental problems. Rationalewith the option of networked collaboration be- and protocols about the use of Virtual Real-tween simultaneous users. The system archi- ity-enhanced treatments, named Integratedtecture of these "characters" contains four Experiential Therapy (lET), will be explained.main components: (1) Bio-behavior is mod- The major aim of this presentation is the de-eled using cellular automata. (2) Bio-morphing scription of a new paradigm of virtual envi-uses vision-based shape tracking techniques ronments (VEs): new possibilities for differentto learn from recordings of real biological dy- clinical protocols will be discussed. The realnamics. (3) Bio-sensing is based on molecular novelty of this new generation of VEs is theprinciples of recognition to identify objects, high level of flexibility and plasticity allowingenvironmental conditions, and progression in therapists to save different versions accord-a process. (4) Bio-dynamics implements ing to the specific users' needs and features.mathematical models of cell growth and fluid- Moreover it is possible to carry on systemic,dynamic properties of biological solutions, dynamic or cognitive-behavioural approachesThe principles are implemented in a simple using different aspects and nuances of VEs.world model of the human vascular systemand a biomedical problem that involves an This research is part of the Prof. Giuseppeinfection by Neisseria meningitides where the Riva's NEUROTIV project - Immersive virtualbiological characters are white and red blood telepresence managed care for the assess-cells and Neisseria cells. Our case studies ment and rehabilitation in neuro-psychologyshow that the system can be used for public and clinical psychology.health education, biomedical simulation andcreative problem solving. Contact:
Gianluca Castelnuovo, Ph. D.Contact: Applied Technology for Neuro-PsychologyYang Cai LabCarnegie Mellon University P.O. BOX 18211Email: ycaipcmu.edu 28921 Verbania, Italy
Tel. +39/0323/514278-.339Fax. +39/0323/514338
Presenter: Gianluca Castelnuovo PhD Email: [email protected]
A NEW GENERATION OF VIRTUAL EN-VIRONMENTS FOR THE TREATMENT Presenter: Gian Luca Cesa MSAND REHABILITATION OF EATINGDISORDERS INTEGRATED EXPERIENTIAL THER-
APY FOR THE TREATMENT OF OBE-Gianluca Castelnuovo, Ph.D.1-2-4, Gianluca SITY AND BINGE EATING DISORDER:Cesa, M.S.-4, Andrea Gaggioli, M.S.1-3 , A CLINICAL TRIALDaniela Villani, Ph.D. 1 Enrico Molinari,Psy.D. 2-4, Giuseppe Rliva, Ph.D.1 2 Gian Luca Cesa, M.S.1 , Gianluca Castel-
nuovo,1 Applied Technology for Neuro-Psychology Ph.D.1 , Andrea Gaggioli, Ph.D.1 , DanielaLab, Istituto Auxologico Italiano Villani, M.S', Giuseppe Riva, Ph.D.2 Department of Psychology, Catholic University,Milan, Italy 1 Applied Technology for Neuro-Psychology Lab.3Laboratory of Psychology, Department of Preclini- Istituto Auxologico Italiano, Verbania, Italycal Sciences LITA Vialba, University of Milan, Mi- 2 Department of Psychology, Universita Cattolicalan, Italy4 Clinical Psychology Lab, Istituto Auxologico Itali- del Sacro Cuore, Milan, Italy
ano, Verbania, Italy The main goal of this work is the description
The cognitive behavioral therapy (CBT) is still of a new Virtual Reality-enhanced treatment
considered the best approach in the treatment named Integrated Experiential Therapy (lET)
of eating disorders, but it could present differ- for the treatment of Obesity and Binge Eating
229

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Disorder. lET for eating disorders and obesity ness, body satisfaction, eating control, socialis a relatively short-term, integrated, patient skills, self-esteem, and motivation to change.oriented approach that focuses on individual In particular, pre-treatment/post-treatmentdiscovery. Integrated Experiential Therapy is comparison seems to indicate that Integratedan integrated approach ranging from cogni- Experiential Therapy is more effective thantive-behavioural therapy to virtual reality ses- traditional approaches in the treatment ofsions for the treatment of eating disorders and Obesity and Binge Eating Disorder. Com-obesity. In this approach VR is mainly used to plete results will be presented in the confer-modify body image perceptions. The use of ence.VR offers two key advantages. On one side, itis possible to integrate all different methods This research is part of the Prof. Giuseppe(cognitive, behavioural, and experiential) com- Riva's NEUROTIV project - Immersive virtualmonly used in the treatment of body experi- telepresence managed care for the assess-ence disturbances within a single virtual ex- ment and rehabilitation in neuro-psychologyperience. On the other side, VR can be used and clinical psychology.to induce in the patient a controlled sensoryrearrangement that unconsciously modifies Contact:his/her bodily awareness (body schema).The Gian Luca Cesa M.S.treatment is a 4-6-week inpatient treatment Applied Technology for Neuro-Psychologyand it is administered by therapists having a Labcognitive-behavioural orientation who work in P.O. BOX 18211conjunction with a psychiatrist as far as the 28921 Verbania, Italypharmacological component is concerned. Tel. +39/0323/514278-.339The individual work regards assessment by Fax. +39/0323/514338means of psychometric tests, weekly suppor- Email: aluca.cesa@_auxglogicoittive psychological talks, 7 sessions for as-sessment, and therapy carried out using Vir-tual Reality (VR), and psycho- Presenter: Sophie C6t0, Ph.D. candidatepharmacological assessment and control. Thepsychological group therapy is based on COGNITIVE MECHANISMS UNDERLY-weekly group meetings (closed group of 5/6 ING VIRTUAL REALITY EXPOSURE'Spersons) of two hours each. The work group EFFICACY IN THE TREATMENT OFaims both at training for development and ac- ARACHNOPHOBIAquisition of assertive skills, and at training forassessment and consolidation of motivation. S PMoreover, the subjects participate to both bi- Sophie C2te 1, Ph.D. candidate & Stephaneweekly psycho-nutritional groups held by nu- Bouchard' , Ph.D.
tritionists and to daily group sessions of physi- 1 Ottawa University, Ottawa, Ontario, Canadacal activity. In order to verify the efficacy of 2 University of Quebec in Outaouais, Gatineau,lET we are realizing a clinical trial with a sam- Quebec, Canadapie of obese patients (with and without BingeEating Disorder). Subjects were randomly Research status: Completed.assigned to the experimental group and to thethree control groups. Subjects were assessed Virtual exposure therapy for phobias is aby one of three independent assessment clini- growing field of interest. Studies have beguncians who were not involved in the direct clini- to demonstrate its efficacy, which is at leastcal care of any subject. All subjects were as- equivalent to in vivo exposure. However,sessed at pre-treatment and upon completion though a majority of studies have addressedof the clinical trial. Patients were administered efficacy itself, few have attempted to under-a battery of outcome measures assessing stand the treatment mechanisms underlyingeating disorders symptoms, attitudes toward this efficacy. In the case of traditional ther-food, body dissatisfaction, level of anxiety, apy, two models are still the object of amotivation for change, level of assertiveness strong debate: the information processingand general psychiatric symptoms. model and the perceived self-efficacy model.
Interestingly, this debate is still fuelled byIn summary, the preliminary results show that their authors' attempts to prove the predictivethe virtual simulation of demanding real life superiority of their model by using predictedsituations is useful to improve patient's aware- variables that are in fact different. Actually,
230
CYBERTHERAPY 2005 ABSTRACTS
no study has yet directly compared the most arachnophobia. It also brings elements of alikely predictors of change, for virtual expo- better understanding of the distinct contribu-sure. tion of each predictive variable in the psycho-
pathological models for phobias. Interest-The goal of this study was to contrast the pre- ingly, this information can be applied to bothdictive value of different treatment mecha- in vivo and virtual reality exposure. Likewise,nisms for specific phobias. The hypotheses both clinicians and researchers can benefitare the following. Changes in information from that knowledge, in order to betterprocessing (measured with a pictorial Stroop choose the exposure treatment targets ortask) will better predict changes in anxiety procedures, according to the type of changesduring a behavioral avoidance test, while they want to observe in clients.changes in perceived self-efficacy will betterpredict changes in avoidance behaviors dur- Referencesing a behavioral avoidance test.
Constantine, R., McNally, R.J., & Hornig,Twenty-eight adult arachnophobics were as- C.D. (2001). Snake fear and the pictorialsessed for standardized inclusion and exclu- emotional Stroop paradigm. Cognitive Ther-sion criteria. General outcome and specific apy and Research, 25(6), 757-764.processes measures included questionnaires Foa, E.B. & McNally, R.J. (1986). Mecha-and a pictorial Stroop task. The main out- nisms of change in exposure therapy, danscome and predicted variables were based on R. M. Rapee (Eds), Current controversies ina behavioral avoidance test (BAT). Avoidance the anxiety disorders, (pp. 329-343). Newbehavior was measured by participants' ca- York: Guilford Press.pacity to approach a live tarantula during the Riva, G., Wiederhold, B.K., & Molinari,BAT and anxiety was measured by recording (1998). Virtual environments in clinical psy-their heart rate during the first minute of the chology and neuroscience: Methods andtask. All measures were completed before techniques in advanced patient-therapist in-treatment (session 1) and at post-treatment teraction. Washington: lOS Press.(session 7). After explanations about the cog- Williams, S.L. (1996). Therapeutic changesnitive-behavioral rationale for phobias and an in phobic behavior are mediated by changesinitiation to the virtual reality equipment in perceived self-efficacy. In R. M. Rapee(session 2), participants went through virtual (Eds), Current controversies in the anxietyexposure for five sessions (60 minutes each) disorders, (pp. 344-368). New York: Guilfordin various virtual environments with spiders. Press.
Repeated measures ANOVAs on outcome Contact:measures revealed that therapy had a posi- Sophie C6tetive impact. Analyses made on the pictorial Ottawa University, OttawaStroop task showed that information process- Ontario, Canadaing of spider-related stimuli is faster after Phone: (819)_76-8045treatment, which also indicates therapeutic Fax: (819) 776-8098success. Psychophysiological data also Email : scote067@(uottawa.cashowed a positive change after treatment,suggesting a decrease in anxiety. In them-selves, these results represent new contribu- Presenter: David Coyle MSctions to the field. Hierarchic regressions wereabout to be made as this abstract was submit- ADAPTABLE COMPUTER GAMINGted; results will be available in the presenta- FOR ADOLESCENT PSYCHOTHER-tion. These regressions will be used to assess APYthe respective predictive capacities of eachkey variable for therapeutic change. David Coyle, MSc1, Dr John Sharry2, Dr
Gavin Doherty 1
This innovative study brings fascinating infor-
mation about the various and deep impacts of 1 Trinity College Dublin, IrelandVRE at physiological, information processing 2 Mater Hospital, Dublin Irelandand cognitive levels. Therefore, VRE doesprovoke significant clinical and statistical Research Status: The Virtually Healthy Pro-therapeutic change for people suffering from ject is exploring the use of computer gaming
231

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
on adolescent mental health care. Details are playing PI in sessions is very helpful in en-given of preliminary clinical trials of a custom gaging adolescents. It can increase thedeveloped game and of ongoing research amount of dialogue between therapists anddirections. adolescents and help in setting therapeutic
goals. The use of 3D had an empoweringReports show that, although mental health effect, allowing the adolescent more controlproblems increase during adolescence, the over the pacing and direction of the thera-majority of disturbed adolescents do not re- peutic process. For full details of the theoreti-ceive professional mental health care and of cal foundations, design, and pilot study of PIthose who do fewer still fully engage with the see Coyle et al. 2005.therapeutic process (Offer et al. 1991; USSurgeon General 1999). Adolescents are gen- PI implemented a therapeutic model in anerally more private and self-conscious than open manner, not tailored to address specificeither younger children or adults. Typically mental health issues or specific adolescenttherapy is imposed upon them (usually by cases. One ongoing aim of the Virtuallytheir parents) and because of this they are Healthy project is to create a toolkit that al-less willing to accept it. Play therapists often lows non-programming, professional thera-engage younger children using materials such pists to adapt and create issue specific com-as puppets, storybooks, and construction ma- puter games. The system should be usableterials. Adolescents can be resistant to these by therapists with wide-ranging levels ofmethods, not liking to be treated as children. computer literacy and be adaptable on manyEqually, many react confrontationally or not at levels, from small fine-tuning of existingall to direct dialogue (Sharry 2004). However games to the creation of new games.adolescents often show a great interest incomputer games. A recent UK survey re- Referencesported that 53% of eleven to fourteen yearolds play games four times a week or more Clark, B. and Schoech, D. (1984) 'A Com-(McFarlane et al. 2002). Computer games puter-assisted Therapeutic Game for Ado-currently constitute a client-centred approach lescents: Initial development and com-to adolescent psychotherapy. ments.' In Schwartz, M. D., Using com-
puters in clinical practice: PsychotherapyPersonal Investigator (PI) is a 3D computer and mental health applications. Newgame specifically designed to help adoles- York:, Haworth Press: pp. 335-353.cents with mental health problems. It incorpo- Coyle, D., Matthews, M., Sharry, J., Nisbet,rates a goal-oriented, strengths based model A. and Doherty, G. (2005)'Personal In-of psychotherapy called Solution Focused vestigator: A Therapeutic 3D Game forTherapy (SFT). Adolescents play the role of a Adolescent Psychotherapy'. Internationalpersonal investigator hunting for the clues that Journal of Interactive Technology andwill help them solve personal problems. By Smart Education In press.engaging adolescents, in a client-centred McFarlane, A., Sparrowhawk, A. and Heald,way, it aims to build stronger therapeutic rela- Y. (2002). Report on Educational Use oftionships between therapists and adolescents. Games. Teachers Evaluating EducationalP1 is the first game to integrate this estal- Multimedia Report., TEEM.ished psychotherapy approach into an engag- Offer, D., Howard, K. I., Schonert, K. A. anding 3D game. PI differs from previous thera- Ostrov, E. (1991) 'To whom do adoles-peutic games by encouraging the adolescent cents turn for help? Differences betweento create a written record of their own discov- disturbed and nondisturbed adolescents'.eries. The player creates a virtual detective Journal of the American Academy of Childnotebook in which they write down all their and Adolescent Psychiatry 30(4): 623-goals, objectives, ideas, and thoughts. Upon 630.completing the game, they receive a printout Sharry, J. (2004) 'Counselling Children, Ado-of their notebook. Clark et al. 1984 reported lescents and Families'. London, Sage.benefits of having a tangible output from a US Surgeon General (1999). Mental Health:game. A pilot study of the game has been A Report of the Surgeon General. Wash-conducted with four adolescents, referred to ington, DC, US Department of Health andclinics for issues including anxiety and behav- Human Services.iour problems, attempted suicide, and socialskills difficulties. Initial results indicate that Contact:
232
CYBERTHERAPY 2005 ABSTRACTS
David Coyle control group points in the recognition of sad-Trinity College Dublin, Ireland ness at 100% of expression and in the recog-Tel: 353-86-8269863 nition of happiness at 60% of expression. InEmail: david~coylej•gmailcom each case depressed patients reached
higher rates.
Presenter: Gabor Csukly MD Contact:Gabor Csukly MD
FACIAL EXPRESSION RECOGNITION Semmelweis UniversityIN PSYCHIATRIC DISORDERS USING Psychiatric and Psychoterapic DepartementANIMATED 3D EMOTIONAL FACIAL Budapest, HungaryEXPRESSIONS Tel: 36302886737
Email: csugabnyahoo.com
Lajos Simon PhD1, G~bor Csukly MD1,Barnabas Takacs PhD2 Presenter: Carlos de las Cuevas MD PhD
Semmelweis University, Psychiatric andPsychoterapic Departement TELEPSYCHIATRY: PSYCH IATRIC2 DigitalElite Inc. CONSULTATION THROUGH VIDEO-
CONFERENCE CLINICAL RESULTSResearch Status: Completed.
Carlos de las Cuevas MD PhDThe first purpose of our investigation is to cre-
ate a screening protocol where repeatable University of La Lagunaand parametric facial stimuli are presentedinteractively to patients in order to character- Telepsychiatry can be conceived as an inte-ize and later identify their respective mental grated system of mental health care deliverydisorders using their measured responses. that employs telecommunications and com-
puterized information technology as an alter-We would like to prove that depressed pa- native to face-to-face conventional alterna-tients may be differentiated based on the deg- tive. Videoconferencing is the central tech-radation in performance of recognition. nology currently used in telepsychiatry, since
it permits live, two-way interactive, full-colour,We have generated 24 faces (12 male - 12 video, audio, and data communication. Thefemale) expressing the 6 basic emotions in effectiveness of a telepsychiatry servicetwo different ways (shown below), and 2 neu- through videoconferencing was evaluatedtral faces (1 male - 1 female). We have from a users' perspective. Ninety (30 male,shown these faces to 117 people. We have 60 female) subjects completed the Symptomaccepted a picture if the recognition rate was Rating Checklist-90-Revised (SCL-90-R) onhigher than 70%. Finally we have chosen the three occasions, once before the first tele-best recognized picture of each emotion and consultation and twice during telepsychiatryused these 7 pictures in the experiment. In treatment. Patients and psychiatrist com-our experiments we evaluated 26 depressed pleted the Clinical Global Impression Scale-patients and used frontal views of the two 3D Severity Index (CGI) after each teleconsulta-animated faces and asked the subjects to tion. Twenty five percent of patients wereidentify the emotion. We generated the 20-40- aged less than 30 years, 44% were aged60-80-100% (expression level of the emo- between 30 and 45 years, 24% between 45tions) sequence of each validated face and 60 years, while 7% were aged over 60(5x7=35 pictures). years. Anxiety disorders were the more
prevalent diagnosis (43.8%), followed by de-ANOVA evaluation of the data shows that de- pression (36%), schizophrenia (7.9%), sub-pressed patients consistently did not show stance disorders (6.1%), and personality dis-differentiable degradation in overall perform- orders (5.6%). The patients' mean SCL-90-Rance when compared to the control group. scores decreased significantly over time, in-Furthermore we found that the higher the dicating less psychiatric distress. Both pa-level of education the more significantly tients and psychiatrist reported patient clini-higher the recognition rate. We have found cal significant improvement over time as as-significant difference between depressed and sessed by the CGI. The mean number of
233

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
teleconsultations in patients discharged was Carlos de las Cuevas MD PhD6. Telepsychiatry showed to be an effective University of La Lagunamean of delivering mental health services to Urbanizaci6n Las Carias 33populations living in remote areas with limited La Laguna, Tenerifer e s o u r c e s Canary Islands 38208, Spain
Phone: 0034609521405Contact: Email: ccuevasrwull.esCarlos de las Cuevas MD PhDUniversity of La LagunaUrbanizaci6n Las Cafias 33 Presenter: JoAnn Difede PhDLa Laguna, Tenerife
Canary Islands 38208, Spain VIRTUAL REALITY THERAPY FORPhone: 0034609521405 POSTTRAUMATIC STRESS DISOR-Email: [email protected] DER FOLLOWING SEPTEMBER 11,
2001
Presenter: Carlos de las Cuevas MD PhD JoAnn Difede PhD1 , Hunter Hoffman, Ph.D,
Judith Cukor, Ph.D., Ivy Patt, Ph.D., CezarTELEPSYCHIATRY: PSYCHIATRIC Giosan, Ph.D.CONSULTATION THROUGH VIDEO-CONFERENCE PATIENTS' PERCEP- 1 Weill Medical College of Cornell UniversityTION AND SATISFACTION
Research status: This abstract presents theCarlos de las Cuevas MD PhD findings of an ongoing study which includes,
to date, 21 subjects.University of La Laguna
BackgroundlProblemA telepsychiatry service, using a videoconfer-encing system, was established to provide Posttraumatic Stress Disorder (PTSD) is apsychiatric consultations for the population of prevalent and often persistent mental illnessLa Gomera, in the Canary Islands. During the which affects approximately 7.8% of the U.S.first year of routine operation, a total of 90 population.1 In the aftermath of the Worldpatients had 90 initial and 224 follow-up tele- Trade Center attacks, studies of residents ofconsultations. The main reason for the con- New York City have found increased rates ofsultation identified in the general practitioner's PTSD,2 with rates among disaster workersreferral form was to establish a diagnosis possibly higher. Expert treatment guidelines(70% of patients); the second most common for PTSD recommend cognitive-behavioralreason was the management of a previously treatment with exposure therapy.3 However,diagnosed patient (20% of patients). Accord- due to avoidance symptoms inherent ining to the results of a questionnaire survey, PTSD, some patients refuse to or are unablepatients' acceptance of and satisfaction with to engage their emotions in treatment,the technology was very high. In their first thereby limiting its efficacy. The use of vir-teleconsultation, about a third of them said tual reality (VR) provides a greater possibilitythat they experienced some initial inconven- of generating patient involvement through theience, but this disappeared after a few min- multiplicity of sensory cues that it af-utes. During the teleconsultations, 90% of fords. The goal of this study is to evaluatepatients felt understood and could explain the efficacy of the use of VR in the treatmentall their worries and fears. Ninety percent of of PTSD directly resulting from the Worldthe patients considered that they received the Trade Center attacks on September 11,follow-up care they required and felt satisfied 2001.with the attention received. Only nine out ofninety patients (10%) stated they liked the Method/Tools'real' doctor better than the 'television doctor';forty five (50%) said they had no preference, Enrolled subjects meet diagnostic criteria forand thirty five (40%) expressed their prefer- PTSD and directly witnessed at least part ofence to telepsychiatry. the attacks of September 11th. Subjects in
the treatment group receive treatment basedContact: upon a 14 -week protocol that incorporates
234

CYBERTHERAPY 2005 ABSTRACTS
exposure using virtual reality with other cogni- comorbidity survey.tive-behavioral techniques. The subject views Archives of General Psychiatry, 52: 1048-scenes of the World Trade Center attacks 1060,1995.through a 3-D headset that progress in sever- 2. DeLisi LE, Maurizio A, Yost M, et al. A sur-ity culminating in two planes hitting the towers vey of New Yorkersand their subsequent collapses, with accom- after the September 11, 2001, terrorist at-panying sounds of screaming and si- tacks. American Journal ofrens. Subjects complete self-report question- Psychiatry. 2003;160:780-783.naires weekly and are assessed prior to and 3. Foa EB, Davidson RT, & Frances A. (eds.)following the treatment by an experienced Expert Consensusclinician. Subjects in the waitlist control are Guideline Series: Treatment of posttraumaticevaluated at baseline and again after 14 stress disorder. Journal ofweeks, at which time they are offered treat- Clinical Psychiatry, 60: 5-76, 1999.Contact:ment. JoAnn Difede, Ph.D.
Weill Medical College of Cornell UniversityResults 525 East 68th St Box 200
New York, NY 10021To date, 7 subjects have completed the treat- Phone: 212-746-3079ment protocol and 14 have been enrolled in Fax: 212-746-0719the waitlist condition. This sample was 91% Email: idifede~med-cornelI.edumale with a mean age of 43 (SD=9). Notably,in the treatment group 5 of the 7 subjectswere disaster workers and 6 of the 7 subjects Presenter: Mario Doulishad failed to respond to imaginal exposuretherapy (i.e., had been in prior treatment for THE AMALGAMATION - PRODUCTtheir PTSD symptoms but still suffered signifi- DESIGN ASPECTS FOR THE DEVEL-cantly from PTSD with a mean baseline OPMENT OF IMMERSIVE VIRTUALCAPS score of 78 +/- 24). Data analysis ENVIRONMENTSshows that scores on the CAPS decreased byan average of 28 points for individuals in theVR group and decreased by an average of 5 Professor Mario Doulis, Andreas Simonpoints for individuals in the waitlist control University of Applied Sciences Aargau, CH(p<.05).Conclusion Interacting in an immersive virtual environ-
ment we refer to the real world. The user getsto expect real world behaviour from virtual
This preliminary data suggests that virtual toepcralwldbhvurfmviulTsrealimy isanaryfdatave suestsmtht virt PTS objects and functions. We explore the idea ofreality is an effective treatment for PTSD. bringing aspects of product design to the de-
Novelty/Discussion: This preliminary study is velopment of input devices and interaction
the first to show that virtual reality is an effica- techniques for virtual environments. We use
cious treatment for individuals suffering from ergnics and prtua gento desiPTSDfolowin terorsm ad, o ou knwl- ergonomics and product language to design
PTSD following terrorism and, to our knowl- the physical input device, the virtual represen-edge, is only the second study of PTSD using tation and the connection between real andvirtual reality. Treatment failures using imagi- virtual parts. This connection, which we callnal exposure may be partially due to the in- amalgamation, is the most important elementability of the patient to emotionally engage in of the design, since it defines, if the userthe exposure work. Virtual reality appears to rather interacts with virtual objects as "virtualaddress this problem by enhancing the pa- products" (via an input device), or rather inter-
tient's capacities with visual, auditory, and a cts w it an input device as a threal tpro
even haptic computer-generated experiences, controlling virtual content.
thereby facilitating the patient's emotional en-
gagement in the exposure treatment. Contact:
References Mario DoulisUniversity of Applied Sciences Aargau, CH
1. Kessler RC, Sonnega A, Bromet E, Hughes Email: [email protected]
M, Nelson CB:Posttraumatic stress disorder in the national Presenter: St6phanie Dumoulin
235

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
vidual (e.g., sense of presence, hypnotisabil-POTENTIAL MECHANISMS UNDERLY- ity, self-efficacy, and outcome expectations)ING THE EFFICACY OF VR TO RE- and pain factors (e.g., pain intensity). We
DUCE ACUTE PAIN: A LITERATURE believe that by highlighting explicitly in this
REVIEW poster the variables that may lead to painmanagement, VR researchers can narrow
St6phanie Dumoulin, B.Sc., Stephane Bou- more effectively their search for treatment
chard, Ph.D. & Vicky Rivard, Ph.D. moderators and mediators.
Cyberpsychology Lab of the University of Quebec Contact:in Outaouais Stephanie Dumoulin, B.Sc.
[email protected] status: Completed. Phone: (819) 771-7761-8419
Fax: (819) 776-8098
Pain is now considered a complex subjectivephenomenon that involves sensorial, motiva-tional, cognitive, and emotional dimensions. Presenter: Natalia FernandezRecent studies have now shown that virtualreality (VR) can be used to control and reduce MOTIVATIONAL TRAINING TOOL TOacute pain; probably because of it's potential PROMOTE HEALTHY LIFESTYLE US-for distracting attention away from the pain. ING VIRTUAL REALITYBut many factors may influence the efficacy ofVR to help manage pain. The aim of this lit- Natalia Fern~ndez, PhD candidateerature review is to summarize the studiesthat assessed the efficacy of VR in experi- Universidad Politecnica de Madridmental and clinical pain management in orderto highlight psychological variables that may One of the main challenges that developedbe involved in the mechanisms of pain man- societies face is the prevention of non-agement using YR. communicable diseases such as diabetes or
obesity. These diseases are responsible forMethod 60% of the registered global deaths and for
45% of the global burden of disease. Un-This systematic review followed a standard healthy diet, together with physical inactivityand structured research approach. It has the and smoking, are among the key risk factorsadvantages of being rigorous, replicable, and for the development of these illnesses. Thethe results can easily be presented in a poster fact that these are preventable leads directlyformat. Journal databases such as MedLine, to the elaboration of prevention strategiesPsycINFO and Web of Science were that aim to empower and motivate the citi-searched with key words such as ((pain)» or zens to be responsible for their own healthopain management>> were crossed with key by, among others, providing them with qualitywords such as ((virtual)) or ((virtual reality)). and personalised information. As the purposeMore than 110 articles were found. Most of is to incorporate healthy lifestyles to the us-them were theoretical. But 17 empirical stud- ers' daily activities, motivational aspectsies using VR to manage pain were found. Six need to be seriously taken into account.used rigorous experimental protocols and 11 Hence, the way the information is presentedwere more exploratory and had no experi- to the user must be carefully analysed.mental protocol.
The development of a virtual reality tool helpsResults and Conclusion to motivate the user and also improves the e-
learning process. The work presented in thisMost studies showed an important and statis- paper contributes partially to solve this situa-tically significant reduction in pain. Although tion by offering the users personalised infor-distraction is considered the key ingredient to mation for their own self-care and further-explain theses results, a detailed analysis re- more, by motivating them to make use of thisveals that several factors might be involved, information and take control of their decisionsThese factors could be grouped in three cate- regarding their lifestyle through the use of agories: task relevant (e.g., attention required, virtual reality tool.task complexity, and emotional content), indi- The tool, based in X3D (eXtensible 3D), a
236
CYBERTHERAPY 2005 ABSTRACTS
virtual 3D technology for the Internet, is inte-grated in an e-learning environment which is Jos6 Gutierrez-Maldonado, PhD, Martaalso interactive and immersive. A training ac- Ferrer-Garcia, PhD candidatetivity in the system consists of an Internet mul-timedia session that shows personalised infor- University of Barcelona, Spainmation by means of an attractive visual inter-face. It is worth mentioning that the tool not This paper describes the effectiveness of vir-only provides citizens specific information tual environments to elicit emotional re-adapted to their profile and needs but also the sponses in eating disordered patients. Thisinterface is personalised accordingly. The in- study is part of a wider research project ana-formation managed throughout the system, lysing the influence of the situation to whichincluding the virtual scenarios, has been subjects are exposed on their performance onstored using the XML format. body image estimation tasks.
Moreover, in order to perform the personalisa- Though it seems self-evident that there is ation of the tool for every single user, the sys- close relation between eating disorders (ED)tem has been programmed to be "intelligent." and altered body image, in the literature onThe process is started by obtaining the user the subject no clear association has in factprofile. This is created the first time the citizen been established, and indeed the results ofaccesses the tool by filling in a structured the studies1' 2, 3' 4' 5 are often contradictory orquestionnaire about nutritional, statistical, mo- inconclusive. A number of hypotheses havetivational and physical activity data. By proc- been proposed to account for these results.essing this data, the information that suits the Some authors have stressed the fact thatuser needs and preferences best, is selected body image may be to a certain extent more afrom a native XML database. In addition, the state than a trait2 '4'8 and may change accord-information is presented to the users in a dif- ing to situational or emotional variables. Sev-ferent way depending on their motivational eral studies have analysed the possible im-state, which is revealed by applying the pact of exposure to specific objects or situa-"Stages of Change" methodology, tions on the stability of the body image.6 '7'8' 9.
10, 11
In order to measure the user response to thesystem, a survey is compiled after the first In this study we designed several virtual envi-training session. The evaluation of the results ronments that were emotionally significant forallows us to conclude that Virtual Reality is subjects with ED in order to generate differ-perceived as an interesting and easy to use ent levels of anxiety and variations in mood.tool. Besides, the users state that the relation Unlike conventional methods (real exposurebetween the scenarios developed and the to the situation, exposure to photographs,information provided in each of them was tai- exposure via guided imagination, and so on),lored to their needs and the contents were virtual reality exposes subjects to interactivemarked as a good educational tool to adopt a three-dimensional environments that simu-healthy lifestyle, late real situation. These environments have
ecological validity but also permit strict con-Contact: trol over the variables and the recording ofNatalia Ferncndez data. Virtual reality offers many of the advan-E.T.S.I.Telecomunicaci6n. tages of the conventional methods men-Ciudad Universitaria tioned above, and also overcomes many ofUniversidad Politecnica de Madrid their drawbacks.Phone: +34 91 549 57 00 ext. 332Fax: +34 91 336 68 28 Thirty female patients with eating disordersEmail: [email protected] were exposed to six virtual environments: a
living-room (neutral situation), a kitchen withhigh-calorie food, a kitchen with low-calorie
Presenter: Marta Ferrer-Garcia food, a restaurant with high-calorie food, arestaurant with low-calorie food, and a swim-
ASSESSMENT OF EMOTIONAL REACTIV- ming-pool. After exposure to each environ-ITY PRODUCED BY EXPOSURE TO VIR- ment the STAI-S (a measurement of stateTUAL ENVIRONMENTS IN PATIENTS WITHEATING DISORDER
237

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
anxiety) and the CDB (a measurement of de- Therapy, 24,195-207.pression) were administered to all subjects. 7. Carter F.A., Bullick C.M., Lawson R.H.,
Sullivan P.F. & Wilson J.S. (1996). Effect ofThe results showed significantly higher levels mood and food cues on body image inof state anxiety in the kitchen with high-calorie women with bulimia and controls. Interna-food (F=13.120; p = 0.001), the restaurant tionaljournal of eating disorders, 20(1), 65-with high-calorie food (F = 14.954; p = 0.001) 76.and the swimming-pool (F = 4.230; p = 0.049) 8. Cash, T.F.; Cash, D.W. & Butters, J.W.than in the neutral environment. Analysing (1983). "Mirror, mirror, on the wall...?": Con-the scores for depression obtained on the trast effects and self-evaluations of physicalCDB, significant differences again appeared attractiveness. Personality and Social Psy-between the high-calorie food environments chology Bulletin, 9 (3), 351-358.(F = 7.187; p = 0.012 in the kitchen and F = 9. Heilbrun, A.B. & Flodin, A. (1989). Food5.933; p = 0.021 in the restaurant) and the cues and perceptual distortion of the femaleneutral environment. In the high-calorie food body: implications for food avoidance in thesituations patients with ED showed a more early dynamics of anorexia nervosa. Journaldepressed mood. of Clinical Psychology, 45 (6), 843-851.
10. Laberg, J.C.; Wilson G.T.; Eldredge K. &Virtual reality thus appears to be a valid in- Nordby H. (1991). Effects of Mood on Heartstrument particularly useful for simulating eve- Rate Reactivity in Bulimia Nervosa. Interna-ryday situations that may provoke emotional tional Journal of Eating Disorders, 10 (2),reactions such as anxiety and depression, in 169-178.patients with ED. Virtual environments in 11. Haimovitz D.; Lansky L.M. & O'Reilly P.which subjects are obliged to ingest high- (1993). Fluctuations in body satisfactioncalorie food provoke the highest levels of across situations. International Journal ofstate anxiety and depression. Previous stud- Eating Disorders, 3 (1), 77-84.ies have shown the capacity of VR to elicit 12. James, L.K., Lin, C. -Y., Steed, A.,states of anxiety in patients with other pa- Swapp, D. & Slater, M. (2003). Social anxietythologies too.12 13,4 in virtual environments: Results of a pilot
study. CyberPsychology & Behavior, 6 (3),References 237-243.
13. Robillard, G., Bouchard, S., Fournier, T.1. Hsu, L.K.G. & Sobkiewick, T.A. (1991). & Renaud, P. (2003). Anxiety and presenceBody image disturbance: Time to abandon de durent virtual reality immersion: A compara-concept for eating disorders? International tive study of the reactions of phobic and non-Journal of Eating Disorders, 10 (1), 15-30. phobic participans in therapeutic virtual envi-2. Slade, P.D. & Brodie, D. (1994). Body ronments derived from computer games. Cy-Image distortion and eating disorder: A recon- berPsychology & Behavior, 6 (5), 467-476.ceptualitation based on recent literature. Eat- Pertaud, D.P., Slater, M. & Baker, C. (2001).ing Disorders Review, 1 (2), 32-46. An experiment on public speaking anxiety in3. Cash, T.F. & Deagle, E.A. (1997). The reponse to three different types of virtual au-nature and extend of body image distur- diences. Presence: Tele-operators and Vir-bances in anorexia nervosa anb bulimia ner- tual Environments, 11, 68-78.vosa: a Meta-analysis. International Journal ofEating Disorders, 22, 107-125. Contact:4. Sepilveda, A.R.; Botella, J. & Le6n, J.K. Marta Ferrer-Garcia(2001). La alteraci6n de la imagen corporal en Departamento de Personalidad, Evaluacion ylos trastomos de la alimentaci6n: un meta- Tratamientos Psicol6gicosan~lisis. Psicothema, 13 (1), 7-16. Facultad de Psicologia. Paseo Valle de5. Skrzypek, S.; Wehmeier, P.M. & Hebron, 171, 08035 Barcelona, SpainRemschmidt, H. (2001). Body image assess- telephone number: +34933125126ment using body size estimation in recent fax number: +34934021362studies on anorexia nervosa. A brief review, e-mail : [email protected] Child & Adolescent Psychiatry, 10,215-221. Presenter: Raymond A. Folen PhD6. McKenzie, S.J.; Williamson, D.A. & Cubic,B.A. (1993). Stable and reactive body image IS VIRTUAL REALITY BETTER THANdisturbances in bulimia nervosa. Behavior NON-VIRTUAL REALITY CLINICAL
238

