
Elimination of Congenital Syphilis Book.cdr - National AIDS ...
Upload
independentCategory
view
0download
0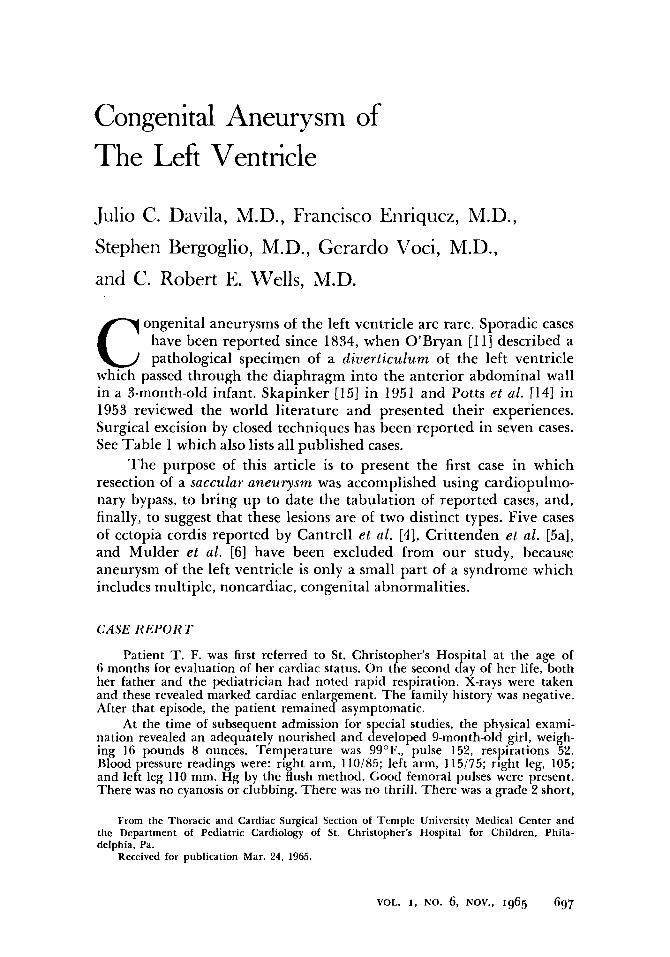
Congenital Aneurysm of The Left Ventricle
Julio C. Davila, M.D., Francisco Enriquez, M.D., Stephen Bergoglio, M.D., Gerard0 Voci, M.D., and C. Robert E. Wells, M.D.
ongenital aneurysms of the left ventricle are rare. Sporadic cases have been reported since 1834, when O'Bryan [l 11 described a C pathological specimen of a diverticulum of the left ventricle
which passed through the diaphragm into the anterior abdominal wall in a 3-month-old infant. Skapinker [15] in 1951 and Potts et al. [14] in 1953 reviewed the world literature and presented their experiences. Surgical excision by closed techniques has been reported in seven cases. See Table 1 which also lists all published cases.
The purpose of this article is to present the first case in which resection of a saccular aneurysm was accomplished using cardiopulmo- nary bypass, to bring up to date the tabulation of reported cases, and, finally, to suggest that these lesions are of two distinct types. Five cases of ectopia cordis reported by Cantrell et al . [4], Crittenden et al. [5a], and Mulder et al. [6] have been excluded from our study, because aneurysm of the left ventricle is only a small part of a syndrome which includes multiple, noncardiac, congenital abnormalities.
CASE R E P O R T
Patient T. F. was first referred to St. Christopher's Hospital at the age of 6 months for evaluation of her cardiac status. On the second day of her life, both her father and the pediatrician had noted rapid respiration. X-rays were taken and these revealed marked cardiac enlargement. The family history was negative. After that episode, the patient remained asymptomatic.
At the time of subsequent admission for special studies, the physical exami- nation revealed an adequately nourished and developed 9-month-old girl, weigh- ing 16 pounds 8 ounces. Temperature was 99"F., pulse 152, respirations 52. Blood pressure readings were: right arm, 110/85; left arm, 115/75; right leg, 105; and left leg 110 mm. Hg by the flush method. Good femoral pulses were present. There was no cyanosis or clubbing. There was no thrill. There was a grade 2 short,
From the Thoracic and Cardiac Surgical Section of Temple University Medical Center and the Department of Pediatric Cardiology of St. Christopher's Hospital for Children, Phila- delphia, Pa.