CYBERTHERAPY 2005 ABSTRACTS
APPLICATIONS? A DISCUSSION OF rion temperature, and rate of change.FIVE STUDIES Chronic pain is the focus of the fourth study
which compares the effectiveness of three
Raymond A. Folen, Ph.D. treatment conditions in reducing the percep-tion of chronic pain: (1) therapist guided im-
Tripler Army Medical Center, Department of agery (standard treatment), (2) audio-tapedPsychology imagery, and (3) therapist guided imagery
enhanced with VR. The outcome measuresResearch Status: In Progress consist of pre- and post- treatment pain per-
ception, self-efficacy ratings of treatment ef-Background/Problem fectiveness, and physiological measures.
The fifth study compares the effectiveness ofVirtual Reality (VR) interventions for behav- VR as a pain and anxiety distraction to theioral health have demonstrated promise for a standard of care for participants undergoingwide variety of clinical concerns.1 At the a cystoscopy examination. Outcome meas-same time, most research to date has lacked ures include the degree of perceived pain,control conditions and comparisons with non- pre- and post-procedure anxiety, and physio-
2VR environments and interventions, making it I o g i c a I m e a s u r e smore challenging to justify the cost of estab- Results, Conclusions, and Novelty: The fivelishing in-house VR services. Research being studies will be discussed in terms of protocolconducted at the Pacific Telehealth & Tech- design and anticipated unique contributionsnology Hui Virtual Reality Behavioral Health to the field of VR in behavioural health. Sev-laboratory compares VR interventions with eral themes will be highlighted, including (1)active treatment controls and standard of care the need to establish the incremental benefitcontrols, and assesses the efficacy of differ- of using VR versus alternative display for-ent display formats. Five controlled compari- mats, such as in the anger reactivity, nicotineson study protocols designed to advance the and biofeedback studies, (2) the need forfield of VR in behavioral health will be pre- controlled comparisons as exemplified by allsented and preliminary findings will be dis- of the studies, (3) the need to generalize find-cussed. ings within clinical domains, e.g., generaliz-
ing pain analgesia findings for cystoscopyMethod examinations, and (4) the benefits of estab-
lishing experimental results that may beTwo of the research projects, a reactivity to transportable to clinical applications, such asanger stimuli study and a nicotine cue expo- the use of VR-enhanced thermal biofeedbacksure study, evaluate the effectiveness of im- training for reducing migraine headaches ormersive panoramic video virtual environment anger reactivity study protocols for anger(VE) displays in evoking physiological and management programs. Preliminary stan-emotional responses to anger stimuli or smok- dardized questionnaire and physiologicaling cues compared to flat screen video dis- findings will also be presented.plays of the same content. Outcome meas-ures include standardized questionnaires and Referencesphysiological measures of heart rate, bloodpressure, skin conductance, temperature, and 1 Wiederhold, B. K. (2000). Virtual reality inr e s p i r a t i o n the 1990's: What did we learn? CyberPsy-The third study, a biofeedback training study, chology & Behavior, 3:311-314.compares the effectiveness of three biofeed- 2 Miyahira, S. D., Folen, R. A., & Mezo, P. G.back training modalities for controlling periph- (2005, January). Use of virtual reality envi-eral body temperature. Participants are ran- ronments and VR technology in behavioraldomly assigned to one of three training condi- health: Is the bang worth the bucks? Postertions: (1) temperature change presented on a session presented at the 13th annual meet-monitor (standard feedback mode), (2) stan- ing of the Medicine Meets Virtual Realitydard feedback presented through a HMD, and Conference, Long Beach, CA.(3) immersive VE with pictorial feedback dis-play presented through a HMD. Outcome Contact:measures include the maximum temperature Raymond A. Folen, Ph.D.difference, time to maximum temperature, Tripler Army Medical Centertime to criterion temperature, duration of crite- Department of Psychology
239

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
1 Jarrett White Road nel soldier surveillance systems. This sys-Honolulu, Hawaii 96859-5000 tem also provides the backbone for futurePhone: 1-808-433-5865 neurocognitive monitoring enhancements.Fax: 1-808-433-1466 These may draw from currently availableEmail: raymondjfolen(ameddarmy.mil sensors such as voice analysis, pupil re-
sponses, saccadic eye movements, sloweyelid closure, electroencephalography, non-
Presenter: Beau J. Freund PhD invasive biochemical measures (e.g., tearanalytes), and nerve conduction velocity.
PHYSIOLOGIC MONITORING OF SOL- The challenge will be the research studies inDIERS: PRESENT AND FUTURE realistic and stressful conditions that lead to
development of valid predictive algorithms ofBeau J. Freund, Mark J. Buller, William A. brain function and behavior. These predic-Latzka and Karl E. Friedl tions of the consequences of information
overload, psychological trauma, and physio-U.S. Army Research Institute of Environmental logical stress consequences to brain functionMedicine will be central to future adaptive displays.
Wearable medical sensors can provide real Contact:time situational awareness to the soldier, Beau J. Freundcommander, and medic. Key to this system is U.S. Army Research Institute of Environ-the algorithms and knowledge displays that mental Medicinelink and interprets sensor information. For the Natick, MA 01760first time ever, the U.S. Army has a prototypesystem that will monitor physiological signalsfrom the soldier and integrate this sensor data Presenter: Andrea Gaggioli PhDthrough algorithms to predict health status.This Warfighter Physiological Status Monitor- THE VIRTUAL REALITY MIRROR:Initial Capability (WPSM-IC) is comprised of a MENTAL PRACTICE WITH AUG-medical hub that hosts a personal area net- MENTED REALITY FOR POST-work of physiologic and medical sensors STROKE REHABILITATION(heart rate, respiration, skin and core tem-perature, body motion, acoustic/impact, sleep Andrea Gaggiolil; Francesca Morgantil; An-history, fluid intake) and algorithms. The algo- drea Meneghini 2; Mariano Alcaniz 3; Jose An-rithms estimate thermal, hydration, cognitive, tonio Lozano3; Javier Montesa 3 , Jose Miguellife signs, and wounding status from the sen- Martinez Saez3; Richard Walker 4; Irene Lo-sors distributed around a soldier's body, uni- russo 4, Giuseppe Riva 1.form and equipment and from other models,databases, and contextual information (e.g., 1Applied Technology for Neuro-Psychology Lab,location, weather, mission, individual data).This system is intended as one component of Istituto Auxologico Italiano, Milan, Italyfuture warrior system of systems with differen-tial displays of the information to the individ- 2 Azienda Ospedaliera dell'Universit6 di Padova,ual, the unit leader, and the medic, ranging Unitb Operativa di Riabilitazione, Italyf g du• 3MedlCLab, Universidad Politecnica of Valencia,from aggregate data on overall status mem- Spainbers of the unit for the leader to specific early 4 Telecom Italia Learning Services, Rome, Italytriage of a wounded soldier for the medic.This physiological monitoring capability lays Research status: in progressthe groundwork for data collection for furtherrefinements, as well as testing a wide range The aim of the project is to apply augmented-of potential useful applications. Further re- reality technology to teach motor skills to pa-search with this system will expand under- tients suffering from stroke. To achieve thisstanding of limits on human tolerance. Appli- goal the project adopts an innovative ap-cations may include safety monitoring in haz- proach based on the use of so-called "motorardous conditions, training to learn and teach imagery." Recent studies in neurosciencesoldier limits, closed loop systems for control have provided converging evidence thatof equipment (e.g., microclimate cooling, exo- "imagining" a motor action involves the sameskeleton, information displays), and as senti- brain areas involved in performing the ac-
240
CYBERTHERAPY 2005 ABSTRACTS
tion.1 This supports the idea - already ex- Applied Technology for Neuro-Psychologyploited by sports trainers - that training with Labmotor imagery (mental practice) could be ef- Istituto Auxologico Italianofective in learning new motor skills or in pro- Via Pelizza da Volpedo 41moting motor recovery after damage to the Milan, Italycentral nervous system. Previous clinical Phone/Fax +39-02-619112892studies have shown that the rehabilitation of Email: [email protected] hemiplegic patients can be mademore effective by combining physical practicewith mental practice.2'3 However, for many Presenter: Enrico Gaia Dr. Ing.patients who suffer from damage to the cen-tral nervous system, mental simulation of VIRTUAL TECNOLOGIES FOR EX-movements can be difficult, even when the TREME ENVIROMENT EFFECT MITI-relevant neural circuitry has not been injured. GATIONStarting from these premises, we have de-signed and developed an augmented-reality Enrico Gaia Dr. Ing.workbench (called "VR Mirror") to help post-stroke hemiplegic patients evoking motor im- Alenia Spazio S.p.A. Torino Italyages. First, the movement is acquired by thesystem from the healthy arm. Second, the This paper examines the demands of amovement is being mirrored and displayed so manned system operating in an extreme envi-that the patient can observe and see as if the ronment where there is the need to enhanceimpaired arm is performing the movement. or at least maintain crew health, team spiritThird, the patient is instructed to rehearse in and cohesion and how new techniques basedhis/her imagination the movement he/she has on Virtual Reality technologies can providejust observed. Last, the patient has to perform some answers. A typical example is athe movement with the affected arm. The sys- manned mission to Mars with a crew of 4-8tem is currently being tested to see if it does astronauts where it is mandatory to maintainhelp patients to recover more quickly and re- their psychological health for a mission that isgain control of arms that have been paralysed envisaged to last from two to three years.following a stroke. Preliminar clinical out- They will have to work and live in an artificialcomes will be presented during the confer- environment with limited resources (for exam-ence. The research is supported by the EU pIe communication capability with ground, dueproject, called I-learning (Immersion/Imagery to the distances involved, cannot be a directEnhanced Learning4), which is funded under two way system) and living volumes. The pa-the FET Program (Future and Emerging per proposes some possible fields of investi-Technologies5 ). gation. It will also consider the fact of how
these innovative technologies based on Vir-References tual Reality will have to be developed and
tested.1. Jeannerod, M., Neural simulation of
action: a unifying mechanism for mo- Contact:tor cognition. Neuroimage, 2001. 14(1 Enrico GaiaPt 2): p. 103-9. Alenia Spazio S.p.A.
2. Stevens, J.A. and M.E. Stoykov, Us- Torino, Italying motor imagery in the rehabilitation Phone: +39 011 7180742of hemiparesis. Arch Phys Med Reha- Email: Enrico. GaiatZaleniaspazio. itbil, 2003. 84(7): p. 1090-2.
3. Page, S.J., et al., A randomized effi-cacy and feasibility study of imagery Presenter: Carlo Galimberti PhDin acute stroke. Clin Rehabil, 2001.15(3): p. 233-40. THE DOMOTIC EVALUATION
4. http://www.tils.com/i-learning/html/objectives.htm. Carlo Galimberti, Ph.D1, Luca Menti, M.S.,
5. http://www.cordis.lu/istlfet/pr2-da.htm. Simona Pegorari, M.S.
Contact: 1Universita Cattolica del Sacro Cuore-MilanoAndrea Gaggioli
241
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Domotic introduces remarkable advantages, and Neuroscience" Amsterdam, lOS Press,above all to impaired persons, and elders, but 2004 - Njord-Tide Project DE4102 httat present the lack of an actual user-oriented njord-tide.arch.kth.sedesign occurs. We planned and put in act anaction-research, now in progress, in the Contact:framework of the "Domus" project (Tuscany Carlo GalimbertiRegion council resolution n.977/2003) with Dept of psychology -Universita Cattolica delthe participation, in the first phase, of 10 cou- Sacro Cuore-Milanopies affected by mobility disorders, each one Milan, Italy 20123living for five days in a domotic apartment. Phone: +39272342660
Fax: +39272342280The aims are to set up a methodology of Email: [email protected] of the user-domotic environmentsinteraction and to supply results concerningthe interaction of an impaired user with a do- Presenter: Carlo Galimberti PhDmotic environment, with the aim both to as-sess the system and to propose new solu- BEYOND INTERFACES: AN INTE-tions. GRATED APPROACH TO THE ERGO-
NOMIC ANALYSIS OF VIRTUAL ENVI-General approach RONMENTS IN PSYCHOTHERAPY OF
An anthropological and ethno-methodological ANXIETY DISORDERS
approach was followed, in terms of an actualuse-orened esin.Int deais, hedomotic Carlo Galimberti, Ph.D', Gloria Belloni, M.A.,user-oriented design. Into details, the dmtc Matteo Cantamesse, M.S., Fabiana Gatti,environments design must follow an iterative Ph.D., Maddalena Grassi, Ph.D., Luca Menti,procedure, foreseeing a continuous loop M.S.among design, ergonomic evaluation, andimplementation. This ergonomic stance to 1Universita Cattolica del Sacro Cuore-Milanoevaluate not only technical and functional re-quirements (conformance testing) but also Research Status: In Progress (analysis ofgeneral usability and usefulness of the envi- first clinical trial data)ronment (usability evaluation), consideringboth the physical and the cognitive affor- Background/Problemdance.
The present study is part of the FIRB-Methodolgy NEUROTIV project whose main objective is
The evaluation phases foresee the analysis of to develop - on the basis of the result and
Ta luatiom projet, imirmentse anai re- applications coming out from VEPSY Project,autonomy project, impairments and funded by EU (Galimberti et al. 2004) - thesources, and interaction with artefacts. technical and clinical viability of using Virtual
Focusing on the interaction analysis we evalu- Reality Therapy in clinical psychology bymeans of portable and shared VR Systems.
ated usability, efficacy, efficiency, satisfaction, The project is providing enhancements ofusefulness, and pleasantness. Vepsy's tools (Telemedicine and Portable
Methods and techniques were constructive tools) for the treatment of patients, new clini-t partici- cal trials to verify their viability, action plans
interaction - thinking aloud modality, ptrview, for dissemination of its results to an extendedpating observation, semi-structured interview, audience and an integrated approach to er-video-recordings of all the interactions, and gonomic analysis of 3D Virtual Environmentsanalysis of the reports supplied by the soft- for psychotherapy.ware controlling the electronic domotic envi-ronments. Method/Tools
References To face the aspects connected with VR envi-
Galimberti, C. et al. (2004) Cybertherapy. ronments' usability for psychotherapeutic
Internet and Virtual Reality as Assesment and applications mean to dare a double chal-Rehabiitatond ViTools forlinical Assesychology lenge from a methodological point of view:
Rehabilitation Tools for Clinical Psychology from one side, the need to adapt and to inte-
242
CYBERTHERAPY 2005 ABSTRACTS
grate on a heuristic basis classic usability only a descriptive function, but to find out solu-evaluation methods to specific artifacts such tions to make the VEs systems more efficient.as 3D Virtual Environments for clinical appli- And this is intended to improve the whole in-cations (Galimberti and Belloni, 2003); from teractive process, abandoning both artifactthe other hand, the problems arisen by inte- and user-artifact centered interaction in favorgration of expert evaluation of VR environ- of a 'situated and context sensible' ergonomicments user-based tests carried out in real analysis.context of use (Riva, 2003; Mantovani, 2000).To face these challenges we have chosen to Referencesbase our analytical stance upon an ethnome-todological approach, a perspective that gives Galimberti C., et al. 2004 "An Integrated Ap-evidence of how people, in specific social proach to the Ergonomic Analysis of VR2 insituations, are able to solve complex tasks Psychotherapy: Panic Disorders, Agorapho-producing shared meanings and achieving bia and Eating Disorders in: G. Riva, C. Bo-their goals during interaction. According to tella et al., Cybertherapy, lOS Press, Amster-this perspective, the methodological objective dam, pp. 231-251.consisted also in the identification of the us- Galimberti C. and Belloni G. 2003 "Three-ability requirements of the specific community Dimensional Virtual Environments for Cy-of practice by whom Virtual environments are bertherapy: A Psychosocial approach to Ef-to be used (Riva and Galimberti, 2001). The fective Usability", in Cyberpsychology andvirtual environments considered were the Behavior, vol. 6, n.3, pp. 229-236.Panic Disorders and Agoraphobia VR mod- Krug, S. 2000 Don't make me think! A com-ules developed in the framework of the FIRB - mon sense approach to Web Usability, Indi-NEUROTIV project, anapolis, Macmillan
Mantovani, G. (edited by) 2000 Ergonomia.Data had been produced by means of differ- Lavoro, sicurezza e nuove tecnologie,ent situations: Bologna, il Mulino
"* functional analysis of VR environments Nielsen, J. 2000 Web usability, Milano, Apo-"* observational analysis of videotaped pa- geo Riva, G. and Galimberti, C. (edited by)
tient-VR environments interactions, thera- 2001 Towards CyberPsychology: Mind, Cog-pist-patient interactions and therapist- nition and Society in the Internet Age, Am-patient-VR environments interactions dur- sterdam, los Pressing therapy sessions G. Riva G. 2002 Web usability revised: a
"* Semi-structured interviews to out-patients situated approach. Psychnology Journal, 1:1."* Usability tests performed by out-patients Available on line: http://www.psychnology.org
Different data analysis technique (Galimberti Contact:et al., 2004; Krug, 2000), both quantitative Carlo Galimbertiand qualitative, are presently applied to data Dept of psychology -Universitti Cattolica delproducted. Sacro Cuore-Milano
Milan, Italy 20123
NoveltylDiscussion Phone: +39272342660Fax: +39272342280
"* The main goal of the study is to go 'beyond Email: [email protected],' extending ergonomic analysisof 3D virtual environments use in psycho- Presenter: Luciano Gamberini, PhDtherapy to such topic as:
"* their pragmatic context of use PLAYSAFETY: VIRTUAL ENVIRON-"* the culture of use featuring the community ETASA PE RSUAS TOOT
of professional users MENTS AS A PERSUASIVE TOOL TO
"* side-effects and by-products of their appli- CONTRAST RISKY BEHAVIORS INcation YOUTH
Obviously without forgetting the outcomes of Adriano Purgato and Luciano Gamberini,traditional usability analysis. The research is Ph.D.thus intended to construct - and not of simpleapplication -new tools for an ergonomic analy- HTLab - Human Technology Laboratories, Univer-sis. One of its main features will be to have not sity of Padova, Italy
243
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
eral clubs. Users were invited to judge theResearch Status: Complete environment and its efficacy through a 24
items questionnaire and a short interview.This paper, following the idea of Persuasive The evaluation addressed persuasiveness ofTechnology proposed by Fogg (2003), pre- the artifact, presence feeling, quantity andsents a way to develop a Virtual Reality (VR) quality of concepts learned, user's perceptioneducational system, Playsafety, capable of of consistency, effectiveness, and usefulnesshaving an impact on risky behaviors in young of the product.people. The participative design of Playsafety,its application in the field and its first evalua- Resultstion will be illustrated.
In general, users declared to have moreBackground competence on drug-related issues and risky
behaviours after the VE experience. TheyCan Virtual Reality work as a means to pre- declared to understand clearly what design-vent drug abuse and to persuade people into ers want to communicate with them (av.adopting safe behaviors? The potentials of 5.50/6 points), to perceive a strong consis-VR as learning or health care environment tency between real situations and virtualhave long been investigated (de Jong, 1991; worlds (av. 4.75/6 points) and to consider theMcComas 2002; Riva, 2002). Virtual Environ- VE useful to educate people on specific drugments offer the opportunity to explore social effects. Perceived usefulness of the productsituations and 'try out' different responses to a was particularly high in the age range 24-29variety of events (Kerr et al, 2002; Alcahiz M., for alcohol abuse (X2 =10.8 1 4 ,p=.013 with2003). As simulations, they also allow to cope d.f. =4 a=.05).with novel situations (Gamberini et al., 2003)and explore cause-and-effect relationships in Conclusiona safe, non-threatening, and compelling envi-ronment (Fogg, 2003). Scenario-based-design seems to be a pre-
cious methods to develop VE educationalMethod and Tools tools for risk prevention: Playsafety provides
a safe educational experience to young p eo-A first step in the creation of Playsafety was pie who potentially could be involved in dan-an ethnographic investigation of dangerous gerous contexts. As a persuasive technologynight situations. A six-month participative ob- working on cause-effect relationships, Play-servation was carried out in the clubs of a safety, effectively communicates what risksummer holiday location in Italy. The field underlies many common situations in youthnotes were organized as 'stories about people life.and how they keep on their projects' (Carroll,2000). Novelty
In a second stage, following the scenario- The tool addresses the lack of persuasivebased design approach (Carroll,2000), four products regarding alcohol and safe-drivingdifferent hazardous situations were extracted problems in young people.from the notes and as many VEs were builtwith 3D Studio Max 4.2 and Virtools DEV 2.5. ReferencesEnvironments included a discotheque, a park,a restroom as place for drug and alcohol Alcaiiz M., Bahos R., Botella C., Rey B. Theabuse, and a motorbike ride (safe drive). The EMMA Project: Emotions as a Determinant ofheuristic method of expert evaluation Presence. Psychnology Journal 1, [2]. 20,03(Nielson, 1993; Hix et al.,1993) was deployed (available on line: bjtp2to test their usability. Within each environ- www svchnologv.org)ment, two avatars interacted with the user. Carroll J.M., Rosson M.B., The developmentParticipants were free to respond to the situa- of cooperation: five years of participatory de-tion in many different ways, each one provok- sign in the virtual school, Publication of theing a different modification in the scene. ACM, 239-251, 2000
De Jong T., Learning and instruction withFinally, the virtual scenarios were tested on- computer simulations, Editions & Computing,site, during a two sessions-evaluation in sev- 6: 217-229, 1991
244

CYBERTHERAPY 2005 ABSTRACTS
Fogg B.J. Persuasive Technology, MorganKaufmann, 2003 Exposure in vivo is a well tested and effectiveGamberini L., Cottone P., Spagnolli A., Va- treatment in anxiety and phobic disorders.rotto D., Mantovani G. (2003) Responding to However, it is not viable to expose patientsa fire emergency in a virtual Environment: with War Post Traumatic Stress Disorderdifferent patterns of action for different situa- (PTSD) to real war environments. Being vir-tions. Ergonomics. 46 (8) pp. 842-858 tual reality exposure the most approximateHix D., Hartson H.R., User Interface Develop- simulation of a real war situation, we hy-ment: Ensuring Usability trough Product and pothesized that treatments of War PTSD thatSoftware, John Wiley and Sons, New York, included virtual reality exposure are better1993. than the current forms of psychotherapeuticKerr S.J., Neale H.R., Cobb S.V.G., Virtual intervention, namely exposure in imagination.Environments for Social Skill Training: The This paper describes the procedures andimportant of Scaffolding in Practice, Publica- presents the up to date development of (VR)tion of the ACM, 104-110, 2002 war environments as a methodology to im-McComas J., MacKay M., Pivik J., Effective- plement immersive virtual reality VR as anness of Virtual Reality for Teaching Pedes- alternative psychotherapeutic course of ac-trian Safety CyberPsychology & Behavior. tion for patients with the diagnostic of WarVol. 5, Page 185-190, 2002 PTSD. The study population of this ongoingNielson J., Usability Engineering, Academic research consists of male subjects with thePress, 1993. diagnostic of War PTSD according to DSM-Riva G., Virtual Reality for Health Care: The IV-TR (APA, 2001) that looked for treatmentStatus of Research. CyberPsycholoci & Be- at Jti1io de Matos Hospital in Lisbon, Portu-havior. Vol.5, Page 219-225. 2002 gal. Participants were distributed through 6
treatments plus placebo (VR; Drug treatment;Acknowledgements Imagination Exposure; VR+Drug Treatment;
VR+lmagination Exposure; Drug Treat-
This work was partly sponsored by Comune di ment+lmagination Exposure). The adequateFaenza within the project "Catcher in the therapeutic dosage with Sertraline (Zoloft,Rye". The authors wish to thank: Dr Edoardo Pfeizer) will be administrated during 16Polidori and all the workers of the SerT weeks to the Drug Treatment groups. VRFaenza, Provincia of Ferrara and "W la Notte" Treatment groups will be using a Headproject for providing a useful space to test the Mounted Device that provides an immersiveproduct, ZeroCento and RicercAzione Asso- experience on the following war virtual sce-ciations (Faenza) for helping us since the narios: mine deflagration, assisting casual-early stage. Finally we would like to thank ties, waiting for a rescue helicopter, and am-Gianluca Borghi, Assessore alle Politiche So- bush. CAPS, BDI, STAI, SCL-90, MCM-I1 forciali, Regione Emilia Romagna for supporting Psychometric measures and TAS, DES, PQ,the project. SUDS, heart rate and blood pressure, ECG,
EEG, and ACTH for VR reactions measuresContact: are the evaluation procedures selected forLuciano Gamberini, PhD assessing the results.Tel: ++39/049/8276605Fax: ++39/049/8276600 Contact:Email: luciano., amberini~uniod.it Pedro Gamito, PhDwwpsjcoloqia~unipd~i/htlab Universidade Lusofona de Humanidades eTecnologias
Rua Prof. Barbosa Sueiro, 5 2B
Presenter: Pedro Gamito PhD 1600 Lisbon PortugalTel: +351966057132
VIRTUAL WAR PTSD - A METHODO- Email: Dramitosapo.otLOGICAL APPROACH
Presenter: Azucena Garcia-Palacios PhDPedro Gamito, PhD, Jos& Pacheco; Carlos
Ribeiro; Cristina Pablo; Tomaz Saraiva OUTCOME PREDICTORS IN VIRTUAL
Universidade Lusofona de Humanidades e REALITY EXPOSURE FOR THETecnologias TREATMENT OF PHOBIAS
245
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
exposure.Garcia-Palacios, A. Ph.D.1 , Quero, S., Ph.D.1 ,Botella, C., Ph.D.' & Banos, R., Ph.D.,2 References
1 Universitat Jaume I Castellon. (Spain). American Psychiatric Association (200,0).2 Universidad de Valencia (Spain). Diagnostic and statistical manual of men-
tal disorders DSM-IV-TR (4 th ed., textVirtual Reality (VR) Exposure has proven to revision). Washington, DC, APA..be efficacious in the treatment of phobias. Botella, C., Baios, R. M., Villa, H., Perpihca,There are an increasing number of controlled C., & Garcia-Palacios, A. (2000). Virtualstudies that support the use of VR as an ef- reality in the treatment of claustrophobicfective tool in the treatment of several specific fear: a controlled multiple baseline de-phobias like acrophobia, claustrophobia, spi- sign. Behaviour and Therapy, 31, 583-der phobia, and flying phobia (i.e., Botella, 595.Bahos, Villa, Perpihi, & Garcia-Palacios, Emmelkamp, P. M. G., Krijn, M., Hulsbosch,2000; Emmelkamp et al. 2002; Garcia- A. M., Vries, S., Schuemie, M. J. & VanPalacios, Hoffman, Carlin, Furness, & Botella, der Mast, C.A.P.G., (2002). Virtual Real-2002; Rothbaum, Hodges, Anderson, Price, & ity Treatment versus exposure in vivo: ASmith, 2002; Wiederhold, Jang, Gevirtz, Kim, Comparative Evaluation in Acrophobia.Kim, & Wiederhold, 2002). The findings sup- Behaviour Research & Therapy, 40(5),port that VR exposure is as effective as in 509-516.vivo exposure and some of the studies offer Garcia-Palacios, A., Hoffman, H., Carlin, A.,long-term efficacy (six and twelve month fol- Furness, T. A. & Botella, C. (2002). Vir-low-ups). Another line of research in the study tual reality in the treatment of spiderof treatment effectiveness is to investigate the phobia: A controlled study. Behaviourmechanisms of change associated to the suc- Research and Therapy, 40, 983-993.cess of VR exposure. The data regarding this Rothbaum, B. 0., Hodges, L., Anderson, P.important issue are very scarce. The aim of L., Price, L. & Smith, S. (2002). Twelve-this work is to contribute to the study of pre- month follow-up of virtual reality anddictors of outcome in the field of VR exposure standard exposure therapies for the feartreatments. VR has some unique features that of flying. Journal of consulting and Clini-may be involved in its efficacy and can play a cal Psychology, 70 (2), 428-432.role as predictors of outcome. One important Wiederhold, B. K.; Jang, D. P.; Gevirtz, R.aspect in VR treatments is the degree of pres- G.; Kim, S. I.; Kim, I. Y. & Wiederhold, D.ence that the patient feels in the virtual envi- (2002). The treatment of fear of flying: Aronment. We could hypothesize that the more controlled study of imaginal and virtualpresence the patients feel the more they will reality graded exposure therapy. IEEEbe involved in the treatment and the more Transactions on Information Technologyeffective it will be. Another set of variables in Biomedicine, 6 (3), 218-223.could influence treatment response. There aresome psychological differences that may be Contact:relevant to the VR experience like hypnotiza- Garcia-Palacios, A. Ph.D.bility, dissociation, absorption, imagery, etc. In Universitat Jaume I Castellon. (Spain).this work we are interested in two of these Phone: +34 964729725variables: Absorption (the tendency to be- Fax: +34 964729267come involved in a perceptual, imaginative, or Email: azLucena(5ipsb.ujiesideational experience) and dissociation (thetendency to experience disruptions in the inte-grated functions of consciousness, memory, Presenter: Azucena Garcia-Palacios PhDor perception of the environment). The aim ofthis work is to study the possible role of pres- VIRTUAL REALITY DISTRACTION VS.ence, absorption, and dissociation in the treat- POST-HYPNOTIC ANALGESIC EF-ment response to VR exposure therapy. The FECTS ON THERMAL PAIN STIMULA-sample was composed by sixty patients meet- TIONing DSM-IV (APA, 2000) criteria for different ONphobias like claustrophobia, acrophobia, in-sect phobia, and flying phobia participating in Garcia-Palacios, A. Ph.D.several investigation testing the efficacy of VR
Universitat Jaume I Castellon. (Spain).
246
CYBERTHERAPY 2005 ABSTRACTS
BackgroundPatients frequently report severe to excruciat-ing pain during medical procedures. The Since 2001, researchers have developed andmedical literature shows post-hypnotic sug- tested virtual reality (VR) software and envi-gestions (PHS) can reduce such procedural ronments across a variety of addictivepain, and recent preliminary clinical studies drugs. Research in addictions has primarilysuggest that virtual reality (VR) distraction focused on testing the feasibility of VR envi-may serve as an even more powerful non- ronments to elicit cued-reactivity (i.e., drugpharmacologic adjunct. The present study is craving and physiological responses). Cue-the first to examine the individual and com- reactivity involves exposing substance ad-bined effects of post-hypnotic suggestions dicted persons to VR drug cues and VR neu-(PHS) and VR. In the present experimental tral cues while assessing subjective cravingpain study, 104 healthy volunteers partici- and physiological reactivity. Cue reactivity ispated in a double-blind between-groups de- based on the theory of classical conditioningsign with four groups: (No PHS, No VR), (No where drug use is repeatedly paired with en-PHS, Yes VR), (No VR, Yes PHS), and (Yes vironmental stimuli and these stimuli can trig-PHS, Yes VR). Each subject provided sub- ger craving and reactivity. Environmentaljective 0-10 ratings of cognitive, sensory, and stimuli are often referred to as cues and mayaffective components of pain. Afterwards consist of objects (i.e., cigarettes, drug para-subjects received a Stanford Hypnotizability phernalia), places (e.g., crack house, bar),test to measure their receptivity to hypnotic people, and scents (i.e., smell of cigarettes orsuggestions. Immersive VR distraction had beer). Several controlled experimental trialsrobust effects on pain intensity, pain unpleas- clearly demonstrate that VR drug environ-antness, and time spent thinking about pain ments can elicit craving and physiologicalregardless of hypnotizability. In contrast, responses compared to neutral VR environ-overall post-hypnotic suggestions had rela- ments in nicotine dependent persons1' 2 andtively weak effects on pain intensity and un- cocaine dependent person.3 Currently VRpleasantness but had robust analgesic effects environments have been developed for nico-for participants with higher hypnotizability tine, cocaine, and alcohol. The marijuana VRscores. For highly hypnotizable subjects environment is being constructed. This pres-there was a pattern suggesting the possibility entation will focus on current results and thethat VR + PHS combined may reduce pain status of VR environments as well as futuremore than either technique alone. Implica- directions in the addiction field.tions for maximizing pain relief are discussed.
MethodsContact:Garcia-Palacios, A. Ph.D. All studies reviewed and presented are con-Universitat Jaume I Castellon. (Spain). trolled experimental trials with substance de-Phone: +34 964729725 pendent samples using strict inclusion andFax: +34 964729267 exclusion criteria. Across trials, participantsEmail: azucena(-psb.uii.es are exposed to both VR neutral stimuli and
VR drug related stimuli using a VFX-3D HMD(Interactive Imaging, Rochester, NY) con-
Presenter: Ken Graap MEd nected to a 2Ghz P-IV PC. VR drug cuesconsisted of both inanimate (i.e., drug para-
VIRTUAL REALITY AND ADDICTION phernalia) and animate cues (i.e., social set-RESEARCH: UPDATES, STATUS, AND tings where participants are offered their drugLESSONS LEARNED of choice) and VR neutral cues (i.e., non-
drug related objects or scenes). In addition
Patrick Bordnick, MSW, MPH, PhD1 , Ken to the visual cues, recent advances in our labGraap, M.Ed. 2, Hilary L. Copp, MSW, Div.1 have led to the addition of olfactory cues intothe VR environments. Current data on olfac-1 University of Georgia - Gwinnett University tion in VR cue reactivity will be presented.2 Center Virtually Better, Inc. & Emory University,
Department of Psychology Results
Research Status: Preliminary clinical trials Data presented will focus on the comparisonof drug craving and autonomic physiological
247

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
reactivity between VR drug cues and VR neu-tral cues. A summary of current data from Ken Graap, M.Ed. 12, Patrick Bordnick3 , Jer-nicotine, alcohol, and cocaine cue reactivity emy Brooks1 , Mirtha Ferrer', Shelley Brund-trials will be presented. age4
Conclusions 1 V i r t u a I I y B e t t e r, In c.2 Emory University, Department of Psychology
This presentation will provide an overview of 3 University of Georgia, Department of SocialVR applications in addiction research and W 0 r ktreapatment.Pst, current andd futurction s r a4 George Washington University, Department oftreatment. Past, current and future directions S p e e c h P a t h o I o g ywill be discussed along with lessons learnedto date. Research Status: Preliminary clinical trials
Novelty/Discussion Background
This presentation will provide the first over- Scent is one of the most salient senses forview of VR cue reactivity research to date, emotional response. The olfactory bulbs pro-including data on controlled alcohol, cocaine, ject into nerve tracts that synapse into theand nicotine trials. The first application of a amygdala. The amygdala is connected bidi-novel olfactory stimuli presentation system in rectionally to the hippocampus, the center ofVR drug research will also be high- many memory functions. These connectionslighted. Future research and treatment appli- suggest that specific smells may be associ-cations will be discussed. ated with accessing emotionally laden
References memories. Herz & Schoolerl and Herz,2
have investigated the associations of scentand memory providing an empirical basis for
1. Bauman, S. B. (2004). Smoking cues in a scent research in virtual reality (VR). In re-virtual world provoke craving in cigarette spondent conditioning, scents can serve assmokers as demonstrated by neurobehavioral powerful cues that trigger physiological and
and fmri data. Paper presented at the Cy- subjective responses to past conditioned
berTherapy, San Diego, CA. events. Building upon these studies, we are
2. Bordnick, P. S., Graap, K. M., Copp, H., exploring the use of scent in virtual reality
Brooks, J., Ferrer, M., & Logue, B. (2004). (VR). The addition of scent will extend our
Utilization of virtual reality to standardize nico- previous work in phobias 3 and enhance ourtine craving research: A pilot study. Addictive research in addictions 4 and speech pathol-Behaviors, 29(9), 1889-1894. ogy.5 This presentation outlines the process3. Graap, K. M. (2004). Cue reactivity in a of adding scents to several immersive envi-virtual crack house. Paper presented at the ronments being tested in controlled researchAssociation for the Advancement of Behavior t r i a I sTherapy, New Orleans, LA.
Contact: Method & Tools
Patrick S. Bordnick, MSW, MPH, Ph.D. Scent is being utilized in two different andVirtual Reality Clinical Research Center related areas. First, it is being applied to fa-University of Georgia- cilitate immersion in VR environments as anGwinnett University Center ambient stimulus in a job interview designed1000 University Lane, Suite 3020 for use with persons who stutter. Second,Lawrenceville, Georgia 30043 USA scent is being applied directly as a primarybordnickcgqgedu stimulus to facilitate craving responses in678-407-5204 controlled trials with substance abusing and
dependent participants. Examples of suchPresenter: Ken Graap MEd implementations using the EnviroScent ma-
chine in conjunction with Virtually Better VRTHE ADDITION OF SCENT TO IMMER- environments will be presented.SIVE VR ENVIRONMENTS IN ADDIC-TION AND SPEECH PATHOLOGY RE- ResultsSEARCH
248

CYBERTHERAPY 2005 ABSTRACTS
Initial data including immersion ratings, and 1Imaging Research, Sunnybrook and Women'ssubjected units of discomfort (SUDs) or crav- College Health Sciences Centre, Toronto, Ontarioing ratings from the trials will be discussed. 2 Department of Medicine, University of Toronto,Qualitative experiences of participants in trials Ontario, Canadawill be discussed. 3Division of Life Sciences, University of Toronto,Ontario, Canada
4 Department of Medical Biophysics, University ofNovelty Toronto, Ontario, Canada
To our knowledge this will be the first time Reserach Status: Completedthat our Enviroscent Machine will have beenused with immersive VR in a clinical setting. Several functional neuroimaging studies
have studied different specific aspects of hu-References man navigation. 1' 2' 3 To further elucidate re-
gions involved during performance of spatial1. Herz, R.S., & Schooler, J.W. (2002). A navigation and to determine how task per-naturalistic study of autobiographical memo- formance influences the identified brain re-ries evoked to olfactory versus visual cues. gions, this study utilized a novel virtual realityAmerican Journal of Psychology, 115, 21-32. (VR) navigation task during functional mag-2. Herz, R.S., (2004). A comparison of auto- netic resonance imaging (fMRI). The taskbiographical memories triggered by olfactory, enabled both learning and recall of routes tovisual and auditory stimuli. Chemical Senses, be assessed. The multivariate Partial Least29, 217-224. Squares analysis (PLS)4 was used to identify3. Glantz, K., Rizzo, A & Graap, K (2003). time-varying distributed activity patterns inVirtual Reality for Psychotherapy: Current Re- the fMRI data.ality and Future Possibilities. Psychotherapy,40, 55-67. MethodslTools4. Bordnick P., Graap, K., Copp, H., Brooks,J., Ferrer, M. Logue, B. (2004). Utilizing virtual The experiment involved navigation throughreality to standardize nicotine craving re- a virtual city using an fMRI-compatible virtualsearch: A pilot study. Journal of Addictive reality platform. The task consisted of a setBehavior, 29, 1889-1994. of 3 learning trials for Path A followed by 15. Brundage, S. & Graap, K. (2004). Virtual learning trial for Path B. Each learning trialReality: An exciting new tool to enhance stut- consisted of two components; passive view-tering treatment Perspective on Fluency Dis- ing of the path by video playback, and activeorders, 14, 4-9. navigation using an fMRI-compatible joystick.
In subsequent short (5 min) and long (20Contact: min) delay recall trials, Path A was navigatedKen Graap, M.Ed. from memory. Twelve, healthy, right-handedVirtually Better subjects participated. Functional MRI experi-2450 Lawrenceville Hwy ments were performed at 1.5T (Signa, GEDecatur, GA 30033 Healthcare). Behavioural metrics includedPhone: 404-634-3400 time to completion and distance travelled.Fax: 404-634-3482 For the primary analysis, learning trials wereEmail: ,qraaprvirtuallybetter.com contrasted with recall trials (task-PLS) follow-
ing motion correction and temporal detrend-ing. Further analysis included a behavioural-
Presenter: Simon J. Graham PhD PLS in which time to completion was used todetermine significant brain-behaviour correla-
AN FMRI STUDY EXAMINING SPATIAL tions.NAVIGATION THROUGH A VIRTUALENVIRONMENT: PARTIAL LEAST ResultsSQUARES ANALYSIS
One significant (p<0.01) latent variable char-Richard Mraz, P.Eng. 1, Nancy J. Lobaugh, acterized differences in brain activity be-Ph.D. 1'2 , Genevieve Quintin, M.A.3 , tween learning trials and recall trials. DesignKonstantine K. Kakzanis, Ph.D., C.Psych.3, scores denoted significant differing neuronalSimon J. Graham, Ph.D., P.Eng. 1 A involvement between conditions. Activation
maps indicated that bilateral frontal regions
249

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
and right hippocampus were more involved Sunnybrook and Women's College Healthduring learning, while parietal and temporal Sciences Centre - S650regions, such as the left parahippocampal Toronto, ONgyrus, bilateral precuneus and cingulate cor- Canadatex, were more active during recall. A second Phone: 416-480-4104task-PLS analysis focused on the 4 learning Fax: 416-480-5714trials, identifying a pattern related to the first Email: sirnon.raharnsw.calearning trial for each path. Areas involved ininitial learning included right precuneus andthe cerebellum. Subsequent trials recruited Presenter: Kay Howell MBAregions surrounding the lateral sulcus bilater-ally as well as the middle and medial frontal IMMUNE ATTACK: BUILDING BIO-gyri. The behaviour-PLS confirmed many of LOGICALLY BASED IMMUNE SYSTEMthese findings among similar brain regions, SIMULATIONS FOR EDUCATION ANDidentifying patterns that were related to gen- TRAININGeral task performance, to initial learning, andthat specifically distinguished learning from Kay Howellrecall.
Conclusion Federation of American ScientistsConclusiond
Findings of posterior activations during recall Background
are consistent with the notion that temporal A growing literature suggests that simulation,regions are involved in spatial information re- visualization, and gaming can play an impor-trieval, whereas initial encoding of a complex tant role in deepening understanding of diffi-route demands increased precuneus involve- cult concepts in mathematics, engineering,ment. The predominant activation of frontal and science. Learning sciences researchand temporal regions in subsequent learning suggests that learning by doing with under-trials can probably be associated with encod- standing produces better transfer than mereing, maintenance, and recall of visual cues, doing alone.1'2 Challenge-based simulationswhich are critical for successful navigation, can provide students opportunities to receive
feedback and revise their thinking, a criticalNovelty part of the learning process.3'4 Immune At-Combining VR-fMRI with PLS proved to be a tack is a simulation game to teach biologicalhighly sensitive technique for examining re- concepts related to immunology and woundgions engaged during spatial navigation, infection, allowing the student to explore the
internal compartments and cells of the hu-man body and visualize immunological proc-
References esses.
Method/Tools[1] EA Maguire, et al. Journal of Cognitive
Neuroscience, 10:61-76 (1998). Immune Attack will combine 3D visualiza-
[2] RPC Kessels, et al. Neuropsychology tions of biological structure and function withReview, 10:101-113 (2000). advanced educational technologies to pro-
vide an introduction to basic concepts in im-[3] E Mellet, et al. Neuroimage, 12:588- munology for high school students. It is in-
600 (2000). tended to be as fun and compelling as the
[4] AR McIntosh, NJ Lobaugh. Neuroi- computer games currently played by manymage, 23:S250-S263 (2004). adolescents and young adults. Students aremotivated with a series of progressively more
[5] R Mraz, et al. Cyberpsychology & difficult challenges in a gaming environmentBehavior, 6:359-368 (2003). in which success depends on increasingly
sophisticated grasp of concepts in immunol-
Contact: ogy. The learning experience will be individu-Simon J. Graham, Ph.D., P.Eng. alized by use of context-sensitive help and
dialogues and continuous assessment tech-
250
CYBERTHERAPY 2005 ABSTRACTS
niques to determine when the learner is ready sons from research on problem and project-to move to a new level, based learning. Journal of Learning Sciences
7 (3 and 4): 271-312.The biological models are being developed 2. John D. Bransford, Sean Brophy, andworking closely with prominent immunology Susan Williams. "When computer technolo-researchers and educators. Experienced gies meet the learning sciences: Issues andvideo game developers are developing the opportunities" in Journal of Applied Develop-game and assisting in integrating the learning mental Psychology, 21 (1) pp. 59-84.tools. The learning objectives and instruc- 3. Black, P., and William D. 1998. Assess-tional strategies are being developed in con- ment and classroom learning. In Assess-sultation with biology teachers, at both the ment and Education. Special issue of As-high school and college freshmen levels, and sessment in Education: Principles, policy andwith learning research scientists. practice 5(1):7-75. Carfax Pub. Co.
4. Vye, N.J. , D.L. Schwartz, J.D. Bransford,Evaluation B.J. Barron, L. Zech, and Cognition
Technology Group at Vanderbilt, 1998.The game will be used to supplement imunol- SMART environments that supportogy taught as a part of biology courses given monitoring, reflection, and revision. Into high school students and will be valuated in Metacognition in Educational Theory andhigh school biology classes. The project will Practice, D. Hacker, J. Dunlosku, and A.be evaluated based on the following criteria: Graesser, eds. Mahwah, NJ: Erbaum.1) Has the project developed biologically cor-rect, visually compelling simulations of the Contact:immune system that can be easily navigated Kay Howellby people without specialized technical profi- Federation of American Scientistsciency? 2) Do the simulations allow revisions 1717 K. St., NW, Suite 209and augmentations and encourage use of Washington, DC 20036simulation components in the work of others? Ph: 202.454.46853) Can the simulations be used in conjunction Fax: 202.6751010with a variety of assessment, feedback, and Email: khowellafas•oraugmentation tools? 4) Does use of the gameincrease students' motivation to learn theclassroom material? Presenter: Eva Hudlicka PhD
Novelty/Discussion A COMPUTATIONAL MODEL OF EMO-TION AND PERSONALITY: APPLICA-
Computer games hold special interest to a TIONS TO PSYCHOTHERAPY RE-generation who has grown up with them, and SEARCH AND PRACTICEas such, they show promise as educationaltools. Whether this is due to the inherent Eva Hudlicka, Ph.D.challenge built into game play, the richness ofgraphics presented to the user, the opportu- Psychometrix Associates, Inc.nity to interact with other users (in web-basedgames), the story or context in which the Research Status: MAMID cognitive-game is couched, or some other feature is an affective architecture is implemented; Appli-important part of this research project. Ex- cations to psychotherapy research areploiting the inherent motivational aspects of planned.games and simulations for education andtraining must be based on a sound under- Backgroundstanding of which features of these systemsare important for learning and why. VR applications in psychotherapy are gaining
prominence in the research community andReferences acceptance among practitioners. However, a
promising technology remains unexplored:1. Barron, B.J., D.L. Schwartz, N.J.; Vye, A. computational models of cognition and emo-Moore, A. Petrosino, I. Zech, J.D. Bransford, tion.and the Cognitive and Technology Group at Cognitive models (also termed cognitive- orVanderbilt. Doing with Understanding: Les- agent-architectures) aim to emulate cognitive
251

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
processing such as attention, perception, and Novelty/Discussiondecision-making, and are used by cognitivescientists to advance understanding of the There is great potential for application of cog-mechanisms and structures mediating cogni- nitive-affective models in psychotherapy re-tion. These models are also used in applied search and practice; both in a "stand-alone"settings to improve training and human- mode, and coupled with synthetic avatars, tosystem design. Recently, architectures have produce more realistic virtual characters.been developed that explicitly represent emo-tions: both emotion appraisal processes, and Research MAMID provides a tool for model-effects of emotions on cognition. ing the etiology and treatment of a variety of
disorders; e.g., the positive feedback cycleIn this paper I first describe a cognitive- characterizing generalized anxiety disordersaffective architecture capable of modeling the and phobias could be modeled by represent-dynamic generation of emotions (affect ap- ing the increasing predominance of anxiety-praisal), and some effects of emotions on related schemas in the patient's long-termcognition. I then describe applications of this memory, increased sensitivity to anxiety-architecture to psychotherapy research and producing stimuli, and generalization acrosspractice. previously neutral stimuli. Results of cogni-
tive restructuring could be modeled byMethod I Tools exposing' models to repeated simulated in-
puts representing therapeutic interventions orThe MAMID cognitive-affective architecture changing social contexts, and modeling thedynamically generates four emotions (anxiety, gradual emergence of more adaptive mem-anger, joy, sadness) from a combination of ory schemas, interpretations, and behavior.external and internal stimuli (e.g., incoming Improved understanding of these processessensory cues, goals, expectations). The archi- would provide opportunities for more finely-tecture then models the effects of these emo- tuned assessment and treatment.tions, as well as four traits (extraversion, neu-roticism, conscientiousness, aggressiveness), Clinical Practice MAMID provides a means ofon the cognitive processes and structures controlling the behavior of avatars in thera-mediating decision-making and action selec- peutic virtual environments, thereby enhanc-tion. For example, anxiety-linked threat-bias ing their believability. The avatars would rep-is modeled by biasing attentional, interpretive resent specific stereotypes (e.g., 'aggressiveand expectation-generation processes to pref- audience member,' 'shy friend'), allowing theerentially process threatening stimuli, and de- construction of virtual social situations rele-rive higher-threat interpretations and expecta- vant for the patient. The use of affectively-tions. MAMID is able to model a broad range realistic avatars, embedded within simulatedof 'stereotypes' by representing emotion ef- situations, would also enhance assessment.fects in terms of parameters controlling thearchitecture structures (memory) and proc- Contact:esses (e.g., attention, situation assessment). Eva Hudlicka
Psychometrix Associates, Inc.Results Blacksburg, VA, USA
Phone: (01) 540 552 4803Feasibility of the model was demonstrated in Email: evahud•_)earthlink.netthe context of a simulated peacekeeping sce-nario, where separate instances of the archi-tecture controlled the behavior of Presenter: Wijnand IJsselsteijn, Ph.D.'stereotypical' unit leaders ('anxious,''aggressive,' 'normal'). The same set of exter- TOWARDS A NEUROPSYCHOLOGI-nal stimuli triggered distinct emotions in the CAL BASIS OF PRESENCEdifferent stereotypes, and their effects on de-cision-making then caused differences in ob- Wijnand lJsselsteijn, Ph.D.servable behaviors. The MAMID architectureis domain-independent, to facilitate transitions Eindhoven University of Technologyto other domains, including psychotherapy.
In this presentation, we will review recentneuropsychological studies regarding tool
252
CYBERTHERAPY 2005 ABSTRACTS
use and body image perception, and highlight case, described by Berti and Frassinetti,4
their importance for understanding presence. where a patient, after a right hemispherestroke, showed a dissociation between near
The experience of presence appears to be a and far spaces in the manifestation of ne-complex perception, formed through an inter- glect. Using a line bisection task, the neglectplay of raw multisensory data, spatial percep- was apparent in near space, but not in fartion, attention, cognition, and motor action, all space when bisection in the far space wascoupled through a constant dynamic loop of performed with a projection light pen. How-sensorimotor correspondence. Presence re- ever, neglect appeared when in the far spacesearch studies the experience of being in a bisection was performed with a stick (used byplace or being with someone as it is mediated the patient to reach the line) and it was asthrough technology, severe as neglect in the near space. Thus,
this study provides evidence that an artificialThe perception of ourselves as part of a extension of a person's body (the stick)space not only depends on a passive percep- causes a remapping of far space as neartion of spatial layout but also on the ability to space - essentially telepresence.actively explore an environment, allowing theperceptual systems to construct a spatial map Referencesbased on sensorimotor dependencies. By in-corporating telepresence technology that sup- 1. Ramachandran, V.S. & Blakeslee, S.ports our bodily perceptual and control move- (1998). Phantoms in the Brain. New York:ments as part of the ongoing perceptual- Harper Collins.motor loop, the correlations between motor 2. Rizzolatti, G., Fadiga, L., Fogassi, L. &actions and multisensory inputs remain intact Gallese, V. (1997). The space around us.and a sense of telepresence or 'distal attribu- Science 277, 190-191.tion' may occur. 3. Previc, F.H.. (1998). The neuropsychology
of 3-D space. Psychological Bulletin 124,The fact that technology can start working as 123-164.a transparent extension of our own bodies is 4. Berti, A. & Frassinetti, F. (2000). When farcritically dependent on the highly plastic na- becomes near: Remapping of space by toolture of our brain, which is continuously able use. Journal of Cognitive Neuroscience 12,and prone to adapt to altered sensorimotor 1215-420.contingencies. This fact finds its basis in thesignificant evolutionary benefit of having a Contact:negotiable body image to accommodate life- Wijnand lJsselsteijn, Ph.D.time development and change, which requires Eindhoven University of Technologya continuous remapping of bodily boundaries. Eindhoven, The NetherlandsA radical example is provided by the amazing Phone: +31 40 2474455adaptation processes that occur in the body- Fax: +31 40 2449875image of people with one or more lost or am- Email: [email protected] limbs.' Although body-image adapta-tions across the lifespan can afford to taketheir time, it is the relative speed of these sen- Presenter: Hee Jeong Jangsorimotor adaptations that enables us to ex-perience man-made technology as, quite liter- INVESTIGATION OF SOCIAL ANXIETYally, part of ourselves - be they a blind per- OF PATIENTS WITH SCHIZOPHRENIAson's cane or an advanced telerobotic arm. USING VIRTUAL AVATAR
In general, the space that surrounds an indi- Hee Jeong Jang, BA, 1, Jeonghun Ku, PhD2,vidual can be meaningfully segmented into Sung Hyouk Park, MS1, So Young Kim, BA1
near or peripersonal space and far or ex- In Y. Kim, MD, PhD2, Chan-Hyung Kim, MD,trapersonal space. Animal and human brain PhD1, Jae-Jin Kim, MD, PhD'studies have confirmed this distinction, show-ing that space is not homogeneously repre- 1Yonsei University College of Medicinesented in the brain.2 3 Telepresence technolo- Severance Mental Health Hospital, Gyunggi-do,gies can be viewed as attempts to overcome Koreathe boundaries of spatial segmentation. Their 2 Dept. of Biomedical Engineering, Hanyang Uni-success in doing so is evidenced by a clinical versity, Seoul, Korea
253

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
avatar conditions compared to the other twoBackgrounds conditions. In a correlation analysis between
patient's anxiety levels and the severity ofPatients with schizophrenia show a tendency their symptoms, social anxiety on "happy"to avoid social interaction because they feel and "neutral" avatars was positively corre-great anxiety during their social interactions. lated with the negative syndrome of PANSSTherefore, they have trouble making social (happy : r=.539, p=.038, neutral : r=.533,relationships. This trouble is largely due to the p=.041). Particularly, the anxiety level byfact that the patients have emotional with- "happy" and "neutral" avatars was positivelydrawal as well as passive/apathetic social correlated with two subscales (NI: bluntedwithdrawal. These social deficits of patients affect, N4: passive/apathetic social with-has been overcome through social skills train- drawal) of the negative syndrome of PANSSing programs, which provide them opportuni- (N1. happy: r=.549, p=.034/ neutral: r=.536,ties to experience previously various social p=.039) (N4. happy: r=.536, p=.039/ neutral:situations by role play method. r=.658, p=.008).
Objectives Conclusion
This study was conducted in order to investi- Through this study, we found that virtual ava-gate whether an interaction with virtual ava- tar's emotional expressions could cause so-tars can evoke patient's social anxiety and the cial anxiety to patients with schizophreniarelationship between patient's symptom se- and that patient's symptom severity was cor-verity and social anxiety traits. related with social anxiety during the time
they coped with avatars. These results showMethod/Tools that the more severe negative symptoms a
patient has, the higher social anxiety theyFifteen patients with schizophrenia and fifteen feel. It might be due to their passive, apa-control people were recruited. A male and a thetic, and isolated traits. Therefore, theyfemale avatar were generated. 2x2x3 (group, tend to recognize even socially positive emo-avatar's gender and avatar's emotional ex- tion as fearful stimuli. This inference could bepression) was used in this experiment. Each supported by the relationship between anxi-avatar has three emotional expressions, ety and subscales of negative symptom ofwhich are happy, neutral, and angry. Subjects PANSS. In this sense, we could say that aperformed an introduction task in six condi- virtual avatar could provide an opportunity fortions (gender x emotional expression) in a patients to experience emotion induced so-random order. The task is composed of cial situations. In addition, it could be used"approach," "listening to an avatar's introduc- for training them to cope effectively by ex-tion," and "introducing oneself to the avatar." periencing emotions close to reality as wellAfter all six tasks were performed, subjects as to find out the clinical characteristics re-completed a State-Trait Anxiety Inventory lated to patient's symptoms.(STAI) questionnaire. In addition, patient'ssymptom severity was evaluated using the Contact:Positive and Negative Syndrome Scale Hee Jeong Jang(PANSS). Mind Mapping Laboratory
Institute of Behavioral Science in MedicineResults Yonsei University College of Medicine
Email: [email protected] social anxiety level to avatar's emotionalrepresentation was significantly different inboth group (p<.001). In control group, the Presenter: Naomi Josman PhDlevel was lowest when subjects coped with anavatar expressing "happy," while the highest VIRTUAL REALITY: INNOVATIVEanxiety level was shown when they faced to TECHNOLOGY FOR THE TREATMENTan avatar expressing "anger." However, in FOR VICTIMS OF TERRORIST BUSpatient groups, the level difference was not BOMBING WITH POST-TRAUMATICsignificant between "neutral" and "happy" ava-tars. Patients only showed a significantly highanxiety level when they experience "angry"
254
CYBERTHERAPY 2005 ABSTRACTS
Naomi Josman1 , Ayelet Reisberg, Eli Somer, ment involves viewing scenes of the terroristHunter Hoffman, Azucena Garcia-Palacios, bus bombing attack through a positionAri Hollander, Russ Shilling, Patrice (Tamar) tracked 3-D VR helmet. The scenes, com-Weiss puter controlled by therapist button pushes,
progress in severity, culminating in a busUniversity of Haifa pulling up to a bus stop in an Israeli town,
exploding into smoke and flame with loudResearch Status: Preliminary clinical trials sound explosion effects (with vibrotactile(case report) currently in progress augmentation via amplified speakers) with
accompanying sounds of screaming and si-Background/Problem rens, and a smouldering limb in the street.
The subject completes self-report question-Cognitive Behavioural Therapy (CBT) with naires and is assessed prior to and followingexposure involves having patients gradually the treatment by two experienced cliniciansremember the traumatic event and process (one clinician blind to treatment condition).the extreme emotions associated with thatmemory so they can eventually remember the Conclusiontraumatic event in a more healthy way. CBTwith exposure is currently the treatment of VR exposure therapy is a promising new me-choice for Post Traumatic Stress Disorder dium for treating PTSD from terrorist bus(PTSD). There is strong empirical support for bombing attacks.the efficacy of CBT interventions for PTSD forthose who seek and complete treatment. Un- Novelty/Discussionfortunately, avoidance of remembering thetraumatic event is a defining symptom of There are currently no controlled studies inPTSD, and the majority of people who de- the literature on the topic of using VR expo-velop PTSD avoid seeking treatment. Those sure therapy for treating PTSD. The currentneeding treatment most may be the most project addresses a completely original re-likely to avoid or drop out of traditional treat- search topic on a rapidly growing patientment. CBT with exposure provides patients population (using VR to help treat PTSD fromwith opportunities to learn to control their own terrorism). In Israel, there have been dozensemotional responses when confronted with of extremely violent deadly terrorist attacksstimuli that elicit physiological and emotional involving civilians causalities and deathsactivation. In order to develop new, healthier (often including women and children) in thepatterns of thinking, feeling, and acting toward past few years alone. PTSD is a very chal-the distressing stimuli, CBT requires the prac- lenging psychological disorder to treat, yettice of new beliefs and actions in the presence the social and economic cost of the currentof stimuli that elicit the anxiety. CBT and Vir- trend of leaving so many PTSD victims un-tual Reality (VR) provide patients with an ideal treated is unacceptable.context for gradually remembering memoriesof the traumatic event. VR may help increase Referencesemotional engagement and treatment suc-cess. VR is proving effective even for difficult 1. Difede, J., Hoffman, H. & Jaysingle, N.patients who have failed to respond to tradi- (2002). Innovative use of virtual reality tech-tional therapy.1 Surveys suggest that patients nology in the treatment of PTSD in the after-with anxiety disorders are much more recep- math of September 11. Psychiatric Services,tive to VR than to traditional therapy, perhaps 53(9), 1083-1085.because VR has fewer stigmas, is more inter-esting, and less threatening than traditional Contact:therapy. Naomi Josman, Ph.D.
Department of Occupational TherapyMethod/Tools University of Haifa
Haifa, IsraelThe patient we treated met diagnostic criteria Tel: +972 4 824-0610for PTSD after directly witnessing a terrorist Email: [email protected] bombing attack in Haifa, Israel, and re-ceived a 9-visit treatment protocol that incor-porates CBT+VR. Among other things, treat- Presenter: Hannes Kaufmann PhD
255

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Research status: CompletedGENERAL TRAINING OF SPATIALABILITIES BY GEOMETRY EDUCA- Virtual Environments (VEs) offer the potentialTION IN AUGMENTED REALITY for users to explore social situations and 'try
out' different behaviour responses for a vari-Hannes Kaufmann', Karin Steinb0gl1, ety of simulated social interactions. The ASAndreas Djnser2, Judith GI0ck2 Interactive project was a three-year pro-
gramme of study to examine the use of vir-'Institute of Software Technology and Interactive tual environments for social skills training ofSystems, Vienna University of Technology young people and adults with autistic spec-2 Institute of Psychology, University of Vienna trum disorders (ASDs) and Asperger's Syn-
drome (AS). The project research team com-Geometry education has proven as one pow- prised computer scientists, virtual environ-erful means of improving spatial abilities, an ment developers, human factors researchers,important component of human intelligence, psychologists, and autism training specialistsIn the first part of this paper we summarize working with individuals from AS socialour development of a system that uses col- groups and students and teachers from au-laborative augmented reality as a medium for tism specialist schools.teaching, and uses 3D dynamic geometry tofacilitate mathematics and geometry educa- The first consideration of the project was thetion. Our immersive collaborative educational feasibility of constructing usable social envi-application, specifically developed for geome- ronments using virtual reality technology.try education, serves as the basis of a com- Two types of virtual environments wereprehensive evaluation study regarding its effi- evaluated; single user virtual environmentscacy in training spatial abilities. The main con- (SVEs) and collaborative virtual environ-tribution is the description of evaluation de- ments (CVEs). In the SVE the user wassign including the test instruments, learning guided through a social interaction task andtasks, and practical experiences with using invited to make choices about what to do andour system for actual training of high school what to say in situations represented within astudents. Results of a pre-study with spatial virtual cafe and a virtual bus. In the CVEability tests in high schools are presented. several users, positioned at different PCs,They point to interesting gender-specific dif- simultaneously shared the same virtual envi-ferences of strategies when solving spatial ronment, representing a virtual caf6 or anability tests, which have not been reported in interview scenario. The intended use of theliterature before. CVE was that a teacher or training advisor
could support the user by taking the role ofContact: one of the other characters and providingHannes Kaufmann guidance using virtual social interaction.Institute of Software Technology and Interac-tive Systems Observation studies found that SVEs wereVienna University of Technology much more successful than CVEs as the lat-Favoritenstr. 9-11/188-2 ter was too complex, technologically, to setA-1040 Vienna, Austria up in school and users tended not to engageEmail: [email protected] with other avatars in conversation. SVEs
however could be used in one to one tuition,which gauged the suitability of the program
Presenter: Steven Kerr MSc for individual students and identifying theirlevel of understanding or in group exploration
AS INTERACTIVE: DEVELOPMENT and reflection (where a teacher led a discus-
AND USE OF VIRTUAL ENVIRON- sion with a small group of students viewing
MENTS FOR SOCIAL SKILLS TRAIN- the VE on a projected screen) which was
ING useful for identifying social cues in the VEand understanding the perspectives of oth-
Steven Kerr and Sue Cobb ers.
Human Factors Research Group, University Of The conclusions drawn from this project wereNottingham that successful VEs for teaching social skills
to people with Asperger's Syndrome (AS),
256
CYBERTHERAPY 2005 ABSTRACTS
will need sufficient scaffolding inbuilt to sup- Method/Toolsport learning whilst also having the flexibilityto adapt for unforeseen problems through We developed a project-based VR systemteacher intervention. Allowing a teacher to because schizophrenic patients feels veryindividualise the content of the VEs in some anxious when wearing a Head-mounted dis-way is important, as it should not be assumed play. Narrative-based contents were con-that a student has understood the lesson by structed to induce schizophrenic patients intoappearing to exhibit the appropriate behaviour proper goals to assess social problem solv-for the given task. Some behaviour might be ing abilities. Survey for selecting 8 compli-individual to that user and only someone who cate social problems among many daily-knows the user will understand this. This pa- happening social problems and setting theirper aims to discuss the issues behind the de- difficulty was conducted for 50 normal peo-sign and development of the SVEs and the pie. The virtual environment and virtual ava-features which can be used to facilitate the tar matched with 8 complicated situationsteaching of social skills to people with AS, were built by using 3D-MAX and were con-who have very individualised needs. verted into MAP or MDL format for rendering
in A6 engine. The behavioural databaseContact: which consists of 15 avatars, 40 apparels, 70Steven Kerr actions and 6 facial expressions was con-Virtual Reality Applications Research Team structed to make a flexible and dynamic ava-Human Factors Research Group tar. Also eye-blinking and lip-synching wasUniversity Of Nottingham roughly implemented to make the virtual ava-Tel: +44 (0) 115 9514070 tar more realistic and live-like. The VR sys-Fax: +44 (0) 115 8466771 tem was designed to give patients the infor-Email: steven~kerrdnottinqhamnac•uk mation that is needed in problem solving be-
cause we want to measure the pure socialproblem solving ability except cognitive as-
Presenter: Jaehun Kim pects such as memory. It was implementedby making an information window in which
DEVELOPMENT OF VR SYSTEM TO patients know what time it is, how muchASSESS SOCIAL PROBLEM SOLVING money I have, today's schedule, and what IABILITY FOR PATIENT WITH SCHIZO- should do. After VR experience in each con-
PHRENIA tent, Q&A panels about the complicatedsituation appeared and patients could select
Jaehun Kim, M.S.; Kwanguk Kim M.S.; Kiwan their own solution about given social prob-
Han, B.S.; Jeonghun Ku, Ph.D.; Hee Jeong lems by using an 8-button joystick.
Jang, B.A.; Sung Hyouk Park, M.D.; SoYoung Kim, B.A.; Chan Hyung Kim, M.D., ResuItsI ConclusionPh.D.; Jae-Jin Kim, M.D., Ph.D.; Jang HanLee, Ph.D.; In Young Kim, M.D., Ph.D.; and In this study, we designed a VR system toSun I. Kim, Ph.D. assess schizophrenic's social problem solv-ing ability except the cognitive ability ofDepartment of Biomedical Engineering, Hanyang schizophrenia. Reaction time responding toU n i v e r s i t y the Q&A panel and problem solution in given
social VR situation is extracted from the pro-Background/Problem posed VR system to assess social problem
abilities. After having experiences in session,Patients with schizophrenia usually lack social schizophrenia answers following questions:skills and have an inability to communicate computer experience scale, immersive ten-effectively with people, confirm and express dencies questionnaire, virtual reality ques-their feelings, and understand interpersonal tionnaire, social problem solving index, posi-boundaries. They may solve their problems in tive and negative syndrome scale, KWIS.an unsuitable manner or they may have few Now we are gathering data from associatedsolutions. In this study, we developed the Vir- hospital and have a plan to validate usabilitytual Reality system to measure social problem and effectiveness of proposed VR contentssolving ability according to the state of illness by showing that VR parameters are closelyof the patient with schizophrenia. correlated with the traditional assessment
257

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
tools e.g. SPSI.Method/Tools
Novelty/DiscussionFor the effective social perception test, VR
In this study we develop a VR system for pa- may be needed to compose various situa-tients with schizophrenia to perceive more tions and contents. So, we used VR Behav-realistic and dynamic situations, which could iour & Facial Data Base architecturebe difficult when constructed from other media (VRBFDB) for easy and fast VR composition.such as text, pictures, or video. However ad- This architecture is composed of predefinedditional research of the usability and validation 93 behaviours and 7 facial expressions dataof the proposed VR system is needed and is base. In this data base, we selected behav-being conducted in our lab. iours and facial expressions according to
contents. And, VR of 35 contents is devel-Contact: oped. The contents can be divided into twoJaehun Kim sub-contents "Attention to and interpretationDepartment of Biomedical Engineering of relevant cue test" and "Emotion Recogni-Hanyang University tion test." "Attention to and interpretation ofEmail: [email protected] relevant cue test" is composed of non-verbal
social situation, recognition, and verbal socialPresenter: Kwanguk Kim MS situation recognition, and "Emotion Recogni-
tion test" is composed of happy, sad, angry,
INVESTIGATION OF SOCIAL CUE PER- and surprise facial expression recognition.CEPTION IN SCHIZOPHRENIA USING The 21 contents are selected from 35 con-
VIRTUAL REALITY tents based on 70% selection of normal sub-jects. The subjects consisted of 17 patients
Kwanguk Kim, M.S.1 , Jaehun Kim, M.S.1 , (12 males and 5 females) and 19 controls (12
Daeun Park, B.S.1 , Jeonghun Ku, Ph.D.1 ; Hee males and 7 females). This study measured
Jeong Jang, B.A.2; Sung Hyouk Park, M.D. 2; VR data, questionnaire data, and symptom
So Young Kim, B.A. 2; Chan Hyung Kim, M.D., data. VR data included participant's response
Ph.D2 ; Jae-Jin Kim, M.D., Ph.D2; Jang Han results, reaction time, presence, and experi-
Lee, Ph.D.'; In Young Kim, M.D., Ph.D.', and ence of computer. Questionnaire data in-
Sun I. Kim, Ph.D' cluded age, education, gender, intelligence(K-WAIS) and so on. Symptom data is meas-
1 Department of Biomedical Engineering, Hanyang ured by PANSS (Positive and Negative Syn-
University drome Scales).2 Institute of Behavioral Science in Medicine, Yon-
sei University Severance Mental Health Hospital Results/Conclusion
BackgroundlProblem According to analyzed results, schizophrenicsubjects perform significantly more poorly
Impairment in social skills is one of the few than normal subjects on the VR testcriteria that all individuals diagnosed with (difference 0.86). In detail, the difference isschizophrenia must meet. Successful social 0.90 in "Attention to and interpretation ofskill requires the coordination of many skills, relevant cue test" and 0.82 in "Emotion rec-including social perception that involve the ognition test." One result shows that emotiondecoding and interpretation of social cues in recognition test corresponds with establishedothers. Previous research on the social per- research on schizophrenia on emotional fa-ception in schizophrenia has focused on the cial recognition. And, the other result showsinterpretation of emotion from facial expres- that relevant cue test is showing that schizo-sions. Recently, there have been reports on phrenia also has a difficulty to recognize so-the potential of virtual reality (VR) in social cial cues.skills training. In this study, we developed VRfor social perception assessment including the NoveltylDiscussioninterpretation of non-facial expressions. Andwe hypothesized that schizophrenic subjects In this study, we developed and used Virtualwould perform significantly more poorly than Reality Behavior & Facial Data Basenormal subjects on the VR test. (VRBFDB) for saving developing times and
costs. And we apply VR to finding the differ-
258