Received for publication Mar. 24, 1965.
VOL. 1, NO. 6, NOV., 1965 697

DAVILA ET A L .
A B FIG. 1. ( A ) Preoperatiue chest x - m y . There is marked cardiac enlargement of the left ventricle. The intrapulnionary uasculature is normal in appearance. (B) Post- operative (18 months) chest x - m y reuealed the heart to be smaller and more normal in contour.
rough, grating, apical systolic murmur. Diastole was clear, and the second sound at the pulmonic area was normal. The liver edge was 1 cm. below the right costal margin. The rest of the physical examination was within normal limits.
X-ray (Fig. 1A) revealed 3+ to 4+ cardiac enlargement of the left ventricular type with a peculiar bulbous form. T h e pulmonary vasculature appeared normal.
ECG (Fig. 2) revealed marked left ventricular hypertrophy with strain. There was a reversal of the T waves across the precordium and inverted T waves in leads I, 11, antl AVF.
At cardiac catheterization, the O2 study failed to reveal intracarcliac shunting of blood. Arterial 0, saturation was within normal limits.
Retrograde catheterization of the left ventricle via the aorta was carried out for cineangiography (Fig. 3A, H , C). The left ventricle seemed to be partitioned into a normal-sized proximal contractile portion antl a relatively noncontractile distal portion, almost as large, which filled secondarily from a small stream from the proximal portion. Sluggish contractility raised the possibility of fibroelastosis. An injection in the root of the aorta revealed normal origin, caliber, and coiirse of the coronary arteries. Pressures within the piilmonary circiilation were at the upper limits of normal. The pulmonary artery wedge pressure was slightly elevated, as was the left ventricular end-diastolic pressure.
When the patient was 14 months old, surgery was performed. The patient was placed in the dorsal decubitus position and the chest was entered through a mitl- line, sternum-splitting incision. The pericardium was opened in the midline and the aneurysm was visualized (Fig. 1A). I t was located on the lateral wall of the left ventricle and measured about 6 cm. in diameter, 2.5 cm. in height; it had a broad base. The wall was very thin and even transparent in several areas. The patient was placed on total bypass using the superior and inferior venae cavae for venous return and the right external iliac artery for the arterial line. The aneurysm was opened, revealing two chambers, one measuring 2.4 cm. and the other 1.5 cm. in diameter (Fig. 4B). There was a communication between the larger chamber and the left ventricle. The smaller chamber communicated with the larger one through a 1.0 cm. hole in the septum between the two. The com- munication with the left ventricle was 1 cm. in diameter. The inner surface of the aneurysm was white and glistening, suggesting the possibility of endocardial fibroelastosis. T h e endocardial surface of the ventricular cavity could be partially
698 1 H E ANNALS 01; lHORACI<; SURGERY

Congetiital b'entrirwlar Aneurysms
FIG. 2 . (Above) Preoperative ECG. Marked left ventricular hypertrophy with strain. There is reversal of the T waves across the precordium and in- verted T waves in leads I , 11, and AVF.
(Left) Postoperative (18 months) ECG. Less left ventricular hypertrophy, but the strain is persistent.
VOL. I , NO. 6, NOV., 1965 Ggg

DAVILA E T AL.
FIG. 3. T h e angiocardiogram rmealed progressiue filling (left to right) of n large aneurysm-like structure arising from the left ventrick. T h e nnrirrysm is noncontractile; the main body of the ventricle does not contract as vigorously ns cxpected. Both coronaries originate from the aorta and appear to ha-oc a norrnnl distribution. Blood gas studies show n o evidence of shun!s.
visualized through the small opening, and it appeared to be normal. The opened aneurysm was resected at its base, and the myocardial defect was closed with five heavy silk mattress sutures and reinforced with a continuous row (Fig. 4C). The bypass was discontinued, and the heart beat was of good quality. The pericardium was closed with a few interrupted stitches, a chest tube was inserted into the pericardial cavity, and the chest was closed.
The postoperative course was uneventful as far as her cardiac condition was concerned. It was complicated, however, by a bout of pneumonia which subsided promptly with antibiotic therapy. Digitalization was started on the first post- operative clay, and the patient was discharged on a maintenance dosage. At this writing, she is 20 months postoperative, in excellent condition, and off medica- tions.