CYBERTHERAPY 2005 ABSTRACTS
ence between schizophrenic subjects and inverse correlation between the distances fromnormal subjects in social cue perception. avatars with angry emotion and negative symp-
toms. These results suggest that negative symp-
Contact: toms of schizophrenic patients may have an asso-
Kwanguk Kim M.S. ciation with deficit of social skills and that negativesymptoms of schizophrenia may have effects on
Department of Biomedical Engineering processing of emotions, especially of negativeHanyang University valence.17 HAENG-DANG DONG SEONG-DONG GUSeoul 133-605, Korea Contact:Phone: +82-2-2290-0693 Sung Hyouk ParkFax: +82-2-2296-5943 Email: inuonechanmail.netEmail: kwang6 bme.hanvana.ac.kr
Presenter: Evelyn KlingerPresenter: So Young Kim VIRTUAL REALITY THERAPY FORTHE RELATIONSHIP BETWEEN INTER- SOCIAL PHOBIA: ITS EFFICACYPERSONAL DISTANCE AND SYMP- THROUGH A CONTROL STUDYTOMS OF SCHIZOPHRENIA ACCORD-ING TO DIFFERENT EMOTIONAL Evelyne Klinger, ENG., PhD.candidate1' 6
CATEGORIES USING VIRTUAL REAL- Stephane Bouchard 2, Ph.D., PatrickITY Legeron, M.D.3 , Stephane Roy, Psy. 3,
Fran oise Lauer, Psy.4, Isabelle Chemin,Sung Hyouk Park1' 2, M.D., So Young Kim 2 , M.A.', and Pierre Nugues, Ph.D.5
B.A.Jeonghun Ku 3 , Ph.D., Hee Jeong Jana2 , B.A., 1 ENSICAEN-GREYC, Caen, FranceWon Yong Hahn 3, MS., In Young Kim , M.D., University of Quebec in Outaouais, Gatineau,
Sun I. Kim 3, Ph.D., Chan-Hyung Kim 1' 2, Quebec, CanadaPh.D., S3 CBT Unit, Sainte-Anne Hospital, Paris, FranceM.D., Ph.D., Jae-Jin Kim 1'2 , M.D., Ph.D. 4 Stimulus, Paris, France
' LTH Department of Computer Science, Lund1Department of Psychiatry, Yonsei University Col- University, Swedenlege of Medicine 6 GET/ENST-Paris, CNRS/LTCI, Paris, France2Mind mapping laboratory, Institute of behavioral
science in medicine,Yonsei University College of Medicine Research status: Completed control study3Department of Biomedical Engineering, HanyangUniversity, Seoul, Korea The efficiency of virtual exposure for phobic
disorders has been confirmed by severalSchizophrenia is a disease characterized by social studies, especially in the case of the fear ofimpairment. Adequate interpersonal distance is public speaking (FOPS). However, FOPS isimportant for good interpersonal relationship and a less severe subtype of social phobia andfor the social rehabilitation of schizophrenia. There does not reflect entirely the diversity of socialhave been few researches about interpersonal situations that could potentially induce anxi-distance of schizophrenia. We tried to improve the ety. In an earlier study, we reported a virtualmethod of presenting stimuli through virtual reality, reality (VR)-based clinical protocol designedWe constructed virtual environment and virtualavatar with gradual facial expressions. Fifteen toease th efiacy of ailRaltyschizophrenic patients and control subjects partici- Therapy (VRT) on a larger set of social pho-pated in this experiment. This experiment is con- bias compared to a validated psychologicalsisted of 6 blocks. In each block, subjects were treatment (group-CBT= Cognitive Behaviorasked to approach the avatar with gradual facial Therapy). The virtual environments (VEs)expressions representing one emotional category, used in the treatment recreate four situationsto the most comfortable place and introduce them- dealing with social anxiety: performance, inti-selves. We measured the distance subjects took macy, assertiveness, and scrutiny. With thefrom the avatars. We explored the characteristics help of the therapist, the patient learnsof interpersonal distances of schizophrenia andthe relationship among the distances, symptoms of adapted cognitions and behaviors in order toschizophrenia and emotional categories (happy, reduce anxiety in the corresponding realneutral or angry). There were major effects of situations.group and emotion on distances. There were an
259

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
The study is based on a pre-post design the full spectrum of social phobia.where the control condition is a gold-standardtreatment. Thirty-six participants, diagnosed Referenceswith social phobia and meeting the inclusionand exclusion criteria, were matched on either North, M., North, S., and Coble, J.R. (1998).VRT or group-CBT. Both treatments lasted Virtual Reality Therapy: An effective Treat-twelve weekly sessions and were delivered ment for the Fear of Public Speaking. Inter-according to a treatment manual in the pres- national Journal of Virtual Reality. 3 (2):2-6.ence of a CB-therapist. In VRT condition, ses- Roy, S., Klinger, E., Legeron, P., Lauer, F.,sions were individual and lasted about 45 Chemin, I., and Nugues, P. (2003). Defini-minutes, with less then 20 minutes of expo- tion of a VR-based protocol to treat socialsure to the four VEs either for assessment or phobia. Cyberpsychology & Behavior. 6therapy, while in group-CBT condition two (4):411-420.hours sessions were delivered with abouteight people, a format which allows creating Contact:multiple social situations. In both cases, fur- Evelyne Klingerther exercises were prescribed in vivo appli- 43, rue Appertcation of the principles developed during the 44100 Nantes Francesessions. The participants were submitted to Tel: +33 2 40 69 59 21 (home)"pre-post" assessment of the full spectrum of Fax: +33 2 40 69 59 21 (home)social phobia, from key symptoms to global Email: klinaeroenst.frfunctioning.
Using repeated measures ANOVAs (2 Condi- Presenter: Manfred Krapp MD PhDtions x 2 Temps), three families of hypotheseswere tested: social phobia (as measured with THE COMPUTER AS A HELPMATELSAS score and subscores), social function- FOR IMAGINATIONing (assertiveness - Rathus and SCIA), andgeneral functioning. Given these hypotheses Dr. med. Manfred Krappand the use of a gold-standard control condi-tion, the results include the effect-sizes of the C.G. Jung-institute ZuerichCondition by Time interactions and the esti-mates these differences' importance. They This paper deals with virtual reality (VR) andindicate that both treatments were highly ef- Cyberspace from a psychoanalytical point offective to reduce social anxiety and social view, especially regarding the analytical psy-avoidance and to improve social as well as chology of C.G. Jung. Electronic media haveglobal functioning, with no significant differ- basically changed the relationship betweenences between the two treatments except the Ego and the unconscious. The discourseassertiveness. of electronic media is right-hemispherical and
imaginal and corresponds to the primaryOur results clearly show the efficacy of virtual process of the unconscious. Flusser empha-reality in the treatment of social phobia. They sises a new faculty of imagination, "computeralso demonstrate that people can react emo- images simulate brain processes. The im-tionally to virtual humans and their behaviors, ages that form there are almost directly pro-even if they are unrealistic representations of jected from the brain to the outside," they arehumans. A promising explanation can be "dreams made exact." This contrasts to thefound in the interplay between believability of secondary process of the Ego which is char-a virtual reality and emotions felt by the user acteristic of the left hemisphere of the brainimmersed in the virtual environment, and of alphabetic writing and print with its
linear-perspectival discourse (Mc Luhan).These statistical analyses represent a new The electronic media has relativised time andstep in the use of our collected data, and in space in the same way as the border be-the comprehension of emotional contexts. tween individuals and between ego and un-Interesting features of our research are the conscious which become more permeableselection of a sample composed of young and flexible.adults showing clinically significant and lastingsocial phobia, the use of VEs that tackle di- Based on this point of view I will reflect onverse social situations, and the assessment of the possibilities and limits of VR and Cyber-
260
CYBERTHERAPY 2005 ABSTRACTS
space. The space of inner images can be rep- tal, Gyunggi-do, Korearesented very well by the means of hypertextwith its manifold refer ability and simultaneity. BackgroundThis is exemplified by a borderline-patient'sinitial imagery which are analysed by the A virtual avatar has been used for variousmeans of the computer-interpretation-support applications that require communicationsystem ATLAS/ti. It is based on the proceed- among persons, or to train or educate peopleings of Grounded Theory and was specifically by demonstrating human-like behavior. Re-developed for the requirements of qualitative, cently, much research has shown an en-hermeneutic research. It is based on semantic hancement of virtual avatar technology, withnetwork representations and realizes in this the avatar perceived as a real person. As away the hypertext structure. result, the technology could begin to be used
for observing human behavior to a virtualReferring to this case the capacity of cy- avatar.bertherapy is discussed, how it could functionlike art therapy in a broader sense fostering Objectivesthe emergence of inner images, and symbolswith their creative potential and self-healing This paper concerns whether a virtual avatarforces. In analytical psychology and art ther- could be perceived as a real human by pa-apy active participation on creating individual tients with a mental illness, particularlymetaphors, images and symbols is necessary schizophrenic patients, as well as whether ain order to strengthen the ego and to restore virtual avatar could acquire patients' behav-the capacity of symbolisation and imagination. ioral characteristics during a short conversa-Cybertherapy could be a therapeutic tool for tion.concretizing and structuring the primary proc-ess material as it emerges in analytical treat- Method/Toolsment offering a symbolic and archetypal im-agery for the patient. For this, we designed a virtual avatar that
was standing in a virtual room, with elevenContact: schizophrenic patients assigned the task ofManfred Krapp, MD, PhD approaching the virtual avatar, initiating aC.G. Jung-institute Zuerich conversation, and providing answers to theBerlin, 10711 avatar's questions. To measure behavioralGermany parameters in the virtual environment, wePhone: ++49308911503 acquired the interpersonal distance and theFax: ++493089096830 verbal response time. In addition, we ratedEmail: [email protected] patients on the Positive and Negative Syn-
drome Scale (PANSS) in order to investigatea relationship between patients' symptomatic
Presenter: Jeonghun Ku PhD characteristic and behavioral parameters.
RELATIONSHIP BETWEEN SOCIAL ResultsRESPONSE TO VIRTUAL AVATARAND SYMPTOM SEVERITY OF PA- Results of this study revealed that the inter-
TIENTS WITH SCHIZOPHRENIA personal distance was negatively correlatedwith the negative syndrome scale, which is a
Jeonghun Ku1 Ph.D., Won Yong Hahn 1, M.S., subscale of PANSS (r=-0.687, p=0.02). By
Hee Jeong Jang2, B. A., Sung Hyouk Park2, contrast, the verbal response time was not
M.D., So Young Kim 2, B.A., Kwang Uk Kim 1, correlated with any other subscale of
M.S., Jae Hun Kim', M.S., Jang Han Lee1, PANSS. However, after analyzing this vari-
Ph.D., Chan-Hyung Kim 2 , M.D., Ph.D., Jae Jin able with sub-items of the negative syndrome
Kim2, M.D., Ph.D., Ing Kimn , M.D., Ph.D., of PANSS, two positive correlations were
andS .Kim', Ph.D. Kfound: one with blunted affect (r=.638,and Sun I. Kp=.035) and the other with poor rapport1Dept. of Biomedical Engineering, Hanyang Univer- (r=.615, p=.044).sity, Seoul, Korea2Department of Psychiatry, College of Medicine, DiscussionYonsei University, Severance Mental Health Hospi-
261

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
The negative correlation between the distance M.D., So Young Kim, B.A., Kwang Uk Kim,and negative symptom severity observed in M.S., Jae Hun Kim, M.S., Jang Han Lee,this study could represent that they keep Ph.D., Chan-Hyung Kim, M.D., Ph.D., Jae Jincloser distance during interacting with an ava- Kim, M.D., Ph.D., In Y. Kim, M.D., Ph.D. andtar due to patient's symptom severity. There- Sun I. Kim, Ph.D.fore, it also could be said that the severernegative symptom patients have, the harder Dept. of Biomedical Engineering, Hanyang Univer-they recognize or interact with the other ex- sity, Seoul, Koreapressing emotion in a social interaction. Thisresult is consistent with previous studies that Backgroundinvestigated the relationship between schizo-phrenic patients' interpersonal distance and Facial expression research has been issuedtheir symptoms. And. the positive correlation on areas such as social psychology, psychia-between the verbal response time acquired try, and so on. Particularly, patients withand subscales in PANSS in this study could mental illness showed deficits in reading andbe explained by the definition of these sub- recognizing facial expression, so that theyscales. The blunted affect score represents suffer from their social life due to the deficit.the amount of emotional change, which is These studies mostly focused on facial rec-characterized as the reduction of facial ex- ognition ability and were conducted with stillpression, emotional modulation, and gesture images of people. However, the still imagesduring communication. By contrast, the poor as stimuli have limitations, which are lack ofrapport score represents the amount of inti- controllability and flexibility, and lack of realitymacy to an interviewer or the level of deficit in due to the inability to give a dynamic image.forming a relationship, which is characterized Actually, dynamic representation of facialas distancing a human relationship and the expressions is necessary because it is morereduction of verbal and nonverbal communi- effective to be recognized.cation. Therefore, this positive correlationmeans that the less a patient's emotional re- Objectivessponse, intimacy, and relationship makingwith a virtual avatar, the slower they answer The objectives of this study were to proposethe avatar's question. Inferring from these a method in order to present dynamic facialresults, we conclude that the virtual avatar expressions having various intensity, to in-could be perceived as a real human by vestigate human's perception to avatar's fa-schizophrenic patients, the avatar could facili- cial expressions divided by gradual strength,tate the schizophrenic patients' behavioral to investigate how the perception varies tocharacteristics, and the avatar could be used the strength of facial expression, as well asas a tool for assessing the behavioral charac- to investigate how different the perceptionteristics of patients with schizophrenia. according to avatar's gender.
Contact: Method/ToolsJeonghun Ku133-605 Dept. of Biomedical Engineering For accomplishing these goals, we generatedHanyang University, a male and a female virtual avatar with fiveSung Dong P.O. Box 55 levels of strength of happy and anger emo-Seoul, Korea, tion using morphing technique, recruited 16Tel: +82-2-2290-0693 healthy and normal subjects and measuringFax: +82-2-2296-5943 the subject's affected emotion by rating affec-Email: kuihbme.hang .ac.kr tive arousal and valence. The presentation of
expressions of virtual faces was not just toshow a still image but to show an animation
Presenter: Jeonghun Ku PhD in order for the subject to recognize the ava-tar's facial expression more realistically.
GENERATION AND VALIDATION OF Therefore, we made a virtual avatar animateDYNAMIC FACIAL EXPRESSION OF so that subjects could see a facial animation
AVATAR changing from neutral into a target expres-sion for one second, subsequently they could
M.S., see the target expression (one of five levels)Jeonghun Ku Ph.D., Won Yong Hahn, MS, for 5 seconds. Then, they scored the em~o-Hee Jeong Jang, B. A., Sung Hyouk Park,
262

CYBERTHERAPY 2005 ABSTRACTS
tional valence or arousal for the stimulus while Ph.D., Chan-Hyung Kim, M.D., Ph.D., Jae Jinbeing shown a black screen for 5 seconds. Kim, M.D., Ph.D., In Y. Kim, M.D., Ph.D. andThe 24 facial expressions of avatars were Sun I. Kim, Ph.D.provided in random order.
Dept. of Biomedical Engineering, Hanyang Univer-Results sity, Seoul, Korea
In this study, we were able to investigate the Backgroundhuman's perceptual characteristics evoked bya male and a female avatar's facial expres- Technological advances make virtual realitysion of happy and anger, and avatar's gradual (VR) able to provide social events by beingfacial expression. In addition, we were able to populated with avatars. Several studies rep-know that the virtual avatar's facial expression resented that the avatar's representationcould affect human's emotion and it showed could influence people's sense of social real-different characteristics varied with avatar's ism. As one of the critical components togender and the strengths of the facial expres- evaluate the effectiveness of virtual environ-sions as well as those characteristics ob- ment for the social interaction, the concept ofserved in previous studies using photos or presence has been used. However, there arevideo clips. However, we could also see that few studies on how emotion works in thevirtual face have some limitations because it 'feeling of presence' during experiences withis not real, so subjects were not influenced as virtual societies, although emotion plays anmuch as they recognized the virtual faces. important role in social interaction.
Conclusion Objectives
This study was meaningful in that it could pro- It focuses on the impact of avatar's emotionsvide new potential for using or manipulating (Happy, Angry, and Neutral Emotion) in co-emotional intensity by controlling a virtual ava- presence, social presence, and tele-tar's facial expression linearly using a morph- presence. Specifically, we hypothesize thating technique, although a virtual avatar has presence, particularly tele-presence, will oc-some limitation to convey its emotion using cur within immersive virtual environments asfacial expressions. Therefore, it is predicted to a function of intensity of emotion. Therefore,be used for assessing emotional characteris- we tried to evaluate the presence producedtics with emotional deficit through a presenta- by emotional value of virtual avatars in virtualtion of dynamic expression having various environments in this study.emotional intensities.
Media/ToolsContact:Jeonghun Ku A total of fifteen healthy subjects were re-133-605 Dept. of Biomedical Engineering cruited for this study. 2 x 3 (avatar gender,Hanyang University, avatar emotion) mixed ANOVA experimental
Sung Dong P.O. Box 55 design was used for this experiment. All sixSeoul, Korea, avatars have emotional appearance, behav-Tel : +82-2-2290-0693 iour, and voice. Each participant experiencedFax: +82-2-2296-5943 all 6 tasks (avatar gender x avatar emotion)Email: kujh•brnehanyang.ac.kr in a random order. Each task was to be intro-
duced with an avatar and then to introduceoneself to the avatar. After participating, sub-
Presenter: Jeonghun Ku PhD jects should complete a presence question-naire and answer the arousal (relax: 0 - exci-
EMOTIONAL INVOLVEMENT IN PRES- tation: 8) and valence (unpleasant: -4 -ENCE DURING INTERACTING WITH pleasant: +4) induced by the experience.
VIRTUAL AVATAR Results
Jeonghun Ku Ph.D., Won Yong Hahn, M.S., In an investigation of self-reported co-Hee Jeong Jang, B. A., Sung Hyouk Park, In an inv eived othereprtedco-M.D., So Young Kim, B.A., Kwang Uk Kim, presence and perceived other's copresence,M.S., Jae Hun Kim, M.S., Jang Han Lee, the scores of both co-presence scales to
263

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
happy emotional avatar were highest, and thescores to neutral emotional avatar were next, DEVELOPMENT OF AVATAR FORand the scores to angry emotion avatar was MEASURING HUMAN'S SOCIAL EMO-lowest (main effect : p<0.001). For social TIONAL RESPONSE IN IMMERSIVEpresence score, the significant main effect VIRTUAL ENVIRONMENTwas also observed (p=0.003). And, the scoreto happy emotional avatar was significantly Jeonghun Ku Ph.D., Won Yong Hahn, M.S.,high to Neutral (p=0.001), and to Angry avatar Hee Jeong Jang, B. A., Sung Hyouk Park,(p=0.007). The scores of tele-presence to M.D., So Young Kim, B.A., Kwang Uk Kim,happy emotional avatar (p=0.014) and angry M.S., Jae Hun Kim, M.S., Jang Han Lee,emotional avatar (p=0.046) were more signifi- Ph.D., Chan-Hyung Kim, M.D., Ph.D., Jae Jincantly higher than the score to neutral emo- Kim, M.D., Ph.D., In Y. Kim, M.D., Ph.D., andtion avatar. Sun I. Kim, Ph.D.
In the results of correlation analysis between Dept. of Biomedical Engineering, Hanyang Univer-emotional value (arousal and valence) and sity, Seoul, Koreapresence score, the correlations between va-lence and self-reported co-presence (r=0.873, Backgroundp<0.001) and perceived others co-presence(r=0.887, p<0.001) were significant, and the Virtual reality (VR) has become a representa-correlation between tele-presence and abso- tive method or tool to intervene between hu-lute value of valence (r=0.327, p=0.002) and man and computer. It has been widely usedvalue of arousal (r=0.228, p=0.031) was also in various fields including medical field, par-statically significant. Also, the correlation be- ticularly for treating people with mental dis-tween social presence and absolute value of ease and training handicapped people. It isvalence was statically significant (r=0.210, because VR has the ability to provide us ap=0.047). well controlled environment as well as a real-
istic, interactive, and immersive environment.Discussion Nowadays, an idea has emerged, which so-
cial stimuli also could be generated using VRThe pattern of self-reported copresence and technique, particularly using avatars. Thisperceived other's copresence to the avatar's idea has been realized and utilized for peo-emotional expression was similar. It is proba- pie with social anxiety. However, there is lackbly due to the fact that the questionnaires of evidence whether a virtual avatar couldmostly include factors regarding intimacy and influence human behaviour and emotion.involvement, which are highly related to emo- Therefore, the goal of this study was to de-tional valence. On the other side, the social velop a virtual avatar and to investigate hu-presence and tele-presence score showed a man's behavioural and emotional response inhigh correlation with absolute value of va- order to examine the possibility to apply it tolence. It might mean that humans feel greater patients with schizophrenia.presence when the other expresses emotionregardless of positive and negative. There- Method/Toolsfore, we could conclude that emotion is animportant factor to evoke 'feeling presence' in A male and a female virtual avatar havingvirtual environments with avatars. emotional expressions (happy, neutral, or
anger) were designed. The arousal & va-Contact: lence of each avatar's facial expression wasJeonghun Ku matched to the same level based on results133-605 Dept. of Biomedical Engineering of a previous study. For the experiment, 2 xHanyang University, 3 (avatar's gender and avatar's emotion)
Sung Dong P.O. Box 55 ANOVA experimental design was used. ForSeoul, Korea, the experiment, fifteen healthy subjects wereTel: +82-2-2290-0693 recruited. Each participant experienced all 6Fax: +82-2-2296-5943 introduction tasks (avatar gender x avatarEmail: kuihfbnme.hanyanq.ac.kr emotion) in random order. As measurements
for this study, behavioural response(interpersonal distance defined as a distance
Presenter: Jeonghun Ku PhD between a subject and an avatar), emotional
264
CYBERTHERAPY 2005 ABSTRACTS
(arousal and valence) measurements, andrecalled memory score were acquired. Presenter: Damini Kumar
Results WEARABLE KINEMATIC ANDPHYSIOLOGICAL BIOFEEDBACK
Through this study, we were able to observe SYSTEM FOR MOVEMENT-BASEDthat an avatar expressing emotion could influ- RELAXATIONence human behaviour, emotion, and mem-ory. In detail, when the interpersonal distance Damini Kumar MSc, John Foody; Brian Caul-was compared in each condition, the signifi- field; Tomas Ward; Charles Markhamcant main effect to avatar's gender was ob-served (p=0.023), while the difference accord- University College Dublining to avatar's gender at each emotional ex-pression was not significant. In addition, fur- In this project we are developing an effectivether distance was set in case of being pre- feedback system for a human interface with asented with an angry avatar regardless of video game designed to promote mental andavatar's gender (happy vs angry: p=0.006/ physical relaxation. Therapies such as Taineutral vs angry: p=0.003). In summary, hu- Chi and Yoga have been shown to havemans keep the interpersonal distance closer many therapeutic benefits in rehabilitationto female avatar than to male avatars and including enhancing postural awareness andfurther from an avatar representing angry reducing chronic pain and hypertension.emotion than to an avatar representing neu-tral or happy emotion. Furthermore, subjects We aim to develop a computer game inrecalled more correctly in a condition having which the player's performance is determinedan angry avatar than in a neutral avatar condi- by their ability to master one of these physi-tion (p=0.006). However, in the case of being cal arts and in doing so bring about a state ofprovided an avatar representing happiness, a mental relaxation. We are developing a vir-higher mean score was shown but was not tual reality application where whole-bodysignificant (p=O. 108). movement, respiration and physiological cor-
relates of relaxation are used as input. SuchConclusion input will be processed to provide changes to
the avatar or its environment in order to af-These results support that the virtual avatar fect appropriate biofeedback for thecould influence human behaviour, emotion, user. The purpose of this biofeedback isand memory, in particular, that those charac- such that they may more easily achieve tar-teristics were varied by emotional expressions geted postures and physiological variableof the virtual avatar. The characteristics re- ranges commensurate with Yoga/Tai Chisuiting from this study coincided with studies philosophy.conducted with real people or other instru-ments. A virtual reality and virtual avatar could A garment based physiological and kinemat-draw human behavioural and emotional char- ics measurement system will provide our pri-acteristics and assess those objectively. mary method of communication with theTherefore, it could provide a potential to be video game. This lightweight garment willused for assessing human's characteristics as monitor heart and breathing rate, muscle ac-well as assessing and enhancing social ability tivity, galvanic skin response, and alignmentof a person who has social function deficits, of body segments. To measure the humane.g., schizophrenia, using virtual avatars. body motion we have designed and imple-
mented a Universal Serial Bus (USB) basedContact: unobtrusive kinematics transducer capable ofJeonghun Ku scalable deployment with minimum instru-133-605 Dept. of Biomedical Engineering mentation.Hanyang University,Sung Dong P.O. Box 55 The player must reproduce physical posturesSeoul, Korea, displayed by a model on screen whilst main-Tel: +82-2-2290-0693 taining a relaxed and controlled breathingFax: +82-2-2296-5943 pattern. Feedback is provided by means ofEmail: kuih(_.bme.hanvanya.ac.kr reproduction of the player's body image on
screen. Quality of movement and posture,
265

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
and degree of mental relaxation will determine A randomized controlled trial was used. Po-the player's performance. The game could diatry undergraduates were randomly as-take the form of a track and field decathlon signed to receive the procedure whilst im-format. This system could benefit patients mersed in VR (Group A=VR) or verbally dis-suffering from many conditions including hy- tracted (Group B=control). Pre and post out-pertension, anxiety disorder, and chronic pain. come measures included VAS(pain), State-
Trait anxiety inventory (STAI), and simulatorReferences sickness questionnaire (SSQ). Blood pres-
sure (BP), heart rate (HR), skin conductance1.Tran MD, Holly RG, Lashbrook J, Amster- (SC), and malaise scale (MS) were meas-dam EA. Effects of Hatha yoga practice on ured pre, during, and post procedure. Within-the health related aspects of physical fitness. group and between-group analyses werePrev Cardiology 2001; 4:165-70 performed.2. David Fontaine, David Dominique -"Sourceless Human Body Motion Capture"- ResultsSOC Grenoble 2003.
There were no significant differences inContact: demographics between groups. No signifi-Damini Kumar MSc cant difference was found between groupsUniversity College Dublin for VAS for pain (p=0.78). Compared toSchool of Physiotherapy, Health Sciences baseline levels, SC was significantly higherBuilding, University College Dublin, Belfield during the procedure in the control groupDublin 4, Ireland (p<0.001). State STAI significantly decreasedTel: 00353861725625 in both groups following the procedureFax: 00441895812446 (Group A p=0.01; Group B p=0.008) and noEmail: [email protected] difference was evident between groups (pre
(p=0.124), post (p=0.065) procedure). Twosubjects reported symptoms (MS) when im-
Presenter: Belinda Lange mersed in VR. There was no significant dif-ference between pre/post SSQ in the VR
THE EFFECTIVENESS OF VIRTUAL group. Diastolic BP was significantly lowerREALITY IN REDUCING PAIN AND (p=0.034) and HR significantly higherANXIETY DURING DIGITAL NERVE (p=0.042) in the VR group. Novelty/ discus-
BLOCK sion: To date the majority of studies investi-gating the use of VR as a distraction tech-
Belinda Lange (PhD candidate) BSc, B nique have concentrated on medical proce-
Physio (Hons), Marie T Williams, Sara Jones dures with high pain levels. Pain associatedwith injections is comparatively low, however
University of South Australia often associated with high anxiety levels. Nosignificant difference in subjective pain may
Background be a result of the action of local anaesthetic,numbing the area after needle insertion. The
Applications of Virtual reality (VR) as a dis- significant increase in SC during the controltraction technique have included situations condition only (p<0.001) suggests that, de-requiring medical procedure for an injury/ spite the presence of local anaesthetic, an-ailment. Common invasive procedures ticipatory anxiety was high when the proce-(injections/venipuncture) involve the learner dure was viewed, compared to distractionpracticing the task. Some health training pro- with VR (p>0.056). STAI results are possiblygrams offer students the opportunity to learn due to an ordering effect; the majority ofinvasive techniques on each other prior to group A subjects received the procedureperforming them in therapeutic situations. The then performed the procedure on anotheraim of this study was to determine if VR was student. Malaise scale results indicate thateffective in reducing pain and anxiety in stu- adverse effects occurred in two subjects. Nodents receiving a digital nerve block from their significant change in SSQ scores for the VRpeers as part of a teaching program. group supports MS findings. However, pre
and post SSQ scores were high for bothMethodltools groups, including the control group where
SSQ scores should be zero since subjects
266
CYBERTHERAPY 2005 ABSTRACTS
were not exposed to VR, suggesting that SSQ North Terrace Adelaidemay be associated with procedural anxiety Adelaide, SA 5000and not adverse VR symptoms. Significant AustraliaBP and HR changes during VR reflect the Phone: 011 61 8 83022083physical activity involved in the intervention. Fax: 011 61 8 83022766
Email:Conclusion: While VR did not significantly Belinda Lang rads.unisaeduauinfluence subjective pain scores, lower SCindicates that VR reduced anticipatory anxietyassociated with the procedure. The MS may Presenter: Belinda Langebe a more appropriate measure of adverseeffects than the SSQ in situations where high SUBJECTIVE, PHYSIOLOGICAL ANDlevels of anxiety exist. ADVERSE EFFECTS OF THE VIRTUAL
REALITY ARQUAKE GAME COM-References PARED TO WATCHING AN ANIMATED
MOVIE IN CHILDREN AGED 6-17Hoffman HG, Doctor JN, Patterson DR, Car- YEARS
rougher GJ, Furness TA. Virtual reality as
an adjunctive pain control during burnwound care in adolescent patients. Pain Belinda Lange (PhD candidate) BSc, Marie T2000b; 85:305-309. Williams, Ian Fulton, Meredith Craigie, &
Hoffman HG, Garcia-Palacios A, Patterson Bruce ThomasDR, Jensen M, Furness TA, Ammons WF.The effectiveness of virtual reality for dental University of South Australiapain control: a case study. CyberPsychol- Backgroundogy & Behaviour 2001 b; 4:527-535.
Hoffman HG, Patterson DR, Carrougher GJ. The Virtual reality (VR) ARQuake game wasUse of virtual reality for adjunctive treatment developed at the Wearable Computer Labo-of adult burn pain during physical therapy: a ratory (UniSA) and is currently being used bycontrolled study. Clin J Pain 2000a; 16:244- researchers as a distraction technique for250. children undergoing painful procedures. ThisHoffman HG, Patterson DR, Carrougher G J, su y w sd sg e ou d rt n o hlNakamura D, Moore M, Garcia-Palacios A, study was designed to understand how chil-Furness TA. The effectiveness of virtual dren react to VR, when not undergoing pain-Furneality pAin coTrol wimtiplesf vtreat s ful situations. The aim of the study was toreality pain control with multiple treatments compare the subjective, physiological andof longer durations: a case study. Int. J. adverse responses of children to the VRHum.-Comput. Interact., 2001 a; 13:1-12. ARQuake game with an animated movie.
Kennedy RS, Lane NB, Berbaum KS, Lilien-thai MG. Simulator sickness questionnaire: Method/toolsan enhanced method for quantifying simula-tor sickness. The Int J Aviat Psychol 1993; A randomized AB/BA crossover design was3: 203-220.
Regan EC, Ramsey AD The efficacy of hyos used. Subjects aged between 6-17 yearswere randomly assigned to 14 minutes of VR
cine hydrobromide in reducing side-effects and a 14 minute section of an animatedinduced during immersion in virtual reality, movie in varying order (Group A=VR/movie;Aviat Space Environ Med 1996; 67:222-226. group B=movieNR). The simulator sickness
Spielberger CD. Stait-Trait Anxiety Inventory questionnaire (SSQ) was completed pre and(Form Y). California: Mind Garden, Inc.; post procedure. Blood pressure (BP), heart1983. p 13. rate (HR), skin conductance (SC), and mal-
Steele E, Grimmer K, Thomas B, Mulley B, aise scale (MS) were measured pre, during,Fulton I, Hoffman HG. Virtual reality as a and post procedure. Subjects completed apediatric pain modulation technique: A casestudy.presence questionnaire (PQ) following bothstudy. VR and movie.CyberPsychol Behav 2003; 6:633-638.
Contact: Results
Belinda Lange Thirty-six subjects were recruited (21 malesUniversity of South Australia and 15 females, mean age 11.89±2.98). Sub-
267

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ject numbers were equal in both groups. No Referencessignificant difference was found in demo-graphic details between groups. Significant Kennedy RS, Lane NB, Berbaum KS, Lilien-treatment effects were present for the level of thai MG. Simulator sickness questionnaire:enjoyment of the game (PQ) (p=0.03) and an enhanced method for quantifying simu-SSQ (p<0.0001). No significant period-by- lator sickness. The Int J Aviat Psycholtreatment interaction was present for any out- 1993; 3:203-220.come measures (p>0.05). The level of pres- Regan EC, Ramsey AD. The efficacy ofence (PQ) was significantly higher during VR hyoscine hydrobromide in reducing side-(p<0.004). No significant difference in SC be- effects induced during immersion in virtualtween VR and movie (>0.051) occurred at any reality. Aviat Space Environ Med 1996;time point. Blood pressure and HR were sig- 67:222-226.nificantly higher during VR (p<0.014), how-ever no significant difference in BP and HR Contact:was present post 5 minutes (p>0.481). Symp- Belinda Langetoms (e.g., HMD heavy, dizziness) were re- University of South Australiaported during VR on the MS by 47% of sub- North Terrace Adelaidejects, compared to 3% during the movie. Mild Adelaide, SA 5000nausea was reported by 6% of subjects dur- Australiaing VR (0% movie). Subjects reported no Phone: 011 61 8 83022083symptoms 5 minutes post VR. Fax: 011 61 8 83022766
Email:Novelty/ discussion Belinda.Lange5astgradsunisa.edu.au
The VR ARQuake game demonstrated higherlevels of presence than the movie with sub- Presenter: Belinda Langejects reporting significantly higher scores inthe PQ (felt like they were really there; felt like VIRTUAL REALITY AS A DISTRAC-they were actually moving; game was more TION TECHNIQUE FOR CHILDRENdifficult and harder to get used to). These re- DURING MINOR MEDICAL PROCE-suits indicate that VR will be an effective dis- DURES IN A PEDIATRIC EMERGENCYtraction DEPARTMENTtechnique during painful procedures becauseof the higher level of presence and greater Belinda Lange PhD candidate, Marie Wil-level of concentration required. Although hams, Ian Fulton, Meredith Craigiegreater symptoms were reported on the MSduring VR, only 6% reported mild nausea and University of South Australiaall symptoms subsided within five minutes. Itappears that the MS is a more appropriate The aim of this study was to determine if Vir-indicator of adverse responses to VR than tual Reality is an effective distraction tech-SSQ in children, possibly as a result of the nique for children undergoing minor medicalwording on the SSQ. The non-significant SC procedures in a Paediatric Emergency De-result between VR and movie supports the partment compared to watching a movie.MS findings. The significant increase in BP Children between 6-17 years undergoingand HR during VR reflect the physical activity minor medical procedures such as bloodinvolved in interacting with the virtual environ- sampling, intravenous cannulae insertion andment. suturing were provided with either Virtual
Conclusion reality or an animated movie excerpt as adistraction technique during the procedure.Pre, post and maximum scores were re-This study provides more information about~ ceived for children's self report pain and anxi-
the physiological and adverse effects of VR in ety and parent's perception of their child's
children and provides support for the use of pai and anty. S taff m b wer askedthe R ARuak gam inchilrenundego- pain and anxiety. Staff members were asked
the VR ARQuake game in children undergo- to provide a score for their perception of theing painful and anxiety provoking procedures child's pain and anxiety. Parental anxiety wasprovided a malaise scale is used to monitor also measured for comparison with thenausea. child's anxiety levels. The brief behavioral
distress scale was used to score the child's
268