The pathological specimen consisted of a bowl-shaped structure 4.0 cm. in its greatest diameter and 2.0 cm. in height. The convex or external surface was smooth and exhibited scattered petechiae. The concave aspect was incompletely divided into a smaller and a larger compartment, lined by thick, opaque endo- cardium. At the site of resection the wall was composed of thin myocardium which varied from 0.2 cm. to 0.7 cm. in thickness. Near the vertex, however, there were two areas where the wall was extremely attenuated, being less than 0.1 cm. in thickness.
Sections were stained with hematoxylin and eosin, Masson’s trichrome, and Verhoeff’s elastic tissue stain. The endocardium consisted of a thick layer of elastic tissue fibers and somewhat smaller amounts of collagen. The elastic was more concentrated toward the luminal aspect of the specimen. Peripherally, bundles of collagen devoid of elastic tissue extended into the myocardium. Coarse trabeculae of collagen also extended from the epicardium into the subjacent myocardium. The thin, apical portions of the specimen consisted almost entirely of fibroelastic tissue with only islands and isolated strands of myocardial fibers; here the tissue was predominantly collagenous, with scant elastic tissue fibers being largely con- fined to the luminal aspect. The arrangement of elastic tissue fibers was somewhat different from that usually encountered in endocardial sclerosis, in which the fibers tend to be located predominantly toward the myocardium rather than luminally as in the present specimen. There was no inflammatory reaction.
T h e lesion is probably best interpreted as simple failure of development of myocardial fibers in a localiied area of the heart, with endocardial sc1erosi.s secondary to the muscular defect.
700 THE ANNALS OF THORACIC SURGERY
A
B
C
FIG. 4. Drawings of the operatiue steps, and photographs of pathological speci- mens. (A) Af ter opening the pericardizim. Pathological specimen: The conilex or serosal surface was smooth and contained sctlttered petechiae. ( B ) T h e aneurysm open, revealing 2 chambers, one measuring 2.4 cm. and t h e other 1.5 cm. i n diameter. Pathological specimen: T h e concaue surface, which is incompletely divided into a smaller and larger compar tment , is lined by thick, opaque endocardium. (C) T h e opened aneurysm was resected at its base and the myocardial defect was closed wi th five heavy silk mattress sutures and reinforced w i th a cont inuous suture. Pathological specimen: T h e thinned-out areas are shown by transillumina- tion.
VOI.. I , NO. 6, NOV., 1965 7 0 1

TA
BL
E 1
. R
EPO
RT
ED
CA
SES
OF
CO
NG
EN
ITA
L A
NEU
RY
SM OF T
HE
LE
FT V
EN
TR
ICL
E
Prop
osed
C
lass
ific
atio
n C
ause
of
Dea
th
Rep
orte
r Y
ear
Age
Se
x A
nato
mic
al D
etai
l of
A
neur
ysm
Fa
te'
O'B
ryan
111
1 18
37
3 m
o.
? D
iver
ticul
um o
f th
e le
ft v
entr
i-
Div
ertic
uloi
d D
ied
cle
pass
ing
thro
ugh
the
dia-
ph
ragm
int
o an
teri
or a
bdom
- in
al w
all
Von
Tha
den
[151
18
65
5 m
o.
M
5.3
cm.
fing
er-l
ike
dive
rtic
ulum
D
iver
ticul
oid
Die
d of
th
e le
ft
vent
ricl
e, p
assi
ng
into
th
e an
teri
or
abdo
min
al
wal
l
Gilb
ert
[151
Arn
old
[151
Asc
hoff
[151
1883
2
mo.
F
3.8
cm.
fing
er-l
ike
dive
rtic
ulum
D
iver
ticul
oid
Die
d of
th
e le
ft
vent
ride
. pa
ssin
g th
roug
h th
e di
aphr
agm
, pr
e-
sent
ing
in t
he e
piga
stri
um
apex
ben
t up
war
d to
the
lef
t lik
e a
hook
1894
1%
mo.
F
1.1
cm.
dive
rtic
ulum
fro
m
the
Div
ertic
uloi
d D
ied
1896
1
? Pa
thol
ogic
al
spec
imen
, di
ver-
D
iver
ticul
oid
Die
d tic
ulum
of
bo
th
cham
bers
, pe
netr
atin
g th
roug
h di
a-
phra
gm;
2.5
cm.
prot
rusi
on
form
ed
hern
ia
3 cm
., ab
ove
umbi
licus
Kol
ler-
Aeb
y [I
51
1907
7
mo.
F
Div
ertic
ulum
of
le
ft
vent
ricl
e D
iver
ticul
oid
Die
d
Wie
ting
[I51
19
12
3 yr
. M
D
iver
ticul
um o
f he
art,
no m
en-
Div
ertic
uloi
d ?
pass
ing
thro
ugh
diap
hrag
m
tion
from
whi
ch c
avity
, whi
ch
pass
ed
thro
ugh
diap
hrag
ni;
dive
rtic
ulum
rep
lace
d in
per
i-
card
ium
and
dia
phra
gm d
osed
Not
men
tione
d
Not
men
tione
d
Not
men
tione
d
Con
geni
tal
syph
ilis
and
bron
chop
neum
onia
Not
men
tione
d
Prem
atur
ity
No
follo
w-u
p

Dre
nnan
I1
51
1928
Mah
rbur
g I1
51
1930
Iffe
rt
[I51
Roe
ssle
r I1
51
1938
1944
Viv
as-S
alas
[ IT
1 19
48
Swye
r [1
51
1950
6 yr
.
3 da
ys
Kew
born
New
born
7 yr
.
3 hr
.
M
M
F F \I
\I
~
Smal
l pc
dunc
ulat
ed
dive
rtic
u-
lum
of
the
left
ven
tric
le c
on-
fine
d w
ithi
n th
e pe
rica
rdiu
m
Div
erti
culu
m
of
the
left
ve
n-
tric
le,
5 cm
. lo
ng,
1 cm
. th
ick
pass
ed t
hrou
gh t
he d
iaph
ragm
to
pr
esen
t as
a
puls
atin
g sw
ellin
g on
th
e co
rd;
had
VSD
,b
hare
lip,
ac
rani
a,
and
othe
r co
ngen
ital
le
sion
s
Dib
crti
culu
m
4.5
cm.
long
, 3.
5 cm
. br
oad
from
bo
th
cham
- be
rs,
pass
ing
thro
ugh
a de
fect
in
th
e di
aphr
agm
Dhe
rtic
ulum
of
the
left
ven
tri-
cl
e 7
X 3
cm
. pa
ssin
g th
roug
h th
e di
aphr
agm
and
pre
sent
ing
abo\
e th
e um
bili
cus,
no
sac;
ha
d ot
her
cong
enit
al
hear
t le
sion
s
Vcn
tric
ular
ane
urys
m o
f th
e le
ft
\ent
ricl
e,
diag
nose
d by
x-
ray
and
EC
G
Bif
urca
ting
di
vert
icul
um
wit
h bu
lbou
s te
rmin
atio
n, 0
.9 c
m.
in
diam
eter
, pe
rfor
atio
n of
on
e sa
c; d
id n
ot p
ass
thro
ugh
diap
hrag
m;
apex
of
the
othe
r sa
c w
as t
issu
e-pa
per
thin
; ha
d PD
Ac
Div
ertic
uloi
d D
ied
Div
crtic
uloi
d D
ied
Div
crtic
uloi
tl D
ied
Rup
ture
d
Mul
tipl
e co
ngen
ital
le
- si
ons
Seco
ndar
y he
mor
rhag
e fr
om u
mbi
licu
s
No
foll
ow-u
p D
ivcr
ticul
oid
Succ
essf
ul li
gati
on
Sacc
u la r
Div
ertic
uloi
d D
ied
No
furt
her
repo
rts
Rup
ture
d
"Pat
ient
s in
whi
ch n
o re
fere
nce
to s
urge
ry i
s m
ade
wer
e no
t op
erat
ed o
n. W
here
que
stio
n m
ark
appe
ars,
no
info
rmat
ion
is a
vaila
ble.
bV
entr
icul
ar s
epta
1 de
fect
. 'P
aten
t du
ctus
art
erio
sus.

TA
BL
E 1
(C
onti
nued
) Prop
osed
C
lass
ific
atio
n R
epor
ter
Yea
r A
ge
Sex
Ana
tom
ical
D
etai
l of
A
neur
ysm
Fa
te"
Cau
se o
f D
eath
Skap
inke
r I1
51
1950
5
mo.