CYBERTHERAPY 2005 ABSTRACTS
behavior during the procedure. Data collection 6 Department of Medical Biophysics, University offor this study is still ongoing and is anticipated Toronto, Toronto, Ontario, Canadatobe completed by June 2005. To date,twenty-two subjects have been recruited with Research Status: Completeda target of at least 100 subjects. The two in-terventions (Virtual reality and animated Background & Significance of the Prob-movie) will be compared using mixed be- lemtween-within subjects analysis of varianceand independent t tests. Baseline pain and Virtual environments (VEs) can be used toanxiety data for these procedures was col- assess spatial memory and navigation skills,lected in a separate study, providing informa- although the behaviour elicited is inherentlytion about the pain and anxiety associated complex. The purpose of this study was towith these procedures without distraction. Pi- investigate the ecological validity and interre-lot testing comparing the level of presence lationship between virtual navigation tasksand enjoyment of the Virtual reality to watch- and several neuropsychological tests.ing an animated movie in healthy children notundergoing procedures has also been com- Methods/Toolspleted. If Virtual reality is found to significantlyreduce pain and anxiety in children during Forty-two participants (mean age: 70.42)minor medical procedures compared to took part in the study, of which eighteen werewatching an animated movie, the technique recruited from the Cognitive Neurology Clinicmay be employed by the Pediatric Emergency at Sunnybrook & Women's College HealthDepartment as a non pharmacological pain Sciences Centre (S&W) based on diagnosismanagement tool. of mild cognitive impairment (MCI). Subjects
completed the Groton Maze Learning TestContact: (GMLT; a hidden maze task developed byBelinda Lange one of the authors [P.J.S.]) and severalUniversity of South Australia neuropsychological tests, including theNorth Terrace Adelaide MMSE, 1 the Rey Complex Figure Test,2 Ben-Adelaide, SA 5000 ton Visual Retention test,3 Trail-Making TestAustralia (Forms A and B), 4 and Digit Span.5 SixteenPhone: 011 61 8 83022083 of the participants (9 normal, 7 MCI) alsoFax: 011 61 8 83022766 undertook a VE navigation task.6 BehaviourEmail: elicited by the VE task was characterized inBelinda.Lanae{[email protected] terms of two components, as estimated by
factor analysis: a VE memory index, and aVE movement index.
Presenter: Jang-Han Lee PhDResults
SPATIAL ABILITY AND NAVIGATIONLEARNING IN A VIRTUAL CITY The VE memory index was significantly asso-
ciated with the results of a conventional
Richard Mraz, P.Eng2, Konstantine K. Zakza- memory test (Rey Complex Figure), and thenis, Ph.D., C.Psych.°, Peter J. Snyder, Ph.D. 4 VE movement index was significantly associ-In Y. Kim, Ph.D.1 , Sun I. Kim, PhD.1 , Sandra ated with measures of the Trail Making Test.E. Black, MD. 5, Simon J. Graham, Ph.D., Compared with normal participants, partici-.Eng.2,6 pants with mild cognitive impairment (MCI)
showed a significant reduction in the mem-1Department of Biomedical Engineering, Hanyang ory-related measures in the PGRD Maze
University, Seoul, Korea Learning Test and memory tests (particularly2Imaging Research, Sunnybrook and Women's RCFT), and the MCI group deviated signifi-
College Health Sciences Centre, Toronto, On- cantly from the correct route, particularly intario, Canada novel environments. Performance in the VE
3Division of Life Sciences, University of Toronto, navigation-learning task was significantlyToronto, Ontario, Canada associated with measures of visual memory
"Department of Psychology, University of Con- and the executive function in conventionalnecticut, Groton, CT, USA neuropsychological tests.
SDepartment of Medicine-Neurology, University ofToronto, Toronto, Ontario, Canada
269
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Conclusion THE APPLICATION OF A VR-TANGIBLE INTERACTION SYSTEM IN
The results of this study demonstrate that VE SENSORY INTEGRATION TRAININGtechnology can be used to assess spatial AND ASSESSMENT FOR CHILDRENmemory and navigation skills, and that meas- WITH AUTISMures of this behavior in a VE are related tothose of conventional neuropsychological Jang-Han Lee, Ph.D., Hyun-Jhin Lee,tests. Our results also demonstrate that the M.Sc.2, Young Sik Lee, M.D.,Ph.D.3, Seong-MCI group showed a significant reduction in 4shi Yong , M.D.,Ph.D.Kw Seong-memory-related measures in the GMLT and shiMK gthe neuropsychological tests. In particular,
differences between the groups were evident 1 Department of Biomedical Engineering, Collegein the immediate and delayed recall in the of Medicine, Hanyang University, Seoul, KoreaRey Test. However, because of the small 2 School of Design and Media, Hongik University,sample size, statistically significant results Seoul, Koreawere not found between groups in the VE 3 Department of Neuropsychiatry, College of Medi-navigation task. cine, Chung-Ang University, Seoul, Korea
4 Seoul Metropolitan Children's Hospital, Seoul,Novelty Korea
' Department of Psychology, Chungbuk National
The interrelationship between the VE task, the University, Seoul, Korea
GMLT, and neuropsychological assessments Research status: Still in progressis important for administration and interpreta-tion of these computerized tests in the future. Children with autism, as well as children with
References other developmental disabilities, may havedysfunctional sensory systems. Sometimesone or more senses are either over- or un-
[1] Folstein, M.F. et al. (1975). Journal of Psy- der-reactive to stimulation in these individu-[2] Meyers, J.E.s, K.R. (1995). Rey als. Sensory processing abnormalities affectComplex Figure Test and Recognition Trial: all aspects of adaptive, cognitive, social, andProfessional Manual. Odessa, FL: PAR academic functioning, and correlate withProfssioan ual.B.(1992. Oes isua, l PRe- higher levels of stereotypic, rigid, and repeti-[31 Sivan, A.B. (1992). Benton Visual Reten- tive behaviours in autism. Thus, sensory
tion Test: Fifth Edition. San Antonio, TX: Psy- proess in ab tisma beimort
chological Corporation. tprocessing abnormalities may be important
[4] Spreen, 0., & Strauss, E. (1998). A Com- to address in therapeutic interventions that
pendium of Neuropsychological Tests: Ad- aim to reduce rigidity and stereotyped behav-
ministration, Norms, and Commentary (2nd iours. Sensory integration therapy is based
ed.). New York: Oxford University Press. which emphasizes the relationship between
[5] Wechsler, D. (1981). Wechsler Adult Intel-
ligence Scale-Revised Manual. San Antonio, sensory experiences and motor and behav-
TX: The Psychological Corporation. ioural performance. Intervention strategies
[6] Mraz, R. et al. (2003). CyberPsychology & involve the use of planned and controlledsensory experiences, including vestibular,
Behavior, 6(4), 359-368. proprioceptive, and somatosensory activities,
Contact: such as swinging, deep pressure touch, andtactile stimulation; that is, the techniques fa-
Jang-Han Lee, Ph.D. cilitate attention and awareness, and reduceDepartment of Biomedical Engineering overall arousal of children with autism.College of Medicine
Hanyang University Virtual reality technology is an exciting toolSeoul, Korea for allowing children with autism to practiceTEL: +82-2-2290-8280 behaviours in role-play situations, while pro-FAX: +82-2-2296-5943 viding a safe environment for rule learning
and repetition of tasks (Parsons & Mitchell,
2002). However, some ethical and technical
Presenter: Jang-Hari Lee PhD concerns surround the use of fully immersivevirtual reality technology (i.e., the use ofhead-mounted displays (HMDs)). HMDs can
270

CYBERTHERAPY 2005 ABSTRACTS
be extremely expensive and people may ex- Parsons, S., & Mitchell, P. (2002). The po-perience 'cybersickness' in the form of nau- tential of virtual reality in social skills train-sea, headache, and dizziness, whereas desk- ing for people with autistic spectrum disor-top or projection virtual environments tend to ders. Journal of Intellectual Disability Re-be much less likely to induce cybersickness. search, 46(5), 430-443.Moreover, because HMDs place some limita-tions on the child's interaction with another Contact:person, the mixed and augmented reality is Jang-Han Lee, Ph.D.more useful for group interactions and sen- Department of Biomedical Engineeringsory experiences. College of Medicine
Hanyang UniversityTherefore, we developed a virtual reality- Seoul, Koreatangible (VR-tangible) interaction system for TEL: +82-2-2290-8280sensory integration training and assessment FAX: +82-2-2296-5943of autism by mixing the virtual environment Email: jclpsvfunite.coqkrwith the natural physical environment. Withthis system, children with autism experiencevestibular, proprioceptive, and somatosensory Presenter: Jang-Han Lee PhDactivities, such as swinging, spinning, androtating, and a social skills training program SEX DIFFERENCES IN HEALTHY ELD-such as eye gaze. In addition, a program that ERLY ADULTS FOR COMPLETING 2-involves breaking virtual balloons with a real DIMENSIONAL HIDDEN MAZE AND 3-stick measures the visuomotor coordination of DIMENSIONAL VIRTUAL REALITYchildren with autism. The participants view NAVIGATION LEARNING TASKSthemselves, virtual balloons, and a real stickon a large screen that displays game-like sce- Jang-Han Lee PhD', Richard Mraz, P.Eng 2
narios. Our VR-tangible interaction system Konstantine K. Zakzanis, Ph.D , C.Psych.Econsists of a Pentium IV PC, a projector, a Pete nyder PhD 2 , In.Di, PhyD.1
screen (200 x 150 cm), an infrared reflector, Peter J. Snyder, Ph.D.2, In Y. Kim, Ph.D. 2and adigial caera.Sun 1. Kim, Ph.D.', Sandra E. Black, M.D.2Simon J. Graham, Ph.D., P.Eng.2
The performances of normal control groups 1Hanyang University, Seoul, Koreaand autistic groups will be compared in the 2Sunnybrook and Women's College Health Sci-visuomotor coordination program and the so- ences Centre, Toronto, Ontario, Canadacial skills training program. The degree that 3University of Toronto, Toronto, Ontario, Canadathe sensory integration training leads autistic 4University of Connecticut, Groton, CT, USAchildren to more productive contacts with an-other individual and environments will also be Background & Significance of the Problemanalyzed.
Sex differences in navigation and mazeAs the study is still in progress, final results learning are well known, with men often out-were not available at the time this abstract performing women on route-learning, spatialwas written. The use of a VR-tangible interac- perception, and visualization.1 4 Some sug-tion system to better understand sensory gest that these differences stem from evolu-processing abnormalities of children with au- tion, while others attempt to further elucidatetism is relatively rare, even in studies with vir- these differences by new experimental meth-tual environments. We hope that this study ods. The present study used a series of non-will clarify sensory processing abnormalities verbal, visually-guided navigation tasks toof children with autism and stimulate further investigate gender differences in healthy,studies on sensory integration training and elderly adults.assessment in the field of VR-tangible inter-action. Methods/Tools
References The three distinct test components were 1)the Groton Maze Learning Test (GMLT), 2)
Ayres, J. (1972). Improving academic scores traditional neuropsychological tests, and 3) athrough sensory integration. Journal of 3D VE navigation-learning task. The GMLT isLearning Disabilities, 5, 338-343. a computerized measure of a participant's
271
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ability to acquire and use efficiently an internal [3] Moffat, S.D. et al. (2001). Neurobiology ofspatial map of a hidden 2D maze. Neuropsy- Aging, 22, 787-796.chological tests included the MMSE, 5 the Rey [4] Sandstrom et al. (1998). Cognitive BrainComplex Figure Test,6 Benton Visual Reten- Research, 6, 351-360.tion test, 7 Trail-Making Test,8 and Digit Span.9 [5] Folstein, M.F. et al. (1975). Journal ofThe 3D VE navigation task10 involves learning Psychiatry Research, 12, 189-198.and recalling routes through a virtual city. [61 Meyers, J.E., & Meyers, K.R. (1995). ReyTwenty-five healthy elderly volunteers partici- Complex Figure Test and Recognition Trial.pated. Odessa, FL: PAR
[7] Sivan, A.B. (1992). Benton Visual Reten-Results tion Test. San Antonio, TX: Psychological
Corporation.Sex differences were found in learning ability [8] Spreen, 0., & Strauss, E. (1998). A Com-with the 2D maze test and the VE navigation. pendium of Neuropsychological Tests. NewMen excelled at maze-learning ability, espe- York: Oxford University Press.cially after the middle trials, although men and [9] Wechsler, D. (1981). WechslerAdult Intel-women did not differ in performance on the ligence Scale-Revised Manual. San Antonio,first learning trial for this test. These results TX: The Psychological Corporation.suggest that men more easily acquired spatial [101 Mraz, R. et al. (2003). CyberPsychologyability and learning than women, and that men & Behavior, 6(4), 359-368.also reached their peak performance abilitymore rapidly than women in the maze- Contact:learning test. Jang-Han Lee, Ph.D.
Department of Biomedical EngineeringMen significantly outperformed the women College of Medicineonly on the first trial of the VE navigation task. Hanyang UniversityThere were no sex differences after a second Seoul, Koreatrial, perhaps due to the relative ease of the TEL: +82-2-2290-8280VE navigation task since no subjects deviated FAX: +82-2-2296-5943significantly from the path following the sec- Email: ckpsya2unitel~co.krond learning trial.
Performance on the GMLT was related to per- Presenter: Elizabeth Lewis M.R.C.Psychformance on both the memory-related neuro-psychological tests and the VE task. WHAT ASPECTS OF VIRTUAL ENVI-
RONMENTS MAKES THE EXPERI-Conclusion ENCE "REAL" FOR AGORAPHOBIC
Men outperform women on the 2D and 3D PATIENTS?
navigation tasks. Future studies should inves- David.G.Walshe1 , Elizabeth J. Lewis 2
tigate sex differences between topographicand Euclidian cues in VE navigation learning 1 St. Stephen's Hospital, Cork, Ireland., Depart-and how these strategies and age affect spa- ment of Psychiatry, University College Cork.tial memory and navigation learning in normal 2 St. Stephen's Hospital, Cork, Ireland. Depart-people. ment of Child Health and Paediatrics, University
College Cork
NoveltyResearch Status: Research in progress
This study suggests that the VE task has eco-logical and comparative validity for measuring Agoraphobia with or without panic disorder isspatial ability and navigation, a disabling mental health problem with an
estimated population prevalence of 6%. It isReferences frequently seen in both primary and secon-
dary mental health settings. Currently, al-[1] Galea, L.A., & Kimura, D. (1993). Person- though the evidence base for behaviour ther-ality and Individual Differences, 14, 53-65. apy for agoraphobia is extensive, the service[2] Holding, C.S., & Holding, D.H. (1989). delivery is poor. It is estimated that 25% ofJournal of General Psychology, 116, 29-41. phobic patients refuse "in vivo" exposure
272
CYBERTHERAPY 2005 ABSTRACTS
therapy or drop out. Consequently behaviour sented at conference together with VR envi-therapy is often difficult to provide in this area. ronments.
Preliminary studies have shown a role for vir- Noveltytual reality (VR) in the treatment of agorapho-bia. Vincelli et al. showed significant reduc- VRET for agoraphobia is at a developmentaltions in the number of panic attacks, level of stage. Information from this study will assistdepression and both state and trait anxiety in tailoring VR software and treatment pro-following VR treatment with Experiental Cog- grams.nitive Therapy (ECT). 1 Botella et al showedVR exposure therapy as effective as in vivo Contact:exposure in a number of outcome measures Dr David Walsheincluding fear, avoidance and panic symp- St Stephens Hospitaltoms. 2 Sarsfield Court
CorkIn this study of 5 agoraphobic patients we in- Tel: 00-353-21-48214211vestigated what aspects of virtual environ- Email: da vidjlg•,fahoq cornments induce presence in agoraphobic pa-tients using VRMRI Virtual World software byPsychology Software Tools, Inc. This software Presenter: Elizabeth Lewis M.R.C.Psychprovides 13 inter-connected VR environmentswhich include: an urban area, apartment, IS VIDEO HOMEWORK OF BENEFITtheatre complex, restaurant, bank, urban sub- WHEN PATIENTS DON'T RESPONDway station, village subway station, village TO VR THERAPY FOR DRIVING PHO-area, house, doctor's office, airport subway BIA?station, and two airports).
We examined which environments induced David.G.Walshel, Elizabeth J. Lewis2
presence with associated subjective distressand physiological anxiety and whether theaddition of background sounds pertinent to 1 St. Stephen's Hospital, Cork, Ireland., Depart-each environment influenced presence and ment of Psychiatry, University College Cork.distress 2 St. Stephen's Hospital, Cork, Ireland. Depart-levels. ment of Child Health and Paediatrics, University
College CorkProcedure
In our Virtual Therapy Clinic, based in Cork,5 subjects with DSM-IV criteria either for ago- we have specialised in developing and evalu-raphobia without history of panic disorder or ating virtual reality environment treatmentpanic disorder with agoraphobia were initially (VRET) programmes for driving phobia inexposed to a neutral VR environment to accli- motor accident victims. Findings have beenmatise to VR. Thereafter patients navigated reported supporting this treatment modality.'-virtual environments with or without the addi- 3 This patient group often has co-morbid psy-tion of background sound over a 3 minute pe- chiatric conditions including major depres-riod unless anxiety symptoms necessitated sion, posttraumatic stress disorder, panictermination of exposure. disorder, and substance abuse which compli-
cates treatment.Ratings of presence (Item from Presence In-ventory), subjective distress (SUDS) and Our standard driving programme involves 8-physiological anxiety (Heart Rate measure- 12 VR sessions, using computer games withments) were recorded once per minute during graded driving in vivo homework tasks follow-exposure to each environment and verbal ing progress in virtual exposure.feedback from each patient following eachexposure was recorded. Presently we are focusing on two clinical
concerns. Patients who do not desensitise/Results reprocess their travel fears despite multiple
virtual exposure sessions and the number ofThis study is ongoing. Results will be pre- treatment sessions required for successful
273
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
VR treatment. CyberPsychology &Behavior 6:329-334.
Aim 3.Walshe, D.G., Lewis, E., Kim SI,O'Sullivan, K., Virtually driving: Are the driv-
To assess whether the addition of video ing environments "real enough" for exposurehomework tasks involving exposure to watch- therapy with accident victims? Submitted foring video clips of driving situations encoun- publication CyberPsychology & Behaviortered in VR therapy will bring about desensi- 2004.tization and thereby symptom resolution inpatients resistant to VR exposure therapy. Contact:
Dr David WalsheProcedure St Stephens Hospital
Sarsfield Court3 patients, with a diagnosis of DSM-IV Spe- Corkcific Phobia-driving, resistant to a VR driving Tel: 00-353-21-48214211programme undertook a "video homework" Email: davidamw @yvahoo.cornprogramme. A video tape containing a 10minute clip of anxiety provoking driving situa-tions derived from the most recent VR session Presenter: J. Harvey Mageewas assigned as homework. These clips wererecorded directly from the VR driving scenes A PRIMER ON TATRC'S MEDICALpresented in therapy. Each patient was re- MODELING & SIMULATION PORTFO-quested to watch the video clip for 30 minutes LIO: THE SERIOUS SIDE OF FUNdaily in a darkened room with earphones andrecord Subjective Units of Distress (SUD) rat- J. Harvey Mageeings daily until anxiety level fell to SUD ratingof 2 or less. As the patient progressed to Portfolio Manager, Medical Modeling & Simulationmore distressing driving scenarios in VR ther- (MM&S)apy the video clip was updated accordingly. Telemedicine and Advanced Technology Re-
search Center (TATRC)The Fear of Driving Inventory (FDI) and the HQ U.S. Army Medical Research and MaterielPosttraumatic Stress Disorder Symptom Command
Scale (PTSS) were documented at entry and As we enter the 21t century, the worlds ofreassessed on completion of the study. military and civilian medical training struggle
Results with critical questions. For the military, howdo we train medical personnel in peace for
This study is ongoing. Results will be pre- the realities of war? For the civilian sector,
sented at conference together with assigned how do we train medical personnel in a way
video clips, that results in increased patient safety... orreduced patient errors? Reports from the
Novelty U.S. General Accounting Office and the Insti-tute of Medicine have dealt with these chal-
This is a novel development in VRET with lenges.
potential clinic benefit. Why serious? Here are a couple of exam-
References ples. First, health care the power to heal orharm patients. How we train to deliver care
1 Walshe, D.G., Lewis, E.J., Kim, S.I., et al is serious too. What if residents actually de-
(2003). Virtual Reality and computer games liver health care the way we teach them to?in the treatment of driving phobia induced by Second, the human body is infinitely chal-
a motor vehicle accident. Cybertherapy Con- lenging... and constantly changing. Every-
ference 2003 p34. body (literally every body) is different. How
2.Walshe, D.G., Lewis, E.J., Kim, S.I., et al much realism is necessary to simulate it?
(2003). Exploring What objective performance metrics are most
the use of computer games and virtual reality appropriate? Simulated environments impact
exposure therapy for fear people, but in what ways?of driving following a motor vehicle accident.
274

CYBERTHERAPY 2005 ABSTRACTS
In 2000, TATRC MM&S leaders (Dr. Moses, MEASUREMENTS IN A REAL-CARMr. Magee), facilitated a 70-person strategic BASED DRIVING-SIMULATORplanning workshop. At its conclusion and inconjunction with "end users" of simulation- Dr. Ralph Magerbased training systems, a strategy was devel-oped. Based on that strategy, collaborations COAT Basel, Switzerlandof academic, government, and industrial re-search groups began to take shape, and net- Objectiveworks of relationships formed. Leadersstepped forward, and funding sources were The goal of the present study was to evalu-
identified to propel research in four general ate physiological measures and objectivecategories of medical simulation research: performance parameters during driving in aPC-based interactive multimedia, digitally en- real-car based driving simulator. Arousinghanced mannequins, part-task trainers, and auditory stimuli were applied to compare dataTotal Immersion Virtual Reality. Key defining prior and after intervention to test the sensi-events and workshops have been funded over tivity of the system.the past five years in support of that strategy.Annual refinements of the strategy have been Design and Methodsmade, always in conjunction with "end users."
Overall 41 subjects were selected matchedFueled by congressionally designated funded for age and driving experience. To createand managed by TATRC, the Center for Inte- realistic traffic scenarios in a laboratory envi-gration of Medicine and Innovative Technol- ronment a passenger car simulator was usedogy (CIMIT) Simulation Group (PI: Dr. Steve emulating the functionality of a modern car.Dawson) embraced the challenge to develop Electroencephalographic (EEG) activity, skinand integrate key enabling technologies into conductance, respiratory and cardiac pa-systems of simulation-based training. Exam- rameters were continuously recorded duringpies are real-time in vivo tissue property driving. Analysis was focused on time inter-measurement, tissue-tool interactions, graph- vals prior and after application of a warningics and visualization, learning systems, met- stimulus intervening a monotonous drivingrics development, learning transfer and as- session. Simultaneously objective driving-sessment. parameters were derived from the simulator
(time to lane crossing, lateral position andExamples of current projects include ad- others).vanced ureteroscopic surgical simulation(TURP procedure), virtual cricothyroidotomy, ResultsVIRGILTM Chest Trauma Training System,Central Venous Catheterization, Exsanguinat- The intervening stimuli induced significanting Hemorrhage, "VR-Demo", Dynamic Injury group effects in respect to EEG activity andCreation Simulator. skin conductance. There was a decline of the
stimulus induced changes within several min-What degree of validation is necessary to utes. Other physiological parameters likedemonstrate transfer-of-training effective- respiratory or cardiac parameters were unaf-ness? What open source standards require fected. Data revealed a strong inter-individualdevelopment enroute to the eventual need for variability. This applied also to the perform-systems to be interoperable with either other ance parameters provided by the simulator.medical simulation systems or more compre- Time to lane crossing and the lateral positionhensive training systems? of the car were determined in different sce-
narios and separated for various types ofIn summary, the presenter will predict some tracks.benefits of medial simulation, and offer someclosing thoughts for success for the MM&S Conclusioncommunity... and the world.
The present study revealed significantphysiological group effects in response to
Presenter: Ralph Mager MD intervening stimuli during driving in a real-carbased simulator. EEG effects, simulator data
VIGILANCE AND PERFORMANCE
275

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
and first applications in psychiatry are dis- phones will synchronise with therapists'cussed. computers during sessions and allow thera-
pists and clients to view and discuss theContact: game information.Dr. Ralph MagerCOAT Basel Trials of this system will be run in the MaterBasel, 4025 Hospital and several of its associated clinicsSwitzerland in Dublin. Research conclusions will bePhone: 0041613255242 made as a result of pre- and post- question-Fax: 0041613255492 naires for therapists and clients, detailedEmail: [email protected] interviews with therapists, client attendance
records, and log data from client's mobilegames. A comparative study of mobile
Presenter: Mark Matthews MSc games versus current materials and ap-proaches will also be undertaken.
WIRELESS THERAPY: MOBILEGAMES AS A MEANS OF ENGAGING It is hoped that this research will ascertain
ADOLESCENT CLIENTS whether mobile games can: effectively in-corporate therapeutic elements, improve thetherapeutic alliance, help increase adoles-
Mark, Matthews BA, M. Sc.1, Dr. Gavin Do- cent engagement in therapeutic activitiesherty1 , Dr. John Sharry2 between sessions with a therapist as well as
in actual sessions, increase the amount of1 Trinity College Dublin, Ireland time clients give between sessions to work-2Mater Hospital, Dublin, Ireland ing on their issues, increase client task com-
pletion rate, and reduce stigma attached to
Research Status: Currently in progress. therapy through positive associations withgaming.The proposed research aims to evaluate the
Therapists have difficulties engaging adoles- potential of mobile therapeutic games tocent clients in therapeutic activities between overcome difficulties faced by therapists insessions. These activities usually require engaging adolescents in therapeutic activi-clients to prepare materials in advance of ties between therapeutic sessions. It alsosessions or chart their feelings between aims to discover whether this approachthem. Typically there is a very low rate of might save therapist session time by bring-task completion in these activities. This ing therapy outside of sessions and intomight be attributed to the use of outmoded adolescents' everyday life.materials or methods which are not concur-rent with adolescent interests. There have been studies of the potential
educational uses of mobile games to facili-Research suggests that client-centered ma- tate cooperative learning and to examineterials have a greater chance of success in their potential as tools for supporting learn-engaging adolescent clients. Mobile gaming ing. There has been little research into therepresents such an approach, allowing ac- therapeutic use of mobile technology. Somecess to adolescents' personal space, but studies have examined the use of text mes-affording adolescent users persistent and saging in client aftercare, while others havecontinual access to therapeutic materials, tentatively explored the use of mobile de-Most importantly it takes advantage of an vices to structure client narratives. To date,existent widespread network in use by ado- there has been a lack of research exploringlescents and therefore requires no extra the effects mobile therapeutic games couldhardware costs. The proposed system will have on adolescent engagement in therapy.allow therapists to send personalised gamemissions to clients' phones at specific agreed Contact:times between sessions. After each level theclient will receive a positive personal mes- Mark, Matthewssage from the therapist. The proposed game Trinity College Dublinwill be similar to the shoot-em-up genre of Ireland.mobile game. During a session clients' Ph: +353-1-6081765
276

CYBERTHERAPY 2005 ABSTRACTS
Fax: +353-1-6772204 Tasks 1 and 2 have been completed. TheEmail: matthemim(tcd.ie system is under Phase 2 development as
part of Task 3. Themes associated with che-motherapy-related alopecia include shock,embarrassment, feeling unprepared, and
Presenter: Elizabeth L. McGarvey EdD anxiety about self and others perceptions. OnINTERACTIVE COMPUTER IMAGINING a scale of 1 = not all easy to 10 = extremelyTO FACILITATE COPING WITH CHE- easy to use, a non-clinical sample rated theMOTHERAPY-RELATED ALOPECIA prototype system no lower than a mean ofDISTRESS 8.66 (SD=1.28) on ease of use in 4 areas.
Health care professionals in oncology ratedElizabeth L. McGarvey, EdD, Adrienne Keller, the realism of images on a similar scale withPhD, David Brenin, MD, Lora Baum, PhD, the lowest score received a mean of 8.94Brian Clark, Scott Acton, PhD, B. Eugene (SD= .93). Phase II is currently underwayParker, Jr, PhD with a 2006 completion date.
Univeristy of Virginia' Charlottesville, VA, USA Conclusion
Background/Problem Interactive computer imaging systems usingvirtual images have a viable place in treat-
As many as 47% to 58% of women with can- ment for distress in cancer patients sufferingcer report alopecia as the most disturbing an- quality of life issues due to alopecia.ticipated aspect of receiving chemotherapy.1
This project develops and evaluates the effec- Referencestiveness of a computer imagining system thatpresents virtually real images of a woman 1. McGarvey, E.L., Baum, L.D., Pinkerton,going through the stages of hair loss/ re- R.C., & Rogers, L.M. (2001). Psycho-growth as part of a strategy to provide psy- logical sequelae and intervention forchosocial support to reduce distress associ- treatment-induced alopecia among fe-ated with chemotherapy-related alopecia. male cancer patients. Cancer Practice,
9(6), 283-289.Methods
Contact:Following Phase I development of a prototype Department of Psychiatric Medicineof a computer imaging system, further devel- University of Virginiaopment of a user-friendly, touch screen, inter- P.O. Box 800623action system that shows hair re-growth and Charlottesville, VA 22908-0623images sufficient for use to provide psychoso- Tel: 434-924-5522
cial support to women with cancer is now un- Fax: 434-982-3764
der development. The project has a number E-Mail: [email protected]
of tasks prior to the final evaluation of the sys-tem: Task 1: Following Phase 1 focus groupswith a sample of patients provided feedback Presenter: Sarah D. Miyahira PhDon the usefulness of such a system. Alopecia-related distress was also further studied. Task THE MATURING OF VIRTUAL REAL-2: A sample of health care professionals were ITY RESEARCH IN BEHAVIORALinterviewed to provide feedback on the accu- HEALTH: A META-ANALYSIS ANDracy of the images and usefulness of the sys- REVIEWtem. Task 3: Complete and refine the com-puter imagining system. Task 4: Conduct a Sarah D. Miyahira, Ph. D.randomized clinical trial comparing quality oflife between patients with chemotherapy- Pacific Telehealth & Technology Hui: A DoD/VArelated alopecia who use the computer imag- Joint Ventureing system to those who receive standardcare. Research Status: In Progress
Results Background/Problem
277

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
for select studies were large in magnitude,Since the early 1990's, the research on virtual and a meta-analysis will be performed withreality (VR) applications for behavioral health the identified controlled VR studies, includinghas progressed from exploratory case studies those published in early 2005.and feasibility studies to comparisons withwait-list and active treatment control Conclusionsgroups. This maturation of the field has setthe foundation for conducting meta-analytic The findings to date suggest that VR for be-and review studies of the research findings to havioral health is a maturing field that holdsdate. The current investigation presents a considerable promise with continued re-comprehensive review of the published VR search. Most of the published studies areresearch in four clinical domains: (1) anxiety either case studies or uncontrolled feasibilitydisorders, (2) eating disorders, (3) pain anal- studies, particularly for novel uses of VR ingesia, and (4) addictions. In addition, a meta- behavioural health. Additionally, some clini-analysis of andomized controlled studies of cal domains have had relatively minimal at-VR applications in behavioral health provides tention (e.g., addictions) as compared to oth-a summary of effect sizes, making it possible ers (e.g., anxiety disorders). Preliminary cal-to draw stronger conclusions regarding the culations of effect sizes indicate high efficacyefficacy of VR interventions than significance of VR, which is not only encouraging for thetesting results alone. As such, this study field, but supports the need for more con-builds and expands upon recently published trolled studies across clinical domains. It isreviews of VR for anxiety disorders1- 3 and eat- essential that there be a better balance be-ing disorders.4 The results of this investigation tween innovation and validation to establishshould be highly relevant and disseminable VR as an effective intervention for behav-for researchers in the area of VR and the ioural health.more general area of behavioral health.
NoveltyMethod
To our knowledge, this is the first statisticalThe investigation consists of a systematic re- meta-analysis of VR for behavioral health. Inview of the research to February 2005 as well addition, this review includes studies andas a meta-analysis of the literature. Utilizing clinical domains that were not included inPsychlnfo and Medline, all of the published previous reviews.and abstracted studies in the four clinical do-mains described earlier were identified and Referencesreviewed. Each study was categorized as (1)a case study/uncontrolled study, (2) a wait- 1 Anderson, P., & Jacobs, C. (2004). Corn-list/attention placebo controlled study, or (3) puter-supported cognitive behavioral treat-an active treatment/standard care controlled ment of anxiety disorders. Journal of Clini-study. The meta-analysis combines the effect cal Psychology, 60:253-267.sizes from all controlled studies to produce 2 Krijn, M., Emmelkamp, P. M. G., Olafsson,general indicators of the efficacy of VR inter- R. P., & Biemond, R. (2004). Virtual realityventions for behavioral health. exposure therapy of anxiety disorders: A
review. Clinical PsychologyResults Review, 24:259-281.
3 Wiederhold, B. K., & Wiederhold, M. D.The review component of the investigation (2005). Virtual Reality Therapy for Anxietyhas been completed of VR studies related to Disorders. Washington, DC: American Psy-behavioral health published through Decem- chological Association.ber 2004. Thus far, the data indicate that 73 4 Myers, T. C., Swan-Kremeier, L., Wonder-outcome studies have been published across lich, S., Lancaster, K., & Mitchell, J. E.the four clinical domains with 19% (14) being (2003). The use of alternative delivery sys-wait-list or attention placebo studies, and 18% tems and new technologies in the treat-(13) active treatment or standard care con- ment of patients with eating disorders. In-trolled trials. A more detailed review of each ternational Journal of Eating Disorders,clinical domain was done to assess the scope 36:123.of the research conducted within the specificdomain. Preliminary effect sizes computed Contact:
278
CYBERTHERAPY 2005 ABSTRACTS
Sarah D. Miyahira tion simulation while thirteen participantsPacific Telehealth & Technology Hui: A DoD/ received VR exposure without motion simu-VA Joint Venture lation.1 Jarrett White RoadMCPA-PO, Tripler AMC Virtual flights consisted out of different flyingHonolulu, Hawaii 96859-5000 phases (start, flying, turbulences, landing)Phone: 1-808-433-1912 and were simulated using a head mountedFax: 1-808-433-1920 display (HMD), a head tracking device andEmail: [email protected] a motion platform to simulate accelerations
and provide proprioceptive stimuli.
Presenter: Andreas Mulhlberger PhD Results
SUBJECTIVE AND PHYSIOLOGIC RE- Overall, subjective fear ratings as well as
ACTIONS OF FLIGHT PHOBICS DUR- skin conductance responses confirmed sub-
ING VR EXPOSURE AND TREATMENT stantial fear of both groups during VR expo-
OUTCOME: WHAT ADDS MOTION sure. However, these responses were sub-
SIMULATION? stantially stronger and habituated slower inthe VR motion group compared to the VRno-motion group. Nevertheless and in con-
Andreas M Phlberger, Ph.D., Georg trast to network theories - which suggestWiedemann and Paul Pauli that stronger activation of fear networks
should result in an enhanced treatment out-Department of Psychology, Biological Psychol- come wesfoun n difrenes betwogy, Clinical Psychology, and Psychotherapy, come - we found no differences betweenUniversity of Wurzburg, Wcrzburg, Germany groups in treatment outcome. There was no
trend of a superior treatment outcome forBackground/Problem the VR-motion compared to the VR-no-
motion group.The efficacy of virtual reality (VR) exposurefor the treatment of fear of flying was con- Conclusions and Noveltyfirmed in more than 8 controlled clinical tri-als. Important goals of future studies are the The present study helps to better under-evaluation of underlying treatment processes stand VR exposure treatment and givesand the identification of crucial treatment hints for future research to evaluate thecomponents, both in order to optimize the treatment process. Based on our results ittreatment. The present study was designed may be speculated that treatment outcometo examine the effect of motion simulation on is more related to the amount of habituationsubjective and physiological fear reactions during exposure than to the strength of theas part of a VR exposure that also included initial fear response.visual and acoustic stimuli. Our hypotheseswere that motion simulation results in Contact:stronger initial subjective and physiological Andreas Muhlberger, Ph.D.fear reactions, and as a consequence is as- Department of Psychologysociated with stronger habituations of fear University of W(rzburgresponses within VR flights and between VR Marcusstr. 9-11flights. Furthermore, we assumed that mo- 97070 WOrzburg, Germanytion simulation enhances treatment efficacy Tel.: +49 (0)931-312843as measured in the fear of flying scale (FFS). Fax: +49 (0)931-312733
E-mail: [email protected] and Tools wuerzburg.de
Twenty five participants with flight phobiareceived a virtual reality exposure treatment Presenter: Sarah Parsons PhDincluding written information about fear offlying and how to cope with it (information USE, UNDERSTANDING AND LEARN-booklet), one hour of cognitive therapy, and ING IN VIRTUAL ENVIRONMENTS BYVR exposure (four flights). However, VR ex- ADOLESCENTS WITH AUTISTICposure included for twelve participants mo- SPECTRUM DISORDERS
279