F
Div
erti
culu
m
of
the
left
ve
n-
tric
le,
3 X
1.
25 cm.,
pass
ing
thro
ugh
dcfe
ct
in
ante
rior
po
rtio
n of
di
aphr
agm
in
to
umbi
licus
; se
rous
-lin
ed
sac
com
mun
icat
ing
wit
h pe
rica
r-
dium
Form
ijne
I5b
l 19
50
30 y
r.
F Pr
olon
gati
on
of
left
ve
ntri
cle
abov
e di
aphr
agm
, te
tral
ogy
of
Fallo
t, in
fund
ibul
ar s
teno
- si
s w
ith
pulm
onar
y at
resi
a,
larg
e le
ft v
entr
icle
and
rud
i-
men
tary
ri
ght
vent
ricl
e w
ith
VSD
b,
tric
uspi
d at
resi
a,
and
ASD
d
Snel
len
et a
l. [
I61
1952
5
mo.
F
Tru
nkli
ke p
rolo
ngat
ion
form
ed
by t
he w
all
of
the
left
ven
tri-
cl
e. T
he
epi-
and
per
icar
dial
co
veri
ngs
abse
nt b
oth
on t
his
prol
onga
tion
and
on
the
low
er
ante
rior
as
pect
of
th
e ve
n-
tric
ular
w
all;
the
mas
s pr
e-
sent
ed o
n th
e ep
igas
triu
m
as
a pu
lsat
ing
swel
ling
whi
ch
exte
nded
dow
n to
the
um
bili
- cu
s; l
arge
VSD
b
Pott
s et
al.
I141
19
52
9 yr
. ?
Div
erti
culu
m w
eigh
ing
42
gm.,
5 X
3.5
cm
., w
all
thic
knes
s 3.
5 cm
., m
ade
up
of
thin
ned
out,
bu
t no
rmal
, ep
icar
dium
, myo
- ca
rdiu
m,
and
endo
card
ium
Div
ertic
uloi
d C
lose
d-he
art
surg
ery;
N
o fo
llow
-up
base
cl
ampe
d, t
ran-
se
cted
, an
d m
argi
ns
over
sew
n
Div
ertic
uloi
d D
ied
Dit
erti
culo
id
Die
d
Mul
tipl
e co
ngen
ital
ca
r-
diov
ascu
lar
defe
cts
Hea
rt f
ailu
re
Di\
crti
culo
id
Clo
sed-
hear
t su
rger
y;
No
foll
ow-u
p ba
se
clam
ped,
tra
n-
sect
ed,
and
mar
gins
ov
erse
wn

Lov
itt
and
Lut
z [7
1
Bai
ley
[I1
Ber
tran
d &
Coo
ley
[21
Gro
ss [
I1
Gal
indo
et
al.
[61
1954
1954
1955
1955
1957
63 y
r.
12 c
lays
37 y
r.
7 45 d
ays
M
? F ? F
Mul
tilo
cula
ted
endo
thel
ium
- li
ned
aneu
rysm
exp
lain
ed
on
the
basi
s of
an
omal
ous
vasc
u-
lar
supp
ly,
enla
rged
the
besi
an
vess
els,
or
myo
card
ial
sinu
soid
de
fect
Div
erti
culu
m
20
cm.
long
, 15
m
m.
wid
e fr
om a
pex
of
left
ve
ntri
cle
pres
enti
ng a
s an
epi
- ga
stri
c pu
lsat
ing
mas
s
Ven
tric
ular
ane
urys
m s
ugge
stiv
e of
con
geni
tal
vari
ety,
as
ther
e w
as n
o ev
iden
ce o
f rh
eum
atic
he
art
dise
ase,
ar
teri
oscl
erot
ic
hear
t di
seas
e,
myo
card
ial
in-
farc
tion
, or
TB
; it
mea
sure
d 35
cm
. and
con
sist
ed o
f a
thic
k ye
llow
en
doca
rdia
1 su
rfac
e an
d hy
alin
ized
fi
brou
s tis
sue
and
mus
cle
fibe
rs
No
det
ails
ava
ilab
le
A s
ausa
ge-s
hape
d st
ruct
ure
con-
ti
nuou
s w
ith
the
vent
ricu
lar
wal
l at
the
reg
ion
of
the
apex
, m
easu
red
2 cm
. lo
ng:
the
card
iac
dive
rtic
ulum
was
cov
- er
ed
by
peri
card
ium
; pe
ne-
trat
ed t
hrou
gh a
n o
peni
ng i
n th
e an
teri
or
port
ion
of
the
diap
hrag
m
Sacc
ular
Di\
ert
icul
oid
Sacc
ular
Die
d R
uptu
red
Clo
sed-
hear
t su
rger
y;
No
foll
ow-u
p ba
se
clam
ped,
tra
n-
sect
ed,
and
mar
gins
ov
erse
wn
Die
d U
rem
ia
?