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
at learning directly and found that partici-Sarah Parsons, Ph.D pants improved in their awareness of social
conventions, both in terms of performance inSchool of Education, University of Birmingham the virtual cafe and in judgments and com-
ments made in relation to some video clipsBackground (which served as approximations of real life
judgments). Study 4 involved case studiesThe potential for using Virtual Environments with two participants and showed that both(VEs) with children with autistic spectrum dis- appeared to learn the target social conven-orders (ASDs) has been recognised by some tions and commented on how the VE couldauthors. The central premise is that interac- be relevant to their lives.tions in VEs may be less threatening for chil-dren with ASDs compared to the 'real world' Conclusionbecause many of the confusing inputs of realworld interaction can be directly controlled The overall findings suggest that some ado-and/or manipulated. The present research lescents with ASDs can use, understand andinvestigated whether single-user VEs could learn social skills/conventions presented insupport the learning of social skills by adoles- VEs. The main challenge now is to reflect oncents with ASDs. these findings in order to shape future work.
Specifically, there is a need to consider theMethod role of the facilitator in 'scaffolding' partici-
pants' use of the VEs. To what extent canA series of quasi-experimental studies was facilitation be separated from the effect of thecarried out to investigate three main research VE itself? If the aim is to provide educationalquestions; would adolescents with ASDs be support, is a separation of factors desirableable to use the VEs appropriately, understand anyway?VEs as representational devices, and/or learnnew information from VEs about social skills? Novelty
Single-user VEs were developed to show dif- This series of studies represents a system-ferent social contexts, such as a bus and a atic and detailed addition to the scant exist-caf6, and participants completed a number of ing literature on the use of VEs by childrentasks such as finding a place to sit, navigating with ASDs. The investigation into representa-to the counter to buy food/drink and queuing. tional understanding, inclusion of carefullyNon-autistic comparison groups were in- matched comparison groups, and considera-cluded where possible and participants were tion of clearly specified social learning objec-also interviewed about their experiences and tives are particularly noteworthy aspects ofunderstanding. All sessions were videotaped the research.for later analysis, such as time taken to com-plete the tasks, navigational paths, and verbal Contact:responses. Independent measures of verbal Sarah Parsons Ph.D(VIQ) and non-verbal (PIQ) understanding, School of Educationand Executive ability were also taken. University of Birmingham Edgbaston
Birmingham UK B15 2TTResults Phone: +44 (0) 121 414 4819
Fax: +44 (0) 121 414 4865In Study 1, participants with ASDs were not Email: s •i.narsonsnbham.ac.uksignificantly different from a PIQ-match groupin time taken to complete VE-based tasks,and the majority understood the VE as having Presenter: Paul Penn PhDbasic representational qualities. Study 2showed that a majority of participants with VIRTUAL REALITY IN MEMORY AS-ASDs behaved in a similar way to non-autistic SESSMENT AND REHABILITATION:comparison groups by treating the VE like a PROGRESS TO DATE AND FUTUREgame in most situations. A third of the ASD POTENTIALgroup (4 out of 12) showed substantial 'off-task' behaviour, which was linked to low VIQand weak executive abilities. Study 3 looked
280
CYBERTHERAPY 2005 ABSTRACTS
Paul Penn. BSc (Hons), Ph.D., Barbara whose physical disabilities restrict their mo-Brooks. BSc, Ph.D., David Rose. BSc, Ph.D. bilityl 5 16' 17; and motivate patients with trau-FBPsS matic brain injury (TBI) to participate in exer-
cise in order to stimulate memory remedia-University of East London. UK tion.18 There has also been some preliminary
research on prospective memory in patientsFrom its inception in 1994, the Virtual Reality who have suffered a stroke19 and older indi-Research Group at the University of East Lon- viduals. 20 Finally, using VR together withdon recognised the enormous potential of vir- fMRI offers exciting opportunities to addresstual reality (VR) as a highly flexible, rigorously the neurophysiological basis of differentcontrollable, yet non-invasive method of di- types of memory. These, and other possibili-rectly assessing and manipulating brain activ- ties, are discussed.ity in order to reduce the impact of brain dam-age. Studies have been conducted to address This paper evaluates the current state of re-whether individuals who have suffered brain search on the applications of VR to memorydamage can use VR, 1 whether what is assessment and rehabilitation, proposeslearned in VR transfers to the real world,2 and some directions for future research, de-the implications of active interaction vs. pas- scribes some recent work on VR and pro-sive manipulation within virtual environments. spective memory being conducted at UEL,Experiments have encompassed individuals and suggests a strategy for turning our re-who have suffered brain damage as a result search findings into real benefits for patients.of vascular,' traumatic, 4 degenerative, 5 anddevelopmental factors.6 References
Memory impairments are one of the most dis- Rose, F. D., Brooks, B. M., Attree, E. A.,abling consequences of brain injury. 7 8 They Parslow, D. M., Leadbetter, A. G., McNeil,can be problematical to assess, as conven- J. E., Jayawardena, S., Greenwood, R., &tional "paper and pencil" neuropsychological Potter, J. (1999). A preliminary investiga-tests of memory and cognitive function do not tion into the use of virtual environments inadequately cover important aspects of every- memory retraining of patients with vascularday memory, such as prospective memory brain injury: Indications for future strategy?(remembering to perform actions in the future) Disability and Rehabilitation, 21; 548-554.and incidental memory (the encoding and re- Rose, F. D., Attree, E. A., Brooks, B. M.,call of memories without any instructions from Parslow, D. M., Penn, P. R., & Ambihaipa-a third party).9 Paper and pencil tests have han, N (2000). Training in virtual environ-also been heavily criticized as lacking ments: Transfer to real world tasks and"ecological validity,"10 Unfortunately, it can be equivalence to real task training. Ergonom-very difficult to achieve ecological validity ics; 43, 494-511.without compromising experimental control. Andrews, T. K., Rose, F. D., Leadbetter, A.
G., Attree, E. A., & Painter, J. (1995). TheVirtual environments provide an elegant solu- use of virtual reality in the assessment oftion to the problem of developing memory cognitive ability. In I. Placencia Porrero andtests and rehabilitation strategies that are R. Puig de la Bellacasa (Eds.), Proceed-valid from both empirical and ecological ings of the 2nd TIDE Congress; 276-279.standpoints. In spite of this, it is probably fair Amsterdam: lOS Press.to argue that research into memory assess- Brooks, B. M., Attree, E. A., Rose, F. D., Clif-ment and rehabilitation in VR has been under- ford, B. R, & Leadbetter, A. G. (1999). Theexploited. However, some progress has been specificity of memory enhancement duringmade; for example, researchers have devel- interaction with a virtual environment.oped VEs to: assess incidental and spatial Memory, 7(1); 65-78.memory via active interaction and passive Andrews, T. K. (1999). Virtual environmentsobservation" 1; enhance the restoration of and memory training: A preliminary investi-memory function in individuals with demen- gation into the feasibility and efficacy oftia 12; facilitate in the reorganisation of memory training amnesic patients in a virtual envi-skills to use unimpaired functions in order to ronment. Unpublished doctoral disserta-train patients with amnesia to navigate around tion, University of East London.a rehabilitation ward13'14; encourage the de- Rose, F. D., Brooks, B. M., & Attree, E. A.velopment of spatial memory in children (2000). Virtual reality in vocational training
281
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
of people with learning disabilities. Proceed- multi-level environments, Proceedings of theings of the International Conference on Dis- 4th International Conference on Disability,ability, Virtual Reality and Associated Tech- Virtual Reality and Associated technologies,nologies-ICDVRAT2000; 129-136. Reading, Hungary, 2002, pp. 13-18.UK: University of Reading. Stanton, D., Wilson, P., Foreman, N., and
Kinsella, G., Murtagh, D., Landry, A., Jomfray, Duffy, H. Virtual environments as spatialK., Hammond, M., Obeirn, L., Dwyer, L., training aids for children and adults withLamont, M., and Ponsford, J. (1996) Every- physical disabilities, Proceedings of the 3rdday memory following traumatic brain injury, International Conference on Disability, Vir-Brain Injury 10; 499-507. tual Reality and Associated technologies,
Thone, A.I.T. Memory rehabilitation - Recent Sardinia, 2000, pp. 123-128.developments and future directions (1996) Grealy, M.A., Johnson, D.A., and Rushton,Restorative Neurology and Neuroscience 9; S.K. Improving cognitive function after brain125-140. injury: The use of exercise and virtual real-
Brooks, B. M., Rose, F. D. (2003) The use of ity, Archives of Physical Medicine and Re-virtual reality in memory rehabilitation: Cur- habilitation 80, 1999, 661-667.rent findings and future directions. Neu- Brooks, B.M., Rose, F.D., Potter, J., Attree,roRehabilitation, Vol 18(2); 147-157. E.A., Jayawardena, S. & Morling, A. (20,02)
Neisser, U. Memory: What are the important Assessing stroke patients' ability to remem-questions? in: Practical Aspects of Memory, ber to perform actions in the future usingM.M. Gruneberg, P.E. Morris and R.N. virtual reality, Proceedings of the 4 th Interna-Sykes, eds., Academic Press, London, tional Conference on Disability, Virtual Real-1978; 3-24. ity and Associated Technologies, Hungary,
Brooks, B.M., Attree, E.A., Rose, F.D., Clif- 2002; 239-245.ford, B.R., & Leadbetter, A.G. (1999). The Brooks, B.M., Rose, F.D. (2003) The effectsspecificity of memory enhancement during of age and cognitive load on time-based,interaction with a virtual environment, Mem- event-based, and activity-based prospec-ory 7; 65-78. tive memory task retrieval in a virtual envi-
Schreiber, M., Schweizer, A., Lutz, K., Kal- ronment. Unpublished data.veram, K.T., and JAncke, L. Potential of an Morris, R.G., Parslow, D. Fleminger, S.,interactive computer-based training in the Brooks, B., Brammer, M., and Rose, D.rehabilitation of dementia: An initial study, (2002) Functional magnetic resonanceNeuropsychological Rehabilitation 9 (1999), imagining investigation of allocentric spatial155-167 memory tested using virtual reality in pa-
Brooks, B. M., McNeil, J. E., Rose, F. D., tients with anoxic hippocampal damage,Greenwood, R. J., Attree, E. A., & Leadbet- Proceedings of the 4 h International Confer-ter, A. G. (1999). Route learning in a case of ence on Disability, Virtual Reality and As-amnesia: The efficacy of training in a virtual sociated Technologies, Hungary, pp. 87-92environment. Neuropsychological Rehabili-tation, 9(1); 63-76. Contact:
Rose, F.D., Attree, E.A., Brooks, B.M., and Paul Penn Ph.DAndrews, T.K. Learning and memory in vir- School of Psychology.tual environments: A role in neurorehabilita- University of East London. UK.tion? Questions (and occasional answers) Telephone: +44(0) 208 223 [44241442514500]from the University of East London, Pres- E-mail: [email protected] 10 (2001), 345-358.
Stanton, D., Foreman, N., and Wilson, P. Usesof virtual reality in training: developing the Presenter: Thomas Penzel PhDspatial skills of children with mobility impair-ments, in: Virtual Environments in Clinical NEW SENSOR DEVELOPMENT FORPsychology and Neuroscience: Methods and THE DETECTION OF SLEEPINESS INTechniques in Advanced Patient Interaction, THE WORK AND TRAFFIC ENVIRON-G. Riva, B.K. Wiederhold and E. Molinari, MENT AND SLEEP LABORATORIESeds. OS Press, Amsterdam, 1998, pp. 219-232. T. Penzel1 , H.F. Becker', I. Lekka 2 , E.
Stanton, D., Foreman, N., Wilson, P., Duffy, H., Bekiaris 3
and Parnell, R. Use of virtual environmentsto acquire spatial understanding of real-world 1 Hospital of Philipps-University, Dept. of Internal
282

CYBERTHERAPY 2005 ABSTRACTS
Medicine, Pneumology, Marburg, Germany The new developed sensors and analysis2Aristoteles University of Thessaloniki, Greece algorithms are then applied in sleep laborato-SCentre for Research and Technology Hellas, Hel- ries and intensive care medicine with moni-lenic Inst. of Transportation, Thessaloniki, Greece toring demands. Wireless data transmission
based on body area network technologies isResearch status: In Progress of major importance for these applications.
Background Novelty
Sleepiness in the work and traffic environment Existing applications in sleep diagnosis arecan cause severe accidents. Sleepiness is based on wired technology and are restrictedeither the consequence of sleep loss or sleep to hospital based sleep laboratories. The newdeprivation or of a sleep disorder. Car acci- systems will allow a medical diagnosis in out-dents have more fatal outcomes at night than patient settings with the same signal qualityduring the day. Drowsy or sleepy drivers and as reached in the hospital until now. The sys-workers at monitoring tasks do have a slower tematic approach to signals and parametersresponse to react adequately to alarms or will enable the development of improved al-dangerous situations. Therefore there is a gorithms for diagnosis. Sensors technologyneed to monitor sleepiness in such circum- developed for automotive purposes can bestances. reused in medical diagnostic environment.
Methods: A European project uses existing Referencestechnologies and sensors to develop new in-tegrated systems in order to detect a lower 1. A. Rechtschaffen and A. Kales, A manualvigilance at an early stage. Definitions for the of standardized terminology, techniques anddifferent levels of sleepiness were developed scoring system for sleep stages of humanbased on monitoring of brain function' and
2 subjects. NIH Publication No. 204. Washing-autonomous nervous system functions. The ton D.C.: U.S. Government Printing Officemost sensitive parameters will be chosen in 1968.order to monitor sleepiness without impair- 2. T. Penzel and R. Conrad, Computer basedment of the driver or worker. An alarm or Sleep Analysis, Sleep Medicine Reviewsother adequate feedback will be developed in 2000; 4: 131-148.order to create awareness to the driver orworker. The same sensors are also used for Contact:the medical applications in order to diagnose Thomas Penzelsleep disorders. The specific challenge is to Hospital of Philipps-Universitydetect sleep disorders at an early stage in Depart. of Internal Medicineorder to initiate prevention programs. Marburg, D-35033
Results GermanyPhone: +49-6421-2866435
A set of important signals for the identification Fax: +49-6421-2865450
of sleepiness has been identified. The electro- Email: [email protected]
encephalogram, the electromyogram, andheart rate are sensitive signals. Among all Presenter: Alessandra Preziosasleep disorders the most prevalent sleep dis-orders are addressed. These are insomnia, MOBILE NARRATIVES TO IMPROVEsleep disordered breathing, periodic limb THE QUALITY OF LIFE: AN EXPERI-movements during sleep, and narcolepsy. T AL RES:ARCRApplication scenarios for work environment as MENTAL RESEARCHwell as for diagnostic and treatment ap-proaches were defined. Preziosa, A., A. Grassi, D. Villani, F.
Mantovani, Ph.D, J. Waterworth Ph.D, J.Conclusions Freeman Ph.D, G. Riva
The definitions reached up to now allow to Applied Technology for Neuro-Psychology Lab
specify systems for use in the work and traffic Istituto Auxologico Italiano
field as well as in the medical environment. Abstract
283

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Schedule)3 and the STAI (State Trait AnxietyThe market of mobile phones is increasing Inventory).4quickly and now account for shipments ofover 400 million units per year. The mobiles of The final results will be presented at the Cy-new generation bring much functionality, as bertherapy 2005 conference.PDA, cameras, gaming devices, or mediaplayers. These innovations will grow in the Referencesnext years, so a new generation of hardware-accelerated mobile devices will soon be http://www.neurotiv.orgljoined by a suite of emerging 3D software Jacobson, E. (1938) Progressive Relaxation.standards that gives developers the ability to Chicago. U. of Chicago Press.create interactive content and applications Watson, D.; Clark, L.A.; Tellegen, A. (1988).that haven't been possible before. Development and validation of brief meas-
ures of positive and negative affect: TheIn this context, mobile narratives are emerg- PANAS scales. Journal of Personality &ing as possible applications. Mobile narratives Social Psychology, 54(6).are interactive multimedia experiences imple- Spielberger, C. D., Gorsuch, R. L., Lushene,mented on mobile devices, in which the narra- R., Vagg, P. R., & Jacobs, G. A. (1983)tive component is a critical aspect to create a Manual for the State-Trait Anxiety Inven-feeling of presence and engagement. tory (Form Y). Palo Alto, CA: Mind Garden.
The mobile narratives, through the link be- Contact:tween the feeling of presence and the emo- Alessandra Preziosational state, may be used to improve the Applied Technology for Neuro-Psychologymood state in the users. In particular, mobile Labnarratives may be used for both modifying the Istituto Auxologico Italianouser's mood and helping him to relax, en- Via Pelizza da Volpedo 41hancing his well-being. Milan, Italy
Ph./Fax +39-02-619112892Relaxing is a difficult activity, especially in Email: [email protected] life. Many of us are usually involvedin stressful situations far away from the con-text required by the classical relaxation tech- Presenter: Patrice Renaud PhDniques. In this study - supported by the Italian"NeuroTiv' MIUR FIRB research project1 wedeveloped a mobile narrative for UMTS THE RECORDING OF GAZING RE-phones to be used by commuters to improve SPONSES IN VIRTUAL IMMERSION: Atheir well-being. The narrative, based on a trip NEW CLINICAL TOOL TO ASSESSin a desert tropical island, relaxes the userthrough different audio-visual experiences. SEXALP ESThey include the exploration of the island and PARAPHILIASdifferent relaxation techniques based on theProgressive Relaxation protocol developed by Patrice Renaud, Ph.D.1, Jean Proulx, Ph.D.2,Jacobson.2 Joanne L. Rouleau, Ph.D.2 , Stephane Bou-
chard, Ph.D.', Gina Madrigrano, Ph.D.3 ,The experimental sample is composed by 90 John Bradford, M.D.3, Paul Fedoroff, M.D. 3
commuting students, aged between 20 an 24,randomly divided in 3 different conditions: the 1 Departement de psychoeducation et deexperimental group, which experienced the ?sychologie, Universit6 du Quebec en Outaouaismobile narrative during their daily train trip; a Universite de Montrealfirst control group, which experienced a relax- 3 Forensic Program, Royal Ottawa Hospitaling new age DVD during their train trip; and asecond control group, which experienced the Research status: In progresstrain trip only. Sexual preferences are usually assessedEach subject was submitted before and after either by resorting on sexual responses re-the experience to the following questionnaires corded with a penile plethysmograph or bythe PANAS (Positive and Negative Affects using visual reaction time from stimuli with
284
CYBERTHERAPY 2005 ABSTRACTS
sexual content. However, numerous short- developed by head-movements definecomings come with penile plethysmography changes in the global scene presented in theand visual reaction time, and notably volun- HMD, the 2 DOF given by the eye-trackingtary erectile control and not paying attention device allow the computation of the exact po-to stimuli, which are important threats to the sition of the line of sight relative to the VMP.internal validity of these assessment proce- As other physiologic signals, we also measuredures. In order to get round these limitations, the subject's distance from the VPR, the pupilwe developed a method that controls gazing size diameter, the blinking response and theactivity relative to sexual avatars. A study is erectile response recorded with a penileconducted using our method that is aiming at plethysmograph. The 3D stimuli that we usedassessing sexual preferences with sex offend- are animated naked human models.ers and control subjects interacting with sex-ual avatars. Results
Background Preliminary results from sex offenders andcontrol subjects will be presented. These
Sexual preferences are usually assessed results will consist in analyses performed oneither by resorting on sexual responses re- time series coming from oculomotor andcorded with a penile plethysmograph or by other physiologic responses recorded in im-using visual reaction time from stimuli with mersion.sexual content. However, numerous short-comings come with penile plethysmography Noveltyand visual reaction time, and notably volun-tary erectile control and not paying attention The novelty of this method for assessing sex-to stimuli, which are important threats to the ual preferences was acknowledged at theinternal validity of these assessment proce- last Conference of the Association for thedures. In order to get round these limitations, Treatment of Sexual Abusers held Octoberwe developed a method that controls gazing 2004 in Albuquerque (NM). These resultsactivity relative to sexual avatars. A study is inscribe themselves in the extension of ourconducted using our method that is aiming at past studies whose goal was mainly to makeassessing sexual preferences with sex offend- sense of the perceptual and motor dimen-ers and control subjects interacting with sex- sions of virtual immersion. 1-5 They also paveual avatars. the way to interactive behavior and percep-
tion modification therapies based on eye-Methods tracking recorded in MR.6'7
Our method relies upon a technological setting Referencesincluding what is usually necessary to presentvirtual environments in immersion plus equip- 1. Renaud, P., Singer, G., & Proulx, R.ments dedicated to eye-movements tracking (2001). Head-tracking fractal dynamics infrom within a head mounted display (HMD). A visually pursuing virtual objects. In Sulis W.,special mounting built from a monocular infra- Trofimova I. (Eds.), Nonlinear Dynamics inred eye-tracking system combined within a Life and Social Sciences (NATO Sciencebinocular HMD is used to track eye- series, Vol. 320), Institute of Science Pressmovements. Head-movements are recorded (lOS Press), Amsterdam, pp 333-346.from a magnetic tracking system rendering the 2. Renaud, P., Cusson, J.-F., Bernier, S.,6 degrees-of-freedom (DOF) of translation and Decarie, J., Gourd, S.-P., & Bouchard, S.rotation. Our method performs gaze analysis (2002). Extracting perceptual and motor in-by the way of virtual measurement points variants using eye-tracking technologies in(VMP) placed on virtual objects for the analysis virtual immersions. Proceedings ofof eye-movements in relation to specific fea- HA VE'2002-/EEE (Institute of Electrical andtures of these objects. Gaze radial angular de- Electronics Engineers) International Work-viation (GRAD) from the VMP is given by the shop on Haptic Virtual Environments andcombinations of the 6 DOF developed by their Applications, Ottawa, pp. 73-78.head-movements and the x and y coordinates 3. Renaud, P., Rouleau, J.-L., Granger, L.,rendered by the eye-tracking system. The VMP Barsetti, I., & Bouchard, S. (2002 c).is locked to virtual objects and moves jointly Measuring sexual preferences in virtualwith them. While the variations in the 6 DOF reality: A pilot sudy. Cyberpsychology and
285
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Behavior, 5 (1), 1-10.4. Renaud, P., Bouchard, S., & Proulx, R. This presentation will review the state of the(2002). Behavioral avoidance dynamics in the art in this research field. In particular, it willpresence of a virtual spider. IEEE (Institute of discuss the result coming from different con-Electrical and Electronics Engineers). trolled trials comparing this approach withTransactions in Information Technology and competing techniques.Biomedecine, 6 (3), 235-243.5. Renaud, P., Decarie, J., Gourd, S.-P., Further, the presentation will address thePaquin, L.-C., & Bouchard, S. (2003). Eye- future directions of this method focusing ontracking in immersive environments : a general the possible opportunities coming from Inter-methodology to analyze affordance-based in- net and mobile devices.teractions from oculomotor dynamics. Cyberp-sychology and Behavior, 6 (5), 519-526.6. Renaud, P. (2004). Moving assessment of Presenter: Albert "Skip" Rizzo PhDsexual interest into the 2 1st century : the po-tential of new information technology. Invited GAMES FOR HEALTH: GAME-BASEDspeaker at The 23 rd Annual Research and VIRTUAL REALITY APPLICATIONSTreatment Conference (Association for the FOR MENTAL DISORDERS & REHA-Treatment of Sexual Abusers), Albuquerque, BILITATION27-30 October 2004.7. Renaud, P., Albert, G., Sauve, L., Renaud, Albert "Skip" Rizzo1 , Jarrell Pair, Galen Buck-L., Dfcarie, J., & Bouchard, S. (2004). As- walter, Jeff Gold, Carolee V\instein, Margaretsessing perceptual learning dynamics during McLaughlin, Ken Graap, Brenda Wiederholdvisual search in virtual immersion using eye-tracking technologies. Cognition and Learning 'University of Southern California Institute forin Digital Age (CELDA 2004), Lisbon, 15-17 Creative TechnologiesDecember, 6 pages.
The rapidly growing popularity of digital gam-Contact: ing has driven advances in game-basedPatrice Renaud, Ph.D. technology that has now added new momen-Laboratoire de cyberpsychologie turn to the vision of creating immersive andUniversitd du Quebec en Outaouais interactive experiential opportunities for aInstitut Philippe-Pinel de Montreal wide range of human needs beyond just theC.P. 1250, Succ. B entertainment value that come from playingGatineau (Quebec) Canada, J8X 3X7 games. In addition to the readily intuitive ap-Tel. : 819 595 3900 plication of game-based earning for educa-Email: Patrice.renaud(&uqo.ca, tion and training purposes (Prensky, 2001),
the mental health and rehabilitation fieldsstand to substantially benefit from advances
Presenter: Giuseppe Riva PhD in this area. The integration of game technol-ogy and experiences with VR-based ap-
VIRTUAL REALITY IN EATING DISOR- proaches for clinical assessment, treatment,DERS AND OBESITY: STATE OF THE and rehabilitation offers powerful options thatART AND FUTURE DIRECTIONS could revolutionize standard practices in
these fields. Thus far, the integration of gam-Prof. Giuseppe Riva, Ph.D. ing features into a VE has been reported to
enhance motivation in adult clients undergo-Applied Technology for Neuro-Psychology Lab ing physical and occupational therapy follow-Istituto Auxologico Italiano ing a stroke (Jack et al, 2001; Kizony, Katz &
Weiss, 2003) and to reduce acute pain dur-The first study describing the possible use of ing medical procedures (Hoffman et al.,virtual reality in the treatment of eating disor- 2000). As well, Strickland (2001) reports thatders and obesity was published in 1995. children with autism were observed to be-Since then, different researchers have been come very engaged in the VR safety trainingstudying the possible advantages of virtual applications that she has developed whichreality as experiential technique able to mod- incorporate game features. Further anecdotalify the body image, self-efficacy and emo- observations suggest that children diagnosedtional control of the patient. with Attention Deficit Hyperactivity Disorder
286
CYBERTHERAPY 2005 ABSTRACTS
often have a fascination for the type of stimu- Contact:lus environments that are presented in Albert "Skip" Rizzocomputer/video games (Greenhill, 1998). Par- University of Southern Californiaents are often puzzled when they observe Institute for Creative Technologiestheir children focusing on computer games 13274 Fiji Wayintently, while teacher reports indicate inatten- Marina del Rey, CA, 90292tion in the classroom. Additionally, in the pre- Phone: 213-610-4737senter's previous clinical experience, it was Email: arizzoc&usc.eduanecdotally observed that certain young adulttraumatic brain injury clients, who had diffi-culty maintaining concentration on traditional Presenter: Albert "Skip" Rizzo PhDcognitive rehabilitation tasks, would easilyspend hours at a time playing the computer FROM TRAINING TO TOY TO TREAT-game "SimCity." These observations suggest MENT: PRELIMINARY RESULTSthat designers of clinical assessment and FROM A VR THERAPY APPLICATIONtreatment tasks could benefit from examining FOR IRAQ WAR MILITARY PERSON-the formulas that commercial game develop- NEL WITH COMBAT-RELATED PTSDers use in the creation of interactive digitalgames. These formulas govern the flow and Albert "Skip" Rizzo', Jarrell Pair, Peter J.variation in stimulus pacing that provide link- McNerney, Ernie Eastlund, Brian Manson,age to a progressive reward and goal struc- Jon Gratch, Randy Hill, Michael Roy*, Billture. When delivered within a highly interac- Swartout, Ken Graap & Brenda WRederholdtive graphics-rich environment, users arecommonly observed to become extremely 1 University of Southern California Institute forengaged in this sort of game play. This pres- Creative Technologiesentation will describe a variety of ongoing pro-jects at USC that integrate game technology In 1997, researchers at Georgia Tech re-with VR-based applications for the assess- leased the first version of the Virtual Vietnamment, treatment and rehabilitation of cogni- VR scenario for use as a graduated exposuretive, psychological, emotional, and physical therapy treatment for PTSD in Vietnam veter-disorders. These projects have focused on ans. This occurred over 20 years followingthe development of applications for: the end of the Vietnam War. During that in-
terval, in spite of valiant efforts to develop1. Attention process assessment in children and apply traditionalwith ADHD psychotherapeutic approaches to PTSD, the2. Pain distraction in children undergoing progression of the disorder in some veteranspainful medical procedures and chemother- severely impaired their functional abilitiesapy and quality of life, as well as that of their fam-3. Exposure therapy in returning Iraq War vet- ily members and friends. Prior to the avail-erans with PTSD ability of VR therapy applications, the existing4. Motor rehabilitation for persons with central standard of care for PTSD was imaginal ex-nervous system dysfunction (i.e. stroke, brain posure therapy. Such treatment typically in-injury) volves the graded and repeated imaginal
reliving of the traumatic event within theThese applications have leveraged the assets therapeutic setting. This approach is believedthat have come from advances in both game to provide a low-threat context where theengine technology and from the unique ex- patient can begin to therapeutically processperience that is fostered from the psychologi- the emotions that are relevant to the trau-cally involving act of game play. Such USC matic event as well as de-condition the learn-initiatives may provide hope that innovative ing cycle of the disorder via a habituation/methods can be created to advance these extinction process. While the efficacy ofareas that have long been mired in the meth- imaginal exposure has been established inods of the past. My presentation will begin multiple studies with diverse trauma popula-with an introduction on how and why game tions (Rothbaum & Schwartz, 2002), manyassets can be used to create applications in patients are unwilling or unable to effectivelymental health and rehabilitation and then will visualize the traumatic event. With this his-review the data/status of our various projects. tory in mind, the USC Institute for Creative
Technologies (ICT) has initiated a project
287

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
that is creating an immersive virtual environ-ment system for the treatment of Iraq War 1 University of Quebec in Outaouaismilitary personnel diagnosed with combat-related PTSD. The treatment environment is Backgroundbased on a creative approach to recyclingvirtual assets that were initially built for a com- Virtual reality (VR) can become a useful toolbat tactical simulation scenario entitled Full to overcome obesity, especially for young-Spectrum Command, and later licensed to sters, considering its similarity to videocreate the commercially available X-Box games. This comparative study aim to as-game, Full Spectrum Warrior. sess what type of immersive display is pre-
ferred by youngsters for using a virtual bicy-Thus far we have created a prototype virtual cle. This is the first step in the developmentenvironment designed to resemble a Middle of a program to enhance motivation in obeseEastern city. We intend to use this VE for ini- youngsters to exercise.tial clinical and patient user testing to gatherfeedback to refine the city scenario and for Method/Toolsthe future expansion of the system to includeother relevant scenarios (e.g. outlying village Twenty-one healthy participants aged 10-18and desert scenes, etc.) and user perspec- years old (mean age = 12.5, 52.4% male)tives. We have also created an initial version were immersed three times (three minutesof a "wizard of oz" type clinical interface. This each) in a virtual environment using a differ-interface is a key element in that it will provide ent type of technology for each immersiona clinician with the capacity to customize the (HMD, projector, television). The order oftherapy experience to the individual needs of immersive technology was randomly as-the patient by placing them in VE locations signed. The hardware used was a 10-speedthat resemble the setting in which the trau- bicycle connected to an I-Magic@ VR trainermatic events initially occurred. The interface steering with an integrated tracker connectedwill also allow the therapist to gradually intro- to a Pentium I1l® 866 Mhz PC. The HMDsduce and control "trigger" stimuli in the envi- used were an I-Visor® for half of the partici-ronment in real time as is required to foster pants and an I-Glass@. An Eiki® LCD multi-the anxiety modulation needed for therapeutic media projector and a Sony® 27-inch televi-habituation. This presentation will discuss the sion were used. Pre-post measures of Im-vision, rationale and user-centered develop- mersive Tendencies and the Simulator Sick-ment status of the Full Spectrum PTSD treat- ness were completed. Subjective measuresment system that is currently in progress at were administered after each immersion forthe ICT. As well, initial results will be pre- presence, cybersickness, and preferences.sented from ongoing user-centered designtrials that are part of the development of this Resultsimmersive VR application for this highly rele-vant mental healthcare problem. Participant significantly preferred the HMD
over the projector and the television. TheyContact: felt more "present" using the HMD but alsoAlbert "Skip" Rizzo more cybersickness. No significant differenceUniversity of Southern California was found in the preference for the televisionInstitute for Creative Technologies vs. projector. Immersive Tendencies corre-13274 Fiji Way lates significantly with presence when HMDMarina del Rey, CA, 90292 was used.Phone: 213-610-4737
Conclusion
Presenter: Genevieve Robillard MSc Results indicate that levels presence, prefer-ence, and cybersickness are higher when
COMPARATIVE STUDY OF IMMER- using a HMD. Considering the purpose ofSION TECHNOLOGY FOR A VIRTUAL this study, cybersickness has to be acknowl-
BICYCLE edge since obese youngsters will use thevirtual bicycle for a longer periods. The pro-
Genevieve Robillard, M.Sc.1, Stephane Bou- jector and television still had a high level of
chard, Ph.D., & Judith Lapierre, Ph.D. interest for participants and low cybersick-
288
CYBERTHERAPY 2005 ABSTRACTS
ness. LCD projectors are the best technology the subject to be effective. To design a suit-to use as an immersive display for virtual ex- able training protocol, it would be interestingercises. to study possible effects that diferent type of
feedback can have on subjects. FeedbackContact: may help subjects to improve their EEG con-Genevieve Robillard, M.Sc. trol, but sometimes its effects can be frustrat-University of Quebec in Outaouais ing. Besides,Cyberpsychology Lab conventional systems of feedback, such asGatineau, Quebec J8X 2B7 cursor control or horizontal bar extension canCanada prove somewhat boring, leading to a lack ofPhone: (819) 776-8045 motivation.Fax: (819) 776-8098Email: [email protected] Method/Tools
To avoid this problem, feedback must be at-Presenter: Ricardo Ron-Angevin tractive, motivating subjects to control their
EEG signals. For this, a good option is theDEVELOPMENT OF A BRAIN- use of techniques based on virtual reality [2],COMPUTER INTERFACE (BCI) BASED combining 3D display, sound and isolation.ON VIRTUAL REALITY TO IMPROVE Using these techniques, a more natural inter-
TRAINING TECHNIQUES action can be achieved, isolating subjectsfrom distraction, and providing a more im-
Ricardo Ron-Angevin, PhD candidate, mersed and motivating environment. Based
Antonio Diaz-Estrella, Arcadio Reyes- on virtual reality techniques, a new type of
Lecuona BCI system to enable to establish the appro-priate feedback allowing subjects to get bet-
Departamento de Tecnologia Electr6nica, ter control of EEG signals, is developed.Universidad de Mlaga Results
Research Status: In progress. This BCI allows to set parameters related to
Background/Problem training paradigm timing (- duration, repeti-tiveness and pause between trials, - duration
A brain-computer interface (BCI) is based on of the feedback period, - duration of the ses-the analysis of the electroencephalographic sion), the type of feedback (continuous orsignals (EEG), recorded during certain mental discrete feedback) and the presentation ofactivities, to control an external device. One of feedback selecting different scenes. Due toits main uses could be in the field of medicine trial repetitiveness, interface were designedand especially in rehabilitation. It could help to to be as appealing and motivating as possi-establish a communication and control chan- ble. It was decided to submit subjects to anel for people with serious motor function more familiar environment, such as control-problems but without brain function disorder. ling a car to avoid crashing it into a wall, to
avoid logs in the road, or to reach a rampPerformance of BCI will depend, especially, that would make the car jump. Preliminaryon the ability of subjects to control their EEG results show how this new system can bepatterns being necessary to provide suitable useful to study and to improve training proto-training. The vast majority of research in the col in BCI.BCI field puts emphasis on the importance ofdeveloping training methods based on bio- Conclusionsfeedback techniques that would improve hu-man performance. The new BCl system is very promising, pro-
viding an attractive training to the subject andTraining in BCI consists on carrying out some allowing to adapt training protocols to be ef-trials, repeated times, being very important to fective.provide some type of feedback allowing sub-jects to see their progress [1]. Training proto- Novelty/Discussioncols must not be chosen at random. On thecontrary, in many cases, they must adapt to
289