Die
d
?
Pncu
tnon
ia
"Pat
ient
s in
whi
ch n
o re
fere
nce
to s
urge
ry i
s m
ade
wer
e no
t op
erat
ed o
n. f
\'hcr
e qu
esti
on m
ark
appe
ars,
no
inf
orm
atio
n is
ava
ilabl
e.
bVen
tric
ular
sep
tal
defe
ct.
'Pat
ent
duct
us a
rter
iosu
s.
'Atr
ial
sept
al d
efec
t.

TA
BL
E 1
(C
onti
nued
)
Rep
orte
r
Pars
ons
1131
Mus
tard
et
ol.
[I01
Low
e et
al.
[81
Yea
r A
ge
Sex
Ana
tom
ical
D
etai
l
1957
1958
1958
18 m
o.
10 y
r.
8 yr
.
F E
norm
ousl
y hy
pert
roph
ied
left
ve
ntri
cle
wit
h a
wal
l 17
mm
. th
ick.
The
ape
x of
th
e he
art
was
fu
sifo
rm
and
was
co
n-
tain
ed d
ownw
ard
as a
mus
cu-
lar
tube
, co
mm
unic
atin
g at
th
e ap
ex
of
both
ve
ntri
cles
“l
ike
an
ante
ater
’s
snou
t” t
o an
ovo
id t
umor
27
X
18 X
10
m
m.
exte
ndin
g in
to t
he u
m-
b i 1 i
c u s
F D
iver
ticu
lum
in
it
s pe
rica
rdia
l sa
c w
itho
ut d
iaph
ragm
atic
de-
fe
ct
F T
he d
iver
ticu
lum
rem
oved
sur
- gi
cally
w
as
a fi
rm
mus
cula
r tu
be w
ith
a lu
men
0.8
cm. in
di
amet
er
and
7.3 cm.
in
leng
th;
hist
olog
ical
ex
amin
a-
tion
reve
aled
no
rmal
ca
rdix
m
uscl
e w
ith
som
e ir
regu
lar
stra
nds
of
fibr
ous
tissu
e sc
at-
tere
d th
roug
h th
e m
uscu
lar
budl
es
and
som
ewha
t th
ick-
en
ed f
ibro
us e
ndoc
ardi
a1 la
yer
wit
h no
rmal
pr
opor
tion
of
el
astic
tis
sue
Prop
osed
C
lass
ific
atio
n of
A
neur
ysm
Fa
tea
Div
ertic
uloi
d;
Die
d mu
1 tip
le
hear
t de
fect
s
Div
ertic
uloi
d
Div
ertic
uloi
d
Clo
sed-
hear
t su
rger
y;
base
cla
mpe
d,
tran
- se
cted
, an
d m
argi
ns
over
sew
n
Clo
sed-
hear
t su
rger
y;
base
cl
ampe
d, t
ran-
se
cted
, an
d m
argi
ns
over
sew
n
Cau
se o
f D
eath
Hea
rt f
ailu
re
NO
fol
low
-up
NO
fol
low
-up

TA
BL
E 1
(C
onti
nued
) Prop
osed
C
lass
ific
atio
n R
epor
ter
Yea
r A
ge
Sex
Ana
tom
ical
Det
ail
of A
neur
ysm
Fa
tea
Cau
se o
f D
eath
Paro
nett
o [1
21
1963
8
mo.
F
Lar
ge
circ
umsc
ribe
d an
eury
sm
Div
ertic
uloi
d D
ied
of
the
left
ven
tric
le a
ssoc
iate
d w
ith
endo
card
ial
fibr
oela
stos
is
conf
ined
to
th
e no
nane
urys
- m
a1 p
art
of
the
vent
ricl
e
Dav
ila e
t al
. [p
rese
nt
repo
rt1
Hea
rt f
ailu
re
1964
9
mo.
F
Sacc
ular
an
eury
sm
mea
suri
ng
Sacc
ular
O
pen-
hear
t su
rger
y;
Liv
ing
and
wel
l, ne
arly
6
X
2.5
cm.
bilo
cula
ted;
con
- tr
anse
cted
at
its
neck
tw
o ye
ars
post
oper
ativ
e si
sted
of
epic
ardi
um,
myo
car-
an
d th
e m
argi
ns
dium
, an
d th
icke
ned
opaq
ue
over
sew
n w
hite
end
ocar
dium
; ev
iden
ce
of
endo
card
ial
scle
rosi
s th
roug
hout
al
l la
yers
'Pat
ient
s in
whi
ch n
o re
fere
nce
to s
urge
ry i
s m
ade
wer
e no
t op
erat
ed o
n. W
here
que
stio
n m
ark
appe
ars,
no
info
rmat
ion
is av
aila
ble.

DAVILA ET AZ..
TYPES OF ANEURYSMS
All reported cases are listed in Table 1. T h e anomalies have been labeled congenital diverticulum by some and congenital aneurysm by others. Perusal of these cases reveals that these lesions are aneurysms of two distinct types. T h e term aneurysm, derived from the Greek aneurynein, to dilate, seems more appropriate for both types than diverticulum, from the Latin devertere, to turn aside.
DIVERTICULOID ANEURYSM
Diverticuloid aneurysms are found in the majority of the cases; they arise in the region of the ventricular apex. In most instances the “diverticulum” then descends through a defect in the diaphragm to present as a pulsatile mass in the epigastrium or is contained in an umbilical hernia. T h e deverticuloid aneurysm is commonly associated with other anomalies. T h e wall consists of a thinned-out portion of normal-appearing ventricular myocardium lined by endocardium and covered by epicardium. T h e sac may be completely or partially enclosed by pericardium. --
Embryologically the ventral pCdtion of the septum transversum- gives rise to the diaphragmatic, ventral portion of the pericardium, the leaf of the diaphragm, and, by fibrous proliferation, the ventral portion of the abdominal wall [3]. Thus it would appear that the congenital “diverticulum” is closely associated with defective development of the septum transversum. T h e left ventricular cavity is formed from the greatest convexity of the cardiac loop. As the cardiac loop is being formed this portion comes into close proximity with the ventral portion of the septum transversum. At this point the epimyocardiuin of the loop fuses with the mesenchyme of the septum transversum, and, as the latter descends, the apical myocardium is pulled ventrally and caudally.
Normally the myocardium is thinnest at the apex in the region of the whorl formed by the spiraling muscle fibers. It is probable that posi- tion as well as traction contributes to formation of these anomalies.
SACCULAR ANEURYSM
Saccular aneurysm is not associated with anomalies of the dia- phragm or of the abdominal wall and has been discovered at necropsy in both adult [2, 71 and child [17]. These appear to be related to defects in development of the ventricular wall in other than the apical region. They are usually asymptomatic and discovered as an accidental roent- genological finding or at necropsy. T h e wall consists of endocardium, scanty or absent myocardium, and epicardium. T h e sac is contained within the pericardium and may be uni- or multiloculated, and its wall is often translucent as in the case presented above.
708 1 H E ANNALS OF THORACIC SURGERY

Congenital Ventricular Aneurysms
These may be the result of abnormal myocardial sinusoids as suggested by Lovitt et al . [7] or simply of excessively thin myocardium in the region of a deep groove between trabeculae carneae. Pulsion would appear to be a significant factor, whereas traction does not play a role. It is not clear whether endocardia1 fibroelastosis plays a primary part or is a secondary or incidental factor in either type of anomaly.
SUMMARY
T h e first successful resection of a congenital saccular aneurysm of the left ventricle with the use of extracorporeal circulation has been reported. An attempt has been made to classify the 27 reported cases into two groups-diverticuloid and saccular aneurysms-in accordance with their embryological, anatomical, and pathological characteristics.
ACKNO IVLEDGMENTS
The authors wish to acknowledge the participation of Dr. J. Kirkpatrick in the radiological study, and Dr. J. Arey in the pathological study of the specimen of the case presented. Drs. A. Caruso and C. Fink contributed to this presenta- tion by their assistance in the operative management of the case presented and in reviewing the literature.