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
One of the differences of this new system, larly, it provides an opportunity to enhancecompared to conventional feedbacks, such as treatment of their patients through such mo-cursor control or horizontal bar extension, is dalities.the use of virtual reality to provide feedbackwith more immersive and motivating effects. We report our experience with the use of
standardized patients (SPs) in educatingReferences physicians regarding the diagnosis and treat-
ment of biological and chemical warfare[1] Guger, C., Edlinguer, G., Harkam, W., agent exposure. We trained professionalNiedermayer, I., actors to serve as SPs representing expo-Pfurtscheller, G., 2003. How many people are sure to the biological agents anthrax, small-able to operate an pox, botulinum toxin, and staphylococcusEEG-Based Brain-Computer Interface (BCI). enterotoxin B (SEB). We conducted work-IEEE Trans. On Neural Systems shops at two national medical meetings, withand Rehabil. Eng. 11, 145-147. workshop participants rotating in small[21 J.A Pineda, D.S. Silverman, A. Vankov, groups through a series of teaching stationsand J. Hestenes, "Learning to where they were able to perform a medicalControl Brain Rhythms: Making a Brain- history and physical examination, order tests,Computer Interface Possible," IEEE make a diagnosis, and establish a manage-Trans. Neural Systems and Rehab. Eng., vol. ment plan. Workshop staff physicians then11, pp. 181-184, June 2003. conducted discussions and emphasized key
teaching points. In addition, we trained SPsContact: to simulate a mass casualty (MASCAL) inci-Ricardo Ron-Angevin dent involving a terrorist spraying a liquid onDepartamento de Tecnologia Electr6nica a city bus, once using sarin, and in anotherUniversidad de Mclaga case using hydrochloric acid. All workshopCampus de Teatinos sin 29071 participants worked together to treat MAS-Mclaga, Spain CAL victims, followed by debriefing and dis-Phone: +34-952132897 cussion.Fax: +34-952131447Email: rraadte.umaes We also describe a current project to develop
computer-based interactive modules of simu-lated patients exposed to smallpox, anthrax,
Presenter: Michael J. Roy MD MPH and other biological and chemical agents.The nature of the program allows the user to
USE OF STANDARDIZED PATIENTS go through the simulation repeatedly, with aAND COMPUTER-BASED SIMULATION different presentation each time, based partlyFOR PHYSICIAN EDUCATION ON on the questions they pose and the way they
BIOTERRORISM ask them, as well as by chance. The pro-gram provides feedback on each question
Michael J. Roy, MD, MPH and on the overall conduct of the interview.
Uniformed Services University, Bethesda, MID The advantages and disadvantages of eachof these methods will be discussed.
Continuing medical education has historically Contact:been provided largely through didactic class- chact:room-style teaching. However, educators Michael J. Roy, MD, MPHhave identified this as one of the least effec- Professor of Medicinetive methods of adult education. Adult learn- Uniformed Services Universityers are far more likely to retain new informa- Bethesda, MDtion that is required through experiential orself-directed learning. In addition, manyyoung adults today havecome of age with sig- Presenter: Jaime SAnchez PhDnificant experience with computer-based or"video" games. Comfort with new technolo-gies renders new physicians and physicians- TRAINING BLIND CHILDREN TO DE-in-training ripe for medical education that en- VELOP MATHEMATICS SKILLSgages them through such technologies. Simi- THROUGH AUDIO
290
CYBERTHERAPY 2005 ABSTRACTS
metric figures.Jaime Sanchez, Ph D.
We have tested these audio-based productsUniversity of Chile with twenty blind learners from 7 to 15 years
old in a school setting by using tests forIt is well known that mathematics allow us to mathematics knowledge and thinking, andabstract and understand our surrounding audio memory. We implemented a caseworld. Thus an early training to people in study by doing cognitive introspection duringmathematics can help to develop better learn- and after each task. Children were exposeding skills. People with visual disabilities can to software with formal activities and solvednot learn mathematics easily. Mathematics is related cognitive tasks during six months. Wedeveloped, represented, and communicated have preliminary evidenced that the use ofbasically through visual means such as in al- audio-based software with related cognitivegebraic expressions, graphs, and geometric tasks can help to develop mathematics think-figures. A few studies have approached this ing and knowledge. Blind children haveissue by studying new interfaces for mathe- shown positive gains in learning addition,matics learning.1-4 subtraction, multiplication, and division after
interaction with audio-based virtual environ-This research analyses how audio-based ments. They have improved the developmenttechnology can be used as a powerful tool to and use of mathematics skills.train blind children to learn mathematics con-cepts. We introduce and analyze three audio- A usability evaluation was also implementedbased software products to develop mathe- during and after the implementation. Childrenmatics skills. enriched the software after evaluating differ-
ent modules during implementation and help-AudioMath is an audio-based interactive ap- ing us to map their mental models.plication that mimics the social board gameMemory. 5'6 The child has to open pairs of to- Finally, this study adds preliminary knowl-kens in a board with several levels of difficulty edge to the field of learning of mathematicsto find the corresponding pair of tokens in ac- in blind children. We are beginning to under-cordance with the mathematical content such stand how audio-based interfaces can help toas correspondence and equivalency relation- develop mathematics knowledge and skills inships, memory development, and differentiat- blind learners.ing tempo-spatial notions.
ReferencesTheo & Seth is an audio-based interactivevirtual environment to enhance learning of Edwards, A. D. N. and Stevens, R. D. Mathe-number and basic operations with different matical representations: Graphs, curves andlevels of complexity. The metaphor used re- formulas. In D. Burger and J.-C. Sperandiosembles a grange with two major virtual envi- (ed.) Non-Visual Human-Computer Interac-ronments: the kitchen and the henhouse. The tions: Prospects for the visually handicapped.kitchen covers cardinality including the num- Paris: John Libbey Eurotext, (1993), pp. 181-ber, the position in the numerical straight line, 194.information about the antecessor and succes- Sahyun, S., Gardner, S., & Gardner, C., Au-sor; and the introduction of ordinal numbers. dio and Haptic Access to Math and Sci-The henhouse is a virtual space where learn- ence - Audio graphs, Triangle, the Math-ers learn how to do sum and rest. Plus Toolbox, and the Tiger printer. Pro-
ceedings of the 15th IFIP World Com-AudioGeometry is based on Van Hiele's puter Congress, Vienna, Septembermodel of geometric thinking and serve as a 1998, pp. 78-86.guide for instruction and evaluation of geo- Karshmer A., Pontelli E., & Gupta, G., Help-metric skills. The software is implemented ing Visually Impaired Students in thewith a useful scheme to organize content Study of Mathematics. 29th ASEE/IEEE(plane figures, area, and perimeter). Audio- Frontiers in Education Conference, No-Geometry consists of identifying, recognizing, vember 10 - 13, 1999 San Juan, Puertoand naming polygons and related elements as Rico.well as measuring geometric figures and cal- Stevens R. D., and Edwards A. D. N. An Ap-culating areas and perimeters of plane geo- proach to the Evaluation of Assistive
291
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDIGINE
Technology. Proceedings of the ACM AS- Telemedicine and Advanced Technology Re-SETS 1996 Conference. Vancouver, Brit- search Center (TATRC)ish Columbia Canada
S&nchez, J., Flores, H. (2004a). Memory Robotics has moved from industry to health-enhancement through audio. Proceedings care, creating a new revolution. The con-of The Sixth International ACM cepts behind this profound revolution areSIGACCESS Conference on Computers discussed, and the various classes of robotsand Accessibility, Assets 2004, Atantla, are demonstrated, along with their remark-Giorgia, USA, October 18-20, pp. 24-31. able capabilities - from 'robotic cells' to re-
Sinchez J., Flores, H. (2004b). AudioMath: placing entire operating room teams, to rov-Blind Children Learning Mathematics ing robotic systems and medevacs on thethrough Audio. Proceedings of The 5th battlefield, to mobile robots (unmanned vehi-International Conference on Disability, cles) to make rounds for the doctor andVirtual Reality and Associated nurse. Finally speculation on the logical fu-Technologies, ICD VRAT 2004, ture that will emerge once these robotic sys-September 20-22, Oxford, United tems are truly embraced by the medical pro-Kingdom, pp. 183-189 fession
Contact:Jaime Sanchez, Ph D. Presenter: Ben SawyerDepartment of Computer ScienceUniversity of Chile GAMES FOR HEALTH: THERAPY ANDBlanco Encalada 2120 BEYONDSantiago, Chile
Ben Sawyer
Presenter: Richard Satava MD Woodrow Wilson International Center for Scholars
ADVANCED TECHNOLOGIES FOR RE- In the therapy field the use of virtual reality
HABILITATION (VR) and game technologies has been agrowing force for some years but the greater
Richard Satava. MD health field is just tuning in to the possibleuses of games and game technologies. The
Telemedicine and Advanced Technology Research Games for Health project is a Robert Wood
Center (TATRC) Johnson Foundation effort designed to bothexplore and identify relevant uses for game
Numerous technologies, such as virtual real- technologies and the talents that produceity, brain-machine devices, nanotechnology, them that could offer breakthroughs inintelligent prosthetics, robotics, and artificial healthcare from training, to healthorgans to name a few, are opening new op- messaging, to direct patient application.portunities for rehabilitation. Current pro-grams which include exoskeletons and intelli- During this presentation Ben Sawyer whogent prostheses for rehabilitation will focus leads day-to-day activities on the games formainly on how the engineering sciences are health project will discuss the current trendsrevolutionizing care of the disabled and disad- in the games for health field. With the assis-vantaged. Finally we are able to bring new tance of several other presenters the sessiontechnologies to restore function and some- will also highlight the logistical and industrialtimes realistic form for those systems which cultural issues which must be hurdled to fur-are lost or incapacitated, ther the promise game technologies and ap-
proaches have shown.
Presenter: Richard Satava MD Attendees will not only get a sense of the
current best practices but also get a keen
THE REVOLUTION IN HEALTHCARE sense of the comparative advantages (and
ROBOTICS disadvantages) game-based approaches areseeking to offer the health field.
Richard Satava, MD
PresenterL Thomas Senn
292
CYBERTHERAPY 2005 ABSTRACTS
Kazuyoshi Wada1 , Takanori Shibata1'3 , To-ISLANDS - E -MENTAL HEALTH - moko Saito1 Kayoko Sakamotol and KazuoTELEPSYCHIATRY Tanie2
Thomas Senn 1Intelligent Systems Research Institute, NationalInstitute Advance Science and Technology (AIST)
COAT-Basel 1-1-1 Umezono, Tsukuba, Ibaraki 305-8568, JA-PAN2 National Institute Advance Science and Technol-
An overview of the European project IS- ogy (AIST)LANDS will be provided. Which services are 3PERESTO, JSTfeasible and which are desired, which arepromising? The ISLANDS project will be em- Backgroundbedded in e-health and e-mental health. Thepersons involved, the services provided and We have proposed Robot-Assisted Therapythe tools used will then be explained. Different and Activity since 1996, and have been de-questions will be touched: How can informa- veloping mental commit robots that providetion of counselling and therapy be formalised psychological, physiological, and social ef-for persons that are indirectly involved fects to human beings through physical inter-(informal carer) in the therapeutic process? action1 )9). The appearances of these robotsWhat are the process dynamics within an look like real animals such as cat and seal.online therapy? Which patient - therapist rela- The seal robot, Paro, was developed espe-tionships can evolve? Which are the limits of cially for therapy. We have applied seal ro-e-mental health service provisions? bots to therapy of children at pediatric hospi-
tals 4) and to assisting activity of elderly peo-Within ISLANDS, a cognitive behavioural ap- pie at a day service center5 )-7). Recently, sev-proach for the therapy module was chosen; eral research groups have tried robot as-other forms of therapy are imaginable. Details sisted therapy and activity. Dautenhahn hasabout our approaches will be delivered, used mobile robots and robotic dolls for ther-
apy of autistic childrenl°). Besides, robot-Counselling is part of a comprehensive model assisted activity that uses commercializedthat is founded on several assumptions about animal type robots (such as AIBO11), Ne-human development: e.g., individuals achieve CoRo, etc.) has been tried 12)14). For exam-optimal functioning when they attain opera- pie, Yokoyama used AIBO in a pediatricstional mastery of fundamental life skills and ward, and observed the interaction betweenneurosis and functional psychosis frequently children and pointed out that the initial stimu-result from failure to develop certain life skills. lus received from AIBO was strong. How-
ever, the long term stability was quite weak,Further an overview of technological means in compared with living animals 1 2). In this pres-which ISLANDS can be embedded in the fu- entation, we will explain the results of theture is given. Visions for the future are out- robot-assisted activity for elderly people at alined. health service facility for the aged for more
than one year.Contact:Thomas Senn MethodCOAT-BaselBasel 4025 CH In order to investigate the effects of seal ro-Tel: +41613255669 bots to the elderly people, we evaluatedEmail: [email protected] moods of elderly people by face scales1 5 ) that
express person's moods by illustration ofperson's faces, questionnaires of Geriatric
Presenter: Takanori Shibata PhD Depression Scales (GDS) 6 ). Seal robotswere provided into the health service facility
A PROGRESS REPORT OF LONG- on two days per a week from Aug. 2003.TERM ROBOT ASSISTED ACTIVITY ATA HEALTH SERVICE FACILITY FOR Results
THE AGED The results of face scale and GDS showedthat feelings and depression of elderly people
293
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
were improved by interaction with the seal T. Shibata, et al., Robot Assisted Activity forrobots, Paro. Regarding a case study, Senior People at Day Service Center, Proc.Hanako (pseudonym), aged 89, was sociable of Int'l Conf. on Information Technology inand comparatively independent. On the first Mechatronics, pp.71-76, (20:01).day of the interaction with Paro, she looked a K. Wada, et al., Effects of Robot Assistedlittle nervous of the experiment. However, she Activity for Elderly People and Nurses at asoon came to like Paro. She treated Paro like Day Service Center, Proc. of the IEEE,her child or grandchild. Her face scale scores Vol.92, No. 11, pp. 1780-1788 (2004).after interaction were always lower than be- T. Saito, et al., Examination of Change offore interaction after the first day. Unfortu- Stress Reaction by Urinary Tests of Eld-nately, she was hospitalized during Dec. 10 to erly before and after Introduction of26, 2003. When she met Paro for the first time Mental Commit Robot to an Elderly Insti-after leaving hospital, she said to Paro "I was tution, Proc. of the 7t Int. Symp. on Arti-lonely, Paro. I wanted to see you again." Her ficial Life and Robotics Vol.1 pp.316-319GDS score then improved. To the present, (2002).she has continued to join the activity and will- T. Shibata, et al., Tabulation and Analysis ofingly interacted with Paro. Caregivers com- Questionnaire Results of Subjectivemented that interaction with Paro made the Evaluation of Seal Robot in Japan, U.K.,people laugh and become more active. For Sweden and Italy, Proc. of the 2004example, their facial expression changed, sof- IEEE Int. Conf. on Robotics and Auto-tened, and brightened. In addition, Paro en- mation, pp.1387-1392, (2004).couraged the people to communicate, both T. Shibata, Ubiquitous Surface Tactile Sen-with each other and caregivers, by becoming sor, 2004 1st IEEE Technical Exhibitiontheir common topic of conversation. Thus, the Based Conf. on Robotics and Automa-general atmosphere became brighter. tion Proc. pp. 5, 6, (2004).
I. Werry and K. Dautenhahn, Applying MobileConclusions Robot Technology to the Rehabilitation
of Autistic Children, Proc. of 7t Int.We have used seal robots, Paro in RAA for Symp. on Intelligent Robotic Systems,elderly people at a health service facility for pp.265-272 (1999).the aged since August 2003. The results M. Fujita and H. Kitano, An Development ofshowed that interaction with Paro improved an Autonomous Quadruped Robot fortheir moods and depression, and then the Robot Entertainment, Autonomous Ro-effects showed up through more than one bots, Vol.5, pp.7-18 (1998).year. Consequently, the seal robots, Paro A. Yokoyama, The Possibility of the Psychiat-were effective for therapy at health service ric Treatment with a Robot as an Inter-facilities. vention -From the Viewpoint of Animal
Therapy-, Proc. of Joint 1st Int'l Conf. onT. Shibata, et al., Emotional Robot for Intelli- SCIS & ISIS, paper number 23Q1-1, in
gent System - Artificial Emotional Creature CD-ROM Proc. (2002).Project, Proc. of 5th IEEE Int'l Workshop on E. Libin, and A. Libin, Robotherapy: Defini-ROMAN, pp. 466-471 (1996). tion, Assessment, and Case Study,
T. Shibata, et al., Emergence of Emotional Proc. of the 8th Int. Conf. on Virtual Sys-Behavior through Physical Interaction be- tems and Multimedia, pp.906-915tween Human and Robot, Procs. of the (2002).1999 IEEE Int'l Conf. on Robotics and Auto- E. Ohkubo, et. al. Studies on necessary con-mation (1999). dition of companion robot in the RAA
T. Shibata, and K. Tanie, Influence of A-Priori application, Proc. of 2003 IEEE Int.Knowledge in Subjective Interpretation and Sympo. on Computational Intelligence inEvaluation by Short-Term Interaction with Robot and Automation, pp. 101-106Mental Commit Robot, Proc. of the IEEE (2003).Int'l Conf. On Intelligent Robot and Systems C. D. Lorish, R. Maisiak, The Face Scale: A(2000) Brief, Nonverbal Method for Assessing
T. Shibata, et al., Mental Commit Robot and Patient Mood, Arthritis and Rheumatism,its Application to Therapy of Children, Proc. Vol.29, No.7, pp.906-909, (1986).of the IEEE/ASME Int'l Conf. on AIM'01 J. A. Yesavage, Geriatric Depression Scale,(July. 2001) paper number 182 and 6 pages Journal of Psychopharmacology Bulle-in CD-ROM Proc. tin, Vol.24, No.4 (1988).
294

CYBERTHERAPY 2005 ABSTRACTS
the audio experience for the game, extensiveContact: consultations were made with leading expertsTakanori Shibata and engineers from the movie and videogameIntelligent Systems Research Institute industry. As a result, the game has receivedNational Institute Advance Science and Tech- high reviews in the videogame industry for thenology (AIST) quality of sound and has helped the game1-1-1 Umezono, Tsukuba gain over 4-million registered users worldwide.
Ibaraki 305-8568, JAPAN These same sound design techniques and
Tel.: +81-29-861-5980 philosophies need to be incorporated in VR
Fax: +81-29-861-5992 therapy applications to help maximize the
Email: [email protected] emotional impact and increase the sense ofimmersion in the simulation. Important les-sons were also learned concerning the video-game development process and how it relatesto creating so-called "serious games" withgoals other than entertainment. Current
THE OFFICE OF NAVAL RESEARCH trends in the "serious" use of videogame tech-PROGRAM IN VR THERAPY AND THE nologies will be discussed, including theUSE OF "SERIOUS GAMES" AND EN- "Games for Health" Project which held its firstTERTAINMENT TECHNOLOGIES FOR annual conference in Madison, Wisconsin inMEDICAL SIMULATION 2004.
CDR Russell Shilling, Ph.D. Contact:CDR Russell Shilling, Ph.D.
Office of Naval Research Biological and Medical Science & TechnologyDivision
Increasingly, virtual reality (VR) and videogame Office of Naval Researchtechnologies are garnering more interest in the Arlington, VA 22217medical community. At the Office of Naval Email: [email protected] (ONR), programs have been initiatedwhich look at treatments for combat-relatedPost-Traumatic Stress Disorder (PTSD) and Presenter: Vikt6ria Simon MDalso evaluate a wide variety of VR medicaltraining platforms. ONR is also assisting the CLINICAL EXPERIENCES IN USINGDefense Advanced Research Project Agency VIRTUAL REALITY (VR) IN PSYCHO-(DARPA) in developing innovative treatment THERAPYoptions for amputees using videogame tech-nology. One of the underlying philosophies 1Vikt6ria Simon 1MD, ' Lajos Simon 1MD,that unify these different programs is the belief Phd, , 2Barnabis Takccs Phdthat emotion is a crucial component for effec-tive simulation and that lessons learned from 1Semmelweis University Budapest, Department ofthe entertainment industry need to be inte- Psychiatry and Psychotherapygrated into the development process. In the 2DigitalElite, Los Angeles (CA)entertainment industry, sound design is recog-nized as a critical component in creating emo- This year our team in the department of psy-tional content. Until recently, little effort was chiatry and psychotherapy of Semmelweismade to adapt professional sound design tech- University Budapest had the opportunity toniques commonly used in the entertainment create and try VR in treating phobic patientsindustry for use in simulation. This talk will for the first time in Hungary. The programssummarize programs sponsored by ONR to that are available for us can be used for thedevelop VR therapy applications for treating therapy of travel-phobia (subway, driving,Sailors, Soldiers, and Marines. These PTSD bus, airplane), acrophobia, claustrophobia.programs will also be discussed in the context Beside learning the conditions and tools weof research and development activities con- make the first steps needed for exposition-ducted by the author while acting as the sound therapy together with the patient. We teachdesigner, audio engineer, and research psy- also relaxation technics. For controlling thechologist working on the popular videogame, relaxation and the process of the expositionAmerica's Army. In the process of developing we are monitoring real-time the data of
295
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
physiological parameters provided by special Referencebiosensors.
1 IST-2000-26089
After this training period, desensitization takes 2Contract no.: 507248-2place in a virtual environment under the con-trol of the therapist. In the different environ-ments the therapist can change the parame- Presenter: Julie St-Jacquesters in order to get the phobic stimuli strongeror weaker. CLINICAL APPLICATIONS OF VIR-
Based on our first pilot-cases and experi- TUAL REALITY AND CYBERSICK-
ences we can enforce that desensitization NESSwith VR:
Julie St-Jacques Ph.D. candidate and St&-- makes the therapy practically easier to carry phane Bouchard Ph.D.out, also easier to controloutalsoeaser t conrolUniversit6 du Quebec en Outaouais- can be less dangerous than standard desen-sitization (thinking about acrophobia for exam- For a few years, virtual reality (VR) has made- easier to engage patients for therapy its entry as a new therapeutic method, anddrp osiswer t hgane ptients snrd therapis more and more studies are documenting its- drop out is lower than in standard therapies effectiveness, especially for the treatment of- the stimuli that reach the patient can be con- anxiety disorders. Cybersickness is the prin-trolled more precisely, the reactions given by cipal counter-indication with the use of thisthe patient to the environment can be meas- therapeutic method and are also a majorured more precisely. concern for many Research Ethics Boards.
Contact: Very few studies have documented cyber-
Vikt6ria Simon MD sickness in clinical populations and research-Semmelweis University Budapest ers as report very low symptoms. Moreover,Dematmens U syhiatry BudaPsyoth y our current knowledge on this question isDepartment of Psychiatry and Psychotherapy often based on studies conducted either withFax: +36/11/2100-336Email: simonviktoria@_nsvch.sote.hu very different populations (e.g., Navy pilots or
astronauts) or with different tasks (e.g.,
search and rescue, complex motor tasks).These may not generalize well to clinicalpopulations and therapeutic tasks. It is there-
fore important to document cybersickness inNEXT GENERATION VIRTUAL REAL- a way that is useful and applicable to clinicalITY SYSTEMS: FUTURE CHALLENGES situations.
Oliver Stefani, Dipl.-Ing. Designer The goal of this study is to document cyber-sickness by collecting systematic data in chil-
COAT-Basel, Switzerland dren and adults. The sample of non phobice brain participants consisted of 23 children and 34
Technologies that directly stimulate the ban adults. Questionnaire and head motion data
to simulate reality still are science fiction. were r eor naore to c ma r if th
Therefore, current VR technologies are bound were re porder to comp are
to the stimulation of the five human physio- cybersickness reported by non phobics are
logical senses. This paper discusses the state ticipants, data from adult phobics are also
of the art of current Virtual Reality (VR) Sys- used.
tems and highlights their barriers and prob-
lems. The focus will be on stereoscopic dis- The results revealed few cybersicknessplay technologies, CAD-VR integration and symptoms. Wen comparing children andinterface technologies. We will give insights in adults separately, there's no signifi-the trends of new VR technologies which we cant difference in cybersickness reported. Aidentified within VIEW of the Future1 and IN- significant correlation is found between dis-TUITION2 and provide some suggestions to comfort related to VR and the amplitude ofimprove current VR systems. head movements performed during the VR
immersion. Finally, the relatively low level of
296
CYBERTHERAPY 2005 ABSTRACTS
cybersickness reported is comparable be- the users, quality of mental health care andtween phobics and non phobics. The results the economic strength of the region shouldobtained illustrate that VR is safe when used improve and overweight the costs of imple-with healthy participants as well as when all mentation and service support. In the projectthe precautions to ensure there comfort are a questionnaire was developed to identify thetaken. needs of the potential user groups of such a
service. This questionnaire was given to pa-Contact: tients, family members, and therapists in fiveJulie St-Jacques Ph.D. candidate European regions to find relevant differencesUniversit6 du Quebec en Outaouais between urban centers and remote rural re-23 Pharand Gatineau J9A 1K7 gions. The results of this survey showed aCanada dissatisfying situation of mental health-careTel: 1-819-771-7761 X 8392 as well as of diffusion of telecommunicationFax: 1-819-776-8098 technologies in remote regions. We foundEmail: iuliestiacques(@netscape. net little knowledge about and little experience
with telepsychiatry and e-mental health, butall potential user groups showed positive atti-
Presenter: Hubert Sulzenbacher MD tudes towards the psychiatric use of telecom-munication media, and most users were in-
TELECOMMUNICATION IN PSYCHIA- terested having a telepsychiatric or e-mentalTRY: A NEEDS ASSESSMENT OF DIF- health service available.
FERENT POTENTIAL USER GROUPSIN THE "ISLANDS" PROJECT Contact:
Dr. Hubert Sulzenbacher
Dr. Hubert Sulzenbacher Department of PsychiatryMedical University
Department of Psychiatry Anichstrasse 35Medical University Innsbruck, Austria Innsbruck 6020, Austria
Phone: 004351250423668Geography influences access to mental Fax: 004351250423628health-care. There are some regions in the Email: [email protected] Union with particular geographicalcharacteristics, which are responsible for theirbeing behind the average socio-economic Presenter: loannis Tarnanas PhDdevelopment in Europe. In such regions thereis a lack of access to modem health-care fa- AROUSED AND IMMERSED: INTRO-cilities, especially psychiatric and psycho- DUCING "VIRTUAL PAIN" INTO ANtherapeutic therapies. Telecommunication EXTREME TEAM TRAINING EXPERI-technologies, such as the telephone, interac- ENCEtive television, and the Internet, can providefeasible tools for diagnostic, counseling and loannis Tarnanas PhDtherapy purposes to improve mental health-care in such disadvantaged areas. One has to Kozani University of Applied Science, Greecedifferentiate between several users' needs.Persons who are suffering from a certain dis- Biocybernetics approaches for promotingorder are looking for different information, human-system compatibility continuouslyseeking different forms and content of help adjust the challenge level of a task to matchthan their family members, partners, or friends the available resources of the human opera-do. All of them are involved in the disorder tor based on his/her psycho physiologicaland its consequences. So are professionals state. This project expands the scope of bio-who sometimes need advice, especially in cybernetics to teams. The objective of thisstate of the art treatment adjusted to their project was to test the effectiveness of a se-specific environment. "ISLANDS", a project lected training intervention enabled by VEfunded by the Commission of the European technology. The training intervention that wasUnion (QLRT-2001-01637), aims to develop selected was the use of an advanced teamservices to provide modular, remote psychiat- human-computer interface to enhance VEric and psychotherapeutic assistance for re- training effectiveness. Specifically, this pro-mote areas. By these means quality of life of ject tested the effects of one operator's psy-
297

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
cho-physiological fear and anxiety measures, EXPLORING ANIMATED NARRATIVEto another operator's explicit display of control VIGNETTE TECHNOLOGY TO UNDER-"difficulty", represented in a force feedback STAND EMPATHY, AGGRESSIONJoystick ("virtual pain"), to handle cues in a AND RACIAL IDEOLOGIES WITH MID-counter strike wargame simulation. Prior re- DLE SCHOOL YOUTHSsearch work indicated that social psychophysiological compliance can predict team Sharon Tettegah, Ph.D., Helen Neville, Ph.D.performance in a projective tracking task(Tarnanas, et al., 2003). Two instructional VE University of Illinois, Urbana Campaignwere presented. One VE was using the ex-plicit biocybernetic interface that challenged Research status: Completed Preliminarythe self-efficacy and team decision making of Clinical Trialsthe operators in a crisis situation scenario, bylinking their heart rates (ECG), electrodermalactivity (EDA) and electromyogram measure-ments of facial muscle tensions (EMG) with a Relational aggression, such as name callingForce Feedback Joystick of controlled "ease" and other epithets, remain in today's schoolof movements while engaged in a joint task. environments. Despite the effort to reduceThe second VE was the same team crisis relational aggression (name-calling, eye roll-situation environment as the above, but with- ing, etc.) in schools, such behaviors continueout the introduction of the advanced biocyber- to pervade our classroom and subject stu-netic interface. In both the scenarios the op- dents to forms of unnecessary victimization.erators had the freedom to communicate ver-bally while engaged in the common task. Two This study begins with a personal narrative of
an eleven year old African American female,performance measures were computed: (a) which was developed into a web-based ani-RMS error, and (b) number of groundings. mated narrative vignette (ANy). An ANV is aAnalyses of RMS error scores indicate that scenario that expresses a real life experienceperformance improved over the three re- that mimics a situation (Tettegah, 2002,peated runs with each VE, as evidence of 2003, 2004). As a research and teachingspecific-channel learning. Similarly, perform- tool, other types ofance improved on the first run from Day 1 to vignettes tend to be positively received byDay 2, as evidence of near-transfer learning, both scholars and educators and the use ofHowever, the advanced biocybernetic inter- vignettes has been empirically validated toface provided to the first experimental group, help students achieve educational goals on aprovided an additional important statistical variety of technical, social, and behavioralperformance improvement relative to the topics (Barter & Renold, 2000; Finch, 1987;"simple" VE group and the control groups. Chau et al., 2001; Mosquera, Manstead &
The mapping between the type of user- Fischer, 2002; Schoenberg & Ravdal, 2000;
operator state and the type of medium re- slee, Durrheriel o aneal,
sponse also had an influence on the level of Sleed, Durrheim, Kriel, Soloman, et al.,presence. This project suggests that social- 2002;). Our research leverages the storytel-presnce.Thyisprojct measuggestsnd that soil- ling process of creating an ANV by usingpsychophysiological measures and team bio- technology and will leverage the deliverablescybernetics merit further investigation in so- of that storytelling process, the vignettes, tociotechnical systems that demand high profi- understand how students perceive, in thisciency and self-efficacy. paper, an incident in the classroom (multiple
Contact: types of ANVs have been created with differ-Ioannis Tarnanas PhD ent foci). This research sought to answer theKozani University of Applied Science following questions: Is ANV technology aThessalonica, 1st Emm. Papa street viable fidelity to measure student responses55236 Kozani, Greece to social, anti-social and behavioral disposi-
Phone: +302310344831 tions?
Fax: +302310344810 MethodEmail: ioannistcauthg.qr
Participants. One hundred and four middle
Presenter: Sharon Tettegah PhD school students (N= 55 males, N = 45 fe-males, 4 unidentified) in the inner city Chi-cago area participated in this study. Students
298
CYBERTHERAPY 2005 ABSTRACTS
were in the 7th and 8th grade (N= 30, 7th Finch, J. (1987). The vignette technique ingraders and N = 70, 8th graders, 4 unidenti- survey research. Sociology, 21(1). 105-114fled). Qualitative data analysis revealed the Chau, J., Chang, A., Lee, I., Ip, W., Lee, D.,following categories: & Wootton, Y. (2001). Effects of using
videotaped vignettes on enhancing stu-Racism = acknowledgement of racism or ra- dents' critical thinking ability in a baccalau-cial prejudice occurring in the vignette (0 = no reate nursing programme. Journal of Ad-acknowledgement; 1 = acknowledgement) vanced Nursing, 36(1), 112-119.Empathy = participant expressed empathy Mosquera, P.M., Manstead, A.S.R., &toward the victim in the vignette (0 = no ex- Fischer, A.H. (2002) the role of honourpressed empathy; 1 = expressed empathy) concerns in emotional reactions to of-Response = how the participant would re- fences. Cognition and Emotion, 16(1). 143-spond to the situation. There are three rows 163representing physical aggression, verbal re- Schoenberg, N.E., & Ravdal, H. (2000). Us-sponse, and tell authority. Physical Aggres- ing vignettes in awareness and attitudinalsion (first row) -- 1 = response includes some research. International Journal of Socialform of physical aggression (e.g., hit, beat up, Research Methodology, 3(1).63-74etc.); 0 = no physical aggression Verbal Re- Sleed, M., Durrheim, K., KrieI,A., Solo-sponse (second row)-- 1 = participant indi- man,V., & Baxter, V. (2002). The effective-cated verbally responding to Scott (e.g., in- ness of vignette methodology: A compari-quired about his intentions and thinking, insult son of written and video vignettes in eleicit-him, etc.); 0 = no verbal response Tell Author- ing responses about date rape. South Afri-ity (third row)-- 1 = participant would respond can Journal of Psychology, 32(3).by telling an authority figure (e.g., teacher, Tettegah, S. (2002b). Teachers, identity,principal, parent); 0 = no mention of telling psychological capital, and electronicallyauthority Affect = self identified affect or per- mediated representations of cultural con-sonal feelings of the participant sciousness. In(e.g., acknowledging personally feeling mad, Proceedings of the 14th Ed-Media Worldangry, hurt, offended, etc.) (0 = no acknowl- Conference on Educational Multimedia,edged affect; 1 = acknowledged affect) Hypermedia and Telecommunications (pp.
337-340).Results Denver, CO. Tettegah, S. & Kien, G. (2003,
April) Identity, Human-Computer-Data analysis suggested that students inter- Interaction, and Teacher Voices. Paperpreted the situation using ANV technology as presented at thea methodological tool was effective. The stu- Annual Meeting of American Educationaldent's were able to take on the perspectives Research Association Conference, Chi-of character(s) in the ANV and respond in cago, ILways that suggest perspective taking and Tettegah, S. (2004, August). Pre-serviceproblem solving, teachers problem solving and victim empa-
thy; What about Jamilah? Poster presentedNovelty/Discussion at the Annual Meeting of the American
Psychological Association.Prior work in this area focused on pre-serviceteachers (Tettegah, 2002, 2003, 2004). Our Contact:research provides the first systematic evalua- Sharon Tettegah, Ph.D.tion of the use of an ANV technology as a University of Illinois, Urbana Campaignmethodological tool with middle school stu- 383 Education, MC 708, 1310 S. Sixth Streetdents to understand how students perceive Illinois, United Statesclassroom conflict. Phone: (217) 265-6206
Fax: (217) 244-4572References Email: stetteqa(aad~uiuc.edu
Barter, C. & Renold, E. (2000). I wanna tellyou a story; exploring the application of vi- Presenter: Dave Thomas PhDgnettes in qualitative research with childrenand young people. International Journal ofSocial Re search, 3(4). 307-323
299

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
NIDA'S VIRTUAL REALITY PAIN RE- BackgroundSEARCH PROGRAM
Autistic Disorder is defined by social andDave Thomas, PhD communicative impairments and restricted,
narrow interests. Impaired motivation is alsoNational Institutes on Health common.National Institute on Drug Abuse
Several investigators have developed com-The National Institute on Drug Abuse (NIDA) puter-based and virtual environment tools tohas an annual budget of about a billion dol- address various issues in autism(I-5). Fourlars, and is the largest drug abuse research projects at CUA address the social impair-funding entity in the world. NIDA supports ment.basic drug abuse research, clinical trials ofanti-addiction medications, and research on Method/Toolscommunity interventions for drug abuse pre-vention and treatment. NIDA also supports Face Processing: The prediction that autisticmany other areas of research that are related face processing impairment involves gazeto drug abuse. One example of this is NIDA's differences was tested in an eye trackingextensive pain research program. NIDA's study using a VR display. A replication ininterest in pain research is many fold, and progress uses a monitor.includes research on why many pain killersare addictive, how to make analgesics that Early Intervention: A virtual environment, withare less addictive, and the development of kiddie-ride, monitor display and eye tracker,effective non- pharmacological pain treat- is being tested. The goal is to induce youngments. Included in this later category are children with autism to attend to faces.treatments using acupuncture, transcutane-ous electrical nerve stimulation (TENS), and Social Navigation: A joystick-navigable, first-virtual reality (VR). NIDA's VR and pain pro- person-perspective shopping mall is pre-gram is in its infancy, yet a number of projects sented on a monitor. To locate objects, thehave been funded that have demonstrated user must move either between or aroundefficacy of VR in the treatment of various social and non-social obstacles. Data includetypes of pain, including dental pain, burn pain, user comments and path records.and pain encountered during physical ther-apy. NIDA is also funding research for the Training in Social Conversation: SIMmersionuse of VR, along with fMRI imaging, to allow LLCTm are collaborating with us to develop apeople with chronic pain to control the brain social conversation module for adults withareas responsible for their pain, thereby re- Asperger's Disorder. A virtual character re-ducing their perception of chronic pain. At members the conversation and responds asNIDA, VR is envisioned as a powerful tool that would an actual interlocutor to the user'scan be used to help many of the millions of speech.people living life with chronic pain.
Results
Presenter: Cheryl Y. Trepagnier PhD Face Processing: Preliminary results (withheadset) confirmed gaze differences(6). The
VIRTUAL ENVIRONMENTS TO AD- replication is in progress. Early intervention:DRESS AUTISTIC SOCIAL DEFICITS Reliability-testing is being completed.
Social Navigation: Controls describe theirCheryl Y. Trepagnier, Ph.D., Marc M. Se- avatar's actions in the first person, and re-brechts, Andreas Finkelmeyer, Maya Cole- frain from walking between conversing char-man, Willie Stewart, Jr., Monica Werner- acters. Data collection with persons with au-Adler. tism has begun. Training in Social Conversa-
tion: Development is in progressThe Catholic University of America
DiscussionResearch Status: The paper describes re-search in progress. The projects described above derive from the
hypothesis that failure to establish species-
300
CYBERTHERAPY 2005 ABSTRACTS
typical face attention and processing itselfundermines cognitive development(7). Ac- The Hong Kong Polytechnic Universitycordingly face processing is targeted in youngchildren, and compensatory training is ad- Background/Problemdressed with older individuals. The challengeis to make the technology not only effective, With increasing life expectancy, the inci-but adequately entertaining to overcome au- dence of chronic illness and chronic pain alsotistic motivational barriers, increase. Chronic pain robs older people of
their quality of life, limits functional mobilityReferences and ambulation, and this lead to muscle atro-
phy. The older persons are reluctant to re-(1) Max ML, Burke JC. (1997). Virtual reality quest pain relief, attempting to endure pain
for autism communication and education, as 'normal' part of ageing. Chronic pain andwith lessons for medical training simulators. mobility difficulties interact among older per-Stud Health Technol Inform. 39:46-53. son; causing a negative feedback loop in
(2) Parsons S, Mitchell P. (2002). The poten- which reducing physical activity to avoid paintial of virtual reality in social skills training for usually ends up a further increase in painpeople with autistic spectrum disorders. J when activity is undertaken. To this end, theIntellect Disabil Res. 46(Pt 5):430-43. innovative non-pharmacological intervention
(3) Parsons S, Mitchell P, Leonard A. (2004). in pain management is appealing.The use and understanding of virtual envi-ronments by adolescents with autistic spec- Method/Tooltrum disorders. J Autism Dev Disord. 34(4):449-66. Affective images and pictures were used in
(4) Strickland D, Marcus LM, Mesibov GB, 15 elderly (12 female and 3 male, agesHogan K. (1996). Brief report: two case ranged 60 to 80, median age 71) in chronicstudies using virtual reality as a learning tool pain and needed to perform stretching andfor autistic children. J Autism Dev Disord. 26 standing exercises in their physiotherapy(6):651-9. session. The affective picture book was
(5) Strickland D. (1997). Virtual reality for the made according to the preference of thetreatment of autism. Stud Health Technol older persons. The images included ChineseInform. 44:81-6. snack food and dim sum; market areas; land-
(6) Trepagnier C, Sebrechts MM, Peterson R. mark of the city; transportation system; flow-(2002). Atypical face gaze in autism. Cy- ers and natural scenery as well as imagesberpsychol Behav. 5(3):213-7. and pictures of previous famous movie
(7)Trepagnier C. (1996). A Possible Origin for stars. There were about 60 images and pic-the Social and Communicative Deficits of tures in the picture book.Autism. Focus on Autism and Other Devel-opmental Disabilities. 11(3):170-82. Pain scores were measured by Visual Ana-
logue Scale (VAS) and health-related qualityContact: of life was measured by Medical OutcomesCheryl Y. Trepagnier, Ph.D., Study Short Form 36 (SF 36). VAS and SF-The Catholic University of America, 36 were taken in week 1 and in week 6. PainWashington, DC, USA scores were measured during physiotherapyTel: 1 (202) 319-5780 session in following weeks.Fax: 1 (202) 319-6162Email: trepagnierccua.edu Results
Before the intervention, pain intensity wasPresenter: Mimi M.Y.Tse PhD found to be severe (median pain scores was
50 on a 100mm VAS). There was a signifi-AFFECTIVE IMAGES: RELIEVING cant decreased of VAS from week 1 to weekCHRONIC PAIN AND ENHANCING 6 (t = 3.607; df = 14; p <0.05). Also, a signifi-QUALITY OF LIFE FOR OLDER PER- cant decreased in VAS when the older per-
SONS sons were watching affective pictures whileperforming the physiotherapy exercise in the
Mimi M.Y.Tse PhD, RN, Sandra P.Y. Pun,, 2nd and 3rd week; but not over the 4th and
BSN, RN, MHA, Iris F.F.Benzie, DPhil, FIBMS 5th week. SF-36 had been increased in
301

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
week 6 which indicated an increased in work for haptic interaction with 3D virtualhealth-related quality of life, despite not statis- scenes automatically generated from a videotically significant. captured by a single camera. The system is
used for training visually impaired users.Discussion/Conclusion
Background/ProblemThe study demonstrated a decreased in painperception and increased in health-related The combination of two different and comple-quality of life among the older persons with mentary modalities like haptics and video is achronic pain. Before the intervention, pain very challenging research area. The potentialwas severe enough to hinder their activities of benefits of such a combination for the visu-daily living, decreasing the desire to partici- ally impaired people are very high [1], sincepate in exercise and social events, they will be able to navigate in unknown for
them places without risking injuries etc., asRegular physical activity is important to will be described in the sequel.health. With the use of affective images andpictures, the older persons tend to report less Method/Toolspain; became more cooperated and increasedthe mobility level during and after the physio- Initially, bi-directional 2D motion estimation istherapy session. In this regard, affective im- performed on the video. Rigid 3D motion andages and pictures appear to be an effective structure is recovered using an object basednon-pharmacological intervention in pain reconstruction approach, which makes use ofmanagement for the older persons, of which, extended Kalman filtering (EKF), utilizingtheir mobility and quality of life would be en- also a basic knowledge of the scene. Thehanced. resulting 3D structure data are used to gen-
erate the 3D model of the processed scene.Novelty This is accomplished either by generating a
single mesh of the scene utilizing the gener-There has not been any research and applica- ated depth maps, or by applying modeling fortion of affective images and pictures as an the objects of the scene using analytical im-adjunct to pain relief for older population. Our plicit functions and non-linear least squaresstudy adds knowledge to existing pain relief minimization. The generated model is used inmethods. order to provide haptic access to the proc-
essed scene for the blind using haptic de-Contact: vices like the PHANToM and the Cyber-Mimi M.Y.Tse Grasp.School of NursingThe Hong Kong Polytechnic University ResultsPhone:852 2766 6541Fax: 852 2364 9663 In order to evaluate the proposed methods,Email: hsmtseCDinet.polyu~edu.hk experiments were performed on 3D real
maps of buildings as well as indoor maps.The camera captures the map and the sys-
Presenter: Dimitrios Tzovaras PhD tem converts the monoscopic video into a 3Dmodel. Finally, the blind user navigates
HAPTIC ACCESS TO VIRTUAL MOD- through the map using the haptic devices [2].The experiments demonstrated the efficiency
ELS OF REAL DATA FOR TRAINING of the proposed methods. The system per-THE VISUALLY IMPAIRED forms in real time and if there exists knowl-
edge about the captured scene, like the caseK. Moustakas, G. Nikolakis, D. Tzovaras and with the 3D maps, the scene can be approxi-M.G. Strintzis mated using implicit functions and computa-
tionally intensive processes like collision de-Informatics and Telematics lnstitute/CERTH tection are performed 20-30 times faster,
when compared to standard mesh basedResearch Status: Completed. methods.
This paper presents a completed novel frame- Usability Studies
302
CYBERTHERAPY 2005 ABSTRACTS
GRAPHY EXAMINATIONThe proposed haptic interaction system hasbeen also evaluated in tests with users of the K. Moustakas, G. Nikolakis, D. Tzovaras andBlind Association in Thessaloniki, Greece. M.G. StrintzisThe system evaluation results have shownthat users consider it very innovative and sat- Informatics and Telematics Institute/CERTHisfactory in terms of providing realistic andsmooth force feedback. The percentage of the Research Status: Completed.satisfied users was reported to be more than96\%. Analysis of variance (ANOVA) test The proposed paper describes a force feed-were also performed and illustrated interest- back control system for the performance ofing statistical results (i.e. the gender does not remote ultrasound examination.affect the performance results of the user,there exists a difference in performance for Background/Problemusers which were born blind). These tests arenot presented in detail due to space restric- During the last few years, there have been ations. lot of efforts to use and integrate virtual envi-
ronments in medical applications. SuchConclusion works have been developed in order to im-
prove the performance of specific medicalIn terms of novelty the proposed framework applications. In our case, a 3D virtual envi-combines video with haptics in a real time ronment is developed to provide the expertframework for the generation of virtual with a realistic simulation of remote ultra-scenes, which are then used to train visually sound examination. The proposed paper de-impaired people, on how to navigate in spe- scribes the force feedback [1] control aspectscific areas. Moreover it extends structure from of a remote ultrasound examination system.motion (SfM) methods and combines them The haptic interface is used by an ultrasoundwith surface approximation schemes using specialist in order to control a robotic systemimplicit surfaces, thus resulting in an efficient, and perform a remote ultrasound examina-realistic and user-friendly system. tion.
References Method/Tools
[1] D. Tzovaras and G. Nikolakis and G. Fer- The PHANToMT [2] fictive probe can providegadis and S. Malasiotis and M. Stavrakis, sufficient data for the control of the robot,"Design and Implementation of Haptic Virtual which is located at the remote site, and offersEnvironments for the Training of Visually Im- the capability to use force feedback to assistpaired", IEEE Transactions on Neural Sys- the expert performing the echography exami-tems and Rehabilitation Engineering, vol. 12, nation. In the proposed virtual reality 3D envi-no. 2, pp. 266-278, June 2004. ronment a menu provides the user/expert[2] G.C. Burdea, "Force and touch feedback with the ability to select between a variety offor virtual reality" Wiley-lnterscience Publica- actions and functionalities. Specifically, thetion 1996. user can view a representation of the work-
space. The user in the expert site can simplyContact: import appropriate 3D geometries fromD. Tzovaras VRML files. The expert can select the exami-Informatics and Telematics Institute/CERTH nation working area using the PHANToMT1st km Thermi Panorama Road Stylus and start/stop the examination proc-Thermi-Thessaloniki, 57001 Greece ess. When the expert selects the examina-Phone: +302310464160 tion area an automatic scaling occurs so thatFax:+302310464164 the active PHANToMT workspace size canEmail: moustakýDitLc[ access all the workspace of the slave robot,
using a uniform scale factor. When the ex-pert starts the examination, the force feed-
Presenter: Dimitrios Tzovaras PhD back is applied to the expert via PHANToMTdepending on the force measured by the
HAPTIC INTERFACE FOR THE PER- slave robot located at the remote station. TheFORMANCE OF A REMOTE ECHO- 3D model can be also used as an alternative
303

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
source for providing this force feedback inputto the PHANToMT device, in cases of weak Dr. Efisia Urrucommunication links. For safety reasons, ifthe PHANToMT probe penetrates the 3D L'Associazione Medica Italiana per lo Studio dellagraphical model over a threshold value, an Ipnosi (A.M.I.S.I)alarm sound is activated to warn the expertfor possible communication failure. The use of This is a time to venture for hypnotherapy. Alla master probe and slave robot brings up the things change in a human being. The strangeproblem that they have different workspaces. link between us and machines is a realityUsing scaling can solve the problem of differ- today. Milton Erickson gives us a lesson forent workspaces. If scaling is applied only to the coming years. His mysterious work, onlythe positions and the forces felt by the human in this millennium appears as a secret coderemain the same, as measured at the remote that will be revealed to the new genera-site, then the appearing stiffness of the envi- tion. With the case of "February Man" it isronment changes due to the scaling factor "s". possible for us to give a new interpretation toIn order to solve this problem scaling is also it. This is a new era for hypnosis. Do weperformed to the force feedback. stand by? Our answer is in this work the
PROJECT IR in which for the first time hyp-Results nosis is utilized with virtual reality. Therapist
and patients together live in a virtual pro-The system was integrated with a communi- gram. In this project synthesis there are twocation system for the transmission of ultra- possible programs. One is the developmentsound images and video and it was tested. of relaxation with a standard program of vir-The results have shown that the doctors ap- tual reality for all people that want to removepreciated the haptic feedback when the com- themselves out of their daily life. This pro-munication bandwidth was good enough to gram is made for a psychologist's clinic or inprovide feedback to the user without noticable the future when it will be available as a video-delay. game in personal homes. Two is a specific
virtual reality program for grave pathologyConclusion such as phobias, depression, psychosis, and
schizophrenia.In this paper, we presented a new 3D virtualreality environment with force feedback con- This virtual reality program is made aftertrol and inspection of ultrasound examination, studying a deep history of patience. EachThe system was successfully integrated and program has the same key of opening andtested to a Tele-Echography environment, closure with particularly pictures.
Reference Contact:Dr. Efisia Urru
[1] G.C. Burdea, "Force and touch feedback L'Associazione Medica Italiana per lo Studiofor virtual reality" Wiley-lnterscience Publica- della lpnosi (A.M.I.S.I)tion 1996. Street lamarmora 38[2] Sensable Technologies Inc., h•ttrl Sardinia Cagliari Italywww.sensable.com/ Tel: 3477762318
Email: efisia.urruwa-inwind.itContact:D. TzovarasInformatics and Telematics Institute/CERTH Presenter: Cecilia Vera MSc1st km Thermi Panorama RoadThermi-Thessaloniki, 57001 Greece WEARABLE SYSTEM FOR AUTO-Phone: +302310464160 MATIC EMOTION DETECTION IN EX-Fax:+302310464164 TREME CONDITIONSEmail: moustakaitixgr
Cecilia Vera MSc
Presenter: Efisia Urru PhD SIEMENS, S.A.
PROJECT IR In the recent years the automatic detection of
304

CYBERTHERAPY 2005 ABSTRACTS
human emotions has been one of the areas of gain knowledge in this area and increasinginterest within the scientific community. Most the efficiency in diagnosis.of the studies published so far are based on acombination of two techniques: advanced im- AUBADE project will develop the next gen-age-processing and codification of expres- eration of the remote emotion's monitoringsions. This second approach is based on the systems, providing health professionals withtheories that postulate the existence of basic an innovative tool that will lead them to aand universal emotions and establish a rela- deep study, analysis, understanding, andtionship between these basic emotions and comprehension of human emotions.certain facial expressions. Up to now, a goodstrategy for detecting a subject emotion has Contact:been the analysis of facial images to deter- Cecilia Vera MScmine the expressions shown by the individual, SIEMENS, S.A.and the subsequent codification of these ex- Ronda de Europa, 5. Tres Cantos.pressions in terms of basic emotions. Never- Madrid 28070, Spaintheless, this abstract brings up an innovative Phone: + 34 91 514 45 84method for the detection and recognition of Fax: +34 91 514 47 87human emotions: the processing of biomedi- Email: [email protected] signals.
This novel technique has been the origin of Presenter: Erik Viirre MD PhDthe AUBADE project (partially funded by theEC IST programme) that aims to develop an ADAPTIVE DISPLAYS: CAN WE PRE-intelligent, multi-sensor and wearable system DICT PERFORMANCE?for the assessment of the emotional state ofhumans under special or extreme conditions. Erik Viirre M.D. Ph.D.1 , Tzyy-Ping JungThe emotions are detected after the process- Ph.D.1 , Bradley Chase Ph.D.2 , Yi-Fang Tsai3 ,ing of electromyogram (EMG) measurements Shawn Wing 3, Christopher Strychacz 3
obtained from the face of the person to beassessed. Additionally other biomedical sig- 1 University of California, San Diegonals are considered: hearth rate variability, 2 University of San Diegoskin conductivity and respiration rate. This 3 Naval Health Research Center, San Diegoapproach means an alternative to the tradi-tional image-processing techniques and Research Status: In Progress.makes possible the application of the systemin a wider number of situations, especially in Backgroundthose were it is not achievable to have facialimages available. The project, now in pro- Adaptive displays are often envisioned asgress, involves the utilization of innovative systems that respond to state changes in antechnologies, such as wearable devices, bio- operator. To date, physiologic measures aresensors, data fusion, medical decision sup- typically averaged over a window of someport systems, 3-D animation and telecommu- duration, often several minutes, to developnications. statistical certainty on the onset of a state
change. We are interested in determining theThe result of the project will be a modular and possibility of using physiologic measures tomultifunctional system to be applicable in di- more directly predict the onset of perform-verse areas. In the health sector, it is ex- ance changes during tasks. To do so, we arepected that it will contribute to improve the examining oculomotor changes as they pre-diagnosis of neurological diseases as well as cede performance on a dual auditory andto get a better comprehension of the psycho- visual tracking task. In line with previouslogical status of patients through the emotion studies in this area (1,2), we anticipate that adetection. It will be used to monitor people number of oculomotor behaviors will changeunder high levels of stress or special condi- with performance and that an aggregatetions, making possible to assess the effects measure will have higher predictive powerthat these conditions produce to their emo- that an individual measure. Our aspiration istional state. The system will also establish to be able to monitor oculomotor activity,relations between facial expressions and cer- perhaps combined with other behavior meas-tain diseases, helping health professionals to ures, to detect work overload conditions
305

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
where errors might occur. Such approaches provements in performance. If predictivewould be applicable to situations such as the measures can be described for our particularcommon driving-while-talking-on-the-phone tracking/audio task, it will be important to de-and could be used to warn drivers that their termine how generalizable our model of cog-attention is overloaded. nitive overload and our metrics can be for
other high work-load conditions.Method/Tools
ReferencesEye movements and head were recordedEyeLink II from SR Research. The interactive Van Orden K., Limbert W., Makeig S., andSTI fixed-base driving simulator developed Jung T-P, "Eye Activity Correlates of Work-by Systems Technology, Inc. with custom load during a Visualspatial Memory Task",visual scenes were used for a curving moun- Human Factors, 43(1):111-21, 2001.tain-driving scenario. Participants were asked Van Orden K, Jung T-P, and Makeig S,to maintain lane position between two moving "Combined eye activity measures accu-vehicles a fixed distance apart. The secon- rately estimate changes in sustained visualdary task was a version of the Paced Auditory task performance," Bio Psych, 52:221-40,Serial Addition Test (PASAT). Subjects hear a 2000series of numbers, mentally add a number tothe previous number and verbally state thesum. Difficulty is varied as a function of num- Contact:ber presentation speed. A typical number Erik Viirre M.D. Ph.D.presentation rate of 1.8 seconds results in University of California, San Diegoapproximately 60% correct responses. The Department of Cognitive Sciencesubjects were instructed to perform three ten- Tel: 858 336-0317minute block trials of driving, auditory, and the Fax: 858 270 0740dual tasks. Eye movement behaviour charac- Email: eviirre~cucsd.eduteristics including those of blinks, saccades,vergence eye movements and pupil diameterare all being examined for their statistical rela-tion to the correct or incorrect responses on Presenter: Daniela Villanithe audio task and to the variability on thedriving performance task. VIRTUAL REALITY TO REDUCE ANXI-
Results ETY IN HEALTHY POPULATION: THERELAXATION ISLAND
Preliminary data analysis has progressed todescription of overall comparisons of perform- Daniela Villanil; Francesco Riva 2 ; Eva L. Wa-ance on the combined task compared to the terworth, Ph.D.3; John Waterworth, Ph.D. 4;individual driving or audio task. Comparison of Jonathan Freeman, Ph.D.S; Giuseppe Riva,performance on the auditory task alone ver- Ph.D.1 .sus with driving showed that there was small,non-significant decrease in performance with 1 Applied Technology for Neuro-Psychology Lab,the dual-task. Blink durations increased in the Istituto Auxologico Italiano, Milan, Italycombined task versus the driving task alone, 2 Center for Communication Psychology, Catholicbut actually substantially increased during the University of the Sacred Heart, Milan, Italyauditory task alone. Further, the variability of 3 Tools for Creativity Studio, The Interactive Insti-blink duration showed a similar pattern. Fur- tute, Umeg, Swedenther analyses are ongoing. 4 Department of Informatics, Ume6 University,
Umea, SwedenConclusion/Discussion 5 Department of Psychology, Goldsmith College,
University of London, UK
We hope that this study will provoke discus- The use of Virtual Reality in therapy is not asion as to the feasibility of using physiologic novelty [11 and we expect that, combined withmeasures as direct predictors of performance different relaxation techniques, it can enhanceas opposed to general indicators of operator the relaxation by visually presenting, andstate. Improved prediction could lead to ad- thereby enhancing, key images for facilitatingvanced adaptive interfaces and direct im- relaxation and acceptance, and enabling par-
306
CYBERTHERAPY 2005 ABSTRACTS
ticipants to practice, and hence master, relaxa- Manual for the State-Trait Anxiety Inven-tion and acceptance techniques in a more real- tory (Form Y). Palo Alto, CA: Mind Gardenistic context. Watson, D.; Clark, L.A.; Tellegen, A. (1988).
Development and validation of brief meas-The aim of the study is to explore whether the ures of positive and negative affect: Theeffects on mood, specifically on anxiety and PANAS scales. Journal of Personality &positive and negative states, of a therapeutic Social Psychology, 54(6)narrative enhance through its presentationwithin a virtual environment [2] in an immer- Contact:sive condition. Daniela Villani
Applied Technology for Neuro-PsychologyTo accomplish this goal we use the Relaxa- Labtion Island in which we apply different relaxa- Istituto Auxologico Italianotion techniques, following a specific protocol Via Pelizza da Volpedo 41that is composed by two sessions. Three Milan, Italyphases compose each session: the first is Ph./Fax +39-02619112892based on immersive navigation in the day, the Email: d.viIlani(auxoloqico.itsecond on imagination and the third on im-mersive navigation in the night.
Presenter: Tamar Weiss PhDThe techniques aim to reduce anxiety linkedto active negative thinking through cognitive THE VIRTUAL MALL: A FUNCTIONALcontrol and to achieve progressive muscular VIRTUAL ENVIRONMENT FORrelaxation following the approach proposed by STROKE REHABILITATIONJacobson [3] and the breathing techniques.To test the enhance of the effects we com- Debbie Rand M.Sc 1,3, Noomi Katz Ph.D2,pare this procedure with an usually video pro- Rachel Kizony M.Sc 1,2,3,4, Meir Shahar MBA3 ,cedure, a new age DVD with relaxing music, Patrice L. (Tamar) Weiss Ph.D 1'3
where participants watch a video and havethe freedom to imagine any sensory element 1 Department of Occupational Therapy, Universityrequired. Some of the questionnaires used of Haifaare Positive and Negative Affect Schedule 2 School of Occupational Therapy, Hadassah-(PANAS), to measure the positive and nega- Hebrew University, Jerusalemtive affects [4], and State Trait Anxiety Inven- 3 Laboratory for Innovations in Rehabilitationtory (STAI), to measure the level of anxiety[5]. TechnologyParticipants, University students, were 30 4 Dept of Occupational Therapy, Sheba Medical
subjects ranging from 21 to 24 years old, split Center, Tel Hashomer
up in two groups. The study is in progress and Research Status: In Progressthe results will be ready in march, thereforepreliminary outcomes will be presented during Backgroundthe conference.
References Patients who have had a stroke constitute alarge population with significant needs for
Riva, G., Wiederlhold K. B. and Molinari E. rehabilitation. To date, even after long, inten-
(Eds), (1998) Virtual Environment in Clinical sive and costly rehabilitation, these patients
Psychology and Neuroscience. Amsterdam: still suffer from many impairments leading to
lOS Press severe restrictions of participation in everyFreeman, J., Lessiter, J., Keogh, E., Bond, day life. In addition, there is insufficient train-
F.W., & Chapman, K. (2004) Relaxation ing of instrumental activities of daily living
Island: virtual, and really relaxino. 7th Inter- (IADL) functioning during the rehabilitation,national Workshop on Presence/Presence since it is both time consuming and techni-2004, 13-15 October, Universitat Polite cnica cally difficult to implement. There is a great2004 13len Octoberin. advantage to remediate motor and executivede Valencia, Spain. function deficits via practicing tasks that are
Jacobson, E. (1938) Progressive Relaxation, functional, meaningful to the patient, andChicago. U. of Chicago Press which can be repeated over and over again
Spielberger, C. D., Gorsuch, R. L., Lushene, in a safe environment. A Virtual Mall (VMalI)R., Vagg, P. R., & Jacobs, G. A. (1983) has been designed to be used for the treat-
307

ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
ment of patients following a stroke who have In comparison to functional virtual environ-motor and/or executive functions deficits (1). ments that are presented on desktop VR sys-
tems or those which use a Head-mountedAims Display, the use of a video capture platform
for the development of a virtual functional1) To describe the development of a func- environment is advantageous since it encour-tional virtual environment, the Virtual Mall. 2) ages patients to actively move their affectedTo present data from a pilot study of stroke upper extremity in a relatively functional man-patients which assessed the suitability of the ner while planning, initiating, and problemVMall for this population, and 3) To present solving when engaged in the shopping task.the data of an initial clinical trial which exam-ines the effectiveness of the VMall environ- Referencesment for the assessment and treatment ofexecutive functions deficits and motor deficits. 1. Weiss, P.L., Rand, D., Katz, N., & Kizony,
R. (2004). Video capture virtual reality as aMethod flexible and effective rehabilitation tool. Jour-
nal of NeuroEngineering and Rehabilitation,Participants: For testing the suitability of the 1:12.VMaII, six patients, aged 50-74 years, who 2. Wilson, B.A., Alderman, N., Burgess,had sustained a stroke more than two years P.W., Emslie, H., & Evans, J.J., (199,6). Be-prior to the study were pilot-tested. For the havioral Assessment of the Dysexecutivepilot clinical trial stroke patients, aged 50-85 syndrome. Bury St. Edmunds: Thames Val-years, who had sustained a stroke at least ley Test Company.three months prior to the study will be re-cruited. The patients all suffer either from aconsiderable motor impairment of their upper Presenter: Marc Wolter PhDextremity (assessed using the Fugl-MeyerMotor Assessment) and/or from deficits in NEUROMAN - A COMPREHENSIVEtheir executive functions (assessed using two SOFTWARE SYSTEM FOR NEURO-subtests from the Behavioral Assessment of PSYCHOLOGICAL EXPERIMENTSthe Dysexecutive syndrome (BADS) (2)). In-struments: The VMall (to date one large store Jakob T. Valvoda, Torsten Kuhlen, Marcwith multiple aisles), has been implemented Wolter, Claudia ArmbrOster, Will Spijkers,via VividGroup's (www.vividgroup.com) video Rene Vohn, Walter Sturm, Bruno Fimm,capture Gesture Xtreme system (GX). The Martina Graf, Ines Ann Heber, Hans-performance of the task provides multiple op- Christoph Nuerk, Klaus Willmesportunities to make decisions, plan strategiesand multitask, all in a fairly intuitive manner. Virtual Reality Group, Center for ComputingShopping for grocery products is done by vir- and Communication, RWTH Aachen Univer-tually touching the different items located on sityshelves in different aisles. Output measuresrecord the user's performance with in the Background/ProblemVMall and the kinematics of the patient'smovements. Procedure: A single case study Virtual Reality (VR) is an established neuro-design (ABA) will be used to assess the effec- scientific instrument. Several approaches totiveness of treatment using the VMaII. develop software systems for particular
neuropsychological experiments exist, likeInitial ResultslConclusion navigation1 or driving assessment.2 An over-
view is given.3 In other studies game enginesInitial performance data and feedback from have been used.4 These systems are in gen-the patients suggest that the VMall provides eral limited to a specific field of application.an interesting and motivating task. Detailed eWhen experimental paradigms are changed,results of the initial clinical trial will be pre- the software has to be re-designed. In neuro-sented and further development of the VMadl psychological studies exact runtime behav-paradigm will be discussed. iour of the software has to be guaranteed
and measured as well as the responses ofNovelty participants within millisecond accuracy, fea-
tures that are not provided in most existing
308
CYBERTHERAPY 2005 ABSTRACTS
approaches. Finally, some of the systems ments described have been carried out ononly allow execution on desktop-based sys- table-like displays, on a HoloBench TM , in a 5-tems, lacking immersive, stereoscopic visuali- sided CAVE-like environment and with azation. head-mounted display. Electro-magnetic and
optical tracking systems have been used.In order to use Virtual Reality in the broadfield of neuropsychological research, and to Conclusionsmeet diverse needs and requirements ofneuropsychological researchers, we have de- NeuroMan has been used successfully inveloped the NeuroMan system, a comprehen- several neuropsychological studies. Thesive software framework. NeuroMan enables script language with its underlying experi-the user to describe experimental set-ups and mental model is capable of describing vari-their runtime behaviour in a versatile and easy ous experimental set-upsway and to monitor the responses of partici-pants. With our approach we have handled Novelty/Discussionthe challenges of diversity of experimentalset-ups, chronological logging, and heteroge- Even though several approaches to the de-neous virtual environments. velopment of software systems for neuropsy-
chological experiments have been utilized, aMethod/Tools comprehensive software framework for VR-
based experiments has not been establishedThe design of NeuroMan is based on the prin- yet. NeuroMan is capable of handling a vari-ciple, that a description of the experimental ety of experiments on a comprehensive andset-up and its chronological performance homogeneous basis.should be separated from the implementationof VR-methods and their particular implemen- Referencetation on VR-hardware. In NeuroMan experi- [1] Mallot, HA und Gillner, S: Route naviga-mental set-ups are defined by scripts.5 The tion without place recognition: What issystem generates a virtual experiment with recognized in recognition-triggered re-the desired application flow, i.e., a sequence sponses? Perception 29, 43-55, 2000of sessions, blocks, trials and multimodal [2] Wald JL, Liu L, Reil S: Concurrent Validitystimuli, which may be influenced by specified of a Virtual Reality Driving Assessmentuser interactions or system events. The re- for Persons with Brain Injury. CyberPsy-suiting experiments can be executed on a chology & Behavior, 3(4): 643-654, 2000variety of VR-hardware, making use of the [3] Riva G: Virtual environments in neurosci-VR-toolkit ViSTA, and its multimedia exten- ence. IEEE Transactions on Informationsions.6 Main features of NeuroMan are the Technology in Biomedicine 2(4), 275 -possibility to log the overall system behaviour 281, 1998with specific timing characteristics 7 and to [4] Burgess N, Maguire EA, Spiers HJ,handle large environmental models as visual O'Keefe J: A temporoparietal and pre-stimuli. Integration of acoustics, human ava- frontal network for retrieving the spatialtars, and fMRI scanner support are being de- context of lifelike events. Neurolmage,veloped in current projects. 14(2):439-453, 2001
[5] Valvoda JT, Assenmacher I, Dohle C,Results Kuhlen T, Bischof C. NeuroVRAC - A
comprehensive approach to virtual real-We have conducted several neuropsychologi- ity-based neurological assessment andcal experiments with NeuroMan, e.g., re- treatment systems. Medicine meets Vir-search on mental representations of num- tual Reality 11, Los Angeles, 2003bers,8 on attentional asymmetries after sleep [6] Assenmacher I, Kuhlen T, Lentz T, Vor-deprivation 9 and for the assessment and treat- lander M.: Integrating Real-Time Acous-ment of disorders of spatial representations. tics into VR-Applications. Proc. Euro-In a further study we investigated distance graphics/ACM SIGGRAPH Symposiumestimation in VR. 10 Studies concerning the Virtual Environments, Grenoble, 2004influence of language properties on object [7] Valvoda JT, Assenmacher I, Kuhlen T,manipulation and the modulatory effects of Bischof CH. Reaction-Time Measure-attention on pointing and grasping move- ment and Real-Time Data Acquisition forments are currently underway. The experi- Neuroscientific Experiments in Virtual
309
ANNUAL REVIEW OF CYBERTHERAPY AND TELEMEDICINE
Environments. Medicine Meets VirtualReality 12, Newport Beach, CA, 2004 Presenter: Brenda K. Wiederhold PhD
[8] Graf M, Nuerk HC, Valvoda JT, Kuhlen T, MBA BCIAWillmes K: Wie sind Zahlen mental im 3D-Raum reprasentiert? In Rammsayer T, et VR FOR BLOOD-INJECTION-INJURYal. (Edt.), 44. Kongress der Deutschen PHOBIAGesellschaft f0r Psychologie, p. 297,Lengerich: Pabst, 2004 Brenda K. Wiederhold' 2 , Megan Mendoza1 ,
[9] Heber IA, Valvoda JT, Kuhlen T, Sturm W, Tadashi Nakatanil,Fimm B: Asymmetries of visuo-spatial Alex H. Bullinger3, Mark D. Wiederhold1
attention in virtual space after sleep depri-vation. 12th Annual Cognitive Neurosci- 1 Virtual Reality Medical Center, San Diego,ence Society (CNS) Meeting, New York, CaliforniaNY, 2005, (accepted abstract) 2 Interactive Media Institute, San Diego, California
[10] Armbruster C, Heber IA, Valvoda JT, 3COAT-Basel/UPKBS, University of Basel,Kuhlen T, Fimm B, Spijkers W: Distance Switzerland, Department of Psychiatry
Estimation in a VR application: inter-individual differences and intra-individual Virtual reality (VR) exposure therapy hasstabilities from a psychological point of been shown to be successful in treatingview. Proccedings of the 110' international many types of specific phobias which areConference on Human-Computer Interac- mostly visual in nature. However, limitedtion, 2005, (in press) research has been completed on the use of
VR therapy for Blood Injection-Injury (BII)
Contact; phobias, one of the subtypes of Specific Pho-
Jakob T. Valvoda, bia listed in the DSM-IV TR. Since BII pho-
Virtual Reality Group, Center for Computing bia may operate by some tactile component,
and Communication, RWTH Aachen Univer- it may respond differently to VR therapy com-
sity pared to other categories of specific phobias
52074 Aachen, Germany that are largely visually activated. This paper
[email protected] discusses initial development and results
Tel: +49 - 241 - 80-243 76 from a study on both subjective and objective
Fax: +49 - 241 - 80-221 34 arousal elicited by a prototype virtual worldwhich has been developed to treat those withBII phobia. The present study evaluated the
Presenter: Christine Youngblut PhD responses of 20 healthy, non-phobic maleand female participants to VR blood and in-
PRESENCE-- SETTING THE SCENE jection stimuli. Initial results are positive andshow that the VR world delivers appropriate
Christine Youngblut PhD cues to elicit physiological and self-reportedarousal when exposed to the injection sce-
Institute for Defense Analyses narios. Correlations between self-reportedanxiety and physiological arousal confirm
Much attention has been focused on feeling a that individuals experiencing greater symp-
sense of presence in a virtual environment toms of fear in conditions involving blood or
(VE). The potential importance of presence is injections will exhibit more intense arousal
based on an assumption that increasing the from the virtual stimuli than those who experi-
sense of presence experienced in a VE leads ence reduced symptoms. Findings suggest
to improved task performance, that the virtual world is an effective method ofcue exposure for individuals who experience
The goal of this informal talk is to set the scene anxiety in situations related to blood and in-
for the following presentations by introducing jections. Future research on the use of VR
the presence construct. It will summarize the exposure therapy in the treatment of BII pho-
results of over 120 studies that have been con- bia is warranted.
ducted by various researchers over the lastdecade. Critical outstanding research ques- Contact:
tions will be identified, along with some recom- Brenda K. Wiederhold
mendations for future presence research. Interactive Media Institute6160 Cornerstone Court East, Suite 161
310

CYBERTHERAPY 2005 ABSTRACTS
San Diego, CA 92121 PARIS FRANCEPh: (866) 822-8762 Phone: + 33 1 42 16 12 59Fax: (858) 642-0285 Fax: + 33 1 53 79 07 70
Email: znaidi.extjussieufr
Presenter: Feryel Zna'fdi
TOWARDS A COGNITIVE AND SENSO-RIAL MODEL OF PRESENCE: ASTUDY IN DIFFERENT VIRTUAL SEN-SORY CONDITIONS
Feryel Zna'idi, MA, Olivier Warusfel, Roland
Jouvent, IsabelleViaud-Delmon
CNRS UMR 7593
Presence is the experience a person has,when in a virtual environment (VE), of 'beingthere.' Presence is an important concept toassess the effectiveness of a virtual environ-ment in clinical applications. We designed anexperiment in which the importance of differ-ent factors that might contribute to the feelingof presence could be evaluated. Three kindsof VEs in which different sensory informationwere provided to the subjects were tested andcompared. Subjects were equipped with ahead-mounted display coupled with an elec-tromagnetic sensor system and immersed in avirtual town in which they could move forwardby pressing a mouse button. Subjects had toturn on their own vertical axis in order tochange the direction of heading in the virtualtown. Their task was to locate different land-marks and become familiar with the town. Af-ter this virtual navigation, they had to fill in apresence scale, a state anxiety scale, a cybersickness symptoms scale, and complete sev-eral spatial memory tests related to their ex-perience. Subjects had to perform this naviga-tion according to three conditions (Vis, Avis,and A) during separate sessions. In the AViscondition subjects were equipped with thehead-mounted display and headphones,which delivered a soundscape updated in realtime according to their movement in the virtualtown. In the third condition, they were askedto navigate in a soundscape in the absence ofvision (A). The sounds were producedthrough tracked binaural rendering (HRTF)and were dependent upon the subject's move-ments. During all conditions, skin conduc-tance was recorded.
Contact:Feryel Zna'fdi, MACNRS UMR 7593
311




