REFERENCES
1. Bailey, C. P. 2. Bertrantl, C. A., and Cooley, R. N. Congenital aneurysm of left ventricle:
Case report. Ann. Intern. Med. 43:426, 1955. 3. Bremer, J . L. Transposition of aorta and pulmonary artery: Embryologic
study of its cause. Arch. Path. 31:1016, 1942. 4. Cantrell, J. R., Haller, J. A., and Ravitch, M. M. A syndrome featuring
defects of the heart, sternum, diaphragm, pericardiiim and heart. Surg. Gynec. Obstrt. 107:602, 1958.
A syndrome featuring defects of the heart, sternum, diaphragm and anterior abdominal wall. Circiilation 20:396, 1959.
Surgery of the Heart. Philadelphia: Lea 8c Febiger, 1955.
5a. Crittenden, I. H., Atlanis, F. A., and Mulder, D. G.
5b. Formijne, P. 6. Galindo, L., Arean, V. M., Stevenson, S. D., and Rivera, C. Congenital
diverticulum of the heart. Amer. J. Clin. Path. 27:84, 1957. 7. Lovitt, W. V., Jr., and Lutz, S., Jr. Embryological aneurysm of the myo-
cardial vessels. Arch. Path. 57: 163, 1954. 8. Lowe, J. B., Williams, J. D. P., Robb, D., and Cole, D. Congenital diverticu-
lum of left ventricle. Brit. Heart J. 21: 101, 1959. 9. Mulcler, D. G., Crittenden, I. H., and Adams, F. A. Complete repair of a
syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium and heart: Excision of left ventricular diverticulum. A n n . Siirg. 151:113, 1960.
10. Mustard, W. T., Duckworth, J. W. A., Rowe, R. D., and Dolan, F. G. Con- genital diverticulum of the left ventricle of the heart. Canad. J . Stirg. 50: 149, 1958.
11. O’Bryan in T. B. Peacock, (Ed.): On Malformations of the Human Heart (2nd ed.). London: J. Churchill and Sons, 1866.
Aangeboren hartebreken. Nederl. T . Geneesk 94:2704, 1950.
VOL. 1 , NO. 6, NOV., 1965 tog

DAVILA ET AL.
12. Paronetto, F., and Strauss, L. Aneurysm of the left ventricle due to con- genital muscle defect in an infant. Amer. J. Cardiol. 12:5, 1963.
13. Parsons, C. Ventricular extension into the abdominal wall. Brit. Heart J. 19:34, 1957.
14. Potts, W. J., DeBoer, A., and Johnson, F. R. Congenital diverticulum of the left ventricle. Surgery 33:301, 1953.
15. Skapinker, S. Diverticulum of left ventricle of the heart. Arch. Surg. 63:629, 1951.
16. Snellen, H. A., Dankmeijer, J., Briums, C., and Collister, R. M. Saccular elongation of the left ventricle into the abdominal wall with persistence of the anterior mesocardium and ventricular septa1 defect. Cardiologia 21 :562, 1952.
Cardiac aneurysm in a child seven years old. Amer. J. Dis. Child. 75:92, 1948.
17. Vivas-Salas, E.
The Editor and members of the Editorial Board are grateful for the assistance given in the review of certain manuscripts during the past year by the following:
BRUCE ARMSTRONG, M.D., Los Angeles, Calif. DAVID L. DEAN, M.D., Sun Fernando, Calif. JOHN H. EDMONDS, JR., M.D., Augusta, Ga. DONALD R. KAHN, M.D., Ann Arbor, Mich. ROBERT I. KATZ, M.D., Sun Fernando, Calif .
AVERILL A. LIEBOW, M.D., New Haven, Conn. EDWARD E. MASON, M.D., Iowa Ci t y , Iowa DONALD L. PAULSO", M.D., Dallas, Tex.
PAUL C. SAMSON, M.D., Oakland, Calif. GERALD WHIPPLE, M.D., Boston, Mass.
THOMAS YEH, M.D., Augusta, Ga.
710 THE ANNALS OF THORACIC SURGERY
Copyright © 2022 FDOKUMEN




















